Alemtuzumab Review SINS Santiago, Chile
70
ALEMTUZUMAB S ETTING NEW HORIZONS IN MULTIPLE SCLEROSIS TREATMENT Professor Gavin Giovannoni Blizard Institute, Barts and The London School of Medicine and Dentistry
-
Upload
gavin-giovannoni -
Category
Health & Medicine
-
view
1.526 -
download
1
description
My presentation at the SINS meeting in Santiiago. The aim of the presentation was to discuss changes in therapeutic strategies in light of the launch of alemtuzumab as a treatment for active MS defined clinically or on MRI.
Transcript of Alemtuzumab Review SINS Santiago, Chile

ALEMTUZUMAB
SETTING NEW HORIZONS IN MULTIPLE SCLEROSIS TREATMENT
Professor Gavin Giovannoni
Blizard Institute, Barts and The London School of Medicine and Dentistry

Disclosures Professor Giovannoni has received personal compensation for participating on
Advisory Boards in relation to clinical trial design, trial steering committees and
data and safety monitoring committees from: Abbvie, Bayer-Schering Healthcare,
Biogen-Idec, Canbex, Eisai, Elan, Fiveprime, Genzyme, Genentech, GSK, GW
Pharma, Ironwood, Merck-Serono, Novartis, Pfizer, Roche, Sanofi-Aventis,
Synthon BV, Teva, UCB Pharma and Vertex Pharmaceuticals.
Regarding www.ms-res.org survey results in this presentation: please note that
no personal identifiers were collected as part of these surveys and that by
completing the surveys participants consented for their anonymous data to be
analysed and presented by Professor Giovannoni.
Professor Giovannoni would like to acknowledge and thank Biogen-Idec,
Genzyme and Novartis for making available data slides on natalizumab,
alemtuzumab and fingolimod for this presentation.

1.Early therapy
2.Effective therapy
3.Induction therapy
Objectives

1.Early therapy
2.Effective therapy
3.Induction therapy
Objectives

Coles et al. J Neurol. 2006 Jan;253(1):98-108..
Window of therapeutic efficacy

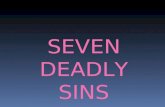
Consequences of increasing EDSS scores: loss of employment1
0
10
20
30
40
50
60
70
80
90
Work Capacity by Disability Level
0.0/1.0 2.0 3.0 4.0 5.0 6.0 6.5 7.0 8.0/9.0
EDSS Score
Pro
po
rtio
n o
f P
ati
en
ts ≤
65
Ye
ars
Old
Wo
rkin
g (
%)
The proportion of patients employed or on long-term sick leave is calculated as a percentage of patients aged 65 or younger.
1. Kobelt G et al. J Neurol Neurosurg Psychiatry. 2006;77:918-926;
2. Pfleger CC et al. Mult Scler. 2010;16:121-126.
Spain
Sweden
Switzerland
United Kingdom
Netherlands
Italy
Germany
Belgium
Austria
~10 yrs2

Survival in MS: a randomized cohort study 21 years
after the start of the pivotal IFN-1b trial
Goodin et al. Neurology 2012;78:1315-1322.

Theoretical model: treat early and effectively
Natural course of disease
Later intervention
Later treatment
Treatment at diagnosis Intervention
at diagnosis
Time Disease Onset
Dis
abili
ty
Time is brain

1.Early therapy
2.Effective therapy
3.Induction therapy
Objectives

Risks vs. Benefits

MS Infographic
www.ms-res.org

No evident disease activity: NEDA
Gd, gadolinium. 1. Havrdova E, et al. Lancet Neurol 2009; 8:254–260; 2. Giovannoni G, et al. Lancet Neurol 2011; 10:329–337.
Treat-2-target
No evidence of disease activity defined as:1,2
× No relapses
× No sustained disability progression
× No MRI activity
× No new or enlarging T2 lesions
× No Gd-enhancing lesions

Treating-2-target
Choosing therapy
X Y Z
Define the
Individual’s MS
No
Treatment failure? Yes
• Patient’s preferences?
• Your choice?
Individual measures:
• Evidence of disease activity?
• Tolerability/safety?
• Adherence?
• Drug or inhibitory markers?
Monitoring
• MS prognosis
• Life style and goals
• Shared goals for therapy
Rebaseline
Rebaseline:
• IFNβ, natalizumab, fingolimod,
teriflunomide, DMF=3-6 months
• Glatiramer acetate=9 months
• Alemtuzumab=24 months
DMF=dimethyl fumarate.

Relapses
Unreported relapses
Clinical disease progression
Subclinical relapses: focal MRI activity
Focal gray and white matter lesions not detected by MRI
Brain atrophy
Spinal fluid neurofilament levels
MS Iceberg
Clinical activity
Focal MRI activity
Hidden focal and diffuse MRI activity
Microscopic or biochemical pathology
Biomarkers

Control Multiple sclerosis

Rheumatoid arthritis End-stage joint disease

Brain atrophy occurs across all stages of the disease
De Stefano, et al. Neurology 2010
n= 963 MSers

Treatment-effect on atrophy correlates with treatment-effect on disability
Sormani et al. Ann Neurol 2014;75:43–49.

Treatment effect on disability predicted by effect on T2-lesion load and brain atrophy
Meta-analysis of treatment effect on EDSS worsening (y) vs effects on MRI lesions
and brain atrophy, individually or combined, in 13 placebo-controlled RRMS trials
(13,500 patients)
Sormani MP et al. Ann Neurol. 2014;75:43-49.

-1.0%
-0.8%
-0.6%
-0.4%
-0.2%
0.0% Years 0-2
-0.82%
-0.80%
P=0.822†
Placebo (N=315) Natalizumab (N=627)
Year 0-1* Year 1-2
-0.40%
-0.56%
-0.43%
-0.24%
P=0.004†
P=0.002†
†Difference between treatments; ‡Change from baseline; Miller DH et al. Neurology 2007;68:1390-1401.
AFFIRM Study: natalizumab and brain atrophy
Mean
(S
E)
perc
en
tag
e c
han
ge i
n B
PF

Fingolimod has an early and sustained effect on the rate of brain atrophy compared with placebo and IFNb-1a IM
FREEDOMS, 2 years
Fingolimod 0.5 mg (n = 356)
Placebo (n = 329)
***
*
**
6 0 12 24
Time (months)
0
-0.4
-0.8
-1.2
-1.6
-2.0
−38%
vs placebo p<0.001
Ch
ange
in m
ean
BV
fro
m
bas
elin
e (%
)
TRANSFORMS, 1 year
0 12
Time (months)
0.0
-0.4
-0.6
-1.0
IFNb-1a IM (n = 359)
Fingolimod 0.5 mg (n = 368)
−40%
vs IFNb-1a IM p<0.001
*** -0.2
-0.8
Ch
ange
in m
ean
BV
fro
m
bas
elin
e (%
)
ITT population with evaluable MRI images. Note: n numbers for FREEDOMS data reflect the number of patients with available data at 24 months. *p<0.05; **p<0.01; ***p<0.001 vs comparator; p-values are for comparisons over Months 0-6, Months 0-12, Months 0-24 BV, brain volume; ITT, intent-to-treat. Gilenya™ Prescribing Information 19 April 2012. Reproduced with permission. Kappos L et al. N Engl J Med 2010; 362: 387-401, and Cohen JA et al. N Engl J Med 2010; 362: 402-415. Copyright © 2011 Massachusetts Medical Society. All rights reserved

Reduction in brain atrophy on alemtuzumab

No evident disease activity: NEDA
Gd, gadolinium. 1. Havrdova E, et al. Lancet Neurol 2009; 8:254–260; 2. Giovannoni G, et al. Lancet Neurol 2011; 10:329–337.
Treat-2-target
No evidence of disease activity defined as:1,2
× No relapses
× No sustained disability progression
× No MRI activity
× No new or enlarging T2 lesions
× No Gd-enhancing lesions
Brain volume loss should be
included in our definition for NEDA

1.Early therapy
2.Effective therapy
3.Induction therapy
Objectives

Pros and cons of maintenance vs. induction therapies
Maintenance therapies
• Continuous treatment
• Low to very high efficacy
• Reversible
• Perceived to be lower risk
• Examples • Laquinimod, GA, IFN-beta, teriflunomide, BG12,
fingolimod, natalizumab, daclizumab
• Breakthrough disease • Suboptimal or failure to respond
• NEDA reliable metric for efficacy
• Rebound activity • Highly likely
• Can be life threatening
• Pregnancy • Contra-indicated
• No potential for a cure • Rebound
• SPMS & progressive brain atrophy
Induction therapies
• Short-courses or pulsed therapy
• Very high efficacy
• Irreversible
• Perceived to be higher risk
• Examples • Mitoxantrone, cladribine, alemtuzumab, anti-
CD20 (?), BMT
• Breakthrough disease • Marker for retreatment
• NEDA unreliable to assess efficacy
• Rebound activity • Less likely
• Unlikely to be life-threatening
• Pregnancy • Strategy of choice
• Potentially curative • 15-20 year experiment
• BMT, alemtuzumab, cladribine

Possible
cure
The Ideal MS Therapy
Reliable
long-term efficacy
Maintaining
QOL
Maintaining
independence
Maintaining the
ability to work
No issue for
pregnancy/fertility
Maximum reduction
of MS disease activity
Maximum
tolerability
Maximum
safety
Ease of
use
Minor impact on
everyday life

Role of T and B lymphocytes in MS
• Activation of autoreactive T cells1,2
• Genetic and environmental
factors involved3
• Increased migration across BBB1,2,4
• Inflammatory response to CNS
antigens1,2
• Release of proinflammatory cytokines
leading to recruitment and activation
of T and B lymphocytes, macrophages,
and microglial cells
• Local release of damaging mediators
by activated cells
• Demyelination, axonal loss1-4
BBB, blood–brain barrier.
1. Hemmer B, et al. Nat Clin Pract Neurol. 2006;2:201-211; 2. Piccio L, et al. In: Primer on Multiple Sclerosis. New York, NY: Oxford
University Press; 2011:47-59; 3. Sospedra M, Martin R. Annu Rev Immunol. 2005;23:683-747; 4. Compston A, Coles A. Lancet.
2008;372:1502-1517.

1.Early therapy
2.Effective therapy
3.Induction therapy
Alemtuzumab

Alemtuzumab for the treatment of RRMS
• Alemtuzumab is indicated for adult patients with
relapsing remitting multiple sclerosis (RRMS) with
active disease defined by clinical or imaging
features1.
• Alemtuzumab is a humanized monoclonal antibody
that selectively targets CD52, a protein abundant
on the surface of B and T lymphocytes2
• A phase 2 & 3 clinical trial program was
implemented to establish efficacy and safety in MS
patients
• Completed 3 head-to-head trials vs. high-dose
subcutaneous interferon beta-1a (SC IFNB-1a)
in patients with active relapsing-remitting
multiple sclerosis (RRMS) 3-6
1. SMPC – EMA label; 2. Hu Y et al. Immunology 2009;128:260-70; 3. Coles AJ et al. N Engl J Med 2008;359:1786-801; 4. Coles AJ et al. Lancet
2012;380:1819-1828; 5. Coles AJ et al. Lancet 2012;380(1829-1839); 6. Brinar V et al. Presented at 21st Meeting of the European Neurological
Society, 2011.

Overview of Alemtuzumab MoA
1. Selection
• In animal studies, innate immune cells that express lower levels of CD52 were affected minimally or transiently by Alemtuzumab2
2. Depletion
Decreases MS inflammation
• Alemtuzumab selectively depletes circulating T and B cells2,3
• Significant numbers of lymphocytes remain present in lymphoid organs after Alemtuzumab treatment2,3
3. Repopulation
Reduces MS disease activity
• CLP cells are presumed unaffected by Alemtuzumab2,4,5
• Distinctive pattern of T-, B-cell repopulation begins within weeks, potentially changing the balance of the immune system2,4,5
CD52 B
CD52 T B T
HSC
CLP
NK/T cell precursor
Pre/Pro B cell
B CD52
T CD52
Monocyte
Macrophage
Neutrophil
NKT
Targets T and B cells thought
to mediate MS inflammation1
The exact mechanism of action of alemtuzumab is not fully elucidated.
CLP, common lymphoid progenitor; HSC, hematopoietic stem cell; MOA, mechanism of action;
NK, natural killer.
1. Weber MS, Hemmer Bl. Results Probl Cell Differ. 2010;51:115-126; 2. Hu Y, et al. Immunology. 2009;128:260-270; 3.Turner MJ, et al. J
Neuroimmunol. 2013;261:29-36; 4. Cox AL, et al. Eur J Immunol. 2005;35:3332-3342; 5. Fox EJ. Exp Rev Neurotherapeutics. 2010;10:1789-1797.

Selective binding to CD52 • Little or no CD52 detected on
neutrophils, plasma cells, BM
stem cells1,2
• Limited, transient effect on innate
immunity3
• Greater effect on circulating cells; lesser
degree of depletion in lymphoid tissue3
CD52 Expression on
Immune Cell Populations2
©2009 Immunology. Used with permission. Placebo Alemtuzumab
To
tal Im
mu
ne
Ce
lls (
×10
8)
3
2
1
Blood
BM
Lymph nodes
Thymus
Spleen
BM, bone marrow; NTG, nontransgenic.
1. Alemtuzumab Summary of Product Characteristics. Oxford, UK: Genzyme Therapeutics, Ltd; 2013. 2. Hu Y, et al. Immunology. 2009;128:260-270; 3. Turner MJ, et al. J
Neuroimmunol. 2013;15;261:29-36.
Post-Alemtuzumab: More Immune Cells Remain
in Lymphoid Tissue vs Peripheral Blood3
6
4
2
0 CD
52
Mo
lecu
les p
er
Ce
ll (×
10
5)
CD
4 s
ingle
pos.
CD
8 s
ing
le p
os.
Do
ub
le p
os.
Do
ub
le n
eg
.
Ma
cro
ph
ag
es
Ne
utr
op
hils
NK
ce
lls
Ste
m c
ells
CD
8 T
ce
lls
NT
G
B c
ells
CD
4 T
ce
lls
CD
4 T
reg
Spleen BM Thymus

Alemtuzumab depletes circulating T and B cells
• Alemtuzumab depleted lymphocytes rapidly and selectively after each treatment course1
• Occurred via antibody-dependent cellular cytolysis, complement-mediated lysis2,3
White Blood Cell Counts
Time After Alemtuzumab, mo
CARE-MS I: White Blood Cell Counts
Following Alemtuzumab1
0 1 2 3 4 5 6 7 8 9 10 11 12
0.0
0.5
1.0
1.5
2.0
4.0
4.5
5.0
Me
an
Ce
ll C
ou
nt (1
09/L
)
Basophils
NR, (0-0.2)4
Eosinophils
NR, (0-0.5)4
Monocytes
NR, (0-0.8)4
Lymphocytes
NR, 0.8-4.15
Neutrophils
NR, 1.8-7.74
NR, normal range.
1. Kovarova I, et al. Presented at: European Neurological Society; 2012; Prague; P341; 2. Minagar A, et al. Expert Opin Biol Ther. 2010;10:421-429; 3. Freedman MS, et
al. J Clin Cell Immunol. 2013;4:152; 4. Coles A, et al. Presented at: American Academy of Neurology; 2010; Toronto; PO6.172. 5. Data on file, Genzyme Therapeutics,
Ltd; Oxford, UK;

Repopulation changes the balance of the immune system
• After Alemtuzumab, distinctive pattern
of T-, B-cell repopulation emerged
within weeks1-3
— B cells return to baseline within 6 months
— T cells generally do not reach baseline by 12
months
• Relative increase in proportion
of Treg cells1,4
• Relative increase in proportion
of memory T, B lymphocytes1,4
• Effects similar after repeated courses4
LLN, lower limit of normal.
1. Alemtuzumab Summary of Product Characteristics. Oxford, UK: Genzyme Therapeutics, Ltd; 2013; 2. Cox AL, et al. Eur J Immunol. 2005;35:3332-3342. 3. Turner MJ,
et al. J Neuroimmunol. 2013;261:29-36; 4. Hartung HP, et al. Presented at: European Committee for Research and Treatment in Multiple Sclerosis; 2012; Lyon; P935; 5.
Kovarova I, et al. Presented at: European Neurological Society; 2012; Prague; P341.
May change balance of
immune system to reduce
MS disease activity1,3
CARE-MS I: Mean Treg Cells as Percentage of Total CD4+ Count4*
2
6
10
14
CD
4+ T
reg C
ell
Count, %
4
8
12
16 Alemtuzumab 12 mg
0.0
1
0.2
0.4
0.6
0.8
1.0
1.2
0 3 6 9 12 13 15 18 21 24
Time, mo
CARE-MS I: Mean Lymphocyte Counts After Alemtuzumab5*
CD4+ T cells
CD19+ B cells
CD19+ LLN
CD4+ LLN
IFNB-1a 44 μg
1 0 3 6 9 12 13 15 18 21 24
Time, mo
Cell
Count (1
09/L
)

Alemtuzumab pharmacokinetics in MS
Clinical effects persist after Alemtuzumab is cleared from circulation
• Alemtuzumab serum concentrations low or undetectable within ~30 days after treatment
Alemtuzumab 12 mg administered at time 0 and 12 months.
Kovarova I, et al. Presented at: European Neurological Society; 2012; Prague; P341.
CARE-MS I: Mean Serum Concentration Over Time
Time on Study, mo
4,000
0
2,000
3,000
1,000
0 1 3 6 9 12 24 15 18 21
Co
nce
ntr
ation
(n
g/m
L)
13
Alemtuzumab
12 mg
Alemtuzumab
12 mg

Efficacy of Alemtuzumab

Clinical development program
2017 2005 2013 2009 2003 2007 2011 2015
CAMMS2231
CARE-MS I3
CAMMS223 Extension2
CARE-MS II4
CARE-MS Extension5
• Included patients with active RRMS who
relapsed on prior therapy and those who
were naïve to treatment1-4
• Efficacy and safety established vs
high-dose IFNB-1a SC (no placebo
used) in 3 rater-blinded RCTs1-4
RCT, randomized controlled trial; SC, subcutaneous.
1. Coles, AJ et al. N Engl J Med. 2008;359:1786-1801; 2. Coles AJ, et al. Neurol. 2012;78:1069-1078; 3. Cohen JA, et al. Lancet. 2012;380:1819-
1828; 4. Coles AJ, et al. Lancet. 2012;380:1829-1839; 5. Data on file, Genzyme Therapeutics, Ltd; Oxford, UK.

Alemtuzumab vs high-dose IFNB-1a SC
MRI inclusion criteria:5
CARE-MS II: MS diagnosis per McDonald criteria; white matter lesions attributable to MS; ≥9 T2 lesions ≥3 mm, any axis;
Gd-enhancing lesion ≥3 mm, any axis, with ≥1 brain T2 lesions; spinal cord lesion with ≥1 brain T2 lesions; CARE–MS I:
MS diagnosis per McDonald criteria; cranial MRI demonstrating white matter lesions attributable to MS (within 5 y of screening);
CAMMS223: MS diagnosis per McDonald criteria, including cranial MRI; ≥1 enhancing lesion on any of ≤4 Gd-enhanced brain
scans during ≤3-mo run-in period (including baseline scan).
NA, not applicable; TIW, 3 times per week. aTreatment with beta interferon or glatiramer acetate for ≥6 months. bThrough month 13.
1. Alemtuzumab Summary of Product Characteristics. Oxford, UK: Genzyme Therapeutics, Ltd; 2013. 2. Coles AJ, et al. Lancet. 2012;380:1829-1839; 3. Cohen JA, et al.
Lancet. 2012;380:1819-1828; 4. Coles AJ, et al. N Engl J Med. 2008;359:1786-1801; 5. Data on file. Genzyme Therapeutics, Ltd; Oxford, UK.
CARE-MS II1,2
Phase III
CARE-MS I1,3
Phase III
CAMMS2231,4
Phase II
Total patients, n
(% completed)
Alemtuzumab
12 mg/d 426 (94) 376 (96) 108 (85b)
IFNB-1a SC
44 μg TIW 202 (78) 187 (88) 107 (62b)
Patient population
Active RRMS,
relapse on prior
therapya
Active RRMS,
treatment-naïve
Active RRMS,
treatment-naïve
Eligibility
≥2 clinical episodes
in prior 2 y,
≥1 relapse in prior y
≥2 clinical episodes
in prior 2 y,
≥1 relapse in prior y
≥2 clinical episodes
in prior 2 y,
≥1 Gd-enhancing
lesion at baseline
Mean age, y 35 33 32
EDSS range (mean) 0.0-5.0 (2.7) 0.0-3.0 (2.0) 0.0-3.0 (1.9)
Mean disease duration, y (median) 4.5 (3.8) 2.0 (1.6) 1.3 (NA)

Phase II study design
CAMMS223
• Rater-blinded, comparator-
controlled trial1
— No placebo used
• 334 treatment-naïve patients
with early, active RRMS1
aReceived study drug.
Note: All treatment arms received 1 g methylprednisolone qd ×3 d at months 0, 12, and 24.
1. Coles AJ, et al. N Engl J Med. 2008;359:1786-1801; 2. Coles AJ, et al. Neurology. 2012;78:1069-1078.
• Co-primary endpoints:
ARR, time to 6-month SAD1
• Safety, efficacy assessments
continued in extension phase
beyond 36 months2
105 QD×3
0 12 24 36
Extension Phase2 Study Duration (mo)1
60
Alemtuzumab
12 mg/d IV 102 101 n=108a
QD×3 QD×5
24
77 92 67
Alemtuzumab
24 mg/d IV 104 n=108a
QD×5
22
82
92 74
IFNB-1a
44 µg TIW SC n=107a 95 80 42 66

Durable efficacy over 5 years
CAMMS223
aCo-primary endpoints.
Coles AJ, et al. Neurology. 2012;76:1069-1078.
0.35
0.12
0
0.1
0.2
0.3
0.4
0.5
38%
16%
0
10
20
30
40
50
0.46
-0.15
-0.4
-0.2
0
0.2
0.4
0.6
0.8
P<0.0001 P=0.0005 P=0.0056
Mean EDSS Score 6-Month SADa ARRa
Months 0-60 Months 0-60 Months 0-60
66% reduction 69% reduction
IFNB-1a 44 μg Alemtuzumab12 mg

Phase III study design
• Rater-blinded RCTs1,2
• Comparator-controlled (no placebo used)
• Scoring by blinded raters1,2
• Relapse, EDSS every 3 months
• MSFC every 6 months
• MRI annually
• Education, safety monitoring program
for patients, physicians1,2
— Surveys, urinalysis, CBC monthly
— Thyroid testing quarterly
• In CARE-MS II only, 24-mg arm included
but discontinued to accelerate recruitment
into other arms; thereafter deemed exploratory1
Both treatment arms received 1 g methylprednisolone qd ×3 d at months 0 and 12.
CBC, complete blood count; IV, intravenous.
1. Coles AJ, et al. Lancet. 2012;380:1829-1839; 2. Cohen JA, et al. Lancet. 2012;380:1819-1828 Image adapted from Hartung HP, Arnold DL.
Presented at: European Neurological Society; 2012; Prague.
Alemtuzumab
12 mg IV Daily
×5
Daily
×3
TIW
IFNB-1a
44 µg SC
Study Duration (mo)
0 12 24
Randomized
Alemtuzumab
24 mg IV Daily
×5
Daily
×3

Phase III efficacy endpoints
ARR, annualised relapse rate; MSFC, Multiple Sclerosis Functional Composite; SAD, sustained accumulation
of disability; SRD, sustained reduction in disability.
1. Cohen JA, et al. Lancet. 2012;380:1819-1828; 2. Coles AJ, et al. Lancet. 2012;380:1829-1839; 3. Data on file. Genzyme Therapeutics, Ltd; Oxford,
UK; 4. Alemtuzumab Summary of Product Characteristics. Oxford, UK: Genzyme Therapeutics, Ltd; 2013.
Co-Primary Endpoints1,2 Secondary Endpoints1,2 Select Tertiary Endpoints1-3
• ARR
• Time to 6-month SAD,
defined as increase of
≥1.0 point on EDSS from
baseline of ≥1.0 (or ≥1.5
point from baseline of 0),
confirmed twice during
6-month period
• Proportion of patients
relapse-free at study
completion
• Change in EDSS score
from baseline
• Percent change in T2
hyperintense lesion volume
from baseline to study
completion
• Change in MSFC
from baseline
• Time to first relapse
• Proportion of patients with
no MS disease activity
(MRI, relapse, SAD) at
years 1, 2
• Time to 6-month SRD
• Change in MSFC
components plus Sloan
charts from baseline
• MRI measures of MS-related
brain measures
• A priori efficacy objective met if statistically significant treatment effect demonstrated
for Alemtuzumab over IFNB-1a SC on either or both co-primary efficacy endpoint(s)4

Significant reduction in ARR
Lower rates of SAD in treatment-naïve patients
CARE-MS I
0.39 0.18
Risk reduction: 55%
P<0.0001
Ad
juste
d A
RR
(9
5%
CI)
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0 Alem
(n=376)
IFNB-1a
(n=187)
187
376
185
376
181
372
177
368
170
368
164
357
162
352
158
345
149
336
25
15
10
5
0
20
Pa
tie
nts
With
SA
D (
%)
8%
11%
30% reduction
P=0.22 (NS)
IFNB-1a 44 μg Alemtuzumab12 mg
ARR: Years 0-21,2a Time to 6-Month SAD1a
Alem
IFNB-1a
0 3 6 9 12 15 18 21 24
Follow-Up Month
aCo-primary endpoints. Alem: alemtuzumab
1. Cohen JA, et al. Lancet. 2012;380:1819-1828; 2. Fox EJ, et al. Presented at: American Academy of Neurology; 2012; New Orleans, LA; PD5.004.

Reduced MRI activity across select markers
CARE-MS I
• Alemtuzumab reduced the proportion of patients with new MRI lesion activity
Endpoint1,2 Alemtuzumab INFB-1a SC P Value
Patients with no new or newly
enlarging T2 lesions, %a 52 42 0.035
Patients with no new
Gd-enhancing lesions, %a 85 73 0.001
Patients with no new T1-hypointense
lesions, %a 76 69 NS
Change from baseline in BPF, %a -0.867 -1.488 <0.0001
Change from baseline in T2
hyperintense lesion volume, %b -9.3 -6.5 NS
aTertiary endpoint.2
bSecondary endpoint.2
1. Alemtuzumab Summary of Product Characteristics; Oxford, UK: Genzyme Therapeutics, Ltd; 2013;
2. Cohen JA, et al. Lancet. 2012;380:1819-1828.

Alemtuzumab patients more likely free of MS disease activity
CARE-MS I
OR: 1.75
P=0.0064
P=0.0388 OR: 2.36
P<0.0001
42
56
27
51
74
39
0
10
20
30
40
50
60
70
80
90
100
Pa
tie
nts
(%
)
MRI
activity-freea
MS disease
activity-freec
Clinical disease
activity-freeb
IFNB-1a 44 μg
Alemtuzumab12 mg
aAbsence of new Gd-enhancing lesion or new or enlarging T2 hyperintense lesion. bAbsence of relapse or SAD. cAbsence of CDA or MRI activity.
CDA, clinical disease activity; OR, odds ratio
Giovanni G, et al. Presented at: European Neurological Society; 2012; Prague.

Alemtuzumab significantly reduced ARR & SAD
CARE-MS II
Time to 6-Month SADa
Alem
IFNB-1a 202
426
200
426
184
412
175
404
167
392
162
384
155
380
145
375
131
354
Pa
tie
nts
With
SA
D (
%)
0 3 6 9 12 15 18 21 24
25
15
10
5
0
20
Follow-Up Month
13%
21% 42% reduction
P=0.0084
aCo-primary endpoints. Alem: alemtuzumab
Coles AJ, et al. Lancet. 2012;380:1829-1839.
0.52 0.26 0.0
0.2
0.4
0.6
0.8
AR
R (
95
% C
I)
ARR: Years 0-2a
Alem
(n=426)
IFNB-1a
(n=202)
IFNB-1a 44 μg Alemtuzumab 12 mg

Alemtuzumab improved pre-existing disability
CARE-MS II
aSecondary endpoint; defined as decrease of ≥1 EDSS point lasting at least 6 months, assessed in patients
with baseline EDSS ≥2.0. bTertiary endpoint. cMeasured by SRD score in relapsing patients.
Coles AJ, et al. Lancet. 2012;380:1829-1839.
IFNB-1a 44 μg Alemtuzumab12 mg
‒0.17
P<0.0001
+0.24
ED
SS
Sco
re, m
ea
n
3.25
3.00
2.75
2.50
2.25
Follow-Up Month
0 3 6 9 12 15 18 21 24
40
30
20
10
0
Pa
tie
nts
With
6-M
on
th S
RD
(%
)
29%
13%
P=0.0002
Mean EDSS Change From Baselinea SRDb
Follow-Up Month
0 3 6 9 12 15 18 21 24
Alemtuzumab is the first and currently only MS therapy to demonstrate sustained improvement
in preexisting disability vs an active comparator (in 2 of 3 clinical trials)

Reduced MRI activity across select markers
CARE-MS II
• Alemtuzumab reduced the proportion of patients with new MRI lesion activity
aTertiary endpoint.2. bSecondary endpoint.2
BPF, brain parenchymal fraction; NS, non significant
1. Alemtuzumab Summary of Product Characteristics; Oxford, UK: Genzyme Therapeutics, Ltd; 2013;
2. Coles AJ, et al. Lancet. 2012;380:1829-1839.
Endpoints1,2 Alemtuzumab INFB-1a SC P Value
Patients with no new or newly
enlarging T2 lesions, %a 54 32 <0.001
Patients with no new
Gd-enhancing lesions, %a 82 66 <0.001
Patients with no new T1-hypointense
lesions, %a 80 62 <0.001
Change from baseline in BPF, %a -0.615 -0.810 0.012
Change from baseline in T2
hyperintense lesion volume, %b -1.3 -1.2 NS

Alemtuzumab patients more likely free of MS disease activity
CARE-MS II
aAbsence of new Gd-enhancing lesion or new or enlarging T2 hyperintense lesion. bAbsence of relapse or SAD. cAbsence of CDA or MRI activity.
CDA, clinical disease activity; OR, odds ratio
Hartung HP, et al. Presented at: American Academy of Neurology; 2013, San Diego, CA; P07.093.
32
41
14
53
60
32
0
10
20
30
40
50
60
70
80
90
100
Pa
tie
nts
(%
)
OR: 3.03
P<0.0001
OR: 2.14
P<0.0001
OR: 0.39
P<0.0001
MRI
activity-freea
MS disease
activity-freec
Clinical disease
activity-freeb
IFNB-1a 44 μg
Alemtuzumab12 mg

Reduction in brain atrophy on Alemtuzumab

ALEMTUZUMAB IMPROVES BRAIN MRI OUTCOMES
IN PATIENTS WITH ACTIVE RELAPSING-REMITTING
MULTIPLE SCLEROSIS: THREE-YEAR FOLLOW-UP OF THE
CARE-MS STUDIES
Douglas L Arnold,1,2 Elizabeth Fisher,3 Jeffrey A Cohen,4 Frederik Barkhof,5 Krzysztof W Selmaj,6 David H Margolin,7 Jeffrey Palmer,7 Edward J Fox8
AAN 2014
Blitz S65-008
1NeuroRx Research, Montréal, Québec, Canada, and 2Department of Neurology and Neurosurgery, Montreal
Neurological Institute, McGill University, Montreal, Québec, Canada; 3Department of Biomedical Engineering,
Cleveland Clinic, Cleveland, OH, USA; 4Cleveland Clinic, Cleveland, OH, USA; 5VU University Medical Centre,
Amsterdam, Netherlands; 6Department of Neurology, Medical University of Łódź, Łódź, Poland; 7Genzyme, a
Sanofi company, Cambridge, MA, USA; 8University of Texas Medical Branch, Round Rock, TX, USA

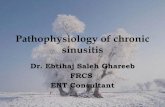
CARE-MS I & II Three-Year MRI Outcomes Change in Brain Parenchymal Fraction (BPF)
Alemtuzumab slowed brain volume loss over 3 years, as assessed by change in BPF
For both patient populations, the median percentage reduction in BPF observed in in Year 3 (0.19% and 0.10%, respectively) was smaller than that observed in Year 1 (0.59% and 0.48%) and Year 2 (0.25% and 0.22%)
Percentage Change in BPF in Formerly Treatment-Naive Patients (CARE-MS I)
Percentage Change in BPF in Patients Who Relapsed on Prior Therapy (CARE-MS II)
Me
dia
n C
ha
ng
e F
rom
Ba
se
lin
e, %
(9
5%
CI)
Year No. of Patients 371 367 351 323
% Change from Previous Year – –0.59% –0.25% –0.19%
Me
dia
n C
ha
ng
e F
rom
Ba
se
lin
e, %
(9
5%
CI)
Year 428 414 405 359
– –0.48% –0.22% –0.10%
No. of Patients
% Change from Previous Year
0 1 2 3
-1 .5 0
-1 .2 5
-1 .0 0
-0 .7 5
-0 .5 0
-0 .2 5
0 .0 0
0 1 2 3
-1 .5 0
-1 .2 5
-1 .0 0
-0 .7 5
-0 .5 0
-0 .2 5
0 .0 0
AAN 2014
Blitz S65-008

CARE-MS I & II Three-Year MRI Outcomes Proportion of Patients Free of Gd Lesions, T2 Lesions, and MRI Activity
The majority of alemtuzumab-treated patients were free of MRI activity (absence of Gd-enhancing lesions and new/enlarging T2 hyperintense lesions) at Year 2 and Year 3
MRI activity-free: absence of both Gd-enhancing and new or enlarging T2 hyperintense lesions; CARE-MS=Comparison of
Alemtuzumab and Rebif® Efficacy in Multiple Sclerosis; CI=confidence interval; DMT=disease-modifying therapy; Gd=gadolinium;
MRI=magnetic resonance imaging; Y=year
No. of Patients 359 370 336 356 370 325 354 369 326
Y1 Y2 Y3 Y1 Y2 Y3 Y1 Y2 Y3
Pro
po
rtio
n o
f P
ati
en
ts,
% (
95
% C
I)
0
20
40
60
80
100
Gd-enhancing
lesion-free
New/enlarging
T2 lesion-free
MRI
activity-free
% MRI Activity Free in Treatment-Naive
Patients (CARE-MS I)
% MRI Activity Free in Patients Who
Relapsed on Prior Therapy (CARE-MS II)
No. of Patients 412 421 364 405 423 361
Gd-enhancing
lesion-free
New/enlarging MRI
activity-free
402 414 361
Pro
po
rtio
n o
f P
ati
en
ts,
% (
95
% C
I)
0
20
40
60
80
100
Y1 Y2 Y3 Y1 Y2 Y3 Y1 Y2 Y3
T2 lesion-free
Patients were treated with alemtuzumab 12 mg at baseline and 12 months later
Re-treatment in Year 3 was administered upon recurrence of disease activity
18% of CARE-MS I patients and 20% of CARE-MS II patients were re-treated with
alemtuzumab in Year 3; <3% were treated with another DMT in Year 3
AAN 2014
Blitz S65-008

Safety of Alemtuzumab

Safety Issues
0 12 24 36
Observation Treatment Cycles Duration (mo)
60 Alemtuzumab
12 mg/d IV
QD×3 QD×5 ? QD×3
Short-term
Infusion reactions
Infections: viral and opportunistic
Travel
Baseline De-risking
VZV
Live vaccines
Latent TB
HPV
Pregnancy
Intermediate-term
2° autoimmunity
Pregnancy
Pulsed steroids
Travel
? Long-term
Immune senescence
2° malignancy
Risks
Monitoring & prophylaxis
Baseline bloods
VZV serology
CXR & quantiferon TB assay
Cervical smear
Pregnancy test
Monthly FBC & urinalysis
3-monthly TFTs
Annual MRI
Pretreatment with steroids, anti-
histamines and paracetamol
Herpes prophylaxis x 28 days
Listeriosis prevention diet Pre-planned rapid access to haematology,
nephrology, dermatology, etc.
Patient education
Baseline counselling Signed consent Engaged with self-monitoring Lifelong monitoring
Active public engagement programme

Overall AE rates in clinical trials
• Rate of AEs with Alemtuzumab 12 mg,
including those leading to treatment
discontinuation, generally similar to
those with IFNB-1a SC
aIncludes CAMMS223, CARE-MS I, and CARE-MS II.
AE, adverse event.
Data on file. Genzyme Therapeutics, Ltd; Oxford, UK.
2-year active-controlled experiencea
• AE profiles similar for treatment-naïve
patients and those who relapsed on
prior therapy
AEs IFNB-1a SC 44 μg
n=496 Alemtuzumab 12 mg
n=919
AEs, n (%) 469 (94.6) 896 (97.5)
Grade 1 (mild) 400 (80.6) 815 (88.7)
Grade 2 (moderate) 402 (81.0) 831 (90.4)
Grade 3 (severe) 106 (21.4) 227 (24.7)
Grade 4 (very severe) 10 (2.0) 27 (2.9)
AEs leading to treatment discontinuation, n (%) 39 (7.9) 21 (2.3)
Serious AEs, n (%) 91 (18.3) 168 (18.3)
Serious AEs leading to treatment discontinuation, n (%) 10 (2.0) 7 (0.8)
Deaths 0 3

Rate of AEs over time
• Rate of AEs was similar in IFNB-1a- and Alemtuzumab-treated patients,
except during month following Alemtuzumab administration, due to IARs1
— IAR rates lower with second vs first treatment course of Alemtuzumab1
• Similar pattern observed in CARE-MS II2 and CAMMS2233
Time, mo
Ra
te o
f A
Es
(to
tal e
ve
nts
/tota
l p
ers
on
-mo
nth
s)
CARE-MS I1
0
1
2
3
4
5
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
Both treatment arms received 1 g methylprednisolone qd ×3 d at months 0 and 12.
1. Coles AJ, et al. Presented at: American Academy of Neurology; 2012; New Orleans, LA; 2. LaGanke CC, et al. Presented at: American
Academy of Neurology; 2013; San Diego, CA. P01.174 3. Data on file, Genzyme Therapeutics, Ltd; Oxford, UK

Overview of IARs in clinical trials
CARE-MS I and II (Pooled)1
Avera
ge N
um
ber
of IA
R S
ym
pto
ms
Infusion Number
Course 1 Course 2
0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
1.6
1.8
2.0
1 2 3 4 5 1 2 3
• To manage IAR severity:
— Pretreat with corticosteroids,
(ie, methylprednisolone)
immediately before infusion
with Alemtuzumab for first 3 days
of any treatment course1
— Consider pretreatment with
antihistamines and/or antipyretics
• Observe patient for IARs
during and for 2 hours after
Alemtuzumab infusion
• Physician and patient education
Premedication and Monitoring2
• Predominantly mild to moderate;decreased with each treatment course3
• 3% serious: pyrexia, urticaria, atrial fibrillation, nausea, chest discomfort,
hypotension2
1. Data on file. Genzyme Therapeutics, Ltd; Oxford, UK; 2. Alemtuzumab Summary of Product Characteristics. Oxford, UK: Genzyme
Therapeutics, Ltd; 2013; 3. Caon C. et al. Presented at: Consortium of Multiple Sclerosis Centers; 2012; San Diego, CA; DX41.

No increase in infection rate over 2 years
Time, mo
Incid
en
ce
of In
fection
s
0.0
0.1
0.2
0.3
0.4
0.5
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
IFNB-1a
Alem12 mg
389
811
388
811
387
811
386
811
384
811
379
811
377
811
375
811
373
811
372
810
371
810
368
810
363
810
362
807
358
807
357
806
355
805
354
804
353
803
352
803
352
797
351
796
349
785
342
761
CARE-MS I and II (pooled data)
IFNB-1a 44g
Alemtuzumab12 mg
Alem: alemtuzumab
Havrdova E, et al. Presented at: European Committee for Research and Treatment in Multiple Sclerosis; 2013, Copenhagen; P603.
• Risk highest in first month after first
treatment; rates decreased over time
• No increase in infection risk that would
indicate cumulative immunosuppressive
effects

Overview of infections in clinical trials
• More frequent with Alemtuzumab
vs INFB-1a (71% vs 53%)1
• Predominately mild to moderate1
• Generally of typical
duration, resolved following
conventional treatment1
• Did not correlate with lymphocyte
counts3
• Total or subgroups CD4,
CD8, CD19
2-year active-controlled experience2a,b
IFNB-1a SC 44 μg
n=496
Alemtuzumab 12 mg n=919
Grade 1, 2 258 (52.0) 618 (67.2)
Grade 3 6 (1.2) 33 (3.6)
Grade 4 0 (0.0) 1 (0.1)
Serious AEs, n (%) 5 (1.0) 25 (2.7)
Nasopharyngitis 82 (16.5) 216 (23.5)
Urinary tract infection 40 (8.1) 162 (17.7)
Upper respiratory tract infection 57 (11.5) 141 (15.3)
Sinusitis 34 (6.9) 100 (10.9)
Oral herpes 6 (1.2) 79 (8.6)
Influenza 25 (5.0) 77 (8.4)
Bronchitis 16 (3.2) 64 (7.0)
Herpes zoster 4 (0.8) 38 (4.1)
Gastroenteritis 5 (1.0) 36 (3.9)
Pharyngitis 7 (1.4) 36 (3.9)
• Prophylaxis with oral
anti-herpes agent (acyclovir
200 mg twice a day used in
clinical trials) starting first day
of treatment, continuing for
1 mo after treatment course
Risk Mitigation (Monitoring)1
aInfections with incidence of ≥5.0% in any
treatment group shown. bIncludes CAMMS223, CARE-MS I, and CARE-MS II. cEvents occurring in ≥5% of Alemtuzumab-treated patients, based on all available follow-up.
1. Alemtuzumab Summary of Product Characteristics. Oxford, UK: Genzyme Therapeutics, Ltd; 2013; 2. Data on file. Oxford, UK: Genzyme Therapeutics, Ltd; 3. Havrdova
E, et al. Presented at: European Committee for Research and Treatment in Multiple Sclerosis; 2013; Copenhagen; P603.

ITP cases in detail (phase II and III studies)
aIndex case excluded. bCR: first recovery of platelet count ≥100 x 109/L after onset of ITP.
CR, complete response.
1. Cuker A, et al. Blood. 2011;118:6299-6305; 2. Data on file, Genzyme Corporation, Ltd; Oxford, UK;
3. Cohen JA, et al. Lancet. 2012;389:1819-1828; 4. Coles AJ, et al. Lancet. 2012;380:1829-1839.
Trial (ITP cases;
Alemtuzumab
patients)
Time from last dose
to ITP onset (mo)
Nadir platelet count
(109/L)
Time from ITP onset
to CRb (mo)
In CR at last follow-up
Yes/No (n)
CAMMS2231
(5; 216)a 1-15 1-41 1-8 Yes (5)
CARE-MS I2
(3; 376) 7-17 1-42 0.4-2.7 Yes (3)
CARE-MS II2
(8; 596) 3-13 1-37 0.2-1
Yes (7)
No (1)
CAMMS2231 CARE-MS I3 CARE-MS II4
Following implementation of mandatory
monitoring (after index case)3:
• 2 cases detected by visible ITP symptoms
• 3 patients diagnosed by monthly CBC
− 2 symptomatic; 1 presented with
cutaneous symptoms
• All in CR at last follow-up (response to
standard therapy or spontaneous
recovery)
• 1 case had initial platelet drop
that resolved spontaneously,
recurred 6 months later, and
responded to prednisolone
• All presented with visible signs
• All in CR at last follow-up
(response to standard
therapy)
• 3 cases initially presented
with visible signs
• 4 cases initially detected
by monthly CBC
• 6 of 7 in CR at last follow-up;
1 patient remained
on corticosteroids

Nephropathy cases in detail
aCreatinine normal range, 0.6-1.1 mg/dL.
CKD, chronic kidney disease; URTI, upper respiratory tract infection.
Wynn D, et al. Presented at: European Committee for Research and Treatment in Multiple Sclerosis; 2013; Copenhagen; P597.
Age/Sex/
Trial
Months
From
Last Dose
Dose (Courses;
Cumulative
Dose)
Serum Creatinine
at Diagnosis
mg/dL (mol/L) Prodrome
Treatment
Outcome
Anti-GBM cases
35 yr/female/
CAMMS223 39
12 mg
(2 courses;
96 mg)
1.8 (163) URTI, rash,
hematuria
Standard Rx
CKD3a
23 yr/female/
Extension 4
12 mg
(3 courses;
132 mg)
0.7 (63)
(Normal)a
Proteinuria;
hematuria
Standard Rx
CKD 1
Membranous nephropathy
26 yr/female/
CARE-MS II 5
12 mg
(2 courses;
96 mg)
0.6 (54)
(Normal)a
Proteinuria,
hematuria,
hypoalbuminemia,
peripheral edema
Furosemide
+ ACEI
Symptoms
improved
58 yr/female/
CAMMS3409
EXT
13
12 mg
(2 courses;
96 mg)
1.5 (135) Proteinuria,
hematuria, edema
Initial: diuretics +
albumin
Ongoing: diuretics
All cases (0.3% in clinical trials) detected by safety monitoring program; none resulted in renal failure
Monitoring, education essential for early detection, effective management

Autoimmune-related thyroid AE incidence Phase II through complete follow-up (6.7 years)
• Occurred in 34% of patients taking Alemtuzumab vs 6.5% of those taking INFB (P<0.0001)1
• Majority were hyperthyroidism1
• 4 events identified as serious (0.4 events per 100 person-years)2
• Delayed onset: peaked in third year after initial Alemtuzumab treatment, declined thereafter1,2
Phase III Studies3
CARE-MS I CARE-MS II
Rebif 44 µg
N=187
Alemtuzumab
12 mg
N=376
Rebif 44 µg
N=202
Alemtuzumab
12 mg
N=435
Any thyroid AEa (n,
%) 12 (6.4) 68 (18.1) 10 (5.0) 69 (15.9)
Hyperthyroidism 3 (1.6) 31 (8.2) 1 (0.5) 19 (4.4)
Hypothyroidism 6 (3.2) 29 (7.7) 3 (1.5) 29 (6.7)
Goiter 0 6 (1.6) 1 (0.5) 6 (1.4)
Thyroid mass 0 1 (0.3) 0 0
Lab investigations 5 (2.7) 21 (5.6) 6 (3.0) 22 (5.1)
Thyroid SAE (n, %) 0 4 (1.1) 0 2 (0.5)
Thyroid
carcinoma (n, %) 0 2 (1) 0 1 (<1)
aSome patients had >1 episode of thyroid dysfunction; for example, treatment of one hyperthyroidism case
in CARE-MS II resulted in development of hypothyroidism.
SAE, serious adverse event.
1. Daniels GH, et al. J Clin Endocrinol Metab. 2014;99:80-89; 2. Coles AJ, et al. Neurology. 2012;78:1069-1078; 3. Habek M, et al. Presented at: European Neurological
Society; 2012; Prague; P340.

Risks identified in clinical trials
aThrough 48 mo after first exposure.
ITP, immune thrombocytopenia; GBM, glomerular basement membrane; mAb, monoclonal antibody.
1. Alemtuzumab Summary of Product Characteristics. Oxford, UK: Genzyme Therapeutics, Ltd; 2013; 2. Wynn D, et al. Presented at: European
Committee for Treatment and Research in Multiple Sclerosis; 2013; Copenhagen; P597; 3. Coles AJ, et al. Neurology. 2012;78:1069-1078.
Identified Risk
Rate in Alemtuzumab-
Treated Patients Notes
ITP A
uto
imm
un
e E
ve
nts
~1% (1 fatality prior
to implementation of
monitoring program)1
• Onset generally occurred 14-36 mo after first exposure1
• Most cases responded to first-line medical therapy1
0.3%
(anti-GBM n=2)1
• Generally occurred within 39 mo after last administration1
• Responded to timely medical treatment and did not develop permanent
kidney failure2 Nephropathies
Thyroid
disorders
(Hypo-/hyper-)
~36%a
(serious, 1%)1
• Onset occurred 6-61 mo after first Alemtuzumab exposure;
peaked in year 3 and declined thereafter3
• Most mild to moderate, most managed with conventional medical
therapy, however, some patients required surgical intervention1
• Higher incidence in patients with history of thyroid disorders1
IARs >90%
(serious, 3%)1
• Occurred within 24 h of Alemtuzumab administration1
• Most mild to moderate; rarely led to treatment discontinuation1
• May be caused by cytokine release following mAb-mediated
cell lysis1
Infections 71%
(serious, 2.7%)1
• Incidence highest during first mo after infusion; rate decreased over time2
• More common with Alemtuzumab; mostly mild to moderate1
• Generally of typical duration; resolved following conventional medical
treatment1

Who should decide?


WWW.MS-RES.ORG

WWW.MS-RES.ORG

survival analysis
“hit hard and early ”
MS is an autoimmune disease hypothesis
15-20 year experiment
What is your treatment philosophy? maintenance-escalation vs. induction

Questions?