
Alcohol – What Can Secondary Care Do Better?
19
Alcohol – What Can Secondary Care Do Better? Dr Paul Richardson Consultant Hepatologist Clinical Alcohol Lead Royal Liverpool University Hospital NHS Trust
description
Alcohol – What Can Secondary Care Do Better?. Dr Paul Richardson Consultant Hepatologist Clinical Alcohol Lead Royal Liverpool University Hospital NHS Trust. What is the Scale of the Problem – Liver deaths. Hospital Admissions for Liver Disease. Alcohol Related Hospital Admissions. - PowerPoint PPT Presentation
Transcript of Alcohol – What Can Secondary Care Do Better?

Alcohol – What Can Secondary Care Do Better?
Dr Paul RichardsonConsultant HepatologistClinical Alcohol Lead
Royal Liverpool University Hospital NHS Trust

What is the Scale of the Problem – Liver deaths

Hospital Admissions for Liver Disease
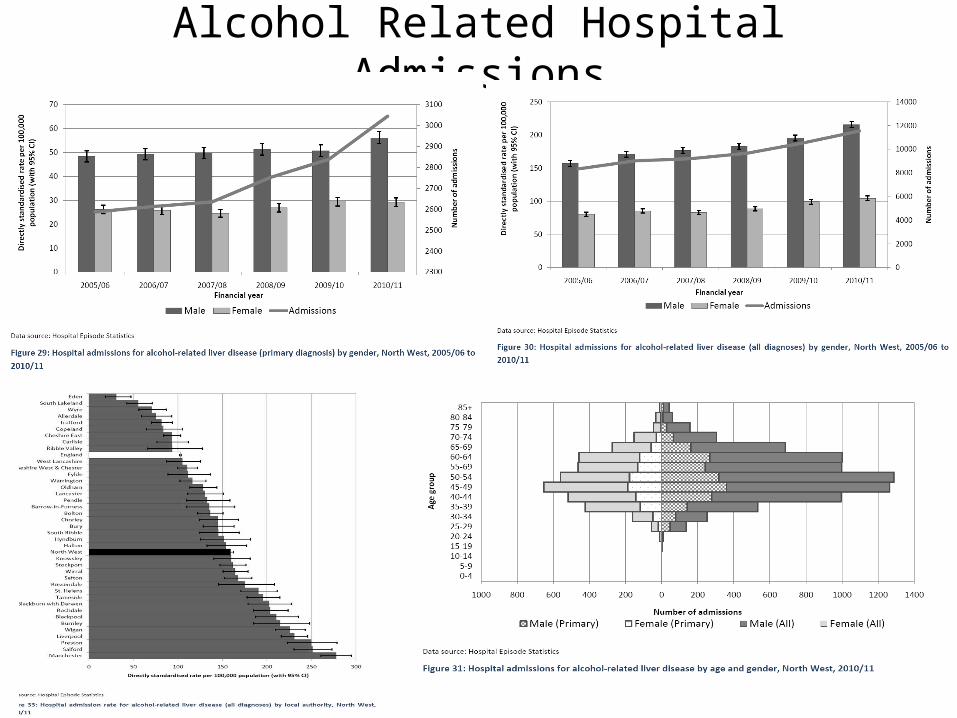
Alcohol Related Hospital Admissions
We All Know The Scale of the Problem!
• Recognition / Screening• Risk stratification - alcohol and end organ
damage• Integrated management by multi-faceted
teams• Patient central and locally centred

Shifting drinking categorisation as a treatment aim10% reduction in units in a dependent and high risk drinker will produce significant health and social benefits
Derived from ONS data for England 2012

Alcohol Specific Treatment PathwaysFrom Neighbourhoods to and through appropriate domains

Pathways 1. Alcohol Interventions Pathway in Acute Care
This pathway signposts to all other pathway options
2. Management of Acute Alcohol Withdrawal3. Early Discharge Policy (EDP)4. Frequent attender (FA) pathway5. End of Life (EOL) pathway6. Prescribing to maintain alcohol abstinence: Adjunct Pharmacotherapy Management (APM)7. Medical Alcohol Clinic (MAC)
And anything else to improve quality and access to timely, appropriate, effective management

Case 1
• 36y Male• First presentation to AMU – Alcohol
withdrawal fit• Referred to alcohol team• Full history
– Short period IV drug use – Low platelets / Mild jaundice– Managed in Early Discharge Clinic– Referred to Medical alcohol clinic for clinical
work-up

Case 1 cont.• Hepatitis C positive• High Fibroscan score – Cirrhosis – started
in surveillance programs.• Pharmacotherapy for maintenance of
abstinence• 3 months later treated for his Hepatitis C• Surveillance ultra-sound scan focal lesion
in liver – hepato-cellular cancer • Seen in satellite transplant clinic – listed
for liver transplantation.

A UNIQUE TECHNOLOGY
FibroScan product range
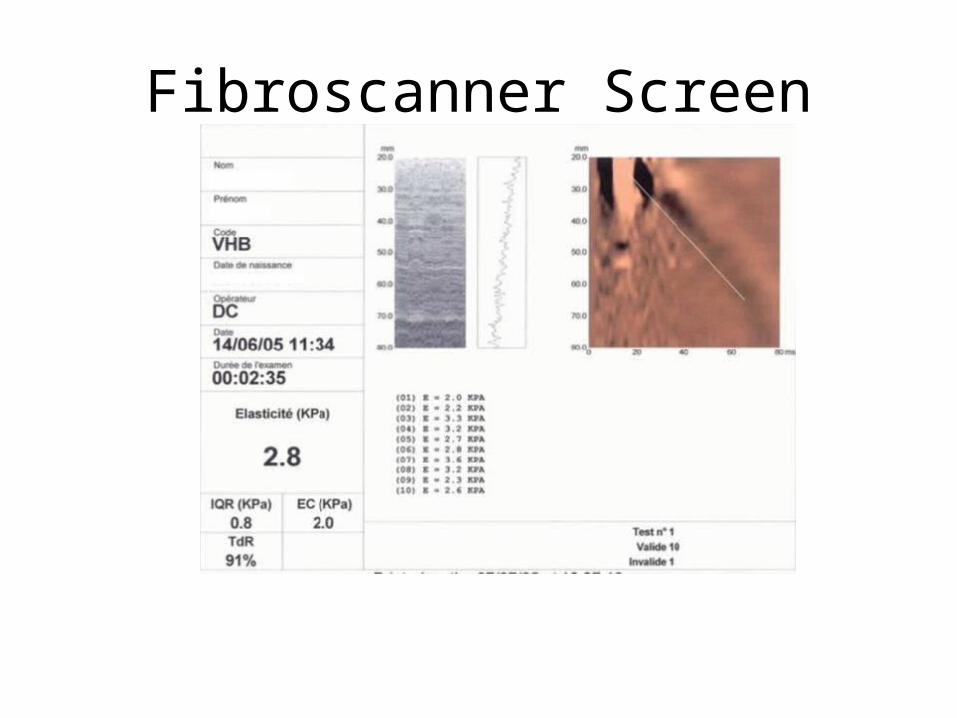
Fibroscanner Screen

Correlation Between TE and Fibrosis Stage

Underutilisation of proven pharmacological benefits

Case 2
• 45y F• Long history alcohol abuse triggered by
life changing event• Died July 2012• July 2011 – April 2012
– 86 days in hospital– 5 CT scans– 8 US scans– 17 X-rays– 8 Endoscopies

Case 2 cont• May – July• End of life care approach• Multi-disciplinary approach• Support for hostel workers – clear management
plan• Early intervention if patient admitted• Full and open discussion with patient and
agreement of plan– 12 hospital days– 8 day case management days– 3 X-rays– Comfortable and dignified death

Case 3
• 42y M• Multiple A+E attendances /MAU• Medical and trauma related• Banned from numerous homeless hostels• “Frequent Flyer” / Recidivist etc• Alcohol team – liaison psychiatrist review• Patient does not have capacity• Placed for long-term management.

Integrated Care Pathways

Summary
• Alcohol services moving in the right direction
• Identify / Stratify / Manage • End organ damage – medical and social –
the top 5-10% of the pyramid.• Integration paramount – in primary /
secondary care• Need to lower the barriers – localism is
key


















