Alcohol septal ablation in hypertrophic obstructive cardiomyopathy
3
Image of the Issue Alcohol septal ablation in hypertrophic obstructive cardiomyopathy Itsik Ben-Dor, Gabriel Maluenda, Zuyue Wang, Joseph Lindsay, Lowell F. Satler, Augusto D. Pichard, Ron Waksman ⁎ Interventional Cardiology, Washington Hospital Center, Washington, DC Received 1 December 2010; accepted 7 December 2010 An 80-year-old female with a history of coronary artery disease and post cardiac bypass surgery was admitted with increasing shortness of breath and fatigue. Electrocardiogram showed left ventricular hypertrophy with marked nonspecific ST-T changes. Transthoracic echocardiography demonstrat- ed normal systolic function with asymmetric septal hyper- trophy (25 mm) and increased left ventricular outflow velocity indicating a gradient up to 144 mmHg (Fig. 1). Coronary angiography demonstrated patent grafts. Hemody- namics demonstrated the classic Brockenbrough–Braunwald phenomenon: a resting gradient of 62 mmHg in left ventricular outflow tract increased the post ventricular premature beat to 160 mmHg; diminution in arterial pressure; and the appearance of a developing spike-and-dome pulse- wave configuration (Fig. 2). In view of the findings, the patient was considered for alcohol septal ablation. The procedure was guided by intraprocedural transesophageal echocardiography during which systolic anterior motion of the anterior mitral leaflet and moderate mitral regurgitation were demonstrated (Fig. 3A). A 5-Fr transvenous temporary pacemaker was placed in the right ventricle apex. Coronary angiography demonstrated a large first septal branch. The branch was cannulated with a 0.018-in. coronary guidewire, then a 2-mm over-the-wire balloon was advanced into the proximal third of the first septal and inflated to occlude the septal branch. After the guidewire was removed, DEFINITY contrast (Lantheus Medical Imaging, N. Billerica, MA, USA) was injected through the balloon to confirm the exact distribution of this branch and thus the potential infarct area (Fig. 3B). A total of 0.8 ml of 98% dehydrated alcohol was injected via the balloon over 10 min. The occluding balloon was then deflated and removed. Repeated coronary angiography showed the branch to be occluded (Fig. 4). The left ventricular outflow gradient was eliminated as well and the Brockenbrough–Braunwald phenomenon disappeared (Fig. 5). The patient had transient atrioventricular block that resolved spontaneously. Echo- cardiography revealed that the left ventricular gradient had declined to 10 mmHg. Mild mitral regurgitation was present. The patient remained stable and was discharged 5 days after the procedure. Cardiovascular Revascularization Medicine 13 (2012) 72 – 74 ⁎ Corresponding author. Washington Hospital Center, 110 Irving Street, NW, Suite 4B-1, Washington, DC 20010, USA. Tel.: +1 202 877 2812; fax: +1 202 877 2715. E-mail address: [email protected] (R. Waksman). 1553-8389/10/$ – see front matter © 2012 Published by Elsevier Inc. doi:10.1016/j.carrev.2010.12.005
-
Upload
itsik-ben-dor -
Category
Documents
-
view
215 -
download
1
Transcript of Alcohol septal ablation in hypertrophic obstructive cardiomyopathy

Cardiovascular Revascularization Medicine 13 (2012) 72–74
Image of the Issue
Alcohol septal ablation in hypertrophic obstructive cardiomyopathy
Itsik Ben-Dor, Gabriel Maluenda, Zuyue Wang, Joseph Lindsay, Lowell F. Satler,Augusto D. Pichard, Ron Waksman⁎
Interventional Cardiology, Washington Hospital Center, Washington, DC
Received 1 December 2010; accepted 7 December 2010
An 80-year-old female with a history of coronary arterydisease and post cardiac bypass surgery was admitted withincreasing shortness of breath and fatigue. Electrocardiogramshowed left ventricular hypertrophy with marked nonspecificST-T changes. Transthoracic echocardiography demonstrat-ed normal systolic function with asymmetric septal hyper-trophy (25 mm) and increased left ventricular outflowvelocity indicating a gradient up to 144 mmHg (Fig. 1).Coronary angiography demonstrated patent grafts. Hemody-namics demonstrated the classic Brockenbrough–Braunwaldphenomenon: a resting gradient of 62 mmHg in leftventricular outflow tract increased the post ventricularpremature beat to 160 mmHg; diminution in arterial pressure;and the appearance of a developing spike-and-dome pulse-wave configuration (Fig. 2).
In view of the findings, the patient was considered foralcohol septal ablation. The procedure was guided byintraprocedural transesophageal echocardiography duringwhich systolic anterior motion of the anterior mitral leafletand moderate mitral regurgitation were demonstrated(Fig. 3A). A 5-Fr transvenous temporary pacemaker was
⁎ Corresponding author. Washington Hospital Center, 110 Irving Street,NW, Suite 4B-1, Washington, DC 20010, USA. Tel.: +1 202 877 2812;fax: +1 202 877 2715.
E-mail address: [email protected] (R. Waksman).
1553-8389/10/$ – see front matter © 2012 Published by Elsevier Inc.doi:10.1016/j.carrev.2010.12.005
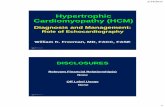
placed in the right ventricle apex. Coronary angiographydemonstrated a large first septal branch. The branch wascannulated with a 0.018-in. coronary guidewire, then a 2-mmover-the-wire balloon was advanced into the proximalthird of the first septal and inflated to occlude the septalbranch. After the guidewire was removed, DEFINITYcontrast (Lantheus Medical Imaging, N. Billerica, MA,USA) was injected through the balloon to confirm theexact distribution of this branch and thus the potentialinfarct area (Fig. 3B). A total of 0.8 ml of 98% dehydratedalcohol was injected via the balloon over 10 min. Theoccluding balloon was then deflated and removed.Repeated coronary angiography showed the branch to beoccluded (Fig. 4). The left ventricular outflow gradient waseliminated as well and the Brockenbrough–Braunwaldphenomenon disappeared (Fig. 5). The patient had transientatrioventricular block that resolved spontaneously. Echo-cardiography revealed that the left ventricular gradient haddeclined to 10 mmHg. Mild mitral regurgitation waspresent. The patient remained stable and was discharged 5days after the procedure.

Fig. 1. Transthoracic echocardiography demonstrated asymmetric septal hypertrophy (25 mm) and a left ventricular outflow gradient of 144 mmHg.
Fig. 2. Surface ECG leads and simultaneous pressure tracings from the left ventricle and aorta. Large post ventricular premature beat gradient with the classicBrockenbrough–Braunwald phenomenon (decline in the arterial pressure in the same beat). PVC, Premature ventricular contraction; LV, left ventricle; Ao, aorta.
Fig. 3. (A) Transesophageal echocardiography demonstrating systolic anterior motion of mitral valve and mitral regurgitation. (B) DEFINITY staining identifiedthe potential infarct area.
73I. Ben-Dor et al. / Cardiovascular Revascularization Medicine 13 (2012) 72–74
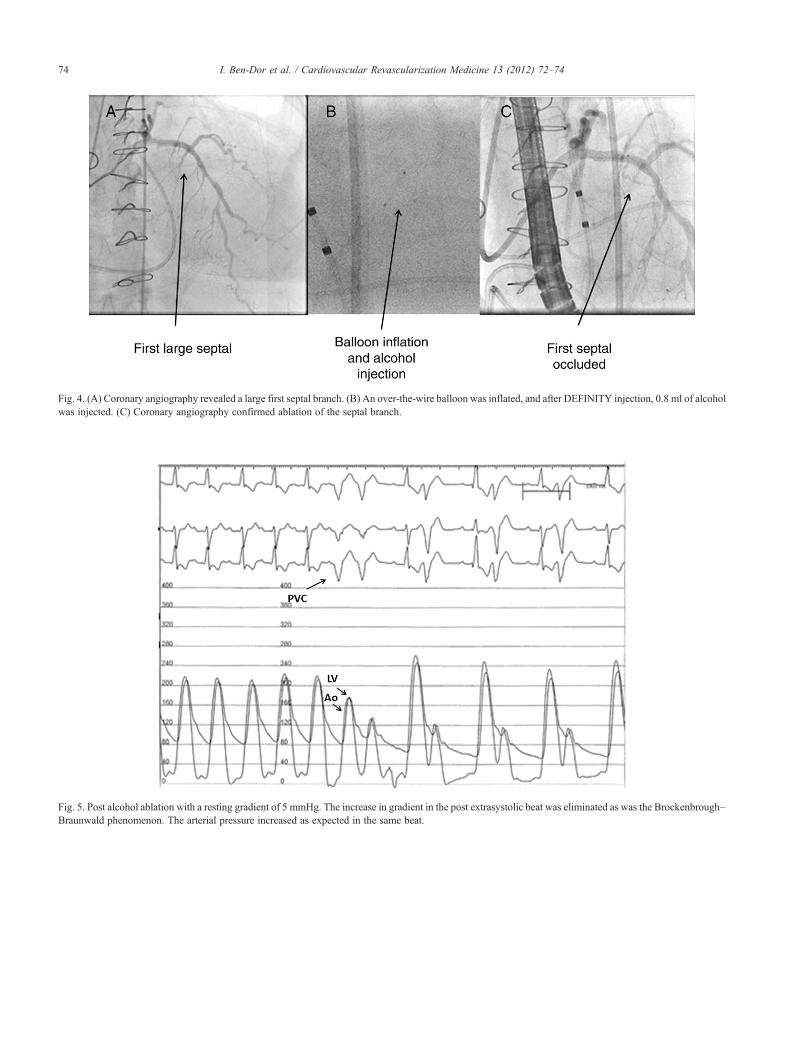
Fig. 4. (A) Coronary angiography revealed a large first septal branch. (B) An over-the-wire balloon was inflated, and after DEFINITY injection, 0.8 ml of alcoholwas injected. (C) Coronary angiography confirmed ablation of the septal branch.
Fig. 5. Post alcohol ablation with a resting gradient of 5 mmHg. The increase in gradient in the post extrasystolic beat was eliminated as was the Brockenbrough–Braunwald phenomenon. The arterial pressure increased as expected in the same beat.
74 I. Ben-Dor et al. / Cardiovascular Revascularization Medicine 13 (2012) 72–74