
ALCOHOL AND DISEASE Alcohol and · PDF fileAlcohol and Disease Dr Bastiaan de Boer School of...
44
Alcohol and Disease Dr Bastiaan de Boer School of Pathology and Laboratory Medicine University of Western Australia ALCOHOL AND DISEASE
Transcript of ALCOHOL AND DISEASE Alcohol and · PDF fileAlcohol and Disease Dr Bastiaan de Boer School of...
Alcohol and Disease
Dr Bastiaan de Boer
School of Pathology and Laboratory Medicine
University of Western Australia
ALCOHOL AND DISEASE
Disclaimer: Yes, I drink

What is alcohol?
Alcohol is more correctly called ethyl alcohol
and also known as ethanol.

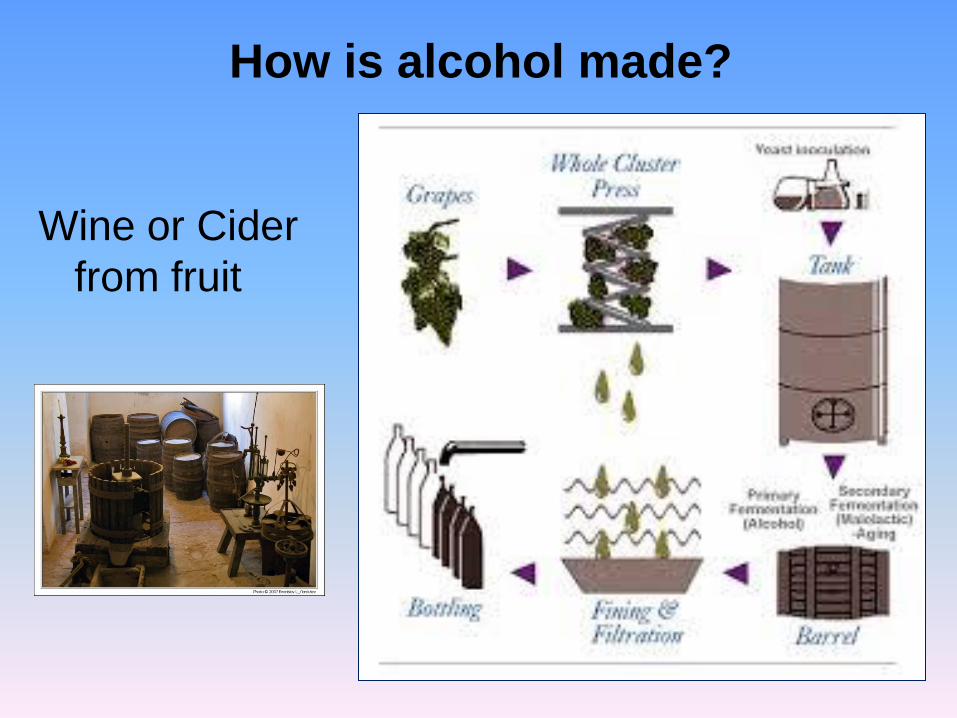
How is alcohol made?
• Fermenting various sources of sugar using
yeast or bacteria
– grains, fruits and vegetables
• turns the sugars into alcohol.
How is alcohol made?
Wine or Cider
from fruit

How is alcohol made?
Beer and spirits from cereals such as barley
and rye
Spirits also go through
distillation – where a
proportion of the water is
removed, leaving a
stronger concentration of
alcohol and flavour.
What is a “standard drink”?
A “standard” drink is an arbitrary unit of
measurement: 10g (12.5ml) of pure alcohol.

What is a “standard drink”?
What is meant by the terms:
• Alcoholism
– Physical dependence
– Tolerance
– Craving
– Loss of control
Dependence on alcohol to function normally
Withdrawal symptoms after stopping drinking
The need to drink greater amounts of alcohol to get “high”
A strong need or urge to drink
Not being able to stop once drinking has begun

What is meant by the terms: • Alcohol abuse
• Intoxication
• Alcohol poisoning
• Binge drinking
• Withdrawal
excitement or dulling of the senses
a dangerously high concentration of alcohol likely to to
induce coma or respiratory depression
drinking heavily on one occasion or continuously over a
period of time
Symptoms such as nausea, sweating, shakiness and
anxiety after stopping drinking (physical dependence).
a pattern of drinking that results in a recurring problem

Do you drink – yes or no?
What are your reasons?

Do you drink? – YES
• Socialise with friends
• Have fun or celebrate
• Relax
• Overcome social awkwardness
• Forget worries or problems
• Experiment
• Relieve boredom
• Because I like the taste
• It’s an important part of my
culture
• Peer pressure
• Decreases your risk of
atherosclerosis
Do you drink? – No
• I do not like the taste
• I do not like the feeling
• My parents tell me not to
• I have had a bad experience
• It is against my religion
• I socialize with people who do
not drink
• I do not have the enzyme
alcohol dehydrogenase

What happens to alcohol when you drink it?

Absorption
• Alcohol enters the blood stream within
minutes of consumption
• It is absorbed unchanged
• The small intestine absorbs much more
alcohol than the stomach
• Peak alcohol levels are reached 30 to 60
minutes after someone stops drinking

Distribution
• Alcohol is distributed throughout all of the
water-containing components of the body
• It distributes rapidly and thoroughly
• The less a person weighs, the smaller the
water content and the more he or she will
be affected

Distribution
• Fat contains less water than muscle so
those with a higher percentage of fat will
be more affected
• On average men are 68% water, woman
are 55% water therefore women are more
affected.
hhhhhh
hhhhhh

Elimination
• Approx. 95 % is metabolized in the liver
• A person metabolizes one standard drink
(10g alcohol) per hour
• It is excreted in urine, tears, sweat, semen,
and saliva
• Alcohol evaporates from the blood into the
lungs and is excreted in breath
– This can be measured in a breath sample
• Metabolism, excretion, and evaporation
occur after approximately 15 to 45 minutes
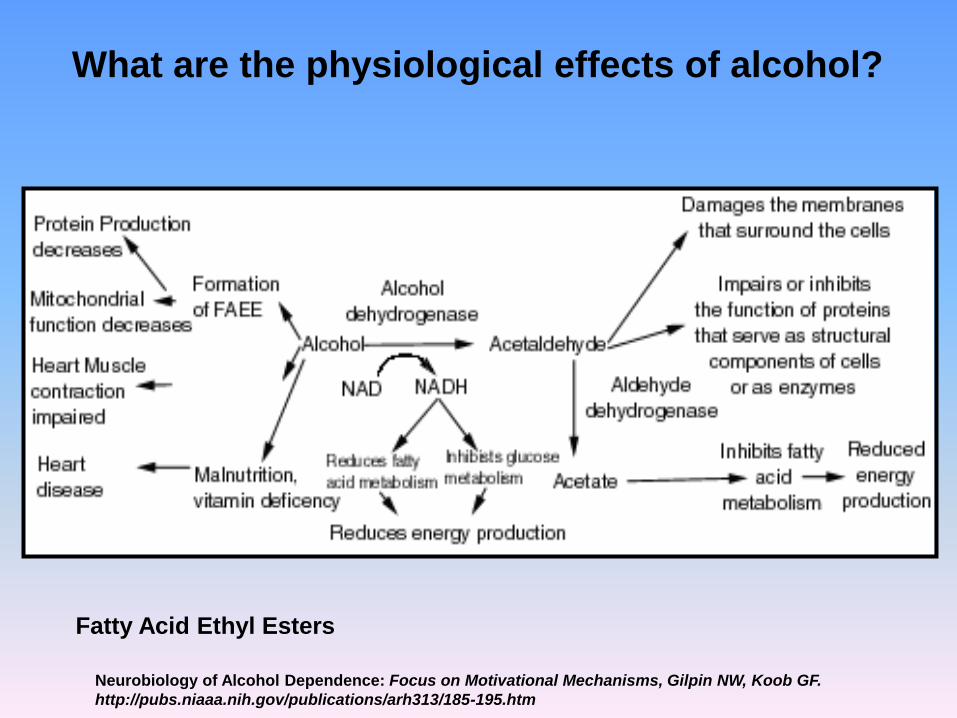
What are the physiological effects of alcohol?
Neurobiology of Alcohol Dependence: Focus on Motivational Mechanisms, Gilpin NW, Koob GF.
http://pubs.niaaa.nih.gov/publications/arh313/185-195.htm
Fatty Acid Ethyl Esters

Mechanism of action
Exact molecular targets and mechanism of
action uncertain
• A central nervous system depressant
• Direct effects on cardiac muscle, thyroid
tissue and hepatic tissue.
• Metabolic effects - Hypoglycaemia

CNS neurotransmitter systems
Enhanced systems:
• binds directly to the gamma-aminobutyric
acid (GABA) receptor in the CNS and
causes sedative effects
• 5-HT receptor agonism responsible for
– GABAergic
– glycinergic
– cholinergic effects
• Nicotinic acetylcholine receptors

CNS neurotransmitter systems
Inhibited systems:
• NMDA
• Ca2+ channels
• K+ channels
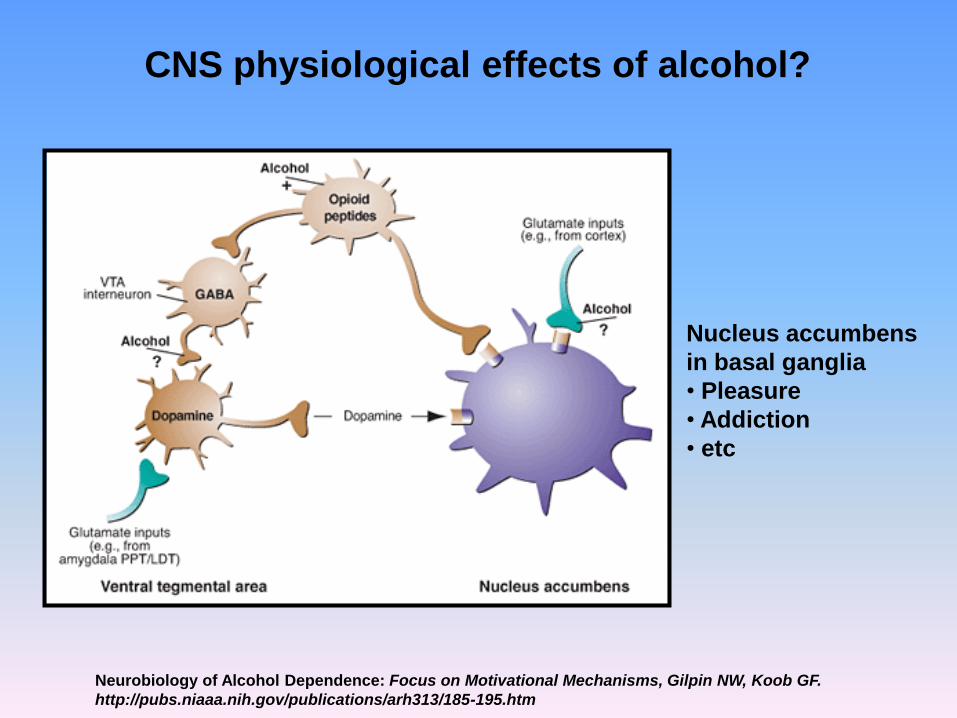
CNS physiological effects of alcohol?
Neurobiology of Alcohol Dependence: Focus on Motivational Mechanisms, Gilpin NW, Koob GF.
http://pubs.niaaa.nih.gov/publications/arh313/185-195.htm
Nucleus accumbens
in basal ganglia
• Pleasure
• Addiction
• etc

Blood alcohol concentrations
effect on CNS
• 20–79 mg/dL – Impaired coordination and euphoria
• 80–199 mg/dL: “Binge drinking” – Ataxia, poor
judgement, labile mood.
• 200–299 mg/dL – Marked ataxia, slurred speech,
poor judgement, labile mood, nausea and vomiting
• 300–399 mg/dL – Stage 1 anaesthesia, memory
lapse, labile mood
• 400+ mg/dL – Respiratory failure, coma

Metabolic effects
• Hypoglycemia occurs secondary to
ethanol's inhibition of gluconeogenesis
– may cause lactic acidosis, ketoacidosis, and
acute renal failure.
• Metabolic acidosis is compounded by
respiratory failure.
• Patients may also present with
hypothermia.
Possible short term consequences of
excess alcohol intake?
Physical consequences
– nausea and vomiting
– impaired judgement and decision making
• slow response time
– memory loss
– blurred vision
– poor muscle co-ordination and reaction
• loss of balance, shakiness
– Inhibition of breathing and gag reflex
– Alcohol poisoning : confusion, drowsiness,
sleep, coma, death
– Hangovers: headache, nausea and vomiting
Social consequences
– Feeling bad about yourself and embarrassed
by your actions
– Losing money that you need for other things
after reckless spending on alcohol
– Having unprotected sex, or unwanted sex.
This might lead to unwanted pregnancy, or
sexually transmitted diseases (STIs)
– Break down of relationships as a result of
your behaviour
– Loss of job

Community consequences
– Increased aggressive behaviour
– Injury to drinker or others
– Drink driving – increased accidents
– Hospital attendance

Possible long term consequences of
excess alcohol intake?
Physical or social and can affect the
surrounding community
• Physical and psychological dependence
(alcoholism)
• Mental health problems - depression and
anxiety
• Problems at school, at work and with
relationships
• Increased risk of sexual problems
(especially male impotency)
• Organ damage

Which organs are damaged by long term
excess alcohol intake?
Organ damage
• CVS: hypertension, myocardial damage
• Liver: fatty liver, inflammation, necrosis,
fibrosis – cirrhosis, liver failure, cancer
• Stomach: inflammation and bleeding
• Pancreas: inflammation ie pancreatitis
• CNS: neuronal damage, dementia,
tremors, stroke
• Endocrine system: problems with blood
sugar control, loss of libido, reduced fertility
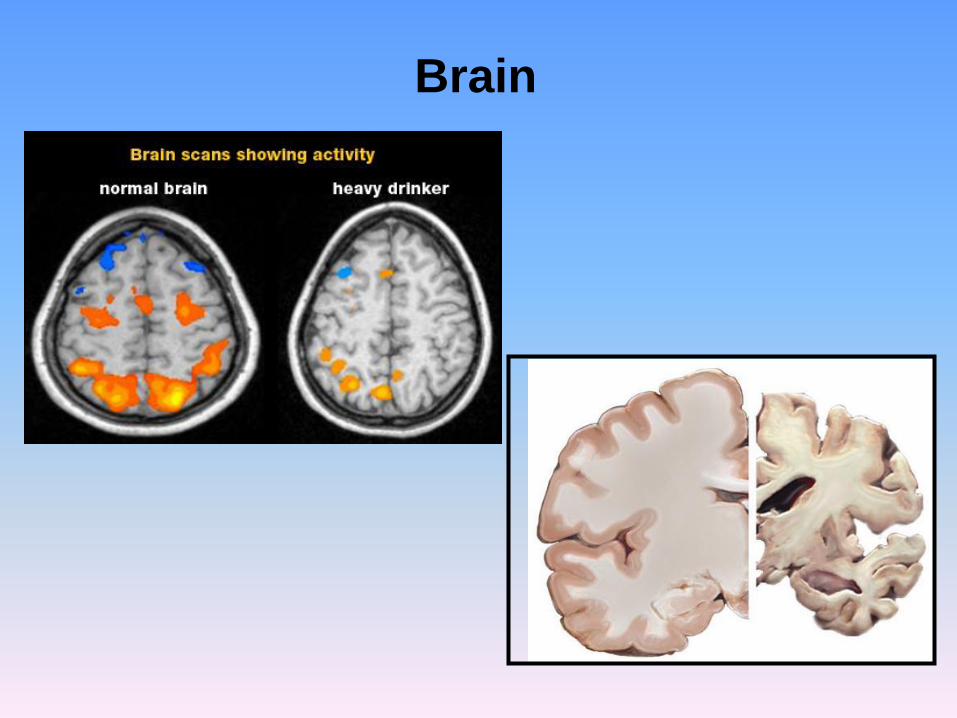
Brain

Heart

Liver
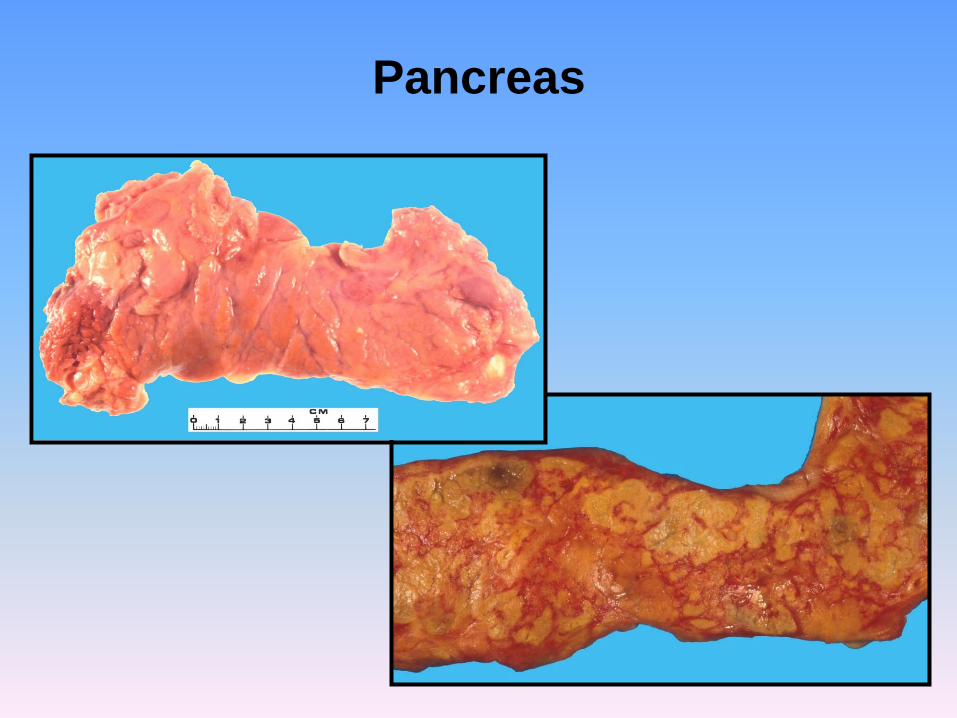
Pancreas
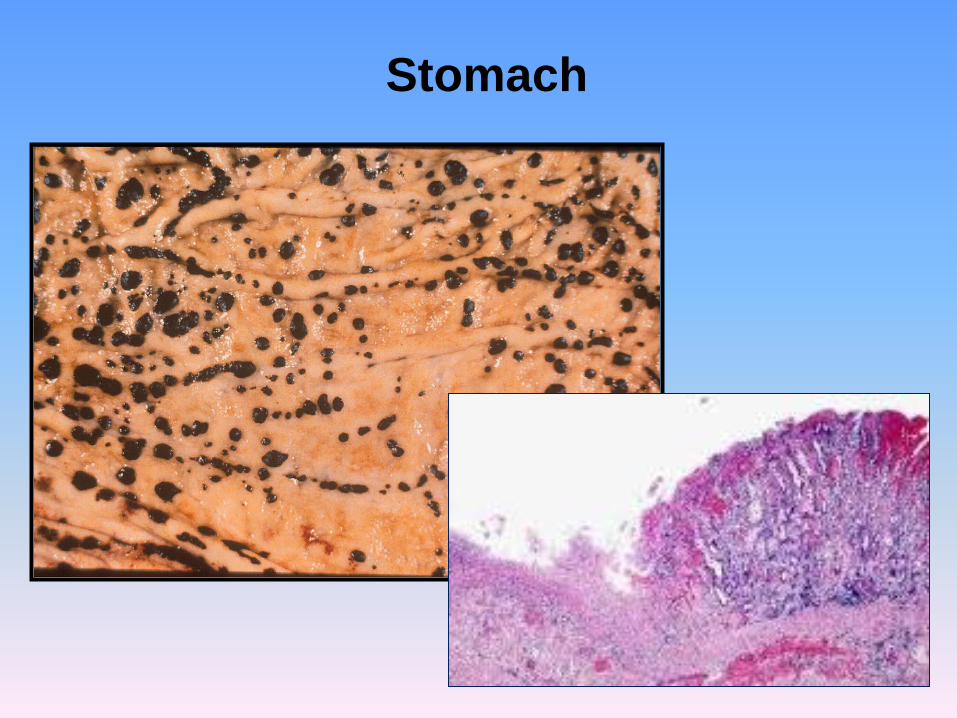
Stomach

• http://edupalm.meddent.uwa.edu.au/museu
m/search.php

Do you know any myths or
misconceptions regarding alcohol?
Myths or misconceptions
You can lower your blood alcohol, ie sober up, by:
– vomiting
– breathing fresh air
– exercise
– having a cold shower
– drinking hot coffee
• The only way to sober up is for your body to
metabolize and eliminate the alcohol in your
system. All of these other manoeuvres have
no effect on your blood alcohol.

Myths or misconceptions
Alcohol is legal so why all the fuss
• This ignores the fact that excessive
consumption of alcohol can be harmful to our
short and long term health
If someone is very drunk or passes out then it’s best
to let them sleep it off.
• As alcohol depresses the CNS, people who
pass out may have problems maintaining their
airways should they vomit. These people
should be watched.

Myths or misconceptions
Teenagers can’t become alcoholics because they
have not been drinking for long enough
• Studies have shown that people that start
drinking earlier are more likely to become
alcohol dependent.
Parent: My child is going to drink anyway whether I
like it or not so I might as well buy them alcohol
so I can control how much and what they drink
• There is very little evidence that parents are
supplying their children with alcohol has the
effect of controlling the amount consumed.
Alcohol and Disease
Dr Bastiaan de Boer
School of Pathology and Laboratory Medicine
University of Western Australia
ALCOHOL AND DISEASE


















