

ALC Cover Jan/Feb - Wound Care...
44
March/April 2016 • Volume 5 • Number 2 www.WoundCareAdvisor.com A Publication No more skin tears Buzz Report: Latest trends How to apply silver nitrate Nutritional considerations in patients with pressure ulcers Comprehensive turning programs can avoid a pain in the back Official journal of Wound Care ADVISOR Practical issues in wound, skin, and ostomy management ®
Transcript of ALC Cover Jan/Feb - Wound Care...

March/April 2016 • Volume 5 • Number 2 www.WoundCareAdvisor.com
A Publication
No more skin tears
Buzz Report: Latest trends
How to apply silver nitrate
Nutritional considerationsin patients with pressure
ulcers
Comprehensive turningprograms can avoid a pain
in the back
Official journal of
WoundCareADVISOR
Practical issues in wound, skin, and ostomy management®

y tiuca-rehgir huor yoe f foraf cy otilaust qehgie hhe tdivor: Pdesturd T Trn, adeste, T TedeirTTr
dey Bpared Thezidiulr Fi® AnortinilC
)rrotacidne ilgnB aOh Htiwn (oitalucitrd aef bd oaeH•
thgied hee blbatsujdjn ah atic wirtcey ellluF•
metsy® Setie Hti® Rnortinilh Ctiy wcneiciffffr eevigerae cvorpmI
1 stisi vomo ryencger emnd alatips horew lox6. 2o tpU•
1ytilicae f faho te tsnepxd eesaerced//dsgnviat sson caem
y ah mcihs wrecle urusserf pg onilaer hetsax f4.o 4p tU•
)tsequ renop uelbaailv ayduts(
:seomct oulacinil cenvor phougrh tksi reucdeR
t, 2005, 51(2):38-68.anagemenound MWy om. Osttsesideners in Nursing Home Re Ulcessurrt PearTo sed tes UfacSur
t ther Suppory with OapherTed luidiz-Fison of Airompar. C, et aln SD, Horchs RF F, HorO1.
calling 800-638-2546.y anager bccount Mom Aill-Rour local Ht ycontac
mation, ore inf foror morvaluation or f for moree patient eor a frF
stneitay p
ENG – US-201526-FEBev 2191289 r.VEDS RESER. ALL RIGHTnc, Iesvicerom Sill-R©2015 H
f dhmpiuqe erae cmor heffefffe oWWe o
s otroffomoe cTh
pet ud sn
sonit opreya pd
stif ltenita pnd asd
e tacovdt aneitam p
snoitidnog cd an,yy,sal palrbegnilaes dtneita
tahs tnoitulot sne
emof h o
om.com-r
y areviele dert fuobk asA•
nd atnemya ptoub anraeL•
de bera ce homr outouba
m Ro-llio a Hy tltcerik dlaTTa•
g nitimi-lytiliboe mrever sehtoere c,seiurjn idro cnalip shtiwaf ps odeee nuqine uht teem
om.com.hill-rwww
yodaUs T Todat ontacC
ENG – US-2014TOC15-ev 1189531 r.VEDS RESER. ALL RIGHTnc, Iesvicerom Sill-R©2014 H

Wound Care Advisor • March/April 2016 • Volume 5, Number 2 www.WoundCareAdvisor.com 1
staffGroup Publisher
Gregory P. OsborneVice President of Publishing & Sales
Sofia GollerDirector, Marketing & Program Mgmt.
Tyra LondonEditor-in-Chief
Donna Sardina, RN, MHA, WCC, CWCMS, DWC, OMS
Editorial DirectorCynthia Saver, RN, MS
EditorKathy E. Goldberg
Copy EditorJulie CullenArt Director
David BeverageProduction Director
Christian Evans GartleyAccount Managers
Susan Schmidt, Renee Artuso,John Travaline
PuBlished ByHealthCom Media
259 Veterans Lane, Doylestown, PA 18901Tel: 215/489-7000 • Fax: 215/230-6931
Chief Executive OfficerGregory P. Osborne
Digital Design Manager Michelle Welliver
Social Media ManagerLizzie Witte
Finance Director/OperationsMaryAnn Fosbenner
Finance Manager/OperationsNancy J. Dengler
Wound Care Advisor (ISSN 2168-4421) is published byHealthCom Media, 259 Veterans Lane, Doylestown, PA18901. Printed in the USA. Copyright © 2016 by Health-Com Media. All rights reserved. No part of this publica-tion may be reproduced, stored, or transmitted in anyform or by any means, electronic or mechanical, includ-ing photocopy, recording, or any information storageand retrieval system, without permission in writing fromthe copyright holder. Send communication to Health-Com Media, 259 Veterans Lane, Doyles town, PA 18901.
The opinions expressed in the editorial and advertis-ing material in this issue are those of the authorsand advertisers and do not necessarily reflect theopinions or recommendations of the National Al-liance of Wound Care and Ostomy®; the EditorialAdvisory Board members; or the Publisher, Editors,and the staff of Wound Care Advisor.
Editorial Mission: Wound Care Advisor providesmultidisciplinary wound care professionals withpractical, evidence-based information on theclinical management of wounds. As the officialjournal of the National Alliance of Wound Careand Ostomy®, we are dedicated to deliveringsuccinct insights and information that our read-ers can immediately apply in practice and useto advance their professional growth.
Wound Care Advisor is written by skin and woundcare experts and presented in a reader-friendly elec-tronic format. Clinical content is peer reviewed.
The publication attempts to select authors who are knowl-edgeable in their fields; however, it does not warrant theexpertise of any author, nor is it responsible for any state-ments made by any author. Certain statements about theuse, dosage, efficacy, and characteristic of some drugsmentioned here reflect the opinions or investigational ex-perience of the author. Any procedures, medications, orother courses of diagnosis or treatment discussed or sug-gested by authors should not be used by clinicians with-out evaluations of their patients’ conditions and possiblecontraindications or danger in use, review of any applica-ble manufacturer’s prescribing information, and compari-son with the recommendations of other authorities.
editor-in-chief
Donna Sardina, RN, MHA, WCC, CWCMS, DWC, OMSCo-Founder, Wound Care Education Institute
Lake Geneva, WI
editorial advisory Board
Nenette L. Brown, RN, PHN,MSN/FNP, WCC
Wound Care Program CoordinatorSheriff’s Medical Services Division
San Diego, CA
Debra Clair, PhD, APN, RN, WOCN,WCC, DWC
Wound Care ProviderAlliance Community Hospital
Alliance, OH
Kulbir Dhillon, NP, WCCWound Care Specialist
Skilled Wound CareSacramento, CA
Fred BergVice President, Marketing/Business
DevelopmentNational Alliance of Wound Care and
OstomySt. Joseph, MI
Cindy Broadus, RN, BSHA, LNHA,CLNC, CLNI, CHCRM, WCC,
DWC, OMSExecutive Director
National Alliance of Wound Care and Ostomy
St. Joseph, MI
Gail Hebert, MS, RN, CWCN, WCC,DWC, OMS
Clinical instructorWound Care Education Institute
Plainfield, IL
Joy Hooper, BSN, RN, CWOCN,OMS, WCC
Owner and manager of MedicalCraft, LLCTifton, GA
Catherine Jackson, RN, MSN, WCCClinical Nurse Manager
Inpatient and Outpatient Wound CareMacNeal Hospital
Berwyn, IL
Jeffrey Jensen, DPM, FACFASDean and Professor of Podiatric
Medicine & SurgeryBarry University School of Podiatric
MedicineMiami Shores, FL
Rosalyn S. Jordan, RN, BSN, MSc,CWOCN, WCC
Director of Clinical EducationRecoverCare, LLC
Louisville, KY
Jeff Kingery, RNVice President of Professional
DevelopmentRestorixHealthTarrytown, NY
Jeri Lundgren, RN, BSN, PHN, CWS,CWCN
Vice President of Clinical ConsultingJoerns
Charlotte, NC
Nancy Morgan, RN, BSN, MBA,WOC, WCC, DWC, OMS
Co-Founder, Wound Care EducationInstitute
Plainfield, IL
Steve Norton, CDT, CLT-LANACo-founder, Lymphedema & Wound Care
Education, LLCPresident, Lymphedema Products, LLC
Matawan, NJ
Bill Richlen, PT, WCC, CWS, DWCOwner
Infinitus, LLCChippewa Falls, WI
Lu Ann Reed, RN, MSN, CRRN,RNC, LNHA, WCC
Adjunct Clinical InstructorUniversity of Cincinnati
Cincinnati, OH
Stanley A. Rynkiewicz III, RN, MSN,WCC, DWC, CCS
AdministratorDeer Meadows Home Health and
Support Services, LLCBHP Services
Philadelphia, PA
Cheryl Robillard, PT, WCC, CLTClinical SpecialistAegis TherapiesMilwaukee WI
Donald A. Wollheim, MD, WCC,DWC, FAPWCA
Owner and Clinician, IMPLEXUS WoundCare Service, LLC
Watertown, WIInstructor, Wound Care Education
InstitutePlainfield, IL

2 www.WoundCareAdvisor.com March/April 2016 • Volume 5, Number 2 • Wound Care Advisor
March/April 2016 • Volume 5 • Number 2www.WoundCareAdvisor.comCONTENTS
page 11
page 14
page 21
page 24
FEATURES
11 Buzz Report: Latest trends, Part 2 By Donna Sardina, RN, MHA, WCC, CWCMS, DWC, OMS
More highlights of the latest trends in wound care.
14 No more skin tears By Gail R. Hebert, MS, RN CWCN, DWC, WCC, OMS
Learn how to prevent, assess, and treat these common injuries.
DEPARTMENTS
4 From the Editor Caution: Checklists may lead to inaccurate documentation
8 Clinical Notes 19 Apple Bites How to apply silver nitrate
21 Best Practices FAQs about support surfaces
Nutritional considerations in patients with pressure ulcers
31 Business Consult Comprehensive turning programs can avoid a pain in the back
Exercise your right to be fit!
36 Clinician Resources 38 NAWCO News
Incontinence Associated Dermatitis (IAD)
t

Dr. Smith’s® Zinc Oxide Adult Barrier Spray
improved quality of care in nursing home usage trial.
To request samples, order product, or obtain a copyof the complete trial study, contact us at:
* This study and its data were provided by a third party. Data on fi le.
Copyright © 2016 Mission Pharmacal Company. All Rights Reserved. Patent Pending. DSL-P155946-5AdultBarrierSpray.com
For External Use Only
Provide a more effi cient way to treat and prevent Incontinence Associated Dermatitis (IAD)
Offer nursing staff a touch-free alternative that saves them time and is easy to clean up with brief changes
Help eliminate risk of cross contamination
Help eliminate product waste and save money
Conduct your own usage trial with Dr. Smith’s Adult Barrier Sprayto improve quality of care in your facility.
Incorporating Dr. Smith’s Adult Barrier Spray into your protocol can:
Study Finding Highlights:
• 80% prefer a new method of application to standard protocol of ointment/creams
• 82% said Dr. Smith’s Adult Barrier Spray has improved the quality of care in their facility
• 88% would recommend Dr. Smith’s Adult Barrier Spray
• There were no instances of UTI or other infection during the course of the study
• Comments received included that it was “easy to use,” “more convenient,” “saved time,” and “provided a no-mess alternative.”
nursing home usage trial.
Nursing Home Usage Study*: After a 30-day nursing home usage study, caregivers indicated that Dr. Smith’s ® Adult Barrier Spray improved the quality of care in their facility, and the vast majority preferred Dr. Smith’s method of application over their previous barrier cream or ointment.

4 www.WoundCareAdvisor.com March/April 2016 • Volume 5, Number 2 • Wound Care Advisor
From theEDITOR
Using a checklist form to documentwound care can make the task easi-er and faster—and help ensure that
you’ve captured all pertinent data neededfor assessment, reimbursement, and legalsupport. But the form itself may not becomprehensive; some important fields maybe missing.
Recently, we at Wound Care Advisor re-ceived a question from a clinician who washaving trouble deciding how to code a pa-tient’s wound in her hospital’s electronichealth record (EHR). Her patient’s specificwound and tissue types weren’t availableoptions in the dropdown menu on the soft-ware system. Luckily, on investigating, wediscovered her system provided the optionto override the checklist and add com-ments in a notes section.
Perhaps you’ve been in a similar position.If so, did you ask for help? Did you find outabout an override option? Or did you just
choose from the only options offered?Whether it’s done with pen and paper, a
computer mouse, a checklist, or a narrativeform, documentation in the medical recordis considered a legal document. Choosingan option that isn’t clinically accurate be-cause it’s the only option you think isavailable doesn’t protect you from legal is-sues or even healthcare fraud.
Think of the problems that could arisefrom this. Suppose, for instance, you classi-fy a dermal lesion as a pressure ulcer; thecomputer software recognizes the pressureulcer code and bills Medicare for pressureulcer reimbursement. Hospitals are reim-bursed at a higher rate for pressure ulcersthan for dermal lesions, so your documen-tation could constitute Medicare fraud.
Here’s another scenario: You code awound as a skin tear in the EHR, but theskin tear actually is a pressure ulcer. Sub-sequently, the patient develops a woundinfection and dies. Your facility is suedfor wrongful death and you lose yourprofessional license due to inaccuratedocumentation.
Checklist tipsTo make your wound care checklist andEHR documentation the best it can be, fol-low these tips:rNotify management about complications
or challenges with current documenta-tion forms.
rAsk the wound care committee to re-view the forms and generate a wish listto present to the information technology
Caution: Checklists may lead to inaccurate documentation
(continued on page 7)

Cl hrofo
TISEMENTADVER
CCClClfo hrr hffofo
e whs thrs eallssis tiyhthlae h
llea s s hhe w t t th thrrs trs tlleall heal hh iissssiissui t t ti tiyy tttthth
ya waesu
aay w w wa wasue
tivceles-ADly Fno
SeasneaglolC
iotalunar gngimrhaeuss tictiorce nsevome rylerbec ditamynzd eevorppa-stin0 u5t 2nemtni O®L®YTNA
yy
eussi tnotuoith wetahr tedir
ehs tg i/s
Use of Collagenas 1 year of treatment systemic hypersens applied outside the been noted in surro Occasional slight tr
dermal ulcers and is indicated for deb Collagenase SANTY
Ointment should be® se SANTYL®
t with collagenase and cortisone. sitivity has been reported after
e wound. One case of ounding tissue when
ythema has ransient ery
severely burned areas. briding chronic
Ointment® YL®
iatmorfn ieor morF
lpmoe cee ssaelP
tissue is well estabterminated when d Use of Collagenas
, Inc. 1 of Smith & Nephew, , ©2015 Smith & Nephew,
.omco.lytna.sw.wwwtis viease pl,oni
ajdn an ooitamrofong inibircseree pte et
blished. debridement is complete and granulati
Ointment should be se SANTYL
TM1672-0615.santyl.comwww -800-441-8227 Inc. SANTYL is a registered trademark
Please swip
y
y
.egat pnec
on
amrofng inibircsere ptetlpmo pe for c
.noita

DESCRIPTION: Collagenase SANTYL® Ointment is a sterile enzymatic debriding ointment which contains 250 collagenase units per gram of white petrolatum USP. The enzyme collagenase is derived from the fermentation by Clostridium histolyti- cum. It possesses the unique ability to digest collagen in necrotic tissue.
CLINICAL PHARMACOLOGY: Since collagen accounts for 75% of the dry weight of skin tissue, the ability of collagenase to digest collagen in the physiological pH and temperature range makes it particularly effective in the removal of detritus.1 Collagenase thus contributes towards the formation of granulation tissue and subsequent epithelization of dermal ulcers and severely burned areas. 2, 3, 4, 5, 6 Collagen in healthy tissue or in newly formed granulation tissue is not attacked. 2, 3,
4, 5, 6, 7, 8 There is no information available on collagenase absorption through skin or its concentration in body fluids associated with therapeutic and/or toxic effects, degree of binding to plasma proteins, degree of uptake by a particular organ or in the fetus, and passage across the blood brain barrier.
INDICATIONS AND USAGE: Collagenase SANTYL® Ointment is indicated for debriding chronic dermal ulcers 2, 3, 4, 5, 6, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18 and severely burned areas. 3, 4, 5, 7, 16, 19, 20, 21
CONTRAINDICATIONS: Collagenase SANTYL® Ointment is contraindicated in patients who have shown local or systemic hypersensitivity to collagenase.
PRECAUTIONS: The optimal pH range of collagenase is 6 to 8. Higher or lower pH conditions will decrease the enzyme’s activity and appropriate precautions should be taken. The enzymatic activity is also adversely affected by certain detergents, and heavy metal ions such as mercury and silver which are used in some antiseptics. When it is suspected such materials have been used, the site should be carefully cleansed by repeated washings with normal saline before Collagenase SANTYL® Ointment is applied. Soaks containing metal ions or acidic solutions should be avoided because of the metal ion and low pH. Cleansing materials such as Dakin’s solution and normal saline are compatible with Collagenase SANTYL® Ointment.
Debilitated patients should be closely monitored for systemic bacterial infections because of the theoretical possibility that debriding enzymes may increase the risk of bacteremia.
A slight transient erythema has been noted occasionally in the surrounding tissue, particularly when Collagenase SANTYL® Ointment was not confined to the wound. Therefore, the ointment should be applied carefully within the area of the wound. Safety and effectiveness in pediatric patients have not been established.
ADVERSE REACTIONS: No allergic sensitivity or toxic reactions have been noted in clinical use when used as directed. However, one case of systemic manifestations of hypersensitivity to collagenase in a patient treated for more than one year with a combination of collagenase and cortisone has been reported.
OVERDOSAGE: No systemic or local reaction attributed to overdose has been observed in clinical investigations and clinical use. If deemed necessary the enzyme may be inactivated by washing the area with povidone iodine.
DOSAGE AND ADMINISTRATION: Collagenase SANTYL® Ointment should be applied once daily (or more frequently if the dressing becomes soiled, as from incontinence). When clinically indicated, crosshatching thick eschar with a #10 blade allows Collagenase SANTYL® Ointment more surface contact with necrotic debris. It is also desirable to remove, with forceps and scissors, as much loosened detritus as can be done readily. Use Collagenase SANTYL® Ointment in the following manner:
Rx only
1 – Prior to application the wound should be cleansed of debris and digested material by gently rubbing with a gauze pad saturated with normal saline solution, or with the desired cleansing agent compatible with Collagenase SANTYL® Ointment (See PRECAUTIONS), followed by a normal saline solution rinse.2 – Whenever infection is present, it is desirable to use an appropriate topical antibiotic powder. The antibiotic should be applied to the wound prior to the application of Collagenase SANTYL® Ointment. Should the infection not respond, therapy with Collagenase SANTYL® Ointment should be discontinued until remission of the infection.3 – Collagenase SANTYL® Ointment may be applied directly to the wound or to a sterile gauze pad which is then applied to the wound and properly secured.4 – Use of Collagenase SANTYL® Ointment should be terminated when debride- ment of necrotic tissue is complete and granulation tissue is well established.
HOW SUPPLIED: Collagenase SANTYL® Ointment contains 250 units of collagenase enzyme per gram of white petrolatum USP.
Do not store above 25˚C (77˚F). Sterility guaranteed until tube is opened.
Collagenase SANTYL® Ointment is available in 15 gram, 30 gram, and 90 gram tubes.
REFERENCES: 1. Mandl, I., Adv Enzymol. 23:163, 1961. 2. Boxer, A.M., Gottesman, N., Bernstein, H., & Mandl, I., Geriatrics. 24:75, 1969. 3. Mazurek, I., Med. Welt. 22:150, 1971. 4. Zimmermann, WE., in “Collagenase,” Mandl, I., ed., Gordon & Breach, Science Publishers, New York, 1971, p. 131, p. 185. 5. Vetra, H., & Whittaker, D., Geriatrics. 30:53, 1975. 6. Rao, D.B., Sane, P.G., & Georgiev, E.L., J. Am. Geriatrics Soc. 23:22, 1975. 7. Vrabec, R., Moserova, J., Konickova, Z., Behounkova, E., & Blaha, J., J. Hyg. Epidemiol. Microbiol. Immunol. 18:496, 1974. 8. Lippmann, H.I., Arch. Phys. Med. Rehabil. 54:588, 1973. 9. German, F. M., in “Collagenase,” Mandl, I., ed., Gordon & Breach, Science Publishers, New York, 1971, p. 165. 10. Haimovici, H. & Strauch, B., in “Collagenase,” Mandl, I., ed., Gordon & Breach, Science Publishers, New York, 1971, p. 177. 11. Lee, L.K., & Ambrus, J. L., Geriatrics. 30:91, 1975. 12. Locke, R.K., & Heifitz, N.M., J. Am. Pod. Assoc. 65:242, 1975. 13. Varma, A.O., Bugatch, E., & German, F.M., Surg. Gynecol. Obstet. 136:281, 1973. 14. Barrett, D., Jr., & Klibanski, A., Am. J. Nurs. 73:849, 1973. 15. Bardfeld, L.A., J. Pod. Ed. 1:41, 1970. 16. Blum, G., Schweiz, Rundschau Med Praxis. 62:820, 1973. Abstr. in Dermatology Digest, Feb. 1974, p. 36. 17. Zaruba, F., Lettl, A., Brozkova, L., Skrdlantova, H., & Krs, V., J. Hyg. Epidemiol. Microbiol. Immunol. 18:499, 1974. 18. Altman, M.I., Goldstein, L., & Horwitz, S., J. Am. Pod. Assoc. 68:11, 1978. 19. Rehn, V.J., Med. Klin. 58:799, 1963. 20. Krauss, H., Koslowski, L., & Zimmermann, W.E., Langenbecks Arch. Klin. Chir. 303:23, 1963. 21. Gruenagel, H.H., Med. Klin. 58:442, 1963.
Manufactured by: Smith & Nephew, Inc. Fort Worth, Texas 76107 US Gov’t License #2004
Marketed by:
1-800-441-8227 Smith & Nephew, Inc. Fort Worth, Texas 76107
Reorder Nos. 0064-5010-15 (15 g tube) 0064-5010-30 (30 g tube) 0064-5010-90 (90 g tube)
© 2014 Smith & Nephew, Inc. SANTYL is a registered trademark of Smith & Nephew, Inc. 140385-0814

department.r Investigate possible use of a commercial
specialty wound documentation moduleA. rAdvocate for staff training on the proper
use of forms and electronic records, aswell as the legal implications of woundcare documentation.
r If your computer system can’t bechanged, work with management tofind an alternative method for properwound documentation.
In addition to commercial wound docu-mentation modules, consider free resources.For example, you can download a pressureulcer documentation formB from the Agencyfor Healthcare Research and Quality.
Having the best possible checklist or
documentation form helps protect youfrom legal action, ensures that your facilityobtains proper reimbursement and, mostimportantly, promotes optimal patient care.
Donna Sardina, RN, MHA, WCC, CWCMS,DWC, OMS
Editor-in-ChiefWound Care Advisor
Cofounder, Wound Care Education InstitutePlainfield, Illinois
Online ResourcesA. woundsource.com/product-category/practice-management-software/emr-systems-health-care-reporting
B. ahrq.gov/sites/default/files/wysiwyg/professionals/systems/long-term-care/resources/pressure-ulcers/pressureulcerhealing/waform2.pdf
(continued from page 4)

Self-management ostomyprogram improves HRQOL
A five-session ostomy self-care programwith a curriculum based on the ChronicCare Model can improve health-relatedquality of life (HRQOL), according to astudy in Psycho-Oncology.
“A chronic care ostomy self-managementprogram for cancer survivorsA” describes re-sults from a longitudinal pilot study of 38people. Participants reported sustained im-provements in patient activation, self-effi-cacy, total HRQOL, and physical and so-cial well-being. Most patients had ahistory of rectal cancer (60.5%) or bladdercancer (28.9%).
Assessment scale may helppredict pressure ulcerdevelopment in patients withfecal incontinence
A study in the International Wound Jour-nal has found that higher scores on theIncontinence-Associated Dermatitis and itsSeverity (IADS) tool are associated withan increased likelihood of developing apressure ulcer in patients with fecal in-continence.
The authors of “Prospective study on In-continence-Associated Dermatitis and itsSeverity instrument for verifying its ability to
predict the development of pressure ulcers inpatients with fecal incontinenceB” suggestthat patients with IADS scores higher than 8points should be classified as being at riskof developing a pressure ulcer and receive“intensive care as a proactive measure” toprevent pressure ulcer development.
Keratin-based products effectivefor burn treatment
Researchers report in Burns that com-pared to standard products, novel keratin-based products facilitate healing with min-imal scarring in patients with superficialand partial thickness burns.
“Keratin-based products for effectivewound care management in superficial andpartial thickness burns injuriesC” notes thatthe keratin products are cost-effective, as-sociated with minimal pain and itch, andeasy to use in community-based care.
8 www.WoundCareAdvisor.com March/April 2016 • Volume 5, Number 2 • Wound Care Advisor
ClinicalNOTES

Sirolimus-eluting stents helpwound healing in patients withischemic PAD
Infrapopliteal sirolimus-eluting stents (SES)accelerate wound healing in patients withischemic peripheral arterial disease (PAD)compared with balloon angioplasty, ac-cording to a study of 200 patients in JACC:Cardiovascular Interventions.
“Wound healing outcomes and health-re-lated quality-of-life changes in the ACHILLESTrial: 1-year results from a prospective ran-domized controlled trial of infrapopliteal bal-loon angioplasty versus sirolimus-elutingstenting in patients with ischemic peripheralarterial diseaseD” also reported a trend ofmore quality-of-life gains for patients re-ceiving an SES.
Incontinence of older personsaffects QOL of their caregivers
“Impact of incontinence on the quality of life
of caregivers of older persons with inconti-nence: A qualitative study in four EuropeancountriesE” concludes that incontinencehas a strong effect on the quality of life(QOL) of caregivers.
The study in Archives of Gerontologyand Geriatrics included 50 interviews withcaregivers in Italy, the Netherlands, theSlovak Republic, and Sweden. The re-searchers discovered that families need tolearn new competencies in caring for theolder person with incontinence and thatincontinence remains “a taboo and a highstigmatizing condition” for caregivers. Theconcept that incontinence is unavoidablein older patients, along with shame andembarrassment, prevents caregivers fromseeking help at an early stage.
Trauma patients vulnerable todevice-related pressure ulcers
“Pressure ulcers in trauma patients with sus-pected spine injury: a prospective cohortstudy with emphasis on device-related pres-sure ulcersF” reports the incidence of pres-sure ulcers in 254 patients with suspectedspine injury as 28.3%, with 60.7% of thoserelated to devices.
The study, published in the Interna-tional Wound Journal, found pressure ul-cers in 16 different locations on the body.The researchers conclude that the propor-tion of device-related pressure ulcers is“very high in trauma patients.”
Wound Care Advisor • March/April 2016 • Volume 5, Number 2 www.WoundCareAdvisor.com 9

Intensive therapy for patientswith diabetes reduces CVcomplications
“Intensive diabetes treatment and cardiovas-cular outcomes in Type 1 Diabetes: The DC-CT/EDIC Study 30-year follow-upG” reportsthat intensive treatment reduced the inci-dence of cardiovascular (CV) disease by
30% and the incidence of major CV events(nonfatal myocardial infarction, stroke, orcardiovascular death) by 32%.
Authors of the study, published in Dia-betes Care, note that lower HbA1c levelsaccounted for the observed treatment ef-fect on CV disease risk, and that increasedalbuminuria was also associated with CVdisease risk. ■
Online ResourcesA. onlinelibrary.wiley.com/doi/10.1002/pon.4078/full
B. onlinelibrary.wiley.com/doi/10.1111/iwj.12549/full
C. burnsjournal.com/article/S0305-4179%2815%2900334-4/abstract
D. interventions.onlinejacc.org/article.aspx?articleID=2480656
E. aggjournal.com/article/S0167-4943%2815%2930077-7/abstract
F. onlinelibrary.wiley.com/doi/10.1111/iwj.12568/abstract?userIsAuthenticated=false&deniedAccessCustomisedMessage=
G. care.diabetesjournals.org/content/early/2016/01/29/dc15-1990.abstract

Wound Care Advisor • March/April 2016 • Volume 5, Number 2 www.WoundCareAdvisor.com 11
Keeping clinicians up-to-date onclinical knowledge is one ofthe main goals of the Wild onWounds (WOW) conference
held each September in Las Vegas. Everyyear, I present the opening session,called “The Buzz Report,” which focuseson the latest-breaking wound carenews—what’s new, what’s now, andwhat’s coming up. I discuss new prod-ucts, practice guidelines, resources, andtools from the last 12 months in skin,wound, and ostomy management.
In the January issue, I discussed someof the updates from my 2015 Buzz Report.Now I’d like to share a few more, alongwith some of my favorite resources.
Product buzzWound dressings withsilicone are designed toreduce pain and traumaduring dressing changesand to protect thewound. Coloplast’s new Biatain® SiliconeLiteA does just that, combining an ab-sorbent polyurethane foam dressing witha semipermeable, water- and bacteria-proof top film and a soft silicone wound-contact layer. The thin foam provides acloser fit at skin level, resulting in in-creased mobility and product comfort.
Anasept® Antimicrobial Wound IrrigationSolutionC provides a new dimension in an-
timicrobial wound careand negative-pressure wound therapy(NPWT). This FDA-cleared solution is aclear isotonic liquid that delivers 0.057%broad-spectrum antimicrobial sodiumhypochlorite via a NPWT device. Kill stud-iesD for Anasept® are fascinating: a 30-second kill time for infections withClostridium difficile, methicillin-resistantStaphylococcus aureus, vanc o mycin-resistant enterococci, Pseudo monas, andmany more. Anasept comes with an easy-to-use spikable container with an integrat-ed hanger that can be quickly attached toan I.V. pole or NPWT device. It can beused with most NPWT systems that haveinstillation or infusion capability.
Cutimed® Sorbact® Hydroactive BF fromBSN Medical provides infection controland fluid management for up to 4 days ina single wound dressing. It helps fight andprevent infection without chemical agentsor antibiotics. The bacteria-binding, ab-
Buzz Report: Latest trends, Part 2
By Donna Sardina, RN, MHA, WCC, CWCMS, DWC, OMS
A wound careclinician’s best
friend
View: Biatain® Silicone LiteB
View: Cutimed® Sorbact® Hydroactive BE

12 www.WoundCareAdvisor.com March/April 2016 • Volume 5, Number 2 • Wound Care Advisor
sorbent gel dressing with an adhesive bor-der absorbs and locks wound exudate andbacteria in a hydropolymer gel core; witheach dressing change, bound bacteria areremoved. The hydrogel matrix helps main-tain a moist wound environment.
No scissors? No problem! Hy-Tape In-ternational, maker of the Original PinkTape®, has come to the rescue with Hy-Tape® Pre-cut Strips and PatchesG. These latex free, waterproof, zinc–oxide-basedadhesive tape products are perfect for ex-tended wear, soothing to delicate skin,and adherent to wet, oily, or hairy skin.The single-use strips measure 1.25" x 6"and come in packs of four. They canquickly be used to secure devices or to“picture-frame” wounds or ostomy barri-ers. The patches are designed to cover alarge area. Available in 4" and 5" squares,they’re perfect for making hydrocolloiddressings completely occlusive.
The American Diabetes Association’sreport “Comprehensive Foot Examinationand Risk AssessmentH” states that all indi-viduals with diabetes should get an annu-al foot exam to assess peripheral neu-ropathy and protective sensation,including a test for vibration perception.Typically, the clinician uses a tuning forkto test for vibration sensation, but thiscan be difficult for those unfamiliar withthe feel; also, the results are totally sub-jective. The new portable, handheld non-invasive Dynamic Neuroscreening DeviceI
(DND) from Prosenex provides objectiveand consistent quantitative testing for vi-bration sensation. It offers five grades ofvibration and temperature discriminationto screen for large- and small-fiber neu-ropathy. FDA approved and made in theUnited States, DND was named the 2014New Hampshire High Tech Product ofthe Year.
Zinc oxide ointmentK is a “go-to” productfor incontinence-associated dermatitis. But its consistency makes it difficult andmessy to spread evenly over the skin.Mission Pharmacal Co. has created a newsolution for this—Dr. Smith’s Adult BarrierSprayL. This 10% zinc oxide solutioncomes as an easy, touch-free, spray appli-cation, offering accurate, uniform cover-age with no rubbing necessary.
Incidence data reveal that the heel isthe most common site of facility-acquiredpressure ulcers. Once a heel pressure ul-cer develops, complete elimination of heelpressure using a pressure-relief device iscritical. The new TruVue™ Heel Protectorfrom EHOB positions a pillow under theAchilles tendon to elevate the heel. Con-structed with an anti-shear pad that servesas a barrier to shearing forces, the devicehas a deep, V-cut heel well that fully off -loads the heel without product interactionand relieves product-to-heel engagementwith foot flexion.
Resource buzz Accessing the Internet forinformation using smart-phones and tablets hasquickly become a hugepart of health care. Twomajor wound care companies have re-leased mobile applications to help health-care professionals and consumers use andorder their products. Several new wound-care books were published in 2015 aswell. (See What’s the buzz on books?)
The iOn Healing™ N mobile app fromAcelity offers a suite of tools to improvecustomer support. In addition to productguides, features include the ability to con-nect and consult directly with an Acelityrepresentative, track outcomes to support
View: ProsenexJ
View: TruVue™ Heel ProtectorM

Wound Care Advisor • March/April 2016 • Volume 5, Number 2 www.WoundCareAdvisor.com 13
documentation of medical necessity, andorder V.A.C.® Therapy and instantly trans-mit the signed prescription to Acelity. TheHIPAA-compliant app offers high-securitydata protection. Designed for use by li-censed clinicians in the United States, it’sfree to download and available for iOSand Android.
The Johnson & Johnson Wound Care Re-source™ O app helps identify new wounds,provides recommendations on wound caretreatment, and keeps track of the dailychecklists that come with continued treat-ment. It’s available free for iOS at iTunesand for Android at GooglePlay.
A dream come true for wound care cli-nicians—an app that measures wounds!With the Mobile Wound Care app from Tis-sue AnalyticsP, you can take a wound pho-to with a smartphone camera and streamit directly to your desktop, where you canmeasure, track, and manage your patients’wounds on a secure web portal. It’s avail-able for iOS at iTunes and for Android atGoogle Play.
The Agency for Healthcare Research &Quality (AHRQ) produces evidence thatcan be used to make health care safer,better, more accessible, more equitable,and more affordable. AHRQ websites of-fer a wealth of useful information for cli-nicians. A few of my favorites are the Patient Safety ChannelQ on YouTube, Inno-vations Exchange, Safety Program for Nurs-ing Homes: On-Time Pressure Ulcer Preven-tionR, and Service Delivery InnovationProfileS, such as this one, which detailsvarious healthcare projects around thecountry. ■
Online ResourcesA. coloplast.us/biatain-silicone-lite-new-en-us.aspx
B. vimeo.com/89699735
C. anacapa-tech.net
D. anacapa-tech.net/live/wp-content/uploads/2014/09/Anasept-Negative-pressure-brochure3.pdf
E. youtube.com/watch?v=kmzKhIiWunE
F. bsnmedical.com/products/wound-care-vascular/category-
product-search/advanced-wound-care/wound-bed-preparation/cutimedr-sorbactr-hydroactive-b.html
G. hytape.com
H. care.diabetesjournals.org/content/31/8/1679.full
I. www.prosenex.com
J. prosenex.com/default.asp
K. woundcareadvisor.com/assessing-risk-of-pressure-and-moisture-related-problems-in-long-term-care-patients_vol2_no3/
L. adultbarrierspray.com
M. ehob.com/education/video_library.html?video_id=28
N. kci1.com/KCI1/ionhealingmobileapp
O. itunes.apple.com/us/app/johnson-johnson-wound-care/id600009964?mt=8&ign-mpt=uo%3D4
P. tissue-analytics.com
Q. youtube.com/user/ahrqpatientsafety
R. ahrq.gov/professionals/systems/long-term-care/resources/ontime/pruprev/index.html
S. innovations.ahrq.gov/profiles/collaborative-health-education-and-access-events-offer-no-cost-screenings-and-navigation
Donna Sardina is editor-in-chief of Wound CareAdvisor and cofounder of the Wound Care Edu-cation Institute in Plainfield, Illinois.
DISCLAIMER: All clinical recommendations are in-tended to assist with determining the appropriatewound therapy for the patient. Responsibility forfinal decisions and actions related to care of spe-cific patients shall remain the obligation of the in-stitution, its staff, and the patients’ attending physi-cians. Nothing in this information shall be deemedto constitute the providing of medical care or thediagnosis of any medical condition. Individualsshould contact their healthcare providers for med-ical-related information.
Check out these new releases in wound and osto-my reference books and textbooks:
• Text and Atlas of Wound Diagnosis and Treat-ment, by Rose Hamm PT, DPT, CWS, FACCWS.(published in 2015 by McGraw-Hill Medical)
• Wound Care at a Glance, by Ian Peate and WynGlencross (published in 2015 by Wiley-Blackwell)
• Wound, Ostomy and Continence Nurses Society®
Core Curriculum: Ostomy Management (pub-lished in 2015 by Lippincott Williams & Wilkins)
What’s the buzz on books?
14 www.WoundCareAdvisor.com March/April 2016 • Volume 5, Number 2 • Wound Care Advisor
Imagine watching your skin tear,bleed, and turn purple. Imagine,too, the pain and disfigurementyou’d feel.
What if you had to live through this ex-perience repeatedly? That’s what manyelderly people go through, suffering withskin tears through no fault of their own.Some go on to develop complications.
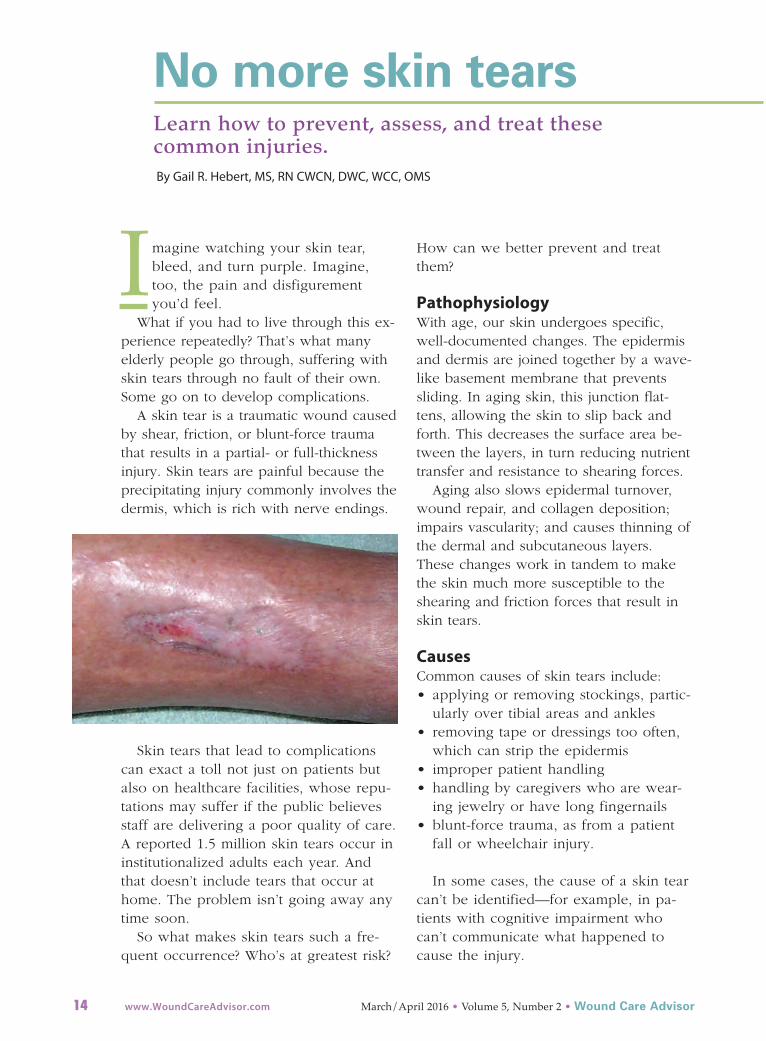
A skin tear is a traumatic wound causedby shear, friction, or blunt-force traumathat results in a partial- or full-thicknessinjury. Skin tears are painful because theprecipitating injury commonly involves thedermis, which is rich with nerve endings.
Skin tears that lead to complicationscan exact a toll not just on patients butalso on healthcare facilities, whose repu-tations may suffer if the public believesstaff are delivering a poor quality of care.A reported 1.5 million skin tears occur ininstitutionalized adults each year. Andthat doesn’t include tears that occur athome. The problem isn’t going away anytime soon.
So what makes skin tears such a fre-quent occurrence? Who’s at greatest risk?
How can we better prevent and treatthem?
Pathophysiology With age, our skin undergoes specific,well-documented changes. The epidermisand dermis are joined together by a wave-like basement membrane that preventssliding. In aging skin, this junction flat-tens, allowing the skin to slip back andforth. This decreases the surface area be-tween the layers, in turn reducing nutrienttransfer and resistance to shearing forces.
Aging also slows epidermal turnover,wound repair, and collagen deposition;impairs vascularity; and causes thinning ofthe dermal and subcutaneous layers.These changes work in tandem to makethe skin much more susceptible to theshearing and friction forces that result inskin tears.
Causes Common causes of skin tears include:• applying or removing stockings, partic-
ularly over tibial areas and ankles• removing tape or dressings too often,
which can strip the epidermis • improper patient handling• handling by caregivers who are wear-
ing jewelry or have long fingernails• blunt-force trauma, as from a patient
fall or wheelchair injury.
In some cases, the cause of a skin tearcan’t be identified—for example, in pa-tients with cognitive impairment whocan’t communicate what happened tocause the injury.
No more skin tears Learn how to prevent, assess, and treat these common injuries. By Gail R. Hebert, MS, RN CWCN, DWC, WCC, OMS

Wound Care Advisor • March/April 2016 • Volume 5, Number 2 www.WoundCareAdvisor.com 15
Risk factors Patients who depend on caregiver assis-tance for activities of daily living are atrisk for skin tears. Assistance with bathing,dressing, positioning, and transferring in-volves significant caregiver handling. Re-search from across many settings showsthat roughly 70% to 80% of skin tears oc-cur on the hands and arms, and mosthappen during peak activity hours (from 6to 11 AM and from 3 to 9 PM).
Very young patients with immature skinalso are at risk. The dermis doesn’t devel-op fully until after birth; even at full-term,it has reached only 60% of its adult thick-ness. In neonates, skin tears commonlyare linked to device trauma or adhesiveuse. In many cases, they occur on thehead, face, and extremities.
Additional at-risk groups include criti-cally ill patients with multiple risk factorsand older adults who ambulate independ-ently, especially those with an unsteadygait. Among these older adults, skin tearsare common on the lower extremities.(See Additional risk factors for skin tears.)
Risk assessment toolYou can use a risk assessment tool to helpidentify patients at risk and guide imple-mentation of a prevention protocol. Calledthe Skin Integrity Risk Assessment Tool byWhite, Karam, and Colwell, it’s the onlytool designed specifically to assess skin in-tegrity risk. Although the instrument issomewhat dated and not used widely inclinical settings, clinicians who’ve adoptedit report it helps reduce skin-tear incidencethrough early identification and immediatetargeted prevention. (Click hereA for moreinformation.)
AssessmentThe Payne-Martin Classification systemprovides a common language for assess-ing and classifying skin tears, promotingbetter communication among cliniciansand helping to guide treatment. Devel-
oped in 1990 and updated in 1993, it hasthree primary classifications based on de-gree of severity. Besides helping cliniciansdifferentiate full-thickness from partial-thickness tears, it addresses the skin flap(if present). For images of skin tears clas-sified by the Payne-Martin system, clickhereB.
In addition to identifying the skin-tearclassification, also check for and documentthe following:• anatomic location and duration of the
tear• dimensions of the tear (length, width,
and depth)• wound bed characteristics and percent-
age of viable vs. nonviable tissue• exudate type and amount • presence of bleeding or hematoma• periwound skin color and condition;
note edema, maceration, and induration• wound-edge approximation and condi-
tion (open vs. closed) • degree of flap necrosis• integrity of surrounding skin• signs and symptoms of infection• associated pain.
PreventionPreventing skin tears requires a multifac-eted approach, described below. Althoughnot all skin tears are preventable, take allnecessary steps to minimize risk. Remem-ber—skin tears are a negative patient out-come. If your healthcare facility has a high
Patients with the following conditions may be athigher risk for skin tears:
• compromised nutritional status
• sensory and cognitive deficits
• visible changes to the skin
• agitated behavior
• incontinence
• cardiac, pulmonary, and vascular disorders
• use of four or more prescribed medications.
Additional risk factors for skin tears

16 www.WoundCareAdvisor.com March/April 2016 • Volume 5, Number 2 • Wound Care Advisor
skin-tear incidence, some people may sus-pect the facility is not doing everything itcan to decrease tears or that its caregiversare too rough when providing direct pa-tient care.
Provide an optimal environmentTo minimize skin tears, start by providinga safe environment. Remove scatter rugsand unclutter walkways. Pad bedrails,wheelchairs, and sharp furniture corners.Provide support for the patient’s depend-ent limbs and ensure adequate lighting.
Keep room temperature on the coolside, as heat tends to dry the skin. Elderlypatients commonly are sensitive to cold, sothis isn’t always realistic—but you can addmoisture to the air by using a humidifier.
Follow bathing guidelinesToo-frequent bathing dries the skin, mak-ing it more vulnerable to tearing. The fol-lowing recommendations help minimizetears.• Decrease bathing frequency.• Advise patients to take shorter showers
with warm to tepid (not hot) water tohelp the skin resist tearing.
• Use pH-balanced cleaning productsthat contain emollients and don’t re-quire rinsing. Know that although abar of soap is inexpensive and re-moves soil, it also alters the skin’sphysical and chemical make-up andmakes it more vulnerable to tears.
• Pat the patient’s skin dry instead ofrubbing it.
• Moisturize the patient’s skin afterbathing while it’s still damp. This trapsmoisture and keeps skin hydrated. Theskin’s top layer, the stratum corneum,requires at least 10% moisture to main-tain its integrity.
• Encourage proper fluid intake to helppatients stay hydrated.
Handle patients gently Learn about the proper way to touch pa-tients to decrease skin trauma risk. Using apracticed, deliberate, gentle touch makesall the difference.
Also, use low-friction repositioningsheets and equipment to decrease skintrauma caused by repositioning. Avoidwearing jewelry, because it can cause skintrauma, and keep your fingernails short.
Dress patients properlyPatient clothing plays a role in preventingskin tears. Dress at-risk patients in longsleeves, long pants, and knee-high socks toprotect the skin below these garments. Youcan use athletic shin guards as protectivedevices on patients who are willing towear them. Specialized products, such asthe DermaSaver™ Arm Tube, Dermatuff®
Protection Socks and Leg Protectors, andPosey® SkinSleeves™ Protectors, also helpsafeguard the skin. If the budget is tight,you can use tube socks to protect the pa-tient’s arms; just cut off the toe section andslip the socks on over your patient’s hands.
ManagementDespite all of our efforts, skin tears do oc-cur. How we treat them can make a bigdifference in our patient’s pain level, howquickly tears resolve, and whether compli-cations arise. Although we lack gold-stan-dard or clinical practice guidelines to iden-tify the ideal treatment regimen, manyapproaches can work well. Choose theone that best fits your individual patient.
Dress at-riskpatients in longsleeves, long pants,and knee-high socksto protect the skinbelow these garments.

Wound Care Advisor • March/April 2016 • Volume 5, Number 2 www.WoundCareAdvisor.com 17
Management goals include: • stopping the bleeding• reapproximating the edges of the skin
flap to maintain integrity withoutstretching
• providing moisture and protection forthe wound
• protecting periwound skin• minimizing pain and discomfort• preventing infection.
Also, if possible, try to determine thecause of the skin tear and remove it tohelp prevent recurrence.
Methods of treating skin tears includeskin glue, skin-closure strips, and dress-ings. (See Applying skin-closure strips.)
Skin glueA specially formulated liquid topical band-age, skin glue creates a clear film thatdries in 15 to 30 seconds. It doesn’t re-quire secondary dressings and allows forroutine inspection. Examples of skin gluesinclude Dermabond®, Surgiseal®, andOctylseal™.
DressingsThe best standard dressing for a skin teardepends on the type of tear, amount ofexudate, skin fragility, and other patientfactors. In general, hydrocolloids or tradi-tional transparent film dressings aren’t rec-ommended, as they may cause skin strip-ping and injure the healing tear if notremoved properly.
To manage a skin-tear dressing, markthe outer dressing with an arrow to indi-cate the preferred direction of removal;document this to help prevent disturbingthe healing wound. Ideally, this stepshould be included in your facility’s policyand procedures to help ensure it’s doneevery time.
When using a dressing over your patient’sskin tear, remember these important points:• Calcium alginates may help control
bleeding and exudate.
• Soft silicone or silicone-impregnateddressings promote flap security and aidnontraumatic removal.
• Foam or hydrofiber dressings aid exu-date management.
• Hydrogel dressings promote pain reliefand a moist wound bed.
• Petroleum-based protective ointmentsand gauze also may be used.
• Antimicrobial dressings aid infectioncontrol.
• If the wound is infected or contaminat-ed, observe it daily.
• Avoid tape whenever possible, because
You can use skin-closure strips to keep the woundedges approximated, which promotes healing byprimary intention. Remember—the skin flap needsto stay intact with no signs of infection. (Becauseof fragile surrounding tissues, staples usuallyaren’t recommended.)
To apply skin-closure strips, follow these steps:
• Clean the wound gently and remove excessblood under the skin flap.
• Gently roll the flap back into place using a mois-tened applicator, making sure not to stretch it.
• To apply a strip, start in the middle of thewound. Apply half of the first strip to the woundmargin; press firmly in place without tension.Using your fingers or forceps, approximate theskin edges as closely as possible.
• Press the other half of the strip firmly on theother side of the wound.
• Close the rest of the wound with additionalstrips spaced approximately 1⁄8" (3 mm) apart,until the edges are completely approximated.
• If needed, apply additional strips parallel to thewound, approximately ½" in from the ends. Thismay reduce stress under the ends, decreasingthe risk of skin-tension blisters and prematurelifting of the strips.
• To allow the skin flap to “take,” don’t disturb itfor approximately 5 days.
• Know that skin sealants (such as benzoin) aren’trequired or recommended.
• For added protection, you can cover skin-closurestrips with a secondary dressing, such as a foamor silicone nonadherent dressing.
Applying skin-closure strips

it may tear the skin on removal. Toprevent this, use an adhesive remover.
• Alternative ways to secure the dressinginclude gauze netting, stockinette, co-hesive bandages, TubiFast™ bandages,and other specialty products, such asTAPEless™ dressings. Be sure to followthe manufacturer’s instructions forproper application to protect patientsfrom harm stemming from circulatorycompromise.
Education is keyWe need more research on skin tears toimprove management. Education is thekey to preventing skin tears. All caregiversshould be well versed in prevention andmanagement strategies and should teachpatients about them. ■
Gail R. Hebert is a clinical instructor with the
Wound Care Education Institute in Plainfield, Illinois.
Selected referencesAyello EA, Sibbald RG. Preventing pressure ulcers andskin tears. In: Boltz M, Capezuti E, Fulmer T, et al, eds.Evidence-Based Geriatric Nursing Protocols for BestPractice. 4th ed. New York: Springer; 2012; 298-323.
LeBlanc K, Baranoski S; Skin Tear Consensus PanelMembers. Skin tears: state of the science: Consen-sus statements for the prevention, prediction, as-sessment and treatment of skin tears. Adv SkinWound Care. 2011;24(9):2-15.
LeBlanc K, Christensen D, Orsted HL, et al. Bestpractice recommendations for the prevention andtreatment of skin tears. Wound Care Canada. 2008;6(1):14-30.
Pennsylvania Patient Safety Authority. Patient SafetyAdvisory. Skin Tears: The Clinical Challenge. 2006.http://goo.gl/QOLw3q
White MW, Karam S, Cowell B. Skin tears in frailelders: a practical approach to prevention. GeriatrNurs. 1994;15(2):95-9.
Online ResourcesA. goo.gl/AhnLFc
B. goo.gl/SHXG0w
C. skintears.org/Education/
Access an audio education programon skin tears.
Wound Care Advisor invites you to consider submitting articles forpublication in the new voice for wound,skin, and ostomy management specialists.
as the official journal of wcc®s, dwc®s, omss,
and lleSMs, the journal is dedicated to delivering
succinct insights and pertinent, up-to-date
information that multidisciplinary wound team
members can immediately apply in their practice
and use to advance their professional growth.
we are currently seeking submissions for these
departments:
• Best Practices, which includes case studies,
clinical tips from wound care specialists, and
other resources for clinical practice
• Business Consult, which is designed to help
wound care specialists manage their careers
and stay current in relevant healthcare issues
that affect skin and wound care.
if you’re considering
writing for us, please
click here to review
our author guidelines.
the guidelines will
help you identify an
appropriate topic and learn how
to prepare and submit your
manuscript. following these
guidelines will increase the
chance that we’ll accept your
manuscript for publication.
if you haven’t written before, please consider
doing so now. our editorial team will be happy
to work with you to develop your article so that
your colleagues can benefit from your
experience.
for more information, click here to send an
email to the managing editor.
A guidetodiabeticfootulcersByDonnaSardina,RN,MH A,WCC ,CWCM S,DW CThischartexplainsthe differencesamong
ischemic,neuropathic,andneuroischemic
diabeticfootulcers,m aking iteasierforyou
toselectthebesttreatmentforyourpatient.�
20www.WoundCareAdvisor.com
July/August2012• Issue1,Number 2 • Wound CareAd visor
BestPRA CTICES
Ischemi c ulcersN europathic ulcers
Neuroischemic ulcers
Anatomiclocation•Betw een toes ortips oftoes •Plantarm etatarsalheads•M argins offoot,especially on
•Overphalangealheads•Plantarheel
medialsurfaceoffirst
•Bordersordorsalaspectof •Overplantarbony prom inencesmetatarsophalangealjoint
feet
and deformities
•O verlateralaspectoffifth
•Areas subjected to weightmetatarsophalangealjoint
bearing on plantarsurface•Tips oftoes;beneath toenails
•Areas subjected to stress (eg,dorsalportion ofham me rtoes)
Wo undcharacteristics•Deep,palew ound bed
•Red base,with healthy•Pale pink oryellow wo und bed
•Even w ound ma rginsgranularappearance
•Even wo und m argins
•Gangrene ornecrosis•Even w ound m argins
•Rounded oroblong shape over
•Rednessatbordersofulcer •Callus forma tion atbordersbony prom inence
•Blanched orpurpuricofulcer
•Callus;m ay orm ay notbe present
periwo und tissue
•Painless,unless com plicated •Painless,ow ing to neuropathy
•Severe pain
by infection
•M inimalexudate
•Cellulitis
•Rounded oroblong shape
•Minima lexudate
overbony prominence•Variableexudate
Associatedfindings•Thin,shiny,dryskin
•Dry skin
•Thin,shiny,dry skin
•Absentordiminished pulses •Bounding pulses
•Absentordiminished pulses
•TBPI< 0.7 mm Hg
•TBPI � 0.7mm Hg
•TBPI< 0.7m m Hg
•TcPO2 < 30 mm Hg
•TcPO2 > 30 m m Hg
•TcPO2 < 30 m m Hg
•Skin cooltotouch,pale,or •W arm foot
•Skin cooltotouch,pale,orm ottled
mo ttled
•Evidence ofperipheral•Evidence ofperipheralneuropathy
•No findings ofperipheralneuropathy
•Hairloss on ankleand foot
neuropathy
•Atrophy ofsmallm usclesoffeet •Thick dystrophictoenails
•Hairlosson ankleand foot •Distended dorsalfootveins •Palloron elevation;dependent
•Thickdystrophic toenails•Cyanosis
rubor
•Palloron elevation;dependentrubor•CyanosisSource:Wou nd CareEducation Institute.TBPI= toebrachialpressureindex;TcPO2 = transcutaneous oxygen pressure.
Differentiating diabeticfootulcers
View:Diabeticfootexam
“ButIleftvoicemessages anda note…”ByNancyJ.Brent,MS,RN,JD
O ftennursesgetnamed in a lawsuitwhen theyareinvolvedinclearlynegligentconductthatcausesaninjuryto orthe deathofa patient.Exam -plesinclude administeringthewrong med-icationto the wrongpatientornotposi-tioninga patientcorrectlyin the operativesuitepriortosurgery.Sometimes,howev-er,thenegligentbehaviorofa nurse isnotasclearto the nurseinvolvedin thecareofthe patient.Thatwasapparently the circumstance inthe reported case,Olsten HealthServices,Incv.Cody.1 InSeptember2000,Mr.Codywas the victimofa crime thatresulted inparaplegia.He wasadmittedto a rehabili-tation centerand dischargedon November15,2000.Hisphysicianordereddaily homehealth care servicesin ordertomonitorhis“almosthealed”Stage2 decubituspressuresore.2 The home healthcare agency as-signed a registerednurse(RN)toMr.Codyand,afterMr.Cody’shealth care insurancewould notapprovedaily visits,a reducedvisitplan wasapprovedby Mr.Cody’sphysician.
A progressiveproblemOn November16,2000,the nursevisitedMr.Cody forthe firsttime.During thatvisit,shedidanadmission assessmentandnotedthatthe pressure sore,locatedatthe areaofthe tailbone,m easured5 cm by 0.4 cmwide and 0.2 cm deep.She believedthepressure ulcercould be completely healedwithin3 weeks.The nurse called M r.Cody’sphysicianandlefthim a voicem es-sageconcerning hervisitand herfindings.On November19,a second visittookplace and the nurse observedand docu-mented thatMr.Cody’spressuresorewas“100%”pink andno odorwasdetected.On November20,she attemptedanoth-ervisitbutdid notseeMr.Cody becausethefrontgatesurrounding hishome waslocked.The nursebuzzed the gate door-bellseveraltimesto no avail.Sheleftanote on the frontgateforthe Cody familyand lefta voicem essage forM r.Cody’sphysician.The nextvisittook placeon November21.The pressureulcerwas now only “90%pink”andhada “fetid”odor;thiscondi-tion did notimproveoverthe next24hours.The nurse documentedthisfactinhernurses’notes.Again,she lefta voicemailm essageforthe physician concerningthese findings.
BusinessCO NSULT
32 www.WoundCareAdvisor.com July/August2012• Issue1,Number 2 • Wound CareAd visor
Consider writing an article

How to applysilver nitrate By Nancy Morgan, RN, BSN, MBA, WOC, WCC,DWC, OMS
Each issue, Apple Bites brings you a toolyou can apply in your daily practice. Hereis how to safely apply silver nitrate.
Topical application of silver nitrate isoften used in wound care to helpremove and debride hypergranula-
tion tissue or calloused rolled edges inwounds or ulcerations. It’s also an effec-tive agent to cauterize bleeding inwounds. Silver nitrate is a highly causticmaterial, so it must be used with cautionto prevent damage to healthy tissues.
Application methodSilver nitrate applicators are firm woodensticks with 75% silver nitrate and 25%potassium nitrate embedded on the tip.Moistening the tip sparks a chemical reac-tion that burns organic matter (skin), coag-ulates tissue, and destroys bacteria.
Precautions• Silver nitrate is very caustic to skin and
clothing. Wear protective equipment asneeded.
• Excess silver nitrate can be neutralizedwith 0.9% or stronger saline and thenwashed away with water.
• Because silver nitrate is a corrosive sub-stance, apply it only to tissue to be
treated. Take care to confine the silvernitrate to the desired area by using asuitable barrier, such as petroleum jelly.Prevent any excess from oozing by cov-ering the application area as necessary.
• Silver nitrate directly reduces fibroblastproliferation, so it is not recommendedfor prolonged or excessive use.
• Some patients report pain or burningduring treatment with silver nitrate.Consider the need for medication be-fore the procedure, including use oftopical anesthetic, to reduce discomfort.
Procedure1. Wash your hands and put on gloves. 2. Remove the wound dressing, following
dressing-removal procedure.3. Wash your hands and put on new
gloves.4. Clean the wound with sterile normal
saline solution according to wound-cleansing procedure.
Wound Care Advisor • March/April 2016 • Volume 5, Number 2 www.WoundCareAdvisor.com 19
AppleBITESBITES
Dose from WCEI

5. Remove your gloves, wash your hands,and put on new gloves.
6. Confine the area to be treated by en-circling it with petroleum jelly orequivalent.
7. Cover the wound base tissue with mois-tened normal saline gauze to protect itfrom any spillage. It is important not toallow drips of silver nitrate to settle onany surface, as they will stain and burn.
8. Slightly moisten the caustic tip of the sil-ver nitrate applicator stick by dipping(tip only) in distilled or deionized water.
9. To apply to tissue, rub and rotate thetip of the applicator along the tissue tobe debrided. Two minutes of contacttime is typically sufficient, keeping inmind that the degree of caustic actiondepends on the quantity of silver nitrateapplied, which in turn is governed bythe length of time the moistened tip isleft in contact with the tissue. Do nottouch any other part of the body, cloth-ing, or furnishings with the tip. De-pending on the size of the area to bedebrided, more than one applicatormay be needed.
10. Monitor the patient closely for responseto the procedure, including pain anddiscomfort. STOP the procedure if thepatient complains of pain.
11. Use damp saline gauze to gently clean
the treated area after application. Patdry to avoid trauma to surrounding tis-sue. Do not rub or apply friction totreated area.
12. Remove gloves and put on new ones.13. Apply any other prescribed treatment to
the wound base as ordered.
Length of treatmentFrequency of application varies based onwound needs. If silver nitrate is beingused for hypergranulation, apply it oncedaily for up to 5 days or until resolutionof hypergranulation. In the case of rollededges/epibole, treatment varies from dailyto 3 times a week until the problem is re-solved.
Use with careSilver nitrate can be an effective tool intreating wounds, but, as with many treat-ments, it must be used with care to obtainthe best results for patients. ■
Nancy Morgan, cofounder of the Wound CareEducation Institute, combines her expertise as aCertified Wound Care Nurse with an extensivebackground in wound care education and pro-gram development as a nurse entrepreneur.
Information in Apple Bites is courtesy of the WoundCare Education Institute (WCEI), © 2016.
Selected referencesCrawley-Coha T. A practical guide for the manage-ment of pediatric gastrostomy tubes based on 14years of experience. J Wound Ostomy ContinenceNurs. 2004;31(4):193-200.
Garten AJ. Keys to diagnosing and addressing hy-pergranulation tissue. Podiatry Today Blog. 2015.www.podiatrytoday.com/blogged/keys-diagnosing-and-addressing-hypergranulation-tissue#sthash.Ounqv9yL.dpuf
Stephen-Haynes J, Hampton S. Achieving effectiveoutcomes in patients with over-granulation. WoundCare Alliance UK. 2010. www.wcauk.org/downloads/booklet_overgranulation.pdf
20 www.WoundCareAdvisor.com March/April 2016 • Volume 5, Number 2 • Wound Care Advisor
Because silver nitrateis a corrosivesubstance, apply it only to tissue to be treated.

FAQs aboutsupport surfaces By Tony Forsberg, RN, BSBA, AMS, WCC, andRosalyn S. Jordan, RN, BSN, MSc, CWOCN, WCC
Support surfaces are consistently rec-ommended for the prevention and
treatment of pressure ulcers. So patientscan derive optimal benefits from supportsurfaces, clinicians must understand howto use them effectively. This article an-swers several questions about these usefultools.
What is a support surface?The National Pressure Ulcer Advisory Pan-el (NPUAP) defines support surfaces as“specialized devices for pressure redistrib-ution designed for the management of tis-sue loads, microclimate, and/or other ther-apeutic functions (i.e., any mattress,integrated bed system, mattress replace-ment, overlay, seat cushion, or seat cush-ion overlay)”.
Support surfaces are designed to redis-tribute pressure on skin, tissue, and bonyprominences. The redistribution of pres-sure (“load”) is achieved by the design ofthe support surface.
Examples of support surface devices fora sleeping surface include mattress re-placement systems, overlays that fit on topof a standard mattress, and specializedmattresses. Examples of support surfacedevices for a seated surface include spe-cialized seat or wheelchair cushions andoverlays. Support surfaces may be con-structed of different materials or combina-tion of materials, such as foam products,air, gel, or liquid.
What are some features of supportsurfaces?Support surfaces fall into one of two cate-gories: • Reactive support surfaces provide redis-
tribution by immersion and envelop-ment. In other words, they conform toa person’s body shape, which decreasesthe pressure over bony prominences.
• Active support surfaces shift the contactover the skin and tissue against thesupport surface periodically or at set in-tervals.
Individual support surfaces may haveadditional features. For example, a reac-tive support surface with a low-air-lossfeature provides not only immersion andenvelopment but also changes the micro-climate (the temperature and humidity ofthe patient) by increasing evaporationand heat transfer from the patient’s skin.
A feature of some active support sur-faces is alternating pressure, whichchanges load periodically: The poweredactive support surface changes the pres-sure on a specific area of the body by al-ternating higher and lower pressures.
How are support surfaces bestused?The 2014 Prevention and Treatment ofPressure Ulcers: Clinical Practice Guide-
Wound Care Advisor • March/April 2016 • Volume 5, Number 2 www.WoundCareAdvisor.com 21
BestPRACTICES

line, from NPUAP, European Pressure Ul-cer Advisory Panel, and Pan Pacific Pres-sure Injury Alliance contains several rec-ommendations related to the use ofsupport surfaces. These guidelines formthe basis for how to manage support sur-faces.
Choose a support surface that meets theperson’s needsFactors to consider include the individual’sactivity, mobility, size, weight, risk for(and existing) pressure ulcers, and theneed for microclimate control and sheerreduction. For example, a mattress mustproperly fit the bed frame. If the mattressis too narrow, the patient could becomeentrapped.
Match the support surface to the caresetting. For example, space, ventilation,door width, and ability to use a continu-ous power source should be considered.
Conduct assessments on a regular basisSupport surfaces require ongoing assess-ment and monitoring:• Assess the function of the support sur-
face when it’s initiated and each timeyou interact with a patient, just as youwould check an infusion pump. For in-stance, the electrical plug for a pow-ered support surface may have beenknocked out of the socket or the settingcould have been changed for transfersfrom the bed to the chair and notchanged back.
• Remember that support surfaces have afinite functional life span, meaning theydo not continue providing the expectedpressure redistribution for an unlimitedperiod of time. Follow the manufactur-er’s guidelines regarding testing func-tion.
Choose materials compatible with thesupport surfaceChoose clothing, linens, and incontinencepads that are compatible with the supportsurface. For instance, specially made dis-posable incontinence pads will allow airmovement, which maximizes the benefitof a low-air-loss mattress.
In addition, limit the number of linensand incontinence pads on support sur-faces. Studies show that excess linens andincontinence pads interfere with supportsurface therapy. For example, Williamsonand others found that multiple layers oflinens and pads increased the interfacepressure between the skin and the top ofthe mattress. In another study, Williamsand others found that each additional layerof linens and/or pads on a low-air-losssupport surface reduced the surface’s abili-ty to manage moisture-vapor transmission,which leads to decreased effectiveness.
Continue to reposition the patientThe patient must be turned and reposi-tioned, unless this is contraindicated by amedical condition. Individualized treat-ment plan and turning schedules shouldbe developed based upon the patient’sgeneral condition related to skin and com-fort measures. The care plan should reflect
22 www.WoundCareAdvisor.com March/April 2016 • Volume 5, Number 2 • Wound Care Advisor
Resources
• Download a table of support surface termsand definitionsA from the National Pres-sure Ulcer Advisory Panel Support Sur-face Standards Initiative.
• Download a quick reference guideB for the2014 Prevention and Treatment of Pres-sure Ulcers: Clinical Practice Guideline.

the turning and repositioning schedule anda rationale if the schedule deviates fromstandard policy.
Consider unique needs based on thesupport surfaceSome support surfaces present circum-stances that require special patient care.For example, dehydration may occur withsome bed systems that are warmer andhave a more intense airflow. When usingthis equipment, the patient’s fluid intakemay need to be increased.
How can I promote optimal use ofsupport surfaces?Staff education is an integral element forproviding appropriate support surfacetherapy. Education should include all staffmembers who care for the individual orthe equipment. Assess the staff’s knowl-edge before developing an educationalplan, so it can be tailored to their specificneeds. After education, reassess to verifystaff’s understanding. (See Suggested topicsfor a support-surfaces education program.)
Through better understanding of sup-port surface therapy and its appropriateuse, you can help provide patients withquality, cost-effective care. ■
Tony Forsberg is senior account executive andRosalyn S. Jordan is clinical director of posta-cute clinical programs and services for JoernsHealth Care in Charlotte, North Carolina.
Selected referencesANSI/RESNA. SS-1 Support Surfaces. Section 1 Vo-cabulary. Arlington, VA: Rehabilitation Engineeringand Assistive Technology Society of North America;2014.
Call E, Deppisch M, Jordan R, et al. Hand CheckMethod: Is it an Effective Method to Monitor for Bot-toming Out? A National Pressure Ulcer Advisory Posi-tion Statement; 2015. www.npuap.org.
McNichol L, Watts C, Mackey D, et al. Identifying theright surface for the right patient at the right time:generation and content validation of an algorithm forsupport surface selection. J Wound, Ostomy, Conti-nence Nurs. 2015;42(1):19-37.
National Pressure Ulcer Advisory Panel, EuropeanPressure Ulcer Advisory Panel and Pan Pacific Pres-sure Injury Alliance. Emily Haesler (Ed). Preventionand Treatment of Pressure Ulcers: Clinical PracticeGuideline. Cambridge Media: Osborne Park, WesternAustralia; 2014.
Stone A, Brienza D, Call E, et al. Standardizing sup-port surface testing and reporting; A National Pres-sure Ulcer Advisory Panel Executive Summary. JWound, Ostomy, Continence Nurs. 2015;42(5):445-49.
Williamson R, Lachenbruch C, VanGilder C. A labora-tory study examining the impact of linen use onlow-air-loss support surface heat and water vaportransmission rates. Ostomy Wound Manage.2013;59(8):32-41.
Williamson R, Lachenbruch C, VanGilder C, et al.The effect of multiple layers of linens on surface in-terface pressure: results of a laboratory study. Osto-my Wound Manage. 2013;59(6):38-47.
Online ResourcesA. npuap.org/wp-content/uploads/2012/03/NPUAP_S3I_TD.pdf
B. npuap.org/wp-content/uploads/2014/08/Quick-Reference-Guide-DIGITAL-NPUAP-EPUAP-PPPIA-Jan2016.pdf
Wound Care Advisor • March/April 2016 • Volume 5, Number 2 www.WoundCareAdvisor.com 23
Here are some topics you might want to in-clude in your education program on supportsurfaces:
• importance of support surface use in theprevention and treatment of pressure ulcers
• review of the organization’s algorithm or de-cision tree for support surfaces. If no suchtool exists, one should be developed.
• demonstration of each support surface• correct assessment and reporting of supportsurface function
• appropriate use of linens and incontinencepads
• turning and repositioning• daily maintenance of support surface• documentation in the patient’s healthrecord.
Suggested topics for a support-surfaces education program

Nutritionalconsiderations inpatients withpressure ulcers Addressing four essentialelements can help youmeet these patients’nutritional needs.
By Jill Cox, PhD, RN, APN-C, CWOCN, and SophiaZigouras, MS, RD, CNSC
Optimizing nutritional status is a keystrategy both in preventing and man-
aging pressure ulcers. In patients acrossall care settings, compromised nutrition—as from poor intake, undesired weightloss, and malnutrition—increases the riskof pressure ulcers. It contributes to alteredimmune function, impaired collagen syn-thesis, and decreased tensile strength. Inmany cases, malnutrition also contributesto wound chronicity and increases the riskfor delayed and impaired wound healing.In patients with chronic wounds, such aspressure ulcers, a chronic inflammatory
state can induce catabolic metabolism,malnutrition, and dehydration.
Adequate nutrition, on the other hand,promotes wound healing in patients withpressure ulcers. Wound healing occurs inthree distinct but overlapping phases—in-flammatory, proliferative, and remodeling.Each phase is time limited and marked bydistinct physiologic events, with specifickey nutrients playing a crucial role duringthat phase. (See Understanding wound-healing phases.)
Pressure-ulcer management must in-clude a comprehensive nutritional careplan based on the latest practice guide-lines. This article describes the four essen-tial elements that help you address thenutritional needs of patients with pressureulcers: • performing a nutrition screening for po-
tential nutrition deficits• identifying malnutrition• addressing the patient’s macronutrient
and fluid needs• determining appropriate micronutrient
supplementation. (See Nutritional ther-apy recommendations for pressure-ulcermanagement.)
Element 1: Nutrition screening The goal of nutrition screening is to iden-tify patients who need a more in-depthnutritional assessment and a comprehen-sive nutritional plan based on identifiednutritional risk factors. On admission to ahealthcare facility, the patient should un-dergo a complete nutrition screening, in-cluding assessment of pressure ulcer riskusing a tool such as the Braden Scale(www.bradenscale.com). In the hospitalsetting, the nurse generally completes thisinitial screening.
Several validated screening tools can be
24 www.WoundCareAdvisor.com March/April 2016 • Volume 5, Number 2 • Wound Care Advisor

used in various settings, including the Nu-trition Risk Classification, Malnutrition Uni-versal Screening Tool, and Nutrition RiskScreening 2002. Screening parameters in-clude malnutrition risk factors, such as: • unintentional weight loss• changes in appetite or food and fluid
intake• poor dental health• chewing and swallowing difficulties• poor self-feeding ability • GI signs and symptoms.
If the screening determines the patientis at nutritional risk, a registered dietitian(RD) conducts a timely and complete nu-trition assessment. The RD determines the
patient’s nutritional status and develops acomprehensive nutritional care plan inconsultation with interdisciplinary teammembers, including the physician or amid level practitioner, a registered nurse,and when appropriate, a speech patholo-gist, occupational therapist, or dentist. TheRD also provides the expertise to ensurethat the plan of care is based on standardnutritional guidelines from the AmericanSociety for Parenteral and Enteral Nutrition(A.S.P.E.N.) and the Academy of Nutritionand Dietetics. This plan must be individu-alized to reflect the patient’s comorbiditiesand malnutrition level. Then the RD imple-ments the plan to address nutritionaldeficits and monitors macro- and micronu-
Wound Care Advisor • March/April 2016 • Volume 5, Number 2 www.WoundCareAdvisor.com 25
The three phases of wound healing—inflammatory, proliferative, and remodeling—overlap. Dur-ing each phase, key physiologic events occur and specific nutrients play a vital role in healing.
Phase, onset, and duration Key events Essential nutrients
Inflammatory phase • Hemostasis • Vitamins A, C, and KStarts at time of injury • Release of pro-inflammatory • Ironand lasts 4 to 6 days cytokines • Zinc • Vasodilation • Protein • Phagocytosis of bacteria • Fat by neutrophils • Carbohydrates • Removal of debris and growth-factor secretion by macrophages
Proliferative phase • Fibroblast proliferation • Vitamins A and CStarts 3 or 4 days after • Angiogenesis • Ironinjury and lasts 2 to 3 • Collagen synthesis • Copperweeks • Collagen deposition and • Zinc cross-linking • Manganese • Development of granulation • Protein tissue and extracellular matrix • Carbohydrates • Epithelialization • Onset of wound closure by myofibroblasts
Maturation/remodeling • Collagen maturation and • Vitamins A and Cphase stabilization • ZincStarts about 21 days after • Increased tensile strength • Proteininjury and lasts up to 2 • Scar-tissue formation years
Understanding wound-healing phases

26 www.WoundCareAdvisor.com March/April 2016 • Volume 5, Number 2 • Wound Care Advisor
This table shows therapeutic nutrition recommendations for each pressure-ulcer stage.
Recommended Stage1: Stage 2: Stage 3: Stage 4:nutritional therapy Nonblanchable Partial- Full-thickness Full-thickness tissueand goal erythema of thickness loss tissue loss; sub- loss with intact skin of dermis cutaneous fat exposed muscle, may be visible bone, or tendon
Total calories ≥ 25 cal/kg 28-30 cal/kg 30 cal/kg 33-35 cal/kg. To optimize anabolism, Maximum: collagen formation, 40 cal/kgnitrogen retention, and angiogenesis
Protein 1-1.2 g/kg 1.25-1.4 g/kg 1.5 g/kg 1.5-2.0 g/kg. To promote cell growth Maximum: 2.2 g/kgand structure, fibroblast proliferation, collagen production, and angiogenesis
Fluid ≥ 30 mL/kg with ≥ 1 mL/cal 30-40 mL/kg with 1-1.5 mL/cal To maintain skin turgor, consumed. Adjust to fluid consumed. Adjust to fluid losses.tissue perfusion and losses. oxygenation, and nutrient transport
Multivitamins with Multivitamin/mineral Add multivitamin/mineral minerals supplement once daily for supplement once daily. To provide many patients with inadequate oral Maximum dose: twice daily. nutrients involved in or enteral intakecollagen production, tissue regeneration, and prothrombin synthesis
Vitamin C 100-200 mg/day 1,000-2,000 mg/day in divided doses To aid collagen for patients who are stressed or at formation, angiogenesis, risk for deficiency; reassess in 10-14 and fibroblast formation days. Maximum dose: 2,000 mg/day.and promote neutrophil activity
Zinc 15 mg elemental zinc/day; give 25-40 mg elemental zinc per day; To promote cell up to 220 mg zinc sulfate daily give up to 220 mg zinc sulfate replication and growth for 10-14 days for suspected up to twice daily for 10-14 days and serve as a cofactor deficiency. for suspected deficiency.for synthesis of collagen and other wound proteins
Vitamin A • If patient is taking concomitant glucocorticoids, supplement with To stimulate 10,000-15,000 units vitamin A daily for 7 days.inflammatory phase of • For patients with suspected deficiency, replete with 10,000-50,000 wound healing, maintain units daily for 10-14 days, based on degree of injury and malnutrition. integrity of mucosal and • Maximum dose: 25,000-50,000 units daily for 10-14 daysepithelial surfaces,increase collagen formation, and inhibit detrimental effects of diabetes and glucocorticoids cal/kg = calories per kilograms of body weight; mL/cal = milliliters of fluid per calorie consumedNote: Requirements can be adjusted based on clinician’s judgment and patient’s overall clinical condition, comorbidities,and medical history.
Nutritional therapy recommendations for pressure-ulcer management

trient interventions until the patient’s nutri-tional status has been optimized.
Element 2: Malnutritionidentification Adult malnutrition (undernutrition) resultsfrom inadequate calories, protein, or othernutrients needed for tissue maintenance andrepair. At least two of the following condi-tions indicate the patient has malnutrition: • insufficient energy intake• weight loss• muscle mass loss• subcutaneous fat loss• localized or generalized fluid accumula-
tion that may mask weight loss• diminished functional status, as meas-
ured by handgrip strength.
The extent of these conditions deter-mines if malnutrition is severe. Based onsymptom duration and inflammation pres-ence, malnutrition is classified further asacute, chronic, or social/environmental.Severe malnutrition of acute or chronic ill-ness is associated with pressure ulcer de-velopment with increased severity, de-layed healing, and chronicity. (SeeClinical features of severe malnutrition.)
Be aware that using serum inflammato-ry biomarkers (such as albumin and preal-bumin) to diagnose malnutrition isn’t rec-ommended. These values can be affectedby inflammation, renal function, hydrationstatus, and other factors (such as comor-bidities and illness severity) and may notaccurately reflect the patient’s nutritionalstatus.
Element 3: Macronutrientrequirements and hydration Calories, protein, fat, and fluids each play aspecific role in supporting wound healing.
MacronutrientsPatients with pressure ulcers require suffi-cient calorie and protein intake to supportanabolism, nitrogen retention, collagenformation, and angiogenesis—all of whichare fundamental for wound healing. The2014 National Pressure Ulcer AdvisoryPanel/European Pressure Ulcer AdvisoryPanel/Pan Pacific Pressure Injury Alliance(NPUAP/EPUAP/PPPIA) Nutrition Guide-lines recommend providing 30 to 35 calo-ries/kg/day to adults who have, or are atrisk for, pressure ulcers and malnutrition.The guidelines suggest adjusting energyintake based on weight change, under-weight, and obesity.
Dietary carbohydrates and fat are thepreferred energy sources because theyspare protein for collagen production andcell structure. According to dietary refer-ence intakes, adults should get 45% to65% of calories from carbohydrates and20% to 35% from fat. No recommenda-tions exist for carbohydrate intake basedon pressure ulcer stage; however, hyper-glycemia is linked to impaired leukocyteproduction, which impedes wound heal-
Wound Care Advisor • March/April 2016 • Volume 5, Number 2 www.WoundCareAdvisor.com 27
Pressure-ulcer healingrequires adequateprotein; increasedprotein intake isassociated withimproved woundhealing rates.

ing and increases susceptibility to infec-tion. In patients with diabetes mellitus orglucocorticoid-induced hyperglycemia, theinterdisciplinary team should maximizeblood glucose control through medicationadjustment and carbohydrate restriction asneeded.
Similarly, no recommendation exists forfat intake specific to patients with pres-sure ulcers. A dense energy source, fatprovides essential fatty acids and carriesfat-soluble vitamins. Nonetheless, its rolein wound healing hasn’t been established.
Protein is needed for cell growth andstructure, collagen production, fibroblastproliferation, and synthesis of enzymes in-volved in wound healing. Pressure-ulcerhealing requires adequate protein; in-creased protein intake is associated withimproved wound healing rates. NPUAP/EPUAP/PPPIA guidelines recommend pro-viding 1.25 to 1.5 g/kg/day of protein foradults who have, or are at risk, for pres-
sure ulcers and malnutrition. Patients withstage III/IV pressure ulcers or multiplewounds may need 1.5 to 2 g/kg/day.Those with a protein intake as high as 2g/kg/day must be monitored for changesin renal function and hydration status.
Current guidelines for patients withpressure ulcers recommend supplementsof specific amino acids, such as arginine,along with high protein supplementationin patients with stage III/IV pressure ul-cers or multiple pressure ulcers whose nu-tritional needs can’t be met with tradition-al high-calorie and protein supplements.According to A.S.P.E.N, recommendationsfor arginine and glutamine supplementa-tion are lacking.
HydrationTo prevent or treat pressure ulcers, pa-tients require adequate hydration. Suffi-cient fluid intake maintains skin turgorand delivery of oxygen and nutrients to
28 www.WoundCareAdvisor.com March/April 2016 • Volume 5, Number 2 • Wound Care Advisor
This chart distinguishes the clinical features of severe malnutrition of acute illness from those ofsevere malnutrition of chronic illness.
Clinical feature Severe malnutrition of acute illness Severe malnutrition of chronic illness
Energy intake • ≤ 50% of estimated needs • ≤ 75% of estimated needs for for ≥ 5 days ≥ 1 month
Weight loss • 2% in 1 week • 5% in 1 month • 5% in 1 month • 7.5% in 3 months • > 7.5% in 3 months • 10% in 6 months • > 20% in 1 year
Body fat wasting Moderate Severe(orbital, triceps, over ribs)
Muscle wasting Moderate Severe(temples, clavicle, scapula, thigh, calf)
Edema Moderate Severe(generalized, ascites, or extremities)
Grip strength Measurably reduced Measurably reduced
Clinical features of severe malnutrition

both healthy and healing tissues. Currentfluid intake recommendations are 30mL/kg/day or 1 to 1.5 mL per caloriesconsumed. The interdisciplinary teammust monitor the patient’s hydration statuscarefully because high protein intake, flu-id losses from draining wounds, elevatedtemperature, diaphoresis, vomiting, anddiarrhea may increase fluid requirements.
Element 4: MicronutrientrequirementsMicronutrients are vitamins, minerals, andtrace elements that the body requires forcell metabolism in small but criticalamounts. Standard multivitamin supple-ments with minerals are recommended forpatients with pressure ulcers and inade-quate oral or enteral intake. In particular,vitamins C and A and zinc play importantroles in wound healing. • Vitamin C is crucial for collagen forma-
tion, angiogenesis, and fibroblast forma-tion; it also acts on neutrophil activity.Patients with stage I or II pressure ul-cers should receive 100 to 200 mg/dayin vitamin C supplementation; thosewith stage III or IV ulcers should re-ceive 1,000 to 2,000 mg/day.
• Vitamin A stimulates the inflammatoryphase of wound healing, maintains in-tegrity of mucosal and epithelial sur-faces, increases collagen formation,and inhibits detrimental effects of glu-cocorticoid therapy, diabetes, radiation,and chemotherapy. Patients with vita-min A deficiencies and pressure ulcersof any stage should receive 10,000 to50,000 units/day for 10 days. Patientsreceiving glucocorticoids should re-ceive 10,000 to 15,000 units/day for 1week prophylactically to counter im-munosuppression.
• Zinc promotes cell replication andgrowth and aids protein and collagensynthesis. Supplements are recommend-ed only for patients with zinc deficien-cy, which commonly accompanies mal-nutrition, malabsorption, diarrhea, and
hypermetabolic states. For patients withzinc deficiency, supplementation at therecommended dose of 220 mg zinc sul-fate twice daily for 10 to 14 days canenhance wound healing.
Strategies to improve nutritionalintakeFor patients with pressure ulcers whocan’t achieve an adequate dietary intake,NPUAP/EPUAP/PPPIA guidelines recom-mend these additional strategies to im-prove overall nutritional status: • Liberalize dietary restrictions if those re-
strictions lead to inadequate nutritionalintake.
• Offer high-calorie, high-protein oralsupplements between meals.
• Consider providing enteral or parenteralnutrition support to patients who can’t
Wound Care Advisor • March/April 2016 • Volume 5, Number 2 www.WoundCareAdvisor.com 29
Standard multivitaminsupplements withminerals arerecommended forpatients with pressureulcers and inadequateoral or enteral intake.

achieve a satisfactory oral nutritional in-take.
When considering whether to imple-ment these strategies, keep in mind thepatient’s comorbidities and overall caregoals.
A comprehensive nutritional planbased on the latest clinical practiceguidelines can improve outcomes for pa-tients who have pressure ulcers or are atrisk for developing them. All healthcareteam members are responsible for opti-mizing nutrition for these patients. TheRD is central to developing and refininga successful nutritional plan. As frontlinecaregivers, nurses are in a unique posi-tion to identify nutritional deficiencies,evaluate pressure-ulcer healing, and com-municate assessment findings to the med-ical team and RD. ■
The authors work at Englewood Hospital andMedical Center, in Englewood, New Jersey. JillCox is an advanced practice nurse and WOCnurse; Sophia Zigouras is a clinical dietitian. Dr. Cox is also an assistant professor of nursingat Rutgers University in Newark.
Selected referencesBergstrom N, Braden BJ, Laguzza A, et al. TheBraden scale for predicting pressure sore risk. NursRes. 1987;36(4):205-10.
Doughty DB, Sparks-DeFriese B. Wound healingphysiology. In: Bryant R, Nix D, eds. Acute andChronic Wounds: Current Management Concepts.4th ed. St. Louis, MO: Elsevier; 2012.
Iizaka S, Okuwa M, Sugama J, et al. The impact ofmalnutrition and nutrition-related factors on the de-velopment and severity of pressure ulcers in olderpatients receiving home care. Clin Nutr. 2010;29(1):47-53.
Institute of Medicine. Panel on Macronutrients, Panelon the Definition of Dietary Fiber, Subcommittee onUpper Reference Levels of Nutrients, Subcommitteeon Interpretation and Uses of Dietary Reference In-takes, and the Standing Committee on the ScientificEvaluation of Dietary Reference Intakes. Food and
Nutrition Board. Dietary Reference Intakes for Ener-gy, Carbohydrate, Fiber, Fat, Fatty Acids, Choles-terol, Protein and Amino Acids. Washington, DC:National Academies Press; 2005.
Kondrup J, Allison SP, Elia M, et al. ESPEN guide-lines for nutrition screening 2002. Clin Nutr.2003;22(4):415-21.
Kovacevich DS, Boney AR, Braunschweig CL, et al.Nutrition risk classification; a reproducible and validtool for nurses. Nutr Clin Pract. 1997;12(1):20-5.
Lee SK, Posthauer ME, Dorner B, et al. Pressure ul-cer healing with a concentrated, fortified, collagenprotein hydrolysate supplement: a randomized con-trolled trial. Adv Skin Wound Care. 2006:19(2):92-6.
National Pressure Ulcer Advisory Panel, EuropeanPressure Ulcer Advisory Panel, and Pan Pacific Pres-sure Injury Alliance. Prevention and Treatment ofPressure Ulcers: Clinical Practice Guideline. HaeslerE (ed.). Perth, Australia: Cambridge Media; 2014.
Patel V, Romano M, Corkins MR, et al; American So-ciety for Parenteral and Enteral Nutrition(A.S.P.E.N.). Nutrition screening and assessment inhospitalized patients: a survey of current practice inthe United States. Nutr Clin Prac. 2014;29(4):483-90.
Posthauer ME, Banks M, Dorner B, et al. The role ofnutrition for pressure ulcer management: NationalPressure Ulcer Advisory Panel, European PressureUlcer Advisory Panel, and Pan Pacific Pressure In-jury Alliance White Paper. Adv Skin Wound Care.2015;28(4):175-88.
Stechmiller JK. Understanding the role of nutritionand wound healing. Nutr Clin Pract. 2010;25(1):61-8.
Stechmiller JK. Wound healing. In: Mueller C, ed.A.S.P.E.N. Adult Nutrition Support Core Curriculum.2nd ed. Silver Spring, MD: American Society for Par-enteral and Enteral Nutrition; 2012: 348-63.
Stotts N. Nutritional assessment and support. In:Bryant R, Nix D, eds. Acute and Chronic Wounds:Current Management Concepts. 4th ed. St Louis,MO: Elsevier; 2012
Todorovic V, Russell C, Elia M. The MUST explana-tory booklet: A Guide to the “Malnutrition UniversalScreening Tool” (“MUST”) for Adults. www.bapen.org.uk/pdfs/must/must_explan.pdf
White JV, Guenter P, Jensen G, Malone A, SchofieldM; Academy Malnutrition Work Group; A.S.P.E.N.Malnutrition Task Force; A.S.P.E.N. Board of Direc-tors. Consensus statement: Academy of Nutritionand Dietetics and American Society for Parenteraland Enteral Nutrition: characteristics recommendedfor the identification and documentation of adultmalnutrition (undernutrition). JPEN J Parenter Enter-al Nutr. 2012;36(3):275-83.
30 www.WoundCareAdvisor.com March/April 2016 • Volume 5, Number 2 • Wound Care Advisor

Comprehensiveturning programscan avoid a painin the back By Jeri Lundgren, BSN, RN, PHN, CWS, CWCN
Turning programs are essential to pre-vent and promote healing of pressure
ulcers and to prevent the many negativeeffects of immobility, ranging from consti-pation to respiratory infections. However,turning a patient often puts a caregiver’sbody in an awkward position, which canlead to musculoskeletal damage, especial-ly back injuries.
According to the U.S. Bureau of LaborStatistics, healthcare workers suffer thehighest rate of musculoskeletal disordersfor all occupational groups and more thanseven times the average rate for all occu-pations. Direct caregivers are the groupmost likely to experience musculoskeletalinjuries. During turning tasks, excessiveforces are imposed on the caregiver’smusculoskeletal structure due to the exter-nal load of the patient and the caregiver’sform and position during the task. Fragalaand Fragala found that turning patients inbed is one of the highest-risk activitiesthat lead to low back pain.
Reducing the riskUsing safe patient handling equipment re-duces the force exerted on musculoskeletalstructures and lowers the risk of injury tothe caregiver. Leaders should consider in-vesting in the following safe patient han-dling equipment as part of the organiza-tion’s comprehensive turning program:
• grab bars and/or a trapeze on the bedso the patient can participate or be-
Wound Care Advisor • March/April 2016 • Volume 5, Number 2 www.WoundCareAdvisor.com 31
BusinessCONSULT
The following tools are a useful additions tosafe turning programs.
Small repositioningsling
Limb liftsling
Photos from JoernsRecoverCare. Used with permission.
Lifting aids

come independent in turning• friction-reducing aids to reduce the
force required to turn patients• mechanical lifts with
• full-body turning/repositioning slings toremove the workload of the caregiver
• a small repositioning sling and a limblift sling to position and hold a patientin place during care or a dressingchange to a wound. (See Lifting aids.)
Investment in this equipment can helpreduce costs associated with musculo -skeletal disorders in caregivers.
Caregivers should choose the rightequipment for the task at hand and usethe equipment appropriately. They shouldremove slings or friction-reducing aidswhen the task is complete, so they don’t
hinder the pressure redistribution proper-ties of the support surface.
Making safe patient handling equipmentavailable encourages caregivers to complywith turning protocols and leads to betteroutcomes for both patients and caregivers. ■
Jeri Lundgren is the president of SeniorProviders Resource in Cape Coral, Florida. Shecan be contacted at [email protected].
Selected referenceFragala G, Fragala, M. Improving the safety of pa-tient turning and repositioning tasks for caregivers.Workplace Health Saf. 2014;62(7):268-73.
Access more informationA about selecting equip-ment from the Association of Rehabilitation Nurses.
Online ResourceA. rehabnurse.org/uploads/files/pdf/sphchap4.pdf
Admission also includes exhibitor showcase & lunch Only $60

Exercise yourright to be fit! The medicine ofmovement
By Tracey Long, PhD, RN, MS, MSN, CDE, CNE,CHUC, CCRN
Nearly all clinicians know exercise isgood for our physical and mental
health. But incorporating it into our busylives can be a challenge. The only typesof exercise some clinicians have time forare working long shifts, juggling life’s de-mands, balancing the books, jumping onthe bandwagon, climbing the ladder ofsuccess, and skipping meals.
Clinicians are in a unique position tohelp patients change their behavior to im-prove their health. Ironically, the first be-havior clinicians need to change is to worktoward improving our own exercise habits.
Jumping through hurdlesClinicians have no problem describing themany benefits of exercise to patients, butmost of us don’t have a regular exerciseprogram for ourselves. Even with strongevidence supporting the benefits of exer-cise, only about 25% of adults follow therecommendation to get at least 30 minutesof moderate-intensity physical activity daily;37% admit they get no exercise at all. Ourhigh-tech society makes it convenient to besedentary; figuring out how to get Ameri-cans out of their seats and away from theirTVs and computers poses a real challenge. Moving in new definitions One barrier that can be overcome may beas simple as semantics. For many, the wordexercise carries the stigma of sweat, pain
and, when neglected, guilt. So simply re-placing exercise with movement may be lib-erating. Movement is any bodily action pro-duced by skeletal muscle contraction thatincreases energy use above the baselinelevel and requires tissue oxygenation.Movements with the most health-promotingand disease-preventing benefits includethose that build cardiorespiratory enduranceand muscle strength, toning, and flexibility.
Get movingAccording to the Department of Healthand Human Services, the more physicallyactive you are, the more health benefitsyou gain for life. Physical activity guideli-nesA established in 2008 can help physicaleducators, policymakers, healthcareproviders, and the public understand theamounts, types, and intensity of physicalactivity needed to achieve health benefitsacross the lifespan. Combined with the Di-etary Guidelines for AmericansB, these evi-dence-based documents support the phys-ical activity objectives established forHealthy People 2020C.
Exercise guidelines andprescriptionsExercise guidelines and prescriptions are
Wound Care Advisor • March/April 2016 • Volume 5, Number 2 www.WoundCareAdvisor.com 33

based on the FITT formula, which stands for: • Frequency (how often you exercise)• Intensity (how hard you exercise)• Time (how long you exercise)• Type (which exercises you do).
Frequency recommendations are basedon multiple research studies that showcardiovascular benefits occur with 2½hours of exercise weekly.
The intensity level must be customizedto each individual’s health, age, and limita-tions. The American Heart Association rec-
ommends reaching target heart rate (THR),calculated with this formula: 220 minusyour age. Reach ing THR helps you achievemaximum cardiovascular exercise, but youmust sustain it for 20 to 30 minutes. Safetyis a priority, though, and not everyoneshould attempt to reach 100% of THR.People taking beta blockers, for instance,may not be able to reach even 70%.
Time recommendations are 20 to 60minutes of continuous aerobic exercise ofmoderate to vigorous intensity 3 to 5 daysper week.
The type of exercise depends on indi-vidual preference and ability. Generally,aerobic exercise is best because it sup-plies oxygen for muscle movements. Aner-obic exercise, done while holding your
breath, may create lactic acidosis and sideaches. Even while doing static exercise orweight training, pay attention to breathing.
Exercise caution How much to exercise depends on yourhealth status, initial fitness level, availabletime, activity preferences, personal goals,and available equipment and facilities. Theminimum caloric expenditure for health is150 kcal/day or 1,000 kcal/week. For themaximum health benefit, you’ll need toperform 5 to 6 hours of physical activityper week and expend 2,000 kcal/weekabove your basal metabolic rate.
For an even higher fitness level or weightloss, you’ll need to exercise in the upperend of the range by expending 300 to 400kcal/day. But be aware that age, gender,and health status can influence the totals.Thirty minutes of moderate activity daily isequivalent to 600 to 1,200 cal/week of ener-gy expenditure. Modify this expenditure ifyou have neuropathy, retinopathy, cardiacdisease, or medication contraindications.People with asthma should carry emergencyinhalers and bronchodilators. Sedatives andantihistamines may cause drow si ness, slowreaction time, and impair balance and coor-dination, creating a safety risk during exer-cise. Stimulants may increase the heart rateand cause unwanted side effects. Exercise iscontraindicated in people with known aorticaneu rysms, aortic stenosis, decompensatedheart failure, pulmonary or systemic em-bolism, thrombo phle bitis, uncontrolledmetabolic disorders, and ventricular tachy-cardia or other dangerous arrhythmias.
Training technologies Although technology might be at the root ofour sedentary lifestyles, we can use it to im-prove our movement and activity level. Nu-
34 www.WoundCareAdvisor.com March/April 2016 • Volume 5, Number 2 • Wound Care Advisor
The morephysically activeyou are, the morehealth benefitsyou gain for life.

merous smartphone apps can track walking,eating, sleeping, and exercise levels to pro-mote self-awareness and progress towardgoals. Finding these tools is as easy as exer-cising your fingers to an online search en-gine. (See Exercise and fitness apps.)
Movement mantras You can help drive a shift toward a moreactive lifestyle by spreading the word thatpublic health officials have been preach-ing—but tone it down to the kinder andgentler philosophy of getting into shapesimply by moving more. And by allmeans, set an example yourself. By be-coming better examples of healthy living,clinicians can help eliminate the mantra“No pain, no gain” and replace it with thissage advice: If you don’t have time foryour health today, you won’t have healthfor your time tomorrow. ■
Tracey Long is on the nursing faculty at the Col-lege of Southern Nevada in Las Vegas.
Selected referencesAhmad T, Chasman DI, Mora S, et al. The fat-massand obesity-associated (FTO) gene, physical activity,and risk of incident cardiovascular events in whitewomen. Am Heart J. 2010;160(6):1163-9.
American College of Sports Medicine. ACSM’s Guide-lines for Exercise Testing and Prescription. 9th ed.Lippincott Williams & Wilkins; 2013.
American Heart Association Recommendations forPhysical Activity in Adults. American Heart Association.Updated May 16, 2014. www.heart.org/HEARTORG/GettingHealthy/PhysicalActivity/FitnessBasics/
American-Heart-Association-Recommendations-for-Physical-Activity-in-Adults_UCM_307976_Article.jsp.
Britton KA, Lee IM, Wang L, et al. Physical activityand the risk of becoming overweight or obese inmiddle-aged and older women. Obesity (SilverSpring). 2012;20(5):1096-103.
Exercise benefit equals drugs for some health prob-lems. Harv Mens Health Watch. 2014;18(6):8.
Five easy ways to start exercising. Get moving bychanging your thinking and working exercise intodaily activity. Harv Health Lett. 2014;39(4):6.
Global recommendations on physical activity for
health. World Health Organization. 2014. www.who.int/dietphysicalactivity/factsheet_recommenda-tions/en. Accessed May 29, 2014.
Haskell WL, Lee IM, Pate RR, et al. Physical activityand public health: updated recommendation foradults from the American College of Sports Medicineand the American Heart Association. Med Sci SportsExerc. 2007;39(8):1423-34.
Healthy People 2020. Physical activity. U.S. Depart-ment of Health and Human Services. May 29, 2014.www.healthypeople.gov/2020/topicsobjectives2020/overview.aspx?topicid=33.
How much physical activity do adults need? Centersfor Disease Control and Prevention. Last reviewed De-cember 1, 2011. www.cdc.gov/physicalactivity/every -one/guidelines/adults.html. Accessed May 29, 2014.
Panel on Macronutrients, Subcommittees on UpperReference Levels of Nutrients and Interpretation andUses of Dietary Reference Intakes, Standing Commit-tee on the Scientific Evaluation of Dietary ReferenceIntakes, Food and Nutrition Board, Institute of Medi-cine. Dietary Reference Intakes for Energy, Carbohy-drates, Fiber, Fat, Fatty Acids, Cholesterol, Protein,and Amino Acids (Macronutrients). Washington, DC:National Academies Press; 2005. www.nap.edu/open-book.php?isbn=0309085373.
2008 Physical Activity Guidelines for Americans. U.S.Department of Health and Human Services. October2008. www.health.gov/paguidelines/pdf/paguide.pdf.
Online ResourcesA. health.gov/PAGuidelines/B. health.gov/dietaryguidelines/2015/default.aspC. healthypeople.gov/2020/topics-objectives/topic/physical-activity?topicid=33
Wound Care Advisor • March/April 2016 • Volume 5, Number 2 www.WoundCareAdvisor.com 35
A multitude of exercise and fitness appsare available for smartphones, computers,and tablets. Here’s just a small sampling.
• MyFitnessPal• Fitness Buddy• iFitness• 1000 Exercises• Daily Workout Apps• FitnessBuilder• GymGoal ABC• iTreadmill• RunKeeper Pro• Women’s Health Personal Trainer• Women’s Health Workouts LITE• Workout Trainer
Exercise and fitness apps

Check out the following resources, all de-signed to help you in your clinical practice.
Human trafficking resources
Victims of human trafficking often suffertremendous physical and psychologicaldamage. Clinicians play an important rolein identifying potential victims so they canobtain help.
Here are some resources to learn moreabout human trafficking.• “Addressing human trafficking in the health
care settingA” is an online course that in-cludes a downloadable quick-referenceguide that can be saved and easily ac-cessed from a mobile device to assistproviders with essential information inthe healthcare setting.
• The National Human Trafficking ResourceCenterB provides an online course forhealthcare professionals on how toidentify human trafficking victims. Youalso can access tools such as a shortsummary of what to look for on exami-nation.
Experts recommend posting the phonenumber for the National Human Traffick-ing Resource Center in a prominent loca-tion: (888) 373-7888. The hotline is staffed24 hours a day, 7 days a week, and helpis available in more than 200 languages.
Resources from NPUAP
The National Pressure Ulcer Advisory Pan-el (NPUAP) website includes links to re-sources, including:• “Do lift slings significantly change the effi-
cacy of therapeutic support surfaces?C”• “The Role of Nutrition for Pressure Ulcer
ManagementD” (from the NPUAP, Euro-pean Pressure Ulcer Advisory Panel,and Pan Pacific Pressure Injury Al-liance).
Patient/caregiver educationbrochure
The European PressureUlcer Advisory Panel’swebsite includes abrochureE for patients andcaregivers that describesthe “RISE” strategy forpreventing pressure ul-cers—Reposition, Inspect,Skin care, and Eat well.
The brochure definespressure ulcer, describes who is at risk,and reviews the elements of the RISE strat-egy, providing caregiver tips for each one.
Online course on ostomy care
“Nursing care of the person with an ostomyF,”an online education course from Hollister,includes types of ostomies, pouching sys-tems, pouching basics, ostomy acces-sories, problem solving, and patient edu-cation and resources.
36 www.WoundCareAdvisor.com March/April 2016 • Volume 5, Number 2 • Wound Care Advisor
ClinicianRESOURCES

New guidelines for use of anti-retroviral agents in HIV
The recently updated “Guidelines for theuse of antiretroviral agents in HIV-1-infectedadults and adolescentsG,” developed by apanel convened by the U.S. Departmentof Health and Human Services, are basedon two large randomized clinical trials.
A summary of key changesH is availableonline and includes information on whento start antiviral therapy (ART):• ART is recommended for all HIV-infect-
ed individuals, regardless of CD4 cellcount, to reduce the morbidity andmortality associated with HIV infection.
• ART is also recommended for HIV-in-fected individuals to prevent HIV trans-mission. ■
Online ResourcesA. catholichealthinitiatives.org/human-trafficking-and-the-role-of-the-health-provider
B. traffickingresourcecenter.org/audience/service-providers
C. npuap.org/wp-content/uploads/2012/01/NPUAP-Lift-Sling-White-Paper-March-2015.pdf
D. journals.lww.com/aswcjournal/Fulltext/2015/04000/The_Role_of_Nutrition_for_Pressure_Ulcer.7.aspx
E. epuap.org/wp-content/uploads/2014/11/RISE-LEaflet-07.05.14-FInal-Version.pdf
F. hollister.com/us/ostomy/hcp/nursing/online_ce.asp
G. aidsinfo.nih.gov/contentfiles/lvguidelines/adultandadolescentgl.pdf
H. aidsinfo.nih.gov/guidelines/html/1/adult-and-adolescent-treat-ment-guidelines/0
Present Your Wound Care CredentialsWith Distinction.
The NAWCO online Print Shop offers custom business materials that you can order online. Each piece is professionally designed to visually promote you and all your active NAWCO credentials.
Business CardsNote CardsPost Cards
To browse the print shop and order 24 hours a day, 7 days a week.
CLICK HERE

Note from Executive Director
By Cindy Broadus, RN, BSHA, LNHA,CLNC, CLNI, CHCRM, WCC, DWC, OMS
It’s hard to believe that it has been over2 years since I was named executive di-rector of NAWCO. What an experience!
During these 2 years, I’ve had the opportu-nity to meet many great individuals whovolunteer their time to make this organiza-tion a success. Last year, I introduced youto the Board of Directors over several is-sues. I wanted our readers and members toget to know the impressive group of peoplewho collaborate with me in leading NAW-CO. Board members volunteer their timeand are instrumental in making decisionsthat positively affect what we do for ourmembers as an organization and, ultimately,for the individuals those members care for.
Equally as impressive are the volunteermembers of the NAWCO Wound Care Certi-fied (WCC) Certification Committee. I couldnot tell you about the board and not men-tion this dedicated and intelligent group ofclinicians who work to ensure that the WCCexamination remains credible, current, andcongruent with the requirements of accred-iting boards.
In this and upcoming issues of WoundCare Advisor, I’ll focus on the CertificationCommittee, including its purpose, who themembers are, the importance of obtainingcertification, and reasons for maintainingyour certification once you have earned it.
Let me begin the series by discussing theprocess the Certification Committee uses todevelop and maintain the WCC examina-tion. Many of our readers are certified, orhave taken examinations in the past, so you
probably can imagine how much work goesinto putting one together. Here’s an over -view of how the exam is developed.
The volunteer members of the Certifica-tion Committee, who are subject matter ex-perts (SMEs), write the questions. The ques-tions are designed to assess cognitive levelsof knowledge, comprehension, application,and analysis related to skin and woundmanagement. Questions are based on jobtask analyses conducted to ensure the con-tent is current, job-related, and representa-tive of the responsibilities of wound carepractitioners.
The members of the Certification Com-mittee strive to ensure that those who re-ceive certification meet or exceed theknowledge of a minimally qualified candi-date. During in-person meetings, the com-mittee members analyze job tasks of woundcare professionals, define criteria for theminimally qualified candidate who can takethe exam, and accomplish other tasks. TheCertification Committee also holds virtualmeetings about every 4 to 6 weeks to de-velop and review test questions. Betweenmeetings, committee members work on thequestions they have been assigned to de-velop or refine. Experts from Alpine TestingSolutions, Inc., which provides NAWCOwith support to ensure the exam is psycho-metrically sound, edit each question forgrammar, potential bias, and technical adequacy.
After the questions are written, they arepilot tested. A total of 100 candidates take
38 www.WoundCareAdvisor.com March/April 2016 • Volume 5, Number 2 • Wound Care Advisor
NAWCONEWS

Wound Care Advisor • March/April 2016 • Volume 5, Number 2 www.WoundCareAdvisor.com 39
the exam consisting of questions previouslytested and approved, plus 10 of the newquestions the committee has developed.Alpine Testing Solutions experts analyze re-sponses to determine which of the pilotquestions meet required standards. Thosequestions meeting the standards are main-tained for future use in the final exam, anda new set of pilot questions, pulled from theones the committee developed, is added foradditional testing. Questions that don’tmeet the standards are returned to the Certi-fication Committee for reevaluation and fur-ther action.
As you can see, the process is quite in-volved and requires many steps, each in-volving experts in wound care and/or testdevelopment. Now that you know a bitabout the process, I’d like to begin introduc-ing you to the members of the CertificationCommittee, starting with the chair.
Jen Pettis, BS, RN, WCC, chair of the Certification Committee Jen is a nurse researcher/associate in theU.S. Division of Abt Associates. Jen, who be-gan her career as a nursing assistant, hasmore than 25 years’ experience in health
care, including experience as a clinical andregulatory consultant to the Division of Nurs-ing Homes at the Centers for Medicare &Medicaid Services (CMS). She has extensiveclinical, managerial, consulting, and trainingexperience, has provided educational ses-sions around the country, and has written orcontributed to multiple publications. Jenjoined the certification committee in 2012.
When I asked Jen why she joined theCertification Committee, she said, “I wantedto get involved in the organization and sawinvolvement in the Certification Committeeas an opportunity to continue to use mywound care expertise while learning newskills related to test development. I have re-ally learned a great deal about developingpsychometrically sound tests and the infor-mation has been very useful in my practice,including when developing educationaltools for others.”
Jen has played a key role in the certifica-tion process and we are pleased to have heras the Committee Chair.
I hope you’ll join me for the next issue ofWound Care Advisor as I continue this se-ries on certification and introduce othermembers of the committee.
Victoria AblesTheresa AcholonuAlice AdamsStephanie AllenRuth Altidor-FloreusLeidy Alvarez-LopezApril Antazo
Sally ArsenaultMarykutty BabuRenee BalboaMonette BarbianNadine BarkmanVeronica BarrazaSusan Bartocci
Shannon BawdenKaren BayLu Ann BeebeElise BelcherJennifer BenderJennifer BishopBelinda BlantonLisa BodemerShelley BorbonusAisha BrackettJudith BrightLashawn BrownHanna Brown
Carla BrownShawna BurksMadalene CalvertTiffany CampbellLilian CardenasKerri CarrAutumn CarterDarlene CelevanteAnitha CherianCourtney ClaiborneJulie ClintonBilinda CollinsDanielle Collord
New certificants
Below are WCC, DWC, and OMS certifi-cants who were certified from December2015 to January 2016.

40 www.WoundCareAdvisor.com March/April 2016 • Volume 5, Number 2 • Wound Care Advisor
Linda CorbittAlma CoronaCathrina CoxCathryn CraigRhonda DaltonRebecca DavidsonBarbara DavignonJohn Carlo De
ChavezElizabeth DeFeoEmily DeLoachJennifer DeTurkKelin DimasDustin DodgeNana DonkorTammy DriscollLydia DunbarJennifer DunnTamesha EatonTowanah EdwardsAnnette FearonEvangeline
FernandezSeptember FosterCaitlin FostesonAnita FranciscoEvamariely Garcia
SolisMelissa GaynorRebekah GerhardsTeresa GoldenAngela GordonAnne GrahamJennifer HackmanHeather HaileyJennifer HamiltonSusan HanniganMary HeatlieJennifer HesterJennifer HobigTracy HoffmanSheri HoneycuttBobbie Honorable
Elizabeth Hope RiesRonald HornerPatricia HoyeckiChristie HsuMary HubbardMindy HundYaritza IslasMargaret JablonskiMarla JimPaulette JohnsonOksana KakurievAmy KelsheimerMichelle KennedySusan KlineCheri KlinghardMelissa KoonceAnna KoziolKaren KruegerCynthia KrystozekJudith LaisLarkland LawrenceRebecca LeBlancJessica LeskoKrista LickeyChristine LogginsBrooke LopezTamara LutsykAyshia MaddenKisun MamonBarbara McFaddenSherin McGovernApril MeyerRachelle MitchellTisha MooreSondra MoseleyCourtney MudrickElizabeth MurphyDonna MyersRebecca NaughtonLiesl NeumannLaura NickelTracy OcchipintiTreva Ockenfels
Kimberly O'learyAylmer OportoBeata PearceChristy PetersonTanya PintadoKaren PowersColleen PriceLeslie PrimeJamie PritchardErica ProvciNina PurtlebaughEdma Quiambao
ValenciaMaybelle RamosJackie RamseyHeather RastelloKenneth RestorHeather RevaleonAmy RickensNora RodgersBrittan RothMichelle RuffnerJose SalvadorSuzanne SchatzerSusan SchaubAnne Schiavoni-
ColucciSharon SchillingsKetlin SchneiderJin SchnitzlerKarin SchrunkWendi ScottMahanee Lei SermonKristine SetterlundJodie ShimpFrances SibongaCatherine SierraTamela SilveiraColleen SkoglundMiriam SmartBrent SmithCarol SmithMaria Soto
Eileen StahlheberMallikarjuna
SuryamoniSuzan TahirKathleen TerleckiBeverly TerregrossaWilliam TerryMary TerryAmber ThackerAmber ThomasNikki ThorntonLinda ThurenRhellen TigleyOfonasaha UdofiaKimberly ValenteMargaret ValenteKeiko VandeBergMonette VirtudazoAmanda WaggTricia WagnerKatoria WestbrookRebecca WhittonVeronica WilhelmMitchelle WilliamsAmanda YaleRoldan YumulShannon Zundel
Louise AlbergDiana AmickChristine AmoleKaren Andrews
Recertified certificants Below are WCC,DWC, and OMS certificants whowere recertifiedfrom December2015 to January2016.

Vicki AndrewsJudith Anthony-
MillerMiguel ArguellesDawn AugerArlene AyugatDonna BailerBobbi BaileyChristina BallingRamon BaneaTina BarkNancy BarkerTommie BassAmy BeightelMolly BerryWendy BordenaveLinda BoyceKimberly BoyettCharleen BrisindiKristian BugaoanCheryl BurkeRegenia ButlerPatricia CabalaMaureen CalnanSara-Scott CappsJessica CarterKathleen CasolinoJill CavaliereTracey CearleyZiping CenLeah ChandlerMique ChappellCathleen ChristyCatherine ChungMaryAnn ClaypooleElizabeth ClupnyWinona CoakerAmber CollinsChristopher CormierTeresa CornwellMary CoyleJacqueline CretserRuthann Crocetto
Robert CrocettoShannon CyphersAshley DamianoShannon DartKyle DeFrainSherry DeMouraNancy DreherLakena DupreePatty EmbersonSue EmmonsShane EnglandQueen EnyogaiMaria EscuadroRosario EscuetaElizabeth EspinMarlo Franklin-
HammTara FrazierEugene Gaertner,
MDKathy GallagherKristi GallegosEleanor GanibiRoberta GauthierKristina GilbertOlga GilillandStephanie GirardAndrea GormanMarina GrigoriantJulie HarringtonStephanie HazzardAutumn HensonAmy HerrmannTanya HodgeDonna Hoffer
HeiseyBeth Hoffmire
HeidemanMohamed JallohJan Johnson-BargerVeronica JonesD Lynn JonesKelly Jorgenson
Loretta KakascikMartina KauckaAntoinette KettnerJudith KlingensmithDebra LaBrecqueSusan LaningRebecca LeathamElizabeth LefflerLynn LesperanceJei-Ing LiuLeonor LopezStacy LoweryStephanie MansfieldAnnet MatovuCandice MayerMelissa McGrailKathleen MedvedoffToby MikkiNexeli MohrmanJane MomohSue MooreMark NeerLam-Quynh NguyenJane Oliver MoodyNormita OredinaCarolyn ParsonsLene PedersenLisa PerssonMichelle PradaJacqueline ProbyCynthia QuinonesShirin RamsiniAmanda RayMichelle ReevesPeggy RennelsCynthia RiceBrenda RobersonCarol RobinsonDeAnn RonkRebecca RoordaVicky RubySherry RunestadMichelle Rung
Karen SalasLatosha SandersChristina SawelskyLaurie SchmittKatie SchroederMary SchrothJeannine SedlacikLori SherlockColleen ShivettsKathleen ShollerRose ShufeltMariclaire SilvermanFarida SitorusLorrie SniderLiza SombritoShellie SonnentagCarol SpencerJill SpenglerLeilani StenbergCynthia StoneVeronica StoryBeth StreckerCheryl SwannHelen TagliaferroPatricia TiddJosette TolbertMarie Torell-AlverioDorothy ValineArturo VillafuerteMonessa WadfordDonna WatsonNancy WeljkovicCarrie WhiteLois WilsonMargaret WoodruffTracey Yap
■


















