Aki in neonate
41
AKI in a neonate Bharathi B
-
Upload
bharathi-balachander -
Category
Documents
-
view
268 -
download
0
Transcript of Aki in neonate

AKI in a neonate
Bharathi B
Sub headings
Definition
Classification – AKIN / RIFLE
Pathophysiology
Evaluation
Management
Medical
Dialysis

Definition
Acute kidney injury (AKI) - a sudden
impairment in kidney function, that
results in the retention of nitrogenous
waste products and alters the
regulation of extracellular fluid volume,
electrolytes, and acid-base
homeostasis.
“ recognize the injury , don’t wait for
the failure” ( Mehta 2007)

Creatinine based definition
Creatinine ≥1.5 mg/dL independent of day of life and regardless of the rate of urine output.
Problems of this approach1. Will not change till 25 – 50 % func loss2. Overestimates renal function3. Varies by muscle mass, age , sex, hydr4. Different methods of est ( Jaffe/
enzymatic)5. Easily dialysed
Avery diseases of the neonate – 9 th edition
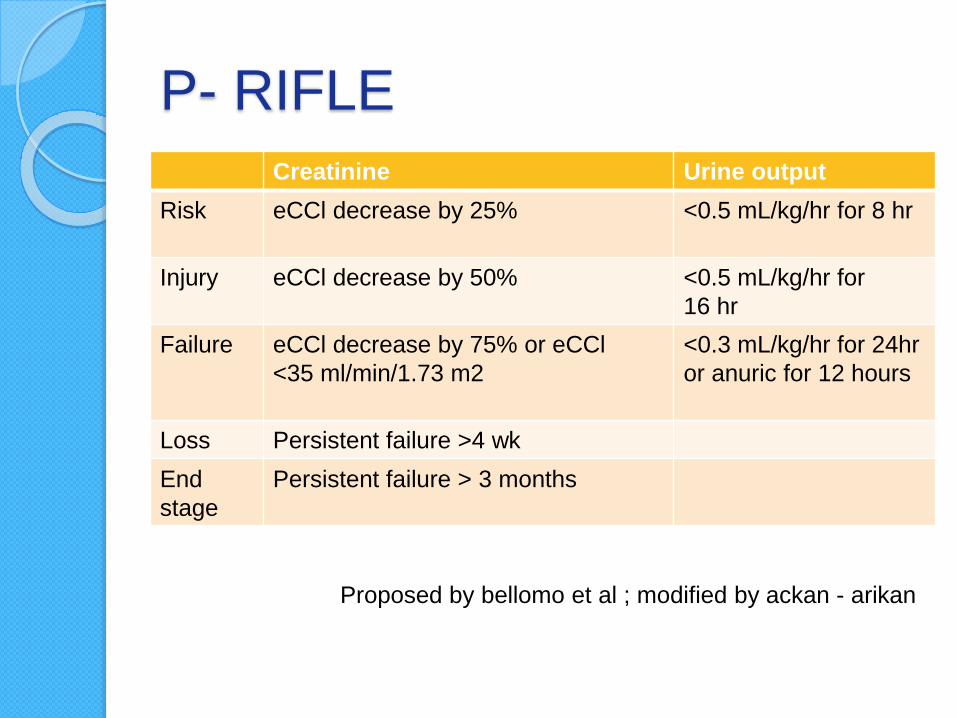
P- RIFLE
Creatinine Urine output
Risk eCCl decrease by 25% <0.5 mL/kg/hr for 8 hr
Injury eCCl decrease by 50% <0.5 mL/kg/hr for
16 hr
Failure eCCl decrease by 75% or eCCl
<35 ml/min/1.73 m2
<0.3 mL/kg/hr for 24hr
or anuric for 12 hours
Loss Persistent failure >4 wk
End
stage
Persistent failure > 3 months
Proposed by bellomo et al ; modified by ackan - arikan

AKIN criteria ( Mehta et al ,
2007)Abrupt (within 48 h) reduction in
kidney function currently defined as an
absolute increase in serum creatinine
of 0.3 mg/dL or more or
A percentage increase in serum
creatinine of 50% or more (1.5-fold
from baseline) or
A reduction in urine output
(documented oliguria of < 0.5 mL/kg/h
for >6 h)

KDIGO staging for AKI severity
( Mehta et al 2007)Creatinine Urine output
Stage 1 1.5-1.9 times
baseline
or
≥0.3 mg/dL
increase
<0.5 mL/kg/hr for 6 hr
Stage 2 2- 2.9 times
baseline
<0.5 mL/kg/hr for 12 hr
Stage 3 3 times baseline
or
Increase in serum
creatinine to ≥4
mg/dL
or
Initiation of renal
< 0.3 mL/kg/h for 24 h
or
Anuria for ≥12 h
Problems
Delineation between the 1st week of life
and changes in SCr level after the 1st
week - needed in a neonatal AKI
classification system.
Despite these working classification
systems, the diagnosis of AKI is
problematic, because current diagnosis
relies on two functional abnormalities:
functional changes in SCr (marker of
GFR) and oliguria.
Avery diseases of the neonate – 9 th edition

Acute Renal Failure in the Neonate
Steven Alan Ringer Neoreviews
2010;11;e243

Etiopathogenesis
Acute Renal Failure in the Neonate
Steven Alan Ringer Neoreviews 2010;11;e243

Prerenal failure – pathophysio
Alteration in
plasma flow
Catecholami
ne surge
Prostagland
in & RAAS
activation
Dilation of
afferent
arteriole /
constric of
efferent
Acute Renal Failure in the Neonate
Steven Alan Ringer Neoreviews 2010;11;e243
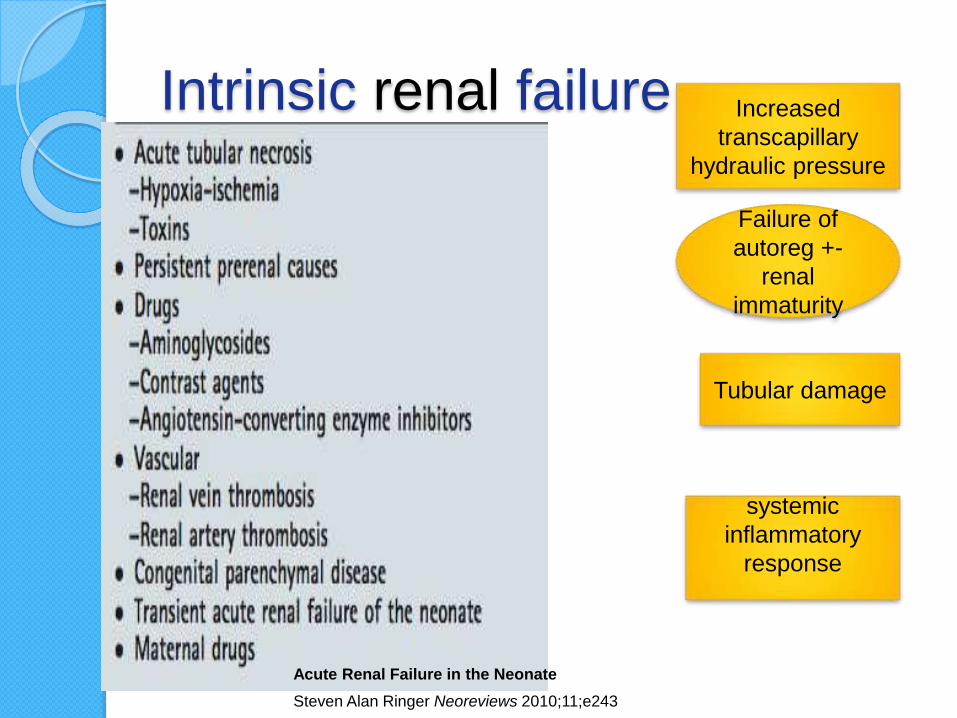
Intrinsic renal failure Increased
transcapillary
hydraulic pressure
Failure of
autoreg +-
renal
immaturity
Tubular damage
systemic
inflammatory
response
Acute Renal Failure in the Neonate
Steven Alan Ringer Neoreviews 2010;11;e243

Post renal
Reversible with
reversal of
obstruction
Acute Renal Failure in the Neonate
Steven Alan Ringer Neoreviews 2010;11;e243
Evaluation
Identify prerenal causes
Is there a volume contraction ?- Inadeq feeding- Dehydration- Large fetomaternal h’hage- Subgaleal bleeds- Warm shocks
Congestive cardiac failure
Acute Renal Failure in the Neonate
Steven Alan Ringer Neoreviews 2010;11;e243

Investigations
Serum sodium, potassium, chloride,
bicarbonate, calcium, phosphorus,
magnesium, urea, creatinine, uric
acid, glucose, blood gases,
hemoglobin, and platelets
S.Cr often does not rise for days after
an injury, thus monitoring these values
for several days after the inciting event
is necessary to determine if AKI
occurred.
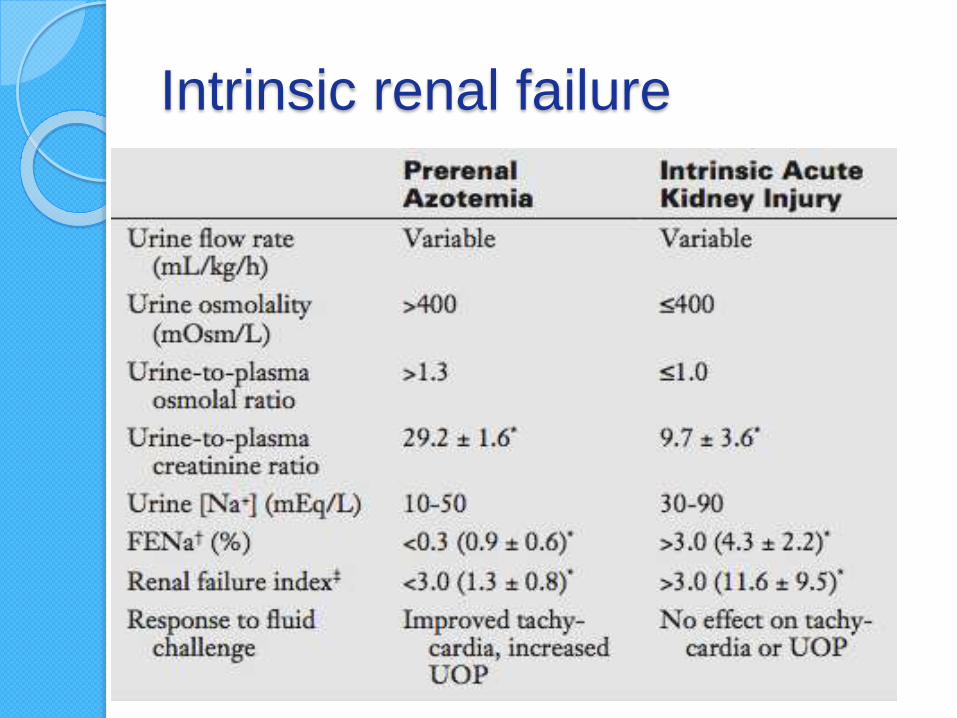
Intrinsic renal failure

Management
Supportive –
keep the kid
and kidney
alive
Acute Renal Failure in the Neonate
Steven Alan Ringer Neoreviews
2010;11;e243
Dopamine
Dopamine can increase renal
perfusion in the sick pre- term and
term infant with prerenal azotemia
caused by hypoxemia, acidosis, or
indomethacin administration (Seri,
1995; Seri et al, 1998, 2002).
Compared with placebo, low-dose
dopamine does not improve survival,
shorten hospital stay, or limit dialysis
use.
Acute Renal Failure in the Neonate
Steven Alan Ringer Neoreviews 2010;11;e243
Fenoldopam is a selective dopamine-1
receptor agonist whose effects include
vasodilation of renal and splanchnic
vasculature, increased renal blood
flow, and increased GFR.
Fenoldopam is approved to treat
severe hypertension in adults, but is
not clinically approved for the
treatment of AKI.
Avery ‘s diseases of newborn – 9th edition
Diuretic
No studies in neonates, children, or
adults have shown that diuretics are
effective in preventing AKI or
improving outcomes once AKI occurs
(Bellomo et al, 2000).
If loop diuretics are to be used in
neonates, continuous doses of
furosemide may be superior to larger
intermittent doses
Volume & electrolyte / acidbase
imbalanceHyponatremia:
Na Required (mEq) =(Na Desired − Na + Actual) × Body weight (kg) × 0.7
Hypocalcemia -100 to 200 mg/kg of calcium gluconate should be infused over 10 to 20 minutes and repeated every 4 to 8 hours as necessary. Hyperphosphatemia - Breastmilk and Simi- lac 60/40 both contain low phosphorous and low potassium compared with other neonatal infant formulas .
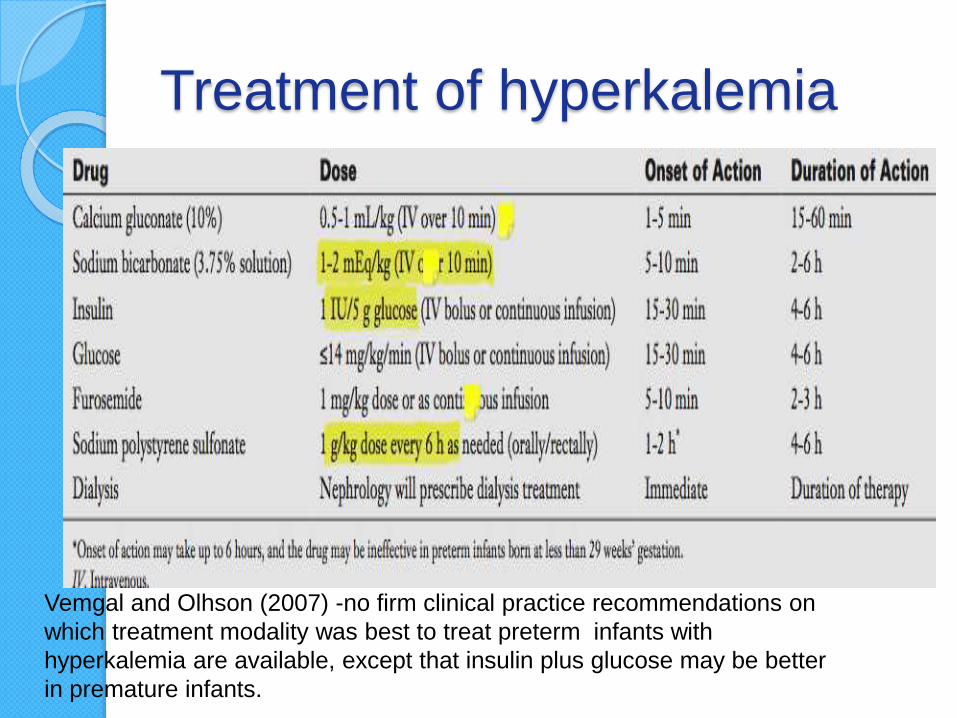
Treatment of hyperkalemia
Vemgal and Olhson (2007) -no firm clinical practice recommendations on
which treatment modality was best to treat preterm infants with
hyperkalemia are available, except that insulin plus glucose may be better
in premature infants.
Nutrition & drugs
Nutritional goals in infants with AKI are similar to those of infants without AKI.
Feeds or parenteral nutrition will need to be concentrated to avoid excessive fluid
a neonate is receiving continuous peritoneal dialysis or hemodialysis, an additional 1 g/kg/day of protein is needed to supplement the protein losses that occur with these forms of dialysis (Zappitelli et al, 2008, 2009).

Indications For Renal Support
Severe electrolyte abnormalities that are
not correctable with medicalinterventions
Life-threatening intoxication by
medications that can be cleared with
dialysis
inborn errors of metabolism
fluid overload
Acidosis – refractory to medical
management
Coma Neonatal Peritoneal Dialysis
Marsha M. Lee, Annabelle N. Chua and Peter D. Yorgin Neoreviews 2005;6;e384
DOI: 10.1542/neo.6-8-e384
Renal replacement therapy
The timing of dialysis initiation in
infants with AKI is controversial.
Several observational studies show a
clear advantage in adults receiving
dialysis early versus late (Liu et al,
2006; Ronco et al, 1986).
Neonatal Peritoneal Dialysis
Marsha M. Lee, Annabelle N. Chua and Peter D. Yorgin
Neoreviews 2005;6;e384
DOI: 10.1542/neo.6-8-e384
Basic Physiology of Dialysis And
Ultrafiltration
Molecular movement across
semipermeable membrane
Basic mechanisms of water and
particle removal include
Diffusion
Convection
Ultrafiltration

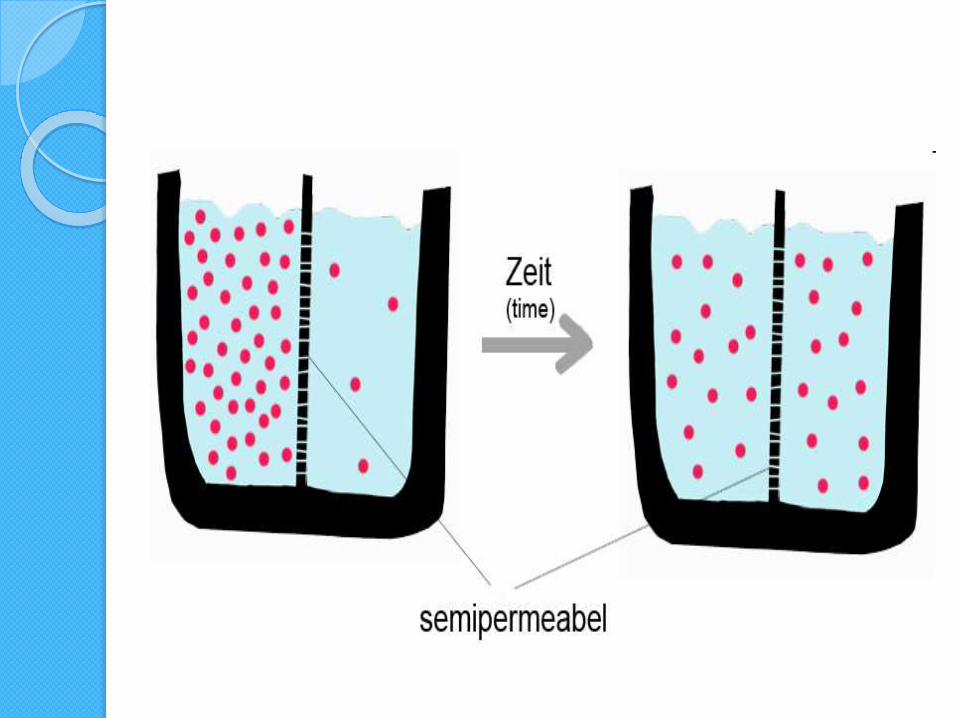
Diffusion
Movement of dissolved particles
across semi- permeable membrane
from area of high concentration to
area of low concentration
Favors movement of smaller particles
Stops when concentration gradient
achieves equilibrium

Convection
Dissolved particles pass across semi
permeable membrane due to effects
of pressure gradient
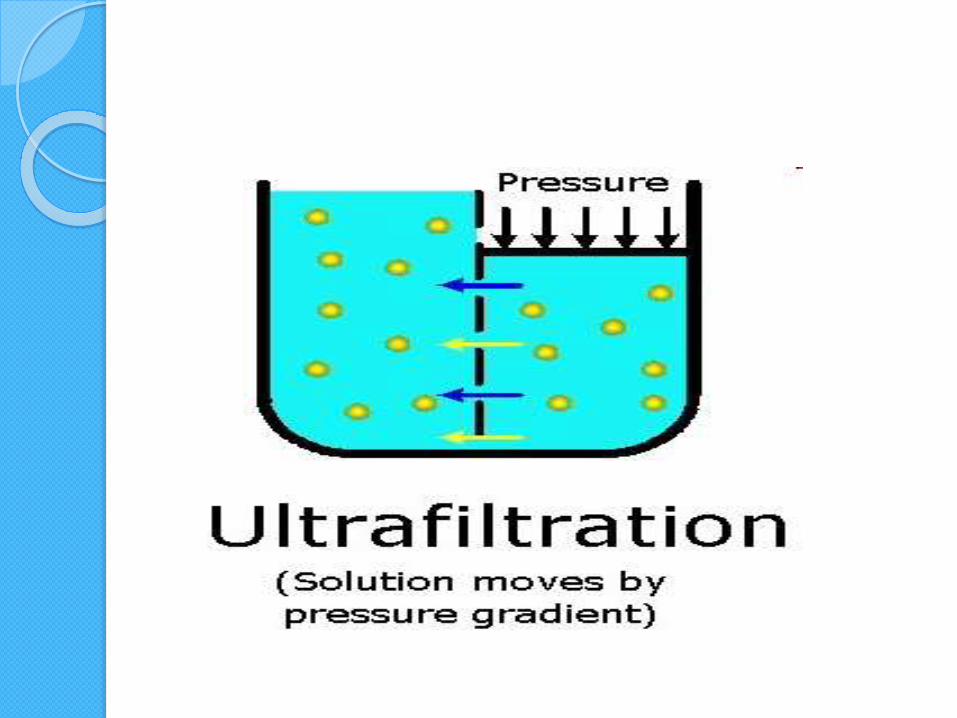
Ultrafiltration
Describes movement of water across
semipermeable due to pressure

3 modalities
Peritoneal dialysis
Intermittent Hemodialysis
Continuous Renal Replacement
Therapy
PERITONEAL DIALYSIS
Physiology
Peritoneum can be used as a dialysing membrane
Instillation of a dialysate into the peritoneal space permits diffusion of particles out of the blood across the peritoneum
Through the use of a hypertonic solution , water also passes across the membrane generating an ultrafiltrate
Water movement tends to drag particles across the peritoneum by convection
After the dwell is complete , the spent dialysate is drained from the abdomen and fresh dialysate may be introduced
Neonatal Peritoneal Dialysis
Marsha M. Lee, Annabelle N. Chua and Peter D. Yorgin
Neoreviews 2005;6;e384
DOI: 10.1542/neo.6-8-e384
Indications
Remove excess fluid and provide
volume control in the patient with
oligoanuria
Much slower than intermittent
hemodialysis
Preferable in the critically ill patient
Provides metabolic control
Neonatal Peritoneal Dialysis
Marsha M. Lee, Annabelle N. Chua and Peter D. Yorgin
Neoreviews 2005;6;e384
DOI: 10.1542/neo.6-8-e384

Technique
Instill sterile dialysate into peritoneal cavity
Allow it to dwell
End of dwell time the dialysate is removed
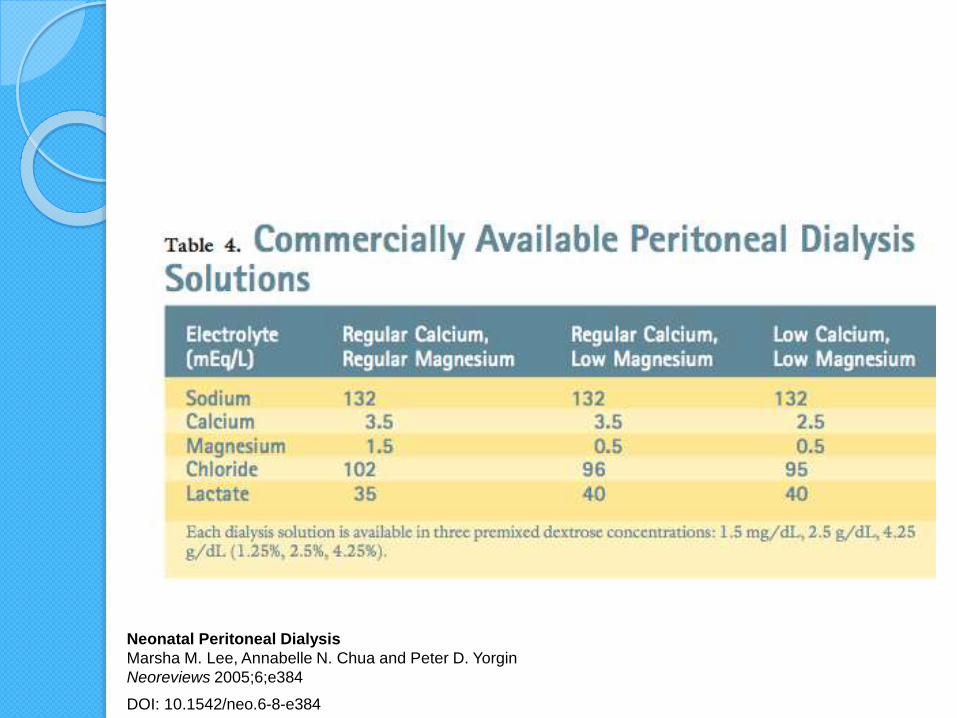
Dialysate contains base in the form of lactate
Ultrafiltration accomplished by osmotic pressure thro dextrose
Should be warmed to body temp
Start with 10 – ml/kg ( 500 ml/m2)
Dwell period of 30 - 60 minNeonatal Peritoneal Dialysis
Marsha M. Lee, Annabelle N. Chua and Peter D. Yorgin
Neoreviews 2005;6;e384
DOI: 10.1542/neo.6-8-e384
Neonatal Peritoneal Dialysis
Marsha M. Lee, Annabelle N. Chua and Peter D. Yorgin
Neoreviews 2005;6;e384
DOI: 10.1542/neo.6-8-e384

Complications
Peritonitis
Leakage around the catheter exit site
Tunnel infection
Catheter malfunction, and obstruction by omentum (Coulthard and Vernon, 1995).
Fluid leakage into other compartments (including the chest in patients without an intact diaphragm) can occur and if suspected, the fluid composition will reveal high glucose levels if a leak is present Neonatal Peritoneal Dialysis
Marsha M. Lee, Annabelle N. Chua and Peter D. Yorgin
Neoreviews 2005;6;e384
DOI: 10.1542/neo.6-8-e384
Issues
Loss of protein – supplement it
Hyperglycemia
GER – stomach comp
Critically ill – inc intra abd pressure
leading to dec Venous return and dec
diaphragm excursion
Neonatal Peritoneal Dialysis
Marsha M. Lee, Annabelle N. Chua and Peter D. Yorgin
Neoreviews 2005;6;e384
DOI: 10.1542/neo.6-8-e384
Poor candidates for PD
worsening respiratory status or
ventilatory
Diaphragmatic hernias
Abdominal wall defects
Neonatal Peritoneal Dialysis
Marsha M. Lee, Annabelle N. Chua and Peter D. Yorgin
Neoreviews 2005;6;e384
DOI: 10.1542/neo.6-8-e384

AKI to CKD
Adult studies – 3- 5 % go on to have
CKD
Stapleton – retrospective study – 40 –
88 % CKD prevalence
Preterms did worse than term babies
![Jaundice in Neonate[1]](https://static.fdocuments.us/doc/165x107/577cdf6d1a28ab9e78b136c3/jaundice-in-neonate1.jpg)