ajph%2E86%2E2%2E214
7
Smoking Cessation in Young Adults: Age at Initiation of Cigarette Smoking and Other Suspected Influences Naomi Breslau, PhD, and Edward L. Peterson, PhD Introduction The dramatic decline in the preva- lence of cigarette smoking in the United States since the 1960s has been achieved primarily by smokers' successful attempts to quit.'-3 Although smoking initiation by young people has declined somewhat, the contribution of the decline to the overall decreased prevalence of smoking has been of secondary importance. As smok- ing cessation programs continue to be a key component of public health efforts to prevent the adverse effects of smoking on health, the identification of factors that predict smoking cessation has implica- tions for public policy. While the initiation of cigarette smok- ing in adolescence appears to fit within a model of progression from legal to illegal substances," the persistence of smoking in the third decade of life is in striking contrast with the sharp decline in the use of alcohol and illicit drugs in the early 20s.7 A maturation process has been proposed to describe the course of alcohol and illicit drug use from adolescence to young adulthood, whereby cessation is linked to transitions in adult social roles- specifically, marriage, parenthood, and employment-that are presumed to be incompatible with drug involvement.8 The persistence of cigarette smoking into adulthood might suggest that cigarette smoking, in contrast with heavy drinking and illicit drug use, has been compatible with the fulfillment of adult social roles. Smoking cessation varies by sex, race, education, and number of cigarettes smoked daily. Higher rates of quitting have been reported for males versus females, Whites versus Blacks, persons with higher versus lower education, and light versus heavy smokers.8lI Older smokers-that is, those over 40 years of age-are more likely to quit than younger smokers, a change attributed to the growing awareness of smoking-related illnesses with advancing age." In fact, there is evidence to suggest that age modifies the relationship between heavy smoking and quitting. Specifically, Coambs et al. report that among older adults, the chance of quitting is higher in heavy smokers, than in light smokers," an opposite trend to that in younger adults. By way of explanation, they suggest that among older adults, light smokers are not necessarily less dependent than heavy smokers, since there are among them formerly heavy smokers who, unable to quit, have cut down "as the best alterna- tive to quitting completely.' "(P244) This interpretation is based on the assumption that level of smoking is an imperfect indicator of nicotine dependence, which is the critical factor in cessation. Nico- tine dependence per se, as distinct from heavy smoking, has not been previously examined. Other potential factors in smoking cessation might include a history of childhood conduct problems and a life- time history of major depression. A history of conduct problems has been related to early smoking initiation and, independent of age of initiation, to the development of nicotine dependence.'2"13 Naomi Breslau is with the Department of Psychiatry, Henry Ford Health Sciences Cen- ter, Detroit, Mich; the Department of Psychia- try, University of Michigan School of Medicine, Ann Arbor; and Case Western Reserve Univer- sity School of Medicine, Cleveland, Ohio. She and Edward L. Peterson are with the Division of Biostatistics and Research Epidemiology, Henry Ford Health Sciences Center. Requests for reprints should be sent to Naomi Breslau, PhD, Henry Ford Health Sciences Center, Psychiatry Research, 1 Ford PI, 3A, Detroit, MI 48202-3450. This paper was accepted September 12, 1995. February 1996, Vol. 86, No. 2
-
Upload
filip-raluca -
Category
Documents
-
view
213 -
download
0
description
ps
Transcript of ajph%2E86%2E2%2E214
-
Smoking Cessation in Young Adults:Age at Initiation of Cigarette Smokingand Other Suspected Influences
Naomi Breslau, PhD, and Edward L. Peterson, PhD
IntroductionThe dramatic decline in the preva-
lence of cigarette smoking in the UnitedStates since the 1960s has been achievedprimarily by smokers' successful attemptsto quit.'-3 Although smoking initiation byyoung people has declined somewhat, thecontribution of the decline to the overalldecreased prevalence of smoking hasbeen of secondary importance. As smok-ing cessation programs continue to be akey component of public health efforts toprevent the adverse effects of smoking onhealth, the identification of factors thatpredict smoking cessation has implica-tions for public policy.
While the initiation of cigarette smok-ing in adolescence appears to fit within amodel of progression from legal to illegalsubstances," the persistence of smokingin the third decade of life is in strikingcontrast with the sharp decline in the useof alcohol and illicit drugs in the early20s.7 A maturation process has beenproposed to describe the course of alcoholand illicit drug use from adolescence toyoung adulthood, whereby cessation islinked to transitions in adult social roles-specifically, marriage, parenthood, andemployment-that are presumed to beincompatible with drug involvement.8 Thepersistence of cigarette smoking intoadulthood might suggest that cigarettesmoking, in contrast with heavy drinkingand illicit drug use, has been compatiblewith the fulfillment of adult social roles.
Smoking cessation varies by sex, race,education, and number of cigarettessmoked daily. Higher rates of quittinghave been reported for males versusfemales, Whites versus Blacks, personswith higher versus lower education, andlight versus heavy smokers.8lI Oldersmokers-that is, those over 40 years ofage-are more likely to quit than younger
smokers, a change attributed to thegrowing awareness of smoking-relatedillnesses with advancing age." In fact,there is evidence to suggest that agemodifies the relationship between heavysmoking and quitting. Specifically, Coambset al. report that among older adults, thechance of quitting is higher in heavysmokers, than in light smokers," anopposite trend to that in younger adults.By way of explanation, they suggest thatamong older adults, light smokers are notnecessarily less dependent than heavysmokers, since there are among themformerly heavy smokers who, unable toquit, have cut down "as the best alterna-tive to quitting completely.' "(P244) Thisinterpretation is based on the assumptionthat level of smoking is an imperfectindicator of nicotine dependence, whichis the critical factor in cessation. Nico-tine dependence per se, as distinct fromheavy smoking, has not been previouslyexamined.
Other potential factors in smokingcessation might include a history ofchildhood conduct problems and a life-time history of major depression. Ahistory of conduct problems has beenrelated to early smoking initiation and,independent of age of initiation, to thedevelopment of nicotine dependence.'2"13
Naomi Breslau is with the Department ofPsychiatry, Henry Ford Health Sciences Cen-ter, Detroit, Mich; the Department of Psychia-try, University of Michigan School of Medicine,Ann Arbor; and Case Western Reserve Univer-sity School of Medicine, Cleveland, Ohio. Sheand Edward L. Peterson are with the Divisionof Biostatistics and Research Epidemiology,Henry Ford Health Sciences Center.
Requests for reprints should be sent toNaomi Breslau, PhD, Henry Ford HealthSciences Center, Psychiatry Research, 1 FordPI, 3A, Detroit, MI 48202-3450.
This paper was accepted September 12,1995.
February 1996, Vol. 86, No. 2
-
Factors in Smoking Cessation
Major depression has been associatedwith nicotine dependence and a lowerprevalence of being an ex-smoker.1446The relationship of these variables to thepotential for smoking cessation has alsonot been previously examined.
As is the case with illicit drug use,early initiation of cigarette smoking hasbeen associated with a greater potentialfor problems, including heavy daily con-sumption, longer duration of smoking,and nicotine dependence.5"2"3"7-19 Thisevidence would suggest that the inverseassociation between age at initiation andcessation, observed in relation to someillicit drugs,8 might apply also to ciga-rettes. However, this hypothesis has notbeen previously examined.
The purpose of this report is toexamine the extent to which smokingcessation varies by age at smoking initia-tion. We address the following questions:(1) Are smokers with late initiation morelikely to quit than smokers with earlyinitiation? (2) Are nicotine-dependentsmokers less likely to quit than nondepen-dent smokers? (3) Does nicotine depen-dence account for the differential likeli-hood of quitting between smokers withlate and early onset, if such an associationis observed? Evidence that the potentialfor quitting is greater for smokers whobegan at an older age compared withthose who began at an early age wouldsupport public policies that delay theonset of smoking. Thus, the relationshipbetween age of smoking initiation andthat of cessation and the role of nicotinedependence were investigated in a longitu-dinal epidemiological study of youngadults and estimated in a multivariatesurvival analytic model that controlled forsex, race, and education.
MethodsA simple random sample of 1200
individuals was selected from all 21- to30-year-old members of a 400 000 mem-ber health maintenance organization(HMO) in southeast Michigan. The HMOserves the tricounty area of Wayne,Oakland, and Macomb, which contains91% of the 4.3 million people in theDetroit standard metropolitan statisticalarea. Of those selected, 1007 respondents(84% of the sample) were interviewed attheir homes in 1989. Compared withnonparticipants, participants were slightlymore likely to be female and older-thatis, between ages 26 and 30. The medianage of the respondents was 26 years,61.7% were female, 80.7% were White,
and 45% were married. A small minority(3.7%) had less than a high schooleducation, 21% had completed highschool, 46% had some college, and 29.3%were college graduates. Twenty-two per-cent of the respondents lived in the city ofDetroit at the time of the interview whilethe remaining respondents resided inother parts of the metropolitan area.Follow-up interviews were conducted in1992, 3.5 years after baseline, with 979(97%) of the original interviewees.
The National Institute of MentalHealth Diagnostic Interview Schedule,20revised to cover diagnoses in the Diagnos-tic and Statistical Manual ofMental Disor-ders, 3rd edition, revised (DSM-III-R),21was used to gather information on sub-jects' history of psychiatric disorders,including nicotine dependence. Data onthe precision and accuracy of the previousversion of the Diagnostic Interview Sched-ule have been reported elsewhere.22-24The Diagnostic Interview Schedule in-quires about age of onset of daily smokingand age of last cigarette. An item on ageat smoking initiation, as defined below,was added for this study. History ofsubjects' lifetime nicotine dependencewas ascertained at baseline, and intervalhistory, covering the 3.5-year period sincebaseline, was ascertained in the follow-upinterview.
Definition ofKey VariablesSmoking cessation was defined as
having last smoked at least 1 year beforethe time of the latest interview. Becausemost relapses occur within the first yearafter quitting, the definition capturessuccessful quitting.25Age ofsmoking initia-tion was defined as the age at which arespondent first smoked a cigarette. Basedon previous research on this issue andnicotine dependence, age at smokinginitiation was classified into three catego-ries: up to and including 13 years, 14 to 16years, and 17 years and older.12 Regardingnicotine dependence, the DSM-III-Radopted a unitary diagnostic definitionacross all psychoactive substances, reflect-ing the current consensus in the field ofaddiction on the key features of substanceuse disorder. At the core of the definitionis the construct of dependence, defined bycognitive, behavioral, and physiologicalsymptoms that characterize compulsiveuse of all substances. The following arethe criterion symptoms of psychoactivesubstance dependence in the DSM-III R:(1) greater use than intended, (2) unsuc-cessful efforts to quit, (3) a great deal oftime spent getting the substance, (4)
intoxication or withdrawal symptomswhenexpected to fulfill a major role obligation,(5) important activities given up, (6)continued use despite knowledge of ad-verse consequences, (7) tolerance, (8)withdrawal symptoms, and (9) use toavoid withdrawal. Nicotine dependence isdefined in the DSM-III-R by the presenceof three or more of these criterionsymptoms.21 Age ofonset ofnicotine depen-dence is defined in the Diagnostic Inter-view Schedule as the age at which the firstdependence symptom occurred.
StatisticalAnalysisThe analysis of smoking cessation
was performed on the combined baselineand follow-up data of the subset of youngadults who had smoked daily for a monthor more at any time in their life (n = 414).(Cessation in persons who had neverprogressed to daily smoking is a separatetopic not covered in this inquiry.) Thecombined data covered lifetime experi-ence up to age 33. The cumulativeincidence of smoking cessation in thethree age-of-initiation groups was esti-mated by standard life-table methods, anonparametric estimator for grouped cen-sored data.26,V7 The censored subjectswere smokers who had continued tosmoke for up to 1 year before the lastinterview.
Cox proportional hazards models forcensored survival data were used toestimate the hazard ratios of quittingassociated with age at smoking initia-tion.28-30 The models included sex, race,and education as fixed covariates. Be-cause the period during which cessationcould have occurred started when dailysmoking began, time was defined asnumber of years since onset of dailysmoking. The use of years rather thandays as the time unit increases the numberof ties in event occurrences. For thatreason, the discrete version of the propor-tional hazard model, which correctlymodels tied data, was used. Two adjustedhazard ratios were calculated in themodel: the hazard ratio of quitting amongsmokers who began smoking at ages 14 to16 compared with those who began beforetheir 14th birthday, and the hazard ratioof quitting among smokers who begansmoking at age 17 or older compared withthose who began before age 14. Thesehazard ratios provide direct estimates ofthe extent to which each of the latesmoking onsets is associated with anadvantage over early smoking onset interms of the potential for cessation. Therole of nicotine dependence in the associa-
American Journal of Public Health 215February 1996, Vol. 86, No. 2
-
Breslau and Petersen
tion between age at initiation and cessa-tion was estimated in an expanded model,which also included time of onset ofnicotine dependence as a time-dependentcovariate. In separate analyses, interac-tions between the key independent vari-ables were tested, and no significantinteractions were detected.
In an additional analysis, the associa-tion of smoking cessation with a history ofconduct problems and major depressionwas explored. The two variables wereadded to the Cox proportional hazardsmodel, the first as a fixed covariate andthe second as a time-dependent covariate.The expanded model estimated and testedthe partial associations of each of thesevariables with smoking cessation, as wellas the partial association of age at
smoking initiation with smoking cessation,with the added variables held constant.
ResultsAge at Smoking Initiation
Of the 414 persons who have eversmoked daily for 1 month or more, 33.6%smoked their first cigarette at age 13 orbefore, 43.2% first smoked at 14 to 16years of age, and 23.2% began at age 17 orlater. Table 1 compares the three smokinginitiation groups on sex, race, education,nicotine dependence, and age at whichdaily smoking began. Race varied signifi-cantly across the three groups, with higherproportions of Whites in the earliersmoking initiation groups than in the later
group. No significant differences weredetected on the other four variables.
Smoking Cessation andAgeat First Cigarette
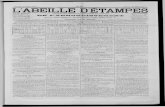
Of those same 414 persons, 145 hadquit and did not smoke for at least 1 yearbefore the last interview. The cumulativeincidence of cessation and the confidenceintervals [CIs] for selected years, up to 13years since daily smoking began, appear inTable 2. (There were not sufficient datafor precise estimation beyond 13 years.)At all time points, the cumulative percent-age of those quitting increased withincreasing age at first cigarette. Thegradient relationship between quittingand age of smoking initiation was evidentas early as 3 years after daily smokingbegan. Specifically, the cumulative per-centage of quitting in smokers with earlyage of smoking initiation ( < 13 years) was4.4%, compared with 9.6% and 13.6% insmokers with intermediate (14 to 16years) and late (>17 years) initiation,respectively. The smoking cessation advan-tage associated with delayed smokinginitiation was maintained throughout theentire 13-year period depicted in Table 2.Figure 1 presents the survival curves ofsmoking cessation in these three groups ofsmokers. The unadjusted hazard ratiosfor cessation up to age 33 in smokers whosmoked their first cigarette at 14 to 16years and at age 17 or later, comparedwith those who first smoked at age 13 orearlier, were 1.5 (95% CI = 1.0, 2.2) and1.9 (95% CI = 1.2,3.0), respectively.
The adjusted hazard ratios for smok-ing cessation associated with age ofsmoking initiation were estimated in adiscrete Cox proportional hazards model,with sex, race, and education as covari-ates. These ratios, or estimated relativerisks, are presented in Table 3 for twoage-of-smoking initiation groups, 14 to 16years and 17 years and older, comparedwith the earliest group, age 13 andyounger, as a reference. Adjusted for sex,race, and education, the hazard ratio forquitting associated with initiation at 14 to16 years of age was 1.6 (95% CI = 1.1,2.3) and that associated with initiation atage 17 or later was 2.0 (95% CI = 1.3,3.2). The results also show that race andsex were not significantly related tosmoking cessation, but that smokers withless than a college education were 60%less likely to quit compared with college-educated smokers (hazard ratio = 0.4;95% CI = 0.3,0.6).
216 American Journal of Public Health
TABLE 1 --Selected Characterlstics of Young Adult Smokers, by Age atSmoking Initiation
Age at Smoking Initiation< 13 Years 14-16 Years 2 17 Years(n = 139) (n = 179) (n = 96)
Female, % 64 67 59White,% 86 93 72Less than college, % 75 81 79Nicotine dependence, % 75 69 54Daily smoking onset, age range, y 11-28 14-30 17-29
Note. Difference in percentage of Whites across groups is statistically significant (x2 = 22.3, 2 df,P < .0001).
TABLE 2-Estimated Probabilities of Smoking Cessation at Selected Years ofDaily Smoking, by Age at Smoking Initiation
Age at Smoking InitiationY13Years (n = 139) 14-16Years (n = 179) >17Years (n = 96)
Years DailySmoking % (95% Cl) % (95% Cl) % (95% Cl)
3 4.4 (1.0, 7.8) 9.6 (5.3, 13.9) 13.6 (6.7, 20.5)(130) (158) (80)
5 6.6 (2.4,10.7) 16.5 (11.0, 22.0) 22.7 (14.1, 31.2)(126) (144) (62)
7 11.0 (5.8,16.4) 24.1 (17.7, 30.4) 30.4 (20.7, 40.1)(115) (127) (49)
9 17.3 (10.9, 23.8) 27.8 (21.1, 34.5) 2.19 (24.6, 45.2)(102) (105) (33)
11 23.0 (15.8, 30.3) 35.0 (27.6, 42.4) '3.1 (31.4, 54.9)(88) (82) (20)
13 29.6 (21.5, 37.7) 39.6 (31.7, 47.4) 43.1 (31.4, 54.9)(66) (55) (1 0)
Note. Numbers on which the estimates are based appear in parentheses below the estimates;estimated probabilities represent cumulative incidence figures from standard life-table methods.
February 1996, Vol. 86, No. 2
-
Factors in Smoking Cessation
The Role ofNicotine DependenceThe relationship of nicotine depen-
dence with smoking cessation and thepotential role of nicotine dependence inthe association between age of initiationand cessation were examined next. Thediscrete proportional hazards model wasexpanded by adding onset of nicotinedependence as a time-dependent covari-ate. The results appear in Table 4.Smokers with nicotine dependence were40% less likely to quit than smokers whowere not dependent, with sex, race,education, and age of initiation controlledfor (hazard ratio = 0.6; 95% CI = 0.4,0.8). Nevertheless, the association be-tween age of smoking initiation andquitting remained statistically significant,with little change in the hazard ratiosfrom the previous estimates as theyappear in Table 3. No significant interac-tions were detected between nicotinedependence and age of smoking initiation(P > .25).Exploring the Effects ofConductProblems and Major Depression
In additional models, the potentialassociation of smoking cessation with ahistory of conduct problems and majordepression was explored.
A history of childhood conduct prob-lems, defined as at least one out of sixconduct problems before age 15, andonset of major depression were addedinto the discrete Cox proportional hazardmodels, the first as a fixed covariate andthe second as a time-dependent r-. drnate.Neither a history of con ;_.t problems norprior major depr,xision were significantlyreltec' 3inoking cessation. A history ofconduct problems was associated with aslight increase in the hazard ratio ofsubsequent quitting (1.3, P = .121), andprior major depression was associatedwith a slight decrease in the hazard ratioof subsequent quitting (0.8, P = .384).Furthermore, neither of these variablesmodified the association between age ofsmoking initiation and cessation.
DiscussionThe results indicate the following:
(1) The likelihood of smoking cessationwas greater in smokers who had beguncigarette smoking after age 13 than inthose who had begun earlier. Comparedwith smokers in the earliest initiationgroup, smokers who began at 14 to 16years were 1.6 times more likely to quit,and those who began at age 17 or laterwere twice as likely to quit. (2) Nicotine-
dependent smokers were 40% less likelyto quit successfully than nondependentsmokers. (3) The relationship betweendelayed uptake of smoking and quittingwas independent of the inhibiting effect ofnicotine dependence. There were twoother results of interest: the strongestpredictor of smoking cessation was levelof education, with smokers who com-pleted college being 2.5 times as likely toquit as those with no college education;and sex and race differences in smokingcessation were trivial and nonsignificant.
The generalizability of the findings islimited in several ways. The samplecomprises young adults, so the findingsmight not apply to older smokers. Itshould, however, be emphasized that theage limitation provides a methodologicaladvantage. Because of the young age ofthe sample, the findings are less likely tobe biased by selective mortality or byrecall errors regarding historical informa-tion on smoking behaviors than theywould be if older adults were included.Furthermore, the restriction of the sample
American Journal of Public Health 217
R
4i
.
.9
104ia
5 10 15
Years Since Daily Smoking Began
INITIATE -17 (n-96)
FIGURE 1-Cumulative probabilities of smoking cessation among young adultdaily smokers, by age at smoking initiation.
TABLE 3-Discrete Cox Proportional Hazard Model (n = 414): Hazard Ratio forSmoking Cessation, by Age at Initlation, with Sex, Race, andEducation Controlled for
95% ConfidenceHazards Ratio Interval P
Initiation, y< 13 1.0 Reference14-16 1.6 1.1, 2.3 .015>17 2.0 1.3,3.2 .002
SexMale 1.0 ReferenceFemale 0.9 0.7,1.3 .618
RaceBlack 1.0 ReferenceWhite 0.8 0.5,1.3 .339
EducationCollege 1.0 ReferenceLess than college 0.4 0.3, 0.6 .0001
Note. Ukelihood ratio test: X2 = 36.87, 5 df, P = .0001.
February 1996, Vol. 86, No. 2
-
Breslau and Peterson
to a relatively narrow age range in youngadulthood avoids complexities due tocohort effects and the effects of advancedage on cessation behavior. Thus, theyoung age of the sample allows a clearerinterpretation of the observed relation-ship between age of smoking initiationand cessation than if a wider age rangewas included.
Drawn from a list of members of alarge HMO, subscribers and dependents,the sample represents the population ofthis age in the area, excluding only theextremes of the socioeconomic range.Available reports on HMO populationsindicate that the members generally repre-sent the population of the geographicarea except that they are slightly moreeducated and healthier.31'32 On indicatorsof general health and health behaviors(e.g., ratings of self-assessed health, preva-lence of cigarette smoking, and alcoholand cocaine use), our sample resemblesthe late 1980s US population of compa-rable age, as described in national re-ports.33-35
It is almost by definition that nicotine-dependent smokers have more difficultyquitting and are therefore less likely toquit successfully than nondependent smok-ers. Previous studies on communitysamples and smoking cessation programshave used the number of cigarettes smokedper day as an indicator of dependence;many (but not all) found that this numberpredicted successful quitting.9'1036-38 An-
other commonly used measure of nicotinedependence is the Fagerstrom ToleranceQuestionnaire,39 which appears to corre-late with biochemical measures of depen-dence (nicotine, cotinine) and, probably,behavioral outcomes such as withdrawalsymptoms and ability to quit.40 The limita-tions of daily cigarette consumption andof the Fagerstrom Tolerance Question-naire for measuring dependence havebeen discussed previously.40
This is the first study to examinesmoking cessation in a community sample,using the current definition of nicotinedependence as formulated in the majorpsychiatric classification systems, theDSM-III-R and the International Classification ofDiseases, 9th revision (ICD-9).21'4' Whilelevel of cigarette consumption and theFagerstrom questionnaire reflect notionsof addiction as a physiological phenom-enon, at the core of the DSM-III-R andthe ICD-9 definition is a cognitive, behav-ioral, and physiological cluster that charac-terizes compulsive use of all substances.The definition reflects the current consen-sus in the field of addiction on thecardinal characteristics of substance usedisorder.42 Our findings support the pre-dictive validity of this definition: control-ling for variables previously observed topredict cessation, we found that nicotine-dependent smokers were less likely to quitthan nondependent smokers. Other find-ings from this study suggest that smokingcessation might vary also by level of
nicotine dependence, with moderatelydependent smokers being less likely toquit than mildly dependent ones.'3 Ourprevious reports on the association ofnicotine dependence with psychiatric dis-orders, including other substance usedisorders, major depression, and anxietydisorders, support the construct validity ofthe definition.14'15 Such associations couldbe expected on the basis of previousfindings on the comorbidity betweenother substance use (i.e., alcohol andillicit drug) disorders and specific mentaldisorders.43
The greater potential for quittingassociated with later smoking initiationwas independent of nicotine dependence.Although dependent smokers were lesslikely to quit than nondependent smokers,dependent smokers who had delayed theinitiation of smoking were more likely toquit than those who had begun to smokeat an earlier age. While previous researchhas reported that age at smoking initia-tion predicts duration or level of smoking,this is the first study to report on theassociation between age at smoking initia-tion and cessation. The association wasnot accounted for by sociodemographiccorrelates of early initiation or nicotinedependence. Moreover, although a his-tory of conduct problems was associatedwith early smoking initiation, such ahistory did not account for the associationbetween early initiation and cessation.Nonetheless, this observational study doesnot permit a causal interpretation of theassociation. Early smoking initiation mightbe a marker of factors that influence thepotential for smoking cessation.
Our finding that the potential forquitting was markedly higher in smokerswith a college education than in smokerswith no college education is in accord withprevious evidence that smoking cessationvaries by indicators of social class."' 4445 Awell-established finding is the inverserelationship between the prevalence ofsmoking and the level of education, withcollege-educated individuals showing thelowest prevalence.246 While it would betempting to attribute the smoking gapbetween the college- and the non-college-educated populations to the enlighteningeffect of education, the explanation islikely to lie elsewhere. National data fromthe Monitoring the Future study, gath-ered over a period of nearly 20 years,indicate that the smoking gap has itsorigins in high school, and that the rate ofsmoking is far lower in college-boundthan in non-college-bound high schoolseniors.46 That the smoking pattern estab-
February 1996, Vol. 86, No. 2218 American Journal of Public Health
TABLE 4-Discrete Cox Proportional Hazard Model (n = 414): Hazard Ratios forSmoking Cessation by Age at Initiation, with Nicotine Dependence,Sex, Race, and Education Controlled for
95% ConfidenceHazards Ratio Interval P
Initiation, y< 13 1.0 Reference14-16 1.6 1.1,2.4 .013.17 2.0 1.3,3.2 .003
SexMale 1.0 ReferenceFemale 0.9 0.6,1.3 .543
RaceBlack 1.0 ReferenceWhite 0.9 0.5,1.4 .572
EducationCollege 1.0 ReferenceLess than college 0.4 0.3, 0.5 .0001
Nicotine dependenceNo 1.0 ReferenceYes 0.6 0.4, 0.8 .001
Note. Likelihood ratio test: X2 = 47.62, 6 df, P = .0001.
-
Factors in Smoking Cessation
lished in high school continues intoadulthood is supported by evidence onenduring cohort differences in smokingrates.47 Our finding that smokers who arecollege graduates are more likely to quitthan smokers with less than a collegeeducation is an additional aspect of thesocial class-smoking association. It mightbe that, because of the lower rate ofsmoking among college-bound adoles-cents (predominantly children of middle-class, college-educated parents), college-educated smokers find themselves insocial environments in which fewer oftheir peers smoke, a condition that wouldenhance the likelihood of cessation. Thus,the smoking gap that originates in highschool is likely to widen over time ascollege graduates, with already lowerrates of smoking, quit at higher rates thannon-college graduates of the same age.Increasing class-related gaps in the preva-lence of smoking, attendant on class-related differences in the cessation ofsmoking, have been reported for theUnitd States, Canada, Great Britain,Norway, and Sweden.48
As smoking has become increasinglyconcentrated within the non-college-educated population, the finding thatdelayed initiation signals an increasedpotential for quitting among all smokers(including those with less than a collegeeducation) has important public healthimplications. Programs that delay smok-ing initiation might have considerablevalue even if they do not succeed in fullypreventing the uptake of smoking. Delay-ing smoking initiation among adolescentscould eventually reduce the rate of smok-ing through increasing the potential forsuccessful cessation. C:
AcknowledgmentThis work was supported by a research grantMH-48802 from the National Institute ofMental Health, Bethesda, Md.
References1. Fiore MC, Novotny TE, Pierce JP, Hatzian-
dreu EJ, Patel KM, Davis RM. Trends incigarette smoking in the United States: thechanging influence of gender and race.JAMA. 1989;261:49-55.
2. Pierce JP, Fiore MC, Novotny TE, Hatzian-dreu EJ, Davis RM. Trends in cigarettesmoking in the United States: educationaldifferences are increasing.JAMA. 1989;261:56-60.
3. Pierce JP, Fiore MC, Novotny TE, Hatzian-dreu EJ, Davis RM. Trends in cigarettesmoking in the United States: projectionsto the Year 2000. JAMA. 1989;261:61-65.
4. Kandel DB, Logan JA. Patterns of druguse from adolescence to early adulthood: I.periods of risk for initiation, continued use
and discontinuation. Am J Public Health.1984;74:660-666.
5. Yamaguchi K, Kandel DB. Patterns ofdrug use from adolescence to young adult-hood: III. predictors of progression. Am JPublic Health. 1984;74:673-681.
6. Henningfield JE, Clayton R, Pollin W.Involvement of tobacco in alcoholism andillicit drug use. Br J Addict. 1990;85:279-292.
7. Raveis VH, Kandel DB. Changes in drugbehavior from the middle to the latetwenties: initiation, persistence, and cessa-tion ofuse.Am JPublic Health. 1987;77:607-611.
8. Kandel DB, Raveis VH. Cessation of illicitdrug use in young adulthood. Arch GenPsychiatry. 1989;46:109-116.
9. Mothersill KJ, McDowell I, Rosser W.Subject characteristics and long-term post-program smoking cessation. Addict Behav.1988;13:29-36.
10. Cohen S, Lichtenstein E, Prochaska JO, etal. Evidence from 10 prospective studies ofpersons who attempt to quit smoking bythemselves: debunking myths about self-quitting.Am Psychol. 1989;44:1355-1365.
11. Coambs RB, Li S, Kozlowski LT. Ageinteracts with heaviness of smoking inpredicting success in cessation of smoking.Am JEpidemiol. 1992;135:240-246.
12. Breslau N, Fenn N, Peterson EL. Earlysmoking initiation and nicotine depen-dence in a cohort of young adults. DrugAlcohol Depend. 1993;33:129-137.
13. Breslau N, Kilbey MM, Andreski P. DSM-III-R nicotine dependence in young adults:prevalence, correlates and associated psy-chiatric disorders. Addiction. 1994;89:743-754.
14. Breslau N, Kilbey MM, Andreski P. Nico-tine dependence, major depression, andanxiety in young adults. Arch Gen Psychia-try. 1991;48:1069-1074.
15. Breslau N, Kilbey MM, Andreski P. Nico-tine dependence and major depression:new evidence from a prospective investiga-tion.Arch Gen Psychiatry. 1993;50:31-35.
16. Glassman AH, Helzer JE, Covey LS, et al.Smoking, smoking cessation, and majordepression.JAMA. 1990;264:1546-1549.
17. Robins LN, Przybeck TR. Age of onset ofdrug use as a factor in drug and otherdisorders. In: Jones CL, Battjes RJ, eds:Etiology of Drug Abuse: Implications forPrevention. Rockville, Md: US Dept ofHealth and Human Services, Alcohol,Drug Abuse, and Mental Health Adminis-tration; 178-192. NIDA Research Mono-gram 56, A Raus Review Report.
18. Taioli E, Wynder EL. Effect of the age atwhich smoking begins on frequency ofsmoking in adulthood. N Engl J Med.1991:325;968-969.
19. Escobedo LG, Anda RF, Smith PF, Rem-ington PL, Mast EE. Sociodemographiccharacteristics of cigarette smoking initia-tion in the United States: implications forsmoking prevention policy.JAMA 1990;264:1550-1555.
20. Robins LN, Helzer JE, Cottler L, GoldingE. NIMH Diagnostic Interview Schedule,Version III, Revised. St Louis, Mo: Washing-ton University; 1989.
21. Diagnostic and Statistical Manual of MentalDisorders. 3rd ed, rev. Washington, DC:American Psychiatric Association; 1987.
22. Robins LN, Helzer JE, Ratcliff KS, Sey-fried W. Validity of the Diagnostic Inter-view Schedule, version II: DSM-III diag-noses. Psychol Med. 1982;12:855-870.
23. Helzer JE, Robins LN, McEvoy LT, et al.A comparison of clinician and DiagnosticInterview Schedule diagnoses. Arch GenPsychiatry. 1985;42:657-666.
24. Anthony JC, Folstein M, Romanoski AJ, etal. Comparison of the lay DiagnosticInterview Schedule and a standardizedpsychiatric diagnosis. Arch Gen Psychiatry.1985;42:667-675.
25. Shumaker SA, Grunberg NE, eds. Proceed-ings of the national working conference onsmoking relapse. Health Psychol. 1986;5(suppl):1-17.
26. Cutler SJ, Ederer F. Maximum utilizationof the lifetable method in analyzing sur-vival. J Chronic Dis. 1958;8:699-712.
27. Gehan EA. Estimating survival functionfrom the lifetable. J Chronic Dis. 1969;21:629-644.
28. Cox DR. Regression models and lifetables. J Royal Stat Soc, Series B. 1972;34:187-220.
29. Cox DR. Partial likelihood. Biometrika.1975;62:269-276.
30. Breslow N. Covariance analysis of cen-sored survival data. Biometrics. 1974;30:89-99.
31. Freeborn DK, Pope CR. Health status,utilization, and satisfaction among enroll-ees in three types of private health insur-ance plans. Group Health J. 1982;3:4-1 1.
32. McFarland BH, Freeborn DK, Mulloly JP,Pope CR. Utilization patterns and mortal-ity of HMO enrollees. Med Care. 1986;24:200-208.
33. US Dept of Health and Human Services.National Household Survey on Drug Abuse:Main Findings, 1985. Washington, DC:National Institute on Drug Abuse; 1988.DHHS publication ADM 88-1586.
34. Moss AJ, Parson VL. Current estimatesfrom the National Health Survey, UnitedStates. Vital Health Stat [10]. 1985.
35. Schoenborn CA, Boyd GM. Smoking andother tobacco use: United States 1987.Vital Health Stat [20]. 1989.
36. Hall SM, Herning RI, Reese TJ, BenowitzNL, Jacob P. Blood cotinine levels asindicators of smoking treatment outcome.Clin Pharmacol Ther. 1984;6:810-814.
37. Schacter S. Recidivism and self-cure ofsmoking and obesity. Am Psychol. 1982;37:436 444.
38. McWhorter WP, Boyd GM, Mattson ME.Predictors of quitting smoking: theNHANES I followup experience. J ClinEpidemiol. 1990;43:1399-1405.
39. Fagerstrom KO. Measuring degree ofphysical dependence to tobacco smokingwith reference to individualization of treat-ment.AddictBehav. 1978;3:235-241.
40. Fagerstrom K-O, Schneider NG. Measur-ing nicotine dependence: a review of theFagerstrom Tolerance Questionnaire. JBehav Med. 1989;12:159-182.
41. World Health Organization IntemationalClassification of Diseases. 9th rev. AnnArbor, Mich: Commission on Professionaland Hospital Activities; 1980.
42. Rounsaville BJ, Kranzler HR. The DSM-III-R diagnosis of alcoholism. In: TasmanA, Hales RE, Frances Al, eds. Review of
February 1996, Vol. 86, No. 2 American Joumal of Public Health 219
-
Breslau and Peterson
Psychiatry. Washington, DC: AmericanPsychiatric Press; 1989;8:323-340.
43. Regier DA, Farmer ME, Rae DS, et al.Comorbidity of mental disorders withalcohol and other drug abuse: results fromthe Epidemiologic Catchment Area (ECA)Study. JAMA. 1990;264:2511-2518.
44. Killen JD, Fortmann SP, Telch MJ, New-man B. Are heavy smokers different fromlight smokers? A comparison after 48
hours without cigarettes. JAMA. 1988;260:1581-1585.
45. Kabat GC, Wynder EL. Determinants ofquitting smoking. Am J Public Health.1987;77:1301-1305.
46. Johnston LD, O'Malley PM, Bachman JG.National Survey Results on Drug Use fromthe Monitoring the Future Study, 1975-1992.Vol II. College Students and Young Adults.Washington, DC: US Dept of Health and
Human Services, Public Health Service;1993. NIH publication 93-3598.
47. O'Malley PM, Bachman JG, Johnston LD.Period, age, and cohort effects on sub-stance use among young Americans: adecade of change, 1976-1986. Am J PublicHealth. 1988;78:1315-1321.
48. Pierce JP. International comparisons oftrends in cigarette smoking prevalence.AmJPublic Health. 1989;79:152-157.
.M.M,M,:
.M. .!..:...i;.,,,..'..'...!.'-..-':...,...,-..,...'-..'..,.-..,...,-....,!.,-...!.,-..,!.!.... .'_'!-'.`.-'_-'.i.;.: . ...-,..,.".,i..,-..-'....:.!....'-..'........-....-...,.-.....,:,--,.9...,...,..,."...,."..;..: .:: ::! :!.:.f,!x!.'.-'.i4i; ;, .!.. .: ,.:.:i.;i: ,:.: :!:;:...,.:-.-!-.i:s:..: .,..:..-.,...::::. -.--': :.: :.. .::. .::....;:-::--, ....!.;:.'!.n!..--..---...-.'...:. ...-.,:.....-.f....'-..-,..l.'s..Ri..'si.1'.- ... ..,.:,.-:..----'--.i..!!.:;:..'._'...-.--...4 :.I:.:. .:, :..,.:;.. ::.::. '.,-
--, ,,.,. .. -...-,- -.:f.:-':.., :..,,..K ... ...::......:: :!.. ,.: ,:, ;..i! ".: .-:.!. .!::!.,-,:..:..:.::...,..:..j..:,.-..i'.'.'..:...-....'.-.....!....-...'-..'...:..'S.i.....'!.::..:..'.-..,i.f:.:.:: ... :%:!
'!.I, :,. ::,.: :.'..::.:%:,-,:.":.:,..-,.- .,...! ::!....".:.".::.:-::,:...,:?:.."..'i..:...;.::,..".i'.-'..'.-,'...."..'..."..'i.:.-.'...i..'-..'....'..,.'...'..'...... .:::;.,.-":.,-,.,..L',.'.'..'.. ::y:::.;?:!: ,:. :.:.-*;. ..---.'.---,.-- .K, ", '. .. -. -"-,:D--",... ..:., ......:........'.,:.::,::..........,:;.::..F-!--..'.:"' .. '!....:,:.::.:...'.....;..%.:%:.f...,..,........:.........::."", :,. .:::.:-.. ...,..,:..:..".,:...:..:j...",..."....,.".,:.:.!.-,'.'. -'S...-'-,'.:::.. :.,:::-":;-.-.; :,.:,:.: :- ..:.....,-.,..'.-'...:..;."...-.,.:.:...."..;........"...'..:.'-.'!..-,."..-.,!,:: :T-:-,F.: ... :::. -,.-".--'.:.:.x:... '!. :":.:::.......:::::,. ----.---. ';..-, --".-" -,...-. -'.,';..,--..,:.:--,.,.-:' ...:....
..: :,,:.. '.. :.. ..'. :..,:.,:, .....:.,...-. .... ..:..:.. .:.:::.:.....'.'-.'..'.'.'...;...".-'..',;.. ::-- .......:..-,.i,-,.i..,.'.i..'..'$.,.:::.,-":,.-,-.".-"..,.,...:. :.. ::f.jf,::%..,:i.:i::: :.. ...'-..,::....-,..:"..,.-..,:.'-.'i.;.i.".,...'...-'.'.-'.i....,-,.,.."..'...-,...%. ::%'-':.:.,,-!--:-:..--.;:--: .... ....: -,-..fZ...'-..::.:?...: .,...,.,..,:....,-..:.,-"..?.i.,.."..,."....:..., .....:; :-.!-;.;;:...:...-.:--.:. :,:.:...:.::..::::::.::.:."::i:.. ..-.: :..::-!...-,. ... "'A.,I....... W,"-.-.......-- Oa "i""N...".". -..'.'.' ..-..-....-..-..I ,..:: ",,:!5,-,..-..,-, .'.!!I.%:- ,i..'i.".'!. .. W. ..-'-.'.-' ..a..., --.,....F-.-,::;i.I.D.,.-:..,,.-.-...;.... .:i.i....:i.,.,i,."..;..,-.-,.,.,.....,.,-.'i..'-..'i'--,:....,.:..!.. ..: :;!::. .!: :::.. ..::!..,.,...:!...!..,..,...,.."...,...".,"
.;;1101'0..:J.q,%..M...,,,,.2-12,106-Irl,:.... ,-.- :: ......-, -,..... .:........,
-:4........
.4.....:..............:-::.''.,:-,::...
.-,.........i.::.
.: ....v.!:.: ..:.,..I-.-..t.......,Ong .11111R.L,0 W.... .:.:.....,
'......%.
--
...:.:;-.-.:.........R.: :. .............,;!....,".,..::.,W:".:!.;!.'::,...."::..,.,..;::....:."...".,.-.-'...-...-..'- ...........__..--.-.-':i-.---......1:..:."..
..,..,....... ..-..:. :,:.:....".:::::-.:::,:,--,--,--,:.'...........
-.......: 6:,: M:.....:..:.-.-..::... ': .,.:.:,..,.,.::,:" ..-..,......p..-4::::..........-.::..`.--,.-, -::,. `.-:,.,:-;::;. .-:.-..-.:-O,:-%M_."I'k'I--'I"'-.4'. ..-:....-..:,!. .-:-:--...-::---.F. ..._.:-:..----,.-.,:-,.-,?--.,:.....::;,:.- ..: ...:.:..
,... :":: ",.,.".,..'.. .............:W....:....--,:......:.......,,........
---i" lk:.:.:..::..:..% .:.:''.... .-,.-I --.... -...............-, ,::::,:. .,.. .-::!...:-.,_.:._... -:. :.....-:-,-,:.,..'%'--.-:1,
....W.......-..... ....... :.--, ... ...:-:.f::.::.:::-:.:-.....V,.-.......-,-.-::..":.::...:;.--'.-...` :::,.,:::..L...':-:.:...:.::.,:.- :..::.?.%-.......::.-,-.-,; :...
..:::,.::",W?.%:......W.-:,::.....:.:. .':-.'-.'-.,-,:".-...-.-::--. ..............-.-...:..-.:-: :.-.-,.:."-::----..'.....: .......- .:., -.....-.....- ..:
..;: %:..-..::...: -::-'-' ,.,. .,. -..........".. :......:-::,..,::%:.:::::.:..........!::r: ....... ..::...:: ,':'.-.'.' .."., ::,.,,,:::.:.:.,,:::...::. -:,: !:...: .:: :'.-.-'.,;.-_-:, .., .:----. -,:.::.:------,-.. ........:::;:.::...:::.". ":::::::.::::..:.::.:::::::..---'.'-'-.-'.::..i.:: .,.,:,.:. -:- ,..,,....
---::.:-:-.'.".'.:: ,-,...:::::.::,.:,. :.. .. ........... ...... .... .:.:. .. .,:,::....:-.. ......:.:.:,:...:::--,:.,:..:.....'."::.. -:-:::::-,..:.i:::-.:-..--::'.:.---:----.;::...-::.::.: :: ...:.-... .:,::,.-".':......:.:Z':%::.,.,:,.....,. .:.:..,.% .. ".::,.: .:: ",--'..-.-::...-. ....,:....' ,:::::: .., ..:W :.........
.,:.:.i::.:...'.. .,-..,'-.-,-.:-:.' -.': -`.-:::. .....................i .:-.-.-I-II'--"::;. ..:.,-.,:%::-,--,: ...:!::.:: .':.i .'.' -,-:.:.-.-...::.'..'...,:.. ::.. :..%: ..: ..'-.'..;..."...'..."..'..,...,!....,..:.... ...... .......,-- :.. .:--:-:..:...:,..:.:::::.:;::....:-:::,::----,,,..
.::..".L :. .:.:.
--.:.:.,::,:j-'::.,,":::%.:..:.-. -..-.--,.-....-...................... -,:,.::.:::.:,.....:.::-..:.:,:.;:...:...- -- ..'. -:.::.-,-:..5.:,.!:.':.....:..i..::::;.:.,..:.:...:..-.:-..;::..:.,....:: ,1..,,::::,.,.",.,..,: ':........-.. ......,.,-..". ------:..::..:-:-.._.......,::.'.-..-.-.-::?.:.'.:: :.i..:.....:::-..::..: :. .,:::.,...:....:,.i.:.i::.:..;::.:...:,:....:i.:!.-..::...::.:;:::,:"...:.:......-::. .. .., :.. .-'--'..:.:.;.,j.j-., -... .,..,:..: -...:,..':'-..:.'--'-:,--:-II- -------..---'--,-,.:..'..:.::::: -'..;::.-.........::i:.::.....,:.,..,.:.i:...,.:......:.:-:::.::..:....:::::.i.:.%::.....:]::.;:--::".."..::.:..,. .,.: .. -.:: .:,.:::.:.,::;!...:.i:.,-.,:.:.- :..f:.'.'-,.::.............:...........'...Z.,...'.:-..:.,.:.:!:':!....ii,.::.,..!:.::.:.: :.!..-.,.--..::..:..:.:.:%.:.....:::.. .....:...:.....::;: .....-:.:i...--'. -....-. -.-..:;:i-.::.;:E.'..::..:.......:.: --:... .... .'.-.'.,.:-,.-:.-:::.::_.-:.. .::....::%.`.:.::. ::..:,:i..:.,..::::.:::..::..i.:.:.'.'.,..::.....:...... .,.. -:--.::..,-::: .:....'...::.::...... .:.-.,..;...,.- ",%",., .....: .:'.,.;-:: -..:.-i,:..'.::. ... %.:.........:-.-'.i."..,:.;..::..-..'.:..-...-..:.-..:.: ........,.'"',.. ::..-
-.-.-.:.:..:.:...:.::.:..:....::...::,::,..:.......::-.i::-::-:.....!..:-.:-.--.--: --,,-..-:--:-,-,--:-. ....::.,-.,:...:.:..:..'..'..,.:..:.!...:.:!.:..,::,.::
--- ....,-,'.j-'--....::.......4::-::-'-.:'....,:%.--'. ": ..:::::.:...:....:.:..'.:....::..,.::.....,-:.:..:.:..:.:...im"::............ li:..:. ...:. ... .-:.: .:....:.......,. ..f. -.1 .,:. ii.::,:.:-:.%:-.-.,-j.!' :f::...'..'..j..::..:.,-.,:.!....::;:.i..: ,;::;::.:j::::,:::;. -.-:.-'.'-..:-::.::::::.:::.:..:.:::..:."-.,..'.-'.-. ,-:.,::,.-.'.'..% -... ..- .. .."'::.:::.: ---'..:.-;'i:.:.-.-'..:::-.-,.!..'...'.--..;.. .::j:::. :.. .::. --. :::.- ..:.,::":::: .....--: :.--'..:.. i:::,-:::;.::.!:!::.:... ----.. ...:..:::.:..:
": ::-.-:::.,.,::...:.........
..:-'f:::..:....:...i;.:...:.;...,........."...'...,...,i.,....:.:.....,....,...,....... .:..:...i..,..f:...-.::::i::.:.;...::,::... .!:....:..... ::.,--,j%.i:.i:.:.::.. :.:.,,.'....,:.i:..:..::,..,.:.:i:.::.:...i:....::...,:,.:.:::.:::.%::..:..-.:..:....: .:,:..:.,..,:.-:-,-.,:-:.::.,-".'.J..::,. :::"::.,.:.::...:::.-.,:::.:f:.:.....'.,........., ...,,_::.a .:;:
..:.:...--.'..--.'.... :;... .:..0 .,....-'..::.."...'...,...:.:.:.;..;!..:::..:..:::::::f:.::.:,::...:..:....:..:.:.:. .:...:..:..:...-,...:.,.::..:.,..,..:::.:::...::::.::..:-..M. ";...,::::!... ,i:..i..;N,, -., -.. ----.----.. ,-..I..` .;'.-'-'i:;:::,.-....---j..,...,. ::: -:-...:........ -.'..-..-...,-...,...;......,..,..--..-':.--..-.:..:..j..::i.:...f:::.:.:ii;i!:!,.!..:::.:..:i.:,.::.,:.i.,..:.....!.::.::::.:.::::.,:,:,::,: -.:.-,!-.:::!.f:.,.-....:....'.-..'.-'..".'.'.--...-.....:..........:.:.::::;:..:..:::::...........,:--.:.-.:.:..:.5. .""","..;:..:.L,.,,.'-.'.'..'.i..-........::....'-..':.::...:..;...:",...:-.','.,.--:......:::%... "'.- ..,.._.:.:,.:,..-.:....:.,..,.:..:::..::.:...j:.:..:::..::.::!...:.:.,-4:;....,....--.,.,.-.,......:....... .,;.,
-::-.:-.,-.,.:,::;::;.,P---..--.... ........:,.E.'.'.'-.'!.-,, ..-..'-.' ..'-...........-.,:.f.:.,..,...,.,.,:.:::.:..:,::,::::.:::.:.:: :]: .:...:K.:: -.$'.';,.-,.i.ii..:....:;!..::.'!.f...,-.'-.-'.i'.-'.i:,:......i:i.",.,..,..:..,......'......'...........::.:.%.i.. ,-,:;-,-"-.,"%:.,...........:-::::,!:i.,.::::;.::..::,::...'.:.j:::::. .........";:.:. ...:..: .... ;.::%-J!%:.:.-. ..;.--' .'---.F ..!.f ..:...:: .i:.:--::;.:..::....::....::...:........;i::i.'ij:..i..!9!...-......:.,.,..'..'...'.'....""'.:... ..:. .%i.t..-...i.'-.'i..'.,'.-.-..:'.-'...'.-..'..'.'.'.......--:.Z.'.-'.:;..3..I::.!:....:.:!.%::.",..:.W.;.::.;:: ..'j-',-j..:.:...".,::i...:.....::::;::L.:i::::;:......:...:....::::;:.::.:..."':,,;,-.n. :-.ii i..... ....,.--1..:..:..'-.'. i,.,.,--i..:.:::. .-'"....-.: j:".-,..,.::i-.-., lia,.h ...,:.......-;,.- _2:..:--......:..."'Is. .I..,I....:.:...- .-..
:-_.:....... :: .!;:-::.:..... ,.".,.-,,-.,-,.,.-.,-.,...':i.':-'..:i:::.....:..:..,.,.,.,.,.,..0!.nI.;....-i-d!.:';'il
''I1;3.tiP i--"--.'-"N'-------".....::::.,..:...:..:.,.,.,.,........-.-'....-...i...i..,.,..-... .,.,.,..,w,.i;,....,.........-!,.. `ii:.:...I-6" .. U,'I:.--".`i.xl. i'-'.:.:.:. """:::.;...:::.:..:....i.:..:..,-,.'i;ii-..'-.-.,..!!'.'.-..'-W 4n----'.....-:.:::. i"fi., -.... -...... ;:.... .:. ..r........-..-.::'-.'.'-2... .?.":.:'.-;:.
.:;........ ..........:.:...:,.,-,...."....,..'",.........-I........,;. I.M.:*:i::.!.:::;..:;:.:.,.11:1,.,:.::-.......,...:........ ....i..i.;i.!!:;.::..::i.....!.::;:.!::.--S-::-:.-:-.-:-.-.---.-.'-.-.....,.., ':.', -J, -.,':..::--,.,!..i.;i;.ii, -':;..:-.::i2'.-,.--..-.--....-...--.:...;."j..:..!.::..W..:.
...-;;. ,,,::.:!.:-.w;::-:.'::.':.%:.... ..aA.; ....14-.::!..::.----,:.:.: .---,-.,-, --,.,-,.,-".-'.- ..-...'.'-...,-.,....".....'.-'..i :.-;.:.i--,-.-,.:..:]--....... .,--.i-..!........'..:.'..'.'..'..:..:...:.:-.--..'.-'......L....'....'....,.?.::;::::-:.:::............:.i,i:;i,i:,.:i:;.:::..::::...:;.:: .......'---- ...ot
-.-":--.---,.---..: ;:..:.,.,.,.,..::...
.;--i.],::
..::-!:-.:-.--':---'.---K:F'11"', ,.,-"., ..", Iii ..U:,:..::""",::.II VIi il -,.11-1, IR-1:1,": ;', ":,--",--- -..,_-.iN,'.." .. .:-;...::...-...
MI.............:'-'--:-.:-:..,::,:::.. ;:..-!mmmo .........:: ::.:. .::::::...I.'-!.:,:-:,!::!:%. -:. .i::;,:,.::.:..:..::: ::...i.Z....-.:J:.-- .:.':..: :...-..':; :..J-.".-...-..'..-:-,.. ,:,;: :..,-,.:,.,...:,. ... :,::.....;,, .....:. :,;:-,.-,.-...-':-" .. .... --::.:........ ...K.N...,.:...;.-:. ...-.:-.. .........
-:`--,..... ..........-...................-.%-.%-.--,'-:.,'.;......,:.,.,.:....:!-,.-,i,.-,...,,.-..,.,,..,.!..",...,!..,..,..,..-..-...,.,.,.,.,..,...,.'.-,..-'..-..'-..,F..,.::, -:;.;xmI-.-...:.-,- :'. .-:.-'.-': .::-:::':.':.--%:----M......-ri ..-I":,.,.,:::...:::::,..:.,-..,:... ...,".,:.: :''
............ ,.. .-...
....:...I ..........., ........','..-. .................. ... !:':.'. .:.:.::....:...'.:.,.,..-.,..:... "" "'.:,...-... .., :.I---------- -- "'-"'' ."o- -.] III------------------d'- :.-......,.%.. ...f.-.I .i---- :-,.-::.%:.. ."..'r....., ., 111-11, F,....
...-:..... ....:-%"....:-:-,-,::::.::::,::.,..,::.-.:,.-4:,:"-.,.,:::.:,...:::::.:"",...-....... ...-,. ...-':.,.:,:..'.''......--m. ........:..........-:::.:,.,.,. :., --: -_-.:-I._I.-I,--'--'--':.-::,-,.'-.'.'..:.....-'.i:.::, ..:..-.:..-.....--,:..-.-..".,-,.,: :.--., ..... ':.f:..'-m: .-..:,-,.......m. ::":%.-':-.-'::'............:-,:,: .::,. .... :;.-,.: .-..'..'-.....'-.-...'..-.-..'..-.,...'.., -..........,,..--:-'*'.':--'.-.:. "''.''.:.::-:'...... .....
......W.............,."..'I.. ,....-.:.,........
...............
.;....':.':.....--..
.-:,.--:..2...h..::..-"I,,:.t:i. .,'.'..-.i i..ii _.. -,""', ....."-.... ,..,::Z.,.. ....i
....,b,............:
...........:...""'-... ...:.
"..-:,?%,:.,-. M....i )g-..... ::, .i..".i.i"'.,..'..
-,.flM.:....,::........aw."I'll d's.,y-..;:::..,*-.-.-.:.::..:.%:......... .................. 1- ..:f.,:'..':..,:,. ...:...... ,.:."....:.:-.-.-,.-.:..,...,:..',-.'..'...-..-...'-..-.-....'.-.:.....-.:;-,.-.,:,-,....:::-.-,:.-..................Y:
.:...%- ..,.... ....... :..::. .-::,-".,::.!::.' '.. m.: .::-..,-W...............::...._.._.;... :. ..-..-...- ni:-'--:- "', 1"..---:,,:::.,.::, .....
.-?-. .."I'i ii,-, ,...,., :::t..g,, -"- %...-M..--.-,,,:,,, "' .1