
AIDS-related malignancies in teenagers horizontally infected with HIV-1 during infancy A.Cupşa¹,...
26
AIDS-related malignancies in teenagers horizontally infected with HIV-1 during infancy A.Cupşa¹, Florentina Dumitrescu ¹, Irina Niculescu¹, L. Giubelan¹, Andreea Cristina Stoian¹, Amalia Romanescu², Cristina Iocu² ¹ University of Medicine and Pharmacy from Craiova, Romania, Infectious Diseases Department ² “Victor Babes” Clinical Hospital of Infectious Diseases and Pneumology, Craiova,
-
Upload
rodney-harrison -
Category
Documents
-
view
216 -
download
0
Transcript of AIDS-related malignancies in teenagers horizontally infected with HIV-1 during infancy A.Cupşa¹,...

AIDS-related malignancies in teenagers horizontally
infected with HIV-1 during infancy
A.Cupşa¹, Florentina Dumitrescu¹, Irina Niculescu¹, L. Giubelan¹, Andreea Cristina Stoian¹, Amalia Romanescu², Cristina Iocu²
¹ University of Medicine and Pharmacy from Craiova, Romania, Infectious Diseases Department ² “Victor Babes” Clinical Hospital of Infectious Diseases and Pneumology, Craiova, Romania

Background• HIV infection predisposes to several neoplastic
conditions, especially non-Hodgkin lymphoma and Kaposi's sarcoma, and also intraepithelial cervical neoplasia, anal neoplasia [1,2]
• For neoplasias associated with oncogenic human viruses, the role of HIV is most probably linked to its immunosuppressive effect and interference with immune-mediated tumour surveillance [2,3,4]
¹ Goedert, J. J., Cote, T. R., et al. (1998). Spectrum of AIDS-associated malignant disorders. Lancet 351(9119), 1833–1839.² Engels, E. A., Biggar, R. J., Hall, H. I., , et al. (2008). Cancer risk in people infected with human immunodeficiency virus in the United States. Int J Cancer123, 187–194.³ Grulich, A., Wan, X., et al. (1999). Risk of cancer in people with AIDS. AIDS 13(7), 839–843.4 Schulz TF, Boshoff CH, Weiss RA HIV infection and neoplasia. Lancet. 1996 Aug 31;348(9027):587-91.

Objectives
To assess :• the spectrum• prevalence • evolution
of AIDS-related malignancies in teenagers horizontally infected with HIV-1 during their infancy

Material and methods • retrospective study, from 01.01.2000 to 31.12.2009,
on a cumulative group of 594 adolescents (according to Tanner classification), born and horizontally infected with HIV-1 (mainly nosocomial) between 1988 and 1990, followed up by Regional Center for Evaluation and Monitoring of HIV/AIDS Infection, Craiova, Romania
• Patients (Px) were clinically, biologically and imaging evaluated; diagnosis of certainty for malignant condition has been histopathologically established

Results-1 • 21 Px (3.5%) have been diagnosed with AIDS-
associated malignancies, gender ratio M/F = 14/7 (66.7% / 33.3%)
• mean age when malignancy has been diagnosed = 15 [12; 18] years
The spectrum and prevalence of malignancies:• 13 Px (61.9%)- non-Hodgkin lymphoma (NHL), of
which: - 8 Px (38.2%)- diffuse large B-cell NHL- 2 Px (9.5%) - primary central nervous system
lymphoma- 2 Px (9.5%) - Burkitt lymphoma- 1 Px (4.7%) – marginal zone B-cell NHL
• 8 Px (38.1%) - Kaposi sarcoma

Results-2 • The average time between diagnosis of HIV infection
and identifying neoplasia has been 6.3 [0; 15] years
At the malignancy diagnosis:• average CD4 count =116.6 [9; 267] cells/mm³ • average HIV-RNA = 5.45 [3.89; 5.89] log10 copies/ml• 11 Px (52.4%) were antiretroviral multiexperienced, 4
other Px (19%) were naïve (neoplasia highlighted HIV infection)
• All Px received ARTc, while chemotherapy courses has been introduced in Px diagnosed with lymphoma

Evolution
• 12 deaths (57.2%) – 11 lymphoma Px, one case of Kaposi sarcoma (also having concomitant pulmonary tuberculosis) - with an average survival time after diagnosis of 5.6 [1; 14] months
• 2 Px (9.5.%) with NHL demonstrated remission• 7 Px (33.3%) with Kaposi sarcoma, treated only with
ARV, were still alive after an average of 5.4 [1; 9] years of follow-up.

Cases presentations

Case 1: Kaposi Sarcoma
• N.A, female, born in 1989• Late diagnosis of HIV
infection in March 2008 (long term non progressor?) with a concomitant diagnosis of palatinal Kaposi sarcoma
• CD4 count=18 cells/mm³• HIV-RNA= 28.800 c/ml• ARTc - 2NRTI+PI/r
(no chemotherapy)August 2008:
• CD4=217 cells/mm³• HIV-RNA< 50 c/ml• Complete remission of the
sarcoma

Case 2: Burkitt lymphoma
• D.N. female, born in 1990• Diagnosed with HIV
infection in 1996, EBV-Ig G anti EBNA, anti VCA-positives
• Burkitt lymphoma in 2001• When malignancy has been
recognized: CD4= 152cells/mm³
ART: • 2 NRTI - 1997• NNRTI+PI since 2000

Case 2: Burkitt lymphoma• The ARTc regimen has
been changed: 2 NRTI+PI/r
• She has received chemotherapy - CHOP (cyclophosphamidum-doxorubicinum-oncovin/vincristinum-prednisonum) regimen (photo has been taken after the first chemotherapy course)
• She died 6 months later due to renal failure

Case 3: Burkitt lymphoma
• D.F, male, born in 1988• Diagnosed with HIV infection -1993, EBV-Ig G anti
EBNA, anti VCA-positives, ART since 1996, 2 NRTI+PI since 2002
• CD4 count=632 cells/mm³-Feb.2006• Diagnosed with Burkitt lymphoma in May 2006 –
mandibular tumour (CD4=212cells/mm³)• Only 4 months survival (mandibular, axilar, iliac
tumours, medular invasion)

Case 3: Burkitt lymphoma

Case 4: Marginal zone B-cell NHL
• V.I, female, born in 1989, diagnosed with HIV infection in 1996
• ART since 1996, 2 NRTI+PI/r since 2007
• May 2008: CD4=431cells/mm³, HIV-RNA <50 copies/ml
• marginal zone B-cell NHL in August 2008

Case 4:Marginal zone B-cell non-Hodgkin lymphoma

Case 4: Marginal zone B-cell NHL
• Px starts radiation, but after two courses the swelling, which has had an initial tendency to remission, shows progression
• CT proves the presence of two intraconjunctival abscesses;
• lymphoma continues to progress and breaches the anterior right eye pole, requiring enucleation

Case 4: Marginal zone B-cell NHL
• A new CT exam rises suspicion of intracranial expansive formations in the frontal right lobe. Reassessment of CD4 lymphocytes shows their fall in (the new value at 148 cells/mm³)
• The Px died in October 2008
• The case shows the fulminating progression of malignant lesions in a special host (previously stabilized in terms of clinical, immunological and virological aspects) and the rapid and profound impact on cellular immunity

Case 5: NHL
• D.N.. Male, born in 1988• Diagnosed with HIV
infection in 1996• ART since 1996• Diagnosed with diffuse
large B cell NHL in 2001 • Chemotherapy:- COMP
(cyclophosphamidum-oncovin/vincristinum -methotrexatum-prednisonum) regimen-18 months
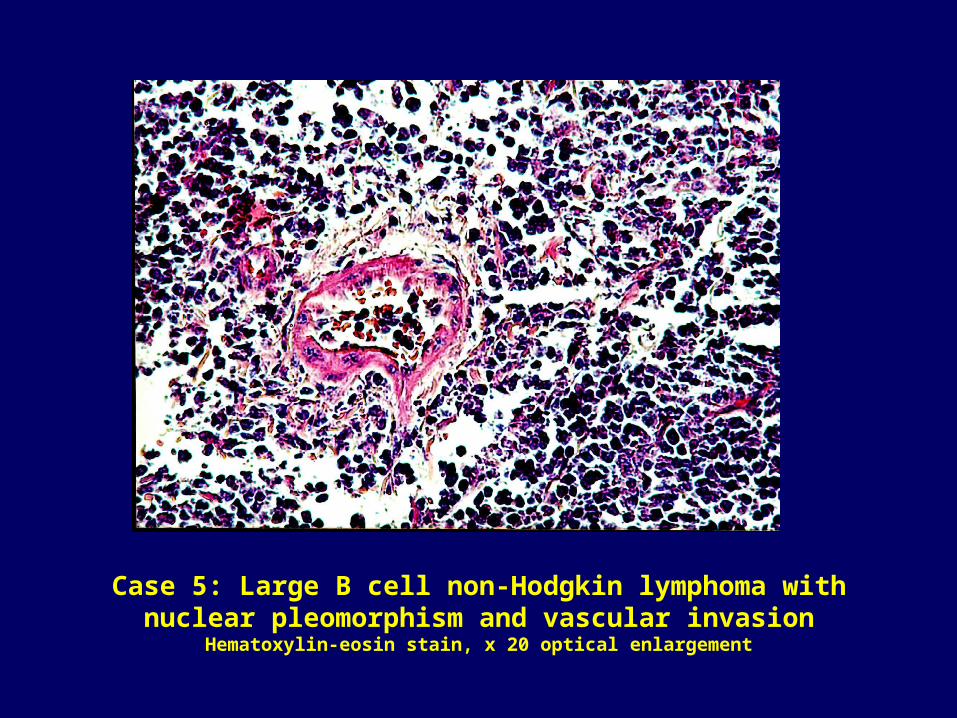
Case 5: Large B cell non-Hodgkin lymphoma with nuclear pleomorphism and vascular invasion
Hematoxylin-eosin stain, x 20 optical enlargement

Evolution, May 2008:
Average well-being, BMI = 19 kg/m², oral thrush
CD4 count = 71cells/mm³, HIV-RNA=31.400 c/ml,
TG=367mg/dl
A genotypic test has been performed and the
following mutations have been revealed:
RT mutation-D67N, T69D, V75T, M184V, T215F, K219Q;
PR mutation- L10V, K20R, L24I, L33F, M36I, M46I, I50V,
I54V, V77I, V82A

• Taking into account the results of the genotypic test and considering the fact that the Px has been exposed, during 1999-2001, to NNRTI (with a subsequent clinical, immunological and virological failure due, probably, to the occurence of NNRTI resistance), the following regimen has been proposed:
RAL + T20 + DRV/r
• After 12 months it is noted: • Two minor episodes of respiratory infections, not requiring
hospitalization• A good immune reconstruction (CD4 count 384 cells/mm³)• HIV-RNA undetectable (< 50 copies/ml after one month of
treatment with the new regimen)

• Due to adverse effects of T20 (occurence of
subcutaneous nodules), a new regimen has been
introduced: ABC + 3TC +RAL+DRV/r
In August 2009:
BMI = 23.7kg/ m²
CD4 count = 541 cells/mm³
HIV-RNA< 50 copies/ml
no signs of opportunistic diseases
without relapses of NHL
following hypolipemiant treatment
maximal well-being and with social integration
(student)

CD4 evolution
0
100
200
300
400
500
600
IDV+EFVAZT+ddc
d4T+3TC+IDV+RTV d4T+ddI+APV+RTV
ABC+3TC+LPV/r
T20+RAL+DRV+RTV
AZT ABC+3TC+RAL+DRV+RTV
Cells/mm³

HIV-RNA evolution
0
50000
100000
150000
200000
250000
c/m
l
Conclusions
in HIV-1 positive teenagers horizontally infected
during infancy, AIDS-related malignancies have a
relatively low prevalence
when present, they are accompanied by an
increased mortality in spite of appropriate diagnosis
and treatment.

Acknowledgement:D. Rodica Costa-TimişoaraD. Polixenia StancuD. Luminţa OcrotealăD. Elena IoniţăD. Surugiu PaulaD. Volosciuc ElenaD. Marinescu MariaD. Georgescu AdrianaD. Lucia GodeanuD. D. EcobiciPsychologist Liliana Marinescu
NursesPatients and their family
Thank you for your attention!


















