
Aide Memoire -MTR and Preparation Missiondocuments.worldbank.org/curated/en/... · Midterm Review...
29
1 AIDE-MEMOIRE Kenya Kenya Health Sector Support Project (P-74091) Midterm Review and Preparation of Additional Financing August 13- September 26, 2013 I. INTRODUCTION AND ACKNOWLEDGEMENTS 1. A World Bank team 1 worked with the officers from Ministry of Health (MoH), Government of Kenya (GoK), during August 13-28, 2013 to conclude the on-going mid-term review and initiate preparation of the proposed additional financing for the Kenya Health Sector Support Project (KHSSP). The mission met with Prof. Fred H. K. Segor, Principal Secretary and discussed the key implementation issues. Dr. S. K. Sharif, Director of Public Health supported by Dr. Peter Kimuu, Coordinator for the Program and Dr. Mary Wangai led the discussions participated by other senior officers from the MoH while Dr. John Munyu led the discussions with the Kenya Medical Supplies Authority (KEMSA). Discussions also with senior officers were held on the proposed areas of support for additional financing which were joined by key partners interested in supporting new health financing reforms to shift emphasis on results and eliminate payment at the point of service delivery through health insurance subsidies for the poor (HISP). The Bank also had follow-on discussions with MoH and the Ministry of Finance (MoF) on September 23 and 26, 2013 regarding funds flow and implementation arrangements for the Project under the devolved health systems. 2. The mission successfully achieved the objectives of: (a) completing the mid-term review of IDA supported Kenya Health Sector Support Project documenting key achievements and lessons learnt including specific areas that need improvement, and those activities that need to be dropped; (b) holding detailed discussions with government counterparts and key stakeholders on design and implementation arrangements for the proposed additional financing including revision of project development objectives and results framework accordingly; and (c) agreeing on next steps in project preparation including dates for appraisal. 3. The key findings of the mission were shared with Prof. Fred H. K. Segor, Principal Secretary Health on October 1, 2013, and his comments on implementation and reporting arrangements were incorporated in the proposed design. The wrap-up meeting chaired by Mr. Moses Kanagi, Head, World Bank Division, External Resources Department, on behalf of the Principal Secretary, Ministry of Finance, GoK was held on October 28 , 2013 where specific actions to be completed for the appraisal of the proposed restructuring and additional financing of the project were agreed. Annex 1 lists the people who 1 The Bank team included Gandham NV Ramana (Task Team Leader); Ms. Rekha Menon (Sector Leader, AFTHD); Ms. Wacuka Ikua (Senior Operations Officer); Ms. Nightingale Rukuba-Ngiaiza (Senior Counsel); Mr. Henry Amuguni (Senior FM Specialist); Mr. Joel Munyori (Senior Procurement Specialist); Ms. Gibwa Kajubi (Senior Social Development Specialist); Dr. Rachael Njeri Mwaura (Operations Officer IFC); Ms. Josphine Gathoni Muigai (Investment Officer IFC); Ms. Kathleen Whimp (Senior Public Sector Specialist); Mr. Michael Munavu (Consultant, Social Protection); Ms. Toni Kuguru (Consultant); and Hope Nanshemeza (Team Assistant). Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized
Transcript of Aide Memoire -MTR and Preparation Missiondocuments.worldbank.org/curated/en/... · Midterm Review...

1
AIDE-MEMOIRE
Kenya
Kenya Health Sector Support Project (P-74091)
Midterm Review and Preparation of Additional Financing
August 13- September 26, 2013
I. INTRODUCTION AND ACKNOWLEDGEMENTS
1. A World Bank team1worked with the officers from Ministry of Health (MoH), Government of
Kenya (GoK), during August 13-28, 2013 to conclude the on-going mid-term review and initiate
preparation of the proposed additional financing for the Kenya Health Sector Support Project (KHSSP).
The mission met with Prof. Fred H. K. Segor, Principal Secretary and discussed the key implementation
issues. Dr. S. K. Sharif, Director of Public Health supported by Dr. Peter Kimuu, Coordinator for the
Program and Dr. Mary Wangai led the discussions participated by other senior officers from the MoH
while Dr. John Munyu led the discussions with the Kenya Medical Supplies Authority (KEMSA).
Discussions also with senior officers were held on the proposed areas of support for additional financing
which were joined by key partners interested in supporting new health financing reforms to shift emphasis
on results and eliminate payment at the point of service delivery through health insurance subsidies for
the poor (HISP). The Bank also had follow-on discussions with MoH and the Ministry of Finance (MoF)
on September 23 and 26, 2013 regarding funds flow and implementation arrangements for the Project
under the devolved health systems.
2. The mission successfully achieved the objectives of: (a) completing the mid-term review of IDA
supported Kenya Health Sector Support Project documenting key achievements and lessons learnt
including specific areas that need improvement, and those activities that need to be dropped; (b) holding
detailed discussions with government counterparts and key stakeholders on design and implementation
arrangements for the proposed additional financing including revision of project development objectives
and results framework accordingly; and (c) agreeing on next steps in project preparation including dates
for appraisal.
3. The key findings of the mission were shared with Prof. Fred H. K. Segor, Principal Secretary
Health on October 1, 2013, and his comments on implementation and reporting arrangements were
incorporated in the proposed design. The wrap-up meeting chaired by Mr. Moses Kanagi, Head, World
Bank Division, External Resources Department, on behalf of the Principal Secretary, Ministry of Finance,
GoK was held on October 28 , 2013 where specific actions to be completed for the appraisal of the
proposed restructuring and additional financing of the project were agreed. Annex 1 lists the people who
1The Bank team included Gandham NV Ramana (Task Team Leader); Ms. Rekha Menon (Sector Leader, AFTHD); Ms. Wacuka
Ikua (Senior Operations Officer); Ms. Nightingale Rukuba-Ngiaiza (Senior Counsel); Mr. Henry Amuguni (Senior FM Specialist); Mr. Joel Munyori (Senior Procurement Specialist); Ms. Gibwa Kajubi (Senior Social Development Specialist); Dr. Rachael Njeri Mwaura (Operations Officer IFC); Ms. Josphine Gathoni Muigai (Investment Officer IFC); Ms. Kathleen Whimp (Senior Public Sector Specialist); Mr. Michael Munavu (Consultant, Social Protection); Ms. Toni Kuguru (Consultant); and Hope Nanshemeza (Team Assistant).
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
wb456288
Typewritten Text
wb456288
Typewritten Text
83820
2
participated in the Mission. Annex 2 presents the status of intermediate results. Annex 3 describes
financial progress by sub activity. Finally, Annex 4 presents the disbursements.
4. The team acknowledges the high quality discussions and constructive suggestions made by senior
officers from the MoH and KEMSA to enhance the implementation of KHSSP under the devolved health
system and to develop much stronger results focused approaches with innovations to improve access of
essential health services to the poor.
II. CONTEXT
5. The KHSSP aims to improve the delivery of essential health services for the Kenyans, especially
the poor and drought affected populations following a Sector Wide Approach (SWAP). The program also
supports improvements in planning, financing and procurement of pharmaceuticals and medical supplies.
The KHSSP supports two key reforms initiated by the Government of Kenya: (a) providing direct cash
transfers to primary health facilities through the Health Sector Services Fund (HSSF) to enhance
participatory decentralized planning of essential health services; and (b) improving the availability of
Essential Medicines and Medical Supplies (EMMS) at the health facility level through scaling up the
“pull system” of supply and reforms in procurement and distribution.
6. The KHSSP (Credit No.4771) for an amount of SDR66.2 million (US$100 million equivalent)
was approved by the Bank on June 29, 2010 and became effective on September 30, 2010. In December
2011, the Bank approved additional financing of SDR35.9 million (US$56.8 million equivalent) for
KHSSP, to support urgent nutrition and health needs of drought affected populations in Kenya and to
complement on-going reforms to strengthen procurement and distribution of EMMS. The Danish
International Development Agency (DANIDA) is co- financing the two key reforms through its Health
Sector Support Program III. The support from DANIDA and IDA are broadly guided by the Joint
Financing Agreement (JFA) and Code of Conduct agreed between the GoK and its development partners
in the health sector.
7. The KHSSP has completed over two and a half years of implementation since its launch in
December 2010 and the mid-term review which started in January 2013 was extended due to the
transformational changes taking place in the health sector that have implications on the design and
implementation arrangements of the project and to be informed by the Public Expenditure Tracking and
Service Delivery Indicators Survey. As of September 2013, 86.5% of the Credit from the original project
and 24% from the IDA CRW has been disbursed and disbursements are expected to further pick-up with
provision of adequate allocations for MoH in the revised budget to process payments for the on-going
procurement. However, the project needs to be appropriately restructured to align with Kenya’s devolved
health systems and new roles and responsibilities to be undertaken by the national and county levels and
also respond to recent policy decisions taken by the Government to eliminate user-fee for primary care
and to offer free-maternity care. The project development objectives also need to be revised to ensure
better focus.
III. ACHIEVEMENT OF PROJECT DEVELOPMENT OBJECTIVES
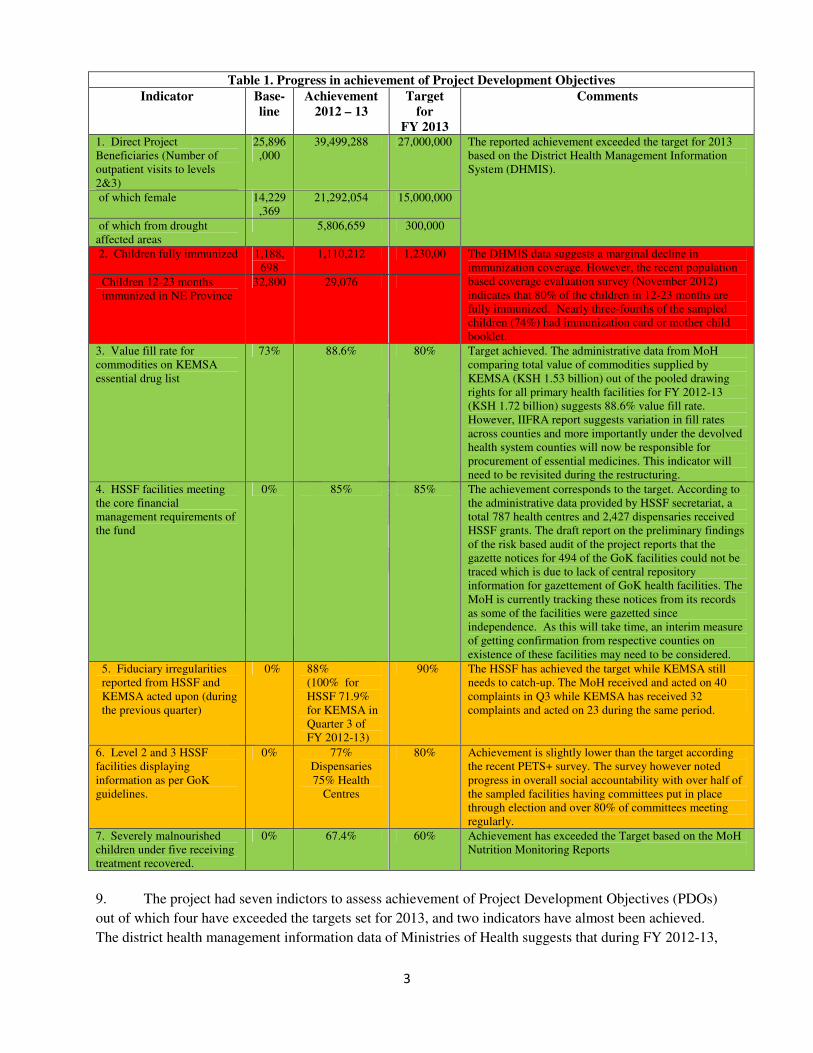
8. A score card summarizing the progress of PDOs is presented in Table 1. Based on the available
data, the progress in achievement of PDOs is considered satisfactory.
3
Table 1. Progress in achievement of Project Development Objectives
Indicator Base-line
Achievement 2012 – 13
Target for
FY 2013
Comments
1. Direct Project Beneficiaries (Number of outpatient visits to levels 2&3)
25,896,000
39,499,288 27,000,000 The reported achievement exceeded the target for 2013 based on the District Health Management Information System (DHMIS).
of which female 14,229,369
21,292,054 15,000,000
of which from drought affected areas
5,806,659 300,000
2. Children fully immunized 1,188,698
1,110,212 1,230,00 The DHMIS data suggests a marginal decline in immunization coverage. However, the recent population based coverage evaluation survey (November 2012) indicates that 80% of the children in 12-23 months are fully immunized. Nearly three-fourths of the sampled children (74%) had immunization card or mother child booklet.
Children 12-23 months immunized in NE Province
32,800 29,076
3. Value fill rate for commodities on KEMSA essential drug list
73% 88.6% 80% Target achieved. The administrative data from MoH comparing total value of commodities supplied by KEMSA (KSH 1.53 billion) out of the pooled drawing rights for all primary health facilities for FY 2012-13 (KSH 1.72 billion) suggests 88.6% value fill rate. However, IIFRA report suggests variation in fill rates across counties and more importantly under the devolved health system counties will now be responsible for procurement of essential medicines. This indicator will need to be revisited during the restructuring.
4. HSSF facilities meeting the core financial management requirements of the fund
0% 85% 85% The achievement corresponds to the target. According to the administrative data provided by HSSF secretariat, a total 787 health centres and 2,427 dispensaries received HSSF grants. The draft report on the preliminary findings of the risk based audit of the project reports that the gazette notices for 494 of the GoK facilities could not be traced which is due to lack of central repository information for gazettement of GoK health facilities. The MoH is currently tracking these notices from its records as some of the facilities were gazetted since independence. As this will take time, an interim measure of getting confirmation from respective counties on existence of these facilities may need to be considered.
5. Fiduciary irregularities reported from HSSF and KEMSA acted upon (during the previous quarter)
0% 88% (100% for HSSF 71.9% for KEMSA in Quarter 3 of FY 2012-13)
90% The HSSF has achieved the target while KEMSA still needs to catch-up. The MoH received and acted on 40 complaints in Q3 while KEMSA has received 32 complaints and acted on 23 during the same period.
6. Level 2 and 3 HSSF facilities displaying information as per GoK guidelines.
0% 77% Dispensaries 75% Health
Centres
80% Achievement is slightly lower than the target according the recent PETS+ survey. The survey however noted progress in overall social accountability with over half of the sampled facilities having committees put in place through election and over 80% of committees meeting regularly.
7. Severely malnourished children under five receiving treatment recovered.
0% 67.4% 60% Achievement has exceeded the Target based on the MoH Nutrition Monitoring Reports
9. The project had seven indictors to assess achievement of Project Development Objectives (PDOs)
out of which four have exceeded the targets set for 2013, and two indicators have almost been achieved.
The district health management information data of Ministries of Health suggests that during FY 2012-13,

4
39.5.million individuals directly benefited from the project and over half of them (21.29 million) were
females. During this period, the value fill rate of the facilities under the pull system of supply was around
88%, and 85% of the facilities receiving the HSSF grants have met the core financial management
requirements. The MoH nutrition surveillance data suggests that nearly two thirds of the children
admitted with severe acute malnutrition have recovered.
10. The number of children reported to be immunized during their first year continues to remain
around 1.1 million2. However, the population based National Immunization Survey (November 2012)
suggests that Kenya has achieved an overall full immunization coverage of 80% which is an improvement
from 68% reported by the Demographic Health Survey of 2008. While the MoH has acted on all cases of
irregularities reported by Integrated Fiduciary Review Agency (IIFRA), KEMSA acted on about three
fourths of the complaints. Over three fourths of the health facilities sampled under the recent Public
Expenditure Tracking Survey (PETS+) have disclosed financial information. While this indicator has
marginally fallen short of the envisaged target of 80%, considering the operational and security
challenges in disclosing such information, this can be considered a reasonable progress.
11. There has been good progress in the intermediate results indicators (Annex 2) especially those on
people with access to basic health services, health personnel receiving training, facilities implementing
results based financing initiatives and number of beneficiaries receiving supplemental feeding in the
drought affected areas. The PETS+ survey has shown that 84% of facility committees meet every
quarter, which is close to the envisaged target of 85% and nearly 95% of the facilities on pull system of
supplying essential medicines and medical supplies (EMMS) have sent their orders in the previous
quarter. The on-going audit of human resources is expected to provide data on health facilities meeting
staffing norms. The HSSF funds however could not reach the facilities within 15 days of the beginning
of the quarter mainly due to delays in submission of facility level financial expenditure returns. To
remedy this, the Ministry of Health has shifted from quarterly to annual authorization to incur expenditure
(AIE), which enabled the facilities to access available resources including user fee to ensure service
delivery. However, these arrangements now need to be revisited in the light of devolved system of
government and abolition of user fee in all public primary care health facilities. While the MoH has
reimbursed KEMSA for three quarters during FY 2012-13 based on documented claims of supply to
primary health facilities, there were delays on both sides.
Implementation of the Joint Financing Agreement (JFA) and evolving challenges:
12. Among several partners supporting the health sector, only two partners (DANIDA and the World
Bank) have signed the JFA so far and a significant part of the external aid to the sector still remains off-
budget. The pooling partners are being engaged in the planning and budgeting process of financing pools
for HSSF and EMMS. A new Health Sector Policy covering the period 2012-30 has been developed and
the draft sector strategy 2012- 2018 was reviewed through a Joint National Assessment of Sector (JANS)
Strategy process involving all key stakeholders. Based on the recommendations from this review, the
strategy is being revised.
2 The health management information system is being upgraded to a web based program (DHIS 2) and currently reporting rates are around 80%. 3 The “pull system” is an ordering mechanism makes the facilities responsible for their orders based on their needs i,e demand driven. In the past the system was operated as a push system by which the Ministry of Health determined the quantity to be received by each facility i.e. supply driven.

5
13. With the on-going devolution mandated by Kenya’s 2010 Constitution, the entire health sector
architecture is changing. The 47 County Governments will now be primarily responsible for the delivery
of essential health services while the National Government will provide the policy framework and
manage national referral hospitals. The GOK share of HSSF basic operating costs and allocations for
procurement of EMMS have been included in the equitable share of revenues allocated to counties. In
addition, the recent policy pronouncements made by the National Government to eliminate payment at
point of service delivery by abolishing user fee at primary health facility and offering free maternity care
at all public health facilities will also have important implications for service delivery. At present, user
fee is estimated to contribute nearly 60% of the operating costs of primary health facilities and the
government’s commitment to improve maternal health outcomes will provide an opportunity for the MoH
to shift emphasis onto outputs and delivery of quality maternal healthcare. The SWAp secretariat is
providing more strategic support for on-going reform initiatives and undertook comprehensive functional
mapping responding to new roles and responsibilities of National and County governments as envisaged
by the Constitution and the proposed draft legislations. A new organogram reflecting the merging of the
two ministries of health is being developed. With these developments there will be changes in the
institutional and implementation arrangements for KHSSP, which requires a comprehensive review
including existing financing arrangements by the pooling partners. Also, the JFA needs to be revisited
while finalizing the proposed restructuring and additional financing.
IV. COMPONENT-WISE IMPLEMENTATION PROGRESS
Component 1: Effective and transparent implementation of the Kenya Essential Package for Health
through HSSF grants and performance strengthening
14. The HSSF program has been expanded to all Government primary health care facilities and is
currently covering 787 health centres and 2,427 dispensaries. As per the information provided by the
HSSF Secretariat, the fund has so far disbursed K.Sh 1.695 billion (about US$20 million) and K.Sh 757
million out of this was disbursed to GoK levels 2 and 3 facilities during FY2012-13. Reports of the IIFRA
noted visible overall improvements in the service delivery at the health facilities. Similar feedback was
received from the independent Citizen’s Report Card exercise undertaken by Family Care International
(October 2012) in Kitui and Nakuru Counties. A majority of the 599 clients interviewed stated that the
overall quality of service, waiting time, cleanliness and the state of the health centres had improved
compared to the past one year.
15. The facility survey covering randomly selected health facilities undertaken by the Kenya Institute
for Public Policy and Research (KIPPRA) as a part of the Public Expenditure Tracking and Service
Indicators Study for the MoH has shown that a majority of the sampled public health centres (95%) and
over three fourths of the public dispensaries (75.7%) received HSSF grants and 92% and 69% of health
centres and dispensaries had annual operational plans in place. This trend could be due to fact that the
inclusion of public dispensaries started only in 2012. All sampled public dispensaries started receiving the
HSSF grants only in FY 2012-13. Most (98%) of primary health facilities had health facility management
committees (HFMCs) in place and over half of such committees were elected. The HFMCs in over 80%
of sampled public primary health facilities met every quarter. Over three fourths of the facilities (77%)
disclosed financial information to the public and there is nearly 20% lesser probability of receiving funds
if a facility failed to submit quarterly financial reports suggesting that the HSSF program has put in place

6
some internal controls. However, the study identified the need to strengthen financial record keeping at
the facility level. Over a quarter of dispensaries and about a tenth of the health centres did not have proper
records. The IIFRA report for the third quarter of FY 2012-13 covering 159 Dispensaries, 76 Health
Centres and 47 DHMTs also highlights this. Around 71% of the health facilities audited during the
quarter (compared to 63% in previous quarter) maintained their Cash Books and 75% had updated
memorandum vote books with 72% maintaining asset inventory records.
16. Based on the feedback received, the MoH has taken some proactive measures to enhance
engagement of the Districts and has made approval by the district health officers for the annual work
plans of facilities mandatory. Also, authorizations to incur expenditure (AIEs), which includes national
HSSF grants and revenues generated through cost sharing, are now being issued on annual basis.
However, failure of nearly two thirds of facilities (64%) to prepare monthly financial statements and over
half of facilities (56%) not undertaking bank reconciliation of their accounts as required by GoK financial
guidelines as reported by IIFRA remain the main weaknesses which need to be addressed. Further, due to
delays in reporting expenditure by facilities and inclusion of the user fee, the HSSF Secretariat was not
able to fully reconcile releases with expenditures and was unable to prepare consolidated reports for
HSSF disbursements to DHMTs and health facilities in a timely manner.
17. With the responsibility of delivering primary and secondary health services with the Counties
and the GoK share of HSSF grants included under the equity based allocations provided to Counties, the
existing implementation arrangements now need to be revisited with the Bank team starting dialogue with
key stakeholders. The IDA Credit for FY 2013-14 seems to be included under the special grants provided
to Counties while allocations made by GoK for compensating health facilities for providing the free
maternity care (K.Sh3.8 billion) and removal of user fee (K.Sh 700 million) have been provided for in
the MoH budget. Going forward, the MoH is considering the option of pooling all resources meant for
primary health facilities available at the national level under the HSSF pool. The MoH is also discussing
with the Counties the option of releasing these funds directly to facilities subject to confirmation received
from Counties regarding the approval of the facility annual plans as well as appropriation of both County
and National shares in the County Budgets. Counties will be issuing the Authorization to Incur
Expenditures and also be taking lead on collecting and compiling expenditure reports from facilities and
sharing consolidated reports with the MoH.
18. The KHSSP supported strengthening of supportive supervision by providing some key missing
inputs such as vehicles and provision of operational costs for supervision visits. A new “supervision
checklist” developed by the Department of Primary Health care through a consultative process was
expected to help to assess the facility performance more objectively. The Health Management
Information System (HMIS) division has created an additional module under the district health
information system to enable on-line data entry and information sharing. Unfortunately, the
implementation of the checklist remains patchy and the module in HMIS is not being regularly updated.
The on-going devolution and shift towards output based approaches for free maternity care and expansion
of results based financing in northern Kenya will provide an excellent opportunity to make supportive
supervision also results based by linking quarterly visits to facilities and updating supervision checklists
as the measure of output. This arrangement needs to be finalized by MoH in consultation with Counties
by appraisal of the proposed restructuring and additional financing of the KHSSP.
7
19. Procurement of Motor Vehicles for supportive supervision has been completed and delivery
completed. As per the GoK guidelines, tracking devices were installed in these vehicles to monitor their
proper use.
20. For the consultancy services for communication strategy, the final review of the tender committee
of MoH is still pending. Procurement of this important consultancy has taken far too long and it was
agreed that MoH will conclude this process by end September 2013 and effectively use this service during
the remainder of the project for providing strategic communication support to the MoH and Counties.
Governance and Stewardship
21. The IIFRA has completed seven quarterly assessments covering the four quarters of FY 2011-12
and three quarters of FY 2012-13. The scope so far covered over 1,200 visits to primary health facilities
and over 250 visits to DHMTs. The MoH has promptly acted on any financial irregularities identified by
the IIFRA. The findings of the reviews are that HSSF and SWAp secretariat have generally maintained
proper books of accounts and prepared interim financial reports on a timely basis. The KEMSA has
integrated the inventory management system with the Enterprise Resource Planning system and has put in
place a well-organized and adequately staffed procurement department. The report however identified
weaknesses in financial reporting of funds disbursed to facilities and DHMTs as well as the need for
regular updating of the master facility list. Very slow implementation of some project activities by the
erstwhile Ministry of Medical Services was also highlighted. These issues need to be addressed under the
devolved health system with Counties taking lead with relevant technical assistance and capacity building
by the MoH.
22. The IIFRA started using the score card for rating the performance of facilities (Green –Well
performing; Amber: Average performing and Red: Poor performing) and providing feedback at the end of
the review. There was a steady improvement in record keeping at facility level with over two thirds of
facilities maintaining cash books and up-to-date vote books while half of the facilities dated and stamped
payment vouchers and supporting documents (IIFRA). The facilities rated poor (red) declined from 21%
to 15% by the third quarter of FY 2012-13. Further, the share of poor performance was much lower
among newly sampled facilities which were re-visited (3%) highlighting the importance of direct
feedback to the facility in-charges and DHMTs by auditors. However, having nearly two-thirds of
facilities under the amber category highlights the importance of sustained capacity building, especially in
the areas of financial reporting and bank reconciliations.
IDA support for Nutrition under Crisis Reponses Window and Pilots:
23. Emergency Nutrition Support to Drought Affected Areas under IDA Crisis Response Window:
To support Government of Kenya’s efforts to address the severe drought conditions among resident
populations in the northern Kenya, the Bank approved additional financing in December 2011. The
nutrition support covered 22 most drought affected districts spread over 18 countries. This intervention is
being implemented through existing GoK partnerships with UNICEF and World Food Program for
procurement and distribution. While UNICEF is responsible for overall procurement and distribution of
Ready to Use Therapeutic Food (RUTF), the World Food Program (WFP) is sub-contracted for
distribution and implementation of Ready to Use Supplemental Food (RUSF). Going forward, WFP will
8
no longer be sub-contracted for distribution and implementation of RUSF, and UNICEF will distribute
both RUTF and RUSF
24. The findings from the nutrition surveillance and reporting system suggest that the proportion of
severely malnourished children under five years of age recovered among those receiving treatment in the
project areas (67.4%) exceeds the project target (60%). The number of admissions of children suffering
from severe acute malnutrition (SAM) has declined to around 3000 per month in 2013 compared to over
5000 per month in 2011. During the year so far 194,417 beneficiaries (moderately malnourished children
under five and pregnant and lactating women) have been enrolled for supplementary feeding. In the light
of reduced number of SAM cases, the division of nutrition proposed to increase allocation for RUSF to
focus on moderately malnourished groups. The planned procurement was delayed due to bacterial
contamination of supplies and the on-going contracts of WFP may end 2 months before the end of
planned nutrition activities. Given that available stocks of nutrition commodities will only last until
November 2013 and the need to maintain adequate stocks in light of a potential drought in later in the
year, the Division of Nutrition recommended: (i) increasing supply of nutrition commodities for
distribution as EMMS and (ii) building capacity at the county level focusing on supply chain
management. It was agreed that the Division of Nutrition will prepare a concept note by October 15
outlining a mutually acceptable way forward to ensure sustained nutrition support during the appraisal.
25. The pilot on Results Based Financing (RBF) in Samburu County started from October 2011
received its second verification in October, 2012. The verification covering the period of January-
September 2012 was carried out by a joint team consisting of staff DHMT and District Hospital and local
implementation partners supporting the district such as African Medical Research Foundation (AMREF)
and World Vision. The verification shows improvements in four antenatal care visits (by 28%), deliveries
at health facilities (by 6%) and children fully immunized (12%). The average utilization rates for growth
monitoring of children in facilities were nearly 30% higher and HIV/AIDS counselling and testing was
nearly double among the RBF facilities compared to those not receiving RBF. However, there was a
decline in use of family planning services. The verification also highlighted major discrepancies in HMIS
data and information available at facility records. An experience sharing work shop was held in
November 2012 where the lessons from the RBF pilot were discussed and a strategy for scale-up was
proposed. The Bank team is pleased to note that the MoH RBF team is working closely with other
partners supporting RBF initiatives in Kenya to ensure effective harmonization. The APHIA-plus
program has been implementing the RBF in two districts in Western Kenya and one more pilot is
proposed in Isiolo.
26. Recently the Bank has awarded a contract to the Population Council Kenya for undertaking an
end-line evaluation to assess the impact of the pilot and to make recommendations for the scaled up
program. In areas with insufficient capacity to provide primary health services or where there is no
access to government facilities, non-government health facilities such as FBOs meeting eligibility
conditions may participate in the RBF scale up. The operational manual is being revised in the light of
on-going devolution so that the institutional and financial arrangements clearly include specific roles and
responsibilities for Counties. To scale-up RBF, a grant of US$20 million has been approved recently
from the partners supporting the Health Results Innovation Trust Fund, which will complement similar
initiatives proposed under the health systems strengthening support from the Global Alliance for Vaccines
Immunization (GAVI). More details on the scale up are provided under the section additional financing.

9
27. The pilot for making non-functional health facilities built under the Constituency Development
Fund (CDF) operational has made little further progress after the initial survey and no decision has been
taken on the Public Private Partnership (PPP) options. With the devolution, this initiative now requires
active engagement of Counties and appropriate technical assistance. The Bank is the process of providing
such TA through the infrastructure financing and public private partnership project to support this
initiative. It was agreed that PPP initiatives will be tested in Counties showing keen interest to improve
service delivery. The potential options include rural Counties service delivery challenges3 and an urban
County4 where priority focus will be given to improving delivery of basic health services urban slum
residents. The draft design for the PPPs will be ready by appraisal.
28. The health financing pilot (Health for all Kenyans through Innovation) to be coordinated by the
German Development Corporation (GDC) could not start due to reasons beyond the control of MoH and
GDC. During the past 6 months, the MoH economic planning team worked closely with the National
Hospital Insurance Fund (NHIF) and prepared a proposal for providing Health Insurance Subsidies for the
Poor (HISP) and the Bank has issued no objection to move forward. A Technical Working Group for
HISP has been established to develop detailed operational guidelines including a comprehensive
operational manual. The progress made under this sub component is summarized under the additional
financing section.
29. The proposed pilot on referral systems has not made any further progress since the baseline
assessment completed in 2011, which was discussed during the previous mission. Unfortunately, the
ambulances could not be procured due to lack of response from bidders even after re-advertisement. It
was agreed that the resources allocated for this sub component will be reallocated to the HISP to cover
300 households in each County during the first phase.
30. Strengthening Social Accountability (SAc). As explained earlier, considerable progress has been
made in the project on promoting overall Social Accountability. As planned, the SWAp Secretariat
contracted the African Development and Emergency Organisation (ADEO) to implement the pilot. The
16-month pilot (November 2011 to February 2013) was implemented in nine (9) locations reflecting
different socio-economic settings in Kenya. These include: arid and semi-arid including pastoral, fishing,
agriculture, semi-urban, and coastal. The nine districts (and corresponding health centres) are Kirinyaga
South (Mutithi), Lamu (Mokowe), Naivasha (Maiella), Garissa (Medina), Turkana South (Makutano),
Mbooni (Kalawa), Suba (Tom Mboya Memorial), Msambweni (LungaLunga) and Nairobi West (Riruta).
Improvements were noted in utilization of services, staff motivation, transparency in use of resources and
harmony between the staff and communities.
31. The pilot tested the operational feasibility of improving transparency in sharing information about
health services, enhancing participation of communities in health service delivery planning and
introducing effective complaint redress mechanisms targeting the user communities. A Community
Score Card was designed to encourage the dialogue between service providers and community to improve
health services in the pilot health centres. The key findings from the pilot are: (a) There has been
demonstrated improvement in information sharing and disclosing behaviour from the health service
3 Kisumu and Lamu
4 Nairobi or Mombasa

10
providers with corresponding information seeking behaviour from the users; (b) An enabling environment
has been created where users and providers have seized the opportunity to build trust and are developing
positive attitude towards each other; (c) In all sites, the community score card showed an overall
improvement in the selected and prioritized performance indicators between the first and the second
scoring; and (d) The community forum has provided an opportunity for the community and health centre
staff to dialogue and plan together on the delivery of health services.
32. A draft of the “Social Accountability Implementer’s Manual and Operating Guidelines” is now
being finalized. This will be shared with Counties and the MoH will provide TA to support
implementation in Counties showing interest to scale-up.
Availability of Essential health Commodities and Strengthening of supply chain management
Essential Medicines and Medical Supplies (EMMS)
33. All public primary health care facilities in Kenya are now covered by the “pull system” of supply
with the facilities making orders based on their drawing rights. The Kenya Medical Supplies Authority
(KEMSA) is supplying the facilities based on their orders placed using commodities procured under GoK
funds provided under the Economic Stimulus Package and IDA through the KHSSP. The MoH is
reimbursing KEMSA based on documented evidence of supply to primary health facilities (proof of
deliveries) using GoK and DANIDA funding. The reimbursement to KEMSA aims at establishing a pool
of fund for supplying EMMS to primary health care facilities. Out of the total invoices of K.Sh2.7 billion
raised by KEMSA, the MoH has reimbursed K.Sh1.6 billion. The MoH needs to reimburse the remaining
balance to KEMSA and also pay for the warehousing and distribution costs.
34. A case study undertaken by the Bank assessed the effect of the reform process in improving the
provision of essential medicines to poor counties. This was done by regressing KEMSA supplies with
district level poverty data. The study has shown that per capita value of supplies made by KEMSA were
marginally higher in districts with highest proportion of the poor (75%) compared to districts where about
a quarter of the population was living below poverty line (K.Sh99 vs. K.Sh86). However, the study has
shown that it costs KEMSA more to ship supplies to poorer districts compared to better-off districts,
probably due to dispersed location of facilities in such districts. Finally, determining the drawing rights
based on utilization trends could be disadvantageous to poorer districts with dispersed populations having
limited transport access to fixed health facilities. While the study advises caution in drawing policy
conclusions, it provides some useful leads such as (a) need for budgeting higher transport costs for poorer
districts; and (b) linking supply chain to community strategy in the poorer districts where communities
are more widely dispersed with limited transport to access fixed health facilities.
35. The total IDA commitment for procurement of EMMS under the original project was US$ 44.29
million and with the additional financing this increased up to US$82.64 million (as of August 19, 2013).
This includes US$ 4 million provided for supporting KEMSA to establish a supplementary services
division to supply essential commodities to district hospitals on a cost recovery basis. KEMSA did a
commendable job in procurement and so far contracts valued at US$68 million have been awarded
(including US$ 3.5 million under the supplementary services) and the remaining contracts are in different
phases of bidding. Out of the contracts awarded, payments have been made for US$36.27 million, special
commitments were issued for US$28.35 million and payments for US$6.64 million are being processed.

11
36. The MoH has successfully established drawing rights for health facilities based on available data
and systematically built facility level capacity for storage, inventory management and ordering under the
pull system. The capacity building is done through Training of Trainers given to District health
Management Teams which in turn trained one staff from each facility responsible for Inventory
Management. Under the KHSSP, a total of 291 out of 329 (88.45%) trainers training programs were held
and 2473 out of 2568 (96.30%) planned facility level health staff received training in managing the pull
system of supply between May 2011 and February 2013. Most of the facilities are now sending their
orders to KEMSA every quarter. While the value fill rates of the orders placed by facilities show
improvement, the order fill rate still low and require attention.
37. While the pull system is still getting institutionalized, major changes are taking place in the
Kenyan Health System as per the new constitutional dispensation. Under the devolved health systems,
Counties are responsible for the procurement of EMMS, and GOK resources for EMMS have been
included in the equitable share allocated to Counties. The recent Gazette notice proposes that the
Counties procure EMMS through KEMSA and only procure from an outside source if KEMSA fails to
supply. However, it is still not clear how the on-going system of reimbursing KEMSA will continue. As
a result, during the first quarter of FY 2013-14, KEMSA has made supplies only to the 13 counties that
did not receive EMMS during the last quarter of the previous financial year. As a result, stock-outs are
being reported from some facilities. To address this immediate need, the MoH has recently authorized
KEMSA to release supplies equivalent to two quarters of drawing rights to the levels 2 and 3 facilities.
However, a more sustained solution needs to be proposed during the next 6 months to sustain this
important reform. Further, the pool funds available for supply of EMMS to primary health care facilities
at KEMSA stands around K.Sh1.6 billion which will enable KEMSA to effectively respond to the EMMS
needs for primary health ensuring efficiency and economy. Further, there are commodities in KEMSA
warehouses and some orders are still being supplied which could take this pool over K Sh. 3 billon. The
MoH through a consultative process involving Counties needs to establish appropriate governance
arrangements for managing this pool in line with the devolved health system ensuring transparency and
efficiency in use.
KEMSA Reforms
38. There has been good progress in the KEMSA reform program which is now receiving support
from several development partners especially the US Government. During the past few years KEMSA has
taken some important steps to strengthen governance and accountability. The Board now has 7
independent members (out of 10) and plans are underway to include Counties in the Board. The internal
audit department established in 2008 has been strengthened and it reports to the Board. An integrity
testing program has been institutionalized with initial support from the Ethics and Anti-Corruption
Commission. Recently, a web-based whistle blower initiative has been started and citizen’s tracking of
KEMSA supplies through mobile phones is now being put in place. With support from the World Bank
Institute, KEMSA is working with a coalition that includes civil society and private sector to improve
transparency in public procurement of pharmaceuticals.
39. Under the project, procurement capacity building of KEMSA was envisaged, but this could not be
undertaken as the selected firm was blacklisted by the Bank. Therefore, an individual consultant familiar
12
with Bank procedures was selected in October 2011 to provide hands on capacity building to KEMSA
procurement team. This assignment was successfully completed in May 2012. The consultancy
assignment for developing a procurement manual for KEMSA was also successfully completed and the
manual is now being used. KEMSA also successfully concluded the procurement of E-filing of records
under its Enterprise Resource Planning (ERP) and filing equipment. The servers and filing equipment
procured under the project are now fully operational. To enhance mutual accountability, performance
based Memorandum of Understanding clearly stating roles and responsibilities of KEMSA and erstwhile
Ministries of Health were prepared by a consultant under the project. However, due to the on-going
devolution and the integration of two Ministries of Health in to one, it was agreed that the scope of this
consultant selected through competitive process will be expanded to specify the role of Counties. The
Logistics Management Information System within the ERP was developed and being used after the
preliminary testing. However, this requires further updating in the light of devolution.
40. Two activities originally envisaged under the project were dropped. As KEMSA has well
established protocol for quality assurance that includes testing of each batch by a WHO pre-qualified
testing laboratory, the pre-shipment inspection envisaged under the project was dropped. Similarly,
USAID has supported the development of a marketing plan for the supplementary services division of
KEMSA and hence this activity was also dropped from the scope of the project. As a result, a saving of
US$ 424,206 is still available with KEMSA which will be reprogramed with focus on responding to the
devolved health system.
Financial Management:
41. The FM arrangements are assessed as adequate. The project has sufficient accounting capacity at
the Health SWAP and HSSF Secretariats and at the County level. There are no outstanding audit issues,
and the quarterly Interim Financial Reports (IFRs) and annual audit reports are submitted to the Bank on
time and in form and content is satisfactory to the Bank.
42. The health sector has been devolved to the County level in line with the implementation of the
new constitution. The MoH is working with various stakeholders to agree on country-level Public
Financial Management (PFM) arrangements that would be applicable in managing funds flows to the
devolved levels in line with the new PFM laws and other relevant laws. In the transition period, the
program will continue to disburse funds in line with the agreed FM arrangements as per the Financing
Agreement and the Project Appraisal Document.
43. The second in-depth review was conducted by the Internal Audit Department (IAD) in May 2013.
Unlike the first in-depth review of FY11/12 done by IAD, this one was conducted with support from
consultants from Deloitte. The draft report has now been consolidated by IAD and validated. The
validation exercise did not reveal any cases of suspected fraud and corruption. Nevertheless, the draft
report reveals certain internal control weaknesses, which the MoH needs to address once the final audit
report is released by IAD after taking management response provided by the Ministry of Health. The
program is subject to stringent audit reviews which include quarterly reviews by IIFRA, half-year audits
by IAD, annual audits by KENAO and risk-based FM reviews by the Bank FM team. These reviews are
deemed to be robust enough to manage the assessed project fiduciary risks.

13
Procurement: 44. To complement the day-to-day implementation support and contract prior reviews, the Bank
conducted a procurement post review mission on June 26, 2013, mainly focusing on KEMSA operations
whose procurement activities had not been reviewed in previous missions. The mission reviewed four out
of thirteen contracts undertaken by KEMSA since the commencement of the Project. Over this period, the
Ministry of Public Health and Sanitation (MOPHS) had not undertaken any post review contracts.
45. The mission noted that KEMSA had made significant progress in the procurement of EMMS
goods and the implementation of the Procurement Plan. Improvements were noted in procurement
processes and compliance mainly in the areas of procurement planning, preparation of bidding
documents, publication of contracts award, and more importantly procurement filing and records
management. Procurement records are stored in a systematic and structured manner and in locations that
are secure and accessible making retrieval of documents faster while maintaining information security
and confidentiality. Internal processing of contract awards has also improved considerably. The mission
advised KEMSA to fast-track the on-going investigations and audit on the losses incurred following the
fire incident so as to obtain a clear picture of its financial and security exposure on the matter. The
mission further observed that the Fiduciary Review conducted by IIFRA for the 3rd quarter of the last
financial year rated the overall procurement performance as ‘satisfactory’. This is in tandem with the
Bank’s review findings.
46. However a few challenges that require KEMSA’s attention were noted during the mission among
them including:
(a) Evaluation of bids. As observed in previous missions, delays in the evaluation of bids still persists
leading to multiple extensions of bid validity. As noted earlier, such delays usually lead to cancellation of bids, lack of confidence in the procurement process and at times suspicions of bid manipulation issues that are likely to erode the gains made in the reform process.
(b) Quality of bid evaluation reports. It was observed that there have been increased instances of cancelations of contracts awarded to suppliers on account of non-performance of contracts. This is mainly attributed to lack of due diligence on the part of the evaluators to establish the reasonableness and consistency in the pricing of bids submitted by bidders and at times inadequate post-qualification of responsive bidders prior to the award of contract.
(c) Weak contract administration and management. It was observed that there is need to improve on the administration, enforcement and monitoring of contract performance to so as to ensure that contracts are not only executed in accordance with the terms and conditions of contract, but that in case of default, penalties and other remedies are instituted against the defaulting suppliers.
(d) Delays in processing payment to suppliers. This was attributed to poor cash flow and administrative bureaucracy in the parent ministry.
Safeguard Policies
47. There has been progress in the implementation of Social Safeguards. The Consultant agency
selected for the development of Vulnerable and Marginalized Peoples Plans (VMPPs) jointly for three on-
going operations in the health sector (KHSSP, Total War Against AIDs and East Africa Public Health
Laboratory Networking Project) has completed the consultations in 13 selected vulnerable and
marginalized communities and prepared draft plans for each of the three health operations. The MoH has
disclosed the draft report and plans at its Web site and a broad set of actions have been identified to
improve services to vulnerable and marginalized populations. With the on-going devolution it is now

14
important for the Ministry of Health to consult with Counties where vulnerable and marginalized
populations are residing and to provide technical assistance for implementation.
48. Environmental and Waste Management. The project was to support the implementation of the
National Health Care Waste Management plan by helping to set up pilot sites in 5 county hospitals
(Narok, Kitale, Isiolo, Makindu and Voi) networking with 25 level 2 and 3 primary health care facilities
per site. The scope of support included provision of incinerators for the hospitals and commodities to
selected facilities and training to the facility staff to improve health care waste management practices
including establishment or strengthening of infection prevention and control committees in these
facilities.
49. The MoH team has completed a rapid situation analysis of the pilot sites agreed in February
2013 and KEMSA has completed procurement of consumables at an estimated cost of KSh 29. 7 million
(US$ 350,000 equivalent). However, the data from situation analysis could not be analysed and procured
commodities could not to be distributed to facilities as the pilot activities were delayed and now the
responsibility for managing these health facilities rests with the Counties. Further, the civil works
required for incinerators were to be provided by the MoH through the Ministry of Public Works. Under
the devolved health system this is no longer possible and it hence was agreed that the MoH team will
consult with respective counties and implement the pilot only in locations where the County governments
are willing to provide civil works infrastructure. It was agreed that the remaining resources allocated for
this component (US$ 650,000) will be retained and a final decision on continuing this sub component will
be made by December 31, 2013. The option of incentivizing desirable health care waste management
practices in health facilities through a systems approach based on results will also be explored which will
call for reprogramming of the allocated resources.
50. The Bank team appreciates the effort made by the RBF core team to include compliance with
health care waste management as one of the crosscutting quality indicators in the Samburu pilot. Based on
positive contribution of RBF in improving practices, the recent decision taken by the MoH to scale-up
this approach to 20 Arid and Semi-Arid Counties is expected to positively contribute to better health care
waste management. Such support will be in line with the devolved health system.
Restructuring of the Project and preparation for the proposed Additional Financing
51. The restructuring of the project and preparation for the proposed additional financing focused on
the four key thematic areas that respond to commitments made by the Government of Kenya to “improve
health outcomes among the poor” and eliminate payments at the point of service delivery for essential
health care, especially maternal health. There will be “stronger results focus” for the proposed activities
with emphasis on quality. They will be complemented by supporting on-going county capacity building
initiatives started by Government of Kenya.
52. Taking into consideration the disbursement and committed expenditures, it is estimated that
around USD50 million will still be available under the original project and IDA supported Crisis
Response Window (CRW). With the proposed additional financing consisting of a USD20 million grant
from Health Results Innovation Trust Fund (HRITF) and USD30 million from IDA, the total resources
available for the proposed program activities will be around USD100 million. It was agreed that the
remaining resources under the CRW will focus on counties prone to drought in northern Kenya and
15
implementation arrangements will be better integrated with existing health systems to ensure better
sustainability.
Free maternity care:
53. The President’s initiative for free maternity care highlights the strong commitment of the
government to improve maternal and new-born health outcomes. The MoH has prepared a comprehensive
concept note with estimated costs for the initiative which proposes to make this important commitment
results-based giving attention to both coverage and quality. There is already positive citizen’s response to
this initiative. The concept note also proposes to address some important barriers for delivering free
maternity care especially the lack of staff with midwifery skills and some gaps in service delivery
infrastructure. While such inputs are important, they should be better aligned with the current devolved
health system. The MoH can encourage facilities and counties to find local solutions by providing
flexibility in using reimbursed resources to improve delivery of maternal health services and by providing
essential commodities, especially family planning products. Partnerships with faith based organizations
and private sector also need to be nurtured to further improve the delivery and innovations such as
contracting in midwives and using under-utilized beds in health centres as maternity waiting facilities
needs to be explored, especially in counties with serious access problems. These measures need to be
complemented by strong demand side interventions to improve community behaviors and network with
traditional birth attendants. The mission is pleased to note priority attention being given to monitoring
and evaluation in this important initiative to inform the progress to all key stakeholders.
54. To move forward on this important initiative, it was agreed that the MoH will develop an
operational manual in consultation with counties and other key stakeholders. This will clarify the roles
and responsibilities of different players and describe how the program will operate. It is also important to
finalize the M&E arrangements with a limited set of indicators which will be a sub set of the Health
Management Information System (HMIS) and complimented by well-targeted independent assessments to
provide assurance on service coverage and quality.
55. Agreed actions for appraisal:
a) Develop an operational manual for the free maternity care initiative building on the concept note.
b) Update the costing and estimates of financing gap covering both reimbursements linked to results
and critical inputs especially midwifery services and demand side strategies.
c) Finalize the M&E arrangements including external verification and semi-annual national maternal
death review.
Results based financing (RBF)
56. The Bank team is very pleased to see on-going efforts of MoH to harmonize all RBF initiatives in
the health sector and systematically build management capacity to implement such initiatives through
international and well-targeted hands on county based training involving actual implementers from the
RBF pilot. During the past few months, the MoH has introduced RBF in West Pokot and Lamu counties
and is preparing plans for further scale-up to cover all arid and semi-arid counties of Kenya.

16
57. There is a strong partnership between the MoH core team leading the RBF initiative and USAID
funded APHIA Plus implementing partners, and protocols being used as well as implementation
challenges being faced are similar. In addition to Samburu, the APHIA Plus Western has been
implementing the RBF in two more districts and another pilot proposed in Isiolo County is in final stages
of design. The Bank team believes that the initial verification process could be well integrated with
supportive supervision rather than creating parallel structures. Such focused approach will strengthen the
supervision and make it more objective as well as reduce costs. This also can be used for making results
based reimbursements to county health teams for effectively performing their supportive supervision role.
The verification, however, needs to be complemented by appropriate arrangements for external and
community validation.
58. With the proposed scale-up of RBF initiatives and government commitment to make the free
maternity care results based, there is need for a stronger institutional base well embedded in the new MoH
structures under the strategic planning and financing division. With the devolved health system, the role
of Counties needs to be clearly articulated in the design of RBF as the purchaser and an appropriate sub
county level entity needs to be identified for leading the quarterly verification process. Further, clearly
defined community and periodic independent validation arrangements need to be introduced. The end-line
survey of the Samburu pilot covering both quantitative and qualitative aspects will be completed by
December 2013 and will provide some useful insights for the future design of RBF in Kenya and the
Bank will also support rigorous independent evaluation of the larger program.
59. Agreed actions for appraisal:
a) Clearly define institutional arrangements for RBF in MoH including engagement of the Counties
and create a technical working group for RBF under the Health Financing Interagency
Consultative Committee (ICC) with a clear TOR.
b) Update operational manual clearly defining roles and responsibilities of counties and
strengthened community validation including refining indicators that posed some challenges in
measurement as observed from the Samburu pilot.
c) Define the role of Independent Integrated Fiduciary Review Agency in RBF and accordingly
enhance their scope of work.
d) Develop a standard protocol for periodic external verification of results from RBF facilities..
Health Insurance Subsidies for the Poor (HISP):
60. As a part of its commitment to achieve Universal Health Care, the Government of Kenya has
begun preparation for the phase I of the Health Insurance Subsidies for the Poor (HISP). The Bank team
met with the National Hospital Insurance Fund (NHIF) to discuss the plans for the HISP rollout. The
team was very impressed with the work that has been completed in preparing for the pilot rollout
including a comprehensive operational manual and well-articulated work plan. The plan is to target 300
households under the pilot program in selected areas identified based on agreed criteria, which match
poor households with pre-qualified health facilities. The proposed mechanism of using the existing social
protection database for identification is quite appropriate and reduces unnecessary duplication. Making
this mechanism work at the operational level and matching the beneficiaries with facilities however still
needs to be explored more carefully during the next few months. Current estimates of the program are
that the scheme will cost approximately $50 per beneficiary which, even accounting for possible

17
economies of scale, may be unsustainable when the program is rolled out nationwide. These estimates
and benefit package need to be carefully reviewed based on experiences of civil servants scheme which
also provides similar package. The work plan for the pilot roll-out is quite comprehensive and most
activities were on track as planned. The team agreed with the Government, that to ensure timely initiation
of the pilot roll-out, a few key steps need to be undertaken. These include:
(i) Review the cost of the basic benefit package based on the data from the civil servants scheme.
(ii) The signing of the Memorandum of Understanding between the NHIF and the MoH.
61. The team also requested that in preparation for the pilot roll-out, field visits be conducted early
October in 2 counties pre-selected for the pilot – one where there are several pre-qualified facilities in an
area where the extreme poor reside and another where there are only limited pre-qualified facilities – to
explore the mechanism for identifying target households with community participation and identify any
issues or bottlenecks that may arise during pilot implementation.
County Capacity Building:
62. The team clarified that Bank Credit could be used for a standardized competency-based County
capacity building initiative systematically implemented through a network of institutions led by the
Kenya School of Government. This can result in a formal competency certification for the health service
managers at County and facility levels. It was agreed that a concept note with work plan and costing will
be prepared. This activity can also support creation of strategic program management units at counties
with expertize in health economics, program management, financial management, procurement and
M&E.
Scaling up nutrition:
63. The Bank has provided support to Kenya through the Crisis Response Window to respond to high
levels of malnutrition in the drought affected areas. This is part of its broader response to the recent horn
of Arica crisis and included targeted support fully integrated with on-going nutrition interventions to 22
districts from 18 counties. This was implemented by the Division of Nutrition, MOH with support from
UNICEF and World Food Program (WFP) in line with existing arrangements. There has been notable
reduction in admission of acute severe malnutrition cases in project supported districts and hence more
emphasis is now being given to community based interventions to deal with moderate malnutrition. This
needs to be sustained for some more time and integrated with existing implementation arrangements for
distribution of essential medicines and medical supplies of KEMSA.
64. The Bank team is pleased to see efforts being made by the division of nutrition to support
counties to implement guidelines for use of multi-nutrient-powder and to develop action plans to improve
nutrition outcomes. These inputs however need to be better integrated with on-going integrated strategic
planning and informed by county specific data for identifying priorities and establishing baseline.
65. The overall child nutrition situation in Kenya however needs continued attention, especially the
stubbornly high levels of stunting that have remained more or less constant during the past 2 decades.
This will result in huge productivity loss known to impact future economic gains. While micro-nutrient
deficiencies can be addressed through periodic supplementation or fortification, stunting requires strong

18
cross sectoral approach. Being one of the early signatories of the Scaling up Nutrition (SUN) initiative,
Kenya can provide good leadership for the region in such approaches. Also, at present the periodic
nutrition surveys are limited to drought affected counties and there is little validated information from
other counties except for the DHS carried out once in five years.
66. Agreed action to be completed by appraisal:
a) The Division of Nutrition will prepare a concept note with estimated costs for future support from
the Bank for nutrition as a part of broader integrated response under the SUN initiative.
Disclosure:
67. As per the Bank’s new Access to Information Policy, it was agreed during the wrap-up meeting
that this aide memoire will be disclosed to the public.

19
AGREEMENTS REACHED
Issue Agreement Timeframe Responsibility 1. HSSF under
devolved health system
• Develop comprehensive operational guidelines for conditional cash transfer after consultations with Counties and other key stakeholders
By Negotiations
SWAp Secretariat
2. Delayed start of PPP pilots
• Develop PPPs pilots in consultation with at least two counties (one rural and one urban) will be ready for discussion
By Appraisal SWAp Secretariat
3. Scale-up of Social Accoutnabity
• Finalize the Social Accountability implementer’s manual and operating guidelines and provide technical assistance to counties to implement
By October 31, 2013
SWAp Secretariat
4. Sustained supply of EMMS
• Develop operational guidelines for continuing the pull system of supply in consultation with Counties and other key stakeholders
By Negotiations
MOH and KEMSA
5. Financial Management
• Share the final report of the in-depth audit review. By September 30, 2013
IAD
6. Procurement • Fast-track on-going investigations and audit on the losses due to fire incident
By Appraisal KEMSA
7. KEMSA engagement with Counties
• Develop strategy to enhance the accountability relationship with counties including performance based MOUs
By Negotiations
KEMSA
8. Healthcare Waste Management
• Confirm final decision on using the remaining resources for providing incinerators to pilot locations in consultation with involved counties.
December 31, 2013
MOH
9. Free maternity services
• Develop an operational manual for the free maternity care initiative building on the concept note.
• Update the costing and estimates of financing gap covering both reimbursements linked to results and critical inputs especially midwifery services and demand side strategies.
• Finalize the M&E arrangements including external verification and semi-annual national maternal death review.
By appraisal MOH
10. Results based financing
• Clearly define institutional arrangements for RBF in MoH including engagement of the Counties and create a technical working group for RBF under the Health Financing Interagency Consultative Committee (ICC) Health Financing with a clear TOR.
• Update operational manual clearly defining roles and responsibilities of counties and strengthened community validation including refining indicators that posed some challenges in measurement.
• Define the role of Independent Integrated Fiduciary Review Agency in RBF and accordingly enhance their scope of work.
• Develop protocols for periodic external verification of pilots.
By appraisal MOH
11. Health Insurance Subsides for the Poor
• Review the cost of the basic benefit package based on the data from the civil servants scheme.
• Sign Memorandum of Understanding between the NHIF and the MoH.
By Negotiations
NHIF and MOH
12. Continued support for nutrition
• Prepare a concept note with estimated costs for future support from the Bank for nutrition as a part of broader integrated response under the SUN initiative.
By Appraisal MOH Division of Nutrition

20
ANNEX 1: MISSION PARTICIPANTS
Name Position Mr. Fred H.K. Segor Principal Secretary, Ministry of Health (MoH)
Dr. S. K. Sharif Director of Public Health and Sanitation
Mr. Jackson Kinyanjui Director, External Resources Division, Ministry of Finance
Dr. Annah Wamae Head, Dept of Family Health / MOH
Dr. Rael Mutai Head, HSSF Secretariat / MOH
Dr. Peter Kimuu SWAp Secretariat, MOH
Dr. Mary Wangai SWAp Secretariat, MOH
Dr. Abel Nyakiongora SWAp Secretariat, MOH
Dr. Ruth Kitetu Technical Planning, MOH
Dr. Jackson Omondi Pharmacy, Department of Primary Health Services / MOH
Dr. Simon Kibias Department of Primary Health Services / MOH
Dr. Charles Nzioka Head, Dept. of Health Information Services/ MOH
Mr. Pepela Wanjala DHIS
Dr. Ayub Manya DHIS
Ms. Sophia Karanja DHIS
Ms. Jane Oburu Department of Primary Health Services / MOH
Ms. Terrie Wefafwa Division of Nutrition/ MOH
Ms. Monica Okoth Division of Nutrition/ MOH
Ms. Lucy Gathigi Division of Nutrition/MOH
Ms. Grace Gichohi Division of Nutrition/ MOH
Mr. Daniel Kongai HSSF / MOH
Mr. Ngari Karani Division of Child Health
Mr. Jackson Mureithi MoH
Mr. D. M. Nzoya Planning/ MOH
Mr. Allan Kobiya HSSF/MOH
Dr. Chris Forshaw TA Dept. of Pharmacy
Mr. Per Clausen TA, HSSF /MOH
Dr. Dirk de Coeyere TA SWAp Secretariat/MOH
Dr. Charles Sigei Consultant, IIFRA
Dr. Daraus Bukenya Country Representative, Management Sciences for Health
Mr. John Munyu CEO, KEMSA
Mr. Philip Omondi KEMSA
Mr. Joshua Obell KEMSA
Mr. Kiumbura Githinji KEMSA
Mr. John Kabuchi Procurement Manager, KEMSA
Mr. Samuel Wataku KEMSA
Ms. Evelyn Wachuka KEMSA
21
Mr. Eluid Muriithi KEMSA
Mr. Charles Juma KEMSA
Dr. Cecilia Wandera KEMSA
Ms. Caroline Gichinga KEMSA
Mr. Joel Lehmann Population Council
Dr. Patrick Onyango APHIA plus- Western
Ms. Josephine Lesiamon AMREF – APHIA plus Imarisha
Mr. John Githiaka AMREF – APHIA plus Imarisha
Dr. Annette Getecha AMREF – APHIA plus Imarisha
Mr. Mathieu Joyeux UNICEF
Mr. Henry Neufville UNICEF
Dr. Tomohiko Sugishita JICA
Ms. Shisho Sasada JICA
Mr. Elijah Kinyanjui JICA
Ms. Juliet Maara NHIF
Ms. Josie Muigai IFC
Dr. Edwine Barasa IFC
Dr. Njeri Mwaura IFC
Dr. G.N.V Ramana Task Team Leader, WB
Ms. Wacuka Ikua Operations Officer, World Bank
Ms. Rekha Menon Sector Leader, WB
Ms. Hope Nanshemeza Team Assistant, WB
Ms. Toni Kuguru Consultant, WB
Ms. Isabel Waiyaki Consultant, WB

22
Annex 2
Progress in achievement of KHSSP Results Framework
Intermediate Results and Indicators
Indicator Baseline Achievem
ent
2012 – 13
Target FY
2013
Comments
1. People with access to a basic
package of health nutrition and
population services
0 38,935,80 27,000,000 The project interventions
have a nationwide impact.
2. Facilities receiving HSSF funds
within 15 days of beginning of quarter.
0% 0% 60% Releases are contingent upon
facilities submitting expenditure
statements to districts which in
turn consolidate and submit to
the MOH. Implementation
experiences (including IIFRA
assessments) show that 15 days
is not realistic. This indicator
will be revised.
3. Facilities management committees
having quarterly meetings with
minutes of meetings.
Level 2: 27%
Level 3: 46%
(2004)
83.7% 85% PETS+ survey data
4. Health Personnel receiving training. 0 13,780 6,000 Includes all trainings
provided
5. Level 2 and 3 facilities meeting
minimum staffing norms.
Level 2: 3%
Level
3=34%
No data 40% Based on current MOH
standards and norms
6. Level 2-3 facilities implementing
results based financing initiatives
(number).
0 117 50 Currently being implemented
in three counties (Samburu,
West Pokot and Lamu)
7. Number of beneficiaries receiving
supplementary feeding in the drought
affected areas. (Moderately
malnourished children under five and
moderately malnourished pregnant and
lactating women)
157,4135 556,810 No specific Target was set
8. Performance contract between
KEMSA and MOMS and client
service agreement between KEMSA
and MOHS, established and monitored
on a quarterly basis.
No Drafts
ready.
Yes Drafts need to be revised in
context of devolution.
9. Facilities under pull system sending
their orders during the previous
quarter.
TBD 95% (Q4) - Information reported by
KEMSA
10. Timely reimbursement to KEMSA
documented claims by Ministries of
Health (Percent).
undefined 0% 75% (3
quarters)
There were still delays both
in submission of invoices and
reimbursement.
5 Baseline is for 2011

1
Annex 3 – Detailed Sub Activity-wise expenditure and agreed way forward
Activity Original Allocation
(USD)
Revised Allocation
(USD)
Utilized Committed Balance Comments and way forward
COMPONENT 1 Sub-comp 1.A
1.A.1: Rolling out of HSSF to levels 1-3 in government facilities
11,300,000.00 11,300,000.00 7,304,079.48 3,995,920.52 To date, 787 health centers and 2,427 dispensaries (all public) are receiving HSSF grants with over Ksh. 1 billion and Ksh. 473 million being disbursed respectively.
1.A.2: Pilot and roll-out of HSSF to FBOs 3,000,000.00 3,000,000.00 - 3,000,000.00 Activity not started. Draft MOU outlining proposed implementation arrangements is being developed and FBOs are expected to participate in the RBF scale up.
1.A.3: Pilot contracting of Private providers to make CDF facilities functional
500,000.00 500,000.00 - 500,000.00 Activity not started. No progress on decision made on PPP options that include (i) group contracting out of service improvement to an NGO for one district; (ii) contracting in staff at specific facilities; and (iii) establishing a private entrepreneurial arrangement where interested individuals (nurses) take on the mgmt of the facility on a for profit basis
1.A.4: Performance incentives to health facility management
2,300,000.00 2,300,000.00 124,841.67 2,175,158.33 RBF pilot successfully implemented in 26 health facilities in Samburu with Samburu East and North selected as controls. Key staff in pilot were trained in RBF and the Population Council provided support for capacity building and is leading the evaluation. During the fiscal year RBF was introduced to additional 91 facilities from Samburu, Lamu and West Pokot Counties. RBF will be scaled up into 20 ASAL counties.
1.A.5: Capacity building of Health facility committees and supervisory functions
5,000,000.00 5,000,000.00 1,508.34 4,998,491.66 15 members of DHMT in RBF pilot have received international training in RBF and sensitization and capacity building meetings have been conducted with DHMTs and HFMCs.
1.A.7: Investment in other office equipment 500,000.00 500,000.00 16,257.72 483,742.28 Start up office equipment procured.

2
1.A.8: Support to DHMTs, secretariats for support supervision and operations for the HSSF secretariats and NHSC committee
2,500,000.00 2,500,000.00 2,500,000.00 - To date, 741 DHMTs have received supportive supervision funds.
1.A.9: Score cards, system for citizen's complaints incl. hotline
2,200,000.00 2,200,000.00 196,924.20 2,003,075.80 A 15 month pilot at the Coast covering 9 sites and a FCI study covering Kitui and Nakuru counties were conducted studying community participation, complaint redress and information sharing. A SAc draft manual has been developed and is being finalized for dissemination to the county health providers and management teams.
1.A.10: Development and dissemination to public through communication strategy
2,000,000.00 2,000,000.00 - 2,000,000.00 Activity not started Consultancy is undergoing procurement.
1.A.11: Periodic impact evaluation 200,000.00 200,000.00 - 200,000.00 Activity not started.
1.A.6: Procurement of vehicles including for DOP
3,100,000.00 3,151,295.00 2,950,469.20 200,825.80 Original allocation was $3,100,000. Consolidated with 2.B.3 ($51,295). Exclusive of taxes $1,593,448.49
PPF Refund 1,000,000.00 1,000,000.00 - 1,000,000.00
Sub Total 33,600,000.00 33,651,295.00 10,143,611.41 - 19,356,388.59
COMPONENT 1 Sub-comp 1.B
1.B.1: Health financing strategy implementation focus on extending access to poor
1,500,000.00 1,500,000.00 - 1,500,000.00 Activity not started. A new concept note for providing health insurance subsidies to the poor has been prepared (HISP). NHIF is working with the SPS in beneficiary selection. Pre-test regions are being determined based on availability of accredited NHIF facilities and OVC enrollment with the aim of enrolling 300 beneficiaries per county.
1.B.2: Household surveys, updating of costing at community level
300,000.00 300,000.00 - 300,000.00 Activity not started. Activity was conducted under a different mechanism.
1.B 3: Capacity building of key HF institutions
500,000.00 500,000.00 17,681.64 482,318.36 A flagship course was offered and Health Financing Workshop (Nanyuki).
1.B.4: Support to district hospitals for improved district referral
2,600,000.00 2,600,000.00 8,109.82 2,591,890.18 Activity not started
1.B.5: Capacity building for referral management
400,000.00 400,000.00 21,273.63 378,726.37 Baseline is complete. No further progress. Poor response to ambulance program.

3
1.B.6: Piloting of model for waste management at health facilities
1,000,000.00 1,000,000.00 399,390.92 600,609.08 5 referral sites have been identified and commodities including personal protection equipment have been procured. A health care worker management training manual and on the job manual are being developed in collaboration with PATH. This activity will be revisited during the AF preparation as the function has been devolved.
1.B.7: Support for SWAp secretariat for strengthened sector coordination
500,000.00 500,000.00 171,971.55 328,028.45 The Bank has provided technical assistance to the Ministry of Medical Services to develop a proposal to provide UHC to indigent populations and short term consultants to support the Joint National Assessment of Sector Strategy Process and SAc and JANS. Other advisors provided by DANIDA.
1.B.8: Ministerial staff trained in WB procurement procedures and financial management
150,000.00 150,000.00 19,307.00 130,693.00 Staff and program managers were sent for procurement training. FM staff received training at the Bank and Kenya School of Gov't.
1.B.9: Strengthening M & E 210,000.00 210,000.00 15,558.89 194,441.11 Mobile phones and SIM cards were provided for DHMIS.
1.B.10: Strengthening HMIS 625,000.00 625,000.00 26,755.60 598,244.40 Data bundles for internet connectivity were procured for the DHMTs.
1.B.11: Regular fiduciary and performance 4,000,000.00 4,000,000.00 1,360,037.31 2,639,962.69 Quarterly, semi-annual and annual fiduciary reports, value for money assessments and procurement audits have been undertaken by IIFRA providing strong oversight and social accountability to the MoH. . The IIFRA has completed 7 quarterly assessments covering 4 quarters of FY 2011-12 and 3 quarters covering FY 2012-13.
1.B.12: Strengthened audit capacity 500,000.00 500,000.00 60,668.21 439,331.79 The IFR are being streamlined and being shared on time. The external audit report covering HSSF 2011-12 by KENAO was received on time. An internal audit team is leading an in-depth review.
Sub total 12,285,000.00 12,285,000.00 2,100,754.58 - 10,184,245.42

4
Procurement of essential health and nutrition supplements through UNICEF
12,800,000.00 12,800,000.00 12,800,000.00 - Supplements cover 18 counties spread over 22 districts. To date over 76,000 boxes of RUSF and 75,000 boxes of RUTF have been procured by UNICEF and WFP respectively. Procurement arrangements were revised to procure less RUTF and more RUSF as cases of SAM have decreased.
Sub total 12,800,000.00 12,800,000.00 12,800,000.00 - -
Component 1 Total 58,685,000.00 58,736,295.00 25,044,365.99 - 29,540,634.01
COMPONENT 2 Sub Comp 2.A
2.A.1: Essential medicines and medical supplies levels 1 to 3 (incl sub-district hosp)
40,000,000.00 40,000,000.00 40,000,000.00 - Pharmaceutical and non-pharmaceutical commodities have been procured (approximately Ksh. 2.87 billion and 1.67 billion respectively). Ksh. 9,165,775 being 20% contract variations moved to CRW.
2.A.3: Supplementary commodities for hospitals
4,000,000.00 4,000,000.00 3,505,409.39 494,590.61 Pharmaceutical and non-pharmaceutical commodities were procured (approximately Ksh. 175 million and 121 million respectively)
2.A.2.: Warehousing and distribution costs 4,000,000.00 4,000,000.00 1,027,194.95 2,972,805.05 KEMSA operation and warehousing costs were covered.
Sub total 48,000,000.00 48,000,000.00 44,532,604.34 - 3,467,395.66
AF CRW
2.A.4: Essential medicines and medical supplies levels
40,000,000.00 40,000,000.00 28,994,505.52 11,005,494.48 First and second line anti-TB drugs were procured.
2.A.5: Warehousing and distribution costs 4,000,000.00 4,000,000.00 - 4,000,000.00
Sub total 44,000,000.00 44,000,000.00 28,994,505.52 - 15,005,494.48
COMPONENT 2 Sub Comp 2.B
2.B.1: Establish drawing rights for all facilities
8,800.00 8,800.00 - 8,800.00 95% of the health facilities place orders for EMMS under the "pull" system.
2.B.2: TA to analyze data from KEMSA ERP system
5,400.00 5,400.00 - 5,400.00 Activity dropped - available for re-allocation
2.B.3: Procurement of 2 vehicles for Pharmacy department
51,295.00 - - - Original allocation of $51,295 was consolidated with 1.A 6
2.B.4: Review and printing of non-pharm specifications
53,300.00 53,300.00 58,464.08 (5,164.08) Dept of Primary care workers attended 3 workshops on reviewing non-pharm specifications.

5
2.B.5: Printing of all transaction forms required for the supply chain
1,402,000.00 1,402,000.00 330,133.33 27,220.51 1,044,646.16 KEMSA - forms delivered (Ksh. 330,133); MoH - final payment pending for procurement of forms (Ksh. 27,220)
2.B.6: Dissemination of STGs, EMLs and other essential guidelines and tools
214,400.00 214,400.00 - 214,400.00 Activity dropped - available for re-allocation
2.B.7: Trainings for health facility workers for capacity building in EMMS management, storage and appropriate use
2,683,200.00 2,683,200.00 345,233.63 2,337,966.37 The last cycle of ToT in managing the pull system was done during January 2013 for 43 district managers and is being following by facility level staff for inventory management. A total of 291/329 ToTs and 2473/2568 health workers were trained between May 2011 and February 2013.
2.B.8 Training and capacity building in EMMS management storage and use country wide
22,800.00 22,800.00 22,800.00 Activity done under 2.B.7 - available for re-allocation
2.B. 9: Training of DHMTs and HMTs on supportive supervision for EMMS nation wide
926,805.00 926,805.00 - 926,805.00 Activity dropped. Now a devolved function to be responsibility of counties.
2.B.10: KEMSA staff trained on WB procurement procedures and financial management
50,000.00 50,000.00 50,000.00 Activity not started.
2.B.11: Hire TA to develop performance-based MOUs between KEMSA and other parties
3,000.00 20,000.00 18,791.09 1,208.91 USD 17,000 re-allocated to this activity. MOU is under review given new context of devolution.
2.B.12: Hire pre-inspection firm for quality assurance testing
460,000.00 0.00 - Activity dropped. Funds re-allocated.
2.B.13: Develop marketing plan for KEMSA for supplementary services for levels 4-5
30,000.00 0.00 - Activity dropped. Funds re-allocated.
2.B.14 Develop SOPs for procurement records and retrieval system.
7,000.00 22,963.00 20,261.60 2,701.40 Re-allocation of $15,963. Contract awarded to Tetralink and Taylor Assoc and procurement manual now in use.
2.B.15 Develop E-filing process and ERP system adapted for e-filing
7,000.00 20,000.00 23,200.00 (3,200.00) Activity redefined to include purchase of servers. E-filing implemented and DMS servers are operational.
2.B.16: Procurement of filing equipment 140,000.00 140,000.00 105,542.34 34,457.66 Items procured delivered and currently in use (i.e. mobile shelving units, boxes and dividers, and metal racks)
2.B.17: Develop LMIS module 50,000.00 50,000.00 41,618.07 8,381.93 Testing of LMIS has been undertaken with stakeholders and module is now in use.

6
Sub Total 6,115,000.00 5,619,668.00 943,244.14 27,220.51 4,649,203.35 -
New Activity
On job training for KEMSA - 30,380.00 30,380.00 - Consultant contracted for training in September 2011 and successfully concluded May 2012.
Funds that have not been re-allocated under reforms (Activities B10-B17)
- 413,657.00 413,657.00 Funds available for re-allocation
Sub Total - 444,037.00 30,380.00 - 413,657.00
Component 2 Total 98,115,000.00 98,063,705.00 74,500,734.00 27,220.51 23,535,750.49
Total Component 1 and 2 156,800,000.00 156,800,000.00 99,545,099.99 27,220.51 53,076,384.50

1
Annex 4: Disbursement for KHSSP
Activity
IDA Allocated
(USD)
IDA Disbursed
(USD)
Special
Commitments
(USD)
Balance
(USD) Comments
HSSF: goods, services, training and
operating costs
Activities 1.A.1 - 1.A.11 (excl. 1.A.6)
29,070,200.00 8,669,103.90 - 20,401,096.10
Vehicles Part A.2 (a)(ii)
Activity 1.A.6
3,652,800.00 3,203,656.08 449,143.92
PPF Refinancing 1,065,400.00 4,425.58 1,060,974.42
Goods, consultants' services, training and operating costs Prt A.2/b/c/d/e & P B2 Activities 1.B.1 - 1.B.12, 2.B.13 - 2.B.17 (incl new KEMSA activity)
18,568,400.00 3,015,718.85 15,552,681.15
EMMS Goods Part B1(a)
Activities 2.A.1 - 2.A.4 (excl 2.A.2)
82,644,600.00 35,411,475.06 3,893,100.41 43,340,024.53
KEMSA Operating Costs Part B1(b)
Activities 2.A.2 and 2.A.5
8,066,600.00 863,473.06 - 7,203,126.94
Goods, services and operating costs
PrtA.3 and A.4
Procurement of essential health and
nutrition supplements through UNICEF
12,328,200.00 - - 12,328,200.00
UN Advances
Procurement of essential health and
nutrition supplements through UNICEF
12,818,697.12 (12,818,697.12) UNICEF has recently submitted the
documented distribution
TOTAL 155,396,200.00 63,986,549.65 3,893,100.41 87,516,549.94 The balance includes Designated
Accounts (advances disbursed)
totalling $32,758,925.72


















