AHM Governance and Regulation
469
AHM 510 : Health Plans : Governance and Regulation AHM 510 Health Plans: Governance and Regulation Page 1 of 469
-
Upload
senthilj82 -
Category
Documents
-
view
51 -
download
6
Transcript of AHM Governance and Regulation

AHM 510 : Health Plans : Governance and Regulation
AHM 510 Health Plans: Governance and Regulation
Page 1 of 469

AHM 510 : Health Plans : Governance and Regulation
AHM 510: Syllabus
AHM 510 describes the formation, types, and structure of health plans. It also addresses the role of health plans in government-sponsored programs, the impact of fraud and abuse, how health plans make decisions about their purpose and overall direction, and the role of public policy in health plans today.
Assignment 1: Environmental ForcesReading A Environmental Forces
Assignment 2: Legal Organization of health plansReading A Legal Organization of health plans
Assignment 3: Formation and Structure of health plansReading A Corporate Restructuring and Corporate TransactionsReading B Health Plan Structures and Arrangements
Assignment 4: Overview of Laws and RegulationsReading A Perspective and Overview of State and Federal LawsReading B Regulatory Agencies and health plan
Assignment 5: State Regulation of Health Plans: Part 1Reading A State HMO and Other Types of Health Plan LawsReading B State Mandates and Regulation of the Health Plan-Provider Relationship
Assignment 6: State Regulation of Health Plans: Part 2Reading A Other Laws That Apply to Health PlansReading B Workers' Compensation ProgramsReading C Pharmacy Laws and Legal IssuesReading D Market Conduct Examinations and Mechanisms for Enforcement
Assignment 7: Federal Regulation of Health PlansReading A Federal Regulation of Health PlansReading B Antitrust Concerns and Health PlansReading C ERISA and Health Plans
Assignment 8: Federal Government as PurchaserReading A Federal Government as Purchaser: Overview, TRICARE, and FEHBPReading B Medicare and Health PlansReading C Joint Federal-State Healthcare Programs (Medicaid, Programs of AllInclusive Care for the Elderly, and the State Children's Health Insurance Program)
Page 2 of 469

AHM 510 : Health Plans : Governance and Regulation
Assignment 9: Fraud and AbuseReading A Fraud and Abuse
Assignment 10: Governance: Structure and StrategyReading A The Components of Governance in a Health PlanReading B Strategic Planning in Health PlansReading C Key Strategic Issues for Health Plans
Assignment 11: Governance: Accountability and LeadershipReading A Governance: Accountability and Leadership
Assignment 12: Key Legal Issues in Health PlanReading A Key Legal Issues in Health Plan
Assignment 13: Public Policy and Changing EnvironmentReading A Public Policy from the Health Plan PerspectiveReading B Changing Environment and Emerging Trends in Health Plan Industry
Page 3 of 469

AHM 510 : Health Plans : Governance and Regulation
AHM 510: Course Objectives
This course describes the formation, types, and structure of MCOs. It addresses the role of health plans in government-sponsored pro-grams, the impact of fraud and abuse, how the purpose of an individual health plan is determined, and the role of public policy in the health plan industry. You will learn:
Assignment 1: Environmental Forces
Reading 1A: Environmental Forces
• Name and describe several major factors shaping the environment of health plans • Describe the players in health plan and how their interests affect the way they influence the healthcare environment • Explain the influences accreditation organizations and the media exert over the financing and delivery of healthcare • Describe several possible governance responses that health plans make to deal with their changing environment
Assignment 2: Legal Organization of Health Plans
Reading 2A: Legal Organization of Health Plans
• Explain the distinguishing features of a corporation and a limited liability company • Describe the key features and differences between a for-profit company and a not-for-profit company • Describe the differences between a publicly traded stock company and a privately held stock company • Describe the key features and differences between a stock company and a mutual company
Assignment 3: Formation and Structure of health plans
Reading 3A: Corporate Restructuring and Corporate Transactions
• Describe the options available to mutual companies seeking access to capital, strategic partnerships, and other corporate transactions • Describe the issues that a not-for-profit entity must address when converting to for-profit status or when engaging in other transactions with for-profit entities • Explain how health plans use reorganization and reengineering to improve performance • Distinguish between strategic partnerships, joint ventures, acquisitions, and mergers
Reading 3B: Health Plan Structures and Arrangements
• Identify and describe the various types of sponsors of health plans
Page 4 of 469

AHM 510 : Health Plans : Governance and Regulation
• Discuss the objectives of providers in health plan structures and arrangements • Discuss the impact of changes in health plan structures and arrangements on regulation • Differentiate between horizontal, vertical, and conglomerate integration • Differentiate between structural, virtual, and operational integration • Explain how strategic, marketplace, and regulatory issues can shape health plan structures and arrangements • Describe various arrangements employers use to provide healthcare benefit plans for their employees
Assignment 4: Overview of Laws and Regulations
Reading 4A: Perspective and Overview of State and Federal Laws
• Describe the sources of law in the United States • Explain the significance of the HMO Act of 1973 in the development of managed care • Name the federal laws that stimulated health plan participation in Medicare and Medicaid • Describe the provisions of the Health Insurance Portability and Accountability Act of 1996 (HIPAA) of major interest to health plans • Describe the aspects of a health plan on which state regulations usually focus
Reading 4B: Regulatory Agencies and Health Plan
• Explain the role of HCFA in regulating healthcare • Describe the role of the Department of Labor in regulating health plans • Explain the methods states use to delegate regulatory authority for health plans to state agencies
Assignment 5: State Regulation of Health Plans: Part I
Reading 5A: State HMO and Other Types of Health Plan Laws
• Describe the major provisions of the NAIC HMO Model Act • Describe the types of state regulation that apply to PPO, URO, TPA, PSO, and POS products • Explain the need for the Risk-Based Capital for Health Organizations Model Act and the risk-based capital formula
Reading 5B: State Mandates and Regulation of the MCO-Provider Relationship
• Describe the difference between a mandated benefit and a mandated provider law • Give examples and explain the purpose of several mandated benefit laws • Describe the problems with applying any willing provider laws to certain types of health plans • Explain why state mandates often increase the cost of healthcare services provided by health plans
Page 5 of 469

AHM 510 : Health Plans : Governance and Regulation
Assignment 6: State Regulation of Health Plans: Part II
Reading 6A: Other Laws That Apply to Health Plans
• Describe the various types of state laws, other than HMO and insurance laws, that apply to health plan products • Explain how states regulate agent licensing, marketing activities, and advertising • Describe common types of general insurance laws that apply to health plans
Reading 6B: Workers' Compensation Programs
• Describe the kinds of benefits injured employees receive under workers' compensation • List several ways in which workers' compensation differs from other types of healthcare coverage • Describe how state laws can limit the use of health plan to provide workers' compensation benefits • Describe some of the common features of workers' compensation managed care plans • Describe the features of an integrated health and disability plan
Reading 6C: Pharmacy Laws and Legal Issues
• Describe the various types of open pharmacy laws • Describe how states regulate mail-order/ mail service pharmacy programs • Describe how states regulate use of formularies and generic substitution • Explain the benefit exclusions for an experimental drug, an investigational drug, and the off-label use of a drug • Describe how the Nonprofit Institutions Act applies to prescription drug pricing • Describe how states regulate an health plan's use of drug utilization review programs
Reading 6D: Market Conduct Examinations and Mechanisms for Enforcement
• List the operations that a state insurance department reviews in conducting a market conduct examination • Describe the enforcement mechanisms available to states to address violations of law
Assignment 7: Federal Regulation of Health Plans
Reading 7A: Federal Regulation of Health Plans
• Describe some of the operational and quality requirements that federally qualified HMOs must meet • Explain some of the administrative burdens that the Health Insurance Portability and Accountability Act of 1996 (HIPAA) imposes on health plans • Describe the general provisions of the Mental Health Parity Act of 1996 and the Newborns' and Mothers' Health Protection Act of 1996
Page 6 of 469

AHM 510 : Health Plans : Governance and Regulation
• Explain several typical applications to health plan of the Americans with Disabilities Act
Reading 7B: Antitrust Concerns and Health Plans
• Describe the three major federal laws that regulate business activities to prevent antitrust actions • Describe the difference between the per se rule and the rule of reason • Explain the applications of antitrust law in health plan-provider contracting • Explain the relevance of antitrust in mergers and acquisitions • Identify the issues that the 1994 DOJ and FTC guidelines addressed • Explain the procedures the DOJ and FTC follow for their enforcement proceedings
Reading 7C: ERISA and Health Plans
• Describe ERISA's documentation, reporting, and disclosure requirements • Describe the minimum standards of conduct (the fiduciary duties) applicable to ERISA plan fiduciaries • Describe the claims procedures required under ERISA and the standards of review that courts apply in deciding disputed claims • Describe how ERISA preemption has been applied by the courts to: utilization review and credentialing decisions made by health plans; mistaken verification of eligibility by an employer or health plan to a healthcare provider; entities that perform administrative functions under an ASO contract; and provider networks that contract to provide healthcare services to either health plans or self-funded employers on a capitated basis
Assignment 8: Federal Government as Purchaser
Reading 8A: Federal Government as Purchaser: Overview, TRICARE, and FEHBP
• Explain the government's dual role as purchaser and regulator of healthcare services • Describe the evolution of the military health services system from CHAMPUS to TRICARE, and describe TRICARE's triple benefit structure • List the primary features of the Federal Employees Health Benefits Program (FEHBP) • Describe how actions taken by the Office of Personnel Management (OPM) have a positive influence on FEHBP
Reading 8B: Medicare and health plan
• Describe the types of Medicare health plan contracts • Explain the certification process for a Medicare PSO • List the three ways that payment rates will be determined for health plans under Medicare + Choice • Explain how a Medicare Medical Savings Account works • Describe health plan contracting standards under the Medicare + Choice program
Page 7 of 469

AHM 510 : Health Plans : Governance and Regulation
• Provide examples of Medicare marketing restrictions
Reading 8C: Joint Federal-State Healthcare Programs
• Explain the roles of the federal and state governments in the operation of the Medicaid program • Describe the Medicaid services mandated by the federal government • Describe effects of the Balanced Budget Act 1997on regulation and operation of Medicaid managed care programs • Name the types of managed care entities that can contract to provide Medicaid services • Explain the purpose of Section 1915(b) and Section 1115 waivers • Explain how states can mandate Medicaid managed care without obtaining a waiver • Explain the role of Programs of All-Inclusive Care for the Elderly (PACE) • Discuss the purpose and options for implementation of the State Children's Health Insurance Program (SCHIP)
Assignment 9: Fraud and Abuse
Reading 9A: Fraud and Abuse
• Define the terms fraud and abuse • Describe how different types of compensation arrangements can lead to different kinds of fraud and abuse • List and describe the federal laws that regulate healthcare fraud and abuse, and identify the federal agency responsible for enforcing them • Describe the penalties that may be imposed for violating the federal fraud and abuse laws • Discuss some of the steps health plans can take to reduce fraud and abuse
Assignment 10: Governance: Structure and Strategy
Reading 10A: The Components of Governance in a Health Plan
• Explain the purpose of governance in a health plan • Describe the roles and responsibilities of the board of directors • Explain how organizational variations affect board structure and operation • List the three steps in a board risk management program • Describe the roles of shareholders/members and providers in governance • Discuss the roles and responsibilities of the CEO and other senior management
Reading 10B: Strategic Planning in Health Plans
• Define strategic planning • Explain why strategic planning is important to a health plan • Describe the four primary activities in strategic planning • Explain the importance of input and ownership in strategic planning
Reading 10C: Key Strategic Issues for Health Plans
Page 8 of 469

AHM 510 : Health Plans : Governance and Regulation
• Identify and describe the key strategic issues faced by health plans • Give examples of how key strategic issues are interrelated in the strategic planning process
Assignment 11: Governance: Accountability and Leadership
Reading 11A: Governance: Accountability and Leadership
• Discuss accountability among the stakeholders in managed care • Explain several implications of accountability on health plan leadership and governance • Describe the essential elements of an effective health plan compliance plan • Define medical necessity and describe how health plans address related governance issues • Describe quality and ethics programs and ombudsman programs
Assignment 12: Key Legal Issues in Managed Care
Reading 12A: Key Legal Issues in Managed Care
• Define breach of contract, negligence, medical malpractice, and punitive damages • Discuss the obligations that health plans owe to plan members in conducting utilization management activities • Describe the standard of care health plans must meet when they credential plan providers • Discuss two theories of liability that may make health plans liable for the medical malpractice of plan providers • Describe how ERISA affects the ability of plan members to bring legal actions against health plans • Identify and describe some legal issues that may arise between health plans and plan providers • Discuss some of the federal and state laws that regulate the business conduct of health plans
Assignment 13: Public Policy and Changing Environment
Reading 13A: Public Policy from the Health Plan Perspective
• Explain some of the ways that health plans influence public policy • Identify primary interest groups in each of the major healthcare sectors that participate in efforts to affect health plan public policy • Describe several types of advocacy and political activities undertaken by interest groups in the health plan policy debate • Discuss the role of litigation in determining health plan public policy • Describe several techniques interest groups use to affect public opinion
Reading 13B: Changing Environment and Emerging Trends in the Health Plan Industry
• Identify several key environmental factors that affect health plans
Page 9 of 469

AHM 510 : Health Plans : Governance and Regulation
• Describe the underlying tension between universal healthcare coverage and comprehensive healthcare benefits • Explain how marketplace reform and regulatory reform have brought about change in the health plan industry
Page 10 of 469

AHM 510 : Health Plans : Governance and Regulation
Chapter 1 A : Environmental Forces
To operate their businesses, health plans must navigate through a complex environment. "Major players move into new markets in a matter of days. Market segments unheard of just a few years ago-such as physician practicemanagement- get major infusions of Wall Street capital and become forces to reckon with overnight. Changes in policy emphasis from Washington create new forms of competition, such as Medicare and Medicaid health plans."¹
Today, health plans must focus on raising capital, addressing competition, and helping to shape or respond to healthcare public policy. In addition, health plans must cope with a rapidly changing market that is regional and national as well as local in nature. Mergers, acquisitions, and business alliances among health plan players who were once avid competitors further complicate the environment. The increase in government mandates dictating the healthcare services that must be covered by health plans drives up costs for health plans. And these are just a few of the environmental forces present in the industry today.
After completing this lesson, you should be able to:
• Name and describe several major factors shaping the environment of managed healthcare
• Describe the players in health plan and how their interests affect the way they influence the healthcare environment
• Explain the influences accreditation organizations and the media exert over the financing and delivery of healthcare
• Describe several possible governance responses that health plans make to deal with their changing environment
The board of directors and senior management of health plans must develop plans to operate their businesses within this constantly changing environment. Business practices that worked well yesterday may not be sufficient today. Healthcare public policy in the form of regulation often impacts and sometimes constricts a health plan's business plan for its operations. For example, health plans must meet state minimum capital requirements in establishing and maintaining their business. In this way, state and federal regulation affects executive management decisions concerning virtually all aspects of a health plan. In addition, business decisions made by health plans may trigger the enactment of new regulations to address new forms of business or new business practices.
Governance is the vehicle health plans use to make decisions about the overall direction or purpose of a company. In this course, we will define governance as the efforts by the health plan's board of directors or other governing body, in conjunction with senior management, to develop corporate policy, to create a corporate mission statement and vision, and to develop strategies in order to achieve the organization's goals and mission. We will discuss corporate vision and mission statements later in this lesson.
Page 11 of 469

AHM 510 : Health Plans : Governance and Regulation
Because regulation and health plan governance decisions share an interdependent relationship, this course combines the presentation of governance issues faced and managed by health plans and the regulations with which health plans must comply.
The environments in which health plans operate can be described as external or internal as discussed in Figure 1A-1. In this lesson, we will discuss the factors that influence the external environment of health plans and the internal responses that health plans make to changes in the environment. Because the health plans' internal responses are covered later in this course, this lesson focuses largely on the external environment affecting health plans.
The Evolving Health Plan MarketThe factors that drive the rapid change and shape the environment in the health plan industry include:
• Extent and level of regulation and legislation (e.g., healthcare reform bills)
• Status of the economy
• Pace and number of mergers and acquisitions
• Changing structure of the health plan market
• Changing demographics (e.g., aging population)
• Consumer expectations for availability of and demand for new and better products and services
• Entrepreneurial and technological innovation (e.g., advances in medical technology including devices, surgical procedures and new pharmaceuticals)
• Politics and election cycles
• Media coverage
• Litigation developments and trends
• Changing interests or needs of the various health plab players (i.e., consumers, competitors, purchasers, providers, payors, etc.) in the marketplace
Page 12 of 469

AHM 510 : Health Plans : Governance and Regulation
All the factors in the preceding list affect a health plan's business decisions and many impact decisions related to formation, organization, and governance of the health plan. In the following sections and throughout this lesson, we will examine how these factors exert influence in the health plan marketplace.
Extent and Level of Regulation and LegislationThe health plan market is unique compared to many other business markets because of the extent to which healthcare is regulated in the United States. For example, few other industries are required to submit quality assurance plans with their applications to operate in a particular state. In addition, few other industries must comply with state and federal requirements regarding the minimum services a company must offer to its customers. Ensuring compliance with regulations requires an allocation of resources and capital to functional areas that would not otherwise need those resources and capital, from a purely business operations standpoint.
Political pressures greatly impact both the regulatory and the legislative processes. In addition, regulation is often the result of legislation. In recent years, the number of health plan bills in the state and federal legislatures has dramatically increased. Legislators have responded to their constituents' healthcare coverage concerns by proposing both benefit mandates for specific healthcare services (e.g., maternity length-of-stay mandates) and comprehensive bills that address numerous concerns (e.g., network adequacy, mental health parity, external review, etc.).
Health plans have a great interest in legislation because of the impact it has on their businesses. Each new mandate and administrative rule or regulation for coverage adds to the health plan's costs for delivering and financing healthcare. These increased costs may make premium hikes a necessity or cause the health plan to discontinue its coverage of some of the "extras" (e.g., vision care or prescription programs) that make health plans attractive to purchasers and consumers.
Status of the EconomyThe state of the economy has a tremendous impact on the formation and operations of health plans. Factors that reflect the state of the economy include the rate of a nation's growth, employment levels, interest rates, spending, production, prices, housing starts, and the money supply.
For health plans, economic factors can influence:
1. The availability of capital for business start-ups or expansions 2. The demand for healthcare services, or the type or amount of those services
desired 3. The accessibility of healthcare coverage
For example, as the United States comes closer to having full employment, the overall population has greater access to healthcare coverage since most coverage is provided through employment relationships. However, an increase in the number of mandates or economic downturns can have a negative effect on the amount of employer-sponsored
Page 13 of 469

AHM 510 : Health Plans : Governance and Regulation
healthcare coverage because employers may buy less healthcare coverage in a period of increased costs or economic instability.
Inflation also plays a role in the health plan environment by influencing the prices of healthcare services, supplies, and coverage.
During an inflationary period, consumers may have less purchasing power because the prices of goods and services increase more quickly than income. Economic factors also influence employers' willingness to purchase coverage for employees and the amount of the premium that employers are willing to pay. If the economy is experiencing increased inflation, consumers and purchasers may choose not to purchase healthcare coverage. During periods of inflation, costs for health plans usually increase more rapidly than the health plan can increase premiums for purchasers to balance the increased costs. The resulting downturn in premium revenue may cause health plans to cut back on employment and/or to reduce expenses by cutting back on employment and/or offering fewer services.
Fast Definition
Economic environment includes all the elements affecting the production, distribution, and consumption of goods and services. 2
Fast Definition
Inflation-a prolonged rise in the average level of prices in an economy
Review Question
In the paragraph below, a statement contains two pairs of terms enclosed in parentheses. Determine which term in each pair correctly completes the statement. Then select the answer choice containing the two terms that you have chosen.
Inflation plays a role in the health plan environment by influencing the prices of healthcare services, supplies, and coverage. During an inflationary period, consumers typically have (more / less) purchasing power because the prices of goods and services increase (more / less) quickly than income.
more / more
more / less
less / more
less / less
Incorrect. Because inflation increases the costs of goods and services, consumers do not have more purchasing power.
Page 14 of 469

AHM 510 : Health Plans : Governance and Regulation
Incorrect. Because inflation increases the costs of goods and services, consumers do not have more purchasing power.
Correct. Inflation typically increases costs, and reduces consumer purchasing power
Incorrect. In an inflationary period, consumers have less purchasing power because inflation increases the costs of goods and services, and consumers do not have more purchasing power.
Mergers and AcquisitionsMergers and acquisitions occur in almost every industry as companies identify business opportunities that will enhance their market position. In the last few years, however, the health plan industry has experienced a large proportion of mergers and acquisitions that have changed the landscape of the market. On one hand, some industry observers express concern that if the pace of consolidations continues there will be a substantial lessening of competition in the health plan industry. For example, when two health plans merge, the result may be a lessening of competition in some of the affected national, regional, state, or local markets for managed healthcare. In addition, a merger may give the newly formed health plan more market power than each participant had individually prior to the merger. Each phenomenon raises antitrust issues.
On the other hand, a merger may result in a health plan being able to realize operational synergies, reduce administrative costs, and expand and develop a better quality provider network. However, health plans typically consider mergers with care because integration of two formerly separate businesses requires a substantial amount of financial and other resources.
Changing Market StructureThe geographical area of the health plan market has changed from a mostly local market structure to a structure that frequently requires local, regional, and national market presence. Employers with operations in multiple locations in different states or regions often want to negotiate and enter into agreements with only one health plan that will handle the financing and delivery of healthcare in all the employer's business locations. Although enrollment in health plans has surged over the last 10 years, the rate of growth varies among different geographical markets, and the strategies that work in one market do not necessarily work in others.
Market maturity also affects business decisions. Market maturity is a measure of the growth or development of a market in terms of the number and types of players present, the relationships among those players, the products available, and consumer acceptance of the products. Market maturity can affect how receptive consumers and providers are to health plan programs, the extent to which employer healthcare purchasing coalitions are present, the types of products the market demands, and the level of competition among health plans in an area. For example, a health plan that operates in a large metropolitan area may have to offer additional services to compete with other health plans in that market. A health plan that is the only health plan available in a rural community might not face the same market challenges. It is not necessarily easy to assess market maturity in managed healthcare markets. Certain aspects of a market may be in more mature phases than other aspects of the market. For example,
Page 15 of 469

AHM 510 : Health Plans : Governance and Regulation
there may be several health plan competitors in a market but the provider networks for one or more of those competitors may be in the initial stages of development. Health plans, therefore, must constantly assess each of the aspects of the market separately and make business decisions based on the level of maturity of each market aspect.
Changing Demographics
Baby boomers are aging, and as they age they will require more healthcare services. As a significant portion of the American population becomes eligible for Medicare, opportunities for health plans to tap into this demographic market will grow. Recent federal legislation expanded the types of health plans that can contract to serve the healthcare needs of the Medicare population.
The increase in the U.S. population of members of certain ethnic groups or races is another demographic factor that presents challenges and opportunities for health plans. For example, some health plans are pursuing marketing programs that are targeted to reach non-English-speaking potential enrollees. Other health plans are creating disease management programs directed to age-based ethnic groups with a high incidence of certain diseases.
Several health plans offer open access plans that allow members to choose in-network coverage for a small copayment or out-of-network coverage that is generally more expensive. In general, such plans are targeted to economically prosperous baby boomers. In addition, women's healthcare issues and special needs have been the focus of some purchasers, and legislative initiatives such as maternity length-of-stay laws and mandated direct access to obstetricians/gynecologists reflect this concern. Health plans may need to reassess their product and service offerings in light of these demographic and associated regulatory changes.
Consumer DemandThe expectations of today's consumers continue to grow- and consumers are clamoring for new and better healthcare products and services. Among these demands are:
• Direct access to specialists
• Increased efforts to ensure the delivery of quality healthcare (e.g., By obtaining more information about plans and their providers)
• Coverage for more and different types of treatment (e.g., Experimental treatments, alternative medicine, etc.)
• Free and open exchange about healthcare treatment options between physicians and other medical personnel and the consumer
• Grievance and appeals procedures for claim denials, and health plan liability for "bad outcomes"
• Convenience in the delivery of healthcare
Consumer demand has a significant effect on healthcare legislation. It also has an impact on health plan operations. For example, most health plans use primary care providers (PCPs) to manage and coordinate care. PCPs also act as conduits to specialists to coordinate patient care and manage healthcare costs by eliminating
Page 16 of 469

AHM 510 : Health Plans : Governance and Regulation
unnecessary visits to specialists. Allowing consumers direct access to specialists requires some modification in a health plan's procedures.
For example, in a direct access plan, usually the primary care provider (PCP) is still responsible for coordinating patient care and monitoring the patient's health. A health plan may notify (or regulators may require that the plan notify) the PCP about care from specialists received without the PCP's knowledge. This notification may increase costs by adding to administrative procedures, and if state-mandated, may subject a plan to monetary or other penalties for noncompliance
Entrepreneurial and Technological InnovationEntrepreneurs can claim credit for many of the innovations that exist in health plans today. By identifying a market need, and finding a way to address that need, entrepreneurs have established new standard industry practices or developed alternative methods for providing healthcare. For example, entrepreneurs created the concept of physician-hospital organizations, physician practice management companies, and firms that offer disease management programs. Entrepreneurs change the way healthcare is financed and delivered by creating new ways of fulfilling needs and providing services. One way that entrepreneurs affect health plans is through the establishment of unique strategic business alliances. We discuss strategic partnerships in Formation and Structure of Health Plans.
Technological innovation is thriving on several fronts. From a clinical standpoint, advances in healthcare abound- from the application of gene research in treating diseases to breakthroughs in the early detection and treatment of certain forms of cancer. New medical devices and new drugs have been created to treat illness and disease.
From an information management standpoint, change is also flourishing. For example, efforts by health plans to involve physicians in managing health risks require a great deal of information technology support. In addition, recently enacted federal legislation requires the Department of Health and Human Services to develop national standards for the electronic transmission of health data. Information technology plays a pivotal role in the maturation of health plans. Health plans are spending money to apply the findings of outcomes research and evidenced-based medicine. Health plans that do not invest in information technology find themselves at a competitive disadvantage.
Entrepreneurs in health plans have also had an impact on marketing. For example, pharmaceutical companies now market new drugs directly to the consumer through television, magazines, and other forms of advertising.
Evidence based medicine the conscientious, explicit, and judicious use of current best evidence in making decisions about the care of individual patients.5
Politics and Election CyclesBecause our legislative representatives are elected every two years, healthcare is a public policy issue raised every two years in connection with political election campaigns. Although voters do not vote on the issues considered by legislatures, they do elect the representatives who vote on such matters. The elected representatives usually feel compelled to try to implement into law the wants and needs of their
Page 17 of 469

AHM 510 : Health Plans : Governance and Regulation
constituents. As evidenced by the Clinton administration's healthcare reform proposal of 1992 and various patient bills of rights currently under consideration in the House, Senate, and state legislatures, healthcare is an issue of some concern to legislators and the voting public.
Litigation Developments and TrendsIn addition to legislative and regulatory activity, court activity and decisions also impact health plans. For example, consumers are bringing lawsuits against health plans as well as providers for treatment decisions that result in bad outcomes. Court rulings often result in precedents being set that are followed in subsequent court decisions. We discuss key legal issues that impact health plans in Key Legal Issues in Health Plans.
Changing Interests of the PlayersThe main players in health plans are the consumers (the end users of the health plan products and services), the purchasers (employers, unions, purchasing coalitions, other large groups, government programs, and individuals), the providers (physicians, hospitals, and other healthcare professionals), and the payors (health plans, insurance companies, and certain self-funded employer groups).
The players in helath plans have diverse and sometimes conflicting interests. For example, the payors and purchasers want to manage costs and deliver quality healthcare, while the end-user consumers are usually concerned with obtaining the best medical care without focusing on the cost. Physicians often want unlimited authority to make decisions concerning patient care, while health plans must maintain utilization management and quality assurance systems. For example, physicians who refer health plan members to an out-of-network provider without obtaining plan approval may undermine the plan's credentialing and quality programs and hamper the health plan's ability to manage costs. In the following sections, we discuss the interests of the major players and how they influence health plans. We will also discuss other stakeholders in the health plan marketplace, such as vendors, the community, and patient advocacy groups.
ConsumersAmericans see healthcare as a social good and expect it to be available to all individuals, whenever it is needed and in whatever quantity it is needed. In this way, healthcare differs from almost every other product or service. Other products and services are generally available only to those consumers who are able to pay for them. Consumer expectations for healthcare services place burdens and unique responsibilities on the suppliers or providers of such services. They also necessitate the involvement of public policy in setting standards for the provision of healthcare services to populations that are unable to pay the market price or even make any contribution to the payment for those services. We will discuss the impact of the uninsured and underserved populations later in this lesson. Let's now consider the end users who are consuming health plan products and services and explore their impact on the health insurance plan environment.
Consumers want affordable, quality healthcare available-where they need it, when they need it. The influence of consumers can be seen in the number of legislative bills concerning healthcare. For example, many states are considering mandating external review for health plan decisions regarding exclusions from coverage to ensure protection
Page 18 of 469

AHM 510 : Health Plans : Governance and Regulation
of members' interests. Consumers are taking a more active role in their personal health. In the past, a consumer may have hesitated to question the diagnosis or treatment prescribed by a provider, but today such interaction is much more common. Consumers are voicing and demonstrating their desires that certain aspects of healthcare be available to them. The demand for greater choice of providers has encouraged health plans to develop direct access plans. The increased interest in alternative medicine has led some health plans to offer coverage for "non-traditional" providers and treatments.
Today's commercial health plan consumers are better educated and have higher disposable incomes and higher standards of living than their predecessors. Employers and other purchasers that buy the healthcare for these consumers are more attuned to the consumer's needs and desires. In a booming economy with unemployment at a low level, offering a generous package of healthcare benefits may make the difference between hiring the candidate of choice or a less qualified substitute.
PurchasersEmployers and other purchasing groups have exerted tremendous influence on the products and services offered by health plans. Employer initiatives that are shaping health plans include an increased focus on quality as well as cost, as evidenced by the formation of organizations such as the Foundation for Accountability (FACCT). FACCT is a coalition of purchasers (mostly large employers) and consumer organizations founded to make an outcome-oriented assessment of health plans' treatment of medical conditions or diseases. Largely as a result of employers' focus on quality, there has been an increase in the number of health plans that seek accreditation from nationally recognized accreditation organizations. To prove that employers' dollars are being well spent, health plans have begun devoting more time and money to outcomes research and other quality-ensuring initiatives. Additionally, employers' efforts to curb the costs of healthcare coverage, such as the establishment of on-site clinics for employees and the creation of wellness programs, have caused health plans to innovate and expand their product and service offerings.
ProvidersSince providers actually supply the healthcare services that health plans deliver to their customers, they are a crucial component of a health plan. A health plan must employ or recruit and contract with many different types of providers for the provision of healthcare services to the health plan's members. Health plans that strive to develop a relationship with providers based on the exchange of mutual expertise are likely to be more successful than health plans that have a less flexible approach. Providers' concerns about the continued growth of health plans usually center on compensation and autonomy issues. Because some physicians have concerns about losing their decision-making autonomy to health plans, a number of physicians have joined physician groups or created alliances with other providers to establish their own health plans, such as physician-hospital organizations or provider-sponsored organizations. These organizations sometimes become competitors of established health plans or insurance companies by contracting directly with a purchaser and bypassing the health plan entirely. Alternatively, they may present a different type of entity with which a health plan or insurance company must negotiate to obtain provider services in a market. Health plans that maintain strong and positive locally based relationships with providers are more likely to prosper in today's environment. For example, providers have the clinical expertise and supporting clinical data that health plans need to demonstrate to
Page 19 of 469

AHM 510 : Health Plans : Governance and Regulation
purchasers their commitment to quality. In addition, providers usually have great influence with their patients. When these patients are members of a health plan, their satisfaction is of prime importance to that health plan.
PayorsInsurance companies that offer a full range of healthcare products, including indemnity products, compete with health plans. These same insurance companies are health plans if they offer health plan products such as health maintenance organizations (HMOs), preferred provider organizations (PPOs), POS options, etc. In certain instances, an insurance company may have a slight advantage in establishing certain types of managed healthcare product offerings. For example, an insurance company that forms an HMO and also has experience in the fee-for-service arena may have an easier time beginning a PPO or offering a POS option than an HMO that is not affiliated with an indemnity insurer, because the indemnity insurer has the experience and ability to process out-of-network claims and more accurately determine premium rates. The HMO can build or acquire these assets and capabilities, but may take more time and use substantial financial resources to do so.
Other StakeholdersIn the preceding sections, we have discussed some of the main players in the managed healthcare marketplace; however, these are not the only participants in this market. The community in which a health plan operates, the uninsured or underserved populations, vendors, academic medical centers, patient advocacy groups, and the federal and state government are also stakeholders in the health plan marketplace. Each of these stakeholders is discussed in the following sections.
The Community
Although the markets for health plans may be expanding to regional or national markets, most health plans are initially established to serve a local community. In addition, the articles of incorporation and the mission statements of not-for-profits, established for charitable purposes, reflect their commitment to provide benefits to the community. Some state laws require community representation on the board of directors for health plans.
Certain not-for-profit organizations are required to serve their community by making membership available to individuals and small employers; by making services available to low-income, high-risk, medically underserved, and elderly populations; and by using community rating to determine their premiums. Other ways that health plans serve their communities include: teaming up with community public health organizations to provide demand management and health promotion activities, joining forces with academic medical centers to perform education and research, and sponsoring community health projects such as childhood immunization initiatives and health fairs. For example, some health plans are partnering with community public health agencies to educate health plan enrollees about the dangers of substance abuse or obesity. Since community public health agencies often are already doing some of the promotion activities that a health plan wishes to provide, a partnership between these two entities makes sense. In some situations, the promotional activities of the public health agency are tailored for the
Page 20 of 469

AHM 510 : Health Plans : Governance and Regulation
health plan enrollee population; in others, the promotion is aimed at the geographic population (which includes health plan enrollees) at large.
Health plans that are active participants in their local communities can gain many benefits. From a public relations perspective, providing additional or tailored services to meet needs in the local community can reap great rewards from increased enrollment in plans to availability of funding sources for expansions. Additionally, individuals, the community, and health plans all reap rewards when health plans participate in activities to improve the health of their members.
Uninsured and Underserved PopulationsThe uninsured population in the United States is a significant social policy concern. Federal and state governments often implement plans to extend insurance coverage or health plan enrollment as an option for these populations. As we will discuss later in this course, major reform initiatives to guarantee insurance for all citizens have not been successful.
The uninsured population has a tremendous impact on the cost of healthcare services in this country. Emergency-room treatment of conditions that would be better served by a primary care provider costs a great deal. Costs of the uninsured cannot always be expressed in monetary terms. For example, no amount of money can compensate the parent of a child who dies after contracting a disease that could have been prevented by an immunization. The basic tenets of health plan education and preventive services- are a natural fit for this population; however, finding the public funding to finance such endeavors is a challenge.
Recently enacted legislation (i.e., the Health Insurance Portability and Accountability Act of 1996), which was intended to make great strides in guaranteeing access to health insurance for some members of the uninsured population, does not seem to be achieving that goal because the cost of coverage is being passed on to individuals. For example, a recently released General Accounting Office report noted that individuals in some states are paying premium rates 140% to 600% higher than standard premiums for individual healthcare products.6
Additional legislation to address this issue at either the state or federal level (or both) is likely. Such legislation can sometimes increase a health plan's costs of providing coverage to members. Health plans that remain active in this public policy debate may be able to suggest solutions that benefit all the participants in this dilemma.
The underserved population in both rural and urban areas presents a somewhat different problem than the uninsured population. Low-income residents in outlying rural communities often suffer from lack of access to healthcare. There may be no hospital and may be only one physician or other healthcare professional that visits such communities once a week as part of a government outreach program. Sometimes, a health plan or insurance company refrains from entering a rural market because there are not enough potential members to make the market a viable business undertaking. Additionally, health plans that desire to enter rural markets may meet resistance from the local physicians or hospitals in those communities. Addressing the needs of underserved markets is not an easy task, yet some health plan innovators have developed methods of serving at least some of the underserved populations in rural areas. One health plan
Page 21 of 469

AHM 510 : Health Plans : Governance and Regulation
builds networks for medium-to-large employers with operations in rural areas across broad geographic regions that allow the health plan to have a large enough potential enrollee market to make the venture worthwhile. Although such a solution does not address the communities where no healthcare facilities are available, it is a step toward making health plans more accessible to a larger portion of the population. In addition, a number of PPOs operate in rural markets.
In metropolitan or urban areas, meeting the needs of the underserved population is also a challenge. For example, many urban Medicaid programs must address transportation issues, lack of providers willing to serve this population, and long waits for care. Finding ways to meet the needs of the uninsured and underserved populations is a responsibility that health plans share with others in the healthcare industry and our country in general.
VendorsVendors, such as organizations that provide billing or other administrative services, can play a significant role in the healthcare market. Companies that produce software for contract or claims management or premium billing are essential to the operation of a health plan. In addition, vendors may provide or manage clinical services such as radiology, and disease management programs targeted to specific diseases such as diabetes. Vendors may also arrange for and administer the provision of carve-out healthcare services such as behavioral healthcare, radiology, chiropractic, oncology, etc. In fact, some health plans have outsourced to vendors their entire information technology function. A vendor often has expertise in a particular area that the health plan has not developed or for which the cost of developing such expertise is not practical. In the managed healthcare industry, there is increasing use of vendors to provide services that are not cost-effective for the health plan to provide. For example, one health plan has outsourced to a vendor its call center for customer service. As another example, an HMO with little expertise in claim processing for a point-of-service product might outsource this activity to a vendor.
As vendors become even more prevalent, they may impact the health plan market in new ways. For example, there are increasing numbers of software firms that want to meet the information needs of all stakeholders in the managed healthcare market. Employers that self-fund their plans already use vendors to perform many functions that are not cost-effective for the employer to undertake. Often the "vendor" to an employer is a health plan; however, as more enterprising firms create market niches for their services some health plans may lose some of their vendor contracts with employers. For example, pharmacy benefit managers (PBMs) act as vendors to employers for pharmaceutical products and services.
Academic Medical CentersAnother stakeholder in the health plan industry is the academic medical center. Academic medical centers (AMCs), also known as academic health centers, are healthcare institutions that offer physician residency programs and include medical schools and other professional healthcare schools such as nursing and dental programs. These institutions train healthcare professionals and perform various clinical and other types of healthcare-related research. Teaching hospitals are usually part of an AMC. Teaching hospitals are institutions that offer physician residency programs. In the past, academic medical centers have had concerns about the growth of health plans. Some of the reasons for this concern are as follows:
Page 22 of 469

AHM 510 : Health Plans : Governance and Regulation
• Often the physician billing practices of AMCs may not mesh with health plan payment structures
• Lack of primary care providers on the staffs of AMCs (usually staffed by specialists) may make such institutions unlikely candidates for health plan approaches
At most teaching hospitals, the physician who supervises the resident bills for his or her services, although it is the resident who provides all or some of the services. In addition, the fee-for-service side of Medicare has largely subsidized AMCs. The proliferation of Medicare health plans may eliminate some of that funding for AMCs. Also, policymakers and legislators are reviewing many aspects of Medicare, including the fee-for-service aspects, and have curbed some of the additional funds that were previously funneled into AMCs.
The environmental pressures that have caused dramatic change in the health plan industry are also impacting AMCs. Some AMCs have merged with other teaching institutions or have entered into relationships with other hospital systems. Other AMCs are beginning to enter into formal relationships with health plans. AMCs are purchasing physician practices to gain access to patients, contracting with non-teaching hospitals to become participants in Integrated Delivery Systems (IDS), or entering into partnerships as providers with HMOs. Some AMCs are even becoming owners/investors in health plans. AMCs can bring unique capabilities and resources to a health plan relationship. Their expertise in education and research is a valuable tool in an era when the health plan market focuses on information. Medical outcomes research and evidence-based medicine are two areas in which AMCs may be able to help health plans.
Review Question
The Sawgrass Health Center is an institution that trains healthcare professionals and performs various clinical and other types of healthcare-related research. Because Sawgrass receives government funding, it is required to provide medical care for the poor. Of the following types of health plans, Sawgrass can best be described as:
a medical foundation
an academic medical center (AMC)
a healthcare cooperative
a community health center (CHC)
Incorrect. A medical foundation is an entity that owns and manages all purchased assets of physician practices, you will read more about this arrangement in the lesson Health Plan Structure and Arrangements.
Correct. An academic medical center is an institution that trains healthcare professionals, performs clinical and other types of healthcare-related research and is required to provide medical care for the poor.
Page 23 of 469

AHM 510 : Health Plans : Governance and Regulation
Incorrect. A healthcare cooperative is a consumer-sponsored, physician-operated medical facility that provides prepaid healthcare to members. You will read more about this arrangement in the lesson Health Plan Structure and Arrangements.
Incorrect. A community health center is a medical facility that recieves federal, state and private grant funding to provide primary care for medically underserved populations. You will read more about this arrangement in the lesson Health Plan Structure and Arrangements.
Patient Advocacy GroupsPatient Advocacy groups are consumer organizations that may provide patient education, coordinate the delivery of or provide care, and/or represent the general political interests of patients or those with certain illnesses. In addition, patient advocacy groups often pursue legislation designed to further the interests of the patients in the group (e.g., mandated coverage of benefits for experimental cancer drugs).
In the past, health plans' relationships with patient advocacy groups have sometimes been adversarial. Health plans often only interacted with a patient advocacy group when the health plan denied coverage for a treatment needed by a member the advocacy group represented. Today, some health plans are partnering with patient advocacy groups to provide certain aspects care. Some patient advocacy groups provide psychosocial or holistic care in partnership with a health plan. A health plan may benefit from such a partnership in several ways, including establishing a better reputation among patients and actually lowering the long term cost of certain treatments by providing care that more closely monitors and treats a patient's condition and over all health.
Federal and State GovernmentsAs we will describe throughout this course, federal and state governments exert tremendous influence over a health plan's formation, operations, and governance. These governments are stakeholders in the managed healthcare industry in two important ways. First, such governments enact and enforce laws to protect and preserve the public's interests.
The second way in which governments act as stakeholders is through their roles as purchasers of healthcare services for government employees and government-sponsored healthcare programs. From this perspective, their needs and concerns more closely parallel those of purchasers described earlier. Governments, through their dual roles as purchasers and regulators, affect the types of laws or regulations enacted or the standards to compete in the marketplace. We will discuss governments' roles as purchasers in more detail in Federal Government as Purchaser.
Review Question
Page 24 of 469

AHM 510 : Health Plans : Governance and Regulation
Regulatory and legislative bodies are among the important environmental forces in the health plan industry. The following statements are about such regulation and legislation. Select the answer choice that contains the correct statement.
Federal guidelines exist to direct health plans on compliance issues when a health plan encounters conflicting state laws in a given service area. Administrative rules and regulations do not carry the force of law.
As stakeholders in the health plan industry, federal and state governments exert tremendous influence over a health plan's formation and operations. In recent years, the number of health plan bills in the state and the federal legislatures has decreased.
Incorrect. Healtrh plans often have to comply with multiple state laws while trying to meet the needs of a single market.
Incorrect. Administrative rules and regulations, prescribed by a federal or state administrative agency, carry the force of law.
Correct. Federal and state governments exert tremendous influence over health plans' formation, operations and governance
Incorrect. In recent years the number of health plan bills in the state and federal legislatures has increased.
Other Environmental ForcesIn addition to the direct environmental forces that impact the market that we have just discussed, other forces also shape health plans. Governments' roles as purchasers, conflicting state and federal regulations, the increasing use of accreditation, and the media all have an impact on health plans and their operations. We briefly discuss each of these below.
1. Governments
2. Accreditation
3. The Media
We mentioned earlier that governments' dual roles as purchasers and regulators sometimes affect the laws or regulations that impact managed healthcare. The dual roles of governments sometimes affect the market in ways not necessarily intended. For example, if the federal agency responsible for purchasing healthcare for federal employees sets a standard that potential contractors must meet to be eligible for consideration as a health plan for those employees, other purchasers in the industry may demand a similar minimum threshold for the health plans with which they contract.
Governments also affect the managed healthcare regulatory environment in other unintended ways. A health plan that serves a multistate community such as Memphis,
Page 25 of 469

AHM 510 : Health Plans : Governance and Regulation
Tennessee (portions of the Memphis metropolitan area are also in the states of Mississippi and Arkansas), may be subject to several sets of state laws that sometimes conflict. Offering the same product in the entire metropolitan area may become a regulatory challenge since there are no guidelines for a health plan to follow to comply with conflicting state laws in a service area. The health plan and its legal counsel must comply with the laws of multiple states while trying to meet the needs of a single market. In addition, there can be conflicts between state and federal laws. For example, a health plan may have to meet a minimum federal standard for the provision of some aspect of healthcare services, such as mental health in accordance with the federal Mental Health Parity Act that we will discuss in Federal Regulation of Health Plans, and meet additional requirements of a state that has regulations affecting the coverage for mental health services.
Complying with regulations requires an allocation of time and money from a health plan. The more complicated or burdensome the laws and regulations become, the more time and resources are required to comply with such laws and regulations. Eventually, these increased costs to the health plan are passed on to the purchaser in the form of increased premiums.
Increased demands by purchasers and consumers for accountability in managed healthcare have spurred growth of a competitive industry for accrediting health plans, the health plans they sponsor, and the separate providers of specialized care within health plans. Accreditation programs develop standards for health plan performance; conduct reviews of the organization, its policies, and procedures; and gather data to determine the extent to which the organizations meet the standards. Most accreditation programs were initially developed by the providers in the industry they accredit in response to pressure for accountability and the need for an independent third-party review. The major accrediting programs for healthcare are now sponsored by independent not-for-profit entities. These entities are governed by boards of directors with a broad representation of providers, insurers, purchasers (private and public), and consumers to help ensure independence, credibility, and responsiveness to the needs of major stakeholders. Accrediting programs confer an accreditation status following their review but generally do not attempt to establish rankings that directly compare health plans, their health plans, or parts of their plans. 7
Many employers will not consider entering into a contract with a health plan that has not been accredited by a nationally recognized accreditation program. In addition, some state governments are requiring health plans to obtain accreditation from a nationally recognized accreditation organization as a condition of licensure in a state. Other states may not require accreditation for licensure but allow accreditation to suffice in place of a mandatory external review for quality.
Today, it is hard to pick up any newspaper or magazine or to tune into network television and not see managed healthcare mentioned. All too often, the articles are not positive. The media has significant influence on public opinion in the choice of topics that it covers and the manner in which the stories are covered. Since public opinion can have an impact on a health plan's business, health plans must consider media coverage as a
Page 26 of 469

AHM 510 : Health Plans : Governance and Regulation
factor in their environment. Insight 1A-3 provides a brief overview of health plan's relationship with the media.
Insight 1A-3. Does the media fuel health plan backlash?
A new survey on media coverage of health plan by the Kaiser Family Foundation points to a significant increase in coverage of health plan issues over the past decade, much of it critical of health plans. The study, which was published in the January/February 1998 issue of Health Affairs, finds that most, two-thirds, of 2,100 news stories that have appeared in newspapers, business publications, and on network television since 1990 are largely neutral in their coverage of health plan. A quarter were critical, whereas 11% praised the system.
However, the more highly visible stories on network TV and in special newspaper series have been much more negative, particularly in the last four years. Coverage involving health plan in the early 1990s tended to emphasize the benefits of this emerging system and its potential to reduce high healthcare costs. During the health reform debate of 1993 to 1994, health plan was the "savior," recalled reporter Susan Dentzer at a Kaiser forum on media coverage of health plan. Competing health plans were going to improve quality and lower costs.
More recently the media has highlighted patient "horror stories" and "high-drama" anecdotes, particularly on TV and in newspaper series. Journalists acknowledge a "herd instinct" among reporters in covering such issues as "drive-through deliveries" and gag clauses. And some have found that editors are interested only in stories with health plan victims and villains. To gain more balance, reporters cited a need for better data and hard information on costs, enrollment, and benefits.
Health Plan Responses to Environmental ForcesWe've discussed many of the external environmental forces at work in the health plan industry and stated that health plans must make business decisions taking these factors and forces into account. Now we'll briefly mention some ways health plans are responding to the various forces in the health plan environment.
In our earlier discussion of the market for health plans, we touched upon many of the ways health plans respond to changes in their environment or the market, such as forming strategic business alliances and participating in mergers or acquisitions. To ensure their survival in the rapidly changing health plan environment, health plans are assessing their strategic options by reviewing their organizational structure, their corporate values and mission, their product portfolio and development process, their strategies to remain or become competitive in a particular market, and the way they respond to consumers' demands.
Page 27 of 469

AHM 510 : Health Plans : Governance and Regulation
Most companies develop a corporate vision and a mission statement. Health plans are no exception.
A mission statement is a statement that succinctly sums up the organization's reason for existence and overall purpose. What is changing with health plans is the focus of their corporate vision and mission statements. In the past, health plan mission statements may have mentioned the customer, but meeting the customer's needs was usually not the focus. Health plans now develop mission statements that center on defining and meeting in an ethical and cost-effective manner the needs of the customer and/or the community. To realize this overall goal of addressing the customer's needs, health plans develop strategic plans. Strategic planning is the process of identifying a company's long-term objectives. Companies use corporate strategies to achieve their plans.
Changes in the environment of a health plan sometimes necessitate governance moves that are not in the normal course of business. Occasionally, a change in a health plan's environment makes it necessary for the health plan to restructure or reorganize its business operations to remain competitive, become more competitive, or enter new markets. A corporate reorganization or restructuring is the process of adjusting the internal structure of an organization by changing reporting relationships; adding, eliminating or changing the responsibilities of functional departments; moving from a centralized to a decentralized business structure (or vice versa); or creating a new subsidiary or holding company. For example, an insurance company that enters the health plan arena may create a subsidiary HMO. Or, an existing health plan may change the functional duties of departments or reporting relationships within its organization to streamline its responses to customer needs or to reduce administrative expenses.
Fast Definition Corporate vision an overall view of what the organization should achieve by its existence.
Fast DefinitionCorporate strategies the methods a company plans to use to achieve its long-term objectives.
Other ways that health plans respond to change include leadership changes, converting from a not-for-profit or mutual organization to a for-profit organization, going public, selling portions of their businesses, acquiring new or existing companies, entering new business ventures, getting out of existing business ventures, or making major changes in plan or product offerings. We will discuss each of these responses later in this course. However, let's now consider an example of one of these environmental responses. See Figure 1A-2.
As you can see, a health plan has many internal governance tools it can use to respond to changes in its external environment. Throughout the remainder of this course, we will discuss the legal and regulatory factors in the health plan environment, as well as the governance planning and responses that allow health plans to thrive in the dynamic environment of health plans today.
Figure 1A-2. An example of one health plan's response to its environment.
Page 28 of 469

AHM 510 : Health Plans : Governance and Regulation
After reviewing demographic characteristics and regulatory factors, the Livwel Company, a health plan, identifies a new business opportunity in the Medicare market. This health plan has ready capital, but no expertise in serving this market. The Livwel Company decides to enter into a business venture with another health plan, called Firstline, that has expertise in serving the Medicare market. This type of joint business venture benefits Firstline by providing a ready source of capital, while the Livwel Company gains expertise in serving this new type of market.
Chapter 2 A : Legal Organization of Health Plans
Because of the rapid pace of change in the health plan industry and the need to constantly reassess strategic plans, determining a health plan's legal form is one of the fundamental issues that must be addressed by the company's leaders. In this lesson, we begin with an overview of the basic forms of legal organization available to health plans, with a focus on corporations, the predominant form. We then examine the for-profit health plan, the not-for-profit health plan, and the mutual insurance company. In this discussion, we examine issues such as legal and formal requirements, owners' liability, tax treatment, long-term stability, allocation of profits, and options for raising operating funds.
After completing this lesson, you should be able to:
Explain the distinguishing features of a corporation and a limited liability company Describe the key features and differences between a for-profit company and a not-
for-profit company Describe the differences between a publicly traded stock company and a privately
held stock company Describe the key features and differences between a stock company and a mutual
company
Basic Forms of Legal OrganizationIn the United States today, business entities can be established in any one of a number of legal forms. For instance, most health plans are corporations, and many healthcare providers and other vendors with whom health plans do business are sole proprietorships, partnerships, or professional corporations. Figure 2A-1 provides an overview of several forms of legal organization.
CorporationsHealth plans are typically established as corporations. This legal form affords owners, directors, and executives the greatest protection from individual liability. Also, in the case of for-profit health plans, the corporation is the legal form that provides the greatest flexibility for raising operating funds. In some states, an entity responsible for financing healthcare, such as an insurance company, is required by law to be organized as a corporation. In many states, however, a health plan, such as an HMO, is not required to be a corporation; it can, for instance, be a limited liability company. Also, as we will see later in this lesson, federal law now allows certain types of provider-owned organizations, which are not all corporations, to operate as health plans in the Medicare and Medicaid markets.
Page 29 of 469

AHM 510 : Health Plans : Governance and Regulation
Figure 2A-1. Sole Proprietorships, Partnerships, and Corporations.
Sole Proprietorships
A sole proprietorship is a business owned by one person. All the debts of the business are the debts of the owner. Business profits or losses are treated as individual income for tax purposes. Although the sole proprietor can leave the assets and liabilities of the business to someone else, continuing the operation of a sole proprietorship after the owner's death is often difficult.
Partnerships
A partnership is a business that has many of the same legal characteristics of a sole proprietorship but is owned by two or more persons. The partners can be individuals or legal entities, such as corporations. A partnership can be established by oral agreement or through a formal partnership agreement. All states have laws that spell out the requirements for establishing a partnership. A partnership can take any one of the following legal forms.
A general partnership is owned by two or more general partners who share responsibility for business operations. General partners, when they are individuals, are responsible for the debts of the whole business and declare the appropriate share of their partnership income or losses on their individual tax returns. The partnership itself does not pay federal income tax, although it is required to file a return for information purposes. A general partnership ends with the death or withdrawal of any general partner; the remaining partners must form a new partnership if they want to continue the business.
Partners can limit the liability of certain owner-investors by forming a limited partnership. A limited partnership consists of limited partners and at least one general partner. Limited partners, who cannot participate in the day-to-day management of the organization, are at personal financial risk only for the amount of their investment in the business. The general partners, on the other hand, have full liability, similar to the liability of sole proprietors. Typically, limited partners can enter into and opt out of a limited partnership with much greater freedom than can general partners, which is an advantage for raising operating funds because the partnership can more easily attract limited partners if it needs additional investors.
When the partners in a limited partnership are individuals, the profits and losses of the business are treated as individual income, and the partners each declare the appropriate share of their partnership income on their individual tax returns. The partnership itself does not pay federal or state income tax. However, if the structure of the limited partnership includes more corporate than partnership characteristics, it may be taxed as a corporation.
Generally, a limited partnership continues upon the death or withdrawal of a limited partner, but it ends with the death or withdrawal of a general partner. However, the partnership agreement can place restrictions on a limited partner's right to withdraw, or can allow for the partnership to continue beyond the withdrawal of a general partner.
Page 30 of 469

AHM 510 : Health Plans : Governance and Regulation
Another type of partnership, permitted by enabling statutes in some states, is the registered limited liability partnership (LLP). A registered limited liability partnership agreement eliminates a partner's personal liability for debts and obligations that result from acts committed by another partner or a representative of the partnership while conducting partnership business. A registered limited liability partnership is similar to a general partnership in most other respects.
Corporations
A corporation, as defined in 1819 by U.S. Supreme Court Chief Justice John Marshall, is "an artificial being, invisible, intangible, and existing only in contemplation of the law."
The owners, directors, and officers of a corporation, unlike the owners of a sole proprietorship or a general partnership, are not individually liable for the debts of the organization. Unlike sole proprietorships and partnerships, many corporations are taxed twice. First, the corporation pays a corporate tax before it distributes earnings to its owner-investors. Then the owner-investors pay individual income tax on the distributed earnings. However, not all corporations are subject to this double-taxation. For example, some smaller businesses can organize as a subchapter S corporation, which is not subject to corporate taxes. To qualify as a subchapter S corporation, an entity must file a formal election with the Internal Revenue Service (IRS) and must meet other criteria, including requirements limiting the number of stockholders.
A corporation continues beyond the death of any or all of its owners. For example, the individual investors in a for-profit corporation may change continually, but the entity itself remains intact.
Review Question
The Surrey Medical Supply Company was formed as a limited partnership. In this partnership, Victoria Lewin is one of the limited partners and Oscar Gould is a general partner. This information indicates that, with respect to the typical characteristics of limited partnerships,
Ms. Lewin has more freedom to opt out of the partnership than does Mr. Gould
Ms. Lewin has more liability for the debts of Surrey than does Mr. Gould
both Ms. Lewin and Mr. Gould participate in the day-to-day management of Surrey
the partnership will continue upon the death of Mr. Gould, whereas it will end with the death of Ms. Lewin
Correct! In a limited partnership the limited partner can enter into and opt out of the limited partnership with much greater freedom than the general partner.
Incorrect. In a limited partnership, the general partner has full liability, where the limited partner is only at personal financial risk for the amount of their investment.
Page 31 of 469

AHM 510 : Health Plans : Governance and Regulation
Incorrect. In a limited partnership, the limited partner, Ms. Lewin, cannot participate in the day-to-day management of the organization.
Incorrect. In a limited partnership, the partnership ends with the death of the general partner
Legal Requirements and GovernanceIn each state, the authority to incorporate businesses is delegated to an administrative agency, typically the Office of the Secretary of State. The exact requirements for incorporating a business vary by state. The usual procedure is to submit proposed articles of incorporation along with the required filing fee. The articles of incorporation describe the essential features of the corporation, including its purpose, its name, the location of its principal place of business, the type of business in which it will engage, the names of the members of its initial board of directors, and whether it will be for-profit or not-for-profit. The articles of incorporation usually describe in a limited way the proposed governance structure of the company. For example, the articles might indicate that the board of directors will be comprised of three or more members. Typically, more detailed governance provisions are included in the corporate bylaws, which are required by state law but do not have to be filed.
In most states, once all statutory incorporation requirements are met, the appropriate state agency approves and maintains a record of the document that was submitted by the company. This document grants the corporation its legal existence and right to operate. In some states, the approved document is called a certificate of incorporation; in other states and federally it is called a corporate charter.
Each state has laws regarding the governance of corporations. These laws generally apply to all corporations, but additional provisions often apply to special types of organizations, such as health plans. For example, laws might specify how health plans can raise operating funds and invest their assets. Laws often stipulate that in order to make certain changes in a corporation's structure, the individuals responsible for governing the organization must comply with specific state requirements and must obtain approval from the Secretary of State or the Attorney General. In most circumstances, the approval of other state agencies is also required. For instance, laws typically require HMOs, as well as corporations and mutual organizations that conduct the business of insurance, to obtain Insurance Department approval.
A corporation's board of directors is composed of individuals- called directors- who serve as the primary governing body of a corporation. Historically, directors of not-for-profit corporations were called trustees, and their actions were governed by trust law. Today, both not-for-profit and not-for-profit organizations are governed by corporate law, but the term trustee is still sometimes used to refer to directors of not-for-profit organizations.
Some laws require a health plan to be governed by at least a minimum number of board members to help ensure a broad governance perspective. Others dictate that a specific number of board members must reside in the state in which the health plan is incorporated to increase the likelihood that the interests of state residents will be represented. Others stipulate that the number of board members from the healthcare industry must be limited to less than 50% to help ensure that interests other than those
Page 32 of 469

AHM 510 : Health Plans : Governance and Regulation
of providers will be represented. For similar reasons, some states require that consumers make up a specified percentage of board members.
Typically, a health plan incorporates only once, in a state of its choosing. It is then said to be domiciled in that state. Later, the company may file applications with other states to do business in those states. In most cases, the health plan does not incorporate in those states, although it is usually subject to applicable laws and regulations and is licensed in those states. From the point of view of any state, a domestic corporation is one that is incorporated under the laws of that state; a foreign corporation is one that is incorporated under the laws of another state; and an alien corporation is one that is incorporated under the laws of another country. For example, assume a health plan is incorporated in New Jersey and does business in New Jersey and Georgia. From New Jersey's point of view, this is a domestic corporation; from Georgia's point of view, it is a foreign corporation. A company incorporated in Canada that does business in New Jersey and Georgia is, from the point of view of both New Jersey and Georgia, an alien corporation.
Review Question
The Tidewater Life and Health Insurance Company is owned by its policy owners, who are entitled to certain rights as owners of the company, and it issues both participating and nonparticipating insurance policies. Tidewater is considering converting to the type of company that is owned by individuals who purchase shares of the company's stock. Tidewater is incorporated under the laws of Illinois, but it conducts business in the Canadian provinces of Ontario and Manitoba.
With regard to the state in which Tidewater is domiciled, it is correct to say that, from the perspective of both Ontario and Manitoba, Tidewater is considered to be the type of corporation known as:
a foreign corporation
an alien corporation
a sister corporation
a domestic corporation
Incorrect. A foreign corporation is incorporated under the laws of another state.
Correct. An alien corporation is one that is incorporated under the laws of another country.
Incorrect. Sister corporations are two corporations having common or substantially common ownership by the shareholders.
Incorrect. A domestic corporation is one that is incorporated under the laws of that state.
Page 33 of 469
AHM 510 : Health Plans : Governance and Regulation
In some states, such as California and New York, all HMOs must be domestic corporations. Therefore, an HMO that is domiciled in another state but wants to do business in one of these states must incorporate a separate subsidiary in the applicable state. Once established, this company can, at its discretion, also file for a license to do business in other states. To illustrate, an HMO domiciled in Pennsylvania that wants to do business in New York must incorporate a subsidiary in New York. If this same HMO also wants to do business in Ohio, either the Pennsylvania company or the New York company can file for a license to do business in Ohio as a foreign company.
Some states provide favorable tax treatment to domestic corporations. A health plan that does business in one of these states as a foreign corporation may wish to voluntarily incorporate a subsidiary as a domestic corporation to obtain the tax advantages.
When a health plan incorporates, it becomes subject to (1) its state of domicile's applicable laws and regulations and (2) the jurisdiction of its state of domicile's courts. State laws seek to ensure that domestic corporations are subject to the authority of the courts by requiring the health plan to register the name and address of an individual the corporation has appointed as its registered agent for purposes of service of process. Service of process is the act of delivering to a party written notice that a lawsuit or other legal action has been filed against that party. Foreign corporations may also be subject to the jurisdiction of the courts of the states in which they do business.
Limited Liability of OwnersA corporation- apart from its owners, directors, or officers- can be considered a "person" under the law and can be a party in a legal action. It can sue and be sued. Any legal actions involving a corporation, however, affect only the assets and liabilities of the corporation. If a corporation goes bankrupt, the organization's creditors must be satisfied with the assets of the corporation only. The creditors cannot legally require the owners, directors, or officers of the corporation to pay the organization's debt out of their own individual property. This feature of limited liability is important to potential owners, directors, or officers, especially if a company has to incur large debts in the course of doing business.
On rare occasions, however, individuals can be held liable for the debts of the corporation. A court that makes such a determination is said to be piercing the corporate veil. Generally, this can happen if the owners, directors, or officers exhibit so much control over the operations of the organization that a court finds it difficult to distinguish between the interests and activities of the company and the interests and activities of the individuals involved. In such cases, these individuals typically display a blatant disregard for corporate formalities and largely ignore the corporate structure in carrying out the business of the corporation. For example, these individuals may never conduct board of director meetings or they may fail to maintain separate bank accounts, expense records, and tax returns for the corporation. Insight 2A-1 reviews a court case in which a plaintiff attempted to pierce the corporate veil of a pharmacy plan administrator.
Insight 2A-1. Piercing the Corporate Veil.
Page 34 of 469

AHM 510 : Health Plans : Governance and Regulation
The United States Court of Appeals for the Second Circuit reversed a district court decision and held that a pharmacy chain may not have been entitled to pierce a pharmacy plan administrator's corporate veil in an attempt to recoup unpaid prescription claims.
The defendant in this case was a pharmacy plan administrator who entered into agreements with "panel pharmacies" such as the plaintiff. Under these agreements, eligible beneficiaries of ERISA welfare plans would have their prescriptions filled at panel pharmacies. The panel pharmacies would accept only a small copayment from beneficiaries, and would then submit the prescription claims to the pharmacy plan administrator for reimbursement.
As a result of cash flow problems (due in part to loans to the sole stockholder of the pharmacy plan administrator to pay personal expenses), the plan administrator failed to reimburse one panel pharmacy for a number of prescriptions. The panel pharmacy sued the plan administrator.
A district court ruled in favor of the panel pharmacy and determined that the pharmacy plan administrator was liable to the panel pharmacy. After a subsequent bench trial, the district court ordered that, under state law, the panel pharmacy could pierce the plan administrator's corporate veil to recover its judgment from the assets of the administrator's sole director and stockholder. In determining that the panel pharmacy could pierce the corporate veil, the district court stated that "where the corporation in fact is run by one person regardless of any corporate form, that person has to be responsible for whatever debt the corporations have."
On appeal, the Second Circuit observed that in order to pierce the corporate veil: (1) the owner must have exercised complete domination over the corporation with respect to the transaction at issue; and (2) such domination was used to commit a fraud or wrong that injured the party seeking to pierce the corporate veil. In this case, the court observed that the first prong of the corporate veil test had been clearly satisfied. However, the district court made no findings as to whether the executive's domination of the company was used to commit a fraud or wrong against the panel pharmacy which resulted in the pharmacy's injury. For this reason, the district court's judgment permitting the pharmacy to pierce the pharmacy plan administrator's corporate veil and to recover damages from its sole director and stockholder was declared legally void and sent back to the district court with instructions to determine whether the second prong of the two-prong test was satisfied.
Long-Term StabilityA corporation is the most permanent form of business organization. This feature gives a corporation a stability that other legal forms cannot guarantee. Furthermore, a well-managed corporation can survive the personal misfortunes of any of its owners, directors, or officers. This fact is reassuring to the corporation's customers and, in the case of a for-profit health plan, its investors.
Recently, new types of legal forms, such as limited liability companies, have emerged to provide additional options for establishing a health plan. These organizational structures
Page 35 of 469

AHM 510 : Health Plans : Governance and Regulation
have certain characteristics of corporations and certain characteristics of limited partnerships.
Limited Liability CompaniesThe limited liability company (LLC) is a relatively new type of legal entity that combines features of both a partnership and a corporation. The owners, who can be either individuals or companies, are called members. As in a partnership, when the LLC's members are individuals, the business profits and losses are treated as individual income for tax purposes. Similar to a corporation, the LLC makes available several options for raising operating funds, and it limits the liability of its owners. When the LLC members manage the organization themselves, the entity is called a member-managed LLC. When the LLC members do not manage the organization, it is called a manager-managed LLC.¹
Some provider groups are formed as limited liability companies, and although it is not common, a health plan can be formed as a limited liability company or can enter a specific business venture by forming a limited liability company with strategic partners. For example, an insurer and a healthcare management company, both corporations, might decide to launch a commercial health plan venture as an LLC. The LLC might benefit from the financial stability and administrative expertise of the insurer and the medical management know-how of the healthcare management company. Or a health plan might decide to expand into a new market, such as Medicaid, and seek a partner with familiarity in this market to jointly establish an LLC.
An LLC is usually established by filing a legal document, typically called articles of organization, with the appropriate state agency. Typically, the LLC also draws up a document, called an operating agreement- similar to a partnership agreement or corporate bylaws- that provides more detailed information about governance issues, such as voting rights, economic rights, and the steps to be taken if a member resigns. LLC statutes provide a great deal of flexibility in these organizational matters, which makes the LLC an attractive legal entity for attaining certain business objectives.
A health plan organized and operated in accordance with state LLC requirements can obtain the benefits of organizational flexibility similar to a partnership, along with the limited ownership liability of a corporation. In addition, for tax purposes, the profits and losses of the business are treated as if it were a partnership; that is, the LLC itself does not pay taxes. It is worth noting, however, that because LLCs are a fairly recent development, many of the enabling state laws have not been reviewed by the Internal Revenue Service (IRS) to determine if, in fact, the tax advantages are permitted.
An LLC is usually established for a limited period of time, such as 30 years, and typically ends with the withdrawal, expulsion, or death of a member. However, the LLC can remain in effect if there is a provision in the state law or the governing agreement that allows for continuation upon approval by a majority of the remaining members
Professional Corporations and Professional Limited Liability CorporationsCertain "special-purpose" corporations, such as professional corporations and professional limited liability corporations, are also available to some players in the healthcare industry.
Page 36 of 469

AHM 510 : Health Plans : Governance and Regulation
For years, practitioners of the "learned" professions, such as law and medicine, were not permitted to establish corporations. In the early 1960s, however, states began enacting laws to permit and regulate professional corporations, and in 1969 the IRS granted professional corporations the same tax status as other types of corporations. Physicians and, in some states, other healthcare practitioners-such as registered nurses, physical therapists, chiropractors, dentists, and pharmacists-may now establish professional corporations. In some states, medical practitioners may also establish professional limited liability companies.3
Because of the variety of state approaches to regulation, it is difficult to generalize about professional corporation laws; however, in almost all states professional corporations differ from business corporations in at least three ways:4
1. Ownership. 2. Directors and officers.3. Liability.
Ownership.
A unique feature of professional corporations is that their shares of stock can only be owned by individuals (and in some states, partnerships or other professional corporations) licensed to practice that corporation's profession. Some states allow the owners to be licensed practitioners in different areas of medicine, such as physicians and dentists. Any sale or transfer of shares must be to a person or entity meeting this requirement. Also, if a shareholder dies or is no longer a qualified shareholder, the stock must be transferred to a qualified shareholder or it must be purchased by the corporation within a specified period of time.
Directors and officers.
Another unique feature of professional corporations is the requirement in most states that all directors and officers be licensed to practice the corporation's profession. In states where nonprofessional directors are permitted, laws typically prohibit them from exercising authority over professional matters.
Liability.
Under the professional corporation laws in most states, professionals who own shares of stock in the corporation are individually liable for improper acts they perform or that are performed under their supervision, but only if the act is related to their profession. In other words, if a lawsuit arises concerning the corporation's purchase of office equipment, the physician involved is not personally liable. However, if a lawsuit arises concerning a medical service, then the physician who performed or supervised the service can be held individually liable, although the risk can be insured against or financially limited by the purchase of liability insurance. In a business corporation, the liability of individual stockholders is limited in virtually all circumstances.
Page 37 of 469

AHM 510 : Health Plans : Governance and Regulation
Corporate Practice of Medicine DoctrineMany jurisdictions have in place, either by specific statute or court decisions, a prohibition against corporate practice of medicine. In general, the corporate practice of medicine doctrine prohibits a physician from practicing medicine for a business corporation. Where this doctrine applies, a physician can only practice medicine as a sole proprietor, as a partner, for another physician, for a professional corporation, or for a professional LLC. In other words, this doctrine prohibits a business corporation from practicing medicine or from employing physicians to practice medicine on its behalf.
Corporate practice of medicine statutes arose largely out of the fear that business organizations would unduly influence the professional judgment of physicians. Some states also apply this doctrine to other healthcare practitioners besides physicians. The corporate practice of medicine doctrine is often modified to allow certain types of organizations to employ physicians when these organizations are licensed to employ physicians, as is the case for hospitals and staff model HMOs.
The application of the corporate practice of medicine doctrine can impact the legal structure of certain types of health plans. As insurers and health plans ally with providers, they must ensure that such alliances are established so as not to invoke corporate practice of medicine laws.
The application of the corporate practice of medicine doctrine varies by state. In practice, only a small number of states have actually applied a prohibition against corporate practice of medicine within the past 15 years, with California being a noteworthy example. Many more states have applied this doctrine at least once, but not within the past 15 years. Also, some states do not have a prohibiting statute, nor have they ever applied the doctrine in court, although this is no guarantee that they never will. 5
For-Profit, Not-for-Profit, and Mutual CompaniesA health plan's organizational structure strongly influences its approach to critical business activities such as allocating profits, obtaining operating funds, and overall governance. In developing a strategy to meet a health plan's mission and objectives, the health plan's leaders must determine, among other things, whether the organization will be a for-profit or not-for-profit company, and in the case of an insurer, whether it will be a stock or mutual company.
For-Profit Health PlansProfit can be defined as a health plan's total income (the amount of money it brings in) minus its total expenses (the amount of money it spends). In this sense, it is possible for a not-for-profit company or a mutual insurance company to make a "profit." However, one feature that clearly distinguishes a for-profit health plan from a not-for-profit health plan or a mutual insurer is the way the entity uses this excess of income over expenses.
A for-profit health plan conducts its business with the goal of making a profit to be distributed to or shared by its owner-investors. A mutual insurance company distributes "profits" to its policyowners. A not-for-profit health plan cannot distribute "profits" to individuals for personal gain, but must instead use its profits to benefit the company and its purpose.
Page 38 of 469

AHM 510 : Health Plans : Governance and Regulation
Obviously, any health plan, whether it is a for-profit company, a not-for-profit company, or a mutual insurance company, seeks to have its income exceed its operating expenses. The excess can be used to generate additional funds, and instills confidence in potential investors and lenders who provide access to even more funds. If a health plan is unable to convince investors, lenders, or donors of its ability to operate "in the black," the health plan is likely to lose access to outside funds that are often critical to continued operation in an increasingly competitive environment.
Stock CompaniesMost for-profit health plans in the United States today are stock companies. A stock company obtains the funds it needs to begin operations from investors who purchase ownership shares of stock in the company. These owner-investors are called shareholders. Although shareholders may receive a portion of the company's earnings through periodic payments, known as dividends, historically health plans have elected not to pay dividends. Shareholders realize capital gains or losses by selling their shares of stock. If shares of stock are offered to the general public, the company is called a publicly traded corporation. If shares of stock are not offered to the public, the company is called a privately held corporation.
In a publicly traded corporation, certain shareholders, called common stockholders, vote on company affairs and are ordinarily granted one vote per share of stock. Common stockholders elect the company's board of directors and influence company operations by voting on matters of company policy. One of the board's primary responsibilities is to select senior management to operate the company. In this type of arrangement, the vast majority of shareholders do not participate in the day-to-day operations of the business. Ultimately, the board of directors and management of the company are accountable to the shareholders for the profitability of the corporation.
Another class of stockholders is known as preferred stockholders. Preferred stockholders must be paid their dividends before common stockholders are paid theirs, but preferred stockholders generally do not have voting rights regarding the company's directors or company policy.
Shares of stock in a privately held corporation are available only to a closed group. A corporation may be privately held for any number of reasons. It may be too small to be publicly traded, it may be a family business, or the owners may not want to give up control and/or income by sharing ownership with outside investors. In these corporations, the number of owner-investors may be small enough so that it is feasible for all of the individuals to sit on the group's governing board. A privately held corporation always has the option of "going public" if it decides this would be in its best interest-for example, if the privately-held corporation needs to generate funds quickly for expansion into new markets or if it seeks to improve its information management capabilities by investing in new systems.
When a stock company is established, the articles of incorporation describe the number of authorized shares of stock and the par value of those shares. Generally, a company does not issue the total number of authorized shares. Instead, it retains some shares for future investment purposes. The par value of the shares is established for state tax purposes, but the actual investment is invariably greater than the par value.
Page 39 of 469

AHM 510 : Health Plans : Governance and Regulation
Governance of For-Profit Health PlansA for-profit health plan is run strictly as a business focused on growth and generating profits for its shareholders. This business focus and the ability to raise needed funds through owner-investors are two primary reasons that for-profit health plans have become more common in recent years. Another advantage that for-profit stock companies have over not-for-profits and mutuals is the ability to attract executive-level managers by offering shares of company stock as part of their compensation packages.
Some analysts believe that publicly traded corporations have a governance advantage over other types of companies because their shareholders often take an active interest in company operations. Shareholders, whose money is at stake, hold the board and senior management accountable. Because of the scrutiny of shareholders, the management of stock companies tends to be more aggressive, growth-oriented, and adaptable to changes in the economy. However, some analysts consider this to be a disadvantage, at times, because the desire for short-term financial results can overshadow the need for long-term investments and strategies.
Regulation of For-Profit Health PlansAt one time, many states placed significant regulatory constraints on the formation of for-profit HMOs, but today Minnesota and Vermont are the only states where for-profit HMOs are prohibited. In other jurisdictions, for-profit health plans are subject to comparatively fewer restrictions than mutual insurers and not-for-profit companies with regard to how profits and surplus funds can be used, although they are often subject to certain regulations, such as limitations on the types of investments they can make. A large number of not-for-profit health plans are converting to for-profit status, a trend that has prompted several states, as well as public interest groups, to pay closer attention to regulation of "for-profit" transactions involving not-for-profit health plans (see Formation and Structure of Health Plans).
Not-for-Profit Health PlansThe distinguishing characteristic of a not-for-profit health plan is that it has no owners or owner-investors, as does a for-profit health plan, and therefore cannot distribute profits for the benefit of individuals. Not-for-profit health plans typically use the term surplus to refer to the excess of income over expenses. Depending on the stated purpose of the health plan, surplus can be used for the benefit of the organization, the community, or a charity, but not private individuals. If a portion of the net earnings of a not-for-profit organization go to the benefit of private individuals, this is called private inurement. Salary and benefits paid to employees of a not-for-profit health plan are part of the organization's operating expenses and are not considered private inurement. However, a not-for-profit company must be cautious in designing its compensation plan because if regulatory authorities determine that the plan is not reasonable, the excess could be deemed unlawful private inurement of profit.
Although one might think that not-for-profit health plans would be less "profitable" than for-profit health plans, this has not been demonstrated. According to one study, the rates of return on assets are not appreciably different between for-profit and not-for-profit HMOs. 6
Taxable and Tax-Exempt Health PlansSome not-for-profit health plans obtain tax advantages by qualifying for tax exempt
Page 40 of 469

AHM 510 : Health Plans : Governance and Regulation
status; however, not all not-for-profit health plans qualify as tax-exempt organizations. A primary reason for tax-exempt status is that "charitable exemptions from income taxation constitute a quid pro quo: the public is willing to relieve an organization from paying income taxes because the organization is providing a benefit to the public." 7 A complex process that involves examination of sections of the Internal Revenue Code (IRC), numerous IRS rulings, and applicable court decisions determine a health plan's federal tax status.
The pertinent IRC sections for not-for-profits are 501(c)(3), 501(c)(4), and 501(m), not all of which confer tax exemption. The most notable court decisions are Sound Health Assn. v. Commissioner and Geisinger Health Plan v. Commissioner.
A health plan that qualifies as a 501(c)(3) charitable organization is tax-exempt on the basis that it promotes health for the benefit of the community. In Sound Health, the court held that an HMO can benefit the community, rather than solely private interests, if it meets certain criteria, such as providing healthcare services and maintaining healthcare facilities and staff, providing services to nonmembers on a fee-for-service basis, providing care for the indigent at reduced rates, providing care for individuals on public assistance programs, making emergency room facilities available to all members of the community without regard to ability to pay, and appointing a board of directors that is broadly representative of the community. Endnote8 Geisinger, the court further narrowed the interpretation of the community benefit standard so that in essence the only types of health plans that could qualify as 501(c)(3) organizations would be staff model HMOs or HMOs owned and operated by providers or healthcare systems.
A health plan that qualifies as a 501(c)(4) social welfare organization is tax-exempt on the basis that it is organized and operated exclusively to promote the general welfare of certain people in the community it serves. A 501(c)(4) exemption is easier to obtain than a 501(c)(3) exemption because 501(c)(4)s are allowed to benefit a comparatively smaller group of individuals such as the members of an HMO. A 501(c)(3) exemption, on the other hand, requires the organization to benefit the community at large. 9
A health plan that qualifies as a 501(c)(3) charitable organization can raise operating funds through the sale of tax-exempt bonds and can accept tax-deductible donations. A 501(c)(3) designation can also help an organization establish exemption from state and local property and sales taxes. Although a 501(c)(4) social welfare organization does not have these advantages, it does have more flexibility in determining use of funds for social or political activities. The choice of whether a health plan is established as a 501(c)(3) or 501(c)(4) organization is typically based on the organization's mission and whether it intends to serve a charitable purpose. Few health plans have qualified as 501(c)(3) organizations.
The Tax Reform Act of 1986 included a provision, Section 501(m) of the IRC, that for the most part eliminated the tax-exempt status for Blue Cross and Blue Shield plans, which until then were typically established as 501(c)(4) organizations. As a result, these plans were permitted to make tax deductions only for the portion of their earnings placed in reserve funds. Although 501(m) has had the greatest impact on Blue Cross and Blue Shield plans, the IRS also uses this section of the IRC in conjunction with sections 501(c)(3) and 501(c)(4) to determine the tax status of other types of health plans.
Page 41 of 469

AHM 510 : Health Plans : Governance and Regulation
Review Question
Some health plans qualify as tax-exempt organizations under Sections 501(c)(3) and 501(c)(4) of the Internal Revenue Code. One true statement regarding a health plan that qualifies as a 501(c)(4) social welfare organization, in comparison to a health plan that qualifies as a 501(c)(3) charitable organization, is that a
501(c)(4) social welfare organization is allowed to distribute profits for the benefit of individuals, whereas a 501(c)(3) charitable organization can use surplus only for the benefit of the organization, the community, or a charity 501(c)(4) social welfare organization can raise operating funds through the sale of tax-exempt bonds, whereas a 501(c)(3) charitable organization does not have this advantage 501(c)(4) social welfare organization has less flexibility in determining use of funds for social or political activities than does a 501(c)(3) charitable organization 501(c)(4) exemption is easier to obtain than a 501(c)(3) exemption, because 501(c)(4) social welfare organizations are allowed to benefit a comparatively smaller group of individuals
Incorrect. A not-for-profit entity cannot distribute profits for the benefit of individuals.
Incorrect. A 501(c)(3)charitable organization can raise operating funds through the sale of tax-exempt bonds, where a 501(c)(4) cannot.
Incorrect. A 501(c)(4) charitable organzation has flexibility in determining use of fund for social or personal activities.
Correct. A 501(c)3(3) charitable organizaton must benefit the community, while a 501(c)(4) charitable organization promotes the general welfare of certain people in the community it serves.
Section 501(m) denies tax-exempt status to any entity for which a "substantial part of its activities consists of providing commercial-type insurance." Furthermore, according to an IRS ruling, if a tax-exempt entity derives a portion of its income from operations that are classified as commercial-type insurance, that portion of its income is treated as taxable unrelated trade or business income.10 In distinguishing between HMOs and commercial insurance companies, IRS rulings suggest that certain indemnity-type features of HMOs, such as non-network emergency care or specialty care, are not considered commercial-type insurance. However, other indemnity-type features, such as POS options, are considered commercial-type insurance.
Some state requirements for tax-exempt status closely resemble federal requirements, while other state requirements are more restrictive. For example, a Massachusetts court ruled that a 501(c)(3) HMO was exempt from local real estate taxes because the HMO's health promotion activities applied to a large enough class of persons to be considered a benefit to the community at large. 11 On the other hand, Maryland courts ruled that a 501(c)(3) HMO was not a charitable organization and was subject to state property
Page 42 of 469

AHM 510 : Health Plans : Governance and Regulation
taxes, finding that the provision of "high quality medical care to . . . members for a fee" is not a charitable, benevolent, or educational activity.12
In most cases, even when a health plan is tax-exempt it is still required to pay a state premium tax, which is levied on premiums collected for certain types of insurance and healthcare coverage. Whether a health plan is subject to state premium tax depends on the type of health plan it is providing and the state in which it is doing business. Typically, premiums for indemnity insurance and PPO plans are subject to premium tax. In some states, POS options, exclusive provider only (EPO) plans, and HMO plans are also subject to premium tax.
Fast Definition
Reserve funds are funds set aside and conservatively invested to enable a health plan or insurer to pay claims as they come due.
Governance of Not-for-Profit Health PlansIn a not-for-profit health plan, governance comes from a board of directors or a board of trustees appointed when the entity is established. In some organizations, directors are replaced by board vote; in others, the board is elected by the health plan membership. Some states require boards to be at least partly elected by members. In a not-for-profit company, the directors or trustees are not accountable to voting shareholders or policyowners, but rather, depending on the stated purpose of the health plan, to the interests of the members, the community, or the charity the company serves.
Although the overall mission is different, the board of a not-for-profit health plan fulfills a role and functions in a manner similar to the board of a for-profit health plan. In the past, not-for-profit board members were often volunteers. Today, however, most board members are paid fees, although the amount is typically less than the amount received by for-profit board members. Later in this lesson, we will take a closer look at similarities and differences between governance of for-profit and not-for-profit health plans.
Evolution of Not-for-Profit Health PlansWhen Blue Cross and Blue Shield Plans and other prepaid health plans such as Kaiser Permanente began to appear in America in the first half of the 20th century, the federal government determined that these plans could be established as tax-exempt not-for-profit organizations. In 1973, the federal HMO Act authorized grants and loans for federally qualified HMOs that, at the time, were required to be "public or nonprofit entities." These tax advantages and funding incentives accounted for the establishment of a large number of not-for-profit HMOs. In the 1980s, however, government funding for HMOs was phased out, and the industry- encouraged by the federal government- began to demonstrate an increased ability to attract private investors.
Although not-for-profit health plans do not have access to shareholders, they do have other alternatives for obtaining operating funds, especially if they are tax-exempt. These alternatives include bond offerings, loans, private donations, surplus from business operations, and, in some cases, funds from for-profit subsidiaries or joint venture partners. It should be noted, however, that these funds are often more difficult to obtain than funds from private investors.
Page 43 of 469

AHM 510 : Health Plans : Governance and Regulation
As Figure 2A-2 demonstrates, not-for-profit health plans are no longer the predominant type of health plan in the United States; however, they remain a significant force.
Insight 2A-2. For-Profit and Not-for-Profit Health Plan Status in the United States.Percentage of For-Profit and Not for Profit PPOs in the United States
For-Profit Not-for-Profit 1993 84% 16%1996 88% 12%Percentage of For-Profit and Not for Profit HMOs in the United States
For-Profit Not-for-Profit 1985 35% 65%1990 66% 34% 1993 68% 32%1996 74% 26%
Mutual Insurance CompaniesSome health plans are organized as mutual insurance companies. The distinguishing characteristic of a mutual insurance company is that technically it is owned and governed not by investors, but by policyowners, and the board is ultimately accountable to the policyowners who elect it. The policyowners elect the board of directors on the basis of one vote for each policyowner, regardless of the amount of insurance or the number of policies a person owns.
Mutual insurers can issue both participating and nonparticipating policies, but only participating policyowners are eligible to elect board members. Participating policyowners are also entitled to receive policy dividends, which are considered a return of part of the premiums that were paid to keep the policy in force.
Most health plan policies issued by mutual companies are nonparticipating. However, even when a health plan policy is participating, the covered individuals are seldom eligible to participate in board elections or to receive policy dividends. Typically, covered individuals do not have these rights because under group policies the empolyer, not each covered employee, is the policy holder.
Review Question
The Tidewater Life and Health Insurance Company is owned by its policy owners, who are entitled to certain rights as owners of the company, and it issues both participating and nonparticipating insurance policies. Tidewater is considering converting to the type of company that is owned by individuals who purchase shares of the company's stock. Tidewater is incorporated under the laws of Illinois, but it conducts business in the Canadian provinces of Ontario and Manitoba.
Tidewater established the Diversified Corporation, which then acquired various subsidiary firms that produce unrelated products and services. Tidewater remains an independent corporation and continues to own Diversified and the subsidiaries. In order
Page 44 of 469

AHM 510 : Health Plans : Governance and Regulation
to create and maintain a common vision and goals among the subsidiaries, the management of Diversified makes decisions about strategic planning and budgeting for each of the businesses.
Tidewater's participating policy owners have the right to
elect the board of directors on the basis of one vote per policy owner
elect the board of directors on the basis of one vote for each policy a person owns
participate in developing a corporate mission statement and strategic plans
receive stock dividends for each policy they own
Correct. Participating policyholders select the board of directors on the basis of one vote per policyholder, regardless of the amount of insurance or the number of policies owned.
Incorrect. Participating policyholders select the board of directors on the basis of one vote per policyholder, regardless of the amount of insurance or the number of policies owned.
Incorrect. Participating policyholders participate by electing a board, and by receiving dividends.
Incorrect. Participating policyholders receive policy dividends, which are considered a return of the part of the premiums that were paid to keep the policy in force.
Similar to not-for-profit health plans, mutual insurers use the term surplus to refer to the excess of income over expenses. The wealth of many mutual insurers lies largely in their accumulated surplus. State regulations typically limit the ways that mutual insurers can use or invest this surplus.
Health plans that are organized as mutual insurers have certain advantages. Similar to not-for-profit health plans, mutual insurers are free from the pressures of stockholders who, according to some analysts, may focus primarily on short-term profits at the expense of long-term initiatives. Mutual insurers are also protected from unwanted takeovers by outside interests because, unlike stock companies, they have no shares of stock that can be acquired by other companies or investors. However, health plans that are organized as mutual insurers also face certain disadvantages. These plans are more difficult to establish and expand because, unlike stock companies, mutual insurers cannot sell shares of stock to raise start-up funds, nor can they sell additional shares to finance expansion or infrastructure improvements. Mutual insurers must raise capital primarily from company operations- that is, by selling policies.
The inability to sell shares of stock also makes it more difficult for mutual insurers, as well as not-for-profit companies, to take advantage of consolidation. Many players in the health plan industry today consider consolidation to be a key strategic advantage. If two for-profit health plans determine that it is in their best interest to merge, they can
Page 45 of 469

AHM 510 : Health Plans : Governance and Regulation
accomplish the transaction through an exchange of stock; however, if one of the entities is a mutual insurer or a not-for-profit health plan, this option is not available.
Although some stock and not-for-profit health plans are converting to mutual insurance companies (a process called mutualization), the trend over the past several years has been for mutual insurers to convert to stock companies (a process called demutualization). Also, some mutual insurers have created mutual holding companies to address some of the difficulties associated with being a mutual company. We discuss these topics in greater detail in Formation and Structure of Health Plans.
Health Plan FundingIn health plans, for-profit, not-for-profit, and mutual insurance companies compete in the same marketplace for the same business. Yet each operates within a somewhat different framework. Generating funds to establish, maintain, and expand operations is critical for all health plans. Access to capital is essential for initiatives such as systems upgrades, development of new products, expansion into new markets, and strategic alliances. The way a health plan raises these funds, however, is strongly influenced by how the health plan is organized. Although this text is not intended to provide a detailed analysis of health plan financing, we will provide a brief review of how each type of entity raises operating funds and a broad overview of funding sources.
A health plan can potentially obtain private sector operating funds from any number of sources. For the purpose of this discussion, we will divide these sources into four general categories: (1) internal sources, such as operating and investing activities; (2) debt markets; (3) equity markets; and (4) donations. In other words, a health plan can:
• Generate funds by using its own resources, that is, its business operations and investments (internal sources)
• Borrow from creditors (debt markets)
• Sell shares of ownership to owner-investors (equity markets)
• Solicit or receive funds (donations)
Different combinations of these options are available to each type of health plan.
All health plans have the potential to generate funds via internal sources of income. For the purpose of this discussion, we have divided internal sources of income into operating activities and investing activities.
1. Operating activities
2. Investing activities
A health plan's investing activities can be both long-term and short-term. Since premiums are prepaid, the funds are available before expenses are incurred. Thus, health plans can use premiums to make investments that can be used as a source of income until the funds are needed to pay healthcare expenses.
Operating activities are those activities associated with a health plan's major lines of business and involve transactions that directly determine the company's profits, including
Page 46 of 469

AHM 510 : Health Plans : Governance and Regulation
selling, administering, delivering, and designing managed healthcare products. 13
Generally, a health plan prefers to generate funds via operating activities. The health plan invests in itself to improve its operations, which results in a healthier organization in terms of funds on-hand, as well as future earnings potential. When it invests in operating activities, a health plan does not have to take outside investment risk, pay interest on debt, or pay the cost of issuing stock, as it might when seeking other sources of funds. At the same time, it strengthens its ability to provide products and services. Of course, such activities are not risk-free. There are no guarantees that a venture will succeed. Also, with increased competition in healthcare, profits are slimmer, and many operating activities require substantial capital investments. These challenges make it increasingly difficult for health plans to generate sufficient income via operations. In addition, health plans must adhere to all regulations governing investment in operating activities. For instance, a not-for-profit health plan that seeks to enter a strategic alliance with a for-profit health plan must comply with the requirements that apply to such transactions, and faces extensive and protracted regulatory scrutiny.
Investing activities a health plan's other internal source of income, are transactions that involve the purchase or sale of assets and the lending of funds to another entity. A health plan's investing activities include (1) purchasing and selling bonds, mortgage loans, stocks, real estate, equipment, certificates of deposit, and other assets, and (2) making loans and collecting the principal and interest on those loans. 14
A company can also raise funds through the debt markets, which are sources of funds loaned in exchange for the receipt of interest income and the promised repayment of the loan at a given future date. Debt instruments, also known as bond issues, represent debts that the issuing corporation owes to the bondholders. The debt markets are available to all health plans, although mutual companies do not usually issue conventional bonds. As we have seen, 501(c)(3) charitable organizations have access to tax-exempt bond offerings and tax-free loans; for tax purposes, they can deduct both the cost of generating a bond offering and the interest paid. Other types of health plans can deduct only the interest payments.
Debt is the most expensive method of obtaining operating funds. Companies must pay interest on debt, whether or not the company is making money. Typically, debt is utilized by health plans that operate medical facilities, such as staff model HMOs, and is used in connection with building or renovating facilities.
A for-profit company can also raise funds in the equity markets. The equity markets are sources of funds obtained by issuing financial instruments that represent an ownership interest (equity) in the issuing corporation. Shareholders invest in and own shares in the issuing corporation.15 A publicly traded or privately held health plan can make a "public offering" to obtain investors. In addition, a health plan that prefers not to "go public" can raise private equity in the equity market. Many analysts consider access to equity markets to be a significant advantage for a health plan. For instance, the cash that stock companies receive from selling stock can be used to buy other companies or to pay for expansion and improvements. Several not-for-profit and mutual companies have converted to for-profit health plans in recent years to obtain access to equity markets.
Page 47 of 469

AHM 510 : Health Plans : Governance and Regulation
Health plans that pay dividends can also generate net income by reducing the dividend amount they pay to their shareholders or policyowners.
Review Question
One way that a health plan can obtain operating funds is by issuing financial instruments that represent an ownership interest in the issuing corporation. By raising funds in this way, a health plan is accessing sources of funds called:
debt markets, which are available to all health plans
debt markets, which are available to for-profit health plans only
equity markets, which are available to all health plans
equity markets, which are available to for-profit health plans only
Incorrect. Debt markets are sources of funds loaned in exchange for the receipt of interest income and the promised repayment of the loan at a given future date. They are available to all types of health plans, although mutual companies do not usually issue conventional bonds
Incorrect. Debt markets are sources of funds loaned in exchange for the receipt of interest income and the promised repayment of the loan at a given future date. They are available to all types of health plans, although mutual companies do not usually issue conventional bonds
Incorrect. Equity markets are sources of funds obtained by issuing financial instruments that represent an ownership interest (equity) in the issuing corporation. They are not available to not-for-profit or mutual companies
Correct! Equity markets are sources of funds obtained by issuing financial instruments that represent an ownership interest (equity) in the issuing corporation. They are only available to for-profit companies.
Theoretically, any type of health plan can solicit and receive private donations. In practice, however, donations are almost never made to health plans other than 501(c)(3) organizations because only contributors to 501(c)(3) organizations can deduct qualified donations from their taxable income.
Figure 2A-3 shows the options available to for-profit, not-for-profit, and mutual companies for obtaining operating funds.
Insight 2A-3. For-Profit, Not-for-Profit, and Mutual Company Access to Operating Funds.
Type of Company
Internal Sources Debt Markets Equity Markets
Donations
Page 48 of 469

AHM 510 : Health Plans : Governance and Regulation
For-Profit
Available via funds generated by opening activities and investments
Available Available
Available, but almost never utilized because there is no tax incentives for donors
Not-for-Profit
Available via funds generated by opening activities and investments
AvailableNot available
Available, but almost never utilized except by 501(c)(3) organizations
Mutual
Available via funds generated by opening activities and investments
Available, but mutuals do not usually issue conventional bonds
Not available
Available, but almost never utilized because there is no tax incentives for donors
Page 49 of 469

AHM 510 : Health Plans : Governance and Regulation
Chapter 3 A : Corporate Restructuring and Corporate Transactions
After completing this lesson, you should be able to:
• Describe the options available to mutual companies seeking access to capital, strategic partnerships, and other corporate transactions
• Describe the issues that a not-for-profit entity must address when converting to for-profit status or when engaging in other transactions with for-profit entities
• Explain how health plans use reorganization and reengineering to improve performance
• Distinguish between strategic partnerships, joint ventures, acquisitions, and mergers
In the 1990s, the managed healthcare industry experienced massive restructuring. The unprecedented rate of corporate activities can be attributed to several factors. For instance, health plans often seek to:
1. Generate funds.
2. Gain market share or offer new products.
3. Reduce expenses.
4. Integrate or improve functions.
The number and nature of strategies for realigning corporate structure and the reasons for pursuing these strategies are virtually unlimited, as illustrated in Insight 3A-1 and Figure 3A-1. In this lesson, we describe how health plans seek to improve their performance through:
1. Corporate restructuring-such as demutualization, conversion from not-for-profit to for-profit status, and reengineering
2. Corporate transactions-such as strategic partnerships, joint ventures, affiliations, acquisitions, and mergers
Our discussion also examines key regulatory issues pertaining to corporate restructuring and corporate transactions.
Fast Fact
1997 closed as a record year, with 1,183 mergers and acquisitions in the healthcare industry, up 18.7% over 1996's 999 transactions. 1
Generate funds.
Managed healthcare is a capital-intensive business, and changes in corporate arrangements can help generate funds needed for activities such as expanding service areas, leasing facilities, purchasing equipment, paying off debt, adding to reserves to
Page 50 of 469

AHM 510 : Health Plans : Governance and Regulation
cover healthcare delivery costs, handling legal expenses, building information systems, and improving key functions and capabilities.
Gain market share or offer new products.
In a rapidly evolving marketplace, health plans restructure or undertake corporate transactions to capture a greater market share, enter new markets, or offer new products.
Reduce expenses.
Companies that restructure or combine organizationally often want to reduce the cost of running the business. They do this by obtaining economies of scale, which means they are able to perform functions on a larger scale and therefore at a lower unit cost than if they operated independently, thereby reducing administrative and medical expenses.
Integrate or improve functions.
Operating a health plan requires integrating several diverse and challenging tasks, such as arranging for the delivery and financing of healthcare, as well as performing many closely regulated administrative, technical, and legal functions. Sometimes it is beneficial for organizations to change structures and processes or join forces to more effectively provide these key services to their customers.
Insight 3-1. Corporate Transactions in the Health Plan Industry.
Following is a "snapshot" of corporate transactions that took place during a period of just one month, as reported in a health plan periodical:
Detroit, Mich.-based The Wellness Plan, which is formally incorporated as Comprehensive Health Services Inc., and Troy, Mich.-based SelectCare HMO are discussing the possibility of an affiliation or merger. The Wellness Plan, a not-for-profit organization, is the Detroit area's third-largest HMO. For-profit SelectCare HMO is the area's seventh-largest HMO.
Magellan Health Services and Merit Behavioral Care Corp. have signed a definitive merger agreement under which Magellan will acquire Merit. The company will become the nation's leading specialty health plan company. Under the agreement, Magellan will purchase all of Merit's outstanding stock. Magellan will also refinance Merit's existing debt.
Foundation Health Systems (FHS) Inc.'s Oregon HMO has completed its acquisition of Clackamas, Oregon-based PACC HMO and PACC health plans. The combined organization, called QualMed Plans for Health of Oregon Inc., serves about 180,000 members throughout Oregon and southwest Washington.
Page 51 of 469

AHM 510 : Health Plans : Governance and Regulation
Western Montana Clinic and Blue Cross and Blue Shield of Montana unveiled a new HMO called Montana Health. Montana Health will emphasize preventative care and freedom to choose providers, along with healthcare cost management.
Sutter Health and PacifiCare of California, the HMO subsidiary of PacifiCare Health Systems, have signed a long-term agreement to create a "systemwide strategic alliance." The agreement includes the FHP/Take Care members being absorbed into PacifiCare as the result of the recent acquisition. The agreement is the first of its kind in Northern California.
Ramsay Health Care Inc.'s managed behavioral care division, FPM Behavioral Health (FPM), has signed a contract with PacifiCare of Utah and Talbert Medical Management Corporation. Under the agreement, FPM will provide integrated behavioral healthcare services to more than 193,000 of PacifiCare of Utah's Medicare and commercial members.
Blue Cross and Blue Shield of Kansas City has acquired Overland Park, Kan.-based Preferred Health Professionals. The acquisition will help Blue Cross and Blue Shield offer health plan options to its 90,000 members. Preferred Health Professionals will retain its name and location and will function as a subsidiary of Blue Cross and Blue Shield.
Source: Excerpted and adapted from NewsFurst (November 1997, III/10)
Figure 3A-1 Examples of Health Plan Realignment Strategies. A national health plan might decide to change its organizational structure by
consolidating its marketing and administrative support regions in an effort to improve efficiency and reduce operating expenses.
Two health plans might decide to join forces because their particular geographic strengths complement each other, and by combining operations they can become a strong regional or national health plan with significant market share.
A national or regional health plan, which has been struggling to obtain market share in a particular city, might decide to enter into a transaction with a local health plan, which is also seeking greater market share; together they seek to significantly improve their market position.
A health plan might determine that it is "behind the curve" in developing a new product critical to its customers-for example, a preferred provider organization or a managed dental product. Rather than spend the time and money to develop the product from the ground up, the health plan might enter into a transaction with a health plan that has already developed such a product.
One health plan may be expert at marketing and administration, another may be expert at healthcare delivery. By combining resources and, in effect, drawing upon the best of both operations, they seek to develop a more effective operation than either could have built on its own.
Two local health plans might decide to join forces because their provider networks effectively complement each other; for example, one might have a strong primary care physician panel and the other might have a strong specialist panel.
Page 52 of 469

AHM 510 : Health Plans : Governance and Regulation
Corporate RestructuringHealth plans, seeking to improve performance and respond to the multitude of environment factors discussed in Environmental Forces, sometimes elect to change their corporate structure. In this section, we describe several corporate restructuring options available to health plans.
Parent Companies, Subsidiaries, Spin-offs, and Holding Companies²The corporate structure of a health plan can take any of a number of forms, from a single corporate entity to a complex arrangement of multiple entities. In this section, we briefly describe the relationship between parent companies, subsidiaries, spin-offs, and holding companies.
A parent company is a company that has a controlling interest in another company, called a subsidiary. A subsidiary is a company whose controlling interest is owned by another company, its parent. For example, some major insurance companies are parent companies that have HMO subsidiaries. Two subsidiaries of the same parent company are known as sister corporations.
Because a not-for-profit health plan cannot be owned, it cannot, technically, be a subsidiary of a parent company. In some instances, however, a parent company controls sole voting membership of a not-for-profit health plan, and the health plan is referred to as an affiliate. In this context, affiliate means a company that is held, but not owned, by a parent company.
In some situations, an organization actually lets a portion of its operations "spin off." A spin-off is a former unit or department of a company that operates as a subsidiary or, more often, as an independent company. If the company becomes completely independent, it may be owned by the same shareholders as the original company, who may be provided shares of the spin-off company's stock. In some cases, the spin-off is sold to certain employees who then own and operate it; this is sometimes referred to as a management buy-out. For example, a national multiline insurer with a health plan division might decide to spin-off its health plan business unit, selling it to the health plan division's senior management staff. Alternatively, the spin-off company's stock may be sold to another company in the same line of business, thereby expanding the purchasing company's business.
Sometimes the former parent company is the primary customer of a spin-off. However, the spin-off can also offer services to other individuals or organizations. For example, a health plan might develop a pharmacy management unit that it uses to provide services to its covered individuals. Later it may decide to make this unit an independent company (via spin-off) whose clients include the former parent company (the health plan from which it was spun off), as well as other health plans. Such spin-offs are established under the assumption that, freed from the restrictions of operating within a larger company, a subsidiary tends to be managed in a more aggressive and competitive manner and with lower administrative expenses. Spin-offs also may be designed to utilize excess resources, to take advantage of unique expertise in a certain area, or to pursue profit opportunities.
Page 53 of 469

AHM 510 : Health Plans : Governance and Regulation
When corporations wish to maintain a connection among a pair or group of separate corporate entities, they often use the mechanism of a holding company system. A holding company, which is a type of parent company, is an entity whose primary business is the holding or "ownership" of controlling interests of other companies, which are its affiliates or subsidiaries. A holding company arrangement can be used to control a group of companies in the same or related lines of business to maximize expertise and market presence in that field. A holding company arrangement can also be used to control subsidiaries in widely differing industries. In this way, the holding company can diversify its interests and protect itself from the risks involved in concentrating on just one kind of business.
As illustrated in Figure 3A-2, there are two basic types of holding companies. A downstream holding company is owned or controlled by the company that forms it. In other words, the parent company establishes a holding company, which then creates or acquires subsidiary firms. The parent that forms the holding company remains an independent corporation and continues to own or control the entire holding company system. Conversely, with an upstream holding company, the parent company forms a holding company and is actually controlled by the holding company it forms. The holding company is then in a position to create or acquire additional subsidiaries. The holding company owns or controls the entire holding company system, including the company that forms it.
Page 54 of 469

AHM 510 : Health Plans : Governance and Regulation
Most companies do not create downstream holding companies unless this is the only option available due to regulatory requirements, as is the case for a mutual insurer. Because a mutual insurer can only be owned and controlled by its policyholders, it cannot form or be purchased by an upstream holding company. Some mutual insurers determine that this restriction limits their ability to compete with other companies, a factor that leads them to consider other alternatives, which we discuss later in this lesson.
In pursuing a holding company arrangement, a not-for-profit health plan must be careful to protect any charitable or community benefit interests in its stated purpose. If a not-for-profit health plan creates an upstream holding company, there may be limits on the assets that can be transferred. If a not-for-profit health plan establishes a for-profit parent, this would likely be deemed a for-profit conversion, subject to applicable state requirements. We discuss issues related to not-for-profit transactions later in this lesson.
In some jurisdictions, organizations have found that forming a holding company can result in fewer restrictions on investments and greater flexibility in raising operating funds. For example, regulations in New York limit the kinds of investments that can be made by licensed insurance companies and their subsidiaries, although a parent company or a holding company that owns or controls a licensed insurer is not subject to the same investment rules, nor are its other subsidiaries. In this case, the holding
Page 55 of 469
AHM 510 : Health Plans : Governance and Regulation
company or one of its subsidiaries can make investments that an insurer cannot make. However, regulators are particularly concerned with preventing a holding company system from separating an insurer's assets and liabilities from that insurer's control. Regulators are aware, for example, that a holding company could "raid" the capital and surplus of an insurance subsidiary to provide funds for the holding company or another subsidiary. State regulation of insurance holding company systems is therefore designed to protect insurers and their customers from any such eventuality.3
All states have enacted some type of holding company act, and most such acts are based in whole or in part on the National Association of Insurance Commissioners' (NAIC) Insurance Holding Company System Regulatory Act (Model Holding Company Act). State holding company acts typically impose a number of registration and reporting requirements on companies that are part of an insurance holding company system. Also, most states have adopted regulations based on the NAIC's Insurance Holding Company System Model Regulation with Reporting Forms and Instructions (Holding Company Model Regulation). Such regulations specify requirements designed to carry out the provisions of the state's holding company act.4
Review Question
The Tidewater Life and Health Insurance Company is owned by its policy owners, who are entitled to certain rights as owners of the company, and it issues both participating and nonparticipating insurance policies. Tidewater is considering converting to the type of company that is owned by individuals who purchase shares of the company's stock. Tidewater is incorporated under the laws of Illinois, but it conducts business in the Canadian provinces of Ontario and Manitoba.
Tidewater established the Diversified Corporation, which then acquired various subsidiary firms that produce unrelated products and services. Tidewater remains an independent corporation and continues to own Diversified and the subsidiaries. In order to create and maintain a common vision and goals among the subsidiaries, the management of Diversified makes decisions about strategic planning and budgeting for each of the businesses.
In creating Diversified, Tidewater formed the type of company known as
a mutual holding company
a spin-off company
an upstream holding company
a downstream holding company
Incorrect. A mutual inurer cannot form or be purchased by an upstream holding company, and can only create downstream holding companies.
Page 56 of 469

AHM 510 : Health Plans : Governance and Regulation
Incorrect. A spin-off is a former unit of department of a company that operates a subsidiary
Incorrect. With an upstream holding company, the parent company forms a holding company and is actually controlled by the holding company it forms
Correct. A downstream holding company is owned or controlled by the company that forms it.
Mutualization and DemutualizationMutualization is the process of converting a stock or not-for-profit company to a mutual insurance company. Of particular note in the healthcare industry is the number of not-for-profit Blue Cross and Blue Shield plans that have changed their legal structure to become mutual insurers. Although the reasons for pursuing this strategy vary, a common advantage is that mutual insurers are subject to fewer regulatory controls than not-for-profit health plans. In addition, one Blue Cross and Blue Shield plan might seek to mutualize to be able to merge with another mutual Blue Cross and Blue Shield plan. Sometimes, mutualization allows a plan to expand its marketing territory into neighboring states or to enter strategic alliances with providers that serve populations in bordering states. Typically, when a Blue Cross and Blue Shield plan pursues mutualization, it must obtain state insurance department approval. Also, because such a conversion involves a change in the status of a not-for-profit health plan, it often raises issues of whether there exists a public benefit or charitable trust (which we address later in this lesson).
Demutualization is the process of changing a mutual company to a stock company. Often, companies that demutualize view this strategy as a way to compete with shareholder-owned entities. Some mutuals, entering the process primarily out of financial need, seek access to additional operating funds through the ability to sell stock. Other mutuals, building on a position of financial strength, seek an organizational structure that allows them to more quickly and easily pursue strategic options such as acquisitions and mergers, which in turn provide greater access to new markets, additional lines of business, and improved operational capacities. As we saw in Legal Organization of Health Plans, a stock company has the ability to pursue consolidation strategies using publicly traded stock as payment, and usually with less regulatory scrutiny than a mutual.
Regulation of demutualization varies by state. Some states have no specific regulations and guidelines for the process; others specifically prohibit it. A company that is demutualizing must be sure to comply with all regulatory requirements. Because of the changing business climate and legislators have been reviewing and in some cases changing applicable mutual insurance laws to be less restrictive.
Demutualization requires the distribution of the company's surplus funds among its policyowners. The company must find an equitable and efficient way to distribute this surplus. The company must also seek the legal opinions of regulators and find answers to several difficult questions. For instance, which policyowners should share in the surplus? Should all living policyowners, as well as the heirs of deceased policyowners, have rights to the surplus? Should only current or recent policyowners have these rights? Once a company determines who is entitled to the surplus, it must also determine how to make the distribution. Should policyowners receive cash, shares of
Page 57 of 469

AHM 510 : Health Plans : Governance and Regulation
stock in the converted company, or both cash and stock? Some consumer advocates have challenged the way that mutual insurers have handled or proposed to handle distributions that result from demutualization.5
A company undergoing demutualization must be prepared to incur substantial legal, accounting, printing, and postage costs as well as a decline in employee morale that is likely to result because of uncertainty about the new direction of the company.6
Recently, a new option has become available for mutual insurers seeking to change to a corporate structure that enables them to compete more effectively with shareholder-owned entities. The mutual holding company is a corporate structure under which the mutual insurer can sell as much as 49% of its ownership to public shareholders. The company gains access to capital markets, yet remains a mutual insurer because policyowners retain majority ownership. A number of jurisdictions have passed new mutual holding company laws or are considering new laws to allow mutual holding companies.
Proponents of the mutual holding company structure contend that it is a valuable option for mutual insurers that need access to capital and strategic alliances to compete with stock companies, but want to preserve the mutual relationship with their policyowners. On the other hand, some stock companies argue that this type of arrangement gives mutuals an unfair advantage in that they can access capital markets and initiate strategic alliances yet remain immune to takeover. In addition, some consumer advocates argue that policyowners as a group suffer because they lose the full ownership available to them under the traditional mutual insurance company structure.
Review Question
The Tidewater Life and Health Insurance Company is owned by its policy owners, who are entitled to certain rights as owners of the company, and it issues both participating and nonparticipating insurance policies. Tidewater is considering converting to the type of company that is owned by individuals who purchase shares of the company's stock. Tidewater is incorporated under the laws of Illinois, but it conducts business in the Canadian provinces of Ontario and Manitoba.
Tidewater established the Diversified Corporation, which then acquired various subsidiary firms that produce unrelated products and services. Tidewater remains an independent corporation and continues to own Diversified and the subsidiaries. In order to create and maintain a common vision and goals among the subsidiaries, the management of Diversified makes decisions about strategic planning and budgeting for each of the businesses.
In order to become the type of company that is owned by people who purchase shares of the company's stock, Tidewater must undergo a process known as
management buy-out
piercing the corporate veil
Page 58 of 469

AHM 510 : Health Plans : Governance and Regulation
demutualization
mutualization
Incorrect. A management buy out is when a spin-off company is sold to certain employees who then own and operate it.
Incorrect. Piercing the corporate veil is when a court determines that individuals can be held held liable for the debts of the corporation.
Correct! Demutualization is the process of changing a mutual insurance company to a stock company
Incorrect. Mutualization is the process of converting a stock, or not-for-profit company to a mutual insurance company
Not-for-Profit Conversions and Other TransactionsA major trend in the healthcare industry today is for hospital systems and health plans, including not-for-profit HMOs and Blue Cross and Blue Shield plans, to convert from not-for-profit to for-profit or mutual status. In addition to outright conversions, not-for-profit health plans sometimes enter into "for-profit-type" transactions, such as:
• Selling assets to raise funds
• Establishing for-profit subsidiaries
• Transferring assets into existing for-profit subsidiaries
• Entering into joint ventures or mergers with for-profit companies
As we noted previously, a key advantage of for-profit status is access to equity markets. To compete effectively, a health plan must make significant investments in administrative and medical management systems as well as in developing provider networks, which might require expensive financial transactions such as the acquisition of physician practices or hospital systems. For both business and regulatory reasons, health plans do not want to carry large amounts of debt to fund these critical activities. Therefore, the ability to raise equity capital becomes increasingly important.7 For those companies that have already incurred these expenses, conversion to for-profit status or a strategic alliance with a for-profit entity can help reduce or eliminate debt and meet ongoing operating expenses. In some cases, an alliance with a for-profit entity can even be used as a means to obtain funds for the not-for-profit charitable or community benefit obligations.
Many not-for-profit health plans are finding that there are few business advantages to retaining not-for-profit status in today's environment. Previously, there were tax exemptions that in many cases are no longer available. In some jurisdictions- New York, for example- not-for-profit health plans are subject to regulatory requirements and restrictions that do not apply to for-profit health plans. Some not-for-profit organizations convert to for-profit status or align with for-profit companies as a way to change the overall governance or strategic focus of the organization.
Page 59 of 469

AHM 510 : Health Plans : Governance and Regulation
If a not-for-profit entity is converting to for-profit status, regulators in some states attempt to apply a to apply a public benefit or charitable trust obligation and determine whether (1) the sale price represents fair market value for the assets sold, and (2) the sale proceeds will be used for charitable purposes. In some cases, the selling health plan may be required to use its assets to establish a charitable foundation for a related healthcare purpose such as provision of free medical care for residents in the community.
If a not-for-profit health plan enters into a "for-profit type" transaction that might impact its status as a not-for-profit entity, then the state Attorney General or the courts may have to determine if the assets are being applied in a manner consistent with the organization's stated purpose. Conversion activities raise concerns that the not-for-profit entity is taking funds generated for charitable or social welfare purposes and putting them into for-profit ventures that benefit individual owner-investors. For example, if a not-for-profit health plan participates in a joint venture with a for-profit health plan, this might raise questions about its ability to continue to fulfill its not-for-profit obligations. Such participation might also raise questions about how the joint venture contributions made by the not-for-profit organization will be used.
In some states, the Attorney General has the responsibility and authority to ensure that any corporate transactions a not-for-profit organization undertakes or enters into are in accordance with the organization's stated purpose. Some state Attorneys General, as well as public interest groups, have attempted to either block not-for-profit transactions or change the terms of the transactions. In effect, the states and public advocates, through the court system, are attempting to become involved in the governance of not-for-profit healthcare organizations, such as hospital systems and health plans. Figure 3A-3 lists some common issues that have arisen concerning not-for-profit transactions.
Figure 3A-3 Common Issues Concerning Not-for-Profit Transactions. Some states are concerned that not-for-profit entities are proceeding with conversions
to for-profit status without seriously considering other alternatives to the transaction which might allow the entity to retain its not-for-profit status.
Some Attorneys General want to require the not-for-profit organization to obtain a court approval prior to proceeding with a transaction that could affect any not-for-profit assets that are "impressed with a charitable trust." In other states, a court approval is clearly required. For example, New York not-for-profit corporation law requires a court order to authorize selling all or substantially all of the assets of a not-for-profit corporation.
A not-for-profit entity may be required to establish a charitable foundation with certain of its public assets, or to donate those assets to an existing charitable foundation. Several questions have been raised with regard to the transfer of assets to foundations. Is the foundation's mission close enough to the not-for-profit entity's stated purpose? Is the foundation far enough removed from the newly established for-profit entity? Is the not-for-profit company undervaluing its assets, thereby donating less than fair market value to the foundation?
States are concerned that a transaction might result in personal financial gain for directors or officers of the not-for-profit company. As we have seen, not-for-profit assets cannot be used for individual gain.
Page 60 of 469

AHM 510 : Health Plans : Governance and Regulation
Some Attorneys General have instituted court action when a not-for-profit entity failed to respond in a timely or thorough manner to requests for information about a transaction. Attorneys general also have expressed concern when a not-for-profit entity failed to disclose the proposed transaction to the public.
In most states, HMO laws are silent on the subject of not-for-profit conversions. As of the date of this writing, no jurisdictions, other than those that prohibit for-profit HMOs, have proposed or enacted an outright ban on not-for-profit to for-profit conversions. However, several jurisdictions have instituted or are considering closer regulatory scrutiny of health plan conversions. In addition, the National Association of Insurance Commissioners (NAIC) has focused on this issue, as have some federal legislators.
The type of legislation or proposed legislation governing conversions that has been developed at the state level requires the health plan to submit an application to the state Attorney General, a state agency, or both. This application is then reviewed to determine that the transaction is in the public interest. In some jurisdictions, actual state approval would be required for the transaction to proceed; in others, if the state does not respond within the specified timeframe, the transaction would be deemed approved.9
There is no consensus as to how to regulate not-for-profit transactions or even who should regulate them. In a number of states, Attorneys General have not addressed these transactions because they have taken the position that the laws in their states do not give them authority to do so. Some analysts recommend federal legislation to address this issue, but it appears federal legislation is not likely any time soon.
Insight 3A-2 provides an example of a not-for-profit transaction that illustrates several of the issues discussed in this lesson.
Insight 3A-2.Case Study: Not-for-Profit Conversions and Community Benefit Issues.
In 1993, Blue Cross of California, a not-for-profit company, restructured itself to transfer substantially all of its assets to a newly formed for-profit subsidiary, WellPoint Health Networks. WellPoint includes both Blue Cross' HMO and its preferred provider network. Blue Cross then raised $517 million when it sold a nearly 20% stake in WellPoint in an initial public offering. California law required that the corporation converting from not-for-profit to for-profit status make a financial contribution to charity equal to the value of its assets. Initially, the California Department of Corporations determined that Blue Cross would not have to make such payment because WellPoint is controlled by Blue Cross, which had itself remained not-for-profit. In response, legislation was introduced that, if enacted, would have required that a restructured not-for-profit public-benefit corporation not only maintain, but also increase corporate charitable expenditures in proportion to any increase in assets owned by the corporation. As a result of the introduction of this legislation, Blue Cross agreed to make charitable contributions of $5 million annually for the next 20 years. However, in late 1992, the Department of Corporations demanded that Blue Cross make additional contributions. In an attempt to settle the matter, Blue Cross of California agreed to donate $100 million in 1994 to healthcare charities and made a tentative offer of donating a total of $500 million to charity. Source: Hall and Brewbaker, 1-122.
Page 61 of 469

AHM 510 : Health Plans : Governance and Regulation
ReengineeringIn a rapidly evolving and increasingly competitive environment, some health plans seek to improve their performance by changing their internal structures and processes through corporate reengineering. Reengineering is defined by Michael Hammer and James Champy as "the fundamental rethinking and radical redesign of business processes to achieve dramatic improvements in critical, contemporary measures of performance such as cost, quality, service, and speed."10
Sometimes, reengineering focuses primarily on corporate structure and internal organization and staffing; this process is also called reorganization as noted in Environmental Forces. Often, however, the reengineering process goes beyond organizational realignment to include a fundamental rethinking of the way the company does business. In this more comprehensive approach to internal alignment, a health plan closely evaluates and redesigns its technology, support systems (such as mechanisms for hiring, training, and communication), competencies (such as the technical and managerial skills of its employees), and overall work environment and ability to change. 11
In other words,
"Reengineering requires companies to look past existing models, assumptions, and infrastructures to see the underlying key processes that bring value to the customer. Cross-functional teams are assembled to ask the following question of each process: 'Would we do it this way if we could start from scratch tomorrow?' If the answer is no, the process is a candidate for reengineering . . . The most successful health plans have used the concepts of reengineering to establish large-scale, highly flexible, integrated organizations that operate with a uniform set of work practices and information systems, significantly lowering transaction costs. These centralized systems could not have been created from existing systems that were built according to outmoded market assumptions."
Typically, the reengineering process focuses on outcomes and results, rather than specific tasks. For example, when looking at how to handle new business for group purchasers, a health plan would not organize its reengineering process around separate tasks performed for the purchaser by various departments. Instead, it would focus on the specific items and services that are delivered to the purchaser (such as information kits, premium notices, the group contract, and member booklets) and seek to find the most effective ways to provide these "deliverables" to the customer. For example, the health plan might decide to assign an employee to each new purchaser; this employee's job would be to coordinate interdepartmental activities and to supply the various areas with the information needed to produce the "deliverables" quickly and accurately.
Reengineering can result in restructuring of departments and job responsibilities, consolidation and closing of work sites, or withdrawal from geographic markets or lines of business. A health plan might decide to focus on its "core businesses" by investing time, effort, and funds on what they do best. Or a health plan might decide that environmental and competitive pressures require a focus on new markets and new lines of business. One health plan might then embark on a reengineering process to develop the required competencies from within. Another health plan might pursue a strategy that involves an alliance with another company, and then utilize corporate reengineering to combine the existing structures and operations of the previously separate entities into a single organization.
Page 62 of 469

AHM 510 : Health Plans : Governance and Regulation
Corporate TransactionsIn the first part of this lesson, we have seen how health plans change corporate structure to respond to environmental factors and to improve performance. In this section, we describe how health plans, for many of the same reasons, pursue corporate transactions with other companies. Here are some examples of what health plans frequently hope to gain from these transactions.
An alliance with a well-financed company might enable a health plan to (1) meet the demands of intense competition for capital and (2) invest this capital in key operational and technological improvements to attract customers and generate revenue.
A health plan can improve its overall financial strength and stability through an effective alliance.
The participants in an alliance can improve their ability to negotiate price with national suppliers as well as local providers by delivering increased volume.
If the participants are in different lines of business, they can diversify risk and be less likely to suffer catastrophic loss in the event of a market downturn.
Health plans can mesh geographical markets to obtain a broader presence. For instance, one health plan might be well established in the east; the other might be well established in the west. A combined broader geographical presence might generate increased business with national employers that seek a single health plan for all of their locations.
Two health plans together might establish a more prominent position in a particular market where each has been unable to make inroads on its own.
Health plans can mesh product strengths and weaknesses to obtain a stronger product mix. For example, one health plan might be strong in group HMO products, the other might be strong in managed workers' compensation programs.
The participants might have provider networks that effectively complement each other and offer greater choice to members. For instance, one might have a strong primary care physician panel, the other might have a strong specialist panel.
An alliance can help obtain economies of scale to reduce operating expense. The participants might have functional strengths and weaknesses that complement
one another. For example, one might be proficient in marketing, claims, and member services; the other might be proficient in provider contracting, provider relations, and medical management.
The participants might combine resources to make improvements in functions such as medical management or marketing. For instance, they might combine their medical outcomes databases to obtain a substantially larger pool of information; or they might combine their marketing survey data to obtain similar advantages.
Strategic Partnerships and Joint VenturesIn the course of doing business, all health plans conduct basic corporate transactions. For example, through aggressive sourcing, health plans seek to obtain the best deals from various vendors for equipment, supplies, and services such as telephones, overnight mail, computer hardware and software, and copy machines. 12
Some health plans also choose to contract with vendors who provide specific functions that would otherwise be performed in-house, such as paying claims. This type of
Page 63 of 469

AHM 510 : Health Plans : Governance and Regulation
corporate transaction, called outsourcing, typically requires more of an emphasis on managing relationships and customizing processes than does aggressive sourcing. 13
Review Question
In the course of doing business, health plans conduct basic corporate transactions. For example, when a health plan engages in the corporate transaction known as aggressive sourcing, the health plan
chooses to contract with vendors who provide specific functions that would otherwise be performed in-house, such as paying claims seeks to obtain the best deals from various vendors for equipment, supplies, and services such as telephones, overnight mail, computer hardware and software, and copy machines merges with one or more companies to form an entirely new company
joins with one or more companies, but retains its autonomy and relies on the other companies to perform specific functions
Incorrect. Outsourcing is when the health plan chooses to contract with vendors who provide specific functions that would otherwise be performed in-house, such as paying claims.
Correct. Aggressive sourcing is when the health plan seeks to obtain the best deals from various vendors for equipment, supplies, and services such as telephones, overnight mail, computer hardware and software, and copy machines.
Incorrect. A consolidation is when the health plan merges with one or more companies to form an entirely new company.
Incorrect. A stratgic partnership is when the health plan joins with one or more companies, but retains its autonomy and relies on the other companies to perform specific functions.
Another type of corporate transaction, which can be viewed as more reciprocal in nature than either aggressive sourcing or outsourcing, is the strategic partnership. For the purpose of this course, we use the term strategic partnership to mean an alliance between two or more entities that are not directly involved in the other entities' operations. Firms that enter into a strategic partnership often do not want to merge operations with or acquire other companies. In fact, a strategic partnership is not the same as the legal form of partnership we discussed in Legal Organization of Health Plans.
Even though the participants in a strategic partnership are not directly involved in each other's operations, the companies typically operate in accordance with a contract or letter agreement. Rather than enter into a full-fledged joint venture (see below), the
Page 64 of 469

AHM 510 : Health Plans : Governance and Regulation
entities elect to retain their autonomy and enter into an arrangement in which they rely upon each other for the specific functions needed.
For example, a physician-hospital organization might enter into a strategic partnership with a management consulting company to gain the expertise needed to help bring a new Medicare health plan product to market. Or an insurer might enter into a strategic partnership with a hospital-physician network to develop a preferred provider organization. We will take a closer look at specific health plan structures and arrangements such as these in Health Plan Structures and Arrangements.
In a joint venture, a company is formed, owned, and operated by two or more entities as a separate business or project for the mutual benefit of the participating entities. Often, a joint venture is formed to share the risks and rewards in developing a new product or entering a new market location, and the joint venture participants possess resources and expertise that complement one another. In most joint ventures, a contract spells out how each joint venture partner participates in the overall management and operations of the venture. One joint venture partner may contribute more to the operation of the venture or may have a greater economic interest in the venture than the others; however, the arrangement is still considered a joint venture as long as no single partner actually controls the venture. Often, the board of directors consists of an equal number of representatives from each of the participating entities.
A national health plan and a local hospital system, which operates its own health plan network, might enter a joint venture in which they share ownership of a newly created health plan operation. The primary objective for the hospital system might be to shift its focus back to hospital operations, while still obtaining patients from the health plan. The primary objective for the health plan might be to gain market share in a geographical area where in the past it has been unable to compete effectively. Eventually, the health plan might buy the hospital system's share of the joint venture, or the companies might merge some or all of their operations. The governance structure for the joint venture would be described in an agreement that specifies the rights and responsibilities of the participants, such as the percentage of the venture that each party owns, the organizational structure, and the decision-making/approval process.
In an environment of constant change, strategic partnerships and joint ventures offer a flexible and cost-efficient way of doing business. An entity can move quickly into a new and potentially profitable endeavor without altering its legal form.
Acquisitions and MergersAn acquisition occurs when one company purchases a controlling interest in another company. Ownership of more than 50% of the stock generally gives the purchaser a controlling interest. Practical control of a company's operations can take place with as little as 10% of a company's stock, if the remaining stock is widely distributed.14
One type of acquisition is called a stock purchase. In a stock purchase, a company acquires 100% of the voting shares of another company's stock, thereby making the acquired company a wholly owned subsidiary. All of the assets and liabilities of the subsidiary, including those that were incurred prior to but not yet realized on the date of the transaction, remain with the acquired subsidiary. 15
Page 65 of 469

AHM 510 : Health Plans : Governance and Regulation
Another type of acquisition is called an asset purchase. In an asset purchase a company acquires all or certain operating assets of another company. The acquisition agreement identifies the assets to be acquired and typically spells out any associated liabilities that would be transferred. An asset purchase can be used when a for-profit company acquires a business from a not-for-profit entity or a mutual company. It can also be used when the company being acquired would otherwise carry with it substantial liabilities such as financial problems or potential regulatory or legal problems. 16
Review Question
In the paragraph below, a statement contains two pairs of terms enclosed in parentheses. Determine which term in each pair correctly completes the statement. Then select the answer choice containing the two terms that you have chosen.
One type of acquisition is called a stock purchase. In a typical stock purchase, a company acquires (51% / 100%) of the voting shares of another company's stock, thereby making the acquired company a subsidiary. The (acquired / acquiring) company holds all of the assets and liabilities of the acquired company.
51% / acquired
51% / acquiring
100% / acquired
100% / acquiring
Incorrect. In a stock purchase, the acquired company becomes a wholey owned subsidiary and retains all its assets and liabilities
Incorrect. In a stock purchase, the acquired company becomes a wholey owned subsidiary, and the aquiring company does not take over the the assets and liabilities of the aquired company
Correct. In a typical stock purchase, a company acquires 100% of the voting shares of another company's stock, thereby making the acquired company a subsidiary. The acquired company holds all of the assets and liabilities of the acquired company.
Incorrect. While the company acquires 100% of the voting shares of another company's stock, the aquiring company does not take over the the assets and liabilities of the aquired company.
A merger occurs when two or more entities decide to pool their resources to form a single legal entity. A merger can be transacted in any of a number of ways. For example, one of the entities can merge into the other, or one of the entities can merge into a new subsidiary formed by the acquiring entity. Frequently, the acquiring entity forms a new subsidiary, which it then merges into the entity being acquired, leaving the acquired
Page 66 of 469

AHM 510 : Health Plans : Governance and Regulation
entity as the surviving entity in the merger. By having the acquired company survive as a legal entity, the acquiring company can sometimes avoid requirements for obtaining new licenses or other government approvals.17 When two or more companies merge to form an entirely new company, and the original companies are dissolved, this type of transaction is called a consolidation.
Because acquisitions and mergers are complex transactions that have the potential to generate substantial financial and legal risks, health plans typically perform a due diligence investigation before proceeding. When performing due diligence, a health plan carefully examines a number of issues, such as potential transferred liabilities and tax and accounting implications, that may determine the type of transaction and how it is structured.
Besides conducting a due diligence investigation to minimize legal and financial risks, a health plan also carefully considers whether a proposed corporate transaction actually meets a strategic or business need. If the answer is yes and the health plan proceeds with the transaction, then it is equally important for the health plan to perform effective post-transaction management. Insight 3A-3 illustrates these points.
Insight 3A-3. Effective Corporate Transactions.
Consolidation in the health plan industry can create value. Yet evidence from the healthcare marketplace and experience in other industries demonstrate that the chances of gaining real value from a merger or acquisition are low unless firms pay careful attention to why and how they pursue business combinations.
Specifically, effective merger management requires the ability to identify merger or acquisition opportunities that fit a real strategic need and create economic value. This means determining the real value of the merger or acquisition and not getting caught up in the "chase" that allows the "purchase price" to reach astronomical levels that exclusively benefit the acquired company's shareholders.
The second requirement for success is the ability to ensure that once the merger or acquisition is consummated, strategic and economic value is captured through rigorous post-transaction management. It is these two skills that are separating the winners from the losers as health plan industry consolidation continues.
As in any other industry, a health plan company must evaluate a business combination with a real eye to clarity of purpose and a hardheaded approach to determining the real value of the merger.
The chance of gaining real value from a merger or an acquisition declines precipitously when companies do not have a clear economic and strategic rationale for the deal. Thus, merging companies need to systematically determine the actual value of each potential synergy so that they can be very sure of not overpaying and then plan sufficiently for how to capture the value through the post-merger integration process.
Page 67 of 469

AHM 510 : Health Plans : Governance and Regulation
Even management teams that have a good rationale for their business combination often fail to capture the identified value after the merger has been consummated. This reflects a fundamental axiom of mergers and acquisitions: Identifying synergy potential is a lot easier than realizing it.
Those who have been most successful have done three things very well. They have:
(1) Planned for the integration and management of the merger or acquisition well before the ink dried on the "deal" papers
(2) Moved quickly to achieve savings, focusing first on the administrative savings and medical cost management areas. These savings include integrating the best approach in the local markets where the networks overlap or leveraging lower HMO-negotiated provider rates for such other products as their PPO
(3) Not let the merger or acquisition distract them from their growth agendas and the value that can be created beyond the basic synergies. The successful mergers are encouraging efforts on the "top-line" as well as the "bottom-line." Too often when a merger occurs, executives focus exclusively on bottom-line savings and lose sight of how much of the strategic and economic rationale for the merger was due to new revenue that could be achieved by the merged entity (top-line growth)
Source: Vivian Riefberg, Susan Stock, and Cyrus Taraporevala, "Getting the Most from Your Health Plan Merger," Health Plan Week (February 23, 1998): 6-7.
Page 68 of 469

AHM 510 : Health Plans : Governance and Regulation
Chapter 3 B
Health Plan Structures and Arrangements
After completing this lesson, you should be able to:
Identify and describe the various types of sponsors of health plans Discuss the objectives of providers in health plan structures and arrangements Discuss the impact of changes in health plan structures and arrangements on
regulation Differentiate between horizontal, vertical, and conglomerate integration Differentiate between structural, virtual, and operational integration Explain how strategic, marketplace, and regulatory issues can shape health plan
structures and arrangements Describe various arrangements employers use to provide healthcare benefit plans for
their employees
In the United States today, as many as a million separate entities may be participating in healthcare and health plans. This number includes organizations such as hospitals, other healthcare institutions, various providers and provider groups, practice management firms, manufacturers and suppliers, insurers, specialty health plans, PPOs, and HMOs.1 As Charles G. Benda and Fay A. Rozovsky describe it: "The phrase "managed health care" or "health plan" has been used in a variety of ways and applied to a variety of organizations and activities. In the past, the term "health plan" was often associated with a type of organization known as a health maintenance organization or HMO. Currently, the term "health plan" has become a veritable circus tent under which numerous and quite different organizational animals reside. Some organizations, such as utilization review firms, do not deliver any type of care but their activities are usually considered fundamental to health plans. Other organizations, such as physician provider groups, appear to the patient to be delivering services in a manner identical to that used in the past even though they may be sharing in the insurance risk traditionally borne exclusively by insurance companies. In addition, there is a whole assortment of health plans going under such acronyms as PPO, IPA, PHO, POS, and the like.
Health plans are best understood as the result of a whole constellation of changes in health care delivery, management, and financing. These changes have spawned a variety of organizations and approaches, as businesses and professionals respond to the changes and adapt to the new health care environment. . . Absent any government-mandated approach that locks a particular program or structure into place, (these changes) and the resulting variety of organizational forms (are) likely to continue."
A new type of health plan might appear when an unmet need is identified in the marketplace. As the market changes, a health plan may decide to build upon a time-tested strategy or to try something new, perhaps borrowing concepts from a number of successful models to form a different type of health plan entity. Existing health plans are constantly looking for new ways to operate and solidify their standing in a very competitive environment. The participants in the health plan industry pay close attention
Page 69 of 469
AHM 510 : Health Plans : Governance and Regulation
to what succeeds and what doesn't, freely borrowing from one another and sometimes forming "hybrid" business entities, further blurring the lines of distinction between the various entities. Insight 3B-1 describes how the variety of health plan structures and arrangements can impact industry researchers as well as participants.
In this lesson, we examine the variety of structures and arrangements in health plans, focusing on who sponsors them, how they operate and interrelate, and the regulatory and governance issues associated with their formation and evolution. Figure 3B-1 provides an overview of several organizational arrangements that have emerged to address the changes, challenges, and opportunities in the healthcare environment.
Insight 3B-1. A Government Agency's Research Agenda for Health Plans.
Probably the greatest challenge to research on health plan is the fact that market realities have evolved far more quickly than has our ability as researchers to conceptualize and classify them. As a result, it is not clear how to isolate and measure those features of the complex new healthcare organizations that are likely to be most important to use of services, customer satisfaction, health status, or costs. The old alphabet soup configurations of HMOs, IPAs, PHOs, and so on no longer do the job, but no generally accepted alternative framework has emerged. To address this issue, the Agency for Health Care Policy and Research (AHCPR) has been leading and encouraging the development of new conceptual frameworks for analyzing the configuration, operation, and impact of emerging health organizations and markets.
Source: Irene Fraser, "Research Agenda for Health Plans," U.S. Department of Health and Human Services, Public Health Service, Agency for Health Care Policy and Research: 675.
Figure 3B-1. Types of Health Plans.
HMO. A health maintenance organization (HMO) is a system designed to deliver healthcare to a voluntarily enrolled population in a particular geographic area, usually in exchange for a fixed, prepaid fee. An HMO brings together the delivery, financing, and administration of healthcare into a single integrated system.
PPO. A preferred provider organization (PPO) is an organization that offers a healthcare benefit arrangement designed to supply services at a discounted cost by providing incentives for members to use network providers, while also providing more limited coverage for services rendered by providers who are not part of the PPO network. Sometimes the product is called a preferred provider arrangement (PPA) to differentiate it from the organization that offers it.
EPO. An exclusive provider organization (EPO), as its name suggests, only covers healthcare rendered by participating providers, and does not cover most healthcare rendered by nonparticipating providers. Typically, an EPO, as opposed to an HMO, is regulated by state insurance laws and is subject to fewer licensing requirements.
Specialty health plans. A specialty health plan is an organization that uses an HMO or PPO model to provide healthcare services to a subset or single specialty of medical care.
Page 70 of 469

AHM 510 : Health Plans : Governance and Regulation
Many states require a licensed HMO to provide a comprehensive set of services and supplies. Some states regulate the establishment of single-service HMOs, such as dental HMOs. Other states do not permit single-service HMOs, although organizers do have other options for offering health plan specialty services, such as dental PPOs and dental POS plans.
Utilization Review Organization. A utilization review organization (URO) is an organization that conducts utilization review activities for health plans and purchasers. A URO may offer medical cost management services in any number of areas, such as inpatient review, outpatient review, and case management of high-risk conditions. Some UROs have expanded their services to include additional functions, such as claims administration, provider contracting, provider credentialing, medical outcomes measurement, member satisfaction surveys, and plan design consulting.
Third party administrator. A third party administrator (TPA) contracts with insurers, health plans, or employers to provide services to help administer healthcare benefits. Because TPAs often perform insurance-like functions, such as claims administration, they are regulated by the insurance department in many states.
At-risk provider organization. Broadly speaking, an at-risk provider organization, also called a provider sponsored organization (PSO), also called a physician-owned organization or provider-owned organization, is a health plan entered into or established by providers to arrange for the delivery, financing, and administration of healthcare. PSOs are often formed as a result of a state authorizing an alternative to securing an HMO license. Typically, PSOs are subject to less rigorous solvency and licensing requirements than HMOs, although regulators are considering changing these requirements. The Medicare PSO, a specific type of PSO, is an entity entered into or established by providers who deliver a substantial proportion of services under a Medicare+Choice contract; these providers share substantial financial risk and have at least a majority financial interest in the entity.
Independent practice association. An independent practice association (IPA) is an association of individual physicians (or physicians in small group practices) that contracts with a health plan to provide healthcare services.
Physician-hospital organization. A physician-hospital organization (PHO) is structurally much the same as an IPA, except that it includes a hospital. The primary purpose of a PHO is to contract with other health plans, payors, and purchasers on behalf of its participating hospitals and medical practices.
Management service organization. A management service organization (MSO) is a legal entity that provides a variety of management and administrative services for participating physicians' practices. These services may include centralized purchasing, administrative support, marketing, and practice management. With regard to these primary functions, an MSO is similar to a physician practice management company (see next item). Some MSOs have begun negotiating contracts with payors. For the most part,
Page 71 of 469

AHM 510 : Health Plans : Governance and Regulation
however, the MSO focuses on the "back office" (i.e., the administrative functions) to free the physicians to focus on the clinical aspects of healthcare.
Physician practice management company. A physician practice management (PPM) company is a legal entity that provides a variety of management and administrative services for participating physicians' practices. Typically, a PPM accomplishes this by purchasing the assets of the practices and entering into long-term contracts with those physicians, often supplying capital for improving and expanding existing assets. The services they provide may include centralized purchasing, administrative support, marketing, practice management, and contract negotiations. Some PPMs perform payer and utilization review/quality management functions; others have acquired HMOs.
Integrated delivery system. An integrated delivery system (IDS) is a combination of two or more legally affiliated health plans, group practices, clinics, or hospitals that combine their assets, efforts, risks, and rewards to deliver comprehensive healthcare and, in certain instances, to arrange for the financing and administration of that care.
Medical foundation. A medical foundation is an entity that owns and manages all purchased assets of physicians' practices. However, unlike an MSO or PPM, a medical foundation is organized as a not-for-profit entity, rather than a partnership, professional corporation, or other for-profit entity. A similar entity, the medical foundation IDS, integrates a hospital and a tax-exempt physician practice, thereby producing tax-exempt status for this organization as well. Typically, a medical foundation IDS consists of a holding company and two not-for-profit subsidiaries: a hospital, and a medical foundation. The medical foundation (not the holding company or hospital) enters into contracts with payors and receives the negotiated fees.
Academic medical center. An academic medical center (AMC), also known as an academic health center (AHC) is an institution that trains healthcare professionals and performs basic and clinical research. In addition, because AMCs receive government funding, they are required to provide medical care for the poor.
Cooperative. A cooperative, sometimes called a healthcare cooperative or a rural cooperative, is a consumer-sponsored, physician-operated medical facility that provides prepaid healthcare to members.
Community health center. A community health center (CHC) is a medical facility, typically located in an inner city or a rural site, that receives federal, state, and often private grant funding to provide primary care for medically underserved populations, such as Medicaid recipients, Medicare recipients, or individuals who do not have health coverage. The federal government first provided grants to establish these programs in the 1960s, at which time they were called neighborhood health centers, and then expanded them to include rural areas, migrant farm workers, and homeless individuals.
The System in Health PlansDespite the variety of participants in health plans, every entity we examine is involved in
Page 72 of 469

AHM 510 : Health Plans : Governance and Regulation
one or more functions comprising a system that delivers, finances, and administers healthcare.
This system coordinates and manages a set of complex tasks or businesses that have a well-established history of operating independently. When fee-for-service, third party payment was prevalent, healthcare delivery and financing were at best only loosely coordinated, and sometimes were at odds with each other because of different perceived missions. Providers delivered healthcare. Insurers designed and administered benefit plans that paid the healthcare bills. Both groups went about their business separately, focusing on their particular areas of interest with limited coordination between them.
Health plans brings together virtually the whole range of services that, in the indemnity environment, were performed by separate businesses and professionals. The goal of health plans is to streamline operations by integrating hospitals, physicians, various other facilities and providers, payors, and administrators so that the various participants can effectively share information, produce economies of scale, and provide continuity of care- thereby improving quality, increasing access, and reducing cost.
The expertise required to operate a successful hospital or physician practice is completely different from the expertise required to operate a successful insurance company. Yet in health plans, these highly complex and diverse functions must work together. What makes this an even greater challenge is the need for healthcare professionals, who have a strong sense of autonomy of professional judgment, to buy in to the health plan system. Thus, this system must combine "a collegium of professionals- highly trained scientists delivering intimate human service- and a business- competitive, entrepreneurial, preoccupied with the 'bottom line,' and therefore absorbed in all the traditional problems of hierarchical organization of corporate authority. Both elements must somehow be made to mesh." 2
The Role of Sponsors in Health PlansA key factor in the development of health plans is how they are sponsored. A sponsor, in this context, means an organization or group of individuals that pays for or plans and carries out a health plan endeavor. Over the years, health plans have been established or funded by many different kinds of sponsors. Figure 3B-2 shows the most common types of sponsors in health plans. The presence of sponsors and the "depth of their pockets" can play a major role in both the number of health plans that are established and the mission of those health plans.
Although some sponsors view their participation primarily as an investment opportunity, as is the case with investor groups, the motivation behind sponsorship often goes beyond finances. The purpose of sponsorship might be to:
1. Improve the accessibility of health service in a local community 2. Control rising costs for health benefit plans 3. Achieve public policy goals 4. Compete effectively with other business entities
Page 73 of 469

AHM 510 : Health Plans : Governance and Regulation
For example, employers concerned about the cost of purchasing healthcare coverage for their employees might consider sponsoring a health plan as a way to gain more control over expenses. Insurance companies might see sponsorship of a health plan as a relatively quick way to stay competitive in a rapidly changing environment. The federal government or a state or municipal government might view sponsorship of health plans as a way to meet a public policy need for affordable, accessible, quality healthcare.
Figure 3B-2. Sponsors in Manage Care.Investor Groups Government Employers Labor Unions Consumer Groups Insurance Companies and Blue Cross and Blue Shield Plans Medical Schools and Universities Hospital and Physician Groups Other Health Plans
Types of SponsorsIn this lesson, we offer a brief overview of various types of sponsors.
1. Investor groups
2. Government
3. Employers
4. Labor Unions
5. Consumer Groups
6. Insurance Companies
7. Medical Schools and Universities
8. Hospital and Physician Groups
9. Other Health Plans
Investor groups.
Investors can invest in any type of health plan except a not-for-profit company or a mutual company. Private sponsors have been a part of the health plan landscape since the late 1970s and early 1980s when the federal government first began to encourage private investment in HMOs. Various types of entities in the health plan industry continue to obtain funds through investors. These include hospitals, physician groups, physician-hospital organizations, physician practice management companies, HMOs, PPOs, and insurers.
Government.
Over the years, municipal, state, and federal government entities have sponsored health plans, sometimes directly founding health plans, sometimes playing a significant role as a
Page 74 of 469

AHM 510 : Health Plans : Governance and Regulation
purchaser or regulator. For example, the municipal government of New York established the Health Insurance Plan of Greater New York (HIP), largely as an effort to put in place a prepaid plan for city employees. Many of the HMOs for Medicaid recipients came about largely as a result of state funding and initiatives to incorporate health plan into Medicaid programs. And through the HMO Act, the federal government has played a major role in the evolution of HMOs in many areas of the country.3
Employers.
Many employers pay a substantial portion of the cost of healthcare for their employees. Consequently, they have a major financial stake in the system. Making premium payments, however, does not constitute direct sponsorship of an insurance or health plan organization. Sponsorship arises when employers accept the financial risk of providing healthcare coverage for their employees. Often employers take on this risk by entering into contractual arrangements with insurers, TPAs, or health plans for use of networks and administrative services, or when employers, either on their own or through coalitions, contract directly with providers. A well-known example of an employer-sponsored health plan is the Kaiser Foundation health plans, established in 1937 when Kaiser, a construction company, sought to finance medical care via a prepaid plan for its employees working on a project in the southern California desert. Other employers, while not sponsors of health plan entities, remain a major influence in the healthcare market by participating in healthcare coalitions that contract with health plans or by contracting directly with providers.
Labor Unions.
Labor unions today are not major sponsors of health plans; however, there was a time when labor and cooperative movements were a driving force behind the establishment of prepaid plans. The medical cooperative at Elk City, Oklahoma, was founded in the late 1920s with the support of the Farmers' Union. In the past, labor sponsored prepaid plans in St. Louis, Detroit, and Providence. 4
Consumer Groups.
Sometimes healthcare consumers decide to pool resources and form a health plan organization for their mutual benefit. Members founded several early HMOs, sometimes requiring that the governing board be comprised of a specified number or percentage of consumer members. A well-known example of a consumer-sponsored health plan is the Group Health Cooperative of Puget Sound, established in 1947 by consumers in Seattle who organized 400 families, each of which contributed $100, to sponsor this group.
Insurance Companies.
Insurance companies, including Blue Cross and Blue Shield Plans and commercial insurers, are major sponsors of health plans. These entities began sponsoring HMOs in the late 1960s and early 1970s when public policymakers were considering a national
Page 75 of 469

AHM 510 : Health Plans : Governance and Regulation
health insurance program that might bypass or eliminate indemnity health insurance plans. Insurers soon found other reasons to continue sponsoring health plans. For instance, as healthcare costs rapidly rose, insurers saw health plans as a way to help control costs for both their health plan and indemnity products. They also saw advantages in diversifying their healthcare product portfolio. And, of course, they considered the sponsorship of health plans to be a profitable business venture in its own right. 5
Medical Schools and Universities.
Universities with medical schools, a form of the academic medical centers (AMCs) discussed earlier, must maintain a sufficient patient base to remain in operation. One way they can do this is by sponsoring a health plan. For example, QualChoice of Arkansas, Inc., is a health plan that is sponsored by Tenet Health Systems and the University of Arkansas for Medical Sciences.
Hospital and Physician Groups.
Historically, when an HMO or other type of health plan was established in an area, hospitals and/or fee-for-service physicians responded by sponsoring similar organizations. Providers have formed some community health plans and Blue Cross and Blue Shield Plans. Hospital and physician groups have established various types of partnerships to sponsor health plans. Providers also sponsor health plans through alliances with other types of entities. For example, in the 1970s, Rush Presbyterian Hospital in Chicago started a group practice HMO, and in the 1990s became 50% owner in the Rush Prudential Health Plan, a joint venture with Prudential. In addition, new types of entities, such as physician practice management companies, have emerged, some of which have gone on to sponsor health plan arrangements. In the past, activities such as these have taken place mostly on a local basis, although multistate corporations and physician practice management companies have recently begun sponsoring health plan arrangements. Physicians and hospitals can also play a key role in the funding and governance of health plans without actually acting as sponsors. For example, some nonprovider sponsors of health plans may offer physicians or hospitals an ownership interest in the health plan.
Other health plans.
Health plans are often sponsored by the expansion activities of existing health plans. For example, a large, multistate HMO operating successfully in one region of the country might establish, merge with, or acquire an HMO in another region.
Providers and Health Plan Structures and ArrangementsIn Formation and Structure of Health Plans, we examined several factors that have driven the restructuring initiatives and corporate transactions in health plans. In this section, we look at another primary driver of change in health plans, the relationship-strategic, financial, and operational-between health plans and providers. As Mark Hall and William Brewbaker describe it,
Page 76 of 469
AHM 510 : Health Plans : Governance and Regulation
"The days of the free-standing hospital and the solo practitioner may soon be no more. Significant pressures are transforming our traditional system of small, independent professional practices and facilities into a competitive marketplace dominated by large businesses consisting of hospitals, physicians, and other entities that have bonded together to deliver broad regional health care services. The consolidation of the health care delivery system in the United States has been brought about by a number of important forces. Among the most significant have been the increasing attention given to health care cost containment by employers (through whom most private health insurance is purchased) and the simultaneous development of health plan entities which blend health care delivery and finance. . . As more patients (and employers) have begun buying their health care coverage through health plans that combine the delivery and finance functions, the pressure on hospitals and physicians to join integrated networks has intensified greatly."
Through consolidation and strategic alliances, hospitals and physicians seek a number of competitive advantages. For example, many hospitals pursue alliances to access health plan contracts and thereby reduce excess capacity of hospital beds, or to obtain capital for investments in information management systems. Physicians often pursue alliances to acquire leverage in negotiating with health plans. They can obtain access to management expertise, advanced information systems, and nurse practitioners and physician's assistants. Physicians can significantly reduce the cost and administrative burden of operating a small practice by relying upon others to manage functions such as tracking and registering patients, obtaining treatment approvals, and providing encounter data.6 In addition, both hospitals and physicians are increasingly willing to accept a portion of healthcare financing risk as a means of obtaining greater involvement in developing and implementing medical management goals and decisions. Figure 3B-3 further explores these and other factors that have led to consolidation and strategic alliances in healthcare.
Figure 3B-3.
Factors Contributing to Consolidation and Strategic Alliances in Healthcare.
Health plan contracting. When health plan patients represented a small portion of the total patient population, providers were not particularly concerned with the impact of health plan arrangements; from the providers' perspective, health plan patients brought a slight increase in patient volume, but were not critical to maintaining a healthcare practice. Today, providers that do not participate in health plan networks find it increasingly difficult to market their services to an adequate volume of patients. Consolidation and strategic alliances ease the burden of evaluating and entering into contractual relationships.
Administrative complexity. Providers are less inclined or able to handle increasingly complicated administrative functions such as electronic billing and collections from a variety of payors. Consolidations and strategic alliances offer healthcare providers the opportunity to access expertise and economies of scale in administrative functions.
Management expertise. Consolidation or strategic alliances enable providers to place the business side of healthcare management with individuals who are more experienced in these matters.
Page 77 of 469

AHM 510 : Health Plans : Governance and Regulation
Information technology. Consolidation or strategic alliances enable providers to obtain access to information technology, which plays an increasingly important role in health plan arrangements and in effectively linking with other components of the healthcare delivery system.
Access to capital. Consolidation can provide greater access to capital. For physicians practicing on their own or in small groups, obtaining operating funds can be difficult. For hospitals, additional funds can be used for ongoing expenses, construction, and strategic investments in medical and information technology.
Lifestyle preferences. Many younger physicians prefer a more stable work environment and the security of working for a large organization.
Increased competition. Changes in the healthcare delivery environment such as the emergence of ambulatory surgical centers and urgent-care centers have increased competition, giving healthcare providers an additional reason to consider consolidation or alliances.
Increased accountability. Providers are less inclined to handle the increasing demands of quality improvement and utilization review processes. The specialization of functions available through consolidations and strategic alliances can ease the burdens on individual providers.
Positioning for the future. Consolidation and strategic alliances better position providers for whatever lies ahead by enabling them to share skills, resources, expertise, and strategies to face the unknown future.
Source: Excerpted and adapted from Hall and Brewbaker, 5-8 through 5-10.
Regulatory Issues from the Regulators' PerspectiveThe changing nature of the organizations and arrangements in the healthcare market is of great concern to regulators, who monitor developments and formulate regulatory responses, as necessary, to address their findings. The primary objective is to enhance competition by accommodating various types of organizations that emerge and evolve, while also applying relevant consumer protection standards for the benefit of the general public.Insight 3B-1, from an article published by the Agency for Health Care Policy and Research, gives an indication of how the variety of health plan structures and arrangements impacts government agencies that monitor and regulate this rapidly changing industry.
According to the National Association of Insurance Commissioners (NAIC), when considering the wide variety of health plans in the market,
"The primary approach used by state insurance regulators is to regulate by function. Almost all states regulate health plans performing similar functions through the same laws. A few states have insurance laws that specifically apply to health plans owned or controlled by providers. Most states do not directly regulate the contracts between health
Page 78 of 469

AHM 510 : Health Plans : Governance and Regulation
plans and providers. States do monitor these arrangements by imposing certain requirements on the regulated health plan organization.
The states, through individual state initiatives and through the NAIC, are constantly adapting to an evolving marketplace as part of the state regulatory process. The state's tools for regulation continue to become more sophisticated. State insurance regulators are reviewing the range of regulatory issues which have arisen from the growing dominance of all forms of health plans in the health insurance market. In their review, states focus on the insurance function performed. The development of a risk-based capital formula (discussed in State Regulation of Health Plans) for health plans based on the level of risk being assumed by a health plan, and the development of a uniform licensing law for health organizations assuming insurance risk (also discussed in State Regulation of Health Plans) are examples of the states' efforts to regulate by function and adapt to an evolving marketplace."7
With the emergence of various health plan structures and arrangements, federal and state regulators have focused on issues such as solvency, quality assurance, benefits, access to care, and provider contracting.
We examine these and other regulatory issues in greater detail later in this lesson.
Insight 3B-1. A Government Agency's Research Agenda for Health Plans.
Probably the greatest challenge to research on health plan is the fact that market realities have evolved far more quickly than has our ability as researchers to conceptualize and classify them. As a result, it is not clear how to isolate and measure those features of the complex new healthcare organizations that are likely to be most important to use of services, customer satisfaction, health status, or costs. The old alphabet soup configurations of HMOs, IPAs, PHOs, and so on no longer do the job, but no generally accepted alternative framework has emerged. To address this issue, the Agency for Health Care Policy and Research (AHCPR) has been leading and encouraging the development of new conceptual frameworks for analyzing the configuration, operation, and impact of emerging health organizations and markets.
Source: Irene Fraser, "Research Agenda for Health Plans," U.S. Department of Health and Human Services, Public Health Service, Agency for Health Care Policy and Research: 675.
Regulatory Issues from the Health Plan's PerspectiveAn existing regulatory framework can result in the evolution of different types of health plan arrangements. For example, providers may be inclined to establish a PSO in a state where PSOs are not subject to HMO licensing and solvency requirements. On the other hand, providers may be more inclined to enter into strategic partnerships with licensed HMOs in states where PSOs are required to comply with comprehensive HMO licensing and solvency requirements. Also, as we saw in Legal Organization of Health Plans, laws such as those relating to corporate practice of medicine and not-for-profit status have an impact on the type of health plan that can be formed.
Although health plans are largely regulated at the state level, it is important to keep in mind that federal regulation also plays a significant role in the evolution of health plan
Page 79 of 469

AHM 510 : Health Plans : Governance and Regulation
arrangements. As various entities consolidate, form strategic alliances, and do business with one another, they must comply with federal laws, regulations, and related court decisions that impact their business relationships.
Integration and GovernanceHealth plan structures and arrangements effectively deliver, finance, and administer healthcare by employing varying degrees of integration. Integration is a combination of two or more endeavors into a single endeavor that pursues common goals, which results in previously separate entities sharing the risks and rewards of the combined endeavor.
According to antitrust law, the three basic types of integration are horizontal integration, vertical integration, and conglomerate integration. Horizontal integration is a combination of two or more entities in the same business segment that may directly compete with one another. Examples of horizontal integration include the acquisition of one HMO by another or a joint venture between two medical groups in the same market. Vertical integration is a combination of two or more entities in different segments of the same industry; the entities may be economically related, but they are dissimilar in nature and do not substantially compete with each other. Examples of vertical integration include a joint venture between an HMO, a hospital, and a medical group or the merger of a hospital and a medical group. Conglomerate integration is a combination of entities that produce unrelated products or services.8 An example of conglomerate integration is the acquisition of a health plan by a holding company that owns various types of businesses.
Structural and Virtual IntegrationA single organization could integrate within it all the tasks that comprise a comprehensive health plan system. This organization could own the healthcare facilities, employ the physicians who provide the care, design the healthcare benefit and funding arrangements, maintain the funds to pay for all covered healthcare expenses, market the products and services, and employ the administrative staff responsible for functions such as calculating and collecting the purchasers' bills, enrolling the members, and issuing benefit description material.
However, as the health plan business becomes more complex, some health plans are finding that they cannot excel at everything. As Derek F. Covert describes it,
"Health plans have been spinning off their provider units at a dizzying rate. FHP sold its hospitals, Foundation Health sold its medical groups, CIGNA sold its medical groups, and even Kaiser is positioning itself to move out of the hospital business. (It should be noted that Kaiser does not own its physician groups, although they are very strongly linked.) These health plans have determined that it is too difficult to effectively operate both a health plan and a provider organization. The underlying operating principles are very different, politics create hurdles effecting change, and the alignment of economic incentives is always a challenge. In most of these transactions, it was determined that in order for the provider organization to be economically feasible, it had to be able to enter into agreements with other payors, and see patients other than those aligned with the sponsoring health plan, which was deemed to be incompatible with the needs of the health plan."9
Also, when staff model HMOs expand their product offerings to include out-of-network features or when health plans move quickly to enter new geographic markets, they often
Page 80 of 469

AHM 510 : Health Plans : Governance and Regulation
find it necessary to enter into arrangements with other entities to bring their health plan products to market. These arrangements and structures are established through the use of many of the concepts we described in Formation and Structure of Health Plans. For example, integration could be achieved through a strategic partnership, a joint venture, an acquisition, or a merger.
Fast Definition
Span of Control an indicator of the number of people or activities being managed.
These different structures and arrangements result in varying degrees of management control for the sponsors of the business venture. No degree of control is inherently better or worse than another. Too great a span of control over a disparate, complex set of functions can hinder effective leadership and management. Too little control can make it difficult to develop and implement a common vision and strategy with focused business objectives.
The type of integration that creates the joint ventures, acquisitions, and mergers presented here and in Formation and Structure of Health Plans is called structural integration. Structural integration, which can be horizontal, vertical, or conglomerate, occurs when previously separate businesses create a legal entity that is either a single organization or a combination of two or more organizations that are under common ownership and control.10
Some attempts at integration begin with structural integration. Others, such as strategic partnerships and outsourcing, do not involve creating a single entity or affiliated organizations under common ownership and control; instead, these arrangements are contractual, and the entities remain separate. This type of arrangement is sometimes called virtual integration.
Operational IntegrationNo integration process- whether horizontal, vertical, conglomerate, structural, or virtual- is likely to succeed without operational integration. Operational integration occurs when the various activities needed to design, sell, administer, and deliver health plans are consolidated. As the term indicates, this consolidation does not have to be legal in nature. Thus, recently merged organizations as well as separate business entities can achieve operational integration. Depending upon the legal relationship between the participants, operational integration may include joint strategic planning, the consolidation of management, or the combining or developing of business systems and processes. The purpose of operational integration is to create a common vision and goals and to realize efficiencies by identifying and implementing best practices.
Health plans, which are a complex and diverse system of financing, administering, and delivering healthcare, involves a certain amount of operational integration, whether it is within a single entity or between separate entities. Greater operational integration is achieved when an endeavor exhibits these characteristics:
• Operating all lines of business under a consolidated budget
Page 81 of 469

AHM 510 : Health Plans : Governance and Regulation
• Unifying governance and management functions and coordinating all lines of business
• Coordinating and making compatible all business functions, such as information systems, accounting, billing, utilization management, and quality management
• Developing and implementing a common vision and common goals
• Implementing a unified strategic plan and marketing program designed to further the best interest of the newly integrated organization as expressed in its common vision and goals11
The important issue to be decided by a health plan's leaders is not whether to pursue structural integration or virtual integration, but to focus on how to deliver value to their customers, and then, through operational integration, establish the structures or arrangements that best support this focus. Insight 3B-2 illustrates the importance of strategic focus in health plan arrangements.
Once a health plan's leaders have established objectives, they consider the functions needed to accomplish those objectives. As part of the process, they might also determine how critical a role each function plays in achieving the organization's major strategic goals. The health plan's leaders then assess the organization's competencies in the various functions compared to the availability and value of obtaining those services from external sources. Put another way, the health plan's leaders might ask questions such as these:
• What are we good at?
• What can we access and manage via a strategic partnership or outsourcing?
• Are there any functions that are so critical that we shouldn't depend upon receiving them from someone outside the organization?
• What should we own and excel at?12
Insight 3B-2. Strategic Focus in Health Plan Integration.
True integration is difficult to define because it is not an end point; rather, it is a continuum- an ongoing process that varies with each organization. Consider, for example, the different approaches of two hypothetical organizations. ABC Integrated Health System might claim, "We have everything you need in health care- a hospital, physician practices in various locales, home health services, and an HMO." This statement focuses on structural integration. Premier XYZ Alliance might say, "Our goal is to provide the patient with the highest quality health care as conveniently as possible. The patient enters our system once, and we take care of everything after that."
Ultimately, integration is much more than an organizational chart; it is the result of a philosophy. Regardless of the specific organizational model involved, true integration embodies several core cultural attributes and operational approaches. It flows from shared values and a common purpose that make up the cultural fabric of an organization.
Page 82 of 469

AHM 510 : Health Plans : Governance and Regulation
Sources: Excerpted and adapted from Suzanne T. Anderson, "How Healthcare Organizations Can Achieve True Integration," Healthcare Financial Management (February 1998): 31-34.
Some health plans encounter difficulties trying to develop and implement effective integration strategies. Difficulties can arise when a health plan's leaders either overestimate or underestimate the organization's abilities to perform certain functions. For example, senior management that has been with an organization for a number of years might have a bias towards keeping functions "in-house" because "that's how we built this company." Conversely, senior management that is new to an organization might have a tendency to outsource or pursue strategic partnerships because these executives lack familiarity with or confidence in the organization's internal capabilities. Other factors that can cause problems for a health plan include a tendency for senior management to simply mirror the latest industry trends, internal systems that support the status quo, strong resistance from the workforce and middle management, and political or community resistance.13
Based on the unique capabilities of the organization and the market in which it operates, the leaders of a health plan can choose from a virtually limitless mix of structures and arrangements in pursuing an integration strategy. Each choice requires the organization to apply a different combination of governance and management expertise and skills. For example, the decision about how to structure or arrange the medical management function is completely different from the decision about how to structure or arrange the marketing function. However, one set of leadership characteristics required for all such decisions is "the focus, toughness and courage to aggressively attack these issues without bias, while maintaining the agility to modify structures as market dynamics change."14
Review Question
The Tidewater Life and Health Insurance Company is owned by its policy owners, who are entitled to certain rights as owners of the company, and it issues both participating and nonparticipating insurance policies. Tidewater is considering converting to the type of company that is owned by individuals who purchase shares of the company's stock. Tidewater is incorporated under the laws of Illinois, but it conducts business in the Canadian provinces of Ontario and Manitoba.
Tidewater established the Diversified Corporation, which then acquired various subsidiary firms that produce unrelated products and services. Tidewater remains an independent corporation and continues to own Diversified and the subsidiaries. In order to create and maintain a common vision and goals among the subsidiaries, the management of Diversified makes decisions about strategic planning and budgeting for each of the businesses.
By combining under Diversified a group of businesses that produce unrelated products and by consolidating the management of the businesses, Tidewater has achieved the type(s) of integration known as
conglomerate integration and operational integration
Page 83 of 469

AHM 510 : Health Plans : Governance and Regulation
horizontal integration and operational integration
horizontal integration and virtual integration
conglomerate integration only
Correct. Conglomerate integration is a combination of entities that produce unrelated products or services. Operational integration occurs when the various activities needed to design, sell, administer, and deliver health plans are consolidated
Incorrect. While operational integration occurs when the various activities needed to design, sell, administer, and deliver health plans are consolidated; horizontal integration is a combination of two or more entities in the same business segment that may directly compete with one another.
Incorrect. Horizontal integration is a combination of two or more entities in the same business segment that may directly compete with one another. Vertical integration is a combination of two or more entities in different segments of the same industry; the entities may be economically related, but they are dissimilar in nature and do not substantially compete with each other.
Incorrect. While conglomerate integration is a combination of entities that produce unrelated products or services, there are other correct answers.
Other Governance and Strategic IssuesThe strategic objectives of an organization's sponsors and executives invariably dictate what type of health plan is formed and the arrangements it enters. For instance, a hospital (or a joint venture between a hospital and physicians) sometimes sponsors an MSO as a way to encourage formation of a physician medical group and to strengthen the relationship between the hospital and physicians. Often the sponsors of an MSO expect that at some point in the future the medical group will integrate with the hospital to form an IDS. As a result, they may be willing to take a loss on the MSO venture so they can realize a strategic gain later.
Historically, healthcare in the United States has been a local industry. In one location, the bulk of the economic and political power with regard to healthcare issues may reside with a hospital or a hospital system; in another location, this power may reside with the physicians. In one area, an HMO may be dominant; in another area, the dominant entity may be a large employer health plan that covers most of the residents. Or there may be no single dominant entity. It follows, then, that the types of health plans and arrangements that evolve in these various locations will vary depending upon the nature of the market.
Some health plans offer ownership interests to participating providers. Ownership can establish a strong financial incentive for providers to effectively manage care; it can also enhance physician loyalty to the health plan. While this strategy can be advantageous to both the health plan and providers, arrangements such as these are subject to regulatory scrutiny, in part because of concerns that financial incentives might influence the type and amount of healthcare services provided.
Page 84 of 469

AHM 510 : Health Plans : Governance and Regulation
The need to respond quickly to market conditions can also influence the form a health plan takes. For example, a provider group may determine that it needs to enter into a contract-based arrangement to respond to competition from other types of health plans. Once it establishes a foothold, it may later decide to enter into a more structurally integrated approach, such as a PHO or an IDS.
Employer-Sponsored PlansAs we mentioned in our discussion of sponsors, an employer's approach to providing healthcare benefits for its employees plays a major role in determining the types of health plan structures and arrangements utilized by health plans. Employers have four options available to them with regard to structuring healthcare benefit plans for their employees. They can
1. Purchase an insurance or prepaid product from an insurer or health plan2. Self-fund a healthcare benefit arrangement and perform all associated administrative services or obtain those services from an insurer, health plan, or third party administrator3. Contract directly with healthcare providers4. Directly provide some or all of the healthcare services (e.g., employ company healthcare providers to look after the healthcare needs of employees)
Employers can pursue each of these options (or a combination thereof) on their own or collectively with other employers. In this section, we examine options 2 and 3, in which employers move beyond the role of healthcare purchaser but stop short of the role of healthcare provider. In other words, employers often assume the role of payor or take on some of the functions typically performed by insurers and prepaid plans.
Self-Funded and Self-Administered PlansAs we discussed in Healthcare Management: An Introduction, self-funding (also called self-insuring) is a method employers use to provide healthcare benefits to their employees by funding the cost of the healthcare themselves, rather than through a payor, such as an insurer or health plan. The employer, rather than the health plan, assumes the financial risk. Figure 3B-4 shows the percentage of employers who provide healthcare benefits to their employees through self-funded plans. Most employers that decide to self-fund do so to improve finances and gain more control of benefit design.
Employers that decide not to self-fund typically do so because of (1) the financial risk of having to pay for catastrophic healthcare costs and (2) the investment in time, effort, and financial resources needed to establish a self-funded arrangement. Also, smaller employers that cannot perform the necessary administrative functions on their own sometimes find that the cost of contracting for these services eliminates many of the financial advantages described above.
In a self-funded arrangement, employers use one of two funding vehicles. They either obtain the funds from their general assets (this is called a nontrusteed plan), or they use a trust to hold plan reserves. Employers that are concerned about claim fluctuation or large-amount claims often minimize their financial risk by purchasing stop-loss insurance. Stop-loss insurance places a dollar limit on the employer's liability for paying claims. However, some states have maintained that in certain situations a self-
Page 85 of 469
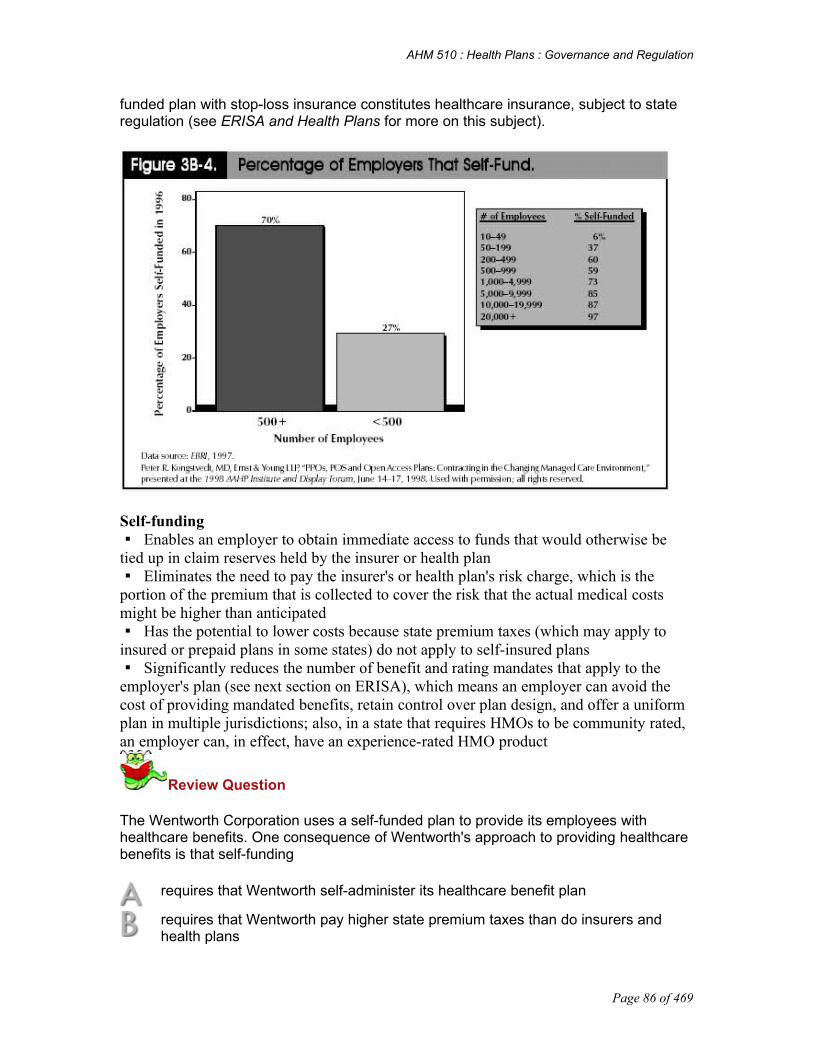
AHM 510 : Health Plans : Governance and Regulation
funded plan with stop-loss insurance constitutes healthcare insurance, subject to state regulation (see ERISA and Health Plans for more on this subject).
Self-funding Enables an employer to obtain immediate access to funds that would otherwise be
tied up in claim reserves held by the insurer or health plan Eliminates the need to pay the insurer's or health plan's risk charge, which is the
portion of the premium that is collected to cover the risk that the actual medical costs might be higher than anticipated
Has the potential to lower costs because state premium taxes (which may apply to insured or prepaid plans in some states) do not apply to self-insured plans
Significantly reduces the number of benefit and rating mandates that apply to the employer's plan (see next section on ERISA), which means an employer can avoid the cost of providing mandated benefits, retain control over plan design, and offer a uniform plan in multiple jurisdictions; also, in a state that requires HMOs to be community rated, an employer can, in effect, have an experience-rated HMO product
Review Question
The Wentworth Corporation uses a self-funded plan to provide its employees with healthcare benefits. One consequence of Wentworth's approach to providing healthcare benefits is that self-funding
requires that Wentworth self-administer its healthcare benefit plan
requires that Wentworth pay higher state premium taxes than do insurers and health plans
Page 86 of 469

AHM 510 : Health Plans : Governance and Regulation
eliminates the need for Wentworth to pay a risk charge to an insurer or health plan
increases the number of benefit and rating mandates that apply to Wentworth's plan
Incorrect. Often, an employer handles the administration of the self-funded plan by hiring an insurer, a health plan, or a third party administrator (TPA) to provide administrative services under the plan, while financial responsibility for funding benefit payments remains with the employer.
Incorrect. Self funding has the potential to lower costs because state premium taxes do not apply to self-insured plans
Correct. Self funding eliminates the need to pay the insurer's or health plan's risk charge.
Incorrect. Self-funding significantly decreases the number of benefit and rating mandates that apply to Wentworth's plan.
ERISA's Impact on Self-Funded and Self-Administered PlansIt is difficult to discuss self-funded plans without taking a quick look at the Employee Retirement Income Security Act of 1974 (ERISA), which governs employee benefit plans. We will do so here, saving a thorough analysis for ERISA and Health Plans.
ERISA is a federal law that regulates most employment-based health benefit plans, not just self-funded plans. One effect of ERISA is that it preempts certain state laws with regard to the regulation of most self-funded plans. In other words, state insurance laws typically do not apply to self-funded plans. Currently, benefits are left largely unregulated by ERISA, which gives employers who provide self-funded plans the freedom to design plans without having to consider requirements that apply to insurance and HMO plans. In addition, ERISA preempts state laws that allow covered individuals to sue their employers and/or plan administrators, although the extent and limits of the ERISA preemption, as interpreted by various court decisions, are not always clear.
ERISA's reach goes far beyond the issue of preemption. However, for the purpose of our discussion of employer-based plans, one other provision is worthy of note. ERISA imposes strict requirements on persons who are fiduciaries of employee benefit plans. A fiduciary is defined under ERISA as a person, regardless of formal title or position, who exercises discretionary authority and control over the operation or administration of the plan, exercises any control over plan assets, or renders investment advice for a fee. Individuals who have fiduciary responsibilities with respect to a self-funded plan and who breach their trust are subject to personal liability to restore to the plan any resulting losses and forfeit any profits. Generally, an insurer, health plan, or TPA has fiduciary responsibility with respect to payment of claims under a self-funded plan, and the employer has all other fiduciary responsibilities. There are, however, different views as to which party has fiduciary responsibility for activities related to establishing and operating a health plan network.
Administration of Self-Funded PlansSelf-funding eliminates or minimizes the employer's need to pay an insurer or health
Page 87 of 469

AHM 510 : Health Plans : Governance and Regulation
plan to assume financial risk. However, the employer must still have a way to administer the healthcare benefit plan: determine eligibility, enroll members, review and pay claims, and perform all the other administrative functions typically performed by a health plan. Often, an employer handles this by hiring an insurer, a health plan, or a third party administrator (TPA) to provide administrative services under the plan, while financial responsibility for funding benefit payments remains with the employer. The contract that describes this arrangement is called an administrative services only (ASO) contract. 15
Some employers choose to self-administer. A self-administered plan is a self-funded plan that is also administered by the employer. Often a large employer can devote staff to perform these administrative activities. An employer that self-funds or both self-funds and self-administers a healthcare benefit plan is performing some or all of the major functions of an insurer; however, it is not required to be licensed as an insurer or health plan as long as it performs these functions only for its employees.16
Self-administration is comparatively simple when the employer is providing an indemnity health plan. A health plan, on the other hand, involves healthcare management functions such as provider contracting, utilization review, and medical management, thereby making the task of self-administration much more daunting and time-consuming.
When an employer decides to contract with a health plan to administer its health plan, there are a number of ways to establish payment. For example, a health plan may set a flat monthly fee for services. Or a health plan may identify specific services such as network administration and utilization management for which it sets separate fees in addition to a flat monthly fee.
A health plan also bills the employer for actual healthcare costs incurred by the covered employees and dependents. Typically, at the end of the plan year, a final payment is calculated to determine the employer's actual "claims" experience for the year. When the healthcare providers are paid under special reimbursement arrangements, such as capitation, the health plan must disclose to the employer that the employer's healthcare payments are not necessarily the actual cost of providing care. This disclosure is required by the Department of Labor in accordance with ERISA.
Employer Direct ContractingBecause large numbers of employers self-fund their health plans and because health plans have become a dominant force in healthcare, it follows that some employers would want to try their hand at direct contracting. Employer direct contracting is when employers elect not to purchase a health plan product from a health plan, but instead provide coverage for their employees by making arrangements directly with providers for the delivery of healthcare. A large employer might structure an exclusive arrangement with a network of providers, making the services of those providers available only to employees of that employer. Or the employer might contract with providers who are also entering into contracts with a number of other health plans and/or employers.
Because few employers have the expertise or resources to take on the complexities of organizing and managing a healthcare network themselves, those that decide to enter into a direct contracting arrangement typically contract with an already established network of providers. However, some large employers do have the capability, not only to contract directly with providers, but also to establish an exclusive or "captive" network
Page 88 of 469

AHM 510 : Health Plans : Governance and Regulation
when doing so. Insight 3B-3 provides an example of one such employer. Other employers have achieved the capability to establish networks by joining with other employers in coalitions, which we will discuss later in this section.
One other alternative available to some employers is the so-called "company clinic" where employers develop their own primary care clinics and specialty care referral networks. However, these types of arrangements will remain relatively few in number because they can only be utilized by employers with large concentrations of employees in a single location and because they are much more expensive to establish and operate than any other type of network arrangement.
Insight 3B-3. Hershey Foods Corporation's "Captive Network."
Hershey Foods Corporation developed a captive network after spending two years analyzing outcomes data for 55 diagnosis-related groups at 23 hospitals in central Pennsylvania. Hospitals were ranked in such categories as length of stay, mortality and morbidity rates, cesarean sections, back surgery, and inappropriate admissions, using a formula of 70 percent quality and 30 percent cost. On the basis of these rankings and certain ease-of-access criteria, Hershey established a point-of-service (POS) network that includes nine hospitals, 180 primary-care physicians and 800 specialists. The company gave employees a $150 bonus and a waiver of the first year's premium as an incentive to choose the captive network.
Sources: J. Montague, Low Fat, Low Cost, Hospitals & Health Networks (Aug. 5, 1993), 76-78. Hall and Brewbaker, 4-5 through 4-6.
Purchasing AlliancesEmployers have also exerted influence on health plan arrangements through purchasing alliances, also known as employer coalitions, employer purchasing coalitions, or health insurance purchasing cooperatives (HIPCs). A purchasing alliance is a collection of employers and/or individuals (in some cases established and assisted by a governmental or quasi-governmental agency) who employ a collective approach to obtaining healthcare for their employees or themselves. Purchasing alliances can be organized in any number of ways. In Other Laws that Apply to Health Plans, we will examine state-initiated small group coalitions. Here we look at employer-sponsored alliances.
One type of employer-sponsored alliance has as its primary objective increased purchasing power when negotiating with health plans. A large number of small employers can come together to form a healthcare benefit purchasing group that is in many ways similar to a large employer. This arrangement gives the group increased flexibility in negotiating plan features and premiums. In exchange, the health plan obtains increased membership in its network. Although often used by small employers, coalitions are also used by medium and large group employers. For instance, a group of large, national employers, coordinated by a national consultant, can establish a coalition to obtain price advantages, implement uniform administration, and standardize plan features in multiple locations.
Another type of employer purchasing alliance, though not as common, involves contracting directly with healthcare providers rather than health plans. Insight 3B-4
Page 89 of 469

AHM 510 : Health Plans : Governance and Regulation
describes one such coalition in Houston. Similar alliances have also been formed in other locations such as Atlanta, Chicago, Cleveland, and Minneapolis.
As we have seen in this lesson, the complex relationships between employers, health plans, hospitals, physicians, and other healthcare facilities and providers will continue to evolve. The leaders of these groups, as well as regulators, will continue to closely monitor the market, and as they do so a variety of health plan structures and arrangements is likely to emerge, followed by a variety of regulatory responses.
Insight 3B-4. The Houston Health Purchasing Organization (HHPO).
"At the end of the day, you still have to go out and compete with the commercial entities," says D. Rick Huntington, who administers the Houston Healthcare Purchasing Organization (HHPO) with Ralph T. Smith, Jr. "It's a coalition that operates like a business. I think that's the key to its success."
Five years ago, a survey of members of the Houston Area Health Care Coalition-all large, self-funded firms-showed that many wanted the group to begin buying coverage. Others argued that they were big enough to have ample bargaining clout on their own. After much debate, Huntington and Smith, the corporate representatives who were most vocal about the need for a purchasing group, got the coalition's blessing to forge ahead.
In 1994, the two men quit their jobs as benefits managers and launched a for-profit operation, Business Health Companies (BHC). They also established the not-for-profit HHPO, which they contracted to manage for the next 10 years under the auspices of a BHC subsidiary.
HHPO set out to "take pricing out of the equation," says Smith, president of BHC. The tactic: Come up with a schedule of payments and offer it to doctors and hospitals on a take-it-or-leave it basis. Initially 15 companies-about a third of the employers in the original Houston area coalition-agreed to go along. Participating companies now number 55.
The fees are discounted but generous enough so that all of Houston's hospitals and some 6,000 doctors-about three-quarters of those in the area-are on the HHPO list. "Our experience really questions the design of narrow PPOs," Smith says. "By including almost everybody, you end up saving more money" since there's seldom a need, even in emergencies, to go out of network.
In 1996, providers under contract with HHPO collectively received $87 million, which works out to 66% of billed charges. The discount was deepest (37%) for the biggest cost component, hospital inpatient services. Doctors' services were discounted the least.
HHPO monitors how good a job the providers are doing. The idea is that eventually employers will go with sub-networks comprising those with the best outcomes, rather than offer the entire list of providers to their workers.
Page 90 of 469

AHM 510 : Health Plans : Governance and Regulation
Huntington and Smith have joined forces with Baltimore, Md.-based HCIA Inc. to collect severity-adjusted data on the outcomes of HHPO patients. The coalition won provider support for this portion of the undertaking by promising to keep the results confidential for the first three years. The period of secrecy expires in 1998, but coalition members have not specified how harsh they'll be with providers who don't measure up.
HHPO's direct payment concept works well for companies big enough to self-insure. But its reach is much broader: John Alden Life Insurance Co. leases the network for an insured product it sells to 5,000 smaller firms. In keeping with the coalition concept, all 5,000 have been required to join the not-for-profit HHPO.
HHPO's success has led to rapid growth. When members wanted to expand the plan to other work sites, Huntington and Smith used the same model to put together a statewide network. With 257 hospitals and 14,000 doctors outside of the Houston area, "We're in every nook and cranny of Texas," Smith boasts.
Source: Excerpted and adapted from Daniel B. Moskowitz, "Going Entrepreneurial," Business and Health (January 1998): 42.
Page 91 of 469

AHM 510 : Health Plans : Governance and Regulation
Chapter 4 APerspective and Overview of State and Federal Laws In Legal Organization of Health Plans and Formation and Structure of Health Plans, we discussed many of the ways health plans are choosing to structure their organizations from a business perspective. We also discussed, from a legal perspective, the forms of organization a health plan can opt to use- i.e., corporation, partnership, limited partnership, limited liability company, etc. In health plan, however, laws and regulations affect much more than an organization's choice of legal structure. Because the regulation of health plan evolved largely from a system designed to regulate indemnity healthcare, there are many laws that may not be specific to health plan which affect the formation and/or operation of health plans. In general, the term law refers to a system of rules, enforceable by a controlling authority, that governs human conduct.1 Throughout this lesson we use the term law to refer to statutes, rules, regulations, and court decisions.
In this lesson, we will discuss laws and regulations affecting health plan. We begin our discussion of laws and regulations affecting health plan in this assignment with a brief review of the origin of laws, rules, and regulations in the United States.
After completing this lesson, you should be able to:
Describe the sources of law in the United States Explain the significance of the HMO Act of 1973 in the development of healthcare Name the federal laws that stimulated health plan participation in Medicare and
Medicaid Describe the provisions of the Health Insurance Portability and Accountability Act of
1996 (HIPAA) of major interest to health plans Describe the aspects of a health plan on which state regulations usually focus
Sources of LawLaws governing health plans come from a number of sources, including constitutions, statutes, administrative rules and regulations, and case law. The following sections describe each of these sources of law and introduce model laws.
ConstitutionsA constitution sets forth in general terms the principles that form the legal foundation of a government. It describes the structure of the government, defines the extent of its powers, and outlines the principles on which it is to operate. In addition, a constitution usually guarantees to citizens certain basic human rights. Because these principles are intended to remain relatively stable and consistent over time, most constitutions include safeguards designed to prevent frequent or ill-considered amendments. Changes to a constitution that must be made to meet the needs of a changing society are generally accomplished through interpretation of its terms by the courts, rather than by amendment. The general language of a constitution makes this flexibility possible.
In the United States, there are two kinds of constitutions: the federal Constitution and the state constitutions. The basic difference between the federal Constitution and a state constitution is that power is delegated by the federal Constitution to the federal government, whereas a state constitution defines and limits the already existing power of the state government. The federal government has no power that is not given to it by the
Page 92 of 469

AHM 510 : Health Plans : Governance and Regulation
federal Constitution. A state government has all powers (i.e., "reserved powers") that are not prohibited by the federal Constitution or by the constitution of that state.
StatutesA statute, or act, is "an act of the legislature declaring, commanding, or prohibiting something; a particular law enacted and established by the will of the legislative department of government." 2 Statutes enacted by Congress are called either federal statutes or acts of Congress. Statutes enacted by state legislatures are called state statutes. If it is not clear whether Congress or the state legislatures have the power to legislate in a given area, the question can be referred to the courts for decision.
Fast Definition
Doctrine a statement of fundamental government policy.3
Administrative Rules and RegulationsBoth federal and state governments operate under a doctrine called separation of powers. Separation of powers means that a government is divided into departments or branches, each of which primarily performs a distinct function. Constitutions in the United States provide for three branches of government-legislative, executive, and judicial-and establish a system of checks and balances to guard against any branch becoming too powerful. A branch of government performs a primarily legislative function when it enacts, or makes, laws; a primarily executive function when it enforces, or carries out, laws; and a primarily judicial function when it interprets laws and adjudicates disputes under the law.
The complexities of modern business have necessitated some overlap among the three branches. Legislators cannot have the necessary technical knowledge about every business that must be regulated. Consequently, they have adopted the practice of enacting regulatory statutes in general terms. They then authorize the administrative officer having the duty of executing the law to fill in the details by enacting administrative rules and regulations that have the force and effect of law. Courts have held that this delegation of rule-making power to administrative officers does not violate the separation of powers doctrine, as long as the rules so made are within the scope of the delegated power, are made following specified procedure, and are subject to judicial review. Administrative rules or administrative regulations are prescribed guides for conduct or action created by an administrative agency that carry the force of law. For example, the Centers for Medicare and Medicaid Services establishes rules and regulations for health plans that wish to participate in Medicare. The agencies that regulate health plans exert great power and influence over whether, and how, a health plan does business.
Administrative officers also perform judicial functions. They hold hearings, make decisions, and impose penalties. Thus, administrative officers function in all three spheres-executive, legislative, and judicial.
The commissioner, director, or superintendent of insurance is a state administrative officer. Today, state legislatures have authorized such officers to adopt appropriate rules and regulations to implement the provisions of the state insurance and health plan
Page 93 of 469

AHM 510 : Health Plans : Governance and Regulation
statutes. Often, such administrative rules and regulations constitute a major part of the law governing the health plan industry. Similarly, Congress authorizes various federal administrative officers to adopt appropriate rules and regulations implementing the provisions of certain federal statutes that affect health plans. For example, the Centers for Medicare and Medicaid Services creates and adopts administrative rules and regulations to implement Medicare. Sometimes the rules and regulations issued by administrative agencies do not provide enough detail for health plans. Often, administrative agencies make informal policy documents available and provide guidance to health plans trying to comply with such rules and regulations.
Model LawsA model law is an act proposed by experts in a particular field for consideration by the states that may be adopted and enacted, in whole or in part, by a state or that may serve as the basis for state legislation, particularly in a technical area. The National Association of Insurance Commissioners (NAIC), a nongovernmental association of state insurance regulators, develops and adopts model laws and regulations for consideration by legislators and regulatory agencies in developing particular state laws and regulations. The model laws and regulations address subjects relating to health plan financial requirements, quality assurance, utilization review, and statutory accounting standards.
A model law or regulation itself is not a law and does not have the force or effect of law. However, many of the NAIC's model laws and regulations directly impact health plans by serving as the basis for state or federal legislation or regulations. For example, NAIC model laws and regulations are often adopted in whole or in part by state legislatures or state administrative agencies.
Another name for model law is uniform law. The term uniform law is sometimes used because an important purpose of a model law is to promote uniformity among state laws.
Case LawA court applies laws to resolve the controversies brought before it. In so doing, a court interprets those laws and thus creates more law. In the United States, federal and state court decisions form a vast and growing body of law called case law or common law. Federal case law is made up of federal trial court decisions, federal intermediate court decisions, and U.S. Supreme Court decisions. State case law consists of state intermediate and supreme court decisions, because most state trial court decisions are not published. The term common law is sometimes used to distinguish case law (court decisions) from statutory or regulatory law. In that sense, the common law of a jurisdiction is made up of the decisions of the courts, but not the enactments of the legislature or administrative regulations.
Health plan case law has evolved from the decisions that state and federal courts have made involving the laws and regulations that impact health plans. For example, case law has been used to interpret how the provisions of the Employee Retirement Income Security Act of 1974 (ERISA) should be applied to employee benefit plans that are governed under ERISA.
History of Regulation of Health PlansEarlier in this assignment we noted that regulation of health plans evolved from an
Page 94 of 469

AHM 510 : Health Plans : Governance and Regulation
environment designed largely to regulate indemnity insurance. It should be no surprise that regulation of health plans also followed in the wake of traditional indemnity insurance laws. In the absence of regulation specific to health plans, states and the federal government have applied insurance and other applicable laws to health plans.
Federal laws that were passed to protect individual citizens or to protect the free market economy in the United States were among the first noninsurance laws applied to health plans. Antitrust laws are one example of this type of federal law. Antitrust became an issue of national concern in the United States after the end of the Civil War. 4 Using pooling arrangements and trusts, "robber barons" created large companies that could dominate a single industry.5 To curtail this type of activity that restrained trade and competition, Congress passed the Sherman Act in 1890. The Clayton Act and the Federal Trade Commission Act were both passed in 1914 to supplement and reinforce the Sherman Act.
Historically, providers and provider groups asserted antitrust violations to combat the development of prepaid group practices and other health plans that seemed to threaten their livelihood. As health plans have evolved, entrepreneurs have created unique partnerships and affiliations among providers, payors, and employers. The subsequent mergers, acquisitions, and affiliations of these players have been subjected to antitrust scrutiny. Antitrust laws and their application to health plans are discussed in Federal Regulation of Health Plans.
Recall from Healthcare Management: An Introduction that prepaid group practices, a forerunner to today's health plans, existed as early as 1910 (e.g., the Western Clinic in Tacoma, Washington). At that time, prepaid group practices, cooperative health plans, and other health plan-type organizations had to comply with state insurance regulations and other state and federal laws that were not specifically designed to regulate such entities. Prepaid group plans and their cost-saving components captured the attention of the Nixon administration in the late 1960s. As described in the following section, health plan-specific regulation was developed shortly thereafter.
Laws Enacted Specifically to Regulate Health PlansHMO Act of 1973The first major attempt by the federal government to influence the development of managed care plans (now known as health plans) was the HMO Act of 1973. In the late 1960s and early 1970s, the Nixon administration was seeking ways to harness drastic increases in healthcare costs. Initially proposed as a way to manage costs of Medicare and Medicaid, health plans soon became a pivotal healthcare strategy for the Nixon administration. Insight 4A-1 provides an explanation of the 1970s' vision of using health plans to control healthcare costs in this country.
The Health Maintenance Organization Act of 1973 ("HMO Act"), Title XIII of the Public Health Service Act, is a federal law that was designed to help contain spiraling healthcare costs by encouraging the development of HMOs. The HMO Act was signed into law on December 29, 1973, and provided requirements that health plans must meet to obtain federal qualification. In addition, for a period of time, the HMO Act provided federal funds for the establishment of HMOs. The HMO Act applied only to health plans that chose to become federally qualified. Federal qualification is not a requirement and state licensure is sufficient for a health plan to operate in a particular state. Initially, many
Page 95 of 469

AHM 510 : Health Plans : Governance and Regulation
health plans chose to become federally qualified because of the federal funds available to establish and operate HMOs. Today, the majority of HMOs do not seek federal qualification.
Insight 4A-1. The HMO Concept is Born.
According to the Consumer Price Index (CPI), from 1962 to 1975, medical costs rose 59 percent--more rapidly than any major category of personal expenses. Thus, both private groups and public agencies looked for mechanisms that would reduce and contain costs.
Several national studies, in particular the 1967 Report to the President, recommended group practice, and especially prepaid group practice, as possible solutions to the cost-of-care crisis. The gestation period for the federal program was relatively short: by March 9, 1970, a position paper was completed by Paul M. Ellwood Jr., M.D., and his associates at the American Rehabilitation Foundation (later to be called InterStudy) in which he coined the phrase "health maintenance organization." As described in this paper, the HMO concept was to become a major issue of the Nixon administration's health program.
First announced before an executive session of the House Ways and Means Committee on March 23, 1970, and through a press release on March 25, 1970, Alternative C, as the proposal was called, would authorize the Social Security Administration to contract with HMOs to guarantee comprehensive health service for the elderly at a fixed rate. The Nixon administration's bill, designed to help establish HMOs, was introduced in March 1971. Initially, the HMO concept was proposed by the Nixon administration as a way to contain the costs of the Medicare and Medicaid programs. But, because of their cost-saving potential and the increasing interest and acceptance of the concept, HMOs became the central issue of President Nixon's health program.
Source: Used with permission, Robert G. Shouldice, An Introduction to Health Plans: HMOs, PPOs, and CMPs (Arlington, VA: Information Resources Press, 1991), 29, 35.
The HMO Act contained provisions that:
• Made funds available for the formation and development of HMOs
• Preempted state laws that contained more stringent standards for HMO development
• Required that employers with 25 or more workers offer a federally qualified HMO as a choice for their employees if the HMO requested inclusion as a choice for employees
• Gave the Department of Health and Human Services the authority to regulate federally qualified HMOs to ensure that quality care was provided 6
Amendments to the HMO Act were passed from 1976 through 1995. These amendments will be discussed in Federal Regulation of Health Plans. Currently, the HMO Act is the only federal legislation enacted specifically to regulate health plans. However, over the years other federal laws have been applied to the formation and operation of health plans. Some of these laws even contain provisions specifically directed at health plans.
Page 96 of 469

AHM 510 : Health Plans : Governance and Regulation
Other Federal Laws Applied to Health PlansFederal laws that impact health plans are often found in broad legislation not specifically enacted to regulate health plans. For example, portions of various budget acts contain provisions that affect health plans. Additionally, amendments to the Social Security Act established the federal programs Medicare and Medicaid; health plans that wish to participate in such programs must comply with requirements set forth in that law. In the following sections we explore several federal laws that contain provisions that are applied to health plans' operations.
Employee Retirement Income Security Act (ERISA)To help contain costs for financing healthcare for their employees or members, employers and other large organizations began self-funding their own health plans. In the early 1960s, the NAIC noted with growing concern the increase in the number of self-funded plans in this country.7 At that time, self-funded plans were unregulated. In 1972, one state insurance department stepped forward to challenge a self-funded plan sponsored by the Monsanto Company, alleging that the plan constituted an insurance transaction and, therefore, should be subject to state regulatory requirements for insurance. The Missouri Supreme Court ruled favor of the Monsanto Company in its 1974 decision on the case, and the challenge was unsuccessful.8 However, in that same year a federal law was passed that addressed, among other things, the regulation of self-funded employee benefit plans.
The Employee Retirement Income Security Act of 1974 (ERISA), a law whose primary purpose was to prevent abuse of employer-sponsored pension benefit plans, included a provision that subjects employment-based health benefit plans to regulation under this act.
As noted in Health Plan Structures and Arrangements, ERISA does not directly regulate health plans; instead it sets standards for most employment-based health benefit plans, whether or not they are self-funded.9 The types of standards that ERISA imposes include: documentation explaining benefits available under the plan and any modifications to those benefits, reporting requirements, and procedures for appeals of denial of claims. ERISA also sets standards that must upheld by anyone who acts as a plan fiduciary. We discuss ERISA in more detail in Federal Regulation of Health Plans.
Omnibus Budget Reconciliation Act of 1981 (OBRA-81) and MedicaidAmendments to the Social Security Act authorized Medicaid, a joint federal/state program that provides medical assistance to low-income individuals. These provisions required states to share the financial burden of this program and provided for matching funds from the federal government. Although enrollment in health plan arrangements was permitted almost from the inception of the Medicaid program in 1966, the Omnibus Budget Reconciliation Act of 1981 (OBRA-81) was the true stimulus for increasing participation by health plans in Medicaid. OBRA-81 amended the Social Security Act to allow states to set their own qualification standards for HMOs that contracted with state Medicaid programs and revised the requirement that participating HMOs have an enrollment mix of no more than 50% combined Medicare and Medicaid members by increasing that percentage to 75%.10 As you will learn later in this lesson, this 75% requirement has been eliminated. OBRA-81 expanded the ability of the Centers for Medicare and Medicaid Services (CMS), the federal agency in the Department of Health
Page 97 of 469
AHM 510 : Health Plans : Governance and Regulation
and Human Services that administers Medicaid, to grant waivers from the rules of the Social Security Act. CMS could grant a waiver that allowed a state to develop a research and demonstration project that served the particular needs of the Medicaid population in that state. These Medicaid demonstration projects allowed states to try different financing and delivery options, including health plan techniques, for serving their Medicaid populations. The Balanced Budget Act of 1997, discussed later in this lesson, includes amendments that streamline the waiver process and allow states to mandate enrollment in health plans for most Medicaid beneficiaries.
Fast Definition
Medicare risk contract - A contract by which an HMO or CMP contracted with CMS to assume the risk of providing medical services to Medicare beneficiaries.11
Competitive medical plan - A federal designation that allowed a health plan to obtain eligibility to receive a Medicare risk contract without having to obtain federal qualification as an HMO; requirements for eligibility were somewhat less restrictive than for an HMO. 12
Tax Equity and Fiscal Responsibility Act of 1982 (TEFRA) and MedicareJust as OBRA-81 made it easier for health plans to serve the Medicaid population, the Tax Equity and Fiscal Responsibility Act (TEFRA) of 1982 made it easier for HMOs to enter into risk contracts to serve the Medicare population. Medicare, authorized by amendments to the Social Security Act, is the federal government's hospital expense and medical expense insurance plan for persons age 65 and older and certain other qualified individuals. TEFRA also allowed competitive medical plans (CMPs) to participate in Medicare risk contracting. As we discuss later in this lesson, the Medicare program has been changed by recent legislation that eliminates CMPs and Medicare risk contracting.
Prior to TEFRA, amendments to the Social Security Act contained provisions that allowed prepaid plans to enter into a cost or risk contract for Medicare; however, only federally qualified HMOs were allowed to participate. In the early stage of the Medicare program, many plans participated through cost contracts. Under these contracts, HMOs were reimbursed for all of their expenses, and although they could not profit, they could cover a portion of their general overhead and were not at any risk. Many HMOs chose not to participate in the Medicare program because the opportunities to make profits in the Medicare program were limited. TEFRA addressed some of these obstacles to participation in Medicare for HMOs.
Review Question
One federal law amended the Social Security Act to allow states to set their own qualification standards for HMOs that contracted with state Medicaid programs and revised the requirement that participating HMOs have an enrollment mix of no more than 50% combined Medicare and Medicaid members. This act, which was the true stimulus for increasing participation by health plans in Medicaid, is called the
Page 98 of 469

AHM 510 : Health Plans : Governance and Regulation
Omnibus Budget Reconciliation Act of 1981 (OBRA-81)
Tax Equity and Fiscal Responsibility Act of 1982 (TEFRA)
Employee Retirement Income Security Act of 1974 (ERISA)
Federal Employees Health Benefits Act of 1958 (FEHB Act)
Correct. OBRA-81 made it easier for health plans to serve the Medicaid population
Incorect. TEFRA was a federal budget act that made it easier for HMOs to enter into risk contracts to serve the Medicare population
Incorrect. ERISA's primary purpose was to prevent abuse of employer-sponsored pension benefit plans.
Incorrect. FEHP established a voluntary program to provide health insurance to federal employees, retirees and their dependents.
Fraud and Abuse LawsIn addition, the federal government has enacted laws and established regulations to prevent fraud and abuse of monies paid for healthcare from the coffers of Medicare and Medicaid. Since Medicaid is a joint federal-state program, states have also enacted and created fraud and abuse laws.
Other Budget ActsLegislation that affects health plans has often been included as part of other federal budget acts as well. Insight 4A-2 describes some provisions of various budget acts that affect health plans. The driving forces behind many of the provisions listed in the following insight were:
• To protect seniors from becoming victims of misleading business practices
• To ensure continuation of health insurance coverage for certain populations (i.e., employer-sponsored coverage upon termination of employment)
• To discourage discrimination in providing healthcare services to lower socioeconomic populations
• To encourage communication of health plan benefits to beneficiaries/members
Insight 4A-2. Budget Act Provisions Affecting Health Plans.
Omnibus Budget Reconciliation Act of 1985 (OBRA-85)
Required that HMOs inform members of their rights when the members join the HMO and annually thereafter
Allowed Medicare HMO members to disenroll from a plan at Social Security offices
Page 99 of 469

AHM 510 : Health Plans : Governance and Regulation
Required Quality Improvement Organizations (QIOs) to review HMO inpatient and ambulatory care
Mandated a study of physician incentive arrangements in hospitals reimbursed under the Medicare prospective payment system
Consolidated Omnibus Budget Reconciliation Act of 1986 (COBRA-86)
Required that group health plans allow employees and certain dependents to continue their group coverage for a stated period of time following a qualifying event that causes the loss of a person's group health coverage.
Required that all Medicare marketing materials be approved by CMS before use
Omnibus Budget Reconciliation Act of 1987 (OBRA-87)
Required that Medicare contracting plans which were terminating service in an area or not renewing a contract arrange for Medigap coverage for affected Medicare beneficiaries
Omnibus Budget Reconciliation Act of 1990 (OBRA-90)
Imposed additional regulatory requirements on Medicare-contracting plans that have incentive arrangements that put physicians at substantial risk for services the physicians do not directly provide
Required that health plans comply with Medicare rules to notify beneficiaries of rights to use advance directives, such as living wills
Allowed retroactive enrollment of retirees who enrolled in a Medicare contracting plan through an employer-sponsored health plan
Required Medicare-risk HMOs to make prompt payment on claims for services provided by non-network providers [Note that the Medicare-risk program is being replaced as of January 1, 1999, with a program called Medicare+Choice which will be discussed in Medicare and Health Plans.
Source: Except as noted above, used with permission and adapted from Peter R. Kongstvedt, The Managed Health Care Handbook, Third Edition (Gaithersburg, MD: Aspen Publishers, Inc., 1996), 721.
Americans with Disabilities Act (ADA)The Americans with Disabilities Act (ADA), which was enacted in 1990 primarily to ensure rights for people with disabilities, is being applied to the activities and facilities of all types of health plans. For example, the ADA requires that a health plan facility must be accessible to wheelchairs. Also, certain plan benefit exclusions have been challenged in court as ADA violations. The health plan implications of the ADA are discussed in Federal Regulation of Health Plans.
Health Insurance Portability and Accountability Act of 1996 (HIPAA)After Congress failed to pass the comprehensive healthcare reform initiative championed by the Clinton administration in 1994, a new approach to reform emerged. Members of Congress began introducing healthcare bills that sought to reform only a portion of the healthcare system in the United States. These efforts are commonly
Page 100 of 469

AHM 510 : Health Plans : Governance and Regulation
referred to as incremental reform bills. The Health Insurance Portability and Accountability Act of 1996 (HIPAA) is an example of incremental reform legislation.
HIPAA affects health plans in many ways. In general, HIPAA contains provisions to ensure that prospective or current enrollees in a group health plan are not discriminated against based on health status (e.g., there are rules and limits on the use of pre-existing condition exclusions). In addition, HIPAA generally requires guaranteed access to health insurance for small businesses and certain eligible individuals that have lost their group health coverage. HIPAA also generally requires guaranteed renewal of insurance once a policy is sold to an individual or group regardless of the health status of the members. 13
Amendments to HIPAA relate to mental health benefits and maternity hospital length of stays covered by insurers including health plans. We discuss HIPAA in more detail in Federal Regulation of Health Plans.
Balanced Budget Act of 1997 (BBA)The Balanced Budget Act of 1997 (BBA) has made significant changes to Medicare and Medicaid health plan programs by making enrolling Medicare and Medicaid beneficiaries in health plans easier. 14 The BBA changes allow Medicare beneficiaries more health plan options under the Medicare+Choice program. Beneficiaries can now enroll in PPOs, POS options, medical savings account plans, provider-sponsored plans, private fee-for-service plans as well as in HMOs. Payment reform provisions in the BBA may encourage health plans to enter traditionally low-payment Medicare markets.15
Funds for expanding health insurance for children whose parents cannot afford health insurance were also allocated as part of the BBA.16 The Medicare Modernization Act of 2003 further encouraged health plans to re-enter the Medicare market, though the creation of the more inclusive Medicare Advantage program (replacing M+C plans) a competitive bidding processs and more favorable risk selection.
Federal Programs Established by Law that Incorporate Health PlansAs we discussed earlier in this lesson, both Medicaid and Medicare allow health insurance plans to offer health plan products to eligible members of those populations. In addition, two other federal programs established by law have significantly incorporated health plans into their product offerings. The Federal Employees Health Benefits Act of 1959 (FEHB Act of 1959) established a voluntary program to provide health insurance to federal employees, retirees, and their dependents and survivors.17 The program established by the FEHB Act of 1959 is called the Federal Employees Health Benefits Program (FEHBP). FEHBP offers a choice of fee-for-service and health plans to more than nine million beneficiaries. 18 Many health plans participate in FEHBP and must comply with rules and requirements for this program set forth by the Office of Personnel Management (OPM).
Amendments to the Dependents Medical Care Act created the Civilian Health and Medical Program of the Uniformed Services (CHAMPUS) in 1967. 19 CHAMPUS authorized a program of medical benefits for families of active-duty military members, certain military retirees and their families, and certain former spouses of members of the military. To incorporate health plans into CHAMPUS, the Department of Defense created TRICARE. TRICARE is a health benefits program that has three options for eligible members: an HMO-type option, a PPO option, or the traditional fee-for-service option. Most of the care provided by TRICARE is through military facilities. The Department of
Page 101 of 469
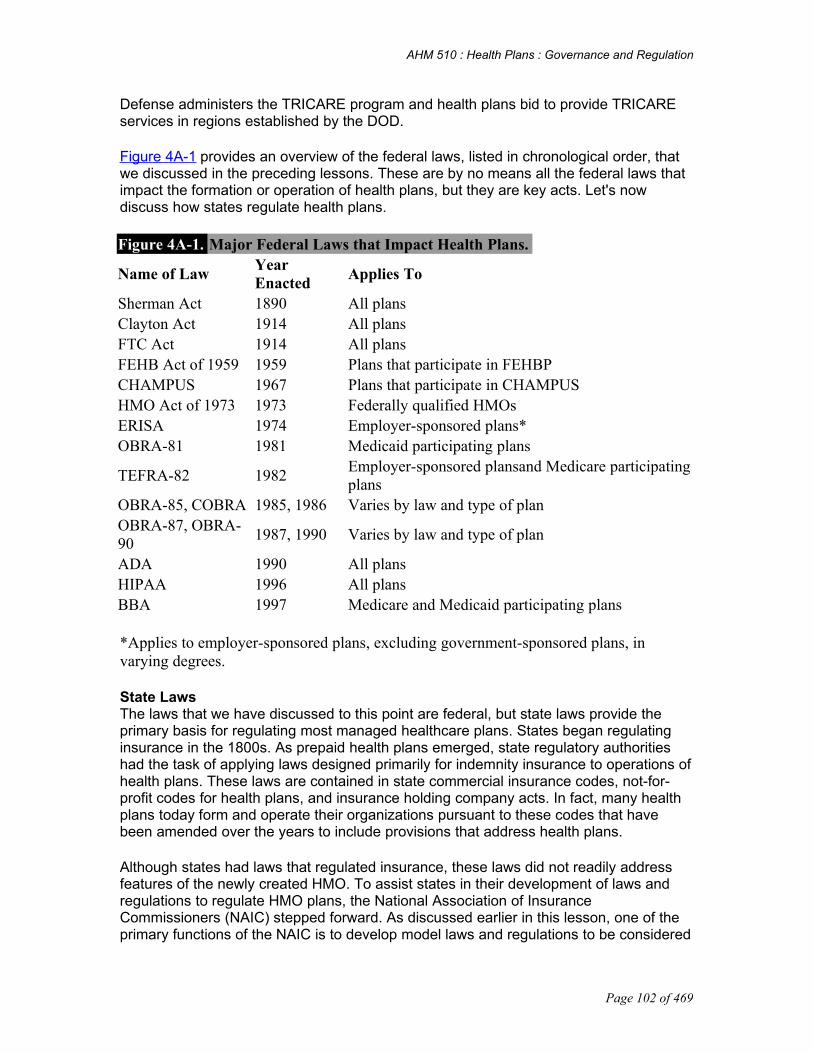
AHM 510 : Health Plans : Governance and Regulation
Defense administers the TRICARE program and health plans bid to provide TRICARE services in regions established by the DOD.
Figure 4A-1 provides an overview of the federal laws, listed in chronological order, that we discussed in the preceding lessons. These are by no means all the federal laws that impact the formation or operation of health plans, but they are key acts. Let's now discuss how states regulate health plans.
Figure 4A-1. Major Federal Laws that Impact Health Plans.
Name of Law Year Enacted
Applies To
Sherman Act 1890 All plansClayton Act 1914 All plansFTC Act 1914 All plansFEHB Act of 1959 1959 Plans that participate in FEHBPCHAMPUS 1967 Plans that participate in CHAMPUS HMO Act of 1973 1973 Federally qualified HMOs ERISA 1974 Employer-sponsored plans*OBRA-81 1981 Medicaid participating plans
TEFRA-82 1982Employer-sponsored plansand Medicare participating plans
OBRA-85, COBRA 1985, 1986 Varies by law and type of plan OBRA-87, OBRA-90
1987, 1990 Varies by law and type of plan
ADA 1990 All plans HIPAA 1996 All plans BBA 1997 Medicare and Medicaid participating plans
*Applies to employer-sponsored plans, excluding government-sponsored plans, in varying degrees.
State LawsThe laws that we have discussed to this point are federal, but state laws provide the primary basis for regulating most managed healthcare plans. States began regulating insurance in the 1800s. As prepaid health plans emerged, state regulatory authorities had the task of applying laws designed primarily for indemnity insurance to operations of health plans. These laws are contained in state commercial insurance codes, not-for-profit codes for health plans, and insurance holding company acts. In fact, many health plans today form and operate their organizations pursuant to these codes that have been amended over the years to include provisions that address health plans.
Although states had laws that regulated insurance, these laws did not readily address features of the newly created HMO. To assist states in their development of laws and regulations to regulate HMO plans, the National Association of Insurance Commissioners (NAIC) stepped forward. As discussed earlier in this lesson, one of the primary functions of the NAIC is to develop model laws and regulations to be considered
Page 102 of 469

AHM 510 : Health Plans : Governance and Regulation
for adoption by states.20 One of the most significant model laws developed by the NAIC in conjunction with another association of state regulators, the National Association of HMO Regulators (NAHMOR)--now the National Association of Health Plan Regulators--is the Health Maintenace Organization Model Act (HMO Model Act). The HMO Model Act, originally drafted in 1972 and modified subsequently as necessary, contains provisions regulating major aspects affecting formation and operation of HMOs. There are provisions in the HMO Model Act concerning licensing, solvency requirements, quality assurance, enrollee information, grievance procedures, enrollment periods, confidentiality of medical information, and reporting requirements. Most states have some form of HMO law that closely mirrors the HMO Model Act.
While risk-bearing PPOs are typically regulated under state insurance law, some states have enacted preferred provider organization (PPO) laws for nonrisk-bearing PPO entities.21 Some states also regulate independent practice associations (IPAs). For example, in New York, IPAs must have corporate purposes limited only to contracting with HMOs. In addition, New York law subjects IPAs to review by the New York State Department of Health. Many states have also enacted laws to regulate independent functions performed by a health plan under contract to another organization.22 The most common examples of these laws are utilization review and third party administrator statutes.
A few states have enacted legislation or issued administrative rules that either create a special licensure category for risk-bearing provider-sponsored organizations (PSOs) or require such organizations to obtain a license as an HMO. However, most states do not currently have specific laws or regulations that apply to at-risk provider organizations. In those states that do not have specific PSO laws, such organizations often are required to comply with the existing HMO or insurance laws that apply to the services or business they are offering. To "level the regulatory playing field" among different types of health plans, the NAIC is developing a model law called Consolidated Licensure for Entities Assuming Risk (CLEAR). CLEAR would establish uniform licensing standards for all health entities assuming insurance risk and is discussed in more detail in State Regulation of Health Plans I.
The HMO Act of 1973 specified the services that a federally qualified HMO must provide or cover. Many states have mirrored their benefit requirements on the federal HMO Act. In addition, some states have passed laws mandating specific benefits to be covered by health plans or mandating the providers who may deliver healthcare services to health plan members. For example, states have enacted mandates that require health plans to cover:
• Certain emergency room services
• A minimum hospital stay for mastectomy patients
• Certain benefits, such as alcoholism/substance abuse, mammograms, and Pap smears
States have also enacted legislation to protect the rights of providers. Several years ago, states began enacting any willing provider legislation. Any willing provider laws generally allow any provider who meets the health plan's terms and conditions of participation to become part of the network or receive payment from the health plan for
Page 103 of 469

AHM 510 : Health Plans : Governance and Regulation
covered services provided to health plan enrollees, whether the provider is a member of the health plan network or not.23
Although quite a few states have any willing provider laws in their legal code, few states have enacted this type of legislation in the last few years. Many of these laws are limited to pharmacists or another specific category of provider.
In general, state and federal laws, rules, and regulations apply to a range of activities performed by health plans. Insight 4A-4 discusses the scope of such regulation.
Review Question
Regulators of health plans have set standards in a number of areas of plan operations. Requirements with which health plans must comply typically include
providing enrollees and prospective enrollees with detailed information about various aspects of health plan policies and operations maintaining internal grievance and appeals processes to resolve enrollee complaints against the organization maintaining quality assurance programs that reflect the plan's activities in monitoring quality all of the above
Incorrect. While providing enrollees and prospective enrollees with detailed information about various aspects of health plan policies and operations is a typical regulatory requirement, other answers are also correct.
Incorrect. While maintaining internal grievance and appeals processes to resolve enrollee complaints against the organization is a typical regulatory requirement, other answers are also correct.
Incorrect. While maintaining quality assurance programs that reflect the plan's activities in monitoring quality is a typical regulatory requirement, other answers are also correct.
Correct
Page 104 of 469
AHM 510 : Health Plans : Governance and Regulation
Chapter 4 BRegulatory Agencies and Health Plans The regulation of healthcare in the United States has developed in a piecemeal fashion over the years. There has not been a master plan; instead, regulators have made attempts to address problems or issues as they arise. This approach has resulted in a patchwork (or segmentation) of regulations enacted by state and federal legislatures and administrative agencies, often making it difficult for health plans to comply.
Rather than a single set of laws and regulations that apply to all health plans, there are separate sets of regulations, both state and federal, applicable to different purchasers (i.e., private employers, Medicare, Medicaid, FEHBP, TRICARE, etc.). Each federal program in which a health plan chooses to participate has unique requirements. In some states, a health plan may have different aspects of its plan regulated by the state Medicaid agency, the state department of health, and the state department of insurance. In some states, a health plan may have different aspects of its operations regulated by the state Medicaid agency, the state department of health, and the state department of insurance. In some states, these departments may regulate the same aspect of a plan with differing standards. For example, a plan may have to meet different quality standards set by each of the three agencies. Because of this regulatory complexity, health plans often work closely with regulatory agencies to ensure compliance with all applicable requirements.
The federal and state governments have created regulatory agencies to implement and enforce federal and state laws and to establish additional rules and regulations, as necessary, to ensure the legislative intent of such laws is put into practice. In addition, some federal agencies provide education and training related to health plan. We discuss several of these agencies and their responsibilities in the following sections.
After completing this lesson, you should be able to:
Explain the roles of CMS in regulating healthcare Describe the role of the DOL in regulating health plans Explain the methods states use to delegate regulatory authority for healthcare plans
to state agencies
Federal Regulatory AgenciesDepartment of Health and Human ServicesThe Centers for Medicare and Medicaid Services (CMS) is a federal agency within the Department of Health and Human Services that was created in 1977 to administer the Medicare and Medicaid programs. 1
While CMS mainly acts as a purchaser of healthcare services for the Medicare and Medicaid beneficiaries, it also:
Assures that Medicare and Medicaid are properly administered by its contractors and state agencies
Establishes policies for the reimbursement of healthcare providers Conducts research on the effectiveness of various methods of healthcare
management, treatment, and financing
Page 105 of 469

AHM 510 : Health Plans : Governance and Regulation
Assesses the quality of healthcare facilities and services
CMS's programs are administered by agency staff working in its Baltimore, Maryland, headquarters and in 10 regional offices nationwide. The headquarters staff are responsible for the national direction of the Medicare and Medicaid programs. The regional office staffs provide CMS with the local presence necessary for quality customer service and oversight.2
In addition, CMS and its sister agency, the Office of Inspector General, regulate federally qualified HMOs and enforce the federal fraud and abuse laws that we will discuss later in this lesson. 3 See Figure 4B-1 for an overview of CMS's organizational structure and specific information on the three centers that serve CMS's main customers.
Within CMS, the Center for Health Plans and Providers (CHPPs) handles the day-to-day responsibilities of monitoring health plans and applying CMS's Medicare rules and regulations to health plans. 4 CHPPs issues operational policy letters addressing Medicare issues and provides technical assistance to health plans in areas such as guidelines for contracts with providers. 5
Another office within CMS is the Center for Medicaid and State Operations. The Department of Health and Human Services has delegated its responsibility for development and oversight of regulations under the Health Insurance Portability and Accountability Act (HIPAA) to CMS's Center for Medicaid and State Operations. The provisions in HIPAA allow for a joint federal/state enforcement scheme to ensure compliance with HIPAA regulations. If a state chooses not to enforce the federal requirements and standards of HIPAA, that job will fall to the Center for Medicaid and State Operations. Some states may choose to share the enforcement responsibilities with the Department of Health and Human Services. In addition, if a state is not adequately enforcing a specific HIPAA requirement, the Center for Medicaid and State Operations can step in and enforce that HIPAA regulation. 6
The Center for Beneficiary Services is an office within CMS that provides Medicare beneficiaries with support and information about health plans and other coverage options. 7 In addition, this office oversees health plan beneficiary appeals activities.
Page 106 of 469

AHM 510 : Health Plans : Governance and Regulation
Review Question
The Department of Health and Human Services (HHS) has delegated its responsibility for development and oversight of regulations under the Health Insurance Portability and Accountability Act (HIPAA) to an office within the Centers for Medicaid & Medicare Services (CMS). The CMS office that is responsible for enforcing the federal requirements of HIPAA is the
Center for Health Plans and Providers (CHPPs)
Center for Medicaid and State Operations
Center for Beneficiary Services
Center for Managed Care
Incorrect. The Center for Health Plan and Providers (CHPPs) handles the day to day responsibilities of monitoring health plans and applying CMS' Medicare Rules and Regulations to health plans.
Page 107 of 469

AHM 510 : Health Plans : Governance and Regulation
Correct. The Center for Medicaid and State Operations has responsibility for the delegation and oversight of regulations under HIPAA.
Incorrect. The Center for Beneficiary Services provides Medicare beneficiaries with support and information about health plans and other coverage options.
Incorrect. The Center for Managed Care falls under HRSA, another division of HHS.
Health Resources and Services Administration (HRSA)The Health Resources and Services Administration (HRSA) is another division of HHS. HRSA assists in providing health resources for medically underserved populations.8 Although HRSA does not regulate health plans, it provides resources and performs activities that are designed to educate and train people about health plans and underserved populations. Within HRSA, a Center for Managed Care has been established. The Center's goals are:
• To ensure that trained primary care providers are available to serve the needs of the underserved populations
• To educate the populations that HRSA serves about health plan systems and encourage active participation in such systems
• To assist in building health plan systems that are responsive to the needs of such underserved populations9
Health and Human Services Office of Inspector General (OIG)The Office of Inspector General (OIG) within HHS was established by the Inspector General Act of 1978. The OIG's primary functions are to prevent fraud and abuse in HHS programs, enforce sanctions for violations of HHS rules and regulations, and perform audits of company practices to ensure compliance with HHS rules and regulations. The OIG has three basic components or operational arms, the Office of Audit Services (OAS), the Office of Evaluations and Inspections, and the Office of Investigations.
Department of LaborPension and Welfare Benefits Administration 10
The Pension and Welfare Benefits Administration (PWBA) of the Department of Labor is responsible for administering and enforcing the fiduciary, reporting, and disclosure provisions of Title I of the Employee Retirement Income Security Act of 1974 (ERISA). Prior to January 1986, PWBA was known as the Pension and Welfare Benefits Program. At the time of its name change, PWBA was upgraded to a sub-cabinet position with the establishment of Assistant Secretary and deputy Assistant Secretary positions.
The administration of ERISA is divided among the Labor Department, the Internal Revenue Service of the Department of the Treasury (IRS), and the Pension Benefit Guaranty Corporation (PBGC). Title I- which contains rules for reporting and disclosure, vesting, participation, funding, fiduciary conduct, and civil enforcement- is administered by the Labor Department.
ERISA authorizes the Secretary of Labor, as well as plan participants and beneficiaries, to bring a civil legal suit to enforce the terms of a health plan governed by ERISA. The
Page 108 of 469

AHM 510 : Health Plans : Governance and Regulation
Secretary of Labor may also seek injunctions barring future violations and may seek criminal penalties for failure to comply with ERISA's disclosure and reporting requirements. 11
Changes in legislation have expanded the DOL's scope of responsibility for ERISA. The Omnibus Budget Reconciliation Act of 1989 contained provisions that require the Secretary of Labor to assess a civil penalty equal to 20% of any amount recovered for violations of fiduciary responsibility under ERISA.12
In addition, the Department of Labor is authorized to enforce the provisions of the Consolidated Omnibus Budget Reconciliation Act of 1986 (COBRA) and shares enforcement of HIPAA with several other federal agencies. 13
Office of Personnel ManagementThe Office of Personnel Management (OPM) is the federal government's human resources agency. OPM administers the Federal Employees Health Benefits Program (FEHBP). The FEHBP is the largest employer-sponsored health insurance program in the United States, serving federal employees, retirees, and their family members.14 To provide federal employees with choices for their healthcare, OPM contracts with health maintenance organizations, preferred provider organizations, plans offering point-of-service products, and fee-for-service plans. OPM is responsible for setting standards for plans that wish to participate in FEHBP. Such standards typically relate to the plan's management experience, enrollment rates, network of providers throughout the proposed service area, and ability to meet proposed budget projections. 15 In addition to setting standards for participation, the OPM conducts audits of health plans that participate in FEHBP. 16 These audits are designed to confirm that contracting health plans use the appropriate rating method in determining the rates charged to FEHBP and that the costs charged to the government are allowable.
Department of Defense (DOD)17
The Department of Defense (DOD) administers the Military Health Services System (MHSS), which provides medical care to active duty military personnel, their families, and retirees who are not yet eligible for Medicare. (Because the MHSS covers Coast Guard personnel and commissioned officers of the U.S. Public Health Service, DOD consults with the Department of Transportation (DOT) and HHS on matters affecting these two populations.) Within DOD, responsibility for administering this program has been delegated to the Assistant Secretary of Defense for Health Affairs.
Much of the care is provided directly through government-owned military treatment facilities (MTFs). This system currently includes about 115 hospitals and 471 clinics around the world and employs more than 43,000 civilian and 103,000 active duty personnel. MTFs are the core of the system. MHSS's recent TRICARE initiative- which is intended to bring health plan principles to the military health services system- uses several private plans to provide administrative services and back-up treatment facilities on an exclusive basis in the 12 regions of the MHSS. For example, MHSS enrollees may receive some care from MTFs and other care from providers under contract with a private plan.
Department of the TreasuryInternal Revenue Service (IRS)
Page 109 of 469

AHM 510 : Health Plans : Governance and Regulation
The Internal Revenue Service (IRS) is the largest agency in the Department of the Treasury. The IRS issues regulations to implement laws enacted by Congress in the Internal Revenue Code. Tax implications affect the choice of forms of legal organization for health plans. The IRS plays a part in many aspects affecting health plans' formation and operations. For example, as we discussed in Legal Organization of Health Plans, a not-for-profit health plan that applies for tax-exempt status must comply with many rules and regulations set forth by the IRS. In addition, a health plan may have interaction with the IRS in determining its federal income tax owed.
Often, tax laws passed by Congress contain provisions that affect many different aspects of government. For example, TEFRA and OBRA-81 have provisions that apply to Medicare and Medicaid as well as provisions that affect taxation. The IRS makes rules and regulations to interpret and apply the tax portions of such laws while other federal agencies, such as CMS in the case of Medicare and Medicaid, implement portions of the law that apply to their particular area of expertise. In addition, the IRS can impose tax penalties for failure to comply with certain laws.
Other Federal Agencies that Impact Health Plan OperationsThere are many federal agencies that impact the operations of health plans. If a question of job discrimination is raised about a health plan, the Equal Employment Opportunity Commission (EEOC) or the National Labor Relations Board (NLRB) may be involved. Healthcare plans must comply with rules and regulations made by the Immigration and Naturalization Service (INS) concerning employment of illegal aliens. Moving closer to the healthcare arena, the Food and Drug Administration (FDA) regulates pharmaceuticals, and health plans must ensure that the pharmacy networks with which it contracts comply with FDA rules and regulations. And the list goes on, depending on the type of issue and the agency that is charged with implementing and enforcing federal laws in that area.
Two other federal agencies that impact the formation and operation of health plans on more regular basis. Those agencies are the United States Department of Justice (DOJ) and the Federal Trade Commission (FTC). The U. S. Department of Justice is the executive department responsible for enforcing federal laws, representing the United States in federal cases, and providing legal advice to other federal officials and departments. 18 The U.S. Attorney General is responsible for directing the work of the DOJ. 19 Of particular interest to health plans is the DOJ's responsibility for enforcing antitrust laws. As we will discuss in greater detail later in this course, antitrust laws can affect formation, merger activities, or acquisition initiatives of a health plan.
Review Question
Antitrust laws can affect the formation, merger activities, or acquisition initiatives of a health plan. In the United States, the two federal agencies that have the primary responsibility for enforcing antitrust laws are the
Internal Revenue Service (IRS) and the Department of Justice (DOJ)
Office of Inspector General (OIG) and the Department of Defense (DOD)
Page 110 of 469

AHM 510 : Health Plans : Governance and Regulation
Federal Trade Commission (FTC) and the Department of Labor (DOL)
Federal Trade Commission (FTC) and the Department of Justice (DOJ)
Incorrect. While the DOJ does have antitrust enforcement responsibility, the IRS focuses on enforcing the Internal Revenue Code
Incorrect. The OIG's primary function is to prevent fraud and abuse in HHS programs, and the DOD is actually a purchaser of health plan services, but not an enforcer of the antitrust laws
Incorrect. While the FTC does have an antitrust role, the DOL is focused on health plans and ERISA
Correct! The FTC and the DOJ are responsible for enforcing antitrust laws.
The DOJ may also take a role in "qui tam" actions (commonly called "whistleblower" actions) brought under the false claims act. "Qui tam" actions are legal actions brought by private parties with direct knowledge of fraud. A private party makes a confidential filing (often referred to as "a filing under seal") in federal court on behalf of the federal government. The DOJ also receives a copy of this complaint. Generally, the DOJ has 60 days to decide whether it will pursue legal action based on the complaint. If the DOJ decides to take action, it has primary responsibility for prosecuting the action. In addition, if the government decides to take action the private party that filed the complaint is usually allowed to share in a portion of the funds recovered from the party that committed fraud. If the government elects not to take action, the private party can pursue action on their own and receive a larger portion of the funds recovered from the party that committed fraud.
The Federal Trade Commission (FTC) is a federal administrative agency, created by the Federal Trade Commission Act, that helps enforce a variety of antitrust and consumer protection laws. The Federal Trade Commission Act, passed in 1914, authorized creation of the FTC and empowered it to work with the U.S. DOJ to enforce the Clayton Act.20 In addition, the FTC enforces a variety of consumer protection laws, such as laws pertaining to the interstate mailing of unfair or deceptive advertising material by an insurer for solicitation purposes.21 The FTC defers to the states where states have adequate laws to protect consumers against such unfair or deceptive trade practices. 22
Overlap sometimes exists in the responsibilities of federal or state agencies in enforcing rules and regulations that affect health plan operations. Insight 4B-1 provides an example of this type of agency overlap at the federal level.
Insight 4B-1. Overlap of Federal Agencies' Responsibilities.
The Health Insurance Portability and Accountability Act (HIPAA) relies on the Department of Labor (DOL) and private parties to enforce its requirements that apply to employee benefit plans and plan sponsors. However, HHS is responsible for enforcing compliance of the insured product, purchased by an employment-based plan, with
Page 111 of 469

AHM 510 : Health Plans : Governance and Regulation
HIPAA and may take action against the product's issuer if a violation occurs. In such cases, DOL becomes involved only if the plan or plan sponsor induces or otherwise causes the issuer's violation-or engages in behavior that, in itself, is a violation. When a group plan self-funds, however, DOL is solely responsible for enforcement. Tax penalties may also be imposed by the IRS for HIPAA violations.
Source: Adapted and used with permission, American Association of Health Plans, 10.
State Regulatory Agencies23
Health plans often are regulated by more than one agency in a state- usually the department of insurance (which generally oversees the financial aspects of health plan operations) and the department of health (which generally regulates the healthcare delivery system, including oversight on access and quality of care). Because states are also purchasers of healthcare for their own employees and through Medicaid programs, other state agencies also may be involved in setting standards for HMOs.
In addition to the state agencies discussed above, a health plan may interact with a state's secretary of state or similar agency responsible for incorporation issues; a state attorney general for legal issues, such as not-for-profit issues, antitrust, or for-profit conversions; the state social or human services department for Medicaid; and the state department of revenue for taxation issues. Managed healthcare plans that offer workers' compensation products are usually subject to regulation by the state Department of Labor or similar state agency.24
Page 112 of 469

AHM 510 : Health Plans : Governance and Regulation
Chapter 5 AState HMO and Other Types of Health Plan Laws When the federal HMO Act was passed, many state laws constrained or restricted the development of HMOs. These state laws were designed to regulate insurance companies, hospital and medical service corporations, or other entities- not health plans.1 For example, some state laws required that an HMO be approved by a medical society. Providers, who were the members of such societies, often saw HMOs as a threat to their method of practicing medicine and put up roadblocks to deter HMO formation. To encourage states to develop HMO-enabling laws in the early 1970s, the now-defunct federal Office of Health Maintenance Organizations provided assistance and conducted educational programs about the HMO Act for audiences of state regulators.2
Over time, almost every state in the United States developed its own HMO statute or included HMO provisions in its general insurance code. Since it is not possible to discuss every state's HMO laws in this assignment, we will use as a framework for our discussion the National Association of Insurance Commissioners (NAIC) HMO Model Act, which has served as the basis for many of the state laws that regulate HMOs.
After completing this lesson, you should be able to:
Describe the major provisions of the NAIC HMO Model Act Describe the types of state regulation that apply to PPOs, UROs, TPAs, PSOs, and
POS products Explain the need for the Risk-Based Capital for Health Organizations Model Act and
the risk-based capital formula
NAIC HMO Model ActIn 1972, the NAIC adopted the Health Maintenance Organization Model Act (HMO Model Act), a model law designed to regulate the licensure and operations of HMOs. In the HMO Model Act, a health maintenance organization is defined as "any person that undertakes to provide or arrange for the delivery of basic healthcare services to enrollees on a prepaid basis, except for enrollee responsibility for copayments and/or deductibles."3 Basic healthcare services are defined under the Model Act as "the following medically necessary services: preventive care, emergency care, inpatient and outpatient hospital and physician care, diagnostic laboratory services, and diagnostic and therapeutic radiological services. It does not include mental health services or services for alcohol or drug abuse, dental or vision services, or long-term rehabilitation treatment." 4
Once it has been determined that an entity meets the definition of an HMO, the entity must comply with the licensing requirements and all other applicable requirements of the particular state's HMO statute.
The main purpose of the HMO Model Act is to provide consumer protection in two critical areas: financial responsibility and healthcare delivery. In the rest of this section, we discuss how the HMO Model Act regulates the licensure of HMOs, then we describe how the HMO Model Act regulates financial responsibility, healthcare delivery, and several other important operational issues with regard to HMOs.
Page 113 of 469
AHM 510 : Health Plans : Governance and Regulation
Obtaining a Certificate of AuthorityUnder the HMO Model Act and most state laws, an entity that wishes to operate as an HMO must obtain a certificate of authority, often called a license. The process of obtaining and maintaining a certificate of authority is often referred to as licensure. A certificate of authority (COA) is a certificate issued by the state authority that regulates HMOs, asserting that all requirements have been met for the establishment of an HMO in accordance with the state's HMO laws. Generally, the purpose of licensing is to ensure that an HMO is a solid, dependable organization, fiscally sound, and able to meet specified quality standards for healthcare delivery.
As we discussed in Legal Organization of Health Plans, some states allow only domestic corporations to obtain a certificate of authority, while others allow both domestic and foreign corporations to obtain a certificate. To obtain a certificate of authority, an HMO applicant must file an application form and additional information with the insurance department or other state agency responsible for HMO regulation. Typically, the submission must include these items.
In many states, the department of insurance and the department of health each have specific responsibilities for regulating HMOs. For instance, the insurance department might have responsibility for matters pertaining to solvency, financial statements, rate filings, group contract filings, evidence of coverage filings, benefit mandates, and member grievances; the health department might have responsibility for matters pertaining to quality assurance, service area expansions, provider networks, and provider relations. In some states, either the insurance department or the health department has responsibility for all matters pertaining to regulation of HMOs. In other states, regulation of HMOs is the responsibility of a different state agency, such as the Department of Commerce in Minnesota.
Organizational documents such as partnership agreements, trust agreements, or articles of incorporation and bylaws, depending on the organizational form under which the applicant operates
Biographical information about the individuals who will be responsible for the HMO's day-to-day operations and copies of all contract forms the HMO will use for agreements with those individuals
Current and historical financial statements and a financial feasibility plan detailing projected enrollments, how the HMO will calculate premium rates, projected financial statements, and sources of working capital or other funding resources
A description of the procedures or processes the HMO will follow to meet the protection against insolvency requirements in the HMO Model Act or state statute
A description of the HMO's quality assurance program Contract forms the HMO will use for agreements with other parties providing
services, such as healthcare providers and third party administrators Copies of the evidence of coverage forms that the HMO will issue to enrollees Contract forms the HMO plans to use for group contracts with employers, unions,
trustees, or other organizations A description or map of the geographic area in which the HMO proposes to operate A list of the names, addresses, and license numbers of all providers in the HMO
network
Page 114 of 469

AHM 510 : Health Plans : Governance and Regulation
A description of the internal grievance procedures the HMO will follow to investigate and resolve enrollee complaints
Other information required by the state regulatory authority to determine whether to issue a COA
Financial ResponsibilityHMO laws seek to apply appropriate net worth or capital requirements to help ensure that members are enrolled in financially viable entities with the resources to pay for their members' current and future healthcare needs. These requirements, along with provisions for financial reporting, accounting, liquidity, investment practices, and related matters, are often referred to as financial standards. HMO laws seek to ensure that members are adequately protected in the event of insolvency, which is when an entity's liabilities exceed its assets or when it is unable to meet its financial obligations on time.
Financial StandardsAdequate capital and surplus is essential to allow HMOs (as well as other types of health plans) to withstand losses incurred due to unexpected fluctuations in operating costs. If a health plan does not have a cushion to absorb such losses, its members may experience adverse consequences. These consequences might include disruption of care, having to pay for medical expenses that should have been covered by the health plan (e.g., referral or out-of-network expenses for emergency or specialty care), or the loss of any premium paid in advance. 5
The HMO Model Act requires an HMO seeking to obtain a COA to have an initial net worth of $1,500,000 and to thereafter maintain the minimum net worth described in Figure 5A-1. Net worth is an HMO's total admitted assets minus its total liabilities (its debts and obligations, including obligations to pay for in-network and out-of-network care for its members). Assets are all things of value owned by an individual or organization. 6
An admitted asset is an asset that state HMO or insurance laws permit on the Assets page of a company's Annual Statement.7 Recall from Healthcare Management: An Introduction that the Annual Statement is a financial report that most health plans have to file to comply with state insurance regulations.
As the health plan industry has matured, the NAIC has developed additional capital standards that were not contemplated in the original HMO Model Act. One example of this type of regulatory evolution can be seen in the NAIC's recent efforts to develop a formula for determining risk-based capital standards that will apply to all healthcare organizations (not just HMOs). Risk-based capital refers to a method of taking into account an organization's size, structure, and risk profile to set the minimum amount of capital needed for that organization to support its overall business operations. The NAIC's RBC formula for all healthcare organizations provides variable capital requirements based on the nature and volatility of an organization's business. It is expected that RBC will not replace, but rather complement, other state law financial requirements.8 We address this regulatory initiative in greater detail later in this lesson.
Figure 5A-1. Minimum Net Worth Requirements in the NAIC HMO Model Act.
Section 13
Page 115 of 469

AHM 510 : Health Plans : Governance and Regulation
* * * * *A (2) Except as provided in Paragraphs (3) and (4) of this subsection, every health maintenance organization must maintain a minimum net worth equal to the greater of:
(a) One million dollars ($1,000,000)(b) Two percent (2%) of annual premium revenues as reported on the most recent annual financial statement filed with the commissioner [director, superintendent] on the first $150,000,000 of premium and one percent of annual premium on the premium in excess of $150,000,000(c) An amount equal to the sum of three months uncovered health care expenditures as reported on the most recent financial statement filed with the commissioner [director, superintendent](d) An amount equal to the sum of: (i) Eight percent (8%) of annual health care expenditures except those paid on a capitated basis or managed hospital payment basis as reported on the most recent financial statement filed with the commissioner [director, superintendent](ii) Four percent (4%) of annual hospital expenditures paid on a managed hospital payment basis as reported on the most recent financial statement filed with the commissioner [director, superintendent].
Source: Section 13, Health Maintenance Organization Model Act (National Association of Insurance Commissioners, 1995).
Protections Against and in the Event of InsolvencyAs we have seen, the HMO Model Act sets capital and surplus requirements to help ensure that members are enrolled in financially viable entities that have the resources to pay for their members' current and future healthcare needs. In addition, regulators can use financial standards to help determine if a health plan is showing signs of deteriorating financial condition. If the state insurance commissioner determines, after a notice and hearing, that the financial condition of an HMO is such that its continued operation might be hazardous to its enrollees, its creditors, or the general public, then the commissioner may proceed with any of a number of interventions to protect against insolvency. These interventions might include monitoring of a corrective plan developed by the company, reducing the volume of new business being accepted, reducing expenses by specified methods, suspending or limiting the writing of new business for a period of time, selling the time or merging it with a financially sound company, or taking over the management of the business.
Although financial standards provide a useful tool for state regulators to assess an organization's financial viability and to intervene when necessary, they cannot completely eliminate the possibility of insolvency. To further safeguard members, state regulators rely upon other regulatory measures, such as deposit requirements, plans for handling insolvency, replacement coverage requirements, administrative supervision laws, receivership, assessments, and guaranty associations.
Deposit RequirementsThe HMO Model Act requires that an HMO place a deposit in trust with the state insurance commissioner that can be used to protect the interests of enrollees of an HMO that becomes financially impaired. At the discretion of the insurance commissioner, the deposit can be placed with an organization or trustee acceptable to the commissioner. The deposit, regardless of where it is placed, must be in cash and/or securities and must
Page 116 of 469

AHM 510 : Health Plans : Governance and Regulation
at all times have a minimum value as specified by law. The amount deposited is treated as an admitted asset for purposes of determining the amount of the HMO's net worth. 9
Sometimes an HMO must make an additional deposit in trust with the state insurance department to protect members from creditors in the event of the HMO's insolvency. The need for this deposit depends on the amount of the HMO's uncovered expenditures. An expenditure is considered to be "covered" if it is the cost of a service provided by a network provider that has a hold-harmless clause in its contract with the HMO. The hold-harmless clause prevents a provider from trying to recover any outstanding payments for covered services from HMO members. Although the HMO Model Act requires that contracts between the HMO and healthcare providers include a hold-harmless clause, not all healthcare expenses are subject to the clause, e.g., emergency services, out-of-area care, and services provided by nonparticipating providers. Uncovered expenditures are the costs to the HMO for healthcare services that are the obligation of the HMO and for which an enrollee may also be liable if the HMO becomes insolvent. Such expenditures are considered to be "uncovered" because if the HMO becomes insolvent, the provider can seek to recover payment from the members. To prevent such an occurrence, the HMO must make some other arrangements for covering those expenses in the event of its insolvency. 10
If an HMO's uncovered expenditures exceed 10 percent of its total healthcare expenditures, then it must place a deposit in trust with the state insurance department. This deposit is called an uncovered expenditures insolvency deposit. If the HMO becomes insolvent, the uncovered expenditures insolvency deposit may be used by the state insurance commissioner on behalf of enrollees in the state to pay claims for uncovered expenditures. For purposes of determining the HMO's net worth, the amount of the uncovered expenditures insolvency deposit is treated as an admitted asset.11
Review Question
The National Association of Insurance Commissioners (NAIC) adopted the Health Maintenance Organization Model Act (HMO Model Act) to regulate the development and operations of HMOs. One true statement regarding the HMO Model Act is that the act
includes mental health services in its definition of basic healthcare services
authorizes only one state agency-the department of insurance-to regulate HMOs
requires HMOs to place a deposit in trust with the state insurance commissioner for the purpose of protecting the interests of enrollees should an HMO become financially impaired requires HMOs that wish to offer a point-of-service (POS) product to contract with a licensed insurance company to provide POS options to plan members
Incorrect. The HMO Model Act does not include, as part of basic healthcare services, mental health services, or services for alcohol or drug abuse, dental or vision services or long-term rehabilitation treatment.
Page 117 of 469

AHM 510 : Health Plans : Governance and Regulation
Incorrect. In many states, the department of insurance and the department of health each have specific responsibilities for regulating HMOs.
Correct. The HMO Model Act does require HMOs to place a deposit in trust with the state insurance commissioner in order to protect the interests of enrollees should an HMO become financially impaired.
Incorrect. A standalone POS product is regulated under the state's HMO Act
Plan for Handling InsolvencyThe HMO Model Act requires each HMO to have a plan for handling insolvency. If the HMO becomes insolvent, this plan must allow for the continuation of benefits (1) for contract periods for which it has received premium payments and (2) for enrollees who are confined in an inpatient facility on the date of insolvency until they are discharged. The state insurance department may require such a plan to include the following types of features:
• Insurance to cover the expenses to be paid for continued benefits
• Provisions in provider contracts requiring healthcare providers to render services the HMO is obligated to provide following an insolvency
• Insolvency reserves
• Acceptable letters of credit
Fast Definition
Reserves - Amounts of money set aside for the purpose of paying future business obligations.
Letters of credit - Documents issued by a bank guaranteeing the payment of a customer's bank drafts or other financial obligation up to a stated amount for a specified period.
Replacement Coverage in the Event of InsolvencyIn the NAIC HMO Model Act the term carrier is often used to refer to organizations or entities that are responsible for paying for benefits or providing services under a group contract. For example, such organizations include HMOs, insurers, and not-for-profit hospital and medical service corporations. 12 We will sometimes refer to carriers in our discussion of the HMO Model Act.
The HMO Model Act prescribes additional regulatory actions to protect consumers in the event an HMO becomes financially impaired or insolvent. For enrollees who were covered under a group contract with an insolvent HMO, the insurance commissioner can order all other carriers that participated in the group's most recent enrollment period to offer their plan to the insolvent HMO's group enrollees. The insolvent HMO's group enrollees are given a thirty-day enrollment period that begins on the date of insolvency to enroll with another carrier. This offer must include the same coverages and rates that were offered by the carrier during the last enrollment period.13
Page 118 of 469

AHM 510 : Health Plans : Governance and Regulation
If no other carriers offered coverage to some groups enrolled in the insolvent HMO, or if the insurance commissioner determines that the other health plans do not have sufficient resources to assume responsibility for all of the group enrollees, then the commissioner can allocate the insolvent HMO's group contracts among all HMOs that operate in the insolvent HMO's service area. This allocation must be made equitably among all the remaining eligible HMOs. In making the allocation, the commissioner considers the healthcare delivery resources of each HMO. Each HMO must offer one of its current benefit plans that provides coverage most similar to the coverage that each group had with the insolvent HMO, at rates determined in accordance with the successor HMO's existing rating methodology.14
Similarly, the commissioner can allocate equitably the insolvent HMO's nongroup enrollees among all HMOs that operate within a portion of the insolvent HMO's service area, taking into account the healthcare delivery resources of each such HMO. Each HMO is required to offer nongroup enrollees one of its current benefit plans that provides individual or conversion coverage as determined by the type of coverage the enrollee had with the insolvent HMO, at rates determined in accordance with the successor HMO's existing rating methodology. Successor HMOs that do not offer direct nongroup enrollment are permitted to include all of the allocated nongroup enrollees in one group for coverage and rating purposes. 15
The HMO Model Act also requires a successor carrier to immediately cover all eligible enrollees, regardless of any provisions in the carrier's contracts that might otherwise deny eligibility due to an individual being hospital confined, pregnant, or not actively at work. Further, a successor carrier cannot reduce or exclude benefits for an eligible enrollee's pre-existing conditions.
Administrative Supervision Laws and ReceivershipThe HMO Model Act gives the insurance commissioner the authority to take action in accordance with sections of the state rehabilitation, liquidation, and administrative supervision laws that apply to insurance companies. Administrative supervision may occur, by order of the insurance commissioner or consensual agreement, when an HMO is in hazardous financial condition, has failed to comply with insurance laws, or for other reasons.
When a state insurance commissioner judges that an HMO's financial difficulties are so severe that more serious action than placing the HMO under supervision is warranted, then the commissioner may choose to place the insurer in receivership. When an HMO is placed in receivership, the state insurance commissioner, acting for a state court, takes control of and administers the HMO's assets and liabilities. The receiver may either try to rehabilitate the HMO or, if that is not possible, liquidate it by collecting the HMO's assets and making sure that the HMO's obligations to customers are fulfilled as much as possible. Rehabilitation occurs when an insolvent HMO continues in existence under receivership; during this period state authorities try to find ways to return the organization to normal operation. Liquidation occurs when the receiver either transfers all of the HMO's business and assets to other carriers or sells the assets to satisfy the HMO's outstanding obligations and terminates the HMO's business.16
Assessments and Guaranty FundsIf a court declares an HMO to be insolvent, the HMO Model Act authorizes the insurance
Page 119 of 469

AHM 510 : Health Plans : Governance and Regulation
commissioner to levy an assessment on other HMOs that operate in the state. This assessment goes towards paying (1) claims for uncovered expenditures of enrollees and (2) continued coverage for a specified period of time for members who are not otherwise eligible for continued coverage. In any one calendar year, an HMO's assessment cannot be more than 2 percent of the aggregate premium written by the HMO in the state during the previous year. An HMO that fails to pay an assessment within 30 days after notice is subject to fines and/or suspension or revocation of its certificate of authority. The insurance commissioner can waive an assessment of an HMO if the commissioner determines that such an assessment would jeopardize the HMO's financial condition. The HMO Model Act does not recommend that all states include this assessment requirement in their statutes, especially if, in a particular state, the HMO premium volume is small or the market is dominated by a few large HMOs.
Similar to the assessment provision in the HMO Model Act, a few states have adopted HMO guaranty association requirements. These requirements, based on the life and health insurance guaranty association requirements that are in effect in all states, provide another way to safeguard consumers in the event of insolvency. As a condition for obtaining an HMO license in these states, each HMO must participate in the HMO guaranty association. This association is governed by a board composed of representatives from all HMOs doing business in the state. If an HMO is declared insolvent, the HMO guaranty association assesses the other HMOs in the amount necessary to cover the failed HMO's responsibility to its members.
Healthcare DeliveryHMO members often rely exclusively on the HMO network for their choice of providers, the quality of healthcare they receive, and their overall satisfaction with healthcare services. To ensure that members are afforded appropriate consumer protections, HMO laws pay particular attention to HMO healthcare delivery issues. Generally, with regard to healthcare delivery, HMO laws focus on three key issues: network adequacy, quality assurance programs, and grievance procedures.
• Network Adequacy
• Quality Assurance
• Member Grievances
Network Adequacy
As discussed earlier, the HMO Model Act requires an HMO seeking to obtain a certificate of authority to file a description or map of the geographic area in which the HMO proposes to operate and a list of the names, addresses, and license numbers of all providers in the HMO network. Typically, state regulators examine this information to ensure that providers are located within a reasonable distance of all locations in the HMO's service area. In addition, regulators seek to ensure that the health plan maintains adequate numbers of providers based on the number of members enrolled in the HMO.
As we mentioned in our discussion of financial responsibility, with the growth of the health plan industry, the NAIC has developed additional standards that were not
Page 120 of 469

AHM 510 : Health Plans : Governance and Regulation
contemplated in the original HMO Model Act. In 1996, the NAIC adopted the Managed Care Network Adequacy Model Act to establish network standards and to assure the adequacy, accessibility, and quality of healthcare services offered under all health plans, including HMOs. We describe the Health Plan Network Adequacy Model Act in more detail later in this lesson.
Quality Assurance
The HMO Model Act also requires an HMO to file a description of its proposed program for quality assurance. A quality assurance program establishes procedures to assure that healthcare services provided to enrollees are rendered under reasonable standards of quality of care consistent with prevailing professionally recognized standards of medical practice. The procedures must include mechanisms to assure availability, accessibility, and continuity of care.17 The purpose of the quality assurance program is to monitor and evaluate the HMO's delivery of healthcare services. The HMO's quality assurance program must include a statement of goals and objectives for evaluating the plan's quality of care that emphasizes improving enrollees' health status. In addition, the program must keep records of quality assurance program activities and make those records available to the commissioner of health or other authorized regulatory official. The HMO Model Act also requires that the HMO have a system for periodic reporting of program activities to the HMO's board, its providers, and other organizational staff. Before a certificate of authority is issued, the insurance department may confer with the health department to assure that the HMO's proposed quality assurance program meets the standards set forth in the HMO law. The NAIC has developed other model acts, such as the Quality Assessment and Improvement Model Act and the Utilization Review Model Act to more specifically regulate various aspects of quality assurance in all health plans, including HMOs. We describe these model acts later in this lesson.
Member Grievances
In addition to requiring an HMO to file a description of the internal grievance procedures that the HMO follows to investigate and resolve enrollee complaints, the HMO Model Act requires the HMO to maintain records regarding all complaints received. These records are subject to review by the appropriate regulatory authority. In addition, the NAIC has developed the Health Carrier Grievance Procedure Model Act, discussed later in this lesson, which more specifically addresses requirements concerning the handling of member grievances.
Filing and Reporting RequirementsAs we have seen, the HMO Model Act requires an HMO seeking to obtain a certificate of authority to submit copies of its proposed provider and group contract forms, evidence of coverage forms, and premium rate methodology. In most states, if an HMO wishes to make changes to its group contract and evidence of coverage forms, it must file the changes with the appropriate state agency. Some states also require HMOs to file changes in premium rates. In many states, an HMO is not permitted to use new forms (or rates, if rate filing is required) until the appropriate state agency reviews and approves the filing. This is called prior approval. Some states, however, operate on a file
Page 121 of 469
AHM 510 : Health Plans : Governance and Regulation
and use basis, which means that the HMO must submit a filing, but prior approval is not required for the HMO to begin using the forms (or rates), although the regulator may later disapprove any forms or rates found to violate state laws.
HMOs must file with the state insurance department or appropriate state agency an annual report detailing financial and operational information. This annual report must be filed on a form approved by the state and must be verified by at least two of the HMO's principal officers. Based on requirements set forth in the HMO Model Act, HMOs also must file the following information each year:
• Audited financial statements
• A list of the healthcare providers who have executed a contract agreeing to provide services to HMO enrollees
• A description of the HMO's grievance procedures, the total number of grievances handled, a compilation of the causes underlying those grievances, and a summary of the final disposition of the grievances
The HMO Model Act also gives the state the authority to require additional reports deemed necessary and appropriate, such as reports that provide information on quality assurance programs.
Note that each state may have in its reporting requirements some variation from the items listed above. For example, some states do not require an annual filing of a list of the HMO's contracted providers. Some states also require that material business changes be reported more frequently than once a year. Such a filing may be required to update the state's records of the HMO's enrollee materials, including the handbooks it uses to describe coverage, provider lists, and sample member identification cards. In addition, some states require regulatory approval of material business changes before the changes are allowed. An HMO may also have to make a filing to obtain state approval to expand its service area.
Enrollee ContractsUnder the HMO Model Act, HMOs are required to provide each group and individual contract holder with a document that specifies the benefits and services available to enrollees. For groups, the HMO typically provides a copy of the contract to the group contract holder. The contract must contain a clear statement of this information.
Most of the foregoing information also must be included in a written statement, known as an evidence of coverage (EOC), also called a certificate of coverage, that is provided to individuals enrolled under group HMO contracts.
Individual HMO contracts also must provide for a 10-day period in which the enrollee may examine and return the contract in exchange for a full premium refund. If an enrollee receives services during the 10-day period and returns the contract for a premium refund, then the enrollee must pay for all services received.
The name and address of the HMO Eligibility requirements
Page 122 of 469

AHM 510 : Health Plans : Governance and Regulation
Benefits and services within the service area Emergency care benefits and services Out-of-area benefits and services, if any Copayments, deductibles, or other out-of-pocket expenses Limitations and exclusions Enrollee termination procedures Enrollee reinstatement procedures, if any Claims procedures Enrollee grievance procedures Continuation of coverage Conversion Extension of benefits, if any Coordination of benefits, if applicable Description of the service area Entire contract provision Term of coverage Cancellation Renewal Grace period Conformity with state law
Disclosure RequirementsWe have noted that the HMO Model Act requires HMOs to provide enrollees with specific information about the HMO, its services, and its providers. Upon enrollment, an enrollee must receive a list of the HMO's healthcare providers. Any "material change" in the operation of an HMO affecting enrollees must be reported to enrollees within 30 days of the change. For example, a major change in the provider network is considered a material change that must be reported to enrollees. By contrast, the termination of one medical care provider from the provider network would not qualify as a material change unless that provider is a primary care provider. When a primary care provider is terminated from the network, the HMO must notify all enrollees who receive primary care from the terminated provider. In addition, the HMO must help those enrollees:
• Transfer to another primary care provider
• Obtain information about HMO services and notify them where additional information on access to services can be found
The HMO must also supply a toll-free telephone number that enrollees can use to contact the HMO. Newly enacted consumer protection laws contain additional disclosure requirements intended to provide members with information about topics such as risk arrangements, plan financial information, and prescription drug formularies.
Review Question
Greenpath Health Services, Inc., an HMO, recently terminated some providers from its network in response to the changing enrollment and geographic needs of the plan. A
Page 123 of 469

AHM 510 : Health Plans : Governance and Regulation
provision in Greenpath's contracts with its healthcare providers states that Greenpath can terminate the contract at any time, without providing any reason for the termination, by giving the other party a specified period of notice.
The state in which Greenpath operates has an HMO statute that is patterned on the NAIC HMO Model Act, which requires Greenpath to notify enrollees of any material change in its provider network. As required by the HMO Model Act, the state insurance department is conducting an examination of Greenpath's operations. The scope of the on-site examination covers all aspects of Greenpath's market conduct operations, including its compliance with regulatory requirements.
With respect to the type of change that constitutes a material change under the HMO Model Act's disclosure requirements, the termination of one healthcare provider from Greenpath's provider network
always qualifies as a material change in the plan, and Greenpath must report the change to all plan enrollees always qualifies as a material change in the plan, and Greenpath must report the change to only those plan enrollees who have received care from the terminated provider qualifies as a material change in the plan only if the provider is a primary care provider, and in such a case Greenpath must report the change to all plan enrollees qualifies as a material change in the plan only if the provider is a primary care provider, and in such a case Greenpath must report the change to only those plan enrollees who receive primary care from the terminated provider
Incorrect. Termination of one physician does not constitute a material change, unless the physician is a primary care provider
Incorrect. Termination of one physician does not constitute a material change, unless the physician is a primary care provider
Incorrect. While termination of a primary care provider is a material change, the health plan does not have to notify all members
Correct. The HMO must only notify enrollees who receive primary care from the terminated provider
Regulatory Supervision and EnforcementTo protect the interests of HMO members, the HMO Model Act authorizes the insurance department to conduct an examination of each HMO's operations as often as is reasonably necessary, but at least once every three years. Similarly, the HMO Model Act authorizes the health department to conduct an examination of each HMO's quality assurance program and its providers as often as is reasonably necessary to protect the interests of the members, but at least once every three years. In lieu of conducting the examination themselves, the insurance department and the health department have the option of accepting the report of an examination made by another state. The insurance department is authorized to take any of a number of actions, including suspending or
Page 124 of 469

AHM 510 : Health Plans : Governance and Regulation
revoking an HMO's certificate of authority, to enforce state laws and regulations and to protect the public. We discuss market conduct examinations and mechanisms for enforcement in more detail in Market Conduct Examinations and Mechanisms for Enforcements.
Accreditation and HMO RegulationBeyond the HMO Model Act requirements, a few states have made accreditation by an external accreditation organization a requirement of licensure. For example, in Florida an HMO must pass a quality-of-care assessment as a condition for doing business.18 In some states, the state agency responsible for regulating HMO quality initiatives will accept an accreditation by a nationally recognized accreditation organization in lieu of a state-conducted quality review. Many states are moving toward adopting the same standards for their quality assurance oversight responsibilities as those used by the National Committee for Quality Assurance (NCQA) in their accreditation process; however, these states are not planning to require accreditation as a condition for licensure. Organizations from which health plans receive accreditation that may be accepted by states in lieu of a state-conducted quality review include: the NCQA, the American Accreditation Health Care Commission (The Commission/URAC-discussed later), and the Joint Commission on Accreditation of Healthcare Organizations (JCAHO). In general, accreditation organizations set minimum quality performance standards and then measure health plans against those standards
Laws Regulating Other Types of Health PlansThe NAIC has developed and adopted a number of other model acts in addition to the HMO Model Act to specifically address various aspects of health plans. These model laws include the Health Care Credentialing Verification Model Act, the Quality Assessment and Improvement Model Act, the Health Plan Network Adequacy Model Act, the Health Carrier Grievance Procedure Model Act, and the Utilization Review Model Act. Figure 5A-2 provides a brief description of these model acts.
Some states have specific regulations that address PPOs, TPAs, POS products, utilization review, and PSOs. However, there is a movement at the NAIC to consolidate licensure of all types of health risk-bearing entities into one regulatory act through the CLEAR model act discussed in Overview of Laws and Regulations. Let's now look at state regulation of preferred provider arrangements.
Figure 5A-2. NAIC Model Acts.
The NAIC defines the term "health carrier," used in the model acts described below, as "an entity (subject to state insurance laws and regulations or to the insurance commissioner's jurisdiction) that offers to contract to provide, arrange for, or reimburse any of the costs of health care services." 19 Some provisions of the model acts apply only to a "health plan," which is broadly defined as one that either requires an enrollee to use or provides incentive to use certain providers. The model acts recognize that states can exclude some plans with large networks and minimal restrictions from the definition of health plan.
Page 125 of 469

AHM 510 : Health Plans : Governance and Regulation
Health Care Credentialing Verification Model Act: All health carriers that offer a health plan are required to establish a comprehensive credential verification program that verifies the credentials of all contracted health care professionals. Health carriers are required to establish written credential verification procedures that they disclose upon written request to any applying healthcare professionals. Health carriers must also allow providers to review and correct any information they submit.
Quality Assessment and Improvement Model Act: This act requires that all health carriers that offer a health plan must develop the systems necessary to measure and report on quality of healthcare services. All health carriers that provide health plans must have a quality assessment program. In addition, closed plans must have a quality improvement plan.
Health Plan Network Adequacy Model Act: Health carriers offering a health plan must meet general requirements pertaining to the provisions included in their provider contracts. In addition, specific requirements related to notice of termination of contracts are included for the plans and providers. Under this act, health carriers must notify a provider's regular patients of the contract termination in writing within 15 business days of the termination. Health carriers must establish provider selection standards and make them available to all healthcare professionals. A prohibition on so-called "gag" clauses is included in this act. Health carriers are required to maintain an adequate network sufficient in number and types of providers. This act also requires the filing of sample contract forms with the state regulatory agency and obtaining approval of any material contract changes.
Health Carrier Grievance Procedure Model Act: Under this act, health carriers offering a health plan must establish a second-level review panel (in addition to the existing mechanism the plan has in place) for addressing grievances. Also, the health carrier must allow members to review relevant information pertaining to their grievance, attend the review panel meeting concerning their grievance, and have representation at the panel meeting. Health carriers must develop written procedures for the expedited review of any grievance where the normal timeframe would jeopardize the life or health of the member. Health carriers must also use clinical peers "in the same or similar specialty," that typically manage the situation under review, to perform expedited and second-level review.
Utilization Review Model Act: Under this act, health carriers are required to cover emergency services needed to screen and stabilize a member, without prior authorization, if a prudent layperson acting reasonably would have believed that an emergency medical condition existed. Health carriers must also cover an emergency visit to a non-contracted provider if a prudent layperson would have believed that the delay in visiting a contracted provider would worsen the emergency. Health carriers must provide written notice of adverse determinations with instructions for filing appeals and for requesting disclosure of the clinical rational, including the clinical review criteria used to make the determination. Health carriers must also use clinical peers "in the same or similar
Page 126 of 469

AHM 510 : Health Plans : Governance and Regulation
specialty," that typically manage the situation under review, to perform expedited and second-level review.
Source: "Key Issues: NAIC Health Plan Accountability Models," Washington Report 23-96, Issue Review, BlueCross BlueShield Association, July 26, 1996, 1-8.
Preferred Provider Arrangements LawsFor regulatory purposes, a preferred provider arrangement (PPA) is a contract between a healthcare insurer and a healthcare provider or group of providers who agree to provide specified services to persons covered under the contract. The healthcare insurer in a PPA can be either a licensed HMO or a licensed insurance company. The providers who enter into such a contract with a healthcare insurer are known as preferred providers or network providers. Providers who have not contracted with a healthcare insurer are known as nonpreferred providers or nonnetwork providers. A preferred provider organization (PPO) is one specific type of health benefit plan that includes a preferred provider arrangement.20
State regulation of PPOs is difficult to summarize primarily because PPOs are regulated in different ways depending upon the state. In addition, the regulatory authority of each state frequently is found in various statutes, rather than in a single statute. Nevertheless, states tend to adopt at least one of the following general regulatory approaches.21
Several states require PPOs to be licensed, registered, or certified. Requirements for licensure may include solvency and grievance procedures or may be limited to registering with state agency.
Other states require that an insurer (most often an indemnity plan) that contracts with a preferred provider network submit documentation that the network is compliant with certain state laws. These requirements may appear in a separate section of the insurance code governing PPOs or they may be included in the carrier section of the insurance code. In either case, this regulatory approach requires indemnity insurers that contract with a PPO network to assure that the network complies with requirements, such as network adequacy, timely claims processing procedures, and grievances and appeals procedures.
In addition, some states require that risk-bearing entities meet specific solvency standards. In other states, risk-bearing entities generally must meet the same solvency standards as an indemnity plan or an HMO.
Many states have adopted laws or regulations that impose additional requirements on preferred provider arrangements. The NAIC has adopted a Preferred Provider Arrangements Model Act (PPA Model Act) that establishes minimum standards for preferred provider arrangements and the health benefit plans that include such arrangements.22
The PPA Model Act permits healthcare organizations to develop health benefit plans that include incentives for PPO members to use the services of preferred providers. Plans must clearly identify the differences in benefit levels for services of preferred providers and for services of nonpreferred providers. The amount of such differences in benefit levels must be no greater than necessary to provide a reasonable incentive for members
Page 127 of 469

AHM 510 : Health Plans : Governance and Regulation
to use preferred providers. Some states prohibit a benefit differential greater than a specified percentage. These plans must also provide benefits for emergency care for covered services rendered by a nonpreferred provider when an insured cannot reasonably reach a preferred provider. In such cases, the cost of emergency care must be covered by the PPO as though the insured had been treated by a preferred provider.23
The PPA Model Act requires a preferred provider arrangement to establish the amount and manner of payment to the preferred providers. The PPA Model Act also requires that the arrangement must include mechanisms designed to minimize the cost of the health benefit plan. These mechanisms may include procedures for reviewing or controlling utilization of healthcare services and for determining whether healthcare services rendered are medically necessary. Preferred provider arrangements must provide PPO members with reasonable access to covered services, and health benefit plans that include a PPA must include an adequate number of preferred providers to render those services. The PPA Model Act also prohibits preferred provider arrangements from unfairly denying health benefits for medically necessary covered services.24
Although only a few states have adopted requirements based closely on the PPA Model Act, a number of states have adopted requirements to regulate PPOs. Also, a significant number of preferred provider arrangements are offered as self-funded plans and, thus, are not subject to state insurance law.
Utilization Review LawsIn addition to HMO and PPA laws, some states regulate certain functions that health plans perform. Utilization review is one example of a health plan function regulated by many states. Recall from Healthcare Management: An Introduction that utilization review (UR) is the evaluation of the medical necessity, efficiency, and/or appropriateness of healthcare services and treatment plans for a given patient. Utilization review may be undertaken by an in-house department of a health plan or an external entity. External entities that perform utilization review functions are called utilization review organizations (UROs).
Utilization review laws in some states require any entity that performs UR functions to be registered with the appropriate regulatory agency, such as the insurance department or health department. Registration can be accomplished by simply filing some basic information about the entity's structure and operations. In other states, full certification is required. In these states, the personnel of any entity performing UR functions must meet certain criteria with regard to experience, training, and education. For example, in Maryland the physician performing utilization review must be in the same specialty as the physician whose treatment plan is being reviewed.25
CertificationMost states that require certification direct health plans and UROs to file a plan with the appropriate state regulatory agency. This plan confirms that the entity's personnel meet the requirements discussed above and provides information about the services to be provided. In general, states require certification to keep track of the entities performing UR services and to maintain an avenue for providers to question or appeal UR decisions.
Page 128 of 469

AHM 510 : Health Plans : Governance and Regulation
Typically, state laws impose some requirements governing the accessibility of UR personnel who make utilization review determinations. For example, most states require that personnel be accessible by telephone during normal business hours, five days a week. In addition, some states require that the entity performing UR establish a toll-free telephone line, staff after-hours coverage for review determinations, and/or meet certain response times for decisions. A typical required response time for UR decisions is two days after receiving all information pertinent to the case.26
To protect the confidentiality of a patient's medical information, an entity performing utilization review must also meet and uphold federal and state requirements concerning the confidentiality of medical information standards. In addition, state laws usually require the inclusion of an appeal procedure for adverse decisions or denials. Some states require a written appeal procedure and set 30 days as the standard amount of time for completing an appeal. A few states even have laws that ban the use of financial incentives that might induce utilization review personnel to deny certain services, reduce a length of stay in an inpatient facility, or otherwise impact a utilization review decision. 27
Licenses or certificates are usually valid for one to two years and are renewable. State laws authorize officials to revoke an entity's license or certification and/or impose fines and penalties for noncompliance with utilization review laws. 28 In addition to requiring that the entity obtain a license, some states also require that the personnel conducting utilization reviews obtain reviewer licenses.
AccreditationIn lieu of following the requirements to obtain a certificate to provide utilization review services, some states allow such entities to submit evidence of their accreditation by a private accreditation organization. The accreditation organization must meet the requirements of the state regulatory agency in charge of utilization review. Several national organizations conduct accreditation programs. The most prominent accrediting organization for utilization review programs is the American Accreditation Health Care Commission (the Commission/URAC), formerly called URAC. The Commission/URAC sets standards that UROs must meet and maintain to obtain accreditation. Standards for accreditation focus on timely review of determinations, efficient and effective use of information to make determinations, maintenance of confidentiality standards, training and qualification of the UR staff, and specific requirements for the appeal process.
Third Party Administrator Laws29
Another health plan function that has been the subject of state regulation is third party administration of certain services, such as claims.
Most states have adopted laws and/or regulations to govern the activities of organizations known as third party administrators (TPAs). As we described in our discussion of self-funded plans, TPAs provide various administrative services to health plans or employers or other large groups, such as unions, that provide health benefit plans to their employees or members. Health plans and such employer groups often obtain the services of TPAs to help administer health plan contracts. In such a case, the health plan or group delegates some of its administrative duties to the TPA and agrees to compensate the TPA for the services it provides. Because TPAs often perform insurance functions-such as underwriting and claims processing-the states have authority to regulate these activities.
Page 129 of 469

AHM 510 : Health Plans : Governance and Regulation
However, in some states, TPAs-using ERISA as the foundation-have challenged the states' regulatory authority over TPAs that contract with self-funded plans. Courts have taken both sides in this controversy so it is not yet clear whether TPA laws will be viewed as preempted under ERISA in the future.
The NAIC Third Party Administrator Model Statute (TPA Model Law) is an NAIC model law designed to regulate operations of third party administrators. Many state laws that regulate TPAs are based on this model. We will base our description of TPA laws on the provisions of this model law, which we refer to as the TPA Model Law.
Fast Fact
In addition to claims administration, some TPAs are offering services in disability management, 24-hour coverages, vocational and physical rehabilitation, return-to-work programs, employee assistance programs, mental health and crisis management, benefit design, and plan document preparation.30
Certificate of AuthorityAccording to the TPA Model Law, a third party administrator subject to the law is any organization that directly or indirectly solicits or effects coverage of, underwrites, collects premiums from, or settles claims on residents of the state or on residents of another state from offices in the state enacting the TPA Model Law. An organization may not act as a TPA unless it has received from the state insurance department a certificate of authority designating it a TPA. Thus, a certificate of authority is required from each state that has enacted such a law and in which a TPA has an office or whose residents are members of plans administered by the TPA. Note that some insurers act as TPAs for self-funded employer plans. In those situations, the licensed insurer does not need to seek additional certification. The TPA Model Law defines insurer as any person who provides life or health insurance coverage in the state. Thus, for purposes of the TPA Model Law, an insurer may be an HMO, an insurance company, or anyone who provides insurance that is subject to state regulation.
To obtain a certificate of authority, a TPA must submit an application to the insurance department and must provide information similar to the information an HMO must provide for a certificate of authority. The state insurance department may also request that a TPA provide additional information, and the TPA must make available documents such as the written agreements it has entered into with health plans and employers.
When evaluating an application for a TPA's certificate of authority, the insurance department will be concerned with ensuring that the TPA is solvent and that the individuals responsible for conducting the TPA's affairs are competent, trustworthy, financially responsible, and of good character.
Some states waive the application requirements for certain TPAs. Typically, a TPA may obtain a waiver from such a state if the TPA has a valid certificate of authority from another state that has similar certification requirements.
Written AgreementWhenever a TPA enters into an agreement to provide administrative services, the agreement must be put into written form. In most instances, a TPA enters into an
Page 130 of 469

AHM 510 : Health Plans : Governance and Regulation
agreement with an employer to administer a self-funded health benefits plan. The written agreement entered into between the employer and the TPA must describe:
• The duties that the TPA will perform
• How the TPA will be compensated for its services-compensation may be based on the amount of premium or charges the TPA collects or on the number of claims it processes
• The health plan's or insurer's underwriting standards and any other standards that pertain to the business the TPA will administer
Certain types of provisions may not be included in a TPA agreement. For example, the TPA Model Law prohibits a TPA from entering into an agreement under which the amount of the TPA's compensation is contingent upon savings the TPA is able to realize from claims payments. Such prohibitions are designed to assure that the TPA is not induced to place its own financial interests above the interests of plan members.
Both the TPA and the health plan or insurer must maintain the written agreement as a business record through the term of the agreement. The insurance department has authority to examine these business records, and the TPA's records of transactions performed on behalf of a health plan or insurer must be made available to the health plan or insurer.
With specific exceptions, the TPA Model Law requires the TPA to maintain such records for at least five years after the termination of such an agreement. If a TPA agreement terminates, however, the TPA and the health plan or insurer may agree for the TPA to transfer all its records to a new administrator. In such a case, the TPA is not required to maintain the records for an additional five years if the new administrator acknowledges in writing that it is responsible for retaining the records for the required time.
Insurer ResponsibilitiesAn insurer does not transfer its responsibilities for administration of its plan even if an agreement between the health plan and a TPA specifies that the TPA will provide certain administrative services. The health plan remains responsible for ensuring that its plans are administered properly. The health plan must determine all premium rates, benefits, underwriting criteria, and claims payment procedures for its plans, and it must provide the TPA with written information on all such matters.
TPA's ResponsibilitiesWhen it acts on behalf of a health plan, a TPA acts in a fiduciary capacity. As a fiduciary, a TPA must hold all funds it receives on behalf of a health plan in trust, must promptly remit all such funds to the proper parties, and must periodically provide the health plan with an accounting of all transactions the TPA has performed on behalf of the health plan. The TPA Model Law also requires a TPA to:
• Provide a written notice, which has been approved by the health plan, to all members identifying the health plan, policyowner, and TPA and describing the relationship among these parties
• Identify all charges that it collects from covered individuals
Page 131 of 469

AHM 510 : Health Plans : Governance and Regulation
• Disclose to the health plan all charges, fees, and commissions the TPA receives in connection with the services it provides to the health plan
• Promptly deliver to covered individuals any certificates, booklets, termination notices, or other written communications that it receives from the health plan
A TPA is required to notify the state insurance department immediately following any material change in its ownership or control. In addition, a TPA must notify the insurance department if any material change occurs that might affect its qualification for a certificate of authority. Each TPA is required to file with the insurance department an annual report, which includes the names and addresses of all health plans that the TPA contracted with during the preceding year.
Suspension or Revocation of Certificate of AuthorityThe TPA Model Law requires the state insurance department to suspend or revoke a TPA's certificate of authority under certain specified conditions. The insurance department must suspend or revoke a TPA's certificate of authority if the TPA (1) is financially unsound, (2) is using practices that are harmful to insured persons or the public, or (3) has failed to pay any judgment rendered against it in the state within 60 days after that judgment became final.
In addition, the insurance department has discretionary authority to suspend or revoke a TPA's certificate of authority if, after notice and a hearing, the department finds such action is warranted.
Review Question
Third party administrators (TPAs) provide various administrative services to health plans or groups that provide health benefit plans to their employees or members. Many state laws that regulate TPAs are based on the NAIC Third Party Administrator Model Statute. One provision of the TPA Model Law is that it
prohibits TPAs from performing insurance functions such as underwriting and claims processing prohibits TPAs from entering into an agreement under which the amount of the TPA's compensation is based on the amount of premium or charges the TPA collects requires TPAs, upon the termination of a TPA agreement with a group, to immediately transfer all its records relating to the group to the new administrator requires TPAs to notify the state insurance department immediately following any material change in the TPA's ownership or control
Incorrect. The TPA Model Law regulates TPAs who peform insurance functions such as underwriting and claims processing
Incorrect. Under the TPA Model Law the TPA is probibited from entering into an agreement under which the amount of a TPA's compensation is contingent upon savings the TPA is able to realize from claims payments
Page 132 of 469

AHM 510 : Health Plans : Governance and Regulation
Incorrect. The TPA Model Laaw requries a TPA to maintain records for five years after the termination of an agreement, unless the TPA and insurer agree to transfer all records to a new administrator
Correct! A TPA is required to notify state insurers immediately following a material change in ownership
Laws Affecting Point-of-Service ProductsRecall from Healthcare Management: An Introduction that with a point-of-service (POS) product, when members need medical care, they choose, at the point of service, whether to go to a provider within that plan's network or to seek medical care out of the network. The regulatory requirements that apply to a POS product depend largely on the way the product is structured. A POS product can be provided:
• Entirely by an HMO • By an HMO and an insurer • Entirely by an insurer
In the past, some states' statutes prohibited HMOs from being the sole sponsors of point-of-service (POS) options. Recently, in response to consumer demand, states have begun to allow HMOs to offer POS options without the involvement of a licensed insurance company as long as the HMO meets certain requirements. Such requirements may include having additional financial reserves related specifically to those services or limiting the percentage of POS option products sold by the HMO to a specified percentage of the overall products sold by the HMO. A few states have begun to mandate that HMOs offer a POS option or product. When an HMO directly underwrites healthcare services rendered by nonparticipating providers, this is sometimes called a standalone POS product. The entire standalone POS product is regulated by the state's HMO Act.
In states with laws that do not allow an HMO to directly underwrite healthcare services rendered by nonparticipating providers, HMOs that wish to offer a POS product must arrange for provision of the non-network care through an insurance contract. These are sometimes referred to as wraparound POS products. An HMO may be a licensed insurance company or may have a parent or sister corporation that is a licensed insurance company, and can issue a separate insurance contract to provide non-network care. Or, an HMO may enter into a contractual arrangement with an unrelated insurer to provide non-network care. For a wraparound POS product, the HMO provides the network benefits. Such benefits are subject to the laws that pertain to HMOs. The non-network benefits for a wraparound POS product are provided by an insurer and are subject to the state's insurance laws.
Sometimes an HMO chooses to develop a wraparound POS product even in a state where it is permitted to provide these benefits entirely through the HMO. The HMO may choose this approach to avoid having its financial condition negatively affected by non-network claims. Since the financial viability of an HMO depends largely on its ability to
Page 133 of 469

AHM 510 : Health Plans : Governance and Regulation
manage costs by using network-based managed care techniques, an HMO that does not want its financial condition impacted by "non-managed" non-network claims can offer a wraparound POS product, where permitted by law.
A gatekeeper PPO, sometimes called an insured POS product, is like a POS product except that the gatekeeper PPO provides network benefits through an insurance contract. Insurers that offer this insured POS product develop provider networks in some states that they use for several health plan arrangements, including POS products. The insured POS looks almost identical to an HMO POS. The only differences result from regulatory requirements; the network portion of the HMO POS product is subject to HMO requirements, while the network portion of the insured POS is subject to state insurance regulatory requirements.
Laws Regulating At-Risk Provider OrganizationsMost at-risk provider organizations (sometimes called provider-sponsored organizations) operate under a state HMO license; however, a few states have developed a special licensure category for these entities. Georgia, Iowa, Kentucky, Minnesota, New Mexico, New York, Oklahoma, and Texas all have separate laws for at-risk provider organizations. Generally, these laws are patterned after state HMO laws, but some contain different standards for solvency and quality assurance programs than their existing HMO laws. For example, in Iowa an at-risk provider organization, called an organized delivery system (ODS), does not have specific quality or access standards that it must meet; however, an HMO in Iowa must have a quality assurance program. In Oklahoma, the State Board of Health has the discretion to set standards for solvency to ensure the at-risk provider organization's ability to deliver the services promised. For HMOs, Oklahoma has set specific requirements for the amount of surety bonds or deposits that must be furnished to the State Board of Health to ensure solvency. Idaho reviews provider arrangements on a case-by-case basis, and North Dakota has a law that allows healthcare provider cooperatives to contract with nonprofit health service plans, HMOs, insurance companies, and the state Medicaid program on a capitated or other risk-sharing basis. The Florida Commission on Integrated Health Care Delivery Systems has recommended that at-risk provider organizations in that state meet the same quality and solvency standards as HMOs.
Uniform LicensureWe mentioned in Overview of Laws and Regulations the NAIC's proposed model law called CLEAR that seeks to reform state legislation by requiring that all health risk-bearing entities that assume health insurance risk- for instance, HMOs, PPOs, and at-risk provider organizations-be subject to the same regulatory licensing standards. Under CLEAR, every health risk-bearing entity applying for licensure and meeting the requirements of the model law would receive the same license as a health carrier. Carriers would also have to meet additional requirements based on their activities or plan design (e.g., plans that use contracted providers would have to meet provider contracting standards).31
The NAIC has not yet adopted CLEAR and, therefore, no states have adopted CLEAR. However, the state of Ohio has developed and passed its own uniform licensure law for all health insuring corporations. The Ohio Health Plan Uniform Licensure Act (Ohio MCULA) regulates health risk-bearing entities based upon how they function in the health plan marketplace. For example, if a PHO meets the definition of a health insuring
Page 134 of 469

AHM 510 : Health Plans : Governance and Regulation
corporation based on the role it plays in the market, then it is required to obtain a license under MCULA. An Ohio Department of Insurance policy statement describes the purpose of MCULA this way: "MCULA was enacted to regulate risk-bearing entities on a functional basis, regardless of the entity's acronym. In enacting MCULA, the Department's goal was to fulfill its regulatory duty to regulate the 'business of insurance.'"32 As regulators struggle to apply laws not designed to regulate many of the recent innovative forms of health plans, uniform licensure acts, such as MCULA in Ohio, may become more prevalent.
Capital Standards for all Health PlansGiven the diversity of organizations and arrangements that have emerged in the rapidly changing healthcare marketplace, regulators have begun to address the original "one size fits all" approach to healthcare financial regulation. As we discussed earlier in this lesson, the HMO Model Act contains uniform solvency standards that all HMOs must meet to obtain and retain a license. However, the nature and volatility of business can vary significantly from one HMO to another. For instance, an HMO's capital and surplus requirements can be affected by factors such as out-of-network coverage provisions and provider compensation/risk-sharing arrangements.
In addition, some regulators and healthcare analysts maintain that because health plans effectively reduce the risks assumed by traditional healthcare insurers, the capital and surplus requirements for health plans should not be the same as those for indemnity insurers. Further, the financial standards contained in the HMO Model Act and various states' HMO and insurance statutes may not apply to at-risk provider organizations or certain other health risk-bearing entities. Insight 5A-1 provides a brief discussion of the evolution of solvency standards to apply to all health risk-bearing entities.
Recognizing the limitations of relying upon a single minimum fixed level of capital and surplus requirements, the NAIC in the early 1990s began developing risk-based capital (RBC)formulas for all life and health insurance companies. However, NAIC members recognized that this formula did not adequately reflect the range of risks present in the health insurance business. The NAIC then began a process to create a separate RBC formula for all health insurers and health plans that accept risk.33
Insight 5A-1.History and Purpose of Risk-Based Capital Requirements for Health Plans.
In the early 1990s, the NAIC began developing RBC formulas for life and health insurance companies. The RBC concept differs from the regulatory approach previously used in many states, which set a minimum fixed-level of capital and surplus requirements for all insurers. NAIC members recognized that the current life and health RBC formula did not adequately reflect the range of risks associated with the variety of coverages available, funding approaches used, and organizational structures present in today's health insurance business. To better reflect the full scope of health insurance risk characteristics, the NAIC began a process to create a separate RBC formula that could be applied to all health insurers and health plans that accept risk.
Source: Excerpted and adapted from "Health Organizations Risk-Based Capital (HORBC) National Association of Insurance Commissioners," information paper prepared by National Association of Insurance Commissioners staff, 1998, p. 1).
Page 135 of 469

AHM 510 : Health Plans : Governance and Regulation
The NAIC's approach to risk-based capital standards has two components: the RBC formula and the enforcement model act. The RBC formula for health plans is a set of calculations, based on information in the health plan's annual financial report, that yields a target capital requirement for the organization. The health plan-RBC formula assesses the risk profiles of specific health plans, gives credit for payment arrangements that reduce risk, and determines appropriate capital requirements based on these risk profiles. As a result, health plans that perform the same or similar functions with similar types of assets, liabilities, and business profiles are subject to the same solvency standards.34
The health plan-RBC formula takes into account five different types of risk:
1. Affiliate risk2. Asset risk3. Underwriting risk (typically, the largest single determinant of a plan's RBC requirement)4. Credit risk5. Business risk
Affiliate risk the risk that the financial condition of an affiliated entity causes an adverse change in capital.
Asset risk the risk of adverse fluctuations in the value of assets.
Underwriting risk (typically, the largest single determinant of a plan's RBC requirement) the risk that premiums will not be sufficient to pay for services or claims.
Credit risk the risk that providers and plan intermediaries paid by capitation will not be able to provide the services contracted for and the risk associated with recoverability of amounts due from reinsurers.
Business risk the general risk of conducting business, including the risk that actual expenses will exceed amounts budgeted. 35
The second component of the NAIC's RBC regulatory framework is a model act that gives regulators authority to take specific actions when the RBC level, as calculated by the formula, reaches certain levels or has negative trends. The model act for the health plan-RBC formula, which is virtually identical to the model act for other lines of insurance, was not yet finalized at the time of this writing. It is titled the Health Organizations Risk-Based Capital Model Act (HORBC), a reference to an earlier version of the health plan-RBC formula. According to the provisions of HORBC, regulators are to compare an organization's capital requirements (as determined by the health plan-RBC formula) with the organization's total adjusted capital (the organization's net worth as shown in the filing of its annual financial statements plus any other items specified in the formula instructions). If the organization's total adjusted capital is insufficient, then one of four levels of regulatory intervention may be triggered. These four levels are (1) company action level, (2) regulatory action level, (3) authorized control level, and (4) mandatory control level. These interventions range from requiring the
Page 136 of 469

AHM 510 : Health Plans : Governance and Regulation
submission of a corrective action plan to placing the plan under regulatory control of the appropriate state agency.
In addition to serving as a tool for state regulators, the health plan-RBC formula provides start-up companies with the information needed to estimate initial RBC levels based on their operating projections for their first full year.
Page 137 of 469
AHM 510 : Health Plans : Governance and Regulation
Chapter 5 BState Mandates and Regulation of the Health Plan-Provider Relationship
After completing this lesson, you should be able to:
Describe the difference between a mandated benefit and a mandated provider law Give examples and explain the purpose of several mandated benefit laws Describe the problems with applying any willing provider laws to certain types of
health plans Explain why state mandates often increase the cost of healthcare services provided
by health plans
State MandatesWebster defines mandate as "an authoritative command."1 In a managed healthcare context, state mandates are "authoritative commands" in the form of laws that require health plans to provide coverage for specific treatments or benefits or that regulate aspects of the health plan-provider relationship. In the last several years, many states have enacted a variety of mandates that affect health plan operations. Although mandates have been around for many years, the recent increase in such mandates may be a response to a public perception that health plans are not providing coverage for certain services seen as necessary and basic. In addition, some mandates are passed because there are strong lobbying efforts made by various interested constituencies, such as healthcare providers, patients with chronic diseases, etc. Regardless of the motivation for their enactment, there are basically two types of state mandates: mandated benefit laws and mandated provider laws.2 Other mandates that affect health plans and do not fit into the two preceding categories include mandates concerning utilization review activities, confidentiality of medical records, network adequacy, direct access to providers, quality assurance, and external review of coverage decisions.
Mandated benefit laws or benefit mandates are laws that contain provisions which require that health plans arrange for the financing and delivery of a particular benefit, such as coverage for a stay in a hospital for a specified length of time. Mandated provider laws are laws that relate to the health plan-provider relationship, including decisions to engage or terminate providers, to include certain types of providers in networks, and to establish certain financial arrangements between health plans and providers.
Sometimes mandates are incorporated into a state's HMO statutes; other times mandates are incorporated into the state insurance laws. Some mandates apply both to entities that are licensed as an HMO and to entities licensed under state insurance law. For the purposes of this lesson, we discuss state mandates in general and do not distinguish between HMO and insurance laws.
In this lesson, we discuss some of the state mandates that affect health plans. Note that not all plans must comply with state benefit mandates. Health plans provided by the federal government and self-funded employee benefit plans are generally exempt from
Page 138 of 469

AHM 510 : Health Plans : Governance and Regulation
state benefit mandates because such plans are governed by federal, not state, law. However, all health plans (including insurance companies), whether government-sponsored, self-funded, or otherwise, must comply with the provisions in the Health Insurance Portability and Accountability Act of 1996 (HIPAA). HIPAA, discussed in more detail in Assignment 7, includes some federal mandates with which all health plans must comply. Plans that are subject to state regulation must comply with both state mandates and the federal mandates included in HIPAA. Such a regulatory system may create a dual and sometimes potentially conflicting regulation of health plans.
In the remainder of this lesson, we discuss in more detail several types of mandates, both benefit and provider, and look at other mandates that impact the benefits offered by health plans. Figure 5B-1 shows a state-by-state comparison of some of the mandates discussed in this lesson.
Mandated Benefit LawsTo attempt to list every mandated benefit that the states have passed would be a daunting task. Figure 5B-2 shows a catalog of some different types of state benefit mandates. Benefits have been mandated for illnesses, conditions, and diseases that range from the diagnosis, treatment, and management of osteoporosis (California) to the treatment of Lyme disease (Minnesota). We discuss a few of the newer types of mandates appearing in state legislatures and mandates that have been passed by more than a few states.
Figure 5B-2. Catalog of State Benefit Mandates.
This list provides a sampling of the types of mandates states have enacted:
• Mental health coverage
Page 139 of 469

AHM 510 : Health Plans : Governance and Regulation
• Length of stay for specific conditions/procedures (e.g., maternity, mastectomy) • Infertility treatment • Experimental treatments for cancer (e.g., bone marrow transplants for treatment
of cancer) • Diabetes management • Off-label uses for drugs to treat cancer and/or HIV/AIDS • Hospice services • Mammograms and pap smears • Phenylketonuria and related metabolic disorders, sickle cell anemia, Lyme disease • Services related to the diagnosis, treatment, and management of osteoporosis
Source: Centers for Medicare and Medicaid Services, Office of Health Plan "A Report to the Governor on State Regulation of Health Maintenance Organizations," 16th ed., Prepared by Aspen Systems Corporation for CMS (Baltimore, MD: CMS, 1996).
Mental Health CoverageConcern that coverage for mental illnesses was not being treated on a par with physical illnesses motivated lawmakers to enact a mental health parity requirement that subsequently was incorporated into HIPAA. The federal mental health coverage requirements bar group health plans from having more restrictive annual and lifetime limits or caps on mental illness coverage than for physical illness coverage if the health plan has annual payment limits or aggregate dollar lifetime caps. The federal mental health coverage law does not mandate coverage for mental illness; it seeks to ensure that- if a health plan covers mental illness- the caps and limits are comparable to caps and limits for physical illness. More than 15 states have enacted their own mental health coverage laws. These laws, similar to HIPAA, vary from mandating coverage of treatment for severe disorders or biologically based illnesses such as schizophrenia, manic-depression, or bipolar disorder to mandating parity for coverage of mental illnesses comparable to caps and limits for physical illnesses.3 Some state laws require that all terms and conditions of coverage (i.e., copayments, deductibles, etc.) be the same for both mental and physical illnesses.
Some state parity laws exclude substance abuse treatment from their mandates for coverage of mental illnesses. Other state laws provide extensive coverage for mental illnesses. For example, the Vermont mental health parity law, which includes in its definition of mental illness any disorder listed in the International Classification of Diseases Manual (ICDM), requires coverage for the treatment of a wide variety of mental illnesses including substance abuse. In addition, as in several other state laws, the Vermont law prohibits separate deductibles, copayments, coinsurance, and other similar types of cost-sharing arrangements for mental and physical illnesses.4 In general, health plans must ensure that they comply with the mental health parity requirements of the federal law as well as any more stringent requirements imposed by the states in which they operate.
Length of Stay LawsTwo types of length of stay (LOS) laws enacted by many states are maternity length of stay and mastectomy length of stay. A federal maternity length of stay mandate was enacted by passage of the Newborns' and Mothers' Health Protection Act of 1996 (NMHPA). The NMHPA was subsequently incorporated into HIPAA. The NMHPA requires that health plans provide coverage for hospital stays for childbirth-at least 48 hours for normal deliveries and 96 hours for cesarean births. Prior to enactment of the
Page 140 of 469

AHM 510 : Health Plans : Governance and Regulation
NMHPA, more than half of the states had enacted maternity length of stay mandates. At a minimum, a health plan must comply with the federal NMHPA law. If the health plan operates in a state with a similar mandate that has more stringent requirements, it must also comply with those additional requirements.
In addition, most states have considered and a number have enacted mastectomy length of stay mandates. Some state mastectomy length of stay laws mandate a specific hospital stay. For example, in New Jersey, health plans and insurers must cover hospital stays for 72 hours for a radical mastectomy and 48 hours for a simple mastectomy. In other states, such as Florida, health plans and insurers must cover the length of the hospital stay as determined by the physician.5
Emergency CareIn the past, some HMOs denied coverage for services provided in an emergency room if it turned out that the illness or injury was not an actual medical emergency as defined by the plan. State mandates for emergency care generally require that health plans cover emergency room services if a "prudent layperson" would have assumed the illness or injury to be an emergency.
Other Benefit MandatesAlthough there are many state mandates that require coverage for specific diseases, one of the newer types of mandates for a specific, prevalent disease is for diabetes. About 23 states have passed mandates requiring health plans and insurers to cover equipment, supplies, and self-care training for members with diabetes. Most of these mandates have been passed in the last three to four years. Diabetes is a disease that can have many complications and can be very expensive if left undetected or untreated for a long period of time. It is estimated that the annual cost for the routine care of one diabetic patient can be $5,000.6 Health plans have developed innovative strategies for the management of diabetes, often incorporating disease management. Many health plans voluntarily provide benefits for self-management of diabetes in the absence of state mandates.
Other benefit mandates that have been enacted include coverage for:
• Experimental medical treatments for diseases such as AIDS and cancer
• Infertility treatments
• Contraceptives
• Chiropractic care
Some state laws have addressed the use of formularies for pharmaceutical management. Mandates pertaining to prescription drugs are discussed in Pharmacy Laws and Legal Issues.
State Benefit Mandates - Are They Free?Most of the mandates that states enact come with a price tag. Some experts believe that legislating coverage for certain procedures often translates into higher premiums that purchasers or plan members ultimately have to pay. The reason for the increased costs associated with mandates is threefold: (1) the health plan must pay for the additional healthcare benefit, (2) the health plan must implement administrative procedures to
Page 141 of 469

AHM 510 : Health Plans : Governance and Regulation
assure that a mandated benefit is provided, and (3) the health plan may have to change other plan policies or procedures to comply with mandates. Increased costs, resulting from benefit mandates, may prompt health plans to raise premiums. In turn, purchasers may raise the contributions required of plan members for participation in a plan. To illustrate, assume that a state mandate requires that all impatient hospital stays for a particular procedure, such as a simple mastectomy, be covered for a minimum of two days. First, the health plan must pay for the hospital charges it might not have paid if the stay was determined to be medically unnecessary. Second, the health plan must make administrative changes to comply with the mandate. These administrative changes may include changing plan literature for current or prospective enrollees, updating the health plan's computer claims payment system to note coverage for that benefit, and amending all existing contracts with purchasers to incorporate coverage for the documents. In addition, the health plan will need to change it's treatment guidelines or medical protocols to note this exception to its rules on medical necessity. Figure 5B-3 provides an analysts perspective on the increase in costs triggered by different types of benefit mandates.
Benefit mandates generally increase costs. One result of such increased costs may be that employers drop healthcare coverage for their employees, which, in turn, may cause the number of uninsureds to increase. States are recognizing the value of performing cost-benefit analyses on proposed mandated benefits. For example, Colorado, Kentucky, and Oklahoma have adopted laws that require an independent financial and social impact study for all proposed mandated benefits bills before they can be passed by the legislatures.8 Insight 5B-1 describes, from a cost perspective, some unintended consequences of state health mandates.
Page 142 of 469

AHM 510 : Health Plans : Governance and Regulation
Insight 5B-1. Unintended Consequences of State Mandates.
Depending on their focus and approach, state healthcare mandates can make it difficult, if not impossible, for health plans to arrange for the delivery of high quality, well-coordinated, and affordable care. This, in turn hinders the ability of individuals and employers to select and purchase benefits based on their healthcare needs and ability to pay. A 1992 study in the Journal of Public Economics (Gabel and Jensen) estimated that mandated benefits prevented one in five small firms that did not offer health insurance to their employees from doing so.
Important, too, is the negative impact of state mandates on the state regulated insurance market. Because self-funded health benefits plans are not subject to state mandates, employers may have an incentive to self-fund to avoid these costs. According to estimates from the Bureau of Labor Statistics, about half of the U.S. firms self-fund their employee health benefits plans, rather than purchase a state regulated insurance product.
However, a more recent study indicated that although some companies chose to self-fund to avoid mandates in the past, more recently self-funded companies are offering the same or similar benefits as those mandated by the states in which they operate.
Ironically, the population most likely to be affected by mandate costs is also the most vulnerable economically: persons working for small firms that are not self-funded; and those who work part-time or are self-employed, who must purchase expensive, non-group coverage.
Source: Adapted, with permission of the publisher, from BlueCross BlueShield Association, "Legislative Report: States Turning To Evaluation Laws to Curb Mandated Benefits," Issue Review, April 18, 1997, 2-4.
Other Types of MandatesAs discussed in State HMO and Other Types of Health Plan Laws, all states have comprehensive HMO licensure statutes and regulations that include protections in key areas such as quality assurance, access to care (i.e., network adequacy, physician credentialing, disclosure of health plan information, utilization review, grievance procedures), coverage for basic health services, emergency services, and financial solvency. In addition to these existing protections, several states have enacted or are considering passage of specific mandates related to network access/adequacy and quality assurance efforts. For example, New Hampshire now has a law that allows the department of insurance to establish rules related to utilization review processes that networks must develop, credentialing of network providers, ensuring the adequacy of provider networks, and setting standards for quality assurance and improvement programs. Sometimes quality assurance mandates are part of a larger health plan bill, such as a consumer bill of rights, discussed later in this lesson.
External Review MandatesOne type of proposed legislation that is appearing frequently before state legislatures mandates external review of a health plan's decisions to deny or limit benefits for certain procedures or treatments. External review refers to a dispute resolution
Page 143 of 469

AHM 510 : Health Plans : Governance and Regulation
mechanism that involves review-by an individual or group of individuals not affiliated with the health plan-of certain disputed decisions made by a health plan, which may include what constitutes medically necessary treatment or denials for experimental treatments. In most cases, the plan enrollee must exhaust the health plan's internal grievance procedures before seeking external review. Some plans set a minimum dollar threshold for the value of services for which coverage disputes can go to external review. In general, external review laws may cover areas such as:
• Qualifications of external reviewers
• Who chooses the external review entity (i.e., the health plan or the state agency responsible for ensuring compliance with the external review mandate)
• The impact of external review determinations
• The type of decisions (i.e., experimental treatment or medical necessity) subject to external review
All health plans have some type of formal, internal grievance procedure through which enrollees can appeal coverage decisions. Some health plans also have less formal processes to review complaints concerning issues that are routine or not as major as coverage decisions. Formal grievance procedures are required by state and federal laws for HMOs. Some health plans have also voluntarily implemented external review programs to review complex coverage decisions (e.g., cases involving coverage for experimental treatments). In addition, some health plans are establishing internal ombudsman programs to resolve disputes between health plans and members regarding benefits provided under a health plan. Ombudsman programs may also be created by state agencies. We discuss ombudsman in more detail in Governance: Accountability and Leadership.
Regulation of the Health Plan-Provider RelationshipTypically, the legal relationship between a health plan and its providers is based on the contracts between these parties. State contract law governs many of the disputes that may arise in relation to the health plan-provider relationship; however, states have also passed health plan-specific laws regulating aspects of this relationship. For example, a recent topic of considerable interest to consumers is the amount or type of any physician financial incentives related to physician performance in meeting quality standards, satisfaction rates of individual physicians' patients, and, in some cases, utilization of certain services. Incentives could relate to underutilization (e.g., for preventive services such as mammography or immunizations) as well as overutilization of some services. Several states have enacted or are considering passage of laws that require disclosure to health plan members of any physician financial incentives. As health plans become more prevalent in the United States, consumers are demanding more information on which to base decisions in choosing or changing health plans. To assist consumers in this effort, legislators have introduced bills that seem to support the consumers' rights in areas that affect the health plan-provider relationship. Thus, legislators have expanded the legal authority over the health plan-provider relationship that was once based almost exclusively on contract law to now encompass mandates that affect the health plans' selection and compensation of providers. Some analysts argue that the purpose of mandated provider laws is to protect the interests of providers, not to assist consumers. Whatever the motivation behind these laws, they exist and affect the health plan's operations. We discuss these types of mandates in the following sections. The elements
Page 144 of 469

AHM 510 : Health Plans : Governance and Regulation
of a contract between a health plan and its network providers will be explored in some detail in the AHM Network Management in Health Plans dealing with network management. We will discuss liability issues arising from this contractual relationship in this lesson in Key Legal Issue in Health Plans.
Mandated Provider LawsAs mentioned earlier, mandated provider laws apply to the health plan-provider relationship. The following sections discuss some of these laws.
Any Willing Provider LawsWe introduced the concept of any willing provider laws in Overview of Laws and Regulations. Recall that such laws allow any provider who meets the health plan's terms and conditions of participation to become part of the health plan's network or receive payment from the health plan for covered services provided to enrollees, whether the provider is part of the health plan network or not. However, not all state any willing provider laws are alike. The definition of what constitutes a provider varies from state to state. For example, in some states "provider" refers only to pharmacists, while in other states the term "provider" includes non-physician healthcare providers and physicians. The following discussion describes the differences among state any willing provider laws and the groups that support and oppose such laws.
Of the 24 states with some type of any willing provider requirements, 22 apply such requirements to PPOs or insurer-based provider networks.11 Seventeen states' any willing provider laws apply to HMOs, and some of these laws provide exceptions for staff/group-model or federally qualified HMOs.12 Also, since many of the laws were enacted several years ago, it is unclear how they will affect new and developing health plan arrangements, such as at-risk provider organizations.
The types of providers affected by any willing provider laws vary from state to state. Pharmacy is the most common type of provider affected. More than 10 states' any willing provider laws apply only to pharmacy providers. Some states, such as Arkansas, Idaho, Kentucky, and Wyoming, include a wide variety of healthcare providers, including physicians, in their any willing provider laws.13
The terms of the contract that a provider is required to meet to be considered a "willing" provider also vary. Some any willing provider laws merely prohibit health plans from "unreasonably discriminating" against providers, while others require that the provider meet all of the health plan's qualifications for participation, or be appropriately licensed, reputable, and in good standing. Some require that the provider be willing to meet more specific standards, including those relating to the provision, utilization review, and cost-containment procedures; the management and administrative procedures; and the provision of cost-effective and clinically efficacious healthcare services.14
The proponents of any willing provider laws all argue that selective contracting by health plans reduces the number of providers, decreases competition, and could sever long-standing relationships between patients and providers. The advocates further argue that in the absence of any willing provider laws, health plans limit access to certain types of providers. Proponents of any willing provider laws include members from pharmacy, chiropractic, dental, home health, physical therapy, outpatient surgical, and clinical lab associations.16
Page 145 of 469

AHM 510 : Health Plans : Governance and Regulation
Opponents of any willing provider laws include individual health plans and health plan associations, the NAIC, the National Governors' Association, the FTC, employers, and many policyholders. In many letters to state legislators, the Federal Trade Commission has described any willing provider laws as anticompetitive.17 In addition, opponents argue that any willing provider laws undermine the quality and affordability of healthcare and limit consumer choice. Listed below are some of the chief reasons for opposition to any willing provider laws. According to some analysts, these laws:
• Increase healthcare costs by eliminating incentives for providers to offer discounts in exchange for patient volume18
• Undercut the quality initiatives of health plans because such laws prevent plans from choosing and contracting with only the most qualified providers
• May increase the number of uninsured Americans (i.e., as a result of the increase in premiums that any willing provider laws bring, some employers drop healthcare coverage for their employees)
• Limit consumer choice to coverage options much more costly than network-based plans
• Decrease quality of care by requiring health plans to accept any provider regardless of whether additional providers are necessary to meet the needs of health plan members
• Allow providers to have mandatory contracting privileges that are not present in any other industry or even elsewhere in the healthcare industry
Review Question
Any willing provider laws have their share of proponents and opponents. Arguments commonly made in opposition to any willing provider laws include
that such laws reduce the number of providers in a health plan's network
that such laws limit consumer choice to coverage options that are more costly than network-based plans that such laws encourage providers to offer discounts in exchange for patient volume all of the above
Incorrect. Opponents argue that AWP laws decrease the quality of care by requiring health plans to accept any provider regardless of whether they are necessary to meet the needs of health plan members.
Correct. Opponents of AWP laws feel that they limit consumer choice to coverage options more costly than network-based plans
Incorrect. Opponents feel the AWP laws increase healthcare costs by eliminating incentives for providers to offer discounts in exhange for patient volume.
Page 146 of 469

AHM 510 : Health Plans : Governance and Regulation
Incorrect. Several of the responses listed above are incorrect
Direct Access Laws Direct access laws allow subscribers to have direct access to certain specialists in the health plan's network without a referral from a primary care provider (PCP). As of mid-1998, thirty-four states require direct access to some type of provider. The vast majority of these direct access laws relate to access to obstetricians/gynecologists. Interestingly, most health plans already provide direct access to in-network obstetrician-gynecologists for routine gynecological and maternity care. Florida and Georgia both have direct access laws that allow enrollees to visit a dermatologist without referral from a PCP. Many states have mandates that require coverage for chiropractic care. Recently, New York has mandated direct access to chiropractors for health plan members. That law requires that plans cover at least 15 chiropractic visits without any ability to deny coverage for lack of medical necessity; after the 15 visits have been made, HMOs and other health plans can deny coverage for further treatment that they do not find medically necessary.22 Mandates such as direct access laws may make it difficult for health plans to ensure the quality coordination of healthcare.
Physician/Patient CommunicationThe term "gag" clauses, or "gag" rules as they are sometimes called, has been used to refer to a statement in a health plan-provider contract that could restrict a provider from discussing alternative treatment options with their patients. In 1996 the American Medical Association (AMA) proposed a Patient Protection Act that among other measures, prohibited health plans from using "gag-clauses" in provider contracts. Shortly after, the General Accounting Office (GAO) studied 529 HMO's provider contracts to determine the presence of these clauses. and they concluded that none of the HMOs studeid used contract clauses that specifically restrict doctors from discussing all appropriate medical treatment with their patients. Many states have enacted legislation barring the use of so-called "gag" clauses in provider contracts. Health plans do encourage physician/patient communication between their network providers and the health plan enrollees. This physician/patient communication includes dialogues between a provider and a health plan enrollee about diagnoses, treatment options, physical examinations, laboratory tests, and other concerns that patient may have about their healthcare.
The so-called "gag" clause mandates in most states bar health plans from including such a provision in their provider contracts and from terminating a provider who violates such a provision if one is included in the contract.
Review Question
Nightingale Health Systems, a health plan, operates in a state that requires health plans to allow enrollees to visit obstetricians and gynecologists without a referral from a primary care provider. This information indicates that Nightingale must comply with a type of mandate known as a:
Page 147 of 469

AHM 510 : Health Plans : Governance and Regulation
direct access law
scope-of-practice law
provider contracting mandate
physician incentive law
Correct! Direct access laws allow subscribers to have direct access to certain specialists in the health plan's network without a referral from a primary care provider
Incorrect. Scope-of-practice legislation is legislation proposed by one type of provider to amend state licensing laws to allow that type of provider to do a procedure or set of procedures typically reserved only to another provider group
Incorrect. A provider contracting mandate requires that a health plan disclose its criteria for selecting or deselecting providers
Incorrect! A physician incentive law requires a health plan to disclose to members any incentive arrangements available to plan provicers, or the law bans types of incentives that may encourage network providers not to refer members to specialists for needed care.
Provider Contracting MandatesProvider contracting mandates, also known as due process laws, require that a health plan disclose its criteria for selecting or deselecting providers. In addition, such laws usually contain certain procedural rules that must be followed when a provider is not selected or is deselected from a health plan's network of providers. Typically, the procedural rules that must be followed by health plans include notification of the selection criteria for network providers, an explanation of the reason(s) that a provider is deselected or rejected, and the provider's right to contest or challenge the health plan's decision to deselect. 23
To help standardize the process of credentialing that health plans use in selecting network providers, the NAIC has developed and adopted a model act that sets standards for credentialing efforts. The act is entitled the Health Care Credentialing Verification Model Act. This model act calls for24
The creation of policies and procedures to be used by health plans to verify the credentials of providers before contracting with them and for reverification every three years
Communication with potential participating providers of the applicable standards for providers who wish to participate in the plan
The creation of a committee comprised of healthcare professionals who would make decisions setting the standards for verification of credentials
Physician Incentive LawsThere are actually two types of physician incentive laws enacted by states. One requires only that health plans disclose to plan members any financial incentives available to
Page 148 of 469

AHM 510 : Health Plans : Governance and Regulation
participating providers in the health plan. The other type of law bans certain compensation arrangements that regulators believe may encourage network providers to not refer members to specialists as necessary or that encourages providers to not provide the appropriate, medically necessary care to plan members. For example, an Arizona law requires that health plans disclose any incentives or penalties that could encourage participating providers to withhold healthcare services or minimize or avoid referral to specialists. In addition, federal law provides specific guidelines regarding permissible and impermissible incentive arrangements that apply to federally qualified HMOs and other plans that provide coverage to participants in the Medicare program.
Mandating a Point-of-Service OptionSome states have adopted legislation requiring that certain health plans offer a point-of-service (POS) option in addition to an HMO. Physicians who are not participants in certain health plan networks generally support this type of legislation because it gives them access to a patient base, members of health plans, that is otherwise not available to them. A recent Johns Hopkins University study found that specialist utilization was no higher in POS products than in closed-panel HMOs.25 The authors of the study suggested that enrollment in a POS product was more for "peace of mind" than for changing actual patterns of using specialists.
Market demand, not legislation, has given a boost to POS options in HMOs in many markets. HMOs have realized the popularity of POS options with consumers and have voluntarily offered POS options in many of their markets. While more than three-quarters of all HMOs already voluntarily offer a POS option, only 22% of insured individuals are enrolled in POS products. POS products typically cost more than a closed-panel HMO, and consumers continue to choose HMOs as a high-quality, affordable healthcare option.
States that mandate the provision of a POS option usually require a mandatory offering by HMOs of a POS option to employers. Some states' POS mandates apply only to employers that employ 50 or more employees or some other threshold number of employees. There is some debate about the applicability of such mandates to group plans governed by ERISA, but there is not yet a definitive answer on this issue.
Utilization Review MandatesSome states (for example, North Dakota) have laws requiring that health plans disclose to both providers and patients the criteria that they use in making utilization review decisions.27
Other states have laws that may require that:
• Only physicians be allowed to make utilization review (UR) decisions
• The physician making the UR decision must be in the same specialty as the physician providing the care
• The physician performing UR be licensed in the state where the patient resides
Page 149 of 469

AHM 510 : Health Plans : Governance and Regulation
In Texas, a law has been passed that establishes standard UR procedures and requires that UR decisions be made only by licensed physicians, nurses, and physician assistants.
Comprehensive Health Plan LegislationSome states have taken the approach of rolling all their benefit mandates, mandated provider laws, and other legislation pertaining to health plans into one comprehensive piece of legislation. Comprehesive legislation may address issues such as:
• Grievance procedures • Coverage of emergency room treatment • External review • Provider credentialing • Direct access • Physician/patient communication • Disclosure of financial incentives • Provider contracting • Point-of-service option mandates • Qualification standards for utilization reviewers • Network adequacy and performance • Confidentiality of medical records • Use of drug formularies • Continuity of healthcare coverage (e.g., laws similar to HIPAA and COBRA)
Many of the provisions included in comprehensive health plan laws are already covered by existing law or regulations. Figure 5B-3 provides an overview of several states' comprehensive health plan bills.
Page 150 of 469

AHM 510 : Health Plans : Governance and Regulation
Page 151 of 469

AHM 510 : Health Plans : Governance and Regulation
Chapter 6 AOther Laws That Apply to Health Plans As we have seen, health plans, like other businesses, must comply with a variety of local, state, and federal laws. Many of these laws do not pertain exclusively to health plans or insurance companies. For instance, in some states, general consumer protection laws apply to the claims payments that are made by health plans. Also, because health plans are employers, they are subject to laws that govern all aspects of the workplace, from employment and hiring practices to workplace health and safety standards. In addition, health plans must comply with laws governing diverse issues, such as civil rights, taxation, and zoning.
We begin this lesson with a brief overview of some of the healthcare-related and antitrust laws that apply to health plans at the state level. We then take a closer look at some of the more common types of insurance laws that apply to health plans yet do not specifically address issues unique to health plans. These laws cover a wide variety of subjects and often vary by state.
After completing this lesson, you should be able to:
Describe the various types of state laws, other than HMO and insurance laws, that apply to health plans
Explain how states regulate agent licensing, marketing activities, and advertising Describe common types of general insurance laws that apply to health plans
Review Question
Certificate of need (CON) laws apply to health plans in a variety of ways, depending upon the state. By definition, CON laws are laws that are designed to
regulate the construction, renovation, and acquisition of healthcare facilities as well as the purchase of major medical equipment in a geographical area protect commerce from unlawful restraint of trade, price discrimination, price fixing, reduced competition, and monopolies determine benefit payments when a person is covered by more than one plan, such as two group health plans license and regulate health plans that wish to establish and operate an HMO
Correct. Certificate of need (CON) laws regulate the construction, renovation, and acquisition of healthcare facilities as well as the purchase of major medical equipment in a geographical area. A primary objective of these laws is to contain healthcare costs by reducing or eliminating unnecessary or duplicate services or capital expenditures
Incorrect. Antitrust laws are designed to protect commerce from unlawful restraint of trade, price discrimination, price fixing, reduced competition, and monopolies
Incorrect. Coordination of benefits (COB) laws are used to determine benefit payments when a person is covered by more than one plan, such as two group
Page 152 of 469

AHM 510 : Health Plans : Governance and Regulation
health plans or a health plan and the medical benefits provisions of an automobile policy.
Incorrect. Under the HMO Model Act, and most state laws, an entity that wishes to operate as an HMO must obtain a certificate of authority.
State Antitrust LawsAntitrust laws are designed to protect commerce from unlawful restraint of trade, price discrimination, price fixing, reduced competition, and monopolies.1 As we saw in Legal Organization of Health Plans, the health plan industry relies heavily on structural and operational integration, strategic partnerships, mergers, and acquisitions. For this reason, health plans must be particularly aware of antitrust laws. In addition to federal antitrust laws, which we address in Federal Regulation of Health Plans, health plans are subject to state antitrust laws. Most states have modeled their antitrust laws on the Sherman Act and the Federal Trade Commission Act. The state antitrust laws apply to all types of businesses, including health plans. In addition, many states address antitrust issues through anticompetition provisions that are found in their insurance holding company laws.
State attorneys general enforce both federal and state antitrust laws. State insurance commissioners enforce insurance holding company laws. In looking at proposed mergers and acquisitions, regulators determine if a particular transaction would result in substantially reduced competition or a monopoly. Typically, they make this determination by looking at the market shares of the entities involved, as well as other factors, such as number of competitors in the market, volatility of ranking of market leaders, and ease of entry into and exit from the market.2
General Insurance Laws that Apply to Health PlansSome of the state laws that affect health plans may be found in general laws applicable to all businesses, others may be found in general insurance laws, and others may be found in HMO acts. At times, a state's general insurance code and HMO act will regulate the same issue, and the requirements for HMOs may be different than the requirements for other types of health plans. For example, some states have different insurance and HMO benefit mandates for treatment of substance abuse. In other instances, statutes from the insurance code apply to HMOs. For example, in some states HMOs are subject to insurance regulations regarding payment of premium taxes, use of unfair trade practices, rehabilitation and liquidation of insurance companies, and establishment of holding companies. For the purpose of our discussion, we have organized general insurance and HMO laws into the categories listed below, although the way these types of laws are codified can vary by state:
• Sales and marketing
• Underwriting
• Records and privacy
• Claims and coordination of benefits
• Antifraud
• Continuation and conversion
Page 153 of 469

AHM 510 : Health Plans : Governance and Regulation
• Small group
• Individual healthcare (direct pay products for individuals)
• States as purchasers
Sales and MarketingAs competition in the health plan environment intensifies, marketing takes on an increasingly important role. So, too, do state and federal laws that regulate marketing and sales practices. Health plans that violate these laws can face liability for damages, restitution, fines, or even criminal charges in cases of extreme misrepresentation or deception. Therefore, it is important for health plans to be aware of the regulatory requirements with regard to sales and marketing. In this lesson we discuss state sales and marketing requirements; in Federal Regulation of Health Plans we address federal requirements.
Typically, health plan products in the commercial market are sold by means of face-to-face interactions between a sales representative or agent and a prospective purchaser, often an employer. Health plan representatives also conduct marketing activities when recruiting providers, such as healthcare practitioners and hospitals. Sales representatives must comply with all applicable licensing requirements to be able to sell the health plan's products. They must also conduct business in accordance with all applicable laws and regulations, and must not engage in any prohibited sales practices. In addition, any marketing and advertising material that a health plan uses must be complete and accurate to comply with state and federal advertising requirements, which are often very detailed.
Corporate Liability Based on Agency3
A corporation can act only by delegating its authority to individuals, such as directors, officers, and employees, who conduct the corporation's business. Because these individuals act on behalf of the corporation, they are, in a sense, agents for the corporation. Agency is a legal relationship in which one party, known as the principal, authorizes another party, known as the agent, to act on the principal's behalf. (See Key Legal Issues in Health Plans for a broader discussion of agency.)
As the principal in an agency relationship, a health plan has the right to determine the scope of the agents' authority. Because agents who act within the scope of their authority have the power to bind the principal, health plans are generally interested in limiting the scope of such authority. For example, health plans want to ensure that their sales representatives do not have authority to enter into binding insurance contracts on the health plan's behalf. Sales representatives typically submit each contract application for underwriting approval, and only specified employees- usually in the health plan's home or regional office- have actual authority to approve an application and issue and sign a contract that is binding on the health plan.
Licensing4
The licensing requirements imposed on sales representatives allow the states to oversee the activities of the individuals who engage in the sale of insurance and health plan products. As with other regulatory requirements, specific licensing requirements vary from state to state but are similar in many respects. We'll use the NAIC Agents
Page 154 of 469

AHM 510 : Health Plans : Governance and Regulation
and Brokers Licensing Model Act to illustrate state licensing requirements. Although most states enacted their licensing laws before the NAIC adopted this Model Act, the model illustrates features that are common to licensing laws.
Who Must Be Licensed?Sales representatives must be licensed in each state in which they do business. Although not all states define exactly what they mean by "doing business" in the state, sales representatives are generally required to obtain a license in each state in which they solicit or negotiate sales, deliver contracts, collect premiums, or have an office that transacts insurance business. State laws typically list a number of individuals who are not required to be licensed sales representatives. The Agents and Brokers Licensing Model Act exempts certain individuals from the licensing requirements, such as:
• A health plan's or insurer's employees who do not negotiate or solicit business
• Persons who assist in administering group health coverage and who do not receive commissions for their services
• Employers that provide employee benefit plans, trustees of employee trusts, and employees who administer such plans and who are not compensated by the health plan or insurers that issued such plans
Agent and Broker LicensesAccording to the Agents and Brokers Licensing Model Act, an insurance agent is an individual, partnership, or corporation appointed by a company to solicit applications for policies or to negotiate policies on the company's behalf. The Model Act defines an insurance broker as a partnership, corporation, or individual who is compensated for helping others to obtain insurance from a company that has not appointed that individual as an agent. Note the distinction the Model Act makes between an insurance agent and an insurance broker. An agent represents and acts on behalf of the health plan, whereas a broker acts on behalf of the purchaser. Agents may place business with a health plan only if they have been appointed as an agent with that company. By contrast, brokers may place business with health plans they have not been appointed to represent.
Most states issue both agent's licenses and broker's licenses. States that do not issue broker's licenses typically require individuals who act as brokers to obtain an agent's license.
In most states, partnerships and corporations are eligible to be licensed agents and brokers. Laws in these states usually require licensed partnerships to register with the insurance department every partnership member and employee who personally engages in the sale of insurance; licensed corporations must register every officer, director, and employee who personally engages in the sale of insurance. In addition, these individuals who are registered by a partnership or corporation must also be licensed as agents or brokers.
Resident and Nonresident LicensesSales representatives typically conduct their business in the state in which they reside. From the state's perspective, these individuals who reside and work in the state are
Page 155 of 469

AHM 510 : Health Plans : Governance and Regulation
known as resident agents and brokers, and the type of license they are required to hold is known as a resident license.
Individuals who do not live in the state or whose principal place of business is located outside the state are known as nonresident agents and nonresident brokers, and must obtain a nonresident license before conducting business in the state. State laws typically require applicants for a nonresident license to hold a similar license from another state or country. In other words, sales representatives usually must hold a resident's license from their home jurisdiction before being eligible to receive a nonresident license from another jurisdiction.
Licensing RequirementsIndividuals must comply with statutory requirements in order to be eligible to receive a license. Figure 6A-1 lists the requirements from the Agents and Brokers Licensing Model Act.
Once the insurance department receives a completed application and all applicable fees, the department may conduct whatever investigation it deems necessary before acting on that application. In most cases, the department approves the application and notifies applicants of the dates and times on which they may take any required examination. If the applicant passes the examination, then the department issues a license to the applicant. If the department disapproves an application, it notifies the applicant of its disapproval and gives the reasons for its decision.
Requirements for a nonresident license are generally the same as the requirements for a resident license. Some states that issue nonresident licenses impose a countersignature requirement under which applications solicited by nonresident sales representatives must also be signed by an individual who holds a resident license.
Figure 6A-1.Licensing Requirements from the Agents and Brokers Licensing Model Act.
The applicant must complete a written application on a form provided by the state insurance department, which provides identifying information.
An application for an agent's license must be accompanied by a written statement, sometimes referred to as an appointment, made by an officer of an insurer or health plan that is licensed to do business in the state. The appointment, made on a form prescribed by the insurance department, indicates that an insurer or health plan appoints the applicant as an agent for the products the applicant will be authorized to market. If a health plan's corporate structure is such that it issues contracts through more than one legal entity, then it must be sure to appoint the applicant for each entity. For instance, if the health plan provides HMO coverage through one legal entity and PPO coverage through another, then it must appoint its applicants for each entity.
Individual applicants must be at least 18 years old. Applicants for a broker's license must have had at least two years' experience as an
insurance agent or in comparable employment with an insurer, health plan, agency, or brokerage firm. This experience must have been during the three-year period before the application.
Page 156 of 469

AHM 510 : Health Plans : Governance and Regulation
An applicant must be competent, trustworthy, and financially responsible, and must have a good personal and business reputation. The insurance department uses information from the application to evaluate the applicant's character and fitness to hold a license. In addition, the application typically includes a section that is to be completed by the entity that has appointed the applicant as its agent. That entity certifies that it has investigated the applicant's qualifications and background and believes the applicant is trustworthy and competent.
Applicants must pass a written examination in each line of business that they propose to sell. Some states waive part of the examination requirement for applicants who have successfully completed applicable courses of industry study. Many states require applicants to complete a specified amount of prelicensing education before sitting for the required written examination.
Source: Excerpted and Adapted form Harriet E. Jones, Regulatory Compliance: Companies, Producers, and Operations (Atlanta: LOMA©1998), Used with permission; all rights reserved.
Review Question
State X issued a nonresident license to Tamara Pensky, a sales representative of the Verity Health Plan. In doing so, State X imposed a countersignature requirement, which requires that
an officer of Verity sign a written statement which indicates that Verity appoints Ms. Pensky as an agent who is authorized to market Verity's products an officer of Verity sign a written statement which certifies that Verity has investigated Ms. Pensky's qualifications and background and believes she is trustworthy and competent applications solicited by Ms. Pensky must be signed by an individual who holds a resident license applications solicited by Ms. Pensky must be signed by an officer of Verity
Incorrect. In order to obtain an agent's license, the license must be accompanied by a written statement from the health plan appointing the applicant as an agent for the health plan's products
Incorrect. In order to obtain an agent's license, an officer of Verity sign a written statement which certifies that Verity has investigated Ms. Pensky's qualifications and background and believes she is trustworthy and competent
Correct. A countersignature requirement requires applications solicited by Ms. Pensky must be signed by an individual who holds a resident license
Incorrect. Applications solicited by Ms. Pensky must be signed by someone other than an officer of Verity
Page 157 of 469

AHM 510 : Health Plans : Governance and Regulation
Duration of LicenseIn many states, as long as required renewal fees are paid, a sales representative's license continues for an indefinite time, and expires only upon the occurrence of specified events, such as termination of the individual's appointment with the health plan. Other states issue a sales representative's license for a stated period, such as one or two years. To renew the license, either the individual or the health plan must complete a request for renewal and pay a renewal fee. In addition, the growing complexity of products has led many states to require that licensed sales representatives complete continuing education requirements in order to maintain their licenses.
The state insurance department has the authority to suspend or revoke a sales representative's license. For example, suspension or revocation can occur when an individual makes materially untrue statements in the license application, mishandles funds, violates an insurance or HMO law, or is convicted of a felony or misdemeanor involving moral turpitude, which is an act or behavior that gravely violates the moral standards of the community. Typically, if the insurance department suspects a sales representative of wrongdoing, it conducts a hearing at which the individual is given the opportunity to present evidence. In the event of suspension or revocation, the insurance department notifies the sales representative and all appointing entities. The insurance department also notifies the NAIC and the insurance department of each state in which the individual holds a license.
Marketing Activities5
Most states have enacted a type of law typically known as an Unfair Trade Practices Act. An Unfair Trade Practices Act defines certain practices as unfair and prohibits those practices in the business of insurance if they are committed (1) flagrantly in conscious disregard of the Act or (2) so frequently as to indicate a general business practice. Such laws generally apply to all individuals and legal entities that engage in the business of insurance, including sales representatives, insurers, third party administrators, and all types of health plans ranging from medical and dental service plans to PPOs and HMOs.
Many such state laws are based on the NAIC Unfair Trade Practices Act, which lists 15 general practices that are prohibited; these prohibited practices are shown in Figure 6A-2.
Figure 6A-2. NAIC Unfair Trade Practices Act Defined.
Section 4. Unfair Trade Practices Defined
Any of the following practices, if committed in violation of Section 3, are hereby defined as unfair trade practices in the business of insurance:
A. Misrepresentations and false advertising of insurance policiesB. False information and advertising generallyC. DefamationD. Boycott, coercion, or intimidationE. False statements and entriesF. Stock operations and advisory board contractsG. Unfair discrimination
Page 158 of 469

AHM 510 : Health Plans : Governance and Regulation
H. RebatesI. Prohibited group enrollmentsJ. Failure to maintain marketing and performance recordsK. Failure to maintain complaint handling proceduresL. Misrepresentation in insurance applicationsM. Unfair financial planning practicesN. Failure to file or to certify information regarding the endorsement or sale of long-term care insuranceO. Failure to provide claims history
*Section 3 prohibits the practices listed in Section4 if committed (1) flagrantly and in coscious disregard of the Act or (2) so frequently as to indicate a general business practice.
Source: Unfair Trade Practices Act, Sections 3 and 4, National Association of Insurance Commissioners, 1993.
State unfair trade practices acts tend to contain broad prohibitions against certain unfair practices; these laws do not attempt to identify every activity that is deemed unfair. Many states have adopted regulations that supplement these acts. In addition, states have enacted laws and regulations that govern specific activities of health plans and sales representatives.
States often prohibit as an unfair trade practice the offering of inducements to enroll. For example, some states would prohibit a health plan from giving out exercise equipment to new members as part of a promotional campaign to increase membership.
State unfair trade practices laws may also pertain to activities between health plans and prospective providers. For instance, a provider may be prohibited from offering the same services at a price more favorable to one health plan than another. Or a health plan may be prohibited from discriminating against a provider based on the types of services typically rendered by the provider.
Advertising Requirements6
A variety of state laws and regulations govern advertising by health plans. General consumer protection statutes in many states regulate all types of advertisements, including those generated by health plans. Unfair trade practices acts broadly prohibit advertisements that are untrue, deceptive, or misleading. Many states' HMO laws have similar prohibitions. The HMO laws in some states require that an HMO's application for a certificate of authority include a description of the proposed method of marketing the plan. Most states also have laws that specifically govern advertising of health coverage.
The NAIC Model Rules Governing Advertisements of Accident and Sickness Insurance provide a good framework for discussing regulation of advertising for health coverage. Most states have adopted rules based on the NAIC model, although there are variations from state to state. The purpose of the model is to "assure the clear and truthful disclosure of the benefits, limitations, and exclusions of policies sold as accident and sickness insurance. This is intended to be accomplished by the establishment of guidelines and permissible and impermissible standards of conduct in the advertising of accident and sickness insurance."7
Page 159 of 469

AHM 510 : Health Plans : Governance and Regulation
The NAIC rule define an advertisement to include:
• Printed and published material, audiovisual material, and descriptive literature of an insurer used in direct mail, newspapers, magazines, radio scripts, TV scripts, billboards, and similar displays
• Descriptive literature and sales aids of all kinds issued by an insurer, agent, producer, broker, or solicitor for presentation to members of the insurance-buying public, including but not limited to circulars, leaflets, booklets, depictions, illustrations, form letters, and lead-generating devices of all kinds
• Prepared sales talks, presentations, and material for use by agents, brokers, producers, and solicitors whether prepared by the insurer or by the agent, broker, producer, or solicitor8
The model act requires health plans to "establish and maintain a system of control over the content, form, and method of dissemination of all advertisements of its policies. All such advertisements, regardless of by whom written, created, designed or presented, shall be the responsibility of the insurer whose policies are so advertised."9 Some states require health plans to maintain an advertising file that contains copies of all advertising pieces generated within a specified timeframe; this file indicates whether each piece was reviewed for compliance with applicable requirements, how it was used, and whether it remains in use. Advertising materials are subject to regulatory market conduct examination.
The specific requirements imposed on any given advertisement depend on the type of advertisement. According to the NAIC Rules, advertisements can be classified into three types.
1. An institutional advertisement is one that is designed to promote either the concept of health insurance or the insurer as a provider of health insurance. Such advertisements do not refer to any specific product.2. An invitation to inquire is an advertisement that is designed to induce the audience to inquire further about a specific health policy and contains the policy form number and a brief description of the coverage provided by the policy. States typically prohibit invitations to inquire from referring to the cost of coverage provided by the policy.3. An invitation to contract is any health policy advertisement other than an institutional advertisement or an invitation to inquire. Such an advertisement contains fairly detailed information about a specific health policy and usually must include the policy form number. Because invitations to contract are designed to create consumer interest in purchasing a particular policy- so that a customer's response to the ad is essentially an application for insurance- the states impose a number of specific disclosure requirements on such ads. For example, if the advertised policy contains exceptions, reductions, or limitations, the advertisement must disclose those provisions. An exception is a policy provision that eliminates coverage for a specific hazard. A reduction is a policy provision that reduces the amount of the benefit payable for a specified loss. A limitation is a provision, other than an exception or a reduction, which restricts the coverage provided by the policy. Figure 6A-3 provides samples of an exception, a reduction, and a limitation.
Page 160 of 469
AHM 510 : Health Plans : Governance and Regulation
Exceptions, reductions, or limitations must be placed conspicuously and in close proximity to the statements to which they relate, or they must be put under prominent headings, such as "Exceptions," "Exclusions," "Conditions Not Covered," or "Limitations." Use of the words "only," "just," or "merely" to downplay the nature of limitations or cost-sharing features is prohibited. For example, an advertisement cannot state that "healthcare expenses are covered in full after you make a copayment of only $15." State advertising regulations also prohibit exaggerated claims. For instance, an HMO that requires members to file a claim form to be reimbursed for emergency care rendered by a nonparticipating provider cannot state that "you never have to file a claim form."
Figure 6A-3. Examples of an Exception, a Reduction, and a Limitation.
Exception: Charges for dental services are not covered.Reduction: Charges for dental exams are limited to $40 per exam and not more than one exam in any calendar year.Limitation: Charges for dental services, other than treatment due to an accident, are not covered.
Review Question
Indigo Health Plan advertised a specific individual health insurance policy through a direct mail advertisement that provided detailed information about the product. In order to comply with the NAIC Model Rules Governing Advertisements of Accident and Sickness Insurance, Indigo must disclose whether the advertised policy contains any exceptions, reductions, or limitations. Thus, Indigo disclosed in the advertisement that one policy provision limits coverage for dental exams to $50 per exam and to one exam per calendar year. This information indicates that, with respect to the definitions in the NAIC Model Rules, Indigo's advertisement is an example of an
invitation to contract, and it discloses a policy provision known as an exception
invitation to contract, and it discloses a policy provision known as a reduction
invitation to inquire, and it discloses a policy provision known as an exception
invitation to inquire, and it discloses a policy provision known as a reduction
Incorrect. An invitation to contract is any health policy advertisement other than an institutional advertisement or an invitation to inquire. An exception is a policy provision that eliminates coverage for a specific hazard.
Correct. An invitation to contract is any health policy advertisement other than an institutional advertisement or an invitation to inquire. A reduction is a policy provision that reduces the amount of the benefit payable for a specified loss.
Page 161 of 469

AHM 510 : Health Plans : Governance and Regulation
Incorrect. An invitation to inquire is an advertisement that is designed to induce the audience to inquire further about a specific health policy and contains the policy form number and a brief description of the coverage provided by the policy. An exception is a policy provision that eliminates coverage for a specific hazard.
Incorrect. An invitation to inquire is an advertisement that is designed to induce the audience to inquire further about a specific health policy and contains the policy form number and a brief description of the coverage provided by the policy. A reduction is a policy provision that reduces the amount of the benefit payable for a specified loss.
Most states require a health plan to disclose its legal entity name on all advertising, applications, policies, and claim forms. In addition, most states prohibit advertisements that disparage other insurers or health plans, or advertisements that provide unfair or incomplete comparisons of plan provisions.
Some states have filing requirements for advertising material. These requirements vary considerably by state. For instance, one state may require filing of all advertising material for HMO products, but may not require filing of advertising material for PPO or indemnity products. Another state may require filing for all small group advertising material, whether the product is HMO, PPO, or indemnity. Some states establish a time frame for health plans to file certain types of advertising. For example, a health plan might be required to file each advertising piece at least 30 days prior to the date it intends to use the piece; if the insurance department does not reply by that date, then the filing is deemed approved.
ReadabilityMany states have readability laws, also called plain language laws or policy simplification laws. The purpose of these laws is to simplify the language in the evidence of coverage and make it easier for members to understand the plan provisions. Readability laws require the health plan or insurer to issue documents that meet or exceed a minimum readability score. This score is determined by a formula that includes the average number of syllables per word and the average number of words per sentence. Typically, the health plan calculates and certifies the score when it submits forms to the state insurance department for approval.
UnderwritingMost state insurance laws contain provisions that in some way regulate the underwriting practices of health plans. Often the purpose of these provisions is to protect consumers from unfair discrimination. For example, most states require that any differences in health plan benefits for members of employer groups must be based on conditions pertaining to employment. An employer group would be permitted to have a $20 office visit copayment for salaried employees and a $15 copayment for hourly employees because these coverage classifications are determined by job-related factors. However, an employer group would not be permitted to have a separate copayment for certain employees listed in a memorandum sent by the company's human resources manager to the health plan.
Many states prohibit discrimination in terms of denying coverage or charging higher premiums based on factors such as race, national origin, marital status, gender, or
Page 162 of 469

AHM 510 : Health Plans : Governance and Regulation
sexual orientation. Some states prohibit such discrimination based on specified physical or mental conditions.
Eligible Groups and IndividualsState group insurance laws specify the types of groups that can be issued group coverage. The definition of an eligible group varies from state to state, but typically includes the following:
• Single employers or trusts established by single employers
• Creditors
• Labor unions
• Trusts established by two or more employers or by employers and labor unions
• Associations or multiple employer welfare groups
Some state insurance commissioners have the authority to approve other types of groups that are substantially similar to those defined in the statute.
In addition to defining eligible groups, state insurance laws typically specify the individuals who can or must be covered under a group policy. For example, eligible employees in an employer group are often defined to include the officers, managers, employees, and retired employees of the employer, a subsidiary corporation, or companies under common control. Most health plans provide coverage for a member's spouse and dependent children. Health plans often consider a spouse to be an individual who is legally recognized as the employee's spouse, and a dependent child to be a natural child, stepchild, or adopted child under a specified age, typically 19. Some states have laws that specify whether or not domestic partners can be covered under a health plan. Many states require a health plan to continue eligibility for handicapped dependent children for as long as the child remains handicapped. Some states require continued eligibility for college students up to a specified age. A number of states require that newborn children of covered employees be provided automatic coverage for 31 days from the moment of birth, even if the coverage would require an increase in contributions; the employee then has those 31 days to enroll the newborn child for contributory coverage. If the employee fails to do so, then the child's coverage ends after the 31-day period and the employee is liable for healthcare costs incurred after that date.
Records and Privacy10
In the course of doing business, health plans gather a large amount of personal information about individuals. General laws and court cases relating to confidentiality of medical information apply to health plans and insurers. In addition, many states have enacted laws designed to protect the privacy of individuals by establishing guidelines for how health plans must treat such personal information. State privacy laws regulate the ways in which companies collect, use, and disclose personal information. Many of these laws are based on NAIC model acts.11
For example, the NAIC HMO Model Act requires HMOs to protect the confidentiality of information that would reveal the health status or treatment of members. HMOs may disclose such information only in the following situations:
Page 163 of 469

AHM 510 : Health Plans : Governance and Regulation
• To carry out the purposes of the HMO Act
• With the express consent of the individual
• Pursuant to a statute or court order requiring the production of evidence
• In litigation between an enrollee and the HMO where the information or data is relevant
In addition, the NAIC has enacted the Health Information Privacy Model Act. The model act sets standards to protect health information from unauthorized collection, use and disclosure by requiring carriers to establish procedures for the treatment of all health information.
Aside from NAIC model acts, some states have enacted laws that:
• Prohibit health plans from selling for commercial purposes the names of their enrollees
• Make all health plan documents and communications related to mental health confidential
• Make all information derived from genetic testing confidential and authorize release only with the consent of the individual tested
Some states also address procedures for maintaining health plan records. For instance, they may require specific methods for filing and retrieving information and a specified period of time for retaining files.
In addition to health plan information, health plans often need access to medical records to perform utilization review and other medical management and quality assurance activities. Recognizing this need, some states allow health plans limited access to medical records. Typically, these laws require the health plan to obtain the appropriate authorization from the member. Health plans often address this authorization requirement by including a statement and signature line on the member enrollment form which gives the member's approval for the health plan to access appropriate medical records.
Several states that have enacted legislation or adopted constitutional amendments to protect privacy of medical records have given patients access to their own medical records, addressed procedures for maintaining health databases, and put in place strict disclosure and authorization procedures.
Claims and Coordination of BenefitsState laws that address handling of claims set out a variety of improper claims practices and prohibit health plans from engaging in those practices. The NAIC Model Unfair Claims Settlement Practices Act defines improper claims practices as those committed "flagrantly or in conscious disregard of this Claims Act" or so often as to appear to be a general business practice.12 Figure 6A-4 provides some examples of acts that would be considered unfair or improper according to the NAIC.
Coordination of benefits (COB) laws are used to determine benefit payments when a person is covered by more than one plan, such as two group health plans or a health
Page 164 of 469

AHM 510 : Health Plans : Governance and Regulation
plan and the medical benefits provisions of an automobile policy. COB laws contain an order of benefit determination to indicate which plan pays its benefits first (the primary payor) and which plan pays its benefits second (the secondary payor). The primary payor pays benefits as if the person had no other coverage. The secondary payor reduces its benefits in a manner described by the COB provision in its contract and/or according to the state's COB law, taking into account the benefits paid by the primary payor.
COB provisions are relatively easy to administer for indemnity carriers. The individual incurs the healthcare expenses and submits a claim to the primary payor, which determines benefit payments; the individual then submits a claim to the secondary payor, which reviews the primary payor's claim payment, then adjusts its payment accordingly.
Figure 6A-4. Improper Claims Practices.
Following are some examples of acts that would be considered improper claims practices according to the NAIC Model Unfair Claims Settlement Practices Act:
• Knowingly misrepresenting relevant facts or policy provisions • Failing to acknowledge with reasonable promptness communications about claims • Failing to adopt and implement reasonable standards for the prompt investigation
and settlement of claims • Not attempting in good faith to effectuate prompt, fair, and equitable settlement of
claims • Compelling insureds or beneficiaries to institute suits to recover amounts due by
offering substantially less than the amounts ultimately recovered in such suites • Refusing to pay claims without conducting a reasonable investigation • Failing to affirm or deny coverage of claims within reasonable time after having
completed an investigation • Attempting to settle claims on the basis of an application that was materially
altered without notice to, or knowledge or consent of, the insured • Making claims payments to an insured or beneficiary without indicating the
coverage under which each payment is being made • Failing, in the case of claims denials or offers of compromise settlement, to
promptly provide reasonable explanations of the basis for such actions
Source: Excerpted and Adapted from Charles G. Benda and Fay A. Rozovsky, Liability and Risk Management in Health Plan (Gaithersburg, MD: Aspen Publishers, Inc., 1998), p. 5:11.
Review Question
Determine whether the following statement is true or false:
Failing to adopt and implement standards for the prompt investigation and settlement of claims is an example of an activity that would be considered an improper claims practice according to the NAIC Model Unfair Claims Settlement Practices Act.
Page 165 of 469

AHM 510 : Health Plans : Governance and Regulation
True
False
Correct. NAIC Model Unfair Claims Settlement Practices Act defines improper claims practices as those committed flagrantly or in conscious disregard of this Claims Act or so often as to appear to be a general business practice
Incorrect. NAIC Model Unfair Claims Settlement Practices Act defines improper claims practices as those committed flagrantly or in conscious disregard of this Claims Act or so often as to appear to be a general business practice
COB provisions present more of a challenge for health plans. For instance, what is the dollar amount of the "benefit" when an individual receives care from a capitated HMO provider? Most COB laws state that when one plan uses capitation or similar reimbursement provisions, then the "reasonable value" of the services will be used as the basis for determining payment for COB purposes. For example, if an individual obtains treatment from a capitated HMO physician and the HMO is the primary payor, the secondary payor must determine the "actual charge" and the "benefit that was paid by the HMO" in order to pay secondary benefits under the COB provision. The secondary payor does this by assuming that the actual charge is the reasonable and customary charge in the area for the care provided. It then determines the HMO "benefit" by reducing the actual charge by the copayment made by the individual.
Another complicating factor arises when the health plan is the secondary payor, and the covered individual obtains treatment from one of the health plan's participating providers. If the provider is capitated, then the health plan has, in effect, already "paid the claim" at the time of treatment, even though it is the secondary payor. The health plan must then work with the primary payor to obtain a reimbursement in the amount that the primary payor would have paid. The health plan, as secondary payor, then determines the total benefit payable to the individual under the COB provision and, if applicable, reimburses the individual. Typically, this means the health plan returns the member's copayment. Health plans sometimes use the term "pay and chase" to refer to this method of handling COB.
If a health plan determines prior to treatment that a member has primary coverage under another plan, it might bill the patient and have the patient submit the bill to the primary payor. After the primary payor pays the claim, the health plan can then determine the total benefit payable under the COB provision and, if applicable, reimburse the individual. However, in some states this practice is prohibited.
AntifraudBecause of the high cost to health plans, purchasers, and consumers, a number of states have enacted legislation designed to reduce insurance fraud. These antifraud laws vary a great deal from state to state, but they include a number of requirements with which health plans must comply. For example, some states require health plans to report all fraudulent activities-including all types of insurance fraud-that they discover. Some states require health plans to establish special fraud units or systems that enable them to detect fraudulent activity. Some states require health plans to include a fraud
Page 166 of 469

AHM 510 : Health Plans : Governance and Regulation
warning on applications for coverage and/or on claims forms. We discuss fraud and abuse in more detail in Key Legal Issues in Health Plans.
Continuation and ConversionWhen a person's eligibility under a group contract would otherwise end, a continuation provision allows the employee and/or dependent to continue eligibility as if still covered under the group contract. Except for the eligibility provision, all of the terms of the group contract remain the same for the person who is continuing coverage. A conversion privilege allows an employee or dependent to convert from or leave the group contract to obtain similar coverage under a separate individual contract.
Several states have continuation laws that either (1) apply to groups not subject to the COBRA continuation requirements or (2) require health plans to provide for continuation not required by COBRA.
Many states have conversion laws that require health plans to offer a contract to members whose eligibility under a group contract ends. Typically these laws specify the circumstances under which the conversion contract need not be offered; for example, if the member's coverage terminates for failure to pay premium contributions or if the member has not been continuously covered under the plan for a minimum number of months. If the member qualifies for and requests a conversion contract, then a contract must be issued and the member does not have to submit evidence of insurability as is typical in many other individual healthcare coverage transactions. The health plan can, however, charge premiums in accordance with its individual rate structure, rather than its group rates. Most states require the insurer or health plan to clearly disclose this conversion right in the evidence of coverage and to issue a new contract to the member upon conversion. If an individual also has a right to continue eligibility under the group plan in accordance with COBRA or a state-mandated continuation law, then the conversion right typically does not go into effect until after the continuation period has ended. Some states, however, give an individual the right to decline the continuation and immediately elect an individual conversion policy.
Fast Fact
According to the Employee Benefit Research Institute, 38 percent of the uninsured are either self-employed, work for a private firm with 25 or fewer employees, or live in a household headed by someone who is self-employed or who works for a small firm. 13
Small GroupA large segment of the U.S. population obtains healthcare coverage through employee benefit plans, but historically many small employers have not offered healthcare benefits to their employees. During the 1990s, in an attempt to increase access to healthcare, many states enacted small group reform laws. Generally, these laws address two major factors: (1) the cost of healthcare, which keeps many small employers and their employees out of the marketplace, and (2) marketplace practices that deny small employers and/or their employees access to coverage.
Although small group laws vary by state, they have certain features in common:
• Standardized benefit design
Page 167 of 469

AHM 510 : Health Plans : Governance and Regulation
• Restrictions on underwriting practices
• Restrictions on premium rating
• Requirements for disclosure of plan and rating information
Typically, states define a small group as an employer with as few as 2 or 3 employees and as many as 49 or 50 employees, whether or not they enroll for coverage. Most states have amended their small group laws to align with the guaranteed access requirements of HIPAA. Some states have elected to apply an expanded definition. For instance, some states consider a self-employed individual to be a small group, and other states consider groups with as many as 99 employees to be a small group.
Uniform Benefit DesignSome states have developed standardized benefit designs that provide limited coverage. Depending on the state, these plans are called low option, basic, essential, or bare bone plans. They typically include features such as a high annual deductible, high copayments, limits on lifetime and annual benefits, and a limited list of covered services and supplies. To make healthcare coverage more affordable and thereby more accessible to to small employers and their employees, a state might exempt small groups from some of the regulatory benefit mandates that apply to other groups.
Many states have also developed standard plans that provide more comprehensive coverage at benefit levels closer to large group products. In addition, some states allow health plans to offer high option plans, which are benefit designs that are identical to the health plans typically offered in the large group market. By allowing this increased flexibility in plan design, states hope to attract small employers and their employees who might be interested in more comprehensive coverage than the low option design provides.
Recognizing health plan's success in controlling healthcare costs, most states have included standardized benefit designs for HMO and PPO products in addition to indemnity products.
Restrictions on Premium RatingAnother way that small group laws attempt to reduce the cost of healthcare coverage is by placing restrictions on the rates that health plans can charge small employers. Typically, these laws prohibit health plans from using experience rating and they prescribe a method that limits the rate spread that health plans can use for all small employer groups.
Many small group laws require health plans to use a rating method that is either pure community rating or adjusted community rating. Other small group laws are based on the rating method contained in the 1991 NAIC model small group laws and regulations. This method allows health plans to use up to nine rating classes with prescribed minimums and maximums in each class. Also, the average premium in each class cannot be more than 120% of the average premium in any other class. The result of these requirements is that the highest rate a health plan can charge a small employer cannot be more than twice the lowest rate. The 1991 NAIC model was amended in 1995 to eliminate the class rating rules and require what the NAIC refers to as adjusted community rating, which allows adjustments only for geography, family composition, and
Page 168 of 469

AHM 510 : Health Plans : Governance and Regulation
age. However, many state laws are based on the 1991 NAIC model and still allow rating classes based on experience factors, subject to the requirements described above.
Restrictions on Underwriting PracticesMany small group laws seek to improve access to healthcare coverage by restricting the underwriting practices that health plans can use to reduce their overall risk. Although these restrictions actually increase the cost of providing healthcare coverage, they directly improve access for groups and individuals who might otherwise be denied coverage. Several of these features have been incorporated into the federal Health Insurance Portability and Accountability Act of 1996 (HIPAA), which we describe in Federal Regulation of Health Plans. These restrictions can be divided into two types, those that apply to employer groups and those that apply to the individuals who are members of the groups.
• Underwriting Practices for Employer Groups • Underwriting Practices for Individual Members of Employer Groups
Another way that health plans can limit risk is by applying waiting periods and pre-existing condition exclusions to individuals who are eligible for group coverage. Small group laws seek to improve access to healthcare by placing restrictions on these provisions.
Fast Fact
According to a 1996 survey, more than 16 million Americans under age 65 have healthcare coverage through plans that are not provided through employer or government programs. 14
Underwriting Practices for Employer Groups
Most small group laws contain a guaranteed issue provision, and HIPAA now mandates guaranteed issue in the small group market. A guaranteed issue provision requires each health plan that participates in a state's small group market to issue a contract to any employer who requests coverage, provided that the employer meets the state's definition of a small group. Typically, in the large group market an insurer or health plan can elect not to issue a contract to a particular group if it determines that the group has had poor claim experience or has a member who is suffering from a catastrophic illness or injury that would result in substantial healthcare expenses. Small group laws prohibit this underwriting practice. State and federal small group laws also contain guaranteed renewal provisions, which prohibit health plans from canceling a group's coverage because of poor claims experience or because of other factors that relate to group underwriting, such as a change in health status of group members.
Underwriting Practices for Individual Members of Employer Groups
Before the small group reform initiatives of the 1990s, group insurance laws often set the minimum number of employees in an eligible employer group at 10 or more. This meant that employers with fewer than the specified number of employees were not considered
Page 169 of 469
AHM 510 : Health Plans : Governance and Regulation
employer groups for the purpose of applying group insurance laws. Therefore, insurers used individual medical underwriting for individuals within these small groups. In other words, insurers were able to accept an employer group for coverage, but determine that certain individuals within that group could not enroll under the plan because of health conditions. The small group reform laws typically changed the definition of an employer group to include employers with as few as two or three emplyees, thereby subjecting each individual in a small group to group, rather than individual, underwriting requirements.
Requirements for Disclosure of Plan and Rating InformationSmall group laws typically include disclosure requirements to help acclimate purchasers who are entering the group market for the first time and are unfamiliar with the issues involved in purchasing group coverage. These requirements are intended to help educate purchasers and enable them to make informed choices. They often require marketing brochures to include information about rating criteria or about benefits that low option plans do not cover.
Purchasing AlliancesThe small group laws in some states establish purchasing alliances. A purchasing alliance, also called a purchasing cooperative or a health insurance purchasing cooperative (HIPC), is a means of increasing healthcare access for small employers by (1) providing economies of scale in marketing and administrative activities and (2) making it easier for small employers to purchase healthcare. In theory, by joining a purchasing alliance, small employers gain purchasing power similar to that of a large employer. The purchasing alliance acts as a liaison between the small employer and the health plans. For example, the alliance might prescribe a uniform format for marketing material and maintain copies of brochures from all participating health plans so that any interested small employer can go to a single source (the purchasing alliance) to obtain information about all available plans. The alliance might also coordinate billing and enrollment activities between the small employer and the participating health plans.
Typically, the purchasing alliance is not a government agency; rather it is operated as a not-for-profit entity that obtains its authority through state law but is governed by a board made up of representatives from the community.
Individual HealthcareMany states have laws intended to improve access and affordability in the individual healthcare market. These laws often employ provisions similar to those found in small group laws. In fact, certain small group laws that define a self-employed individual as a "small group" are actually applying their small group laws to individuals.
A number of individual healthcare laws include guaranteed issue provisions, which require health plans participating in the individual market to issue a contract to any individual who requests coverage. In some states, the health plan is only required to issue a contract to individuals who meet established criteria, such as individuals who have had continuous healthcare coverage for the past 12 months or more. In a few states, the health plan must agree to issue every product it markets in the state. Elsewhere, the insurer or health plan must agree to issue at least one of the products it markets in the state or to issue a standardized benefit design developed by the state.15
Page 170 of 469

AHM 510 : Health Plans : Governance and Regulation
Individual healthcare laws in many states seek to improve access to healthcare by placing restrictions on pre-existing conditions exclusions, similar to those found in small group reform laws. To address the problem of affordability, several states apply rating restrictions to limit variations in premium rates or to prohibit the use of rate factors, such as health status, claims experience, age, or gender. For example, New York requires all health plans to use community rating with variations based only on product, family composition, and geographic location. In Washington, the highest rate a health plan can charge an individual cannot be more than four times the lowest rate it charges, and rates can vary based only on age and geographic location, but not health status or claims experience.16
Several states have not enacted any individual healthcare reform laws. In these states, the only reforms that apply are those imposed by HIPAA.
Fast Definitions
Waiting period (also called probationary period, service waiting period, or employment waiting period) - the length of time that a new member must wait before becoming eligible to enroll in the plan.
Pre-existing condition exclusion - a policy exclusion that denies coverage for a condition for which an individual received treatment during a specified period of time prior to the effective date of his or her current plan. Although the individual is eligible to enroll in the plan, the expenses relating specifically to the pre-existing condition are not covered.
States as PurchasersIn their role as purchasers of healthcare, states also regulate health plans. For example, states employ thousands of workers for whom they purchase group healthcare coverage. Sometimes state employee healthcare plans are subject to unique bidding and contractual requirements that are specified in laws, regulations, or administrative guidelines. States also serve as purchasers of healthcare through their Medicaid programs and the Children's Health Insurance Program (CHIP), both of which we address in Federal Government as Purchaser. States arrange for workers' compensation coverage for employees in their jurisdiction as well. These programs must comply with unique requirements under workers' compensation laws that are enforced by state Departments of Labor or similar agencies. We discuss Workers' Compensation in the next lesson.
Page 171 of 469

AHM 510 : Health Plans : Governance and Regulation
Chapter 6 BWorkers' Compensation Programs Before states required workers' compensation insurance, employees who were injured on the job were not automatically entitled to receive compensation from their employers. As a result, injured employees often had to sue their employers for their medical expenses and lost wages. In 1911, Wisconsin became the first state to adopt a workers' compensation law. Every state now has a workers' compensation law, and 47 states require employers to offer workers' compensation benefits.
After completing this lesson, you should be able to:
Describe the kinds of benefits injured employees receive under workers’ compensation
List several ways in which workers’ compensation differs from other types of healthcare coverage
Describe how state laws can limit the use of health plans to provide workers’ compensation benefits
Describe some of the common features of workers’ compensation health plans Describe the features of an integrated health and disability plan
Workers' compensation is a state-mandated insurance program that provides benefits for healthcare costs and lost wages to qualified employees and their dependents. If an employee suffers a work-related injury or disease, his or her employer will pay the cost of the related medical expenses through workers' compensation.1
The workers' compensation system is a compromise between the needs of injured employees and the needs of employers. Workers' compensation protects employees who are injured on the job by assuring that they will receive benefits for medical expenses and lost wages. Workers' compensation also protects employers from lawsuits by injured workers by imposing what is known as the exclusive remedy doctrine. The exclusive remedy doctrine is a rule that states that employees who are injured on the job are entitled to the benefits provided by workers' compensation but cannot sue their employers for any additional amounts. In exchange for this protection, though, employers are not allowed to deny liability for work-related injuries and must provide benefits for work-related injuries even if the injuries are not their fault. As we will discuss later in this lesson, the workers' compensation system also regulates how those benefits must be provided.
In this lesson, we describe the ways in which workers' compensation differs from group healthcare coverage and how workers' compensation plans have incorporated health plan techniques. We conclude the lesson with a discussion of some of the challenges facing the employers, insurers, and health plans involved in workers' compensation programs.
How Workers' Compensation Differs from Group HealthcareAlthough healthcare in workers' compensation programs and the group healthcare market both provide medical benefits to injured or ill employees, there are many differences between the two benefit systems. Some of these differences arise from the fact that workers' compensation laws were first enacted decades ago- before managed
Page 172 of 469

AHM 510 : Health Plans : Governance and Regulation
healthcare became prevalent- and have not been revised to reflect modern ways of providing healthcare. Some of the differences result from the compromises that were built into the workers' compensation system when it was first designed. Understanding these differences is important because they often affect the ability to use managed healthcare techniques in providing workers' compensation benefits. These differences are summarized in Figure 6B-1.
Free and Unlimited Coverage for All EmployeesOne of the basic distinctions between workers' compensation and group healthcare is that employers in almost every state are required to provide workers' compensation coverage for all employees, regardless of the number of hours worked. Group plans typically limit coverage to eligible full-time employees.
Workers' compensation laws also require employers to provide coverage at no cost to their employees. This means there can be no employee contributions and no cost-sharing features, such as deductibles and copayments. In group healthcare, employees often pay contributions toward the employer's total premium and share the cost of their medical care by paying deductibles and copayments. Most use cost-sharing features to help manage utilization, which can lower plan costs.
In addition, workers' compensation programs do not contain coverage restrictions, such as those that specify an annual or lifetime benefit maximum or that limit benefits to a predetermined number of days or visits. Workers' compensation laws require coverage for as long as treatment is necessary. Many group plans limit benefits for certain types of conditions or for certain services and supplies.
Page 173 of 469

AHM 510 : Health Plans : Governance and Regulation
Coverage for Work-Related InjuriesAnother key difference between workers' compensation programs and group healthcare is that workers' compensation provides benefits only if an injury or disease is work-related. An employer or health plan, therefore, can contest a workers' compensation claim if it feels that an injury or disease is not related to work. As we will discuss later, employees sometimes fraudulently claim that their medical conditions are work-related to gain access to workers' compensation benefits. Only a small percentage of workers' compensation claims are contested, but resolving the contested claims can be expensive and time consuming. Group healthcare plans, on the other hand, provide care regardless of the cause of the injury or illness, although they typically exclude charges for work-related injury or illness covered by any workers' compensation law.
Benefits for Lost Wages Workers' compensation not only covers medical expenses resulting from work-related injuries or illnesses, it also provides indemnity benefits. Workers' compensation indemnity benefits are workers' compensation benefits that replace an employee's wages while the employee is unable to work because of a work-related injury or illness. Indemnity benefits are a concern for employers and workers' compensation carriers because they account for almost half of all workers' compensation expenses. 2
Employees May Choose ProvidersMost workers' compensation laws give injured employees a great deal of freedom to choose their own medical providers. Injured workers frequently have the right to select any provider they choose and to change providers whenever they like. Even in states that allow employers to set up networks of providers to treat workers' compensation patients, injured employees can usually opt out of the networks and obtain care from providers of their own choice. In health plans, employees are often encouraged or required to use providers who are part of the health plan network.
Fast Fact
By one estimate, employers in the United States spent over $90 billion to provide workers' compensation benefits in 1996. 4
Cost Pressures on Workers' CompensationWorkers' compensation represents only a small portion of the total cost of providing employee healthcare coverage, but employers still pay billions of dollars a year to provide this coverage. Employers have become especially concerned about the inflationary pressures that affect workers' compensation because the costs of providing workers' compensation medical benefits have increased more quickly than the costs of providing benefits under group healthcare plans. One reason for this is that injured employees who do not have to pay deductibles or copayments have little incentive to use cost-effective providers. Another reason for faster-rising costs for workers' compensation is that workers' compensation coverage has grown in recent years to include new types of injuries and illnesses. Today, workers' compensation often provides benefits for conditions such as carpal-tunnel injuries and work-related stress disorders that were not covered just a few years ago. Workers' compensation costs may continue to increase even more quickly as the population continues to age, because older people tend to require more time off the job when they are injured.
Page 174 of 469

AHM 510 : Health Plans : Governance and Regulation
The Cost of Employee FraudWe have already learned that workers' compensation must be provided free to all employees, with no deductibles or copayments, and that employees receive benefits for lost wages in addition to health care. Some employees attempt to take advantage of this generous coverage by claiming that their injuries are work-related when they are not. For example, part-time employees who are not covered by group healthcare policies may claim that their injuries are work-related so they can gain access to medical benefits they would not otherwise receive. Employees who are covered by group healthcare policies may claim that their injuries are work-related to avoid copayments and deductibles. And since workers' compensation replaces lost wages while injured employees are out of work, some employees receiving workers' compensation are able to obtain statements from their physicians that allow them to stay off the job longer than necessary. Even though most employees and physicians are honest, workers' compensation fraud costs employers and insurers billions of dollars a year.3
State Responses to Rising Costs To help control workers' compensation costs, states commonly use fee schedules that specify the maximum amount providers may charge for treating workers' compensation patients. One advantage of fee schedules is that they can regulate increases in medical costs by limiting how much medical fees may increase from year to year. Fee schedules also help ensure that the fees paid by employers and health plans for medical treatments are consistent from provider to provider. Most workers' compensation fee schedules are based on the schedules used in Medicare and Medicaid.
As an additional way of controlling workers' compensation costs, several states have adopted clinical practice guidelines, or treatment guidelines, for treating workers' compensation injuries. A clinical practice guideline, or treatment guideline, is a utilization management and quality management mechanism designed to aid providers in making decisions about the most appropriate course of treatment for a specific case. These guidelines help providers determine the most cost-effective methods of treating work-related injuries.
In the next lesson, we discuss how some states are beginning to use health plans to help control workers' compensation costs.
Review Question
Several states have adopted clinical practice guidelines for treating workers' compensation injuries. Clinical practice guidelines can best be described as
fee schedules that specify the maximum amount providers may charge for treating workers' compensation patients a utilization management and quality management mechanism designed to aid providers in making decisions about the most appropriate course of treatment for a specific case detailed plans of medical treatment designed to facilitate a patient's return to the workplace payment practices that might technically violate the provisions of the anti-kickback statute but that will not be considered illegal and for which providers and health
Page 175 of 469

AHM 510 : Health Plans : Governance and Regulation
plans will not be subject to penalties
Incorrect. Clinical practice guidelines refer to the provision of approriate medical services, not the payment of physicians
Correct! A clinical practice guideline, or treatment guideline, is a utilization management and quality management mechanism designed to aid providers in making decisions about the most appropriate course of treatment for a specific case. These guidelines help providers determine the most cost-effective methods of treating work-related injuries
Incorrect. A return-to-work protocol is a detailed plan of medical treatment designed to facilitate the patient's return to the workplace
Incorrect. As you will learn in the lesson titled Fraud and Abuse, safe harbor regulations describe payment practices that might technically violate the provisions of the anti-kickback statute but that will not be considered illegal and for which providers and health plans will not be subject to penalties
The Move to Managed CareAs the cost of providing workers' compensation benefits increases, employers and states are looking to managed care way to help reduce expenses while ensuring quality. The use of managed care not only helps control the cost of workers' compensation medical benefits, it also helps reduce the cost of indemnity (wage replacement) benefits by coordinating care to enable injured employees to return to work more quickly.
Until recently, workers' compensation laws often restricted the use of managed care techniques, such as copayments and deductibles, or prevented employers from limiting employees' choice of provider. Now, almost half the states allow managed workers' compensation, and in a few states, the use of health plans are required. For example, since January 1, 1997, Florida has required that all workers' compensation medical benefits be provided using health plans. Many states have encouraged demonstration projects to establish standards for new approaches to workers' compensation, including the use of selective networks, utilization review, and case management.
Fast Fact
Using health plans can help employers save as much as 40% on workers' compensation medical costs and 25% on costs for lost wages 5
Features of Managed Workers' CompensationDescribing the "typical" managed care workers' compensation product is difficult, because like group healthcare plans, they may be structured in many different ways. And because workers' compensation laws vary so much from state to state, a health plan arrangement that is used in some states may not be allowed in others. In this section, we discuss some of the most common characteristics of managed workers' compensation and point out how state laws may affect their usefulness. These characteristics are summarized in Figure 6B-2.
Page 176 of 469

AHM 510 : Health Plans : Governance and Regulation
Figure 6B-2. Common Characteristics of Managed Workers' Compensation. Use of preferred provider organizations (PPOs) to encourage employees to choose
providers who deliver affordable, quality care Use of utilization review and case management to ensure the most appropriate,
coordinated care Reliance on total disability management to control indemnity (wage replacement)
benefits Focus on occupational health services to return employees to work quickly
Review Question
While traditional workers' compensation laws have restricted the use of managed care techniques, many states now allow managed workers' compensation. One common characteristic of managed workers' compensation plans is that they
discourage injured employees from returning to work until they are able to assume all the duties of their jobs use low copayments to encourage employees to choose preferred providers
cover an employee's medical costs, but they do not provide coverage for lost wages rely on total disability management to control indemnity benefits
Incorrect. Managed worker's compensation programs use return to work protocols, detailed plans of medical treatment designed to facilitate the patient's return to the workplace. Case managers often find ways of returning employees to work even if they cannot assume all the duties of their job.
Incorrect. Under workers' compensation copayments are not permitted
Incorrect. Workers compensation provides coverage for an employee's medical cost as well as for lost wages
Correct! Managed workers compensation relies on total disability management to control indemnity (wage replacement) benefits. Total disability management is a type of case management that controls both medical and wage benefits by developing treatment plans to emphasize the early return to work.
Use of Preferred Provider OrganizationsIn some states, workers' compensation laws allow insurers and health plans to direct employees to certain providers. However, in many states, employees can seek care from any provider they choose. The laws in these states prevent the use of some kinds of health plans, such as HMOs and EPOs, which may require employees to use only participating providers. Although HMOs are sometimes used in states that allow employers to limit employee choice of provider, the most common type of health plan used to provide workers' compensation benefits is the PPO.
Page 177 of 469

AHM 510 : Health Plans : Governance and Regulation
Under group healthcare plans using PPOs, the benefit incentives that encourage members to use preferred providers include lower copayments and limits on the out-of-pocket costs for in-network care. Under workers' compensation, however, copayments are not permitted and employees are not responsible for out-of-pocket expenses, so employers and health plans must rely on other incentives to encourage employees to use preferred providers. For example, some employers give cash payments, while others provide information about the high quality of in-network care.
Fast Fact
PPOs are used in 70% of all health plans providing workers' compensation benefits. 6
Reliance on Utilization Review and Case ManagementWorkers' compensation health plans often rely on utilization review techniques to help manage cost and oversee quality. For example, plans that offer services through provider networks can reduce unnecessary medical expenses through the use of prospective review procedures, such as preadmission certifications and second opinion requirements. They can also monitor ongoing treatment with concurrent review procedures.
In managed workers' compensation, case management is especially important because of the emphasis on returning injured employees to work quickly. To manage indemnity (lost wages) benefits and medical benefits more effectively, managed workers' compensation plans often practice total disability management. Total disability management is a type of case management that controls both medical and indemnity workers' compensation benefits by developing treatment plans that emphasize the early return to work.
One way workers' compensation health plans enable their case managers to use total disability management is to develop return-to-work protocols. Return-to-work protocols are detailed plans of medical treatment designed to facilitate the patient's return to the workplace. A skilled case manager can often find ways of returning employees to work even if they are not able to assume all the duties of their jobs. A case manager might develop a treatment plan, for example, that allows an employee to return to work on a "light duty" or "limited hours" basis while still receiving treatment for an injury.
Case management can also help control workers' compensation costs by reducing the number of workplace accidents. By asking injured workers what caused their injuries, case managers can aid in loss prevention by helping employers identify and correct situations that contribute to workplace accidents.
Fast Definition
Case management - the process of developing healthcare strategies by assessing the patient's needs and developing an appropriate plan of treatment and then monitoring and coordinating care to achieve the optimum healthcare outcome in an efficient and cost-effective manner.
Page 178 of 469

AHM 510 : Health Plans : Governance and Regulation
Focus on Occupational Health and Returning Employees to Work Health plans that treat workers' compensation cases pay careful attention to selecting providers who are trained in occupational health services. Occupational health services are health services designed to protect the health and safety of employees at work and, if necessary, to treat work-related injuries and illnesses. Some primary care providers in group healthcare networks may not have a background in occupational health services and may not be experienced in treating work-related injuries and illnesses. Those providers may not place the same importance on returning employees to work as providers who are experienced in treating workers' compensation cases, and they may not be as aware of the different options for returning to work, such as the "light duty" programs we mentioned earlier.
Challenges in Complying with State RegulationsEmployers, insurers, and health plans face a difficult challenge in complying with the state laws that regulate workers' compensation. Workers' compensation is closely regulated, and the laws vary widely from state to state. The administrative costs of ensuring compliance with these state regulations can be high, especially for health plans that operate in several states. Many insurers and health plans find that they must add staff to keep abreast of changing regulations.
Most states that allow the use of health plans in providing workers' compensation benefits impose certification requirements on health plans to ensure that they provide high quality care. Employers and health plans have developed national accreditation standards for workers' compensation PPOs and workers' compensation utilization review organizations through the American Accreditation Health Care Commission (AAHCC/URAC). Several states that have certification requirements now allow health plans to satisfy those requirements by achieving accreditation through the AAHCC/URAC.
Integrating Workers' Compensation With Other Benefit PlansWe learned earlier that workers' compensation is similar to group healthcare plans because it provides medical benefits to injured or ill employees. Worker's compensation is also like short-term and long-term disability programs because it provides benefits for lost wages. The key difference is that workers' compensation provides benefits only if an injury or illness is work-related, and group healthcare plans typically exclude coverage for work-related injury or illness.
Because of the similarities between workers' compensation, group healthcare, and disability benefit plans, some employers are looking for ways to create integrated health and disability plans. An integrated health and disability plan is a health plan that provides medical or lost wage benefits to employees for all covered injuries or illnesses, whether they are work-related or not. One reason for the interest in integrated health and disability plans is that employers can reduce their administrative expenses if they administer only one integrated benefit plan instead of several separate plans. In addition, under integrated plans employers no longer have to devote time and resources determining whether injuries are work-related as they do under workers' compensation. Instead, they can focus their attention on promptly providing the care necessary to return injured employees to work.
Page 179 of 469

AHM 510 : Health Plans : Governance and Regulation
24-Hour CoverageOne type of integrated health and disability plan is called 24-hour coverage. Under 24-hour coverage, an employer's group health plan, disability plan, and workers' compensation program are merged, integrated, or coordinated (depending on state regulations) into a single health benefit plan that covers employees 24 hours a day. Twenty-four-hour coverage provides all eligible benefits whether an illness or injury occurs on the job or not.
The application of health plan principles to 24-hour coverage is called 24-hour managed care. An advantage of 24-hour coverage or 24-hour managed care is the coordination of claims processing. In some integrated plans, for example, claims examiners who are trained in handling both healthcare claims and workers' compensation claims use their knowledge and experience to select the most appropriate treatment for injured workers from the wide range of treatment options that are available. Coordinating the claims processing function also helps prevent situations in which plan members receive duplicate workers' compensation and group healthcare benefits.
Obstacles to Developing Integrated CoverageIn large organizations, the administration of different health, disability, and workers' compensation plans is often handled by more than one department. Integrating these plans can require additional coordination between the employee benefits department, which may oversee an employer's group health plan, and the risk management department, which may oversee workers' compensation coverage. In addition, although integrating the plans may result in administrative savings over the long run, the process of initially designing and implementing an integrated program can be expensive. Finally, until very recently, few insurance companies and health plans offered products that combined group health, disability, and workers' compensation coverage. As illustrated in Insight 6B-1 , however, more of these integrated products are now being introduced.
Insight 6B-1. Insurers Are Developing New Integrated Products.
Today health plans are offering innovative new programs that not only combine coverage for workers' compensation and employee health benefits, but also provide top-notch care for people with work-related injuries or illnesses. Two of these programs are discussed below.
Kaiser Permanente's "Kaiser-on-the-job": This integrated health and disability plan was recently introduced in the Pacific Northwest. "We're a health plan delivering preventive and treatment services to injured workers," says Adrianne Feldstein, M.D., a Kaiser Permanente physician who manages Kaiser Permanente's occupational medicine operations. "We can provide integrated medical care-that is, care for injured or ill workers and care for standard family practice patients-because we're one medical group. We have one unified medical record, the same clinical guidelines covering both primary care and occupational care-and we communicate."
Workers see physicians and nurses with full-time expertise in occupational medicine at Kaiser Permanente's nine clinics-professionals who assess workplace risk, minimize disability, and treat conditions common to workplace injury and illness every day. The health plan sends its occupational care professionals through special training covering
Page 180 of 469

AHM 510 : Health Plans : Governance and Regulation
treatment protocols, with an emphasis on disability management-an important focus, since in workers' compensation the big costs come not while the worker recovers from an illness or injury, but later on, during disability.
"Although from Kaiser Permanente's overall perspective, workers' comp is only about 2% of all medical care visits," Dr. Feldstein says, "to the employer who pays for both group medical care and workers' comp, workers' comp is very important. In some high risk areas, the cost of worker's comp, including indemnity costs, can come very near the cost of [other] care."
Employers get consistent, quality care throughout the system, Feldstein says. Physicians, nurses, and other professionals follow up-to-date treatment protocols, and the case managers stay in touch with everybody concerned, including the employer, to get the injured worker back to a productive life on the job as quickly as possible.
"And employers know they're saving money-something in the range of 30% to 50% compared to unmanaged care," Feldstein says.
United Wisconsin Services' "United 24": United 24 is a "24-hour plan" that incorporates all three health-related benefit programs offered by employers: health, disability (both short-term and long-term), and workers' compensation. The plan is currently offered in parts of Wisconsin by United Wisconsin Services (UWS), but may soon expand to other parts of the country, according to Roger Formisano, executive vice president and COO of UWS.
UWS is able to offer an integrated product like United 24 because it owns the three insurers that offer the different kinds of coverage. Each of these insurers has its own case managers, but all are cross-trained on the issues and approaches of the other insurers. They meet weekly to discuss cases and coordinate care, regardless of whether the case involves occupational or nonoccupational illness or injury. Employees have only one point of contact, no matter which kind of coverage is involved.
Formisano explains that in traditional insurance settings, the health plan may prefer to "go easy" on services so nature can take its course, while the disability plan may prefer to see intensive services applied up front in order to spur an early return to work. But in United 24, all care uses "medical management and back-to-work technology," he says. Even the health plan is on the back-to-work track. The result, Formisano says, is that on an injury, such as that resulting from a slip and fall, "all the physical therapy is done quickly, to get the person back to work, regardless of where the fall occurred." If the person can return to work only on a light-duty basis, the plan will arrange for it. This may increase some of the healthcare costs, he concedes, but the program is managed with an eye on the total dollars spent under all three insurance plans. The extra healthcare costs may be more than offset by the savings on the disability side of the plan.
Because of regulatory boundaries between the three types of insurance coverage, the insurance products are offered as individual modules, not one unified insurance contract.
Page 181 of 469

AHM 510 : Health Plans : Governance and Regulation
But Formisano says that United 24 functions in every other way as one product, managed by a United 24 service team. There is one point of contact for claims, one toll-free phone number, one enrollment person, one human resources training program, and one bill. And, Formisano says, the integrated approach of United 24 is projected to save employers something in the neighborhood of 15% over the cost of separate health, workers' compensation, and disability policies.
Source: Adapted from Linda Koco, "24-Hour Plan Offers Health, Disability and Workers' Comp," National Underwriter, 2 March 1998, 29. Reprinted with permission of the publisher.
Page 182 of 469

AHM 510 : Health Plans : Governance and Regulation
Chapter 6 CPharmacy Laws and Legal Issues As the number of available medications has risen, the prescription drug benefit has become an increasingly important part of health plans. Federal and state laws and regulations address nearly every facet of drug therapy, including drug selection, pricing, discounts, patient counseling, and utilization review. Further, states are regulating the manner in which health plan entities administer the prescription drug benefit by establishing legislative limits on the relationships between plans and pharmaceutical providers in the form of open pharmacy laws. As health plans attempt to control costs by streamlining the prescribing and dispensing process, state laws and regulations outline which practitioners may prescribe and dispense medications. Each health plan offering a prescription drug benefit must be closely familiar with federal and state laws and regulations.
After completing this lesson, you should be able to:
Describe the various types of open pharmacy laws Describe how states regulate mail-order/mail service pharmacy programs Describe how states regulate use of formularies and generic substitution Explain the benefit exclusions for an experimental drug, an investigational drug, and
the off-label use of a drug Describe how the Nonprofit Institutions Act applies to prescription drug pricing Describe how states regulate a health plan’s use of drug utilization review programs
Selecting Pharmacy ProvidersSelecting a network of healthcare providers is a primary method of cost containment for health plans. Many health plans have adopted benefit plans limiting or eliminating a subscriber’s medication coverage if the patientdoes not purchase medications at a pharmacy within a network of providers. These restrictions reduce drug benefit costs because pharmacists who join a network accept a reduced reimbursement rate in return for an anticipated increase in their volume of customers. In response, many states have enacted legislation, either opening the networks to pharmaceutical providers who are willing to participate, or prohibiting health plans from limiting a subscriber’s choice of pharmacy. Some states have passed laws precluding the exclusive use of mail-order pharmacies.
Health plans also may attempt to reduce administrative costs by allowing healthcare providers to dispense drugs. These entities must observe state regulations concerning the practice of pharmacy.
Open Pharmacy LawsOpen pharmacy laws are aimed at allowing health plan subscribers to choose their own pharmacists. An any willing provider law requires health plans to allow any provider who meets the terms and conditions of the health plan to participate in the plan. A typical AWP law might state that any “pharmacy or pharmacist has the right to participate as a contract provider under a plan or policy if the pharmacy or pharmacist agrees to accept the terms and reimbursement set forth by the insurer.”1 Legislation also may effectively ban preferred provider networks by prohibiting favorable reimbursements for participating pharmacists, thus placing nonparticipating pharmacists on equal financial
Page 183 of 469

AHM 510 : Health Plans : Governance and Regulation
ground. In Alabama, for example, insurers may not reimburse pharmacists at a rate lower than the “usual and customary rates.”2
Freedom of choice laws focus on the patient, rather than on the pharmacists. Some states have enacted broad statutes that allow health plan subscribers to choose even a nonparticipating pharmacist without a monetary penalty. In Virginia, for example, no insurer or corporation offering a preferred provider plan may require subscribers to pay an additional copayment or penalty for choosing a nonpreferred pharmacy, as long as the pharmacy provider is willing to accept reimbursement at preferred provider rates.3
Some states have passed legislation that is a hybrid of any willing provider and freedom of choice law. In South Carolina, a health plan must allow subscribers to choose any participating pharmacy and must admit any eligible pharmacy into the network or plan.4
State open pharmacy laws also vary in terms of the types of health plan entities they regulate. Virginia freedom of choice law, for example, applies to preferred provider organizations (PPOs) and health maintenance organizations (HMOs).5 Several states exempt HMOs with in-house pharmacies from open pharmacy regulation.6 Health plans should assess the open pharmacy laws of the states in which they practice to determine whether the laws apply to various aspects of their operations.
The legality of some open pharmacy laws has been successfully challenged by health plans on the grounds that these laws relate to employee benefit plans and, as such, are preempted by ERISA.7 (See Federal Regulation of Health Plans for a detailed discussion of ERISA preemption.) At least one state has attempted to resolve this problem by excluding "health maintenance organizations which are both state-certified and federally qualified and self-insured plans under the Employee Retirement Income Security Act of 1974" from its pharmacy choice statute. 8
Mail-Order and Out-of-State PharmaciesHealth plans often encourage subscribers to obtain certain "maintenance" medications from mail-order pharmacies (also called mail service pharmacies). Contractual provisions or monetary incentives favoring this practice may come under scrutiny, however, as many states have enacted legislation proscribing this method of reducing medication costs. Some states simply provide that health plans may not require subscribers to obtain drugs from a mail order pharmacy as a condition of coverage.9
Other state laws prohibit reimbursement schemes that induce subscribers to use mail-order pharmacists. The Nebraska law provides an example:
A medical benefit contract . . . which provides reimbursement for prescription drugs and other pharmacy services shall not impose upon any person . . . a fee or copayment not equally imposed upon any party . . . utilizing a mail order pharmacy, and no such contract shall provide differences in coverage or impose any different conditions upon any person . . . not equally imposed upon any party . . . utilizing a mail order pharmacy. 10
Some states have passed laws that apply only to out-of-state pharmacies (also called nonresident pharmacies), allowing health plans to encourage the use of mail order within the state.11 Many states have additional laws regulating the practice of out-of-state pharmacists who provide medications to people in the state, mail order or otherwise. These laws generally require the out-of-state pharmacy to register within the state. Many states focus primarily on registration and disclosure requirements, but a few states also require out-of-state pharmacies to be licensed in and to follow the drug laws of the state.
Page 184 of 469

AHM 510 : Health Plans : Governance and Regulation
This requirement poses a problem for a pharmacist with an interstate practice if the laws of the state in which the pharmacist is located conflict with the laws of a state where customers reside. Conflicts are more likely to occur in states with extensive out-of-state pharmacy laws. Idaho, for example, requires out-of-state mail-order pharmacies to be licensed in Idaho, as well as in the state where the facility is located, provide detailed information on prescriptions or submit to inspection, identify all pharmacists, and comply with Idaho substitution laws. 12
Health plans with mail order pharmacies should be alert to patient counseling requirements and ensure that mail-order facilities comply with the patient counseling requirements of states in which customers are located. Some states have enacted patient counseling laws specifically directed at mail-order pharmacies. Florida and Kentucky, for example, require out of state mail-order pharmacies to provide a 40-hour-per-week toll-free service to allow customers to speak with a pharmacist. 13 California requires mail-order pharmacies to satisfy the same standards as state pharmacies with regard to patient counseling, except that face-to-face counseling is not required for mail-order transactions. 14
Regulation of Pharmacy PersonnelState and federal authorities regulate the qualifications and permissible activities of individuals participating in pharmacy practice. Violations of these laws and regulations could lead not only to enforcement procedures by state and federal authorities, but also to increased risk of liability, should a patient be injured by a medication error. Pharmacists are licensed professionals who must meet state qualification requirements in order to practice pharmacy lawfully. State laws specify the training and education required for a pharmacist to be licensed. The appropriate designation for the licensed pharmacists is "registered pharmacist." Licensing requirements generally include minimum standards of education, training, and experience; and evidence of competency through examination.
Drug SelectionEstablishing a formulary, adopting a policy of substituting generic drugs for brand name drugs, and excluding experimental and investigational drugs from coverage are common methods of managing pharmacy benefits.
FormulariesA formulary is a list of drugs, classified by therapeutic category or disease class, that is continually updated to represent the current clinical judgment of providers and experts in the diagnosis and treatment of disease.15 A formulary can reduce costs by promoting a uniform approach to prescribing and dispensing medication. Further, for health plans that operate their own pharmacy, a formulary eliminates the costs associated with stocking all available brands of a drug and permits economic savings associated with large volume purchases from just one supplier. Formularies are not a recent development; for years, they have been used by hospitals, government agencies, self-funded employers, pharmacy benefit management companies, and health plans. In 2003, 97% of HMOs used formularies.16 Thus, the formulary plays an important role in drug selection.
Federal law allows states to establish Medicaid drug formularies that identify pharmaceuticals for which Medicaid will provide payment.17 A state formulary must be
Page 185 of 469

AHM 510 : Health Plans : Governance and Regulation
established by a committee that includes physicians and pharmacists. A drug may be excluded from the formulary if, based on the labeling, it does not have a significant, clinically meaningful therapeutic advantage over other drugs in the formulary. Medicaid outpatient drug reimbursement plans may exclude or restrict coverage for anorectic agents, fertility drugs, antismoking agents, drugs intended for cosmetic use, and certain other substances.18 Many private health plans also exclude coverage for these medications.
Health plans have taken a variety of approaches with regard to implementing formularies. A health plan may cover only formulary drugs (known as a "closed formulary"), present the formulary as a recommendation (known as an "open formulary"), require preauthorization for nonformulary drugs, or offer financial incentives for prescribers and patients to use listed drugs. Over the past several years, the number of HMOs with closed formularies has increased significantly.19 Figure 6C-1 describes three key areas that health plans address in developing formulary policy.
Figure 6C-1. Liability Issues in Developing a Formulary Policy.
When developing a formulary policy, health plans should be aware that liability may arise in three areas:
1. Negligent Drug Selection: Traditionally, physicians have borne the responsibility for drug product selection. If a health plan requires a physician to choose a medication from a predetermined list of approved drugs, however, the plan injects itself into the drug selection process and exposes itself to the liability that may result if a patient is harmed by the formulary drug. Similarly, if a pharmacist substitutes a formulary drug for a prescribed drug, causing a patient injury, the health plan could be liable not only on the basis of the formulary policy, but also for the pharmacist's conduct. To reduce the potential liability, health plans at the least should establish a procedure for allowing physicians to prescribe medications outside the formulary and require pharmacists to contact prescribing physicians before substituting. Correspondence between the health plan and participating physicians and pharmacists should stress the medical, rather than cost, effectiveness of formulary drugs and should indicate that drug selection is a matter of the physicians' discretion. Health plans also should ensure that the formulary committee updates the formulary regularly, makes decisions based on medical effectiveness, and documents the decision process carefully.
2. Inadequate Disclosure: A patient not properly apprised of the scope of the drug benefit may sue on the basis of fraud or breach of contract. Health plans should review promotional materials and subscriber contracts to ensure that these materials are consistent with reliance on a formulary. A health plan that promotes its full prescription drug coverage, for example, may be open to suit if a patient is unable to obtain coverage for a medication not included in the formulary.
3. Effective Exclusion of a Condition: When developing a formulary, health plans must consider not only the effectiveness and cost of individual drugs, but also whether the formulary as a whole adequately addresses the variety of conditions for which subscribers will seek drug therapy. A health plan that does not cover the only drug therapy for a
Page 186 of 469

AHM 510 : Health Plans : Governance and Regulation
particular disease, for example, effectively excludes coverage for that disease and may be liable for breach of contract. Further, offering a reduced form of coverage for certain conditions by not covering drug therapy may run afoul of the Americans with Disabilities Act a federal law prohibiting differential treatment on the basis of disability.
Therapeutic SubstitutionTherapeutic substitution takes place when a pharmacist, with the prescribing physician's approval, replaces the drug originally prescribed with a drug that is the therapeutic equivalent. A drug is a therapeutic equivalent if it can be expected to produce an identical level of clinical effectiveness and sound medical outcomes.19 The formulary itself might list therapeutic equivalents. Or, to assess whether the medication prescribed is the therapeutic equivalent of a formulary drug, the pharmacist might consult clinically based prescribing guidelines developed and administered by a team of physicians, pharmacists, and other medical practitioners who are experts in the diagnosis and treatment of disease. Although state laws generally address only substitution of generic drugs for brand name drugs (see discussion below), the practice of pharmacy has included therapeutic substitution for many years, particularly in hospitals and HMOs. The Delaware legislature has acknowledged the practice by defining the role of the pharmacist to include therapeutic substitution20
Generic SubstitutionA generic medication or generic drug is a chemically equivalent version of a brand name drug. Substitution of generic medications for prescribed brand name drugs is a widely used method of healthcare cost containment. Some 73 percent of HMOs required generic drug substitution in 1993. 21 At one time, pharmacists in every state were prohibited from substituting one brand of a drug for another, unless the pharmacist obtained the express consent of the prescriber. With the growth of the consumer movement and the widespread view that antisubstitution laws were forcing the public to pay unwarranted higher prices for brand name products, every state has enacted legislation permitting pharmacists to disperse less expensive generic equivalents or, in some cases, requiring the substitution.
Health plan pharmacy providers must determine whether generic substitution is permissive or mandatory under state law. In Florida, substitution is mandatory, as the law states that "A pharmacist who receives a prescription for a brand name drug shall, unless requested otherwise by the purchaser, substitute a less expensive, generically equivalent drug product . . . "22 Maine provides an example of permissive substitution language: "Any pharmacist . . . may substitute a generic and therapeutically equivalent drug for the drug specified on the prescription, provided . . . that the price of the substituted drug does not exceed the price of the drug specified by the practitioner." 23
In every state, the prescriber can prevent the pharmacist from substituting a generic drug, although the method varies. In many states, prescribers use a two line prescription form. The prescriber signs the prescription on either a "substitution permitted" or "brand necessary" line. In other states, a physician who wishes to prevent substitution must hand-write a message such as "Do not substitute," or "Dispense as written" on the prescription. Some states allow prescription forms on which a physician may check a box prohibiting substitution.
Page 187 of 469

AHM 510 : Health Plans : Governance and Regulation
In most states, the pharmacist or a pharmacy employee must notify the patient or obtain the patient's consent before substituting a generic drug. For example, in Oregon, "The pharmacist, or the pharmacist's agent, assistant, or employee shall inform the person receiving the drug pursuant to the prescription of the selection of a lower cost generically equivalent drug, of the price difference between the brand name drug and the generically equivalent drug, and of the person's right to refuse the drug selected." 24
Further, pharmacies must label drug containers with the name of the generic drug dispensed, or risk violating misbranding provisions of the federal Food, Drug, and Cosmetic Act (FDCA), and state drug labeling law. Under the FDCA, a drug is misbranded if its label is "false or misleading in any particular."25 Violations of the FDCA can lead to civil or criminal penalties.26 State laws may contain labeling provisions specific to generic substitution. In addition to requiring labeling that reflects the name of the substituted generic medication, some states require additional notations, such as "Generic substitution made," 27 or "Interchange." 28
As a result of generic substitution, pharmacists and health plans assume increased responsibility, and increased potential for liability, as discussed previously in the context of therapeutic substitution. In the case of generic substitution, however, more than half of the state substitution statutes include language purporting to exempt the pharmacist from liability for selecting a generic equivalent. The Illinois statute states:
The selection of any drug product by a pharmacist shall not constitute evidence of negligence if the selected nonlegend drug product was of the same dosage form and each of its active ingredients did not vary by more than 1% from the active ingredients of the prescribed, brand name, nonlegend drug product or if the selected legend drug product was included in the Illinois Drug Product Selection Formulary at the time the prescription was dispensed.29
At least one state court has held that a pharmacist who selected brands pursuant to the state's generic drug law was not liable to a patient alleging injury as a result of taking the medication selected by the pharmacist.30 The court stated that a pharmacist is not negligent in selecting an alternate product unless an inferior or defective drug is knowingly dispensed. Nevertheless, pharmacists and health plans should evaluate substitution policies with an eye to potential liability that could result from a drug induced patient injury.
Coverage for Particular DrugsIn addition to developing a drug selection process, health plans may control drug benefit expenditure by limiting coverage of medications for which effectiveness has not been proved conclusively. The conflict between a health plan's need to spend funds wisely and patients' demand for promising innovative therapies requires careful drafting of the benefit contract.
Experimental and Investigational DrugsInsurance companies and health plans usually do not provide coverage for experimental and investigational therapies. There is a fine line between experimentation, investigational research, and treatment. Generally speaking, an experimental procedure or experimental drug is one that has not been tested for safety or effectiveness, or is being tested outside standard clinical trials. An investigational procedure or investigational drug is one that is being tested in humans for safety and effectiveness, in accordance with Food and Drug Administration requirements. Patients with life-threatening medical conditions not likely to respond to conventional treatments are likely
Page 188 of 469

AHM 510 : Health Plans : Governance and Regulation
to consider experimental and investigational drugs to be medical treatment that should be covered by their health plan. Although innovative drugs are extremely costly, and of uncertain therapeutic value, a court faced with a coverage decision may have difficulty denying a patient the only possibly successful treatment for a fatal condition. Thus, health plans must draft subscriber contracts and other benefit description material carefully to avoid litigation concerning coverage for experimental and investigational "treatments."
One way to exclude coverage for questionable treatments is to specifically identify the drugs that are not covered. Advancing technology makes it necessary to update the list of exclusions continuously, however, making subscriber notification a daunting task. Periodic lists of newly excluded treatments also may have a negative impact on subscribers' perception of the plan's coverage.
Legal challenges to experimental exclusions have occurred, specifically in the area of high dose chemotherapy and autologous bone marrow transplant (HDC/ABMT) as a treatment for breast cancer. The particular treatments that lead to litigation change over time, however. Advancing medical technology creates new treatments that will be sought by subscribers before insurers and health plans are willing to provide coverage. Older treatments lead to less litigation, as clinical data on the efficacy of a particular treatment either results in increased coverage or less demand for the treatment. Further, legislation may resolve disputes concerning the effectiveness of certain experimental or investigational treatments by mandating coverage. For example, at least two states have mandated coverage for high dose chemotherapy in conjunction with autologous bone marrow transplant.31 Before denying coverage for an experimental drug, particularly for terminal diseases such as cancer or AIDS, health plans should consult state law to determine whether coverage is mandated.
Health Plans should assess not only contract provisions, but also the decision making process involved in refusing coverage for an experimental drug. In addition to a suit for breach of contract, a patient denied access to a particular drug may sue a health plan based on negligent denial or bad faith denial of a claim. (See Key Legal Issues in Health Plans for a discussion of these types of legal risks.)
Off-Label Uses of Approved DrugsEven after a drug has been approved by the FDA, coverage disputes may arise when a healthcare provider prescribes a drug for a use not approved by the FDA. This type of prescription is known as an off label use (also called unlabeled or unapproved use). Off-label use refers to the use of a drug for clinical indications other than those stated in the labeling approved by the FDA. For example, using a drug for one form of cancer (e.g., prostate) when the drug had originally been approved by the FDA to treat other forms of cancer (e.g., breast, lung, etc.) is an off-label use. The FDA's long standing policy has been not to interfere with off label uses, citing a reluctance to interfere with the practice of medicine.32
The Omnibus Reconciliation Act of 1990 (OBRA '90) allows states to exclude Medicaid coverage of outpatient drugs when they are prescribed for a use other than a "medically accepted indication." 33 Similarly, many health plans exclude off label uses in the subscriber contract. Health plans should be cautious when denying coverage for the off-label use of approved drugs, however, as state law may mandate coverage. In
Page 189 of 469

AHM 510 : Health Plans : Governance and Regulation
Maryland, the law prohibits health insurance policies that provide drug coverage from excluding coverage of an FDA approved drug on the ground that the drug has not been approved for that particular indication, if medical literature recognizes the off label use.34
Other states have enacted narrower statutes, requiring coverage of off label drug use for treatment of cancer or AIDS only.35
Review Question
The following statements describe various state benefit mandates. Select the answer choice that describes a state law pertaining to off-label uses for drugs.
State A mandates that health plans provide benefits for experimental drugs for the treatment of terminal diseases such as AIDS and cancer. State B mandates that health plans have a procedure in place to allow a patient to have a non-formulary drug covered under certain conditions. State C mandates that, in dispensing generic drugs, pharmacies must label drug containers with the name of the substituted generic medication. State D mandates that health plans provide benefits for the treatment of one form of cancer with specific drugs that had originally been approved by the Food and Drug Administration (FDA) to treat other forms of cancer.
Incorrect. This type of mandate refers to experimental drugs
Incorrect. This type of mandate refers to therapeutic substitution
Incorrect. This type of mandate refers to generic substitution
Correct. Off-label use refers to the use of a drug for clinical indications other than those stated in the labeling approved by the FDA.
Drug PricingHealth plans have produced a heightened interest in the sales arrangements between drug manufacturers and healthcare providers. The increased networking of caregivers has resulted in a differential pricing structure. Entities that can engender competition among drug manufacturers, for example through formulary inclusion, can purchase medications at discounted prices.
Motivated in part by lobbying by retail pharmacists, legislatures at the state and federal level have considered measures that would place regulatory controls on manufacturer pricing practices. Litigation challenging differential drug pricing has also occurred as retail pharmacies sue manufacturers under long standing federal antitrust laws, such as the Robinson-Patman Act. (See Federal Regulation of Health Plans for a discussion of federal antitrust laws.)
Not-for-Profit ExemptionThe Nonprofit Institutions Act, an amendment to the Robinson Patman Act, allows not-for-profit hospitals and other not-for-profit charitable institutions to purchase drugs
Page 190 of 469
AHM 510 : Health Plans : Governance and Regulation
and other supplies at a discount, for their "own use."36 The primary issue under this exemption from antitrust/price discrimination enforcement is the definition of "own use."
The Supreme Court of the United States has considered the scope of this exemption and determined that the following sales of drugs were not for a not-for-profit hospital's own use (and therefore were subject to antitrust enforcement):
1. Sales to former patients of the hospital renewing prescriptions originally dispensed when patients were discharged from the hospital.
2. Sales to nondependents, e.g., friends of employees or medical staff members.
3. Sales to walk in customers with no connection with the hospital, e.g., patrons of a physician's office building.37
Review Question
The Nonprofit Institutions Act allows the Neighbor Hospital, a not-for-profit hospital, to purchase at a discount drugs for its 'own use'. Consider whether the following sales of drugs were not for Neighbor's own use and therefore were subject to antitrust enforcement:
• Elijah Jamison, a former patient of Neighbor, renewed a prescription that was originally dispensed when he was discharged from Neighbor.
• Neighbor filled a prescription for Camille Raynaud, who has no connection to Neighbor other than that her prescribing physician is located in a nearby physician's office building.
• Neighbor filled a prescription for Nigel Dixon, who is a friend of a Neighbor medical staff member.
With respect to the United States Supreme Court's definition of 'own use,' the drug sales that were not for Neighbor's own use were the sales that Neighbor made to
Mr. Jamison, Ms. Raynaud, and Mr. Dixon
Mr. Jamison and Ms. Raynaud only
Mr. Dixon only
none of these individuals
CorrectIncorrectIncorrectIncorrect
Not-for-profit hospitals selling drugs to customers in those three classes must purchase the drugs at the supplier's usual (not discounted) rate and must account separately for the sales or they will be outside the protection of the Nonprofit Institutions Act and subject to antitrust enforcement.38
Page 191 of 469

AHM 510 : Health Plans : Governance and Regulation
A not-for-profit HMO may sell pharmaceuticals to its members at a discount under the "own use" exemptions, the Ninth Circuit has held.39 The court cautioned, however, that sales to walk in customers who are not members are not exempt. As not-for-profit healthcare institutions move into related markets, such as home health agencies and ambulatory surgicenters, new issues may arise concerning the applicability of the exemption.
Other Drug Pricing RegulationsPharmaceutical pricing practices are regulated by a variety of other laws, such as the federal Prescription Drug Marketing Act, state and federal unitary pricing laws, and the Medicare and Medicaid fraud antikickback statute. These laws are discussed in Figure 6C-2.
Figure 6C-2. Other Drug Pricing Regulations.
Prescription Drug Marketing Act. In 1988, Congress enacted the Prescription Drug Marketing Act in response to concern that both public and private hospitals were continuing to receive drug discounts and resell drugs at a profit, thus competing unfairly with pharmaceutical retailers and wholesalers who are not entitled to such discounts. The law forbids hospitals and other healthcare entities to resell prescription pharmaceuticals. However, there are exceptions to the ban that allow resales under certain circumstances. The Act does not apply to:
1. The sale or dispensing of a drug pursuant to a valid prescription. 2. The purchase of drugs for a provider's own use from a group purchasing
organization of which it is a member. 3. The temporary transfer of drugs to a retail pharmacy for a medical emergency. 4. Sales among facilities under common control. 5. Sales between nonprofit affiliates.
The Prescription Drug Marketing Act also prohibits the sale, purchase, and trade of prescription drug samples. Drug samples are distributed without charge by manufacturers to promote their sale. Licensed practitioners, as well as healthcare professionals and hospital pharmacies acting at the direction of a licensed practitioner, may provide drug samples to patients.
Unitary Pricing Laws. Not satisfied with the provisions of the Robinson Patman Act and Prescription Drug Marketing Act, legislatures on the state and federal level have attempted in the past to eliminate manufacturer price differentials by enacting laws that directly mandate a single price for pharmaceutical sales. These statutes commonly are known as "best price" or "unitary pricing" laws. As of the date of this writing, Maine is the only state that has enacted such a law.
Federal Antikickback Law. The Medicare and Medicaid fraud antikickback statute prohibits certain financial inducements to purchase medical goods and services. With some exceptions, the law forbids offers and payments of remuneration (including rebates)
Page 192 of 469

AHM 510 : Health Plans : Governance and Regulation
made to induce any person to order, purchase, or recommend any good or service that may be paid for, in whole or in part, directly or indirectly, by Medicare or Medicaid.
Although this broadly worded statute could encompass many discounting practices common to prescription drug sales, the Department of Health and Human Services has established "safe harbors" that outline legal procedures for discounting goods. Entities complying with the safe-harbor requirements will not be subject to civil or criminal penalties.
Prescription drug marketing has come under scrutiny recently, however. The Health and Human Services Office of the Inspector General (OIG), responsible for prosecuting Medicare and Medicaid fraud, has issued a "Special Fraud Alert" outlining prescription drug marketing activities that the OIG may investigate under the federal antikickback statute. The alert specifically identifies three marketing activities that may implicate the antikickback statute:
1. Product conversion programs that offer cash rewards to pharmacies for switching prescriptions from one drug to another
2. Frequent flier campaigns that give physicians credit toward airline mileage for each new patient placed on a certain drug
3. Bogus research programs in which manufacturers pay physicians for providing minimal information, sometimes a single word, concerning the treatment outcome of patients placed on a drug
The OIG warns that violations of the antikickback law can result in exclusion from Medicare and Medicaid participation, as well as criminal prosecution. According to the alert, OIG investigation may be warranted based on the following marketing plan features: a prize, gift, cash payment, coupon, or bonus based on choice of drug product; cash or other benefits in exchange for pharmacist marketing activities under the guise of "counseling"; grants for product-related research of questionable scientific value; and payments to patients, providers, and suppliers for changing prescriptions. The alert urges individuals to contact their local OIG regional office with any information concerning possible violations.
Drug Utilization ReviewIn the past, pharmacy practice was focused primarily on the accurate delivery of drug products as specified by prescribers. Today, the practice of pharmacy is patient oriented. The pharmacist takes an active role in advising practitioners and patients about drug therapy. This role expansion was facilitated by recent federal legislation. Specifically, the Omnibus Budget Reconciliation Act of 1990 (OBRA '90) mandates prospective and retrospective drug utilization review (DUR) for Medicaid providers of outpatient drugs.40
Although OBRA '90 does not apply to hospitals (as long as the institutions use a formulary system and do not bill Medicaid more than their purchasing cost for the drug) or HMOs, it has brought DUR to the forefront.Prospective drug utilization review (prospective DUR) focuses on the drug therapy for a single patient, rather than on overall usage patterns. The purpose of prospective DUR is to allow the pharmacist to intervene before a drug is administered or dispensed to a patient, thus avoiding undesirable results. Although OBRA '90 mandated
Page 193 of 469

AHM 510 : Health Plans : Governance and Regulation
prospective DUR for Medicaid patients only, most states have extended the requirement to all patients, either by statute or rule.41 Prospective DUR consists of three components: documentation, screening, and counseling.
Documentation is a key component of prospective DUR because it serves as the basis for both screening and counseling. Many states require pharmacists to maintain patient profiles. In New Jersey, a broad statute requires all pharmacies to maintain patient profiles that allow "immediate retrieval" of information including the patient's identity, address, and telephone number, age, gender, known allergies, drug reaction, previously prescribed drugs, dispensing dates, initials of dispensing pharmacist, prescription number, prescriber, and drug dispensed.42 Massachusetts and Virginia require pharmacists to make "reasonable efforts" to maintain a similar list of information for each patient.43 By maintaining complete patient drug histories that include both prescribed and over the counter medications, the pharmacist can improve the quality of drug therapy. Failure to maintain proper patient documentation also may result in liability. A Tennessee appeals court has ruled that failing to maintain and review drug profiles may lead to liability.44
The second component of prospective DUR is screening. If the pharmacist's review of the patient's record yields problem findings or observations, they then are relayed to the attending practitioner during consultation. A Florida regulation specifically identifies the potential problems for which pharmacists should screen the patient profile: overutilization, underutilization, therapeutic duplication, drug drug interactions, drug disease contraindications, drug food interactions, incorrect dosage, incorrect duration of drug treatment, drug allergies, and drug abuse or misuse.45 Facilities that maintain records but fail to review them may be liable for failing to act.46
Prospective DUR culminates with patient counseling. A pharmacist may make an offer of counseling to a patient face to face, in writing, or by telephone, depending on both the circumstances and state law. Virginia, for example, allows the pharmacist to choose among face-to-face communication, a sign, a notation on the prescription bag or container, or by telephone.47 Florida requires both a written and verbal offer to counsel for patients present in the pharmacy, but allows a written offer for toll-free telephone counseling for delivered prescriptions.48 Pharmacists should ensure that their procedures comply with applicable state law.
The content of the counseling itself usually is left to the professional judgment of the pharmacist, although state laws and regulations may list subjects that a pharmacist might discuss. The pharmacist may address the name of the drug dispensed, dosage and route of administration, expected effects, special directions and precautions, potential interactions with other substances, common side effects, what to do in the event of a missed dose, and storage instructions. Most states require that a pharmacist meet face-to-face with the patient whenever possible.49
The pharmacist also may consult directly with prescribers in the planning of drug therapy, advising them on matters such as product selection, expected patient responses, and drug interactions. Consultation with prescribers may be required by state law if the pharmacist identifies a potential problem when screening a patient's drug profile.50 In addition, pharmacists may provide consultative services to nurses and others
Page 194 of 469

AHM 510 : Health Plans : Governance and Regulation
as to the proper techniques to use in preparing injectables, the administration of drugs requiring special handling, and other matters.
In addition to prospective review, focusing on each prescription for individual patients, retrospective drug utilization review (retrospective DUR) is necessary to determine whether a health plan is using drug therapy to its best advantage. For example, OBRA '90 requires that each state establish a board to conduct periodic review of Medicaid prescription drug claims.51 The goal of this retrospective review is to determine whether covered outpatient drugs are being used efficiently and appropriately. Health plans also conduct retrospective DUR to monitor practitioner prescribing practices and to determine the expense of the prescription drug benefit. Although hospitals are exempt from OBRA '90 requirements, Joint Commission standards now require a similar continuing review of drug use in hospitals.52
Review Question
The Good & Well Pharmacy, a Medicaid provider of outpatient drugs, is subject to the prospective drug utilization review (DUR) mandates of the Omnibus Budget Reconciliation Act of 1990 (OBRA '90). One component of prospective DUR is screening. In this context, when Good & Well is involved in the process of screening, the pharmacy is
updating a formulary to represent the current clinical judgment of providers and experts in the diagnosis and treatment of disease reviewing patient profiles for the purpose of identifying potential problems
consulting directly with prescribers and patients in the planning of drug therapy
denying coverage for the off-label use of approved drugs
IncorrectCorrectIncorrectIncorrect
Page 195 of 469

AHM 510 : Health Plans : Governance and Regulation
Chapter 6 DMarket Conduct Examinations and Mechanisms for Enforcement We conclude our review of state regulation of health plans with a discussion of market conduct examinations and the enforcement mechanisms that are available to state regulators to address violations of law.
After completing this lesson, you should be able to:
List the operations that a state insurance department reviews in conducting a market conduct examination
Describe the enforcement mechanisms available to states to address violations of law
Market Conduct ExaminationsFrom a regulatory perspective, market conduct is one of the most critical issues facing the insurance and health plan industries. A market conduct examination is a formal review that is carried out by one or more state insurance departments and is designed to determine whether a health plan's operations are conducted in compliance with applicable state laws and regulations.
With regard to health plans, the NAIC Market Conduct Examiners Handbook states, "Examinations are performed to determine treatment of enrollees, to measure the quality of care procedures employed by an HMO in conjunction with any other appropriate health regulatory agency, and to determine compliance with statutory provisions relating to contractual arrangements for both providers and enrollees."1
The states have developed procedures that insurance departments follow to examine health plan operations to determine whether these operations are conducting business in compliance with state laws and regulations. The procedures that are followed in undertaking market conduct examinations are designed to provide state regulators with information they can use to detect when a health plan is not in compliance with state laws and regulations and, if necessary, to determine what enforcement action is appropriate. Following some well-publicized cases of market conduct violations in the insurance industry, the NAIC has developed a number of new model laws, and state regulators have imposed new regulatory requirements on the activities of insurers and health plans. Insight 6D-1 provides an NAIC view of the growth of market conduct examinations for all risk-bearing entities in the United States.
Insight 6D-1. The Growth of Market Conduct Oversight in the 1990s.
By John C. ManciniIt has been said many times over the past few years: Market conduct is the issue of the decade. In 1990, state insurance departments conducted 1,018 market conduct examinations with 286 staff and 71 contract market conduct examiners. Contrast these statistics to 1995 when state insurance departments conducted 1,511 market conduct examinations with 364 staff and 85 contract market conduct examiners. Over this period, the number of examinations increased 48% and the total number of market conduct
Page 196 of 469

AHM 510 : Health Plans : Governance and Regulation
examiners increased 26%. Clearly there has been increased attention to market conduct because this growth occurred during a period when total state insurance department staffs only grew 4.5%, from 9,323 to 9,751. In the 1990s, has greater attention been focused on market conduct, consumer protection, and compliance? You bet it has. Are state insurance departments, like most other business sectors, more efficient and productive today than they were in 1990? Certainly.
What are the reasons for this growth? I think there are several reasons that stand out. In the late 1980s and early 1990s, some members of Congress were espousing federal regulation of insurance. This threat brought greater attention to several areas of state insurance regulation, including consumer protection. A second reason for the increased attention focuses on the methods used to sell insurance products. Recently, allegations of churning and misrepresentation by agents and companies in the sale and marketing of life insurance products have been in the forefront, including a number of nationwide class actions. However, in the 1990s market conduct attention has been extended to all lines of business and touched virtually every segment of the insurance industry. Problems with the sale of Medicare supplement policies led to reforms in that area earlier this decade. In the early and mid-1990s, state insurance regulators and other agencies, such as the U.S. Department of Housing and Urban Development (HUD), investigated allegations of redlining by property/casualty insurers, particularly in urban areas. Finally, the information revolution and improved technology of the 1990s have changed the way that the insurance business is conducted. There is more information available and it flows much faster and more efficiently than it ever has. Regulators have had to keep up.
Not only has this heightened attention resulted in more examiners and more examinations, but it has also resulted in increased attention to market conduct at the NAIC. The NAIC's Market Conduct Examiners Handbook has been completely overhauled since 1994. An annual Chief Examiners Forum is held to bring the top state personnel working in the Market Conduct area together to discuss issues of common concern. And, the amount of information in the NAIC's Market Information Systems (MIS) is increasing proportionally. Today, the NAIC maintains market conduct databases with over 100,000 regulatory actions and over 1.2 million consumer complaint records, allowing insurance regulators and the public to get a good picture of the market behaviors of agents and companies.
Where are we going from here? Many changes are likely to occur over the remainder of the decade of the 1990s. These changes will take many forms, including information technology improvements both by the insurance industry and by insurance regulators. The Internet, expansion into new products and services, and financial services modernization will all have a significant impact on the business of insurance and the business of insurance regulation.
Source: John C. Mancini is Market Affairs Manager for the National Association of Insurance Commissioners.
To carry out a market conduct examination, representatives of a state insurance department, called examiners, visit the insurer or health plan's home or regional office and examine the business records of the company. The team of examiners is composed
Page 197 of 469

AHM 510 : Health Plans : Governance and Regulation
of specially trained insurance department employees or independent examiners hired by the insurance department, or both. One individual functions as the examiner-in-charge and is responsible for the conduct of the examination and supervision of the team of examiners. The insurer or health plan usually appoints one of its employees to serve as the examination coordinator, with responsibility for facilitating the examination. For example, if the examiners have questions or need additional information, they make those requests to the examination coordinator, who is responsible for obtaining the information.
The specific types of business records the examiners review vary depending on the scope of the examination. An on-site market conduct examination may be either a comprehensive examination of all market conduct operations or a target examination of one or only a few facets of a health plan's conduct operations. For example, a target examination might focus on one line of a health plan's business or on specific functions such as underwriting or claims. We describe the scope of a comprehensive market conduct examination later in this lesson.
Many state insurance departments conduct a follow-up examination, known as a reexamination, some time after the completion of a comprehensive or target examination. An insurance department's focus in a reexamination is to determine whether an insurer or health plan has complied with recommendations or directives contained in a previous examination.
In addition to on-site examinations, state insurance departments sometimes conduct desk examinations in which they review some of a health plan's business records in the offices of the insurance department. A health plan that is the subject of a desk examination is required to provide all necessary materials to the insurance department. A desk examination is generally limited in scope as compared to an on-site examination. For example, an insurance department might request that a health plan send a list of all contract forms and evidence of coverage forms used within a specified time period to determine if the health plan is in compliance with state filing requirements. Or an insurance department may receive a series of consumer complaints about a specific aspect of a health plan's operations. The insurance department then might require the health plan to provide the department with its files and correspondence relating to those complaints. The department would use those records to conduct a desk examination as part of its investigation of the consumer complaints.
Multistate Cooperative ExaminationsEvery state in which a health plan is licensed to conduct business has authority to examine the health plan's market conduct practices within its jurisdictional boundaries. States cooperate extensively in performing financial examinations of insurers and health plans to avoid duplication of effort. In the case of financial examinations, multistate examinations are appropriate because the focus of each state's concern is the entity's financial condition, and that condition does not vary from state to state. In addition, regulatory requirements concerning a health plan's financial condition tend to be quite similar from state to state.
In contrast, a health plan's market conduct practices may not be exactly the same in each jurisdiction or geographic region in which it operates. A health plan, for example, will likely sell different products in different geographic locations, and its market conduct
Page 198 of 469

AHM 510 : Health Plans : Governance and Regulation
practices might vary from product to product. Similarly, regulatory requirements concerning market conduct vary from state to state more than do requirements concerning solvency. Nevertheless, it may be appropriate in some cases for the insurance departments of several states to perform a multistate cooperative examination-that is, a market conduct examination performed on behalf of a number of states that have agreed upon the standards against which the health plan will be evaluated. The NAIC Market Conduct Examiners Handbook identifies three situations in which an insurer or health plan is a candidate for a multistate cooperative examination:
1. Examination of an insurer's or health plan's group business. A multistate examination is appropriate when an insurer or health plan maintains a sufficiently large block of group insurance covering individuals in a number of jurisdictions.
2. Examination of an insurer's or health plan's national business. A multistate examination is appropriate when an insurer or health plan issues large blocks of business across the country using consistent underwriting, pricing, advertising, and claims processing practices.
3. Examination of an insurer's or health plan's regionalized business. A multistate examination is appropriate when an insurer's or health plan's regional office conducts business in a number of states.
Examination SchedulingMost states' laws require the state insurance department to perform periodic examinations-including financial and market conduct examinations-of each insurer or health plan licensed to conduct business in the state. The HMO Model Act requires the state department of insurance to conduct a comprehensive examination of an HMO's operations at least every three years. Many states require each licensed insurer to be examined at least every three to five years. Other states conduct market conduct examinations when they identify specific complaints about a health plan's market conduct activities or have some specific concern about a health plan's operations. The insurer or health plan is required to bear all costs of the examination.
The NAIC has developed an electronic system, known as the Examination Tracking System (ETS), that enables the states to schedule and coordinate market conduct examinations, as well as financial examinations. A state that plans to schedule an examination may notify the other states by entering the information into the ETS. Other states then have the opportunity to participate in the examination.
Review Question
Greenpath Health Services, Inc., an HMO, recently terminated some providers from its network in response to the changing enrollment and geographic needs of the plan. A provision in Greenpath's contracts with its healthcare providers states that Greenpath can terminate the contract at any time, without providing any reason for the termination, by giving the other party a specified period of notice.
The state in which Greenpath operates has an HMO statute that is patterned on the NAIC HMO Model Act, which requires Greenpath to notify enrollees of any material change in its provider network. As required by the HMO Model Act, the state insurance
Page 199 of 469

AHM 510 : Health Plans : Governance and Regulation
department is conducting an examination of Greenpath's operations. The scope of the on-site examination covers all aspects of Greenpath's market conduct operations, including its compliance with regulatory requirements.
From the following answer choices, select the response that identifies the type of market conduct examination that is being performed on Greenpath and the frequency with which the HMO Model Act requires state insurance departments to conduct an examination of an HMO's operations.
Type of examination: comprehensive; Required frequency: annually
Type of examination: comprehensive; Required frequency: at least every three years Type of examination: target; Required frequency: annually
Type of examination: target; Required frequency: at least every three years
Incorrect. The HMO Model Act requires state insurance departments conduct a comprehensive exam of the HMO's operations at least every three years
Correct! The HMO Model Act requires state insurance departments conduct a comprehensive exam of the HMO's operations at least every three years
Incorrect. A target examination covers only a few facets of the health plan's conduct operations. HMO Model Act requires state insurance departments to conduct comprehensive market conduct examination every three years
Incorrect. While the HMO Model Act requires state insurance departments to conduct comprehensive market conduct examination every three years, a target examination covers only a few facets of the health plan's conduct operations.
A state insurance department that schedules a comprehensive examination typically notifies the health plan in writing in advance of the examination to allow time to prepare. The length of this notice period varies from state to state and ranges from a few weeks to as much as 60 days. The notification letter, which can be several pages long, usually includes the following types of information:
• A description of the scope of the examination, including the types of market conduct activities and the time period that will be reviewed (for example, all member and claims activities that took place from January 1, 2003 through June 31, 2004)
• The date the examination will begin and the date estimated for completion • The estimated cost of the examination and how that cost will be billed to the
health plan • Identification of the types of materials the insurer or health plan must provide,
such as its procedural guidelines, manuals, policy forms with notices of approval, advertising materials, and sales representatives' records
• Requests for information that will take time for the insurer or health plan to compile
Page 200 of 469

AHM 510 : Health Plans : Governance and Regulation
• Identification of the office space, supplies, and equipment the insurer or health plan is to provide for the examiners
In some cases, an insurance department has the right to perform an examination without giving prior notice. For example, if an insurance department has reason to believe that the rights of a member might be harmed if it delays conducting an examination, then the department is not required to provide advance notice of an examination. Similarly, if a health plan has a valid reason for needing more time to prepare, state insurance departments generally postpone the scheduled start date of an examination.
Examination TechniquesBefore beginning an on-site market conduct examination, the team of examiners will review a variety of documents to familiarize themselves with the health plan's operations. Examiners generally review the results of previous examinations of the health plan and note problem areas that should be reexamined. They also review the health plan's Annual Statements so that they can assess its financial condition.
Once the examiners arrive at the health plan's offices, they begin to review the business records. Because of the volume of those records, examiners usually are not physically able to review them all. Instead, examiners use statistical sampling techniques that enable them to review a representative sample of the records. For example, in order to review a PPO's records concerning non-network claims payments, the examiners would evaluate the total set of records and determine the appropriate method for selecting a portion of those records to examine. The examiners' goal is to select a sample that will lead them to the same conclusions about the PPO's claims payment procedures as they would have reached had they evaluated all of the records.
Scope of Market Conduct ExaminationsAll nonfinancial aspects of a health plan's operations are considered within the purview of market conduct. In this section, we identify and describe specific aspects of a health plan's operations that may be the subject of a market conduct examination. Although we describe the scope of a comprehensive market conduct examination here, keep in mind that specific operations might be the subject of a target examination.
If a health plan is part of a legal entity licensed as an insurer, then the health plan's operations might be included in a market conduct examination of the insurer's total book of business. If a health plan is a separate legal entity, such as an HMO that is a subsidiary of a parent insurance company, then that health plan would likely be subject to a separate market conduct examination.
During review of each aspect of a health plan's operations, market conduct examiners generally make the following determinations:
1. Has the health plan established standards to assure the activity is carried out effectively?
2. Do the health plan's standards comply with applicable regulatory requirements? 3. Is the activity being carried out so as to meet the established standards?
Company Plan Structure and ManagementIn evaluating a health plan's plan structure, operations, and management, examiners are
Page 201 of 469

AHM 510 : Health Plans : Governance and Regulation
concerned with whether the health plan is structured and governed to assure regulatory compliance. The types of records the examiners review include the certificate of authority, structure and contractual arrangements, audit plan materials, computer systems, and antifraud plans.
Certificate of AuthorityExaminers typically evaluate whether the health plan's operations conform to its certificate of authority. For example, they determine whether the entity is licensed as an HMO, a PPO, or another type of health plan and then determine if it is has been operating accordingly.
Structure and Contractual ArrangementsExaminers review the health plan's operations to determine if and how administrative activities are delegated. They also examine other structural features, such as the fee arrangements for reimbursing participating providers, provider referral procedures and constraints, ratio of physicians to members, availability and choice of physicians, and procedures for maintaining records.
Audit Plan MaterialsExaminers will want to know whether the health plan has established an internal audit system and/or compliance program by which it can detect and correct market conduct problems. Businesses have long used audits-both internal and external-to review their accounting and financial records for accuracy and appropriateness. Audits traditionally have included an evaluation of the effectiveness of the organization's internal financial control systems. Internal audit results are communicated to top management along with recommendations, if necessary, for corrective action.
Market conduct examiners review the health plan's audit plan and all accompanying procedures manuals. They also review audit reports to determine whether those reports provide management with meaningful information about regulatory compliance issues. Finally, examiners look at how management uses the information provided in audit reports. For example, does management respond to audit recommendations by adopting new procedures or modifying existing procedures? If not, then the examiners will want an explanation of management's response.
Computer SystemsHealth plans must keep a large volume of business records, and, thus, they have developed computer systems to assist them in maintaining those business records. Market conduct examiners evaluate the systems and procedures that are in place to maintain data. Examiners evaluate whether there are adequate safeguards and controls to assure the integrity of the information contained in the computerized records. Examiners also evaluate the health plan's disaster recovery plans. Should a health plan's records be lost following a disaster, the health plan must be able to recover the information and continue operations without significant interruptions.Antifraud PlanExaminers determine whether the health plan has established any required antifraud plan. Examiners then evaluate the plan to determine whether (1) it complies with statutory requirements and (2) written antifraud manuals and procedures provide enough detail for employees to understand how to perform their jobs in conformance with management's intent.
Page 202 of 469

AHM 510 : Health Plans : Governance and Regulation
Complaints and Grievance ProceduresMost states have laws that require insurers and health plans to maintain marketing and performance records, including complaint records. Examiners review the health plan's complaint logs and make the following determinations about its complaint handling procedures:
• Do the health plan's complaint records reflect all consumer complaints, including those received by the state insurance department? Do complaint records include all required information?
• Are there any patterns in the types of complaints received about the health plan? For example, do a significant number of complaints concern a specific product or are complaints concentrated in a specific geographic location? If examiners detect a pattern in complaints, they will follow up to locate the source of the complaints and may be required to broaden the scope of the market conduct examination.
• Has the health plan handled the complaints adequately and in compliance with regulatory requirements? For example, if the state imposes a time limit within which health plans must respond to complaints, examiners will study the health plan's response times.
In addition, many state HMO laws specify procedures for handling member grievances or appeals. In reviewing a health plan's grievance procedures, examiners typically seek to determine members' awareness of these procedures. They also review the health plan's grievance process, the minutes of the health plan's Grievance Committee, and other documentation supporting the process and the resolution of member appeals.
Marketing and SalesAll states impose regulatory requirements on the advertising and sales materials health plans use to market their products. Market conduct examination of advertising material includes comparing the materials to the policy forms they advertise to assure that the materials accurately represent the terms of the policy forms and comply with the applicable laws.
States hold health plans responsible for the content of all advertisements, whether the advertisements originate from the company's home office, an individual agent, or even an employer that is purchasing coverage from the health plan. A market conduct examination includes a review of procedures and controls the health plan has in place for reviewing all advertising and sales materials.
Sales Representative LicensingMarket conduct examinations include an evaluation of the health plan's compliance with sales representative licensing requirements and whether or not outside brokers were used. In this component of an examination, the health plan's records of licensing and appointment are compared to the state insurance department's records to verify that the records agree. The reasons for any discrepancies must be discovered to determine whether regulatory requirements have been violated.
Review Question
Page 203 of 469

AHM 510 : Health Plans : Governance and Regulation
The following statements are about market conduct examinations of health plans. Select the answer choice that contains the correct statement.
Multistate examinations are not appropriate for financial examinations, because regulatory requirements concerning a health plan's financial condition tend to vary from state to state. Market conduct examinations of a health plan's advertising and sales materials include comparing the advertising materials to the policies they advertise. Once an examination report is provided to the state insurance department, a health plan is not given an opportunity to present a formal objection to the report. In imposing sanctions on health plans, state insurance departments are required to follow federal sentencing guidelines.
Incorrect
Correct
Incorrect
Incorrect
OperationsExamination of health plan operations consists of evaluating compliance with regulatory requirements regarding all policy transactions other than claims payments. Examiners review files and periodic reports to evaluate how the health plan handled transactions such as billing, member enrollment, and member termination. Examinations focus on two primary issues:
1. Did the health plan handle policy transactions in a timely manner? 2. Did the health plan handle policy transactions in accordance with applicable
policy provisions and regulatory requirements?
Examiners may review the correspondence received by the health plan and the health plan's responses to that correspondence to determine if the health plan responded in a timely and appropriate manner.
Premium Rating, Underwriting, and Policy FormsA market conduct examination typically includes evaluation of the health plan's practices regarding premium rates and underwriting. In order to evaluate the health plan's rating practices, examiners review a variety of materials, including rate manuals, rate cards, and policy files. Examiners determine whether the health plan has filed premium rates, if required, and is applying premium rates consistently and in accordance with filed rates and its own rating methods. Examiners evaluate whether the health plan is charging the proper premiums and implementing premium rate increases properly.
Examiners review the health plan's underwriting practices to assure that they are not unfairly discriminatory and that they comply with applicable regulatory requirements. This step includes a review of the underwriting files to assure that underwriting is being
Page 204 of 469

AHM 510 : Health Plans : Governance and Regulation
performed in accordance with the health plan's guidelines. If underwriting guidelines are required to be filed with the state insurance department, examiners review the health plan's records to verify that required filings were made.
Examiners also review the health plan's policy filings to verify that, where required, the insurer has filed policy forms and received approval from the state insurance department before using those forms.
ClaimsMarket conduct examiners review the health plan's claims handling practices to verify that those practices comply with regulatory requirements and policy provisions. Examiners review the health plan's claims systems, procedures manuals, and available internal documents that describe claims handling practices. Then they review the methods the health plan uses to process claims. Examiners also review claims files to evaluate:
• The length of time required to investigate and settle claims
• Whether files contain adequate and accurate documentation
• Whether the amounts of claim payments made are accurately calculated
• Whether claims are paid to the correct payees
Examiners review the health plan's claim forms to verify that they are appropriate for the product and are used appropriately. Claim forms should request only information the health plan reasonably needs to evaluate the claim, and claimants should be able to complete the forms without unreasonable hardship.
Market conduct examiners also review the health plan's files of litigated claims-that is, claims that resulted in lawsuits. The focus of this review is to determine whether the health plan has improperly denied claims. Examiners also look for patterns in how the health plan handles claims and evaluate those patterns to verify that proper claims handling procedures have been followed.
Quality Assurance and Utilization ReviewExaminers determine the nature and scope of medical directors' responsibilities. They also determine if the health plan uses a Peer Review Committee and a Professional Review Committee and, if so, how frequently these committees meet, what activities they oversee, and how they are operated. Examiners determine if the health plan has established a system for medical audits and, if so, how management uses the information provided in audit reports. Examiners also evaluate a health plan's utilization review procedures by examining the appropriate information systems and by looking at how the health plan reviews and acts upon physician practice patterns and hospital utilization.
Anticompetitive PracticesIn some states, the market conduct exam also includes a review of operating or marketing practices that might have an anticompetitive impact. Whether or not an insurance department conducts such a review depends largely on the scope of its statutory authority.
Page 205 of 469

AHM 510 : Health Plans : Governance and Regulation
After the Market Conduct ExaminationMarket conduct examiners document their findings throughout an examination and complete an exception form each time their findings indicate possible noncompliance. Following completion of a market conduct examination, the team of examiners is responsible for summarizing its findings into a written examination report. The report lists the problems noted on all exception forms and makes recommendations as to steps the health plan should take to comply.
The examination report is provided to the state insurance department and the health plan. Although procedures vary from state to state, the health plan has the opportunity to discuss the report with the insurance department and, where appropriate, the report is corrected.
If the health plan objects to the report, it has the right to request a formal hearing before a hearing officer who is authorized to evaluate testimony and make a decision as to the contents of the final report. Once the report is finalized, the insurance department adopts it and places it on file. In most instances, the filed examination report becomes a public document. The insurance department typically provides a copy of the report to the appropriate health regulatory agency in the state and to the NAIC, which maintains the report in its information system.
Once an examination report is filed, the insurance department, where appropriate, issues an order to the health plan. This order lists the recommendations contained in the examination report and, in some cases, provides a date by which the health plan must provide the department with evidence that it has complied with the order.
Mechanisms for EnforcementAt times, a market conduct examination reveals that a health plan has violated certain insurance or HMO laws. Complaints from members, purchasers, or providers or an investigation by other regulatory authorities could lead to similar findings. For example, the office of the attorney general might receive a complaint from a competitor alleging antitrust activities on the part of a health plan. When a state determines that a health plan has violated a law or regulation, it has available to it several mechanisms for enforcement.
Most state laws give the appropriate regulatory agency the authority to order a health plan to "cease and desist" from violating a particular requirement. For example, if a health plan is found to be using a television commercial prior to obtaining applicable regulatory approval, the state can order the health plan to stop running that commercial. In addition, regulators can sanction a health plan. Sanctions often take the form of fines. The amount of the fine varies depending on the seriousness and frequency of the violation. State laws sometimes provide the insurance department with guidance on the amount of the fine that may be imposed for each specific violation. For example, the NAIC Unfair Claims Settlement Practices Act recommends fines of $1,000 for each violation up to a total limit of $100,000; in the event of a flagrant violation, the Claims Act recommends fines of $25,000 for each violation up to a total limit of $250,000.2 In extreme situations, a state might seek to suspend or revoke a health plan's certificate of authority.
Page 206 of 469

AHM 510 : Health Plans : Governance and Regulation
Failure to comply with applicable regulatory requirements could also lead to civil litigation, either as a breach of contract or a breach of a standard or duty of care, as Insight 6D-2 illustrates.
Insight 6D-2.
Failure to Comply with Advertising Requirements Can Lead to Significant Liability for a health plan
An unreported Idaho court decision (Warne v. Lincoln Natl. Admin. Serv. Corp., No. 96932) illustrates a health plan's liability with regard to marketing activities. In this situation, a health plan was sued for bad faith and fraud when it denied coverage for a liver transplant. The plaintiff, relying on a brochure that indicated that organ transplants were considered a covered benefit, was able to convince the jury that she had relied to her detriment on the advertised coverage. The defense was unable to convince the jury that other plan documentation, which denied almost all coverage for liver transplant procedures, was controlling. The jury found for the plaintiff and awarded her $25 million in punitive damages and $1.5 million for pain and suffering. In addition, the plaintiff was awarded over $300,000 for the denied covered benefit.
Although this case was subsequently settled, it does paint a threatening scenario for health plans that do not pay attention to the content of advertising and promotional materials. Source: Liability and Risk Management in Health Plan, p. 12:5
State laws require health plans to oversee their operations to assure regulatory compliance. In imposing sanctions on health plans, several state insurance departments have followed the lead the federal government has taken in its sentencing guidelines. Federal sentencing guidelines are used by federal courts to determine specific punishments that are to be imposed on organizations and individuals who violate federal laws. Note that state insurance departments are not required to follow the federal sentencing guidelines; rather, they voluntarily follow some of the practices contained in the guidelines. The primary influence of the federal sentencing guidelines on state insurance departments has been the policy of assessing the degree of blame to place on a company for allowing illegal activities to occur.
The guidelines recognize that all illegal behavior cannot be prevented, and they recommend less severe punishments for companies that have taken steps to prevent illegal activities. Thus, companies that have made good faith efforts to prevent employees from engaging in illegal activities receive a lesser fine than do companies that have not taken steps to assure regulatory compliance. We will examine the federal sentencing guidelines in greater detail in Goverance: Accountability and Leadership.
Review Question
SoundCare Health Services, a health plan, recently conducted a situation analysis. One step in this analysis required SoundCare to examine its current activities, its strengths and weaknesses, and its ability to respond to potential threats and opportunities in the environment. This activity provided SoundCare with a realistic appraisal of its capabilities. One weakness that SoundCare identified during this process was that it
Page 207 of 469

AHM 510 : Health Plans : Governance and Regulation
lacked an effective program for preventing and detecting violations of law. SoundCare decided to remedy this weakness by using the 1991 Federal Sentencing Guidelines for Organizations as a model for its compliance program.
By definition, the activity that SoundCare conducted when it examined its strengths, weaknesses, and capabilities is known as
an environmental analysis
an internal assessment
an environmental forecast
a community analysis
IncorrectCorrectIncorrectIncorrect
Page 208 of 469

AHM 510 : Health Plans : Governance and Regulation
Chapter 7 AFederal Regulation of Health Plans In Overview of Laws and Regulations, we introduced the HMO Act of 1973 and described its history and its major provisions. In this lesson, we explore the major amendments to the HMO Act and discuss the advantages and disadvantages of federal qualification as well as the operational and quality requirements with which federally qualified HMOs must comply. We conclude the lesson with an examination of Centers for Medicare and Medicaid (CMS)'s role as the enforcer of federal HMO standards.
After completing this lesson, you should be able to:
Describe some of the operational and quality requirements that federally qualified HMOs must meet
Explain some of the administrative burdens that the Health Insurance Portability and Accountability Act of 1996 (HIPAA) imposes on health plans
Describe the general provisions of the Mental Health Parity Act of 1996 and the Newborns’ and Mothers’ Health Protection Act of 1996
Explain several typical applications to health plans of the Americans with Disabilities Act
Federal Qualification and the HMO Act of 1973The HMO Act, enacted in 1973, defined the standards for developing and operating HMOs. The HMO Act also established the requirements necessary for HMOs to be federally qualified. An HMO that applies for and meets the federal qualification requirements whose application is approved becomes a federally qualified HMO. Amendments to the HMO Act were made from 1976 to 1996. The 1976 amendments allowed some flexibility related to community rating, open enrollment, and medical staffing.1 Subsequent amendments addressed such issues as financial disclosure and solvency protection. A 1986 amendment eliminated the federal grant and loan program, created to encourage the development of HMOs. Amendments added in 1988 made several significant changes to the HMO Act. These changes included:
• Allowing federally qualified HMOs to provide up to 10% of physician services through nonaffiliated physicians and allowing reasonable deductibles for such services
• Allowing federally qualified HMOs to establish non-federally qualifiable separate lines of business
• Authorizing the repeal-effective in 1995-of the mandate requiring that employers who offered a health insurance option also offer an HMO if one was available in the geographic area (often referred to as the "dual-choice" mandate)
• Expanding the definition of restrictive state laws that are preempted by the HMO Act
• Requiring disclosure of the data and methods HMOs use to set their rates
• Addressing nondiscrimination in the financing of employee plans
• Eliminating the requirements that at least one-third of an HMO's policy-making body be comprised of HMO members
• Abolishing the provision that required representation of underserved communities on the HMO's policy-making body2
Page 209 of 469
AHM 510 : Health Plans : Governance and Regulation
In 1996, another amendment to the HMO Act was included as a provision of HIPAA. This amendment allows federally qualified HMOs to offer high-deductible plans.3 In the following lessons, we will discuss the requirements for federal qualification and look at the pros and cons of obtaining federal qualification. As described in the following lessons, the federal qualification program played a much more important role for HMOs in the past than it does today.Operational Requirements for Qualification4
HMOs sought federal qualification had to meet requirements in four basic operational areas. First, the HMO had to offer a comprehensive basic benefits package that included outpatient and inpatient services, unlimited home health benefits, and outpatient mental health visits. HMOs could deliver these services through one of four permissible delivery models: staff, group, individual practice association, or direct contract. Second, the HMO had to enroll individuals eligible for group coverage without regard to health status and established their prepayment charges on a community-rated basis with nominal copayments by members.
Third, HMOs needed to have a fiscally sound operation and adequate protections against the risk of insolvency. For example, one measure of fiscal soundness was for the HMO to demonstrate that its total assets are greater than its total unsubordinated liabilities. Finally, with respect to the quality of the care that federally qualified HMOs provided, the HMO had arrangements for an ongoing quality assurance program that met CMS (formerly HCFA) requirements, stressed outcomes, and provided for review by physicians and other health professionals.
Fast Definition
Unsubordinated liabilities-A "subordinated liability" is a liability that is payable only after all other liabilities hare paid. Unsubordinated liabilities are all other liabilities.
Review Question
Health maintenance organizations (HMOs) seeking federal qualification under the HMO Act of 1973 and its amendments must meet requirements in four basic operational areas. One operational requirement for qualification is that an HMO must
ensure that at least 1/3 of its policy-making body is comprised of HMO members
ensure that there is adequate representation of underserved communities on its policy-making body have an ongoing quality assurance program that meets the requirements of the Centers for Medicaid & Medicare Services (CMS), stresses health outcomes, and provides for review by health professionals test, safeguard, and promote quality of care by following detailed programmatic techniques that are explained in CMS's Federally Qualified HMO (FQHMO) Manual
Page 210 of 469

AHM 510 : Health Plans : Governance and Regulation
Incorrect. While a basic qualification requirement is that an HMO must have a fiscally sound operation, the make-up of the board is not specifically prescribed
Incorrect. While a basic qualification requirement is that an HMO must have a fiscally sound operation, the make-up of the board is not specifically prescribed
Correct! A basic qualification requirement was that an HMO had arrangements for an ongoing quality assurance program that met CMS (formerly HCFA) requirements, stressed outcomes, and provided for review by physicians and other health professionals.
Incorrect. The quality assurance program regulations adopted by HCFA at the time focused on process, access, and continuity of care. These regulations are explained further in the Federally Qualified HMO (FQHMO) Manual. In addition, the FQHMO Manual provided detailed optional 'programmatic techniques' that HMOs could use 'to test, safeguard, and promote quality of care.' While the techniques are optional, the HMO had to meet underlying quality assurance requirements to retain federal HMO qualification.
Quality of Care Requirements for Qualification5
The quality assurance program regulations adopted by HCFA at the time focused on process, access, and continuity of care. These regulations are explained further in the Federally Qualified HMO (FQHMO) Manual. In addition, the FQHMO Manual provided detailed optional "programmatic techniques" that HMOs could use "to test, safeguard, and promote quality of care." While the techniques are optional, the HMO had to meet underlying quality assurance requirements to retain federal HMO qualification.
Regarding process, federally qualified HMOs needed to have an ongoing quality assurance (QA) program that
1. Stressed health outcomes to the extent consistent with the state of the art 2. Provided review by physicians and other health professionals of the process
followed to provide health services 3. Collected data on performance and patient results and provides interpretations to
its professionals and institutes change as necessary 4. Had written procedures to take appropriate remedial action whenever
substandard services are provided or whenever necessary care was not provided
Under the FQHMO Manual, the QA program needed a written plan that was reviewed annually by the HMO's board. In addition, the program must be directed by an HMO physician, be adequately staffed, and report regularly to the policy-making body of the HMO about its activities and actions taken in response to its findings. Federally qualified HMOs also needed to provide to enrollees services that were available and accessible with "reasonable promptness" and "within generally accepted norms for meeting projected enrollment needs." The HMO was explicitly required to make medically necessary emergency services available 24 hours a day, seven days a week. With respect to continuity of care, federally qualified HMOs required enrollees to use a single health professional, usually known as a gatekeeper, to coordinate each enrollee's overall
Page 211 of 469

AHM 510 : Health Plans : Governance and Regulation
care. While this system is often seen as a utilization control, which it is, it began as (and in its best iterations continues to be) a powerful technique to assure continuity in the delivery system. The HMO also was required to keep necessary medical and nonmedical records and assure their confidentiality.
Enforcement for Federally Qualified HMOs6
CMS does not conduct regular surveys to assure that the HMO continues to meet federal qualification standards; however, CMS will conduct necessary investigations, generally in response to enrollee complaints. These complaints are brought to CMS's attention through complaints by enrollees or competing health plans.
Federal Qualification: Then and Now7
While federal qualification is entirely voluntary, HMOs that elected to meet federal qualification requirements historically gained two basic advantages. First, HMOs were eligible to participate in Medicare as risk or cost contractors without submitting additional documentation to qualify as Medicare contractors. Second, certain employers used federal qualification status to determine which HMOs to offer to their employees, viewing federal qualification as a "stamp of approval" from the federal government.
The Balanced Budget Act of 1997 (BBA) made changes to the Medicare law that, in effect, eliminate the first advantage cited above. As for the second advantage, employers are increasingly looking to private accreditation status, rather than federal qualification, as an indicator of a high quality health plan.
Until October 1995, the federal HMO law gave federally qualified HMOs the right to require certain employers to offer the HMO as part of their health benefits program if the employers were not already offering a federally qualified HMO. If the employer offered a health insurance option and a federally qualified HMO was available in that area, the employer had to offer it, too, through this "dual choice mandate" if requested by the federally qualified HMO. Although the mandate lapsed, employers that contribute to the cost of health insurance for their employees may not discriminate in the amount of the contribution the employer will make toward health care costs if the employee selects a federally qualified HMO as opposed to other plans offered by the employer.
In the past, the federal HMO Act gave federally qualified HMOs the right to require certain employers to offer the HMO as part of their health benefits program if the employers were not already offering a federally qualified HMO. If the employer offered a health insurance option and a federally qualified HMO was available in that area, the employer had to offer it, too, through this "dual choice mandate" if requested by the federally qualified HMO. Although the "dual choice mandate" lapsed in 1995, employers that contributed to the cost of health insurance for their employees may not discriminate in the amount of the contribution the employer will make toward healthcare costs if the employee selects a federally qualified HMO as opposed to other plans offered by the employer.
The HMO Act initially required a federally qualified HMO to be a distinct legal entity and not part of a non-federally qualified HMO. This requirement, which was repealed by Congress in 1988, stifled the flexibility of HMOs that wanted to offer product lines that were not federally qualified. Under current law, federally qualified HMOs can now market nonqualified product lines separate and apart from the federally qualified HMO, with
Page 212 of 469

AHM 510 : Health Plans : Governance and Regulation
benefits and rates that would not be permitted for a federally qualified HMO. This change allowed HMOs to offer benefit plans without conforming to the rigid benefit and community rating requirements. Some HMOs viewed these requirements as burdensome. Although federal qualification is voluntary, and newly created HMOs may not seek federal qualification, about one third of the operational HMOs in the US currently meet qualification requirements.
Health Insurance Portability and Accountability Act of 1996 (HIPAA)A federal law that more significantly impacts health plans today is the Health Insurance Portability and Accountability Act of 1996 (HIPAA). HIPAA is a federal law that includes provisions designed to make healthcare coverage available and portable by creating standardds applicable to access, portability, and renewability in both the group and individual markets. As noted in Overview of Laws and Regulations, HIPAA affects health plans in several ways, many of which are discussed in the following lessons.
Portability and Pre-Existing ConditionsHIPAA eliminates one obstacle for many individuals who desire to leave their current jobs but who are concerned that a potential employer's health plan may exclude pre-existing conditions. In effect, health coverage is made portable for individuals and their dependents. Such individuals and their dependents are considered to be continuously covered (as discussed below) under employer-sponsored plans.
The following federal requirements are related to health insurance portability. However, these requirements serve as a "floor" for protecting individuals and groups seeking insurance coverage. State law may be more protective, e.g., may require shorter periods of pre-existing condition exclusion or may allow for longer breaks in coverage.
Group health plans and health insurance issuers offering group health coverage may only impose pre-existing condition exclusions if the exclusion is related to a condition for which medical advice, diagnosis, or treatment was given within the prior six months. Under HIPAA, the term health insurance issuer means an insurance company, insurance service, or insurance organization; insurance organizations include HMOs and other risk-bearing health plans.
Pre-existing condition exclusions may only be applied for a period of 12 months, in the case of employer group coverage-18 months for a late enrollee (defined below)-and the period must be reduced by the length of the aggregate period of prior creditable coverage. Creditable coverage is continuous healthcare coverage under a plan that reduces the amount of time a pre-existing condition clause in a plan can apply to an individual. Therefore, if an enrollee has 12 months of prior creditable coverage without a significant break in coverage (or a late enrollee has 18 months of prior creditable coverage without such a break), a plan may not impose a pre-existing condition exclusion period. A break in coverage of more than 63 days is considered a significant break in coverage. The following further clarify creditable coverage and the use of pre-existing condition exclusions:
• Plans may not impose a pre-existing condition exclusion period on a newborn, an adopted child, or a child under 18 placed for adoption as long as the individual becomes covered under creditable coverage within 20 days of
Page 213 of 469

AHM 510 : Health Plans : Governance and Regulation
birth, adoption, or placement for adoption. Pre-existing condition exclusions cannot apply to pregnancies.
• Creditable coverage includes coverage of the individual under a group health plan, health insurance coverage, Medicare, Medicaid, military-sponsored health care, an Indian Health Service program, a state risk pool, FEHBP, a public health plan, or health plan under the Peace Corps.
• A late enrollee is a person who enrolls under an employer group plan other than during the first period in which the person is eligible or other than during a "special enrollment period" during which HIPAA requires a plan to accept the person's enrollment.
• A person establishes creditable coverage through presentation of certifications describing previous coverage or other procedures set forth in the implementing regulations.
Health insurance issuers offering coverage in the individual market may not impose exclusions for pre-existing conditions on eligible individuals. Individual-market-eligible individuals are persons:
• With at least 18 or more months of aggregate creditable coverage
• With their most recent prior coverage from a group health plan, governmental plan, or church plan
• Who are ineligible for Medicare Parts A or B and Medicaid
• Without any other health insurance coverag
• Who were not terminated from their most recent prior coverage for nonpayment of premiums or fraud
• Who-if eligible for continuation coverage under COBRA or a similar state program-elected and exhausted this coverage
States have flexibility in assuring this guarantee is met through a variety of mechanisms-known as "alternative mechanisms"-including health insurance coverage pools or programs, mandatory group conversion policies, open enrollment to individuals by one or more insurers, or laws requiring guaranteed issue. If the state does not have a mechanism to ensure group-to-individual portability, the federal requirement applies.
Affiliation PeriodsAn affiliation period is a period of time that must expire before coverage becomes effective. A group health plan that offers coverage through an HMO may impose affiliation periods of up to two months (three months for late enrollees) if the plan does not impose a pre-existing condition limitation and the period is applied uniformly without respect to any health status-related factors. An affiliation period is a period of time that must expire before coverage becomes effective. During this period, no premium is paid and no benefits or services are provided.
Administrative RequirementsGroup health plans and health insurance issuers must provide each plan member with a certificate of creditable coverage, a document that verifies the creditable coverage earned by the member, at the time the member ceases to be covered under a plan or
Page 214 of 469

AHM 510 : Health Plans : Governance and Regulation
begins COBRA continuation coverage. Such certificates must also be provided when COBRA coverage ends and at the request of a former enrollee if that request is made within 24 months of the expiration of that enrollee's health coverage.Guaranteed IssueIn general, HIPAA requires that issuers offering coverage in the small group market (defined as employers with two to 50 employees) must guarantee issue of health insurance to every small employer applying for coverage. An issuer cannot exclude an employee or his or her dependents from coverage or discriminate with respect to premiums on the basis of health status.
A network plan may limit employers that may apply for coverage to those in the plan's service area or may deny coverage based on network capacity. A network plan may also limit the individuals applying for coverage to those who live or work in the plan's service area or deny coverage based on network capacity.
Issuers offering coverage in the individual market must guarantee issue to individual-market-eligible individuals (discussed earlier).
Similar to the ban on imposing pre-existing condition exclusions on individual-market-eligible individuals, the requirement that issuers guarantee issue to individuals only applies in states that have not implemented "alternative mechanisms" to ensure group-to-individual portability.
Guaranteed RenewalWith limited exceptions, issuers offering group health coverage must renew group health policies in both small and large group markets, regardless of the health status of any member. Issuers offering coverage in the individual market must also renew individual policies, except in limited circumstances. This requirement applies regardless of whether the state has implemented an "alternative mechanism."
Review Question
A federal law that significantly affects health plans is the Health Insurance Portability and Accountability Act of 1996 (HIPAA). In order to comply with HIPAA provisions, issuers offering group health coverage generally must.
A. Renew group health policies in both small and large group markets, regardless of the health status of any group member
B. Provide a plan member with a certificate of creditable coverage at the time the member enrolls in the group plan
Both A and B
A only
B only
Neither A nor B
Page 215 of 469

AHM 510 : Health Plans : Governance and Regulation
Incorrect. While HIPAA does require insurers offering group health coverage to renew group health policies in small and large group markets, regardless of the health status of any group member, it does not require the insurer provide a certificate of creditable coverage when the member enrolls in the group plan.
Correct. HIPAA does require insurers offering group health coverage to renew group health policies in small and large group markets, regardless of the health status of any group member and does not require the insurer provide a certificate of creditable coverage when the member enrolls in the group plan.
Incorrect. HIPAA does not require the insurer provide a certificate of creditable coverage when the member enrolls in the group plan.
Incorrect. While HIPAA does require insurers offering group health coverage to renew group health policies in small and large group markets, regardless of the health status of any group member, it does not require the insurer provide a certificate of creditable coverage when the member enrolls in the group plan.
Health Information PrivacyHIPAA required the Secretary to issue privacy regulations governing individually identifiable health information, if Congress did not enact privacy legislation within three years of the passage of HIPAA. Because Congress did not enact privacy legislation, HHS promulgated regulations for individually identifiable electronic health information that healthcare providers, health plans, and healthcare clearinghouses must follow. HHS developed a proposed rule and released it for public comment on November 3, 1999. The final regulation, the Privacy Rule, was published December 28, 2000 and final modifications were published in final form on August 14, 2002.
Individually identifiable health information is information, including demographic data, that relates to:
• the individual's past, present or future physical or mental health or condition, • the provision of health care to the individual, or t • he past, present, or future payment for the provision of health care to the
individual, and that identifies the individual or for which there is a reasonable basis to believe can be used to identify the individual.
Individually identifiable health information includes many common identifiers (e.g., name, address, birth date, Social Security Number).
A major purpose of the Privacy Rule is to define and limit the circumstances in which an individual's protected health information may be used or disclosed by covered entities. A covered entity may not use or disclose protected health information, except either: (1) as the Privacy Rule permits or requires; or (2) as the individual who is the subject of the information (or the individual's personal representative) authorizes in writing.
Page 216 of 469

AHM 510 : Health Plans : Governance and Regulation
Required Disclosures. A covered entity must disclose protected health information in only two situations:
a. to individuals (or their personal representatives) specifically when they request access to, or an accounting of disclosures of, their protected health information
b. to HHS when it is undertaking a compliance investigation or review or enforcement action.
Permitted Uses and Disclosures. A covered entity is permitted, but not required, to use and disclose protected health information, without an individual's authorization, for the following purposes or situations:
1. To the Individual (unless required for access or accounting of disclosures) A covered entity may disclose protected health information to the individual who is the subject of the information.
2. Treatment, Payment, and Health Care Operations; A covered entity may use and disclose protected health information for its own treatment, payment, and health care operations activities. A covered entity also may disclose protected health information for the treatment activities of any health care provider, the payment activities of another covered entity and of any health care provider, or the health care operations of another covered entity involving either quality or competency assurance activities or fraud and abuse detection and compliance activities, if both covered entities have or had a relationship with the individual and the protected health information pertains to the relationship. Treatment is the provision, coordination, or management of health care and related services for an individual by one or more health care providers, including consultation between providers regarding a patient and referral of a patient by one provider to another. Payment encompasses activities of a health plan to obtain premiums, determine or fulfill responsibilities for coverage and provision of benefits, and furnish or obtain reimbursement for health care delivered to an individual and activities of a health care provider to obtain payment or be reimbursed for the provision of health care to an individual. Health care operations are any of the following activities: (a) quality assessment and improvement activities, including case management and care coordination; (b) competency assurance activities, including provider or health plan performance evaluation, credentialing, and accreditation; (c) conducting or arranging for medical reviews, audits, or legal services, including fraud and abuse detection and compliance programs; (d) specified insurance functions, such as underwriting, risk rating, and reinsuring risk; (e) business planning, development, management, and administration; and (f) business management and general administrative activities of the entity, including but not limited to: de-identifying protected health information, creating a limited data set, and certain fundraising for the benefit of the covered entity. Most uses and disclosures of psychotherapy notes for treatment, payment, and health care operations purposes require an authorization as described below. Obtaining consent (written permission from individuals to use and disclose their protected health information for treatment, payment, and health care operations) is optional under the Privacy Rule for all covered entities.
3. Opportunity to Agree or Object; Informal permission may be obtained by asking the individual outright, or by circumstances that clearly give the individual the opportunity to agree, acquiesce, or object. Where the individual is incapacitated,
Page 217 of 469

AHM 510 : Health Plans : Governance and Regulation
in an emergency situation, or not available, covered entities generally may make such uses and disclosures, if in the exercise of their professional judgment, the use or disclosure is determined to be in the best interests of the individual.
4. Incident to an otherwise permitted use and disclosure; The Privacy Rule does not require that every risk of an incidental use or disclosure of protected health information be eliminated. A use or disclosure of this information that occurs as a result of, or as incident to, an otherwise permitted use or disclosure is permitted as long as the covered entity has adopted reasonable safeguards as required by the Privacy Rule, and the information being shared was limited to the minimum necessary as required by the Privacy Rule
5. Public Interest and Benefit Activities; The Privacy Rule permits use and disclosure of protected health information, without an individual's authorization or permission, for 12 national priority purposes.28 These disclosures are permitted, although not required, by the Rule in recognition of the important uses made of health information outside of the health care context. Specific conditions or limitations apply to each public interest purpose, striking the balance between the individual privacy interest and the public interest need for this information.
6. Limited Data Set for the purposes of research, public health or health care operations. A limited data set is protected health information from which certain specified direct identifiers of individuals and their relatives, household members, and employers have been removed. A limited data set may be used and disclosed for research, health care operations, and public health purposes, provided the recipient enters into a data use agreement promising specified safeguards for the protected health information within the limited data set.
Administrative SimplificationAll healthcare providers and health plans that engage in electronic administrative and financial transactions must use a single uniform set of national standards-to be developed and adopted by CMS-for the electronic transmission of the following information:8
• Health insurance enrollment and eligibility
• Health insurance claims and equivalent information for encounters in health plan settings
• Identification numbers for providers, health plans, employers, and individuals
• Health data codes and classification systems
• Security standards and safeguards
Electronic health information systems must meet security standards, which should result in more cost-effective electronic claims processing and coordination of benefits.9
Other Areas of RegulationIn addition to the provisions described above, HIPAA contains provisions concerning the establishment of Medical Savings Accounts (discussed in Healthcare Management: An Introduction), long-term care insurance, changes in the notice requirements associated with benefit payments under Medigap insurance, and tax deductions for insurance costs of self-employed individuals. HIPAA also amended the Employee Retirement Income Security Act of 1974, which we discussed in ERISA and Health Plans.
Page 218 of 469

AHM 510 : Health Plans : Governance and Regulation
Some HIPAA provisions are of special interest to health plans. The provision that requires health plans, as well as other payors, to develop information systems that support electronic claims processing and comply with uniform national standards to be established by the Department of Health and Human Services may require some planning and additional allocation of resources.11 Note that CMS has experienced substantial obstacles in developing a uniform numerical identifier for individuals for electronic transactions due to concerns about confidentiality and, therefore, has delayed implementation and enforcement of this requirement. However, CMS has recently taken steps to propose a uniform numerical identifier for providers
A health plan or group plan also has to send a letter to inform newly enrolled plan members about HIPAA's provisions and their rights under that law. Self-funded plans may not pass their responsibility to issue certificates of creditable coverage to a TPA. Even if they try, the self-funded plan retains ultimate responsibility for the issuance of certificates under the law.12
HIPAA also requires special open enrollment periods for people who lose other health coverage or when an individual becomes a dependent of an employee through marriage, birth, or adoption. Health plans or employers must provide a notice of the special enrollment rights to any individual who declines coverage.13
One other area of regulation that HIPAA impacts is fraud and abuse. HIPAA strengthened the existing fraud and abuse laws in a number of ways. We discuss these changes in Fraud and Abuse.
EnforcementStates have primary responsibility to enforce the protections provided under HIPAA. If states fail to act, the HHS Secretary can impose civil monetary penalties on health plans or health insurance issuers who violate the provisions of HIPAA.14 HHS shares federal regulatory responsibility for oversight and enforcement of HIPAA—with the Department of Labor (DOL) and the Internal Revenue Service (IRS). For example, in addition to any penalties or other enforcement actions taken by the DOL or HHS, the IRS may impose tax penalties on employers or the employer’s benefit plans that do not comply with HIPAA. The IRS may also impose tax penalties for violations of two other federal acts—the Mental Health Parity Act of 1996 and the Newborns’ and Mothers’ Health Protection Act of 1996—discussed in the following lessons.
Mental Health Parity ActAmendments to HIPAA created the Mental Health Parity Act of 1996 and the Newborns' and Mothers' Health Protection Act of 1996. Through these acts, HIPAA is the first law that sets federal benefit mandates for group healthcare. In general, the Mental Health Parity Act of 1996 (MHPA) prohibits certain group health plans that provide both medical benefits and mental health benefits from imposing lower annual or lifetime dollar limits or caps for mental illness than for physical illness, if the health plan has established an annual payment limit or aggregate dollar lifetime cap for mental health benefits.
Until September 30, 2001, the MHPA applies to both fully funded and self-funded group health plans, but does not apply to group health plans for small employers (defined as those with at least two but no more than 50 employees).15 The law also does not apply to
Page 219 of 469

AHM 510 : Health Plans : Governance and Regulation
substance abuse, often subject to stricter limits on annual and lifetime caps than mental health. 16
Under the law, group health plans cannot, for example, set a cap of $1 million for a group member's lifetime medical health benefits while limiting the member's lifetime mental health benefits to $50,000. Rather, plans must either (1) set one lifetime limit that applies to both medical and mental health benefits or (2) set separate but equal lifetime limits each for medical health benefits and mental health benefits or (3) set higher limits for mental health benefits than for medical health benefits. These same requirements for lifetime limits apply to annual limits for group medical and mental health benefits.17
Fast Facts
In 1997, an estimated 168.5 million people had mental health benefits through a health plan behavioral health program.10
Note that the MHPA does not require group health plans to offer mental health benefits; it imposes requirements on those plans that do offer mental health benefits.18 In addition, the MHPA
• Does not prevent group health plans from imposing annual limits on the number of outpatient visits and inpatient hospital stays for mental health services. For instance, many group health plans limit group members to 20 outpatient visits and 30 days of inpatient hospital stays for mental health services per year. The Act allows such limitations.19
• Permits health plans to charge different copayments and deductibles for mental health benefits than for medical/surgical benefits. "Different" may mean higher copays and deductibles.20
• Allows an exemption from compliance for employers who can prove (after six months) that providing parity would result in an increase in costs under the plan of at least 1 percent. As we mentioned earlier, there is also an exemption for employers with at least two but no more than 50 employees.
• Does not ban limits on the number of days or visits for mental health treatment, or place restrictions on medical necessity determinations.21
• Does not preempt more stringent state mental health parity laws.
• Will sunset (i.e., the Act will no longer be effective) on September 30, 2001.*
The MHPA will require some employers to make difficult decisions regarding the mental health benefits that they provide to their employees. Most health plans are not affected by the MHPA because relatively few benefit plans are out of compliance with the law. Those plans that are not in compliance are principally self-funded plans. Health plans will be affected primarily if they are performing administrative services for a self-funded plan.
* On January 10, 2002, President Bush signed legislation extending the sunset date on the Mental Health Parity Act until December 31, 2002.
Page 220 of 469

AHM 510 : Health Plans : Governance and Regulation
Review Question
One provision of the Mental Health Parity Act of 1996 (MHPA) is that the MHPA prohibits group health plans from
setting a cap for a group member's lifetime medical health benefits that is higher than the cap for the member's lifetime mental health benefits imposing limits on the number of days or visits for mental health treatment
charging deductibles for mental health benefits that are higher than the deductibles for medical benefits imposing annual limits on the number of outpatient visits and inpatient hospital stays for mental health services
Correct. The MHPA prohibits certain group health plans that provide both medical benefits and mental health benefits from imposing lower annual or lifetime dollar limits or caps for mental illness than for physical illness, if the health plan has established an annual payment limit or aggregate dollar lifetime cap for mental health benefits.
Incorrect. The MHPA does not ban limits on the number of days or visits for mental health treatment, or place restrictions on medical necessity determinations.
Incorrect. The MHPA permits health plans to charge different copayments and deductibles for mental health benefits than for medical/surgical benefits. 'Different' may mean higher copays and deductibles.
Incorrect. The MHPA does not prevent group health plans from imposing annual limits on the number of outpatient visits and inpatient hospital stays for mental health services. For instance, many group health plans limit group members to 20 outpatient visits and 30 days of inpatient hospital stays for mental health services per year.
Newborns' and Mothers' Health Protection Act of 1996The Newborns' and Mothers' Health Protection Act of 1996 (NMHPA) requires that group health plans cover hospital stays for childbirth for both the mother and the newborn for at least 48 hours for normal deliveries and 96 hours for cesarean births. An attending physician is permitted to make a decision for an earlier discharge after consulting with the mother. Similar to the MHPA, the NMHPA mandate applies only to those group plans that provide benefits for childbirth-related hospital stays. The law does not require plans to offer benefits for childbirth-related hospital stays.
Review Question
The Opal Health Plan complies with all of the provisions of the Newborns' and Mothers' Health Protection Act of 1996 (NMHPA). Samantha Hill and Debra Chao are Opal
Page 221 of 469

AHM 510 : Health Plans : Governance and Regulation
enrollees. Ms. Hill was hospitalized for a cesarean birth, and Ms. Chao was hospitalized for a normal delivery. From the following answer choices, select the response that indicates the minimum hospital stay for which Opal, under NMHPA, must provide benefits for Ms. Hill and Ms. Chao.
Ms. Hill: 72 hours; Ms. Chao: 24 hours
Ms. Hill: 72 hours; Ms. Chao: 48 hours
Ms. Hill: 96 hours; Ms. Chao: 24 hours
Ms. Hill: 96 hours; Ms. Chao: 48 hours
Incorrect. The NMHPA requires more thana 24 hour minimum for normal deliveries, and more than a 72 hour minimum for cesareans.
Incorrect. While the NMHPA requires a minimum stay of at least 48 hours for normal deliveries, it requires morre than a 72 hour minimum for cesareans.
Incorrect. The NMHPA requires a minimum stay of 96 hours for cesarean births, and requires more than a 1 day stay for normnal deliveries.
Correct! The NMHPA requires a minimum stay of at least 48 hours for normal deliveries and 96 hours for cesarean births.
Confidentiality LawsHealthcare reform laws such as the MHPA and NMHPA reflect social concerns. Technological advances in medicine and information systems that offer new options for prevention and treatment of illnesses and disease are also drawing legislative attention. For example, gene research is beginning to be used to identify individuals susceptible to certain chronic or terminal illnesses. That information, along with the patient's medical history, can be loaded into a computer database to assist in future diagnoses and planning for preventive treatment. But many people are concerned about who will have access to such confidential medical information. This concern has made assuring confidentiality of medical records a top public policy priority as evidenced by the HIPAA provision that allows HHS to develop regulations for health information privacy if Congress does not enact such privacy legislation.22 HHS has made recommendations to Congress regarding the privacy of confidential medical information, but, to date, no legislation has been passed. Most states currently have in place confidentiality or privacy laws. Federal confidentiality legislation will have to address these laws and resolve potential conflicts. The question is: Will federal legislation preempt state laws on privacy or will state laws with standards more stringent than the yet-to-be-enacted federal law be allowed to prevail? Another major challenge to the drafters of federal confidentiality of medical information legislation is balancing quality improvement and research with privacy concerns. Figure 7A-1 illustrates the results of one consumer survey about the confidentiality of medical information.
Page 222 of 469

AHM 510 : Health Plans : Governance and Regulation
Applications of the Americans with Disabilities Act to Health Plan OperationsThe Americans with Disabilities Act (ADA) enacted in 1990 is a federal law that addresses discrimination against people with disabilities in areas such as employment, health services, access to public services, public accommodations, institutionalization, education, vocational training, housing, communication, recreation, transportation, and voting. The ADA expanded the nondiscrimination requirements of the Rehabilitation Act of 1973. The Rehabilitation Act of 1973 was passed to prohibit discrimination against disabled persons. Specifically, Section 504 of the 1973 Act requires agencies or organizations that receive U.S. government money to open jobs, education, and services to disabled persons. Health plans that have federal grants, loans, or contracts are subject to the requirements of Section 504 of the Rehabilitation Act.
The ADA impacts health plans and their network providers mainly in the areas of health services, public accommodation, and employment. Plaintiffs have brought lawsuits against health plans for ADA violations in the following areas:
• Credentialing and/or termination of providers
• Reduction in plan benefits or denials of claims
• Access to provider facilities
• Employment-related claims of discrimination
In addition, the ADA has provisions regarding the confidentiality of medical records maintained by employers.23
Under the ADA, a disability is defined as a physical or mental impairment that substantially limits one or more of an individual's major life activities. Major life activities include communication, ambulation, self-care, employment, housing issues,
Page 223 of 469

AHM 510 : Health Plans : Governance and Regulation
socialization, education, vocational training, and transportation. The ADA provides protections for any individual with a physical or mental impairment, anyone who has a record of such impairment, or anyone who is regarded as having such an impairment. A person does not have to currently have a disability or to ever have had a disability to be covered under the ADA. In addition, the ADA protects people who live with someone who has a disability.
A major area of interest for health plans is the application of the ADA in the area of employment discrimination. The ADA applies to private sector employment organizations that employ 15 or more employees. The Equal Employment Opportunity Commission enforces the ADA, and other EEOC-related protections apply to persons covered under the ADA.
Under the ADA, employers must reasonably accommodate the known disability of a disabled person who is qualified to fill a position unless such accommodation represents significant undue hardship for the employer. A qualified disabled person is one who has the skills, experience, education, and other job-related abilities necessary for an employment position, who can perform the essential duties of the position, and whose employment does not pose a direct threat to the health and safety of other employees. A qualified disabled person is protected by the ADA.
Employment activities that are subject to the ADA's provisions include job application procedures, hiring, promotions, terminations, employee compensation, and training.
Outside the employment area, credentialing and termination of providers are two of a health plan's activities most greatly affected by the ADA. These activities are discussed in the following section.
Credentialing, Termination, and the ADAA health plan or integrated delivery system must not discriminate against qualified persons with disabilities through its credentialing program under the ADA, yet at the same time the health plan or IDS must ensure patients of a high level of quality care. The requirements of the ADA appear to be, in some instances, in conflict with this duty to provide quality care. This is most evident in cases of providers with alcohol or drug dependency. With respect to the ADA's application to credentialing, so long as the health plan or IDS can show that the adverse employment (contract) action is directly and necessarily related to quality of care issues, it may be able to reconcile its duty with the ADA requirements. By questioning specific job-related functions rather than general health status, the health plan or IDS should be able to achieve ADA compliance in its application process.
Another health plan activity subject to ADA litigation is termination of providers or other related action that may be viewed as ADA discrimination. A provider with a disability may sue a health plan that terminates his or her contract without cause alleging ADA discrimination. Health plans must carefully consider such decisions and document their criteria for the termination. In lieu of termination, some health plans may require that a provider disclose his or her disability to the provider's patients if the health plan perceives a direct threat to patient care associated with the disability. For example, in Pennsylvania, a health plan successfully required a surgeon to notify all his former and potential patients of his HIV-positive status. This decision was upheld by a federal court
Page 224 of 469

AHM 510 : Health Plans : Governance and Regulation
on the grounds that the physician's disability posed a direct threat to his patients that could not be solved by reasonable accommodation.24
Reduction in Plan BenefitsHealth plans that change the level of benefits for a specific disease and not for others may find themselves the subject of ADA lawsuits. A plan that reduces benefits for a certain service or treatment that does not discriminate against a certain group or class of enrollees would generally not be in violation of the ADA. Also, a plan that does reduce or eliminate benefits that impacts only individuals with a particular disease or disability may not be in violation of the ADA if the health plan has a sound underwriting reason for eliminating or reducing that benefit. For example, a plan that eliminates coverage for allergy shots for asthmatics may be faced with a successful ADA lawsuit. However, if the health plan reduces the benefits for prescription drugs that affects all classes of enrollees, a successful ADA lawsuit would be unlikely.
Provider Facilities and the ADAAnother area in which health plans have faced litigation is access to provider facilities. Since health plans contract with providers and have a duty to credential those providers, access to the facilities of the provider becomes a responsibility of the health plan as well as the provider. Most health plans include a site visit to a provider's facilities in their credentialing processes to ensure that accommodations for people with disabilities are available. In parts of New York, there have been demands by patients for the provider to supply interpreters for deaf people under the ADA. It is not clear who should be responsible for paying for these interpreters.
Federal Marketing LawsSeveral federal laws have requirements that affect marketing. The Federal Trade Commission Act (FTCA) focuses largely on antitrust issues, but it also prohibits unfair or deceptive acts or practices related to commerce. Under this law, a marketing practice is considered deceptive if it has the capacity or the tendency to deceive or mislead some members of the public. One court has determined that the FTCA must be applied more closely in the healthcare context than in business in general. In FTC v American Medical Association, the court stated that "what may be false and deceptive for doctors may be permissible for sellers of other products and services. Harmless puffery for a household product may be deceptive in a medical context." Violations of the FTCA can result in a cease-and desist-order, as well as fines, from the FTC.25
Under the Lanham Act, a consumer or a competitor can sue for false advertising. The party that files suit can recover compensatory or punitive damages if a court determines that the advertising has deceived the public.26
With limited exceptions, the Medicare law requires managed Medicare plans to submit all advertising material to CMS for review and approval prior to use. In addition, federal Medicaid law prohibits health plan entities from distributing marketing materials without prior approval of the state. We discuss other regulatory requirements related to Medicare and Medicaid marketing later in this lesson.
Other Federal Laws There are other federal laws that affect healthcare benefits. In Healthcare Management: An Introduction, we discussed that the Age Discrimination in Employment Act (ADEA),
Page 225 of 469

AHM 510 : Health Plans : Governance and Regulation
the Family and Medical Leave Act, COBRA, and Title VII of the Civil Rights Act all contain provisions that affect the provision of healthcare benefits. In Overview of Laws and Regulations, we described provisions of various federal budget and tax acts that include provisions relating to healthcare that may impact health plans.
Some federal laws regulate activities associated with providers. The Health Care Quality Improvement Act of 1986 provides rules that health plans must follow in peer review activities to avoid antitrust violations. The Act creates a preferred set of provider contracting procedures for peer review that, if followed, provides liability protection to those conducting the peer review. The Act also requires the reporting of adverse peer review determinations to state medical boards and the National Practitioner Data Bank.
In addition, government programs such as FEHBP, TRICARE, Medicare, and Medicaid were all created by federal law and have federal regulation components. We discuss the use and regulation of health plans in each of these programs in the next few lessons.
Page 226 of 469

AHM 510 : Health Plans : Governance and Regulation
Chapter 7 BAntitrust Concerns and Health Plans As we discussed in Overview of Laws and Regulations, antitrust laws emerged in the late part of the 19th century to promote competitive business practices and to curb efforts to restrain trade. Antitrust laws are laws that address competition, price fixing, and monopolies in business practices. Insight 7B-1 describes how for many years the healthcare industry was thought to be outside the reach of such laws.
Health plans now routinely consider the impact antitrust laws and regulations may have on their businesses in the area of provider contracting. Regulators also scrutinize joint ventures, mergers, and acquisitions that might create a monopoly or substantially lessen competition in a given market. In addition, courts and other regulatory agencies scrutinize the business practices of health plans or health plan business ventures that have a sizeable market share to guard against potential monopolistic practices. In this lesson, we describe the major federal laws that pertain to antitrust: the Sherman Antitrust Act, the Clayton Act, and the Federal Trade Commission Act. Next, we explain the standards used to review business practices to determine if antitrust violations have occurred. Then, we look at the typical applications of antitrust laws in health plans.
After completing this lesson, you should be able to:
Describe the three major federal laws that regulate business activities to prevent antitrust actions
Describe the difference between the per se rule and the rule of reason Explain the applications of antitrust law in health plan-provider contracting Explain the relevance of antitrust in mergers and acquisitions Identify the issues that the 1994 DOJ and FTC guidelines addressed Explain the procedures the DOJ and FTC follow for their enforcement proceedings
Insight 7B-1. Application of Antitrust Laws to Healthcare.
For a long time, the healthcare industry was widely believed to be exempt from antitrust laws. The activities of individual healthcare providers, such as physicians, were considered outside the scope of antitrust laws because they involved a "learned profession," as distinguished from trade or business. Over the years, the scope of this "exemption" was limited, and its validity often was challenged. The challenges reflected a growing public perception that the activities of those in learned professions were not entirely different from the activities of those in trade or business and that some such activities were anticompetitive in purpose and effect. It was not until 1975, however, that the Supreme Court, in Goldfarb v. Virginia State Bar, abolished any remnants of a blanket exemption from the federal antitrust laws for the learned professions. Although Goldfarb involved the activities of lawyers, its reasoning has been applied to other professions, including healthcare.
Another reason the healthcare industry was thought to be exempt from the antitrust laws was the tendency of courts to give broad construction to the McCarran-Ferguson Act exemption for the "business of insurance." However, in 1979, the U.S. Supreme Court
Page 227 of 469

AHM 510 : Health Plans : Governance and Regulation
reversed that judicial tendency by narrowly construing the Act in Group Life and Health Ins. Co. v. Royal Drug Co. In that case, the Court held that agreements between a health plan and pharmacies that fixed prices but did not involve underwriting or the spreading of risk did not constitute the business of insurance and therefore were not exempt from antitrust scrutiny. A few years later, the Supreme Court ruled that the use of peer review committees to determine reasonableness of chiropractic charges did not constitute the business of insurance. Later cases reiterated that, for activities to be exempt under the McCarran-Ferguson Act, challenged practices must constitute the "business of insurance," must be regulated by state law, and must not amount to boycott, coercion, or intimidation. The market for private healthcare financing, which embraces HMOs, PPOs, and TPAs, generally is not considered to fall within the exemption.
Source: Jane Garwood et al., Managed Care Law Manual, vol. 1, 1998, "Antitrust", Supplement #1, April 1995, pp. 4-5 (Gaithersburg, MD: Aspen Publishers, Inc.)
Determination of Antitrust ActivitiesFigure 7B-1 describes the three federal acts that govern antitrust activities-the Sherman Act, the Clayton Act, and the Federal Trade Commission Act. An important test used to determine if monopolization exists is the presence of market power. Market power is the power to control prices or exclude competition in a given market. We will reference the concept of market power throughout this lesson.
Antitrust activities are measured under two standards. One is the per se rule, which applies to restraints of trade that are so obvious as to be presumed unreasonable and therefore illegal. There is no requirement that harm to competition be proven for a per se violation. Restraints of trade are not permitted regardless of the business justification or pro-competitive effect. Included as per se illegal are price-fixing agreements among competitors, horizontal division of markets.
The second standard is less onerous and uses a "rule of reason" analysis to determine if the purpose or effect of the activity or agreement actually harms competition or if the arrangement has redeeming economic benefits. A party must show actual and unreasonable harm to competition under this standard. The existence of market power is an essential ingredient in the analysis.
Figure 7B-1. Federal Acts that Impact Antitrust.
The Sherman Antitrust ActThe Sherman Antitrust Act prohibits actions that constitute unreasonable restraints of trade. Section 1 of the Act provides that "Every contract, combination in the form of trust or otherwise, or conspiracy, in the restraint of trade or commerce among the several States, or with foreign nations, is hereby declared to be illegal." Section 2 of the Act prohibits monopolization or attempts to monopolize and provides that "Every person who shall monopolize, or attempt to monopolize, or combine or conspire with any other person or persons, to monopolize any part of the trade or commerce among the several States, or with foreign nations, shall be deemed guilty of a felony."
Page 228 of 469

AHM 510 : Health Plans : Governance and Regulation
The elements of restraint of trade under Section 1 of the Sherman Antitrust Act concern (1) a concerted action by distinct entities (2) that has an unreasonable anticompetitive effect (3) on interstate commerce.
The elements of monopolization under the Sherman Antitrust Act include (1) market power and (2) the willful acquisition or maintenance of that power as distinguished from growth or development arising from a superior product, business acumen, or historic accident. Attempted monopolization under Section 2 of the Sherman Antitrust Act includes intent to monopolize and actions in furtherance of that intent that have the probability of success.
The Clayton ActThe Clayton Act addresses specific practices of single entities that would tend to lessen competition or create a monopoly. Section 3 [15 USC § 14] prohibits exclusive dealing arrangements, tying arrangements, and requirement contracts involving the sale of commodities where the effect may be to substantially lessen competition. Section 7 [15 USC § 18] prohibits mergers, joint ventures, consolidations, or acquisitions of stock or assets where the effect may be to substantially lessen competition or tend to create a monopoly or to otherwise unreasonably restrain trade. In addition, Section 7a [15 USC § 18a], known as the Hart-Scott-Rodino Act of 1976, requires that certain proposed mergers and acquisitions involving a specified level of stock/assets receive approval from the FTC and the Justice Department before consummation. Section 2 of the Clayton Act, which originally prohibited price discrimination in sales of commodities, was amended by the Robinson-Patman Act and affects sales of products by nonprofit organizations. The Robinson-Patman Act prohibits certain practices that result in discriminatory pricing.
Under the Sherman Act, an activity must have an actual adverse effect on competition before it is considered illegal. Under the Clayton Act, if the activity might have an effect on competition, it is illegal.
The Federal Trade Commission ActThe Federal Trade Commission Act (FTC Act) declares that unfair methods of competition and unfair or deceptive acts or practices are illegal. The FTC Act's broad proscription of unfair methods of competition was intended to ensure that antitrust enforcement would not be limited to specific activities prohibited under the Clayton Act. Consequently, the FTC Act is interpreted quite broadly, and violations of the Sherman and Clayton Acts are also violations of the FTC Act.
Source: Excerpted and adapted, used with permission of the publisher, from Sheryl Tatar Dacso and Clifford C. Dacso, Managed Care Answer Book, Second Edition (New York: Panel Publishers, 1997), pp. 5-3-5-4.
Review Question
The following situations illustrate per se violations of federal antitrust laws:
Page 229 of 469

AHM 510 : Health Plans : Governance and Regulation
• Situation A - Two groups of providers agreed among themselves that each provider will do business with health plans only on a fee-for-service basis.
• Situation B - In order to avoid competing with each other, two independent, competing physician-hospital organizations (PHOs) divide the geographic areas in which they will market their services.
From the following answer choices, select the response that correctly identifies the types of per se violations illustrated by these situations.
Situation A: price fixing; Situation B: horizontal division of markets
Situation A: price fixing; Situation B: tying arrangement
Situation A: horizontal group boycott; Situation B: horizontal division of markets
Situation A: horizontal group boycott; Situation B: tying arrangement
Correct. Price fixing involves the agreement by two or more independent competitors on the prices or fees that they will charge for services. A horizontal division of markets is when two or more independent competitors to agree not to compete by dividing (a) geographic areas in which each will market and sell its products, (b) the products that each will offer, or (c) the customers that each will service.
Incorrect. While Situation A does describe price fixing, tying arrangements exist when a competitor conditions the sale of one of its products or services, for which it has market power, upon the purchase of a second.
Incorrect. While Situation B does describe a horizontal division of markets, a horizontal group boycott occurs when two competitors agree not to do business with another competitor or purchaser.
Incorrect. A horizontal group boycott occurs when two competitors agree not to do business with another competitor or purchaser, and tying arrangements exist when a competitor conditions the sale of one of its products or services, for which it has market power, upon the purchase of a second.
Per Se Violations in AntitrustAs discussed earlier, some activities are per se (which means "taken alone") violations of the federal antitrust laws. The four types of per se violations-price fixing, horizontal group boycotts, tying arrangements, and horizontal division of markets-are discussed in more detail below. The U.S. Supreme Court has ruled that tying arrangements and horizontal group boycotts will be considered per se violations only if the entities under scrutiny have market power.1
Price FixingPrice fixing involves the agreement by two or more independent competitors on the prices or fees that they will charge for services. For example, independent physicians, hospitals, or other healthcare providers may not agree on the fees they will individually charge health plan providers. Nor may they agree on other practices that influence price.
Page 230 of 469

AHM 510 : Health Plans : Governance and Regulation
For example, it would be unlawful for two or more providers or groups of providers (whether IPAs, PPOs, physician networks, PHOs, or hospitals) to get together and agree among themselves that each will do business with health plan providers only on a fee-for-service basis. This agreement would restrict the manner in which competitors compete on the basis of price or fees and would have the same effect on competition as an agreement on particular prices or fees. Nor may health plans agree among themselves to accept only capitated contracts, or a certain level of reimbursement.
The principle here is that, for competition to work, buyers and sellers (providers and health plans) must each bargain freely and independently based upon the particular merits of the goods and services involved, and the economic needs of both parties. The Department of Justice/FTC guidelines, discussed later in this assignment, provide information regarding how these agencies analyze agreements related to price between or among providers as part of physician or multiprovider joint ventures.
Horizontal Group BoycottsA horizontal group boycott occurs when two competitors agree not to do business with another competitor or purchaser. Horizontal group boycotts are almost always unlawful. For example, two health plans may not agree to each refuse to do business with a particular nonprofit hospital until that hospital ceases merger talks with a private hospital corporation. Nor may a PHO deny membership to a physician solely because that physician has admitting privileges at a competing hospital. This type of joint pressure reduces the free market choices or disadvantages a competitor.
Tying ArrangementsIn most cases, tying arrangements are unlawful. A tying arrangement exists when a competitor conditions the sale of one of its products or services, for which it has market power, upon the purchase of a second. This would force the purchaser to purchase an unwanted product or service to obtain the desired product or service. For example, a health plan with substantial market share may not require its contracting providers to offer its health plan product to the provider's employees as a condition of contracting with that provider. Each product or service must be permitted to compete on its own merits. Likewise, a provider-owned IDS controlling most or all providers in a particular specialty, for example, oncology services, will be vulnerable to an unlawful tying claim if it refuses to reasonably contract (or to permit the specialty providers themselves to contract) with competing provider networks or health plans that need the oncology services, but not all of the services provided by the IDS.
Horizontal Division of MarketsIt is unlawful for two or more independent competitors to agree not to compete by dividing (a) geographic areas in which each will market and sell its products, (b) the products that each will offer, or (c) the customers that each will service. The preceding sentence describes a horizontal division of markets. For example, two competing PHOs may not split the geographic areas in which they will market their services to health plans. Nor may two health plans split large employer subscribers by agreeing that one will market to certain employers and the second will market to different employers. Horizontal division of markets represents an agreement not to compete and is thus, by definition, anticompetitive.
Page 231 of 469

AHM 510 : Health Plans : Governance and Regulation
The Application and Elements of Market PowerWe defined market power as the power to control prices or exclude competition in a given market. Market power is used as a basis for evaluating a variety of potential antitrust activities. First, market power is assessed to determine if certain businesses are monopolies or certain business combinations are attempts to monopolize a market. Second, in examining mergers and acquisitions for antitrust violations, market power is an important factor. Third, market power is also examined in suits alleging illegal price discrimination, illegal tying arrangements, exclusive dealing arrangements, and illegal agreements that unreasonably restrain trade between or among two or more entities.2 To determine if an entity or venture has market power, two elements must be assessed: (1) the relevant product market and (2) the relevant geographical market.
The Product MarketThe relevant product market for antitrust purposes consists of the product or service under debate and all close substitutes. A close substitute is a product that is reasonably interchangeable with the original product. The Managed Care Law Manual explains the relevant product market for health plans in this way:
"The relevant product market for health plans is the market for healthcare financing. Broadly defined, this market includes traditional insurers, HMOs, PPOs, IPAs, etc., and their subscriber members. Participants in the market are considered to be purchasers of healthcare benefit packages. Characteristics of this market include few barriers to entry and great mobility. As a result, the market share necessary to demonstrate market power is extremely high."3
However, others dispute this broad market as the product market for health plans. These opponents say that HMOs and/or health plans are a separate market from that of the traditional insurers.
The Geographical MarketAs explained in Tampa Elec. Co. v. Nashville Coal Co., the relevant geographical market for antitrust purposes is the "market area in which the seller operates, and to which the purchaser can practically turn for supplies."4 To determine the geographical market, courts look at economic and physical barriers to expansion such as transportation costs, delivery limitations, and customer convenience.5 Courts may use other applicable factors to determine the geographical market. Once the relevant product and geographical markets are confirmed, the market share can be determined and a decision can be made as to the entity's market power.
Now that we know the elements and standards of antitrust regulation, we can examine their application in health plan scenarios. First, we'll look at antitrust issues that arise in provider contracting.
Antitrust Issues in Provider ContractingMany antitrust issues in health plans involve providers and provider contracting. In developing provider networks, health plans may be charged with excluding providers or excluding specific groups of providers in violation of antitrust laws. In addition, a health plan that enters into exclusive contracts with providers should be prepared for antitrust scrutiny. Provider-controlled health plans such as PSOs may also have to contend with price fixing allegations, discussed in DOJ/FTC guidelines later in this lesson.
Page 232 of 469

AHM 510 : Health Plans : Governance and Regulation
We introduced the concept of price fixing earlier in this lesson. However, not all joint agreements related to price are considered anticompetitive or violations under antitrust laws. The U.S. Supreme Court has ruled favorably on joint venture agreements among competitors that pertain to price which are necessary for the creation of a new product.6
In defined instances, courts will use the rule of reason instead of the per se rule to analyze such joint ventures. For example, provider joint ventures that compensate their providers by capitation enter into an agreement with those providers and pay a fixed rate or price per member per month to all participating providers (who would normally be competitors) in that market. However, courts do not view these types of agreements as a violation of the per se rule because the independent providers share a substantial risk of financial loss.7 As noted in the antitrust guidelines for healthcare (discussed later in this lesson), such financial risk demonstrates integration that is likely to produce significant efficiencies that benefit consumers.
Most-Favored-Nation ClausesMost-favored-nation clauses are clauses sometimes found in contracts between health plans and healthcare providers. Under a most-favored-nation (MFN) clause, if a provider offers a price to any other health plan that is more favorable than the price offered to the contracting health plan, then the provider must offer the same price to the contracting health plan.8 The Seventh Circuit Court of Appeals ruled that MFN clauses are not per se illegal and that they violate antitrust laws only if they have a predatory purpose and an anticompetitive effect.9 If these clauses are not per se illegal, then the other elements of antitrust behavior must be present for such a clause to violate antitrust laws. Although MFN clauses included in health plan-provider contracts relate to price, they do not involve decisions by providers concerning the level of fees to charge. Since this is the case, such clauses are not per se illegal but should be reviewed under the rule of reason analysis for antitrust purposes.10 The FTC takes a hard stand against MFN clauses and there have been circumstances in which health plans have agreed not to use them.
Review Question
Determine whether the following statement is true or false:
Although most-favored-nation (MFN) clauses in contracts between health plans and healthcare providers are not per se illegal, they should be reviewed under the rule of reason analysis for antitrust purposes.
True, because the Federal Trade Commission (FTC) ruled that MFN clauses are not per se illegal and the FTC encourages health plans to include them in provider contracts. True, because although MFN clauses are not per se illegal, they violate antitrust laws if they have a predatory purpose and an anticompetitive effect. False, because MFN clauses involve decisions by providers concerning the level of fees to charge, and thus they are per se illegal. False, because MFN clauses are not per se illegal, and thus they are exempt from antitrust laws and regulation by the FTC.
Page 233 of 469

AHM 510 : Health Plans : Governance and Regulation
Incorrect. The FTC takes a hard stance against MFN clauses, and there have been circumstances where health plans have agreed not to use them.
Correct. The 7th Circuit Court of Appeals ruled that while MFN clauses are not per se illegal, they violate antitrust laws if they have a predatory purpose and an anticompetitive effect.
Incorrect. The 7th Circuit Court of Appeals ruled that MFN clauses are not per se illegal
Incorrect. While MFN clauses are not per se illegal, the FTC takes a hard stand against MFN clauses and there have been circumstances in which health plans have agreed not to use them.
Provider ExclusionIn general, the federal regulatory agencies that enforce the antitrust laws recognize that health plans may enter into selective or exclusive contracts with provider groups without violating antitrust laws. Such arrangements result in greater competition among providers. However, if the provider groups are required to contract with only one health plan in an area, anticompetitive results may occur and antitrust claims may be made. Antitrust claims relating to provider exclusion focus on the effect the exclusion has on the relevant market (e.g., will the services offered to consumers be adversely affected), not harm to providers. For example, a health plan may contract with only one hospital and two IPAs in a market, excluding all other providers, with no antitrust effects. However, if that same health plan requires those contracted providers to contract exclusively with that health plan, competition may be adversely affected and antitrust claims successfully made.
In some cases, certain groups of providers-such as podiatrists, chiropractors, or psychologists-have alleged that health plan provider exclusion from a network results in a group boycott of providers in those specialties. The decision as to whether antitrust laws have been violated depends on the particular factors in the relevant case. Generally, if there is no legitimate business purpose for the exclusion, a violation of antitrust laws may be found.11
Antitrust Issues in Mergers and AcquisitionsAntitrust regulators scrutinize mergers and acquisitions in healthcare to ensure that no one entity assumes too much market power as a result of such business activities. We discussed mergers as a means of integrating business operations in Formation and Structures of Health Plans and described the three basic types of organizational integration: horizontal, vertical, and conglomerate. These three types of integration strategies affect the type of antitrust standard used to evaluate each type of merger. Regulators are concerned primarily with determining whether (1) the resulting entity in a potential merger or acquisition will retain too much market power and (2) the merger or acquisition will create market concentration. For antitrust purposes, market concentration occurs when one independent competitor's business decision affects the market interdependently, allowing all the competitors in that market to exercise collective market power.
Page 234 of 469

AHM 510 : Health Plans : Governance and Regulation
The Antitrust Division of the Department of Justice (DOJ) has primary responsibility for enforcing federal antitrust laws, which includes investigation of possible violations of both the criminal and civil provisions of the Sherman, Clayton, and Robinson-Patman acts. The Federal Trade Commission (FTC) enforces certain sections of the Clayton Act, described in more detail later in this lesson, and a section of the FTC Act that prohibits unfair methods of competition and unfair or deceptive acts or practices. In the following sections, we describe the analysis the DOJ and the FTC undertake in reviewing horizontal and vertical mergers for antitrust violations. Because conglomerate mergers involve companies that produce unrelated products or services and there is little integration, there is very little antitrust risk.12
One part of the premerger regulatory filings that many health plans make is a Hart-Scott-Rodino Act of 1976 (H-S-R Act) requires that certain mergers receive DOJ and FTC approval before consummation. If a proposed health plan merger falls within the parameters of the H-S-R Act, the parties to the transactions often make a filing with the DOJ and FTC. This filing is made on forms provided by the DOJ and FTC and requires supporting documentation detailing the particulars of the proposed transaction. The DOJ and FTC review the H-S-R filing to determine if the proposed merger may create any anticompetitive results. After a prescribed waiting period to allow for the agencies' review of the filing, the parties to the proposed merger may proceed with the transaction as long as neither the DOJ nor the FTC has intervened. However, a filing made under the H-S-R Act does not preclude the DOJ and the FTC from subsequent investigation of any anticompetitive behavior related to the merger or the merging parties.
Analysis for Horizontal MergersMarket power and market concentration are two factors that regulatory agencies assess in reviewing horizontal mergers for antitrust violations. In their examination of horizontal mergers, such as the acquisition of one HMO by another HMO or one hospital by another, the DOJ and the FTC follow their 1992 Horizontal Merger Guidelines, updated in 1997. These steps that the DOJ and FTC take in analyzing a merger are outlined in Figure 7B-2.
Figure 7B-2. DOJ and FTC 1992 Horizontal Merger Guidelines.
Overview: The Guidelines describe the analytical process that the DOJ (the Agency) employs in determining whether to challenge a horizontal merger. First, the Agency assesses whether the merger would significantly increase concentration and result in a concentrated market, properly defined and measured. Second, the Agency assesses whether the merger, in light of market concentration and other factors that characterize the market, raises concern about potential adverse competitive effects. Third, the Agency assesses whether entry would be timely, likely, and sufficient either to deter or to counteract the competitive effects of concern. Fourth, the Agency assesses any efficiency gains that reasonably cannot be achieved by the parties through other means. Finally, the Agency assesses whether, but for the merger, either party to the transaction would be likely to fail, causing its assets to exit the market. The process of assessing market concentration, potential adverse competitive effects, entry, efficiency, and failure is a tool that allows the Agency to answer the ultimate inquiry in merger analysis: whether the merger is likely to create or enhance market power or to facilitate its exercise.
Page 235 of 469

AHM 510 : Health Plans : Governance and Regulation
In analyzing a horizontal merger, the Agency takes the following steps:
1. Define the relevant product market, especially from the perspective of the health plans that purchase services from the merging groups.
2. Define the relevant geographic market. 3. Identify competitors in the relevant market. 4. Compute all competitors' market shares in each relevant market based on
capacity, sales, and production. 5. Compute the postmerger market share of the merging parties. 6. Apply the Merger Guidelines concentration standards to determine how serious a
problem, if any, the merger might raise. 7. Determine if the postmerger market share of the merging parties is more than 35
percent, which is the general benchmark used to determine market power. 8. If the level of concentration is significantly above Merger Guidelines levels or the
postmerger market share is above 35 percent, examine other factors. 9. Examine the level of entry barriers-that is, how difficult and likely would it be
that new entrants would enter the market if those already in the market attempted to exercise market power by raising prices.
10. If the only issue is the group's postmerger market share, examine how difficult it would be for competing groups in the market to increase their capacity and output quickly if the merged firm increased prices.
11. Examine other factors suggesting whether collusion would occur and, if so, whether it would be successful.
12. Examine the extent of efficiencies in the new, merged system. 13. Balance the procompetitive with anticompetitive effects.
Source: Excerpted from Sheryl Tatar Dacso and Clifford C. Dacso, MD, Managed Care Answer Book, Second Edition (New York: Panel Publishers, 1997), p. 5-14
Analysis for Vertical MergersThe same factors, market power and market concentration, used to analyze a horizontal merger for antitrust violations are also used to analyze a vertical merger, such as the merger of a hospital with an IPA. Particular antitrust concerns associated with vertical mergers are: (1) that the merger will close off a large part of the market to competitors at either the purchaser or seller levels, thereby creating market dominance for the merged entity at one of those levels; (2) that it can create barriers to market entry because either customers or suppliers will be unavailable to them as a result of the merger; and (3) the number of competitors in the market may diminish.13
Developments in Antitrust RegulationIn September 1993, the DOJ and the FTC issued the first healthcare-specific antitrust guidelines. These guidelines set forth six policy statements regarding:
• Hospital mergers
• Hospital joint ventures involving high technology or other expensive medical equipment
• Physicians' provision of information to purchasers of healthcare services
• Hospital participation in exchanges of price and cost information
Page 236 of 469

AHM 510 : Health Plans : Governance and Regulation
• Joint purchasing arrangement among healthcare providers
• Physician network joint ventures
In these guidelines, the DOJ and FTC established antitrust safety zones by describing circumstances they would not challenge, absent extraordinary circumstances. In addition, the statements provided an outline of the analysis the agencies would use to review conduct falling outside the antitrust safety zones. The statements also committed the agencies to respond to requests for business reviews or advisory opinions from the healthcare community.
In 1994, the same regulatory agencies revised and expanded the 1993 policy statements with superseding guidelines. The resulting guidelines cover:
• Hospital joint ventures involving specialized or expensive healthcare services
• Providers' collective provision of information about fees to purchasers of healthcare services
• Analytical principles relating to multiprovider networks
The new multiprovider network statement applied to networks that include providers other than physicians, such as multihospital systems or physician hospital organizations (PHOs). However, the statement did not include antitrust safety zones for such arrangements. In their revised guidelines, the agencies emphasized that just because they have established safety zones, it doesn't mean that activity outside the safety zones is likely to be challenged.
The most significant change in the new guidelines is the explicit statement that networks that engage in joint pricing but do not involve shared risk may receive rule-of-reason treatment. The old guidelines took a narrow approach to joint pricing among competitors participating in multiprovider networks; such activities had to be related to significant economic integration or were deemed per se illegal. The agencies took a broader approach with physician networks, stating that they would review joint pricing among physicians under rule-of-reason analysis either if the physicians in the joint venture shared substantial financial risk or if the combining of physicians into a joint venture enabled them to offer a new product producing substantial efficiencies.
Review Question
In 1994, the Department of Justice (DOJ) and the Federal Trade Commission (FTC) revised their 1993 healthcare-specific antitrust guidelines to include analytical principles relating to multiprovider networks. Under the new guidelines, the regulatory agencies will use the rule of reason to analyze joint pricing activities by competitors in physician or multiprovider networks only if
provider integration under the network is likely to produce significant efficiencies that benefit consumers the providers in a network share substantial financial risk
Page 237 of 469

AHM 510 : Health Plans : Governance and Regulation
the combining of providers into a joint venture enables the providers to offer a new product all of the above
Correct. The 1994 guidelines focus on the efficiencies produced that benefit consumers.
Incorrect. The 1994 guidelines focus on physicians in the joint venture sharing substantive risk, and the rule of reason will apply if the provider integration is likely to produce significant efficiencies to benefit consumers.
Incorrect. The rule of reason will apply if combining providers into a joint venture enables the providers to offer a new product that produces significant efficiencies to benefit consumers
Incorrect. More than one of the responses above are incorrect.
The guidelines also apply the broader approach to multiprovider networks and explicitly focus only on the efficiencies likely to be produced, rather than whether a new product is created. The agencies now analyze joint pricing activities by competitors in physician or multiprovider networks under the rule of reason if provider integration under the network is likely to produce significant efficiencies that benefit consumers, and any price agreements by providers are reasonably necessary to realize those efficiencies.
The guidelines provide that sufficient integration to produce efficiencies can be demonstrated through an active and ongoing program to evaluate and modify the participants' practice patterns and create a high degree of interdependence and cooperation between participants to control cost and ensure quality, including:
• Establishing mechanisms to monitor utilization, control costs, and assure quality of care
• Selecting network participants who are likely to further efficiency objectives
• Investing significant amounts of human and monetary capital in infrastructure to achieve efficiencies, such as clinical information systems
The agencies' analysis focuses on substance, rather than form, in assessing a network's likelihood of producing significant efficiencies. Networks whose purpose or effect are little more than efforts to prevent or impede competition are not likely to produce efficiencies and remain per se illegal according to the agencies.
The FTC and DOJ addressed some of the concerns about the balance of antitrust and competititon in a July 2004 report described in Insight 7B-1.
Insight 7B-1 FTC-DOJ Report on Competition in the Health Care System
The Federal Trade Commission (FTC) and the Department of Justice (DOJ issued a report on July 26, 2004 addressing the state of competition in the U.S. health care system. This report was the result of numerous joint hearings the FTC and DOJ held
Page 238 of 469

AHM 510 : Health Plans : Governance and Regulation
over the past two years to examine the health care marketplace and issues relating to competition, antitrust enforcement, and consumer protection. The report addressed two basic questions. First, what is the current role of competition in health care, and how can be enhanced to increase consumer welfare? Second, how has, and how should antitrust enforcement work to protect existing and potential competition in health care?
Key recommendations from the report include:
• Payment methods should be developed for "aligning providers' incentives with consumers' interests in lower prices, quality improvements and innovation";
• Consumers should be provided with "more information on prices and quality" and "greater incentives to use such information";
• Legislation should not be enacted to permit independent physicians to collectively bargain; and
• Governments should consider whether coverage mandates serve consumers' health care needs, given that "mandates are likely to limit consumer choice, eliminate product diversity, raise the cost of health insurance, and increase the number of uninsured Americans."
For more information and to retrieve a copy of the FTC-DOJ report, Improving Health Care: A Dose of Competition, please access the FTC's website at www.ftc.gov/reports. The 361 page report includes an executive summary.
Review Question
Antitrust laws can affect the formation, merger activities, or acquisition initiatives of a health plan. In the United States, the two federal agencies that have the primary responsibility for enforcing antitrust laws are the
Internal Revenue Service (IRS) and the Department of Justice (DOJ)
Office of Inspector General (OIG) and the Department of Defense (DOD)
Federal Trade Commission (FTC) and the Department of Labor (DOL)
Federal Trade Commission (FTC) and the Department of Justice (DOJ)
Incorrect. The IRS does not have primary responsibility for enforcing antitrust laws
Incorrect. The OIG enforces fraud and abuse statutes, and the DOD is a purchaser of healthcare services
Incorrect. The DOL does not have primary responsibility for enforcing antitrust laws
Page 239 of 469

AHM 510 : Health Plans : Governance and Regulation
Correct. Both the FTC and the DOJ have primary responsibility for enforcing antitrust laws.
Enforcement of Antitrust LawsThe potential plaintiffs that must be considered in an antitrust suit include the DOJ, the FTC, state attorneys general, and individuals harmed by anticompetitive actions. The likelihood that either a government or private suit will be initiated depends on statutory limitations or the degree of the potential plaintiff's interest in the particular activity. Thus, each activity must be evaluated on the basis of its facts.
Justice DepartmentThe Antitrust Division of the DOJ has primary responsibility for enforcing federal antitrust laws, which includes investigation of possible violations of both the criminal and civil provisions of the Sherman, Clayton, and Robinson-Patman acts.
The DOJ investigates possible criminal violations of antitrust laws by initiating a proceeding before a grand jury. The grand jury has broad investigative powers; it may compel witnesses to testify and may require the presentation of books, documents, records, and other information. Unlike trial juries, which determine guilt or innocence, a grand jury merely determines whether a party charged with violating an antitrust law should stand trial. If, after the examination of witnesses, documents, records, and other information, the grand jury finds probable cause to believe that a criminal antitrust violation has occurred, it returns an indictment setting forth the practices alleged to be in violation of the law. If no indictment is returned, the DOJ still may use the evidence obtained by the grand jury in a civil action.14
If the indictment results in a criminal conviction under the Sherman Act, a corporation may be fined a maximum of $10 million. Individuals and representatives of partnerships and unincorporated associations are subject to imprisonment not exceeding three years and/or a maximum fine of $350,000.15
The DOJ also may initiate investigations to determine whether a party has violated any civil provision of the antitrust laws.16 If the civil investigation indicates that a violation has occurred, the DOJ may bring a civil suit, seeking an injunction or damages. In such civil actions, only actual damages may be recovered.
A defendant that loses in a government enforcement suit faces the possibility that a private plaintiff will employ the decision in a subsequent treble damage action. Either a criminal or civil conviction constitutes prima facie evidence of liability in such a suit. A plaintiff will be required only to prove damages. In addition, almost any type of antitrust legal action is lengthy and expensive to defend.
Fast Definitions
Actual damages - in legal terms damages refer to losses or injuries; courts award actual damages to compensate for losses or injuries that have actually occurred (e.g., loss of income because of a medical injury, specific business losses due to a breach in a contract, etc.).
Page 240 of 469

AHM 510 : Health Plans : Governance and Regulation
Treble damages - damages, in connection with certain types of wrongs, that by statute are allowed to be multiplied by three to determine total damages payable.
Prima facie evidence - evidence sufficient to entitle the party presenting the evidence to a verdict in that party's favor if the other party does not refute the evidence.21
Divestiture - a remedy the court orders against the offending party to dispose of property or assets before the party would normally have done so.22
Interlocking directorates - the situation that occurs when an individual serves as an officer or director of two or more competing corporations.23
Because of this additional exposure, defendants often enter into a consent decree under the Antitrust Procedures and Penalties Act.17 In essence, consent decrees are negotiated settlements entered before any testimony is taken. These decrees not only save both parties substantial time and expense, but also provide a wide range of enforcement remedies, including divestiture or dissolution. 18 Although consent decrees are made without admissions by any party, once the court enters the final order, these decrees have the same force and effect as decrees entered in litigated cases 19 except that they do not constitute prima facie evidence in any subsequent private treble damages action.
The DOJ monitors compliance with antitrust judgments by means of the civil investigative process. Through this process, it can compel a hospital against which an antitrust judgment has been entered to produce records that indicate whether the hospital is in compliance with the judgment. Noncompliance can result in the initiation of contempt of court proceedings.20
Federal Trade CommissionThe FTC is authorized to enforce Section 5 of the FTC Act, which prohibits unfair methods of competition and unfair or deceptive acts or practices. Together with the DOJ, the FTC also enforces those sections of the Clayton Act that prohibit discrimination (e.g., in price), exclusive dealings and similar arrangements, certain corporate acquisitions of stock or assets, and interlocking directorates.
The FTC may investigate an alleged antitrust violation on its own initiative or at the request of the president, Congress, another government agency, the attorney general, courts, 25 or other persons.26 This broad investigative authority extends throughout FTC activities, from investigations of alleged violations of antitrust laws to investigations of compliance with antitrust decrees issued under the Clayton or FTC acts.27
FTC enforcement proceedings begin in an administrative setting. A trial is held before an administrative law judge. Both the FTC staff and the party sued have a right of appeal to the full Commission.28 Decisions of the Commission that are adverse to the party can be appealed to a federal appeals court, while decisions adverse to the FTC cannot be appealed. If the Commission finds a practice to be unlawful, it enters a cease-and-desist order that may require that the practice be stopped and also may require affirmative action by the violator.
Page 241 of 469

AHM 510 : Health Plans : Governance and Regulation
Prior to adjudication on the case's merits, an FTC investigation may be terminated by the entry of a consent order.29 Like consent decrees, consent orders that are entered before adjudicative proceedings are conducted have the same force and effect as a court order.30
The FTC also is authorized to institute civil penalty actions against those who knowingly violate the FTC Act, 31 and to petition a court for a temporary restraining order or a preliminary injunction in appropriate circumstances.32 Courts generally have interpreted this power as authorization for the FTC to seek any equitable remedy judicially appropriate. 33 The FTC does not, however, have the power to seek damages for antitrust violations.
State attorneys general also have antitrust enforcement responsibility. State regulation of antitrust, including enforcement mechanisms, was discussed in State Regulation of Health Plans.
Fast Definitions
Temporary restraining order (TRO) - an emergency remedy that a court can grant, without a hearing, to prohibit a person or entity from engaging in certain conduct that is likely to cause irreparable harm to another party. A TRO is of short duration, and is effective only until the court can determine what long-term relief, if any, may be appropriate. 24
Preliminary injunction - a remedy that a court can grant, after a preliminary hearing, to prohibit a person or entity from engaging in certain conduct that might harm another party. The purpose of a preliminary injunction is to preserve the existing status of the parties until the court can determine the merits of the controversy.
Private EnforcementThe universe of potential private plaintiffs is large, and the exposure to treble damages can be disastrous. Hospitals and physicians, as well as vendors, are potential antitrust plaintiffs. To assert an antitrust claim, a private party is required to demonstrate three "standing" requirements:
• A violation of the antitrust laws
• Injury to its business or property or, in the case of injunction, threatened loss or damage
• A causal relationship between the antitrust violation and the injury34
Probably the most important of the three standing requirements is injury to business or property, i.e., injury to commercial interests or enterprises.35 In actions for treble damages, private parties' access to the courts is limited when they are injured only indirectly by the antitrust activity.36 For example, a hospital that had a contract with a mechanical contractor was found not to have standing to sue subcontractors for unlawful price fixing when the hospital was not the direct purchaser of the subcontractor's goods.37
When the injury is direct, however, courts have held that private parties have standing under the antitrust laws in a variety of different situations involving diverse injuries, including those that cause increases in the cost of doing business38; those that cause
Page 242 of 469

AHM 510 : Health Plans : Governance and Regulation
loss of business, including goodwill and reputation39; and those that frustrate a serious potential competitor's attempts to enter the healthcare market.
Indeed, the Supreme Court held in Blue Shield of Virginia v. McCready that, as long as the injury is direct and flows from that which makes the defendant's acts illegal, it is an injury within the meaning of the antitrust laws even though the injury is not part of the alleged anticompetitive effect.41 In McCready, the Supreme Court ruled that the patient had standing to sue an insurer that had engaged in an unlawful boycott against psychologists because the patient's injury was direct and provable. As a result of the boycott, patients seeking treatment by psychologists were required to see a physician as well. That discouraged the use of psychologists and increased the patients' out-of-pocket costs.
In actions seeking injunctive relief, proof of a threatened injury loss may be sufficient to constitute injury to business or property.42 Actual injury need not be shown; to obtain relief, a private party need demonstrate only a significant threat of injury from an impending, continuing, or recurring antitrust violation.43 In a unanimous decision in California v. American Stores Co., the U.S. Supreme Court ruled that a private party, including a state, can sue for injunctive relief against a merger.44 The Court held that divestiture is a form of "injunctive relief" authorized by Section 16 of the Clayton Act.
The American Stores case also indicates that having a transaction approved by the FTC or the DOJ (even by consent decree) will not eliminate all antitrust risks. A state or a private litigant still may have grounds for pursuing a private right of action. On the other hand, because of American Stores, hospitals can directly challenge and possibly prevent a merger or seek divestiture of a completed merger.
Fast Definitions
Preliminary injunction - a remedy that a court can grant requiring a party to either perform, or refrain from engaging in, certain conduct. Injunctive relief can be in the form of a temporary restraining order, preliminary injunction, or a permanent injunction. A permanent injunction is a final order that requires a party to do something or to refrain from doing something.
Page 243 of 469

AHM 510 : Health Plans : Governance and Regulation
Chapter 7 CERISA and Health Plans Few federal laws have a greater impact on the operations of health plans than the Employee Retirement Income Security Act (ERISA) of 1974, as amended.1 Although ERISA does not directly regulate health plans, it does regulate most employer-sponsored employee benefit plans to which health plans market their products. ERISA will affect the nature, design, and administration of such products by health plans. Moreover, ERISA will determine what state laws can be applied to such products as well as what legal challenges can be made to the administration of such products.
This lesson is designed to provide a working knowledge of the provisions of ERISA that are likely to affect health plan operations. Topics addressed include ERISA's documentation, reporting, and disclosure requirements; benefit plan design considerations; the amendment of benefit plans; the duties of ERISA fiduciaries, which may include health plans; challenges to benefit denials; ERISA's civil enforcement scheme and remedies; and the effect of ERISA preemption of state laws and causes of actions on health plans' operations.
After completing this lesson, you should be able to:
Describe ERISA’s documentation, reporting, and disclosure requirements Describe the minimum standards of conduct (the fiduciary duties) applicable to
ERISA plan fiduciaries Describe the claims procedures required under ERISA and the standards of review
that courts apply in deciding disputed claims Describe how ERISA preemption has been applied by the courts to:
utilization review and credentialing decisions made by health plans; mistaken verification of eligibility by an employer or health plan to a healthcare provider; entities that perform administrative functions under an ASO contract; and provider networks that contract to provide healthcare services to either health plans or self-funded employers on a capitated basis
Documentation, Reporting, and Disclosure RequirementsA plan maintained by a nongovernment employer that provides healthcare or healthcare benefits to employees (including plans providing coverage or benefits through a health plan arrangement) generally constitutes an employee benefit plan subject to ERISA.2
Such plans must meet the documentation, reporting, and disclosure requirements set forth in ERISA.
Plan DocumentEvery employee benefit plan governed by ERISA is required to be set forth in a written plan document (or documents) that detail the operative provisions governing benefits under the plan.3 In the case of healthcare benefits that are provided through an insurance contract or a contract with a health plan, the sponsoring employer might maintain a simple plan document that describes certain of the plan's rules, such as a description of the plan's eligibility and amendment provisions, but that otherwise refers to the insurance or health plan contract for the description of plan benefits.
Summary Plan DescriptionA summary plan description (SPD) is a booklet that describes the operative provisions
Page 244 of 469

AHM 510 : Health Plans : Governance and Regulation
of a plan in lay language. The Department of Labor has prescribed the types of information that are required to be included in the summary plan description.4 For insured or health plans, employers often use the booklet published by the insurance company or health plan as the basis for the summary plan description, although the employer generally will have to add certain administrative information to comply with the Department of Labor requirements concerning summary plan descriptions. In some cases, a healthcare plan contains detailed benefit schedules that are difficult to summarize. In lieu of repeating the benefit schedules, the summary plan description may provide a general description of the types of benefits provided if the summary informs participants that the complete schedules are available for their review.5
As a result of the Health Insurance Portability and Accountability Act (HIPAA), other SPD disclosure requirements were added. The SPD must include information on whether the insurer, health plan, or third party administrator (TPA) is responsible for the financing or administration of the plan. When this is the case, the SPD must show the name and address of the insurer, health plan, or TPA, and must indicate to what extent, if any, the benefits under the plan are guaranteed under an insurance or HMO contract. The SPD must also indicate the nature of any administrative services provided by the insurer, health plan, or TPA under an administrative services only (ASO) contract. In addition, the SPD must include information about the HIPAA requirements for length of hospital stay in connection with childbirth. Finally, the SPD must disclose the office of the Department of Labor from which plan participants can obtain assistance regarding their rights under HIPAA.
The summary plan description must be distributed to participants within 120 days after the date on which the plan is adopted or made effective (or, in the case of an employee who becomes a participant after the adoption or effective date of the plan, within 90 days after the date on which the employee becomes a participant).6 In general, a new summary plan description must be issued every five years, although if there have been no amendments to the plan, distribution of a new summary plan description can be made every 10 years.7
Review Question
In the paragraph below, a statement contains two pairs of terms enclosed in parentheses. Determine which term in each pair correctly completes the statement. Then select the answer choice containing the two terms that you have chosen.
Every employee benefit plan governed by the Employee Retirement Income Security Act (ERISA) must distribute a summary plan description (SPD) to participants within (90 / 120) days after the date on which the plan is adopted or made effective. Thereafter, if the plan is amended, a new SPD must be distributed every (5 / 10) years.
90 / 5
90 / 10
120 / 5
Page 245 of 469

AHM 510 : Health Plans : Governance and Regulation
120 / 10
Incorrect. While when the plan is amended a new SPD must be distributed every 5 years, the first distribution can be made in a longer period of time than 90 days
Incorrect. When the plan is amended a new SPD must be distributed sooner than every 10 years, and the first distribution can be made in a longer period of time than 90 days.
Correct. Every employee benefit plan governed by ERISA must distribute a summary plan description (SPD) to participants within 120 days after the date on which the plan is adopted or made effective. Thereafter, if the plan is amended, a new SPD must be distributed every 5 years
Incorrect. While the first distribution must be made in 120 days, subsequent distributions need to be made sooner than every 10 years.
Summary of Material ModificationsIf there are changes in the plan that affect the information provided in the summary plan description at a time when the plan sponsor is not required to publish a new summary plan description, the employer must publish a summary of material modifications.8 The summary of material modifications (SMM) explains the plan changes and acts as a supplement to the summary plan description until a revised summary plan description is distributed. The summary of material modifications must be distributed to plan participants within 210 days after the close of the plan year in which the plan amendment is adopted.9 However, as a result of changes made by HIPAA and described in interim final regulations (issued by the departments of Health and Human Services, Labor, and Treasury), if there is a "material reduction in covered services or benefits provided under a health plan," the plan sponsor must furnish a summary of material modifications no later than 60 days after the adoption of the reduction. Alternatively, to comply with the disclosure requirements for material reductions, the employer can furnish SMMs at regular intervals of not more than 90 days. Also, the plan sponsor may at any time publish an updated summary plan description in lieu of the summary of material modifications.
The interim final regulations describe a material reduction as a modification that "would be considered by the average plan participant to be an important reduction in covered services or benefits under the plan," such as elimination of a benefit, increase in deductible or copayment, or reduction of an HMO service area.
Discrepancies in Plan DocumentationAlthough the summary plan description and summary of material modifications are intended, as their names suggest, as summaries of the actual plan document, some courts have held that the summaries override the terms of the plan where the plan and the summaries conflict.10 Thus, where the summary plan description provides for benefits in a situation not covered under the formal plan document, the summary plan description might govern, particularly if the participant or beneficiary is able to demonstrate reliance on the faulty summary plan description.
Page 246 of 469

AHM 510 : Health Plans : Governance and Regulation
Government Reporting RequirementsThe plan administrator of an ERISA welfare benefit plan (including plans that provide benefits pursuant to a health plan contract) must file a variety of documents with either the Department of Labor or the Internal Revenue Service. Each year, unless the plan is exempt from filing, the plan administrator must file an annual return.11 The annual return (form 5500) is a standard form that includes information pertaining to the plan, such as plan year, plan number, employer identification number, type of coverage provided, approximate number of plan participants, and financial information. The annual return is due on or before the last day of the seventh month after the close of the plan year, although certain extensions are possible.12 The return is filed with the Internal Revenue Service and is provided by the IRS to the Department of Labor. The annual return is not distributed to plan participants as a general matter, although a plan participant must be allowed to review and make copies of the annual return.13
Plan Design ConsiderationsSubstantive Regulation under ERISAERISA provides little regulation of the content of employee welfare benefit plans (a category that includes health benefit plans). In stark contrast to the regulation of pension plans, where ERISA provides detailed requirements, the only areas in which ERISA substantively regulates the terms and conditions of employer-sponsored health benefit plans are as follows:
1. An employer-sponsored health plan is required to comply with the terms of a qualified medical child support order. A qualified medical child support order is a court order or court approved property settlement agreement that is entered pursuant to state domestic relations law or certain state Medicaid laws and that provides for health insurance coverage for a child of an employee.14
2. A group health plan, if it otherwise provides coverage for dependent natural children, is required to provide identical coverage for children who are placed for adoption with the covered employee.15
3. A group health plan may not reduce its coverage of pediatric vaccines below the level of coverage that it provided as of 1 May, 1993.16
4. A plan of an employer with 20 or more employees is required to provide employees and their covered dependents whose coverage under the plan would otherwise cease as a result of termination of employment or certain other "qualifying events" the opportunity to purchase continued coverage under the plan for a limited period of time.17
5. An employer-sponsored health plan must comply with the requirements of HIPAA, described earlier in this assignment.
Despite the limited regulation of the content of employee welfare benefit plans, ERISA's impact is considerable.
ERISA Preemption of State Insurance Laws Affecting Plan DesignGenerally As is explained in more detail in the section of this lesson devoted to ERISA preemption, ERISA broadly preempts all state law (and lawsuits under state law causes of action) that relate to ERISA plans.18 Although limited exceptions exist for state laws that regulate insurance, banking, or securities as well as for certain generally applicable laws, ERISA's preemptive scope provides plan sponsors with great flexibility with respect to
Page 247 of 469

AHM 510 : Health Plans : Governance and Regulation
the design of their benefit programs, because ERISA generally will preempt state law attempts to regulate the terms and conditions of ERISA plans.
Distinction between Insured and Self-Funded PlansThe exception for state laws that regulate the "business of insurance" creates an interesting distinction between health benefit plans that purchase insurance and those for which the plan sponsor self-insures (or self funds) the benefits. So-called mandated benefits laws-that is, state laws that mandate that health insurance contracts subject to the state's jurisdiction provide coverage or benefits for certain conditions or illnesses-constitute laws that regulate the business of insurance, and are saved from preemption.19
A self-funded plan does not purchase insurance, however, and a provision of ERISA known as the "deemer clause" prevents a state from directly applying its insurance regulation to the employee benefit plan.20 The result is a significant distinction between insured and self funded plans. Although a state may not directly regulate an employee benefit plan, the state may indirectly regulate the content of an insured plan by regulating the terms and conditions of the insurance contract that the plan purchases. A state may not, however, directly or indirectly regulate the terms and conditions of a self funded plan.
When Is a Plan Self-Funded?Historically, most health plan programs were insured arrangements, although today a growing number of plan sponsors have adopted self-funded arrangements that incorporate a preferred provider organization (PPO), point-of-service product, or other feature generally associated within the rubric of health plans. Because of the significance of the distinction between insured and self-funded plans, courts and state regulators have been called upon to determine whether certain plans are insured or self-funded.
This issue typically arises when the plan claims to be self-funded, but the plan or the plan sponsor then purchases stop loss or excess loss insurance to protect the plan or plan sponsor from large losses. Stop loss or excess loss insurance provides reimbursement to the plan or plan sponsor in the event that benefits paid by the plan to or on behalf of a plan participant or all plan participants as a group exceed thresholds established in the insurance policy. Stop loss coverage is written with either or both a specific or individual attachment point and an aggregate attachment point. Above the specific or individual attachment point, the plan or plan sponsor is entitled to reimbursement for claims paid during the policy year with respect to a single plan participant. Above the aggregate attachment point, the plan or the plan sponsor is entitled to reimbursement for claims paid during the policy year with respect to all plan participants.
Plans that purchase stop loss or excess loss insurance coverage generally have been considered self-funded for the purposes of the preemption rules described above, so that a state is not allowed to regulate the plan indirectly through application of its mandated benefit or other health insurance laws to the terms and conditions of the insurance contract.21 Rather, the stop loss or excess loss contract typically is viewed as property and casualty insurance that is subject to the state's rules and regulations for such insurance. This characterization is subject to two caveats. First, the plan participant should have no rights to claim benefits directly against the stop-loss or excess loss insurer. Stop-loss or excess loss insurance is intended to provide reimbursement to the plan or the plan sponsor for losses incurred beyond certain thresholds. If the plan
Page 248 of 469

AHM 510 : Health Plans : Governance and Regulation
participant has a direct claim against the insurer, however, the stop-loss or excess loss contract arguably constitutes a direct health insurance contract that the state could regulate as such.
Second, the thresholds at which the insurance company reimburses the plan or the plan sponsor should be sufficient so that the plan or the plan sponsor bears substantial risk for the provision of benefits under the plan (other than the risk of the insurance carrier's bankruptcy). A number of courts have suggested that, if the thresholds are set so low that they constitute a disguised deductible, the insurance contract, even though treated by the parties as providing stop loss or excess loss coverage, might be treated as direct health insurance.22 Similarly, several states have promulgated regulations to the effect that stop-loss or excess loss policies with threshold points below certain amounts would be regulated as direct health insurance contracts, allowing the state to assert the applicability of its mandated benefit laws to the contract.23 More recently in 1995, the National Association of Insurance Commissioners adopted a Stop-Loss Insurance Model Act, under which a self-funded plan would be treated as having purchased health insurance, which would be subject to all state insurance mandates, if the specific attachment point is less than $20,000. Similar rules would apply with respect to the aggregate attachment point. For groups of 50 or more, the plan will be treated as fully insured if the aggregate attachment point is less than 110% of expected claims. For groups of 50 or less, the aggregate attachment point must be at least equal to the greater of $4,000 times the number of employees, 120% of expected claims, or $20,000.24
Limits on ERISA PreemptionERISA's preemptive reach is extremely broad, although not all encompassing. For example, a New York law that imposed surcharges on hospital bills was not preempted by ERISA.25 Although the surcharges undoubtedly had an impact on a self-funded plan by increasing the cost of the benefits provided by the plan, the New York surcharge system did not relate to ERISA plans and therefore was not preempted. Although this type of indirect impact law may survive preemption, a state law that attempts to regulate the benefits provided by the plan will be preempted unless saved, in the case of an insured plan, as a law regulating the business of insurance. Thus, plan sponsors have significant flexibility with respect to the design of health benefit plans.
Also, as was noted in the section of this lesson that discusses documentation, reporting, and disclosure requirements, ERISA does not apply to government plans, such as municipal or county governments; thus, ERISA preemption of state law does not apply to a government plan. Even if such a plan is self-funded, state laws that regulate "the business of insurance" still apply.
Other Federal Laws Affecting Plan DesignAlthough ERISA grants plan sponsors considerable flexibility with respect to the design of their healthcare plans, other federal laws may restrict a plan sponsor's discretion to some extent. For example, a plan may not discriminate on the basis of age or other protected classification.26 Moreover, a plan may not discriminate on the basis of disability in a manner that violates the Americans with Disabilities Act (ADA).27
Amendment of Plans
Page 249 of 469

AHM 510 : Health Plans : Governance and Regulation
ERISA requires that every employee benefit plan provide a procedure for amending the plan and for identifying the persons who have authority to amend the plan.28 Generally, a plan sponsor reserves to itself the power and authority to amend (or even terminate) a plan. The employer's reserved amendment authority and the process by which the employer exercises that authority have been the subject of considerable debate.
Benefit ReductionsMany employers provide health plan coverage to former employees who retired after attaining a certain age and after completing a minimum period of service specified in the plan (e.g., age 55 and 10 years of service). Traditionally, the employer had few retirees relative to active employees, and healthcare costs were reasonable. As healthcare costs escalated, however, and as the employer's population shifted to include a greater number of retirees relative to active employees, employers began to modify (and in some cases terminate) the coverage provided to retirees.
Predictably, retirees whose coverage was modified or eliminated challenged many of the benefit cut-backs. Although early cases were far from uniform-some favoring the employer, some applying a rebuttable presumption in favor of the retiree-more recent cases, although still not entirely uniform, have become more homogenous in their approach. In particular, the cases have rejected a per se rule and have instead viewed the issue as a question of plan interpretation. Where the employer (plan sponsor) has reserved to itself the authority to amend, modify, or terminate the plan, the employer's exercise of that right has been upheld.29 Where the employer has not reserved to itself the authority to amend, modify, or terminate the plan, however, or if the plan language is ambiguous, the courts will seek to ascertain the parties' intent when creating the plan (i.e., did the employer or, in the case of a collectively bargained arrangement, the parties to the contract intend to create vested benefit rights that cannot thereafter be modified by the employer?).30 The starting point, however, is the plan language concerning the employer's right to amend the plan.
There is also a line of cases holding that, even where the plan documents reserve to the employer the right to amend, modify, or terminate the plan, the employer might be estopped from implementing the change as a result of prior assurances provided to plan participants. For example, in Sprague v. General Motors Corp., the court determined that General Motors had agreed to provide lifetime benefits as part of an early retirement program, a commitment that in the court's opinion overrode the employer's rights under the plan document.31 Similarly, in a case involving Unisys Corporation retirees, the U.S. Court of Appeals for the Third Circuit permitted a retiree challenge to proceed based on a breach of fiduciary duty theory (see "Fiduciary Duties" later in this lesson), despite the fact that the plan document had at all times reserved to the employer the right to amend, modify, or terminate benefits.32 The retirees alleged that plan fiduciaries had violated their fiduciary duties by consistently misrepresenting to plan participants over a period of years that retiree benefits were lifetime benefits.
Fast Definitions
Estop - a legal term meaning to stop, bar, prevent, or preclude.
Page 250 of 469

AHM 510 : Health Plans : Governance and Regulation
Amendment ProcedureEven where a plan document reserves to the employer the right to amend the plan, employees and retirees have challenged the process by which amendments have been adopted. In Schoonejongen v. Curtiss Wright Corp., the employer terminated a retiree health insurance program.33 The plan reserved to the employer the right to amend or terminate the plan but did not specify the process by which amendments could be adopted or the persons or person with the authority to amend the plan. The U.S. Court of Appeals for the Third Circuit held that the plan amendment procedure, and thus the amendment terminating the plan, was invalid under ERISA.
The Third Circuit position was short lived. The U.S. Supreme Court reversed, holding that the plan amendment procedure was valid even though it did not specifically identify the person or persons with the authority to amend the plan.34 Also, the U.S. Court of Appeals for the Seventh Circuit refused to set aside an amendment terminating a retiree welfare plan even though the plan did not contain an adequate amendment procedure under ERISA.35 It would thus appear that the courts will not easily set aside plan changes communicated by the employer to plan participants. Nevertheless. a plan sponsor would be well advised to avoid the issue altogether by specifying the amendment procedure in the plan document and, having done so, to follow that procedure.
Fiduciary DutiesERISA imposes special duties on plan fiduciaries. ERISA's definition of fiduciary is functional, that is, a person, regardless of formal title or position, is a fiduciary to the extent that he or she exercises discretionary authority and control over the operation or administration of the plan, exercises any control over plan assets, or renders investment advice for a fee.36
ERISA prescribes the minimum standard of conduct applicable to fiduciaries, the so-called fiduciary duties. A fiduciary with respect to a plan must discharge his or her obligations with respect to a plan solely in the interests of the plan participants and beneficiaries and for the exclusive purpose of providing benefits to plan participants and their beneficiaries and defraying reasonable expenses of administering the plan.37
Furthermore, the fiduciary must act in accordance with the plan documents (except to the extent that the documents are themselves inconsistent with ERISA) and with the care, skill, and diligence that a prudent person familiar with such matters would use in a similar enterprise.38 Finally, if the plan is funded, plan investment must be diversified to minimize the risk of large losses.39
Often, a plan fiduciary is also an officer of the sponsoring employer, raising the question of when such a person is wearing his or her "fiduciary hat," and thus is required to act in the sole interest of plan participants and their beneficiaries, and when the fiduciary is wearing his or her "corporate hat," and thus is able to act in the best interests of the plan sponsor. Although the distinction is not always clear, the authority to amend or even terminate the plan is a "settlor function"; that is, an employer is not acting in a fiduciary capacity when deciding to amend or terminate a plan.40 Thus, an employer might prospectively amend its group health plan to eliminate certain coverages (assuming that such elimination does not violate the ADA), and this action, although not in the best interest of plan participants, does not implicate the fiduciary's obligations under ERISA. Similarly, the decision to terminate a plan is a "settlor" or business decision of the plan
Page 251 of 469

AHM 510 : Health Plans : Governance and Regulation
sponsor. Although certain aspects of the termination process might constitute fiduciary functions, the decision to terminate does not.
In addition to ERISA's general fiduciary responsibility rules, ERISA also prohibits a plan fiduciary from engaging in a number of transactions known as prohibited transactions.41
There are two sets of prohibited transactions. The first set prohibits a plan fiduciary from causing a plan to engage in certain transactions (such as sale or lease of property or extension of credit) between a plan and a party in interest. A party in interest includes a fiduciary with respect to the plan, persons who perform services for a plan, and other persons or entities related to such fiduciaries or service providers.42 Unless advance approval is obtained from the Department of Labor, this type of related party transaction is prohibited without regard to the economic benefits of the transaction to the plan.
A second branch of the prohibited transaction rules proscribes a fiduciary from acting in certain conflict-of-interest situations or from receiving compensation from a third party in connection with a transaction involving the assets of the plan. For example, a fiduciary with respect to the plan may not cause the plan to retain the fiduciary (or a related party) to perform additional services for a fee. Where a fiduciary uses the authority, discretion, and control that makes him or her a fiduciary to cause the plan to pay an additional fee to the fiduciary, the fiduciary has engaged in a prohibited act of self-dealing.43
Challenges to Benefit DenialsClaims ProcedureEvery employee benefit plan under ERISA is required to establish a procedure whereby a plan participant or beneficiary may challenge a denial of his or her claim for benefits.44
A claims procedure will be deemed reasonable if a plan participant's or beneficiary's claim is answered in writing, with explanation of the reasons for the decision and references to pertinent plan provisions, within 90 days. If the claim is denied and the plan participant or beneficiary wishes to pursue the matter further, an appeal may be filed with the appropriate fiduciary designated by the plan. The appeal must be answered in writing, again with explanation of the reasons for the decision and references to pertinent plan provisions, within 60 days after the date on which the appeal is filed. In certain cases, the 90-day and 60-day periods can be extended if the plan participant or beneficiary is notified of the need for additional time before expiration of the initial period.45
Standard of Review in Court ActionIf the plan participant is not satisfied with the disposition of his or her claim at the plan level, he or she can file suit in state or federal court. An important threshold question involves the standard of review that the court will apply in reviewing the plan administrator's denial of the plan participant's claim.
In Firestone Tire & Rubber Co. v. Bruch, the U.S. Supreme Court determined that, in accordance with established principles of trust law, a plan participant's or beneficiary's challenge to a denial of benefits is to be reviewed under a de novo standard- that is, the court independently reviews and weighs the evidence and makes its decision accordingly, with deference to the decision made by the plan administrator- unless the plan document grants to the plan administrator or other appropriate fiduciary the discretionary authority and control to determine eligibility for benefits or to construe the terms of the plan.46 Where the plan grants the administrator such discretionary authority
Page 252 of 469

AHM 510 : Health Plans : Governance and Regulation
and control, the court is to review the benefit denial under the more deferential arbitrary and capricious standard of review. Under this standard, the court reviews the evidence but overturns the plan administrator's decision only if it represents a clearly unreasonable interpretation or construction of the plan.
The Supreme Court's decision, although based upon principles of trust law, is a puzzlement to many. Although the general rule is de novo review, the Supreme Court's decision creates an exception that potentially eliminates the general rule. By including appropriate language in the plan document, a plan sponsor changes the standard of review that a court will apply in the event that a plan participant challenges a benefit denial. More generally, why should a plan sponsor be allowed to select the standard of review through its decision to include or not include certain language in the plan document?
In the years after the Supreme Court's Bruch decision, the lower federal courts have struggled with the implications of the decision. In a number of decisions, courts have applied the de novo standard even though the document contained evidence that the plan administrator (or other fiduciary) was intended to have considerable authority and control with respect to the plan. For example, in Michael Reese Hospital & Medical Center v. Solo Cup Employee Health Benefit Plan, even though the plan document gave the administrator the authority to control and manage the operation and administration of the plan, it was held that the plan demonstrated insufficient intent to grant to the administrator discretionary authority to determine eligibility or to construe the terms of the plan.47 Similarly, in Nelson v. EG&G Energy Measurements Group, the plan document granted to the administrator the authority to "control and manage the operation and administration of the plan and to promulgate rules and regulations as deemed necessary and proper to interpret or administer the plan," yet the court applied the de novo standard.48 Although it is not necessary that the plan document contain "magic words" to demonstrate an appropriate grant of discretion, the arbitrary and capricious standard will apply only if there is evidence to show that the administrator has the power to construe uncertain terms or that eligibility and benefit determinations are to be given deference.49
In other cases, particularly those involving self funded arrangements for which benefits are payable from the plan sponsor's general corporate assets, courts have focused on the conflict of interest under which a plan fiduciary may operate because a denial of benefits is directly beneficial to the plan sponsor's treasury.50 If a plan fiduciary with the discretion to construe plan terms and make eligibility and benefit determinations also has a conflict of interest, courts will apply a less deferential standard of review than the arbitrary and capricious standard that would normally be applicable.51
Right to Jury TrialMost courts have held that ERISA does not provide a right to a jury trial, reasoning that benefit claims under ERISA are equitable in nature. The decisions are not uniform, however, and a minority of courts have found a right to jury trial.
Fast Definitions
Equitable relief - legal remedy available to a plaintiff who does not have an adequate remedy in an action at law. The function of equity is to supplement, not to replace, the
Page 253 of 469

AHM 510 : Health Plans : Governance and Regulation
law. It can include legal principles such as a mandatory injunction (a command that a person or entity do something) or a prohibitory injunction (a command that a person or entity stop doing something).
ERISA'S Civil Enforcement Scheme And RemediesIn addition to suits for benefits brought by a plan participant or beneficiary, ERISA authorizes a plan participant, beneficiary, fiduciary, or the secretary of the Department of Labor to bring a variety of civil actions. Among the more important suits are those that involve the right of a plan participant, beneficiary, fiduciary, or the secretary to bring an action for breach of fiduciary duty under Section 502(a)(2) of ERISA.54 Also, a plan participant, beneficiary, or fiduciary may bring an action under Section 502(a)(3) of ERISA to enjoin any act or practice that violates (or to enforce the provisions of) Title I of ERISA or the terms of the plan or to obtain other appropriate equitable relief.55
Although ERISA authorizes a variety of civil actions, the remedies that are available to a successful plaintiff have been quite limited. An action for breach of fiduciary duty under Section 502(a)(2) of ERISA is an action brought on behalf of the plan and all recovery runs in favor of the plan. Accordingly, the U.S. Supreme Court in Massachusetts Mutual Life Insurance Co. v. Russell, held that a plan participant or beneficiary could not recover extracontractual or punitive damages.56 Later, the Supreme Court in Mertens v. Hewitt Associates held that Section 502(a)(3) authorizes only traditional forms of equitable relief, not monetary damages.57
The Supreme Court's restrictive interpretation of Sections 502(a)(2) and 502(a)(3) takes on added significance in light of ERISA's preemption of state laws and state law causes of action that relate to ERISA governed employee benefit plans. Because of ERISA's preemptive reach, plaintiffs may not forego ERISA's civil enforcement scheme in favor of state law remedies, which might, if not preempted, include punitive or extracontractual damages.58
After the Supreme Court's holding in Russell and Mertens, the lower federal courts have struggled to attempt to provide meaningful remedies to plan participants and beneficiaries in actions brought under Section 502(a)(3) of ERISA. For example, in Watkins v. Westinghouse Hanford Co., the U.S. Court of Appeals for the Ninth Circuit ruled that a plan participant could not recover under Section 502(a)(3) benefits allegedly due the plan participant as a result of a misrepresentation.59 In other cases, such as Howe v. Varity Corp., successful plaintiffs have recovered what are, in effect, monetary damages by framing the action for benefits as a claim for restitution, an equitable remedy.60 As a result, recovery under Section 502(a)(3) remains an open issue.
ERISA PreemptionArguably, no provision of ERISA has more of an effect on the operations of health plans than ERISA's preemption clause. This section explains the general principles of preemption and discusses the impact of preemption on the following activities of health plans: utilization review determinations; the establishment of provider networks; the provision of healthcare services, either directly or by contract; representations of eligibility and coverage to healthcare providers; and the provision of administrative and other noninsurance services to ERISA plans.
Page 254 of 469

AHM 510 : Health Plans : Governance and Regulation
General Principles of PreemptionWhen Congress enacted ERISA, it intended to make the regulation of employee benefit plans an exclusively federal concern. Congress, however, also did not want to divest the states of their traditional power to regulate insurance. Pursuant to this scheme, Congress enacted three clauses relating to the preemptive effect of ERISA:
1. The preemption clause-This clause provides that ERISA supersedes any and all state laws insofar as they may relate to any employee benefit plan subject to ERISA, except to the extent that such laws may be "saved" from preemption by the savings clause. 61
2. The savings clause-This clause preserves from preemption any law of any state that regulates insurance, banking, or securities except as provided in the deemer clause.62
3. The deemer clause-This clause provides that an employee benefit plan shall not be deemed to be an insurance company or other insurer, bank, trust company, or investment company or to be engaged in the business of insurance or banking for the purposes of any law of any state purporting to regulate insurance companies, insurance contracts, banks, trust companies, or investment companies. 63
The Preemption ClauseAs noted above, Section 514(a) of ERISA preempts "any and all State laws insofar as they may now or hereafter relate to any employee benefit plan." A law relates to an employee benefit plan if it has "a connection with or reference to such a plan."64 The preemption clause is "conspicuous for its breadth," however, preempting not only state laws that are specifically designed to affect employee benefit plans but also those that may only indirectly affect such plans.65, 66 Those state laws that courts have found not to be preempted under Section 514(a) are generally limited to laws of general applicability that only tangentially affect ERISA plans.67
The Savings ClauseA state law that relates to an ERISA plan may be saved from preemption if it falls within Section 514(b)(2)(A), which excepts from preemption those state laws that regulate the "business of insurance." In Pilot Life Insurance Co. v. Dedeaux, the U.S. Supreme Court used a two-part analysis to determine whether a state law regulates the business of insurance.68, 69 First, the Supreme Court took a common-sense approach, determining that, in order to regulate insurance, a law must be specifically directed toward the insurance industry. Second, the Supreme Court applied the three part test for determining whether a practice constituted the business of insurance formulated for the McCarran Ferguson Act, namely, whether the practice had the effect of transferring or spreading a policyholder's risk, whether the practice was an integral part of the policy relationship between the insured and the insurer, and whether the practice was limited to entities within the insurance industry.70 Since Pilot Life, courts have recognized the necessity of a state law meeting both parts of the test to fall within the protection of the savings clause. 71
Review Question
Page 255 of 469

AHM 510 : Health Plans : Governance and Regulation
Congress enacted three clauses relating to the preemptive effect of the Employee Retirement Income Security Act of 1974 (ERISA). One of these clauses preserves from ERISA preemption any state law that regulates insurance, banking, or securities, with the exception of the exemption for self-funded employee benefit plans. This clause is called the
savings clause
preemption clause
deemer clause
de novo clause
Correct. The savings clause preserves from preemption any state law that regulates insurance, banking or securities except as provided by the deemer clause.
Incorrect. The preemption clause provides that ERISA supercedes any and all state laws as they may be related to any employee benefit plan subject to ERISA, except to the extent that such laws may be saved from preemption by the saving clause.
Incorrect. The deemer clause provides that an employee benefit plan shall not be deemed to be an insurance company or other insurer, bank, trust company or investment company or to be engaged in the business of insurance or banking
Incorrect. A de novo standard is a standard of evaluating a plan administrator's decision to deny benefits in which the court independently reviews and weighs evidence and makes its decision accoridingly, with deference to the decision made by the plan administrator.
The Deemer ClauseThe deemer clause exempts from any direct or indirect state regulation self-funded employee benefit plans. All power to regulate insurance reserved to the states under the savings clause is taken away with respect to self-funded plans under the deemer clause.72 The language of the deemer clause, according to the U.S. Supreme Court, is either coextensive with or broader, not narrower, than that of the savings clause.73 Thus state laws that relate to employee benefit plans but that are saved from preemption under Section 514(b)(2)(A) are still preempted as applied to self funded ERISA plans. Although, as discussed above in regard to the benefit design of ERISA plans, this interpretation establishes a disparity between the regulation of insured and uninsured plans, the U.S. Supreme Court has determined that such a dichotomy was the intent of Congress when it enacted the statute.74
Utilization Review DecisionsThe consensus among courts seems to be that utilization review decisions by health plans, even when they involve medical decisions, are an integral part of the administration of ERISA plans. Consequently, they relate to such plans and are preempted by ERISA.
Page 256 of 469

AHM 510 : Health Plans : Governance and Regulation
The U.S. Court of Appeals for the Sixth Circuit recently had occasion to reaffirm this conclusion. In Tolton v. American Biodyne, Inc., the coadministrators of the estate of a mental patient who had committed suicide sued, among others, the patient's ERISA plan administrator, the plan's mental health utilization review company, and the psychologists performing utilization review on behalf of the utilization review company, alleging that the plan administrator wrongfully denied benefits for inpatient psychiatric care based upon the utilization review company's refusal to authorize such care.75 Plaintiffs' state law claims based on such utilization review decision included wrongful death, improper refusal to authorize benefits, medical malpractice, and insurance bad faith. The court held that such claims clearly related to the ERISA plan and were preempted by ERISA.
In reaching its decision, the Tolton court relied on an earlier opinion of the U.S. Court of Appeals for the Fifth Circuit, Corcoran v. United Health Care, Inc.76 In Corcoran, the utilization review decision at issue was the refusal by the defendant utilization review company to precertify hospitalization for a high risk pregnancy despite the recommendation of the patient's physician. Instead, the defendant authorized 10 hours per day of home nursing care. The patient, who had already been admitted to the hospital, returned home when she learned that the expenses for her hospitalization would not be covered. At a time when no nurse was on duty, her fetus went into distress and died. The patient and her husband then sued the defendant, alleging wrongful death and medical malpractice.
The Fifth Circuit Court acknowledged that utilization reviewers make medical decisions despite any disclaimers to the contrary in policy manuals or promotional materials. The court found, however, that the medical decisions made by the defendant were inseparable from its determinations regarding what benefits were available under the plan. The court found that the wrongful death claim related to a denial of benefits under the plan and so was preempted by ERISA. Other courts have followed the reasoning of the Corcoran case and have preempted claims arising out of utilization review decisions.77
Credentialing DecisionsLike the analogous duty imposed on hospitals to exercise reasonable care in the selection and granting of privileges to its medical staff, a health plan has a duty to conduct a reasonable investigation of the qualifications and competence of the healthcare providers to whom they refer patients. 78, 79 Courts have declined to describe what will constitute a reasonable investigation of a provider's credentials, stating that its scope will vary from case to case.80 Recent cases have focused not on the nature or extent of the investigation of a provider's qualifications, but on whether a claim that a health plan did not conduct the requisite investigation is preempted by ERISA. Most courts that have considered the issue have ruled in favor of ERISA preemption.
A representative case is Kearney v. U.S. Healthcare, Inc.81 In Kearney, plaintiff filed wrongful death and survival claims against an HMO, alleging that decedent's primary care physician failed to diagnose properly decedent's condition or to refer decedent to a hospital for specialized treatment. Plaintiff claimed that the HMO breached its contract to provide needed specialized care by limiting or discouraging the use of specialists, hospitalization, and state of the art diagnostic procedures; misrepresented the primary care physician's competence; and was negligent in selecting and supervising the primary care physician. Plaintiff also claimed that the HMO was vicariously liable for the
Page 257 of 469

AHM 510 : Health Plans : Governance and Regulation
malpractice of the primary care physician. The court held that a "claim that an operator or administrator of a plan failed to use due care in selecting those with whom it contracted to perform services relates to the manner in which benefits are administered or provided and is preempted."82 The court dismissed not only plaintiff's claims of negligent selection but also the claim for misrepresentation and breach of contract. As discussed further below, however, the court held that plaintiff's claim that the HMO was vicariously liable for the malpractice of the primary care physician on ostensible agency grounds was not preempted
Although the list of courts in agreement with the preemption of negligent selection claims is impressive, there is some authority to the contrary.83 For example, in Jackson v. Roseman, plaintiff brought a medical malpractice case against his physicians and the HMO with which they contracted.84 Plaintiff alleged that the HMO was vicariously liable for the negligence of his physicians in allowing the growth and ultimate metastasis of a malignant cancer in his mouth. The court noted that the complaint could also be read as asserting a claim of direct negligence on the part of the HMO for negligent hiring and supervision of its contracting physicians.85 Although the court declined to address the merits of whether a negligent hiring and/or supervision claim went to the heart of the benefit plan's administration, the court indicated that it agreed with the reasoning of the U.S. Court of Appeals for the Second Circuit in a case involving claims of negligent hiring and/or supervision of a psychologist.86 In that case, the Second Circuit rejected defendant's argument that claims of negligent hiring and supervision of healthcare providers so resembled a denial of benefits or a denial of some other plan-created right as to support the removal of such claims from state court to federal court.87
Despite the cases to the contrary, a health plan can take some comfort from the likelihood that a court will find that claims that a health plan has negligently selected or retained a participating provider who committed malpractice are preempted. The same court, however, may not preempt a claim against the health plan based on vicarious liability for the malpractice of a provider, as discussed below.
Vicarious Liability for Medical MalpracticeOf the various tort theories used to impose liability on health plans for the medical malpractice of healthcare providers to whom they refer patients, none has generated more recent litigation than that of apparent or ostensible agency. Although the elements of apparent or ostensible agency vary from jurisdiction to jurisdiction, a common allegation is that the patient reasonably relied upon actions or representations of the health plan, which "held out" the negligent provider as its employee or agent, the degree of reliance required of the patient being subject to judicial debate.88
As in the area of negligent credentialing, ERISA plays a crucial role in determining whether a health plan will be vicariously liable for the malpractice of healthcare providers. The courts have been sharply divided as to whether ERISA preempts such claims, however.
Courts holding that medical malpractice claims against health plans are not preempted have found that such claims do not sufficiently relate to the employee plan to warrant preemption.89 Such courts point out that such claims do not involve the administration of benefits or the level or quality of benefits provided under plan; they merely allege negligence by a physician and an agency relationship between the physician and the
Page 258 of 469

AHM 510 : Health Plans : Governance and Regulation
health plan. Courts reaching the opposite conclusion have reasoned that a vicarious liability malpractice claim concerns the delivery of benefits under the ERISA plan and that the claim requires the examination of the terms of the ERISA plan to determine the quality and quantity of services required of physicians and the relationship between the ERISA plan and the physicians.90
Fast Definitions
Tort - a violation of a duty to another person imposed by law, rather than by contract, causing harm to the other person and for which the law provides a remedy.
Although the lower courts have been almost evenly split as to whether ERISA preempts medical malpractice claims against health plans based on vicarious liability theories, two recent Circuit Court decisions indicate that the trend may be against preemption. The U.S. Court of Appeals for the Tenth Circuit in the case of Pacificare of Oklahoma, Inc. v. Burrage identified four categories of laws that related to an employee benefit plan: laws that regulated the type of benefits or terms of ERISA plans; laws that created reporting, disclosure, funding, or vesting requirements for ERISA plans; laws that provided rules for the calculation of the amount of benefits to be paid under ERISA plans; and laws and common law rules that provided remedies for misconduct growing out of the administration of ERISA plans.91 The Tenth Circuit held that a claim that an HMO was vicariously liable for the malpractice of one of its primary care physicians did not involve the administration of benefits or the level or quality of benefits promised by the plan; it merely alleged negligent care by the physician and an agency relationship between the physician and the HMO. The court pointed out that ERISA would not preempt the malpractice claim against the physician and concluded that ERISA should similarly not preempt the vicarious liability claim against the HMO if the HMO held the physician out as its agent. Reference to the ERISA plan to resolve the agency issue did not "implicate the concerns of ERISA preemption." 92
Review Question
In the paragraph below, a statement contains two pairs of terms enclosed in parentheses. Determine which term in each pair correctly completes the statement. Then select the answer choice containing the two terms that you have chosen.
In the case of Pacificare of Oklahoma, Inc. v. Burrage, the U.S. Court of Appeals for the Tenth Circuit considered whether ERISA preempts medical malpractice claims against health plans based on certain liability theories. In this case, the Tenth Circuit court held that ERISA (should / should not) preempt a liability claim against an HMO for the malpractice of one of its primary care physicians, and therefore the HMO was subject to a claim of (subordinated / vicarious) liability.
should / subordinated
should / vicarious
should not / subordinated
Page 259 of 469

AHM 510 : Health Plans : Governance and Regulation
should not / vicarious
Incorrect. The Tenth Circuit Court did not hold that ERISA should preempt a liability claim for the malpractice of one of its primary care physicians, and is not subordinated.
Incorrect. While the Tenth Circuit court held that the HMO was subject to a claim of vicarious liability, it did not hold that ERISA should preempt a liability claim for the malpractice of one of its primary care physicians
Incorrect. While the Tenth Circuit court held that ERISA should not preempt a liability claim against an HMO for the malpractice of one of its primary care physicians, and is not subordinated.
Correct. In the case of PacifiCare of Oklahoma, Inc. v. Burrage, the Tenth Circuit court held that ERISA should not preempt a liability claim against an HMO for the malpractice of one of its primary care physicians, and therefore the HMO was subject to a claim of vicarious liability.
In Dukes v. U.S. Healthcare. Inc., the U.S. Court of Appeals for the Third Circuit addressed the issue of whether vicarious liability malpractice claims against the defendant HMO could be removed from the state court to federal court.93 The lower federal courts had allowed such a removal and then had dismissed the claims, holding that they were preempted by ERISA. The Third Circuit reversed, noting that not all claims preempted by ERISA were subject to removal. The court held that removal was improper where plaintiffs were merely attacking the quality of the benefits received and were not claiming that the ERISA plans had erroneously withheld benefits that were due or were not seeking to enforce rights under the terms of their respective plans or to clarify rights to future benefits. The court expressly distinguished the situation where the HMO denied benefits in its utilization review role.94, 95
It should be noted that the Third Circuit's decision in Dukes was limited to the issue of whether a defendant health plan can remove a medical malpractice claim from state court to federal court.96 That court's discussion of the distinction between the quantity of benefits due under an ERISA plan and the quality of the benefits provided under such plan, however, will probably be cited by other courts as authority for a refusal to preempt malpractice claims challenging the quality of services provided to plan participants and beneficiaries.
Negligent Representations by Health Plans to ProvidersWhether claims by a provider that a health plan misrepresented the existence or extent of coverage is preempted by ERISA may hinge or whether the provider is suing in its own capacity or as assignee of the health plan's insured or member. A majority of courts have held that state law causes of action brought by a provider suing in its own capacity are not preempted by ERISA, even though such causes of action would be preempted if the provider was suing in a derivative capacity as assignee for the insured or member.
For example, in the influential case of Memorial Hospital System v. Northbrook Life Insurance Company, the plaintiff hospital had treated a patient after the hospital had
Page 260 of 469

AHM 510 : Health Plans : Governance and Regulation
called the employer of the patient's husband and verified that the patient had coverage for the hospital care under a group insurance policy issued and administered by defendant.97 Subsequently, the patient and her husband assigned their benefits to the hospital. Upon the hospital's request for payment, however, defendant informed the hospital that the patient had not been eligible for benefits on the date of her hospitalization and denied benefits. The hospital subsequently sued, alleging that the employer acted as defendant's agent in verifying coverage and asserting state law causes of deceptive and unfair trade practices under the Texas insurance code, breach of contract, negligent misrepresentation, and equitable estoppel.
Fast Definitions
Equitable estoppel - a court's bar to a party from exercising a right or from asserting a fact because of something the party said or did that misled a second party to act so that harm resulted to the second party.
The lower court dismissed the hospital's claims for breach of contract and deceptive and unfair trade practices, finding that those claims were brought by the hospital in a derivative capacity, were related to a claim for benefits under an ERISA plan, and were consequently preempted. The lower court reached the opposite conclusion with respect to the claims of misrepresentation and estoppel, however, finding that those claims were based on the hospital's independent position as a third party healthcare provider, were not related to the ERISA plan, and thus "were not caught in the broad net of ERISA preemption.98
The hospital appealed the dismissal of the deceptive and unfair trade practices claim, alleging that the lower court had mischaracterized it as a derivative claim for benefits. The U.S. Court of Appeals for the Fifth Circuit agreed, holding that it was merely a Texas codification of the common law doctrine of negligent misrepresentation. Nevertheless, the Fifth Circuit felt "compelled to enter the preemption thicket" and determine whether such cause of action was sufficiently related to the employee benefit plan at issue so as to be preempted.99 The court ultimately held that it was not sufficiently related to be preempted. It is worthwhile, however, to examine in some detail the court's analysis of the policy issues involved in determining whether to preempt a provider's claims based on an erroneous verification of a patient's eligibility and coverage because the same reasoning has been adopted by courts in subsequent cases.
Before determining the legal issue of preemption, the court found it necessary to examine the "commercial realities" of the hospital's position as a healthcare provider.
The scenario depicted in Memorial's appeal is one that is reenacted each day across the country. A patient in need of medical care requests admission to a hospital (or seeks treatment from a physician). The costs of medical care are high, and many providers have only limited budget allocations for indigent care and for losses from patient nonpayment. Naturally, the provider wants to know if payment reasonably can be expected. Thus, one of the first steps in accepting a patient for treatment is to determine a financial source for the cost of care to be provided.100
The court recognized that it was customary practice for a provider to communicate with plan agents to verify eligibility and coverage and viewed the issue of a mistaken
Page 261 of 469

AHM 510 : Health Plans : Governance and Regulation
verification of eligibility and coverage by such plan agents as solely one of allocation of risks, namely, whether the risk of nonpayment of the provider's costs "should remain with the provider or be shifted to the insurance company, which through its agents misrepresented to the provider the patient's coverage under the plan," noting that enforcing "the allocation of risks between commercial entities that conduct business in a state is a classically important state interest." 101
The court remained unconvinced that "either the commercial scenario described above, or its state law vindication, raises any issue concerning the matters that Congress intended to be regulated exclusively by ERISA."102 Moreover, the court was unpersuaded that "insulating plan fiduciaries from the consequences of their commercial dealings with third-party providers would further any of ERISA's goals."103
According to the court, a one-time recovery by the hospital against the insurer or its putative agent, the employer, would not affect the ongoing administration or obligations of an ERISA plan. In addition, the court found that, if providers were held to have no recourse under either ERISA or state law in situations where there was no coverage under the express terms of the plan but providers had relied on assurances that there was such coverage, providers would be understandably reluctant to accept the risk of nonpayment and might require upfront payment by beneficiaries or impose other inconveniences before treatment would be rendered: "This does not serve, but rather directly defeats, the purpose of Congress in enacting ERISA." 104
Finally, noting that a healthcare provider did not have independent standing to seek redress under ERISA, the Fifth Circuit found that, although employees had received protection under ERISA in exchange for certain rights to sue under previous federal and state law, the plaintiff and "the countless other healthcare providers were not a party to this bargain."105 The court stated that it could not believe that "Congress intended the preemptive scope of ERISA to shield welfare plan fiduciaries from the consequences of their acts toward non-ERISA healthcare providers when a cause of action based on such conduct would not relate to the terms or conditions of a welfare plan, nor affect-or affect only tangentially-the ongoing administration of the plan."106 The court concluded that ERISA's "preemption provision designed to prevent state interference with federal control of ERISA plans does not require the creation of a fully insulated legal world that excludes these plans from regulation of any purely local transaction."107 Other courts have adopted the reasoning of the Memorial Hospital System case and refused to insulate ERISA plans, their sponsors, or their administrators from liability when they mistakenly verify eligibility or coverage to a healthcare provider. 108
Preemption of State Insurance RegulationState insurance laws and regulations often expressly exempt ERISA employee benefit plans from their application.109 In the absence of such express exemption, however, it has been increasingly common for state insurance authorities to attempt to apply insurance laws and regulations directly to noninsurance products of health plans as well as to integrated delivery systems and other entities that have contracted to provide services to ERISA plans. Whether state insurance laws and regulations are preempted by ERISA depends on a combination of the nature of the state law or regulation at issue and the nature of the services being provided to the ERISA plan.
Page 262 of 469

AHM 510 : Health Plans : Governance and Regulation
Under the traditional preemption analysis, the first issue to be addressed is whether the state law or regulation relates to the ERISA plan. If so, the law or regulation will be preempted unless it is "saved" from preemption because it regulates the "business of insurance." The nature of the services being provided to the ERISA plan and that the state is seeking to regulate, however, must constitute the "business of insurance"; it is not sufficient that the services are being provided by an insurance company or other entity subject to insurance regulation or that the state law or regulation is part of the insurance code.
The U.S. Supreme Court has held that the underwriting or spreading of risk is an indispensable characteristic of insurance.110 According to the Supreme Court, the spreading of risk means that the entity engaged in the business of insurance accepts a number of risks, some of which involve losses, and spreads such losses over all the risks to enable the entity to accept each risk at a slight fraction of the possible liability upon it.111 Courts also have held, however, that an incidental element of insurance in a contract does not bring the contract within the regulatory power of the insurance laws.112
Because some element of risk is inherent in any business transaction, the primary effect of the contract at issue must be assumption and spreading of risk.
Administrative Services Only ContractsIn the situation where the entity contracting with the ERISA plan merely provided administrative services to such plan, courts have determined that such services did not constitute the business of insurance, and therefore ERISA preempted the application of state insurance laws and regulations to such services. For example, the U.S. Court of Appeals for the Fifth Circuit held that a third party administrator of an ERISA plan was not engaged in the business of insurance where it performed no risk bearing function.113
Consequently, ERISA preempted a Texas statute imposing regulations, fees, and taxes to the extent that the statute applied to such third party administrator.
Similarly, the U.S. Court of Appeals for the Fourth Circuit held that, where an insurer acted as a third party administrator, providing purely claims processing functions for an ERISA plan pursuant to an administrative services agreement with the employer, the insurer was not engaged in the business of insurance.114 According to the court, the ERISA savings clause covered the same category of state insurance regulation as the McCarran-Ferguson Act,115 which preserves to the states the right to regulate insurance, and the McCarran-Ferguson Act did not "purport to make the States supreme in regulating all the activities of insurance companies; … only when they are engaged in the 'business of insurance' does the statute apply."116
Finally, the U.S. Court of Appeals for the Third Circuit, in the often-cited case Insurance Board of Bethlehem Steel Corp. v. Muir, found that the Pennsylvania Blue Cross and Blue Shield (BCBS) plans were not engaged in the business of insurance where they performed no underwriting function and received only an administrative fee based on the number and type of plan participants, regardless of the fact that plan participants and beneficiaries used BCBS claim forms, BCBS staff processed the claims, BCBS made initial determinations regarding coverage, and BCBS paid plan participants and beneficiaries directly and was reimbursed by the employer.117 According to the court, because "ERISA creates a scheme in which any entity engaged in the business of insurance, except an ERISA employee benefit plan, is subject to state insurance regulation," the controlling question was whether BCBS was engaging in the business of
Page 263 of 469

AHM 510 : Health Plans : Governance and Regulation
insurance when it sold administrative services to the ERISA plan.118 The court held that it was not because it did not assume any financial risk of a valid claim, it did not provide a service that was an essential part of the insurance relationship but instead merely provided administrative services, and other entities outside the insurance industry provided the same administrative services provided by BCBS.
In summary, so long as the services being provided by contract to the ERISA plan do not constitute the assumption and spreading of risk (i.e., "the business of insurance"), any attempted state regulation of those services, including regulation under the insurance code, will be preempted by ERISA.119 As the discussion below of the preemption of state any willing provider (AWP) laws demonstrates, however, the dividing line between the "business of insurance" and the provision of professional services is not always clear.
Any Willing Provider LawsA key legal battle in the health plan arena is the fight between states and health plans over the applicability of AWP laws to networks that contract with ERISA plans. Although the terms of AWP statutes differ from state to state, in general AWP statutes require that health plans and other entities establishing provider networks include the provider in the network so long as the provider meets the network's general qualifications and is willing to be compensated at the network's payment rate. Under some state statutes, patients also cannot be penalized through reduced benefits if they seek treatment from providers outside their designated network.
The debate over AWP statutes centers on ERISA and whether health plans that service ERISA plans are subject to state AWP statutes. As explained above, under ERISA, any state law that relates to an ERISA employee benefits plan is preempted. ERISA makes an exception to its broad preemption provision, however, for any state law that regulates the "business of insurance." Courts have interpreted that phrase to require a two part analysis. First, courts look to whether common sense dictates that the state statute regulates insurance. Then they decide whether a state statute affects a practice that has the effect of transferring or spreading a policyholder's risk, is an integral part of the relationship between the insurer and the insured, and is limited to entities within the insurance industry. If it does, then the statute is not preempted by ERISA as applied to a fully insured ERISA plan. As applied to a self funded ERISA plan, however, the statute is still preempted.
The difference of opinion regarding the scope of ERISA with respect to AWP statutes arises from the uncertainty as to whether regulating the identities of a network's participating providers is a regulation of the business of insurance or a regulation of noninsurance business.
Defenders of AWP statutes argue that AWP statutes regulate the business of insurance because they define the type of policy that can be issued. HMOs and other health plans that maintain closed provider networks increase the costs to patients who use nonparticipating providers by reducing or eliminating benefits for services received from those providers. An AWP statute allows a patient to obtain care from a provider who might otherwise be excluded from a network without a reduction of benefits. This prohibition on closed networks, it is argued, spreads the policyholders' risk insofar as it shifts to health plans and physician groups the costs to patients of seeking treatment from providers who otherwise would be excluded from a network.
Page 264 of 469
AHM 510 : Health Plans : Governance and Regulation
In addition to spreading policyholder risk, defenders of AWP statutes argue that such statutes affect an integral part of the relationship between the insurer and the insured: treatment and cost. AWP statutes help define the nature of the available services, who can provide them, and how those providers will be paid. In this respect, AWP statutes have been analogized to mandated benefits laws, which require insurers to include certain types of benefits in their insurance policies. Mandated benefits laws were found to be saved from ERISA preemption because they regulate the scope of the insurance coverage and the availability of services. In the same manner, it is argued, AWP statutes affect the type of benefits that an insured receives by determining who can provide covered services and how those providers are selected. Opponents of preemption assert that such regulation touches upon a vital part of the insurer insured relationship.
On the other hand, proponents of ERISA preemption contend that such statutes do not regulate the business of insurance, although they may regulate the business of insurance companies. They argue that the practice of limiting the providers with which a health plan contracts does not spread policyholder risk. Instead, the practice is merely a cost-saving mechanism. According to this argument, contracts between health plans and providers, whereby the provider receives a reduced rate of compensation in exchange for a certain volume of patients, are merely contracts for the purchase of goods and services. The transfer of risk occurs when an HMO insures an ERISA plan, not when it or another health plan attempts to minimize costs through its contracts with providers. The provider contracts are seen as identical to many other arrangements whereby health plans try to reduce costs.
Second, proponents of preemption argue that the practice of choosing the providers through whom it will provide services does not affect an integral part of the relationship between an insurer and the insured. The agreements at issue are between the insurer and the providers. They do not affect the amount or the type of benefit that a patient receives, only the vehicle through which such services are rendered.
Because of the runaway costs of healthcare and the concerted effort to find means by which to curb healthcare expenses, there are also strong policy reasons for finding ERISA preemption of AWP statutes. As discussed above, if health plans are prohibited from closing their networks, they can no longer ensure a certain volume of business. In this manner, AWP statutes eliminate any leverage health plans may have had to bargain with providers for reduced rates of compensation, effectively eliminating the benefits of establishing a provider network.
Thus far, courts have reached different conclusions as to whether particular AWP statutes regulate "the business of insurance." One of the first AWP statutes to be challenged by the health plan industry was in Virginia.120 Virginia's AWP statute allowed insurers to form PPOs and establish terms and conditions that physicians, hospitals, or other providers had to meet to qualify as a preferred provider. The statute, however, prohibited insurers from both unreasonably discriminating against and among such providers and from excluding providers willing to meet the terms and conditions for participation in the PPO. The challenge to the Virginia statute arose after a PPO established by Aetna, which provided services exclusively to employee benefit plans, refused to allow a hospital to participate in its network. Instead, the PPO only contracted with hospitals that were already participants in Aetna's HMO. The hospital sued Aetna for failing to comply with the AWP statute and excluding it from the PPO network for the
Page 265 of 469

AHM 510 : Health Plans : Governance and Regulation
sole reason that it was not a member of Aetna's HMO. Aetna defended on the ground that the statute was preempted by ERISA.
In the Virginia case, the court first found that the AWP statute related to ERISA plans. The statute not only expressly provided that it applied to health benefit programs offered or administered by insurers but also restricted the ability of an insurer to limit the choice of providers that would otherwise confine the plan participants of an ERISA plan to those preferred by the insurer.
Next, the court held that the statute was rescued from preemption because it regulated the business of insurance and consequently fell under the ERISA savings clause. According to the court, the statute spread policyholder risk because insureds whose benefits otherwise would be reduced or denied if they sought treatment from nonparticipating providers would receive full benefits under the statute. In addition, the court asserted, the statute affected an integral part of the relationship between the insured and the insurer because the statute affected the provision for treatment and cost. Finally, the Virginia statute was explicitly limited to entities within the insurance industry, thus satisfying the third McCarran Ferguson criterion. Consequently, the court held that Virginia AWP statute was not preempted by ERISA.121
A federal court in Louisiana reached the opposite conclusion in a challenge to Louisiana's AWP statute.122 Like the Virginia court, it held that the Louisiana statute related to ERISA plans. Indeed, the statute explicitly mentioned employee benefit plans. In addition, the court found that application of the statute affected the employer's or plan sponsor's discretion as to how health benefits could be structured under its employee benefit plans, pointing out that the statute explicitly directed that it could not structure its programs to exclude any provider willing and able to participate. The court then found, however, that the Louisiana statute did not regulate the business of insurance. The statute was not specifically addressed to the insurance industry but applied to entities such as employers and Taft Hartley trusts. Consequently, the court held that it did not meet the common definition of insurance test or the third prong of the McCarran Ferguson test. The legal challenges to the application of state AWP statutes to networks established by health plans and provided to ERISA plans are certain to increase.
Capitated Administrative Services Only ContractsAnother legal battle is brewing over the extent to which providers who have contracted to provide healthcare services to either health plans or self-funded employers on a capitated basis are subject to the insurance laws. The answer depends on whether such capitated contracts are construed as insurance contracts.
In an opinion dated 19 June 1990, the Maryland Attorney General addressed whether a third party administrator that had established a provider network and offered that network to self-funded ERISA plans was engaged in the business of insurance and, thus, needed an insurance license.123 The Attorney General opined that it was not. The Attorney General warned, however, that the providers might need an insurance license if they agreed to be paid on a capitated basis. The rationale for the Attorney General's opinion was that, by agreeing to be paid on a capitated basis, the providers had assumed risk and, therefore, were engaged in the business of insurance. The Attorney General concluded that an employer's creation of a self-funded employee benefit plan,
Page 266 of 469

AHM 510 : Health Plans : Governance and Regulation
protected from state regulation by ERISA, did not also exempt the providers of services to that plan from state insurance regulation.
On May 18, 1995, the Office of the Georgia Commissioner of Insurance notified a physician-hospital organization that offered its services on a capitated basis that the Georgia insurance statutes "do not permit a hospital or medical group or combination of both to provide healthcare services or benefits directly to patients for a monthly capitation fee unless fully licensed as an insurer by this department."124 The commissioner ordered the immediate discontinuance of the physician-hospital organization's healthcare program unless it was being underwritten by a licensed insurer. With respect to the issue of ERISA preemption, the commissioner took the position that the healthcare program at issue was being offered to multiple employers but did not meet ERISA's definition of an employee benefit plan.
Similarly, the Virginia Bureau of Insurance notified the health plan industry that healthcare providers and other entities that provide healthcare services to self-funded employers on a capitated basis either would have to obtain insurance licenses or would have to provide such services through licensed entities, such a HMOs.125 If the healthcare services were provided on a capitated basis by means of a contract with a health plan that in turn contracted with a self-funded employer for administrative services only (a so-called capitated administrative services only contract), then the capitated administrative services only contract would be considered an at-risk contract by the Bureau of Insurance and would be subject to the full panoply of the insurance code, including reserves requirements and assessments. The Bureau of Insurance took the position that capitated administrative services only contracts were insurance contracts and, therefore, were saved from ERISA preemption by the savings clause.
It seems likely that health plans and integrated delivery systems will seek both legislative and judicial relief from insurance commissioners' efforts to regulate capitated arrangements and that ERISA will continue to play a prominent role.
Page 267 of 469

AHM 510 : Health Plans : Governance and Regulation
Chapter 8 AFederal Government as Purchaser: Overview, TRICARE, and FEHBP
After completing this lesson, you should be able to:
Explain the government's dual role as purchaser and regulator of healthcare services Describe the evolution of the military health services system from CHAMPUS to
TRICARE, and describe TRICARE's triple benefit structure List the primary features of the Federal Employees Health Benefits Program
(FEHBP) Describe how actions taken by the Office of Personnel Management (OPM) have a
positive influence on FEHBP
Role as PurchaserIn Overview of Laws and Regulations and Federal Regulations of Health Plans, we discussed the federal government's role as a regulator of healthcare. The federal government also acts as a purchaser of healthcare benefits by operating healthcare programs that serve federal employees, the military, the poor, and the elderly. As we discussed in Overview of Laws and Regulations, federal employees have healthcare coverage options under the Federal Employees Health Benefits Program (FEHBP). Through TRICARE, formerly called CHAMPUS, healthcare benefits are available to families of active-duty service members of the military and certain other individuals who have an association with the military. Medicaid is a joint federal-state program that provides medical benefits for low-income individuals, and Medicare covers certain health expenses and benefits for persons age 65 and older. All are government-sponsored healthcare benefits programs in which the federal government is the purchaser of healthcare benefits or services.
Because the federal government is such a large purchaser of healthcare benefits and services, the standards and rules it sets for the health plans with which it contracts often become industry standards for all health plans or a large portion of a company's business. For example, in areas where federal employees make up a large part of the population, the volume of business a provider gains by participating in a plan that serves federal employees allows the health plan to negotiate with providers to form a more extensive network. The health plan can often negotiate favorable rates from the providers who will be able to spread their financial risk among a larger pool of health plan participants.
Fast Fact
Forty-seven percent of the total healthcare spending in the United States can be attributed to government purchasers.1
Approximately 5.5 million people are eligible for TRICARE benefits.2
Page 268 of 469

AHM 510 : Health Plans : Governance and Regulation
However, in February 1998, former President Clinton instructed the Secretaries of Health and Human Services, Labor, Defense, and Veterans Affairs and the Director of the Office of Personnel Management to determine the extent of their compliance with the Consumer Bill of Rights and Responsibilities and to initiate actions consistent with the Patient Bill of Rights. FEHBP was created by the Federal Employees Health Benefits Act of 1958 and is administered by the Office of Personnel Management (OPM), the human resources agency of the U.S. government. Subsequently, the following actions occurred:
• The Secretary of Health and Human Services notified all state Medicaid directors that emergency room care protections should be consistent with the Consumer Bill of Rights.
• The Secretary of Defense issued a policy directive to ban all so-called "gag" clauses and to ensure that all patients in the military health system can fully discuss all treatment options.
• The Secretary of Veterans Affairs ensured that a sufficient appeals process is in place throughout the Veterans Health System.
• The Director of OPM issued regulations for plans that participate in FEHBP to prohibit practices that restrict physician-patient communications about medically necessary treatment options.
• In March 1998, the Director of OPM announced an initiative to bring FEHBP plans into compliance with the Patient Bill of Rights within the next two years. Plans were required to report on their current compliance with the standards and submit a proposal describing how they will bring their plans into compliance.
The Federal Employees Health Benefits Program (FEHBP)As we discussed in Perspective and Overview of State and Federal Laws, the Federal Employees Health Benefits Program (FEHBP) was created by the Federal Employees Health Benefits Act of 1959 (FEHB Act) and is administered by the Office of Personnel Management (OPM), the human resources agency of the U.S. government. Through the FEHBP, the U.S. government provides health benefits to federal employees, retirees, and their family members. FEHBP is the largest employer-sponsored health benefits program in the United States. Federal employees enjoy the widest selection of health plans in the country. The choices that FEHBP offers include managed fee-for-service (FFS) plans, plans offering point-of-service (POS) options, and health maintenance organizations (HMOs). Eighty percent of the FFS plans in FEHBP offer participants a preferred provider organization (PPO) option. Figure 8A-1 describes some features of FEHBP for beneficiaries.
Figure 8A-1 Features of FEHBP
1. Voluntary, annual enrollment 2. No pre-existing conditions, physical exam, or age requirements 3. Choice of HMOs, POS options, and fee-for-service plans 4. Self-only or self-and-family coverage is available, and coverage begins
immediately upon enrollment 5. Payroll deduction for premium contributions
Page 269 of 469

AHM 510 : Health Plans : Governance and Regulation
To help employees select the right kind and quality of care at the right price, the OPM develops and distributes an annual Guide to Federal Employees Health Benefits Plans for Federal Civilian Employees. This Guide is a clear, well-written presentation of both general information, such as the OPM's statement of commitment to its customers, and specific plan report cards. The plan report cards include premium and deductible amounts, information on accreditation, status designations from the National Committee for Quality Assurance (NCQA), and the results of recent surveys measuring the satisfaction of plan participants. In addition to examining overall customer satisfaction, the surveys measure consumer satisfaction on a number of specific issues, such as those listed in Figure 8A-2. The Guide indicates which plans have received an overall satisfaction score that is significantly higher than other plans.
All prepaid plans offered by FEHBP have health plan features such as preadmission certification, the use of primary care providers as gatekeepers to coordinate medical care, and a network of physicians and other providers. The minimum benefits that FEHBP plans provide include hospital benefits, surgical benefits, physician services benefits, ambulatory patient benefits, supplemental benefits, and obstetrical benefits.
Figure 8A-2. Measures of Customer Satisfaction with FEHBP.
1. Ability to see the same doctor on most visits 2. Access to medical care (arranging for and getting care) 3. Access to medical care in an emergency (POS and HMO only) 4. Choice of doctors available through the plan (plan members' ability to find
doctors they are satisfied with) 5. Costs that beneficiaries personally have to pay (FFS only) 6. Coverage (range of services covered) 7. Explanation of care (what is wrong, what is being done, and what to expect) 8. Getting appointments when sick 9. How quickly claims are processed (FFS only) 10. Quality of care (from doctors and other medical professionals) 11. Results of care
Source: Adapted, with permission of the publisher, from 1998 Guide to Federal Employees Health Benefits Plans for Federal Civilian Employees, 1997, online, United States Office of Personnel Management, Available: http://www.opm.gov/insure.
Preemption IssuesIn drafting the FEHB Act of 1958, Congress took steps to protect the uniformity of services provided under FEHBP. Concerned about the effect of requirements that differ from state to state, Congress specified in Section 8902(m)(1) that FEHBP contract provisions "which relate to the nature or extent of coverage or benefits" preempt any inconsistent state law. The preemption provision allows the federal government to preempt state laws that relate to (a) the nature or extent of coverage or benefits or (b) taxes, fees, or other monetary payments, imposed on a carrier, when such state requirements are inconsistent with the provisions of the FEHBP contract.
Congress intended for this preemption to be broad to cover state law requirements that destroyed the uniformity of FEHBP benefits or any rates or taxes. However, no one knows the absolute breadth of federal preemption of state laws. Case law generally upholds the broad scope of the preemption.
Page 270 of 469
AHM 510 : Health Plans : Governance and Regulation
Funding for FEHBPLike most employers, the U.S. government makes a monetary contribution for health benefits for its employees. The FEHP Manual states the the Government pays "72 percent of the average premium" toward the cost of health insurance premiums, but not more than 75 percent of the total premium for any plan. For example, in 2002, the biweekly average premium amounts are $135.61 for self-only and $309.66 for self-and-family coverage. Accordingly, the maximum biweekly Government contribution is $97.68 for self and $223.41 for family.4 For some plans the actual figure the government pays is a lower amount, because the FEHB Act specifies that the government's contribution cannot exceed 75 percent of a plan's total premium.5 Therefore, for some plans with relatively inexpensive premiums, the government may have to pay less than it otherwise would to keep from exceeding the 75% limit. Federal employees contribute their portion of the premium through payroll deduction.
OPM Administration of FEHB ProgramWith an administrative staff of 150, OPM manages health benefits worth more than $16 billion at an administrative cost of $20 million.6 OPM is responsible for:
• Determining which plans will be part of FEHBP
• Communicating a wealth of information to plan members so plan members can make informed choices and so participating plans will compete to offer the best care to federal employees
• Requiring participating plans to perform a large share of the administrative tasks
• Demanding attractive premium rates and auditing the plans periodically to ensure that premiums were properly developed
These tasks, plus the creation and administration of a reserve fund, allow OPM to keep FEHBP premiums as low as possible.
Selecting Participants for FEHBPOPM is responsible for determining which plans will be offered as part of FEHBP. By law, OPM must offer any federally qualified HMO that meets its requirements. In principle, OPM accepts any plan that can satisfy its requirements. To be eligible to participate in FEHBP, a plan must:
1. Demonstrate financial stability and have a management team that has experience pertinent to the prepaid healthcare provider industry
2. Possess an enrollment of at least 300 subscribers (exceptions are made for new plans and plans in rural areas with limited numbers of government workers), and sufficient subscriber income to operate within a budget
3. Have a healthcare delivery system that provides reasonable access to and choice of quality primary care and specialty care throughout the service area
4. Be able to establish firm budget projections that can be met on a regular basis 5. Comply with OPM's minimum standards for benefit design
Once a plan is accepted, it can stay in FEHBP as long as it continues to meet the minimum standards as they are specified each year. Each spring, OPM sends all plan providers its call letter, a document that specifies, among other things, the kinds of benefits that must be available to plan participants and cost goals and procedural
Page 271 of 469

AHM 510 : Health Plans : Governance and Regulation
changes that the plans need to adopt. Figure 8A-3 provides a list of examples of expanded benefits or other benefit changes in the last few years.
Figure 8A-3. Expanded benefits/benefit changes to FEHBP.
1. Minimum of 48 hours inpatient care for normal childbirth and 96 hours of inpatient care for Cesarean deliveries
2. Option of inpatient care with stay of at least 48 hours for mastectomy patients 3. Mammography screenings according to the National Cancer Institute's minimum
standard 4. The elimination of annual dollar limits on mental healthcare coverage, in
accordance with the new Mental Health Parity Act 5. Better access to specialists for treatment of complex or serious conditions, and
improved continuity of care for such conditions when either the participant or the provider leaves the plan
Source: Eric Minton, "Purchasing Lessons From the Feds," Business & Health, February 1998, 21-28.
Setting Premium Rates and Auditing PlansFor FFS plans, including PPOs, OPM actuaries annually determine the lowest premium that is actuarially sound, and then OPM negotiates to establish that premium rate. In each instance, the negotiated premium rate allows the plan to earn a fixed profit for every subscriber; however, that profit per subscriber is a fraction of 1% of the premium. This profit structure gives the FFS plans an incentive to compete for subscribers.
For HMOs and POS options, OPM uses a different approach to set premium rates. If OPM attempted to negotiate premium rates with every health plan with which it contracts, the staff of OPM would have to be much larger than it is now. Instead, OPM requires each health plan or plan with a POS product to use the same rating methodology (adjusted for differences in benefits) for FEHBP members that it would use to determine rates for other similarly sized subscriber groups (SSSGs). For a health plan, similarly sized subscriber groups (SSSGs) are two employer groups with which the health plan contracts that:
• Have similar numbers of enrolled members (as would enroll under FEHBP)
• Use any rating method other than retrospective experience rating
• Meet other OPM rate criteria for this classification
Review Question
The following statements are about the Federal Employees Health Benefits Program (FEHBP), which is administered by the Office of Personnel Management (OPM). Three of the statements are true and one statement is false. Select the answer choice that contains the FALSE statement.
Page 272 of 469

AHM 510 : Health Plans : Governance and Regulation
For every plan in the FEHBP, OPM annually determines the lowest premium that is actuarially sound and then negotiates with each plan to establish that premium rate. Once a health plan has submitted its rate proposals for a contract year to the OPM, it cannot adjust its premium rate for any reason. To cover its administrative costs, OPM sets aside 1% of all FEHBP premiums.
Each spring, OPM sends all plan providers its call letter, a document that specifies the kinds of benefits that must be available to plan participants and cost goals and procedural changes that the plans need to adopt.
Correct. If OPM attempted to negotiate premium rates with every health plan with which it contracts, the staff of OPM would have to be much larger than it is now. Instead, OPM requires each health plan or plan with a POS product to use the same rating methodology (adjusted for differences in benefits) for FEHBP members that it would use to determine rates for other similarly sized subscriber groups (SSSGs).
Incorrect. It is true that once a health plan has submitted its rate proposals for a contract year to the OPM, it cannot adjust its premium rate for any reason.
Incorrect. To cover administrative costs OPM DOES set aside 1% of all FEHBP premiums
Incorrect. Each spring, OPM DOES sends all plan providers call letter, a document that specifies the kinds of benefits that must be available to plan participants and cost goals and procedural changes that the plans need to adopt.
Historically, OPM required participating plans (i.e., the nonexperience-rated plans) to use prospective community rating to determine premium rates for FEHBP. There was some confusion over the definition of a community rate and the way plans were to determine such a rate. To simplify program administration, OPM shifted the focus of its premium negotiations to SSSGs.
Health plans must be careful and accurate in setting premium rates for FEHBP. Once a health plan has submitted its rate proposals, due annually by May 31 of the year preceding the contract year, it cannot adjust its premium rate for any reason. In addition, the OPM has the authority to conduct periodic audits of any health plans participating in FEHBP. The purpose of these audits is to verify that the rate was determined in accordance with FEHBP requirements and that any benefit or loading added to the FEHBP premium rate was reasonable and appropriate. If OPM auditors determine that a health plan’s premium development process was defective, the auditors will recommend that the health plan refund any overcharges to FEHBP. If the auditors determine that a health plan intentionally presented a false claim to the U.S. government, the health plan could be liable for a substantial civil penalty, including treble damages for each violation.
Fast Definition
Page 273 of 469

AHM 510 : Health Plans : Governance and Regulation
Loading - The charge added to a net premium to cover the plan's or insurer's costs of doing business. 14
Creating and Administering a Reserve FundOPM creates a special rollover reserve fund and uses the amounts in this fund either to increase the benefits it offers or to decrease the premium that must be charged. The money in this reserve fund comes from two primary sources:
• To cover its administrative costs, OPM sets aside 1% of all FEHBP premiums. As a result of the money-saving strategies applied by OPM, the cost of administering FEHBP is only about two-tenths of that 1%, and OPM puts the remainder in the reserve fund.8
• OPM sets aside 3% of every premium and specifically tags this money for the carrier that collects that premium.9
Each year at rate-setting time, OPM takes everything above two months of reserves and uses this amount either to add an extra benefit to the coverage or to decrease the premium for the plan.
TRICARE The military health services system (MHSS) is a worldwide healthcare system comprised of more than 500 medical and dental treatment facilities called military treatment facilities (MTFs), including 124 hospitals, that provide medical care to people entitled to such care as defined by the Department of Defense (DOD).12 People entitled to such medical care include members of the armed forces on active duty, other armed forces members, their dependents, and certain other persons specified as eligible by the DOD.13
In addition to providing direct medical care for eligible participants, the DOD also offers healthcare benefits to certain qualifying individuals under a program entitled TRICARE. Qualifying individuals include:
• Families of active-duty service members
• Retired service members, their spouses, and certain unmarried children
• Certain former spouses of members of the military
TRICARE is a regional managed healthcare program available to eligible beneficiaries, as defined by the DOD. Insight 8A-1 provides a brief history of the development of TRICARE. TRICARE offers three options for healthcare services: TRICARE Prime, TRICARE Extra, and TRICARE Standard.
1. TRICARE Prime 2. TRICARE Extra 3. TRICARE Standard
TRICARE is unique because it is not insurance and, therefore, is not subject to state regulation of insurance. Under TRICARE, the federal government pays for healthcare services delivered by authorized providers to eligible individuals except under the
Page 274 of 469

AHM 510 : Health Plans : Governance and Regulation
demonstration programs where TRICARE Management Activity (TMA), discussed in the following section, contracts with health plans to finance and deliver care.18
Insight 8A-1. The Development of TRICARE.
As early as 1884, Congress directed that "medical officers of the Army and contract surgeons shall whenever possible attend the families of officers and soldiers free of charge." This system remained in place with very little change for nearly 50 years.
World War II and the Korean conflict strained the ability of the military medical care to meet the medical needs of family members of active-duty service members. In 1943, Congress authorized the Emergency Maternal and Infant Care Program (EMIC). EMIC provided for maternity care and the care of infants up to one year of age for wives and children of service members in the lower four pay grades. It was administered by the "Children's Bureau," through state health departments.
On December 7, 1956, the Dependents' Medical Care Act was signed into law. In 1966, Congress proposed amendments to this act that created the Civilian Health and Medical Program for the Uniformed Services (CHAMPUS). Beginning in 1967, active-duty family members and retirees and their family members were all eligible for medical treatment under CHAMPUS. The CHAMPUS budget for Fiscal Year (FY) 1967 was $106 million. The MHSS has converted the CHAMPUS program to a program that incorporates the use of a health plan, called TRICARE. In FY 1996, the TRICARE budget was more than $3.5 billion, and more than 20 million claims were received. Today, nearly 5.5 million people are eligible for TRICARE benefits.
Source: Adapted and used with permission, THE HISTORY OF CHAMPUS AND ITS EVOLVING ROLE IN TRICARE, online, Tricare Management Activity, hp, Available: http://www.ochampus.mil/Fact_Sheets/Historyoftricare.htm, 11 Mar. 1998.
TRICARE Prime - a voluntary, annual enrollment option similar to a civilian HMO that offers the full range of benefits formerly available under CHAMPUS plus additional preventive and primary care services, such as physical screenings. A point-of-service (POS) option is also available. If the beneficiary receives care from the civilian and military providers who make up the Prime network, there are no deductibles to meet, no claims filings, and cost-sharing is low. If the beneficiary receives care outside the Prime network under the POS option, there are annual deductible requirements, claims must be filed, and cost-sharing is 50% of the TRICARE allowable charge. Although active-duty service members are automatically enrolled in the TRICARE Prime option, these personnel are strongly encouraged to complete an enrollment form. Active-duty dependents and eligible retirees and their families who wish to be covered under TRICARE Prime must apply for enrollment. Active Duty service members and their families pay no enrollment fee for TRICARE Prime. Retirees and their families pay an annual enrollment fee to participate in TRICARE Prime.15
TRICARE Extra - A Preferred Provider Organization (PPO) option that does not require enrollment and offers low out-of-pocket costs for those beneficiaries who choose to obtain care from network providers. There are annual deductible requirements but no claims filings as long as the care is delivered by a PPO provider.16
Page 275 of 469

AHM 510 : Health Plans : Governance and Regulation
TRICARE Standard - the same as the current CHAMPUS benefit and cost-sharing structure. Under this option, TRICARE pays a share of the cost of covered health services that are obtained from non-network providers. The cost-sharing for the beneficiary under this option is higher than the other two options, but the beneficiary has the most freedom to choose providers. No enrollment is required, but there are annual deductible and claims filing requirements.17
Review Question
TRICARE, a military healthcare program, offers eligible beneficiaries three options for healthcare services: TRICARE Prime, TRICARE Extra, and TRICARE Standard. With respect to plan features, both an annual deductible and claims filing requirements must be met, regardless of whether care is delivered by network providers, under
TRICARE Prime and TRICARE Extra only
TRICARE Extra and TRICARE Standard only
TRICARE Standard only
none of these healthcare options
Incorrect. TRICARE and Extra offer no claims filings, and TRICARE Prime has no deductible.
Incorrect. TRICARE Extra does not have claims filing
Correct. TRICARE Standard has both deductibles and claims filings
Incorrect. One of the three TRICARE options has deductibles and claims filing
Administration, Funding, and Benefits of TRICAREAlthough three different cabinet secretaries-the Secretary of Defense, the Secretary of Health and Human Services, and the Secretary of Transportation-share the regulatory authority over TRICARE, the responsibility for providing policy guidance, management control, and coordination for TRICARE belongs to the Assistant Secretary of Defense for health affairs.19 TRICARE is administered by TRICARE Management Activity (TMA), formerly called the Office of CHAMPUS (OCHAMPUS), and the TRICARE Support Office (TSO).
Through its annual appropriations to the DOD and the Department of Health and Human Services, Congress provides the funds used by TRICARE to pay benefits. Fiscal intermediaries (FIs), who are disbursing agents under contract to the federal government or TRICARE contractors, use these federal funds to pay TRICARE benefits only; such funds are not used to pay claims under any other programs.
TRICARE benefits include most inpatient and outpatient health services, a large portion of provider charges, medical supplies and equipment, and mental health services. In
Page 276 of 469

AHM 510 : Health Plans : Governance and Regulation
recent years, TRICARE benefits have been expanded to include liver, heart, lung, and heart-lung transplants, as well as hospice care. Ambulatory surgical centers and free-standing birthing centers have also been added to the list of authorized providers of care for TRICARE.20
Transition to TRICAREBetween 1985 and 1990, CHAMPUS expenditures and CHAMPUS claims more than doubled.21 To address these factors, the DOD began several demonstration projects in various parts of the United States through a project called the CHAMPUS Reform Initiative (CRI). Each demonstration experimented with applying certain health plan techniques to the services available under CHAMPUS.
Additionally, by enacting the National Defense Authorization Act for Fiscal 1994, Congress directed the DOD to develop and implement a health benefit option under CHAMPUS patterned after private-sector HMOs and other similar government health insurance programs. Based on the demonstration programs initiated in the late 1980s through CRI and following Congress' directive in 1994, TRICARE was developed.
Administration and Payment Mechanisms of TRICAREBefore attempting to implement TRICARE, the DOD divided the United States into 12 health services regions. Each health services region is administered by a Lead Agent who works with the region's military treatment facility (MTF) commanders to develop an integrated plan for the delivery of healthcare to eligible beneficiaries.22 A Lead Agent's responsibilities include ensuring the appropriate referral of patients between the direct care system and civilian providers, especially managing specialized treatment services. The nature of the TRICARE program is regional as evidenced by the seven health services regions. Due to its regional nature, some TRICARE features vary from one region to the next, but other TRICARE features are the same in every region. Figure 8A-4 describes features that are the same in every TRICARE region.
Figure 8A-4. Uniform TRICARE Features.
• Incentives based on enrollment status and network provider use—Beneficiaries have financial incentives to enroll in managed care plans and to use network providers. Such differentials are designed as incentives to use the system that better ensures high-quality care and low costs.
• Primary care managers—MTF commanders have the flexibility to assign each enrolled beneficiary to, or to allow each beneficiary to choose, a primary care manager who has overall responsibility for managing the care provided to the beneficiary and family.
• Greater uniformity in scope of covered services—To minimize beneficiary confusion, the services covered under TRICARE will be as uniform as possible.
• Utilization management and quality assurance programs— Refinement and expansions of existing utilization management and quality assurance policies throughout the MHSS permit the DOD and the military service medical departments to ensure quality improvement and cost effectiveness of TRICARE within and among geographic regions.
Page 277 of 469

AHM 510 : Health Plans : Governance and Regulation
• Marketing strategies—A critical responsibility of managers at alllevels is to communicate all changes in the way healthcare is delivered and received in the TRICARE program to all those affected. An extensive education program for both beneficiaries and healthcare providers is being [used to accompany the transition from CHAMPUS to TRICARE.] This education program focuses on informing beneficiaries of the options available in seeking healthcare and ensuring that beneficiaries understand how they can maintain and improve their own health status through family risk management, diet, exercise, and appropriate use of health services.
Source: Reprinted from Peter R. Kongstvedt, MD, ed., The Managed Health Care Handbook, Third Edition, © 1996, p. 785, with permission from Aspen Publishers, Inc., Gaithersburg, MD (1-800-638-8437).
Enrollment-based Capitation Capitation23
A major component of TRICARE is the series of health plan support contracts that supplement the capabilities of regional military healthcare delivery networks. These contracts have been developed in coordination with the Lead Agents and procured by the Department of Defense on a competitive basis. The TRICARE support contractors develop networks of civilian providers around the MTFs and other prime service areas, facilitate locating providers for beneficiaries, perform utilization management functions, process claims, and provide beneficiary support functions. There are seven fixed-price, at-risk contracts supporting the TRICARE regions.
Enrollment-based capitation (EBC) is being initiated throughout the MHSS to allow MTF commanders full accountability for all resources used by the TRICARE Prime enrolled populations. Under EBC, commanders commanders will know exactly which TRICARE Prime patients they are responsible for and how much money they are being given to care for these patients. There are essentially three components of EBC:
1. A per member per month (PMPM) “premium” earned by the MTF for each TRICARE Prime patient enrolled
2. Additional revenues earned by the MTF for providing care for patients on a space-available basis, as capacity permits
3. A system of referrals under which the referring institution is billed for the treatment provided TRICARE Prime enrollees who are sent out for specialty care
This earning of revenues and purchasing of care will be reconciled on a monthly basis and could result in a transfer of funds within and between the military departments.
Page 278 of 469

AHM 510 : Health Plans : Governance and Regulation
Chapter 8 BMedicare and Health Plans
After completing this lesson, you should be able to:
Describe the three major types of Medicare+Choice plans Explain the certification process for a Medicare PSO List the three ways that payment rates will be determined for health plans under
Medicare+Choice Explain how a Medicare Medical Savings Account works Describe health plan contracting standards under the Medicare+Choice program Provide examples of Medicare marketing restrictions
Editor's Note
On December 8, 2003, President George W. Bush signed into law the Medicare Modernization Act of 2003 (MMA), taking steps to expand private sector health care choices for current and future generations of Medicare beneficiaries. The MMA proposes short-term and long-term reforms that build upon more than 30 years of private sector participation in Medicare.
The centerpiece of the legislation is the new voluntary prescription drug benefit that will be made available to all Medicare beneficiaries in 2006. Additional changes to the Medicare+Choice (M+C) program include:
• Medicare+Choice program’s name is changed to Medicare Advantage (MA);
• Increased funding is provided for MA plans in 2004 and 2005;
• MA regional plans are established effective 2006.
On January 16, 2004 CMS announced new county base payment rates for the MA program. Beginning March 1, 2004, all county MA base rates received an increase which plans are required to use for enhanced benefits. Plans may use the extra money in one of four ways:
• Reduce enrollee cost sharing;
• Enhance benefits for enrollees;
• Increase access to providers;
• Utilize the stabilization fund.
The short-term reforms have already improved benefits and reduced out-of-pocket costs for millions of Medicare beneficiaries who are covered by health plans in the Medicare Advantage program, previously known as the Medicare+Choice program. These coverage improvements became effective on March 1, 2004.
Page 279 of 469

AHM 510 : Health Plans : Governance and Regulation
Beginning in 2006, the MMA will provide beneficiaries with a broader range of private health plan choices similar to those that are available to working-age Americans and federal employees. In addition to the locally-based health plans that currently cover more than 4.6 million Medicare beneficiaries, regional PPO-style plans will be available as a permanent option under the Medicare Advantage program.
Final regulations were released in January, 2005, and this chapter's content will be updated in July, 2005 to reflect the new regulatory changes.
Overview and BackgroundIn 1965, President Lyndon B. Johnson signed Medicare into law. Medicare is a federal government hospital expense and medical expense plan for persons age 65 and older and for certain other persons as specified by law. Under the Act that established Medicare, the Medicare program was to be funded by payroll deductions, federal subsidies, and (initially) $3.00 per month in individual premiums. In 1972, the Medicare program was extended to include persons of all ages with end-stage renal disease and those receiving Social Security disability payments.1
Over the years since Medicare was initiated, a growing percentage of the nation's elderly population has received health insurance through the program. Figure 8B-1 illustrates the growth Medicare has experienced since its inception.
Originally, Medicare consisted of two parts: Hospital Insurance (Part A) and Medical Insurance (Part B). Medicare Part A provides coverage of inpatient hospital services, skilled nursing facilities, and hospice care.2 Medicare Part B helps pay for the cost of physician services, outpatient hospital services, home health care, medical equipment, and other health services and supplies.
In 1997, a Congressional budget act, entitled the Balanced Budget Act of 1997, added a Part C (also called Medicare+Choice) to Medicare. Medicare+Choice is a portion of the Medicare program, and is designed to (1) expand the healthcare coverage choices available to Medicare beneficiaries by allowing more types of health plans to apply for Medicare contracts, and (2) change the system for determining the rates that will be paid to health plans with Medicare contracts. We will examine these changes in more detail later in this lesson.
Page 280 of 469

AHM 510 : Health Plans : Governance and Regulation
Figure 8B-1. Medicare Enrollment Trends.
65+
EnrollmentDisability
EnrollmentTotal
EnrollmentJuly (In millions) 1966 19.1 -- 19.11970 20.5 -- 20.51975 22.8 2.2 25.01980 25.5 3.0 28.51985 28.2 2.9 31.11990 30.9 3.3 34.21991 31.5 3.4 34.91992 32.0 3.6 35.61993 32.4 3.8 36.31994 32.8 4.1 36.91995 33.0 4.3 37.31996 33.4 4.7 38.11997 33.6 5.0 38.61998 33.8 5.3 39.1
Source: CMS Statistics: Populations, Centers for Medicare and Medicaid Services, online, Available: http://www.hcfa.gov/stats/hstats96/blustats.htm, 9 Sept. 1998.
Administration of the Medicare ProgramAs we discussed in Overview of Laws and Regulations, the Centers for Medicare and Medicaid Services (CMS), a division of the Department of Health and Human Services (HHS), administers the Medicare program. CMS is responsible for contracting with health plans that wish to participate in the Medicare program. In addition, CMS develops rules and regulations to implement various laws, such as the Balanced Budget Act of 1997, that impact the Medicare program. In a later section of this lesson, we will discuss CMS's role in more detail.
Why Use Health Plans for Medicare?Although Medicare covers hospitalization and many other medical services, it does not usually pay the full costs of those services. Coverage is subject to both deductible and coinsurance provisions. Also, a number of healthcare services are not covered under Medicare. For example, fee-for-service (FFS) Medicare generally does not pay for benefits such as prescription drugs, eyeglasses, hearing aids, routine physical exams, and basic dental services.3 Medicare beneficiaries often purchase supplemental insurance for healthcare expenses or services that are not covered by FFS Medicare. This supplemental insurance is called Medigap. In the large majority of Medicare markets where qualified HMOs have provided services, however, HMO enrollees have seen a reduced need for Medigap insurance because HMOs offer more comprehensive coverage to their Medicare enrollees than FFS Medicare.
Page 281 of 469

AHM 510 : Health Plans : Governance and Regulation
Another important reason the federal government has passed laws encouraging health plans in the Medicare market is that, under the predominantly FFS system, Medicare outlays have been growing rapidly. In fiscal year 1980, Medicare spending totaled $33.9 billion.4 By 1998, this amount had increased to $231.1 billion.5 With the baby-boomer generation entering the Medicare program, many experts believe that without significant reform Medicare Part A will become insolvent around the year 2010. Because health plans have proven to be an instrumental tool in managing commercial healthcare costs, the federal government is increasingly turning to health plans to help contain Medicare costs.
Although the original Medicare law included opportunities for health plans to participate in Medicare on a cost-reimbursement basis, in many markets this program was of limited attractiveness to health plans. In 1972, Section 1876 of the Social Security Act was enacted. Section 1876 allowed both cost-based and partial-risk Medicare health plan contracts. The Tax Equity and Fiscal Responsibility Act of 1982 (TEFRA) amended Section 1876 to include provisions that enabled health plans to participate in the Medicare program on a full-risk basis. Figure 8B-2 describes the differences between risk and cost contracts. Increasingly, Congress and CMS, in its role as administrator, are focusing on a risk-based approach for the Medicare program. And, as described in Figure 8B-2, cost contracts will be completely phased out of the program by the end of the year 2002.
Figure 8B-2. Risk vs. Cost Contracts.
Since 1972, the federal government has provided payment to Medicare health plans through two main types of contracts: risk contracts and cost contracts. Provisions in Section 1876 of the Social Security Act allow for the formation of Medicare risk and cost contracts. As a result, Medicare risk and cost contracts are sometimes referred to as "Section 1876" contracts.
All Medicare-contracting health plans (both cost and risk plans) are required to provide Medicare covered benefits. In addition, as an optional benefits package, services that are not covered by Medicare may be offered by such plans. The plans may charge enrollees an additional premium for those benefits packages.
Medicare Risk ContractsHealth plans with Medicare risk contracts are considered to be "at risk" because they are financially responsible for providing beneficiaries with all necessary healthcare services covered by Medicare. Risk plans receive a set amount of money from CMS each month for each plan member, regardless of the amount of services the beneficiary requires in any given month. The amount paid to the health plan varies depending on the category of the enrollee, e.g., the enrollee's age, sex, institutional status, and Medicaid status.
Each year, a Medicare risk contracting plan is required to submit to CMS its adjusted community rate (ACR). The ACR is the estimated premium that the plan would have to charge Medicare enrollees for Medicare covered services, independent of Medicare payments, less coinsurance and deductibles. The plan bases the ACR on the same rates it charges to its non-Medicare enrollees, adjusting for Medicare enrollees' utilization.
Page 282 of 469

AHM 510 : Health Plans : Governance and Regulation
A risk contracting health plan may be required to offer "additional benefits" at no additional charge or to lower its premium if the organization achieves a "savings" from its Medicare payments. A savings is achieved when the plan's ACR is less than the plan's average Medicare payment rate. A risk contracting plan may elect not to pass back all of its savings to enrollees but to instead have the saving withheld and placed by CMS in a benefit stabilization fund. A benefit stabilization fund is a fund established by CMS, at the request of a risk HMO or CMP, to withhold a portion of the per capita payments available to the HMO or CMP and to pay that withheld portion in a subsequent contract period for the purpose of stabilizing fluctuations in the additional benefits the HMO or CMP provides to its Medicare enrollees.
Medicare risk contracting health plans may also choose to offer mandatory supplemental benefits, which are benefits that are not paid for by Medicare but that the plan requires its members to accept and pay extra for as a condition of membership. Required supplemental services must be approved by CMS. Unless an enrollee is enrolled in a point-of-service (POS) plan, an enrollee of a risk contracting health plan is required to obtain all Medicare services (except hospice, emergency, and urgently needed services) from the plan. This is called the "lock-in rule." If the enrollee obtains such items or services outside the risk plan's network, neither the plan nor Medicare is required to pay for them. Electing a risk plan with a POS option provides enrollees with the right to receive a limited amount of healthcare services outside the plan's provider network.
According to CMS statistics, as of July 1, 1998, risk contract plans accounted for 76.9% of all Medicare health plans, and enrolled nearly 90% of those beneficiaries who were in Medicare health plans.
On May 1, 1998, CMS discontinued accepting applications from plans to enter into Medicare risk contracts because on January 1, 1999, the Medicare risk contracting program will be replaced with the Medicare+Choice program, which we discuss later in this lesson.
Medicare Cost ContractsOrganizations with cost contracts are reimbursed for health services by the government using an allocation-of-costs system that is ultimately based on the amount of services provided rather than on the number of enrollees served by the organization. (Health Care Prepayment Plans--HCPPs--which cover part or all of the Medicare Part B services, but not Part A services, also are reimbursed for health services on an allocation-of-costs basis.) Administrative costs not related to health services are allocated based on the ratio of the number of Medicare enrollees the plan serves to the number of total enrollees the plan serves.
Enrollees of cost-based plans are not "locked in" to using the plan's network providers, unless the enrollees elect to obtain non-Medicare covered supplemental benefits. Enrollees of cost-based plans may receive services from non-network providers subject to the usual Medicare deductible and coinsurance obligations.
Page 283 of 469

AHM 510 : Health Plans : Governance and Regulation
A provision of the Balanced Budget Act of 1997 calls for the phase out of cost contracts by the end of 2002, and provides for the phase out of the HCPP program for health plans by the end of 1998.
Medicare Choices Demonstration ProjectMedicare Choices demonstration project was authorized by CMS in 1995. The project's purposes were to provide Medicare beneficiaries with more delivery system choices and to test alternative payment methods. Some of these payment methods involved risk-adjusted payments, in which payments were adjusted to reflect diagnoses or the health status of plan enrollees. In many particulars, these demonstration projects were a precursor to the much broader changes in Medicare that came about through the Balanced Budget Act of 1997, which we examine next.
Medicare and The Balanced Budget Act of 1997 (BBA)The Balanced Budget Act (BBA) of 1997 (Public Law 105-33) has made the most sweeping changes in federal healthcare programs since the inception of Medicare in 1965. The goal of the legislation is to reduce the federal budget by $115 billion over the next 5 years and, in the process, protect the Medicare Part A fund to provide solvency through at least the year 2007.6
One of the most significant changes in Medicare brought on by the BBA is the creation of Medicare+Choice. All individuals who are enrolled in Medicare Part B and are entitled to benefits under Medicare Part A are eligible to enroll in any Medicare+Choice plan available in their area or residence, except those people with end-stage renal disease who were not already enrolled in a Medicare+Choice plan at the time of diagnosis.7
Where Medicare Parts A and B address covered services under the traditional FFS system, Part C addresses alternative methods of delivery of Medicare services and increases beneficiaries' choices of Medicare delivery systems. A Medicare+Choice plan can be any one of the following:
1. Coordinated care plan (i.e., an HMO with or without a point-of-service option, a preferred provider organization [PPO], a provider sponsored organization [PSO], or a plan offered by a religious/fraternal organization)2. Private, fee-for-service plan3. Combination of a medical savings account (MSA) plan and contributions to a Medicare+Choice MSA
Major Provisions of the BBA under Medicare+ChoiceProvisions of the BBA specify the types of organizations that are eligible to participate in Medicare+Choice and outline the steps in the process by which health plans can seek approval for participation in Medicare.
New Types of Contracting EntitiesUnder Section 1876 (prior to enactment of the BBA), a health plan had to qualify as a competitive medical plan (CMP) or as a federally qualified HMO in order to participate in the Medicare program as a Medicare risk entity. Through Medicare+Choice, the BBA expanded the types of health plans that may qualify to contract with CMS for the purposes of providing covered services to Medicare beneficiaries. As noted above, organizations that may qualify for such contracts include, but are not limited to, HMOs,
Page 284 of 469

AHM 510 : Health Plans : Governance and Regulation
PPOs, PSOs, and religious/fraternal benefit societies that meet the requirements of the law.
Requirements for Medicare+Choice Organizations Many of the new provisions outlined in the BBA directly affect how health plans are required to qualify and operate as Medicare+Choice providers. For example, the BBA establishes new rules for qualifying for a Medicare contract as a coordinated care plan. All Medicare+Choice coordinated care plans must comply with requirements for Medicare benefit packages, marketing, enrollment, appeals and grievances, solvency, quality assurance (QA), reporting, and other processes. Health plans with Medicare contracts have always had to meet requirements in these categories, but in some cases the Medicare+Choice requirements within specific categories have changed. For example, health plans have always been subject to solvency requirements, but as we will discuss later in this lesson, the solvency requirements have been changed for some PSOs in specific situations defined under the Medicare+Choice program. The following sections describe the requirements that contracting entities must meet to participate in Medicare+Choice. Because the provisions in Medicare+Choice set forth provisions specific to PSOs for the first time, later in this lesson we will also discuss some specific requirements that apply to PSOs.
Health Plan Medicare+Choice ContractingCMS oversees Medicare contracting with all Medicare+Choice organizations. All Medicare+Choice coordinated care plans must comply with the interim final regulations published by CMS in June 1998. These regulations are based on the regulations that implemented Section 1876. Plans that had risk contracts in "good standing" before the Medicare+Choice program and that submit the required supplemental information to demonstrate compliance with Medicare+Choice requirements will be transitioned to the Medicare+Choice program January 1, 1999.
LicensingCoordinated care plans under the Medicare+Choice program must be state licensed as risk-bearing entities. Medicare PSOs, however, may seek a waiver of this requirement under certain conditions, which we will discuss later in this lesson. State licensure laws govern the solvency standards that apply to such entities.
PSO Solvency and LicensureA Medicare Provider-Sponsored Organization (Medicare PSO) is an organization operated by hospitals or other affiliated groups of healthcare providers that provides a substantial portion of healthcare treatments and services under its Medicare contract through its affiliated providers. Medicare PSOs must also accept substantial financial risk in delivering this healthcare, and the affiliated providers must have a majority financial ownership in the PSO. PSOs "provide a way for doctors and hospitals to contract with Medicare and to take capitated risk directly from Medicare for the patients to whom they provide services. It is the combination of provider control and the direct provision of services" by the owner-providers and affiliated providers that distinguishes PSOs from many HMOs.8
Medicare PSO Solvency RequirementsMedicare PSO solvency standards are divided into three parts: the (1) initial stage, (2) ongoing stage, and (3) insolvency. In the initial stage, prior to CMS approval, the PSO typically must have a minimum net worth of $1.5 million. CMS, however, may reduce this required amount to $1 million if the PSO can demonstrate that its start-up costs will be
Page 285 of 469

AHM 510 : Health Plans : Governance and Regulation
reduced as a result of its administrative infrastructure. In addition, the PSO must have a financial plan that demonstrates that it has sufficient resources to cover losses through a period 12 months beyond its projected break-even point.
To meet the ongoing net worth requirements, the PSO must have a minimum net worth that meets the greater of four amounts. Figure 8B-3 defines these four amounts.
To meet the liquidity requirements, the PSO must demonstrate that it can meet its financial obligations as they come due and that it has the greater of $750,000 in cash or cash equivalents or 40% of the minimum net worth required.
With regard to the insolvency portion of the requirements, the PSO must make a $100,000 insolvency deposit in accordance with CMS instructions. In addition, consistent with the NAIC HMO Model Act (see State HMO and Other Types of Health Plan Laws), the PSO is obligated to have hold-harmless clauses in its provider contracts and have a plan for the continuation of benefits for a specified period in the event of insolvency.
Review Question
Solvency standards for Medicare provider-sponsored organizations (PSOs) are divided into three parts: (1) the initial stage, (2) the ongoing stage, and (3) insolvency. In the initial stage, prior to CMS approval, a Medicare PSO typically must have a minimum net worth of
$750,000
$1,000,000
Page 286 of 469

AHM 510 : Health Plans : Governance and Regulation
$1,500,000
$2,000,000
Incorrect. To meet the liquidity requirements, the PSO must demonstrate that it can meet its financial obligations as they come due and that it has the greater of $750,000 in cash or cash equivalents or 40% of the minimum net worth required
Incorrect. In the initial stage prior to CMS approval, a PSOs minimum net work must be an amount greater than $1 million. CMS, however, may reduce this required amount to $1 million if the PSO can demonstrate that its start-up costs will be reduced as a result of its administrative infrastructure.
Correct. In the initial stage, prior to CMS approval, the PSO typically must have a minimum net worth of $1.5 million
Incorrect. A Medicare PSOs net worth in the initial stage can be less than $2 million
Medicare PSO Licensure RequirementsAs a general rule, Medicare PSOs must secure state licensure as risk-bearing entities. However, the HHS Secretary may grant a PSO a waiver from this requirement through November 2002 under certain conditions. The HHS Secretary will grant a waiver if the state:
1) Fails to complete action on the PSO's licensure application within 90 days2) Denies the PSO's application and the state standards or review process imposes material requirements or procedures on PSOs that are not required of other entities engaged in substantially similar business, or the state requires the PSO to offer a product or plan other than Medicare+Choice3) Denies the PSO's application based on the PSO's failure to meet solvency requirements that are different from those developed and published by the HHS secretary, or the state imposes documentation or information requirements relating to solvency that are different from the standards promulgated by the HHS secretary.
Under the BBA, a waiver is effective for a maximum of 36 months and is nonrenewable. PSOs that submit a waiver request must do so no later than November 1, 2002. The HHS secretary must grant or deny a waiver within 60 days of the time the PSO files a substantially complete waiver application. PSOs that have received waivers must submit an application to the secretary for certification (and periodic recertification) that the PSO meets federal solvency standards. The secretary must act upon each of these applications within 90 days.
As noted above, by the end of 2002, this waiver process will be discontinued.
Minimum Enrollment RequirementsNew minimum Medicare+Choice enrollment requirements for PSOs are 1,500 members in urban areas and 500 in rural areas. In certain circumstances, PSOs may request that Medicare waive this requirement for the first three years. This enrollment standard for PSOs differs from the Medicare+Choice enrollment standards for other plans, which are
Page 287 of 469

AHM 510 : Health Plans : Governance and Regulation
required to have a minimum enrollment of 5,000 (or 1,500 if the organization primarily operates in nonurban areas). Under the BBA, the old "50/50" rule requiring that health plans enroll 50% Medicare and 50% non-Medicare beneficiaries has been eliminated for all health plans including PSOs.
Option to Use Medical Savings Accounts (MSAs)The BBA also created the Medical Savings Account (MSA) national demonstration project. The Medicare MSA demonstration project is limited to 390,000 beneficiaries, with no new enrollment accepted after January 1, 2003.9 Medical Savings Accounts (MSAs) are "health insurance arrangements that give consumers a financial incentive to control their own healthcare costs by combining a high-deductible health insurance policy with an individual savings account."10 A Medicare+Choice Medical Savings Account is a tax-preferred account set up for individual Medicare beneficiaries and to which CMS makes contributions on behalf of the beneficiary. Individuals who choose to establish Medicare+Choice MSAs purchase a catastrophic MSA health policy with high deductibles and out-of-pocket expenses of not more than $6,000 in 1999. After the deductible and out-of-pocket expenses are met, Medicare covered services are paid at 100%.
Beneficiaries are not allowed to deposit their own funds in their MSA account. Instead, Medicare+Choice MSAs may only receive funds from CMS. Deposits and earnings are not taxable. Likewise, withdrawals are free from federal income tax if used for qualified medical expenses, as defined by the Internal Revenue Code, for the beneficiary. Withdrawals can be used to pay medical expenses that are not covered under the high-deductible health insurance policy.
MSA plans are the high-deductible plans that beneficiaries must obtain in conjunction with the establishment of an MSA. In general, MSA plans are subject to the same requirements as other Medicare+Choice plans.
MSA plans are required to cover at least 100% of the cost of Medicare-covered items and services or 100% of the amounts that would have been paid under Medicare, but only after the enrollee incurs accountable expenses equal to the amount of the annual deductible. If the Medicare+Choice payment exceeds the MSA plan premium, the difference is deposited in the beneficiary's MSA.
Benefit RequirementsCoordinated care plans with Medicare contracts are required to offer members standard covered items and services available in the basic fee-for-service Medicare benefit package. Additional services may be offered as part of the benefit package, or as a supplement for which members may be required to pay extra. Coordinated care plans with Medicare contracts must also cover out-of-network services as follows:
1. Provide coverage of emergency services based on the "prudent layperson" standard
2. Provide coverage of urgently needed services received outside the plan's network when such services are medically necessary and immediately required because of unforeseen illness or injury and it was not reasonable, given the circumstances, to obtain the services through the plan
Page 288 of 469

AHM 510 : Health Plans : Governance and Regulation
3. Provide renal dialysis treatment to eligible members who are temporarily out of the network area
4. Provide post-stabilization care covered under guidelines established by the HHS secretary
The BBA expanded Medicare coverage of preventive benefits for members. Figure 8B-4 outlines the expanded coverage and the effective dates. The BBA also provides for Medicare coverage of outpatient diabetes self-management training services and blood glucose strips. In addition, the National Academy of Sciences has been directed to study the desirability of requiring coverage for other preventive care benefits including nutritional therapy, skin cancer screening, and additional coverage for immunosuppressive drugs.11
Figure 8B-4. New Preventive Health Benefits Requirements.Benefit Effective DateAnnual Screening Mammography (for women over 40) January 1, 1998Screening PAP Smear and Pelvic Exam (every 3 years) January 1, 1998Colorectal Cancer Screening Exam January 1, 1998Bone Density Measurement (to rule out osteoporosis) July 1, 1998Diabetic Test Strips July 1, 1998Prostate Cancer Screening Exam (for men over 50) January 1, 2000
Rate DeterminationsMedicare reforms under the BBA make significant changes in payment rates to Medicare coordinated care plans. Historically, payments to Medicare risk plans were based on 95% of the adjusted average per capita cost (AAPCC). The adjusted average per capita cost (AAPCC) is the estimated cost, adjusted for certain demographic factors such as age, gender, and health status, of covering Medicare beneficiaries under the fee-for-service system in a particular county. In 1998, CMS implemented a new payment methodology, authorized under the BBA for the Medicare+Choice program.
Changes in Payment Rates for Medicare+Choice PlansIn creating Medicare Part C, and eliminating the AAPCC, the BBA made several significant changes in the way in which payment rates for Medicare health plans are determined:
1. Payments in local markets will be based on the highest of three rates: a minimum percentage increase over the previous year's rates; a blended rate using a weighted average of the local rate and national rates; and a minimum rate that sets a "floor" payment for markets with historically low rates. Figure 8B-5 describes this process.
2. Over time, Medicare payments for medical education costs will be carved out of the new rate calculations
3. Beginning in 2000, the HHS Secretary must implement a risk adjustment methodology to account for variations in per capita costs resulting from the health status of enrollees
Figure 8B- Determining Medicare's Monthly Payment Rate under the
Page 289 of 469

AHM 510 : Health Plans : Governance and Regulation
5. Medicare+Choice Program.
Starting January 1, 1998, Medicare's payment rate for any given geographical area will equal the largest of the following three amounts:
1. Blended rate (a rate determined by blending a weighted average of an area-specific rate and a national rate)2. A floor amount (a minimum monthly payment rate per enrollee) of $367 in 1998. In following years, this floor amount will equal the previous year's floor amount increased by the national per capita Medicare+Choice growth percentage.3. The previous year's rate increased by 2%.
For 1998 and 1999, the majority of plans will receive a 2% increase over the previous year's rate. Additional BBA provisions stipulate that, over time, the calculation of blended rates will change so that the national rate component will increase in weight compared to the local rate component. Eventually the blended rate will move to a fifty-fifty blend of national and local costs. For example, the blend will move from 90% local and 10% national in 1998 to 50% local and 50% national by 2003.
States can also request a geographic adjustment to a Medicare payment area. These adjustments can seek to create a single statewide payment area, metropolitan payment areas, or consolidate into a single payment area noncontiguous counties within the state. However, these adjustments in payment areas must be budget neutral.
One result of these changes in the ways that payment rates are determined is that annual adjustments to the payment rates will no longer be based solely on Medicare spending for fee-for-service beneficiaries in a given geographic area. Instead, as noted above, in some cases national payment averages will affect local payment rates, some local areas will be paid the "floor" rate, and some areas will be affected by the minimum percentage increase rate.12
Congress's intent in making the changes in payment methodology under the BBA as described above and in Figure 8B-5 appears to have been to:
• Increase rates in rural, traditionally low payment areas
• Reduce, over time, geographic variations in payment rates
These changes have important implications for organizations with Medicare+Choice contracts. The new BBA payment methodology narrows the geographic variations in payments by both lowering the growth rate of payments in high-payment counties and raising the rates in low-payment counties. As a result, the BBA reduces the growth in rates in many markets relative to what the payment rates in those markets would have been without BBA implementation. Furthermore, average payment rates for coordinated care plans under Medicare+Choice will fall relative to payment rates in the fee-for-service side of the program. The implementation of a risk adjustment methodology in 2000 is expected to further reduce Medicare+Choice payments relative to the FFS
Page 290 of 469

AHM 510 : Health Plans : Governance and Regulation
program. As a result of these constraints in Medicare+Choice payment rates, many coordinated care plans may have to cut benefits, raise premiums, or do both.
The BBA also provides for testing of changes to payment methodologies in the future. For example, Section 4012 of the BBA requires HHS to establish a Competitive Pricing Advisory Committee (CPAC). CPAC will recommend geographic areas and will consult with the HHS secretary to develop price-setting methodologies to be used in a demonstration project that is designed to test competitive pricing.13 Other demonstration projects and committees will be discussed in more detail later in this lesson
Review Question
The Balanced Budget Act (BBA) of 1997 created the Medicare+Choice plan. One provision of the BBA under Medicare+Choice is that the BBA
requires health plans to qualify as either a competitive medical plan (CMP) or a federally qualified HMO in order to participate in the Medicare program eliminates funding for demonstration projects such as the Medicare Enrollment Demonstration Project narrows the geographic variations in payments to Medicare health plans by lowering the growth rate of payments in high-payment counties and raising the rates in low-payment counties increases Graduate Medical Education (GME) payments to hospitals for the training and cost of educating and training residents
Incorrect. Through Medicare+Choice, the BBA expanded the types of health plans that may qualify to contract with CMS including, but are not limited to, HMOs, PPOs, PSOs, and religious/fraternal benefit societies that meet the requirements of the law.
Incorrect. In addition to the Medeicare Enrollment Demonstration Project, the BBA funds several other demonstration projects
Correct. The BBA payment methodology narrows the geographic variations in payments by both lowering the growth rate of payments in high-payment counties and raising the rates in low-payment counties. As a result, the BBA reduces the growth in rates in many markets relative to what the payment rates in those markets would have been without BBA .
Incorrect. The BBA reduces these payments and limits the number of residents supported by Medicare.
Provider Payment ReformsIn addition to significant changes in health plan payments under Medicare, the BBA also changes some aspects of its fee-for-service provider payment systems. The BBA caps the rate of growth in payments to hospitals that operate under the prospective payment system (PPS). A PPS system will be applied for payments to skilled nursing facilities (SNF) as well. The bulk of Medicare payments to SNFs in the past were made on a
Page 291 of 469

AHM 510 : Health Plans : Governance and Regulation
"reasonable cost" basis after the care was provided. Under the new PPS, these facilities will be paid on a per diem basis.14
Graduate Medical Education PaymentsMedicare provides financial support called Graduate Medical Education (GME) payments to hospitals for the training and cost of educating and training residents. The BBA reduces these payments and limits the number of residents supported by Medicare. Payments are based on medical education factors, which are being reduced from 7.7% to 7% in 1998, to 6.5% in 1999, to 6% in 2000, and 5.5% thereafter.
Plan EnrollmentIn general, Medicare+Choice plans will be obligated to accept new members during annual coordinated election periods, special enrollment periods, and a beneficiary's initial election period. The annual coordinated election period is held each November, during which time a Medicare beneficiary may choose to enroll in a Medicare+Choice plan or change his or her election from one plan to another. Enrollment during the annual coordinated election period becomes effective the following January 1. An initial election period is the time period during which a person who is newly eligible for Medicare benefits may elect to enroll in a plan.
In November 1998, CMS begins conducting an education and publicity campaign in selected geographic regions aimed at those who are Medicare+Choice eligible. This campaign's goal is to focus on informing beneficiaries of their options under Medicare+Choice beginning in 1999.
Those who are eligible for Medicare+Choice will receive election forms, information on disenrollment, member satisfaction data, health records, and compliance information from CMS prior to their initial Medicare+Choice eligibility and prior to each annual coordinated election period. Those eligible for Medicare+Choice will have the ability to enroll and disenroll on a monthly basis until 2002. A beneficiary who fails to make a choice will automatically be assigned to traditional FFS Medicare. Figure 8B-6 outlines the disenrollment options available in 2002 and thereafter for those who are eligible for Medicare+Choice.
Figure 8B-6. Medicare+Choice Disenrollment Options.
During 2002 - An individual may disenroll:
1. At any time during the first six months of the year or the first six months after making an initial election if the individual has not previously changed his or her election during this period
2. During the annual coordinated election period in November 3. At any time during a special election period
Beneficiaries first becoming eligible for benefits under Part A at age 65 may discontinue their election and enroll under the traditional fee-for-service program at any time during the 12-month period beginning on the effective date of enrollment.
Page 292 of 469

AHM 510 : Health Plans : Governance and Regulation
2003 and thereafter - An individual may disenroll:
1. At any time during the first three months of the year or the first three months after making an initial election if the individual has not previously changed his or her election during this period
2. During the annual coordinated election period in November 3. At any time during a special election period
Beneficiaries first becoming eligible for benefits under Part A at age 65 may discontinue their election and enroll under the traditional fee-for-service program at any time during the 12-month period beginning on the effective date of enrollment. (Sec. 1851[e][2]-[4])
Fast Definition
Special election period- Effective January 1, 2002, the time period during which a currently enrolled Medicare+Choice enrollee may disenroll and make a new election. Special election is allowed if
1. the enrollee loses eligibility because of a change in residence, 2. the plan violates terms or conditions of its contract or makes misrepresentations in
its marketing materials, 3. the plan loses its certification as a Medicare+Choice contractor or terminates the
plan, or 4. the enrollee meets other special conditions set by the HHS Secretary.
MarketingCMS's The Medicare Health Plan National Marketing Guide contains rules related to marketing products to Medicare beneficiaries. One CMS requirement is that health plans submit proposed marketing materials to CMS for approval at least 45 days in advance of dissemination. However, the guide provides for a "use and file" program for plans that meet certain criteria. A use and file program allows health plans meeting specified criteria that demonstrate ongoing compliance with marketing criteria to streamline the market materials review process. Under the program, approved plans may use materials marketing the plan to non-plan members without prior approval as long as they provide CMS with copies of the materials within 10 days of their use. All other materials (e.g., those that describe membership rules and benefits such as member notices and the member handbook) remain subject to prior approval. In addition, a "lead region" policy guarantees that materials approved by a plan's lead CMS regional office automatically meet approval in other CMS regions in which the plan contracts to provide Medicare Coverage.
The Medicare Health Plan National Marketing Guide serves a number of purposes. Its rules help to assure that beneficiaries receive current, accurate, and reader-friendly marketing materials. It assists CMS in conducting uniform national marketing reviews. Finally, it provides guidance for new health plan applicants submitting such materials to CMS and for their overall marketing efforts. The guide addresses marketing activities such as the following:
Page 293 of 469

AHM 510 : Health Plans : Governance and Regulation
1. Giveaways to potential enrollees may not have a value of more than $10 and may not be conditioned upon enrollment (e.g., a coffee mug or day planner would be acceptable). The goal of this rule is to prevent health plans from inducing potential enrollees to join their plan with the promise of a gift.
2. Health plans may not advertise or provide "value-added services" (e.g. discounts on health-related items such as over-the-counter medications and devices, memberships in health clubs, etc.). However, in some circumstances, plans may provide incentives to encourage preventative care. Again, CMS's goal is to assure that an enrollee is making the decision to join a plan based on actual plan merits.
3. No promotional language on quality rating may be used in any advertising efforts conducted by the health plan without citing the source of the rating. CMS's experience has shown that elderly beneficiaries are particularly susceptible to false and/or misleading advertising.
In addition, marketing materials may not claim that the health plan is the "Centers for Medicare and Medicaid Services" or the "Medicare Program," or that plan employees are agents or employees of the federal government.15 For example, plans are not allowed to describe their Medicare products as "a special contract with Medicare," or as "certified or endorsed by Medicare," or as a "special plan for Medicare beneficiaries."16 A health plan may tell its members it is:
• An HMO with a Medicare contract
• A Medicare-approved HMO
• A federally qualified HMO with a Medicare contract
• A federally qualified Medicare-contracting HMO17
The Guide also contains model letters for routine communications between a plan and its members. A "Must Use/Can't Use" chart of marketing language is also available for health plans and covers subjects such as eligibility, benefits, premiums, providers, enrollment periods, etc.
Quality AssuranceQuality improvement organizations are already in place to monitor quality issues relating to health plans. Quality improvement organizations (QIOs) are organizations or groups of practicing physicians and other healthcare professionals paid by the federal government to review services ordered or furnished by other practitioners in the same medical fields for the purpose of determining whether medical services provided were reasonable and necessary, and of monitoring the quality of care given to Medicare patients.18
The BBA reinforces the changes that have occurred in the quality assurance monitoring area, particularly under the purview of QIOs and CMS's Health Care Quality Improvement Program. The Health Care Quality Improvement Program (HCQIP) is a program initiated by CMS that seeks to improve the quality of care provided to Medicare beneficiaries. Medicare+Choice coordinated care plans must have an agreement with a QIO and undergo periodic quality reviews. The BBA allows external review requirements to be waived if the plan has an excellent record of quality assurance (QA) and compliance with other Medicare+Choice requirements. Furthermore, a plan may be
Page 294 of 469

AHM 510 : Health Plans : Governance and Regulation
deemed to have met requirements regarding confidentiality and accuracy of patient records if the plan is accredited by a private organization approved by the state.19
Review Question
From the following answer choices, choose the term that best corresponds to this description. The SureQual Group is a group of practicing physicians and other healthcare professionals paid by the federal government to review services ordered or furnished by other practitioners in the same medical fields for the purpose of determining whether medical services provided were reasonable and necessary, and to monitor the quality of care given to Medicare patients.
Health insuring organization (HIO)
Independent practice association (IPA)
Physician practice management (PPM) company
Peer review organization (PRO)
Incorrect. A Health insuring organization contracts with state Medicaid agencies as a fiscal intermediary.
Incorrect. An IPA is an association of individual physicians that that contracts with health plans to provide healthcare services
Incorrect. A PPM is a legal entity that provides a variety of management and administrative services for participating physicians' practices.
Correct. A PRO is an organization or group of practicing physicians and other healthcare professioanls paid by the federal government to review services ordered or furnished by other practitioners in the same medical field to determine whether the medical services provided were reasonable and necessary.
The Medicare+Choice regulations identify five general requirements for a Medicare+Choice plans quality assessment and performance improvement program. Section 422.152(b) of the Medicare+Choice regulations identifies the following five general requirements for a Medicare+Choice plan's quality assessment and performance improvement program:
1. Meet the requirements contained in the rule concerning performance measurement and reporting (including use of standard measures required by CMS) and the requirements of the rule concerning the achievement of minimum performance levels
2. Conduct performance improvement projects that achieve demonstrable and sustained improvement in significant aspects of clinical care and nonclinical areas
Page 295 of 469

AHM 510 : Health Plans : Governance and Regulation
3. Follow written policies and procedures that reflect current standards of medical practice in processing requests for initial or continued authorization of services
4. Have in effect mechanisms to detect both underutilization and overutilization of services
5. Make available to CMS information on quality and outcomes measures that will enable beneficiaries to compare health coverage options and select among them
Medicare+Choice regulations require that the organization maintain a health information system that collects, analyzes, and integrates the data necessary to implement its program. Also, for each plan, a process for formal evaluation must take place at least annually and it must address the impact and effectiveness of its quality assessment and performance improvement program.
Appeals and GrievancesIssues subject to appeal include those involving a health plan's denial of payment or reimbursement for provider services, or the health plan's refusal to provide medical services that are covered by Medicare.22 The BBA and its implementing regulations include a number of requirements regarding beneficiary appeals including:
• Explanations of appeal rights
• Provisions for expedited appeals
In general, when a party has made a request for a service, a Medicare+Choice organization must notify the enrollee of its determination as expeditiously as the enrollee's health requires, but not later than 14 days after the date the organization receives the request. The BBA's language on expedited determination/reconsideration is similar to the regulations already adopted by CMS. A Medicare+Choice organization must provide an expedited appeal upon request by an enrollee if the organization determines that the standard timeframe could seriously jeopardize the life or health of the enrollee or the enrollee's ability to regain full function. The organization must grant an expedited appeal upon the request of a physician if the physician indicates that the above standard is met. Health plans must respond to such appeals within 72 hours. Any notice of an adverse determination must include the reasons for the determination and information on appeal rights and processes.
Health plans are also required to have grievance procedures for nonappealable disputes. Instances of these grievance issues may include enrollment and disenrollment practices, long waiting periods for appointment and referrals, care complaints, etc. 23
Anti-Fraud and Abuse ProvisionsThe BBA reinforces existing Medicare anti-fraud and abuse provisions and includes new provisions such as giving HHS authority to refuse to enter into Medicare agreements with providers who are convicted felons. In 1997, anti-fraud and abuse activities yielded nearly $1 billion in savings and excluded more than 2,700 individuals and entities from federal health care programs. Several new anti-fraud and abuse provisions affect Medicare under Subtitle D, Section 4301 of the BBA.24 (See Fraud and Abuse for a detailed discussion of fraud and abuse).
Page 296 of 469

AHM 510 : Health Plans : Governance and Regulation
CMS's Evolving Role under the Balanced Budget ActAs noted earlier, the Centers for Medicare and Medicaid Services (CMS) is the federal agency that administers the Medicare program. CMS oversees and regulates health insurance provided to over 74 million Americans through Medicare and other programs. The majority of these individuals receive benefits through a traditional fee-for-service plan. However, an increasing number are choosing health plans.
"The creation of the new Medicare+Choice program imposes substantial short-term and ongoing burdens for CMS. These burdens are separate from the obligations placed on the agency by other changes to Medicare made by the BBA. In addition to developing new solvency requirements for PSOs and other nonsolvency standards as required under Section 1856 of the Balanced Budget Act, CMS has to develop additional regulations and guidance involving, among other things, enrollments and disenrollment procedures; appeals and grievance procedures; rates and rate-setting mechanisms."25
The BBA has created a number of initiatives that CMS must address as part of implementing the Act. These key initiatives include the following:
• Medicare+Choice - As a result of the creation of the Medicare+Choice program, CMS has had to issue hundreds of new Medicare regulations, such as solvency standards for PSOs. Additionally, CMS has responsibility for developing new Medicare+Choice contract documents. Existing Medicare risk-based contractors transitioning to the Medicare+Choice organization types are required to execute a new Medicare+Choice contract. These contract documents will replace the current Section 1876 risk-based contract.26
• Medicare Beneficiary Information - To help meet the BBA's directive of increasing beneficiary understanding of Medicare options, CMS is required to coordinate a national educational and publicity campaign. This campaign focuses on distributing comprehensive, user-friendly information about health plans and other coverage options to every Medicare beneficiary.
• New Payment Requirements - The move to Medicare+Choice requires that CMS develop risk adjusters to apply to the payment methodology used to compensate health plans.
• Anti-Fraud Efforts - To continue its efforts to crack down on fraud and abuse, CMS plans to increase claims reviews, screen home health agencies more carefully, and encourage beneficiaries to phone in fraudulent activities.27
• The "Quality Agenda" - CMS's Medicare Quality Improvement (QI) System for health plans also require risk contractors to report performance data according to standardized measures, to meet minimum specified performance standards, and to develop internal QI programs."28 CMS is also making efforts to put Medicare in compliance with the proposed Consumer Bill of Rights and Responsibilities (discussed in Federal Government as Purchaser) as far as the existing law allows
Operational Issues for Health PlansHealth plans in the Medicare market face unique challenges. To enter into and operate within Medicare markets, health plans must "create the infrastructure and management systems to effectively manage a very high-risk population represented by Medicare
Page 297 of 469

AHM 510 : Health Plans : Governance and Regulation
beneficiaries."29 This lesson provides a brief discussion of those operational areas. Figure 8B-7 offers some practical tips on developing a Medicare health plan strategy.
Figure 8B-7. Medicare Health Plan: Tips for Health Plans.
1. Be one of the first health plans in your market. Elderly patients are more likely to switch to your plan from a FFS plan than from another health plan with which they are satisfied.
2. Grow quickly after you start. A plan with 25,000 or more members has the best chance for success.
3. Get your capital and marketing plans together. Expect to spend at least $500+ to sign up each new enrollee. In addition, keep in mind that plans usually lose money the first two or three years.
4. Hire additional support staff. You'll need extra staff to field questions from older enrollees. They telephone more often and spend more time on the telephone when they do.
5. Work closely with providers to help them succeed under capitation. Make sure that both your health plan and those providing care have the same incentives to do so cost-effectively.
6. Some plans find it more efficient to use internists sd primary care doctors for seniors. Interists often are comfortable treating many chronic conditions and refer patients less often to specialists than do other primary care physicians.
Source: Reprinted from Hospitals & Health Networks, vol. 71, no. 7, by permission, April 5, 1997, copyright 1997, American Hospital Publishing, Inc.
Marketing and EducationA large portion of the start-up costs of a Medicare program go toward sales and marketing, and these costs are significant. Health plans must also be aware of the new rules and regulations for how plans are allowed to market Medicare. With increased competition, marketing and sales are critical areas; it is generally agreed that success is "typically bestowed on [plans] with a large enrollment....with those of at least 25,000 best suited for survival."31
Beneficiaries will be subject to a large amount of information regarding health plans, Medicare, and Medicare+Choice. Therefore, education is an essential factor in attracting and keeping Medicare beneficiaries in health plans. Beneficiaries are often skeptical of health plans offering "zero premiums" since they may not understand that health plans are able to offer these packages, not by offering an inferior product, but rather by managing dollars.32 According to Kevin Shanklin, a practice director with the Blue Cross and Blue Shield Association's Strategic Consulting Services, "The need for education is critical. Health plan companies have to develop and, in fact, are developing major educational programs in order to make their health plan programs work in the Medicare and Medicaid markets."
Fast Definition
"Zero Premium" Plan - A plan that offers extra or supplemental benefit features (e. g., prescription benefits) at no additional cost to the Medicare health plan enrollee.37
Page 298 of 469

AHM 510 : Health Plans : Governance and Regulation
Member Services and BenefitsHealth plans have discovered a high volume of care is needed for an over-65 population, not only in the provision of healthcare services, but also in member services. According to Craig Schub, former president of Secure Horizons, a health plan in California, "Whenever we announce a change in a Medicare plan, our phones light up. Seniors want to understand those changes."34 Health plans need to consider their communications and information systems and the personnel they currently have for handling the increased demand for information.
Competition for the Medicare market means health plans need to develop flexible benefit packages for seniors and the disabled. For example, Blue Cross and Blue Shield (BCBS), among several other organizations, offers a portable Medicare health plan product for their senior market. According to BCBS, this plan "has generated a lot of excitement within the Association and among Plans because it's expected to meet an important need of the senior market."35
Studies also show that beneficiaries join health plans because of comprehensive benefit packages. For example, according to a 1996 Physicians Payment Review Commission (PPRC) survey, nearly half of beneficiaries polled cited the risk plan's reduced costs and increased benefits as their primary reasons for enrolling.36 The second most common reason was the plan's provider list.
The BBA seeks to expand Medicare coverage of preventative health care services. While coverage of certain health screenings is required, health plans may wish to follow the HMO industry's lead in creating Health Improvement Programs. These programs provide help with managing member health and managing costs, and they are also popular with senior members. These programs usually include senior seminars, cholesterol and high blood pressure screenings, smoking cessation or weight loss clinics, and other initiatives for members to maintain their health and quality of life.
Medical Management It is generally agreed that seniors need two to three times the care of a commercial member. As a result, plans will need more utilization management staff to manage this care and more programs designed specifically for the healthcare needs of this population.Network Development and Provider RelationsOne key to success for health plans in developing Medicare+Choice plans is establishing and maintaining strong physician networks. Seniors tend to develop lasting relationships with their physicians, and most seniors who have an established relationship with a physician are not receptive to leaving that physician. In addition, plans may need to increase their provider contracting efforts to include more physicians and organizations that can manage chronic and terminal conditions, such as home health care and cancer centers. A typical rule of thumb is, “a primary care doctor typically can handle 2,000 patients under age 65, but only 800 over 65.”38 Another factor to consider is that the scope of managed care contracting with physicians has changed significantly. For example, physicians with health plan contracts rose from 61% in 1990 to 83% in 1995.
Page 299 of 469

AHM 510 : Health Plans : Governance and Regulation
With respect to provider relations, the BBA requires that health plans maintain certain communications with their participating providers. For instance, health plans must supply providers with Medicare+Choice participation rules and regulations. Health plans must supply written notices of adverse participation decisions and the processes required to appeal those decisions. Health plans must also have procedures and systems in place to provide ongoing communications with providers regarding medical policies, quality, and medical management.
Management Information Services (MIS)The BBA requires the collection and reporting of encounter information, enrollment/ disenrollment information, HEDIS® and CAHPS information, among other data. Much of this information must be collected, stored, and submitted electronically. Health plans will need the information services equipment, personnel, and resources to maintainand compete in the world of “electronic commerce.”
CMS requires its contracted health plans to transmit most data and information electronically. CMS is encouraging contractors to adapt new and existing information systems to prepare for Year 2000 programming changes. Though a costly and difficult effort even for CMS, failure to do so could result in “massive breakdowns in information flows” between health plans and CMS.39 CMS plans to provide health plans with additional information on this issue in the future.
The National Bipartisan Commission on the Future of MedicareThe BBA includes provisions for a commission to monitor Medicare and develop recommendations for ensuring the long-term financial reliability of the Medicare program. This group, the National Bipartisan Commission on the Future of Medicare, is composed of 17 members: 4 appointed by the President, 6 each appointed by the Senate Majority Leader and the Speaker of the House (no more than 4 of whom are from the same party), and an additional member who serves as Chairperson and was jointly appointed by the President, the Majority Leader, and the Speaker of the House. The commission's report is due in March of 1999.
The commission has created task forces to work on new program designs, build on the system that is already in place, and examine the role Medicare plays in America's healthcare system.
In addition to the National Bipartisan Commission, the BBA also established various Demonstration Projects as outlined next.
Medicare Subvention Demonstration ProjectThe BBA authorized "six sites for Medicare health plan subvention demonstrations between CMS and the Department of Defense (DOD)."40 Military retirees who are Medicare eligible will be able to receive healthcare through military healthcare facilities. Facilities must meet the same requirements as health plans that serve Medicare and will be paid a percentage of Medicare reimbursement. Therefore, under military subvention projects, the BBA gives veterans more freedom to choose where they receive their medical care. 41
Military retirees in these areas are allowed to begin enrolling after the above healthcare facilities are accepted into the Medicare program. A similar demonstration project has
Page 300 of 469

AHM 510 : Health Plans : Governance and Regulation
been proposed for the Department of Veterans Affairs (VA). Veterans would have a choice of healthcare providers many do not currently have. "The three-year pilot, designed to be at least cost-neutral, would cap Medicare payments to the VA at $50 million annually. The VA could determine which services it currently can make available and target its service delivery to veterans who need them."42
Fast Definition
Medicare subvention — a proposal that “would allow CMS to reimburse military MTFs for the medical care provided to Medicareeligible beneficiaries.”43
Medicare Enrollment Demonstration Project The Medicare Enrollment Demonstration Project is a three-year project, authorized by the BBA, that is designed to study the use of third-party contractors to oversee and conduct Medicare+Choice enrollment and disenrollment. Third-party contractors will be evaluated on their adherence to performance standards. If the contractor does not comply with these standards, enrollment/ disenrollment functions will be carried out by Medicare+Choice plans until a new contractor is secured.
Medicare Coordinated Care Demonstration ProjectThe Medicare Coordinated Care Demonstration Project is designed to study case management and coordination of care for beneficiaries with chronic illnesses. The project will be implemented in nine sites: five urban, three rural, and one within the District of Columbia. If project components prove to be cost-effective while maintaining quality and beneficiary satisfaction, they will be implemented for the Medicare program.
PrivatizationThe BBA has a tremendous capacity to lead Medicare toward privatization through the availability of Medicare+Choice plans. The potential for increased enrollment by seniors in large group healthcare plans could create competition among plans which, ultimately, could lead to increased plan offerings to seniors. Therefore, privatization would benefit the Medicare consumer as well.
Page 301 of 469

AHM 510 : Health Plans : Governance and Regulation
Chapter 8 CJoint Federal-State Healthcare Programs (Medicaid, Programs of All-Inclusive Care for the Elderly, and the State Children’s Health Insurance Program)
After completing this lesson, you should be able to:
Explain the roles of the federal and state governments in the operation of the Medicaid program
Describe the Medicaid services mandated by the federal government Describe the effects of the Balanced Budget Act of 1997 (BBA) on regulation and
operation of Medicaid health plan programs Name the types of health plan entities that can contract to provide Medicaid services Explain the purpose of Section 1915(b) and Section 1115 waivers Explain how states can mandate Medicaid health plans without obtaining a waiver Explain the role of Programs of All-Inclusive Care for the Elderly (PACE) Discuss the purpose and options for implementation of the State Children’s Health
Insurance Program (SCHIP)
In its efforts to ensure that needy populations have access to and coverage for healthcare services, the federal government often enters into joint programs with state governments. In this lesson, we discuss three joint federal-state programs that target specific populations:
1. Medicaid. The Medicaid program targets the low-income population, including certain aged and disabled individuals.
2. Programs of All-Inclusive Care for the Elderly (PACE). PACE is a combined Medicaid and Medicare program that targets people aged 55 or older who require a nursing-facility level of care.
3. State Children’s Health Insurance Program (SCHIP). SCHIP targets uninsured, low-income children who traditionally have not been eligible for healthcare coverage under Medicaid
MedicaidThe Medicaid program was established in 1965 as a joint federal-state matching entitlement program under Title XIX of the Social Security Act (SSA) to provide healthcare coverage to low-income families and certain categories of aged and disabled individuals. Medicaid is the largest source of funding for medical and healthrelated services for America’s poorest populations.
In this lesson, we discuss the purpose and operation of the Medicaid program and the steadily increasing role of health plans in what was once almost entirely a fee-for-service insurance program. Figure 8C-1 shows the breakdown of the Medicaid population by fee-for-service (FFS) and health plans.
Page 302 of 469

AHM 510 : Health Plans : Governance and Regulation
This lesson includes the roles of the federal and state governments in establishing the level of benefits, selecting and regulating health plan entities that contract to participate in the Medicaid program, and determining eligibility for Medicaid benefits. As you will learn, in recent years there have been a number of changes in the regulation of the Medicaid program.
Fast Fact
In 1996, Medicaid provided healthcare assistance to more than 36 million individuals, at a cost of $147.7 billion. 1
Joint Federal-State Nature of ProgramThe Medicaid program is jointly financed by the federal and state governments. The role of the federal government in Medicaid is to establish broad federal guidelines for the program, to provide partial funding to the states, and to set minimum standards regarding eligibility, benefit coverage, and provider participation and reimbursement. The individual states administer the Medicaid program. The federal funds contributed to a state Medicaid program are called federal financial participation (FFP), or the Federal Medical Assistance Percentage. FFP ranges from 50 percent to 80 percent of the state’s total Medicaid costs, with poorer states (based on per capita income) receiving a higher percentage of federal matching funds. States have considerable latitude to expand the benefits offered under Medicaid, as long as they meet the minimum federal standards. Because states have the option to expand their programs beyond the minimum standards set by the federal government, Medicaid programs vary from state to state. Later in this lesson, we discuss how states determine eligibility and benefits for Medicaid programs. First, we look at traditional Medicaid and examine why the Medicaid program has embraced health plans in recent years.
Traditional MedicaidTraditionally, Medicaid has operated as a fee-for-service insurance program. State Medicaid agencies either (1) negotiate with physicians and other providers to render care for a reduced fee for each service or (2) establish a fee schedule without negotiation for the rates they will pay providers for each service rendered. These providers are referred to as traditional Medicaid providers. Under Medicaid, a traditional Medicaid provider is defined as one who has treated Medicaid beneficiaries within the past year and has demonstrated expertise and experience in dealing with the Medicaid population through participation in the Medicaid program.
The reduced FFS payment system established by the states has helped to manage the costs of healthcare; however, the impact of the reduced FFS approach has presented some difficulties in meeting the needs of certain Medicaid beneficiaries. State Medicaid provider reimbursement rates have typically been lower compared to those of commercial insurance plans. As a result, many medical providers have chosen not to participate in the Medicaid program. Since there are fewer primary care providers willing to treat Medicaid beneficiaries, the beneficiaries often have access to a limited selection of providers. Frequently, this lack of providers leads Medicaid beneficiaries to use inner-city hospitals (especially emergency departments), community health centers, public health programs, and a sparse number of private practitioners for their medical care. As a result, Medicaid beneficiaries may overuse emergency departments for routine care rather than establish an ongoing relationship with a primary care provider.
Page 303 of 469

AHM 510 : Health Plans : Governance and Regulation
A large percentage of the Medicaid population consists of:
• Children under age 18 who have a need for well-child care
• Women of childbearing age who have a disproportionately high need for obstetrical and perinatal services
The socioeconomic circumstances of this population often limit their access to a routine source of care and their utilization of available services.
Determining Reimbursement for Providers and Medicaid Benefit LevelsProviders participating in Medicaid must accept Medicaid’s established payment rates as payment in full for services rendered to Medicaid beneficiaries. Federal guidelines require that payment rates be adequate to attract a sufficient number of providers to serve the Medicaid population.
With a few exceptions, each state has relatively broad discretion (within federally imposed upper limits and specific restrictions) to determine the reimbursement methodology and resulting payment rates.
States may impose nominal deductibles, coinsurance, or copayments on some Medicaid recipients for certain services. The state cannot, however, require copayments for emergency services and family planning services. In addition, states may not require cost-sharing by certain Medicaid recipients, who include:
• Pregnant women (for services related to pregnancy or another condition that could complicate pregnancy)
• Children under age 18
• Hospital or nursing-home patients who are expected to contribute most of their income to institutional care
• Individuals receiving hospice care
Review Question
States may impose nominal deductibles, coinsurance, or copayments on some Medicaid recipients for certain services. Services for which states can require copayments from Medicaid recipients include
A. Emergency servicesB. Family planning services
Both A and B
A only
B only
Neither A nor B
Page 304 of 469

AHM 510 : Health Plans : Governance and Regulation
Incorrect. Services for which states can require copayments from Medicaid recipients cannot include emergency services or family planning services.
Incorrect. Services for which states can require copayments from Medicaid recipients cannot include emergency services
Incorrect. Services for which states can require copayments from Medicaid recipients cannot include family planning services
Correct. Services for which states can require copayments from Medicaid recipients cannot include emergency services or family planning services.
Health Plans Under MedicaidMedicaid programs have faced financial crises over the past several years. As a result, states have found it necessary to find ways to contain increases in expenditures. In an effort to manage the costs and usage of Medicaid services and to make quality care more accessible to beneficiaries, in the mid-1980s many states began applying health plan techniques to their traditional Medicaid programs.
Almost from the beginning of the Medicaid program, states have had the option to enroll Medicaid beneficiaries in a managed care plan on a voluntary basis. As we will discuss, the need to manage costs and improve access to care have resulted in a move toward mandatory enrollment of many beneficiaries in health plan programs. Under health plans, the Medicaid program still covers the broad range of services previously covered, with an emphasis on health maintenance and preventive care, especially for children and pregnant women. The Balanced Budget Act of 1997 made several significant changes to the Medicaid program.
Impact of the Balanced Budget Act of 1997 on Medicaid Health PlansThe Balanced Budget Act (BBA) of 1997 made sweeping changes in the ways states contract with health plans and gave states greater flexibility in administering their Medicaid programs. The BBA added Section 1932 to the Social Security Act (SSA). Section 1932 of the SSA addresses virtually every area of Medicaid health plan contracts, including definitions of Medicaid health plan entities, eligibility for benefits, states’ ability to mandate health plans, regulation of MCE performance, marketing by Medicaid MCEs, and protection of Medicaid enrollees’ rights. We will discuss some of these changes in the following lessons.
Health Plans Eligible to Participate in the Medicaid ProgramIn Healthcare Management: An Introduction, we explained that there are three models of health plans commonly used for Medicaid programs. These models are
1. Entities that contract with a state to provide or arrange for comprehensive services on a risk basis—that is, health maintenance organizations (HMOs), health insuring organizations (HIOs), and provider-sponsored organizations
2. Entities that contract for less than comprehensive services, contract on a nonrisk or partial risk basis, or are otherwise exempt from the requirements a health plan must meet to contract under Medicaid laws and regulations, i.e., prepaid health plans (PHPs)
Page 305 of 469

AHM 510 : Health Plans : Governance and Regulation
3. Primary care case management programs (PCCMs), under which “freedom of choice” of providers is restricted and all services must be approved by a primary care provider or “gatekeeper”
In addition to HMOs, HIOs, PHPs, and PCCMs, the BBA amended Medicaid law to explicitly allow states to enter Medicaid contracts with provider-sponsored organizations (PSOs), discussed in Medicare and Health Plans. The BBA also created a new name or term—health plan entities— for certain entities providing Medicaid health plan services. As shown in Figure 8C-2, the term health plan entities refers to Medicaid health plans (discussed in the following lesson) and PCCMs.
As we discussed earlier, health insuring organizations are one of the three main models used in Medicaid health plan arrangements. Health insuring organizations (HIOs) are entities that contract with the state Medicaid agency as a fiscal intermediary. The HIO does not provide medical services but contracts with medical providers on behalf of the Medicaid agency. In the states of California, Minnesota, and Washington, several HIOs provide countywide healthcare coverage for all Medicaid participants. Since 1985, Congress has subjected HIOs engaged in full-risk contracting to the same strict regulatory standards as HMOs.
The BBA did not address the status of prepaid health plans (PHPs). Therefore, PHPs are not subject to the Medicaid health plan contracting requirements found in section 1903(m) of the SSA, discussed in the following section. A prepaid health plan (PHP) is a public or private entity under contract with a state Medicaid agency that provides a noncomprehensive set of medical services to enrolled beneficiaries on either a capitated risk or nonrisk basis or the entity provides a comprehensive set of medical services on a nonrisk or partial risk basis. PHPs also include a few risk-comprehensive organizations that have received statutory exceptions from section 1903(m).
Page 306 of 469

AHM 510 : Health Plans : Governance and Regulation
Review Question
From the following answer choices, choose the term that best corresponds to this description.
Barrington Health Services, Inc. contracts with a state Medicaid agency as a fiscal intermediary. Barrington does not provide medical services, but contracts with medical providers on behalf of the state Medicaid agency.
Health insuring organization (HIO)
Independent practice association (IPA)
Physician practice management (PPM) company
Peer review organization (PRO)
Correct. Health insuring organizations (HIOs) are entities that contract with the state Medicaid agency as a fiscal intermediary. The HIO does not provide medical services but contracts with medical providers on behalf of the Medicaid agency.
Incorrect. An independent practice association is an assoication of physicians (or physicians in small group practices) that contracts with a health plans to provide healthcare services.
Incorrect. A physician practice management company is a legal entity that provides a variety if management and administrative services for participating physicians' practices.
Incorrect. PROs are organizations or groups of practicing physicians or other healthcare professionals who review services ordered or furnished by other practitioners in the same medical field to determine whether the medical services provided were reasonable and necessary.
The following four types of entities meet the definition of PHP:
• Entities that do not accept risk for the comprehensive range of Medicaid services
• Entities that accept less than full risk for Medicaid services
• A narrow range of entities receiving Public Health Service Act grants since July 1, 1976, that contract with state Medicaid agencies to provide Medicaid services on a risk basis
• Entities that contracted to provide Medicaid services (but not inpatient hospital services) to Medicaid-eligible persons on a prepaid risk basis prior to 1970
Page 307 of 469

AHM 510 : Health Plans : Governance and Regulation
For example, a PHP may assume risk for only physician services or only ambulatory care. PHPs are frequently clinics or large group practices that do not accept risk for inpatient services or plans that provide only a single service, such as behavioral health.
Medicaid Health PlansMedicaid Health Plans are entities qualified by either the federal or the state government to contract on a prepaid, fully capitated basis to provide comprehensive healthcare services to Medicaid beneficiaries. The Medicaid health plan determines the reimbursement to be paid to providers. A Medicaid health plan integrates both the contracting entity and the providers of medical services into one organization. Medicaid health plans include HMOs, organizations with a current risk contract under Section 1876 or a Medicare+Choice contract, provider-sponsored organizations, or any other managed care risk-bearing organizations. The term, Medicaid health plan, refers to those managed care risk-bearing organizations that meet the requirements of Section 1903(m) of the SSA and that meet certain other regulatory requirements (e.g., relating to solvency, access, coverage area, etc.) for contracting under the authority of the Medicaid provisions in the SSA. To participate in the Medicaid program, a Medicaid health plan must meet a broad range of standards set forth in the Medicaid law and regulations. For example, a health plan’s services must be accessible to Medicaid beneficiaries within a service area equivalent to that provided for Medicaid beneficiaries not enrolled in the plan. Medicaid health plans, like commercial HMOs, must provide safeguards against the risk of insolvency.
States have some flexibility in defining Medicaid health plans, but the definition must require such health plans to give Medicaid enrollees the same access to care as the health plan’s other plan participants. Medicaid health plans accept full risk for a comprehensive range of healthcare services that they provide to enrollees. The benefits provided by Medicaid health plans are often more extensive than those provided by commercial HMOs because of the broad coverage mandated by the Medicaid program. For example, Medicaid health plans almost always include pharmacy and vision benefits, and may also provide dental benefits.
Primary Care Case Management ProgramsUnder a primary care case management program (PCCM program), states contract directly with providers who serve as primary care case managers. Primary care case managers (PCCMs) are responsible for locating, coordinating, and monitoring covered primary care and other services to all their Medicaid enrollees. An MCE’s primary care case management may be provided by a physician, a physician group practice, an entity2
that contracts with or employs physicians or—at a state’s option —a nurse practitioner, nurse midwife, or physician assistant. Usually, general practitioners, family practitioners, internal medicine practitioners, obstetrician/gynecologists, or pediatricians serve as PCCMs.
Most state PCCM programs pay the primary care provider a monthly case management fee in addition to paying for medical services on a reduced FFS basis. PCCM programs seek to reduce emergency room use and increase utilization of preventive care by fostering ongoing interaction between PCPs and their Medicaid patients.
State contracts must require that the PCCM provide reasonable and adequate hours of operation and a reasonable geographic location. The PCCM must have arrangements
Page 308 of 469

AHM 510 : Health Plans : Governance and Regulation
with, or the ability to refer to, a sufficient supply of providers other than the primary case manager.
Who Is Eligible for Medicaid?The Centers for Medicare and Medicaid Services (CMS), which we discussed in Regulatory Agencies and Health Plans, is the federal agency that provides guidelines for operating the Medicaid program. These guidelines include specific requirements for Medicaid eligibility and covered benefits. The Balanced Budget Act of 1997 (BBA) and the Personal Responsibility and Work Opportunity Reconciliation Act (PRWORA) of 1996, a welfare reform law, have made recent changes in the categories of people eligible for Medicaid. To understand how these laws affect eligibility for Medicaid, it is helpful to have a general understanding of:
• Who was eligible for Medicaid prior to the passage of the BBA and welfare reform
• Who is eligible for Medicaid now that the BBA and welfare reform are in place
It is important to keep in mind that rules and regulations for Medicaid eligibility frequently change at the federal level. In addition, the states have flexibility in setting some eligibility requirements for their Medicaid programs. The following information is intended to give a broad overview of Medicaid eligibility. CMS or state Medicaid agencies can provide more specific information on eligibility requirements.
Overview of ChangesBasically, prior to passage of the BBA, people who were eligible for welfare were eligible for Medicaid benefits. Recently passed welfare reform laws unlinked the automatic connection between these two programs. In some instances, it became more difficult for certain categories of people to qualify for welfare assistance; however, most of these people were still eligible for Medicaid.
Eligibility Before Welfare Reform and the BBAThree broad categories of individuals were eligible for Medicaid prior to the BBA and welfare reform:
• The categorically needy
• The medically needy
• “Expansion populations”
The Categorically NeedyCategorically needy individuals are those individuals who meet a state’s requirements for certain categories that the federal and state governments have determined need welfare coverage. Categorically needy individuals have Medicaid automatically because they receive welfare (often called “cash assistance” or “cash-grants-in-aid”). Prior to the passage of the BBA and welfare reform, there were two main welfare categories that contained individuals considered to be categorically needy:
1. Individuals who qualified for a statefederal program called Aid to Families with Dependent Children (AFDC). As a result of welfare reform laws, AFDC has
Page 309 of 469

AHM 510 : Health Plans : Governance and Regulation
been replaced with a new federal program called Temporary Assistance for Needy Families (TANF); however, states still use the eligibility criteria in AFDC to determine Medicaid eligibility for singleparent households. We discuss AFDC and TANF in Figure 8C-3.
2. Individuals who qualified for a federal assistance program called Supplemental Security Income (SSI). Figure 8C-4 describes individuals who are eligible for SSI. Note that neither the BBA nor welfare reform laws currently unlink the connection between eligibility for SSI and eligibility for Medicaid. Welfare reform laws briefly unlinked this connection for certain categories of immigrants, but that change was then reversed by provisions in the BBA, as we discuss later in this lesson.
Figure 8C-3. Medicaid Eligibility and the AFDC and TANF Programs.
The Personal Responsibility and Work Opportunity Reconciliation Act (PRWORA) of 1996 (Public Law 104-193) was basically a welfare reform act. PRWORA established time limits and work requirements for low-income individuals and families receiving cash assistance. Signed into law on August 22, 1996, the PRWORA replaced several cash welfare benefit programs. Aid to Families with Dependent Children (AFDC) was one of the programs that was replaced. The AFDC program was a federally funded welfare program that provided assistance to one-parent households with one or more children which households met certain financial eligibility requirements.
AFDC was replaced with the Temporary Assistance for Needy Families (TANF) program. Under TANF, each state receives a block grant for providing income support and work programs to needy individuals. TANF gives states greater latitude than AFDC did in determining who is eligible to receive cash grants. Because the purpose of PRWORA is to encourage individuals to become self-supporting, the law generally limits states to paying benefits to families for a maximum of five years; however, this limit does not apply to Medicaid benefits.
Figure 8C-4. What is Supplemental Security Income (SSI)?
Supplemental Security Income (SSI) is an ongoing federal program that provides cash assistance to the following groups:
• The aged (i.e., individuals aged 65 and older), called Old Age Assistance • Individuals who are blind and/or permanently and totally disabled, called Aid to
the Blind and Aid to the Disabled, respectively
Individuals who qualify for SSI are also eligible for Medicaid benefits. The federal government establishes income eligibility criteria for SSI benefits.
In addition to meeting the categorical requirements (e.g., single-parent household, elderly, blind or disabled), individuals must meet certain financial resource requirements
Page 310 of 469

AHM 510 : Health Plans : Governance and Regulation
and monthly income requirements to be considered eligible as categorically needy for Medicaid benefits. These financial eligibility criteria require that individuals’ financial resources (assets) and monthly income not exceed specified limits, based on household size. When the AFDC program was in effect, states set the resource and income limits for the AFDC programs, subject to CMS approval. The Social Security Administration sets the resource and income limits for the SSI program.
Medically Needy IndividualsThe second group of people for which Medicaid benefits were available prior to the BBA and welfare reform is the medically needy group. Medically needy individuals are individuals who meet the categorical and financial resource requirements, described above, to be deemed categorically needy—but whose income is too high to meet the monthly income requirement. States can choose to provide Medicaid coverage to such individuals and have the flexibility to provide such coverage to individuals whose incomes are up to 100% of the federal poverty level. The federal poverty level (FPL) is the income level at which an individual or family is considered “poor” by the federal government. States may also choose to provide Medicaid coverage on a monthly basis to individuals who “spend down” their excess income on medical care costs. The “spending down” process works like a deductible; once an individual meets the threshold maximum income level by incurring healthcare expenses, he or she becomes eligible for Medicaid coverage as medically needy. Individuals can “spend down” by incurring medical and/or remedial care expenses to offset their excess income. In this way, individuals reduce their income to a level below the maximum allowed by a state’s Medicaid program for eligibility under this category.
Expansion PopulationsIn the late 1980s, Congress expanded Medicaid coverage to certain populations—children and pregnant women—who did not meet the requirements for the categorically needy groups. The coverage for children includes all services available to children under the AFDC program. The coverage for pregnant women is limited to pregnancyrelated services throughout the pregnancy and continuing up through a 60-day postpartum period. Congress later extended this coverage to include family planning services for a period of one year after the birth of the child.
The laws that Congress passed to enact coverage for these “expansion populations” do not require a financial resource test for eligibility; however, states can choose to impose a financial resource test within specified limits. To be eligible for the “expansion populations” category, an individual must meet an income test based on federal poverty guidelines. Note that the income test sets a maximum income a household may earn to be considered eligible for Medicaid under the “expansion population” category; however, states may allow individuals or households with higher incomes to qualify for their state Medicaid programs at their discretion. The standard income requirements, based on the FPL, are as follows:
• For children up to age one and pregnant women, the household income level is below 185% of the FPL guidelines
• For children aged one to five, the household income level is below 133% of the FPL
Page 311 of 469

AHM 510 : Health Plans : Governance and Regulation
• For children aged six to 19, the household income level is below 100% of the FPL guidelines
Dual EligiblesDual eligibles are people who are eligible for both Medicare and Medicaid benefits. Almost 100% of people who are eligible for Medicaid because they receive Old Age Assistance and approximately 40% of people who are eligible for Medicaid because they receive Aid to the Blind/Aid to the Disabled also have Medicare coverage. For these people, Medicare coverage is primary and Medicaid coverage is secondary, and Medicaid pays the Medicare Part B premium. In addition, for a small group of dual eligibles, Medicaid pays their Part A premium. Figure 8C-5 describes several categories of dual eligibles and what the Medicaid program covers for these individuals.
Figure 8C-5. Medicaid-Eligible Medicare Beneficiaries.
State Medicaid programs are required to pay the Medicare premiums and the cost-sharing (e.g., copayments, deductibles) on Medicare services for Medicare beneficiaries whose income is below 100% of the poverty level and whose assets do not exceed two times (200%) the amount allowed by the Supplemental Security Income program. The Medicare beneficiaries who qualify for this costsharing are called qualified Medicare beneficiaries (QMBs).
State Medicaid programs are also required to pay Part B premiums for individuals with income between 100% and 120% of the FPL and whose assets do not exceed 200% of the allowable SSI amount. These beneficiaries are known as specified low-income Medicare beneficiaries (SLMBs). In general, SLMBs are people with slightly higher incomes than QMBs.
States are also obligated to pay all or a portion of the Part A premium for a group of beneficiaries known as called qualified disabled working individuals (QDWIs). QDWIs are people who formerly qualified for Social Security disability income and have lost eligibility but are exercising the option of keeping Medicare by paying the Part A premium. These individuals have incomes of less than 200% of the FPL and assets that do not exceed 200% of the allowable SSI amount. Medicaid pays the Part A premiums for these individuals. QDWIs are a very small portion of the dual eligible population.
Medicaid Eligibility for Immigrants with Permanent Resident StatusBecause we discuss changes that PRWORA and the BBA made in Medicaid eligibility later in this section, it is important to note that prior to PRWORA, immigrants with permanent resident status (i.e., “those who had qualified for and received a green card”) had the same entitlement to Medicaid as didU.S. citizens.
Eligibility After Welfare Reform and Passage of the BBAAs described in Figure 8C-2, PRWORA was basically a welfare reform act; Congress chose not to deal with Medicaid reform directly. However, welfare reform had certain impacts on the Medicaid program. In the final analysis some of the changes that
Page 312 of 469

AHM 510 : Health Plans : Governance and Regulation
PRWORA made on Medicaid eligibility were unintended. The BBA corrected some of those changes and made further changes to eligibility for the Medicaid program.
Effects of Unlinking TANF and MedicaidAs we discussed earlier, PRWORA abolished the AFDC welfare entitlement program and established TANF in its place. The link between welfare and Medicaid for the AFDC population was broken. As we mentioned earlier in this lesson, being eligible for TANF does not make an individual automatically eligible for Medicaid.
Unless the states choose to implement a single application and facilitate submission of the application to both the TANF and Medicaid programs, eligible individuals have to apply separately for benefits under TANF and Medicaid. Medicaid advocates have been concerned that the separate application process will result in fewer eligible individuals applying for Medicaid. For example, people who find out that they are not eligible for TANF may assume that they are not eligible for Medicaid, or they just may not apply for Medicaid benefits.
States' Flexibility to Change Eligibility RequirementsStates still have to make Medicaid, not welfare, available to people who meet the AFDC categorical and financial eligibility criteria in place as of July 16, 1996. However, states have flexibility to adjust the financial eligibility criteria by one of two methods:
• Reducing the income standards to the levels they had in effect on May 1, 1988
• Increasing the income standards in accordance with changes in the Consumer Price Index
In addition, the BBA offers states the opportunity to implement 12-month, rather than six-month, continuous eligibility for children up to 19 years of age.
BBA Corrects Unintended Changes Made by PRWORAAs we discussed earlier, the BBA corrected some unintended effects of PRWORA. One such change related to Medicaid coverage for disabled children. PRWORA changed the disability determination criteria for children under the SSI program. This change could have resulted in certain children losing their SSI welfare status and their Medicaid benefits. The BBA softened the impact of the provisions of PRWORA by requiring that states continue Medicaid coverage for children who were receiving SSI benefits on August 22, 1996, and who subsequently lost those benefits as a result of the more restrictive disability definition in PRWORA. The BBA also ensures that children who began receiving SSI benefits after August 22, 1996, will be covered by state Medicaid programs.
Medicaid Eligibility for Immigrants with Permanent Resident StatusAs previously mentioned, prior to passage of PRWORA, immigrants with permanent resident status were entitled to the same Medicaid benefits as U. S. citizens. PRWORA contained provisions that
• Required that immigrants who attained permanent resident status after the passage of PRWORA were subject to a five-year waiting period before becoming eligible for any Medicaid benefits, with certain limited exceptions
Page 313 of 469

AHM 510 : Health Plans : Governance and Regulation
• Gave states the option not to provide Medicaid to immigrants—who had attained permanent resident status prior to PRWORA—that met AFDC eligibility criteria
• Ceased cash grant assistance and Medicaid coverage to immigrants— who had attained permanent resident status prior to PRWORA—that were receiving SSI. However, the BBA restored SSI eligibility and Medicaid to this population
Dual EligibleThe BBA provided for additional allocations to the states in the form of five-year block grants for paying Medicare Part B premiums for low-income, low-resource individuals who do not qualify for Old Age Assistance under Medicaid. Unlike other Medicaid eligibility categories, assistance funded by the block grants is available on a first-come, first-served basis until the state allotment is depleted.
Medicaid Eligibility for Other PopulationsIn the preceding lessons, we have discussed Medicaid eligibility for certain populations; however, the Medicaid program contains flexibility that allows states to cover other populations outside the groups we discussed. There are three major populations for which states have chosen to allow eligibility for their Medicaid program which we have not discussed:
• States that have obtained waivers of Medicaid rules to extend eligibility to populations that would not ordinarily be covered by Medicaid. Tennessee has a Medicaid-waiver program called TennCare that is an example of such a waiver program. The states that have these waivers determine the eligibility criteria, subject to CMS approval, for the additional populations who will be eligible to receive Medicaid benefits under their program.
• States that have chosen to implement the State Children’s Health Insurance Program (SCHIP)—Title XXI of the Social Security Act, created by the Balanced Budget Act—through their Medicaid programs. Eligibility criteria for these children are determined by the state, subject to CMS approval. We discuss SCHIP later in this lesson.
• States that provide health services to persons not eligible for federal Medicaid through their Medicaid programs. The states set the eligibility criteria for these individuals, who are often called Home Relief or General Relief recipients. These criteria are not subject to CMS approval since there is no federal funding for the services provided.
As mentioned above, we discuss SCHIP and how it can be implemented using an existing Medicaid program or a separate non- Medicaid program later in this lesson. Information on eligibility for Medicaidwaiver programs and programs for other populations not ordinarily eligible for Medicaid can be obtained from state or county Medicaid agencies or CMS.
States’ Responsibilities Under Medicaid Managed Care ProgramsAs we mentioned earlier in this lesson, the BBA made changes that allow states to contract with additional types of MCEs, such as provider-sponsored organizations. The BBA also lifted the need for states to obtain a waiver of certain requirements for state Medicaid programs in order to implement certain mandatory health plan programs.
Page 314 of 469

AHM 510 : Health Plans : Governance and Regulation
However, states may still file a waiver to implement their Medicaid managed care programs and must follow the rules for that process; such waivers must be renewed every three years.
Under the nonwaiver option, states that file a satisfactory state plan amendment, discussed later in this lesson, may continue their Medicaid managed care program indefinitely. The following lessons describe waivers and the waiver process. Then we focus on the role of the states in connection with Medicaid managed care initiatives.
WaiversInitially, federal law prohibited states from making enrollment in health plans mandatory for Medicaid beneficiaries without obtaining a special waiver of the Medicaid law and regulations. By requiring beneficiaries to enroll in a health plan, their choice of providers was effectively limited. Limiting choice of providers was considered a violation of beneficiaries’ rights. Therefore, states were only allowed to encourage voluntary enrollment in managed care programs. However, it became clear that PCCM programs and voluntary enrollment were not going to stem the tide of increasing costs for the Medicaid programs. The federal government encouraged states to apply for “waivers” of certain requirements for state Medicaid programs. The requirements for such waivers were already defined in Sections 1915(b) and 1115 of the SSA.
Section 1915(b) WaiverSection 1915(b) of the SSA gives the Secretary of Health and Human Services (HHS Secretary) authority to waive the requirements of the section of the SSA3 that sets forth state plan requirements for Medicaid programs. Such waivers are very common and obtaining them is routine. Exceptions can be allowed for any portions of the requirements that prohibit a state from limiting the providers from whom a beneficiary may choose to receive services. However, states are required to apply for a waiver to require their Medicaid beneficiaries to enroll in health plans. The BBA amended Medicaid law to provide that state Medicaid programs may mandate enrollment in a health plan entity without seeking a Section 1915(b) waiver.4
States must still obtain or renew an existing 1915(b) waiver to implement programs that do not meet the 1915(b) requirements of the SSA. For example, those programs that allow enrollment by special-needs children or Medicare beneficiaries or have default enrollment processes (discussed later in this lesson) that give priority based on the lowest cost provider must still obtain a waiver.
Many states have health plan Medicaid programs that currently operate under a Section 1915(b)(1) waiver known as a “freedom of choice” waiver. Figure 8C-6 describes the 1915(b)(1) waiver and several other types of 1915(b) waivers.
Figure 8C-6. Section 1915(b) Waivers.
Section 1915(b) has four subsections:
1. Subsection (1) is commonly referred to as the “freedom of choice” waiver. This provision allows a state to restrict a Medicaid beneficiary’s choice of providers by using a PCCM system or other arrangement. The beneficiary may also be offered
Page 315 of 469
AHM 510 : Health Plans : Governance and Regulation
a choice between enrolling in an HMO or choosing an independent practitioner or clinic.
2. Subsection (2) permits a state to act as a central broker in helping Medicaid clients to choose among competing health plans.
3. Subsection (3) allows the state to share with providers some of the savings from a Medicaid health plan by providing coverage of enhanced services to Medicaid beneficiaries. For example, Alabama has implemented a 1915(b)(3) waiver to offer an enriched maternity benefit package to pregnant women.
4. Subsection (4) is commonly called the “selective contracting” section and allows the state to limit eligible providers of a certain service to those who can demonstrate effectiveness and efficiency. Some states have received 1915(b)(4) waivers to contract for such services as inpatient maternity care, transportation services, oxygen therapy, or mail-order prescription drugs.
To receive a Section 1915(b) waiver, a state is required, among other conditions, to
1. Demonstrate sufficient Medicaid health plan capacity 2. Show that Medicaid health plan payments did not exceed payments under the
state’s FFS plan 3. Comply with quality assurance and grievance requirements
The federal government monitors and evaluates states’ activities under Section 1115 waivers. Much of early Medicaid health plans evolved under Section 1115 waivers. As of May 1998, seventeen states5 had received and implemented Section 1115 projects, three additional states6 have received Section 1115 waivers but have not yet implemented their programs; and one state7 has had its proposal approved in concept.
States often use a Section 1115 waiver to extend Medicaid eligibility to low-income individuals not covered under federal Medicaid rules. Each waiver differs in the new population covered, the scope of coverage, and the nature of the participating health plans. The federal Medicaid requirements most commonly waived under Section 1115 are described in Figure 8C-7.
Figure 8C-7. Requirements Most Commonly Waived Under Section 1115.
The requirements of Title XIX of the SSA that are most commonly waived under Section 1115 include the following seven categories:
1. Statewideness: A Section 1115 waiver can permit variations in the Medicaid program in different areas of the state.
2. Comparability: A Section 1115 waiver can allow benefits to be provided to one group and not to another and/or can permit the state to use different eligibility methods and standards for different classes of beneficiaries.
3. Eligibility: A Section 1115 waiver can allow a state to revise its Medicaid eligibility criteria and standards.
Page 316 of 469
AHM 510 : Health Plans : Governance and Regulation
4. Freedom of Choice: A Section 1115 waiver can allow a state to restrict beneficiaries’ freedom of provider choice and can allow a state to make health plan enrollment mandatory.
5. Health Plans: A Section 1115 waiver can allow Medicaid beneficiaries to receive services through alternative delivery systems that otherwise would not meet existing state and federal requirements.
6. Reimbursement: A Section 1115 waiver can allow reasonable alterations in Medicaid payment requirements.
7. Benefits: A Section 1115 waiver can allow states to expand benefits beyond those traditionally covered in the Medicaid program.
The Medicaid statute does not allow Section 1115 waivers to be used for the following purposes:
1. To alter the medical assistance given to children and pregnant women 2. To change the drug rebate provisions that apply to drug manufacturers 3. To impose copayments on Medicaid-eligible individuals 4. To waive spousal impoverishment protections for institutionalized people 5. To change coverage of certain low-income beneficiaries or disabled individuals
who qualify for Medicaid assistance in paying the premiums for their Medicare Part A or Part B premiums
Most statewide demonstration programs have attempted to expand Medicaid eligibility and to increase the use of managed care in Medicaid programs. Some states have also used Section 1115 waivers to move Medicaid beneficiaries with more complex healthcare needs (e.g., the disabled or the elderly) into health plans. Arizona has implemented the most comprehensive program of this type, encompassing all eligibility groups and almost all services. Tennessee and Oregon have taken steps to cover their entire Medicaid populations under health plans, although they specifically exempt individuals who are residents in long-term care facilities.
States that currently operate Medicaid programs under Section 1115 waivers may continue to do so. The BBA amended Medicaid law to create new authority to extend the five-year waiver period. A state may submit a request for extension of a Section 1115 demonstration waiver 12 to 18 months before the waiver is due to expire. The extension may be granted for up to three years. The HHS Secretary reviews requests and approves or disapproves waiver extensions. If the HHS Secretary fails to respond within six months, the request is automatically granted. All terms and conditions that applied to the original waiver also apply to the extension.
Figure 8C-7. Requirements Most Commonly Waived Under Section 1115.
The requirements of Title XIX of the SSA that are most commonly waived under Section 1115 include the following seven categories:
1. Statewideness: A Section 1115 waiver can permit variations in the Medicaid program in different areas of the state.
Page 317 of 469

AHM 510 : Health Plans : Governance and Regulation
2. Comparability: A Section 1115 waiver can allow benefits to be provided to one group and not to another and/or can permit the state to use different eligibility methods and standards for different classes of beneficiaries.
3. Eligibility: A Section 1115 waiver can allow a state to revise its Medicaid eligibility criteria and standards.
4. Freedom of Choice: A Section 1115 waiver can allow a state to restrict beneficiaries’ freedom of provider choice and can allow a state to make health plan enrollment mandatory.
5. Health Plans: A Section 1115 waiver can allow Medicaid beneficiaries to receive services through alternative delivery systems that otherwise would not meet existing state and federal requirements.
6. Reimbursement: A Section 1115 waiver can allow reasonable alterations in Medicaid payment requirements.
7. Benefits: A Section 1115 waiver can allow states to expand benefits beyond those traditionally covered in the Medicaid program.
The Medicaid statute does not allow Section 1115 waivers to be used for the following purposes:
1. To alter the medical assistance given to children and pregnant women 2. To change the drug rebate provisions that apply to drug manufacturers 3. To impose copayments on Medicaid-eligible individuals 4. To waive spousal impoverishment protections for institutionalized people 5. To change coverage of certain low-income beneficiaries or disabled individuals
who qualify for Medicaid assistance in paying the premiums for their Medicare Part A or Part B premiums
Section 1115 WaiverSection 1115 of the SSA gives the HHS Secretary broad authority to waive provisions in the Medicaid law in order to offer more comprehensive services for the following categories:
• Aged individuals
• Blind individuals
• Dependent and crippled children
• Maternal and child welfare
• Public health
Although both the 1915(b) and 1115 waivers allow states to mandate enrollment in Medicaid managed care plans, Section 1115 research and demonstration waivers allow states more flexibility than Section 1915(b) waivers. Section 1115 allows the HHS Secretary to waive compliance with sections of the SSA that establish basic requirements for state Medicaid plans. In addition, Section 1115 allows the HHS Secretary to approve and provide federal financial participation (FFP) for healthcare coverage arrangements not ordinarily eligible for federal funds. States use Section 1115 waivers to test, or demonstrate, various innovative methods of covering uninsured
Page 318 of 469
AHM 510 : Health Plans : Governance and Regulation
populations and to test new healthcare delivery systems. These demonstration projects can be statewide or can focus on a specific area of the state.
To receive a Section 1115 waiver, a state must demonstrate to the federal government that the project will cost no more than the state’s current Medicaid program. The state must also offer assurances that the demonstration project will maintain the quality of care, prevent unnecessary utilization of services, and reimburse providers at adequate rates, and that the participating health plans will meet the requirements of federal rules.
The federal government monitors and evaluates states’ activities under Section 1115 waivers. Much of early Medicaid health plans evolved under Section 1115 waivers. As of May 1998, seventeen states5 had received and implemented Section 1115 projects, three additional states6 have received Section 1115 waivers but have not yet implemented their programs; and one state7 has had its proposal approved in concept.
States often use a Section 1115 waiver to extend Medicaid eligibility to low-income individuals not covered under federal Medicaid rules. Each waiver differs in the new population covered, the scope of coverage, and the nature of the participating health plans. The federal Medicaid requirements most commonly waived under Section 1115 are described in Figure 8C-7.
Most statewide demonstration programs have attempted to expand Medicaid eligibility and to increase the use of managed care in Medicaid programs. Some states have also used Section 1115 waivers to move Medicaid beneficiaries with more complex healthcare needs (e.g., the disabled or the elderly) into health plans. Arizona has implemented the most comprehensive program of this type, encompassing all eligibility groups and almost all services. Tennessee and Oregon have taken steps to cover their entire Medicaid populations under health plans, although they specifically exempt individuals who are residents in long-term care facilities.
States that currently operate Medicaid programs under Section 1115 waivers may continue to do so. The BBA amended Medicaid law to create new authority to extend the five-year waiver period. A state may submit a request for extension of a Section 1115 demonstration waiver 12 to 18 months before the waiver is due to expire. The extension may be granted for up to three years. The HHS Secretary reviews requests and approves or disapproves waiver extensions. If the HHS Secretary fails to respond within six months, the request is automatically granted. All terms and conditions that applied to the original waiver also apply to the extension.
Implementing State Mandatory Medicaid Managed Care Programs Without WaiversAs we discussed earlier in this lesson, the BBA contains provisions to allow states to implement a mandatory health plan program without obtaining a 1915(b) waiver. States must file a state plan amendment (SPA) with the HHS secretary to make Medicaid health plans mandatory. A state plan amendment (SPA) must describe how the state will meet the requirements for mandating health plans. States may not require special-needs children, dually enrolled Medicare and Medicaid beneficiaries, or native Americans (in certain cases) to enroll in a health plan program unless they apply for a Section 1915(b) waiver.
Page 319 of 469

AHM 510 : Health Plans : Governance and Regulation
To mandate health plan enrollment, states must offer enrollees a choice between at least two MCEs, except in rural areas, where a state could offer beneficiaries a choice of at least two providers in one MCE. The states must also give enrollees the right to change plans or PCPs for cause at any time and without cause within the first 90 days following enrollment. Enrollees must also have the opportunity to make a change in plans at least once during any 12-month period. In effect, this allows states to limit disenrollment from a health plan to only once per calendar year. Prior to the BBA, enrollment could only be “locked in” for six months under a 1915(b) waiver.
States must establish an enrollment priority system that gives first choice for enrollment to Medicaid beneficiaries who are currently enrolled in a health plan if the new plan that they choose is full. States that implement programs to mandate health plan coverage for Medicaid beneficiaries must ask beneficiaries to select a plan from the plans qualified by the state.
If a beneficiary fails to select a plan or a PCP, the state is allowed to automatically assign a beneficiary to a plan. States must establish a default enrollment process to assign beneficiaries to a plan if they do not exercise their right to choose a plan or PCP. This default process must attempt to maintain existing provider-beneficiary relationships or relationships with traditional Medicaid pro-viders. If the default process cannot maintain such relationships, the state’s process must try to equitably distribute beneficiaries among the available health plans. Some states use criteria other than provider relationships, such as plan quality performance, availability of additional benefits, etc., to assign beneficiaries to health plans.
Requirements for Notices and InformationAll notices and information provided to Medicaid enrollees by the states, its brokers, and the health plan entities must be presented in a manner that is easily understood by Medicaid enrollees and potential enrollees. For example, notices and information must be written at no more than a sixth-grade reading level. The BBA requires MCES to provide detailed information to prospective enrollees, including the following:
• The names of providers who are included in the entity’s network
• Enrollees’ rights and responsibilities
• Grievance procedures
• Covered items and services
Annually, or on the request of the enrollee, states must provide a list of available MCES, including information about each entity’s benefits, service areas, and quality and performance indicators.8
Requirements for State Quality Assurance ProgramsAs we have seen, the Medicaid program seeks to manage the costs of healthcare. In addition, the Medicaid program seeks to ensure the quality of healthcare provided to Medicaid beneficiaries. Specifically, each state must develop and implement a quality assessment and improvement strategy, applicable to contracting Medicaid MCEs, which includes the following:
• Standards for access to care
Page 320 of 469

AHM 510 : Health Plans : Governance and Regulation
• Examination of other aspects of care and service directly related to quality such as grievance procedures and marketing and information standards
• Procedures for monitoring the quality and appropriateness of care
• Requirements for providing quality assurance data to the state using the data and information standards required by Medicare
CMS has been working closely with other federal and state officials, as well as representatives of beneficiary advocacy groups and the health plan industry, to develop quality standards that can better ensure that health plans which contract with CMS protect and improve the health and satisfaction of their enrollees. The Quality Assessment Performance Improvement (QAPI) is the product of these efforts. It builds on a variety of recent CMS and state efforts to promote the assessment and improvement of health plan quality. Once complete, QAPI will offer a uniform set of quality assurance standards that can be used by CMS and the state Medicaid agencies to determine whether a health plan can meet the quality assurance requirements necessary to become and remain eligible as a Medicaid contractor.
Although the requirement for plans to undergo external quality review was in place prior to passage of the BBA, the BBA requires that a standard protocol be developed for such reviews. The HHS Secretary and the National Governor’s Association are charged with contracting with an independent quality review organization to develop protocols to be used in external independent reviews conducted on or after January 1, 1999. In addition, the BBA gave states the authority to ensure that such external reviews do not duplicate review activities performed by a private accreditation organization or a review under the Medicare+Choice program. States may choose to “deem compliance”9 with the external review requirement for Medicare+ Choice organizations that have had a Medicaid risk contract in effect for at least two years.
The BBA also repealed a rule that required health plans to limit their Medicaid and Medicare enrollment to less than 75% of total enrollment. This rule was intended to ensure that Medicaid enrollees received the same level of quality healthcare that plans provided to commercial enrollees. Since this rule has been repealed, Medicaid MCEs are no longer required to serve commercial enrollees. The 75/25 composition rule, as this rule was called, was repealed in part because new quality indicators have been developed that help assure Medicaid managed care enrollees receive quality healthcare. In addition, the composition rule was cumbersome to enforce and posed a problem for health plans in areas with a large proportion of Medicaid recipients.
Oversight of Marketing EffortsAlthough states had many regulatory requirements related to marketing prior to 1997, there was very little federal regulation of Medicaid health plan marketing and enrollment practices. Federal regulations did not require advance approval of marketing materials and did not prohibit Medicaid HMOs from marketing door-todoor or from offering gifts or payments to attract enrollees. Federal regulations addressed only general marketing practices.
With passage of the BBA, the federal government demanded closer management of Medicaid health plan marketing practices. For example, the federal Medicaid law now prohibits health plans from distributing marketing materials without prior state approval.
Page 321 of 469

AHM 510 : Health Plans : Governance and Regulation
Medicaid marketing materials may not contain false or misleading information, and no other insurance products may be marketed in conjunction with the health plan. Each plan must distribute marketing materials to its entire service area. Both oral and written marketing materials must conform to the standards of accuracy and understandability set by the HHS Secretary so that enrollees can make an informed choice among health plans. “Cold calls”—either door-to-door or by telephone—are prohibited.
The state must consult a medical care advisory committee as a part of the review of marketing materials. In addition, states must distribute, either directly or through its Medicaid MCEs, information in a chartlike format that compares the benefits, costsharing, service area, and instructions on accessing any covered services not included in the health plan benefit package.
If available, the comparative information must also include each health plan’s quality and performance indicators. In addition, Medicaid marketing practices are heavily regulated by state Medicaid agencies and, in some cases, the state agency responsible for regulating commercial HMOs. State regulations specify where marketing activities may take place and include provisions for certification and oversight of marketing agents. Figure 8C-8 describes one state’s regulations for Medicaid marketing materials.
The Office of the Inspector General of the U.S. Department of Health and Human Services, the U.S. General Accounting Office (on the request of a member of Congress), the U.S. Attorney General, and in some states the State Attorney General and/or Department of Insurance all can investigate Medicaid health plan marketing abuses.
Figure 8C-8. An Example of State Regulation of Marketing Materials.
The state of Tennessee has set the following standards for marketing materials used by Medicaid managed care plans:
1. The state must preapprove written marketing materials. 2. Materials cannot mislead, confuse, or defraud. 3. Materials must be written on a reading level no higher than sixth grade. 4. Enrollment forms cannot be attached to marketing materials. 5. If the plan is advertising special benefits, it must explain clearly which health
services are required by the state and which are additional benefits. 6. Materials cannot give the appearance that the state endorses a particular plan. For
instance, plans cannot display the state seal on their materials. 7. Since Tennessee’s TennCare program requires certain people to pay premiums,
plans cannot use the word “free” on their marketing materials. 8. If plans fail to comply with these or other marketing restrictions, Tennessee may
suspend new enrollments, inform misinformed enrollees that they may disenroll, and/or withhold capitation payments.
Source: Excerpted and adapted from Families USA Foundation, A Guide to Marketing and Enrollment in Medicaid Health Plan. June 1997, p. 9.
Determining Services to Be OfferedEach state determines the amount and duration of services offered under its Medicaid
Page 322 of 469
AHM 510 : Health Plans : Governance and Regulation
program, within broad federal guidelines (described later in this lesson). For example, a state may limit the number of days of hospital care or the number of physician visits. However, the limits must be sufficient to include a level of service to reasonably achieve the purpose of the benefits. Limits on mandatory benefits may not be different for different medical diagnoses or conditions.
States may also receive federal matching funds for providing certain optional services to Medicaid recipients. The most common of the 34 currently approved optional Medicaid services include the following:
• Diagnostic services
• Clinical services
• Intermediate care facilities for the mentally retarded
• Prescribed drugs and prosthetic devices
• Optometrist services and eyeglasses
• Nursing facility services for children under 21
• Transportation services
• Rehabilitation and physical therapy services
• Home and community-based care to certain persons with chronic impairments (only 1915[b] waiver)
Role of State Regulatory AgenciesA survey of state insurance, Medicaid, and public health agencies conducted by the National Academy for State Health Policy revealed that in a majority of states two or more agencies have simultaneous regulatory authority over MCEs. State insurance and health departments often regulate MCEs and publish review standards for purchasers to consider. State Medicaid agencies have both regulatory and purchasing responsibilities. Insurance departments typically monitor the financial aspects of MCE operations. Health departments tend to monitor quality and consumer protection. Medicaid agencies are more likely to monitor both the financial and quality assurance aspects of MCEs. The Medicaid agencies’ dual responsibilities reflect their accountability to federal regulation of the Medicaid program. If there are any gaps in a state’s oversight of its Medicaid program, they tend to be in the area of quality assurance standards. The reason for this gap is most likely the recent evolution of increasing emphasis on quality within the healthcare industry and among consumer groups that demands more detailed oversight of plans for quality assurance.
There are several approaches to the interagency division of responsibility for MCE oversight. In one approach, the concurrent model, various state agencies exert authority over similar aspects of MCE operations among the same group of MCEs. For example, a state Medicaid agency and a state health department may both be responsible for ensuring quality improvement programs are in place to meet each agency’s rules and regulations for such programs. In this approach, there is considerable overlap of the functions performed by the various agencies. States using this approach include New Jersey, Rhode Island, and Vermont.
Page 323 of 469

AHM 510 : Health Plans : Governance and Regulation
Another approach is the parallel model, in which each agency regulates both financial and quality aspects of MCE operations for distinctly different MCE types. For example, one agency might focus on HMOs, the second on PCCMs, and the third on PHPs.
A third approach is the shared model, in which each agency focuses on its particular area of expertise in regulating managed care. The health department focuses on quality assurance; the insurance department focuses on financial operation; the Medicaid agency focuses on those aspects of financial operation and quality assurance that are beyond the expertise of the insurance or health department. Alternatively, the Medicaid agency may focus more exclusively on program administration, including contracting, rate-setting, and contract compliance. While this approach is still in development, the states of Florida, Illinois, and Tennessee each have implemented a version of the shared model.10
Enforcement and Sanctions for NoncomplianceState Medicaid agencies must monitor MCEs and take action if MCEs fail to meet Medicaid’s standards and requirements. However, states must allow MCEs due process prior to terminating their participation in the Medicaid program. Federal law outlines the intermediate sanctions a state may impose on an MCE. These sanctions may include civil monetary penalties or other remedies. The state may impose sanctions if the MCE:
• Fails substantially to provide medically necessary items and services that are required under law or under contract (penalty of up to $25,000 for each determination)
• Imposes excessive premiums and charges (penalty is double the excess amount charged)
• Acts to discriminate among enrollees on the basis of health status or other requirements for health services except as permitted under applicable sections of the SSA (penalty must not be more than $100,000 for each determination)
• Engages in a practice that reasonably could be expected to have the effect of denying or discouraging enrollment by people who may need substantial future medical services (penalty of up to $100,000 for each determination)
• Misrepresents or falsifies information furnished to the state, HHS, an enrollee, a potential enrollee, or a provider (penalty of up to $100,000 for each determination)
• Violates marketing requirements outlined in Section 1932(d) of the SSA (penalty of up to $25,000 for each determination)
Review Question
There are several approaches to the interagency division of responsibility for managed care entity (MCE) oversight. In State M, the state Medicaid agency, the state department of health, and the state insurance department are all responsible for ensuring that quality improvement programs are in place among the same group of MCEs and that these programs meet each agency's rules and regulations for such programs. This information indicates that State M uses the approach known as the
Page 324 of 469
AHM 510 : Health Plans : Governance and Regulation
parallel model
shared model
concurrent model
PACE model
Incorrect. The parallel model is when each agency regulates both financial and quality aspects of MCE operations for distinctly different MCE types. For example, one agency might focus on HMOs, the second on PCCMs, and the third on PHPs
Incorrect. The shared model is when each agency focuses on its particular area of expertise in regulating managed care. The health department focuses on quality assurance; the insurance department focuses on financial operation; the Medicaid agency focuses on those aspects of financial operation and quality assurance that are beyond the expertise of the insurance or health department
Correct. In one approach, the concurrent model, various state agencies exert authority over similar aspects of MCE operations among the same group of MCEs.
Incorrect. PACE is a joint federal-state program that states have the option of implementing to provide ann alternative to institutional care for persons age 55 or older who require nursing facility levels of care.
In addition to, or instead of, imposing monetary penalties, a state may choose to take any or all of the following actions:
• Permit beneficiaries to disenroll from the plan without cause
• Suspend default enrollment
• Suspend payment for individuals enrolled after the plan was notified of the determination
• Appoint temporary management to oversee the plan (1) if there is a finding of continued conspicuously bad behavior; (2) if there is a substantial risk to the health of enrollees; or (3) to assure the health of enrollees while there is an orderly termination or reorganization of the organization or while improvements are made to remedy violations for which intermediate sanctions could be imposed
Before imposing any sanctions other than termination, the state must provide the entity with notice and any other due process protections that the state ordinarily provides. In addition, before terminating a contract with an MCE, the state must grant the plan a hearing. The state may notify plan enrollees of the hearing and permit them to disenroll without cause.
Responsibilities of Health Plans Participating in Medicaid ProgramsThe following sections describe the services and certain protections that Medicaid health plans must provide to beneficiaries. Requirements for quality assurance and prohibition of certain marketing activities were discussed in the previous lessons.
Page 325 of 469
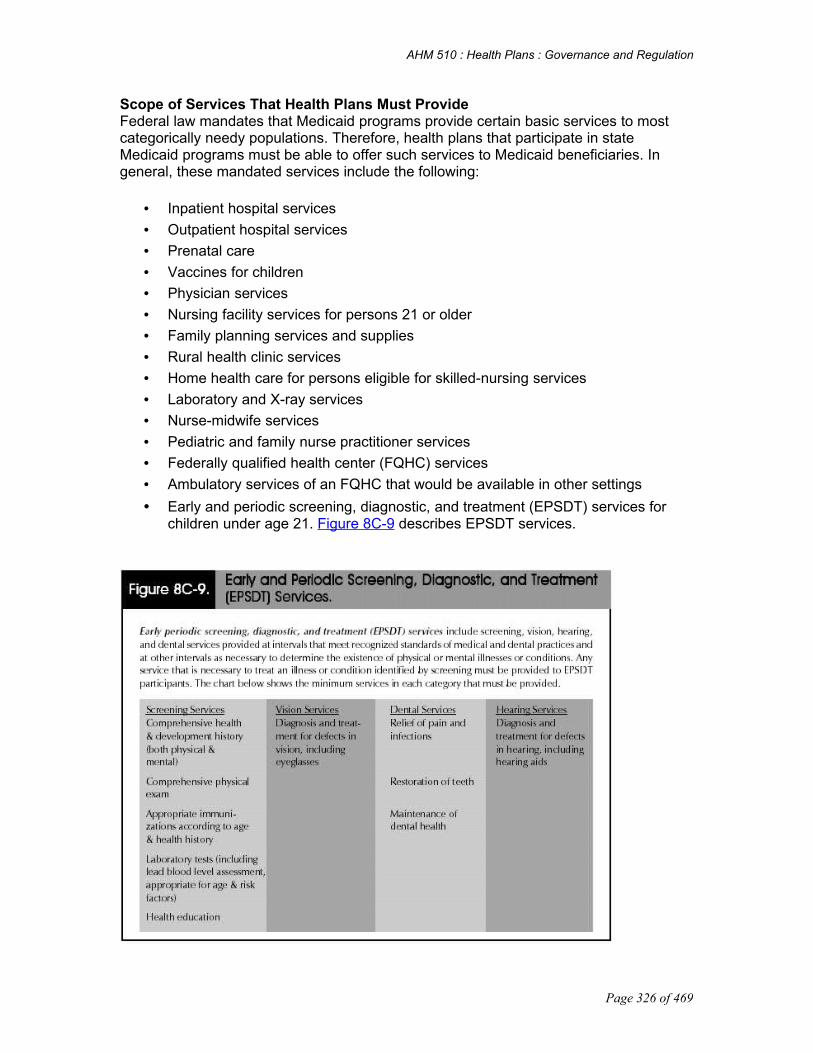
AHM 510 : Health Plans : Governance and Regulation
Scope of Services That Health Plans Must ProvideFederal law mandates that Medicaid programs provide certain basic services to most categorically needy populations. Therefore, health plans that participate in state Medicaid programs must be able to offer such services to Medicaid beneficiaries. In general, these mandated services include the following:
• Inpatient hospital services
• Outpatient hospital services
• Prenatal care
• Vaccines for children
• Physician services
• Nursing facility services for persons 21 or older
• Family planning services and supplies
• Rural health clinic services
• Home health care for persons eligible for skilled-nursing services
• Laboratory and X-ray services
• Nurse-midwife services
• Pediatric and family nurse practitioner services
• Federally qualified health center (FQHC) services
• Ambulatory services of an FQHC that would be available in other settings
• Early and periodic screening, diagnostic, and treatment (EPSDT) services for children under age 21. Figure 8C-9 describes EPSDT services.
Page 326 of 469

AHM 510 : Health Plans : Governance and Regulation
Protections for Medicaid BeneficiariesEach Medicaid managed care plan contract must cover emergency services under the “prudent layperson” standard without regard to whether prior authorization for such services was obtained from the health plan. Health plans must also comply with Medicare guidelines for coverage of post-stabilization care. To protect enrollee-provider communications, under a health plan/Medicaid health plan contract, healthcare professionals must not be restricted from advising a beneficiary about his or her health status, medical care, or treatment, regardless of whether benefits for this care or treatment are provided by the contract. In addition, each Medicaid managed care plan must establish an internal appeals procedure by which an enrollee may appeal coverage or payment decisions. Medicaid managed care plans must also provide the HHS secretary and the state with assurances that the plan has the capacity to serve the expected enrollment in the service area.
Medicaid managed care contracts must include a hold harmless provision that protects enrollees against liability for payment. If the state does not make payment to a provider or plan, in the event of the plan’s insolvency, the enrollee cannot be held liable for those payments.
The plan must also offer an appropriate range of services, access to preventive and primary care services, with a sufficient number, mix, and geographic distribution of providers for those services.
New Programs Established Under the BBAIn addition to making changes to the existing Medicaid program, the BBA established two new programs. One is an extension of a Medicare program and a demonstration project serving the elderly poor; the other is an entirely new approach to providing healthcare to uninsured low-income children.
Programs of All-Inclusive Care for the Elderly (PACE)The BBA established Programs of All-Inclusive Care for the Elderly, which may be implemented as a state option. This program has operated under demonstration waivers in the past. Programs of All-Inclusive Care for the Elderly (PACE) provides an alternative to institutional care for persons aged 55 or older who require a nursing-facility level of care. PACE operates within both the Medicare and the Medicaid programs. States may elect to provide PACE program services to individuals who are Medicaid-eligible and are enrolled in PACE program. These individuals are not required to be enrolled in Medicare to be eligible for a state’s PACE program.
To participate in PACE a public entity or private, not-for-profit organization that seeks to provide, on a capitated basis, health and long-term care services to frail elderly people who are at risk for institutional care files an application with the HHS Secretary. Upon approval of such application, a PACE provider enters into an agreement with either:
• The state Medicaid agency responsible for administering the operation of the PACE program
• The HHS Secretary
Page 327 of 469

AHM 510 : Health Plans : Governance and Regulation
This agreement, which defines the service area and describes other relevant information related to the provision of PACE services, is called the PACE program agreement. Each state determines eligibility for its PACE program in accordance with the PACE program agreement. Individuals are eligible for PACE if they are 55 years of age or older, require a nursing-facility level of care, reside in the service area of the PACE program, and meet other requirements outlined in the agreement. An individual is considered to be eligible for PACE if he or she could reasonably be expected to requalify for a nursing-home level of care within the following six months if PACE services were denied. The individual’s health status is determined using indicators such as medical diagnosis, activities of daily living (ADLs), and cognitive impairment.
PACE enrollees must undergo an annual eligibility recertification to ensure that they are being appropriately served in a PACE setting. Enrollees may voluntarily disenroll from the program at any time. However, the PACE program may not disenroll individuals except in cases of nonpayment of premiums (if applicable) or in cases where the individual is engaging in disruptive or threatening behavior. Involuntary disenrollment is subject to review by the HHS Secretary or the state Medicaid agency.
The individuals enrolled in PACE receive benefits solely through the PACE program. Regardless of the source of payment (i.e., state Medicaid funds, matching Medicaid funds, or Medicare funds), PACE providers receive capitated payment only through the PACE program agreement. PACE providers must make available to PACE enrollees all items and services covered under both Medicare and Medicaid, without limiting the amount, duration, or scope of services, and without imposing on eligible enrollees any deductibles, copayments, or other cost-sharing mechanisms that might otherwise apply under Medicaid or Medicare. PACE enrollees must have access to benefits 24 hours a day, every day of the year, and services must be provided through a comprehensive, multidisciplinary system that integrates acute and long-term care services. The PACE program agreement must include a written plan of quality assurance and improvement and a set of written safeguards (including a patient bill of rights and procedures for filing grievances and appeals).
During the initial three-year trial period of a state’s PACE program, the HHS Secretary will conduct a comprehensive annual review of PACE providers to ensure compliance with the requirements and regulations governing the program. The HHS Secretary may terminate PACE provider agreements if this annual review identifies significant deficiencies in the quality of care or if the provider is substantially out of compliance with the conditions of the PACE program and fails to initiate a corrective action plan.
State Children’s Health Insurance Program (SCHIP)In addition to making changes to Medicare and Medicaid, the BBA of 1997 established a new title in the SSA: Title XXI. Title XXI of the SSA established the State Children’s Health Insurance Program (SCHIP) to enable states to initiate and expand child health assistance to uninsured, low-income children. Title XXI provides $47 billion in funding to states over a tenyear period, $40 billion of which will be available in the form of matching funds. Effective October 1, 1997, the states were charged with establishing programs in one or both of the following ways:
Page 328 of 469

AHM 510 : Health Plans : Governance and Regulation
1. By establishing a separate program (in addition to an existing Medicaid program) to provide health insurance coverage that meets the requirements of SCHIP. These requirements relate to the amount, duration, and scope of benefits
2. By expanding eligibility for children under the State’s Medicaid program
State Children’s Health Insurance Program (SCHIP)To be eligible for funds, states must submit a State Child Health Plan to the secretary of HHS for approval. A State Child Health Plan must include general background on the extent to which children currently have coverage, current state efforts to obtain coverage, how the plan will be coordinated with other efforts, the proposed delivery methods, and methods to assure quality and access to covered services. The plan must describe standards and methods used to establish and continue eligibility and enrollment for targeted low-income children. In addition, the plan must describe procedures for outreach to inform and enroll families of children who are likely to be eligible for assistance under the plan or under other public or private coverage.
Separate Program OptionIf the state chooses to implement a separate, non-Medicaid option, the benefit package must be structured in compliance with one of four options: benchmark coverage, benchmark-equivalent coverage, existing comprehensive state-based coverage, or HHS Secretary-approved coverage. Figure 8C-10 describes each of these options. States are allowed to collect premiums consistent with the SCHIP guidelines for the separate program option; however, the program’s cost-sharing must not favor higher-income children over lower-income children. In addition, the State Child Health Plan may not impose any pre-existing condition exclusions for covered benefits.
Figure 8C-10. SCHIP Separate Program Options.
Option 1/Benchmark CoverageBenefit plans must be equivalent to one of the following healthcare plans:
1. The standard Blue Cross/Blue Shield Preferred Provider option offered under FEHBP
2. A health benefits plan that is offered and generally is available to state employees 3. The HMO plan with the largest commercial enrollment in the state
Option 2/Benchmark- Equivalent CoverageThe health benefit coverage must have an aggregate actuarial value (determined by a member of the American Academy of Actuaries) that is at least equal to one of the benchmark coverage packages described above. The coverage under the benchmark-equivalent package must include benefits in the following categories of basic services:
1. Inpatient and outpatient hospital services 2. Physicians’ surgical and medical services 3. Laboratory and x-ray services 4. Well-baby and well-child care, including age-appropriate immunizations
Page 329 of 469

AHM 510 : Health Plans : Governance and Regulation
If the state chooses to implement a benchmark-equivalent coverage package that includes prescription drugs, mental health, vision, or hearing services, then the actuarial value of each of these categories of service must be at least 75% of the actuarial value of the benchmark package value. If the benchmark- equivalent package does not cover one of the categories of services listed in the preceding sentence, then the equivalent plan may, but does not have to, provide coverage for that category of service.
Option 3/Existing Comprehensive State-Based CoverageHealth benefit coverage under an existing comprehensive statewide program is defined as a program that
1. Provides a range of benefits 2. Is administered by the state and receives state funds 3. Is offered in New York, Florida, or Pennsylvania 4. Was offered on the date of enactment of Title XXI 5. If modified, still includes a range of benefits and has an actuarial value equal to or
greater than either its value on August 5, 1997, or the value of one of the benchmark packages
Option 4/HHS Secretary- Approved CoverageAny health benefit coverage package that the secretary of HHS determines, upon application by a state, provides appropriate coverage for targeted low-income children.
Medicaid Expansion OptionStates may also choose to expand their Medicaid programs to meet the needs of targeted low-income children. States that elect to expand children’s health insurance through the Medicaid option are required to provide the state-mandated Medicaid benefit package. If a state chooses to implement SCHIP by expanding its Medicaid program, the state must submit a plan amendment, as well as submitting specified information required by Title XXI. The advantage of choosing Medicaid expansion over a separate program option is that even after the federal allocation of funds provided through SCHIP is exhausted, states may continue to receive federal matching funds at their normal Medicaid rate for children covered by a Medicaid expansion program.
Federal Funding for SCHIPUnder the law, a state must have an approved state plan for a fiscal year to receive an allotment from SCHIP funds. Allotments are determined by a complex formula that takes into account the total number of uninsured, low-income children in the state, multiplied by a geographic cost factor. Like Medicaid, SCHIP is a matching program, under which the states’ receipt of federal funds depends on state expenditures. As with the Medicaid program, the federal percentage of contribution varies by state, based on the state’s relative wealth. However, there is a cap on the federal contribution.
Administration of SCHIPThe Center for Medicaid and State Operations (CMSO) within CMS has primary responsibility for administering the federal aspects of Title XXI. There is a team composed of staff from other HHS offices providing support for the SCHIP program. Among other coordination efforts, HHS works closely with states through the National Governors Association.
Page 330 of 469
AHM 510 : Health Plans : Governance and Regulation
Eligibility for SCHIP AssistanceThe SCHIP program is designed to assist targeted low-income children. A targeted low-income child is considered to be a child who:
• Meets the eligibility standards set by the state
• Is under 19 years of age
• Is not currently eligible for Medicaid or covered under other health insurance coverage
• Resides in a family with income below the greater of the following: 200% of the FPL or, for states with Medicaid-eligible levels for children above 150% of the FPL as of June 1, 1997, 50 percentage points above the state’s Medicaid eligibility limit as of that date
One exception to these requirements is that the term targeted low-income child may include children covered under a health insurance program in operation since before July 1, 1997, that is offered by the state and receives no federal funds. Children who might otherwise be included are excluded if they are inmates of public institutions, patients in an institution for mental disease (IMD), or children whose families are eligible for the state employee benefits plan.
Evaluation of SCHIP ProgramsStates must assess the operation of their plan, including progress made in reducing the number of low-income children not covered by insurance, and report annually to the HHS Secretary by January 1 of each year. By March 31, 2000, each state with an approved State Child health plan must submit to the HHS Secretary an evaluation addressing the effectiveness of the plan in a number of areas. The HHS Secretary will submit to Congress by December 31, 2001, a report based on the state evaluations.
The Future of Medicaid Managed Care and SCHIPCongress has targeted Medicaid spending for a $13 billion reduction between 1997 and 2002. The PRWORA and the BBA are the first steps toward achieving that goal. Because of the extensive changes implemented by this legislation, it is logical to assume that there will be additional legislation to fine-tune the operation of Medicaid health plans. This prediction is supported by the fact that the BBA made several amendments to the PRWORA.
Congress has not been concerned only with cost. The trend in government-sponsored healthcare in the mid-to-late 1990s has been to give states greater flexibility and accountability for providing medical care to their poor, with an emphasis on providing care to poor children. The PRWORA has placed greater responsibility on poor adults to improve their own situation, creating motivation for these individuals to become selfsupporting. Yet, the federal and state governments have taken care not to disenfranchise poor children, creating options for the well-being of the truly needy under managed healthcare. MCEs must keep a watchful eye on what develops to remain effective and competitive in Medicaid managed care.
Page 331 of 469

AHM 510 : Health Plans : Governance and Regulation
Page 332 of 469
AHM 510 : Health Plans : Governance and Regulation
Chapter 9 AFraud and Abuse
The amount spent annually on healthcare in the United States now exceeds one trillion dollars. With this amount of money at stake, it is not surprising that some of the players involved in delivering, financing, or consuming healthcare engage in dishonest or even criminal conduct to obtain money or other benefits to which they are not entitled. These improper activities-known as fraud and abuse-not only make healthcare more expensive, they also diminish its quality.
In this assignment, we describe the kinds of fraud and abuse that occur in managed healthcare plans, both in federally funded programs such as Medicare and Medicaid and in commercial plans. We also discuss the major federal laws that regulate healthcare fraud and abuse and describe the penalties that can be imposed for violating them. We end by examining some of the steps that health plans take to identify and reduce healthcare fraud and abuse.
After completing this lesson, you should be able to:
Define the terms fraud and abuse Describe how different types of compensation arrangements can lead to different
kinds of fraud and abuse List and describe the federal laws that regulate healthcare fraud and abuse, and
identify the federal agency responsible for enforcing them Describe the penalties that may be imposed for violating the federal fraud and abuse
laws Discuss some of the steps health plans can take to reduce fraud and abuse
What Is Fraud and Abuse?The phrase fraud and abuse is used to describe a wide range of improper healthcare activities. Fraud and abuse do have distinctive meanings, however. The more general of the terms- abuse- is any improper practice that results in excessive or unreasonable healthcare costs. Fraud, which is a specific kind of abuse, is a knowing and willful deception or misrepresentation, or a reckless disregard of the facts, done with the intent to receive an unauthorized benefit. The distinctive feature of fraud is the element of misrepresentation or deception. For example, in a healthcare/health plan context, abuse occurs when a doctor orders unnecessary tests, and fraud occurs when a provider submits a bill to a managed healthcare plan or to the government requesting payment for services that the provider knows were not actually provided.
Because of the element of deception or misrepresentation involved in fraud, it is usually considered to be a crime. At the federal level, the Health Insurance Portability and Accountability Act of 1996, which we will discuss in more detail later in this lesson, makes it a federal crime to obtain money from a healthcare plan by fraud or false pretenses. Penalties include fines up to $250,000 and terms in federal prison. Most states also have laws that make healthcare fraud a crime, and in many states healthcare fraud is considered to be a felony.
Page 333 of 469

AHM 510 : Health Plans : Governance and Regulation
We will use the phrase fraud and abuse in this lesson as it is commonly used-as a catch-all way of describing the variety of improper activities that drive up the costs of healthcare. You should keep in mind, though, that fraud often has a very specific meaning under the criminal laws, while abuse describes conduct that is improper but not necessarily criminal.
How Compensation Arrangements Affect Fraud and AbuseYou may recall from Healthcare Management: An Introduction that compensation arrangements in health plans form a continuum, with fee-for-service (FFS) arrangements at one end of the spectrum and capitation arrangements at the other. Under fee-for-service compensation plans, providers are paid after the fact for services that have been performed. Therefore, a provider's income increases with the volume and variety of the services that he or she generates. Under capitation arrangements, on the other hand, providers are paid in advance for all of the services that they have agreed to provide. A provider is paid the same monthly amount for each member regardless of how often (if at all) the member receives care during that month and regardless of the cost of that care. The compensation arrangements used by a health plan can be at either end of this continuum or somewhere in the middle, and the same health plan may use different arrangements to pay for different services. Understanding these arrangements is important, because the different types of arrangements generally lead to different kinds of fraud and abuse. You may find it helpful to refer to Figure 9-1 as we discuss these differences in the following lessons.
How Compensation Arrangements Affect Fraud and AbuseYou may recall from Healthcare Management: An Introduction that compensation arrangements in health plans form a continuum, with fee-for-service (FFS) arrangements at one end of the spectrum and capitation arrangements at the other. Under fee-for-service compensation plans, providers are paid after the fact for services that have been performed. Therefore, a provider's income increases with the volume and variety of the services that he or she generates. Under capitation arrangements, on the other hand, providers are paid in advance for all of the services that they have agreed to provide. A provider is paid the same monthly amount for each member regardless of how often (if at all) the member receives care during that month and regardless of the cost of that care. The compensation arrangements used by a health plan can be at either end of this continuum or somewhere in the middle, and the same health plan may use different arrangements to pay for different services. Understanding these arrangements is important, because the different types of arrangements generally lead to different kinds
Page 334 of 469
AHM 510 : Health Plans : Governance and Regulation
of fraud and abuse. You may find it helpful to refer to Figure 9-1 as we discuss these differences in the following lessons.
Review Question
Arthur Dace, a plan member of the Bloom health plan, tried repeatedly over an extended period to schedule an appointment with Dr. Pyle, his primary care physician (PCP). Mr. Dace informally surveyed other Bloom plan members and found that many people were experiencing similar problems getting an appointment with this particular provider. Mr. Dace threatened to take legal action against Bloom, alleging that the health plan had deliberately allowed a large number of patients to select Dr. Pyle as their PCP, thus making it difficult for patients to make appointments with Dr. Pyle.
Bloom recommended, and Mr. Dace agreed to use, an alternative dispute resolution (ADR) method that is quicker and less expensive than litigation. Under this ADR method, both Bloom and Mr. Dace presented their evidence to a panel of medical and legal experts, who issued a decision that Bloom's utilization management practices in this case did not constitute a form of abuse. The panel's decision is legally binding on both parties.
Different types of compensation arrangements in managed care plans, from fee-for-service (FFS) arrangements to capitation arrangements, lead to different types of fraud and abuse. From the answer choices below, select the response that identifies the form of abuse in which Bloom is allegedly engaging, according to Mr. Dace's complaint, and whether this form of abuse is more likely to occur in FFS compensation arrangements or in capitation arrangements.
Type of abuse underutilizationType of compensation arrangement FFS arrangement Type of abuse underutilizationType of compensation arrangement capitation arrangement Type of abuse overutilizationType of compensation arrangement FFS arrangement Type of abuse overutilizationType of compensation arrangement capitation arrangement
Incorrect. Underutilization occurs when services that are covered under a health plan are provided to a lesser extent than was medically necessary. Plans with FFS arrangements are not subject to this type of abuse.
Correct. Underutilization occurs when services that are covered under a health plan are provided to a lesser extent than was medically necessary. Plans with capitation arrangements may be subject to this form of abuse.
Incorrect. Overutilization occurs when services under a health plan are provided at a greater extent than is medically necessary. Plans with FFS arrangements are subject to this type of abuse.
Page 335 of 469

AHM 510 : Health Plans : Governance and Regulation
Incorrect. Overutilization occurs when services under a health plan are provided at a greater extent than is medically necessary. Plans with capitation arrangements are not subject to this type of abuse
Fraud and Abuse in Fee-for-Service ArrangementsIn FFS arrangements, as healthcare services increase so do the incomes of providers. With such strong financial incentives, there are typically more concerns regarding fraud and abuse under plans with FFS arrangements than under plans with other types of compensation arrangements. Also, plans with FFS arrangements seldom use health plan techniques such as specialty referral or preauthorization requirements that can sometimes prevent certain types of fraud. Because providers under FFS plans are paid each time they submit a bill for services, much of the fraud and abuse under FFS plans results from false billing practices. Most often, a false billing involves providers submitting fraudulent bills for services that were not provided. False billing can also involve upcoding.
Upcoding occurs when a provider requests payment for a service that has a higher reimbursement to the provider than the service that was actually performed. For example, upcoding occurs when a physician performs a minor nonsurgical procedure but requests payment for surgery, or when a patient is seen by a nurse but the health plan is charged for an office visit with a physician. In some cases, providers share the money they receive from fraudulent claims with dishonest patients who provide them with the insurance information they use to file the claims.
In addition to the fraud that results from submitting false claims, FFS arrangements can also be subject to a form of abuse known as overutilization. Overutilization occurs when services under a health plan are provided to a greater extent than is either medically necessary or authorized by the plan. Overutilization may occur, for example, when a physician sees a patient more often or provides for a certain condition a greater number of treatments than are medically necessary. Providers under FFS arrangements have an incentive to practice overutilization because their incomes increase with the volume of services they provide.
Providers engage in underutilization when they undertreat the medical conditions of plan members, either by providing fewer office visits than are medically necessary or by providing substandard care. For example, some providers may improperly allow patients to be examined by physician assistants or nurses when a higher level of care is needed. Underutilization can also be practiced in more subtle ways, such as by delaying the scheduling of appointments.
Another type of fraud and abuse that may occur under capitated fee arrangements is for providers to overstate the number of patient encounters they have when they file encounter reports with health plans. Health plans rely on encounter reports from providers to establish how large future capitation payments will be. A provider who overstates his or her encounters does not receive any additional income at the time, but in the future may receive capitation payments that are larger than justified.
Fraud and Abuse by Health PlansBecause health plans often rely upon compensation arrangements as well as utilization
Page 336 of 469

AHM 510 : Health Plans : Governance and Regulation
review and quality assurance programs to help manage the delivery of healthcare, the incidence of fraud and abuse is generally less frequent in health plans than in FFS plans. However, one way that fraud and abuse can be committed by a health plan is through the practice of underutilization, especially when the health plan shares part of the financial risk. For example, a health plan might allow a large number of patients to select a particular primary care physician, making it difficult for patients to make appointments; or a health plan might try to limit patient access to high-cost treatments or specialists by engaging in over-restrictive utilization management practices. We will discuss the legal issues that can arise from inappropriate utilization management practices in Key Legal Issues in Health Plans.
The Impact on Cost and Quality of Care An enormous amount of money is lost to health care fraud and abuse each year. The costs of fraud and abuse are felt both by health plans, which compensate providers for services under health plans, and by the employers and individuals who ultimately pay the premiums under those plans. And although the increased costs resulting from fraudulent billing and overutilization may be easier to visualize, underutilization drives up the cost of healthcare as well. When providers practice underutilization, plan sponsors and members end up receiving fewer services than they pay for, so they pay more than they should for the services they do receive.
Overutilization and underutilization can both be harmful to the health of plan members. When providers practice overutilization, plan members may receive more extensive treatment than is medically necessary or appropriate, and at times this can present unnecessary health risks. When providers practice underutilization, plan members typically receive fewer health services than they need, and as a result, their health can be compromised.
Fast Fact
By some estimates, healthcare fraud amounted to $100 billion in 1997, or 10% of the total national healthcare budget.1
Fraud and Abuse in Federal Healthcare ProgramsAs we mentioned in Federal Government as Purchaser, the federal government is a purchaser of healthcare benefits for a significant number of Americans through the Medicare and Medicaid programs. Because Medicare and Medicaid are still largely fee-for-service (FFS) programs, they are subject to the same forms of fraud and abuse present in other FFS plans. Much of this fraud and abuse is in the form of false billings and overutilization. As Medicare and Medicaid continue to move toward health plans, however, other kinds of fraud and abuse may become more common. To combat the fraud and abuse in federally funded healthcare programs, Congress has enacted a variety of laws that regulate the activities of participants in those programs. We discuss the most important of these laws in this section. Other federal laws that do not apply specifically to healthcare but that are sometimes used to fight healthcare fraud and abuse are summarized in Figure 9A-2.
Figure 9A-2.
Other Federal Laws That Can Be Used Against Healthcare Fraud and Abuse.
Page 337 of 469

AHM 510 : Health Plans : Governance and Regulation
The False Claims Act makes it illegal to present a false, fictitious, or fraudulent claim against the United States. Although the Act was not enacted specifically to combat healthcare fraud, it has been used to prosecute fraudulent billings under FEHBP, the Medicare and Medicaid programs, and other federal contracts as well. Sanctions include fines and prison terms, plus additional penalties equal to three times the amount of the false claim.
The mail fraud statute makes it illegal to use the mail to further a scheme to defraud. This statute is especially useful in fighting healthcare fraud because healthcare fraud often involves using the mail to submit false bills and invoices. Sanctions include fines of up to $250,000 and prison terms.
The Racketeer Influenced and Corrupt Organizations Act (RICO) was originally enacted to fight organized crime, but it has also been used against healthcare fraud. RICO makes it illegal to associate with a criminal enterprise and participate in its activities. Sanctions include fines of up to $25,000 and prison terms of up to 20 years.
The Anti-Kickback StatuteThe federal anti-kickback statute, which is part of the Social Security Act, prohibits the exchange of kickbacks in any federal healthcare program. The definition of kickback under the federal anti-kickback statute is complex, but in general terms related to healthcare a kickback occurs when one party directly or indirectly gives another party money or some other benefit in exchange for receiving increased business under a federal healthcare program. Kickbacks are undesirable because they may influence providers and health plans to take actions that are not in the best interest of patients and because they increase the costs of federal healthcare.
The anti-kickback statute applies to a wide variety of healthcare business activities, and a comprehensive discussion of its provisions is beyond the scope of this lesson. By way of example, however, illegal kickbacks may take the form of:
1. Payments or other benefits given to physicians or health plans in exchange for patient referrals
2. Rebates and discounts given to health plans or providers to encourage them to buy particular goods, services, or other items
3. Payments by drug manufacturers to physicians in exchange for prescribing the manufacturers' drugs to patients
Safe HarborsThe Department of Health and Human Services (HHS) has issued regulations that establish a number of "safe harbors" under the anti-kickback statute, which implement the exceptions provided under the law and set forth additional exceptions. These safe harbor regulations describe payment practices that might technically violate the provisions of the anti-kickback statute but that will not be considered illegal and for which providers and health plans will not be subject to penalties.
Page 338 of 469

AHM 510 : Health Plans : Governance and Regulation
The safe harbor regulations cover several types of conduct, a few of which have particular application to health plans. For example, one of the safe harbors allows health plans with Medicare or Medicaid contracts to offer increased benefits and reduced copayments, deductibles, and premiums to Medicare and Medicaid beneficiaries enrolled under the contracts, as long as the benefits and reductions are offered to all such Medicare and Medicaid enrollees covered under the contract, and as long as any other applicable requirements are met. Another safe harbor authorizes providers to give health plans price reductions meeting the specific criteria of the safe harbor on treatments and services provided to the plan's enrollees. A new provision enacted by the Health Insurance Portability and Accountability Act of 1996 provides a few additional exceptions to the anti-kickback law for certain provider contracting arrangements.
The safe harbor regulations are extremely detailed and describe many practices that do not violate the anti-kickback statute, but they do not cover every type of permissible conduct. Therefore, practices that are not specifically covered by the safe harbor regulations are not necessarily illegal; they are simply not entitled to the automatic protection provided by the regulations. To be safe, however, many health plans try to structure their practices so that they fall squarely within one of the safe harbors.
The Ethics in Patient Referrals Act ("Stark laws")The Ethics in Patient Referrals Act of 1989 and its amendments, commonly called the Stark laws or Stark I and Stark II, prohibit a physician from referring Medicare or Medicaid patients for certain designated services or supplies provided by entities in which the physician or the physician's family member has a direct or indirect financial interest. These designated services and supplies include but are not limited to laboratory services, radiology, diagnostic services, physical therapy, home health services, prescription drugs, occupational therapy, and durable medical equipment. Under the Stark laws, there are two ways that a physician may have a financial interest in a healthcare facility. First, a financial interest can arise if the physician has an ownership or investment interest in a facility that provides services. A financial interest can also result because there is some kind of compensation arrangement between the physician and the healthcare facility. The definition of compensation arrangement is very broad, and almost any kind of payment between the physician and the facility could be considered to create a financial interest. For example, a physician might have a financial interest in a clinic simply because the clinic leases office space or equipment from the physician.
If a physician makes a referral that is prohibited by the Stark laws, the healthcare facility receiving the referral may not present a bill to Medicare or Medicaid for the services that were provided. In addition, a physician who violates the Stark laws may be required to pay a penalty of up to $15,000 and be excluded from participating in the Medicare and Medicaid programs.
The Stark laws were enacted to avoid the conflict of interest that might result when a physician refers patients to healthcare facilities in which the physician has a financial interest. The laws can also apply to a physician who belongs to a health plan network and has a financial relationship with the health plan arising from the health plan's compensation of the physician.
Page 339 of 469
AHM 510 : Health Plans : Governance and Regulation
There are numerous exceptions to the Stark laws, however, including an exception that applies to prepaid health plans. This exception states that health services provided to plan members by some prepaid healthcare plans, including federally qualified HMOs and plans with Medicare contracts, are not subject to the ownership and compensation prohibitions. Another important exception exempts certain physician incentive arrangements complying with the Medicare/Medicaid physician incentive requirements. This exception is important because it may protect health plan payment arrangements for Medicare enrollees not covered under the Medicare Advantage program. Provider compensation arrangements for services provided under the Medicare Advantage program are exempt under the prepaid health plan exception. These exceptions recognize that some referrals to services or laboratories in which the referring physician has a financial interest are not necessarily fraudulent or abusive.
The Stark laws also impose reporting requirements on each entity that provides Medicare or Medicaid services. The entities must provide the Department of Health and Human Services with detailed information about the identity of all the physicians who have an ownership interest in the entity or who have a compensation arrangement with it. An entity that fails to comply with these requirements can be fined up to $10,000 per day.
The Health Insurance Portability and Accountability ActThe Health Insurance Portability and Accountability Act of 1996 (HIPAA) expands the scope of the federal fraud and abuse laws by amending and strengthening existing law and by creating a new category of federal healthcare crimes, called federal healthcare offenses, that apply to private healthcare plans as well as federally funded health programs. Under the provisions of HIPAA, it is now a federal crime to engage in a scheme to defraud a healthcare plan or to obtain money from a healthcare plan under false pretenses. This new law covers many of the fraudulent billing practices we discussed earlier in this lesson. Some of the practices that are federal crimes under HIPAA include:
• Requesting payment for services that were not provided
• Misrepresenting the nature of services that were provided
• Falsely certifying that provided services were medically necessary
Review Question
There are several exceptions to the Ethics in Patient Referrals Act and its amendments (the Stark laws), which prohibit a physician from referring Medicare or Medicaid patients for certain designated services or supplies provided by entities in which the physician has a financial interest. Consider whether the situations described below qualify as exceptions to the Stark laws:
• Situation A: Dr. Wong is a physician in the Marvel Health Plan's provider network and has a financial relationship with Marvel arising from the health plan's compensation for his services. Marvel is not a prepaid health plan.
• Situation B: Dr. Ryder is a physician in the provider network of the Glen Health Plan, which is not a prepaid health plan. In situations of medical necessity, Dr.
Page 340 of 469

AHM 510 : Health Plans : Governance and Regulation
Ryder refers Glen patients to a physical therapy clinic that leases office space from him.
• Situation C: Dr. Yost has a compensation arrangement with a health plan for providing health services under the Medicare+Choice program.
An arrangement that is exempt from the Stark laws is described in all of these situations
Situations A and C only
Situation B only
Situation C only
Incorrect. Stark allows an exemption that applies to prepaid health plans. This exception states that health services provided to plan members by some prepaid healthcare plans, including federally qualified HMOs and plans with Medicare contracts, are not subject to the ownership and compensation prohibitions.
Incorrect. There are numerous exceptions to the Stark laws, however, including an exception that applies to prepaid health plans. This exception states that health services provided to plan members by some prepaid healthcare plans, including federally qualified HMOs and plans with Medicare contracts, are not subject to the ownership and compensation prohibitions.
Incorrect. There are numerous exceptions to the Stark laws, however, including an exception that applies to prepaid health plans. This exception states that health services provided to plan members by some prepaid healthcare plans, including federally qualified HMOs and plans with Medicare contracts, are not subject to the ownership and compensation prohibitions.
Correct. Provider compensation arrangements for services provided under the Medicare Advantage program are exempt under the prepaid health plan exception
In addition to defining these new federal healthcare crimes, HIPAA provides additional sources of funding for federal investigations into healthcare fraud and abuse. For example, HIPAA provides that any fines and penalties recovered through regulatory proceedings to enforce the federal fraud and abuse statutes will be turned over to enforcement agencies to conduct additional investigations.
Section 231(h) of HIPAA amended the Social Security Act to prohibit offering or transferring remuneration to a Medicare or Medicaid beneficiary when that remuneration is likely to influence the beneficiary to order or receive from a particular provider a Medicare- or Medicaid-reimbursable service. Under this law, remuneration includes the waiver of all or part of coinsurance or deductible amounts, as well as transfers of items or services for free, or for other than fair market value. Exceptions to the definition of remuneration include differentials in coinsurance and deductible amounts as part of a benefit plan if disclosed in writing in accordance with applicable standards, as well as
Page 341 of 469

AHM 510 : Health Plans : Governance and Regulation
incentives given to individuals to promote the delivery of preventive care in accordance with applicable regulations. An important effect on the law has been with regard to the offering of value-added services by health plans. As we saw in Medicare and Health Plans, the law has been interpreted to prohibit health plans with Medicare contracts from providing to enrollees value-added services such as discounted memberships to health clubs or access to networks of discounted dental or optical providers.
Review Question
The following statements are about various provisions of the Health Insurance Portability and Accountability Act of 1996 (HIPAA). Three of the statements are true and one statement is false. Select the answer choice that contains the FALSE statement.
HIPAA permits group health plans that offer coverage through an HMO to impose affiliation periods during which no benefits or services are provided to a plan member. HIPAA created a new category of federal healthcare crimes, called federal healthcare offenses, that apply to private healthcare plans as well as to federally funded healthcare programs. One effect of Section 231(h) of HIPAA, which amended the Social Security Act, has been to permit health plans with Medicare contracts to provide enrollees with value-added services such as discounted memberships to health clubs. HIPAA provides that any fines and penalties recovered through regulatory proceedings to enforce the federal fraud and abuse statutes will be turned over to enforcement agencies to conduct additional investigations.
Incorrect. Is is true to say that HIPAA permits group health plans that offer coverage through an HMO to impose affiliation periods during which no benefits or services are provided to a plan member.
Incorrect. It is true to say that HIPAA created a new category of federal healthcare crimes, called federal healthcare offenses, that apply to private healthcare plans as well as to federally funded healthcare programs.
Correct. One effect of Section 231(h) of HIPAA, which amended the Social Security Act, has been to PROHIBIT health plans with Medicare contracts to provide enrollees with value-added services such as discounted memberships to health clubs.
Incorrect. It is true to say that HIPAA provides that any fines and penalties recovered through regulatory proceedings to enforce the federal fraud and abuse statutes will be turned over to enforcement agencies to conduct additional investigations.
Enforcement MechanismsAt the federal level, primary responsibility for enforcing the fraud and abuse statutes rests with the Office of the Inspector General (OIG), which was established by Congress in 1976 to assist federal agencies, including the Department of Health and Human
Page 342 of 469
AHM 510 : Health Plans : Governance and Regulation
Services (HHS). The OIG's mission is to identify and eliminate fraud and abuse in programs administered by HHS, including Medicare and Medicaid. It carries out this mission through a nationwide program of audits, investigations, and inspections. The Department of Justice and the FBI also investigate violations of the federal fraud and abuse laws that may result in criminal penalties.
One of the OIG's most effective initiatives in combating fraud and abuse is known as Operation Restore Trust. The OIG started Operation Restore Trust in five states in 1995 to help identify providers who overbill the Medicare program and to recover fines and other financial penalties from them. Operation Restore Trust has been very successful during its first few years of existence, and the OIG now plans to expand it to other states and eventually implement it nationwide.
At the state level, states have established Medicaid fraud control units. A Medicaid fraud control unit (MFCU) is a state program, jointly funded by federal and state money, established to investigate and prosecute fraud under the Medicaid program. MFCUs have enforcement authority under the Medicaid program similar to the OIG's authority under Medicare.
Fast Fact
In 1997, the Office of the Inspector General recovered $1.2 billion in fines and settlements with healthcare providers that overcharged government insurance programs such as Medicare.3 Operation Restore Trust identified $23 in fraud and abuse for every $1 it spent on investigation.4
Criminal and Civil Penalties Federal fraud and abuse laws provide a wide range of criminal and civil penalties that can be imposed against individuals and organizations that violate those laws. The criminal penalties are often severe. For example, an individual who violates the general prohibition on defrauding any healthcare benefit program (Section 1347 added to Title 18, Chapter 63 of the U.S. Code by HIPAA) can be fined and sentenced to prison for up to 10 years.2 If the violation causes someone to suffer a serious bodily injury, the maximum prison sentence can be up to 20 years, and if the violation causes someone to die, the maximum prison sentence can be life imprisonment.
The federal laws we discussed earlier also authorize the imposition of civil monetary penalties. A civil monetary penalty (CMP) is a fine that may be imposed against individuals and organizations for violating the federal fraud and abuse laws. One important source for civil monetary penalties is the Balanced Budget Act of 1997 (BBA). The BBA amended Medicare law to provide for civil monetary penalties of up to $50,000 for violations of the anti-kickback law. CMPs are in addition to the amounts assessed for criminal fraud and abuse violations.
Another civil penalty that can be imposed under the federal fraud and abuse laws is exclusion. For example, a provider or health plan that is convicted of a healthcare crime may be excluded from participating in any federal healthcare program for up to five years. Such an exclusion can have a serious financial impact on a health plan that derives a significant portion of its income from federal programs.
Page 343 of 469

AHM 510 : Health Plans : Governance and Regulation
Health Plan Responses to Fraud and AbuseWe have discussed some of the adverse financial impacts that healthcare fraud and abuse can have on health plans. Recall, for example, that fraud and abuse by providers costs health plans billions of dollars a year. To help minimize these financial impacts, many health plans are developing programs to detect and prevent fraud and abuse.
Because false billing practices represent the largest source of healthcare fraud, health plans often focus their efforts on detecting fraudulent bills. An important part of this process is auditing claims to identify those that might be questionable. Special training can help claims examiners pick out suspicious claims, and many health plans employ Certified Fraud Examiners, who have received specialized training in fraud detection, as part of their programs. New fraud-detection software can also help health plans identify suspicious billings and claims. Health plans that detect fraudulent billing practices often share this information with law enforcement officials to assist in criminal investigations and with other health plans and insurers to alert them to those practices.
Fast Fact
Health insurers reported total savings of $260 million, or an average of $2.3 million per insurer, as a result of their antifraud efforts in 1995. They also reported savings of $7.50 for each dollar spent on fraud detection.5
Fraud and abuse resulting from underutilization are often harder to detect than fraud resulting from false billings. Some health plans use statistical analysis to monitor utilization levels and identify utilization rates that appear unusually low. Other health plans rely on feedback from plan members to identify incidents of underutilization. Underutilization might be suspected, for example, when plan members report that they have difficulty getting appointments with providers or when a large number of plan members want to drop a particular primary care physician. Performance information gathered in the process of reporting on Health Plan Employee Data and Information Set (HEDIS) measures (required by Medicare, by many states under Medicaid, and by many employers) may highlight unusual practice patterns and help plans identify underutilization.
Corporate Compliance Programs
Many health plans are instituting or enhancing compliance programs to help them avoid the penalties that can result from violating the federal fraud and abuse laws. An important feature of these programs is that they do not have to prevent all violations to be beneficial. Even if a violation occurs, the penalties for violating the federal fraud and abuse laws may be reduced if the health plan committing the violation has an effective compliance program in place. We take a closer look at health plan compliance programs in Governance: Accountability and Leadership.
We mentioned earlier that the Office of the Inspector General (OIG) enforces the federal fraud and abuse statutes. In addition to conducting these enforcement activities, the OIG administers programs that assist corporations in their voluntary programs to comply with the federal fraud and abuse laws. Some of the OIG services that help health plans and providers avoid violating the fraud and abuse laws include:
Page 344 of 469

AHM 510 : Health Plans : Governance and Regulation
• Issuing Special Fraud Alerts that identify segments of the healthcare industry that are particularly vulnerable to abuse
• Issuing advisory opinions to providers who are seeking guidance on questions arising under the federal fraud and abuse statutes
• Developing guidance for model compliance programs for hospitals and other providers that health plans can customize to meet their individual needs
The advisory opinion process may be useful to a health plan in its compliance efforts, if the health plan is seeking assurance that an activity in which it intends to engage won't violate fraud and abuse prohibitions. However, the OIG is unlikely to be willing to issue a favorable opinion regarding activities that are in the "gray area." To date, the advisory opinion has not been a commonly used tool, likely due to the burden and expense related to requesting such an opinion.
Page 345 of 469

AHM 510 : Health Plans : Governance and Regulation
Chapter 10 AThe Components of Governance in a Health Plan
After completing this lesson, you should be able to:
Explain the purpose of governance in a health plan Describe the roles and responsibilities of the board of directors Explain how organizational variations affect board structure and operation List the three steps in a board risk management program Describe the roles of shareholders/members and providers in governance Discuss the roles and responsibilities of the CEO and other senior management
What Is Governance and Why Is It Needed?In Environmental Forces, we defined governance as the efforts by the health plan’s board of directors working with senior management to develop corporate policy, create a corporate mission statement and vision, and develop strategies in order to achieve the organization’s goals and mission. Simply put, governance guides a health plan’s decisions about how to operate its business. A health plan’s board of directors provides much of this guidance. The board and senior management are not the only participants in governing a health plan. Shareholders, members, policyholders, consumers, and providers may all have roles in the governance of a health plan.
A health plan’s board of directors plays a vital role in governing the organization’s strategic operations. Senior management could make the decisions that boards typically handle. But if senior management becomes too involved in “implementing” policies, they may lose sight of strategic goals. The board provides valuable perspective on the health plan’s business. Since the board as a whole is not involved in the day-to-day decisions of operating the business, the board members have more objectivity to view the organization’s efforts to meet the corporate mission or vision.
How Does Governance in Health Plans Differ From Governance in Other Industries?In the health plan industry, for-profit, not-for-profit, and charitable organizations work alongside each other trying to achieve similar goals. Some of today's for-profit health plans are subsidiaries of not-for-profit organizations or healthcare cooperatives. These for-profit companies may face challenges in board establishment since they emerged from a not-for-profit entity. They also may face challenges from state regulatory agencies relating to the conversion of any charitable assets. Although the goals of for-profit and not-for-profit health plans may be driven by different factors, the ultimate goal for both types of organizations is often the same-to establish and maintain a successful health plan. Figure 10A-1 provides an example of a business goal that illustrates one of the unique governance relationships that a health plan must manage.
As described in Figure 10A-1, health plans govern multiple interdependent relationships. A health plan, such as an HMO, combines all the functions that were present in the fee-for-service healthcare system into one organizational structure.1 The HMO is responsible for financing and ensuring the delivery of quality healthcare services for its members. This combination of formerly separate functions into one organization can present
Page 346 of 469

AHM 510 : Health Plans : Governance and Regulation
governance challenges for a health plan. For example, an HMO that contracts with an IPA must ensure that the IPA adheres to practices and procedures set by the HMO. The IPA itself often has its own separate corporate vision, culture, and organizational goals that may not be identical to the HMO's vision, culture, and goals.
One example of a governance challenge that some integrated delivery systems (IDSs) face is the presence of a representational rather than an enterprise-focused board. IDS directors usually include physicians or hospital representatives who may feel compelled to represent a specific constituency or organization that is only one part of the IDS. This may lead to representational governance-a situation in which the members of the enterprise board focus on the best interests of component parts of the enterprise rather than on the best interests of the enterprise as a whole.1 In addition, although constituent interests can and should be represented by directors, a focus on representational governance violates directors' fiduciary duty to represent the best interests of the entire company. To overcome representational governance, a health plan must stress the organization's mission and its identity as a whole unit instead of its separate components.2
Figure 10A-1. The Health Plan-Provider Relationship.
A specific goal developed by a health plan board may be to increase membership in the health plan’s health plans. To achieve this goal, one action the health plan may need to take is to provide purchasers with more detailed information about medical outcomes data for its members. The health plan’s providers often have the raw data concerning medical outcomes. To achieve its stated goal, the health plan needs to obtain this data from providers. The health plan must have in place a system that fosters a cooperative environment between the health plan and its providers that will allow the health plan to obtain the needed information. Health plans constantly govern the interdependent relationships they create among providers, other vendors, purchasers, and consumers.
Review Question
The board of directors of the Garnet Health Plan, an integrated delivery system (IDS), includes physicians and hospital representatives who sometimes feel compelled to represent a specific organization that is only one part of the IDS. Such a circumstance can lead to ___________, which is a situation in which the members of the board focus on the best interests of component parts of the enterprise rather than on the best interests of Garnet as a whole.
an enterprise-focused board
representational governance
enterprise liability
boundary spanning
Page 347 of 469

AHM 510 : Health Plans : Governance and Regulation
Incorrect. An enterprise focused board centers its decision on the best interests of the entire organization
Correct. Representational governance is a situation in which the members of the board focus on the best interests of component parts of the enterprise rather than on the best interests of Garnet as a whole.
Incorrect. Enterprise liability is a legal theory that creates a system where a health plan is liable for any torts commited by plan providers against plan members while they are enrolled in the plan, even if there is no employment or agency relationship.
Incorrect. Boundary spanning is an aspect of leadership that requires an individual to relate an organization or department to its environment.
The Board of DirectorsIn Healthcare Management: An Introduction, the variety in governance structures among different types of health plans was discussed. For instance, most health plans have established a board of directors (board) that is responsible for governance of the organization. But not all health plans have boards. In health plans that have boards, the number and types of board committees and board functions vary from one organization to another. Further, regulations often require that certain groups or entities be represented on the board or that board composition include those groups or entities. In addition, the roles and responsibilities of senior management are not standard among plans. In the following sections, we discuss some forms of board organization that are found in many health plans and the duties and responsibilities of boards and board members.
Board OrganizationAs we discussed in Legal Organization of Health Plans, a corporation’s board of directors is composed of individuals—called directors— who serve as the primary governing body of a corporation. A company’s articles of incorporation usually set a minimum number of directors. State laws may also set a minimum. A chairperson is often elected to facilitate direction of board activities; however, sometimes a chairperson is appointed by the board and is paid additionally for his or her services. A chairperson’s duties typically include scheduling board meetings, developing agendas, presiding at meetings, overseeing the board evaluation process, and planning for leadership succession. 5 Sometimes the chairperson is also the CEO of the organization, but often a separation of these two roles is desired, or even mandated by regulatory requirements.
Boards sometimes include both inside and outside directors. The proportion of inside to outside directors varies from organization to organization.
Fast Definition
Inside directors — board members who hold positions with the company in addition to their positions on the board.3
Page 348 of 469

AHM 510 : Health Plans : Governance and Regulation
Outside directors — board members who do not hold other positions with the company.4
Differences in Boards Based on Organizational VariationsNot all boards are alike. Boards vary in size and structure among different types of organizations. The board structure and the board process are very similar between for-profit and not-for-profit boards. However, one clear difference exists between for-profit and not-for-profit boards. For-profit boards are accountable to shareholders, and at least part of their corporate mission is to earn a return on shareholder investments. Not-for-profit boards do not answer to shareholders, nor do their organizations have a corporate mission focused on return on investment. However, not-for-profit boards may be required to answer to health plan members, regulators, and/or the community if return on assets is not adequate or if goals are not met; however, their duty is to the corporation as a whole, not members or other interested parties. Figure 10A-2 describes some of the differences between for-profit and not-for-profit boards.
Not only are there differences among boards based on their for-profit or not-for-profit status, variations also occur based on who sponsors the organization. Provider-sponsored organizations face some unique challenges in board operation because their historical role as providers sometimes conflicts with their new role as managers of healthcare. For example, for-profit PSO boards often have several provider directors, as well as outside directors who are not providers. Sometimes, the provider directors want to run the health plan like a medical institution, while the directors with a financial or business background want to run the health plan like a business.
For-profit boards of organizations with a not-for-profit parent or an organization established through a joint venture among for-profit and not-for-profit companies may suffer governance growing pains. Although for-profit and not-for-profit boards operate similarly, their cultures are often very different and their perspective on organizational goals and strategic plans may clash.
Figure 10A-2.
Typical Differences Between For-Profit and Not-For-Profit Boards of Directors.
For-Profit Boards:
1. Elected by shareholders 2. Directly accountable to shareholders 3. Small in size 4. Highly structured 5. Directors’ terms of service often limited by age only 6. Directors compensated for board participation 7. Directors do not participate directly in raising capital
Not-for-Profit Boards:
1. Self-perpetuating or elected or approved by other organization members 2. Duty is to corporation as a whole, but may be accountable to members, regulators,
and/or the community
Page 349 of 469

AHM 510 : Health Plans : Governance and Regulation
3. Large in size 4. Loosely structured 5. Directors’ terms of service often preset by number of years and age 6. Directors compensated for board participation at lower rate than for-profit
counterparts 7. Directors may participate in raising capital themselves
Review Question
One typical difference between a for-profit health plan's board of directors and a not-for-profit health plan's board of directors is that the directors in a for-profit health plan
can serve on the board for a period of no more than ten years, whereas the terms of service for a not-for-profit board's directors are usually unlimited by the director's age or by a preset maximum number of years of service must participate in raising capital for the health plan, whereas a not-for-profit board's directors are prohibited from participating directly in raising capital for the health plan are directly accountable to shareholders, whereas a not-for-profit board's directors are accountable to plan members and the community are not compensated for board participation, whereas a not-for-profit board's directors are compensated for board participation
Incorrect. Terms of service for a not-for-profit board's directors are usually limited by the director's age or by a preset maximum number of years of service. For-profit board members face terms of service limited by age only.
Incorrect. For-profit boards do not participate directly in raising capital for the health plan, whereas a not-for-profit board's directors may participate in raising capital for the health plan.
Correct. For-profit boards are directly accountable to shareholders, whereas a not-for-profit board's directors are accountable to plan members and the community.
Incorrect. For profit board members are compensated for board participation, whereas a not-for-profit board's directors are compensated for board participation at a lower rate than for-profit board members.
Board CommitteesTo help the board fulfill its responsibilities for ensuring survival of the company, the board is usually divided into a number of standing committees. These standing committees can make decisions and take actions to recommend to the full board. Board members may participate on more than one committee. Often, the background and experience of directors dictate on which committees they will serve. Typical standing committees for health plan boards include the executive committee (which may be authorized to take actions between full board meetings), the finance committee, the audit
Page 350 of 469

AHM 510 : Health Plans : Governance and Regulation
or compliance committee, the compensation committee, a quality management committee, a nominating committee, and a strategic planning committee. Figure 10A-3 provides a brief description of the purposes and responsibilities of each of these committees.
In addition to standing committees, the board may be authorized by the bylaws to create one or more special or ad hoc committees. Special committees may be composed of board members and nonboard members. Members of a special committee usually have expertise in a particular area. These committees may be standing or ad hoc entities. For example, a special litigation committee may be temporarily established to oversee a legal challenge regarding breach of fiduciary duty.
Figure 10A-3. Standing Committees of Health Plan Boards.
Members of standing committees of health plan boards are composed solely of board members.
Executive Committee-handles issues related to overall policy for the organization including such areas as the lines of business the organization participates in, employment policies, locations in which the organization operates, etc. The executive committee often acts on behalf of the full board between board meetings or when emergencies arise. This committee may also be responsible for strategic planning for the organization if a separate strategic planning committee does not exist.
Strategic Planning Committee - responsible for developing the strategic direction for the health plan. This committee receives recommendations from management on the strategic goals of the company and is responsible for reviewing and approving the business plan. In addition, this committee considers proposed transactions such as mergers and acquisitions.
Compensation Committee - handles issues related to compensation of the CEO and sets general compensation and benefits policies for the organization.8 The compensation committee may also function as the nominating committee for the board and executive officers if a separate nominating committee does not exist.
Nominating Committee - responsible for annually recommending to the full board nominations for the company officers as required in bylaws.
Audit and/or Compliance Committee -responsible for arranging for external audits of the organization's operations and receiving regular reports from the external auditors. Its duties may include review of regular reports by internal audit personnel to assess the organization's various risks. The audit committee is responsible for reporting significant risks to the full board. In some companies, this committee is also responsible for compliance functions; in other companies, a separate compliance committee performs compliance oversight. Compliance responsibilities include ensuring that a compliance program is instituted and followed throughout the organization and that an annual review of the effectiveness of the compliance program is conducted.
Page 351 of 469

AHM 510 : Health Plans : Governance and Regulation
Finance Committee - determines the broad investment policy of the organization and is responsible for approval of budgets, review of health plan financial results, review of the annual audit, approval of outside funding sources, and determination of the types of investments in which the organization will place its funds.9
Quality Committee - health plan boards usually establish a standing quality management committee (QM committee) to put in place and oversee companywide quality improvement programs and receive reports on quality initiatives from staff-level committees.
Many health plans have a staff-level quality management committee that works closely with the plan's medical director and makes regular reports to the full board. Staff-level quality management committees are usually composed of staff members, outside physicians, and sometimes board members.
Fast Definition
Standing committee — permanent committees that are used by company executives and the board as sources of continuing advice.6
Ad hoc committee — a non-permanent committee that is established for a specific purpose or project.7
Legal Requirements Affecting Board Structure Federally qualified HMOs must meet requirements for board composition set forth in the HMO Act of 1973 and related regulations. As we discussed in State Regulation of Health Plans, some state laws require representation of health plan members, consumers, or providers on boards of directors or limit the number of providers on a board. For example, in California a task force formed to make recommendations related to health plan laws has developed guidelines for board composition for health plans. Arkansas has a law that requires that certain categories of providers and consumers be represented on HMO boards.
Board Duties and ResponsibilitiesThe board exercises control over the company by approving or not approving actions performed or proposed by the executive officers. Most health plan boards, whether for-profit or not-for-profit, perform the following functions:
• Participate in developing the overall corporate strategic plan
• Set major policies for the company (e.g., Assuring high customer satisfaction, employee morale, and quality performance goals)
• Evaluate the results of the company's operations (the methods used for evaluation differ between not-for-profit and for-profit companies)
• Authorize major transactions, such as mergers and acquisitions
• Appoint and evaluate the performance of the executive officers (including the chief executive) who actually operate the company
• Hire external auditors
Page 352 of 469

AHM 510 : Health Plans : Governance and Regulation
• Recruit and orient new board members and assess board performance10
Individual Directors' Roles and ResponsibilitiesCorporate directors are bound by several specific legal duties and obligations as defined in the state corporate codes, the corporation's articles of incorporation, bylaws, and in other governing rules. As a threshold matter, corporate directors are required to act within the scope of the corporation's and their own authority. They must act only within the particular power and authority of their positions as directors. Corporate management is the responsibility of the entire board; individual directors generally do not have independent legal authority to govern the corporation. Rather, the board's combined judgment is to be relied upon to protect the corporation from unwise decisions.
Directors, as a group, can be held liable for the decisions of the board. In unusual circumstances, directors can be held individually liable for board decisions; however, most state laws and corporate charters limit directors' individual liability. To minimize the risk of such liability, individual directors must exercise good faith business judgment. To meet this requirement of exercising good faith business judgment, directors must demonstrate their compliance with three duties in all their decisions: the duty of care, the duty of loyalty, and the duty to supervise.
The Duty of CareBoth for-profit and not-for-profit corporate law in most states requires that directors exercise their duties in good faith and with the same degree of diligence, care, and skill that an ordinary, reasonable person would be expected to display in the same situation.11
This is known as the duty of care. Figure 10A-4 describes some key criteria that are used by regulators to evaluate meeting the duty of care.
Figure 10A-4. Key Criteria to Evaluate Meeting the Duty of Care. The director's exercise of independent business judgment (e.g., did the director
critically evaluate the recommendations of the corporation's officers and employees and make an independent decision, or did he or she simply follow the recommendations of another without independent thought?)
The director's decision-making based on knowledge of the facts and circumstances related to the issue under consideration (e.g., was the director's decision based upon a consideration of the facts relevant to a particular issue, or was it based upon other factors?)
The director's attendance at meetings at which a decision was to be made, and other relevant meetings and activities that were required for an informed decision (e.g., did the director attend meetings at which relevant information was presented and discussions held, or was he or she chronically absent?)
Source: Excerpted and adapted from Bruce A. Johnson, JD, MPA, Gerald A. Niederman, JD, Managed Care Legal Issues (Englewood, CO: Medical Group Management Association, 1996), 238. Reprinted with permission from the Medical Group Management Association, 104 Inverness Terrace East, Englewood, Colorado 80112-5306; 303-799-1111. Copyright 1996.
The Duty of LoyaltyBecause directors hold positions of special trust and confidence (i.e., they act as fiduciaries), they have certain special obligations to the company. Fiduciaries must carry
Page 353 of 469

AHM 510 : Health Plans : Governance and Regulation
out their duties by acting in the best interests of the organization. That is, a director must put the interests of the organization before his or her personal interests. In this way, a director meets the duty of loyalty. For example, directors may not use their roles as directors to further their personal business interests to the detriment of the organization. In addition, directors may not try to win business away from the organization to further their personal business or interests. These types of situations are generally referred to as conflicts of interest.
To uphold their duty of loyalty, directors must notify the organization of potential conflicts of interest that arise and may have to abstain from participation in board decisions on such matters. Many boards develop policies that address conflicts of interest. In addition, some state laws allow boards to excuse themselves from obligations made by a director who had a conflict of interest and did not disclose that conflict to the board, unless the action is shown to be fair despite the conflict of interest.12
The Duty to SuperviseA board of directors cannot undertake every action to manage and operate the organization's business and affairs, but must necessarily rely on the actions of others. Accordingly, directors also have a duty to supervise. If the board is notified that its officers or outside advisers (e.g., accountants, attorneys, or others) may not be adequately performing their duties, then the board must use reasonable care to investigate and correct such conduct. The board must exercise its duty of care to supervise the corporation's officers and others who act on the corporation's behalf.
A corporate board of directors can also delegate some powers to executive or other committees. Provisions of state law, the corporation's articles, or bylaws typically provide for committees that have the power to exercise the authority of the board except with respect to certain substantial matters (e.g., a committee may generally not authorize distributions, approve proposed shareholders, fill board vacancies, amend the articles or bylaws, or undertake certain other actions). The board and its committees can also use and rely upon the advice provided by lawyers, accountants, and others to assist in the exercise of their authority. The creation of a committee and the delegation of authority does not, however, relieve the board or any of its members from their ultimate responsibility as the corporation's governing body.
Excerpted and adapted from Bruce A. Johnson, JD, MPA, Gerald A. Niederman, JD, Managed Care Legal Issues (Englewood, CO: Medical Group Management Association, 1996), 240. Reprinted with permission from the Medical Group Management Association, 104 Inverness Terrace East, Englewood, Colorado 80112-5306; 303-799-1111. Copyright 1996.
Review Question
Directors on a health plan's board must demonstrate their compliance with three duties in all their decisions. Directors who exercise their duties in good faith and with the same degree of diligence and skill that an ordinary, reasonable person would be expected to display in the same situation are meeting the duty known as the
duty of loyalty
duty to supervise
Page 354 of 469

AHM 510 : Health Plans : Governance and Regulation
duty of care
trustee duty
Incorrect. The duty of loyalty dictates that a director must put the interests of the organziation before his or her personal needs
Incorrect. The duty to supervise states that the board of directors, if aware that its officers or advisors may not be adequately performing their duties, they must use reasonable care to investigate and correct such conduct
Correct. The duty of care states that the director exercise their duties in good faith and with the same degree of diligence and skill that an ordinary, reasonable person would be expected to display in the same situation
Incorrect. This term refers to the duties of a not-for-profit board member.
Liability Issues for Board MembersIncreased board responsibility and accountability bring increased exposure to liability. The liability of the governing board and the company's officers is called directors' and officers' liability, and there are two separate categories: (1) the organization's liability for the actions of its governing board and/or officers and (2) the personal liability of individual board members and/or officers. There are four types of protection from directors' and officers' liability:
1. Indemnification provisions in bylaws 2. Liability insurance 3. State statutory limitations on liability 4. Corporate risk management
Figure 10A-5 shows the type of liability (organization or individual) to which each protection applies.
An indemnification provision in the healthcare organization’s bylaws may provide that board members will be compensated by the organization for losses that board members are legally obligated to pay and that are related to their being members of the board, as well as legal defense costs.
Adapted and reprinted from Robert J. Taylor and Susan B. Taylor, editors, The AUPHA Manual of Health Services Management, © 1994, p. 177, with permission from Aspen Publishers, Inc., Gaithersburg, MD (1-800-638-8437).
Page 355 of 469

AHM 510 : Health Plans : Governance and Regulation
An indemnification provision in the healthcare organization's bylaws may provide that board members will be compensated by the organization for losses that board members are legally obligated to pay and that are related to their being members of the board, as well as legal defense costs.
In addition to the indemnification provision, most organizations purchase liability insurance for their directors and key officers. As with most insurance policies, these policies contain coverage limitations and exclusions. Therefore, such insurance is not total protection for board members.
States often provide some protection for director liability. Many states have passed legislation to provide immunity from liability for directors of nonprofit organizations. However, many state statutes contain limitations and exclusions, vague language, and loopholes.
The fourth method of protecting boards and trustees from liability is corporate risk management. Corporate risk management consists of a series of activities designed to minimize the corporation's and the board's liability exposure and reduce the risks of lawsuits, while enabling the board to govern the organization effectively. A corporate risk management program usually has three steps: (1) determine potential areas of board liability exposure, (2) assess the degree of liability exposure in each area, and (3) implement actions to minimize liability exposure in high-risk areas.
Effective BoardsSimply establishing a board of directors for a health plan does not ensure successful governance. A board that exists only to comply with regulatory requirements or as a figurehead does not help a health plan meet its goals. To be useful to the health plan, a board must be effective in its duties. Characteristics of effective boards include:13
Page 356 of 469

AHM 510 : Health Plans : Governance and Regulation
• A commitment to the continuing education of board members, including information about the health plan, the industry, and the board's duties and responsibilities within that framework
• A self-evaluation process for improvement of individual board members
• An effort to develop itself and act as a single governing body, not just component parts
• The ability to analyze and dissect complex problems and develop appropriate responses
• An understanding of the environment in which the board and the organization operate
• A vision of where the organization stands and where it is headed in the industry
• The ability to keep the organization on course in meeting its goals, using the corporate mission as a guide
Shareholders' Role in GovernanceAs we discussed in Legal Organization of Health Plans, many health plans are legally organized as for-profit, stock corporations. In exchange for their purchase of a share or shares of ownership of a health plan, most shareholders obtain voting rights that allow them to exercise a voice in the governance of a health plan.
Common shareholders participate in health plan governance by electing the board of directors. Shareholders may also call for a vote for termination of the current board if they are dissatisfied with the company's performance. Another way that shareholders participate in health plan governance is by approving board actions at annual or special meetings of the shareholders. Shareholders also have the right to approve mergers and acquisitions by vote.
Members' and Providers' Roles in GovernanceMembers of health plan health plans often sit on the health plan board to represent customers' interests. Many states have laws that require representation of members on health plan boards. In addition, most health plans have consumer representatives on their grievance and appeals committee.
Members have a less direct, but possibly greater, influence on governance through their buying power. The needs and desires of members often drive governance decisions made by health plans. State laws often require representation of key constituencies on health plan boards of directors. Providers constitute a key constituency. As we discussed in Legal Organization of Health Plans, some state laws also limit the amount of provider representation on boards.
Overview of Executive LeadershipWe have used the term governance throughout this lesson to refer to actions taken by boards to steer health plans in achieving their corporate mission. Sometimes, the terms governance and management are used interchangeably, but they are not the same. Recognizing the distinctions between these two terms makes it easier to understand the roles and responsibilities of the board versus the roles and responsibilities of the chief executive officer (CEO) and senior management team of an organization.
Page 357 of 469

AHM 510 : Health Plans : Governance and Regulation
Governance is frequently equated with policy development, and management is equated with the implementation of policy. Put another way, the board decides if an organization will do something, and management decides how it will be done. Does this mean that management does not participate in policy development or that the board does not monitor the implementation of the policy or occasionally fine-tune it? No, there is rarely an absolute division of these two intertwined functions. The practical distinction between governance and management must be tailored to fit each individual organization, and it must be revisited and revised as new circumstances and issues arise.
Recall that one of the primary responsibilities of a board of directors is hiring a chief executive officer. The chief executive officer (CEO), called chief operating officer (COO) in some companies, is the officer of an organization that the board of directors entrusts with broad administrative powers. The CEO is also the primary liaison between the board and other members of management and is responsible for leading the organization in the pursuit of the goals outlined in the strategic plan. The CEO is responsible for recruiting and developing a management team that can successfully implement the policies created by the board. CEO's duties vary by organization but many of their concerns are the same.
Choosing the right CEO for a particular organization depends on the type of organization and the maturity of the organization. For example, a start-up IDS requires a different kind of chief executive officer than an established HMO. The start-up company often needs a leader who can make decisions with no precedents to rely on, build the business, and build coalitions with groups who are resistant to change and new approaches.14
The Roles and Responsibilities of Senior ManagementChoosing a senior management team for a health plan can be a challenging task. We noted that it is the board's responsibility to select the chief executive officer. It is also crucial for health plans to select the right candidates for other senior management positions.
One of the most important responsibilities of the key officers and senior management of a health plan is the duty to report information to the board of directors. Presenting relevant, concise reports to the board on strategic issues affecting the organization aids a health plan in meeting its corporate goals.
In most companies, the board hires the chief executive officer (CEO) and annually appoints the officer positions of president, treasurer, and secretary. The CEO hires and appoints other officer positions in the organization. These key officers include vice presidents, a chief financial officer (CFO), a chief information officer (CIO), chief medical officer (CMO), and general counsel.
In Healthcare Management: An Introduction, we introduced the key management positions in a health plan. Figure 10A-6 outlines some of those roles and responsibilities for your review. Although titles and duties vary from one organization to another, senior management is a crucial link in the management chain descending from the board and the CEO.
Figure 10A-6. Key Management Positions.
Page 358 of 469

AHM 510 : Health Plans : Governance and Regulation
MEDICAL DIRECTOR - Almost by definition, health plans will have a medical director. Whether that position is a full-time manager or a community physician who comes in a few hours per week is determined by the needs of the plan. The medical director usually has responsibility for provider relations, provider recruiting, quality management, utilization management, and medical policy.
FINANCE DIRECTOR - In free-standing plans or large operations, it is common to have a finance director or chief financial officer. That individual is generally responsible for oversight of all financial and accounting operations. In some plans, that may include functions such as billing, management information services, enrollment, and underwriting as well as accounting, fiscal reporting, and budget preparation. This position usually reports to the executive director, although once again some national companies use vertical reporting.
MARKETING DIRECTOR - This person is responsible for marketing the plan. Responsibility generally includes oversight of marketing representatives, advertising, client relations, and enrollment forecasting. A few plans have marketing generating initial premium rates, which are then sent to finance or underwriting for review, but that is uncommon. This position reports to the executive director or vertically, depending on the company.
OPERATIONS DIRECTOR - In larger plans, it is not uncommon to have an operations director. This position usually oversees claims, management information services, enrollment, underwriting (unless finance is doing so), member services, office management, and any other additional backroom functions. This position usually reports to the executive director.
Source: Reprinted from Peter R. Kongstvedt, MD, ed., Essentials of Managed Health Care, Second Edition, © 1997, pp. 73–74, with permission from Aspen Publishers, Inc., Gaithersburg, MD (1-800-638-8437).
Page 359 of 469

AHM 510 : Health Plans : Governance and Regulation
Chapter 10 BStrategic Planning in Health Plans
What Is Strategic Planning?2
As we saw in the lesson Environmental Forces, strategic planning is the process of identifying an organization’s long-term objectives and the broad, overall courses of action that the company will take to achieve those objectives. Strategic planning forces a company to look beyond tomorrow or next year and establish a long-term plan. Most companies today develop a long-term strategic plan for at least the next three to five years as well as a short-term tactical or business plan (with measurable objectives) for the first one or two years of the strategic plan.
Effective strategic plans are developed to accommodate change and to be revised as circumstances warrant. The farther a company plans into the future, the less exact its planning can be because of unanticipated changes that may occur both within the company and in its external environment. Therefore, it is important for a health plan to re-evaluate corporate goals on a regular basis to determine whether the goals remain valid. Health plans must also re-evaluate corporate strategies to determine whether these strategies can still achieve a company's long-term goals. Consequently, each year when a company develops its business plan, it usually conducts a strategic review of current long-term objectives and strategies. Many companies update their strategic plans by first evaluating the past year (comparing the actual results to the business objectives), and then adding a new "final" year to the long-term plan. This annual review process keeps the strategic plan current on a "rolling basis."3
Strategic planning is conducted by the board of directors, senior executives, or the board and executives working together. Sometimes the board establishes a long-term planning committee as a way to maintain board involvement in the planning process and to keep the board apprised of the organization's progress in attaining its goals. Typically, these committees report on a regular basis at board meetings.
When strategic planning is driven by senior management, control of the process resides with the chief executive officer (CEO) and key senior executives, who may work with a few members of the board of directors or with a board planning committee. This group develops a strategic plan that it presents to the full board for review and approval. Some CEOs choose to work alone on a preliminary draft of the strategic plan and then obtain input from key board members and executives. Others schedule a few days or a week-long "retreat" devoted exclusively to strategic planning with senior executives and/or board members where they develop or update the organization's plan for presentation to the full board. 4
In contrast to a senior-management-driven approach, some health plans engage in a strategic planning process that is more participatory in nature by involving most, if not all, of the board members as well as key senior management staff. This group conducts an in-depth analysis of market conditions, organizational strengths and weaknesses, and resource requirements before coming together as a complete or representative group to develop an overall plan. Often the task of developing the written plan is assigned to a work group and the draft plan is presented at board and senior management meetings for review and revision.5
Page 360 of 469

AHM 510 : Health Plans : Governance and Regulation
The time required to effectively complete the planning process and develop a written strategic plan varies, depending on the type of plan and the manner in which it is conducted. Obviously, an initial strategic plan requires more time to complete than an update to an existing plan. Also, a plan developed solely by the CEO, which is then revised based on input from key senior management and board members, takes less time to complete than a plan developed in a participatory manner. Some health plans take several months or as long as a year every three to five years to update their overall strategic plans. Others, as we have mentioned, allocate intensive time to the planning process and can update a plan in a few days or weeks.
Why Is Strategic Planning Important?At first glance, it might seem that long-term planning makes little sense in the rapidly changing environment of health plans. Urgent, day-to-day business pressures can easily push aside a long-term planning process. An organization may slip into a reactive rather than a proactive approach to the challenges it faces, and may simply follow the competition or the latest industry trends. A health plan's leaders may decide that the results of strategic planning just don't justify the time and effort it takes to complete a formal plan. Or they may conclude that it is pointless to prepare for five years in the future when marketplace and regulatory uncertainties make it difficult to predict what will happen in the next five months, let alone five years.
However, the sense of urgency and uncertainty in healthcare today is all the more reason that successful health plans choose to devote their time and efforts to strategic planning, which can be used as a "compass" to maintain the right direction in an environment of constant change. Effective strategic planning often brings about practical business decisions and improved results. For example, in response to the need for greater choice, health plans developed out-of-network options and direct access to specialists, and they provided more flexibility with regard to the number and types of healthcare providers available within their networks. Studies have shown that when health plans implement a strategic planning process, their results are typically better than the results of health plans that do not use strategic planning or that do not follow through with implementation. For example, according to a 1998 study, health plans that are actively involved in strategic planning are more likely to have lower administrative costs than health plans that are not involved in strategic planning.6
Strategic planning can also produce other tangible benefits for an organization. Potential board members and executives, as well as investors or donors, sometimes examine a health plan's strategic plan before deciding to become involved with the organization. They review the plan to find out the organization's mission and how it is implemented. The presence of a well-thought-out strategic plan can help a health plan recruit key personnel or obtain important funding.7
Strategic planning can "translate" the goals of the organization into specific day-to-day actions and objectives for each employee in the organization. If done in a participatory manner, strategic planning can enhance teamwork and morale. Some organizations use strategic planning as a way to not only focus on challenges, objectives, and actions, but to shape organizational culture. Organizational culture, also called corporate culture, is "a collection of shared values, beliefs, and language that creates a common identity and
Page 361 of 469

AHM 510 : Health Plans : Governance and Regulation
sense of community among organization members."8 A health plan's culture can have a subtle but significant influence on the results the organization achieves.
The Strategic Planning Process9
As illustrated in Figure 10B-1, the strategic planning process includes four primary activities:
1. Defining or redefining the company mission2. Conducting a situation analysis3. Establishing or revising corporate objectives4. Developing or revising corporate strategies
As shown in the figure, each activity performed in the strategic planning process provides input for the activities that follow, and the entire strategic planning process provides the basis for tactical planning.
Defining or Redefining the Company's Mission10
As we noted in Environmental Forces, a mission statement is a statement that succinctly sums up the organization’s reason for existence and overall fundamental purpose. A mission statement defines the scope or domain of an organization’s activities and answers the question, “What business are we in?” Although a company is not likely to change its mission regularly, a company still needs to consider making such a change each time it conducts strategic planning. As we saw in Formation and Structure of Health Plans, some notfor- profit health plans in effect changed their mission when they converted to for-profit status.
Page 362 of 469

AHM 510 : Health Plans : Governance and Regulation
Many organizations develop formal mission statements to provide all employees with a clear, unified sense of the organization’s purpose and direction. According to marketing expert Peter Drucker, a mission statement should answer the following questions:
(1) What is our business?(2) Who is our customer?(3) What constitutes value for our customer?(4) What will our business be?(5) What should our business be?11
An effective mission statement is broad enough to encompass the types of business a company is engaged in, but specific enough to provide a meaningful focus for the company’s activities. A mission statement also defines the scope and nature of a company’s business, both as it is today and as it could be in the future, yet it is realistic about the company’s ability to enact the mission statement. In some companies, each functional area develops its own mission statement based on the organization’s overall mission.
Most companies today are moving toward a market-oriented philosophy. To help transition to a market-oriented philosophy, companies often develop a mission statement that focuses on the customer needs that the company plans to satisfy, not just on the products that the company plans to sell. For example, a product-oriented health plan in the early 1990s might have focused its mission on “striving to be a market leader by managing the quality and cost of healthcare through strong group model HMOs.” Such a mission may have been effective at one time, but if a health plan neglected to adjust its focus as healthcare consumers and purchasers began to seek additional choice of providers in health plans, that health plan might have run into difficulties during the next few years. A health plan that focuses its mission on “striving to be a leading health plan by meeting the needs of midsize employers and their employees and families with products and delivery systems that provide healthcare quality and value” is more likely to attract and keep customers and to maintain the flexibility to refocus its mission as products and needs change.
Market-oriented mission statements also carefully define their markets in terms of customers who value the abilities and strengths of the company. Companies must attract customers whom they can satisfy and be willing to turn away customers whose patronage will not be cost-effective for the company. A company that tries to serve all potential consumers will spend too much money trying to attract and keep consumers that it will not be able to satisfy in the long run anyway.
For example, a health plan that is successful in the small-employer market where purchasers typically select healthcare based on cost would find it difficult to attract and retain large national employers that expect customized reports and similar services. An effective mission statement recognizes its most suitable market segments.
To be effective, a mission statement should not only define the scope of a company's operations, but should also be motivating and relevant to employees. Often motivation results from defining the company vision. A vision is an ideal that a company would like to achieve and what it would like to be. A vision is intended to inspire enthusiasm and commitment in employees. Such energy is needed for a company to make the vision
Page 363 of 469

AHM 510 : Health Plans : Governance and Regulation
become a reality. An example of a company mission statement is shown in Figure 10B-2.
Figure 10B-2. Mission Statement: QualChoice of Arkansas, Inc.
QualChoice of Arkansas, Inc. is a full service health plan dedicated to delivering affordable, high quality, patient-centered healthcare to its members. We are committed to:
1. superior service to members 2. active partnership with providers 3. accountability for the cost and quality of care 4. developing and recognizing employees
Central to achieving our mission is our partnership with the University of Arkansas for Medical Sciences, the state’s only academic health center.
Source: Reprinted with permission from QualChoice of Arkansas, Inc.
Situation Analysis12
After a company has focused its operations on a specific mission, the company ordinarily conducts a situation analysis. Situation analysis, which involves examining the environments that affect a company, provides many of the assumptions an organization needs to develop its strategic plan. The primary steps involved in situation analysis are (1) conducting an environmental analysis, (2) developing an environmental forecast, and (3) conducting an internal assessment.
Environmental analysis is the ongoing compilation and examination of information about events and relationships in the external environment, and the ways these events and relationships are likely to affect a company. Since monitoring and analyzing the whole environment would be a monumental task, most companies concentrate their efforts on specific areas they know are relevant to their business activities. These specific external areas might include (1) the company's current target market, (2) competitors' activities, (3) legal and regulatory developments, and (4) other major environmental factors that affect purchaser behavior, such as demographic changes, attitudes/beliefs about the healthcare and health plan industry and products, economic conditions, and technological advances. Many of the topics addressed in Environmental Forces are examples of events and relationships that would be examined in a health plan's environmental analysis.
Information gained in the environmental analysis is used to develop an environmental forecast, which is a prediction of the major environmental trends that will affect a company's business activities. By conducting an environmental analysis and developing an environmental forecast, a company can reduce uncertainty and risk by estimating the character, magnitude, and timing of anticipated environmental changes and predicting the effects those changes may have on the company's performance and operations.
For example, changes in the environment that result from mergers or acquisitions might mean that a health plan is faced with a new competitor that has different strengths and
Page 364 of 469

AHM 510 : Health Plans : Governance and Regulation
weaknesses than existing competitors. The newly formed entity might offer a popular product that was previously not available in the market, requiring the health plan to adjust its strategic plan by introducing new products or perhaps seeking a strategic alliance of its own to meet the challenge of new and more formidable competition
To further illustrate this point, consider how changes in laws and regulations might present a health plan with new and different competition. As we discussed in Federal Government as Purchaser, recent changes in Medicare now allow PSOs to contract with the federal government to offer health plan products for Medicare beneficiaries. For a health plan that contracts with Medicare, an environmental analysis and forecast might lead the senior management team to address this new type of competition by re-examining the organization's current products and services. Or the health plan might seek a strategic alliance or identify a new business opportunity such as offering administrative services to PSOs that are unfamiliar with the managed Medicare business. However, before senior management seriously considers responses to environmental factors, they typically conduct an internal assessment to realistically determine the organization's capabilities in the changing external environment.
A company analyzes its internal environment by conducting an internal assessment. An internal assessment is an examination of a company's current activities, its strengths and weaknesses, and its ability to respond to potential threats and opportunities in the environment. Determining its strengths and weaknesses helps a company develop corporate objectives that will allow it to take advantage of its strengths and to avoid or remedy its weaknesses. Examples of strengths might include efficient billing and eligibility processes, underwriting expertise, a productive sales force, and knowledgeable and responsive member services staff. Examples of weaknesses might include insufficient financial resources and outdated computer systems.
Review Question
SoundCare Health Services, an MCO, recently conducted a situation analysis. One step in this analysis required SoundCare to examine its current activities, its strengths and weaknesses, and its ability to respond to potential threats and opportunities in the environment. This activity provided SoundCare with a realistic appraisal of its capabilities. One weakness that SoundCare identified during this process was that it lacked an effective program for preventing and detecting violations of law. SoundCare decided to remedy this weakness by using the 1991 Federal Sentencing Guidelines for Organizations as a model for its compliance program.
By definition, the activity that SoundCare conducted when it examined its strengths, weaknesses, and capabilities is known as
an environmental analysis
an internal assessment
an environmental forecast
Page 365 of 469

AHM 510 : Health Plans : Governance and Regulation
a community analysis
Incorrect. An environmental analysis involves examining the environments that affect a company
Correct. An internal assessment is an examination of a company's current activities, stengths and weaknesses and ability to respond to potential threats and opportunities.
Incorrect. An environmental forecast is a prediction of environmental trends that will affect a company's business activities
Incorrect. A community analysis is the process that allows not-for-profit health plans to gather informion and evaluate trends related to chartiable mission or community benefit
Among the internal factors that have a significant impact on a health plan's strategic planning are the company's mission and vision, governance and leadership capabilities, financial condition, product portfolio, sales and marketing capabilities, provider networks, medical management techniques, claims and member services capabilities, and technological resources.
Tools of AnalysisGathering the enormous quantity of information required to conduct a situation analysis is only half the process. If the information is not organized in a useful manner, it is worthless. In this case, "useful" means in a way that will help the senior management team decide where and how to focus efforts and resources. In the next lessons, we describe several methods used to highlight information so senior management can gain useful insights and not be burdened with irrelevant data.
SWOT AnalysisThe acronym SWOT stands for strengths, weaknesses, opportunities, and threats. As we discussed, companies undergoing a situation analysis attempt to identify their strengths and weaknesses as well as the current and upcoming opportunities and threats posed by environmental forces. SWOT analysis is a means of organizing this information so planners can easily identify matches between a company's strengths and specific marketing opportunities. A marketing opportunity arises when the right combination of circumstances occurs to allow a company to use its strengths or capabilities to take advantage of an environmental opportunity. The term strategic window is often used to describe the time period during which an optimum "fit" exists between a company's distinctive capabilities and the key requirements of an opportunity. Use of SWOT analysis helps a company identify the best possible places to devote resources so strategic windows are exploited before they begin to close.
Business Portfolio AnalysisCompanies that engage in more than one business or offer more than one product line can use business portfolio analysis when conducting an internal assessment. For example, this tool might be valuable to health plans that provide health plan products in the commercial market and in government programs such as Medicare, Medicaid, or workers' compensation.
Page 366 of 469

AHM 510 : Health Plans : Governance and Regulation
Business portfolio analysis is a process that allows a company to evaluate its individual business units according to their potential contribution to the firm, given their strengths and weaknesses in comparison to trends in their markets. Business portfolio analysis helps senior management determine each unit's potential for (1) generating financial resources for the firm and (2) requiring financial resources from the firm. Generally, companies will want to invest more of their resources in units that are already profitable or that have the potential to grow and become more profitable. Companies usually will want to withdraw from units that lack such potential.
To conduct business portfolio analysis, a company typically must identify its major business units. In this text, we use the term strategic business unit to refer to these units. A strategic business unit (SBU) is an area of business that is distinct from other areas within a company in that it:
• Is operated as a separate profit center
• Has its own separate set or share of customers and competitors
• Generally has its own management
• Is capable of having its own marketing strategy
Not all companies label their organizational units as SBUs. Other labels that are commonly used are profit centers, divisions, subsidiaries, product lines, teams, or lines of business. An SBU may be an entire company, a division, a product line, a single product department, or a major market. For example, a health plan's sub-business units might consist of several divisions organized according to geographic markets (e.g., west, central, and east), demographic markets (e.g., employer groups, Medicare beneficiaries, and the Medicaid population), or products and services (e.g., HMO/PPO, third party administration, pharmacy management, and behavioral healthcare). Although SBUs are separate profit centers, they are usually dependent on their parent company for allocation of their financial resources.
Once a company's SBUs have been identified, a business portfolio analysis considers factors related to (1) the market in which the SBU competes and (2) the strength of the SBU in that market. With regard to the market, the portfolio analysis might examine market growth rate, market size, government regulation, market stability, competitive intensity, and technological requirements. With regard to the SBU, the portfolio analysis might examine relative market share, price competitiveness, product quality, customer loyalty, technological and financial resources, and management effectiveness.
Based on this analysis, the senior management team is in a position to determine the role each business unit will play in the company's future. Although a company can seldom do much to affect the market's growth rate, it can take action to improve a business unit's market share in a particular market. A company can follow four basic strategies with a business unit:
1. Build strategy. Under a build strategy, a company seeks to increase a business unit's market share. This strategy usually requires that a company sacrifice immediate earnings in order to fund the growth required to improve a business unit's market position.2. Hold strategy. When following a hold strategy, a company tries to maintain a
Page 367 of 469
AHM 510 : Health Plans : Governance and Regulation
business unit's market position. The company generally invests only enough to hold promotional activities and customer services constant, though occasionally a company will increase short-term investment in the business unit in an attempt to enhance profits.3. Harvest strategy. Under a harvest strategy, a company seeks to maximize a business unit's short-term earning and cash flow. Usually, the harvest strategy entails reducing the amount of resources expended on the business unit and, thus, allowing its market share to decline. For example, a company may stop allocating money to the business unit for promotional activities, or it may cut the staff serving the business unit.
4. Withdrawal strategy. Under a withdrawal strategy, a company sells or discontinues a business unit because the resources required to support it can be more profitably employed elsewhere.
Review Question
After conducting a business portfolio analysis, the Acorn Health Plan decided to pursue a harvest strategy with one of its strategic business units (SBUs)-Guest Behavioral Healthcare. By following a harvest strategy with Guest, Acorn most likely is seeking to
maximize Guest's short-term earnings and cash flow
increase Guest's market share
maintain Guest's market position
sacrifice immediate earnings in order to fund Guest's growth
Correct. A harvest strategy maximizes Guest's short-term earnings and cash flow.
Incorrect. Under a harvest strategy a plan reduces the amount of money expended on the business unit, allowing its market share to decline.
Incorrect. Under a harvest strategy a plan reduces the amount of money expended on the business unit, allowing its market share to decline
Incorrect. A build strategy sacrifices immediate earnings to fund growth required to improve a business unit's market position.
Community AnalysisIn the case of many not-for-profit health plans, an additional element in strategic planning is the community analysis. Community analysis is a process that allows a not-for-profit health plan to gather information and evaluate trends related to charitable mission or community benefit. Community analysis helps the board and senior management team determine demand for services and programs, environmental forces that may have an impact on demand, and the emergence of additional opportunities for the health plan to fulfill its charitable/community benefit mission.13
Page 368 of 469

AHM 510 : Health Plans : Governance and Regulation
Establishing and Revising Corporate Objectives14
After developing the company mission statement and conducting a situation analysis, the next step in the strategic planning process is to establish specific goals for addressing the threats and opportunities uncovered during the situation analysis. Corporate objectives, also known as organizational objectives or corporate goals, are statements that describe the long-term results that a company plans to achieve in carrying out its mission. Corporate objectives add a sense of purpose to the activities undertaken by the organization and, in turn, increase employee motivation. Corporate objectives also increase the consistency with which decisions are made throughout the company and, thus, increase management control over operations.
Corporate objectives, which normally cover a period of three to five years, are established for a whole company. Such objectives often deal with profit, growth, use of technology, quality of services, and sales and market share; in the case of not-for-profit health plans, the objectives might also focus on any community benefit or charitable purpose. Effective corporate objectives are (1) clearly stated, (2) specific and measurable, and (3) realistic. Whenever possible, each objective specifies in quantifiable terms what is to be accomplished and the time period over which the objective is to be achieved. For example, rather than stating, "To increase sales" as a goal, an effective corporate objective makes a quantitative statement such as "To increase total corporate sales by 10% within four years" or "To achieve a market share of 20% within the next four years." Figure 10B-3 provides some examples of corporate objectives health plans might develop.
Figure 10B-3. Examples of a Health Plan Corporate Objectives.
1. Obtain full NCQA accreditation within three years 2. Increase the percentage of preventive health interventions for total eligible
membership during each of the next three calendar years for the following services: mammography, Pap smears, immunizations, and first trimester visits for prenatal mothers
3. Improve high-impact health and satisfaction outcomes during each of the next three calendar years for the following medical conditions: asthma, depression, cardiovascular disease, diabetes, and end-stage renal disease
4. Improve customer satisfaction on an annual basis for each of the next three calendar years, as measured by satisfaction surveys for members, providers, and employer groups
5. Attain top three market share position within the next three years 6. Increase by 30% the number of claims processed by the automated claims
payment system and reduce by 10% the cost of paying claims during the next three years
7. Reduce overall administrative expenses by 10% over the next three years 8. Reduce voluntary turnover to less than 9% for all employees each calendar year
Review Question
The following statements appear in the Twilight Health Plan's strategic plan:
Page 369 of 469

AHM 510 : Health Plans : Governance and Regulation
• Increase the percentage of preventive health interventions for total eligible membership during each of the next three calendar years for the following services: mammography, Pap smears, immunizations, and first trimester visits for prenatal mothers
• Improve customer satisfaction on an annual basis for each of the next three calendar years, as measured by satisfaction surveys for members, providers, and employer groups
• Increase by 30% the number of claims processed by the automated claim payment system and reduce by 10% the cost of paying claims during the next three years
These statements are examples of Twilight's corporate objectives
company mission
company vision
corporate strategies
Correct. Corporate objectives, also known as organizational objectives or corporate goals, are statements that describe the long-term results that a company plans to achieve in carrying out its mission.
Incorrect. A corporate mission succinctly sums up the organization's reason for existence and overall fundamental purpose
Incorrect. A company vision is an ideal that the company would like to achieve
Incorrect. Corporate strategies define long-term methods by which an organization plans to achieve its corporate objectives.
Corporate objectives form the basis for the objectives of each functional area of the company. For example, a health plan's marketing objectives are based on overall corporate objectives, as are the objectives of accounting, claims, finance (investments), human resources, information systems, legal, member services, provider relations, underwriting, and other functional areas. As corporate objectives are translated into functional area objectives, they become more specific and more short-term and are, thus, easier to plan and control.
In light of increased attention in the area of market conduct, most health plans today are including objectives related to market conduct and compliance in their strategic plans. In Governance: Accountability and Leadership, we take a closer look at how health plans approach compliance.
Developing and Re-evaluating Corporate Strategies15
After a company has established its corporate objectives, the next step in strategic planning is to develop the corporate strategies required to achieve those objectives. Corporate strategies define the long-term methods by which an organization plans to achieve its corporate objectives.
Page 370 of 469

AHM 510 : Health Plans : Governance and Regulation
Companies generally can choose among several alternative strategies to accomplish their objectives. Further, companies can apply different strategies to different SBUs. In our discussion of business portfolio analysis, we discussed the strategies associated with the development of business units. The combination of strategies required by one company may be different from the combination of strategies required by another company, even when both are trying to reach the same or similar goals. In addition, the combination of strategies that is best for a company today may not be the best combination in the future. Consequently, companies regularly re-evaluate their strategies to make sure that their present strategies are still appropriate in the context of their current environments. In addition, organizations often establish contingency plans for use in the event that current conditions radically change.
In the next lesson, we discuss overall corporate strategies that focus on growth.
Corporate Strategies That Focus on GrowthAlthough most companies develop corporate strategies that seek growth, a company can pursue a number of different strategies to attain their objectives. These strategies are categorized as:
(1) Intensive growth strategies(2) Integrated growth strategies(3) Diversified growth strategies
Intensive growth strategies are those available to a company that has not yet exhausted the sales or market potential in its current products or current markets. Intensive growth strategies focus on market penetration, market development, and product development. These strategies require significant financial capital.
1. Market penetration focuses on increasing sales of current products to current purchasers. A company using a market penetration strategy usually increases its sales by increasing its promotion efforts significantly. For example, as a market penetration strategy, a health plan can simultaneously increase its advertising in business periodicals, increase the size of its sales force, and offer additional incentives to its sales associates.
2. Market development focuses on increasing sales of current products by introducing them in new markets. This type of strategy often involves expansion into new geographic areas. In recent years, several health plans that established themselves in one region of the country have sought new markets by setting up operations in other regions.
3. Product development focuses on increasing sales by modifying current products or developing new, but related, products for current markets or segments within current markets. When a health plan develops a new type of health plan product and then markets that product to its current customers, the company is following a product development strategy. For example, a health plan that decides to offer an open access plan or a managed dental plan is following a product development strategy.
Page 371 of 469

AHM 510 : Health Plans : Governance and Regulation
Integrated growth strategies are strategies that involve taking over or entering a strategic alliance with another area or level of a company's industry. Integrated growth strategies include horizontal integration and vertical integration, as discussed inFormation and Structure of Health Plans.
Diversified growth strategies are strategies that require companies to venture outside the industry in which they conduct business to seek growth opportunities in industries that produce products or services unrelated to their existing business. Diversification can be a risky strategy because a company must employ knowledge, skills, and processes that are substantially different from those with which it is generally familiar, but diversification can soften the blow of a dramatic downturn in a market.
Review Question
In developing its corporate strategies, the Haven Health Plan decided to implement a growth strategy that is focused on increasing the percentage of preventive health office visits from its current plan members. To accomplish this objective, Haven will send a direct mail kit to existing plan members to remind them of the variety of preventive health services that Haven currently offers, including physical exams, cholesterol tests, and mammograms. This information illustrates Haven's use of
an intensive growth strategy known as market penetration
an integrated growth strategy known as product development
an integrated growth strategy known as market development
a diversified growth strategy known as market penetration
Correct
Incorrect. Product development is considered an intensive growth strategy. Product development focuses on increasing sales by modifying current products or by developing new products for current markets.
Incorrect. Market development is considered an intensive growth strategy. Market development focuses on increasing sales of current products by introducing them to new markets.
Incorrect. Diversified growth strategies are strategies that require companies to venture outside the industry in which they conduct business to seek growth opportunities in other markets.
Linking Corporate Strategies with Tactical PlanningAs noted earlier in this lesson, strategic planning focuses on a health plan’s long-term corporate goals and the broad, overall courses of action that the company will follow to
Page 372 of 469

AHM 510 : Health Plans : Governance and Regulation
achieve those goals. These longterm goals provide a framework for developing a tactical plan with short-term objectives that are tied to the corporate strategy. This framework helps coordinate the efforts of the health plan’s various functional areas and strategic partners in implementing the organization’s overall strategy. Each functional area within the health plan (and ideally, each strategic partner outside the health plan) develops specific plans based on the health plan’s overall strategic goals and business objectives.
A comprehensive discussion of all functional area plans in a health plan is beyond the scope of this lesson. From a governance perspective, however, an important point to keep in mind is that strategic planning must be integrated and coordinated with tactical planning in the various functional areas. Each functional area determines what its role is in the overall corporate strategic plan and then sets its own objectives, strategies, and tactics accordingly.
It is also important to keep in mind that for the purpose of this discussion, we have classified strategic planning and tactical planning as distinct and separate processes. In reality, however, these planning processes often overlap. For example, marketing is a functional area with activities that are typically a major focus in a health plan’s strategic plan. Because marketing forms a health plan’s primary link to potential customers, the strategic planning process relies heavily upon input from marketing. Without marketing input, the board and senior management would have no way to realistically estimate future revenue, nor would they be able to estimate future workloads in each of the functional areas to help plan for equipment purchases and staffing. Figure 10B-4 illustrates how corporate strategy can be linked to tactical planning.
Figure 10B-4. Linking Corporate Strategy and Tactical Planning.A provider group developing a corporate strategy for building a preferred provider organization will give careful consideration to the overall effort involved, which should be broken down into tasks and subtasks. The major tasks in the corporate strategy might include:
1. Developing the provider network and negotiating provider contracts2. Establishing a sales and marketing organization3. Developing a utilization management and quality assurance capability4. Developing a management information system5. Establishing an organizational infrastructure
Each of these major tasks then would be broken down into individual subtasks (i.e., tactical planning in the appropriate functional areas). The major task of developing a provider network (item 1 above) could be further broken down into subtasks that might include:
1. Analyze provider admission and cost information2. Identify desired providers3. Develop model provider contract4. Negotiate provider contracts5. Establish ongoing provider relations function
Source: Reprinted from Peter Boland, editor, Making Managed Healthcare Work, © 1993, p. 219, with permission from Aspen Publishers, Inc., Gaithersburg, MD (1-800-638-8437).
Page 373 of 469

AHM 510 : Health Plans : Governance and Regulation
Corporate Strategies: Resource Requirements and Project Management ToolsThe implementation of a health plan strategy can be labor intensive and slow to produce results. Therefore, the board and senior management pay close attention to the resources that will be needed in terms of capital investment, areas of expertise, staffing allocations, and management oversight. Strategic planners resist the tendency to underestimate needed resources. They try to anticipate problems and build flexibility into their planning.
Corporate strategies include specific action plans identifying who will do what and when. These strategies include cost and staffing projections for start-up activities as well as ongoing activities. The projections are reviewed and approved by the board of directors and/or senior management to assure that adequate funds and staff are appropriated for successful implementation of the plan. These projections are typically integrated into the annual budgeting process to assure that needed resources are available to the appropriate functional areas. Strategic planners typically use project management tools to plan and monitor progress and to report results to the board of directors and senior management. These tools help coordinate efforts and also identify problems that the original plan may not have anticipated.
Risk Assessment in Corporate StrategiesSenior management, recognizing that there is no such thing as a risk-free strategy, tries to anticipate (1) the likelihood that a strategy will create problems and (2) the consequences of such problems. Sometimes the negative consequences can be quantified. For example, a health plan might determine that failure to successfully develop a new POS product would result in the loss of the startup capital required to launch this project. Other times the risk may be difficult to quantify. For example, a strategy to contract with a new physician group could seriously damage a health plan’s existing relationship with its providers. Once the board and senior management have assessed the risk, they re-examine the strategy and determine whether the potential rewards justify the risk.16
The “Human Element” in Corporate StrategiesAs we have seen, strategic planners often link corporate strategies to tactical planning and allocate the necessary financial and staffing resources to improve the chances for success. However, effective planners also realize that the “human element” is critical to the success of any strategy. Some organizations develop a formal human resource strategy to help determine the number of associates and the types of skills that will be needed to successfully implement the corporate strategy. A human resource strategy might specify ways to retrain existing staff or to hire additional staff from outside the organization. A carefully developed human resource strategy helps ensure that the organization is staffed with associates who have the necessary skills and motivation to support the goals of the strategic plan.17
Successful implementation of a strategic plan not only requires the commitment of key associates such as board members, senior management, and middle management, it also requires an organizational climate in which as many associates as possible understand the reasons behind the strategy and their individual roles in implementing it. One of the keys to obtaining this understanding is effective communication.
The need for effective communication is particularly important when health plans pursue aggressive strategies such as joint ventures, mergers, vertical integration, and targeting
Page 374 of 469

AHM 510 : Health Plans : Governance and Regulation
of new markets. Strategies such as these in an environment that has become increasingly competitive and uncertain can directly impact the jobs and personal lives of many of a health plan’s associates as well as its strategic partners.
For example, a not-for-profit health plan that is seeking access to equity markets by converting to for-profit status will improve its chances for success if it has the cooperation and commitment of the many people who will be involved in or affected by this strategic initiative. Some associates might view the overall strategy as a mistake. Others might understand the business need, but have concerns that their departments will have to reassign associates from critical day-to-day operations to help implement the strategy. Others might view the strategy and the associated changes as a threat to their current jobs, or they might be concerned that their salary and benefit packages will be affected.
Often when a health plan decides to pursue a market-driven strategy, its associates have to make significant changes in the way they approach their jobs. A company, which in the past has been successful with a product-oriented focus, may have difficulty shifting to an organizational culture that focuses on customer needs. Some companies have decided to change from a traditional top-down structure organized in separate functional areas to a matrix management system that relies upon much more communication and cooperation than associates may be accustomed to. Changes such as these are often unsettling to employees. If the board and senior management do not attempt to gauge the impact and plan appropriately, many associates within the organization will not respond well to the new strategy.18
A carefully considered strategic plan recognizes that associates will perform in a more positive and effective manner if they understand the reasons for change and they have an opportunity to provide input and ask questions about their new or changing responsibilities. An effective strategic plan provides for frequent communication in as many ways as possible, such as in newsletters, electronic-mail messages, “town hall meetings,” work group meetings, and individual objective-setting sessions that link each employee’s compensation level and performance review to the strategic plan. These efforts to communicate and encourage participation help build consensus and increase the likelihood of obtaining “buy-in” from the many associates responsible for implementing the corporate strategy on a daily basis.
Page 375 of 469

AHM 510 : Health Plans : Governance and Regulation
Chapter 10 CKey Strategic Issues for Health Plans
After completing this lesson, you should be able to:
Identify and describe the key strategic issues faced by health plans Give examples of how key strategic issues are interrelated in the strategic planning
process
As we have seen, an effective board of directors and senior management team (1) define the organization’s mission, (2) assess the external environment and the organization’s own capabilities and limitations, (3) establish corporate objectives, and (4) develop strategies to meet the objectives. Although the strategic planning process for each health plan is based on a unique blend of corporate mission and objectives, internal capabilities, and external environmental factors, there are several key issues that most health plans consider when developing a strategic plan. These key strategic issues are:
• Markets and product portfolio
• Pricing
• Financial management
• Provider networks
• Medical management
• Customer services
• Information technology
• Corporate transactions
In this lesson, we provide a brief overview of each of these issues. As we do so, keep in mind that the overall objective of the strategic planning process is to assemble these separate but interrelated issues into a cohesive and effective corporate strategy. When the board and senior management consider one key issue, they often must consider other related issues. For instance, a health plan’s market strategy can be significantly influenced by its capabilities to perform certain types of functions such as medical management and member services. Also, in the “information age” there are few operational issues that are not in some way impacted by information technology. For example, a health plan’s ability to provide effective member services is closely related to the effectiveness of its supporting systems. Finally, although we have not listed legislative and regulatory activities as a separate strategic area, the regulatory issues associated with markets and products, pricing, provider networks, medical management, customer services, information technology, financial management, and organizational structure require careful attention because they can have a significant impact on a health plan’s strategic plan.
Markets and Product PortfolioAn effective strategic plan includes an assessment and selection of target markets. Health plans can target any one or a combination of the following markets: non-government groups, government employee groups, government- sponsored programs,
Page 376 of 469

AHM 510 : Health Plans : Governance and Regulation
and individual purchasers. Within each of these larger markets are market segments. For instance, a health plan that is considering nongovernment groups can target singleemployer groups, multiple-employer associations, or certain sized groups, such as large, midsize, or small employers. A health plan that is considering government employee groups might target municipal entities, state employee plans, FEHBP, or TRICARE. When considering government-sponsored programs, a health plan might target workers’ compensation plans, Medicaid, or Medicare.
To effectively determine market strategies in the planning process, a health plan looks at both the external and internal environment. The board and senior management team consider external issues such as the needs and buying behavior of the purchasers, medical needs that may be unique to a particular population, the amount and nature of the competition in the market, and any state and federal regulatory requirements. For example, many large employers expect a health plan to duplicate product features that they had under a prior plan. Also, large employers often expect customized contracts, benefit description material, and year-end reports. Small employers, on the other hand, typically purchase healthcare based on price, and do not expect customized products and services. When considering target markets, a health plan must determine what the market expects and then realistically assess the organization’s abilities to deliver on those expectations. If a health plan does not have the personnel or information systems needed to provide the customized products and services that large employers demand, then its strategic plan would likely focus on the small and midsize employer markets.
As this example demonstrates, the strategic issues involved in a health plan’s choice of markets can touch upon several other key areas such as customer services, pricing, and information systems.
Closely related to a health plan’s assessment of its markets is an assessment of its product portfolio. A product portfolio (also called lines of business or health plan products) is the number and variety of product designs or plans that the health plan makes available to its customers. The only constraints on a health plan’s product portfolio are regulatory requirements and the organization’s ability to effectively deliver and administer the products to its customers. Some of the issues health plans address in developing their product portfolios are the:
• Number and types of healthcare services and supplies that will be covered
• Benefits or cost-sharing features, such as deductibles, copayments, coinsurance, limitations, and maximums
• Protocols for delivery of healthcare services and supplies (for example, which healthcare services and supplies require preauthorization)
• Out-of-network coverage, if any, including the number and types of healthcare services and supplies that will be covered and the applicable benefits or cost-sharing features
• Breadth of the product portfolio (the number of “plans” that will be standardly offered to the health plan’s customers, based on variations of the above features)
• Willingness to customize products at the request of specific customers
Page 377 of 469
AHM 510 : Health Plans : Governance and Regulation
Some health plans develop products that are based on the networks or delivery systems available within a particular geographic area. For example, a health plan might offer two types of HMO products: one that delivers healthcare services via a network that consists solely of group model practices and another that delivers healthcare services via a network of both group model practices and individual practices.
To effectively address product issues in its strategic plan, a health plan looks at the external environment by conducting market research and considering the strengths and weaknesses of its competitors. The objective of this external assessment is to develop a strategy that meets the customers’ needs and differentiates the company from the competition. Because the results of this assessment can vary, depending upon the location, a health plan that operates in multiple locations may develop different products or product features in different markets. In addition to this external assessment, a health plan evaluates its internal strengths and weaknesses to determine the number and variety of products it is capable of delivering effectively and at a competitive price.
For example, as a result of its environmental assessment a health plan might conclude that purchasers and members consider “easy access to specialty providers” to be a valuable plan feature. The health plan would then determine the number of competitors that offer this type of plan and the actions it must take to be capable of providing a competitively priced product that offers open access to specialists. This decision might be based in large part on the organization’s relationship with and confidence in its network specialists as well as its ability to monitor the frequency and cost of specialty care. Using this internal and external assessment, the health plan can then determine whether to include an open access plan in its product portfolio.
A health plan’s structure and the applicable regulatory requirements can also affect the organization’s product strategy. State or federal regulations can require certain types of health plans to offer certain healthcare services or benefits, sometimes subject to specified rating requirements. As we saw in Federal Regulation of health plans, federally qualified HMOs are subject to benefit requirements that do not apply to other types of health plans. Another example that illustrates this point is the variation in plan design between POS and PPO products. These products are similar in that they each provide in-network and out-of-network benefits. However, the product design varies depending on the regulations that apply to the offering health plan. For instance, the in-network benefits provided by an HMO’s POS product are subject to the requirements of that state’s HMO act. However, in the same state, the in-network benefits provided by a PPO organization are subject to the requirements of that state’s insurance code. Differences in benefit and rating mandates in the state’s HMO act and the insurance code could result in a difference in premiums, covered services, and benefit levels—all of which could result in a product that would be more or less likely to generate business. Yet the product concept—in-network and out-of-network benefits—is the same for both the HMO and the PPO.
Similarly, a traditional HMO product and an EPO product both require members to obtain in-network services, for the most part, but the benefit mandates that apply to the HMO are typically found in the state’s HMO act, whereas the benefit mandates that apply to the EPO are often found in the state’s insurance code. Entities that offer an EPO product are sometimes preferred provider organizations that are competing with HMOs. These PPOs develop a strategy to offer both the EPO product and a PPO product. In this way,
Page 378 of 469

AHM 510 : Health Plans : Governance and Regulation
a PPO organization can offer two health plan products, one of which is a less expensive “network only” product (the EPO) that competes directly with similar HMO products in the marketplace.
PricingBasically, when a health plan considers a pricing strategy it tries to determine the market’s perception of value. In other words, how much are customers willing to pay for the health plan’s products and services? Included in this assessment is a determination of competitive pricing pressures. Once this marketplace evaluation is complete, the health plan performs an internal assessment to determine the cost of providing these products and services.
Health plans typically divide their costs into medical and administrative expenses. Medical expenses are payments to providers for the delivery of healthcare. Administrative expenses are all other costs associated with providing healthcare coverage, such as office leases, equipment costs, sales and marketing costs, and salaries and benefits for executives and for all functional areas.
Review Question
Health plans typically divide their costs into medical and administrative expenses. Examples of medical expenses are.
equipment costs
salaries and benefits for executives and for all functional areas
sales and marketing costs
payments to providers for the delivery of healthcare
Incorrect. Equipment costs would be an example of administrative costs
Incorrect. Salaries and benefits would be an example of administrative costs
Incorrect. Sales and marketing costs would be an example of administrative costs
Correct! Medical expenses are payments to providers for the delivery of healthcare.
Once a health plan knows how much the market is willing to pay and how much the organization must spend to provide the proposed products and services, it has the necessary information to establish a pricing strategy. Often, health plans base premiums on the estimated cost of providing the product and services, plus a targeted profit margin (or, in the case of a not-for-profit health plan, the excess of income over expenses). Figure 10C-1 examines two other types of pricing strategies that are used by health plans: buying market share and market skimming.
Page 379 of 469

AHM 510 : Health Plans : Governance and Regulation
Pricing is not always controlled by the health plan. For example, the health plan does not determine the rates for Medicare and Medicaid products. However, for these products, a key strategic issue for the health plan is to determine whether it can provide the products and services at the established price.
Figure 10C-1. Pricing Strategies.Buying Market Share
Many health plans have used a strategy of buying market share, also called penetration pricing, by setting a low price in a highly price-sensitive market to stimulate revenue growth. The objective of this strategy is to sacrifice near-term profits for fast growth as a means of quickly building critical mass and establishing a market position. This is a relatively high-risk strategy, and careful consideration must be given to determining capital requirements and ensuring that capital is available to sustain the organization organization through this high-growth, low-profit stage. However, caution must be exercised to avoid a price war in which the competition simply matches the low price and thus lowers the price level of the entire industry at the expense of industry profits.
Market Skimming
Another pricing strategy frequently used is market skimming, also called price skimming. Under this strategy, the highest price possible is established given the comparative benefits of the product versus those of the competition. Even at this relatively high price, certain segments of the market will still buy the product. Each time sales slow down, the price is lowered to draw in the next price-sensitive layer of customers. This strategy results in slower growth. The significant risk inherent in this type of strategy is the limited market available to the product. Clearly, the product must be substantially differentiated from that of lower-priced competitors to justify its higher price in the eyes of the consumer.
Source: Reprinted from Peter Boland, editor, Making Managed Healthcare Work, © 1993, pp. 225–226, with permission from Aspen Publishers, Inc., Gaithersburg, MD (1-800-638-8437).
Review Question
The Westchester Health Plan is using a pricing strategy that involves setting a low price in a highly price-sensitive market to stimulate revenue growth. In following this strategy, Westchester is sacrificing short-term profits for fast growth in selected markets. This information indicates that Westchester is following the pricing strategy known as
market skimming
buying market share
price skimming
Page 380 of 469

AHM 510 : Health Plans : Governance and Regulation
unitary pricing
Incorrect. Under this strategy, the highest price possible is established given the comparative benefits of the product versus those of the competition.
Correct. Buying market share is a strategy where health plans set a low price in a highly price-sensitive market to stimulate revenue growth.
Incorrect. Under price skimming, also called market skimming, the highest price possible is established given the comparative benefits of the product versus those of the competition
Incorrect. One of the responses above is the correct choice.
Financial ManagementA strategic plan that recognizes the importance of timely and accurate financial data can significantly improve a health plan’s chances for success. Basically, when a health plan considers financial management issues, its goal is to obtain information to determine past and current expenses and revenues, to project future expenses and revenues, and to effectively evaluate and utilize this information in developing its overall strategy.
If financial management systems are unable to detect (or do not detect quickly enough) that revenues are outpacing expenses, a health plan might miss an opportunity to pursue a key strategic initiative. For instance, on the mistaken notion that they do not have access to needed capital, the board and senior management might decide to delay pursuing a market expansion initiative or delay developing a new product that might have provided a competitive advantage. Conversely, if a health plan’s financial management systems are unable to detect (or do not detect quickly enough) that the health plan has been operating at a loss, the board and senior management might overextend the organization by pursuing a strategy they otherwise might not have considered. For example, on the mistaken notion that they have access to needed capital, a health plan might decide to invest in a new technology without adequate funds to support such an investment.
Further, if a health plan fails to develop effective financial management systems, it can waste critical time needed to redirect its strategies to reduce exposure to loss or to support growth. For example, suppose a health plan begins losing money on a particular market segment (such as large self-funded plans) or a particular product line (such as managed dental).
If this information is not made available in a timely manner, the health plan’s board and senior management team might not be able to make the necessary adjustments to turn things around or to prevent additional losses that otherwise might have been prevented. Alternatively, if a health plan is experiencing a period of rapid growth, but its financial management systems cannot effectively evaluate the impact of the projected growth on the organization’s capital requirements, the health plan will be unable to support the infrastructure it will need to maintain its customers.
Page 381 of 469

AHM 510 : Health Plans : Governance and Regulation
Effective financial management strategies rely heavily upon information captured and monitored by the various functional areas within the health plan, particularly areas such as medical management, claims, and provider contracting.1 It is important for the medical management and claims areas to effectively communicate to the financial management/ accounting area the actual and estimated medical costs based on claims paid, claims reported but not paid, and claims incurred but not reported.2 It is also important for the financial management/accounting area to be aware of potential expenses resulting from provider reimbursement arrangements such as physician and hospital withholds.3
A key component of effective financial management is the ability of a health plan to analyze financial requirements/results for each of its market segments and product lines. This information enables a health plan to determine specific strategic initiatives. For instance, based in part on information obtained through its financial management systems, a health plan might decide to withdraw from a particular market or it might decide to redirect resources to bolster a particular market or product that has excellent long-term prospects.
Provider NetworksWhen a health plan’s strategic planners prepare to address provider networks, they consider the geographic coverage of the network and the number and types of providers to be included. In most cases, their objective is to obtain a full continuum of healthcare services, from acute care hospitals and physicians to outpatient care to various specialties such as rehabilitation services, home healthcare, mental health and chemical dependency services, and vision care. They often decide on first choices and back-up choices for each type of provider or service.4
Recognizing the importance of providers, many health plans make a concerted effort to recruit and retain quality providers who will reflect favorably on the health plan in both the way that they deliver healthcare and their attitude toward the plan. Many health plans approach provider recruitment as they would an important customer. For example, they market their health plan to providers by stressing that when providers become part of their organization they realize an increase in patient volume and prompt provider reimbursements.
To strengthen ties with providers, health plans might pursue strategies that involve increased sharing of data with providers or seeking ways to help providers improve the quality and effectiveness of their practice. Some health plans involve providers in the strategic planning process as they would an important strategic partner. At a minimum, they communicate promptly and effectively to keep providers apprised of important governance decisions.
Medical ManagementAn effective strategic plan also establishes objectives and strategies for medical management that monitor and address the utilization and quality of healthcare services. These strategies recognize the need for clinical quality measures and performance improvement, as well as the need for quality medical personnel to oversee the medical management programs and processes. These strategies also incorporate the use of state-of-the-art information systems to facilitate processes such as authorizations, large case management, and discharge planning. In addition, these strategies recognize the need to respond quickly and effectively to the rapidly changing healthcare environment.
Page 382 of 469

AHM 510 : Health Plans : Governance and Regulation
A health plan must develop the capability to address a complex array of medical issues, such as treatment of new diseases and the appropriate use of newly developed prescription drugs, medical technologies, and medical procedures.
Some health plans do not have the resources to develop the medical or systems expertise and equipment needed for an effective medical management program. Other health plans have the resources but decide to outsource this function. In both instances, these health plans develop a strategy to provide medical management services by contracting with a third party vendor. As the health plan business becomes increasingly complex and competitive, more health plans include outsourcing in their strategies, and more vendors emerge to provide services such as claims payment, systems support, and medical management. Many third party utilization and quality management organizations offer experienced personnel, tested medical protocols, and large databases of information that enable them to perform this critical function more effectively and at a lower cost than it can be performed within some health plans.5
Customer ServicesBecause most healthcare is provided through group plans, marketing and sales strategies initially focus on group purchasers and the brokers and consultants that support group purchasers. However, many employers provide their employees with more than one healthcare option, and in this situation health plans must make a “second sale” to the employees at enrollment meetings and through the services provided to members throughout the year. Even in the case of a health plan that is the sole healthcare plan for an employer, health plans seek to keep member trust and satisfaction high as part of their strategy to conserve business. Many group purchasers solicit input from their employees about their health plans. If member satisfaction is low, the health plan could lose the business.
One way that health plans seek to retain members is by ensuring timely and efficient service through their member services functions. An effective strategic plan considers the staffing, training, and equipment necessary to ensure that phone calls will be answered promptly, hold times will be kept to a minimum, and concerns will be resolved to the members’ satisfaction. In addition, health plans seek to maintain the trust of their members through a complaint and appeals process that handles member grievances in a timely and impartial manner.
Information TechnologyMost health plans have developed unique information systems within their organizations; like most other businesses, health plans have become increasingly dependent on information technology. In a worst-case scenario, a strategic plan that does not adequately consider information technology can result in catastrophic operational problems. In a best-case scenario, a strategic plan that takes full advantage of advances in information technology can deliver world-class service in all aspects of its operations. For example, with the right information systems the member services function can quickly access the specific plan information needed to provide telephone support to members. Member enrollments and claims, provider reimbursements, and purchaser billing can all be handled more quickly and accurately.
Effective use of information technology can also extend outside the organization through information sharing with strategic partners. For example, medical outcomes can be
Page 383 of 469

AHM 510 : Health Plans : Governance and Regulation
tracked and applied by medical management and providers to improve the quality of healthcare. In addition, a health plan with effective information systems can produce the types of reports that purchasing groups, particularly large employers and government purchasers, often require as a condition for doing business with a health plan.
Corporate TransactionsMany health plans use corporate transactions such as strategic partnerships, joint ventures, mergers or acquisitions to achieve the strategic objectives related to the issues we have examined in this lesson.
For example, a health plan that is considering adding an open access HMO plan to its product portfolio has several options. The health plan can develop the product internally, utilizing its existing resources, or it can look outside the organization, perhaps forming a strategic partnership with a provider network or perhaps merging with a health plan that already has an open access product in its portfolio.
A health plan that has a strategic goal to enter new markets might consider an alliance as a means of attaining that goal, particularly when the new markets differ significantly from the organization’s existing markets in areas such as buying behavior, medical needs, administrative demands, and regulatory requirements.
For example, consider a commercial health plan that plans to enter the Medicare market within a specified period of time. Based on a situation analysis, the strategic planners conclude that:
• Existing provider networks and medical management functions are not in a position to handle the unique needs of a large elderly population
• Existing member services staff would require considerable training to be able to effectively handle the types of issues and questions typical of a Medicare population
• The compliance area does not have enough familiarity with Medicare filing procedures to obtain the required regulatory approvals within the proposed timeframe
Before abandoning a promising strategic option, however, this health plan might consider whether it can proceed by way of a strategic partnership, joint venture, merger, or acquisition. If the health plan merges with or acquires a health plan that is already established in the Medicare market, not only does it gain the expertise it previously lacked, but also it immediately acquires a Medicare book of business.
As this example illustrates, the right alliance can result in “instant expertise” and “instant market share” for a health plan that is considering a new market, whether that market is Medicare, Medicaid, workers’ compensation, small employer groups, or large employer groups with locations in several different states or regions of the country.
The right alliance can also increase an health plan’s ability to address a number of other key strategic issues we have examined in this lesson. For example, a health plan that wants to become more competitive in a price-sensitive market might determine that a
Page 384 of 469

AHM 510 : Health Plans : Governance and Regulation
merger or acquisition could produce economies of scale that would better enable it to meet this strategic objective. A health plan that determines the need to offer a wider choice in terms of the number or types of providers in its network could pursue a strategic partnership with a health plan or provider group that provides a good match. A health plan seeking to improve its medical management or member services functions might consider an alliance with a health plan that has demonstrated strengths in these areas.
As we mentioned at the beginning of this lesson, each health plan addresses a unique combination of key strategic issues depending on the organization’s mission, objectives, external environment, and internal capabilities. However, there are several issues that are common to the strategic plans of most health plans.
Page 385 of 469

AHM 510 : Health Plans : Governance and Regulation
Chapter 11 A Governance: Accountability and Leadership
After completing this lesson, you should be able to:
Discuss accountability among the stakeholders in health plans Explain several implications of accountability on health plan leadership and
governance Describe the essential elements of an effective health plan compliance plan Define medical necessity and describe how health plans address related governance
issues Describe quality and ethics programs and ombudsman programs
Accountability in Health PlansA primary driver of leadership and decision- making in health plans today is the demand for accountability. Indeed, the demand for accountability “has become one of the mantras of the 1990s in health care.”1 Accountability is the process by which one party is required to justify its actions and policies to another party.2 Healthcare analysts sometimes describe accountability as a “motivational state” to emphasize the expectation that accountability will motivate behavior to ensure certain minimal standards of quality.
To examine accountability in the world of health plans, we begin by considering these questions:
• Who is accountable?
• To whom are they accountable?
• What behaviors are being examined?
• What standards of performance apply?
Who Is Accountable and to Whom Are They Accountable?We address these questions together because we can answer both with the same set of parties or stakeholders. In the context of health plans, stakeholders are any individuals or institutions with whom an health plan interacts. Many of these stakeholders can be held accountable and can hold others accountable. The accountable stakeholders in health plans include3:
• Health plans
• Hospitals and other institutional providers such as skilled nursing facilities
• Physicians and nonphysician healthcare providers
• Professional medical associations
• Purchasers
• Private investors in for-profit health plans
• Individual members
Page 386 of 469

AHM 510 : Health Plans : Governance and Regulation
• Lawyers and courts
• The government
What Behaviors Are Being Examined and What Standards of Performance Apply?Each accountable stakeholder has accountability in one or more of the following areas:
• Professional competence (how well the stakeholder does the job)
• Legal and ethical conduct (the stakeholder’s adherence to legal and ethical standards)
• Financial performance (obtaining a return for investors)
• Equity of access (giving equal opportunity to obtain healthcare)
• Public health promotion (making a contribution to prevention of illness and accidents)
• Community benefit (being a good “corporate citizen” and, in the case of certain not-for-profit health plans, adhering to a charitable or community benefit mission)4
Within each of these areas of accountability are a number of sets of behavioral or quality standards against which performance is measured. Within a particular area for a particular stakeholder, there may be multiple sets of behavioral standards for accountability, each tied to a different stakeholder. For example, in the area of professional competence for health plans, there is one set of performance standards established by the courts (see Key Legal Issues in Health Plans), another established by employers (directly through their agents or through the accreditation organizations), and yet another established by the government (in the form of state and federal regulatory oversight of health plan quality).
Creating Balanced Accountability SystemsThe challenge for health plans is to meet the need for organizational control in a way that fosters, rather than erodes, personal responsibility. Traditional notions of accountability tend to emphasize external control. Under this view, as long as the standards are high and individuals are held accountable to their superiors for meeting—or failing to meet—those standards, people will be motivated to perform. The problem with this approach is that people who work in an organization they perceive as unsupportive or for leaders they perceive as unfair tend to shrink their self-definition of the job and are less likely to engage in helpful behaviors outside their perceived job descriptions. 5 The results are similar when work is too structured or too formal.6 Figure 11A-1 provides a few examples to illustrate this point.
Leaders of a health plan need to balance the way they structure expectations for employees and other stakeholders: too much or too little structure will reduce individuals’ levels of perceived responsibility, while balanced structure will increase those levels. They need to increase employees’ sense of control over their ability to meet expectations, their resources, and their choice of methods of task production. Finally, the health plan’s leaders need to structure stakeholders’ activities so that stakeholders see the importance of what they are doing.7
Figure 11A- The Need For Organizational Control that Fosters Personal
Page 387 of 469

AHM 510 : Health Plans : Governance and Regulation
1. Responsibility.
As the following examples illustrate, health plans need their employees and others who work for the health plan to define their jobs broadly and operate flexibly across departments, functions, and roles.
An employee of a health plan’s marketing department defines the job so narrowly (“Sell, sell, sell!”) as to ignore the need to run a change in benefit design by the legal department to obtain regulatory approval (“Compliance is the legal department’s job, not mine!”). This practice could result in fines or even a cease-and-desist order from the state insurance department.
A lawyer charged with assuring that customer service representatives give the proper description of how the health plan is complying with a newly enacted benefit mandate simply photocopies the law and sends it to the director of the customer service department (“It’s their job to train their staff, not mine!”). This approach could result in noncompliance and possible fines or a cease-and-desist order. A physician in a health plan’s network views the responsibilities of a participating provider as being limited to treating patients, not responding to the health plan’s practice patterns survey or providing requested encounter data. This behavior impairs the health plan’s quality improvement efforts and perhaps its legal reporting requirements.
Models of AccountabilityOutside the world of healthcare, organizations typically establish accountability through selection, training, job design, goal setting, performance development/appraisal, and corporate climate. However, these challenges are made more complex within the healthcare environment because accountability has typically been defined by the professional model of accountability. The professional model of accountability, designed for individuals and focused on the relationship between a physician and a patient, relies extensively on personal relationships and trust. This paradigm does not work well with large institutions,8 yet most participants in the healthcare system have been raised on that professional model. These providers often perceive the network of external controls imposed by health plans, government regulators, private accreditation organizations, hospital or physician practice risk management policies, and payment and reimbursement decisions as interfering with professional accountability and eroding the clinical and ethical quality of care.9
As an alternative to the professional model of accountability, health plans and other participants in health plans are turning to the economic model of accountability and the political model of accountability. The economic model of accountability suggests that the delivery of healthcare should be more like a business—patients are just specialized consumers, shopping for some optimal combination of price and quality. Under this model, the primary mechanisms for accountability are the mechanisms of the marketplace; failure to meet standards will result in a loss of demand for services.10 In other words, patients are “cost-conscious buyers shop[ping] for the lowest price,” and the health plans are “the provider community… divided into competing economic units.”11
Page 388 of 469
AHM 510 : Health Plans : Governance and Regulation
Review Question
In examining accountability in the current managed care environment, one is likely to find that combinations of various models of accountability are in operation. Under one model of accountability, the primary mechanisms for accountability are the mechanisms of the marketplace-failure to meet standards will result in a loss of demand for services. By definition, this model of accountability is called the
professional model of accountability
political model of accountability
due diligence model of accountability
economic model of accountability
Incorrect. The professional model of accountability, designed for individuals and focused on the relationship between a physician and a patient, relies extensively on personal relationships and trust.
Incorrect. The political model of accountability is achieved, not through exit, as is the case in the economic model, but through voice.
Incorrect. There are only three models of accountability, professional, political and economic
Correct. The economic model of accountability suggests that the delivery of healthcare should be more like a business.
The political model of accountability, on the other hand, sees the health plan as less of a business and more a community of stakeholders. In this view, accountability is achieved, not through exit, as is the case in the economic model, but through voice. In other words, instead of withdrawing business from a stakeholder who does not meet the standards (exit), the other participants can complain, protest, and offer an alternative (voice). Note that political does not necessarily mean governmental—under this model, stakeholders can express themselves through a variety of mechanisms, only one of which is governmental. Community boards, physician committees, and citizen advisory groups are other mechanisms for the expression of this voice and the exercise of organizational control.12
All three of these models of accountability are in operation in the current healthcare environment; various stakeholders, whether organizations or individuals, have some level of influence over the models and systems of accountability under which they operate. For example, health plans can choose a primarily economic model of governance through a shareholder-dominant board of directors or they can elect a political model of governance through member and provider participation on the board of directors and advisory committees.13
Page 389 of 469

AHM 510 : Health Plans : Governance and Regulation
It is unlikely, however, that an entire health insurance plan system —including all its stakeholders —can operate under a single model of accountability. The advantages and disadvantages of each of the models vary from one set of accountability relationships to the next. Most healthcare systems feature some combination of two or even all three of these models of accountability. However, some health plans, recognizing for the first time that they have choices about models of accountability, are modifying their structures of organizational control to optimize the strengths of each model in particular settings. For example, it may be in a hospital-based health plan that quality improvement efforts are better served by the inclusion of physicians in governance than by the inclusion of senior management in that governance, as is suggested in a recent study.14
On the other hand, it seems likely that the economic model of accountability will continue to be the optimal model in the relationship between investors and health plans. In other words, by recognizing that they have choices regarding models and structures of accountability, and by developing rational methods of assessing the appropriateness of particular models for particular relationships, health plans and other participants are moving toward a more informed selection among organizational control systems.
Leadership in Health PlansLeaders of organizations have a special function. Some analysts maintain that “executive work is not that of the organization, but the specialized work of maintaining the organization in operation.”15 As one healthcare CEO recently put it, “My job is to create a milieu in which other people can function. I do very little when you get right down to it. But I create an environment that’s conducive to people doing their thing.”16
This view of executive leadership, however, paints only a part of the picture, that of the internal management of the company. Some analysts view organizations as open systems whose fates are intertwined with their environments; these analysts focus on the boundary-spanning functions of leaders.17 Boundary-spanning requires an individual to relate an organization or department to its environment.18 Boundary-spanning leadership functions include such roles as “scout,” “ambassador,” “sentry,” and “guard.” One cannot overstate the importance of these functions. There is growing support that the external leadership functions are more closely related to organizational success than the internal administrative functions.19 The extent to which any of these functions is necessary for leadership of a particular organization depends largely on the nature of the environment in which the organization operates.20
Most modern models now assume both the internal and boundary-spanning functions of leadership.21 This dual-orientation view applies to leaders at all levels organization. The nature of their functions, however, may vary depending on their within the organization.22
All leaders, regardless of organizational level, engage in direction setting ( setting, planning, envisioning) and boundary spanning. The qualitative nature direction setting does not vary substantially with organizational level. Further, nature of boundary-spanning activities differ from one level to the next, remain an essential component of leadership. For example, while a director of information services department need to span the health plan’s boundary great frequency, this individual much involved in negotiating the environment in which the department is embedded, spanning the boundary of the department to negotiate for resources and accountability relationships. The the other hand, is more likely to engage activities that relate to the management the health plan’s boundary, such as negotiations with business partners, regulators, external
Page 390 of 469

AHM 510 : Health Plans : Governance and Regulation
stakeholders. This boundary-spanning function may even extend to managing the boundary of the industry as Public advocacy on behalf of the care industry, which we discuss in Public Policy and Changing Environment, is the responsibility of in many organizations.
In addition, all leaders, regardless of level, are responsible for “operational maintenance and coordination within the organization.” 23 Where there is accountability, there is a leader charged with designing or maintaining the organizational control structures by which that line of accountability is managed.
What kinds of skills, then, are important for a health plan executive? In short, leaders must have a high ability to process and respond to environmental complexity. As S. J. Zaccaro explains in Models and Theories of Executive Leadership,
[the] operating environment for organizational leaders becomes increasingly complex at higher levels. . . . The different internal and external stakeholders to whom the executive is beholden, as well as the range of dynamic environmental forces and influences (e.g., economic, political, legal, technological...) acting on the organization, virtually guarantee that top organizational executives will have to generate, attend to, and choose from multiple solution paths. Further, the diversity within and between constituencies and the fluid character of most organizational environments create multiple outcome possibilities, conflicting or interconnected solution paths, and ambiguous associations between defined solution paths and organizational outcomes. These characteristics of executive work result in higher information-processing demands and hence greater complexity.24
The environmental factors that increase the need for these skills are very much present in the health plan industry. The first of these factors is environmental munificence. Environmental munificence is the degree of richness or scarcity of resources in the environment; it is important because executive mistakes are less critical in a resourceabundant environment than in a resourcescarce environment.25 In the past, health plans operated in an abundant environment where the primary competitors were traditional, fee-for-service indemnity carriers, but this is no longer the case in most regions of the country. Mistakes in a highly competitive environment can be catastrophic, as profit margins shrink or, in some cases, are replaced by losses.
A second environmental factor weighing heavily on health plan leaders is environmental complexity. Environmental complexity is the degree of complexity in an organization’s internal and external environment in terms of stakeholders, markets, and geography. Few modern economic environments are as complex as the health plan industry today. Similarly, environmental dynamism, or the rate of change in an industry, can place great demands on an organization’s leaders in terms of the need for effective strategic planning. Dynamism in the managed care environment is pervasive—the entire landscape of health plans, including competition, regulation, purchasing, the provider sector, and consumer involvement, is in a constant state of flux. For example, many entities that are part of the healthcare delivery system today are downsizing or “right-sizing.” Flexibility is becoming the watchword in the structure of entities, whether they are health plans or companies that provide services under a broader healthcare system.
Page 391 of 469

AHM 510 : Health Plans : Governance and Regulation
Some nearly inevitable consequences of downsizing are that employees operate with reduced managerial supervision and less specific job descriptions. In addition, employees are expected to exhibit greater flexibility in the face of unpredictable demands on their time and skills. This environment expands the need for approaches to accountability that promote diverse and creative responses, rather than “by the book” solutions.26
This consequence of downsizing—the increased need for flexibility and broad skill sets—argues for the expanded use by health plan leaders of cross-training and interdisciplinary teams in the performance of essential health plan functions. Increasingly, health plans are creating teams that span closely related departments, such as customer service, utilization review, and claims processing. Not only do these highly interdependent teams possess an expanded ability to address multidimensional issues raised by members, but the individual members of the teams see a broader set of solutions they can apply to particular member issues. Over time, cross-functional learning occurs, providing the health plan with employees who are more capable and willing to take flexible approaches to organizational problem solving.
Another leadership challenge posed by the rise in downsizing in the health plan industry is the need for the senior executive to respond to the inevitable shock and grief that follows downsizing, even among the “survivors” of the layoffs. The complex organizational and interpersonal needs of an organization that has been through the shock of a downsizing process expand the requisite skills of health plan executives to include emotional leadership skills, introspection, and an enhanced ability to learn.27
Systems of Organizational ControlBecause health plans function within a complex web of accountabilities to a wide array of stakeholders, their leaders must rely upon systems of organizational control. Such systems allow health plans to:
• Maximize individual initiative and creativity yet create a climate for cooperation toward common goals28
• Ensure that all participants in the organization follow a coordinated agenda in the face of the various pulls and pushes stemming from the disparate and often conflicting goals of multiple stakeholders29
• Enhance predictability so that the organization can meet its social, legal, and fiduciary responsibilities and requirements30
In this lesson, we examine a few of the more prominent health plan control systems: compliance programs, utilization review and quality oversight programs, ethics programs, and ombudsman programs.
Compliance ProgramsAs we have seen, health plan structures are quite complex and the industry must comply with a large number of complicated state and federal laws and regulations. Not surprisingly, compliance presents a substantial management challenge. Therefore, many health plans today have established compliance programs to prevent, detect, and address conduct by the health plan and its agents that violates legal requirements.
Page 392 of 469

AHM 510 : Health Plans : Governance and Regulation
The Office of Inspector General’s (OIG’s) Compliance Program Guidance for Hospitals defines a corporate compliance program as, “Effective internal controls that promote adherence to applicable federal and state law, and the program requirements of federal, state and private health plans.”31 An effective compliance program uses employee education, training, and oversight to ensure compliance with laws and regulations applicable to the ongoing operation of an organization. A compliance program can be all-encompassing—covering all lines of business in which an organization is involved—or it can be limited in scope to one or more specific lines of business.
Why Implement a Corporate Compliance Program?A compliance program is not just good corporate practice, it is a necessity. Healthcare misconduct is clearly the focus of increased attention by the government and the media. In the 1980s, the federal government began to intensify its efforts to address criminal activity and misconduct in the delivery of healthcare. This trend has continued to the present with a daunting assortment of federal and state agencies engaged in the investigation and prosecution of healthcare wrongs.
Obviously, it is better to prevent adverse events than to have to respond to them. Although the OIG is expected to eventually publish compliance guidelines for health plans, there are no such guidelines at the time of this writing, and there are few laws that explicitly require that a company establish a compliance program. However, in the absence of clear guidance outside the realm of fraud, prosecutors and practitioners alike turn to the 1991 Federal Sentencing Guidelines for Organizations (“Guidelines”) and comparable state laws for direction.
The Guidelines can be a valuable tool for establishing and maintaining an effective compliance program. Also, federal prosecutors now routinely insist that a company seeking to settle a fraud case set up a corporate compliance program modeled on the Guidelines. Further, entities that have a compliance plan can sometimes lessen potential penalities by voluntarily reporting a criminal offense to the government.
The Guidelines, which became effective November 1, 1991, furnish a strong incentive for companies to develop compliance plans. By establishing a compliance program that incorporates the features required by the Guidelines, an organization diminishes the potential for criminal activity by its employees and agents. It also reduces the potential criminal and civil consequences of criminal conviction should an employee commit a crime despite the compliance program.
The Guidelines, which became effective November 1, 1991, furnish a strong incentive for companies to develop compliance plans. By establishing a compliance program that incorporates the features required by the Guidelines, an organization diminishes the potential for criminal activity by its employees and agents. It also reduces the potential criminal and civil consequences of criminal conviction should an employee commit a crime despite the compliance program.
The Guidelines govern the sentencing of all organizations, including corporations, partnerships, joint-stock companies, union, trusts, pension funds, unincorporated organizations, and nonprofit organizations. They impose severe economic sanctions on organizations convicted in federal courts of criminal offenses. Several mitigating factors can temper the severity of the sanctions imposed by the Guidelines. The most significant
Page 393 of 469

AHM 510 : Health Plans : Governance and Regulation
mitigating factor is the maintenance of a corporate compliance program. The Guidelines describe the essential features that a compliance program must include to be considered “effective” and thereby qualify as a mitigating factor during sentencing.
Criminal and civil liability may attach to the directors and officers of the company as well as the corporation itself. An officer “may be convicted for the criminal acts of lower level company employees simply because of the officer’s responsible relation to the situation and failure to correct or prevent the criminal violations.”32 Certainly, under this theory an officer or director would be more vulnerable in the event he or she did little or nothing to prevent the employee misdeeds by way of establishing an effective corporate compliance program. Still further, one easily could argue that shareholders’ civil actions against directors and officers that failed to take reasonable steps to prevent employee misconduct would be seriously considered by the courts.33
It is important to note that it will not be enough for a corporation to plead in its defense that it did not sanction the illegal activities of its employees. There is no requirement in the law that there be a finding of corporate willfulness or fault. Rather, the law-breaking employee’s intent will be attributed to the corporation, as long as it involves conduct that is within the ordinary duties of employment and will inure to the benefit of the organization.34
Obviously, an organization would prefer to discover an internal problem before regulators and prosecutors do. Besides mitigating any penalties ultimately imposed, such discovery could avoid a costly investigation. In addition, self-policing through use of a compliance plan can avert the possibility of a lawsuit being filed against the health plan under the False Claims Act. Under the False Claims Act, introduced in Fraud and Abuse any person having knowledge of a false or fraudulent claim, or the use of a false record or statement to obtain government payment or approval, may bring a “qui tam” action (as described in Regulatory Agencies and Health Plans) in federal district court on behalf of himself and the government.35 If the government proceeds with the action, or if the individual elects to continue it, the person is entitled to share in a portion of the proceeds or settlement of the action. The “whistleblower” is entitled to costs, expenses, and attorney fees.
Virtually anyone can file a qui tam suit: a disgruntled current or former employee, competitors, physicians, or patients. People who may potentially bring a “qui tam” action are called relators. A corporate compliance program can heighten employee awareness of fraud and abuse concerns and thus may expand the pool of potential qui tam relators. This places an even greater premium on self-policing to avoid improper activities and, when necessary, to detect improper activities at an early stage and undertake remedial action as soon as possible.
Some states have adopted requirements similar to those found in the Guidelines. For example, Maryland’s insurance laws and regulations specifically require every authorized insurer to “institute, implement and maintain an insurance antifraud plan” that it must file with the State.36
Developing a Corporate Compliance ProgramAs we discussed earlier, the Guidelines can provide a framework for the development of a health plan’s compliance program. The Guidelines include seven minimum objectives
Page 394 of 469

AHM 510 : Health Plans : Governance and Regulation
that an organization must meet for its corporate compliance program to be considered an effective program to prevent and detect violations of law. This framework requires an organization to exercise due diligence in attempting to deter and, if a violation occurs, detect misconduct. Recall that in Health Plan Structure we discussed due diligence in relation to acquisitions and mergers. In an organization’s compliance effort, exercising due diligence requires, at a minimum, these actions.
1. Putting in place written standards and procedures for the corporation’s employees and other agents that could reduce the prospect of criminal conduct.
2. The assignment of high-level personnel to oversee compliance with such standards and procedures.
3. The use of due care to avoid the delegation of substantial authority to persons whom the corporation knows, or reasonably should know, have a propensity to engage in illegal activities.
4. The effective communication of the corporation’s standards and procedures to its employees and agents (e.g., through training programs or publications that explain in practical terms what the company requires).
5. The implementation of reasonable measures or steps to achieve compliance with the corporation’s standards (e.g., establishing a monitoring or auditing system designed to detect misconduct, establishing and publicizing a reporting system by which employees and agents could report misconduct without fear of retribution).
6. Consistent enforcement of the corporation’s standards through appropriate disciplinary mechanisms, including, as appropriate, discipline of individuals responsible for the failure to detect an offense. Adequate discipline of individuals responsible for an offense is a necessary component of enforcement; however, the form of discipline that will be appropriate will be case-specific.
7. When and if the entity detects misconduct, taking all reasonable steps to respond appropriately and prevent further misconduct, including modifying the corporation’s compliance program.37
The nature and complexity of a compliance program depends on several factors. These factors include: (1) the size and financial condition of the organization, (2) the vulnerability of the organization to misconduct, and (3) whether the organization has a history of being a party to or the victim of fraud or other misconduct. In addition, answers to the following important questions help establish the scope of the compliance effort:
1. Is the organization primarily engaged in government contracting, Medicare contracting, or Medicaid?
2. Is the organization in a growth phase, i.e., actively acquiring physician practices and other network providers?
3. Are there problems that require immediate review and corrective action or is the organization taking a proactive approach to its compliance efforts?
Page 395 of 469

AHM 510 : Health Plans : Governance and Regulation
Enlisting the support of essential employees is important to a successful compliance effort. Depending upon the scope of the program, the organization can best develop the compliance program through a committee of individuals with diverse views of the company’s business, e.g., operations, finance, human resources, marketing, medical management, claims, internal audit, and legal. This group could include directors, executive officers, managers of important operating units or divisions, and legal counsel. By participating in such a work group, employees not only feel a part of the process, but help create companywide support for the compliance program.
The following lessons describe important elements of an effective compliance program.
Establishment of Legal Standards and ProceduresEffective standards and procedures that govern a compliance program are tailored to the particular industry. Therefore, the team or work group formulating such standards and procedures typically begins the process by taking an inventory of all laws and regulations that govern the business. For example, a health plan hospital will examine such regulations as those promulgated by CMS, the state health department, or the state insurance department. Although not all of these regulations carry criminal penalties, the organization usually incorporates all of them into the organization’s standards so that one integrated document governs all corporate conduct. Finally, besides these industry-specific standards, the organization’s compliance standards might also include workplace standards that are generally applicable to all businesses. For example, these might include standards governing use of company property and proprietary information, accuracy in recordkeeping, and company policies regarding harassment and discrimination.
The organization can use the inventory for two purposes: (1) to identify those departments and departmental activities likely to fall within the reach of each particular law or regulation, and (2) to conduct a comprehensive internal evaluation of each key department.
Review Question
SoundCare Health Services, a health plan, recently conducted a situation analysis. One step in this analysis required SoundCare to examine its current activities, its strengths and weaknesses, and its ability to respond to potential threats and opportunities in the environment. This activity provided SoundCare with a realistic appraisal of its capabilities. One weakness that SoundCare identified during this process was that it lacked an effective program for preventing and detecting violations of law. SoundCare decided to remedy this weakness by using the 1991 Federal Sentencing Guidelines for Organizations as a model for its compliance program.
With respect to the Federal Sentencing Guidelines, actions that SoundCare should take in developing its compliance program include
creating a system through which employees and other agents can report suspected misconduct without fear of retribution holding management accountable for the misconduct of their subordinates
Page 396 of 469

AHM 510 : Health Plans : Governance and Regulation
assigning a high-level member of management to the position of compliance coordinator or administrator all of the above
Incorrect. With respect to the Federal Sentencing Guidelines, actions that SoundCare should take in developing its compliance program should include creating a system through which employees and other agents can report suspected misconduct without fear of retribution, as well as other actions listed on this page.
Incorrect. With respect to the Federal Sentencing Guidelines, actions that SoundCare should take in developing its compliance program should include holding management accountable for the misconduct of their subordinates, as well as other actions listed on this page.
Incorrect. With respect to the Federal Sentencing Guidelines, actions that SoundCare should take in developing its compliance program should include assigning a high-level member of management to the position of compliance coordinator or administrator, as well as other actions listed on this page.
Correct! With respect to the Federal Sentencing Guidelines, actions that SoundCare should take in developing its compliance program include all of the above
Initial Internal Departmental Evaluation and Monitoring ProceduresThe group creating the compliance plan may conduct a comprehensive internal audit at the time it develops the compliance program. After the company has identified the relevant legal standards with which the company must comply, the next step is to conduct a thorough self-evaluation.
This self-evaluation can be accomplished by asking that the group members use the inventory of applicable laws and regulations as a resource to review all of the functions and procedures in their departments and to identify those risk areas where misconduct could occur. For example, such risks could relate to billing for items and services not provided, improper diversion of payment intended for compensating a provider, and misrepresentation of types of services provided. By identifying risk areas, each department can develop monitoring procedures that specifically address the risk areas of that department, and design specific procedures to detect misconduct unique to that department.
Detection/Reporting SystemTo satisfy the Guidelines, a company generally does more than establish compliance standards and procedures; it takes steps to achieve actual compliance with those standards and procedures. The Guidelines expressly recommend the creation of a system through which employees and other agents can report suspected misconduct without fear of retribution.
Page 397 of 469

AHM 510 : Health Plans : Governance and Regulation
An internal detection/reporting system benefits the company in at least two ways. First, it provides constant evaluation of the company by its own employees and agents. Second, it encourages employees and agents, who might otherwise go directly to governmental authorities, to report suspected misconduct to the company instead.
In an effective internal detection/reporting system, the company conveys to all personnel its ongoing genuine interest in operating a legal and ethical business. The company also designs a system that fosters a sense of confidence in the system. Finally, the procedures for detecting and reporting misconduct are not so intricate and detailed that they are difficult for individuals to follow consistently.
Sometimes, there is a mechanism for anonymous reporting, which makes it much more likely that employees will report suspected misconduct. In addition, an anonymous reporting system shows that the company is more interested in learning about misconduct than about the identity of the person reporting it. Mechanisms for creating such a system can include a standard reporting tool, a toll-free hotline number, and a mail-drop for those individuals who want to report incidents of suspected misconduct but wish to maintain anonymity.
Besides providing this information to its employees and agents, the organization may distribute this information to enrollees and participating providers. The reason for extending the reporting system to include enrollees and participating providers is twofold; it conveys (to enrollees and providers) the organization’s interest in operating a legal and ethical business, and it provides an additional avenue for learning about suspected misconduct before governmental intervention.
In the end, health plans generally cannot guarantee anonymity even to those who report misconduct through an apparently anonymous procedure. At some point, the company may need to reveal the identity of the person who initiated the complaint, or that identity may become obvious. Typically, health plans strive to assure discretion, but also endeavor not to mislead individuals with promises of absolute anonymity. Some health plans address this issue before the onset of an investigation by sending a formal notice to the department from which a complaint has originated. Among other things, this notice includes a statement that the law may require that the organization reveal the identity of the individual who reported the misconduct. The organization can also incorporate a similar statement into the company’s standard reporting tool or in the taped message on the toll-free hotline.
Program OversightUnder effective compliance programs, a high-level member of management is responsible for overseeing the company’s compliance program. The Guidelines expressly state that this compliance coordinator or administrator must be a “director; an executive officer; an individual in charge of a major business or functional unit of the organization; or an individual with a substantial ownership interest.” To strengthen the compliance officer’s ability to carry out the duties of the position and assure a commitment to this effort, the individual reports periodically to the company’s board of directors, preferably, or at minimum to the company’s chief executive officer. The Inspector General and a number of commentators have recommended that the chief compliance officer neither be the general counsel nor report to the general counsel.38
Page 398 of 469

AHM 510 : Health Plans : Governance and Regulation
A typical compliance program includes the establishment of a formal compliance committee to oversee its implementation. Such a committee, chaired by the compliance officer, often consists of individuals selected from major departments. Under such a structure the committee is responsible for coordinating the detection, referral, and investigation of all suspected misconduct that occurs against or by the company. Among other things, the committee is responsible for reviewing all complaints to decide whether they warrant a full fraud investigation. The committee also maintains a database that tracks all incidents of suspected misconduct and the disposition of each complaint, and considers whether mandatory reporting requirements (to the appropriate regulatory or law enforcement agency) apply.
InvestigationsOnce an organization becomes aware that misconduct may have been committed, the Guidelines require the organization to respond appropriately. While the Guidelines do not state specifically what an appropriate response to suspected misconduct would be, it is clear that the organization must begin by conducting a thorough internal investigation.
An organization can obtain mitigation credit, in addition to the credit available for maintaining a corporate compliance program, if it voluntarily reports a criminal offense to the government and subsequently reveals the results of the internal investigation.
Some states have similar provisions. For example, Maryland’s fraud statute provides that “if an insurer, in good faith, has cause to believe that insurance fraud has been or is being committed, the insurer shall report the suspected fraud to the Insurance Fraud Division or to the appropriate federal, State or local law enforcement authority.”39
The benefits of internally investigating possible misconduct extend beyond reducing the organization’s ultimate fine, if any. Through the internal investigation, the company gains an understanding of the facts, which it can then use to prevent further similar offenses.
An effective compliance program includes extensive fraud investigation procedures. Under one popular model, the compliance committee refers those complaints that warrant a full investigation to an investigation unit. That unit will then investigate the complaint and submit a written report of its findings to the committee. Several days before an investigation begins, the investigation unit sends a memorandum to the appropriate department head, which includes the following:
• Notification that the unit will conduct a full investigation of a complaint
• The duration of the investigation
• The nature of the complaint
• A statement that the investigators may interview and ask departmental personnel to provide information (which will be considered confidential)
• A statement that the unit may refer the matter to federal, state, or local regulatory or law enforcement officials, and that cooperation with such officials, which may include court room testimony, may be a result of the investigation
Finally, if the investigation unit determines that fraud has been or is being committed, the compliance committee reports the incident to the applicable federal and/or state governmental agency within fifteen days of receiving the investigation unit’s report.
Page 399 of 469
AHM 510 : Health Plans : Governance and Regulation
Auditing SystemThe Guidelines also suggest that an effective compliance program include an auditing system that will ensure that the company has followed its policies and procedures. Ideally, someone independent of line management conducts the audits.
A sound compliance program might include a two-tiered auditing system that includes annual and random audits. The compliance program could require each department to conduct its own internal audit at least once a year. The purpose of the audit is to: (1) decide whether fraud has been or is being committed by or against the organization, (2) assess whether the department’s current monitoring procedures adequately detect fraud committed by or against the organization, and (3) assess the department’s current functions and systems to decide if they adequately deter misconduct committed by or against the organization.
Effective compliance programs also typically provide for random audits. The compliance committee oversees such audits and establishes guidelines and procedures for the conduct of the audits. One ground for the initiation of an audit would be if a department has a high incidence of misconduct or is a department in which the committee determines that misconduct is most likely to occur.
Disciplinary and Corrective ActionThe Guidelines require organizations to discipline individuals who violate compliance standards. The Guidelines do not mandate, however, specific sanctions that the company must apply. An organization, therefore, has discretion to decide the nature and severity of the discipline depending on the facts and circumstances, as long as it applies the sanctions consistently. For an unintentional and minor infraction, an informal reprimand often is an appropriate sanction. Such a reprimand puts the employee on notice that the conduct engaged in is a violation of the company’s compliance standards and that further misconduct may lead to more severe sanctions.
For serious, intentional violations of the company’s compliance standards, firings and referrals to the relevant governmental agency or law enforcement unit are appropriate. For violations that fall between these two extremes, the company may discipline an employee by demoting or transferring the employee, or suspending the employee without pay. Effective but less severe sanctions might include financial penalties, such as a temporary salary reduction, a denial of a salary increase, or denial of a bonus or incentive compensation.
The Guidelines also specifically state that management must be accountable for the misconduct of their subordinates. Managers are subject to discipline for failure to detect compliance violations that occur within their departments. If a manager’s negligence, carelessness or inattention facilitates or prolongs misconduct within an operating unit, the organization disciplines that manager in a way that is commensurate with the seriousness of the violation that has occurred.
The compliance committee notifies the human resources department (HRD) of every instance of employee misconduct. The committee’s notice includes a description of the misconduct and a recommendation of the appropriate sanction warranted. Although most HRDs have much discretion over the imposition of sanctions against employees,
Page 400 of 469

AHM 510 : Health Plans : Governance and Regulation
the compliance program usually provides that the HRD confer with the employee’s line manager and/or department head before imposing a sanction.
Employees are not the only individuals against whom health plans can take disciplinary actions. Others in this category include enrollees, agents, and participating providers, under the contractual arrangements between the health plan and such individuals. In such a case of disciplinary action, the compliance committee sends a notice to the applicable department head, including a recommendation as to the appropriate sanction warranted. The department head would then have discretion over the type of sanction imposed against the enrollee, agent, or participating provider. For example, if a participating provider is found to have violated the company’s compliance standards, the compliance committee would send to the applicable department head—perhaps the director of provider relations—a notice that would include a description of the misconduct and a recommendation of the appropriate sanction.
Finally, it is particularly important that the organization handle any disciplinary actions in a way that affords the individual some form of due process, i.e., advance notice, and an opportunity to respond to the charges, and the availability of any appeal procedures previously established by the organization for terminating or suspending employees, agents, enrollees, and providers.
Incentive ProgramTo encourage the reporting of suspected misconduct, some organizations maintain a program that gives recognition to employees whose reports of suspected misconduct lead to the successful detection, investigation, and referral of misconduct. A compliance program might also include an employee reward program that disburses a cash award for each well-founded complaint of fraud or serious misconduct that is made to the compliance committee.
Education and TrainingOnce the company has developed and written compliance standards and procedures, it typically distributes them to all employees and agents of the company. The organization can include these standards and procedures in a separate compliance manual or as an additional section in the company’s employee handbook. Either way, many health plans require all employees who receive a copy of the company’s compliance standards and procedures to sign a written certification that they have received, read, and understood them. In addition, the company generally gives all employees and agents updated and new material whenever a change in law or a change in compliance standards or procedures makes it necessary.
Distribution of written compliance standards and procedures, however, is not enough. An effective compliance program uses a variety of training and other interactive activities to communicate the company’s policies and procedures. New employees receive a copy of the company’s compliance standards and procedures immediately upon hiring with the same certification requirements described above. The company typically requires that new employees attend an introductory training session that:
• Presents an overview of the applicable laws and regulations that regulate the company
Page 401 of 469
AHM 510 : Health Plans : Governance and Regulation
• Addresses the specific aspects of fraud associated with the company’s various lines of business, if applicable
• Thoroughly educates all personnel about the company’s compliance program, including a review of all standards and procedures. More specifically, the training sessions will ensure that employees and agents (a) know how to report misconduct, anonymously or otherwise, (b) know what happens to complaints after the initial report, and (c) know what happens to people who use the reporting system
The sound compliance program includes an annual “refresher course” for all current employees and agents. Such a course reviews the company’s standards and procedures, highlights any particular problems or concerns in the company or in the industry generally, and explains any changes to the applicable laws or changes in company procedures that employees need to know to ensure compliance.
Trainers for the introductory training sessions and the refresher courses can be internal or external. Large, well-developed HRD training programs can usually accept this responsibility. In any event, an effective program includes documentation and maintenance of records of attendance. Maintaining records of attendance by topic and date ensures that all personnel receive sufficient compliance training and creates a record of the company’s efforts to carry out an effective compliance program.
Periodic Compliance Program ReviewsNothing in the world of health plan compliance is static. Laws, regulations, and court decisions affecting health plans, both state and federal, are in a constant state of flux. Thus, corporate compliance programs designed to remain useful require a regularly scheduled, reasonably frequent, and comprehensive review of the law. This will typically involve both an ongoing monitoring of state and federal developments and an annual or biannual audit of the adequacy of the compliance standards.
Changes in law are not the only source of potentially hazardous change. Company practices and products, if anything, are changing even more rapidly than laws and regulations. Health plans are creating new contractual relationships with provider organizations, designing new products that involve radically different operational approaches than typical health plan products, and making a host of other operational changes that can have profound legal implications. Compliance officers must ensure that the business changes that the organization undertakes are handled in compliance with existing laws.
Governing the Compliant Health Plan: The Role of LeadershipA health plan can follow every recommendation of every compliance expert, develop a plan that anticipates every regulator’s and every prosecutor’s objections, and create a structure that the authors of the Guidelines themselves could have written, and still fall short. The essential ingredient to any compliance plan is that the company’s leadership —from the board of directors to the CEO and president on down—must be committed to compliance and fully aware of the risks involved in noncompliance. For example, they must take care not to be too single-minded in their oversight of the company’s bottom line that they neglect to calculate compliance risks. Executives sometimes face
Page 402 of 469

AHM 510 : Health Plans : Governance and Regulation
situations that call for a choice between maximizing a business opportunity or strictly complying with the demands of regulation, as Insight 11A-1 illustrates.
Insight 11A-1. Business Opportunity and Compliance Risk.
A new product is ready to be launched. The state requires a health plan to obtain insurance department approval of policy forms before issuing any new product. If the health plan unveils this product by the first of the next month it will (1) have the first such product in the market and (2) be just in time to offer the product to a large employer coalition that is putting its healthcare benefit business out to bid. The competitive advantage could be worth millions of dollars, but only if the product “hits the streets” next month. Regulators have approved all but a single, minor aspect of the policy form, but will not grant approval in time for the product to be available for the client. In short, to comply with the law is to hand millions of dollars of business over to competitors, miss corporate profit targets, and cost many employees of the company a year-end bonus.
Obviously, the executive’s question to the compliance officer will be “what are the costs of noncompliance?” If the issue were one of public safety, the commission of a fraudulent act, or some act of similar severity, it is likely to be an easier issue for the executive than the above example. Few people will risk imprisonment, a corporate death sentence, or injury to life or limb for profits. Yet, this example, with neither life nor limb nor criminal statutes at stake, illustrates the type of issues a health plan’s leaders must sometimes address.
Compliance officers who are asked to assess the risk of noncompliance can shrug their shoulders and say, “This is too subjective to predict.” Alternatively, they can hazard a guess. Or they can perform some sort of rigorous analysis to formulate an educated guess. While some might argue that regulatory penalties are too arbitrary for an outsider to calculate, there is evidence to the contrary. A recent analysis of one state’s market conduct administrative penalties assessed against HMOs over a 10- year period was able to explain, with a rather simple formula, nearly 96 percent of the variance among those penalties.40 That formula was based in large part on a calculation of maximum penalty allowed by law per violation that the HMO was alleged to have committed.
However, regulatory standards of punishment have been on the rise as public scrutiny of both health plans and regulators has grown in intensity. Calculations based on even recent regulatory experience may not predict regulatory penalties in the future as well as they would have, absent this elevated scrutiny. Furthermore, regulators sometimes react quite strongly to the idea that corporate executives would calculate the cost of noncompliance, then decide it was worth it. A health plan’s leaders must consider the risk of fines or a cease-anddesist order from regulators. Also, a health plan’s leaders must consider the risk of damage to its client relationships and of negative publicity.
As we have seen, compliance programs are a critical system of organizational control for health plans; in the remainder of this lesson we examine several other systems.
Utilization Review and Quality Oversight ProgramsOne of the most sensitive issues in the world of health plans is the question of medical necessity as a condition for covering a medical service or supply. Most health plans
Page 403 of 469

AHM 510 : Health Plans : Governance and Regulation
exclude from coverage any service or supply that is not medically necessary. Therefore, the notion of medical necessity comes up in the context, not of clinical decisions about treatment alternatives (which are made by the healthcare practitioner), but of coverage decisions (which are made by the health plan). In other words, medical necessity is a contractual issue; the health plan must decide whether the service or supply is covered under the terms of the contract’s medical necessity requirement.
While medical necessity has been defined in a number of ways, most definitions include requirements that the proposed treatment be (1) medical (provided or ordered by a licensed healthcare practitioner), (2) effective (supported by scientific literature that suggests the treatment will result in a benefit to the patient), (3) individualized (likely to be effective for this particular patient, given that patient’s clinical indications), and (4) economical (as compared to other available, equally effective treatment alternatives).
Returning to our earlier analysis of accountability in health plans, we may ask,
• “Who is accountable for decisions of medical necessity?
• To whom are they accountable?
• In what domains are they accountable?
• Who establishes the standards for accountability?”
The mechanisms and structures employed by health plans to make determinations of medical necessity vary from organization to organization.
However, we can generalize about the most common structures. Typically, medical management is under the supervision of a medical director, assisted in larger plans by assistant medical directors or local medical directors who report to a national medical director. Other licensed healthcare professionals, notably nurses, are typically quite heavily involved, at least initially, in reviewing claims for determining the medical necessity of the treatment.
Accountability for decisions of medical necessity is owed to several stakeholders. First, the medical director typically reports to the chief executive officer of the health plan. Furthermore, state law often requires not only that each health plan have a medical director, but that the medical director be a physician licensed in the health plan’s state, raising the specter of accountability not only to professional medical societies but also to the state medical board or other state regulator. Many health plans have utilization review committees, to whom the medical director brings questions such as those of medical necessity. Increasingly, as health plans grow and as public demands for accountability increase, health plans are using specialized utilization review panels; for example, pediatricians are assisting the medical director in difficult cases involving pediatric medical necessity, cardiologists are assisting with cardiological medical necessity, and so on. Additionally, state and federal governments increasingly demand some form of external review of such decisions. Finally and most significantly, health plans are accountable to their members—the patients—for their determinations of medical necessity.
Page 404 of 469

AHM 510 : Health Plans : Governance and Regulation
A number of areas of accountability are involved in determining medical necessity. Certainly, the primary area is professional competence. Another significant area of accountability in determining medical necessity is financial performance, i.e., the economic obligations of the participants in the decision. The interest of government and the relevance of ethical questions to the decision also bring that area of accountability into the fray. Even access is an issue, particularly in the face of behavioral health professionals who charge that the standard of medical necessity is an inappropriate standard for judging coverage for behavioral healthcare treatments.41
As we have seen, within each of these domains, each stakeholder has a separate claim on establishing the standards for performance. For example, professional organizations may attempt to assert jurisdiction over medical directors’ professional competence in making determinations of medical necessity. Chief executives may establish economic targets that affect assessments of the economic portion of the medical necessity determination.
Related to the issue of utilization review and medical necessity is the overlapping issue of clinical quality management. As we saw in Healthcare Management: An Introduction, clinical quality management has traditionally been defined in terms of:
(1) assessing a healthcare organization’s structure (whether the entity is capable of delivering quality care by means of certification, licensure, recordkeeping, etc.)(2) process (whether the way care is provided is consistent with quality)(3) outcomes (whether the end result of treatment is consistent with standards of quality healthcare delivery).42
Essentially, the same stakeholders and areas of accountability apply in quality management as apply in determining medical necessity, since medical necessity is a component of quality management. The greater breadth of the subject matter involved in quality management, however, brings into play additional mechanisms of organizational control. Quality committees, which oversee clinical quality, and perhaps include questions of peer review and provider credentialing, are a common mechanism for the exercise of health plans’ organizational control. Such committees typically set standards, provide feedback and administer sanctions to providers, and advise the medical director and the management team on clinical quality improvement initiatives
An important and relatively recent development has been the systematic development of clinical practice guidelines. As we discussed in Workers' Compensation Programs, a clinical practice guideline is a utilization management and quality management mechanism designed to aid providers in making decisions about the most appropriate course of treatment for a specific case. Clinical practice guidelines are a particularly powerful tool in establishing accountability for relatively specific behaviors of providers. Indeed, the specificity of the standards may make it particularly important that providers who are accountable to those standards feel that the standards have been arrived at by competent, unbiased parties. Clinical practice guidelines that are so developed, preferably by or in consultation with providers themselves, are more likely to be accepted by physicians than those perceived to be designed and imposed by the health plan.
To date, over 1,800 guidelines have been catalogued, although a complete assessment of their impact on cost and quality of healthcare services has yet to be conducted. 43
Page 405 of 469

AHM 510 : Health Plans : Governance and Regulation
While over 82% of HMOs claimed in a recent survey to use clinical practice guidelines to reduce variability in practice patterns of participating providers, there is still a great deal of uncertainty as to the extent these patterns actually represent optimal clinical practice or have been diluted with considerations of patient preferences and socioeconomic factors.44 In any event, clinical practice guidelines are just that— guidelines, which may be modified to meet the special circumstances of a patient.
Ethics ProgramsBiomedical ethics, a field with a long and respected history, recently has gained a specific focus—the ethics of health plans. Rather than the exclusive domain of academics and consultants, the field has taken up residence in the form of health plan ethics committees. Ethics committees review health plan policies for consistency with principles of ethics and recommend changes where needed.45 Accepted in hospitals the 1980s, ethics committees are emerging in health plans. They can provide valuable assistance to health plan executives by providing forum for the discussion of difficult issues, reviewing or generating statements health plan policy, and assisting in the education of health plan employees and participating providers.46
Ethics committees are only one component of a broader corporate commitment to ethical organizational behavior, sometimes described as ethics programs. Ethics programs represent an across-the-board effort to foster exemplary ethical behavior throughout the health plan by seeking to:
• Continuously improve efforts to communicate the health plan’s mission and core values
• Train executives and staff on how to weave ethical behavior into daily organizational activities, including all organizational meetings
• Develop tools and techniques for using ethical considerations as a criterion in selection processes for hiring, promotion, and training47
• Codify and measure standards of ethical behavior48
• Recognize health plans’ clinical responsibilities in addition to their business obligations49
Some analysts have expressed concerns about the ethical problems specific to managed care. These concerns involve the potential for conflict—apparent or real—between the financial objectives of the health plan and the health interests of the patient. In other words, the concern is over the collision between medical ethics and business ethics.50 The distinction between the business world generally and the world of health plans specifically is that the product— healthcare—suggests the need for a higher standard of ethical behavior,51 and the providers of care—physicians and other professionals—operate under their own sets of ethical standards. The challenge, then, is for health plans to adopt ethics systems in a highly competitive environment.52
Another concern has to do with the privacy of the traditional doctor-patient relationship, and the potential impact of managed care programs, such as utilization review and member appeals, which rely upon the sharing of patient-specific medical information. 53
This concern suggests that an important task of health plan ethics programs is to assure
Page 406 of 469

AHM 510 : Health Plans : Governance and Regulation
that health plan employees preserve patient privacy as a top priority throughout the organization.
Ombudsman ProgramsAs we have seen, the ombudsman program is a method to have complaints against an health plan investigated by a neutral third party, thereby helping to ensure health plan accountability to healthcare consumers. Webster defines ombudsman as “a public official appointed to investigate citizens’ complaints against the government.”54 Common usage and the practice of governments and nongovernmental organizations have expanded the definition to include any official appointed to investigate complaints against the official’s organization.
Analysts disagree as to the precise role an ombudsman plays. They have described an ombudsman in a number of ways:
• A neutral, third-party fact-finder55
• A person who helps the aggrieved person gather information in preparation for an appeal56
• A person who is not necessarily neutral as he or she helps the aggrieved party pursue justice57
One can see legislators’ affinity for ombudsman programs in healthcare laws approved by legislatures at all levels. For example, the Congress, in funding activities to protect the rights of vulnerable elderly users of long-term care, saw state and local ombudsman programs as being an essential component of that program.58 Indeed, ombudsman programs can be found throughout the U.S. Code.
Similarly, states have turned to ombudsman programs to help consumers of healthcare services. States, responding to the federal government’s invitation to establish longterm care ombudsman programs, have gone well beyond the domain of long-term care in the establishment of such programs. For example, Florida has a Statewide Managed Care Ombudsman Committee, charged with acting “as a consumer protection and advocacy organization on behalf of all healthcare consumers receiving services through health plan programs in the state.”59
Healthcare entities of all sorts have established ombudsman programs. For example, Pennsylvania’s public health department has established such a program throughout its mental hospitals.60 Health plans are employing psychiatrists as ombudsmen.61 Some health organizations have established specialized ombudsman programs targeting specific types of grievances, such as sexual harassment.62
Experience in HMOs and other healthcare organizations have left practitioners with a number of guidelines on how to operate such programs:
1. Establish a clear mission and objectives 2. Empower the program to resolve problems other departments cannot 3. Build programs on existing resources, using available skill sets
Page 407 of 469

AHM 510 : Health Plans : Governance and Regulation
4. Empower the program with independence and the authority to identify the root of and facilitate the resolution of the problem
5. Gain the buy-in of all the relevant stakeholders within and outside of the health plan
6. Use documentation of accomplishments to build confidence in stakeholders 7. Use the program to identify organization developmental needs 8. Keep an eye on cost effectiveness of the program
9. Maintain a client-centered focus63
Ombudsman programs are seen as yet another tool for creating organizational control, emphasizing the organization’s accountability to the clients of the programs, whether they are health plan members, employees, providers, or other stakeholders. Their flexibility makes them uniquely adapted to a variety of accountability domains and sets of performance standards. Insight 11A-2 describes one health plan’s ombudsman program.
Insight 11A-2. An Ombudsman Program at BCBSMA.
Ask Ron Romano of Blue Cross Blue Shield of Massachusetts (BCBSMA) how his role as ombudsman works for health plan members, and he’ll tell you the story of Peter.
Peter (not his real name), a member of HMO Blue, BCBSMA’s principal managed health care plan, was a man with a serious alcoholism problem. Peter had shown signs of alcohol-based impairment at work and home, causing concern to friends, family, and colleagues, but he had always denied his problem.
Finally, one day earlier this year, Peter became irate and started smashing furniture at the small business he owns. Panicked and unsure what to do, his coworkers called a detoxification and rehabilitation center. The center urged the coworkers to get Peter into a car and drive him over immediately. Fortunately, after intensive detoxification and rehabilitation, Peter overcame his alcoholism and has been sober for over a year.
Unfortunately, the center turned out not to be part of HMO Blue’s provider network, and when the facility submitted claims to the plan, they were denied. Any of BCBSMA’s customer service reps could have explained the plan’s policies in this case, but none were authorized to override them. Ron Romano is authorized and empowered to use his experience-based judgment (he’s been in the position for seven years and with the company for nearly 17) to resolve cases just like Peter’s.
Romano, in his role as ombudsman, is one example of a creative, flexible strategy that’s being employed to help health plan members navigate the system that delivers their care.
When Peter was referred to Romano on appeal of his claims denial, Romano sat down with him, heard his story, and realized that there was excellent precedent for paying this claim based on a case from several years ago. Peter “didn’t realize he was in crisis, and of course, his coworkers didn’t know what his health plan covered,” Romano notes. Even more importantly, he says, here was a plan member who took responsibility for his
Page 408 of 469

AHM 510 : Health Plans : Governance and Regulation
situation, and for whom the clinical treatment worked. It wasn’t difficult for Romano to make a judgment in Peter’s favor.
Nor did Romano have to ask permission, which is another key aspect of his role. While customer service representatives are empowered to make certain exceptions, Romano, as ombudsman, has no contractual, procedural, or financial limit.
His role is also different from the kind of proactive patient advocacy naturally practiced by physicians and other clinicians in their day-today provision of patient care. In contrast to providers, his involvement is usually retrospective; most of his interventions come about as the result of a plan member’s appeal for coverage denied. In making his judgments, Romano says he has a single criterion: What is the most reasonable solution to a disagreement or confusion between the plan and a member, and the closest to a win-win for both parties possible?
And that explains the core of the ombudsman’s role as it’s evolving in managed health care, as a goodfaith mediator between members and health plans, someone who uses his or her judgment to find the best answers to questions about coverage issues, and who is able to bring knowledge, experience, and resources to such problems. Though ombudsmen differ widely in their affiliation (some are set up by health plans themselves; others by external agencies), funding, scope of authority, and scope of practice, all focus on educating health plan members about their rights and responsibilities, and resolving issues to achieve the best outcomes for plan members and health plans alike.
At BCBSMA, the ombudsman program actually began in the early 1970s, when the company was primarily fee-for-service, but in the past decade it has shifted almost entirely over to the company’s health plans, primarily HMO Blue. This is a natural response, Romano says, to the fact that more and more people are choosing HMOs and thus many plan members are new to managed care. In a sense, the ombudsman’s role is helping people navigate in a changing health care system.
The same phenomenon has helped spur the creation of ombudsman programs in other venues, primarily for Medicaid managed care plan members in states where large numbers of (or even almost all) Medicaid recipients have switched to health plans in recent years. Gradually, the whole ombudsman phenomenon is moving into the spotlight.
Source: Adapted from Mark Hagland, “Seven Lessons of the Ombudsman,” Healthplan (July/August 1997): 70–71. Used with permission; all rights reserved.
Page 409 of 469

AHM 510 : Health Plans : Governance and Regulation
Chapter 12 AKey Legal Issues in Health Plans In previous lessons, you learned about many of the federal and state regulations that govern the activities of health plans. These regulations impose obligations that health plans must satisfy to remain qualified to operate under federal and state law. In administering health plans, however, health plans also have legal obligations to members who receive plan services, as well as obligations to physicians and others who provide services under the plan. And like all businesses, health plans are subject to antitrust laws and other business regulations that govern how they may interact with their competitors. In this lesson, we discuss some of the key legal issues that arise from these obligations.
After completing this lesson, you should be able to:
Define breach of contract, negligence, medical malpractice, and punitive damages Discuss the obligations that health plans owe to plan members in conducting
utilization management activities Describe the standard of care health plans must meet when they credential plan
providers Discuss two theories of liability that may make health plans liable for the medical
malpractice of plan providers Describe how ERISA affects the ability of plan members to bring legal actions
against health plans Identify and describe some legal issues that may arise between health plans and
plan providers Discuss some of the federal and state laws that regulate the business conduct of
health plans
An Overview of Contract and Tort LawMany of the legal issues that health plans encounter in administering health plans arise from contracts. A contract is a binding promise or an agreement enforceable at law. For example, the terms and provisions of a healthcare plan are considered to form a contract that creates obligations on the part of the health plan that are enforceable by plan members. Health plans also enter into contracts with healthcare providers and others, such as pharmacists, who provide services to plan members. A health plan may be required to pay money damages if it commits a breach of any of these contracts. A breach of contract is the failure of a party to perform a contract according to its terms without a legal excuse.
In addition to liabilities arising from breach of contract, health plans may be liable for damages if they commit a tort. A tort is a violation of a duty to another person imposed by law, rather than contract, causing harm to the other person and for which the law provides a remedy. One type of tort is known as negligence. Negligence is the failure to exercise the amount of care that a reasonably prudent and careful person would exercise under similar circumstances.
The duty to exercise reasonable care applies both to individuals and corporations, such as health plans, and both individuals and corporations are liable for damages when their negligence harms someone.
Page 410 of 469

AHM 510 : Health Plans : Governance and Regulation
One type of negligence most of us are familiar with in the field of healthcare is medical malpractice. Medical malpractice is a type of negligence that occurs when a patient is harmed because a healthcare provider failed to exercise reasonable care in providing medical treatment.
We mentioned that health plans may be required to pay damages if they commit a breach of contract or a tort. Damages are the sum of money that the law awards as compensation for a legal wrong. In most contract and tort cases, damages are the amount of money that will compensate the injured party for his or her injuries. In some tort cases, however, courts may also award the injured party a kind of damages known as punitive damages. Punitive damages are damages awarded to punish and make an example of the wrongdoer and not to compensate the injured party for an injury. They are usually permitted only when a tort is outrageous or intentional. Because punitive damages are intended as punishment and not as compensation, they are typically awarded in very large amounts—sometimes in the millions of dollars.
Fast Fact
Medical malpractice costs account for as much as 5% of the total healthcare bill in the United States. These costs include direct costs resulting from malpractice lawsuits and indirect costs resulting from doctors practicing unnecessary “defensive medicine.”1
Between 1990 and 1994, there were at least 33 awards of punitive damages against health insurers and health plans, and almost half of these awards were for $1 million or more.2
Issues That Can Be Raised by Plan MembersPlan members can raise a number of legal issues, including claims that result from utilization management decisions, claims that arise from credentialing decisions, vicarious liability, and ERISA claims. In this section, we take a look at each of these legal issues. We also look at arbitration as an alternative to litigation.
Claims Resulting from Utilization Management DecisionsRecall that a key feature of health plans is utilization management, which is the process of managing the use of medical services so that patients receive necessary, appropriate, high-quality care in a costeffective manner. Utilization management may be performed either by healthcare professionals who are employees of the health plan or by outside organizations, such as utilization review organizations (UROs), who are under contract with the health plan. In this section, we discuss some of the ways that a health plan’s utilization management activities can give rise to liabilities to plan members.
Breach of Contract ClaimsManaged healthcare contracts contain exclusions and other provisions limiting the kind of benefits that are available to plan members. Some of these limits are clear and specific, such as limitations on the number of covered home health visits. Others require the exercise of judgment, such as when covered treatments are limited to those that are medically necessary. These determinations are made through utilization management activities.
In exercising sound utilization management practices, health plans sometimes find it necessary to deny coverage for some treatments or services. A common example
Page 411 of 469

AHM 510 : Health Plans : Governance and Regulation
occurs when a contract excludes coverage for experimental or investigative medical treatments. Medical advances sometimes produce new treatments that may be requested by plan members before they are proven to be effective. When a health plan denies coverage for those treatments, a plan member might bring a lawsuit claiming that the healthcare contract requires the health plan to cover the treatments. In that type of lawsuit, the court must determine whether the health plan properly excluded the treatment from coverage under the policy.
When the language in a health plan contract is unclear or ambiguous, a court will interpret the language against the party that selected the language and wrote the contract —in this case, the health plan. As we noted in Pharmacy Laws and Legal Issues, health plans must pay careful attention to drafting their contracts to ensure that they clearly and unambiguously specify what types of treatments are excluded, because ambiguities will be interpreted in favor of plan members. Some health plans define coverage for drugs based on whether treatment has been approved by the Food and Drug Administration, for example, because determining whether a treatment is FDA-approved is an objective decision and leaves little room for ambiguity. Some plans also voluntarily seek third party review of these claims to assure plan members that the decisions are objective.
Negligence ClaimsIn addition to claims for breach of contract, health plans may also face negligence claims as a result of their utilization management activities. Recall that negligence is the failure to exercise the amount of care that a reasonable person would exercise under similar circumstances. Plan members have sometimes claimed that health plans are negligent for designing utilization management systems in such a way that they result in decisions that are not in the best interests of plan members. For example, a plan member might argue that a health plan is negligent because its utilization review program is designed so that physicians are not allowed to have input into coverage issues regarding treatments they feel are medically necessary for their patients.
Plan members have also claimed that the process of making utilization management decisions is subject to a standard of care and that the failure to meet that standard constitutes negligence. To help minimize the risk of such claims, health plans adopt processes to assure that decisions are made by personnel who are competent to make them and only after gathering the information necessary to reach a sound medical judgment. Figure 12A-1 contains a checklist of some other steps health plans can take to help ensure that they minimize the risk of liability from their utilization management processes.
Figure 12A-1.
Ways to Help Minimize Liability Risks from Utilization Management Decisions.
1. Develop clear utilization management policies and procedures and follow them consistently.
2. Make sure that cases are reviewed by proper personnel. For example, if the initial reviewer is a nurse, have denials reviewed by a physician reviewer as well.
Page 412 of 469

AHM 510 : Health Plans : Governance and Regulation
3. Make sure that physician reviewers practice in areas of medicine relevant to the cases they review.
4. Discuss cases with the patient’s physician before issuing a denial. 5. Document the basis for all denials. 6. Allow patients and physicians to appeal denials. 7. Communicate denials to patients and inform them of their rights.
Source: Adapted from Mark Hagland, “Seven Lessons of the Ombudsman,” Healthplan (July/August 1997): 70–71. Used with permission; all rights reserved.
If a health plan’s utilization management is performed by an outside organization such as a utilization review organization, the health plan must use reasonable care in selecting and monitoring the performance of the URO to ensure that the URO’s procedures are appropriate and that its personnel are qualified to conduct utilization review. The health plan should also ensure that the URO is properly licensed and accredited. The leading organization that accredits UROs is the American Accreditation Health Care Commission/ URAC (the Commission/URAC).
Claims for Bad FaithSome courts have held that health plans owe plan members a duty to act in good faith when making utilization management decisions. The duty to act in good faith means that an health plan may not act maliciously, recklessly, or purely in its own economic self-interest when it denies coverage for a treatment or service. If a health plan violates this standard of conduct, a court may find that the health plan is liable for the tort of bad faith rather than only for breach of contract or mere negligence. This distinction is significant because the tort of bad faith—unlike the breach of contract and negligence liabilities we discussed earlier—can justify an award of punitive damages. Recall that punitive damages are intended to serve as punishment and are often awarded in large amounts. Some states also have laws that impose monetary penalties in addition to punitive damages against insurers that are guilty of bad faith.
In deciding whether a health plan acted in bad faith in denying coverage, a court will determine from the terms of the plan whether the health plan had a reasonable basis for the denial. If the health plan’s interpretation of the plan is not reasonable, the court is more likely to find that the health plan acted in bad faith. The court may also examine the health plan’s conduct for evidence of bad faith. Courts are especially likely to find bad faith when a health plan allows its own financial selfinterest to outweigh the welfare of plan members or considerations of medical necessity. Other conduct that might indicate that a health plan acted in bad faith includes:
• Unreasonably delaying a decision on a request for coverage until the plan member dies or is no longer eligible for coverage
• Denying a request for coverage without observing the health plan’s own utilization management policies and procedures
• Misleading a plan member about the reasons for denying coverage or about the procedures the health plan used in reaching a decision
Page 413 of 469
AHM 510 : Health Plans : Governance and Regulation
To avoid the potential liability for punitive damages and other penalties that can result from a finding of bad faith, health plans should scrupulously avoid conduct that might appear to be self-serving or indifferent to the medical needs of plan members. Health plans should also comply with state laws regulating the handling of claims. For example, most states have adopted variations on the Unfair Claims Settlement Practices Model Regulation, drafted by the National Association of Insurance Commissioners (NAIC).
As we saw in Market Conduct Examinations and Mechanisms for Enforcement, this model regulation specifies how insurers should process claims and notify beneficiaries of claim determinations. The regulation requires that claims be evaluated in a fair and timely manner and provides that when a claim is denied, the denial should be in writing and give a reason. Health plans can help establish that they did not act in bad faith by showing that they complied with laws modeled on this regulation.
Claims Arising from Credentialing DecisionsAn important feature of many health plans is that health plans either limit plan members’ choice of provider or provide incentives for plan members to select from panels of preferred providers. Because plan members may be injured if a health plan selects providers who are incompetent or unqualified to provide quality care, courts have held that health plans have a duty to use reasonable care in credentialing providers. Recall that credentialing is a review process conducted to determine the current clinical competence of providers and to ensure that providers meet the organization’s criteria. If a plan member is injured because a health plan fails to exercise reasonable care in credentialing providers, the health plan may be required to pay damages for negligence.
Various organizations, including the National Committee for Quality Assurance (NCQA) and the American Association of Preferred Provider Organizations (AAPPO), have adopted standards for conducting provider credentialing. The NCQA standards list the kinds of information health plans should obtain about providers during the initial credentialing process and suggest that health plans recredential all providers every two years. These standards are not mandatory for health plans, but courts sometimes find that health plans have satisfied their duty to use reasonable care in their credentialing activities if they comply with them. In addition, some states have enacted laws that specify the criteria health plans should consider in making credentialing decisions. Compliance with these laws may help a health plan show that it has satisfied its standard of care.
Health plans sometimes delegate the credentialing of providers to a third party known as a credential verification organization (CVO). When contracting with a facility, such as a hospital, the health plan may delegate credentialing of the hospital’s staff to the hospital administration, which must credential its staff to obtain Joint Commission on Accreditation of Healthcare Organizations (JCAHO) accreditation. The NCQA has certified a number of CVOs that have met NCQA’s requirements for performing certain activities of the credentialing function.
Refer to Figure 12A-2 for the standards that the NCQA has established for delegated credentialing. The Commission/URAC has also established guidelines for delegation of credentialing.
Page 414 of 469

AHM 510 : Health Plans : Governance and Regulation
When a health plan delegates credentialing activities to a third party, the health plan typically agrees to assume the following responsibilities:
• Review the third party’s credentialing policies and procedures for compliance with the health plan’s standards, state and federal laws, and accreditation agency regulations
• Provide the third party with the health plan’s credentialing policies and procedures
• Maintain the confidentiality of the third party’s files, reports, and recommendations, and permit access only to authorized parties
• Share with the third party any utilization management (UM), quality management (QM), member satisfaction, and member complaint information that relates to the delegated credentialing or recredentialing activities
• Retain the right to approve, reject, suspend, or terminate any individual provider or healthcare delivery site not in compliance with the health plan’s policies and procedures
• Notify the third party prior to the termination of a provider or site
• Determine the effective date and the termination date of all providers added to the network by the third party
• Perform an annual audit of the third party’s credentialing and recredentialing program and records to assess effectiveness and compliance with regulations
The third party generally accepts the following responsibilities under the delegation agreement:
Page 415 of 469

AHM 510 : Health Plans : Governance and Regulation
• Review the health plan’s policies and procedures and conduct the delegated credentialing and recredentialing activities in accordance with these policies and procedures
• Provide the health plan with the third party’s policies and procedures
• Maintain the confidentiality of documents, reports, and other information provided by the health plan, and permit access only to authorized parties
• Allow the health plan to review the minutes from meetings of the third party’s credentialing committee or other designated decision-making body
• Provide specific information on all individual providers in the network and revise the information on a monthly basis
• Notify the health plan immediately of any provider who has been terminated or placed on probation, or whose practice has been restricted in any way
• Notify the health plan immediately of any provider who fails to meet credentialing or recredentialing standards, or who has been sanctioned by a hospital, licensing board, professional association, or regulatory agency
• Share with the health plan any information on UM, member satisfaction, claims, or other functions that may be relevant to the health plan’s QM program
Although health plans sometimes delegate their credentialing decisions to third parties, many states consider a health plan’s duty to use reasonable care in credentialing providers and monitoring their performance to be a nondelegable duty. A nondelegable duty is a duty that cannot be assigned or entrusted to someone else. If the duty is nondelegable, a health plan that relies on a third party for credentialing might still be liable to plan members who are injured by the third party’s negligent credentialing decision.
Vicarious LiabilityA patient who is injured by medical malpractice can bring a claim for damages against the individual provider whose negligence caused the injuries. When the negligent medical treatment was provided under a health plan, however, the injured patient may also be able to present a claim against the health plan that administers the plan. One reason patients find such claims advantageous is that health plans are usually corporations, so they often have more resources from which to pay damages than the individual provider who committed the malpractice.
The legal basis for a claim against a health plan for the negligence of a plan provider is known as vicarious liability. Vicarious liability is a kind of liability that arises when one party is held responsible for the actions of another party because of the existence of a special relationship between those two parties. The key characteristic of vicarious liability is that it makes a health plan liable for a plan member’s injuries not because of any negligence committed by the health plan, but simply because of the relationship between the health plan and the negligent provider. This means that a health plan can be responsible for medical malpractice committed by a plan physician even if the health plan had no direct involvement in providing the medical treatment that caused the injuries.
Review Question
Page 416 of 469
AHM 510 : Health Plans : Governance and Regulation
The Hanford Health Plan has delegated the credentialing of its providers to the Sienna Group, a credential verification organization (CVO). If the contract between Hanford and Sienna complies with all of the National Committee for Quality Assurance (NCQA) guidelines for delegation of credentialing, then this contract
A. Transfers to Sienna all rights to terminate or suspend individual practitioners or providers in Hanford's provider network
B. Describes the process by which Hanford evaluates Sienna's performance in credentialing providers
Both A and B
A only
B only
Neither A nor B
Incorrect. When a health plan delegates credentialing activities to a third party, the health plan retains the right to approve, reject, suspend, or terminate any individual provider or healthcare delivery site not in compliance with the health plan’s policies and procedures.
Incorrect. When a health plan delegates credentialing activities to a third party, the health plan retains the right to approve, reject, suspend, or terminate any individual provider or healthcare delivery site not in compliance with the health plan’s policies and procedures.
Correct. When a health plan delegates credentialing activities to a third party, the health plan typically agrees to review the third party’s credentialing policies and procedures for compliance with the health plan’s standards, state and federal laws, and accreditation agency regulations.
Incorrect. When a health plan delegates credentialing activities to a third party, the health plan typically agrees to review the third party’s credentialing policies and procedures for compliance with the health plan’s standards, state and federal laws, and accreditation agency regulations.
Claims Based on the Respondeat Superior DoctrineHealth plans may be liable for the actions of their employees under a doctrine of vicarious liability called respondeat superior, which is a Latin term meaning “let the master answer.” Respondeat superior stands for the principle that an employer is responsible for torts its employees commit in the course of their employment and within the scope of their authority. The rationale for this rule is that because an employer has the right to control the conduct of its employees, the employer should be responsible for the employees’ actions.
Respondeat superior applies only when there is an employment relationship between the health plan and the provider who committed the medical malpractice. Traditionally, physicians have been considered to be independent contractors rather than employees
Page 417 of 469
AHM 510 : Health Plans : Governance and Regulation
because of their high degree of skill and the independence they exercise in making medical decisions. However, some kinds of health plans such as staff-model HMOs have formal employment relationships with physicians. When such an employment relationship exists, the health plan is responsible if a physician-employee commits a tort that injures a plan member.
Respondeat superior may apply even when there is no formal employment relationship between the physician and the health plan if the circumstances show that the health plan actually treated the physician like an employee. One important consideration in making this determination is the amount of control the health plan exercises over the physician’s medical decisions and judgments. Other considerations include whether the physician controls the financial and operational aspects of his or her practice and whether the physician also treats patients who are not enrollees of the health plan. We mentioned earlier that physicians have traditionally been considered to be independent contractors because they exercise independence in doing their work. If that traditional independence in making medical and other decisions is not present because the health plan exercises too much control, the physician might be considered to be the health plan’s employee.
Claims Based on AgencyA health plan may also be subject to vicarious liability under principles of agency. As we saw in Other Laws that Apply to Health Plans, an agent is someone who acts on behalf of another person (known as the principal) in dealings with third parties. For example, an insurance agent acts on behalf of an insurance company (the principal) in dealing with clients who are buying insurance. Under the laws of agency, the principal is responsible for actions the agent takes while acting within the scope of the agency relationship. A health plan may be liable for the negligence of a plan provider if the provider is considered to be the health plan’s agent. Ordinarily, an agency relationship arises only if the principal and the agent mutually agree that there will be such a relationship. In the case of an insurance agent, for example, the insurance company and the agent typically sign a written contract that establishes the agency relationship, and both parties intend that an agency relationship will come into effect.
Another type of agency, called ostensible (or apparent) agency, may occur even when there is no agency agreement and the principal does not intend to create an agency relationship. Ostensible (or apparent) agency is a type of agency that occurs when one party negligently or intentionally creates the impression that another party is its agent. Ostensible agency can arise in the health plan context when a health plan somehow gives plan members the impression that plan providers are its agents. An health plan can be responsible for injuries committed by a plan provider if the health plan causes a plan member to reasonably believe that a provider is the health plan’s agent and the plan member is injured by the provider’s malpractice.
As with respondeat superior, the element of control is important in determining whether a health plan is liable under principles of ostensible agency, because plan members are more likely to believe that providers are agents of the health plan when the health plan exercises significant control over the providers’ activities. A plan member might also get the impression that providers are agents of the health plan from statements in the health plan’s advertising or marketing brochures indicating that healthcare is being provided by the health plan and not the individual providers. In one case, for example, a health plan’s advertising materials stated that the health plan itself provided healthcare, that the health
Page 418 of 469
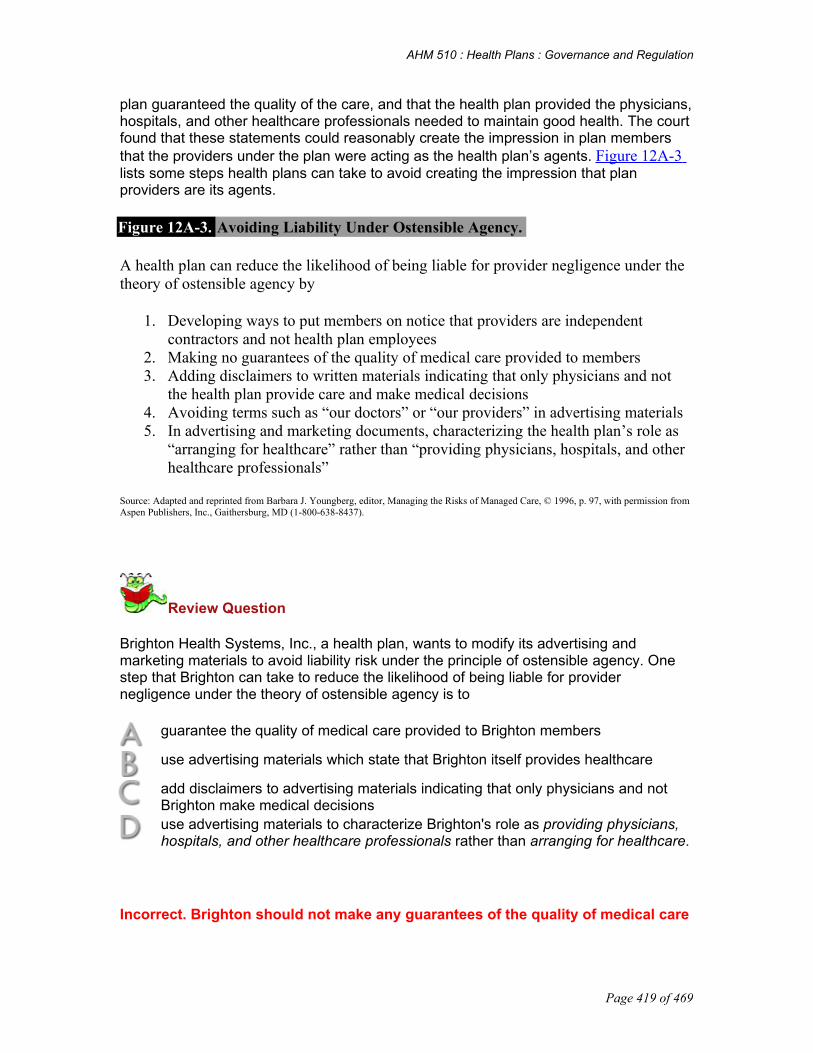
AHM 510 : Health Plans : Governance and Regulation
plan guaranteed the quality of the care, and that the health plan provided the physicians, hospitals, and other healthcare professionals needed to maintain good health. The court found that these statements could reasonably create the impression in plan members that the providers under the plan were acting as the health plan’s agents. Figure 12A-3 lists some steps health plans can take to avoid creating the impression that plan providers are its agents.
Figure 12A-3. Avoiding Liability Under Ostensible Agency.
A health plan can reduce the likelihood of being liable for provider negligence under the theory of ostensible agency by
1. Developing ways to put members on notice that providers are independent contractors and not health plan employees
2. Making no guarantees of the quality of medical care provided to members 3. Adding disclaimers to written materials indicating that only physicians and not
the health plan provide care and make medical decisions 4. Avoiding terms such as “our doctors” or “our providers” in advertising materials 5. In advertising and marketing documents, characterizing the health plan’s role as
“arranging for healthcare” rather than “providing physicians, hospitals, and other healthcare professionals”
Source: Adapted and reprinted from Barbara J. Youngberg, editor, Managing the Risks of Managed Care, © 1996, p. 97, with permission from Aspen Publishers, Inc., Gaithersburg, MD (1-800-638-8437).
Review Question
Brighton Health Systems, Inc., a health plan, wants to modify its advertising and marketing materials to avoid liability risk under the principle of ostensible agency. One step that Brighton can take to reduce the likelihood of being liable for provider negligence under the theory of ostensible agency is to
guarantee the quality of medical care provided to Brighton members
use advertising materials which state that Brighton itself provides healthcare
add disclaimers to advertising materials indicating that only physicians and not Brighton make medical decisions use advertising materials to characterize Brighton's role as providing physicians, hospitals, and other healthcare professionals rather than arranging for healthcare.
Incorrect. Brighton should not make any guarantees of the quality of medical care
Page 419 of 469

AHM 510 : Health Plans : Governance and Regulation
Incorrect. A health plan does not provide healthcare itself, but contracts with providers to provide the healthcare
Correct. Because Brighton does not provide healthcare, Brighton shoild make it clear that the physicians are ultimately responsibile for medical decision-making, not the health plan.
Incorrect. Brighton should have materials stating that it arranges for healthcare, rather than providing physicians, hospitals and other healthcare professionals
Statutes Affecting Vicarious LiabilityIn some states, health plans receive protection from vicarious liability claims by laws that exempt health plans from responsibility for medical malpractice. For example, some states have laws stating that furnishing healthcare under a health plan is not considered the practice of medicine. Courts have sometimes decided that these laws mean that a health plan cannot be sued for medical malpractice. Other states have laws that prohibit corporations from practicing medicine, and courts in these states sometimes apply the corporate practice of medicine doctrine. As we discussed in Legal Organizations of Health Plans, the corporate practice of medicine doctrine is a rule stating that a corporation cannot legally engage in the practice of medicine.
On the other hand, the legislature in one state has enacted a law that makes it easier to sue health plans for medical malpractice, and several other states are considering enacting such laws. In 1997, Texas enacted a law providing that health plans have a duty to exercise ordinary care when making healthcare treatment decisions and providing that health plans are liable for damages if their failure to exercise ordinary care causes harm to plan members. More importantly, the law also allows plan members to sue a health plan for damages if they are harmed by the negligence of the health plan’s employees, agents, ostensible agents, or representatives who are under the health plan’s control.
In such a lawsuit, a health plan cannot use the corporate practice of medicine doctrine as a defense.
Enterprise LiabilityThe two theories of vicarious liability we have discussed so far—respondeat superior and ostensible agency—depend on the existence of an employment or agency relationship as the basis for making a health plan liable for a provider’s negligence. Some people have argued for a theory of liability that would make health plans responsible for the actions of plan providers regardless of the existence of such a relationship. This theory, known as enterprise liability, would create a system in which a health plan is liable for any torts committed by plan providers against plan members while they are enrolled in the plan, even if there is no employment or agency relationship between the health plan and the providers.
Statutes that would impose enterprise liability on health plans have been proposed at the federal level. Enterprise liability was part of the unsuccessful Clinton administration healthcare reform plan of the early 1990s, for example. Recent bills in Congress do not
Page 420 of 469

AHM 510 : Health Plans : Governance and Regulation
provide for this type of liability. Instead, those bills take away ERISA preemption of state law for wrongful coverage decisions. None of these proposals has yet become law.
ERISA’s Impact on Claims by Plan MembersRecall that most employer-sponsored health plans are governed by ERISA. As we discussed previously, one of the most significant features of ERISA is that it contains a preemption provision, which means that the terms of ERISA generally take precedence over state laws that regulate employee welfare benefit plans, including most employer-sponsored health plans. When a state law is preempted by ERISA, a person may not seek a remedy or file a lawsuit under state law, but must rely instead on the remedies provided by ERISA. The remedies under ERISA are less generous in some ways than those allowed under state law. For example, ERISA does not permit the recovery of compensatory or punitive damages, which are often permitted by state law.
In 1987, the U.S. Supreme Court decided in Pilot Life Insurance Co. v. Dedeaux3 that ERISA preempts state lawsuits claiming that an employer-sponsored benefit plan acted in bad faith in denying benefits. Under ERISA, therefore, state law claims based on the denial of a plan benefit are preempted.
With regard to state lawsuits seeking to recover for plan negligence, however, lower courts have issued conflicting rulings when applying the Pilot Life decision. Under some of these decisions, claims that an health plan was negligent in credentialing providers or performing utilization review are preempted. Other decisions have held that these kinds of claims are not preempted. Similarly, it is not clear whether ERISA preempts state claims seeking to hold health plans liable for the negligence of their providers under principles of vicarious liability. The courts that have addressed this issue have reached conflicting results, but the trend seems to be that ERISA does not preempt vicarious liability claims.
Overall, recent court decisions have tended to reduce the protections provided to health plans by the preemption doctrine. Federal legislation has also been proposed (but not yet passed) that would remove ERISA as an obstacle to bad faith denial claims against health plans. As the protections afforded by ERISA preemption continue to erode, health plans can expect to face greater exposure to liability for state law claims.
Even when state claims are preempted by ERISA, plan members may still bring claims against health plans under the provisions of ERISA itself. Although some kinds of damages that are available under state law are not available in ERISA actions, a health plan that loses an ERISA claim may still be required to pay damages to the plan member who brought the claim. For example, the plan might have to pay the value of any services or benefits that were improperly denied to the plan member, and it may be required to pay any attorney’s fees and expenses the plan member incurred in bringing the claim.
Arbitration as an Alternative to LitigationTraditionally, parties who were unable to settle legal disputes themselves had little choice but to go to court to seek a resolution. Using litigation to resolve disputes can be time consuming and expensive, however, because court proceedings often take months or years to conclude and the attorney’s fees for such prolonged proceedings can be substantial. Litigation also involves a great deal of uncertainty because it is difficult to
Page 421 of 469

AHM 510 : Health Plans : Governance and Regulation
predict how a jury will rule in any given case or what damages it will award. And in cases involving physical injuries, such as medical malpractice, juries can sometimes be affected by feelings of sympathy toward the injured party and award damages that seem out of proportion to the party’s injuries.
In an attempt to resolve disputes with plan members more quickly and with less expense and uncertainty, some health plans are using alternative dispute resolution (ADR) methods such as arbitration. Arbitration is a method of dispute resolution in which the dispute is submitted to a person or panel of persons, known as arbitrators, who are either chosen by the parties or selected as provided by law. After conducting a proceeding in which the parties are allowed to present their evidence, the arbitrator issues a decision. This decision is usually binding on both parties, although some arbitration procedures permit a party who is dissatisfied with the arbitrator’s decision to seek further review in court.
Review Question
Arthur Dace, a plan member of the Bloom Health Plan, tried repeatedly over an extended period to schedule an appointment with Dr. Pyle, his primary care physician (PCP). Mr. Dace informally surveyed other Bloom plan members and found that many people were experiencing similar problems getting an appointment with this particular provider. Mr. Dace threatened to take legal action against Bloom, alleging that the health plan had deliberately allowed a large number of patients to select Dr. Pyle as their PCP, thus making it difficult for patients to make appointments with Dr. Pyle.
Bloom recommended, and Mr. Dace agreed to use, an alternative dispute resolution (ADR) method that is quicker and less expensive than litigation. Under this ADR method, both Bloom and Mr. Dace presented their evidence to a panel of medical and legal experts, who issued a decision that Bloom's utilization management practices in this case did not constitute a form of abuse. The panel's decision is legally binding on both parties.
This information indicates that Bloom resolved its dispute with Mr. Dace by using an ADR method known as:
corporate risk management
an ombudsman program
an ethics committee
arbitration
Incorrect. Corporate risk management is a series of activities undertaken by an organization to minimize the organization's and board's liability exposure and to reduce the risk of lawsuits.
Page 422 of 469

AHM 510 : Health Plans : Governance and Regulation
Incorrect. An ombudsman program is a mechanism of ensuring accountability to healthcare consumers by providing members with methods of having complaints against a health plan investigated by a third neutral party.
Incorrect. An ethics committee reviews health plan policies for consistency with principles of ethics and recommends changes where needed.
Correct. Arbitration is a method of dispute resolution in which the dispute is submitted to a person or panel, called arbitrators, who are either chosen by the parties or selected by law. The arbitrators weigh evidence and produce a (usually) binding decision.
A key feature of arbitration is that arbitrators are often medical experts, retired judges, or lawyers. Using arbitrators to resolve disputes can help ensure that decisions are reached rationally and based on the facts, without the emotional influences that can sometimes affect the decisions of juries. In addition, arbitration is quicker and less expensive than litigation, so it can be beneficial to plan members as well as to health plans.
Health plans have established arbitration procedures to resolve both medical malpractice claims and disputes involving utilization management decisions. In some states, health plans are allowed to require plan members to use arbitration to resolve those disputes, while in others health plans may offer arbitration as an option but may not require plan members to use it. Insight 12A-1 illustrates how one health plan uses arbitration to resolve disputes with plan members.
Insight 12A-1. Arbitration: A New Approach to Dispute Resolution.
Kaiser Permanente’s Southern California Region has used binding arbitration to resolve disputes for almost 20 years.
Under this system, claimants choose one arbitrator, respondents choose another, and those two agree on a third, neutral arbitrator. Hearings are much like a trial, with expert as well as factual witnesses. The decision of the three arbitrators is final, with extremely limited statutory grounds (such as a failure to hear relevant evidence) for overturning an award.
“In general, this system is costeffective and works extremely well,” says Trischa O’Hanlon, senior counsel for the region. “Cases are resolved much more quickly than in the courts—typically in about 19 months, compared to an average of 33 months for malpractice lawsuits handled by the court system.”
“In emergency situations we have gotten cases to arbitration within a week. For example, in one instance a cancer patient wanted a bone marrow transplant, and she needed it very quickly if she was going to have it at all. In this particular situation it wasn’t clear whether the procedure was experimental or not, so we went to arbitration very quickly—
Page 423 of 469

AHM 510 : Health Plans : Governance and Regulation
and ended up paying for the treatment.” Kaiser probably ends up paying more judgments than it would in court, O’Hanlon says, but the judgments are lower than jury awards.
“In arbitration you don’t have these enormous, irrational awards. Arbitrators will give a lower amount, but they will give something.”
Source: Adapted from Elaine Zablocki, “Tort Reform,” HMO Magazine (May/June 1994): 74–77. Used with permission; all rights reserved.
Issues That Can Be Raised by Plan ProvidersIn addition to the issues that arise in dealing with plan members, health plans also encounter legal issues when dealing with entities that provide benefits or services to plan members. These entities include healthcare professionals, physicians, hospitals, and others who contract with health plans to provide medical treatment or benefits to members. As in any contractual relationship, care must be taken in drafting these contracts to ensure that they comply with applicable laws and regulations and appropriately define the obligations of all parties. When these obligations are not clearly defined, disputes may arise. For example, providers may claim that the health plan is not paying them for their services in the way their contracts require.
Claims Arising from Selection and Termination DecisionsAs we discussed earlier, health plans owe plan members a duty to use reasonable care in selecting providers. Health plans also have other legal obligations when selecting providers. Some of these obligations are imposed by antitrust laws. A provider who is excluded from a health plan network may claim that the exclusion is a violation of these laws if the exclusion adversely affects competition.
A provider who is excluded or terminated from a healthcare network may also bring a claim against the health plan under state law for the tort of defamation. A defamation is a false communication that tends to harm the reputation of the defamed person so as to lower the defamed person in the estimation of others and to deter others from associating or dealing with that person. A provider might bring a claim for defamation, for example, if a health plan damages the provider’s reputation or ability to attract referrals by communicating the reason for the exclusion to the provider’s patients or peers.
Without-Cause Terminations and Obligations of Fair ProcessContracts between health plans and healthcare providers sometimes contain “without cause” or “at will” termination provisions. A “without cause” (or “at will”) termination provision states that a party can terminate the contract at any time, without providing any reason for the termination, simply by giving the other party a specified period of notice. One reason these provisions are used by health plans is that they allow health plans to terminate providers in response to the changing enrollment and geographic needs of the plan. Historically, courts found that “without cause” termination provisions were enforceable, reasoning that parties should be bound by agreements they freely entered into.
More recently, some providers who have been terminated under “without cause” termination provisions have claimed that because of the financial impact termination will have on their practices, they should have the right to receive a reason for the termination and a chance to present information relevant to the termination decision. Other providers have claimed that they were terminated for reasons that might violate public policy. For
Page 424 of 469

AHM 510 : Health Plans : Governance and Regulation
example, some providers have claimed that they were terminated for advocating for their patients during utilization review or for advising patients about alternative treatment options.
In response to these claims, courts in a few states have ruled that providers who will suffer an adverse financial impact from termination or who claim that their terminations are based on reasons that violate public policy may not be terminated from health plan networks without receiving what is known as “fair procedure” or “due process.” Although the courts have not always defined specifically what “fair procedure” is, in this context fair procedure (or due process) typically means that a provider who is being terminated from a health plan has the right to receive an explanation for the termination and an opportunity to present reasons that the termination should not take place. Some states have enacted laws that restrict the use of “without cause” termination provisions.
Generally, these laws require health plans to give a terminated provider written notice of the termination, to provide a written list of reasons for the termination, and to allow the provider to respond to the allegations or to appeal an adverse decision. Some laws prohibit health plans from basing termination decisions on reasons that violate public policy, such as for engaging in patient advocacy. Other laws regulate the use of economic credentialing in making termination decisions. Economic credentialing is credentialing that considers economic factors (such as the provider’s utilization rate and cost-effectiveness in providing care) in determining whether the provider meets the health plan’s selection criteria.
Some states prohibit health plans from terminating or excluding providers for purely economic reasons, while other states that permit the use of economic credentialing require health plans to share with providers the economic criteria that will be used to make credentialing decisions.
Review Question
Greenpath Health Services, Inc., an HMO, recently terminated some providers from its network in response to the changing enrollment and geographic needs of the plan. A provision in Greenpath's contracts with its healthcare providers states that Greenpath can terminate the contract at any time, without providing any reason for the termination, by giving the other party a specified period of notice.
The state in which Greenpath operates has an HMO statute that is patterned on the NAIC HMO Model Act, which requires Greenpath to notify enrollees of any material change in its provider network. As required by the HMO Model Act, the state insurance department is conducting an examination of Greenpath's operations. The scope of the on-site examination covers all aspects of Greenpath's market conduct operations, including its compliance with regulatory requirements.
The contracts between Greenpath and its healthcare providers contain a termination provision known as
an 'economic credentialing' termination provision
Page 425 of 469

AHM 510 : Health Plans : Governance and Regulation
a 'breach of contract' termination provision
a 'fair procedure' termination provision
a 'without cause' termination provision
Incorrect. Economic credentialing is credentialing that considers economic factors (such as the provider’s utilization rate and cost-effectiveness in providing care) in determining whether the provider meets the health plan’s selection criteria.
Incorrect. Breech of contract is the failure of a party to perform a contract according to its terms without a legal excuse
Incorrect. Fair procedure (or due process) typically means that a provider who is being terminated from a health plan has the right to receive an explanation for the termination and an opportunity to present reasons that the termination should not take place
Correct! A 'without cause' (or 'at will') termination provision states that a party can terminate the contract at any time, without providing any reason for the termination, simply by giving the other party a specified period of notice.
Federal laws also impact the use of “without cause” terminations. For example, the Medicare+Choice health plans, created by the federal Balanced Budget Act of 1997, are required to give providers notice of adverse selection decisions and must allow hearings so that providers can appeal unfavorable decisions. The law also prohibits these plans from excluding providers simply because they advise patients about alternative treatment options. Another federal law, the Health Care Quality Improvement Act (HCQIA), exempts some health plans from liability arising from the credentialing and peer review process. To receive the benefits of this exemption, however, health plans must adhere to certain due process standards. For example, a health plan that declines to retain a physician in its provider network—because of the physician’s professional misconduct or incompetence, which could adversely affect patient health—must provide the physician with timely notice of its decision so the physician can prepare a response.
Business Conduct IssuesIn Antitrust Concerns and Health Plans, you learned about some of the federal antitrust laws that have been enacted to help maintain a competitive business environment. Health plans must ensure that their business activities do not result in anticompetitive activities that might violate these laws. Health plans must use special care to avoid violating the federal antitrust laws because violations can result in large awards of damages. And because the laws are so complex, professional legal advice is often necessary to ensure compliance. As we discussed in Medicare and Health Plans, federal regulatory agencies establish rules and regulations that also affect business conduct of health plans (e.g., the Medicare marketing guidelines).
As we saw in Other Laws that Apply to Health Plans, state laws also impose restrictions on the business conduct of health plans. For example, most states have laws that prohibit unfair or deceptive trade practices. The business practices prohibited by these
Page 426 of 469

AHM 510 : Health Plans : Governance and Regulation
laws vary widely from state to state, but many states prohibit unfair marketing practices such as false advertising and making misrepresentations in promotional materials. More than half the states have adopted variations of the National Association of Insurance Commissioners (NAIC) Health Maintenance Organization Model Act, which provides that an HMO’s certificate of authority may be suspended or revoked if it advertises its services in an “untrue, misrepresentative, misleading, deceptive, or unfair” manner.
In some states, health plans are also subject to laws that specifically regulate other types of business conduct by insurance companies or health plans. Several states prohibit as an unfair trade practice the offering of inducements to enroll in a health plan, for example. A health plan might violate this kind of restriction by giving out items of more than nominal value, such as bike helmets or exercise equipment, as part of a promotion to increase membership. As with federal antitrust law, health plans must rely on professional legal advice to avoid violating these laws.
The Importance of Risk ManagementWe have discussed some of the legal damages and financial penalties that can result when claims are asserted against health plans. It is important to remember, however, that health plans may suffer other indirect consequences, such as action by regulatory agencies and adverse public relations, when dissatisfied plan members or providers bring claims against them. A health plan that is accused of negligence or other wrongdoing may also suffer damage to its reputation and, as a result, find it more difficult to secure business from employers and other plan sponsors. For all these reasons, many health plans are relying more heavily on risk management programs to help prevent claims from occurring and to minimize the damage from claims that do occur.
We have already discussed some of the steps health plans can take to help avoid claims by plan members and providers. In addition to these steps, as we saw in Governance: Accountability and Leadership, health plans have implemented compliance programs to help ensure compliance with regulatory requirements and to monitor member satisfaction. An important goal of compliance programs is to identify and correct potential liabilities before they result in claims or litigation. As part of the compliance process, health plans rely on legal counsel to help them keep abreast of court decisions and proposed legislation that may affect the legal relationships between health plans and their members and providers.
As we discussed in The Components of Governance in a Health Plan, health plans can obtain insurance to protect them against many of the risks we have discussed in this lesson. Insurance is available that will protect health plans against liability for breach of contract and negligence, for example, and some insurers offer policies that will protect against vicarious liability claims, including those that arise as a result of medical management activities. Health plans in many areas can also obtain insurance against punitive damages, although some states prohibit on public policy grounds insurance against punitive damages.
The Importance of Risk ManagementWe have discussed some of the legal damages and financial penalties that can result when claims are asserted against health plans. It is important to remember, however, that health plans may suffer other indirect consequences, such as action by regulatory agencies and adverse public relations, when dissatisfied plan members or providers
Page 427 of 469
AHM 510 : Health Plans : Governance and Regulation
bring claims against them. A health plan that is accused of negligence or other wrongdoing may also suffer damage to its reputation and, as a result, find it more difficult to secure business from employers and other plan sponsors. For all these reasons, many health plans are relying more heavily on risk management programs to help prevent claims from occurring and to minimize the damage from claims that do occur.
We have already discussed some of the steps health plans can take to help avoid claims by plan members and providers. In addition to these steps, as we saw in Governance: Accountability and Leadership, health plans have implemented compliance programs to help ensure compliance with regulatory requirements and to monitor member satisfaction. An important goal of compliance programs is to identify and correct potential liabilities before they result in claims or litigation. As part of the compliance process, health plans rely on legal counsel to help them keep abreast of court decisions and proposed legislation that may affect the legal relationships between health plans and their members and providers.
As we discussed in The Components of Governance in a Health Plan, health plans can obtain insurance to protect them against many of the risks we have discussed in this lesson. Insurance is available that will protect health plans against liability for breach of contract and negligence, for example, and some insurers offer policies that will protect against vicarious liability claims, including those that arise as a result of medical management activities. Health plans in many areas can also obtain insurance against punitive damages, although some states prohibit on public policy grounds insurance against punitive damages.
Page 428 of 469
AHM 510 : Health Plans : Governance and Regulation
Chapter 13 APublic Policy and Changing Environment
After completing this lesson, you should be able to:
Explain some of the ways that health plans influence public policy Identify primary interest groups in each of the major healthcare sectors that
participate in efforts to affect health plan public policy Describe several types of advocacy and political activities undertaken by interest
groups in the health plan policy debate Discuss the role of litigation in determining health plan public policy Describe several techniques interest groups use to affect public opinion
Public Policy from the Health Plan Perspective How do we expand health benefit coverage to include more medical conditions and more treatment alternatives? And, how do we continue to improve the quality of healthcare delivered in this country? On the other hand, how do we control costs and make coverage available to the roughly 42 million Americans who currently lack health insurance coverage. How do we slow (or even halt) the growth of the uninsured population? How do we make the healthcare system easier to navigate?
Each side of this healthcare dilemma has its own supporters, and those supporters have varying political resources and constraints that affect their abilities to influence policy. These resources and constraints change over time with changes in market, budgetary, and political conditions.1 Some of these issues are at center stage in health care public policy; other issues are in the wings. In this lesson, we define what public policy is and examine some of the major factors that influence the public policy process.
What Is Public Policy?For purposes of this discussion, we define public policy as any law, regulation, principle, or plan established by an agency, arm, or branch of government. It can apply at the federal, state, or local level. Most often, public policy involves action and is shaped by many players, including privatesector entities, interested in its outcome. However, the choice not to act is also an element of public policy, as “absence of action is not the absence of policy.”2
Governments have six types of tools they can exercise in the domain of public policy: legislation, regulation, taxation, funding of public programs, purchase of services, and collection and provision of information.3 Historically, they have used these tools within the realm of two broad categories of public policy—allocative policies and regulatory policies.
Types of Public PolicyIn the context of public policy, allocative policies are those that determine the allocation of public funding. Regulatory policies include all other policies that affect the delivery and financing of healthcare in both the public and private sectors.
At the broadest level, Medicaid and Medicare are examples of allocative policies— government programs that allocate public funds to members of the population eligible for
Page 429 of 469

AHM 510 : Health Plans : Governance and Regulation
such programs. Medicare laws have always recognized that health plans were fundamentally different modes of financing healthcare and provided that health plans could receive payment for services on a basis other than standard fee-for-service. Over time, the federal government has enacted a number of laws designed to attract health plans into the Medicare market. These laws, ranging from amendments to the Social Security Act (Section 1876 of the Social Security Act) to the Balanced Budget Act of 1997, are discussed in earlier assignments in this course manual. All of these laws are allocative in that they change how health plans participating in the Medicare program do business and they shift the way public money is spent in the provision of healthcare.
Similarly, the federal and state governments, acting in loose concert, have adopted a number of allocative laws and regulations affecting health plans by switching state Medicaid systems from fee-for-service to health plans. As we have seen, Congress laid the groundwork for this series of laws in 1981 by expanding the authority of the Centers for Medicare and Medicaid Services (CMS), formerly known as the Health Care Financing Administration, to grant waivers to states seeking to experiment with ways of providing healthcare to the indigent. Arizona was the first state to create a health plan Medicaid system, and dozens of states have followed suit in the intervening years. While these laws and regulations affect how health plans operate, they are essentially allocative in their purpose and content, since they modify how public funds are spent in the financing of healthcare.
Although most allocative policy is set by the legislature, the legislature is not the sole government agency that is engaged in such allocative actions. For example, when former President Clinton announced an Executive Order expanding federal efforts to enroll children in Medicaid, he proposed a public policy action that will change the allocation of public resources devoted to healthcare.
Other laws and regulations, which are regulatory in nature, control how health plans do business. State and federal officials, both legislative and regulatory, have been engaged in a nearly constant process of adopting new regulations in the last few years. Laws ranging from the Health Insurance Portability and Accountability Act (HIPAA) of 1996—that contains provisions designed to ensure access to portability of healthcare coverage—to laws affecting health plan quality oversight and how health plans may contract with providers fall into this category of regulatory policy. Examples of regulatory policy include mandated healthcare benefits, laws specifying procedures for health plan handling of consumer appeals and grievances, and laws and regulations addressing the solvency of health plans.
Allocative policy is limited because only a portion of the population receives direct benefit from the allocation of public funds for healthcare. In contrast, regulatory policy is nearly unlimited in its range. The regulation of the financing and delivery of healthcare affects nearly every American. Health plans have their greatest impact on public policy in the arena of regulatory policy where they help set legislative agendas and develop laws.
Review Question
Page 430 of 469

AHM 510 : Health Plans : Governance and Regulation
The government uses various tools within the realm of two broad categories of public policy-allocative policies and regulatory policies. In the context of public policy, laws that fall into the category of allocative policy include
the Balanced Budget Act (BBA) of 1997
the Health Insurance Portability and Accountability Act (HIPAA) of 1996
laws affecting health plan quality oversight
laws specifying procedures for health plan handling of consumer appeals and grievances
Correct. Allocative policies are those that determine the allocation of public funding.
Incorrect. HIPAA is an example of regulatory policy.
Incorrect. Laws that affect health plan quality oversight are examples of regulatory policy
Incorrect. Laws specifying consumer appeals and grievance procedures are examples of regulatory policy
How Health Plans Exert Influence on Agenda SettingHealth plans help set the agenda for regulatory policy in a variety of ways. At the passive end of the spectrum, a health plan can simply comply with the laws and regulations that apply to its organization. At the active end of the spectrum, health plans can choose to devote resources in a variety of ways to influence the content of the relevant laws and regulations. Even the most passive health plans can influence the course of public policy through their day-to-day operations. The failure to act can also shape policy. An omission so seemingly minor as a failure to train health plan employees to properly answer members’ questions about how the health plan is complying with a new state law can inadvertently trigger legislative and regulatory activity. In addition, much of today’s legislative and regulatory activity seems to be driven more by politics than by the actions or nonactions of health plans.
One example of the influence of individual health plans on regulatory policy relates to so-called “gag” clauses. In 1996, a few reports of the presence of these clauses in some contracts led to state and federal government action. In a span of a few months, state and federal governmental bodies prohibited such clauses. In November 1996, CMS sent a letter to health plans explaining that federal law prohibited the restriction of a physician’s responsibility to explain all treatment options.4 By the end of 1997, over 40 states had adopted laws or regulations prohibiting or limiting the use of these clauses. Yet, despite this nearly universal public policy activity in opposition to such clauses, the U.S. General Accounting Office’s examination of the issue found that the clauses were virtually nonexistent in provider contracts.5
Health plan public policy activity, especially in the last few years, also has broader roots. That portion of policy activity that is responsive to broad changes in the market is
Page 431 of 469

AHM 510 : Health Plans : Governance and Regulation
growing rapidly, as government becomes increasingly responsive to constituencies injured or fearing injury by changes in the health plan market.6
Exerting Influence Through Policy ModificationAs we discussed in the preceding lesson, health plans can influence public policy through acts or omissions at the policy or operational level. They also influence public policy by modifying their policies or practices. A recent example illustrates this point. In 1995, the Maryland General Assembly threatened to force health plans to pay for all medical care provided to health plan members in Maryland emergency rooms, even when the condition underlying the care was not considered an emergency under the state’s “reasonable layperson” standard. Legislators were particularly interested in situations in which the member’s primary care physician referred the member to the emergency room. Reports indicated that some health plans were not covering medical care administered in emergency rooms after such a referral. Health plans argued that such policies denying coverage for emergency room referrals may have existed in the past, but no longer existed. By surveying its members, the Maryland Association of Health Maintenance Organizations (MAHMO) confirmed that no members of MAHMO had such a policy, blunting the pressure for the General Assembly to act on the subject.
One observer explains health plans’ ability to anticipate the issues that will be the subject of policy debate and perhaps shape that policy in this way:
Federal policy is often mentioned as an important force behind increasingly competitive health care markets. But if this is the case, it is not through policies that have been enacted, but through a process of market participants taking anticipatory steps to prepare for policies that might be enacted.7
In the wake of the Clinton administration’s healthcare reform initiatives in the 90s and the more recent Republican initiatives for Medicare in 2004, health plans anticipated and shaped public policy on those issues.8
Exerting Influence in the Development of LegislationHealth plans have an even greater impact on public policy when they participate in the process of developing legislation. This participation can be formal or informal, and includes bill drafting and voicing opinions on legislation through written or oral testimony, informal advocacy, or undertaking grassroots efforts. In the following lesson we discuss these methods of influencing legislation. Later in this lesson we discuss influences on overall public policy that are not necessarily limited to specific legislation.
Drafting LegislationWhen a health plan or an association of health plans wants government to take a specific action, they may actually write the proposed law and present it to one or more legislators for introduction. The chief advantage to this approach is that it provides the drafting organization with an opportunity to start the policy discussion with its own language, so that any subsequent versions will simply be amendments to the organization’s starting position. In some situations, the final product may be closer to the health plan’s position than it would have been if others initially drafted the bill.
A bill drafted by a health plan may also be easier to implement than a similar bill drafted by legislators and their staffs. Health plan employees often have a greater understanding of operational nuances than do legislators. While this may not be an important consideration when the time comes to pass or reject a bill, it could be vital at the point of implementing the law.
Page 432 of 469

AHM 510 : Health Plans : Governance and Regulation
One argument against health plan bill-drafting is the assumption that the drafting is driven by self-interest. However, the health plan can argue that while its proposed changes certainly are in its own best interests, a health plandrafted bill also serves the public interest. The success of this argument depends on the nature of the proposal itself, the credibility of the organization, and the political climate in the state or the nation. Proposals to change health plan laws vary based on the extent to which other groups and the public would be affected by the change. Some proposals impact the relationship between health plans and all their members, suppliers, and providers—impact many people and/or many interest groups. Other proposals impact only the relationship between the government and health plans. For example, proposals such as those to simplify the procedure for market conduct impact only regulators and health plans.
Similarly, the credibility of the health plan introducing the proposal will affect its ability to persuade legislators that its proposal is in the public interest. This credibility is a product of many factors. One factor is the organization’s reputation with legislators. If the health plan and its representatives are perceived by legislators as providing objective information about the industry and their operations, their credibility will be high. Credibility can also be affected by the health plan’s behavior in the marketplace. In general, health plans that serve their members well will have greater success persuading legislators that their proposals are in the public interest. Another factor that affects credibility is personal relationships between legislators and the health plan’s leaders and lobbyists.
The political climate surrounding the introduction of the health plan’s proposal also influences the likelihood that the health plan’s proposal will lead to legislation. In some markets, the history of healthcare issues is so contentious that no health plan’s proposal is accepted, no matter how limited the proposal or how credible the organization.
If an individual health plan has credibility problems with legislators, it can ask an industry trade association to sponsor legislation that the health plan supports. A health plan that wants an industry trade association to sponsor legislation generally participates on the association’s legislative committee. Such committees, typically composed of public policy specialists from each of the member organizations of the association, make all recommendations concerning legislative matters for the association. Health plan association legislative committees are good venues for the drafting of legislation because of the diverse expertise of the committee members. If an entire industry has credibility problems with legislators, the industry participants may ask another organization or group of organizations outside the industry to sponsor legislation or to work jointly to secure passage of specific legislation.
Voicing Opinions on LegislationHealth plans that wish to express their opinion on their own or other proposals may express their views through both formal and informal processes. The most formal method of voicing opinions is through the submission of written and oral testimony in a legislative hearing. A health plan faces several decisions in pursuing this approach.
First, it must decide whether to submit that testimony on its own or through its association or other interested parties. The health plan’s credibility with legislators, discussed in the previous section, affects this decision. Second, if the health plan decides to present its own testimony, it must decide who should present that testimony.
Page 433 of 469

AHM 510 : Health Plans : Governance and Regulation
Most often, the choice is between a medical director or a government relations professional.
The decision depends on both the position and the individual, and in both cases the issue is credibility. Some professional occupations lend more credibility than others, particularly on certain issues. For example, for issues concerning how an health plan makes medical necessity decisions, a good argument could be made that the health plan’s representative should be its Chief Medical Officer.
While legislators, like their constituents, are influenced by the credibility of physicians, they are also influenced by other issues —such as the expertise of the witness. In optimal testimony, this expertise should be both substantive and procedural. Certainly, the health plan’s witness should have unquestionable understanding of the subject of the proposed legislation. Additionally, the witness should have a solid understanding of the legislative process generally and the legislative committee hearing process specifically. Not only should the witness understand what is going on, he or she should be comfortable as a participant in the process.
In general, it may make sense to have the medical director testify at more technical, less emotional hearings and the government relations professional testify at less technical, more heated hearings. Sometimes, however, health plans are faced with an acute need for substantive expertise found only among its senior management and medical directors on an issue over which emotions are inflamed. Most health plans train their executives and clinical professionals to present oral legislative testimony in a hostile environment. While many health plans and trade associations have the expertise in-house to provide such training, many are turning to a growing body of consultants who specialize in preparing employees for legislative committee hearings.
Many experts, however, question the value of appearing before a legislative committee to make one’s case. Some believe that a health plan or its association can accomplish much more through informal advocacy. Informal advocacy which is a form of lobbying (discussed later in this lesson) involves the promotion of a position in ways other than providing formal legislative testimony. Such advocacy may be limited by state open meeting laws. These laws, present in most jurisdictions, place some restrictions on the ability of advocates to present their case to groups of legislators behind closed doors. However, some forms of informal advocacy are still permitted under these laws.
The most commonly used type of informal advocacy is the face-to-face meeting between the health plan’s representative and a legislator and his or her staff. Such encounters between lobbyists and legislators occur while the legislature is in session. Sometimes health plans bring a clinical leader or senior executive to such meetings to provide substantive information. Usually, the health plan’s lobbyist accompanies the health plan executive, to provide an interpersonal liaison between the legislator and the executive and to help provide political context to which the executive may not be privy.
Grassroots lobbying efforts can have a substantial impact on the development of legislation. For purposes of our discussion, a grassroots lobbying campaign is a connected series of efforts or actions directed at generating public support on a particular issue which an organization or group supports. We discuss this concept in more detail later in this lesson.
Page 434 of 469
AHM 510 : Health Plans : Governance and Regulation
A variation of the face-to-face meeting between health plan executives and legislators is the “lobby day.” Typically coordinated through a trade association, lobby day is an all-day affair during which health plan employees at all levels and from all departments move from appointment to appointment with individual legislators, accompanied where possible by a lobbyist or other government relations professional. The value of such a series of meetings is that the legislators meet their constituents in the health plan industry and can develop a better understanding of their needs and the challenges they face.
A similar form of advocacy is the “site visit.” In a site visit, an individual legislator, a legislative subcommittee, or even a full committee pays a visit to a major facility of the health plan. During the visit, the legislators meet with employees at all levels of the company, both at their desks and in open meetings. Where a lobby day allows a health plan to put a handful of its employees in front of the legislators, a site visit can put hundreds of employee-voters in face-to-face contact with lawmakers, for a longer period of time than is usually available on a lobby day. The site visit is also a forum that is amenable to highlighting some of the pro-consumer achievements of the health plan, such as a disease-management program, a high-achieving quality improvement department, or community service.
Effective advocacy does not start or end with legislators. Legislative staff may be an even more important audience for the advocacy methods described in this section. As translators and interpreters for legislators and committees, legislative staff members spend time reading testimony, listening to detailed concerns about bill drafting, and balancing competing interests. They often serve as the “gatekeeper” to the legislator.
In addition to face-to-face meetings, the written word is influential in the legislative process. Individual letters, including electronic mail, from constituents are often effective in making a case for or against legislation. health plans can seek participation in their letter-writing campaigns to legislators from their enrollees and other interested parties.
Exerting Influence in RulemakingAs we have seen, much of the regulatory policy that affects health plans stems from administrative rules and regulations, discussed in Overview of Laws and Regulations, rather than laws. Rulemaking and regulation drafting offer health plans an opportunity to shape health plan policy.
Most state legal codes include an administrative procedures act, which establishes the requirements that agencies must follow to establish and enforce regulations. They also often mandate that certain procedures must be established through formal rulemaking or regulation as outlined in the administrative procedures act, to prevent agencies from circumventing the guidelines set forth in the act. In general, rulemaking requirements are designed to ensure adequate public notice and opportunity for public comment prior to the finalization of a proposed rule or regulation.
Administrative procedures acts typically require administrative agencies to take the following steps to establish rules or regulations:
• Notify a central state agency (such as the Office of the Secretary of State) of the agency’s intent to promulgate a rule or regulation
Page 435 of 469

AHM 510 : Health Plans : Governance and Regulation
• Publish in the official state administrative publication (usually known as the Register) and/or in a newspaper of general circulation, and notify any parties that have requested notification, of the agency’s intent to promulgate a rule or regulation, the text of the proposed rule or regulation, and the date or dates of public hearings
• Prepare (and perhaps publish) an analysis of regulatory impact
• Allow oral and written testimony to be submitted to the agency, either in the public hearing(s) provided for such purpose or directly in writing to the agency
• Decide whether to adopt, amend, or withdraw the proposed rule or regulation
• Publish (as described above) notice of adoption or amendment of the proposed rule or regulation
In most states, interested parties may influence the process at several points along the way. The first opportunity is in the decision to promulgate. If, for example, a state agency is engaged in a regulatory practice that, in the view of a health plan, would not withstand the public scrutiny that is built into the formal promulgation process, it might seek to induce the agency to promulgate a rule or regulation that formalizes that practice. It may use informal direct persuasion in discussions with regulators, exert pressure on regulators through other public officials in the legislative or executive branches, or threaten or even bring litigation to force the initiation of the statutory rulemaking process.
If relationships between a health plan and its regulators are sufficiently positive, a health plan can provide technical assistance to the regulators as they draft the proposed regulation. Most states do not prohibit such informal consultations, although state law should be consulted. In some cases, informal participation prior to the initiation of formal rulemaking procedures is encouraged by regulators through the formation of informal working groups and advisory committees. The drafting stage of the rulemaking process is a good opportunity to anticipate and avoid potential technical problems that may be difficult to address in a more formal process. It is also the last opportunity for a health plan to participate informally in the rulemaking process. Once the process has begun, and notice of intent to establish rules is published, there is substantial pressure on interested parties to participate exclusively through the statutory process. If the agency accepts input through avenues other than those specified in the governing statutes, the legality of the process may be threatened.
The formal rulemaking process is very much like the legislative hearing process described earlier in this lesson except that the hearing is before an administrative law judge rather than a legislative committee.
Health plans participating in the formal hearings on a proposed rule or regulation face the same questions of mode of testifying, who should testify, and whether to involve allied organizations. The primary difference between hearings in the two settings is that the regulatory hearing is likely to be more substantive and less emotionally charged, because most regulators have more expertise in the particular area of regulation than most legislators. A health plan typically will send its most technically proficient experts to regulatory hearings, paying less attention to the public relations and oratorial skills than it would pay in connection with a legislative hearing.
Page 436 of 469

AHM 510 : Health Plans : Governance and Regulation
Once the regulators adopt a rule or regulation, health plans can continue to participate in the process by appealing the decision. In some states, the first appeal after the formal adoption of a rule is to the same agency, in the form of a request for reconsideration. In others, the first appeal is to an external agency, either executive (such as to a commission that oversees the regulatory agency), legislative (to a special committee that oversees the state’s administrative process), or judicial (either an administrative law judge whose jurisdiction is primarily over such appeals from regulatory bodies, or to a court of general jurisdiction). Generally, the grounds for such an appeal are limited either to procedural grounds or jurisdictional grounds. Procedural grounds for appeal are usually in the form of objections to the process by which the rule or regulation was adopted, such as a claim of inadequate opportunity to be heard, improper publication of the notice of intent to establish rules, or some other nonsubstantive objective. Jurisdictional grounds for appeal generally are objections that the subject matter is outside the realm of issues that are legal for inclusion in that agency’s rules or regulations, or that the regulations are contrary to or inconsistent with the law.
Beyond procedural and jurisdictional grounds, bases for appeal are usually extremely limited. Those states that do permit appeals on other grounds than these limit the grounds for appeal to a claim that the regulatory agency abused its discretion and imposed substantial burden-of-proof requirements on the party appealing the regulatory decision.
Review Question
Health plans are allowed to appeal rules or regulations that affect them. Generally, the grounds for such appeals are limited either to procedural grounds or jurisdictional grounds. The Kabyle Health Plan appealed the following new regulations:
• Appeal 1 - Kabyle objected to this regulation on the ground that this regulation is inconsistent with the law.
• Appeal 2 - Kabyle objected to this regulation because it believed that the subject matter was outside the realm of issues that are legal for inclusion in the regulatory agency's regulations.
• Appeal 3 - Kabyle objected to the process by which this regulation was adopted.
Of these appeals, the ones that Kabyle appealed on jurisdictional grounds were
Appeals 1, 2, and 3
Appeals 1 and 2 only
Appeals 1 and 3 only
Appeals 2 and 3 only
Incorrect. Jurisdictional grounds for appeal generally are objections that the subject matter is outside the realm of issues that are legal for inclusion in that
Page 437 of 469
AHM 510 : Health Plans : Governance and Regulation
agency’s rules or regulations, or that the regulations are contrary to or inconsistent with the law.
Correct! Jurisdictional grounds for appeal generally are objections that the subject matter is outside the realm of issues that are legal for inclusion in that agency’s rules or regulations, or that the regulations are contrary to or inconsistent with the law.
Incorrect. Jurisdictional grounds for appeal generally are objections that the subject matter is outside the realm of issues that are legal for inclusion in that agency’s rules or regulations, or that the regulations are contrary to or inconsistent with the law
Incorrect. Jurisdictional grounds for appeal generally are objections that the subject matter is outside the realm of issues that are legal for inclusion in that agency’s rules or regulations, or that the regulations are contrary to or inconsistent with the law.
Appeals of regulations are relatively rare. First, as we have just seen, the grounds for appeal are usually limited to procedural and jurisdictional grounds, providing potential appellants with a narrow target for an appeal. Second, courts are reluctant to impinge on the ability of regulators to exercise their legal discretion in establishing rules and regulations. Third, interested parties—particularly those, like health plans, who have an ongoing relationship with regulators and therefore an ongoing need for the continued good will of the regulators —are generally reluctant to threaten the regulators’ good will by appealing a regulatory decision.
Exerting Influence at the Stage of Policy OperationPolicymaking does not end with adoption of a law or regulation. It extends into the administration of the policy as well. Most laws and regulations are vaguely written to garner broad-based support, allow for contingencies, and reduce the threat of challenge. This drafting ambiguity gives regulators enormous flexibility in administering laws that apply to health plans. It also gives health plans opportunity to influence administrative decisions.
Frequent contact between regulators and health plan employees tends to increase familiarity and can help the health plan in its effort to make an impact on how a law is administered by regulators.9 If it appears that the health plan can bring substantial expertise in a hearing before an administrative law judge, and is likely to prevail in that hearing on the basis of that expertise, the regulator is more likely to be responsive to the health plan’s arguments.
A health plan’s direct influence over regulators is augmented by its ability to take its case elsewhere. Regulators do not operate in a policy vacuum, despite the presence of a wide variety of legal mechanisms to ensure their independence from the influence of other branches of government, or even other parts of the executive branch of government. Regulators make their decisions about how to implement health plan laws and regulations with an eye on the governor, other regulators, the legislature, and the courts.
Page 438 of 469
AHM 510 : Health Plans : Governance and Regulation
Most state health plan regulators, whether in insurance departments, health departments, or elsewhere, are accountable to the state governor. Only a dozen insurance commissioners are elected directly by the people, and fewer chief health regulators are elected. Most of the chief regulators are appointed by the governor. When the actions of regulators seem grossly unfair, health plans have the option of pleading their cases with the governor. While this avenue is rarely pursued except in situations where the stakes are high and the regulatory conduct is extreme, the existence of this option helps to temper regulatory conduct to some extent. While not all health plan regulators report to the state’s governor, all are accountable to legislatures for their authority, funding, and staffing. This means the legislature is also a potential forum for a health plan to air disputes with a regulator. However, the regulators can also appeal to the legislature for support or the passage of further legislation to bolster their position.
Regulators are also accountable to the judicial branch of state government. This accountability provides health plans with another forum for appeal of perceived regulatory abuses. Judicial appeal is the most direct route for a health plan to seek redress for grievance it may have against a regulator, but it is often the least likely to succeed and the slowest. Regulators have a great deal of legal discretion in the administration of the laws within the scope of their jurisdiction. As a result, courts are reluctant to overturn regulatory judgments except in cases of clear abuse of that discretion or a reasonably clear showing that the regulators misapplied the law or regulation.
Health plans rarely seek any of these avenues of relief from regulatory burdens. An appeal is likely to diminish good will between the health plan and its regulators, good will that the health plan needs to function in a highly regulated environment. For the most part, health plans rely on their expertise and the good will of regulators in its exercise of influence on policy.
Participation on Government-Sponsored Task ForcesWhen government officials face a difficult challenge, they often advocate the creation of task forces to research and resolve the issue. A task force is a special, ad hoc committee established to research and report on a specific problem or issue. A task force typically consists of multilevel and/or crossfunctional personnel.
The Formation and Purposes of Task ForcesPolicy makers can form task forces in a number of different ways. The variety can be attributed to differences in state laws, disparate political dynamics in various legislative and regulatory environments, and differing levels of interest among members of the executive and legislative branches. For example, a governor or the President can call for a task force to be formed. In addition, the legislature sometimes convenes a task force to deal with complex or volatile issues.
Task forces are formed for a variety of purposes. For example, a task force can be formed to address broad issues, such as health plan accountability, the costs and benefits of expanding a health plan’s tort liability, or reviewing various proposals for mandates and determining if mandates are the best way to ensure access and quality care.
Page 439 of 469

AHM 510 : Health Plans : Governance and Regulation
Alternatively, a task force can focus on narrower issues, such as ways to amend state laws to allow plan members to bring suit against the health plan for tort liability. In cases such as this, the basic issue has been decided in advance (e.g., plan members must be able to bring suit for tort liability against a health plan), leaving the task force to decide only on its implementation.
Composition of Task ForcesThe composition of a task force can often determine the outcome of the process. The interests and policy preferences of the participants on a task force, as well as the number of representatives from each viewpoint, may decide the task force’s ultimate results. For example, a task force that is formed to address health plan issues, and that has minimal representation from the health plan industry may make recommendations that are not practical to implement. health plans often work to assure representation on task forces.
Work StructureTask forces may structure their duties in at least two different ways. They may form subcommittees and delegate specific tasks enumerated in the task force’s purpose to each subcommittee for research and recommendation to the full task force. On the other hand, the task force may operate as a group to perform the research and make recommendations to its founders. The timeframe and number of participants on a task force may determine the work structure.
Insight 13A-1 describes two task forces that were created to address health plan public policy.
Insight 13A-1. Examples of a Federal and a State Task Force.
In the following examples, the clamor in the Congress and the California legislature, respectively, for changes in health plan law induced the president and California's governor to move the proposed changes into task forces that could consider all the issues together.
The President's Advisory Commission on Consumer Protection and Quality in the Health Care Industry
President Clinton established the Advisory Commission on Consumer Protection and Quality in the Health Care Industry (President's Commission) by Executive Order 13040 on March 26, 1997. Because he established the commission by executive order, he had complete discretion over the Commission's composition, purpose, and work plan.
Purpose: The president's task force focused on implementing a public policy directive (i.e., to make recommendations concerning consumer protection and quality in healthcare). The objectives of the president's commission were to:
1. Review the available data addressing consumer information and protection for health plan members and to recommend any necessary improvements
Page 440 of 469

AHM 510 : Health Plans : Governance and Regulation
2. Review existing and proposed efforts to define, measure, and promote healthcare quality, and attempt to build consensus on approaches to promote healthcare quality
3. Collect and evaluate information on changes in the availability of healthcare treatment and services and to recommend any necessary improvements
Composition: The president's commission was comprised of 32 members drawn from a broad array of stakeholders: seven members that represented academics, foundations, and experts, one consumer advocate, three representatives of labor unions, two lawyers, five representatives from health plans, four private purchasers, eight providers, one research organization, and one representative of state government officials.
Work Structure: This commission held public hearings, took testimony, and reviewed and commissioned extensive research. It conducted the bulk of its work through subcommittees.
The California Managed Health Care Improvement Task Force
The California task force was produced through actions of the governor and the legislature. California Governor Pete Wilson expressed his opposition to piecemeal reform of the health plan industry by threatening to veto most health plans legal reform bills in 1996. This led the legislature to approve Assembly Bill 2343, to require the governor to create a task force on health plans to research and report on certain aspects of the effect of healthcare plans. During the year while the task force met, the governor continued to veto legislation aimed at health plan practices, citing his desire to await the recommendations of the task force.
Purpose: This task force took a broad-based approach and focused on establishing the policy itself. Its objectives were to research and report on:
1. An overall descriptive analysis of the world of health plans, including a review of the types, modes of operation, and structure of health plans, health plan regulation, the trends and changes in healthcare and their impact on the economy, academic medical centers, and the education of healthcare professionals
2. Whether health plans are succeeding in controlling costs and improving quality and access to care
3. An examination of the impact of provider financial incentive systems on the delivery of healthcare
4. The effect of health plans on the patient-physician relationship, if any, and on academic medical centers and health professions education
Composition: Twenty of the California Task Force's 30 members were gubernatorial appointees - four representatives of each of five groups: healthcare plans, employer purchasers, healthcare plan enrollees, providers of healthcare, and consumer groups. The Senate Rules Committee and the Assembly Speaker each had five appointments, one
Page 441 of 469

AHM 510 : Health Plans : Governance and Regulation
from each of these groups. The governor also appointed five ex-officio members and the Senate appointed two ex-officio members.
Work Structure: The California task force held public hearings, with agendas posted, and minutes and transcripts made available to the public. The task force itself consulted with experts, reviewed existing policy research, and conducted a public opinion survey.
Other Participants in PolicymakingSo far, we have discussed the influence that health plans have on the development and implementation of public policy. In this section, we address the roles of two other major participants in the policy making process: organized interest groups and politicians. Organized interest groups are groups that “have discernible stakes in or positions on the policy status quo or policy alternatives to it. They each naturally wish to manipulate policy making to the advantage of their group or clients.”10 Politicians “are the elected officials who possess the formal public authority to decide the course of government policy and who regularly suffer the consequences of their decisions by standing for reelection in their constituencies.11
Interest GroupsIn the context of health plan policy, interest groups consist of payors, providers, purchasers, and consumers. Each group is typically motivated by some blend of self-interest and the public interest. In addition, each group vies to be heard in the health plan policy discussion.
PayorsHealth plans are payors, as are indemnity insurers and self-funded employer groups that provide healthcare coverage. (Self-funded employer groups can be either payors or purchasers depending on which tasks they perform themselves and which tasks they contract to third parties.) Although payors as a group would seem to have the same interests in health plan policy, this is not always the case. For example, a substantial number of individuals in group plans still are not covered under health plans. Employees in these plans receive their coverage from indemnity carriers. Indemnity carriers sometimes find themselves opposing health plans on policy positions that would alter the way health plans and indemnity carriers are regulated relative to one another. An example of such an issue would be a law specifying that the state employees’ health benefit plan contract only with health plans accredited by a national accreditation organization. Such a decidedly pro-managed care slant would split traditional allies within the payor community.
Often, indemnity carriers are organized separately from health plans into trade associations restricted to representing the interests of these indemnity carriers. For example, in Maryland you will find both the Maryland Association of Health Maintenance Organizations and the Maryland League of Life and Health Insurers. However, in many cases, insurers that provide traditional indemnity coverage also provide PPO, point-of-service, and HMO options. What’s more, companies that traditionally offered only “pure” HMO products are now offering a full line of health products including indemnity, PPO, and point-of-service products. As a result, the lines between health plans and indemnity payor trade associations become increasingly blurry each year. On the national level, trade associations that represent the interests of health plans include the America's
Page 442 of 469

AHM 510 : Health Plans : Governance and Regulation
Health Insurance Plans (AHIP) and the Blue Cross and Blue Shield Association (BCBSA).
Employers that offer self-funded plans to their employees have policy interests distinct from indemnity carriers, and other employers that purchase healthcare coverage from indemnity carriers and health plans. As we discussed earlier in this lesson, the most significant policy distinction is that self-funded plans are not subject to state insurance laws. ERISA’s preemption of such state insurance laws has profound consequences in the area of health plan policy. For example, if a state’s oversight of health plans becomes so rigorous that it imposes an undue burden or cost on health coverage, employers may decide to selffund and thereby escape the regulatory burden.
Similarly, self-funded employers often have an entirely different reaction to state legislative proposals affecting health plans (which laws would not apply to them) than the employers that purchase health coverage from regulated carriers and health plans. Finally, while a state-regulated health plan could conceivably support some forms of federal regulation of health plans if the law helped to level the competitive playing field without damaging its ability to operate profitably, it is less likely that self-funded employers would support an expanded federal regulatory role that subjects them to additional regulation.
Fast Fact
In 2003, HRET/KFF estimated that only 7% of covered employees were still in conventional indemnity plans.12
The government also acts as a payor for healthcare programs such as Medicare, Medicaid, CHAMPUS, and FEHBP. However, the government is a different kind of payor than those we have already discussed. Unlike other payors, government can—for the most part—unilaterally change the terms under which it operates as a payor. One of the few constraints on this power, other than traditional mechanisms of accountability to the public, is the extent to which a state is constrained in some important respects by federal Medicaid law.
ProvidersAs we discussed earlier in this lesson, increasing numbers of physicians and hospitals have begun to band together to create risk-bearing entities similar to health plans. This blurring of roles in the healthcare market has had an impact on health plan politics and policy. Providers that once opposed all policies that furthered the spread or enhanced the operations of HMOs may now support such policies. Indeed, state health plan associations are finding that traditional political opponents are taking different political stands than they did only a couple of years prior, and these former opponents are now becoming members of the health plan association.
However, it is still valid to consider providers as a separate interest group with policy interests that are often in direct opposition to health plan policy interests. Increasingly, employers that are demanding more services for a lower cost have health plans searching for ways to cut costs while continuing to deliver a quality healthcare product.
Page 443 of 469

AHM 510 : Health Plans : Governance and Regulation
ProvidersLike health plans, providers operate in the policy arena both as individuals and as institutions. The most visible provider policy participants are the physician professional associations, such as the American Medical Association (AMA) and the National Medical Association (NMA). Specialists such as obstetricians, pediatricians, and emergency physicians are also represented by national and state professional associations.
Physician societies often face challenges in representing the interests of all of their members. For example, some physician members have fared well in the modern healthcare marketplace while others have not. Reaching a consensus on a medical society legislative committee or executive committee on health plan policy issues can be challenging. As a result, some societies have lost members, and societies tend to take the middle road in policy positions. These same issues are also present in the organizations representing other providers, such as hospital or nurse associations.
Specialty physician organizations provide an opportunity to pursue specialty-specific issues that may not be the priority of a broader organization. For example, while only a small minority of the overall physician population is concerned with questions involving compensation for emergency services, these issues can be pursued with single-minded intensity by the American College of Emergency Physicians (ACEP) and its state affiliates.
Additionally, not all health plan policy issues are provider-versus-payor issues. Sometimes, they pit providers against each other. For example, scope-of-practice legislation can be both a health plan issue and a clear provider-versus-provider issue. Typically, scope-of-practice legislation is an attempt by one type of provider (not necessarily a physician) to amend state healthcare licensing laws to allow another type of provider to do a procedure or set of procedures typically reserved only to another provider group. One example is chiropractors’, psychologists’, and podiatrists’ efforts to expand their domain into areas previously thought to be the domain only of physicians. On the surface, these appear to be turf issues among providers. However, when coupled with state laws that prohibit health plans from discriminating among healthcare professionals that are licensed to provide a service covered by the health plan, these issues also become managed care policy issues.
Another example of a provider-versus-provider dispute can be found in health plans’ use of preferred pharmacies. Drug manufacturers, chain pharmacies, and locally operated pharmacies have often found themselves with opposing viewpoints or interests pertaining to health plans and pharmacy benefit managers (PBMs). For example, chain pharmacies have challenged local pharmacies over the ability of health plans to selectively contract with some pharmacies and exclude others—the any-willing-provider dispute. More recently, the use of formularies by health plans and PBMs has given rise to efforts to curb or eliminate their use. These issues have split the pharmacy world, with the chain pharmacies and manufacturers siding with the health plans and PBMs against the efforts of the local pharmacies.
Page 444 of 469

AHM 510 : Health Plans : Governance and Regulation
One advantage provider interest groups have over payor organizations is the number of providers represented by interest groups. The majority of people employed in the healthcare industry are engaged in the provision of healthcare, not the financing of it. The impact in terms of numbers of constituents that can become involved in an effort to lobby legislators translates directly into a larger number of:
• Votes, phone calls, and letters to legislators
• Face-to-face meetings between constituents and legislators
• Campaign contributions
PurchasersTypically, purchasers of health plans are strong allies of health plans. The business community has been supportive of health plans, both in purchasing decisions and in the political domain.13 One major reason for this support is the ability of health plans to help purchasers contain the increase in costs for healthcare coverage for their employees. Inflation in health plan premiums has been in the low- to mid-single digits for the last several years due largely to the rise of health plans as the dominant means of healthcare financing. Purchasers’ satisfaction with health plans and a fear of a return to rampant inflation fuel purchasers’ political support for health plans.
Political support for health plans often stem from organizations supported by large corporations. State and national chambers of commerce frequently have served as the coordinating bodies for business efforts to provide political support to health plans. Other organizations with substantial membership in large companies that have been important pro-health plan players have included the National Association of Manufacturers, the Health Benefits Coalition for Affordable Choice & Quality, and the The Washington Business Group on Health (WBGH). These organizations are all composed of payors and purchasers supportive of the health plans’ position in the public policy debate.
Small businesses sometimes have different concerns than large businesses when it comes to health plans. Small businesses may place more emphasis on aspects of health plans, such as accessibility and renewability, than larger corporations
Fast Fact
From 1993–1996, health insurance premiums lagged behind the rise in consumer prices.18
ConsumersAll the players in the public policy process contend that their positions are in the best interests of consumers. On one hand, the supporters of health plans claim, with some legitimacy, that:
• Health plans are pro-consumer because they have increased the affordability of health coverage for the average consumer
• Health plans, especially HMOs, are actively engaged in quality initiatives and support preventive care
Page 445 of 469

AHM 510 : Health Plans : Governance and Regulation
• Health plans slowed the tendency of employers to shift the cost of that coverage to employees
• Health plans established accountability for healthcare providers that was largely absent in the pre-health plan era
On the other hand, health plan opponents argue that:
• Health plans have restricted consumers’ ability to go to any healthcare provider they desire and have that visit covered by their health plans
• Government oversight of health plans is not uniform across the nation and suffers from serious gaps
The arguments about the consumer-friendliness of health plans have ample support on both sides. There are basically two types of organizations that seek to represent consumer interests: unaffiliated consumer groups and consumer advocacy organizations. Unaffiliated consumer groups consist of consumer advocacy organizations, such as the Consumers Union (CU), the Consumer Federation of America (CFA), Community Catalyst, and Public Citizen, that have a long history across a broad array of issues. These groups are less likely to represent a single special interest than consumer advocacy organizations. Consumer advocacy organizations are consumer organizations created by special interests with a more direct stake in the outcome of particular policy issues. For example, the American Association of Retired Persons (AARP) seeks to represent the consumer interests of retired persons. In addition, patient advocacy groups, discussed in Environmental Forces, can have an impact on healthcare public policy by advocating for the passage of laws to protect their members’ interests.
GovernmentAs we discussed previously, government acts as both a purchaser and regulator of healthcare services. In its role as a purchaser, government is a stakeholder in the health plan public policy debate. As a regulator, it has information often gathered through government-sponsored healthcare programs (e.g., Medicare and Medicaid) that impacts public policy for health plans.
State public officials are often members of not-for-profit organizations of state officials, divided along lines of job description. The oldest of these state associations, the National Association of Insurance Commissioners (NAIC), is a key participant in managed care debates because of the central role played by most insurance regulators in the oversight of health plans. The National Conference of State Legislatures (NCSL), representing over 8,000 state legislators across the nation, has a very active health policy component that often influences managed care issues. The National Governors Association (NGA) has taken positions on health plan issues such as any-willing-provider laws and consumer disclosure laws.15
Federal government officials are less likely than state public officials to be informally organized in not-for-profit associations. The need for organization at the federal level is filled by more formal governmental structures (e.g., the Department of Health and Human Services and the Department of Labor). However, one vehicle for participation of federal officials that is specifically focused on health plans is the National Association for
Page 446 of 469

AHM 510 : Health Plans : Governance and Regulation
Managed Care Regulators. The members are both state and federal officials involved in health plan oversight. Most of these officials are employees of the federal Centers for Medicare and Medicaid Services (CMS) and state insurance and health departments.
These organizations of state and federal officials participate in the health plan policy process primarily as experts. This has been particularly true in the 1990s, as the federal government has expanded its jurisdiction into areas, such as health insurance regulation for non-government programs, that have typically been the nearly-exclusive domain of state regulators.
Influences on PolicymakingIn this lesson we examine several ways that healthcare policymaking can be influenced. These influences are lobbying, political activities, litigation, and public opinion.
LobbyingLobbying, which we mentioned in our earlier discussion of informal advocacy, is the act of “communicating with public policymakers for the purpose of influencing their decisions to be more favorable to, or at least consistent with, the preferences of those doing the lobbying.”16 A lobbyist is a person employed or retained by a client to perform lobbying for compensation.
Both state and federal laws address lobbying. For example, federal lobbying laws do not consider a person a lobbyist if less than 20 percent of his or her time over a sixmonth period is spent lobbying. For the most part, federal and state lobbying laws exclude certain activities from the definition of lobbying, such as presenting testimony, participating in advisory commissions, and advocating on behalf of one’s own personal interests that are exclusive to that person.
Lobbyists play important roles in policy debates. They serve as educators, mediators, bill-drafters, facilitators, advocates, and fundraisers, to mention just a few of their roles. While many lobbyists are lawyers (legal training may assist their billdrafting), the number of nonlawyer lobbyists has grown over time.
Lobbying is big business. In the first six months of 1997, federal lobbying alone involved over 7,000 organizations spending an annual sum of $1.2 billion on over 9,000 lobbyists.17 Although it is difficult to assess what portion of these organizations performed lobbying on health plan issues, 2,531 organizations listed health issues as a subject on which they lobbied Congress— ranked third among all issues. Insurance issues were listed by 558 organizations, ranking 24th on the list of issues.18
Health plan lobbyists typically work for the health plans directly or for trade associations of health plans, or both. It is common practice in both the state legislatures and the Congress for health plan lobbyists to work in tandem with health plan association lobbyists. In some states, the association lobbyist will coordinate the efforts of the lobbyists representing the individual health plans. In other states, the lobbyists operate more independently of each other.
Most health plan lobbying efforts are coordinated through the relevant health plan association’s legislative committee. Such committees are typically populated by in-house government relations specialists from the member health plans who (1) lobby directly
Page 447 of 469

AHM 510 : Health Plans : Governance and Regulation
and (2) oversee the activities of outside lobbyists representing their respective health plans.
Political ActivitiesInterest groups can influence policy making by participating in the political election process. Most organizations, like health plans, that are profoundly affected by policy, participate in campaign financing to the extent permitted by law. American politics has always been dominated by money, and most of that money has come from organized groups, such as social, political, and business organizations. Institutional interests and many wealthy individuals typically finance the bulk of American electoral campaigns.
Before 1972, restrictions on campaign contributions were few. In the post-Watergate reform, however, Congress and a number of state legislatures began to limit substantially the extent to which organizations, both for-profit and not-for profit, could contribute to campaigns out of general organizational funds. Instead, political action committees (PACs) became the funding vehicle of choice for interest groups. Political action committees (PACs), organized under various state and federal laws, allow individuals and organizations to pool their resources to contribute to electoral campaigns. The laws under which these state and federal PACs operate usually limit or even prohibit certain kinds of organizational contributions, and usually establish incentives for funding to come from individuals rather than corporate or union treasuries. Organizations, therefore, fund the PACs they sponsor through individual, voluntary contributions from their employees, members, or other individual stakeholders.
PAC dollars go directly to candidates’ campaign committees, and, along with other contributions made directly to campaigns, are known as hard money. In contrast to hard money, soft money is not subject to state and federal restrictions on campaign financing. The U.S. Supreme Court drew this distinction in a 1976 decision that declared unconstitutional a federal effort to limit “independent expenditure” or soft money. Soft money is money used in connection with a candidate’s election but not contributed directly to the campaign or controlled by the campaign.19 As a result of the Supreme Court ruling, attempts to constrain soft money to fund independent efforts— that have an increasing impact on electoral politics—have been challenged based on freedom of expression conferred by the Bill of Rights.
Health plans, like other organizations greatly impacted by changes in the political arena, must decide whether it makes good economic, legal, and ethical sense to be involved in financing campaigns for public office. Those that choose to participate have a number of options. The more limited level of participation is to encourage employees to contribute to already-existing PACs, or to encourage employees to donate to a particular candidate or set of candidates deemed to be supportive of the organization’s interests. Greater involvement might take the form of establishing a PAC for employees’ contributions. Even greater involvement might involve soliciting outside the organization for contributions to the PAC (to such groups as the organization’s vendors), or to use corporate or individual funds to support soft-money efforts.
The importance of a health plan’s employees in the legislative process is often overlooked. As mentioned above, employees are frequently encouraged to participate in the legislative process by contributing to PACs and/or by writing letters to their representatives to support the health plan’s positions on policy issues. Many health
Page 448 of 469

AHM 510 : Health Plans : Governance and Regulation
plans invest a considerable amount of time and resources to educate their employees about the policy issues that impact their business.
LitigationMost discussions about public policy revolve around the executive and legislative branches of government. However, the judiciary also plays an important role in the public policy process.
Litigation has both a direct and an indirect impact on public policy. Direct impact can be seen in the changes in law brought about by appellate court rulings on sub-stantive issues. Indirect impact can be seen when litigation or the threat of litigation influences public officials’ decisions about public policy development and/or implementation.
One of the central functions of courts is to interpret the laws approved by the legislature. An additional function for courts is to test laws against the standard of the federal and state constitutions. Because legislation often deals with broad concepts instead of the details required for implementation, courts have had the task of interpreting the policy intended to be contained in legislation.
Where statutes are vague or too sparsely written, the courts must work especially hard. For example, the ERISA preemption clause gives rise to much court involvement in interpretation of ERISA. As we have seen, the preemption does not apply to “any law of any State which regulates insurance.” 20 The question of “what constitutes the business of insurance” defines the boundary between whether state insurance laws or federal laws under ERISA apply to the particular case. The courts, almost exclusively, have dealt with this question with little or no help from Congress.
Shaping Public OpinionPublic opinion is one of the more potent influences on policymaking. However, as we saw at the beginning of this lesson, public understanding of many healthcare issues is sometimes low, at least in the view of many policymakers and academics.For example, public support for the Clinton administration’s failed healthcare reform plan dropped from a high of 59 percent in September 1993 to 43 percent in April 1994, a 16-point drop in only six months.21 While members of the public may not have been particularly well informed on the details of the plan, it is undeniable that this collapse of support contributed to the political failure to act.
There are two basic approaches to lobbying through the vehicle known as public opinion: grassroots lobbying and media relations. A grassroots lobbying campaign includes a set of activities designed to encourage people or entities who share that same “desired” public opinion to contact key decision makers and voice their support for the opinion. In many instances, the “desired” public opinion is representative of the actual majority public opinion on an issue. Media relations, on the other hand, involve a direct effort to change public opinion through the vehicle of a wide variety of media, both paid and free.
There is an important distinction between these two concepts. While grassroots lobbying campaigns may have an impact on public opinion, those efforts are generally designed to give exposure to a public opinion that may or may not reflect the actual majority opinion on an issue. However, interest groups can broaden their efforts beyond
Page 449 of 469

AHM 510 : Health Plans : Governance and Regulation
straightforward grassroots tactics to try to influence public opinion at large. For the most part, this broader approach involves the use of mass media.
In a grassroots lobbying campaign, an organization has a number of potential sources of sympathetic individuals to tap. They include the organization’s employees, vendors, customers, business partners, and other stakeholders. In the case of a health plan, the array of potential contacts includes not only the company’s employees and vendors, but that part of the provider network that might be favorably inclined toward the health plan side of policy issues (e.g., primary care providers) and members and insureds of the health plan.
Grassroots efforts involve a variety of techniques. Direct mail, telephone banks, announcements in company literature, advertisements in the popular press are all means of attempting to mobilize grassroots activity. The activity that the health plan wants to mobilize might be related to specific policy issue (e.g., “call your legislators today and tell them to vote no Senator Smith’s anti-health plan bill”) or to more general issue (e.g., “call your legislators today and tell them to draw the on all the anti-health plan legislation pending the legislature”). A grassroots campaign may target all employees, or all vendors, or may be more narrowly targeted geographically to focus resources on a few legislators (e.g., health committee chairpersons), depending on the organization’s available resources.
If there is time and money to do so, ambitious health plan or association might try sway public opinion. This is a difficult thing to do once people have made up their minds on an issue. However, on many issues, public’s level of awareness of, understanding of, or involvement with the issue is low that there is still an opportunity to move public opinion. Under the best of circumstances, such an effort involves a significant expenditure of time and money.
Review Question
The following answer choices describe various approaches that a health plan can take to voice its opinions on legislation. Select the answer choice that best describes a health plan's use of grassroots lobbying.
The Delancey Health Plan is launching a media campaign in an effort to persuade the public that proposed health care legislation will increase the cost of healthcare. The Stellar Health Plan is using direct mail and telephone calls to encourage people who support a patient rights bill to contact key legislators and voice their support for the bill. The Bestway Health Plan is encouraging its employees to contribute to a political action committee (PAC) that is funding the political campaign of a pro-health plan candidate. A representative of the Palmer Health Plan is attending a one-on-one meeting with a legislator to present Palmer's position on pending managed care legislation.
Page 450 of 469

AHM 510 : Health Plans : Governance and Regulation
Incorrect. Public opinion lobbying can be done through grassroots lobbying, or media relations. Media relations goes beyond grassroots lobbying by trying to influence public opinion at large.
Correct. A grassroots lobby campaign includes a set of activities designed to encourage people or entities that share the same desired public opinion to contact key decision makers and voice their support for their opinion.
Incorrect. PAC donations are used by health plans to donate money to canditate's campaigns, where those canditates are deemed to be supportive of of the organization's interests.
Incorrect. Health plans use lobbyists to meet with legislators to present the health plan's position on pending legislation.
Traditionally, media relations are divided into “paid media” and “free media.” Paid media or advertising is any form of promotion or media exposure that is generated and controlled by a paying sponsor and presented by the mass media. The most famous use of paid media in connection with healthcare policy is the campaign featuring a fictional couple known as “Harry and Louise.” This couple’s concerned chats over the breakfast table about their objections to the Clinton administration’s healthcare reform effort of 1993 and 1994 have been credited with a substantial portion of the decline in public support for the proposal.
Free media or publicity is any form of promotion or media exposure that is transmitted by the mass media but is not directly generated, controlled, and paid for by a sponsor. Free media campaigns involve using the media to persuade the public. The tools of such campaigns are news releases, news conferences, speeches covered by the media, media “events” such as protests or demonstrations, and visits with the editorial boards of media organizations. The use of “free” is a misnomer in the sense that such campaigns can involve substantial amounts of time and money. Nevertheless, they are generally only a fraction of the cost of paid media campaigns.
One advantage of free media over paid media is that of credibility. While Americans may have an inherent suspicion of such obviously self-interested modes of communications as paid advertising, they are less suspicious of information delivered through presumably independent third parties such as journalists. The chief disadvantage of free media, on the other hand, is that the organization has substantially less control over the content of the message.
Like other forms of communications efforts, paid and free media campaigns can be made more efficient through the use of public opinion polling, focus groups, and targeting. Through polls and focus groups, media professionals are increasingly proficient at identifying the themes that will be most persuasive to the target public—the so-called “magic bullet” themes that may make the difference in public opinion.
Targeting subsets of the population can also improve the efficiency of the media campaign. Such targeting can be geographically based, focusing on important legislative districts or media markets. An alternative targeting method is demographically based, allowing certain “narrow-band” messages to be delivered to certain audiences. For
Page 451 of 469

AHM 510 : Health Plans : Governance and Regulation
example, if a specific message is more effective for certain age, gender, or socioeconomic groups, advances in direct mail now allow organizations to deliver that message only to the receptive group.
Page 452 of 469

AHM 510 : Health Plans : Governance and Regulation
Chapter 13 BChanging Environment and Emerging Trends in Health Plans In Environmental Forces, we examined the current environment in health plans and the ways that health plans respond to the many challenges and opportunities in their environment. In the assignments that followed, we addressed topics such as formation and evolution of health plans, regulations, government programs, governance of health plans, key legal issues, and public policy. In our last lesson, we focus exclusively on changes and emerging trends. We begin with a look at the overall environment within which all healthcare organizations, including health plans, must operate, and we examine some of the underlying tensions that drive change in health plans. We then look at recent events in healthcare reform and provide an overview of emerging trends.
After completing this lesson, you should be able to:
Identify several key environmental factors that affect health plans Describe the underlying tension between universal healthcare coverage and
comprehensive healthcare benefits Explain how marketplace reform and regulatory reform have brought about change in
the health plan industry
Changing Environment and Underlying Tensions in Health PlansHealthcare is inextricably woven into the economic and social fabric of the United States, and over the past several years health plans have played an increasingly important role in healthcare. It stands to reason, then, that changes in society will affect the health plan industry, and vice versa.
In this lesson, we look at some of the overriding factors and underlying tensions that are driving change in the environment in which health plans operate.
Demographics Aging PopulationThe cost of providing healthcare for the aging population is exerting considerable financial pressure on America’s healthcare system. According to the Bureau of Labor Statistics,
A major component of spending among the elderly is for health care. In general, those age 75 and older are presumably at the greatest risk for incurring health care costs. The overall increase in real total health care expenditures from 1984 to 1995 is much higher for older consumers than for younger ones. For example: the overall increase in real total health care expenditures from 1984 to 1995 is much higher for older consumers than for younger ones. Expenditures rose about 8% for the younger group, while the older groups each increased their health care expenditures by more than 20%.
Between 1984 and 1986, shares for health insurance for all groups decreased. They then began to increase and have done so more or less continuously…. The rate of increase in the share for the oldest group (75 and older) has been steeper than for the 65- to 74-year-old group in the last few years.1
Page 453 of 469

AHM 510 : Health Plans : Governance and Regulation
Many health plans, which now have a relatively high percentage of younger, healthier members, will face rising healthcare costs as their membership ages. The Medicare program will have to address an even greater challenge, since it will not only have to provide coverage for an aging population, but will have to do so with a decreasing tax base because of the lower birthrate in the “post-baby boom” generation.
The aging population and the American Association of Retired Persons (AARP) will have a lot to say in the healthcare policy debate. As the “baby boomers” encounter the inevitable health problems associated with aging, they are likely to focus intently on healthcare as a public policy issue. With their economic and political power, this group will be a key participant in the public dialogue that shapes the future of healthcare.
Fast Fact
By 2030, the proportion of people over age 65 will reach 20% of the population, up from 13% today, and the 85- and-older group will be the fastest growing segment of the population.2
DiversityAs minority and immigrant populations continue to make up a greater percentage of the U.S. population, racial and ethnic diversity will present an increasing challenge for health plans. Because racial and ethnic groups sometimes have unique sets of health factors, medical conditions, and healthcare access issues, successful health plans will need to develop “cultural competency” to recognize and respond to an increasingly complex variety of member needs. In addition, health plans, in their role as employers, will have to address the cultural and language issues associated with employing a diverse workforce.
The Role of WomenFor a number of reasons, women are likely to become an increasingly important constituency for health plans. Because women as a group have a higher incidence of illness and a longer life span than men, they receive more healthcare and interact more often with health plans over the course of a lifetime. Women are also more likely than men to coordinate healthcare for other family members. Also, because large numbers of women have entered the workforce during the past two decades, a greater percentage of the subscribers in employee group health plans are women. These demographic factors indicate that health plans, as part of their efforts to compete effectively, are likely to focus more of their marketing, customer service, and healthcare efforts on women.
Review Question
Health plans should monitor changes in the environment and emerging trends, because changes in society will affect the managed care industry. One true statement regarding recent changes in the environment in which health plans operate is that
women as a group receive more healthcare and interact more often with health plans than do men over the course of a lifetime
Page 454 of 469

AHM 510 : Health Plans : Governance and Regulation
the focus of healthcare during the past decade has shifted away from outpatient care to inpatient hospital treatment the uninsured population in the United States has been decreasing in recent years
the decline in overall inflation in the 1990s failed to slow the growth in healthcare inflation
Correct. Women, as a group, have a higher incidence of illness and a longer life span than men, and are more lkely than men to coordinate healthcare for other family members.
Incorrect. The focus of healthcare has shifted from inpatient to outpatient care
Incorrect. The uninsured population has continued to increase in recent years
Incorrect. The decline in overall inflation in the 1990s has contributed to an impressive reduction in healthcare inflation.
Consumer AttitudesSince most health plans operate in the group market, in the past they looked upon the employer as their primary customer. Recently, however, health plans have begun to pay closer attention to the individual consumer. The focus has shifted, in part, because health plans need to educate a large number of individuals who are new to health plans and unfamiliar with network protocols, such as PCP authorizations, referrals, and emergency procedures. However, as we pointed out in Environmental Forces, this shift in focus is also due to the growing influence of consumerism among plan members, legislators and regulators, and public interest groups.
Members now expect more from their healthcare providers and their health plans. In response, health plans, policymakers and the government agencies that regulate health plans have tried to anticipate and address consumer needs and concerns. Health plans are developing member material that is easier to read and understand. They are emphasizing excellent customer service to assure that questions are answered quickly and correctly and that appropriate action is taken on member requests. Like other businesses, the health plan industry increasingly refers to “delighting the customer” by providing responsive service, high quality, and competitive prices.
On the legislative and regulatory front, a large number of laws and regulations have been proposed and enacted in the name of consumer, member, and patient satisfaction and rights. Government agencies have established consumer “hotlines,” which members can call to register complaints and ask questions. Government programs, such as Medicare, are making a concerted effort to improve beneficiary education and communication.
Public interest groups and the media have also focused on consumerism in healthcare. Some consumer “watchdog groups” have made healthcare a top priority in their advocacy efforts. Several periodicals now evaluate and rank hospitals and health plans on a variety of consumer-oriented criteria.
Page 455 of 469

AHM 510 : Health Plans : Governance and Regulation
In the future, health plans will continue to be challenged by the increasing influence of consumerism and the importance of adjusting products and services to meet the needs of the individual healthcare consumer. Insight 13B-1 illustrates how some of these trends are taking shape.
Insight 13B-1. A Consumer “Voice” Will Drive Health Plans as a Service Industry.
Consumers have a growing influence on the healthcare industry, according to a study by KPMG Peat Marwick. Furthermore, consumer satisfaction and preferences drive product design, development, and innovation.
“New Voices: Consumerism in Healthcare” examines the impact of consumers on the healthcare industry and the industry’s response. Eighty-three percent of healthcare executives in all segments of the industry “agreed” or “strongly agreed” that consumers influence the policy, strategy, operations, and investment decisions of healthcare organizations.
“While health plan companies still view large employers as their primary customers, they are more often looking to reach out to individual consumers to pull them through the system,” says Richard A. D’Amaro, national managing partner, healthcare, at KPMG Peat Marwick.
“The growth of ‘choice-enhancing’ products such as point-of-service plans is a direct manifestation of this, as are the growth in consumer- focused advertising, interactive websites, and health information services,” he adds.
Consumerism in many ways is the root cause of much of the regulation or pending regulation that has and will continue to impact health plans, such as 48-hour maternity-stay requirements, antigag- rule regulations and, perhaps most visibly, the Patient Bill of Rights.
In touch with consumers. Virtually all of the healthcare organizations surveyed will increase investments in feedback mechanisms to assure they are “in touch” with consumer needs. For example:
1. 99% of the healthcare organizations responding referred to new services as indications of consumer influence, including facility renovations, improved patient access, and new informational/ educational services.
2. 95.7% of organizations responding have at least one patient satisfaction initiative. 3. 72.9% report going beyond conventional patient feedback mechanisms, such as
questionnaires, patient and member surveys, and toll-free numbers.
“Health plan companies cannot be held exempt from a movement that is sweeping every other sector of the economy,” D’Amaro says. “For years, many health plans and providers operated under the premise that simple customer service could be sacrificed as long as the medical care was good. Now they are realizing that both are required to maintain retention and customer loyalty.”
Page 456 of 469

AHM 510 : Health Plans : Governance and Regulation
Most health plan companies are starting only now to make organizational and operational changes to address these problems, according to D’Amaro. These changes, most of which already have been implemented in other service industries, include empowering front-line workers, providing more detailed and meaningful customer service training, linking everyone’s compensation to customer service, and undertaking more rigorous hiring and recruiting to identify people who are more apt to be successful in a “customerinterface” position.
“The lessons that health plan can learn from other service industries should have tremendous benefit,” he says.
COPYRIGHT NOTICE:Reproduced with permission of the publisher, from Tracey Walker, “Health Maintenance Organizations Can Run, But They Can’t Hide: A Consumer ‘Voice’ Will Drive Health Plan as a Service Industry,” Managed Healthcare, (Vol. 8, Number 3, March 1998), pp. 13, 15. Copyright by Advanstar Communications Inc. Advanstar Communications Inc. retains all rights to this material.
The EconomyHealthcare and the health of the economy are closely interrelated. The decline in overall inflation in the 1990s has contributed to the impressive reduction in healthcare inflation, while the success of health plans in controlling runaway healthcare costs has contributed significantly to lowering the overall inflation rate and improving the economy. Simply stated, changes in the economy are bound to affect the healthcare industry, and changes in the healthcare industry are bound to affect the economy.
One way to view the impact healthcare has on the economy is to look at it from the employer/industry perspective. Since a large percentage of the healthcare bills are paid by employers, a rise or decline in the cost of healthcare can affect the wages paid by employers, which impacts the ability of most Americans to make purchases. Also, a change in the cost of healthcare can impact the cost of producing products and providing services, which in turn affects prices. In a global marketplace, where many competitors are not funding employee healthcare coverage, the cost of healthcare is a critical competitive issue for U.S. employers.
Fast Fact
The United States has “the most costly health delivery system in the world. Health care consumes 14% of the gross domestic product, or almost oneseventh of the nation’s output, a percentage that has remained unchanged for four years.”3
Growth in the nation’s healthcare spending reached a 37-year low in 1996.4
Healthcare inflation during the past few years has been as low as it has been in decades, but there are signs that prices may not hold much longer. During the past several years, as health plans have replaced traditional fee-for-service insurance, it has achieved significant cost reductions. Recently, however, factors such as advances in medical and pharmaceutical treatments, increased competition among health plans, benefit mandates, and consumer and purchaser demand for better benefits and greater choice in providers have led to reduced profits and even significant losses for many health plans. These factors combine to create price pressures on the cost of healthcare and healthcare coverage.
Page 457 of 469

AHM 510 : Health Plans : Governance and Regulation
Advances in Information ManagementInformation management is critical to an health plan’s ability to operate effectively. It can be used to improve functions as diverse as maintaining eligibility lists, authorizing medical procedures, paying member and provider claims, issuing contracts, measuring customer service and satisfaction, analyzing medical outcomes, and monitoring medical and administrative costs. Information management can be used to improve a health plan’s ability to meet the demands of purchasers, consumers, regulators, and accrediting agencies, all of which require accurate information about quality, cost, responsiveness, and customer satisfaction to help evaluate health plans. In fact, “Of all the truths that have emerged from managed care’s evolution in recent years, one clearly stands out: Information management has moved from the basement to the boardroom. The ability of health plans to manage this strategic resource is fast becoming a fundamental driver of care quality and industry performance.”5
Unfortunately, because technology typically changes faster than laws, there is often a period of time during which existing regulations do not address issues that arise as a result of new technologies. Therefore, as health plans employ the latest information management tools to maintain a competitive edge, they must be well versed in the associated regulatory and liability issues.
A case in point is the increased use by health plans of electronic data interchange (EDI), which is the computer-to-computer exchange of data between two or more organizations. Although health plans must comply with all applicable federal and state regulations regarding privacy, specific compliance issues may not always be clear because most existing privacy laws address presentation in the paper medium, but do not yet address the specific intricacies of EDI.
Changes in the Practice of MedicineThe practice of medicine is changing at an amazing rate. For example, researchers are developing new types of imaging technology for diagnostic use, improving laser and radio-frequency technology for surgery, producing new drugs, and making advances in genetics that could lead to enhanced diagnosis and treatment capabilities. This rapid rate of change presents a variety of challenges for health plans, purchasers, regulators, and society as a whole.
In the United States, we sometimes take for granted the availability of state-of-the-art medical treatments, but since most advances come with a high price tag, they exert considerable cost pressures on the financing and delivery of healthcare. As we have seen, healthcare inflation has a negative impact on the overall economy, and high costs make it difficult or impossible for some purchasers and consumers to obtain healthcare coverage.
Advances in medicine present non-economic dilemmas as well. For instance, when researchers develop a promising new treatment for a life-threatening illness, health plans, purchasers, and regulators face intense public pressure to immediately begin paying for the treatment, regardless of whether it has been proven to be safe and effective.
Page 458 of 469

AHM 510 : Health Plans : Governance and Regulation
Health plans and regulators often have to scramble to keep up with changes in medical technology, as was demonstrated by the debate over coverage for treatment of impotency using the prescription drug Viagra. Another example of the impact of advances in medical technology was when the medical community began to use high-dose chemotherapy and autologous bone marrow transplants (ABMT) as a method for treating cancer. Some state insurance departments struggled to develop regulatory requirements to effectively address this complex medical issue. Florida, for example, convened a statewide task force to decide questions about the medical appropriateness of ABMT for specific types of cancer. Health plans had to contend with these same issues.
Advances in medical technology also raise ethical issues. Medical practitioners sometimes use extraordinary measures to keep patients alive. The cost of these life-prolonging procedures is often enormous, and some analysts contend that healthcare dollars would be better spent on patients who are more likely to survive.
The practice of medicine is also changing due to the influence of health plans. For instance, during the past decade, the focus of healthcare has shifted away from inpatient hospital treatment to outpatient care and demand management, in which the patient obtains decision-making information, designed to reduce the overall need for healthcare services.
Review Question
One example of health plan's influence on the practice of medicine is that, during the past decade, the focus of healthcare has moved toward __________________, which is designed to reduce the overall need for healthcare services by providing patients with decision-making information.
demand management
managed competition
comprehensive coverage
private inurement
Correct. Demand management is when the patient obtains decision-making information designed to reduce the overall need for healthcare services.
Incorrect. Managed competititon tries to keep healthcare coverage largely in the private sector to achieve the benefits and efficiencies of marketplace competititon.
Incorrect. Universal coverage provides healthcare benefits to the entire populationIncorrect. Private inurement is the net earnings of a not-for-profit organization that go to the benfefit of a private individual.
Page 459 of 469

AHM 510 : Health Plans : Governance and Regulation
Role of the MediaAccording to a survey conducted by the Kaiser Family Foundation, media coverage of health plans increased sevenfold during the period from 1990 through mid- 1997, while the media’s portrayal of HMOs and the health plan industry became increasingly negative.
The increasingly negative coverage has contributed to an explosion of proposed and enacted legislation at the state and federal level to regulate health plans. Along with this increase in legislative activity has come an increase in media coverage of legislative activity. The Kaiser Family Foundation survey indicated that in 1990 only 3% of health plan stories in the media covered regulatory issues, but the number jumped to 16% by mid-1997.
Universal Coverage vs. Comprehensive Healthcare BenefitsSome people might describe the “ideal” healthcare system as one that provides both universal coverage and comprehensive healthcare benefits. In other words, it would protect the entire population (universal coverage) and give all individuals complete choice of healthcare practitioners and facilities, while providing full, unlimited benefits for every medical condition and every type of service or supply that patients and providers deem necessary (comprehensive healthcare benefits). However, the purchasers and taxpayers who pay for healthcare in America would likely be reluctant to finance such a system.
Today the majority of Americans have some form of healthcare coverage, through individual policies, group plans, or public health programs. However, 42 million Americans do not have healthcare coverage.
With the rise in healthcare costs, many employers are now requiring their employees to pay a larger percentage of group healthcare premiums. A number of employees, who can’t afford the contributions or don’t think they need coverage, are choosing not to participate. Americans often do not obtain individual coverage because they can’t afford the premiums. As a result, many Americans tend to seek coverage only when they are seriously ill or expecting a serious illness, driving the cost of healthcare coverage even higher.
Even if policymakers were to agree that healthcare coverage should be provided to all Americans, they would have to determine a system for achieving that goal. The alternatives proposed so far are controversial. Greater coverage could be achieved through an employer-sponsored system, such as the one in place now, by mandating that all employers provide coverage. This approach, however, would leave many of the unemployed without coverage. Another option would be to implement a national program, such as Medicare, for all Americans. Recently, some analysts have proposed an individual voucher system for healthcare. Beyond this, policymakers would have to agree on whether to mandate a minimum level of benefits. If benefits were not sufficient, all Americans might be eligible but coverage for many of their medical conditions would be limited or excluded. On the other hand, with comprehensive healthcare benefits, the cost of providing healthcare to all Americans might be prohibitive. Since there are only so many dollars available to pay for healthcare, a key issue in the public policy debate is to determine how those funds will be spent. Over the years, this underlying tension
Page 460 of 469

AHM 510 : Health Plans : Governance and Regulation
between the desire for universal coverage and the desire for comprehensive healthcare benefits has been behind many legislative initiatives, such as Medicare, Medicaid, HIPAA, and SCHIP.
Regulatory Reform vs. Marketplace ReformProponents of increased regulation contend that the business of health plans and insurance is a business affected with a public interest. In other words, “insurance is of such importance to so many people that it is in the public interest to enact whatever laws are necessary to assure that the great trust vested in insurers is not abused.”7
These analysts contend that the rapid rate of change in the industry requires new regulations to oversee evolving entities and practices, and to ensure fairness and adequate access to healthcare coverage for all Americans.
Few, if any, analysts would argue that managed care should be completely free of regulation. However, proponents of marketplace reform argue that too much regulation hampers competition and makes it difficult for businesses to operate efficiently. In a competitive environment, these analysts contend, the health plans that are most capable of providing high quality and competitively priced services will find ways to do so.8
Often the goals of regulators and the managed care industry are the same, but the industry believes it can attain these goals voluntarily. Industry advocates maintain that new mandates and the diversity of mandates among the state and the federal governments often have unintended consequences, placing a cumulative burden on health plans by stifling innovation, causing confusion and delays in service, and increasing medical, administrative, and compliance costs. Also, proponents of less regulation point to federal and state agencies that have recognized the success of managed care innovation in managing healthcare costs and improving quality, and have turned to the private sector to improve government- sponsored programs, such as Medicare, Medicaid, workers’ compensation/ programs, and coverage for government employees. Insight 13B-2 describes the “blend” of regulatory and marketplace influence that makes up the healthcare system in the United States today.
Insight 13B-2. Healthcare in America.
Back in 1960, nearly one of every two dollars spent on health care (49.2 percent) came from the pockets of private individuals. Doctors charged higher fees to patients who could afford it and lower fees to those who couldn’t. As a nation, we could have continued this direct economic relationship between doctor and patient. Or we could have adopted an insurance system with large deductibles and copayments, meant to protect against “catastrophic” medical expenses.
Instead, we built a system of relatively generous private and public insurance. One compelling reason was that this type of insurance encouraged the spread of lifesaving but expensive medical innovations.
By 1993, total health care expenditures were 33 times their level in 1960, but less than one dollar in five (17.8 percent) came from private pockets. (These figures come from the Congressional Budget Office and the Centers for Medicare and Medicaid Services.)
Page 461 of 469

AHM 510 : Health Plans : Governance and Regulation
At some point we might have phased out most private health insurance and instituted a nationalized system such as those of almost all other Western nations. Medicare and Medicaid could have been (as many expected) the first step towards comprehensive, government- financed health coverage.
But, again, we did not take that route, nor did we embrace the private- public solution—“managed competition”—proposed by the Clinton administration.
What we as a nation have chosen, instead, is to let the marketplace determine the shape of our health care system. To be sure, there is still state regulation of insurance companies, both from a fiscal and consumer-rights perspective. Nonetheless, the present system is neither as neat and centralized, nor as political and bureaucratic, as a federally directed solution would be. It is a kind of “unmanaged” competition. Unlike a “single-payer” system, in which one organization has responsibility for all medical spending, hundreds of health plans do much the same thing on a smaller scale for their own members.
Source: Michael L. Millenson, The New American Health System (Washington, DC: American Association of Health Plans, 1997), 19.
Federal vs. State RegulationAlthough the authority for regulating insurance rests with the federal government, the McCarran-Ferguson Act gives states the authority to regulate insurance as long as Congress considers regulation to be adequate and in the public interest. “By leaving the door open to federal oversight of insurance, the McCarran-Ferguson Act created a certain tension between the federal and state governments. The Act gives the states an incentive to oversee the insurance industry adequately and fairly; that incentive is the threat of federal legislation. Thus, historically, when specific concerns have been raised about state regulation of industry practices, the states have increased their efforts to regulate in the areas affected by those concerns. As a result, the regulation of insurance continues to reside with the states, but that situation could change at any time.”9
From the time the McCarran-Ferguson Act became effective in 1945, Congress has enacted a growing body of legislation to regulate healthcare coverage. Also, the topic of sweeping national healthcare reform is almost always on the agendas of at least a handful of federal legislators, and at times it has received considerable attention.
Insight 13B-3 presents arguments in favor of comprehensive federal regulation and in favor of continued state regulation.
Insight 13B-3. Federal vs. State Regulation of Healthcare Coverage.
Why Federal Regulation?People have a variety of reasons for wanting to shift the regulation of healthcare coverage to the federal government. A reason that has been stated for many years is that federal regulation would result in uniformity. Health plans would no longer be required to comply with laws that vary from state to state, and consumers in all states would have the same legal rights and the same access to quality medical services at an affordable price.
Page 462 of 469

AHM 510 : Health Plans : Governance and Regulation
The increasing complexity of the healthcare industry has led some people to support federal regulation.
The healthcare industry today is characterized by intense competition. health plans must find new ways to attract and satisfy customers and bolster profits. Some companies have increased the amount of risk they are willing to take in order to meet their objectives. The increased risk causes some people to worry that these companies either will not be able to pay benefits when due or will not be able to stay in business. Many companies have undertaken efforts to cut costs, often resulting in the downsizing of their operations. The industry has seen a flurry of mergers and acquisitions between companies seeking to improve their solvency and profitability. All of this activity has led some to conclude that the states are unable to effectively regulate the solvency of an industry undergoing this level of change.
Why State Regulation?Proponents of state regulation believe that the states have been relatively effective in regulating the insurance and health plan industries, and that federal regulation is not always in the public interest. The states have many years of experience in overseeing insurance.
The states continue to respond to the changing environment in which the industry operates by escalating their regulatory efforts. For example, the NAIC is now taking a more active role in encouraging states to enact laws based on NAIC model bills. Risk-based capital requirements have strengthened the states’ ability to make sure that insurers and health plans remain solvent. State regulators are also placing increasing emphasis on market conduct examinations.
Source: Excerpted and adapted from Harriett E. Jones, Regulatory Compliance: Companies, Producers, and Operations (Atlanta: LOMA, © 1998), 10–11. Used with permission; all rights reserved.
Recent Events and Emerging Trends in the Health Plan EnvironmentIn the early 1990s, healthcare premiums had been rising for years and healthcare inflation seemed to be a problem that might never be solved. The federal budget and most state budgets were running deficits, and many Americans lacked confidence in the U.S. economy. In this climate of economic uncertainty, healthcare became an important “security” issue for many voters, worried that if they lost their jobs they would have no coverage. Against this backdrop, national healthcare reform became a high-profile issue, but then faded. Seemingly overnight, health plans came to prominence. Meanwhile, incremental reform continued in the marketplace and in state legislatures, and soon emerged again at the federal level in the form of new and proposed regulations. Today most experts agree that the American healthcare system is in the midst of significant change (some would say revolution); however, there is no consensus on where this change will lead.
National Healthcare ReformIn 1993, the Clinton administration proposed a national system of managed competition to address the issues of rising medical costs, the uninsured, and the quality of healthcare. The goal of managed competition is to keep healthcare coverage largely in the private sector to achieve the benefits and efficiencies of marketplace competition.
Page 463 of 469

AHM 510 : Health Plans : Governance and Regulation
However, to ensure consistency, fairness, and effective communication, this competitive environment is “managed” by the government or a government- sponsored entity, similar to the way the market is managed in states that sponsor small group purchasing coalitions (see Other Laws that Apply to Health Plans).
Recognizing the successes of health plans in the marketplace, the Clinton proposal relied heavily upon the participation and innovation of health plans. As a result, managed care received a great deal of attention, and “[w]ith health reform seemingly inevitable, enrollment in HMOs and other managed care plans surged. HMOs alone added more than seven million new members between July 1, 1994 and July 1, 1995, a record increase.” 10 Yet, around the time that managed care enrollments were soaring, Americans made it clear that they did not intend to support national healthcare reform. Why? Although, there are rarely simple answers to complex policy issues, analysts point to several key factors:
• When it became apparent that there were no easy solutions to obtaining universal coverage, Americans chose to keep the status quo
• Americans were worried about placing their healthcare coverage in the hands of a federal bureaucracy
• As the economy improved and managed care reined in healthcare inflation, Americans were less concerned about losing healthcare
• Americans were worried their choice of providers might be restricted
Although the Clinton administration’s proposal for national healthcare reform was never sent to Congress, it did succeed in placing healthcare issues in the public spotlight. As the next round of the public policy debate began, the healthcare landscape was in the process of changing in three significant ways: (1) healthcare inflation was coming under control, (2) health plans were replacing fee-for-service as the main system for financing and administering coverage, and (3) purchasers were becoming more informed and aggressive in their approach to obtaining healthcare coverage. Increasingly, the successes and shortcomings of the American healthcare system became, in the eyes of much of the American public and many politicians, the successes and shortcomings of health plans. This was the beginning of what some analysts call the health plan “backlash.”
The Health Plan “Backlash”In some ways, health plans became a victim of their own success. Once consumers, purchasers, policymakers, and other healthcare players were no longer occupied with the problem of rising costs, they started to focus on other problems, many of which were laid at the doorstep of health plans. Several of the factors that contributed to this health plan “backlash” are listed below. Some of these factors had also contributed to the rejection of managed competition, while others were unique to managed care:
• Members became concerned about losing their ability to choose providers and the procedures covered by their plans, as employers increasingly switched from indemnity to managed care plans.
Page 464 of 469

AHM 510 : Health Plans : Governance and Regulation
• Doctors and hospitals were concerned about the increasing number of patients covered by health plans and the potential for reduced income as a result of reimbursement agreements with health plans.
• Hospitals were concerned about losing inpatient revenues due to an increased focus on outpatient care.
• Specialists were concerned about fewer referrals as a result of tighter utilization review procedures.
• Primary care doctors were concerned that they would lose their autonomy if they participated in health plans.
• The media—picking up on anecdotal complaints from patients, consumers, consumer groups, providers, and their lobbyists—started to focus on concerns with (rather than benefits of) health plans.
• Politicians began proposing legislation to address concerns they were hearing from constituents, lobbyists, and the media.
Marketplace ReformAlthough large-scale national healthcare reform was dormant, incremental reform continued in the marketplace, as managed care evolved as the predominant system for healthcare financing and delivery. Health plans, competing on cost and quality, quickly replaced most of the fee-for-service healthcare business in the commercial market.
Health plans also made impressive gains with health plans that covered state and federal government employees, and with government purchasing programs, such as Medicaid and Medicare. The cost of healthcare coverage remained level, and competition among health plans became more intense. Increased competition drove health plans to seek new ways to attract and retain purchasers and consumers. Before long, health plans were providing plan features such as outof- network options and direct access to specialists, and they were providing more flexibility with regard to the number and types of healthcare providers available within their networks.
As we noted in Formation and Structure of Health Plans, the participants in the health plan marketplace also changed dramatically. Large health plans moved quickly into new markets, often establishing a local or regional presence by merging with or acquiring other health plans. New competitors, such as physician practice management companies, appeared seemingly out of nowhere and became major players, due in part to large capital infusions from the stock market. Employers became more informed and aggressive in their negotiations with health plans, focusing increasingly on measurement and quality issues and applying vendor management techniques to their purchasing decisions.
In some mature health plan markets, employers even formed purchasing coalitions to contract directly with providers. Accreditation organizations, which for years were part of the healthcare marketplace, became an important participant in the health plan industry and a way for purchasers to determine the quality of health plans. More recently, some states have turned to accreditation organizations for regulatory purposes.
Page 465 of 469

AHM 510 : Health Plans : Governance and Regulation
Regulatory ReformReform continued in state legislatures in an explosion of healthcare legislation. From 1994 through 1996 more than a thousand bills to regulate health plans were introduced into state legislatures,11 and many were enacted into law. States initiated special task forces to investigate problems in healthcare and to recommend solutions. At the federal level, the President appointed an advisory commission out of which came a Consumer Bill of Rights and Responsibilities, which now applies to all federal employee healthcare plans (such as FEHBP and CHAMPUS) and to federal healthcare programs (such as Medicare). Congress passed HIPAA, MHPA, NMHPA, and SCHIP all of which seek to reform particular aspects of healthcare coverage. In addition, numerous proposals have been introduced or proposed by federal legislators.
Recently, Congress’ focus has been on providing coverage for specific segments of the population, such as uninsured children (SCHIP) or individuals who are between jobs (HIPAA). These laws outline general requirements and authorize a federal agency to establish specific national standards. However, rather than preempt state law, these federal laws have established national standards as a “baseline” and given each state the option to decide whether to (1) defer regulation to the federal government, (2) enforce the federal standards themselves, or (3) develop their own standards, using the federal standards as a foundation. In the case of HIPAA, over forty states elected the third option (the “acceptable alternative mechanism”) to avoid transferring state authority to the federal government.
Legislators and policymakers are also looking closely at ERISA. Those who contend that ERISA should be amended point out that it “is a law enacted before the advent of health plans and is being used by the courts in a way Congress never intended.” 12 Proponents of change argue that ERISA does not go far enough to protect the rights of members and patients. They point out that ERISA’s disclosure requirements apply to the relationship between members and employers, not health plans.
Also, although ERISA requires health plan sponsors to act solely in the interest of their employees, many analysts contend that this fiduciary duty is weakly enforced. In addition, under ERISA, plaintiffs who challenge benefit denials must meet a far more stringent standard to demonstrate harm than plaintiffs in most other types of civil cases. Perhaps the most contentious issue with ERISA is that it generally does not allow patients to recover punitive or compensatory damages.
Those who contend that ERISA should not be amended point out that ERISA “has played a key role in making health care coverage available to millions of Americans.” 13
These analysts point out that the American healthcare system is based largely on employer-sponsored benefit plans. The premise of ERISA, they argue, is that employers voluntarily sponsor benefit plans for their employees in exchange for limiting the employer’s risk to whatever benefits should have been provided.
If this protection is removed, then employers will be less inclined to provide coverage for their employees. In addition, ERISA’s defenders point out that this federal law allows multistate employers to provide uniform benefits to their employees through self-funded plans that are exempt from state benefit mandates. ERISA’s defenders argue that weakening the law would do nothing to improve the quality of healthcare, it would only encourage costly lawsuits, increase the cost of healthcare, and reduce the number of
Page 466 of 469

AHM 510 : Health Plans : Governance and Regulation
Americans able to afford coverage, all for the financial benefit of a small number of plaintiffs and their attorneys. They contend that a major restructuring of ERISA would endanger America’s employer-based healthcare system that provides coverage to the majority of the population.
One key element that has largely been missing from the recent round of proposed legislation and enacted laws is any attempt to address the cost of healthcare. “Unfortunately, much of the public believes that more care equals better care. Yet health plans cannot just loosen cost controls, because the public is not prepared to accept the fiscal consequences of its demands, that is, higher taxes, higher health insurance premiums, or lower wages. Given global economic pressures, corporate purchasers aren’t about to let healthcare costs slip out of control, either.”14 With healthcare costs and premiums starting to exert upward pressure, it’s only a matter of time before cost again becomes an issue, particularly if reform policy is to address the continuing problem of the uninsured. It remains to be seen if these difficult issues will be addressed from a regulatory standpoint.
Emerging TrendsRecognizing that in health plans, this morning’s “emerging trends” are often this afternoon’s “recent history,” we now briefly examine some of the issues that are likely to trigger change. Many industry experts believe that issues important to consumers are at the top of the list: choice of plans, choice of providers, access to providers and healthcare services, affordability, and customer service in both the delivery and administration of healthcare.
Consumer groups, health plans, and regulators all agree that it is critical for a healthcare system to give purchasers and consumers useful information to make informed choices. This information enhances competition and is likely to lower costs and improve quality and customer service. Also, with the advent of automated medical records, we can expect to see legislative activity as well as voluntary industry initiatives concerning methods for disclosure and communication of medical information.
Surprisingly, quality of healthcare is not a major factor in a large number of healthcare purchasing decisions. In part, this may be because existing information on quality of care is not always adequate for purchasers and consumers to make choices. Increasingly, however, employers are using HEDIS® and other data about quality to make and guide purchasing decisions. Because this is an area where there is opportunity for improvement, we are likely to see increased activity to develop meaningful healthcare quality criteria through a combination of industry-initiated efforts and regulatory requirements.15
Issues important to the provider community will be another important source of change. Providers, especially physicians, have a lot to say about the future of healthcare in America. “If everyone seems to be trying to control the actions of physicians, that is because doctors’ orders determine where 80 cents of each healthcare dollar is spent—or roughly $800 billion a year.”16 With the rapid shift from a fee-forservice to a health plan system, hospitals and physicians have seen their roles change quickly and dramatically. Both are working hard to regain the leadership position that was theirs before the ascendance of health plans. For instance, providers have become increasingly willing to
Page 467 of 469

AHM 510 : Health Plans : Governance and Regulation
take on the risk of financing healthcare coverage, and advocacy efforts by the AMA have been behind many recent regulatory reform initiatives.
Recently, physicians have shown an increased interest in organizing through labor unions to strengthen their bargaining position with health plans. Typically, they are taking this step with the goal of obtaining a stronger, more united voice in healthcare policy discussions. As we saw in Formation and Structure of health plans, the consolidation of healthcare providers through various types of business entities is likely to continue. This consolidation has the potential to make the delivery of healthcare more efficient and cost effective through economies of scale. Conversely, it has the potential to increase healthcare costs by reducing competition and giving providers greater leverage in negotiating price with health plans.
In addition, issues important to purchasers are likely to continue producing change. In some markets, intense competition and increased merger and acquisition activities have narrowed the playing field to a few dominant health plans. Employers, concerned that less competition among health plans will lead to rising prices and less product innovation, have joined forces to contract directly with providers. So far, the results of these initiatives are mixed. Some analysts doubt that employer purchasing coalitions will succeed nationwide because the markets where they have been implemented are mature health plan markets with many large employers, a combination that is not typical in most locations.
The intense competition in health plans has forced health plans to operate more like entrepreneurial small companies in terms of efficiency, innovation, and responsiveness to the marketplace. At the same time, competition has placed substantial pressures on health plans to enter joint ventures and mergers and acquisitions to obtain economies of scale, “instant” local market share, and the additional capital needed to improve infrastructure and enter into new ventures. The successful health plans of the future will likely be those that efficiently address these critical governance issues, while meeting the expectations of consumers and purchasers through effective partnerships with providers.
ConclusionAs we have seen, healthcare reform has come about through a combination of government regulation and marketplace innovation. Since the majority of patients are now covered under health plans, “the call for more regulation of managed care is tantamount to asking…government to step in and expand regulation of the entire health care system.”17
Legislators and health plans frequently have the same goals, but the industry prefers to attain these goals voluntarily. Through the marketplace, new initiatives have emerged such as HMO report cards to provide more information to purchasers and consumers in selecting health plans, ombudsman programs to assist members with problems they encounter within their health plans, and adoption of patient-oriented principles and practices. Referring to health plan’s early days as a largely not-for-profit industry, some analysts point out that the perspective of health plans has shifted from doing “social good” to “consumer good.”
Page 468 of 469

AHM 510 : Health Plans : Governance and Regulation
In this lesson, we have examined two different but closely related aspects of the health plan industry. First, the structure, governance, and leadership of health plans constitute the internal environment within which health plans operate. Second, regulatory, legal, and marketplace realities make up the external environment. We have seen the way that each can affect the other. Regulations and laws often impact how health plans are structured and governed, and health plans often exert influence on public policy and regulations through marketplace innovations and advocacy efforts.
No one can say for sure what the future holds for health plans. It is virtually impossible to predict the types of entities that will emerge in the marketplace, the focus and degree of legislation that will come from federal and state government, or the rulings that the courts will make in their interpretation of health plan-related laws and regulations. Almost everyone agrees, however, that the industry will continue to undergo dramatic change, either through marketplace innovation, regulation, or a combination of the two.
Page 469 of 469