
AHA SHAPE Symposium 2017 Dr. Slomka Presentation
21
Piotr J. Slomka, PhD, FACC Scientist , Artificial Intelligence in Medicine Cedars Sinai Medical Center Professor of Medicine, UCLA school of Medicine Cedars-Sinai Medical Center Machine learning improves image analysis, diagnosis and prognostic risk assessment in cardiac imaging: an update” [email protected] Some software described in this presentation is owned by Cedars-Sinai Medical Center, which receives or may receive royalties from its licensing. A minority portion of those royalties is shared by the authors
-
Upload
society-for-heart-attack-prevention-and-eradication -
Category
Health & Medicine
-
view
7 -
download
0
Transcript of AHA SHAPE Symposium 2017 Dr. Slomka Presentation
Piotr J. Slomka, PhD, FACCScientist , Artificial Intelligence in Medicine
Cedars Sinai Medical CenterProfessor of Medicine, UCLA school of Medicine
Cedars-Sinai Medical Center
Machine learning improves image analysis, diagnosis and prognostic risk assessment in cardiac imaging: an update”
Some software described in this presentation is owned by Cedars-Sinai Medical Center, which receives or may receive royalties from its licensing. A minority portion of those royalties is shared by the authors
Machine learning
Predicitng anything that can be predictedNo particular model is assumed unlike in statisticsTesting data always separate from training data
• Predicting death from CTA and clinical data EHJ 2016• Predicting MACE from fast MPS JACC Imaging 2017• Predicting cardiac/cardiovascular death from large registry• AHA 2017 (Nakanishi Slomka AHA 2017)• Deep learning SCCT, RSNA 2017• Predicting CAD by Deep learning from MPI images ASNC 2017
AN UPDATE
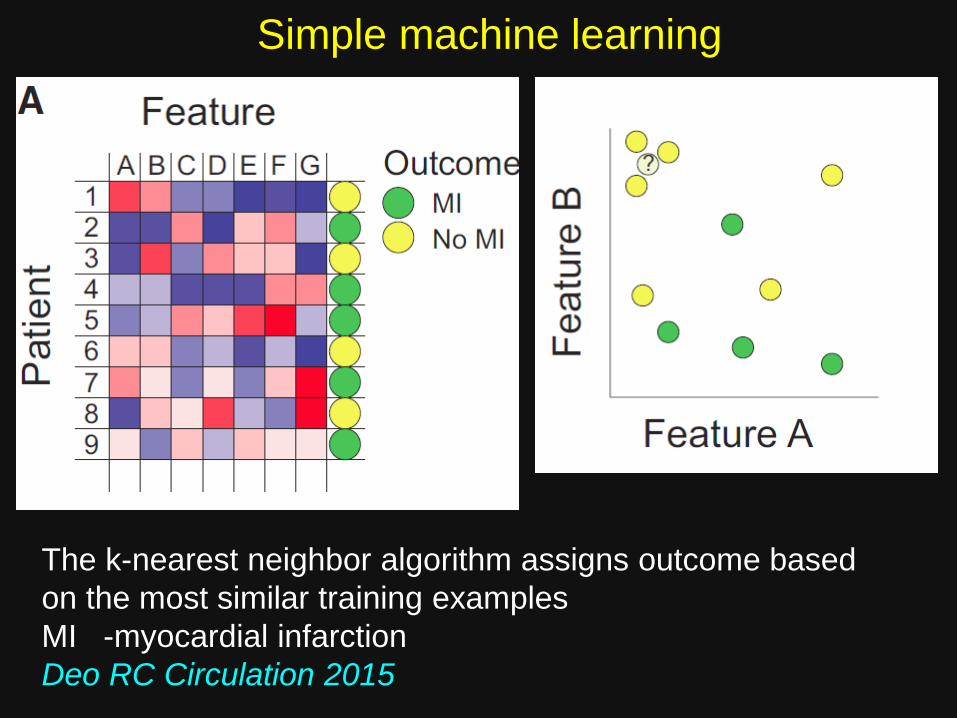
Simple machine learning
The k-nearest neighbor algorithm assigns outcome based on the most similar training examplesMI -myocardial infarction Deo RC Circulation 2015
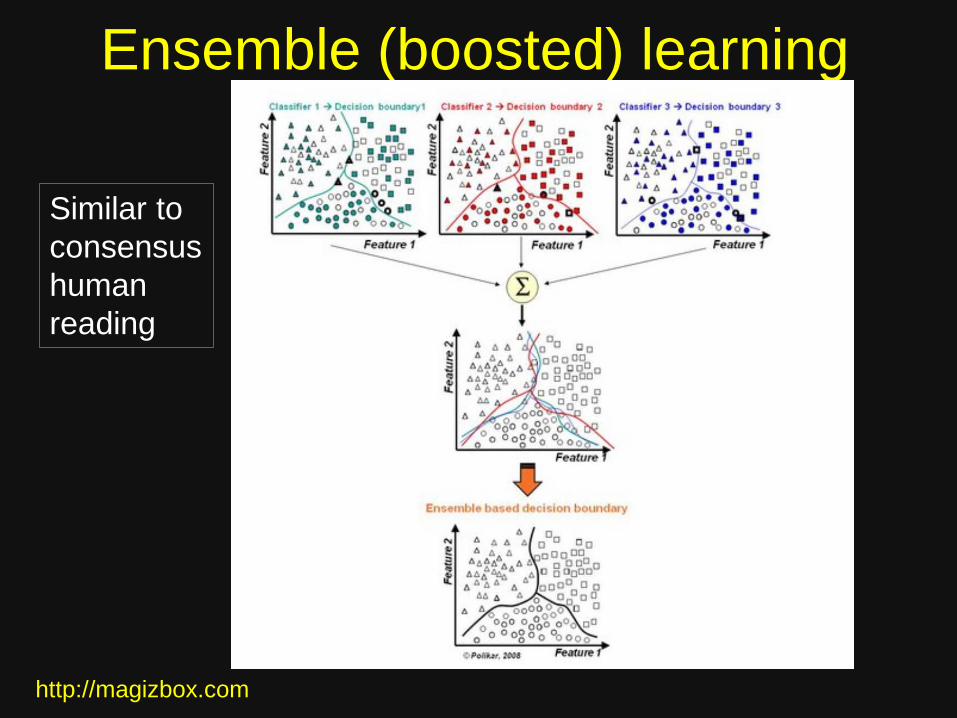
Ensemble (boosted) learning
http://magizbox.com
Similar to consensushumanreading
Motwani M, EHJ 2016
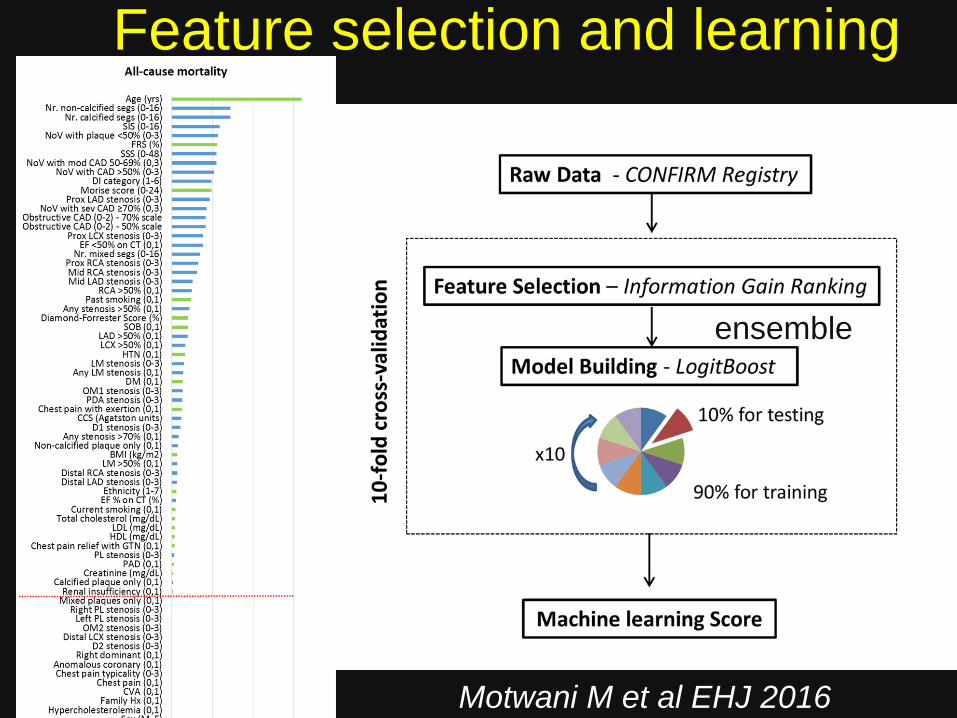
Feature selection and learning
(ensemble
Motwani M et al EHJ 2016
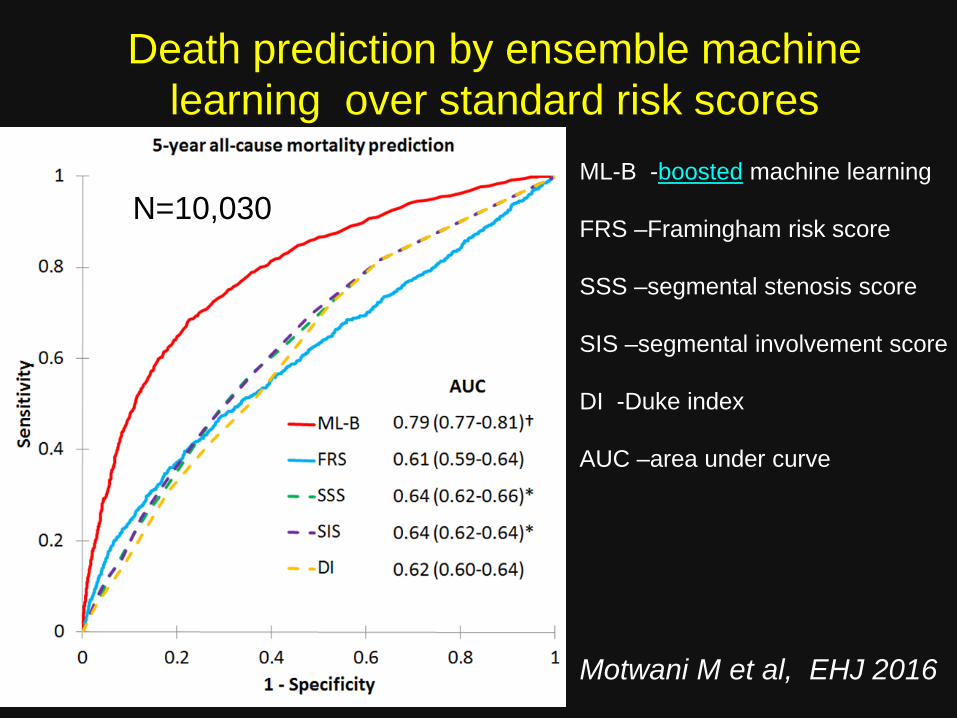
Death prediction by ensemble machine learning over standard risk scores
ML-B -boosted machine learning
FRS –Framingham risk score
SSS –segmental stenosis score
SIS –segmental involvement score
DI -Duke index
AUC –area under curve
N=10,030
Motwani M et al, EHJ 2016
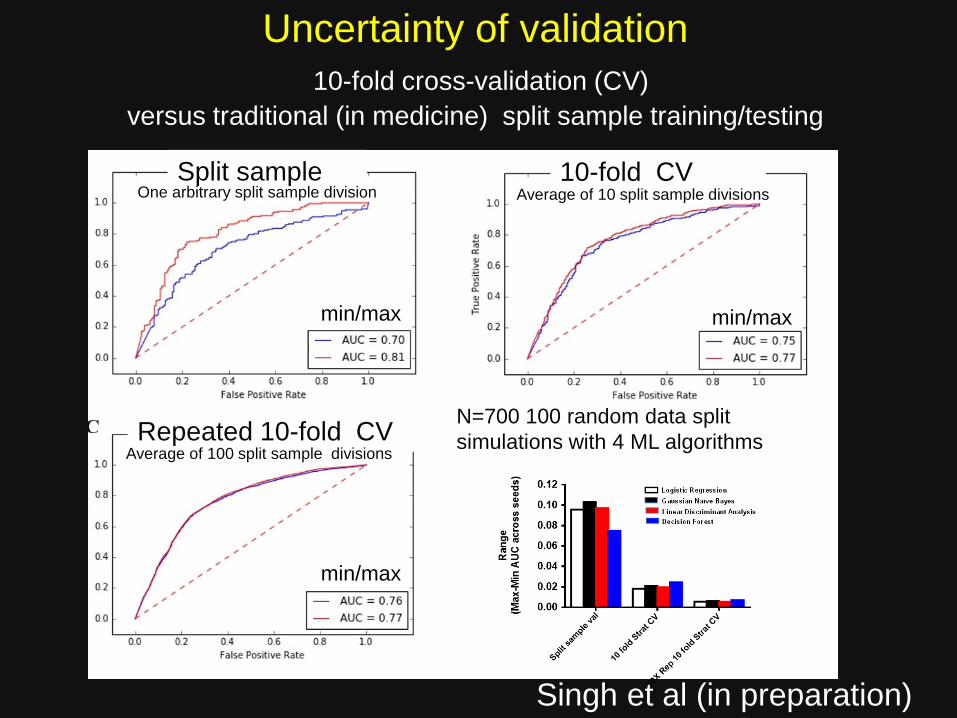
Uncertainty of validation10-fold cross-validation (CV)
versus traditional (in medicine) split sample training/testing
Singh et al (in preparation)
Split sample
N=700 100 random data split simulations with 4 ML algorithms
10-fold CV
Repeated 10-fold CV
min/max min/max
min/max
Average of 100 split sample divisions
Average of 10 split sample divisions One arbitrary split sample division
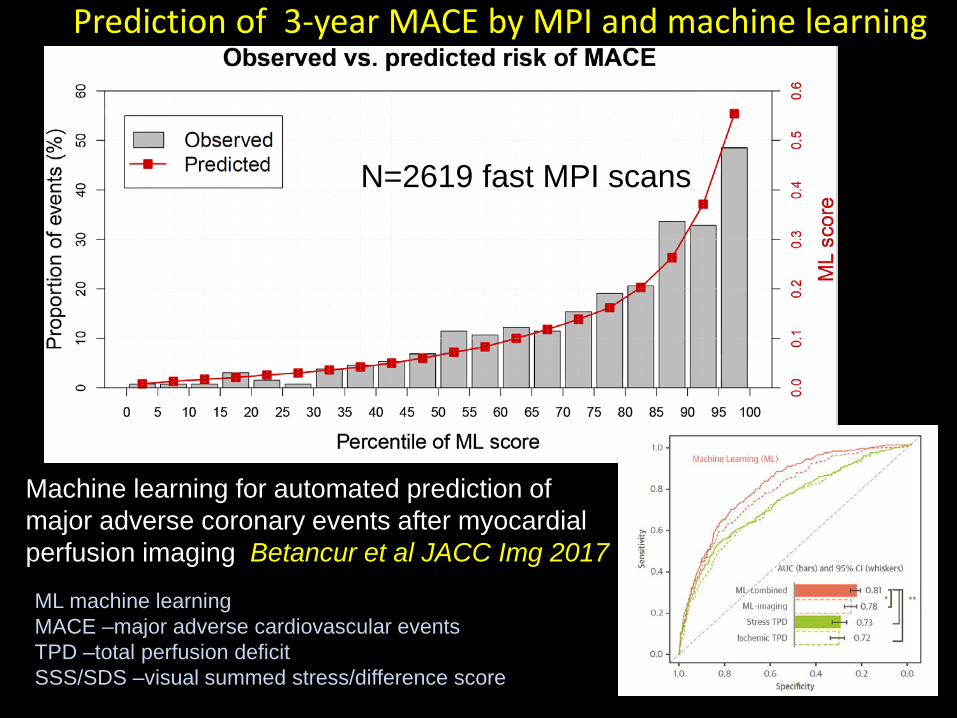
Prediction of 3-year MACE by MPI and machine learning
Stress TPD< 4 %
Stress TPD≥ 4 %
ML score ≥0.15
N= 1965
SSS ≥1
SSS= 0
N= 653
N=1993
N= 625
N= 1956Machine learning for automated prediction of major adverse coronary events after myocardial perfusion imaging Betancur et al JACC Img 2017
N=2619 fast MPI scans
ML machine learning MACE –major adverse cardiovascular eventsTPD –total perfusion deficit SSS/SDS –visual summed stress/difference score
12
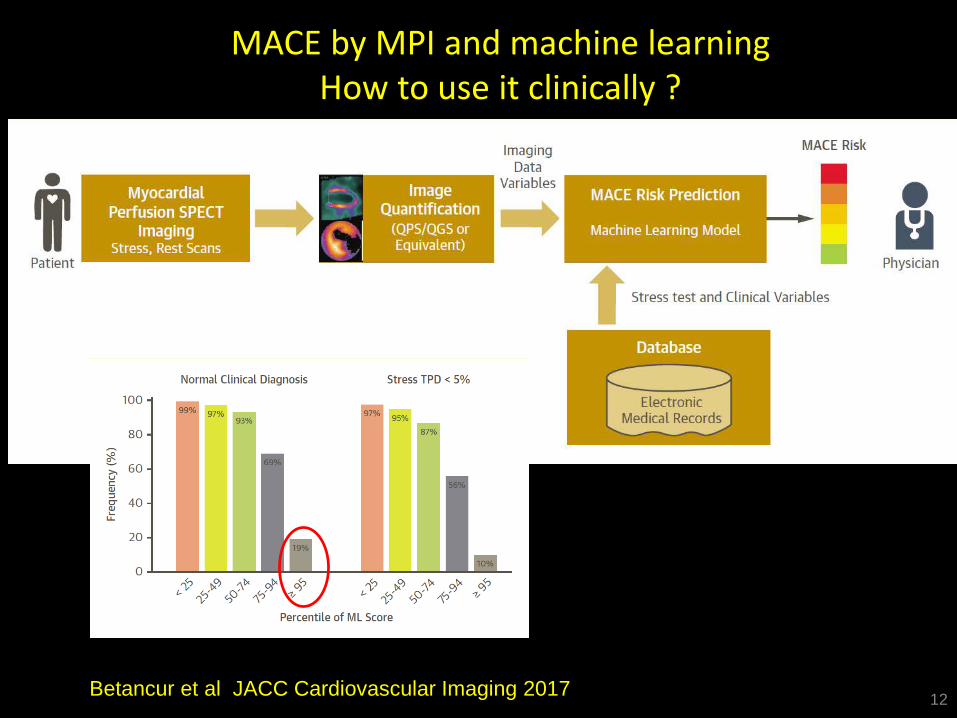
MACE by MPI and machine learningHow to use it clinically ?
Betancur et al JACC Cardiovascular Imaging 2017
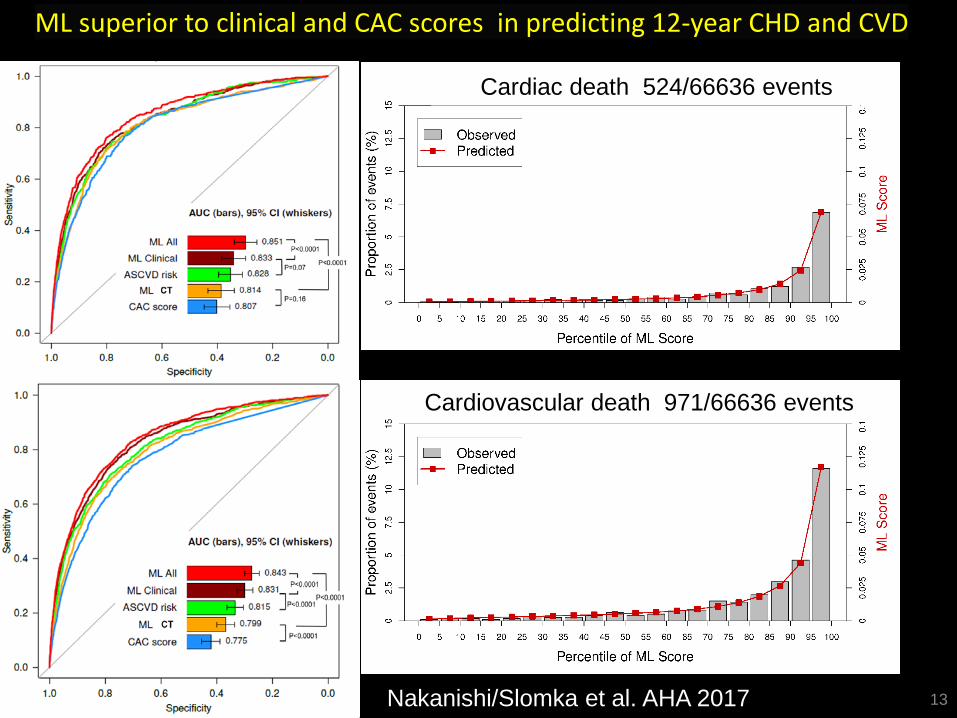
ML superior to clinical and CAC scores in predicting 12-year CHD and CVD
13
Cardiovascular death 971/66636 events
Cardiac death 524/66636 events
Nakanishi/Slomka et al. AHA 2017
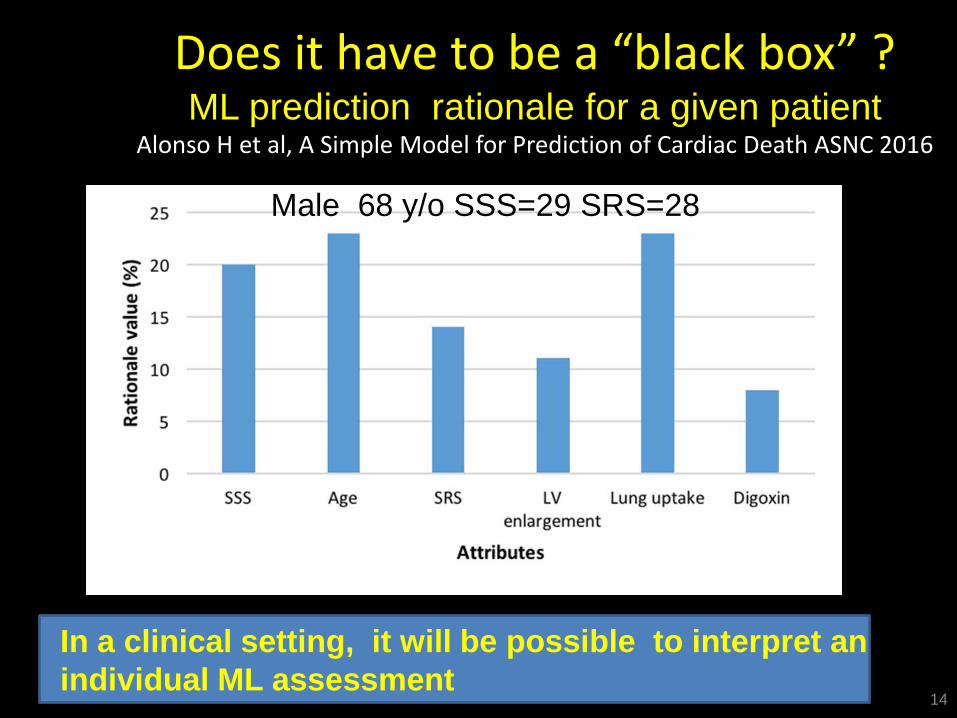
Does it have to be a “black box” ?ML prediction rationale for a given patient
Alonso H et al, A Simple Model for Prediction of Cardiac Death ASNC 2016
14
In a clinical setting, it will be possible to interpret an individual ML assessment
Male 68 y/o SSS=29 SRS=28
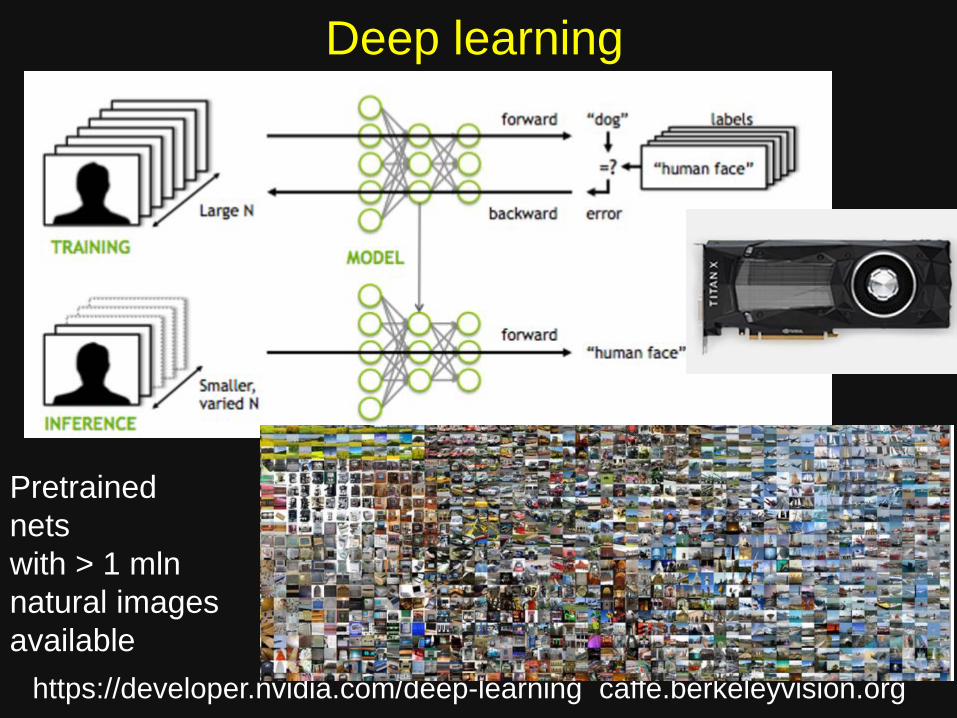
Deep learning
https://developer.nvidia.com/deep-learning caffe.berkeleyvision.org
Pretrainednetswith > 1 mlnnatural imagesavailable
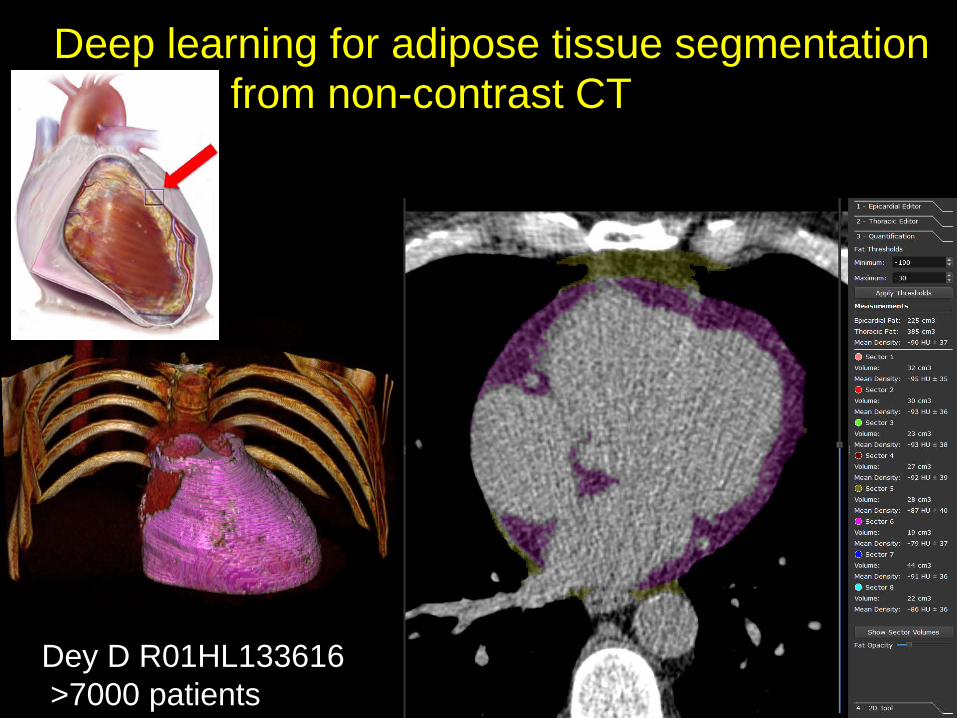
Deep learning for adipose tissue segmentationfrom non-contrast CT
Dey D R01HL133616>7000 patients
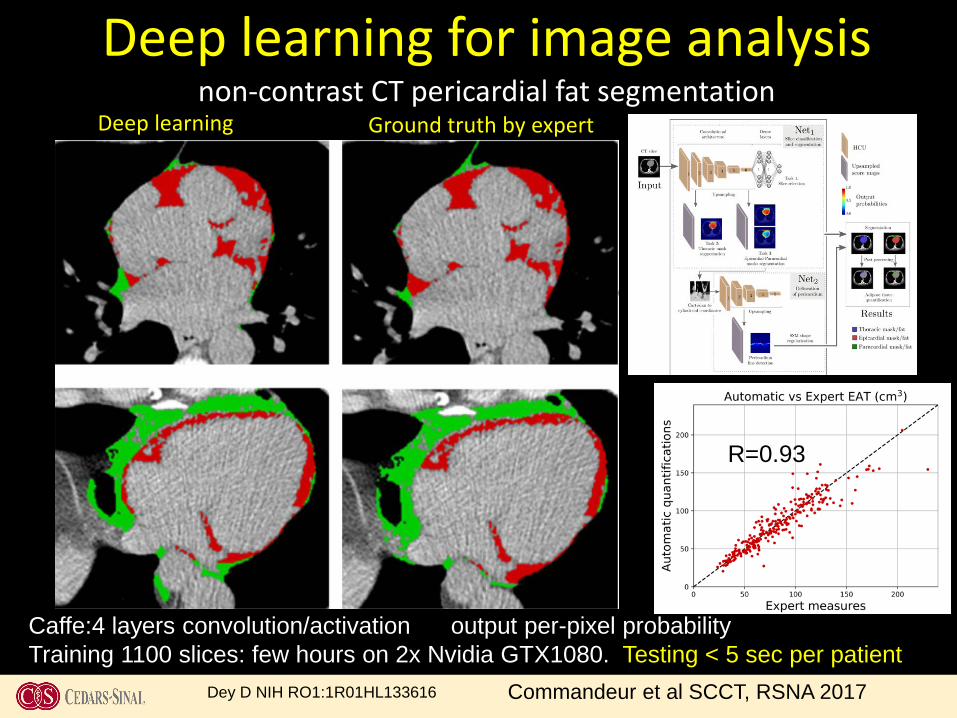
Deep learning for image analysisnon-contrast CT pericardial fat segmentation
Ground truth by expertDeep learning
Dey D NIH RO1:1R01HL133616
Caffe:4 layers convolution/activation output per-pixel probabilityTraining 1100 slices: few hours on 2x Nvidia GTX1080. Testing < 5 sec per patient
Commandeur et al SCCT, RSNA 2017
R=0.93
R=0.95
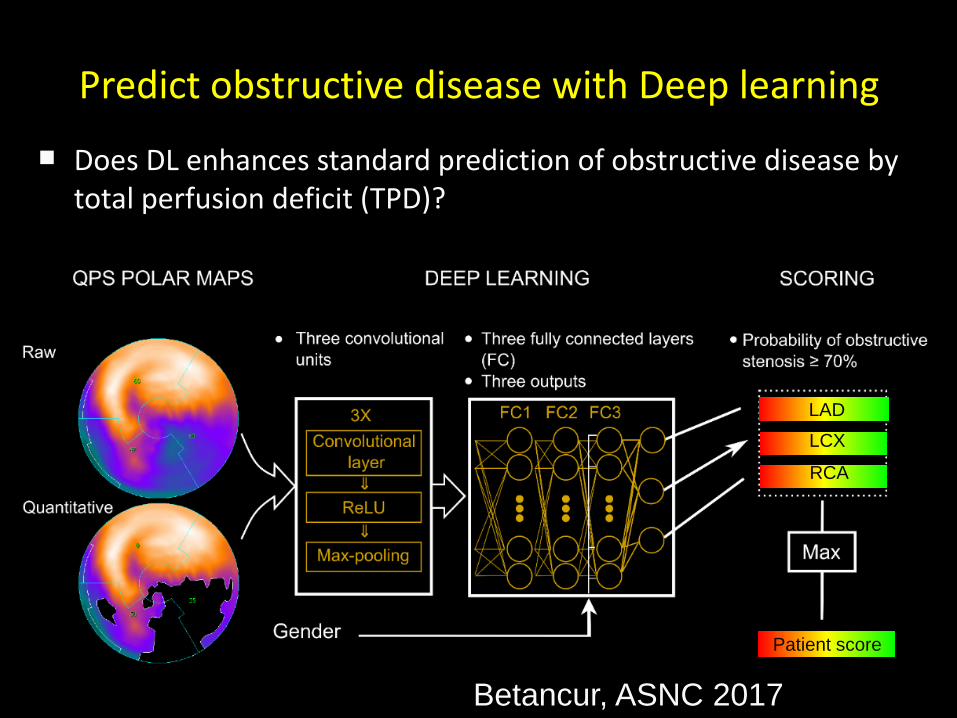
Predict obstructive disease with Deep learning
Does DL enhances standard prediction of obstructive disease by total perfusion deficit (TPD)?
Betancur, ASNC 2017
LADLCX
RCA
Patient score
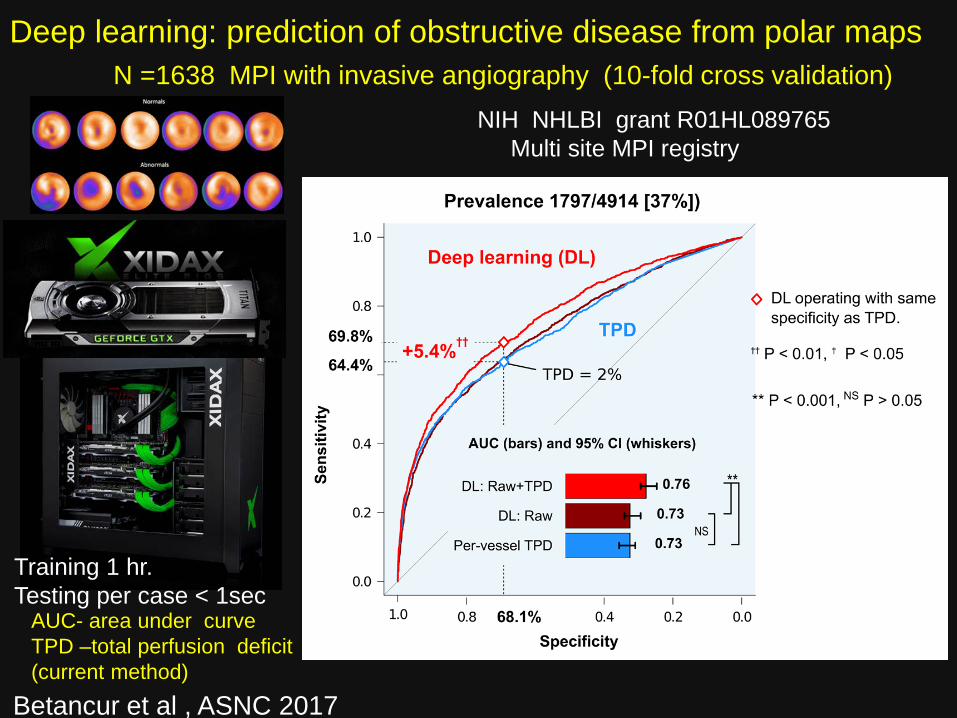
Deep learning: prediction of obstructive disease from polar maps
AUC- area under curveTPD –total perfusion deficit (current method)
N =1638 MPI with invasive angiography (10-fold cross validation)
Betancur et al , ASNC 2017
NIH NHLBI grant R01HL089765Multi site MPI registry
Training 1 hr. Testing per case < 1sec
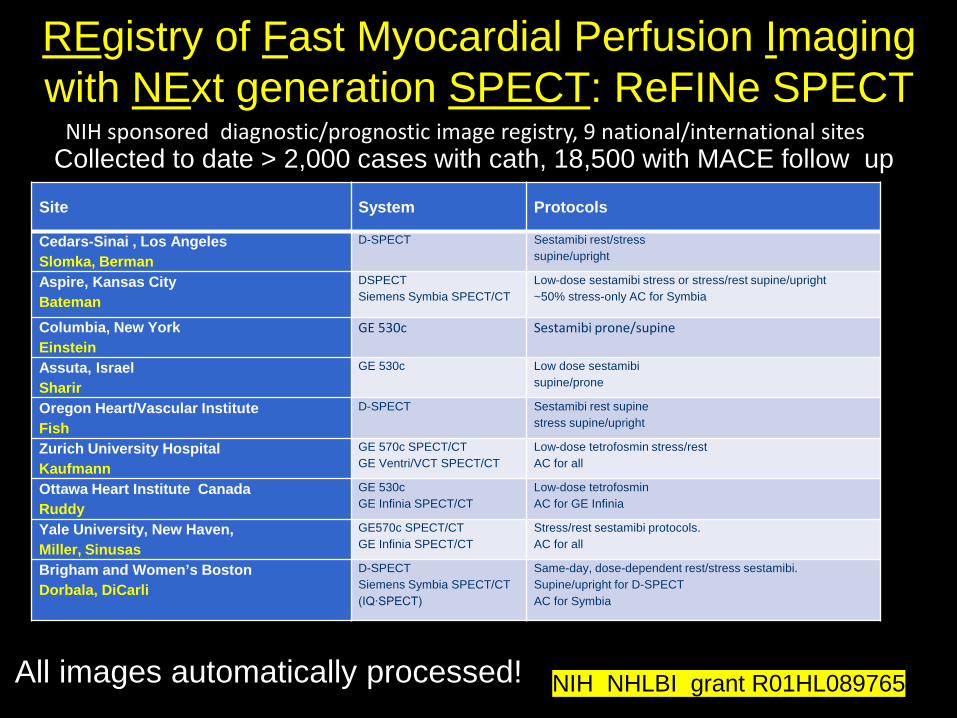
Collected to date > 2,000 cases with cath, 18,500 with MACE follow up Site System Protocols
Cedars-Sinai , Los AngelesSlomka, Berman
D-SPECT Sestamibi rest/stresssupine/upright
Aspire, Kansas CityBateman
DSPECTSiemens Symbia SPECT/CT
Low-dose sestamibi stress or stress/rest supine/upright~50% stress-only AC for Symbia
Columbia, New York Einstein
GE 530c Sestamibi prone/supine
Assuta, IsraelSharir
GE 530c Low dose sestamibi supine/prone
Oregon Heart/Vascular InstituteFish
D-SPECT Sestamibi rest supinestress supine/upright
Zurich University HospitalKaufmann
GE 570c SPECT/CTGE Ventri/VCT SPECT/CT
Low-dose tetrofosmin stress/restAC for all
Ottawa Heart Institute CanadaRuddy
GE 530cGE Infinia SPECT/CT
Low-dose tetrofosmin AC for GE Infinia
Yale University, New Haven,Miller, Sinusas
GE570c SPECT/CTGE Infinia SPECT/CT
Stress/rest sestamibi protocols. AC for all
Brigham and Women’s BostonDorbala, DiCarli
D-SPECTSiemens Symbia SPECT/CT (IQ∙SPECT)
Same-day, dose-dependent rest/stress sestamibi. Supine/upright for D-SPECT AC for Symbia
NIH NHLBI grant R01HL089765
REgistry of Fast Myocardial Perfusion Imaging with NExt generation SPECT: ReFINe SPECT
NIH sponsored diagnostic/prognostic image registry, 9 national/international sites
All images automatically processed!
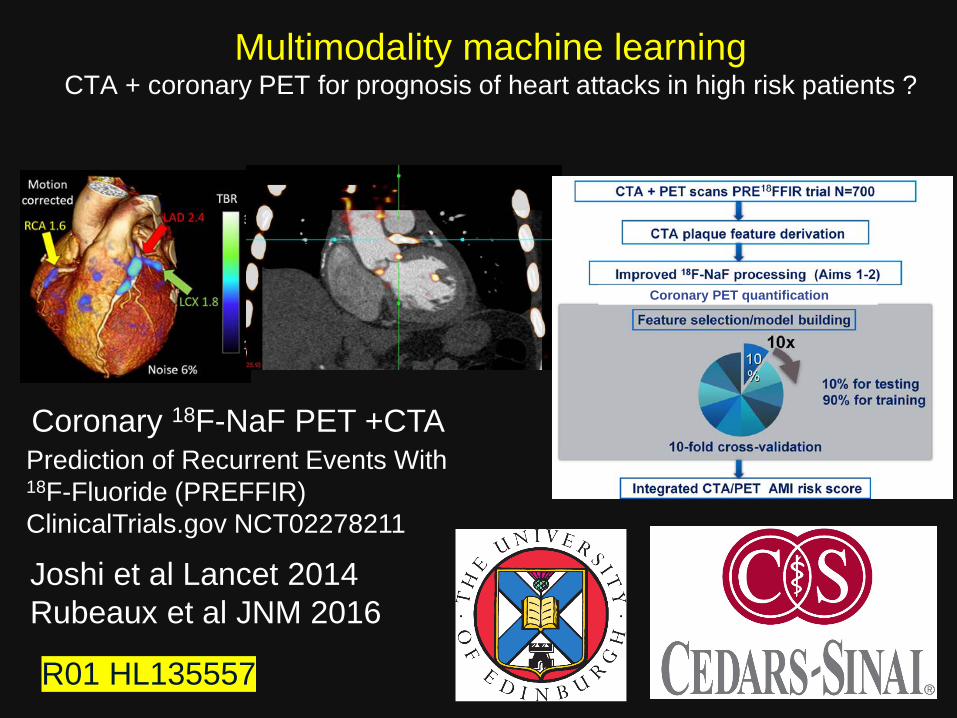
Multimodality machine learning CTA + coronary PET for prognosis of heart attacks in high risk patients ?
Coronary 18F-NaF PET +CTA
Coronary PET quantification
Prediction of Recurrent Events With 18F-Fluoride (PREFFIR)ClinicalTrials.gov NCT02278211
Joshi et al Lancet 2014Rubeaux et al JNM 2016
R01 HL135557
Software vs physician?
“Patients whose lives and medical histories shape the algorithms, will emerge the biggest winners as machine learning transforms clinical medicine”
Obermayer and Emanuel New England Journal of Medicine 2016
Machine learning in cardiac imaging
• Machine learning (ML) combines multiple imaging and clinical datapoints in one score.
• Deep learning perform image segmentation
• ML can predict disease, intervention, or outcomes in terms of post-test probability
• Quantitative computer interpretation will help clinicians find the right answer for a given patient






![₪[martin gardner] aha aha insight](https://static.fdocuments.us/doc/165x107/568cad201a28ab186daa6515/martin-gardner-aha-aha-insight.jpg)











