Agua Extravascular Pulmonar Periopera
9
7/24/2019 Agua Extravascular Pulmonar Periopera http://slidepdf.com/reader/full/agua-extravascular-pulmonar-periopera 1/9 Critical Care Medicine www.ccmjournal.org 665 Objective: Robust markers of subclinical perioperative lung injury are lacking. Extravascular lung water indexed to predicted body weight and pulmonary vascular permeability index are two promising early markers of lung edema. We aimed to evaluate whether extravascular lung water indexed to predicted body weight and pulmonary vascular permeability index would iden- tify patients at risk for clinically significant postoperative pul- monary edema, particularly resulting from the acute respiratory distress syndrome. Design: Prospective cohort study. Setting: Tertiary care academic medical center. Patients: Adults undergoing high-risk cardiac or aortic vascular surgery (or both) with risk of acute respiratory distress syndrome. Interventions: None. Measurements and Main Results: Extravascular lung water indexed to predicted body weight and pulmonary vascular per- meability index measurements were obtained intraoperatively and in the early postoperative period. We assessed the accuracy of peak extravascular lung water indexed to predicted body weight and pulmonary vascular permeability index as predictive markers of clinically significant pulmonary edema (defined as acute respi- ratory distress syndrome or cardiogenic pulmonary edema) using area under the receiver-operating characteristic curves. Associa- tions between extravascular lung water indexed to predicted body weight and pulmonary vascular permeability patient-important with important outcomes were assessed. Of 150 eligible patients, 132 patients (88%) had extravascular lung water indexed to pre- dicted body weight and pulmonary vascular permeability index measurements. Of these, 13 patients (9.8%) had postoperative acute respiratory distress syndrome and 15 patients (11.4%) had cardiogenic pulmonary edema. Extravascular lung water indexed to predicted body weight effectively predicted development of clinically significant pulmonary edema (area under the receiver- operating characteristic curve, 0.79; 95% CI, 0.70–0.89). Pulmo- nary vascular permeability index discriminated acute respiratory Copyright © 2015 by the Society of Critical Care Medicine and Wolters Kluwer Health, Inc. All Rights Reserved. DOI: 10.1097/CCM.0000000000000765 *See also p. 721. 1 Department of Anesthesiology, Mayo Clinic, Rochester, MN. 2 Department of Physiology and Biomedical Engineering, Mayo Clinic, Rochester, MN. 3 Department of Health Sciences Research, Mayo Clinic, Rochester, MN. 4 Division of Pulmonary and Critical Care Medicine, Mayo Clinic, Rochester, MN. 5 Department of Information Technology, Mayo Clinic, Rochester, MN. 6 Department of Cardiovascular Surgery, Mayo Clinic, Rochester, MN. Mayo Clinic does not endorse the products mentioned in this article. Supplemental digital content is available for this article. Direct URL citations appear in the printed text and are provided in the HTML and PDF versions of this article on the journal’s website (http://journals.lww.com/ccmjournal). Supported, in part, by grants UL1 TR000135 and KL2 TR000136 from the National Institutes of Health and the Mayo Clinic Critical Care Research Committee. Dr. Kor consulted for the National Institutes of Health (NIH) Recipient Epi- demiology and Donor Evaluation Study-III (National Heart, Lung and Blood Institute [NHLBI] funded research network), lectured for America’s Blood Centers (presentation on Transfusion-associated circulatory overload for annual America’s Blood Centers meeting, 2012), received royalties from UpToDate (Transfusion-related acute lung injury topic description), received support for article research from the NIH, and has disclosed work for hire. His institution received grant support from the NIH KL2 Career Development Training Grant (KL2 TR000136) and the NIH K23 award (K23HL112855-01). Dr. Warner served as a board member for the American Board of Anesthesiology (member of Board of Directors) and has disclosed work for hire. His institution received grant support from the NIH (multiple grants), Clearway Minnesota, and Pfizer. Dr. Carter received support for article research from the NIH (UL1 TR000135) and has dis- closed work for hire. Ms. Meade is employed by the Mayo Clinic, received support for travel from Spectral and Allocure, and has disclosed work for hire. Her institution received grant support from the NI H (Kl2 TR000136). Mr. Wilson, Ms. Li, and Mr. Hamersma have disclosed work for hire. Dr. Hubmayr served as a board member for Respithera, consulted for Phil- lips, is employed by the Mayo Clinic, and has disclosed work for hire. His institution received grant support from the NHLBI. Drs. Mauermann and Gajic have disclosed work for hire. Address requests for reprints to: Daryl J. Kor, MD, Department of Anes- thesiology, Mayo Clinic, 200 First St SW, Rochester, MN 55905. E-mail: [email protected] Extravascular Lung Water and Pulmonary Vascular Permeability Index as Markers Predictive of Postoperative Acute Respiratory Distress Syndrome: A Prospective Cohort Investigation* Daryl J. Kor, MD 1 ; David O. Warner, MD 1,2 ; Rickey E. Carter, PhD 3 ; Laurie A. Meade, RN 1 ; Greg A. Wilson, RRT 4 ; Man Li, MD 5 ; Marvin J. Hamersma, CVMT 6 ; Rolf D. Hubmayr, MD 2,4 ; William J. Mauermann, MD 1 ; Ognjen Gajic, MD 3,4
-
Upload
patty-alarcon-parra -
Category
Documents
-
view
213 -
download
0
Transcript of Agua Extravascular Pulmonar Periopera

7/24/2019 Agua Extravascular Pulmonar Periopera
http://slidepdf.com/reader/full/agua-extravascular-pulmonar-periopera 1/9
Critical Care Medicine www.ccmjournal.org 665
Objective: Robust markers of subclinical perioperative lung
injury are lacking. Extravascular lung water indexed to predicted
body weight and pulmonary vascular permeability index are two
promising early markers of lung edema. We aimed to evaluate
whether extravascular lung water indexed to predicted body
weight and pulmonary vascular permeability index would iden-
tify patients at risk for clinically significant postoperative pul-
monary edema, particularly resulting from the acute respiratory
distress syndrome.
Design: Prospective cohort study.
Setting: Tertiary care academic medical center.Patients: Adults undergoing high-risk cardiac or aortic vascular
surgery (or both) with risk of acute respiratory distress syndrome.
Interventions: None.
Measurements and Main Results: Extravascular lung water
indexed to predicted body weight and pulmonary vascular per-
meability index measurements were obtained intraoperatively and
in the early postoperative period. We assessed the accuracy of
peak extravascular lung water indexed to predicted body weight
and pulmonary vascular permeability index as predictive markers
of clinically significant pulmonary edema (defined as acute respi-
ratory distress syndrome or cardiogenic pulmonary edema) using
area under the receiver-operating characteristic curves. Associa-tions between extravascular lung water indexed to predicted body
weight and pulmonary vascular permeability patient-important
with important outcomes were assessed. Of 150 eligible patients,
132 patients (88%) had extravascular lung water indexed to pre-
dicted body weight and pulmonary vascular permeability index
measurements. Of these, 13 patients (9.8%) had postoperative
acute respiratory distress syndrome and 15 patients (11.4%) had
cardiogenic pulmonary edema. Extravascular lung water indexed
to predicted body weight effectively predicted development of
clinically significant pulmonary edema (area under the receiver-
operating characteristic curve, 0.79; 95% CI, 0.70–0.89). Pulmo-
nary vascular permeability index discriminated acute respiratory
Copyright © 2015 by the Society of Critical Care Medicine and WoltersKluwer Health, Inc. All Rights Reserved.
DOI: 10.1097/CCM.0000000000000765
*See also p. 721.
1Department of Anesthesiology, Mayo Clinic, Rochester, MN.2Department of Physiology and Biomedical Engineering, Mayo Clinic,Rochester, MN.
3Department of Health Sciences Research, Mayo Clinic, Rochester, MN.4Division of Pulmonary and Critical Care Medicine, Mayo Clinic, Rochester, MN.5Department of Information Technology, Mayo Clinic, Rochester, MN.6Department of Cardiovascular Surgery, Mayo Clinic, Rochester, MN.
Mayo Clinic does not endorse the products mentioned in this article.
Supplemental digital content is available for this article. Direct URL citationsappear in the printed text and are provided in the HTML and PDF versions
of this article on the journal’s website (http://journals.lww.com/ccmjournal).Supported, in part, by grants UL1 TR000135 and KL2 TR000136from the National Institutes of Health and the Mayo Clinic Critical CareResearch Committee.
Dr. Kor consulted for the National Institutes of Health (NIH) Recipient Epi-demiology and Donor Evaluation Study-III (National Heart, Lung and BloodInstitute [NHLBI] funded research network), lectured for America’s BloodCenters (presentation on Transfusion-associated circulatory overloadfor annual America’s Blood Centers meeting, 2012), received royaltiesfrom UpToDate (Transfusion-related acute lung injury topic description),received support for article research from the NIH, and has disclosedwork for hire. His institution received grant support from the NIH KL2Career Development Training Grant (KL2 TR000136) and the NIH K23award (K23HL112855-01). Dr. Warner served as a board member for theAmerican Board of Anesthesiology (member of Board of Directors) andhas disclosed work for hire. His institution received grant support from the
NIH (multiple grants), Clearway Minnesota, and Pfizer. Dr. Carter receivedsupport for article research from the NIH (UL1 TR000135) and has dis-closed work for hire. Ms. Meade is employed by the Mayo Clinic, receivedsupport for travel from Spectral and Allocure, and has disclosed work forhire. Her institution received grant support from the NIH (Kl2 TR000136).Mr. Wilson, Ms. Li, and Mr. Hamersma have disclosed work for hire. Dr.Hubmayr served as a board member for Respithera, consulted for Phil-lips, is employed by the Mayo Clinic, and has disclosed work for hire. Hisinstitution received grant support from the NHLBI. Drs. Mauermann andGajic have disclosed work for hire.
Address requests for reprints to: Daryl J. Kor, MD, Department of Anes-thesiology, Mayo Clinic, 200 First St SW, Rochester, MN 55905. E-mail:[email protected]
Extravascular Lung Water and PulmonaryVascular Permeability Index as Markers Predictiveof Postoperative Acute Respiratory DistressSyndrome: A Prospective Cohort Investigation*
Daryl J. Kor, MD1; David O. Warner, MD1,2; Rickey E. Carter, PhD3; Laurie A. Meade, RN1;
Greg A. Wilson, RRT4; Man Li, MD5; Marvin J. Hamersma, CVMT6; Rolf D. Hubmayr, MD2,4;
William J. Mauermann, MD1; Ognjen Gajic, MD3,4

7/24/2019 Agua Extravascular Pulmonar Periopera
http://slidepdf.com/reader/full/agua-extravascular-pulmonar-periopera 2/9
Kor et al
666 www.ccmjournal.org March 2015 • Volume 43 • Number 3
distress syndrome from cardiogenic pulmonary edema alone or
no edema (area under the receiver-operating characteristic curve,
0.77; 95% CI, 0.62–0.93). Extravascular lung water indexed to
predicted body weight was associated with the worst postopera-
tive PaO2/FIO
2, duration of mechanical ventilation, ICU stay, and
hospital stay. Peak values for extravascular lung water indexed to
predicted body weight and pulmonary vascular permeability index
were obtained within 2 hours of the primary intraoperative insultfor the majority of patients (> 80%).
Conclusions: Perioperative extravascular lung water indexed to
predicted body weight is an early marker that predicts risk of clini-
cally significant postoperative pulmonary edema in at-risk surgi-
cal patients. Pulmonary vascular permeability index effectively
discriminated postoperative acute respiratory distress syndrome
from cardiogenic pulmonary edema. These measures will aid in
the early detection of subclinical lung injury in at-risk surgical pop-
ulations. (Crit Care Med 2015; 43:665–673)
Key Words: acute respiratory distress syndrome; biologic markers;
critical care; outcomes; perioperative care; prevention; pulmonary
edema; technology
Acute respiratory distress syndrome (ARDS) is a postop-
erative complication with few treatment options andsignificant associated morbidity and mortality (1–5).
ARDS is rarely present before an elective surgical procedure,
and it should be viewed as potentially preventable. Few clinical
investigations have addressed ARDS prevention (6). The lack
of robust markers of subclinical lung injury poses a major bar-rier to studying ARDS prevention and early treatment. Identi-
fication of reliable early markers of lung injury could thus beof considerable value.
Extravascular lung water (EVLW) and the pulmonary
vascular permeability index (PVPI) are two promising early
markers of lung edema and increased lung microvascular per-meability, respectively. Extravascular lung water indexed to
predicted body weight (EVLWi) has been identified as an early
indicator of subclinical lung injury in patients with severe sep-
sis (7). It also provides prognostic information in ICU patients
with established ARDS (7–9). EVLW has been correlated with
late markers of ARDS, such as the ratio of partial pressure of
arterial oxygen to fraction of inspired oxygen (PaO2/FIO
2) (10),
lung injury score (9, 11, 12), and chest radiograph findings
(13, 14). PVPI has been used as a surrogate marker of alveolar-
capillary barrier dysfunction. Although not as well studied as
EVLW, PVPI may help differentiate between hydrostatic and
nonhydrostatic lung edema (10, 15).
We aimed to evaluate the predictive validity of EVLWi as anearly marker of clinically significant postoperative pulmonary
edema and PVPI as a discriminator of ARDS. We hypothesized
that intraoperative and early postoperative EVLWi measure-
ments would be greater in patients with clinically significant
postoperative pulmonary edema; we further hypothesized that
PVPI would help distinguish between ARDS and cardiogenic
pulmonary edema (CPE) in patients with pulmonary edema.
MATERIALS AND METHODSThe Mayo Clinic Institutional Review Board approved this
study, and written informed consent was obtained from allstudy participants.
Study Design
This was a prospective cohort investigation. The Strengthen-
ing the Reporting of Observational Studies in Epidemiology
guidelines were followed in the design and reporting of this
observational study (11).
Study Participants
Study participants included adult patients (≥ 18 yr old) under-
going nonemergent cardiac or aortic vascular surgery with a
predicted risk of early postoperative ARDS more than or equalto 10%, as estimated using the previously described secondary
surgical lung injury prediction model (4). The exclusion crite-
ria for this study protocol and justification for each are noted
in Table 1.
Outcome Variables
The primary outcome was development of clinically significant
pulmonary edema resulting from ARDS or CPE. Clinically sig-
nificant pulmonary edema was defined as pulmonary edema
TABLE 1. Study Participant Exclusion Criteria With Justification for Their Inclusion
Exclusion Criteria Justification
Moderate or severe cardiac valve regurgitation Unreliable extravascular lung water and pulmonaryvascular permeability index measurements
Preexisting ARDS Inability to assess outcome
Emergency surgery Unable to obtain consent
Anesthetic plan does not include the placement of arterial and central venouscatheters
Risk of catheter placement
Presence of preoperative polytrauma, sepsis, aspiration, shock, acutecongestive heart failure, or respiratory failure
Potential confounding from major ARDS risk factors
Recent high-risk surgery (within 30 d before the current surgical procedure) Potential confounding from a major ARDS risk factor
ARDS = acute respiratory distress syndrome.

7/24/2019 Agua Extravascular Pulmonar Periopera
http://slidepdf.com/reader/full/agua-extravascular-pulmonar-periopera 3/9
Clinical Investigations
Critical Care Medicine www.ccmjournal.org 667
manifesting with acute bilateral infiltrates on chest radiogra-
phy (not fully explained by effusions, lobar or lung collapse, or
nodules) with associated hypoxemia (PaO2/FIO
2 ≤ 300) and the
need for ventilatory support (including noninvasive modes of
mechanical ventilation).
The more specific diagnosis of ARDS was defined according
to the recently endorsed Berlin criteria (14). As recommended
by this new definition of ARDS (14), the assessment for evi-dence of hydrostatic pulmonary edema was not restricted to
pulmonary artery catheter measurements. Rather, all available
clinical data were considered, including the following measures
(when available): 1) evidence of left atrial hypertension as
determined by pulmonary artery catheterization (pulmonary
artery capillary wedge pressure > 18 cm H2O), echocardiog-
raphy (left ventricular ejection fraction < 45%), or the ratio
of mitral peak velocity of early filling to early diastolic mitral
annular velocity more than 15; 2) clinical context (e.g., pres-
ence of myocardial ischemia, valvular pathology, and absence
of nonsurgical major risk factors for ARDS); 3) volume sta-
tus; and 4) clinical course (e.g., rapid resolution with volumereduction is considered suggestive of hydrostatic pulmonary
edema). In the current study, the presence of hydrostatic pul-
monary edema resulted in a diagnosis of either CPE alone or
CPE plus ARDS when ARDS was judged to coexist.
ARDS and CPE ascertainment proceeded in three steps.
First, screening was performed by a member of the study team.
Patients with a PaO2/FIO
2 value less than or equal to 300 and
a chest radiograph with any findings suggestive of bilateral
infiltrates, edema, or congestion were considered screen posi-
tive and were sent to two experts in ARDS and CPE adjudica-
tion (D.J.K., O.G.) who independently reviewed each case and
assigned one of four conditions: ARDS, CPE, both, or neither.Disagreements in the outcome of ARDS were resolved by a
third expert (R.D.H.). Interobserver agreement for ARDS adju-
dication was determined with κ values. Secondary outcome
variables included the worst postoperative PaO2/FIO
2, duration
of mechanical ventilation, ICU stay, and hospital stay. All study
personnel involved in outcome adjudication remained blinded
to the EVLW and PVPI measurement results until all outcome
determinations were complete.
Predictor Variables
EVLW and PVPI were measured with the PiCCO system
(Pulsion Medical Systems, Munich, Germany). Proceduraldetails for obtaining these measurements have been previ-
ously described (7) and are briefly summarized here. EVLW
and PVPI measurements were obtained by triplicate central
venous injections of 20 mL of iced (< 8°C) 0.9% NaCl (saline)
and recorded as the mean of the three measurements. Volu-
metric variables were derived as previously described (7).
EVLW was calculated as the difference between the thermal
indicator distribution in the chest and the blood volume of the
chest: EVLW = intrathoracic thermal volume – intrathoracic
blood volume (ITBV) (measured in mL) (7, 16, 17). EVLW is
expressed in mL and as mL/kg when indexed to predicted body
weight (EVLWi), which more accurately characterizes lung
edema (9, 18). PVPI has been variably described as the ratio
of absolute (unindexed) EVLW to ITBV or pulmonary blood
volume (7, 10, 19–21). In the present investigation, PVPI is cal-
culated as the ratio of EVLW:ITBV. All EVLW and PVPI mea-
surements were obtained by certified monitoring technicians
or licensed respiratory therapists who were specifically trained
to use the PiCCO device. Standard operating procedures were
developed before study onset, and multiple focused trainingsessions were completed before initiating patient enrollment.
Measurements were obtained at the following time points.
The first measurement followed the induction of anesthesia
after insertion of the catheters (baseline). The timing of the
second and third measurements depended on the surgical
procedure. For cardiac surgery patients, the second and third
measurements were obtained immediately before initiation
of cardiopulmonary bypass (CPB) and within 30 minutes of
separation from CPB, respectively. For aortic vascular surgery
patients, the second measurement was obtained just before
aortic cross-clamp placement and the third was obtained
within 30 minutes after aortic cross-clamp removal. Thus, forall patients, the third measurement was timed to immediately
follow a defined major surgical event. Additional measure-
ments were planned 2, 4, 6, 12, and 24 hours after the third
measurement.
Statistical Analyses
Sample Size Determination . Measurements of EVLWi and
PVPI were planned for 150 eligible patients with a calcu-
lated risk of early postoperative ARDS more than or equal
to 10%. Therefore, we estimated 15 study participants would
have ARDS. In a previous study comparing patients with and
without ARDS (n = 15 and n = 14, respectively), the medianEVLW
i was 15 and 7 mL/kg, respectively (7). Similarly, in a trial
comparing salmeterol with placebo in patients with ARDS
(n = 19 and n = 21, respectively), mean (SD) EVLWi at baseline
was 14 mL/kg (8 mL/kg) (22). Using the method of Hsieh et al
(23), 15 patients with events and 135 patients without events
were estimated to provide 80% power (two-tailed, α = 0.05)
to detect a between-group difference of 0.8 SD units. Assuming
the SD of peak EVLWi is 8 mL/kg, a sample size of 150 was esti-
mated to provide 80% power to detect a 6.5 mL/kg difference
in EVLWi between groups.
Analysis Plan . Dichotomous variables are presented as
number (%); continuous data are presented as median (inter-quartile range [IQR]). Preliminary analyses compared patients
with and without ARDS by using Pearson chi-square tests,
Fisher exact tests, or Wilcoxon rank-sum test (Mann-Whitney
U statistic), as appropriate.
The primary goal of this investigation was to evaluate EVLWi
as a predictor of clinically significant postoperative pulmonary
edema (ARDS or CPE) and PVPI as a discriminator of ARDS.
Peak EVLWi and PVPI values among all available measurements
were determined for each patient. These values were compared
among subjects who had development of ARDS or CPE (alone
or in combination) or no postoperative pulmonary edema.
The validity of peak EVLWi and PVPI as predictive markers of

7/24/2019 Agua Extravascular Pulmonar Periopera
http://slidepdf.com/reader/full/agua-extravascular-pulmonar-periopera 4/9
Kor et al
668 www.ccmjournal.org March 2015 • Volume 43 • Number 3
clinically significant pulmonary edema and ARDS were assessed
by calculating the area under the receiver-operating character-istics curve (AUC). The threshold score that maximized the
Youden index (24) was determined. The corresponding positiveand negative likelihood ratios at this optimal threshold were
calculated. To improve the functionality of the prediction mod-els, sensitivity analyses were performed to determine model
performance at two additional thresholds.The association of these peak measurements with secondary
outcome measures (worst postoperative PaO2/FIO
2, duration
of mechanical ventilation, ICU stay, and hospitalization) was
assessed by evaluating Spearman rank correlation coefficientsfor the associations of interest. Two-sided tests were used, with p values less than or equal to 0.05 being statistically significant.All statistical analyses were conducted using SAS software v9.3
(SAS Institute, Cary, NC).
RESULTSFrom October 2010 to March 2013, 150 study subjects were
enrolled (Fig. 1). Of these, 132 subjects (88%) had at least oneEVLW
i and PVPI measurement. The primary reason for absent
measurements was difficult catheter placement (n = 12). Ofthe 132 patients with EVLW
i and PVPI measurements, seven
patients (5.3%) had postoperative ARDS without CPE, ninepatients (6.8%) had postoperative CPE without ARDS, and
six patients (4.5%) had combined ARDS and CPE. Thus, 22patients (16.7%) had clinically significant postoperative pul-
monary edema and 13 patients (9.8%) had ARDS. The κ value(95% CI) for the adjudication of ARDS was 0.66 (0.47–0.86).
Baseline information for the 132 study participants areshown in Supplemental Table 1 (Supplemental Digital
Content 1, http://links.lww.com/CCM/B147). Compared withthose who did not have postoperative ARDS, patients with
ARDS appeared to have more extensive surgical procedures, as
evidenced by longer operative duration, greater time on CPB,
and a greater volume of fluid and blood product administra-
tion. Those who ultimately had development of postoperative
ARDS received lower tidal volume ventilation in the operating
room environment.
For all patients, peak EVLWi and PVPI values ranged from
6.97 to 38.78 and from 0.27 to 3.05, respectively. Peak EVLW i was higher in patients who subsequently had pulmonary
edema (median [IQR], 15.06 mL/kg [13.74–19.01 mL/kg])
than in patients who did not (10.82 mL/kg [9.36–13.51 mL/
kg]) ( p < 0.001). Peak PVPI was greater in those who subse-
quently had ARDS (median [IQR], 0.64 [0.49–0.84]) than in
those who did not (0.44 [0.39–0.52]) ( p = 0.001). EVLWi and
PVPI measurements from the four groups evaluated are pre-
sented in Table 2.
The measurement time points at which peak values were
noted for both EVLWi and the PVPI are shown in Figure 2.
Peak EVLWi and PVPI values occurred within 2 hours of sepa-
rating from either CPB (cardiac surgery) or removal of the aor-tic cross clamp (aortic vascular surgery) in more than 80% of
patients and within 6 hours in more than 90% of patients. Peak
EVLWi and PVPI measurements were noted at the baseline
measurements for 19.7% and 23.5% of the cohort, respectively.
In comparison, the median (IQR) time from the end of CPB
(cardiac surgery) or removal of the aortic cross clamp (aortic
vascular surgery) to ARDS onset using the Berlin criteria was
20.4 hours (10.6–40.8 hr). In 10 of 13 ARDS cases, the chest
imaging study was the final variable met to fulfill all ARDS cri-
teria. In the remaining three cases, PaO2/FIO
2 was the final cri-
teria used to determine ARDS onset time. Median (IQR) time
to CPE using the qualifying chest radiograph as the onset timewas 13.0 hours (4.9–32.9 hr). Although the worst PaO
2/FIO
2
most often occurred on the first
postoperative day (n = 91/131
[69.5%]), the worst ratio was
observed on the second post-
operative day in approximately
one quarter of the patients
(n = 33/131 [25.2%]), with the
remaining worst values being
spread over the last 3 days of the
5-day evaluation interval.
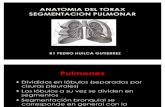
Results from the AUC analy-ses are presented in Figure 3.
Peak EVLWi effectively discrim-
inated between those with and
without clinically significant
pulmonary edema (Fig. 3A )
(AUC [95% CI], 0.79 [0.70–
0.89]). EVLWi was also an
effective discriminator of both
ARDS versus no ARDS (Fig.
3B ) (AUC [95% CI], 0.76 [0.63–
0.89]) and CPE versus no CPE
(Fig. 3C ) (0.75 [0.63–0.87]).Figure 1. Study participant flow diagram.

7/24/2019 Agua Extravascular Pulmonar Periopera
http://slidepdf.com/reader/full/agua-extravascular-pulmonar-periopera 5/9

7/24/2019 Agua Extravascular Pulmonar Periopera
http://slidepdf.com/reader/full/agua-extravascular-pulmonar-periopera 6/9
Kor et al
670 www.ccmjournal.org March 2015 • Volume 43 • Number 3
In light of the barriers identified above, interest has focused
on identifying biologic markers of subclinical lung injury thatpredict risk of ARDS (30–38). Although numerous mark-
ers have been associated with ARDS development and sub-sequent outcome, the robustness of these relationships has
often been limited by inconsistent findings (39). In part, thismay be due to the syndromic nature of ARDS, as the clini-
cal events that portend risk for this syndrome can be quiteheterogeneous (31). Indeed, investigations suggest that bio-
marker profiles associated with ARDS may differ, depending
on the clinical context (40). Additionally, the lack of point-of-care testing for most of these assays significantly limits their
use in clinical medicine and the study of ARDS prevention orearly treatment.
In contrast to risk factors and specific mechanisms under-lying ARDS, the primary pathophysiologic events of alveo-
lar flooding and hypoxemia remain consistent, regardlessof the clinical context. Therefore, readily available interme-
diate physiologic markers may prove more robust in iden-
tifying heterogeneous populations at risk for ARDS. Recent
Figure 3. Receiver-operating characteristics curves for predicting postoperative pulmonary edema. A, Pulmonary edema (acute respiratory distresssyndrome [ARDS] with or without cardiogenic pulmonary edema [CPE]) versus no edema. B, ARDS (with or without CPE) versus no ARDS (CPE aloneor no edema). C, CPE (with or without ARDS) versus no CPE (ARDS alone or no edema). AUC = area under the receiver-operating characteristic curve,EVLW
i = extravascular lung water indexed to predicted body weight, PVPI = pulmonary vascular permeability index.
TABLE 3. Sensitivity Analyses Evaluating the Diagnostic Performance of evlwI for the
Prediction of Clinically Significant Pulmonary Edema and PVPI for the Prediction of
Acute Respiratory Distress Syndrome
Variable
EVLWi, mL/kg PVPI
≥ 12.50 ≥ 14.25 ≥ 15.75 ≥ 0.48 ≥ 0.54 ≥ 0.60
Sensitivity, % (95% CI) 81.8(61.5–92.7)
72.7(51.8–86.8)
40.9(23.3–61.3)
84.6(57.8–95.7)
69.2(42.4–87.3)
53.8(29.1–76.8)
Specificity, % (95% CI) 64.5(55.3–72.9)
81.8(73.6–87.9)
85.5(77.7–90.8)
62.2(53.2–70.4)
78.2(69.9–84.6)
84.0(76.4–89.5)
Positive likelihood ratio 2.31 4.00 2.81 2.24 3.17 3.37
Negative likelihood ratio 0.28 0.33 0.69 0.25 0.39 0.55
EVLWi = extravascular lung water indexed to predicted body weight, PVPI = pulmonary vascular permeability index.
TABLE 4. Correlation of EVLWi and PVPI With Secondary Patient Outcomes
Outcome
Peak EVLWi
Peak PVPI
ρa p ρ
a p
Worst postoperative ratio of PaO2 to FIO
2–0.314 < 0.001 –0.250 0.04
Duration of mechanical ventilation 0.357 < 0.001 0.140 0.11
Duration of ICU stay 0.438 < 0.001 0.149 0.09
Duration of hospital stay 0.186 0.01 0.114 0.19
EVLWi = extravascular lung water indexed to predicted body weight, PVPI = pulmonary vascular permeability index.aSpearman rank correlation coefficients.

7/24/2019 Agua Extravascular Pulmonar Periopera
http://slidepdf.com/reader/full/agua-extravascular-pulmonar-periopera 7/9
Clinical Investigations
Critical Care Medicine www.ccmjournal.org 671
investigations evaluating patients requiring acute care ser-
vices (e.g., emergency department and ICU) note the poten-
tial utility of FIO2 (34, 35), SpO
2 (41), respiratory rate (35),
serum lactate (37), and lung ultrasonography (42, 43) in esti-
mating risk of ARDS. However, the standards of care in the
setting of high-risk cardiac and aortic vascular surgery (e.g.,
high FIO2 and pharmacologic paralysis with controlled respi-
ratory rates) minimize the utility of these physiologic mark-ers. Additionally, intraoperative lung ultrasonography can be
technically challenging in patients with highest risk of post-
operative ARDS (e.g., cardiac, thoracic, and aortic vascular
surgery). Similarly, point-of-care laboratory tests for serum
lactate are frequently not available in the operating room
environment. Therefore, the need persists for an accurate and
reliable marker of subclinical lung injury that can be feasibly
implemented in the operating room environment.
EVLWi is proposed as an early marker of subclinical ARDS
(7, 15, 44–46). As with the protein biologic markers, it has
primarily been evaluated as a marker predicting outcome in
patients with established ARDS (45). However, recent evi-dence suggests that EVLW
i may also be useful in predicting
risk of ARDS development (7, 15, 46). Martin et al (7) identi-
fied EVLWi as a useful marker of subclinical lung injury in
patients with severe sepsis, correlating higher EVLWi mea-
surements with more severe hypoxemia and reduced survival.
Similarly, LeTourneau et al (46) identified EVLWi on day 1
of ICU admission to be predictive of subsequent develop-
ment of ARDS in a population of at-risk patients; specifically,
mean (SD) EVLWi on day 1 was 15.5 mL/kg (7.4 mL/kg) and
8.7 mL/kg (2.3 mL/kg) for those who did and did not have
ARDS development, respectively ( p = 0.04). In contrast, no
other physiologic markers tested in that study (physiologicdead space, PaO
2/FIO
2, or static lung compliance) predicted
progression to ARDS.
PVPI has been proposed as a useful early marker of ARDS
(15, 45, 47). Jozwiak et al (45) identified PVPI as an indepen-
dent risk factor for 28-day mortality in patients with ARDS.
Similarly, Kushimoto et al (15) noted the utility of PVPI
as a diagnostic tool for ARDS in patients with hypoxemic
respiratory insufficiency. However, other investigations have
not confirmed these findings (19, 46). Perhaps, the greatest
value of PVPI is its ability to differentiate hydrostatic from
nonhydrostatic lung edema. Indeed, numerous investiga-
tions have suggested the utility of PVPI in this regard (10,15). Preliminary data suggest that PVPI may be particularly
useful when assessing patients with concomitant increases in
EVLWi (17).
Notably, greater than 90% of the current study popula-
tion had their peak EVLWi and PVPI measurements within 6
hours of separation from CPB (cardiac surgery) or removal of
the aortic cross clamp (aortic vascular surgery). Although the
early rise in EVLWi and PVPI was unexpected, particularly for
those with baseline elevations, we believe this may simply con-
firm the ability of EVLWi and PVPI to detect subclinical lung
edema in a cohort of patients with clear baseline risk. Indeed,
these findings suggest that EVLWi and PVPI may be very early
markers of risk for progression to clinically significant pulmo-
nary edema and lung injury. If confirmed, EVLWi and PVPI
would be particularly attractive markers of subclinical lung
injury when studying time-sensitive therapeutic interventions.
Interestingly, in the study by LeTourneau et al (46), EVLWi
measurements were similar for those with prevalent ARDS and
those who later progressed to ARDS, perhaps corroborating
our findings that increased EVLWi is a very early change in the
progression from healthy lungs to the full ARDS phenotype.
Although the prospective design, rigorous training of the
investigative team, and specific focus on at-risk surgical popu-
lations are notable strengths of this investigation, important
limitations must be discussed. First is the single-center nature
of the study. Second, we had a limited sample size and small
number of ARDS outcomes (n = 13), which prevents us from
drawing firm conclusions regarding the validity of the study
findings. Nonetheless, our findings are consistent with those
reported in the multicenter study of ICU patients with risk of
ARDS (46), as well as with the study by Martin et al (7) in
patients with sepsis. A third concern relates to the reproducibil-
ity of the diagnosis of ARDS and differentiating this outcome
from CPE. Although these challenges affect all clinical ARDS
studies, they are particularly relevant in the study of postop-
erative ARDS, in which atelectasis and ventilatory support are
common after surgery. To address this concern, we had two
independent evaluations of the outcomes of interest, and when
disagreements arose, a third consulting expert made the final
determination. Nonetheless, we acknowledge the remaining
potential for misclassification of ARDS and CPE. Finally, the
requirement for both central venous and arterial catheteriza-
tion may limit the use of the PiCCO device in patients with lowrisk of ARDS. However, we emphasize that surgical patients
with high risk of postoperative ARDS (e.g., those undergoing
cardiac, aortic vascular, and high-risk thoracic surgery) often
have both of these procedures performed as a routine part of
their anesthetic care.
CONCLUSIONSPerioperative EVLW
i is an effective early marker that predicts
risk of clinically significant postoperative pulmonary edema in
at-risk surgical patients. PVPI will aid in discriminating post-
operative ARDS from CPE. If validated in a larger cohort, these
measures may prove useful in the early detection of subclinical
lung injury in at-risk surgical populations.
ACKNOWLEDGMENTSWe acknowledge Lavonne M. Liedl, RRT; Brenda K. Anderson,
RN; Anita Baumgartner, RN; and Melissa A. Passe, RRT, for
their passion, perseverance, and excellence serving as study
coordinators for this project. We also acknowledge Pulsion
Medical Systems SE for their willingness to provide the PiCCO
equipment used to obtain the extravascular lung water indexed
to predicted body weight and pulmonary vascular permeabil-
ity index measurements in this study.

7/24/2019 Agua Extravascular Pulmonar Periopera
http://slidepdf.com/reader/full/agua-extravascular-pulmonar-periopera 8/9
Kor et al
672 www.ccmjournal.org March 2015 • Volume 43 • Number 3
REFERENCES 1. Alam N, Park BJ, Wilton A, et al: Incidence and risk factors for
lung injury after lung cancer resection. Ann Thorac Surg 2007;84:1085–1091
2. Fernández-Pérez ER, Sprung J, Afessa B, et al: Intraoperative ventila-tor settings and acute lung injury after elective surgery: A nested casecontrol study. Thorax 2009; 64:121–127
3. Herridge MS, Tansey CM, Matté A, et al; Canadian Critical Care Trials
Group: Functional disability 5 years after acute respiratory distresssyndrome. N Engl J Med 2011; 364:1293–1304
4. Kor DJ, Warner DO, Alsara A, et al: Derivation and diagnostic accu-racy of the surgical lung injury prediction model. Anesthesiology 2011;115:117–128
5. Sen S, Sen S, Sentürk E, et al: Postresectional lung injury in thoracicsurgery pre and intraoperative risk factors: A retrospective clinicalstudy of a hundred forty-three cases. J Cardiothorac Surg 2010; 5:62
6. Spragg RG, Bernard GR, Checkley W, et al: Beyond mortality: Futureclinical research in acute lung injury. Am J Respir Crit Care Med 2010; 181:1121–1127
7. Martin GS, Eaton S, Mealer M, et al: Extravascular lung water inpatients with severe sepsis: A prospective cohort study. Crit Care 2005; 9:R74–R82
8. Berkowitz DM, Danai PA, Eaton S, et al: Alcohol abuse enhances pul-
monary edema in acute respiratory distress syndrome. Alcohol ClinExp Res 2009; 33:1690–1696
9. Berkowitz DM, Danai PA, Eaton S, et al: Accurate characterization ofextravascular lung water in acute respiratory distress syndrome. CritCare Med 2008; 36:1803–1809
10. Monnet X, Anguel N, Osman D, et al: Assessing pulmonary perme-ability by transpulmonary thermodilution allows differentiation of hydro-static pulmonary edema from ALI/ARDS. Intensive Care Med 2007;33:448–453
11. von Elm E, Altman DG, Egger M, et al; STROBE Initiative: TheStrengthening the Reporting of Observational Studies in Epidemiology(STROBE) statement: Guidelines for reporting observational studies.Ann Intern Med 2007; 147:573–577. Erratum in Ann Intern Med 2008; 148:168
12. Licker M, de Perrot M, Spiliopoulos A, et al: Risk factors for acutelung injury after thoracic surgery for lung cancer. Anesth Analg 2003;97:1558–1565
13. Fernández-Pérez ER, Keegan MT, Brown DR, et al: Intraoperative tidalvolume as a risk factor for respiratory failure after pneumonectomy.Anesthesiology 2006; 105:14–18
14. Ranieri VM, Rubenfeld GD, Thompson BT, et al; ARDS Denition TaskForce: Acute respiratory distress syndrome: The Berlin Definition.JAMA 2012; 307:2526–2533
15. Kushimoto S, Taira Y, Kitazawa Y, et al; PiCCO Pulmonary EdemaStudy Group: The clinical usefulness of extravascular lung water andpulmonary vascular permeability index to diagnose and characterizepulmonary edema: A prospective multicenter study on the quantitativedifferential diagnostic definition for acute lung injury/acute respiratorydistress syndrome. Crit Care 2012; 16:R232
16. Neumann P: Extravascular lung water and intrathoracic blood volume:Double versus single indicator dilution technique. Intensive Care Med
1999; 25:216–219 17. Sakka SG, Rühl CC, Pfeiffer UJ, et al: Assessment of cardiac preload
and extravascular lung water by single transpulmonary thermodilution.Intensive Care Med 2000; 26:180–187
18. Phillips CR, Chesnutt MS, Smith SM: Extravascular lung water insepsis-associated acute respiratory distress syndrome: Indexing withpredicted body weight improves correlation with severity of illnessand survival. Crit Care Med 2008; 36:69–73
19. Groeneveld AB, Verheij J: Extravascular lung water to blood volumeratios as measures of permeability in sepsis-induced ALI/ARDS.Intensive Care Med 2006; 32:1315–1321
20. Holm C, Tegeler J, Mayr M, et al: Effect of crystalloid resuscitationand inhalation injury on extravascular lung water: Clinical implications.Chest 2002; 121:1956–1962
21. Honore PM, Jacquet LM, Beale RJ, et al: Effects of normothermia
versus hypothermia on extravascular lung water and serum cytokines
during cardiopulmonary bypass: A randomized, controlled trial. CritCare Med 2001; 29:1903–1909
22. Perkins GD, McAuley DF, Thickett DR, et al: The beta-agonist lunginjury trial (BALTI): A randomized placebo-controlled clinical trial. AmJ Respir Crit Care Med 2006; 173:281–287
23. Hsieh FY, Bloch DA, Larsen MD: A simple method of sample sizecalculation for linear and logistic regression. Stat Med 1998;17:1623–1634
24. Ray P, Le Manach Y, Riou B, et al: Statistical evaluation of a bio-marker. Anesthesiology 2010; 112:1023–1040
25. Jepsen S, Herlevsen P, Knudsen P, et al: Antioxidant treatmentwith N-acetylcysteine during adult respiratory distress syndrome: Aprospective, randomized, placebo-controlled study. Crit Care Med 1992; 20:918–923
26. Matthay MA, Brower RG, Carson S, et al; National Heart, Lung, andBlood Institute Acute Respiratory Distress Syndrome (ARDS) ClinicalTrials Network: Randomized, placebo-controlled clinical trial of anaerosolized β2-agonist for treatment of acute lung injury. Am J RespirCrit Care Med 2011; 184:561–568
27. The ARDS Network: Ketoconazole for early treatment of acute lunginjury and acute respiratory distress syndrome: A randomized con-trolled trial. JAMA 2000; 283:1995–2002. Errata in JAMA 2000;284:2450; JAMA 2001; 286:1578; JAMA 2000; 284:2597
28. Randomized, placebo-controlled trial of lisofylline for early treatmentof acute lung injury and acute respiratory distress syndrome. CritCare Med 2002; 30:1–6
29. Zeiher BG, Artigas A, Vincent JL, et al; STRIVE Study Group:Neutrophil elastase inhibition in acute lung injury: Results of theSTRIVE study. Crit Care Med 2004; 32:1695–1702
30. Agrawal A, Matthay MA, Kangelaris KN, et al: Plasma angiopoietin-2predicts the onset of acute lung injury in critically ill patients. Am JRespir Crit Care Med 2013; 187:736–742
31. Binnie A, Tsang JL, dos Santos CC: Biomarkers in acute respiratorydistress syndrome. Curr Opin Crit Care 2014; 20:47–55
32. Cepkova M, Brady S, Sapru A, et al: Biological markers of lung injurybefore and after the institution of positive pressure ventilation inpatients with acute lung injury. Crit Care 2006; 10:R126
33. Fremont RD, Koyama T, Calfee CS, et al: Acute lung injury in patientswith traumatic injuries: Utility of a panel of biomarkers for diagnosisand pathogenesis. J Trauma 2010; 68:1121–1127
34. Levitt JE, Bedi H, Calfee CS, et al: Identification of early acute lunginjury at initial evaluation in an acute care setting prior to the onset ofrespiratory failure. Chest 2009; 135:936–943
35. Levitt JE, Calfee CS, Goldstein BA, et al: Early acute lung injury:Criteria for identifying lung injury prior to the need for positive pres-sure ventilation. Crit Care Med 2013; 41:1929–1937
36. Liu X, Chen Q, Shi S, et al: Plasma sRAGE enables prediction ofacute lung injury after cardiac surgery in children. Crit Care 2012;16:R91
37. Mikkelsen ME, Shah CV, Meyer NJ, et al: The epidemiology of acuterespiratory distress syndrome in patients presenting to the emer-gency department with severe sepsis. Shock 2013; 40:375–381
38. Rubin DB, Wiener-Kronish JP, Murray JF, et al: Elevated vonWillebrand factor antigen is an early plasma predictor of acutelung injury in nonpulmonary sepsis syndrome. J Clin Invest 1990;86:474–480
39. Terpstra ML, Aman J, van Nieuw Amerongen GP, et al: Plasma bio-markers for acute respiratory distress syndrome: A systematic reviewand meta-analysis. Crit Care Med 2014; 42:691–700
40. Calfee CS, Eisner MD, Ware LB, et al; Acute Respiratory DistressSyndrome Network, National Heart, Lung, and Blood Institute:Trauma-associated lung injury differs clinically and biologically fromacute lung injury due to other clinical disorders. Crit Care Med 2007;35:2243–2250
41. Gajic O, Dabbagh O, Park PK, et al; U.S. Critical Illness andInjury Trials Group: Lung Injury Prevention Study Investigators(USCIITG-LIPS): Early identification of patients at risk ofacute lung injury: Evaluation of lung injury prediction score ina multicenter cohort study. Am J Respir Crit Care Med 2011;
183:462–470

7/24/2019 Agua Extravascular Pulmonar Periopera
http://slidepdf.com/reader/full/agua-extravascular-pulmonar-periopera 9/9