Aging of the Male Reproductive System Spring 2007 PS Timiras.
19
Aging of the Male Reproductive System Spring 2007 PS Timiras
-
date post
21-Dec-2015 -
Category
Documents
-
view
216 -
download
2
Transcript of Aging of the Male Reproductive System Spring 2007 PS Timiras.

Aging of theMale Reproductive
SystemSpring 2007PS Timiras

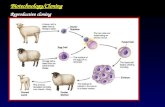
Dr. Brown Sequard (Physiologist, Univ. Sorbonne, Paris) introduced the idea that some glands secrete internally (in the blood) potent substances that affect the whole organism.
In 1905, these substances were called “hormones” by the British physiologist E.H. Starling.

Comparison between the relative simplicity of the male reproductivesystem and the complexity of the female reproductive system.
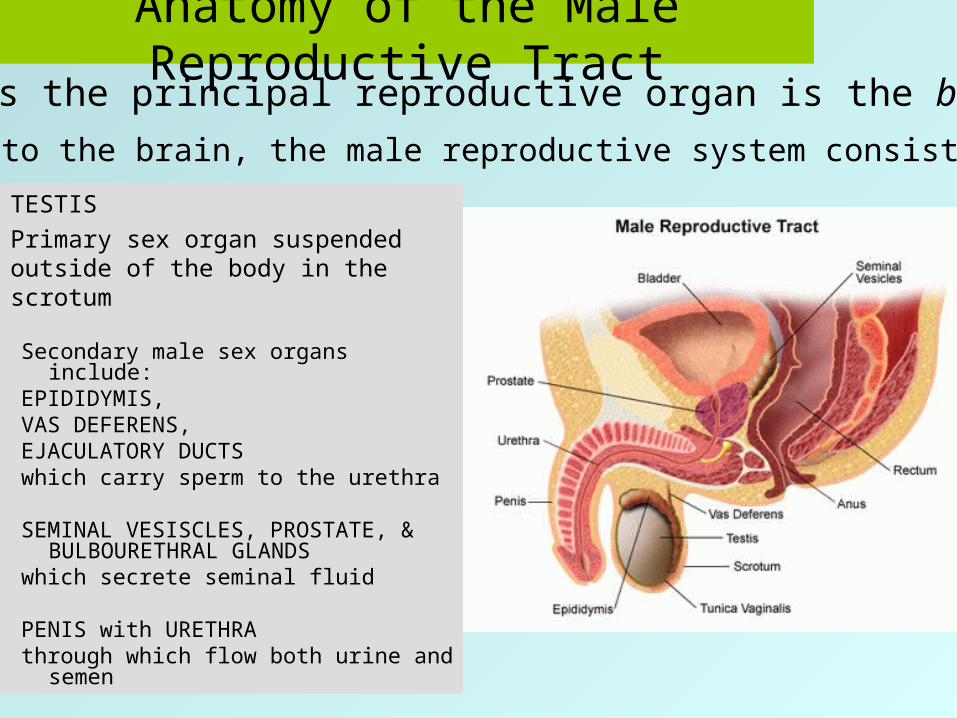
Anatomy of the Male Reproductive Tract
TESTISPrimary sex organ suspended outside of the body in the scrotum
Secondary male sex organs include:
EPIDIDYMIS,VAS DEFERENS,EJACULATORY DUCTSwhich carry sperm to the urethra
SEMINAL VESISCLES, PROSTATE, & BULBOURETHRAL GLANDS
which secrete seminal fluid
PENIS with URETHRAthrough which flow both urine
and semen
In humans the principal reproductive organ is the brain
In addition to the brain, the male reproductive system consists of the:

A simplified version of the
male reproductive endocrinology:
The hypothalamus releases GnRH into the circulatory system and, through blood, directly into the pituitary.
GnRH triggers the release of the pituitary LH and FSH that stimulate the testes to testosterone secretion and sperm production.

the GERM CELLS or GAMETES,involved in fertilization.
the INTERSTITIAL CELLS of LEYDIGthat secrete testosterone, the
major androgen
the SERTOLI CELLSwith secretory and reproductive
functions
The testis, the male primary reproductive
organ, contains three types of cells, all
necessary for reproduction:

With Age:
• On the average, the male reproductive function remains normal (or only slightly diminished in some individuals) until advanced old age (80+ years) when it decreases
• Subtle changes include: GnRHSensitivity of androgen secretion
to LHSensitivity of negative feedback
between GnRH and LH

Figure 12.2Differences in
levels (total,
bioavailable, and percentage)
of free/bioavailable
testosterone
Young
Young
Young
Old
Old
Old

Serum LH concentration
With aging, loss of high-amplitude LH pulses despite normal or increased pituitary LH stores
Serum testosterone concentration
With aging, decreased responsiveness of testis androgen secretion to LH
Young OlderYoung Older

TABLE 12-2SELECTED NEUROENDOCRINE MODELING ISSUES IN THE
AGING MALE REPRODUCTIVE AXIS
1. How does the timing of GnRH pulse-generator change with age?
2. Which alterations in the aging male reproductive axis reflect pathophysiology versus secondary adaptations?
3. What mechanisms account for greater inter-subject heterogeneity in aging of GnRH-LH testosterone secretion?
Aging of the Prostate

Figure 19.7

Table 19-12 The Prostate and Testosterone
The healthy prostate is dependent on androgens for growth
In the prostate: testosterone dihydrotestosterone (DHT)
The enzyme catalyzing this reaction is 5--reductase
DHT stimulates growth of the prostate
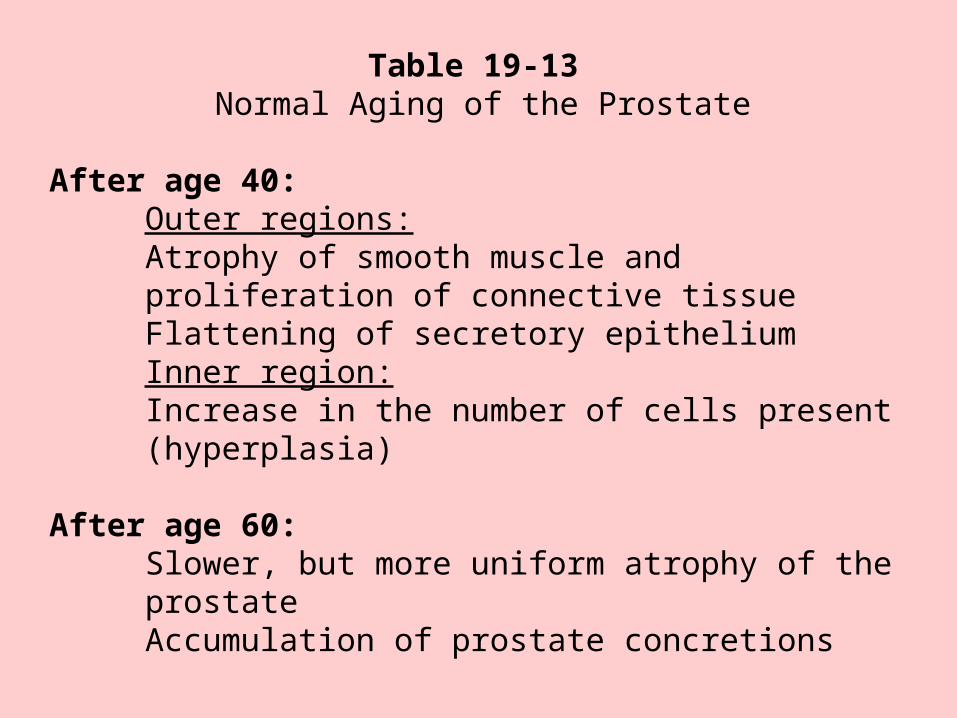
Table 19-13 Normal Aging of the Prostate
After age 40:Outer regions:Atrophy of smooth muscle and proliferation of connective tissueFlattening of secretory epitheliumInner region:Increase in the number of cells present (hyperplasia)
After age 60:Slower, but more uniform atrophy of the prostateAccumulation of prostate concretions
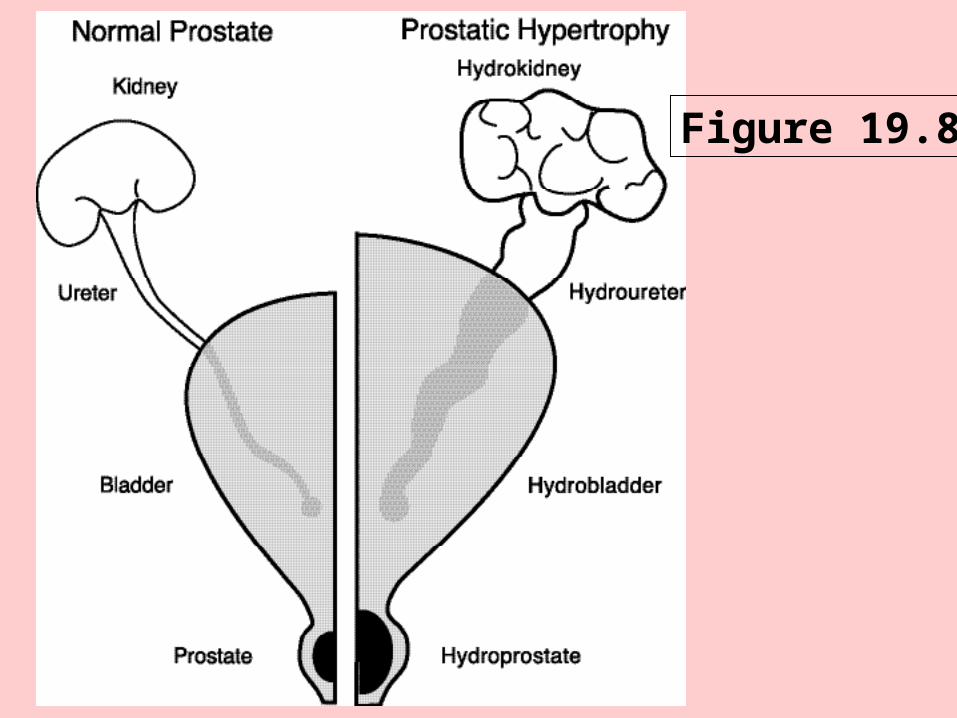
Figure 19.8

Table 19-14 Synopsis of Benign Prostatic Hyperplasia (BPH)Characteristics
• Caused by g rowt h of th e prost at e f rom about age 40 un t il deat h• Af fect s 50 % of m en > 50 years o ld• Af fect s 95 % of m en > 70 years o ld• Clinical sympt oms due t o obstru cti on of th e ureth ra are present up to
25% of men w it h histo logic evidence of BPH• BPH t issue resembles normal prosta t e t issue wit h increased am ount s
of smoot h muscle, g landular, and/ or str omal component s• An enlarged prost at e can str angle th e ureth ra
• BPH is not found in men who have been castr at ed or men who lack 5-α-reducta se

Table 19-15 Possible Risk Factors for Benign ProstaticHyperplasia (BPH) and Prostate Cancer
Possible Risk Factors for BPH Possible Risk Factors for Prostate Cancer• Aging • Genet ic predisposit ion• Use of a nabolic st eroids • To bacco exposure• Dieta ry f act ors • Cadmium exposure• Genet ic predisposit ion • Vit amin A def iciency• Environment al to xins • Vasecto my• No oth er major risk fa cto rs • Sexually t ransmit t ed d iseases
• Muta genic hormonal facto rs• Dieta ry f act ors (part icularly h igh level of
animal fa t)

Treatment of Prostate CancerDepends on
Life expectancyOverall health statusPersonal preferencesSize of the prostate
State of disease
Treatments include:Watchful waiting
SurgeryRadiation TherapyHormonal Therapy
Cryotherapy
**PSA controversy pp. 353, 354**