
Agents Used in Anemias.his 2009.ppt...
39
Agents Used in Anemias; Agents Used in Anemias; Hematopoietic Growth Factors Tri Widyawati-Zulkarnain Rangkuty Blok HIS, Senin, 13 April 2009
-
Upload
nguyenliem -
Category
Documents
-
view
218 -
download
0
Transcript of Agents Used in Anemias.his 2009.ppt...
![Page 1: Agents Used in Anemias.his 2009.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000096-hematology-and... · Eritropoesis (120 h ) Lambung ...](https://reader042.fdocuments.us/reader042/viewer/2022022806/5ccd0a4788c993b2538d66a0/html5/page/1.jpg)
Agents Used in Anemias;Agents Used in Anemias;Hematopoietic Growth Factors
Tri Widyawati-Zulkarnain Rangkutyy g y
Blok HIS, Senin, 13 April 2009
![Page 2: Agents Used in Anemias.his 2009.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000096-hematology-and... · Eritropoesis (120 h ) Lambung ...](https://reader042.fdocuments.us/reader042/viewer/2022022806/5ccd0a4788c993b2538d66a0/html5/page/2.jpg)
IntroductionIntroductionAnemia : a deficiency in oxygen-carrying
erythrocytes.
Hematopoietic machinery residesHematopoietic machinery resides primarily in the bone marrow, requires a constant supply of :constant supply of :
- Iron- Vitamin B- Vitamin B12- Folic acid
And : hematopoietic growth factorAnd : hematopoietic growth factor.
![Page 3: Agents Used in Anemias.his 2009.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000096-hematology-and... · Eritropoesis (120 h ) Lambung ...](https://reader042.fdocuments.us/reader042/viewer/2022022806/5ccd0a4788c993b2538d66a0/html5/page/3.jpg)
Agents Used in Anemias
• Iron• Vitamin B12• Folic acid
![Page 4: Agents Used in Anemias.his 2009.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000096-hematology-and... · Eritropoesis (120 h ) Lambung ...](https://reader042.fdocuments.us/reader042/viewer/2022022806/5ccd0a4788c993b2538d66a0/html5/page/4.jpg)
Iron : Basic Pharmacology
• Iron form the nucleus of the iron porphyrin heme ring t th ith l bi h i h l bitogether with globin chains hemoglobin
• Hb reversibly binds O2 and provides the critical mechanism for O2 delivery from the lungs to other 2 y gtissues
![Page 5: Agents Used in Anemias.his 2009.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000096-hematology-and... · Eritropoesis (120 h ) Lambung ...](https://reader042.fdocuments.us/reader042/viewer/2022022806/5ccd0a4788c993b2538d66a0/html5/page/5.jpg)
Iron Distribution in normal adultsIron Distribution in normal adults
Iron content (mg)Men Women
H l biHemoglobin 3050 1700Myoglobin 430 300Enzymes 10 8Enzymes 10 8Transport (transferrin) 8 6Storage (ferritin and other forms) 750 300Storage (ferritin and other forms) 750 300
Total 4248 2314
![Page 6: Agents Used in Anemias.his 2009.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000096-hematology-and... · Eritropoesis (120 h ) Lambung ...](https://reader042.fdocuments.us/reader042/viewer/2022022806/5ccd0a4788c993b2538d66a0/html5/page/6.jpg)
Estimated Dietary Iron RequirementsAbsorbed iron requirement mg/day
Daily food iron requirement* mg/day
Normal men and non menstruating women
0,5-1 5-10
Menstruating women 0,7-2 7-20g ,
Pregnant women 2-4,8 20-48#
Adolescent 1-2 10-20
Children 0,4-1 4-10
Infants 0,5-1,5 1,5mg/kg**
* Assuming 10% absorption# This amount of iron can’t be derived from diet and should be met by iron supplementation in the latter half of pregnancy** To a maximum of 15 mg
![Page 7: Agents Used in Anemias.his 2009.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000096-hematology-and... · Eritropoesis (120 h ) Lambung ...](https://reader042.fdocuments.us/reader042/viewer/2022022806/5ccd0a4788c993b2538d66a0/html5/page/7.jpg)
Iron Requirements for Pregnancyg y
Average(mg)
Range (mg)( g) ( g)
External iron loss 170 150-200
Expansion of red-blood-cell mass 450 200-600
Fetal iron 270 200-370
Iron in placenta and cord 90 30-170
Blood loss at delivery 150 90-310-Total requirement *-Cost of pregnancy #
980680
580-1340440-1050
* Blood loss at delivery not included# Expansion of red-cell mass no included
![Page 8: Agents Used in Anemias.his 2009.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000096-hematology-and... · Eritropoesis (120 h ) Lambung ...](https://reader042.fdocuments.us/reader042/viewer/2022022806/5ccd0a4788c993b2538d66a0/html5/page/8.jpg)
Iron : PharmacokineticIron : Pharmacokinetic• Absorption
N ll i d d d i l j j- Normally in duodenum and proximal jejunum.- Usually absorption ± 5-10% of average diet daily.- In menstruating women : ↑ to 1-2 mg/day and 3-4 mg/day in
pregnant women.• Iron in:
- meat protein easily absorbed.meat protein easily absorbed.- vegetables & grain tightly bound to phytates or other complexing agents less available for absorption.
• Non heme iron in foods and Iron in organic iron salts and• Non heme iron in foods and Iron in organic iron salts and complexes :
must be reduced to ferrous (Fe2+) before absorbedcan be inhibited b chelatorscan be inhibited by chelatorsincreased by HCl and vit. C.
![Page 9: Agents Used in Anemias.his 2009.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000096-hematology-and... · Eritropoesis (120 h ) Lambung ...](https://reader042.fdocuments.us/reader042/viewer/2022022806/5ccd0a4788c993b2538d66a0/html5/page/9.jpg)
Iron : PharmacokineticIron : Pharmacokinetic• Transport
I i t t d i th l b d t t f i ( β l b li- Iron is transported in the plasma bound to transferrin (a β-globulin that specially binds ferric iron).- The transferrin-ferric iron complex enters maturing erythroid
ll b ifi t h i (t f i t )cells by a spesific receptor mechanism (transferrin receptors)- The transferrin and transferrin receptors are then recycled → incorporating iron into hemoglobin in developing red blood cells
• Storage- Iron binds avidly to a protein, apoferritin → form the complex ferritin
- Iron stored as ferritin in: intestinal mucosal cells and in the macrophages in the liver, spleen, and bone.
- Apoferritin synthesis is regulated by the levels of free iron.p y g y
![Page 10: Agents Used in Anemias.his 2009.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000096-hematology-and... · Eritropoesis (120 h ) Lambung ...](https://reader042.fdocuments.us/reader042/viewer/2022022806/5ccd0a4788c993b2538d66a0/html5/page/10.jpg)
Iron : PharmacokineticIron : Pharmacokinetic• EliminationElimination
- small amounts : exfoliation of intestinal mucosal cells into the stool- trace amounts : bile, urine, and sweat. - 0 5 – 1 mg/day0,5 1 mg/day
![Page 11: Agents Used in Anemias.his 2009.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000096-hematology-and... · Eritropoesis (120 h ) Lambung ...](https://reader042.fdocuments.us/reader042/viewer/2022022806/5ccd0a4788c993b2538d66a0/html5/page/11.jpg)
![Page 12: Agents Used in Anemias.his 2009.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000096-hematology-and... · Eritropoesis (120 h ) Lambung ...](https://reader042.fdocuments.us/reader042/viewer/2022022806/5ccd0a4788c993b2538d66a0/html5/page/12.jpg)
Iron Therapy : OralIron Therapy : OralPreparation Tablet size Elemental iron per Usual adult
(mg) tablet (mg) dosage (tablets per day)
Ferrous sulfate, h drated
325 65 3-4hydratedFerrous sulfate, desiccated
200 65 3-4
F l t 325 36 3 4Ferrous gluconate 325 36 3-4Ferrous fumarate 200 66 3-4Ferrous fumarate 325 106 2-3
• 200-400 mg of elemental iron should be given daily to correct iron deficiency
• 3-6 months
![Page 13: Agents Used in Anemias.his 2009.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000096-hematology-and... · Eritropoesis (120 h ) Lambung ...](https://reader042.fdocuments.us/reader042/viewer/2022022806/5ccd0a4788c993b2538d66a0/html5/page/13.jpg)
Iron Therapy: ParenteralIron Therapy: Parenteral
• anemic patients unable to tolerate oral therapyanemic patients unable to tolerate oral therapy.• extensive chronic blood loss
![Page 14: Agents Used in Anemias.his 2009.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000096-hematology-and... · Eritropoesis (120 h ) Lambung ...](https://reader042.fdocuments.us/reader042/viewer/2022022806/5ccd0a4788c993b2538d66a0/html5/page/14.jpg)
Preparation
• Iron dextran 5% (IM/IV): ferric hydroxide and low-molecular-weight dextran ( 50 mg of elemental iron/ml solution)
• Iron sucrose complex.• Iron sodium gluconate complexIron sodium gluconate complex.
Dosage : 1-2 g of replacement iron,or 20-40 mL of iron dextran
![Page 15: Agents Used in Anemias.his 2009.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000096-hematology-and... · Eritropoesis (120 h ) Lambung ...](https://reader042.fdocuments.us/reader042/viewer/2022022806/5ccd0a4788c993b2538d66a0/html5/page/15.jpg)
Iron : Adverse Effect
• Oral: nausea epigastric discomfortOral: nausea, epigastric discomfort, abdominal cramps, constipation, diarrhea, black stoolsblack stools
• Parenteral: local pain, tissue staining, headache fever arthralgia nauseaheadache, fever, arthralgia, nausea, vomiting, back pain, flushing, urticaria, bronchospasm and rarely anaphylaxis andbronchospasm and rarely anaphylaxis and death.
![Page 16: Agents Used in Anemias.his 2009.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000096-hematology-and... · Eritropoesis (120 h ) Lambung ...](https://reader042.fdocuments.us/reader042/viewer/2022022806/5ccd0a4788c993b2538d66a0/html5/page/16.jpg)
Iron : Acute ToxicityIron : Acute Toxicity• Usually in ChildrenUsually in Children
ingested iron tablets → necrotizing gastroenteritis :g- Vomitting.- Abdominal painAbdominal pain.- Bloody diarrhealethargy shock & dyspnealethargy, shock & dyspnea.
![Page 17: Agents Used in Anemias.his 2009.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000096-hematology-and... · Eritropoesis (120 h ) Lambung ...](https://reader042.fdocuments.us/reader042/viewer/2022022806/5ccd0a4788c993b2538d66a0/html5/page/17.jpg)
Iron : Acute ToxicityIron : Acute Toxicity• TreatmentTreatment
- Charcoal ineffective because does not bind iron.- Deferoxamine potent iron-chelating.- Supportive therapySupportive therapy.
![Page 18: Agents Used in Anemias.his 2009.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000096-hematology-and... · Eritropoesis (120 h ) Lambung ...](https://reader042.fdocuments.us/reader042/viewer/2022022806/5ccd0a4788c993b2538d66a0/html5/page/18.jpg)
Iron : Chronic ToxicityIron : Chronic Toxicity
• HemochromatosisHemochromatosis• In patients with :
I h it d h h t i ( i- Inherited hemochromatosis (excessive iron absorption)- too many blood, transfusion over a long period of time.
• Treatment : intermittent phlebotomy
![Page 19: Agents Used in Anemias.his 2009.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000096-hematology-and... · Eritropoesis (120 h ) Lambung ...](https://reader042.fdocuments.us/reader042/viewer/2022022806/5ccd0a4788c993b2538d66a0/html5/page/19.jpg)
Vitamin B12Vitamin B12
• Cofactor for several essential biochemicalCofactor for several essential biochemical reactions.
• Deficiency of vit B12 :• Deficiency of vit. B12 :anemiagastrointestinal symptomsneurologic abnormalitiesg
![Page 20: Agents Used in Anemias.his 2009.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000096-hematology-and... · Eritropoesis (120 h ) Lambung ...](https://reader042.fdocuments.us/reader042/viewer/2022022806/5ccd0a4788c993b2538d66a0/html5/page/20.jpg)
Vitamin B12Vitamin B12• Chemistry :Chemistry :- Porphyrin – like ring with a central cobalt atom
attached to a nucleotide.• In human : active form → - deoxyadenosylcobalamine→ deoxyadenosylcobalamine
- methylcobalamin• Therapeutic use: cyanocobalamin and• Therapeutic use: cyanocobalamin and
hydroxycobalamin
![Page 21: Agents Used in Anemias.his 2009.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000096-hematology-and... · Eritropoesis (120 h ) Lambung ...](https://reader042.fdocuments.us/reader042/viewer/2022022806/5ccd0a4788c993b2538d66a0/html5/page/21.jpg)
Vitamin B12 : PharmacokineticsVitamin B12 : Pharmacokinetics
• Stored in the liver (3000-5000 μg)Stored in the liver (3000 5000 μg)• Normal daily requirement ± 2 μg• Vit B12 in food bind to intrinsic factor ( aVit. B12 in food, bind to intrinsic factor ( a
glycoprotein secreted by the parietal cells of the gastic mucosa) absorbed in distal ileum by g ) yhighly specific receptor mediated transport system.
![Page 22: Agents Used in Anemias.his 2009.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000096-hematology-and... · Eritropoesis (120 h ) Lambung ...](https://reader042.fdocuments.us/reader042/viewer/2022022806/5ccd0a4788c993b2538d66a0/html5/page/22.jpg)
Vitamin B12 : PharmacokineticsVitamin B12 : Pharmacokinetics• After absorption :p
- Transported to the various organ cells bound to plasma glycoprotein → transcobalamin II (beta globulin)globulin) - Excess vit. B12 stored in the liver
• Metabolism : hati ⇒ hydroxycobalamin and y ycyanocobalamin → coenzim B12
![Page 23: Agents Used in Anemias.his 2009.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000096-hematology-and... · Eritropoesis (120 h ) Lambung ...](https://reader042.fdocuments.us/reader042/viewer/2022022806/5ccd0a4788c993b2538d66a0/html5/page/23.jpg)
Vitamin B12 : PharmacokineticsVitamin B12 : Pharmacokinetics• Excretion : empedup
urin (bentuk tdk terikat protein)• 80-95% diretensi tubuh sampai dosis 50 mcg
K it ik t t i d i h ti j i d• Kapasitas ikatan protein dari hati, jaringan dan darah jenuh ⇒ dikeluarkan melalui urin
• Vitamin B12 dapat melewati sawar uriVitamin B12 dapat melewati sawar uri• Vit. B12 deficiency often results from :- Malabsorption of Vit. B12 due to ⇒ Lack of intrinsic factor⇒ Malfunction of specific absorptive mechanism.
![Page 24: Agents Used in Anemias.his 2009.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000096-hematology-and... · Eritropoesis (120 h ) Lambung ...](https://reader042.fdocuments.us/reader042/viewer/2022022806/5ccd0a4788c993b2538d66a0/html5/page/24.jpg)
Vitamin B12 : Pharmacodynamics
• Methylfolate trap: def Vit B12 corrected : folic acid• Neurologic manifestations : def vit B12
![Page 25: Agents Used in Anemias.his 2009.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000096-hematology-and... · Eritropoesis (120 h ) Lambung ...](https://reader042.fdocuments.us/reader042/viewer/2022022806/5ccd0a4788c993b2538d66a0/html5/page/25.jpg)
Vit i B12 Cli i l Ph lVitamin B12 : Clinical Pharmacology
• Vitamin B12 is used to treat or prevent deficiency megaloblastic anemiadeficiency megaloblastic anemia (macrocytic anemia)
![Page 26: Agents Used in Anemias.his 2009.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000096-hematology-and... · Eritropoesis (120 h ) Lambung ...](https://reader042.fdocuments.us/reader042/viewer/2022022806/5ccd0a4788c993b2538d66a0/html5/page/26.jpg)
Preparation
• Tablet : oral • Solution : par enteral (IM/SK) → lebih baik
1. sol. Cyanocobalamin 10-1000 mcg/mlJ i b lk k i l i⇒ Jarang menimbulkan reaksi alergi
2. sol. Eksrak hati dalam air⇒ Sering reaksi alergi⇒ Sering reaksi alergi
3. suntikan depot vit. B12⇒Mengurangi frekuensi pemberian ⇒ e gu a g e ue s pe be a• Solution : hidroxycobalamin 100 mcg : efek
lebih lama
![Page 27: Agents Used in Anemias.his 2009.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000096-hematology-and... · Eritropoesis (120 h ) Lambung ...](https://reader042.fdocuments.us/reader042/viewer/2022022806/5ccd0a4788c993b2538d66a0/html5/page/27.jpg)
Folic AcidFolic AcidPrecursors for the synthesis
f i id i dof amino acids, purines, and DNADNA
![Page 28: Agents Used in Anemias.his 2009.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000096-hematology-and... · Eritropoesis (120 h ) Lambung ...](https://reader042.fdocuments.us/reader042/viewer/2022022806/5ccd0a4788c993b2538d66a0/html5/page/28.jpg)
Folic Acid
![Page 29: Agents Used in Anemias.his 2009.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000096-hematology-and... · Eritropoesis (120 h ) Lambung ...](https://reader042.fdocuments.us/reader042/viewer/2022022806/5ccd0a4788c993b2538d66a0/html5/page/29.jpg)
Folic Acid : PharmacokineticsFolic Acid : Pharmacokinetics
• The average diets : 500-700 μg daily ⇒The average diets : 500 700 μg daily ⇒50-200 μg of which is usually absorbed
• Sources :• Sources : - plant and animal tissues- richest : yeast, liver, kidney and green vegetables
• Normally : 5 – 20 mg stored in the liver and other tissues
![Page 30: Agents Used in Anemias.his 2009.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000096-hematology-and... · Eritropoesis (120 h ) Lambung ...](https://reader042.fdocuments.us/reader042/viewer/2022022806/5ccd0a4788c993b2538d66a0/html5/page/30.jpg)
Folic Acid : PharmacokineticsFolic Acid : Pharmacokinetics
• Excreted : urine and stoolExcreted : urine and stool destroyed by catabolism
F li id d fi i d l bl ti• Folic acid deficiency and megaloblastic anemia : develop within 1-6 months after th i t k f li id tthe intake folic acid stops
![Page 31: Agents Used in Anemias.his 2009.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000096-hematology-and... · Eritropoesis (120 h ) Lambung ...](https://reader042.fdocuments.us/reader042/viewer/2022022806/5ccd0a4788c993b2538d66a0/html5/page/31.jpg)
Folic Acid : TherapyFolic Acid : Therapy
• Oral : - well absorbedOral : well absorbed- 1 mg/day for anemia megaloblastic
C ti d til th d l i f⇒ Continued until the underlying cause of deficiency is removed or corrected
• Parenteral : rarely
![Page 32: Agents Used in Anemias.his 2009.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000096-hematology-and... · Eritropoesis (120 h ) Lambung ...](https://reader042.fdocuments.us/reader042/viewer/2022022806/5ccd0a4788c993b2538d66a0/html5/page/32.jpg)
Hematopoietic Growth FactorsE h i iErythropoietin
E th i ti• Erythropoietin :- Glycoprotein- a growth hormone- a growth hormone
• stimulates erythroid proliferation and differentiation by interacting with spesificdifferentiation by interacting with spesific eryhropoietin receptors on red cell progenitors
• induces release of reticulocytes from the boneinduces release of reticulocytes from the bone marrow
![Page 33: Agents Used in Anemias.his 2009.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000096-hematology-and... · Eritropoesis (120 h ) Lambung ...](https://reader042.fdocuments.us/reader042/viewer/2022022806/5ccd0a4788c993b2538d66a0/html5/page/33.jpg)
ErythropoietinErythropoietin
• Recombinant human erythropoietin used in clinic.
• Epoitin alfa : - I.V t ½ 4-13 hrs in CRF- Not cleared by dialysis.y y
• Darbopoietin alfa : - Glycosylated form of erythropoietiny y y p- t ½ 2-3 x epoitin.
![Page 34: Agents Used in Anemias.his 2009.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000096-hematology-and... · Eritropoesis (120 h ) Lambung ...](https://reader042.fdocuments.us/reader042/viewer/2022022806/5ccd0a4788c993b2538d66a0/html5/page/34.jpg)
ErythropoietinErythropoietinI di ti• Indication :
- Anaemia in chronic renal failure → can maintained a hematocrit of 35% with erythropoietin 50-150 IU/kg I.V. or S C 3 x a weekS.C. 3 x a week.
• Anaemia in :- Bone marrow disorders.
Ch i i fl ti- Chronic inflammation- AIDS- CancerSid ff t rapid increase in hematocrit & Hb• Side effect : rapid increase in hematocrit & Hb
- hypertension- thrombotic complication.
![Page 35: Agents Used in Anemias.his 2009.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000096-hematology-and... · Eritropoesis (120 h ) Lambung ...](https://reader042.fdocuments.us/reader042/viewer/2022022806/5ccd0a4788c993b2538d66a0/html5/page/35.jpg)
![Page 36: Agents Used in Anemias.his 2009.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000096-hematology-and... · Eritropoesis (120 h ) Lambung ...](https://reader042.fdocuments.us/reader042/viewer/2022022806/5ccd0a4788c993b2538d66a0/html5/page/36.jpg)
Vitamin B12 : PharmacokineticsVitamin B12 : Pharmacokinetics• Absorption :
- B12-FIC (Faktor intrinsik Castle)- Langsung : mass action effect- cyanocobalamin : IM/SK ⇒ well absorptioncyanocobalamin : IM/SK ⇒ well absorption
Cmax (IM): 1 hour- hydroxycobalamin : lebih lambat ~ ikatan protein kuat
oral : lambat (Cmax: 8 12 jam)- oral : lambat (Cmax: 8-12 jam)• Sekresi FIC ↑ : obat kolinergik, histamin, ACH,
coricoseroid, hormon tiroid → B12 absorption ↑B12 b ti ↓ k l k l i d bit l• B12 absoprtion ↓ : pengkela kalsium dan sorbitol
![Page 37: Agents Used in Anemias.his 2009.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000096-hematology-and... · Eritropoesis (120 h ) Lambung ...](https://reader042.fdocuments.us/reader042/viewer/2022022806/5ccd0a4788c993b2538d66a0/html5/page/37.jpg)
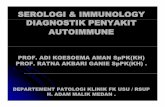
Metabolisme ferrum di dalam tubuh
ABSORBSI TRANSPORT KEBUTUHAN Simpan
apoferritin → ferritin
Oral Ferrum
pHati, lien, sumsum tulang
Ferrum
TransferinPlasma, protein
Eritropoesis(120 h )
Lambung → HCL → ferro
Plasma, protein ( )
Pe cah
D d f iti f iti
Darah plasmaprotein
Duodenum, apoferritin → ferritin
Hemosiderin
![Page 38: Agents Used in Anemias.his 2009.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000096-hematology-and... · Eritropoesis (120 h ) Lambung ...](https://reader042.fdocuments.us/reader042/viewer/2022022806/5ccd0a4788c993b2538d66a0/html5/page/38.jpg)
![Page 39: Agents Used in Anemias.his 2009.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000096-hematology-and... · Eritropoesis (120 h ) Lambung ...](https://reader042.fdocuments.us/reader042/viewer/2022022806/5ccd0a4788c993b2538d66a0/html5/page/39.jpg)
The great majority of iron in the body is found in red cells where it is incorporated into hemoglobin tocells where it is incorporated into hemoglobin to function as an oxygen carrier. Smaller amounts are incorporated into myoglobin (muscle) and cytochromes (all tissues). As red cells turnover incytochromes (all tissues). As red cells turnover in the spleen, iron is recycled back to the bone marrow where it is re-incorporated into hemoglobin. Iron is transported through the plasma bound to transferrin
d t k b ll i th t f i tand taken up by cells via the transferrin receptor. Iron is concentrated and stored within the cell encased by ferritin. Excess iron is stored primarily in the macrophages of the liver spleen and bonethe macrophages of the liver, spleen and bone marrow Very little iron is lost except through bleeding and menstruation. Therefore, homeostasis of total body iron is maintained by regulatingof total body iron is maintained by regulating intestinal iron absorption.

![meningitis bakterialis.ppt [Read-Only]ocw.usu.ac.id/...PEDIATRIC-NEURO/...meningitis_in_infant_and_children.pdfBacterial meningitis Is an acute purulent infection in the subarachnoid](https://static.fdocuments.us/doc/165x107/5d1407a988c993f1238cb07e/meningitis-read-onlyocwusuacidpediatric-neuromeningitisininfantandchildrenpdfbacterial.jpg)

![Organizational Change and Development.ppt [Read-Only]ocw.usu.ac.id/course/download/127-PLO/plo_slide_chapter... · Title: Microsoft PowerPoint - Organizational_Change_and_Development.ppt](https://static.fdocuments.us/doc/165x107/5fa8c4785f3ae726d1270292/organizational-change-and-read-onlyocwusuacidcoursedownload127-ploploslidechapter.jpg)







![MEASLES ((campakcampak,, rubeolarubeola,, gabakgabak ...ocw.usu.ac.id/course/download/1110000141-tropical-medicine/tmd175... · Microsoft PowerPoint - CAMPAK.ppt [Read-Only] [Compatibility](https://static.fdocuments.us/doc/165x107/5bc96d4009d3f2ca288cff62/measles-campakcampak-rubeolarubeola-gabakgabak-ocwusuacidcoursedownload1110000141-tropical-medicinetmd175.jpg)



![Congenital toxoplasmosis kbk-1.ppt [Read-Only]ocw.usu.ac.id/.../tmd175_slide_congenital_toxoplasmosis.pdf · (symptomatic congenital toxoplasmosis infection) PyrimethaminePyrimethamine1](https://static.fdocuments.us/doc/165x107/5e11e77d573e9002e5752212/congenital-toxoplasmosis-kbk-1ppt-read-onlyocwusuacidtmd175slidecongenital.jpg)

