
Agenda Spondyloarthropathies Early Rheumatoid Arthritis Established Rheumatoid Arthritis Benefit -...
58
-
Upload
harold-whitehead -
Category
Documents
-
view
220 -
download
1
Transcript of Agenda Spondyloarthropathies Early Rheumatoid Arthritis Established Rheumatoid Arthritis Benefit -...


Agenda
• Spondyloarthropathies• Early Rheumatoid Arthritis• Established Rheumatoid Arthritis• Benefit - Risk
Dr. Jad OKAISHDF 2009

Agenda
• Spondyloarthropathies• Early Rheumatoid Arthritis• Established Rheumatoid Arthritis• Benefit - Risk

Spondyloarthropathies
Early treatmentBy Anti-TNF
Inflammation Ankylosis
Year 1 Year 10 Year 20
Late treatmentBy Anti-TNF

Arthritis & Enthesopathies
Anti-TNF treatment in AS
• In general, about half of the patients gain 50% improvement of disease activity as assessed by the Bath Ankylosing Spondylitis Activity Index (BASDAI).
• 30–40% show an increase in function as assessed by the Bath Ankylosing Spondylitis Functional Index (BASFI).
• Applying the ASAS outcome criteria usually >60% reach ASAS 20, and >40% the ASAS 40 and ASAS 5/6 criteria, while 20–30% even achieve ASAS partial remission.
• Furthermore, AS patients treated with TNF blockers report an improved quality of life and reach higher productivity scores.
• There is very good efficacy on clinical disease activity, acute-phase reactants an inflammation visible on MRI.
1- Braun J,et al. Improvement in patientreported outcomes for patients with ankylosing spondylitis treated with etanercept 50mg once-weekly and 25mg twice-weekly. Rheumatology 2007;46:999–1004.2- Davis JC et al. Health-related quality of life outcomes in patients with active ankylosing spondylitis treated with adalimumab: results from a randomized controlled study. Arthritis Rheum 2007;57:1050–7.3- Van der Heide et al. Infliximab improves productivity and reduces workday loss in patients with ankylosing spondylitis: results from a randomized, placebo-controlled trial. Arthritis Rheum 2006;55:569–74.4- Rudwaleit M et al. Prediction of a major clinical response (BASDAI 50) to tumour necrosis factor alpha blockers in ankylosing spondylitis. Ann Rheum Dis 2004;63:665–70.

Better response to TNF blockers with early treatment
10
30
50
70
90
< 10 yearsN=37
11-20 yearsN=33
>20 yearsN=29
Patients with AS treated with INFLIXIMAB
Pat
ien
ts a
chie
vin
g B
AS
DA
I 50
Rudwaleit M, et al. Ann Rheum. Dis. 2004;63:665-70

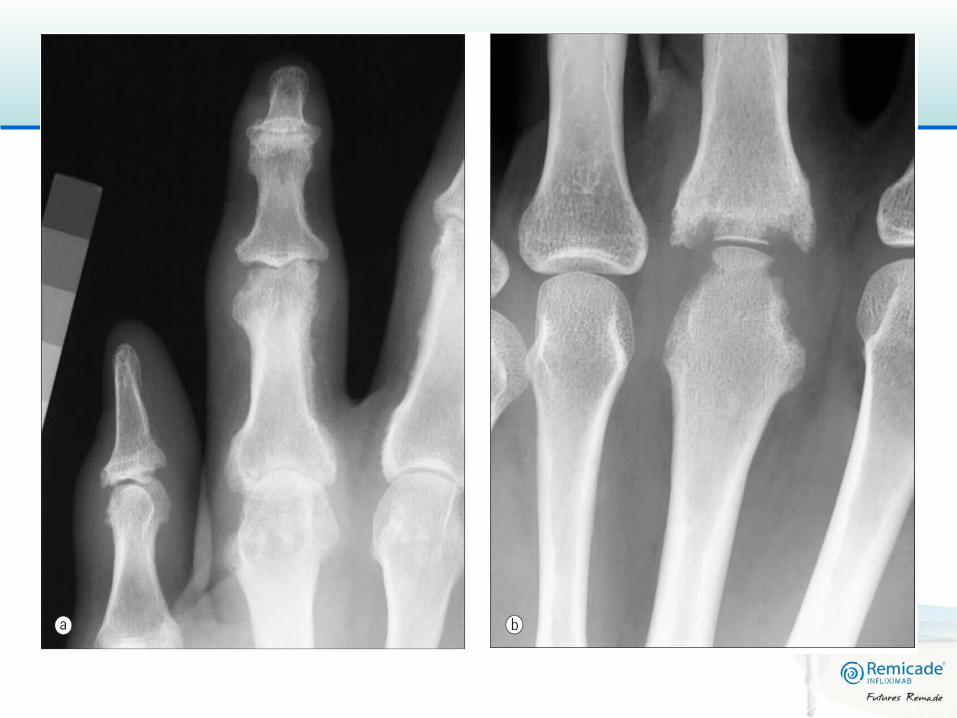
Anti-TNF and Syndesmophytes
• Growing syndesmophytes and ankylosis seems not to be inhibited by anti-TNF therapy
• some unresolved methodological issues :
– historical cohorts are only included – the inability to assess the thoracic spine by
standard radiography– the low sensitivity of the currently used
modified Stokes AS spinal score scoring– the degree of damage: one (mean) new
syndesmophyte developing in the whole spine over two years.
– continuous NSAID therapy may reduce radiographic progression in AS ( placebo group)
Baraliakos X, Listing J, Rudwaleit M et al. Progression of radiographic damage in patients with ankylosing spondylitis: defining the central role of syndesmophytes.Ann Rheum Dis 2007;66:910–5.Baraliakos X, Listing J, Brandt J et al. Radiographic progression in patients with ankylosing spondylitis after 4 yrs of treatment with the anti-TNF-alpha antibody infliximab. Rheumatology 2007;46:1450–3.van der Heijde D, Landewe´ R, Braun J et al. Radiographic progression of ankylosing spondylitis after up to two years of treatment with infliximab. Arthritis Rheum 2008.Wanders A, van der Heijde D, Landewe´ R, et al. Nonsteroidal antiinflammatory drugs reduce radiographic progression in patients with ankylosing spondylitis.Arthritis Rheum 2005; 52:1756–1765.

Link between the presence of inflammation at the vertebral corner on the MRI and
sydesmophytes on plain rx • The presence of inflammation is associated with the
development of new syndesmophytes• The presence of inflammation is associated with the
development of new syndesmophytes even when inflammation is suppressed with anti-TNF treatment
• A new syndesmophyte can occur even when initial RX and MRI are normal
Walter P. et al. inflammatory lesions of the spine on MRI predict the development of new syndesmophytes in SA. A&R, 60;1; 2009 pp 93-102

Infliximab lessens cellular infiltration in bone marrow

RA SA

Wnt proteins and Dickkopf-1 (DKK-1)
Diarra D et al. Dickkopf-1 is a master regulator of joint remodeling. Nat Med 2007;13:156–63.

DKK (Dickkopf) Level in RA and AS
Diarra D, et al. Nature Medicine 2007;13(2):156
0
5
10
15
20
25
30
350
wee
k an
ti-TN
F
2 w
eek
anti-
TNF
6 w
eek
anti-
TNF
Healthy RA AS
DK
K-1
Ser
um le
vel (
pg/m
l)
*
**
**
*

Conclusion :
• TNF blockers indeed do not inhibit syndesmophyte formation in AS.
• Data with longer follow-up, with the antibodies against TNF in patients with early disease, will give us the final answer concerning the inhibition of syndesmophyte formation.

Ankylosing Spondylitis Ankylosing Spondylitis
Early Pre-radiographic Axial SpA

The Inflixispine Study
Barkham et al. Arthritis Rheum. 2009; 60(4):946-954
Objective: To evaluate the efficacy of IFX in HLA-B27 + pts with MRI-determined
early sacroiliitis
Patients: HLA B27+, Inflammatory Back Pain (Calin criteria) and MRI determined
sacroiliitis 40 pts included, mean age: 28.8 years, 75% male, mean symptom
duration: 15.3 months.
Protocol: Infliximab 5 mg/kg (n=20) or placebo (n=19/20) infusions at 0, 2, 6 and
12 weeks FU every 4 wks from wk 16 to wk 40 or time to active disease
(BASDAI>4)
Pts with active disease open label IFX infusions after wk 16

Baseline characteristicsBaseline characteristics
InflixiSpine(n=40)
Age, mean years 28.8 (±7.6)
% female 25
HLA-B27 positive 100
Disease duration, years mean (range)* or median (±SD)
1.3 (±0.73)
% MRI positive 100
% Both HLA-B27 and MRI positive
100
% with IBP 100
BASDAI, mean (range) 5.86 (±0.73)
Haibel et al. Arthritis Rheum. 2008; 58(7):1981-1991; Barkham et al. ACR 2007. Abstract L11.

.
HLA-B27HLA-B27++ Very Early Pre-radiographic AS - Very Early Pre-radiographic AS - Treatment with IFX*Treatment with IFX*
Primary endpoint: change in MRI scores from baseline to week 16
62.7%
29.4%
P=0.001
0
50
100
% o
f le
sion
s re
solv
ing
47/7520/68
Sacroiliac MRI lesions resolved
New sacroiliac MRI lesions
1.2% 12% 0
50
100
% n
ew le
sion
s
P=0.004
PBO (n=20)
IFX (n=20)
Patients with spinal lesions resolved
0
50
100
% o
f pa
tien
ts 60%
25%3/5
1/4
n=9 (pts with spinal lesions at BL)
P=0.016
Barkham et al. EULAR 08 FRI0310Barkham et al. Ghent SpA 08 poster
• All 3 criteria – IBP – HLA-B27 – MRI inflammation of spine or SI joints
* IFX 5mg/kg w0, w2, w6, w12

Infliximab Therapy in Patients with HLA B27 Positive Very Early Ankylosing Spondylitis
13
56
Placebo(n=19)
Infliximab(n=20)A
SA
S P
art
ial R
em
iss
ion
(%)
**
**p=0.009
Pts treated with PBO or IFX 5 mg/kg at 0, 2, 6 and 12 weeks (RCT), FU from week 16-40. If pts developed active disease (BASDAI>4), they received OL IFX after week 16
-0.75
-3.41
Re
du
cti
on
in
BA
SD
AI
*p=0.002*
Week 16
Barkham et al. EULAR 09 OP-0016
Week 16

Remicade Therapy in Patients with HLA B27 Positive Very Early Ankylosing Spondylitis
13
56
Placebo(n=19)
Infliximab(n=20)A
SA
S P
art
ial R
em
iss
ion
(%
)
**
**p=0.009
Pts treated with PBO or IFX 5 mg/kg at 0, 2, 6 and 12 weeks (RCT), FU from week 16-40. If pts developed active disease (BASDAI>4), they received OL IFX after week 16
-0.75
-3.41
Re
du
cti
on
in B
AS
DA
I
*p=0.002*
Week 16
Barkham et al. EULAR 09 OP-0016
12/196/20
17/1912/20
PBO IFX
Wk 16Wk 40
Remission induction approach works in early AS, (8/20) 40% of the patients are biologic-free
Week 16
PBO IFX
Short course of IFX continued suppression of disease activity in early AS pts with sustained benefit in QoL, function and disease activity. 40% of the pts remained in a low disease activity state for 28 weeks off IFX after 4 IFX infusions.
*
*p=0.035 vs PBO
Number of pts requiring OL IFX
Barkham et al. Arthritis Rheum. 2009; 60(4):946-954
Clinical Efficacy of IFX in HLA-B27+ Very Early AS: Conclusions
Remicade appears to be an effective therapy for very early inflammatory back
pain.
This is the first therapy to show suppression of the inflammatory lesions on
MRI in very early Ankylosing Spondylitis.
Compared to studies of TNF blockers in established disease, the proportion of
patients achieving ASAS partial remission was much higher suggesting a clear
benefit for early treatment.

Ankylosing Spondylitis Ankylosing Spondylitis
Long-Term Efficacy
EASICEASIC – – EEuropean uropean AAnkylosing nkylosing SSpondylitis pondylitis IInfliximab nfliximab CCohortohort
Three abstracts submitted to EULAR 09:
• EASIC 5 years:
– Outcomes (European Ankylosing Spondylitis Infliximab
Cohort (EASIC): Outcome of patients who had
discontinued infliximab after the end of ASSERT)
– Long-Term efficacy (European Ankylosing Spondylitis
Infliximab Cohort (EASIC): Long-Term (5 years) Efficacy of
Remicade on disease activity and function – A real life
experience after the end of ASSERT
– Safety (European Ankylosing Spondylitis Infliximab Cohort
(EASIC): Safety of long term therapy with Remicade in
patients with ankylosing spondylitis (AS)

EASIC – European Ankylosing Spondylitis Infliximab Cohort
• Background: insufficient knowledge of long term safety and efficacy of anti-TNF therapy in AS
• EASIC-study: Open label extension of ASSERT
Brandt et al. EULAR 08 FRI0305, ClinicalTrials.gov identifier: NCT00237419

A Randomized, Double-blind Trial of the Efficacy of REMICADE ® (Infliximab) Compared with Placebo in
Subjects with Ankylosing Spondylitis Receiving Standard Anti-inflammatory Drug Therapy

ASSERT Study DesignASSERT Study Design
Screening Patients (N=357)
RANDOMIZATION
Placebo (N=78)
Infliximab 5 mg/kg(N=201)
Wk 0 Wk 2 Wk 6 Wk 12 Wk 18 Wk 24
Endpoint
Assigned to treatment (N=279)
Failed Screening (N=78)
Van der Heijde et al., Arthritis & Rheumatism 2005, 52: 582
3/8 ratio

EASIC – European Ankylosing Spondylitis Infliximab Cohort• Background: insufficient knowledge of long term safety and efficacy
of anti-TNF therapy in AS • EASIC-study: Open label extension of ASSERT • Time course:
ASSERTN=279
2 years Mean: 1,3 + 0.9 yrs 96 weeks
EASICN=10315% did not receive IFX
continuously between ASSERT and EASIC
Brandt et al. EULAR 08 FRI0305, ClinicalTrials.gov identifier: NCT00237419
5 years total

EASICEASIC – – EEuropean uropean AAnkylosing nkylosing SSpondylitis pondylitis IInfliximab nfliximab CCohortohort
ClinicalTrials.gov identifier: NCT00237419
Completers at 96 weeks n=4 n=5 n=76

EASIC – European Ankylosing Spondylitis Infliximab Cohort: Outcomes at 96 weeks in Group 1
Group 1A: discontinuation and relapse (n=9)
44% (4/9) patients still on IFX Mean BASDAI 6.7 + 2.4 start of
EASIC 3.5 + 2.4 Reasons for dropping:
• 3/5 = infusions reactions 97 + 22 days after screening
• 1/5 = lack of efficacy
• 1/5 = lost to FU
Group 1B: discontinuation and remission (n=5)
1/5 remains on remission at week 96
4/5 relapses after 61+ 50 days
1 switched to ADA
3/4 treated with IFX
Overall 5 patients in Group 1 completed the study under therapy with IFX,
mean BASDAI = 1.8 + 1.3 after 96 weeks. One pt remained in drug-free
remission.
2/3 dropped out after 89 + 29 days of Tx (1 IR and 1 lack of efficacy)
Heldmann et al. EULAR 09 SAT0259

EASIC – European Ankylosing Spondylitis Infliximab Cohort: Long-Term efficacy in Group 2
Completers Group 2 (n=76/88)
At the end of EASIC: 78% pts had no arthritis and 85% no enthesitis
0
20
40
60
80
100
End of ASSERT wk 0 wk 48 wk 96
ASAS 20
ASAS 40
ASAS Partial remission
0
2
4
6
8
10BASDAI
BASFI
BASMI
Heldmann et al. EULAR 09 SAT0258

Long-term efficacy of aTNFs in patients with Long-term efficacy of aTNFs in patients with active Spondyloarthritisactive Spondyloarthritis
ETN1 IFX2 IFX3 ADA4 ETN1 IFX2
3 yrs 4 yrs 6 yrs 8 yrs
Adherence (%)
81.0 62.3 77.8 67.3 65.4 53.6
BASDAI 50 (%)
63.0 67.5 58.0 67.6
ASAS 20 (%)
81.8 81
PR (%) 35.0 39.4 35.5 35.1
1Baraliakos et al. EULAR 09 AB0428, 2Baraliakos et al. EULAR 09 SAT0284, 3Devinck et al. EULAR 09 SAT0278, 4van der Heijde et al. EULAR 09 SAT0254.
Similar therapy adherence and efficacy data for the TNF blockers

Devinck et al. EULAR 09 SAT0278
Long-term efficacy/safety of IFX in patients with Long-term efficacy/safety of IFX in patients with active Spondyloarthritis: Results of an 8-Year FUactive Spondyloarthritis: Results of an 8-Year FUSpA with active axial and/or peripheral disease were treated with 5 mg/kg IFX q8 (AS: 63 pts; PsA: 36 pts; und. SpA: 10 pts). Dec. 2008: 617 patient-yrs reached.
A highly significant improvement in all disease manifestations was maintained over a FU period up to 8 years. No new safety signals.
Baseline Yr 1 Yr 2 Yr 3 Yr 4 Yr 5 Yr 6 Yr 7 Yr 8
Nr pts 107 101 90 90 77 61 49 32 11
Pt global 66 20 17 12 20 20 20 30 20
Pt pain 61 22 16 11 20 20 20 25 25
ESR 20 10 10 8 9 7 7 9 5
CRP 2,00 0,60 0,40 0,30 0,25 0,20 0,30 0,20 0,20
Nr AS pts 63 59 53 49 41 30 23 11 6
BASDAI 51 21 16 9 10 13 12 22 8
BASFI 58 39 27 27 23 27 21 39 20
Belgian Cohort
47 patients had peripheral arthritis at baseline (25 oligo-, 22 polyarticular), mostly were PsA and IBD related SpA
All patients reached the 6 yrs evaluation
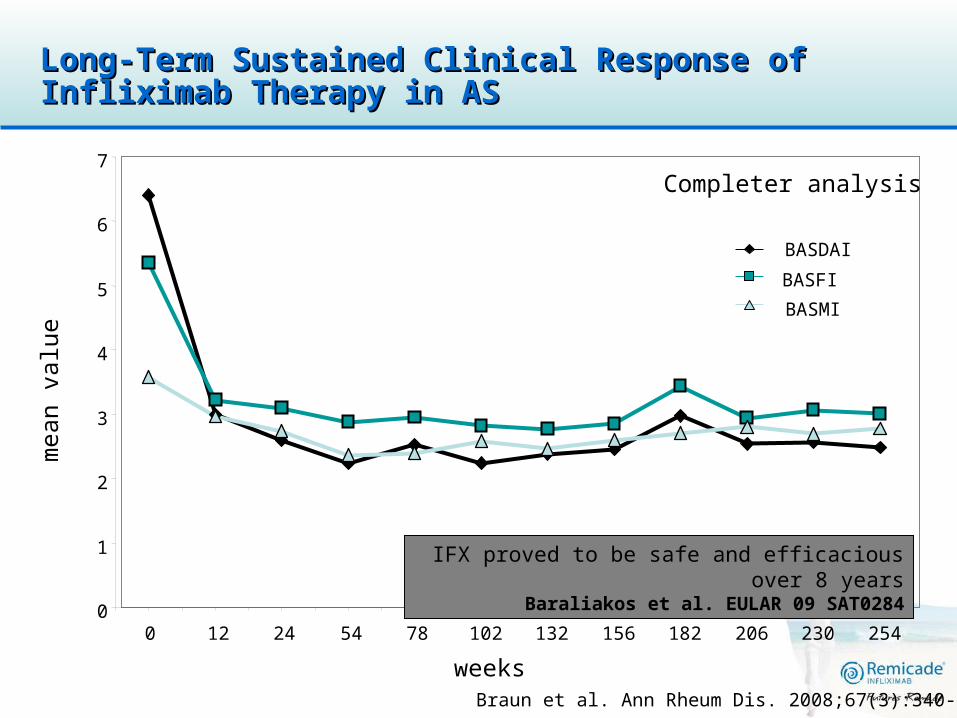
0
1
2
3
4
5
6
7
0 12 24 54 78 102 132 156 182 206 230 254
weeks
mea
n va
lue
BASDAI
BASFI
BASMI
Long-Term Sustained Clinical Response of Long-Term Sustained Clinical Response of Infliximab Therapy in ASInfliximab Therapy in AS
Braun et al. Ann Rheum Dis. 2008;67(3):340-345
Completer analysis
IFX proved to be safe and efficacious over 8 yearsBaraliakos et al. EULAR 09 SAT0284
% p
ts tr
eate
d in
par
tial
rem
issi
on
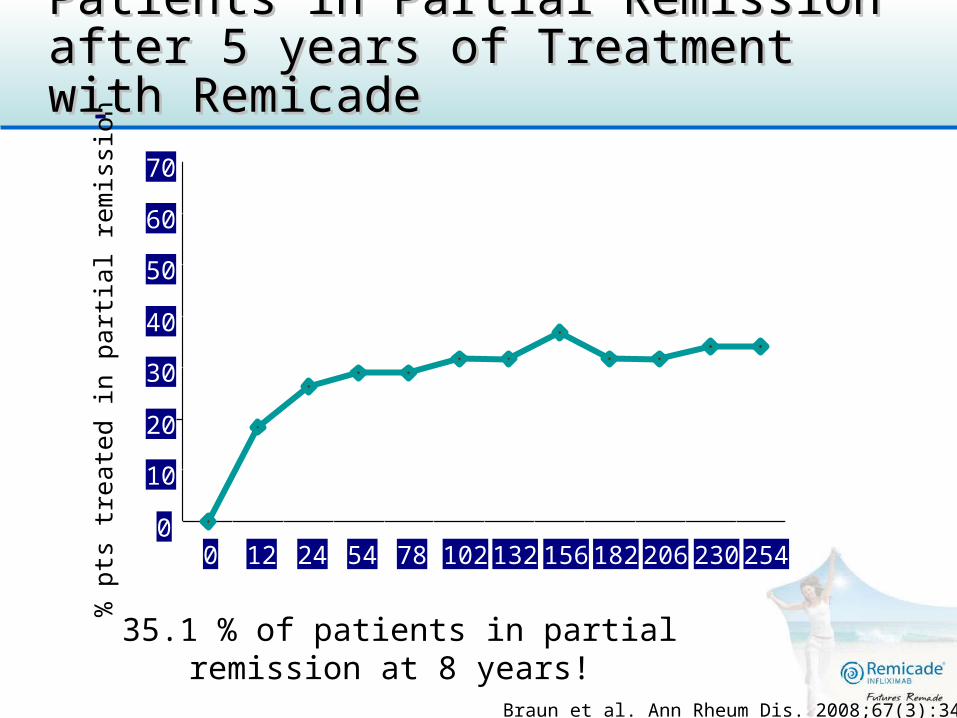
Patients in Partial Remission after 5 years of Patients in Partial Remission after 5 years of Treatment with RemicadeTreatment with Remicade
0
10
20
30
40
50
60
70
0 12 24 54 78 102 132 156 182 206 230 254weeks
Completer analysis
Braun et al. Ann Rheum Dis. 2008;67(3):340-345
35.1 % of patients in partial remission at 8 years!
Baraliakos et al. EULAR 09 SAT0284

Psoriatic ArthritisPsoriatic Arthritis
Efficacy of Treatment in Early Polyarticular PsA

REmicade Study in Psoriatic arthritis patients Of methotrexate-Naïve Disease: The RESPOND Study
PsA pts, naïve to MTX and anti-TNFs
n=115
IFX 5 mg/kg; wk 0, 2, 6, 14 + MTX 15 mg/week
n=57
0 Week
MTX 15 mg/weekn=58
2 6 14 16 Study visits
PE: ACR 20 at wk 16
Study design: Randomized, prospective, open-label, multi-center, multi-national studyInclusion criteria:
• Patients >18 years of age • Diagnosis of Psoriatic Arthritis with peripheral polyarticular involvement• Disease duration 3 months prior to screening. • Active PsA = ≥5 swollen and tender joints, + one of the following:
ESR≥28 mm/hr, CRP≥15 mg/L or morning stiffness≥45 min• Pts naïve to MTX, anti-TNF agents, and could not be on DMARDS
Nasonov et al. EULAR 09 OP0196
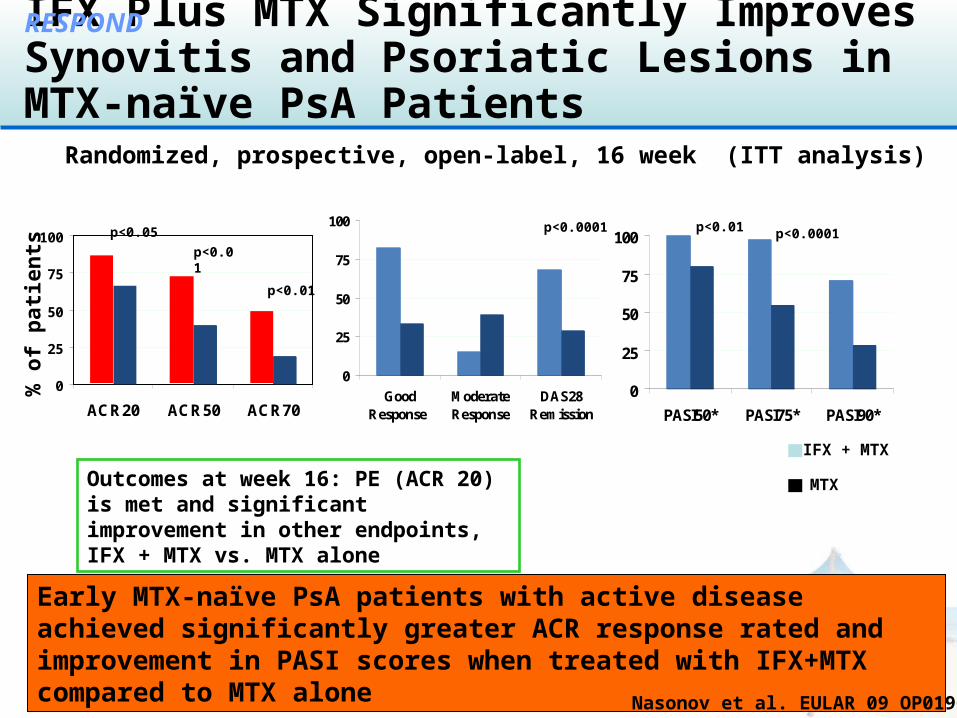
IFX Plus MTX Significantly Improves Synovitis and Psoriatic Lesions in MTX-naïve PsA Patients
Outcomes at week 16: PE (ACR 20) is met and significant improvement in other endpoints, IFX + MTX vs. MTX alone
Early MTX-naïve PsA patients with active disease achieved significantly greater ACR response rated and improvement in PASI scores when treated with IFX+MTX compared to MTX alone
0
25
50
75
100
ACR20 ACR50 ACR70
% o
f p
atie
nts
p<0.05
p<0.01
p<0.01
0
25
50
75
100
PASI50* PASI75* PASI90*
p<0.01
p<0.01
p<0.0001
0
25
50
75
100
GoodResponse
ModerateResponse
DAS28Remission
p<0.0001
Nasonov et al. EULAR 09 OP0196
RESPOND
Randomized, prospective, open-label, 16 week (ITT analysis)
IFX + MTX
MTX

MTX-naïve PsA Patients Respond Rapidly to IFX+MTX Therapy
Outcomes at week 6: IFX + MTX treated pts attain a response significantly more rapid then MTX alone treated pts
A significantly greater proportion of MTX naïve PsA patients – when treated with IFX+MTX – attain an early response to treatment in terms of arthritic and psoriatic signs and symptoms compared to MTX alone
Nasonov et al. EULAR 09 SAT0353
RESPOND
Randomized, prospective, open-label, 16 week (ITT analysis)
IFX + MTX
MTX
0
25
50
75
100
ACR50 ACR700
25
50
75
100
0 2 4 6 8 10 12 14 16 18Weeks
p<0.0001
p=0.0042
p=0.003
p<0.0001
p<0.0001
PASI 75*
*Pts with BL PASI 2.5
6 weeks
Psoriatic ArthritisPsoriatic Arthritis
Efficacy

Mak et al. EULAR 09 SAT0345
The Best The Best Biologic for Pso and PsA - UST ( for Pso and PsA - UST (ustekinumab) 90 mg shows superior efficacy compared to all biologics 90 mg shows superior efficacy compared to all biologics except Remicadeexcept Remicade
Meta-analysis of 25 RCTs (n=9889 pts, mean age 44.1 yrs)
8.19
5.99
2.451.31
0
2
4
6
8
10
EFA1mg/kg
QW
ETA 50mgQW
ADA 40mgEOW
UST 45mgw 0, 4
IFX 5mg/kgQ8
No superiority
OR for PASI 75 vs UST 90 mg at wks 0 and 4 For PsARC Remicade better than ADA (OR 1.51) with no stat. difference between ADA, ETN, EFA, ALE
• PsO: UST 90mg is superior to all biologics except Remicade
• PsA: Remicade is the best biologic
•Toxicity and safety profiles of all biologics are comparable
Summary
Ankylosing Spondylitis
•Short course IFX – Biologic-free remission induction in early axial AS• EASIC – long-term data• 8 years long-term data: q8 (Belgian cohort)• 8 years long-term data: q6 (Braun)
Psoriatic Arthritis
•2 abstracts on RESPOND - MTX-naïve PsA • Best biologic of choice
Agenda
• Spondyloarthropathies• Early Rheumatoid Arthritis• Established Rheumatoid Arthritis• Benefit - Risk
1. Sequential monotherapy
2. Step-up combination therapy
Initial MTX
Initial Combo
3. Initial combination with high prednisone
4. Initial combination with infliximab
BeSt BeSt Comparison of Four Treatment StrategiesComparison of Four Treatment Strategies
Group 4Group 3Group 2Group 1
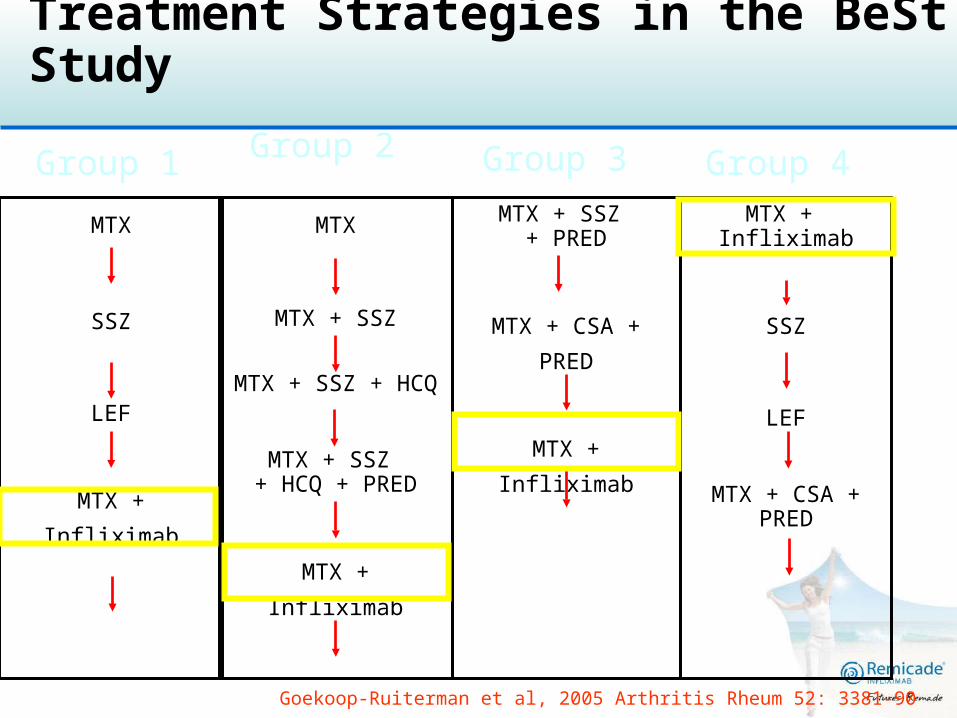
Treatment Strategies in the BeSt Study
MTX + Infliximab
SSZ
LEF
MTX + CSA + PRED
MTX + SSZ + PRED
MTX + CSA + PRED
MTX + Infliximab
MTX
MTX + SSZ
MTX + SSZ + HCQ
MTX + SSZ + HCQ + PRED
MTX + Infliximab
MTX
SSZ
LEF
MTX + Infliximab
Goekoop-Ruiterman et al, 2005 Arthritis Rheum 52: 3381-90

2 to 3-monthly treatment adjustments based on DAS44-scores:DAS44 >2.4 next step
DAS44 < 2.4 continue therapy
Taper/Discontinuation Restart:
DAS44 < 2.4 for ≥6 months medication Taper to maintenance dose
DAS was ≤1.6 for ≥6 months after 2 yrs Discontinuation last DMARD
DAS increased to ≥1.6 Restart with last DMARD
Treatment Strategies in the BeSt Treatment Strategies in the BeSt StudyStudy
Goekoop-Ruiterman YPM et al., Arthritis Rheum 2005;52(11):3381-3390

0%
20%
40%
60%
80%
100%
Group 1 Group 2 Group 3 Group 4
% o
f pa
tient
s
DAS<1.6**
Pts on IFX+ MTX after at least 3 DMARDS
21%5% 11%
0%
50%
100%
Group 1 Group 2 Group 3
Klarenbeek et al. EULAR 08 THU0162
BeSt 5 Year Results: Remission**BeSt 5 Year Results: Remission**
** Includes ALL patients in remission
(on drugs and off IFX and DMARDs)
“With DAS-steered, tight-controlled treatment, 48%
of all patients achieved biologic free remission”
Achieved with initial
treatment step
81%
39% 46%
65%
**p<0.001 Gr 4 vs Gr 1&2

Sustained benefit of initial combination therapy in Sustained benefit of initial combination therapy in the amount of joint damage after 5 yearsthe amount of joint damage after 5 years
14
11
7.66
0
2
4
6
8
10
12
14
16
Mea
n v
dH
-S p
rog
ress
ion
Seq. Monotherapy
Step-up
Modified COBRA
IFX + MTX
Median Change in vdH-S Score after 5 years of FU
1 and 2 vs 4 p<0.01
Median change 3.5 2.5 1.0 1.0
Even a short period of early better suppression of disease activity still defines the amount of joint damage 5 yrs later
Klarenbeek N. et al. EULAR 09 SAT0013

Agenda
• Spondyloarthropathies• Early Rheumatoid Arthritis• Established Rheumatoid Arthritis• Benefit - Risk
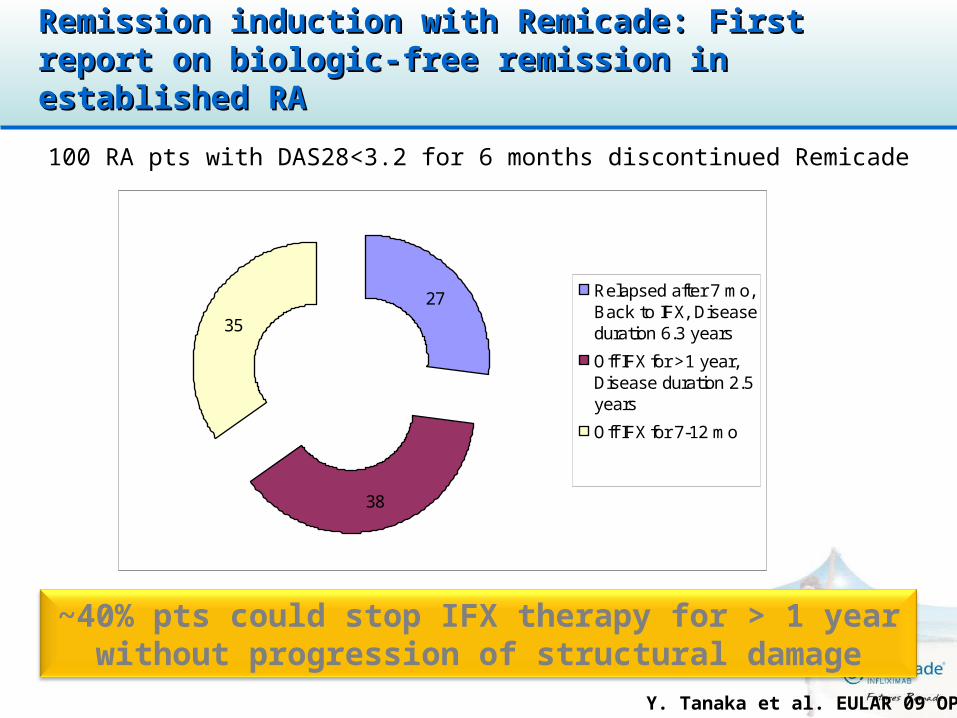
Remission induction with Remicade: First report Remission induction with Remicade: First report on biologic-free remission in established RAon biologic-free remission in established RA
100 RA pts with DAS28<3.2 for 6 months discontinued Remicade
~40% pts could stop IFX therapy for > 1 year without progression of structural damage
Y. Tanaka et al. EULAR 09 OP-0150
27
38
35
Relapsed after 7 mo,Back to IFX, Diseaseduration 6.3 years
Off IFX for >1 year,Disease duration 2.5years
Off IFX for 7-12 mo
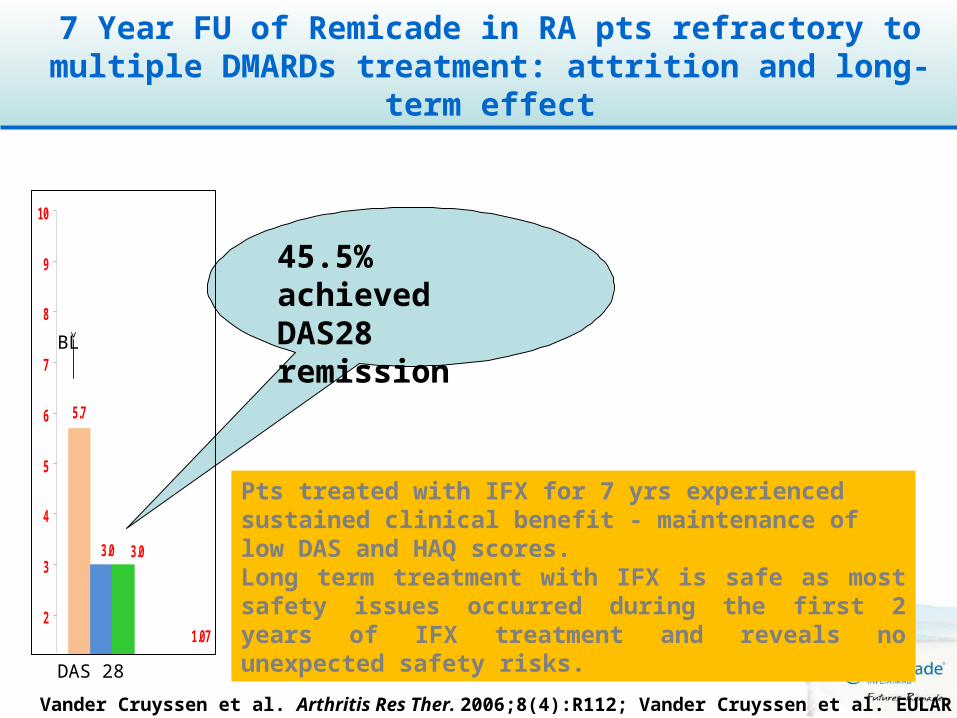
7 Year FU of Remicade in RA pts refractory to multiple DMARDs treatment: attrition and long-
term effect
Vander Cruyssen et al. Arthritis Res Ther. 2006;8(4):R112; Vander Cruyssen et al. EULAR 09 THU0181
Pts treated with IFX for 7 yrs experienced sustained clinical benefit - maintenance of low DAS and HAQ scores. Long term treatment with IFX is safe as most safety issues occurred during the first 2 years of IFX treatment and reveals no unexpected safety risks.
45.5% achieved DAS28 remission
1.07
5.7
3.0 3.0
0
1
2
3
4
5
6
7
8
9
10
DAS28 Mean HAQ
DAS 28
BL

RAISE surveyRAISE survey
Agenda
• Spondyloarthropathies• Early Rheumatoid Arthritis• Established Rheumatoid Arthritis• Benefit - Risk

Contraindications, Warnings and Precautions of TNFα inhibitors
TNF Inhibitors:EU Summary of Product Characteristics
Infusion / injection reactions /
Hypersensitivity/ allergy
Infections, TB*, Sepsis Malignancies/ Lymphoma Caution
Congestive Heart failure* (NYHA class III/IV)
Autoimmune processes/ auto-antibodies
Neurological events
Haematologic reactions†
Hepatobiliary event
EMEA Product specific SPCs 2008.
* contraindicated for adalimumab and infliximab, special warning for etanercept † special warning for adalimumab and etanercept

Active treatment Follow-up period
1st 90 days duration of Tx + 90 days
Ever treatedReceiving of Tx
time
British Society of Rheumatology (BSR) Registry: Serious British Society of Rheumatology (BSR) Registry: Serious Infections with anti-TNF Agents Using Different ModelsInfections with anti-TNF Agents Using Different Models
0.1 1 10 100
1st 90 days of treatment
currently receiving treatment
Duration of treatment +90 days
ever treated
Adjusted incidence rate of Serious infections of anti-TNFs vs. DMARDS using various models. OR (95% CI)
DMARDS
Different models used, including varying lengths of follow up time
Treatment period
Model
Registry
Dixon WG, et al. Arthritis Rheum 2007;56:2896-2904.
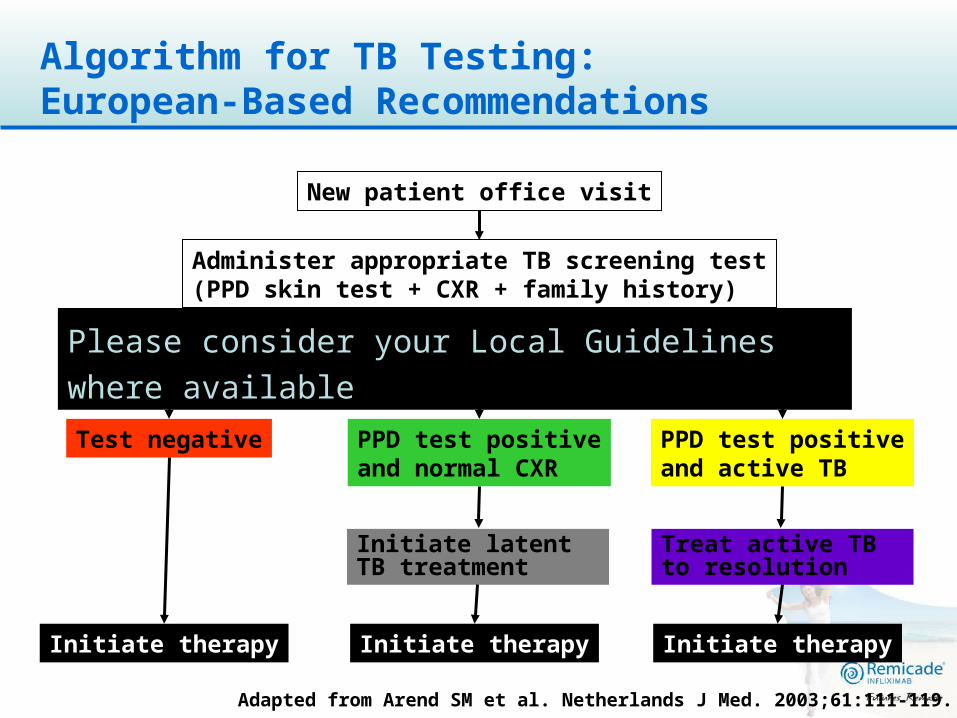
Algorithm for TB Testing:European-Based Recommendations
Treat active TB to resolution
New patient office visit
PPD test positiveand active TB
Initiate latent TB treatment
Initiate therapyInitiate therapy
Administer appropriate TB screening test(PPD skin test + CXR + family history)
Evaluate test results
Test negative
Initiate therapy
PPD test positiveand normal CXR
Adapted from Arend SM et al. Netherlands J Med. 2003;61:111-119.
Please consider your Local Guidelines where available


Remicade Benefit:Risk - Conclusions
• Remicade, with 7 approved indications, is the most widely used TNF inhibitor
– More than 15 years of safety data collected in clinical trials
– Estimated exposure since commercial launch on 24 August 1998
• >1.1 million patients• >4.2 million patient-years since first exposure
• Remicade is effective in patients with inflammatory diseases who have failed conventional therapies in RA, AS, PsA, Pso, CD, Ped CD, and UC
• When given to appropriately selected patients, Remicade’s benefit-risk profile continues to be favorable
Data on file, Centocor (PSUR 18, October 2008).










