AGENDA COUNCIL OF ONTARIO MEDICAL OFFICERS … · Gemmill, Allen Heimann, Jin-Hee Kim, Jessica...
58
I information; D discussion; A approval; P presentation 2 Carlton Street, Suite 1306 Toronto ON M5B 1J3 Tel: (416) 595-0006 Fax: (416) 595-0030 E-mail: [email protected]Providing leadership in public health management AGENDA COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH SECTION MEETING Friday November 15 2013 10:30 AM – 12:30 PM Champagne Ballroom East Novotel Toronto Centre 45 The Esplanade **PLEASE NOTE THAT THIS MEETING IS PART OF THE alPHa FALL SYMPOSIUM . REGISTRATION IS REQUIRED** TO JOIN BY TELECONFERENCE: DIAL: 1-866-518-0789. CONFERENCE ID: 624258# # TOPIC MRP ATTACHMENT / NOTE OUTCOME 1.0 Call to Order / Approval of Agenda JAEGER A 2.0 Approval of Minutes, September 18 h 2013 ALL Minutes A 3.0 COMOH BUSINESS 3.1 COMOH Priorities / Strategic Planning JAEGER alPHa Strategic Plan – COMOH Considerations ; COMOH Terms of Reference ; COMOH Survey Report D 4.0 PUBLIC HEALTH ISSUES 4.1 Mandatory Immunization GEMMILL Work Group Update D 4.2 Lyme Disease Testing JAEGER Expanded PHO communications role D 4.3 SFOA Violations Ministry e-mail D 4.4 CWS Fluoridation GARDNER Proposal for COMOH Action D/A 4.5 Panorama LEVY e-mail background 4.6 Smoke-Free Patios KURJI Briefing Note
Transcript of AGENDA COUNCIL OF ONTARIO MEDICAL OFFICERS … · Gemmill, Allen Heimann, Jin-Hee Kim, Jessica...
I information D discussion A approval P presentation
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
AGENDA COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH SECTION MEETING
Friday November 15 2013 1030 AM ndash 1230 PM
Champagne Ballroom East Novotel Toronto Centre
45 The Esplanade
PLEASE NOTE THAT THIS MEETING IS PART OF THE alPHa FALL SYMPOSIUM REGISTRATION IS REQUIRED
TO JOIN BY TELECONFERENCE
DIAL 1-866-518-0789 CONFERENCE ID 624258
TOPIC MRP ATTACHMENT NOTE OUTCOME 10 Call to Order Approval of Agenda JAEGER A 20 Approval of Minutes September
18h 2013 ALL Minutes A
30 COMOH BUSINESS
31 COMOH Priorities Strategic
Planning JAEGER alPHa Strategic Plan ndash
COMOH Considerations COMOH Terms of Reference
COMOH Survey Report
D
40 PUBLIC HEALTH ISSUES
41 Mandatory Immunization GEMMILL Work Group Update D
42 Lyme Disease Testing JAEGER Expanded PHO communications role
D
43 SFOA Violations Ministry e-mail D
44 CWS Fluoridation GARDNER Proposal for COMOH Action DA 45 Panorama LEVY e-mail background
46 Smoke-Free Patios KURJI Briefing Note
I information D discussion A approval P presentation
47 Ontario Regulation 565 Public
Pools KURJI Briefing Note
50 Provincial Partners
51 CODE - COMOH project on
School BoardPHU Partnerships FINKELSTEIN Joint Code-COMOH Letter
(attached) I
52 Public Health Ontario PASUT D 60 UPDATES INFORMATION ITEMS REPORTS
61 Public Health Leadership
Council JAEGER I
611 ndash PHLC Update JAEGER Update I 612 ndash PHSSP
Implementation Tables JAEGER CMOH Memo I
62 COMOH Executive Committee JAEGER Minutes October 8 I 63 COMOH Built Environment
Work Group GARDNER Update I
64 HIV Non-Disclosure JAEGER Update following COMOH Chair disc W CMOH
I
65 Access to Oral Contraceptives PELLIZZARI Report back from disc W Erika Bontovics
I
66 Child and Youth Data Strategy JAEGER Update I 67 Public Health Early Years
Group FELLER Meeting Notes I
68 iPHIS Panorama FINKELSTEIN Update I 69 Joint OPHAalPHa Health
Equity Working Group PELLIZZARI Submission to Minimum
Wage Review I
610 COMOH Electronic Mailing List
FLEMING List of Subscribers I
611 COMOH Correspondence FLEMING Summary of COMOH Letters
I
70 Next MeetingAdjournment
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
SECTION TELECONFERENCE September 18th 2013
900 ndash 1100 AM Please dial 1-866-518-0789 or 416-443-4586 and enter Conference ID 624258 to participate
PRESENT Valerie Jaeger (Chair) Kim Barker Lisa Berger Jim Chirico Janet DeMille Andrea Feller Ian Gemmill Allen Heimann Jin-Hee Kim Jessica Hopkins Miriam Klassen Karim Kurji Isra Levy Rosamund Lewis Hazel Lynn David McKeown Nicola Mercer Lynn Noseworthy Rosana Pellizzari Carolyn Pim Sudit Ranade Lisa Simon Richard Schabas Marlene Spruyt Paula Stewart Penny Sutcliffe Monir Taha Hsiu-Li Wang Bryna Warshawsky David Williams Lilian Yuan Gordon Fleming (alPHa Staff Recorder) Linda Stewart (alPHa Staff)
10 Call to Order Approval of Agenda Meeting called to order at 904 Agenda approved as circulated 20 Approval of Minutes June 4th 2013 Minutes Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning V Jaeger reported that the Executive has met four times since the last Section meeting and this remains a standing item on the Executive agenda It is their opinion that this process needs to be executed in concert with the plan that is being developed by alPHa at this time and decisions about processes and directions for COMOH will need to be informed by those taken by the parent Association There is a strong agreement about the importance of COMOH strengthening it as a group and reinforcing its relationships with public health sector partners including but not limited to the CMOH PHO and the MOHLTC The Executive will continue these discussions and keep the Section informed as appropriate 40 PUBLIC HEALTH ISSUES
41 Mandatory Immunization I Gemmill reported that the issue of Health Care Worker influenza immunization rates which remain quite low despite best efforts was discussed at a session at the most recent Canadian Immunization Conference Having accepted that mandatory HCW immunization is very unlikely to become public policy anytime soon the discussion focused on how to convince more HCWs that this is important He observed that only 10 of 36 public health units have policies for their own employees which may be rendering our
argument that hospitals should be developing policies of their own less convincing He suggested that COMOH might for a start consider facilitating the development of a template for policies on mandatory immunization of public health staff (subject to exemptions for people with no contact with others people already under contract etc) which could increase the number of health units with policies thereby increasing the credibility of the case He also suggested a process whereby the existing policies and procedures could be collected examined and synthesized into a legally defensible practical but non-binding template which would be palatable to health unit staff and their unions He agreed that a COMOH working group would be the most appropriate mechanism to do this but asked that alPHa begin the process by collecting the existing policies A Heimann reported that Windsor is discussing this issue ahead of its local public campaign and he thinks this is an excellent idea Rosana Pellizzari added that this process is a good opportunity for those who have policies in place to share lessons learned about unintended consequences experiences with grievances sorting out the NACI definition of high-risk groups and identifying classes of employees that could reasonably be exempt due to the nature of their work ACTION V Jaeger to invite members to submit questions and expressions of interest in participating on the proposed working group directly to I Gemmill and to forward existing policies and related information to G Fleming at alPHa for collection and assembly 42 HIV Non-Disclosure PHLC Briefing Note V Jaeger reminded the group that this was raised at the June Section meeting where it was determined that COMOH should take the lead on developing a procedure that would ensure greater consistency in how and under what circumstances Section 22 orders are used in cases of HIV non-disclosure She has since raised this with the CMOH who agreed that an Associate CMOH at the MOHLTC would be an appropriate person to take the lead on this but until those positions are filled this isnrsquot an available option She also reported that George Pasut has offered PHO support in the form of logistics and meeting space to support a COMOH working group if it is decided to create one She then indicated that L Yuan and R Shahin who have been the COMOH leads on this issue on previous agendas are unable to participate in this process right now so she invited expressions of interest R Schabas observed that this is an issue for which the Provincial public health leadership should take responsibility He suggested that COMOH can present recommendations but they should be framed by an expectation of the CMOH to exercise leadership and provide clear direction V Jaeger agreed to articulate this to Arlene but reiterated that the present request is for volunteers people are willing to sit and do the work R Schabas I Gemmill and A Heimann indicated interest ACTION V Jaeger to discuss the foregoing with the CMOH whose response will inform next steps including development of process and confirmation of expressions of interest 43 Supervised Injection Sites Draft COMOH Letter V Jaeger referred to the attached and stated that it is meant more as a starting point for discussion than to make any suggestions about what COMOHrsquos position should be and invited D McKeown to speak to the issues
D McKeown reported that this is something that Toronto has been looking at for some time and they have concluded that it would be beneficial to have this service available alongside others related to serving the health needs of injection drug users Hersquos looking for an expression of COMOH support for the idea of Safe Injection Sites (SIS) that will in turn support his case for a pilot site in Toronto that can be practically evaluated Responding to R Schabasrsquos question about why TPH isnrsquot just going ahead and doing it D McKeown noted that Provincial support will likely be required for funding (partly because it is considered a health service) and for obtaining the required federal exemption under the Controlled Substances Act Some members expressed discomfort with the idea of expressing specific support for one element of the broader strategy of harm reduction as it is a more downstream intervention than is the usual for public health is not one that is required or practical in many areas of the province and has significant political implications I Gemmill also indicated concerns with some of the papers that are most commonly used to support SIS which are predominantly policy papers and not scientific ones R Schabas observed that from a public health perspective harm reduction has been extremely effective in reducing blood-borne diseases and SIS appears to be an example if an area where we have an opportunity to make a difference As the evidence is so strongly in favour of harm reduction as a public health strategy he believes that COMOH should in fact have a voice on this D McKeown clarified that he is not asking for COMOH to take a position that public health should be responsible for SIS he is simply asking that COMOH take a position that this service should be available alongside the other elements of a comprehensive harm reduction strategy He agreed that this position need not elevate SIS above the other components of harm reduction nor does it need to make any statement of support for specific sites In the end it was agreed that COMOH should proceed in drafting an expression of support V Jaeger invited members to provide suggestions about what should and should not be included D McKeown indicated that this is not time sensitive but he would appreciate a response sooner than later ACTION V Jaeger to synthesize feedback into a document for initial review by the Executive prior to full review and endorsement by the Section 44 Access to Oral Contraceptives Briefing Note R Pellizzari referred to the attached briefing note reminding the group that HUs are required to provide low-cost contraceptives under the OPHS Her board is having trouble with this now that the compassionate contraceptives assistance program is no longer available and that samples are becoming scarcer She suggested that options for a purchasing co-op might be considered by COMOH She noted that Erika Bontovics at the PHD has done a survey on this issue but she has not seen it and isnrsquot sure if any of the data would be useful for this discussion It was suggested that the Government Pharmacy be considered as a bulk purchaser but it was pointed out that this is not an option given that public health charges for these products alPHa was also suggested but acting as a clearing house for pharmaceuticals would be far outside of the Associationrsquos scope and mandate R Pellizzari added that larger health units are able to negotiate good deals based on volume and wondered if there is a potential for them to make purchases on behalf of the smaller health units that do not enjoy this advantage
There was support for further exploration but it was agreed that more information would be beneficial As an initial step RPellizzari will contact Erika Bontovics in an effort to examine the date described above with a view to determining what further information (eg costs negotiated by each HU) might be needed 45 Children and Youth Data Strategy Slide Deck ndash Aug 15 Teleconference amp ICES
Privacy Code V Jaeger referred to the linked ICES presentation and reported that discussions are underway on how to develop a data sharing strategy for the purposes of the attached by way of a working group of ICES COMOH and PHO She Robert Kyle and Michael Finkelstein have already agreed to participate but she invited others to express interest She will bring this up at PHLC and report back 46 Lyme Disease Testing Backgrounder J Hopkins reported that an increasing amount of staff time in Niagara is being devoted to responding to inquiries from the public regarding the different diagnostic methods being used to confirm Lyme disease in the US and Canada She is therefore asking COMOH if this is a prevalent enough issue that a request should be made to PHO to develop some explanatory materials that could be used to address them She clarified that they arenrsquot having much of a problem with physicians itrsquos more a matter of educating the public regarding the accepted approach to the prevention diagnosis and treatment of the disease R Schabas cautioned that public education is a double-edged sword as it has the potential to create the impression that Lyme disease is a bigger problem than it is P Stewart reported that her health unit had a good in-service by a PHO lab person that has been very helpful for the odd questions that come up There were differing opinions of how much effort should be devoted to this as it appears to be another example of ill-informed public opinion on a public health issue akin to anti-vaccination and anti-fluoridation attitudes While these attitudes should not be ignored therersquos not much we can do in the near term to alter them V Jaeger offered to raise this during her next monthly conversation with George Pasut 50 Addendum
51 MOH Retirement I Gemmill noted that Mike Corriveau (MOH ndash Renfrew) will be retiring in December after over thirty years of service He asked that the COMOH Executive consider some form of recognition 60 UPDATES INFORMATION ITEMS REPORTS
61 Public Health Leadership
Council
611 ndash PHLC Update e-Mail Update
612 ndash PHSSP Implementation Tables CMOH Memo ndash PHSSP Tables V Jaeger referred to the linked memo which the result of the desire for clarity and openness on how the topic-specific implementation tables would be assembled The PHLC has already received a number of expressions of interest and will be communicating next steps soon 62 COMOH Executive Committee Minutes June 11
Notes July 9 Minutes July 31
Minutes September 10
63 COMOH Built Environment Work Group
The BEWG has not met since the last meeting but will meet on October 7 During the summer that group led by C Gardner and Nikhil Rajaram developed the paper (COMOHrsquos Advice for the Provincersquos Review of its Long-Term Energy Plan) that was the basis for the letter that went to the province (see item 68 below) V Jaeger expressed appreciation for the work that went into that C Gardner has expressed interest in being a member of the Promoting Healthy Environments ndash Both Natural and Built PHSSP implementation table 64 Public Health Early Years Group Aug 9 Meeting Notes A Feller reported that this group is putting together a November 5 Grand Rounds at PHO 65 iPHIS Panorama
July 8 Update
66 Joint OPHAalPHa Health Equity Working Group R Pellizzari reminded that this is a joint initiative of alPHa and OPHA She will ensure that L Stewart provides minutes of these meetings for future updates She and L Simon are the COMOH reps on this group L Simon circulated a paper by the Wellesley Institute that examines the health equity impacts of cessation of community water fluoridation which was requested by the HEWG She added that Bob Gardner Director of Policy at the Wellesley Institute is now participating in this group and he would welcome suggestions for other subjects for health equity impact assessments M Klassen suggested that Radon might be a good one She also reported that the National Collaborating Centre for Determinants of Health hosted a discussion for the nurses that have been hired under the SDOH portfolio in order to more clearly identify what the specific mandate of public health is in this area and to identify reasonable evaluative measurements This is being proposed as the basis of a Locally Driven Collaborative project and three health units are already involved (PCCHU Toronto and Durham) but more are required and any assistance would be welcome HEWG is also working on positions on the minimum wage review and the poverty strategy Both of these will be circulated once complete and approved
It is also working on a TOPHC session on Cultural Safety related to working with aboriginal populations Feedback was also invited on this with a note that the deadline for abstract submission is September 27 Finally work is also being done with PHO on developing resources and supports for work with Priority Populations 67 COMOH Electronic Mailing List List of Subscribers 68 COMOH Correspondence Aug 26 COMOH Letter ndash Energy Policy
Aug 8 COMOH Letter ndash CMA Poverty Report
July 22 COMOH Letter ndash Immunization Data
70 Next MeetingAdjournment Meeting adjourned at 1035 Next Section meeting will be on November 15 2013 in Toronto part of the alPHa Fall Symposium
Page 1 of 8 ndash DRAFT FOR COMOH DISCUSSION
alPHa Membership Survey hello
Draft Report ndash COMOH Version hello
alPHarsquos membership was surveyed in the fall of 2013 Similar surveys were administered to all member groups ie COMOH BOH Section and Affiliates using the online survey tool Survey Monkey Small alterations were made to group-specific surveys to ensure that the survey questions were relevant to each group A total of 84 responses were received from alPHa members The breakdown of respondents was as follows This draft report is provided for discussion purposes to COMOH members and therefore focuses on the responses provided by COMOH members To provide additional information overall survey responses are also provided for some questions
SECTION 1 RESPONDENT PROFILE
Survey Question What region is your health unit located in
For COMOH members responses came from 6 of the 7 regions of Ontario All 7 regions were represented in the full set of survey responses
Summary of Respondents COMOH 27 32 BOH Section 34 40 Affiliates 23 27 Totals 84 100
All ResponsesEastern 24 29South West 12 14Central East 13 15Central West 15 18North East 11 13Toronto 5 6Not Sure 3 4North West 1 1Totals 84 100
All COMOH ResponsesEastern 3 11South West 5 19Central East 6 22Central West 6 22North East 3 11Toronto 4 15North West 0 0Totals 27 100
Page 2 of 8 ndash DRAFT FOR COMOH DISCUSSION
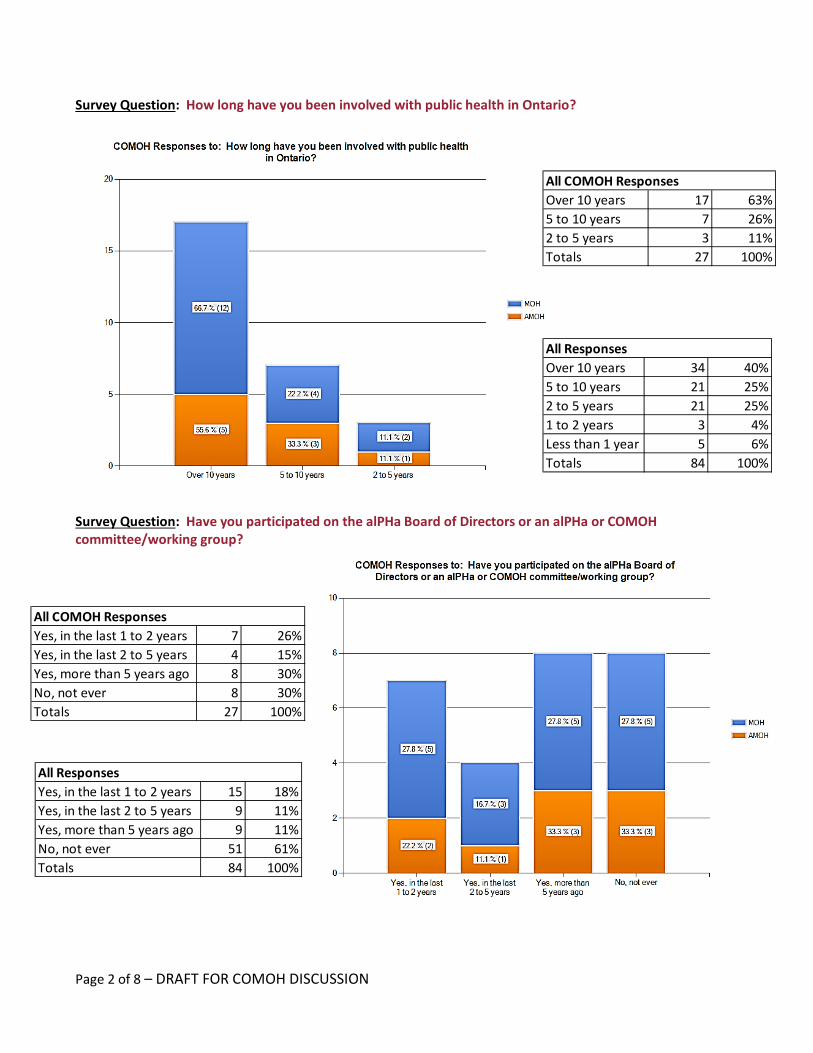
Survey Question How long have you been involved with public health in Ontario
Survey Question Have you participated on the alPHa Board of Directors or an alPHa or COMOH committeeworking group
All ResponsesYes in the last 1 to 2 years 15 18Yes in the last 2 to 5 years 9 11Yes more than 5 years ago 9 11No not ever 51 61Totals 84 100
All COMOH ResponsesOver 10 years 17 635 to 10 years 7 262 to 5 years 3 11Totals 27 100
All ResponsesOver 10 years 34 405 to 10 years 21 252 to 5 years 21 251 to 2 years 3 4Less than 1 year 5 6Totals 84 100
All COMOH ResponsesYes in the last 1 to 2 years 7 26Yes in the last 2 to 5 years 4 15Yes more than 5 years ago 8 30No not ever 8 30Totals 27 100
Page 3 of 8 ndash DRAFT FOR COMOH DISCUSSION
SECTION 2 PROFESSIONAL DEVELOPMENT
Survey Question Which of the following events have you attended at least once in the past two years
Survey Question Overall how satisfied have you been with alPHa events ie conferences meetings
Survey Question How much value do alPHarsquos events provide for the money
Survey Question How can alPHa make its events more valuable to you Please share any suggestions regarding future topics speakers formats duration locations or any other event component that is important to you
Comments about content bull Expert speakerpanels on emerging or hot topics
(2) bull More engaged dialogue with Ministry rather than
just updates bull Fewer Ministry updates (3) bull Content on medicalPH issues is better left to PHO
TOPHC and joint conferences (2) bull alPHa should stick to Ministrypoliticspolicysenior
PH supportPHU support on key priorities (eg November practical conference on HKP report)
bull For COMOH more discussion bull More time for section activities like face-to-face
COMOH meetings
bull More facilitated work groups of COMOH members to respond to public health practice questions
bull More focus on rural and northern issues bull Infection Control Logistical Considerations bull Consider partnering with other groups bull More collaboration with PHO and OPHA events bull Use of video conferencing bull Less frequentfewer meetings (2) bull Connect with CME Location bull Consider other venues than TO
( ) brackets indicate that more than one response included a similar comment
More than enough value 7 11A lot of value 34 52Some value 22 34A little value 2 3Not enough value 0 0Totals 65 100
All Responses for those who Attended at least One Event in the Last 2 Years
All COMOH ResponsesMore than enough value 4 15A lot of value 13 48Some value 9 33A little value 1 4Not enough value 0 0Totals 27 100
Page 5 of 8 ndash DRAFT FOR COMOH DISCUSSION
SECTION 3 VALUE FOR MEMBERSHIP
Survey Question What do you value the most about your alPHa membership
The comments provided in response to the text response question What is the most important benefit of alPHa membership for you personally supported the answers illustrated in the chart above 15 of the 20 comments provided focussed on the importance of opportunities to interact with colleagues across the province The next most important benefit mentioned was the support for COMOH members to work on public health issues together When asked What is the most important benefit of alPHa membership for your health unit COMOH members emphasized the following bull A coordinated and collective voice in advocating for public health issues and the public health sector (9) bull Opportunities to connect with other public health units to share experiences and best practices (8) bull Maintaining relationships with government both politicians and bureaucrats (3) and bull Support for boards of health (3)
Page 6 of 8 ndash DRAFT FOR COMOH DISCUSSION
Overall Level of Satisfaction
SECTION 4 LOOKING TO THE FUTURE
The questions in this section were asked to obtain input from alPHa members regarding a proposal from alPHarsquos Board of Directors to focus the Association on five service areas COMOH members were asked to indicate their level of agreement with the proposed areas of focus COMOH responses compared to the overall survey responses were as follows
To explore some proposed changes to Association services COMOH members were asked to provide their level of agreement with the following questions
COMOH Responses BOH Section Affiliates All Survey Responses
Strongly Agree
AgreeNeither Agree or Disagree
DisagreeStrongly Disagree
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1Promoting the role and value of local public health units
15 9 2 0 0 26 92 93 95 94
2
Providing important information to members about trends and events that will impact the public health system and management of public health units
10 8 8 0 0 26 69 97 86 85
3Facilitating professional networking and information sharing
13 10 3 0 0 26 88 83 82 85
4
Providing professional development to support excellence in public health unit leadership management and governance
3 15 7 1 0 26 69 83 86 79
5
Responding to public health sector issues when it makes the most sense to have a collective voice ie issues that impact the structure and funding of the public health sector and public health units and issues that have a broad focus on population health
15 8 2 0 1 26 88 97 95 93
PROPOSED AREAS OF FOCUS
COMOH Responses BOH Section Affiliates All Survey Responses
Strongly Agree
AgreeNeither Agree or Disagree
DisagreeStrongly Disagree
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1
COMOH and other professional groups within alPHa should do their own advocacy while alPHa supports members to share and support each others advocacy efforts
7 6 6 6 1 26 50 58 45 52
2
alPHa should provide support to action-oriented inter-professional work groups on priority public health unit issues and member resolutions
4 13 5 3 1 26 65 81 86 77
PROPOSALS
Page 8 of 8 ndash DRAFT FOR COMOH DISCUSSION
COMOH members were also asked to indicate the level of acceptability for some possible changes to alPHarsquos services and way of doing business
COMOH Responses BOH Section Affiliates All Survey Responses
Very Acceptable
Somewhat Acceptable
Neither Acceptable or Unacceptable
Somewhat Unacceptable
Very Unaccept
able
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1Single conference with additional face-to-face section meetings
21 2 0 1 0 24 96 68 80 81
2alPHa to offer alternatives like webinars on focussed topics
13 6 1 4 0 24 79 50 90 71
3Coordinate COMOH meetings with PHO OMA or Ministry events
16 4 2 0 0 22 91 na na --
4
Increase focus on building leadership and management capacity for health unit CEOs and senior management
7 9 4 3 0 23 70 na 70 70
5
Would it be acceptable for alPHa to request voluntary financial contributions from member PHUs in addition to annual fees
3 5 5 4 5 22 36 7 26 21
6
Would it be acceptable for alPHa to request voluntary in-kind staff contributions from member PHUs to expand alPHas capacity eg communications policy work group support
7 11 1 1 3 23 78 31 45 50
7Would it be acceptable to you for alPHa to discontinue staff support for COMOH (BOH Section)
0 4 1 5 14 24 17 11 na 14
8
Would it be acceptable to you for alPHa to reduce the amount of staff support for COMOH (BOH Section)
1 6 1 8 6 22 32 26 na 29
9
Would it be acceptable to you for alPHa to provide supports to MOHs and AMOHs (BOH Members) without maintaining COMOH (BOHs) as a section of the association
3 2 3 2 12 22 23 17 na 20
10
Would it be acceptable to you for alPHas Board of Directors to move from the current representational model to a skills-based strategic model ie board membership would be based on the skills needed to carry out alPHas strategic plan
6 11 2 1 3 23 74 56 56 62
11
Would it be acceptable to you for alPHas President Vice-President and Treasurer to be elected from the full membership of the alPHa Board of Directors (rather than the current model of alternating between BOH and COMOH members)
10 8 1 2 2 23 78 70 70 73
PROPOSED CHANGES
1 Council of Ontario Medical Officers of Health Terms of Reference
ASSOCIATION OF LOCAL PUBLIC HEALTH AGENCIES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
TERMS OF REFERENCE NAME 1 The name of the organization shall be ldquoThe Council of Ontario Medical Officers of
Health a section of the Association of Local Public Health Agencies (alPHa)rdquo hereinafter referred to as ldquothe Councilrdquo
MISSION 2 As local leaders in public health we are committed to improving the health of
Ontarians and increasing health equity by strengthening Ontariorsquos public health system We achieve this through system leadership and coordination in collaboration with the provincial government and other organizations and through evidence-informed advocacy on public health policy
OBJECTIVES 3 The objectives of the Council shall be
a) To provide strong province-wide leadership in public health
b) To advocate for health protection and promotion policies and programs that maintain and improve the health of Ontarians
c) To promote and maintain the highest standards for Ontariorsquos public health
programs and services
d) To support the planning implementation and evaluation of effective and efficiently run public health programs and services
e) To act as a forum for sharing information and resources and for addressing and
discussing public health issues both amongst the Councilrsquos members and other agencies that support the goals of alPHa eg Ontario Medical Association Ontario Public Health Association etc
f) To engage with and to provide public health and related policy advice to alPHa
the Chief Medical Officer of Health the Ontario Ministries of Health and Long-Term Care (including the Health Promotion and Public Health Divisions) Children
2 Council of Ontario Medical Officers of Health Terms of Reference
and Youth Services and other provincial ministries Public Health Ontario Health Canada the Public Health Agency of Canada and other public health partners
g) To promote and protect the professional interests of its members
h) To provide support to individual members as needed
i) To seek recognition for outstanding practice from among the members
j) To support evidence based practice of public health medicine
k) To engage and involve the membership to participate in COMOHrsquos endeavours
l) To mentor Public Health and Preventive Medicine Residents
MEMBERSHIP 4 Membership on the Council in each of the following categories is subject to the
limitations imposed by the current terms of reference and all policies and governing documents of the Association of Local Public Health Agencies Benefits of membership in each category are included in Appendix A These shall be subject to regular review and may be suspended under certain circumstances
Active membership in the Council shall be open to all Associate Medical Officers of Health and all full-time Medical Officers of Health whose Boards of Health are members of alPHa Such members shall have full voting privileges and may hold office in the Council Associate membership shall be open to all full and part-time physicians employed by a Board of Health that is a member of alPHa Such members shall not have voting privileges nor hold office
Affiliate membership shall be open to the following individuals interested in furthering the objectives of the Council
bull Public Health and Preventive Medicine Residents and Public Health and Preventive Medicine Residency Program Directors
bull Federal public health physicians working in Ontariorsquos First Nations communities
bull other public health or related physicians including those employed by a Board of Health that is not a member of alPHa
Such members shall not have voting privileges nor hold office
3 Council of Ontario Medical Officers of Health Terms of Reference
Emeritus membership shall be open to all former members who have retired after five (5) or more years of Active membership subject to the nomination in writing of two (2) active members in good standing endorsement of the Executive Committee and approval of the Council by majority vote at a general meeting Such members shall have neither voting privileges nor hold office but may be invited to attend general meetings Honorary membership shall be open to any non-active or associate member subject to the nomination in writing of two (2) active members in good standing endorsement of the Executive Committee and approval of the Council Such members shall have neither voting privileges nor hold office but may be invited to attend general meetings
OFFICERS 5 The Officers of the Council shall be the Chair Vice-Chair and immediate Past Chair
6 The Chair shall prepare the agendas of all Council meetings She shall preside and
preserve order at all such meetings shall ensure that these Terms of Reference are upheld and enforced and shall contribute to the supervision and evaluation of any Public Health and Preventive Medicine Resident who is on a placement with alPHa
7 The Vice-Chair shall fulfill the duties of the Chair in hisher absence The immediate
Past Chair may fulfill the duties of the Chair or Vice-Chair in their absences 8 The Chair shall normally serve a term of one (1) year which is renewable once and
after which the Vice-Chair shall normally assume the vacated office COMMITTEES 9 The Council shall elect seven (7) active members one from each of alPHarsquos regions
and the active member who is scheduled to serve as the President or immediate Past-President of alPHa to represent it on the alPHa Board of Directors These seven (7) members shall constitute the Councilrsquos Executive Committee and shall serve a term of at least one (1) year The Chair and Vice-Chair shall be elected from among the Executive Committee members If alPHarsquos immediate Past President is an active member she shall be an ex-officio member of the Executive Committee
10 The mandate of the Executive Committee shall be to facilitate the achievement of
the objectives of the Council by fulfilling the following
a Identifying priorities 1
1 See Appendix B Planning Cycle to Identify Priorities for COMOH
and ensuring the development of briefing documents and or recommendations as appropriate for the consideration of the Council
4 Council of Ontario Medical Officers of Health Terms of Reference
b Setting agendas and otherwise ensuring preparations for Council meetings c Ensuring the fulfillment of the direction of Council d Responding in a timely fashion to time-sensitive public health matters in
accordance with the Executive Committeersquos understanding of the perspective of the Council
e Engaging with the Chief Medical Officer of Health Associate Chief Medical Officers of Health and other provincial public health leaders and
f Representing Council at public and partner agency forums including the Public Health Leadership Council which shall normally include membership from the Officers of the Council and two other Executive Committee members as selected by agreement among the Executive
g Identifying opportunities for the recognition of outstanding practice from among the members including the annual nomination of at least one member for the alPHa Distinguished Service Award
11 The Executive Committee shall meet and correspond in the manner and at the times
and if required places as deemed necessary by the Chair to conduct the business of the Council A quorum shall consist of four (4) members
12 The Executive Committee shall have the power to strike committeestask or working
groups to assist it in carrying out the business of the Council 13 The Council may by special resolution remove a member of the Executive
Committee before the completion of hisher term of office and may elect a successor to complete the term The special resolution shall require a majority vote of 67 of the members present and voting at the meeting at which the special resolution is considered
14 A Nominating Committee shall consist of the three (3) most recent Past Chairs who
are able to serve and shall be chaired by the immediate Past Chair The Nominating Committee shall prepare a list of proposed Officers and Executive Committee members for the consideration of the Council at its Annual General Meeting
MEETINGS 15 The Council shall hold at least four (4) general meetings per year in a manner and at
the times and if required places as deemed necessary by the Executive Committee to share information direct and assist the Executive Committee in conducting the business of the Council
16 The Council shall hold its Annual General Meeting during and at the same place as
the alPHarsquos Annual Conference
5 Council of Ontario Medical Officers of Health Terms of Reference
17 The Council shall hold a special meeting at the call of the Chair or upon the written request specifying the purpose of such meeting of at least five (5) active members Council members must be given at least 48 hours notice of any special meeting
18 Only Councilrsquos active and associate members and alPHa staff are entitled to attend
general and special meetings of the Council Other members and non-members may be invited to attend all or part of such meetings as determined by the Chair preferably in consultation with the Executive Committee Non-members who come to such meetings without an invitation may attend all or part of the meeting by a majority vote of the active members present and voting
19 The Chair shall prepare the agendas for such meetings and shall normally include
reports from the Chair and the Councilrsquos committeestask or working groups and representatives to external bodies alPHarsquos Executive Director shall ensure that the minutes shall be recorded and promptly distributed to the Section
20 A quorum for all such meetings shall be ten (10) active members 21 The Council shall normally be notified in a manner deemed appropriate by the Chair
of such meetings at least one (1) month prior to their being held 22 A majority vote of the members present at such meetings and voting shall make
Council decisions In the case of a tied vote the Chair shall cast the deciding vote The Executive Committee shall ensure that actions arising from such decisions at such meetings are implemented and monitored
23 The Chair may solicit advice from the Council through the use of teleconferencing
and alPHarsquos electronic mailing lists in order to gain an understanding of the overall perspective of the Council (see 10d)
ELECTIONS 24 The Officers and Executive Committee members shall be elected at the Sectionrsquos
Annual General Meeting The Nominating Committee Chair or hisher designate shall present a list of nominations Additional nominations from the floor shall also be considered Each Officer and Executive Committee member shall be elected by secret ballot if necessary by a majority of the active members present and voting In the case of a tie the Chair shall cast the deciding vote
AMENDMENTS 25 The Councilrsquos Terms of Reference may be amended from time to time by the
Executive Committee provided the Committee receives notice of such proposed amendments at least one (1) month prior to the meeting at which the amendments
6 Council of Ontario Medical Officers of Health Terms of Reference
will be considered Such amendments shall be ratified by the Council at the next general meeting or the Annual General Meeting as the case may be
26 The Executive Committee shall review the Terms of Reference as required and not
less than once every two years Original September 1987 1st Revision October 2000 2nd Revision July 2001 3rd Revision December 2003 4th Revision February 2008 5th Revision June 2009 6th Revision June 2011 7th Revision June 2013
7 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX A
COMOH Membership Benefits Active Membership
bull Entitled to attend all meetings of the Section bull May hold office on the COMOH Executive Committee alPHa Board of Directors
Standing Committees bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Associate Membership
bull Entitled to attend all meetings of the Section bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Affiliate Membership
bull May attend meetings or parts thereof subject to approval of Chair bull May serve on ad-hoc committees of the Section subject to the approval of the
Executive Committee bull Discounted registration rates for alPHa Conferences (for Public Health and
Preventive Medicine Residents) bull Upon written request and subject to COMOH Executive approval Affiliate
Members may subscribe to comohlistsalphaweborg The approval will be reviewed on an annual basis in order to determine if the Affiliate Member can remain a subscriber to mohsalphaweborg
Emeritus Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair bull Enjoy discounted registration rates for alPHa Conferences and regular COMOH
meetings bull Subscription to comohlistsalphaweborg electronic mailing list bull Full access to alPHa Web site bull May represent alPHa COMOH on selected external committees and working
groups Honorary Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair
8 Council of Ontario Medical Officers of Health Terms of Reference
bull May represent alPHa COMOH on selected external committees and working groups subject to the approval of the COMOH or alPHa Executive Committee as appropriate
9 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX B
Planning Cycle to Identify Priorities for COMOH
1 There shall normally be a COMOH membership strategic planning retreat every four years In recognition of the dynamic environment of public health the need for and timing of such a retreat shall be at the discretion of the Executive Committee in consultation with the membership
2 The COMOH Executive is responsible (through the creation of a subcommittee of COMOH members) for ensuring the preparation for the COMOH retreats with resources to include those provided by alPHa
3 Leadership for action on COMOH priorities will be recruited from among the COMOH membership in order to make good use of the full base of capacity of the membership The resources to support actions will be recruited from both within and beyond the COMOH membership employing other public health professionals that reside within the broader public health system and community
4 The COMOH Executive shall ensure an annual review of strategic priorities and initiatives and the development of a draft report of the same for the review of the members at the June meeting
2013 Strategic Planning
Considerations for COMOH
As part of its strategic planning discussions alPHarsquos Board has been considering changes to the level of support provided to member sections A member survey is being carried out over the fall to determine options acceptable to alPHa members The following approach to support is put forward as a proposal for the consideration of COMOH Note that the feasibility of the points below depend upon future decisions of the alPHa board They assume that COMOH remains part of alPHa but becomes more independent in administering meetings
1 alPHa can provide to COMOH staff support (Gord Fleming) amounting to 02 FTE or one day per week This is a reduction from the current level of 35 days per week COMOH can choose to use the support any way it wants writing COMOH letters meeting minutes agenda support special projects etc
2 In addition to 02 FTE alPHa staff would provide support for up to 4 face-to-face meetings per year One meeting would be concurrent to alPHarsquos annual conference in June The timing of other meetings could be negotiated The support includes consulting on the development of the program arranging for speakers registration for the event arranging venue AV support and hospitality services
3 In addition to 02 FTE alPHa staff would provide support for setting meeting dates and any polling required to establish dates Note that the individual supporting this function would be Karen Reece
4 COMOHrsquos Executive and Section would continue to have access to online supports through the alPHa including the COMOH Listserve and a group page for posting agendas minutes and other resources on the alPHa website
5 alPHa staff (Linda Stewart and Gord Fleming) can also start participating on CMOH calls as a way to be up-to-date on issues related to COMOH
6 Other than what is outlined above COMOH would be expected to prepare agendas and take minutes for its Executive and Section meetings The Executive would be expected to operate more independently than it does now but would be able to access the supports outlined above
Prepared by Linda Stewart Executive Director
From comoh-bounceslistsalphaweborg on behalf of Christopher MackieTo MOH ListserveSubject [comoh] Fw URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)Date Wednesday October 30 2013 91241 AMAttachments ATT00249txt
For AMOHs and PHPM residents who didnt receive the initial email
Chris
Christopher Mackie MD MHSc FRCPCMedical Officer of Health and CEOMiddlesex-London Health Unit50 King St LondonON N6A 5L7 O 519 663 5317 ext 2444 wwwhealthunitcomFrom Pisko Laura (MOHLTC)Sent Tuesday October 29 2013 759 PMTo kbarkeralgomapublichealthcom malcolmlockbchuorg davidcchatham-kentcarobertkyledurhamca proumeliotiseohuca fwarshelginhealthonca mohelginhealthoncahlynnpublichealthgreybruceonca malcolmlockhnhuorg hnmohhnhuorglnoseworthyhkpronca bobnosalhaltonca elizabethrichardsonhamiltoncarschabashpechuonca ncameronhuroncountyca drimgemmillkflapublichealthcamohkflapublichealthca suditranadecounty-lambtononca paulastewarthealthunitorgChristopher Mackie valeriejaegerniagararegionca jimchiriconbpsdhuca jarthursnwhuoncaisralevyottawaca dnealoxfordcountyca davidmowatpeelregionca mklassenpdhuoncarpellizzaripcchuca rosemarieramsinghporcupinehuonca mcorriveaurcdhucomcharlesgardnersmdhuorg sutcliffepsdhucom davidwilliamstbdhucomspruytmtimiskaminghucom dmckeowntorontoca lnolanregionofwaterloocanicolamercerwdghuorg aheimannwechealthunitorg karimkurjiyorkcaCc coreywesleytbdhucom CindyBaker-Barillsmdhuorg Donna Kosmack pilonlsdhucomPaulaMuiskflapublichealthca sthibautorontoca Mueller Daina (MOHLTC) Gordon Marcus(MOHLTC) andreakitahamiltoncaSubject URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)
Dear Colleagues The ministry has received reports that some tobacco vendors across the province aregiving away single cigarettes with the purchase of tobacco products It is the ministryrsquosposition that giving out free single cigarettes does not violate subsection 31(3) of theSmoke-Free Ontario Act (ldquoSFOArdquo) Although the practice of giving out free singlecigarettes may promote the sale of tobacco products it does not take the form of aldquoproduct enhancement product association or promotional materialrdquo and therefore doesnot fall within the scope of subsection 31(3) of the SFOA We have confirmed with Health Canada that this practice may violate section 29(b) of thefederal Tobacco Act As such Health Canada is requesting that you notify them in writingand I am directing you to communicate with them via email and provide to them as manydetails as possible Emails should be sent to Tobacco-Ontariohc-scgcca and thesubject line should read ldquoViolation of Section 29(b) of Tobacco Actrdquo This will ensurethat the complaints are given priority status by Health Canada We will continue to monitor
this situation and liaise with our colleagues at Health Canada Please share this information with your tobacco control staff and contact me or DainaMueller Manager Tobacco Control Unit Health Promotion Implementation Branch atdainamuellerontarioca with any questions RegardsLaura Laura A PiskoDirectorHealth Promotion Implementation BranchHealth Promotion DivisionMinistry of Health and Long Term Care416-327-7445 (office)416-451-3185 (mobile) Marcus Gordon - EA (416)326-0625 for urgent issues
========= Middlesex-London Health Unit E-Mail Disclaimer =============______________________________________________________________
Private and confidential intended only for named recipient If otherwisereceived please destroy immediately Health information in this email isonly general information and is not intended to replace an in personconsultation with a medical professional nor is it intended to providemedical advice Individual circumstances of which we are not aware mayaffect the information provided herein and as such the Middlesex-LondonHealth Unit assumes no liability or responsibility for your reliancethereon The Middlesex-London Health Unit works under the authority of theHealth Protection and Promotion Act and this correspondence may be used toassess your needs for public health services (519-663-5317 ext 2448)______________________________________________________________
From Gardner CharlesTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes (RayCopesoahppca)
George Pasut (GeorgePasutoahppca) Peter Cooney (petercooneyhc-scgcca)Cc Ito DickSubject Discontinuation of Fluoridation in MuskokaDate Tuesday October 22 2013 125254 PM
Hello Colleagues
As I reported in my email below on September 26th fluoridation has come under challenge again inSimcoe Muskoka I am now very unhappy to report that despite our best efforts last night theDistrict Council of Muskoka voted to remove fluoride from municipal drinking supplies across theDistrict This brings to an end fluoridation in all of Simcoe and Muskoka (with the exception of Base Borden)ndash though New Tecumseth will be conducting a plebiscite on the question of fluoridation with themunicipal election next October Defending community water fluoridation has drained a great deal of time human resources andcommitment from other priorities and has been exhausting here in SMDHU as I am sure it hasbeen in many other health units While the outcomes have been very disappointing I have beenimpressed by the professionalism and dedication that SMDHU staff members have shown inshouldering this burden In particular our dental consultant Dr Ito has provided us with much ofthe foundational knowledge and the local research essential to our efforts and has very frequentlyattended and presented at council meetings and other public events I would also like to thank themany of you who have offer and provided support including advocacy letters and informationresources Over the years Dr Peter Cooney Chief Dental Officer of Health of Canada has beenvery helpful attending and presenting with us at council meetings and at public consultationevents We will of course continue our oral health surveillance of the children of Muskoka documentingand reporting in future years on the increase in dental decay that we anticipate will occur Suchsurveillance is the foundation of our advocacy both to municipal politicians and to the province I am very concerned that our experience will continue to repeat itself across the province unlessthere is strong leadership provincially It is with this in mind that I raise the followingrecommendations for your consideration
1 That we collectively (with PHOrsquos leadership) conduct high quality publish-worthy researchdocumenting the impact on dental decay that occurs in those municipalities throughoutOntario that in recent years have discontinued community water fluoridation This could bepart of a larger study on such municipalities across the country and it could also be part ofa study documenting overall oral health (including fluoridation coverage) in the province(and possibly across the country)
2 That COMOH engage with our Chief MOH to advocate for the province to require allmunicipal water supplies to be fluoridated (the exception of course being those withnaturally sufficient fluoride concentrations) This could built upon the alPHa position to
Gordon
Highlight
Gordon
Highlight
date (A11-00 - Community Water Fluoridation) on the CMOH position (Oral Health ndash) and on theemail discussion generated on the COMOH listserv some months back re Richardrsquosproposal (calling on the province to fund municipal water fluoridation)
Valerie I request that this be an item for our COMOH meeting on November 15th Sincerely Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorg From Gardner Charles Sent Thursday September 26 2013 245 PMTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes(RayCopesoahppca)Subject Community Water Fluoridation Under Challenge Again in Simcoe Muskoka Hello Colleagues You may wish to know that community water fluoridation (CWF) is again under challenge in SimcoeMuskoka specifically both in Tottenham (Town of New Tecumseth in Simcoe County) and for theentire District of Muskoka On Monday September 23 Committee of the Whole Council of theTown of New Tecumseth voted to submit application to discontinue community water fluoridation(CWF) in the town of Tottenham despite presentations to the contrary from our dental consultantDr Ito and from me The next Council meeting is scheduled for Monday Sept 30 at which lastMondayrsquos (Sept 23) votes will be ratified
Since Monday I have spoken with the Mayor of the Town of New Tecumseth and with most of thecouncilors encouraging deferral of a decision on Monday to allow the town more time to make afully informed decision
This is the second time in recent years that the issue of discontinuing CWF in Tottenham has beenraised at council This issue is also scheduled to return again to the District of Muskoka Council on
October 21st where I will be presenting in response to deputations in opposition to fluoridation
Outside of Base Borden Tottenham is the only community with fluoridated water in SimcoeCounty The health unitrsquos own screening data between 2011 and 2013 shows that Tottenhamrsquos
Gordon
Highlight
children as well as those in Muskoka have a lower rate of dental decay than Simcoe Muskokacommunities without CWF
Sincerely
Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorgChuck Gardner MOH
November 04 2013
Mandatory State Laws on Fluoridation Thirteen states Puerto Rico and the District of Columbia have laws intended to provide
statewide fluoridation These states and the year that the fluoridation legislation was passed are
District of Columbia (1952) Connecticut (1965) Kentucky (1966) Illinois (1967) Minnesota
(1967) Ohio (1969) South Dakota (1969) Georgia (1973) Nebraska (1973 and 2008)
California (1995) Delaware (1998) Puerto Rico (1998) Nevada (1999) Louisiana (2008) and
Arkansas (2011) (see Table 1) The sizes of the public water systems or countiescommunities
affected and exemption provisions vary by state Table 1
STATES THAT HAVE MANDATORY LAWS ON FLUORIDATION -2011
State (1) Year of
Fluoridation
Legislation (1)
Population
served by
Fluoridated
CWS (2)
Persons
receiving
fluoridated
water (2)
State
Average
Caries
Experience
of Grade 3
Students (3)
Arkansas 2011 647 1724131 64
California 1995 621 22812721 709
Connecticut 1965 910 2370423 406
Delaware 1998 862 705344 545
Georgia 1973 921 8924598 52
Illinois 1967 993 11325132 532
Kentucky 1966 999 4334223 598
Louisiana 2008 407 1846149 657
Minnesota 1967 988 4117266 549
Nebraska 1973 and 2008 702 1001665 593
Nevada 1999 702 1001665 649
Ohio 1969 877 8772683 512
South Dakota 1969 948 642942 623
District of
Columbia
1952 1000 595000
Puerto Rico 1998
United States 739 204283554
2010 Statistics for population fluoridated and number of people
1 Communication with Jane McGinley RDH MBA Manager Fluoridation and Preventive Health
Activities Council on Access Prevention and Interprofessional Relations
2 Centers for Disease Control and Prevention Department of Health and Human Services
accessed Oct 21 2013 httpwwwcdcgovfluoridationstatistics2010statshtm
3 Centers for Disease Control and Prevention National Oral Health Surveillance System Caries
Experience - Percentage of 3rd Grade students with Caries Experience (treated or untreated tooth
If data from 43 states for the percentage of Grade 3 children with experience of dental decay is
compared with the 2008 percentages of the population in a state with Community Water
Fluoridation then the percentage of children with experience of dental decay decreases as the
percentage of the state population with Community Water Fluoridation increases (see Figure 1)
Figure 1
Correlation of Percentage of Grade 3 Children with Caries Experience and
Percentage of Population With Community Water Fluoridation for 43
Reporting States
0
10
20
30
40
50
60
70
80
0 10 20 30 40 50 60 70 80 90 100
State of Population With Community Water Fluoridation
Sta
te
of
Gra
de 3
Stu
den
ts w
ith
Cari
es E
xp
eri
en
ce
Data from CDC (2 3)
The description of the fluoridation laws in California Illinois and Nevada can be found on the
Association of State amp Territorial Dental Directors website(4 7 8)
The California fluoridation law AB 733 came into effect in 1995 requiring communities of 10
000 residents or more be supplied with fluoridated drinking water However the state did not
provide any funding to implement the legislation (California is unique in requiring fluoridation
without funding the practice)(4) The California Department of Health Services therefore had to
fund fluoridation initiatives from non-governmental sources ie the California Endowment
California Dental Association Foundation the First 5 Commission and others(5) From 1995 to
2011 the percentage of the California population receiving fluoridated drinking water has risen
from 17 to 625(6) 4 Dental Public Health Activities amp Practices Office of Oral Health California Department of Health
Services April 2002 httpwwwastddorgbestpracticesDES06002CAfluoridationpdf
5 Stock M Pollick H The CDA Foundation Model to Fluoridate Communities California Dental
Association Journal vol 40 no 8 649 - 655
httpwwwcdaorgPortals0journaljournal_082012pdf
6 California Dental Association Foundation
httpwwwcdafoundationorglearnadvocacyfluoridation
The State of Illinois passed a mandatory fluoridation state in 1967 and required all community
water systems to adjust fluoride levels in the drinking water to optimal levels within 1 year(7)
From 1962 when over 5000000 residents had optimally fluoridated drinking water by 2010
the number had risen to 11325132 (993 of the population on community water systems)(2)
7 Dental Public Health Activities amp Practices Division of Oral Health Illinois Department of Public
Health April 2002 httpwwwastddorgbestpracticesDES16007ILfluoridationpdf
The State of Nevada passed a mandatory fluoridation statute in 2000 for communities with
400000 or more residents(8) This was a result of the work of a statewide coalition that
included the Nevada Dental and Dental Hygienist Associations the Washoe and Clark County
District Health Departments the Clark County School District Junior League of Las Vegas
Head Start the Community College of Southern Nevada Dental Hygiene Program Health
Access Washoe County and Saint Maryrsquos Hospital For communities with less than 400000 the
implementation of fluoridation still required the vote of the majority voters in the community
The Las Vegas Water Authority and the City of Henderson started fluoridation in 2000
increasing the percentage of the population with fluoridated drinking water from 2 to 65 (8) 8 Dental Public Health Activities amp Practices Bureau of Family Health Services Nevada State Health
Division April 2002 httpwwwastddorgbestpracticesDES31002NVfluoridationbillpdf
Countries with Mandatory Laws on Fluoridation Countries that have mandated Community Water Fluoridation are Brazil Hong Kong
Malaysia Singapore Ireland Israel and some of the states in Australia
Singapore started fluoridating its water in 1956 based on the success of the fluoridation trials in
Grand Rapids Newburgh Evanston and Brantford Singapore became the first Asian country to
have 100 of its population benefitting from the implementation of fluoridated drinking water
Loh reported that ldquoThe ten year study on the effects of water fluoridation in Singapore showed
a decrease in caries prevalence in the children In the permanent dentition the reduction was
523 per cent for Chinese and 31 per cent for Malays in the 7 to 9 year old age group A similar
trend was observed in the mixed dentition in which the decrease was 325 per cent for Chinese
and 306 per cent for Malaysrdquo(9) By 2010 the population of the country was 5080000(10)
9 Loh T Thirty-eight years of water fluoridation--the Singapore scenario Community Dent
Health 1996 Sep13 Suppl 247-50
10 British Fluoridation Society One in a Million the facts about water fluoridation 3rd Edition
published March 2012) httpwwwbfsweborgonemillion0920One20in20a20Million20-
20The20Extent20of20Fluoridationpdf
Hong Kong started implementing community water fluoridation in 1961 and similar to
Singapore 100 of the population received access to fluoridated drinking water Lo and Wong
reported that ldquoThe mean DMFT score of the children deceased from 44 in 1960 to 15 in 1968
stayed at this level in the 1980 and 1986 surveys and further deceased to 08 in 2001 The
prevalence of dental fluorosis among the children surveyed in 1960 was 1 and this increased
to 59 and 70 in 1968 and 1980 respectively It was found in the 1986 and 2001 surveys that
the prevalences of fluorosis were 47 and 9 among children whose teeth developed at the
time when the respective water fluoride concentrations were 07 ppm and 05 ppmrdquo(11) The
population of Hong Kong was 6968000 in 2009(10) 11 LO ECM and WONG AHH Water fluoride concentration and fluorosis in Hong Kong in 1960-
2001 84th General Session and Exhibition of the International Association for Dental Research amp
1st Meeting of the Pan-Asian-Pacific Federation Brisbane Australia 28 June-1 July 2006 v 85 n
Sp B
The Malaysian cabinet approved a nationwide community water fluoridation program in 1972
(12) One of the states Sabah decided to stop fluoridation in 1989 due to concerns about
inadequate supervision in adding fluoride to the drinking water Oral Health Surveys in 2009
and 2007 indicated that children in Sabah had the worst oral health with 50 of 12 year-olds
having decay in their permanent teeth and children having an average of 3 teeth being(13)
Under the 10th Malaysian Plan in 2011 the federal and the Sabah state governments
reintroduced water fluoridation in Sabah(1314) In 2010 about 755 of the Malaysian
population or 20700000 people had fluoridated drinking water(1013) 12 Malaysian Dental Association Fluoride in Water
httpwwwmdaorgmy07_public_01healthcare_12htm
13 Sachdev N Fluoridation in Sabah Water for Cleaner Teeth French Tribunecom 28022011
From Levy IsraTo Jaeger ValerieCc Pim Carolyn gordonalphaweborg Diallo Aicha Penny Sutcliffe Paul Roumeliotis Michael Finkelstein
Hazel Lynn Robert KyleSubject FW Panorama - Privacy Security and other issuesDate Wednesday October 16 2013 122110 PM
Hello ValerieOttawa is part of Wave 4 Panorama implementation and we are gearing up increasingly to use thesystem where and if possible Thinking about it I am anticipating that this may need to be on theCOMOH (and alPHa) radar as it is something that will impact all health units and implies a majoroperational shift in vaccine delivery programs for all health units I have asked Carolyn Pim toconnect with our sister wave 4 units to share common experiences as we move forward ndash when wehave a roll up could I bring to COMOH Exec for discussion to explore whether there are broaderimplications for all members As an aside I have also asked the Ministry and their CIO to share with me any roll up learnings thatthey may have had already from previous waves (I understand that Niagara HU was a wave 1participant so if there is such a roll up of common experiences that others could learn fromperhaps you have it already and that could come to the exec too)Thanks Isra From Pim Carolyn Sent October 10 2013 1228 PMTo Christopher Mackie (christophermackiemlhuonca) Elizabeth Richardson(Elizabethrichardsonhamiltonca) H BSc M D F R C P (C) MPH Jim Chirico(jimchiriconbpsdhuca) Marlene Spruyt (spruytmtimiskaminghucom) Robert Kyle (Durham)Cc Levy IsraSubject Panorama - Privacy Security and other issues Dear colleagues Irsquom reaching out to you as fellow Panorama Wave 4 health units to ask about where yourorganizations are at in the process of signing agreements and completing Privacy ImpactAssessments and Threat Risk Assessments (TRAs) Ottawa Public Healthrsquos IT legal and informationsecurity advisors have made numerous requests to the MOHLTC for information (in particular theprovincial TRA) that we consider essential to develop our own risk assessment and PIA but havebeen told that information cannot be shared even with strict confidentiality and access controlsSo we are at somewhat of an impasse Isra emailed Arlene yesterday Arlene has forwarded ourconcerns to the Ministryrsquos CIO and Panorama lead but we havenrsquot had any response or discussionswith either of them yet Have your organizations identified similar concerns andor had interactions with the MOHLTC inthis respect Irsquod also be interested in knowing if your health units have flagged other (egoperational) implementation concerns Thanks
Carolyn ps Robert ndash you can ignore this request I talked with Sharan this morning about Durhamrsquos issuesso am including you now just for information Carolyn Pim MD FRCPC Associate Medical Officer of Health Meacutedecin adjointe en santeacute publique Ottawa Public Health Santeacute publique Ottawa 100 Constellation Cr Ottawa ON K2G 6J8 Tel teacutel (613) 580-6744 ext 23684Fax (613) 580-9641Connect With Ottawa Public Health
Suivez Santeacute publique Ottawa
This e-mail originates from the City of Ottawa e-mail system Any distribution use orcopying of this e-mail or the information it contains by other than the intendedrecipient(s) is unauthorized If you are not the intended recipient please notify meat the telephone number shown above or by return e-mail and delete thiscommunication and any copy immediately Thank you
Le preacutesent courriel a eacuteteacute expeacutedieacute par le systegraveme de courriels de la Ville dOttawaToute distribution utilisation ou reproduction du courriel ou des renseignements quisy trouvent par une personne autre que son destinataire preacutevu est interdite Si vousavez reccedilu le message par erreur veuillez men aviser par teacuteleacutephone (au numeacuteropreacuteciteacute) ou par courriel puis supprimer sans deacutelai la version originale de lacommunication ainsi que toutes ses copies Je vous remercie de votre collaboration
1
Smoke-Free Patios ndash An Amendment to the Smoke-Free Ontario Act
Date November 15 2013 Prepared for Council of Ontario Medical Officers of Health Prepared by York Region Public Health _____________________________________________________________________________ Issue
The Smoke-Free Ontario Act is the current provincial legislation that imposes smoking restrictions in workplaces and public places It prohibits smoking on restaurant and bar patios in instances where any portion of the seating area is covered by a roof With recent studies illustrating that exposure to second hand smoke outdoors poses similar risks to indoor exposure there has been growing public support to enhance smoking restrictions and make patios completely smoke-free
Background
With the implementation of the Smoke-Free Ontario Act in 2006 restaurant and bar patios became subject to smoking restrictions if any portion of the seating area was covered by a roof This allowed for patios without roof coverings to continue to allow smoking and as a result did not provide significant protection to patrons or staff from exposure to second hand smoke outdoors Many businesses chose to alter the design of their patios to allow smoking to continue In some cases patios became more crowded since smoking patrons who dine indoors often proceed outside onto licensed patios with their beverages to smoke York Region like most municipalities in Ontario is host to hundreds of patios being operated by restaurant owners and businesses With smoking prohibitions affecting only a small portion of these patios specifically ones with coverings the vast majority of patios still allow smoking to take place Patrons and employees on patios where smoking is not restricted are exposed to second hand smoke frequently This can contribute to increased disease and aggravation of existing health conditions From a business perspective the existing legislation has been viewed by many operators as unfair because some patios have permanent coverings which cannot be removed requiring a smoke-free status These business owners feel this creates an uneven playing field since they cannot provide an outdoor dining area for their smoking customers There is strong community support for smoke-free patios in Ontario A 2009 Rapid Risk Factor Surveillance System survey revealed 754 percent support in York Region while a Toronto Health Survey in 2011 indicated 74 percent public support
2
Current Status
Smoking is currently prohibited on restaurant and bar patios province-wide in four Canadian provinces and territories Alberta Newfoundland and Labrador Nova Scotia and Yukon A fifth province Prince Edward Island prohibits smoking on patios until 10 pm Since Ontario enacted legislation restricting smoking on patios in 2006 eight municipalities in Ontario have chosen to create bylaws that go beyond the Smoke-Free Ontario Act and enhance outdoor protection from second hand smoke by prohibiting smoking on patios completely The largest of those municipalities is the City of Ottawa Recently the Toronto Board of Health unanimously endorsed a report presented by their Medical Officer of Health recommending that restaurant and bar patios be made smoke-free through an amendment to the Smoke-Free Ontario Act
Key Considerations
There should be no significant financial burden to local Boards of Health resulting from a smoke-free patio amendment to the Smoke-Free Ontario Act Inspection and enforcement for the Smoke-Free Ontario Act is currently 100 percent funded by the Ministry of Health and Long-Term Care Following an introductory period of education on the amendment a complaint response model of service delivery would ensure ongoing compliance with smoke-free requirements A complete ban of smoking on patios would eliminate the widely-held perception by business owners that the current legislation creates an uneven playing field for business Since Smoke-Free Ontario Act inspections of patios began in 2006 operators have expressed the opinion that if patios need to be smoke-free for the protection of the public they should all be smoke-free to avoid undue hardship for individual businesses and to provide protection uniformly across the Province
Next steps
York Region Public Health intends to seek support from Medical Officers of Health across the Central East Tobacco Control Area Network (CETCAN) to advocate to the Ministry of Health and Long-Term Care for an amendment to the Smoke-Free Ontario Act prohibiting smoking on all restaurant and bar patios York Region is also in the process of requesting that its Regional Council advocate to the Minister of Health and Long-Term Care on the issue
Updating and Modernizing O Regulation 565 (Public Pools)
Date November 15 2013
Prepared for Council of Ontario Medical Officers of Health
Prepared by York Region Public Health _____________________________________________________________________________ Background Recent drownings at public pools in Ontario have highlighted the issue of water-borne illness and injury The current pool regulation under Ontariorsquos Health Protection and Promotion Act O Regulation 565 (Public Pools) is outdated It does not accurately reflect new pool technology and design or the changing use of public pools Neither does it incorporate admissions standards recommended by the Office of the Chief Coroner Further O Regulation 565 does not have short-form wording or set fines associated with it This limits public health enforcement capabilities What is the impact Updating O Regulation 565 (Public Pools) to address recent changes in pool technology design and uses and to include Coroner-recommended admissions standards would help improve pool safety Establishing short-form wording for O Regulation 565 would enhance enforcement related to public pools Currently the only enforcement available to Public Health Inspectors for dealing with non-critical regulatory infractions in public pools is the issuance of a Part III summons This involves a considerable amount of resources for a possible small fine With the development of inspection disclosure systems such as YorkSafe there is an even greater need to develop a method to effectively address repeated pool operator non-compliance with non-critical issues Next steps Public health units should advocate to the Province to 1) Conduct a review of O Regulation 565 (Public Pools) to address shortcomings Proposed changes to the
regulation should include a requirement for ownersoperators of public pools to advise the local Medical Officer of Health of any change in the use of a facility and the addition of the Coronerrsquos recommended admission standards
2) Provide short-form wording for O Regulation 565 so that public health inspectors can better deal with pool operator non-compliance
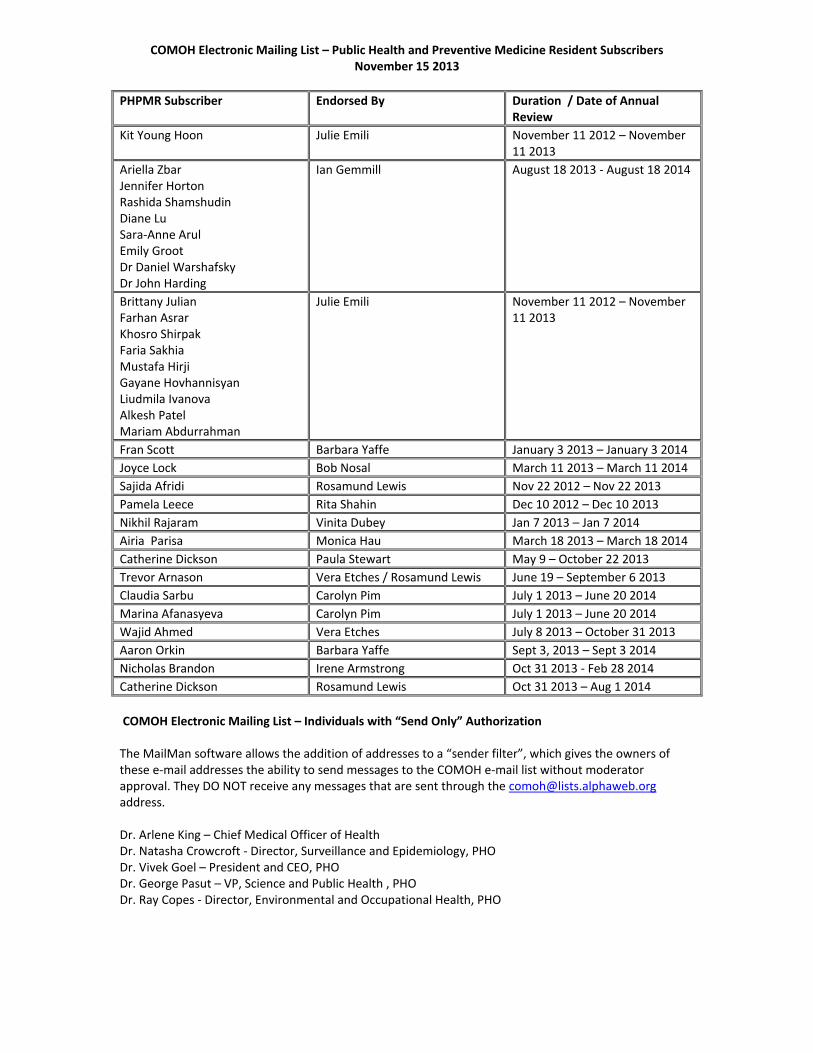
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
I information D discussion A approval P presentation
47 Ontario Regulation 565 Public
Pools KURJI Briefing Note
50 Provincial Partners
51 CODE - COMOH project on
School BoardPHU Partnerships FINKELSTEIN Joint Code-COMOH Letter
(attached) I
52 Public Health Ontario PASUT D 60 UPDATES INFORMATION ITEMS REPORTS
61 Public Health Leadership
Council JAEGER I
611 ndash PHLC Update JAEGER Update I 612 ndash PHSSP
Implementation Tables JAEGER CMOH Memo I
62 COMOH Executive Committee JAEGER Minutes October 8 I 63 COMOH Built Environment
Work Group GARDNER Update I
64 HIV Non-Disclosure JAEGER Update following COMOH Chair disc W CMOH
I
65 Access to Oral Contraceptives PELLIZZARI Report back from disc W Erika Bontovics
I
66 Child and Youth Data Strategy JAEGER Update I 67 Public Health Early Years
Group FELLER Meeting Notes I
68 iPHIS Panorama FINKELSTEIN Update I 69 Joint OPHAalPHa Health
Equity Working Group PELLIZZARI Submission to Minimum
Wage Review I
610 COMOH Electronic Mailing List
FLEMING List of Subscribers I
611 COMOH Correspondence FLEMING Summary of COMOH Letters
I
70 Next MeetingAdjournment
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
SECTION TELECONFERENCE September 18th 2013
900 ndash 1100 AM Please dial 1-866-518-0789 or 416-443-4586 and enter Conference ID 624258 to participate
PRESENT Valerie Jaeger (Chair) Kim Barker Lisa Berger Jim Chirico Janet DeMille Andrea Feller Ian Gemmill Allen Heimann Jin-Hee Kim Jessica Hopkins Miriam Klassen Karim Kurji Isra Levy Rosamund Lewis Hazel Lynn David McKeown Nicola Mercer Lynn Noseworthy Rosana Pellizzari Carolyn Pim Sudit Ranade Lisa Simon Richard Schabas Marlene Spruyt Paula Stewart Penny Sutcliffe Monir Taha Hsiu-Li Wang Bryna Warshawsky David Williams Lilian Yuan Gordon Fleming (alPHa Staff Recorder) Linda Stewart (alPHa Staff)
10 Call to Order Approval of Agenda Meeting called to order at 904 Agenda approved as circulated 20 Approval of Minutes June 4th 2013 Minutes Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning V Jaeger reported that the Executive has met four times since the last Section meeting and this remains a standing item on the Executive agenda It is their opinion that this process needs to be executed in concert with the plan that is being developed by alPHa at this time and decisions about processes and directions for COMOH will need to be informed by those taken by the parent Association There is a strong agreement about the importance of COMOH strengthening it as a group and reinforcing its relationships with public health sector partners including but not limited to the CMOH PHO and the MOHLTC The Executive will continue these discussions and keep the Section informed as appropriate 40 PUBLIC HEALTH ISSUES
41 Mandatory Immunization I Gemmill reported that the issue of Health Care Worker influenza immunization rates which remain quite low despite best efforts was discussed at a session at the most recent Canadian Immunization Conference Having accepted that mandatory HCW immunization is very unlikely to become public policy anytime soon the discussion focused on how to convince more HCWs that this is important He observed that only 10 of 36 public health units have policies for their own employees which may be rendering our
argument that hospitals should be developing policies of their own less convincing He suggested that COMOH might for a start consider facilitating the development of a template for policies on mandatory immunization of public health staff (subject to exemptions for people with no contact with others people already under contract etc) which could increase the number of health units with policies thereby increasing the credibility of the case He also suggested a process whereby the existing policies and procedures could be collected examined and synthesized into a legally defensible practical but non-binding template which would be palatable to health unit staff and their unions He agreed that a COMOH working group would be the most appropriate mechanism to do this but asked that alPHa begin the process by collecting the existing policies A Heimann reported that Windsor is discussing this issue ahead of its local public campaign and he thinks this is an excellent idea Rosana Pellizzari added that this process is a good opportunity for those who have policies in place to share lessons learned about unintended consequences experiences with grievances sorting out the NACI definition of high-risk groups and identifying classes of employees that could reasonably be exempt due to the nature of their work ACTION V Jaeger to invite members to submit questions and expressions of interest in participating on the proposed working group directly to I Gemmill and to forward existing policies and related information to G Fleming at alPHa for collection and assembly 42 HIV Non-Disclosure PHLC Briefing Note V Jaeger reminded the group that this was raised at the June Section meeting where it was determined that COMOH should take the lead on developing a procedure that would ensure greater consistency in how and under what circumstances Section 22 orders are used in cases of HIV non-disclosure She has since raised this with the CMOH who agreed that an Associate CMOH at the MOHLTC would be an appropriate person to take the lead on this but until those positions are filled this isnrsquot an available option She also reported that George Pasut has offered PHO support in the form of logistics and meeting space to support a COMOH working group if it is decided to create one She then indicated that L Yuan and R Shahin who have been the COMOH leads on this issue on previous agendas are unable to participate in this process right now so she invited expressions of interest R Schabas observed that this is an issue for which the Provincial public health leadership should take responsibility He suggested that COMOH can present recommendations but they should be framed by an expectation of the CMOH to exercise leadership and provide clear direction V Jaeger agreed to articulate this to Arlene but reiterated that the present request is for volunteers people are willing to sit and do the work R Schabas I Gemmill and A Heimann indicated interest ACTION V Jaeger to discuss the foregoing with the CMOH whose response will inform next steps including development of process and confirmation of expressions of interest 43 Supervised Injection Sites Draft COMOH Letter V Jaeger referred to the attached and stated that it is meant more as a starting point for discussion than to make any suggestions about what COMOHrsquos position should be and invited D McKeown to speak to the issues
D McKeown reported that this is something that Toronto has been looking at for some time and they have concluded that it would be beneficial to have this service available alongside others related to serving the health needs of injection drug users Hersquos looking for an expression of COMOH support for the idea of Safe Injection Sites (SIS) that will in turn support his case for a pilot site in Toronto that can be practically evaluated Responding to R Schabasrsquos question about why TPH isnrsquot just going ahead and doing it D McKeown noted that Provincial support will likely be required for funding (partly because it is considered a health service) and for obtaining the required federal exemption under the Controlled Substances Act Some members expressed discomfort with the idea of expressing specific support for one element of the broader strategy of harm reduction as it is a more downstream intervention than is the usual for public health is not one that is required or practical in many areas of the province and has significant political implications I Gemmill also indicated concerns with some of the papers that are most commonly used to support SIS which are predominantly policy papers and not scientific ones R Schabas observed that from a public health perspective harm reduction has been extremely effective in reducing blood-borne diseases and SIS appears to be an example if an area where we have an opportunity to make a difference As the evidence is so strongly in favour of harm reduction as a public health strategy he believes that COMOH should in fact have a voice on this D McKeown clarified that he is not asking for COMOH to take a position that public health should be responsible for SIS he is simply asking that COMOH take a position that this service should be available alongside the other elements of a comprehensive harm reduction strategy He agreed that this position need not elevate SIS above the other components of harm reduction nor does it need to make any statement of support for specific sites In the end it was agreed that COMOH should proceed in drafting an expression of support V Jaeger invited members to provide suggestions about what should and should not be included D McKeown indicated that this is not time sensitive but he would appreciate a response sooner than later ACTION V Jaeger to synthesize feedback into a document for initial review by the Executive prior to full review and endorsement by the Section 44 Access to Oral Contraceptives Briefing Note R Pellizzari referred to the attached briefing note reminding the group that HUs are required to provide low-cost contraceptives under the OPHS Her board is having trouble with this now that the compassionate contraceptives assistance program is no longer available and that samples are becoming scarcer She suggested that options for a purchasing co-op might be considered by COMOH She noted that Erika Bontovics at the PHD has done a survey on this issue but she has not seen it and isnrsquot sure if any of the data would be useful for this discussion It was suggested that the Government Pharmacy be considered as a bulk purchaser but it was pointed out that this is not an option given that public health charges for these products alPHa was also suggested but acting as a clearing house for pharmaceuticals would be far outside of the Associationrsquos scope and mandate R Pellizzari added that larger health units are able to negotiate good deals based on volume and wondered if there is a potential for them to make purchases on behalf of the smaller health units that do not enjoy this advantage
There was support for further exploration but it was agreed that more information would be beneficial As an initial step RPellizzari will contact Erika Bontovics in an effort to examine the date described above with a view to determining what further information (eg costs negotiated by each HU) might be needed 45 Children and Youth Data Strategy Slide Deck ndash Aug 15 Teleconference amp ICES
Privacy Code V Jaeger referred to the linked ICES presentation and reported that discussions are underway on how to develop a data sharing strategy for the purposes of the attached by way of a working group of ICES COMOH and PHO She Robert Kyle and Michael Finkelstein have already agreed to participate but she invited others to express interest She will bring this up at PHLC and report back 46 Lyme Disease Testing Backgrounder J Hopkins reported that an increasing amount of staff time in Niagara is being devoted to responding to inquiries from the public regarding the different diagnostic methods being used to confirm Lyme disease in the US and Canada She is therefore asking COMOH if this is a prevalent enough issue that a request should be made to PHO to develop some explanatory materials that could be used to address them She clarified that they arenrsquot having much of a problem with physicians itrsquos more a matter of educating the public regarding the accepted approach to the prevention diagnosis and treatment of the disease R Schabas cautioned that public education is a double-edged sword as it has the potential to create the impression that Lyme disease is a bigger problem than it is P Stewart reported that her health unit had a good in-service by a PHO lab person that has been very helpful for the odd questions that come up There were differing opinions of how much effort should be devoted to this as it appears to be another example of ill-informed public opinion on a public health issue akin to anti-vaccination and anti-fluoridation attitudes While these attitudes should not be ignored therersquos not much we can do in the near term to alter them V Jaeger offered to raise this during her next monthly conversation with George Pasut 50 Addendum
51 MOH Retirement I Gemmill noted that Mike Corriveau (MOH ndash Renfrew) will be retiring in December after over thirty years of service He asked that the COMOH Executive consider some form of recognition 60 UPDATES INFORMATION ITEMS REPORTS
61 Public Health Leadership
Council
611 ndash PHLC Update e-Mail Update
612 ndash PHSSP Implementation Tables CMOH Memo ndash PHSSP Tables V Jaeger referred to the linked memo which the result of the desire for clarity and openness on how the topic-specific implementation tables would be assembled The PHLC has already received a number of expressions of interest and will be communicating next steps soon 62 COMOH Executive Committee Minutes June 11
Notes July 9 Minutes July 31
Minutes September 10
63 COMOH Built Environment Work Group
The BEWG has not met since the last meeting but will meet on October 7 During the summer that group led by C Gardner and Nikhil Rajaram developed the paper (COMOHrsquos Advice for the Provincersquos Review of its Long-Term Energy Plan) that was the basis for the letter that went to the province (see item 68 below) V Jaeger expressed appreciation for the work that went into that C Gardner has expressed interest in being a member of the Promoting Healthy Environments ndash Both Natural and Built PHSSP implementation table 64 Public Health Early Years Group Aug 9 Meeting Notes A Feller reported that this group is putting together a November 5 Grand Rounds at PHO 65 iPHIS Panorama
July 8 Update
66 Joint OPHAalPHa Health Equity Working Group R Pellizzari reminded that this is a joint initiative of alPHa and OPHA She will ensure that L Stewart provides minutes of these meetings for future updates She and L Simon are the COMOH reps on this group L Simon circulated a paper by the Wellesley Institute that examines the health equity impacts of cessation of community water fluoridation which was requested by the HEWG She added that Bob Gardner Director of Policy at the Wellesley Institute is now participating in this group and he would welcome suggestions for other subjects for health equity impact assessments M Klassen suggested that Radon might be a good one She also reported that the National Collaborating Centre for Determinants of Health hosted a discussion for the nurses that have been hired under the SDOH portfolio in order to more clearly identify what the specific mandate of public health is in this area and to identify reasonable evaluative measurements This is being proposed as the basis of a Locally Driven Collaborative project and three health units are already involved (PCCHU Toronto and Durham) but more are required and any assistance would be welcome HEWG is also working on positions on the minimum wage review and the poverty strategy Both of these will be circulated once complete and approved
It is also working on a TOPHC session on Cultural Safety related to working with aboriginal populations Feedback was also invited on this with a note that the deadline for abstract submission is September 27 Finally work is also being done with PHO on developing resources and supports for work with Priority Populations 67 COMOH Electronic Mailing List List of Subscribers 68 COMOH Correspondence Aug 26 COMOH Letter ndash Energy Policy
Aug 8 COMOH Letter ndash CMA Poverty Report
July 22 COMOH Letter ndash Immunization Data
70 Next MeetingAdjournment Meeting adjourned at 1035 Next Section meeting will be on November 15 2013 in Toronto part of the alPHa Fall Symposium
Page 1 of 8 ndash DRAFT FOR COMOH DISCUSSION
alPHa Membership Survey hello
Draft Report ndash COMOH Version hello
alPHarsquos membership was surveyed in the fall of 2013 Similar surveys were administered to all member groups ie COMOH BOH Section and Affiliates using the online survey tool Survey Monkey Small alterations were made to group-specific surveys to ensure that the survey questions were relevant to each group A total of 84 responses were received from alPHa members The breakdown of respondents was as follows This draft report is provided for discussion purposes to COMOH members and therefore focuses on the responses provided by COMOH members To provide additional information overall survey responses are also provided for some questions
SECTION 1 RESPONDENT PROFILE
Survey Question What region is your health unit located in
For COMOH members responses came from 6 of the 7 regions of Ontario All 7 regions were represented in the full set of survey responses
Summary of Respondents COMOH 27 32 BOH Section 34 40 Affiliates 23 27 Totals 84 100
All ResponsesEastern 24 29South West 12 14Central East 13 15Central West 15 18North East 11 13Toronto 5 6Not Sure 3 4North West 1 1Totals 84 100
All COMOH ResponsesEastern 3 11South West 5 19Central East 6 22Central West 6 22North East 3 11Toronto 4 15North West 0 0Totals 27 100
Page 2 of 8 ndash DRAFT FOR COMOH DISCUSSION
Survey Question How long have you been involved with public health in Ontario
Survey Question Have you participated on the alPHa Board of Directors or an alPHa or COMOH committeeworking group
All ResponsesYes in the last 1 to 2 years 15 18Yes in the last 2 to 5 years 9 11Yes more than 5 years ago 9 11No not ever 51 61Totals 84 100
All COMOH ResponsesOver 10 years 17 635 to 10 years 7 262 to 5 years 3 11Totals 27 100
All ResponsesOver 10 years 34 405 to 10 years 21 252 to 5 years 21 251 to 2 years 3 4Less than 1 year 5 6Totals 84 100
All COMOH ResponsesYes in the last 1 to 2 years 7 26Yes in the last 2 to 5 years 4 15Yes more than 5 years ago 8 30No not ever 8 30Totals 27 100
Page 3 of 8 ndash DRAFT FOR COMOH DISCUSSION
SECTION 2 PROFESSIONAL DEVELOPMENT
Survey Question Which of the following events have you attended at least once in the past two years
Survey Question Overall how satisfied have you been with alPHa events ie conferences meetings
Survey Question How much value do alPHarsquos events provide for the money
Survey Question How can alPHa make its events more valuable to you Please share any suggestions regarding future topics speakers formats duration locations or any other event component that is important to you
Comments about content bull Expert speakerpanels on emerging or hot topics
(2) bull More engaged dialogue with Ministry rather than
just updates bull Fewer Ministry updates (3) bull Content on medicalPH issues is better left to PHO
TOPHC and joint conferences (2) bull alPHa should stick to Ministrypoliticspolicysenior
PH supportPHU support on key priorities (eg November practical conference on HKP report)
bull For COMOH more discussion bull More time for section activities like face-to-face
COMOH meetings
bull More facilitated work groups of COMOH members to respond to public health practice questions
bull More focus on rural and northern issues bull Infection Control Logistical Considerations bull Consider partnering with other groups bull More collaboration with PHO and OPHA events bull Use of video conferencing bull Less frequentfewer meetings (2) bull Connect with CME Location bull Consider other venues than TO
( ) brackets indicate that more than one response included a similar comment
More than enough value 7 11A lot of value 34 52Some value 22 34A little value 2 3Not enough value 0 0Totals 65 100
All Responses for those who Attended at least One Event in the Last 2 Years
All COMOH ResponsesMore than enough value 4 15A lot of value 13 48Some value 9 33A little value 1 4Not enough value 0 0Totals 27 100
Page 5 of 8 ndash DRAFT FOR COMOH DISCUSSION
SECTION 3 VALUE FOR MEMBERSHIP
Survey Question What do you value the most about your alPHa membership
The comments provided in response to the text response question What is the most important benefit of alPHa membership for you personally supported the answers illustrated in the chart above 15 of the 20 comments provided focussed on the importance of opportunities to interact with colleagues across the province The next most important benefit mentioned was the support for COMOH members to work on public health issues together When asked What is the most important benefit of alPHa membership for your health unit COMOH members emphasized the following bull A coordinated and collective voice in advocating for public health issues and the public health sector (9) bull Opportunities to connect with other public health units to share experiences and best practices (8) bull Maintaining relationships with government both politicians and bureaucrats (3) and bull Support for boards of health (3)
Page 6 of 8 ndash DRAFT FOR COMOH DISCUSSION
Overall Level of Satisfaction
SECTION 4 LOOKING TO THE FUTURE
The questions in this section were asked to obtain input from alPHa members regarding a proposal from alPHarsquos Board of Directors to focus the Association on five service areas COMOH members were asked to indicate their level of agreement with the proposed areas of focus COMOH responses compared to the overall survey responses were as follows
To explore some proposed changes to Association services COMOH members were asked to provide their level of agreement with the following questions
COMOH Responses BOH Section Affiliates All Survey Responses
Strongly Agree
AgreeNeither Agree or Disagree
DisagreeStrongly Disagree
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1Promoting the role and value of local public health units
15 9 2 0 0 26 92 93 95 94
2
Providing important information to members about trends and events that will impact the public health system and management of public health units
10 8 8 0 0 26 69 97 86 85
3Facilitating professional networking and information sharing
13 10 3 0 0 26 88 83 82 85
4
Providing professional development to support excellence in public health unit leadership management and governance
3 15 7 1 0 26 69 83 86 79
5
Responding to public health sector issues when it makes the most sense to have a collective voice ie issues that impact the structure and funding of the public health sector and public health units and issues that have a broad focus on population health
15 8 2 0 1 26 88 97 95 93
PROPOSED AREAS OF FOCUS
COMOH Responses BOH Section Affiliates All Survey Responses
Strongly Agree
AgreeNeither Agree or Disagree
DisagreeStrongly Disagree
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1
COMOH and other professional groups within alPHa should do their own advocacy while alPHa supports members to share and support each others advocacy efforts
7 6 6 6 1 26 50 58 45 52
2
alPHa should provide support to action-oriented inter-professional work groups on priority public health unit issues and member resolutions
4 13 5 3 1 26 65 81 86 77
PROPOSALS
Page 8 of 8 ndash DRAFT FOR COMOH DISCUSSION
COMOH members were also asked to indicate the level of acceptability for some possible changes to alPHarsquos services and way of doing business
COMOH Responses BOH Section Affiliates All Survey Responses
Very Acceptable
Somewhat Acceptable
Neither Acceptable or Unacceptable
Somewhat Unacceptable
Very Unaccept
able
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1Single conference with additional face-to-face section meetings
21 2 0 1 0 24 96 68 80 81
2alPHa to offer alternatives like webinars on focussed topics
13 6 1 4 0 24 79 50 90 71
3Coordinate COMOH meetings with PHO OMA or Ministry events
16 4 2 0 0 22 91 na na --
4
Increase focus on building leadership and management capacity for health unit CEOs and senior management
7 9 4 3 0 23 70 na 70 70
5
Would it be acceptable for alPHa to request voluntary financial contributions from member PHUs in addition to annual fees
3 5 5 4 5 22 36 7 26 21
6
Would it be acceptable for alPHa to request voluntary in-kind staff contributions from member PHUs to expand alPHas capacity eg communications policy work group support
7 11 1 1 3 23 78 31 45 50
7Would it be acceptable to you for alPHa to discontinue staff support for COMOH (BOH Section)
0 4 1 5 14 24 17 11 na 14
8
Would it be acceptable to you for alPHa to reduce the amount of staff support for COMOH (BOH Section)
1 6 1 8 6 22 32 26 na 29
9
Would it be acceptable to you for alPHa to provide supports to MOHs and AMOHs (BOH Members) without maintaining COMOH (BOHs) as a section of the association
3 2 3 2 12 22 23 17 na 20
10
Would it be acceptable to you for alPHas Board of Directors to move from the current representational model to a skills-based strategic model ie board membership would be based on the skills needed to carry out alPHas strategic plan
6 11 2 1 3 23 74 56 56 62
11
Would it be acceptable to you for alPHas President Vice-President and Treasurer to be elected from the full membership of the alPHa Board of Directors (rather than the current model of alternating between BOH and COMOH members)
10 8 1 2 2 23 78 70 70 73
PROPOSED CHANGES
1 Council of Ontario Medical Officers of Health Terms of Reference
ASSOCIATION OF LOCAL PUBLIC HEALTH AGENCIES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
TERMS OF REFERENCE NAME 1 The name of the organization shall be ldquoThe Council of Ontario Medical Officers of
Health a section of the Association of Local Public Health Agencies (alPHa)rdquo hereinafter referred to as ldquothe Councilrdquo
MISSION 2 As local leaders in public health we are committed to improving the health of
Ontarians and increasing health equity by strengthening Ontariorsquos public health system We achieve this through system leadership and coordination in collaboration with the provincial government and other organizations and through evidence-informed advocacy on public health policy
OBJECTIVES 3 The objectives of the Council shall be
a) To provide strong province-wide leadership in public health
b) To advocate for health protection and promotion policies and programs that maintain and improve the health of Ontarians
c) To promote and maintain the highest standards for Ontariorsquos public health
programs and services
d) To support the planning implementation and evaluation of effective and efficiently run public health programs and services
e) To act as a forum for sharing information and resources and for addressing and
discussing public health issues both amongst the Councilrsquos members and other agencies that support the goals of alPHa eg Ontario Medical Association Ontario Public Health Association etc
f) To engage with and to provide public health and related policy advice to alPHa
the Chief Medical Officer of Health the Ontario Ministries of Health and Long-Term Care (including the Health Promotion and Public Health Divisions) Children
2 Council of Ontario Medical Officers of Health Terms of Reference
and Youth Services and other provincial ministries Public Health Ontario Health Canada the Public Health Agency of Canada and other public health partners
g) To promote and protect the professional interests of its members
h) To provide support to individual members as needed
i) To seek recognition for outstanding practice from among the members
j) To support evidence based practice of public health medicine
k) To engage and involve the membership to participate in COMOHrsquos endeavours
l) To mentor Public Health and Preventive Medicine Residents
MEMBERSHIP 4 Membership on the Council in each of the following categories is subject to the
limitations imposed by the current terms of reference and all policies and governing documents of the Association of Local Public Health Agencies Benefits of membership in each category are included in Appendix A These shall be subject to regular review and may be suspended under certain circumstances
Active membership in the Council shall be open to all Associate Medical Officers of Health and all full-time Medical Officers of Health whose Boards of Health are members of alPHa Such members shall have full voting privileges and may hold office in the Council Associate membership shall be open to all full and part-time physicians employed by a Board of Health that is a member of alPHa Such members shall not have voting privileges nor hold office
Affiliate membership shall be open to the following individuals interested in furthering the objectives of the Council
bull Public Health and Preventive Medicine Residents and Public Health and Preventive Medicine Residency Program Directors
bull Federal public health physicians working in Ontariorsquos First Nations communities
bull other public health or related physicians including those employed by a Board of Health that is not a member of alPHa
Such members shall not have voting privileges nor hold office
3 Council of Ontario Medical Officers of Health Terms of Reference
Emeritus membership shall be open to all former members who have retired after five (5) or more years of Active membership subject to the nomination in writing of two (2) active members in good standing endorsement of the Executive Committee and approval of the Council by majority vote at a general meeting Such members shall have neither voting privileges nor hold office but may be invited to attend general meetings Honorary membership shall be open to any non-active or associate member subject to the nomination in writing of two (2) active members in good standing endorsement of the Executive Committee and approval of the Council Such members shall have neither voting privileges nor hold office but may be invited to attend general meetings
OFFICERS 5 The Officers of the Council shall be the Chair Vice-Chair and immediate Past Chair
6 The Chair shall prepare the agendas of all Council meetings She shall preside and
preserve order at all such meetings shall ensure that these Terms of Reference are upheld and enforced and shall contribute to the supervision and evaluation of any Public Health and Preventive Medicine Resident who is on a placement with alPHa
7 The Vice-Chair shall fulfill the duties of the Chair in hisher absence The immediate
Past Chair may fulfill the duties of the Chair or Vice-Chair in their absences 8 The Chair shall normally serve a term of one (1) year which is renewable once and
after which the Vice-Chair shall normally assume the vacated office COMMITTEES 9 The Council shall elect seven (7) active members one from each of alPHarsquos regions
and the active member who is scheduled to serve as the President or immediate Past-President of alPHa to represent it on the alPHa Board of Directors These seven (7) members shall constitute the Councilrsquos Executive Committee and shall serve a term of at least one (1) year The Chair and Vice-Chair shall be elected from among the Executive Committee members If alPHarsquos immediate Past President is an active member she shall be an ex-officio member of the Executive Committee
10 The mandate of the Executive Committee shall be to facilitate the achievement of
the objectives of the Council by fulfilling the following
a Identifying priorities 1
1 See Appendix B Planning Cycle to Identify Priorities for COMOH
and ensuring the development of briefing documents and or recommendations as appropriate for the consideration of the Council
4 Council of Ontario Medical Officers of Health Terms of Reference
b Setting agendas and otherwise ensuring preparations for Council meetings c Ensuring the fulfillment of the direction of Council d Responding in a timely fashion to time-sensitive public health matters in
accordance with the Executive Committeersquos understanding of the perspective of the Council
e Engaging with the Chief Medical Officer of Health Associate Chief Medical Officers of Health and other provincial public health leaders and
f Representing Council at public and partner agency forums including the Public Health Leadership Council which shall normally include membership from the Officers of the Council and two other Executive Committee members as selected by agreement among the Executive
g Identifying opportunities for the recognition of outstanding practice from among the members including the annual nomination of at least one member for the alPHa Distinguished Service Award
11 The Executive Committee shall meet and correspond in the manner and at the times
and if required places as deemed necessary by the Chair to conduct the business of the Council A quorum shall consist of four (4) members
12 The Executive Committee shall have the power to strike committeestask or working
groups to assist it in carrying out the business of the Council 13 The Council may by special resolution remove a member of the Executive
Committee before the completion of hisher term of office and may elect a successor to complete the term The special resolution shall require a majority vote of 67 of the members present and voting at the meeting at which the special resolution is considered
14 A Nominating Committee shall consist of the three (3) most recent Past Chairs who
are able to serve and shall be chaired by the immediate Past Chair The Nominating Committee shall prepare a list of proposed Officers and Executive Committee members for the consideration of the Council at its Annual General Meeting
MEETINGS 15 The Council shall hold at least four (4) general meetings per year in a manner and at
the times and if required places as deemed necessary by the Executive Committee to share information direct and assist the Executive Committee in conducting the business of the Council
16 The Council shall hold its Annual General Meeting during and at the same place as
the alPHarsquos Annual Conference
5 Council of Ontario Medical Officers of Health Terms of Reference
17 The Council shall hold a special meeting at the call of the Chair or upon the written request specifying the purpose of such meeting of at least five (5) active members Council members must be given at least 48 hours notice of any special meeting
18 Only Councilrsquos active and associate members and alPHa staff are entitled to attend
general and special meetings of the Council Other members and non-members may be invited to attend all or part of such meetings as determined by the Chair preferably in consultation with the Executive Committee Non-members who come to such meetings without an invitation may attend all or part of the meeting by a majority vote of the active members present and voting
19 The Chair shall prepare the agendas for such meetings and shall normally include
reports from the Chair and the Councilrsquos committeestask or working groups and representatives to external bodies alPHarsquos Executive Director shall ensure that the minutes shall be recorded and promptly distributed to the Section
20 A quorum for all such meetings shall be ten (10) active members 21 The Council shall normally be notified in a manner deemed appropriate by the Chair
of such meetings at least one (1) month prior to their being held 22 A majority vote of the members present at such meetings and voting shall make
Council decisions In the case of a tied vote the Chair shall cast the deciding vote The Executive Committee shall ensure that actions arising from such decisions at such meetings are implemented and monitored
23 The Chair may solicit advice from the Council through the use of teleconferencing
and alPHarsquos electronic mailing lists in order to gain an understanding of the overall perspective of the Council (see 10d)
ELECTIONS 24 The Officers and Executive Committee members shall be elected at the Sectionrsquos
Annual General Meeting The Nominating Committee Chair or hisher designate shall present a list of nominations Additional nominations from the floor shall also be considered Each Officer and Executive Committee member shall be elected by secret ballot if necessary by a majority of the active members present and voting In the case of a tie the Chair shall cast the deciding vote
AMENDMENTS 25 The Councilrsquos Terms of Reference may be amended from time to time by the
Executive Committee provided the Committee receives notice of such proposed amendments at least one (1) month prior to the meeting at which the amendments
6 Council of Ontario Medical Officers of Health Terms of Reference
will be considered Such amendments shall be ratified by the Council at the next general meeting or the Annual General Meeting as the case may be
26 The Executive Committee shall review the Terms of Reference as required and not
less than once every two years Original September 1987 1st Revision October 2000 2nd Revision July 2001 3rd Revision December 2003 4th Revision February 2008 5th Revision June 2009 6th Revision June 2011 7th Revision June 2013
7 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX A
COMOH Membership Benefits Active Membership
bull Entitled to attend all meetings of the Section bull May hold office on the COMOH Executive Committee alPHa Board of Directors
Standing Committees bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Associate Membership
bull Entitled to attend all meetings of the Section bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Affiliate Membership
bull May attend meetings or parts thereof subject to approval of Chair bull May serve on ad-hoc committees of the Section subject to the approval of the
Executive Committee bull Discounted registration rates for alPHa Conferences (for Public Health and
Preventive Medicine Residents) bull Upon written request and subject to COMOH Executive approval Affiliate
Members may subscribe to comohlistsalphaweborg The approval will be reviewed on an annual basis in order to determine if the Affiliate Member can remain a subscriber to mohsalphaweborg
Emeritus Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair bull Enjoy discounted registration rates for alPHa Conferences and regular COMOH
meetings bull Subscription to comohlistsalphaweborg electronic mailing list bull Full access to alPHa Web site bull May represent alPHa COMOH on selected external committees and working
groups Honorary Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair
8 Council of Ontario Medical Officers of Health Terms of Reference
bull May represent alPHa COMOH on selected external committees and working groups subject to the approval of the COMOH or alPHa Executive Committee as appropriate
9 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX B
Planning Cycle to Identify Priorities for COMOH
1 There shall normally be a COMOH membership strategic planning retreat every four years In recognition of the dynamic environment of public health the need for and timing of such a retreat shall be at the discretion of the Executive Committee in consultation with the membership
2 The COMOH Executive is responsible (through the creation of a subcommittee of COMOH members) for ensuring the preparation for the COMOH retreats with resources to include those provided by alPHa
3 Leadership for action on COMOH priorities will be recruited from among the COMOH membership in order to make good use of the full base of capacity of the membership The resources to support actions will be recruited from both within and beyond the COMOH membership employing other public health professionals that reside within the broader public health system and community
4 The COMOH Executive shall ensure an annual review of strategic priorities and initiatives and the development of a draft report of the same for the review of the members at the June meeting
2013 Strategic Planning
Considerations for COMOH
As part of its strategic planning discussions alPHarsquos Board has been considering changes to the level of support provided to member sections A member survey is being carried out over the fall to determine options acceptable to alPHa members The following approach to support is put forward as a proposal for the consideration of COMOH Note that the feasibility of the points below depend upon future decisions of the alPHa board They assume that COMOH remains part of alPHa but becomes more independent in administering meetings
1 alPHa can provide to COMOH staff support (Gord Fleming) amounting to 02 FTE or one day per week This is a reduction from the current level of 35 days per week COMOH can choose to use the support any way it wants writing COMOH letters meeting minutes agenda support special projects etc
2 In addition to 02 FTE alPHa staff would provide support for up to 4 face-to-face meetings per year One meeting would be concurrent to alPHarsquos annual conference in June The timing of other meetings could be negotiated The support includes consulting on the development of the program arranging for speakers registration for the event arranging venue AV support and hospitality services
3 In addition to 02 FTE alPHa staff would provide support for setting meeting dates and any polling required to establish dates Note that the individual supporting this function would be Karen Reece
4 COMOHrsquos Executive and Section would continue to have access to online supports through the alPHa including the COMOH Listserve and a group page for posting agendas minutes and other resources on the alPHa website
5 alPHa staff (Linda Stewart and Gord Fleming) can also start participating on CMOH calls as a way to be up-to-date on issues related to COMOH
6 Other than what is outlined above COMOH would be expected to prepare agendas and take minutes for its Executive and Section meetings The Executive would be expected to operate more independently than it does now but would be able to access the supports outlined above
Prepared by Linda Stewart Executive Director
From comoh-bounceslistsalphaweborg on behalf of Christopher MackieTo MOH ListserveSubject [comoh] Fw URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)Date Wednesday October 30 2013 91241 AMAttachments ATT00249txt
For AMOHs and PHPM residents who didnt receive the initial email
Chris
Christopher Mackie MD MHSc FRCPCMedical Officer of Health and CEOMiddlesex-London Health Unit50 King St LondonON N6A 5L7 O 519 663 5317 ext 2444 wwwhealthunitcomFrom Pisko Laura (MOHLTC)Sent Tuesday October 29 2013 759 PMTo kbarkeralgomapublichealthcom malcolmlockbchuorg davidcchatham-kentcarobertkyledurhamca proumeliotiseohuca fwarshelginhealthonca mohelginhealthoncahlynnpublichealthgreybruceonca malcolmlockhnhuorg hnmohhnhuorglnoseworthyhkpronca bobnosalhaltonca elizabethrichardsonhamiltoncarschabashpechuonca ncameronhuroncountyca drimgemmillkflapublichealthcamohkflapublichealthca suditranadecounty-lambtononca paulastewarthealthunitorgChristopher Mackie valeriejaegerniagararegionca jimchiriconbpsdhuca jarthursnwhuoncaisralevyottawaca dnealoxfordcountyca davidmowatpeelregionca mklassenpdhuoncarpellizzaripcchuca rosemarieramsinghporcupinehuonca mcorriveaurcdhucomcharlesgardnersmdhuorg sutcliffepsdhucom davidwilliamstbdhucomspruytmtimiskaminghucom dmckeowntorontoca lnolanregionofwaterloocanicolamercerwdghuorg aheimannwechealthunitorg karimkurjiyorkcaCc coreywesleytbdhucom CindyBaker-Barillsmdhuorg Donna Kosmack pilonlsdhucomPaulaMuiskflapublichealthca sthibautorontoca Mueller Daina (MOHLTC) Gordon Marcus(MOHLTC) andreakitahamiltoncaSubject URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)
Dear Colleagues The ministry has received reports that some tobacco vendors across the province aregiving away single cigarettes with the purchase of tobacco products It is the ministryrsquosposition that giving out free single cigarettes does not violate subsection 31(3) of theSmoke-Free Ontario Act (ldquoSFOArdquo) Although the practice of giving out free singlecigarettes may promote the sale of tobacco products it does not take the form of aldquoproduct enhancement product association or promotional materialrdquo and therefore doesnot fall within the scope of subsection 31(3) of the SFOA We have confirmed with Health Canada that this practice may violate section 29(b) of thefederal Tobacco Act As such Health Canada is requesting that you notify them in writingand I am directing you to communicate with them via email and provide to them as manydetails as possible Emails should be sent to Tobacco-Ontariohc-scgcca and thesubject line should read ldquoViolation of Section 29(b) of Tobacco Actrdquo This will ensurethat the complaints are given priority status by Health Canada We will continue to monitor
this situation and liaise with our colleagues at Health Canada Please share this information with your tobacco control staff and contact me or DainaMueller Manager Tobacco Control Unit Health Promotion Implementation Branch atdainamuellerontarioca with any questions RegardsLaura Laura A PiskoDirectorHealth Promotion Implementation BranchHealth Promotion DivisionMinistry of Health and Long Term Care416-327-7445 (office)416-451-3185 (mobile) Marcus Gordon - EA (416)326-0625 for urgent issues
========= Middlesex-London Health Unit E-Mail Disclaimer =============______________________________________________________________
Private and confidential intended only for named recipient If otherwisereceived please destroy immediately Health information in this email isonly general information and is not intended to replace an in personconsultation with a medical professional nor is it intended to providemedical advice Individual circumstances of which we are not aware mayaffect the information provided herein and as such the Middlesex-LondonHealth Unit assumes no liability or responsibility for your reliancethereon The Middlesex-London Health Unit works under the authority of theHealth Protection and Promotion Act and this correspondence may be used toassess your needs for public health services (519-663-5317 ext 2448)______________________________________________________________
From Gardner CharlesTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes (RayCopesoahppca)
George Pasut (GeorgePasutoahppca) Peter Cooney (petercooneyhc-scgcca)Cc Ito DickSubject Discontinuation of Fluoridation in MuskokaDate Tuesday October 22 2013 125254 PM
Hello Colleagues
As I reported in my email below on September 26th fluoridation has come under challenge again inSimcoe Muskoka I am now very unhappy to report that despite our best efforts last night theDistrict Council of Muskoka voted to remove fluoride from municipal drinking supplies across theDistrict This brings to an end fluoridation in all of Simcoe and Muskoka (with the exception of Base Borden)ndash though New Tecumseth will be conducting a plebiscite on the question of fluoridation with themunicipal election next October Defending community water fluoridation has drained a great deal of time human resources andcommitment from other priorities and has been exhausting here in SMDHU as I am sure it hasbeen in many other health units While the outcomes have been very disappointing I have beenimpressed by the professionalism and dedication that SMDHU staff members have shown inshouldering this burden In particular our dental consultant Dr Ito has provided us with much ofthe foundational knowledge and the local research essential to our efforts and has very frequentlyattended and presented at council meetings and other public events I would also like to thank themany of you who have offer and provided support including advocacy letters and informationresources Over the years Dr Peter Cooney Chief Dental Officer of Health of Canada has beenvery helpful attending and presenting with us at council meetings and at public consultationevents We will of course continue our oral health surveillance of the children of Muskoka documentingand reporting in future years on the increase in dental decay that we anticipate will occur Suchsurveillance is the foundation of our advocacy both to municipal politicians and to the province I am very concerned that our experience will continue to repeat itself across the province unlessthere is strong leadership provincially It is with this in mind that I raise the followingrecommendations for your consideration
1 That we collectively (with PHOrsquos leadership) conduct high quality publish-worthy researchdocumenting the impact on dental decay that occurs in those municipalities throughoutOntario that in recent years have discontinued community water fluoridation This could bepart of a larger study on such municipalities across the country and it could also be part ofa study documenting overall oral health (including fluoridation coverage) in the province(and possibly across the country)
2 That COMOH engage with our Chief MOH to advocate for the province to require allmunicipal water supplies to be fluoridated (the exception of course being those withnaturally sufficient fluoride concentrations) This could built upon the alPHa position to
Gordon
Highlight
Gordon
Highlight
date (A11-00 - Community Water Fluoridation) on the CMOH position (Oral Health ndash) and on theemail discussion generated on the COMOH listserv some months back re Richardrsquosproposal (calling on the province to fund municipal water fluoridation)
Valerie I request that this be an item for our COMOH meeting on November 15th Sincerely Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorg From Gardner Charles Sent Thursday September 26 2013 245 PMTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes(RayCopesoahppca)Subject Community Water Fluoridation Under Challenge Again in Simcoe Muskoka Hello Colleagues You may wish to know that community water fluoridation (CWF) is again under challenge in SimcoeMuskoka specifically both in Tottenham (Town of New Tecumseth in Simcoe County) and for theentire District of Muskoka On Monday September 23 Committee of the Whole Council of theTown of New Tecumseth voted to submit application to discontinue community water fluoridation(CWF) in the town of Tottenham despite presentations to the contrary from our dental consultantDr Ito and from me The next Council meeting is scheduled for Monday Sept 30 at which lastMondayrsquos (Sept 23) votes will be ratified
Since Monday I have spoken with the Mayor of the Town of New Tecumseth and with most of thecouncilors encouraging deferral of a decision on Monday to allow the town more time to make afully informed decision
This is the second time in recent years that the issue of discontinuing CWF in Tottenham has beenraised at council This issue is also scheduled to return again to the District of Muskoka Council on
October 21st where I will be presenting in response to deputations in opposition to fluoridation
Outside of Base Borden Tottenham is the only community with fluoridated water in SimcoeCounty The health unitrsquos own screening data between 2011 and 2013 shows that Tottenhamrsquos
Gordon
Highlight
children as well as those in Muskoka have a lower rate of dental decay than Simcoe Muskokacommunities without CWF
Sincerely
Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorgChuck Gardner MOH
November 04 2013
Mandatory State Laws on Fluoridation Thirteen states Puerto Rico and the District of Columbia have laws intended to provide
statewide fluoridation These states and the year that the fluoridation legislation was passed are
District of Columbia (1952) Connecticut (1965) Kentucky (1966) Illinois (1967) Minnesota
(1967) Ohio (1969) South Dakota (1969) Georgia (1973) Nebraska (1973 and 2008)
California (1995) Delaware (1998) Puerto Rico (1998) Nevada (1999) Louisiana (2008) and
Arkansas (2011) (see Table 1) The sizes of the public water systems or countiescommunities
affected and exemption provisions vary by state Table 1
STATES THAT HAVE MANDATORY LAWS ON FLUORIDATION -2011
State (1) Year of
Fluoridation
Legislation (1)
Population
served by
Fluoridated
CWS (2)
Persons
receiving
fluoridated
water (2)
State
Average
Caries
Experience
of Grade 3
Students (3)
Arkansas 2011 647 1724131 64
California 1995 621 22812721 709
Connecticut 1965 910 2370423 406
Delaware 1998 862 705344 545
Georgia 1973 921 8924598 52
Illinois 1967 993 11325132 532
Kentucky 1966 999 4334223 598
Louisiana 2008 407 1846149 657
Minnesota 1967 988 4117266 549
Nebraska 1973 and 2008 702 1001665 593
Nevada 1999 702 1001665 649
Ohio 1969 877 8772683 512
South Dakota 1969 948 642942 623
District of
Columbia
1952 1000 595000
Puerto Rico 1998
United States 739 204283554
2010 Statistics for population fluoridated and number of people
1 Communication with Jane McGinley RDH MBA Manager Fluoridation and Preventive Health
Activities Council on Access Prevention and Interprofessional Relations
2 Centers for Disease Control and Prevention Department of Health and Human Services
accessed Oct 21 2013 httpwwwcdcgovfluoridationstatistics2010statshtm
3 Centers for Disease Control and Prevention National Oral Health Surveillance System Caries
Experience - Percentage of 3rd Grade students with Caries Experience (treated or untreated tooth
If data from 43 states for the percentage of Grade 3 children with experience of dental decay is
compared with the 2008 percentages of the population in a state with Community Water
Fluoridation then the percentage of children with experience of dental decay decreases as the
percentage of the state population with Community Water Fluoridation increases (see Figure 1)
Figure 1
Correlation of Percentage of Grade 3 Children with Caries Experience and
Percentage of Population With Community Water Fluoridation for 43
Reporting States
0
10
20
30
40
50
60
70
80
0 10 20 30 40 50 60 70 80 90 100
State of Population With Community Water Fluoridation
Sta
te
of
Gra
de 3
Stu
den
ts w
ith
Cari
es E
xp
eri
en
ce
Data from CDC (2 3)
The description of the fluoridation laws in California Illinois and Nevada can be found on the
Association of State amp Territorial Dental Directors website(4 7 8)
The California fluoridation law AB 733 came into effect in 1995 requiring communities of 10
000 residents or more be supplied with fluoridated drinking water However the state did not
provide any funding to implement the legislation (California is unique in requiring fluoridation
without funding the practice)(4) The California Department of Health Services therefore had to
fund fluoridation initiatives from non-governmental sources ie the California Endowment
California Dental Association Foundation the First 5 Commission and others(5) From 1995 to
2011 the percentage of the California population receiving fluoridated drinking water has risen
from 17 to 625(6) 4 Dental Public Health Activities amp Practices Office of Oral Health California Department of Health
Services April 2002 httpwwwastddorgbestpracticesDES06002CAfluoridationpdf
5 Stock M Pollick H The CDA Foundation Model to Fluoridate Communities California Dental
Association Journal vol 40 no 8 649 - 655
httpwwwcdaorgPortals0journaljournal_082012pdf
6 California Dental Association Foundation
httpwwwcdafoundationorglearnadvocacyfluoridation
The State of Illinois passed a mandatory fluoridation state in 1967 and required all community
water systems to adjust fluoride levels in the drinking water to optimal levels within 1 year(7)
From 1962 when over 5000000 residents had optimally fluoridated drinking water by 2010
the number had risen to 11325132 (993 of the population on community water systems)(2)
7 Dental Public Health Activities amp Practices Division of Oral Health Illinois Department of Public
Health April 2002 httpwwwastddorgbestpracticesDES16007ILfluoridationpdf
The State of Nevada passed a mandatory fluoridation statute in 2000 for communities with
400000 or more residents(8) This was a result of the work of a statewide coalition that
included the Nevada Dental and Dental Hygienist Associations the Washoe and Clark County
District Health Departments the Clark County School District Junior League of Las Vegas
Head Start the Community College of Southern Nevada Dental Hygiene Program Health
Access Washoe County and Saint Maryrsquos Hospital For communities with less than 400000 the
implementation of fluoridation still required the vote of the majority voters in the community
The Las Vegas Water Authority and the City of Henderson started fluoridation in 2000
increasing the percentage of the population with fluoridated drinking water from 2 to 65 (8) 8 Dental Public Health Activities amp Practices Bureau of Family Health Services Nevada State Health
Division April 2002 httpwwwastddorgbestpracticesDES31002NVfluoridationbillpdf
Countries with Mandatory Laws on Fluoridation Countries that have mandated Community Water Fluoridation are Brazil Hong Kong
Malaysia Singapore Ireland Israel and some of the states in Australia
Singapore started fluoridating its water in 1956 based on the success of the fluoridation trials in
Grand Rapids Newburgh Evanston and Brantford Singapore became the first Asian country to
have 100 of its population benefitting from the implementation of fluoridated drinking water
Loh reported that ldquoThe ten year study on the effects of water fluoridation in Singapore showed
a decrease in caries prevalence in the children In the permanent dentition the reduction was
523 per cent for Chinese and 31 per cent for Malays in the 7 to 9 year old age group A similar
trend was observed in the mixed dentition in which the decrease was 325 per cent for Chinese
and 306 per cent for Malaysrdquo(9) By 2010 the population of the country was 5080000(10)
9 Loh T Thirty-eight years of water fluoridation--the Singapore scenario Community Dent
Health 1996 Sep13 Suppl 247-50
10 British Fluoridation Society One in a Million the facts about water fluoridation 3rd Edition
published March 2012) httpwwwbfsweborgonemillion0920One20in20a20Million20-
20The20Extent20of20Fluoridationpdf
Hong Kong started implementing community water fluoridation in 1961 and similar to
Singapore 100 of the population received access to fluoridated drinking water Lo and Wong
reported that ldquoThe mean DMFT score of the children deceased from 44 in 1960 to 15 in 1968
stayed at this level in the 1980 and 1986 surveys and further deceased to 08 in 2001 The
prevalence of dental fluorosis among the children surveyed in 1960 was 1 and this increased
to 59 and 70 in 1968 and 1980 respectively It was found in the 1986 and 2001 surveys that
the prevalences of fluorosis were 47 and 9 among children whose teeth developed at the
time when the respective water fluoride concentrations were 07 ppm and 05 ppmrdquo(11) The
population of Hong Kong was 6968000 in 2009(10) 11 LO ECM and WONG AHH Water fluoride concentration and fluorosis in Hong Kong in 1960-
2001 84th General Session and Exhibition of the International Association for Dental Research amp
1st Meeting of the Pan-Asian-Pacific Federation Brisbane Australia 28 June-1 July 2006 v 85 n
Sp B
The Malaysian cabinet approved a nationwide community water fluoridation program in 1972
(12) One of the states Sabah decided to stop fluoridation in 1989 due to concerns about
inadequate supervision in adding fluoride to the drinking water Oral Health Surveys in 2009
and 2007 indicated that children in Sabah had the worst oral health with 50 of 12 year-olds
having decay in their permanent teeth and children having an average of 3 teeth being(13)
Under the 10th Malaysian Plan in 2011 the federal and the Sabah state governments
reintroduced water fluoridation in Sabah(1314) In 2010 about 755 of the Malaysian
population or 20700000 people had fluoridated drinking water(1013) 12 Malaysian Dental Association Fluoride in Water
httpwwwmdaorgmy07_public_01healthcare_12htm
13 Sachdev N Fluoridation in Sabah Water for Cleaner Teeth French Tribunecom 28022011
From Levy IsraTo Jaeger ValerieCc Pim Carolyn gordonalphaweborg Diallo Aicha Penny Sutcliffe Paul Roumeliotis Michael Finkelstein
Hazel Lynn Robert KyleSubject FW Panorama - Privacy Security and other issuesDate Wednesday October 16 2013 122110 PM
Hello ValerieOttawa is part of Wave 4 Panorama implementation and we are gearing up increasingly to use thesystem where and if possible Thinking about it I am anticipating that this may need to be on theCOMOH (and alPHa) radar as it is something that will impact all health units and implies a majoroperational shift in vaccine delivery programs for all health units I have asked Carolyn Pim toconnect with our sister wave 4 units to share common experiences as we move forward ndash when wehave a roll up could I bring to COMOH Exec for discussion to explore whether there are broaderimplications for all members As an aside I have also asked the Ministry and their CIO to share with me any roll up learnings thatthey may have had already from previous waves (I understand that Niagara HU was a wave 1participant so if there is such a roll up of common experiences that others could learn fromperhaps you have it already and that could come to the exec too)Thanks Isra From Pim Carolyn Sent October 10 2013 1228 PMTo Christopher Mackie (christophermackiemlhuonca) Elizabeth Richardson(Elizabethrichardsonhamiltonca) H BSc M D F R C P (C) MPH Jim Chirico(jimchiriconbpsdhuca) Marlene Spruyt (spruytmtimiskaminghucom) Robert Kyle (Durham)Cc Levy IsraSubject Panorama - Privacy Security and other issues Dear colleagues Irsquom reaching out to you as fellow Panorama Wave 4 health units to ask about where yourorganizations are at in the process of signing agreements and completing Privacy ImpactAssessments and Threat Risk Assessments (TRAs) Ottawa Public Healthrsquos IT legal and informationsecurity advisors have made numerous requests to the MOHLTC for information (in particular theprovincial TRA) that we consider essential to develop our own risk assessment and PIA but havebeen told that information cannot be shared even with strict confidentiality and access controlsSo we are at somewhat of an impasse Isra emailed Arlene yesterday Arlene has forwarded ourconcerns to the Ministryrsquos CIO and Panorama lead but we havenrsquot had any response or discussionswith either of them yet Have your organizations identified similar concerns andor had interactions with the MOHLTC inthis respect Irsquod also be interested in knowing if your health units have flagged other (egoperational) implementation concerns Thanks
Carolyn ps Robert ndash you can ignore this request I talked with Sharan this morning about Durhamrsquos issuesso am including you now just for information Carolyn Pim MD FRCPC Associate Medical Officer of Health Meacutedecin adjointe en santeacute publique Ottawa Public Health Santeacute publique Ottawa 100 Constellation Cr Ottawa ON K2G 6J8 Tel teacutel (613) 580-6744 ext 23684Fax (613) 580-9641Connect With Ottawa Public Health
Suivez Santeacute publique Ottawa
This e-mail originates from the City of Ottawa e-mail system Any distribution use orcopying of this e-mail or the information it contains by other than the intendedrecipient(s) is unauthorized If you are not the intended recipient please notify meat the telephone number shown above or by return e-mail and delete thiscommunication and any copy immediately Thank you
Le preacutesent courriel a eacuteteacute expeacutedieacute par le systegraveme de courriels de la Ville dOttawaToute distribution utilisation ou reproduction du courriel ou des renseignements quisy trouvent par une personne autre que son destinataire preacutevu est interdite Si vousavez reccedilu le message par erreur veuillez men aviser par teacuteleacutephone (au numeacuteropreacuteciteacute) ou par courriel puis supprimer sans deacutelai la version originale de lacommunication ainsi que toutes ses copies Je vous remercie de votre collaboration
1
Smoke-Free Patios ndash An Amendment to the Smoke-Free Ontario Act
Date November 15 2013 Prepared for Council of Ontario Medical Officers of Health Prepared by York Region Public Health _____________________________________________________________________________ Issue
The Smoke-Free Ontario Act is the current provincial legislation that imposes smoking restrictions in workplaces and public places It prohibits smoking on restaurant and bar patios in instances where any portion of the seating area is covered by a roof With recent studies illustrating that exposure to second hand smoke outdoors poses similar risks to indoor exposure there has been growing public support to enhance smoking restrictions and make patios completely smoke-free
Background
With the implementation of the Smoke-Free Ontario Act in 2006 restaurant and bar patios became subject to smoking restrictions if any portion of the seating area was covered by a roof This allowed for patios without roof coverings to continue to allow smoking and as a result did not provide significant protection to patrons or staff from exposure to second hand smoke outdoors Many businesses chose to alter the design of their patios to allow smoking to continue In some cases patios became more crowded since smoking patrons who dine indoors often proceed outside onto licensed patios with their beverages to smoke York Region like most municipalities in Ontario is host to hundreds of patios being operated by restaurant owners and businesses With smoking prohibitions affecting only a small portion of these patios specifically ones with coverings the vast majority of patios still allow smoking to take place Patrons and employees on patios where smoking is not restricted are exposed to second hand smoke frequently This can contribute to increased disease and aggravation of existing health conditions From a business perspective the existing legislation has been viewed by many operators as unfair because some patios have permanent coverings which cannot be removed requiring a smoke-free status These business owners feel this creates an uneven playing field since they cannot provide an outdoor dining area for their smoking customers There is strong community support for smoke-free patios in Ontario A 2009 Rapid Risk Factor Surveillance System survey revealed 754 percent support in York Region while a Toronto Health Survey in 2011 indicated 74 percent public support
2
Current Status
Smoking is currently prohibited on restaurant and bar patios province-wide in four Canadian provinces and territories Alberta Newfoundland and Labrador Nova Scotia and Yukon A fifth province Prince Edward Island prohibits smoking on patios until 10 pm Since Ontario enacted legislation restricting smoking on patios in 2006 eight municipalities in Ontario have chosen to create bylaws that go beyond the Smoke-Free Ontario Act and enhance outdoor protection from second hand smoke by prohibiting smoking on patios completely The largest of those municipalities is the City of Ottawa Recently the Toronto Board of Health unanimously endorsed a report presented by their Medical Officer of Health recommending that restaurant and bar patios be made smoke-free through an amendment to the Smoke-Free Ontario Act
Key Considerations
There should be no significant financial burden to local Boards of Health resulting from a smoke-free patio amendment to the Smoke-Free Ontario Act Inspection and enforcement for the Smoke-Free Ontario Act is currently 100 percent funded by the Ministry of Health and Long-Term Care Following an introductory period of education on the amendment a complaint response model of service delivery would ensure ongoing compliance with smoke-free requirements A complete ban of smoking on patios would eliminate the widely-held perception by business owners that the current legislation creates an uneven playing field for business Since Smoke-Free Ontario Act inspections of patios began in 2006 operators have expressed the opinion that if patios need to be smoke-free for the protection of the public they should all be smoke-free to avoid undue hardship for individual businesses and to provide protection uniformly across the Province
Next steps
York Region Public Health intends to seek support from Medical Officers of Health across the Central East Tobacco Control Area Network (CETCAN) to advocate to the Ministry of Health and Long-Term Care for an amendment to the Smoke-Free Ontario Act prohibiting smoking on all restaurant and bar patios York Region is also in the process of requesting that its Regional Council advocate to the Minister of Health and Long-Term Care on the issue
Updating and Modernizing O Regulation 565 (Public Pools)
Date November 15 2013
Prepared for Council of Ontario Medical Officers of Health
Prepared by York Region Public Health _____________________________________________________________________________ Background Recent drownings at public pools in Ontario have highlighted the issue of water-borne illness and injury The current pool regulation under Ontariorsquos Health Protection and Promotion Act O Regulation 565 (Public Pools) is outdated It does not accurately reflect new pool technology and design or the changing use of public pools Neither does it incorporate admissions standards recommended by the Office of the Chief Coroner Further O Regulation 565 does not have short-form wording or set fines associated with it This limits public health enforcement capabilities What is the impact Updating O Regulation 565 (Public Pools) to address recent changes in pool technology design and uses and to include Coroner-recommended admissions standards would help improve pool safety Establishing short-form wording for O Regulation 565 would enhance enforcement related to public pools Currently the only enforcement available to Public Health Inspectors for dealing with non-critical regulatory infractions in public pools is the issuance of a Part III summons This involves a considerable amount of resources for a possible small fine With the development of inspection disclosure systems such as YorkSafe there is an even greater need to develop a method to effectively address repeated pool operator non-compliance with non-critical issues Next steps Public health units should advocate to the Province to 1) Conduct a review of O Regulation 565 (Public Pools) to address shortcomings Proposed changes to the
regulation should include a requirement for ownersoperators of public pools to advise the local Medical Officer of Health of any change in the use of a facility and the addition of the Coronerrsquos recommended admission standards
2) Provide short-form wording for O Regulation 565 so that public health inspectors can better deal with pool operator non-compliance
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
SECTION TELECONFERENCE September 18th 2013
900 ndash 1100 AM Please dial 1-866-518-0789 or 416-443-4586 and enter Conference ID 624258 to participate
PRESENT Valerie Jaeger (Chair) Kim Barker Lisa Berger Jim Chirico Janet DeMille Andrea Feller Ian Gemmill Allen Heimann Jin-Hee Kim Jessica Hopkins Miriam Klassen Karim Kurji Isra Levy Rosamund Lewis Hazel Lynn David McKeown Nicola Mercer Lynn Noseworthy Rosana Pellizzari Carolyn Pim Sudit Ranade Lisa Simon Richard Schabas Marlene Spruyt Paula Stewart Penny Sutcliffe Monir Taha Hsiu-Li Wang Bryna Warshawsky David Williams Lilian Yuan Gordon Fleming (alPHa Staff Recorder) Linda Stewart (alPHa Staff)
10 Call to Order Approval of Agenda Meeting called to order at 904 Agenda approved as circulated 20 Approval of Minutes June 4th 2013 Minutes Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning V Jaeger reported that the Executive has met four times since the last Section meeting and this remains a standing item on the Executive agenda It is their opinion that this process needs to be executed in concert with the plan that is being developed by alPHa at this time and decisions about processes and directions for COMOH will need to be informed by those taken by the parent Association There is a strong agreement about the importance of COMOH strengthening it as a group and reinforcing its relationships with public health sector partners including but not limited to the CMOH PHO and the MOHLTC The Executive will continue these discussions and keep the Section informed as appropriate 40 PUBLIC HEALTH ISSUES
41 Mandatory Immunization I Gemmill reported that the issue of Health Care Worker influenza immunization rates which remain quite low despite best efforts was discussed at a session at the most recent Canadian Immunization Conference Having accepted that mandatory HCW immunization is very unlikely to become public policy anytime soon the discussion focused on how to convince more HCWs that this is important He observed that only 10 of 36 public health units have policies for their own employees which may be rendering our
argument that hospitals should be developing policies of their own less convincing He suggested that COMOH might for a start consider facilitating the development of a template for policies on mandatory immunization of public health staff (subject to exemptions for people with no contact with others people already under contract etc) which could increase the number of health units with policies thereby increasing the credibility of the case He also suggested a process whereby the existing policies and procedures could be collected examined and synthesized into a legally defensible practical but non-binding template which would be palatable to health unit staff and their unions He agreed that a COMOH working group would be the most appropriate mechanism to do this but asked that alPHa begin the process by collecting the existing policies A Heimann reported that Windsor is discussing this issue ahead of its local public campaign and he thinks this is an excellent idea Rosana Pellizzari added that this process is a good opportunity for those who have policies in place to share lessons learned about unintended consequences experiences with grievances sorting out the NACI definition of high-risk groups and identifying classes of employees that could reasonably be exempt due to the nature of their work ACTION V Jaeger to invite members to submit questions and expressions of interest in participating on the proposed working group directly to I Gemmill and to forward existing policies and related information to G Fleming at alPHa for collection and assembly 42 HIV Non-Disclosure PHLC Briefing Note V Jaeger reminded the group that this was raised at the June Section meeting where it was determined that COMOH should take the lead on developing a procedure that would ensure greater consistency in how and under what circumstances Section 22 orders are used in cases of HIV non-disclosure She has since raised this with the CMOH who agreed that an Associate CMOH at the MOHLTC would be an appropriate person to take the lead on this but until those positions are filled this isnrsquot an available option She also reported that George Pasut has offered PHO support in the form of logistics and meeting space to support a COMOH working group if it is decided to create one She then indicated that L Yuan and R Shahin who have been the COMOH leads on this issue on previous agendas are unable to participate in this process right now so she invited expressions of interest R Schabas observed that this is an issue for which the Provincial public health leadership should take responsibility He suggested that COMOH can present recommendations but they should be framed by an expectation of the CMOH to exercise leadership and provide clear direction V Jaeger agreed to articulate this to Arlene but reiterated that the present request is for volunteers people are willing to sit and do the work R Schabas I Gemmill and A Heimann indicated interest ACTION V Jaeger to discuss the foregoing with the CMOH whose response will inform next steps including development of process and confirmation of expressions of interest 43 Supervised Injection Sites Draft COMOH Letter V Jaeger referred to the attached and stated that it is meant more as a starting point for discussion than to make any suggestions about what COMOHrsquos position should be and invited D McKeown to speak to the issues
D McKeown reported that this is something that Toronto has been looking at for some time and they have concluded that it would be beneficial to have this service available alongside others related to serving the health needs of injection drug users Hersquos looking for an expression of COMOH support for the idea of Safe Injection Sites (SIS) that will in turn support his case for a pilot site in Toronto that can be practically evaluated Responding to R Schabasrsquos question about why TPH isnrsquot just going ahead and doing it D McKeown noted that Provincial support will likely be required for funding (partly because it is considered a health service) and for obtaining the required federal exemption under the Controlled Substances Act Some members expressed discomfort with the idea of expressing specific support for one element of the broader strategy of harm reduction as it is a more downstream intervention than is the usual for public health is not one that is required or practical in many areas of the province and has significant political implications I Gemmill also indicated concerns with some of the papers that are most commonly used to support SIS which are predominantly policy papers and not scientific ones R Schabas observed that from a public health perspective harm reduction has been extremely effective in reducing blood-borne diseases and SIS appears to be an example if an area where we have an opportunity to make a difference As the evidence is so strongly in favour of harm reduction as a public health strategy he believes that COMOH should in fact have a voice on this D McKeown clarified that he is not asking for COMOH to take a position that public health should be responsible for SIS he is simply asking that COMOH take a position that this service should be available alongside the other elements of a comprehensive harm reduction strategy He agreed that this position need not elevate SIS above the other components of harm reduction nor does it need to make any statement of support for specific sites In the end it was agreed that COMOH should proceed in drafting an expression of support V Jaeger invited members to provide suggestions about what should and should not be included D McKeown indicated that this is not time sensitive but he would appreciate a response sooner than later ACTION V Jaeger to synthesize feedback into a document for initial review by the Executive prior to full review and endorsement by the Section 44 Access to Oral Contraceptives Briefing Note R Pellizzari referred to the attached briefing note reminding the group that HUs are required to provide low-cost contraceptives under the OPHS Her board is having trouble with this now that the compassionate contraceptives assistance program is no longer available and that samples are becoming scarcer She suggested that options for a purchasing co-op might be considered by COMOH She noted that Erika Bontovics at the PHD has done a survey on this issue but she has not seen it and isnrsquot sure if any of the data would be useful for this discussion It was suggested that the Government Pharmacy be considered as a bulk purchaser but it was pointed out that this is not an option given that public health charges for these products alPHa was also suggested but acting as a clearing house for pharmaceuticals would be far outside of the Associationrsquos scope and mandate R Pellizzari added that larger health units are able to negotiate good deals based on volume and wondered if there is a potential for them to make purchases on behalf of the smaller health units that do not enjoy this advantage
There was support for further exploration but it was agreed that more information would be beneficial As an initial step RPellizzari will contact Erika Bontovics in an effort to examine the date described above with a view to determining what further information (eg costs negotiated by each HU) might be needed 45 Children and Youth Data Strategy Slide Deck ndash Aug 15 Teleconference amp ICES
Privacy Code V Jaeger referred to the linked ICES presentation and reported that discussions are underway on how to develop a data sharing strategy for the purposes of the attached by way of a working group of ICES COMOH and PHO She Robert Kyle and Michael Finkelstein have already agreed to participate but she invited others to express interest She will bring this up at PHLC and report back 46 Lyme Disease Testing Backgrounder J Hopkins reported that an increasing amount of staff time in Niagara is being devoted to responding to inquiries from the public regarding the different diagnostic methods being used to confirm Lyme disease in the US and Canada She is therefore asking COMOH if this is a prevalent enough issue that a request should be made to PHO to develop some explanatory materials that could be used to address them She clarified that they arenrsquot having much of a problem with physicians itrsquos more a matter of educating the public regarding the accepted approach to the prevention diagnosis and treatment of the disease R Schabas cautioned that public education is a double-edged sword as it has the potential to create the impression that Lyme disease is a bigger problem than it is P Stewart reported that her health unit had a good in-service by a PHO lab person that has been very helpful for the odd questions that come up There were differing opinions of how much effort should be devoted to this as it appears to be another example of ill-informed public opinion on a public health issue akin to anti-vaccination and anti-fluoridation attitudes While these attitudes should not be ignored therersquos not much we can do in the near term to alter them V Jaeger offered to raise this during her next monthly conversation with George Pasut 50 Addendum
51 MOH Retirement I Gemmill noted that Mike Corriveau (MOH ndash Renfrew) will be retiring in December after over thirty years of service He asked that the COMOH Executive consider some form of recognition 60 UPDATES INFORMATION ITEMS REPORTS
61 Public Health Leadership
Council
611 ndash PHLC Update e-Mail Update
612 ndash PHSSP Implementation Tables CMOH Memo ndash PHSSP Tables V Jaeger referred to the linked memo which the result of the desire for clarity and openness on how the topic-specific implementation tables would be assembled The PHLC has already received a number of expressions of interest and will be communicating next steps soon 62 COMOH Executive Committee Minutes June 11
Notes July 9 Minutes July 31
Minutes September 10
63 COMOH Built Environment Work Group
The BEWG has not met since the last meeting but will meet on October 7 During the summer that group led by C Gardner and Nikhil Rajaram developed the paper (COMOHrsquos Advice for the Provincersquos Review of its Long-Term Energy Plan) that was the basis for the letter that went to the province (see item 68 below) V Jaeger expressed appreciation for the work that went into that C Gardner has expressed interest in being a member of the Promoting Healthy Environments ndash Both Natural and Built PHSSP implementation table 64 Public Health Early Years Group Aug 9 Meeting Notes A Feller reported that this group is putting together a November 5 Grand Rounds at PHO 65 iPHIS Panorama
July 8 Update
66 Joint OPHAalPHa Health Equity Working Group R Pellizzari reminded that this is a joint initiative of alPHa and OPHA She will ensure that L Stewart provides minutes of these meetings for future updates She and L Simon are the COMOH reps on this group L Simon circulated a paper by the Wellesley Institute that examines the health equity impacts of cessation of community water fluoridation which was requested by the HEWG She added that Bob Gardner Director of Policy at the Wellesley Institute is now participating in this group and he would welcome suggestions for other subjects for health equity impact assessments M Klassen suggested that Radon might be a good one She also reported that the National Collaborating Centre for Determinants of Health hosted a discussion for the nurses that have been hired under the SDOH portfolio in order to more clearly identify what the specific mandate of public health is in this area and to identify reasonable evaluative measurements This is being proposed as the basis of a Locally Driven Collaborative project and three health units are already involved (PCCHU Toronto and Durham) but more are required and any assistance would be welcome HEWG is also working on positions on the minimum wage review and the poverty strategy Both of these will be circulated once complete and approved
It is also working on a TOPHC session on Cultural Safety related to working with aboriginal populations Feedback was also invited on this with a note that the deadline for abstract submission is September 27 Finally work is also being done with PHO on developing resources and supports for work with Priority Populations 67 COMOH Electronic Mailing List List of Subscribers 68 COMOH Correspondence Aug 26 COMOH Letter ndash Energy Policy
Aug 8 COMOH Letter ndash CMA Poverty Report
July 22 COMOH Letter ndash Immunization Data
70 Next MeetingAdjournment Meeting adjourned at 1035 Next Section meeting will be on November 15 2013 in Toronto part of the alPHa Fall Symposium
Page 1 of 8 ndash DRAFT FOR COMOH DISCUSSION
alPHa Membership Survey hello
Draft Report ndash COMOH Version hello
alPHarsquos membership was surveyed in the fall of 2013 Similar surveys were administered to all member groups ie COMOH BOH Section and Affiliates using the online survey tool Survey Monkey Small alterations were made to group-specific surveys to ensure that the survey questions were relevant to each group A total of 84 responses were received from alPHa members The breakdown of respondents was as follows This draft report is provided for discussion purposes to COMOH members and therefore focuses on the responses provided by COMOH members To provide additional information overall survey responses are also provided for some questions
SECTION 1 RESPONDENT PROFILE
Survey Question What region is your health unit located in
For COMOH members responses came from 6 of the 7 regions of Ontario All 7 regions were represented in the full set of survey responses
Summary of Respondents COMOH 27 32 BOH Section 34 40 Affiliates 23 27 Totals 84 100
All ResponsesEastern 24 29South West 12 14Central East 13 15Central West 15 18North East 11 13Toronto 5 6Not Sure 3 4North West 1 1Totals 84 100
All COMOH ResponsesEastern 3 11South West 5 19Central East 6 22Central West 6 22North East 3 11Toronto 4 15North West 0 0Totals 27 100
Page 2 of 8 ndash DRAFT FOR COMOH DISCUSSION
Survey Question How long have you been involved with public health in Ontario
Survey Question Have you participated on the alPHa Board of Directors or an alPHa or COMOH committeeworking group
All ResponsesYes in the last 1 to 2 years 15 18Yes in the last 2 to 5 years 9 11Yes more than 5 years ago 9 11No not ever 51 61Totals 84 100
All COMOH ResponsesOver 10 years 17 635 to 10 years 7 262 to 5 years 3 11Totals 27 100
All ResponsesOver 10 years 34 405 to 10 years 21 252 to 5 years 21 251 to 2 years 3 4Less than 1 year 5 6Totals 84 100
All COMOH ResponsesYes in the last 1 to 2 years 7 26Yes in the last 2 to 5 years 4 15Yes more than 5 years ago 8 30No not ever 8 30Totals 27 100
Page 3 of 8 ndash DRAFT FOR COMOH DISCUSSION
SECTION 2 PROFESSIONAL DEVELOPMENT
Survey Question Which of the following events have you attended at least once in the past two years
Survey Question Overall how satisfied have you been with alPHa events ie conferences meetings
Survey Question How much value do alPHarsquos events provide for the money
Survey Question How can alPHa make its events more valuable to you Please share any suggestions regarding future topics speakers formats duration locations or any other event component that is important to you
Comments about content bull Expert speakerpanels on emerging or hot topics
(2) bull More engaged dialogue with Ministry rather than
just updates bull Fewer Ministry updates (3) bull Content on medicalPH issues is better left to PHO
TOPHC and joint conferences (2) bull alPHa should stick to Ministrypoliticspolicysenior
PH supportPHU support on key priorities (eg November practical conference on HKP report)
bull For COMOH more discussion bull More time for section activities like face-to-face
COMOH meetings
bull More facilitated work groups of COMOH members to respond to public health practice questions
bull More focus on rural and northern issues bull Infection Control Logistical Considerations bull Consider partnering with other groups bull More collaboration with PHO and OPHA events bull Use of video conferencing bull Less frequentfewer meetings (2) bull Connect with CME Location bull Consider other venues than TO
( ) brackets indicate that more than one response included a similar comment
More than enough value 7 11A lot of value 34 52Some value 22 34A little value 2 3Not enough value 0 0Totals 65 100
All Responses for those who Attended at least One Event in the Last 2 Years
All COMOH ResponsesMore than enough value 4 15A lot of value 13 48Some value 9 33A little value 1 4Not enough value 0 0Totals 27 100
Page 5 of 8 ndash DRAFT FOR COMOH DISCUSSION
SECTION 3 VALUE FOR MEMBERSHIP
Survey Question What do you value the most about your alPHa membership
The comments provided in response to the text response question What is the most important benefit of alPHa membership for you personally supported the answers illustrated in the chart above 15 of the 20 comments provided focussed on the importance of opportunities to interact with colleagues across the province The next most important benefit mentioned was the support for COMOH members to work on public health issues together When asked What is the most important benefit of alPHa membership for your health unit COMOH members emphasized the following bull A coordinated and collective voice in advocating for public health issues and the public health sector (9) bull Opportunities to connect with other public health units to share experiences and best practices (8) bull Maintaining relationships with government both politicians and bureaucrats (3) and bull Support for boards of health (3)
Page 6 of 8 ndash DRAFT FOR COMOH DISCUSSION
Overall Level of Satisfaction
SECTION 4 LOOKING TO THE FUTURE
The questions in this section were asked to obtain input from alPHa members regarding a proposal from alPHarsquos Board of Directors to focus the Association on five service areas COMOH members were asked to indicate their level of agreement with the proposed areas of focus COMOH responses compared to the overall survey responses were as follows
To explore some proposed changes to Association services COMOH members were asked to provide their level of agreement with the following questions
COMOH Responses BOH Section Affiliates All Survey Responses
Strongly Agree
AgreeNeither Agree or Disagree
DisagreeStrongly Disagree
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1Promoting the role and value of local public health units
15 9 2 0 0 26 92 93 95 94
2
Providing important information to members about trends and events that will impact the public health system and management of public health units
10 8 8 0 0 26 69 97 86 85
3Facilitating professional networking and information sharing
13 10 3 0 0 26 88 83 82 85
4
Providing professional development to support excellence in public health unit leadership management and governance
3 15 7 1 0 26 69 83 86 79
5
Responding to public health sector issues when it makes the most sense to have a collective voice ie issues that impact the structure and funding of the public health sector and public health units and issues that have a broad focus on population health
15 8 2 0 1 26 88 97 95 93
PROPOSED AREAS OF FOCUS
COMOH Responses BOH Section Affiliates All Survey Responses
Strongly Agree
AgreeNeither Agree or Disagree
DisagreeStrongly Disagree
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1
COMOH and other professional groups within alPHa should do their own advocacy while alPHa supports members to share and support each others advocacy efforts
7 6 6 6 1 26 50 58 45 52
2
alPHa should provide support to action-oriented inter-professional work groups on priority public health unit issues and member resolutions
4 13 5 3 1 26 65 81 86 77
PROPOSALS
Page 8 of 8 ndash DRAFT FOR COMOH DISCUSSION
COMOH members were also asked to indicate the level of acceptability for some possible changes to alPHarsquos services and way of doing business
COMOH Responses BOH Section Affiliates All Survey Responses
Very Acceptable
Somewhat Acceptable
Neither Acceptable or Unacceptable
Somewhat Unacceptable
Very Unaccept
able
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1Single conference with additional face-to-face section meetings
21 2 0 1 0 24 96 68 80 81
2alPHa to offer alternatives like webinars on focussed topics
13 6 1 4 0 24 79 50 90 71
3Coordinate COMOH meetings with PHO OMA or Ministry events
16 4 2 0 0 22 91 na na --
4
Increase focus on building leadership and management capacity for health unit CEOs and senior management
7 9 4 3 0 23 70 na 70 70
5
Would it be acceptable for alPHa to request voluntary financial contributions from member PHUs in addition to annual fees
3 5 5 4 5 22 36 7 26 21
6
Would it be acceptable for alPHa to request voluntary in-kind staff contributions from member PHUs to expand alPHas capacity eg communications policy work group support
7 11 1 1 3 23 78 31 45 50
7Would it be acceptable to you for alPHa to discontinue staff support for COMOH (BOH Section)
0 4 1 5 14 24 17 11 na 14
8
Would it be acceptable to you for alPHa to reduce the amount of staff support for COMOH (BOH Section)
1 6 1 8 6 22 32 26 na 29
9
Would it be acceptable to you for alPHa to provide supports to MOHs and AMOHs (BOH Members) without maintaining COMOH (BOHs) as a section of the association
3 2 3 2 12 22 23 17 na 20
10
Would it be acceptable to you for alPHas Board of Directors to move from the current representational model to a skills-based strategic model ie board membership would be based on the skills needed to carry out alPHas strategic plan
6 11 2 1 3 23 74 56 56 62
11
Would it be acceptable to you for alPHas President Vice-President and Treasurer to be elected from the full membership of the alPHa Board of Directors (rather than the current model of alternating between BOH and COMOH members)
10 8 1 2 2 23 78 70 70 73
PROPOSED CHANGES
1 Council of Ontario Medical Officers of Health Terms of Reference
ASSOCIATION OF LOCAL PUBLIC HEALTH AGENCIES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
TERMS OF REFERENCE NAME 1 The name of the organization shall be ldquoThe Council of Ontario Medical Officers of
Health a section of the Association of Local Public Health Agencies (alPHa)rdquo hereinafter referred to as ldquothe Councilrdquo
MISSION 2 As local leaders in public health we are committed to improving the health of
Ontarians and increasing health equity by strengthening Ontariorsquos public health system We achieve this through system leadership and coordination in collaboration with the provincial government and other organizations and through evidence-informed advocacy on public health policy
OBJECTIVES 3 The objectives of the Council shall be
a) To provide strong province-wide leadership in public health
b) To advocate for health protection and promotion policies and programs that maintain and improve the health of Ontarians
c) To promote and maintain the highest standards for Ontariorsquos public health
programs and services
d) To support the planning implementation and evaluation of effective and efficiently run public health programs and services
e) To act as a forum for sharing information and resources and for addressing and
discussing public health issues both amongst the Councilrsquos members and other agencies that support the goals of alPHa eg Ontario Medical Association Ontario Public Health Association etc
f) To engage with and to provide public health and related policy advice to alPHa
the Chief Medical Officer of Health the Ontario Ministries of Health and Long-Term Care (including the Health Promotion and Public Health Divisions) Children
2 Council of Ontario Medical Officers of Health Terms of Reference
and Youth Services and other provincial ministries Public Health Ontario Health Canada the Public Health Agency of Canada and other public health partners
g) To promote and protect the professional interests of its members
h) To provide support to individual members as needed
i) To seek recognition for outstanding practice from among the members
j) To support evidence based practice of public health medicine
k) To engage and involve the membership to participate in COMOHrsquos endeavours
l) To mentor Public Health and Preventive Medicine Residents
MEMBERSHIP 4 Membership on the Council in each of the following categories is subject to the
limitations imposed by the current terms of reference and all policies and governing documents of the Association of Local Public Health Agencies Benefits of membership in each category are included in Appendix A These shall be subject to regular review and may be suspended under certain circumstances
Active membership in the Council shall be open to all Associate Medical Officers of Health and all full-time Medical Officers of Health whose Boards of Health are members of alPHa Such members shall have full voting privileges and may hold office in the Council Associate membership shall be open to all full and part-time physicians employed by a Board of Health that is a member of alPHa Such members shall not have voting privileges nor hold office
Affiliate membership shall be open to the following individuals interested in furthering the objectives of the Council
bull Public Health and Preventive Medicine Residents and Public Health and Preventive Medicine Residency Program Directors
bull Federal public health physicians working in Ontariorsquos First Nations communities
bull other public health or related physicians including those employed by a Board of Health that is not a member of alPHa
Such members shall not have voting privileges nor hold office
3 Council of Ontario Medical Officers of Health Terms of Reference
Emeritus membership shall be open to all former members who have retired after five (5) or more years of Active membership subject to the nomination in writing of two (2) active members in good standing endorsement of the Executive Committee and approval of the Council by majority vote at a general meeting Such members shall have neither voting privileges nor hold office but may be invited to attend general meetings Honorary membership shall be open to any non-active or associate member subject to the nomination in writing of two (2) active members in good standing endorsement of the Executive Committee and approval of the Council Such members shall have neither voting privileges nor hold office but may be invited to attend general meetings
OFFICERS 5 The Officers of the Council shall be the Chair Vice-Chair and immediate Past Chair
6 The Chair shall prepare the agendas of all Council meetings She shall preside and
preserve order at all such meetings shall ensure that these Terms of Reference are upheld and enforced and shall contribute to the supervision and evaluation of any Public Health and Preventive Medicine Resident who is on a placement with alPHa
7 The Vice-Chair shall fulfill the duties of the Chair in hisher absence The immediate
Past Chair may fulfill the duties of the Chair or Vice-Chair in their absences 8 The Chair shall normally serve a term of one (1) year which is renewable once and
after which the Vice-Chair shall normally assume the vacated office COMMITTEES 9 The Council shall elect seven (7) active members one from each of alPHarsquos regions
and the active member who is scheduled to serve as the President or immediate Past-President of alPHa to represent it on the alPHa Board of Directors These seven (7) members shall constitute the Councilrsquos Executive Committee and shall serve a term of at least one (1) year The Chair and Vice-Chair shall be elected from among the Executive Committee members If alPHarsquos immediate Past President is an active member she shall be an ex-officio member of the Executive Committee
10 The mandate of the Executive Committee shall be to facilitate the achievement of
the objectives of the Council by fulfilling the following
a Identifying priorities 1
1 See Appendix B Planning Cycle to Identify Priorities for COMOH
and ensuring the development of briefing documents and or recommendations as appropriate for the consideration of the Council
4 Council of Ontario Medical Officers of Health Terms of Reference
b Setting agendas and otherwise ensuring preparations for Council meetings c Ensuring the fulfillment of the direction of Council d Responding in a timely fashion to time-sensitive public health matters in
accordance with the Executive Committeersquos understanding of the perspective of the Council
e Engaging with the Chief Medical Officer of Health Associate Chief Medical Officers of Health and other provincial public health leaders and
f Representing Council at public and partner agency forums including the Public Health Leadership Council which shall normally include membership from the Officers of the Council and two other Executive Committee members as selected by agreement among the Executive
g Identifying opportunities for the recognition of outstanding practice from among the members including the annual nomination of at least one member for the alPHa Distinguished Service Award
11 The Executive Committee shall meet and correspond in the manner and at the times
and if required places as deemed necessary by the Chair to conduct the business of the Council A quorum shall consist of four (4) members
12 The Executive Committee shall have the power to strike committeestask or working
groups to assist it in carrying out the business of the Council 13 The Council may by special resolution remove a member of the Executive
Committee before the completion of hisher term of office and may elect a successor to complete the term The special resolution shall require a majority vote of 67 of the members present and voting at the meeting at which the special resolution is considered
14 A Nominating Committee shall consist of the three (3) most recent Past Chairs who
are able to serve and shall be chaired by the immediate Past Chair The Nominating Committee shall prepare a list of proposed Officers and Executive Committee members for the consideration of the Council at its Annual General Meeting
MEETINGS 15 The Council shall hold at least four (4) general meetings per year in a manner and at
the times and if required places as deemed necessary by the Executive Committee to share information direct and assist the Executive Committee in conducting the business of the Council
16 The Council shall hold its Annual General Meeting during and at the same place as
the alPHarsquos Annual Conference
5 Council of Ontario Medical Officers of Health Terms of Reference
17 The Council shall hold a special meeting at the call of the Chair or upon the written request specifying the purpose of such meeting of at least five (5) active members Council members must be given at least 48 hours notice of any special meeting
18 Only Councilrsquos active and associate members and alPHa staff are entitled to attend
general and special meetings of the Council Other members and non-members may be invited to attend all or part of such meetings as determined by the Chair preferably in consultation with the Executive Committee Non-members who come to such meetings without an invitation may attend all or part of the meeting by a majority vote of the active members present and voting
19 The Chair shall prepare the agendas for such meetings and shall normally include
reports from the Chair and the Councilrsquos committeestask or working groups and representatives to external bodies alPHarsquos Executive Director shall ensure that the minutes shall be recorded and promptly distributed to the Section
20 A quorum for all such meetings shall be ten (10) active members 21 The Council shall normally be notified in a manner deemed appropriate by the Chair
of such meetings at least one (1) month prior to their being held 22 A majority vote of the members present at such meetings and voting shall make
Council decisions In the case of a tied vote the Chair shall cast the deciding vote The Executive Committee shall ensure that actions arising from such decisions at such meetings are implemented and monitored
23 The Chair may solicit advice from the Council through the use of teleconferencing
and alPHarsquos electronic mailing lists in order to gain an understanding of the overall perspective of the Council (see 10d)
ELECTIONS 24 The Officers and Executive Committee members shall be elected at the Sectionrsquos
Annual General Meeting The Nominating Committee Chair or hisher designate shall present a list of nominations Additional nominations from the floor shall also be considered Each Officer and Executive Committee member shall be elected by secret ballot if necessary by a majority of the active members present and voting In the case of a tie the Chair shall cast the deciding vote
AMENDMENTS 25 The Councilrsquos Terms of Reference may be amended from time to time by the
Executive Committee provided the Committee receives notice of such proposed amendments at least one (1) month prior to the meeting at which the amendments
6 Council of Ontario Medical Officers of Health Terms of Reference
will be considered Such amendments shall be ratified by the Council at the next general meeting or the Annual General Meeting as the case may be
26 The Executive Committee shall review the Terms of Reference as required and not
less than once every two years Original September 1987 1st Revision October 2000 2nd Revision July 2001 3rd Revision December 2003 4th Revision February 2008 5th Revision June 2009 6th Revision June 2011 7th Revision June 2013
7 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX A
COMOH Membership Benefits Active Membership
bull Entitled to attend all meetings of the Section bull May hold office on the COMOH Executive Committee alPHa Board of Directors
Standing Committees bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Associate Membership
bull Entitled to attend all meetings of the Section bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Affiliate Membership
bull May attend meetings or parts thereof subject to approval of Chair bull May serve on ad-hoc committees of the Section subject to the approval of the
Executive Committee bull Discounted registration rates for alPHa Conferences (for Public Health and
Preventive Medicine Residents) bull Upon written request and subject to COMOH Executive approval Affiliate
Members may subscribe to comohlistsalphaweborg The approval will be reviewed on an annual basis in order to determine if the Affiliate Member can remain a subscriber to mohsalphaweborg
Emeritus Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair bull Enjoy discounted registration rates for alPHa Conferences and regular COMOH
meetings bull Subscription to comohlistsalphaweborg electronic mailing list bull Full access to alPHa Web site bull May represent alPHa COMOH on selected external committees and working
groups Honorary Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair
8 Council of Ontario Medical Officers of Health Terms of Reference
bull May represent alPHa COMOH on selected external committees and working groups subject to the approval of the COMOH or alPHa Executive Committee as appropriate
9 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX B
Planning Cycle to Identify Priorities for COMOH
1 There shall normally be a COMOH membership strategic planning retreat every four years In recognition of the dynamic environment of public health the need for and timing of such a retreat shall be at the discretion of the Executive Committee in consultation with the membership
2 The COMOH Executive is responsible (through the creation of a subcommittee of COMOH members) for ensuring the preparation for the COMOH retreats with resources to include those provided by alPHa
3 Leadership for action on COMOH priorities will be recruited from among the COMOH membership in order to make good use of the full base of capacity of the membership The resources to support actions will be recruited from both within and beyond the COMOH membership employing other public health professionals that reside within the broader public health system and community
4 The COMOH Executive shall ensure an annual review of strategic priorities and initiatives and the development of a draft report of the same for the review of the members at the June meeting
2013 Strategic Planning
Considerations for COMOH
As part of its strategic planning discussions alPHarsquos Board has been considering changes to the level of support provided to member sections A member survey is being carried out over the fall to determine options acceptable to alPHa members The following approach to support is put forward as a proposal for the consideration of COMOH Note that the feasibility of the points below depend upon future decisions of the alPHa board They assume that COMOH remains part of alPHa but becomes more independent in administering meetings
1 alPHa can provide to COMOH staff support (Gord Fleming) amounting to 02 FTE or one day per week This is a reduction from the current level of 35 days per week COMOH can choose to use the support any way it wants writing COMOH letters meeting minutes agenda support special projects etc
2 In addition to 02 FTE alPHa staff would provide support for up to 4 face-to-face meetings per year One meeting would be concurrent to alPHarsquos annual conference in June The timing of other meetings could be negotiated The support includes consulting on the development of the program arranging for speakers registration for the event arranging venue AV support and hospitality services
3 In addition to 02 FTE alPHa staff would provide support for setting meeting dates and any polling required to establish dates Note that the individual supporting this function would be Karen Reece
4 COMOHrsquos Executive and Section would continue to have access to online supports through the alPHa including the COMOH Listserve and a group page for posting agendas minutes and other resources on the alPHa website
5 alPHa staff (Linda Stewart and Gord Fleming) can also start participating on CMOH calls as a way to be up-to-date on issues related to COMOH
6 Other than what is outlined above COMOH would be expected to prepare agendas and take minutes for its Executive and Section meetings The Executive would be expected to operate more independently than it does now but would be able to access the supports outlined above
Prepared by Linda Stewart Executive Director
From comoh-bounceslistsalphaweborg on behalf of Christopher MackieTo MOH ListserveSubject [comoh] Fw URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)Date Wednesday October 30 2013 91241 AMAttachments ATT00249txt
For AMOHs and PHPM residents who didnt receive the initial email
Chris
Christopher Mackie MD MHSc FRCPCMedical Officer of Health and CEOMiddlesex-London Health Unit50 King St LondonON N6A 5L7 O 519 663 5317 ext 2444 wwwhealthunitcomFrom Pisko Laura (MOHLTC)Sent Tuesday October 29 2013 759 PMTo kbarkeralgomapublichealthcom malcolmlockbchuorg davidcchatham-kentcarobertkyledurhamca proumeliotiseohuca fwarshelginhealthonca mohelginhealthoncahlynnpublichealthgreybruceonca malcolmlockhnhuorg hnmohhnhuorglnoseworthyhkpronca bobnosalhaltonca elizabethrichardsonhamiltoncarschabashpechuonca ncameronhuroncountyca drimgemmillkflapublichealthcamohkflapublichealthca suditranadecounty-lambtononca paulastewarthealthunitorgChristopher Mackie valeriejaegerniagararegionca jimchiriconbpsdhuca jarthursnwhuoncaisralevyottawaca dnealoxfordcountyca davidmowatpeelregionca mklassenpdhuoncarpellizzaripcchuca rosemarieramsinghporcupinehuonca mcorriveaurcdhucomcharlesgardnersmdhuorg sutcliffepsdhucom davidwilliamstbdhucomspruytmtimiskaminghucom dmckeowntorontoca lnolanregionofwaterloocanicolamercerwdghuorg aheimannwechealthunitorg karimkurjiyorkcaCc coreywesleytbdhucom CindyBaker-Barillsmdhuorg Donna Kosmack pilonlsdhucomPaulaMuiskflapublichealthca sthibautorontoca Mueller Daina (MOHLTC) Gordon Marcus(MOHLTC) andreakitahamiltoncaSubject URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)
Dear Colleagues The ministry has received reports that some tobacco vendors across the province aregiving away single cigarettes with the purchase of tobacco products It is the ministryrsquosposition that giving out free single cigarettes does not violate subsection 31(3) of theSmoke-Free Ontario Act (ldquoSFOArdquo) Although the practice of giving out free singlecigarettes may promote the sale of tobacco products it does not take the form of aldquoproduct enhancement product association or promotional materialrdquo and therefore doesnot fall within the scope of subsection 31(3) of the SFOA We have confirmed with Health Canada that this practice may violate section 29(b) of thefederal Tobacco Act As such Health Canada is requesting that you notify them in writingand I am directing you to communicate with them via email and provide to them as manydetails as possible Emails should be sent to Tobacco-Ontariohc-scgcca and thesubject line should read ldquoViolation of Section 29(b) of Tobacco Actrdquo This will ensurethat the complaints are given priority status by Health Canada We will continue to monitor
this situation and liaise with our colleagues at Health Canada Please share this information with your tobacco control staff and contact me or DainaMueller Manager Tobacco Control Unit Health Promotion Implementation Branch atdainamuellerontarioca with any questions RegardsLaura Laura A PiskoDirectorHealth Promotion Implementation BranchHealth Promotion DivisionMinistry of Health and Long Term Care416-327-7445 (office)416-451-3185 (mobile) Marcus Gordon - EA (416)326-0625 for urgent issues
========= Middlesex-London Health Unit E-Mail Disclaimer =============______________________________________________________________
Private and confidential intended only for named recipient If otherwisereceived please destroy immediately Health information in this email isonly general information and is not intended to replace an in personconsultation with a medical professional nor is it intended to providemedical advice Individual circumstances of which we are not aware mayaffect the information provided herein and as such the Middlesex-LondonHealth Unit assumes no liability or responsibility for your reliancethereon The Middlesex-London Health Unit works under the authority of theHealth Protection and Promotion Act and this correspondence may be used toassess your needs for public health services (519-663-5317 ext 2448)______________________________________________________________
From Gardner CharlesTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes (RayCopesoahppca)
George Pasut (GeorgePasutoahppca) Peter Cooney (petercooneyhc-scgcca)Cc Ito DickSubject Discontinuation of Fluoridation in MuskokaDate Tuesday October 22 2013 125254 PM
Hello Colleagues
As I reported in my email below on September 26th fluoridation has come under challenge again inSimcoe Muskoka I am now very unhappy to report that despite our best efforts last night theDistrict Council of Muskoka voted to remove fluoride from municipal drinking supplies across theDistrict This brings to an end fluoridation in all of Simcoe and Muskoka (with the exception of Base Borden)ndash though New Tecumseth will be conducting a plebiscite on the question of fluoridation with themunicipal election next October Defending community water fluoridation has drained a great deal of time human resources andcommitment from other priorities and has been exhausting here in SMDHU as I am sure it hasbeen in many other health units While the outcomes have been very disappointing I have beenimpressed by the professionalism and dedication that SMDHU staff members have shown inshouldering this burden In particular our dental consultant Dr Ito has provided us with much ofthe foundational knowledge and the local research essential to our efforts and has very frequentlyattended and presented at council meetings and other public events I would also like to thank themany of you who have offer and provided support including advocacy letters and informationresources Over the years Dr Peter Cooney Chief Dental Officer of Health of Canada has beenvery helpful attending and presenting with us at council meetings and at public consultationevents We will of course continue our oral health surveillance of the children of Muskoka documentingand reporting in future years on the increase in dental decay that we anticipate will occur Suchsurveillance is the foundation of our advocacy both to municipal politicians and to the province I am very concerned that our experience will continue to repeat itself across the province unlessthere is strong leadership provincially It is with this in mind that I raise the followingrecommendations for your consideration
1 That we collectively (with PHOrsquos leadership) conduct high quality publish-worthy researchdocumenting the impact on dental decay that occurs in those municipalities throughoutOntario that in recent years have discontinued community water fluoridation This could bepart of a larger study on such municipalities across the country and it could also be part ofa study documenting overall oral health (including fluoridation coverage) in the province(and possibly across the country)
2 That COMOH engage with our Chief MOH to advocate for the province to require allmunicipal water supplies to be fluoridated (the exception of course being those withnaturally sufficient fluoride concentrations) This could built upon the alPHa position to
Gordon
Highlight
Gordon
Highlight
date (A11-00 - Community Water Fluoridation) on the CMOH position (Oral Health ndash) and on theemail discussion generated on the COMOH listserv some months back re Richardrsquosproposal (calling on the province to fund municipal water fluoridation)
Valerie I request that this be an item for our COMOH meeting on November 15th Sincerely Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorg From Gardner Charles Sent Thursday September 26 2013 245 PMTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes(RayCopesoahppca)Subject Community Water Fluoridation Under Challenge Again in Simcoe Muskoka Hello Colleagues You may wish to know that community water fluoridation (CWF) is again under challenge in SimcoeMuskoka specifically both in Tottenham (Town of New Tecumseth in Simcoe County) and for theentire District of Muskoka On Monday September 23 Committee of the Whole Council of theTown of New Tecumseth voted to submit application to discontinue community water fluoridation(CWF) in the town of Tottenham despite presentations to the contrary from our dental consultantDr Ito and from me The next Council meeting is scheduled for Monday Sept 30 at which lastMondayrsquos (Sept 23) votes will be ratified
Since Monday I have spoken with the Mayor of the Town of New Tecumseth and with most of thecouncilors encouraging deferral of a decision on Monday to allow the town more time to make afully informed decision
This is the second time in recent years that the issue of discontinuing CWF in Tottenham has beenraised at council This issue is also scheduled to return again to the District of Muskoka Council on
October 21st where I will be presenting in response to deputations in opposition to fluoridation
Outside of Base Borden Tottenham is the only community with fluoridated water in SimcoeCounty The health unitrsquos own screening data between 2011 and 2013 shows that Tottenhamrsquos
Gordon
Highlight
children as well as those in Muskoka have a lower rate of dental decay than Simcoe Muskokacommunities without CWF
Sincerely
Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorgChuck Gardner MOH
November 04 2013
Mandatory State Laws on Fluoridation Thirteen states Puerto Rico and the District of Columbia have laws intended to provide
statewide fluoridation These states and the year that the fluoridation legislation was passed are
District of Columbia (1952) Connecticut (1965) Kentucky (1966) Illinois (1967) Minnesota
(1967) Ohio (1969) South Dakota (1969) Georgia (1973) Nebraska (1973 and 2008)
California (1995) Delaware (1998) Puerto Rico (1998) Nevada (1999) Louisiana (2008) and
Arkansas (2011) (see Table 1) The sizes of the public water systems or countiescommunities
affected and exemption provisions vary by state Table 1
STATES THAT HAVE MANDATORY LAWS ON FLUORIDATION -2011
State (1) Year of
Fluoridation
Legislation (1)
Population
served by
Fluoridated
CWS (2)
Persons
receiving
fluoridated
water (2)
State
Average
Caries
Experience
of Grade 3
Students (3)
Arkansas 2011 647 1724131 64
California 1995 621 22812721 709
Connecticut 1965 910 2370423 406
Delaware 1998 862 705344 545
Georgia 1973 921 8924598 52
Illinois 1967 993 11325132 532
Kentucky 1966 999 4334223 598
Louisiana 2008 407 1846149 657
Minnesota 1967 988 4117266 549
Nebraska 1973 and 2008 702 1001665 593
Nevada 1999 702 1001665 649
Ohio 1969 877 8772683 512
South Dakota 1969 948 642942 623
District of
Columbia
1952 1000 595000
Puerto Rico 1998
United States 739 204283554
2010 Statistics for population fluoridated and number of people
1 Communication with Jane McGinley RDH MBA Manager Fluoridation and Preventive Health
Activities Council on Access Prevention and Interprofessional Relations
2 Centers for Disease Control and Prevention Department of Health and Human Services
accessed Oct 21 2013 httpwwwcdcgovfluoridationstatistics2010statshtm
3 Centers for Disease Control and Prevention National Oral Health Surveillance System Caries
Experience - Percentage of 3rd Grade students with Caries Experience (treated or untreated tooth
If data from 43 states for the percentage of Grade 3 children with experience of dental decay is
compared with the 2008 percentages of the population in a state with Community Water
Fluoridation then the percentage of children with experience of dental decay decreases as the
percentage of the state population with Community Water Fluoridation increases (see Figure 1)
Figure 1
Correlation of Percentage of Grade 3 Children with Caries Experience and
Percentage of Population With Community Water Fluoridation for 43
Reporting States
0
10
20
30
40
50
60
70
80
0 10 20 30 40 50 60 70 80 90 100
State of Population With Community Water Fluoridation
Sta
te
of
Gra
de 3
Stu
den
ts w
ith
Cari
es E
xp
eri
en
ce
Data from CDC (2 3)
The description of the fluoridation laws in California Illinois and Nevada can be found on the
Association of State amp Territorial Dental Directors website(4 7 8)
The California fluoridation law AB 733 came into effect in 1995 requiring communities of 10
000 residents or more be supplied with fluoridated drinking water However the state did not
provide any funding to implement the legislation (California is unique in requiring fluoridation
without funding the practice)(4) The California Department of Health Services therefore had to
fund fluoridation initiatives from non-governmental sources ie the California Endowment
California Dental Association Foundation the First 5 Commission and others(5) From 1995 to
2011 the percentage of the California population receiving fluoridated drinking water has risen
from 17 to 625(6) 4 Dental Public Health Activities amp Practices Office of Oral Health California Department of Health
Services April 2002 httpwwwastddorgbestpracticesDES06002CAfluoridationpdf
5 Stock M Pollick H The CDA Foundation Model to Fluoridate Communities California Dental
Association Journal vol 40 no 8 649 - 655
httpwwwcdaorgPortals0journaljournal_082012pdf
6 California Dental Association Foundation
httpwwwcdafoundationorglearnadvocacyfluoridation
The State of Illinois passed a mandatory fluoridation state in 1967 and required all community
water systems to adjust fluoride levels in the drinking water to optimal levels within 1 year(7)
From 1962 when over 5000000 residents had optimally fluoridated drinking water by 2010
the number had risen to 11325132 (993 of the population on community water systems)(2)
7 Dental Public Health Activities amp Practices Division of Oral Health Illinois Department of Public
Health April 2002 httpwwwastddorgbestpracticesDES16007ILfluoridationpdf
The State of Nevada passed a mandatory fluoridation statute in 2000 for communities with
400000 or more residents(8) This was a result of the work of a statewide coalition that
included the Nevada Dental and Dental Hygienist Associations the Washoe and Clark County
District Health Departments the Clark County School District Junior League of Las Vegas
Head Start the Community College of Southern Nevada Dental Hygiene Program Health
Access Washoe County and Saint Maryrsquos Hospital For communities with less than 400000 the
implementation of fluoridation still required the vote of the majority voters in the community
The Las Vegas Water Authority and the City of Henderson started fluoridation in 2000
increasing the percentage of the population with fluoridated drinking water from 2 to 65 (8) 8 Dental Public Health Activities amp Practices Bureau of Family Health Services Nevada State Health
Division April 2002 httpwwwastddorgbestpracticesDES31002NVfluoridationbillpdf
Countries with Mandatory Laws on Fluoridation Countries that have mandated Community Water Fluoridation are Brazil Hong Kong
Malaysia Singapore Ireland Israel and some of the states in Australia
Singapore started fluoridating its water in 1956 based on the success of the fluoridation trials in
Grand Rapids Newburgh Evanston and Brantford Singapore became the first Asian country to
have 100 of its population benefitting from the implementation of fluoridated drinking water
Loh reported that ldquoThe ten year study on the effects of water fluoridation in Singapore showed
a decrease in caries prevalence in the children In the permanent dentition the reduction was
523 per cent for Chinese and 31 per cent for Malays in the 7 to 9 year old age group A similar
trend was observed in the mixed dentition in which the decrease was 325 per cent for Chinese
and 306 per cent for Malaysrdquo(9) By 2010 the population of the country was 5080000(10)
9 Loh T Thirty-eight years of water fluoridation--the Singapore scenario Community Dent
Health 1996 Sep13 Suppl 247-50
10 British Fluoridation Society One in a Million the facts about water fluoridation 3rd Edition
published March 2012) httpwwwbfsweborgonemillion0920One20in20a20Million20-
20The20Extent20of20Fluoridationpdf
Hong Kong started implementing community water fluoridation in 1961 and similar to
Singapore 100 of the population received access to fluoridated drinking water Lo and Wong
reported that ldquoThe mean DMFT score of the children deceased from 44 in 1960 to 15 in 1968
stayed at this level in the 1980 and 1986 surveys and further deceased to 08 in 2001 The
prevalence of dental fluorosis among the children surveyed in 1960 was 1 and this increased
to 59 and 70 in 1968 and 1980 respectively It was found in the 1986 and 2001 surveys that
the prevalences of fluorosis were 47 and 9 among children whose teeth developed at the
time when the respective water fluoride concentrations were 07 ppm and 05 ppmrdquo(11) The
population of Hong Kong was 6968000 in 2009(10) 11 LO ECM and WONG AHH Water fluoride concentration and fluorosis in Hong Kong in 1960-
2001 84th General Session and Exhibition of the International Association for Dental Research amp
1st Meeting of the Pan-Asian-Pacific Federation Brisbane Australia 28 June-1 July 2006 v 85 n
Sp B
The Malaysian cabinet approved a nationwide community water fluoridation program in 1972
(12) One of the states Sabah decided to stop fluoridation in 1989 due to concerns about
inadequate supervision in adding fluoride to the drinking water Oral Health Surveys in 2009
and 2007 indicated that children in Sabah had the worst oral health with 50 of 12 year-olds
having decay in their permanent teeth and children having an average of 3 teeth being(13)
Under the 10th Malaysian Plan in 2011 the federal and the Sabah state governments
reintroduced water fluoridation in Sabah(1314) In 2010 about 755 of the Malaysian
population or 20700000 people had fluoridated drinking water(1013) 12 Malaysian Dental Association Fluoride in Water
httpwwwmdaorgmy07_public_01healthcare_12htm
13 Sachdev N Fluoridation in Sabah Water for Cleaner Teeth French Tribunecom 28022011
From Levy IsraTo Jaeger ValerieCc Pim Carolyn gordonalphaweborg Diallo Aicha Penny Sutcliffe Paul Roumeliotis Michael Finkelstein
Hazel Lynn Robert KyleSubject FW Panorama - Privacy Security and other issuesDate Wednesday October 16 2013 122110 PM
Hello ValerieOttawa is part of Wave 4 Panorama implementation and we are gearing up increasingly to use thesystem where and if possible Thinking about it I am anticipating that this may need to be on theCOMOH (and alPHa) radar as it is something that will impact all health units and implies a majoroperational shift in vaccine delivery programs for all health units I have asked Carolyn Pim toconnect with our sister wave 4 units to share common experiences as we move forward ndash when wehave a roll up could I bring to COMOH Exec for discussion to explore whether there are broaderimplications for all members As an aside I have also asked the Ministry and their CIO to share with me any roll up learnings thatthey may have had already from previous waves (I understand that Niagara HU was a wave 1participant so if there is such a roll up of common experiences that others could learn fromperhaps you have it already and that could come to the exec too)Thanks Isra From Pim Carolyn Sent October 10 2013 1228 PMTo Christopher Mackie (christophermackiemlhuonca) Elizabeth Richardson(Elizabethrichardsonhamiltonca) H BSc M D F R C P (C) MPH Jim Chirico(jimchiriconbpsdhuca) Marlene Spruyt (spruytmtimiskaminghucom) Robert Kyle (Durham)Cc Levy IsraSubject Panorama - Privacy Security and other issues Dear colleagues Irsquom reaching out to you as fellow Panorama Wave 4 health units to ask about where yourorganizations are at in the process of signing agreements and completing Privacy ImpactAssessments and Threat Risk Assessments (TRAs) Ottawa Public Healthrsquos IT legal and informationsecurity advisors have made numerous requests to the MOHLTC for information (in particular theprovincial TRA) that we consider essential to develop our own risk assessment and PIA but havebeen told that information cannot be shared even with strict confidentiality and access controlsSo we are at somewhat of an impasse Isra emailed Arlene yesterday Arlene has forwarded ourconcerns to the Ministryrsquos CIO and Panorama lead but we havenrsquot had any response or discussionswith either of them yet Have your organizations identified similar concerns andor had interactions with the MOHLTC inthis respect Irsquod also be interested in knowing if your health units have flagged other (egoperational) implementation concerns Thanks
Carolyn ps Robert ndash you can ignore this request I talked with Sharan this morning about Durhamrsquos issuesso am including you now just for information Carolyn Pim MD FRCPC Associate Medical Officer of Health Meacutedecin adjointe en santeacute publique Ottawa Public Health Santeacute publique Ottawa 100 Constellation Cr Ottawa ON K2G 6J8 Tel teacutel (613) 580-6744 ext 23684Fax (613) 580-9641Connect With Ottawa Public Health
Suivez Santeacute publique Ottawa
This e-mail originates from the City of Ottawa e-mail system Any distribution use orcopying of this e-mail or the information it contains by other than the intendedrecipient(s) is unauthorized If you are not the intended recipient please notify meat the telephone number shown above or by return e-mail and delete thiscommunication and any copy immediately Thank you
Le preacutesent courriel a eacuteteacute expeacutedieacute par le systegraveme de courriels de la Ville dOttawaToute distribution utilisation ou reproduction du courriel ou des renseignements quisy trouvent par une personne autre que son destinataire preacutevu est interdite Si vousavez reccedilu le message par erreur veuillez men aviser par teacuteleacutephone (au numeacuteropreacuteciteacute) ou par courriel puis supprimer sans deacutelai la version originale de lacommunication ainsi que toutes ses copies Je vous remercie de votre collaboration
1
Smoke-Free Patios ndash An Amendment to the Smoke-Free Ontario Act
Date November 15 2013 Prepared for Council of Ontario Medical Officers of Health Prepared by York Region Public Health _____________________________________________________________________________ Issue
The Smoke-Free Ontario Act is the current provincial legislation that imposes smoking restrictions in workplaces and public places It prohibits smoking on restaurant and bar patios in instances where any portion of the seating area is covered by a roof With recent studies illustrating that exposure to second hand smoke outdoors poses similar risks to indoor exposure there has been growing public support to enhance smoking restrictions and make patios completely smoke-free
Background
With the implementation of the Smoke-Free Ontario Act in 2006 restaurant and bar patios became subject to smoking restrictions if any portion of the seating area was covered by a roof This allowed for patios without roof coverings to continue to allow smoking and as a result did not provide significant protection to patrons or staff from exposure to second hand smoke outdoors Many businesses chose to alter the design of their patios to allow smoking to continue In some cases patios became more crowded since smoking patrons who dine indoors often proceed outside onto licensed patios with their beverages to smoke York Region like most municipalities in Ontario is host to hundreds of patios being operated by restaurant owners and businesses With smoking prohibitions affecting only a small portion of these patios specifically ones with coverings the vast majority of patios still allow smoking to take place Patrons and employees on patios where smoking is not restricted are exposed to second hand smoke frequently This can contribute to increased disease and aggravation of existing health conditions From a business perspective the existing legislation has been viewed by many operators as unfair because some patios have permanent coverings which cannot be removed requiring a smoke-free status These business owners feel this creates an uneven playing field since they cannot provide an outdoor dining area for their smoking customers There is strong community support for smoke-free patios in Ontario A 2009 Rapid Risk Factor Surveillance System survey revealed 754 percent support in York Region while a Toronto Health Survey in 2011 indicated 74 percent public support
2
Current Status
Smoking is currently prohibited on restaurant and bar patios province-wide in four Canadian provinces and territories Alberta Newfoundland and Labrador Nova Scotia and Yukon A fifth province Prince Edward Island prohibits smoking on patios until 10 pm Since Ontario enacted legislation restricting smoking on patios in 2006 eight municipalities in Ontario have chosen to create bylaws that go beyond the Smoke-Free Ontario Act and enhance outdoor protection from second hand smoke by prohibiting smoking on patios completely The largest of those municipalities is the City of Ottawa Recently the Toronto Board of Health unanimously endorsed a report presented by their Medical Officer of Health recommending that restaurant and bar patios be made smoke-free through an amendment to the Smoke-Free Ontario Act
Key Considerations
There should be no significant financial burden to local Boards of Health resulting from a smoke-free patio amendment to the Smoke-Free Ontario Act Inspection and enforcement for the Smoke-Free Ontario Act is currently 100 percent funded by the Ministry of Health and Long-Term Care Following an introductory period of education on the amendment a complaint response model of service delivery would ensure ongoing compliance with smoke-free requirements A complete ban of smoking on patios would eliminate the widely-held perception by business owners that the current legislation creates an uneven playing field for business Since Smoke-Free Ontario Act inspections of patios began in 2006 operators have expressed the opinion that if patios need to be smoke-free for the protection of the public they should all be smoke-free to avoid undue hardship for individual businesses and to provide protection uniformly across the Province
Next steps
York Region Public Health intends to seek support from Medical Officers of Health across the Central East Tobacco Control Area Network (CETCAN) to advocate to the Ministry of Health and Long-Term Care for an amendment to the Smoke-Free Ontario Act prohibiting smoking on all restaurant and bar patios York Region is also in the process of requesting that its Regional Council advocate to the Minister of Health and Long-Term Care on the issue
Updating and Modernizing O Regulation 565 (Public Pools)
Date November 15 2013
Prepared for Council of Ontario Medical Officers of Health
Prepared by York Region Public Health _____________________________________________________________________________ Background Recent drownings at public pools in Ontario have highlighted the issue of water-borne illness and injury The current pool regulation under Ontariorsquos Health Protection and Promotion Act O Regulation 565 (Public Pools) is outdated It does not accurately reflect new pool technology and design or the changing use of public pools Neither does it incorporate admissions standards recommended by the Office of the Chief Coroner Further O Regulation 565 does not have short-form wording or set fines associated with it This limits public health enforcement capabilities What is the impact Updating O Regulation 565 (Public Pools) to address recent changes in pool technology design and uses and to include Coroner-recommended admissions standards would help improve pool safety Establishing short-form wording for O Regulation 565 would enhance enforcement related to public pools Currently the only enforcement available to Public Health Inspectors for dealing with non-critical regulatory infractions in public pools is the issuance of a Part III summons This involves a considerable amount of resources for a possible small fine With the development of inspection disclosure systems such as YorkSafe there is an even greater need to develop a method to effectively address repeated pool operator non-compliance with non-critical issues Next steps Public health units should advocate to the Province to 1) Conduct a review of O Regulation 565 (Public Pools) to address shortcomings Proposed changes to the
regulation should include a requirement for ownersoperators of public pools to advise the local Medical Officer of Health of any change in the use of a facility and the addition of the Coronerrsquos recommended admission standards
2) Provide short-form wording for O Regulation 565 so that public health inspectors can better deal with pool operator non-compliance
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
argument that hospitals should be developing policies of their own less convincing He suggested that COMOH might for a start consider facilitating the development of a template for policies on mandatory immunization of public health staff (subject to exemptions for people with no contact with others people already under contract etc) which could increase the number of health units with policies thereby increasing the credibility of the case He also suggested a process whereby the existing policies and procedures could be collected examined and synthesized into a legally defensible practical but non-binding template which would be palatable to health unit staff and their unions He agreed that a COMOH working group would be the most appropriate mechanism to do this but asked that alPHa begin the process by collecting the existing policies A Heimann reported that Windsor is discussing this issue ahead of its local public campaign and he thinks this is an excellent idea Rosana Pellizzari added that this process is a good opportunity for those who have policies in place to share lessons learned about unintended consequences experiences with grievances sorting out the NACI definition of high-risk groups and identifying classes of employees that could reasonably be exempt due to the nature of their work ACTION V Jaeger to invite members to submit questions and expressions of interest in participating on the proposed working group directly to I Gemmill and to forward existing policies and related information to G Fleming at alPHa for collection and assembly 42 HIV Non-Disclosure PHLC Briefing Note V Jaeger reminded the group that this was raised at the June Section meeting where it was determined that COMOH should take the lead on developing a procedure that would ensure greater consistency in how and under what circumstances Section 22 orders are used in cases of HIV non-disclosure She has since raised this with the CMOH who agreed that an Associate CMOH at the MOHLTC would be an appropriate person to take the lead on this but until those positions are filled this isnrsquot an available option She also reported that George Pasut has offered PHO support in the form of logistics and meeting space to support a COMOH working group if it is decided to create one She then indicated that L Yuan and R Shahin who have been the COMOH leads on this issue on previous agendas are unable to participate in this process right now so she invited expressions of interest R Schabas observed that this is an issue for which the Provincial public health leadership should take responsibility He suggested that COMOH can present recommendations but they should be framed by an expectation of the CMOH to exercise leadership and provide clear direction V Jaeger agreed to articulate this to Arlene but reiterated that the present request is for volunteers people are willing to sit and do the work R Schabas I Gemmill and A Heimann indicated interest ACTION V Jaeger to discuss the foregoing with the CMOH whose response will inform next steps including development of process and confirmation of expressions of interest 43 Supervised Injection Sites Draft COMOH Letter V Jaeger referred to the attached and stated that it is meant more as a starting point for discussion than to make any suggestions about what COMOHrsquos position should be and invited D McKeown to speak to the issues
D McKeown reported that this is something that Toronto has been looking at for some time and they have concluded that it would be beneficial to have this service available alongside others related to serving the health needs of injection drug users Hersquos looking for an expression of COMOH support for the idea of Safe Injection Sites (SIS) that will in turn support his case for a pilot site in Toronto that can be practically evaluated Responding to R Schabasrsquos question about why TPH isnrsquot just going ahead and doing it D McKeown noted that Provincial support will likely be required for funding (partly because it is considered a health service) and for obtaining the required federal exemption under the Controlled Substances Act Some members expressed discomfort with the idea of expressing specific support for one element of the broader strategy of harm reduction as it is a more downstream intervention than is the usual for public health is not one that is required or practical in many areas of the province and has significant political implications I Gemmill also indicated concerns with some of the papers that are most commonly used to support SIS which are predominantly policy papers and not scientific ones R Schabas observed that from a public health perspective harm reduction has been extremely effective in reducing blood-borne diseases and SIS appears to be an example if an area where we have an opportunity to make a difference As the evidence is so strongly in favour of harm reduction as a public health strategy he believes that COMOH should in fact have a voice on this D McKeown clarified that he is not asking for COMOH to take a position that public health should be responsible for SIS he is simply asking that COMOH take a position that this service should be available alongside the other elements of a comprehensive harm reduction strategy He agreed that this position need not elevate SIS above the other components of harm reduction nor does it need to make any statement of support for specific sites In the end it was agreed that COMOH should proceed in drafting an expression of support V Jaeger invited members to provide suggestions about what should and should not be included D McKeown indicated that this is not time sensitive but he would appreciate a response sooner than later ACTION V Jaeger to synthesize feedback into a document for initial review by the Executive prior to full review and endorsement by the Section 44 Access to Oral Contraceptives Briefing Note R Pellizzari referred to the attached briefing note reminding the group that HUs are required to provide low-cost contraceptives under the OPHS Her board is having trouble with this now that the compassionate contraceptives assistance program is no longer available and that samples are becoming scarcer She suggested that options for a purchasing co-op might be considered by COMOH She noted that Erika Bontovics at the PHD has done a survey on this issue but she has not seen it and isnrsquot sure if any of the data would be useful for this discussion It was suggested that the Government Pharmacy be considered as a bulk purchaser but it was pointed out that this is not an option given that public health charges for these products alPHa was also suggested but acting as a clearing house for pharmaceuticals would be far outside of the Associationrsquos scope and mandate R Pellizzari added that larger health units are able to negotiate good deals based on volume and wondered if there is a potential for them to make purchases on behalf of the smaller health units that do not enjoy this advantage
There was support for further exploration but it was agreed that more information would be beneficial As an initial step RPellizzari will contact Erika Bontovics in an effort to examine the date described above with a view to determining what further information (eg costs negotiated by each HU) might be needed 45 Children and Youth Data Strategy Slide Deck ndash Aug 15 Teleconference amp ICES
Privacy Code V Jaeger referred to the linked ICES presentation and reported that discussions are underway on how to develop a data sharing strategy for the purposes of the attached by way of a working group of ICES COMOH and PHO She Robert Kyle and Michael Finkelstein have already agreed to participate but she invited others to express interest She will bring this up at PHLC and report back 46 Lyme Disease Testing Backgrounder J Hopkins reported that an increasing amount of staff time in Niagara is being devoted to responding to inquiries from the public regarding the different diagnostic methods being used to confirm Lyme disease in the US and Canada She is therefore asking COMOH if this is a prevalent enough issue that a request should be made to PHO to develop some explanatory materials that could be used to address them She clarified that they arenrsquot having much of a problem with physicians itrsquos more a matter of educating the public regarding the accepted approach to the prevention diagnosis and treatment of the disease R Schabas cautioned that public education is a double-edged sword as it has the potential to create the impression that Lyme disease is a bigger problem than it is P Stewart reported that her health unit had a good in-service by a PHO lab person that has been very helpful for the odd questions that come up There were differing opinions of how much effort should be devoted to this as it appears to be another example of ill-informed public opinion on a public health issue akin to anti-vaccination and anti-fluoridation attitudes While these attitudes should not be ignored therersquos not much we can do in the near term to alter them V Jaeger offered to raise this during her next monthly conversation with George Pasut 50 Addendum
51 MOH Retirement I Gemmill noted that Mike Corriveau (MOH ndash Renfrew) will be retiring in December after over thirty years of service He asked that the COMOH Executive consider some form of recognition 60 UPDATES INFORMATION ITEMS REPORTS
61 Public Health Leadership
Council
611 ndash PHLC Update e-Mail Update
612 ndash PHSSP Implementation Tables CMOH Memo ndash PHSSP Tables V Jaeger referred to the linked memo which the result of the desire for clarity and openness on how the topic-specific implementation tables would be assembled The PHLC has already received a number of expressions of interest and will be communicating next steps soon 62 COMOH Executive Committee Minutes June 11
Notes July 9 Minutes July 31
Minutes September 10
63 COMOH Built Environment Work Group
The BEWG has not met since the last meeting but will meet on October 7 During the summer that group led by C Gardner and Nikhil Rajaram developed the paper (COMOHrsquos Advice for the Provincersquos Review of its Long-Term Energy Plan) that was the basis for the letter that went to the province (see item 68 below) V Jaeger expressed appreciation for the work that went into that C Gardner has expressed interest in being a member of the Promoting Healthy Environments ndash Both Natural and Built PHSSP implementation table 64 Public Health Early Years Group Aug 9 Meeting Notes A Feller reported that this group is putting together a November 5 Grand Rounds at PHO 65 iPHIS Panorama
July 8 Update
66 Joint OPHAalPHa Health Equity Working Group R Pellizzari reminded that this is a joint initiative of alPHa and OPHA She will ensure that L Stewart provides minutes of these meetings for future updates She and L Simon are the COMOH reps on this group L Simon circulated a paper by the Wellesley Institute that examines the health equity impacts of cessation of community water fluoridation which was requested by the HEWG She added that Bob Gardner Director of Policy at the Wellesley Institute is now participating in this group and he would welcome suggestions for other subjects for health equity impact assessments M Klassen suggested that Radon might be a good one She also reported that the National Collaborating Centre for Determinants of Health hosted a discussion for the nurses that have been hired under the SDOH portfolio in order to more clearly identify what the specific mandate of public health is in this area and to identify reasonable evaluative measurements This is being proposed as the basis of a Locally Driven Collaborative project and three health units are already involved (PCCHU Toronto and Durham) but more are required and any assistance would be welcome HEWG is also working on positions on the minimum wage review and the poverty strategy Both of these will be circulated once complete and approved
It is also working on a TOPHC session on Cultural Safety related to working with aboriginal populations Feedback was also invited on this with a note that the deadline for abstract submission is September 27 Finally work is also being done with PHO on developing resources and supports for work with Priority Populations 67 COMOH Electronic Mailing List List of Subscribers 68 COMOH Correspondence Aug 26 COMOH Letter ndash Energy Policy
Aug 8 COMOH Letter ndash CMA Poverty Report
July 22 COMOH Letter ndash Immunization Data
70 Next MeetingAdjournment Meeting adjourned at 1035 Next Section meeting will be on November 15 2013 in Toronto part of the alPHa Fall Symposium
Page 1 of 8 ndash DRAFT FOR COMOH DISCUSSION
alPHa Membership Survey hello
Draft Report ndash COMOH Version hello
alPHarsquos membership was surveyed in the fall of 2013 Similar surveys were administered to all member groups ie COMOH BOH Section and Affiliates using the online survey tool Survey Monkey Small alterations were made to group-specific surveys to ensure that the survey questions were relevant to each group A total of 84 responses were received from alPHa members The breakdown of respondents was as follows This draft report is provided for discussion purposes to COMOH members and therefore focuses on the responses provided by COMOH members To provide additional information overall survey responses are also provided for some questions
SECTION 1 RESPONDENT PROFILE
Survey Question What region is your health unit located in
For COMOH members responses came from 6 of the 7 regions of Ontario All 7 regions were represented in the full set of survey responses
Summary of Respondents COMOH 27 32 BOH Section 34 40 Affiliates 23 27 Totals 84 100
All ResponsesEastern 24 29South West 12 14Central East 13 15Central West 15 18North East 11 13Toronto 5 6Not Sure 3 4North West 1 1Totals 84 100
All COMOH ResponsesEastern 3 11South West 5 19Central East 6 22Central West 6 22North East 3 11Toronto 4 15North West 0 0Totals 27 100
Page 2 of 8 ndash DRAFT FOR COMOH DISCUSSION
Survey Question How long have you been involved with public health in Ontario
Survey Question Have you participated on the alPHa Board of Directors or an alPHa or COMOH committeeworking group
All ResponsesYes in the last 1 to 2 years 15 18Yes in the last 2 to 5 years 9 11Yes more than 5 years ago 9 11No not ever 51 61Totals 84 100
All COMOH ResponsesOver 10 years 17 635 to 10 years 7 262 to 5 years 3 11Totals 27 100
All ResponsesOver 10 years 34 405 to 10 years 21 252 to 5 years 21 251 to 2 years 3 4Less than 1 year 5 6Totals 84 100
All COMOH ResponsesYes in the last 1 to 2 years 7 26Yes in the last 2 to 5 years 4 15Yes more than 5 years ago 8 30No not ever 8 30Totals 27 100
Page 3 of 8 ndash DRAFT FOR COMOH DISCUSSION
SECTION 2 PROFESSIONAL DEVELOPMENT
Survey Question Which of the following events have you attended at least once in the past two years
Survey Question Overall how satisfied have you been with alPHa events ie conferences meetings
Survey Question How much value do alPHarsquos events provide for the money
Survey Question How can alPHa make its events more valuable to you Please share any suggestions regarding future topics speakers formats duration locations or any other event component that is important to you
Comments about content bull Expert speakerpanels on emerging or hot topics
(2) bull More engaged dialogue with Ministry rather than
just updates bull Fewer Ministry updates (3) bull Content on medicalPH issues is better left to PHO
TOPHC and joint conferences (2) bull alPHa should stick to Ministrypoliticspolicysenior
PH supportPHU support on key priorities (eg November practical conference on HKP report)
bull For COMOH more discussion bull More time for section activities like face-to-face
COMOH meetings
bull More facilitated work groups of COMOH members to respond to public health practice questions
bull More focus on rural and northern issues bull Infection Control Logistical Considerations bull Consider partnering with other groups bull More collaboration with PHO and OPHA events bull Use of video conferencing bull Less frequentfewer meetings (2) bull Connect with CME Location bull Consider other venues than TO
( ) brackets indicate that more than one response included a similar comment
More than enough value 7 11A lot of value 34 52Some value 22 34A little value 2 3Not enough value 0 0Totals 65 100
All Responses for those who Attended at least One Event in the Last 2 Years
All COMOH ResponsesMore than enough value 4 15A lot of value 13 48Some value 9 33A little value 1 4Not enough value 0 0Totals 27 100
Page 5 of 8 ndash DRAFT FOR COMOH DISCUSSION
SECTION 3 VALUE FOR MEMBERSHIP
Survey Question What do you value the most about your alPHa membership
The comments provided in response to the text response question What is the most important benefit of alPHa membership for you personally supported the answers illustrated in the chart above 15 of the 20 comments provided focussed on the importance of opportunities to interact with colleagues across the province The next most important benefit mentioned was the support for COMOH members to work on public health issues together When asked What is the most important benefit of alPHa membership for your health unit COMOH members emphasized the following bull A coordinated and collective voice in advocating for public health issues and the public health sector (9) bull Opportunities to connect with other public health units to share experiences and best practices (8) bull Maintaining relationships with government both politicians and bureaucrats (3) and bull Support for boards of health (3)
Page 6 of 8 ndash DRAFT FOR COMOH DISCUSSION
Overall Level of Satisfaction
SECTION 4 LOOKING TO THE FUTURE
The questions in this section were asked to obtain input from alPHa members regarding a proposal from alPHarsquos Board of Directors to focus the Association on five service areas COMOH members were asked to indicate their level of agreement with the proposed areas of focus COMOH responses compared to the overall survey responses were as follows
To explore some proposed changes to Association services COMOH members were asked to provide their level of agreement with the following questions
COMOH Responses BOH Section Affiliates All Survey Responses
Strongly Agree
AgreeNeither Agree or Disagree
DisagreeStrongly Disagree
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1Promoting the role and value of local public health units
15 9 2 0 0 26 92 93 95 94
2
Providing important information to members about trends and events that will impact the public health system and management of public health units
10 8 8 0 0 26 69 97 86 85
3Facilitating professional networking and information sharing
13 10 3 0 0 26 88 83 82 85
4
Providing professional development to support excellence in public health unit leadership management and governance
3 15 7 1 0 26 69 83 86 79
5
Responding to public health sector issues when it makes the most sense to have a collective voice ie issues that impact the structure and funding of the public health sector and public health units and issues that have a broad focus on population health
15 8 2 0 1 26 88 97 95 93
PROPOSED AREAS OF FOCUS
COMOH Responses BOH Section Affiliates All Survey Responses
Strongly Agree
AgreeNeither Agree or Disagree
DisagreeStrongly Disagree
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1
COMOH and other professional groups within alPHa should do their own advocacy while alPHa supports members to share and support each others advocacy efforts
7 6 6 6 1 26 50 58 45 52
2
alPHa should provide support to action-oriented inter-professional work groups on priority public health unit issues and member resolutions
4 13 5 3 1 26 65 81 86 77
PROPOSALS
Page 8 of 8 ndash DRAFT FOR COMOH DISCUSSION
COMOH members were also asked to indicate the level of acceptability for some possible changes to alPHarsquos services and way of doing business
COMOH Responses BOH Section Affiliates All Survey Responses
Very Acceptable
Somewhat Acceptable
Neither Acceptable or Unacceptable
Somewhat Unacceptable
Very Unaccept
able
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1Single conference with additional face-to-face section meetings
21 2 0 1 0 24 96 68 80 81
2alPHa to offer alternatives like webinars on focussed topics
13 6 1 4 0 24 79 50 90 71
3Coordinate COMOH meetings with PHO OMA or Ministry events
16 4 2 0 0 22 91 na na --
4
Increase focus on building leadership and management capacity for health unit CEOs and senior management
7 9 4 3 0 23 70 na 70 70
5
Would it be acceptable for alPHa to request voluntary financial contributions from member PHUs in addition to annual fees
3 5 5 4 5 22 36 7 26 21
6
Would it be acceptable for alPHa to request voluntary in-kind staff contributions from member PHUs to expand alPHas capacity eg communications policy work group support
7 11 1 1 3 23 78 31 45 50
7Would it be acceptable to you for alPHa to discontinue staff support for COMOH (BOH Section)
0 4 1 5 14 24 17 11 na 14
8
Would it be acceptable to you for alPHa to reduce the amount of staff support for COMOH (BOH Section)
1 6 1 8 6 22 32 26 na 29
9
Would it be acceptable to you for alPHa to provide supports to MOHs and AMOHs (BOH Members) without maintaining COMOH (BOHs) as a section of the association
3 2 3 2 12 22 23 17 na 20
10
Would it be acceptable to you for alPHas Board of Directors to move from the current representational model to a skills-based strategic model ie board membership would be based on the skills needed to carry out alPHas strategic plan
6 11 2 1 3 23 74 56 56 62
11
Would it be acceptable to you for alPHas President Vice-President and Treasurer to be elected from the full membership of the alPHa Board of Directors (rather than the current model of alternating between BOH and COMOH members)
10 8 1 2 2 23 78 70 70 73
PROPOSED CHANGES
1 Council of Ontario Medical Officers of Health Terms of Reference
ASSOCIATION OF LOCAL PUBLIC HEALTH AGENCIES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
TERMS OF REFERENCE NAME 1 The name of the organization shall be ldquoThe Council of Ontario Medical Officers of
Health a section of the Association of Local Public Health Agencies (alPHa)rdquo hereinafter referred to as ldquothe Councilrdquo
MISSION 2 As local leaders in public health we are committed to improving the health of
Ontarians and increasing health equity by strengthening Ontariorsquos public health system We achieve this through system leadership and coordination in collaboration with the provincial government and other organizations and through evidence-informed advocacy on public health policy
OBJECTIVES 3 The objectives of the Council shall be
a) To provide strong province-wide leadership in public health
b) To advocate for health protection and promotion policies and programs that maintain and improve the health of Ontarians
c) To promote and maintain the highest standards for Ontariorsquos public health
programs and services
d) To support the planning implementation and evaluation of effective and efficiently run public health programs and services
e) To act as a forum for sharing information and resources and for addressing and
discussing public health issues both amongst the Councilrsquos members and other agencies that support the goals of alPHa eg Ontario Medical Association Ontario Public Health Association etc
f) To engage with and to provide public health and related policy advice to alPHa
the Chief Medical Officer of Health the Ontario Ministries of Health and Long-Term Care (including the Health Promotion and Public Health Divisions) Children
2 Council of Ontario Medical Officers of Health Terms of Reference
and Youth Services and other provincial ministries Public Health Ontario Health Canada the Public Health Agency of Canada and other public health partners
g) To promote and protect the professional interests of its members
h) To provide support to individual members as needed
i) To seek recognition for outstanding practice from among the members
j) To support evidence based practice of public health medicine
k) To engage and involve the membership to participate in COMOHrsquos endeavours
l) To mentor Public Health and Preventive Medicine Residents
MEMBERSHIP 4 Membership on the Council in each of the following categories is subject to the
limitations imposed by the current terms of reference and all policies and governing documents of the Association of Local Public Health Agencies Benefits of membership in each category are included in Appendix A These shall be subject to regular review and may be suspended under certain circumstances
Active membership in the Council shall be open to all Associate Medical Officers of Health and all full-time Medical Officers of Health whose Boards of Health are members of alPHa Such members shall have full voting privileges and may hold office in the Council Associate membership shall be open to all full and part-time physicians employed by a Board of Health that is a member of alPHa Such members shall not have voting privileges nor hold office
Affiliate membership shall be open to the following individuals interested in furthering the objectives of the Council
bull Public Health and Preventive Medicine Residents and Public Health and Preventive Medicine Residency Program Directors
bull Federal public health physicians working in Ontariorsquos First Nations communities
bull other public health or related physicians including those employed by a Board of Health that is not a member of alPHa
Such members shall not have voting privileges nor hold office
3 Council of Ontario Medical Officers of Health Terms of Reference
Emeritus membership shall be open to all former members who have retired after five (5) or more years of Active membership subject to the nomination in writing of two (2) active members in good standing endorsement of the Executive Committee and approval of the Council by majority vote at a general meeting Such members shall have neither voting privileges nor hold office but may be invited to attend general meetings Honorary membership shall be open to any non-active or associate member subject to the nomination in writing of two (2) active members in good standing endorsement of the Executive Committee and approval of the Council Such members shall have neither voting privileges nor hold office but may be invited to attend general meetings
OFFICERS 5 The Officers of the Council shall be the Chair Vice-Chair and immediate Past Chair
6 The Chair shall prepare the agendas of all Council meetings She shall preside and
preserve order at all such meetings shall ensure that these Terms of Reference are upheld and enforced and shall contribute to the supervision and evaluation of any Public Health and Preventive Medicine Resident who is on a placement with alPHa
7 The Vice-Chair shall fulfill the duties of the Chair in hisher absence The immediate
Past Chair may fulfill the duties of the Chair or Vice-Chair in their absences 8 The Chair shall normally serve a term of one (1) year which is renewable once and
after which the Vice-Chair shall normally assume the vacated office COMMITTEES 9 The Council shall elect seven (7) active members one from each of alPHarsquos regions
and the active member who is scheduled to serve as the President or immediate Past-President of alPHa to represent it on the alPHa Board of Directors These seven (7) members shall constitute the Councilrsquos Executive Committee and shall serve a term of at least one (1) year The Chair and Vice-Chair shall be elected from among the Executive Committee members If alPHarsquos immediate Past President is an active member she shall be an ex-officio member of the Executive Committee
10 The mandate of the Executive Committee shall be to facilitate the achievement of
the objectives of the Council by fulfilling the following
a Identifying priorities 1
1 See Appendix B Planning Cycle to Identify Priorities for COMOH
and ensuring the development of briefing documents and or recommendations as appropriate for the consideration of the Council
4 Council of Ontario Medical Officers of Health Terms of Reference
b Setting agendas and otherwise ensuring preparations for Council meetings c Ensuring the fulfillment of the direction of Council d Responding in a timely fashion to time-sensitive public health matters in
accordance with the Executive Committeersquos understanding of the perspective of the Council
e Engaging with the Chief Medical Officer of Health Associate Chief Medical Officers of Health and other provincial public health leaders and
f Representing Council at public and partner agency forums including the Public Health Leadership Council which shall normally include membership from the Officers of the Council and two other Executive Committee members as selected by agreement among the Executive
g Identifying opportunities for the recognition of outstanding practice from among the members including the annual nomination of at least one member for the alPHa Distinguished Service Award
11 The Executive Committee shall meet and correspond in the manner and at the times
and if required places as deemed necessary by the Chair to conduct the business of the Council A quorum shall consist of four (4) members
12 The Executive Committee shall have the power to strike committeestask or working
groups to assist it in carrying out the business of the Council 13 The Council may by special resolution remove a member of the Executive
Committee before the completion of hisher term of office and may elect a successor to complete the term The special resolution shall require a majority vote of 67 of the members present and voting at the meeting at which the special resolution is considered
14 A Nominating Committee shall consist of the three (3) most recent Past Chairs who
are able to serve and shall be chaired by the immediate Past Chair The Nominating Committee shall prepare a list of proposed Officers and Executive Committee members for the consideration of the Council at its Annual General Meeting
MEETINGS 15 The Council shall hold at least four (4) general meetings per year in a manner and at
the times and if required places as deemed necessary by the Executive Committee to share information direct and assist the Executive Committee in conducting the business of the Council
16 The Council shall hold its Annual General Meeting during and at the same place as
the alPHarsquos Annual Conference
5 Council of Ontario Medical Officers of Health Terms of Reference
17 The Council shall hold a special meeting at the call of the Chair or upon the written request specifying the purpose of such meeting of at least five (5) active members Council members must be given at least 48 hours notice of any special meeting
18 Only Councilrsquos active and associate members and alPHa staff are entitled to attend
general and special meetings of the Council Other members and non-members may be invited to attend all or part of such meetings as determined by the Chair preferably in consultation with the Executive Committee Non-members who come to such meetings without an invitation may attend all or part of the meeting by a majority vote of the active members present and voting
19 The Chair shall prepare the agendas for such meetings and shall normally include
reports from the Chair and the Councilrsquos committeestask or working groups and representatives to external bodies alPHarsquos Executive Director shall ensure that the minutes shall be recorded and promptly distributed to the Section
20 A quorum for all such meetings shall be ten (10) active members 21 The Council shall normally be notified in a manner deemed appropriate by the Chair
of such meetings at least one (1) month prior to their being held 22 A majority vote of the members present at such meetings and voting shall make
Council decisions In the case of a tied vote the Chair shall cast the deciding vote The Executive Committee shall ensure that actions arising from such decisions at such meetings are implemented and monitored
23 The Chair may solicit advice from the Council through the use of teleconferencing
and alPHarsquos electronic mailing lists in order to gain an understanding of the overall perspective of the Council (see 10d)
ELECTIONS 24 The Officers and Executive Committee members shall be elected at the Sectionrsquos
Annual General Meeting The Nominating Committee Chair or hisher designate shall present a list of nominations Additional nominations from the floor shall also be considered Each Officer and Executive Committee member shall be elected by secret ballot if necessary by a majority of the active members present and voting In the case of a tie the Chair shall cast the deciding vote
AMENDMENTS 25 The Councilrsquos Terms of Reference may be amended from time to time by the
Executive Committee provided the Committee receives notice of such proposed amendments at least one (1) month prior to the meeting at which the amendments
6 Council of Ontario Medical Officers of Health Terms of Reference
will be considered Such amendments shall be ratified by the Council at the next general meeting or the Annual General Meeting as the case may be
26 The Executive Committee shall review the Terms of Reference as required and not
less than once every two years Original September 1987 1st Revision October 2000 2nd Revision July 2001 3rd Revision December 2003 4th Revision February 2008 5th Revision June 2009 6th Revision June 2011 7th Revision June 2013
7 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX A
COMOH Membership Benefits Active Membership
bull Entitled to attend all meetings of the Section bull May hold office on the COMOH Executive Committee alPHa Board of Directors
Standing Committees bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Associate Membership
bull Entitled to attend all meetings of the Section bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Affiliate Membership
bull May attend meetings or parts thereof subject to approval of Chair bull May serve on ad-hoc committees of the Section subject to the approval of the
Executive Committee bull Discounted registration rates for alPHa Conferences (for Public Health and
Preventive Medicine Residents) bull Upon written request and subject to COMOH Executive approval Affiliate
Members may subscribe to comohlistsalphaweborg The approval will be reviewed on an annual basis in order to determine if the Affiliate Member can remain a subscriber to mohsalphaweborg
Emeritus Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair bull Enjoy discounted registration rates for alPHa Conferences and regular COMOH
meetings bull Subscription to comohlistsalphaweborg electronic mailing list bull Full access to alPHa Web site bull May represent alPHa COMOH on selected external committees and working
groups Honorary Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair
8 Council of Ontario Medical Officers of Health Terms of Reference
bull May represent alPHa COMOH on selected external committees and working groups subject to the approval of the COMOH or alPHa Executive Committee as appropriate
9 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX B
Planning Cycle to Identify Priorities for COMOH
1 There shall normally be a COMOH membership strategic planning retreat every four years In recognition of the dynamic environment of public health the need for and timing of such a retreat shall be at the discretion of the Executive Committee in consultation with the membership
2 The COMOH Executive is responsible (through the creation of a subcommittee of COMOH members) for ensuring the preparation for the COMOH retreats with resources to include those provided by alPHa
3 Leadership for action on COMOH priorities will be recruited from among the COMOH membership in order to make good use of the full base of capacity of the membership The resources to support actions will be recruited from both within and beyond the COMOH membership employing other public health professionals that reside within the broader public health system and community
4 The COMOH Executive shall ensure an annual review of strategic priorities and initiatives and the development of a draft report of the same for the review of the members at the June meeting
2013 Strategic Planning
Considerations for COMOH
As part of its strategic planning discussions alPHarsquos Board has been considering changes to the level of support provided to member sections A member survey is being carried out over the fall to determine options acceptable to alPHa members The following approach to support is put forward as a proposal for the consideration of COMOH Note that the feasibility of the points below depend upon future decisions of the alPHa board They assume that COMOH remains part of alPHa but becomes more independent in administering meetings
1 alPHa can provide to COMOH staff support (Gord Fleming) amounting to 02 FTE or one day per week This is a reduction from the current level of 35 days per week COMOH can choose to use the support any way it wants writing COMOH letters meeting minutes agenda support special projects etc
2 In addition to 02 FTE alPHa staff would provide support for up to 4 face-to-face meetings per year One meeting would be concurrent to alPHarsquos annual conference in June The timing of other meetings could be negotiated The support includes consulting on the development of the program arranging for speakers registration for the event arranging venue AV support and hospitality services
3 In addition to 02 FTE alPHa staff would provide support for setting meeting dates and any polling required to establish dates Note that the individual supporting this function would be Karen Reece
4 COMOHrsquos Executive and Section would continue to have access to online supports through the alPHa including the COMOH Listserve and a group page for posting agendas minutes and other resources on the alPHa website
5 alPHa staff (Linda Stewart and Gord Fleming) can also start participating on CMOH calls as a way to be up-to-date on issues related to COMOH
6 Other than what is outlined above COMOH would be expected to prepare agendas and take minutes for its Executive and Section meetings The Executive would be expected to operate more independently than it does now but would be able to access the supports outlined above
Prepared by Linda Stewart Executive Director
From comoh-bounceslistsalphaweborg on behalf of Christopher MackieTo MOH ListserveSubject [comoh] Fw URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)Date Wednesday October 30 2013 91241 AMAttachments ATT00249txt
For AMOHs and PHPM residents who didnt receive the initial email
Chris
Christopher Mackie MD MHSc FRCPCMedical Officer of Health and CEOMiddlesex-London Health Unit50 King St LondonON N6A 5L7 O 519 663 5317 ext 2444 wwwhealthunitcomFrom Pisko Laura (MOHLTC)Sent Tuesday October 29 2013 759 PMTo kbarkeralgomapublichealthcom malcolmlockbchuorg davidcchatham-kentcarobertkyledurhamca proumeliotiseohuca fwarshelginhealthonca mohelginhealthoncahlynnpublichealthgreybruceonca malcolmlockhnhuorg hnmohhnhuorglnoseworthyhkpronca bobnosalhaltonca elizabethrichardsonhamiltoncarschabashpechuonca ncameronhuroncountyca drimgemmillkflapublichealthcamohkflapublichealthca suditranadecounty-lambtononca paulastewarthealthunitorgChristopher Mackie valeriejaegerniagararegionca jimchiriconbpsdhuca jarthursnwhuoncaisralevyottawaca dnealoxfordcountyca davidmowatpeelregionca mklassenpdhuoncarpellizzaripcchuca rosemarieramsinghporcupinehuonca mcorriveaurcdhucomcharlesgardnersmdhuorg sutcliffepsdhucom davidwilliamstbdhucomspruytmtimiskaminghucom dmckeowntorontoca lnolanregionofwaterloocanicolamercerwdghuorg aheimannwechealthunitorg karimkurjiyorkcaCc coreywesleytbdhucom CindyBaker-Barillsmdhuorg Donna Kosmack pilonlsdhucomPaulaMuiskflapublichealthca sthibautorontoca Mueller Daina (MOHLTC) Gordon Marcus(MOHLTC) andreakitahamiltoncaSubject URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)
Dear Colleagues The ministry has received reports that some tobacco vendors across the province aregiving away single cigarettes with the purchase of tobacco products It is the ministryrsquosposition that giving out free single cigarettes does not violate subsection 31(3) of theSmoke-Free Ontario Act (ldquoSFOArdquo) Although the practice of giving out free singlecigarettes may promote the sale of tobacco products it does not take the form of aldquoproduct enhancement product association or promotional materialrdquo and therefore doesnot fall within the scope of subsection 31(3) of the SFOA We have confirmed with Health Canada that this practice may violate section 29(b) of thefederal Tobacco Act As such Health Canada is requesting that you notify them in writingand I am directing you to communicate with them via email and provide to them as manydetails as possible Emails should be sent to Tobacco-Ontariohc-scgcca and thesubject line should read ldquoViolation of Section 29(b) of Tobacco Actrdquo This will ensurethat the complaints are given priority status by Health Canada We will continue to monitor
this situation and liaise with our colleagues at Health Canada Please share this information with your tobacco control staff and contact me or DainaMueller Manager Tobacco Control Unit Health Promotion Implementation Branch atdainamuellerontarioca with any questions RegardsLaura Laura A PiskoDirectorHealth Promotion Implementation BranchHealth Promotion DivisionMinistry of Health and Long Term Care416-327-7445 (office)416-451-3185 (mobile) Marcus Gordon - EA (416)326-0625 for urgent issues
========= Middlesex-London Health Unit E-Mail Disclaimer =============______________________________________________________________
Private and confidential intended only for named recipient If otherwisereceived please destroy immediately Health information in this email isonly general information and is not intended to replace an in personconsultation with a medical professional nor is it intended to providemedical advice Individual circumstances of which we are not aware mayaffect the information provided herein and as such the Middlesex-LondonHealth Unit assumes no liability or responsibility for your reliancethereon The Middlesex-London Health Unit works under the authority of theHealth Protection and Promotion Act and this correspondence may be used toassess your needs for public health services (519-663-5317 ext 2448)______________________________________________________________
From Gardner CharlesTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes (RayCopesoahppca)
George Pasut (GeorgePasutoahppca) Peter Cooney (petercooneyhc-scgcca)Cc Ito DickSubject Discontinuation of Fluoridation in MuskokaDate Tuesday October 22 2013 125254 PM
Hello Colleagues
As I reported in my email below on September 26th fluoridation has come under challenge again inSimcoe Muskoka I am now very unhappy to report that despite our best efforts last night theDistrict Council of Muskoka voted to remove fluoride from municipal drinking supplies across theDistrict This brings to an end fluoridation in all of Simcoe and Muskoka (with the exception of Base Borden)ndash though New Tecumseth will be conducting a plebiscite on the question of fluoridation with themunicipal election next October Defending community water fluoridation has drained a great deal of time human resources andcommitment from other priorities and has been exhausting here in SMDHU as I am sure it hasbeen in many other health units While the outcomes have been very disappointing I have beenimpressed by the professionalism and dedication that SMDHU staff members have shown inshouldering this burden In particular our dental consultant Dr Ito has provided us with much ofthe foundational knowledge and the local research essential to our efforts and has very frequentlyattended and presented at council meetings and other public events I would also like to thank themany of you who have offer and provided support including advocacy letters and informationresources Over the years Dr Peter Cooney Chief Dental Officer of Health of Canada has beenvery helpful attending and presenting with us at council meetings and at public consultationevents We will of course continue our oral health surveillance of the children of Muskoka documentingand reporting in future years on the increase in dental decay that we anticipate will occur Suchsurveillance is the foundation of our advocacy both to municipal politicians and to the province I am very concerned that our experience will continue to repeat itself across the province unlessthere is strong leadership provincially It is with this in mind that I raise the followingrecommendations for your consideration
1 That we collectively (with PHOrsquos leadership) conduct high quality publish-worthy researchdocumenting the impact on dental decay that occurs in those municipalities throughoutOntario that in recent years have discontinued community water fluoridation This could bepart of a larger study on such municipalities across the country and it could also be part ofa study documenting overall oral health (including fluoridation coverage) in the province(and possibly across the country)
2 That COMOH engage with our Chief MOH to advocate for the province to require allmunicipal water supplies to be fluoridated (the exception of course being those withnaturally sufficient fluoride concentrations) This could built upon the alPHa position to
Gordon
Highlight
Gordon
Highlight
date (A11-00 - Community Water Fluoridation) on the CMOH position (Oral Health ndash) and on theemail discussion generated on the COMOH listserv some months back re Richardrsquosproposal (calling on the province to fund municipal water fluoridation)
Valerie I request that this be an item for our COMOH meeting on November 15th Sincerely Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorg From Gardner Charles Sent Thursday September 26 2013 245 PMTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes(RayCopesoahppca)Subject Community Water Fluoridation Under Challenge Again in Simcoe Muskoka Hello Colleagues You may wish to know that community water fluoridation (CWF) is again under challenge in SimcoeMuskoka specifically both in Tottenham (Town of New Tecumseth in Simcoe County) and for theentire District of Muskoka On Monday September 23 Committee of the Whole Council of theTown of New Tecumseth voted to submit application to discontinue community water fluoridation(CWF) in the town of Tottenham despite presentations to the contrary from our dental consultantDr Ito and from me The next Council meeting is scheduled for Monday Sept 30 at which lastMondayrsquos (Sept 23) votes will be ratified
Since Monday I have spoken with the Mayor of the Town of New Tecumseth and with most of thecouncilors encouraging deferral of a decision on Monday to allow the town more time to make afully informed decision
This is the second time in recent years that the issue of discontinuing CWF in Tottenham has beenraised at council This issue is also scheduled to return again to the District of Muskoka Council on
October 21st where I will be presenting in response to deputations in opposition to fluoridation
Outside of Base Borden Tottenham is the only community with fluoridated water in SimcoeCounty The health unitrsquos own screening data between 2011 and 2013 shows that Tottenhamrsquos
Gordon
Highlight
children as well as those in Muskoka have a lower rate of dental decay than Simcoe Muskokacommunities without CWF
Sincerely
Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorgChuck Gardner MOH
November 04 2013
Mandatory State Laws on Fluoridation Thirteen states Puerto Rico and the District of Columbia have laws intended to provide
statewide fluoridation These states and the year that the fluoridation legislation was passed are
District of Columbia (1952) Connecticut (1965) Kentucky (1966) Illinois (1967) Minnesota
(1967) Ohio (1969) South Dakota (1969) Georgia (1973) Nebraska (1973 and 2008)
California (1995) Delaware (1998) Puerto Rico (1998) Nevada (1999) Louisiana (2008) and
Arkansas (2011) (see Table 1) The sizes of the public water systems or countiescommunities
affected and exemption provisions vary by state Table 1
STATES THAT HAVE MANDATORY LAWS ON FLUORIDATION -2011
State (1) Year of
Fluoridation
Legislation (1)
Population
served by
Fluoridated
CWS (2)
Persons
receiving
fluoridated
water (2)
State
Average
Caries
Experience
of Grade 3
Students (3)
Arkansas 2011 647 1724131 64
California 1995 621 22812721 709
Connecticut 1965 910 2370423 406
Delaware 1998 862 705344 545
Georgia 1973 921 8924598 52
Illinois 1967 993 11325132 532
Kentucky 1966 999 4334223 598
Louisiana 2008 407 1846149 657
Minnesota 1967 988 4117266 549
Nebraska 1973 and 2008 702 1001665 593
Nevada 1999 702 1001665 649
Ohio 1969 877 8772683 512
South Dakota 1969 948 642942 623
District of
Columbia
1952 1000 595000
Puerto Rico 1998
United States 739 204283554
2010 Statistics for population fluoridated and number of people
1 Communication with Jane McGinley RDH MBA Manager Fluoridation and Preventive Health
Activities Council on Access Prevention and Interprofessional Relations
2 Centers for Disease Control and Prevention Department of Health and Human Services
accessed Oct 21 2013 httpwwwcdcgovfluoridationstatistics2010statshtm
3 Centers for Disease Control and Prevention National Oral Health Surveillance System Caries
Experience - Percentage of 3rd Grade students with Caries Experience (treated or untreated tooth
If data from 43 states for the percentage of Grade 3 children with experience of dental decay is
compared with the 2008 percentages of the population in a state with Community Water
Fluoridation then the percentage of children with experience of dental decay decreases as the
percentage of the state population with Community Water Fluoridation increases (see Figure 1)
Figure 1
Correlation of Percentage of Grade 3 Children with Caries Experience and
Percentage of Population With Community Water Fluoridation for 43
Reporting States
0
10
20
30
40
50
60
70
80
0 10 20 30 40 50 60 70 80 90 100
State of Population With Community Water Fluoridation
Sta
te
of
Gra
de 3
Stu
den
ts w
ith
Cari
es E
xp
eri
en
ce
Data from CDC (2 3)
The description of the fluoridation laws in California Illinois and Nevada can be found on the
Association of State amp Territorial Dental Directors website(4 7 8)
The California fluoridation law AB 733 came into effect in 1995 requiring communities of 10
000 residents or more be supplied with fluoridated drinking water However the state did not
provide any funding to implement the legislation (California is unique in requiring fluoridation
without funding the practice)(4) The California Department of Health Services therefore had to
fund fluoridation initiatives from non-governmental sources ie the California Endowment
California Dental Association Foundation the First 5 Commission and others(5) From 1995 to
2011 the percentage of the California population receiving fluoridated drinking water has risen
from 17 to 625(6) 4 Dental Public Health Activities amp Practices Office of Oral Health California Department of Health
Services April 2002 httpwwwastddorgbestpracticesDES06002CAfluoridationpdf
5 Stock M Pollick H The CDA Foundation Model to Fluoridate Communities California Dental
Association Journal vol 40 no 8 649 - 655
httpwwwcdaorgPortals0journaljournal_082012pdf
6 California Dental Association Foundation
httpwwwcdafoundationorglearnadvocacyfluoridation
The State of Illinois passed a mandatory fluoridation state in 1967 and required all community
water systems to adjust fluoride levels in the drinking water to optimal levels within 1 year(7)
From 1962 when over 5000000 residents had optimally fluoridated drinking water by 2010
the number had risen to 11325132 (993 of the population on community water systems)(2)
7 Dental Public Health Activities amp Practices Division of Oral Health Illinois Department of Public
Health April 2002 httpwwwastddorgbestpracticesDES16007ILfluoridationpdf
The State of Nevada passed a mandatory fluoridation statute in 2000 for communities with
400000 or more residents(8) This was a result of the work of a statewide coalition that
included the Nevada Dental and Dental Hygienist Associations the Washoe and Clark County
District Health Departments the Clark County School District Junior League of Las Vegas
Head Start the Community College of Southern Nevada Dental Hygiene Program Health
Access Washoe County and Saint Maryrsquos Hospital For communities with less than 400000 the
implementation of fluoridation still required the vote of the majority voters in the community
The Las Vegas Water Authority and the City of Henderson started fluoridation in 2000
increasing the percentage of the population with fluoridated drinking water from 2 to 65 (8) 8 Dental Public Health Activities amp Practices Bureau of Family Health Services Nevada State Health
Division April 2002 httpwwwastddorgbestpracticesDES31002NVfluoridationbillpdf
Countries with Mandatory Laws on Fluoridation Countries that have mandated Community Water Fluoridation are Brazil Hong Kong
Malaysia Singapore Ireland Israel and some of the states in Australia
Singapore started fluoridating its water in 1956 based on the success of the fluoridation trials in
Grand Rapids Newburgh Evanston and Brantford Singapore became the first Asian country to
have 100 of its population benefitting from the implementation of fluoridated drinking water
Loh reported that ldquoThe ten year study on the effects of water fluoridation in Singapore showed
a decrease in caries prevalence in the children In the permanent dentition the reduction was
523 per cent for Chinese and 31 per cent for Malays in the 7 to 9 year old age group A similar
trend was observed in the mixed dentition in which the decrease was 325 per cent for Chinese
and 306 per cent for Malaysrdquo(9) By 2010 the population of the country was 5080000(10)
9 Loh T Thirty-eight years of water fluoridation--the Singapore scenario Community Dent
Health 1996 Sep13 Suppl 247-50
10 British Fluoridation Society One in a Million the facts about water fluoridation 3rd Edition
published March 2012) httpwwwbfsweborgonemillion0920One20in20a20Million20-
20The20Extent20of20Fluoridationpdf
Hong Kong started implementing community water fluoridation in 1961 and similar to
Singapore 100 of the population received access to fluoridated drinking water Lo and Wong
reported that ldquoThe mean DMFT score of the children deceased from 44 in 1960 to 15 in 1968
stayed at this level in the 1980 and 1986 surveys and further deceased to 08 in 2001 The
prevalence of dental fluorosis among the children surveyed in 1960 was 1 and this increased
to 59 and 70 in 1968 and 1980 respectively It was found in the 1986 and 2001 surveys that
the prevalences of fluorosis were 47 and 9 among children whose teeth developed at the
time when the respective water fluoride concentrations were 07 ppm and 05 ppmrdquo(11) The
population of Hong Kong was 6968000 in 2009(10) 11 LO ECM and WONG AHH Water fluoride concentration and fluorosis in Hong Kong in 1960-
2001 84th General Session and Exhibition of the International Association for Dental Research amp
1st Meeting of the Pan-Asian-Pacific Federation Brisbane Australia 28 June-1 July 2006 v 85 n
Sp B
The Malaysian cabinet approved a nationwide community water fluoridation program in 1972
(12) One of the states Sabah decided to stop fluoridation in 1989 due to concerns about
inadequate supervision in adding fluoride to the drinking water Oral Health Surveys in 2009
and 2007 indicated that children in Sabah had the worst oral health with 50 of 12 year-olds
having decay in their permanent teeth and children having an average of 3 teeth being(13)
Under the 10th Malaysian Plan in 2011 the federal and the Sabah state governments
reintroduced water fluoridation in Sabah(1314) In 2010 about 755 of the Malaysian
population or 20700000 people had fluoridated drinking water(1013) 12 Malaysian Dental Association Fluoride in Water
httpwwwmdaorgmy07_public_01healthcare_12htm
13 Sachdev N Fluoridation in Sabah Water for Cleaner Teeth French Tribunecom 28022011
From Levy IsraTo Jaeger ValerieCc Pim Carolyn gordonalphaweborg Diallo Aicha Penny Sutcliffe Paul Roumeliotis Michael Finkelstein
Hazel Lynn Robert KyleSubject FW Panorama - Privacy Security and other issuesDate Wednesday October 16 2013 122110 PM
Hello ValerieOttawa is part of Wave 4 Panorama implementation and we are gearing up increasingly to use thesystem where and if possible Thinking about it I am anticipating that this may need to be on theCOMOH (and alPHa) radar as it is something that will impact all health units and implies a majoroperational shift in vaccine delivery programs for all health units I have asked Carolyn Pim toconnect with our sister wave 4 units to share common experiences as we move forward ndash when wehave a roll up could I bring to COMOH Exec for discussion to explore whether there are broaderimplications for all members As an aside I have also asked the Ministry and their CIO to share with me any roll up learnings thatthey may have had already from previous waves (I understand that Niagara HU was a wave 1participant so if there is such a roll up of common experiences that others could learn fromperhaps you have it already and that could come to the exec too)Thanks Isra From Pim Carolyn Sent October 10 2013 1228 PMTo Christopher Mackie (christophermackiemlhuonca) Elizabeth Richardson(Elizabethrichardsonhamiltonca) H BSc M D F R C P (C) MPH Jim Chirico(jimchiriconbpsdhuca) Marlene Spruyt (spruytmtimiskaminghucom) Robert Kyle (Durham)Cc Levy IsraSubject Panorama - Privacy Security and other issues Dear colleagues Irsquom reaching out to you as fellow Panorama Wave 4 health units to ask about where yourorganizations are at in the process of signing agreements and completing Privacy ImpactAssessments and Threat Risk Assessments (TRAs) Ottawa Public Healthrsquos IT legal and informationsecurity advisors have made numerous requests to the MOHLTC for information (in particular theprovincial TRA) that we consider essential to develop our own risk assessment and PIA but havebeen told that information cannot be shared even with strict confidentiality and access controlsSo we are at somewhat of an impasse Isra emailed Arlene yesterday Arlene has forwarded ourconcerns to the Ministryrsquos CIO and Panorama lead but we havenrsquot had any response or discussionswith either of them yet Have your organizations identified similar concerns andor had interactions with the MOHLTC inthis respect Irsquod also be interested in knowing if your health units have flagged other (egoperational) implementation concerns Thanks
Carolyn ps Robert ndash you can ignore this request I talked with Sharan this morning about Durhamrsquos issuesso am including you now just for information Carolyn Pim MD FRCPC Associate Medical Officer of Health Meacutedecin adjointe en santeacute publique Ottawa Public Health Santeacute publique Ottawa 100 Constellation Cr Ottawa ON K2G 6J8 Tel teacutel (613) 580-6744 ext 23684Fax (613) 580-9641Connect With Ottawa Public Health
Suivez Santeacute publique Ottawa
This e-mail originates from the City of Ottawa e-mail system Any distribution use orcopying of this e-mail or the information it contains by other than the intendedrecipient(s) is unauthorized If you are not the intended recipient please notify meat the telephone number shown above or by return e-mail and delete thiscommunication and any copy immediately Thank you
Le preacutesent courriel a eacuteteacute expeacutedieacute par le systegraveme de courriels de la Ville dOttawaToute distribution utilisation ou reproduction du courriel ou des renseignements quisy trouvent par une personne autre que son destinataire preacutevu est interdite Si vousavez reccedilu le message par erreur veuillez men aviser par teacuteleacutephone (au numeacuteropreacuteciteacute) ou par courriel puis supprimer sans deacutelai la version originale de lacommunication ainsi que toutes ses copies Je vous remercie de votre collaboration
1
Smoke-Free Patios ndash An Amendment to the Smoke-Free Ontario Act
Date November 15 2013 Prepared for Council of Ontario Medical Officers of Health Prepared by York Region Public Health _____________________________________________________________________________ Issue
The Smoke-Free Ontario Act is the current provincial legislation that imposes smoking restrictions in workplaces and public places It prohibits smoking on restaurant and bar patios in instances where any portion of the seating area is covered by a roof With recent studies illustrating that exposure to second hand smoke outdoors poses similar risks to indoor exposure there has been growing public support to enhance smoking restrictions and make patios completely smoke-free
Background
With the implementation of the Smoke-Free Ontario Act in 2006 restaurant and bar patios became subject to smoking restrictions if any portion of the seating area was covered by a roof This allowed for patios without roof coverings to continue to allow smoking and as a result did not provide significant protection to patrons or staff from exposure to second hand smoke outdoors Many businesses chose to alter the design of their patios to allow smoking to continue In some cases patios became more crowded since smoking patrons who dine indoors often proceed outside onto licensed patios with their beverages to smoke York Region like most municipalities in Ontario is host to hundreds of patios being operated by restaurant owners and businesses With smoking prohibitions affecting only a small portion of these patios specifically ones with coverings the vast majority of patios still allow smoking to take place Patrons and employees on patios where smoking is not restricted are exposed to second hand smoke frequently This can contribute to increased disease and aggravation of existing health conditions From a business perspective the existing legislation has been viewed by many operators as unfair because some patios have permanent coverings which cannot be removed requiring a smoke-free status These business owners feel this creates an uneven playing field since they cannot provide an outdoor dining area for their smoking customers There is strong community support for smoke-free patios in Ontario A 2009 Rapid Risk Factor Surveillance System survey revealed 754 percent support in York Region while a Toronto Health Survey in 2011 indicated 74 percent public support
2
Current Status
Smoking is currently prohibited on restaurant and bar patios province-wide in four Canadian provinces and territories Alberta Newfoundland and Labrador Nova Scotia and Yukon A fifth province Prince Edward Island prohibits smoking on patios until 10 pm Since Ontario enacted legislation restricting smoking on patios in 2006 eight municipalities in Ontario have chosen to create bylaws that go beyond the Smoke-Free Ontario Act and enhance outdoor protection from second hand smoke by prohibiting smoking on patios completely The largest of those municipalities is the City of Ottawa Recently the Toronto Board of Health unanimously endorsed a report presented by their Medical Officer of Health recommending that restaurant and bar patios be made smoke-free through an amendment to the Smoke-Free Ontario Act
Key Considerations
There should be no significant financial burden to local Boards of Health resulting from a smoke-free patio amendment to the Smoke-Free Ontario Act Inspection and enforcement for the Smoke-Free Ontario Act is currently 100 percent funded by the Ministry of Health and Long-Term Care Following an introductory period of education on the amendment a complaint response model of service delivery would ensure ongoing compliance with smoke-free requirements A complete ban of smoking on patios would eliminate the widely-held perception by business owners that the current legislation creates an uneven playing field for business Since Smoke-Free Ontario Act inspections of patios began in 2006 operators have expressed the opinion that if patios need to be smoke-free for the protection of the public they should all be smoke-free to avoid undue hardship for individual businesses and to provide protection uniformly across the Province
Next steps
York Region Public Health intends to seek support from Medical Officers of Health across the Central East Tobacco Control Area Network (CETCAN) to advocate to the Ministry of Health and Long-Term Care for an amendment to the Smoke-Free Ontario Act prohibiting smoking on all restaurant and bar patios York Region is also in the process of requesting that its Regional Council advocate to the Minister of Health and Long-Term Care on the issue
Updating and Modernizing O Regulation 565 (Public Pools)
Date November 15 2013
Prepared for Council of Ontario Medical Officers of Health
Prepared by York Region Public Health _____________________________________________________________________________ Background Recent drownings at public pools in Ontario have highlighted the issue of water-borne illness and injury The current pool regulation under Ontariorsquos Health Protection and Promotion Act O Regulation 565 (Public Pools) is outdated It does not accurately reflect new pool technology and design or the changing use of public pools Neither does it incorporate admissions standards recommended by the Office of the Chief Coroner Further O Regulation 565 does not have short-form wording or set fines associated with it This limits public health enforcement capabilities What is the impact Updating O Regulation 565 (Public Pools) to address recent changes in pool technology design and uses and to include Coroner-recommended admissions standards would help improve pool safety Establishing short-form wording for O Regulation 565 would enhance enforcement related to public pools Currently the only enforcement available to Public Health Inspectors for dealing with non-critical regulatory infractions in public pools is the issuance of a Part III summons This involves a considerable amount of resources for a possible small fine With the development of inspection disclosure systems such as YorkSafe there is an even greater need to develop a method to effectively address repeated pool operator non-compliance with non-critical issues Next steps Public health units should advocate to the Province to 1) Conduct a review of O Regulation 565 (Public Pools) to address shortcomings Proposed changes to the
regulation should include a requirement for ownersoperators of public pools to advise the local Medical Officer of Health of any change in the use of a facility and the addition of the Coronerrsquos recommended admission standards
2) Provide short-form wording for O Regulation 565 so that public health inspectors can better deal with pool operator non-compliance
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
D McKeown reported that this is something that Toronto has been looking at for some time and they have concluded that it would be beneficial to have this service available alongside others related to serving the health needs of injection drug users Hersquos looking for an expression of COMOH support for the idea of Safe Injection Sites (SIS) that will in turn support his case for a pilot site in Toronto that can be practically evaluated Responding to R Schabasrsquos question about why TPH isnrsquot just going ahead and doing it D McKeown noted that Provincial support will likely be required for funding (partly because it is considered a health service) and for obtaining the required federal exemption under the Controlled Substances Act Some members expressed discomfort with the idea of expressing specific support for one element of the broader strategy of harm reduction as it is a more downstream intervention than is the usual for public health is not one that is required or practical in many areas of the province and has significant political implications I Gemmill also indicated concerns with some of the papers that are most commonly used to support SIS which are predominantly policy papers and not scientific ones R Schabas observed that from a public health perspective harm reduction has been extremely effective in reducing blood-borne diseases and SIS appears to be an example if an area where we have an opportunity to make a difference As the evidence is so strongly in favour of harm reduction as a public health strategy he believes that COMOH should in fact have a voice on this D McKeown clarified that he is not asking for COMOH to take a position that public health should be responsible for SIS he is simply asking that COMOH take a position that this service should be available alongside the other elements of a comprehensive harm reduction strategy He agreed that this position need not elevate SIS above the other components of harm reduction nor does it need to make any statement of support for specific sites In the end it was agreed that COMOH should proceed in drafting an expression of support V Jaeger invited members to provide suggestions about what should and should not be included D McKeown indicated that this is not time sensitive but he would appreciate a response sooner than later ACTION V Jaeger to synthesize feedback into a document for initial review by the Executive prior to full review and endorsement by the Section 44 Access to Oral Contraceptives Briefing Note R Pellizzari referred to the attached briefing note reminding the group that HUs are required to provide low-cost contraceptives under the OPHS Her board is having trouble with this now that the compassionate contraceptives assistance program is no longer available and that samples are becoming scarcer She suggested that options for a purchasing co-op might be considered by COMOH She noted that Erika Bontovics at the PHD has done a survey on this issue but she has not seen it and isnrsquot sure if any of the data would be useful for this discussion It was suggested that the Government Pharmacy be considered as a bulk purchaser but it was pointed out that this is not an option given that public health charges for these products alPHa was also suggested but acting as a clearing house for pharmaceuticals would be far outside of the Associationrsquos scope and mandate R Pellizzari added that larger health units are able to negotiate good deals based on volume and wondered if there is a potential for them to make purchases on behalf of the smaller health units that do not enjoy this advantage
There was support for further exploration but it was agreed that more information would be beneficial As an initial step RPellizzari will contact Erika Bontovics in an effort to examine the date described above with a view to determining what further information (eg costs negotiated by each HU) might be needed 45 Children and Youth Data Strategy Slide Deck ndash Aug 15 Teleconference amp ICES
Privacy Code V Jaeger referred to the linked ICES presentation and reported that discussions are underway on how to develop a data sharing strategy for the purposes of the attached by way of a working group of ICES COMOH and PHO She Robert Kyle and Michael Finkelstein have already agreed to participate but she invited others to express interest She will bring this up at PHLC and report back 46 Lyme Disease Testing Backgrounder J Hopkins reported that an increasing amount of staff time in Niagara is being devoted to responding to inquiries from the public regarding the different diagnostic methods being used to confirm Lyme disease in the US and Canada She is therefore asking COMOH if this is a prevalent enough issue that a request should be made to PHO to develop some explanatory materials that could be used to address them She clarified that they arenrsquot having much of a problem with physicians itrsquos more a matter of educating the public regarding the accepted approach to the prevention diagnosis and treatment of the disease R Schabas cautioned that public education is a double-edged sword as it has the potential to create the impression that Lyme disease is a bigger problem than it is P Stewart reported that her health unit had a good in-service by a PHO lab person that has been very helpful for the odd questions that come up There were differing opinions of how much effort should be devoted to this as it appears to be another example of ill-informed public opinion on a public health issue akin to anti-vaccination and anti-fluoridation attitudes While these attitudes should not be ignored therersquos not much we can do in the near term to alter them V Jaeger offered to raise this during her next monthly conversation with George Pasut 50 Addendum
51 MOH Retirement I Gemmill noted that Mike Corriveau (MOH ndash Renfrew) will be retiring in December after over thirty years of service He asked that the COMOH Executive consider some form of recognition 60 UPDATES INFORMATION ITEMS REPORTS
61 Public Health Leadership
Council
611 ndash PHLC Update e-Mail Update
612 ndash PHSSP Implementation Tables CMOH Memo ndash PHSSP Tables V Jaeger referred to the linked memo which the result of the desire for clarity and openness on how the topic-specific implementation tables would be assembled The PHLC has already received a number of expressions of interest and will be communicating next steps soon 62 COMOH Executive Committee Minutes June 11
Notes July 9 Minutes July 31
Minutes September 10
63 COMOH Built Environment Work Group
The BEWG has not met since the last meeting but will meet on October 7 During the summer that group led by C Gardner and Nikhil Rajaram developed the paper (COMOHrsquos Advice for the Provincersquos Review of its Long-Term Energy Plan) that was the basis for the letter that went to the province (see item 68 below) V Jaeger expressed appreciation for the work that went into that C Gardner has expressed interest in being a member of the Promoting Healthy Environments ndash Both Natural and Built PHSSP implementation table 64 Public Health Early Years Group Aug 9 Meeting Notes A Feller reported that this group is putting together a November 5 Grand Rounds at PHO 65 iPHIS Panorama
July 8 Update
66 Joint OPHAalPHa Health Equity Working Group R Pellizzari reminded that this is a joint initiative of alPHa and OPHA She will ensure that L Stewart provides minutes of these meetings for future updates She and L Simon are the COMOH reps on this group L Simon circulated a paper by the Wellesley Institute that examines the health equity impacts of cessation of community water fluoridation which was requested by the HEWG She added that Bob Gardner Director of Policy at the Wellesley Institute is now participating in this group and he would welcome suggestions for other subjects for health equity impact assessments M Klassen suggested that Radon might be a good one She also reported that the National Collaborating Centre for Determinants of Health hosted a discussion for the nurses that have been hired under the SDOH portfolio in order to more clearly identify what the specific mandate of public health is in this area and to identify reasonable evaluative measurements This is being proposed as the basis of a Locally Driven Collaborative project and three health units are already involved (PCCHU Toronto and Durham) but more are required and any assistance would be welcome HEWG is also working on positions on the minimum wage review and the poverty strategy Both of these will be circulated once complete and approved
It is also working on a TOPHC session on Cultural Safety related to working with aboriginal populations Feedback was also invited on this with a note that the deadline for abstract submission is September 27 Finally work is also being done with PHO on developing resources and supports for work with Priority Populations 67 COMOH Electronic Mailing List List of Subscribers 68 COMOH Correspondence Aug 26 COMOH Letter ndash Energy Policy
Aug 8 COMOH Letter ndash CMA Poverty Report
July 22 COMOH Letter ndash Immunization Data
70 Next MeetingAdjournment Meeting adjourned at 1035 Next Section meeting will be on November 15 2013 in Toronto part of the alPHa Fall Symposium
Page 1 of 8 ndash DRAFT FOR COMOH DISCUSSION
alPHa Membership Survey hello
Draft Report ndash COMOH Version hello
alPHarsquos membership was surveyed in the fall of 2013 Similar surveys were administered to all member groups ie COMOH BOH Section and Affiliates using the online survey tool Survey Monkey Small alterations were made to group-specific surveys to ensure that the survey questions were relevant to each group A total of 84 responses were received from alPHa members The breakdown of respondents was as follows This draft report is provided for discussion purposes to COMOH members and therefore focuses on the responses provided by COMOH members To provide additional information overall survey responses are also provided for some questions
SECTION 1 RESPONDENT PROFILE
Survey Question What region is your health unit located in
For COMOH members responses came from 6 of the 7 regions of Ontario All 7 regions were represented in the full set of survey responses
Summary of Respondents COMOH 27 32 BOH Section 34 40 Affiliates 23 27 Totals 84 100
All ResponsesEastern 24 29South West 12 14Central East 13 15Central West 15 18North East 11 13Toronto 5 6Not Sure 3 4North West 1 1Totals 84 100
All COMOH ResponsesEastern 3 11South West 5 19Central East 6 22Central West 6 22North East 3 11Toronto 4 15North West 0 0Totals 27 100
Page 2 of 8 ndash DRAFT FOR COMOH DISCUSSION
Survey Question How long have you been involved with public health in Ontario
Survey Question Have you participated on the alPHa Board of Directors or an alPHa or COMOH committeeworking group
All ResponsesYes in the last 1 to 2 years 15 18Yes in the last 2 to 5 years 9 11Yes more than 5 years ago 9 11No not ever 51 61Totals 84 100
All COMOH ResponsesOver 10 years 17 635 to 10 years 7 262 to 5 years 3 11Totals 27 100
All ResponsesOver 10 years 34 405 to 10 years 21 252 to 5 years 21 251 to 2 years 3 4Less than 1 year 5 6Totals 84 100
All COMOH ResponsesYes in the last 1 to 2 years 7 26Yes in the last 2 to 5 years 4 15Yes more than 5 years ago 8 30No not ever 8 30Totals 27 100
Page 3 of 8 ndash DRAFT FOR COMOH DISCUSSION
SECTION 2 PROFESSIONAL DEVELOPMENT
Survey Question Which of the following events have you attended at least once in the past two years
Survey Question Overall how satisfied have you been with alPHa events ie conferences meetings
Survey Question How much value do alPHarsquos events provide for the money
Survey Question How can alPHa make its events more valuable to you Please share any suggestions regarding future topics speakers formats duration locations or any other event component that is important to you
Comments about content bull Expert speakerpanels on emerging or hot topics
(2) bull More engaged dialogue with Ministry rather than
just updates bull Fewer Ministry updates (3) bull Content on medicalPH issues is better left to PHO
TOPHC and joint conferences (2) bull alPHa should stick to Ministrypoliticspolicysenior
PH supportPHU support on key priorities (eg November practical conference on HKP report)
bull For COMOH more discussion bull More time for section activities like face-to-face
COMOH meetings
bull More facilitated work groups of COMOH members to respond to public health practice questions
bull More focus on rural and northern issues bull Infection Control Logistical Considerations bull Consider partnering with other groups bull More collaboration with PHO and OPHA events bull Use of video conferencing bull Less frequentfewer meetings (2) bull Connect with CME Location bull Consider other venues than TO
( ) brackets indicate that more than one response included a similar comment
More than enough value 7 11A lot of value 34 52Some value 22 34A little value 2 3Not enough value 0 0Totals 65 100
All Responses for those who Attended at least One Event in the Last 2 Years
All COMOH ResponsesMore than enough value 4 15A lot of value 13 48Some value 9 33A little value 1 4Not enough value 0 0Totals 27 100
Page 5 of 8 ndash DRAFT FOR COMOH DISCUSSION
SECTION 3 VALUE FOR MEMBERSHIP
Survey Question What do you value the most about your alPHa membership
The comments provided in response to the text response question What is the most important benefit of alPHa membership for you personally supported the answers illustrated in the chart above 15 of the 20 comments provided focussed on the importance of opportunities to interact with colleagues across the province The next most important benefit mentioned was the support for COMOH members to work on public health issues together When asked What is the most important benefit of alPHa membership for your health unit COMOH members emphasized the following bull A coordinated and collective voice in advocating for public health issues and the public health sector (9) bull Opportunities to connect with other public health units to share experiences and best practices (8) bull Maintaining relationships with government both politicians and bureaucrats (3) and bull Support for boards of health (3)
Page 6 of 8 ndash DRAFT FOR COMOH DISCUSSION
Overall Level of Satisfaction
SECTION 4 LOOKING TO THE FUTURE
The questions in this section were asked to obtain input from alPHa members regarding a proposal from alPHarsquos Board of Directors to focus the Association on five service areas COMOH members were asked to indicate their level of agreement with the proposed areas of focus COMOH responses compared to the overall survey responses were as follows
To explore some proposed changes to Association services COMOH members were asked to provide their level of agreement with the following questions
COMOH Responses BOH Section Affiliates All Survey Responses
Strongly Agree
AgreeNeither Agree or Disagree
DisagreeStrongly Disagree
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1Promoting the role and value of local public health units
15 9 2 0 0 26 92 93 95 94
2
Providing important information to members about trends and events that will impact the public health system and management of public health units
10 8 8 0 0 26 69 97 86 85
3Facilitating professional networking and information sharing
13 10 3 0 0 26 88 83 82 85
4
Providing professional development to support excellence in public health unit leadership management and governance
3 15 7 1 0 26 69 83 86 79
5
Responding to public health sector issues when it makes the most sense to have a collective voice ie issues that impact the structure and funding of the public health sector and public health units and issues that have a broad focus on population health
15 8 2 0 1 26 88 97 95 93
PROPOSED AREAS OF FOCUS
COMOH Responses BOH Section Affiliates All Survey Responses
Strongly Agree
AgreeNeither Agree or Disagree
DisagreeStrongly Disagree
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1
COMOH and other professional groups within alPHa should do their own advocacy while alPHa supports members to share and support each others advocacy efforts
7 6 6 6 1 26 50 58 45 52
2
alPHa should provide support to action-oriented inter-professional work groups on priority public health unit issues and member resolutions
4 13 5 3 1 26 65 81 86 77
PROPOSALS
Page 8 of 8 ndash DRAFT FOR COMOH DISCUSSION
COMOH members were also asked to indicate the level of acceptability for some possible changes to alPHarsquos services and way of doing business
COMOH Responses BOH Section Affiliates All Survey Responses
Very Acceptable
Somewhat Acceptable
Neither Acceptable or Unacceptable
Somewhat Unacceptable
Very Unaccept
able
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1Single conference with additional face-to-face section meetings
21 2 0 1 0 24 96 68 80 81
2alPHa to offer alternatives like webinars on focussed topics
13 6 1 4 0 24 79 50 90 71
3Coordinate COMOH meetings with PHO OMA or Ministry events
16 4 2 0 0 22 91 na na --
4
Increase focus on building leadership and management capacity for health unit CEOs and senior management
7 9 4 3 0 23 70 na 70 70
5
Would it be acceptable for alPHa to request voluntary financial contributions from member PHUs in addition to annual fees
3 5 5 4 5 22 36 7 26 21
6
Would it be acceptable for alPHa to request voluntary in-kind staff contributions from member PHUs to expand alPHas capacity eg communications policy work group support
7 11 1 1 3 23 78 31 45 50
7Would it be acceptable to you for alPHa to discontinue staff support for COMOH (BOH Section)
0 4 1 5 14 24 17 11 na 14
8
Would it be acceptable to you for alPHa to reduce the amount of staff support for COMOH (BOH Section)
1 6 1 8 6 22 32 26 na 29
9
Would it be acceptable to you for alPHa to provide supports to MOHs and AMOHs (BOH Members) without maintaining COMOH (BOHs) as a section of the association
3 2 3 2 12 22 23 17 na 20
10
Would it be acceptable to you for alPHas Board of Directors to move from the current representational model to a skills-based strategic model ie board membership would be based on the skills needed to carry out alPHas strategic plan
6 11 2 1 3 23 74 56 56 62
11
Would it be acceptable to you for alPHas President Vice-President and Treasurer to be elected from the full membership of the alPHa Board of Directors (rather than the current model of alternating between BOH and COMOH members)
10 8 1 2 2 23 78 70 70 73
PROPOSED CHANGES
1 Council of Ontario Medical Officers of Health Terms of Reference
ASSOCIATION OF LOCAL PUBLIC HEALTH AGENCIES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
TERMS OF REFERENCE NAME 1 The name of the organization shall be ldquoThe Council of Ontario Medical Officers of
Health a section of the Association of Local Public Health Agencies (alPHa)rdquo hereinafter referred to as ldquothe Councilrdquo
MISSION 2 As local leaders in public health we are committed to improving the health of
Ontarians and increasing health equity by strengthening Ontariorsquos public health system We achieve this through system leadership and coordination in collaboration with the provincial government and other organizations and through evidence-informed advocacy on public health policy
OBJECTIVES 3 The objectives of the Council shall be
a) To provide strong province-wide leadership in public health
b) To advocate for health protection and promotion policies and programs that maintain and improve the health of Ontarians
c) To promote and maintain the highest standards for Ontariorsquos public health
programs and services
d) To support the planning implementation and evaluation of effective and efficiently run public health programs and services
e) To act as a forum for sharing information and resources and for addressing and
discussing public health issues both amongst the Councilrsquos members and other agencies that support the goals of alPHa eg Ontario Medical Association Ontario Public Health Association etc
f) To engage with and to provide public health and related policy advice to alPHa
the Chief Medical Officer of Health the Ontario Ministries of Health and Long-Term Care (including the Health Promotion and Public Health Divisions) Children
2 Council of Ontario Medical Officers of Health Terms of Reference
and Youth Services and other provincial ministries Public Health Ontario Health Canada the Public Health Agency of Canada and other public health partners
g) To promote and protect the professional interests of its members
h) To provide support to individual members as needed
i) To seek recognition for outstanding practice from among the members
j) To support evidence based practice of public health medicine
k) To engage and involve the membership to participate in COMOHrsquos endeavours
l) To mentor Public Health and Preventive Medicine Residents
MEMBERSHIP 4 Membership on the Council in each of the following categories is subject to the
limitations imposed by the current terms of reference and all policies and governing documents of the Association of Local Public Health Agencies Benefits of membership in each category are included in Appendix A These shall be subject to regular review and may be suspended under certain circumstances
Active membership in the Council shall be open to all Associate Medical Officers of Health and all full-time Medical Officers of Health whose Boards of Health are members of alPHa Such members shall have full voting privileges and may hold office in the Council Associate membership shall be open to all full and part-time physicians employed by a Board of Health that is a member of alPHa Such members shall not have voting privileges nor hold office
Affiliate membership shall be open to the following individuals interested in furthering the objectives of the Council
bull Public Health and Preventive Medicine Residents and Public Health and Preventive Medicine Residency Program Directors
bull Federal public health physicians working in Ontariorsquos First Nations communities
bull other public health or related physicians including those employed by a Board of Health that is not a member of alPHa
Such members shall not have voting privileges nor hold office
3 Council of Ontario Medical Officers of Health Terms of Reference
Emeritus membership shall be open to all former members who have retired after five (5) or more years of Active membership subject to the nomination in writing of two (2) active members in good standing endorsement of the Executive Committee and approval of the Council by majority vote at a general meeting Such members shall have neither voting privileges nor hold office but may be invited to attend general meetings Honorary membership shall be open to any non-active or associate member subject to the nomination in writing of two (2) active members in good standing endorsement of the Executive Committee and approval of the Council Such members shall have neither voting privileges nor hold office but may be invited to attend general meetings
OFFICERS 5 The Officers of the Council shall be the Chair Vice-Chair and immediate Past Chair
6 The Chair shall prepare the agendas of all Council meetings She shall preside and
preserve order at all such meetings shall ensure that these Terms of Reference are upheld and enforced and shall contribute to the supervision and evaluation of any Public Health and Preventive Medicine Resident who is on a placement with alPHa
7 The Vice-Chair shall fulfill the duties of the Chair in hisher absence The immediate
Past Chair may fulfill the duties of the Chair or Vice-Chair in their absences 8 The Chair shall normally serve a term of one (1) year which is renewable once and
after which the Vice-Chair shall normally assume the vacated office COMMITTEES 9 The Council shall elect seven (7) active members one from each of alPHarsquos regions
and the active member who is scheduled to serve as the President or immediate Past-President of alPHa to represent it on the alPHa Board of Directors These seven (7) members shall constitute the Councilrsquos Executive Committee and shall serve a term of at least one (1) year The Chair and Vice-Chair shall be elected from among the Executive Committee members If alPHarsquos immediate Past President is an active member she shall be an ex-officio member of the Executive Committee
10 The mandate of the Executive Committee shall be to facilitate the achievement of
the objectives of the Council by fulfilling the following
a Identifying priorities 1
1 See Appendix B Planning Cycle to Identify Priorities for COMOH
and ensuring the development of briefing documents and or recommendations as appropriate for the consideration of the Council
4 Council of Ontario Medical Officers of Health Terms of Reference
b Setting agendas and otherwise ensuring preparations for Council meetings c Ensuring the fulfillment of the direction of Council d Responding in a timely fashion to time-sensitive public health matters in
accordance with the Executive Committeersquos understanding of the perspective of the Council
e Engaging with the Chief Medical Officer of Health Associate Chief Medical Officers of Health and other provincial public health leaders and
f Representing Council at public and partner agency forums including the Public Health Leadership Council which shall normally include membership from the Officers of the Council and two other Executive Committee members as selected by agreement among the Executive
g Identifying opportunities for the recognition of outstanding practice from among the members including the annual nomination of at least one member for the alPHa Distinguished Service Award
11 The Executive Committee shall meet and correspond in the manner and at the times
and if required places as deemed necessary by the Chair to conduct the business of the Council A quorum shall consist of four (4) members
12 The Executive Committee shall have the power to strike committeestask or working
groups to assist it in carrying out the business of the Council 13 The Council may by special resolution remove a member of the Executive
Committee before the completion of hisher term of office and may elect a successor to complete the term The special resolution shall require a majority vote of 67 of the members present and voting at the meeting at which the special resolution is considered
14 A Nominating Committee shall consist of the three (3) most recent Past Chairs who
are able to serve and shall be chaired by the immediate Past Chair The Nominating Committee shall prepare a list of proposed Officers and Executive Committee members for the consideration of the Council at its Annual General Meeting
MEETINGS 15 The Council shall hold at least four (4) general meetings per year in a manner and at
the times and if required places as deemed necessary by the Executive Committee to share information direct and assist the Executive Committee in conducting the business of the Council
16 The Council shall hold its Annual General Meeting during and at the same place as
the alPHarsquos Annual Conference
5 Council of Ontario Medical Officers of Health Terms of Reference
17 The Council shall hold a special meeting at the call of the Chair or upon the written request specifying the purpose of such meeting of at least five (5) active members Council members must be given at least 48 hours notice of any special meeting
18 Only Councilrsquos active and associate members and alPHa staff are entitled to attend
general and special meetings of the Council Other members and non-members may be invited to attend all or part of such meetings as determined by the Chair preferably in consultation with the Executive Committee Non-members who come to such meetings without an invitation may attend all or part of the meeting by a majority vote of the active members present and voting
19 The Chair shall prepare the agendas for such meetings and shall normally include
reports from the Chair and the Councilrsquos committeestask or working groups and representatives to external bodies alPHarsquos Executive Director shall ensure that the minutes shall be recorded and promptly distributed to the Section
20 A quorum for all such meetings shall be ten (10) active members 21 The Council shall normally be notified in a manner deemed appropriate by the Chair
of such meetings at least one (1) month prior to their being held 22 A majority vote of the members present at such meetings and voting shall make
Council decisions In the case of a tied vote the Chair shall cast the deciding vote The Executive Committee shall ensure that actions arising from such decisions at such meetings are implemented and monitored
23 The Chair may solicit advice from the Council through the use of teleconferencing
and alPHarsquos electronic mailing lists in order to gain an understanding of the overall perspective of the Council (see 10d)
ELECTIONS 24 The Officers and Executive Committee members shall be elected at the Sectionrsquos
Annual General Meeting The Nominating Committee Chair or hisher designate shall present a list of nominations Additional nominations from the floor shall also be considered Each Officer and Executive Committee member shall be elected by secret ballot if necessary by a majority of the active members present and voting In the case of a tie the Chair shall cast the deciding vote
AMENDMENTS 25 The Councilrsquos Terms of Reference may be amended from time to time by the
Executive Committee provided the Committee receives notice of such proposed amendments at least one (1) month prior to the meeting at which the amendments
6 Council of Ontario Medical Officers of Health Terms of Reference
will be considered Such amendments shall be ratified by the Council at the next general meeting or the Annual General Meeting as the case may be
26 The Executive Committee shall review the Terms of Reference as required and not
less than once every two years Original September 1987 1st Revision October 2000 2nd Revision July 2001 3rd Revision December 2003 4th Revision February 2008 5th Revision June 2009 6th Revision June 2011 7th Revision June 2013
7 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX A
COMOH Membership Benefits Active Membership
bull Entitled to attend all meetings of the Section bull May hold office on the COMOH Executive Committee alPHa Board of Directors
Standing Committees bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Associate Membership
bull Entitled to attend all meetings of the Section bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Affiliate Membership
bull May attend meetings or parts thereof subject to approval of Chair bull May serve on ad-hoc committees of the Section subject to the approval of the
Executive Committee bull Discounted registration rates for alPHa Conferences (for Public Health and
Preventive Medicine Residents) bull Upon written request and subject to COMOH Executive approval Affiliate
Members may subscribe to comohlistsalphaweborg The approval will be reviewed on an annual basis in order to determine if the Affiliate Member can remain a subscriber to mohsalphaweborg
Emeritus Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair bull Enjoy discounted registration rates for alPHa Conferences and regular COMOH
meetings bull Subscription to comohlistsalphaweborg electronic mailing list bull Full access to alPHa Web site bull May represent alPHa COMOH on selected external committees and working
groups Honorary Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair
8 Council of Ontario Medical Officers of Health Terms of Reference
bull May represent alPHa COMOH on selected external committees and working groups subject to the approval of the COMOH or alPHa Executive Committee as appropriate
9 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX B
Planning Cycle to Identify Priorities for COMOH
1 There shall normally be a COMOH membership strategic planning retreat every four years In recognition of the dynamic environment of public health the need for and timing of such a retreat shall be at the discretion of the Executive Committee in consultation with the membership
2 The COMOH Executive is responsible (through the creation of a subcommittee of COMOH members) for ensuring the preparation for the COMOH retreats with resources to include those provided by alPHa
3 Leadership for action on COMOH priorities will be recruited from among the COMOH membership in order to make good use of the full base of capacity of the membership The resources to support actions will be recruited from both within and beyond the COMOH membership employing other public health professionals that reside within the broader public health system and community
4 The COMOH Executive shall ensure an annual review of strategic priorities and initiatives and the development of a draft report of the same for the review of the members at the June meeting
2013 Strategic Planning
Considerations for COMOH
As part of its strategic planning discussions alPHarsquos Board has been considering changes to the level of support provided to member sections A member survey is being carried out over the fall to determine options acceptable to alPHa members The following approach to support is put forward as a proposal for the consideration of COMOH Note that the feasibility of the points below depend upon future decisions of the alPHa board They assume that COMOH remains part of alPHa but becomes more independent in administering meetings
1 alPHa can provide to COMOH staff support (Gord Fleming) amounting to 02 FTE or one day per week This is a reduction from the current level of 35 days per week COMOH can choose to use the support any way it wants writing COMOH letters meeting minutes agenda support special projects etc
2 In addition to 02 FTE alPHa staff would provide support for up to 4 face-to-face meetings per year One meeting would be concurrent to alPHarsquos annual conference in June The timing of other meetings could be negotiated The support includes consulting on the development of the program arranging for speakers registration for the event arranging venue AV support and hospitality services
3 In addition to 02 FTE alPHa staff would provide support for setting meeting dates and any polling required to establish dates Note that the individual supporting this function would be Karen Reece
4 COMOHrsquos Executive and Section would continue to have access to online supports through the alPHa including the COMOH Listserve and a group page for posting agendas minutes and other resources on the alPHa website
5 alPHa staff (Linda Stewart and Gord Fleming) can also start participating on CMOH calls as a way to be up-to-date on issues related to COMOH
6 Other than what is outlined above COMOH would be expected to prepare agendas and take minutes for its Executive and Section meetings The Executive would be expected to operate more independently than it does now but would be able to access the supports outlined above
Prepared by Linda Stewart Executive Director
From comoh-bounceslistsalphaweborg on behalf of Christopher MackieTo MOH ListserveSubject [comoh] Fw URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)Date Wednesday October 30 2013 91241 AMAttachments ATT00249txt
For AMOHs and PHPM residents who didnt receive the initial email
Chris
Christopher Mackie MD MHSc FRCPCMedical Officer of Health and CEOMiddlesex-London Health Unit50 King St LondonON N6A 5L7 O 519 663 5317 ext 2444 wwwhealthunitcomFrom Pisko Laura (MOHLTC)Sent Tuesday October 29 2013 759 PMTo kbarkeralgomapublichealthcom malcolmlockbchuorg davidcchatham-kentcarobertkyledurhamca proumeliotiseohuca fwarshelginhealthonca mohelginhealthoncahlynnpublichealthgreybruceonca malcolmlockhnhuorg hnmohhnhuorglnoseworthyhkpronca bobnosalhaltonca elizabethrichardsonhamiltoncarschabashpechuonca ncameronhuroncountyca drimgemmillkflapublichealthcamohkflapublichealthca suditranadecounty-lambtononca paulastewarthealthunitorgChristopher Mackie valeriejaegerniagararegionca jimchiriconbpsdhuca jarthursnwhuoncaisralevyottawaca dnealoxfordcountyca davidmowatpeelregionca mklassenpdhuoncarpellizzaripcchuca rosemarieramsinghporcupinehuonca mcorriveaurcdhucomcharlesgardnersmdhuorg sutcliffepsdhucom davidwilliamstbdhucomspruytmtimiskaminghucom dmckeowntorontoca lnolanregionofwaterloocanicolamercerwdghuorg aheimannwechealthunitorg karimkurjiyorkcaCc coreywesleytbdhucom CindyBaker-Barillsmdhuorg Donna Kosmack pilonlsdhucomPaulaMuiskflapublichealthca sthibautorontoca Mueller Daina (MOHLTC) Gordon Marcus(MOHLTC) andreakitahamiltoncaSubject URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)
Dear Colleagues The ministry has received reports that some tobacco vendors across the province aregiving away single cigarettes with the purchase of tobacco products It is the ministryrsquosposition that giving out free single cigarettes does not violate subsection 31(3) of theSmoke-Free Ontario Act (ldquoSFOArdquo) Although the practice of giving out free singlecigarettes may promote the sale of tobacco products it does not take the form of aldquoproduct enhancement product association or promotional materialrdquo and therefore doesnot fall within the scope of subsection 31(3) of the SFOA We have confirmed with Health Canada that this practice may violate section 29(b) of thefederal Tobacco Act As such Health Canada is requesting that you notify them in writingand I am directing you to communicate with them via email and provide to them as manydetails as possible Emails should be sent to Tobacco-Ontariohc-scgcca and thesubject line should read ldquoViolation of Section 29(b) of Tobacco Actrdquo This will ensurethat the complaints are given priority status by Health Canada We will continue to monitor
this situation and liaise with our colleagues at Health Canada Please share this information with your tobacco control staff and contact me or DainaMueller Manager Tobacco Control Unit Health Promotion Implementation Branch atdainamuellerontarioca with any questions RegardsLaura Laura A PiskoDirectorHealth Promotion Implementation BranchHealth Promotion DivisionMinistry of Health and Long Term Care416-327-7445 (office)416-451-3185 (mobile) Marcus Gordon - EA (416)326-0625 for urgent issues
========= Middlesex-London Health Unit E-Mail Disclaimer =============______________________________________________________________
Private and confidential intended only for named recipient If otherwisereceived please destroy immediately Health information in this email isonly general information and is not intended to replace an in personconsultation with a medical professional nor is it intended to providemedical advice Individual circumstances of which we are not aware mayaffect the information provided herein and as such the Middlesex-LondonHealth Unit assumes no liability or responsibility for your reliancethereon The Middlesex-London Health Unit works under the authority of theHealth Protection and Promotion Act and this correspondence may be used toassess your needs for public health services (519-663-5317 ext 2448)______________________________________________________________
From Gardner CharlesTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes (RayCopesoahppca)
George Pasut (GeorgePasutoahppca) Peter Cooney (petercooneyhc-scgcca)Cc Ito DickSubject Discontinuation of Fluoridation in MuskokaDate Tuesday October 22 2013 125254 PM
Hello Colleagues
As I reported in my email below on September 26th fluoridation has come under challenge again inSimcoe Muskoka I am now very unhappy to report that despite our best efforts last night theDistrict Council of Muskoka voted to remove fluoride from municipal drinking supplies across theDistrict This brings to an end fluoridation in all of Simcoe and Muskoka (with the exception of Base Borden)ndash though New Tecumseth will be conducting a plebiscite on the question of fluoridation with themunicipal election next October Defending community water fluoridation has drained a great deal of time human resources andcommitment from other priorities and has been exhausting here in SMDHU as I am sure it hasbeen in many other health units While the outcomes have been very disappointing I have beenimpressed by the professionalism and dedication that SMDHU staff members have shown inshouldering this burden In particular our dental consultant Dr Ito has provided us with much ofthe foundational knowledge and the local research essential to our efforts and has very frequentlyattended and presented at council meetings and other public events I would also like to thank themany of you who have offer and provided support including advocacy letters and informationresources Over the years Dr Peter Cooney Chief Dental Officer of Health of Canada has beenvery helpful attending and presenting with us at council meetings and at public consultationevents We will of course continue our oral health surveillance of the children of Muskoka documentingand reporting in future years on the increase in dental decay that we anticipate will occur Suchsurveillance is the foundation of our advocacy both to municipal politicians and to the province I am very concerned that our experience will continue to repeat itself across the province unlessthere is strong leadership provincially It is with this in mind that I raise the followingrecommendations for your consideration
1 That we collectively (with PHOrsquos leadership) conduct high quality publish-worthy researchdocumenting the impact on dental decay that occurs in those municipalities throughoutOntario that in recent years have discontinued community water fluoridation This could bepart of a larger study on such municipalities across the country and it could also be part ofa study documenting overall oral health (including fluoridation coverage) in the province(and possibly across the country)
2 That COMOH engage with our Chief MOH to advocate for the province to require allmunicipal water supplies to be fluoridated (the exception of course being those withnaturally sufficient fluoride concentrations) This could built upon the alPHa position to
Gordon
Highlight
Gordon
Highlight
date (A11-00 - Community Water Fluoridation) on the CMOH position (Oral Health ndash) and on theemail discussion generated on the COMOH listserv some months back re Richardrsquosproposal (calling on the province to fund municipal water fluoridation)
Valerie I request that this be an item for our COMOH meeting on November 15th Sincerely Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorg From Gardner Charles Sent Thursday September 26 2013 245 PMTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes(RayCopesoahppca)Subject Community Water Fluoridation Under Challenge Again in Simcoe Muskoka Hello Colleagues You may wish to know that community water fluoridation (CWF) is again under challenge in SimcoeMuskoka specifically both in Tottenham (Town of New Tecumseth in Simcoe County) and for theentire District of Muskoka On Monday September 23 Committee of the Whole Council of theTown of New Tecumseth voted to submit application to discontinue community water fluoridation(CWF) in the town of Tottenham despite presentations to the contrary from our dental consultantDr Ito and from me The next Council meeting is scheduled for Monday Sept 30 at which lastMondayrsquos (Sept 23) votes will be ratified
Since Monday I have spoken with the Mayor of the Town of New Tecumseth and with most of thecouncilors encouraging deferral of a decision on Monday to allow the town more time to make afully informed decision
This is the second time in recent years that the issue of discontinuing CWF in Tottenham has beenraised at council This issue is also scheduled to return again to the District of Muskoka Council on
October 21st where I will be presenting in response to deputations in opposition to fluoridation
Outside of Base Borden Tottenham is the only community with fluoridated water in SimcoeCounty The health unitrsquos own screening data between 2011 and 2013 shows that Tottenhamrsquos
Gordon
Highlight
children as well as those in Muskoka have a lower rate of dental decay than Simcoe Muskokacommunities without CWF
Sincerely
Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorgChuck Gardner MOH
November 04 2013
Mandatory State Laws on Fluoridation Thirteen states Puerto Rico and the District of Columbia have laws intended to provide
statewide fluoridation These states and the year that the fluoridation legislation was passed are
District of Columbia (1952) Connecticut (1965) Kentucky (1966) Illinois (1967) Minnesota
(1967) Ohio (1969) South Dakota (1969) Georgia (1973) Nebraska (1973 and 2008)
California (1995) Delaware (1998) Puerto Rico (1998) Nevada (1999) Louisiana (2008) and
Arkansas (2011) (see Table 1) The sizes of the public water systems or countiescommunities
affected and exemption provisions vary by state Table 1
STATES THAT HAVE MANDATORY LAWS ON FLUORIDATION -2011
State (1) Year of
Fluoridation
Legislation (1)
Population
served by
Fluoridated
CWS (2)
Persons
receiving
fluoridated
water (2)
State
Average
Caries
Experience
of Grade 3
Students (3)
Arkansas 2011 647 1724131 64
California 1995 621 22812721 709
Connecticut 1965 910 2370423 406
Delaware 1998 862 705344 545
Georgia 1973 921 8924598 52
Illinois 1967 993 11325132 532
Kentucky 1966 999 4334223 598
Louisiana 2008 407 1846149 657
Minnesota 1967 988 4117266 549
Nebraska 1973 and 2008 702 1001665 593
Nevada 1999 702 1001665 649
Ohio 1969 877 8772683 512
South Dakota 1969 948 642942 623
District of
Columbia
1952 1000 595000
Puerto Rico 1998
United States 739 204283554
2010 Statistics for population fluoridated and number of people
1 Communication with Jane McGinley RDH MBA Manager Fluoridation and Preventive Health
Activities Council on Access Prevention and Interprofessional Relations
2 Centers for Disease Control and Prevention Department of Health and Human Services
accessed Oct 21 2013 httpwwwcdcgovfluoridationstatistics2010statshtm
3 Centers for Disease Control and Prevention National Oral Health Surveillance System Caries
Experience - Percentage of 3rd Grade students with Caries Experience (treated or untreated tooth
If data from 43 states for the percentage of Grade 3 children with experience of dental decay is
compared with the 2008 percentages of the population in a state with Community Water
Fluoridation then the percentage of children with experience of dental decay decreases as the
percentage of the state population with Community Water Fluoridation increases (see Figure 1)
Figure 1
Correlation of Percentage of Grade 3 Children with Caries Experience and
Percentage of Population With Community Water Fluoridation for 43
Reporting States
0
10
20
30
40
50
60
70
80
0 10 20 30 40 50 60 70 80 90 100
State of Population With Community Water Fluoridation
Sta
te
of
Gra
de 3
Stu
den
ts w
ith
Cari
es E
xp
eri
en
ce
Data from CDC (2 3)
The description of the fluoridation laws in California Illinois and Nevada can be found on the
Association of State amp Territorial Dental Directors website(4 7 8)
The California fluoridation law AB 733 came into effect in 1995 requiring communities of 10
000 residents or more be supplied with fluoridated drinking water However the state did not
provide any funding to implement the legislation (California is unique in requiring fluoridation
without funding the practice)(4) The California Department of Health Services therefore had to
fund fluoridation initiatives from non-governmental sources ie the California Endowment
California Dental Association Foundation the First 5 Commission and others(5) From 1995 to
2011 the percentage of the California population receiving fluoridated drinking water has risen
from 17 to 625(6) 4 Dental Public Health Activities amp Practices Office of Oral Health California Department of Health
Services April 2002 httpwwwastddorgbestpracticesDES06002CAfluoridationpdf
5 Stock M Pollick H The CDA Foundation Model to Fluoridate Communities California Dental
Association Journal vol 40 no 8 649 - 655
httpwwwcdaorgPortals0journaljournal_082012pdf
6 California Dental Association Foundation
httpwwwcdafoundationorglearnadvocacyfluoridation
The State of Illinois passed a mandatory fluoridation state in 1967 and required all community
water systems to adjust fluoride levels in the drinking water to optimal levels within 1 year(7)
From 1962 when over 5000000 residents had optimally fluoridated drinking water by 2010
the number had risen to 11325132 (993 of the population on community water systems)(2)
7 Dental Public Health Activities amp Practices Division of Oral Health Illinois Department of Public
Health April 2002 httpwwwastddorgbestpracticesDES16007ILfluoridationpdf
The State of Nevada passed a mandatory fluoridation statute in 2000 for communities with
400000 or more residents(8) This was a result of the work of a statewide coalition that
included the Nevada Dental and Dental Hygienist Associations the Washoe and Clark County
District Health Departments the Clark County School District Junior League of Las Vegas
Head Start the Community College of Southern Nevada Dental Hygiene Program Health
Access Washoe County and Saint Maryrsquos Hospital For communities with less than 400000 the
implementation of fluoridation still required the vote of the majority voters in the community
The Las Vegas Water Authority and the City of Henderson started fluoridation in 2000
increasing the percentage of the population with fluoridated drinking water from 2 to 65 (8) 8 Dental Public Health Activities amp Practices Bureau of Family Health Services Nevada State Health
Division April 2002 httpwwwastddorgbestpracticesDES31002NVfluoridationbillpdf
Countries with Mandatory Laws on Fluoridation Countries that have mandated Community Water Fluoridation are Brazil Hong Kong
Malaysia Singapore Ireland Israel and some of the states in Australia
Singapore started fluoridating its water in 1956 based on the success of the fluoridation trials in
Grand Rapids Newburgh Evanston and Brantford Singapore became the first Asian country to
have 100 of its population benefitting from the implementation of fluoridated drinking water
Loh reported that ldquoThe ten year study on the effects of water fluoridation in Singapore showed
a decrease in caries prevalence in the children In the permanent dentition the reduction was
523 per cent for Chinese and 31 per cent for Malays in the 7 to 9 year old age group A similar
trend was observed in the mixed dentition in which the decrease was 325 per cent for Chinese
and 306 per cent for Malaysrdquo(9) By 2010 the population of the country was 5080000(10)
9 Loh T Thirty-eight years of water fluoridation--the Singapore scenario Community Dent
Health 1996 Sep13 Suppl 247-50
10 British Fluoridation Society One in a Million the facts about water fluoridation 3rd Edition
published March 2012) httpwwwbfsweborgonemillion0920One20in20a20Million20-
20The20Extent20of20Fluoridationpdf
Hong Kong started implementing community water fluoridation in 1961 and similar to
Singapore 100 of the population received access to fluoridated drinking water Lo and Wong
reported that ldquoThe mean DMFT score of the children deceased from 44 in 1960 to 15 in 1968
stayed at this level in the 1980 and 1986 surveys and further deceased to 08 in 2001 The
prevalence of dental fluorosis among the children surveyed in 1960 was 1 and this increased
to 59 and 70 in 1968 and 1980 respectively It was found in the 1986 and 2001 surveys that
the prevalences of fluorosis were 47 and 9 among children whose teeth developed at the
time when the respective water fluoride concentrations were 07 ppm and 05 ppmrdquo(11) The
population of Hong Kong was 6968000 in 2009(10) 11 LO ECM and WONG AHH Water fluoride concentration and fluorosis in Hong Kong in 1960-
2001 84th General Session and Exhibition of the International Association for Dental Research amp
1st Meeting of the Pan-Asian-Pacific Federation Brisbane Australia 28 June-1 July 2006 v 85 n
Sp B
The Malaysian cabinet approved a nationwide community water fluoridation program in 1972
(12) One of the states Sabah decided to stop fluoridation in 1989 due to concerns about
inadequate supervision in adding fluoride to the drinking water Oral Health Surveys in 2009
and 2007 indicated that children in Sabah had the worst oral health with 50 of 12 year-olds
having decay in their permanent teeth and children having an average of 3 teeth being(13)
Under the 10th Malaysian Plan in 2011 the federal and the Sabah state governments
reintroduced water fluoridation in Sabah(1314) In 2010 about 755 of the Malaysian
population or 20700000 people had fluoridated drinking water(1013) 12 Malaysian Dental Association Fluoride in Water
httpwwwmdaorgmy07_public_01healthcare_12htm
13 Sachdev N Fluoridation in Sabah Water for Cleaner Teeth French Tribunecom 28022011
From Levy IsraTo Jaeger ValerieCc Pim Carolyn gordonalphaweborg Diallo Aicha Penny Sutcliffe Paul Roumeliotis Michael Finkelstein
Hazel Lynn Robert KyleSubject FW Panorama - Privacy Security and other issuesDate Wednesday October 16 2013 122110 PM
Hello ValerieOttawa is part of Wave 4 Panorama implementation and we are gearing up increasingly to use thesystem where and if possible Thinking about it I am anticipating that this may need to be on theCOMOH (and alPHa) radar as it is something that will impact all health units and implies a majoroperational shift in vaccine delivery programs for all health units I have asked Carolyn Pim toconnect with our sister wave 4 units to share common experiences as we move forward ndash when wehave a roll up could I bring to COMOH Exec for discussion to explore whether there are broaderimplications for all members As an aside I have also asked the Ministry and their CIO to share with me any roll up learnings thatthey may have had already from previous waves (I understand that Niagara HU was a wave 1participant so if there is such a roll up of common experiences that others could learn fromperhaps you have it already and that could come to the exec too)Thanks Isra From Pim Carolyn Sent October 10 2013 1228 PMTo Christopher Mackie (christophermackiemlhuonca) Elizabeth Richardson(Elizabethrichardsonhamiltonca) H BSc M D F R C P (C) MPH Jim Chirico(jimchiriconbpsdhuca) Marlene Spruyt (spruytmtimiskaminghucom) Robert Kyle (Durham)Cc Levy IsraSubject Panorama - Privacy Security and other issues Dear colleagues Irsquom reaching out to you as fellow Panorama Wave 4 health units to ask about where yourorganizations are at in the process of signing agreements and completing Privacy ImpactAssessments and Threat Risk Assessments (TRAs) Ottawa Public Healthrsquos IT legal and informationsecurity advisors have made numerous requests to the MOHLTC for information (in particular theprovincial TRA) that we consider essential to develop our own risk assessment and PIA but havebeen told that information cannot be shared even with strict confidentiality and access controlsSo we are at somewhat of an impasse Isra emailed Arlene yesterday Arlene has forwarded ourconcerns to the Ministryrsquos CIO and Panorama lead but we havenrsquot had any response or discussionswith either of them yet Have your organizations identified similar concerns andor had interactions with the MOHLTC inthis respect Irsquod also be interested in knowing if your health units have flagged other (egoperational) implementation concerns Thanks
Carolyn ps Robert ndash you can ignore this request I talked with Sharan this morning about Durhamrsquos issuesso am including you now just for information Carolyn Pim MD FRCPC Associate Medical Officer of Health Meacutedecin adjointe en santeacute publique Ottawa Public Health Santeacute publique Ottawa 100 Constellation Cr Ottawa ON K2G 6J8 Tel teacutel (613) 580-6744 ext 23684Fax (613) 580-9641Connect With Ottawa Public Health
Suivez Santeacute publique Ottawa
This e-mail originates from the City of Ottawa e-mail system Any distribution use orcopying of this e-mail or the information it contains by other than the intendedrecipient(s) is unauthorized If you are not the intended recipient please notify meat the telephone number shown above or by return e-mail and delete thiscommunication and any copy immediately Thank you
Le preacutesent courriel a eacuteteacute expeacutedieacute par le systegraveme de courriels de la Ville dOttawaToute distribution utilisation ou reproduction du courriel ou des renseignements quisy trouvent par une personne autre que son destinataire preacutevu est interdite Si vousavez reccedilu le message par erreur veuillez men aviser par teacuteleacutephone (au numeacuteropreacuteciteacute) ou par courriel puis supprimer sans deacutelai la version originale de lacommunication ainsi que toutes ses copies Je vous remercie de votre collaboration
1
Smoke-Free Patios ndash An Amendment to the Smoke-Free Ontario Act
Date November 15 2013 Prepared for Council of Ontario Medical Officers of Health Prepared by York Region Public Health _____________________________________________________________________________ Issue
The Smoke-Free Ontario Act is the current provincial legislation that imposes smoking restrictions in workplaces and public places It prohibits smoking on restaurant and bar patios in instances where any portion of the seating area is covered by a roof With recent studies illustrating that exposure to second hand smoke outdoors poses similar risks to indoor exposure there has been growing public support to enhance smoking restrictions and make patios completely smoke-free
Background
With the implementation of the Smoke-Free Ontario Act in 2006 restaurant and bar patios became subject to smoking restrictions if any portion of the seating area was covered by a roof This allowed for patios without roof coverings to continue to allow smoking and as a result did not provide significant protection to patrons or staff from exposure to second hand smoke outdoors Many businesses chose to alter the design of their patios to allow smoking to continue In some cases patios became more crowded since smoking patrons who dine indoors often proceed outside onto licensed patios with their beverages to smoke York Region like most municipalities in Ontario is host to hundreds of patios being operated by restaurant owners and businesses With smoking prohibitions affecting only a small portion of these patios specifically ones with coverings the vast majority of patios still allow smoking to take place Patrons and employees on patios where smoking is not restricted are exposed to second hand smoke frequently This can contribute to increased disease and aggravation of existing health conditions From a business perspective the existing legislation has been viewed by many operators as unfair because some patios have permanent coverings which cannot be removed requiring a smoke-free status These business owners feel this creates an uneven playing field since they cannot provide an outdoor dining area for their smoking customers There is strong community support for smoke-free patios in Ontario A 2009 Rapid Risk Factor Surveillance System survey revealed 754 percent support in York Region while a Toronto Health Survey in 2011 indicated 74 percent public support
2
Current Status
Smoking is currently prohibited on restaurant and bar patios province-wide in four Canadian provinces and territories Alberta Newfoundland and Labrador Nova Scotia and Yukon A fifth province Prince Edward Island prohibits smoking on patios until 10 pm Since Ontario enacted legislation restricting smoking on patios in 2006 eight municipalities in Ontario have chosen to create bylaws that go beyond the Smoke-Free Ontario Act and enhance outdoor protection from second hand smoke by prohibiting smoking on patios completely The largest of those municipalities is the City of Ottawa Recently the Toronto Board of Health unanimously endorsed a report presented by their Medical Officer of Health recommending that restaurant and bar patios be made smoke-free through an amendment to the Smoke-Free Ontario Act
Key Considerations
There should be no significant financial burden to local Boards of Health resulting from a smoke-free patio amendment to the Smoke-Free Ontario Act Inspection and enforcement for the Smoke-Free Ontario Act is currently 100 percent funded by the Ministry of Health and Long-Term Care Following an introductory period of education on the amendment a complaint response model of service delivery would ensure ongoing compliance with smoke-free requirements A complete ban of smoking on patios would eliminate the widely-held perception by business owners that the current legislation creates an uneven playing field for business Since Smoke-Free Ontario Act inspections of patios began in 2006 operators have expressed the opinion that if patios need to be smoke-free for the protection of the public they should all be smoke-free to avoid undue hardship for individual businesses and to provide protection uniformly across the Province
Next steps
York Region Public Health intends to seek support from Medical Officers of Health across the Central East Tobacco Control Area Network (CETCAN) to advocate to the Ministry of Health and Long-Term Care for an amendment to the Smoke-Free Ontario Act prohibiting smoking on all restaurant and bar patios York Region is also in the process of requesting that its Regional Council advocate to the Minister of Health and Long-Term Care on the issue
Updating and Modernizing O Regulation 565 (Public Pools)
Date November 15 2013
Prepared for Council of Ontario Medical Officers of Health
Prepared by York Region Public Health _____________________________________________________________________________ Background Recent drownings at public pools in Ontario have highlighted the issue of water-borne illness and injury The current pool regulation under Ontariorsquos Health Protection and Promotion Act O Regulation 565 (Public Pools) is outdated It does not accurately reflect new pool technology and design or the changing use of public pools Neither does it incorporate admissions standards recommended by the Office of the Chief Coroner Further O Regulation 565 does not have short-form wording or set fines associated with it This limits public health enforcement capabilities What is the impact Updating O Regulation 565 (Public Pools) to address recent changes in pool technology design and uses and to include Coroner-recommended admissions standards would help improve pool safety Establishing short-form wording for O Regulation 565 would enhance enforcement related to public pools Currently the only enforcement available to Public Health Inspectors for dealing with non-critical regulatory infractions in public pools is the issuance of a Part III summons This involves a considerable amount of resources for a possible small fine With the development of inspection disclosure systems such as YorkSafe there is an even greater need to develop a method to effectively address repeated pool operator non-compliance with non-critical issues Next steps Public health units should advocate to the Province to 1) Conduct a review of O Regulation 565 (Public Pools) to address shortcomings Proposed changes to the
regulation should include a requirement for ownersoperators of public pools to advise the local Medical Officer of Health of any change in the use of a facility and the addition of the Coronerrsquos recommended admission standards
2) Provide short-form wording for O Regulation 565 so that public health inspectors can better deal with pool operator non-compliance
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
There was support for further exploration but it was agreed that more information would be beneficial As an initial step RPellizzari will contact Erika Bontovics in an effort to examine the date described above with a view to determining what further information (eg costs negotiated by each HU) might be needed 45 Children and Youth Data Strategy Slide Deck ndash Aug 15 Teleconference amp ICES
Privacy Code V Jaeger referred to the linked ICES presentation and reported that discussions are underway on how to develop a data sharing strategy for the purposes of the attached by way of a working group of ICES COMOH and PHO She Robert Kyle and Michael Finkelstein have already agreed to participate but she invited others to express interest She will bring this up at PHLC and report back 46 Lyme Disease Testing Backgrounder J Hopkins reported that an increasing amount of staff time in Niagara is being devoted to responding to inquiries from the public regarding the different diagnostic methods being used to confirm Lyme disease in the US and Canada She is therefore asking COMOH if this is a prevalent enough issue that a request should be made to PHO to develop some explanatory materials that could be used to address them She clarified that they arenrsquot having much of a problem with physicians itrsquos more a matter of educating the public regarding the accepted approach to the prevention diagnosis and treatment of the disease R Schabas cautioned that public education is a double-edged sword as it has the potential to create the impression that Lyme disease is a bigger problem than it is P Stewart reported that her health unit had a good in-service by a PHO lab person that has been very helpful for the odd questions that come up There were differing opinions of how much effort should be devoted to this as it appears to be another example of ill-informed public opinion on a public health issue akin to anti-vaccination and anti-fluoridation attitudes While these attitudes should not be ignored therersquos not much we can do in the near term to alter them V Jaeger offered to raise this during her next monthly conversation with George Pasut 50 Addendum
51 MOH Retirement I Gemmill noted that Mike Corriveau (MOH ndash Renfrew) will be retiring in December after over thirty years of service He asked that the COMOH Executive consider some form of recognition 60 UPDATES INFORMATION ITEMS REPORTS
61 Public Health Leadership
Council
611 ndash PHLC Update e-Mail Update
612 ndash PHSSP Implementation Tables CMOH Memo ndash PHSSP Tables V Jaeger referred to the linked memo which the result of the desire for clarity and openness on how the topic-specific implementation tables would be assembled The PHLC has already received a number of expressions of interest and will be communicating next steps soon 62 COMOH Executive Committee Minutes June 11
Notes July 9 Minutes July 31
Minutes September 10
63 COMOH Built Environment Work Group
The BEWG has not met since the last meeting but will meet on October 7 During the summer that group led by C Gardner and Nikhil Rajaram developed the paper (COMOHrsquos Advice for the Provincersquos Review of its Long-Term Energy Plan) that was the basis for the letter that went to the province (see item 68 below) V Jaeger expressed appreciation for the work that went into that C Gardner has expressed interest in being a member of the Promoting Healthy Environments ndash Both Natural and Built PHSSP implementation table 64 Public Health Early Years Group Aug 9 Meeting Notes A Feller reported that this group is putting together a November 5 Grand Rounds at PHO 65 iPHIS Panorama
July 8 Update
66 Joint OPHAalPHa Health Equity Working Group R Pellizzari reminded that this is a joint initiative of alPHa and OPHA She will ensure that L Stewart provides minutes of these meetings for future updates She and L Simon are the COMOH reps on this group L Simon circulated a paper by the Wellesley Institute that examines the health equity impacts of cessation of community water fluoridation which was requested by the HEWG She added that Bob Gardner Director of Policy at the Wellesley Institute is now participating in this group and he would welcome suggestions for other subjects for health equity impact assessments M Klassen suggested that Radon might be a good one She also reported that the National Collaborating Centre for Determinants of Health hosted a discussion for the nurses that have been hired under the SDOH portfolio in order to more clearly identify what the specific mandate of public health is in this area and to identify reasonable evaluative measurements This is being proposed as the basis of a Locally Driven Collaborative project and three health units are already involved (PCCHU Toronto and Durham) but more are required and any assistance would be welcome HEWG is also working on positions on the minimum wage review and the poverty strategy Both of these will be circulated once complete and approved
It is also working on a TOPHC session on Cultural Safety related to working with aboriginal populations Feedback was also invited on this with a note that the deadline for abstract submission is September 27 Finally work is also being done with PHO on developing resources and supports for work with Priority Populations 67 COMOH Electronic Mailing List List of Subscribers 68 COMOH Correspondence Aug 26 COMOH Letter ndash Energy Policy
Aug 8 COMOH Letter ndash CMA Poverty Report
July 22 COMOH Letter ndash Immunization Data
70 Next MeetingAdjournment Meeting adjourned at 1035 Next Section meeting will be on November 15 2013 in Toronto part of the alPHa Fall Symposium
Page 1 of 8 ndash DRAFT FOR COMOH DISCUSSION
alPHa Membership Survey hello
Draft Report ndash COMOH Version hello
alPHarsquos membership was surveyed in the fall of 2013 Similar surveys were administered to all member groups ie COMOH BOH Section and Affiliates using the online survey tool Survey Monkey Small alterations were made to group-specific surveys to ensure that the survey questions were relevant to each group A total of 84 responses were received from alPHa members The breakdown of respondents was as follows This draft report is provided for discussion purposes to COMOH members and therefore focuses on the responses provided by COMOH members To provide additional information overall survey responses are also provided for some questions
SECTION 1 RESPONDENT PROFILE
Survey Question What region is your health unit located in
For COMOH members responses came from 6 of the 7 regions of Ontario All 7 regions were represented in the full set of survey responses
Summary of Respondents COMOH 27 32 BOH Section 34 40 Affiliates 23 27 Totals 84 100
All ResponsesEastern 24 29South West 12 14Central East 13 15Central West 15 18North East 11 13Toronto 5 6Not Sure 3 4North West 1 1Totals 84 100
All COMOH ResponsesEastern 3 11South West 5 19Central East 6 22Central West 6 22North East 3 11Toronto 4 15North West 0 0Totals 27 100
Page 2 of 8 ndash DRAFT FOR COMOH DISCUSSION
Survey Question How long have you been involved with public health in Ontario
Survey Question Have you participated on the alPHa Board of Directors or an alPHa or COMOH committeeworking group
All ResponsesYes in the last 1 to 2 years 15 18Yes in the last 2 to 5 years 9 11Yes more than 5 years ago 9 11No not ever 51 61Totals 84 100
All COMOH ResponsesOver 10 years 17 635 to 10 years 7 262 to 5 years 3 11Totals 27 100
All ResponsesOver 10 years 34 405 to 10 years 21 252 to 5 years 21 251 to 2 years 3 4Less than 1 year 5 6Totals 84 100
All COMOH ResponsesYes in the last 1 to 2 years 7 26Yes in the last 2 to 5 years 4 15Yes more than 5 years ago 8 30No not ever 8 30Totals 27 100
Page 3 of 8 ndash DRAFT FOR COMOH DISCUSSION
SECTION 2 PROFESSIONAL DEVELOPMENT
Survey Question Which of the following events have you attended at least once in the past two years
Survey Question Overall how satisfied have you been with alPHa events ie conferences meetings
Survey Question How much value do alPHarsquos events provide for the money
Survey Question How can alPHa make its events more valuable to you Please share any suggestions regarding future topics speakers formats duration locations or any other event component that is important to you
Comments about content bull Expert speakerpanels on emerging or hot topics
(2) bull More engaged dialogue with Ministry rather than
just updates bull Fewer Ministry updates (3) bull Content on medicalPH issues is better left to PHO
TOPHC and joint conferences (2) bull alPHa should stick to Ministrypoliticspolicysenior
PH supportPHU support on key priorities (eg November practical conference on HKP report)
bull For COMOH more discussion bull More time for section activities like face-to-face
COMOH meetings
bull More facilitated work groups of COMOH members to respond to public health practice questions
bull More focus on rural and northern issues bull Infection Control Logistical Considerations bull Consider partnering with other groups bull More collaboration with PHO and OPHA events bull Use of video conferencing bull Less frequentfewer meetings (2) bull Connect with CME Location bull Consider other venues than TO
( ) brackets indicate that more than one response included a similar comment
More than enough value 7 11A lot of value 34 52Some value 22 34A little value 2 3Not enough value 0 0Totals 65 100
All Responses for those who Attended at least One Event in the Last 2 Years
All COMOH ResponsesMore than enough value 4 15A lot of value 13 48Some value 9 33A little value 1 4Not enough value 0 0Totals 27 100
Page 5 of 8 ndash DRAFT FOR COMOH DISCUSSION
SECTION 3 VALUE FOR MEMBERSHIP
Survey Question What do you value the most about your alPHa membership
The comments provided in response to the text response question What is the most important benefit of alPHa membership for you personally supported the answers illustrated in the chart above 15 of the 20 comments provided focussed on the importance of opportunities to interact with colleagues across the province The next most important benefit mentioned was the support for COMOH members to work on public health issues together When asked What is the most important benefit of alPHa membership for your health unit COMOH members emphasized the following bull A coordinated and collective voice in advocating for public health issues and the public health sector (9) bull Opportunities to connect with other public health units to share experiences and best practices (8) bull Maintaining relationships with government both politicians and bureaucrats (3) and bull Support for boards of health (3)
Page 6 of 8 ndash DRAFT FOR COMOH DISCUSSION
Overall Level of Satisfaction
SECTION 4 LOOKING TO THE FUTURE
The questions in this section were asked to obtain input from alPHa members regarding a proposal from alPHarsquos Board of Directors to focus the Association on five service areas COMOH members were asked to indicate their level of agreement with the proposed areas of focus COMOH responses compared to the overall survey responses were as follows
To explore some proposed changes to Association services COMOH members were asked to provide their level of agreement with the following questions
COMOH Responses BOH Section Affiliates All Survey Responses
Strongly Agree
AgreeNeither Agree or Disagree
DisagreeStrongly Disagree
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1Promoting the role and value of local public health units
15 9 2 0 0 26 92 93 95 94
2
Providing important information to members about trends and events that will impact the public health system and management of public health units
10 8 8 0 0 26 69 97 86 85
3Facilitating professional networking and information sharing
13 10 3 0 0 26 88 83 82 85
4
Providing professional development to support excellence in public health unit leadership management and governance
3 15 7 1 0 26 69 83 86 79
5
Responding to public health sector issues when it makes the most sense to have a collective voice ie issues that impact the structure and funding of the public health sector and public health units and issues that have a broad focus on population health
15 8 2 0 1 26 88 97 95 93
PROPOSED AREAS OF FOCUS
COMOH Responses BOH Section Affiliates All Survey Responses
Strongly Agree
AgreeNeither Agree or Disagree
DisagreeStrongly Disagree
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1
COMOH and other professional groups within alPHa should do their own advocacy while alPHa supports members to share and support each others advocacy efforts
7 6 6 6 1 26 50 58 45 52
2
alPHa should provide support to action-oriented inter-professional work groups on priority public health unit issues and member resolutions
4 13 5 3 1 26 65 81 86 77
PROPOSALS
Page 8 of 8 ndash DRAFT FOR COMOH DISCUSSION
COMOH members were also asked to indicate the level of acceptability for some possible changes to alPHarsquos services and way of doing business
COMOH Responses BOH Section Affiliates All Survey Responses
Very Acceptable
Somewhat Acceptable
Neither Acceptable or Unacceptable
Somewhat Unacceptable
Very Unaccept
able
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1Single conference with additional face-to-face section meetings
21 2 0 1 0 24 96 68 80 81
2alPHa to offer alternatives like webinars on focussed topics
13 6 1 4 0 24 79 50 90 71
3Coordinate COMOH meetings with PHO OMA or Ministry events
16 4 2 0 0 22 91 na na --
4
Increase focus on building leadership and management capacity for health unit CEOs and senior management
7 9 4 3 0 23 70 na 70 70
5
Would it be acceptable for alPHa to request voluntary financial contributions from member PHUs in addition to annual fees
3 5 5 4 5 22 36 7 26 21
6
Would it be acceptable for alPHa to request voluntary in-kind staff contributions from member PHUs to expand alPHas capacity eg communications policy work group support
7 11 1 1 3 23 78 31 45 50
7Would it be acceptable to you for alPHa to discontinue staff support for COMOH (BOH Section)
0 4 1 5 14 24 17 11 na 14
8
Would it be acceptable to you for alPHa to reduce the amount of staff support for COMOH (BOH Section)
1 6 1 8 6 22 32 26 na 29
9
Would it be acceptable to you for alPHa to provide supports to MOHs and AMOHs (BOH Members) without maintaining COMOH (BOHs) as a section of the association
3 2 3 2 12 22 23 17 na 20
10
Would it be acceptable to you for alPHas Board of Directors to move from the current representational model to a skills-based strategic model ie board membership would be based on the skills needed to carry out alPHas strategic plan
6 11 2 1 3 23 74 56 56 62
11
Would it be acceptable to you for alPHas President Vice-President and Treasurer to be elected from the full membership of the alPHa Board of Directors (rather than the current model of alternating between BOH and COMOH members)
10 8 1 2 2 23 78 70 70 73
PROPOSED CHANGES
1 Council of Ontario Medical Officers of Health Terms of Reference
ASSOCIATION OF LOCAL PUBLIC HEALTH AGENCIES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
TERMS OF REFERENCE NAME 1 The name of the organization shall be ldquoThe Council of Ontario Medical Officers of
Health a section of the Association of Local Public Health Agencies (alPHa)rdquo hereinafter referred to as ldquothe Councilrdquo
MISSION 2 As local leaders in public health we are committed to improving the health of
Ontarians and increasing health equity by strengthening Ontariorsquos public health system We achieve this through system leadership and coordination in collaboration with the provincial government and other organizations and through evidence-informed advocacy on public health policy
OBJECTIVES 3 The objectives of the Council shall be
a) To provide strong province-wide leadership in public health
b) To advocate for health protection and promotion policies and programs that maintain and improve the health of Ontarians
c) To promote and maintain the highest standards for Ontariorsquos public health
programs and services
d) To support the planning implementation and evaluation of effective and efficiently run public health programs and services
e) To act as a forum for sharing information and resources and for addressing and
discussing public health issues both amongst the Councilrsquos members and other agencies that support the goals of alPHa eg Ontario Medical Association Ontario Public Health Association etc
f) To engage with and to provide public health and related policy advice to alPHa
the Chief Medical Officer of Health the Ontario Ministries of Health and Long-Term Care (including the Health Promotion and Public Health Divisions) Children
2 Council of Ontario Medical Officers of Health Terms of Reference
and Youth Services and other provincial ministries Public Health Ontario Health Canada the Public Health Agency of Canada and other public health partners
g) To promote and protect the professional interests of its members
h) To provide support to individual members as needed
i) To seek recognition for outstanding practice from among the members
j) To support evidence based practice of public health medicine
k) To engage and involve the membership to participate in COMOHrsquos endeavours
l) To mentor Public Health and Preventive Medicine Residents
MEMBERSHIP 4 Membership on the Council in each of the following categories is subject to the
limitations imposed by the current terms of reference and all policies and governing documents of the Association of Local Public Health Agencies Benefits of membership in each category are included in Appendix A These shall be subject to regular review and may be suspended under certain circumstances
Active membership in the Council shall be open to all Associate Medical Officers of Health and all full-time Medical Officers of Health whose Boards of Health are members of alPHa Such members shall have full voting privileges and may hold office in the Council Associate membership shall be open to all full and part-time physicians employed by a Board of Health that is a member of alPHa Such members shall not have voting privileges nor hold office
Affiliate membership shall be open to the following individuals interested in furthering the objectives of the Council
bull Public Health and Preventive Medicine Residents and Public Health and Preventive Medicine Residency Program Directors
bull Federal public health physicians working in Ontariorsquos First Nations communities
bull other public health or related physicians including those employed by a Board of Health that is not a member of alPHa
Such members shall not have voting privileges nor hold office
3 Council of Ontario Medical Officers of Health Terms of Reference
Emeritus membership shall be open to all former members who have retired after five (5) or more years of Active membership subject to the nomination in writing of two (2) active members in good standing endorsement of the Executive Committee and approval of the Council by majority vote at a general meeting Such members shall have neither voting privileges nor hold office but may be invited to attend general meetings Honorary membership shall be open to any non-active or associate member subject to the nomination in writing of two (2) active members in good standing endorsement of the Executive Committee and approval of the Council Such members shall have neither voting privileges nor hold office but may be invited to attend general meetings
OFFICERS 5 The Officers of the Council shall be the Chair Vice-Chair and immediate Past Chair
6 The Chair shall prepare the agendas of all Council meetings She shall preside and
preserve order at all such meetings shall ensure that these Terms of Reference are upheld and enforced and shall contribute to the supervision and evaluation of any Public Health and Preventive Medicine Resident who is on a placement with alPHa
7 The Vice-Chair shall fulfill the duties of the Chair in hisher absence The immediate
Past Chair may fulfill the duties of the Chair or Vice-Chair in their absences 8 The Chair shall normally serve a term of one (1) year which is renewable once and
after which the Vice-Chair shall normally assume the vacated office COMMITTEES 9 The Council shall elect seven (7) active members one from each of alPHarsquos regions
and the active member who is scheduled to serve as the President or immediate Past-President of alPHa to represent it on the alPHa Board of Directors These seven (7) members shall constitute the Councilrsquos Executive Committee and shall serve a term of at least one (1) year The Chair and Vice-Chair shall be elected from among the Executive Committee members If alPHarsquos immediate Past President is an active member she shall be an ex-officio member of the Executive Committee
10 The mandate of the Executive Committee shall be to facilitate the achievement of
the objectives of the Council by fulfilling the following
a Identifying priorities 1
1 See Appendix B Planning Cycle to Identify Priorities for COMOH
and ensuring the development of briefing documents and or recommendations as appropriate for the consideration of the Council
4 Council of Ontario Medical Officers of Health Terms of Reference
b Setting agendas and otherwise ensuring preparations for Council meetings c Ensuring the fulfillment of the direction of Council d Responding in a timely fashion to time-sensitive public health matters in
accordance with the Executive Committeersquos understanding of the perspective of the Council
e Engaging with the Chief Medical Officer of Health Associate Chief Medical Officers of Health and other provincial public health leaders and
f Representing Council at public and partner agency forums including the Public Health Leadership Council which shall normally include membership from the Officers of the Council and two other Executive Committee members as selected by agreement among the Executive
g Identifying opportunities for the recognition of outstanding practice from among the members including the annual nomination of at least one member for the alPHa Distinguished Service Award
11 The Executive Committee shall meet and correspond in the manner and at the times
and if required places as deemed necessary by the Chair to conduct the business of the Council A quorum shall consist of four (4) members
12 The Executive Committee shall have the power to strike committeestask or working
groups to assist it in carrying out the business of the Council 13 The Council may by special resolution remove a member of the Executive
Committee before the completion of hisher term of office and may elect a successor to complete the term The special resolution shall require a majority vote of 67 of the members present and voting at the meeting at which the special resolution is considered
14 A Nominating Committee shall consist of the three (3) most recent Past Chairs who
are able to serve and shall be chaired by the immediate Past Chair The Nominating Committee shall prepare a list of proposed Officers and Executive Committee members for the consideration of the Council at its Annual General Meeting
MEETINGS 15 The Council shall hold at least four (4) general meetings per year in a manner and at
the times and if required places as deemed necessary by the Executive Committee to share information direct and assist the Executive Committee in conducting the business of the Council
16 The Council shall hold its Annual General Meeting during and at the same place as
the alPHarsquos Annual Conference
5 Council of Ontario Medical Officers of Health Terms of Reference
17 The Council shall hold a special meeting at the call of the Chair or upon the written request specifying the purpose of such meeting of at least five (5) active members Council members must be given at least 48 hours notice of any special meeting
18 Only Councilrsquos active and associate members and alPHa staff are entitled to attend
general and special meetings of the Council Other members and non-members may be invited to attend all or part of such meetings as determined by the Chair preferably in consultation with the Executive Committee Non-members who come to such meetings without an invitation may attend all or part of the meeting by a majority vote of the active members present and voting
19 The Chair shall prepare the agendas for such meetings and shall normally include
reports from the Chair and the Councilrsquos committeestask or working groups and representatives to external bodies alPHarsquos Executive Director shall ensure that the minutes shall be recorded and promptly distributed to the Section
20 A quorum for all such meetings shall be ten (10) active members 21 The Council shall normally be notified in a manner deemed appropriate by the Chair
of such meetings at least one (1) month prior to their being held 22 A majority vote of the members present at such meetings and voting shall make
Council decisions In the case of a tied vote the Chair shall cast the deciding vote The Executive Committee shall ensure that actions arising from such decisions at such meetings are implemented and monitored
23 The Chair may solicit advice from the Council through the use of teleconferencing
and alPHarsquos electronic mailing lists in order to gain an understanding of the overall perspective of the Council (see 10d)
ELECTIONS 24 The Officers and Executive Committee members shall be elected at the Sectionrsquos
Annual General Meeting The Nominating Committee Chair or hisher designate shall present a list of nominations Additional nominations from the floor shall also be considered Each Officer and Executive Committee member shall be elected by secret ballot if necessary by a majority of the active members present and voting In the case of a tie the Chair shall cast the deciding vote
AMENDMENTS 25 The Councilrsquos Terms of Reference may be amended from time to time by the
Executive Committee provided the Committee receives notice of such proposed amendments at least one (1) month prior to the meeting at which the amendments
6 Council of Ontario Medical Officers of Health Terms of Reference
will be considered Such amendments shall be ratified by the Council at the next general meeting or the Annual General Meeting as the case may be
26 The Executive Committee shall review the Terms of Reference as required and not
less than once every two years Original September 1987 1st Revision October 2000 2nd Revision July 2001 3rd Revision December 2003 4th Revision February 2008 5th Revision June 2009 6th Revision June 2011 7th Revision June 2013
7 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX A
COMOH Membership Benefits Active Membership
bull Entitled to attend all meetings of the Section bull May hold office on the COMOH Executive Committee alPHa Board of Directors
Standing Committees bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Associate Membership
bull Entitled to attend all meetings of the Section bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Affiliate Membership
bull May attend meetings or parts thereof subject to approval of Chair bull May serve on ad-hoc committees of the Section subject to the approval of the
Executive Committee bull Discounted registration rates for alPHa Conferences (for Public Health and
Preventive Medicine Residents) bull Upon written request and subject to COMOH Executive approval Affiliate
Members may subscribe to comohlistsalphaweborg The approval will be reviewed on an annual basis in order to determine if the Affiliate Member can remain a subscriber to mohsalphaweborg
Emeritus Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair bull Enjoy discounted registration rates for alPHa Conferences and regular COMOH
meetings bull Subscription to comohlistsalphaweborg electronic mailing list bull Full access to alPHa Web site bull May represent alPHa COMOH on selected external committees and working
groups Honorary Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair
8 Council of Ontario Medical Officers of Health Terms of Reference
bull May represent alPHa COMOH on selected external committees and working groups subject to the approval of the COMOH or alPHa Executive Committee as appropriate
9 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX B
Planning Cycle to Identify Priorities for COMOH
1 There shall normally be a COMOH membership strategic planning retreat every four years In recognition of the dynamic environment of public health the need for and timing of such a retreat shall be at the discretion of the Executive Committee in consultation with the membership
2 The COMOH Executive is responsible (through the creation of a subcommittee of COMOH members) for ensuring the preparation for the COMOH retreats with resources to include those provided by alPHa
3 Leadership for action on COMOH priorities will be recruited from among the COMOH membership in order to make good use of the full base of capacity of the membership The resources to support actions will be recruited from both within and beyond the COMOH membership employing other public health professionals that reside within the broader public health system and community
4 The COMOH Executive shall ensure an annual review of strategic priorities and initiatives and the development of a draft report of the same for the review of the members at the June meeting
2013 Strategic Planning
Considerations for COMOH
As part of its strategic planning discussions alPHarsquos Board has been considering changes to the level of support provided to member sections A member survey is being carried out over the fall to determine options acceptable to alPHa members The following approach to support is put forward as a proposal for the consideration of COMOH Note that the feasibility of the points below depend upon future decisions of the alPHa board They assume that COMOH remains part of alPHa but becomes more independent in administering meetings
1 alPHa can provide to COMOH staff support (Gord Fleming) amounting to 02 FTE or one day per week This is a reduction from the current level of 35 days per week COMOH can choose to use the support any way it wants writing COMOH letters meeting minutes agenda support special projects etc
2 In addition to 02 FTE alPHa staff would provide support for up to 4 face-to-face meetings per year One meeting would be concurrent to alPHarsquos annual conference in June The timing of other meetings could be negotiated The support includes consulting on the development of the program arranging for speakers registration for the event arranging venue AV support and hospitality services
3 In addition to 02 FTE alPHa staff would provide support for setting meeting dates and any polling required to establish dates Note that the individual supporting this function would be Karen Reece
4 COMOHrsquos Executive and Section would continue to have access to online supports through the alPHa including the COMOH Listserve and a group page for posting agendas minutes and other resources on the alPHa website
5 alPHa staff (Linda Stewart and Gord Fleming) can also start participating on CMOH calls as a way to be up-to-date on issues related to COMOH
6 Other than what is outlined above COMOH would be expected to prepare agendas and take minutes for its Executive and Section meetings The Executive would be expected to operate more independently than it does now but would be able to access the supports outlined above
Prepared by Linda Stewart Executive Director
From comoh-bounceslistsalphaweborg on behalf of Christopher MackieTo MOH ListserveSubject [comoh] Fw URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)Date Wednesday October 30 2013 91241 AMAttachments ATT00249txt
For AMOHs and PHPM residents who didnt receive the initial email
Chris
Christopher Mackie MD MHSc FRCPCMedical Officer of Health and CEOMiddlesex-London Health Unit50 King St LondonON N6A 5L7 O 519 663 5317 ext 2444 wwwhealthunitcomFrom Pisko Laura (MOHLTC)Sent Tuesday October 29 2013 759 PMTo kbarkeralgomapublichealthcom malcolmlockbchuorg davidcchatham-kentcarobertkyledurhamca proumeliotiseohuca fwarshelginhealthonca mohelginhealthoncahlynnpublichealthgreybruceonca malcolmlockhnhuorg hnmohhnhuorglnoseworthyhkpronca bobnosalhaltonca elizabethrichardsonhamiltoncarschabashpechuonca ncameronhuroncountyca drimgemmillkflapublichealthcamohkflapublichealthca suditranadecounty-lambtononca paulastewarthealthunitorgChristopher Mackie valeriejaegerniagararegionca jimchiriconbpsdhuca jarthursnwhuoncaisralevyottawaca dnealoxfordcountyca davidmowatpeelregionca mklassenpdhuoncarpellizzaripcchuca rosemarieramsinghporcupinehuonca mcorriveaurcdhucomcharlesgardnersmdhuorg sutcliffepsdhucom davidwilliamstbdhucomspruytmtimiskaminghucom dmckeowntorontoca lnolanregionofwaterloocanicolamercerwdghuorg aheimannwechealthunitorg karimkurjiyorkcaCc coreywesleytbdhucom CindyBaker-Barillsmdhuorg Donna Kosmack pilonlsdhucomPaulaMuiskflapublichealthca sthibautorontoca Mueller Daina (MOHLTC) Gordon Marcus(MOHLTC) andreakitahamiltoncaSubject URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)
Dear Colleagues The ministry has received reports that some tobacco vendors across the province aregiving away single cigarettes with the purchase of tobacco products It is the ministryrsquosposition that giving out free single cigarettes does not violate subsection 31(3) of theSmoke-Free Ontario Act (ldquoSFOArdquo) Although the practice of giving out free singlecigarettes may promote the sale of tobacco products it does not take the form of aldquoproduct enhancement product association or promotional materialrdquo and therefore doesnot fall within the scope of subsection 31(3) of the SFOA We have confirmed with Health Canada that this practice may violate section 29(b) of thefederal Tobacco Act As such Health Canada is requesting that you notify them in writingand I am directing you to communicate with them via email and provide to them as manydetails as possible Emails should be sent to Tobacco-Ontariohc-scgcca and thesubject line should read ldquoViolation of Section 29(b) of Tobacco Actrdquo This will ensurethat the complaints are given priority status by Health Canada We will continue to monitor
this situation and liaise with our colleagues at Health Canada Please share this information with your tobacco control staff and contact me or DainaMueller Manager Tobacco Control Unit Health Promotion Implementation Branch atdainamuellerontarioca with any questions RegardsLaura Laura A PiskoDirectorHealth Promotion Implementation BranchHealth Promotion DivisionMinistry of Health and Long Term Care416-327-7445 (office)416-451-3185 (mobile) Marcus Gordon - EA (416)326-0625 for urgent issues
========= Middlesex-London Health Unit E-Mail Disclaimer =============______________________________________________________________
Private and confidential intended only for named recipient If otherwisereceived please destroy immediately Health information in this email isonly general information and is not intended to replace an in personconsultation with a medical professional nor is it intended to providemedical advice Individual circumstances of which we are not aware mayaffect the information provided herein and as such the Middlesex-LondonHealth Unit assumes no liability or responsibility for your reliancethereon The Middlesex-London Health Unit works under the authority of theHealth Protection and Promotion Act and this correspondence may be used toassess your needs for public health services (519-663-5317 ext 2448)______________________________________________________________
From Gardner CharlesTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes (RayCopesoahppca)
George Pasut (GeorgePasutoahppca) Peter Cooney (petercooneyhc-scgcca)Cc Ito DickSubject Discontinuation of Fluoridation in MuskokaDate Tuesday October 22 2013 125254 PM
Hello Colleagues
As I reported in my email below on September 26th fluoridation has come under challenge again inSimcoe Muskoka I am now very unhappy to report that despite our best efforts last night theDistrict Council of Muskoka voted to remove fluoride from municipal drinking supplies across theDistrict This brings to an end fluoridation in all of Simcoe and Muskoka (with the exception of Base Borden)ndash though New Tecumseth will be conducting a plebiscite on the question of fluoridation with themunicipal election next October Defending community water fluoridation has drained a great deal of time human resources andcommitment from other priorities and has been exhausting here in SMDHU as I am sure it hasbeen in many other health units While the outcomes have been very disappointing I have beenimpressed by the professionalism and dedication that SMDHU staff members have shown inshouldering this burden In particular our dental consultant Dr Ito has provided us with much ofthe foundational knowledge and the local research essential to our efforts and has very frequentlyattended and presented at council meetings and other public events I would also like to thank themany of you who have offer and provided support including advocacy letters and informationresources Over the years Dr Peter Cooney Chief Dental Officer of Health of Canada has beenvery helpful attending and presenting with us at council meetings and at public consultationevents We will of course continue our oral health surveillance of the children of Muskoka documentingand reporting in future years on the increase in dental decay that we anticipate will occur Suchsurveillance is the foundation of our advocacy both to municipal politicians and to the province I am very concerned that our experience will continue to repeat itself across the province unlessthere is strong leadership provincially It is with this in mind that I raise the followingrecommendations for your consideration
1 That we collectively (with PHOrsquos leadership) conduct high quality publish-worthy researchdocumenting the impact on dental decay that occurs in those municipalities throughoutOntario that in recent years have discontinued community water fluoridation This could bepart of a larger study on such municipalities across the country and it could also be part ofa study documenting overall oral health (including fluoridation coverage) in the province(and possibly across the country)
2 That COMOH engage with our Chief MOH to advocate for the province to require allmunicipal water supplies to be fluoridated (the exception of course being those withnaturally sufficient fluoride concentrations) This could built upon the alPHa position to
Gordon
Highlight
Gordon
Highlight
date (A11-00 - Community Water Fluoridation) on the CMOH position (Oral Health ndash) and on theemail discussion generated on the COMOH listserv some months back re Richardrsquosproposal (calling on the province to fund municipal water fluoridation)
Valerie I request that this be an item for our COMOH meeting on November 15th Sincerely Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorg From Gardner Charles Sent Thursday September 26 2013 245 PMTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes(RayCopesoahppca)Subject Community Water Fluoridation Under Challenge Again in Simcoe Muskoka Hello Colleagues You may wish to know that community water fluoridation (CWF) is again under challenge in SimcoeMuskoka specifically both in Tottenham (Town of New Tecumseth in Simcoe County) and for theentire District of Muskoka On Monday September 23 Committee of the Whole Council of theTown of New Tecumseth voted to submit application to discontinue community water fluoridation(CWF) in the town of Tottenham despite presentations to the contrary from our dental consultantDr Ito and from me The next Council meeting is scheduled for Monday Sept 30 at which lastMondayrsquos (Sept 23) votes will be ratified
Since Monday I have spoken with the Mayor of the Town of New Tecumseth and with most of thecouncilors encouraging deferral of a decision on Monday to allow the town more time to make afully informed decision
This is the second time in recent years that the issue of discontinuing CWF in Tottenham has beenraised at council This issue is also scheduled to return again to the District of Muskoka Council on
October 21st where I will be presenting in response to deputations in opposition to fluoridation
Outside of Base Borden Tottenham is the only community with fluoridated water in SimcoeCounty The health unitrsquos own screening data between 2011 and 2013 shows that Tottenhamrsquos
Gordon
Highlight
children as well as those in Muskoka have a lower rate of dental decay than Simcoe Muskokacommunities without CWF
Sincerely
Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorgChuck Gardner MOH
November 04 2013
Mandatory State Laws on Fluoridation Thirteen states Puerto Rico and the District of Columbia have laws intended to provide
statewide fluoridation These states and the year that the fluoridation legislation was passed are
District of Columbia (1952) Connecticut (1965) Kentucky (1966) Illinois (1967) Minnesota
(1967) Ohio (1969) South Dakota (1969) Georgia (1973) Nebraska (1973 and 2008)
California (1995) Delaware (1998) Puerto Rico (1998) Nevada (1999) Louisiana (2008) and
Arkansas (2011) (see Table 1) The sizes of the public water systems or countiescommunities
affected and exemption provisions vary by state Table 1
STATES THAT HAVE MANDATORY LAWS ON FLUORIDATION -2011
State (1) Year of
Fluoridation
Legislation (1)
Population
served by
Fluoridated
CWS (2)
Persons
receiving
fluoridated
water (2)
State
Average
Caries
Experience
of Grade 3
Students (3)
Arkansas 2011 647 1724131 64
California 1995 621 22812721 709
Connecticut 1965 910 2370423 406
Delaware 1998 862 705344 545
Georgia 1973 921 8924598 52
Illinois 1967 993 11325132 532
Kentucky 1966 999 4334223 598
Louisiana 2008 407 1846149 657
Minnesota 1967 988 4117266 549
Nebraska 1973 and 2008 702 1001665 593
Nevada 1999 702 1001665 649
Ohio 1969 877 8772683 512
South Dakota 1969 948 642942 623
District of
Columbia
1952 1000 595000
Puerto Rico 1998
United States 739 204283554
2010 Statistics for population fluoridated and number of people
1 Communication with Jane McGinley RDH MBA Manager Fluoridation and Preventive Health
Activities Council on Access Prevention and Interprofessional Relations
2 Centers for Disease Control and Prevention Department of Health and Human Services
accessed Oct 21 2013 httpwwwcdcgovfluoridationstatistics2010statshtm
3 Centers for Disease Control and Prevention National Oral Health Surveillance System Caries
Experience - Percentage of 3rd Grade students with Caries Experience (treated or untreated tooth
If data from 43 states for the percentage of Grade 3 children with experience of dental decay is
compared with the 2008 percentages of the population in a state with Community Water
Fluoridation then the percentage of children with experience of dental decay decreases as the
percentage of the state population with Community Water Fluoridation increases (see Figure 1)
Figure 1
Correlation of Percentage of Grade 3 Children with Caries Experience and
Percentage of Population With Community Water Fluoridation for 43
Reporting States
0
10
20
30
40
50
60
70
80
0 10 20 30 40 50 60 70 80 90 100
State of Population With Community Water Fluoridation
Sta
te
of
Gra
de 3
Stu
den
ts w
ith
Cari
es E
xp
eri
en
ce
Data from CDC (2 3)
The description of the fluoridation laws in California Illinois and Nevada can be found on the
Association of State amp Territorial Dental Directors website(4 7 8)
The California fluoridation law AB 733 came into effect in 1995 requiring communities of 10
000 residents or more be supplied with fluoridated drinking water However the state did not
provide any funding to implement the legislation (California is unique in requiring fluoridation
without funding the practice)(4) The California Department of Health Services therefore had to
fund fluoridation initiatives from non-governmental sources ie the California Endowment
California Dental Association Foundation the First 5 Commission and others(5) From 1995 to
2011 the percentage of the California population receiving fluoridated drinking water has risen
from 17 to 625(6) 4 Dental Public Health Activities amp Practices Office of Oral Health California Department of Health
Services April 2002 httpwwwastddorgbestpracticesDES06002CAfluoridationpdf
5 Stock M Pollick H The CDA Foundation Model to Fluoridate Communities California Dental
Association Journal vol 40 no 8 649 - 655
httpwwwcdaorgPortals0journaljournal_082012pdf
6 California Dental Association Foundation
httpwwwcdafoundationorglearnadvocacyfluoridation
The State of Illinois passed a mandatory fluoridation state in 1967 and required all community
water systems to adjust fluoride levels in the drinking water to optimal levels within 1 year(7)
From 1962 when over 5000000 residents had optimally fluoridated drinking water by 2010
the number had risen to 11325132 (993 of the population on community water systems)(2)
7 Dental Public Health Activities amp Practices Division of Oral Health Illinois Department of Public
Health April 2002 httpwwwastddorgbestpracticesDES16007ILfluoridationpdf
The State of Nevada passed a mandatory fluoridation statute in 2000 for communities with
400000 or more residents(8) This was a result of the work of a statewide coalition that
included the Nevada Dental and Dental Hygienist Associations the Washoe and Clark County
District Health Departments the Clark County School District Junior League of Las Vegas
Head Start the Community College of Southern Nevada Dental Hygiene Program Health
Access Washoe County and Saint Maryrsquos Hospital For communities with less than 400000 the
implementation of fluoridation still required the vote of the majority voters in the community
The Las Vegas Water Authority and the City of Henderson started fluoridation in 2000
increasing the percentage of the population with fluoridated drinking water from 2 to 65 (8) 8 Dental Public Health Activities amp Practices Bureau of Family Health Services Nevada State Health
Division April 2002 httpwwwastddorgbestpracticesDES31002NVfluoridationbillpdf
Countries with Mandatory Laws on Fluoridation Countries that have mandated Community Water Fluoridation are Brazil Hong Kong
Malaysia Singapore Ireland Israel and some of the states in Australia
Singapore started fluoridating its water in 1956 based on the success of the fluoridation trials in
Grand Rapids Newburgh Evanston and Brantford Singapore became the first Asian country to
have 100 of its population benefitting from the implementation of fluoridated drinking water
Loh reported that ldquoThe ten year study on the effects of water fluoridation in Singapore showed
a decrease in caries prevalence in the children In the permanent dentition the reduction was
523 per cent for Chinese and 31 per cent for Malays in the 7 to 9 year old age group A similar
trend was observed in the mixed dentition in which the decrease was 325 per cent for Chinese
and 306 per cent for Malaysrdquo(9) By 2010 the population of the country was 5080000(10)
9 Loh T Thirty-eight years of water fluoridation--the Singapore scenario Community Dent
Health 1996 Sep13 Suppl 247-50
10 British Fluoridation Society One in a Million the facts about water fluoridation 3rd Edition
published March 2012) httpwwwbfsweborgonemillion0920One20in20a20Million20-
20The20Extent20of20Fluoridationpdf
Hong Kong started implementing community water fluoridation in 1961 and similar to
Singapore 100 of the population received access to fluoridated drinking water Lo and Wong
reported that ldquoThe mean DMFT score of the children deceased from 44 in 1960 to 15 in 1968
stayed at this level in the 1980 and 1986 surveys and further deceased to 08 in 2001 The
prevalence of dental fluorosis among the children surveyed in 1960 was 1 and this increased
to 59 and 70 in 1968 and 1980 respectively It was found in the 1986 and 2001 surveys that
the prevalences of fluorosis were 47 and 9 among children whose teeth developed at the
time when the respective water fluoride concentrations were 07 ppm and 05 ppmrdquo(11) The
population of Hong Kong was 6968000 in 2009(10) 11 LO ECM and WONG AHH Water fluoride concentration and fluorosis in Hong Kong in 1960-
2001 84th General Session and Exhibition of the International Association for Dental Research amp
1st Meeting of the Pan-Asian-Pacific Federation Brisbane Australia 28 June-1 July 2006 v 85 n
Sp B
The Malaysian cabinet approved a nationwide community water fluoridation program in 1972
(12) One of the states Sabah decided to stop fluoridation in 1989 due to concerns about
inadequate supervision in adding fluoride to the drinking water Oral Health Surveys in 2009
and 2007 indicated that children in Sabah had the worst oral health with 50 of 12 year-olds
having decay in their permanent teeth and children having an average of 3 teeth being(13)
Under the 10th Malaysian Plan in 2011 the federal and the Sabah state governments
reintroduced water fluoridation in Sabah(1314) In 2010 about 755 of the Malaysian
population or 20700000 people had fluoridated drinking water(1013) 12 Malaysian Dental Association Fluoride in Water
httpwwwmdaorgmy07_public_01healthcare_12htm
13 Sachdev N Fluoridation in Sabah Water for Cleaner Teeth French Tribunecom 28022011
From Levy IsraTo Jaeger ValerieCc Pim Carolyn gordonalphaweborg Diallo Aicha Penny Sutcliffe Paul Roumeliotis Michael Finkelstein
Hazel Lynn Robert KyleSubject FW Panorama - Privacy Security and other issuesDate Wednesday October 16 2013 122110 PM
Hello ValerieOttawa is part of Wave 4 Panorama implementation and we are gearing up increasingly to use thesystem where and if possible Thinking about it I am anticipating that this may need to be on theCOMOH (and alPHa) radar as it is something that will impact all health units and implies a majoroperational shift in vaccine delivery programs for all health units I have asked Carolyn Pim toconnect with our sister wave 4 units to share common experiences as we move forward ndash when wehave a roll up could I bring to COMOH Exec for discussion to explore whether there are broaderimplications for all members As an aside I have also asked the Ministry and their CIO to share with me any roll up learnings thatthey may have had already from previous waves (I understand that Niagara HU was a wave 1participant so if there is such a roll up of common experiences that others could learn fromperhaps you have it already and that could come to the exec too)Thanks Isra From Pim Carolyn Sent October 10 2013 1228 PMTo Christopher Mackie (christophermackiemlhuonca) Elizabeth Richardson(Elizabethrichardsonhamiltonca) H BSc M D F R C P (C) MPH Jim Chirico(jimchiriconbpsdhuca) Marlene Spruyt (spruytmtimiskaminghucom) Robert Kyle (Durham)Cc Levy IsraSubject Panorama - Privacy Security and other issues Dear colleagues Irsquom reaching out to you as fellow Panorama Wave 4 health units to ask about where yourorganizations are at in the process of signing agreements and completing Privacy ImpactAssessments and Threat Risk Assessments (TRAs) Ottawa Public Healthrsquos IT legal and informationsecurity advisors have made numerous requests to the MOHLTC for information (in particular theprovincial TRA) that we consider essential to develop our own risk assessment and PIA but havebeen told that information cannot be shared even with strict confidentiality and access controlsSo we are at somewhat of an impasse Isra emailed Arlene yesterday Arlene has forwarded ourconcerns to the Ministryrsquos CIO and Panorama lead but we havenrsquot had any response or discussionswith either of them yet Have your organizations identified similar concerns andor had interactions with the MOHLTC inthis respect Irsquod also be interested in knowing if your health units have flagged other (egoperational) implementation concerns Thanks
Carolyn ps Robert ndash you can ignore this request I talked with Sharan this morning about Durhamrsquos issuesso am including you now just for information Carolyn Pim MD FRCPC Associate Medical Officer of Health Meacutedecin adjointe en santeacute publique Ottawa Public Health Santeacute publique Ottawa 100 Constellation Cr Ottawa ON K2G 6J8 Tel teacutel (613) 580-6744 ext 23684Fax (613) 580-9641Connect With Ottawa Public Health
Suivez Santeacute publique Ottawa
This e-mail originates from the City of Ottawa e-mail system Any distribution use orcopying of this e-mail or the information it contains by other than the intendedrecipient(s) is unauthorized If you are not the intended recipient please notify meat the telephone number shown above or by return e-mail and delete thiscommunication and any copy immediately Thank you
Le preacutesent courriel a eacuteteacute expeacutedieacute par le systegraveme de courriels de la Ville dOttawaToute distribution utilisation ou reproduction du courriel ou des renseignements quisy trouvent par une personne autre que son destinataire preacutevu est interdite Si vousavez reccedilu le message par erreur veuillez men aviser par teacuteleacutephone (au numeacuteropreacuteciteacute) ou par courriel puis supprimer sans deacutelai la version originale de lacommunication ainsi que toutes ses copies Je vous remercie de votre collaboration
1
Smoke-Free Patios ndash An Amendment to the Smoke-Free Ontario Act
Date November 15 2013 Prepared for Council of Ontario Medical Officers of Health Prepared by York Region Public Health _____________________________________________________________________________ Issue
The Smoke-Free Ontario Act is the current provincial legislation that imposes smoking restrictions in workplaces and public places It prohibits smoking on restaurant and bar patios in instances where any portion of the seating area is covered by a roof With recent studies illustrating that exposure to second hand smoke outdoors poses similar risks to indoor exposure there has been growing public support to enhance smoking restrictions and make patios completely smoke-free
Background
With the implementation of the Smoke-Free Ontario Act in 2006 restaurant and bar patios became subject to smoking restrictions if any portion of the seating area was covered by a roof This allowed for patios without roof coverings to continue to allow smoking and as a result did not provide significant protection to patrons or staff from exposure to second hand smoke outdoors Many businesses chose to alter the design of their patios to allow smoking to continue In some cases patios became more crowded since smoking patrons who dine indoors often proceed outside onto licensed patios with their beverages to smoke York Region like most municipalities in Ontario is host to hundreds of patios being operated by restaurant owners and businesses With smoking prohibitions affecting only a small portion of these patios specifically ones with coverings the vast majority of patios still allow smoking to take place Patrons and employees on patios where smoking is not restricted are exposed to second hand smoke frequently This can contribute to increased disease and aggravation of existing health conditions From a business perspective the existing legislation has been viewed by many operators as unfair because some patios have permanent coverings which cannot be removed requiring a smoke-free status These business owners feel this creates an uneven playing field since they cannot provide an outdoor dining area for their smoking customers There is strong community support for smoke-free patios in Ontario A 2009 Rapid Risk Factor Surveillance System survey revealed 754 percent support in York Region while a Toronto Health Survey in 2011 indicated 74 percent public support
2
Current Status
Smoking is currently prohibited on restaurant and bar patios province-wide in four Canadian provinces and territories Alberta Newfoundland and Labrador Nova Scotia and Yukon A fifth province Prince Edward Island prohibits smoking on patios until 10 pm Since Ontario enacted legislation restricting smoking on patios in 2006 eight municipalities in Ontario have chosen to create bylaws that go beyond the Smoke-Free Ontario Act and enhance outdoor protection from second hand smoke by prohibiting smoking on patios completely The largest of those municipalities is the City of Ottawa Recently the Toronto Board of Health unanimously endorsed a report presented by their Medical Officer of Health recommending that restaurant and bar patios be made smoke-free through an amendment to the Smoke-Free Ontario Act
Key Considerations
There should be no significant financial burden to local Boards of Health resulting from a smoke-free patio amendment to the Smoke-Free Ontario Act Inspection and enforcement for the Smoke-Free Ontario Act is currently 100 percent funded by the Ministry of Health and Long-Term Care Following an introductory period of education on the amendment a complaint response model of service delivery would ensure ongoing compliance with smoke-free requirements A complete ban of smoking on patios would eliminate the widely-held perception by business owners that the current legislation creates an uneven playing field for business Since Smoke-Free Ontario Act inspections of patios began in 2006 operators have expressed the opinion that if patios need to be smoke-free for the protection of the public they should all be smoke-free to avoid undue hardship for individual businesses and to provide protection uniformly across the Province
Next steps
York Region Public Health intends to seek support from Medical Officers of Health across the Central East Tobacco Control Area Network (CETCAN) to advocate to the Ministry of Health and Long-Term Care for an amendment to the Smoke-Free Ontario Act prohibiting smoking on all restaurant and bar patios York Region is also in the process of requesting that its Regional Council advocate to the Minister of Health and Long-Term Care on the issue
Updating and Modernizing O Regulation 565 (Public Pools)
Date November 15 2013
Prepared for Council of Ontario Medical Officers of Health
Prepared by York Region Public Health _____________________________________________________________________________ Background Recent drownings at public pools in Ontario have highlighted the issue of water-borne illness and injury The current pool regulation under Ontariorsquos Health Protection and Promotion Act O Regulation 565 (Public Pools) is outdated It does not accurately reflect new pool technology and design or the changing use of public pools Neither does it incorporate admissions standards recommended by the Office of the Chief Coroner Further O Regulation 565 does not have short-form wording or set fines associated with it This limits public health enforcement capabilities What is the impact Updating O Regulation 565 (Public Pools) to address recent changes in pool technology design and uses and to include Coroner-recommended admissions standards would help improve pool safety Establishing short-form wording for O Regulation 565 would enhance enforcement related to public pools Currently the only enforcement available to Public Health Inspectors for dealing with non-critical regulatory infractions in public pools is the issuance of a Part III summons This involves a considerable amount of resources for a possible small fine With the development of inspection disclosure systems such as YorkSafe there is an even greater need to develop a method to effectively address repeated pool operator non-compliance with non-critical issues Next steps Public health units should advocate to the Province to 1) Conduct a review of O Regulation 565 (Public Pools) to address shortcomings Proposed changes to the
regulation should include a requirement for ownersoperators of public pools to advise the local Medical Officer of Health of any change in the use of a facility and the addition of the Coronerrsquos recommended admission standards
2) Provide short-form wording for O Regulation 565 so that public health inspectors can better deal with pool operator non-compliance
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
612 ndash PHSSP Implementation Tables CMOH Memo ndash PHSSP Tables V Jaeger referred to the linked memo which the result of the desire for clarity and openness on how the topic-specific implementation tables would be assembled The PHLC has already received a number of expressions of interest and will be communicating next steps soon 62 COMOH Executive Committee Minutes June 11
Notes July 9 Minutes July 31
Minutes September 10
63 COMOH Built Environment Work Group
The BEWG has not met since the last meeting but will meet on October 7 During the summer that group led by C Gardner and Nikhil Rajaram developed the paper (COMOHrsquos Advice for the Provincersquos Review of its Long-Term Energy Plan) that was the basis for the letter that went to the province (see item 68 below) V Jaeger expressed appreciation for the work that went into that C Gardner has expressed interest in being a member of the Promoting Healthy Environments ndash Both Natural and Built PHSSP implementation table 64 Public Health Early Years Group Aug 9 Meeting Notes A Feller reported that this group is putting together a November 5 Grand Rounds at PHO 65 iPHIS Panorama
July 8 Update
66 Joint OPHAalPHa Health Equity Working Group R Pellizzari reminded that this is a joint initiative of alPHa and OPHA She will ensure that L Stewart provides minutes of these meetings for future updates She and L Simon are the COMOH reps on this group L Simon circulated a paper by the Wellesley Institute that examines the health equity impacts of cessation of community water fluoridation which was requested by the HEWG She added that Bob Gardner Director of Policy at the Wellesley Institute is now participating in this group and he would welcome suggestions for other subjects for health equity impact assessments M Klassen suggested that Radon might be a good one She also reported that the National Collaborating Centre for Determinants of Health hosted a discussion for the nurses that have been hired under the SDOH portfolio in order to more clearly identify what the specific mandate of public health is in this area and to identify reasonable evaluative measurements This is being proposed as the basis of a Locally Driven Collaborative project and three health units are already involved (PCCHU Toronto and Durham) but more are required and any assistance would be welcome HEWG is also working on positions on the minimum wage review and the poverty strategy Both of these will be circulated once complete and approved
It is also working on a TOPHC session on Cultural Safety related to working with aboriginal populations Feedback was also invited on this with a note that the deadline for abstract submission is September 27 Finally work is also being done with PHO on developing resources and supports for work with Priority Populations 67 COMOH Electronic Mailing List List of Subscribers 68 COMOH Correspondence Aug 26 COMOH Letter ndash Energy Policy
Aug 8 COMOH Letter ndash CMA Poverty Report
July 22 COMOH Letter ndash Immunization Data
70 Next MeetingAdjournment Meeting adjourned at 1035 Next Section meeting will be on November 15 2013 in Toronto part of the alPHa Fall Symposium
Page 1 of 8 ndash DRAFT FOR COMOH DISCUSSION
alPHa Membership Survey hello
Draft Report ndash COMOH Version hello
alPHarsquos membership was surveyed in the fall of 2013 Similar surveys were administered to all member groups ie COMOH BOH Section and Affiliates using the online survey tool Survey Monkey Small alterations were made to group-specific surveys to ensure that the survey questions were relevant to each group A total of 84 responses were received from alPHa members The breakdown of respondents was as follows This draft report is provided for discussion purposes to COMOH members and therefore focuses on the responses provided by COMOH members To provide additional information overall survey responses are also provided for some questions
SECTION 1 RESPONDENT PROFILE
Survey Question What region is your health unit located in
For COMOH members responses came from 6 of the 7 regions of Ontario All 7 regions were represented in the full set of survey responses
Summary of Respondents COMOH 27 32 BOH Section 34 40 Affiliates 23 27 Totals 84 100
All ResponsesEastern 24 29South West 12 14Central East 13 15Central West 15 18North East 11 13Toronto 5 6Not Sure 3 4North West 1 1Totals 84 100
All COMOH ResponsesEastern 3 11South West 5 19Central East 6 22Central West 6 22North East 3 11Toronto 4 15North West 0 0Totals 27 100
Page 2 of 8 ndash DRAFT FOR COMOH DISCUSSION
Survey Question How long have you been involved with public health in Ontario
Survey Question Have you participated on the alPHa Board of Directors or an alPHa or COMOH committeeworking group
All ResponsesYes in the last 1 to 2 years 15 18Yes in the last 2 to 5 years 9 11Yes more than 5 years ago 9 11No not ever 51 61Totals 84 100
All COMOH ResponsesOver 10 years 17 635 to 10 years 7 262 to 5 years 3 11Totals 27 100
All ResponsesOver 10 years 34 405 to 10 years 21 252 to 5 years 21 251 to 2 years 3 4Less than 1 year 5 6Totals 84 100
All COMOH ResponsesYes in the last 1 to 2 years 7 26Yes in the last 2 to 5 years 4 15Yes more than 5 years ago 8 30No not ever 8 30Totals 27 100
Page 3 of 8 ndash DRAFT FOR COMOH DISCUSSION
SECTION 2 PROFESSIONAL DEVELOPMENT
Survey Question Which of the following events have you attended at least once in the past two years
Survey Question Overall how satisfied have you been with alPHa events ie conferences meetings
Survey Question How much value do alPHarsquos events provide for the money
Survey Question How can alPHa make its events more valuable to you Please share any suggestions regarding future topics speakers formats duration locations or any other event component that is important to you
Comments about content bull Expert speakerpanels on emerging or hot topics
(2) bull More engaged dialogue with Ministry rather than
just updates bull Fewer Ministry updates (3) bull Content on medicalPH issues is better left to PHO
TOPHC and joint conferences (2) bull alPHa should stick to Ministrypoliticspolicysenior
PH supportPHU support on key priorities (eg November practical conference on HKP report)
bull For COMOH more discussion bull More time for section activities like face-to-face
COMOH meetings
bull More facilitated work groups of COMOH members to respond to public health practice questions
bull More focus on rural and northern issues bull Infection Control Logistical Considerations bull Consider partnering with other groups bull More collaboration with PHO and OPHA events bull Use of video conferencing bull Less frequentfewer meetings (2) bull Connect with CME Location bull Consider other venues than TO
( ) brackets indicate that more than one response included a similar comment
More than enough value 7 11A lot of value 34 52Some value 22 34A little value 2 3Not enough value 0 0Totals 65 100
All Responses for those who Attended at least One Event in the Last 2 Years
All COMOH ResponsesMore than enough value 4 15A lot of value 13 48Some value 9 33A little value 1 4Not enough value 0 0Totals 27 100
Page 5 of 8 ndash DRAFT FOR COMOH DISCUSSION
SECTION 3 VALUE FOR MEMBERSHIP
Survey Question What do you value the most about your alPHa membership
The comments provided in response to the text response question What is the most important benefit of alPHa membership for you personally supported the answers illustrated in the chart above 15 of the 20 comments provided focussed on the importance of opportunities to interact with colleagues across the province The next most important benefit mentioned was the support for COMOH members to work on public health issues together When asked What is the most important benefit of alPHa membership for your health unit COMOH members emphasized the following bull A coordinated and collective voice in advocating for public health issues and the public health sector (9) bull Opportunities to connect with other public health units to share experiences and best practices (8) bull Maintaining relationships with government both politicians and bureaucrats (3) and bull Support for boards of health (3)
Page 6 of 8 ndash DRAFT FOR COMOH DISCUSSION
Overall Level of Satisfaction
SECTION 4 LOOKING TO THE FUTURE
The questions in this section were asked to obtain input from alPHa members regarding a proposal from alPHarsquos Board of Directors to focus the Association on five service areas COMOH members were asked to indicate their level of agreement with the proposed areas of focus COMOH responses compared to the overall survey responses were as follows
To explore some proposed changes to Association services COMOH members were asked to provide their level of agreement with the following questions
COMOH Responses BOH Section Affiliates All Survey Responses
Strongly Agree
AgreeNeither Agree or Disagree
DisagreeStrongly Disagree
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1Promoting the role and value of local public health units
15 9 2 0 0 26 92 93 95 94
2
Providing important information to members about trends and events that will impact the public health system and management of public health units
10 8 8 0 0 26 69 97 86 85
3Facilitating professional networking and information sharing
13 10 3 0 0 26 88 83 82 85
4
Providing professional development to support excellence in public health unit leadership management and governance
3 15 7 1 0 26 69 83 86 79
5
Responding to public health sector issues when it makes the most sense to have a collective voice ie issues that impact the structure and funding of the public health sector and public health units and issues that have a broad focus on population health
15 8 2 0 1 26 88 97 95 93
PROPOSED AREAS OF FOCUS
COMOH Responses BOH Section Affiliates All Survey Responses
Strongly Agree
AgreeNeither Agree or Disagree
DisagreeStrongly Disagree
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1
COMOH and other professional groups within alPHa should do their own advocacy while alPHa supports members to share and support each others advocacy efforts
7 6 6 6 1 26 50 58 45 52
2
alPHa should provide support to action-oriented inter-professional work groups on priority public health unit issues and member resolutions
4 13 5 3 1 26 65 81 86 77
PROPOSALS
Page 8 of 8 ndash DRAFT FOR COMOH DISCUSSION
COMOH members were also asked to indicate the level of acceptability for some possible changes to alPHarsquos services and way of doing business
COMOH Responses BOH Section Affiliates All Survey Responses
Very Acceptable
Somewhat Acceptable
Neither Acceptable or Unacceptable
Somewhat Unacceptable
Very Unaccept
able
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1Single conference with additional face-to-face section meetings
21 2 0 1 0 24 96 68 80 81
2alPHa to offer alternatives like webinars on focussed topics
13 6 1 4 0 24 79 50 90 71
3Coordinate COMOH meetings with PHO OMA or Ministry events
16 4 2 0 0 22 91 na na --
4
Increase focus on building leadership and management capacity for health unit CEOs and senior management
7 9 4 3 0 23 70 na 70 70
5
Would it be acceptable for alPHa to request voluntary financial contributions from member PHUs in addition to annual fees
3 5 5 4 5 22 36 7 26 21
6
Would it be acceptable for alPHa to request voluntary in-kind staff contributions from member PHUs to expand alPHas capacity eg communications policy work group support
7 11 1 1 3 23 78 31 45 50
7Would it be acceptable to you for alPHa to discontinue staff support for COMOH (BOH Section)
0 4 1 5 14 24 17 11 na 14
8
Would it be acceptable to you for alPHa to reduce the amount of staff support for COMOH (BOH Section)
1 6 1 8 6 22 32 26 na 29
9
Would it be acceptable to you for alPHa to provide supports to MOHs and AMOHs (BOH Members) without maintaining COMOH (BOHs) as a section of the association
3 2 3 2 12 22 23 17 na 20
10
Would it be acceptable to you for alPHas Board of Directors to move from the current representational model to a skills-based strategic model ie board membership would be based on the skills needed to carry out alPHas strategic plan
6 11 2 1 3 23 74 56 56 62
11
Would it be acceptable to you for alPHas President Vice-President and Treasurer to be elected from the full membership of the alPHa Board of Directors (rather than the current model of alternating between BOH and COMOH members)
10 8 1 2 2 23 78 70 70 73
PROPOSED CHANGES
1 Council of Ontario Medical Officers of Health Terms of Reference
ASSOCIATION OF LOCAL PUBLIC HEALTH AGENCIES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
TERMS OF REFERENCE NAME 1 The name of the organization shall be ldquoThe Council of Ontario Medical Officers of
Health a section of the Association of Local Public Health Agencies (alPHa)rdquo hereinafter referred to as ldquothe Councilrdquo
MISSION 2 As local leaders in public health we are committed to improving the health of
Ontarians and increasing health equity by strengthening Ontariorsquos public health system We achieve this through system leadership and coordination in collaboration with the provincial government and other organizations and through evidence-informed advocacy on public health policy
OBJECTIVES 3 The objectives of the Council shall be
a) To provide strong province-wide leadership in public health
b) To advocate for health protection and promotion policies and programs that maintain and improve the health of Ontarians
c) To promote and maintain the highest standards for Ontariorsquos public health
programs and services
d) To support the planning implementation and evaluation of effective and efficiently run public health programs and services
e) To act as a forum for sharing information and resources and for addressing and
discussing public health issues both amongst the Councilrsquos members and other agencies that support the goals of alPHa eg Ontario Medical Association Ontario Public Health Association etc
f) To engage with and to provide public health and related policy advice to alPHa
the Chief Medical Officer of Health the Ontario Ministries of Health and Long-Term Care (including the Health Promotion and Public Health Divisions) Children
2 Council of Ontario Medical Officers of Health Terms of Reference
and Youth Services and other provincial ministries Public Health Ontario Health Canada the Public Health Agency of Canada and other public health partners
g) To promote and protect the professional interests of its members
h) To provide support to individual members as needed
i) To seek recognition for outstanding practice from among the members
j) To support evidence based practice of public health medicine
k) To engage and involve the membership to participate in COMOHrsquos endeavours
l) To mentor Public Health and Preventive Medicine Residents
MEMBERSHIP 4 Membership on the Council in each of the following categories is subject to the
limitations imposed by the current terms of reference and all policies and governing documents of the Association of Local Public Health Agencies Benefits of membership in each category are included in Appendix A These shall be subject to regular review and may be suspended under certain circumstances
Active membership in the Council shall be open to all Associate Medical Officers of Health and all full-time Medical Officers of Health whose Boards of Health are members of alPHa Such members shall have full voting privileges and may hold office in the Council Associate membership shall be open to all full and part-time physicians employed by a Board of Health that is a member of alPHa Such members shall not have voting privileges nor hold office
Affiliate membership shall be open to the following individuals interested in furthering the objectives of the Council
bull Public Health and Preventive Medicine Residents and Public Health and Preventive Medicine Residency Program Directors
bull Federal public health physicians working in Ontariorsquos First Nations communities
bull other public health or related physicians including those employed by a Board of Health that is not a member of alPHa
Such members shall not have voting privileges nor hold office
3 Council of Ontario Medical Officers of Health Terms of Reference
Emeritus membership shall be open to all former members who have retired after five (5) or more years of Active membership subject to the nomination in writing of two (2) active members in good standing endorsement of the Executive Committee and approval of the Council by majority vote at a general meeting Such members shall have neither voting privileges nor hold office but may be invited to attend general meetings Honorary membership shall be open to any non-active or associate member subject to the nomination in writing of two (2) active members in good standing endorsement of the Executive Committee and approval of the Council Such members shall have neither voting privileges nor hold office but may be invited to attend general meetings
OFFICERS 5 The Officers of the Council shall be the Chair Vice-Chair and immediate Past Chair
6 The Chair shall prepare the agendas of all Council meetings She shall preside and
preserve order at all such meetings shall ensure that these Terms of Reference are upheld and enforced and shall contribute to the supervision and evaluation of any Public Health and Preventive Medicine Resident who is on a placement with alPHa
7 The Vice-Chair shall fulfill the duties of the Chair in hisher absence The immediate
Past Chair may fulfill the duties of the Chair or Vice-Chair in their absences 8 The Chair shall normally serve a term of one (1) year which is renewable once and
after which the Vice-Chair shall normally assume the vacated office COMMITTEES 9 The Council shall elect seven (7) active members one from each of alPHarsquos regions
and the active member who is scheduled to serve as the President or immediate Past-President of alPHa to represent it on the alPHa Board of Directors These seven (7) members shall constitute the Councilrsquos Executive Committee and shall serve a term of at least one (1) year The Chair and Vice-Chair shall be elected from among the Executive Committee members If alPHarsquos immediate Past President is an active member she shall be an ex-officio member of the Executive Committee
10 The mandate of the Executive Committee shall be to facilitate the achievement of
the objectives of the Council by fulfilling the following
a Identifying priorities 1
1 See Appendix B Planning Cycle to Identify Priorities for COMOH
and ensuring the development of briefing documents and or recommendations as appropriate for the consideration of the Council
4 Council of Ontario Medical Officers of Health Terms of Reference
b Setting agendas and otherwise ensuring preparations for Council meetings c Ensuring the fulfillment of the direction of Council d Responding in a timely fashion to time-sensitive public health matters in
accordance with the Executive Committeersquos understanding of the perspective of the Council
e Engaging with the Chief Medical Officer of Health Associate Chief Medical Officers of Health and other provincial public health leaders and
f Representing Council at public and partner agency forums including the Public Health Leadership Council which shall normally include membership from the Officers of the Council and two other Executive Committee members as selected by agreement among the Executive
g Identifying opportunities for the recognition of outstanding practice from among the members including the annual nomination of at least one member for the alPHa Distinguished Service Award
11 The Executive Committee shall meet and correspond in the manner and at the times
and if required places as deemed necessary by the Chair to conduct the business of the Council A quorum shall consist of four (4) members
12 The Executive Committee shall have the power to strike committeestask or working
groups to assist it in carrying out the business of the Council 13 The Council may by special resolution remove a member of the Executive
Committee before the completion of hisher term of office and may elect a successor to complete the term The special resolution shall require a majority vote of 67 of the members present and voting at the meeting at which the special resolution is considered
14 A Nominating Committee shall consist of the three (3) most recent Past Chairs who
are able to serve and shall be chaired by the immediate Past Chair The Nominating Committee shall prepare a list of proposed Officers and Executive Committee members for the consideration of the Council at its Annual General Meeting
MEETINGS 15 The Council shall hold at least four (4) general meetings per year in a manner and at
the times and if required places as deemed necessary by the Executive Committee to share information direct and assist the Executive Committee in conducting the business of the Council
16 The Council shall hold its Annual General Meeting during and at the same place as
the alPHarsquos Annual Conference
5 Council of Ontario Medical Officers of Health Terms of Reference
17 The Council shall hold a special meeting at the call of the Chair or upon the written request specifying the purpose of such meeting of at least five (5) active members Council members must be given at least 48 hours notice of any special meeting
18 Only Councilrsquos active and associate members and alPHa staff are entitled to attend
general and special meetings of the Council Other members and non-members may be invited to attend all or part of such meetings as determined by the Chair preferably in consultation with the Executive Committee Non-members who come to such meetings without an invitation may attend all or part of the meeting by a majority vote of the active members present and voting
19 The Chair shall prepare the agendas for such meetings and shall normally include
reports from the Chair and the Councilrsquos committeestask or working groups and representatives to external bodies alPHarsquos Executive Director shall ensure that the minutes shall be recorded and promptly distributed to the Section
20 A quorum for all such meetings shall be ten (10) active members 21 The Council shall normally be notified in a manner deemed appropriate by the Chair
of such meetings at least one (1) month prior to their being held 22 A majority vote of the members present at such meetings and voting shall make
Council decisions In the case of a tied vote the Chair shall cast the deciding vote The Executive Committee shall ensure that actions arising from such decisions at such meetings are implemented and monitored
23 The Chair may solicit advice from the Council through the use of teleconferencing
and alPHarsquos electronic mailing lists in order to gain an understanding of the overall perspective of the Council (see 10d)
ELECTIONS 24 The Officers and Executive Committee members shall be elected at the Sectionrsquos
Annual General Meeting The Nominating Committee Chair or hisher designate shall present a list of nominations Additional nominations from the floor shall also be considered Each Officer and Executive Committee member shall be elected by secret ballot if necessary by a majority of the active members present and voting In the case of a tie the Chair shall cast the deciding vote
AMENDMENTS 25 The Councilrsquos Terms of Reference may be amended from time to time by the
Executive Committee provided the Committee receives notice of such proposed amendments at least one (1) month prior to the meeting at which the amendments
6 Council of Ontario Medical Officers of Health Terms of Reference
will be considered Such amendments shall be ratified by the Council at the next general meeting or the Annual General Meeting as the case may be
26 The Executive Committee shall review the Terms of Reference as required and not
less than once every two years Original September 1987 1st Revision October 2000 2nd Revision July 2001 3rd Revision December 2003 4th Revision February 2008 5th Revision June 2009 6th Revision June 2011 7th Revision June 2013
7 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX A
COMOH Membership Benefits Active Membership
bull Entitled to attend all meetings of the Section bull May hold office on the COMOH Executive Committee alPHa Board of Directors
Standing Committees bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Associate Membership
bull Entitled to attend all meetings of the Section bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Affiliate Membership
bull May attend meetings or parts thereof subject to approval of Chair bull May serve on ad-hoc committees of the Section subject to the approval of the
Executive Committee bull Discounted registration rates for alPHa Conferences (for Public Health and
Preventive Medicine Residents) bull Upon written request and subject to COMOH Executive approval Affiliate
Members may subscribe to comohlistsalphaweborg The approval will be reviewed on an annual basis in order to determine if the Affiliate Member can remain a subscriber to mohsalphaweborg
Emeritus Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair bull Enjoy discounted registration rates for alPHa Conferences and regular COMOH
meetings bull Subscription to comohlistsalphaweborg electronic mailing list bull Full access to alPHa Web site bull May represent alPHa COMOH on selected external committees and working
groups Honorary Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair
8 Council of Ontario Medical Officers of Health Terms of Reference
bull May represent alPHa COMOH on selected external committees and working groups subject to the approval of the COMOH or alPHa Executive Committee as appropriate
9 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX B
Planning Cycle to Identify Priorities for COMOH
1 There shall normally be a COMOH membership strategic planning retreat every four years In recognition of the dynamic environment of public health the need for and timing of such a retreat shall be at the discretion of the Executive Committee in consultation with the membership
2 The COMOH Executive is responsible (through the creation of a subcommittee of COMOH members) for ensuring the preparation for the COMOH retreats with resources to include those provided by alPHa
3 Leadership for action on COMOH priorities will be recruited from among the COMOH membership in order to make good use of the full base of capacity of the membership The resources to support actions will be recruited from both within and beyond the COMOH membership employing other public health professionals that reside within the broader public health system and community
4 The COMOH Executive shall ensure an annual review of strategic priorities and initiatives and the development of a draft report of the same for the review of the members at the June meeting
2013 Strategic Planning
Considerations for COMOH
As part of its strategic planning discussions alPHarsquos Board has been considering changes to the level of support provided to member sections A member survey is being carried out over the fall to determine options acceptable to alPHa members The following approach to support is put forward as a proposal for the consideration of COMOH Note that the feasibility of the points below depend upon future decisions of the alPHa board They assume that COMOH remains part of alPHa but becomes more independent in administering meetings
1 alPHa can provide to COMOH staff support (Gord Fleming) amounting to 02 FTE or one day per week This is a reduction from the current level of 35 days per week COMOH can choose to use the support any way it wants writing COMOH letters meeting minutes agenda support special projects etc
2 In addition to 02 FTE alPHa staff would provide support for up to 4 face-to-face meetings per year One meeting would be concurrent to alPHarsquos annual conference in June The timing of other meetings could be negotiated The support includes consulting on the development of the program arranging for speakers registration for the event arranging venue AV support and hospitality services
3 In addition to 02 FTE alPHa staff would provide support for setting meeting dates and any polling required to establish dates Note that the individual supporting this function would be Karen Reece
4 COMOHrsquos Executive and Section would continue to have access to online supports through the alPHa including the COMOH Listserve and a group page for posting agendas minutes and other resources on the alPHa website
5 alPHa staff (Linda Stewart and Gord Fleming) can also start participating on CMOH calls as a way to be up-to-date on issues related to COMOH
6 Other than what is outlined above COMOH would be expected to prepare agendas and take minutes for its Executive and Section meetings The Executive would be expected to operate more independently than it does now but would be able to access the supports outlined above
Prepared by Linda Stewart Executive Director
From comoh-bounceslistsalphaweborg on behalf of Christopher MackieTo MOH ListserveSubject [comoh] Fw URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)Date Wednesday October 30 2013 91241 AMAttachments ATT00249txt
For AMOHs and PHPM residents who didnt receive the initial email
Chris
Christopher Mackie MD MHSc FRCPCMedical Officer of Health and CEOMiddlesex-London Health Unit50 King St LondonON N6A 5L7 O 519 663 5317 ext 2444 wwwhealthunitcomFrom Pisko Laura (MOHLTC)Sent Tuesday October 29 2013 759 PMTo kbarkeralgomapublichealthcom malcolmlockbchuorg davidcchatham-kentcarobertkyledurhamca proumeliotiseohuca fwarshelginhealthonca mohelginhealthoncahlynnpublichealthgreybruceonca malcolmlockhnhuorg hnmohhnhuorglnoseworthyhkpronca bobnosalhaltonca elizabethrichardsonhamiltoncarschabashpechuonca ncameronhuroncountyca drimgemmillkflapublichealthcamohkflapublichealthca suditranadecounty-lambtononca paulastewarthealthunitorgChristopher Mackie valeriejaegerniagararegionca jimchiriconbpsdhuca jarthursnwhuoncaisralevyottawaca dnealoxfordcountyca davidmowatpeelregionca mklassenpdhuoncarpellizzaripcchuca rosemarieramsinghporcupinehuonca mcorriveaurcdhucomcharlesgardnersmdhuorg sutcliffepsdhucom davidwilliamstbdhucomspruytmtimiskaminghucom dmckeowntorontoca lnolanregionofwaterloocanicolamercerwdghuorg aheimannwechealthunitorg karimkurjiyorkcaCc coreywesleytbdhucom CindyBaker-Barillsmdhuorg Donna Kosmack pilonlsdhucomPaulaMuiskflapublichealthca sthibautorontoca Mueller Daina (MOHLTC) Gordon Marcus(MOHLTC) andreakitahamiltoncaSubject URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)
Dear Colleagues The ministry has received reports that some tobacco vendors across the province aregiving away single cigarettes with the purchase of tobacco products It is the ministryrsquosposition that giving out free single cigarettes does not violate subsection 31(3) of theSmoke-Free Ontario Act (ldquoSFOArdquo) Although the practice of giving out free singlecigarettes may promote the sale of tobacco products it does not take the form of aldquoproduct enhancement product association or promotional materialrdquo and therefore doesnot fall within the scope of subsection 31(3) of the SFOA We have confirmed with Health Canada that this practice may violate section 29(b) of thefederal Tobacco Act As such Health Canada is requesting that you notify them in writingand I am directing you to communicate with them via email and provide to them as manydetails as possible Emails should be sent to Tobacco-Ontariohc-scgcca and thesubject line should read ldquoViolation of Section 29(b) of Tobacco Actrdquo This will ensurethat the complaints are given priority status by Health Canada We will continue to monitor
this situation and liaise with our colleagues at Health Canada Please share this information with your tobacco control staff and contact me or DainaMueller Manager Tobacco Control Unit Health Promotion Implementation Branch atdainamuellerontarioca with any questions RegardsLaura Laura A PiskoDirectorHealth Promotion Implementation BranchHealth Promotion DivisionMinistry of Health and Long Term Care416-327-7445 (office)416-451-3185 (mobile) Marcus Gordon - EA (416)326-0625 for urgent issues
========= Middlesex-London Health Unit E-Mail Disclaimer =============______________________________________________________________
Private and confidential intended only for named recipient If otherwisereceived please destroy immediately Health information in this email isonly general information and is not intended to replace an in personconsultation with a medical professional nor is it intended to providemedical advice Individual circumstances of which we are not aware mayaffect the information provided herein and as such the Middlesex-LondonHealth Unit assumes no liability or responsibility for your reliancethereon The Middlesex-London Health Unit works under the authority of theHealth Protection and Promotion Act and this correspondence may be used toassess your needs for public health services (519-663-5317 ext 2448)______________________________________________________________
From Gardner CharlesTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes (RayCopesoahppca)
George Pasut (GeorgePasutoahppca) Peter Cooney (petercooneyhc-scgcca)Cc Ito DickSubject Discontinuation of Fluoridation in MuskokaDate Tuesday October 22 2013 125254 PM
Hello Colleagues
As I reported in my email below on September 26th fluoridation has come under challenge again inSimcoe Muskoka I am now very unhappy to report that despite our best efforts last night theDistrict Council of Muskoka voted to remove fluoride from municipal drinking supplies across theDistrict This brings to an end fluoridation in all of Simcoe and Muskoka (with the exception of Base Borden)ndash though New Tecumseth will be conducting a plebiscite on the question of fluoridation with themunicipal election next October Defending community water fluoridation has drained a great deal of time human resources andcommitment from other priorities and has been exhausting here in SMDHU as I am sure it hasbeen in many other health units While the outcomes have been very disappointing I have beenimpressed by the professionalism and dedication that SMDHU staff members have shown inshouldering this burden In particular our dental consultant Dr Ito has provided us with much ofthe foundational knowledge and the local research essential to our efforts and has very frequentlyattended and presented at council meetings and other public events I would also like to thank themany of you who have offer and provided support including advocacy letters and informationresources Over the years Dr Peter Cooney Chief Dental Officer of Health of Canada has beenvery helpful attending and presenting with us at council meetings and at public consultationevents We will of course continue our oral health surveillance of the children of Muskoka documentingand reporting in future years on the increase in dental decay that we anticipate will occur Suchsurveillance is the foundation of our advocacy both to municipal politicians and to the province I am very concerned that our experience will continue to repeat itself across the province unlessthere is strong leadership provincially It is with this in mind that I raise the followingrecommendations for your consideration
1 That we collectively (with PHOrsquos leadership) conduct high quality publish-worthy researchdocumenting the impact on dental decay that occurs in those municipalities throughoutOntario that in recent years have discontinued community water fluoridation This could bepart of a larger study on such municipalities across the country and it could also be part ofa study documenting overall oral health (including fluoridation coverage) in the province(and possibly across the country)
2 That COMOH engage with our Chief MOH to advocate for the province to require allmunicipal water supplies to be fluoridated (the exception of course being those withnaturally sufficient fluoride concentrations) This could built upon the alPHa position to
Gordon
Highlight
Gordon
Highlight
date (A11-00 - Community Water Fluoridation) on the CMOH position (Oral Health ndash) and on theemail discussion generated on the COMOH listserv some months back re Richardrsquosproposal (calling on the province to fund municipal water fluoridation)
Valerie I request that this be an item for our COMOH meeting on November 15th Sincerely Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorg From Gardner Charles Sent Thursday September 26 2013 245 PMTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes(RayCopesoahppca)Subject Community Water Fluoridation Under Challenge Again in Simcoe Muskoka Hello Colleagues You may wish to know that community water fluoridation (CWF) is again under challenge in SimcoeMuskoka specifically both in Tottenham (Town of New Tecumseth in Simcoe County) and for theentire District of Muskoka On Monday September 23 Committee of the Whole Council of theTown of New Tecumseth voted to submit application to discontinue community water fluoridation(CWF) in the town of Tottenham despite presentations to the contrary from our dental consultantDr Ito and from me The next Council meeting is scheduled for Monday Sept 30 at which lastMondayrsquos (Sept 23) votes will be ratified
Since Monday I have spoken with the Mayor of the Town of New Tecumseth and with most of thecouncilors encouraging deferral of a decision on Monday to allow the town more time to make afully informed decision
This is the second time in recent years that the issue of discontinuing CWF in Tottenham has beenraised at council This issue is also scheduled to return again to the District of Muskoka Council on
October 21st where I will be presenting in response to deputations in opposition to fluoridation
Outside of Base Borden Tottenham is the only community with fluoridated water in SimcoeCounty The health unitrsquos own screening data between 2011 and 2013 shows that Tottenhamrsquos
Gordon
Highlight
children as well as those in Muskoka have a lower rate of dental decay than Simcoe Muskokacommunities without CWF
Sincerely
Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorgChuck Gardner MOH
November 04 2013
Mandatory State Laws on Fluoridation Thirteen states Puerto Rico and the District of Columbia have laws intended to provide
statewide fluoridation These states and the year that the fluoridation legislation was passed are
District of Columbia (1952) Connecticut (1965) Kentucky (1966) Illinois (1967) Minnesota
(1967) Ohio (1969) South Dakota (1969) Georgia (1973) Nebraska (1973 and 2008)
California (1995) Delaware (1998) Puerto Rico (1998) Nevada (1999) Louisiana (2008) and
Arkansas (2011) (see Table 1) The sizes of the public water systems or countiescommunities
affected and exemption provisions vary by state Table 1
STATES THAT HAVE MANDATORY LAWS ON FLUORIDATION -2011
State (1) Year of
Fluoridation
Legislation (1)
Population
served by
Fluoridated
CWS (2)
Persons
receiving
fluoridated
water (2)
State
Average
Caries
Experience
of Grade 3
Students (3)
Arkansas 2011 647 1724131 64
California 1995 621 22812721 709
Connecticut 1965 910 2370423 406
Delaware 1998 862 705344 545
Georgia 1973 921 8924598 52
Illinois 1967 993 11325132 532
Kentucky 1966 999 4334223 598
Louisiana 2008 407 1846149 657
Minnesota 1967 988 4117266 549
Nebraska 1973 and 2008 702 1001665 593
Nevada 1999 702 1001665 649
Ohio 1969 877 8772683 512
South Dakota 1969 948 642942 623
District of
Columbia
1952 1000 595000
Puerto Rico 1998
United States 739 204283554
2010 Statistics for population fluoridated and number of people
1 Communication with Jane McGinley RDH MBA Manager Fluoridation and Preventive Health
Activities Council on Access Prevention and Interprofessional Relations
2 Centers for Disease Control and Prevention Department of Health and Human Services
accessed Oct 21 2013 httpwwwcdcgovfluoridationstatistics2010statshtm
3 Centers for Disease Control and Prevention National Oral Health Surveillance System Caries
Experience - Percentage of 3rd Grade students with Caries Experience (treated or untreated tooth
If data from 43 states for the percentage of Grade 3 children with experience of dental decay is
compared with the 2008 percentages of the population in a state with Community Water
Fluoridation then the percentage of children with experience of dental decay decreases as the
percentage of the state population with Community Water Fluoridation increases (see Figure 1)
Figure 1
Correlation of Percentage of Grade 3 Children with Caries Experience and
Percentage of Population With Community Water Fluoridation for 43
Reporting States
0
10
20
30
40
50
60
70
80
0 10 20 30 40 50 60 70 80 90 100
State of Population With Community Water Fluoridation
Sta
te
of
Gra
de 3
Stu
den
ts w
ith
Cari
es E
xp
eri
en
ce
Data from CDC (2 3)
The description of the fluoridation laws in California Illinois and Nevada can be found on the
Association of State amp Territorial Dental Directors website(4 7 8)
The California fluoridation law AB 733 came into effect in 1995 requiring communities of 10
000 residents or more be supplied with fluoridated drinking water However the state did not
provide any funding to implement the legislation (California is unique in requiring fluoridation
without funding the practice)(4) The California Department of Health Services therefore had to
fund fluoridation initiatives from non-governmental sources ie the California Endowment
California Dental Association Foundation the First 5 Commission and others(5) From 1995 to
2011 the percentage of the California population receiving fluoridated drinking water has risen
from 17 to 625(6) 4 Dental Public Health Activities amp Practices Office of Oral Health California Department of Health
Services April 2002 httpwwwastddorgbestpracticesDES06002CAfluoridationpdf
5 Stock M Pollick H The CDA Foundation Model to Fluoridate Communities California Dental
Association Journal vol 40 no 8 649 - 655
httpwwwcdaorgPortals0journaljournal_082012pdf
6 California Dental Association Foundation
httpwwwcdafoundationorglearnadvocacyfluoridation
The State of Illinois passed a mandatory fluoridation state in 1967 and required all community
water systems to adjust fluoride levels in the drinking water to optimal levels within 1 year(7)
From 1962 when over 5000000 residents had optimally fluoridated drinking water by 2010
the number had risen to 11325132 (993 of the population on community water systems)(2)
7 Dental Public Health Activities amp Practices Division of Oral Health Illinois Department of Public
Health April 2002 httpwwwastddorgbestpracticesDES16007ILfluoridationpdf
The State of Nevada passed a mandatory fluoridation statute in 2000 for communities with
400000 or more residents(8) This was a result of the work of a statewide coalition that
included the Nevada Dental and Dental Hygienist Associations the Washoe and Clark County
District Health Departments the Clark County School District Junior League of Las Vegas
Head Start the Community College of Southern Nevada Dental Hygiene Program Health
Access Washoe County and Saint Maryrsquos Hospital For communities with less than 400000 the
implementation of fluoridation still required the vote of the majority voters in the community
The Las Vegas Water Authority and the City of Henderson started fluoridation in 2000
increasing the percentage of the population with fluoridated drinking water from 2 to 65 (8) 8 Dental Public Health Activities amp Practices Bureau of Family Health Services Nevada State Health
Division April 2002 httpwwwastddorgbestpracticesDES31002NVfluoridationbillpdf
Countries with Mandatory Laws on Fluoridation Countries that have mandated Community Water Fluoridation are Brazil Hong Kong
Malaysia Singapore Ireland Israel and some of the states in Australia
Singapore started fluoridating its water in 1956 based on the success of the fluoridation trials in
Grand Rapids Newburgh Evanston and Brantford Singapore became the first Asian country to
have 100 of its population benefitting from the implementation of fluoridated drinking water
Loh reported that ldquoThe ten year study on the effects of water fluoridation in Singapore showed
a decrease in caries prevalence in the children In the permanent dentition the reduction was
523 per cent for Chinese and 31 per cent for Malays in the 7 to 9 year old age group A similar
trend was observed in the mixed dentition in which the decrease was 325 per cent for Chinese
and 306 per cent for Malaysrdquo(9) By 2010 the population of the country was 5080000(10)
9 Loh T Thirty-eight years of water fluoridation--the Singapore scenario Community Dent
Health 1996 Sep13 Suppl 247-50
10 British Fluoridation Society One in a Million the facts about water fluoridation 3rd Edition
published March 2012) httpwwwbfsweborgonemillion0920One20in20a20Million20-
20The20Extent20of20Fluoridationpdf
Hong Kong started implementing community water fluoridation in 1961 and similar to
Singapore 100 of the population received access to fluoridated drinking water Lo and Wong
reported that ldquoThe mean DMFT score of the children deceased from 44 in 1960 to 15 in 1968
stayed at this level in the 1980 and 1986 surveys and further deceased to 08 in 2001 The
prevalence of dental fluorosis among the children surveyed in 1960 was 1 and this increased
to 59 and 70 in 1968 and 1980 respectively It was found in the 1986 and 2001 surveys that
the prevalences of fluorosis were 47 and 9 among children whose teeth developed at the
time when the respective water fluoride concentrations were 07 ppm and 05 ppmrdquo(11) The
population of Hong Kong was 6968000 in 2009(10) 11 LO ECM and WONG AHH Water fluoride concentration and fluorosis in Hong Kong in 1960-
2001 84th General Session and Exhibition of the International Association for Dental Research amp
1st Meeting of the Pan-Asian-Pacific Federation Brisbane Australia 28 June-1 July 2006 v 85 n
Sp B
The Malaysian cabinet approved a nationwide community water fluoridation program in 1972
(12) One of the states Sabah decided to stop fluoridation in 1989 due to concerns about
inadequate supervision in adding fluoride to the drinking water Oral Health Surveys in 2009
and 2007 indicated that children in Sabah had the worst oral health with 50 of 12 year-olds
having decay in their permanent teeth and children having an average of 3 teeth being(13)
Under the 10th Malaysian Plan in 2011 the federal and the Sabah state governments
reintroduced water fluoridation in Sabah(1314) In 2010 about 755 of the Malaysian
population or 20700000 people had fluoridated drinking water(1013) 12 Malaysian Dental Association Fluoride in Water
httpwwwmdaorgmy07_public_01healthcare_12htm
13 Sachdev N Fluoridation in Sabah Water for Cleaner Teeth French Tribunecom 28022011
From Levy IsraTo Jaeger ValerieCc Pim Carolyn gordonalphaweborg Diallo Aicha Penny Sutcliffe Paul Roumeliotis Michael Finkelstein
Hazel Lynn Robert KyleSubject FW Panorama - Privacy Security and other issuesDate Wednesday October 16 2013 122110 PM
Hello ValerieOttawa is part of Wave 4 Panorama implementation and we are gearing up increasingly to use thesystem where and if possible Thinking about it I am anticipating that this may need to be on theCOMOH (and alPHa) radar as it is something that will impact all health units and implies a majoroperational shift in vaccine delivery programs for all health units I have asked Carolyn Pim toconnect with our sister wave 4 units to share common experiences as we move forward ndash when wehave a roll up could I bring to COMOH Exec for discussion to explore whether there are broaderimplications for all members As an aside I have also asked the Ministry and their CIO to share with me any roll up learnings thatthey may have had already from previous waves (I understand that Niagara HU was a wave 1participant so if there is such a roll up of common experiences that others could learn fromperhaps you have it already and that could come to the exec too)Thanks Isra From Pim Carolyn Sent October 10 2013 1228 PMTo Christopher Mackie (christophermackiemlhuonca) Elizabeth Richardson(Elizabethrichardsonhamiltonca) H BSc M D F R C P (C) MPH Jim Chirico(jimchiriconbpsdhuca) Marlene Spruyt (spruytmtimiskaminghucom) Robert Kyle (Durham)Cc Levy IsraSubject Panorama - Privacy Security and other issues Dear colleagues Irsquom reaching out to you as fellow Panorama Wave 4 health units to ask about where yourorganizations are at in the process of signing agreements and completing Privacy ImpactAssessments and Threat Risk Assessments (TRAs) Ottawa Public Healthrsquos IT legal and informationsecurity advisors have made numerous requests to the MOHLTC for information (in particular theprovincial TRA) that we consider essential to develop our own risk assessment and PIA but havebeen told that information cannot be shared even with strict confidentiality and access controlsSo we are at somewhat of an impasse Isra emailed Arlene yesterday Arlene has forwarded ourconcerns to the Ministryrsquos CIO and Panorama lead but we havenrsquot had any response or discussionswith either of them yet Have your organizations identified similar concerns andor had interactions with the MOHLTC inthis respect Irsquod also be interested in knowing if your health units have flagged other (egoperational) implementation concerns Thanks
Carolyn ps Robert ndash you can ignore this request I talked with Sharan this morning about Durhamrsquos issuesso am including you now just for information Carolyn Pim MD FRCPC Associate Medical Officer of Health Meacutedecin adjointe en santeacute publique Ottawa Public Health Santeacute publique Ottawa 100 Constellation Cr Ottawa ON K2G 6J8 Tel teacutel (613) 580-6744 ext 23684Fax (613) 580-9641Connect With Ottawa Public Health
Suivez Santeacute publique Ottawa
This e-mail originates from the City of Ottawa e-mail system Any distribution use orcopying of this e-mail or the information it contains by other than the intendedrecipient(s) is unauthorized If you are not the intended recipient please notify meat the telephone number shown above or by return e-mail and delete thiscommunication and any copy immediately Thank you
Le preacutesent courriel a eacuteteacute expeacutedieacute par le systegraveme de courriels de la Ville dOttawaToute distribution utilisation ou reproduction du courriel ou des renseignements quisy trouvent par une personne autre que son destinataire preacutevu est interdite Si vousavez reccedilu le message par erreur veuillez men aviser par teacuteleacutephone (au numeacuteropreacuteciteacute) ou par courriel puis supprimer sans deacutelai la version originale de lacommunication ainsi que toutes ses copies Je vous remercie de votre collaboration
1
Smoke-Free Patios ndash An Amendment to the Smoke-Free Ontario Act
Date November 15 2013 Prepared for Council of Ontario Medical Officers of Health Prepared by York Region Public Health _____________________________________________________________________________ Issue
The Smoke-Free Ontario Act is the current provincial legislation that imposes smoking restrictions in workplaces and public places It prohibits smoking on restaurant and bar patios in instances where any portion of the seating area is covered by a roof With recent studies illustrating that exposure to second hand smoke outdoors poses similar risks to indoor exposure there has been growing public support to enhance smoking restrictions and make patios completely smoke-free
Background
With the implementation of the Smoke-Free Ontario Act in 2006 restaurant and bar patios became subject to smoking restrictions if any portion of the seating area was covered by a roof This allowed for patios without roof coverings to continue to allow smoking and as a result did not provide significant protection to patrons or staff from exposure to second hand smoke outdoors Many businesses chose to alter the design of their patios to allow smoking to continue In some cases patios became more crowded since smoking patrons who dine indoors often proceed outside onto licensed patios with their beverages to smoke York Region like most municipalities in Ontario is host to hundreds of patios being operated by restaurant owners and businesses With smoking prohibitions affecting only a small portion of these patios specifically ones with coverings the vast majority of patios still allow smoking to take place Patrons and employees on patios where smoking is not restricted are exposed to second hand smoke frequently This can contribute to increased disease and aggravation of existing health conditions From a business perspective the existing legislation has been viewed by many operators as unfair because some patios have permanent coverings which cannot be removed requiring a smoke-free status These business owners feel this creates an uneven playing field since they cannot provide an outdoor dining area for their smoking customers There is strong community support for smoke-free patios in Ontario A 2009 Rapid Risk Factor Surveillance System survey revealed 754 percent support in York Region while a Toronto Health Survey in 2011 indicated 74 percent public support
2
Current Status
Smoking is currently prohibited on restaurant and bar patios province-wide in four Canadian provinces and territories Alberta Newfoundland and Labrador Nova Scotia and Yukon A fifth province Prince Edward Island prohibits smoking on patios until 10 pm Since Ontario enacted legislation restricting smoking on patios in 2006 eight municipalities in Ontario have chosen to create bylaws that go beyond the Smoke-Free Ontario Act and enhance outdoor protection from second hand smoke by prohibiting smoking on patios completely The largest of those municipalities is the City of Ottawa Recently the Toronto Board of Health unanimously endorsed a report presented by their Medical Officer of Health recommending that restaurant and bar patios be made smoke-free through an amendment to the Smoke-Free Ontario Act
Key Considerations
There should be no significant financial burden to local Boards of Health resulting from a smoke-free patio amendment to the Smoke-Free Ontario Act Inspection and enforcement for the Smoke-Free Ontario Act is currently 100 percent funded by the Ministry of Health and Long-Term Care Following an introductory period of education on the amendment a complaint response model of service delivery would ensure ongoing compliance with smoke-free requirements A complete ban of smoking on patios would eliminate the widely-held perception by business owners that the current legislation creates an uneven playing field for business Since Smoke-Free Ontario Act inspections of patios began in 2006 operators have expressed the opinion that if patios need to be smoke-free for the protection of the public they should all be smoke-free to avoid undue hardship for individual businesses and to provide protection uniformly across the Province
Next steps
York Region Public Health intends to seek support from Medical Officers of Health across the Central East Tobacco Control Area Network (CETCAN) to advocate to the Ministry of Health and Long-Term Care for an amendment to the Smoke-Free Ontario Act prohibiting smoking on all restaurant and bar patios York Region is also in the process of requesting that its Regional Council advocate to the Minister of Health and Long-Term Care on the issue
Updating and Modernizing O Regulation 565 (Public Pools)
Date November 15 2013
Prepared for Council of Ontario Medical Officers of Health
Prepared by York Region Public Health _____________________________________________________________________________ Background Recent drownings at public pools in Ontario have highlighted the issue of water-borne illness and injury The current pool regulation under Ontariorsquos Health Protection and Promotion Act O Regulation 565 (Public Pools) is outdated It does not accurately reflect new pool technology and design or the changing use of public pools Neither does it incorporate admissions standards recommended by the Office of the Chief Coroner Further O Regulation 565 does not have short-form wording or set fines associated with it This limits public health enforcement capabilities What is the impact Updating O Regulation 565 (Public Pools) to address recent changes in pool technology design and uses and to include Coroner-recommended admissions standards would help improve pool safety Establishing short-form wording for O Regulation 565 would enhance enforcement related to public pools Currently the only enforcement available to Public Health Inspectors for dealing with non-critical regulatory infractions in public pools is the issuance of a Part III summons This involves a considerable amount of resources for a possible small fine With the development of inspection disclosure systems such as YorkSafe there is an even greater need to develop a method to effectively address repeated pool operator non-compliance with non-critical issues Next steps Public health units should advocate to the Province to 1) Conduct a review of O Regulation 565 (Public Pools) to address shortcomings Proposed changes to the
regulation should include a requirement for ownersoperators of public pools to advise the local Medical Officer of Health of any change in the use of a facility and the addition of the Coronerrsquos recommended admission standards
2) Provide short-form wording for O Regulation 565 so that public health inspectors can better deal with pool operator non-compliance
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
It is also working on a TOPHC session on Cultural Safety related to working with aboriginal populations Feedback was also invited on this with a note that the deadline for abstract submission is September 27 Finally work is also being done with PHO on developing resources and supports for work with Priority Populations 67 COMOH Electronic Mailing List List of Subscribers 68 COMOH Correspondence Aug 26 COMOH Letter ndash Energy Policy
Aug 8 COMOH Letter ndash CMA Poverty Report
July 22 COMOH Letter ndash Immunization Data
70 Next MeetingAdjournment Meeting adjourned at 1035 Next Section meeting will be on November 15 2013 in Toronto part of the alPHa Fall Symposium
Page 1 of 8 ndash DRAFT FOR COMOH DISCUSSION
alPHa Membership Survey hello
Draft Report ndash COMOH Version hello
alPHarsquos membership was surveyed in the fall of 2013 Similar surveys were administered to all member groups ie COMOH BOH Section and Affiliates using the online survey tool Survey Monkey Small alterations were made to group-specific surveys to ensure that the survey questions were relevant to each group A total of 84 responses were received from alPHa members The breakdown of respondents was as follows This draft report is provided for discussion purposes to COMOH members and therefore focuses on the responses provided by COMOH members To provide additional information overall survey responses are also provided for some questions
SECTION 1 RESPONDENT PROFILE
Survey Question What region is your health unit located in
For COMOH members responses came from 6 of the 7 regions of Ontario All 7 regions were represented in the full set of survey responses
Summary of Respondents COMOH 27 32 BOH Section 34 40 Affiliates 23 27 Totals 84 100
All ResponsesEastern 24 29South West 12 14Central East 13 15Central West 15 18North East 11 13Toronto 5 6Not Sure 3 4North West 1 1Totals 84 100
All COMOH ResponsesEastern 3 11South West 5 19Central East 6 22Central West 6 22North East 3 11Toronto 4 15North West 0 0Totals 27 100
Page 2 of 8 ndash DRAFT FOR COMOH DISCUSSION
Survey Question How long have you been involved with public health in Ontario
Survey Question Have you participated on the alPHa Board of Directors or an alPHa or COMOH committeeworking group
All ResponsesYes in the last 1 to 2 years 15 18Yes in the last 2 to 5 years 9 11Yes more than 5 years ago 9 11No not ever 51 61Totals 84 100
All COMOH ResponsesOver 10 years 17 635 to 10 years 7 262 to 5 years 3 11Totals 27 100
All ResponsesOver 10 years 34 405 to 10 years 21 252 to 5 years 21 251 to 2 years 3 4Less than 1 year 5 6Totals 84 100
All COMOH ResponsesYes in the last 1 to 2 years 7 26Yes in the last 2 to 5 years 4 15Yes more than 5 years ago 8 30No not ever 8 30Totals 27 100
Page 3 of 8 ndash DRAFT FOR COMOH DISCUSSION
SECTION 2 PROFESSIONAL DEVELOPMENT
Survey Question Which of the following events have you attended at least once in the past two years
Survey Question Overall how satisfied have you been with alPHa events ie conferences meetings
Survey Question How much value do alPHarsquos events provide for the money
Survey Question How can alPHa make its events more valuable to you Please share any suggestions regarding future topics speakers formats duration locations or any other event component that is important to you
Comments about content bull Expert speakerpanels on emerging or hot topics
(2) bull More engaged dialogue with Ministry rather than
just updates bull Fewer Ministry updates (3) bull Content on medicalPH issues is better left to PHO
TOPHC and joint conferences (2) bull alPHa should stick to Ministrypoliticspolicysenior
PH supportPHU support on key priorities (eg November practical conference on HKP report)
bull For COMOH more discussion bull More time for section activities like face-to-face
COMOH meetings
bull More facilitated work groups of COMOH members to respond to public health practice questions
bull More focus on rural and northern issues bull Infection Control Logistical Considerations bull Consider partnering with other groups bull More collaboration with PHO and OPHA events bull Use of video conferencing bull Less frequentfewer meetings (2) bull Connect with CME Location bull Consider other venues than TO
( ) brackets indicate that more than one response included a similar comment
More than enough value 7 11A lot of value 34 52Some value 22 34A little value 2 3Not enough value 0 0Totals 65 100
All Responses for those who Attended at least One Event in the Last 2 Years
All COMOH ResponsesMore than enough value 4 15A lot of value 13 48Some value 9 33A little value 1 4Not enough value 0 0Totals 27 100
Page 5 of 8 ndash DRAFT FOR COMOH DISCUSSION
SECTION 3 VALUE FOR MEMBERSHIP
Survey Question What do you value the most about your alPHa membership
The comments provided in response to the text response question What is the most important benefit of alPHa membership for you personally supported the answers illustrated in the chart above 15 of the 20 comments provided focussed on the importance of opportunities to interact with colleagues across the province The next most important benefit mentioned was the support for COMOH members to work on public health issues together When asked What is the most important benefit of alPHa membership for your health unit COMOH members emphasized the following bull A coordinated and collective voice in advocating for public health issues and the public health sector (9) bull Opportunities to connect with other public health units to share experiences and best practices (8) bull Maintaining relationships with government both politicians and bureaucrats (3) and bull Support for boards of health (3)
Page 6 of 8 ndash DRAFT FOR COMOH DISCUSSION
Overall Level of Satisfaction
SECTION 4 LOOKING TO THE FUTURE
The questions in this section were asked to obtain input from alPHa members regarding a proposal from alPHarsquos Board of Directors to focus the Association on five service areas COMOH members were asked to indicate their level of agreement with the proposed areas of focus COMOH responses compared to the overall survey responses were as follows
To explore some proposed changes to Association services COMOH members were asked to provide their level of agreement with the following questions
COMOH Responses BOH Section Affiliates All Survey Responses
Strongly Agree
AgreeNeither Agree or Disagree
DisagreeStrongly Disagree
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1Promoting the role and value of local public health units
15 9 2 0 0 26 92 93 95 94
2
Providing important information to members about trends and events that will impact the public health system and management of public health units
10 8 8 0 0 26 69 97 86 85
3Facilitating professional networking and information sharing
13 10 3 0 0 26 88 83 82 85
4
Providing professional development to support excellence in public health unit leadership management and governance
3 15 7 1 0 26 69 83 86 79
5
Responding to public health sector issues when it makes the most sense to have a collective voice ie issues that impact the structure and funding of the public health sector and public health units and issues that have a broad focus on population health
15 8 2 0 1 26 88 97 95 93
PROPOSED AREAS OF FOCUS
COMOH Responses BOH Section Affiliates All Survey Responses
Strongly Agree
AgreeNeither Agree or Disagree
DisagreeStrongly Disagree
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1
COMOH and other professional groups within alPHa should do their own advocacy while alPHa supports members to share and support each others advocacy efforts
7 6 6 6 1 26 50 58 45 52
2
alPHa should provide support to action-oriented inter-professional work groups on priority public health unit issues and member resolutions
4 13 5 3 1 26 65 81 86 77
PROPOSALS
Page 8 of 8 ndash DRAFT FOR COMOH DISCUSSION
COMOH members were also asked to indicate the level of acceptability for some possible changes to alPHarsquos services and way of doing business
COMOH Responses BOH Section Affiliates All Survey Responses
Very Acceptable
Somewhat Acceptable
Neither Acceptable or Unacceptable
Somewhat Unacceptable
Very Unaccept
able
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1Single conference with additional face-to-face section meetings
21 2 0 1 0 24 96 68 80 81
2alPHa to offer alternatives like webinars on focussed topics
13 6 1 4 0 24 79 50 90 71
3Coordinate COMOH meetings with PHO OMA or Ministry events
16 4 2 0 0 22 91 na na --
4
Increase focus on building leadership and management capacity for health unit CEOs and senior management
7 9 4 3 0 23 70 na 70 70
5
Would it be acceptable for alPHa to request voluntary financial contributions from member PHUs in addition to annual fees
3 5 5 4 5 22 36 7 26 21
6
Would it be acceptable for alPHa to request voluntary in-kind staff contributions from member PHUs to expand alPHas capacity eg communications policy work group support
7 11 1 1 3 23 78 31 45 50
7Would it be acceptable to you for alPHa to discontinue staff support for COMOH (BOH Section)
0 4 1 5 14 24 17 11 na 14
8
Would it be acceptable to you for alPHa to reduce the amount of staff support for COMOH (BOH Section)
1 6 1 8 6 22 32 26 na 29
9
Would it be acceptable to you for alPHa to provide supports to MOHs and AMOHs (BOH Members) without maintaining COMOH (BOHs) as a section of the association
3 2 3 2 12 22 23 17 na 20
10
Would it be acceptable to you for alPHas Board of Directors to move from the current representational model to a skills-based strategic model ie board membership would be based on the skills needed to carry out alPHas strategic plan
6 11 2 1 3 23 74 56 56 62
11
Would it be acceptable to you for alPHas President Vice-President and Treasurer to be elected from the full membership of the alPHa Board of Directors (rather than the current model of alternating between BOH and COMOH members)
10 8 1 2 2 23 78 70 70 73
PROPOSED CHANGES
1 Council of Ontario Medical Officers of Health Terms of Reference
ASSOCIATION OF LOCAL PUBLIC HEALTH AGENCIES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
TERMS OF REFERENCE NAME 1 The name of the organization shall be ldquoThe Council of Ontario Medical Officers of
Health a section of the Association of Local Public Health Agencies (alPHa)rdquo hereinafter referred to as ldquothe Councilrdquo
MISSION 2 As local leaders in public health we are committed to improving the health of
Ontarians and increasing health equity by strengthening Ontariorsquos public health system We achieve this through system leadership and coordination in collaboration with the provincial government and other organizations and through evidence-informed advocacy on public health policy
OBJECTIVES 3 The objectives of the Council shall be
a) To provide strong province-wide leadership in public health
b) To advocate for health protection and promotion policies and programs that maintain and improve the health of Ontarians
c) To promote and maintain the highest standards for Ontariorsquos public health
programs and services
d) To support the planning implementation and evaluation of effective and efficiently run public health programs and services
e) To act as a forum for sharing information and resources and for addressing and
discussing public health issues both amongst the Councilrsquos members and other agencies that support the goals of alPHa eg Ontario Medical Association Ontario Public Health Association etc
f) To engage with and to provide public health and related policy advice to alPHa
the Chief Medical Officer of Health the Ontario Ministries of Health and Long-Term Care (including the Health Promotion and Public Health Divisions) Children
2 Council of Ontario Medical Officers of Health Terms of Reference
and Youth Services and other provincial ministries Public Health Ontario Health Canada the Public Health Agency of Canada and other public health partners
g) To promote and protect the professional interests of its members
h) To provide support to individual members as needed
i) To seek recognition for outstanding practice from among the members
j) To support evidence based practice of public health medicine
k) To engage and involve the membership to participate in COMOHrsquos endeavours
l) To mentor Public Health and Preventive Medicine Residents
MEMBERSHIP 4 Membership on the Council in each of the following categories is subject to the
limitations imposed by the current terms of reference and all policies and governing documents of the Association of Local Public Health Agencies Benefits of membership in each category are included in Appendix A These shall be subject to regular review and may be suspended under certain circumstances
Active membership in the Council shall be open to all Associate Medical Officers of Health and all full-time Medical Officers of Health whose Boards of Health are members of alPHa Such members shall have full voting privileges and may hold office in the Council Associate membership shall be open to all full and part-time physicians employed by a Board of Health that is a member of alPHa Such members shall not have voting privileges nor hold office
Affiliate membership shall be open to the following individuals interested in furthering the objectives of the Council
bull Public Health and Preventive Medicine Residents and Public Health and Preventive Medicine Residency Program Directors
bull Federal public health physicians working in Ontariorsquos First Nations communities
bull other public health or related physicians including those employed by a Board of Health that is not a member of alPHa
Such members shall not have voting privileges nor hold office
3 Council of Ontario Medical Officers of Health Terms of Reference
Emeritus membership shall be open to all former members who have retired after five (5) or more years of Active membership subject to the nomination in writing of two (2) active members in good standing endorsement of the Executive Committee and approval of the Council by majority vote at a general meeting Such members shall have neither voting privileges nor hold office but may be invited to attend general meetings Honorary membership shall be open to any non-active or associate member subject to the nomination in writing of two (2) active members in good standing endorsement of the Executive Committee and approval of the Council Such members shall have neither voting privileges nor hold office but may be invited to attend general meetings
OFFICERS 5 The Officers of the Council shall be the Chair Vice-Chair and immediate Past Chair
6 The Chair shall prepare the agendas of all Council meetings She shall preside and
preserve order at all such meetings shall ensure that these Terms of Reference are upheld and enforced and shall contribute to the supervision and evaluation of any Public Health and Preventive Medicine Resident who is on a placement with alPHa
7 The Vice-Chair shall fulfill the duties of the Chair in hisher absence The immediate
Past Chair may fulfill the duties of the Chair or Vice-Chair in their absences 8 The Chair shall normally serve a term of one (1) year which is renewable once and
after which the Vice-Chair shall normally assume the vacated office COMMITTEES 9 The Council shall elect seven (7) active members one from each of alPHarsquos regions
and the active member who is scheduled to serve as the President or immediate Past-President of alPHa to represent it on the alPHa Board of Directors These seven (7) members shall constitute the Councilrsquos Executive Committee and shall serve a term of at least one (1) year The Chair and Vice-Chair shall be elected from among the Executive Committee members If alPHarsquos immediate Past President is an active member she shall be an ex-officio member of the Executive Committee
10 The mandate of the Executive Committee shall be to facilitate the achievement of
the objectives of the Council by fulfilling the following
a Identifying priorities 1
1 See Appendix B Planning Cycle to Identify Priorities for COMOH
and ensuring the development of briefing documents and or recommendations as appropriate for the consideration of the Council
4 Council of Ontario Medical Officers of Health Terms of Reference
b Setting agendas and otherwise ensuring preparations for Council meetings c Ensuring the fulfillment of the direction of Council d Responding in a timely fashion to time-sensitive public health matters in
accordance with the Executive Committeersquos understanding of the perspective of the Council
e Engaging with the Chief Medical Officer of Health Associate Chief Medical Officers of Health and other provincial public health leaders and
f Representing Council at public and partner agency forums including the Public Health Leadership Council which shall normally include membership from the Officers of the Council and two other Executive Committee members as selected by agreement among the Executive
g Identifying opportunities for the recognition of outstanding practice from among the members including the annual nomination of at least one member for the alPHa Distinguished Service Award
11 The Executive Committee shall meet and correspond in the manner and at the times
and if required places as deemed necessary by the Chair to conduct the business of the Council A quorum shall consist of four (4) members
12 The Executive Committee shall have the power to strike committeestask or working
groups to assist it in carrying out the business of the Council 13 The Council may by special resolution remove a member of the Executive
Committee before the completion of hisher term of office and may elect a successor to complete the term The special resolution shall require a majority vote of 67 of the members present and voting at the meeting at which the special resolution is considered
14 A Nominating Committee shall consist of the three (3) most recent Past Chairs who
are able to serve and shall be chaired by the immediate Past Chair The Nominating Committee shall prepare a list of proposed Officers and Executive Committee members for the consideration of the Council at its Annual General Meeting
MEETINGS 15 The Council shall hold at least four (4) general meetings per year in a manner and at
the times and if required places as deemed necessary by the Executive Committee to share information direct and assist the Executive Committee in conducting the business of the Council
16 The Council shall hold its Annual General Meeting during and at the same place as
the alPHarsquos Annual Conference
5 Council of Ontario Medical Officers of Health Terms of Reference
17 The Council shall hold a special meeting at the call of the Chair or upon the written request specifying the purpose of such meeting of at least five (5) active members Council members must be given at least 48 hours notice of any special meeting
18 Only Councilrsquos active and associate members and alPHa staff are entitled to attend
general and special meetings of the Council Other members and non-members may be invited to attend all or part of such meetings as determined by the Chair preferably in consultation with the Executive Committee Non-members who come to such meetings without an invitation may attend all or part of the meeting by a majority vote of the active members present and voting
19 The Chair shall prepare the agendas for such meetings and shall normally include
reports from the Chair and the Councilrsquos committeestask or working groups and representatives to external bodies alPHarsquos Executive Director shall ensure that the minutes shall be recorded and promptly distributed to the Section
20 A quorum for all such meetings shall be ten (10) active members 21 The Council shall normally be notified in a manner deemed appropriate by the Chair
of such meetings at least one (1) month prior to their being held 22 A majority vote of the members present at such meetings and voting shall make
Council decisions In the case of a tied vote the Chair shall cast the deciding vote The Executive Committee shall ensure that actions arising from such decisions at such meetings are implemented and monitored
23 The Chair may solicit advice from the Council through the use of teleconferencing
and alPHarsquos electronic mailing lists in order to gain an understanding of the overall perspective of the Council (see 10d)
ELECTIONS 24 The Officers and Executive Committee members shall be elected at the Sectionrsquos
Annual General Meeting The Nominating Committee Chair or hisher designate shall present a list of nominations Additional nominations from the floor shall also be considered Each Officer and Executive Committee member shall be elected by secret ballot if necessary by a majority of the active members present and voting In the case of a tie the Chair shall cast the deciding vote
AMENDMENTS 25 The Councilrsquos Terms of Reference may be amended from time to time by the
Executive Committee provided the Committee receives notice of such proposed amendments at least one (1) month prior to the meeting at which the amendments
6 Council of Ontario Medical Officers of Health Terms of Reference
will be considered Such amendments shall be ratified by the Council at the next general meeting or the Annual General Meeting as the case may be
26 The Executive Committee shall review the Terms of Reference as required and not
less than once every two years Original September 1987 1st Revision October 2000 2nd Revision July 2001 3rd Revision December 2003 4th Revision February 2008 5th Revision June 2009 6th Revision June 2011 7th Revision June 2013
7 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX A
COMOH Membership Benefits Active Membership
bull Entitled to attend all meetings of the Section bull May hold office on the COMOH Executive Committee alPHa Board of Directors
Standing Committees bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Associate Membership
bull Entitled to attend all meetings of the Section bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Affiliate Membership
bull May attend meetings or parts thereof subject to approval of Chair bull May serve on ad-hoc committees of the Section subject to the approval of the
Executive Committee bull Discounted registration rates for alPHa Conferences (for Public Health and
Preventive Medicine Residents) bull Upon written request and subject to COMOH Executive approval Affiliate
Members may subscribe to comohlistsalphaweborg The approval will be reviewed on an annual basis in order to determine if the Affiliate Member can remain a subscriber to mohsalphaweborg
Emeritus Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair bull Enjoy discounted registration rates for alPHa Conferences and regular COMOH
meetings bull Subscription to comohlistsalphaweborg electronic mailing list bull Full access to alPHa Web site bull May represent alPHa COMOH on selected external committees and working
groups Honorary Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair
8 Council of Ontario Medical Officers of Health Terms of Reference
bull May represent alPHa COMOH on selected external committees and working groups subject to the approval of the COMOH or alPHa Executive Committee as appropriate
9 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX B
Planning Cycle to Identify Priorities for COMOH
1 There shall normally be a COMOH membership strategic planning retreat every four years In recognition of the dynamic environment of public health the need for and timing of such a retreat shall be at the discretion of the Executive Committee in consultation with the membership
2 The COMOH Executive is responsible (through the creation of a subcommittee of COMOH members) for ensuring the preparation for the COMOH retreats with resources to include those provided by alPHa
3 Leadership for action on COMOH priorities will be recruited from among the COMOH membership in order to make good use of the full base of capacity of the membership The resources to support actions will be recruited from both within and beyond the COMOH membership employing other public health professionals that reside within the broader public health system and community
4 The COMOH Executive shall ensure an annual review of strategic priorities and initiatives and the development of a draft report of the same for the review of the members at the June meeting
2013 Strategic Planning
Considerations for COMOH
As part of its strategic planning discussions alPHarsquos Board has been considering changes to the level of support provided to member sections A member survey is being carried out over the fall to determine options acceptable to alPHa members The following approach to support is put forward as a proposal for the consideration of COMOH Note that the feasibility of the points below depend upon future decisions of the alPHa board They assume that COMOH remains part of alPHa but becomes more independent in administering meetings
1 alPHa can provide to COMOH staff support (Gord Fleming) amounting to 02 FTE or one day per week This is a reduction from the current level of 35 days per week COMOH can choose to use the support any way it wants writing COMOH letters meeting minutes agenda support special projects etc
2 In addition to 02 FTE alPHa staff would provide support for up to 4 face-to-face meetings per year One meeting would be concurrent to alPHarsquos annual conference in June The timing of other meetings could be negotiated The support includes consulting on the development of the program arranging for speakers registration for the event arranging venue AV support and hospitality services
3 In addition to 02 FTE alPHa staff would provide support for setting meeting dates and any polling required to establish dates Note that the individual supporting this function would be Karen Reece
4 COMOHrsquos Executive and Section would continue to have access to online supports through the alPHa including the COMOH Listserve and a group page for posting agendas minutes and other resources on the alPHa website
5 alPHa staff (Linda Stewart and Gord Fleming) can also start participating on CMOH calls as a way to be up-to-date on issues related to COMOH
6 Other than what is outlined above COMOH would be expected to prepare agendas and take minutes for its Executive and Section meetings The Executive would be expected to operate more independently than it does now but would be able to access the supports outlined above
Prepared by Linda Stewart Executive Director
From comoh-bounceslistsalphaweborg on behalf of Christopher MackieTo MOH ListserveSubject [comoh] Fw URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)Date Wednesday October 30 2013 91241 AMAttachments ATT00249txt
For AMOHs and PHPM residents who didnt receive the initial email
Chris
Christopher Mackie MD MHSc FRCPCMedical Officer of Health and CEOMiddlesex-London Health Unit50 King St LondonON N6A 5L7 O 519 663 5317 ext 2444 wwwhealthunitcomFrom Pisko Laura (MOHLTC)Sent Tuesday October 29 2013 759 PMTo kbarkeralgomapublichealthcom malcolmlockbchuorg davidcchatham-kentcarobertkyledurhamca proumeliotiseohuca fwarshelginhealthonca mohelginhealthoncahlynnpublichealthgreybruceonca malcolmlockhnhuorg hnmohhnhuorglnoseworthyhkpronca bobnosalhaltonca elizabethrichardsonhamiltoncarschabashpechuonca ncameronhuroncountyca drimgemmillkflapublichealthcamohkflapublichealthca suditranadecounty-lambtononca paulastewarthealthunitorgChristopher Mackie valeriejaegerniagararegionca jimchiriconbpsdhuca jarthursnwhuoncaisralevyottawaca dnealoxfordcountyca davidmowatpeelregionca mklassenpdhuoncarpellizzaripcchuca rosemarieramsinghporcupinehuonca mcorriveaurcdhucomcharlesgardnersmdhuorg sutcliffepsdhucom davidwilliamstbdhucomspruytmtimiskaminghucom dmckeowntorontoca lnolanregionofwaterloocanicolamercerwdghuorg aheimannwechealthunitorg karimkurjiyorkcaCc coreywesleytbdhucom CindyBaker-Barillsmdhuorg Donna Kosmack pilonlsdhucomPaulaMuiskflapublichealthca sthibautorontoca Mueller Daina (MOHLTC) Gordon Marcus(MOHLTC) andreakitahamiltoncaSubject URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)
Dear Colleagues The ministry has received reports that some tobacco vendors across the province aregiving away single cigarettes with the purchase of tobacco products It is the ministryrsquosposition that giving out free single cigarettes does not violate subsection 31(3) of theSmoke-Free Ontario Act (ldquoSFOArdquo) Although the practice of giving out free singlecigarettes may promote the sale of tobacco products it does not take the form of aldquoproduct enhancement product association or promotional materialrdquo and therefore doesnot fall within the scope of subsection 31(3) of the SFOA We have confirmed with Health Canada that this practice may violate section 29(b) of thefederal Tobacco Act As such Health Canada is requesting that you notify them in writingand I am directing you to communicate with them via email and provide to them as manydetails as possible Emails should be sent to Tobacco-Ontariohc-scgcca and thesubject line should read ldquoViolation of Section 29(b) of Tobacco Actrdquo This will ensurethat the complaints are given priority status by Health Canada We will continue to monitor
this situation and liaise with our colleagues at Health Canada Please share this information with your tobacco control staff and contact me or DainaMueller Manager Tobacco Control Unit Health Promotion Implementation Branch atdainamuellerontarioca with any questions RegardsLaura Laura A PiskoDirectorHealth Promotion Implementation BranchHealth Promotion DivisionMinistry of Health and Long Term Care416-327-7445 (office)416-451-3185 (mobile) Marcus Gordon - EA (416)326-0625 for urgent issues
========= Middlesex-London Health Unit E-Mail Disclaimer =============______________________________________________________________
Private and confidential intended only for named recipient If otherwisereceived please destroy immediately Health information in this email isonly general information and is not intended to replace an in personconsultation with a medical professional nor is it intended to providemedical advice Individual circumstances of which we are not aware mayaffect the information provided herein and as such the Middlesex-LondonHealth Unit assumes no liability or responsibility for your reliancethereon The Middlesex-London Health Unit works under the authority of theHealth Protection and Promotion Act and this correspondence may be used toassess your needs for public health services (519-663-5317 ext 2448)______________________________________________________________
From Gardner CharlesTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes (RayCopesoahppca)
George Pasut (GeorgePasutoahppca) Peter Cooney (petercooneyhc-scgcca)Cc Ito DickSubject Discontinuation of Fluoridation in MuskokaDate Tuesday October 22 2013 125254 PM
Hello Colleagues
As I reported in my email below on September 26th fluoridation has come under challenge again inSimcoe Muskoka I am now very unhappy to report that despite our best efforts last night theDistrict Council of Muskoka voted to remove fluoride from municipal drinking supplies across theDistrict This brings to an end fluoridation in all of Simcoe and Muskoka (with the exception of Base Borden)ndash though New Tecumseth will be conducting a plebiscite on the question of fluoridation with themunicipal election next October Defending community water fluoridation has drained a great deal of time human resources andcommitment from other priorities and has been exhausting here in SMDHU as I am sure it hasbeen in many other health units While the outcomes have been very disappointing I have beenimpressed by the professionalism and dedication that SMDHU staff members have shown inshouldering this burden In particular our dental consultant Dr Ito has provided us with much ofthe foundational knowledge and the local research essential to our efforts and has very frequentlyattended and presented at council meetings and other public events I would also like to thank themany of you who have offer and provided support including advocacy letters and informationresources Over the years Dr Peter Cooney Chief Dental Officer of Health of Canada has beenvery helpful attending and presenting with us at council meetings and at public consultationevents We will of course continue our oral health surveillance of the children of Muskoka documentingand reporting in future years on the increase in dental decay that we anticipate will occur Suchsurveillance is the foundation of our advocacy both to municipal politicians and to the province I am very concerned that our experience will continue to repeat itself across the province unlessthere is strong leadership provincially It is with this in mind that I raise the followingrecommendations for your consideration
1 That we collectively (with PHOrsquos leadership) conduct high quality publish-worthy researchdocumenting the impact on dental decay that occurs in those municipalities throughoutOntario that in recent years have discontinued community water fluoridation This could bepart of a larger study on such municipalities across the country and it could also be part ofa study documenting overall oral health (including fluoridation coverage) in the province(and possibly across the country)
2 That COMOH engage with our Chief MOH to advocate for the province to require allmunicipal water supplies to be fluoridated (the exception of course being those withnaturally sufficient fluoride concentrations) This could built upon the alPHa position to
Gordon
Highlight
Gordon
Highlight
date (A11-00 - Community Water Fluoridation) on the CMOH position (Oral Health ndash) and on theemail discussion generated on the COMOH listserv some months back re Richardrsquosproposal (calling on the province to fund municipal water fluoridation)
Valerie I request that this be an item for our COMOH meeting on November 15th Sincerely Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorg From Gardner Charles Sent Thursday September 26 2013 245 PMTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes(RayCopesoahppca)Subject Community Water Fluoridation Under Challenge Again in Simcoe Muskoka Hello Colleagues You may wish to know that community water fluoridation (CWF) is again under challenge in SimcoeMuskoka specifically both in Tottenham (Town of New Tecumseth in Simcoe County) and for theentire District of Muskoka On Monday September 23 Committee of the Whole Council of theTown of New Tecumseth voted to submit application to discontinue community water fluoridation(CWF) in the town of Tottenham despite presentations to the contrary from our dental consultantDr Ito and from me The next Council meeting is scheduled for Monday Sept 30 at which lastMondayrsquos (Sept 23) votes will be ratified
Since Monday I have spoken with the Mayor of the Town of New Tecumseth and with most of thecouncilors encouraging deferral of a decision on Monday to allow the town more time to make afully informed decision
This is the second time in recent years that the issue of discontinuing CWF in Tottenham has beenraised at council This issue is also scheduled to return again to the District of Muskoka Council on
October 21st where I will be presenting in response to deputations in opposition to fluoridation
Outside of Base Borden Tottenham is the only community with fluoridated water in SimcoeCounty The health unitrsquos own screening data between 2011 and 2013 shows that Tottenhamrsquos
Gordon
Highlight
children as well as those in Muskoka have a lower rate of dental decay than Simcoe Muskokacommunities without CWF
Sincerely
Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorgChuck Gardner MOH
November 04 2013
Mandatory State Laws on Fluoridation Thirteen states Puerto Rico and the District of Columbia have laws intended to provide
statewide fluoridation These states and the year that the fluoridation legislation was passed are
District of Columbia (1952) Connecticut (1965) Kentucky (1966) Illinois (1967) Minnesota
(1967) Ohio (1969) South Dakota (1969) Georgia (1973) Nebraska (1973 and 2008)
California (1995) Delaware (1998) Puerto Rico (1998) Nevada (1999) Louisiana (2008) and
Arkansas (2011) (see Table 1) The sizes of the public water systems or countiescommunities
affected and exemption provisions vary by state Table 1
STATES THAT HAVE MANDATORY LAWS ON FLUORIDATION -2011
State (1) Year of
Fluoridation
Legislation (1)
Population
served by
Fluoridated
CWS (2)
Persons
receiving
fluoridated
water (2)
State
Average
Caries
Experience
of Grade 3
Students (3)
Arkansas 2011 647 1724131 64
California 1995 621 22812721 709
Connecticut 1965 910 2370423 406
Delaware 1998 862 705344 545
Georgia 1973 921 8924598 52
Illinois 1967 993 11325132 532
Kentucky 1966 999 4334223 598
Louisiana 2008 407 1846149 657
Minnesota 1967 988 4117266 549
Nebraska 1973 and 2008 702 1001665 593
Nevada 1999 702 1001665 649
Ohio 1969 877 8772683 512
South Dakota 1969 948 642942 623
District of
Columbia
1952 1000 595000
Puerto Rico 1998
United States 739 204283554
2010 Statistics for population fluoridated and number of people
1 Communication with Jane McGinley RDH MBA Manager Fluoridation and Preventive Health
Activities Council on Access Prevention and Interprofessional Relations
2 Centers for Disease Control and Prevention Department of Health and Human Services
accessed Oct 21 2013 httpwwwcdcgovfluoridationstatistics2010statshtm
3 Centers for Disease Control and Prevention National Oral Health Surveillance System Caries
Experience - Percentage of 3rd Grade students with Caries Experience (treated or untreated tooth
If data from 43 states for the percentage of Grade 3 children with experience of dental decay is
compared with the 2008 percentages of the population in a state with Community Water
Fluoridation then the percentage of children with experience of dental decay decreases as the
percentage of the state population with Community Water Fluoridation increases (see Figure 1)
Figure 1
Correlation of Percentage of Grade 3 Children with Caries Experience and
Percentage of Population With Community Water Fluoridation for 43
Reporting States
0
10
20
30
40
50
60
70
80
0 10 20 30 40 50 60 70 80 90 100
State of Population With Community Water Fluoridation
Sta
te
of
Gra
de 3
Stu
den
ts w
ith
Cari
es E
xp
eri
en
ce
Data from CDC (2 3)
The description of the fluoridation laws in California Illinois and Nevada can be found on the
Association of State amp Territorial Dental Directors website(4 7 8)
The California fluoridation law AB 733 came into effect in 1995 requiring communities of 10
000 residents or more be supplied with fluoridated drinking water However the state did not
provide any funding to implement the legislation (California is unique in requiring fluoridation
without funding the practice)(4) The California Department of Health Services therefore had to
fund fluoridation initiatives from non-governmental sources ie the California Endowment
California Dental Association Foundation the First 5 Commission and others(5) From 1995 to
2011 the percentage of the California population receiving fluoridated drinking water has risen
from 17 to 625(6) 4 Dental Public Health Activities amp Practices Office of Oral Health California Department of Health
Services April 2002 httpwwwastddorgbestpracticesDES06002CAfluoridationpdf
5 Stock M Pollick H The CDA Foundation Model to Fluoridate Communities California Dental
Association Journal vol 40 no 8 649 - 655
httpwwwcdaorgPortals0journaljournal_082012pdf
6 California Dental Association Foundation
httpwwwcdafoundationorglearnadvocacyfluoridation
The State of Illinois passed a mandatory fluoridation state in 1967 and required all community
water systems to adjust fluoride levels in the drinking water to optimal levels within 1 year(7)
From 1962 when over 5000000 residents had optimally fluoridated drinking water by 2010
the number had risen to 11325132 (993 of the population on community water systems)(2)
7 Dental Public Health Activities amp Practices Division of Oral Health Illinois Department of Public
Health April 2002 httpwwwastddorgbestpracticesDES16007ILfluoridationpdf
The State of Nevada passed a mandatory fluoridation statute in 2000 for communities with
400000 or more residents(8) This was a result of the work of a statewide coalition that
included the Nevada Dental and Dental Hygienist Associations the Washoe and Clark County
District Health Departments the Clark County School District Junior League of Las Vegas
Head Start the Community College of Southern Nevada Dental Hygiene Program Health
Access Washoe County and Saint Maryrsquos Hospital For communities with less than 400000 the
implementation of fluoridation still required the vote of the majority voters in the community
The Las Vegas Water Authority and the City of Henderson started fluoridation in 2000
increasing the percentage of the population with fluoridated drinking water from 2 to 65 (8) 8 Dental Public Health Activities amp Practices Bureau of Family Health Services Nevada State Health
Division April 2002 httpwwwastddorgbestpracticesDES31002NVfluoridationbillpdf
Countries with Mandatory Laws on Fluoridation Countries that have mandated Community Water Fluoridation are Brazil Hong Kong
Malaysia Singapore Ireland Israel and some of the states in Australia
Singapore started fluoridating its water in 1956 based on the success of the fluoridation trials in
Grand Rapids Newburgh Evanston and Brantford Singapore became the first Asian country to
have 100 of its population benefitting from the implementation of fluoridated drinking water
Loh reported that ldquoThe ten year study on the effects of water fluoridation in Singapore showed
a decrease in caries prevalence in the children In the permanent dentition the reduction was
523 per cent for Chinese and 31 per cent for Malays in the 7 to 9 year old age group A similar
trend was observed in the mixed dentition in which the decrease was 325 per cent for Chinese
and 306 per cent for Malaysrdquo(9) By 2010 the population of the country was 5080000(10)
9 Loh T Thirty-eight years of water fluoridation--the Singapore scenario Community Dent
Health 1996 Sep13 Suppl 247-50
10 British Fluoridation Society One in a Million the facts about water fluoridation 3rd Edition
published March 2012) httpwwwbfsweborgonemillion0920One20in20a20Million20-
20The20Extent20of20Fluoridationpdf
Hong Kong started implementing community water fluoridation in 1961 and similar to
Singapore 100 of the population received access to fluoridated drinking water Lo and Wong
reported that ldquoThe mean DMFT score of the children deceased from 44 in 1960 to 15 in 1968
stayed at this level in the 1980 and 1986 surveys and further deceased to 08 in 2001 The
prevalence of dental fluorosis among the children surveyed in 1960 was 1 and this increased
to 59 and 70 in 1968 and 1980 respectively It was found in the 1986 and 2001 surveys that
the prevalences of fluorosis were 47 and 9 among children whose teeth developed at the
time when the respective water fluoride concentrations were 07 ppm and 05 ppmrdquo(11) The
population of Hong Kong was 6968000 in 2009(10) 11 LO ECM and WONG AHH Water fluoride concentration and fluorosis in Hong Kong in 1960-
2001 84th General Session and Exhibition of the International Association for Dental Research amp
1st Meeting of the Pan-Asian-Pacific Federation Brisbane Australia 28 June-1 July 2006 v 85 n
Sp B
The Malaysian cabinet approved a nationwide community water fluoridation program in 1972
(12) One of the states Sabah decided to stop fluoridation in 1989 due to concerns about
inadequate supervision in adding fluoride to the drinking water Oral Health Surveys in 2009
and 2007 indicated that children in Sabah had the worst oral health with 50 of 12 year-olds
having decay in their permanent teeth and children having an average of 3 teeth being(13)
Under the 10th Malaysian Plan in 2011 the federal and the Sabah state governments
reintroduced water fluoridation in Sabah(1314) In 2010 about 755 of the Malaysian
population or 20700000 people had fluoridated drinking water(1013) 12 Malaysian Dental Association Fluoride in Water
httpwwwmdaorgmy07_public_01healthcare_12htm
13 Sachdev N Fluoridation in Sabah Water for Cleaner Teeth French Tribunecom 28022011
From Levy IsraTo Jaeger ValerieCc Pim Carolyn gordonalphaweborg Diallo Aicha Penny Sutcliffe Paul Roumeliotis Michael Finkelstein
Hazel Lynn Robert KyleSubject FW Panorama - Privacy Security and other issuesDate Wednesday October 16 2013 122110 PM
Hello ValerieOttawa is part of Wave 4 Panorama implementation and we are gearing up increasingly to use thesystem where and if possible Thinking about it I am anticipating that this may need to be on theCOMOH (and alPHa) radar as it is something that will impact all health units and implies a majoroperational shift in vaccine delivery programs for all health units I have asked Carolyn Pim toconnect with our sister wave 4 units to share common experiences as we move forward ndash when wehave a roll up could I bring to COMOH Exec for discussion to explore whether there are broaderimplications for all members As an aside I have also asked the Ministry and their CIO to share with me any roll up learnings thatthey may have had already from previous waves (I understand that Niagara HU was a wave 1participant so if there is such a roll up of common experiences that others could learn fromperhaps you have it already and that could come to the exec too)Thanks Isra From Pim Carolyn Sent October 10 2013 1228 PMTo Christopher Mackie (christophermackiemlhuonca) Elizabeth Richardson(Elizabethrichardsonhamiltonca) H BSc M D F R C P (C) MPH Jim Chirico(jimchiriconbpsdhuca) Marlene Spruyt (spruytmtimiskaminghucom) Robert Kyle (Durham)Cc Levy IsraSubject Panorama - Privacy Security and other issues Dear colleagues Irsquom reaching out to you as fellow Panorama Wave 4 health units to ask about where yourorganizations are at in the process of signing agreements and completing Privacy ImpactAssessments and Threat Risk Assessments (TRAs) Ottawa Public Healthrsquos IT legal and informationsecurity advisors have made numerous requests to the MOHLTC for information (in particular theprovincial TRA) that we consider essential to develop our own risk assessment and PIA but havebeen told that information cannot be shared even with strict confidentiality and access controlsSo we are at somewhat of an impasse Isra emailed Arlene yesterday Arlene has forwarded ourconcerns to the Ministryrsquos CIO and Panorama lead but we havenrsquot had any response or discussionswith either of them yet Have your organizations identified similar concerns andor had interactions with the MOHLTC inthis respect Irsquod also be interested in knowing if your health units have flagged other (egoperational) implementation concerns Thanks
Carolyn ps Robert ndash you can ignore this request I talked with Sharan this morning about Durhamrsquos issuesso am including you now just for information Carolyn Pim MD FRCPC Associate Medical Officer of Health Meacutedecin adjointe en santeacute publique Ottawa Public Health Santeacute publique Ottawa 100 Constellation Cr Ottawa ON K2G 6J8 Tel teacutel (613) 580-6744 ext 23684Fax (613) 580-9641Connect With Ottawa Public Health
Suivez Santeacute publique Ottawa
This e-mail originates from the City of Ottawa e-mail system Any distribution use orcopying of this e-mail or the information it contains by other than the intendedrecipient(s) is unauthorized If you are not the intended recipient please notify meat the telephone number shown above or by return e-mail and delete thiscommunication and any copy immediately Thank you
Le preacutesent courriel a eacuteteacute expeacutedieacute par le systegraveme de courriels de la Ville dOttawaToute distribution utilisation ou reproduction du courriel ou des renseignements quisy trouvent par une personne autre que son destinataire preacutevu est interdite Si vousavez reccedilu le message par erreur veuillez men aviser par teacuteleacutephone (au numeacuteropreacuteciteacute) ou par courriel puis supprimer sans deacutelai la version originale de lacommunication ainsi que toutes ses copies Je vous remercie de votre collaboration
1
Smoke-Free Patios ndash An Amendment to the Smoke-Free Ontario Act
Date November 15 2013 Prepared for Council of Ontario Medical Officers of Health Prepared by York Region Public Health _____________________________________________________________________________ Issue
The Smoke-Free Ontario Act is the current provincial legislation that imposes smoking restrictions in workplaces and public places It prohibits smoking on restaurant and bar patios in instances where any portion of the seating area is covered by a roof With recent studies illustrating that exposure to second hand smoke outdoors poses similar risks to indoor exposure there has been growing public support to enhance smoking restrictions and make patios completely smoke-free
Background
With the implementation of the Smoke-Free Ontario Act in 2006 restaurant and bar patios became subject to smoking restrictions if any portion of the seating area was covered by a roof This allowed for patios without roof coverings to continue to allow smoking and as a result did not provide significant protection to patrons or staff from exposure to second hand smoke outdoors Many businesses chose to alter the design of their patios to allow smoking to continue In some cases patios became more crowded since smoking patrons who dine indoors often proceed outside onto licensed patios with their beverages to smoke York Region like most municipalities in Ontario is host to hundreds of patios being operated by restaurant owners and businesses With smoking prohibitions affecting only a small portion of these patios specifically ones with coverings the vast majority of patios still allow smoking to take place Patrons and employees on patios where smoking is not restricted are exposed to second hand smoke frequently This can contribute to increased disease and aggravation of existing health conditions From a business perspective the existing legislation has been viewed by many operators as unfair because some patios have permanent coverings which cannot be removed requiring a smoke-free status These business owners feel this creates an uneven playing field since they cannot provide an outdoor dining area for their smoking customers There is strong community support for smoke-free patios in Ontario A 2009 Rapid Risk Factor Surveillance System survey revealed 754 percent support in York Region while a Toronto Health Survey in 2011 indicated 74 percent public support
2
Current Status
Smoking is currently prohibited on restaurant and bar patios province-wide in four Canadian provinces and territories Alberta Newfoundland and Labrador Nova Scotia and Yukon A fifth province Prince Edward Island prohibits smoking on patios until 10 pm Since Ontario enacted legislation restricting smoking on patios in 2006 eight municipalities in Ontario have chosen to create bylaws that go beyond the Smoke-Free Ontario Act and enhance outdoor protection from second hand smoke by prohibiting smoking on patios completely The largest of those municipalities is the City of Ottawa Recently the Toronto Board of Health unanimously endorsed a report presented by their Medical Officer of Health recommending that restaurant and bar patios be made smoke-free through an amendment to the Smoke-Free Ontario Act
Key Considerations
There should be no significant financial burden to local Boards of Health resulting from a smoke-free patio amendment to the Smoke-Free Ontario Act Inspection and enforcement for the Smoke-Free Ontario Act is currently 100 percent funded by the Ministry of Health and Long-Term Care Following an introductory period of education on the amendment a complaint response model of service delivery would ensure ongoing compliance with smoke-free requirements A complete ban of smoking on patios would eliminate the widely-held perception by business owners that the current legislation creates an uneven playing field for business Since Smoke-Free Ontario Act inspections of patios began in 2006 operators have expressed the opinion that if patios need to be smoke-free for the protection of the public they should all be smoke-free to avoid undue hardship for individual businesses and to provide protection uniformly across the Province
Next steps
York Region Public Health intends to seek support from Medical Officers of Health across the Central East Tobacco Control Area Network (CETCAN) to advocate to the Ministry of Health and Long-Term Care for an amendment to the Smoke-Free Ontario Act prohibiting smoking on all restaurant and bar patios York Region is also in the process of requesting that its Regional Council advocate to the Minister of Health and Long-Term Care on the issue
Updating and Modernizing O Regulation 565 (Public Pools)
Date November 15 2013
Prepared for Council of Ontario Medical Officers of Health
Prepared by York Region Public Health _____________________________________________________________________________ Background Recent drownings at public pools in Ontario have highlighted the issue of water-borne illness and injury The current pool regulation under Ontariorsquos Health Protection and Promotion Act O Regulation 565 (Public Pools) is outdated It does not accurately reflect new pool technology and design or the changing use of public pools Neither does it incorporate admissions standards recommended by the Office of the Chief Coroner Further O Regulation 565 does not have short-form wording or set fines associated with it This limits public health enforcement capabilities What is the impact Updating O Regulation 565 (Public Pools) to address recent changes in pool technology design and uses and to include Coroner-recommended admissions standards would help improve pool safety Establishing short-form wording for O Regulation 565 would enhance enforcement related to public pools Currently the only enforcement available to Public Health Inspectors for dealing with non-critical regulatory infractions in public pools is the issuance of a Part III summons This involves a considerable amount of resources for a possible small fine With the development of inspection disclosure systems such as YorkSafe there is an even greater need to develop a method to effectively address repeated pool operator non-compliance with non-critical issues Next steps Public health units should advocate to the Province to 1) Conduct a review of O Regulation 565 (Public Pools) to address shortcomings Proposed changes to the
regulation should include a requirement for ownersoperators of public pools to advise the local Medical Officer of Health of any change in the use of a facility and the addition of the Coronerrsquos recommended admission standards
2) Provide short-form wording for O Regulation 565 so that public health inspectors can better deal with pool operator non-compliance
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
Page 1 of 8 ndash DRAFT FOR COMOH DISCUSSION
alPHa Membership Survey hello
Draft Report ndash COMOH Version hello
alPHarsquos membership was surveyed in the fall of 2013 Similar surveys were administered to all member groups ie COMOH BOH Section and Affiliates using the online survey tool Survey Monkey Small alterations were made to group-specific surveys to ensure that the survey questions were relevant to each group A total of 84 responses were received from alPHa members The breakdown of respondents was as follows This draft report is provided for discussion purposes to COMOH members and therefore focuses on the responses provided by COMOH members To provide additional information overall survey responses are also provided for some questions
SECTION 1 RESPONDENT PROFILE
Survey Question What region is your health unit located in
For COMOH members responses came from 6 of the 7 regions of Ontario All 7 regions were represented in the full set of survey responses
Summary of Respondents COMOH 27 32 BOH Section 34 40 Affiliates 23 27 Totals 84 100
All ResponsesEastern 24 29South West 12 14Central East 13 15Central West 15 18North East 11 13Toronto 5 6Not Sure 3 4North West 1 1Totals 84 100
All COMOH ResponsesEastern 3 11South West 5 19Central East 6 22Central West 6 22North East 3 11Toronto 4 15North West 0 0Totals 27 100
Page 2 of 8 ndash DRAFT FOR COMOH DISCUSSION
Survey Question How long have you been involved with public health in Ontario
Survey Question Have you participated on the alPHa Board of Directors or an alPHa or COMOH committeeworking group
All ResponsesYes in the last 1 to 2 years 15 18Yes in the last 2 to 5 years 9 11Yes more than 5 years ago 9 11No not ever 51 61Totals 84 100
All COMOH ResponsesOver 10 years 17 635 to 10 years 7 262 to 5 years 3 11Totals 27 100
All ResponsesOver 10 years 34 405 to 10 years 21 252 to 5 years 21 251 to 2 years 3 4Less than 1 year 5 6Totals 84 100
All COMOH ResponsesYes in the last 1 to 2 years 7 26Yes in the last 2 to 5 years 4 15Yes more than 5 years ago 8 30No not ever 8 30Totals 27 100
Page 3 of 8 ndash DRAFT FOR COMOH DISCUSSION
SECTION 2 PROFESSIONAL DEVELOPMENT
Survey Question Which of the following events have you attended at least once in the past two years
Survey Question Overall how satisfied have you been with alPHa events ie conferences meetings
Survey Question How much value do alPHarsquos events provide for the money
Survey Question How can alPHa make its events more valuable to you Please share any suggestions regarding future topics speakers formats duration locations or any other event component that is important to you
Comments about content bull Expert speakerpanels on emerging or hot topics
(2) bull More engaged dialogue with Ministry rather than
just updates bull Fewer Ministry updates (3) bull Content on medicalPH issues is better left to PHO
TOPHC and joint conferences (2) bull alPHa should stick to Ministrypoliticspolicysenior
PH supportPHU support on key priorities (eg November practical conference on HKP report)
bull For COMOH more discussion bull More time for section activities like face-to-face
COMOH meetings
bull More facilitated work groups of COMOH members to respond to public health practice questions
bull More focus on rural and northern issues bull Infection Control Logistical Considerations bull Consider partnering with other groups bull More collaboration with PHO and OPHA events bull Use of video conferencing bull Less frequentfewer meetings (2) bull Connect with CME Location bull Consider other venues than TO
( ) brackets indicate that more than one response included a similar comment
More than enough value 7 11A lot of value 34 52Some value 22 34A little value 2 3Not enough value 0 0Totals 65 100
All Responses for those who Attended at least One Event in the Last 2 Years
All COMOH ResponsesMore than enough value 4 15A lot of value 13 48Some value 9 33A little value 1 4Not enough value 0 0Totals 27 100
Page 5 of 8 ndash DRAFT FOR COMOH DISCUSSION
SECTION 3 VALUE FOR MEMBERSHIP
Survey Question What do you value the most about your alPHa membership
The comments provided in response to the text response question What is the most important benefit of alPHa membership for you personally supported the answers illustrated in the chart above 15 of the 20 comments provided focussed on the importance of opportunities to interact with colleagues across the province The next most important benefit mentioned was the support for COMOH members to work on public health issues together When asked What is the most important benefit of alPHa membership for your health unit COMOH members emphasized the following bull A coordinated and collective voice in advocating for public health issues and the public health sector (9) bull Opportunities to connect with other public health units to share experiences and best practices (8) bull Maintaining relationships with government both politicians and bureaucrats (3) and bull Support for boards of health (3)
Page 6 of 8 ndash DRAFT FOR COMOH DISCUSSION
Overall Level of Satisfaction
SECTION 4 LOOKING TO THE FUTURE
The questions in this section were asked to obtain input from alPHa members regarding a proposal from alPHarsquos Board of Directors to focus the Association on five service areas COMOH members were asked to indicate their level of agreement with the proposed areas of focus COMOH responses compared to the overall survey responses were as follows
To explore some proposed changes to Association services COMOH members were asked to provide their level of agreement with the following questions
COMOH Responses BOH Section Affiliates All Survey Responses
Strongly Agree
AgreeNeither Agree or Disagree
DisagreeStrongly Disagree
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1Promoting the role and value of local public health units
15 9 2 0 0 26 92 93 95 94
2
Providing important information to members about trends and events that will impact the public health system and management of public health units
10 8 8 0 0 26 69 97 86 85
3Facilitating professional networking and information sharing
13 10 3 0 0 26 88 83 82 85
4
Providing professional development to support excellence in public health unit leadership management and governance
3 15 7 1 0 26 69 83 86 79
5
Responding to public health sector issues when it makes the most sense to have a collective voice ie issues that impact the structure and funding of the public health sector and public health units and issues that have a broad focus on population health
15 8 2 0 1 26 88 97 95 93
PROPOSED AREAS OF FOCUS
COMOH Responses BOH Section Affiliates All Survey Responses
Strongly Agree
AgreeNeither Agree or Disagree
DisagreeStrongly Disagree
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1
COMOH and other professional groups within alPHa should do their own advocacy while alPHa supports members to share and support each others advocacy efforts
7 6 6 6 1 26 50 58 45 52
2
alPHa should provide support to action-oriented inter-professional work groups on priority public health unit issues and member resolutions
4 13 5 3 1 26 65 81 86 77
PROPOSALS
Page 8 of 8 ndash DRAFT FOR COMOH DISCUSSION
COMOH members were also asked to indicate the level of acceptability for some possible changes to alPHarsquos services and way of doing business
COMOH Responses BOH Section Affiliates All Survey Responses
Very Acceptable
Somewhat Acceptable
Neither Acceptable or Unacceptable
Somewhat Unacceptable
Very Unaccept
able
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1Single conference with additional face-to-face section meetings
21 2 0 1 0 24 96 68 80 81
2alPHa to offer alternatives like webinars on focussed topics
13 6 1 4 0 24 79 50 90 71
3Coordinate COMOH meetings with PHO OMA or Ministry events
16 4 2 0 0 22 91 na na --
4
Increase focus on building leadership and management capacity for health unit CEOs and senior management
7 9 4 3 0 23 70 na 70 70
5
Would it be acceptable for alPHa to request voluntary financial contributions from member PHUs in addition to annual fees
3 5 5 4 5 22 36 7 26 21
6
Would it be acceptable for alPHa to request voluntary in-kind staff contributions from member PHUs to expand alPHas capacity eg communications policy work group support
7 11 1 1 3 23 78 31 45 50
7Would it be acceptable to you for alPHa to discontinue staff support for COMOH (BOH Section)
0 4 1 5 14 24 17 11 na 14
8
Would it be acceptable to you for alPHa to reduce the amount of staff support for COMOH (BOH Section)
1 6 1 8 6 22 32 26 na 29
9
Would it be acceptable to you for alPHa to provide supports to MOHs and AMOHs (BOH Members) without maintaining COMOH (BOHs) as a section of the association
3 2 3 2 12 22 23 17 na 20
10
Would it be acceptable to you for alPHas Board of Directors to move from the current representational model to a skills-based strategic model ie board membership would be based on the skills needed to carry out alPHas strategic plan
6 11 2 1 3 23 74 56 56 62
11
Would it be acceptable to you for alPHas President Vice-President and Treasurer to be elected from the full membership of the alPHa Board of Directors (rather than the current model of alternating between BOH and COMOH members)
10 8 1 2 2 23 78 70 70 73
PROPOSED CHANGES
1 Council of Ontario Medical Officers of Health Terms of Reference
ASSOCIATION OF LOCAL PUBLIC HEALTH AGENCIES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
TERMS OF REFERENCE NAME 1 The name of the organization shall be ldquoThe Council of Ontario Medical Officers of
Health a section of the Association of Local Public Health Agencies (alPHa)rdquo hereinafter referred to as ldquothe Councilrdquo
MISSION 2 As local leaders in public health we are committed to improving the health of
Ontarians and increasing health equity by strengthening Ontariorsquos public health system We achieve this through system leadership and coordination in collaboration with the provincial government and other organizations and through evidence-informed advocacy on public health policy
OBJECTIVES 3 The objectives of the Council shall be
a) To provide strong province-wide leadership in public health
b) To advocate for health protection and promotion policies and programs that maintain and improve the health of Ontarians
c) To promote and maintain the highest standards for Ontariorsquos public health
programs and services
d) To support the planning implementation and evaluation of effective and efficiently run public health programs and services
e) To act as a forum for sharing information and resources and for addressing and
discussing public health issues both amongst the Councilrsquos members and other agencies that support the goals of alPHa eg Ontario Medical Association Ontario Public Health Association etc
f) To engage with and to provide public health and related policy advice to alPHa
the Chief Medical Officer of Health the Ontario Ministries of Health and Long-Term Care (including the Health Promotion and Public Health Divisions) Children
2 Council of Ontario Medical Officers of Health Terms of Reference
and Youth Services and other provincial ministries Public Health Ontario Health Canada the Public Health Agency of Canada and other public health partners
g) To promote and protect the professional interests of its members
h) To provide support to individual members as needed
i) To seek recognition for outstanding practice from among the members
j) To support evidence based practice of public health medicine
k) To engage and involve the membership to participate in COMOHrsquos endeavours
l) To mentor Public Health and Preventive Medicine Residents
MEMBERSHIP 4 Membership on the Council in each of the following categories is subject to the
limitations imposed by the current terms of reference and all policies and governing documents of the Association of Local Public Health Agencies Benefits of membership in each category are included in Appendix A These shall be subject to regular review and may be suspended under certain circumstances
Active membership in the Council shall be open to all Associate Medical Officers of Health and all full-time Medical Officers of Health whose Boards of Health are members of alPHa Such members shall have full voting privileges and may hold office in the Council Associate membership shall be open to all full and part-time physicians employed by a Board of Health that is a member of alPHa Such members shall not have voting privileges nor hold office
Affiliate membership shall be open to the following individuals interested in furthering the objectives of the Council
bull Public Health and Preventive Medicine Residents and Public Health and Preventive Medicine Residency Program Directors
bull Federal public health physicians working in Ontariorsquos First Nations communities
bull other public health or related physicians including those employed by a Board of Health that is not a member of alPHa
Such members shall not have voting privileges nor hold office
3 Council of Ontario Medical Officers of Health Terms of Reference
Emeritus membership shall be open to all former members who have retired after five (5) or more years of Active membership subject to the nomination in writing of two (2) active members in good standing endorsement of the Executive Committee and approval of the Council by majority vote at a general meeting Such members shall have neither voting privileges nor hold office but may be invited to attend general meetings Honorary membership shall be open to any non-active or associate member subject to the nomination in writing of two (2) active members in good standing endorsement of the Executive Committee and approval of the Council Such members shall have neither voting privileges nor hold office but may be invited to attend general meetings
OFFICERS 5 The Officers of the Council shall be the Chair Vice-Chair and immediate Past Chair
6 The Chair shall prepare the agendas of all Council meetings She shall preside and
preserve order at all such meetings shall ensure that these Terms of Reference are upheld and enforced and shall contribute to the supervision and evaluation of any Public Health and Preventive Medicine Resident who is on a placement with alPHa
7 The Vice-Chair shall fulfill the duties of the Chair in hisher absence The immediate
Past Chair may fulfill the duties of the Chair or Vice-Chair in their absences 8 The Chair shall normally serve a term of one (1) year which is renewable once and
after which the Vice-Chair shall normally assume the vacated office COMMITTEES 9 The Council shall elect seven (7) active members one from each of alPHarsquos regions
and the active member who is scheduled to serve as the President or immediate Past-President of alPHa to represent it on the alPHa Board of Directors These seven (7) members shall constitute the Councilrsquos Executive Committee and shall serve a term of at least one (1) year The Chair and Vice-Chair shall be elected from among the Executive Committee members If alPHarsquos immediate Past President is an active member she shall be an ex-officio member of the Executive Committee
10 The mandate of the Executive Committee shall be to facilitate the achievement of
the objectives of the Council by fulfilling the following
a Identifying priorities 1
1 See Appendix B Planning Cycle to Identify Priorities for COMOH
and ensuring the development of briefing documents and or recommendations as appropriate for the consideration of the Council
4 Council of Ontario Medical Officers of Health Terms of Reference
b Setting agendas and otherwise ensuring preparations for Council meetings c Ensuring the fulfillment of the direction of Council d Responding in a timely fashion to time-sensitive public health matters in
accordance with the Executive Committeersquos understanding of the perspective of the Council
e Engaging with the Chief Medical Officer of Health Associate Chief Medical Officers of Health and other provincial public health leaders and
f Representing Council at public and partner agency forums including the Public Health Leadership Council which shall normally include membership from the Officers of the Council and two other Executive Committee members as selected by agreement among the Executive
g Identifying opportunities for the recognition of outstanding practice from among the members including the annual nomination of at least one member for the alPHa Distinguished Service Award
11 The Executive Committee shall meet and correspond in the manner and at the times
and if required places as deemed necessary by the Chair to conduct the business of the Council A quorum shall consist of four (4) members
12 The Executive Committee shall have the power to strike committeestask or working
groups to assist it in carrying out the business of the Council 13 The Council may by special resolution remove a member of the Executive
Committee before the completion of hisher term of office and may elect a successor to complete the term The special resolution shall require a majority vote of 67 of the members present and voting at the meeting at which the special resolution is considered
14 A Nominating Committee shall consist of the three (3) most recent Past Chairs who
are able to serve and shall be chaired by the immediate Past Chair The Nominating Committee shall prepare a list of proposed Officers and Executive Committee members for the consideration of the Council at its Annual General Meeting
MEETINGS 15 The Council shall hold at least four (4) general meetings per year in a manner and at
the times and if required places as deemed necessary by the Executive Committee to share information direct and assist the Executive Committee in conducting the business of the Council
16 The Council shall hold its Annual General Meeting during and at the same place as
the alPHarsquos Annual Conference
5 Council of Ontario Medical Officers of Health Terms of Reference
17 The Council shall hold a special meeting at the call of the Chair or upon the written request specifying the purpose of such meeting of at least five (5) active members Council members must be given at least 48 hours notice of any special meeting
18 Only Councilrsquos active and associate members and alPHa staff are entitled to attend
general and special meetings of the Council Other members and non-members may be invited to attend all or part of such meetings as determined by the Chair preferably in consultation with the Executive Committee Non-members who come to such meetings without an invitation may attend all or part of the meeting by a majority vote of the active members present and voting
19 The Chair shall prepare the agendas for such meetings and shall normally include
reports from the Chair and the Councilrsquos committeestask or working groups and representatives to external bodies alPHarsquos Executive Director shall ensure that the minutes shall be recorded and promptly distributed to the Section
20 A quorum for all such meetings shall be ten (10) active members 21 The Council shall normally be notified in a manner deemed appropriate by the Chair
of such meetings at least one (1) month prior to their being held 22 A majority vote of the members present at such meetings and voting shall make
Council decisions In the case of a tied vote the Chair shall cast the deciding vote The Executive Committee shall ensure that actions arising from such decisions at such meetings are implemented and monitored
23 The Chair may solicit advice from the Council through the use of teleconferencing
and alPHarsquos electronic mailing lists in order to gain an understanding of the overall perspective of the Council (see 10d)
ELECTIONS 24 The Officers and Executive Committee members shall be elected at the Sectionrsquos
Annual General Meeting The Nominating Committee Chair or hisher designate shall present a list of nominations Additional nominations from the floor shall also be considered Each Officer and Executive Committee member shall be elected by secret ballot if necessary by a majority of the active members present and voting In the case of a tie the Chair shall cast the deciding vote
AMENDMENTS 25 The Councilrsquos Terms of Reference may be amended from time to time by the
Executive Committee provided the Committee receives notice of such proposed amendments at least one (1) month prior to the meeting at which the amendments
6 Council of Ontario Medical Officers of Health Terms of Reference
will be considered Such amendments shall be ratified by the Council at the next general meeting or the Annual General Meeting as the case may be
26 The Executive Committee shall review the Terms of Reference as required and not
less than once every two years Original September 1987 1st Revision October 2000 2nd Revision July 2001 3rd Revision December 2003 4th Revision February 2008 5th Revision June 2009 6th Revision June 2011 7th Revision June 2013
7 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX A
COMOH Membership Benefits Active Membership
bull Entitled to attend all meetings of the Section bull May hold office on the COMOH Executive Committee alPHa Board of Directors
Standing Committees bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Associate Membership
bull Entitled to attend all meetings of the Section bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Affiliate Membership
bull May attend meetings or parts thereof subject to approval of Chair bull May serve on ad-hoc committees of the Section subject to the approval of the
Executive Committee bull Discounted registration rates for alPHa Conferences (for Public Health and
Preventive Medicine Residents) bull Upon written request and subject to COMOH Executive approval Affiliate
Members may subscribe to comohlistsalphaweborg The approval will be reviewed on an annual basis in order to determine if the Affiliate Member can remain a subscriber to mohsalphaweborg
Emeritus Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair bull Enjoy discounted registration rates for alPHa Conferences and regular COMOH
meetings bull Subscription to comohlistsalphaweborg electronic mailing list bull Full access to alPHa Web site bull May represent alPHa COMOH on selected external committees and working
groups Honorary Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair
8 Council of Ontario Medical Officers of Health Terms of Reference
bull May represent alPHa COMOH on selected external committees and working groups subject to the approval of the COMOH or alPHa Executive Committee as appropriate
9 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX B
Planning Cycle to Identify Priorities for COMOH
1 There shall normally be a COMOH membership strategic planning retreat every four years In recognition of the dynamic environment of public health the need for and timing of such a retreat shall be at the discretion of the Executive Committee in consultation with the membership
2 The COMOH Executive is responsible (through the creation of a subcommittee of COMOH members) for ensuring the preparation for the COMOH retreats with resources to include those provided by alPHa
3 Leadership for action on COMOH priorities will be recruited from among the COMOH membership in order to make good use of the full base of capacity of the membership The resources to support actions will be recruited from both within and beyond the COMOH membership employing other public health professionals that reside within the broader public health system and community
4 The COMOH Executive shall ensure an annual review of strategic priorities and initiatives and the development of a draft report of the same for the review of the members at the June meeting
2013 Strategic Planning
Considerations for COMOH
As part of its strategic planning discussions alPHarsquos Board has been considering changes to the level of support provided to member sections A member survey is being carried out over the fall to determine options acceptable to alPHa members The following approach to support is put forward as a proposal for the consideration of COMOH Note that the feasibility of the points below depend upon future decisions of the alPHa board They assume that COMOH remains part of alPHa but becomes more independent in administering meetings
1 alPHa can provide to COMOH staff support (Gord Fleming) amounting to 02 FTE or one day per week This is a reduction from the current level of 35 days per week COMOH can choose to use the support any way it wants writing COMOH letters meeting minutes agenda support special projects etc
2 In addition to 02 FTE alPHa staff would provide support for up to 4 face-to-face meetings per year One meeting would be concurrent to alPHarsquos annual conference in June The timing of other meetings could be negotiated The support includes consulting on the development of the program arranging for speakers registration for the event arranging venue AV support and hospitality services
3 In addition to 02 FTE alPHa staff would provide support for setting meeting dates and any polling required to establish dates Note that the individual supporting this function would be Karen Reece
4 COMOHrsquos Executive and Section would continue to have access to online supports through the alPHa including the COMOH Listserve and a group page for posting agendas minutes and other resources on the alPHa website
5 alPHa staff (Linda Stewart and Gord Fleming) can also start participating on CMOH calls as a way to be up-to-date on issues related to COMOH
6 Other than what is outlined above COMOH would be expected to prepare agendas and take minutes for its Executive and Section meetings The Executive would be expected to operate more independently than it does now but would be able to access the supports outlined above
Prepared by Linda Stewart Executive Director
From comoh-bounceslistsalphaweborg on behalf of Christopher MackieTo MOH ListserveSubject [comoh] Fw URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)Date Wednesday October 30 2013 91241 AMAttachments ATT00249txt
For AMOHs and PHPM residents who didnt receive the initial email
Chris
Christopher Mackie MD MHSc FRCPCMedical Officer of Health and CEOMiddlesex-London Health Unit50 King St LondonON N6A 5L7 O 519 663 5317 ext 2444 wwwhealthunitcomFrom Pisko Laura (MOHLTC)Sent Tuesday October 29 2013 759 PMTo kbarkeralgomapublichealthcom malcolmlockbchuorg davidcchatham-kentcarobertkyledurhamca proumeliotiseohuca fwarshelginhealthonca mohelginhealthoncahlynnpublichealthgreybruceonca malcolmlockhnhuorg hnmohhnhuorglnoseworthyhkpronca bobnosalhaltonca elizabethrichardsonhamiltoncarschabashpechuonca ncameronhuroncountyca drimgemmillkflapublichealthcamohkflapublichealthca suditranadecounty-lambtononca paulastewarthealthunitorgChristopher Mackie valeriejaegerniagararegionca jimchiriconbpsdhuca jarthursnwhuoncaisralevyottawaca dnealoxfordcountyca davidmowatpeelregionca mklassenpdhuoncarpellizzaripcchuca rosemarieramsinghporcupinehuonca mcorriveaurcdhucomcharlesgardnersmdhuorg sutcliffepsdhucom davidwilliamstbdhucomspruytmtimiskaminghucom dmckeowntorontoca lnolanregionofwaterloocanicolamercerwdghuorg aheimannwechealthunitorg karimkurjiyorkcaCc coreywesleytbdhucom CindyBaker-Barillsmdhuorg Donna Kosmack pilonlsdhucomPaulaMuiskflapublichealthca sthibautorontoca Mueller Daina (MOHLTC) Gordon Marcus(MOHLTC) andreakitahamiltoncaSubject URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)
Dear Colleagues The ministry has received reports that some tobacco vendors across the province aregiving away single cigarettes with the purchase of tobacco products It is the ministryrsquosposition that giving out free single cigarettes does not violate subsection 31(3) of theSmoke-Free Ontario Act (ldquoSFOArdquo) Although the practice of giving out free singlecigarettes may promote the sale of tobacco products it does not take the form of aldquoproduct enhancement product association or promotional materialrdquo and therefore doesnot fall within the scope of subsection 31(3) of the SFOA We have confirmed with Health Canada that this practice may violate section 29(b) of thefederal Tobacco Act As such Health Canada is requesting that you notify them in writingand I am directing you to communicate with them via email and provide to them as manydetails as possible Emails should be sent to Tobacco-Ontariohc-scgcca and thesubject line should read ldquoViolation of Section 29(b) of Tobacco Actrdquo This will ensurethat the complaints are given priority status by Health Canada We will continue to monitor
this situation and liaise with our colleagues at Health Canada Please share this information with your tobacco control staff and contact me or DainaMueller Manager Tobacco Control Unit Health Promotion Implementation Branch atdainamuellerontarioca with any questions RegardsLaura Laura A PiskoDirectorHealth Promotion Implementation BranchHealth Promotion DivisionMinistry of Health and Long Term Care416-327-7445 (office)416-451-3185 (mobile) Marcus Gordon - EA (416)326-0625 for urgent issues
========= Middlesex-London Health Unit E-Mail Disclaimer =============______________________________________________________________
Private and confidential intended only for named recipient If otherwisereceived please destroy immediately Health information in this email isonly general information and is not intended to replace an in personconsultation with a medical professional nor is it intended to providemedical advice Individual circumstances of which we are not aware mayaffect the information provided herein and as such the Middlesex-LondonHealth Unit assumes no liability or responsibility for your reliancethereon The Middlesex-London Health Unit works under the authority of theHealth Protection and Promotion Act and this correspondence may be used toassess your needs for public health services (519-663-5317 ext 2448)______________________________________________________________
From Gardner CharlesTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes (RayCopesoahppca)
George Pasut (GeorgePasutoahppca) Peter Cooney (petercooneyhc-scgcca)Cc Ito DickSubject Discontinuation of Fluoridation in MuskokaDate Tuesday October 22 2013 125254 PM
Hello Colleagues
As I reported in my email below on September 26th fluoridation has come under challenge again inSimcoe Muskoka I am now very unhappy to report that despite our best efforts last night theDistrict Council of Muskoka voted to remove fluoride from municipal drinking supplies across theDistrict This brings to an end fluoridation in all of Simcoe and Muskoka (with the exception of Base Borden)ndash though New Tecumseth will be conducting a plebiscite on the question of fluoridation with themunicipal election next October Defending community water fluoridation has drained a great deal of time human resources andcommitment from other priorities and has been exhausting here in SMDHU as I am sure it hasbeen in many other health units While the outcomes have been very disappointing I have beenimpressed by the professionalism and dedication that SMDHU staff members have shown inshouldering this burden In particular our dental consultant Dr Ito has provided us with much ofthe foundational knowledge and the local research essential to our efforts and has very frequentlyattended and presented at council meetings and other public events I would also like to thank themany of you who have offer and provided support including advocacy letters and informationresources Over the years Dr Peter Cooney Chief Dental Officer of Health of Canada has beenvery helpful attending and presenting with us at council meetings and at public consultationevents We will of course continue our oral health surveillance of the children of Muskoka documentingand reporting in future years on the increase in dental decay that we anticipate will occur Suchsurveillance is the foundation of our advocacy both to municipal politicians and to the province I am very concerned that our experience will continue to repeat itself across the province unlessthere is strong leadership provincially It is with this in mind that I raise the followingrecommendations for your consideration
1 That we collectively (with PHOrsquos leadership) conduct high quality publish-worthy researchdocumenting the impact on dental decay that occurs in those municipalities throughoutOntario that in recent years have discontinued community water fluoridation This could bepart of a larger study on such municipalities across the country and it could also be part ofa study documenting overall oral health (including fluoridation coverage) in the province(and possibly across the country)
2 That COMOH engage with our Chief MOH to advocate for the province to require allmunicipal water supplies to be fluoridated (the exception of course being those withnaturally sufficient fluoride concentrations) This could built upon the alPHa position to
Gordon
Highlight
Gordon
Highlight
date (A11-00 - Community Water Fluoridation) on the CMOH position (Oral Health ndash) and on theemail discussion generated on the COMOH listserv some months back re Richardrsquosproposal (calling on the province to fund municipal water fluoridation)
Valerie I request that this be an item for our COMOH meeting on November 15th Sincerely Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorg From Gardner Charles Sent Thursday September 26 2013 245 PMTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes(RayCopesoahppca)Subject Community Water Fluoridation Under Challenge Again in Simcoe Muskoka Hello Colleagues You may wish to know that community water fluoridation (CWF) is again under challenge in SimcoeMuskoka specifically both in Tottenham (Town of New Tecumseth in Simcoe County) and for theentire District of Muskoka On Monday September 23 Committee of the Whole Council of theTown of New Tecumseth voted to submit application to discontinue community water fluoridation(CWF) in the town of Tottenham despite presentations to the contrary from our dental consultantDr Ito and from me The next Council meeting is scheduled for Monday Sept 30 at which lastMondayrsquos (Sept 23) votes will be ratified
Since Monday I have spoken with the Mayor of the Town of New Tecumseth and with most of thecouncilors encouraging deferral of a decision on Monday to allow the town more time to make afully informed decision
This is the second time in recent years that the issue of discontinuing CWF in Tottenham has beenraised at council This issue is also scheduled to return again to the District of Muskoka Council on
October 21st where I will be presenting in response to deputations in opposition to fluoridation
Outside of Base Borden Tottenham is the only community with fluoridated water in SimcoeCounty The health unitrsquos own screening data between 2011 and 2013 shows that Tottenhamrsquos
Gordon
Highlight
children as well as those in Muskoka have a lower rate of dental decay than Simcoe Muskokacommunities without CWF
Sincerely
Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorgChuck Gardner MOH
November 04 2013
Mandatory State Laws on Fluoridation Thirteen states Puerto Rico and the District of Columbia have laws intended to provide
statewide fluoridation These states and the year that the fluoridation legislation was passed are
District of Columbia (1952) Connecticut (1965) Kentucky (1966) Illinois (1967) Minnesota
(1967) Ohio (1969) South Dakota (1969) Georgia (1973) Nebraska (1973 and 2008)
California (1995) Delaware (1998) Puerto Rico (1998) Nevada (1999) Louisiana (2008) and
Arkansas (2011) (see Table 1) The sizes of the public water systems or countiescommunities
affected and exemption provisions vary by state Table 1
STATES THAT HAVE MANDATORY LAWS ON FLUORIDATION -2011
State (1) Year of
Fluoridation
Legislation (1)
Population
served by
Fluoridated
CWS (2)
Persons
receiving
fluoridated
water (2)
State
Average
Caries
Experience
of Grade 3
Students (3)
Arkansas 2011 647 1724131 64
California 1995 621 22812721 709
Connecticut 1965 910 2370423 406
Delaware 1998 862 705344 545
Georgia 1973 921 8924598 52
Illinois 1967 993 11325132 532
Kentucky 1966 999 4334223 598
Louisiana 2008 407 1846149 657
Minnesota 1967 988 4117266 549
Nebraska 1973 and 2008 702 1001665 593
Nevada 1999 702 1001665 649
Ohio 1969 877 8772683 512
South Dakota 1969 948 642942 623
District of
Columbia
1952 1000 595000
Puerto Rico 1998
United States 739 204283554
2010 Statistics for population fluoridated and number of people
1 Communication with Jane McGinley RDH MBA Manager Fluoridation and Preventive Health
Activities Council on Access Prevention and Interprofessional Relations
2 Centers for Disease Control and Prevention Department of Health and Human Services
accessed Oct 21 2013 httpwwwcdcgovfluoridationstatistics2010statshtm
3 Centers for Disease Control and Prevention National Oral Health Surveillance System Caries
Experience - Percentage of 3rd Grade students with Caries Experience (treated or untreated tooth
If data from 43 states for the percentage of Grade 3 children with experience of dental decay is
compared with the 2008 percentages of the population in a state with Community Water
Fluoridation then the percentage of children with experience of dental decay decreases as the
percentage of the state population with Community Water Fluoridation increases (see Figure 1)
Figure 1
Correlation of Percentage of Grade 3 Children with Caries Experience and
Percentage of Population With Community Water Fluoridation for 43
Reporting States
0
10
20
30
40
50
60
70
80
0 10 20 30 40 50 60 70 80 90 100
State of Population With Community Water Fluoridation
Sta
te
of
Gra
de 3
Stu
den
ts w
ith
Cari
es E
xp
eri
en
ce
Data from CDC (2 3)
The description of the fluoridation laws in California Illinois and Nevada can be found on the
Association of State amp Territorial Dental Directors website(4 7 8)
The California fluoridation law AB 733 came into effect in 1995 requiring communities of 10
000 residents or more be supplied with fluoridated drinking water However the state did not
provide any funding to implement the legislation (California is unique in requiring fluoridation
without funding the practice)(4) The California Department of Health Services therefore had to
fund fluoridation initiatives from non-governmental sources ie the California Endowment
California Dental Association Foundation the First 5 Commission and others(5) From 1995 to
2011 the percentage of the California population receiving fluoridated drinking water has risen
from 17 to 625(6) 4 Dental Public Health Activities amp Practices Office of Oral Health California Department of Health
Services April 2002 httpwwwastddorgbestpracticesDES06002CAfluoridationpdf
5 Stock M Pollick H The CDA Foundation Model to Fluoridate Communities California Dental
Association Journal vol 40 no 8 649 - 655
httpwwwcdaorgPortals0journaljournal_082012pdf
6 California Dental Association Foundation
httpwwwcdafoundationorglearnadvocacyfluoridation
The State of Illinois passed a mandatory fluoridation state in 1967 and required all community
water systems to adjust fluoride levels in the drinking water to optimal levels within 1 year(7)
From 1962 when over 5000000 residents had optimally fluoridated drinking water by 2010
the number had risen to 11325132 (993 of the population on community water systems)(2)
7 Dental Public Health Activities amp Practices Division of Oral Health Illinois Department of Public
Health April 2002 httpwwwastddorgbestpracticesDES16007ILfluoridationpdf
The State of Nevada passed a mandatory fluoridation statute in 2000 for communities with
400000 or more residents(8) This was a result of the work of a statewide coalition that
included the Nevada Dental and Dental Hygienist Associations the Washoe and Clark County
District Health Departments the Clark County School District Junior League of Las Vegas
Head Start the Community College of Southern Nevada Dental Hygiene Program Health
Access Washoe County and Saint Maryrsquos Hospital For communities with less than 400000 the
implementation of fluoridation still required the vote of the majority voters in the community
The Las Vegas Water Authority and the City of Henderson started fluoridation in 2000
increasing the percentage of the population with fluoridated drinking water from 2 to 65 (8) 8 Dental Public Health Activities amp Practices Bureau of Family Health Services Nevada State Health
Division April 2002 httpwwwastddorgbestpracticesDES31002NVfluoridationbillpdf
Countries with Mandatory Laws on Fluoridation Countries that have mandated Community Water Fluoridation are Brazil Hong Kong
Malaysia Singapore Ireland Israel and some of the states in Australia
Singapore started fluoridating its water in 1956 based on the success of the fluoridation trials in
Grand Rapids Newburgh Evanston and Brantford Singapore became the first Asian country to
have 100 of its population benefitting from the implementation of fluoridated drinking water
Loh reported that ldquoThe ten year study on the effects of water fluoridation in Singapore showed
a decrease in caries prevalence in the children In the permanent dentition the reduction was
523 per cent for Chinese and 31 per cent for Malays in the 7 to 9 year old age group A similar
trend was observed in the mixed dentition in which the decrease was 325 per cent for Chinese
and 306 per cent for Malaysrdquo(9) By 2010 the population of the country was 5080000(10)
9 Loh T Thirty-eight years of water fluoridation--the Singapore scenario Community Dent
Health 1996 Sep13 Suppl 247-50
10 British Fluoridation Society One in a Million the facts about water fluoridation 3rd Edition
published March 2012) httpwwwbfsweborgonemillion0920One20in20a20Million20-
20The20Extent20of20Fluoridationpdf
Hong Kong started implementing community water fluoridation in 1961 and similar to
Singapore 100 of the population received access to fluoridated drinking water Lo and Wong
reported that ldquoThe mean DMFT score of the children deceased from 44 in 1960 to 15 in 1968
stayed at this level in the 1980 and 1986 surveys and further deceased to 08 in 2001 The
prevalence of dental fluorosis among the children surveyed in 1960 was 1 and this increased
to 59 and 70 in 1968 and 1980 respectively It was found in the 1986 and 2001 surveys that
the prevalences of fluorosis were 47 and 9 among children whose teeth developed at the
time when the respective water fluoride concentrations were 07 ppm and 05 ppmrdquo(11) The
population of Hong Kong was 6968000 in 2009(10) 11 LO ECM and WONG AHH Water fluoride concentration and fluorosis in Hong Kong in 1960-
2001 84th General Session and Exhibition of the International Association for Dental Research amp
1st Meeting of the Pan-Asian-Pacific Federation Brisbane Australia 28 June-1 July 2006 v 85 n
Sp B
The Malaysian cabinet approved a nationwide community water fluoridation program in 1972
(12) One of the states Sabah decided to stop fluoridation in 1989 due to concerns about
inadequate supervision in adding fluoride to the drinking water Oral Health Surveys in 2009
and 2007 indicated that children in Sabah had the worst oral health with 50 of 12 year-olds
having decay in their permanent teeth and children having an average of 3 teeth being(13)
Under the 10th Malaysian Plan in 2011 the federal and the Sabah state governments
reintroduced water fluoridation in Sabah(1314) In 2010 about 755 of the Malaysian
population or 20700000 people had fluoridated drinking water(1013) 12 Malaysian Dental Association Fluoride in Water
httpwwwmdaorgmy07_public_01healthcare_12htm
13 Sachdev N Fluoridation in Sabah Water for Cleaner Teeth French Tribunecom 28022011
From Levy IsraTo Jaeger ValerieCc Pim Carolyn gordonalphaweborg Diallo Aicha Penny Sutcliffe Paul Roumeliotis Michael Finkelstein
Hazel Lynn Robert KyleSubject FW Panorama - Privacy Security and other issuesDate Wednesday October 16 2013 122110 PM
Hello ValerieOttawa is part of Wave 4 Panorama implementation and we are gearing up increasingly to use thesystem where and if possible Thinking about it I am anticipating that this may need to be on theCOMOH (and alPHa) radar as it is something that will impact all health units and implies a majoroperational shift in vaccine delivery programs for all health units I have asked Carolyn Pim toconnect with our sister wave 4 units to share common experiences as we move forward ndash when wehave a roll up could I bring to COMOH Exec for discussion to explore whether there are broaderimplications for all members As an aside I have also asked the Ministry and their CIO to share with me any roll up learnings thatthey may have had already from previous waves (I understand that Niagara HU was a wave 1participant so if there is such a roll up of common experiences that others could learn fromperhaps you have it already and that could come to the exec too)Thanks Isra From Pim Carolyn Sent October 10 2013 1228 PMTo Christopher Mackie (christophermackiemlhuonca) Elizabeth Richardson(Elizabethrichardsonhamiltonca) H BSc M D F R C P (C) MPH Jim Chirico(jimchiriconbpsdhuca) Marlene Spruyt (spruytmtimiskaminghucom) Robert Kyle (Durham)Cc Levy IsraSubject Panorama - Privacy Security and other issues Dear colleagues Irsquom reaching out to you as fellow Panorama Wave 4 health units to ask about where yourorganizations are at in the process of signing agreements and completing Privacy ImpactAssessments and Threat Risk Assessments (TRAs) Ottawa Public Healthrsquos IT legal and informationsecurity advisors have made numerous requests to the MOHLTC for information (in particular theprovincial TRA) that we consider essential to develop our own risk assessment and PIA but havebeen told that information cannot be shared even with strict confidentiality and access controlsSo we are at somewhat of an impasse Isra emailed Arlene yesterday Arlene has forwarded ourconcerns to the Ministryrsquos CIO and Panorama lead but we havenrsquot had any response or discussionswith either of them yet Have your organizations identified similar concerns andor had interactions with the MOHLTC inthis respect Irsquod also be interested in knowing if your health units have flagged other (egoperational) implementation concerns Thanks
Carolyn ps Robert ndash you can ignore this request I talked with Sharan this morning about Durhamrsquos issuesso am including you now just for information Carolyn Pim MD FRCPC Associate Medical Officer of Health Meacutedecin adjointe en santeacute publique Ottawa Public Health Santeacute publique Ottawa 100 Constellation Cr Ottawa ON K2G 6J8 Tel teacutel (613) 580-6744 ext 23684Fax (613) 580-9641Connect With Ottawa Public Health
Suivez Santeacute publique Ottawa
This e-mail originates from the City of Ottawa e-mail system Any distribution use orcopying of this e-mail or the information it contains by other than the intendedrecipient(s) is unauthorized If you are not the intended recipient please notify meat the telephone number shown above or by return e-mail and delete thiscommunication and any copy immediately Thank you
Le preacutesent courriel a eacuteteacute expeacutedieacute par le systegraveme de courriels de la Ville dOttawaToute distribution utilisation ou reproduction du courriel ou des renseignements quisy trouvent par une personne autre que son destinataire preacutevu est interdite Si vousavez reccedilu le message par erreur veuillez men aviser par teacuteleacutephone (au numeacuteropreacuteciteacute) ou par courriel puis supprimer sans deacutelai la version originale de lacommunication ainsi que toutes ses copies Je vous remercie de votre collaboration
1
Smoke-Free Patios ndash An Amendment to the Smoke-Free Ontario Act
Date November 15 2013 Prepared for Council of Ontario Medical Officers of Health Prepared by York Region Public Health _____________________________________________________________________________ Issue
The Smoke-Free Ontario Act is the current provincial legislation that imposes smoking restrictions in workplaces and public places It prohibits smoking on restaurant and bar patios in instances where any portion of the seating area is covered by a roof With recent studies illustrating that exposure to second hand smoke outdoors poses similar risks to indoor exposure there has been growing public support to enhance smoking restrictions and make patios completely smoke-free
Background
With the implementation of the Smoke-Free Ontario Act in 2006 restaurant and bar patios became subject to smoking restrictions if any portion of the seating area was covered by a roof This allowed for patios without roof coverings to continue to allow smoking and as a result did not provide significant protection to patrons or staff from exposure to second hand smoke outdoors Many businesses chose to alter the design of their patios to allow smoking to continue In some cases patios became more crowded since smoking patrons who dine indoors often proceed outside onto licensed patios with their beverages to smoke York Region like most municipalities in Ontario is host to hundreds of patios being operated by restaurant owners and businesses With smoking prohibitions affecting only a small portion of these patios specifically ones with coverings the vast majority of patios still allow smoking to take place Patrons and employees on patios where smoking is not restricted are exposed to second hand smoke frequently This can contribute to increased disease and aggravation of existing health conditions From a business perspective the existing legislation has been viewed by many operators as unfair because some patios have permanent coverings which cannot be removed requiring a smoke-free status These business owners feel this creates an uneven playing field since they cannot provide an outdoor dining area for their smoking customers There is strong community support for smoke-free patios in Ontario A 2009 Rapid Risk Factor Surveillance System survey revealed 754 percent support in York Region while a Toronto Health Survey in 2011 indicated 74 percent public support
2
Current Status
Smoking is currently prohibited on restaurant and bar patios province-wide in four Canadian provinces and territories Alberta Newfoundland and Labrador Nova Scotia and Yukon A fifth province Prince Edward Island prohibits smoking on patios until 10 pm Since Ontario enacted legislation restricting smoking on patios in 2006 eight municipalities in Ontario have chosen to create bylaws that go beyond the Smoke-Free Ontario Act and enhance outdoor protection from second hand smoke by prohibiting smoking on patios completely The largest of those municipalities is the City of Ottawa Recently the Toronto Board of Health unanimously endorsed a report presented by their Medical Officer of Health recommending that restaurant and bar patios be made smoke-free through an amendment to the Smoke-Free Ontario Act
Key Considerations
There should be no significant financial burden to local Boards of Health resulting from a smoke-free patio amendment to the Smoke-Free Ontario Act Inspection and enforcement for the Smoke-Free Ontario Act is currently 100 percent funded by the Ministry of Health and Long-Term Care Following an introductory period of education on the amendment a complaint response model of service delivery would ensure ongoing compliance with smoke-free requirements A complete ban of smoking on patios would eliminate the widely-held perception by business owners that the current legislation creates an uneven playing field for business Since Smoke-Free Ontario Act inspections of patios began in 2006 operators have expressed the opinion that if patios need to be smoke-free for the protection of the public they should all be smoke-free to avoid undue hardship for individual businesses and to provide protection uniformly across the Province
Next steps
York Region Public Health intends to seek support from Medical Officers of Health across the Central East Tobacco Control Area Network (CETCAN) to advocate to the Ministry of Health and Long-Term Care for an amendment to the Smoke-Free Ontario Act prohibiting smoking on all restaurant and bar patios York Region is also in the process of requesting that its Regional Council advocate to the Minister of Health and Long-Term Care on the issue
Updating and Modernizing O Regulation 565 (Public Pools)
Date November 15 2013
Prepared for Council of Ontario Medical Officers of Health
Prepared by York Region Public Health _____________________________________________________________________________ Background Recent drownings at public pools in Ontario have highlighted the issue of water-borne illness and injury The current pool regulation under Ontariorsquos Health Protection and Promotion Act O Regulation 565 (Public Pools) is outdated It does not accurately reflect new pool technology and design or the changing use of public pools Neither does it incorporate admissions standards recommended by the Office of the Chief Coroner Further O Regulation 565 does not have short-form wording or set fines associated with it This limits public health enforcement capabilities What is the impact Updating O Regulation 565 (Public Pools) to address recent changes in pool technology design and uses and to include Coroner-recommended admissions standards would help improve pool safety Establishing short-form wording for O Regulation 565 would enhance enforcement related to public pools Currently the only enforcement available to Public Health Inspectors for dealing with non-critical regulatory infractions in public pools is the issuance of a Part III summons This involves a considerable amount of resources for a possible small fine With the development of inspection disclosure systems such as YorkSafe there is an even greater need to develop a method to effectively address repeated pool operator non-compliance with non-critical issues Next steps Public health units should advocate to the Province to 1) Conduct a review of O Regulation 565 (Public Pools) to address shortcomings Proposed changes to the
regulation should include a requirement for ownersoperators of public pools to advise the local Medical Officer of Health of any change in the use of a facility and the addition of the Coronerrsquos recommended admission standards
2) Provide short-form wording for O Regulation 565 so that public health inspectors can better deal with pool operator non-compliance
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
Page 2 of 8 ndash DRAFT FOR COMOH DISCUSSION
Survey Question How long have you been involved with public health in Ontario
Survey Question Have you participated on the alPHa Board of Directors or an alPHa or COMOH committeeworking group
All ResponsesYes in the last 1 to 2 years 15 18Yes in the last 2 to 5 years 9 11Yes more than 5 years ago 9 11No not ever 51 61Totals 84 100
All COMOH ResponsesOver 10 years 17 635 to 10 years 7 262 to 5 years 3 11Totals 27 100
All ResponsesOver 10 years 34 405 to 10 years 21 252 to 5 years 21 251 to 2 years 3 4Less than 1 year 5 6Totals 84 100
All COMOH ResponsesYes in the last 1 to 2 years 7 26Yes in the last 2 to 5 years 4 15Yes more than 5 years ago 8 30No not ever 8 30Totals 27 100
Page 3 of 8 ndash DRAFT FOR COMOH DISCUSSION
SECTION 2 PROFESSIONAL DEVELOPMENT
Survey Question Which of the following events have you attended at least once in the past two years
Survey Question Overall how satisfied have you been with alPHa events ie conferences meetings
Survey Question How much value do alPHarsquos events provide for the money
Survey Question How can alPHa make its events more valuable to you Please share any suggestions regarding future topics speakers formats duration locations or any other event component that is important to you
Comments about content bull Expert speakerpanels on emerging or hot topics
(2) bull More engaged dialogue with Ministry rather than
just updates bull Fewer Ministry updates (3) bull Content on medicalPH issues is better left to PHO
TOPHC and joint conferences (2) bull alPHa should stick to Ministrypoliticspolicysenior
PH supportPHU support on key priorities (eg November practical conference on HKP report)
bull For COMOH more discussion bull More time for section activities like face-to-face
COMOH meetings
bull More facilitated work groups of COMOH members to respond to public health practice questions
bull More focus on rural and northern issues bull Infection Control Logistical Considerations bull Consider partnering with other groups bull More collaboration with PHO and OPHA events bull Use of video conferencing bull Less frequentfewer meetings (2) bull Connect with CME Location bull Consider other venues than TO
( ) brackets indicate that more than one response included a similar comment
More than enough value 7 11A lot of value 34 52Some value 22 34A little value 2 3Not enough value 0 0Totals 65 100
All Responses for those who Attended at least One Event in the Last 2 Years
All COMOH ResponsesMore than enough value 4 15A lot of value 13 48Some value 9 33A little value 1 4Not enough value 0 0Totals 27 100
Page 5 of 8 ndash DRAFT FOR COMOH DISCUSSION
SECTION 3 VALUE FOR MEMBERSHIP
Survey Question What do you value the most about your alPHa membership
The comments provided in response to the text response question What is the most important benefit of alPHa membership for you personally supported the answers illustrated in the chart above 15 of the 20 comments provided focussed on the importance of opportunities to interact with colleagues across the province The next most important benefit mentioned was the support for COMOH members to work on public health issues together When asked What is the most important benefit of alPHa membership for your health unit COMOH members emphasized the following bull A coordinated and collective voice in advocating for public health issues and the public health sector (9) bull Opportunities to connect with other public health units to share experiences and best practices (8) bull Maintaining relationships with government both politicians and bureaucrats (3) and bull Support for boards of health (3)
Page 6 of 8 ndash DRAFT FOR COMOH DISCUSSION
Overall Level of Satisfaction
SECTION 4 LOOKING TO THE FUTURE
The questions in this section were asked to obtain input from alPHa members regarding a proposal from alPHarsquos Board of Directors to focus the Association on five service areas COMOH members were asked to indicate their level of agreement with the proposed areas of focus COMOH responses compared to the overall survey responses were as follows
To explore some proposed changes to Association services COMOH members were asked to provide their level of agreement with the following questions
COMOH Responses BOH Section Affiliates All Survey Responses
Strongly Agree
AgreeNeither Agree or Disagree
DisagreeStrongly Disagree
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1Promoting the role and value of local public health units
15 9 2 0 0 26 92 93 95 94
2
Providing important information to members about trends and events that will impact the public health system and management of public health units
10 8 8 0 0 26 69 97 86 85
3Facilitating professional networking and information sharing
13 10 3 0 0 26 88 83 82 85
4
Providing professional development to support excellence in public health unit leadership management and governance
3 15 7 1 0 26 69 83 86 79
5
Responding to public health sector issues when it makes the most sense to have a collective voice ie issues that impact the structure and funding of the public health sector and public health units and issues that have a broad focus on population health
15 8 2 0 1 26 88 97 95 93
PROPOSED AREAS OF FOCUS
COMOH Responses BOH Section Affiliates All Survey Responses
Strongly Agree
AgreeNeither Agree or Disagree
DisagreeStrongly Disagree
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1
COMOH and other professional groups within alPHa should do their own advocacy while alPHa supports members to share and support each others advocacy efforts
7 6 6 6 1 26 50 58 45 52
2
alPHa should provide support to action-oriented inter-professional work groups on priority public health unit issues and member resolutions
4 13 5 3 1 26 65 81 86 77
PROPOSALS
Page 8 of 8 ndash DRAFT FOR COMOH DISCUSSION
COMOH members were also asked to indicate the level of acceptability for some possible changes to alPHarsquos services and way of doing business
COMOH Responses BOH Section Affiliates All Survey Responses
Very Acceptable
Somewhat Acceptable
Neither Acceptable or Unacceptable
Somewhat Unacceptable
Very Unaccept
able
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1Single conference with additional face-to-face section meetings
21 2 0 1 0 24 96 68 80 81
2alPHa to offer alternatives like webinars on focussed topics
13 6 1 4 0 24 79 50 90 71
3Coordinate COMOH meetings with PHO OMA or Ministry events
16 4 2 0 0 22 91 na na --
4
Increase focus on building leadership and management capacity for health unit CEOs and senior management
7 9 4 3 0 23 70 na 70 70
5
Would it be acceptable for alPHa to request voluntary financial contributions from member PHUs in addition to annual fees
3 5 5 4 5 22 36 7 26 21
6
Would it be acceptable for alPHa to request voluntary in-kind staff contributions from member PHUs to expand alPHas capacity eg communications policy work group support
7 11 1 1 3 23 78 31 45 50
7Would it be acceptable to you for alPHa to discontinue staff support for COMOH (BOH Section)
0 4 1 5 14 24 17 11 na 14
8
Would it be acceptable to you for alPHa to reduce the amount of staff support for COMOH (BOH Section)
1 6 1 8 6 22 32 26 na 29
9
Would it be acceptable to you for alPHa to provide supports to MOHs and AMOHs (BOH Members) without maintaining COMOH (BOHs) as a section of the association
3 2 3 2 12 22 23 17 na 20
10
Would it be acceptable to you for alPHas Board of Directors to move from the current representational model to a skills-based strategic model ie board membership would be based on the skills needed to carry out alPHas strategic plan
6 11 2 1 3 23 74 56 56 62
11
Would it be acceptable to you for alPHas President Vice-President and Treasurer to be elected from the full membership of the alPHa Board of Directors (rather than the current model of alternating between BOH and COMOH members)
10 8 1 2 2 23 78 70 70 73
PROPOSED CHANGES
1 Council of Ontario Medical Officers of Health Terms of Reference
ASSOCIATION OF LOCAL PUBLIC HEALTH AGENCIES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
TERMS OF REFERENCE NAME 1 The name of the organization shall be ldquoThe Council of Ontario Medical Officers of
Health a section of the Association of Local Public Health Agencies (alPHa)rdquo hereinafter referred to as ldquothe Councilrdquo
MISSION 2 As local leaders in public health we are committed to improving the health of
Ontarians and increasing health equity by strengthening Ontariorsquos public health system We achieve this through system leadership and coordination in collaboration with the provincial government and other organizations and through evidence-informed advocacy on public health policy
OBJECTIVES 3 The objectives of the Council shall be
a) To provide strong province-wide leadership in public health
b) To advocate for health protection and promotion policies and programs that maintain and improve the health of Ontarians
c) To promote and maintain the highest standards for Ontariorsquos public health
programs and services
d) To support the planning implementation and evaluation of effective and efficiently run public health programs and services
e) To act as a forum for sharing information and resources and for addressing and
discussing public health issues both amongst the Councilrsquos members and other agencies that support the goals of alPHa eg Ontario Medical Association Ontario Public Health Association etc
f) To engage with and to provide public health and related policy advice to alPHa
the Chief Medical Officer of Health the Ontario Ministries of Health and Long-Term Care (including the Health Promotion and Public Health Divisions) Children
2 Council of Ontario Medical Officers of Health Terms of Reference
and Youth Services and other provincial ministries Public Health Ontario Health Canada the Public Health Agency of Canada and other public health partners
g) To promote and protect the professional interests of its members
h) To provide support to individual members as needed
i) To seek recognition for outstanding practice from among the members
j) To support evidence based practice of public health medicine
k) To engage and involve the membership to participate in COMOHrsquos endeavours
l) To mentor Public Health and Preventive Medicine Residents
MEMBERSHIP 4 Membership on the Council in each of the following categories is subject to the
limitations imposed by the current terms of reference and all policies and governing documents of the Association of Local Public Health Agencies Benefits of membership in each category are included in Appendix A These shall be subject to regular review and may be suspended under certain circumstances
Active membership in the Council shall be open to all Associate Medical Officers of Health and all full-time Medical Officers of Health whose Boards of Health are members of alPHa Such members shall have full voting privileges and may hold office in the Council Associate membership shall be open to all full and part-time physicians employed by a Board of Health that is a member of alPHa Such members shall not have voting privileges nor hold office
Affiliate membership shall be open to the following individuals interested in furthering the objectives of the Council
bull Public Health and Preventive Medicine Residents and Public Health and Preventive Medicine Residency Program Directors
bull Federal public health physicians working in Ontariorsquos First Nations communities
bull other public health or related physicians including those employed by a Board of Health that is not a member of alPHa
Such members shall not have voting privileges nor hold office
3 Council of Ontario Medical Officers of Health Terms of Reference
Emeritus membership shall be open to all former members who have retired after five (5) or more years of Active membership subject to the nomination in writing of two (2) active members in good standing endorsement of the Executive Committee and approval of the Council by majority vote at a general meeting Such members shall have neither voting privileges nor hold office but may be invited to attend general meetings Honorary membership shall be open to any non-active or associate member subject to the nomination in writing of two (2) active members in good standing endorsement of the Executive Committee and approval of the Council Such members shall have neither voting privileges nor hold office but may be invited to attend general meetings
OFFICERS 5 The Officers of the Council shall be the Chair Vice-Chair and immediate Past Chair
6 The Chair shall prepare the agendas of all Council meetings She shall preside and
preserve order at all such meetings shall ensure that these Terms of Reference are upheld and enforced and shall contribute to the supervision and evaluation of any Public Health and Preventive Medicine Resident who is on a placement with alPHa
7 The Vice-Chair shall fulfill the duties of the Chair in hisher absence The immediate
Past Chair may fulfill the duties of the Chair or Vice-Chair in their absences 8 The Chair shall normally serve a term of one (1) year which is renewable once and
after which the Vice-Chair shall normally assume the vacated office COMMITTEES 9 The Council shall elect seven (7) active members one from each of alPHarsquos regions
and the active member who is scheduled to serve as the President or immediate Past-President of alPHa to represent it on the alPHa Board of Directors These seven (7) members shall constitute the Councilrsquos Executive Committee and shall serve a term of at least one (1) year The Chair and Vice-Chair shall be elected from among the Executive Committee members If alPHarsquos immediate Past President is an active member she shall be an ex-officio member of the Executive Committee
10 The mandate of the Executive Committee shall be to facilitate the achievement of
the objectives of the Council by fulfilling the following
a Identifying priorities 1
1 See Appendix B Planning Cycle to Identify Priorities for COMOH
and ensuring the development of briefing documents and or recommendations as appropriate for the consideration of the Council
4 Council of Ontario Medical Officers of Health Terms of Reference
b Setting agendas and otherwise ensuring preparations for Council meetings c Ensuring the fulfillment of the direction of Council d Responding in a timely fashion to time-sensitive public health matters in
accordance with the Executive Committeersquos understanding of the perspective of the Council
e Engaging with the Chief Medical Officer of Health Associate Chief Medical Officers of Health and other provincial public health leaders and
f Representing Council at public and partner agency forums including the Public Health Leadership Council which shall normally include membership from the Officers of the Council and two other Executive Committee members as selected by agreement among the Executive
g Identifying opportunities for the recognition of outstanding practice from among the members including the annual nomination of at least one member for the alPHa Distinguished Service Award
11 The Executive Committee shall meet and correspond in the manner and at the times
and if required places as deemed necessary by the Chair to conduct the business of the Council A quorum shall consist of four (4) members
12 The Executive Committee shall have the power to strike committeestask or working
groups to assist it in carrying out the business of the Council 13 The Council may by special resolution remove a member of the Executive
Committee before the completion of hisher term of office and may elect a successor to complete the term The special resolution shall require a majority vote of 67 of the members present and voting at the meeting at which the special resolution is considered
14 A Nominating Committee shall consist of the three (3) most recent Past Chairs who
are able to serve and shall be chaired by the immediate Past Chair The Nominating Committee shall prepare a list of proposed Officers and Executive Committee members for the consideration of the Council at its Annual General Meeting
MEETINGS 15 The Council shall hold at least four (4) general meetings per year in a manner and at
the times and if required places as deemed necessary by the Executive Committee to share information direct and assist the Executive Committee in conducting the business of the Council
16 The Council shall hold its Annual General Meeting during and at the same place as
the alPHarsquos Annual Conference
5 Council of Ontario Medical Officers of Health Terms of Reference
17 The Council shall hold a special meeting at the call of the Chair or upon the written request specifying the purpose of such meeting of at least five (5) active members Council members must be given at least 48 hours notice of any special meeting
18 Only Councilrsquos active and associate members and alPHa staff are entitled to attend
general and special meetings of the Council Other members and non-members may be invited to attend all or part of such meetings as determined by the Chair preferably in consultation with the Executive Committee Non-members who come to such meetings without an invitation may attend all or part of the meeting by a majority vote of the active members present and voting
19 The Chair shall prepare the agendas for such meetings and shall normally include
reports from the Chair and the Councilrsquos committeestask or working groups and representatives to external bodies alPHarsquos Executive Director shall ensure that the minutes shall be recorded and promptly distributed to the Section
20 A quorum for all such meetings shall be ten (10) active members 21 The Council shall normally be notified in a manner deemed appropriate by the Chair
of such meetings at least one (1) month prior to their being held 22 A majority vote of the members present at such meetings and voting shall make
Council decisions In the case of a tied vote the Chair shall cast the deciding vote The Executive Committee shall ensure that actions arising from such decisions at such meetings are implemented and monitored
23 The Chair may solicit advice from the Council through the use of teleconferencing
and alPHarsquos electronic mailing lists in order to gain an understanding of the overall perspective of the Council (see 10d)
ELECTIONS 24 The Officers and Executive Committee members shall be elected at the Sectionrsquos
Annual General Meeting The Nominating Committee Chair or hisher designate shall present a list of nominations Additional nominations from the floor shall also be considered Each Officer and Executive Committee member shall be elected by secret ballot if necessary by a majority of the active members present and voting In the case of a tie the Chair shall cast the deciding vote
AMENDMENTS 25 The Councilrsquos Terms of Reference may be amended from time to time by the
Executive Committee provided the Committee receives notice of such proposed amendments at least one (1) month prior to the meeting at which the amendments
6 Council of Ontario Medical Officers of Health Terms of Reference
will be considered Such amendments shall be ratified by the Council at the next general meeting or the Annual General Meeting as the case may be
26 The Executive Committee shall review the Terms of Reference as required and not
less than once every two years Original September 1987 1st Revision October 2000 2nd Revision July 2001 3rd Revision December 2003 4th Revision February 2008 5th Revision June 2009 6th Revision June 2011 7th Revision June 2013
7 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX A
COMOH Membership Benefits Active Membership
bull Entitled to attend all meetings of the Section bull May hold office on the COMOH Executive Committee alPHa Board of Directors
Standing Committees bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Associate Membership
bull Entitled to attend all meetings of the Section bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Affiliate Membership
bull May attend meetings or parts thereof subject to approval of Chair bull May serve on ad-hoc committees of the Section subject to the approval of the
Executive Committee bull Discounted registration rates for alPHa Conferences (for Public Health and
Preventive Medicine Residents) bull Upon written request and subject to COMOH Executive approval Affiliate
Members may subscribe to comohlistsalphaweborg The approval will be reviewed on an annual basis in order to determine if the Affiliate Member can remain a subscriber to mohsalphaweborg
Emeritus Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair bull Enjoy discounted registration rates for alPHa Conferences and regular COMOH
meetings bull Subscription to comohlistsalphaweborg electronic mailing list bull Full access to alPHa Web site bull May represent alPHa COMOH on selected external committees and working
groups Honorary Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair
8 Council of Ontario Medical Officers of Health Terms of Reference
bull May represent alPHa COMOH on selected external committees and working groups subject to the approval of the COMOH or alPHa Executive Committee as appropriate
9 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX B
Planning Cycle to Identify Priorities for COMOH
1 There shall normally be a COMOH membership strategic planning retreat every four years In recognition of the dynamic environment of public health the need for and timing of such a retreat shall be at the discretion of the Executive Committee in consultation with the membership
2 The COMOH Executive is responsible (through the creation of a subcommittee of COMOH members) for ensuring the preparation for the COMOH retreats with resources to include those provided by alPHa
3 Leadership for action on COMOH priorities will be recruited from among the COMOH membership in order to make good use of the full base of capacity of the membership The resources to support actions will be recruited from both within and beyond the COMOH membership employing other public health professionals that reside within the broader public health system and community
4 The COMOH Executive shall ensure an annual review of strategic priorities and initiatives and the development of a draft report of the same for the review of the members at the June meeting
2013 Strategic Planning
Considerations for COMOH
As part of its strategic planning discussions alPHarsquos Board has been considering changes to the level of support provided to member sections A member survey is being carried out over the fall to determine options acceptable to alPHa members The following approach to support is put forward as a proposal for the consideration of COMOH Note that the feasibility of the points below depend upon future decisions of the alPHa board They assume that COMOH remains part of alPHa but becomes more independent in administering meetings
1 alPHa can provide to COMOH staff support (Gord Fleming) amounting to 02 FTE or one day per week This is a reduction from the current level of 35 days per week COMOH can choose to use the support any way it wants writing COMOH letters meeting minutes agenda support special projects etc
2 In addition to 02 FTE alPHa staff would provide support for up to 4 face-to-face meetings per year One meeting would be concurrent to alPHarsquos annual conference in June The timing of other meetings could be negotiated The support includes consulting on the development of the program arranging for speakers registration for the event arranging venue AV support and hospitality services
3 In addition to 02 FTE alPHa staff would provide support for setting meeting dates and any polling required to establish dates Note that the individual supporting this function would be Karen Reece
4 COMOHrsquos Executive and Section would continue to have access to online supports through the alPHa including the COMOH Listserve and a group page for posting agendas minutes and other resources on the alPHa website
5 alPHa staff (Linda Stewart and Gord Fleming) can also start participating on CMOH calls as a way to be up-to-date on issues related to COMOH
6 Other than what is outlined above COMOH would be expected to prepare agendas and take minutes for its Executive and Section meetings The Executive would be expected to operate more independently than it does now but would be able to access the supports outlined above
Prepared by Linda Stewart Executive Director
From comoh-bounceslistsalphaweborg on behalf of Christopher MackieTo MOH ListserveSubject [comoh] Fw URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)Date Wednesday October 30 2013 91241 AMAttachments ATT00249txt
For AMOHs and PHPM residents who didnt receive the initial email
Chris
Christopher Mackie MD MHSc FRCPCMedical Officer of Health and CEOMiddlesex-London Health Unit50 King St LondonON N6A 5L7 O 519 663 5317 ext 2444 wwwhealthunitcomFrom Pisko Laura (MOHLTC)Sent Tuesday October 29 2013 759 PMTo kbarkeralgomapublichealthcom malcolmlockbchuorg davidcchatham-kentcarobertkyledurhamca proumeliotiseohuca fwarshelginhealthonca mohelginhealthoncahlynnpublichealthgreybruceonca malcolmlockhnhuorg hnmohhnhuorglnoseworthyhkpronca bobnosalhaltonca elizabethrichardsonhamiltoncarschabashpechuonca ncameronhuroncountyca drimgemmillkflapublichealthcamohkflapublichealthca suditranadecounty-lambtononca paulastewarthealthunitorgChristopher Mackie valeriejaegerniagararegionca jimchiriconbpsdhuca jarthursnwhuoncaisralevyottawaca dnealoxfordcountyca davidmowatpeelregionca mklassenpdhuoncarpellizzaripcchuca rosemarieramsinghporcupinehuonca mcorriveaurcdhucomcharlesgardnersmdhuorg sutcliffepsdhucom davidwilliamstbdhucomspruytmtimiskaminghucom dmckeowntorontoca lnolanregionofwaterloocanicolamercerwdghuorg aheimannwechealthunitorg karimkurjiyorkcaCc coreywesleytbdhucom CindyBaker-Barillsmdhuorg Donna Kosmack pilonlsdhucomPaulaMuiskflapublichealthca sthibautorontoca Mueller Daina (MOHLTC) Gordon Marcus(MOHLTC) andreakitahamiltoncaSubject URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)
Dear Colleagues The ministry has received reports that some tobacco vendors across the province aregiving away single cigarettes with the purchase of tobacco products It is the ministryrsquosposition that giving out free single cigarettes does not violate subsection 31(3) of theSmoke-Free Ontario Act (ldquoSFOArdquo) Although the practice of giving out free singlecigarettes may promote the sale of tobacco products it does not take the form of aldquoproduct enhancement product association or promotional materialrdquo and therefore doesnot fall within the scope of subsection 31(3) of the SFOA We have confirmed with Health Canada that this practice may violate section 29(b) of thefederal Tobacco Act As such Health Canada is requesting that you notify them in writingand I am directing you to communicate with them via email and provide to them as manydetails as possible Emails should be sent to Tobacco-Ontariohc-scgcca and thesubject line should read ldquoViolation of Section 29(b) of Tobacco Actrdquo This will ensurethat the complaints are given priority status by Health Canada We will continue to monitor
this situation and liaise with our colleagues at Health Canada Please share this information with your tobacco control staff and contact me or DainaMueller Manager Tobacco Control Unit Health Promotion Implementation Branch atdainamuellerontarioca with any questions RegardsLaura Laura A PiskoDirectorHealth Promotion Implementation BranchHealth Promotion DivisionMinistry of Health and Long Term Care416-327-7445 (office)416-451-3185 (mobile) Marcus Gordon - EA (416)326-0625 for urgent issues
========= Middlesex-London Health Unit E-Mail Disclaimer =============______________________________________________________________
Private and confidential intended only for named recipient If otherwisereceived please destroy immediately Health information in this email isonly general information and is not intended to replace an in personconsultation with a medical professional nor is it intended to providemedical advice Individual circumstances of which we are not aware mayaffect the information provided herein and as such the Middlesex-LondonHealth Unit assumes no liability or responsibility for your reliancethereon The Middlesex-London Health Unit works under the authority of theHealth Protection and Promotion Act and this correspondence may be used toassess your needs for public health services (519-663-5317 ext 2448)______________________________________________________________
From Gardner CharlesTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes (RayCopesoahppca)
George Pasut (GeorgePasutoahppca) Peter Cooney (petercooneyhc-scgcca)Cc Ito DickSubject Discontinuation of Fluoridation in MuskokaDate Tuesday October 22 2013 125254 PM
Hello Colleagues
As I reported in my email below on September 26th fluoridation has come under challenge again inSimcoe Muskoka I am now very unhappy to report that despite our best efforts last night theDistrict Council of Muskoka voted to remove fluoride from municipal drinking supplies across theDistrict This brings to an end fluoridation in all of Simcoe and Muskoka (with the exception of Base Borden)ndash though New Tecumseth will be conducting a plebiscite on the question of fluoridation with themunicipal election next October Defending community water fluoridation has drained a great deal of time human resources andcommitment from other priorities and has been exhausting here in SMDHU as I am sure it hasbeen in many other health units While the outcomes have been very disappointing I have beenimpressed by the professionalism and dedication that SMDHU staff members have shown inshouldering this burden In particular our dental consultant Dr Ito has provided us with much ofthe foundational knowledge and the local research essential to our efforts and has very frequentlyattended and presented at council meetings and other public events I would also like to thank themany of you who have offer and provided support including advocacy letters and informationresources Over the years Dr Peter Cooney Chief Dental Officer of Health of Canada has beenvery helpful attending and presenting with us at council meetings and at public consultationevents We will of course continue our oral health surveillance of the children of Muskoka documentingand reporting in future years on the increase in dental decay that we anticipate will occur Suchsurveillance is the foundation of our advocacy both to municipal politicians and to the province I am very concerned that our experience will continue to repeat itself across the province unlessthere is strong leadership provincially It is with this in mind that I raise the followingrecommendations for your consideration
1 That we collectively (with PHOrsquos leadership) conduct high quality publish-worthy researchdocumenting the impact on dental decay that occurs in those municipalities throughoutOntario that in recent years have discontinued community water fluoridation This could bepart of a larger study on such municipalities across the country and it could also be part ofa study documenting overall oral health (including fluoridation coverage) in the province(and possibly across the country)
2 That COMOH engage with our Chief MOH to advocate for the province to require allmunicipal water supplies to be fluoridated (the exception of course being those withnaturally sufficient fluoride concentrations) This could built upon the alPHa position to
Gordon
Highlight
Gordon
Highlight
date (A11-00 - Community Water Fluoridation) on the CMOH position (Oral Health ndash) and on theemail discussion generated on the COMOH listserv some months back re Richardrsquosproposal (calling on the province to fund municipal water fluoridation)
Valerie I request that this be an item for our COMOH meeting on November 15th Sincerely Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorg From Gardner Charles Sent Thursday September 26 2013 245 PMTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes(RayCopesoahppca)Subject Community Water Fluoridation Under Challenge Again in Simcoe Muskoka Hello Colleagues You may wish to know that community water fluoridation (CWF) is again under challenge in SimcoeMuskoka specifically both in Tottenham (Town of New Tecumseth in Simcoe County) and for theentire District of Muskoka On Monday September 23 Committee of the Whole Council of theTown of New Tecumseth voted to submit application to discontinue community water fluoridation(CWF) in the town of Tottenham despite presentations to the contrary from our dental consultantDr Ito and from me The next Council meeting is scheduled for Monday Sept 30 at which lastMondayrsquos (Sept 23) votes will be ratified
Since Monday I have spoken with the Mayor of the Town of New Tecumseth and with most of thecouncilors encouraging deferral of a decision on Monday to allow the town more time to make afully informed decision
This is the second time in recent years that the issue of discontinuing CWF in Tottenham has beenraised at council This issue is also scheduled to return again to the District of Muskoka Council on
October 21st where I will be presenting in response to deputations in opposition to fluoridation
Outside of Base Borden Tottenham is the only community with fluoridated water in SimcoeCounty The health unitrsquos own screening data between 2011 and 2013 shows that Tottenhamrsquos
Gordon
Highlight
children as well as those in Muskoka have a lower rate of dental decay than Simcoe Muskokacommunities without CWF
Sincerely
Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorgChuck Gardner MOH
November 04 2013
Mandatory State Laws on Fluoridation Thirteen states Puerto Rico and the District of Columbia have laws intended to provide
statewide fluoridation These states and the year that the fluoridation legislation was passed are
District of Columbia (1952) Connecticut (1965) Kentucky (1966) Illinois (1967) Minnesota
(1967) Ohio (1969) South Dakota (1969) Georgia (1973) Nebraska (1973 and 2008)
California (1995) Delaware (1998) Puerto Rico (1998) Nevada (1999) Louisiana (2008) and
Arkansas (2011) (see Table 1) The sizes of the public water systems or countiescommunities
affected and exemption provisions vary by state Table 1
STATES THAT HAVE MANDATORY LAWS ON FLUORIDATION -2011
State (1) Year of
Fluoridation
Legislation (1)
Population
served by
Fluoridated
CWS (2)
Persons
receiving
fluoridated
water (2)
State
Average
Caries
Experience
of Grade 3
Students (3)
Arkansas 2011 647 1724131 64
California 1995 621 22812721 709
Connecticut 1965 910 2370423 406
Delaware 1998 862 705344 545
Georgia 1973 921 8924598 52
Illinois 1967 993 11325132 532
Kentucky 1966 999 4334223 598
Louisiana 2008 407 1846149 657
Minnesota 1967 988 4117266 549
Nebraska 1973 and 2008 702 1001665 593
Nevada 1999 702 1001665 649
Ohio 1969 877 8772683 512
South Dakota 1969 948 642942 623
District of
Columbia
1952 1000 595000
Puerto Rico 1998
United States 739 204283554
2010 Statistics for population fluoridated and number of people
1 Communication with Jane McGinley RDH MBA Manager Fluoridation and Preventive Health
Activities Council on Access Prevention and Interprofessional Relations
2 Centers for Disease Control and Prevention Department of Health and Human Services
accessed Oct 21 2013 httpwwwcdcgovfluoridationstatistics2010statshtm
3 Centers for Disease Control and Prevention National Oral Health Surveillance System Caries
Experience - Percentage of 3rd Grade students with Caries Experience (treated or untreated tooth
If data from 43 states for the percentage of Grade 3 children with experience of dental decay is
compared with the 2008 percentages of the population in a state with Community Water
Fluoridation then the percentage of children with experience of dental decay decreases as the
percentage of the state population with Community Water Fluoridation increases (see Figure 1)
Figure 1
Correlation of Percentage of Grade 3 Children with Caries Experience and
Percentage of Population With Community Water Fluoridation for 43
Reporting States
0
10
20
30
40
50
60
70
80
0 10 20 30 40 50 60 70 80 90 100
State of Population With Community Water Fluoridation
Sta
te
of
Gra
de 3
Stu
den
ts w
ith
Cari
es E
xp
eri
en
ce
Data from CDC (2 3)
The description of the fluoridation laws in California Illinois and Nevada can be found on the
Association of State amp Territorial Dental Directors website(4 7 8)
The California fluoridation law AB 733 came into effect in 1995 requiring communities of 10
000 residents or more be supplied with fluoridated drinking water However the state did not
provide any funding to implement the legislation (California is unique in requiring fluoridation
without funding the practice)(4) The California Department of Health Services therefore had to
fund fluoridation initiatives from non-governmental sources ie the California Endowment
California Dental Association Foundation the First 5 Commission and others(5) From 1995 to
2011 the percentage of the California population receiving fluoridated drinking water has risen
from 17 to 625(6) 4 Dental Public Health Activities amp Practices Office of Oral Health California Department of Health
Services April 2002 httpwwwastddorgbestpracticesDES06002CAfluoridationpdf
5 Stock M Pollick H The CDA Foundation Model to Fluoridate Communities California Dental
Association Journal vol 40 no 8 649 - 655
httpwwwcdaorgPortals0journaljournal_082012pdf
6 California Dental Association Foundation
httpwwwcdafoundationorglearnadvocacyfluoridation
The State of Illinois passed a mandatory fluoridation state in 1967 and required all community
water systems to adjust fluoride levels in the drinking water to optimal levels within 1 year(7)
From 1962 when over 5000000 residents had optimally fluoridated drinking water by 2010
the number had risen to 11325132 (993 of the population on community water systems)(2)
7 Dental Public Health Activities amp Practices Division of Oral Health Illinois Department of Public
Health April 2002 httpwwwastddorgbestpracticesDES16007ILfluoridationpdf
The State of Nevada passed a mandatory fluoridation statute in 2000 for communities with
400000 or more residents(8) This was a result of the work of a statewide coalition that
included the Nevada Dental and Dental Hygienist Associations the Washoe and Clark County
District Health Departments the Clark County School District Junior League of Las Vegas
Head Start the Community College of Southern Nevada Dental Hygiene Program Health
Access Washoe County and Saint Maryrsquos Hospital For communities with less than 400000 the
implementation of fluoridation still required the vote of the majority voters in the community
The Las Vegas Water Authority and the City of Henderson started fluoridation in 2000
increasing the percentage of the population with fluoridated drinking water from 2 to 65 (8) 8 Dental Public Health Activities amp Practices Bureau of Family Health Services Nevada State Health
Division April 2002 httpwwwastddorgbestpracticesDES31002NVfluoridationbillpdf
Countries with Mandatory Laws on Fluoridation Countries that have mandated Community Water Fluoridation are Brazil Hong Kong
Malaysia Singapore Ireland Israel and some of the states in Australia
Singapore started fluoridating its water in 1956 based on the success of the fluoridation trials in
Grand Rapids Newburgh Evanston and Brantford Singapore became the first Asian country to
have 100 of its population benefitting from the implementation of fluoridated drinking water
Loh reported that ldquoThe ten year study on the effects of water fluoridation in Singapore showed
a decrease in caries prevalence in the children In the permanent dentition the reduction was
523 per cent for Chinese and 31 per cent for Malays in the 7 to 9 year old age group A similar
trend was observed in the mixed dentition in which the decrease was 325 per cent for Chinese
and 306 per cent for Malaysrdquo(9) By 2010 the population of the country was 5080000(10)
9 Loh T Thirty-eight years of water fluoridation--the Singapore scenario Community Dent
Health 1996 Sep13 Suppl 247-50
10 British Fluoridation Society One in a Million the facts about water fluoridation 3rd Edition
published March 2012) httpwwwbfsweborgonemillion0920One20in20a20Million20-
20The20Extent20of20Fluoridationpdf
Hong Kong started implementing community water fluoridation in 1961 and similar to
Singapore 100 of the population received access to fluoridated drinking water Lo and Wong
reported that ldquoThe mean DMFT score of the children deceased from 44 in 1960 to 15 in 1968
stayed at this level in the 1980 and 1986 surveys and further deceased to 08 in 2001 The
prevalence of dental fluorosis among the children surveyed in 1960 was 1 and this increased
to 59 and 70 in 1968 and 1980 respectively It was found in the 1986 and 2001 surveys that
the prevalences of fluorosis were 47 and 9 among children whose teeth developed at the
time when the respective water fluoride concentrations were 07 ppm and 05 ppmrdquo(11) The
population of Hong Kong was 6968000 in 2009(10) 11 LO ECM and WONG AHH Water fluoride concentration and fluorosis in Hong Kong in 1960-
2001 84th General Session and Exhibition of the International Association for Dental Research amp
1st Meeting of the Pan-Asian-Pacific Federation Brisbane Australia 28 June-1 July 2006 v 85 n
Sp B
The Malaysian cabinet approved a nationwide community water fluoridation program in 1972
(12) One of the states Sabah decided to stop fluoridation in 1989 due to concerns about
inadequate supervision in adding fluoride to the drinking water Oral Health Surveys in 2009
and 2007 indicated that children in Sabah had the worst oral health with 50 of 12 year-olds
having decay in their permanent teeth and children having an average of 3 teeth being(13)
Under the 10th Malaysian Plan in 2011 the federal and the Sabah state governments
reintroduced water fluoridation in Sabah(1314) In 2010 about 755 of the Malaysian
population or 20700000 people had fluoridated drinking water(1013) 12 Malaysian Dental Association Fluoride in Water
httpwwwmdaorgmy07_public_01healthcare_12htm
13 Sachdev N Fluoridation in Sabah Water for Cleaner Teeth French Tribunecom 28022011
From Levy IsraTo Jaeger ValerieCc Pim Carolyn gordonalphaweborg Diallo Aicha Penny Sutcliffe Paul Roumeliotis Michael Finkelstein
Hazel Lynn Robert KyleSubject FW Panorama - Privacy Security and other issuesDate Wednesday October 16 2013 122110 PM
Hello ValerieOttawa is part of Wave 4 Panorama implementation and we are gearing up increasingly to use thesystem where and if possible Thinking about it I am anticipating that this may need to be on theCOMOH (and alPHa) radar as it is something that will impact all health units and implies a majoroperational shift in vaccine delivery programs for all health units I have asked Carolyn Pim toconnect with our sister wave 4 units to share common experiences as we move forward ndash when wehave a roll up could I bring to COMOH Exec for discussion to explore whether there are broaderimplications for all members As an aside I have also asked the Ministry and their CIO to share with me any roll up learnings thatthey may have had already from previous waves (I understand that Niagara HU was a wave 1participant so if there is such a roll up of common experiences that others could learn fromperhaps you have it already and that could come to the exec too)Thanks Isra From Pim Carolyn Sent October 10 2013 1228 PMTo Christopher Mackie (christophermackiemlhuonca) Elizabeth Richardson(Elizabethrichardsonhamiltonca) H BSc M D F R C P (C) MPH Jim Chirico(jimchiriconbpsdhuca) Marlene Spruyt (spruytmtimiskaminghucom) Robert Kyle (Durham)Cc Levy IsraSubject Panorama - Privacy Security and other issues Dear colleagues Irsquom reaching out to you as fellow Panorama Wave 4 health units to ask about where yourorganizations are at in the process of signing agreements and completing Privacy ImpactAssessments and Threat Risk Assessments (TRAs) Ottawa Public Healthrsquos IT legal and informationsecurity advisors have made numerous requests to the MOHLTC for information (in particular theprovincial TRA) that we consider essential to develop our own risk assessment and PIA but havebeen told that information cannot be shared even with strict confidentiality and access controlsSo we are at somewhat of an impasse Isra emailed Arlene yesterday Arlene has forwarded ourconcerns to the Ministryrsquos CIO and Panorama lead but we havenrsquot had any response or discussionswith either of them yet Have your organizations identified similar concerns andor had interactions with the MOHLTC inthis respect Irsquod also be interested in knowing if your health units have flagged other (egoperational) implementation concerns Thanks
Carolyn ps Robert ndash you can ignore this request I talked with Sharan this morning about Durhamrsquos issuesso am including you now just for information Carolyn Pim MD FRCPC Associate Medical Officer of Health Meacutedecin adjointe en santeacute publique Ottawa Public Health Santeacute publique Ottawa 100 Constellation Cr Ottawa ON K2G 6J8 Tel teacutel (613) 580-6744 ext 23684Fax (613) 580-9641Connect With Ottawa Public Health
Suivez Santeacute publique Ottawa
This e-mail originates from the City of Ottawa e-mail system Any distribution use orcopying of this e-mail or the information it contains by other than the intendedrecipient(s) is unauthorized If you are not the intended recipient please notify meat the telephone number shown above or by return e-mail and delete thiscommunication and any copy immediately Thank you
Le preacutesent courriel a eacuteteacute expeacutedieacute par le systegraveme de courriels de la Ville dOttawaToute distribution utilisation ou reproduction du courriel ou des renseignements quisy trouvent par une personne autre que son destinataire preacutevu est interdite Si vousavez reccedilu le message par erreur veuillez men aviser par teacuteleacutephone (au numeacuteropreacuteciteacute) ou par courriel puis supprimer sans deacutelai la version originale de lacommunication ainsi que toutes ses copies Je vous remercie de votre collaboration
1
Smoke-Free Patios ndash An Amendment to the Smoke-Free Ontario Act
Date November 15 2013 Prepared for Council of Ontario Medical Officers of Health Prepared by York Region Public Health _____________________________________________________________________________ Issue
The Smoke-Free Ontario Act is the current provincial legislation that imposes smoking restrictions in workplaces and public places It prohibits smoking on restaurant and bar patios in instances where any portion of the seating area is covered by a roof With recent studies illustrating that exposure to second hand smoke outdoors poses similar risks to indoor exposure there has been growing public support to enhance smoking restrictions and make patios completely smoke-free
Background
With the implementation of the Smoke-Free Ontario Act in 2006 restaurant and bar patios became subject to smoking restrictions if any portion of the seating area was covered by a roof This allowed for patios without roof coverings to continue to allow smoking and as a result did not provide significant protection to patrons or staff from exposure to second hand smoke outdoors Many businesses chose to alter the design of their patios to allow smoking to continue In some cases patios became more crowded since smoking patrons who dine indoors often proceed outside onto licensed patios with their beverages to smoke York Region like most municipalities in Ontario is host to hundreds of patios being operated by restaurant owners and businesses With smoking prohibitions affecting only a small portion of these patios specifically ones with coverings the vast majority of patios still allow smoking to take place Patrons and employees on patios where smoking is not restricted are exposed to second hand smoke frequently This can contribute to increased disease and aggravation of existing health conditions From a business perspective the existing legislation has been viewed by many operators as unfair because some patios have permanent coverings which cannot be removed requiring a smoke-free status These business owners feel this creates an uneven playing field since they cannot provide an outdoor dining area for their smoking customers There is strong community support for smoke-free patios in Ontario A 2009 Rapid Risk Factor Surveillance System survey revealed 754 percent support in York Region while a Toronto Health Survey in 2011 indicated 74 percent public support
2
Current Status
Smoking is currently prohibited on restaurant and bar patios province-wide in four Canadian provinces and territories Alberta Newfoundland and Labrador Nova Scotia and Yukon A fifth province Prince Edward Island prohibits smoking on patios until 10 pm Since Ontario enacted legislation restricting smoking on patios in 2006 eight municipalities in Ontario have chosen to create bylaws that go beyond the Smoke-Free Ontario Act and enhance outdoor protection from second hand smoke by prohibiting smoking on patios completely The largest of those municipalities is the City of Ottawa Recently the Toronto Board of Health unanimously endorsed a report presented by their Medical Officer of Health recommending that restaurant and bar patios be made smoke-free through an amendment to the Smoke-Free Ontario Act
Key Considerations
There should be no significant financial burden to local Boards of Health resulting from a smoke-free patio amendment to the Smoke-Free Ontario Act Inspection and enforcement for the Smoke-Free Ontario Act is currently 100 percent funded by the Ministry of Health and Long-Term Care Following an introductory period of education on the amendment a complaint response model of service delivery would ensure ongoing compliance with smoke-free requirements A complete ban of smoking on patios would eliminate the widely-held perception by business owners that the current legislation creates an uneven playing field for business Since Smoke-Free Ontario Act inspections of patios began in 2006 operators have expressed the opinion that if patios need to be smoke-free for the protection of the public they should all be smoke-free to avoid undue hardship for individual businesses and to provide protection uniformly across the Province
Next steps
York Region Public Health intends to seek support from Medical Officers of Health across the Central East Tobacco Control Area Network (CETCAN) to advocate to the Ministry of Health and Long-Term Care for an amendment to the Smoke-Free Ontario Act prohibiting smoking on all restaurant and bar patios York Region is also in the process of requesting that its Regional Council advocate to the Minister of Health and Long-Term Care on the issue
Updating and Modernizing O Regulation 565 (Public Pools)
Date November 15 2013
Prepared for Council of Ontario Medical Officers of Health
Prepared by York Region Public Health _____________________________________________________________________________ Background Recent drownings at public pools in Ontario have highlighted the issue of water-borne illness and injury The current pool regulation under Ontariorsquos Health Protection and Promotion Act O Regulation 565 (Public Pools) is outdated It does not accurately reflect new pool technology and design or the changing use of public pools Neither does it incorporate admissions standards recommended by the Office of the Chief Coroner Further O Regulation 565 does not have short-form wording or set fines associated with it This limits public health enforcement capabilities What is the impact Updating O Regulation 565 (Public Pools) to address recent changes in pool technology design and uses and to include Coroner-recommended admissions standards would help improve pool safety Establishing short-form wording for O Regulation 565 would enhance enforcement related to public pools Currently the only enforcement available to Public Health Inspectors for dealing with non-critical regulatory infractions in public pools is the issuance of a Part III summons This involves a considerable amount of resources for a possible small fine With the development of inspection disclosure systems such as YorkSafe there is an even greater need to develop a method to effectively address repeated pool operator non-compliance with non-critical issues Next steps Public health units should advocate to the Province to 1) Conduct a review of O Regulation 565 (Public Pools) to address shortcomings Proposed changes to the
regulation should include a requirement for ownersoperators of public pools to advise the local Medical Officer of Health of any change in the use of a facility and the addition of the Coronerrsquos recommended admission standards
2) Provide short-form wording for O Regulation 565 so that public health inspectors can better deal with pool operator non-compliance
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
Page 3 of 8 ndash DRAFT FOR COMOH DISCUSSION
SECTION 2 PROFESSIONAL DEVELOPMENT
Survey Question Which of the following events have you attended at least once in the past two years
Survey Question Overall how satisfied have you been with alPHa events ie conferences meetings
Survey Question How much value do alPHarsquos events provide for the money
Survey Question How can alPHa make its events more valuable to you Please share any suggestions regarding future topics speakers formats duration locations or any other event component that is important to you
Comments about content bull Expert speakerpanels on emerging or hot topics
(2) bull More engaged dialogue with Ministry rather than
just updates bull Fewer Ministry updates (3) bull Content on medicalPH issues is better left to PHO
TOPHC and joint conferences (2) bull alPHa should stick to Ministrypoliticspolicysenior
PH supportPHU support on key priorities (eg November practical conference on HKP report)
bull For COMOH more discussion bull More time for section activities like face-to-face
COMOH meetings
bull More facilitated work groups of COMOH members to respond to public health practice questions
bull More focus on rural and northern issues bull Infection Control Logistical Considerations bull Consider partnering with other groups bull More collaboration with PHO and OPHA events bull Use of video conferencing bull Less frequentfewer meetings (2) bull Connect with CME Location bull Consider other venues than TO
( ) brackets indicate that more than one response included a similar comment
More than enough value 7 11A lot of value 34 52Some value 22 34A little value 2 3Not enough value 0 0Totals 65 100
All Responses for those who Attended at least One Event in the Last 2 Years
All COMOH ResponsesMore than enough value 4 15A lot of value 13 48Some value 9 33A little value 1 4Not enough value 0 0Totals 27 100
Page 5 of 8 ndash DRAFT FOR COMOH DISCUSSION
SECTION 3 VALUE FOR MEMBERSHIP
Survey Question What do you value the most about your alPHa membership
The comments provided in response to the text response question What is the most important benefit of alPHa membership for you personally supported the answers illustrated in the chart above 15 of the 20 comments provided focussed on the importance of opportunities to interact with colleagues across the province The next most important benefit mentioned was the support for COMOH members to work on public health issues together When asked What is the most important benefit of alPHa membership for your health unit COMOH members emphasized the following bull A coordinated and collective voice in advocating for public health issues and the public health sector (9) bull Opportunities to connect with other public health units to share experiences and best practices (8) bull Maintaining relationships with government both politicians and bureaucrats (3) and bull Support for boards of health (3)
Page 6 of 8 ndash DRAFT FOR COMOH DISCUSSION
Overall Level of Satisfaction
SECTION 4 LOOKING TO THE FUTURE
The questions in this section were asked to obtain input from alPHa members regarding a proposal from alPHarsquos Board of Directors to focus the Association on five service areas COMOH members were asked to indicate their level of agreement with the proposed areas of focus COMOH responses compared to the overall survey responses were as follows
To explore some proposed changes to Association services COMOH members were asked to provide their level of agreement with the following questions
COMOH Responses BOH Section Affiliates All Survey Responses
Strongly Agree
AgreeNeither Agree or Disagree
DisagreeStrongly Disagree
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1Promoting the role and value of local public health units
15 9 2 0 0 26 92 93 95 94
2
Providing important information to members about trends and events that will impact the public health system and management of public health units
10 8 8 0 0 26 69 97 86 85
3Facilitating professional networking and information sharing
13 10 3 0 0 26 88 83 82 85
4
Providing professional development to support excellence in public health unit leadership management and governance
3 15 7 1 0 26 69 83 86 79
5
Responding to public health sector issues when it makes the most sense to have a collective voice ie issues that impact the structure and funding of the public health sector and public health units and issues that have a broad focus on population health
15 8 2 0 1 26 88 97 95 93
PROPOSED AREAS OF FOCUS
COMOH Responses BOH Section Affiliates All Survey Responses
Strongly Agree
AgreeNeither Agree or Disagree
DisagreeStrongly Disagree
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1
COMOH and other professional groups within alPHa should do their own advocacy while alPHa supports members to share and support each others advocacy efforts
7 6 6 6 1 26 50 58 45 52
2
alPHa should provide support to action-oriented inter-professional work groups on priority public health unit issues and member resolutions
4 13 5 3 1 26 65 81 86 77
PROPOSALS
Page 8 of 8 ndash DRAFT FOR COMOH DISCUSSION
COMOH members were also asked to indicate the level of acceptability for some possible changes to alPHarsquos services and way of doing business
COMOH Responses BOH Section Affiliates All Survey Responses
Very Acceptable
Somewhat Acceptable
Neither Acceptable or Unacceptable
Somewhat Unacceptable
Very Unaccept
able
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1Single conference with additional face-to-face section meetings
21 2 0 1 0 24 96 68 80 81
2alPHa to offer alternatives like webinars on focussed topics
13 6 1 4 0 24 79 50 90 71
3Coordinate COMOH meetings with PHO OMA or Ministry events
16 4 2 0 0 22 91 na na --
4
Increase focus on building leadership and management capacity for health unit CEOs and senior management
7 9 4 3 0 23 70 na 70 70
5
Would it be acceptable for alPHa to request voluntary financial contributions from member PHUs in addition to annual fees
3 5 5 4 5 22 36 7 26 21
6
Would it be acceptable for alPHa to request voluntary in-kind staff contributions from member PHUs to expand alPHas capacity eg communications policy work group support
7 11 1 1 3 23 78 31 45 50
7Would it be acceptable to you for alPHa to discontinue staff support for COMOH (BOH Section)
0 4 1 5 14 24 17 11 na 14
8
Would it be acceptable to you for alPHa to reduce the amount of staff support for COMOH (BOH Section)
1 6 1 8 6 22 32 26 na 29
9
Would it be acceptable to you for alPHa to provide supports to MOHs and AMOHs (BOH Members) without maintaining COMOH (BOHs) as a section of the association
3 2 3 2 12 22 23 17 na 20
10
Would it be acceptable to you for alPHas Board of Directors to move from the current representational model to a skills-based strategic model ie board membership would be based on the skills needed to carry out alPHas strategic plan
6 11 2 1 3 23 74 56 56 62
11
Would it be acceptable to you for alPHas President Vice-President and Treasurer to be elected from the full membership of the alPHa Board of Directors (rather than the current model of alternating between BOH and COMOH members)
10 8 1 2 2 23 78 70 70 73
PROPOSED CHANGES
1 Council of Ontario Medical Officers of Health Terms of Reference
ASSOCIATION OF LOCAL PUBLIC HEALTH AGENCIES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
TERMS OF REFERENCE NAME 1 The name of the organization shall be ldquoThe Council of Ontario Medical Officers of
Health a section of the Association of Local Public Health Agencies (alPHa)rdquo hereinafter referred to as ldquothe Councilrdquo
MISSION 2 As local leaders in public health we are committed to improving the health of
Ontarians and increasing health equity by strengthening Ontariorsquos public health system We achieve this through system leadership and coordination in collaboration with the provincial government and other organizations and through evidence-informed advocacy on public health policy
OBJECTIVES 3 The objectives of the Council shall be
a) To provide strong province-wide leadership in public health
b) To advocate for health protection and promotion policies and programs that maintain and improve the health of Ontarians
c) To promote and maintain the highest standards for Ontariorsquos public health
programs and services
d) To support the planning implementation and evaluation of effective and efficiently run public health programs and services
e) To act as a forum for sharing information and resources and for addressing and
discussing public health issues both amongst the Councilrsquos members and other agencies that support the goals of alPHa eg Ontario Medical Association Ontario Public Health Association etc
f) To engage with and to provide public health and related policy advice to alPHa
the Chief Medical Officer of Health the Ontario Ministries of Health and Long-Term Care (including the Health Promotion and Public Health Divisions) Children
2 Council of Ontario Medical Officers of Health Terms of Reference
and Youth Services and other provincial ministries Public Health Ontario Health Canada the Public Health Agency of Canada and other public health partners
g) To promote and protect the professional interests of its members
h) To provide support to individual members as needed
i) To seek recognition for outstanding practice from among the members
j) To support evidence based practice of public health medicine
k) To engage and involve the membership to participate in COMOHrsquos endeavours
l) To mentor Public Health and Preventive Medicine Residents
MEMBERSHIP 4 Membership on the Council in each of the following categories is subject to the
limitations imposed by the current terms of reference and all policies and governing documents of the Association of Local Public Health Agencies Benefits of membership in each category are included in Appendix A These shall be subject to regular review and may be suspended under certain circumstances
Active membership in the Council shall be open to all Associate Medical Officers of Health and all full-time Medical Officers of Health whose Boards of Health are members of alPHa Such members shall have full voting privileges and may hold office in the Council Associate membership shall be open to all full and part-time physicians employed by a Board of Health that is a member of alPHa Such members shall not have voting privileges nor hold office
Affiliate membership shall be open to the following individuals interested in furthering the objectives of the Council
bull Public Health and Preventive Medicine Residents and Public Health and Preventive Medicine Residency Program Directors
bull Federal public health physicians working in Ontariorsquos First Nations communities
bull other public health or related physicians including those employed by a Board of Health that is not a member of alPHa
Such members shall not have voting privileges nor hold office
3 Council of Ontario Medical Officers of Health Terms of Reference
Emeritus membership shall be open to all former members who have retired after five (5) or more years of Active membership subject to the nomination in writing of two (2) active members in good standing endorsement of the Executive Committee and approval of the Council by majority vote at a general meeting Such members shall have neither voting privileges nor hold office but may be invited to attend general meetings Honorary membership shall be open to any non-active or associate member subject to the nomination in writing of two (2) active members in good standing endorsement of the Executive Committee and approval of the Council Such members shall have neither voting privileges nor hold office but may be invited to attend general meetings
OFFICERS 5 The Officers of the Council shall be the Chair Vice-Chair and immediate Past Chair
6 The Chair shall prepare the agendas of all Council meetings She shall preside and
preserve order at all such meetings shall ensure that these Terms of Reference are upheld and enforced and shall contribute to the supervision and evaluation of any Public Health and Preventive Medicine Resident who is on a placement with alPHa
7 The Vice-Chair shall fulfill the duties of the Chair in hisher absence The immediate
Past Chair may fulfill the duties of the Chair or Vice-Chair in their absences 8 The Chair shall normally serve a term of one (1) year which is renewable once and
after which the Vice-Chair shall normally assume the vacated office COMMITTEES 9 The Council shall elect seven (7) active members one from each of alPHarsquos regions
and the active member who is scheduled to serve as the President or immediate Past-President of alPHa to represent it on the alPHa Board of Directors These seven (7) members shall constitute the Councilrsquos Executive Committee and shall serve a term of at least one (1) year The Chair and Vice-Chair shall be elected from among the Executive Committee members If alPHarsquos immediate Past President is an active member she shall be an ex-officio member of the Executive Committee
10 The mandate of the Executive Committee shall be to facilitate the achievement of
the objectives of the Council by fulfilling the following
a Identifying priorities 1
1 See Appendix B Planning Cycle to Identify Priorities for COMOH
and ensuring the development of briefing documents and or recommendations as appropriate for the consideration of the Council
4 Council of Ontario Medical Officers of Health Terms of Reference
b Setting agendas and otherwise ensuring preparations for Council meetings c Ensuring the fulfillment of the direction of Council d Responding in a timely fashion to time-sensitive public health matters in
accordance with the Executive Committeersquos understanding of the perspective of the Council
e Engaging with the Chief Medical Officer of Health Associate Chief Medical Officers of Health and other provincial public health leaders and
f Representing Council at public and partner agency forums including the Public Health Leadership Council which shall normally include membership from the Officers of the Council and two other Executive Committee members as selected by agreement among the Executive
g Identifying opportunities for the recognition of outstanding practice from among the members including the annual nomination of at least one member for the alPHa Distinguished Service Award
11 The Executive Committee shall meet and correspond in the manner and at the times
and if required places as deemed necessary by the Chair to conduct the business of the Council A quorum shall consist of four (4) members
12 The Executive Committee shall have the power to strike committeestask or working
groups to assist it in carrying out the business of the Council 13 The Council may by special resolution remove a member of the Executive
Committee before the completion of hisher term of office and may elect a successor to complete the term The special resolution shall require a majority vote of 67 of the members present and voting at the meeting at which the special resolution is considered
14 A Nominating Committee shall consist of the three (3) most recent Past Chairs who
are able to serve and shall be chaired by the immediate Past Chair The Nominating Committee shall prepare a list of proposed Officers and Executive Committee members for the consideration of the Council at its Annual General Meeting
MEETINGS 15 The Council shall hold at least four (4) general meetings per year in a manner and at
the times and if required places as deemed necessary by the Executive Committee to share information direct and assist the Executive Committee in conducting the business of the Council
16 The Council shall hold its Annual General Meeting during and at the same place as
the alPHarsquos Annual Conference
5 Council of Ontario Medical Officers of Health Terms of Reference
17 The Council shall hold a special meeting at the call of the Chair or upon the written request specifying the purpose of such meeting of at least five (5) active members Council members must be given at least 48 hours notice of any special meeting
18 Only Councilrsquos active and associate members and alPHa staff are entitled to attend
general and special meetings of the Council Other members and non-members may be invited to attend all or part of such meetings as determined by the Chair preferably in consultation with the Executive Committee Non-members who come to such meetings without an invitation may attend all or part of the meeting by a majority vote of the active members present and voting
19 The Chair shall prepare the agendas for such meetings and shall normally include
reports from the Chair and the Councilrsquos committeestask or working groups and representatives to external bodies alPHarsquos Executive Director shall ensure that the minutes shall be recorded and promptly distributed to the Section
20 A quorum for all such meetings shall be ten (10) active members 21 The Council shall normally be notified in a manner deemed appropriate by the Chair
of such meetings at least one (1) month prior to their being held 22 A majority vote of the members present at such meetings and voting shall make
Council decisions In the case of a tied vote the Chair shall cast the deciding vote The Executive Committee shall ensure that actions arising from such decisions at such meetings are implemented and monitored
23 The Chair may solicit advice from the Council through the use of teleconferencing
and alPHarsquos electronic mailing lists in order to gain an understanding of the overall perspective of the Council (see 10d)
ELECTIONS 24 The Officers and Executive Committee members shall be elected at the Sectionrsquos
Annual General Meeting The Nominating Committee Chair or hisher designate shall present a list of nominations Additional nominations from the floor shall also be considered Each Officer and Executive Committee member shall be elected by secret ballot if necessary by a majority of the active members present and voting In the case of a tie the Chair shall cast the deciding vote
AMENDMENTS 25 The Councilrsquos Terms of Reference may be amended from time to time by the
Executive Committee provided the Committee receives notice of such proposed amendments at least one (1) month prior to the meeting at which the amendments
6 Council of Ontario Medical Officers of Health Terms of Reference
will be considered Such amendments shall be ratified by the Council at the next general meeting or the Annual General Meeting as the case may be
26 The Executive Committee shall review the Terms of Reference as required and not
less than once every two years Original September 1987 1st Revision October 2000 2nd Revision July 2001 3rd Revision December 2003 4th Revision February 2008 5th Revision June 2009 6th Revision June 2011 7th Revision June 2013
7 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX A
COMOH Membership Benefits Active Membership
bull Entitled to attend all meetings of the Section bull May hold office on the COMOH Executive Committee alPHa Board of Directors
Standing Committees bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Associate Membership
bull Entitled to attend all meetings of the Section bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Affiliate Membership
bull May attend meetings or parts thereof subject to approval of Chair bull May serve on ad-hoc committees of the Section subject to the approval of the
Executive Committee bull Discounted registration rates for alPHa Conferences (for Public Health and
Preventive Medicine Residents) bull Upon written request and subject to COMOH Executive approval Affiliate
Members may subscribe to comohlistsalphaweborg The approval will be reviewed on an annual basis in order to determine if the Affiliate Member can remain a subscriber to mohsalphaweborg
Emeritus Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair bull Enjoy discounted registration rates for alPHa Conferences and regular COMOH
meetings bull Subscription to comohlistsalphaweborg electronic mailing list bull Full access to alPHa Web site bull May represent alPHa COMOH on selected external committees and working
groups Honorary Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair
8 Council of Ontario Medical Officers of Health Terms of Reference
bull May represent alPHa COMOH on selected external committees and working groups subject to the approval of the COMOH or alPHa Executive Committee as appropriate
9 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX B
Planning Cycle to Identify Priorities for COMOH
1 There shall normally be a COMOH membership strategic planning retreat every four years In recognition of the dynamic environment of public health the need for and timing of such a retreat shall be at the discretion of the Executive Committee in consultation with the membership
2 The COMOH Executive is responsible (through the creation of a subcommittee of COMOH members) for ensuring the preparation for the COMOH retreats with resources to include those provided by alPHa
3 Leadership for action on COMOH priorities will be recruited from among the COMOH membership in order to make good use of the full base of capacity of the membership The resources to support actions will be recruited from both within and beyond the COMOH membership employing other public health professionals that reside within the broader public health system and community
4 The COMOH Executive shall ensure an annual review of strategic priorities and initiatives and the development of a draft report of the same for the review of the members at the June meeting
2013 Strategic Planning
Considerations for COMOH
As part of its strategic planning discussions alPHarsquos Board has been considering changes to the level of support provided to member sections A member survey is being carried out over the fall to determine options acceptable to alPHa members The following approach to support is put forward as a proposal for the consideration of COMOH Note that the feasibility of the points below depend upon future decisions of the alPHa board They assume that COMOH remains part of alPHa but becomes more independent in administering meetings
1 alPHa can provide to COMOH staff support (Gord Fleming) amounting to 02 FTE or one day per week This is a reduction from the current level of 35 days per week COMOH can choose to use the support any way it wants writing COMOH letters meeting minutes agenda support special projects etc
2 In addition to 02 FTE alPHa staff would provide support for up to 4 face-to-face meetings per year One meeting would be concurrent to alPHarsquos annual conference in June The timing of other meetings could be negotiated The support includes consulting on the development of the program arranging for speakers registration for the event arranging venue AV support and hospitality services
3 In addition to 02 FTE alPHa staff would provide support for setting meeting dates and any polling required to establish dates Note that the individual supporting this function would be Karen Reece
4 COMOHrsquos Executive and Section would continue to have access to online supports through the alPHa including the COMOH Listserve and a group page for posting agendas minutes and other resources on the alPHa website
5 alPHa staff (Linda Stewart and Gord Fleming) can also start participating on CMOH calls as a way to be up-to-date on issues related to COMOH
6 Other than what is outlined above COMOH would be expected to prepare agendas and take minutes for its Executive and Section meetings The Executive would be expected to operate more independently than it does now but would be able to access the supports outlined above
Prepared by Linda Stewart Executive Director
From comoh-bounceslistsalphaweborg on behalf of Christopher MackieTo MOH ListserveSubject [comoh] Fw URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)Date Wednesday October 30 2013 91241 AMAttachments ATT00249txt
For AMOHs and PHPM residents who didnt receive the initial email
Chris
Christopher Mackie MD MHSc FRCPCMedical Officer of Health and CEOMiddlesex-London Health Unit50 King St LondonON N6A 5L7 O 519 663 5317 ext 2444 wwwhealthunitcomFrom Pisko Laura (MOHLTC)Sent Tuesday October 29 2013 759 PMTo kbarkeralgomapublichealthcom malcolmlockbchuorg davidcchatham-kentcarobertkyledurhamca proumeliotiseohuca fwarshelginhealthonca mohelginhealthoncahlynnpublichealthgreybruceonca malcolmlockhnhuorg hnmohhnhuorglnoseworthyhkpronca bobnosalhaltonca elizabethrichardsonhamiltoncarschabashpechuonca ncameronhuroncountyca drimgemmillkflapublichealthcamohkflapublichealthca suditranadecounty-lambtononca paulastewarthealthunitorgChristopher Mackie valeriejaegerniagararegionca jimchiriconbpsdhuca jarthursnwhuoncaisralevyottawaca dnealoxfordcountyca davidmowatpeelregionca mklassenpdhuoncarpellizzaripcchuca rosemarieramsinghporcupinehuonca mcorriveaurcdhucomcharlesgardnersmdhuorg sutcliffepsdhucom davidwilliamstbdhucomspruytmtimiskaminghucom dmckeowntorontoca lnolanregionofwaterloocanicolamercerwdghuorg aheimannwechealthunitorg karimkurjiyorkcaCc coreywesleytbdhucom CindyBaker-Barillsmdhuorg Donna Kosmack pilonlsdhucomPaulaMuiskflapublichealthca sthibautorontoca Mueller Daina (MOHLTC) Gordon Marcus(MOHLTC) andreakitahamiltoncaSubject URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)
Dear Colleagues The ministry has received reports that some tobacco vendors across the province aregiving away single cigarettes with the purchase of tobacco products It is the ministryrsquosposition that giving out free single cigarettes does not violate subsection 31(3) of theSmoke-Free Ontario Act (ldquoSFOArdquo) Although the practice of giving out free singlecigarettes may promote the sale of tobacco products it does not take the form of aldquoproduct enhancement product association or promotional materialrdquo and therefore doesnot fall within the scope of subsection 31(3) of the SFOA We have confirmed with Health Canada that this practice may violate section 29(b) of thefederal Tobacco Act As such Health Canada is requesting that you notify them in writingand I am directing you to communicate with them via email and provide to them as manydetails as possible Emails should be sent to Tobacco-Ontariohc-scgcca and thesubject line should read ldquoViolation of Section 29(b) of Tobacco Actrdquo This will ensurethat the complaints are given priority status by Health Canada We will continue to monitor
this situation and liaise with our colleagues at Health Canada Please share this information with your tobacco control staff and contact me or DainaMueller Manager Tobacco Control Unit Health Promotion Implementation Branch atdainamuellerontarioca with any questions RegardsLaura Laura A PiskoDirectorHealth Promotion Implementation BranchHealth Promotion DivisionMinistry of Health and Long Term Care416-327-7445 (office)416-451-3185 (mobile) Marcus Gordon - EA (416)326-0625 for urgent issues
========= Middlesex-London Health Unit E-Mail Disclaimer =============______________________________________________________________
Private and confidential intended only for named recipient If otherwisereceived please destroy immediately Health information in this email isonly general information and is not intended to replace an in personconsultation with a medical professional nor is it intended to providemedical advice Individual circumstances of which we are not aware mayaffect the information provided herein and as such the Middlesex-LondonHealth Unit assumes no liability or responsibility for your reliancethereon The Middlesex-London Health Unit works under the authority of theHealth Protection and Promotion Act and this correspondence may be used toassess your needs for public health services (519-663-5317 ext 2448)______________________________________________________________
From Gardner CharlesTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes (RayCopesoahppca)
George Pasut (GeorgePasutoahppca) Peter Cooney (petercooneyhc-scgcca)Cc Ito DickSubject Discontinuation of Fluoridation in MuskokaDate Tuesday October 22 2013 125254 PM
Hello Colleagues
As I reported in my email below on September 26th fluoridation has come under challenge again inSimcoe Muskoka I am now very unhappy to report that despite our best efforts last night theDistrict Council of Muskoka voted to remove fluoride from municipal drinking supplies across theDistrict This brings to an end fluoridation in all of Simcoe and Muskoka (with the exception of Base Borden)ndash though New Tecumseth will be conducting a plebiscite on the question of fluoridation with themunicipal election next October Defending community water fluoridation has drained a great deal of time human resources andcommitment from other priorities and has been exhausting here in SMDHU as I am sure it hasbeen in many other health units While the outcomes have been very disappointing I have beenimpressed by the professionalism and dedication that SMDHU staff members have shown inshouldering this burden In particular our dental consultant Dr Ito has provided us with much ofthe foundational knowledge and the local research essential to our efforts and has very frequentlyattended and presented at council meetings and other public events I would also like to thank themany of you who have offer and provided support including advocacy letters and informationresources Over the years Dr Peter Cooney Chief Dental Officer of Health of Canada has beenvery helpful attending and presenting with us at council meetings and at public consultationevents We will of course continue our oral health surveillance of the children of Muskoka documentingand reporting in future years on the increase in dental decay that we anticipate will occur Suchsurveillance is the foundation of our advocacy both to municipal politicians and to the province I am very concerned that our experience will continue to repeat itself across the province unlessthere is strong leadership provincially It is with this in mind that I raise the followingrecommendations for your consideration
1 That we collectively (with PHOrsquos leadership) conduct high quality publish-worthy researchdocumenting the impact on dental decay that occurs in those municipalities throughoutOntario that in recent years have discontinued community water fluoridation This could bepart of a larger study on such municipalities across the country and it could also be part ofa study documenting overall oral health (including fluoridation coverage) in the province(and possibly across the country)
2 That COMOH engage with our Chief MOH to advocate for the province to require allmunicipal water supplies to be fluoridated (the exception of course being those withnaturally sufficient fluoride concentrations) This could built upon the alPHa position to
Gordon
Highlight
Gordon
Highlight
date (A11-00 - Community Water Fluoridation) on the CMOH position (Oral Health ndash) and on theemail discussion generated on the COMOH listserv some months back re Richardrsquosproposal (calling on the province to fund municipal water fluoridation)
Valerie I request that this be an item for our COMOH meeting on November 15th Sincerely Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorg From Gardner Charles Sent Thursday September 26 2013 245 PMTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes(RayCopesoahppca)Subject Community Water Fluoridation Under Challenge Again in Simcoe Muskoka Hello Colleagues You may wish to know that community water fluoridation (CWF) is again under challenge in SimcoeMuskoka specifically both in Tottenham (Town of New Tecumseth in Simcoe County) and for theentire District of Muskoka On Monday September 23 Committee of the Whole Council of theTown of New Tecumseth voted to submit application to discontinue community water fluoridation(CWF) in the town of Tottenham despite presentations to the contrary from our dental consultantDr Ito and from me The next Council meeting is scheduled for Monday Sept 30 at which lastMondayrsquos (Sept 23) votes will be ratified
Since Monday I have spoken with the Mayor of the Town of New Tecumseth and with most of thecouncilors encouraging deferral of a decision on Monday to allow the town more time to make afully informed decision
This is the second time in recent years that the issue of discontinuing CWF in Tottenham has beenraised at council This issue is also scheduled to return again to the District of Muskoka Council on
October 21st where I will be presenting in response to deputations in opposition to fluoridation
Outside of Base Borden Tottenham is the only community with fluoridated water in SimcoeCounty The health unitrsquos own screening data between 2011 and 2013 shows that Tottenhamrsquos
Gordon
Highlight
children as well as those in Muskoka have a lower rate of dental decay than Simcoe Muskokacommunities without CWF
Sincerely
Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorgChuck Gardner MOH
November 04 2013
Mandatory State Laws on Fluoridation Thirteen states Puerto Rico and the District of Columbia have laws intended to provide
statewide fluoridation These states and the year that the fluoridation legislation was passed are
District of Columbia (1952) Connecticut (1965) Kentucky (1966) Illinois (1967) Minnesota
(1967) Ohio (1969) South Dakota (1969) Georgia (1973) Nebraska (1973 and 2008)
California (1995) Delaware (1998) Puerto Rico (1998) Nevada (1999) Louisiana (2008) and
Arkansas (2011) (see Table 1) The sizes of the public water systems or countiescommunities
affected and exemption provisions vary by state Table 1
STATES THAT HAVE MANDATORY LAWS ON FLUORIDATION -2011
State (1) Year of
Fluoridation
Legislation (1)
Population
served by
Fluoridated
CWS (2)
Persons
receiving
fluoridated
water (2)
State
Average
Caries
Experience
of Grade 3
Students (3)
Arkansas 2011 647 1724131 64
California 1995 621 22812721 709
Connecticut 1965 910 2370423 406
Delaware 1998 862 705344 545
Georgia 1973 921 8924598 52
Illinois 1967 993 11325132 532
Kentucky 1966 999 4334223 598
Louisiana 2008 407 1846149 657
Minnesota 1967 988 4117266 549
Nebraska 1973 and 2008 702 1001665 593
Nevada 1999 702 1001665 649
Ohio 1969 877 8772683 512
South Dakota 1969 948 642942 623
District of
Columbia
1952 1000 595000
Puerto Rico 1998
United States 739 204283554
2010 Statistics for population fluoridated and number of people
1 Communication with Jane McGinley RDH MBA Manager Fluoridation and Preventive Health
Activities Council on Access Prevention and Interprofessional Relations
2 Centers for Disease Control and Prevention Department of Health and Human Services
accessed Oct 21 2013 httpwwwcdcgovfluoridationstatistics2010statshtm
3 Centers for Disease Control and Prevention National Oral Health Surveillance System Caries
Experience - Percentage of 3rd Grade students with Caries Experience (treated or untreated tooth
If data from 43 states for the percentage of Grade 3 children with experience of dental decay is
compared with the 2008 percentages of the population in a state with Community Water
Fluoridation then the percentage of children with experience of dental decay decreases as the
percentage of the state population with Community Water Fluoridation increases (see Figure 1)
Figure 1
Correlation of Percentage of Grade 3 Children with Caries Experience and
Percentage of Population With Community Water Fluoridation for 43
Reporting States
0
10
20
30
40
50
60
70
80
0 10 20 30 40 50 60 70 80 90 100
State of Population With Community Water Fluoridation
Sta
te
of
Gra
de 3
Stu
den
ts w
ith
Cari
es E
xp
eri
en
ce
Data from CDC (2 3)
The description of the fluoridation laws in California Illinois and Nevada can be found on the
Association of State amp Territorial Dental Directors website(4 7 8)
The California fluoridation law AB 733 came into effect in 1995 requiring communities of 10
000 residents or more be supplied with fluoridated drinking water However the state did not
provide any funding to implement the legislation (California is unique in requiring fluoridation
without funding the practice)(4) The California Department of Health Services therefore had to
fund fluoridation initiatives from non-governmental sources ie the California Endowment
California Dental Association Foundation the First 5 Commission and others(5) From 1995 to
2011 the percentage of the California population receiving fluoridated drinking water has risen
from 17 to 625(6) 4 Dental Public Health Activities amp Practices Office of Oral Health California Department of Health
Services April 2002 httpwwwastddorgbestpracticesDES06002CAfluoridationpdf
5 Stock M Pollick H The CDA Foundation Model to Fluoridate Communities California Dental
Association Journal vol 40 no 8 649 - 655
httpwwwcdaorgPortals0journaljournal_082012pdf
6 California Dental Association Foundation
httpwwwcdafoundationorglearnadvocacyfluoridation
The State of Illinois passed a mandatory fluoridation state in 1967 and required all community
water systems to adjust fluoride levels in the drinking water to optimal levels within 1 year(7)
From 1962 when over 5000000 residents had optimally fluoridated drinking water by 2010
the number had risen to 11325132 (993 of the population on community water systems)(2)
7 Dental Public Health Activities amp Practices Division of Oral Health Illinois Department of Public
Health April 2002 httpwwwastddorgbestpracticesDES16007ILfluoridationpdf
The State of Nevada passed a mandatory fluoridation statute in 2000 for communities with
400000 or more residents(8) This was a result of the work of a statewide coalition that
included the Nevada Dental and Dental Hygienist Associations the Washoe and Clark County
District Health Departments the Clark County School District Junior League of Las Vegas
Head Start the Community College of Southern Nevada Dental Hygiene Program Health
Access Washoe County and Saint Maryrsquos Hospital For communities with less than 400000 the
implementation of fluoridation still required the vote of the majority voters in the community
The Las Vegas Water Authority and the City of Henderson started fluoridation in 2000
increasing the percentage of the population with fluoridated drinking water from 2 to 65 (8) 8 Dental Public Health Activities amp Practices Bureau of Family Health Services Nevada State Health
Division April 2002 httpwwwastddorgbestpracticesDES31002NVfluoridationbillpdf
Countries with Mandatory Laws on Fluoridation Countries that have mandated Community Water Fluoridation are Brazil Hong Kong
Malaysia Singapore Ireland Israel and some of the states in Australia
Singapore started fluoridating its water in 1956 based on the success of the fluoridation trials in
Grand Rapids Newburgh Evanston and Brantford Singapore became the first Asian country to
have 100 of its population benefitting from the implementation of fluoridated drinking water
Loh reported that ldquoThe ten year study on the effects of water fluoridation in Singapore showed
a decrease in caries prevalence in the children In the permanent dentition the reduction was
523 per cent for Chinese and 31 per cent for Malays in the 7 to 9 year old age group A similar
trend was observed in the mixed dentition in which the decrease was 325 per cent for Chinese
and 306 per cent for Malaysrdquo(9) By 2010 the population of the country was 5080000(10)
9 Loh T Thirty-eight years of water fluoridation--the Singapore scenario Community Dent
Health 1996 Sep13 Suppl 247-50
10 British Fluoridation Society One in a Million the facts about water fluoridation 3rd Edition
published March 2012) httpwwwbfsweborgonemillion0920One20in20a20Million20-
20The20Extent20of20Fluoridationpdf
Hong Kong started implementing community water fluoridation in 1961 and similar to
Singapore 100 of the population received access to fluoridated drinking water Lo and Wong
reported that ldquoThe mean DMFT score of the children deceased from 44 in 1960 to 15 in 1968
stayed at this level in the 1980 and 1986 surveys and further deceased to 08 in 2001 The
prevalence of dental fluorosis among the children surveyed in 1960 was 1 and this increased
to 59 and 70 in 1968 and 1980 respectively It was found in the 1986 and 2001 surveys that
the prevalences of fluorosis were 47 and 9 among children whose teeth developed at the
time when the respective water fluoride concentrations were 07 ppm and 05 ppmrdquo(11) The
population of Hong Kong was 6968000 in 2009(10) 11 LO ECM and WONG AHH Water fluoride concentration and fluorosis in Hong Kong in 1960-
2001 84th General Session and Exhibition of the International Association for Dental Research amp
1st Meeting of the Pan-Asian-Pacific Federation Brisbane Australia 28 June-1 July 2006 v 85 n
Sp B
The Malaysian cabinet approved a nationwide community water fluoridation program in 1972
(12) One of the states Sabah decided to stop fluoridation in 1989 due to concerns about
inadequate supervision in adding fluoride to the drinking water Oral Health Surveys in 2009
and 2007 indicated that children in Sabah had the worst oral health with 50 of 12 year-olds
having decay in their permanent teeth and children having an average of 3 teeth being(13)
Under the 10th Malaysian Plan in 2011 the federal and the Sabah state governments
reintroduced water fluoridation in Sabah(1314) In 2010 about 755 of the Malaysian
population or 20700000 people had fluoridated drinking water(1013) 12 Malaysian Dental Association Fluoride in Water
httpwwwmdaorgmy07_public_01healthcare_12htm
13 Sachdev N Fluoridation in Sabah Water for Cleaner Teeth French Tribunecom 28022011
From Levy IsraTo Jaeger ValerieCc Pim Carolyn gordonalphaweborg Diallo Aicha Penny Sutcliffe Paul Roumeliotis Michael Finkelstein
Hazel Lynn Robert KyleSubject FW Panorama - Privacy Security and other issuesDate Wednesday October 16 2013 122110 PM
Hello ValerieOttawa is part of Wave 4 Panorama implementation and we are gearing up increasingly to use thesystem where and if possible Thinking about it I am anticipating that this may need to be on theCOMOH (and alPHa) radar as it is something that will impact all health units and implies a majoroperational shift in vaccine delivery programs for all health units I have asked Carolyn Pim toconnect with our sister wave 4 units to share common experiences as we move forward ndash when wehave a roll up could I bring to COMOH Exec for discussion to explore whether there are broaderimplications for all members As an aside I have also asked the Ministry and their CIO to share with me any roll up learnings thatthey may have had already from previous waves (I understand that Niagara HU was a wave 1participant so if there is such a roll up of common experiences that others could learn fromperhaps you have it already and that could come to the exec too)Thanks Isra From Pim Carolyn Sent October 10 2013 1228 PMTo Christopher Mackie (christophermackiemlhuonca) Elizabeth Richardson(Elizabethrichardsonhamiltonca) H BSc M D F R C P (C) MPH Jim Chirico(jimchiriconbpsdhuca) Marlene Spruyt (spruytmtimiskaminghucom) Robert Kyle (Durham)Cc Levy IsraSubject Panorama - Privacy Security and other issues Dear colleagues Irsquom reaching out to you as fellow Panorama Wave 4 health units to ask about where yourorganizations are at in the process of signing agreements and completing Privacy ImpactAssessments and Threat Risk Assessments (TRAs) Ottawa Public Healthrsquos IT legal and informationsecurity advisors have made numerous requests to the MOHLTC for information (in particular theprovincial TRA) that we consider essential to develop our own risk assessment and PIA but havebeen told that information cannot be shared even with strict confidentiality and access controlsSo we are at somewhat of an impasse Isra emailed Arlene yesterday Arlene has forwarded ourconcerns to the Ministryrsquos CIO and Panorama lead but we havenrsquot had any response or discussionswith either of them yet Have your organizations identified similar concerns andor had interactions with the MOHLTC inthis respect Irsquod also be interested in knowing if your health units have flagged other (egoperational) implementation concerns Thanks
Carolyn ps Robert ndash you can ignore this request I talked with Sharan this morning about Durhamrsquos issuesso am including you now just for information Carolyn Pim MD FRCPC Associate Medical Officer of Health Meacutedecin adjointe en santeacute publique Ottawa Public Health Santeacute publique Ottawa 100 Constellation Cr Ottawa ON K2G 6J8 Tel teacutel (613) 580-6744 ext 23684Fax (613) 580-9641Connect With Ottawa Public Health
Suivez Santeacute publique Ottawa
This e-mail originates from the City of Ottawa e-mail system Any distribution use orcopying of this e-mail or the information it contains by other than the intendedrecipient(s) is unauthorized If you are not the intended recipient please notify meat the telephone number shown above or by return e-mail and delete thiscommunication and any copy immediately Thank you
Le preacutesent courriel a eacuteteacute expeacutedieacute par le systegraveme de courriels de la Ville dOttawaToute distribution utilisation ou reproduction du courriel ou des renseignements quisy trouvent par une personne autre que son destinataire preacutevu est interdite Si vousavez reccedilu le message par erreur veuillez men aviser par teacuteleacutephone (au numeacuteropreacuteciteacute) ou par courriel puis supprimer sans deacutelai la version originale de lacommunication ainsi que toutes ses copies Je vous remercie de votre collaboration
1
Smoke-Free Patios ndash An Amendment to the Smoke-Free Ontario Act
Date November 15 2013 Prepared for Council of Ontario Medical Officers of Health Prepared by York Region Public Health _____________________________________________________________________________ Issue
The Smoke-Free Ontario Act is the current provincial legislation that imposes smoking restrictions in workplaces and public places It prohibits smoking on restaurant and bar patios in instances where any portion of the seating area is covered by a roof With recent studies illustrating that exposure to second hand smoke outdoors poses similar risks to indoor exposure there has been growing public support to enhance smoking restrictions and make patios completely smoke-free
Background
With the implementation of the Smoke-Free Ontario Act in 2006 restaurant and bar patios became subject to smoking restrictions if any portion of the seating area was covered by a roof This allowed for patios without roof coverings to continue to allow smoking and as a result did not provide significant protection to patrons or staff from exposure to second hand smoke outdoors Many businesses chose to alter the design of their patios to allow smoking to continue In some cases patios became more crowded since smoking patrons who dine indoors often proceed outside onto licensed patios with their beverages to smoke York Region like most municipalities in Ontario is host to hundreds of patios being operated by restaurant owners and businesses With smoking prohibitions affecting only a small portion of these patios specifically ones with coverings the vast majority of patios still allow smoking to take place Patrons and employees on patios where smoking is not restricted are exposed to second hand smoke frequently This can contribute to increased disease and aggravation of existing health conditions From a business perspective the existing legislation has been viewed by many operators as unfair because some patios have permanent coverings which cannot be removed requiring a smoke-free status These business owners feel this creates an uneven playing field since they cannot provide an outdoor dining area for their smoking customers There is strong community support for smoke-free patios in Ontario A 2009 Rapid Risk Factor Surveillance System survey revealed 754 percent support in York Region while a Toronto Health Survey in 2011 indicated 74 percent public support
2
Current Status
Smoking is currently prohibited on restaurant and bar patios province-wide in four Canadian provinces and territories Alberta Newfoundland and Labrador Nova Scotia and Yukon A fifth province Prince Edward Island prohibits smoking on patios until 10 pm Since Ontario enacted legislation restricting smoking on patios in 2006 eight municipalities in Ontario have chosen to create bylaws that go beyond the Smoke-Free Ontario Act and enhance outdoor protection from second hand smoke by prohibiting smoking on patios completely The largest of those municipalities is the City of Ottawa Recently the Toronto Board of Health unanimously endorsed a report presented by their Medical Officer of Health recommending that restaurant and bar patios be made smoke-free through an amendment to the Smoke-Free Ontario Act
Key Considerations
There should be no significant financial burden to local Boards of Health resulting from a smoke-free patio amendment to the Smoke-Free Ontario Act Inspection and enforcement for the Smoke-Free Ontario Act is currently 100 percent funded by the Ministry of Health and Long-Term Care Following an introductory period of education on the amendment a complaint response model of service delivery would ensure ongoing compliance with smoke-free requirements A complete ban of smoking on patios would eliminate the widely-held perception by business owners that the current legislation creates an uneven playing field for business Since Smoke-Free Ontario Act inspections of patios began in 2006 operators have expressed the opinion that if patios need to be smoke-free for the protection of the public they should all be smoke-free to avoid undue hardship for individual businesses and to provide protection uniformly across the Province
Next steps
York Region Public Health intends to seek support from Medical Officers of Health across the Central East Tobacco Control Area Network (CETCAN) to advocate to the Ministry of Health and Long-Term Care for an amendment to the Smoke-Free Ontario Act prohibiting smoking on all restaurant and bar patios York Region is also in the process of requesting that its Regional Council advocate to the Minister of Health and Long-Term Care on the issue
Updating and Modernizing O Regulation 565 (Public Pools)
Date November 15 2013
Prepared for Council of Ontario Medical Officers of Health
Prepared by York Region Public Health _____________________________________________________________________________ Background Recent drownings at public pools in Ontario have highlighted the issue of water-borne illness and injury The current pool regulation under Ontariorsquos Health Protection and Promotion Act O Regulation 565 (Public Pools) is outdated It does not accurately reflect new pool technology and design or the changing use of public pools Neither does it incorporate admissions standards recommended by the Office of the Chief Coroner Further O Regulation 565 does not have short-form wording or set fines associated with it This limits public health enforcement capabilities What is the impact Updating O Regulation 565 (Public Pools) to address recent changes in pool technology design and uses and to include Coroner-recommended admissions standards would help improve pool safety Establishing short-form wording for O Regulation 565 would enhance enforcement related to public pools Currently the only enforcement available to Public Health Inspectors for dealing with non-critical regulatory infractions in public pools is the issuance of a Part III summons This involves a considerable amount of resources for a possible small fine With the development of inspection disclosure systems such as YorkSafe there is an even greater need to develop a method to effectively address repeated pool operator non-compliance with non-critical issues Next steps Public health units should advocate to the Province to 1) Conduct a review of O Regulation 565 (Public Pools) to address shortcomings Proposed changes to the
regulation should include a requirement for ownersoperators of public pools to advise the local Medical Officer of Health of any change in the use of a facility and the addition of the Coronerrsquos recommended admission standards
2) Provide short-form wording for O Regulation 565 so that public health inspectors can better deal with pool operator non-compliance
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
Page 4 of 8 ndash DRAFT FOR COMOH DISCUSSION
Survey Question How much value do alPHarsquos events provide for the money
Survey Question How can alPHa make its events more valuable to you Please share any suggestions regarding future topics speakers formats duration locations or any other event component that is important to you
Comments about content bull Expert speakerpanels on emerging or hot topics
(2) bull More engaged dialogue with Ministry rather than
just updates bull Fewer Ministry updates (3) bull Content on medicalPH issues is better left to PHO
TOPHC and joint conferences (2) bull alPHa should stick to Ministrypoliticspolicysenior
PH supportPHU support on key priorities (eg November practical conference on HKP report)
bull For COMOH more discussion bull More time for section activities like face-to-face
COMOH meetings
bull More facilitated work groups of COMOH members to respond to public health practice questions
bull More focus on rural and northern issues bull Infection Control Logistical Considerations bull Consider partnering with other groups bull More collaboration with PHO and OPHA events bull Use of video conferencing bull Less frequentfewer meetings (2) bull Connect with CME Location bull Consider other venues than TO
( ) brackets indicate that more than one response included a similar comment
More than enough value 7 11A lot of value 34 52Some value 22 34A little value 2 3Not enough value 0 0Totals 65 100
All Responses for those who Attended at least One Event in the Last 2 Years
All COMOH ResponsesMore than enough value 4 15A lot of value 13 48Some value 9 33A little value 1 4Not enough value 0 0Totals 27 100
Page 5 of 8 ndash DRAFT FOR COMOH DISCUSSION
SECTION 3 VALUE FOR MEMBERSHIP
Survey Question What do you value the most about your alPHa membership
The comments provided in response to the text response question What is the most important benefit of alPHa membership for you personally supported the answers illustrated in the chart above 15 of the 20 comments provided focussed on the importance of opportunities to interact with colleagues across the province The next most important benefit mentioned was the support for COMOH members to work on public health issues together When asked What is the most important benefit of alPHa membership for your health unit COMOH members emphasized the following bull A coordinated and collective voice in advocating for public health issues and the public health sector (9) bull Opportunities to connect with other public health units to share experiences and best practices (8) bull Maintaining relationships with government both politicians and bureaucrats (3) and bull Support for boards of health (3)
Page 6 of 8 ndash DRAFT FOR COMOH DISCUSSION
Overall Level of Satisfaction
SECTION 4 LOOKING TO THE FUTURE
The questions in this section were asked to obtain input from alPHa members regarding a proposal from alPHarsquos Board of Directors to focus the Association on five service areas COMOH members were asked to indicate their level of agreement with the proposed areas of focus COMOH responses compared to the overall survey responses were as follows
To explore some proposed changes to Association services COMOH members were asked to provide their level of agreement with the following questions
COMOH Responses BOH Section Affiliates All Survey Responses
Strongly Agree
AgreeNeither Agree or Disagree
DisagreeStrongly Disagree
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1Promoting the role and value of local public health units
15 9 2 0 0 26 92 93 95 94
2
Providing important information to members about trends and events that will impact the public health system and management of public health units
10 8 8 0 0 26 69 97 86 85
3Facilitating professional networking and information sharing
13 10 3 0 0 26 88 83 82 85
4
Providing professional development to support excellence in public health unit leadership management and governance
3 15 7 1 0 26 69 83 86 79
5
Responding to public health sector issues when it makes the most sense to have a collective voice ie issues that impact the structure and funding of the public health sector and public health units and issues that have a broad focus on population health
15 8 2 0 1 26 88 97 95 93
PROPOSED AREAS OF FOCUS
COMOH Responses BOH Section Affiliates All Survey Responses
Strongly Agree
AgreeNeither Agree or Disagree
DisagreeStrongly Disagree
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1
COMOH and other professional groups within alPHa should do their own advocacy while alPHa supports members to share and support each others advocacy efforts
7 6 6 6 1 26 50 58 45 52
2
alPHa should provide support to action-oriented inter-professional work groups on priority public health unit issues and member resolutions
4 13 5 3 1 26 65 81 86 77
PROPOSALS
Page 8 of 8 ndash DRAFT FOR COMOH DISCUSSION
COMOH members were also asked to indicate the level of acceptability for some possible changes to alPHarsquos services and way of doing business
COMOH Responses BOH Section Affiliates All Survey Responses
Very Acceptable
Somewhat Acceptable
Neither Acceptable or Unacceptable
Somewhat Unacceptable
Very Unaccept
able
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1Single conference with additional face-to-face section meetings
21 2 0 1 0 24 96 68 80 81
2alPHa to offer alternatives like webinars on focussed topics
13 6 1 4 0 24 79 50 90 71
3Coordinate COMOH meetings with PHO OMA or Ministry events
16 4 2 0 0 22 91 na na --
4
Increase focus on building leadership and management capacity for health unit CEOs and senior management
7 9 4 3 0 23 70 na 70 70
5
Would it be acceptable for alPHa to request voluntary financial contributions from member PHUs in addition to annual fees
3 5 5 4 5 22 36 7 26 21
6
Would it be acceptable for alPHa to request voluntary in-kind staff contributions from member PHUs to expand alPHas capacity eg communications policy work group support
7 11 1 1 3 23 78 31 45 50
7Would it be acceptable to you for alPHa to discontinue staff support for COMOH (BOH Section)
0 4 1 5 14 24 17 11 na 14
8
Would it be acceptable to you for alPHa to reduce the amount of staff support for COMOH (BOH Section)
1 6 1 8 6 22 32 26 na 29
9
Would it be acceptable to you for alPHa to provide supports to MOHs and AMOHs (BOH Members) without maintaining COMOH (BOHs) as a section of the association
3 2 3 2 12 22 23 17 na 20
10
Would it be acceptable to you for alPHas Board of Directors to move from the current representational model to a skills-based strategic model ie board membership would be based on the skills needed to carry out alPHas strategic plan
6 11 2 1 3 23 74 56 56 62
11
Would it be acceptable to you for alPHas President Vice-President and Treasurer to be elected from the full membership of the alPHa Board of Directors (rather than the current model of alternating between BOH and COMOH members)
10 8 1 2 2 23 78 70 70 73
PROPOSED CHANGES
1 Council of Ontario Medical Officers of Health Terms of Reference
ASSOCIATION OF LOCAL PUBLIC HEALTH AGENCIES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
TERMS OF REFERENCE NAME 1 The name of the organization shall be ldquoThe Council of Ontario Medical Officers of
Health a section of the Association of Local Public Health Agencies (alPHa)rdquo hereinafter referred to as ldquothe Councilrdquo
MISSION 2 As local leaders in public health we are committed to improving the health of
Ontarians and increasing health equity by strengthening Ontariorsquos public health system We achieve this through system leadership and coordination in collaboration with the provincial government and other organizations and through evidence-informed advocacy on public health policy
OBJECTIVES 3 The objectives of the Council shall be
a) To provide strong province-wide leadership in public health
b) To advocate for health protection and promotion policies and programs that maintain and improve the health of Ontarians
c) To promote and maintain the highest standards for Ontariorsquos public health
programs and services
d) To support the planning implementation and evaluation of effective and efficiently run public health programs and services
e) To act as a forum for sharing information and resources and for addressing and
discussing public health issues both amongst the Councilrsquos members and other agencies that support the goals of alPHa eg Ontario Medical Association Ontario Public Health Association etc
f) To engage with and to provide public health and related policy advice to alPHa
the Chief Medical Officer of Health the Ontario Ministries of Health and Long-Term Care (including the Health Promotion and Public Health Divisions) Children
2 Council of Ontario Medical Officers of Health Terms of Reference
and Youth Services and other provincial ministries Public Health Ontario Health Canada the Public Health Agency of Canada and other public health partners
g) To promote and protect the professional interests of its members
h) To provide support to individual members as needed
i) To seek recognition for outstanding practice from among the members
j) To support evidence based practice of public health medicine
k) To engage and involve the membership to participate in COMOHrsquos endeavours
l) To mentor Public Health and Preventive Medicine Residents
MEMBERSHIP 4 Membership on the Council in each of the following categories is subject to the
limitations imposed by the current terms of reference and all policies and governing documents of the Association of Local Public Health Agencies Benefits of membership in each category are included in Appendix A These shall be subject to regular review and may be suspended under certain circumstances
Active membership in the Council shall be open to all Associate Medical Officers of Health and all full-time Medical Officers of Health whose Boards of Health are members of alPHa Such members shall have full voting privileges and may hold office in the Council Associate membership shall be open to all full and part-time physicians employed by a Board of Health that is a member of alPHa Such members shall not have voting privileges nor hold office
Affiliate membership shall be open to the following individuals interested in furthering the objectives of the Council
bull Public Health and Preventive Medicine Residents and Public Health and Preventive Medicine Residency Program Directors
bull Federal public health physicians working in Ontariorsquos First Nations communities
bull other public health or related physicians including those employed by a Board of Health that is not a member of alPHa
Such members shall not have voting privileges nor hold office
3 Council of Ontario Medical Officers of Health Terms of Reference
Emeritus membership shall be open to all former members who have retired after five (5) or more years of Active membership subject to the nomination in writing of two (2) active members in good standing endorsement of the Executive Committee and approval of the Council by majority vote at a general meeting Such members shall have neither voting privileges nor hold office but may be invited to attend general meetings Honorary membership shall be open to any non-active or associate member subject to the nomination in writing of two (2) active members in good standing endorsement of the Executive Committee and approval of the Council Such members shall have neither voting privileges nor hold office but may be invited to attend general meetings
OFFICERS 5 The Officers of the Council shall be the Chair Vice-Chair and immediate Past Chair
6 The Chair shall prepare the agendas of all Council meetings She shall preside and
preserve order at all such meetings shall ensure that these Terms of Reference are upheld and enforced and shall contribute to the supervision and evaluation of any Public Health and Preventive Medicine Resident who is on a placement with alPHa
7 The Vice-Chair shall fulfill the duties of the Chair in hisher absence The immediate
Past Chair may fulfill the duties of the Chair or Vice-Chair in their absences 8 The Chair shall normally serve a term of one (1) year which is renewable once and
after which the Vice-Chair shall normally assume the vacated office COMMITTEES 9 The Council shall elect seven (7) active members one from each of alPHarsquos regions
and the active member who is scheduled to serve as the President or immediate Past-President of alPHa to represent it on the alPHa Board of Directors These seven (7) members shall constitute the Councilrsquos Executive Committee and shall serve a term of at least one (1) year The Chair and Vice-Chair shall be elected from among the Executive Committee members If alPHarsquos immediate Past President is an active member she shall be an ex-officio member of the Executive Committee
10 The mandate of the Executive Committee shall be to facilitate the achievement of
the objectives of the Council by fulfilling the following
a Identifying priorities 1
1 See Appendix B Planning Cycle to Identify Priorities for COMOH
and ensuring the development of briefing documents and or recommendations as appropriate for the consideration of the Council
4 Council of Ontario Medical Officers of Health Terms of Reference
b Setting agendas and otherwise ensuring preparations for Council meetings c Ensuring the fulfillment of the direction of Council d Responding in a timely fashion to time-sensitive public health matters in
accordance with the Executive Committeersquos understanding of the perspective of the Council
e Engaging with the Chief Medical Officer of Health Associate Chief Medical Officers of Health and other provincial public health leaders and
f Representing Council at public and partner agency forums including the Public Health Leadership Council which shall normally include membership from the Officers of the Council and two other Executive Committee members as selected by agreement among the Executive
g Identifying opportunities for the recognition of outstanding practice from among the members including the annual nomination of at least one member for the alPHa Distinguished Service Award
11 The Executive Committee shall meet and correspond in the manner and at the times
and if required places as deemed necessary by the Chair to conduct the business of the Council A quorum shall consist of four (4) members
12 The Executive Committee shall have the power to strike committeestask or working
groups to assist it in carrying out the business of the Council 13 The Council may by special resolution remove a member of the Executive
Committee before the completion of hisher term of office and may elect a successor to complete the term The special resolution shall require a majority vote of 67 of the members present and voting at the meeting at which the special resolution is considered
14 A Nominating Committee shall consist of the three (3) most recent Past Chairs who
are able to serve and shall be chaired by the immediate Past Chair The Nominating Committee shall prepare a list of proposed Officers and Executive Committee members for the consideration of the Council at its Annual General Meeting
MEETINGS 15 The Council shall hold at least four (4) general meetings per year in a manner and at
the times and if required places as deemed necessary by the Executive Committee to share information direct and assist the Executive Committee in conducting the business of the Council
16 The Council shall hold its Annual General Meeting during and at the same place as
the alPHarsquos Annual Conference
5 Council of Ontario Medical Officers of Health Terms of Reference
17 The Council shall hold a special meeting at the call of the Chair or upon the written request specifying the purpose of such meeting of at least five (5) active members Council members must be given at least 48 hours notice of any special meeting
18 Only Councilrsquos active and associate members and alPHa staff are entitled to attend
general and special meetings of the Council Other members and non-members may be invited to attend all or part of such meetings as determined by the Chair preferably in consultation with the Executive Committee Non-members who come to such meetings without an invitation may attend all or part of the meeting by a majority vote of the active members present and voting
19 The Chair shall prepare the agendas for such meetings and shall normally include
reports from the Chair and the Councilrsquos committeestask or working groups and representatives to external bodies alPHarsquos Executive Director shall ensure that the minutes shall be recorded and promptly distributed to the Section
20 A quorum for all such meetings shall be ten (10) active members 21 The Council shall normally be notified in a manner deemed appropriate by the Chair
of such meetings at least one (1) month prior to their being held 22 A majority vote of the members present at such meetings and voting shall make
Council decisions In the case of a tied vote the Chair shall cast the deciding vote The Executive Committee shall ensure that actions arising from such decisions at such meetings are implemented and monitored
23 The Chair may solicit advice from the Council through the use of teleconferencing
and alPHarsquos electronic mailing lists in order to gain an understanding of the overall perspective of the Council (see 10d)
ELECTIONS 24 The Officers and Executive Committee members shall be elected at the Sectionrsquos
Annual General Meeting The Nominating Committee Chair or hisher designate shall present a list of nominations Additional nominations from the floor shall also be considered Each Officer and Executive Committee member shall be elected by secret ballot if necessary by a majority of the active members present and voting In the case of a tie the Chair shall cast the deciding vote
AMENDMENTS 25 The Councilrsquos Terms of Reference may be amended from time to time by the
Executive Committee provided the Committee receives notice of such proposed amendments at least one (1) month prior to the meeting at which the amendments
6 Council of Ontario Medical Officers of Health Terms of Reference
will be considered Such amendments shall be ratified by the Council at the next general meeting or the Annual General Meeting as the case may be
26 The Executive Committee shall review the Terms of Reference as required and not
less than once every two years Original September 1987 1st Revision October 2000 2nd Revision July 2001 3rd Revision December 2003 4th Revision February 2008 5th Revision June 2009 6th Revision June 2011 7th Revision June 2013
7 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX A
COMOH Membership Benefits Active Membership
bull Entitled to attend all meetings of the Section bull May hold office on the COMOH Executive Committee alPHa Board of Directors
Standing Committees bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Associate Membership
bull Entitled to attend all meetings of the Section bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Affiliate Membership
bull May attend meetings or parts thereof subject to approval of Chair bull May serve on ad-hoc committees of the Section subject to the approval of the
Executive Committee bull Discounted registration rates for alPHa Conferences (for Public Health and
Preventive Medicine Residents) bull Upon written request and subject to COMOH Executive approval Affiliate
Members may subscribe to comohlistsalphaweborg The approval will be reviewed on an annual basis in order to determine if the Affiliate Member can remain a subscriber to mohsalphaweborg
Emeritus Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair bull Enjoy discounted registration rates for alPHa Conferences and regular COMOH
meetings bull Subscription to comohlistsalphaweborg electronic mailing list bull Full access to alPHa Web site bull May represent alPHa COMOH on selected external committees and working
groups Honorary Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair
8 Council of Ontario Medical Officers of Health Terms of Reference
bull May represent alPHa COMOH on selected external committees and working groups subject to the approval of the COMOH or alPHa Executive Committee as appropriate
9 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX B
Planning Cycle to Identify Priorities for COMOH
1 There shall normally be a COMOH membership strategic planning retreat every four years In recognition of the dynamic environment of public health the need for and timing of such a retreat shall be at the discretion of the Executive Committee in consultation with the membership
2 The COMOH Executive is responsible (through the creation of a subcommittee of COMOH members) for ensuring the preparation for the COMOH retreats with resources to include those provided by alPHa
3 Leadership for action on COMOH priorities will be recruited from among the COMOH membership in order to make good use of the full base of capacity of the membership The resources to support actions will be recruited from both within and beyond the COMOH membership employing other public health professionals that reside within the broader public health system and community
4 The COMOH Executive shall ensure an annual review of strategic priorities and initiatives and the development of a draft report of the same for the review of the members at the June meeting
2013 Strategic Planning
Considerations for COMOH
As part of its strategic planning discussions alPHarsquos Board has been considering changes to the level of support provided to member sections A member survey is being carried out over the fall to determine options acceptable to alPHa members The following approach to support is put forward as a proposal for the consideration of COMOH Note that the feasibility of the points below depend upon future decisions of the alPHa board They assume that COMOH remains part of alPHa but becomes more independent in administering meetings
1 alPHa can provide to COMOH staff support (Gord Fleming) amounting to 02 FTE or one day per week This is a reduction from the current level of 35 days per week COMOH can choose to use the support any way it wants writing COMOH letters meeting minutes agenda support special projects etc
2 In addition to 02 FTE alPHa staff would provide support for up to 4 face-to-face meetings per year One meeting would be concurrent to alPHarsquos annual conference in June The timing of other meetings could be negotiated The support includes consulting on the development of the program arranging for speakers registration for the event arranging venue AV support and hospitality services
3 In addition to 02 FTE alPHa staff would provide support for setting meeting dates and any polling required to establish dates Note that the individual supporting this function would be Karen Reece
4 COMOHrsquos Executive and Section would continue to have access to online supports through the alPHa including the COMOH Listserve and a group page for posting agendas minutes and other resources on the alPHa website
5 alPHa staff (Linda Stewart and Gord Fleming) can also start participating on CMOH calls as a way to be up-to-date on issues related to COMOH
6 Other than what is outlined above COMOH would be expected to prepare agendas and take minutes for its Executive and Section meetings The Executive would be expected to operate more independently than it does now but would be able to access the supports outlined above
Prepared by Linda Stewart Executive Director
From comoh-bounceslistsalphaweborg on behalf of Christopher MackieTo MOH ListserveSubject [comoh] Fw URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)Date Wednesday October 30 2013 91241 AMAttachments ATT00249txt
For AMOHs and PHPM residents who didnt receive the initial email
Chris
Christopher Mackie MD MHSc FRCPCMedical Officer of Health and CEOMiddlesex-London Health Unit50 King St LondonON N6A 5L7 O 519 663 5317 ext 2444 wwwhealthunitcomFrom Pisko Laura (MOHLTC)Sent Tuesday October 29 2013 759 PMTo kbarkeralgomapublichealthcom malcolmlockbchuorg davidcchatham-kentcarobertkyledurhamca proumeliotiseohuca fwarshelginhealthonca mohelginhealthoncahlynnpublichealthgreybruceonca malcolmlockhnhuorg hnmohhnhuorglnoseworthyhkpronca bobnosalhaltonca elizabethrichardsonhamiltoncarschabashpechuonca ncameronhuroncountyca drimgemmillkflapublichealthcamohkflapublichealthca suditranadecounty-lambtononca paulastewarthealthunitorgChristopher Mackie valeriejaegerniagararegionca jimchiriconbpsdhuca jarthursnwhuoncaisralevyottawaca dnealoxfordcountyca davidmowatpeelregionca mklassenpdhuoncarpellizzaripcchuca rosemarieramsinghporcupinehuonca mcorriveaurcdhucomcharlesgardnersmdhuorg sutcliffepsdhucom davidwilliamstbdhucomspruytmtimiskaminghucom dmckeowntorontoca lnolanregionofwaterloocanicolamercerwdghuorg aheimannwechealthunitorg karimkurjiyorkcaCc coreywesleytbdhucom CindyBaker-Barillsmdhuorg Donna Kosmack pilonlsdhucomPaulaMuiskflapublichealthca sthibautorontoca Mueller Daina (MOHLTC) Gordon Marcus(MOHLTC) andreakitahamiltoncaSubject URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)
Dear Colleagues The ministry has received reports that some tobacco vendors across the province aregiving away single cigarettes with the purchase of tobacco products It is the ministryrsquosposition that giving out free single cigarettes does not violate subsection 31(3) of theSmoke-Free Ontario Act (ldquoSFOArdquo) Although the practice of giving out free singlecigarettes may promote the sale of tobacco products it does not take the form of aldquoproduct enhancement product association or promotional materialrdquo and therefore doesnot fall within the scope of subsection 31(3) of the SFOA We have confirmed with Health Canada that this practice may violate section 29(b) of thefederal Tobacco Act As such Health Canada is requesting that you notify them in writingand I am directing you to communicate with them via email and provide to them as manydetails as possible Emails should be sent to Tobacco-Ontariohc-scgcca and thesubject line should read ldquoViolation of Section 29(b) of Tobacco Actrdquo This will ensurethat the complaints are given priority status by Health Canada We will continue to monitor
this situation and liaise with our colleagues at Health Canada Please share this information with your tobacco control staff and contact me or DainaMueller Manager Tobacco Control Unit Health Promotion Implementation Branch atdainamuellerontarioca with any questions RegardsLaura Laura A PiskoDirectorHealth Promotion Implementation BranchHealth Promotion DivisionMinistry of Health and Long Term Care416-327-7445 (office)416-451-3185 (mobile) Marcus Gordon - EA (416)326-0625 for urgent issues
========= Middlesex-London Health Unit E-Mail Disclaimer =============______________________________________________________________
Private and confidential intended only for named recipient If otherwisereceived please destroy immediately Health information in this email isonly general information and is not intended to replace an in personconsultation with a medical professional nor is it intended to providemedical advice Individual circumstances of which we are not aware mayaffect the information provided herein and as such the Middlesex-LondonHealth Unit assumes no liability or responsibility for your reliancethereon The Middlesex-London Health Unit works under the authority of theHealth Protection and Promotion Act and this correspondence may be used toassess your needs for public health services (519-663-5317 ext 2448)______________________________________________________________
From Gardner CharlesTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes (RayCopesoahppca)
George Pasut (GeorgePasutoahppca) Peter Cooney (petercooneyhc-scgcca)Cc Ito DickSubject Discontinuation of Fluoridation in MuskokaDate Tuesday October 22 2013 125254 PM
Hello Colleagues
As I reported in my email below on September 26th fluoridation has come under challenge again inSimcoe Muskoka I am now very unhappy to report that despite our best efforts last night theDistrict Council of Muskoka voted to remove fluoride from municipal drinking supplies across theDistrict This brings to an end fluoridation in all of Simcoe and Muskoka (with the exception of Base Borden)ndash though New Tecumseth will be conducting a plebiscite on the question of fluoridation with themunicipal election next October Defending community water fluoridation has drained a great deal of time human resources andcommitment from other priorities and has been exhausting here in SMDHU as I am sure it hasbeen in many other health units While the outcomes have been very disappointing I have beenimpressed by the professionalism and dedication that SMDHU staff members have shown inshouldering this burden In particular our dental consultant Dr Ito has provided us with much ofthe foundational knowledge and the local research essential to our efforts and has very frequentlyattended and presented at council meetings and other public events I would also like to thank themany of you who have offer and provided support including advocacy letters and informationresources Over the years Dr Peter Cooney Chief Dental Officer of Health of Canada has beenvery helpful attending and presenting with us at council meetings and at public consultationevents We will of course continue our oral health surveillance of the children of Muskoka documentingand reporting in future years on the increase in dental decay that we anticipate will occur Suchsurveillance is the foundation of our advocacy both to municipal politicians and to the province I am very concerned that our experience will continue to repeat itself across the province unlessthere is strong leadership provincially It is with this in mind that I raise the followingrecommendations for your consideration
1 That we collectively (with PHOrsquos leadership) conduct high quality publish-worthy researchdocumenting the impact on dental decay that occurs in those municipalities throughoutOntario that in recent years have discontinued community water fluoridation This could bepart of a larger study on such municipalities across the country and it could also be part ofa study documenting overall oral health (including fluoridation coverage) in the province(and possibly across the country)
2 That COMOH engage with our Chief MOH to advocate for the province to require allmunicipal water supplies to be fluoridated (the exception of course being those withnaturally sufficient fluoride concentrations) This could built upon the alPHa position to
Gordon
Highlight
Gordon
Highlight
date (A11-00 - Community Water Fluoridation) on the CMOH position (Oral Health ndash) and on theemail discussion generated on the COMOH listserv some months back re Richardrsquosproposal (calling on the province to fund municipal water fluoridation)
Valerie I request that this be an item for our COMOH meeting on November 15th Sincerely Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorg From Gardner Charles Sent Thursday September 26 2013 245 PMTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes(RayCopesoahppca)Subject Community Water Fluoridation Under Challenge Again in Simcoe Muskoka Hello Colleagues You may wish to know that community water fluoridation (CWF) is again under challenge in SimcoeMuskoka specifically both in Tottenham (Town of New Tecumseth in Simcoe County) and for theentire District of Muskoka On Monday September 23 Committee of the Whole Council of theTown of New Tecumseth voted to submit application to discontinue community water fluoridation(CWF) in the town of Tottenham despite presentations to the contrary from our dental consultantDr Ito and from me The next Council meeting is scheduled for Monday Sept 30 at which lastMondayrsquos (Sept 23) votes will be ratified
Since Monday I have spoken with the Mayor of the Town of New Tecumseth and with most of thecouncilors encouraging deferral of a decision on Monday to allow the town more time to make afully informed decision
This is the second time in recent years that the issue of discontinuing CWF in Tottenham has beenraised at council This issue is also scheduled to return again to the District of Muskoka Council on
October 21st where I will be presenting in response to deputations in opposition to fluoridation
Outside of Base Borden Tottenham is the only community with fluoridated water in SimcoeCounty The health unitrsquos own screening data between 2011 and 2013 shows that Tottenhamrsquos
Gordon
Highlight
children as well as those in Muskoka have a lower rate of dental decay than Simcoe Muskokacommunities without CWF
Sincerely
Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorgChuck Gardner MOH
November 04 2013
Mandatory State Laws on Fluoridation Thirteen states Puerto Rico and the District of Columbia have laws intended to provide
statewide fluoridation These states and the year that the fluoridation legislation was passed are
District of Columbia (1952) Connecticut (1965) Kentucky (1966) Illinois (1967) Minnesota
(1967) Ohio (1969) South Dakota (1969) Georgia (1973) Nebraska (1973 and 2008)
California (1995) Delaware (1998) Puerto Rico (1998) Nevada (1999) Louisiana (2008) and
Arkansas (2011) (see Table 1) The sizes of the public water systems or countiescommunities
affected and exemption provisions vary by state Table 1
STATES THAT HAVE MANDATORY LAWS ON FLUORIDATION -2011
State (1) Year of
Fluoridation
Legislation (1)
Population
served by
Fluoridated
CWS (2)
Persons
receiving
fluoridated
water (2)
State
Average
Caries
Experience
of Grade 3
Students (3)
Arkansas 2011 647 1724131 64
California 1995 621 22812721 709
Connecticut 1965 910 2370423 406
Delaware 1998 862 705344 545
Georgia 1973 921 8924598 52
Illinois 1967 993 11325132 532
Kentucky 1966 999 4334223 598
Louisiana 2008 407 1846149 657
Minnesota 1967 988 4117266 549
Nebraska 1973 and 2008 702 1001665 593
Nevada 1999 702 1001665 649
Ohio 1969 877 8772683 512
South Dakota 1969 948 642942 623
District of
Columbia
1952 1000 595000
Puerto Rico 1998
United States 739 204283554
2010 Statistics for population fluoridated and number of people
1 Communication with Jane McGinley RDH MBA Manager Fluoridation and Preventive Health
Activities Council on Access Prevention and Interprofessional Relations
2 Centers for Disease Control and Prevention Department of Health and Human Services
accessed Oct 21 2013 httpwwwcdcgovfluoridationstatistics2010statshtm
3 Centers for Disease Control and Prevention National Oral Health Surveillance System Caries
Experience - Percentage of 3rd Grade students with Caries Experience (treated or untreated tooth
If data from 43 states for the percentage of Grade 3 children with experience of dental decay is
compared with the 2008 percentages of the population in a state with Community Water
Fluoridation then the percentage of children with experience of dental decay decreases as the
percentage of the state population with Community Water Fluoridation increases (see Figure 1)
Figure 1
Correlation of Percentage of Grade 3 Children with Caries Experience and
Percentage of Population With Community Water Fluoridation for 43
Reporting States
0
10
20
30
40
50
60
70
80
0 10 20 30 40 50 60 70 80 90 100
State of Population With Community Water Fluoridation
Sta
te
of
Gra
de 3
Stu
den
ts w
ith
Cari
es E
xp
eri
en
ce
Data from CDC (2 3)
The description of the fluoridation laws in California Illinois and Nevada can be found on the
Association of State amp Territorial Dental Directors website(4 7 8)
The California fluoridation law AB 733 came into effect in 1995 requiring communities of 10
000 residents or more be supplied with fluoridated drinking water However the state did not
provide any funding to implement the legislation (California is unique in requiring fluoridation
without funding the practice)(4) The California Department of Health Services therefore had to
fund fluoridation initiatives from non-governmental sources ie the California Endowment
California Dental Association Foundation the First 5 Commission and others(5) From 1995 to
2011 the percentage of the California population receiving fluoridated drinking water has risen
from 17 to 625(6) 4 Dental Public Health Activities amp Practices Office of Oral Health California Department of Health
Services April 2002 httpwwwastddorgbestpracticesDES06002CAfluoridationpdf
5 Stock M Pollick H The CDA Foundation Model to Fluoridate Communities California Dental
Association Journal vol 40 no 8 649 - 655
httpwwwcdaorgPortals0journaljournal_082012pdf
6 California Dental Association Foundation
httpwwwcdafoundationorglearnadvocacyfluoridation
The State of Illinois passed a mandatory fluoridation state in 1967 and required all community
water systems to adjust fluoride levels in the drinking water to optimal levels within 1 year(7)
From 1962 when over 5000000 residents had optimally fluoridated drinking water by 2010
the number had risen to 11325132 (993 of the population on community water systems)(2)
7 Dental Public Health Activities amp Practices Division of Oral Health Illinois Department of Public
Health April 2002 httpwwwastddorgbestpracticesDES16007ILfluoridationpdf
The State of Nevada passed a mandatory fluoridation statute in 2000 for communities with
400000 or more residents(8) This was a result of the work of a statewide coalition that
included the Nevada Dental and Dental Hygienist Associations the Washoe and Clark County
District Health Departments the Clark County School District Junior League of Las Vegas
Head Start the Community College of Southern Nevada Dental Hygiene Program Health
Access Washoe County and Saint Maryrsquos Hospital For communities with less than 400000 the
implementation of fluoridation still required the vote of the majority voters in the community
The Las Vegas Water Authority and the City of Henderson started fluoridation in 2000
increasing the percentage of the population with fluoridated drinking water from 2 to 65 (8) 8 Dental Public Health Activities amp Practices Bureau of Family Health Services Nevada State Health
Division April 2002 httpwwwastddorgbestpracticesDES31002NVfluoridationbillpdf
Countries with Mandatory Laws on Fluoridation Countries that have mandated Community Water Fluoridation are Brazil Hong Kong
Malaysia Singapore Ireland Israel and some of the states in Australia
Singapore started fluoridating its water in 1956 based on the success of the fluoridation trials in
Grand Rapids Newburgh Evanston and Brantford Singapore became the first Asian country to
have 100 of its population benefitting from the implementation of fluoridated drinking water
Loh reported that ldquoThe ten year study on the effects of water fluoridation in Singapore showed
a decrease in caries prevalence in the children In the permanent dentition the reduction was
523 per cent for Chinese and 31 per cent for Malays in the 7 to 9 year old age group A similar
trend was observed in the mixed dentition in which the decrease was 325 per cent for Chinese
and 306 per cent for Malaysrdquo(9) By 2010 the population of the country was 5080000(10)
9 Loh T Thirty-eight years of water fluoridation--the Singapore scenario Community Dent
Health 1996 Sep13 Suppl 247-50
10 British Fluoridation Society One in a Million the facts about water fluoridation 3rd Edition
published March 2012) httpwwwbfsweborgonemillion0920One20in20a20Million20-
20The20Extent20of20Fluoridationpdf
Hong Kong started implementing community water fluoridation in 1961 and similar to
Singapore 100 of the population received access to fluoridated drinking water Lo and Wong
reported that ldquoThe mean DMFT score of the children deceased from 44 in 1960 to 15 in 1968
stayed at this level in the 1980 and 1986 surveys and further deceased to 08 in 2001 The
prevalence of dental fluorosis among the children surveyed in 1960 was 1 and this increased
to 59 and 70 in 1968 and 1980 respectively It was found in the 1986 and 2001 surveys that
the prevalences of fluorosis were 47 and 9 among children whose teeth developed at the
time when the respective water fluoride concentrations were 07 ppm and 05 ppmrdquo(11) The
population of Hong Kong was 6968000 in 2009(10) 11 LO ECM and WONG AHH Water fluoride concentration and fluorosis in Hong Kong in 1960-
2001 84th General Session and Exhibition of the International Association for Dental Research amp
1st Meeting of the Pan-Asian-Pacific Federation Brisbane Australia 28 June-1 July 2006 v 85 n
Sp B
The Malaysian cabinet approved a nationwide community water fluoridation program in 1972
(12) One of the states Sabah decided to stop fluoridation in 1989 due to concerns about
inadequate supervision in adding fluoride to the drinking water Oral Health Surveys in 2009
and 2007 indicated that children in Sabah had the worst oral health with 50 of 12 year-olds
having decay in their permanent teeth and children having an average of 3 teeth being(13)
Under the 10th Malaysian Plan in 2011 the federal and the Sabah state governments
reintroduced water fluoridation in Sabah(1314) In 2010 about 755 of the Malaysian
population or 20700000 people had fluoridated drinking water(1013) 12 Malaysian Dental Association Fluoride in Water
httpwwwmdaorgmy07_public_01healthcare_12htm
13 Sachdev N Fluoridation in Sabah Water for Cleaner Teeth French Tribunecom 28022011
From Levy IsraTo Jaeger ValerieCc Pim Carolyn gordonalphaweborg Diallo Aicha Penny Sutcliffe Paul Roumeliotis Michael Finkelstein
Hazel Lynn Robert KyleSubject FW Panorama - Privacy Security and other issuesDate Wednesday October 16 2013 122110 PM
Hello ValerieOttawa is part of Wave 4 Panorama implementation and we are gearing up increasingly to use thesystem where and if possible Thinking about it I am anticipating that this may need to be on theCOMOH (and alPHa) radar as it is something that will impact all health units and implies a majoroperational shift in vaccine delivery programs for all health units I have asked Carolyn Pim toconnect with our sister wave 4 units to share common experiences as we move forward ndash when wehave a roll up could I bring to COMOH Exec for discussion to explore whether there are broaderimplications for all members As an aside I have also asked the Ministry and their CIO to share with me any roll up learnings thatthey may have had already from previous waves (I understand that Niagara HU was a wave 1participant so if there is such a roll up of common experiences that others could learn fromperhaps you have it already and that could come to the exec too)Thanks Isra From Pim Carolyn Sent October 10 2013 1228 PMTo Christopher Mackie (christophermackiemlhuonca) Elizabeth Richardson(Elizabethrichardsonhamiltonca) H BSc M D F R C P (C) MPH Jim Chirico(jimchiriconbpsdhuca) Marlene Spruyt (spruytmtimiskaminghucom) Robert Kyle (Durham)Cc Levy IsraSubject Panorama - Privacy Security and other issues Dear colleagues Irsquom reaching out to you as fellow Panorama Wave 4 health units to ask about where yourorganizations are at in the process of signing agreements and completing Privacy ImpactAssessments and Threat Risk Assessments (TRAs) Ottawa Public Healthrsquos IT legal and informationsecurity advisors have made numerous requests to the MOHLTC for information (in particular theprovincial TRA) that we consider essential to develop our own risk assessment and PIA but havebeen told that information cannot be shared even with strict confidentiality and access controlsSo we are at somewhat of an impasse Isra emailed Arlene yesterday Arlene has forwarded ourconcerns to the Ministryrsquos CIO and Panorama lead but we havenrsquot had any response or discussionswith either of them yet Have your organizations identified similar concerns andor had interactions with the MOHLTC inthis respect Irsquod also be interested in knowing if your health units have flagged other (egoperational) implementation concerns Thanks
Carolyn ps Robert ndash you can ignore this request I talked with Sharan this morning about Durhamrsquos issuesso am including you now just for information Carolyn Pim MD FRCPC Associate Medical Officer of Health Meacutedecin adjointe en santeacute publique Ottawa Public Health Santeacute publique Ottawa 100 Constellation Cr Ottawa ON K2G 6J8 Tel teacutel (613) 580-6744 ext 23684Fax (613) 580-9641Connect With Ottawa Public Health
Suivez Santeacute publique Ottawa
This e-mail originates from the City of Ottawa e-mail system Any distribution use orcopying of this e-mail or the information it contains by other than the intendedrecipient(s) is unauthorized If you are not the intended recipient please notify meat the telephone number shown above or by return e-mail and delete thiscommunication and any copy immediately Thank you
Le preacutesent courriel a eacuteteacute expeacutedieacute par le systegraveme de courriels de la Ville dOttawaToute distribution utilisation ou reproduction du courriel ou des renseignements quisy trouvent par une personne autre que son destinataire preacutevu est interdite Si vousavez reccedilu le message par erreur veuillez men aviser par teacuteleacutephone (au numeacuteropreacuteciteacute) ou par courriel puis supprimer sans deacutelai la version originale de lacommunication ainsi que toutes ses copies Je vous remercie de votre collaboration
1
Smoke-Free Patios ndash An Amendment to the Smoke-Free Ontario Act
Date November 15 2013 Prepared for Council of Ontario Medical Officers of Health Prepared by York Region Public Health _____________________________________________________________________________ Issue
The Smoke-Free Ontario Act is the current provincial legislation that imposes smoking restrictions in workplaces and public places It prohibits smoking on restaurant and bar patios in instances where any portion of the seating area is covered by a roof With recent studies illustrating that exposure to second hand smoke outdoors poses similar risks to indoor exposure there has been growing public support to enhance smoking restrictions and make patios completely smoke-free
Background
With the implementation of the Smoke-Free Ontario Act in 2006 restaurant and bar patios became subject to smoking restrictions if any portion of the seating area was covered by a roof This allowed for patios without roof coverings to continue to allow smoking and as a result did not provide significant protection to patrons or staff from exposure to second hand smoke outdoors Many businesses chose to alter the design of their patios to allow smoking to continue In some cases patios became more crowded since smoking patrons who dine indoors often proceed outside onto licensed patios with their beverages to smoke York Region like most municipalities in Ontario is host to hundreds of patios being operated by restaurant owners and businesses With smoking prohibitions affecting only a small portion of these patios specifically ones with coverings the vast majority of patios still allow smoking to take place Patrons and employees on patios where smoking is not restricted are exposed to second hand smoke frequently This can contribute to increased disease and aggravation of existing health conditions From a business perspective the existing legislation has been viewed by many operators as unfair because some patios have permanent coverings which cannot be removed requiring a smoke-free status These business owners feel this creates an uneven playing field since they cannot provide an outdoor dining area for their smoking customers There is strong community support for smoke-free patios in Ontario A 2009 Rapid Risk Factor Surveillance System survey revealed 754 percent support in York Region while a Toronto Health Survey in 2011 indicated 74 percent public support
2
Current Status
Smoking is currently prohibited on restaurant and bar patios province-wide in four Canadian provinces and territories Alberta Newfoundland and Labrador Nova Scotia and Yukon A fifth province Prince Edward Island prohibits smoking on patios until 10 pm Since Ontario enacted legislation restricting smoking on patios in 2006 eight municipalities in Ontario have chosen to create bylaws that go beyond the Smoke-Free Ontario Act and enhance outdoor protection from second hand smoke by prohibiting smoking on patios completely The largest of those municipalities is the City of Ottawa Recently the Toronto Board of Health unanimously endorsed a report presented by their Medical Officer of Health recommending that restaurant and bar patios be made smoke-free through an amendment to the Smoke-Free Ontario Act
Key Considerations
There should be no significant financial burden to local Boards of Health resulting from a smoke-free patio amendment to the Smoke-Free Ontario Act Inspection and enforcement for the Smoke-Free Ontario Act is currently 100 percent funded by the Ministry of Health and Long-Term Care Following an introductory period of education on the amendment a complaint response model of service delivery would ensure ongoing compliance with smoke-free requirements A complete ban of smoking on patios would eliminate the widely-held perception by business owners that the current legislation creates an uneven playing field for business Since Smoke-Free Ontario Act inspections of patios began in 2006 operators have expressed the opinion that if patios need to be smoke-free for the protection of the public they should all be smoke-free to avoid undue hardship for individual businesses and to provide protection uniformly across the Province
Next steps
York Region Public Health intends to seek support from Medical Officers of Health across the Central East Tobacco Control Area Network (CETCAN) to advocate to the Ministry of Health and Long-Term Care for an amendment to the Smoke-Free Ontario Act prohibiting smoking on all restaurant and bar patios York Region is also in the process of requesting that its Regional Council advocate to the Minister of Health and Long-Term Care on the issue
Updating and Modernizing O Regulation 565 (Public Pools)
Date November 15 2013
Prepared for Council of Ontario Medical Officers of Health
Prepared by York Region Public Health _____________________________________________________________________________ Background Recent drownings at public pools in Ontario have highlighted the issue of water-borne illness and injury The current pool regulation under Ontariorsquos Health Protection and Promotion Act O Regulation 565 (Public Pools) is outdated It does not accurately reflect new pool technology and design or the changing use of public pools Neither does it incorporate admissions standards recommended by the Office of the Chief Coroner Further O Regulation 565 does not have short-form wording or set fines associated with it This limits public health enforcement capabilities What is the impact Updating O Regulation 565 (Public Pools) to address recent changes in pool technology design and uses and to include Coroner-recommended admissions standards would help improve pool safety Establishing short-form wording for O Regulation 565 would enhance enforcement related to public pools Currently the only enforcement available to Public Health Inspectors for dealing with non-critical regulatory infractions in public pools is the issuance of a Part III summons This involves a considerable amount of resources for a possible small fine With the development of inspection disclosure systems such as YorkSafe there is an even greater need to develop a method to effectively address repeated pool operator non-compliance with non-critical issues Next steps Public health units should advocate to the Province to 1) Conduct a review of O Regulation 565 (Public Pools) to address shortcomings Proposed changes to the
regulation should include a requirement for ownersoperators of public pools to advise the local Medical Officer of Health of any change in the use of a facility and the addition of the Coronerrsquos recommended admission standards
2) Provide short-form wording for O Regulation 565 so that public health inspectors can better deal with pool operator non-compliance
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
Page 5 of 8 ndash DRAFT FOR COMOH DISCUSSION
SECTION 3 VALUE FOR MEMBERSHIP
Survey Question What do you value the most about your alPHa membership
The comments provided in response to the text response question What is the most important benefit of alPHa membership for you personally supported the answers illustrated in the chart above 15 of the 20 comments provided focussed on the importance of opportunities to interact with colleagues across the province The next most important benefit mentioned was the support for COMOH members to work on public health issues together When asked What is the most important benefit of alPHa membership for your health unit COMOH members emphasized the following bull A coordinated and collective voice in advocating for public health issues and the public health sector (9) bull Opportunities to connect with other public health units to share experiences and best practices (8) bull Maintaining relationships with government both politicians and bureaucrats (3) and bull Support for boards of health (3)
Page 6 of 8 ndash DRAFT FOR COMOH DISCUSSION
Overall Level of Satisfaction
SECTION 4 LOOKING TO THE FUTURE
The questions in this section were asked to obtain input from alPHa members regarding a proposal from alPHarsquos Board of Directors to focus the Association on five service areas COMOH members were asked to indicate their level of agreement with the proposed areas of focus COMOH responses compared to the overall survey responses were as follows
To explore some proposed changes to Association services COMOH members were asked to provide their level of agreement with the following questions
COMOH Responses BOH Section Affiliates All Survey Responses
Strongly Agree
AgreeNeither Agree or Disagree
DisagreeStrongly Disagree
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1Promoting the role and value of local public health units
15 9 2 0 0 26 92 93 95 94
2
Providing important information to members about trends and events that will impact the public health system and management of public health units
10 8 8 0 0 26 69 97 86 85
3Facilitating professional networking and information sharing
13 10 3 0 0 26 88 83 82 85
4
Providing professional development to support excellence in public health unit leadership management and governance
3 15 7 1 0 26 69 83 86 79
5
Responding to public health sector issues when it makes the most sense to have a collective voice ie issues that impact the structure and funding of the public health sector and public health units and issues that have a broad focus on population health
15 8 2 0 1 26 88 97 95 93
PROPOSED AREAS OF FOCUS
COMOH Responses BOH Section Affiliates All Survey Responses
Strongly Agree
AgreeNeither Agree or Disagree
DisagreeStrongly Disagree
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1
COMOH and other professional groups within alPHa should do their own advocacy while alPHa supports members to share and support each others advocacy efforts
7 6 6 6 1 26 50 58 45 52
2
alPHa should provide support to action-oriented inter-professional work groups on priority public health unit issues and member resolutions
4 13 5 3 1 26 65 81 86 77
PROPOSALS
Page 8 of 8 ndash DRAFT FOR COMOH DISCUSSION
COMOH members were also asked to indicate the level of acceptability for some possible changes to alPHarsquos services and way of doing business
COMOH Responses BOH Section Affiliates All Survey Responses
Very Acceptable
Somewhat Acceptable
Neither Acceptable or Unacceptable
Somewhat Unacceptable
Very Unaccept
able
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1Single conference with additional face-to-face section meetings
21 2 0 1 0 24 96 68 80 81
2alPHa to offer alternatives like webinars on focussed topics
13 6 1 4 0 24 79 50 90 71
3Coordinate COMOH meetings with PHO OMA or Ministry events
16 4 2 0 0 22 91 na na --
4
Increase focus on building leadership and management capacity for health unit CEOs and senior management
7 9 4 3 0 23 70 na 70 70
5
Would it be acceptable for alPHa to request voluntary financial contributions from member PHUs in addition to annual fees
3 5 5 4 5 22 36 7 26 21
6
Would it be acceptable for alPHa to request voluntary in-kind staff contributions from member PHUs to expand alPHas capacity eg communications policy work group support
7 11 1 1 3 23 78 31 45 50
7Would it be acceptable to you for alPHa to discontinue staff support for COMOH (BOH Section)
0 4 1 5 14 24 17 11 na 14
8
Would it be acceptable to you for alPHa to reduce the amount of staff support for COMOH (BOH Section)
1 6 1 8 6 22 32 26 na 29
9
Would it be acceptable to you for alPHa to provide supports to MOHs and AMOHs (BOH Members) without maintaining COMOH (BOHs) as a section of the association
3 2 3 2 12 22 23 17 na 20
10
Would it be acceptable to you for alPHas Board of Directors to move from the current representational model to a skills-based strategic model ie board membership would be based on the skills needed to carry out alPHas strategic plan
6 11 2 1 3 23 74 56 56 62
11
Would it be acceptable to you for alPHas President Vice-President and Treasurer to be elected from the full membership of the alPHa Board of Directors (rather than the current model of alternating between BOH and COMOH members)
10 8 1 2 2 23 78 70 70 73
PROPOSED CHANGES
1 Council of Ontario Medical Officers of Health Terms of Reference
ASSOCIATION OF LOCAL PUBLIC HEALTH AGENCIES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
TERMS OF REFERENCE NAME 1 The name of the organization shall be ldquoThe Council of Ontario Medical Officers of
Health a section of the Association of Local Public Health Agencies (alPHa)rdquo hereinafter referred to as ldquothe Councilrdquo
MISSION 2 As local leaders in public health we are committed to improving the health of
Ontarians and increasing health equity by strengthening Ontariorsquos public health system We achieve this through system leadership and coordination in collaboration with the provincial government and other organizations and through evidence-informed advocacy on public health policy
OBJECTIVES 3 The objectives of the Council shall be
a) To provide strong province-wide leadership in public health
b) To advocate for health protection and promotion policies and programs that maintain and improve the health of Ontarians
c) To promote and maintain the highest standards for Ontariorsquos public health
programs and services
d) To support the planning implementation and evaluation of effective and efficiently run public health programs and services
e) To act as a forum for sharing information and resources and for addressing and
discussing public health issues both amongst the Councilrsquos members and other agencies that support the goals of alPHa eg Ontario Medical Association Ontario Public Health Association etc
f) To engage with and to provide public health and related policy advice to alPHa
the Chief Medical Officer of Health the Ontario Ministries of Health and Long-Term Care (including the Health Promotion and Public Health Divisions) Children
2 Council of Ontario Medical Officers of Health Terms of Reference
and Youth Services and other provincial ministries Public Health Ontario Health Canada the Public Health Agency of Canada and other public health partners
g) To promote and protect the professional interests of its members
h) To provide support to individual members as needed
i) To seek recognition for outstanding practice from among the members
j) To support evidence based practice of public health medicine
k) To engage and involve the membership to participate in COMOHrsquos endeavours
l) To mentor Public Health and Preventive Medicine Residents
MEMBERSHIP 4 Membership on the Council in each of the following categories is subject to the
limitations imposed by the current terms of reference and all policies and governing documents of the Association of Local Public Health Agencies Benefits of membership in each category are included in Appendix A These shall be subject to regular review and may be suspended under certain circumstances
Active membership in the Council shall be open to all Associate Medical Officers of Health and all full-time Medical Officers of Health whose Boards of Health are members of alPHa Such members shall have full voting privileges and may hold office in the Council Associate membership shall be open to all full and part-time physicians employed by a Board of Health that is a member of alPHa Such members shall not have voting privileges nor hold office
Affiliate membership shall be open to the following individuals interested in furthering the objectives of the Council
bull Public Health and Preventive Medicine Residents and Public Health and Preventive Medicine Residency Program Directors
bull Federal public health physicians working in Ontariorsquos First Nations communities
bull other public health or related physicians including those employed by a Board of Health that is not a member of alPHa
Such members shall not have voting privileges nor hold office
3 Council of Ontario Medical Officers of Health Terms of Reference
Emeritus membership shall be open to all former members who have retired after five (5) or more years of Active membership subject to the nomination in writing of two (2) active members in good standing endorsement of the Executive Committee and approval of the Council by majority vote at a general meeting Such members shall have neither voting privileges nor hold office but may be invited to attend general meetings Honorary membership shall be open to any non-active or associate member subject to the nomination in writing of two (2) active members in good standing endorsement of the Executive Committee and approval of the Council Such members shall have neither voting privileges nor hold office but may be invited to attend general meetings
OFFICERS 5 The Officers of the Council shall be the Chair Vice-Chair and immediate Past Chair
6 The Chair shall prepare the agendas of all Council meetings She shall preside and
preserve order at all such meetings shall ensure that these Terms of Reference are upheld and enforced and shall contribute to the supervision and evaluation of any Public Health and Preventive Medicine Resident who is on a placement with alPHa
7 The Vice-Chair shall fulfill the duties of the Chair in hisher absence The immediate
Past Chair may fulfill the duties of the Chair or Vice-Chair in their absences 8 The Chair shall normally serve a term of one (1) year which is renewable once and
after which the Vice-Chair shall normally assume the vacated office COMMITTEES 9 The Council shall elect seven (7) active members one from each of alPHarsquos regions
and the active member who is scheduled to serve as the President or immediate Past-President of alPHa to represent it on the alPHa Board of Directors These seven (7) members shall constitute the Councilrsquos Executive Committee and shall serve a term of at least one (1) year The Chair and Vice-Chair shall be elected from among the Executive Committee members If alPHarsquos immediate Past President is an active member she shall be an ex-officio member of the Executive Committee
10 The mandate of the Executive Committee shall be to facilitate the achievement of
the objectives of the Council by fulfilling the following
a Identifying priorities 1
1 See Appendix B Planning Cycle to Identify Priorities for COMOH
and ensuring the development of briefing documents and or recommendations as appropriate for the consideration of the Council
4 Council of Ontario Medical Officers of Health Terms of Reference
b Setting agendas and otherwise ensuring preparations for Council meetings c Ensuring the fulfillment of the direction of Council d Responding in a timely fashion to time-sensitive public health matters in
accordance with the Executive Committeersquos understanding of the perspective of the Council
e Engaging with the Chief Medical Officer of Health Associate Chief Medical Officers of Health and other provincial public health leaders and
f Representing Council at public and partner agency forums including the Public Health Leadership Council which shall normally include membership from the Officers of the Council and two other Executive Committee members as selected by agreement among the Executive
g Identifying opportunities for the recognition of outstanding practice from among the members including the annual nomination of at least one member for the alPHa Distinguished Service Award
11 The Executive Committee shall meet and correspond in the manner and at the times
and if required places as deemed necessary by the Chair to conduct the business of the Council A quorum shall consist of four (4) members
12 The Executive Committee shall have the power to strike committeestask or working
groups to assist it in carrying out the business of the Council 13 The Council may by special resolution remove a member of the Executive
Committee before the completion of hisher term of office and may elect a successor to complete the term The special resolution shall require a majority vote of 67 of the members present and voting at the meeting at which the special resolution is considered
14 A Nominating Committee shall consist of the three (3) most recent Past Chairs who
are able to serve and shall be chaired by the immediate Past Chair The Nominating Committee shall prepare a list of proposed Officers and Executive Committee members for the consideration of the Council at its Annual General Meeting
MEETINGS 15 The Council shall hold at least four (4) general meetings per year in a manner and at
the times and if required places as deemed necessary by the Executive Committee to share information direct and assist the Executive Committee in conducting the business of the Council
16 The Council shall hold its Annual General Meeting during and at the same place as
the alPHarsquos Annual Conference
5 Council of Ontario Medical Officers of Health Terms of Reference
17 The Council shall hold a special meeting at the call of the Chair or upon the written request specifying the purpose of such meeting of at least five (5) active members Council members must be given at least 48 hours notice of any special meeting
18 Only Councilrsquos active and associate members and alPHa staff are entitled to attend
general and special meetings of the Council Other members and non-members may be invited to attend all or part of such meetings as determined by the Chair preferably in consultation with the Executive Committee Non-members who come to such meetings without an invitation may attend all or part of the meeting by a majority vote of the active members present and voting
19 The Chair shall prepare the agendas for such meetings and shall normally include
reports from the Chair and the Councilrsquos committeestask or working groups and representatives to external bodies alPHarsquos Executive Director shall ensure that the minutes shall be recorded and promptly distributed to the Section
20 A quorum for all such meetings shall be ten (10) active members 21 The Council shall normally be notified in a manner deemed appropriate by the Chair
of such meetings at least one (1) month prior to their being held 22 A majority vote of the members present at such meetings and voting shall make
Council decisions In the case of a tied vote the Chair shall cast the deciding vote The Executive Committee shall ensure that actions arising from such decisions at such meetings are implemented and monitored
23 The Chair may solicit advice from the Council through the use of teleconferencing
and alPHarsquos electronic mailing lists in order to gain an understanding of the overall perspective of the Council (see 10d)
ELECTIONS 24 The Officers and Executive Committee members shall be elected at the Sectionrsquos
Annual General Meeting The Nominating Committee Chair or hisher designate shall present a list of nominations Additional nominations from the floor shall also be considered Each Officer and Executive Committee member shall be elected by secret ballot if necessary by a majority of the active members present and voting In the case of a tie the Chair shall cast the deciding vote
AMENDMENTS 25 The Councilrsquos Terms of Reference may be amended from time to time by the
Executive Committee provided the Committee receives notice of such proposed amendments at least one (1) month prior to the meeting at which the amendments
6 Council of Ontario Medical Officers of Health Terms of Reference
will be considered Such amendments shall be ratified by the Council at the next general meeting or the Annual General Meeting as the case may be
26 The Executive Committee shall review the Terms of Reference as required and not
less than once every two years Original September 1987 1st Revision October 2000 2nd Revision July 2001 3rd Revision December 2003 4th Revision February 2008 5th Revision June 2009 6th Revision June 2011 7th Revision June 2013
7 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX A
COMOH Membership Benefits Active Membership
bull Entitled to attend all meetings of the Section bull May hold office on the COMOH Executive Committee alPHa Board of Directors
Standing Committees bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Associate Membership
bull Entitled to attend all meetings of the Section bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Affiliate Membership
bull May attend meetings or parts thereof subject to approval of Chair bull May serve on ad-hoc committees of the Section subject to the approval of the
Executive Committee bull Discounted registration rates for alPHa Conferences (for Public Health and
Preventive Medicine Residents) bull Upon written request and subject to COMOH Executive approval Affiliate
Members may subscribe to comohlistsalphaweborg The approval will be reviewed on an annual basis in order to determine if the Affiliate Member can remain a subscriber to mohsalphaweborg
Emeritus Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair bull Enjoy discounted registration rates for alPHa Conferences and regular COMOH
meetings bull Subscription to comohlistsalphaweborg electronic mailing list bull Full access to alPHa Web site bull May represent alPHa COMOH on selected external committees and working
groups Honorary Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair
8 Council of Ontario Medical Officers of Health Terms of Reference
bull May represent alPHa COMOH on selected external committees and working groups subject to the approval of the COMOH or alPHa Executive Committee as appropriate
9 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX B
Planning Cycle to Identify Priorities for COMOH
1 There shall normally be a COMOH membership strategic planning retreat every four years In recognition of the dynamic environment of public health the need for and timing of such a retreat shall be at the discretion of the Executive Committee in consultation with the membership
2 The COMOH Executive is responsible (through the creation of a subcommittee of COMOH members) for ensuring the preparation for the COMOH retreats with resources to include those provided by alPHa
3 Leadership for action on COMOH priorities will be recruited from among the COMOH membership in order to make good use of the full base of capacity of the membership The resources to support actions will be recruited from both within and beyond the COMOH membership employing other public health professionals that reside within the broader public health system and community
4 The COMOH Executive shall ensure an annual review of strategic priorities and initiatives and the development of a draft report of the same for the review of the members at the June meeting
2013 Strategic Planning
Considerations for COMOH
As part of its strategic planning discussions alPHarsquos Board has been considering changes to the level of support provided to member sections A member survey is being carried out over the fall to determine options acceptable to alPHa members The following approach to support is put forward as a proposal for the consideration of COMOH Note that the feasibility of the points below depend upon future decisions of the alPHa board They assume that COMOH remains part of alPHa but becomes more independent in administering meetings
1 alPHa can provide to COMOH staff support (Gord Fleming) amounting to 02 FTE or one day per week This is a reduction from the current level of 35 days per week COMOH can choose to use the support any way it wants writing COMOH letters meeting minutes agenda support special projects etc
2 In addition to 02 FTE alPHa staff would provide support for up to 4 face-to-face meetings per year One meeting would be concurrent to alPHarsquos annual conference in June The timing of other meetings could be negotiated The support includes consulting on the development of the program arranging for speakers registration for the event arranging venue AV support and hospitality services
3 In addition to 02 FTE alPHa staff would provide support for setting meeting dates and any polling required to establish dates Note that the individual supporting this function would be Karen Reece
4 COMOHrsquos Executive and Section would continue to have access to online supports through the alPHa including the COMOH Listserve and a group page for posting agendas minutes and other resources on the alPHa website
5 alPHa staff (Linda Stewart and Gord Fleming) can also start participating on CMOH calls as a way to be up-to-date on issues related to COMOH
6 Other than what is outlined above COMOH would be expected to prepare agendas and take minutes for its Executive and Section meetings The Executive would be expected to operate more independently than it does now but would be able to access the supports outlined above
Prepared by Linda Stewart Executive Director
From comoh-bounceslistsalphaweborg on behalf of Christopher MackieTo MOH ListserveSubject [comoh] Fw URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)Date Wednesday October 30 2013 91241 AMAttachments ATT00249txt
For AMOHs and PHPM residents who didnt receive the initial email
Chris
Christopher Mackie MD MHSc FRCPCMedical Officer of Health and CEOMiddlesex-London Health Unit50 King St LondonON N6A 5L7 O 519 663 5317 ext 2444 wwwhealthunitcomFrom Pisko Laura (MOHLTC)Sent Tuesday October 29 2013 759 PMTo kbarkeralgomapublichealthcom malcolmlockbchuorg davidcchatham-kentcarobertkyledurhamca proumeliotiseohuca fwarshelginhealthonca mohelginhealthoncahlynnpublichealthgreybruceonca malcolmlockhnhuorg hnmohhnhuorglnoseworthyhkpronca bobnosalhaltonca elizabethrichardsonhamiltoncarschabashpechuonca ncameronhuroncountyca drimgemmillkflapublichealthcamohkflapublichealthca suditranadecounty-lambtononca paulastewarthealthunitorgChristopher Mackie valeriejaegerniagararegionca jimchiriconbpsdhuca jarthursnwhuoncaisralevyottawaca dnealoxfordcountyca davidmowatpeelregionca mklassenpdhuoncarpellizzaripcchuca rosemarieramsinghporcupinehuonca mcorriveaurcdhucomcharlesgardnersmdhuorg sutcliffepsdhucom davidwilliamstbdhucomspruytmtimiskaminghucom dmckeowntorontoca lnolanregionofwaterloocanicolamercerwdghuorg aheimannwechealthunitorg karimkurjiyorkcaCc coreywesleytbdhucom CindyBaker-Barillsmdhuorg Donna Kosmack pilonlsdhucomPaulaMuiskflapublichealthca sthibautorontoca Mueller Daina (MOHLTC) Gordon Marcus(MOHLTC) andreakitahamiltoncaSubject URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)
Dear Colleagues The ministry has received reports that some tobacco vendors across the province aregiving away single cigarettes with the purchase of tobacco products It is the ministryrsquosposition that giving out free single cigarettes does not violate subsection 31(3) of theSmoke-Free Ontario Act (ldquoSFOArdquo) Although the practice of giving out free singlecigarettes may promote the sale of tobacco products it does not take the form of aldquoproduct enhancement product association or promotional materialrdquo and therefore doesnot fall within the scope of subsection 31(3) of the SFOA We have confirmed with Health Canada that this practice may violate section 29(b) of thefederal Tobacco Act As such Health Canada is requesting that you notify them in writingand I am directing you to communicate with them via email and provide to them as manydetails as possible Emails should be sent to Tobacco-Ontariohc-scgcca and thesubject line should read ldquoViolation of Section 29(b) of Tobacco Actrdquo This will ensurethat the complaints are given priority status by Health Canada We will continue to monitor
this situation and liaise with our colleagues at Health Canada Please share this information with your tobacco control staff and contact me or DainaMueller Manager Tobacco Control Unit Health Promotion Implementation Branch atdainamuellerontarioca with any questions RegardsLaura Laura A PiskoDirectorHealth Promotion Implementation BranchHealth Promotion DivisionMinistry of Health and Long Term Care416-327-7445 (office)416-451-3185 (mobile) Marcus Gordon - EA (416)326-0625 for urgent issues
========= Middlesex-London Health Unit E-Mail Disclaimer =============______________________________________________________________
Private and confidential intended only for named recipient If otherwisereceived please destroy immediately Health information in this email isonly general information and is not intended to replace an in personconsultation with a medical professional nor is it intended to providemedical advice Individual circumstances of which we are not aware mayaffect the information provided herein and as such the Middlesex-LondonHealth Unit assumes no liability or responsibility for your reliancethereon The Middlesex-London Health Unit works under the authority of theHealth Protection and Promotion Act and this correspondence may be used toassess your needs for public health services (519-663-5317 ext 2448)______________________________________________________________
From Gardner CharlesTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes (RayCopesoahppca)
George Pasut (GeorgePasutoahppca) Peter Cooney (petercooneyhc-scgcca)Cc Ito DickSubject Discontinuation of Fluoridation in MuskokaDate Tuesday October 22 2013 125254 PM
Hello Colleagues
As I reported in my email below on September 26th fluoridation has come under challenge again inSimcoe Muskoka I am now very unhappy to report that despite our best efforts last night theDistrict Council of Muskoka voted to remove fluoride from municipal drinking supplies across theDistrict This brings to an end fluoridation in all of Simcoe and Muskoka (with the exception of Base Borden)ndash though New Tecumseth will be conducting a plebiscite on the question of fluoridation with themunicipal election next October Defending community water fluoridation has drained a great deal of time human resources andcommitment from other priorities and has been exhausting here in SMDHU as I am sure it hasbeen in many other health units While the outcomes have been very disappointing I have beenimpressed by the professionalism and dedication that SMDHU staff members have shown inshouldering this burden In particular our dental consultant Dr Ito has provided us with much ofthe foundational knowledge and the local research essential to our efforts and has very frequentlyattended and presented at council meetings and other public events I would also like to thank themany of you who have offer and provided support including advocacy letters and informationresources Over the years Dr Peter Cooney Chief Dental Officer of Health of Canada has beenvery helpful attending and presenting with us at council meetings and at public consultationevents We will of course continue our oral health surveillance of the children of Muskoka documentingand reporting in future years on the increase in dental decay that we anticipate will occur Suchsurveillance is the foundation of our advocacy both to municipal politicians and to the province I am very concerned that our experience will continue to repeat itself across the province unlessthere is strong leadership provincially It is with this in mind that I raise the followingrecommendations for your consideration
1 That we collectively (with PHOrsquos leadership) conduct high quality publish-worthy researchdocumenting the impact on dental decay that occurs in those municipalities throughoutOntario that in recent years have discontinued community water fluoridation This could bepart of a larger study on such municipalities across the country and it could also be part ofa study documenting overall oral health (including fluoridation coverage) in the province(and possibly across the country)
2 That COMOH engage with our Chief MOH to advocate for the province to require allmunicipal water supplies to be fluoridated (the exception of course being those withnaturally sufficient fluoride concentrations) This could built upon the alPHa position to
Gordon
Highlight
Gordon
Highlight
date (A11-00 - Community Water Fluoridation) on the CMOH position (Oral Health ndash) and on theemail discussion generated on the COMOH listserv some months back re Richardrsquosproposal (calling on the province to fund municipal water fluoridation)
Valerie I request that this be an item for our COMOH meeting on November 15th Sincerely Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorg From Gardner Charles Sent Thursday September 26 2013 245 PMTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes(RayCopesoahppca)Subject Community Water Fluoridation Under Challenge Again in Simcoe Muskoka Hello Colleagues You may wish to know that community water fluoridation (CWF) is again under challenge in SimcoeMuskoka specifically both in Tottenham (Town of New Tecumseth in Simcoe County) and for theentire District of Muskoka On Monday September 23 Committee of the Whole Council of theTown of New Tecumseth voted to submit application to discontinue community water fluoridation(CWF) in the town of Tottenham despite presentations to the contrary from our dental consultantDr Ito and from me The next Council meeting is scheduled for Monday Sept 30 at which lastMondayrsquos (Sept 23) votes will be ratified
Since Monday I have spoken with the Mayor of the Town of New Tecumseth and with most of thecouncilors encouraging deferral of a decision on Monday to allow the town more time to make afully informed decision
This is the second time in recent years that the issue of discontinuing CWF in Tottenham has beenraised at council This issue is also scheduled to return again to the District of Muskoka Council on
October 21st where I will be presenting in response to deputations in opposition to fluoridation
Outside of Base Borden Tottenham is the only community with fluoridated water in SimcoeCounty The health unitrsquos own screening data between 2011 and 2013 shows that Tottenhamrsquos
Gordon
Highlight
children as well as those in Muskoka have a lower rate of dental decay than Simcoe Muskokacommunities without CWF
Sincerely
Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorgChuck Gardner MOH
November 04 2013
Mandatory State Laws on Fluoridation Thirteen states Puerto Rico and the District of Columbia have laws intended to provide
statewide fluoridation These states and the year that the fluoridation legislation was passed are
District of Columbia (1952) Connecticut (1965) Kentucky (1966) Illinois (1967) Minnesota
(1967) Ohio (1969) South Dakota (1969) Georgia (1973) Nebraska (1973 and 2008)
California (1995) Delaware (1998) Puerto Rico (1998) Nevada (1999) Louisiana (2008) and
Arkansas (2011) (see Table 1) The sizes of the public water systems or countiescommunities
affected and exemption provisions vary by state Table 1
STATES THAT HAVE MANDATORY LAWS ON FLUORIDATION -2011
State (1) Year of
Fluoridation
Legislation (1)
Population
served by
Fluoridated
CWS (2)
Persons
receiving
fluoridated
water (2)
State
Average
Caries
Experience
of Grade 3
Students (3)
Arkansas 2011 647 1724131 64
California 1995 621 22812721 709
Connecticut 1965 910 2370423 406
Delaware 1998 862 705344 545
Georgia 1973 921 8924598 52
Illinois 1967 993 11325132 532
Kentucky 1966 999 4334223 598
Louisiana 2008 407 1846149 657
Minnesota 1967 988 4117266 549
Nebraska 1973 and 2008 702 1001665 593
Nevada 1999 702 1001665 649
Ohio 1969 877 8772683 512
South Dakota 1969 948 642942 623
District of
Columbia
1952 1000 595000
Puerto Rico 1998
United States 739 204283554
2010 Statistics for population fluoridated and number of people
1 Communication with Jane McGinley RDH MBA Manager Fluoridation and Preventive Health
Activities Council on Access Prevention and Interprofessional Relations
2 Centers for Disease Control and Prevention Department of Health and Human Services
accessed Oct 21 2013 httpwwwcdcgovfluoridationstatistics2010statshtm
3 Centers for Disease Control and Prevention National Oral Health Surveillance System Caries
Experience - Percentage of 3rd Grade students with Caries Experience (treated or untreated tooth
If data from 43 states for the percentage of Grade 3 children with experience of dental decay is
compared with the 2008 percentages of the population in a state with Community Water
Fluoridation then the percentage of children with experience of dental decay decreases as the
percentage of the state population with Community Water Fluoridation increases (see Figure 1)
Figure 1
Correlation of Percentage of Grade 3 Children with Caries Experience and
Percentage of Population With Community Water Fluoridation for 43
Reporting States
0
10
20
30
40
50
60
70
80
0 10 20 30 40 50 60 70 80 90 100
State of Population With Community Water Fluoridation
Sta
te
of
Gra
de 3
Stu
den
ts w
ith
Cari
es E
xp
eri
en
ce
Data from CDC (2 3)
The description of the fluoridation laws in California Illinois and Nevada can be found on the
Association of State amp Territorial Dental Directors website(4 7 8)
The California fluoridation law AB 733 came into effect in 1995 requiring communities of 10
000 residents or more be supplied with fluoridated drinking water However the state did not
provide any funding to implement the legislation (California is unique in requiring fluoridation
without funding the practice)(4) The California Department of Health Services therefore had to
fund fluoridation initiatives from non-governmental sources ie the California Endowment
California Dental Association Foundation the First 5 Commission and others(5) From 1995 to
2011 the percentage of the California population receiving fluoridated drinking water has risen
from 17 to 625(6) 4 Dental Public Health Activities amp Practices Office of Oral Health California Department of Health
Services April 2002 httpwwwastddorgbestpracticesDES06002CAfluoridationpdf
5 Stock M Pollick H The CDA Foundation Model to Fluoridate Communities California Dental
Association Journal vol 40 no 8 649 - 655
httpwwwcdaorgPortals0journaljournal_082012pdf
6 California Dental Association Foundation
httpwwwcdafoundationorglearnadvocacyfluoridation
The State of Illinois passed a mandatory fluoridation state in 1967 and required all community
water systems to adjust fluoride levels in the drinking water to optimal levels within 1 year(7)
From 1962 when over 5000000 residents had optimally fluoridated drinking water by 2010
the number had risen to 11325132 (993 of the population on community water systems)(2)
7 Dental Public Health Activities amp Practices Division of Oral Health Illinois Department of Public
Health April 2002 httpwwwastddorgbestpracticesDES16007ILfluoridationpdf
The State of Nevada passed a mandatory fluoridation statute in 2000 for communities with
400000 or more residents(8) This was a result of the work of a statewide coalition that
included the Nevada Dental and Dental Hygienist Associations the Washoe and Clark County
District Health Departments the Clark County School District Junior League of Las Vegas
Head Start the Community College of Southern Nevada Dental Hygiene Program Health
Access Washoe County and Saint Maryrsquos Hospital For communities with less than 400000 the
implementation of fluoridation still required the vote of the majority voters in the community
The Las Vegas Water Authority and the City of Henderson started fluoridation in 2000
increasing the percentage of the population with fluoridated drinking water from 2 to 65 (8) 8 Dental Public Health Activities amp Practices Bureau of Family Health Services Nevada State Health
Division April 2002 httpwwwastddorgbestpracticesDES31002NVfluoridationbillpdf
Countries with Mandatory Laws on Fluoridation Countries that have mandated Community Water Fluoridation are Brazil Hong Kong
Malaysia Singapore Ireland Israel and some of the states in Australia
Singapore started fluoridating its water in 1956 based on the success of the fluoridation trials in
Grand Rapids Newburgh Evanston and Brantford Singapore became the first Asian country to
have 100 of its population benefitting from the implementation of fluoridated drinking water
Loh reported that ldquoThe ten year study on the effects of water fluoridation in Singapore showed
a decrease in caries prevalence in the children In the permanent dentition the reduction was
523 per cent for Chinese and 31 per cent for Malays in the 7 to 9 year old age group A similar
trend was observed in the mixed dentition in which the decrease was 325 per cent for Chinese
and 306 per cent for Malaysrdquo(9) By 2010 the population of the country was 5080000(10)
9 Loh T Thirty-eight years of water fluoridation--the Singapore scenario Community Dent
Health 1996 Sep13 Suppl 247-50
10 British Fluoridation Society One in a Million the facts about water fluoridation 3rd Edition
published March 2012) httpwwwbfsweborgonemillion0920One20in20a20Million20-
20The20Extent20of20Fluoridationpdf
Hong Kong started implementing community water fluoridation in 1961 and similar to
Singapore 100 of the population received access to fluoridated drinking water Lo and Wong
reported that ldquoThe mean DMFT score of the children deceased from 44 in 1960 to 15 in 1968
stayed at this level in the 1980 and 1986 surveys and further deceased to 08 in 2001 The
prevalence of dental fluorosis among the children surveyed in 1960 was 1 and this increased
to 59 and 70 in 1968 and 1980 respectively It was found in the 1986 and 2001 surveys that
the prevalences of fluorosis were 47 and 9 among children whose teeth developed at the
time when the respective water fluoride concentrations were 07 ppm and 05 ppmrdquo(11) The
population of Hong Kong was 6968000 in 2009(10) 11 LO ECM and WONG AHH Water fluoride concentration and fluorosis in Hong Kong in 1960-
2001 84th General Session and Exhibition of the International Association for Dental Research amp
1st Meeting of the Pan-Asian-Pacific Federation Brisbane Australia 28 June-1 July 2006 v 85 n
Sp B
The Malaysian cabinet approved a nationwide community water fluoridation program in 1972
(12) One of the states Sabah decided to stop fluoridation in 1989 due to concerns about
inadequate supervision in adding fluoride to the drinking water Oral Health Surveys in 2009
and 2007 indicated that children in Sabah had the worst oral health with 50 of 12 year-olds
having decay in their permanent teeth and children having an average of 3 teeth being(13)
Under the 10th Malaysian Plan in 2011 the federal and the Sabah state governments
reintroduced water fluoridation in Sabah(1314) In 2010 about 755 of the Malaysian
population or 20700000 people had fluoridated drinking water(1013) 12 Malaysian Dental Association Fluoride in Water
httpwwwmdaorgmy07_public_01healthcare_12htm
13 Sachdev N Fluoridation in Sabah Water for Cleaner Teeth French Tribunecom 28022011
From Levy IsraTo Jaeger ValerieCc Pim Carolyn gordonalphaweborg Diallo Aicha Penny Sutcliffe Paul Roumeliotis Michael Finkelstein
Hazel Lynn Robert KyleSubject FW Panorama - Privacy Security and other issuesDate Wednesday October 16 2013 122110 PM
Hello ValerieOttawa is part of Wave 4 Panorama implementation and we are gearing up increasingly to use thesystem where and if possible Thinking about it I am anticipating that this may need to be on theCOMOH (and alPHa) radar as it is something that will impact all health units and implies a majoroperational shift in vaccine delivery programs for all health units I have asked Carolyn Pim toconnect with our sister wave 4 units to share common experiences as we move forward ndash when wehave a roll up could I bring to COMOH Exec for discussion to explore whether there are broaderimplications for all members As an aside I have also asked the Ministry and their CIO to share with me any roll up learnings thatthey may have had already from previous waves (I understand that Niagara HU was a wave 1participant so if there is such a roll up of common experiences that others could learn fromperhaps you have it already and that could come to the exec too)Thanks Isra From Pim Carolyn Sent October 10 2013 1228 PMTo Christopher Mackie (christophermackiemlhuonca) Elizabeth Richardson(Elizabethrichardsonhamiltonca) H BSc M D F R C P (C) MPH Jim Chirico(jimchiriconbpsdhuca) Marlene Spruyt (spruytmtimiskaminghucom) Robert Kyle (Durham)Cc Levy IsraSubject Panorama - Privacy Security and other issues Dear colleagues Irsquom reaching out to you as fellow Panorama Wave 4 health units to ask about where yourorganizations are at in the process of signing agreements and completing Privacy ImpactAssessments and Threat Risk Assessments (TRAs) Ottawa Public Healthrsquos IT legal and informationsecurity advisors have made numerous requests to the MOHLTC for information (in particular theprovincial TRA) that we consider essential to develop our own risk assessment and PIA but havebeen told that information cannot be shared even with strict confidentiality and access controlsSo we are at somewhat of an impasse Isra emailed Arlene yesterday Arlene has forwarded ourconcerns to the Ministryrsquos CIO and Panorama lead but we havenrsquot had any response or discussionswith either of them yet Have your organizations identified similar concerns andor had interactions with the MOHLTC inthis respect Irsquod also be interested in knowing if your health units have flagged other (egoperational) implementation concerns Thanks
Carolyn ps Robert ndash you can ignore this request I talked with Sharan this morning about Durhamrsquos issuesso am including you now just for information Carolyn Pim MD FRCPC Associate Medical Officer of Health Meacutedecin adjointe en santeacute publique Ottawa Public Health Santeacute publique Ottawa 100 Constellation Cr Ottawa ON K2G 6J8 Tel teacutel (613) 580-6744 ext 23684Fax (613) 580-9641Connect With Ottawa Public Health
Suivez Santeacute publique Ottawa
This e-mail originates from the City of Ottawa e-mail system Any distribution use orcopying of this e-mail or the information it contains by other than the intendedrecipient(s) is unauthorized If you are not the intended recipient please notify meat the telephone number shown above or by return e-mail and delete thiscommunication and any copy immediately Thank you
Le preacutesent courriel a eacuteteacute expeacutedieacute par le systegraveme de courriels de la Ville dOttawaToute distribution utilisation ou reproduction du courriel ou des renseignements quisy trouvent par une personne autre que son destinataire preacutevu est interdite Si vousavez reccedilu le message par erreur veuillez men aviser par teacuteleacutephone (au numeacuteropreacuteciteacute) ou par courriel puis supprimer sans deacutelai la version originale de lacommunication ainsi que toutes ses copies Je vous remercie de votre collaboration
1
Smoke-Free Patios ndash An Amendment to the Smoke-Free Ontario Act
Date November 15 2013 Prepared for Council of Ontario Medical Officers of Health Prepared by York Region Public Health _____________________________________________________________________________ Issue
The Smoke-Free Ontario Act is the current provincial legislation that imposes smoking restrictions in workplaces and public places It prohibits smoking on restaurant and bar patios in instances where any portion of the seating area is covered by a roof With recent studies illustrating that exposure to second hand smoke outdoors poses similar risks to indoor exposure there has been growing public support to enhance smoking restrictions and make patios completely smoke-free
Background
With the implementation of the Smoke-Free Ontario Act in 2006 restaurant and bar patios became subject to smoking restrictions if any portion of the seating area was covered by a roof This allowed for patios without roof coverings to continue to allow smoking and as a result did not provide significant protection to patrons or staff from exposure to second hand smoke outdoors Many businesses chose to alter the design of their patios to allow smoking to continue In some cases patios became more crowded since smoking patrons who dine indoors often proceed outside onto licensed patios with their beverages to smoke York Region like most municipalities in Ontario is host to hundreds of patios being operated by restaurant owners and businesses With smoking prohibitions affecting only a small portion of these patios specifically ones with coverings the vast majority of patios still allow smoking to take place Patrons and employees on patios where smoking is not restricted are exposed to second hand smoke frequently This can contribute to increased disease and aggravation of existing health conditions From a business perspective the existing legislation has been viewed by many operators as unfair because some patios have permanent coverings which cannot be removed requiring a smoke-free status These business owners feel this creates an uneven playing field since they cannot provide an outdoor dining area for their smoking customers There is strong community support for smoke-free patios in Ontario A 2009 Rapid Risk Factor Surveillance System survey revealed 754 percent support in York Region while a Toronto Health Survey in 2011 indicated 74 percent public support
2
Current Status
Smoking is currently prohibited on restaurant and bar patios province-wide in four Canadian provinces and territories Alberta Newfoundland and Labrador Nova Scotia and Yukon A fifth province Prince Edward Island prohibits smoking on patios until 10 pm Since Ontario enacted legislation restricting smoking on patios in 2006 eight municipalities in Ontario have chosen to create bylaws that go beyond the Smoke-Free Ontario Act and enhance outdoor protection from second hand smoke by prohibiting smoking on patios completely The largest of those municipalities is the City of Ottawa Recently the Toronto Board of Health unanimously endorsed a report presented by their Medical Officer of Health recommending that restaurant and bar patios be made smoke-free through an amendment to the Smoke-Free Ontario Act
Key Considerations
There should be no significant financial burden to local Boards of Health resulting from a smoke-free patio amendment to the Smoke-Free Ontario Act Inspection and enforcement for the Smoke-Free Ontario Act is currently 100 percent funded by the Ministry of Health and Long-Term Care Following an introductory period of education on the amendment a complaint response model of service delivery would ensure ongoing compliance with smoke-free requirements A complete ban of smoking on patios would eliminate the widely-held perception by business owners that the current legislation creates an uneven playing field for business Since Smoke-Free Ontario Act inspections of patios began in 2006 operators have expressed the opinion that if patios need to be smoke-free for the protection of the public they should all be smoke-free to avoid undue hardship for individual businesses and to provide protection uniformly across the Province
Next steps
York Region Public Health intends to seek support from Medical Officers of Health across the Central East Tobacco Control Area Network (CETCAN) to advocate to the Ministry of Health and Long-Term Care for an amendment to the Smoke-Free Ontario Act prohibiting smoking on all restaurant and bar patios York Region is also in the process of requesting that its Regional Council advocate to the Minister of Health and Long-Term Care on the issue
Updating and Modernizing O Regulation 565 (Public Pools)
Date November 15 2013
Prepared for Council of Ontario Medical Officers of Health
Prepared by York Region Public Health _____________________________________________________________________________ Background Recent drownings at public pools in Ontario have highlighted the issue of water-borne illness and injury The current pool regulation under Ontariorsquos Health Protection and Promotion Act O Regulation 565 (Public Pools) is outdated It does not accurately reflect new pool technology and design or the changing use of public pools Neither does it incorporate admissions standards recommended by the Office of the Chief Coroner Further O Regulation 565 does not have short-form wording or set fines associated with it This limits public health enforcement capabilities What is the impact Updating O Regulation 565 (Public Pools) to address recent changes in pool technology design and uses and to include Coroner-recommended admissions standards would help improve pool safety Establishing short-form wording for O Regulation 565 would enhance enforcement related to public pools Currently the only enforcement available to Public Health Inspectors for dealing with non-critical regulatory infractions in public pools is the issuance of a Part III summons This involves a considerable amount of resources for a possible small fine With the development of inspection disclosure systems such as YorkSafe there is an even greater need to develop a method to effectively address repeated pool operator non-compliance with non-critical issues Next steps Public health units should advocate to the Province to 1) Conduct a review of O Regulation 565 (Public Pools) to address shortcomings Proposed changes to the
regulation should include a requirement for ownersoperators of public pools to advise the local Medical Officer of Health of any change in the use of a facility and the addition of the Coronerrsquos recommended admission standards
2) Provide short-form wording for O Regulation 565 so that public health inspectors can better deal with pool operator non-compliance
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
Page 6 of 8 ndash DRAFT FOR COMOH DISCUSSION
Overall Level of Satisfaction
SECTION 4 LOOKING TO THE FUTURE
The questions in this section were asked to obtain input from alPHa members regarding a proposal from alPHarsquos Board of Directors to focus the Association on five service areas COMOH members were asked to indicate their level of agreement with the proposed areas of focus COMOH responses compared to the overall survey responses were as follows
To explore some proposed changes to Association services COMOH members were asked to provide their level of agreement with the following questions
COMOH Responses BOH Section Affiliates All Survey Responses
Strongly Agree
AgreeNeither Agree or Disagree
DisagreeStrongly Disagree
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1Promoting the role and value of local public health units
15 9 2 0 0 26 92 93 95 94
2
Providing important information to members about trends and events that will impact the public health system and management of public health units
10 8 8 0 0 26 69 97 86 85
3Facilitating professional networking and information sharing
13 10 3 0 0 26 88 83 82 85
4
Providing professional development to support excellence in public health unit leadership management and governance
3 15 7 1 0 26 69 83 86 79
5
Responding to public health sector issues when it makes the most sense to have a collective voice ie issues that impact the structure and funding of the public health sector and public health units and issues that have a broad focus on population health
15 8 2 0 1 26 88 97 95 93
PROPOSED AREAS OF FOCUS
COMOH Responses BOH Section Affiliates All Survey Responses
Strongly Agree
AgreeNeither Agree or Disagree
DisagreeStrongly Disagree
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1
COMOH and other professional groups within alPHa should do their own advocacy while alPHa supports members to share and support each others advocacy efforts
7 6 6 6 1 26 50 58 45 52
2
alPHa should provide support to action-oriented inter-professional work groups on priority public health unit issues and member resolutions
4 13 5 3 1 26 65 81 86 77
PROPOSALS
Page 8 of 8 ndash DRAFT FOR COMOH DISCUSSION
COMOH members were also asked to indicate the level of acceptability for some possible changes to alPHarsquos services and way of doing business
COMOH Responses BOH Section Affiliates All Survey Responses
Very Acceptable
Somewhat Acceptable
Neither Acceptable or Unacceptable
Somewhat Unacceptable
Very Unaccept
able
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1Single conference with additional face-to-face section meetings
21 2 0 1 0 24 96 68 80 81
2alPHa to offer alternatives like webinars on focussed topics
13 6 1 4 0 24 79 50 90 71
3Coordinate COMOH meetings with PHO OMA or Ministry events
16 4 2 0 0 22 91 na na --
4
Increase focus on building leadership and management capacity for health unit CEOs and senior management
7 9 4 3 0 23 70 na 70 70
5
Would it be acceptable for alPHa to request voluntary financial contributions from member PHUs in addition to annual fees
3 5 5 4 5 22 36 7 26 21
6
Would it be acceptable for alPHa to request voluntary in-kind staff contributions from member PHUs to expand alPHas capacity eg communications policy work group support
7 11 1 1 3 23 78 31 45 50
7Would it be acceptable to you for alPHa to discontinue staff support for COMOH (BOH Section)
0 4 1 5 14 24 17 11 na 14
8
Would it be acceptable to you for alPHa to reduce the amount of staff support for COMOH (BOH Section)
1 6 1 8 6 22 32 26 na 29
9
Would it be acceptable to you for alPHa to provide supports to MOHs and AMOHs (BOH Members) without maintaining COMOH (BOHs) as a section of the association
3 2 3 2 12 22 23 17 na 20
10
Would it be acceptable to you for alPHas Board of Directors to move from the current representational model to a skills-based strategic model ie board membership would be based on the skills needed to carry out alPHas strategic plan
6 11 2 1 3 23 74 56 56 62
11
Would it be acceptable to you for alPHas President Vice-President and Treasurer to be elected from the full membership of the alPHa Board of Directors (rather than the current model of alternating between BOH and COMOH members)
10 8 1 2 2 23 78 70 70 73
PROPOSED CHANGES
1 Council of Ontario Medical Officers of Health Terms of Reference
ASSOCIATION OF LOCAL PUBLIC HEALTH AGENCIES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
TERMS OF REFERENCE NAME 1 The name of the organization shall be ldquoThe Council of Ontario Medical Officers of
Health a section of the Association of Local Public Health Agencies (alPHa)rdquo hereinafter referred to as ldquothe Councilrdquo
MISSION 2 As local leaders in public health we are committed to improving the health of
Ontarians and increasing health equity by strengthening Ontariorsquos public health system We achieve this through system leadership and coordination in collaboration with the provincial government and other organizations and through evidence-informed advocacy on public health policy
OBJECTIVES 3 The objectives of the Council shall be
a) To provide strong province-wide leadership in public health
b) To advocate for health protection and promotion policies and programs that maintain and improve the health of Ontarians
c) To promote and maintain the highest standards for Ontariorsquos public health
programs and services
d) To support the planning implementation and evaluation of effective and efficiently run public health programs and services
e) To act as a forum for sharing information and resources and for addressing and
discussing public health issues both amongst the Councilrsquos members and other agencies that support the goals of alPHa eg Ontario Medical Association Ontario Public Health Association etc
f) To engage with and to provide public health and related policy advice to alPHa
the Chief Medical Officer of Health the Ontario Ministries of Health and Long-Term Care (including the Health Promotion and Public Health Divisions) Children
2 Council of Ontario Medical Officers of Health Terms of Reference
and Youth Services and other provincial ministries Public Health Ontario Health Canada the Public Health Agency of Canada and other public health partners
g) To promote and protect the professional interests of its members
h) To provide support to individual members as needed
i) To seek recognition for outstanding practice from among the members
j) To support evidence based practice of public health medicine
k) To engage and involve the membership to participate in COMOHrsquos endeavours
l) To mentor Public Health and Preventive Medicine Residents
MEMBERSHIP 4 Membership on the Council in each of the following categories is subject to the
limitations imposed by the current terms of reference and all policies and governing documents of the Association of Local Public Health Agencies Benefits of membership in each category are included in Appendix A These shall be subject to regular review and may be suspended under certain circumstances
Active membership in the Council shall be open to all Associate Medical Officers of Health and all full-time Medical Officers of Health whose Boards of Health are members of alPHa Such members shall have full voting privileges and may hold office in the Council Associate membership shall be open to all full and part-time physicians employed by a Board of Health that is a member of alPHa Such members shall not have voting privileges nor hold office
Affiliate membership shall be open to the following individuals interested in furthering the objectives of the Council
bull Public Health and Preventive Medicine Residents and Public Health and Preventive Medicine Residency Program Directors
bull Federal public health physicians working in Ontariorsquos First Nations communities
bull other public health or related physicians including those employed by a Board of Health that is not a member of alPHa
Such members shall not have voting privileges nor hold office
3 Council of Ontario Medical Officers of Health Terms of Reference
Emeritus membership shall be open to all former members who have retired after five (5) or more years of Active membership subject to the nomination in writing of two (2) active members in good standing endorsement of the Executive Committee and approval of the Council by majority vote at a general meeting Such members shall have neither voting privileges nor hold office but may be invited to attend general meetings Honorary membership shall be open to any non-active or associate member subject to the nomination in writing of two (2) active members in good standing endorsement of the Executive Committee and approval of the Council Such members shall have neither voting privileges nor hold office but may be invited to attend general meetings
OFFICERS 5 The Officers of the Council shall be the Chair Vice-Chair and immediate Past Chair
6 The Chair shall prepare the agendas of all Council meetings She shall preside and
preserve order at all such meetings shall ensure that these Terms of Reference are upheld and enforced and shall contribute to the supervision and evaluation of any Public Health and Preventive Medicine Resident who is on a placement with alPHa
7 The Vice-Chair shall fulfill the duties of the Chair in hisher absence The immediate
Past Chair may fulfill the duties of the Chair or Vice-Chair in their absences 8 The Chair shall normally serve a term of one (1) year which is renewable once and
after which the Vice-Chair shall normally assume the vacated office COMMITTEES 9 The Council shall elect seven (7) active members one from each of alPHarsquos regions
and the active member who is scheduled to serve as the President or immediate Past-President of alPHa to represent it on the alPHa Board of Directors These seven (7) members shall constitute the Councilrsquos Executive Committee and shall serve a term of at least one (1) year The Chair and Vice-Chair shall be elected from among the Executive Committee members If alPHarsquos immediate Past President is an active member she shall be an ex-officio member of the Executive Committee
10 The mandate of the Executive Committee shall be to facilitate the achievement of
the objectives of the Council by fulfilling the following
a Identifying priorities 1
1 See Appendix B Planning Cycle to Identify Priorities for COMOH
and ensuring the development of briefing documents and or recommendations as appropriate for the consideration of the Council
4 Council of Ontario Medical Officers of Health Terms of Reference
b Setting agendas and otherwise ensuring preparations for Council meetings c Ensuring the fulfillment of the direction of Council d Responding in a timely fashion to time-sensitive public health matters in
accordance with the Executive Committeersquos understanding of the perspective of the Council
e Engaging with the Chief Medical Officer of Health Associate Chief Medical Officers of Health and other provincial public health leaders and
f Representing Council at public and partner agency forums including the Public Health Leadership Council which shall normally include membership from the Officers of the Council and two other Executive Committee members as selected by agreement among the Executive
g Identifying opportunities for the recognition of outstanding practice from among the members including the annual nomination of at least one member for the alPHa Distinguished Service Award
11 The Executive Committee shall meet and correspond in the manner and at the times
and if required places as deemed necessary by the Chair to conduct the business of the Council A quorum shall consist of four (4) members
12 The Executive Committee shall have the power to strike committeestask or working
groups to assist it in carrying out the business of the Council 13 The Council may by special resolution remove a member of the Executive
Committee before the completion of hisher term of office and may elect a successor to complete the term The special resolution shall require a majority vote of 67 of the members present and voting at the meeting at which the special resolution is considered
14 A Nominating Committee shall consist of the three (3) most recent Past Chairs who
are able to serve and shall be chaired by the immediate Past Chair The Nominating Committee shall prepare a list of proposed Officers and Executive Committee members for the consideration of the Council at its Annual General Meeting
MEETINGS 15 The Council shall hold at least four (4) general meetings per year in a manner and at
the times and if required places as deemed necessary by the Executive Committee to share information direct and assist the Executive Committee in conducting the business of the Council
16 The Council shall hold its Annual General Meeting during and at the same place as
the alPHarsquos Annual Conference
5 Council of Ontario Medical Officers of Health Terms of Reference
17 The Council shall hold a special meeting at the call of the Chair or upon the written request specifying the purpose of such meeting of at least five (5) active members Council members must be given at least 48 hours notice of any special meeting
18 Only Councilrsquos active and associate members and alPHa staff are entitled to attend
general and special meetings of the Council Other members and non-members may be invited to attend all or part of such meetings as determined by the Chair preferably in consultation with the Executive Committee Non-members who come to such meetings without an invitation may attend all or part of the meeting by a majority vote of the active members present and voting
19 The Chair shall prepare the agendas for such meetings and shall normally include
reports from the Chair and the Councilrsquos committeestask or working groups and representatives to external bodies alPHarsquos Executive Director shall ensure that the minutes shall be recorded and promptly distributed to the Section
20 A quorum for all such meetings shall be ten (10) active members 21 The Council shall normally be notified in a manner deemed appropriate by the Chair
of such meetings at least one (1) month prior to their being held 22 A majority vote of the members present at such meetings and voting shall make
Council decisions In the case of a tied vote the Chair shall cast the deciding vote The Executive Committee shall ensure that actions arising from such decisions at such meetings are implemented and monitored
23 The Chair may solicit advice from the Council through the use of teleconferencing
and alPHarsquos electronic mailing lists in order to gain an understanding of the overall perspective of the Council (see 10d)
ELECTIONS 24 The Officers and Executive Committee members shall be elected at the Sectionrsquos
Annual General Meeting The Nominating Committee Chair or hisher designate shall present a list of nominations Additional nominations from the floor shall also be considered Each Officer and Executive Committee member shall be elected by secret ballot if necessary by a majority of the active members present and voting In the case of a tie the Chair shall cast the deciding vote
AMENDMENTS 25 The Councilrsquos Terms of Reference may be amended from time to time by the
Executive Committee provided the Committee receives notice of such proposed amendments at least one (1) month prior to the meeting at which the amendments
6 Council of Ontario Medical Officers of Health Terms of Reference
will be considered Such amendments shall be ratified by the Council at the next general meeting or the Annual General Meeting as the case may be
26 The Executive Committee shall review the Terms of Reference as required and not
less than once every two years Original September 1987 1st Revision October 2000 2nd Revision July 2001 3rd Revision December 2003 4th Revision February 2008 5th Revision June 2009 6th Revision June 2011 7th Revision June 2013
7 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX A
COMOH Membership Benefits Active Membership
bull Entitled to attend all meetings of the Section bull May hold office on the COMOH Executive Committee alPHa Board of Directors
Standing Committees bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Associate Membership
bull Entitled to attend all meetings of the Section bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Affiliate Membership
bull May attend meetings or parts thereof subject to approval of Chair bull May serve on ad-hoc committees of the Section subject to the approval of the
Executive Committee bull Discounted registration rates for alPHa Conferences (for Public Health and
Preventive Medicine Residents) bull Upon written request and subject to COMOH Executive approval Affiliate
Members may subscribe to comohlistsalphaweborg The approval will be reviewed on an annual basis in order to determine if the Affiliate Member can remain a subscriber to mohsalphaweborg
Emeritus Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair bull Enjoy discounted registration rates for alPHa Conferences and regular COMOH
meetings bull Subscription to comohlistsalphaweborg electronic mailing list bull Full access to alPHa Web site bull May represent alPHa COMOH on selected external committees and working
groups Honorary Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair
8 Council of Ontario Medical Officers of Health Terms of Reference
bull May represent alPHa COMOH on selected external committees and working groups subject to the approval of the COMOH or alPHa Executive Committee as appropriate
9 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX B
Planning Cycle to Identify Priorities for COMOH
1 There shall normally be a COMOH membership strategic planning retreat every four years In recognition of the dynamic environment of public health the need for and timing of such a retreat shall be at the discretion of the Executive Committee in consultation with the membership
2 The COMOH Executive is responsible (through the creation of a subcommittee of COMOH members) for ensuring the preparation for the COMOH retreats with resources to include those provided by alPHa
3 Leadership for action on COMOH priorities will be recruited from among the COMOH membership in order to make good use of the full base of capacity of the membership The resources to support actions will be recruited from both within and beyond the COMOH membership employing other public health professionals that reside within the broader public health system and community
4 The COMOH Executive shall ensure an annual review of strategic priorities and initiatives and the development of a draft report of the same for the review of the members at the June meeting
2013 Strategic Planning
Considerations for COMOH
As part of its strategic planning discussions alPHarsquos Board has been considering changes to the level of support provided to member sections A member survey is being carried out over the fall to determine options acceptable to alPHa members The following approach to support is put forward as a proposal for the consideration of COMOH Note that the feasibility of the points below depend upon future decisions of the alPHa board They assume that COMOH remains part of alPHa but becomes more independent in administering meetings
1 alPHa can provide to COMOH staff support (Gord Fleming) amounting to 02 FTE or one day per week This is a reduction from the current level of 35 days per week COMOH can choose to use the support any way it wants writing COMOH letters meeting minutes agenda support special projects etc
2 In addition to 02 FTE alPHa staff would provide support for up to 4 face-to-face meetings per year One meeting would be concurrent to alPHarsquos annual conference in June The timing of other meetings could be negotiated The support includes consulting on the development of the program arranging for speakers registration for the event arranging venue AV support and hospitality services
3 In addition to 02 FTE alPHa staff would provide support for setting meeting dates and any polling required to establish dates Note that the individual supporting this function would be Karen Reece
4 COMOHrsquos Executive and Section would continue to have access to online supports through the alPHa including the COMOH Listserve and a group page for posting agendas minutes and other resources on the alPHa website
5 alPHa staff (Linda Stewart and Gord Fleming) can also start participating on CMOH calls as a way to be up-to-date on issues related to COMOH
6 Other than what is outlined above COMOH would be expected to prepare agendas and take minutes for its Executive and Section meetings The Executive would be expected to operate more independently than it does now but would be able to access the supports outlined above
Prepared by Linda Stewart Executive Director
From comoh-bounceslistsalphaweborg on behalf of Christopher MackieTo MOH ListserveSubject [comoh] Fw URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)Date Wednesday October 30 2013 91241 AMAttachments ATT00249txt
For AMOHs and PHPM residents who didnt receive the initial email
Chris
Christopher Mackie MD MHSc FRCPCMedical Officer of Health and CEOMiddlesex-London Health Unit50 King St LondonON N6A 5L7 O 519 663 5317 ext 2444 wwwhealthunitcomFrom Pisko Laura (MOHLTC)Sent Tuesday October 29 2013 759 PMTo kbarkeralgomapublichealthcom malcolmlockbchuorg davidcchatham-kentcarobertkyledurhamca proumeliotiseohuca fwarshelginhealthonca mohelginhealthoncahlynnpublichealthgreybruceonca malcolmlockhnhuorg hnmohhnhuorglnoseworthyhkpronca bobnosalhaltonca elizabethrichardsonhamiltoncarschabashpechuonca ncameronhuroncountyca drimgemmillkflapublichealthcamohkflapublichealthca suditranadecounty-lambtononca paulastewarthealthunitorgChristopher Mackie valeriejaegerniagararegionca jimchiriconbpsdhuca jarthursnwhuoncaisralevyottawaca dnealoxfordcountyca davidmowatpeelregionca mklassenpdhuoncarpellizzaripcchuca rosemarieramsinghporcupinehuonca mcorriveaurcdhucomcharlesgardnersmdhuorg sutcliffepsdhucom davidwilliamstbdhucomspruytmtimiskaminghucom dmckeowntorontoca lnolanregionofwaterloocanicolamercerwdghuorg aheimannwechealthunitorg karimkurjiyorkcaCc coreywesleytbdhucom CindyBaker-Barillsmdhuorg Donna Kosmack pilonlsdhucomPaulaMuiskflapublichealthca sthibautorontoca Mueller Daina (MOHLTC) Gordon Marcus(MOHLTC) andreakitahamiltoncaSubject URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)
Dear Colleagues The ministry has received reports that some tobacco vendors across the province aregiving away single cigarettes with the purchase of tobacco products It is the ministryrsquosposition that giving out free single cigarettes does not violate subsection 31(3) of theSmoke-Free Ontario Act (ldquoSFOArdquo) Although the practice of giving out free singlecigarettes may promote the sale of tobacco products it does not take the form of aldquoproduct enhancement product association or promotional materialrdquo and therefore doesnot fall within the scope of subsection 31(3) of the SFOA We have confirmed with Health Canada that this practice may violate section 29(b) of thefederal Tobacco Act As such Health Canada is requesting that you notify them in writingand I am directing you to communicate with them via email and provide to them as manydetails as possible Emails should be sent to Tobacco-Ontariohc-scgcca and thesubject line should read ldquoViolation of Section 29(b) of Tobacco Actrdquo This will ensurethat the complaints are given priority status by Health Canada We will continue to monitor
this situation and liaise with our colleagues at Health Canada Please share this information with your tobacco control staff and contact me or DainaMueller Manager Tobacco Control Unit Health Promotion Implementation Branch atdainamuellerontarioca with any questions RegardsLaura Laura A PiskoDirectorHealth Promotion Implementation BranchHealth Promotion DivisionMinistry of Health and Long Term Care416-327-7445 (office)416-451-3185 (mobile) Marcus Gordon - EA (416)326-0625 for urgent issues
========= Middlesex-London Health Unit E-Mail Disclaimer =============______________________________________________________________
Private and confidential intended only for named recipient If otherwisereceived please destroy immediately Health information in this email isonly general information and is not intended to replace an in personconsultation with a medical professional nor is it intended to providemedical advice Individual circumstances of which we are not aware mayaffect the information provided herein and as such the Middlesex-LondonHealth Unit assumes no liability or responsibility for your reliancethereon The Middlesex-London Health Unit works under the authority of theHealth Protection and Promotion Act and this correspondence may be used toassess your needs for public health services (519-663-5317 ext 2448)______________________________________________________________
From Gardner CharlesTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes (RayCopesoahppca)
George Pasut (GeorgePasutoahppca) Peter Cooney (petercooneyhc-scgcca)Cc Ito DickSubject Discontinuation of Fluoridation in MuskokaDate Tuesday October 22 2013 125254 PM
Hello Colleagues
As I reported in my email below on September 26th fluoridation has come under challenge again inSimcoe Muskoka I am now very unhappy to report that despite our best efforts last night theDistrict Council of Muskoka voted to remove fluoride from municipal drinking supplies across theDistrict This brings to an end fluoridation in all of Simcoe and Muskoka (with the exception of Base Borden)ndash though New Tecumseth will be conducting a plebiscite on the question of fluoridation with themunicipal election next October Defending community water fluoridation has drained a great deal of time human resources andcommitment from other priorities and has been exhausting here in SMDHU as I am sure it hasbeen in many other health units While the outcomes have been very disappointing I have beenimpressed by the professionalism and dedication that SMDHU staff members have shown inshouldering this burden In particular our dental consultant Dr Ito has provided us with much ofthe foundational knowledge and the local research essential to our efforts and has very frequentlyattended and presented at council meetings and other public events I would also like to thank themany of you who have offer and provided support including advocacy letters and informationresources Over the years Dr Peter Cooney Chief Dental Officer of Health of Canada has beenvery helpful attending and presenting with us at council meetings and at public consultationevents We will of course continue our oral health surveillance of the children of Muskoka documentingand reporting in future years on the increase in dental decay that we anticipate will occur Suchsurveillance is the foundation of our advocacy both to municipal politicians and to the province I am very concerned that our experience will continue to repeat itself across the province unlessthere is strong leadership provincially It is with this in mind that I raise the followingrecommendations for your consideration
1 That we collectively (with PHOrsquos leadership) conduct high quality publish-worthy researchdocumenting the impact on dental decay that occurs in those municipalities throughoutOntario that in recent years have discontinued community water fluoridation This could bepart of a larger study on such municipalities across the country and it could also be part ofa study documenting overall oral health (including fluoridation coverage) in the province(and possibly across the country)
2 That COMOH engage with our Chief MOH to advocate for the province to require allmunicipal water supplies to be fluoridated (the exception of course being those withnaturally sufficient fluoride concentrations) This could built upon the alPHa position to
Gordon
Highlight
Gordon
Highlight
date (A11-00 - Community Water Fluoridation) on the CMOH position (Oral Health ndash) and on theemail discussion generated on the COMOH listserv some months back re Richardrsquosproposal (calling on the province to fund municipal water fluoridation)
Valerie I request that this be an item for our COMOH meeting on November 15th Sincerely Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorg From Gardner Charles Sent Thursday September 26 2013 245 PMTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes(RayCopesoahppca)Subject Community Water Fluoridation Under Challenge Again in Simcoe Muskoka Hello Colleagues You may wish to know that community water fluoridation (CWF) is again under challenge in SimcoeMuskoka specifically both in Tottenham (Town of New Tecumseth in Simcoe County) and for theentire District of Muskoka On Monday September 23 Committee of the Whole Council of theTown of New Tecumseth voted to submit application to discontinue community water fluoridation(CWF) in the town of Tottenham despite presentations to the contrary from our dental consultantDr Ito and from me The next Council meeting is scheduled for Monday Sept 30 at which lastMondayrsquos (Sept 23) votes will be ratified
Since Monday I have spoken with the Mayor of the Town of New Tecumseth and with most of thecouncilors encouraging deferral of a decision on Monday to allow the town more time to make afully informed decision
This is the second time in recent years that the issue of discontinuing CWF in Tottenham has beenraised at council This issue is also scheduled to return again to the District of Muskoka Council on
October 21st where I will be presenting in response to deputations in opposition to fluoridation
Outside of Base Borden Tottenham is the only community with fluoridated water in SimcoeCounty The health unitrsquos own screening data between 2011 and 2013 shows that Tottenhamrsquos
Gordon
Highlight
children as well as those in Muskoka have a lower rate of dental decay than Simcoe Muskokacommunities without CWF
Sincerely
Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorgChuck Gardner MOH
November 04 2013
Mandatory State Laws on Fluoridation Thirteen states Puerto Rico and the District of Columbia have laws intended to provide
statewide fluoridation These states and the year that the fluoridation legislation was passed are
District of Columbia (1952) Connecticut (1965) Kentucky (1966) Illinois (1967) Minnesota
(1967) Ohio (1969) South Dakota (1969) Georgia (1973) Nebraska (1973 and 2008)
California (1995) Delaware (1998) Puerto Rico (1998) Nevada (1999) Louisiana (2008) and
Arkansas (2011) (see Table 1) The sizes of the public water systems or countiescommunities
affected and exemption provisions vary by state Table 1
STATES THAT HAVE MANDATORY LAWS ON FLUORIDATION -2011
State (1) Year of
Fluoridation
Legislation (1)
Population
served by
Fluoridated
CWS (2)
Persons
receiving
fluoridated
water (2)
State
Average
Caries
Experience
of Grade 3
Students (3)
Arkansas 2011 647 1724131 64
California 1995 621 22812721 709
Connecticut 1965 910 2370423 406
Delaware 1998 862 705344 545
Georgia 1973 921 8924598 52
Illinois 1967 993 11325132 532
Kentucky 1966 999 4334223 598
Louisiana 2008 407 1846149 657
Minnesota 1967 988 4117266 549
Nebraska 1973 and 2008 702 1001665 593
Nevada 1999 702 1001665 649
Ohio 1969 877 8772683 512
South Dakota 1969 948 642942 623
District of
Columbia
1952 1000 595000
Puerto Rico 1998
United States 739 204283554
2010 Statistics for population fluoridated and number of people
1 Communication with Jane McGinley RDH MBA Manager Fluoridation and Preventive Health
Activities Council on Access Prevention and Interprofessional Relations
2 Centers for Disease Control and Prevention Department of Health and Human Services
accessed Oct 21 2013 httpwwwcdcgovfluoridationstatistics2010statshtm
3 Centers for Disease Control and Prevention National Oral Health Surveillance System Caries
Experience - Percentage of 3rd Grade students with Caries Experience (treated or untreated tooth
If data from 43 states for the percentage of Grade 3 children with experience of dental decay is
compared with the 2008 percentages of the population in a state with Community Water
Fluoridation then the percentage of children with experience of dental decay decreases as the
percentage of the state population with Community Water Fluoridation increases (see Figure 1)
Figure 1
Correlation of Percentage of Grade 3 Children with Caries Experience and
Percentage of Population With Community Water Fluoridation for 43
Reporting States
0
10
20
30
40
50
60
70
80
0 10 20 30 40 50 60 70 80 90 100
State of Population With Community Water Fluoridation
Sta
te
of
Gra
de 3
Stu
den
ts w
ith
Cari
es E
xp
eri
en
ce
Data from CDC (2 3)
The description of the fluoridation laws in California Illinois and Nevada can be found on the
Association of State amp Territorial Dental Directors website(4 7 8)
The California fluoridation law AB 733 came into effect in 1995 requiring communities of 10
000 residents or more be supplied with fluoridated drinking water However the state did not
provide any funding to implement the legislation (California is unique in requiring fluoridation
without funding the practice)(4) The California Department of Health Services therefore had to
fund fluoridation initiatives from non-governmental sources ie the California Endowment
California Dental Association Foundation the First 5 Commission and others(5) From 1995 to
2011 the percentage of the California population receiving fluoridated drinking water has risen
from 17 to 625(6) 4 Dental Public Health Activities amp Practices Office of Oral Health California Department of Health
Services April 2002 httpwwwastddorgbestpracticesDES06002CAfluoridationpdf
5 Stock M Pollick H The CDA Foundation Model to Fluoridate Communities California Dental
Association Journal vol 40 no 8 649 - 655
httpwwwcdaorgPortals0journaljournal_082012pdf
6 California Dental Association Foundation
httpwwwcdafoundationorglearnadvocacyfluoridation
The State of Illinois passed a mandatory fluoridation state in 1967 and required all community
water systems to adjust fluoride levels in the drinking water to optimal levels within 1 year(7)
From 1962 when over 5000000 residents had optimally fluoridated drinking water by 2010
the number had risen to 11325132 (993 of the population on community water systems)(2)
7 Dental Public Health Activities amp Practices Division of Oral Health Illinois Department of Public
Health April 2002 httpwwwastddorgbestpracticesDES16007ILfluoridationpdf
The State of Nevada passed a mandatory fluoridation statute in 2000 for communities with
400000 or more residents(8) This was a result of the work of a statewide coalition that
included the Nevada Dental and Dental Hygienist Associations the Washoe and Clark County
District Health Departments the Clark County School District Junior League of Las Vegas
Head Start the Community College of Southern Nevada Dental Hygiene Program Health
Access Washoe County and Saint Maryrsquos Hospital For communities with less than 400000 the
implementation of fluoridation still required the vote of the majority voters in the community
The Las Vegas Water Authority and the City of Henderson started fluoridation in 2000
increasing the percentage of the population with fluoridated drinking water from 2 to 65 (8) 8 Dental Public Health Activities amp Practices Bureau of Family Health Services Nevada State Health
Division April 2002 httpwwwastddorgbestpracticesDES31002NVfluoridationbillpdf
Countries with Mandatory Laws on Fluoridation Countries that have mandated Community Water Fluoridation are Brazil Hong Kong
Malaysia Singapore Ireland Israel and some of the states in Australia
Singapore started fluoridating its water in 1956 based on the success of the fluoridation trials in
Grand Rapids Newburgh Evanston and Brantford Singapore became the first Asian country to
have 100 of its population benefitting from the implementation of fluoridated drinking water
Loh reported that ldquoThe ten year study on the effects of water fluoridation in Singapore showed
a decrease in caries prevalence in the children In the permanent dentition the reduction was
523 per cent for Chinese and 31 per cent for Malays in the 7 to 9 year old age group A similar
trend was observed in the mixed dentition in which the decrease was 325 per cent for Chinese
and 306 per cent for Malaysrdquo(9) By 2010 the population of the country was 5080000(10)
9 Loh T Thirty-eight years of water fluoridation--the Singapore scenario Community Dent
Health 1996 Sep13 Suppl 247-50
10 British Fluoridation Society One in a Million the facts about water fluoridation 3rd Edition
published March 2012) httpwwwbfsweborgonemillion0920One20in20a20Million20-
20The20Extent20of20Fluoridationpdf
Hong Kong started implementing community water fluoridation in 1961 and similar to
Singapore 100 of the population received access to fluoridated drinking water Lo and Wong
reported that ldquoThe mean DMFT score of the children deceased from 44 in 1960 to 15 in 1968
stayed at this level in the 1980 and 1986 surveys and further deceased to 08 in 2001 The
prevalence of dental fluorosis among the children surveyed in 1960 was 1 and this increased
to 59 and 70 in 1968 and 1980 respectively It was found in the 1986 and 2001 surveys that
the prevalences of fluorosis were 47 and 9 among children whose teeth developed at the
time when the respective water fluoride concentrations were 07 ppm and 05 ppmrdquo(11) The
population of Hong Kong was 6968000 in 2009(10) 11 LO ECM and WONG AHH Water fluoride concentration and fluorosis in Hong Kong in 1960-
2001 84th General Session and Exhibition of the International Association for Dental Research amp
1st Meeting of the Pan-Asian-Pacific Federation Brisbane Australia 28 June-1 July 2006 v 85 n
Sp B
The Malaysian cabinet approved a nationwide community water fluoridation program in 1972
(12) One of the states Sabah decided to stop fluoridation in 1989 due to concerns about
inadequate supervision in adding fluoride to the drinking water Oral Health Surveys in 2009
and 2007 indicated that children in Sabah had the worst oral health with 50 of 12 year-olds
having decay in their permanent teeth and children having an average of 3 teeth being(13)
Under the 10th Malaysian Plan in 2011 the federal and the Sabah state governments
reintroduced water fluoridation in Sabah(1314) In 2010 about 755 of the Malaysian
population or 20700000 people had fluoridated drinking water(1013) 12 Malaysian Dental Association Fluoride in Water
httpwwwmdaorgmy07_public_01healthcare_12htm
13 Sachdev N Fluoridation in Sabah Water for Cleaner Teeth French Tribunecom 28022011
From Levy IsraTo Jaeger ValerieCc Pim Carolyn gordonalphaweborg Diallo Aicha Penny Sutcliffe Paul Roumeliotis Michael Finkelstein
Hazel Lynn Robert KyleSubject FW Panorama - Privacy Security and other issuesDate Wednesday October 16 2013 122110 PM
Hello ValerieOttawa is part of Wave 4 Panorama implementation and we are gearing up increasingly to use thesystem where and if possible Thinking about it I am anticipating that this may need to be on theCOMOH (and alPHa) radar as it is something that will impact all health units and implies a majoroperational shift in vaccine delivery programs for all health units I have asked Carolyn Pim toconnect with our sister wave 4 units to share common experiences as we move forward ndash when wehave a roll up could I bring to COMOH Exec for discussion to explore whether there are broaderimplications for all members As an aside I have also asked the Ministry and their CIO to share with me any roll up learnings thatthey may have had already from previous waves (I understand that Niagara HU was a wave 1participant so if there is such a roll up of common experiences that others could learn fromperhaps you have it already and that could come to the exec too)Thanks Isra From Pim Carolyn Sent October 10 2013 1228 PMTo Christopher Mackie (christophermackiemlhuonca) Elizabeth Richardson(Elizabethrichardsonhamiltonca) H BSc M D F R C P (C) MPH Jim Chirico(jimchiriconbpsdhuca) Marlene Spruyt (spruytmtimiskaminghucom) Robert Kyle (Durham)Cc Levy IsraSubject Panorama - Privacy Security and other issues Dear colleagues Irsquom reaching out to you as fellow Panorama Wave 4 health units to ask about where yourorganizations are at in the process of signing agreements and completing Privacy ImpactAssessments and Threat Risk Assessments (TRAs) Ottawa Public Healthrsquos IT legal and informationsecurity advisors have made numerous requests to the MOHLTC for information (in particular theprovincial TRA) that we consider essential to develop our own risk assessment and PIA but havebeen told that information cannot be shared even with strict confidentiality and access controlsSo we are at somewhat of an impasse Isra emailed Arlene yesterday Arlene has forwarded ourconcerns to the Ministryrsquos CIO and Panorama lead but we havenrsquot had any response or discussionswith either of them yet Have your organizations identified similar concerns andor had interactions with the MOHLTC inthis respect Irsquod also be interested in knowing if your health units have flagged other (egoperational) implementation concerns Thanks
Carolyn ps Robert ndash you can ignore this request I talked with Sharan this morning about Durhamrsquos issuesso am including you now just for information Carolyn Pim MD FRCPC Associate Medical Officer of Health Meacutedecin adjointe en santeacute publique Ottawa Public Health Santeacute publique Ottawa 100 Constellation Cr Ottawa ON K2G 6J8 Tel teacutel (613) 580-6744 ext 23684Fax (613) 580-9641Connect With Ottawa Public Health
Suivez Santeacute publique Ottawa
This e-mail originates from the City of Ottawa e-mail system Any distribution use orcopying of this e-mail or the information it contains by other than the intendedrecipient(s) is unauthorized If you are not the intended recipient please notify meat the telephone number shown above or by return e-mail and delete thiscommunication and any copy immediately Thank you
Le preacutesent courriel a eacuteteacute expeacutedieacute par le systegraveme de courriels de la Ville dOttawaToute distribution utilisation ou reproduction du courriel ou des renseignements quisy trouvent par une personne autre que son destinataire preacutevu est interdite Si vousavez reccedilu le message par erreur veuillez men aviser par teacuteleacutephone (au numeacuteropreacuteciteacute) ou par courriel puis supprimer sans deacutelai la version originale de lacommunication ainsi que toutes ses copies Je vous remercie de votre collaboration
1
Smoke-Free Patios ndash An Amendment to the Smoke-Free Ontario Act
Date November 15 2013 Prepared for Council of Ontario Medical Officers of Health Prepared by York Region Public Health _____________________________________________________________________________ Issue
The Smoke-Free Ontario Act is the current provincial legislation that imposes smoking restrictions in workplaces and public places It prohibits smoking on restaurant and bar patios in instances where any portion of the seating area is covered by a roof With recent studies illustrating that exposure to second hand smoke outdoors poses similar risks to indoor exposure there has been growing public support to enhance smoking restrictions and make patios completely smoke-free
Background
With the implementation of the Smoke-Free Ontario Act in 2006 restaurant and bar patios became subject to smoking restrictions if any portion of the seating area was covered by a roof This allowed for patios without roof coverings to continue to allow smoking and as a result did not provide significant protection to patrons or staff from exposure to second hand smoke outdoors Many businesses chose to alter the design of their patios to allow smoking to continue In some cases patios became more crowded since smoking patrons who dine indoors often proceed outside onto licensed patios with their beverages to smoke York Region like most municipalities in Ontario is host to hundreds of patios being operated by restaurant owners and businesses With smoking prohibitions affecting only a small portion of these patios specifically ones with coverings the vast majority of patios still allow smoking to take place Patrons and employees on patios where smoking is not restricted are exposed to second hand smoke frequently This can contribute to increased disease and aggravation of existing health conditions From a business perspective the existing legislation has been viewed by many operators as unfair because some patios have permanent coverings which cannot be removed requiring a smoke-free status These business owners feel this creates an uneven playing field since they cannot provide an outdoor dining area for their smoking customers There is strong community support for smoke-free patios in Ontario A 2009 Rapid Risk Factor Surveillance System survey revealed 754 percent support in York Region while a Toronto Health Survey in 2011 indicated 74 percent public support
2
Current Status
Smoking is currently prohibited on restaurant and bar patios province-wide in four Canadian provinces and territories Alberta Newfoundland and Labrador Nova Scotia and Yukon A fifth province Prince Edward Island prohibits smoking on patios until 10 pm Since Ontario enacted legislation restricting smoking on patios in 2006 eight municipalities in Ontario have chosen to create bylaws that go beyond the Smoke-Free Ontario Act and enhance outdoor protection from second hand smoke by prohibiting smoking on patios completely The largest of those municipalities is the City of Ottawa Recently the Toronto Board of Health unanimously endorsed a report presented by their Medical Officer of Health recommending that restaurant and bar patios be made smoke-free through an amendment to the Smoke-Free Ontario Act
Key Considerations
There should be no significant financial burden to local Boards of Health resulting from a smoke-free patio amendment to the Smoke-Free Ontario Act Inspection and enforcement for the Smoke-Free Ontario Act is currently 100 percent funded by the Ministry of Health and Long-Term Care Following an introductory period of education on the amendment a complaint response model of service delivery would ensure ongoing compliance with smoke-free requirements A complete ban of smoking on patios would eliminate the widely-held perception by business owners that the current legislation creates an uneven playing field for business Since Smoke-Free Ontario Act inspections of patios began in 2006 operators have expressed the opinion that if patios need to be smoke-free for the protection of the public they should all be smoke-free to avoid undue hardship for individual businesses and to provide protection uniformly across the Province
Next steps
York Region Public Health intends to seek support from Medical Officers of Health across the Central East Tobacco Control Area Network (CETCAN) to advocate to the Ministry of Health and Long-Term Care for an amendment to the Smoke-Free Ontario Act prohibiting smoking on all restaurant and bar patios York Region is also in the process of requesting that its Regional Council advocate to the Minister of Health and Long-Term Care on the issue
Updating and Modernizing O Regulation 565 (Public Pools)
Date November 15 2013
Prepared for Council of Ontario Medical Officers of Health
Prepared by York Region Public Health _____________________________________________________________________________ Background Recent drownings at public pools in Ontario have highlighted the issue of water-borne illness and injury The current pool regulation under Ontariorsquos Health Protection and Promotion Act O Regulation 565 (Public Pools) is outdated It does not accurately reflect new pool technology and design or the changing use of public pools Neither does it incorporate admissions standards recommended by the Office of the Chief Coroner Further O Regulation 565 does not have short-form wording or set fines associated with it This limits public health enforcement capabilities What is the impact Updating O Regulation 565 (Public Pools) to address recent changes in pool technology design and uses and to include Coroner-recommended admissions standards would help improve pool safety Establishing short-form wording for O Regulation 565 would enhance enforcement related to public pools Currently the only enforcement available to Public Health Inspectors for dealing with non-critical regulatory infractions in public pools is the issuance of a Part III summons This involves a considerable amount of resources for a possible small fine With the development of inspection disclosure systems such as YorkSafe there is an even greater need to develop a method to effectively address repeated pool operator non-compliance with non-critical issues Next steps Public health units should advocate to the Province to 1) Conduct a review of O Regulation 565 (Public Pools) to address shortcomings Proposed changes to the
regulation should include a requirement for ownersoperators of public pools to advise the local Medical Officer of Health of any change in the use of a facility and the addition of the Coronerrsquos recommended admission standards
2) Provide short-form wording for O Regulation 565 so that public health inspectors can better deal with pool operator non-compliance
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
Page 7 of 8 ndash DRAFT FOR COMOH DISCUSSION
To explore some proposed changes to Association services COMOH members were asked to provide their level of agreement with the following questions
COMOH Responses BOH Section Affiliates All Survey Responses
Strongly Agree
AgreeNeither Agree or Disagree
DisagreeStrongly Disagree
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1Promoting the role and value of local public health units
15 9 2 0 0 26 92 93 95 94
2
Providing important information to members about trends and events that will impact the public health system and management of public health units
10 8 8 0 0 26 69 97 86 85
3Facilitating professional networking and information sharing
13 10 3 0 0 26 88 83 82 85
4
Providing professional development to support excellence in public health unit leadership management and governance
3 15 7 1 0 26 69 83 86 79
5
Responding to public health sector issues when it makes the most sense to have a collective voice ie issues that impact the structure and funding of the public health sector and public health units and issues that have a broad focus on population health
15 8 2 0 1 26 88 97 95 93
PROPOSED AREAS OF FOCUS
COMOH Responses BOH Section Affiliates All Survey Responses
Strongly Agree
AgreeNeither Agree or Disagree
DisagreeStrongly Disagree
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1
COMOH and other professional groups within alPHa should do their own advocacy while alPHa supports members to share and support each others advocacy efforts
7 6 6 6 1 26 50 58 45 52
2
alPHa should provide support to action-oriented inter-professional work groups on priority public health unit issues and member resolutions
4 13 5 3 1 26 65 81 86 77
PROPOSALS
Page 8 of 8 ndash DRAFT FOR COMOH DISCUSSION
COMOH members were also asked to indicate the level of acceptability for some possible changes to alPHarsquos services and way of doing business
COMOH Responses BOH Section Affiliates All Survey Responses
Very Acceptable
Somewhat Acceptable
Neither Acceptable or Unacceptable
Somewhat Unacceptable
Very Unaccept
able
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1Single conference with additional face-to-face section meetings
21 2 0 1 0 24 96 68 80 81
2alPHa to offer alternatives like webinars on focussed topics
13 6 1 4 0 24 79 50 90 71
3Coordinate COMOH meetings with PHO OMA or Ministry events
16 4 2 0 0 22 91 na na --
4
Increase focus on building leadership and management capacity for health unit CEOs and senior management
7 9 4 3 0 23 70 na 70 70
5
Would it be acceptable for alPHa to request voluntary financial contributions from member PHUs in addition to annual fees
3 5 5 4 5 22 36 7 26 21
6
Would it be acceptable for alPHa to request voluntary in-kind staff contributions from member PHUs to expand alPHas capacity eg communications policy work group support
7 11 1 1 3 23 78 31 45 50
7Would it be acceptable to you for alPHa to discontinue staff support for COMOH (BOH Section)
0 4 1 5 14 24 17 11 na 14
8
Would it be acceptable to you for alPHa to reduce the amount of staff support for COMOH (BOH Section)
1 6 1 8 6 22 32 26 na 29
9
Would it be acceptable to you for alPHa to provide supports to MOHs and AMOHs (BOH Members) without maintaining COMOH (BOHs) as a section of the association
3 2 3 2 12 22 23 17 na 20
10
Would it be acceptable to you for alPHas Board of Directors to move from the current representational model to a skills-based strategic model ie board membership would be based on the skills needed to carry out alPHas strategic plan
6 11 2 1 3 23 74 56 56 62
11
Would it be acceptable to you for alPHas President Vice-President and Treasurer to be elected from the full membership of the alPHa Board of Directors (rather than the current model of alternating between BOH and COMOH members)
10 8 1 2 2 23 78 70 70 73
PROPOSED CHANGES
1 Council of Ontario Medical Officers of Health Terms of Reference
ASSOCIATION OF LOCAL PUBLIC HEALTH AGENCIES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
TERMS OF REFERENCE NAME 1 The name of the organization shall be ldquoThe Council of Ontario Medical Officers of
Health a section of the Association of Local Public Health Agencies (alPHa)rdquo hereinafter referred to as ldquothe Councilrdquo
MISSION 2 As local leaders in public health we are committed to improving the health of
Ontarians and increasing health equity by strengthening Ontariorsquos public health system We achieve this through system leadership and coordination in collaboration with the provincial government and other organizations and through evidence-informed advocacy on public health policy
OBJECTIVES 3 The objectives of the Council shall be
a) To provide strong province-wide leadership in public health
b) To advocate for health protection and promotion policies and programs that maintain and improve the health of Ontarians
c) To promote and maintain the highest standards for Ontariorsquos public health
programs and services
d) To support the planning implementation and evaluation of effective and efficiently run public health programs and services
e) To act as a forum for sharing information and resources and for addressing and
discussing public health issues both amongst the Councilrsquos members and other agencies that support the goals of alPHa eg Ontario Medical Association Ontario Public Health Association etc
f) To engage with and to provide public health and related policy advice to alPHa
the Chief Medical Officer of Health the Ontario Ministries of Health and Long-Term Care (including the Health Promotion and Public Health Divisions) Children
2 Council of Ontario Medical Officers of Health Terms of Reference
and Youth Services and other provincial ministries Public Health Ontario Health Canada the Public Health Agency of Canada and other public health partners
g) To promote and protect the professional interests of its members
h) To provide support to individual members as needed
i) To seek recognition for outstanding practice from among the members
j) To support evidence based practice of public health medicine
k) To engage and involve the membership to participate in COMOHrsquos endeavours
l) To mentor Public Health and Preventive Medicine Residents
MEMBERSHIP 4 Membership on the Council in each of the following categories is subject to the
limitations imposed by the current terms of reference and all policies and governing documents of the Association of Local Public Health Agencies Benefits of membership in each category are included in Appendix A These shall be subject to regular review and may be suspended under certain circumstances
Active membership in the Council shall be open to all Associate Medical Officers of Health and all full-time Medical Officers of Health whose Boards of Health are members of alPHa Such members shall have full voting privileges and may hold office in the Council Associate membership shall be open to all full and part-time physicians employed by a Board of Health that is a member of alPHa Such members shall not have voting privileges nor hold office
Affiliate membership shall be open to the following individuals interested in furthering the objectives of the Council
bull Public Health and Preventive Medicine Residents and Public Health and Preventive Medicine Residency Program Directors
bull Federal public health physicians working in Ontariorsquos First Nations communities
bull other public health or related physicians including those employed by a Board of Health that is not a member of alPHa
Such members shall not have voting privileges nor hold office
3 Council of Ontario Medical Officers of Health Terms of Reference
Emeritus membership shall be open to all former members who have retired after five (5) or more years of Active membership subject to the nomination in writing of two (2) active members in good standing endorsement of the Executive Committee and approval of the Council by majority vote at a general meeting Such members shall have neither voting privileges nor hold office but may be invited to attend general meetings Honorary membership shall be open to any non-active or associate member subject to the nomination in writing of two (2) active members in good standing endorsement of the Executive Committee and approval of the Council Such members shall have neither voting privileges nor hold office but may be invited to attend general meetings
OFFICERS 5 The Officers of the Council shall be the Chair Vice-Chair and immediate Past Chair
6 The Chair shall prepare the agendas of all Council meetings She shall preside and
preserve order at all such meetings shall ensure that these Terms of Reference are upheld and enforced and shall contribute to the supervision and evaluation of any Public Health and Preventive Medicine Resident who is on a placement with alPHa
7 The Vice-Chair shall fulfill the duties of the Chair in hisher absence The immediate
Past Chair may fulfill the duties of the Chair or Vice-Chair in their absences 8 The Chair shall normally serve a term of one (1) year which is renewable once and
after which the Vice-Chair shall normally assume the vacated office COMMITTEES 9 The Council shall elect seven (7) active members one from each of alPHarsquos regions
and the active member who is scheduled to serve as the President or immediate Past-President of alPHa to represent it on the alPHa Board of Directors These seven (7) members shall constitute the Councilrsquos Executive Committee and shall serve a term of at least one (1) year The Chair and Vice-Chair shall be elected from among the Executive Committee members If alPHarsquos immediate Past President is an active member she shall be an ex-officio member of the Executive Committee
10 The mandate of the Executive Committee shall be to facilitate the achievement of
the objectives of the Council by fulfilling the following
a Identifying priorities 1
1 See Appendix B Planning Cycle to Identify Priorities for COMOH
and ensuring the development of briefing documents and or recommendations as appropriate for the consideration of the Council
4 Council of Ontario Medical Officers of Health Terms of Reference
b Setting agendas and otherwise ensuring preparations for Council meetings c Ensuring the fulfillment of the direction of Council d Responding in a timely fashion to time-sensitive public health matters in
accordance with the Executive Committeersquos understanding of the perspective of the Council
e Engaging with the Chief Medical Officer of Health Associate Chief Medical Officers of Health and other provincial public health leaders and
f Representing Council at public and partner agency forums including the Public Health Leadership Council which shall normally include membership from the Officers of the Council and two other Executive Committee members as selected by agreement among the Executive
g Identifying opportunities for the recognition of outstanding practice from among the members including the annual nomination of at least one member for the alPHa Distinguished Service Award
11 The Executive Committee shall meet and correspond in the manner and at the times
and if required places as deemed necessary by the Chair to conduct the business of the Council A quorum shall consist of four (4) members
12 The Executive Committee shall have the power to strike committeestask or working
groups to assist it in carrying out the business of the Council 13 The Council may by special resolution remove a member of the Executive
Committee before the completion of hisher term of office and may elect a successor to complete the term The special resolution shall require a majority vote of 67 of the members present and voting at the meeting at which the special resolution is considered
14 A Nominating Committee shall consist of the three (3) most recent Past Chairs who
are able to serve and shall be chaired by the immediate Past Chair The Nominating Committee shall prepare a list of proposed Officers and Executive Committee members for the consideration of the Council at its Annual General Meeting
MEETINGS 15 The Council shall hold at least four (4) general meetings per year in a manner and at
the times and if required places as deemed necessary by the Executive Committee to share information direct and assist the Executive Committee in conducting the business of the Council
16 The Council shall hold its Annual General Meeting during and at the same place as
the alPHarsquos Annual Conference
5 Council of Ontario Medical Officers of Health Terms of Reference
17 The Council shall hold a special meeting at the call of the Chair or upon the written request specifying the purpose of such meeting of at least five (5) active members Council members must be given at least 48 hours notice of any special meeting
18 Only Councilrsquos active and associate members and alPHa staff are entitled to attend
general and special meetings of the Council Other members and non-members may be invited to attend all or part of such meetings as determined by the Chair preferably in consultation with the Executive Committee Non-members who come to such meetings without an invitation may attend all or part of the meeting by a majority vote of the active members present and voting
19 The Chair shall prepare the agendas for such meetings and shall normally include
reports from the Chair and the Councilrsquos committeestask or working groups and representatives to external bodies alPHarsquos Executive Director shall ensure that the minutes shall be recorded and promptly distributed to the Section
20 A quorum for all such meetings shall be ten (10) active members 21 The Council shall normally be notified in a manner deemed appropriate by the Chair
of such meetings at least one (1) month prior to their being held 22 A majority vote of the members present at such meetings and voting shall make
Council decisions In the case of a tied vote the Chair shall cast the deciding vote The Executive Committee shall ensure that actions arising from such decisions at such meetings are implemented and monitored
23 The Chair may solicit advice from the Council through the use of teleconferencing
and alPHarsquos electronic mailing lists in order to gain an understanding of the overall perspective of the Council (see 10d)
ELECTIONS 24 The Officers and Executive Committee members shall be elected at the Sectionrsquos
Annual General Meeting The Nominating Committee Chair or hisher designate shall present a list of nominations Additional nominations from the floor shall also be considered Each Officer and Executive Committee member shall be elected by secret ballot if necessary by a majority of the active members present and voting In the case of a tie the Chair shall cast the deciding vote
AMENDMENTS 25 The Councilrsquos Terms of Reference may be amended from time to time by the
Executive Committee provided the Committee receives notice of such proposed amendments at least one (1) month prior to the meeting at which the amendments
6 Council of Ontario Medical Officers of Health Terms of Reference
will be considered Such amendments shall be ratified by the Council at the next general meeting or the Annual General Meeting as the case may be
26 The Executive Committee shall review the Terms of Reference as required and not
less than once every two years Original September 1987 1st Revision October 2000 2nd Revision July 2001 3rd Revision December 2003 4th Revision February 2008 5th Revision June 2009 6th Revision June 2011 7th Revision June 2013
7 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX A
COMOH Membership Benefits Active Membership
bull Entitled to attend all meetings of the Section bull May hold office on the COMOH Executive Committee alPHa Board of Directors
Standing Committees bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Associate Membership
bull Entitled to attend all meetings of the Section bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Affiliate Membership
bull May attend meetings or parts thereof subject to approval of Chair bull May serve on ad-hoc committees of the Section subject to the approval of the
Executive Committee bull Discounted registration rates for alPHa Conferences (for Public Health and
Preventive Medicine Residents) bull Upon written request and subject to COMOH Executive approval Affiliate
Members may subscribe to comohlistsalphaweborg The approval will be reviewed on an annual basis in order to determine if the Affiliate Member can remain a subscriber to mohsalphaweborg
Emeritus Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair bull Enjoy discounted registration rates for alPHa Conferences and regular COMOH
meetings bull Subscription to comohlistsalphaweborg electronic mailing list bull Full access to alPHa Web site bull May represent alPHa COMOH on selected external committees and working
groups Honorary Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair
8 Council of Ontario Medical Officers of Health Terms of Reference
bull May represent alPHa COMOH on selected external committees and working groups subject to the approval of the COMOH or alPHa Executive Committee as appropriate
9 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX B
Planning Cycle to Identify Priorities for COMOH
1 There shall normally be a COMOH membership strategic planning retreat every four years In recognition of the dynamic environment of public health the need for and timing of such a retreat shall be at the discretion of the Executive Committee in consultation with the membership
2 The COMOH Executive is responsible (through the creation of a subcommittee of COMOH members) for ensuring the preparation for the COMOH retreats with resources to include those provided by alPHa
3 Leadership for action on COMOH priorities will be recruited from among the COMOH membership in order to make good use of the full base of capacity of the membership The resources to support actions will be recruited from both within and beyond the COMOH membership employing other public health professionals that reside within the broader public health system and community
4 The COMOH Executive shall ensure an annual review of strategic priorities and initiatives and the development of a draft report of the same for the review of the members at the June meeting
2013 Strategic Planning
Considerations for COMOH
As part of its strategic planning discussions alPHarsquos Board has been considering changes to the level of support provided to member sections A member survey is being carried out over the fall to determine options acceptable to alPHa members The following approach to support is put forward as a proposal for the consideration of COMOH Note that the feasibility of the points below depend upon future decisions of the alPHa board They assume that COMOH remains part of alPHa but becomes more independent in administering meetings
1 alPHa can provide to COMOH staff support (Gord Fleming) amounting to 02 FTE or one day per week This is a reduction from the current level of 35 days per week COMOH can choose to use the support any way it wants writing COMOH letters meeting minutes agenda support special projects etc
2 In addition to 02 FTE alPHa staff would provide support for up to 4 face-to-face meetings per year One meeting would be concurrent to alPHarsquos annual conference in June The timing of other meetings could be negotiated The support includes consulting on the development of the program arranging for speakers registration for the event arranging venue AV support and hospitality services
3 In addition to 02 FTE alPHa staff would provide support for setting meeting dates and any polling required to establish dates Note that the individual supporting this function would be Karen Reece
4 COMOHrsquos Executive and Section would continue to have access to online supports through the alPHa including the COMOH Listserve and a group page for posting agendas minutes and other resources on the alPHa website
5 alPHa staff (Linda Stewart and Gord Fleming) can also start participating on CMOH calls as a way to be up-to-date on issues related to COMOH
6 Other than what is outlined above COMOH would be expected to prepare agendas and take minutes for its Executive and Section meetings The Executive would be expected to operate more independently than it does now but would be able to access the supports outlined above
Prepared by Linda Stewart Executive Director
From comoh-bounceslistsalphaweborg on behalf of Christopher MackieTo MOH ListserveSubject [comoh] Fw URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)Date Wednesday October 30 2013 91241 AMAttachments ATT00249txt
For AMOHs and PHPM residents who didnt receive the initial email
Chris
Christopher Mackie MD MHSc FRCPCMedical Officer of Health and CEOMiddlesex-London Health Unit50 King St LondonON N6A 5L7 O 519 663 5317 ext 2444 wwwhealthunitcomFrom Pisko Laura (MOHLTC)Sent Tuesday October 29 2013 759 PMTo kbarkeralgomapublichealthcom malcolmlockbchuorg davidcchatham-kentcarobertkyledurhamca proumeliotiseohuca fwarshelginhealthonca mohelginhealthoncahlynnpublichealthgreybruceonca malcolmlockhnhuorg hnmohhnhuorglnoseworthyhkpronca bobnosalhaltonca elizabethrichardsonhamiltoncarschabashpechuonca ncameronhuroncountyca drimgemmillkflapublichealthcamohkflapublichealthca suditranadecounty-lambtononca paulastewarthealthunitorgChristopher Mackie valeriejaegerniagararegionca jimchiriconbpsdhuca jarthursnwhuoncaisralevyottawaca dnealoxfordcountyca davidmowatpeelregionca mklassenpdhuoncarpellizzaripcchuca rosemarieramsinghporcupinehuonca mcorriveaurcdhucomcharlesgardnersmdhuorg sutcliffepsdhucom davidwilliamstbdhucomspruytmtimiskaminghucom dmckeowntorontoca lnolanregionofwaterloocanicolamercerwdghuorg aheimannwechealthunitorg karimkurjiyorkcaCc coreywesleytbdhucom CindyBaker-Barillsmdhuorg Donna Kosmack pilonlsdhucomPaulaMuiskflapublichealthca sthibautorontoca Mueller Daina (MOHLTC) Gordon Marcus(MOHLTC) andreakitahamiltoncaSubject URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)
Dear Colleagues The ministry has received reports that some tobacco vendors across the province aregiving away single cigarettes with the purchase of tobacco products It is the ministryrsquosposition that giving out free single cigarettes does not violate subsection 31(3) of theSmoke-Free Ontario Act (ldquoSFOArdquo) Although the practice of giving out free singlecigarettes may promote the sale of tobacco products it does not take the form of aldquoproduct enhancement product association or promotional materialrdquo and therefore doesnot fall within the scope of subsection 31(3) of the SFOA We have confirmed with Health Canada that this practice may violate section 29(b) of thefederal Tobacco Act As such Health Canada is requesting that you notify them in writingand I am directing you to communicate with them via email and provide to them as manydetails as possible Emails should be sent to Tobacco-Ontariohc-scgcca and thesubject line should read ldquoViolation of Section 29(b) of Tobacco Actrdquo This will ensurethat the complaints are given priority status by Health Canada We will continue to monitor
this situation and liaise with our colleagues at Health Canada Please share this information with your tobacco control staff and contact me or DainaMueller Manager Tobacco Control Unit Health Promotion Implementation Branch atdainamuellerontarioca with any questions RegardsLaura Laura A PiskoDirectorHealth Promotion Implementation BranchHealth Promotion DivisionMinistry of Health and Long Term Care416-327-7445 (office)416-451-3185 (mobile) Marcus Gordon - EA (416)326-0625 for urgent issues
========= Middlesex-London Health Unit E-Mail Disclaimer =============______________________________________________________________
Private and confidential intended only for named recipient If otherwisereceived please destroy immediately Health information in this email isonly general information and is not intended to replace an in personconsultation with a medical professional nor is it intended to providemedical advice Individual circumstances of which we are not aware mayaffect the information provided herein and as such the Middlesex-LondonHealth Unit assumes no liability or responsibility for your reliancethereon The Middlesex-London Health Unit works under the authority of theHealth Protection and Promotion Act and this correspondence may be used toassess your needs for public health services (519-663-5317 ext 2448)______________________________________________________________
From Gardner CharlesTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes (RayCopesoahppca)
George Pasut (GeorgePasutoahppca) Peter Cooney (petercooneyhc-scgcca)Cc Ito DickSubject Discontinuation of Fluoridation in MuskokaDate Tuesday October 22 2013 125254 PM
Hello Colleagues
As I reported in my email below on September 26th fluoridation has come under challenge again inSimcoe Muskoka I am now very unhappy to report that despite our best efforts last night theDistrict Council of Muskoka voted to remove fluoride from municipal drinking supplies across theDistrict This brings to an end fluoridation in all of Simcoe and Muskoka (with the exception of Base Borden)ndash though New Tecumseth will be conducting a plebiscite on the question of fluoridation with themunicipal election next October Defending community water fluoridation has drained a great deal of time human resources andcommitment from other priorities and has been exhausting here in SMDHU as I am sure it hasbeen in many other health units While the outcomes have been very disappointing I have beenimpressed by the professionalism and dedication that SMDHU staff members have shown inshouldering this burden In particular our dental consultant Dr Ito has provided us with much ofthe foundational knowledge and the local research essential to our efforts and has very frequentlyattended and presented at council meetings and other public events I would also like to thank themany of you who have offer and provided support including advocacy letters and informationresources Over the years Dr Peter Cooney Chief Dental Officer of Health of Canada has beenvery helpful attending and presenting with us at council meetings and at public consultationevents We will of course continue our oral health surveillance of the children of Muskoka documentingand reporting in future years on the increase in dental decay that we anticipate will occur Suchsurveillance is the foundation of our advocacy both to municipal politicians and to the province I am very concerned that our experience will continue to repeat itself across the province unlessthere is strong leadership provincially It is with this in mind that I raise the followingrecommendations for your consideration
1 That we collectively (with PHOrsquos leadership) conduct high quality publish-worthy researchdocumenting the impact on dental decay that occurs in those municipalities throughoutOntario that in recent years have discontinued community water fluoridation This could bepart of a larger study on such municipalities across the country and it could also be part ofa study documenting overall oral health (including fluoridation coverage) in the province(and possibly across the country)
2 That COMOH engage with our Chief MOH to advocate for the province to require allmunicipal water supplies to be fluoridated (the exception of course being those withnaturally sufficient fluoride concentrations) This could built upon the alPHa position to
Gordon
Highlight
Gordon
Highlight
date (A11-00 - Community Water Fluoridation) on the CMOH position (Oral Health ndash) and on theemail discussion generated on the COMOH listserv some months back re Richardrsquosproposal (calling on the province to fund municipal water fluoridation)
Valerie I request that this be an item for our COMOH meeting on November 15th Sincerely Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorg From Gardner Charles Sent Thursday September 26 2013 245 PMTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes(RayCopesoahppca)Subject Community Water Fluoridation Under Challenge Again in Simcoe Muskoka Hello Colleagues You may wish to know that community water fluoridation (CWF) is again under challenge in SimcoeMuskoka specifically both in Tottenham (Town of New Tecumseth in Simcoe County) and for theentire District of Muskoka On Monday September 23 Committee of the Whole Council of theTown of New Tecumseth voted to submit application to discontinue community water fluoridation(CWF) in the town of Tottenham despite presentations to the contrary from our dental consultantDr Ito and from me The next Council meeting is scheduled for Monday Sept 30 at which lastMondayrsquos (Sept 23) votes will be ratified
Since Monday I have spoken with the Mayor of the Town of New Tecumseth and with most of thecouncilors encouraging deferral of a decision on Monday to allow the town more time to make afully informed decision
This is the second time in recent years that the issue of discontinuing CWF in Tottenham has beenraised at council This issue is also scheduled to return again to the District of Muskoka Council on
October 21st where I will be presenting in response to deputations in opposition to fluoridation
Outside of Base Borden Tottenham is the only community with fluoridated water in SimcoeCounty The health unitrsquos own screening data between 2011 and 2013 shows that Tottenhamrsquos
Gordon
Highlight
children as well as those in Muskoka have a lower rate of dental decay than Simcoe Muskokacommunities without CWF
Sincerely
Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorgChuck Gardner MOH
November 04 2013
Mandatory State Laws on Fluoridation Thirteen states Puerto Rico and the District of Columbia have laws intended to provide
statewide fluoridation These states and the year that the fluoridation legislation was passed are
District of Columbia (1952) Connecticut (1965) Kentucky (1966) Illinois (1967) Minnesota
(1967) Ohio (1969) South Dakota (1969) Georgia (1973) Nebraska (1973 and 2008)
California (1995) Delaware (1998) Puerto Rico (1998) Nevada (1999) Louisiana (2008) and
Arkansas (2011) (see Table 1) The sizes of the public water systems or countiescommunities
affected and exemption provisions vary by state Table 1
STATES THAT HAVE MANDATORY LAWS ON FLUORIDATION -2011
State (1) Year of
Fluoridation
Legislation (1)
Population
served by
Fluoridated
CWS (2)
Persons
receiving
fluoridated
water (2)
State
Average
Caries
Experience
of Grade 3
Students (3)
Arkansas 2011 647 1724131 64
California 1995 621 22812721 709
Connecticut 1965 910 2370423 406
Delaware 1998 862 705344 545
Georgia 1973 921 8924598 52
Illinois 1967 993 11325132 532
Kentucky 1966 999 4334223 598
Louisiana 2008 407 1846149 657
Minnesota 1967 988 4117266 549
Nebraska 1973 and 2008 702 1001665 593
Nevada 1999 702 1001665 649
Ohio 1969 877 8772683 512
South Dakota 1969 948 642942 623
District of
Columbia
1952 1000 595000
Puerto Rico 1998
United States 739 204283554
2010 Statistics for population fluoridated and number of people
1 Communication with Jane McGinley RDH MBA Manager Fluoridation and Preventive Health
Activities Council on Access Prevention and Interprofessional Relations
2 Centers for Disease Control and Prevention Department of Health and Human Services
accessed Oct 21 2013 httpwwwcdcgovfluoridationstatistics2010statshtm
3 Centers for Disease Control and Prevention National Oral Health Surveillance System Caries
Experience - Percentage of 3rd Grade students with Caries Experience (treated or untreated tooth
If data from 43 states for the percentage of Grade 3 children with experience of dental decay is
compared with the 2008 percentages of the population in a state with Community Water
Fluoridation then the percentage of children with experience of dental decay decreases as the
percentage of the state population with Community Water Fluoridation increases (see Figure 1)
Figure 1
Correlation of Percentage of Grade 3 Children with Caries Experience and
Percentage of Population With Community Water Fluoridation for 43
Reporting States
0
10
20
30
40
50
60
70
80
0 10 20 30 40 50 60 70 80 90 100
State of Population With Community Water Fluoridation
Sta
te
of
Gra
de 3
Stu
den
ts w
ith
Cari
es E
xp
eri
en
ce
Data from CDC (2 3)
The description of the fluoridation laws in California Illinois and Nevada can be found on the
Association of State amp Territorial Dental Directors website(4 7 8)
The California fluoridation law AB 733 came into effect in 1995 requiring communities of 10
000 residents or more be supplied with fluoridated drinking water However the state did not
provide any funding to implement the legislation (California is unique in requiring fluoridation
without funding the practice)(4) The California Department of Health Services therefore had to
fund fluoridation initiatives from non-governmental sources ie the California Endowment
California Dental Association Foundation the First 5 Commission and others(5) From 1995 to
2011 the percentage of the California population receiving fluoridated drinking water has risen
from 17 to 625(6) 4 Dental Public Health Activities amp Practices Office of Oral Health California Department of Health
Services April 2002 httpwwwastddorgbestpracticesDES06002CAfluoridationpdf
5 Stock M Pollick H The CDA Foundation Model to Fluoridate Communities California Dental
Association Journal vol 40 no 8 649 - 655
httpwwwcdaorgPortals0journaljournal_082012pdf
6 California Dental Association Foundation
httpwwwcdafoundationorglearnadvocacyfluoridation
The State of Illinois passed a mandatory fluoridation state in 1967 and required all community
water systems to adjust fluoride levels in the drinking water to optimal levels within 1 year(7)
From 1962 when over 5000000 residents had optimally fluoridated drinking water by 2010
the number had risen to 11325132 (993 of the population on community water systems)(2)
7 Dental Public Health Activities amp Practices Division of Oral Health Illinois Department of Public
Health April 2002 httpwwwastddorgbestpracticesDES16007ILfluoridationpdf
The State of Nevada passed a mandatory fluoridation statute in 2000 for communities with
400000 or more residents(8) This was a result of the work of a statewide coalition that
included the Nevada Dental and Dental Hygienist Associations the Washoe and Clark County
District Health Departments the Clark County School District Junior League of Las Vegas
Head Start the Community College of Southern Nevada Dental Hygiene Program Health
Access Washoe County and Saint Maryrsquos Hospital For communities with less than 400000 the
implementation of fluoridation still required the vote of the majority voters in the community
The Las Vegas Water Authority and the City of Henderson started fluoridation in 2000
increasing the percentage of the population with fluoridated drinking water from 2 to 65 (8) 8 Dental Public Health Activities amp Practices Bureau of Family Health Services Nevada State Health
Division April 2002 httpwwwastddorgbestpracticesDES31002NVfluoridationbillpdf
Countries with Mandatory Laws on Fluoridation Countries that have mandated Community Water Fluoridation are Brazil Hong Kong
Malaysia Singapore Ireland Israel and some of the states in Australia
Singapore started fluoridating its water in 1956 based on the success of the fluoridation trials in
Grand Rapids Newburgh Evanston and Brantford Singapore became the first Asian country to
have 100 of its population benefitting from the implementation of fluoridated drinking water
Loh reported that ldquoThe ten year study on the effects of water fluoridation in Singapore showed
a decrease in caries prevalence in the children In the permanent dentition the reduction was
523 per cent for Chinese and 31 per cent for Malays in the 7 to 9 year old age group A similar
trend was observed in the mixed dentition in which the decrease was 325 per cent for Chinese
and 306 per cent for Malaysrdquo(9) By 2010 the population of the country was 5080000(10)
9 Loh T Thirty-eight years of water fluoridation--the Singapore scenario Community Dent
Health 1996 Sep13 Suppl 247-50
10 British Fluoridation Society One in a Million the facts about water fluoridation 3rd Edition
published March 2012) httpwwwbfsweborgonemillion0920One20in20a20Million20-
20The20Extent20of20Fluoridationpdf
Hong Kong started implementing community water fluoridation in 1961 and similar to
Singapore 100 of the population received access to fluoridated drinking water Lo and Wong
reported that ldquoThe mean DMFT score of the children deceased from 44 in 1960 to 15 in 1968
stayed at this level in the 1980 and 1986 surveys and further deceased to 08 in 2001 The
prevalence of dental fluorosis among the children surveyed in 1960 was 1 and this increased
to 59 and 70 in 1968 and 1980 respectively It was found in the 1986 and 2001 surveys that
the prevalences of fluorosis were 47 and 9 among children whose teeth developed at the
time when the respective water fluoride concentrations were 07 ppm and 05 ppmrdquo(11) The
population of Hong Kong was 6968000 in 2009(10) 11 LO ECM and WONG AHH Water fluoride concentration and fluorosis in Hong Kong in 1960-
2001 84th General Session and Exhibition of the International Association for Dental Research amp
1st Meeting of the Pan-Asian-Pacific Federation Brisbane Australia 28 June-1 July 2006 v 85 n
Sp B
The Malaysian cabinet approved a nationwide community water fluoridation program in 1972
(12) One of the states Sabah decided to stop fluoridation in 1989 due to concerns about
inadequate supervision in adding fluoride to the drinking water Oral Health Surveys in 2009
and 2007 indicated that children in Sabah had the worst oral health with 50 of 12 year-olds
having decay in their permanent teeth and children having an average of 3 teeth being(13)
Under the 10th Malaysian Plan in 2011 the federal and the Sabah state governments
reintroduced water fluoridation in Sabah(1314) In 2010 about 755 of the Malaysian
population or 20700000 people had fluoridated drinking water(1013) 12 Malaysian Dental Association Fluoride in Water
httpwwwmdaorgmy07_public_01healthcare_12htm
13 Sachdev N Fluoridation in Sabah Water for Cleaner Teeth French Tribunecom 28022011
From Levy IsraTo Jaeger ValerieCc Pim Carolyn gordonalphaweborg Diallo Aicha Penny Sutcliffe Paul Roumeliotis Michael Finkelstein
Hazel Lynn Robert KyleSubject FW Panorama - Privacy Security and other issuesDate Wednesday October 16 2013 122110 PM
Hello ValerieOttawa is part of Wave 4 Panorama implementation and we are gearing up increasingly to use thesystem where and if possible Thinking about it I am anticipating that this may need to be on theCOMOH (and alPHa) radar as it is something that will impact all health units and implies a majoroperational shift in vaccine delivery programs for all health units I have asked Carolyn Pim toconnect with our sister wave 4 units to share common experiences as we move forward ndash when wehave a roll up could I bring to COMOH Exec for discussion to explore whether there are broaderimplications for all members As an aside I have also asked the Ministry and their CIO to share with me any roll up learnings thatthey may have had already from previous waves (I understand that Niagara HU was a wave 1participant so if there is such a roll up of common experiences that others could learn fromperhaps you have it already and that could come to the exec too)Thanks Isra From Pim Carolyn Sent October 10 2013 1228 PMTo Christopher Mackie (christophermackiemlhuonca) Elizabeth Richardson(Elizabethrichardsonhamiltonca) H BSc M D F R C P (C) MPH Jim Chirico(jimchiriconbpsdhuca) Marlene Spruyt (spruytmtimiskaminghucom) Robert Kyle (Durham)Cc Levy IsraSubject Panorama - Privacy Security and other issues Dear colleagues Irsquom reaching out to you as fellow Panorama Wave 4 health units to ask about where yourorganizations are at in the process of signing agreements and completing Privacy ImpactAssessments and Threat Risk Assessments (TRAs) Ottawa Public Healthrsquos IT legal and informationsecurity advisors have made numerous requests to the MOHLTC for information (in particular theprovincial TRA) that we consider essential to develop our own risk assessment and PIA but havebeen told that information cannot be shared even with strict confidentiality and access controlsSo we are at somewhat of an impasse Isra emailed Arlene yesterday Arlene has forwarded ourconcerns to the Ministryrsquos CIO and Panorama lead but we havenrsquot had any response or discussionswith either of them yet Have your organizations identified similar concerns andor had interactions with the MOHLTC inthis respect Irsquod also be interested in knowing if your health units have flagged other (egoperational) implementation concerns Thanks
Carolyn ps Robert ndash you can ignore this request I talked with Sharan this morning about Durhamrsquos issuesso am including you now just for information Carolyn Pim MD FRCPC Associate Medical Officer of Health Meacutedecin adjointe en santeacute publique Ottawa Public Health Santeacute publique Ottawa 100 Constellation Cr Ottawa ON K2G 6J8 Tel teacutel (613) 580-6744 ext 23684Fax (613) 580-9641Connect With Ottawa Public Health
Suivez Santeacute publique Ottawa
This e-mail originates from the City of Ottawa e-mail system Any distribution use orcopying of this e-mail or the information it contains by other than the intendedrecipient(s) is unauthorized If you are not the intended recipient please notify meat the telephone number shown above or by return e-mail and delete thiscommunication and any copy immediately Thank you
Le preacutesent courriel a eacuteteacute expeacutedieacute par le systegraveme de courriels de la Ville dOttawaToute distribution utilisation ou reproduction du courriel ou des renseignements quisy trouvent par une personne autre que son destinataire preacutevu est interdite Si vousavez reccedilu le message par erreur veuillez men aviser par teacuteleacutephone (au numeacuteropreacuteciteacute) ou par courriel puis supprimer sans deacutelai la version originale de lacommunication ainsi que toutes ses copies Je vous remercie de votre collaboration
1
Smoke-Free Patios ndash An Amendment to the Smoke-Free Ontario Act
Date November 15 2013 Prepared for Council of Ontario Medical Officers of Health Prepared by York Region Public Health _____________________________________________________________________________ Issue
The Smoke-Free Ontario Act is the current provincial legislation that imposes smoking restrictions in workplaces and public places It prohibits smoking on restaurant and bar patios in instances where any portion of the seating area is covered by a roof With recent studies illustrating that exposure to second hand smoke outdoors poses similar risks to indoor exposure there has been growing public support to enhance smoking restrictions and make patios completely smoke-free
Background
With the implementation of the Smoke-Free Ontario Act in 2006 restaurant and bar patios became subject to smoking restrictions if any portion of the seating area was covered by a roof This allowed for patios without roof coverings to continue to allow smoking and as a result did not provide significant protection to patrons or staff from exposure to second hand smoke outdoors Many businesses chose to alter the design of their patios to allow smoking to continue In some cases patios became more crowded since smoking patrons who dine indoors often proceed outside onto licensed patios with their beverages to smoke York Region like most municipalities in Ontario is host to hundreds of patios being operated by restaurant owners and businesses With smoking prohibitions affecting only a small portion of these patios specifically ones with coverings the vast majority of patios still allow smoking to take place Patrons and employees on patios where smoking is not restricted are exposed to second hand smoke frequently This can contribute to increased disease and aggravation of existing health conditions From a business perspective the existing legislation has been viewed by many operators as unfair because some patios have permanent coverings which cannot be removed requiring a smoke-free status These business owners feel this creates an uneven playing field since they cannot provide an outdoor dining area for their smoking customers There is strong community support for smoke-free patios in Ontario A 2009 Rapid Risk Factor Surveillance System survey revealed 754 percent support in York Region while a Toronto Health Survey in 2011 indicated 74 percent public support
2
Current Status
Smoking is currently prohibited on restaurant and bar patios province-wide in four Canadian provinces and territories Alberta Newfoundland and Labrador Nova Scotia and Yukon A fifth province Prince Edward Island prohibits smoking on patios until 10 pm Since Ontario enacted legislation restricting smoking on patios in 2006 eight municipalities in Ontario have chosen to create bylaws that go beyond the Smoke-Free Ontario Act and enhance outdoor protection from second hand smoke by prohibiting smoking on patios completely The largest of those municipalities is the City of Ottawa Recently the Toronto Board of Health unanimously endorsed a report presented by their Medical Officer of Health recommending that restaurant and bar patios be made smoke-free through an amendment to the Smoke-Free Ontario Act
Key Considerations
There should be no significant financial burden to local Boards of Health resulting from a smoke-free patio amendment to the Smoke-Free Ontario Act Inspection and enforcement for the Smoke-Free Ontario Act is currently 100 percent funded by the Ministry of Health and Long-Term Care Following an introductory period of education on the amendment a complaint response model of service delivery would ensure ongoing compliance with smoke-free requirements A complete ban of smoking on patios would eliminate the widely-held perception by business owners that the current legislation creates an uneven playing field for business Since Smoke-Free Ontario Act inspections of patios began in 2006 operators have expressed the opinion that if patios need to be smoke-free for the protection of the public they should all be smoke-free to avoid undue hardship for individual businesses and to provide protection uniformly across the Province
Next steps
York Region Public Health intends to seek support from Medical Officers of Health across the Central East Tobacco Control Area Network (CETCAN) to advocate to the Ministry of Health and Long-Term Care for an amendment to the Smoke-Free Ontario Act prohibiting smoking on all restaurant and bar patios York Region is also in the process of requesting that its Regional Council advocate to the Minister of Health and Long-Term Care on the issue
Updating and Modernizing O Regulation 565 (Public Pools)
Date November 15 2013
Prepared for Council of Ontario Medical Officers of Health
Prepared by York Region Public Health _____________________________________________________________________________ Background Recent drownings at public pools in Ontario have highlighted the issue of water-borne illness and injury The current pool regulation under Ontariorsquos Health Protection and Promotion Act O Regulation 565 (Public Pools) is outdated It does not accurately reflect new pool technology and design or the changing use of public pools Neither does it incorporate admissions standards recommended by the Office of the Chief Coroner Further O Regulation 565 does not have short-form wording or set fines associated with it This limits public health enforcement capabilities What is the impact Updating O Regulation 565 (Public Pools) to address recent changes in pool technology design and uses and to include Coroner-recommended admissions standards would help improve pool safety Establishing short-form wording for O Regulation 565 would enhance enforcement related to public pools Currently the only enforcement available to Public Health Inspectors for dealing with non-critical regulatory infractions in public pools is the issuance of a Part III summons This involves a considerable amount of resources for a possible small fine With the development of inspection disclosure systems such as YorkSafe there is an even greater need to develop a method to effectively address repeated pool operator non-compliance with non-critical issues Next steps Public health units should advocate to the Province to 1) Conduct a review of O Regulation 565 (Public Pools) to address shortcomings Proposed changes to the
regulation should include a requirement for ownersoperators of public pools to advise the local Medical Officer of Health of any change in the use of a facility and the addition of the Coronerrsquos recommended admission standards
2) Provide short-form wording for O Regulation 565 so that public health inspectors can better deal with pool operator non-compliance
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
Page 8 of 8 ndash DRAFT FOR COMOH DISCUSSION
COMOH members were also asked to indicate the level of acceptability for some possible changes to alPHarsquos services and way of doing business
COMOH Responses BOH Section Affiliates All Survey Responses
Very Acceptable
Somewhat Acceptable
Neither Acceptable or Unacceptable
Somewhat Unacceptable
Very Unaccept
able
Total COMOH
Responses
COMOH Respondents Who Strongly Agree or
Agree
BOH Members Who Strongly Agree or
Agree
Affiliates Who Strongly Agree or
Agree
All Respondents Who Strongly Agree
or Agree
1Single conference with additional face-to-face section meetings
21 2 0 1 0 24 96 68 80 81
2alPHa to offer alternatives like webinars on focussed topics
13 6 1 4 0 24 79 50 90 71
3Coordinate COMOH meetings with PHO OMA or Ministry events
16 4 2 0 0 22 91 na na --
4
Increase focus on building leadership and management capacity for health unit CEOs and senior management
7 9 4 3 0 23 70 na 70 70
5
Would it be acceptable for alPHa to request voluntary financial contributions from member PHUs in addition to annual fees
3 5 5 4 5 22 36 7 26 21
6
Would it be acceptable for alPHa to request voluntary in-kind staff contributions from member PHUs to expand alPHas capacity eg communications policy work group support
7 11 1 1 3 23 78 31 45 50
7Would it be acceptable to you for alPHa to discontinue staff support for COMOH (BOH Section)
0 4 1 5 14 24 17 11 na 14
8
Would it be acceptable to you for alPHa to reduce the amount of staff support for COMOH (BOH Section)
1 6 1 8 6 22 32 26 na 29
9
Would it be acceptable to you for alPHa to provide supports to MOHs and AMOHs (BOH Members) without maintaining COMOH (BOHs) as a section of the association
3 2 3 2 12 22 23 17 na 20
10
Would it be acceptable to you for alPHas Board of Directors to move from the current representational model to a skills-based strategic model ie board membership would be based on the skills needed to carry out alPHas strategic plan
6 11 2 1 3 23 74 56 56 62
11
Would it be acceptable to you for alPHas President Vice-President and Treasurer to be elected from the full membership of the alPHa Board of Directors (rather than the current model of alternating between BOH and COMOH members)
10 8 1 2 2 23 78 70 70 73
PROPOSED CHANGES
1 Council of Ontario Medical Officers of Health Terms of Reference
ASSOCIATION OF LOCAL PUBLIC HEALTH AGENCIES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
TERMS OF REFERENCE NAME 1 The name of the organization shall be ldquoThe Council of Ontario Medical Officers of
Health a section of the Association of Local Public Health Agencies (alPHa)rdquo hereinafter referred to as ldquothe Councilrdquo
MISSION 2 As local leaders in public health we are committed to improving the health of
Ontarians and increasing health equity by strengthening Ontariorsquos public health system We achieve this through system leadership and coordination in collaboration with the provincial government and other organizations and through evidence-informed advocacy on public health policy
OBJECTIVES 3 The objectives of the Council shall be
a) To provide strong province-wide leadership in public health
b) To advocate for health protection and promotion policies and programs that maintain and improve the health of Ontarians
c) To promote and maintain the highest standards for Ontariorsquos public health
programs and services
d) To support the planning implementation and evaluation of effective and efficiently run public health programs and services
e) To act as a forum for sharing information and resources and for addressing and
discussing public health issues both amongst the Councilrsquos members and other agencies that support the goals of alPHa eg Ontario Medical Association Ontario Public Health Association etc
f) To engage with and to provide public health and related policy advice to alPHa
the Chief Medical Officer of Health the Ontario Ministries of Health and Long-Term Care (including the Health Promotion and Public Health Divisions) Children
2 Council of Ontario Medical Officers of Health Terms of Reference
and Youth Services and other provincial ministries Public Health Ontario Health Canada the Public Health Agency of Canada and other public health partners
g) To promote and protect the professional interests of its members
h) To provide support to individual members as needed
i) To seek recognition for outstanding practice from among the members
j) To support evidence based practice of public health medicine
k) To engage and involve the membership to participate in COMOHrsquos endeavours
l) To mentor Public Health and Preventive Medicine Residents
MEMBERSHIP 4 Membership on the Council in each of the following categories is subject to the
limitations imposed by the current terms of reference and all policies and governing documents of the Association of Local Public Health Agencies Benefits of membership in each category are included in Appendix A These shall be subject to regular review and may be suspended under certain circumstances
Active membership in the Council shall be open to all Associate Medical Officers of Health and all full-time Medical Officers of Health whose Boards of Health are members of alPHa Such members shall have full voting privileges and may hold office in the Council Associate membership shall be open to all full and part-time physicians employed by a Board of Health that is a member of alPHa Such members shall not have voting privileges nor hold office
Affiliate membership shall be open to the following individuals interested in furthering the objectives of the Council
bull Public Health and Preventive Medicine Residents and Public Health and Preventive Medicine Residency Program Directors
bull Federal public health physicians working in Ontariorsquos First Nations communities
bull other public health or related physicians including those employed by a Board of Health that is not a member of alPHa
Such members shall not have voting privileges nor hold office
3 Council of Ontario Medical Officers of Health Terms of Reference
Emeritus membership shall be open to all former members who have retired after five (5) or more years of Active membership subject to the nomination in writing of two (2) active members in good standing endorsement of the Executive Committee and approval of the Council by majority vote at a general meeting Such members shall have neither voting privileges nor hold office but may be invited to attend general meetings Honorary membership shall be open to any non-active or associate member subject to the nomination in writing of two (2) active members in good standing endorsement of the Executive Committee and approval of the Council Such members shall have neither voting privileges nor hold office but may be invited to attend general meetings
OFFICERS 5 The Officers of the Council shall be the Chair Vice-Chair and immediate Past Chair
6 The Chair shall prepare the agendas of all Council meetings She shall preside and
preserve order at all such meetings shall ensure that these Terms of Reference are upheld and enforced and shall contribute to the supervision and evaluation of any Public Health and Preventive Medicine Resident who is on a placement with alPHa
7 The Vice-Chair shall fulfill the duties of the Chair in hisher absence The immediate
Past Chair may fulfill the duties of the Chair or Vice-Chair in their absences 8 The Chair shall normally serve a term of one (1) year which is renewable once and
after which the Vice-Chair shall normally assume the vacated office COMMITTEES 9 The Council shall elect seven (7) active members one from each of alPHarsquos regions
and the active member who is scheduled to serve as the President or immediate Past-President of alPHa to represent it on the alPHa Board of Directors These seven (7) members shall constitute the Councilrsquos Executive Committee and shall serve a term of at least one (1) year The Chair and Vice-Chair shall be elected from among the Executive Committee members If alPHarsquos immediate Past President is an active member she shall be an ex-officio member of the Executive Committee
10 The mandate of the Executive Committee shall be to facilitate the achievement of
the objectives of the Council by fulfilling the following
a Identifying priorities 1
1 See Appendix B Planning Cycle to Identify Priorities for COMOH
and ensuring the development of briefing documents and or recommendations as appropriate for the consideration of the Council
4 Council of Ontario Medical Officers of Health Terms of Reference
b Setting agendas and otherwise ensuring preparations for Council meetings c Ensuring the fulfillment of the direction of Council d Responding in a timely fashion to time-sensitive public health matters in
accordance with the Executive Committeersquos understanding of the perspective of the Council
e Engaging with the Chief Medical Officer of Health Associate Chief Medical Officers of Health and other provincial public health leaders and
f Representing Council at public and partner agency forums including the Public Health Leadership Council which shall normally include membership from the Officers of the Council and two other Executive Committee members as selected by agreement among the Executive
g Identifying opportunities for the recognition of outstanding practice from among the members including the annual nomination of at least one member for the alPHa Distinguished Service Award
11 The Executive Committee shall meet and correspond in the manner and at the times
and if required places as deemed necessary by the Chair to conduct the business of the Council A quorum shall consist of four (4) members
12 The Executive Committee shall have the power to strike committeestask or working
groups to assist it in carrying out the business of the Council 13 The Council may by special resolution remove a member of the Executive
Committee before the completion of hisher term of office and may elect a successor to complete the term The special resolution shall require a majority vote of 67 of the members present and voting at the meeting at which the special resolution is considered
14 A Nominating Committee shall consist of the three (3) most recent Past Chairs who
are able to serve and shall be chaired by the immediate Past Chair The Nominating Committee shall prepare a list of proposed Officers and Executive Committee members for the consideration of the Council at its Annual General Meeting
MEETINGS 15 The Council shall hold at least four (4) general meetings per year in a manner and at
the times and if required places as deemed necessary by the Executive Committee to share information direct and assist the Executive Committee in conducting the business of the Council
16 The Council shall hold its Annual General Meeting during and at the same place as
the alPHarsquos Annual Conference
5 Council of Ontario Medical Officers of Health Terms of Reference
17 The Council shall hold a special meeting at the call of the Chair or upon the written request specifying the purpose of such meeting of at least five (5) active members Council members must be given at least 48 hours notice of any special meeting
18 Only Councilrsquos active and associate members and alPHa staff are entitled to attend
general and special meetings of the Council Other members and non-members may be invited to attend all or part of such meetings as determined by the Chair preferably in consultation with the Executive Committee Non-members who come to such meetings without an invitation may attend all or part of the meeting by a majority vote of the active members present and voting
19 The Chair shall prepare the agendas for such meetings and shall normally include
reports from the Chair and the Councilrsquos committeestask or working groups and representatives to external bodies alPHarsquos Executive Director shall ensure that the minutes shall be recorded and promptly distributed to the Section
20 A quorum for all such meetings shall be ten (10) active members 21 The Council shall normally be notified in a manner deemed appropriate by the Chair
of such meetings at least one (1) month prior to their being held 22 A majority vote of the members present at such meetings and voting shall make
Council decisions In the case of a tied vote the Chair shall cast the deciding vote The Executive Committee shall ensure that actions arising from such decisions at such meetings are implemented and monitored
23 The Chair may solicit advice from the Council through the use of teleconferencing
and alPHarsquos electronic mailing lists in order to gain an understanding of the overall perspective of the Council (see 10d)
ELECTIONS 24 The Officers and Executive Committee members shall be elected at the Sectionrsquos
Annual General Meeting The Nominating Committee Chair or hisher designate shall present a list of nominations Additional nominations from the floor shall also be considered Each Officer and Executive Committee member shall be elected by secret ballot if necessary by a majority of the active members present and voting In the case of a tie the Chair shall cast the deciding vote
AMENDMENTS 25 The Councilrsquos Terms of Reference may be amended from time to time by the
Executive Committee provided the Committee receives notice of such proposed amendments at least one (1) month prior to the meeting at which the amendments
6 Council of Ontario Medical Officers of Health Terms of Reference
will be considered Such amendments shall be ratified by the Council at the next general meeting or the Annual General Meeting as the case may be
26 The Executive Committee shall review the Terms of Reference as required and not
less than once every two years Original September 1987 1st Revision October 2000 2nd Revision July 2001 3rd Revision December 2003 4th Revision February 2008 5th Revision June 2009 6th Revision June 2011 7th Revision June 2013
7 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX A
COMOH Membership Benefits Active Membership
bull Entitled to attend all meetings of the Section bull May hold office on the COMOH Executive Committee alPHa Board of Directors
Standing Committees bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Associate Membership
bull Entitled to attend all meetings of the Section bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Affiliate Membership
bull May attend meetings or parts thereof subject to approval of Chair bull May serve on ad-hoc committees of the Section subject to the approval of the
Executive Committee bull Discounted registration rates for alPHa Conferences (for Public Health and
Preventive Medicine Residents) bull Upon written request and subject to COMOH Executive approval Affiliate
Members may subscribe to comohlistsalphaweborg The approval will be reviewed on an annual basis in order to determine if the Affiliate Member can remain a subscriber to mohsalphaweborg
Emeritus Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair bull Enjoy discounted registration rates for alPHa Conferences and regular COMOH
meetings bull Subscription to comohlistsalphaweborg electronic mailing list bull Full access to alPHa Web site bull May represent alPHa COMOH on selected external committees and working
groups Honorary Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair
8 Council of Ontario Medical Officers of Health Terms of Reference
bull May represent alPHa COMOH on selected external committees and working groups subject to the approval of the COMOH or alPHa Executive Committee as appropriate
9 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX B
Planning Cycle to Identify Priorities for COMOH
1 There shall normally be a COMOH membership strategic planning retreat every four years In recognition of the dynamic environment of public health the need for and timing of such a retreat shall be at the discretion of the Executive Committee in consultation with the membership
2 The COMOH Executive is responsible (through the creation of a subcommittee of COMOH members) for ensuring the preparation for the COMOH retreats with resources to include those provided by alPHa
3 Leadership for action on COMOH priorities will be recruited from among the COMOH membership in order to make good use of the full base of capacity of the membership The resources to support actions will be recruited from both within and beyond the COMOH membership employing other public health professionals that reside within the broader public health system and community
4 The COMOH Executive shall ensure an annual review of strategic priorities and initiatives and the development of a draft report of the same for the review of the members at the June meeting
2013 Strategic Planning
Considerations for COMOH
As part of its strategic planning discussions alPHarsquos Board has been considering changes to the level of support provided to member sections A member survey is being carried out over the fall to determine options acceptable to alPHa members The following approach to support is put forward as a proposal for the consideration of COMOH Note that the feasibility of the points below depend upon future decisions of the alPHa board They assume that COMOH remains part of alPHa but becomes more independent in administering meetings
1 alPHa can provide to COMOH staff support (Gord Fleming) amounting to 02 FTE or one day per week This is a reduction from the current level of 35 days per week COMOH can choose to use the support any way it wants writing COMOH letters meeting minutes agenda support special projects etc
2 In addition to 02 FTE alPHa staff would provide support for up to 4 face-to-face meetings per year One meeting would be concurrent to alPHarsquos annual conference in June The timing of other meetings could be negotiated The support includes consulting on the development of the program arranging for speakers registration for the event arranging venue AV support and hospitality services
3 In addition to 02 FTE alPHa staff would provide support for setting meeting dates and any polling required to establish dates Note that the individual supporting this function would be Karen Reece
4 COMOHrsquos Executive and Section would continue to have access to online supports through the alPHa including the COMOH Listserve and a group page for posting agendas minutes and other resources on the alPHa website
5 alPHa staff (Linda Stewart and Gord Fleming) can also start participating on CMOH calls as a way to be up-to-date on issues related to COMOH
6 Other than what is outlined above COMOH would be expected to prepare agendas and take minutes for its Executive and Section meetings The Executive would be expected to operate more independently than it does now but would be able to access the supports outlined above
Prepared by Linda Stewart Executive Director
From comoh-bounceslistsalphaweborg on behalf of Christopher MackieTo MOH ListserveSubject [comoh] Fw URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)Date Wednesday October 30 2013 91241 AMAttachments ATT00249txt
For AMOHs and PHPM residents who didnt receive the initial email
Chris
Christopher Mackie MD MHSc FRCPCMedical Officer of Health and CEOMiddlesex-London Health Unit50 King St LondonON N6A 5L7 O 519 663 5317 ext 2444 wwwhealthunitcomFrom Pisko Laura (MOHLTC)Sent Tuesday October 29 2013 759 PMTo kbarkeralgomapublichealthcom malcolmlockbchuorg davidcchatham-kentcarobertkyledurhamca proumeliotiseohuca fwarshelginhealthonca mohelginhealthoncahlynnpublichealthgreybruceonca malcolmlockhnhuorg hnmohhnhuorglnoseworthyhkpronca bobnosalhaltonca elizabethrichardsonhamiltoncarschabashpechuonca ncameronhuroncountyca drimgemmillkflapublichealthcamohkflapublichealthca suditranadecounty-lambtononca paulastewarthealthunitorgChristopher Mackie valeriejaegerniagararegionca jimchiriconbpsdhuca jarthursnwhuoncaisralevyottawaca dnealoxfordcountyca davidmowatpeelregionca mklassenpdhuoncarpellizzaripcchuca rosemarieramsinghporcupinehuonca mcorriveaurcdhucomcharlesgardnersmdhuorg sutcliffepsdhucom davidwilliamstbdhucomspruytmtimiskaminghucom dmckeowntorontoca lnolanregionofwaterloocanicolamercerwdghuorg aheimannwechealthunitorg karimkurjiyorkcaCc coreywesleytbdhucom CindyBaker-Barillsmdhuorg Donna Kosmack pilonlsdhucomPaulaMuiskflapublichealthca sthibautorontoca Mueller Daina (MOHLTC) Gordon Marcus(MOHLTC) andreakitahamiltoncaSubject URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)
Dear Colleagues The ministry has received reports that some tobacco vendors across the province aregiving away single cigarettes with the purchase of tobacco products It is the ministryrsquosposition that giving out free single cigarettes does not violate subsection 31(3) of theSmoke-Free Ontario Act (ldquoSFOArdquo) Although the practice of giving out free singlecigarettes may promote the sale of tobacco products it does not take the form of aldquoproduct enhancement product association or promotional materialrdquo and therefore doesnot fall within the scope of subsection 31(3) of the SFOA We have confirmed with Health Canada that this practice may violate section 29(b) of thefederal Tobacco Act As such Health Canada is requesting that you notify them in writingand I am directing you to communicate with them via email and provide to them as manydetails as possible Emails should be sent to Tobacco-Ontariohc-scgcca and thesubject line should read ldquoViolation of Section 29(b) of Tobacco Actrdquo This will ensurethat the complaints are given priority status by Health Canada We will continue to monitor
this situation and liaise with our colleagues at Health Canada Please share this information with your tobacco control staff and contact me or DainaMueller Manager Tobacco Control Unit Health Promotion Implementation Branch atdainamuellerontarioca with any questions RegardsLaura Laura A PiskoDirectorHealth Promotion Implementation BranchHealth Promotion DivisionMinistry of Health and Long Term Care416-327-7445 (office)416-451-3185 (mobile) Marcus Gordon - EA (416)326-0625 for urgent issues
========= Middlesex-London Health Unit E-Mail Disclaimer =============______________________________________________________________
Private and confidential intended only for named recipient If otherwisereceived please destroy immediately Health information in this email isonly general information and is not intended to replace an in personconsultation with a medical professional nor is it intended to providemedical advice Individual circumstances of which we are not aware mayaffect the information provided herein and as such the Middlesex-LondonHealth Unit assumes no liability or responsibility for your reliancethereon The Middlesex-London Health Unit works under the authority of theHealth Protection and Promotion Act and this correspondence may be used toassess your needs for public health services (519-663-5317 ext 2448)______________________________________________________________
From Gardner CharlesTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes (RayCopesoahppca)
George Pasut (GeorgePasutoahppca) Peter Cooney (petercooneyhc-scgcca)Cc Ito DickSubject Discontinuation of Fluoridation in MuskokaDate Tuesday October 22 2013 125254 PM
Hello Colleagues
As I reported in my email below on September 26th fluoridation has come under challenge again inSimcoe Muskoka I am now very unhappy to report that despite our best efforts last night theDistrict Council of Muskoka voted to remove fluoride from municipal drinking supplies across theDistrict This brings to an end fluoridation in all of Simcoe and Muskoka (with the exception of Base Borden)ndash though New Tecumseth will be conducting a plebiscite on the question of fluoridation with themunicipal election next October Defending community water fluoridation has drained a great deal of time human resources andcommitment from other priorities and has been exhausting here in SMDHU as I am sure it hasbeen in many other health units While the outcomes have been very disappointing I have beenimpressed by the professionalism and dedication that SMDHU staff members have shown inshouldering this burden In particular our dental consultant Dr Ito has provided us with much ofthe foundational knowledge and the local research essential to our efforts and has very frequentlyattended and presented at council meetings and other public events I would also like to thank themany of you who have offer and provided support including advocacy letters and informationresources Over the years Dr Peter Cooney Chief Dental Officer of Health of Canada has beenvery helpful attending and presenting with us at council meetings and at public consultationevents We will of course continue our oral health surveillance of the children of Muskoka documentingand reporting in future years on the increase in dental decay that we anticipate will occur Suchsurveillance is the foundation of our advocacy both to municipal politicians and to the province I am very concerned that our experience will continue to repeat itself across the province unlessthere is strong leadership provincially It is with this in mind that I raise the followingrecommendations for your consideration
1 That we collectively (with PHOrsquos leadership) conduct high quality publish-worthy researchdocumenting the impact on dental decay that occurs in those municipalities throughoutOntario that in recent years have discontinued community water fluoridation This could bepart of a larger study on such municipalities across the country and it could also be part ofa study documenting overall oral health (including fluoridation coverage) in the province(and possibly across the country)
2 That COMOH engage with our Chief MOH to advocate for the province to require allmunicipal water supplies to be fluoridated (the exception of course being those withnaturally sufficient fluoride concentrations) This could built upon the alPHa position to
Gordon
Highlight
Gordon
Highlight
date (A11-00 - Community Water Fluoridation) on the CMOH position (Oral Health ndash) and on theemail discussion generated on the COMOH listserv some months back re Richardrsquosproposal (calling on the province to fund municipal water fluoridation)
Valerie I request that this be an item for our COMOH meeting on November 15th Sincerely Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorg From Gardner Charles Sent Thursday September 26 2013 245 PMTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes(RayCopesoahppca)Subject Community Water Fluoridation Under Challenge Again in Simcoe Muskoka Hello Colleagues You may wish to know that community water fluoridation (CWF) is again under challenge in SimcoeMuskoka specifically both in Tottenham (Town of New Tecumseth in Simcoe County) and for theentire District of Muskoka On Monday September 23 Committee of the Whole Council of theTown of New Tecumseth voted to submit application to discontinue community water fluoridation(CWF) in the town of Tottenham despite presentations to the contrary from our dental consultantDr Ito and from me The next Council meeting is scheduled for Monday Sept 30 at which lastMondayrsquos (Sept 23) votes will be ratified
Since Monday I have spoken with the Mayor of the Town of New Tecumseth and with most of thecouncilors encouraging deferral of a decision on Monday to allow the town more time to make afully informed decision
This is the second time in recent years that the issue of discontinuing CWF in Tottenham has beenraised at council This issue is also scheduled to return again to the District of Muskoka Council on
October 21st where I will be presenting in response to deputations in opposition to fluoridation
Outside of Base Borden Tottenham is the only community with fluoridated water in SimcoeCounty The health unitrsquos own screening data between 2011 and 2013 shows that Tottenhamrsquos
Gordon
Highlight
children as well as those in Muskoka have a lower rate of dental decay than Simcoe Muskokacommunities without CWF
Sincerely
Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorgChuck Gardner MOH
November 04 2013
Mandatory State Laws on Fluoridation Thirteen states Puerto Rico and the District of Columbia have laws intended to provide
statewide fluoridation These states and the year that the fluoridation legislation was passed are
District of Columbia (1952) Connecticut (1965) Kentucky (1966) Illinois (1967) Minnesota
(1967) Ohio (1969) South Dakota (1969) Georgia (1973) Nebraska (1973 and 2008)
California (1995) Delaware (1998) Puerto Rico (1998) Nevada (1999) Louisiana (2008) and
Arkansas (2011) (see Table 1) The sizes of the public water systems or countiescommunities
affected and exemption provisions vary by state Table 1
STATES THAT HAVE MANDATORY LAWS ON FLUORIDATION -2011
State (1) Year of
Fluoridation
Legislation (1)
Population
served by
Fluoridated
CWS (2)
Persons
receiving
fluoridated
water (2)
State
Average
Caries
Experience
of Grade 3
Students (3)
Arkansas 2011 647 1724131 64
California 1995 621 22812721 709
Connecticut 1965 910 2370423 406
Delaware 1998 862 705344 545
Georgia 1973 921 8924598 52
Illinois 1967 993 11325132 532
Kentucky 1966 999 4334223 598
Louisiana 2008 407 1846149 657
Minnesota 1967 988 4117266 549
Nebraska 1973 and 2008 702 1001665 593
Nevada 1999 702 1001665 649
Ohio 1969 877 8772683 512
South Dakota 1969 948 642942 623
District of
Columbia
1952 1000 595000
Puerto Rico 1998
United States 739 204283554
2010 Statistics for population fluoridated and number of people
1 Communication with Jane McGinley RDH MBA Manager Fluoridation and Preventive Health
Activities Council on Access Prevention and Interprofessional Relations
2 Centers for Disease Control and Prevention Department of Health and Human Services
accessed Oct 21 2013 httpwwwcdcgovfluoridationstatistics2010statshtm
3 Centers for Disease Control and Prevention National Oral Health Surveillance System Caries
Experience - Percentage of 3rd Grade students with Caries Experience (treated or untreated tooth
If data from 43 states for the percentage of Grade 3 children with experience of dental decay is
compared with the 2008 percentages of the population in a state with Community Water
Fluoridation then the percentage of children with experience of dental decay decreases as the
percentage of the state population with Community Water Fluoridation increases (see Figure 1)
Figure 1
Correlation of Percentage of Grade 3 Children with Caries Experience and
Percentage of Population With Community Water Fluoridation for 43
Reporting States
0
10
20
30
40
50
60
70
80
0 10 20 30 40 50 60 70 80 90 100
State of Population With Community Water Fluoridation
Sta
te
of
Gra
de 3
Stu
den
ts w
ith
Cari
es E
xp
eri
en
ce
Data from CDC (2 3)
The description of the fluoridation laws in California Illinois and Nevada can be found on the
Association of State amp Territorial Dental Directors website(4 7 8)
The California fluoridation law AB 733 came into effect in 1995 requiring communities of 10
000 residents or more be supplied with fluoridated drinking water However the state did not
provide any funding to implement the legislation (California is unique in requiring fluoridation
without funding the practice)(4) The California Department of Health Services therefore had to
fund fluoridation initiatives from non-governmental sources ie the California Endowment
California Dental Association Foundation the First 5 Commission and others(5) From 1995 to
2011 the percentage of the California population receiving fluoridated drinking water has risen
from 17 to 625(6) 4 Dental Public Health Activities amp Practices Office of Oral Health California Department of Health
Services April 2002 httpwwwastddorgbestpracticesDES06002CAfluoridationpdf
5 Stock M Pollick H The CDA Foundation Model to Fluoridate Communities California Dental
Association Journal vol 40 no 8 649 - 655
httpwwwcdaorgPortals0journaljournal_082012pdf
6 California Dental Association Foundation
httpwwwcdafoundationorglearnadvocacyfluoridation
The State of Illinois passed a mandatory fluoridation state in 1967 and required all community
water systems to adjust fluoride levels in the drinking water to optimal levels within 1 year(7)
From 1962 when over 5000000 residents had optimally fluoridated drinking water by 2010
the number had risen to 11325132 (993 of the population on community water systems)(2)
7 Dental Public Health Activities amp Practices Division of Oral Health Illinois Department of Public
Health April 2002 httpwwwastddorgbestpracticesDES16007ILfluoridationpdf
The State of Nevada passed a mandatory fluoridation statute in 2000 for communities with
400000 or more residents(8) This was a result of the work of a statewide coalition that
included the Nevada Dental and Dental Hygienist Associations the Washoe and Clark County
District Health Departments the Clark County School District Junior League of Las Vegas
Head Start the Community College of Southern Nevada Dental Hygiene Program Health
Access Washoe County and Saint Maryrsquos Hospital For communities with less than 400000 the
implementation of fluoridation still required the vote of the majority voters in the community
The Las Vegas Water Authority and the City of Henderson started fluoridation in 2000
increasing the percentage of the population with fluoridated drinking water from 2 to 65 (8) 8 Dental Public Health Activities amp Practices Bureau of Family Health Services Nevada State Health
Division April 2002 httpwwwastddorgbestpracticesDES31002NVfluoridationbillpdf
Countries with Mandatory Laws on Fluoridation Countries that have mandated Community Water Fluoridation are Brazil Hong Kong
Malaysia Singapore Ireland Israel and some of the states in Australia
Singapore started fluoridating its water in 1956 based on the success of the fluoridation trials in
Grand Rapids Newburgh Evanston and Brantford Singapore became the first Asian country to
have 100 of its population benefitting from the implementation of fluoridated drinking water
Loh reported that ldquoThe ten year study on the effects of water fluoridation in Singapore showed
a decrease in caries prevalence in the children In the permanent dentition the reduction was
523 per cent for Chinese and 31 per cent for Malays in the 7 to 9 year old age group A similar
trend was observed in the mixed dentition in which the decrease was 325 per cent for Chinese
and 306 per cent for Malaysrdquo(9) By 2010 the population of the country was 5080000(10)
9 Loh T Thirty-eight years of water fluoridation--the Singapore scenario Community Dent
Health 1996 Sep13 Suppl 247-50
10 British Fluoridation Society One in a Million the facts about water fluoridation 3rd Edition
published March 2012) httpwwwbfsweborgonemillion0920One20in20a20Million20-
20The20Extent20of20Fluoridationpdf
Hong Kong started implementing community water fluoridation in 1961 and similar to
Singapore 100 of the population received access to fluoridated drinking water Lo and Wong
reported that ldquoThe mean DMFT score of the children deceased from 44 in 1960 to 15 in 1968
stayed at this level in the 1980 and 1986 surveys and further deceased to 08 in 2001 The
prevalence of dental fluorosis among the children surveyed in 1960 was 1 and this increased
to 59 and 70 in 1968 and 1980 respectively It was found in the 1986 and 2001 surveys that
the prevalences of fluorosis were 47 and 9 among children whose teeth developed at the
time when the respective water fluoride concentrations were 07 ppm and 05 ppmrdquo(11) The
population of Hong Kong was 6968000 in 2009(10) 11 LO ECM and WONG AHH Water fluoride concentration and fluorosis in Hong Kong in 1960-
2001 84th General Session and Exhibition of the International Association for Dental Research amp
1st Meeting of the Pan-Asian-Pacific Federation Brisbane Australia 28 June-1 July 2006 v 85 n
Sp B
The Malaysian cabinet approved a nationwide community water fluoridation program in 1972
(12) One of the states Sabah decided to stop fluoridation in 1989 due to concerns about
inadequate supervision in adding fluoride to the drinking water Oral Health Surveys in 2009
and 2007 indicated that children in Sabah had the worst oral health with 50 of 12 year-olds
having decay in their permanent teeth and children having an average of 3 teeth being(13)
Under the 10th Malaysian Plan in 2011 the federal and the Sabah state governments
reintroduced water fluoridation in Sabah(1314) In 2010 about 755 of the Malaysian
population or 20700000 people had fluoridated drinking water(1013) 12 Malaysian Dental Association Fluoride in Water
httpwwwmdaorgmy07_public_01healthcare_12htm
13 Sachdev N Fluoridation in Sabah Water for Cleaner Teeth French Tribunecom 28022011
From Levy IsraTo Jaeger ValerieCc Pim Carolyn gordonalphaweborg Diallo Aicha Penny Sutcliffe Paul Roumeliotis Michael Finkelstein
Hazel Lynn Robert KyleSubject FW Panorama - Privacy Security and other issuesDate Wednesday October 16 2013 122110 PM
Hello ValerieOttawa is part of Wave 4 Panorama implementation and we are gearing up increasingly to use thesystem where and if possible Thinking about it I am anticipating that this may need to be on theCOMOH (and alPHa) radar as it is something that will impact all health units and implies a majoroperational shift in vaccine delivery programs for all health units I have asked Carolyn Pim toconnect with our sister wave 4 units to share common experiences as we move forward ndash when wehave a roll up could I bring to COMOH Exec for discussion to explore whether there are broaderimplications for all members As an aside I have also asked the Ministry and their CIO to share with me any roll up learnings thatthey may have had already from previous waves (I understand that Niagara HU was a wave 1participant so if there is such a roll up of common experiences that others could learn fromperhaps you have it already and that could come to the exec too)Thanks Isra From Pim Carolyn Sent October 10 2013 1228 PMTo Christopher Mackie (christophermackiemlhuonca) Elizabeth Richardson(Elizabethrichardsonhamiltonca) H BSc M D F R C P (C) MPH Jim Chirico(jimchiriconbpsdhuca) Marlene Spruyt (spruytmtimiskaminghucom) Robert Kyle (Durham)Cc Levy IsraSubject Panorama - Privacy Security and other issues Dear colleagues Irsquom reaching out to you as fellow Panorama Wave 4 health units to ask about where yourorganizations are at in the process of signing agreements and completing Privacy ImpactAssessments and Threat Risk Assessments (TRAs) Ottawa Public Healthrsquos IT legal and informationsecurity advisors have made numerous requests to the MOHLTC for information (in particular theprovincial TRA) that we consider essential to develop our own risk assessment and PIA but havebeen told that information cannot be shared even with strict confidentiality and access controlsSo we are at somewhat of an impasse Isra emailed Arlene yesterday Arlene has forwarded ourconcerns to the Ministryrsquos CIO and Panorama lead but we havenrsquot had any response or discussionswith either of them yet Have your organizations identified similar concerns andor had interactions with the MOHLTC inthis respect Irsquod also be interested in knowing if your health units have flagged other (egoperational) implementation concerns Thanks
Carolyn ps Robert ndash you can ignore this request I talked with Sharan this morning about Durhamrsquos issuesso am including you now just for information Carolyn Pim MD FRCPC Associate Medical Officer of Health Meacutedecin adjointe en santeacute publique Ottawa Public Health Santeacute publique Ottawa 100 Constellation Cr Ottawa ON K2G 6J8 Tel teacutel (613) 580-6744 ext 23684Fax (613) 580-9641Connect With Ottawa Public Health
Suivez Santeacute publique Ottawa
This e-mail originates from the City of Ottawa e-mail system Any distribution use orcopying of this e-mail or the information it contains by other than the intendedrecipient(s) is unauthorized If you are not the intended recipient please notify meat the telephone number shown above or by return e-mail and delete thiscommunication and any copy immediately Thank you
Le preacutesent courriel a eacuteteacute expeacutedieacute par le systegraveme de courriels de la Ville dOttawaToute distribution utilisation ou reproduction du courriel ou des renseignements quisy trouvent par une personne autre que son destinataire preacutevu est interdite Si vousavez reccedilu le message par erreur veuillez men aviser par teacuteleacutephone (au numeacuteropreacuteciteacute) ou par courriel puis supprimer sans deacutelai la version originale de lacommunication ainsi que toutes ses copies Je vous remercie de votre collaboration
1
Smoke-Free Patios ndash An Amendment to the Smoke-Free Ontario Act
Date November 15 2013 Prepared for Council of Ontario Medical Officers of Health Prepared by York Region Public Health _____________________________________________________________________________ Issue
The Smoke-Free Ontario Act is the current provincial legislation that imposes smoking restrictions in workplaces and public places It prohibits smoking on restaurant and bar patios in instances where any portion of the seating area is covered by a roof With recent studies illustrating that exposure to second hand smoke outdoors poses similar risks to indoor exposure there has been growing public support to enhance smoking restrictions and make patios completely smoke-free
Background
With the implementation of the Smoke-Free Ontario Act in 2006 restaurant and bar patios became subject to smoking restrictions if any portion of the seating area was covered by a roof This allowed for patios without roof coverings to continue to allow smoking and as a result did not provide significant protection to patrons or staff from exposure to second hand smoke outdoors Many businesses chose to alter the design of their patios to allow smoking to continue In some cases patios became more crowded since smoking patrons who dine indoors often proceed outside onto licensed patios with their beverages to smoke York Region like most municipalities in Ontario is host to hundreds of patios being operated by restaurant owners and businesses With smoking prohibitions affecting only a small portion of these patios specifically ones with coverings the vast majority of patios still allow smoking to take place Patrons and employees on patios where smoking is not restricted are exposed to second hand smoke frequently This can contribute to increased disease and aggravation of existing health conditions From a business perspective the existing legislation has been viewed by many operators as unfair because some patios have permanent coverings which cannot be removed requiring a smoke-free status These business owners feel this creates an uneven playing field since they cannot provide an outdoor dining area for their smoking customers There is strong community support for smoke-free patios in Ontario A 2009 Rapid Risk Factor Surveillance System survey revealed 754 percent support in York Region while a Toronto Health Survey in 2011 indicated 74 percent public support
2
Current Status
Smoking is currently prohibited on restaurant and bar patios province-wide in four Canadian provinces and territories Alberta Newfoundland and Labrador Nova Scotia and Yukon A fifth province Prince Edward Island prohibits smoking on patios until 10 pm Since Ontario enacted legislation restricting smoking on patios in 2006 eight municipalities in Ontario have chosen to create bylaws that go beyond the Smoke-Free Ontario Act and enhance outdoor protection from second hand smoke by prohibiting smoking on patios completely The largest of those municipalities is the City of Ottawa Recently the Toronto Board of Health unanimously endorsed a report presented by their Medical Officer of Health recommending that restaurant and bar patios be made smoke-free through an amendment to the Smoke-Free Ontario Act
Key Considerations
There should be no significant financial burden to local Boards of Health resulting from a smoke-free patio amendment to the Smoke-Free Ontario Act Inspection and enforcement for the Smoke-Free Ontario Act is currently 100 percent funded by the Ministry of Health and Long-Term Care Following an introductory period of education on the amendment a complaint response model of service delivery would ensure ongoing compliance with smoke-free requirements A complete ban of smoking on patios would eliminate the widely-held perception by business owners that the current legislation creates an uneven playing field for business Since Smoke-Free Ontario Act inspections of patios began in 2006 operators have expressed the opinion that if patios need to be smoke-free for the protection of the public they should all be smoke-free to avoid undue hardship for individual businesses and to provide protection uniformly across the Province
Next steps
York Region Public Health intends to seek support from Medical Officers of Health across the Central East Tobacco Control Area Network (CETCAN) to advocate to the Ministry of Health and Long-Term Care for an amendment to the Smoke-Free Ontario Act prohibiting smoking on all restaurant and bar patios York Region is also in the process of requesting that its Regional Council advocate to the Minister of Health and Long-Term Care on the issue
Updating and Modernizing O Regulation 565 (Public Pools)
Date November 15 2013
Prepared for Council of Ontario Medical Officers of Health
Prepared by York Region Public Health _____________________________________________________________________________ Background Recent drownings at public pools in Ontario have highlighted the issue of water-borne illness and injury The current pool regulation under Ontariorsquos Health Protection and Promotion Act O Regulation 565 (Public Pools) is outdated It does not accurately reflect new pool technology and design or the changing use of public pools Neither does it incorporate admissions standards recommended by the Office of the Chief Coroner Further O Regulation 565 does not have short-form wording or set fines associated with it This limits public health enforcement capabilities What is the impact Updating O Regulation 565 (Public Pools) to address recent changes in pool technology design and uses and to include Coroner-recommended admissions standards would help improve pool safety Establishing short-form wording for O Regulation 565 would enhance enforcement related to public pools Currently the only enforcement available to Public Health Inspectors for dealing with non-critical regulatory infractions in public pools is the issuance of a Part III summons This involves a considerable amount of resources for a possible small fine With the development of inspection disclosure systems such as YorkSafe there is an even greater need to develop a method to effectively address repeated pool operator non-compliance with non-critical issues Next steps Public health units should advocate to the Province to 1) Conduct a review of O Regulation 565 (Public Pools) to address shortcomings Proposed changes to the
regulation should include a requirement for ownersoperators of public pools to advise the local Medical Officer of Health of any change in the use of a facility and the addition of the Coronerrsquos recommended admission standards
2) Provide short-form wording for O Regulation 565 so that public health inspectors can better deal with pool operator non-compliance
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
1 Council of Ontario Medical Officers of Health Terms of Reference
ASSOCIATION OF LOCAL PUBLIC HEALTH AGENCIES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
TERMS OF REFERENCE NAME 1 The name of the organization shall be ldquoThe Council of Ontario Medical Officers of
Health a section of the Association of Local Public Health Agencies (alPHa)rdquo hereinafter referred to as ldquothe Councilrdquo
MISSION 2 As local leaders in public health we are committed to improving the health of
Ontarians and increasing health equity by strengthening Ontariorsquos public health system We achieve this through system leadership and coordination in collaboration with the provincial government and other organizations and through evidence-informed advocacy on public health policy
OBJECTIVES 3 The objectives of the Council shall be
a) To provide strong province-wide leadership in public health
b) To advocate for health protection and promotion policies and programs that maintain and improve the health of Ontarians
c) To promote and maintain the highest standards for Ontariorsquos public health
programs and services
d) To support the planning implementation and evaluation of effective and efficiently run public health programs and services
e) To act as a forum for sharing information and resources and for addressing and
discussing public health issues both amongst the Councilrsquos members and other agencies that support the goals of alPHa eg Ontario Medical Association Ontario Public Health Association etc
f) To engage with and to provide public health and related policy advice to alPHa
the Chief Medical Officer of Health the Ontario Ministries of Health and Long-Term Care (including the Health Promotion and Public Health Divisions) Children
2 Council of Ontario Medical Officers of Health Terms of Reference
and Youth Services and other provincial ministries Public Health Ontario Health Canada the Public Health Agency of Canada and other public health partners
g) To promote and protect the professional interests of its members
h) To provide support to individual members as needed
i) To seek recognition for outstanding practice from among the members
j) To support evidence based practice of public health medicine
k) To engage and involve the membership to participate in COMOHrsquos endeavours
l) To mentor Public Health and Preventive Medicine Residents
MEMBERSHIP 4 Membership on the Council in each of the following categories is subject to the
limitations imposed by the current terms of reference and all policies and governing documents of the Association of Local Public Health Agencies Benefits of membership in each category are included in Appendix A These shall be subject to regular review and may be suspended under certain circumstances
Active membership in the Council shall be open to all Associate Medical Officers of Health and all full-time Medical Officers of Health whose Boards of Health are members of alPHa Such members shall have full voting privileges and may hold office in the Council Associate membership shall be open to all full and part-time physicians employed by a Board of Health that is a member of alPHa Such members shall not have voting privileges nor hold office
Affiliate membership shall be open to the following individuals interested in furthering the objectives of the Council
bull Public Health and Preventive Medicine Residents and Public Health and Preventive Medicine Residency Program Directors
bull Federal public health physicians working in Ontariorsquos First Nations communities
bull other public health or related physicians including those employed by a Board of Health that is not a member of alPHa
Such members shall not have voting privileges nor hold office
3 Council of Ontario Medical Officers of Health Terms of Reference
Emeritus membership shall be open to all former members who have retired after five (5) or more years of Active membership subject to the nomination in writing of two (2) active members in good standing endorsement of the Executive Committee and approval of the Council by majority vote at a general meeting Such members shall have neither voting privileges nor hold office but may be invited to attend general meetings Honorary membership shall be open to any non-active or associate member subject to the nomination in writing of two (2) active members in good standing endorsement of the Executive Committee and approval of the Council Such members shall have neither voting privileges nor hold office but may be invited to attend general meetings
OFFICERS 5 The Officers of the Council shall be the Chair Vice-Chair and immediate Past Chair
6 The Chair shall prepare the agendas of all Council meetings She shall preside and
preserve order at all such meetings shall ensure that these Terms of Reference are upheld and enforced and shall contribute to the supervision and evaluation of any Public Health and Preventive Medicine Resident who is on a placement with alPHa
7 The Vice-Chair shall fulfill the duties of the Chair in hisher absence The immediate
Past Chair may fulfill the duties of the Chair or Vice-Chair in their absences 8 The Chair shall normally serve a term of one (1) year which is renewable once and
after which the Vice-Chair shall normally assume the vacated office COMMITTEES 9 The Council shall elect seven (7) active members one from each of alPHarsquos regions
and the active member who is scheduled to serve as the President or immediate Past-President of alPHa to represent it on the alPHa Board of Directors These seven (7) members shall constitute the Councilrsquos Executive Committee and shall serve a term of at least one (1) year The Chair and Vice-Chair shall be elected from among the Executive Committee members If alPHarsquos immediate Past President is an active member she shall be an ex-officio member of the Executive Committee
10 The mandate of the Executive Committee shall be to facilitate the achievement of
the objectives of the Council by fulfilling the following
a Identifying priorities 1
1 See Appendix B Planning Cycle to Identify Priorities for COMOH
and ensuring the development of briefing documents and or recommendations as appropriate for the consideration of the Council
4 Council of Ontario Medical Officers of Health Terms of Reference
b Setting agendas and otherwise ensuring preparations for Council meetings c Ensuring the fulfillment of the direction of Council d Responding in a timely fashion to time-sensitive public health matters in
accordance with the Executive Committeersquos understanding of the perspective of the Council
e Engaging with the Chief Medical Officer of Health Associate Chief Medical Officers of Health and other provincial public health leaders and
f Representing Council at public and partner agency forums including the Public Health Leadership Council which shall normally include membership from the Officers of the Council and two other Executive Committee members as selected by agreement among the Executive
g Identifying opportunities for the recognition of outstanding practice from among the members including the annual nomination of at least one member for the alPHa Distinguished Service Award
11 The Executive Committee shall meet and correspond in the manner and at the times
and if required places as deemed necessary by the Chair to conduct the business of the Council A quorum shall consist of four (4) members
12 The Executive Committee shall have the power to strike committeestask or working
groups to assist it in carrying out the business of the Council 13 The Council may by special resolution remove a member of the Executive
Committee before the completion of hisher term of office and may elect a successor to complete the term The special resolution shall require a majority vote of 67 of the members present and voting at the meeting at which the special resolution is considered
14 A Nominating Committee shall consist of the three (3) most recent Past Chairs who
are able to serve and shall be chaired by the immediate Past Chair The Nominating Committee shall prepare a list of proposed Officers and Executive Committee members for the consideration of the Council at its Annual General Meeting
MEETINGS 15 The Council shall hold at least four (4) general meetings per year in a manner and at
the times and if required places as deemed necessary by the Executive Committee to share information direct and assist the Executive Committee in conducting the business of the Council
16 The Council shall hold its Annual General Meeting during and at the same place as
the alPHarsquos Annual Conference
5 Council of Ontario Medical Officers of Health Terms of Reference
17 The Council shall hold a special meeting at the call of the Chair or upon the written request specifying the purpose of such meeting of at least five (5) active members Council members must be given at least 48 hours notice of any special meeting
18 Only Councilrsquos active and associate members and alPHa staff are entitled to attend
general and special meetings of the Council Other members and non-members may be invited to attend all or part of such meetings as determined by the Chair preferably in consultation with the Executive Committee Non-members who come to such meetings without an invitation may attend all or part of the meeting by a majority vote of the active members present and voting
19 The Chair shall prepare the agendas for such meetings and shall normally include
reports from the Chair and the Councilrsquos committeestask or working groups and representatives to external bodies alPHarsquos Executive Director shall ensure that the minutes shall be recorded and promptly distributed to the Section
20 A quorum for all such meetings shall be ten (10) active members 21 The Council shall normally be notified in a manner deemed appropriate by the Chair
of such meetings at least one (1) month prior to their being held 22 A majority vote of the members present at such meetings and voting shall make
Council decisions In the case of a tied vote the Chair shall cast the deciding vote The Executive Committee shall ensure that actions arising from such decisions at such meetings are implemented and monitored
23 The Chair may solicit advice from the Council through the use of teleconferencing
and alPHarsquos electronic mailing lists in order to gain an understanding of the overall perspective of the Council (see 10d)
ELECTIONS 24 The Officers and Executive Committee members shall be elected at the Sectionrsquos
Annual General Meeting The Nominating Committee Chair or hisher designate shall present a list of nominations Additional nominations from the floor shall also be considered Each Officer and Executive Committee member shall be elected by secret ballot if necessary by a majority of the active members present and voting In the case of a tie the Chair shall cast the deciding vote
AMENDMENTS 25 The Councilrsquos Terms of Reference may be amended from time to time by the
Executive Committee provided the Committee receives notice of such proposed amendments at least one (1) month prior to the meeting at which the amendments
6 Council of Ontario Medical Officers of Health Terms of Reference
will be considered Such amendments shall be ratified by the Council at the next general meeting or the Annual General Meeting as the case may be
26 The Executive Committee shall review the Terms of Reference as required and not
less than once every two years Original September 1987 1st Revision October 2000 2nd Revision July 2001 3rd Revision December 2003 4th Revision February 2008 5th Revision June 2009 6th Revision June 2011 7th Revision June 2013
7 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX A
COMOH Membership Benefits Active Membership
bull Entitled to attend all meetings of the Section bull May hold office on the COMOH Executive Committee alPHa Board of Directors
Standing Committees bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Associate Membership
bull Entitled to attend all meetings of the Section bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Affiliate Membership
bull May attend meetings or parts thereof subject to approval of Chair bull May serve on ad-hoc committees of the Section subject to the approval of the
Executive Committee bull Discounted registration rates for alPHa Conferences (for Public Health and
Preventive Medicine Residents) bull Upon written request and subject to COMOH Executive approval Affiliate
Members may subscribe to comohlistsalphaweborg The approval will be reviewed on an annual basis in order to determine if the Affiliate Member can remain a subscriber to mohsalphaweborg
Emeritus Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair bull Enjoy discounted registration rates for alPHa Conferences and regular COMOH
meetings bull Subscription to comohlistsalphaweborg electronic mailing list bull Full access to alPHa Web site bull May represent alPHa COMOH on selected external committees and working
groups Honorary Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair
8 Council of Ontario Medical Officers of Health Terms of Reference
bull May represent alPHa COMOH on selected external committees and working groups subject to the approval of the COMOH or alPHa Executive Committee as appropriate
9 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX B
Planning Cycle to Identify Priorities for COMOH
1 There shall normally be a COMOH membership strategic planning retreat every four years In recognition of the dynamic environment of public health the need for and timing of such a retreat shall be at the discretion of the Executive Committee in consultation with the membership
2 The COMOH Executive is responsible (through the creation of a subcommittee of COMOH members) for ensuring the preparation for the COMOH retreats with resources to include those provided by alPHa
3 Leadership for action on COMOH priorities will be recruited from among the COMOH membership in order to make good use of the full base of capacity of the membership The resources to support actions will be recruited from both within and beyond the COMOH membership employing other public health professionals that reside within the broader public health system and community
4 The COMOH Executive shall ensure an annual review of strategic priorities and initiatives and the development of a draft report of the same for the review of the members at the June meeting
2013 Strategic Planning
Considerations for COMOH
As part of its strategic planning discussions alPHarsquos Board has been considering changes to the level of support provided to member sections A member survey is being carried out over the fall to determine options acceptable to alPHa members The following approach to support is put forward as a proposal for the consideration of COMOH Note that the feasibility of the points below depend upon future decisions of the alPHa board They assume that COMOH remains part of alPHa but becomes more independent in administering meetings
1 alPHa can provide to COMOH staff support (Gord Fleming) amounting to 02 FTE or one day per week This is a reduction from the current level of 35 days per week COMOH can choose to use the support any way it wants writing COMOH letters meeting minutes agenda support special projects etc
2 In addition to 02 FTE alPHa staff would provide support for up to 4 face-to-face meetings per year One meeting would be concurrent to alPHarsquos annual conference in June The timing of other meetings could be negotiated The support includes consulting on the development of the program arranging for speakers registration for the event arranging venue AV support and hospitality services
3 In addition to 02 FTE alPHa staff would provide support for setting meeting dates and any polling required to establish dates Note that the individual supporting this function would be Karen Reece
4 COMOHrsquos Executive and Section would continue to have access to online supports through the alPHa including the COMOH Listserve and a group page for posting agendas minutes and other resources on the alPHa website
5 alPHa staff (Linda Stewart and Gord Fleming) can also start participating on CMOH calls as a way to be up-to-date on issues related to COMOH
6 Other than what is outlined above COMOH would be expected to prepare agendas and take minutes for its Executive and Section meetings The Executive would be expected to operate more independently than it does now but would be able to access the supports outlined above
Prepared by Linda Stewart Executive Director
From comoh-bounceslistsalphaweborg on behalf of Christopher MackieTo MOH ListserveSubject [comoh] Fw URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)Date Wednesday October 30 2013 91241 AMAttachments ATT00249txt
For AMOHs and PHPM residents who didnt receive the initial email
Chris
Christopher Mackie MD MHSc FRCPCMedical Officer of Health and CEOMiddlesex-London Health Unit50 King St LondonON N6A 5L7 O 519 663 5317 ext 2444 wwwhealthunitcomFrom Pisko Laura (MOHLTC)Sent Tuesday October 29 2013 759 PMTo kbarkeralgomapublichealthcom malcolmlockbchuorg davidcchatham-kentcarobertkyledurhamca proumeliotiseohuca fwarshelginhealthonca mohelginhealthoncahlynnpublichealthgreybruceonca malcolmlockhnhuorg hnmohhnhuorglnoseworthyhkpronca bobnosalhaltonca elizabethrichardsonhamiltoncarschabashpechuonca ncameronhuroncountyca drimgemmillkflapublichealthcamohkflapublichealthca suditranadecounty-lambtononca paulastewarthealthunitorgChristopher Mackie valeriejaegerniagararegionca jimchiriconbpsdhuca jarthursnwhuoncaisralevyottawaca dnealoxfordcountyca davidmowatpeelregionca mklassenpdhuoncarpellizzaripcchuca rosemarieramsinghporcupinehuonca mcorriveaurcdhucomcharlesgardnersmdhuorg sutcliffepsdhucom davidwilliamstbdhucomspruytmtimiskaminghucom dmckeowntorontoca lnolanregionofwaterloocanicolamercerwdghuorg aheimannwechealthunitorg karimkurjiyorkcaCc coreywesleytbdhucom CindyBaker-Barillsmdhuorg Donna Kosmack pilonlsdhucomPaulaMuiskflapublichealthca sthibautorontoca Mueller Daina (MOHLTC) Gordon Marcus(MOHLTC) andreakitahamiltoncaSubject URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)
Dear Colleagues The ministry has received reports that some tobacco vendors across the province aregiving away single cigarettes with the purchase of tobacco products It is the ministryrsquosposition that giving out free single cigarettes does not violate subsection 31(3) of theSmoke-Free Ontario Act (ldquoSFOArdquo) Although the practice of giving out free singlecigarettes may promote the sale of tobacco products it does not take the form of aldquoproduct enhancement product association or promotional materialrdquo and therefore doesnot fall within the scope of subsection 31(3) of the SFOA We have confirmed with Health Canada that this practice may violate section 29(b) of thefederal Tobacco Act As such Health Canada is requesting that you notify them in writingand I am directing you to communicate with them via email and provide to them as manydetails as possible Emails should be sent to Tobacco-Ontariohc-scgcca and thesubject line should read ldquoViolation of Section 29(b) of Tobacco Actrdquo This will ensurethat the complaints are given priority status by Health Canada We will continue to monitor
this situation and liaise with our colleagues at Health Canada Please share this information with your tobacco control staff and contact me or DainaMueller Manager Tobacco Control Unit Health Promotion Implementation Branch atdainamuellerontarioca with any questions RegardsLaura Laura A PiskoDirectorHealth Promotion Implementation BranchHealth Promotion DivisionMinistry of Health and Long Term Care416-327-7445 (office)416-451-3185 (mobile) Marcus Gordon - EA (416)326-0625 for urgent issues
========= Middlesex-London Health Unit E-Mail Disclaimer =============______________________________________________________________
Private and confidential intended only for named recipient If otherwisereceived please destroy immediately Health information in this email isonly general information and is not intended to replace an in personconsultation with a medical professional nor is it intended to providemedical advice Individual circumstances of which we are not aware mayaffect the information provided herein and as such the Middlesex-LondonHealth Unit assumes no liability or responsibility for your reliancethereon The Middlesex-London Health Unit works under the authority of theHealth Protection and Promotion Act and this correspondence may be used toassess your needs for public health services (519-663-5317 ext 2448)______________________________________________________________
From Gardner CharlesTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes (RayCopesoahppca)
George Pasut (GeorgePasutoahppca) Peter Cooney (petercooneyhc-scgcca)Cc Ito DickSubject Discontinuation of Fluoridation in MuskokaDate Tuesday October 22 2013 125254 PM
Hello Colleagues
As I reported in my email below on September 26th fluoridation has come under challenge again inSimcoe Muskoka I am now very unhappy to report that despite our best efforts last night theDistrict Council of Muskoka voted to remove fluoride from municipal drinking supplies across theDistrict This brings to an end fluoridation in all of Simcoe and Muskoka (with the exception of Base Borden)ndash though New Tecumseth will be conducting a plebiscite on the question of fluoridation with themunicipal election next October Defending community water fluoridation has drained a great deal of time human resources andcommitment from other priorities and has been exhausting here in SMDHU as I am sure it hasbeen in many other health units While the outcomes have been very disappointing I have beenimpressed by the professionalism and dedication that SMDHU staff members have shown inshouldering this burden In particular our dental consultant Dr Ito has provided us with much ofthe foundational knowledge and the local research essential to our efforts and has very frequentlyattended and presented at council meetings and other public events I would also like to thank themany of you who have offer and provided support including advocacy letters and informationresources Over the years Dr Peter Cooney Chief Dental Officer of Health of Canada has beenvery helpful attending and presenting with us at council meetings and at public consultationevents We will of course continue our oral health surveillance of the children of Muskoka documentingand reporting in future years on the increase in dental decay that we anticipate will occur Suchsurveillance is the foundation of our advocacy both to municipal politicians and to the province I am very concerned that our experience will continue to repeat itself across the province unlessthere is strong leadership provincially It is with this in mind that I raise the followingrecommendations for your consideration
1 That we collectively (with PHOrsquos leadership) conduct high quality publish-worthy researchdocumenting the impact on dental decay that occurs in those municipalities throughoutOntario that in recent years have discontinued community water fluoridation This could bepart of a larger study on such municipalities across the country and it could also be part ofa study documenting overall oral health (including fluoridation coverage) in the province(and possibly across the country)
2 That COMOH engage with our Chief MOH to advocate for the province to require allmunicipal water supplies to be fluoridated (the exception of course being those withnaturally sufficient fluoride concentrations) This could built upon the alPHa position to
Gordon
Highlight
Gordon
Highlight
date (A11-00 - Community Water Fluoridation) on the CMOH position (Oral Health ndash) and on theemail discussion generated on the COMOH listserv some months back re Richardrsquosproposal (calling on the province to fund municipal water fluoridation)
Valerie I request that this be an item for our COMOH meeting on November 15th Sincerely Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorg From Gardner Charles Sent Thursday September 26 2013 245 PMTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes(RayCopesoahppca)Subject Community Water Fluoridation Under Challenge Again in Simcoe Muskoka Hello Colleagues You may wish to know that community water fluoridation (CWF) is again under challenge in SimcoeMuskoka specifically both in Tottenham (Town of New Tecumseth in Simcoe County) and for theentire District of Muskoka On Monday September 23 Committee of the Whole Council of theTown of New Tecumseth voted to submit application to discontinue community water fluoridation(CWF) in the town of Tottenham despite presentations to the contrary from our dental consultantDr Ito and from me The next Council meeting is scheduled for Monday Sept 30 at which lastMondayrsquos (Sept 23) votes will be ratified
Since Monday I have spoken with the Mayor of the Town of New Tecumseth and with most of thecouncilors encouraging deferral of a decision on Monday to allow the town more time to make afully informed decision
This is the second time in recent years that the issue of discontinuing CWF in Tottenham has beenraised at council This issue is also scheduled to return again to the District of Muskoka Council on
October 21st where I will be presenting in response to deputations in opposition to fluoridation
Outside of Base Borden Tottenham is the only community with fluoridated water in SimcoeCounty The health unitrsquos own screening data between 2011 and 2013 shows that Tottenhamrsquos
Gordon
Highlight
children as well as those in Muskoka have a lower rate of dental decay than Simcoe Muskokacommunities without CWF
Sincerely
Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorgChuck Gardner MOH
November 04 2013
Mandatory State Laws on Fluoridation Thirteen states Puerto Rico and the District of Columbia have laws intended to provide
statewide fluoridation These states and the year that the fluoridation legislation was passed are
District of Columbia (1952) Connecticut (1965) Kentucky (1966) Illinois (1967) Minnesota
(1967) Ohio (1969) South Dakota (1969) Georgia (1973) Nebraska (1973 and 2008)
California (1995) Delaware (1998) Puerto Rico (1998) Nevada (1999) Louisiana (2008) and
Arkansas (2011) (see Table 1) The sizes of the public water systems or countiescommunities
affected and exemption provisions vary by state Table 1
STATES THAT HAVE MANDATORY LAWS ON FLUORIDATION -2011
State (1) Year of
Fluoridation
Legislation (1)
Population
served by
Fluoridated
CWS (2)
Persons
receiving
fluoridated
water (2)
State
Average
Caries
Experience
of Grade 3
Students (3)
Arkansas 2011 647 1724131 64
California 1995 621 22812721 709
Connecticut 1965 910 2370423 406
Delaware 1998 862 705344 545
Georgia 1973 921 8924598 52
Illinois 1967 993 11325132 532
Kentucky 1966 999 4334223 598
Louisiana 2008 407 1846149 657
Minnesota 1967 988 4117266 549
Nebraska 1973 and 2008 702 1001665 593
Nevada 1999 702 1001665 649
Ohio 1969 877 8772683 512
South Dakota 1969 948 642942 623
District of
Columbia
1952 1000 595000
Puerto Rico 1998
United States 739 204283554
2010 Statistics for population fluoridated and number of people
1 Communication with Jane McGinley RDH MBA Manager Fluoridation and Preventive Health
Activities Council on Access Prevention and Interprofessional Relations
2 Centers for Disease Control and Prevention Department of Health and Human Services
accessed Oct 21 2013 httpwwwcdcgovfluoridationstatistics2010statshtm
3 Centers for Disease Control and Prevention National Oral Health Surveillance System Caries
Experience - Percentage of 3rd Grade students with Caries Experience (treated or untreated tooth
If data from 43 states for the percentage of Grade 3 children with experience of dental decay is
compared with the 2008 percentages of the population in a state with Community Water
Fluoridation then the percentage of children with experience of dental decay decreases as the
percentage of the state population with Community Water Fluoridation increases (see Figure 1)
Figure 1
Correlation of Percentage of Grade 3 Children with Caries Experience and
Percentage of Population With Community Water Fluoridation for 43
Reporting States
0
10
20
30
40
50
60
70
80
0 10 20 30 40 50 60 70 80 90 100
State of Population With Community Water Fluoridation
Sta
te
of
Gra
de 3
Stu
den
ts w
ith
Cari
es E
xp
eri
en
ce
Data from CDC (2 3)
The description of the fluoridation laws in California Illinois and Nevada can be found on the
Association of State amp Territorial Dental Directors website(4 7 8)
The California fluoridation law AB 733 came into effect in 1995 requiring communities of 10
000 residents or more be supplied with fluoridated drinking water However the state did not
provide any funding to implement the legislation (California is unique in requiring fluoridation
without funding the practice)(4) The California Department of Health Services therefore had to
fund fluoridation initiatives from non-governmental sources ie the California Endowment
California Dental Association Foundation the First 5 Commission and others(5) From 1995 to
2011 the percentage of the California population receiving fluoridated drinking water has risen
from 17 to 625(6) 4 Dental Public Health Activities amp Practices Office of Oral Health California Department of Health
Services April 2002 httpwwwastddorgbestpracticesDES06002CAfluoridationpdf
5 Stock M Pollick H The CDA Foundation Model to Fluoridate Communities California Dental
Association Journal vol 40 no 8 649 - 655
httpwwwcdaorgPortals0journaljournal_082012pdf
6 California Dental Association Foundation
httpwwwcdafoundationorglearnadvocacyfluoridation
The State of Illinois passed a mandatory fluoridation state in 1967 and required all community
water systems to adjust fluoride levels in the drinking water to optimal levels within 1 year(7)
From 1962 when over 5000000 residents had optimally fluoridated drinking water by 2010
the number had risen to 11325132 (993 of the population on community water systems)(2)
7 Dental Public Health Activities amp Practices Division of Oral Health Illinois Department of Public
Health April 2002 httpwwwastddorgbestpracticesDES16007ILfluoridationpdf
The State of Nevada passed a mandatory fluoridation statute in 2000 for communities with
400000 or more residents(8) This was a result of the work of a statewide coalition that
included the Nevada Dental and Dental Hygienist Associations the Washoe and Clark County
District Health Departments the Clark County School District Junior League of Las Vegas
Head Start the Community College of Southern Nevada Dental Hygiene Program Health
Access Washoe County and Saint Maryrsquos Hospital For communities with less than 400000 the
implementation of fluoridation still required the vote of the majority voters in the community
The Las Vegas Water Authority and the City of Henderson started fluoridation in 2000
increasing the percentage of the population with fluoridated drinking water from 2 to 65 (8) 8 Dental Public Health Activities amp Practices Bureau of Family Health Services Nevada State Health
Division April 2002 httpwwwastddorgbestpracticesDES31002NVfluoridationbillpdf
Countries with Mandatory Laws on Fluoridation Countries that have mandated Community Water Fluoridation are Brazil Hong Kong
Malaysia Singapore Ireland Israel and some of the states in Australia
Singapore started fluoridating its water in 1956 based on the success of the fluoridation trials in
Grand Rapids Newburgh Evanston and Brantford Singapore became the first Asian country to
have 100 of its population benefitting from the implementation of fluoridated drinking water
Loh reported that ldquoThe ten year study on the effects of water fluoridation in Singapore showed
a decrease in caries prevalence in the children In the permanent dentition the reduction was
523 per cent for Chinese and 31 per cent for Malays in the 7 to 9 year old age group A similar
trend was observed in the mixed dentition in which the decrease was 325 per cent for Chinese
and 306 per cent for Malaysrdquo(9) By 2010 the population of the country was 5080000(10)
9 Loh T Thirty-eight years of water fluoridation--the Singapore scenario Community Dent
Health 1996 Sep13 Suppl 247-50
10 British Fluoridation Society One in a Million the facts about water fluoridation 3rd Edition
published March 2012) httpwwwbfsweborgonemillion0920One20in20a20Million20-
20The20Extent20of20Fluoridationpdf
Hong Kong started implementing community water fluoridation in 1961 and similar to
Singapore 100 of the population received access to fluoridated drinking water Lo and Wong
reported that ldquoThe mean DMFT score of the children deceased from 44 in 1960 to 15 in 1968
stayed at this level in the 1980 and 1986 surveys and further deceased to 08 in 2001 The
prevalence of dental fluorosis among the children surveyed in 1960 was 1 and this increased
to 59 and 70 in 1968 and 1980 respectively It was found in the 1986 and 2001 surveys that
the prevalences of fluorosis were 47 and 9 among children whose teeth developed at the
time when the respective water fluoride concentrations were 07 ppm and 05 ppmrdquo(11) The
population of Hong Kong was 6968000 in 2009(10) 11 LO ECM and WONG AHH Water fluoride concentration and fluorosis in Hong Kong in 1960-
2001 84th General Session and Exhibition of the International Association for Dental Research amp
1st Meeting of the Pan-Asian-Pacific Federation Brisbane Australia 28 June-1 July 2006 v 85 n
Sp B
The Malaysian cabinet approved a nationwide community water fluoridation program in 1972
(12) One of the states Sabah decided to stop fluoridation in 1989 due to concerns about
inadequate supervision in adding fluoride to the drinking water Oral Health Surveys in 2009
and 2007 indicated that children in Sabah had the worst oral health with 50 of 12 year-olds
having decay in their permanent teeth and children having an average of 3 teeth being(13)
Under the 10th Malaysian Plan in 2011 the federal and the Sabah state governments
reintroduced water fluoridation in Sabah(1314) In 2010 about 755 of the Malaysian
population or 20700000 people had fluoridated drinking water(1013) 12 Malaysian Dental Association Fluoride in Water
httpwwwmdaorgmy07_public_01healthcare_12htm
13 Sachdev N Fluoridation in Sabah Water for Cleaner Teeth French Tribunecom 28022011
From Levy IsraTo Jaeger ValerieCc Pim Carolyn gordonalphaweborg Diallo Aicha Penny Sutcliffe Paul Roumeliotis Michael Finkelstein
Hazel Lynn Robert KyleSubject FW Panorama - Privacy Security and other issuesDate Wednesday October 16 2013 122110 PM
Hello ValerieOttawa is part of Wave 4 Panorama implementation and we are gearing up increasingly to use thesystem where and if possible Thinking about it I am anticipating that this may need to be on theCOMOH (and alPHa) radar as it is something that will impact all health units and implies a majoroperational shift in vaccine delivery programs for all health units I have asked Carolyn Pim toconnect with our sister wave 4 units to share common experiences as we move forward ndash when wehave a roll up could I bring to COMOH Exec for discussion to explore whether there are broaderimplications for all members As an aside I have also asked the Ministry and their CIO to share with me any roll up learnings thatthey may have had already from previous waves (I understand that Niagara HU was a wave 1participant so if there is such a roll up of common experiences that others could learn fromperhaps you have it already and that could come to the exec too)Thanks Isra From Pim Carolyn Sent October 10 2013 1228 PMTo Christopher Mackie (christophermackiemlhuonca) Elizabeth Richardson(Elizabethrichardsonhamiltonca) H BSc M D F R C P (C) MPH Jim Chirico(jimchiriconbpsdhuca) Marlene Spruyt (spruytmtimiskaminghucom) Robert Kyle (Durham)Cc Levy IsraSubject Panorama - Privacy Security and other issues Dear colleagues Irsquom reaching out to you as fellow Panorama Wave 4 health units to ask about where yourorganizations are at in the process of signing agreements and completing Privacy ImpactAssessments and Threat Risk Assessments (TRAs) Ottawa Public Healthrsquos IT legal and informationsecurity advisors have made numerous requests to the MOHLTC for information (in particular theprovincial TRA) that we consider essential to develop our own risk assessment and PIA but havebeen told that information cannot be shared even with strict confidentiality and access controlsSo we are at somewhat of an impasse Isra emailed Arlene yesterday Arlene has forwarded ourconcerns to the Ministryrsquos CIO and Panorama lead but we havenrsquot had any response or discussionswith either of them yet Have your organizations identified similar concerns andor had interactions with the MOHLTC inthis respect Irsquod also be interested in knowing if your health units have flagged other (egoperational) implementation concerns Thanks
Carolyn ps Robert ndash you can ignore this request I talked with Sharan this morning about Durhamrsquos issuesso am including you now just for information Carolyn Pim MD FRCPC Associate Medical Officer of Health Meacutedecin adjointe en santeacute publique Ottawa Public Health Santeacute publique Ottawa 100 Constellation Cr Ottawa ON K2G 6J8 Tel teacutel (613) 580-6744 ext 23684Fax (613) 580-9641Connect With Ottawa Public Health
Suivez Santeacute publique Ottawa
This e-mail originates from the City of Ottawa e-mail system Any distribution use orcopying of this e-mail or the information it contains by other than the intendedrecipient(s) is unauthorized If you are not the intended recipient please notify meat the telephone number shown above or by return e-mail and delete thiscommunication and any copy immediately Thank you
Le preacutesent courriel a eacuteteacute expeacutedieacute par le systegraveme de courriels de la Ville dOttawaToute distribution utilisation ou reproduction du courriel ou des renseignements quisy trouvent par une personne autre que son destinataire preacutevu est interdite Si vousavez reccedilu le message par erreur veuillez men aviser par teacuteleacutephone (au numeacuteropreacuteciteacute) ou par courriel puis supprimer sans deacutelai la version originale de lacommunication ainsi que toutes ses copies Je vous remercie de votre collaboration
1
Smoke-Free Patios ndash An Amendment to the Smoke-Free Ontario Act
Date November 15 2013 Prepared for Council of Ontario Medical Officers of Health Prepared by York Region Public Health _____________________________________________________________________________ Issue
The Smoke-Free Ontario Act is the current provincial legislation that imposes smoking restrictions in workplaces and public places It prohibits smoking on restaurant and bar patios in instances where any portion of the seating area is covered by a roof With recent studies illustrating that exposure to second hand smoke outdoors poses similar risks to indoor exposure there has been growing public support to enhance smoking restrictions and make patios completely smoke-free
Background
With the implementation of the Smoke-Free Ontario Act in 2006 restaurant and bar patios became subject to smoking restrictions if any portion of the seating area was covered by a roof This allowed for patios without roof coverings to continue to allow smoking and as a result did not provide significant protection to patrons or staff from exposure to second hand smoke outdoors Many businesses chose to alter the design of their patios to allow smoking to continue In some cases patios became more crowded since smoking patrons who dine indoors often proceed outside onto licensed patios with their beverages to smoke York Region like most municipalities in Ontario is host to hundreds of patios being operated by restaurant owners and businesses With smoking prohibitions affecting only a small portion of these patios specifically ones with coverings the vast majority of patios still allow smoking to take place Patrons and employees on patios where smoking is not restricted are exposed to second hand smoke frequently This can contribute to increased disease and aggravation of existing health conditions From a business perspective the existing legislation has been viewed by many operators as unfair because some patios have permanent coverings which cannot be removed requiring a smoke-free status These business owners feel this creates an uneven playing field since they cannot provide an outdoor dining area for their smoking customers There is strong community support for smoke-free patios in Ontario A 2009 Rapid Risk Factor Surveillance System survey revealed 754 percent support in York Region while a Toronto Health Survey in 2011 indicated 74 percent public support
2
Current Status
Smoking is currently prohibited on restaurant and bar patios province-wide in four Canadian provinces and territories Alberta Newfoundland and Labrador Nova Scotia and Yukon A fifth province Prince Edward Island prohibits smoking on patios until 10 pm Since Ontario enacted legislation restricting smoking on patios in 2006 eight municipalities in Ontario have chosen to create bylaws that go beyond the Smoke-Free Ontario Act and enhance outdoor protection from second hand smoke by prohibiting smoking on patios completely The largest of those municipalities is the City of Ottawa Recently the Toronto Board of Health unanimously endorsed a report presented by their Medical Officer of Health recommending that restaurant and bar patios be made smoke-free through an amendment to the Smoke-Free Ontario Act
Key Considerations
There should be no significant financial burden to local Boards of Health resulting from a smoke-free patio amendment to the Smoke-Free Ontario Act Inspection and enforcement for the Smoke-Free Ontario Act is currently 100 percent funded by the Ministry of Health and Long-Term Care Following an introductory period of education on the amendment a complaint response model of service delivery would ensure ongoing compliance with smoke-free requirements A complete ban of smoking on patios would eliminate the widely-held perception by business owners that the current legislation creates an uneven playing field for business Since Smoke-Free Ontario Act inspections of patios began in 2006 operators have expressed the opinion that if patios need to be smoke-free for the protection of the public they should all be smoke-free to avoid undue hardship for individual businesses and to provide protection uniformly across the Province
Next steps
York Region Public Health intends to seek support from Medical Officers of Health across the Central East Tobacco Control Area Network (CETCAN) to advocate to the Ministry of Health and Long-Term Care for an amendment to the Smoke-Free Ontario Act prohibiting smoking on all restaurant and bar patios York Region is also in the process of requesting that its Regional Council advocate to the Minister of Health and Long-Term Care on the issue
Updating and Modernizing O Regulation 565 (Public Pools)
Date November 15 2013
Prepared for Council of Ontario Medical Officers of Health
Prepared by York Region Public Health _____________________________________________________________________________ Background Recent drownings at public pools in Ontario have highlighted the issue of water-borne illness and injury The current pool regulation under Ontariorsquos Health Protection and Promotion Act O Regulation 565 (Public Pools) is outdated It does not accurately reflect new pool technology and design or the changing use of public pools Neither does it incorporate admissions standards recommended by the Office of the Chief Coroner Further O Regulation 565 does not have short-form wording or set fines associated with it This limits public health enforcement capabilities What is the impact Updating O Regulation 565 (Public Pools) to address recent changes in pool technology design and uses and to include Coroner-recommended admissions standards would help improve pool safety Establishing short-form wording for O Regulation 565 would enhance enforcement related to public pools Currently the only enforcement available to Public Health Inspectors for dealing with non-critical regulatory infractions in public pools is the issuance of a Part III summons This involves a considerable amount of resources for a possible small fine With the development of inspection disclosure systems such as YorkSafe there is an even greater need to develop a method to effectively address repeated pool operator non-compliance with non-critical issues Next steps Public health units should advocate to the Province to 1) Conduct a review of O Regulation 565 (Public Pools) to address shortcomings Proposed changes to the
regulation should include a requirement for ownersoperators of public pools to advise the local Medical Officer of Health of any change in the use of a facility and the addition of the Coronerrsquos recommended admission standards
2) Provide short-form wording for O Regulation 565 so that public health inspectors can better deal with pool operator non-compliance
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
2 Council of Ontario Medical Officers of Health Terms of Reference
and Youth Services and other provincial ministries Public Health Ontario Health Canada the Public Health Agency of Canada and other public health partners
g) To promote and protect the professional interests of its members
h) To provide support to individual members as needed
i) To seek recognition for outstanding practice from among the members
j) To support evidence based practice of public health medicine
k) To engage and involve the membership to participate in COMOHrsquos endeavours
l) To mentor Public Health and Preventive Medicine Residents
MEMBERSHIP 4 Membership on the Council in each of the following categories is subject to the
limitations imposed by the current terms of reference and all policies and governing documents of the Association of Local Public Health Agencies Benefits of membership in each category are included in Appendix A These shall be subject to regular review and may be suspended under certain circumstances
Active membership in the Council shall be open to all Associate Medical Officers of Health and all full-time Medical Officers of Health whose Boards of Health are members of alPHa Such members shall have full voting privileges and may hold office in the Council Associate membership shall be open to all full and part-time physicians employed by a Board of Health that is a member of alPHa Such members shall not have voting privileges nor hold office
Affiliate membership shall be open to the following individuals interested in furthering the objectives of the Council
bull Public Health and Preventive Medicine Residents and Public Health and Preventive Medicine Residency Program Directors
bull Federal public health physicians working in Ontariorsquos First Nations communities
bull other public health or related physicians including those employed by a Board of Health that is not a member of alPHa
Such members shall not have voting privileges nor hold office
3 Council of Ontario Medical Officers of Health Terms of Reference
Emeritus membership shall be open to all former members who have retired after five (5) or more years of Active membership subject to the nomination in writing of two (2) active members in good standing endorsement of the Executive Committee and approval of the Council by majority vote at a general meeting Such members shall have neither voting privileges nor hold office but may be invited to attend general meetings Honorary membership shall be open to any non-active or associate member subject to the nomination in writing of two (2) active members in good standing endorsement of the Executive Committee and approval of the Council Such members shall have neither voting privileges nor hold office but may be invited to attend general meetings
OFFICERS 5 The Officers of the Council shall be the Chair Vice-Chair and immediate Past Chair
6 The Chair shall prepare the agendas of all Council meetings She shall preside and
preserve order at all such meetings shall ensure that these Terms of Reference are upheld and enforced and shall contribute to the supervision and evaluation of any Public Health and Preventive Medicine Resident who is on a placement with alPHa
7 The Vice-Chair shall fulfill the duties of the Chair in hisher absence The immediate
Past Chair may fulfill the duties of the Chair or Vice-Chair in their absences 8 The Chair shall normally serve a term of one (1) year which is renewable once and
after which the Vice-Chair shall normally assume the vacated office COMMITTEES 9 The Council shall elect seven (7) active members one from each of alPHarsquos regions
and the active member who is scheduled to serve as the President or immediate Past-President of alPHa to represent it on the alPHa Board of Directors These seven (7) members shall constitute the Councilrsquos Executive Committee and shall serve a term of at least one (1) year The Chair and Vice-Chair shall be elected from among the Executive Committee members If alPHarsquos immediate Past President is an active member she shall be an ex-officio member of the Executive Committee
10 The mandate of the Executive Committee shall be to facilitate the achievement of
the objectives of the Council by fulfilling the following
a Identifying priorities 1
1 See Appendix B Planning Cycle to Identify Priorities for COMOH
and ensuring the development of briefing documents and or recommendations as appropriate for the consideration of the Council
4 Council of Ontario Medical Officers of Health Terms of Reference
b Setting agendas and otherwise ensuring preparations for Council meetings c Ensuring the fulfillment of the direction of Council d Responding in a timely fashion to time-sensitive public health matters in
accordance with the Executive Committeersquos understanding of the perspective of the Council
e Engaging with the Chief Medical Officer of Health Associate Chief Medical Officers of Health and other provincial public health leaders and
f Representing Council at public and partner agency forums including the Public Health Leadership Council which shall normally include membership from the Officers of the Council and two other Executive Committee members as selected by agreement among the Executive
g Identifying opportunities for the recognition of outstanding practice from among the members including the annual nomination of at least one member for the alPHa Distinguished Service Award
11 The Executive Committee shall meet and correspond in the manner and at the times
and if required places as deemed necessary by the Chair to conduct the business of the Council A quorum shall consist of four (4) members
12 The Executive Committee shall have the power to strike committeestask or working
groups to assist it in carrying out the business of the Council 13 The Council may by special resolution remove a member of the Executive
Committee before the completion of hisher term of office and may elect a successor to complete the term The special resolution shall require a majority vote of 67 of the members present and voting at the meeting at which the special resolution is considered
14 A Nominating Committee shall consist of the three (3) most recent Past Chairs who
are able to serve and shall be chaired by the immediate Past Chair The Nominating Committee shall prepare a list of proposed Officers and Executive Committee members for the consideration of the Council at its Annual General Meeting
MEETINGS 15 The Council shall hold at least four (4) general meetings per year in a manner and at
the times and if required places as deemed necessary by the Executive Committee to share information direct and assist the Executive Committee in conducting the business of the Council
16 The Council shall hold its Annual General Meeting during and at the same place as
the alPHarsquos Annual Conference
5 Council of Ontario Medical Officers of Health Terms of Reference
17 The Council shall hold a special meeting at the call of the Chair or upon the written request specifying the purpose of such meeting of at least five (5) active members Council members must be given at least 48 hours notice of any special meeting
18 Only Councilrsquos active and associate members and alPHa staff are entitled to attend
general and special meetings of the Council Other members and non-members may be invited to attend all or part of such meetings as determined by the Chair preferably in consultation with the Executive Committee Non-members who come to such meetings without an invitation may attend all or part of the meeting by a majority vote of the active members present and voting
19 The Chair shall prepare the agendas for such meetings and shall normally include
reports from the Chair and the Councilrsquos committeestask or working groups and representatives to external bodies alPHarsquos Executive Director shall ensure that the minutes shall be recorded and promptly distributed to the Section
20 A quorum for all such meetings shall be ten (10) active members 21 The Council shall normally be notified in a manner deemed appropriate by the Chair
of such meetings at least one (1) month prior to their being held 22 A majority vote of the members present at such meetings and voting shall make
Council decisions In the case of a tied vote the Chair shall cast the deciding vote The Executive Committee shall ensure that actions arising from such decisions at such meetings are implemented and monitored
23 The Chair may solicit advice from the Council through the use of teleconferencing
and alPHarsquos electronic mailing lists in order to gain an understanding of the overall perspective of the Council (see 10d)
ELECTIONS 24 The Officers and Executive Committee members shall be elected at the Sectionrsquos
Annual General Meeting The Nominating Committee Chair or hisher designate shall present a list of nominations Additional nominations from the floor shall also be considered Each Officer and Executive Committee member shall be elected by secret ballot if necessary by a majority of the active members present and voting In the case of a tie the Chair shall cast the deciding vote
AMENDMENTS 25 The Councilrsquos Terms of Reference may be amended from time to time by the
Executive Committee provided the Committee receives notice of such proposed amendments at least one (1) month prior to the meeting at which the amendments
6 Council of Ontario Medical Officers of Health Terms of Reference
will be considered Such amendments shall be ratified by the Council at the next general meeting or the Annual General Meeting as the case may be
26 The Executive Committee shall review the Terms of Reference as required and not
less than once every two years Original September 1987 1st Revision October 2000 2nd Revision July 2001 3rd Revision December 2003 4th Revision February 2008 5th Revision June 2009 6th Revision June 2011 7th Revision June 2013
7 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX A
COMOH Membership Benefits Active Membership
bull Entitled to attend all meetings of the Section bull May hold office on the COMOH Executive Committee alPHa Board of Directors
Standing Committees bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Associate Membership
bull Entitled to attend all meetings of the Section bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Affiliate Membership
bull May attend meetings or parts thereof subject to approval of Chair bull May serve on ad-hoc committees of the Section subject to the approval of the
Executive Committee bull Discounted registration rates for alPHa Conferences (for Public Health and
Preventive Medicine Residents) bull Upon written request and subject to COMOH Executive approval Affiliate
Members may subscribe to comohlistsalphaweborg The approval will be reviewed on an annual basis in order to determine if the Affiliate Member can remain a subscriber to mohsalphaweborg
Emeritus Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair bull Enjoy discounted registration rates for alPHa Conferences and regular COMOH
meetings bull Subscription to comohlistsalphaweborg electronic mailing list bull Full access to alPHa Web site bull May represent alPHa COMOH on selected external committees and working
groups Honorary Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair
8 Council of Ontario Medical Officers of Health Terms of Reference
bull May represent alPHa COMOH on selected external committees and working groups subject to the approval of the COMOH or alPHa Executive Committee as appropriate
9 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX B
Planning Cycle to Identify Priorities for COMOH
1 There shall normally be a COMOH membership strategic planning retreat every four years In recognition of the dynamic environment of public health the need for and timing of such a retreat shall be at the discretion of the Executive Committee in consultation with the membership
2 The COMOH Executive is responsible (through the creation of a subcommittee of COMOH members) for ensuring the preparation for the COMOH retreats with resources to include those provided by alPHa
3 Leadership for action on COMOH priorities will be recruited from among the COMOH membership in order to make good use of the full base of capacity of the membership The resources to support actions will be recruited from both within and beyond the COMOH membership employing other public health professionals that reside within the broader public health system and community
4 The COMOH Executive shall ensure an annual review of strategic priorities and initiatives and the development of a draft report of the same for the review of the members at the June meeting
2013 Strategic Planning
Considerations for COMOH
As part of its strategic planning discussions alPHarsquos Board has been considering changes to the level of support provided to member sections A member survey is being carried out over the fall to determine options acceptable to alPHa members The following approach to support is put forward as a proposal for the consideration of COMOH Note that the feasibility of the points below depend upon future decisions of the alPHa board They assume that COMOH remains part of alPHa but becomes more independent in administering meetings
1 alPHa can provide to COMOH staff support (Gord Fleming) amounting to 02 FTE or one day per week This is a reduction from the current level of 35 days per week COMOH can choose to use the support any way it wants writing COMOH letters meeting minutes agenda support special projects etc
2 In addition to 02 FTE alPHa staff would provide support for up to 4 face-to-face meetings per year One meeting would be concurrent to alPHarsquos annual conference in June The timing of other meetings could be negotiated The support includes consulting on the development of the program arranging for speakers registration for the event arranging venue AV support and hospitality services
3 In addition to 02 FTE alPHa staff would provide support for setting meeting dates and any polling required to establish dates Note that the individual supporting this function would be Karen Reece
4 COMOHrsquos Executive and Section would continue to have access to online supports through the alPHa including the COMOH Listserve and a group page for posting agendas minutes and other resources on the alPHa website
5 alPHa staff (Linda Stewart and Gord Fleming) can also start participating on CMOH calls as a way to be up-to-date on issues related to COMOH
6 Other than what is outlined above COMOH would be expected to prepare agendas and take minutes for its Executive and Section meetings The Executive would be expected to operate more independently than it does now but would be able to access the supports outlined above
Prepared by Linda Stewart Executive Director
From comoh-bounceslistsalphaweborg on behalf of Christopher MackieTo MOH ListserveSubject [comoh] Fw URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)Date Wednesday October 30 2013 91241 AMAttachments ATT00249txt
For AMOHs and PHPM residents who didnt receive the initial email
Chris
Christopher Mackie MD MHSc FRCPCMedical Officer of Health and CEOMiddlesex-London Health Unit50 King St LondonON N6A 5L7 O 519 663 5317 ext 2444 wwwhealthunitcomFrom Pisko Laura (MOHLTC)Sent Tuesday October 29 2013 759 PMTo kbarkeralgomapublichealthcom malcolmlockbchuorg davidcchatham-kentcarobertkyledurhamca proumeliotiseohuca fwarshelginhealthonca mohelginhealthoncahlynnpublichealthgreybruceonca malcolmlockhnhuorg hnmohhnhuorglnoseworthyhkpronca bobnosalhaltonca elizabethrichardsonhamiltoncarschabashpechuonca ncameronhuroncountyca drimgemmillkflapublichealthcamohkflapublichealthca suditranadecounty-lambtononca paulastewarthealthunitorgChristopher Mackie valeriejaegerniagararegionca jimchiriconbpsdhuca jarthursnwhuoncaisralevyottawaca dnealoxfordcountyca davidmowatpeelregionca mklassenpdhuoncarpellizzaripcchuca rosemarieramsinghporcupinehuonca mcorriveaurcdhucomcharlesgardnersmdhuorg sutcliffepsdhucom davidwilliamstbdhucomspruytmtimiskaminghucom dmckeowntorontoca lnolanregionofwaterloocanicolamercerwdghuorg aheimannwechealthunitorg karimkurjiyorkcaCc coreywesleytbdhucom CindyBaker-Barillsmdhuorg Donna Kosmack pilonlsdhucomPaulaMuiskflapublichealthca sthibautorontoca Mueller Daina (MOHLTC) Gordon Marcus(MOHLTC) andreakitahamiltoncaSubject URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)
Dear Colleagues The ministry has received reports that some tobacco vendors across the province aregiving away single cigarettes with the purchase of tobacco products It is the ministryrsquosposition that giving out free single cigarettes does not violate subsection 31(3) of theSmoke-Free Ontario Act (ldquoSFOArdquo) Although the practice of giving out free singlecigarettes may promote the sale of tobacco products it does not take the form of aldquoproduct enhancement product association or promotional materialrdquo and therefore doesnot fall within the scope of subsection 31(3) of the SFOA We have confirmed with Health Canada that this practice may violate section 29(b) of thefederal Tobacco Act As such Health Canada is requesting that you notify them in writingand I am directing you to communicate with them via email and provide to them as manydetails as possible Emails should be sent to Tobacco-Ontariohc-scgcca and thesubject line should read ldquoViolation of Section 29(b) of Tobacco Actrdquo This will ensurethat the complaints are given priority status by Health Canada We will continue to monitor
this situation and liaise with our colleagues at Health Canada Please share this information with your tobacco control staff and contact me or DainaMueller Manager Tobacco Control Unit Health Promotion Implementation Branch atdainamuellerontarioca with any questions RegardsLaura Laura A PiskoDirectorHealth Promotion Implementation BranchHealth Promotion DivisionMinistry of Health and Long Term Care416-327-7445 (office)416-451-3185 (mobile) Marcus Gordon - EA (416)326-0625 for urgent issues
========= Middlesex-London Health Unit E-Mail Disclaimer =============______________________________________________________________
Private and confidential intended only for named recipient If otherwisereceived please destroy immediately Health information in this email isonly general information and is not intended to replace an in personconsultation with a medical professional nor is it intended to providemedical advice Individual circumstances of which we are not aware mayaffect the information provided herein and as such the Middlesex-LondonHealth Unit assumes no liability or responsibility for your reliancethereon The Middlesex-London Health Unit works under the authority of theHealth Protection and Promotion Act and this correspondence may be used toassess your needs for public health services (519-663-5317 ext 2448)______________________________________________________________
From Gardner CharlesTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes (RayCopesoahppca)
George Pasut (GeorgePasutoahppca) Peter Cooney (petercooneyhc-scgcca)Cc Ito DickSubject Discontinuation of Fluoridation in MuskokaDate Tuesday October 22 2013 125254 PM
Hello Colleagues
As I reported in my email below on September 26th fluoridation has come under challenge again inSimcoe Muskoka I am now very unhappy to report that despite our best efforts last night theDistrict Council of Muskoka voted to remove fluoride from municipal drinking supplies across theDistrict This brings to an end fluoridation in all of Simcoe and Muskoka (with the exception of Base Borden)ndash though New Tecumseth will be conducting a plebiscite on the question of fluoridation with themunicipal election next October Defending community water fluoridation has drained a great deal of time human resources andcommitment from other priorities and has been exhausting here in SMDHU as I am sure it hasbeen in many other health units While the outcomes have been very disappointing I have beenimpressed by the professionalism and dedication that SMDHU staff members have shown inshouldering this burden In particular our dental consultant Dr Ito has provided us with much ofthe foundational knowledge and the local research essential to our efforts and has very frequentlyattended and presented at council meetings and other public events I would also like to thank themany of you who have offer and provided support including advocacy letters and informationresources Over the years Dr Peter Cooney Chief Dental Officer of Health of Canada has beenvery helpful attending and presenting with us at council meetings and at public consultationevents We will of course continue our oral health surveillance of the children of Muskoka documentingand reporting in future years on the increase in dental decay that we anticipate will occur Suchsurveillance is the foundation of our advocacy both to municipal politicians and to the province I am very concerned that our experience will continue to repeat itself across the province unlessthere is strong leadership provincially It is with this in mind that I raise the followingrecommendations for your consideration
1 That we collectively (with PHOrsquos leadership) conduct high quality publish-worthy researchdocumenting the impact on dental decay that occurs in those municipalities throughoutOntario that in recent years have discontinued community water fluoridation This could bepart of a larger study on such municipalities across the country and it could also be part ofa study documenting overall oral health (including fluoridation coverage) in the province(and possibly across the country)
2 That COMOH engage with our Chief MOH to advocate for the province to require allmunicipal water supplies to be fluoridated (the exception of course being those withnaturally sufficient fluoride concentrations) This could built upon the alPHa position to
Gordon
Highlight
Gordon
Highlight
date (A11-00 - Community Water Fluoridation) on the CMOH position (Oral Health ndash) and on theemail discussion generated on the COMOH listserv some months back re Richardrsquosproposal (calling on the province to fund municipal water fluoridation)
Valerie I request that this be an item for our COMOH meeting on November 15th Sincerely Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorg From Gardner Charles Sent Thursday September 26 2013 245 PMTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes(RayCopesoahppca)Subject Community Water Fluoridation Under Challenge Again in Simcoe Muskoka Hello Colleagues You may wish to know that community water fluoridation (CWF) is again under challenge in SimcoeMuskoka specifically both in Tottenham (Town of New Tecumseth in Simcoe County) and for theentire District of Muskoka On Monday September 23 Committee of the Whole Council of theTown of New Tecumseth voted to submit application to discontinue community water fluoridation(CWF) in the town of Tottenham despite presentations to the contrary from our dental consultantDr Ito and from me The next Council meeting is scheduled for Monday Sept 30 at which lastMondayrsquos (Sept 23) votes will be ratified
Since Monday I have spoken with the Mayor of the Town of New Tecumseth and with most of thecouncilors encouraging deferral of a decision on Monday to allow the town more time to make afully informed decision
This is the second time in recent years that the issue of discontinuing CWF in Tottenham has beenraised at council This issue is also scheduled to return again to the District of Muskoka Council on
October 21st where I will be presenting in response to deputations in opposition to fluoridation
Outside of Base Borden Tottenham is the only community with fluoridated water in SimcoeCounty The health unitrsquos own screening data between 2011 and 2013 shows that Tottenhamrsquos
Gordon
Highlight
children as well as those in Muskoka have a lower rate of dental decay than Simcoe Muskokacommunities without CWF
Sincerely
Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorgChuck Gardner MOH
November 04 2013
Mandatory State Laws on Fluoridation Thirteen states Puerto Rico and the District of Columbia have laws intended to provide
statewide fluoridation These states and the year that the fluoridation legislation was passed are
District of Columbia (1952) Connecticut (1965) Kentucky (1966) Illinois (1967) Minnesota
(1967) Ohio (1969) South Dakota (1969) Georgia (1973) Nebraska (1973 and 2008)
California (1995) Delaware (1998) Puerto Rico (1998) Nevada (1999) Louisiana (2008) and
Arkansas (2011) (see Table 1) The sizes of the public water systems or countiescommunities
affected and exemption provisions vary by state Table 1
STATES THAT HAVE MANDATORY LAWS ON FLUORIDATION -2011
State (1) Year of
Fluoridation
Legislation (1)
Population
served by
Fluoridated
CWS (2)
Persons
receiving
fluoridated
water (2)
State
Average
Caries
Experience
of Grade 3
Students (3)
Arkansas 2011 647 1724131 64
California 1995 621 22812721 709
Connecticut 1965 910 2370423 406
Delaware 1998 862 705344 545
Georgia 1973 921 8924598 52
Illinois 1967 993 11325132 532
Kentucky 1966 999 4334223 598
Louisiana 2008 407 1846149 657
Minnesota 1967 988 4117266 549
Nebraska 1973 and 2008 702 1001665 593
Nevada 1999 702 1001665 649
Ohio 1969 877 8772683 512
South Dakota 1969 948 642942 623
District of
Columbia
1952 1000 595000
Puerto Rico 1998
United States 739 204283554
2010 Statistics for population fluoridated and number of people
1 Communication with Jane McGinley RDH MBA Manager Fluoridation and Preventive Health
Activities Council on Access Prevention and Interprofessional Relations
2 Centers for Disease Control and Prevention Department of Health and Human Services
accessed Oct 21 2013 httpwwwcdcgovfluoridationstatistics2010statshtm
3 Centers for Disease Control and Prevention National Oral Health Surveillance System Caries
Experience - Percentage of 3rd Grade students with Caries Experience (treated or untreated tooth
If data from 43 states for the percentage of Grade 3 children with experience of dental decay is
compared with the 2008 percentages of the population in a state with Community Water
Fluoridation then the percentage of children with experience of dental decay decreases as the
percentage of the state population with Community Water Fluoridation increases (see Figure 1)
Figure 1
Correlation of Percentage of Grade 3 Children with Caries Experience and
Percentage of Population With Community Water Fluoridation for 43
Reporting States
0
10
20
30
40
50
60
70
80
0 10 20 30 40 50 60 70 80 90 100
State of Population With Community Water Fluoridation
Sta
te
of
Gra
de 3
Stu
den
ts w
ith
Cari
es E
xp
eri
en
ce
Data from CDC (2 3)
The description of the fluoridation laws in California Illinois and Nevada can be found on the
Association of State amp Territorial Dental Directors website(4 7 8)
The California fluoridation law AB 733 came into effect in 1995 requiring communities of 10
000 residents or more be supplied with fluoridated drinking water However the state did not
provide any funding to implement the legislation (California is unique in requiring fluoridation
without funding the practice)(4) The California Department of Health Services therefore had to
fund fluoridation initiatives from non-governmental sources ie the California Endowment
California Dental Association Foundation the First 5 Commission and others(5) From 1995 to
2011 the percentage of the California population receiving fluoridated drinking water has risen
from 17 to 625(6) 4 Dental Public Health Activities amp Practices Office of Oral Health California Department of Health
Services April 2002 httpwwwastddorgbestpracticesDES06002CAfluoridationpdf
5 Stock M Pollick H The CDA Foundation Model to Fluoridate Communities California Dental
Association Journal vol 40 no 8 649 - 655
httpwwwcdaorgPortals0journaljournal_082012pdf
6 California Dental Association Foundation
httpwwwcdafoundationorglearnadvocacyfluoridation
The State of Illinois passed a mandatory fluoridation state in 1967 and required all community
water systems to adjust fluoride levels in the drinking water to optimal levels within 1 year(7)
From 1962 when over 5000000 residents had optimally fluoridated drinking water by 2010
the number had risen to 11325132 (993 of the population on community water systems)(2)
7 Dental Public Health Activities amp Practices Division of Oral Health Illinois Department of Public
Health April 2002 httpwwwastddorgbestpracticesDES16007ILfluoridationpdf
The State of Nevada passed a mandatory fluoridation statute in 2000 for communities with
400000 or more residents(8) This was a result of the work of a statewide coalition that
included the Nevada Dental and Dental Hygienist Associations the Washoe and Clark County
District Health Departments the Clark County School District Junior League of Las Vegas
Head Start the Community College of Southern Nevada Dental Hygiene Program Health
Access Washoe County and Saint Maryrsquos Hospital For communities with less than 400000 the
implementation of fluoridation still required the vote of the majority voters in the community
The Las Vegas Water Authority and the City of Henderson started fluoridation in 2000
increasing the percentage of the population with fluoridated drinking water from 2 to 65 (8) 8 Dental Public Health Activities amp Practices Bureau of Family Health Services Nevada State Health
Division April 2002 httpwwwastddorgbestpracticesDES31002NVfluoridationbillpdf
Countries with Mandatory Laws on Fluoridation Countries that have mandated Community Water Fluoridation are Brazil Hong Kong
Malaysia Singapore Ireland Israel and some of the states in Australia
Singapore started fluoridating its water in 1956 based on the success of the fluoridation trials in
Grand Rapids Newburgh Evanston and Brantford Singapore became the first Asian country to
have 100 of its population benefitting from the implementation of fluoridated drinking water
Loh reported that ldquoThe ten year study on the effects of water fluoridation in Singapore showed
a decrease in caries prevalence in the children In the permanent dentition the reduction was
523 per cent for Chinese and 31 per cent for Malays in the 7 to 9 year old age group A similar
trend was observed in the mixed dentition in which the decrease was 325 per cent for Chinese
and 306 per cent for Malaysrdquo(9) By 2010 the population of the country was 5080000(10)
9 Loh T Thirty-eight years of water fluoridation--the Singapore scenario Community Dent
Health 1996 Sep13 Suppl 247-50
10 British Fluoridation Society One in a Million the facts about water fluoridation 3rd Edition
published March 2012) httpwwwbfsweborgonemillion0920One20in20a20Million20-
20The20Extent20of20Fluoridationpdf
Hong Kong started implementing community water fluoridation in 1961 and similar to
Singapore 100 of the population received access to fluoridated drinking water Lo and Wong
reported that ldquoThe mean DMFT score of the children deceased from 44 in 1960 to 15 in 1968
stayed at this level in the 1980 and 1986 surveys and further deceased to 08 in 2001 The
prevalence of dental fluorosis among the children surveyed in 1960 was 1 and this increased
to 59 and 70 in 1968 and 1980 respectively It was found in the 1986 and 2001 surveys that
the prevalences of fluorosis were 47 and 9 among children whose teeth developed at the
time when the respective water fluoride concentrations were 07 ppm and 05 ppmrdquo(11) The
population of Hong Kong was 6968000 in 2009(10) 11 LO ECM and WONG AHH Water fluoride concentration and fluorosis in Hong Kong in 1960-
2001 84th General Session and Exhibition of the International Association for Dental Research amp
1st Meeting of the Pan-Asian-Pacific Federation Brisbane Australia 28 June-1 July 2006 v 85 n
Sp B
The Malaysian cabinet approved a nationwide community water fluoridation program in 1972
(12) One of the states Sabah decided to stop fluoridation in 1989 due to concerns about
inadequate supervision in adding fluoride to the drinking water Oral Health Surveys in 2009
and 2007 indicated that children in Sabah had the worst oral health with 50 of 12 year-olds
having decay in their permanent teeth and children having an average of 3 teeth being(13)
Under the 10th Malaysian Plan in 2011 the federal and the Sabah state governments
reintroduced water fluoridation in Sabah(1314) In 2010 about 755 of the Malaysian
population or 20700000 people had fluoridated drinking water(1013) 12 Malaysian Dental Association Fluoride in Water
httpwwwmdaorgmy07_public_01healthcare_12htm
13 Sachdev N Fluoridation in Sabah Water for Cleaner Teeth French Tribunecom 28022011
From Levy IsraTo Jaeger ValerieCc Pim Carolyn gordonalphaweborg Diallo Aicha Penny Sutcliffe Paul Roumeliotis Michael Finkelstein
Hazel Lynn Robert KyleSubject FW Panorama - Privacy Security and other issuesDate Wednesday October 16 2013 122110 PM
Hello ValerieOttawa is part of Wave 4 Panorama implementation and we are gearing up increasingly to use thesystem where and if possible Thinking about it I am anticipating that this may need to be on theCOMOH (and alPHa) radar as it is something that will impact all health units and implies a majoroperational shift in vaccine delivery programs for all health units I have asked Carolyn Pim toconnect with our sister wave 4 units to share common experiences as we move forward ndash when wehave a roll up could I bring to COMOH Exec for discussion to explore whether there are broaderimplications for all members As an aside I have also asked the Ministry and their CIO to share with me any roll up learnings thatthey may have had already from previous waves (I understand that Niagara HU was a wave 1participant so if there is such a roll up of common experiences that others could learn fromperhaps you have it already and that could come to the exec too)Thanks Isra From Pim Carolyn Sent October 10 2013 1228 PMTo Christopher Mackie (christophermackiemlhuonca) Elizabeth Richardson(Elizabethrichardsonhamiltonca) H BSc M D F R C P (C) MPH Jim Chirico(jimchiriconbpsdhuca) Marlene Spruyt (spruytmtimiskaminghucom) Robert Kyle (Durham)Cc Levy IsraSubject Panorama - Privacy Security and other issues Dear colleagues Irsquom reaching out to you as fellow Panorama Wave 4 health units to ask about where yourorganizations are at in the process of signing agreements and completing Privacy ImpactAssessments and Threat Risk Assessments (TRAs) Ottawa Public Healthrsquos IT legal and informationsecurity advisors have made numerous requests to the MOHLTC for information (in particular theprovincial TRA) that we consider essential to develop our own risk assessment and PIA but havebeen told that information cannot be shared even with strict confidentiality and access controlsSo we are at somewhat of an impasse Isra emailed Arlene yesterday Arlene has forwarded ourconcerns to the Ministryrsquos CIO and Panorama lead but we havenrsquot had any response or discussionswith either of them yet Have your organizations identified similar concerns andor had interactions with the MOHLTC inthis respect Irsquod also be interested in knowing if your health units have flagged other (egoperational) implementation concerns Thanks
Carolyn ps Robert ndash you can ignore this request I talked with Sharan this morning about Durhamrsquos issuesso am including you now just for information Carolyn Pim MD FRCPC Associate Medical Officer of Health Meacutedecin adjointe en santeacute publique Ottawa Public Health Santeacute publique Ottawa 100 Constellation Cr Ottawa ON K2G 6J8 Tel teacutel (613) 580-6744 ext 23684Fax (613) 580-9641Connect With Ottawa Public Health
Suivez Santeacute publique Ottawa
This e-mail originates from the City of Ottawa e-mail system Any distribution use orcopying of this e-mail or the information it contains by other than the intendedrecipient(s) is unauthorized If you are not the intended recipient please notify meat the telephone number shown above or by return e-mail and delete thiscommunication and any copy immediately Thank you
Le preacutesent courriel a eacuteteacute expeacutedieacute par le systegraveme de courriels de la Ville dOttawaToute distribution utilisation ou reproduction du courriel ou des renseignements quisy trouvent par une personne autre que son destinataire preacutevu est interdite Si vousavez reccedilu le message par erreur veuillez men aviser par teacuteleacutephone (au numeacuteropreacuteciteacute) ou par courriel puis supprimer sans deacutelai la version originale de lacommunication ainsi que toutes ses copies Je vous remercie de votre collaboration
1
Smoke-Free Patios ndash An Amendment to the Smoke-Free Ontario Act
Date November 15 2013 Prepared for Council of Ontario Medical Officers of Health Prepared by York Region Public Health _____________________________________________________________________________ Issue
The Smoke-Free Ontario Act is the current provincial legislation that imposes smoking restrictions in workplaces and public places It prohibits smoking on restaurant and bar patios in instances where any portion of the seating area is covered by a roof With recent studies illustrating that exposure to second hand smoke outdoors poses similar risks to indoor exposure there has been growing public support to enhance smoking restrictions and make patios completely smoke-free
Background
With the implementation of the Smoke-Free Ontario Act in 2006 restaurant and bar patios became subject to smoking restrictions if any portion of the seating area was covered by a roof This allowed for patios without roof coverings to continue to allow smoking and as a result did not provide significant protection to patrons or staff from exposure to second hand smoke outdoors Many businesses chose to alter the design of their patios to allow smoking to continue In some cases patios became more crowded since smoking patrons who dine indoors often proceed outside onto licensed patios with their beverages to smoke York Region like most municipalities in Ontario is host to hundreds of patios being operated by restaurant owners and businesses With smoking prohibitions affecting only a small portion of these patios specifically ones with coverings the vast majority of patios still allow smoking to take place Patrons and employees on patios where smoking is not restricted are exposed to second hand smoke frequently This can contribute to increased disease and aggravation of existing health conditions From a business perspective the existing legislation has been viewed by many operators as unfair because some patios have permanent coverings which cannot be removed requiring a smoke-free status These business owners feel this creates an uneven playing field since they cannot provide an outdoor dining area for their smoking customers There is strong community support for smoke-free patios in Ontario A 2009 Rapid Risk Factor Surveillance System survey revealed 754 percent support in York Region while a Toronto Health Survey in 2011 indicated 74 percent public support
2
Current Status
Smoking is currently prohibited on restaurant and bar patios province-wide in four Canadian provinces and territories Alberta Newfoundland and Labrador Nova Scotia and Yukon A fifth province Prince Edward Island prohibits smoking on patios until 10 pm Since Ontario enacted legislation restricting smoking on patios in 2006 eight municipalities in Ontario have chosen to create bylaws that go beyond the Smoke-Free Ontario Act and enhance outdoor protection from second hand smoke by prohibiting smoking on patios completely The largest of those municipalities is the City of Ottawa Recently the Toronto Board of Health unanimously endorsed a report presented by their Medical Officer of Health recommending that restaurant and bar patios be made smoke-free through an amendment to the Smoke-Free Ontario Act
Key Considerations
There should be no significant financial burden to local Boards of Health resulting from a smoke-free patio amendment to the Smoke-Free Ontario Act Inspection and enforcement for the Smoke-Free Ontario Act is currently 100 percent funded by the Ministry of Health and Long-Term Care Following an introductory period of education on the amendment a complaint response model of service delivery would ensure ongoing compliance with smoke-free requirements A complete ban of smoking on patios would eliminate the widely-held perception by business owners that the current legislation creates an uneven playing field for business Since Smoke-Free Ontario Act inspections of patios began in 2006 operators have expressed the opinion that if patios need to be smoke-free for the protection of the public they should all be smoke-free to avoid undue hardship for individual businesses and to provide protection uniformly across the Province
Next steps
York Region Public Health intends to seek support from Medical Officers of Health across the Central East Tobacco Control Area Network (CETCAN) to advocate to the Ministry of Health and Long-Term Care for an amendment to the Smoke-Free Ontario Act prohibiting smoking on all restaurant and bar patios York Region is also in the process of requesting that its Regional Council advocate to the Minister of Health and Long-Term Care on the issue
Updating and Modernizing O Regulation 565 (Public Pools)
Date November 15 2013
Prepared for Council of Ontario Medical Officers of Health
Prepared by York Region Public Health _____________________________________________________________________________ Background Recent drownings at public pools in Ontario have highlighted the issue of water-borne illness and injury The current pool regulation under Ontariorsquos Health Protection and Promotion Act O Regulation 565 (Public Pools) is outdated It does not accurately reflect new pool technology and design or the changing use of public pools Neither does it incorporate admissions standards recommended by the Office of the Chief Coroner Further O Regulation 565 does not have short-form wording or set fines associated with it This limits public health enforcement capabilities What is the impact Updating O Regulation 565 (Public Pools) to address recent changes in pool technology design and uses and to include Coroner-recommended admissions standards would help improve pool safety Establishing short-form wording for O Regulation 565 would enhance enforcement related to public pools Currently the only enforcement available to Public Health Inspectors for dealing with non-critical regulatory infractions in public pools is the issuance of a Part III summons This involves a considerable amount of resources for a possible small fine With the development of inspection disclosure systems such as YorkSafe there is an even greater need to develop a method to effectively address repeated pool operator non-compliance with non-critical issues Next steps Public health units should advocate to the Province to 1) Conduct a review of O Regulation 565 (Public Pools) to address shortcomings Proposed changes to the
regulation should include a requirement for ownersoperators of public pools to advise the local Medical Officer of Health of any change in the use of a facility and the addition of the Coronerrsquos recommended admission standards
2) Provide short-form wording for O Regulation 565 so that public health inspectors can better deal with pool operator non-compliance
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
3 Council of Ontario Medical Officers of Health Terms of Reference
Emeritus membership shall be open to all former members who have retired after five (5) or more years of Active membership subject to the nomination in writing of two (2) active members in good standing endorsement of the Executive Committee and approval of the Council by majority vote at a general meeting Such members shall have neither voting privileges nor hold office but may be invited to attend general meetings Honorary membership shall be open to any non-active or associate member subject to the nomination in writing of two (2) active members in good standing endorsement of the Executive Committee and approval of the Council Such members shall have neither voting privileges nor hold office but may be invited to attend general meetings
OFFICERS 5 The Officers of the Council shall be the Chair Vice-Chair and immediate Past Chair
6 The Chair shall prepare the agendas of all Council meetings She shall preside and
preserve order at all such meetings shall ensure that these Terms of Reference are upheld and enforced and shall contribute to the supervision and evaluation of any Public Health and Preventive Medicine Resident who is on a placement with alPHa
7 The Vice-Chair shall fulfill the duties of the Chair in hisher absence The immediate
Past Chair may fulfill the duties of the Chair or Vice-Chair in their absences 8 The Chair shall normally serve a term of one (1) year which is renewable once and
after which the Vice-Chair shall normally assume the vacated office COMMITTEES 9 The Council shall elect seven (7) active members one from each of alPHarsquos regions
and the active member who is scheduled to serve as the President or immediate Past-President of alPHa to represent it on the alPHa Board of Directors These seven (7) members shall constitute the Councilrsquos Executive Committee and shall serve a term of at least one (1) year The Chair and Vice-Chair shall be elected from among the Executive Committee members If alPHarsquos immediate Past President is an active member she shall be an ex-officio member of the Executive Committee
10 The mandate of the Executive Committee shall be to facilitate the achievement of
the objectives of the Council by fulfilling the following
a Identifying priorities 1
1 See Appendix B Planning Cycle to Identify Priorities for COMOH
and ensuring the development of briefing documents and or recommendations as appropriate for the consideration of the Council
4 Council of Ontario Medical Officers of Health Terms of Reference
b Setting agendas and otherwise ensuring preparations for Council meetings c Ensuring the fulfillment of the direction of Council d Responding in a timely fashion to time-sensitive public health matters in
accordance with the Executive Committeersquos understanding of the perspective of the Council
e Engaging with the Chief Medical Officer of Health Associate Chief Medical Officers of Health and other provincial public health leaders and
f Representing Council at public and partner agency forums including the Public Health Leadership Council which shall normally include membership from the Officers of the Council and two other Executive Committee members as selected by agreement among the Executive
g Identifying opportunities for the recognition of outstanding practice from among the members including the annual nomination of at least one member for the alPHa Distinguished Service Award
11 The Executive Committee shall meet and correspond in the manner and at the times
and if required places as deemed necessary by the Chair to conduct the business of the Council A quorum shall consist of four (4) members
12 The Executive Committee shall have the power to strike committeestask or working
groups to assist it in carrying out the business of the Council 13 The Council may by special resolution remove a member of the Executive
Committee before the completion of hisher term of office and may elect a successor to complete the term The special resolution shall require a majority vote of 67 of the members present and voting at the meeting at which the special resolution is considered
14 A Nominating Committee shall consist of the three (3) most recent Past Chairs who
are able to serve and shall be chaired by the immediate Past Chair The Nominating Committee shall prepare a list of proposed Officers and Executive Committee members for the consideration of the Council at its Annual General Meeting
MEETINGS 15 The Council shall hold at least four (4) general meetings per year in a manner and at
the times and if required places as deemed necessary by the Executive Committee to share information direct and assist the Executive Committee in conducting the business of the Council
16 The Council shall hold its Annual General Meeting during and at the same place as
the alPHarsquos Annual Conference
5 Council of Ontario Medical Officers of Health Terms of Reference
17 The Council shall hold a special meeting at the call of the Chair or upon the written request specifying the purpose of such meeting of at least five (5) active members Council members must be given at least 48 hours notice of any special meeting
18 Only Councilrsquos active and associate members and alPHa staff are entitled to attend
general and special meetings of the Council Other members and non-members may be invited to attend all or part of such meetings as determined by the Chair preferably in consultation with the Executive Committee Non-members who come to such meetings without an invitation may attend all or part of the meeting by a majority vote of the active members present and voting
19 The Chair shall prepare the agendas for such meetings and shall normally include
reports from the Chair and the Councilrsquos committeestask or working groups and representatives to external bodies alPHarsquos Executive Director shall ensure that the minutes shall be recorded and promptly distributed to the Section
20 A quorum for all such meetings shall be ten (10) active members 21 The Council shall normally be notified in a manner deemed appropriate by the Chair
of such meetings at least one (1) month prior to their being held 22 A majority vote of the members present at such meetings and voting shall make
Council decisions In the case of a tied vote the Chair shall cast the deciding vote The Executive Committee shall ensure that actions arising from such decisions at such meetings are implemented and monitored
23 The Chair may solicit advice from the Council through the use of teleconferencing
and alPHarsquos electronic mailing lists in order to gain an understanding of the overall perspective of the Council (see 10d)
ELECTIONS 24 The Officers and Executive Committee members shall be elected at the Sectionrsquos
Annual General Meeting The Nominating Committee Chair or hisher designate shall present a list of nominations Additional nominations from the floor shall also be considered Each Officer and Executive Committee member shall be elected by secret ballot if necessary by a majority of the active members present and voting In the case of a tie the Chair shall cast the deciding vote
AMENDMENTS 25 The Councilrsquos Terms of Reference may be amended from time to time by the
Executive Committee provided the Committee receives notice of such proposed amendments at least one (1) month prior to the meeting at which the amendments
6 Council of Ontario Medical Officers of Health Terms of Reference
will be considered Such amendments shall be ratified by the Council at the next general meeting or the Annual General Meeting as the case may be
26 The Executive Committee shall review the Terms of Reference as required and not
less than once every two years Original September 1987 1st Revision October 2000 2nd Revision July 2001 3rd Revision December 2003 4th Revision February 2008 5th Revision June 2009 6th Revision June 2011 7th Revision June 2013
7 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX A
COMOH Membership Benefits Active Membership
bull Entitled to attend all meetings of the Section bull May hold office on the COMOH Executive Committee alPHa Board of Directors
Standing Committees bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Associate Membership
bull Entitled to attend all meetings of the Section bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Affiliate Membership
bull May attend meetings or parts thereof subject to approval of Chair bull May serve on ad-hoc committees of the Section subject to the approval of the
Executive Committee bull Discounted registration rates for alPHa Conferences (for Public Health and
Preventive Medicine Residents) bull Upon written request and subject to COMOH Executive approval Affiliate
Members may subscribe to comohlistsalphaweborg The approval will be reviewed on an annual basis in order to determine if the Affiliate Member can remain a subscriber to mohsalphaweborg
Emeritus Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair bull Enjoy discounted registration rates for alPHa Conferences and regular COMOH
meetings bull Subscription to comohlistsalphaweborg electronic mailing list bull Full access to alPHa Web site bull May represent alPHa COMOH on selected external committees and working
groups Honorary Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair
8 Council of Ontario Medical Officers of Health Terms of Reference
bull May represent alPHa COMOH on selected external committees and working groups subject to the approval of the COMOH or alPHa Executive Committee as appropriate
9 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX B
Planning Cycle to Identify Priorities for COMOH
1 There shall normally be a COMOH membership strategic planning retreat every four years In recognition of the dynamic environment of public health the need for and timing of such a retreat shall be at the discretion of the Executive Committee in consultation with the membership
2 The COMOH Executive is responsible (through the creation of a subcommittee of COMOH members) for ensuring the preparation for the COMOH retreats with resources to include those provided by alPHa
3 Leadership for action on COMOH priorities will be recruited from among the COMOH membership in order to make good use of the full base of capacity of the membership The resources to support actions will be recruited from both within and beyond the COMOH membership employing other public health professionals that reside within the broader public health system and community
4 The COMOH Executive shall ensure an annual review of strategic priorities and initiatives and the development of a draft report of the same for the review of the members at the June meeting
2013 Strategic Planning
Considerations for COMOH
As part of its strategic planning discussions alPHarsquos Board has been considering changes to the level of support provided to member sections A member survey is being carried out over the fall to determine options acceptable to alPHa members The following approach to support is put forward as a proposal for the consideration of COMOH Note that the feasibility of the points below depend upon future decisions of the alPHa board They assume that COMOH remains part of alPHa but becomes more independent in administering meetings
1 alPHa can provide to COMOH staff support (Gord Fleming) amounting to 02 FTE or one day per week This is a reduction from the current level of 35 days per week COMOH can choose to use the support any way it wants writing COMOH letters meeting minutes agenda support special projects etc
2 In addition to 02 FTE alPHa staff would provide support for up to 4 face-to-face meetings per year One meeting would be concurrent to alPHarsquos annual conference in June The timing of other meetings could be negotiated The support includes consulting on the development of the program arranging for speakers registration for the event arranging venue AV support and hospitality services
3 In addition to 02 FTE alPHa staff would provide support for setting meeting dates and any polling required to establish dates Note that the individual supporting this function would be Karen Reece
4 COMOHrsquos Executive and Section would continue to have access to online supports through the alPHa including the COMOH Listserve and a group page for posting agendas minutes and other resources on the alPHa website
5 alPHa staff (Linda Stewart and Gord Fleming) can also start participating on CMOH calls as a way to be up-to-date on issues related to COMOH
6 Other than what is outlined above COMOH would be expected to prepare agendas and take minutes for its Executive and Section meetings The Executive would be expected to operate more independently than it does now but would be able to access the supports outlined above
Prepared by Linda Stewart Executive Director
From comoh-bounceslistsalphaweborg on behalf of Christopher MackieTo MOH ListserveSubject [comoh] Fw URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)Date Wednesday October 30 2013 91241 AMAttachments ATT00249txt
For AMOHs and PHPM residents who didnt receive the initial email
Chris
Christopher Mackie MD MHSc FRCPCMedical Officer of Health and CEOMiddlesex-London Health Unit50 King St LondonON N6A 5L7 O 519 663 5317 ext 2444 wwwhealthunitcomFrom Pisko Laura (MOHLTC)Sent Tuesday October 29 2013 759 PMTo kbarkeralgomapublichealthcom malcolmlockbchuorg davidcchatham-kentcarobertkyledurhamca proumeliotiseohuca fwarshelginhealthonca mohelginhealthoncahlynnpublichealthgreybruceonca malcolmlockhnhuorg hnmohhnhuorglnoseworthyhkpronca bobnosalhaltonca elizabethrichardsonhamiltoncarschabashpechuonca ncameronhuroncountyca drimgemmillkflapublichealthcamohkflapublichealthca suditranadecounty-lambtononca paulastewarthealthunitorgChristopher Mackie valeriejaegerniagararegionca jimchiriconbpsdhuca jarthursnwhuoncaisralevyottawaca dnealoxfordcountyca davidmowatpeelregionca mklassenpdhuoncarpellizzaripcchuca rosemarieramsinghporcupinehuonca mcorriveaurcdhucomcharlesgardnersmdhuorg sutcliffepsdhucom davidwilliamstbdhucomspruytmtimiskaminghucom dmckeowntorontoca lnolanregionofwaterloocanicolamercerwdghuorg aheimannwechealthunitorg karimkurjiyorkcaCc coreywesleytbdhucom CindyBaker-Barillsmdhuorg Donna Kosmack pilonlsdhucomPaulaMuiskflapublichealthca sthibautorontoca Mueller Daina (MOHLTC) Gordon Marcus(MOHLTC) andreakitahamiltoncaSubject URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)
Dear Colleagues The ministry has received reports that some tobacco vendors across the province aregiving away single cigarettes with the purchase of tobacco products It is the ministryrsquosposition that giving out free single cigarettes does not violate subsection 31(3) of theSmoke-Free Ontario Act (ldquoSFOArdquo) Although the practice of giving out free singlecigarettes may promote the sale of tobacco products it does not take the form of aldquoproduct enhancement product association or promotional materialrdquo and therefore doesnot fall within the scope of subsection 31(3) of the SFOA We have confirmed with Health Canada that this practice may violate section 29(b) of thefederal Tobacco Act As such Health Canada is requesting that you notify them in writingand I am directing you to communicate with them via email and provide to them as manydetails as possible Emails should be sent to Tobacco-Ontariohc-scgcca and thesubject line should read ldquoViolation of Section 29(b) of Tobacco Actrdquo This will ensurethat the complaints are given priority status by Health Canada We will continue to monitor
this situation and liaise with our colleagues at Health Canada Please share this information with your tobacco control staff and contact me or DainaMueller Manager Tobacco Control Unit Health Promotion Implementation Branch atdainamuellerontarioca with any questions RegardsLaura Laura A PiskoDirectorHealth Promotion Implementation BranchHealth Promotion DivisionMinistry of Health and Long Term Care416-327-7445 (office)416-451-3185 (mobile) Marcus Gordon - EA (416)326-0625 for urgent issues
========= Middlesex-London Health Unit E-Mail Disclaimer =============______________________________________________________________
Private and confidential intended only for named recipient If otherwisereceived please destroy immediately Health information in this email isonly general information and is not intended to replace an in personconsultation with a medical professional nor is it intended to providemedical advice Individual circumstances of which we are not aware mayaffect the information provided herein and as such the Middlesex-LondonHealth Unit assumes no liability or responsibility for your reliancethereon The Middlesex-London Health Unit works under the authority of theHealth Protection and Promotion Act and this correspondence may be used toassess your needs for public health services (519-663-5317 ext 2448)______________________________________________________________
From Gardner CharlesTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes (RayCopesoahppca)
George Pasut (GeorgePasutoahppca) Peter Cooney (petercooneyhc-scgcca)Cc Ito DickSubject Discontinuation of Fluoridation in MuskokaDate Tuesday October 22 2013 125254 PM
Hello Colleagues
As I reported in my email below on September 26th fluoridation has come under challenge again inSimcoe Muskoka I am now very unhappy to report that despite our best efforts last night theDistrict Council of Muskoka voted to remove fluoride from municipal drinking supplies across theDistrict This brings to an end fluoridation in all of Simcoe and Muskoka (with the exception of Base Borden)ndash though New Tecumseth will be conducting a plebiscite on the question of fluoridation with themunicipal election next October Defending community water fluoridation has drained a great deal of time human resources andcommitment from other priorities and has been exhausting here in SMDHU as I am sure it hasbeen in many other health units While the outcomes have been very disappointing I have beenimpressed by the professionalism and dedication that SMDHU staff members have shown inshouldering this burden In particular our dental consultant Dr Ito has provided us with much ofthe foundational knowledge and the local research essential to our efforts and has very frequentlyattended and presented at council meetings and other public events I would also like to thank themany of you who have offer and provided support including advocacy letters and informationresources Over the years Dr Peter Cooney Chief Dental Officer of Health of Canada has beenvery helpful attending and presenting with us at council meetings and at public consultationevents We will of course continue our oral health surveillance of the children of Muskoka documentingand reporting in future years on the increase in dental decay that we anticipate will occur Suchsurveillance is the foundation of our advocacy both to municipal politicians and to the province I am very concerned that our experience will continue to repeat itself across the province unlessthere is strong leadership provincially It is with this in mind that I raise the followingrecommendations for your consideration
1 That we collectively (with PHOrsquos leadership) conduct high quality publish-worthy researchdocumenting the impact on dental decay that occurs in those municipalities throughoutOntario that in recent years have discontinued community water fluoridation This could bepart of a larger study on such municipalities across the country and it could also be part ofa study documenting overall oral health (including fluoridation coverage) in the province(and possibly across the country)
2 That COMOH engage with our Chief MOH to advocate for the province to require allmunicipal water supplies to be fluoridated (the exception of course being those withnaturally sufficient fluoride concentrations) This could built upon the alPHa position to
Gordon
Highlight
Gordon
Highlight
date (A11-00 - Community Water Fluoridation) on the CMOH position (Oral Health ndash) and on theemail discussion generated on the COMOH listserv some months back re Richardrsquosproposal (calling on the province to fund municipal water fluoridation)
Valerie I request that this be an item for our COMOH meeting on November 15th Sincerely Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorg From Gardner Charles Sent Thursday September 26 2013 245 PMTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes(RayCopesoahppca)Subject Community Water Fluoridation Under Challenge Again in Simcoe Muskoka Hello Colleagues You may wish to know that community water fluoridation (CWF) is again under challenge in SimcoeMuskoka specifically both in Tottenham (Town of New Tecumseth in Simcoe County) and for theentire District of Muskoka On Monday September 23 Committee of the Whole Council of theTown of New Tecumseth voted to submit application to discontinue community water fluoridation(CWF) in the town of Tottenham despite presentations to the contrary from our dental consultantDr Ito and from me The next Council meeting is scheduled for Monday Sept 30 at which lastMondayrsquos (Sept 23) votes will be ratified
Since Monday I have spoken with the Mayor of the Town of New Tecumseth and with most of thecouncilors encouraging deferral of a decision on Monday to allow the town more time to make afully informed decision
This is the second time in recent years that the issue of discontinuing CWF in Tottenham has beenraised at council This issue is also scheduled to return again to the District of Muskoka Council on
October 21st where I will be presenting in response to deputations in opposition to fluoridation
Outside of Base Borden Tottenham is the only community with fluoridated water in SimcoeCounty The health unitrsquos own screening data between 2011 and 2013 shows that Tottenhamrsquos
Gordon
Highlight
children as well as those in Muskoka have a lower rate of dental decay than Simcoe Muskokacommunities without CWF
Sincerely
Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorgChuck Gardner MOH
November 04 2013
Mandatory State Laws on Fluoridation Thirteen states Puerto Rico and the District of Columbia have laws intended to provide
statewide fluoridation These states and the year that the fluoridation legislation was passed are
District of Columbia (1952) Connecticut (1965) Kentucky (1966) Illinois (1967) Minnesota
(1967) Ohio (1969) South Dakota (1969) Georgia (1973) Nebraska (1973 and 2008)
California (1995) Delaware (1998) Puerto Rico (1998) Nevada (1999) Louisiana (2008) and
Arkansas (2011) (see Table 1) The sizes of the public water systems or countiescommunities
affected and exemption provisions vary by state Table 1
STATES THAT HAVE MANDATORY LAWS ON FLUORIDATION -2011
State (1) Year of
Fluoridation
Legislation (1)
Population
served by
Fluoridated
CWS (2)
Persons
receiving
fluoridated
water (2)
State
Average
Caries
Experience
of Grade 3
Students (3)
Arkansas 2011 647 1724131 64
California 1995 621 22812721 709
Connecticut 1965 910 2370423 406
Delaware 1998 862 705344 545
Georgia 1973 921 8924598 52
Illinois 1967 993 11325132 532
Kentucky 1966 999 4334223 598
Louisiana 2008 407 1846149 657
Minnesota 1967 988 4117266 549
Nebraska 1973 and 2008 702 1001665 593
Nevada 1999 702 1001665 649
Ohio 1969 877 8772683 512
South Dakota 1969 948 642942 623
District of
Columbia
1952 1000 595000
Puerto Rico 1998
United States 739 204283554
2010 Statistics for population fluoridated and number of people
1 Communication with Jane McGinley RDH MBA Manager Fluoridation and Preventive Health
Activities Council on Access Prevention and Interprofessional Relations
2 Centers for Disease Control and Prevention Department of Health and Human Services
accessed Oct 21 2013 httpwwwcdcgovfluoridationstatistics2010statshtm
3 Centers for Disease Control and Prevention National Oral Health Surveillance System Caries
Experience - Percentage of 3rd Grade students with Caries Experience (treated or untreated tooth
If data from 43 states for the percentage of Grade 3 children with experience of dental decay is
compared with the 2008 percentages of the population in a state with Community Water
Fluoridation then the percentage of children with experience of dental decay decreases as the
percentage of the state population with Community Water Fluoridation increases (see Figure 1)
Figure 1
Correlation of Percentage of Grade 3 Children with Caries Experience and
Percentage of Population With Community Water Fluoridation for 43
Reporting States
0
10
20
30
40
50
60
70
80
0 10 20 30 40 50 60 70 80 90 100
State of Population With Community Water Fluoridation
Sta
te
of
Gra
de 3
Stu
den
ts w
ith
Cari
es E
xp
eri
en
ce
Data from CDC (2 3)
The description of the fluoridation laws in California Illinois and Nevada can be found on the
Association of State amp Territorial Dental Directors website(4 7 8)
The California fluoridation law AB 733 came into effect in 1995 requiring communities of 10
000 residents or more be supplied with fluoridated drinking water However the state did not
provide any funding to implement the legislation (California is unique in requiring fluoridation
without funding the practice)(4) The California Department of Health Services therefore had to
fund fluoridation initiatives from non-governmental sources ie the California Endowment
California Dental Association Foundation the First 5 Commission and others(5) From 1995 to
2011 the percentage of the California population receiving fluoridated drinking water has risen
from 17 to 625(6) 4 Dental Public Health Activities amp Practices Office of Oral Health California Department of Health
Services April 2002 httpwwwastddorgbestpracticesDES06002CAfluoridationpdf
5 Stock M Pollick H The CDA Foundation Model to Fluoridate Communities California Dental
Association Journal vol 40 no 8 649 - 655
httpwwwcdaorgPortals0journaljournal_082012pdf
6 California Dental Association Foundation
httpwwwcdafoundationorglearnadvocacyfluoridation
The State of Illinois passed a mandatory fluoridation state in 1967 and required all community
water systems to adjust fluoride levels in the drinking water to optimal levels within 1 year(7)
From 1962 when over 5000000 residents had optimally fluoridated drinking water by 2010
the number had risen to 11325132 (993 of the population on community water systems)(2)
7 Dental Public Health Activities amp Practices Division of Oral Health Illinois Department of Public
Health April 2002 httpwwwastddorgbestpracticesDES16007ILfluoridationpdf
The State of Nevada passed a mandatory fluoridation statute in 2000 for communities with
400000 or more residents(8) This was a result of the work of a statewide coalition that
included the Nevada Dental and Dental Hygienist Associations the Washoe and Clark County
District Health Departments the Clark County School District Junior League of Las Vegas
Head Start the Community College of Southern Nevada Dental Hygiene Program Health
Access Washoe County and Saint Maryrsquos Hospital For communities with less than 400000 the
implementation of fluoridation still required the vote of the majority voters in the community
The Las Vegas Water Authority and the City of Henderson started fluoridation in 2000
increasing the percentage of the population with fluoridated drinking water from 2 to 65 (8) 8 Dental Public Health Activities amp Practices Bureau of Family Health Services Nevada State Health
Division April 2002 httpwwwastddorgbestpracticesDES31002NVfluoridationbillpdf
Countries with Mandatory Laws on Fluoridation Countries that have mandated Community Water Fluoridation are Brazil Hong Kong
Malaysia Singapore Ireland Israel and some of the states in Australia
Singapore started fluoridating its water in 1956 based on the success of the fluoridation trials in
Grand Rapids Newburgh Evanston and Brantford Singapore became the first Asian country to
have 100 of its population benefitting from the implementation of fluoridated drinking water
Loh reported that ldquoThe ten year study on the effects of water fluoridation in Singapore showed
a decrease in caries prevalence in the children In the permanent dentition the reduction was
523 per cent for Chinese and 31 per cent for Malays in the 7 to 9 year old age group A similar
trend was observed in the mixed dentition in which the decrease was 325 per cent for Chinese
and 306 per cent for Malaysrdquo(9) By 2010 the population of the country was 5080000(10)
9 Loh T Thirty-eight years of water fluoridation--the Singapore scenario Community Dent
Health 1996 Sep13 Suppl 247-50
10 British Fluoridation Society One in a Million the facts about water fluoridation 3rd Edition
published March 2012) httpwwwbfsweborgonemillion0920One20in20a20Million20-
20The20Extent20of20Fluoridationpdf
Hong Kong started implementing community water fluoridation in 1961 and similar to
Singapore 100 of the population received access to fluoridated drinking water Lo and Wong
reported that ldquoThe mean DMFT score of the children deceased from 44 in 1960 to 15 in 1968
stayed at this level in the 1980 and 1986 surveys and further deceased to 08 in 2001 The
prevalence of dental fluorosis among the children surveyed in 1960 was 1 and this increased
to 59 and 70 in 1968 and 1980 respectively It was found in the 1986 and 2001 surveys that
the prevalences of fluorosis were 47 and 9 among children whose teeth developed at the
time when the respective water fluoride concentrations were 07 ppm and 05 ppmrdquo(11) The
population of Hong Kong was 6968000 in 2009(10) 11 LO ECM and WONG AHH Water fluoride concentration and fluorosis in Hong Kong in 1960-
2001 84th General Session and Exhibition of the International Association for Dental Research amp
1st Meeting of the Pan-Asian-Pacific Federation Brisbane Australia 28 June-1 July 2006 v 85 n
Sp B
The Malaysian cabinet approved a nationwide community water fluoridation program in 1972
(12) One of the states Sabah decided to stop fluoridation in 1989 due to concerns about
inadequate supervision in adding fluoride to the drinking water Oral Health Surveys in 2009
and 2007 indicated that children in Sabah had the worst oral health with 50 of 12 year-olds
having decay in their permanent teeth and children having an average of 3 teeth being(13)
Under the 10th Malaysian Plan in 2011 the federal and the Sabah state governments
reintroduced water fluoridation in Sabah(1314) In 2010 about 755 of the Malaysian
population or 20700000 people had fluoridated drinking water(1013) 12 Malaysian Dental Association Fluoride in Water
httpwwwmdaorgmy07_public_01healthcare_12htm
13 Sachdev N Fluoridation in Sabah Water for Cleaner Teeth French Tribunecom 28022011
From Levy IsraTo Jaeger ValerieCc Pim Carolyn gordonalphaweborg Diallo Aicha Penny Sutcliffe Paul Roumeliotis Michael Finkelstein
Hazel Lynn Robert KyleSubject FW Panorama - Privacy Security and other issuesDate Wednesday October 16 2013 122110 PM
Hello ValerieOttawa is part of Wave 4 Panorama implementation and we are gearing up increasingly to use thesystem where and if possible Thinking about it I am anticipating that this may need to be on theCOMOH (and alPHa) radar as it is something that will impact all health units and implies a majoroperational shift in vaccine delivery programs for all health units I have asked Carolyn Pim toconnect with our sister wave 4 units to share common experiences as we move forward ndash when wehave a roll up could I bring to COMOH Exec for discussion to explore whether there are broaderimplications for all members As an aside I have also asked the Ministry and their CIO to share with me any roll up learnings thatthey may have had already from previous waves (I understand that Niagara HU was a wave 1participant so if there is such a roll up of common experiences that others could learn fromperhaps you have it already and that could come to the exec too)Thanks Isra From Pim Carolyn Sent October 10 2013 1228 PMTo Christopher Mackie (christophermackiemlhuonca) Elizabeth Richardson(Elizabethrichardsonhamiltonca) H BSc M D F R C P (C) MPH Jim Chirico(jimchiriconbpsdhuca) Marlene Spruyt (spruytmtimiskaminghucom) Robert Kyle (Durham)Cc Levy IsraSubject Panorama - Privacy Security and other issues Dear colleagues Irsquom reaching out to you as fellow Panorama Wave 4 health units to ask about where yourorganizations are at in the process of signing agreements and completing Privacy ImpactAssessments and Threat Risk Assessments (TRAs) Ottawa Public Healthrsquos IT legal and informationsecurity advisors have made numerous requests to the MOHLTC for information (in particular theprovincial TRA) that we consider essential to develop our own risk assessment and PIA but havebeen told that information cannot be shared even with strict confidentiality and access controlsSo we are at somewhat of an impasse Isra emailed Arlene yesterday Arlene has forwarded ourconcerns to the Ministryrsquos CIO and Panorama lead but we havenrsquot had any response or discussionswith either of them yet Have your organizations identified similar concerns andor had interactions with the MOHLTC inthis respect Irsquod also be interested in knowing if your health units have flagged other (egoperational) implementation concerns Thanks
Carolyn ps Robert ndash you can ignore this request I talked with Sharan this morning about Durhamrsquos issuesso am including you now just for information Carolyn Pim MD FRCPC Associate Medical Officer of Health Meacutedecin adjointe en santeacute publique Ottawa Public Health Santeacute publique Ottawa 100 Constellation Cr Ottawa ON K2G 6J8 Tel teacutel (613) 580-6744 ext 23684Fax (613) 580-9641Connect With Ottawa Public Health
Suivez Santeacute publique Ottawa
This e-mail originates from the City of Ottawa e-mail system Any distribution use orcopying of this e-mail or the information it contains by other than the intendedrecipient(s) is unauthorized If you are not the intended recipient please notify meat the telephone number shown above or by return e-mail and delete thiscommunication and any copy immediately Thank you
Le preacutesent courriel a eacuteteacute expeacutedieacute par le systegraveme de courriels de la Ville dOttawaToute distribution utilisation ou reproduction du courriel ou des renseignements quisy trouvent par une personne autre que son destinataire preacutevu est interdite Si vousavez reccedilu le message par erreur veuillez men aviser par teacuteleacutephone (au numeacuteropreacuteciteacute) ou par courriel puis supprimer sans deacutelai la version originale de lacommunication ainsi que toutes ses copies Je vous remercie de votre collaboration
1
Smoke-Free Patios ndash An Amendment to the Smoke-Free Ontario Act
Date November 15 2013 Prepared for Council of Ontario Medical Officers of Health Prepared by York Region Public Health _____________________________________________________________________________ Issue
The Smoke-Free Ontario Act is the current provincial legislation that imposes smoking restrictions in workplaces and public places It prohibits smoking on restaurant and bar patios in instances where any portion of the seating area is covered by a roof With recent studies illustrating that exposure to second hand smoke outdoors poses similar risks to indoor exposure there has been growing public support to enhance smoking restrictions and make patios completely smoke-free
Background
With the implementation of the Smoke-Free Ontario Act in 2006 restaurant and bar patios became subject to smoking restrictions if any portion of the seating area was covered by a roof This allowed for patios without roof coverings to continue to allow smoking and as a result did not provide significant protection to patrons or staff from exposure to second hand smoke outdoors Many businesses chose to alter the design of their patios to allow smoking to continue In some cases patios became more crowded since smoking patrons who dine indoors often proceed outside onto licensed patios with their beverages to smoke York Region like most municipalities in Ontario is host to hundreds of patios being operated by restaurant owners and businesses With smoking prohibitions affecting only a small portion of these patios specifically ones with coverings the vast majority of patios still allow smoking to take place Patrons and employees on patios where smoking is not restricted are exposed to second hand smoke frequently This can contribute to increased disease and aggravation of existing health conditions From a business perspective the existing legislation has been viewed by many operators as unfair because some patios have permanent coverings which cannot be removed requiring a smoke-free status These business owners feel this creates an uneven playing field since they cannot provide an outdoor dining area for their smoking customers There is strong community support for smoke-free patios in Ontario A 2009 Rapid Risk Factor Surveillance System survey revealed 754 percent support in York Region while a Toronto Health Survey in 2011 indicated 74 percent public support
2
Current Status
Smoking is currently prohibited on restaurant and bar patios province-wide in four Canadian provinces and territories Alberta Newfoundland and Labrador Nova Scotia and Yukon A fifth province Prince Edward Island prohibits smoking on patios until 10 pm Since Ontario enacted legislation restricting smoking on patios in 2006 eight municipalities in Ontario have chosen to create bylaws that go beyond the Smoke-Free Ontario Act and enhance outdoor protection from second hand smoke by prohibiting smoking on patios completely The largest of those municipalities is the City of Ottawa Recently the Toronto Board of Health unanimously endorsed a report presented by their Medical Officer of Health recommending that restaurant and bar patios be made smoke-free through an amendment to the Smoke-Free Ontario Act
Key Considerations
There should be no significant financial burden to local Boards of Health resulting from a smoke-free patio amendment to the Smoke-Free Ontario Act Inspection and enforcement for the Smoke-Free Ontario Act is currently 100 percent funded by the Ministry of Health and Long-Term Care Following an introductory period of education on the amendment a complaint response model of service delivery would ensure ongoing compliance with smoke-free requirements A complete ban of smoking on patios would eliminate the widely-held perception by business owners that the current legislation creates an uneven playing field for business Since Smoke-Free Ontario Act inspections of patios began in 2006 operators have expressed the opinion that if patios need to be smoke-free for the protection of the public they should all be smoke-free to avoid undue hardship for individual businesses and to provide protection uniformly across the Province
Next steps
York Region Public Health intends to seek support from Medical Officers of Health across the Central East Tobacco Control Area Network (CETCAN) to advocate to the Ministry of Health and Long-Term Care for an amendment to the Smoke-Free Ontario Act prohibiting smoking on all restaurant and bar patios York Region is also in the process of requesting that its Regional Council advocate to the Minister of Health and Long-Term Care on the issue
Updating and Modernizing O Regulation 565 (Public Pools)
Date November 15 2013
Prepared for Council of Ontario Medical Officers of Health
Prepared by York Region Public Health _____________________________________________________________________________ Background Recent drownings at public pools in Ontario have highlighted the issue of water-borne illness and injury The current pool regulation under Ontariorsquos Health Protection and Promotion Act O Regulation 565 (Public Pools) is outdated It does not accurately reflect new pool technology and design or the changing use of public pools Neither does it incorporate admissions standards recommended by the Office of the Chief Coroner Further O Regulation 565 does not have short-form wording or set fines associated with it This limits public health enforcement capabilities What is the impact Updating O Regulation 565 (Public Pools) to address recent changes in pool technology design and uses and to include Coroner-recommended admissions standards would help improve pool safety Establishing short-form wording for O Regulation 565 would enhance enforcement related to public pools Currently the only enforcement available to Public Health Inspectors for dealing with non-critical regulatory infractions in public pools is the issuance of a Part III summons This involves a considerable amount of resources for a possible small fine With the development of inspection disclosure systems such as YorkSafe there is an even greater need to develop a method to effectively address repeated pool operator non-compliance with non-critical issues Next steps Public health units should advocate to the Province to 1) Conduct a review of O Regulation 565 (Public Pools) to address shortcomings Proposed changes to the
regulation should include a requirement for ownersoperators of public pools to advise the local Medical Officer of Health of any change in the use of a facility and the addition of the Coronerrsquos recommended admission standards
2) Provide short-form wording for O Regulation 565 so that public health inspectors can better deal with pool operator non-compliance
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
4 Council of Ontario Medical Officers of Health Terms of Reference
b Setting agendas and otherwise ensuring preparations for Council meetings c Ensuring the fulfillment of the direction of Council d Responding in a timely fashion to time-sensitive public health matters in
accordance with the Executive Committeersquos understanding of the perspective of the Council
e Engaging with the Chief Medical Officer of Health Associate Chief Medical Officers of Health and other provincial public health leaders and
f Representing Council at public and partner agency forums including the Public Health Leadership Council which shall normally include membership from the Officers of the Council and two other Executive Committee members as selected by agreement among the Executive
g Identifying opportunities for the recognition of outstanding practice from among the members including the annual nomination of at least one member for the alPHa Distinguished Service Award
11 The Executive Committee shall meet and correspond in the manner and at the times
and if required places as deemed necessary by the Chair to conduct the business of the Council A quorum shall consist of four (4) members
12 The Executive Committee shall have the power to strike committeestask or working
groups to assist it in carrying out the business of the Council 13 The Council may by special resolution remove a member of the Executive
Committee before the completion of hisher term of office and may elect a successor to complete the term The special resolution shall require a majority vote of 67 of the members present and voting at the meeting at which the special resolution is considered
14 A Nominating Committee shall consist of the three (3) most recent Past Chairs who
are able to serve and shall be chaired by the immediate Past Chair The Nominating Committee shall prepare a list of proposed Officers and Executive Committee members for the consideration of the Council at its Annual General Meeting
MEETINGS 15 The Council shall hold at least four (4) general meetings per year in a manner and at
the times and if required places as deemed necessary by the Executive Committee to share information direct and assist the Executive Committee in conducting the business of the Council
16 The Council shall hold its Annual General Meeting during and at the same place as
the alPHarsquos Annual Conference
5 Council of Ontario Medical Officers of Health Terms of Reference
17 The Council shall hold a special meeting at the call of the Chair or upon the written request specifying the purpose of such meeting of at least five (5) active members Council members must be given at least 48 hours notice of any special meeting
18 Only Councilrsquos active and associate members and alPHa staff are entitled to attend
general and special meetings of the Council Other members and non-members may be invited to attend all or part of such meetings as determined by the Chair preferably in consultation with the Executive Committee Non-members who come to such meetings without an invitation may attend all or part of the meeting by a majority vote of the active members present and voting
19 The Chair shall prepare the agendas for such meetings and shall normally include
reports from the Chair and the Councilrsquos committeestask or working groups and representatives to external bodies alPHarsquos Executive Director shall ensure that the minutes shall be recorded and promptly distributed to the Section
20 A quorum for all such meetings shall be ten (10) active members 21 The Council shall normally be notified in a manner deemed appropriate by the Chair
of such meetings at least one (1) month prior to their being held 22 A majority vote of the members present at such meetings and voting shall make
Council decisions In the case of a tied vote the Chair shall cast the deciding vote The Executive Committee shall ensure that actions arising from such decisions at such meetings are implemented and monitored
23 The Chair may solicit advice from the Council through the use of teleconferencing
and alPHarsquos electronic mailing lists in order to gain an understanding of the overall perspective of the Council (see 10d)
ELECTIONS 24 The Officers and Executive Committee members shall be elected at the Sectionrsquos
Annual General Meeting The Nominating Committee Chair or hisher designate shall present a list of nominations Additional nominations from the floor shall also be considered Each Officer and Executive Committee member shall be elected by secret ballot if necessary by a majority of the active members present and voting In the case of a tie the Chair shall cast the deciding vote
AMENDMENTS 25 The Councilrsquos Terms of Reference may be amended from time to time by the
Executive Committee provided the Committee receives notice of such proposed amendments at least one (1) month prior to the meeting at which the amendments
6 Council of Ontario Medical Officers of Health Terms of Reference
will be considered Such amendments shall be ratified by the Council at the next general meeting or the Annual General Meeting as the case may be
26 The Executive Committee shall review the Terms of Reference as required and not
less than once every two years Original September 1987 1st Revision October 2000 2nd Revision July 2001 3rd Revision December 2003 4th Revision February 2008 5th Revision June 2009 6th Revision June 2011 7th Revision June 2013
7 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX A
COMOH Membership Benefits Active Membership
bull Entitled to attend all meetings of the Section bull May hold office on the COMOH Executive Committee alPHa Board of Directors
Standing Committees bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Associate Membership
bull Entitled to attend all meetings of the Section bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Affiliate Membership
bull May attend meetings or parts thereof subject to approval of Chair bull May serve on ad-hoc committees of the Section subject to the approval of the
Executive Committee bull Discounted registration rates for alPHa Conferences (for Public Health and
Preventive Medicine Residents) bull Upon written request and subject to COMOH Executive approval Affiliate
Members may subscribe to comohlistsalphaweborg The approval will be reviewed on an annual basis in order to determine if the Affiliate Member can remain a subscriber to mohsalphaweborg
Emeritus Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair bull Enjoy discounted registration rates for alPHa Conferences and regular COMOH
meetings bull Subscription to comohlistsalphaweborg electronic mailing list bull Full access to alPHa Web site bull May represent alPHa COMOH on selected external committees and working
groups Honorary Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair
8 Council of Ontario Medical Officers of Health Terms of Reference
bull May represent alPHa COMOH on selected external committees and working groups subject to the approval of the COMOH or alPHa Executive Committee as appropriate
9 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX B
Planning Cycle to Identify Priorities for COMOH
1 There shall normally be a COMOH membership strategic planning retreat every four years In recognition of the dynamic environment of public health the need for and timing of such a retreat shall be at the discretion of the Executive Committee in consultation with the membership
2 The COMOH Executive is responsible (through the creation of a subcommittee of COMOH members) for ensuring the preparation for the COMOH retreats with resources to include those provided by alPHa
3 Leadership for action on COMOH priorities will be recruited from among the COMOH membership in order to make good use of the full base of capacity of the membership The resources to support actions will be recruited from both within and beyond the COMOH membership employing other public health professionals that reside within the broader public health system and community
4 The COMOH Executive shall ensure an annual review of strategic priorities and initiatives and the development of a draft report of the same for the review of the members at the June meeting
2013 Strategic Planning
Considerations for COMOH
As part of its strategic planning discussions alPHarsquos Board has been considering changes to the level of support provided to member sections A member survey is being carried out over the fall to determine options acceptable to alPHa members The following approach to support is put forward as a proposal for the consideration of COMOH Note that the feasibility of the points below depend upon future decisions of the alPHa board They assume that COMOH remains part of alPHa but becomes more independent in administering meetings
1 alPHa can provide to COMOH staff support (Gord Fleming) amounting to 02 FTE or one day per week This is a reduction from the current level of 35 days per week COMOH can choose to use the support any way it wants writing COMOH letters meeting minutes agenda support special projects etc
2 In addition to 02 FTE alPHa staff would provide support for up to 4 face-to-face meetings per year One meeting would be concurrent to alPHarsquos annual conference in June The timing of other meetings could be negotiated The support includes consulting on the development of the program arranging for speakers registration for the event arranging venue AV support and hospitality services
3 In addition to 02 FTE alPHa staff would provide support for setting meeting dates and any polling required to establish dates Note that the individual supporting this function would be Karen Reece
4 COMOHrsquos Executive and Section would continue to have access to online supports through the alPHa including the COMOH Listserve and a group page for posting agendas minutes and other resources on the alPHa website
5 alPHa staff (Linda Stewart and Gord Fleming) can also start participating on CMOH calls as a way to be up-to-date on issues related to COMOH
6 Other than what is outlined above COMOH would be expected to prepare agendas and take minutes for its Executive and Section meetings The Executive would be expected to operate more independently than it does now but would be able to access the supports outlined above
Prepared by Linda Stewart Executive Director
From comoh-bounceslistsalphaweborg on behalf of Christopher MackieTo MOH ListserveSubject [comoh] Fw URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)Date Wednesday October 30 2013 91241 AMAttachments ATT00249txt
For AMOHs and PHPM residents who didnt receive the initial email
Chris
Christopher Mackie MD MHSc FRCPCMedical Officer of Health and CEOMiddlesex-London Health Unit50 King St LondonON N6A 5L7 O 519 663 5317 ext 2444 wwwhealthunitcomFrom Pisko Laura (MOHLTC)Sent Tuesday October 29 2013 759 PMTo kbarkeralgomapublichealthcom malcolmlockbchuorg davidcchatham-kentcarobertkyledurhamca proumeliotiseohuca fwarshelginhealthonca mohelginhealthoncahlynnpublichealthgreybruceonca malcolmlockhnhuorg hnmohhnhuorglnoseworthyhkpronca bobnosalhaltonca elizabethrichardsonhamiltoncarschabashpechuonca ncameronhuroncountyca drimgemmillkflapublichealthcamohkflapublichealthca suditranadecounty-lambtononca paulastewarthealthunitorgChristopher Mackie valeriejaegerniagararegionca jimchiriconbpsdhuca jarthursnwhuoncaisralevyottawaca dnealoxfordcountyca davidmowatpeelregionca mklassenpdhuoncarpellizzaripcchuca rosemarieramsinghporcupinehuonca mcorriveaurcdhucomcharlesgardnersmdhuorg sutcliffepsdhucom davidwilliamstbdhucomspruytmtimiskaminghucom dmckeowntorontoca lnolanregionofwaterloocanicolamercerwdghuorg aheimannwechealthunitorg karimkurjiyorkcaCc coreywesleytbdhucom CindyBaker-Barillsmdhuorg Donna Kosmack pilonlsdhucomPaulaMuiskflapublichealthca sthibautorontoca Mueller Daina (MOHLTC) Gordon Marcus(MOHLTC) andreakitahamiltoncaSubject URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)
Dear Colleagues The ministry has received reports that some tobacco vendors across the province aregiving away single cigarettes with the purchase of tobacco products It is the ministryrsquosposition that giving out free single cigarettes does not violate subsection 31(3) of theSmoke-Free Ontario Act (ldquoSFOArdquo) Although the practice of giving out free singlecigarettes may promote the sale of tobacco products it does not take the form of aldquoproduct enhancement product association or promotional materialrdquo and therefore doesnot fall within the scope of subsection 31(3) of the SFOA We have confirmed with Health Canada that this practice may violate section 29(b) of thefederal Tobacco Act As such Health Canada is requesting that you notify them in writingand I am directing you to communicate with them via email and provide to them as manydetails as possible Emails should be sent to Tobacco-Ontariohc-scgcca and thesubject line should read ldquoViolation of Section 29(b) of Tobacco Actrdquo This will ensurethat the complaints are given priority status by Health Canada We will continue to monitor
this situation and liaise with our colleagues at Health Canada Please share this information with your tobacco control staff and contact me or DainaMueller Manager Tobacco Control Unit Health Promotion Implementation Branch atdainamuellerontarioca with any questions RegardsLaura Laura A PiskoDirectorHealth Promotion Implementation BranchHealth Promotion DivisionMinistry of Health and Long Term Care416-327-7445 (office)416-451-3185 (mobile) Marcus Gordon - EA (416)326-0625 for urgent issues
========= Middlesex-London Health Unit E-Mail Disclaimer =============______________________________________________________________
Private and confidential intended only for named recipient If otherwisereceived please destroy immediately Health information in this email isonly general information and is not intended to replace an in personconsultation with a medical professional nor is it intended to providemedical advice Individual circumstances of which we are not aware mayaffect the information provided herein and as such the Middlesex-LondonHealth Unit assumes no liability or responsibility for your reliancethereon The Middlesex-London Health Unit works under the authority of theHealth Protection and Promotion Act and this correspondence may be used toassess your needs for public health services (519-663-5317 ext 2448)______________________________________________________________
From Gardner CharlesTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes (RayCopesoahppca)
George Pasut (GeorgePasutoahppca) Peter Cooney (petercooneyhc-scgcca)Cc Ito DickSubject Discontinuation of Fluoridation in MuskokaDate Tuesday October 22 2013 125254 PM
Hello Colleagues
As I reported in my email below on September 26th fluoridation has come under challenge again inSimcoe Muskoka I am now very unhappy to report that despite our best efforts last night theDistrict Council of Muskoka voted to remove fluoride from municipal drinking supplies across theDistrict This brings to an end fluoridation in all of Simcoe and Muskoka (with the exception of Base Borden)ndash though New Tecumseth will be conducting a plebiscite on the question of fluoridation with themunicipal election next October Defending community water fluoridation has drained a great deal of time human resources andcommitment from other priorities and has been exhausting here in SMDHU as I am sure it hasbeen in many other health units While the outcomes have been very disappointing I have beenimpressed by the professionalism and dedication that SMDHU staff members have shown inshouldering this burden In particular our dental consultant Dr Ito has provided us with much ofthe foundational knowledge and the local research essential to our efforts and has very frequentlyattended and presented at council meetings and other public events I would also like to thank themany of you who have offer and provided support including advocacy letters and informationresources Over the years Dr Peter Cooney Chief Dental Officer of Health of Canada has beenvery helpful attending and presenting with us at council meetings and at public consultationevents We will of course continue our oral health surveillance of the children of Muskoka documentingand reporting in future years on the increase in dental decay that we anticipate will occur Suchsurveillance is the foundation of our advocacy both to municipal politicians and to the province I am very concerned that our experience will continue to repeat itself across the province unlessthere is strong leadership provincially It is with this in mind that I raise the followingrecommendations for your consideration
1 That we collectively (with PHOrsquos leadership) conduct high quality publish-worthy researchdocumenting the impact on dental decay that occurs in those municipalities throughoutOntario that in recent years have discontinued community water fluoridation This could bepart of a larger study on such municipalities across the country and it could also be part ofa study documenting overall oral health (including fluoridation coverage) in the province(and possibly across the country)
2 That COMOH engage with our Chief MOH to advocate for the province to require allmunicipal water supplies to be fluoridated (the exception of course being those withnaturally sufficient fluoride concentrations) This could built upon the alPHa position to
Gordon
Highlight
Gordon
Highlight
date (A11-00 - Community Water Fluoridation) on the CMOH position (Oral Health ndash) and on theemail discussion generated on the COMOH listserv some months back re Richardrsquosproposal (calling on the province to fund municipal water fluoridation)
Valerie I request that this be an item for our COMOH meeting on November 15th Sincerely Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorg From Gardner Charles Sent Thursday September 26 2013 245 PMTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes(RayCopesoahppca)Subject Community Water Fluoridation Under Challenge Again in Simcoe Muskoka Hello Colleagues You may wish to know that community water fluoridation (CWF) is again under challenge in SimcoeMuskoka specifically both in Tottenham (Town of New Tecumseth in Simcoe County) and for theentire District of Muskoka On Monday September 23 Committee of the Whole Council of theTown of New Tecumseth voted to submit application to discontinue community water fluoridation(CWF) in the town of Tottenham despite presentations to the contrary from our dental consultantDr Ito and from me The next Council meeting is scheduled for Monday Sept 30 at which lastMondayrsquos (Sept 23) votes will be ratified
Since Monday I have spoken with the Mayor of the Town of New Tecumseth and with most of thecouncilors encouraging deferral of a decision on Monday to allow the town more time to make afully informed decision
This is the second time in recent years that the issue of discontinuing CWF in Tottenham has beenraised at council This issue is also scheduled to return again to the District of Muskoka Council on
October 21st where I will be presenting in response to deputations in opposition to fluoridation
Outside of Base Borden Tottenham is the only community with fluoridated water in SimcoeCounty The health unitrsquos own screening data between 2011 and 2013 shows that Tottenhamrsquos
Gordon
Highlight
children as well as those in Muskoka have a lower rate of dental decay than Simcoe Muskokacommunities without CWF
Sincerely
Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorgChuck Gardner MOH
November 04 2013
Mandatory State Laws on Fluoridation Thirteen states Puerto Rico and the District of Columbia have laws intended to provide
statewide fluoridation These states and the year that the fluoridation legislation was passed are
District of Columbia (1952) Connecticut (1965) Kentucky (1966) Illinois (1967) Minnesota
(1967) Ohio (1969) South Dakota (1969) Georgia (1973) Nebraska (1973 and 2008)
California (1995) Delaware (1998) Puerto Rico (1998) Nevada (1999) Louisiana (2008) and
Arkansas (2011) (see Table 1) The sizes of the public water systems or countiescommunities
affected and exemption provisions vary by state Table 1
STATES THAT HAVE MANDATORY LAWS ON FLUORIDATION -2011
State (1) Year of
Fluoridation
Legislation (1)
Population
served by
Fluoridated
CWS (2)
Persons
receiving
fluoridated
water (2)
State
Average
Caries
Experience
of Grade 3
Students (3)
Arkansas 2011 647 1724131 64
California 1995 621 22812721 709
Connecticut 1965 910 2370423 406
Delaware 1998 862 705344 545
Georgia 1973 921 8924598 52
Illinois 1967 993 11325132 532
Kentucky 1966 999 4334223 598
Louisiana 2008 407 1846149 657
Minnesota 1967 988 4117266 549
Nebraska 1973 and 2008 702 1001665 593
Nevada 1999 702 1001665 649
Ohio 1969 877 8772683 512
South Dakota 1969 948 642942 623
District of
Columbia
1952 1000 595000
Puerto Rico 1998
United States 739 204283554
2010 Statistics for population fluoridated and number of people
1 Communication with Jane McGinley RDH MBA Manager Fluoridation and Preventive Health
Activities Council on Access Prevention and Interprofessional Relations
2 Centers for Disease Control and Prevention Department of Health and Human Services
accessed Oct 21 2013 httpwwwcdcgovfluoridationstatistics2010statshtm
3 Centers for Disease Control and Prevention National Oral Health Surveillance System Caries
Experience - Percentage of 3rd Grade students with Caries Experience (treated or untreated tooth
If data from 43 states for the percentage of Grade 3 children with experience of dental decay is
compared with the 2008 percentages of the population in a state with Community Water
Fluoridation then the percentage of children with experience of dental decay decreases as the
percentage of the state population with Community Water Fluoridation increases (see Figure 1)
Figure 1
Correlation of Percentage of Grade 3 Children with Caries Experience and
Percentage of Population With Community Water Fluoridation for 43
Reporting States
0
10
20
30
40
50
60
70
80
0 10 20 30 40 50 60 70 80 90 100
State of Population With Community Water Fluoridation
Sta
te
of
Gra
de 3
Stu
den
ts w
ith
Cari
es E
xp
eri
en
ce
Data from CDC (2 3)
The description of the fluoridation laws in California Illinois and Nevada can be found on the
Association of State amp Territorial Dental Directors website(4 7 8)
The California fluoridation law AB 733 came into effect in 1995 requiring communities of 10
000 residents or more be supplied with fluoridated drinking water However the state did not
provide any funding to implement the legislation (California is unique in requiring fluoridation
without funding the practice)(4) The California Department of Health Services therefore had to
fund fluoridation initiatives from non-governmental sources ie the California Endowment
California Dental Association Foundation the First 5 Commission and others(5) From 1995 to
2011 the percentage of the California population receiving fluoridated drinking water has risen
from 17 to 625(6) 4 Dental Public Health Activities amp Practices Office of Oral Health California Department of Health
Services April 2002 httpwwwastddorgbestpracticesDES06002CAfluoridationpdf
5 Stock M Pollick H The CDA Foundation Model to Fluoridate Communities California Dental
Association Journal vol 40 no 8 649 - 655
httpwwwcdaorgPortals0journaljournal_082012pdf
6 California Dental Association Foundation
httpwwwcdafoundationorglearnadvocacyfluoridation
The State of Illinois passed a mandatory fluoridation state in 1967 and required all community
water systems to adjust fluoride levels in the drinking water to optimal levels within 1 year(7)
From 1962 when over 5000000 residents had optimally fluoridated drinking water by 2010
the number had risen to 11325132 (993 of the population on community water systems)(2)
7 Dental Public Health Activities amp Practices Division of Oral Health Illinois Department of Public
Health April 2002 httpwwwastddorgbestpracticesDES16007ILfluoridationpdf
The State of Nevada passed a mandatory fluoridation statute in 2000 for communities with
400000 or more residents(8) This was a result of the work of a statewide coalition that
included the Nevada Dental and Dental Hygienist Associations the Washoe and Clark County
District Health Departments the Clark County School District Junior League of Las Vegas
Head Start the Community College of Southern Nevada Dental Hygiene Program Health
Access Washoe County and Saint Maryrsquos Hospital For communities with less than 400000 the
implementation of fluoridation still required the vote of the majority voters in the community
The Las Vegas Water Authority and the City of Henderson started fluoridation in 2000
increasing the percentage of the population with fluoridated drinking water from 2 to 65 (8) 8 Dental Public Health Activities amp Practices Bureau of Family Health Services Nevada State Health
Division April 2002 httpwwwastddorgbestpracticesDES31002NVfluoridationbillpdf
Countries with Mandatory Laws on Fluoridation Countries that have mandated Community Water Fluoridation are Brazil Hong Kong
Malaysia Singapore Ireland Israel and some of the states in Australia
Singapore started fluoridating its water in 1956 based on the success of the fluoridation trials in
Grand Rapids Newburgh Evanston and Brantford Singapore became the first Asian country to
have 100 of its population benefitting from the implementation of fluoridated drinking water
Loh reported that ldquoThe ten year study on the effects of water fluoridation in Singapore showed
a decrease in caries prevalence in the children In the permanent dentition the reduction was
523 per cent for Chinese and 31 per cent for Malays in the 7 to 9 year old age group A similar
trend was observed in the mixed dentition in which the decrease was 325 per cent for Chinese
and 306 per cent for Malaysrdquo(9) By 2010 the population of the country was 5080000(10)
9 Loh T Thirty-eight years of water fluoridation--the Singapore scenario Community Dent
Health 1996 Sep13 Suppl 247-50
10 British Fluoridation Society One in a Million the facts about water fluoridation 3rd Edition
published March 2012) httpwwwbfsweborgonemillion0920One20in20a20Million20-
20The20Extent20of20Fluoridationpdf
Hong Kong started implementing community water fluoridation in 1961 and similar to
Singapore 100 of the population received access to fluoridated drinking water Lo and Wong
reported that ldquoThe mean DMFT score of the children deceased from 44 in 1960 to 15 in 1968
stayed at this level in the 1980 and 1986 surveys and further deceased to 08 in 2001 The
prevalence of dental fluorosis among the children surveyed in 1960 was 1 and this increased
to 59 and 70 in 1968 and 1980 respectively It was found in the 1986 and 2001 surveys that
the prevalences of fluorosis were 47 and 9 among children whose teeth developed at the
time when the respective water fluoride concentrations were 07 ppm and 05 ppmrdquo(11) The
population of Hong Kong was 6968000 in 2009(10) 11 LO ECM and WONG AHH Water fluoride concentration and fluorosis in Hong Kong in 1960-
2001 84th General Session and Exhibition of the International Association for Dental Research amp
1st Meeting of the Pan-Asian-Pacific Federation Brisbane Australia 28 June-1 July 2006 v 85 n
Sp B
The Malaysian cabinet approved a nationwide community water fluoridation program in 1972
(12) One of the states Sabah decided to stop fluoridation in 1989 due to concerns about
inadequate supervision in adding fluoride to the drinking water Oral Health Surveys in 2009
and 2007 indicated that children in Sabah had the worst oral health with 50 of 12 year-olds
having decay in their permanent teeth and children having an average of 3 teeth being(13)
Under the 10th Malaysian Plan in 2011 the federal and the Sabah state governments
reintroduced water fluoridation in Sabah(1314) In 2010 about 755 of the Malaysian
population or 20700000 people had fluoridated drinking water(1013) 12 Malaysian Dental Association Fluoride in Water
httpwwwmdaorgmy07_public_01healthcare_12htm
13 Sachdev N Fluoridation in Sabah Water for Cleaner Teeth French Tribunecom 28022011
From Levy IsraTo Jaeger ValerieCc Pim Carolyn gordonalphaweborg Diallo Aicha Penny Sutcliffe Paul Roumeliotis Michael Finkelstein
Hazel Lynn Robert KyleSubject FW Panorama - Privacy Security and other issuesDate Wednesday October 16 2013 122110 PM
Hello ValerieOttawa is part of Wave 4 Panorama implementation and we are gearing up increasingly to use thesystem where and if possible Thinking about it I am anticipating that this may need to be on theCOMOH (and alPHa) radar as it is something that will impact all health units and implies a majoroperational shift in vaccine delivery programs for all health units I have asked Carolyn Pim toconnect with our sister wave 4 units to share common experiences as we move forward ndash when wehave a roll up could I bring to COMOH Exec for discussion to explore whether there are broaderimplications for all members As an aside I have also asked the Ministry and their CIO to share with me any roll up learnings thatthey may have had already from previous waves (I understand that Niagara HU was a wave 1participant so if there is such a roll up of common experiences that others could learn fromperhaps you have it already and that could come to the exec too)Thanks Isra From Pim Carolyn Sent October 10 2013 1228 PMTo Christopher Mackie (christophermackiemlhuonca) Elizabeth Richardson(Elizabethrichardsonhamiltonca) H BSc M D F R C P (C) MPH Jim Chirico(jimchiriconbpsdhuca) Marlene Spruyt (spruytmtimiskaminghucom) Robert Kyle (Durham)Cc Levy IsraSubject Panorama - Privacy Security and other issues Dear colleagues Irsquom reaching out to you as fellow Panorama Wave 4 health units to ask about where yourorganizations are at in the process of signing agreements and completing Privacy ImpactAssessments and Threat Risk Assessments (TRAs) Ottawa Public Healthrsquos IT legal and informationsecurity advisors have made numerous requests to the MOHLTC for information (in particular theprovincial TRA) that we consider essential to develop our own risk assessment and PIA but havebeen told that information cannot be shared even with strict confidentiality and access controlsSo we are at somewhat of an impasse Isra emailed Arlene yesterday Arlene has forwarded ourconcerns to the Ministryrsquos CIO and Panorama lead but we havenrsquot had any response or discussionswith either of them yet Have your organizations identified similar concerns andor had interactions with the MOHLTC inthis respect Irsquod also be interested in knowing if your health units have flagged other (egoperational) implementation concerns Thanks
Carolyn ps Robert ndash you can ignore this request I talked with Sharan this morning about Durhamrsquos issuesso am including you now just for information Carolyn Pim MD FRCPC Associate Medical Officer of Health Meacutedecin adjointe en santeacute publique Ottawa Public Health Santeacute publique Ottawa 100 Constellation Cr Ottawa ON K2G 6J8 Tel teacutel (613) 580-6744 ext 23684Fax (613) 580-9641Connect With Ottawa Public Health
Suivez Santeacute publique Ottawa
This e-mail originates from the City of Ottawa e-mail system Any distribution use orcopying of this e-mail or the information it contains by other than the intendedrecipient(s) is unauthorized If you are not the intended recipient please notify meat the telephone number shown above or by return e-mail and delete thiscommunication and any copy immediately Thank you
Le preacutesent courriel a eacuteteacute expeacutedieacute par le systegraveme de courriels de la Ville dOttawaToute distribution utilisation ou reproduction du courriel ou des renseignements quisy trouvent par une personne autre que son destinataire preacutevu est interdite Si vousavez reccedilu le message par erreur veuillez men aviser par teacuteleacutephone (au numeacuteropreacuteciteacute) ou par courriel puis supprimer sans deacutelai la version originale de lacommunication ainsi que toutes ses copies Je vous remercie de votre collaboration
1
Smoke-Free Patios ndash An Amendment to the Smoke-Free Ontario Act
Date November 15 2013 Prepared for Council of Ontario Medical Officers of Health Prepared by York Region Public Health _____________________________________________________________________________ Issue
The Smoke-Free Ontario Act is the current provincial legislation that imposes smoking restrictions in workplaces and public places It prohibits smoking on restaurant and bar patios in instances where any portion of the seating area is covered by a roof With recent studies illustrating that exposure to second hand smoke outdoors poses similar risks to indoor exposure there has been growing public support to enhance smoking restrictions and make patios completely smoke-free
Background
With the implementation of the Smoke-Free Ontario Act in 2006 restaurant and bar patios became subject to smoking restrictions if any portion of the seating area was covered by a roof This allowed for patios without roof coverings to continue to allow smoking and as a result did not provide significant protection to patrons or staff from exposure to second hand smoke outdoors Many businesses chose to alter the design of their patios to allow smoking to continue In some cases patios became more crowded since smoking patrons who dine indoors often proceed outside onto licensed patios with their beverages to smoke York Region like most municipalities in Ontario is host to hundreds of patios being operated by restaurant owners and businesses With smoking prohibitions affecting only a small portion of these patios specifically ones with coverings the vast majority of patios still allow smoking to take place Patrons and employees on patios where smoking is not restricted are exposed to second hand smoke frequently This can contribute to increased disease and aggravation of existing health conditions From a business perspective the existing legislation has been viewed by many operators as unfair because some patios have permanent coverings which cannot be removed requiring a smoke-free status These business owners feel this creates an uneven playing field since they cannot provide an outdoor dining area for their smoking customers There is strong community support for smoke-free patios in Ontario A 2009 Rapid Risk Factor Surveillance System survey revealed 754 percent support in York Region while a Toronto Health Survey in 2011 indicated 74 percent public support
2
Current Status
Smoking is currently prohibited on restaurant and bar patios province-wide in four Canadian provinces and territories Alberta Newfoundland and Labrador Nova Scotia and Yukon A fifth province Prince Edward Island prohibits smoking on patios until 10 pm Since Ontario enacted legislation restricting smoking on patios in 2006 eight municipalities in Ontario have chosen to create bylaws that go beyond the Smoke-Free Ontario Act and enhance outdoor protection from second hand smoke by prohibiting smoking on patios completely The largest of those municipalities is the City of Ottawa Recently the Toronto Board of Health unanimously endorsed a report presented by their Medical Officer of Health recommending that restaurant and bar patios be made smoke-free through an amendment to the Smoke-Free Ontario Act
Key Considerations
There should be no significant financial burden to local Boards of Health resulting from a smoke-free patio amendment to the Smoke-Free Ontario Act Inspection and enforcement for the Smoke-Free Ontario Act is currently 100 percent funded by the Ministry of Health and Long-Term Care Following an introductory period of education on the amendment a complaint response model of service delivery would ensure ongoing compliance with smoke-free requirements A complete ban of smoking on patios would eliminate the widely-held perception by business owners that the current legislation creates an uneven playing field for business Since Smoke-Free Ontario Act inspections of patios began in 2006 operators have expressed the opinion that if patios need to be smoke-free for the protection of the public they should all be smoke-free to avoid undue hardship for individual businesses and to provide protection uniformly across the Province
Next steps
York Region Public Health intends to seek support from Medical Officers of Health across the Central East Tobacco Control Area Network (CETCAN) to advocate to the Ministry of Health and Long-Term Care for an amendment to the Smoke-Free Ontario Act prohibiting smoking on all restaurant and bar patios York Region is also in the process of requesting that its Regional Council advocate to the Minister of Health and Long-Term Care on the issue
Updating and Modernizing O Regulation 565 (Public Pools)
Date November 15 2013
Prepared for Council of Ontario Medical Officers of Health
Prepared by York Region Public Health _____________________________________________________________________________ Background Recent drownings at public pools in Ontario have highlighted the issue of water-borne illness and injury The current pool regulation under Ontariorsquos Health Protection and Promotion Act O Regulation 565 (Public Pools) is outdated It does not accurately reflect new pool technology and design or the changing use of public pools Neither does it incorporate admissions standards recommended by the Office of the Chief Coroner Further O Regulation 565 does not have short-form wording or set fines associated with it This limits public health enforcement capabilities What is the impact Updating O Regulation 565 (Public Pools) to address recent changes in pool technology design and uses and to include Coroner-recommended admissions standards would help improve pool safety Establishing short-form wording for O Regulation 565 would enhance enforcement related to public pools Currently the only enforcement available to Public Health Inspectors for dealing with non-critical regulatory infractions in public pools is the issuance of a Part III summons This involves a considerable amount of resources for a possible small fine With the development of inspection disclosure systems such as YorkSafe there is an even greater need to develop a method to effectively address repeated pool operator non-compliance with non-critical issues Next steps Public health units should advocate to the Province to 1) Conduct a review of O Regulation 565 (Public Pools) to address shortcomings Proposed changes to the
regulation should include a requirement for ownersoperators of public pools to advise the local Medical Officer of Health of any change in the use of a facility and the addition of the Coronerrsquos recommended admission standards
2) Provide short-form wording for O Regulation 565 so that public health inspectors can better deal with pool operator non-compliance
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
5 Council of Ontario Medical Officers of Health Terms of Reference
17 The Council shall hold a special meeting at the call of the Chair or upon the written request specifying the purpose of such meeting of at least five (5) active members Council members must be given at least 48 hours notice of any special meeting
18 Only Councilrsquos active and associate members and alPHa staff are entitled to attend
general and special meetings of the Council Other members and non-members may be invited to attend all or part of such meetings as determined by the Chair preferably in consultation with the Executive Committee Non-members who come to such meetings without an invitation may attend all or part of the meeting by a majority vote of the active members present and voting
19 The Chair shall prepare the agendas for such meetings and shall normally include
reports from the Chair and the Councilrsquos committeestask or working groups and representatives to external bodies alPHarsquos Executive Director shall ensure that the minutes shall be recorded and promptly distributed to the Section
20 A quorum for all such meetings shall be ten (10) active members 21 The Council shall normally be notified in a manner deemed appropriate by the Chair
of such meetings at least one (1) month prior to their being held 22 A majority vote of the members present at such meetings and voting shall make
Council decisions In the case of a tied vote the Chair shall cast the deciding vote The Executive Committee shall ensure that actions arising from such decisions at such meetings are implemented and monitored
23 The Chair may solicit advice from the Council through the use of teleconferencing
and alPHarsquos electronic mailing lists in order to gain an understanding of the overall perspective of the Council (see 10d)
ELECTIONS 24 The Officers and Executive Committee members shall be elected at the Sectionrsquos
Annual General Meeting The Nominating Committee Chair or hisher designate shall present a list of nominations Additional nominations from the floor shall also be considered Each Officer and Executive Committee member shall be elected by secret ballot if necessary by a majority of the active members present and voting In the case of a tie the Chair shall cast the deciding vote
AMENDMENTS 25 The Councilrsquos Terms of Reference may be amended from time to time by the
Executive Committee provided the Committee receives notice of such proposed amendments at least one (1) month prior to the meeting at which the amendments
6 Council of Ontario Medical Officers of Health Terms of Reference
will be considered Such amendments shall be ratified by the Council at the next general meeting or the Annual General Meeting as the case may be
26 The Executive Committee shall review the Terms of Reference as required and not
less than once every two years Original September 1987 1st Revision October 2000 2nd Revision July 2001 3rd Revision December 2003 4th Revision February 2008 5th Revision June 2009 6th Revision June 2011 7th Revision June 2013
7 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX A
COMOH Membership Benefits Active Membership
bull Entitled to attend all meetings of the Section bull May hold office on the COMOH Executive Committee alPHa Board of Directors
Standing Committees bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Associate Membership
bull Entitled to attend all meetings of the Section bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Affiliate Membership
bull May attend meetings or parts thereof subject to approval of Chair bull May serve on ad-hoc committees of the Section subject to the approval of the
Executive Committee bull Discounted registration rates for alPHa Conferences (for Public Health and
Preventive Medicine Residents) bull Upon written request and subject to COMOH Executive approval Affiliate
Members may subscribe to comohlistsalphaweborg The approval will be reviewed on an annual basis in order to determine if the Affiliate Member can remain a subscriber to mohsalphaweborg
Emeritus Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair bull Enjoy discounted registration rates for alPHa Conferences and regular COMOH
meetings bull Subscription to comohlistsalphaweborg electronic mailing list bull Full access to alPHa Web site bull May represent alPHa COMOH on selected external committees and working
groups Honorary Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair
8 Council of Ontario Medical Officers of Health Terms of Reference
bull May represent alPHa COMOH on selected external committees and working groups subject to the approval of the COMOH or alPHa Executive Committee as appropriate
9 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX B
Planning Cycle to Identify Priorities for COMOH
1 There shall normally be a COMOH membership strategic planning retreat every four years In recognition of the dynamic environment of public health the need for and timing of such a retreat shall be at the discretion of the Executive Committee in consultation with the membership
2 The COMOH Executive is responsible (through the creation of a subcommittee of COMOH members) for ensuring the preparation for the COMOH retreats with resources to include those provided by alPHa
3 Leadership for action on COMOH priorities will be recruited from among the COMOH membership in order to make good use of the full base of capacity of the membership The resources to support actions will be recruited from both within and beyond the COMOH membership employing other public health professionals that reside within the broader public health system and community
4 The COMOH Executive shall ensure an annual review of strategic priorities and initiatives and the development of a draft report of the same for the review of the members at the June meeting
2013 Strategic Planning
Considerations for COMOH
As part of its strategic planning discussions alPHarsquos Board has been considering changes to the level of support provided to member sections A member survey is being carried out over the fall to determine options acceptable to alPHa members The following approach to support is put forward as a proposal for the consideration of COMOH Note that the feasibility of the points below depend upon future decisions of the alPHa board They assume that COMOH remains part of alPHa but becomes more independent in administering meetings
1 alPHa can provide to COMOH staff support (Gord Fleming) amounting to 02 FTE or one day per week This is a reduction from the current level of 35 days per week COMOH can choose to use the support any way it wants writing COMOH letters meeting minutes agenda support special projects etc
2 In addition to 02 FTE alPHa staff would provide support for up to 4 face-to-face meetings per year One meeting would be concurrent to alPHarsquos annual conference in June The timing of other meetings could be negotiated The support includes consulting on the development of the program arranging for speakers registration for the event arranging venue AV support and hospitality services
3 In addition to 02 FTE alPHa staff would provide support for setting meeting dates and any polling required to establish dates Note that the individual supporting this function would be Karen Reece
4 COMOHrsquos Executive and Section would continue to have access to online supports through the alPHa including the COMOH Listserve and a group page for posting agendas minutes and other resources on the alPHa website
5 alPHa staff (Linda Stewart and Gord Fleming) can also start participating on CMOH calls as a way to be up-to-date on issues related to COMOH
6 Other than what is outlined above COMOH would be expected to prepare agendas and take minutes for its Executive and Section meetings The Executive would be expected to operate more independently than it does now but would be able to access the supports outlined above
Prepared by Linda Stewart Executive Director
From comoh-bounceslistsalphaweborg on behalf of Christopher MackieTo MOH ListserveSubject [comoh] Fw URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)Date Wednesday October 30 2013 91241 AMAttachments ATT00249txt
For AMOHs and PHPM residents who didnt receive the initial email
Chris
Christopher Mackie MD MHSc FRCPCMedical Officer of Health and CEOMiddlesex-London Health Unit50 King St LondonON N6A 5L7 O 519 663 5317 ext 2444 wwwhealthunitcomFrom Pisko Laura (MOHLTC)Sent Tuesday October 29 2013 759 PMTo kbarkeralgomapublichealthcom malcolmlockbchuorg davidcchatham-kentcarobertkyledurhamca proumeliotiseohuca fwarshelginhealthonca mohelginhealthoncahlynnpublichealthgreybruceonca malcolmlockhnhuorg hnmohhnhuorglnoseworthyhkpronca bobnosalhaltonca elizabethrichardsonhamiltoncarschabashpechuonca ncameronhuroncountyca drimgemmillkflapublichealthcamohkflapublichealthca suditranadecounty-lambtononca paulastewarthealthunitorgChristopher Mackie valeriejaegerniagararegionca jimchiriconbpsdhuca jarthursnwhuoncaisralevyottawaca dnealoxfordcountyca davidmowatpeelregionca mklassenpdhuoncarpellizzaripcchuca rosemarieramsinghporcupinehuonca mcorriveaurcdhucomcharlesgardnersmdhuorg sutcliffepsdhucom davidwilliamstbdhucomspruytmtimiskaminghucom dmckeowntorontoca lnolanregionofwaterloocanicolamercerwdghuorg aheimannwechealthunitorg karimkurjiyorkcaCc coreywesleytbdhucom CindyBaker-Barillsmdhuorg Donna Kosmack pilonlsdhucomPaulaMuiskflapublichealthca sthibautorontoca Mueller Daina (MOHLTC) Gordon Marcus(MOHLTC) andreakitahamiltoncaSubject URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)
Dear Colleagues The ministry has received reports that some tobacco vendors across the province aregiving away single cigarettes with the purchase of tobacco products It is the ministryrsquosposition that giving out free single cigarettes does not violate subsection 31(3) of theSmoke-Free Ontario Act (ldquoSFOArdquo) Although the practice of giving out free singlecigarettes may promote the sale of tobacco products it does not take the form of aldquoproduct enhancement product association or promotional materialrdquo and therefore doesnot fall within the scope of subsection 31(3) of the SFOA We have confirmed with Health Canada that this practice may violate section 29(b) of thefederal Tobacco Act As such Health Canada is requesting that you notify them in writingand I am directing you to communicate with them via email and provide to them as manydetails as possible Emails should be sent to Tobacco-Ontariohc-scgcca and thesubject line should read ldquoViolation of Section 29(b) of Tobacco Actrdquo This will ensurethat the complaints are given priority status by Health Canada We will continue to monitor
this situation and liaise with our colleagues at Health Canada Please share this information with your tobacco control staff and contact me or DainaMueller Manager Tobacco Control Unit Health Promotion Implementation Branch atdainamuellerontarioca with any questions RegardsLaura Laura A PiskoDirectorHealth Promotion Implementation BranchHealth Promotion DivisionMinistry of Health and Long Term Care416-327-7445 (office)416-451-3185 (mobile) Marcus Gordon - EA (416)326-0625 for urgent issues
========= Middlesex-London Health Unit E-Mail Disclaimer =============______________________________________________________________
Private and confidential intended only for named recipient If otherwisereceived please destroy immediately Health information in this email isonly general information and is not intended to replace an in personconsultation with a medical professional nor is it intended to providemedical advice Individual circumstances of which we are not aware mayaffect the information provided herein and as such the Middlesex-LondonHealth Unit assumes no liability or responsibility for your reliancethereon The Middlesex-London Health Unit works under the authority of theHealth Protection and Promotion Act and this correspondence may be used toassess your needs for public health services (519-663-5317 ext 2448)______________________________________________________________
From Gardner CharlesTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes (RayCopesoahppca)
George Pasut (GeorgePasutoahppca) Peter Cooney (petercooneyhc-scgcca)Cc Ito DickSubject Discontinuation of Fluoridation in MuskokaDate Tuesday October 22 2013 125254 PM
Hello Colleagues
As I reported in my email below on September 26th fluoridation has come under challenge again inSimcoe Muskoka I am now very unhappy to report that despite our best efforts last night theDistrict Council of Muskoka voted to remove fluoride from municipal drinking supplies across theDistrict This brings to an end fluoridation in all of Simcoe and Muskoka (with the exception of Base Borden)ndash though New Tecumseth will be conducting a plebiscite on the question of fluoridation with themunicipal election next October Defending community water fluoridation has drained a great deal of time human resources andcommitment from other priorities and has been exhausting here in SMDHU as I am sure it hasbeen in many other health units While the outcomes have been very disappointing I have beenimpressed by the professionalism and dedication that SMDHU staff members have shown inshouldering this burden In particular our dental consultant Dr Ito has provided us with much ofthe foundational knowledge and the local research essential to our efforts and has very frequentlyattended and presented at council meetings and other public events I would also like to thank themany of you who have offer and provided support including advocacy letters and informationresources Over the years Dr Peter Cooney Chief Dental Officer of Health of Canada has beenvery helpful attending and presenting with us at council meetings and at public consultationevents We will of course continue our oral health surveillance of the children of Muskoka documentingand reporting in future years on the increase in dental decay that we anticipate will occur Suchsurveillance is the foundation of our advocacy both to municipal politicians and to the province I am very concerned that our experience will continue to repeat itself across the province unlessthere is strong leadership provincially It is with this in mind that I raise the followingrecommendations for your consideration
1 That we collectively (with PHOrsquos leadership) conduct high quality publish-worthy researchdocumenting the impact on dental decay that occurs in those municipalities throughoutOntario that in recent years have discontinued community water fluoridation This could bepart of a larger study on such municipalities across the country and it could also be part ofa study documenting overall oral health (including fluoridation coverage) in the province(and possibly across the country)
2 That COMOH engage with our Chief MOH to advocate for the province to require allmunicipal water supplies to be fluoridated (the exception of course being those withnaturally sufficient fluoride concentrations) This could built upon the alPHa position to
Gordon
Highlight
Gordon
Highlight
date (A11-00 - Community Water Fluoridation) on the CMOH position (Oral Health ndash) and on theemail discussion generated on the COMOH listserv some months back re Richardrsquosproposal (calling on the province to fund municipal water fluoridation)
Valerie I request that this be an item for our COMOH meeting on November 15th Sincerely Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorg From Gardner Charles Sent Thursday September 26 2013 245 PMTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes(RayCopesoahppca)Subject Community Water Fluoridation Under Challenge Again in Simcoe Muskoka Hello Colleagues You may wish to know that community water fluoridation (CWF) is again under challenge in SimcoeMuskoka specifically both in Tottenham (Town of New Tecumseth in Simcoe County) and for theentire District of Muskoka On Monday September 23 Committee of the Whole Council of theTown of New Tecumseth voted to submit application to discontinue community water fluoridation(CWF) in the town of Tottenham despite presentations to the contrary from our dental consultantDr Ito and from me The next Council meeting is scheduled for Monday Sept 30 at which lastMondayrsquos (Sept 23) votes will be ratified
Since Monday I have spoken with the Mayor of the Town of New Tecumseth and with most of thecouncilors encouraging deferral of a decision on Monday to allow the town more time to make afully informed decision
This is the second time in recent years that the issue of discontinuing CWF in Tottenham has beenraised at council This issue is also scheduled to return again to the District of Muskoka Council on
October 21st where I will be presenting in response to deputations in opposition to fluoridation
Outside of Base Borden Tottenham is the only community with fluoridated water in SimcoeCounty The health unitrsquos own screening data between 2011 and 2013 shows that Tottenhamrsquos
Gordon
Highlight
children as well as those in Muskoka have a lower rate of dental decay than Simcoe Muskokacommunities without CWF
Sincerely
Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorgChuck Gardner MOH
November 04 2013
Mandatory State Laws on Fluoridation Thirteen states Puerto Rico and the District of Columbia have laws intended to provide
statewide fluoridation These states and the year that the fluoridation legislation was passed are
District of Columbia (1952) Connecticut (1965) Kentucky (1966) Illinois (1967) Minnesota
(1967) Ohio (1969) South Dakota (1969) Georgia (1973) Nebraska (1973 and 2008)
California (1995) Delaware (1998) Puerto Rico (1998) Nevada (1999) Louisiana (2008) and
Arkansas (2011) (see Table 1) The sizes of the public water systems or countiescommunities
affected and exemption provisions vary by state Table 1
STATES THAT HAVE MANDATORY LAWS ON FLUORIDATION -2011
State (1) Year of
Fluoridation
Legislation (1)
Population
served by
Fluoridated
CWS (2)
Persons
receiving
fluoridated
water (2)
State
Average
Caries
Experience
of Grade 3
Students (3)
Arkansas 2011 647 1724131 64
California 1995 621 22812721 709
Connecticut 1965 910 2370423 406
Delaware 1998 862 705344 545
Georgia 1973 921 8924598 52
Illinois 1967 993 11325132 532
Kentucky 1966 999 4334223 598
Louisiana 2008 407 1846149 657
Minnesota 1967 988 4117266 549
Nebraska 1973 and 2008 702 1001665 593
Nevada 1999 702 1001665 649
Ohio 1969 877 8772683 512
South Dakota 1969 948 642942 623
District of
Columbia
1952 1000 595000
Puerto Rico 1998
United States 739 204283554
2010 Statistics for population fluoridated and number of people
1 Communication with Jane McGinley RDH MBA Manager Fluoridation and Preventive Health
Activities Council on Access Prevention and Interprofessional Relations
2 Centers for Disease Control and Prevention Department of Health and Human Services
accessed Oct 21 2013 httpwwwcdcgovfluoridationstatistics2010statshtm
3 Centers for Disease Control and Prevention National Oral Health Surveillance System Caries
Experience - Percentage of 3rd Grade students with Caries Experience (treated or untreated tooth
If data from 43 states for the percentage of Grade 3 children with experience of dental decay is
compared with the 2008 percentages of the population in a state with Community Water
Fluoridation then the percentage of children with experience of dental decay decreases as the
percentage of the state population with Community Water Fluoridation increases (see Figure 1)
Figure 1
Correlation of Percentage of Grade 3 Children with Caries Experience and
Percentage of Population With Community Water Fluoridation for 43
Reporting States
0
10
20
30
40
50
60
70
80
0 10 20 30 40 50 60 70 80 90 100
State of Population With Community Water Fluoridation
Sta
te
of
Gra
de 3
Stu
den
ts w
ith
Cari
es E
xp
eri
en
ce
Data from CDC (2 3)
The description of the fluoridation laws in California Illinois and Nevada can be found on the
Association of State amp Territorial Dental Directors website(4 7 8)
The California fluoridation law AB 733 came into effect in 1995 requiring communities of 10
000 residents or more be supplied with fluoridated drinking water However the state did not
provide any funding to implement the legislation (California is unique in requiring fluoridation
without funding the practice)(4) The California Department of Health Services therefore had to
fund fluoridation initiatives from non-governmental sources ie the California Endowment
California Dental Association Foundation the First 5 Commission and others(5) From 1995 to
2011 the percentage of the California population receiving fluoridated drinking water has risen
from 17 to 625(6) 4 Dental Public Health Activities amp Practices Office of Oral Health California Department of Health
Services April 2002 httpwwwastddorgbestpracticesDES06002CAfluoridationpdf
5 Stock M Pollick H The CDA Foundation Model to Fluoridate Communities California Dental
Association Journal vol 40 no 8 649 - 655
httpwwwcdaorgPortals0journaljournal_082012pdf
6 California Dental Association Foundation
httpwwwcdafoundationorglearnadvocacyfluoridation
The State of Illinois passed a mandatory fluoridation state in 1967 and required all community
water systems to adjust fluoride levels in the drinking water to optimal levels within 1 year(7)
From 1962 when over 5000000 residents had optimally fluoridated drinking water by 2010
the number had risen to 11325132 (993 of the population on community water systems)(2)
7 Dental Public Health Activities amp Practices Division of Oral Health Illinois Department of Public
Health April 2002 httpwwwastddorgbestpracticesDES16007ILfluoridationpdf
The State of Nevada passed a mandatory fluoridation statute in 2000 for communities with
400000 or more residents(8) This was a result of the work of a statewide coalition that
included the Nevada Dental and Dental Hygienist Associations the Washoe and Clark County
District Health Departments the Clark County School District Junior League of Las Vegas
Head Start the Community College of Southern Nevada Dental Hygiene Program Health
Access Washoe County and Saint Maryrsquos Hospital For communities with less than 400000 the
implementation of fluoridation still required the vote of the majority voters in the community
The Las Vegas Water Authority and the City of Henderson started fluoridation in 2000
increasing the percentage of the population with fluoridated drinking water from 2 to 65 (8) 8 Dental Public Health Activities amp Practices Bureau of Family Health Services Nevada State Health
Division April 2002 httpwwwastddorgbestpracticesDES31002NVfluoridationbillpdf
Countries with Mandatory Laws on Fluoridation Countries that have mandated Community Water Fluoridation are Brazil Hong Kong
Malaysia Singapore Ireland Israel and some of the states in Australia
Singapore started fluoridating its water in 1956 based on the success of the fluoridation trials in
Grand Rapids Newburgh Evanston and Brantford Singapore became the first Asian country to
have 100 of its population benefitting from the implementation of fluoridated drinking water
Loh reported that ldquoThe ten year study on the effects of water fluoridation in Singapore showed
a decrease in caries prevalence in the children In the permanent dentition the reduction was
523 per cent for Chinese and 31 per cent for Malays in the 7 to 9 year old age group A similar
trend was observed in the mixed dentition in which the decrease was 325 per cent for Chinese
and 306 per cent for Malaysrdquo(9) By 2010 the population of the country was 5080000(10)
9 Loh T Thirty-eight years of water fluoridation--the Singapore scenario Community Dent
Health 1996 Sep13 Suppl 247-50
10 British Fluoridation Society One in a Million the facts about water fluoridation 3rd Edition
published March 2012) httpwwwbfsweborgonemillion0920One20in20a20Million20-
20The20Extent20of20Fluoridationpdf
Hong Kong started implementing community water fluoridation in 1961 and similar to
Singapore 100 of the population received access to fluoridated drinking water Lo and Wong
reported that ldquoThe mean DMFT score of the children deceased from 44 in 1960 to 15 in 1968
stayed at this level in the 1980 and 1986 surveys and further deceased to 08 in 2001 The
prevalence of dental fluorosis among the children surveyed in 1960 was 1 and this increased
to 59 and 70 in 1968 and 1980 respectively It was found in the 1986 and 2001 surveys that
the prevalences of fluorosis were 47 and 9 among children whose teeth developed at the
time when the respective water fluoride concentrations were 07 ppm and 05 ppmrdquo(11) The
population of Hong Kong was 6968000 in 2009(10) 11 LO ECM and WONG AHH Water fluoride concentration and fluorosis in Hong Kong in 1960-
2001 84th General Session and Exhibition of the International Association for Dental Research amp
1st Meeting of the Pan-Asian-Pacific Federation Brisbane Australia 28 June-1 July 2006 v 85 n
Sp B
The Malaysian cabinet approved a nationwide community water fluoridation program in 1972
(12) One of the states Sabah decided to stop fluoridation in 1989 due to concerns about
inadequate supervision in adding fluoride to the drinking water Oral Health Surveys in 2009
and 2007 indicated that children in Sabah had the worst oral health with 50 of 12 year-olds
having decay in their permanent teeth and children having an average of 3 teeth being(13)
Under the 10th Malaysian Plan in 2011 the federal and the Sabah state governments
reintroduced water fluoridation in Sabah(1314) In 2010 about 755 of the Malaysian
population or 20700000 people had fluoridated drinking water(1013) 12 Malaysian Dental Association Fluoride in Water
httpwwwmdaorgmy07_public_01healthcare_12htm
13 Sachdev N Fluoridation in Sabah Water for Cleaner Teeth French Tribunecom 28022011
From Levy IsraTo Jaeger ValerieCc Pim Carolyn gordonalphaweborg Diallo Aicha Penny Sutcliffe Paul Roumeliotis Michael Finkelstein
Hazel Lynn Robert KyleSubject FW Panorama - Privacy Security and other issuesDate Wednesday October 16 2013 122110 PM
Hello ValerieOttawa is part of Wave 4 Panorama implementation and we are gearing up increasingly to use thesystem where and if possible Thinking about it I am anticipating that this may need to be on theCOMOH (and alPHa) radar as it is something that will impact all health units and implies a majoroperational shift in vaccine delivery programs for all health units I have asked Carolyn Pim toconnect with our sister wave 4 units to share common experiences as we move forward ndash when wehave a roll up could I bring to COMOH Exec for discussion to explore whether there are broaderimplications for all members As an aside I have also asked the Ministry and their CIO to share with me any roll up learnings thatthey may have had already from previous waves (I understand that Niagara HU was a wave 1participant so if there is such a roll up of common experiences that others could learn fromperhaps you have it already and that could come to the exec too)Thanks Isra From Pim Carolyn Sent October 10 2013 1228 PMTo Christopher Mackie (christophermackiemlhuonca) Elizabeth Richardson(Elizabethrichardsonhamiltonca) H BSc M D F R C P (C) MPH Jim Chirico(jimchiriconbpsdhuca) Marlene Spruyt (spruytmtimiskaminghucom) Robert Kyle (Durham)Cc Levy IsraSubject Panorama - Privacy Security and other issues Dear colleagues Irsquom reaching out to you as fellow Panorama Wave 4 health units to ask about where yourorganizations are at in the process of signing agreements and completing Privacy ImpactAssessments and Threat Risk Assessments (TRAs) Ottawa Public Healthrsquos IT legal and informationsecurity advisors have made numerous requests to the MOHLTC for information (in particular theprovincial TRA) that we consider essential to develop our own risk assessment and PIA but havebeen told that information cannot be shared even with strict confidentiality and access controlsSo we are at somewhat of an impasse Isra emailed Arlene yesterday Arlene has forwarded ourconcerns to the Ministryrsquos CIO and Panorama lead but we havenrsquot had any response or discussionswith either of them yet Have your organizations identified similar concerns andor had interactions with the MOHLTC inthis respect Irsquod also be interested in knowing if your health units have flagged other (egoperational) implementation concerns Thanks
Carolyn ps Robert ndash you can ignore this request I talked with Sharan this morning about Durhamrsquos issuesso am including you now just for information Carolyn Pim MD FRCPC Associate Medical Officer of Health Meacutedecin adjointe en santeacute publique Ottawa Public Health Santeacute publique Ottawa 100 Constellation Cr Ottawa ON K2G 6J8 Tel teacutel (613) 580-6744 ext 23684Fax (613) 580-9641Connect With Ottawa Public Health
Suivez Santeacute publique Ottawa
This e-mail originates from the City of Ottawa e-mail system Any distribution use orcopying of this e-mail or the information it contains by other than the intendedrecipient(s) is unauthorized If you are not the intended recipient please notify meat the telephone number shown above or by return e-mail and delete thiscommunication and any copy immediately Thank you
Le preacutesent courriel a eacuteteacute expeacutedieacute par le systegraveme de courriels de la Ville dOttawaToute distribution utilisation ou reproduction du courriel ou des renseignements quisy trouvent par une personne autre que son destinataire preacutevu est interdite Si vousavez reccedilu le message par erreur veuillez men aviser par teacuteleacutephone (au numeacuteropreacuteciteacute) ou par courriel puis supprimer sans deacutelai la version originale de lacommunication ainsi que toutes ses copies Je vous remercie de votre collaboration
1
Smoke-Free Patios ndash An Amendment to the Smoke-Free Ontario Act
Date November 15 2013 Prepared for Council of Ontario Medical Officers of Health Prepared by York Region Public Health _____________________________________________________________________________ Issue
The Smoke-Free Ontario Act is the current provincial legislation that imposes smoking restrictions in workplaces and public places It prohibits smoking on restaurant and bar patios in instances where any portion of the seating area is covered by a roof With recent studies illustrating that exposure to second hand smoke outdoors poses similar risks to indoor exposure there has been growing public support to enhance smoking restrictions and make patios completely smoke-free
Background
With the implementation of the Smoke-Free Ontario Act in 2006 restaurant and bar patios became subject to smoking restrictions if any portion of the seating area was covered by a roof This allowed for patios without roof coverings to continue to allow smoking and as a result did not provide significant protection to patrons or staff from exposure to second hand smoke outdoors Many businesses chose to alter the design of their patios to allow smoking to continue In some cases patios became more crowded since smoking patrons who dine indoors often proceed outside onto licensed patios with their beverages to smoke York Region like most municipalities in Ontario is host to hundreds of patios being operated by restaurant owners and businesses With smoking prohibitions affecting only a small portion of these patios specifically ones with coverings the vast majority of patios still allow smoking to take place Patrons and employees on patios where smoking is not restricted are exposed to second hand smoke frequently This can contribute to increased disease and aggravation of existing health conditions From a business perspective the existing legislation has been viewed by many operators as unfair because some patios have permanent coverings which cannot be removed requiring a smoke-free status These business owners feel this creates an uneven playing field since they cannot provide an outdoor dining area for their smoking customers There is strong community support for smoke-free patios in Ontario A 2009 Rapid Risk Factor Surveillance System survey revealed 754 percent support in York Region while a Toronto Health Survey in 2011 indicated 74 percent public support
2
Current Status
Smoking is currently prohibited on restaurant and bar patios province-wide in four Canadian provinces and territories Alberta Newfoundland and Labrador Nova Scotia and Yukon A fifth province Prince Edward Island prohibits smoking on patios until 10 pm Since Ontario enacted legislation restricting smoking on patios in 2006 eight municipalities in Ontario have chosen to create bylaws that go beyond the Smoke-Free Ontario Act and enhance outdoor protection from second hand smoke by prohibiting smoking on patios completely The largest of those municipalities is the City of Ottawa Recently the Toronto Board of Health unanimously endorsed a report presented by their Medical Officer of Health recommending that restaurant and bar patios be made smoke-free through an amendment to the Smoke-Free Ontario Act
Key Considerations
There should be no significant financial burden to local Boards of Health resulting from a smoke-free patio amendment to the Smoke-Free Ontario Act Inspection and enforcement for the Smoke-Free Ontario Act is currently 100 percent funded by the Ministry of Health and Long-Term Care Following an introductory period of education on the amendment a complaint response model of service delivery would ensure ongoing compliance with smoke-free requirements A complete ban of smoking on patios would eliminate the widely-held perception by business owners that the current legislation creates an uneven playing field for business Since Smoke-Free Ontario Act inspections of patios began in 2006 operators have expressed the opinion that if patios need to be smoke-free for the protection of the public they should all be smoke-free to avoid undue hardship for individual businesses and to provide protection uniformly across the Province
Next steps
York Region Public Health intends to seek support from Medical Officers of Health across the Central East Tobacco Control Area Network (CETCAN) to advocate to the Ministry of Health and Long-Term Care for an amendment to the Smoke-Free Ontario Act prohibiting smoking on all restaurant and bar patios York Region is also in the process of requesting that its Regional Council advocate to the Minister of Health and Long-Term Care on the issue
Updating and Modernizing O Regulation 565 (Public Pools)
Date November 15 2013
Prepared for Council of Ontario Medical Officers of Health
Prepared by York Region Public Health _____________________________________________________________________________ Background Recent drownings at public pools in Ontario have highlighted the issue of water-borne illness and injury The current pool regulation under Ontariorsquos Health Protection and Promotion Act O Regulation 565 (Public Pools) is outdated It does not accurately reflect new pool technology and design or the changing use of public pools Neither does it incorporate admissions standards recommended by the Office of the Chief Coroner Further O Regulation 565 does not have short-form wording or set fines associated with it This limits public health enforcement capabilities What is the impact Updating O Regulation 565 (Public Pools) to address recent changes in pool technology design and uses and to include Coroner-recommended admissions standards would help improve pool safety Establishing short-form wording for O Regulation 565 would enhance enforcement related to public pools Currently the only enforcement available to Public Health Inspectors for dealing with non-critical regulatory infractions in public pools is the issuance of a Part III summons This involves a considerable amount of resources for a possible small fine With the development of inspection disclosure systems such as YorkSafe there is an even greater need to develop a method to effectively address repeated pool operator non-compliance with non-critical issues Next steps Public health units should advocate to the Province to 1) Conduct a review of O Regulation 565 (Public Pools) to address shortcomings Proposed changes to the
regulation should include a requirement for ownersoperators of public pools to advise the local Medical Officer of Health of any change in the use of a facility and the addition of the Coronerrsquos recommended admission standards
2) Provide short-form wording for O Regulation 565 so that public health inspectors can better deal with pool operator non-compliance
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
6 Council of Ontario Medical Officers of Health Terms of Reference
will be considered Such amendments shall be ratified by the Council at the next general meeting or the Annual General Meeting as the case may be
26 The Executive Committee shall review the Terms of Reference as required and not
less than once every two years Original September 1987 1st Revision October 2000 2nd Revision July 2001 3rd Revision December 2003 4th Revision February 2008 5th Revision June 2009 6th Revision June 2011 7th Revision June 2013
7 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX A
COMOH Membership Benefits Active Membership
bull Entitled to attend all meetings of the Section bull May hold office on the COMOH Executive Committee alPHa Board of Directors
Standing Committees bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Associate Membership
bull Entitled to attend all meetings of the Section bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Affiliate Membership
bull May attend meetings or parts thereof subject to approval of Chair bull May serve on ad-hoc committees of the Section subject to the approval of the
Executive Committee bull Discounted registration rates for alPHa Conferences (for Public Health and
Preventive Medicine Residents) bull Upon written request and subject to COMOH Executive approval Affiliate
Members may subscribe to comohlistsalphaweborg The approval will be reviewed on an annual basis in order to determine if the Affiliate Member can remain a subscriber to mohsalphaweborg
Emeritus Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair bull Enjoy discounted registration rates for alPHa Conferences and regular COMOH
meetings bull Subscription to comohlistsalphaweborg electronic mailing list bull Full access to alPHa Web site bull May represent alPHa COMOH on selected external committees and working
groups Honorary Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair
8 Council of Ontario Medical Officers of Health Terms of Reference
bull May represent alPHa COMOH on selected external committees and working groups subject to the approval of the COMOH or alPHa Executive Committee as appropriate
9 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX B
Planning Cycle to Identify Priorities for COMOH
1 There shall normally be a COMOH membership strategic planning retreat every four years In recognition of the dynamic environment of public health the need for and timing of such a retreat shall be at the discretion of the Executive Committee in consultation with the membership
2 The COMOH Executive is responsible (through the creation of a subcommittee of COMOH members) for ensuring the preparation for the COMOH retreats with resources to include those provided by alPHa
3 Leadership for action on COMOH priorities will be recruited from among the COMOH membership in order to make good use of the full base of capacity of the membership The resources to support actions will be recruited from both within and beyond the COMOH membership employing other public health professionals that reside within the broader public health system and community
4 The COMOH Executive shall ensure an annual review of strategic priorities and initiatives and the development of a draft report of the same for the review of the members at the June meeting
2013 Strategic Planning
Considerations for COMOH
As part of its strategic planning discussions alPHarsquos Board has been considering changes to the level of support provided to member sections A member survey is being carried out over the fall to determine options acceptable to alPHa members The following approach to support is put forward as a proposal for the consideration of COMOH Note that the feasibility of the points below depend upon future decisions of the alPHa board They assume that COMOH remains part of alPHa but becomes more independent in administering meetings
1 alPHa can provide to COMOH staff support (Gord Fleming) amounting to 02 FTE or one day per week This is a reduction from the current level of 35 days per week COMOH can choose to use the support any way it wants writing COMOH letters meeting minutes agenda support special projects etc
2 In addition to 02 FTE alPHa staff would provide support for up to 4 face-to-face meetings per year One meeting would be concurrent to alPHarsquos annual conference in June The timing of other meetings could be negotiated The support includes consulting on the development of the program arranging for speakers registration for the event arranging venue AV support and hospitality services
3 In addition to 02 FTE alPHa staff would provide support for setting meeting dates and any polling required to establish dates Note that the individual supporting this function would be Karen Reece
4 COMOHrsquos Executive and Section would continue to have access to online supports through the alPHa including the COMOH Listserve and a group page for posting agendas minutes and other resources on the alPHa website
5 alPHa staff (Linda Stewart and Gord Fleming) can also start participating on CMOH calls as a way to be up-to-date on issues related to COMOH
6 Other than what is outlined above COMOH would be expected to prepare agendas and take minutes for its Executive and Section meetings The Executive would be expected to operate more independently than it does now but would be able to access the supports outlined above
Prepared by Linda Stewart Executive Director
From comoh-bounceslistsalphaweborg on behalf of Christopher MackieTo MOH ListserveSubject [comoh] Fw URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)Date Wednesday October 30 2013 91241 AMAttachments ATT00249txt
For AMOHs and PHPM residents who didnt receive the initial email
Chris
Christopher Mackie MD MHSc FRCPCMedical Officer of Health and CEOMiddlesex-London Health Unit50 King St LondonON N6A 5L7 O 519 663 5317 ext 2444 wwwhealthunitcomFrom Pisko Laura (MOHLTC)Sent Tuesday October 29 2013 759 PMTo kbarkeralgomapublichealthcom malcolmlockbchuorg davidcchatham-kentcarobertkyledurhamca proumeliotiseohuca fwarshelginhealthonca mohelginhealthoncahlynnpublichealthgreybruceonca malcolmlockhnhuorg hnmohhnhuorglnoseworthyhkpronca bobnosalhaltonca elizabethrichardsonhamiltoncarschabashpechuonca ncameronhuroncountyca drimgemmillkflapublichealthcamohkflapublichealthca suditranadecounty-lambtononca paulastewarthealthunitorgChristopher Mackie valeriejaegerniagararegionca jimchiriconbpsdhuca jarthursnwhuoncaisralevyottawaca dnealoxfordcountyca davidmowatpeelregionca mklassenpdhuoncarpellizzaripcchuca rosemarieramsinghporcupinehuonca mcorriveaurcdhucomcharlesgardnersmdhuorg sutcliffepsdhucom davidwilliamstbdhucomspruytmtimiskaminghucom dmckeowntorontoca lnolanregionofwaterloocanicolamercerwdghuorg aheimannwechealthunitorg karimkurjiyorkcaCc coreywesleytbdhucom CindyBaker-Barillsmdhuorg Donna Kosmack pilonlsdhucomPaulaMuiskflapublichealthca sthibautorontoca Mueller Daina (MOHLTC) Gordon Marcus(MOHLTC) andreakitahamiltoncaSubject URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)
Dear Colleagues The ministry has received reports that some tobacco vendors across the province aregiving away single cigarettes with the purchase of tobacco products It is the ministryrsquosposition that giving out free single cigarettes does not violate subsection 31(3) of theSmoke-Free Ontario Act (ldquoSFOArdquo) Although the practice of giving out free singlecigarettes may promote the sale of tobacco products it does not take the form of aldquoproduct enhancement product association or promotional materialrdquo and therefore doesnot fall within the scope of subsection 31(3) of the SFOA We have confirmed with Health Canada that this practice may violate section 29(b) of thefederal Tobacco Act As such Health Canada is requesting that you notify them in writingand I am directing you to communicate with them via email and provide to them as manydetails as possible Emails should be sent to Tobacco-Ontariohc-scgcca and thesubject line should read ldquoViolation of Section 29(b) of Tobacco Actrdquo This will ensurethat the complaints are given priority status by Health Canada We will continue to monitor
this situation and liaise with our colleagues at Health Canada Please share this information with your tobacco control staff and contact me or DainaMueller Manager Tobacco Control Unit Health Promotion Implementation Branch atdainamuellerontarioca with any questions RegardsLaura Laura A PiskoDirectorHealth Promotion Implementation BranchHealth Promotion DivisionMinistry of Health and Long Term Care416-327-7445 (office)416-451-3185 (mobile) Marcus Gordon - EA (416)326-0625 for urgent issues
========= Middlesex-London Health Unit E-Mail Disclaimer =============______________________________________________________________
Private and confidential intended only for named recipient If otherwisereceived please destroy immediately Health information in this email isonly general information and is not intended to replace an in personconsultation with a medical professional nor is it intended to providemedical advice Individual circumstances of which we are not aware mayaffect the information provided herein and as such the Middlesex-LondonHealth Unit assumes no liability or responsibility for your reliancethereon The Middlesex-London Health Unit works under the authority of theHealth Protection and Promotion Act and this correspondence may be used toassess your needs for public health services (519-663-5317 ext 2448)______________________________________________________________
From Gardner CharlesTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes (RayCopesoahppca)
George Pasut (GeorgePasutoahppca) Peter Cooney (petercooneyhc-scgcca)Cc Ito DickSubject Discontinuation of Fluoridation in MuskokaDate Tuesday October 22 2013 125254 PM
Hello Colleagues
As I reported in my email below on September 26th fluoridation has come under challenge again inSimcoe Muskoka I am now very unhappy to report that despite our best efforts last night theDistrict Council of Muskoka voted to remove fluoride from municipal drinking supplies across theDistrict This brings to an end fluoridation in all of Simcoe and Muskoka (with the exception of Base Borden)ndash though New Tecumseth will be conducting a plebiscite on the question of fluoridation with themunicipal election next October Defending community water fluoridation has drained a great deal of time human resources andcommitment from other priorities and has been exhausting here in SMDHU as I am sure it hasbeen in many other health units While the outcomes have been very disappointing I have beenimpressed by the professionalism and dedication that SMDHU staff members have shown inshouldering this burden In particular our dental consultant Dr Ito has provided us with much ofthe foundational knowledge and the local research essential to our efforts and has very frequentlyattended and presented at council meetings and other public events I would also like to thank themany of you who have offer and provided support including advocacy letters and informationresources Over the years Dr Peter Cooney Chief Dental Officer of Health of Canada has beenvery helpful attending and presenting with us at council meetings and at public consultationevents We will of course continue our oral health surveillance of the children of Muskoka documentingand reporting in future years on the increase in dental decay that we anticipate will occur Suchsurveillance is the foundation of our advocacy both to municipal politicians and to the province I am very concerned that our experience will continue to repeat itself across the province unlessthere is strong leadership provincially It is with this in mind that I raise the followingrecommendations for your consideration
1 That we collectively (with PHOrsquos leadership) conduct high quality publish-worthy researchdocumenting the impact on dental decay that occurs in those municipalities throughoutOntario that in recent years have discontinued community water fluoridation This could bepart of a larger study on such municipalities across the country and it could also be part ofa study documenting overall oral health (including fluoridation coverage) in the province(and possibly across the country)
2 That COMOH engage with our Chief MOH to advocate for the province to require allmunicipal water supplies to be fluoridated (the exception of course being those withnaturally sufficient fluoride concentrations) This could built upon the alPHa position to
Gordon
Highlight
Gordon
Highlight
date (A11-00 - Community Water Fluoridation) on the CMOH position (Oral Health ndash) and on theemail discussion generated on the COMOH listserv some months back re Richardrsquosproposal (calling on the province to fund municipal water fluoridation)
Valerie I request that this be an item for our COMOH meeting on November 15th Sincerely Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorg From Gardner Charles Sent Thursday September 26 2013 245 PMTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes(RayCopesoahppca)Subject Community Water Fluoridation Under Challenge Again in Simcoe Muskoka Hello Colleagues You may wish to know that community water fluoridation (CWF) is again under challenge in SimcoeMuskoka specifically both in Tottenham (Town of New Tecumseth in Simcoe County) and for theentire District of Muskoka On Monday September 23 Committee of the Whole Council of theTown of New Tecumseth voted to submit application to discontinue community water fluoridation(CWF) in the town of Tottenham despite presentations to the contrary from our dental consultantDr Ito and from me The next Council meeting is scheduled for Monday Sept 30 at which lastMondayrsquos (Sept 23) votes will be ratified
Since Monday I have spoken with the Mayor of the Town of New Tecumseth and with most of thecouncilors encouraging deferral of a decision on Monday to allow the town more time to make afully informed decision
This is the second time in recent years that the issue of discontinuing CWF in Tottenham has beenraised at council This issue is also scheduled to return again to the District of Muskoka Council on
October 21st where I will be presenting in response to deputations in opposition to fluoridation
Outside of Base Borden Tottenham is the only community with fluoridated water in SimcoeCounty The health unitrsquos own screening data between 2011 and 2013 shows that Tottenhamrsquos
Gordon
Highlight
children as well as those in Muskoka have a lower rate of dental decay than Simcoe Muskokacommunities without CWF
Sincerely
Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorgChuck Gardner MOH
November 04 2013
Mandatory State Laws on Fluoridation Thirteen states Puerto Rico and the District of Columbia have laws intended to provide
statewide fluoridation These states and the year that the fluoridation legislation was passed are
District of Columbia (1952) Connecticut (1965) Kentucky (1966) Illinois (1967) Minnesota
(1967) Ohio (1969) South Dakota (1969) Georgia (1973) Nebraska (1973 and 2008)
California (1995) Delaware (1998) Puerto Rico (1998) Nevada (1999) Louisiana (2008) and
Arkansas (2011) (see Table 1) The sizes of the public water systems or countiescommunities
affected and exemption provisions vary by state Table 1
STATES THAT HAVE MANDATORY LAWS ON FLUORIDATION -2011
State (1) Year of
Fluoridation
Legislation (1)
Population
served by
Fluoridated
CWS (2)
Persons
receiving
fluoridated
water (2)
State
Average
Caries
Experience
of Grade 3
Students (3)
Arkansas 2011 647 1724131 64
California 1995 621 22812721 709
Connecticut 1965 910 2370423 406
Delaware 1998 862 705344 545
Georgia 1973 921 8924598 52
Illinois 1967 993 11325132 532
Kentucky 1966 999 4334223 598
Louisiana 2008 407 1846149 657
Minnesota 1967 988 4117266 549
Nebraska 1973 and 2008 702 1001665 593
Nevada 1999 702 1001665 649
Ohio 1969 877 8772683 512
South Dakota 1969 948 642942 623
District of
Columbia
1952 1000 595000
Puerto Rico 1998
United States 739 204283554
2010 Statistics for population fluoridated and number of people
1 Communication with Jane McGinley RDH MBA Manager Fluoridation and Preventive Health
Activities Council on Access Prevention and Interprofessional Relations
2 Centers for Disease Control and Prevention Department of Health and Human Services
accessed Oct 21 2013 httpwwwcdcgovfluoridationstatistics2010statshtm
3 Centers for Disease Control and Prevention National Oral Health Surveillance System Caries
Experience - Percentage of 3rd Grade students with Caries Experience (treated or untreated tooth
If data from 43 states for the percentage of Grade 3 children with experience of dental decay is
compared with the 2008 percentages of the population in a state with Community Water
Fluoridation then the percentage of children with experience of dental decay decreases as the
percentage of the state population with Community Water Fluoridation increases (see Figure 1)
Figure 1
Correlation of Percentage of Grade 3 Children with Caries Experience and
Percentage of Population With Community Water Fluoridation for 43
Reporting States
0
10
20
30
40
50
60
70
80
0 10 20 30 40 50 60 70 80 90 100
State of Population With Community Water Fluoridation
Sta
te
of
Gra
de 3
Stu
den
ts w
ith
Cari
es E
xp
eri
en
ce
Data from CDC (2 3)
The description of the fluoridation laws in California Illinois and Nevada can be found on the
Association of State amp Territorial Dental Directors website(4 7 8)
The California fluoridation law AB 733 came into effect in 1995 requiring communities of 10
000 residents or more be supplied with fluoridated drinking water However the state did not
provide any funding to implement the legislation (California is unique in requiring fluoridation
without funding the practice)(4) The California Department of Health Services therefore had to
fund fluoridation initiatives from non-governmental sources ie the California Endowment
California Dental Association Foundation the First 5 Commission and others(5) From 1995 to
2011 the percentage of the California population receiving fluoridated drinking water has risen
from 17 to 625(6) 4 Dental Public Health Activities amp Practices Office of Oral Health California Department of Health
Services April 2002 httpwwwastddorgbestpracticesDES06002CAfluoridationpdf
5 Stock M Pollick H The CDA Foundation Model to Fluoridate Communities California Dental
Association Journal vol 40 no 8 649 - 655
httpwwwcdaorgPortals0journaljournal_082012pdf
6 California Dental Association Foundation
httpwwwcdafoundationorglearnadvocacyfluoridation
The State of Illinois passed a mandatory fluoridation state in 1967 and required all community
water systems to adjust fluoride levels in the drinking water to optimal levels within 1 year(7)
From 1962 when over 5000000 residents had optimally fluoridated drinking water by 2010
the number had risen to 11325132 (993 of the population on community water systems)(2)
7 Dental Public Health Activities amp Practices Division of Oral Health Illinois Department of Public
Health April 2002 httpwwwastddorgbestpracticesDES16007ILfluoridationpdf
The State of Nevada passed a mandatory fluoridation statute in 2000 for communities with
400000 or more residents(8) This was a result of the work of a statewide coalition that
included the Nevada Dental and Dental Hygienist Associations the Washoe and Clark County
District Health Departments the Clark County School District Junior League of Las Vegas
Head Start the Community College of Southern Nevada Dental Hygiene Program Health
Access Washoe County and Saint Maryrsquos Hospital For communities with less than 400000 the
implementation of fluoridation still required the vote of the majority voters in the community
The Las Vegas Water Authority and the City of Henderson started fluoridation in 2000
increasing the percentage of the population with fluoridated drinking water from 2 to 65 (8) 8 Dental Public Health Activities amp Practices Bureau of Family Health Services Nevada State Health
Division April 2002 httpwwwastddorgbestpracticesDES31002NVfluoridationbillpdf
Countries with Mandatory Laws on Fluoridation Countries that have mandated Community Water Fluoridation are Brazil Hong Kong
Malaysia Singapore Ireland Israel and some of the states in Australia
Singapore started fluoridating its water in 1956 based on the success of the fluoridation trials in
Grand Rapids Newburgh Evanston and Brantford Singapore became the first Asian country to
have 100 of its population benefitting from the implementation of fluoridated drinking water
Loh reported that ldquoThe ten year study on the effects of water fluoridation in Singapore showed
a decrease in caries prevalence in the children In the permanent dentition the reduction was
523 per cent for Chinese and 31 per cent for Malays in the 7 to 9 year old age group A similar
trend was observed in the mixed dentition in which the decrease was 325 per cent for Chinese
and 306 per cent for Malaysrdquo(9) By 2010 the population of the country was 5080000(10)
9 Loh T Thirty-eight years of water fluoridation--the Singapore scenario Community Dent
Health 1996 Sep13 Suppl 247-50
10 British Fluoridation Society One in a Million the facts about water fluoridation 3rd Edition
published March 2012) httpwwwbfsweborgonemillion0920One20in20a20Million20-
20The20Extent20of20Fluoridationpdf
Hong Kong started implementing community water fluoridation in 1961 and similar to
Singapore 100 of the population received access to fluoridated drinking water Lo and Wong
reported that ldquoThe mean DMFT score of the children deceased from 44 in 1960 to 15 in 1968
stayed at this level in the 1980 and 1986 surveys and further deceased to 08 in 2001 The
prevalence of dental fluorosis among the children surveyed in 1960 was 1 and this increased
to 59 and 70 in 1968 and 1980 respectively It was found in the 1986 and 2001 surveys that
the prevalences of fluorosis were 47 and 9 among children whose teeth developed at the
time when the respective water fluoride concentrations were 07 ppm and 05 ppmrdquo(11) The
population of Hong Kong was 6968000 in 2009(10) 11 LO ECM and WONG AHH Water fluoride concentration and fluorosis in Hong Kong in 1960-
2001 84th General Session and Exhibition of the International Association for Dental Research amp
1st Meeting of the Pan-Asian-Pacific Federation Brisbane Australia 28 June-1 July 2006 v 85 n
Sp B
The Malaysian cabinet approved a nationwide community water fluoridation program in 1972
(12) One of the states Sabah decided to stop fluoridation in 1989 due to concerns about
inadequate supervision in adding fluoride to the drinking water Oral Health Surveys in 2009
and 2007 indicated that children in Sabah had the worst oral health with 50 of 12 year-olds
having decay in their permanent teeth and children having an average of 3 teeth being(13)
Under the 10th Malaysian Plan in 2011 the federal and the Sabah state governments
reintroduced water fluoridation in Sabah(1314) In 2010 about 755 of the Malaysian
population or 20700000 people had fluoridated drinking water(1013) 12 Malaysian Dental Association Fluoride in Water
httpwwwmdaorgmy07_public_01healthcare_12htm
13 Sachdev N Fluoridation in Sabah Water for Cleaner Teeth French Tribunecom 28022011
From Levy IsraTo Jaeger ValerieCc Pim Carolyn gordonalphaweborg Diallo Aicha Penny Sutcliffe Paul Roumeliotis Michael Finkelstein
Hazel Lynn Robert KyleSubject FW Panorama - Privacy Security and other issuesDate Wednesday October 16 2013 122110 PM
Hello ValerieOttawa is part of Wave 4 Panorama implementation and we are gearing up increasingly to use thesystem where and if possible Thinking about it I am anticipating that this may need to be on theCOMOH (and alPHa) radar as it is something that will impact all health units and implies a majoroperational shift in vaccine delivery programs for all health units I have asked Carolyn Pim toconnect with our sister wave 4 units to share common experiences as we move forward ndash when wehave a roll up could I bring to COMOH Exec for discussion to explore whether there are broaderimplications for all members As an aside I have also asked the Ministry and their CIO to share with me any roll up learnings thatthey may have had already from previous waves (I understand that Niagara HU was a wave 1participant so if there is such a roll up of common experiences that others could learn fromperhaps you have it already and that could come to the exec too)Thanks Isra From Pim Carolyn Sent October 10 2013 1228 PMTo Christopher Mackie (christophermackiemlhuonca) Elizabeth Richardson(Elizabethrichardsonhamiltonca) H BSc M D F R C P (C) MPH Jim Chirico(jimchiriconbpsdhuca) Marlene Spruyt (spruytmtimiskaminghucom) Robert Kyle (Durham)Cc Levy IsraSubject Panorama - Privacy Security and other issues Dear colleagues Irsquom reaching out to you as fellow Panorama Wave 4 health units to ask about where yourorganizations are at in the process of signing agreements and completing Privacy ImpactAssessments and Threat Risk Assessments (TRAs) Ottawa Public Healthrsquos IT legal and informationsecurity advisors have made numerous requests to the MOHLTC for information (in particular theprovincial TRA) that we consider essential to develop our own risk assessment and PIA but havebeen told that information cannot be shared even with strict confidentiality and access controlsSo we are at somewhat of an impasse Isra emailed Arlene yesterday Arlene has forwarded ourconcerns to the Ministryrsquos CIO and Panorama lead but we havenrsquot had any response or discussionswith either of them yet Have your organizations identified similar concerns andor had interactions with the MOHLTC inthis respect Irsquod also be interested in knowing if your health units have flagged other (egoperational) implementation concerns Thanks
Carolyn ps Robert ndash you can ignore this request I talked with Sharan this morning about Durhamrsquos issuesso am including you now just for information Carolyn Pim MD FRCPC Associate Medical Officer of Health Meacutedecin adjointe en santeacute publique Ottawa Public Health Santeacute publique Ottawa 100 Constellation Cr Ottawa ON K2G 6J8 Tel teacutel (613) 580-6744 ext 23684Fax (613) 580-9641Connect With Ottawa Public Health
Suivez Santeacute publique Ottawa
This e-mail originates from the City of Ottawa e-mail system Any distribution use orcopying of this e-mail or the information it contains by other than the intendedrecipient(s) is unauthorized If you are not the intended recipient please notify meat the telephone number shown above or by return e-mail and delete thiscommunication and any copy immediately Thank you
Le preacutesent courriel a eacuteteacute expeacutedieacute par le systegraveme de courriels de la Ville dOttawaToute distribution utilisation ou reproduction du courriel ou des renseignements quisy trouvent par une personne autre que son destinataire preacutevu est interdite Si vousavez reccedilu le message par erreur veuillez men aviser par teacuteleacutephone (au numeacuteropreacuteciteacute) ou par courriel puis supprimer sans deacutelai la version originale de lacommunication ainsi que toutes ses copies Je vous remercie de votre collaboration
1
Smoke-Free Patios ndash An Amendment to the Smoke-Free Ontario Act
Date November 15 2013 Prepared for Council of Ontario Medical Officers of Health Prepared by York Region Public Health _____________________________________________________________________________ Issue
The Smoke-Free Ontario Act is the current provincial legislation that imposes smoking restrictions in workplaces and public places It prohibits smoking on restaurant and bar patios in instances where any portion of the seating area is covered by a roof With recent studies illustrating that exposure to second hand smoke outdoors poses similar risks to indoor exposure there has been growing public support to enhance smoking restrictions and make patios completely smoke-free
Background
With the implementation of the Smoke-Free Ontario Act in 2006 restaurant and bar patios became subject to smoking restrictions if any portion of the seating area was covered by a roof This allowed for patios without roof coverings to continue to allow smoking and as a result did not provide significant protection to patrons or staff from exposure to second hand smoke outdoors Many businesses chose to alter the design of their patios to allow smoking to continue In some cases patios became more crowded since smoking patrons who dine indoors often proceed outside onto licensed patios with their beverages to smoke York Region like most municipalities in Ontario is host to hundreds of patios being operated by restaurant owners and businesses With smoking prohibitions affecting only a small portion of these patios specifically ones with coverings the vast majority of patios still allow smoking to take place Patrons and employees on patios where smoking is not restricted are exposed to second hand smoke frequently This can contribute to increased disease and aggravation of existing health conditions From a business perspective the existing legislation has been viewed by many operators as unfair because some patios have permanent coverings which cannot be removed requiring a smoke-free status These business owners feel this creates an uneven playing field since they cannot provide an outdoor dining area for their smoking customers There is strong community support for smoke-free patios in Ontario A 2009 Rapid Risk Factor Surveillance System survey revealed 754 percent support in York Region while a Toronto Health Survey in 2011 indicated 74 percent public support
2
Current Status
Smoking is currently prohibited on restaurant and bar patios province-wide in four Canadian provinces and territories Alberta Newfoundland and Labrador Nova Scotia and Yukon A fifth province Prince Edward Island prohibits smoking on patios until 10 pm Since Ontario enacted legislation restricting smoking on patios in 2006 eight municipalities in Ontario have chosen to create bylaws that go beyond the Smoke-Free Ontario Act and enhance outdoor protection from second hand smoke by prohibiting smoking on patios completely The largest of those municipalities is the City of Ottawa Recently the Toronto Board of Health unanimously endorsed a report presented by their Medical Officer of Health recommending that restaurant and bar patios be made smoke-free through an amendment to the Smoke-Free Ontario Act
Key Considerations
There should be no significant financial burden to local Boards of Health resulting from a smoke-free patio amendment to the Smoke-Free Ontario Act Inspection and enforcement for the Smoke-Free Ontario Act is currently 100 percent funded by the Ministry of Health and Long-Term Care Following an introductory period of education on the amendment a complaint response model of service delivery would ensure ongoing compliance with smoke-free requirements A complete ban of smoking on patios would eliminate the widely-held perception by business owners that the current legislation creates an uneven playing field for business Since Smoke-Free Ontario Act inspections of patios began in 2006 operators have expressed the opinion that if patios need to be smoke-free for the protection of the public they should all be smoke-free to avoid undue hardship for individual businesses and to provide protection uniformly across the Province
Next steps
York Region Public Health intends to seek support from Medical Officers of Health across the Central East Tobacco Control Area Network (CETCAN) to advocate to the Ministry of Health and Long-Term Care for an amendment to the Smoke-Free Ontario Act prohibiting smoking on all restaurant and bar patios York Region is also in the process of requesting that its Regional Council advocate to the Minister of Health and Long-Term Care on the issue
Updating and Modernizing O Regulation 565 (Public Pools)
Date November 15 2013
Prepared for Council of Ontario Medical Officers of Health
Prepared by York Region Public Health _____________________________________________________________________________ Background Recent drownings at public pools in Ontario have highlighted the issue of water-borne illness and injury The current pool regulation under Ontariorsquos Health Protection and Promotion Act O Regulation 565 (Public Pools) is outdated It does not accurately reflect new pool technology and design or the changing use of public pools Neither does it incorporate admissions standards recommended by the Office of the Chief Coroner Further O Regulation 565 does not have short-form wording or set fines associated with it This limits public health enforcement capabilities What is the impact Updating O Regulation 565 (Public Pools) to address recent changes in pool technology design and uses and to include Coroner-recommended admissions standards would help improve pool safety Establishing short-form wording for O Regulation 565 would enhance enforcement related to public pools Currently the only enforcement available to Public Health Inspectors for dealing with non-critical regulatory infractions in public pools is the issuance of a Part III summons This involves a considerable amount of resources for a possible small fine With the development of inspection disclosure systems such as YorkSafe there is an even greater need to develop a method to effectively address repeated pool operator non-compliance with non-critical issues Next steps Public health units should advocate to the Province to 1) Conduct a review of O Regulation 565 (Public Pools) to address shortcomings Proposed changes to the
regulation should include a requirement for ownersoperators of public pools to advise the local Medical Officer of Health of any change in the use of a facility and the addition of the Coronerrsquos recommended admission standards
2) Provide short-form wording for O Regulation 565 so that public health inspectors can better deal with pool operator non-compliance
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
7 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX A
COMOH Membership Benefits Active Membership
bull Entitled to attend all meetings of the Section bull May hold office on the COMOH Executive Committee alPHa Board of Directors
Standing Committees bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Associate Membership
bull Entitled to attend all meetings of the Section bull May serve on any ad-hoc committee of the section bull May represent alPHa on selected external committees and working groups bull Subscription to comohlistsalphaweborg and bull Full access to all areas of the alPHa Web Site
Affiliate Membership
bull May attend meetings or parts thereof subject to approval of Chair bull May serve on ad-hoc committees of the Section subject to the approval of the
Executive Committee bull Discounted registration rates for alPHa Conferences (for Public Health and
Preventive Medicine Residents) bull Upon written request and subject to COMOH Executive approval Affiliate
Members may subscribe to comohlistsalphaweborg The approval will be reviewed on an annual basis in order to determine if the Affiliate Member can remain a subscriber to mohsalphaweborg
Emeritus Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair bull Enjoy discounted registration rates for alPHa Conferences and regular COMOH
meetings bull Subscription to comohlistsalphaweborg electronic mailing list bull Full access to alPHa Web site bull May represent alPHa COMOH on selected external committees and working
groups Honorary Membership
bull May attend COMOH meetings or parts thereof subject to approval of Chair
8 Council of Ontario Medical Officers of Health Terms of Reference
bull May represent alPHa COMOH on selected external committees and working groups subject to the approval of the COMOH or alPHa Executive Committee as appropriate
9 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX B
Planning Cycle to Identify Priorities for COMOH
1 There shall normally be a COMOH membership strategic planning retreat every four years In recognition of the dynamic environment of public health the need for and timing of such a retreat shall be at the discretion of the Executive Committee in consultation with the membership
2 The COMOH Executive is responsible (through the creation of a subcommittee of COMOH members) for ensuring the preparation for the COMOH retreats with resources to include those provided by alPHa
3 Leadership for action on COMOH priorities will be recruited from among the COMOH membership in order to make good use of the full base of capacity of the membership The resources to support actions will be recruited from both within and beyond the COMOH membership employing other public health professionals that reside within the broader public health system and community
4 The COMOH Executive shall ensure an annual review of strategic priorities and initiatives and the development of a draft report of the same for the review of the members at the June meeting
2013 Strategic Planning
Considerations for COMOH
As part of its strategic planning discussions alPHarsquos Board has been considering changes to the level of support provided to member sections A member survey is being carried out over the fall to determine options acceptable to alPHa members The following approach to support is put forward as a proposal for the consideration of COMOH Note that the feasibility of the points below depend upon future decisions of the alPHa board They assume that COMOH remains part of alPHa but becomes more independent in administering meetings
1 alPHa can provide to COMOH staff support (Gord Fleming) amounting to 02 FTE or one day per week This is a reduction from the current level of 35 days per week COMOH can choose to use the support any way it wants writing COMOH letters meeting minutes agenda support special projects etc
2 In addition to 02 FTE alPHa staff would provide support for up to 4 face-to-face meetings per year One meeting would be concurrent to alPHarsquos annual conference in June The timing of other meetings could be negotiated The support includes consulting on the development of the program arranging for speakers registration for the event arranging venue AV support and hospitality services
3 In addition to 02 FTE alPHa staff would provide support for setting meeting dates and any polling required to establish dates Note that the individual supporting this function would be Karen Reece
4 COMOHrsquos Executive and Section would continue to have access to online supports through the alPHa including the COMOH Listserve and a group page for posting agendas minutes and other resources on the alPHa website
5 alPHa staff (Linda Stewart and Gord Fleming) can also start participating on CMOH calls as a way to be up-to-date on issues related to COMOH
6 Other than what is outlined above COMOH would be expected to prepare agendas and take minutes for its Executive and Section meetings The Executive would be expected to operate more independently than it does now but would be able to access the supports outlined above
Prepared by Linda Stewart Executive Director
From comoh-bounceslistsalphaweborg on behalf of Christopher MackieTo MOH ListserveSubject [comoh] Fw URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)Date Wednesday October 30 2013 91241 AMAttachments ATT00249txt
For AMOHs and PHPM residents who didnt receive the initial email
Chris
Christopher Mackie MD MHSc FRCPCMedical Officer of Health and CEOMiddlesex-London Health Unit50 King St LondonON N6A 5L7 O 519 663 5317 ext 2444 wwwhealthunitcomFrom Pisko Laura (MOHLTC)Sent Tuesday October 29 2013 759 PMTo kbarkeralgomapublichealthcom malcolmlockbchuorg davidcchatham-kentcarobertkyledurhamca proumeliotiseohuca fwarshelginhealthonca mohelginhealthoncahlynnpublichealthgreybruceonca malcolmlockhnhuorg hnmohhnhuorglnoseworthyhkpronca bobnosalhaltonca elizabethrichardsonhamiltoncarschabashpechuonca ncameronhuroncountyca drimgemmillkflapublichealthcamohkflapublichealthca suditranadecounty-lambtononca paulastewarthealthunitorgChristopher Mackie valeriejaegerniagararegionca jimchiriconbpsdhuca jarthursnwhuoncaisralevyottawaca dnealoxfordcountyca davidmowatpeelregionca mklassenpdhuoncarpellizzaripcchuca rosemarieramsinghporcupinehuonca mcorriveaurcdhucomcharlesgardnersmdhuorg sutcliffepsdhucom davidwilliamstbdhucomspruytmtimiskaminghucom dmckeowntorontoca lnolanregionofwaterloocanicolamercerwdghuorg aheimannwechealthunitorg karimkurjiyorkcaCc coreywesleytbdhucom CindyBaker-Barillsmdhuorg Donna Kosmack pilonlsdhucomPaulaMuiskflapublichealthca sthibautorontoca Mueller Daina (MOHLTC) Gordon Marcus(MOHLTC) andreakitahamiltoncaSubject URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)
Dear Colleagues The ministry has received reports that some tobacco vendors across the province aregiving away single cigarettes with the purchase of tobacco products It is the ministryrsquosposition that giving out free single cigarettes does not violate subsection 31(3) of theSmoke-Free Ontario Act (ldquoSFOArdquo) Although the practice of giving out free singlecigarettes may promote the sale of tobacco products it does not take the form of aldquoproduct enhancement product association or promotional materialrdquo and therefore doesnot fall within the scope of subsection 31(3) of the SFOA We have confirmed with Health Canada that this practice may violate section 29(b) of thefederal Tobacco Act As such Health Canada is requesting that you notify them in writingand I am directing you to communicate with them via email and provide to them as manydetails as possible Emails should be sent to Tobacco-Ontariohc-scgcca and thesubject line should read ldquoViolation of Section 29(b) of Tobacco Actrdquo This will ensurethat the complaints are given priority status by Health Canada We will continue to monitor
this situation and liaise with our colleagues at Health Canada Please share this information with your tobacco control staff and contact me or DainaMueller Manager Tobacco Control Unit Health Promotion Implementation Branch atdainamuellerontarioca with any questions RegardsLaura Laura A PiskoDirectorHealth Promotion Implementation BranchHealth Promotion DivisionMinistry of Health and Long Term Care416-327-7445 (office)416-451-3185 (mobile) Marcus Gordon - EA (416)326-0625 for urgent issues
========= Middlesex-London Health Unit E-Mail Disclaimer =============______________________________________________________________
Private and confidential intended only for named recipient If otherwisereceived please destroy immediately Health information in this email isonly general information and is not intended to replace an in personconsultation with a medical professional nor is it intended to providemedical advice Individual circumstances of which we are not aware mayaffect the information provided herein and as such the Middlesex-LondonHealth Unit assumes no liability or responsibility for your reliancethereon The Middlesex-London Health Unit works under the authority of theHealth Protection and Promotion Act and this correspondence may be used toassess your needs for public health services (519-663-5317 ext 2448)______________________________________________________________
From Gardner CharlesTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes (RayCopesoahppca)
George Pasut (GeorgePasutoahppca) Peter Cooney (petercooneyhc-scgcca)Cc Ito DickSubject Discontinuation of Fluoridation in MuskokaDate Tuesday October 22 2013 125254 PM
Hello Colleagues
As I reported in my email below on September 26th fluoridation has come under challenge again inSimcoe Muskoka I am now very unhappy to report that despite our best efforts last night theDistrict Council of Muskoka voted to remove fluoride from municipal drinking supplies across theDistrict This brings to an end fluoridation in all of Simcoe and Muskoka (with the exception of Base Borden)ndash though New Tecumseth will be conducting a plebiscite on the question of fluoridation with themunicipal election next October Defending community water fluoridation has drained a great deal of time human resources andcommitment from other priorities and has been exhausting here in SMDHU as I am sure it hasbeen in many other health units While the outcomes have been very disappointing I have beenimpressed by the professionalism and dedication that SMDHU staff members have shown inshouldering this burden In particular our dental consultant Dr Ito has provided us with much ofthe foundational knowledge and the local research essential to our efforts and has very frequentlyattended and presented at council meetings and other public events I would also like to thank themany of you who have offer and provided support including advocacy letters and informationresources Over the years Dr Peter Cooney Chief Dental Officer of Health of Canada has beenvery helpful attending and presenting with us at council meetings and at public consultationevents We will of course continue our oral health surveillance of the children of Muskoka documentingand reporting in future years on the increase in dental decay that we anticipate will occur Suchsurveillance is the foundation of our advocacy both to municipal politicians and to the province I am very concerned that our experience will continue to repeat itself across the province unlessthere is strong leadership provincially It is with this in mind that I raise the followingrecommendations for your consideration
1 That we collectively (with PHOrsquos leadership) conduct high quality publish-worthy researchdocumenting the impact on dental decay that occurs in those municipalities throughoutOntario that in recent years have discontinued community water fluoridation This could bepart of a larger study on such municipalities across the country and it could also be part ofa study documenting overall oral health (including fluoridation coverage) in the province(and possibly across the country)
2 That COMOH engage with our Chief MOH to advocate for the province to require allmunicipal water supplies to be fluoridated (the exception of course being those withnaturally sufficient fluoride concentrations) This could built upon the alPHa position to
Gordon
Highlight
Gordon
Highlight
date (A11-00 - Community Water Fluoridation) on the CMOH position (Oral Health ndash) and on theemail discussion generated on the COMOH listserv some months back re Richardrsquosproposal (calling on the province to fund municipal water fluoridation)
Valerie I request that this be an item for our COMOH meeting on November 15th Sincerely Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorg From Gardner Charles Sent Thursday September 26 2013 245 PMTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes(RayCopesoahppca)Subject Community Water Fluoridation Under Challenge Again in Simcoe Muskoka Hello Colleagues You may wish to know that community water fluoridation (CWF) is again under challenge in SimcoeMuskoka specifically both in Tottenham (Town of New Tecumseth in Simcoe County) and for theentire District of Muskoka On Monday September 23 Committee of the Whole Council of theTown of New Tecumseth voted to submit application to discontinue community water fluoridation(CWF) in the town of Tottenham despite presentations to the contrary from our dental consultantDr Ito and from me The next Council meeting is scheduled for Monday Sept 30 at which lastMondayrsquos (Sept 23) votes will be ratified
Since Monday I have spoken with the Mayor of the Town of New Tecumseth and with most of thecouncilors encouraging deferral of a decision on Monday to allow the town more time to make afully informed decision
This is the second time in recent years that the issue of discontinuing CWF in Tottenham has beenraised at council This issue is also scheduled to return again to the District of Muskoka Council on
October 21st where I will be presenting in response to deputations in opposition to fluoridation
Outside of Base Borden Tottenham is the only community with fluoridated water in SimcoeCounty The health unitrsquos own screening data between 2011 and 2013 shows that Tottenhamrsquos
Gordon
Highlight
children as well as those in Muskoka have a lower rate of dental decay than Simcoe Muskokacommunities without CWF
Sincerely
Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorgChuck Gardner MOH
November 04 2013
Mandatory State Laws on Fluoridation Thirteen states Puerto Rico and the District of Columbia have laws intended to provide
statewide fluoridation These states and the year that the fluoridation legislation was passed are
District of Columbia (1952) Connecticut (1965) Kentucky (1966) Illinois (1967) Minnesota
(1967) Ohio (1969) South Dakota (1969) Georgia (1973) Nebraska (1973 and 2008)
California (1995) Delaware (1998) Puerto Rico (1998) Nevada (1999) Louisiana (2008) and
Arkansas (2011) (see Table 1) The sizes of the public water systems or countiescommunities
affected and exemption provisions vary by state Table 1
STATES THAT HAVE MANDATORY LAWS ON FLUORIDATION -2011
State (1) Year of
Fluoridation
Legislation (1)
Population
served by
Fluoridated
CWS (2)
Persons
receiving
fluoridated
water (2)
State
Average
Caries
Experience
of Grade 3
Students (3)
Arkansas 2011 647 1724131 64
California 1995 621 22812721 709
Connecticut 1965 910 2370423 406
Delaware 1998 862 705344 545
Georgia 1973 921 8924598 52
Illinois 1967 993 11325132 532
Kentucky 1966 999 4334223 598
Louisiana 2008 407 1846149 657
Minnesota 1967 988 4117266 549
Nebraska 1973 and 2008 702 1001665 593
Nevada 1999 702 1001665 649
Ohio 1969 877 8772683 512
South Dakota 1969 948 642942 623
District of
Columbia
1952 1000 595000
Puerto Rico 1998
United States 739 204283554
2010 Statistics for population fluoridated and number of people
1 Communication with Jane McGinley RDH MBA Manager Fluoridation and Preventive Health
Activities Council on Access Prevention and Interprofessional Relations
2 Centers for Disease Control and Prevention Department of Health and Human Services
accessed Oct 21 2013 httpwwwcdcgovfluoridationstatistics2010statshtm
3 Centers for Disease Control and Prevention National Oral Health Surveillance System Caries
Experience - Percentage of 3rd Grade students with Caries Experience (treated or untreated tooth
If data from 43 states for the percentage of Grade 3 children with experience of dental decay is
compared with the 2008 percentages of the population in a state with Community Water
Fluoridation then the percentage of children with experience of dental decay decreases as the
percentage of the state population with Community Water Fluoridation increases (see Figure 1)
Figure 1
Correlation of Percentage of Grade 3 Children with Caries Experience and
Percentage of Population With Community Water Fluoridation for 43
Reporting States
0
10
20
30
40
50
60
70
80
0 10 20 30 40 50 60 70 80 90 100
State of Population With Community Water Fluoridation
Sta
te
of
Gra
de 3
Stu
den
ts w
ith
Cari
es E
xp
eri
en
ce
Data from CDC (2 3)
The description of the fluoridation laws in California Illinois and Nevada can be found on the
Association of State amp Territorial Dental Directors website(4 7 8)
The California fluoridation law AB 733 came into effect in 1995 requiring communities of 10
000 residents or more be supplied with fluoridated drinking water However the state did not
provide any funding to implement the legislation (California is unique in requiring fluoridation
without funding the practice)(4) The California Department of Health Services therefore had to
fund fluoridation initiatives from non-governmental sources ie the California Endowment
California Dental Association Foundation the First 5 Commission and others(5) From 1995 to
2011 the percentage of the California population receiving fluoridated drinking water has risen
from 17 to 625(6) 4 Dental Public Health Activities amp Practices Office of Oral Health California Department of Health
Services April 2002 httpwwwastddorgbestpracticesDES06002CAfluoridationpdf
5 Stock M Pollick H The CDA Foundation Model to Fluoridate Communities California Dental
Association Journal vol 40 no 8 649 - 655
httpwwwcdaorgPortals0journaljournal_082012pdf
6 California Dental Association Foundation
httpwwwcdafoundationorglearnadvocacyfluoridation
The State of Illinois passed a mandatory fluoridation state in 1967 and required all community
water systems to adjust fluoride levels in the drinking water to optimal levels within 1 year(7)
From 1962 when over 5000000 residents had optimally fluoridated drinking water by 2010
the number had risen to 11325132 (993 of the population on community water systems)(2)
7 Dental Public Health Activities amp Practices Division of Oral Health Illinois Department of Public
Health April 2002 httpwwwastddorgbestpracticesDES16007ILfluoridationpdf
The State of Nevada passed a mandatory fluoridation statute in 2000 for communities with
400000 or more residents(8) This was a result of the work of a statewide coalition that
included the Nevada Dental and Dental Hygienist Associations the Washoe and Clark County
District Health Departments the Clark County School District Junior League of Las Vegas
Head Start the Community College of Southern Nevada Dental Hygiene Program Health
Access Washoe County and Saint Maryrsquos Hospital For communities with less than 400000 the
implementation of fluoridation still required the vote of the majority voters in the community
The Las Vegas Water Authority and the City of Henderson started fluoridation in 2000
increasing the percentage of the population with fluoridated drinking water from 2 to 65 (8) 8 Dental Public Health Activities amp Practices Bureau of Family Health Services Nevada State Health
Division April 2002 httpwwwastddorgbestpracticesDES31002NVfluoridationbillpdf
Countries with Mandatory Laws on Fluoridation Countries that have mandated Community Water Fluoridation are Brazil Hong Kong
Malaysia Singapore Ireland Israel and some of the states in Australia
Singapore started fluoridating its water in 1956 based on the success of the fluoridation trials in
Grand Rapids Newburgh Evanston and Brantford Singapore became the first Asian country to
have 100 of its population benefitting from the implementation of fluoridated drinking water
Loh reported that ldquoThe ten year study on the effects of water fluoridation in Singapore showed
a decrease in caries prevalence in the children In the permanent dentition the reduction was
523 per cent for Chinese and 31 per cent for Malays in the 7 to 9 year old age group A similar
trend was observed in the mixed dentition in which the decrease was 325 per cent for Chinese
and 306 per cent for Malaysrdquo(9) By 2010 the population of the country was 5080000(10)
9 Loh T Thirty-eight years of water fluoridation--the Singapore scenario Community Dent
Health 1996 Sep13 Suppl 247-50
10 British Fluoridation Society One in a Million the facts about water fluoridation 3rd Edition
published March 2012) httpwwwbfsweborgonemillion0920One20in20a20Million20-
20The20Extent20of20Fluoridationpdf
Hong Kong started implementing community water fluoridation in 1961 and similar to
Singapore 100 of the population received access to fluoridated drinking water Lo and Wong
reported that ldquoThe mean DMFT score of the children deceased from 44 in 1960 to 15 in 1968
stayed at this level in the 1980 and 1986 surveys and further deceased to 08 in 2001 The
prevalence of dental fluorosis among the children surveyed in 1960 was 1 and this increased
to 59 and 70 in 1968 and 1980 respectively It was found in the 1986 and 2001 surveys that
the prevalences of fluorosis were 47 and 9 among children whose teeth developed at the
time when the respective water fluoride concentrations were 07 ppm and 05 ppmrdquo(11) The
population of Hong Kong was 6968000 in 2009(10) 11 LO ECM and WONG AHH Water fluoride concentration and fluorosis in Hong Kong in 1960-
2001 84th General Session and Exhibition of the International Association for Dental Research amp
1st Meeting of the Pan-Asian-Pacific Federation Brisbane Australia 28 June-1 July 2006 v 85 n
Sp B
The Malaysian cabinet approved a nationwide community water fluoridation program in 1972
(12) One of the states Sabah decided to stop fluoridation in 1989 due to concerns about
inadequate supervision in adding fluoride to the drinking water Oral Health Surveys in 2009
and 2007 indicated that children in Sabah had the worst oral health with 50 of 12 year-olds
having decay in their permanent teeth and children having an average of 3 teeth being(13)
Under the 10th Malaysian Plan in 2011 the federal and the Sabah state governments
reintroduced water fluoridation in Sabah(1314) In 2010 about 755 of the Malaysian
population or 20700000 people had fluoridated drinking water(1013) 12 Malaysian Dental Association Fluoride in Water
httpwwwmdaorgmy07_public_01healthcare_12htm
13 Sachdev N Fluoridation in Sabah Water for Cleaner Teeth French Tribunecom 28022011
From Levy IsraTo Jaeger ValerieCc Pim Carolyn gordonalphaweborg Diallo Aicha Penny Sutcliffe Paul Roumeliotis Michael Finkelstein
Hazel Lynn Robert KyleSubject FW Panorama - Privacy Security and other issuesDate Wednesday October 16 2013 122110 PM
Hello ValerieOttawa is part of Wave 4 Panorama implementation and we are gearing up increasingly to use thesystem where and if possible Thinking about it I am anticipating that this may need to be on theCOMOH (and alPHa) radar as it is something that will impact all health units and implies a majoroperational shift in vaccine delivery programs for all health units I have asked Carolyn Pim toconnect with our sister wave 4 units to share common experiences as we move forward ndash when wehave a roll up could I bring to COMOH Exec for discussion to explore whether there are broaderimplications for all members As an aside I have also asked the Ministry and their CIO to share with me any roll up learnings thatthey may have had already from previous waves (I understand that Niagara HU was a wave 1participant so if there is such a roll up of common experiences that others could learn fromperhaps you have it already and that could come to the exec too)Thanks Isra From Pim Carolyn Sent October 10 2013 1228 PMTo Christopher Mackie (christophermackiemlhuonca) Elizabeth Richardson(Elizabethrichardsonhamiltonca) H BSc M D F R C P (C) MPH Jim Chirico(jimchiriconbpsdhuca) Marlene Spruyt (spruytmtimiskaminghucom) Robert Kyle (Durham)Cc Levy IsraSubject Panorama - Privacy Security and other issues Dear colleagues Irsquom reaching out to you as fellow Panorama Wave 4 health units to ask about where yourorganizations are at in the process of signing agreements and completing Privacy ImpactAssessments and Threat Risk Assessments (TRAs) Ottawa Public Healthrsquos IT legal and informationsecurity advisors have made numerous requests to the MOHLTC for information (in particular theprovincial TRA) that we consider essential to develop our own risk assessment and PIA but havebeen told that information cannot be shared even with strict confidentiality and access controlsSo we are at somewhat of an impasse Isra emailed Arlene yesterday Arlene has forwarded ourconcerns to the Ministryrsquos CIO and Panorama lead but we havenrsquot had any response or discussionswith either of them yet Have your organizations identified similar concerns andor had interactions with the MOHLTC inthis respect Irsquod also be interested in knowing if your health units have flagged other (egoperational) implementation concerns Thanks
Carolyn ps Robert ndash you can ignore this request I talked with Sharan this morning about Durhamrsquos issuesso am including you now just for information Carolyn Pim MD FRCPC Associate Medical Officer of Health Meacutedecin adjointe en santeacute publique Ottawa Public Health Santeacute publique Ottawa 100 Constellation Cr Ottawa ON K2G 6J8 Tel teacutel (613) 580-6744 ext 23684Fax (613) 580-9641Connect With Ottawa Public Health
Suivez Santeacute publique Ottawa
This e-mail originates from the City of Ottawa e-mail system Any distribution use orcopying of this e-mail or the information it contains by other than the intendedrecipient(s) is unauthorized If you are not the intended recipient please notify meat the telephone number shown above or by return e-mail and delete thiscommunication and any copy immediately Thank you
Le preacutesent courriel a eacuteteacute expeacutedieacute par le systegraveme de courriels de la Ville dOttawaToute distribution utilisation ou reproduction du courriel ou des renseignements quisy trouvent par une personne autre que son destinataire preacutevu est interdite Si vousavez reccedilu le message par erreur veuillez men aviser par teacuteleacutephone (au numeacuteropreacuteciteacute) ou par courriel puis supprimer sans deacutelai la version originale de lacommunication ainsi que toutes ses copies Je vous remercie de votre collaboration
1
Smoke-Free Patios ndash An Amendment to the Smoke-Free Ontario Act
Date November 15 2013 Prepared for Council of Ontario Medical Officers of Health Prepared by York Region Public Health _____________________________________________________________________________ Issue
The Smoke-Free Ontario Act is the current provincial legislation that imposes smoking restrictions in workplaces and public places It prohibits smoking on restaurant and bar patios in instances where any portion of the seating area is covered by a roof With recent studies illustrating that exposure to second hand smoke outdoors poses similar risks to indoor exposure there has been growing public support to enhance smoking restrictions and make patios completely smoke-free
Background
With the implementation of the Smoke-Free Ontario Act in 2006 restaurant and bar patios became subject to smoking restrictions if any portion of the seating area was covered by a roof This allowed for patios without roof coverings to continue to allow smoking and as a result did not provide significant protection to patrons or staff from exposure to second hand smoke outdoors Many businesses chose to alter the design of their patios to allow smoking to continue In some cases patios became more crowded since smoking patrons who dine indoors often proceed outside onto licensed patios with their beverages to smoke York Region like most municipalities in Ontario is host to hundreds of patios being operated by restaurant owners and businesses With smoking prohibitions affecting only a small portion of these patios specifically ones with coverings the vast majority of patios still allow smoking to take place Patrons and employees on patios where smoking is not restricted are exposed to second hand smoke frequently This can contribute to increased disease and aggravation of existing health conditions From a business perspective the existing legislation has been viewed by many operators as unfair because some patios have permanent coverings which cannot be removed requiring a smoke-free status These business owners feel this creates an uneven playing field since they cannot provide an outdoor dining area for their smoking customers There is strong community support for smoke-free patios in Ontario A 2009 Rapid Risk Factor Surveillance System survey revealed 754 percent support in York Region while a Toronto Health Survey in 2011 indicated 74 percent public support
2
Current Status
Smoking is currently prohibited on restaurant and bar patios province-wide in four Canadian provinces and territories Alberta Newfoundland and Labrador Nova Scotia and Yukon A fifth province Prince Edward Island prohibits smoking on patios until 10 pm Since Ontario enacted legislation restricting smoking on patios in 2006 eight municipalities in Ontario have chosen to create bylaws that go beyond the Smoke-Free Ontario Act and enhance outdoor protection from second hand smoke by prohibiting smoking on patios completely The largest of those municipalities is the City of Ottawa Recently the Toronto Board of Health unanimously endorsed a report presented by their Medical Officer of Health recommending that restaurant and bar patios be made smoke-free through an amendment to the Smoke-Free Ontario Act
Key Considerations
There should be no significant financial burden to local Boards of Health resulting from a smoke-free patio amendment to the Smoke-Free Ontario Act Inspection and enforcement for the Smoke-Free Ontario Act is currently 100 percent funded by the Ministry of Health and Long-Term Care Following an introductory period of education on the amendment a complaint response model of service delivery would ensure ongoing compliance with smoke-free requirements A complete ban of smoking on patios would eliminate the widely-held perception by business owners that the current legislation creates an uneven playing field for business Since Smoke-Free Ontario Act inspections of patios began in 2006 operators have expressed the opinion that if patios need to be smoke-free for the protection of the public they should all be smoke-free to avoid undue hardship for individual businesses and to provide protection uniformly across the Province
Next steps
York Region Public Health intends to seek support from Medical Officers of Health across the Central East Tobacco Control Area Network (CETCAN) to advocate to the Ministry of Health and Long-Term Care for an amendment to the Smoke-Free Ontario Act prohibiting smoking on all restaurant and bar patios York Region is also in the process of requesting that its Regional Council advocate to the Minister of Health and Long-Term Care on the issue
Updating and Modernizing O Regulation 565 (Public Pools)
Date November 15 2013
Prepared for Council of Ontario Medical Officers of Health
Prepared by York Region Public Health _____________________________________________________________________________ Background Recent drownings at public pools in Ontario have highlighted the issue of water-borne illness and injury The current pool regulation under Ontariorsquos Health Protection and Promotion Act O Regulation 565 (Public Pools) is outdated It does not accurately reflect new pool technology and design or the changing use of public pools Neither does it incorporate admissions standards recommended by the Office of the Chief Coroner Further O Regulation 565 does not have short-form wording or set fines associated with it This limits public health enforcement capabilities What is the impact Updating O Regulation 565 (Public Pools) to address recent changes in pool technology design and uses and to include Coroner-recommended admissions standards would help improve pool safety Establishing short-form wording for O Regulation 565 would enhance enforcement related to public pools Currently the only enforcement available to Public Health Inspectors for dealing with non-critical regulatory infractions in public pools is the issuance of a Part III summons This involves a considerable amount of resources for a possible small fine With the development of inspection disclosure systems such as YorkSafe there is an even greater need to develop a method to effectively address repeated pool operator non-compliance with non-critical issues Next steps Public health units should advocate to the Province to 1) Conduct a review of O Regulation 565 (Public Pools) to address shortcomings Proposed changes to the
regulation should include a requirement for ownersoperators of public pools to advise the local Medical Officer of Health of any change in the use of a facility and the addition of the Coronerrsquos recommended admission standards
2) Provide short-form wording for O Regulation 565 so that public health inspectors can better deal with pool operator non-compliance
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
8 Council of Ontario Medical Officers of Health Terms of Reference
bull May represent alPHa COMOH on selected external committees and working groups subject to the approval of the COMOH or alPHa Executive Committee as appropriate
9 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX B
Planning Cycle to Identify Priorities for COMOH
1 There shall normally be a COMOH membership strategic planning retreat every four years In recognition of the dynamic environment of public health the need for and timing of such a retreat shall be at the discretion of the Executive Committee in consultation with the membership
2 The COMOH Executive is responsible (through the creation of a subcommittee of COMOH members) for ensuring the preparation for the COMOH retreats with resources to include those provided by alPHa
3 Leadership for action on COMOH priorities will be recruited from among the COMOH membership in order to make good use of the full base of capacity of the membership The resources to support actions will be recruited from both within and beyond the COMOH membership employing other public health professionals that reside within the broader public health system and community
4 The COMOH Executive shall ensure an annual review of strategic priorities and initiatives and the development of a draft report of the same for the review of the members at the June meeting
2013 Strategic Planning
Considerations for COMOH
As part of its strategic planning discussions alPHarsquos Board has been considering changes to the level of support provided to member sections A member survey is being carried out over the fall to determine options acceptable to alPHa members The following approach to support is put forward as a proposal for the consideration of COMOH Note that the feasibility of the points below depend upon future decisions of the alPHa board They assume that COMOH remains part of alPHa but becomes more independent in administering meetings
1 alPHa can provide to COMOH staff support (Gord Fleming) amounting to 02 FTE or one day per week This is a reduction from the current level of 35 days per week COMOH can choose to use the support any way it wants writing COMOH letters meeting minutes agenda support special projects etc
2 In addition to 02 FTE alPHa staff would provide support for up to 4 face-to-face meetings per year One meeting would be concurrent to alPHarsquos annual conference in June The timing of other meetings could be negotiated The support includes consulting on the development of the program arranging for speakers registration for the event arranging venue AV support and hospitality services
3 In addition to 02 FTE alPHa staff would provide support for setting meeting dates and any polling required to establish dates Note that the individual supporting this function would be Karen Reece
4 COMOHrsquos Executive and Section would continue to have access to online supports through the alPHa including the COMOH Listserve and a group page for posting agendas minutes and other resources on the alPHa website
5 alPHa staff (Linda Stewart and Gord Fleming) can also start participating on CMOH calls as a way to be up-to-date on issues related to COMOH
6 Other than what is outlined above COMOH would be expected to prepare agendas and take minutes for its Executive and Section meetings The Executive would be expected to operate more independently than it does now but would be able to access the supports outlined above
Prepared by Linda Stewart Executive Director
From comoh-bounceslistsalphaweborg on behalf of Christopher MackieTo MOH ListserveSubject [comoh] Fw URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)Date Wednesday October 30 2013 91241 AMAttachments ATT00249txt
For AMOHs and PHPM residents who didnt receive the initial email
Chris
Christopher Mackie MD MHSc FRCPCMedical Officer of Health and CEOMiddlesex-London Health Unit50 King St LondonON N6A 5L7 O 519 663 5317 ext 2444 wwwhealthunitcomFrom Pisko Laura (MOHLTC)Sent Tuesday October 29 2013 759 PMTo kbarkeralgomapublichealthcom malcolmlockbchuorg davidcchatham-kentcarobertkyledurhamca proumeliotiseohuca fwarshelginhealthonca mohelginhealthoncahlynnpublichealthgreybruceonca malcolmlockhnhuorg hnmohhnhuorglnoseworthyhkpronca bobnosalhaltonca elizabethrichardsonhamiltoncarschabashpechuonca ncameronhuroncountyca drimgemmillkflapublichealthcamohkflapublichealthca suditranadecounty-lambtononca paulastewarthealthunitorgChristopher Mackie valeriejaegerniagararegionca jimchiriconbpsdhuca jarthursnwhuoncaisralevyottawaca dnealoxfordcountyca davidmowatpeelregionca mklassenpdhuoncarpellizzaripcchuca rosemarieramsinghporcupinehuonca mcorriveaurcdhucomcharlesgardnersmdhuorg sutcliffepsdhucom davidwilliamstbdhucomspruytmtimiskaminghucom dmckeowntorontoca lnolanregionofwaterloocanicolamercerwdghuorg aheimannwechealthunitorg karimkurjiyorkcaCc coreywesleytbdhucom CindyBaker-Barillsmdhuorg Donna Kosmack pilonlsdhucomPaulaMuiskflapublichealthca sthibautorontoca Mueller Daina (MOHLTC) Gordon Marcus(MOHLTC) andreakitahamiltoncaSubject URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)
Dear Colleagues The ministry has received reports that some tobacco vendors across the province aregiving away single cigarettes with the purchase of tobacco products It is the ministryrsquosposition that giving out free single cigarettes does not violate subsection 31(3) of theSmoke-Free Ontario Act (ldquoSFOArdquo) Although the practice of giving out free singlecigarettes may promote the sale of tobacco products it does not take the form of aldquoproduct enhancement product association or promotional materialrdquo and therefore doesnot fall within the scope of subsection 31(3) of the SFOA We have confirmed with Health Canada that this practice may violate section 29(b) of thefederal Tobacco Act As such Health Canada is requesting that you notify them in writingand I am directing you to communicate with them via email and provide to them as manydetails as possible Emails should be sent to Tobacco-Ontariohc-scgcca and thesubject line should read ldquoViolation of Section 29(b) of Tobacco Actrdquo This will ensurethat the complaints are given priority status by Health Canada We will continue to monitor
this situation and liaise with our colleagues at Health Canada Please share this information with your tobacco control staff and contact me or DainaMueller Manager Tobacco Control Unit Health Promotion Implementation Branch atdainamuellerontarioca with any questions RegardsLaura Laura A PiskoDirectorHealth Promotion Implementation BranchHealth Promotion DivisionMinistry of Health and Long Term Care416-327-7445 (office)416-451-3185 (mobile) Marcus Gordon - EA (416)326-0625 for urgent issues
========= Middlesex-London Health Unit E-Mail Disclaimer =============______________________________________________________________
Private and confidential intended only for named recipient If otherwisereceived please destroy immediately Health information in this email isonly general information and is not intended to replace an in personconsultation with a medical professional nor is it intended to providemedical advice Individual circumstances of which we are not aware mayaffect the information provided herein and as such the Middlesex-LondonHealth Unit assumes no liability or responsibility for your reliancethereon The Middlesex-London Health Unit works under the authority of theHealth Protection and Promotion Act and this correspondence may be used toassess your needs for public health services (519-663-5317 ext 2448)______________________________________________________________
From Gardner CharlesTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes (RayCopesoahppca)
George Pasut (GeorgePasutoahppca) Peter Cooney (petercooneyhc-scgcca)Cc Ito DickSubject Discontinuation of Fluoridation in MuskokaDate Tuesday October 22 2013 125254 PM
Hello Colleagues
As I reported in my email below on September 26th fluoridation has come under challenge again inSimcoe Muskoka I am now very unhappy to report that despite our best efforts last night theDistrict Council of Muskoka voted to remove fluoride from municipal drinking supplies across theDistrict This brings to an end fluoridation in all of Simcoe and Muskoka (with the exception of Base Borden)ndash though New Tecumseth will be conducting a plebiscite on the question of fluoridation with themunicipal election next October Defending community water fluoridation has drained a great deal of time human resources andcommitment from other priorities and has been exhausting here in SMDHU as I am sure it hasbeen in many other health units While the outcomes have been very disappointing I have beenimpressed by the professionalism and dedication that SMDHU staff members have shown inshouldering this burden In particular our dental consultant Dr Ito has provided us with much ofthe foundational knowledge and the local research essential to our efforts and has very frequentlyattended and presented at council meetings and other public events I would also like to thank themany of you who have offer and provided support including advocacy letters and informationresources Over the years Dr Peter Cooney Chief Dental Officer of Health of Canada has beenvery helpful attending and presenting with us at council meetings and at public consultationevents We will of course continue our oral health surveillance of the children of Muskoka documentingand reporting in future years on the increase in dental decay that we anticipate will occur Suchsurveillance is the foundation of our advocacy both to municipal politicians and to the province I am very concerned that our experience will continue to repeat itself across the province unlessthere is strong leadership provincially It is with this in mind that I raise the followingrecommendations for your consideration
1 That we collectively (with PHOrsquos leadership) conduct high quality publish-worthy researchdocumenting the impact on dental decay that occurs in those municipalities throughoutOntario that in recent years have discontinued community water fluoridation This could bepart of a larger study on such municipalities across the country and it could also be part ofa study documenting overall oral health (including fluoridation coverage) in the province(and possibly across the country)
2 That COMOH engage with our Chief MOH to advocate for the province to require allmunicipal water supplies to be fluoridated (the exception of course being those withnaturally sufficient fluoride concentrations) This could built upon the alPHa position to
Gordon
Highlight
Gordon
Highlight
date (A11-00 - Community Water Fluoridation) on the CMOH position (Oral Health ndash) and on theemail discussion generated on the COMOH listserv some months back re Richardrsquosproposal (calling on the province to fund municipal water fluoridation)
Valerie I request that this be an item for our COMOH meeting on November 15th Sincerely Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorg From Gardner Charles Sent Thursday September 26 2013 245 PMTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes(RayCopesoahppca)Subject Community Water Fluoridation Under Challenge Again in Simcoe Muskoka Hello Colleagues You may wish to know that community water fluoridation (CWF) is again under challenge in SimcoeMuskoka specifically both in Tottenham (Town of New Tecumseth in Simcoe County) and for theentire District of Muskoka On Monday September 23 Committee of the Whole Council of theTown of New Tecumseth voted to submit application to discontinue community water fluoridation(CWF) in the town of Tottenham despite presentations to the contrary from our dental consultantDr Ito and from me The next Council meeting is scheduled for Monday Sept 30 at which lastMondayrsquos (Sept 23) votes will be ratified
Since Monday I have spoken with the Mayor of the Town of New Tecumseth and with most of thecouncilors encouraging deferral of a decision on Monday to allow the town more time to make afully informed decision
This is the second time in recent years that the issue of discontinuing CWF in Tottenham has beenraised at council This issue is also scheduled to return again to the District of Muskoka Council on
October 21st where I will be presenting in response to deputations in opposition to fluoridation
Outside of Base Borden Tottenham is the only community with fluoridated water in SimcoeCounty The health unitrsquos own screening data between 2011 and 2013 shows that Tottenhamrsquos
Gordon
Highlight
children as well as those in Muskoka have a lower rate of dental decay than Simcoe Muskokacommunities without CWF
Sincerely
Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorgChuck Gardner MOH
November 04 2013
Mandatory State Laws on Fluoridation Thirteen states Puerto Rico and the District of Columbia have laws intended to provide
statewide fluoridation These states and the year that the fluoridation legislation was passed are
District of Columbia (1952) Connecticut (1965) Kentucky (1966) Illinois (1967) Minnesota
(1967) Ohio (1969) South Dakota (1969) Georgia (1973) Nebraska (1973 and 2008)
California (1995) Delaware (1998) Puerto Rico (1998) Nevada (1999) Louisiana (2008) and
Arkansas (2011) (see Table 1) The sizes of the public water systems or countiescommunities
affected and exemption provisions vary by state Table 1
STATES THAT HAVE MANDATORY LAWS ON FLUORIDATION -2011
State (1) Year of
Fluoridation
Legislation (1)
Population
served by
Fluoridated
CWS (2)
Persons
receiving
fluoridated
water (2)
State
Average
Caries
Experience
of Grade 3
Students (3)
Arkansas 2011 647 1724131 64
California 1995 621 22812721 709
Connecticut 1965 910 2370423 406
Delaware 1998 862 705344 545
Georgia 1973 921 8924598 52
Illinois 1967 993 11325132 532
Kentucky 1966 999 4334223 598
Louisiana 2008 407 1846149 657
Minnesota 1967 988 4117266 549
Nebraska 1973 and 2008 702 1001665 593
Nevada 1999 702 1001665 649
Ohio 1969 877 8772683 512
South Dakota 1969 948 642942 623
District of
Columbia
1952 1000 595000
Puerto Rico 1998
United States 739 204283554
2010 Statistics for population fluoridated and number of people
1 Communication with Jane McGinley RDH MBA Manager Fluoridation and Preventive Health
Activities Council on Access Prevention and Interprofessional Relations
2 Centers for Disease Control and Prevention Department of Health and Human Services
accessed Oct 21 2013 httpwwwcdcgovfluoridationstatistics2010statshtm
3 Centers for Disease Control and Prevention National Oral Health Surveillance System Caries
Experience - Percentage of 3rd Grade students with Caries Experience (treated or untreated tooth
If data from 43 states for the percentage of Grade 3 children with experience of dental decay is
compared with the 2008 percentages of the population in a state with Community Water
Fluoridation then the percentage of children with experience of dental decay decreases as the
percentage of the state population with Community Water Fluoridation increases (see Figure 1)
Figure 1
Correlation of Percentage of Grade 3 Children with Caries Experience and
Percentage of Population With Community Water Fluoridation for 43
Reporting States
0
10
20
30
40
50
60
70
80
0 10 20 30 40 50 60 70 80 90 100
State of Population With Community Water Fluoridation
Sta
te
of
Gra
de 3
Stu
den
ts w
ith
Cari
es E
xp
eri
en
ce
Data from CDC (2 3)
The description of the fluoridation laws in California Illinois and Nevada can be found on the
Association of State amp Territorial Dental Directors website(4 7 8)
The California fluoridation law AB 733 came into effect in 1995 requiring communities of 10
000 residents or more be supplied with fluoridated drinking water However the state did not
provide any funding to implement the legislation (California is unique in requiring fluoridation
without funding the practice)(4) The California Department of Health Services therefore had to
fund fluoridation initiatives from non-governmental sources ie the California Endowment
California Dental Association Foundation the First 5 Commission and others(5) From 1995 to
2011 the percentage of the California population receiving fluoridated drinking water has risen
from 17 to 625(6) 4 Dental Public Health Activities amp Practices Office of Oral Health California Department of Health
Services April 2002 httpwwwastddorgbestpracticesDES06002CAfluoridationpdf
5 Stock M Pollick H The CDA Foundation Model to Fluoridate Communities California Dental
Association Journal vol 40 no 8 649 - 655
httpwwwcdaorgPortals0journaljournal_082012pdf
6 California Dental Association Foundation
httpwwwcdafoundationorglearnadvocacyfluoridation
The State of Illinois passed a mandatory fluoridation state in 1967 and required all community
water systems to adjust fluoride levels in the drinking water to optimal levels within 1 year(7)
From 1962 when over 5000000 residents had optimally fluoridated drinking water by 2010
the number had risen to 11325132 (993 of the population on community water systems)(2)
7 Dental Public Health Activities amp Practices Division of Oral Health Illinois Department of Public
Health April 2002 httpwwwastddorgbestpracticesDES16007ILfluoridationpdf
The State of Nevada passed a mandatory fluoridation statute in 2000 for communities with
400000 or more residents(8) This was a result of the work of a statewide coalition that
included the Nevada Dental and Dental Hygienist Associations the Washoe and Clark County
District Health Departments the Clark County School District Junior League of Las Vegas
Head Start the Community College of Southern Nevada Dental Hygiene Program Health
Access Washoe County and Saint Maryrsquos Hospital For communities with less than 400000 the
implementation of fluoridation still required the vote of the majority voters in the community
The Las Vegas Water Authority and the City of Henderson started fluoridation in 2000
increasing the percentage of the population with fluoridated drinking water from 2 to 65 (8) 8 Dental Public Health Activities amp Practices Bureau of Family Health Services Nevada State Health
Division April 2002 httpwwwastddorgbestpracticesDES31002NVfluoridationbillpdf
Countries with Mandatory Laws on Fluoridation Countries that have mandated Community Water Fluoridation are Brazil Hong Kong
Malaysia Singapore Ireland Israel and some of the states in Australia
Singapore started fluoridating its water in 1956 based on the success of the fluoridation trials in
Grand Rapids Newburgh Evanston and Brantford Singapore became the first Asian country to
have 100 of its population benefitting from the implementation of fluoridated drinking water
Loh reported that ldquoThe ten year study on the effects of water fluoridation in Singapore showed
a decrease in caries prevalence in the children In the permanent dentition the reduction was
523 per cent for Chinese and 31 per cent for Malays in the 7 to 9 year old age group A similar
trend was observed in the mixed dentition in which the decrease was 325 per cent for Chinese
and 306 per cent for Malaysrdquo(9) By 2010 the population of the country was 5080000(10)
9 Loh T Thirty-eight years of water fluoridation--the Singapore scenario Community Dent
Health 1996 Sep13 Suppl 247-50
10 British Fluoridation Society One in a Million the facts about water fluoridation 3rd Edition
published March 2012) httpwwwbfsweborgonemillion0920One20in20a20Million20-
20The20Extent20of20Fluoridationpdf
Hong Kong started implementing community water fluoridation in 1961 and similar to
Singapore 100 of the population received access to fluoridated drinking water Lo and Wong
reported that ldquoThe mean DMFT score of the children deceased from 44 in 1960 to 15 in 1968
stayed at this level in the 1980 and 1986 surveys and further deceased to 08 in 2001 The
prevalence of dental fluorosis among the children surveyed in 1960 was 1 and this increased
to 59 and 70 in 1968 and 1980 respectively It was found in the 1986 and 2001 surveys that
the prevalences of fluorosis were 47 and 9 among children whose teeth developed at the
time when the respective water fluoride concentrations were 07 ppm and 05 ppmrdquo(11) The
population of Hong Kong was 6968000 in 2009(10) 11 LO ECM and WONG AHH Water fluoride concentration and fluorosis in Hong Kong in 1960-
2001 84th General Session and Exhibition of the International Association for Dental Research amp
1st Meeting of the Pan-Asian-Pacific Federation Brisbane Australia 28 June-1 July 2006 v 85 n
Sp B
The Malaysian cabinet approved a nationwide community water fluoridation program in 1972
(12) One of the states Sabah decided to stop fluoridation in 1989 due to concerns about
inadequate supervision in adding fluoride to the drinking water Oral Health Surveys in 2009
and 2007 indicated that children in Sabah had the worst oral health with 50 of 12 year-olds
having decay in their permanent teeth and children having an average of 3 teeth being(13)
Under the 10th Malaysian Plan in 2011 the federal and the Sabah state governments
reintroduced water fluoridation in Sabah(1314) In 2010 about 755 of the Malaysian
population or 20700000 people had fluoridated drinking water(1013) 12 Malaysian Dental Association Fluoride in Water
httpwwwmdaorgmy07_public_01healthcare_12htm
13 Sachdev N Fluoridation in Sabah Water for Cleaner Teeth French Tribunecom 28022011
From Levy IsraTo Jaeger ValerieCc Pim Carolyn gordonalphaweborg Diallo Aicha Penny Sutcliffe Paul Roumeliotis Michael Finkelstein
Hazel Lynn Robert KyleSubject FW Panorama - Privacy Security and other issuesDate Wednesday October 16 2013 122110 PM
Hello ValerieOttawa is part of Wave 4 Panorama implementation and we are gearing up increasingly to use thesystem where and if possible Thinking about it I am anticipating that this may need to be on theCOMOH (and alPHa) radar as it is something that will impact all health units and implies a majoroperational shift in vaccine delivery programs for all health units I have asked Carolyn Pim toconnect with our sister wave 4 units to share common experiences as we move forward ndash when wehave a roll up could I bring to COMOH Exec for discussion to explore whether there are broaderimplications for all members As an aside I have also asked the Ministry and their CIO to share with me any roll up learnings thatthey may have had already from previous waves (I understand that Niagara HU was a wave 1participant so if there is such a roll up of common experiences that others could learn fromperhaps you have it already and that could come to the exec too)Thanks Isra From Pim Carolyn Sent October 10 2013 1228 PMTo Christopher Mackie (christophermackiemlhuonca) Elizabeth Richardson(Elizabethrichardsonhamiltonca) H BSc M D F R C P (C) MPH Jim Chirico(jimchiriconbpsdhuca) Marlene Spruyt (spruytmtimiskaminghucom) Robert Kyle (Durham)Cc Levy IsraSubject Panorama - Privacy Security and other issues Dear colleagues Irsquom reaching out to you as fellow Panorama Wave 4 health units to ask about where yourorganizations are at in the process of signing agreements and completing Privacy ImpactAssessments and Threat Risk Assessments (TRAs) Ottawa Public Healthrsquos IT legal and informationsecurity advisors have made numerous requests to the MOHLTC for information (in particular theprovincial TRA) that we consider essential to develop our own risk assessment and PIA but havebeen told that information cannot be shared even with strict confidentiality and access controlsSo we are at somewhat of an impasse Isra emailed Arlene yesterday Arlene has forwarded ourconcerns to the Ministryrsquos CIO and Panorama lead but we havenrsquot had any response or discussionswith either of them yet Have your organizations identified similar concerns andor had interactions with the MOHLTC inthis respect Irsquod also be interested in knowing if your health units have flagged other (egoperational) implementation concerns Thanks
Carolyn ps Robert ndash you can ignore this request I talked with Sharan this morning about Durhamrsquos issuesso am including you now just for information Carolyn Pim MD FRCPC Associate Medical Officer of Health Meacutedecin adjointe en santeacute publique Ottawa Public Health Santeacute publique Ottawa 100 Constellation Cr Ottawa ON K2G 6J8 Tel teacutel (613) 580-6744 ext 23684Fax (613) 580-9641Connect With Ottawa Public Health
Suivez Santeacute publique Ottawa
This e-mail originates from the City of Ottawa e-mail system Any distribution use orcopying of this e-mail or the information it contains by other than the intendedrecipient(s) is unauthorized If you are not the intended recipient please notify meat the telephone number shown above or by return e-mail and delete thiscommunication and any copy immediately Thank you
Le preacutesent courriel a eacuteteacute expeacutedieacute par le systegraveme de courriels de la Ville dOttawaToute distribution utilisation ou reproduction du courriel ou des renseignements quisy trouvent par une personne autre que son destinataire preacutevu est interdite Si vousavez reccedilu le message par erreur veuillez men aviser par teacuteleacutephone (au numeacuteropreacuteciteacute) ou par courriel puis supprimer sans deacutelai la version originale de lacommunication ainsi que toutes ses copies Je vous remercie de votre collaboration
1
Smoke-Free Patios ndash An Amendment to the Smoke-Free Ontario Act
Date November 15 2013 Prepared for Council of Ontario Medical Officers of Health Prepared by York Region Public Health _____________________________________________________________________________ Issue
The Smoke-Free Ontario Act is the current provincial legislation that imposes smoking restrictions in workplaces and public places It prohibits smoking on restaurant and bar patios in instances where any portion of the seating area is covered by a roof With recent studies illustrating that exposure to second hand smoke outdoors poses similar risks to indoor exposure there has been growing public support to enhance smoking restrictions and make patios completely smoke-free
Background
With the implementation of the Smoke-Free Ontario Act in 2006 restaurant and bar patios became subject to smoking restrictions if any portion of the seating area was covered by a roof This allowed for patios without roof coverings to continue to allow smoking and as a result did not provide significant protection to patrons or staff from exposure to second hand smoke outdoors Many businesses chose to alter the design of their patios to allow smoking to continue In some cases patios became more crowded since smoking patrons who dine indoors often proceed outside onto licensed patios with their beverages to smoke York Region like most municipalities in Ontario is host to hundreds of patios being operated by restaurant owners and businesses With smoking prohibitions affecting only a small portion of these patios specifically ones with coverings the vast majority of patios still allow smoking to take place Patrons and employees on patios where smoking is not restricted are exposed to second hand smoke frequently This can contribute to increased disease and aggravation of existing health conditions From a business perspective the existing legislation has been viewed by many operators as unfair because some patios have permanent coverings which cannot be removed requiring a smoke-free status These business owners feel this creates an uneven playing field since they cannot provide an outdoor dining area for their smoking customers There is strong community support for smoke-free patios in Ontario A 2009 Rapid Risk Factor Surveillance System survey revealed 754 percent support in York Region while a Toronto Health Survey in 2011 indicated 74 percent public support
2
Current Status
Smoking is currently prohibited on restaurant and bar patios province-wide in four Canadian provinces and territories Alberta Newfoundland and Labrador Nova Scotia and Yukon A fifth province Prince Edward Island prohibits smoking on patios until 10 pm Since Ontario enacted legislation restricting smoking on patios in 2006 eight municipalities in Ontario have chosen to create bylaws that go beyond the Smoke-Free Ontario Act and enhance outdoor protection from second hand smoke by prohibiting smoking on patios completely The largest of those municipalities is the City of Ottawa Recently the Toronto Board of Health unanimously endorsed a report presented by their Medical Officer of Health recommending that restaurant and bar patios be made smoke-free through an amendment to the Smoke-Free Ontario Act
Key Considerations
There should be no significant financial burden to local Boards of Health resulting from a smoke-free patio amendment to the Smoke-Free Ontario Act Inspection and enforcement for the Smoke-Free Ontario Act is currently 100 percent funded by the Ministry of Health and Long-Term Care Following an introductory period of education on the amendment a complaint response model of service delivery would ensure ongoing compliance with smoke-free requirements A complete ban of smoking on patios would eliminate the widely-held perception by business owners that the current legislation creates an uneven playing field for business Since Smoke-Free Ontario Act inspections of patios began in 2006 operators have expressed the opinion that if patios need to be smoke-free for the protection of the public they should all be smoke-free to avoid undue hardship for individual businesses and to provide protection uniformly across the Province
Next steps
York Region Public Health intends to seek support from Medical Officers of Health across the Central East Tobacco Control Area Network (CETCAN) to advocate to the Ministry of Health and Long-Term Care for an amendment to the Smoke-Free Ontario Act prohibiting smoking on all restaurant and bar patios York Region is also in the process of requesting that its Regional Council advocate to the Minister of Health and Long-Term Care on the issue
Updating and Modernizing O Regulation 565 (Public Pools)
Date November 15 2013
Prepared for Council of Ontario Medical Officers of Health
Prepared by York Region Public Health _____________________________________________________________________________ Background Recent drownings at public pools in Ontario have highlighted the issue of water-borne illness and injury The current pool regulation under Ontariorsquos Health Protection and Promotion Act O Regulation 565 (Public Pools) is outdated It does not accurately reflect new pool technology and design or the changing use of public pools Neither does it incorporate admissions standards recommended by the Office of the Chief Coroner Further O Regulation 565 does not have short-form wording or set fines associated with it This limits public health enforcement capabilities What is the impact Updating O Regulation 565 (Public Pools) to address recent changes in pool technology design and uses and to include Coroner-recommended admissions standards would help improve pool safety Establishing short-form wording for O Regulation 565 would enhance enforcement related to public pools Currently the only enforcement available to Public Health Inspectors for dealing with non-critical regulatory infractions in public pools is the issuance of a Part III summons This involves a considerable amount of resources for a possible small fine With the development of inspection disclosure systems such as YorkSafe there is an even greater need to develop a method to effectively address repeated pool operator non-compliance with non-critical issues Next steps Public health units should advocate to the Province to 1) Conduct a review of O Regulation 565 (Public Pools) to address shortcomings Proposed changes to the
regulation should include a requirement for ownersoperators of public pools to advise the local Medical Officer of Health of any change in the use of a facility and the addition of the Coronerrsquos recommended admission standards
2) Provide short-form wording for O Regulation 565 so that public health inspectors can better deal with pool operator non-compliance
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
9 Council of Ontario Medical Officers of Health Terms of Reference
APPENDIX B
Planning Cycle to Identify Priorities for COMOH
1 There shall normally be a COMOH membership strategic planning retreat every four years In recognition of the dynamic environment of public health the need for and timing of such a retreat shall be at the discretion of the Executive Committee in consultation with the membership
2 The COMOH Executive is responsible (through the creation of a subcommittee of COMOH members) for ensuring the preparation for the COMOH retreats with resources to include those provided by alPHa
3 Leadership for action on COMOH priorities will be recruited from among the COMOH membership in order to make good use of the full base of capacity of the membership The resources to support actions will be recruited from both within and beyond the COMOH membership employing other public health professionals that reside within the broader public health system and community
4 The COMOH Executive shall ensure an annual review of strategic priorities and initiatives and the development of a draft report of the same for the review of the members at the June meeting
2013 Strategic Planning
Considerations for COMOH
As part of its strategic planning discussions alPHarsquos Board has been considering changes to the level of support provided to member sections A member survey is being carried out over the fall to determine options acceptable to alPHa members The following approach to support is put forward as a proposal for the consideration of COMOH Note that the feasibility of the points below depend upon future decisions of the alPHa board They assume that COMOH remains part of alPHa but becomes more independent in administering meetings
1 alPHa can provide to COMOH staff support (Gord Fleming) amounting to 02 FTE or one day per week This is a reduction from the current level of 35 days per week COMOH can choose to use the support any way it wants writing COMOH letters meeting minutes agenda support special projects etc
2 In addition to 02 FTE alPHa staff would provide support for up to 4 face-to-face meetings per year One meeting would be concurrent to alPHarsquos annual conference in June The timing of other meetings could be negotiated The support includes consulting on the development of the program arranging for speakers registration for the event arranging venue AV support and hospitality services
3 In addition to 02 FTE alPHa staff would provide support for setting meeting dates and any polling required to establish dates Note that the individual supporting this function would be Karen Reece
4 COMOHrsquos Executive and Section would continue to have access to online supports through the alPHa including the COMOH Listserve and a group page for posting agendas minutes and other resources on the alPHa website
5 alPHa staff (Linda Stewart and Gord Fleming) can also start participating on CMOH calls as a way to be up-to-date on issues related to COMOH
6 Other than what is outlined above COMOH would be expected to prepare agendas and take minutes for its Executive and Section meetings The Executive would be expected to operate more independently than it does now but would be able to access the supports outlined above
Prepared by Linda Stewart Executive Director
From comoh-bounceslistsalphaweborg on behalf of Christopher MackieTo MOH ListserveSubject [comoh] Fw URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)Date Wednesday October 30 2013 91241 AMAttachments ATT00249txt
For AMOHs and PHPM residents who didnt receive the initial email
Chris
Christopher Mackie MD MHSc FRCPCMedical Officer of Health and CEOMiddlesex-London Health Unit50 King St LondonON N6A 5L7 O 519 663 5317 ext 2444 wwwhealthunitcomFrom Pisko Laura (MOHLTC)Sent Tuesday October 29 2013 759 PMTo kbarkeralgomapublichealthcom malcolmlockbchuorg davidcchatham-kentcarobertkyledurhamca proumeliotiseohuca fwarshelginhealthonca mohelginhealthoncahlynnpublichealthgreybruceonca malcolmlockhnhuorg hnmohhnhuorglnoseworthyhkpronca bobnosalhaltonca elizabethrichardsonhamiltoncarschabashpechuonca ncameronhuroncountyca drimgemmillkflapublichealthcamohkflapublichealthca suditranadecounty-lambtononca paulastewarthealthunitorgChristopher Mackie valeriejaegerniagararegionca jimchiriconbpsdhuca jarthursnwhuoncaisralevyottawaca dnealoxfordcountyca davidmowatpeelregionca mklassenpdhuoncarpellizzaripcchuca rosemarieramsinghporcupinehuonca mcorriveaurcdhucomcharlesgardnersmdhuorg sutcliffepsdhucom davidwilliamstbdhucomspruytmtimiskaminghucom dmckeowntorontoca lnolanregionofwaterloocanicolamercerwdghuorg aheimannwechealthunitorg karimkurjiyorkcaCc coreywesleytbdhucom CindyBaker-Barillsmdhuorg Donna Kosmack pilonlsdhucomPaulaMuiskflapublichealthca sthibautorontoca Mueller Daina (MOHLTC) Gordon Marcus(MOHLTC) andreakitahamiltoncaSubject URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)
Dear Colleagues The ministry has received reports that some tobacco vendors across the province aregiving away single cigarettes with the purchase of tobacco products It is the ministryrsquosposition that giving out free single cigarettes does not violate subsection 31(3) of theSmoke-Free Ontario Act (ldquoSFOArdquo) Although the practice of giving out free singlecigarettes may promote the sale of tobacco products it does not take the form of aldquoproduct enhancement product association or promotional materialrdquo and therefore doesnot fall within the scope of subsection 31(3) of the SFOA We have confirmed with Health Canada that this practice may violate section 29(b) of thefederal Tobacco Act As such Health Canada is requesting that you notify them in writingand I am directing you to communicate with them via email and provide to them as manydetails as possible Emails should be sent to Tobacco-Ontariohc-scgcca and thesubject line should read ldquoViolation of Section 29(b) of Tobacco Actrdquo This will ensurethat the complaints are given priority status by Health Canada We will continue to monitor
this situation and liaise with our colleagues at Health Canada Please share this information with your tobacco control staff and contact me or DainaMueller Manager Tobacco Control Unit Health Promotion Implementation Branch atdainamuellerontarioca with any questions RegardsLaura Laura A PiskoDirectorHealth Promotion Implementation BranchHealth Promotion DivisionMinistry of Health and Long Term Care416-327-7445 (office)416-451-3185 (mobile) Marcus Gordon - EA (416)326-0625 for urgent issues
========= Middlesex-London Health Unit E-Mail Disclaimer =============______________________________________________________________
Private and confidential intended only for named recipient If otherwisereceived please destroy immediately Health information in this email isonly general information and is not intended to replace an in personconsultation with a medical professional nor is it intended to providemedical advice Individual circumstances of which we are not aware mayaffect the information provided herein and as such the Middlesex-LondonHealth Unit assumes no liability or responsibility for your reliancethereon The Middlesex-London Health Unit works under the authority of theHealth Protection and Promotion Act and this correspondence may be used toassess your needs for public health services (519-663-5317 ext 2448)______________________________________________________________
From Gardner CharlesTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes (RayCopesoahppca)
George Pasut (GeorgePasutoahppca) Peter Cooney (petercooneyhc-scgcca)Cc Ito DickSubject Discontinuation of Fluoridation in MuskokaDate Tuesday October 22 2013 125254 PM
Hello Colleagues
As I reported in my email below on September 26th fluoridation has come under challenge again inSimcoe Muskoka I am now very unhappy to report that despite our best efforts last night theDistrict Council of Muskoka voted to remove fluoride from municipal drinking supplies across theDistrict This brings to an end fluoridation in all of Simcoe and Muskoka (with the exception of Base Borden)ndash though New Tecumseth will be conducting a plebiscite on the question of fluoridation with themunicipal election next October Defending community water fluoridation has drained a great deal of time human resources andcommitment from other priorities and has been exhausting here in SMDHU as I am sure it hasbeen in many other health units While the outcomes have been very disappointing I have beenimpressed by the professionalism and dedication that SMDHU staff members have shown inshouldering this burden In particular our dental consultant Dr Ito has provided us with much ofthe foundational knowledge and the local research essential to our efforts and has very frequentlyattended and presented at council meetings and other public events I would also like to thank themany of you who have offer and provided support including advocacy letters and informationresources Over the years Dr Peter Cooney Chief Dental Officer of Health of Canada has beenvery helpful attending and presenting with us at council meetings and at public consultationevents We will of course continue our oral health surveillance of the children of Muskoka documentingand reporting in future years on the increase in dental decay that we anticipate will occur Suchsurveillance is the foundation of our advocacy both to municipal politicians and to the province I am very concerned that our experience will continue to repeat itself across the province unlessthere is strong leadership provincially It is with this in mind that I raise the followingrecommendations for your consideration
1 That we collectively (with PHOrsquos leadership) conduct high quality publish-worthy researchdocumenting the impact on dental decay that occurs in those municipalities throughoutOntario that in recent years have discontinued community water fluoridation This could bepart of a larger study on such municipalities across the country and it could also be part ofa study documenting overall oral health (including fluoridation coverage) in the province(and possibly across the country)
2 That COMOH engage with our Chief MOH to advocate for the province to require allmunicipal water supplies to be fluoridated (the exception of course being those withnaturally sufficient fluoride concentrations) This could built upon the alPHa position to
Gordon
Highlight
Gordon
Highlight
date (A11-00 - Community Water Fluoridation) on the CMOH position (Oral Health ndash) and on theemail discussion generated on the COMOH listserv some months back re Richardrsquosproposal (calling on the province to fund municipal water fluoridation)
Valerie I request that this be an item for our COMOH meeting on November 15th Sincerely Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorg From Gardner Charles Sent Thursday September 26 2013 245 PMTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes(RayCopesoahppca)Subject Community Water Fluoridation Under Challenge Again in Simcoe Muskoka Hello Colleagues You may wish to know that community water fluoridation (CWF) is again under challenge in SimcoeMuskoka specifically both in Tottenham (Town of New Tecumseth in Simcoe County) and for theentire District of Muskoka On Monday September 23 Committee of the Whole Council of theTown of New Tecumseth voted to submit application to discontinue community water fluoridation(CWF) in the town of Tottenham despite presentations to the contrary from our dental consultantDr Ito and from me The next Council meeting is scheduled for Monday Sept 30 at which lastMondayrsquos (Sept 23) votes will be ratified
Since Monday I have spoken with the Mayor of the Town of New Tecumseth and with most of thecouncilors encouraging deferral of a decision on Monday to allow the town more time to make afully informed decision
This is the second time in recent years that the issue of discontinuing CWF in Tottenham has beenraised at council This issue is also scheduled to return again to the District of Muskoka Council on
October 21st where I will be presenting in response to deputations in opposition to fluoridation
Outside of Base Borden Tottenham is the only community with fluoridated water in SimcoeCounty The health unitrsquos own screening data between 2011 and 2013 shows that Tottenhamrsquos
Gordon
Highlight
children as well as those in Muskoka have a lower rate of dental decay than Simcoe Muskokacommunities without CWF
Sincerely
Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorgChuck Gardner MOH
November 04 2013
Mandatory State Laws on Fluoridation Thirteen states Puerto Rico and the District of Columbia have laws intended to provide
statewide fluoridation These states and the year that the fluoridation legislation was passed are
District of Columbia (1952) Connecticut (1965) Kentucky (1966) Illinois (1967) Minnesota
(1967) Ohio (1969) South Dakota (1969) Georgia (1973) Nebraska (1973 and 2008)
California (1995) Delaware (1998) Puerto Rico (1998) Nevada (1999) Louisiana (2008) and
Arkansas (2011) (see Table 1) The sizes of the public water systems or countiescommunities
affected and exemption provisions vary by state Table 1
STATES THAT HAVE MANDATORY LAWS ON FLUORIDATION -2011
State (1) Year of
Fluoridation
Legislation (1)
Population
served by
Fluoridated
CWS (2)
Persons
receiving
fluoridated
water (2)
State
Average
Caries
Experience
of Grade 3
Students (3)
Arkansas 2011 647 1724131 64
California 1995 621 22812721 709
Connecticut 1965 910 2370423 406
Delaware 1998 862 705344 545
Georgia 1973 921 8924598 52
Illinois 1967 993 11325132 532
Kentucky 1966 999 4334223 598
Louisiana 2008 407 1846149 657
Minnesota 1967 988 4117266 549
Nebraska 1973 and 2008 702 1001665 593
Nevada 1999 702 1001665 649
Ohio 1969 877 8772683 512
South Dakota 1969 948 642942 623
District of
Columbia
1952 1000 595000
Puerto Rico 1998
United States 739 204283554
2010 Statistics for population fluoridated and number of people
1 Communication with Jane McGinley RDH MBA Manager Fluoridation and Preventive Health
Activities Council on Access Prevention and Interprofessional Relations
2 Centers for Disease Control and Prevention Department of Health and Human Services
accessed Oct 21 2013 httpwwwcdcgovfluoridationstatistics2010statshtm
3 Centers for Disease Control and Prevention National Oral Health Surveillance System Caries
Experience - Percentage of 3rd Grade students with Caries Experience (treated or untreated tooth
If data from 43 states for the percentage of Grade 3 children with experience of dental decay is
compared with the 2008 percentages of the population in a state with Community Water
Fluoridation then the percentage of children with experience of dental decay decreases as the
percentage of the state population with Community Water Fluoridation increases (see Figure 1)
Figure 1
Correlation of Percentage of Grade 3 Children with Caries Experience and
Percentage of Population With Community Water Fluoridation for 43
Reporting States
0
10
20
30
40
50
60
70
80
0 10 20 30 40 50 60 70 80 90 100
State of Population With Community Water Fluoridation
Sta
te
of
Gra
de 3
Stu
den
ts w
ith
Cari
es E
xp
eri
en
ce
Data from CDC (2 3)
The description of the fluoridation laws in California Illinois and Nevada can be found on the
Association of State amp Territorial Dental Directors website(4 7 8)
The California fluoridation law AB 733 came into effect in 1995 requiring communities of 10
000 residents or more be supplied with fluoridated drinking water However the state did not
provide any funding to implement the legislation (California is unique in requiring fluoridation
without funding the practice)(4) The California Department of Health Services therefore had to
fund fluoridation initiatives from non-governmental sources ie the California Endowment
California Dental Association Foundation the First 5 Commission and others(5) From 1995 to
2011 the percentage of the California population receiving fluoridated drinking water has risen
from 17 to 625(6) 4 Dental Public Health Activities amp Practices Office of Oral Health California Department of Health
Services April 2002 httpwwwastddorgbestpracticesDES06002CAfluoridationpdf
5 Stock M Pollick H The CDA Foundation Model to Fluoridate Communities California Dental
Association Journal vol 40 no 8 649 - 655
httpwwwcdaorgPortals0journaljournal_082012pdf
6 California Dental Association Foundation
httpwwwcdafoundationorglearnadvocacyfluoridation
The State of Illinois passed a mandatory fluoridation state in 1967 and required all community
water systems to adjust fluoride levels in the drinking water to optimal levels within 1 year(7)
From 1962 when over 5000000 residents had optimally fluoridated drinking water by 2010
the number had risen to 11325132 (993 of the population on community water systems)(2)
7 Dental Public Health Activities amp Practices Division of Oral Health Illinois Department of Public
Health April 2002 httpwwwastddorgbestpracticesDES16007ILfluoridationpdf
The State of Nevada passed a mandatory fluoridation statute in 2000 for communities with
400000 or more residents(8) This was a result of the work of a statewide coalition that
included the Nevada Dental and Dental Hygienist Associations the Washoe and Clark County
District Health Departments the Clark County School District Junior League of Las Vegas
Head Start the Community College of Southern Nevada Dental Hygiene Program Health
Access Washoe County and Saint Maryrsquos Hospital For communities with less than 400000 the
implementation of fluoridation still required the vote of the majority voters in the community
The Las Vegas Water Authority and the City of Henderson started fluoridation in 2000
increasing the percentage of the population with fluoridated drinking water from 2 to 65 (8) 8 Dental Public Health Activities amp Practices Bureau of Family Health Services Nevada State Health
Division April 2002 httpwwwastddorgbestpracticesDES31002NVfluoridationbillpdf
Countries with Mandatory Laws on Fluoridation Countries that have mandated Community Water Fluoridation are Brazil Hong Kong
Malaysia Singapore Ireland Israel and some of the states in Australia
Singapore started fluoridating its water in 1956 based on the success of the fluoridation trials in
Grand Rapids Newburgh Evanston and Brantford Singapore became the first Asian country to
have 100 of its population benefitting from the implementation of fluoridated drinking water
Loh reported that ldquoThe ten year study on the effects of water fluoridation in Singapore showed
a decrease in caries prevalence in the children In the permanent dentition the reduction was
523 per cent for Chinese and 31 per cent for Malays in the 7 to 9 year old age group A similar
trend was observed in the mixed dentition in which the decrease was 325 per cent for Chinese
and 306 per cent for Malaysrdquo(9) By 2010 the population of the country was 5080000(10)
9 Loh T Thirty-eight years of water fluoridation--the Singapore scenario Community Dent
Health 1996 Sep13 Suppl 247-50
10 British Fluoridation Society One in a Million the facts about water fluoridation 3rd Edition
published March 2012) httpwwwbfsweborgonemillion0920One20in20a20Million20-
20The20Extent20of20Fluoridationpdf
Hong Kong started implementing community water fluoridation in 1961 and similar to
Singapore 100 of the population received access to fluoridated drinking water Lo and Wong
reported that ldquoThe mean DMFT score of the children deceased from 44 in 1960 to 15 in 1968
stayed at this level in the 1980 and 1986 surveys and further deceased to 08 in 2001 The
prevalence of dental fluorosis among the children surveyed in 1960 was 1 and this increased
to 59 and 70 in 1968 and 1980 respectively It was found in the 1986 and 2001 surveys that
the prevalences of fluorosis were 47 and 9 among children whose teeth developed at the
time when the respective water fluoride concentrations were 07 ppm and 05 ppmrdquo(11) The
population of Hong Kong was 6968000 in 2009(10) 11 LO ECM and WONG AHH Water fluoride concentration and fluorosis in Hong Kong in 1960-
2001 84th General Session and Exhibition of the International Association for Dental Research amp
1st Meeting of the Pan-Asian-Pacific Federation Brisbane Australia 28 June-1 July 2006 v 85 n
Sp B
The Malaysian cabinet approved a nationwide community water fluoridation program in 1972
(12) One of the states Sabah decided to stop fluoridation in 1989 due to concerns about
inadequate supervision in adding fluoride to the drinking water Oral Health Surveys in 2009
and 2007 indicated that children in Sabah had the worst oral health with 50 of 12 year-olds
having decay in their permanent teeth and children having an average of 3 teeth being(13)
Under the 10th Malaysian Plan in 2011 the federal and the Sabah state governments
reintroduced water fluoridation in Sabah(1314) In 2010 about 755 of the Malaysian
population or 20700000 people had fluoridated drinking water(1013) 12 Malaysian Dental Association Fluoride in Water
httpwwwmdaorgmy07_public_01healthcare_12htm
13 Sachdev N Fluoridation in Sabah Water for Cleaner Teeth French Tribunecom 28022011
From Levy IsraTo Jaeger ValerieCc Pim Carolyn gordonalphaweborg Diallo Aicha Penny Sutcliffe Paul Roumeliotis Michael Finkelstein
Hazel Lynn Robert KyleSubject FW Panorama - Privacy Security and other issuesDate Wednesday October 16 2013 122110 PM
Hello ValerieOttawa is part of Wave 4 Panorama implementation and we are gearing up increasingly to use thesystem where and if possible Thinking about it I am anticipating that this may need to be on theCOMOH (and alPHa) radar as it is something that will impact all health units and implies a majoroperational shift in vaccine delivery programs for all health units I have asked Carolyn Pim toconnect with our sister wave 4 units to share common experiences as we move forward ndash when wehave a roll up could I bring to COMOH Exec for discussion to explore whether there are broaderimplications for all members As an aside I have also asked the Ministry and their CIO to share with me any roll up learnings thatthey may have had already from previous waves (I understand that Niagara HU was a wave 1participant so if there is such a roll up of common experiences that others could learn fromperhaps you have it already and that could come to the exec too)Thanks Isra From Pim Carolyn Sent October 10 2013 1228 PMTo Christopher Mackie (christophermackiemlhuonca) Elizabeth Richardson(Elizabethrichardsonhamiltonca) H BSc M D F R C P (C) MPH Jim Chirico(jimchiriconbpsdhuca) Marlene Spruyt (spruytmtimiskaminghucom) Robert Kyle (Durham)Cc Levy IsraSubject Panorama - Privacy Security and other issues Dear colleagues Irsquom reaching out to you as fellow Panorama Wave 4 health units to ask about where yourorganizations are at in the process of signing agreements and completing Privacy ImpactAssessments and Threat Risk Assessments (TRAs) Ottawa Public Healthrsquos IT legal and informationsecurity advisors have made numerous requests to the MOHLTC for information (in particular theprovincial TRA) that we consider essential to develop our own risk assessment and PIA but havebeen told that information cannot be shared even with strict confidentiality and access controlsSo we are at somewhat of an impasse Isra emailed Arlene yesterday Arlene has forwarded ourconcerns to the Ministryrsquos CIO and Panorama lead but we havenrsquot had any response or discussionswith either of them yet Have your organizations identified similar concerns andor had interactions with the MOHLTC inthis respect Irsquod also be interested in knowing if your health units have flagged other (egoperational) implementation concerns Thanks
Carolyn ps Robert ndash you can ignore this request I talked with Sharan this morning about Durhamrsquos issuesso am including you now just for information Carolyn Pim MD FRCPC Associate Medical Officer of Health Meacutedecin adjointe en santeacute publique Ottawa Public Health Santeacute publique Ottawa 100 Constellation Cr Ottawa ON K2G 6J8 Tel teacutel (613) 580-6744 ext 23684Fax (613) 580-9641Connect With Ottawa Public Health
Suivez Santeacute publique Ottawa
This e-mail originates from the City of Ottawa e-mail system Any distribution use orcopying of this e-mail or the information it contains by other than the intendedrecipient(s) is unauthorized If you are not the intended recipient please notify meat the telephone number shown above or by return e-mail and delete thiscommunication and any copy immediately Thank you
Le preacutesent courriel a eacuteteacute expeacutedieacute par le systegraveme de courriels de la Ville dOttawaToute distribution utilisation ou reproduction du courriel ou des renseignements quisy trouvent par une personne autre que son destinataire preacutevu est interdite Si vousavez reccedilu le message par erreur veuillez men aviser par teacuteleacutephone (au numeacuteropreacuteciteacute) ou par courriel puis supprimer sans deacutelai la version originale de lacommunication ainsi que toutes ses copies Je vous remercie de votre collaboration
1
Smoke-Free Patios ndash An Amendment to the Smoke-Free Ontario Act
Date November 15 2013 Prepared for Council of Ontario Medical Officers of Health Prepared by York Region Public Health _____________________________________________________________________________ Issue
The Smoke-Free Ontario Act is the current provincial legislation that imposes smoking restrictions in workplaces and public places It prohibits smoking on restaurant and bar patios in instances where any portion of the seating area is covered by a roof With recent studies illustrating that exposure to second hand smoke outdoors poses similar risks to indoor exposure there has been growing public support to enhance smoking restrictions and make patios completely smoke-free
Background
With the implementation of the Smoke-Free Ontario Act in 2006 restaurant and bar patios became subject to smoking restrictions if any portion of the seating area was covered by a roof This allowed for patios without roof coverings to continue to allow smoking and as a result did not provide significant protection to patrons or staff from exposure to second hand smoke outdoors Many businesses chose to alter the design of their patios to allow smoking to continue In some cases patios became more crowded since smoking patrons who dine indoors often proceed outside onto licensed patios with their beverages to smoke York Region like most municipalities in Ontario is host to hundreds of patios being operated by restaurant owners and businesses With smoking prohibitions affecting only a small portion of these patios specifically ones with coverings the vast majority of patios still allow smoking to take place Patrons and employees on patios where smoking is not restricted are exposed to second hand smoke frequently This can contribute to increased disease and aggravation of existing health conditions From a business perspective the existing legislation has been viewed by many operators as unfair because some patios have permanent coverings which cannot be removed requiring a smoke-free status These business owners feel this creates an uneven playing field since they cannot provide an outdoor dining area for their smoking customers There is strong community support for smoke-free patios in Ontario A 2009 Rapid Risk Factor Surveillance System survey revealed 754 percent support in York Region while a Toronto Health Survey in 2011 indicated 74 percent public support
2
Current Status
Smoking is currently prohibited on restaurant and bar patios province-wide in four Canadian provinces and territories Alberta Newfoundland and Labrador Nova Scotia and Yukon A fifth province Prince Edward Island prohibits smoking on patios until 10 pm Since Ontario enacted legislation restricting smoking on patios in 2006 eight municipalities in Ontario have chosen to create bylaws that go beyond the Smoke-Free Ontario Act and enhance outdoor protection from second hand smoke by prohibiting smoking on patios completely The largest of those municipalities is the City of Ottawa Recently the Toronto Board of Health unanimously endorsed a report presented by their Medical Officer of Health recommending that restaurant and bar patios be made smoke-free through an amendment to the Smoke-Free Ontario Act
Key Considerations
There should be no significant financial burden to local Boards of Health resulting from a smoke-free patio amendment to the Smoke-Free Ontario Act Inspection and enforcement for the Smoke-Free Ontario Act is currently 100 percent funded by the Ministry of Health and Long-Term Care Following an introductory period of education on the amendment a complaint response model of service delivery would ensure ongoing compliance with smoke-free requirements A complete ban of smoking on patios would eliminate the widely-held perception by business owners that the current legislation creates an uneven playing field for business Since Smoke-Free Ontario Act inspections of patios began in 2006 operators have expressed the opinion that if patios need to be smoke-free for the protection of the public they should all be smoke-free to avoid undue hardship for individual businesses and to provide protection uniformly across the Province
Next steps
York Region Public Health intends to seek support from Medical Officers of Health across the Central East Tobacco Control Area Network (CETCAN) to advocate to the Ministry of Health and Long-Term Care for an amendment to the Smoke-Free Ontario Act prohibiting smoking on all restaurant and bar patios York Region is also in the process of requesting that its Regional Council advocate to the Minister of Health and Long-Term Care on the issue
Updating and Modernizing O Regulation 565 (Public Pools)
Date November 15 2013
Prepared for Council of Ontario Medical Officers of Health
Prepared by York Region Public Health _____________________________________________________________________________ Background Recent drownings at public pools in Ontario have highlighted the issue of water-borne illness and injury The current pool regulation under Ontariorsquos Health Protection and Promotion Act O Regulation 565 (Public Pools) is outdated It does not accurately reflect new pool technology and design or the changing use of public pools Neither does it incorporate admissions standards recommended by the Office of the Chief Coroner Further O Regulation 565 does not have short-form wording or set fines associated with it This limits public health enforcement capabilities What is the impact Updating O Regulation 565 (Public Pools) to address recent changes in pool technology design and uses and to include Coroner-recommended admissions standards would help improve pool safety Establishing short-form wording for O Regulation 565 would enhance enforcement related to public pools Currently the only enforcement available to Public Health Inspectors for dealing with non-critical regulatory infractions in public pools is the issuance of a Part III summons This involves a considerable amount of resources for a possible small fine With the development of inspection disclosure systems such as YorkSafe there is an even greater need to develop a method to effectively address repeated pool operator non-compliance with non-critical issues Next steps Public health units should advocate to the Province to 1) Conduct a review of O Regulation 565 (Public Pools) to address shortcomings Proposed changes to the
regulation should include a requirement for ownersoperators of public pools to advise the local Medical Officer of Health of any change in the use of a facility and the addition of the Coronerrsquos recommended admission standards
2) Provide short-form wording for O Regulation 565 so that public health inspectors can better deal with pool operator non-compliance
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
2013 Strategic Planning
Considerations for COMOH
As part of its strategic planning discussions alPHarsquos Board has been considering changes to the level of support provided to member sections A member survey is being carried out over the fall to determine options acceptable to alPHa members The following approach to support is put forward as a proposal for the consideration of COMOH Note that the feasibility of the points below depend upon future decisions of the alPHa board They assume that COMOH remains part of alPHa but becomes more independent in administering meetings
1 alPHa can provide to COMOH staff support (Gord Fleming) amounting to 02 FTE or one day per week This is a reduction from the current level of 35 days per week COMOH can choose to use the support any way it wants writing COMOH letters meeting minutes agenda support special projects etc
2 In addition to 02 FTE alPHa staff would provide support for up to 4 face-to-face meetings per year One meeting would be concurrent to alPHarsquos annual conference in June The timing of other meetings could be negotiated The support includes consulting on the development of the program arranging for speakers registration for the event arranging venue AV support and hospitality services
3 In addition to 02 FTE alPHa staff would provide support for setting meeting dates and any polling required to establish dates Note that the individual supporting this function would be Karen Reece
4 COMOHrsquos Executive and Section would continue to have access to online supports through the alPHa including the COMOH Listserve and a group page for posting agendas minutes and other resources on the alPHa website
5 alPHa staff (Linda Stewart and Gord Fleming) can also start participating on CMOH calls as a way to be up-to-date on issues related to COMOH
6 Other than what is outlined above COMOH would be expected to prepare agendas and take minutes for its Executive and Section meetings The Executive would be expected to operate more independently than it does now but would be able to access the supports outlined above
Prepared by Linda Stewart Executive Director
From comoh-bounceslistsalphaweborg on behalf of Christopher MackieTo MOH ListserveSubject [comoh] Fw URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)Date Wednesday October 30 2013 91241 AMAttachments ATT00249txt
For AMOHs and PHPM residents who didnt receive the initial email
Chris
Christopher Mackie MD MHSc FRCPCMedical Officer of Health and CEOMiddlesex-London Health Unit50 King St LondonON N6A 5L7 O 519 663 5317 ext 2444 wwwhealthunitcomFrom Pisko Laura (MOHLTC)Sent Tuesday October 29 2013 759 PMTo kbarkeralgomapublichealthcom malcolmlockbchuorg davidcchatham-kentcarobertkyledurhamca proumeliotiseohuca fwarshelginhealthonca mohelginhealthoncahlynnpublichealthgreybruceonca malcolmlockhnhuorg hnmohhnhuorglnoseworthyhkpronca bobnosalhaltonca elizabethrichardsonhamiltoncarschabashpechuonca ncameronhuroncountyca drimgemmillkflapublichealthcamohkflapublichealthca suditranadecounty-lambtononca paulastewarthealthunitorgChristopher Mackie valeriejaegerniagararegionca jimchiriconbpsdhuca jarthursnwhuoncaisralevyottawaca dnealoxfordcountyca davidmowatpeelregionca mklassenpdhuoncarpellizzaripcchuca rosemarieramsinghporcupinehuonca mcorriveaurcdhucomcharlesgardnersmdhuorg sutcliffepsdhucom davidwilliamstbdhucomspruytmtimiskaminghucom dmckeowntorontoca lnolanregionofwaterloocanicolamercerwdghuorg aheimannwechealthunitorg karimkurjiyorkcaCc coreywesleytbdhucom CindyBaker-Barillsmdhuorg Donna Kosmack pilonlsdhucomPaulaMuiskflapublichealthca sthibautorontoca Mueller Daina (MOHLTC) Gordon Marcus(MOHLTC) andreakitahamiltoncaSubject URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)
Dear Colleagues The ministry has received reports that some tobacco vendors across the province aregiving away single cigarettes with the purchase of tobacco products It is the ministryrsquosposition that giving out free single cigarettes does not violate subsection 31(3) of theSmoke-Free Ontario Act (ldquoSFOArdquo) Although the practice of giving out free singlecigarettes may promote the sale of tobacco products it does not take the form of aldquoproduct enhancement product association or promotional materialrdquo and therefore doesnot fall within the scope of subsection 31(3) of the SFOA We have confirmed with Health Canada that this practice may violate section 29(b) of thefederal Tobacco Act As such Health Canada is requesting that you notify them in writingand I am directing you to communicate with them via email and provide to them as manydetails as possible Emails should be sent to Tobacco-Ontariohc-scgcca and thesubject line should read ldquoViolation of Section 29(b) of Tobacco Actrdquo This will ensurethat the complaints are given priority status by Health Canada We will continue to monitor
this situation and liaise with our colleagues at Health Canada Please share this information with your tobacco control staff and contact me or DainaMueller Manager Tobacco Control Unit Health Promotion Implementation Branch atdainamuellerontarioca with any questions RegardsLaura Laura A PiskoDirectorHealth Promotion Implementation BranchHealth Promotion DivisionMinistry of Health and Long Term Care416-327-7445 (office)416-451-3185 (mobile) Marcus Gordon - EA (416)326-0625 for urgent issues
========= Middlesex-London Health Unit E-Mail Disclaimer =============______________________________________________________________
Private and confidential intended only for named recipient If otherwisereceived please destroy immediately Health information in this email isonly general information and is not intended to replace an in personconsultation with a medical professional nor is it intended to providemedical advice Individual circumstances of which we are not aware mayaffect the information provided herein and as such the Middlesex-LondonHealth Unit assumes no liability or responsibility for your reliancethereon The Middlesex-London Health Unit works under the authority of theHealth Protection and Promotion Act and this correspondence may be used toassess your needs for public health services (519-663-5317 ext 2448)______________________________________________________________
From Gardner CharlesTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes (RayCopesoahppca)
George Pasut (GeorgePasutoahppca) Peter Cooney (petercooneyhc-scgcca)Cc Ito DickSubject Discontinuation of Fluoridation in MuskokaDate Tuesday October 22 2013 125254 PM
Hello Colleagues
As I reported in my email below on September 26th fluoridation has come under challenge again inSimcoe Muskoka I am now very unhappy to report that despite our best efforts last night theDistrict Council of Muskoka voted to remove fluoride from municipal drinking supplies across theDistrict This brings to an end fluoridation in all of Simcoe and Muskoka (with the exception of Base Borden)ndash though New Tecumseth will be conducting a plebiscite on the question of fluoridation with themunicipal election next October Defending community water fluoridation has drained a great deal of time human resources andcommitment from other priorities and has been exhausting here in SMDHU as I am sure it hasbeen in many other health units While the outcomes have been very disappointing I have beenimpressed by the professionalism and dedication that SMDHU staff members have shown inshouldering this burden In particular our dental consultant Dr Ito has provided us with much ofthe foundational knowledge and the local research essential to our efforts and has very frequentlyattended and presented at council meetings and other public events I would also like to thank themany of you who have offer and provided support including advocacy letters and informationresources Over the years Dr Peter Cooney Chief Dental Officer of Health of Canada has beenvery helpful attending and presenting with us at council meetings and at public consultationevents We will of course continue our oral health surveillance of the children of Muskoka documentingand reporting in future years on the increase in dental decay that we anticipate will occur Suchsurveillance is the foundation of our advocacy both to municipal politicians and to the province I am very concerned that our experience will continue to repeat itself across the province unlessthere is strong leadership provincially It is with this in mind that I raise the followingrecommendations for your consideration
1 That we collectively (with PHOrsquos leadership) conduct high quality publish-worthy researchdocumenting the impact on dental decay that occurs in those municipalities throughoutOntario that in recent years have discontinued community water fluoridation This could bepart of a larger study on such municipalities across the country and it could also be part ofa study documenting overall oral health (including fluoridation coverage) in the province(and possibly across the country)
2 That COMOH engage with our Chief MOH to advocate for the province to require allmunicipal water supplies to be fluoridated (the exception of course being those withnaturally sufficient fluoride concentrations) This could built upon the alPHa position to
Gordon
Highlight
Gordon
Highlight
date (A11-00 - Community Water Fluoridation) on the CMOH position (Oral Health ndash) and on theemail discussion generated on the COMOH listserv some months back re Richardrsquosproposal (calling on the province to fund municipal water fluoridation)
Valerie I request that this be an item for our COMOH meeting on November 15th Sincerely Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorg From Gardner Charles Sent Thursday September 26 2013 245 PMTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes(RayCopesoahppca)Subject Community Water Fluoridation Under Challenge Again in Simcoe Muskoka Hello Colleagues You may wish to know that community water fluoridation (CWF) is again under challenge in SimcoeMuskoka specifically both in Tottenham (Town of New Tecumseth in Simcoe County) and for theentire District of Muskoka On Monday September 23 Committee of the Whole Council of theTown of New Tecumseth voted to submit application to discontinue community water fluoridation(CWF) in the town of Tottenham despite presentations to the contrary from our dental consultantDr Ito and from me The next Council meeting is scheduled for Monday Sept 30 at which lastMondayrsquos (Sept 23) votes will be ratified
Since Monday I have spoken with the Mayor of the Town of New Tecumseth and with most of thecouncilors encouraging deferral of a decision on Monday to allow the town more time to make afully informed decision
This is the second time in recent years that the issue of discontinuing CWF in Tottenham has beenraised at council This issue is also scheduled to return again to the District of Muskoka Council on
October 21st where I will be presenting in response to deputations in opposition to fluoridation
Outside of Base Borden Tottenham is the only community with fluoridated water in SimcoeCounty The health unitrsquos own screening data between 2011 and 2013 shows that Tottenhamrsquos
Gordon
Highlight
children as well as those in Muskoka have a lower rate of dental decay than Simcoe Muskokacommunities without CWF
Sincerely
Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorgChuck Gardner MOH
November 04 2013
Mandatory State Laws on Fluoridation Thirteen states Puerto Rico and the District of Columbia have laws intended to provide
statewide fluoridation These states and the year that the fluoridation legislation was passed are
District of Columbia (1952) Connecticut (1965) Kentucky (1966) Illinois (1967) Minnesota
(1967) Ohio (1969) South Dakota (1969) Georgia (1973) Nebraska (1973 and 2008)
California (1995) Delaware (1998) Puerto Rico (1998) Nevada (1999) Louisiana (2008) and
Arkansas (2011) (see Table 1) The sizes of the public water systems or countiescommunities
affected and exemption provisions vary by state Table 1
STATES THAT HAVE MANDATORY LAWS ON FLUORIDATION -2011
State (1) Year of
Fluoridation
Legislation (1)
Population
served by
Fluoridated
CWS (2)
Persons
receiving
fluoridated
water (2)
State
Average
Caries
Experience
of Grade 3
Students (3)
Arkansas 2011 647 1724131 64
California 1995 621 22812721 709
Connecticut 1965 910 2370423 406
Delaware 1998 862 705344 545
Georgia 1973 921 8924598 52
Illinois 1967 993 11325132 532
Kentucky 1966 999 4334223 598
Louisiana 2008 407 1846149 657
Minnesota 1967 988 4117266 549
Nebraska 1973 and 2008 702 1001665 593
Nevada 1999 702 1001665 649
Ohio 1969 877 8772683 512
South Dakota 1969 948 642942 623
District of
Columbia
1952 1000 595000
Puerto Rico 1998
United States 739 204283554
2010 Statistics for population fluoridated and number of people
1 Communication with Jane McGinley RDH MBA Manager Fluoridation and Preventive Health
Activities Council on Access Prevention and Interprofessional Relations
2 Centers for Disease Control and Prevention Department of Health and Human Services
accessed Oct 21 2013 httpwwwcdcgovfluoridationstatistics2010statshtm
3 Centers for Disease Control and Prevention National Oral Health Surveillance System Caries
Experience - Percentage of 3rd Grade students with Caries Experience (treated or untreated tooth
If data from 43 states for the percentage of Grade 3 children with experience of dental decay is
compared with the 2008 percentages of the population in a state with Community Water
Fluoridation then the percentage of children with experience of dental decay decreases as the
percentage of the state population with Community Water Fluoridation increases (see Figure 1)
Figure 1
Correlation of Percentage of Grade 3 Children with Caries Experience and
Percentage of Population With Community Water Fluoridation for 43
Reporting States
0
10
20
30
40
50
60
70
80
0 10 20 30 40 50 60 70 80 90 100
State of Population With Community Water Fluoridation
Sta
te
of
Gra
de 3
Stu
den
ts w
ith
Cari
es E
xp
eri
en
ce
Data from CDC (2 3)
The description of the fluoridation laws in California Illinois and Nevada can be found on the
Association of State amp Territorial Dental Directors website(4 7 8)
The California fluoridation law AB 733 came into effect in 1995 requiring communities of 10
000 residents or more be supplied with fluoridated drinking water However the state did not
provide any funding to implement the legislation (California is unique in requiring fluoridation
without funding the practice)(4) The California Department of Health Services therefore had to
fund fluoridation initiatives from non-governmental sources ie the California Endowment
California Dental Association Foundation the First 5 Commission and others(5) From 1995 to
2011 the percentage of the California population receiving fluoridated drinking water has risen
from 17 to 625(6) 4 Dental Public Health Activities amp Practices Office of Oral Health California Department of Health
Services April 2002 httpwwwastddorgbestpracticesDES06002CAfluoridationpdf
5 Stock M Pollick H The CDA Foundation Model to Fluoridate Communities California Dental
Association Journal vol 40 no 8 649 - 655
httpwwwcdaorgPortals0journaljournal_082012pdf
6 California Dental Association Foundation
httpwwwcdafoundationorglearnadvocacyfluoridation
The State of Illinois passed a mandatory fluoridation state in 1967 and required all community
water systems to adjust fluoride levels in the drinking water to optimal levels within 1 year(7)
From 1962 when over 5000000 residents had optimally fluoridated drinking water by 2010
the number had risen to 11325132 (993 of the population on community water systems)(2)
7 Dental Public Health Activities amp Practices Division of Oral Health Illinois Department of Public
Health April 2002 httpwwwastddorgbestpracticesDES16007ILfluoridationpdf
The State of Nevada passed a mandatory fluoridation statute in 2000 for communities with
400000 or more residents(8) This was a result of the work of a statewide coalition that
included the Nevada Dental and Dental Hygienist Associations the Washoe and Clark County
District Health Departments the Clark County School District Junior League of Las Vegas
Head Start the Community College of Southern Nevada Dental Hygiene Program Health
Access Washoe County and Saint Maryrsquos Hospital For communities with less than 400000 the
implementation of fluoridation still required the vote of the majority voters in the community
The Las Vegas Water Authority and the City of Henderson started fluoridation in 2000
increasing the percentage of the population with fluoridated drinking water from 2 to 65 (8) 8 Dental Public Health Activities amp Practices Bureau of Family Health Services Nevada State Health
Division April 2002 httpwwwastddorgbestpracticesDES31002NVfluoridationbillpdf
Countries with Mandatory Laws on Fluoridation Countries that have mandated Community Water Fluoridation are Brazil Hong Kong
Malaysia Singapore Ireland Israel and some of the states in Australia
Singapore started fluoridating its water in 1956 based on the success of the fluoridation trials in
Grand Rapids Newburgh Evanston and Brantford Singapore became the first Asian country to
have 100 of its population benefitting from the implementation of fluoridated drinking water
Loh reported that ldquoThe ten year study on the effects of water fluoridation in Singapore showed
a decrease in caries prevalence in the children In the permanent dentition the reduction was
523 per cent for Chinese and 31 per cent for Malays in the 7 to 9 year old age group A similar
trend was observed in the mixed dentition in which the decrease was 325 per cent for Chinese
and 306 per cent for Malaysrdquo(9) By 2010 the population of the country was 5080000(10)
9 Loh T Thirty-eight years of water fluoridation--the Singapore scenario Community Dent
Health 1996 Sep13 Suppl 247-50
10 British Fluoridation Society One in a Million the facts about water fluoridation 3rd Edition
published March 2012) httpwwwbfsweborgonemillion0920One20in20a20Million20-
20The20Extent20of20Fluoridationpdf
Hong Kong started implementing community water fluoridation in 1961 and similar to
Singapore 100 of the population received access to fluoridated drinking water Lo and Wong
reported that ldquoThe mean DMFT score of the children deceased from 44 in 1960 to 15 in 1968
stayed at this level in the 1980 and 1986 surveys and further deceased to 08 in 2001 The
prevalence of dental fluorosis among the children surveyed in 1960 was 1 and this increased
to 59 and 70 in 1968 and 1980 respectively It was found in the 1986 and 2001 surveys that
the prevalences of fluorosis were 47 and 9 among children whose teeth developed at the
time when the respective water fluoride concentrations were 07 ppm and 05 ppmrdquo(11) The
population of Hong Kong was 6968000 in 2009(10) 11 LO ECM and WONG AHH Water fluoride concentration and fluorosis in Hong Kong in 1960-
2001 84th General Session and Exhibition of the International Association for Dental Research amp
1st Meeting of the Pan-Asian-Pacific Federation Brisbane Australia 28 June-1 July 2006 v 85 n
Sp B
The Malaysian cabinet approved a nationwide community water fluoridation program in 1972
(12) One of the states Sabah decided to stop fluoridation in 1989 due to concerns about
inadequate supervision in adding fluoride to the drinking water Oral Health Surveys in 2009
and 2007 indicated that children in Sabah had the worst oral health with 50 of 12 year-olds
having decay in their permanent teeth and children having an average of 3 teeth being(13)
Under the 10th Malaysian Plan in 2011 the federal and the Sabah state governments
reintroduced water fluoridation in Sabah(1314) In 2010 about 755 of the Malaysian
population or 20700000 people had fluoridated drinking water(1013) 12 Malaysian Dental Association Fluoride in Water
httpwwwmdaorgmy07_public_01healthcare_12htm
13 Sachdev N Fluoridation in Sabah Water for Cleaner Teeth French Tribunecom 28022011
From Levy IsraTo Jaeger ValerieCc Pim Carolyn gordonalphaweborg Diallo Aicha Penny Sutcliffe Paul Roumeliotis Michael Finkelstein
Hazel Lynn Robert KyleSubject FW Panorama - Privacy Security and other issuesDate Wednesday October 16 2013 122110 PM
Hello ValerieOttawa is part of Wave 4 Panorama implementation and we are gearing up increasingly to use thesystem where and if possible Thinking about it I am anticipating that this may need to be on theCOMOH (and alPHa) radar as it is something that will impact all health units and implies a majoroperational shift in vaccine delivery programs for all health units I have asked Carolyn Pim toconnect with our sister wave 4 units to share common experiences as we move forward ndash when wehave a roll up could I bring to COMOH Exec for discussion to explore whether there are broaderimplications for all members As an aside I have also asked the Ministry and their CIO to share with me any roll up learnings thatthey may have had already from previous waves (I understand that Niagara HU was a wave 1participant so if there is such a roll up of common experiences that others could learn fromperhaps you have it already and that could come to the exec too)Thanks Isra From Pim Carolyn Sent October 10 2013 1228 PMTo Christopher Mackie (christophermackiemlhuonca) Elizabeth Richardson(Elizabethrichardsonhamiltonca) H BSc M D F R C P (C) MPH Jim Chirico(jimchiriconbpsdhuca) Marlene Spruyt (spruytmtimiskaminghucom) Robert Kyle (Durham)Cc Levy IsraSubject Panorama - Privacy Security and other issues Dear colleagues Irsquom reaching out to you as fellow Panorama Wave 4 health units to ask about where yourorganizations are at in the process of signing agreements and completing Privacy ImpactAssessments and Threat Risk Assessments (TRAs) Ottawa Public Healthrsquos IT legal and informationsecurity advisors have made numerous requests to the MOHLTC for information (in particular theprovincial TRA) that we consider essential to develop our own risk assessment and PIA but havebeen told that information cannot be shared even with strict confidentiality and access controlsSo we are at somewhat of an impasse Isra emailed Arlene yesterday Arlene has forwarded ourconcerns to the Ministryrsquos CIO and Panorama lead but we havenrsquot had any response or discussionswith either of them yet Have your organizations identified similar concerns andor had interactions with the MOHLTC inthis respect Irsquod also be interested in knowing if your health units have flagged other (egoperational) implementation concerns Thanks
Carolyn ps Robert ndash you can ignore this request I talked with Sharan this morning about Durhamrsquos issuesso am including you now just for information Carolyn Pim MD FRCPC Associate Medical Officer of Health Meacutedecin adjointe en santeacute publique Ottawa Public Health Santeacute publique Ottawa 100 Constellation Cr Ottawa ON K2G 6J8 Tel teacutel (613) 580-6744 ext 23684Fax (613) 580-9641Connect With Ottawa Public Health
Suivez Santeacute publique Ottawa
This e-mail originates from the City of Ottawa e-mail system Any distribution use orcopying of this e-mail or the information it contains by other than the intendedrecipient(s) is unauthorized If you are not the intended recipient please notify meat the telephone number shown above or by return e-mail and delete thiscommunication and any copy immediately Thank you
Le preacutesent courriel a eacuteteacute expeacutedieacute par le systegraveme de courriels de la Ville dOttawaToute distribution utilisation ou reproduction du courriel ou des renseignements quisy trouvent par une personne autre que son destinataire preacutevu est interdite Si vousavez reccedilu le message par erreur veuillez men aviser par teacuteleacutephone (au numeacuteropreacuteciteacute) ou par courriel puis supprimer sans deacutelai la version originale de lacommunication ainsi que toutes ses copies Je vous remercie de votre collaboration
1
Smoke-Free Patios ndash An Amendment to the Smoke-Free Ontario Act
Date November 15 2013 Prepared for Council of Ontario Medical Officers of Health Prepared by York Region Public Health _____________________________________________________________________________ Issue
The Smoke-Free Ontario Act is the current provincial legislation that imposes smoking restrictions in workplaces and public places It prohibits smoking on restaurant and bar patios in instances where any portion of the seating area is covered by a roof With recent studies illustrating that exposure to second hand smoke outdoors poses similar risks to indoor exposure there has been growing public support to enhance smoking restrictions and make patios completely smoke-free
Background
With the implementation of the Smoke-Free Ontario Act in 2006 restaurant and bar patios became subject to smoking restrictions if any portion of the seating area was covered by a roof This allowed for patios without roof coverings to continue to allow smoking and as a result did not provide significant protection to patrons or staff from exposure to second hand smoke outdoors Many businesses chose to alter the design of their patios to allow smoking to continue In some cases patios became more crowded since smoking patrons who dine indoors often proceed outside onto licensed patios with their beverages to smoke York Region like most municipalities in Ontario is host to hundreds of patios being operated by restaurant owners and businesses With smoking prohibitions affecting only a small portion of these patios specifically ones with coverings the vast majority of patios still allow smoking to take place Patrons and employees on patios where smoking is not restricted are exposed to second hand smoke frequently This can contribute to increased disease and aggravation of existing health conditions From a business perspective the existing legislation has been viewed by many operators as unfair because some patios have permanent coverings which cannot be removed requiring a smoke-free status These business owners feel this creates an uneven playing field since they cannot provide an outdoor dining area for their smoking customers There is strong community support for smoke-free patios in Ontario A 2009 Rapid Risk Factor Surveillance System survey revealed 754 percent support in York Region while a Toronto Health Survey in 2011 indicated 74 percent public support
2
Current Status
Smoking is currently prohibited on restaurant and bar patios province-wide in four Canadian provinces and territories Alberta Newfoundland and Labrador Nova Scotia and Yukon A fifth province Prince Edward Island prohibits smoking on patios until 10 pm Since Ontario enacted legislation restricting smoking on patios in 2006 eight municipalities in Ontario have chosen to create bylaws that go beyond the Smoke-Free Ontario Act and enhance outdoor protection from second hand smoke by prohibiting smoking on patios completely The largest of those municipalities is the City of Ottawa Recently the Toronto Board of Health unanimously endorsed a report presented by their Medical Officer of Health recommending that restaurant and bar patios be made smoke-free through an amendment to the Smoke-Free Ontario Act
Key Considerations
There should be no significant financial burden to local Boards of Health resulting from a smoke-free patio amendment to the Smoke-Free Ontario Act Inspection and enforcement for the Smoke-Free Ontario Act is currently 100 percent funded by the Ministry of Health and Long-Term Care Following an introductory period of education on the amendment a complaint response model of service delivery would ensure ongoing compliance with smoke-free requirements A complete ban of smoking on patios would eliminate the widely-held perception by business owners that the current legislation creates an uneven playing field for business Since Smoke-Free Ontario Act inspections of patios began in 2006 operators have expressed the opinion that if patios need to be smoke-free for the protection of the public they should all be smoke-free to avoid undue hardship for individual businesses and to provide protection uniformly across the Province
Next steps
York Region Public Health intends to seek support from Medical Officers of Health across the Central East Tobacco Control Area Network (CETCAN) to advocate to the Ministry of Health and Long-Term Care for an amendment to the Smoke-Free Ontario Act prohibiting smoking on all restaurant and bar patios York Region is also in the process of requesting that its Regional Council advocate to the Minister of Health and Long-Term Care on the issue
Updating and Modernizing O Regulation 565 (Public Pools)
Date November 15 2013
Prepared for Council of Ontario Medical Officers of Health
Prepared by York Region Public Health _____________________________________________________________________________ Background Recent drownings at public pools in Ontario have highlighted the issue of water-borne illness and injury The current pool regulation under Ontariorsquos Health Protection and Promotion Act O Regulation 565 (Public Pools) is outdated It does not accurately reflect new pool technology and design or the changing use of public pools Neither does it incorporate admissions standards recommended by the Office of the Chief Coroner Further O Regulation 565 does not have short-form wording or set fines associated with it This limits public health enforcement capabilities What is the impact Updating O Regulation 565 (Public Pools) to address recent changes in pool technology design and uses and to include Coroner-recommended admissions standards would help improve pool safety Establishing short-form wording for O Regulation 565 would enhance enforcement related to public pools Currently the only enforcement available to Public Health Inspectors for dealing with non-critical regulatory infractions in public pools is the issuance of a Part III summons This involves a considerable amount of resources for a possible small fine With the development of inspection disclosure systems such as YorkSafe there is an even greater need to develop a method to effectively address repeated pool operator non-compliance with non-critical issues Next steps Public health units should advocate to the Province to 1) Conduct a review of O Regulation 565 (Public Pools) to address shortcomings Proposed changes to the
regulation should include a requirement for ownersoperators of public pools to advise the local Medical Officer of Health of any change in the use of a facility and the addition of the Coronerrsquos recommended admission standards
2) Provide short-form wording for O Regulation 565 so that public health inspectors can better deal with pool operator non-compliance
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
From comoh-bounceslistsalphaweborg on behalf of Christopher MackieTo MOH ListserveSubject [comoh] Fw URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)Date Wednesday October 30 2013 91241 AMAttachments ATT00249txt
For AMOHs and PHPM residents who didnt receive the initial email
Chris
Christopher Mackie MD MHSc FRCPCMedical Officer of Health and CEOMiddlesex-London Health Unit50 King St LondonON N6A 5L7 O 519 663 5317 ext 2444 wwwhealthunitcomFrom Pisko Laura (MOHLTC)Sent Tuesday October 29 2013 759 PMTo kbarkeralgomapublichealthcom malcolmlockbchuorg davidcchatham-kentcarobertkyledurhamca proumeliotiseohuca fwarshelginhealthonca mohelginhealthoncahlynnpublichealthgreybruceonca malcolmlockhnhuorg hnmohhnhuorglnoseworthyhkpronca bobnosalhaltonca elizabethrichardsonhamiltoncarschabashpechuonca ncameronhuroncountyca drimgemmillkflapublichealthcamohkflapublichealthca suditranadecounty-lambtononca paulastewarthealthunitorgChristopher Mackie valeriejaegerniagararegionca jimchiriconbpsdhuca jarthursnwhuoncaisralevyottawaca dnealoxfordcountyca davidmowatpeelregionca mklassenpdhuoncarpellizzaripcchuca rosemarieramsinghporcupinehuonca mcorriveaurcdhucomcharlesgardnersmdhuorg sutcliffepsdhucom davidwilliamstbdhucomspruytmtimiskaminghucom dmckeowntorontoca lnolanregionofwaterloocanicolamercerwdghuorg aheimannwechealthunitorg karimkurjiyorkcaCc coreywesleytbdhucom CindyBaker-Barillsmdhuorg Donna Kosmack pilonlsdhucomPaulaMuiskflapublichealthca sthibautorontoca Mueller Daina (MOHLTC) Gordon Marcus(MOHLTC) andreakitahamiltoncaSubject URGENT Potential violation of s 29(b) of federal Tobacco Act (single cigarette samples)
Dear Colleagues The ministry has received reports that some tobacco vendors across the province aregiving away single cigarettes with the purchase of tobacco products It is the ministryrsquosposition that giving out free single cigarettes does not violate subsection 31(3) of theSmoke-Free Ontario Act (ldquoSFOArdquo) Although the practice of giving out free singlecigarettes may promote the sale of tobacco products it does not take the form of aldquoproduct enhancement product association or promotional materialrdquo and therefore doesnot fall within the scope of subsection 31(3) of the SFOA We have confirmed with Health Canada that this practice may violate section 29(b) of thefederal Tobacco Act As such Health Canada is requesting that you notify them in writingand I am directing you to communicate with them via email and provide to them as manydetails as possible Emails should be sent to Tobacco-Ontariohc-scgcca and thesubject line should read ldquoViolation of Section 29(b) of Tobacco Actrdquo This will ensurethat the complaints are given priority status by Health Canada We will continue to monitor
this situation and liaise with our colleagues at Health Canada Please share this information with your tobacco control staff and contact me or DainaMueller Manager Tobacco Control Unit Health Promotion Implementation Branch atdainamuellerontarioca with any questions RegardsLaura Laura A PiskoDirectorHealth Promotion Implementation BranchHealth Promotion DivisionMinistry of Health and Long Term Care416-327-7445 (office)416-451-3185 (mobile) Marcus Gordon - EA (416)326-0625 for urgent issues
========= Middlesex-London Health Unit E-Mail Disclaimer =============______________________________________________________________
Private and confidential intended only for named recipient If otherwisereceived please destroy immediately Health information in this email isonly general information and is not intended to replace an in personconsultation with a medical professional nor is it intended to providemedical advice Individual circumstances of which we are not aware mayaffect the information provided herein and as such the Middlesex-LondonHealth Unit assumes no liability or responsibility for your reliancethereon The Middlesex-London Health Unit works under the authority of theHealth Protection and Promotion Act and this correspondence may be used toassess your needs for public health services (519-663-5317 ext 2448)______________________________________________________________
From Gardner CharlesTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes (RayCopesoahppca)
George Pasut (GeorgePasutoahppca) Peter Cooney (petercooneyhc-scgcca)Cc Ito DickSubject Discontinuation of Fluoridation in MuskokaDate Tuesday October 22 2013 125254 PM
Hello Colleagues
As I reported in my email below on September 26th fluoridation has come under challenge again inSimcoe Muskoka I am now very unhappy to report that despite our best efforts last night theDistrict Council of Muskoka voted to remove fluoride from municipal drinking supplies across theDistrict This brings to an end fluoridation in all of Simcoe and Muskoka (with the exception of Base Borden)ndash though New Tecumseth will be conducting a plebiscite on the question of fluoridation with themunicipal election next October Defending community water fluoridation has drained a great deal of time human resources andcommitment from other priorities and has been exhausting here in SMDHU as I am sure it hasbeen in many other health units While the outcomes have been very disappointing I have beenimpressed by the professionalism and dedication that SMDHU staff members have shown inshouldering this burden In particular our dental consultant Dr Ito has provided us with much ofthe foundational knowledge and the local research essential to our efforts and has very frequentlyattended and presented at council meetings and other public events I would also like to thank themany of you who have offer and provided support including advocacy letters and informationresources Over the years Dr Peter Cooney Chief Dental Officer of Health of Canada has beenvery helpful attending and presenting with us at council meetings and at public consultationevents We will of course continue our oral health surveillance of the children of Muskoka documentingand reporting in future years on the increase in dental decay that we anticipate will occur Suchsurveillance is the foundation of our advocacy both to municipal politicians and to the province I am very concerned that our experience will continue to repeat itself across the province unlessthere is strong leadership provincially It is with this in mind that I raise the followingrecommendations for your consideration
1 That we collectively (with PHOrsquos leadership) conduct high quality publish-worthy researchdocumenting the impact on dental decay that occurs in those municipalities throughoutOntario that in recent years have discontinued community water fluoridation This could bepart of a larger study on such municipalities across the country and it could also be part ofa study documenting overall oral health (including fluoridation coverage) in the province(and possibly across the country)
2 That COMOH engage with our Chief MOH to advocate for the province to require allmunicipal water supplies to be fluoridated (the exception of course being those withnaturally sufficient fluoride concentrations) This could built upon the alPHa position to
Gordon
Highlight
Gordon
Highlight
date (A11-00 - Community Water Fluoridation) on the CMOH position (Oral Health ndash) and on theemail discussion generated on the COMOH listserv some months back re Richardrsquosproposal (calling on the province to fund municipal water fluoridation)
Valerie I request that this be an item for our COMOH meeting on November 15th Sincerely Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorg From Gardner Charles Sent Thursday September 26 2013 245 PMTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes(RayCopesoahppca)Subject Community Water Fluoridation Under Challenge Again in Simcoe Muskoka Hello Colleagues You may wish to know that community water fluoridation (CWF) is again under challenge in SimcoeMuskoka specifically both in Tottenham (Town of New Tecumseth in Simcoe County) and for theentire District of Muskoka On Monday September 23 Committee of the Whole Council of theTown of New Tecumseth voted to submit application to discontinue community water fluoridation(CWF) in the town of Tottenham despite presentations to the contrary from our dental consultantDr Ito and from me The next Council meeting is scheduled for Monday Sept 30 at which lastMondayrsquos (Sept 23) votes will be ratified
Since Monday I have spoken with the Mayor of the Town of New Tecumseth and with most of thecouncilors encouraging deferral of a decision on Monday to allow the town more time to make afully informed decision
This is the second time in recent years that the issue of discontinuing CWF in Tottenham has beenraised at council This issue is also scheduled to return again to the District of Muskoka Council on
October 21st where I will be presenting in response to deputations in opposition to fluoridation
Outside of Base Borden Tottenham is the only community with fluoridated water in SimcoeCounty The health unitrsquos own screening data between 2011 and 2013 shows that Tottenhamrsquos
Gordon
Highlight
children as well as those in Muskoka have a lower rate of dental decay than Simcoe Muskokacommunities without CWF
Sincerely
Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorgChuck Gardner MOH
November 04 2013
Mandatory State Laws on Fluoridation Thirteen states Puerto Rico and the District of Columbia have laws intended to provide
statewide fluoridation These states and the year that the fluoridation legislation was passed are
District of Columbia (1952) Connecticut (1965) Kentucky (1966) Illinois (1967) Minnesota
(1967) Ohio (1969) South Dakota (1969) Georgia (1973) Nebraska (1973 and 2008)
California (1995) Delaware (1998) Puerto Rico (1998) Nevada (1999) Louisiana (2008) and
Arkansas (2011) (see Table 1) The sizes of the public water systems or countiescommunities
affected and exemption provisions vary by state Table 1
STATES THAT HAVE MANDATORY LAWS ON FLUORIDATION -2011
State (1) Year of
Fluoridation
Legislation (1)
Population
served by
Fluoridated
CWS (2)
Persons
receiving
fluoridated
water (2)
State
Average
Caries
Experience
of Grade 3
Students (3)
Arkansas 2011 647 1724131 64
California 1995 621 22812721 709
Connecticut 1965 910 2370423 406
Delaware 1998 862 705344 545
Georgia 1973 921 8924598 52
Illinois 1967 993 11325132 532
Kentucky 1966 999 4334223 598
Louisiana 2008 407 1846149 657
Minnesota 1967 988 4117266 549
Nebraska 1973 and 2008 702 1001665 593
Nevada 1999 702 1001665 649
Ohio 1969 877 8772683 512
South Dakota 1969 948 642942 623
District of
Columbia
1952 1000 595000
Puerto Rico 1998
United States 739 204283554
2010 Statistics for population fluoridated and number of people
1 Communication with Jane McGinley RDH MBA Manager Fluoridation and Preventive Health
Activities Council on Access Prevention and Interprofessional Relations
2 Centers for Disease Control and Prevention Department of Health and Human Services
accessed Oct 21 2013 httpwwwcdcgovfluoridationstatistics2010statshtm
3 Centers for Disease Control and Prevention National Oral Health Surveillance System Caries
Experience - Percentage of 3rd Grade students with Caries Experience (treated or untreated tooth
If data from 43 states for the percentage of Grade 3 children with experience of dental decay is
compared with the 2008 percentages of the population in a state with Community Water
Fluoridation then the percentage of children with experience of dental decay decreases as the
percentage of the state population with Community Water Fluoridation increases (see Figure 1)
Figure 1
Correlation of Percentage of Grade 3 Children with Caries Experience and
Percentage of Population With Community Water Fluoridation for 43
Reporting States
0
10
20
30
40
50
60
70
80
0 10 20 30 40 50 60 70 80 90 100
State of Population With Community Water Fluoridation
Sta
te
of
Gra
de 3
Stu
den
ts w
ith
Cari
es E
xp
eri
en
ce
Data from CDC (2 3)
The description of the fluoridation laws in California Illinois and Nevada can be found on the
Association of State amp Territorial Dental Directors website(4 7 8)
The California fluoridation law AB 733 came into effect in 1995 requiring communities of 10
000 residents or more be supplied with fluoridated drinking water However the state did not
provide any funding to implement the legislation (California is unique in requiring fluoridation
without funding the practice)(4) The California Department of Health Services therefore had to
fund fluoridation initiatives from non-governmental sources ie the California Endowment
California Dental Association Foundation the First 5 Commission and others(5) From 1995 to
2011 the percentage of the California population receiving fluoridated drinking water has risen
from 17 to 625(6) 4 Dental Public Health Activities amp Practices Office of Oral Health California Department of Health
Services April 2002 httpwwwastddorgbestpracticesDES06002CAfluoridationpdf
5 Stock M Pollick H The CDA Foundation Model to Fluoridate Communities California Dental
Association Journal vol 40 no 8 649 - 655
httpwwwcdaorgPortals0journaljournal_082012pdf
6 California Dental Association Foundation
httpwwwcdafoundationorglearnadvocacyfluoridation
The State of Illinois passed a mandatory fluoridation state in 1967 and required all community
water systems to adjust fluoride levels in the drinking water to optimal levels within 1 year(7)
From 1962 when over 5000000 residents had optimally fluoridated drinking water by 2010
the number had risen to 11325132 (993 of the population on community water systems)(2)
7 Dental Public Health Activities amp Practices Division of Oral Health Illinois Department of Public
Health April 2002 httpwwwastddorgbestpracticesDES16007ILfluoridationpdf
The State of Nevada passed a mandatory fluoridation statute in 2000 for communities with
400000 or more residents(8) This was a result of the work of a statewide coalition that
included the Nevada Dental and Dental Hygienist Associations the Washoe and Clark County
District Health Departments the Clark County School District Junior League of Las Vegas
Head Start the Community College of Southern Nevada Dental Hygiene Program Health
Access Washoe County and Saint Maryrsquos Hospital For communities with less than 400000 the
implementation of fluoridation still required the vote of the majority voters in the community
The Las Vegas Water Authority and the City of Henderson started fluoridation in 2000
increasing the percentage of the population with fluoridated drinking water from 2 to 65 (8) 8 Dental Public Health Activities amp Practices Bureau of Family Health Services Nevada State Health
Division April 2002 httpwwwastddorgbestpracticesDES31002NVfluoridationbillpdf
Countries with Mandatory Laws on Fluoridation Countries that have mandated Community Water Fluoridation are Brazil Hong Kong
Malaysia Singapore Ireland Israel and some of the states in Australia
Singapore started fluoridating its water in 1956 based on the success of the fluoridation trials in
Grand Rapids Newburgh Evanston and Brantford Singapore became the first Asian country to
have 100 of its population benefitting from the implementation of fluoridated drinking water
Loh reported that ldquoThe ten year study on the effects of water fluoridation in Singapore showed
a decrease in caries prevalence in the children In the permanent dentition the reduction was
523 per cent for Chinese and 31 per cent for Malays in the 7 to 9 year old age group A similar
trend was observed in the mixed dentition in which the decrease was 325 per cent for Chinese
and 306 per cent for Malaysrdquo(9) By 2010 the population of the country was 5080000(10)
9 Loh T Thirty-eight years of water fluoridation--the Singapore scenario Community Dent
Health 1996 Sep13 Suppl 247-50
10 British Fluoridation Society One in a Million the facts about water fluoridation 3rd Edition
published March 2012) httpwwwbfsweborgonemillion0920One20in20a20Million20-
20The20Extent20of20Fluoridationpdf
Hong Kong started implementing community water fluoridation in 1961 and similar to
Singapore 100 of the population received access to fluoridated drinking water Lo and Wong
reported that ldquoThe mean DMFT score of the children deceased from 44 in 1960 to 15 in 1968
stayed at this level in the 1980 and 1986 surveys and further deceased to 08 in 2001 The
prevalence of dental fluorosis among the children surveyed in 1960 was 1 and this increased
to 59 and 70 in 1968 and 1980 respectively It was found in the 1986 and 2001 surveys that
the prevalences of fluorosis were 47 and 9 among children whose teeth developed at the
time when the respective water fluoride concentrations were 07 ppm and 05 ppmrdquo(11) The
population of Hong Kong was 6968000 in 2009(10) 11 LO ECM and WONG AHH Water fluoride concentration and fluorosis in Hong Kong in 1960-
2001 84th General Session and Exhibition of the International Association for Dental Research amp
1st Meeting of the Pan-Asian-Pacific Federation Brisbane Australia 28 June-1 July 2006 v 85 n
Sp B
The Malaysian cabinet approved a nationwide community water fluoridation program in 1972
(12) One of the states Sabah decided to stop fluoridation in 1989 due to concerns about
inadequate supervision in adding fluoride to the drinking water Oral Health Surveys in 2009
and 2007 indicated that children in Sabah had the worst oral health with 50 of 12 year-olds
having decay in their permanent teeth and children having an average of 3 teeth being(13)
Under the 10th Malaysian Plan in 2011 the federal and the Sabah state governments
reintroduced water fluoridation in Sabah(1314) In 2010 about 755 of the Malaysian
population or 20700000 people had fluoridated drinking water(1013) 12 Malaysian Dental Association Fluoride in Water
httpwwwmdaorgmy07_public_01healthcare_12htm
13 Sachdev N Fluoridation in Sabah Water for Cleaner Teeth French Tribunecom 28022011
From Levy IsraTo Jaeger ValerieCc Pim Carolyn gordonalphaweborg Diallo Aicha Penny Sutcliffe Paul Roumeliotis Michael Finkelstein
Hazel Lynn Robert KyleSubject FW Panorama - Privacy Security and other issuesDate Wednesday October 16 2013 122110 PM
Hello ValerieOttawa is part of Wave 4 Panorama implementation and we are gearing up increasingly to use thesystem where and if possible Thinking about it I am anticipating that this may need to be on theCOMOH (and alPHa) radar as it is something that will impact all health units and implies a majoroperational shift in vaccine delivery programs for all health units I have asked Carolyn Pim toconnect with our sister wave 4 units to share common experiences as we move forward ndash when wehave a roll up could I bring to COMOH Exec for discussion to explore whether there are broaderimplications for all members As an aside I have also asked the Ministry and their CIO to share with me any roll up learnings thatthey may have had already from previous waves (I understand that Niagara HU was a wave 1participant so if there is such a roll up of common experiences that others could learn fromperhaps you have it already and that could come to the exec too)Thanks Isra From Pim Carolyn Sent October 10 2013 1228 PMTo Christopher Mackie (christophermackiemlhuonca) Elizabeth Richardson(Elizabethrichardsonhamiltonca) H BSc M D F R C P (C) MPH Jim Chirico(jimchiriconbpsdhuca) Marlene Spruyt (spruytmtimiskaminghucom) Robert Kyle (Durham)Cc Levy IsraSubject Panorama - Privacy Security and other issues Dear colleagues Irsquom reaching out to you as fellow Panorama Wave 4 health units to ask about where yourorganizations are at in the process of signing agreements and completing Privacy ImpactAssessments and Threat Risk Assessments (TRAs) Ottawa Public Healthrsquos IT legal and informationsecurity advisors have made numerous requests to the MOHLTC for information (in particular theprovincial TRA) that we consider essential to develop our own risk assessment and PIA but havebeen told that information cannot be shared even with strict confidentiality and access controlsSo we are at somewhat of an impasse Isra emailed Arlene yesterday Arlene has forwarded ourconcerns to the Ministryrsquos CIO and Panorama lead but we havenrsquot had any response or discussionswith either of them yet Have your organizations identified similar concerns andor had interactions with the MOHLTC inthis respect Irsquod also be interested in knowing if your health units have flagged other (egoperational) implementation concerns Thanks
Carolyn ps Robert ndash you can ignore this request I talked with Sharan this morning about Durhamrsquos issuesso am including you now just for information Carolyn Pim MD FRCPC Associate Medical Officer of Health Meacutedecin adjointe en santeacute publique Ottawa Public Health Santeacute publique Ottawa 100 Constellation Cr Ottawa ON K2G 6J8 Tel teacutel (613) 580-6744 ext 23684Fax (613) 580-9641Connect With Ottawa Public Health
Suivez Santeacute publique Ottawa
This e-mail originates from the City of Ottawa e-mail system Any distribution use orcopying of this e-mail or the information it contains by other than the intendedrecipient(s) is unauthorized If you are not the intended recipient please notify meat the telephone number shown above or by return e-mail and delete thiscommunication and any copy immediately Thank you
Le preacutesent courriel a eacuteteacute expeacutedieacute par le systegraveme de courriels de la Ville dOttawaToute distribution utilisation ou reproduction du courriel ou des renseignements quisy trouvent par une personne autre que son destinataire preacutevu est interdite Si vousavez reccedilu le message par erreur veuillez men aviser par teacuteleacutephone (au numeacuteropreacuteciteacute) ou par courriel puis supprimer sans deacutelai la version originale de lacommunication ainsi que toutes ses copies Je vous remercie de votre collaboration
1
Smoke-Free Patios ndash An Amendment to the Smoke-Free Ontario Act
Date November 15 2013 Prepared for Council of Ontario Medical Officers of Health Prepared by York Region Public Health _____________________________________________________________________________ Issue
The Smoke-Free Ontario Act is the current provincial legislation that imposes smoking restrictions in workplaces and public places It prohibits smoking on restaurant and bar patios in instances where any portion of the seating area is covered by a roof With recent studies illustrating that exposure to second hand smoke outdoors poses similar risks to indoor exposure there has been growing public support to enhance smoking restrictions and make patios completely smoke-free
Background
With the implementation of the Smoke-Free Ontario Act in 2006 restaurant and bar patios became subject to smoking restrictions if any portion of the seating area was covered by a roof This allowed for patios without roof coverings to continue to allow smoking and as a result did not provide significant protection to patrons or staff from exposure to second hand smoke outdoors Many businesses chose to alter the design of their patios to allow smoking to continue In some cases patios became more crowded since smoking patrons who dine indoors often proceed outside onto licensed patios with their beverages to smoke York Region like most municipalities in Ontario is host to hundreds of patios being operated by restaurant owners and businesses With smoking prohibitions affecting only a small portion of these patios specifically ones with coverings the vast majority of patios still allow smoking to take place Patrons and employees on patios where smoking is not restricted are exposed to second hand smoke frequently This can contribute to increased disease and aggravation of existing health conditions From a business perspective the existing legislation has been viewed by many operators as unfair because some patios have permanent coverings which cannot be removed requiring a smoke-free status These business owners feel this creates an uneven playing field since they cannot provide an outdoor dining area for their smoking customers There is strong community support for smoke-free patios in Ontario A 2009 Rapid Risk Factor Surveillance System survey revealed 754 percent support in York Region while a Toronto Health Survey in 2011 indicated 74 percent public support
2
Current Status
Smoking is currently prohibited on restaurant and bar patios province-wide in four Canadian provinces and territories Alberta Newfoundland and Labrador Nova Scotia and Yukon A fifth province Prince Edward Island prohibits smoking on patios until 10 pm Since Ontario enacted legislation restricting smoking on patios in 2006 eight municipalities in Ontario have chosen to create bylaws that go beyond the Smoke-Free Ontario Act and enhance outdoor protection from second hand smoke by prohibiting smoking on patios completely The largest of those municipalities is the City of Ottawa Recently the Toronto Board of Health unanimously endorsed a report presented by their Medical Officer of Health recommending that restaurant and bar patios be made smoke-free through an amendment to the Smoke-Free Ontario Act
Key Considerations
There should be no significant financial burden to local Boards of Health resulting from a smoke-free patio amendment to the Smoke-Free Ontario Act Inspection and enforcement for the Smoke-Free Ontario Act is currently 100 percent funded by the Ministry of Health and Long-Term Care Following an introductory period of education on the amendment a complaint response model of service delivery would ensure ongoing compliance with smoke-free requirements A complete ban of smoking on patios would eliminate the widely-held perception by business owners that the current legislation creates an uneven playing field for business Since Smoke-Free Ontario Act inspections of patios began in 2006 operators have expressed the opinion that if patios need to be smoke-free for the protection of the public they should all be smoke-free to avoid undue hardship for individual businesses and to provide protection uniformly across the Province
Next steps
York Region Public Health intends to seek support from Medical Officers of Health across the Central East Tobacco Control Area Network (CETCAN) to advocate to the Ministry of Health and Long-Term Care for an amendment to the Smoke-Free Ontario Act prohibiting smoking on all restaurant and bar patios York Region is also in the process of requesting that its Regional Council advocate to the Minister of Health and Long-Term Care on the issue
Updating and Modernizing O Regulation 565 (Public Pools)
Date November 15 2013
Prepared for Council of Ontario Medical Officers of Health
Prepared by York Region Public Health _____________________________________________________________________________ Background Recent drownings at public pools in Ontario have highlighted the issue of water-borne illness and injury The current pool regulation under Ontariorsquos Health Protection and Promotion Act O Regulation 565 (Public Pools) is outdated It does not accurately reflect new pool technology and design or the changing use of public pools Neither does it incorporate admissions standards recommended by the Office of the Chief Coroner Further O Regulation 565 does not have short-form wording or set fines associated with it This limits public health enforcement capabilities What is the impact Updating O Regulation 565 (Public Pools) to address recent changes in pool technology design and uses and to include Coroner-recommended admissions standards would help improve pool safety Establishing short-form wording for O Regulation 565 would enhance enforcement related to public pools Currently the only enforcement available to Public Health Inspectors for dealing with non-critical regulatory infractions in public pools is the issuance of a Part III summons This involves a considerable amount of resources for a possible small fine With the development of inspection disclosure systems such as YorkSafe there is an even greater need to develop a method to effectively address repeated pool operator non-compliance with non-critical issues Next steps Public health units should advocate to the Province to 1) Conduct a review of O Regulation 565 (Public Pools) to address shortcomings Proposed changes to the
regulation should include a requirement for ownersoperators of public pools to advise the local Medical Officer of Health of any change in the use of a facility and the addition of the Coronerrsquos recommended admission standards
2) Provide short-form wording for O Regulation 565 so that public health inspectors can better deal with pool operator non-compliance
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
this situation and liaise with our colleagues at Health Canada Please share this information with your tobacco control staff and contact me or DainaMueller Manager Tobacco Control Unit Health Promotion Implementation Branch atdainamuellerontarioca with any questions RegardsLaura Laura A PiskoDirectorHealth Promotion Implementation BranchHealth Promotion DivisionMinistry of Health and Long Term Care416-327-7445 (office)416-451-3185 (mobile) Marcus Gordon - EA (416)326-0625 for urgent issues
========= Middlesex-London Health Unit E-Mail Disclaimer =============______________________________________________________________
Private and confidential intended only for named recipient If otherwisereceived please destroy immediately Health information in this email isonly general information and is not intended to replace an in personconsultation with a medical professional nor is it intended to providemedical advice Individual circumstances of which we are not aware mayaffect the information provided herein and as such the Middlesex-LondonHealth Unit assumes no liability or responsibility for your reliancethereon The Middlesex-London Health Unit works under the authority of theHealth Protection and Promotion Act and this correspondence may be used toassess your needs for public health services (519-663-5317 ext 2448)______________________________________________________________
From Gardner CharlesTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes (RayCopesoahppca)
George Pasut (GeorgePasutoahppca) Peter Cooney (petercooneyhc-scgcca)Cc Ito DickSubject Discontinuation of Fluoridation in MuskokaDate Tuesday October 22 2013 125254 PM
Hello Colleagues
As I reported in my email below on September 26th fluoridation has come under challenge again inSimcoe Muskoka I am now very unhappy to report that despite our best efforts last night theDistrict Council of Muskoka voted to remove fluoride from municipal drinking supplies across theDistrict This brings to an end fluoridation in all of Simcoe and Muskoka (with the exception of Base Borden)ndash though New Tecumseth will be conducting a plebiscite on the question of fluoridation with themunicipal election next October Defending community water fluoridation has drained a great deal of time human resources andcommitment from other priorities and has been exhausting here in SMDHU as I am sure it hasbeen in many other health units While the outcomes have been very disappointing I have beenimpressed by the professionalism and dedication that SMDHU staff members have shown inshouldering this burden In particular our dental consultant Dr Ito has provided us with much ofthe foundational knowledge and the local research essential to our efforts and has very frequentlyattended and presented at council meetings and other public events I would also like to thank themany of you who have offer and provided support including advocacy letters and informationresources Over the years Dr Peter Cooney Chief Dental Officer of Health of Canada has beenvery helpful attending and presenting with us at council meetings and at public consultationevents We will of course continue our oral health surveillance of the children of Muskoka documentingand reporting in future years on the increase in dental decay that we anticipate will occur Suchsurveillance is the foundation of our advocacy both to municipal politicians and to the province I am very concerned that our experience will continue to repeat itself across the province unlessthere is strong leadership provincially It is with this in mind that I raise the followingrecommendations for your consideration
1 That we collectively (with PHOrsquos leadership) conduct high quality publish-worthy researchdocumenting the impact on dental decay that occurs in those municipalities throughoutOntario that in recent years have discontinued community water fluoridation This could bepart of a larger study on such municipalities across the country and it could also be part ofa study documenting overall oral health (including fluoridation coverage) in the province(and possibly across the country)
2 That COMOH engage with our Chief MOH to advocate for the province to require allmunicipal water supplies to be fluoridated (the exception of course being those withnaturally sufficient fluoride concentrations) This could built upon the alPHa position to
Gordon
Highlight
Gordon
Highlight
date (A11-00 - Community Water Fluoridation) on the CMOH position (Oral Health ndash) and on theemail discussion generated on the COMOH listserv some months back re Richardrsquosproposal (calling on the province to fund municipal water fluoridation)
Valerie I request that this be an item for our COMOH meeting on November 15th Sincerely Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorg From Gardner Charles Sent Thursday September 26 2013 245 PMTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes(RayCopesoahppca)Subject Community Water Fluoridation Under Challenge Again in Simcoe Muskoka Hello Colleagues You may wish to know that community water fluoridation (CWF) is again under challenge in SimcoeMuskoka specifically both in Tottenham (Town of New Tecumseth in Simcoe County) and for theentire District of Muskoka On Monday September 23 Committee of the Whole Council of theTown of New Tecumseth voted to submit application to discontinue community water fluoridation(CWF) in the town of Tottenham despite presentations to the contrary from our dental consultantDr Ito and from me The next Council meeting is scheduled for Monday Sept 30 at which lastMondayrsquos (Sept 23) votes will be ratified
Since Monday I have spoken with the Mayor of the Town of New Tecumseth and with most of thecouncilors encouraging deferral of a decision on Monday to allow the town more time to make afully informed decision
This is the second time in recent years that the issue of discontinuing CWF in Tottenham has beenraised at council This issue is also scheduled to return again to the District of Muskoka Council on
October 21st where I will be presenting in response to deputations in opposition to fluoridation
Outside of Base Borden Tottenham is the only community with fluoridated water in SimcoeCounty The health unitrsquos own screening data between 2011 and 2013 shows that Tottenhamrsquos
Gordon
Highlight
children as well as those in Muskoka have a lower rate of dental decay than Simcoe Muskokacommunities without CWF
Sincerely
Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorgChuck Gardner MOH
November 04 2013
Mandatory State Laws on Fluoridation Thirteen states Puerto Rico and the District of Columbia have laws intended to provide
statewide fluoridation These states and the year that the fluoridation legislation was passed are
District of Columbia (1952) Connecticut (1965) Kentucky (1966) Illinois (1967) Minnesota
(1967) Ohio (1969) South Dakota (1969) Georgia (1973) Nebraska (1973 and 2008)
California (1995) Delaware (1998) Puerto Rico (1998) Nevada (1999) Louisiana (2008) and
Arkansas (2011) (see Table 1) The sizes of the public water systems or countiescommunities
affected and exemption provisions vary by state Table 1
STATES THAT HAVE MANDATORY LAWS ON FLUORIDATION -2011
State (1) Year of
Fluoridation
Legislation (1)
Population
served by
Fluoridated
CWS (2)
Persons
receiving
fluoridated
water (2)
State
Average
Caries
Experience
of Grade 3
Students (3)
Arkansas 2011 647 1724131 64
California 1995 621 22812721 709
Connecticut 1965 910 2370423 406
Delaware 1998 862 705344 545
Georgia 1973 921 8924598 52
Illinois 1967 993 11325132 532
Kentucky 1966 999 4334223 598
Louisiana 2008 407 1846149 657
Minnesota 1967 988 4117266 549
Nebraska 1973 and 2008 702 1001665 593
Nevada 1999 702 1001665 649
Ohio 1969 877 8772683 512
South Dakota 1969 948 642942 623
District of
Columbia
1952 1000 595000
Puerto Rico 1998
United States 739 204283554
2010 Statistics for population fluoridated and number of people
1 Communication with Jane McGinley RDH MBA Manager Fluoridation and Preventive Health
Activities Council on Access Prevention and Interprofessional Relations
2 Centers for Disease Control and Prevention Department of Health and Human Services
accessed Oct 21 2013 httpwwwcdcgovfluoridationstatistics2010statshtm
3 Centers for Disease Control and Prevention National Oral Health Surveillance System Caries
Experience - Percentage of 3rd Grade students with Caries Experience (treated or untreated tooth
If data from 43 states for the percentage of Grade 3 children with experience of dental decay is
compared with the 2008 percentages of the population in a state with Community Water
Fluoridation then the percentage of children with experience of dental decay decreases as the
percentage of the state population with Community Water Fluoridation increases (see Figure 1)
Figure 1
Correlation of Percentage of Grade 3 Children with Caries Experience and
Percentage of Population With Community Water Fluoridation for 43
Reporting States
0
10
20
30
40
50
60
70
80
0 10 20 30 40 50 60 70 80 90 100
State of Population With Community Water Fluoridation
Sta
te
of
Gra
de 3
Stu
den
ts w
ith
Cari
es E
xp
eri
en
ce
Data from CDC (2 3)
The description of the fluoridation laws in California Illinois and Nevada can be found on the
Association of State amp Territorial Dental Directors website(4 7 8)
The California fluoridation law AB 733 came into effect in 1995 requiring communities of 10
000 residents or more be supplied with fluoridated drinking water However the state did not
provide any funding to implement the legislation (California is unique in requiring fluoridation
without funding the practice)(4) The California Department of Health Services therefore had to
fund fluoridation initiatives from non-governmental sources ie the California Endowment
California Dental Association Foundation the First 5 Commission and others(5) From 1995 to
2011 the percentage of the California population receiving fluoridated drinking water has risen
from 17 to 625(6) 4 Dental Public Health Activities amp Practices Office of Oral Health California Department of Health
Services April 2002 httpwwwastddorgbestpracticesDES06002CAfluoridationpdf
5 Stock M Pollick H The CDA Foundation Model to Fluoridate Communities California Dental
Association Journal vol 40 no 8 649 - 655
httpwwwcdaorgPortals0journaljournal_082012pdf
6 California Dental Association Foundation
httpwwwcdafoundationorglearnadvocacyfluoridation
The State of Illinois passed a mandatory fluoridation state in 1967 and required all community
water systems to adjust fluoride levels in the drinking water to optimal levels within 1 year(7)
From 1962 when over 5000000 residents had optimally fluoridated drinking water by 2010
the number had risen to 11325132 (993 of the population on community water systems)(2)
7 Dental Public Health Activities amp Practices Division of Oral Health Illinois Department of Public
Health April 2002 httpwwwastddorgbestpracticesDES16007ILfluoridationpdf
The State of Nevada passed a mandatory fluoridation statute in 2000 for communities with
400000 or more residents(8) This was a result of the work of a statewide coalition that
included the Nevada Dental and Dental Hygienist Associations the Washoe and Clark County
District Health Departments the Clark County School District Junior League of Las Vegas
Head Start the Community College of Southern Nevada Dental Hygiene Program Health
Access Washoe County and Saint Maryrsquos Hospital For communities with less than 400000 the
implementation of fluoridation still required the vote of the majority voters in the community
The Las Vegas Water Authority and the City of Henderson started fluoridation in 2000
increasing the percentage of the population with fluoridated drinking water from 2 to 65 (8) 8 Dental Public Health Activities amp Practices Bureau of Family Health Services Nevada State Health
Division April 2002 httpwwwastddorgbestpracticesDES31002NVfluoridationbillpdf
Countries with Mandatory Laws on Fluoridation Countries that have mandated Community Water Fluoridation are Brazil Hong Kong
Malaysia Singapore Ireland Israel and some of the states in Australia
Singapore started fluoridating its water in 1956 based on the success of the fluoridation trials in
Grand Rapids Newburgh Evanston and Brantford Singapore became the first Asian country to
have 100 of its population benefitting from the implementation of fluoridated drinking water
Loh reported that ldquoThe ten year study on the effects of water fluoridation in Singapore showed
a decrease in caries prevalence in the children In the permanent dentition the reduction was
523 per cent for Chinese and 31 per cent for Malays in the 7 to 9 year old age group A similar
trend was observed in the mixed dentition in which the decrease was 325 per cent for Chinese
and 306 per cent for Malaysrdquo(9) By 2010 the population of the country was 5080000(10)
9 Loh T Thirty-eight years of water fluoridation--the Singapore scenario Community Dent
Health 1996 Sep13 Suppl 247-50
10 British Fluoridation Society One in a Million the facts about water fluoridation 3rd Edition
published March 2012) httpwwwbfsweborgonemillion0920One20in20a20Million20-
20The20Extent20of20Fluoridationpdf
Hong Kong started implementing community water fluoridation in 1961 and similar to
Singapore 100 of the population received access to fluoridated drinking water Lo and Wong
reported that ldquoThe mean DMFT score of the children deceased from 44 in 1960 to 15 in 1968
stayed at this level in the 1980 and 1986 surveys and further deceased to 08 in 2001 The
prevalence of dental fluorosis among the children surveyed in 1960 was 1 and this increased
to 59 and 70 in 1968 and 1980 respectively It was found in the 1986 and 2001 surveys that
the prevalences of fluorosis were 47 and 9 among children whose teeth developed at the
time when the respective water fluoride concentrations were 07 ppm and 05 ppmrdquo(11) The
population of Hong Kong was 6968000 in 2009(10) 11 LO ECM and WONG AHH Water fluoride concentration and fluorosis in Hong Kong in 1960-
2001 84th General Session and Exhibition of the International Association for Dental Research amp
1st Meeting of the Pan-Asian-Pacific Federation Brisbane Australia 28 June-1 July 2006 v 85 n
Sp B
The Malaysian cabinet approved a nationwide community water fluoridation program in 1972
(12) One of the states Sabah decided to stop fluoridation in 1989 due to concerns about
inadequate supervision in adding fluoride to the drinking water Oral Health Surveys in 2009
and 2007 indicated that children in Sabah had the worst oral health with 50 of 12 year-olds
having decay in their permanent teeth and children having an average of 3 teeth being(13)
Under the 10th Malaysian Plan in 2011 the federal and the Sabah state governments
reintroduced water fluoridation in Sabah(1314) In 2010 about 755 of the Malaysian
population or 20700000 people had fluoridated drinking water(1013) 12 Malaysian Dental Association Fluoride in Water
httpwwwmdaorgmy07_public_01healthcare_12htm
13 Sachdev N Fluoridation in Sabah Water for Cleaner Teeth French Tribunecom 28022011
From Levy IsraTo Jaeger ValerieCc Pim Carolyn gordonalphaweborg Diallo Aicha Penny Sutcliffe Paul Roumeliotis Michael Finkelstein
Hazel Lynn Robert KyleSubject FW Panorama - Privacy Security and other issuesDate Wednesday October 16 2013 122110 PM
Hello ValerieOttawa is part of Wave 4 Panorama implementation and we are gearing up increasingly to use thesystem where and if possible Thinking about it I am anticipating that this may need to be on theCOMOH (and alPHa) radar as it is something that will impact all health units and implies a majoroperational shift in vaccine delivery programs for all health units I have asked Carolyn Pim toconnect with our sister wave 4 units to share common experiences as we move forward ndash when wehave a roll up could I bring to COMOH Exec for discussion to explore whether there are broaderimplications for all members As an aside I have also asked the Ministry and their CIO to share with me any roll up learnings thatthey may have had already from previous waves (I understand that Niagara HU was a wave 1participant so if there is such a roll up of common experiences that others could learn fromperhaps you have it already and that could come to the exec too)Thanks Isra From Pim Carolyn Sent October 10 2013 1228 PMTo Christopher Mackie (christophermackiemlhuonca) Elizabeth Richardson(Elizabethrichardsonhamiltonca) H BSc M D F R C P (C) MPH Jim Chirico(jimchiriconbpsdhuca) Marlene Spruyt (spruytmtimiskaminghucom) Robert Kyle (Durham)Cc Levy IsraSubject Panorama - Privacy Security and other issues Dear colleagues Irsquom reaching out to you as fellow Panorama Wave 4 health units to ask about where yourorganizations are at in the process of signing agreements and completing Privacy ImpactAssessments and Threat Risk Assessments (TRAs) Ottawa Public Healthrsquos IT legal and informationsecurity advisors have made numerous requests to the MOHLTC for information (in particular theprovincial TRA) that we consider essential to develop our own risk assessment and PIA but havebeen told that information cannot be shared even with strict confidentiality and access controlsSo we are at somewhat of an impasse Isra emailed Arlene yesterday Arlene has forwarded ourconcerns to the Ministryrsquos CIO and Panorama lead but we havenrsquot had any response or discussionswith either of them yet Have your organizations identified similar concerns andor had interactions with the MOHLTC inthis respect Irsquod also be interested in knowing if your health units have flagged other (egoperational) implementation concerns Thanks
Carolyn ps Robert ndash you can ignore this request I talked with Sharan this morning about Durhamrsquos issuesso am including you now just for information Carolyn Pim MD FRCPC Associate Medical Officer of Health Meacutedecin adjointe en santeacute publique Ottawa Public Health Santeacute publique Ottawa 100 Constellation Cr Ottawa ON K2G 6J8 Tel teacutel (613) 580-6744 ext 23684Fax (613) 580-9641Connect With Ottawa Public Health
Suivez Santeacute publique Ottawa
This e-mail originates from the City of Ottawa e-mail system Any distribution use orcopying of this e-mail or the information it contains by other than the intendedrecipient(s) is unauthorized If you are not the intended recipient please notify meat the telephone number shown above or by return e-mail and delete thiscommunication and any copy immediately Thank you
Le preacutesent courriel a eacuteteacute expeacutedieacute par le systegraveme de courriels de la Ville dOttawaToute distribution utilisation ou reproduction du courriel ou des renseignements quisy trouvent par une personne autre que son destinataire preacutevu est interdite Si vousavez reccedilu le message par erreur veuillez men aviser par teacuteleacutephone (au numeacuteropreacuteciteacute) ou par courriel puis supprimer sans deacutelai la version originale de lacommunication ainsi que toutes ses copies Je vous remercie de votre collaboration
1
Smoke-Free Patios ndash An Amendment to the Smoke-Free Ontario Act
Date November 15 2013 Prepared for Council of Ontario Medical Officers of Health Prepared by York Region Public Health _____________________________________________________________________________ Issue
The Smoke-Free Ontario Act is the current provincial legislation that imposes smoking restrictions in workplaces and public places It prohibits smoking on restaurant and bar patios in instances where any portion of the seating area is covered by a roof With recent studies illustrating that exposure to second hand smoke outdoors poses similar risks to indoor exposure there has been growing public support to enhance smoking restrictions and make patios completely smoke-free
Background
With the implementation of the Smoke-Free Ontario Act in 2006 restaurant and bar patios became subject to smoking restrictions if any portion of the seating area was covered by a roof This allowed for patios without roof coverings to continue to allow smoking and as a result did not provide significant protection to patrons or staff from exposure to second hand smoke outdoors Many businesses chose to alter the design of their patios to allow smoking to continue In some cases patios became more crowded since smoking patrons who dine indoors often proceed outside onto licensed patios with their beverages to smoke York Region like most municipalities in Ontario is host to hundreds of patios being operated by restaurant owners and businesses With smoking prohibitions affecting only a small portion of these patios specifically ones with coverings the vast majority of patios still allow smoking to take place Patrons and employees on patios where smoking is not restricted are exposed to second hand smoke frequently This can contribute to increased disease and aggravation of existing health conditions From a business perspective the existing legislation has been viewed by many operators as unfair because some patios have permanent coverings which cannot be removed requiring a smoke-free status These business owners feel this creates an uneven playing field since they cannot provide an outdoor dining area for their smoking customers There is strong community support for smoke-free patios in Ontario A 2009 Rapid Risk Factor Surveillance System survey revealed 754 percent support in York Region while a Toronto Health Survey in 2011 indicated 74 percent public support
2
Current Status
Smoking is currently prohibited on restaurant and bar patios province-wide in four Canadian provinces and territories Alberta Newfoundland and Labrador Nova Scotia and Yukon A fifth province Prince Edward Island prohibits smoking on patios until 10 pm Since Ontario enacted legislation restricting smoking on patios in 2006 eight municipalities in Ontario have chosen to create bylaws that go beyond the Smoke-Free Ontario Act and enhance outdoor protection from second hand smoke by prohibiting smoking on patios completely The largest of those municipalities is the City of Ottawa Recently the Toronto Board of Health unanimously endorsed a report presented by their Medical Officer of Health recommending that restaurant and bar patios be made smoke-free through an amendment to the Smoke-Free Ontario Act
Key Considerations
There should be no significant financial burden to local Boards of Health resulting from a smoke-free patio amendment to the Smoke-Free Ontario Act Inspection and enforcement for the Smoke-Free Ontario Act is currently 100 percent funded by the Ministry of Health and Long-Term Care Following an introductory period of education on the amendment a complaint response model of service delivery would ensure ongoing compliance with smoke-free requirements A complete ban of smoking on patios would eliminate the widely-held perception by business owners that the current legislation creates an uneven playing field for business Since Smoke-Free Ontario Act inspections of patios began in 2006 operators have expressed the opinion that if patios need to be smoke-free for the protection of the public they should all be smoke-free to avoid undue hardship for individual businesses and to provide protection uniformly across the Province
Next steps
York Region Public Health intends to seek support from Medical Officers of Health across the Central East Tobacco Control Area Network (CETCAN) to advocate to the Ministry of Health and Long-Term Care for an amendment to the Smoke-Free Ontario Act prohibiting smoking on all restaurant and bar patios York Region is also in the process of requesting that its Regional Council advocate to the Minister of Health and Long-Term Care on the issue
Updating and Modernizing O Regulation 565 (Public Pools)
Date November 15 2013
Prepared for Council of Ontario Medical Officers of Health
Prepared by York Region Public Health _____________________________________________________________________________ Background Recent drownings at public pools in Ontario have highlighted the issue of water-borne illness and injury The current pool regulation under Ontariorsquos Health Protection and Promotion Act O Regulation 565 (Public Pools) is outdated It does not accurately reflect new pool technology and design or the changing use of public pools Neither does it incorporate admissions standards recommended by the Office of the Chief Coroner Further O Regulation 565 does not have short-form wording or set fines associated with it This limits public health enforcement capabilities What is the impact Updating O Regulation 565 (Public Pools) to address recent changes in pool technology design and uses and to include Coroner-recommended admissions standards would help improve pool safety Establishing short-form wording for O Regulation 565 would enhance enforcement related to public pools Currently the only enforcement available to Public Health Inspectors for dealing with non-critical regulatory infractions in public pools is the issuance of a Part III summons This involves a considerable amount of resources for a possible small fine With the development of inspection disclosure systems such as YorkSafe there is an even greater need to develop a method to effectively address repeated pool operator non-compliance with non-critical issues Next steps Public health units should advocate to the Province to 1) Conduct a review of O Regulation 565 (Public Pools) to address shortcomings Proposed changes to the
regulation should include a requirement for ownersoperators of public pools to advise the local Medical Officer of Health of any change in the use of a facility and the addition of the Coronerrsquos recommended admission standards
2) Provide short-form wording for O Regulation 565 so that public health inspectors can better deal with pool operator non-compliance
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
From Gardner CharlesTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes (RayCopesoahppca)
George Pasut (GeorgePasutoahppca) Peter Cooney (petercooneyhc-scgcca)Cc Ito DickSubject Discontinuation of Fluoridation in MuskokaDate Tuesday October 22 2013 125254 PM
Hello Colleagues
As I reported in my email below on September 26th fluoridation has come under challenge again inSimcoe Muskoka I am now very unhappy to report that despite our best efforts last night theDistrict Council of Muskoka voted to remove fluoride from municipal drinking supplies across theDistrict This brings to an end fluoridation in all of Simcoe and Muskoka (with the exception of Base Borden)ndash though New Tecumseth will be conducting a plebiscite on the question of fluoridation with themunicipal election next October Defending community water fluoridation has drained a great deal of time human resources andcommitment from other priorities and has been exhausting here in SMDHU as I am sure it hasbeen in many other health units While the outcomes have been very disappointing I have beenimpressed by the professionalism and dedication that SMDHU staff members have shown inshouldering this burden In particular our dental consultant Dr Ito has provided us with much ofthe foundational knowledge and the local research essential to our efforts and has very frequentlyattended and presented at council meetings and other public events I would also like to thank themany of you who have offer and provided support including advocacy letters and informationresources Over the years Dr Peter Cooney Chief Dental Officer of Health of Canada has beenvery helpful attending and presenting with us at council meetings and at public consultationevents We will of course continue our oral health surveillance of the children of Muskoka documentingand reporting in future years on the increase in dental decay that we anticipate will occur Suchsurveillance is the foundation of our advocacy both to municipal politicians and to the province I am very concerned that our experience will continue to repeat itself across the province unlessthere is strong leadership provincially It is with this in mind that I raise the followingrecommendations for your consideration
1 That we collectively (with PHOrsquos leadership) conduct high quality publish-worthy researchdocumenting the impact on dental decay that occurs in those municipalities throughoutOntario that in recent years have discontinued community water fluoridation This could bepart of a larger study on such municipalities across the country and it could also be part ofa study documenting overall oral health (including fluoridation coverage) in the province(and possibly across the country)
2 That COMOH engage with our Chief MOH to advocate for the province to require allmunicipal water supplies to be fluoridated (the exception of course being those withnaturally sufficient fluoride concentrations) This could built upon the alPHa position to
Gordon
Highlight
Gordon
Highlight
date (A11-00 - Community Water Fluoridation) on the CMOH position (Oral Health ndash) and on theemail discussion generated on the COMOH listserv some months back re Richardrsquosproposal (calling on the province to fund municipal water fluoridation)
Valerie I request that this be an item for our COMOH meeting on November 15th Sincerely Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorg From Gardner Charles Sent Thursday September 26 2013 245 PMTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes(RayCopesoahppca)Subject Community Water Fluoridation Under Challenge Again in Simcoe Muskoka Hello Colleagues You may wish to know that community water fluoridation (CWF) is again under challenge in SimcoeMuskoka specifically both in Tottenham (Town of New Tecumseth in Simcoe County) and for theentire District of Muskoka On Monday September 23 Committee of the Whole Council of theTown of New Tecumseth voted to submit application to discontinue community water fluoridation(CWF) in the town of Tottenham despite presentations to the contrary from our dental consultantDr Ito and from me The next Council meeting is scheduled for Monday Sept 30 at which lastMondayrsquos (Sept 23) votes will be ratified
Since Monday I have spoken with the Mayor of the Town of New Tecumseth and with most of thecouncilors encouraging deferral of a decision on Monday to allow the town more time to make afully informed decision
This is the second time in recent years that the issue of discontinuing CWF in Tottenham has beenraised at council This issue is also scheduled to return again to the District of Muskoka Council on
October 21st where I will be presenting in response to deputations in opposition to fluoridation
Outside of Base Borden Tottenham is the only community with fluoridated water in SimcoeCounty The health unitrsquos own screening data between 2011 and 2013 shows that Tottenhamrsquos
Gordon
Highlight
children as well as those in Muskoka have a lower rate of dental decay than Simcoe Muskokacommunities without CWF
Sincerely
Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorgChuck Gardner MOH
November 04 2013
Mandatory State Laws on Fluoridation Thirteen states Puerto Rico and the District of Columbia have laws intended to provide
statewide fluoridation These states and the year that the fluoridation legislation was passed are
District of Columbia (1952) Connecticut (1965) Kentucky (1966) Illinois (1967) Minnesota
(1967) Ohio (1969) South Dakota (1969) Georgia (1973) Nebraska (1973 and 2008)
California (1995) Delaware (1998) Puerto Rico (1998) Nevada (1999) Louisiana (2008) and
Arkansas (2011) (see Table 1) The sizes of the public water systems or countiescommunities
affected and exemption provisions vary by state Table 1
STATES THAT HAVE MANDATORY LAWS ON FLUORIDATION -2011
State (1) Year of
Fluoridation
Legislation (1)
Population
served by
Fluoridated
CWS (2)
Persons
receiving
fluoridated
water (2)
State
Average
Caries
Experience
of Grade 3
Students (3)
Arkansas 2011 647 1724131 64
California 1995 621 22812721 709
Connecticut 1965 910 2370423 406
Delaware 1998 862 705344 545
Georgia 1973 921 8924598 52
Illinois 1967 993 11325132 532
Kentucky 1966 999 4334223 598
Louisiana 2008 407 1846149 657
Minnesota 1967 988 4117266 549
Nebraska 1973 and 2008 702 1001665 593
Nevada 1999 702 1001665 649
Ohio 1969 877 8772683 512
South Dakota 1969 948 642942 623
District of
Columbia
1952 1000 595000
Puerto Rico 1998
United States 739 204283554
2010 Statistics for population fluoridated and number of people
1 Communication with Jane McGinley RDH MBA Manager Fluoridation and Preventive Health
Activities Council on Access Prevention and Interprofessional Relations
2 Centers for Disease Control and Prevention Department of Health and Human Services
accessed Oct 21 2013 httpwwwcdcgovfluoridationstatistics2010statshtm
3 Centers for Disease Control and Prevention National Oral Health Surveillance System Caries
Experience - Percentage of 3rd Grade students with Caries Experience (treated or untreated tooth
If data from 43 states for the percentage of Grade 3 children with experience of dental decay is
compared with the 2008 percentages of the population in a state with Community Water
Fluoridation then the percentage of children with experience of dental decay decreases as the
percentage of the state population with Community Water Fluoridation increases (see Figure 1)
Figure 1
Correlation of Percentage of Grade 3 Children with Caries Experience and
Percentage of Population With Community Water Fluoridation for 43
Reporting States
0
10
20
30
40
50
60
70
80
0 10 20 30 40 50 60 70 80 90 100
State of Population With Community Water Fluoridation
Sta
te
of
Gra
de 3
Stu
den
ts w
ith
Cari
es E
xp
eri
en
ce
Data from CDC (2 3)
The description of the fluoridation laws in California Illinois and Nevada can be found on the
Association of State amp Territorial Dental Directors website(4 7 8)
The California fluoridation law AB 733 came into effect in 1995 requiring communities of 10
000 residents or more be supplied with fluoridated drinking water However the state did not
provide any funding to implement the legislation (California is unique in requiring fluoridation
without funding the practice)(4) The California Department of Health Services therefore had to
fund fluoridation initiatives from non-governmental sources ie the California Endowment
California Dental Association Foundation the First 5 Commission and others(5) From 1995 to
2011 the percentage of the California population receiving fluoridated drinking water has risen
from 17 to 625(6) 4 Dental Public Health Activities amp Practices Office of Oral Health California Department of Health
Services April 2002 httpwwwastddorgbestpracticesDES06002CAfluoridationpdf
5 Stock M Pollick H The CDA Foundation Model to Fluoridate Communities California Dental
Association Journal vol 40 no 8 649 - 655
httpwwwcdaorgPortals0journaljournal_082012pdf
6 California Dental Association Foundation
httpwwwcdafoundationorglearnadvocacyfluoridation
The State of Illinois passed a mandatory fluoridation state in 1967 and required all community
water systems to adjust fluoride levels in the drinking water to optimal levels within 1 year(7)
From 1962 when over 5000000 residents had optimally fluoridated drinking water by 2010
the number had risen to 11325132 (993 of the population on community water systems)(2)
7 Dental Public Health Activities amp Practices Division of Oral Health Illinois Department of Public
Health April 2002 httpwwwastddorgbestpracticesDES16007ILfluoridationpdf
The State of Nevada passed a mandatory fluoridation statute in 2000 for communities with
400000 or more residents(8) This was a result of the work of a statewide coalition that
included the Nevada Dental and Dental Hygienist Associations the Washoe and Clark County
District Health Departments the Clark County School District Junior League of Las Vegas
Head Start the Community College of Southern Nevada Dental Hygiene Program Health
Access Washoe County and Saint Maryrsquos Hospital For communities with less than 400000 the
implementation of fluoridation still required the vote of the majority voters in the community
The Las Vegas Water Authority and the City of Henderson started fluoridation in 2000
increasing the percentage of the population with fluoridated drinking water from 2 to 65 (8) 8 Dental Public Health Activities amp Practices Bureau of Family Health Services Nevada State Health
Division April 2002 httpwwwastddorgbestpracticesDES31002NVfluoridationbillpdf
Countries with Mandatory Laws on Fluoridation Countries that have mandated Community Water Fluoridation are Brazil Hong Kong
Malaysia Singapore Ireland Israel and some of the states in Australia
Singapore started fluoridating its water in 1956 based on the success of the fluoridation trials in
Grand Rapids Newburgh Evanston and Brantford Singapore became the first Asian country to
have 100 of its population benefitting from the implementation of fluoridated drinking water
Loh reported that ldquoThe ten year study on the effects of water fluoridation in Singapore showed
a decrease in caries prevalence in the children In the permanent dentition the reduction was
523 per cent for Chinese and 31 per cent for Malays in the 7 to 9 year old age group A similar
trend was observed in the mixed dentition in which the decrease was 325 per cent for Chinese
and 306 per cent for Malaysrdquo(9) By 2010 the population of the country was 5080000(10)
9 Loh T Thirty-eight years of water fluoridation--the Singapore scenario Community Dent
Health 1996 Sep13 Suppl 247-50
10 British Fluoridation Society One in a Million the facts about water fluoridation 3rd Edition
published March 2012) httpwwwbfsweborgonemillion0920One20in20a20Million20-
20The20Extent20of20Fluoridationpdf
Hong Kong started implementing community water fluoridation in 1961 and similar to
Singapore 100 of the population received access to fluoridated drinking water Lo and Wong
reported that ldquoThe mean DMFT score of the children deceased from 44 in 1960 to 15 in 1968
stayed at this level in the 1980 and 1986 surveys and further deceased to 08 in 2001 The
prevalence of dental fluorosis among the children surveyed in 1960 was 1 and this increased
to 59 and 70 in 1968 and 1980 respectively It was found in the 1986 and 2001 surveys that
the prevalences of fluorosis were 47 and 9 among children whose teeth developed at the
time when the respective water fluoride concentrations were 07 ppm and 05 ppmrdquo(11) The
population of Hong Kong was 6968000 in 2009(10) 11 LO ECM and WONG AHH Water fluoride concentration and fluorosis in Hong Kong in 1960-
2001 84th General Session and Exhibition of the International Association for Dental Research amp
1st Meeting of the Pan-Asian-Pacific Federation Brisbane Australia 28 June-1 July 2006 v 85 n
Sp B
The Malaysian cabinet approved a nationwide community water fluoridation program in 1972
(12) One of the states Sabah decided to stop fluoridation in 1989 due to concerns about
inadequate supervision in adding fluoride to the drinking water Oral Health Surveys in 2009
and 2007 indicated that children in Sabah had the worst oral health with 50 of 12 year-olds
having decay in their permanent teeth and children having an average of 3 teeth being(13)
Under the 10th Malaysian Plan in 2011 the federal and the Sabah state governments
reintroduced water fluoridation in Sabah(1314) In 2010 about 755 of the Malaysian
population or 20700000 people had fluoridated drinking water(1013) 12 Malaysian Dental Association Fluoride in Water
httpwwwmdaorgmy07_public_01healthcare_12htm
13 Sachdev N Fluoridation in Sabah Water for Cleaner Teeth French Tribunecom 28022011
From Levy IsraTo Jaeger ValerieCc Pim Carolyn gordonalphaweborg Diallo Aicha Penny Sutcliffe Paul Roumeliotis Michael Finkelstein
Hazel Lynn Robert KyleSubject FW Panorama - Privacy Security and other issuesDate Wednesday October 16 2013 122110 PM
Hello ValerieOttawa is part of Wave 4 Panorama implementation and we are gearing up increasingly to use thesystem where and if possible Thinking about it I am anticipating that this may need to be on theCOMOH (and alPHa) radar as it is something that will impact all health units and implies a majoroperational shift in vaccine delivery programs for all health units I have asked Carolyn Pim toconnect with our sister wave 4 units to share common experiences as we move forward ndash when wehave a roll up could I bring to COMOH Exec for discussion to explore whether there are broaderimplications for all members As an aside I have also asked the Ministry and their CIO to share with me any roll up learnings thatthey may have had already from previous waves (I understand that Niagara HU was a wave 1participant so if there is such a roll up of common experiences that others could learn fromperhaps you have it already and that could come to the exec too)Thanks Isra From Pim Carolyn Sent October 10 2013 1228 PMTo Christopher Mackie (christophermackiemlhuonca) Elizabeth Richardson(Elizabethrichardsonhamiltonca) H BSc M D F R C P (C) MPH Jim Chirico(jimchiriconbpsdhuca) Marlene Spruyt (spruytmtimiskaminghucom) Robert Kyle (Durham)Cc Levy IsraSubject Panorama - Privacy Security and other issues Dear colleagues Irsquom reaching out to you as fellow Panorama Wave 4 health units to ask about where yourorganizations are at in the process of signing agreements and completing Privacy ImpactAssessments and Threat Risk Assessments (TRAs) Ottawa Public Healthrsquos IT legal and informationsecurity advisors have made numerous requests to the MOHLTC for information (in particular theprovincial TRA) that we consider essential to develop our own risk assessment and PIA but havebeen told that information cannot be shared even with strict confidentiality and access controlsSo we are at somewhat of an impasse Isra emailed Arlene yesterday Arlene has forwarded ourconcerns to the Ministryrsquos CIO and Panorama lead but we havenrsquot had any response or discussionswith either of them yet Have your organizations identified similar concerns andor had interactions with the MOHLTC inthis respect Irsquod also be interested in knowing if your health units have flagged other (egoperational) implementation concerns Thanks
Carolyn ps Robert ndash you can ignore this request I talked with Sharan this morning about Durhamrsquos issuesso am including you now just for information Carolyn Pim MD FRCPC Associate Medical Officer of Health Meacutedecin adjointe en santeacute publique Ottawa Public Health Santeacute publique Ottawa 100 Constellation Cr Ottawa ON K2G 6J8 Tel teacutel (613) 580-6744 ext 23684Fax (613) 580-9641Connect With Ottawa Public Health
Suivez Santeacute publique Ottawa
This e-mail originates from the City of Ottawa e-mail system Any distribution use orcopying of this e-mail or the information it contains by other than the intendedrecipient(s) is unauthorized If you are not the intended recipient please notify meat the telephone number shown above or by return e-mail and delete thiscommunication and any copy immediately Thank you
Le preacutesent courriel a eacuteteacute expeacutedieacute par le systegraveme de courriels de la Ville dOttawaToute distribution utilisation ou reproduction du courriel ou des renseignements quisy trouvent par une personne autre que son destinataire preacutevu est interdite Si vousavez reccedilu le message par erreur veuillez men aviser par teacuteleacutephone (au numeacuteropreacuteciteacute) ou par courriel puis supprimer sans deacutelai la version originale de lacommunication ainsi que toutes ses copies Je vous remercie de votre collaboration
1
Smoke-Free Patios ndash An Amendment to the Smoke-Free Ontario Act
Date November 15 2013 Prepared for Council of Ontario Medical Officers of Health Prepared by York Region Public Health _____________________________________________________________________________ Issue
The Smoke-Free Ontario Act is the current provincial legislation that imposes smoking restrictions in workplaces and public places It prohibits smoking on restaurant and bar patios in instances where any portion of the seating area is covered by a roof With recent studies illustrating that exposure to second hand smoke outdoors poses similar risks to indoor exposure there has been growing public support to enhance smoking restrictions and make patios completely smoke-free
Background
With the implementation of the Smoke-Free Ontario Act in 2006 restaurant and bar patios became subject to smoking restrictions if any portion of the seating area was covered by a roof This allowed for patios without roof coverings to continue to allow smoking and as a result did not provide significant protection to patrons or staff from exposure to second hand smoke outdoors Many businesses chose to alter the design of their patios to allow smoking to continue In some cases patios became more crowded since smoking patrons who dine indoors often proceed outside onto licensed patios with their beverages to smoke York Region like most municipalities in Ontario is host to hundreds of patios being operated by restaurant owners and businesses With smoking prohibitions affecting only a small portion of these patios specifically ones with coverings the vast majority of patios still allow smoking to take place Patrons and employees on patios where smoking is not restricted are exposed to second hand smoke frequently This can contribute to increased disease and aggravation of existing health conditions From a business perspective the existing legislation has been viewed by many operators as unfair because some patios have permanent coverings which cannot be removed requiring a smoke-free status These business owners feel this creates an uneven playing field since they cannot provide an outdoor dining area for their smoking customers There is strong community support for smoke-free patios in Ontario A 2009 Rapid Risk Factor Surveillance System survey revealed 754 percent support in York Region while a Toronto Health Survey in 2011 indicated 74 percent public support
2
Current Status
Smoking is currently prohibited on restaurant and bar patios province-wide in four Canadian provinces and territories Alberta Newfoundland and Labrador Nova Scotia and Yukon A fifth province Prince Edward Island prohibits smoking on patios until 10 pm Since Ontario enacted legislation restricting smoking on patios in 2006 eight municipalities in Ontario have chosen to create bylaws that go beyond the Smoke-Free Ontario Act and enhance outdoor protection from second hand smoke by prohibiting smoking on patios completely The largest of those municipalities is the City of Ottawa Recently the Toronto Board of Health unanimously endorsed a report presented by their Medical Officer of Health recommending that restaurant and bar patios be made smoke-free through an amendment to the Smoke-Free Ontario Act
Key Considerations
There should be no significant financial burden to local Boards of Health resulting from a smoke-free patio amendment to the Smoke-Free Ontario Act Inspection and enforcement for the Smoke-Free Ontario Act is currently 100 percent funded by the Ministry of Health and Long-Term Care Following an introductory period of education on the amendment a complaint response model of service delivery would ensure ongoing compliance with smoke-free requirements A complete ban of smoking on patios would eliminate the widely-held perception by business owners that the current legislation creates an uneven playing field for business Since Smoke-Free Ontario Act inspections of patios began in 2006 operators have expressed the opinion that if patios need to be smoke-free for the protection of the public they should all be smoke-free to avoid undue hardship for individual businesses and to provide protection uniformly across the Province
Next steps
York Region Public Health intends to seek support from Medical Officers of Health across the Central East Tobacco Control Area Network (CETCAN) to advocate to the Ministry of Health and Long-Term Care for an amendment to the Smoke-Free Ontario Act prohibiting smoking on all restaurant and bar patios York Region is also in the process of requesting that its Regional Council advocate to the Minister of Health and Long-Term Care on the issue
Updating and Modernizing O Regulation 565 (Public Pools)
Date November 15 2013
Prepared for Council of Ontario Medical Officers of Health
Prepared by York Region Public Health _____________________________________________________________________________ Background Recent drownings at public pools in Ontario have highlighted the issue of water-borne illness and injury The current pool regulation under Ontariorsquos Health Protection and Promotion Act O Regulation 565 (Public Pools) is outdated It does not accurately reflect new pool technology and design or the changing use of public pools Neither does it incorporate admissions standards recommended by the Office of the Chief Coroner Further O Regulation 565 does not have short-form wording or set fines associated with it This limits public health enforcement capabilities What is the impact Updating O Regulation 565 (Public Pools) to address recent changes in pool technology design and uses and to include Coroner-recommended admissions standards would help improve pool safety Establishing short-form wording for O Regulation 565 would enhance enforcement related to public pools Currently the only enforcement available to Public Health Inspectors for dealing with non-critical regulatory infractions in public pools is the issuance of a Part III summons This involves a considerable amount of resources for a possible small fine With the development of inspection disclosure systems such as YorkSafe there is an even greater need to develop a method to effectively address repeated pool operator non-compliance with non-critical issues Next steps Public health units should advocate to the Province to 1) Conduct a review of O Regulation 565 (Public Pools) to address shortcomings Proposed changes to the
regulation should include a requirement for ownersoperators of public pools to advise the local Medical Officer of Health of any change in the use of a facility and the addition of the Coronerrsquos recommended admission standards
2) Provide short-form wording for O Regulation 565 so that public health inspectors can better deal with pool operator non-compliance
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
date (A11-00 - Community Water Fluoridation) on the CMOH position (Oral Health ndash) and on theemail discussion generated on the COMOH listserv some months back re Richardrsquosproposal (calling on the province to fund municipal water fluoridation)
Valerie I request that this be an item for our COMOH meeting on November 15th Sincerely Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorg From Gardner Charles Sent Thursday September 26 2013 245 PMTo MOH Listserv Arlene King (CMOHontarioca) (presidentoahppca) Ray Copes(RayCopesoahppca)Subject Community Water Fluoridation Under Challenge Again in Simcoe Muskoka Hello Colleagues You may wish to know that community water fluoridation (CWF) is again under challenge in SimcoeMuskoka specifically both in Tottenham (Town of New Tecumseth in Simcoe County) and for theentire District of Muskoka On Monday September 23 Committee of the Whole Council of theTown of New Tecumseth voted to submit application to discontinue community water fluoridation(CWF) in the town of Tottenham despite presentations to the contrary from our dental consultantDr Ito and from me The next Council meeting is scheduled for Monday Sept 30 at which lastMondayrsquos (Sept 23) votes will be ratified
Since Monday I have spoken with the Mayor of the Town of New Tecumseth and with most of thecouncilors encouraging deferral of a decision on Monday to allow the town more time to make afully informed decision
This is the second time in recent years that the issue of discontinuing CWF in Tottenham has beenraised at council This issue is also scheduled to return again to the District of Muskoka Council on
October 21st where I will be presenting in response to deputations in opposition to fluoridation
Outside of Base Borden Tottenham is the only community with fluoridated water in SimcoeCounty The health unitrsquos own screening data between 2011 and 2013 shows that Tottenhamrsquos
Gordon
Highlight
children as well as those in Muskoka have a lower rate of dental decay than Simcoe Muskokacommunities without CWF
Sincerely
Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorgChuck Gardner MOH
November 04 2013
Mandatory State Laws on Fluoridation Thirteen states Puerto Rico and the District of Columbia have laws intended to provide
statewide fluoridation These states and the year that the fluoridation legislation was passed are
District of Columbia (1952) Connecticut (1965) Kentucky (1966) Illinois (1967) Minnesota
(1967) Ohio (1969) South Dakota (1969) Georgia (1973) Nebraska (1973 and 2008)
California (1995) Delaware (1998) Puerto Rico (1998) Nevada (1999) Louisiana (2008) and
Arkansas (2011) (see Table 1) The sizes of the public water systems or countiescommunities
affected and exemption provisions vary by state Table 1
STATES THAT HAVE MANDATORY LAWS ON FLUORIDATION -2011
State (1) Year of
Fluoridation
Legislation (1)
Population
served by
Fluoridated
CWS (2)
Persons
receiving
fluoridated
water (2)
State
Average
Caries
Experience
of Grade 3
Students (3)
Arkansas 2011 647 1724131 64
California 1995 621 22812721 709
Connecticut 1965 910 2370423 406
Delaware 1998 862 705344 545
Georgia 1973 921 8924598 52
Illinois 1967 993 11325132 532
Kentucky 1966 999 4334223 598
Louisiana 2008 407 1846149 657
Minnesota 1967 988 4117266 549
Nebraska 1973 and 2008 702 1001665 593
Nevada 1999 702 1001665 649
Ohio 1969 877 8772683 512
South Dakota 1969 948 642942 623
District of
Columbia
1952 1000 595000
Puerto Rico 1998
United States 739 204283554
2010 Statistics for population fluoridated and number of people
1 Communication with Jane McGinley RDH MBA Manager Fluoridation and Preventive Health
Activities Council on Access Prevention and Interprofessional Relations
2 Centers for Disease Control and Prevention Department of Health and Human Services
accessed Oct 21 2013 httpwwwcdcgovfluoridationstatistics2010statshtm
3 Centers for Disease Control and Prevention National Oral Health Surveillance System Caries
Experience - Percentage of 3rd Grade students with Caries Experience (treated or untreated tooth
If data from 43 states for the percentage of Grade 3 children with experience of dental decay is
compared with the 2008 percentages of the population in a state with Community Water
Fluoridation then the percentage of children with experience of dental decay decreases as the
percentage of the state population with Community Water Fluoridation increases (see Figure 1)
Figure 1
Correlation of Percentage of Grade 3 Children with Caries Experience and
Percentage of Population With Community Water Fluoridation for 43
Reporting States
0
10
20
30
40
50
60
70
80
0 10 20 30 40 50 60 70 80 90 100
State of Population With Community Water Fluoridation
Sta
te
of
Gra
de 3
Stu
den
ts w
ith
Cari
es E
xp
eri
en
ce
Data from CDC (2 3)
The description of the fluoridation laws in California Illinois and Nevada can be found on the
Association of State amp Territorial Dental Directors website(4 7 8)
The California fluoridation law AB 733 came into effect in 1995 requiring communities of 10
000 residents or more be supplied with fluoridated drinking water However the state did not
provide any funding to implement the legislation (California is unique in requiring fluoridation
without funding the practice)(4) The California Department of Health Services therefore had to
fund fluoridation initiatives from non-governmental sources ie the California Endowment
California Dental Association Foundation the First 5 Commission and others(5) From 1995 to
2011 the percentage of the California population receiving fluoridated drinking water has risen
from 17 to 625(6) 4 Dental Public Health Activities amp Practices Office of Oral Health California Department of Health
Services April 2002 httpwwwastddorgbestpracticesDES06002CAfluoridationpdf
5 Stock M Pollick H The CDA Foundation Model to Fluoridate Communities California Dental
Association Journal vol 40 no 8 649 - 655
httpwwwcdaorgPortals0journaljournal_082012pdf
6 California Dental Association Foundation
httpwwwcdafoundationorglearnadvocacyfluoridation
The State of Illinois passed a mandatory fluoridation state in 1967 and required all community
water systems to adjust fluoride levels in the drinking water to optimal levels within 1 year(7)
From 1962 when over 5000000 residents had optimally fluoridated drinking water by 2010
the number had risen to 11325132 (993 of the population on community water systems)(2)
7 Dental Public Health Activities amp Practices Division of Oral Health Illinois Department of Public
Health April 2002 httpwwwastddorgbestpracticesDES16007ILfluoridationpdf
The State of Nevada passed a mandatory fluoridation statute in 2000 for communities with
400000 or more residents(8) This was a result of the work of a statewide coalition that
included the Nevada Dental and Dental Hygienist Associations the Washoe and Clark County
District Health Departments the Clark County School District Junior League of Las Vegas
Head Start the Community College of Southern Nevada Dental Hygiene Program Health
Access Washoe County and Saint Maryrsquos Hospital For communities with less than 400000 the
implementation of fluoridation still required the vote of the majority voters in the community
The Las Vegas Water Authority and the City of Henderson started fluoridation in 2000
increasing the percentage of the population with fluoridated drinking water from 2 to 65 (8) 8 Dental Public Health Activities amp Practices Bureau of Family Health Services Nevada State Health
Division April 2002 httpwwwastddorgbestpracticesDES31002NVfluoridationbillpdf
Countries with Mandatory Laws on Fluoridation Countries that have mandated Community Water Fluoridation are Brazil Hong Kong
Malaysia Singapore Ireland Israel and some of the states in Australia
Singapore started fluoridating its water in 1956 based on the success of the fluoridation trials in
Grand Rapids Newburgh Evanston and Brantford Singapore became the first Asian country to
have 100 of its population benefitting from the implementation of fluoridated drinking water
Loh reported that ldquoThe ten year study on the effects of water fluoridation in Singapore showed
a decrease in caries prevalence in the children In the permanent dentition the reduction was
523 per cent for Chinese and 31 per cent for Malays in the 7 to 9 year old age group A similar
trend was observed in the mixed dentition in which the decrease was 325 per cent for Chinese
and 306 per cent for Malaysrdquo(9) By 2010 the population of the country was 5080000(10)
9 Loh T Thirty-eight years of water fluoridation--the Singapore scenario Community Dent
Health 1996 Sep13 Suppl 247-50
10 British Fluoridation Society One in a Million the facts about water fluoridation 3rd Edition
published March 2012) httpwwwbfsweborgonemillion0920One20in20a20Million20-
20The20Extent20of20Fluoridationpdf
Hong Kong started implementing community water fluoridation in 1961 and similar to
Singapore 100 of the population received access to fluoridated drinking water Lo and Wong
reported that ldquoThe mean DMFT score of the children deceased from 44 in 1960 to 15 in 1968
stayed at this level in the 1980 and 1986 surveys and further deceased to 08 in 2001 The
prevalence of dental fluorosis among the children surveyed in 1960 was 1 and this increased
to 59 and 70 in 1968 and 1980 respectively It was found in the 1986 and 2001 surveys that
the prevalences of fluorosis were 47 and 9 among children whose teeth developed at the
time when the respective water fluoride concentrations were 07 ppm and 05 ppmrdquo(11) The
population of Hong Kong was 6968000 in 2009(10) 11 LO ECM and WONG AHH Water fluoride concentration and fluorosis in Hong Kong in 1960-
2001 84th General Session and Exhibition of the International Association for Dental Research amp
1st Meeting of the Pan-Asian-Pacific Federation Brisbane Australia 28 June-1 July 2006 v 85 n
Sp B
The Malaysian cabinet approved a nationwide community water fluoridation program in 1972
(12) One of the states Sabah decided to stop fluoridation in 1989 due to concerns about
inadequate supervision in adding fluoride to the drinking water Oral Health Surveys in 2009
and 2007 indicated that children in Sabah had the worst oral health with 50 of 12 year-olds
having decay in their permanent teeth and children having an average of 3 teeth being(13)
Under the 10th Malaysian Plan in 2011 the federal and the Sabah state governments
reintroduced water fluoridation in Sabah(1314) In 2010 about 755 of the Malaysian
population or 20700000 people had fluoridated drinking water(1013) 12 Malaysian Dental Association Fluoride in Water
httpwwwmdaorgmy07_public_01healthcare_12htm
13 Sachdev N Fluoridation in Sabah Water for Cleaner Teeth French Tribunecom 28022011
From Levy IsraTo Jaeger ValerieCc Pim Carolyn gordonalphaweborg Diallo Aicha Penny Sutcliffe Paul Roumeliotis Michael Finkelstein
Hazel Lynn Robert KyleSubject FW Panorama - Privacy Security and other issuesDate Wednesday October 16 2013 122110 PM
Hello ValerieOttawa is part of Wave 4 Panorama implementation and we are gearing up increasingly to use thesystem where and if possible Thinking about it I am anticipating that this may need to be on theCOMOH (and alPHa) radar as it is something that will impact all health units and implies a majoroperational shift in vaccine delivery programs for all health units I have asked Carolyn Pim toconnect with our sister wave 4 units to share common experiences as we move forward ndash when wehave a roll up could I bring to COMOH Exec for discussion to explore whether there are broaderimplications for all members As an aside I have also asked the Ministry and their CIO to share with me any roll up learnings thatthey may have had already from previous waves (I understand that Niagara HU was a wave 1participant so if there is such a roll up of common experiences that others could learn fromperhaps you have it already and that could come to the exec too)Thanks Isra From Pim Carolyn Sent October 10 2013 1228 PMTo Christopher Mackie (christophermackiemlhuonca) Elizabeth Richardson(Elizabethrichardsonhamiltonca) H BSc M D F R C P (C) MPH Jim Chirico(jimchiriconbpsdhuca) Marlene Spruyt (spruytmtimiskaminghucom) Robert Kyle (Durham)Cc Levy IsraSubject Panorama - Privacy Security and other issues Dear colleagues Irsquom reaching out to you as fellow Panorama Wave 4 health units to ask about where yourorganizations are at in the process of signing agreements and completing Privacy ImpactAssessments and Threat Risk Assessments (TRAs) Ottawa Public Healthrsquos IT legal and informationsecurity advisors have made numerous requests to the MOHLTC for information (in particular theprovincial TRA) that we consider essential to develop our own risk assessment and PIA but havebeen told that information cannot be shared even with strict confidentiality and access controlsSo we are at somewhat of an impasse Isra emailed Arlene yesterday Arlene has forwarded ourconcerns to the Ministryrsquos CIO and Panorama lead but we havenrsquot had any response or discussionswith either of them yet Have your organizations identified similar concerns andor had interactions with the MOHLTC inthis respect Irsquod also be interested in knowing if your health units have flagged other (egoperational) implementation concerns Thanks
Carolyn ps Robert ndash you can ignore this request I talked with Sharan this morning about Durhamrsquos issuesso am including you now just for information Carolyn Pim MD FRCPC Associate Medical Officer of Health Meacutedecin adjointe en santeacute publique Ottawa Public Health Santeacute publique Ottawa 100 Constellation Cr Ottawa ON K2G 6J8 Tel teacutel (613) 580-6744 ext 23684Fax (613) 580-9641Connect With Ottawa Public Health
Suivez Santeacute publique Ottawa
This e-mail originates from the City of Ottawa e-mail system Any distribution use orcopying of this e-mail or the information it contains by other than the intendedrecipient(s) is unauthorized If you are not the intended recipient please notify meat the telephone number shown above or by return e-mail and delete thiscommunication and any copy immediately Thank you
Le preacutesent courriel a eacuteteacute expeacutedieacute par le systegraveme de courriels de la Ville dOttawaToute distribution utilisation ou reproduction du courriel ou des renseignements quisy trouvent par une personne autre que son destinataire preacutevu est interdite Si vousavez reccedilu le message par erreur veuillez men aviser par teacuteleacutephone (au numeacuteropreacuteciteacute) ou par courriel puis supprimer sans deacutelai la version originale de lacommunication ainsi que toutes ses copies Je vous remercie de votre collaboration
1
Smoke-Free Patios ndash An Amendment to the Smoke-Free Ontario Act
Date November 15 2013 Prepared for Council of Ontario Medical Officers of Health Prepared by York Region Public Health _____________________________________________________________________________ Issue
The Smoke-Free Ontario Act is the current provincial legislation that imposes smoking restrictions in workplaces and public places It prohibits smoking on restaurant and bar patios in instances where any portion of the seating area is covered by a roof With recent studies illustrating that exposure to second hand smoke outdoors poses similar risks to indoor exposure there has been growing public support to enhance smoking restrictions and make patios completely smoke-free
Background
With the implementation of the Smoke-Free Ontario Act in 2006 restaurant and bar patios became subject to smoking restrictions if any portion of the seating area was covered by a roof This allowed for patios without roof coverings to continue to allow smoking and as a result did not provide significant protection to patrons or staff from exposure to second hand smoke outdoors Many businesses chose to alter the design of their patios to allow smoking to continue In some cases patios became more crowded since smoking patrons who dine indoors often proceed outside onto licensed patios with their beverages to smoke York Region like most municipalities in Ontario is host to hundreds of patios being operated by restaurant owners and businesses With smoking prohibitions affecting only a small portion of these patios specifically ones with coverings the vast majority of patios still allow smoking to take place Patrons and employees on patios where smoking is not restricted are exposed to second hand smoke frequently This can contribute to increased disease and aggravation of existing health conditions From a business perspective the existing legislation has been viewed by many operators as unfair because some patios have permanent coverings which cannot be removed requiring a smoke-free status These business owners feel this creates an uneven playing field since they cannot provide an outdoor dining area for their smoking customers There is strong community support for smoke-free patios in Ontario A 2009 Rapid Risk Factor Surveillance System survey revealed 754 percent support in York Region while a Toronto Health Survey in 2011 indicated 74 percent public support
2
Current Status
Smoking is currently prohibited on restaurant and bar patios province-wide in four Canadian provinces and territories Alberta Newfoundland and Labrador Nova Scotia and Yukon A fifth province Prince Edward Island prohibits smoking on patios until 10 pm Since Ontario enacted legislation restricting smoking on patios in 2006 eight municipalities in Ontario have chosen to create bylaws that go beyond the Smoke-Free Ontario Act and enhance outdoor protection from second hand smoke by prohibiting smoking on patios completely The largest of those municipalities is the City of Ottawa Recently the Toronto Board of Health unanimously endorsed a report presented by their Medical Officer of Health recommending that restaurant and bar patios be made smoke-free through an amendment to the Smoke-Free Ontario Act
Key Considerations
There should be no significant financial burden to local Boards of Health resulting from a smoke-free patio amendment to the Smoke-Free Ontario Act Inspection and enforcement for the Smoke-Free Ontario Act is currently 100 percent funded by the Ministry of Health and Long-Term Care Following an introductory period of education on the amendment a complaint response model of service delivery would ensure ongoing compliance with smoke-free requirements A complete ban of smoking on patios would eliminate the widely-held perception by business owners that the current legislation creates an uneven playing field for business Since Smoke-Free Ontario Act inspections of patios began in 2006 operators have expressed the opinion that if patios need to be smoke-free for the protection of the public they should all be smoke-free to avoid undue hardship for individual businesses and to provide protection uniformly across the Province
Next steps
York Region Public Health intends to seek support from Medical Officers of Health across the Central East Tobacco Control Area Network (CETCAN) to advocate to the Ministry of Health and Long-Term Care for an amendment to the Smoke-Free Ontario Act prohibiting smoking on all restaurant and bar patios York Region is also in the process of requesting that its Regional Council advocate to the Minister of Health and Long-Term Care on the issue
Updating and Modernizing O Regulation 565 (Public Pools)
Date November 15 2013
Prepared for Council of Ontario Medical Officers of Health
Prepared by York Region Public Health _____________________________________________________________________________ Background Recent drownings at public pools in Ontario have highlighted the issue of water-borne illness and injury The current pool regulation under Ontariorsquos Health Protection and Promotion Act O Regulation 565 (Public Pools) is outdated It does not accurately reflect new pool technology and design or the changing use of public pools Neither does it incorporate admissions standards recommended by the Office of the Chief Coroner Further O Regulation 565 does not have short-form wording or set fines associated with it This limits public health enforcement capabilities What is the impact Updating O Regulation 565 (Public Pools) to address recent changes in pool technology design and uses and to include Coroner-recommended admissions standards would help improve pool safety Establishing short-form wording for O Regulation 565 would enhance enforcement related to public pools Currently the only enforcement available to Public Health Inspectors for dealing with non-critical regulatory infractions in public pools is the issuance of a Part III summons This involves a considerable amount of resources for a possible small fine With the development of inspection disclosure systems such as YorkSafe there is an even greater need to develop a method to effectively address repeated pool operator non-compliance with non-critical issues Next steps Public health units should advocate to the Province to 1) Conduct a review of O Regulation 565 (Public Pools) to address shortcomings Proposed changes to the
regulation should include a requirement for ownersoperators of public pools to advise the local Medical Officer of Health of any change in the use of a facility and the addition of the Coronerrsquos recommended admission standards
2) Provide short-form wording for O Regulation 565 so that public health inspectors can better deal with pool operator non-compliance
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
children as well as those in Muskoka have a lower rate of dental decay than Simcoe Muskokacommunities without CWF
Sincerely
Chuck
Dr Charles Gardner MD CCFP MHSc FRCPCMedical Officer of Health and Chief Executive OfficerSimcoe Muskoka District Health Unit15 Sperling DrBarrie OntarioL4M 6K9telephone 705-721-7520 ex 7219fax 705-721-1495email charlesgardnersmdhuorgChuck Gardner MOH
November 04 2013
Mandatory State Laws on Fluoridation Thirteen states Puerto Rico and the District of Columbia have laws intended to provide
statewide fluoridation These states and the year that the fluoridation legislation was passed are
District of Columbia (1952) Connecticut (1965) Kentucky (1966) Illinois (1967) Minnesota
(1967) Ohio (1969) South Dakota (1969) Georgia (1973) Nebraska (1973 and 2008)
California (1995) Delaware (1998) Puerto Rico (1998) Nevada (1999) Louisiana (2008) and
Arkansas (2011) (see Table 1) The sizes of the public water systems or countiescommunities
affected and exemption provisions vary by state Table 1
STATES THAT HAVE MANDATORY LAWS ON FLUORIDATION -2011
State (1) Year of
Fluoridation
Legislation (1)
Population
served by
Fluoridated
CWS (2)
Persons
receiving
fluoridated
water (2)
State
Average
Caries
Experience
of Grade 3
Students (3)
Arkansas 2011 647 1724131 64
California 1995 621 22812721 709
Connecticut 1965 910 2370423 406
Delaware 1998 862 705344 545
Georgia 1973 921 8924598 52
Illinois 1967 993 11325132 532
Kentucky 1966 999 4334223 598
Louisiana 2008 407 1846149 657
Minnesota 1967 988 4117266 549
Nebraska 1973 and 2008 702 1001665 593
Nevada 1999 702 1001665 649
Ohio 1969 877 8772683 512
South Dakota 1969 948 642942 623
District of
Columbia
1952 1000 595000
Puerto Rico 1998
United States 739 204283554
2010 Statistics for population fluoridated and number of people
1 Communication with Jane McGinley RDH MBA Manager Fluoridation and Preventive Health
Activities Council on Access Prevention and Interprofessional Relations
2 Centers for Disease Control and Prevention Department of Health and Human Services
accessed Oct 21 2013 httpwwwcdcgovfluoridationstatistics2010statshtm
3 Centers for Disease Control and Prevention National Oral Health Surveillance System Caries
Experience - Percentage of 3rd Grade students with Caries Experience (treated or untreated tooth
If data from 43 states for the percentage of Grade 3 children with experience of dental decay is
compared with the 2008 percentages of the population in a state with Community Water
Fluoridation then the percentage of children with experience of dental decay decreases as the
percentage of the state population with Community Water Fluoridation increases (see Figure 1)
Figure 1
Correlation of Percentage of Grade 3 Children with Caries Experience and
Percentage of Population With Community Water Fluoridation for 43
Reporting States
0
10
20
30
40
50
60
70
80
0 10 20 30 40 50 60 70 80 90 100
State of Population With Community Water Fluoridation
Sta
te
of
Gra
de 3
Stu
den
ts w
ith
Cari
es E
xp
eri
en
ce
Data from CDC (2 3)
The description of the fluoridation laws in California Illinois and Nevada can be found on the
Association of State amp Territorial Dental Directors website(4 7 8)
The California fluoridation law AB 733 came into effect in 1995 requiring communities of 10
000 residents or more be supplied with fluoridated drinking water However the state did not
provide any funding to implement the legislation (California is unique in requiring fluoridation
without funding the practice)(4) The California Department of Health Services therefore had to
fund fluoridation initiatives from non-governmental sources ie the California Endowment
California Dental Association Foundation the First 5 Commission and others(5) From 1995 to
2011 the percentage of the California population receiving fluoridated drinking water has risen
from 17 to 625(6) 4 Dental Public Health Activities amp Practices Office of Oral Health California Department of Health
Services April 2002 httpwwwastddorgbestpracticesDES06002CAfluoridationpdf
5 Stock M Pollick H The CDA Foundation Model to Fluoridate Communities California Dental
Association Journal vol 40 no 8 649 - 655
httpwwwcdaorgPortals0journaljournal_082012pdf
6 California Dental Association Foundation
httpwwwcdafoundationorglearnadvocacyfluoridation
The State of Illinois passed a mandatory fluoridation state in 1967 and required all community
water systems to adjust fluoride levels in the drinking water to optimal levels within 1 year(7)
From 1962 when over 5000000 residents had optimally fluoridated drinking water by 2010
the number had risen to 11325132 (993 of the population on community water systems)(2)
7 Dental Public Health Activities amp Practices Division of Oral Health Illinois Department of Public
Health April 2002 httpwwwastddorgbestpracticesDES16007ILfluoridationpdf
The State of Nevada passed a mandatory fluoridation statute in 2000 for communities with
400000 or more residents(8) This was a result of the work of a statewide coalition that
included the Nevada Dental and Dental Hygienist Associations the Washoe and Clark County
District Health Departments the Clark County School District Junior League of Las Vegas
Head Start the Community College of Southern Nevada Dental Hygiene Program Health
Access Washoe County and Saint Maryrsquos Hospital For communities with less than 400000 the
implementation of fluoridation still required the vote of the majority voters in the community
The Las Vegas Water Authority and the City of Henderson started fluoridation in 2000
increasing the percentage of the population with fluoridated drinking water from 2 to 65 (8) 8 Dental Public Health Activities amp Practices Bureau of Family Health Services Nevada State Health
Division April 2002 httpwwwastddorgbestpracticesDES31002NVfluoridationbillpdf
Countries with Mandatory Laws on Fluoridation Countries that have mandated Community Water Fluoridation are Brazil Hong Kong
Malaysia Singapore Ireland Israel and some of the states in Australia
Singapore started fluoridating its water in 1956 based on the success of the fluoridation trials in
Grand Rapids Newburgh Evanston and Brantford Singapore became the first Asian country to
have 100 of its population benefitting from the implementation of fluoridated drinking water
Loh reported that ldquoThe ten year study on the effects of water fluoridation in Singapore showed
a decrease in caries prevalence in the children In the permanent dentition the reduction was
523 per cent for Chinese and 31 per cent for Malays in the 7 to 9 year old age group A similar
trend was observed in the mixed dentition in which the decrease was 325 per cent for Chinese
and 306 per cent for Malaysrdquo(9) By 2010 the population of the country was 5080000(10)
9 Loh T Thirty-eight years of water fluoridation--the Singapore scenario Community Dent
Health 1996 Sep13 Suppl 247-50
10 British Fluoridation Society One in a Million the facts about water fluoridation 3rd Edition
published March 2012) httpwwwbfsweborgonemillion0920One20in20a20Million20-
20The20Extent20of20Fluoridationpdf
Hong Kong started implementing community water fluoridation in 1961 and similar to
Singapore 100 of the population received access to fluoridated drinking water Lo and Wong
reported that ldquoThe mean DMFT score of the children deceased from 44 in 1960 to 15 in 1968
stayed at this level in the 1980 and 1986 surveys and further deceased to 08 in 2001 The
prevalence of dental fluorosis among the children surveyed in 1960 was 1 and this increased
to 59 and 70 in 1968 and 1980 respectively It was found in the 1986 and 2001 surveys that
the prevalences of fluorosis were 47 and 9 among children whose teeth developed at the
time when the respective water fluoride concentrations were 07 ppm and 05 ppmrdquo(11) The
population of Hong Kong was 6968000 in 2009(10) 11 LO ECM and WONG AHH Water fluoride concentration and fluorosis in Hong Kong in 1960-
2001 84th General Session and Exhibition of the International Association for Dental Research amp
1st Meeting of the Pan-Asian-Pacific Federation Brisbane Australia 28 June-1 July 2006 v 85 n
Sp B
The Malaysian cabinet approved a nationwide community water fluoridation program in 1972
(12) One of the states Sabah decided to stop fluoridation in 1989 due to concerns about
inadequate supervision in adding fluoride to the drinking water Oral Health Surveys in 2009
and 2007 indicated that children in Sabah had the worst oral health with 50 of 12 year-olds
having decay in their permanent teeth and children having an average of 3 teeth being(13)
Under the 10th Malaysian Plan in 2011 the federal and the Sabah state governments
reintroduced water fluoridation in Sabah(1314) In 2010 about 755 of the Malaysian
population or 20700000 people had fluoridated drinking water(1013) 12 Malaysian Dental Association Fluoride in Water
httpwwwmdaorgmy07_public_01healthcare_12htm
13 Sachdev N Fluoridation in Sabah Water for Cleaner Teeth French Tribunecom 28022011
From Levy IsraTo Jaeger ValerieCc Pim Carolyn gordonalphaweborg Diallo Aicha Penny Sutcliffe Paul Roumeliotis Michael Finkelstein
Hazel Lynn Robert KyleSubject FW Panorama - Privacy Security and other issuesDate Wednesday October 16 2013 122110 PM
Hello ValerieOttawa is part of Wave 4 Panorama implementation and we are gearing up increasingly to use thesystem where and if possible Thinking about it I am anticipating that this may need to be on theCOMOH (and alPHa) radar as it is something that will impact all health units and implies a majoroperational shift in vaccine delivery programs for all health units I have asked Carolyn Pim toconnect with our sister wave 4 units to share common experiences as we move forward ndash when wehave a roll up could I bring to COMOH Exec for discussion to explore whether there are broaderimplications for all members As an aside I have also asked the Ministry and their CIO to share with me any roll up learnings thatthey may have had already from previous waves (I understand that Niagara HU was a wave 1participant so if there is such a roll up of common experiences that others could learn fromperhaps you have it already and that could come to the exec too)Thanks Isra From Pim Carolyn Sent October 10 2013 1228 PMTo Christopher Mackie (christophermackiemlhuonca) Elizabeth Richardson(Elizabethrichardsonhamiltonca) H BSc M D F R C P (C) MPH Jim Chirico(jimchiriconbpsdhuca) Marlene Spruyt (spruytmtimiskaminghucom) Robert Kyle (Durham)Cc Levy IsraSubject Panorama - Privacy Security and other issues Dear colleagues Irsquom reaching out to you as fellow Panorama Wave 4 health units to ask about where yourorganizations are at in the process of signing agreements and completing Privacy ImpactAssessments and Threat Risk Assessments (TRAs) Ottawa Public Healthrsquos IT legal and informationsecurity advisors have made numerous requests to the MOHLTC for information (in particular theprovincial TRA) that we consider essential to develop our own risk assessment and PIA but havebeen told that information cannot be shared even with strict confidentiality and access controlsSo we are at somewhat of an impasse Isra emailed Arlene yesterday Arlene has forwarded ourconcerns to the Ministryrsquos CIO and Panorama lead but we havenrsquot had any response or discussionswith either of them yet Have your organizations identified similar concerns andor had interactions with the MOHLTC inthis respect Irsquod also be interested in knowing if your health units have flagged other (egoperational) implementation concerns Thanks
Carolyn ps Robert ndash you can ignore this request I talked with Sharan this morning about Durhamrsquos issuesso am including you now just for information Carolyn Pim MD FRCPC Associate Medical Officer of Health Meacutedecin adjointe en santeacute publique Ottawa Public Health Santeacute publique Ottawa 100 Constellation Cr Ottawa ON K2G 6J8 Tel teacutel (613) 580-6744 ext 23684Fax (613) 580-9641Connect With Ottawa Public Health
Suivez Santeacute publique Ottawa
This e-mail originates from the City of Ottawa e-mail system Any distribution use orcopying of this e-mail or the information it contains by other than the intendedrecipient(s) is unauthorized If you are not the intended recipient please notify meat the telephone number shown above or by return e-mail and delete thiscommunication and any copy immediately Thank you
Le preacutesent courriel a eacuteteacute expeacutedieacute par le systegraveme de courriels de la Ville dOttawaToute distribution utilisation ou reproduction du courriel ou des renseignements quisy trouvent par une personne autre que son destinataire preacutevu est interdite Si vousavez reccedilu le message par erreur veuillez men aviser par teacuteleacutephone (au numeacuteropreacuteciteacute) ou par courriel puis supprimer sans deacutelai la version originale de lacommunication ainsi que toutes ses copies Je vous remercie de votre collaboration
1
Smoke-Free Patios ndash An Amendment to the Smoke-Free Ontario Act
Date November 15 2013 Prepared for Council of Ontario Medical Officers of Health Prepared by York Region Public Health _____________________________________________________________________________ Issue
The Smoke-Free Ontario Act is the current provincial legislation that imposes smoking restrictions in workplaces and public places It prohibits smoking on restaurant and bar patios in instances where any portion of the seating area is covered by a roof With recent studies illustrating that exposure to second hand smoke outdoors poses similar risks to indoor exposure there has been growing public support to enhance smoking restrictions and make patios completely smoke-free
Background
With the implementation of the Smoke-Free Ontario Act in 2006 restaurant and bar patios became subject to smoking restrictions if any portion of the seating area was covered by a roof This allowed for patios without roof coverings to continue to allow smoking and as a result did not provide significant protection to patrons or staff from exposure to second hand smoke outdoors Many businesses chose to alter the design of their patios to allow smoking to continue In some cases patios became more crowded since smoking patrons who dine indoors often proceed outside onto licensed patios with their beverages to smoke York Region like most municipalities in Ontario is host to hundreds of patios being operated by restaurant owners and businesses With smoking prohibitions affecting only a small portion of these patios specifically ones with coverings the vast majority of patios still allow smoking to take place Patrons and employees on patios where smoking is not restricted are exposed to second hand smoke frequently This can contribute to increased disease and aggravation of existing health conditions From a business perspective the existing legislation has been viewed by many operators as unfair because some patios have permanent coverings which cannot be removed requiring a smoke-free status These business owners feel this creates an uneven playing field since they cannot provide an outdoor dining area for their smoking customers There is strong community support for smoke-free patios in Ontario A 2009 Rapid Risk Factor Surveillance System survey revealed 754 percent support in York Region while a Toronto Health Survey in 2011 indicated 74 percent public support
2
Current Status
Smoking is currently prohibited on restaurant and bar patios province-wide in four Canadian provinces and territories Alberta Newfoundland and Labrador Nova Scotia and Yukon A fifth province Prince Edward Island prohibits smoking on patios until 10 pm Since Ontario enacted legislation restricting smoking on patios in 2006 eight municipalities in Ontario have chosen to create bylaws that go beyond the Smoke-Free Ontario Act and enhance outdoor protection from second hand smoke by prohibiting smoking on patios completely The largest of those municipalities is the City of Ottawa Recently the Toronto Board of Health unanimously endorsed a report presented by their Medical Officer of Health recommending that restaurant and bar patios be made smoke-free through an amendment to the Smoke-Free Ontario Act
Key Considerations
There should be no significant financial burden to local Boards of Health resulting from a smoke-free patio amendment to the Smoke-Free Ontario Act Inspection and enforcement for the Smoke-Free Ontario Act is currently 100 percent funded by the Ministry of Health and Long-Term Care Following an introductory period of education on the amendment a complaint response model of service delivery would ensure ongoing compliance with smoke-free requirements A complete ban of smoking on patios would eliminate the widely-held perception by business owners that the current legislation creates an uneven playing field for business Since Smoke-Free Ontario Act inspections of patios began in 2006 operators have expressed the opinion that if patios need to be smoke-free for the protection of the public they should all be smoke-free to avoid undue hardship for individual businesses and to provide protection uniformly across the Province
Next steps
York Region Public Health intends to seek support from Medical Officers of Health across the Central East Tobacco Control Area Network (CETCAN) to advocate to the Ministry of Health and Long-Term Care for an amendment to the Smoke-Free Ontario Act prohibiting smoking on all restaurant and bar patios York Region is also in the process of requesting that its Regional Council advocate to the Minister of Health and Long-Term Care on the issue
Updating and Modernizing O Regulation 565 (Public Pools)
Date November 15 2013
Prepared for Council of Ontario Medical Officers of Health
Prepared by York Region Public Health _____________________________________________________________________________ Background Recent drownings at public pools in Ontario have highlighted the issue of water-borne illness and injury The current pool regulation under Ontariorsquos Health Protection and Promotion Act O Regulation 565 (Public Pools) is outdated It does not accurately reflect new pool technology and design or the changing use of public pools Neither does it incorporate admissions standards recommended by the Office of the Chief Coroner Further O Regulation 565 does not have short-form wording or set fines associated with it This limits public health enforcement capabilities What is the impact Updating O Regulation 565 (Public Pools) to address recent changes in pool technology design and uses and to include Coroner-recommended admissions standards would help improve pool safety Establishing short-form wording for O Regulation 565 would enhance enforcement related to public pools Currently the only enforcement available to Public Health Inspectors for dealing with non-critical regulatory infractions in public pools is the issuance of a Part III summons This involves a considerable amount of resources for a possible small fine With the development of inspection disclosure systems such as YorkSafe there is an even greater need to develop a method to effectively address repeated pool operator non-compliance with non-critical issues Next steps Public health units should advocate to the Province to 1) Conduct a review of O Regulation 565 (Public Pools) to address shortcomings Proposed changes to the
regulation should include a requirement for ownersoperators of public pools to advise the local Medical Officer of Health of any change in the use of a facility and the addition of the Coronerrsquos recommended admission standards
2) Provide short-form wording for O Regulation 565 so that public health inspectors can better deal with pool operator non-compliance
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
November 04 2013
Mandatory State Laws on Fluoridation Thirteen states Puerto Rico and the District of Columbia have laws intended to provide
statewide fluoridation These states and the year that the fluoridation legislation was passed are
District of Columbia (1952) Connecticut (1965) Kentucky (1966) Illinois (1967) Minnesota
(1967) Ohio (1969) South Dakota (1969) Georgia (1973) Nebraska (1973 and 2008)
California (1995) Delaware (1998) Puerto Rico (1998) Nevada (1999) Louisiana (2008) and
Arkansas (2011) (see Table 1) The sizes of the public water systems or countiescommunities
affected and exemption provisions vary by state Table 1
STATES THAT HAVE MANDATORY LAWS ON FLUORIDATION -2011
State (1) Year of
Fluoridation
Legislation (1)
Population
served by
Fluoridated
CWS (2)
Persons
receiving
fluoridated
water (2)
State
Average
Caries
Experience
of Grade 3
Students (3)
Arkansas 2011 647 1724131 64
California 1995 621 22812721 709
Connecticut 1965 910 2370423 406
Delaware 1998 862 705344 545
Georgia 1973 921 8924598 52
Illinois 1967 993 11325132 532
Kentucky 1966 999 4334223 598
Louisiana 2008 407 1846149 657
Minnesota 1967 988 4117266 549
Nebraska 1973 and 2008 702 1001665 593
Nevada 1999 702 1001665 649
Ohio 1969 877 8772683 512
South Dakota 1969 948 642942 623
District of
Columbia
1952 1000 595000
Puerto Rico 1998
United States 739 204283554
2010 Statistics for population fluoridated and number of people
1 Communication with Jane McGinley RDH MBA Manager Fluoridation and Preventive Health
Activities Council on Access Prevention and Interprofessional Relations
2 Centers for Disease Control and Prevention Department of Health and Human Services
accessed Oct 21 2013 httpwwwcdcgovfluoridationstatistics2010statshtm
3 Centers for Disease Control and Prevention National Oral Health Surveillance System Caries
Experience - Percentage of 3rd Grade students with Caries Experience (treated or untreated tooth
If data from 43 states for the percentage of Grade 3 children with experience of dental decay is
compared with the 2008 percentages of the population in a state with Community Water
Fluoridation then the percentage of children with experience of dental decay decreases as the
percentage of the state population with Community Water Fluoridation increases (see Figure 1)
Figure 1
Correlation of Percentage of Grade 3 Children with Caries Experience and
Percentage of Population With Community Water Fluoridation for 43
Reporting States
0
10
20
30
40
50
60
70
80
0 10 20 30 40 50 60 70 80 90 100
State of Population With Community Water Fluoridation
Sta
te
of
Gra
de 3
Stu
den
ts w
ith
Cari
es E
xp
eri
en
ce
Data from CDC (2 3)
The description of the fluoridation laws in California Illinois and Nevada can be found on the
Association of State amp Territorial Dental Directors website(4 7 8)
The California fluoridation law AB 733 came into effect in 1995 requiring communities of 10
000 residents or more be supplied with fluoridated drinking water However the state did not
provide any funding to implement the legislation (California is unique in requiring fluoridation
without funding the practice)(4) The California Department of Health Services therefore had to
fund fluoridation initiatives from non-governmental sources ie the California Endowment
California Dental Association Foundation the First 5 Commission and others(5) From 1995 to
2011 the percentage of the California population receiving fluoridated drinking water has risen
from 17 to 625(6) 4 Dental Public Health Activities amp Practices Office of Oral Health California Department of Health
Services April 2002 httpwwwastddorgbestpracticesDES06002CAfluoridationpdf
5 Stock M Pollick H The CDA Foundation Model to Fluoridate Communities California Dental
Association Journal vol 40 no 8 649 - 655
httpwwwcdaorgPortals0journaljournal_082012pdf
6 California Dental Association Foundation
httpwwwcdafoundationorglearnadvocacyfluoridation
The State of Illinois passed a mandatory fluoridation state in 1967 and required all community
water systems to adjust fluoride levels in the drinking water to optimal levels within 1 year(7)
From 1962 when over 5000000 residents had optimally fluoridated drinking water by 2010
the number had risen to 11325132 (993 of the population on community water systems)(2)
7 Dental Public Health Activities amp Practices Division of Oral Health Illinois Department of Public
Health April 2002 httpwwwastddorgbestpracticesDES16007ILfluoridationpdf
The State of Nevada passed a mandatory fluoridation statute in 2000 for communities with
400000 or more residents(8) This was a result of the work of a statewide coalition that
included the Nevada Dental and Dental Hygienist Associations the Washoe and Clark County
District Health Departments the Clark County School District Junior League of Las Vegas
Head Start the Community College of Southern Nevada Dental Hygiene Program Health
Access Washoe County and Saint Maryrsquos Hospital For communities with less than 400000 the
implementation of fluoridation still required the vote of the majority voters in the community
The Las Vegas Water Authority and the City of Henderson started fluoridation in 2000
increasing the percentage of the population with fluoridated drinking water from 2 to 65 (8) 8 Dental Public Health Activities amp Practices Bureau of Family Health Services Nevada State Health
Division April 2002 httpwwwastddorgbestpracticesDES31002NVfluoridationbillpdf
Countries with Mandatory Laws on Fluoridation Countries that have mandated Community Water Fluoridation are Brazil Hong Kong
Malaysia Singapore Ireland Israel and some of the states in Australia
Singapore started fluoridating its water in 1956 based on the success of the fluoridation trials in
Grand Rapids Newburgh Evanston and Brantford Singapore became the first Asian country to
have 100 of its population benefitting from the implementation of fluoridated drinking water
Loh reported that ldquoThe ten year study on the effects of water fluoridation in Singapore showed
a decrease in caries prevalence in the children In the permanent dentition the reduction was
523 per cent for Chinese and 31 per cent for Malays in the 7 to 9 year old age group A similar
trend was observed in the mixed dentition in which the decrease was 325 per cent for Chinese
and 306 per cent for Malaysrdquo(9) By 2010 the population of the country was 5080000(10)
9 Loh T Thirty-eight years of water fluoridation--the Singapore scenario Community Dent
Health 1996 Sep13 Suppl 247-50
10 British Fluoridation Society One in a Million the facts about water fluoridation 3rd Edition
published March 2012) httpwwwbfsweborgonemillion0920One20in20a20Million20-
20The20Extent20of20Fluoridationpdf
Hong Kong started implementing community water fluoridation in 1961 and similar to
Singapore 100 of the population received access to fluoridated drinking water Lo and Wong
reported that ldquoThe mean DMFT score of the children deceased from 44 in 1960 to 15 in 1968
stayed at this level in the 1980 and 1986 surveys and further deceased to 08 in 2001 The
prevalence of dental fluorosis among the children surveyed in 1960 was 1 and this increased
to 59 and 70 in 1968 and 1980 respectively It was found in the 1986 and 2001 surveys that
the prevalences of fluorosis were 47 and 9 among children whose teeth developed at the
time when the respective water fluoride concentrations were 07 ppm and 05 ppmrdquo(11) The
population of Hong Kong was 6968000 in 2009(10) 11 LO ECM and WONG AHH Water fluoride concentration and fluorosis in Hong Kong in 1960-
2001 84th General Session and Exhibition of the International Association for Dental Research amp
1st Meeting of the Pan-Asian-Pacific Federation Brisbane Australia 28 June-1 July 2006 v 85 n
Sp B
The Malaysian cabinet approved a nationwide community water fluoridation program in 1972
(12) One of the states Sabah decided to stop fluoridation in 1989 due to concerns about
inadequate supervision in adding fluoride to the drinking water Oral Health Surveys in 2009
and 2007 indicated that children in Sabah had the worst oral health with 50 of 12 year-olds
having decay in their permanent teeth and children having an average of 3 teeth being(13)
Under the 10th Malaysian Plan in 2011 the federal and the Sabah state governments
reintroduced water fluoridation in Sabah(1314) In 2010 about 755 of the Malaysian
population or 20700000 people had fluoridated drinking water(1013) 12 Malaysian Dental Association Fluoride in Water
httpwwwmdaorgmy07_public_01healthcare_12htm
13 Sachdev N Fluoridation in Sabah Water for Cleaner Teeth French Tribunecom 28022011
From Levy IsraTo Jaeger ValerieCc Pim Carolyn gordonalphaweborg Diallo Aicha Penny Sutcliffe Paul Roumeliotis Michael Finkelstein
Hazel Lynn Robert KyleSubject FW Panorama - Privacy Security and other issuesDate Wednesday October 16 2013 122110 PM
Hello ValerieOttawa is part of Wave 4 Panorama implementation and we are gearing up increasingly to use thesystem where and if possible Thinking about it I am anticipating that this may need to be on theCOMOH (and alPHa) radar as it is something that will impact all health units and implies a majoroperational shift in vaccine delivery programs for all health units I have asked Carolyn Pim toconnect with our sister wave 4 units to share common experiences as we move forward ndash when wehave a roll up could I bring to COMOH Exec for discussion to explore whether there are broaderimplications for all members As an aside I have also asked the Ministry and their CIO to share with me any roll up learnings thatthey may have had already from previous waves (I understand that Niagara HU was a wave 1participant so if there is such a roll up of common experiences that others could learn fromperhaps you have it already and that could come to the exec too)Thanks Isra From Pim Carolyn Sent October 10 2013 1228 PMTo Christopher Mackie (christophermackiemlhuonca) Elizabeth Richardson(Elizabethrichardsonhamiltonca) H BSc M D F R C P (C) MPH Jim Chirico(jimchiriconbpsdhuca) Marlene Spruyt (spruytmtimiskaminghucom) Robert Kyle (Durham)Cc Levy IsraSubject Panorama - Privacy Security and other issues Dear colleagues Irsquom reaching out to you as fellow Panorama Wave 4 health units to ask about where yourorganizations are at in the process of signing agreements and completing Privacy ImpactAssessments and Threat Risk Assessments (TRAs) Ottawa Public Healthrsquos IT legal and informationsecurity advisors have made numerous requests to the MOHLTC for information (in particular theprovincial TRA) that we consider essential to develop our own risk assessment and PIA but havebeen told that information cannot be shared even with strict confidentiality and access controlsSo we are at somewhat of an impasse Isra emailed Arlene yesterday Arlene has forwarded ourconcerns to the Ministryrsquos CIO and Panorama lead but we havenrsquot had any response or discussionswith either of them yet Have your organizations identified similar concerns andor had interactions with the MOHLTC inthis respect Irsquod also be interested in knowing if your health units have flagged other (egoperational) implementation concerns Thanks
Carolyn ps Robert ndash you can ignore this request I talked with Sharan this morning about Durhamrsquos issuesso am including you now just for information Carolyn Pim MD FRCPC Associate Medical Officer of Health Meacutedecin adjointe en santeacute publique Ottawa Public Health Santeacute publique Ottawa 100 Constellation Cr Ottawa ON K2G 6J8 Tel teacutel (613) 580-6744 ext 23684Fax (613) 580-9641Connect With Ottawa Public Health
Suivez Santeacute publique Ottawa
This e-mail originates from the City of Ottawa e-mail system Any distribution use orcopying of this e-mail or the information it contains by other than the intendedrecipient(s) is unauthorized If you are not the intended recipient please notify meat the telephone number shown above or by return e-mail and delete thiscommunication and any copy immediately Thank you
Le preacutesent courriel a eacuteteacute expeacutedieacute par le systegraveme de courriels de la Ville dOttawaToute distribution utilisation ou reproduction du courriel ou des renseignements quisy trouvent par une personne autre que son destinataire preacutevu est interdite Si vousavez reccedilu le message par erreur veuillez men aviser par teacuteleacutephone (au numeacuteropreacuteciteacute) ou par courriel puis supprimer sans deacutelai la version originale de lacommunication ainsi que toutes ses copies Je vous remercie de votre collaboration
1
Smoke-Free Patios ndash An Amendment to the Smoke-Free Ontario Act
Date November 15 2013 Prepared for Council of Ontario Medical Officers of Health Prepared by York Region Public Health _____________________________________________________________________________ Issue
The Smoke-Free Ontario Act is the current provincial legislation that imposes smoking restrictions in workplaces and public places It prohibits smoking on restaurant and bar patios in instances where any portion of the seating area is covered by a roof With recent studies illustrating that exposure to second hand smoke outdoors poses similar risks to indoor exposure there has been growing public support to enhance smoking restrictions and make patios completely smoke-free
Background
With the implementation of the Smoke-Free Ontario Act in 2006 restaurant and bar patios became subject to smoking restrictions if any portion of the seating area was covered by a roof This allowed for patios without roof coverings to continue to allow smoking and as a result did not provide significant protection to patrons or staff from exposure to second hand smoke outdoors Many businesses chose to alter the design of their patios to allow smoking to continue In some cases patios became more crowded since smoking patrons who dine indoors often proceed outside onto licensed patios with their beverages to smoke York Region like most municipalities in Ontario is host to hundreds of patios being operated by restaurant owners and businesses With smoking prohibitions affecting only a small portion of these patios specifically ones with coverings the vast majority of patios still allow smoking to take place Patrons and employees on patios where smoking is not restricted are exposed to second hand smoke frequently This can contribute to increased disease and aggravation of existing health conditions From a business perspective the existing legislation has been viewed by many operators as unfair because some patios have permanent coverings which cannot be removed requiring a smoke-free status These business owners feel this creates an uneven playing field since they cannot provide an outdoor dining area for their smoking customers There is strong community support for smoke-free patios in Ontario A 2009 Rapid Risk Factor Surveillance System survey revealed 754 percent support in York Region while a Toronto Health Survey in 2011 indicated 74 percent public support
2
Current Status
Smoking is currently prohibited on restaurant and bar patios province-wide in four Canadian provinces and territories Alberta Newfoundland and Labrador Nova Scotia and Yukon A fifth province Prince Edward Island prohibits smoking on patios until 10 pm Since Ontario enacted legislation restricting smoking on patios in 2006 eight municipalities in Ontario have chosen to create bylaws that go beyond the Smoke-Free Ontario Act and enhance outdoor protection from second hand smoke by prohibiting smoking on patios completely The largest of those municipalities is the City of Ottawa Recently the Toronto Board of Health unanimously endorsed a report presented by their Medical Officer of Health recommending that restaurant and bar patios be made smoke-free through an amendment to the Smoke-Free Ontario Act
Key Considerations
There should be no significant financial burden to local Boards of Health resulting from a smoke-free patio amendment to the Smoke-Free Ontario Act Inspection and enforcement for the Smoke-Free Ontario Act is currently 100 percent funded by the Ministry of Health and Long-Term Care Following an introductory period of education on the amendment a complaint response model of service delivery would ensure ongoing compliance with smoke-free requirements A complete ban of smoking on patios would eliminate the widely-held perception by business owners that the current legislation creates an uneven playing field for business Since Smoke-Free Ontario Act inspections of patios began in 2006 operators have expressed the opinion that if patios need to be smoke-free for the protection of the public they should all be smoke-free to avoid undue hardship for individual businesses and to provide protection uniformly across the Province
Next steps
York Region Public Health intends to seek support from Medical Officers of Health across the Central East Tobacco Control Area Network (CETCAN) to advocate to the Ministry of Health and Long-Term Care for an amendment to the Smoke-Free Ontario Act prohibiting smoking on all restaurant and bar patios York Region is also in the process of requesting that its Regional Council advocate to the Minister of Health and Long-Term Care on the issue
Updating and Modernizing O Regulation 565 (Public Pools)
Date November 15 2013
Prepared for Council of Ontario Medical Officers of Health
Prepared by York Region Public Health _____________________________________________________________________________ Background Recent drownings at public pools in Ontario have highlighted the issue of water-borne illness and injury The current pool regulation under Ontariorsquos Health Protection and Promotion Act O Regulation 565 (Public Pools) is outdated It does not accurately reflect new pool technology and design or the changing use of public pools Neither does it incorporate admissions standards recommended by the Office of the Chief Coroner Further O Regulation 565 does not have short-form wording or set fines associated with it This limits public health enforcement capabilities What is the impact Updating O Regulation 565 (Public Pools) to address recent changes in pool technology design and uses and to include Coroner-recommended admissions standards would help improve pool safety Establishing short-form wording for O Regulation 565 would enhance enforcement related to public pools Currently the only enforcement available to Public Health Inspectors for dealing with non-critical regulatory infractions in public pools is the issuance of a Part III summons This involves a considerable amount of resources for a possible small fine With the development of inspection disclosure systems such as YorkSafe there is an even greater need to develop a method to effectively address repeated pool operator non-compliance with non-critical issues Next steps Public health units should advocate to the Province to 1) Conduct a review of O Regulation 565 (Public Pools) to address shortcomings Proposed changes to the
regulation should include a requirement for ownersoperators of public pools to advise the local Medical Officer of Health of any change in the use of a facility and the addition of the Coronerrsquos recommended admission standards
2) Provide short-form wording for O Regulation 565 so that public health inspectors can better deal with pool operator non-compliance
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
1 Communication with Jane McGinley RDH MBA Manager Fluoridation and Preventive Health
Activities Council on Access Prevention and Interprofessional Relations
2 Centers for Disease Control and Prevention Department of Health and Human Services
accessed Oct 21 2013 httpwwwcdcgovfluoridationstatistics2010statshtm
3 Centers for Disease Control and Prevention National Oral Health Surveillance System Caries
Experience - Percentage of 3rd Grade students with Caries Experience (treated or untreated tooth
If data from 43 states for the percentage of Grade 3 children with experience of dental decay is
compared with the 2008 percentages of the population in a state with Community Water
Fluoridation then the percentage of children with experience of dental decay decreases as the
percentage of the state population with Community Water Fluoridation increases (see Figure 1)
Figure 1
Correlation of Percentage of Grade 3 Children with Caries Experience and
Percentage of Population With Community Water Fluoridation for 43
Reporting States
0
10
20
30
40
50
60
70
80
0 10 20 30 40 50 60 70 80 90 100
State of Population With Community Water Fluoridation
Sta
te
of
Gra
de 3
Stu
den
ts w
ith
Cari
es E
xp
eri
en
ce
Data from CDC (2 3)
The description of the fluoridation laws in California Illinois and Nevada can be found on the
Association of State amp Territorial Dental Directors website(4 7 8)
The California fluoridation law AB 733 came into effect in 1995 requiring communities of 10
000 residents or more be supplied with fluoridated drinking water However the state did not
provide any funding to implement the legislation (California is unique in requiring fluoridation
without funding the practice)(4) The California Department of Health Services therefore had to
fund fluoridation initiatives from non-governmental sources ie the California Endowment
California Dental Association Foundation the First 5 Commission and others(5) From 1995 to
2011 the percentage of the California population receiving fluoridated drinking water has risen
from 17 to 625(6) 4 Dental Public Health Activities amp Practices Office of Oral Health California Department of Health
Services April 2002 httpwwwastddorgbestpracticesDES06002CAfluoridationpdf
5 Stock M Pollick H The CDA Foundation Model to Fluoridate Communities California Dental
Association Journal vol 40 no 8 649 - 655
httpwwwcdaorgPortals0journaljournal_082012pdf
6 California Dental Association Foundation
httpwwwcdafoundationorglearnadvocacyfluoridation
The State of Illinois passed a mandatory fluoridation state in 1967 and required all community
water systems to adjust fluoride levels in the drinking water to optimal levels within 1 year(7)
From 1962 when over 5000000 residents had optimally fluoridated drinking water by 2010
the number had risen to 11325132 (993 of the population on community water systems)(2)
7 Dental Public Health Activities amp Practices Division of Oral Health Illinois Department of Public
Health April 2002 httpwwwastddorgbestpracticesDES16007ILfluoridationpdf
The State of Nevada passed a mandatory fluoridation statute in 2000 for communities with
400000 or more residents(8) This was a result of the work of a statewide coalition that
included the Nevada Dental and Dental Hygienist Associations the Washoe and Clark County
District Health Departments the Clark County School District Junior League of Las Vegas
Head Start the Community College of Southern Nevada Dental Hygiene Program Health
Access Washoe County and Saint Maryrsquos Hospital For communities with less than 400000 the
implementation of fluoridation still required the vote of the majority voters in the community
The Las Vegas Water Authority and the City of Henderson started fluoridation in 2000
increasing the percentage of the population with fluoridated drinking water from 2 to 65 (8) 8 Dental Public Health Activities amp Practices Bureau of Family Health Services Nevada State Health
Division April 2002 httpwwwastddorgbestpracticesDES31002NVfluoridationbillpdf
Countries with Mandatory Laws on Fluoridation Countries that have mandated Community Water Fluoridation are Brazil Hong Kong
Malaysia Singapore Ireland Israel and some of the states in Australia
Singapore started fluoridating its water in 1956 based on the success of the fluoridation trials in
Grand Rapids Newburgh Evanston and Brantford Singapore became the first Asian country to
have 100 of its population benefitting from the implementation of fluoridated drinking water
Loh reported that ldquoThe ten year study on the effects of water fluoridation in Singapore showed
a decrease in caries prevalence in the children In the permanent dentition the reduction was
523 per cent for Chinese and 31 per cent for Malays in the 7 to 9 year old age group A similar
trend was observed in the mixed dentition in which the decrease was 325 per cent for Chinese
and 306 per cent for Malaysrdquo(9) By 2010 the population of the country was 5080000(10)
9 Loh T Thirty-eight years of water fluoridation--the Singapore scenario Community Dent
Health 1996 Sep13 Suppl 247-50
10 British Fluoridation Society One in a Million the facts about water fluoridation 3rd Edition
published March 2012) httpwwwbfsweborgonemillion0920One20in20a20Million20-
20The20Extent20of20Fluoridationpdf
Hong Kong started implementing community water fluoridation in 1961 and similar to
Singapore 100 of the population received access to fluoridated drinking water Lo and Wong
reported that ldquoThe mean DMFT score of the children deceased from 44 in 1960 to 15 in 1968
stayed at this level in the 1980 and 1986 surveys and further deceased to 08 in 2001 The
prevalence of dental fluorosis among the children surveyed in 1960 was 1 and this increased
to 59 and 70 in 1968 and 1980 respectively It was found in the 1986 and 2001 surveys that
the prevalences of fluorosis were 47 and 9 among children whose teeth developed at the
time when the respective water fluoride concentrations were 07 ppm and 05 ppmrdquo(11) The
population of Hong Kong was 6968000 in 2009(10) 11 LO ECM and WONG AHH Water fluoride concentration and fluorosis in Hong Kong in 1960-
2001 84th General Session and Exhibition of the International Association for Dental Research amp
1st Meeting of the Pan-Asian-Pacific Federation Brisbane Australia 28 June-1 July 2006 v 85 n
Sp B
The Malaysian cabinet approved a nationwide community water fluoridation program in 1972
(12) One of the states Sabah decided to stop fluoridation in 1989 due to concerns about
inadequate supervision in adding fluoride to the drinking water Oral Health Surveys in 2009
and 2007 indicated that children in Sabah had the worst oral health with 50 of 12 year-olds
having decay in their permanent teeth and children having an average of 3 teeth being(13)
Under the 10th Malaysian Plan in 2011 the federal and the Sabah state governments
reintroduced water fluoridation in Sabah(1314) In 2010 about 755 of the Malaysian
population or 20700000 people had fluoridated drinking water(1013) 12 Malaysian Dental Association Fluoride in Water
httpwwwmdaorgmy07_public_01healthcare_12htm
13 Sachdev N Fluoridation in Sabah Water for Cleaner Teeth French Tribunecom 28022011
From Levy IsraTo Jaeger ValerieCc Pim Carolyn gordonalphaweborg Diallo Aicha Penny Sutcliffe Paul Roumeliotis Michael Finkelstein
Hazel Lynn Robert KyleSubject FW Panorama - Privacy Security and other issuesDate Wednesday October 16 2013 122110 PM
Hello ValerieOttawa is part of Wave 4 Panorama implementation and we are gearing up increasingly to use thesystem where and if possible Thinking about it I am anticipating that this may need to be on theCOMOH (and alPHa) radar as it is something that will impact all health units and implies a majoroperational shift in vaccine delivery programs for all health units I have asked Carolyn Pim toconnect with our sister wave 4 units to share common experiences as we move forward ndash when wehave a roll up could I bring to COMOH Exec for discussion to explore whether there are broaderimplications for all members As an aside I have also asked the Ministry and their CIO to share with me any roll up learnings thatthey may have had already from previous waves (I understand that Niagara HU was a wave 1participant so if there is such a roll up of common experiences that others could learn fromperhaps you have it already and that could come to the exec too)Thanks Isra From Pim Carolyn Sent October 10 2013 1228 PMTo Christopher Mackie (christophermackiemlhuonca) Elizabeth Richardson(Elizabethrichardsonhamiltonca) H BSc M D F R C P (C) MPH Jim Chirico(jimchiriconbpsdhuca) Marlene Spruyt (spruytmtimiskaminghucom) Robert Kyle (Durham)Cc Levy IsraSubject Panorama - Privacy Security and other issues Dear colleagues Irsquom reaching out to you as fellow Panorama Wave 4 health units to ask about where yourorganizations are at in the process of signing agreements and completing Privacy ImpactAssessments and Threat Risk Assessments (TRAs) Ottawa Public Healthrsquos IT legal and informationsecurity advisors have made numerous requests to the MOHLTC for information (in particular theprovincial TRA) that we consider essential to develop our own risk assessment and PIA but havebeen told that information cannot be shared even with strict confidentiality and access controlsSo we are at somewhat of an impasse Isra emailed Arlene yesterday Arlene has forwarded ourconcerns to the Ministryrsquos CIO and Panorama lead but we havenrsquot had any response or discussionswith either of them yet Have your organizations identified similar concerns andor had interactions with the MOHLTC inthis respect Irsquod also be interested in knowing if your health units have flagged other (egoperational) implementation concerns Thanks
Carolyn ps Robert ndash you can ignore this request I talked with Sharan this morning about Durhamrsquos issuesso am including you now just for information Carolyn Pim MD FRCPC Associate Medical Officer of Health Meacutedecin adjointe en santeacute publique Ottawa Public Health Santeacute publique Ottawa 100 Constellation Cr Ottawa ON K2G 6J8 Tel teacutel (613) 580-6744 ext 23684Fax (613) 580-9641Connect With Ottawa Public Health
Suivez Santeacute publique Ottawa
This e-mail originates from the City of Ottawa e-mail system Any distribution use orcopying of this e-mail or the information it contains by other than the intendedrecipient(s) is unauthorized If you are not the intended recipient please notify meat the telephone number shown above or by return e-mail and delete thiscommunication and any copy immediately Thank you
Le preacutesent courriel a eacuteteacute expeacutedieacute par le systegraveme de courriels de la Ville dOttawaToute distribution utilisation ou reproduction du courriel ou des renseignements quisy trouvent par une personne autre que son destinataire preacutevu est interdite Si vousavez reccedilu le message par erreur veuillez men aviser par teacuteleacutephone (au numeacuteropreacuteciteacute) ou par courriel puis supprimer sans deacutelai la version originale de lacommunication ainsi que toutes ses copies Je vous remercie de votre collaboration
1
Smoke-Free Patios ndash An Amendment to the Smoke-Free Ontario Act
Date November 15 2013 Prepared for Council of Ontario Medical Officers of Health Prepared by York Region Public Health _____________________________________________________________________________ Issue
The Smoke-Free Ontario Act is the current provincial legislation that imposes smoking restrictions in workplaces and public places It prohibits smoking on restaurant and bar patios in instances where any portion of the seating area is covered by a roof With recent studies illustrating that exposure to second hand smoke outdoors poses similar risks to indoor exposure there has been growing public support to enhance smoking restrictions and make patios completely smoke-free
Background
With the implementation of the Smoke-Free Ontario Act in 2006 restaurant and bar patios became subject to smoking restrictions if any portion of the seating area was covered by a roof This allowed for patios without roof coverings to continue to allow smoking and as a result did not provide significant protection to patrons or staff from exposure to second hand smoke outdoors Many businesses chose to alter the design of their patios to allow smoking to continue In some cases patios became more crowded since smoking patrons who dine indoors often proceed outside onto licensed patios with their beverages to smoke York Region like most municipalities in Ontario is host to hundreds of patios being operated by restaurant owners and businesses With smoking prohibitions affecting only a small portion of these patios specifically ones with coverings the vast majority of patios still allow smoking to take place Patrons and employees on patios where smoking is not restricted are exposed to second hand smoke frequently This can contribute to increased disease and aggravation of existing health conditions From a business perspective the existing legislation has been viewed by many operators as unfair because some patios have permanent coverings which cannot be removed requiring a smoke-free status These business owners feel this creates an uneven playing field since they cannot provide an outdoor dining area for their smoking customers There is strong community support for smoke-free patios in Ontario A 2009 Rapid Risk Factor Surveillance System survey revealed 754 percent support in York Region while a Toronto Health Survey in 2011 indicated 74 percent public support
2
Current Status
Smoking is currently prohibited on restaurant and bar patios province-wide in four Canadian provinces and territories Alberta Newfoundland and Labrador Nova Scotia and Yukon A fifth province Prince Edward Island prohibits smoking on patios until 10 pm Since Ontario enacted legislation restricting smoking on patios in 2006 eight municipalities in Ontario have chosen to create bylaws that go beyond the Smoke-Free Ontario Act and enhance outdoor protection from second hand smoke by prohibiting smoking on patios completely The largest of those municipalities is the City of Ottawa Recently the Toronto Board of Health unanimously endorsed a report presented by their Medical Officer of Health recommending that restaurant and bar patios be made smoke-free through an amendment to the Smoke-Free Ontario Act
Key Considerations
There should be no significant financial burden to local Boards of Health resulting from a smoke-free patio amendment to the Smoke-Free Ontario Act Inspection and enforcement for the Smoke-Free Ontario Act is currently 100 percent funded by the Ministry of Health and Long-Term Care Following an introductory period of education on the amendment a complaint response model of service delivery would ensure ongoing compliance with smoke-free requirements A complete ban of smoking on patios would eliminate the widely-held perception by business owners that the current legislation creates an uneven playing field for business Since Smoke-Free Ontario Act inspections of patios began in 2006 operators have expressed the opinion that if patios need to be smoke-free for the protection of the public they should all be smoke-free to avoid undue hardship for individual businesses and to provide protection uniformly across the Province
Next steps
York Region Public Health intends to seek support from Medical Officers of Health across the Central East Tobacco Control Area Network (CETCAN) to advocate to the Ministry of Health and Long-Term Care for an amendment to the Smoke-Free Ontario Act prohibiting smoking on all restaurant and bar patios York Region is also in the process of requesting that its Regional Council advocate to the Minister of Health and Long-Term Care on the issue
Updating and Modernizing O Regulation 565 (Public Pools)
Date November 15 2013
Prepared for Council of Ontario Medical Officers of Health
Prepared by York Region Public Health _____________________________________________________________________________ Background Recent drownings at public pools in Ontario have highlighted the issue of water-borne illness and injury The current pool regulation under Ontariorsquos Health Protection and Promotion Act O Regulation 565 (Public Pools) is outdated It does not accurately reflect new pool technology and design or the changing use of public pools Neither does it incorporate admissions standards recommended by the Office of the Chief Coroner Further O Regulation 565 does not have short-form wording or set fines associated with it This limits public health enforcement capabilities What is the impact Updating O Regulation 565 (Public Pools) to address recent changes in pool technology design and uses and to include Coroner-recommended admissions standards would help improve pool safety Establishing short-form wording for O Regulation 565 would enhance enforcement related to public pools Currently the only enforcement available to Public Health Inspectors for dealing with non-critical regulatory infractions in public pools is the issuance of a Part III summons This involves a considerable amount of resources for a possible small fine With the development of inspection disclosure systems such as YorkSafe there is an even greater need to develop a method to effectively address repeated pool operator non-compliance with non-critical issues Next steps Public health units should advocate to the Province to 1) Conduct a review of O Regulation 565 (Public Pools) to address shortcomings Proposed changes to the
regulation should include a requirement for ownersoperators of public pools to advise the local Medical Officer of Health of any change in the use of a facility and the addition of the Coronerrsquos recommended admission standards
2) Provide short-form wording for O Regulation 565 so that public health inspectors can better deal with pool operator non-compliance
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
The California fluoridation law AB 733 came into effect in 1995 requiring communities of 10
000 residents or more be supplied with fluoridated drinking water However the state did not
provide any funding to implement the legislation (California is unique in requiring fluoridation
without funding the practice)(4) The California Department of Health Services therefore had to
fund fluoridation initiatives from non-governmental sources ie the California Endowment
California Dental Association Foundation the First 5 Commission and others(5) From 1995 to
2011 the percentage of the California population receiving fluoridated drinking water has risen
from 17 to 625(6) 4 Dental Public Health Activities amp Practices Office of Oral Health California Department of Health
Services April 2002 httpwwwastddorgbestpracticesDES06002CAfluoridationpdf
5 Stock M Pollick H The CDA Foundation Model to Fluoridate Communities California Dental
Association Journal vol 40 no 8 649 - 655
httpwwwcdaorgPortals0journaljournal_082012pdf
6 California Dental Association Foundation
httpwwwcdafoundationorglearnadvocacyfluoridation
The State of Illinois passed a mandatory fluoridation state in 1967 and required all community
water systems to adjust fluoride levels in the drinking water to optimal levels within 1 year(7)
From 1962 when over 5000000 residents had optimally fluoridated drinking water by 2010
the number had risen to 11325132 (993 of the population on community water systems)(2)
7 Dental Public Health Activities amp Practices Division of Oral Health Illinois Department of Public
Health April 2002 httpwwwastddorgbestpracticesDES16007ILfluoridationpdf
The State of Nevada passed a mandatory fluoridation statute in 2000 for communities with
400000 or more residents(8) This was a result of the work of a statewide coalition that
included the Nevada Dental and Dental Hygienist Associations the Washoe and Clark County
District Health Departments the Clark County School District Junior League of Las Vegas
Head Start the Community College of Southern Nevada Dental Hygiene Program Health
Access Washoe County and Saint Maryrsquos Hospital For communities with less than 400000 the
implementation of fluoridation still required the vote of the majority voters in the community
The Las Vegas Water Authority and the City of Henderson started fluoridation in 2000
increasing the percentage of the population with fluoridated drinking water from 2 to 65 (8) 8 Dental Public Health Activities amp Practices Bureau of Family Health Services Nevada State Health
Division April 2002 httpwwwastddorgbestpracticesDES31002NVfluoridationbillpdf
Countries with Mandatory Laws on Fluoridation Countries that have mandated Community Water Fluoridation are Brazil Hong Kong
Malaysia Singapore Ireland Israel and some of the states in Australia
Singapore started fluoridating its water in 1956 based on the success of the fluoridation trials in
Grand Rapids Newburgh Evanston and Brantford Singapore became the first Asian country to
have 100 of its population benefitting from the implementation of fluoridated drinking water
Loh reported that ldquoThe ten year study on the effects of water fluoridation in Singapore showed
a decrease in caries prevalence in the children In the permanent dentition the reduction was
523 per cent for Chinese and 31 per cent for Malays in the 7 to 9 year old age group A similar
trend was observed in the mixed dentition in which the decrease was 325 per cent for Chinese
and 306 per cent for Malaysrdquo(9) By 2010 the population of the country was 5080000(10)
9 Loh T Thirty-eight years of water fluoridation--the Singapore scenario Community Dent
Health 1996 Sep13 Suppl 247-50
10 British Fluoridation Society One in a Million the facts about water fluoridation 3rd Edition
published March 2012) httpwwwbfsweborgonemillion0920One20in20a20Million20-
20The20Extent20of20Fluoridationpdf
Hong Kong started implementing community water fluoridation in 1961 and similar to
Singapore 100 of the population received access to fluoridated drinking water Lo and Wong
reported that ldquoThe mean DMFT score of the children deceased from 44 in 1960 to 15 in 1968
stayed at this level in the 1980 and 1986 surveys and further deceased to 08 in 2001 The
prevalence of dental fluorosis among the children surveyed in 1960 was 1 and this increased
to 59 and 70 in 1968 and 1980 respectively It was found in the 1986 and 2001 surveys that
the prevalences of fluorosis were 47 and 9 among children whose teeth developed at the
time when the respective water fluoride concentrations were 07 ppm and 05 ppmrdquo(11) The
population of Hong Kong was 6968000 in 2009(10) 11 LO ECM and WONG AHH Water fluoride concentration and fluorosis in Hong Kong in 1960-
2001 84th General Session and Exhibition of the International Association for Dental Research amp
1st Meeting of the Pan-Asian-Pacific Federation Brisbane Australia 28 June-1 July 2006 v 85 n
Sp B
The Malaysian cabinet approved a nationwide community water fluoridation program in 1972
(12) One of the states Sabah decided to stop fluoridation in 1989 due to concerns about
inadequate supervision in adding fluoride to the drinking water Oral Health Surveys in 2009
and 2007 indicated that children in Sabah had the worst oral health with 50 of 12 year-olds
having decay in their permanent teeth and children having an average of 3 teeth being(13)
Under the 10th Malaysian Plan in 2011 the federal and the Sabah state governments
reintroduced water fluoridation in Sabah(1314) In 2010 about 755 of the Malaysian
population or 20700000 people had fluoridated drinking water(1013) 12 Malaysian Dental Association Fluoride in Water
httpwwwmdaorgmy07_public_01healthcare_12htm
13 Sachdev N Fluoridation in Sabah Water for Cleaner Teeth French Tribunecom 28022011
From Levy IsraTo Jaeger ValerieCc Pim Carolyn gordonalphaweborg Diallo Aicha Penny Sutcliffe Paul Roumeliotis Michael Finkelstein
Hazel Lynn Robert KyleSubject FW Panorama - Privacy Security and other issuesDate Wednesday October 16 2013 122110 PM
Hello ValerieOttawa is part of Wave 4 Panorama implementation and we are gearing up increasingly to use thesystem where and if possible Thinking about it I am anticipating that this may need to be on theCOMOH (and alPHa) radar as it is something that will impact all health units and implies a majoroperational shift in vaccine delivery programs for all health units I have asked Carolyn Pim toconnect with our sister wave 4 units to share common experiences as we move forward ndash when wehave a roll up could I bring to COMOH Exec for discussion to explore whether there are broaderimplications for all members As an aside I have also asked the Ministry and their CIO to share with me any roll up learnings thatthey may have had already from previous waves (I understand that Niagara HU was a wave 1participant so if there is such a roll up of common experiences that others could learn fromperhaps you have it already and that could come to the exec too)Thanks Isra From Pim Carolyn Sent October 10 2013 1228 PMTo Christopher Mackie (christophermackiemlhuonca) Elizabeth Richardson(Elizabethrichardsonhamiltonca) H BSc M D F R C P (C) MPH Jim Chirico(jimchiriconbpsdhuca) Marlene Spruyt (spruytmtimiskaminghucom) Robert Kyle (Durham)Cc Levy IsraSubject Panorama - Privacy Security and other issues Dear colleagues Irsquom reaching out to you as fellow Panorama Wave 4 health units to ask about where yourorganizations are at in the process of signing agreements and completing Privacy ImpactAssessments and Threat Risk Assessments (TRAs) Ottawa Public Healthrsquos IT legal and informationsecurity advisors have made numerous requests to the MOHLTC for information (in particular theprovincial TRA) that we consider essential to develop our own risk assessment and PIA but havebeen told that information cannot be shared even with strict confidentiality and access controlsSo we are at somewhat of an impasse Isra emailed Arlene yesterday Arlene has forwarded ourconcerns to the Ministryrsquos CIO and Panorama lead but we havenrsquot had any response or discussionswith either of them yet Have your organizations identified similar concerns andor had interactions with the MOHLTC inthis respect Irsquod also be interested in knowing if your health units have flagged other (egoperational) implementation concerns Thanks
Carolyn ps Robert ndash you can ignore this request I talked with Sharan this morning about Durhamrsquos issuesso am including you now just for information Carolyn Pim MD FRCPC Associate Medical Officer of Health Meacutedecin adjointe en santeacute publique Ottawa Public Health Santeacute publique Ottawa 100 Constellation Cr Ottawa ON K2G 6J8 Tel teacutel (613) 580-6744 ext 23684Fax (613) 580-9641Connect With Ottawa Public Health
Suivez Santeacute publique Ottawa
This e-mail originates from the City of Ottawa e-mail system Any distribution use orcopying of this e-mail or the information it contains by other than the intendedrecipient(s) is unauthorized If you are not the intended recipient please notify meat the telephone number shown above or by return e-mail and delete thiscommunication and any copy immediately Thank you
Le preacutesent courriel a eacuteteacute expeacutedieacute par le systegraveme de courriels de la Ville dOttawaToute distribution utilisation ou reproduction du courriel ou des renseignements quisy trouvent par une personne autre que son destinataire preacutevu est interdite Si vousavez reccedilu le message par erreur veuillez men aviser par teacuteleacutephone (au numeacuteropreacuteciteacute) ou par courriel puis supprimer sans deacutelai la version originale de lacommunication ainsi que toutes ses copies Je vous remercie de votre collaboration
1
Smoke-Free Patios ndash An Amendment to the Smoke-Free Ontario Act
Date November 15 2013 Prepared for Council of Ontario Medical Officers of Health Prepared by York Region Public Health _____________________________________________________________________________ Issue
The Smoke-Free Ontario Act is the current provincial legislation that imposes smoking restrictions in workplaces and public places It prohibits smoking on restaurant and bar patios in instances where any portion of the seating area is covered by a roof With recent studies illustrating that exposure to second hand smoke outdoors poses similar risks to indoor exposure there has been growing public support to enhance smoking restrictions and make patios completely smoke-free
Background
With the implementation of the Smoke-Free Ontario Act in 2006 restaurant and bar patios became subject to smoking restrictions if any portion of the seating area was covered by a roof This allowed for patios without roof coverings to continue to allow smoking and as a result did not provide significant protection to patrons or staff from exposure to second hand smoke outdoors Many businesses chose to alter the design of their patios to allow smoking to continue In some cases patios became more crowded since smoking patrons who dine indoors often proceed outside onto licensed patios with their beverages to smoke York Region like most municipalities in Ontario is host to hundreds of patios being operated by restaurant owners and businesses With smoking prohibitions affecting only a small portion of these patios specifically ones with coverings the vast majority of patios still allow smoking to take place Patrons and employees on patios where smoking is not restricted are exposed to second hand smoke frequently This can contribute to increased disease and aggravation of existing health conditions From a business perspective the existing legislation has been viewed by many operators as unfair because some patios have permanent coverings which cannot be removed requiring a smoke-free status These business owners feel this creates an uneven playing field since they cannot provide an outdoor dining area for their smoking customers There is strong community support for smoke-free patios in Ontario A 2009 Rapid Risk Factor Surveillance System survey revealed 754 percent support in York Region while a Toronto Health Survey in 2011 indicated 74 percent public support
2
Current Status
Smoking is currently prohibited on restaurant and bar patios province-wide in four Canadian provinces and territories Alberta Newfoundland and Labrador Nova Scotia and Yukon A fifth province Prince Edward Island prohibits smoking on patios until 10 pm Since Ontario enacted legislation restricting smoking on patios in 2006 eight municipalities in Ontario have chosen to create bylaws that go beyond the Smoke-Free Ontario Act and enhance outdoor protection from second hand smoke by prohibiting smoking on patios completely The largest of those municipalities is the City of Ottawa Recently the Toronto Board of Health unanimously endorsed a report presented by their Medical Officer of Health recommending that restaurant and bar patios be made smoke-free through an amendment to the Smoke-Free Ontario Act
Key Considerations
There should be no significant financial burden to local Boards of Health resulting from a smoke-free patio amendment to the Smoke-Free Ontario Act Inspection and enforcement for the Smoke-Free Ontario Act is currently 100 percent funded by the Ministry of Health and Long-Term Care Following an introductory period of education on the amendment a complaint response model of service delivery would ensure ongoing compliance with smoke-free requirements A complete ban of smoking on patios would eliminate the widely-held perception by business owners that the current legislation creates an uneven playing field for business Since Smoke-Free Ontario Act inspections of patios began in 2006 operators have expressed the opinion that if patios need to be smoke-free for the protection of the public they should all be smoke-free to avoid undue hardship for individual businesses and to provide protection uniformly across the Province
Next steps
York Region Public Health intends to seek support from Medical Officers of Health across the Central East Tobacco Control Area Network (CETCAN) to advocate to the Ministry of Health and Long-Term Care for an amendment to the Smoke-Free Ontario Act prohibiting smoking on all restaurant and bar patios York Region is also in the process of requesting that its Regional Council advocate to the Minister of Health and Long-Term Care on the issue
Updating and Modernizing O Regulation 565 (Public Pools)
Date November 15 2013
Prepared for Council of Ontario Medical Officers of Health
Prepared by York Region Public Health _____________________________________________________________________________ Background Recent drownings at public pools in Ontario have highlighted the issue of water-borne illness and injury The current pool regulation under Ontariorsquos Health Protection and Promotion Act O Regulation 565 (Public Pools) is outdated It does not accurately reflect new pool technology and design or the changing use of public pools Neither does it incorporate admissions standards recommended by the Office of the Chief Coroner Further O Regulation 565 does not have short-form wording or set fines associated with it This limits public health enforcement capabilities What is the impact Updating O Regulation 565 (Public Pools) to address recent changes in pool technology design and uses and to include Coroner-recommended admissions standards would help improve pool safety Establishing short-form wording for O Regulation 565 would enhance enforcement related to public pools Currently the only enforcement available to Public Health Inspectors for dealing with non-critical regulatory infractions in public pools is the issuance of a Part III summons This involves a considerable amount of resources for a possible small fine With the development of inspection disclosure systems such as YorkSafe there is an even greater need to develop a method to effectively address repeated pool operator non-compliance with non-critical issues Next steps Public health units should advocate to the Province to 1) Conduct a review of O Regulation 565 (Public Pools) to address shortcomings Proposed changes to the
regulation should include a requirement for ownersoperators of public pools to advise the local Medical Officer of Health of any change in the use of a facility and the addition of the Coronerrsquos recommended admission standards
2) Provide short-form wording for O Regulation 565 so that public health inspectors can better deal with pool operator non-compliance
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
Countries with Mandatory Laws on Fluoridation Countries that have mandated Community Water Fluoridation are Brazil Hong Kong
Malaysia Singapore Ireland Israel and some of the states in Australia
Singapore started fluoridating its water in 1956 based on the success of the fluoridation trials in
Grand Rapids Newburgh Evanston and Brantford Singapore became the first Asian country to
have 100 of its population benefitting from the implementation of fluoridated drinking water
Loh reported that ldquoThe ten year study on the effects of water fluoridation in Singapore showed
a decrease in caries prevalence in the children In the permanent dentition the reduction was
523 per cent for Chinese and 31 per cent for Malays in the 7 to 9 year old age group A similar
trend was observed in the mixed dentition in which the decrease was 325 per cent for Chinese
and 306 per cent for Malaysrdquo(9) By 2010 the population of the country was 5080000(10)
9 Loh T Thirty-eight years of water fluoridation--the Singapore scenario Community Dent
Health 1996 Sep13 Suppl 247-50
10 British Fluoridation Society One in a Million the facts about water fluoridation 3rd Edition
published March 2012) httpwwwbfsweborgonemillion0920One20in20a20Million20-
20The20Extent20of20Fluoridationpdf
Hong Kong started implementing community water fluoridation in 1961 and similar to
Singapore 100 of the population received access to fluoridated drinking water Lo and Wong
reported that ldquoThe mean DMFT score of the children deceased from 44 in 1960 to 15 in 1968
stayed at this level in the 1980 and 1986 surveys and further deceased to 08 in 2001 The
prevalence of dental fluorosis among the children surveyed in 1960 was 1 and this increased
to 59 and 70 in 1968 and 1980 respectively It was found in the 1986 and 2001 surveys that
the prevalences of fluorosis were 47 and 9 among children whose teeth developed at the
time when the respective water fluoride concentrations were 07 ppm and 05 ppmrdquo(11) The
population of Hong Kong was 6968000 in 2009(10) 11 LO ECM and WONG AHH Water fluoride concentration and fluorosis in Hong Kong in 1960-
2001 84th General Session and Exhibition of the International Association for Dental Research amp
1st Meeting of the Pan-Asian-Pacific Federation Brisbane Australia 28 June-1 July 2006 v 85 n
Sp B
The Malaysian cabinet approved a nationwide community water fluoridation program in 1972
(12) One of the states Sabah decided to stop fluoridation in 1989 due to concerns about
inadequate supervision in adding fluoride to the drinking water Oral Health Surveys in 2009
and 2007 indicated that children in Sabah had the worst oral health with 50 of 12 year-olds
having decay in their permanent teeth and children having an average of 3 teeth being(13)
Under the 10th Malaysian Plan in 2011 the federal and the Sabah state governments
reintroduced water fluoridation in Sabah(1314) In 2010 about 755 of the Malaysian
population or 20700000 people had fluoridated drinking water(1013) 12 Malaysian Dental Association Fluoride in Water
httpwwwmdaorgmy07_public_01healthcare_12htm
13 Sachdev N Fluoridation in Sabah Water for Cleaner Teeth French Tribunecom 28022011
From Levy IsraTo Jaeger ValerieCc Pim Carolyn gordonalphaweborg Diallo Aicha Penny Sutcliffe Paul Roumeliotis Michael Finkelstein
Hazel Lynn Robert KyleSubject FW Panorama - Privacy Security and other issuesDate Wednesday October 16 2013 122110 PM
Hello ValerieOttawa is part of Wave 4 Panorama implementation and we are gearing up increasingly to use thesystem where and if possible Thinking about it I am anticipating that this may need to be on theCOMOH (and alPHa) radar as it is something that will impact all health units and implies a majoroperational shift in vaccine delivery programs for all health units I have asked Carolyn Pim toconnect with our sister wave 4 units to share common experiences as we move forward ndash when wehave a roll up could I bring to COMOH Exec for discussion to explore whether there are broaderimplications for all members As an aside I have also asked the Ministry and their CIO to share with me any roll up learnings thatthey may have had already from previous waves (I understand that Niagara HU was a wave 1participant so if there is such a roll up of common experiences that others could learn fromperhaps you have it already and that could come to the exec too)Thanks Isra From Pim Carolyn Sent October 10 2013 1228 PMTo Christopher Mackie (christophermackiemlhuonca) Elizabeth Richardson(Elizabethrichardsonhamiltonca) H BSc M D F R C P (C) MPH Jim Chirico(jimchiriconbpsdhuca) Marlene Spruyt (spruytmtimiskaminghucom) Robert Kyle (Durham)Cc Levy IsraSubject Panorama - Privacy Security and other issues Dear colleagues Irsquom reaching out to you as fellow Panorama Wave 4 health units to ask about where yourorganizations are at in the process of signing agreements and completing Privacy ImpactAssessments and Threat Risk Assessments (TRAs) Ottawa Public Healthrsquos IT legal and informationsecurity advisors have made numerous requests to the MOHLTC for information (in particular theprovincial TRA) that we consider essential to develop our own risk assessment and PIA but havebeen told that information cannot be shared even with strict confidentiality and access controlsSo we are at somewhat of an impasse Isra emailed Arlene yesterday Arlene has forwarded ourconcerns to the Ministryrsquos CIO and Panorama lead but we havenrsquot had any response or discussionswith either of them yet Have your organizations identified similar concerns andor had interactions with the MOHLTC inthis respect Irsquod also be interested in knowing if your health units have flagged other (egoperational) implementation concerns Thanks
Carolyn ps Robert ndash you can ignore this request I talked with Sharan this morning about Durhamrsquos issuesso am including you now just for information Carolyn Pim MD FRCPC Associate Medical Officer of Health Meacutedecin adjointe en santeacute publique Ottawa Public Health Santeacute publique Ottawa 100 Constellation Cr Ottawa ON K2G 6J8 Tel teacutel (613) 580-6744 ext 23684Fax (613) 580-9641Connect With Ottawa Public Health
Suivez Santeacute publique Ottawa
This e-mail originates from the City of Ottawa e-mail system Any distribution use orcopying of this e-mail or the information it contains by other than the intendedrecipient(s) is unauthorized If you are not the intended recipient please notify meat the telephone number shown above or by return e-mail and delete thiscommunication and any copy immediately Thank you
Le preacutesent courriel a eacuteteacute expeacutedieacute par le systegraveme de courriels de la Ville dOttawaToute distribution utilisation ou reproduction du courriel ou des renseignements quisy trouvent par une personne autre que son destinataire preacutevu est interdite Si vousavez reccedilu le message par erreur veuillez men aviser par teacuteleacutephone (au numeacuteropreacuteciteacute) ou par courriel puis supprimer sans deacutelai la version originale de lacommunication ainsi que toutes ses copies Je vous remercie de votre collaboration
1
Smoke-Free Patios ndash An Amendment to the Smoke-Free Ontario Act
Date November 15 2013 Prepared for Council of Ontario Medical Officers of Health Prepared by York Region Public Health _____________________________________________________________________________ Issue
The Smoke-Free Ontario Act is the current provincial legislation that imposes smoking restrictions in workplaces and public places It prohibits smoking on restaurant and bar patios in instances where any portion of the seating area is covered by a roof With recent studies illustrating that exposure to second hand smoke outdoors poses similar risks to indoor exposure there has been growing public support to enhance smoking restrictions and make patios completely smoke-free
Background
With the implementation of the Smoke-Free Ontario Act in 2006 restaurant and bar patios became subject to smoking restrictions if any portion of the seating area was covered by a roof This allowed for patios without roof coverings to continue to allow smoking and as a result did not provide significant protection to patrons or staff from exposure to second hand smoke outdoors Many businesses chose to alter the design of their patios to allow smoking to continue In some cases patios became more crowded since smoking patrons who dine indoors often proceed outside onto licensed patios with their beverages to smoke York Region like most municipalities in Ontario is host to hundreds of patios being operated by restaurant owners and businesses With smoking prohibitions affecting only a small portion of these patios specifically ones with coverings the vast majority of patios still allow smoking to take place Patrons and employees on patios where smoking is not restricted are exposed to second hand smoke frequently This can contribute to increased disease and aggravation of existing health conditions From a business perspective the existing legislation has been viewed by many operators as unfair because some patios have permanent coverings which cannot be removed requiring a smoke-free status These business owners feel this creates an uneven playing field since they cannot provide an outdoor dining area for their smoking customers There is strong community support for smoke-free patios in Ontario A 2009 Rapid Risk Factor Surveillance System survey revealed 754 percent support in York Region while a Toronto Health Survey in 2011 indicated 74 percent public support
2
Current Status
Smoking is currently prohibited on restaurant and bar patios province-wide in four Canadian provinces and territories Alberta Newfoundland and Labrador Nova Scotia and Yukon A fifth province Prince Edward Island prohibits smoking on patios until 10 pm Since Ontario enacted legislation restricting smoking on patios in 2006 eight municipalities in Ontario have chosen to create bylaws that go beyond the Smoke-Free Ontario Act and enhance outdoor protection from second hand smoke by prohibiting smoking on patios completely The largest of those municipalities is the City of Ottawa Recently the Toronto Board of Health unanimously endorsed a report presented by their Medical Officer of Health recommending that restaurant and bar patios be made smoke-free through an amendment to the Smoke-Free Ontario Act
Key Considerations
There should be no significant financial burden to local Boards of Health resulting from a smoke-free patio amendment to the Smoke-Free Ontario Act Inspection and enforcement for the Smoke-Free Ontario Act is currently 100 percent funded by the Ministry of Health and Long-Term Care Following an introductory period of education on the amendment a complaint response model of service delivery would ensure ongoing compliance with smoke-free requirements A complete ban of smoking on patios would eliminate the widely-held perception by business owners that the current legislation creates an uneven playing field for business Since Smoke-Free Ontario Act inspections of patios began in 2006 operators have expressed the opinion that if patios need to be smoke-free for the protection of the public they should all be smoke-free to avoid undue hardship for individual businesses and to provide protection uniformly across the Province
Next steps
York Region Public Health intends to seek support from Medical Officers of Health across the Central East Tobacco Control Area Network (CETCAN) to advocate to the Ministry of Health and Long-Term Care for an amendment to the Smoke-Free Ontario Act prohibiting smoking on all restaurant and bar patios York Region is also in the process of requesting that its Regional Council advocate to the Minister of Health and Long-Term Care on the issue
Updating and Modernizing O Regulation 565 (Public Pools)
Date November 15 2013
Prepared for Council of Ontario Medical Officers of Health
Prepared by York Region Public Health _____________________________________________________________________________ Background Recent drownings at public pools in Ontario have highlighted the issue of water-borne illness and injury The current pool regulation under Ontariorsquos Health Protection and Promotion Act O Regulation 565 (Public Pools) is outdated It does not accurately reflect new pool technology and design or the changing use of public pools Neither does it incorporate admissions standards recommended by the Office of the Chief Coroner Further O Regulation 565 does not have short-form wording or set fines associated with it This limits public health enforcement capabilities What is the impact Updating O Regulation 565 (Public Pools) to address recent changes in pool technology design and uses and to include Coroner-recommended admissions standards would help improve pool safety Establishing short-form wording for O Regulation 565 would enhance enforcement related to public pools Currently the only enforcement available to Public Health Inspectors for dealing with non-critical regulatory infractions in public pools is the issuance of a Part III summons This involves a considerable amount of resources for a possible small fine With the development of inspection disclosure systems such as YorkSafe there is an even greater need to develop a method to effectively address repeated pool operator non-compliance with non-critical issues Next steps Public health units should advocate to the Province to 1) Conduct a review of O Regulation 565 (Public Pools) to address shortcomings Proposed changes to the
regulation should include a requirement for ownersoperators of public pools to advise the local Medical Officer of Health of any change in the use of a facility and the addition of the Coronerrsquos recommended admission standards
2) Provide short-form wording for O Regulation 565 so that public health inspectors can better deal with pool operator non-compliance
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
reintroduced water fluoridation in Sabah(1314) In 2010 about 755 of the Malaysian
population or 20700000 people had fluoridated drinking water(1013) 12 Malaysian Dental Association Fluoride in Water
httpwwwmdaorgmy07_public_01healthcare_12htm
13 Sachdev N Fluoridation in Sabah Water for Cleaner Teeth French Tribunecom 28022011
From Levy IsraTo Jaeger ValerieCc Pim Carolyn gordonalphaweborg Diallo Aicha Penny Sutcliffe Paul Roumeliotis Michael Finkelstein
Hazel Lynn Robert KyleSubject FW Panorama - Privacy Security and other issuesDate Wednesday October 16 2013 122110 PM
Hello ValerieOttawa is part of Wave 4 Panorama implementation and we are gearing up increasingly to use thesystem where and if possible Thinking about it I am anticipating that this may need to be on theCOMOH (and alPHa) radar as it is something that will impact all health units and implies a majoroperational shift in vaccine delivery programs for all health units I have asked Carolyn Pim toconnect with our sister wave 4 units to share common experiences as we move forward ndash when wehave a roll up could I bring to COMOH Exec for discussion to explore whether there are broaderimplications for all members As an aside I have also asked the Ministry and their CIO to share with me any roll up learnings thatthey may have had already from previous waves (I understand that Niagara HU was a wave 1participant so if there is such a roll up of common experiences that others could learn fromperhaps you have it already and that could come to the exec too)Thanks Isra From Pim Carolyn Sent October 10 2013 1228 PMTo Christopher Mackie (christophermackiemlhuonca) Elizabeth Richardson(Elizabethrichardsonhamiltonca) H BSc M D F R C P (C) MPH Jim Chirico(jimchiriconbpsdhuca) Marlene Spruyt (spruytmtimiskaminghucom) Robert Kyle (Durham)Cc Levy IsraSubject Panorama - Privacy Security and other issues Dear colleagues Irsquom reaching out to you as fellow Panorama Wave 4 health units to ask about where yourorganizations are at in the process of signing agreements and completing Privacy ImpactAssessments and Threat Risk Assessments (TRAs) Ottawa Public Healthrsquos IT legal and informationsecurity advisors have made numerous requests to the MOHLTC for information (in particular theprovincial TRA) that we consider essential to develop our own risk assessment and PIA but havebeen told that information cannot be shared even with strict confidentiality and access controlsSo we are at somewhat of an impasse Isra emailed Arlene yesterday Arlene has forwarded ourconcerns to the Ministryrsquos CIO and Panorama lead but we havenrsquot had any response or discussionswith either of them yet Have your organizations identified similar concerns andor had interactions with the MOHLTC inthis respect Irsquod also be interested in knowing if your health units have flagged other (egoperational) implementation concerns Thanks
Carolyn ps Robert ndash you can ignore this request I talked with Sharan this morning about Durhamrsquos issuesso am including you now just for information Carolyn Pim MD FRCPC Associate Medical Officer of Health Meacutedecin adjointe en santeacute publique Ottawa Public Health Santeacute publique Ottawa 100 Constellation Cr Ottawa ON K2G 6J8 Tel teacutel (613) 580-6744 ext 23684Fax (613) 580-9641Connect With Ottawa Public Health
Suivez Santeacute publique Ottawa
This e-mail originates from the City of Ottawa e-mail system Any distribution use orcopying of this e-mail or the information it contains by other than the intendedrecipient(s) is unauthorized If you are not the intended recipient please notify meat the telephone number shown above or by return e-mail and delete thiscommunication and any copy immediately Thank you
Le preacutesent courriel a eacuteteacute expeacutedieacute par le systegraveme de courriels de la Ville dOttawaToute distribution utilisation ou reproduction du courriel ou des renseignements quisy trouvent par une personne autre que son destinataire preacutevu est interdite Si vousavez reccedilu le message par erreur veuillez men aviser par teacuteleacutephone (au numeacuteropreacuteciteacute) ou par courriel puis supprimer sans deacutelai la version originale de lacommunication ainsi que toutes ses copies Je vous remercie de votre collaboration
1
Smoke-Free Patios ndash An Amendment to the Smoke-Free Ontario Act
Date November 15 2013 Prepared for Council of Ontario Medical Officers of Health Prepared by York Region Public Health _____________________________________________________________________________ Issue
The Smoke-Free Ontario Act is the current provincial legislation that imposes smoking restrictions in workplaces and public places It prohibits smoking on restaurant and bar patios in instances where any portion of the seating area is covered by a roof With recent studies illustrating that exposure to second hand smoke outdoors poses similar risks to indoor exposure there has been growing public support to enhance smoking restrictions and make patios completely smoke-free
Background
With the implementation of the Smoke-Free Ontario Act in 2006 restaurant and bar patios became subject to smoking restrictions if any portion of the seating area was covered by a roof This allowed for patios without roof coverings to continue to allow smoking and as a result did not provide significant protection to patrons or staff from exposure to second hand smoke outdoors Many businesses chose to alter the design of their patios to allow smoking to continue In some cases patios became more crowded since smoking patrons who dine indoors often proceed outside onto licensed patios with their beverages to smoke York Region like most municipalities in Ontario is host to hundreds of patios being operated by restaurant owners and businesses With smoking prohibitions affecting only a small portion of these patios specifically ones with coverings the vast majority of patios still allow smoking to take place Patrons and employees on patios where smoking is not restricted are exposed to second hand smoke frequently This can contribute to increased disease and aggravation of existing health conditions From a business perspective the existing legislation has been viewed by many operators as unfair because some patios have permanent coverings which cannot be removed requiring a smoke-free status These business owners feel this creates an uneven playing field since they cannot provide an outdoor dining area for their smoking customers There is strong community support for smoke-free patios in Ontario A 2009 Rapid Risk Factor Surveillance System survey revealed 754 percent support in York Region while a Toronto Health Survey in 2011 indicated 74 percent public support
2
Current Status
Smoking is currently prohibited on restaurant and bar patios province-wide in four Canadian provinces and territories Alberta Newfoundland and Labrador Nova Scotia and Yukon A fifth province Prince Edward Island prohibits smoking on patios until 10 pm Since Ontario enacted legislation restricting smoking on patios in 2006 eight municipalities in Ontario have chosen to create bylaws that go beyond the Smoke-Free Ontario Act and enhance outdoor protection from second hand smoke by prohibiting smoking on patios completely The largest of those municipalities is the City of Ottawa Recently the Toronto Board of Health unanimously endorsed a report presented by their Medical Officer of Health recommending that restaurant and bar patios be made smoke-free through an amendment to the Smoke-Free Ontario Act
Key Considerations
There should be no significant financial burden to local Boards of Health resulting from a smoke-free patio amendment to the Smoke-Free Ontario Act Inspection and enforcement for the Smoke-Free Ontario Act is currently 100 percent funded by the Ministry of Health and Long-Term Care Following an introductory period of education on the amendment a complaint response model of service delivery would ensure ongoing compliance with smoke-free requirements A complete ban of smoking on patios would eliminate the widely-held perception by business owners that the current legislation creates an uneven playing field for business Since Smoke-Free Ontario Act inspections of patios began in 2006 operators have expressed the opinion that if patios need to be smoke-free for the protection of the public they should all be smoke-free to avoid undue hardship for individual businesses and to provide protection uniformly across the Province
Next steps
York Region Public Health intends to seek support from Medical Officers of Health across the Central East Tobacco Control Area Network (CETCAN) to advocate to the Ministry of Health and Long-Term Care for an amendment to the Smoke-Free Ontario Act prohibiting smoking on all restaurant and bar patios York Region is also in the process of requesting that its Regional Council advocate to the Minister of Health and Long-Term Care on the issue
Updating and Modernizing O Regulation 565 (Public Pools)
Date November 15 2013
Prepared for Council of Ontario Medical Officers of Health
Prepared by York Region Public Health _____________________________________________________________________________ Background Recent drownings at public pools in Ontario have highlighted the issue of water-borne illness and injury The current pool regulation under Ontariorsquos Health Protection and Promotion Act O Regulation 565 (Public Pools) is outdated It does not accurately reflect new pool technology and design or the changing use of public pools Neither does it incorporate admissions standards recommended by the Office of the Chief Coroner Further O Regulation 565 does not have short-form wording or set fines associated with it This limits public health enforcement capabilities What is the impact Updating O Regulation 565 (Public Pools) to address recent changes in pool technology design and uses and to include Coroner-recommended admissions standards would help improve pool safety Establishing short-form wording for O Regulation 565 would enhance enforcement related to public pools Currently the only enforcement available to Public Health Inspectors for dealing with non-critical regulatory infractions in public pools is the issuance of a Part III summons This involves a considerable amount of resources for a possible small fine With the development of inspection disclosure systems such as YorkSafe there is an even greater need to develop a method to effectively address repeated pool operator non-compliance with non-critical issues Next steps Public health units should advocate to the Province to 1) Conduct a review of O Regulation 565 (Public Pools) to address shortcomings Proposed changes to the
regulation should include a requirement for ownersoperators of public pools to advise the local Medical Officer of Health of any change in the use of a facility and the addition of the Coronerrsquos recommended admission standards
2) Provide short-form wording for O Regulation 565 so that public health inspectors can better deal with pool operator non-compliance
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
implemented only 5 of Queensland had fluoridated drinking water however by 2012 this had
risen to 86(18) With a change in government in 2012 Queensland reversed the mandated
state fluoridation requirement and again left the decision to local councils The results
according to Dr Alexander President of the Australian Dental Association ldquoEighteen
Queensland councils have since opted out of fluoridation after relentless scare campaigns from
eccentric and dangerous fringe groupsrdquo(19) Dr Alexander also disagreed with the decision
made by Queensland government stating that ldquoThe greatest public health and scientific
expertise lies at state and federal levels of government and decision making on complex public
health issues should therefore also rest at these levels Public health policy in Australia must be
driven by the best health interests of Australians not by misinformation and conspiracy theory
websitesrdquo(19)
Comparisons of children residing in fluoridated and nonfluoridated areas in Australia indicate
the following according to the Australian Institute of Health and Welfare ldquohellipthe average dmft
of children residing in areas where drinking water contained less than 03 ppm fluoride with
dmft in areas where drinking water contained 07 ppm fluoride or more Across all age groups
mean dmft was higher for children living in areas with the low concentration of fluoride Apart
from 4-year-olds the average dmft per child and the average number of missing teeth were all
higher for children residing in areas with a lower fluoride concentration than for children
residing in areas with a higher fluoride concentration Relative differences in mean dmft ranged
from 71 (4-year-olds) to 658 (7-year-olds) A similar pattern can also be seen in the
permanent teeth with higher average DMFT for children in areas with low concentration of
fluoride in drinking water compared to areas with a higher concentration of fluoride (Figure 15)
Differences ranged between 127 (11-year-olds) and 506 (12-year-olds)rdquo (20)
Table 2
State of Population with CWF
2012 (18)
State Mandate (18)
Tasmania 83 Fluoridation Act 1968
New South Wales 95 Fluoridation of Public Water Supplies Act 1957 Fluoridation of Public Water Supplies Regulation 2007
Australian Capital Territory 100 Electricity and Water (Amendment) Act (No 2) 1989 Public
Health (Drinking Water) Code of Practice 2007 (No 1)
Western Australia 92 Fluoridation of Public Water Supplies Act 1966
South Australia 90 none
Northern Territory 70 none
Victoria 90 Health (Fluoridation) Act 1973
Queensland 86 Water Fluoridation Act 2008
(2012 reversed mandated fluoridation) 18 Wikipedia the free encyclopedia Water Fluoridation in Australia
From Levy IsraTo Jaeger ValerieCc Pim Carolyn gordonalphaweborg Diallo Aicha Penny Sutcliffe Paul Roumeliotis Michael Finkelstein
Hazel Lynn Robert KyleSubject FW Panorama - Privacy Security and other issuesDate Wednesday October 16 2013 122110 PM
Hello ValerieOttawa is part of Wave 4 Panorama implementation and we are gearing up increasingly to use thesystem where and if possible Thinking about it I am anticipating that this may need to be on theCOMOH (and alPHa) radar as it is something that will impact all health units and implies a majoroperational shift in vaccine delivery programs for all health units I have asked Carolyn Pim toconnect with our sister wave 4 units to share common experiences as we move forward ndash when wehave a roll up could I bring to COMOH Exec for discussion to explore whether there are broaderimplications for all members As an aside I have also asked the Ministry and their CIO to share with me any roll up learnings thatthey may have had already from previous waves (I understand that Niagara HU was a wave 1participant so if there is such a roll up of common experiences that others could learn fromperhaps you have it already and that could come to the exec too)Thanks Isra From Pim Carolyn Sent October 10 2013 1228 PMTo Christopher Mackie (christophermackiemlhuonca) Elizabeth Richardson(Elizabethrichardsonhamiltonca) H BSc M D F R C P (C) MPH Jim Chirico(jimchiriconbpsdhuca) Marlene Spruyt (spruytmtimiskaminghucom) Robert Kyle (Durham)Cc Levy IsraSubject Panorama - Privacy Security and other issues Dear colleagues Irsquom reaching out to you as fellow Panorama Wave 4 health units to ask about where yourorganizations are at in the process of signing agreements and completing Privacy ImpactAssessments and Threat Risk Assessments (TRAs) Ottawa Public Healthrsquos IT legal and informationsecurity advisors have made numerous requests to the MOHLTC for information (in particular theprovincial TRA) that we consider essential to develop our own risk assessment and PIA but havebeen told that information cannot be shared even with strict confidentiality and access controlsSo we are at somewhat of an impasse Isra emailed Arlene yesterday Arlene has forwarded ourconcerns to the Ministryrsquos CIO and Panorama lead but we havenrsquot had any response or discussionswith either of them yet Have your organizations identified similar concerns andor had interactions with the MOHLTC inthis respect Irsquod also be interested in knowing if your health units have flagged other (egoperational) implementation concerns Thanks
Carolyn ps Robert ndash you can ignore this request I talked with Sharan this morning about Durhamrsquos issuesso am including you now just for information Carolyn Pim MD FRCPC Associate Medical Officer of Health Meacutedecin adjointe en santeacute publique Ottawa Public Health Santeacute publique Ottawa 100 Constellation Cr Ottawa ON K2G 6J8 Tel teacutel (613) 580-6744 ext 23684Fax (613) 580-9641Connect With Ottawa Public Health
Suivez Santeacute publique Ottawa
This e-mail originates from the City of Ottawa e-mail system Any distribution use orcopying of this e-mail or the information it contains by other than the intendedrecipient(s) is unauthorized If you are not the intended recipient please notify meat the telephone number shown above or by return e-mail and delete thiscommunication and any copy immediately Thank you
Le preacutesent courriel a eacuteteacute expeacutedieacute par le systegraveme de courriels de la Ville dOttawaToute distribution utilisation ou reproduction du courriel ou des renseignements quisy trouvent par une personne autre que son destinataire preacutevu est interdite Si vousavez reccedilu le message par erreur veuillez men aviser par teacuteleacutephone (au numeacuteropreacuteciteacute) ou par courriel puis supprimer sans deacutelai la version originale de lacommunication ainsi que toutes ses copies Je vous remercie de votre collaboration
1
Smoke-Free Patios ndash An Amendment to the Smoke-Free Ontario Act
Date November 15 2013 Prepared for Council of Ontario Medical Officers of Health Prepared by York Region Public Health _____________________________________________________________________________ Issue
The Smoke-Free Ontario Act is the current provincial legislation that imposes smoking restrictions in workplaces and public places It prohibits smoking on restaurant and bar patios in instances where any portion of the seating area is covered by a roof With recent studies illustrating that exposure to second hand smoke outdoors poses similar risks to indoor exposure there has been growing public support to enhance smoking restrictions and make patios completely smoke-free
Background
With the implementation of the Smoke-Free Ontario Act in 2006 restaurant and bar patios became subject to smoking restrictions if any portion of the seating area was covered by a roof This allowed for patios without roof coverings to continue to allow smoking and as a result did not provide significant protection to patrons or staff from exposure to second hand smoke outdoors Many businesses chose to alter the design of their patios to allow smoking to continue In some cases patios became more crowded since smoking patrons who dine indoors often proceed outside onto licensed patios with their beverages to smoke York Region like most municipalities in Ontario is host to hundreds of patios being operated by restaurant owners and businesses With smoking prohibitions affecting only a small portion of these patios specifically ones with coverings the vast majority of patios still allow smoking to take place Patrons and employees on patios where smoking is not restricted are exposed to second hand smoke frequently This can contribute to increased disease and aggravation of existing health conditions From a business perspective the existing legislation has been viewed by many operators as unfair because some patios have permanent coverings which cannot be removed requiring a smoke-free status These business owners feel this creates an uneven playing field since they cannot provide an outdoor dining area for their smoking customers There is strong community support for smoke-free patios in Ontario A 2009 Rapid Risk Factor Surveillance System survey revealed 754 percent support in York Region while a Toronto Health Survey in 2011 indicated 74 percent public support
2
Current Status
Smoking is currently prohibited on restaurant and bar patios province-wide in four Canadian provinces and territories Alberta Newfoundland and Labrador Nova Scotia and Yukon A fifth province Prince Edward Island prohibits smoking on patios until 10 pm Since Ontario enacted legislation restricting smoking on patios in 2006 eight municipalities in Ontario have chosen to create bylaws that go beyond the Smoke-Free Ontario Act and enhance outdoor protection from second hand smoke by prohibiting smoking on patios completely The largest of those municipalities is the City of Ottawa Recently the Toronto Board of Health unanimously endorsed a report presented by their Medical Officer of Health recommending that restaurant and bar patios be made smoke-free through an amendment to the Smoke-Free Ontario Act
Key Considerations
There should be no significant financial burden to local Boards of Health resulting from a smoke-free patio amendment to the Smoke-Free Ontario Act Inspection and enforcement for the Smoke-Free Ontario Act is currently 100 percent funded by the Ministry of Health and Long-Term Care Following an introductory period of education on the amendment a complaint response model of service delivery would ensure ongoing compliance with smoke-free requirements A complete ban of smoking on patios would eliminate the widely-held perception by business owners that the current legislation creates an uneven playing field for business Since Smoke-Free Ontario Act inspections of patios began in 2006 operators have expressed the opinion that if patios need to be smoke-free for the protection of the public they should all be smoke-free to avoid undue hardship for individual businesses and to provide protection uniformly across the Province
Next steps
York Region Public Health intends to seek support from Medical Officers of Health across the Central East Tobacco Control Area Network (CETCAN) to advocate to the Ministry of Health and Long-Term Care for an amendment to the Smoke-Free Ontario Act prohibiting smoking on all restaurant and bar patios York Region is also in the process of requesting that its Regional Council advocate to the Minister of Health and Long-Term Care on the issue
Updating and Modernizing O Regulation 565 (Public Pools)
Date November 15 2013
Prepared for Council of Ontario Medical Officers of Health
Prepared by York Region Public Health _____________________________________________________________________________ Background Recent drownings at public pools in Ontario have highlighted the issue of water-borne illness and injury The current pool regulation under Ontariorsquos Health Protection and Promotion Act O Regulation 565 (Public Pools) is outdated It does not accurately reflect new pool technology and design or the changing use of public pools Neither does it incorporate admissions standards recommended by the Office of the Chief Coroner Further O Regulation 565 does not have short-form wording or set fines associated with it This limits public health enforcement capabilities What is the impact Updating O Regulation 565 (Public Pools) to address recent changes in pool technology design and uses and to include Coroner-recommended admissions standards would help improve pool safety Establishing short-form wording for O Regulation 565 would enhance enforcement related to public pools Currently the only enforcement available to Public Health Inspectors for dealing with non-critical regulatory infractions in public pools is the issuance of a Part III summons This involves a considerable amount of resources for a possible small fine With the development of inspection disclosure systems such as YorkSafe there is an even greater need to develop a method to effectively address repeated pool operator non-compliance with non-critical issues Next steps Public health units should advocate to the Province to 1) Conduct a review of O Regulation 565 (Public Pools) to address shortcomings Proposed changes to the
regulation should include a requirement for ownersoperators of public pools to advise the local Medical Officer of Health of any change in the use of a facility and the addition of the Coronerrsquos recommended admission standards
2) Provide short-form wording for O Regulation 565 so that public health inspectors can better deal with pool operator non-compliance
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
19 Dr Karin Alexander ldquoSinking our teeth into fluoridationrdquo Medical observer8th Oct 2013
From Levy IsraTo Jaeger ValerieCc Pim Carolyn gordonalphaweborg Diallo Aicha Penny Sutcliffe Paul Roumeliotis Michael Finkelstein
Hazel Lynn Robert KyleSubject FW Panorama - Privacy Security and other issuesDate Wednesday October 16 2013 122110 PM
Hello ValerieOttawa is part of Wave 4 Panorama implementation and we are gearing up increasingly to use thesystem where and if possible Thinking about it I am anticipating that this may need to be on theCOMOH (and alPHa) radar as it is something that will impact all health units and implies a majoroperational shift in vaccine delivery programs for all health units I have asked Carolyn Pim toconnect with our sister wave 4 units to share common experiences as we move forward ndash when wehave a roll up could I bring to COMOH Exec for discussion to explore whether there are broaderimplications for all members As an aside I have also asked the Ministry and their CIO to share with me any roll up learnings thatthey may have had already from previous waves (I understand that Niagara HU was a wave 1participant so if there is such a roll up of common experiences that others could learn fromperhaps you have it already and that could come to the exec too)Thanks Isra From Pim Carolyn Sent October 10 2013 1228 PMTo Christopher Mackie (christophermackiemlhuonca) Elizabeth Richardson(Elizabethrichardsonhamiltonca) H BSc M D F R C P (C) MPH Jim Chirico(jimchiriconbpsdhuca) Marlene Spruyt (spruytmtimiskaminghucom) Robert Kyle (Durham)Cc Levy IsraSubject Panorama - Privacy Security and other issues Dear colleagues Irsquom reaching out to you as fellow Panorama Wave 4 health units to ask about where yourorganizations are at in the process of signing agreements and completing Privacy ImpactAssessments and Threat Risk Assessments (TRAs) Ottawa Public Healthrsquos IT legal and informationsecurity advisors have made numerous requests to the MOHLTC for information (in particular theprovincial TRA) that we consider essential to develop our own risk assessment and PIA but havebeen told that information cannot be shared even with strict confidentiality and access controlsSo we are at somewhat of an impasse Isra emailed Arlene yesterday Arlene has forwarded ourconcerns to the Ministryrsquos CIO and Panorama lead but we havenrsquot had any response or discussionswith either of them yet Have your organizations identified similar concerns andor had interactions with the MOHLTC inthis respect Irsquod also be interested in knowing if your health units have flagged other (egoperational) implementation concerns Thanks
Carolyn ps Robert ndash you can ignore this request I talked with Sharan this morning about Durhamrsquos issuesso am including you now just for information Carolyn Pim MD FRCPC Associate Medical Officer of Health Meacutedecin adjointe en santeacute publique Ottawa Public Health Santeacute publique Ottawa 100 Constellation Cr Ottawa ON K2G 6J8 Tel teacutel (613) 580-6744 ext 23684Fax (613) 580-9641Connect With Ottawa Public Health
Suivez Santeacute publique Ottawa
This e-mail originates from the City of Ottawa e-mail system Any distribution use orcopying of this e-mail or the information it contains by other than the intendedrecipient(s) is unauthorized If you are not the intended recipient please notify meat the telephone number shown above or by return e-mail and delete thiscommunication and any copy immediately Thank you
Le preacutesent courriel a eacuteteacute expeacutedieacute par le systegraveme de courriels de la Ville dOttawaToute distribution utilisation ou reproduction du courriel ou des renseignements quisy trouvent par une personne autre que son destinataire preacutevu est interdite Si vousavez reccedilu le message par erreur veuillez men aviser par teacuteleacutephone (au numeacuteropreacuteciteacute) ou par courriel puis supprimer sans deacutelai la version originale de lacommunication ainsi que toutes ses copies Je vous remercie de votre collaboration
1
Smoke-Free Patios ndash An Amendment to the Smoke-Free Ontario Act
Date November 15 2013 Prepared for Council of Ontario Medical Officers of Health Prepared by York Region Public Health _____________________________________________________________________________ Issue
The Smoke-Free Ontario Act is the current provincial legislation that imposes smoking restrictions in workplaces and public places It prohibits smoking on restaurant and bar patios in instances where any portion of the seating area is covered by a roof With recent studies illustrating that exposure to second hand smoke outdoors poses similar risks to indoor exposure there has been growing public support to enhance smoking restrictions and make patios completely smoke-free
Background
With the implementation of the Smoke-Free Ontario Act in 2006 restaurant and bar patios became subject to smoking restrictions if any portion of the seating area was covered by a roof This allowed for patios without roof coverings to continue to allow smoking and as a result did not provide significant protection to patrons or staff from exposure to second hand smoke outdoors Many businesses chose to alter the design of their patios to allow smoking to continue In some cases patios became more crowded since smoking patrons who dine indoors often proceed outside onto licensed patios with their beverages to smoke York Region like most municipalities in Ontario is host to hundreds of patios being operated by restaurant owners and businesses With smoking prohibitions affecting only a small portion of these patios specifically ones with coverings the vast majority of patios still allow smoking to take place Patrons and employees on patios where smoking is not restricted are exposed to second hand smoke frequently This can contribute to increased disease and aggravation of existing health conditions From a business perspective the existing legislation has been viewed by many operators as unfair because some patios have permanent coverings which cannot be removed requiring a smoke-free status These business owners feel this creates an uneven playing field since they cannot provide an outdoor dining area for their smoking customers There is strong community support for smoke-free patios in Ontario A 2009 Rapid Risk Factor Surveillance System survey revealed 754 percent support in York Region while a Toronto Health Survey in 2011 indicated 74 percent public support
2
Current Status
Smoking is currently prohibited on restaurant and bar patios province-wide in four Canadian provinces and territories Alberta Newfoundland and Labrador Nova Scotia and Yukon A fifth province Prince Edward Island prohibits smoking on patios until 10 pm Since Ontario enacted legislation restricting smoking on patios in 2006 eight municipalities in Ontario have chosen to create bylaws that go beyond the Smoke-Free Ontario Act and enhance outdoor protection from second hand smoke by prohibiting smoking on patios completely The largest of those municipalities is the City of Ottawa Recently the Toronto Board of Health unanimously endorsed a report presented by their Medical Officer of Health recommending that restaurant and bar patios be made smoke-free through an amendment to the Smoke-Free Ontario Act
Key Considerations
There should be no significant financial burden to local Boards of Health resulting from a smoke-free patio amendment to the Smoke-Free Ontario Act Inspection and enforcement for the Smoke-Free Ontario Act is currently 100 percent funded by the Ministry of Health and Long-Term Care Following an introductory period of education on the amendment a complaint response model of service delivery would ensure ongoing compliance with smoke-free requirements A complete ban of smoking on patios would eliminate the widely-held perception by business owners that the current legislation creates an uneven playing field for business Since Smoke-Free Ontario Act inspections of patios began in 2006 operators have expressed the opinion that if patios need to be smoke-free for the protection of the public they should all be smoke-free to avoid undue hardship for individual businesses and to provide protection uniformly across the Province
Next steps
York Region Public Health intends to seek support from Medical Officers of Health across the Central East Tobacco Control Area Network (CETCAN) to advocate to the Ministry of Health and Long-Term Care for an amendment to the Smoke-Free Ontario Act prohibiting smoking on all restaurant and bar patios York Region is also in the process of requesting that its Regional Council advocate to the Minister of Health and Long-Term Care on the issue
Updating and Modernizing O Regulation 565 (Public Pools)
Date November 15 2013
Prepared for Council of Ontario Medical Officers of Health
Prepared by York Region Public Health _____________________________________________________________________________ Background Recent drownings at public pools in Ontario have highlighted the issue of water-borne illness and injury The current pool regulation under Ontariorsquos Health Protection and Promotion Act O Regulation 565 (Public Pools) is outdated It does not accurately reflect new pool technology and design or the changing use of public pools Neither does it incorporate admissions standards recommended by the Office of the Chief Coroner Further O Regulation 565 does not have short-form wording or set fines associated with it This limits public health enforcement capabilities What is the impact Updating O Regulation 565 (Public Pools) to address recent changes in pool technology design and uses and to include Coroner-recommended admissions standards would help improve pool safety Establishing short-form wording for O Regulation 565 would enhance enforcement related to public pools Currently the only enforcement available to Public Health Inspectors for dealing with non-critical regulatory infractions in public pools is the issuance of a Part III summons This involves a considerable amount of resources for a possible small fine With the development of inspection disclosure systems such as YorkSafe there is an even greater need to develop a method to effectively address repeated pool operator non-compliance with non-critical issues Next steps Public health units should advocate to the Province to 1) Conduct a review of O Regulation 565 (Public Pools) to address shortcomings Proposed changes to the
regulation should include a requirement for ownersoperators of public pools to advise the local Medical Officer of Health of any change in the use of a facility and the addition of the Coronerrsquos recommended admission standards
2) Provide short-form wording for O Regulation 565 so that public health inspectors can better deal with pool operator non-compliance
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
From Levy IsraTo Jaeger ValerieCc Pim Carolyn gordonalphaweborg Diallo Aicha Penny Sutcliffe Paul Roumeliotis Michael Finkelstein
Hazel Lynn Robert KyleSubject FW Panorama - Privacy Security and other issuesDate Wednesday October 16 2013 122110 PM
Hello ValerieOttawa is part of Wave 4 Panorama implementation and we are gearing up increasingly to use thesystem where and if possible Thinking about it I am anticipating that this may need to be on theCOMOH (and alPHa) radar as it is something that will impact all health units and implies a majoroperational shift in vaccine delivery programs for all health units I have asked Carolyn Pim toconnect with our sister wave 4 units to share common experiences as we move forward ndash when wehave a roll up could I bring to COMOH Exec for discussion to explore whether there are broaderimplications for all members As an aside I have also asked the Ministry and their CIO to share with me any roll up learnings thatthey may have had already from previous waves (I understand that Niagara HU was a wave 1participant so if there is such a roll up of common experiences that others could learn fromperhaps you have it already and that could come to the exec too)Thanks Isra From Pim Carolyn Sent October 10 2013 1228 PMTo Christopher Mackie (christophermackiemlhuonca) Elizabeth Richardson(Elizabethrichardsonhamiltonca) H BSc M D F R C P (C) MPH Jim Chirico(jimchiriconbpsdhuca) Marlene Spruyt (spruytmtimiskaminghucom) Robert Kyle (Durham)Cc Levy IsraSubject Panorama - Privacy Security and other issues Dear colleagues Irsquom reaching out to you as fellow Panorama Wave 4 health units to ask about where yourorganizations are at in the process of signing agreements and completing Privacy ImpactAssessments and Threat Risk Assessments (TRAs) Ottawa Public Healthrsquos IT legal and informationsecurity advisors have made numerous requests to the MOHLTC for information (in particular theprovincial TRA) that we consider essential to develop our own risk assessment and PIA but havebeen told that information cannot be shared even with strict confidentiality and access controlsSo we are at somewhat of an impasse Isra emailed Arlene yesterday Arlene has forwarded ourconcerns to the Ministryrsquos CIO and Panorama lead but we havenrsquot had any response or discussionswith either of them yet Have your organizations identified similar concerns andor had interactions with the MOHLTC inthis respect Irsquod also be interested in knowing if your health units have flagged other (egoperational) implementation concerns Thanks
Carolyn ps Robert ndash you can ignore this request I talked with Sharan this morning about Durhamrsquos issuesso am including you now just for information Carolyn Pim MD FRCPC Associate Medical Officer of Health Meacutedecin adjointe en santeacute publique Ottawa Public Health Santeacute publique Ottawa 100 Constellation Cr Ottawa ON K2G 6J8 Tel teacutel (613) 580-6744 ext 23684Fax (613) 580-9641Connect With Ottawa Public Health
Suivez Santeacute publique Ottawa
This e-mail originates from the City of Ottawa e-mail system Any distribution use orcopying of this e-mail or the information it contains by other than the intendedrecipient(s) is unauthorized If you are not the intended recipient please notify meat the telephone number shown above or by return e-mail and delete thiscommunication and any copy immediately Thank you
Le preacutesent courriel a eacuteteacute expeacutedieacute par le systegraveme de courriels de la Ville dOttawaToute distribution utilisation ou reproduction du courriel ou des renseignements quisy trouvent par une personne autre que son destinataire preacutevu est interdite Si vousavez reccedilu le message par erreur veuillez men aviser par teacuteleacutephone (au numeacuteropreacuteciteacute) ou par courriel puis supprimer sans deacutelai la version originale de lacommunication ainsi que toutes ses copies Je vous remercie de votre collaboration
1
Smoke-Free Patios ndash An Amendment to the Smoke-Free Ontario Act
Date November 15 2013 Prepared for Council of Ontario Medical Officers of Health Prepared by York Region Public Health _____________________________________________________________________________ Issue
The Smoke-Free Ontario Act is the current provincial legislation that imposes smoking restrictions in workplaces and public places It prohibits smoking on restaurant and bar patios in instances where any portion of the seating area is covered by a roof With recent studies illustrating that exposure to second hand smoke outdoors poses similar risks to indoor exposure there has been growing public support to enhance smoking restrictions and make patios completely smoke-free
Background
With the implementation of the Smoke-Free Ontario Act in 2006 restaurant and bar patios became subject to smoking restrictions if any portion of the seating area was covered by a roof This allowed for patios without roof coverings to continue to allow smoking and as a result did not provide significant protection to patrons or staff from exposure to second hand smoke outdoors Many businesses chose to alter the design of their patios to allow smoking to continue In some cases patios became more crowded since smoking patrons who dine indoors often proceed outside onto licensed patios with their beverages to smoke York Region like most municipalities in Ontario is host to hundreds of patios being operated by restaurant owners and businesses With smoking prohibitions affecting only a small portion of these patios specifically ones with coverings the vast majority of patios still allow smoking to take place Patrons and employees on patios where smoking is not restricted are exposed to second hand smoke frequently This can contribute to increased disease and aggravation of existing health conditions From a business perspective the existing legislation has been viewed by many operators as unfair because some patios have permanent coverings which cannot be removed requiring a smoke-free status These business owners feel this creates an uneven playing field since they cannot provide an outdoor dining area for their smoking customers There is strong community support for smoke-free patios in Ontario A 2009 Rapid Risk Factor Surveillance System survey revealed 754 percent support in York Region while a Toronto Health Survey in 2011 indicated 74 percent public support
2
Current Status
Smoking is currently prohibited on restaurant and bar patios province-wide in four Canadian provinces and territories Alberta Newfoundland and Labrador Nova Scotia and Yukon A fifth province Prince Edward Island prohibits smoking on patios until 10 pm Since Ontario enacted legislation restricting smoking on patios in 2006 eight municipalities in Ontario have chosen to create bylaws that go beyond the Smoke-Free Ontario Act and enhance outdoor protection from second hand smoke by prohibiting smoking on patios completely The largest of those municipalities is the City of Ottawa Recently the Toronto Board of Health unanimously endorsed a report presented by their Medical Officer of Health recommending that restaurant and bar patios be made smoke-free through an amendment to the Smoke-Free Ontario Act
Key Considerations
There should be no significant financial burden to local Boards of Health resulting from a smoke-free patio amendment to the Smoke-Free Ontario Act Inspection and enforcement for the Smoke-Free Ontario Act is currently 100 percent funded by the Ministry of Health and Long-Term Care Following an introductory period of education on the amendment a complaint response model of service delivery would ensure ongoing compliance with smoke-free requirements A complete ban of smoking on patios would eliminate the widely-held perception by business owners that the current legislation creates an uneven playing field for business Since Smoke-Free Ontario Act inspections of patios began in 2006 operators have expressed the opinion that if patios need to be smoke-free for the protection of the public they should all be smoke-free to avoid undue hardship for individual businesses and to provide protection uniformly across the Province
Next steps
York Region Public Health intends to seek support from Medical Officers of Health across the Central East Tobacco Control Area Network (CETCAN) to advocate to the Ministry of Health and Long-Term Care for an amendment to the Smoke-Free Ontario Act prohibiting smoking on all restaurant and bar patios York Region is also in the process of requesting that its Regional Council advocate to the Minister of Health and Long-Term Care on the issue
Updating and Modernizing O Regulation 565 (Public Pools)
Date November 15 2013
Prepared for Council of Ontario Medical Officers of Health
Prepared by York Region Public Health _____________________________________________________________________________ Background Recent drownings at public pools in Ontario have highlighted the issue of water-borne illness and injury The current pool regulation under Ontariorsquos Health Protection and Promotion Act O Regulation 565 (Public Pools) is outdated It does not accurately reflect new pool technology and design or the changing use of public pools Neither does it incorporate admissions standards recommended by the Office of the Chief Coroner Further O Regulation 565 does not have short-form wording or set fines associated with it This limits public health enforcement capabilities What is the impact Updating O Regulation 565 (Public Pools) to address recent changes in pool technology design and uses and to include Coroner-recommended admissions standards would help improve pool safety Establishing short-form wording for O Regulation 565 would enhance enforcement related to public pools Currently the only enforcement available to Public Health Inspectors for dealing with non-critical regulatory infractions in public pools is the issuance of a Part III summons This involves a considerable amount of resources for a possible small fine With the development of inspection disclosure systems such as YorkSafe there is an even greater need to develop a method to effectively address repeated pool operator non-compliance with non-critical issues Next steps Public health units should advocate to the Province to 1) Conduct a review of O Regulation 565 (Public Pools) to address shortcomings Proposed changes to the
regulation should include a requirement for ownersoperators of public pools to advise the local Medical Officer of Health of any change in the use of a facility and the addition of the Coronerrsquos recommended admission standards
2) Provide short-form wording for O Regulation 565 so that public health inspectors can better deal with pool operator non-compliance
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
Carolyn ps Robert ndash you can ignore this request I talked with Sharan this morning about Durhamrsquos issuesso am including you now just for information Carolyn Pim MD FRCPC Associate Medical Officer of Health Meacutedecin adjointe en santeacute publique Ottawa Public Health Santeacute publique Ottawa 100 Constellation Cr Ottawa ON K2G 6J8 Tel teacutel (613) 580-6744 ext 23684Fax (613) 580-9641Connect With Ottawa Public Health
Suivez Santeacute publique Ottawa
This e-mail originates from the City of Ottawa e-mail system Any distribution use orcopying of this e-mail or the information it contains by other than the intendedrecipient(s) is unauthorized If you are not the intended recipient please notify meat the telephone number shown above or by return e-mail and delete thiscommunication and any copy immediately Thank you
Le preacutesent courriel a eacuteteacute expeacutedieacute par le systegraveme de courriels de la Ville dOttawaToute distribution utilisation ou reproduction du courriel ou des renseignements quisy trouvent par une personne autre que son destinataire preacutevu est interdite Si vousavez reccedilu le message par erreur veuillez men aviser par teacuteleacutephone (au numeacuteropreacuteciteacute) ou par courriel puis supprimer sans deacutelai la version originale de lacommunication ainsi que toutes ses copies Je vous remercie de votre collaboration
1
Smoke-Free Patios ndash An Amendment to the Smoke-Free Ontario Act
Date November 15 2013 Prepared for Council of Ontario Medical Officers of Health Prepared by York Region Public Health _____________________________________________________________________________ Issue
The Smoke-Free Ontario Act is the current provincial legislation that imposes smoking restrictions in workplaces and public places It prohibits smoking on restaurant and bar patios in instances where any portion of the seating area is covered by a roof With recent studies illustrating that exposure to second hand smoke outdoors poses similar risks to indoor exposure there has been growing public support to enhance smoking restrictions and make patios completely smoke-free
Background
With the implementation of the Smoke-Free Ontario Act in 2006 restaurant and bar patios became subject to smoking restrictions if any portion of the seating area was covered by a roof This allowed for patios without roof coverings to continue to allow smoking and as a result did not provide significant protection to patrons or staff from exposure to second hand smoke outdoors Many businesses chose to alter the design of their patios to allow smoking to continue In some cases patios became more crowded since smoking patrons who dine indoors often proceed outside onto licensed patios with their beverages to smoke York Region like most municipalities in Ontario is host to hundreds of patios being operated by restaurant owners and businesses With smoking prohibitions affecting only a small portion of these patios specifically ones with coverings the vast majority of patios still allow smoking to take place Patrons and employees on patios where smoking is not restricted are exposed to second hand smoke frequently This can contribute to increased disease and aggravation of existing health conditions From a business perspective the existing legislation has been viewed by many operators as unfair because some patios have permanent coverings which cannot be removed requiring a smoke-free status These business owners feel this creates an uneven playing field since they cannot provide an outdoor dining area for their smoking customers There is strong community support for smoke-free patios in Ontario A 2009 Rapid Risk Factor Surveillance System survey revealed 754 percent support in York Region while a Toronto Health Survey in 2011 indicated 74 percent public support
2
Current Status
Smoking is currently prohibited on restaurant and bar patios province-wide in four Canadian provinces and territories Alberta Newfoundland and Labrador Nova Scotia and Yukon A fifth province Prince Edward Island prohibits smoking on patios until 10 pm Since Ontario enacted legislation restricting smoking on patios in 2006 eight municipalities in Ontario have chosen to create bylaws that go beyond the Smoke-Free Ontario Act and enhance outdoor protection from second hand smoke by prohibiting smoking on patios completely The largest of those municipalities is the City of Ottawa Recently the Toronto Board of Health unanimously endorsed a report presented by their Medical Officer of Health recommending that restaurant and bar patios be made smoke-free through an amendment to the Smoke-Free Ontario Act
Key Considerations
There should be no significant financial burden to local Boards of Health resulting from a smoke-free patio amendment to the Smoke-Free Ontario Act Inspection and enforcement for the Smoke-Free Ontario Act is currently 100 percent funded by the Ministry of Health and Long-Term Care Following an introductory period of education on the amendment a complaint response model of service delivery would ensure ongoing compliance with smoke-free requirements A complete ban of smoking on patios would eliminate the widely-held perception by business owners that the current legislation creates an uneven playing field for business Since Smoke-Free Ontario Act inspections of patios began in 2006 operators have expressed the opinion that if patios need to be smoke-free for the protection of the public they should all be smoke-free to avoid undue hardship for individual businesses and to provide protection uniformly across the Province
Next steps
York Region Public Health intends to seek support from Medical Officers of Health across the Central East Tobacco Control Area Network (CETCAN) to advocate to the Ministry of Health and Long-Term Care for an amendment to the Smoke-Free Ontario Act prohibiting smoking on all restaurant and bar patios York Region is also in the process of requesting that its Regional Council advocate to the Minister of Health and Long-Term Care on the issue
Updating and Modernizing O Regulation 565 (Public Pools)
Date November 15 2013
Prepared for Council of Ontario Medical Officers of Health
Prepared by York Region Public Health _____________________________________________________________________________ Background Recent drownings at public pools in Ontario have highlighted the issue of water-borne illness and injury The current pool regulation under Ontariorsquos Health Protection and Promotion Act O Regulation 565 (Public Pools) is outdated It does not accurately reflect new pool technology and design or the changing use of public pools Neither does it incorporate admissions standards recommended by the Office of the Chief Coroner Further O Regulation 565 does not have short-form wording or set fines associated with it This limits public health enforcement capabilities What is the impact Updating O Regulation 565 (Public Pools) to address recent changes in pool technology design and uses and to include Coroner-recommended admissions standards would help improve pool safety Establishing short-form wording for O Regulation 565 would enhance enforcement related to public pools Currently the only enforcement available to Public Health Inspectors for dealing with non-critical regulatory infractions in public pools is the issuance of a Part III summons This involves a considerable amount of resources for a possible small fine With the development of inspection disclosure systems such as YorkSafe there is an even greater need to develop a method to effectively address repeated pool operator non-compliance with non-critical issues Next steps Public health units should advocate to the Province to 1) Conduct a review of O Regulation 565 (Public Pools) to address shortcomings Proposed changes to the
regulation should include a requirement for ownersoperators of public pools to advise the local Medical Officer of Health of any change in the use of a facility and the addition of the Coronerrsquos recommended admission standards
2) Provide short-form wording for O Regulation 565 so that public health inspectors can better deal with pool operator non-compliance
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
1
Smoke-Free Patios ndash An Amendment to the Smoke-Free Ontario Act
Date November 15 2013 Prepared for Council of Ontario Medical Officers of Health Prepared by York Region Public Health _____________________________________________________________________________ Issue
The Smoke-Free Ontario Act is the current provincial legislation that imposes smoking restrictions in workplaces and public places It prohibits smoking on restaurant and bar patios in instances where any portion of the seating area is covered by a roof With recent studies illustrating that exposure to second hand smoke outdoors poses similar risks to indoor exposure there has been growing public support to enhance smoking restrictions and make patios completely smoke-free
Background
With the implementation of the Smoke-Free Ontario Act in 2006 restaurant and bar patios became subject to smoking restrictions if any portion of the seating area was covered by a roof This allowed for patios without roof coverings to continue to allow smoking and as a result did not provide significant protection to patrons or staff from exposure to second hand smoke outdoors Many businesses chose to alter the design of their patios to allow smoking to continue In some cases patios became more crowded since smoking patrons who dine indoors often proceed outside onto licensed patios with their beverages to smoke York Region like most municipalities in Ontario is host to hundreds of patios being operated by restaurant owners and businesses With smoking prohibitions affecting only a small portion of these patios specifically ones with coverings the vast majority of patios still allow smoking to take place Patrons and employees on patios where smoking is not restricted are exposed to second hand smoke frequently This can contribute to increased disease and aggravation of existing health conditions From a business perspective the existing legislation has been viewed by many operators as unfair because some patios have permanent coverings which cannot be removed requiring a smoke-free status These business owners feel this creates an uneven playing field since they cannot provide an outdoor dining area for their smoking customers There is strong community support for smoke-free patios in Ontario A 2009 Rapid Risk Factor Surveillance System survey revealed 754 percent support in York Region while a Toronto Health Survey in 2011 indicated 74 percent public support
2
Current Status
Smoking is currently prohibited on restaurant and bar patios province-wide in four Canadian provinces and territories Alberta Newfoundland and Labrador Nova Scotia and Yukon A fifth province Prince Edward Island prohibits smoking on patios until 10 pm Since Ontario enacted legislation restricting smoking on patios in 2006 eight municipalities in Ontario have chosen to create bylaws that go beyond the Smoke-Free Ontario Act and enhance outdoor protection from second hand smoke by prohibiting smoking on patios completely The largest of those municipalities is the City of Ottawa Recently the Toronto Board of Health unanimously endorsed a report presented by their Medical Officer of Health recommending that restaurant and bar patios be made smoke-free through an amendment to the Smoke-Free Ontario Act
Key Considerations
There should be no significant financial burden to local Boards of Health resulting from a smoke-free patio amendment to the Smoke-Free Ontario Act Inspection and enforcement for the Smoke-Free Ontario Act is currently 100 percent funded by the Ministry of Health and Long-Term Care Following an introductory period of education on the amendment a complaint response model of service delivery would ensure ongoing compliance with smoke-free requirements A complete ban of smoking on patios would eliminate the widely-held perception by business owners that the current legislation creates an uneven playing field for business Since Smoke-Free Ontario Act inspections of patios began in 2006 operators have expressed the opinion that if patios need to be smoke-free for the protection of the public they should all be smoke-free to avoid undue hardship for individual businesses and to provide protection uniformly across the Province
Next steps
York Region Public Health intends to seek support from Medical Officers of Health across the Central East Tobacco Control Area Network (CETCAN) to advocate to the Ministry of Health and Long-Term Care for an amendment to the Smoke-Free Ontario Act prohibiting smoking on all restaurant and bar patios York Region is also in the process of requesting that its Regional Council advocate to the Minister of Health and Long-Term Care on the issue
Updating and Modernizing O Regulation 565 (Public Pools)
Date November 15 2013
Prepared for Council of Ontario Medical Officers of Health
Prepared by York Region Public Health _____________________________________________________________________________ Background Recent drownings at public pools in Ontario have highlighted the issue of water-borne illness and injury The current pool regulation under Ontariorsquos Health Protection and Promotion Act O Regulation 565 (Public Pools) is outdated It does not accurately reflect new pool technology and design or the changing use of public pools Neither does it incorporate admissions standards recommended by the Office of the Chief Coroner Further O Regulation 565 does not have short-form wording or set fines associated with it This limits public health enforcement capabilities What is the impact Updating O Regulation 565 (Public Pools) to address recent changes in pool technology design and uses and to include Coroner-recommended admissions standards would help improve pool safety Establishing short-form wording for O Regulation 565 would enhance enforcement related to public pools Currently the only enforcement available to Public Health Inspectors for dealing with non-critical regulatory infractions in public pools is the issuance of a Part III summons This involves a considerable amount of resources for a possible small fine With the development of inspection disclosure systems such as YorkSafe there is an even greater need to develop a method to effectively address repeated pool operator non-compliance with non-critical issues Next steps Public health units should advocate to the Province to 1) Conduct a review of O Regulation 565 (Public Pools) to address shortcomings Proposed changes to the
regulation should include a requirement for ownersoperators of public pools to advise the local Medical Officer of Health of any change in the use of a facility and the addition of the Coronerrsquos recommended admission standards
2) Provide short-form wording for O Regulation 565 so that public health inspectors can better deal with pool operator non-compliance
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
2
Current Status
Smoking is currently prohibited on restaurant and bar patios province-wide in four Canadian provinces and territories Alberta Newfoundland and Labrador Nova Scotia and Yukon A fifth province Prince Edward Island prohibits smoking on patios until 10 pm Since Ontario enacted legislation restricting smoking on patios in 2006 eight municipalities in Ontario have chosen to create bylaws that go beyond the Smoke-Free Ontario Act and enhance outdoor protection from second hand smoke by prohibiting smoking on patios completely The largest of those municipalities is the City of Ottawa Recently the Toronto Board of Health unanimously endorsed a report presented by their Medical Officer of Health recommending that restaurant and bar patios be made smoke-free through an amendment to the Smoke-Free Ontario Act
Key Considerations
There should be no significant financial burden to local Boards of Health resulting from a smoke-free patio amendment to the Smoke-Free Ontario Act Inspection and enforcement for the Smoke-Free Ontario Act is currently 100 percent funded by the Ministry of Health and Long-Term Care Following an introductory period of education on the amendment a complaint response model of service delivery would ensure ongoing compliance with smoke-free requirements A complete ban of smoking on patios would eliminate the widely-held perception by business owners that the current legislation creates an uneven playing field for business Since Smoke-Free Ontario Act inspections of patios began in 2006 operators have expressed the opinion that if patios need to be smoke-free for the protection of the public they should all be smoke-free to avoid undue hardship for individual businesses and to provide protection uniformly across the Province
Next steps
York Region Public Health intends to seek support from Medical Officers of Health across the Central East Tobacco Control Area Network (CETCAN) to advocate to the Ministry of Health and Long-Term Care for an amendment to the Smoke-Free Ontario Act prohibiting smoking on all restaurant and bar patios York Region is also in the process of requesting that its Regional Council advocate to the Minister of Health and Long-Term Care on the issue
Updating and Modernizing O Regulation 565 (Public Pools)
Date November 15 2013
Prepared for Council of Ontario Medical Officers of Health
Prepared by York Region Public Health _____________________________________________________________________________ Background Recent drownings at public pools in Ontario have highlighted the issue of water-borne illness and injury The current pool regulation under Ontariorsquos Health Protection and Promotion Act O Regulation 565 (Public Pools) is outdated It does not accurately reflect new pool technology and design or the changing use of public pools Neither does it incorporate admissions standards recommended by the Office of the Chief Coroner Further O Regulation 565 does not have short-form wording or set fines associated with it This limits public health enforcement capabilities What is the impact Updating O Regulation 565 (Public Pools) to address recent changes in pool technology design and uses and to include Coroner-recommended admissions standards would help improve pool safety Establishing short-form wording for O Regulation 565 would enhance enforcement related to public pools Currently the only enforcement available to Public Health Inspectors for dealing with non-critical regulatory infractions in public pools is the issuance of a Part III summons This involves a considerable amount of resources for a possible small fine With the development of inspection disclosure systems such as YorkSafe there is an even greater need to develop a method to effectively address repeated pool operator non-compliance with non-critical issues Next steps Public health units should advocate to the Province to 1) Conduct a review of O Regulation 565 (Public Pools) to address shortcomings Proposed changes to the
regulation should include a requirement for ownersoperators of public pools to advise the local Medical Officer of Health of any change in the use of a facility and the addition of the Coronerrsquos recommended admission standards
2) Provide short-form wording for O Regulation 565 so that public health inspectors can better deal with pool operator non-compliance
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
Updating and Modernizing O Regulation 565 (Public Pools)
Date November 15 2013
Prepared for Council of Ontario Medical Officers of Health
Prepared by York Region Public Health _____________________________________________________________________________ Background Recent drownings at public pools in Ontario have highlighted the issue of water-borne illness and injury The current pool regulation under Ontariorsquos Health Protection and Promotion Act O Regulation 565 (Public Pools) is outdated It does not accurately reflect new pool technology and design or the changing use of public pools Neither does it incorporate admissions standards recommended by the Office of the Chief Coroner Further O Regulation 565 does not have short-form wording or set fines associated with it This limits public health enforcement capabilities What is the impact Updating O Regulation 565 (Public Pools) to address recent changes in pool technology design and uses and to include Coroner-recommended admissions standards would help improve pool safety Establishing short-form wording for O Regulation 565 would enhance enforcement related to public pools Currently the only enforcement available to Public Health Inspectors for dealing with non-critical regulatory infractions in public pools is the issuance of a Part III summons This involves a considerable amount of resources for a possible small fine With the development of inspection disclosure systems such as YorkSafe there is an even greater need to develop a method to effectively address repeated pool operator non-compliance with non-critical issues Next steps Public health units should advocate to the Province to 1) Conduct a review of O Regulation 565 (Public Pools) to address shortcomings Proposed changes to the
regulation should include a requirement for ownersoperators of public pools to advise the local Medical Officer of Health of any change in the use of a facility and the addition of the Coronerrsquos recommended admission standards
2) Provide short-form wording for O Regulation 565 so that public health inspectors can better deal with pool operator non-compliance
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
COMOH Electronic Mailing List ndash Public Health and Preventive Medicine Resident Subscribers November 15 2013
PHPMR Subscriber Endorsed By Duration Date of Annual
Review Kit Young Hoon Julie Emili November 11 2012 ndash November
11 2013 Ariella Zbar Jennifer Horton Rashida Shamshudin Diane Lu Sara-Anne Arul Emily Groot Dr Daniel Warshafsky Dr John Harding
Julie Emili November 11 2012 ndash November 11 2013
Fran Scott Barbara Yaffe January 3 2013 ndash January 3 2014 Joyce Lock Bob Nosal March 11 2013 ndash March 11 2014 Sajida Afridi Rosamund Lewis Nov 22 2012 ndash Nov 22 2013 Pamela Leece Rita Shahin Dec 10 2012 ndash Dec 10 2013 Nikhil Rajaram Vinita Dubey Jan 7 2013 ndash Jan 7 2014 Airia Parisa Monica Hau March 18 2013 ndash March 18 2014 Catherine Dickson Paula Stewart May 9 ndash October 22 2013 Trevor Arnason Vera Etches Rosamund Lewis June 19 ndash September 6 2013 Claudia Sarbu Carolyn Pim July 1 2013 ndash June 20 2014 Marina Afanasyeva Carolyn Pim July 1 2013 ndash June 20 2014 Wajid Ahmed Vera Etches July 8 2013 ndash October 31 2013 Aaron Orkin Barbara Yaffe Sept 3 2013 ndash Sept 3 2014 Nicholas Brandon Irene Armstrong Oct 31 2013 - Feb 28 2014 Catherine Dickson Rosamund Lewis Oct 31 2013 ndash Aug 1 2014 COMOH Electronic Mailing List ndash Individuals with ldquoSend Onlyrdquo Authorization
The MailMan software allows the addition of addresses to a ldquosender filterrdquo which gives the owners of these e-mail addresses the ability to send messages to the COMOH e-mail list without moderator approval They DO NOT receive any messages that are sent through the comohlistsalphaweborg address Dr Arlene King ndash Chief Medical Officer of Health Dr Natasha Crowcroft - Director Surveillance and Epidemiology PHO Dr Vivek Goel ndash President and CEO PHO Dr George Pasut ndash VP Science and Public Health PHO Dr Ray Copes - Director Environmental and Occupational Health PHO
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
Application for Inclusion on the Council of Ontario Medical Officers of Health Electronic Mailing List As a service to its members the Association of Local Public Health Agencies hosts a number of subscriber-only electronic mailing lists which enable instantaneous two-way communication among subscribers Although the comohlistsalphaweborg list has historically been strictly limited to Medical Officers of Health and Associate MOHs working in Ontariorsquos health units it has been acknowledged that expanding eligibility to Public Health and Preventive Medicine Residents would be of mutual benefit In June 2009 the Council of Ontario Medical Officers of Health (COMOH) approved changes in its Terms of Reference to enable PHPMRs to request inclusion on the comohlistsalphaweborg electronic mailing list as Affiliate Members by written request Requirements
bull All below fields must be completed (Please over-write the examples given in the right column) bull The application must be endorsed by an Active or Associate member of COMOH bull The application must be accompanied by a brief covering letter or e-mail including
o Full contact information o A brief description of the reason for the request
bull The application should be submitted to the COMOH Chair co Gordon Fleming at alPHa ndash Gordonalphaweborg 416-595-0030 fax
Name
Your Name
Institution and Year Name of your medical school level
Location
Name of Public Health Unit agency First Nation Community etc hosting your current rotation
E-mail address
e-mail address for sending and receiving messages via
comohlistsalphaweborg
Endorsement
Name and e-mail of sponsoring Active or Associate COMOH member
Expected duration of subscription (if less than one year)
Memberships will be reviewed by the COMOH Executive annually Please indicate the length of time you expect to be subscribed if less
than one year
Inquiries Gordon Fleming BA BASc CPHI(C) Manager Public Health Issues Association of Local Public Health Agencies (alPHa) 2 Carlton St Suite 1306 Toronto Ontario M5B-1J3 (416) 595-0006 ext 23 (416) 595-0030 Fax gordonalphaweborg
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
2 Carlton Street Suite 1306 Toronto ON M5B 1J3
Tel (416) 595-0006 Fax (416) 595-0030
E-mail infoalphaweborg
Providing leadership in public health management
DRAFT MINUTES COUNCIL OF ONTARIO MEDICAL OFFICERS OF HEALTH
EXECUTIVE COMMITTEE TELECONFERENCE Tuesday October 8th 2013
830 ndash 930 AM PRESENT Valerie Jaeger (Chair) Michael Finkelstein Robert Kyle Isra Levy Hazel Lynn Penny Sutcliffe Gordon Fleming (alPHa Staff Recorder) REGRETS Paul Roumeliotis
10 Call to Order Approval of Agenda Meeting called to order at 0831 AM Agenda approved with the addition of Item 55 ADM Health Promotion 20 Approval of Minutes September 10th 2013 Minutes September 10 Minutes approved as circulated 30 COMOH BUSINESS
31 COMOH Priorities Strategic Planning alPHa StratPlan Summary The attached was discussed at the alPHa Board meeting on September 28 prior to which COMOH Executive members met to discuss its implications on COMOHrsquos own evolving plan V Jaeger invited further comment R Kyle suggested that some current meeting practices could be altered in order to prepare for eventual changes to the nature and quantity of support provided to COMOH by alPHa staff Less detailed minutes fewer teleconferences more concise agendas and eliminating support for subcommittees work groups were given as examples of areas where efficiencies could be found M Finkelstein suggested that the Executiversquos function should be to assign work to eventual working groups and H Lynn recommended reducing the number of agenda items to allow more fulsome discussion of a small number of key issues while identifying ways of dealing with other matters outside of regularly scheduled routine meetings I levy suggested that COMOH is probably still going to want to meet for a variety of reasons and that alPHarsquos primary role should be to ensure that relevant policy information is available in order to determine interventions on important issues 32 COMOH Community of Practice e-Mail Suggestion V Jaeger referred to the suggestion made in the attached e-mail from Sudit Ranade which was sent
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
following the last COMOH Section meeting which refers to a mechanism for creating and maintaining a repository of information G Fleming indicated that there are features in the alPHa Web site infrastructure that would probably serve the purpose once alPHa staff becomes more familiar with the technical capacities and comfort with developing and communicating ideal processes H Lynn confirmed that the alPHa-supported Low Risk Drinking Guidelines work group is already experimenting with this A suggestion that alPHa think about pursuing a grant to make this possible for COMOH was made 33 Emeritus MOH Designation Criteria Conferring Emeritus status to retiring MOHs was discussed in light of an upcoming retirement and it was agreed on principle that COMOH should do so in all but exceptional cases subject to the present COMOH ToR V Jaeger to begin work with alPHa Staff on a process for communicating Emeritus designation to eligible individuals 34 COMOH Section Agenda November 15 2013 Draft Agenda
alPHa Symposium Details V Jaeger referred to the attached draft agenda noting that there will be a Ministry update in plenary prior to the COMOH meeting M Finkelstein observed that the number of hours devoted to these meetings appears to have decreased over time and that it might be a good idea to have an environmental scan of members as to what their feelings are on this V Jaeger noted that she has heard from some members that the meetings are indeed too short especially where items requiring substantive discussion are included She referred to H Lynnrsquos earlier suggestion of reducing the number of agenda items as a possible means of rectifying this R Kyle suggested that the amount of time devoted to these meetings has expanded and contracted in cycles and depends in large part on how the current Chair wishes to conduct COMOH business He agreed that agendas could be shorter or at least clearer on what items are meant for discussion as opposed to those that are for information only It was also noted that in the past more COMOH meeting time was devoted to dialogue with Provincial partners This dialogue has been moved into plenary more recently but it was agreed that the nature of the dialogue is not necessarily the same as it would be in the confines of a COMOH meeting I Levy observed that the plenary sessions have largely been presentations of information rather than discussions of policy mechanics that need clarification or about which there are concerns He suggested that COMOH needs to pursue opportunities for the latter G Fleming indicated that the COMOH meeting could likely continue in the afternoon following lunch if it is determined that more time is needed ACTION V Jaeger to contact Arlene King and Kate Manson-Smith to request information about what they intend to address in plenary on November 15 in order to inform questions and discussions
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
40 PUBLIC HEALTH ISSUES
41 HIV Non-Disclosure S22 Orders COMOH Minutes Sept 18 V Jaeger reported that this has been re-introduced at the PHLC and PHO has agreed to provide secretariat facilities and technical support for a COMOH working group to develop guidelines The MOHLTC has offered some legal resources if necessary but has not committed to anything specific otherwise She reminded the group that there is agreement that COMOH should be taking the lead on this initiative but also that the end product is going to require central (ie PHD MOHLTC) endorsement I Levy suggested that R Schabas I Gemmill and A Heimann (the MOHs who have agreed to do this work) be asked to draft guidelines for comment and eventual endorsement by the COMOH membership Even if central endorsement is not forthcoming a COMOH-supported set of guidelines may at least build in the procedural consistency that is being sought ACTION V Jaeger to communicate this request to the three volunteers 42 Supervised Injection Sites COMOH Feedback
COMOH Minutes Sept 18 V Jaeger referred to the feedback that she had received from a few MOHs on the potential wording of a COMOH position on this issue I Levy stated that the final product will not only need to be principled and widely accepted by the membership but also framed in such a way that accounts for the political realities that surround it It was suggested that reference to crime rates may be superfluous to the public health arguments that can reasonably be made ACTION V Jaeger to revise the statement in light of the most recent feedback and re-circulate for further comment 43 Campaign for Justice on Tobacco Fraud Draft Letters and Endorsements V Jaeger asked for Executive comment on the attached including consideration of whether this should be a COMOH issue or an alPHa one G Fleming reminded the group that this is the continuation of a process that was introduced at the November 2012 COMOH meeting and that the Campaignrsquos intent was most likely to secure the support of the public health physicians specifically It was agreed that there will need to be absolute clarity on what COMOH is putting its signature on and it was suggested that Garfield Mahood be asked to provide a written update of what has happened since this issue was first introduced ACTION V Jaeger to contact Garfield Mahood in an effort to get the required information 44 Student Immunization Data Minutes September 10 V Jaeger stated that there has already been a change to the regulations but work still needs to be done on the privacy issues
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
45 Children and Youth Data Strategy Minutes September 10 V Jaeger has communicated the COMOH executiversquos willingness to participate in this discussion and George Pasut will circle back with ICES to arrange future discussion having agreed that PHO and ICES should take the lead 46 Low Risk Drinking Guidelines Letters to OMA amp TCFCP H Lynn referred to the attached letters that originated from the SW and CW MOH groups which relate to the promotion of the Low Risk Alcohol Drinking Guidelines in clinical settings Discussion centred on the idea of a billable OHIP code that could be added for intervention and referral similar to the one used for tobacco V Jaeger reported that she has discussed this with John Wellner (Director Health Promotion Research amp Emerging Issues OMA) further suggesting that a more general code forrdquomessages of public health importancerdquo could be considered Although it was agreed that it was unlikely that this idea would be resolved as part of the next round of negotiations members supported getting this issue on the radar as it fits well with the Governmentrsquos current emphasis on health promotion and disease prevention in many of its healt-related policy initiatives 50 Public Health Partners
51 Public Health Ontario
511 Strengthening COMOHPHO working relationship V Jaeger indicated that her next regular meeting with George Pasut is scheduled for this week 512 PHO Support - Toxicology e-Mail Backgrounder DEFERRED 52 Public Health Sector Strategic Plan V Jaeger reported that the implementation table co-chairs have been named and that they will be responsible for determining membership work plans and terms of reference for each respectively She is expecting a general communication from the CMOH about this soon 53 COMOH ndash CODE Initiative Proposal e-Mail M Finkelstein reported that he and V Jaeger met with Director-level representatives from the Ministry of Education along with the Executive Director of CODE (Frank Kelly) to introduce the composition and purpose of the two organizations and begin discussions about working together Specifically legislative changes have recently been made that have incorporated ldquostudent wellbeingrdquo into the Education
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
mandate and they are now looking to public health with a view to creating a relationship that will serve this mutual purpose The smaller boards are especially interested in taking advantage of structures and processes that the larger ones have already established They are therefore proposing a joint-committee that would start by doing an environmental scan of best practices An introductory letter (circulated separately to the COMOH Executive) has been drafted 54 Ontario Medical Association Further to what was reported under item 46 V Jaeger indicated that she and John Wellner have agreed to keep in regular contact (every 6-8 weeks) to keep each other informed on issues of mutual interest 55 ADM Health Promotion V Jaeger informed the group that she has met with Kate Manson Smith who impressed upon her that over 80 of the HPDrsquos budget goes directly to public health units but that she reports to people who are not familiar with what public health does and as such are very outcome-oriented She has therefore indicated a need for support on educating government on the much longer horizons involved in population health interventions and outcomes 60 Addendum
70 UPDATES INFORMATION ITEMS REPORTS
71 Public Health Leadership Council PHLC TC Summary 72 COMOH Electronic Mailing List List of Subscribers 80 Next MeetingAdjournment Meeting adjourned at 0936 Next meeting Tuesday November 19 0830-0930 AM
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
1
For COMOH Information COMOH Section Meeting
November 15th 2013
COMOH Correspondence Sept ndash Nov 2013 COMOH - CODE Letter November 12 2013 joint letter from the Executive Director of the Council of Ontario Directors of Education (CODE) and Chair of the Council of Ontario Medical Officers of Health (COMOH)introducing a cooperative project to provide resources and supports that will further enable public health units and district school boards to develop stronger and mutually beneficial partnerships for the delivery of student health and well being services for schools and students
COMOH Letter - Food Safety and Nutrition November 1 2013 correspondence to the federal Minister of Health from the Chair of the Council of Ontario Medical Officers of Health regarding recent federal food safety and nutrition activities MNRG Response - Ontarios Energy Plan October 21 2003 Minister of Energy response to COMOHs August 26 Letter providing input to the Environmental Review of Ontarios Long-Term Energy Plan COMOH Letter - OMA Policy Paper on Alcohol October 17 2013 COMOH response to the Ontario Medical Association (OMA) Policy Paper Mitigating Harm Associated with Alcohol COMOH Letter - Alcohol SBIR October 17 2013 - COMOH Letter commending the College of Family Physicians of Canada for its work in developing the new Alcohol Screening Brief Intervention amp Referral A Clinical Guide and for offering the self-directed Mainpro-C credits to support Family Physicians in applying these tools and guidelines COMOH Letter - Safe Injection Services October 16 2013 COMOH letter to the MOHLTC expressing support for the provision of safe injection services as part of a continuum of harm reduction strategies in Ontario
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
Submission to the Minimum Wage Advisory Panel Ontario Ministry of Labour
by
The Association for Local Public Health AgenciesOntario Public Health Association (alPHa-OPHA) Health Equity Workgroup (HEWG)
October 9 2013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
1
On behalf of the Association of Local Public Health Agencies (alPHa) and the Ontario Public Health Association ndashtwo organizations representing public health leadership in Ontario ndash we are pleased to provide feedback on the consultation paper on Ontariorsquos minimum wage (Ontario Ministry of Labour 2013) Collectively our associations have over 80 years of experience providing leadership in the provincial public health sector As not-for-profit member-based organizations we represent Ontariorsquos 36 local boards of health and public and community health professionals in Ontario We have a long history of supporting policy options that promote health and prevent disease and our membership base includes professionals with the knowledge and skills to assess the health impacts of social and economic policies One of the key priorities of our associations is supporting programs and policies that reduce health inequities Health inequities have been defined as differences which are unnecessary and avoidable but moreover are also considered unfair and unjust (Whitehead 1992) Beginning with the landmark Whitehall I study of British civil servants (Marmot et al 1978) a substantive body of evidence indicates that those living in poverty and occupying lower positions in socio-economic hierarchies have a greater risk of poor health outcomes including lower life expectancy higher infant mortality and increased risk of heart disease stroke diseases related to the digestive tract kidneys and lung tuberculosis HIV and suicide (Marmot 2004 World Health Organization 2008) Evidence indicates that inequities in health are best addressed through a mix of strategies including a minimum wage that enables individuals and families to access the fundamental determinants of health (eg food shelter and clothing) Accordingly we welcome the recent initiative by the Ontario Ministry of Labour to re-assess the provincial minimum wage rates In Ontario the percentage of adult employees earning minimum wage doubled between 2003 and 2011 Almost a million Ontario employees earned between $1025 and $1425 an hour in 2011 Sixty percent of these employees are 25 years of age and over (Block 2013) Proportionately Ontario workers are more reliant on minimum-wage jobs than any other region of Canada except Prince Edward Island and New Brunswick (Yalnizyan 2013) Since rates have remained frozen since March 2010 inflation has eroded minimum wage earnersrsquo purchasing power by 65 percent (Yalnizyan 2013) In practical terms this means that Ontarians relying on minimum wage are increasingly challenged to afford healthy nutritious food safe housing and other essentials for an optimal level of health and well-being To ensure a minimum wage level that reduces health inequities alPHa and OPHA support a policy that ties minimum wage rates to a combination of the consumer price index and average weekly earnings A formula combining both indicators would ensure that the minimum wage rates incorporate considerations of both absolute poverty (experienced when income levels are inadequate to maintain a minimum standard of living) and relative poverty (poverty defined in relation to the overall standard of living in society)
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
2
Relative poverty is an important public health indicator as evidence indicates that preventable health problems are more prevalent in unequal societies For example Wilkinson and Pickett (2009) compiled data from all advanced industrialized nations to explore the relationship between levels of income inequality and performance in key health and social indicators including life expectancy infant mortality and obesity The study consistently found that countries with higher levels of inequality had higher levels of health and social problems at all income levels Simply living in a more unequal society puts individuals at greater risk of negative health outcomes (Wilkinson and Pickett 2009) Setting the minimum wage rates at a level that decreases inequality within Ontariorsquos communities therefore is a healthy public policy We also recognize the importance of food security as a key consideration for calculating a minimum wage that has a positive impact on health inequities The Nutritious Food Basket (NFB) survey tool based upon the purchase price of 67 nutritious foods is administered by all public health units in Ontario and provides a measure of the minimum cost of an adequate diet (Tarasuk Yeudall and Khan 2013) We support the OPHA food security workgrouprsquos recommendation that an annual assessment of Nutritious Food Basket (NFB) data be considered as a factor in determining minimum wage increases (OPHA 2013) We hope that our submission will assist you in considering the public health impacts of minimum wage rates We would be more than happy to get in touch with you if you have any questions or require additional information Sincerely
___________________________________ ___________________________________ Mary Johnson Susan Makin President President Association of Local Public Health Agencies Ontario Public Health Association
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy
10_COMOH_Draft_Agenda_111513
Providing leadership in public health management
2 0_COMOH_Draft_Minutes_091813
Providing leadership in public health management
31_COMOH DRAFT Summary Report
31_COMOH_Terms_of_Reference_June__2013
TERMS OF REFERENCE
NAME
MISSION
OBJECTIVES
MEMBERSHIP
OFFICERS
COMMITTEES
MEETINGS
ELECTIONS
AMENDMENTS
Original September 1987
31_Considerations for COMOH
43_SFOA
44_CWS_Recommendations
45_Panorama
46_SFOA
47_Pools
612_PHSSP_Tables
610_COMOHList_Affiliate_Subscriptions
611_COMOH_Correspondence
For COMOH Information
62_COMOH_EXEC_MINUTES_08101
Providing leadership in public health management
68_COMOH_Correspondence
For COMOH Information
69_alpha_OPHA_minwagesubmission_091013
3
References Block S (2013) Who is working for minimum wage in Ontario Toronto The Wellesley Institute Marmot M G Rose G Shipley M and Hamilton P J (1978) ldquoEmployment grade and coronary heart disease in British civil servantsrdquo Journal of Epidemiology and Community Health 32 (4) 244ndash249 Marmot M (2004) Status Syndrome How your social standing directly affects your health and life expectancy London Bloomsbury Ontario Public Health Association (2013) Submission to the minimum wage advisory panel on behalf of the Ontario Public Health Association Food Security Working Group Toronto OPHA Tarasuk V Yeudall F amp Khan A (2013) Provincial Food Insecurity Status Nutrition Food Basket Analysis and Household Food Insecurity webinar Retrieved from httpophaoncaOPHAmediaResourcesEventsOPHA-fs-webinarpdfext=pdf Whitehead M (1992) ldquoThe concepts and principles of equity and healthrdquo International Journal of Health Services 22 429ndash45 Wilkinson R and Pickett K (2009) The Spirit Level Why equality is better for everyone London Penguin Books World Health Organization (2008) Closing the gap in a generation Health equity through action on the social determinants of health Geneva WHO Yalnizyan A (2013) ldquoBoost the minimum wage boost the economyrdquo Progressive Economics Forum httpwwwprogressive-economicsca20130227boost-the-minimum-wage-boost-the-economy