Afp 30.07.2014
63
Acute Flaccid Paralysis (AFP) Dr . AJAYAN.P JIPMER
-
Upload
lakshmi-mahadevan -
Category
Health & Medicine
-
view
333 -
download
0
Transcript of Afp 30.07.2014

Acute Flaccid Paralysis
(AFP)
Dr . AJAYAN.P
JIPMER
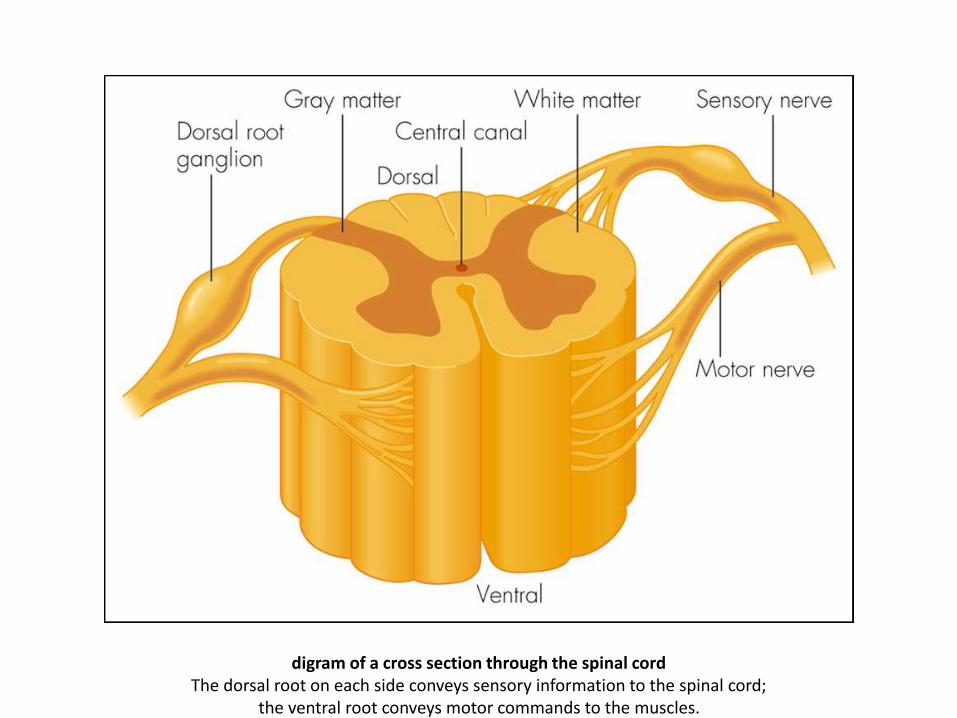
digram of a cross section through the spinal cordThe dorsal root on each side conveys sensory information to the spinal cord;
the ventral root conveys motor commands to the muscles.

Cerebral: Bilateral strokes, Hysteria…
Cerebellar : Acute cerebellar ataxia syndromes.
Spinal: Compressive myolopathy ,
Transverse myelitis .
Peripheral nerve: Acute inflammatory demyelinating
neuropathy,
Toxic neuropathy,
Diphtheria,
Tick paralysis
Differential Diagnosis of Acute Weakness:

Neuromuscular junction:
Botulism,
Myasthenia Gravis…
Muscle disease: Acute myositis.
Acute inflammatory myopathies
Metabolic myopathies ,
Periodic paralysis…
DD of Acute Weakness (cont):
Acute Flaccid Paralysis
Acute Flaccid Paralysis
WHO defines AFP syndrome as “ Rapid onset of weakness of an individual’s extremities, often including weakness of muscles of respiration & swallowing, progressing to maximum severity within 1-10 days. The term ‘flaccid’ indicates the absence of : Spasticity. Other signs of disordered CNS motor tracts such as :
Hyperflexia, Clonus, Extensor plantar response .
Clinically spasticity is defined as velocity dependent resistance to stretch, where a lack of inhibition results in excessive contraction of the muscles, ultimately leading to hyperflexia (overly flexed joints).
AFP is an emergency in which
management priorities are to
support vital functions and reach
a specific diagnosis in a timely
manner with a focused history
and physical examination.

Guillain-Barré Syndrome.
Poliomyelitis.
Transverse Myelitis.
DD of Acute Flaccid Paralysis

Fever at onset - Polio or enteroviral myelitis,
Transverse
myelitis, myositis, epidural abscess, and
Koch spine (prolonged history)
Trauma: head/neck Trivial trauma may lead to
spinal
compression in patients with cervical
vertebral instability (Patients with
Downs syndrome, congenital
cervicovertebral anomalies or juvenile
idiopathic arthritis)
Exposure Toxins: lead, arsenic
Snake envenomation
Dog bite: Rabies
Preceding infectious
prodrome/vaccination
Guillain Barre syndrome or transverse
myelitis
Sore throat, neck swelling- diphtheretic
polyneuropathy (non/partly immunized
Precipitating factors Diarrhea: Hypokalemia,
enteroviral
myelitis
Exertion or post parandial: Hypokalemic
periodic paralysis
Intramuscular injection: Polio, traumatic
sciatic neuritis
Sensory loss/level -Compressive myelopathy,
transverse
myelitis

Early bowel/bladder
involvement
Compressive myelopathy, transverse
myelitis
Constipation in <1 y Botulism (H/o honey
exposure)
Prominent autonomic
signs/symptoms
Guillain Barre syndrome, Rabies, acute
myelopathy

Ascending weakness Guillain Barre syndrome,
Rabies,
Varicella zoster virus, ascending myelitis
Descending weakness ---Diphtheria, Botulism
Prominent and earl
ptosis
Myasthenia Gravis, Botulism

Facial weakness Guillain Barre syndrome,
Myasthenia
Gravis, Botulism
Fluctuating symptoms,
fatigability
Myasthenia Gravis
Muscle tenderness ----Myositis, inflammatory
myopathy,
(myalgias may be severe in Guillain
Barre syndrome

Muscle stretch reflexes
Absent: Guillain Barre syndrome, Polio,
Diphtheria, spinal shock, at level of
spinal cord damage
Preserved : Myasthenia Gravis, periodic
paralysis, Botulism
Exaggerated : Below level of spinal lesion,
Upper motor neuron lesion
Spinal tenderness,
painful spine
movement
Spinal trauma, epidural abscess
1)Spinal cord -Compressive -Traumatic spinal
injury, epidural
abscess, hematoma, discitis
inflammatory-- Transverse myelitis
2)Anterior horn
cell
Viral - Poliomyelitis, vaccine associated
poliomyelitis, Enteroviral
myelitis, Japanese encephalitis
Vascular ----Anterior spinal artery infarction

3)Roots/nerves- Immune mediated-- Guillain
Barre syndrome,
Toxin-- Post diphtheritic, porphyria,
arsenic
Viral ------Rabies
Trauma ----Injection related sciatic neuritis

4)Neuromuscular
junction
Immune mediated--- Myasthenia Gravis
Drugs, toxins-- Organophosphates, snake venom,
drugs (aminoglycosides),
Botulism
Dyselectrolytemia ------Hypermagnesemia
5
5) Muscle ----Infection Viral myositis
Inflammation --nflammatory myopathy
(polymyositis)
Channelopathy ---Hypokalemic periodic
paralysis
Dyselectrolytemia -------------------Hypokalemia

Guillain-Barré Syndrome
• It is an acute idiopathic monophasic acquired
inflammatory demyelinating polyradiculo-
neuropathy.
• Polyradiculopathy refers to damage to multiple nerve roots sufficient to produce neurologic symptoms & signs such as pain, weakness, and sensory affection.
• GBS is the most common cause of acute flaccid
paralysis in healthy infants and children.
Guillain-Barré Syndrome :

(1826-1865 )
French neurologists and physicians first started describing Guillain-Barré Syndrome in 1859
Georges Charles Guillain, neurologist (1876-1961),
André Strohl, physicien (1887-
1977)
Jean-Alexandre Barré, neurologist (1880-1967)
• The annual incidence 0.6 to 2.4 cases / 100,000 population and occurs at all ages and in both sexes.
• The incidence is lower in children, 0.38 and 0.91 cases / 100,000 in two reports.
• Occurs rarely in children younger than 2 years of age, but can occur in infants.
• Males are affected 1.5 times <females in all ages.
Epidemiology :
• Immune mediated disease.
• There is no known genetic factors.
• 2/3 of cases follow a respiratory or GI infection.
• Campylobacter infection is the most common, but other
organisms include CMV, EBV, HSV, Enteroviruses,…
• Guillain-Barré syndrome has been reported to follow :
– vaccinations .
– epidural anesthesia.
– thrombolytic agents.
GBS.Pathophysiology :
The pathophysiologic mechanism of an antecedent illness and of GBS can be typified by Campylobacter jejuniinfections. The virulence of C jejuni is thought to be based on the presence of specific antigens in its capsule that are shared with nerves. Immune responses directed against lipopolysaccharideantigens in the capsule of C jejuni result in antibodies that cross-react with ganglioside GM1 in myelin, resulting in the immunologic damage to the peripheral nervous system. This process has been termed molecular mimicry.

• The main lesions are acute inflammatory
demyelinating polyradiculopathy, with acute
axonal degeneration in some cases,
particularly those following campylobacter
infection.
• A variety of auto-antibodies to gangliosides
have been identified especially with axonal
forms of the disease.
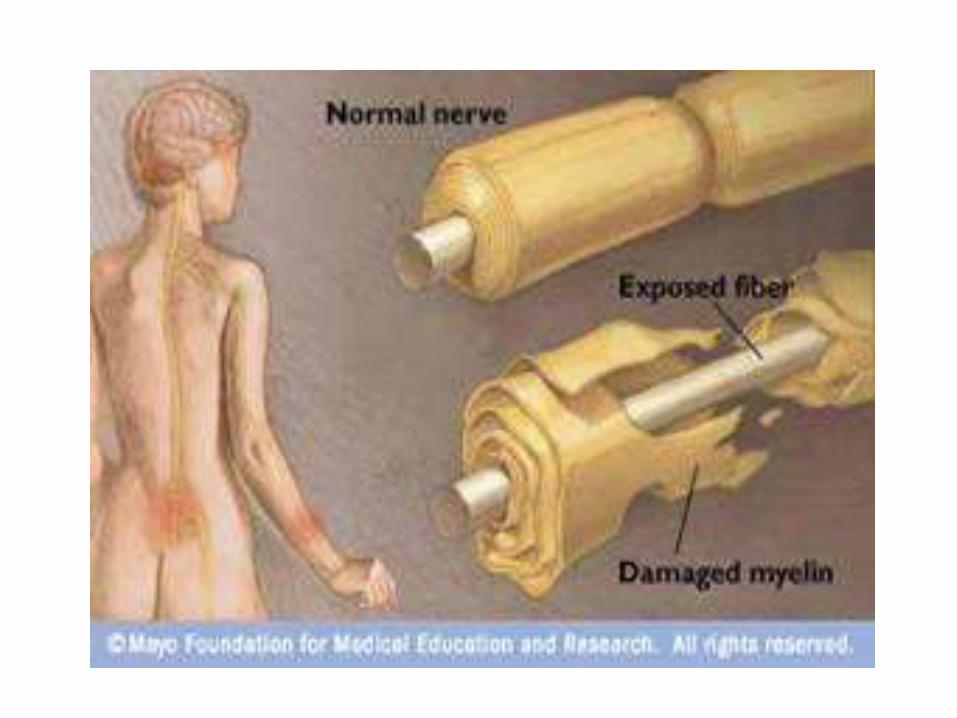
GBS.Pathophysiology :
Pathologic findings in GBS include : lymphocytic infiltration of spinal roots and peripheral nerves (cranial nerves may be involved as well), followed by macrophage-mediated, multifocal stripping of myelin. This phenomenon results in defects in the propagation of electrical nerve impulses, with eventual absence or profound delay in conduction, causing flaccid paralysis. Recovery is typically associated with remyelination.
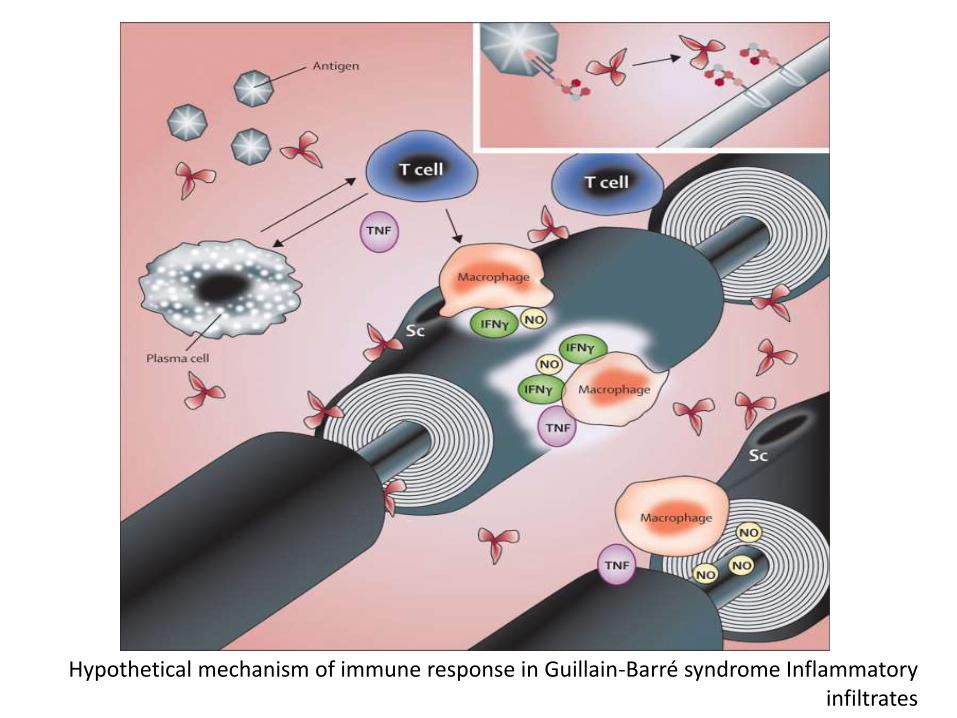
Hypothetical mechanism of immune response in Guillain-Barré syndrome Inflammatory infiltrates
Usually 2 - 4 weeks following respiratory or GI infection.
• The classic presentation:
* Fine paresthesias in the toes and fingertips.
* Lower extremity weakness: symmetric & ascending.
* Gait unsteadiness.
* Inability to walk.
* Respiratory muscles involvement.
* Neuropathic pain… low back pain.
• Cranial Neuropathy:
Facial nerve is most commonly affected, resulting in
bilateral facial weakness.
Clinical Features of GBS :
By the peak of the illness, the frequency of
symptoms was as follows:
- 79% had neuropathic pain.
- 60% could not walk .
- 51% had autonomic dysfunction.
- 46% had cranial nerve involvement.
- 24% could not use their arms.
- 13% required mechanical ventilation.
Clinical Features… cont :
46%
had
cranial
nerve
involve
ment.

Physical Examination
• Symmetric limb weakness.
• diminished or absent reflexes.
• Vibration and position sensation are affected in 40% of cases.
• Autonomic dysfunction:
* Cardiac dysrhythmias.
* Orthostatic hypotension,
* Hypertension.
* Paralytic ileus .
* Bladder dysfunction.
Physical Examination :

A reflex is an involuntary and nearly immediate movement in response to a stimulus mediated via the reflex arc.
reflexes = peripheral problem.
reflexes = central problem.
Human reflexes
:Stretch reflexes• Jaw jerk reflex: (CN V)• Biceps reflex (C5, C6)• Brachio-radialis reflex (C5, C6, C7)• Extensor digitorum reflex (C6, C7)• Triceps reflex (C6, C7, C8)• Patellar reflex or knee-jerk reflex L2, L3, L4)• Ankle jerk reflex (Achilles reflex) (S1, S2)
While the reflexes above are stimulated mechanically, the term H-reflex refers to the analogous reflex stimulated electrically, and Tonic vibration reflex for those stimulated to vibration.
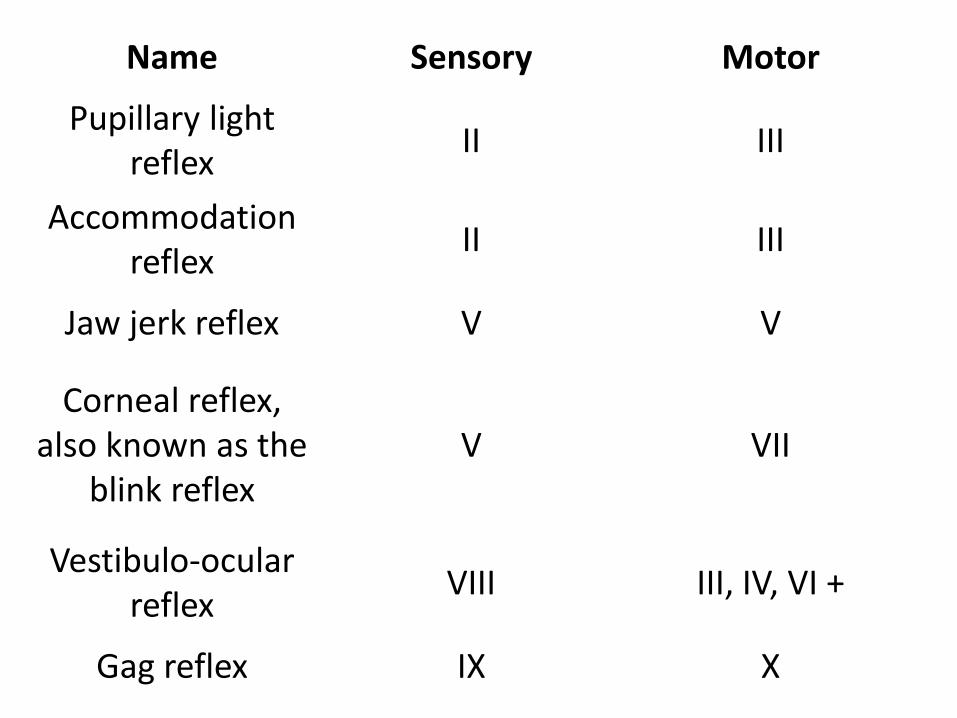
Name Sensory Motor
Pupillary light reflex
II III
Accommodation reflex
II III
Jaw jerk reflex V V
Corneal reflex, also known as the
blink reflexV VII
Vestibulo-ocular reflex
VIII III, IV, VI +
Gag reflex IX X
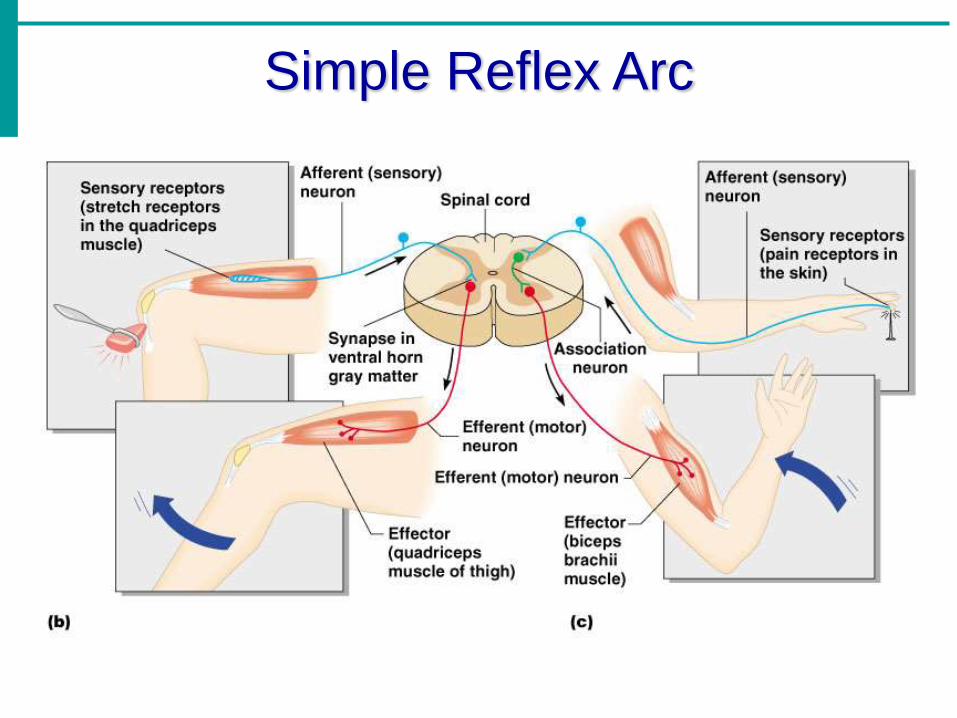
Simple Reflex Arc
• >90% of patients reach the lowest point of their function within 2 - 4 weeks, with return of function occurring slowly over the course of weeks to months.
• The clinical course of GBS in children is shorter than in adults and recovery is more complete.
• In patients who did not require mechanical ventilation, the median time to recovery of independent walking was 43 to 52 days in children compared to 85 days in adults.
Clinical Course :

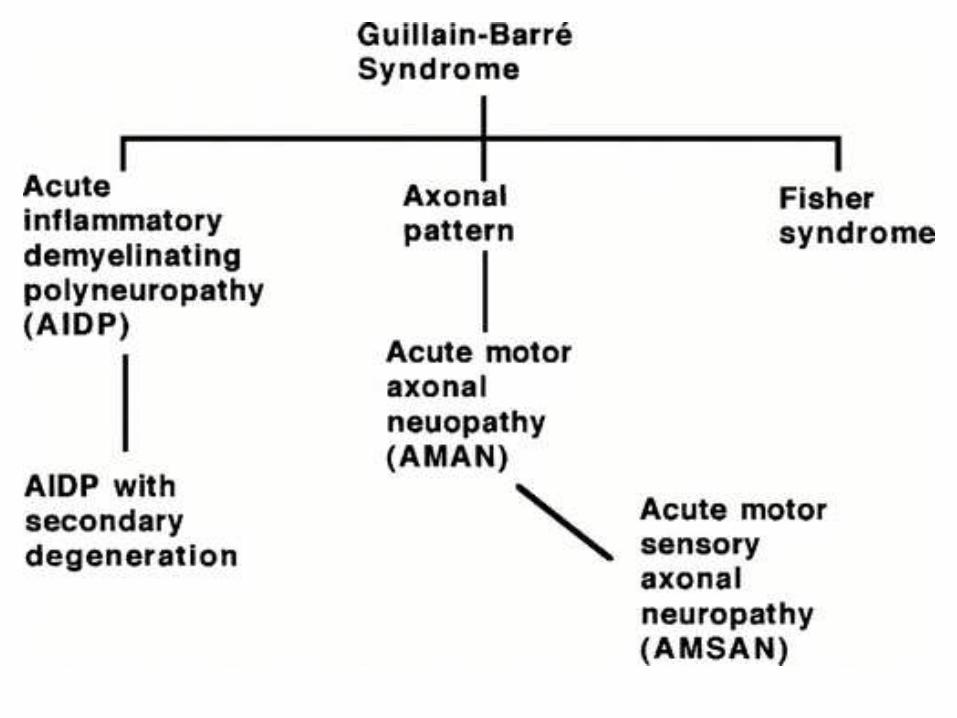
• Acute inflammatory demyelinating polyneuropathy(AIDP): the most common form in developed countries.
• Acute motor axonal neuropathy: more common in developing countries. More severe with common respiratory involvement. Strong association with campylobacter.
• Acute motor-sensory axonal neuropathy.
• Miller Fisher syndrome: triad of external ophthalmo-plegia, Ataxia, areflexia with muscle weakness.
• Polyneuritis cranialis: associated with CMV infection.
Forms of GBS :

Cerebrospinal Fluid:
- After the first week of symptoms typically reveals:
normal pressure,
normal cell count.
elevated proteins (greater than 50 mg/dL)
- Early in the course (less than one week), protein levels may not yet be elevated, ( rarely remain persistently normal) .
Diagnosis :
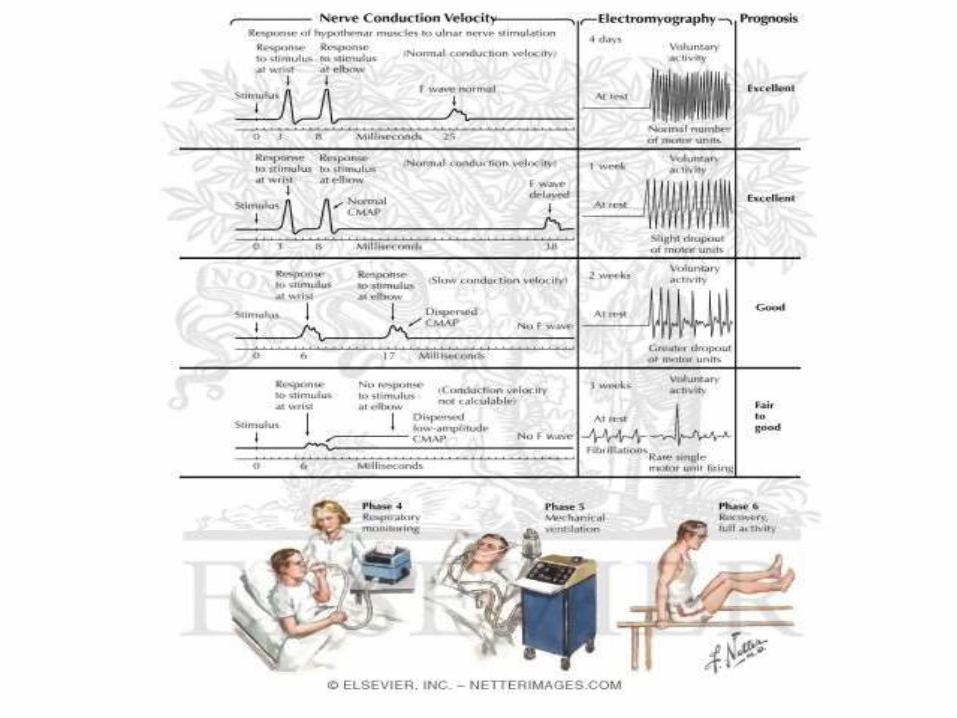
Diagnosis:
Electro-physiologic studies:- Most specific and sensitive tests
for diagnosis.- Evidence evolving multifocal
demyelination.- A normal study after several days
of symptoms, makes the diagnosis of Guillain-Barré syndrome unlikely.
• Marked persistent asymmetry of weakness.
• Persistent bladder or bowel dysfunction.
• Bladder or bowel dysfunction at the onset.
• Mononuclear leukocytosis in the CSF > 50.
• Sharp sensory level.
• Pupillary abnormalities are not seen in GBS.
Doubt the Diagnosis of GBS IF:
GBS Management
• Critical care monitoring for autonomic and respiratory dysfunction.
• Children with the following should be admitted to PICU:
a. Flaccid quadriparesis.
b. Rapidly progressive weakness.
c. Reduced vital capacity (≤20 mL/kg)
d. Bulbar palsy.
e. Autonomic cardiovascular instability.
N.B: Sedation and neuromuscular blockade should be avoided in ventilated patients because they obscure the course of the illness.
GBS Management:
Risk factors for respiratory failure in GBS:
Cranial nerve involvement.
Short time from preceding respiratory illness.
Rapid progression over less than 7 days.
Elevated CSF protein in the first week.
Severe weakness: unable to lift elbows above the bed
unable to lift head above the bed
unable to stand.
20% of children with GBS require mechanical
ventilation for respiratory failure.
GBS Management:

Immune modulatory therapy:
Intravenous Immunoglobulins.
Plasmapheresis.
• Both therapies have been shown to shorten recovery time by as much 50%.
• Combining plasma exchange and IVIG neither improved outcomes nor shortened the duration of illness.
Special Therapy :
INTRAVENOUS
IMMUNE GLOBULIN
• IVIG is preferred to plasma exchange in children because of the relative safety and ease of administration, although it has not been shown to have better results.
• Randomized trials in severe disease show that IVIG started within 4 weeks from onset hastens recovery as much as plasmapheresis.
• Long-term outcome, however, may not be affected.
• Studies have demonstrated that one effect of the IVIG is to neutralize neuromuscular blocking antibodies.
I V. IMMUNE GLOBULIN :
• Several IVIG regimens have been utilized. One regimen includes daily IVIG for 5 days at a dose of 0.4 gm/kg /day, which results in an improvement within a mean of 2 to 3 days after the start of therapy. Other authors use 2 gm/kg of IVIG given as a single dose or 1gm/kg/day for 2 days.
• One study compared the outcome of 0.4 gm/kg/day given for 3 days versus 6 days. In that study, the 6 days of IVIG was superior when “time to walking” was used as an endpoint.
• When comparing treatments of 1gm/kg for 2 days versus 0.4gm/kg over 5 days, no significant difference in the effectiveness was noted in the 2 treatment regimens. However, early “relapses” were more frequently observed in the shorter treatment group.
IVIG Regimens :

• Studies in children indicate that plasmapheresis may decrease the severity and shorten the duration of GBS.
• It is most beneficial when started within 7 days of the onset of symptoms but is still beneficial in patients treated up to 30 days after disease onset.
Plasmapheresis :
• Corticosteroids are not effective and
not indicated
• Interferon-ß reported to be beneficial
in individual cases, but its safety and
efficacy have not been established in
clinical trials.
Management…cont :
Prognosis
• In general, the prognosis in affected children is better than adults.
• Recurrences are uncommon but can occur in children. Some may have a chronic progressive course, whereas others may show recurrences or relapses.
Prognosis :
Prognosis :
At long-term follow up, 93% were free of symptoms, and the remainder were able to walk unaided.
50% are ambulatory by 6 mo, 70% walk within ayear of onset of the disease.Mortality is approximately 3 to 4%, and usually is secondary to autonomic dysfunction and respiratory failure.

Please don’t miss the diagnosis of GBS. By noting: Symptoms begin 2 - 4 weeks following
respiratory or GI infection. Diminished or absent reflexes. Symmetric & ascending lower
extremity weakness. Sensations intact : Fine paresthesias in
the toes and fingertips. No bladder or bowel dysfunction at
the onset.