Aetiology of Running-Related Gastrointestinal Dysfunction
14
Aetiology of Running-Related Gastrointestinal Dysfunction How Far is the Finishing Line? Susana M. Gil, Etsuro Yazaki and David F. Evans St Bartholomew’s and the Royal London School of Medicine and Dentistry, London, England Abstract 30 to 65% of long distance runners experience gastrointestinal (GI) symptoms related to exercise. Several hypotheses have been postulated; however, the aeti- ology and pathophysiology are far from clear. The mechanical effect of running on the viscera must be involved in the devel- opment of GI symptoms in this sport. Reduction of splanchnic blood flow due to visceral vasoconstriction is another widely supported theory; nevertheless, it does not explain many of the clinical findings. Examination of the GI tract during exercise is a difficult task, and measurements of both orocaecal and whole-gut transit time have shown equivocal results. GI hormones, and especially prosta- glandins, may be of crucial importance for the production of symptoms. Intestinal absorption, secretion and permeability may also be altered during exercise, pro- voking intestinal dysfunction. Factors such as stress, diet, dehydration, infections and other factors need to be analysed in order to present a global view of the hypo- theses regarding the aetiology of this common and often overlooked problem. LEADING ARTICLE Sports Med 1998 Dec; 26 (6): 365-378 0112-1642/98/0012-0365/$07.00/0 © Adis International Limited. All rights reserved. 1. Incidence of Gastrointestinal (GI) Disturbances Related to Exercise Since the introduction to the literature of the term ‘runner’s diarrhoea’ in the 1970s and 1980s, [1,2] many attempts have been made to specify the inci- dence of gastrointestinal (GI) disturbances related to running. Although their results (based on sur- veys and questionnaires voluntarily answered by athletes) may be biased, most studies show that GI symptoms are a common feature among long dis- tance runners. Lower GI symptoms (diarrhoea, urgency, the need to stop for a bowel movement, rectal inconti- nence, rectal bleeding and abdominal cramps) are more commonly experienced than upper GI symp- toms (heartburn, reflux, nausea). [3-5] The latter are more likely to occur at rest and in sedentary indi- viduals. [6] The most common complaint is the urge to def- ecate while running, affecting 36 to 63% of run- ners, [3-5,7,8] whereas diarrhoea is experienced by 8 to 54% [4,5,7-9] and abdominal cramps are experi- enced by about a third of the athletes involved in this sport. [3-5,7-10] The need to stop to move the bowels occurs in 16 to 62% of runners and rectal bleeding and incontinence in 2 to 16%. [4,5,7-9] Women were more severely affected in 2 sur- veys [4,5,7,8] and less than half believed that GI symptoms were aggravated during the time of their menses. [6] Young athletes had more GI distur- bances than older runners in 2 studies. [5,7] The relationship with the intensity of running is inconclusive: 2 reports found a positive relation- ship between the intensity of exercise and the
-
Upload
david-f-evans -
Category
Documents
-
view
213 -
download
1
Transcript of Aetiology of Running-Related Gastrointestinal Dysfunction

Aetiology of Running-RelatedGastrointestinal DysfunctionHow Far is the Finishing Line?
Susana M. Gil, Etsuro Yazaki and David F. EvansSt Bartholomew’s and the Royal London School of Medicine and Dentistry, London, England
Abstract 30 to 65% of long distance runners experience gastrointestinal (GI) symptomsrelated to exercise. Several hypotheses have been postulated; however, the aeti-ology and pathophysiology are far from clear.
The mechanical effect of running on the viscera must be involved in the devel-opment of GI symptoms in this sport. Reduction of splanchnic blood flow due tovisceral vasoconstriction is another widely supported theory; nevertheless, it doesnot explain many of the clinical findings. Examination of the GI tract duringexercise is a difficult task, and measurements of both orocaecal and whole-guttransit time have shown equivocal results. GI hormones, and especially prosta-glandins, may be of crucial importance for the production of symptoms. Intestinalabsorption, secretion and permeability may also be altered during exercise, pro-voking intestinal dysfunction. Factors such as stress, diet, dehydration, infectionsand other factors need to be analysed in order to present a global view of the hypo-theses regarding the aetiology of this common and often overlooked problem.
LEADING ARTICLE Sports Med 1998 Dec; 26 (6): 365-3780112-1642/98/0012-0365/$07.00/0
© Adis International Limited. All rights reserved.
1. Incidence of Gastrointestinal (GI)Disturbances Related to Exercise
Since the introduction to the literature of theterm ‘runner’s diarrhoea’ in the 1970s and 1980s,[1,2]
many attempts have been made to specify the inci-dence of gastrointestinal (GI) disturbances relatedto running. Although their results (based on sur-veys and questionnaires voluntarily answered byathletes) may be biased, most studies show that GIsymptoms are a common feature among long dis-tance runners.
Lower GI symptoms (diarrhoea, urgency, theneed to stop for a bowel movement, rectal inconti-nence, rectal bleeding and abdominal cramps) aremore commonly experienced than upper GI symp-toms (heartburn, reflux, nausea).[3-5] The latter are
more likely to occur at rest and in sedentary indi-viduals.[6]
The most common complaint is the urge to def-ecate while running, affecting 36 to 63% of run-ners,[3-5,7,8] whereas diarrhoea is experienced by 8to 54%[4,5,7-9] and abdominal cramps are experi-enced by about a third of the athletes involved inthis sport.[3-5,7-10] The need to stop to move thebowels occurs in 16 to 62% of runners and rectalbleeding and incontinence in 2 to 16%.[4,5,7-9]
Women were more severely affected in 2 sur-veys[4,5,7,8] and less than half believed that GIsymptoms were aggravated during the time of theirmenses.[6] Young athletes had more GI distur-bances than older runners in 2 studies.[5,7]
The relationship with the intensity of running isinconclusive: 2 reports found a positive relation-ship between the intensity of exercise and the

symptoms,[5,10] while another 3 studies failed todemonstrate any connection.[6,7,9]
The incidence of irritable bowel syndrome andalso lactose intolerance is similar to that in studiesof other populations (13 to 16%).[6,8,9] Pre-race di-arrhoea occurs in 40% of athletes; it is more com-mon in women and in those with irritable bowelsyndrome or lactose intolerance.[9]
Running appears to cause a greater degree of GIdisturbance than other activities involving high en-ergy output. During triathlon events, GI complaintsare generally more frequent than musculoskeletalinjuries, and stitch, bowel dysfunction, abdominalcramps and gastroesophageal reflux have been re-ported to be more common during the runningstages than in the swimming and cycling events.[10]
2. Aetiology of GI Dysfunction
2.1 Mechanical Factors
GI symptoms prevail in running compared withother sports where the body remains in a more sta-ble position, such as cross-country skiing, swim-ming or cycling.[11] The pounding effect or intesti-nal jarring is widely cited as a positive direct causefor the development of exercise-related GI symp-toms.[11-14] Rehrer and Meijer[15] measured the me-chanical vibration of the body using an exerciseaccelerometer and found that acceleration/deceler-ation was more than doubled in running comparedwith cycling.
This mechanical theory is supported by the ob-servation that GI disturbances are experiencedmainly during the running part of triathlon events[10]
and the running stages of a study of alternate run-ning and cycling.[16]
On the other hand, mechanical stimulation ofthe intestinal mucosa by rubbing[17] and disten-sion[18,19] releases vasoactive intestinal peptide (VIP)and prostaglandins (PG) [see sections 2.3 and 2.4],causing intestinal secretion which may produce asecretory type of diarrhoea.
Following the report of a runner with right ab-dominal pain on palpation and diarrhoea after amarathon race, the ‘caecal slap syndrome’ was intro-
duced.[20] The same author later admitted that therunner had ingested nonsteroidal anti-inflammatorydrugs (NSAIDs) and a small amount of alcohol.The interaction of these factors was questioned,[21]
but the caecal slap became a widely used hypothe-sis.
Hypertrophy of the psoas muscle, pressing onthe GI tract, has also been postulated as a cause ofGI symptoms due to running.[22]
Two competitive runners who presented withGI symptoms after exercise were intraoperativelyfound to have a caecal volvulus and also a thinmesentery. The ‘up and down’ movement of ab-dominal viscera while running was thought to bethe cause of the volvulus and the symptoms.[23]
GI complaints have not been reported in othersports such as boxing, horse riding, dancing ortrampolining, where theoretically a bouncingmovement of the intestinal contents would occur:however, this may not be entirely due to the factthat they do not occur, but rather that such distur-bances have not been investigated in these activi-ties. A prospective, structured questionnaire-basedstudy of GI disturbances in a wide variety of sport-ing activities is lacking but would help to increaseour understanding of the prevalence of this condi-tion.
2.2 Mesenteric Circulation and Exercise
2.2.1 Exercise-Associated GI BleedingGI bleeding is not an uncommon finding after
long distance races. Macroscopic faecal blood isexperienced by 1 to 16% of runners[6-9] and micro-scopic bleeding has been found in 8 to 87% of run-ners.[24-29] This wide range in the latter inci-dence may be due to differences in the length ofthe events after which faecal blood was measured.Using qualitative techniques after 42.6km mara-thon races[25,27,28,30-32] and a short triathlon,[33] 8 to36% of runners converted from negative to positivefaecal blood, whereas in much longer events suchas a 100-mile (160.9km) ultramarathon[26,28] anda long triathlon of 3.8km swim, 180km ride and42.2km run,[24] 80 to 87.5% of athletes had micro-scopic bleeding.
366 Gil et al.
© Adis International Limited. All rights reserved. Sports Med 1998 Dec; 26 (6)

Using quantitative tests, the amount of faecalhaemoglobin increases in 71 to 83% of athletesafter marathon running,[27,34] whereas using animmunochemical technique (‘OC-Hemodia’) 33%of marathon finishers had positive faecal occultblood on the first post-race stool specimen.[35]
By comparison, lower results were observed incyclists during a 1 week cycling race, of whom 1.2%had positive findings.[36] In a different study, a37km walk on 4 consecutive days did not produceany changes in the amount of faecal haemoglo-bin.[27]
Faecal blood loss occurs more frequently aftera race than during training,[37,38] but no relation-ship has been found between faecal blood loss andfinishing times,[24,27-29,36] age,[25,27,29,30] sex,[29,30]
weekly mileage[25-28] or training experience.[28] Theappearance of blood in stools is correlated withlower GI disturbances.[25,28,35] Nonetheless, thisfinding is not consistent in all reports.[29,30,39]
Not only is the ingestion of aspirin (acetylsali-cylic acid) and NSAIDs unrelated to the incidenceof occult GI bleeding in runners,[26,29] but in somecases it offers a degree of protection. Runners tak-ing such medicines have fewer positive results thannonmedicated athletes after races.[28,32,36] Thus,PG may have an important role in the productionof GI bleeding related to exercise.
The effect of histamine H2 receptor antagonistson running-associated faecal bleeding is inconclu-sive. During a prospective study in a marathonrace, cimetidine reduced slightly, but not signifi-cantly, the incidence of positive faecal occult blood(FOB) using ‘Hemoccult’ tests. The incidence re-mained similar to that in other reports wheremedication was not taken.[25,27,28,30-32] With ‘Hemo-Quant’ tests, the amount of FOB in cimetidine re-cipients did not differ from that found in the run-ners taking a placebo.[39]
During an ultramarathon, 87.5% of runners nottaking cimetidine had positive FOB, whereas ofthose who were voluntarily taking the drug, 11%had blood in the stools.[26] The only difference inthese 2 groups of runners was that the first hadmore running experience; perhaps to avoid dehy-
dration they drank more water during the race, pro-ducing more hydrated faeces and giving more falsepositive results.[40]
However, all these results need careful interpre-tation. Qualitative tests (‘Hemoccult 11’, ‘Hema-Chek’, ‘Hemofec’ measure haemoglobin peroxi-dase activity and can produce false positive resultsin the presence of animal blood, vegetables, stoolhydration, ferrous sulfate and cimetidine,[27,35,40,41]
and false negative results with ascorbic acid, ant-acids and gut enzymes and bacteria.[27,40,42] Quan-titative tests, such as ‘HemoQuant’, are based onthe conversion of nonfluorescing haem to fluoresc-ing porphyrins[43] and may be affected by alter-ations of gut transit time.[37]
Running-related GI changes have been obser-ved endoscopically[29,44-47] and intraoperatively[48-49]
as gastric antral ulcer,[50] haemorrhagic gastritis,[44]
erosive gastritis,[29] ischaemic colitis,[47,49] non-specific colitis[48] and haemorrhagic colitis.[51] Histo-logical findings include decreased gastric mucosalsecretions, oedema, congestion, capillary dilationand red cell extravasation.[29,46-47] Such findingsare transient[13,32,35] and occur in the immediatepostexercise period,[46] improving with reductionof the amount of training,[47] rest[44,51,48] and theadministration of cimetidine/ranitidine.[45,50] Insome cases a full diagnostic GI series failed toshow any abnormalities in the GI tract.[29,52,53] Thiscould have been due to the time lapse between theGI bleeding and the diagnostic investigations,which were performed 4 to 11 days after the bleed-ing episode.
2.2.2 Reduction of Splanchnic Blood FlowExercise produces vasoconstriction of the
splanchnic vascular bed by the action of noradren-aline (norepinephrine) on the α-adrenoceptors viathe sympathetic nervous system.[54] This stimula-tion increases blood flow to the working musclesand skin (for thermoregulation) and maintainsblood flow to the heart and brain.[55,56] Table Ishows the effect of different types and intensitiesof exercise on mesenteric blood flow. As can beseen from table I, using the indocyanine green(ICG) hepatic clearance technique, estimated
Running-Related GI Dysfunction 367
© Adis International Limited. All rights reserved. Sports Med 1998 Dec; 26 (6)

splanchnic blood flow (SBF) decreases in aninversely proportional manner in relation to thepercentage of maximal oxygen consumption(V
.O2max) achieved,[57-60,62-63] duration of exer-
cise[60,62,63] and ambient heat.[58-60] Estimated he-patic blood flow (EHBF) with low intensity exer-cise (30 to 35% V
.O2max) is decreased by 12 to
14%[60] or unchanged;[64] with more severe exer-cise (35 to 60% V
.O2max) it decreases by 30 to 45%
for exercise lasting less than 50 minutes, and moreif the exercise lasts longer.[60,62,63]
Rowell et al.,[57] in their widely cited paper, es-timated that EHBF decreases by approximately80% of resting values during exercise; nonetheless,this was calculated by extrapolating the resultsfrom the ICG clearance due to the difficulties inobtaining hepatic venous samples during high in-tensity exercise. Such results have not been repro-
duced using the same technique, even when volun-teers approached exhaustion with attendant nauseaand vomiting.[59] Using other techniques, differentresults have been produced. Portal vein blood flowwas measured in moderately trained cyclists usingDoppler ultrasound techniques. After 20 minutesof cycling at 70% V
.O2max, SBF decreased by 57%,
and after 1 hour, by 80%. In 2 volunteers the SBFactually approached zero, therefore, the methodol-ogy must be questioned.[65]
Severe exercise (15 minutes at 5 km/h, 20% in-cline) reduced blood flow of the superior mesen-teric artery (SMA) by 43% from resting values.[66]
Abdominal blood flow measured by 99technetium-labelled red cells decreased to 96, 88 and 81% ofresting values at 50, 70 and 100% of maximumoxygen uptake.[67]
Table I. Effect of different types and intensities of exercise on the mesenteric blood flow
Population Exercise type Method Results Reference17M untrained 3.5 mph × 4.5 min, 7 mph to exhaustion ICG CL EHBF ↓ at ↑ V
.O2max 57
11M untrained 3.5 mph × 4.5 min at 25 and 43°C ICG CL EHBF ↓ at ↑ V.O2max and at 40°C 58
11M7 sedentary, 4 active
3.5 mph × 4.5 min at 48-48.9°C and 50% V
.O2max
ICG CL Small ↓ EHBF↑ O2 consumption
59
12M6 young (20-32y,sedentary)6 elderly (59-71y, fit)
20 min at 35% V.O2max, 30 min at
60% V.O2max, at 22 and 36°C
ICG CL 35%: SBF ↓ 12-14% (22 and 36°C; young and elderly)60% at 36°C young: SBF ↓ 45%, elderly: SBF ↓ 33%60% at 22°C young: SBF ↓ 31%, elderly: SBF ↓ 36%
60
13M Arm or leg training for 15 min/day over 5wk (mean heart rate of 130 and 170 bpm, respectively)
ICG CL ↓↓ EHBF with nontrained muscles arm > leg
61
6M 130 min cycling at 50% V.O2max,
140-150 bpmICG CL SBF ↓ 43% (more after 50 min) 62
20M 58% V.O2max × 3.5h ICG CL SBF ↓ 45% at 40 min; ↓ 20% at 90 min
O2 ↑ 70% at 40 min63
6sedentary
4h at 30% V.O2max, 129 bpm ICG CL EHBF ↔
O2 uptake ↑ 120% at 180 min64
8moderately trainedcyclists
Cycling at 70% V.O2max Portal vein USS
Doppler20 min ↓ 57%1h ↓ 80%2 individuals = 0
65
16M 15 min × 5 km/h walk SMA USSDoppler
↓ 43% SMA postexercise 66
14 (4F, 10M)4 sedentary, 10 active
Cycling: 50% × 10 min, 75% × 15 min,100% × 20 min
99Technetium-labelled red cells
Abdominal blood flow ↓ 96%, 88% and 81% of baseline, respectively
67
bpm = beats/min; EHBF = estimated hepatic blood flow; F = female; ICG CL = indocyanine green clearance; M = male; mph = miles/hour;SBF = splanchnic blood flow; SMA = superior mesenteric artery; USS Doppler = Doppler ultrasonography; V
.O2max = maximal oxygen
consumption; ↓ = decreased; ↓↓ = greatly decreased; ↑ = increased; ↑↑ = greatly increased; ↔ = unchanged; > = more than.
368 Gil et al.
© Adis International Limited. All rights reserved. Sports Med 1998 Dec; 26 (6)

Training attenuates the reduction of SBF,[61]
possibly due to adaptation of the sympathetic nerv-ous system.[68] Young, untrained men have agreater reduction than older fit men,[60] but it is notknown whether the different response is due to theage or the fitness of the participants.
Increased blood flow raises the rate of absorp-tion of substances by reducing their concentrationin the interstitial space.[69] Therefore, a decreasedblood flow may reduce absorption and the washouteffect of the substances of the interstitial fluid;hence, more substances accumulate in the colon,producing an osmotic effect with possible diar-rhoea and GI dysfunction.
Hypoperfusion and ischaemia of the splanchnicregion produced during cardiopulmonary bypassoperations reduce the permeability of 3-O-methyl-D-glucose (3-MG), mediated by an active andpassive carrier and D-xylose, and increase thepermeability of lactulose [absorbed through tightjunctions, adenosine triphosphate (ATP)-depend-ent]. Thus, decreased blood flow to the mesentericarea may impair the permeability and absorptionof some carbohydrates, thereby increasing levelsof these substances in the lumen and producingdiarrhoea.[70]
This theory is also supported by the fact that80% of marathon finishers with more than 4% ofweight loss due to dehydration experienced GI dis-turbances.[71] Dehydration reduces blood volume,possibly aggravating the reduction of splanchnicblood flow.
Experimental ischaemia of the GI tract, due toan impaired delivery of oxygen and metabolites,reduces cellular cytochromes,[72,73] mitochondrialrespiratory chains[72] and nucleotides,[73] produc-ing morphological and functional derangement ofthe mucosa and ultimately necrosis in mucosalgastric cells,[72] hepatocytes[73] and intestinalcells.[72,74-77] During reperfusion after ischaemia,more damage occurs due to the release of oxygen-derived free radicals.[78-80] Another possible mech-anism involved is the renin-angiotensin axis, whichconstricts mesenteric vessels during experimental
hypovolaemia[81-84] and is increased during exer-cise[85,86] in an intensity-dependent fashion.[87]
Moreover levels of endothelin, which is a potentsplanchnic vasoconstrictor[88,89] and produces mu-cosal damage and ischaemia,[90,91] are increasedduring dehydration[92] and exercise.[93] This is in-dependent of the duration and the intensity of theexercise.[94]
These mechanisms are also thought to be respon-sible for the stress ulceration found in patients withsevere trauma, major operations or thermal burns.[72]
The physiological splanchnic vasoconstriction as-sociated with exercise has been compared with theresponse occurring in these patients,[11,14,16,95] butthere are a number of differences:(1) Such severely ill patients have profound hypo-tension and decreased stroke volume whereas dur-ing exercise, blood pressure (particularly systolic),stroke volume and cardiac output are increased.[96]
Significant ischaemia is unlikely to occur inhealthy, trained, well hydrated runners.[97] On theother hand, nonocclusive ischaemic colitis is asso-ciated with haemorrhagic shock, low cardiac out-put, aortic stenosis, aortic insufficiency, acutemyocardial infarction, myocardiopathies, conges-tive cardiac failure and hypovolaemia.[98] None ofthese predisposing factors is present in the athleteswith running-associated colitis.[48,49,51]
(2) Physical endurance training is associated withan adaptive reduced sympathetic activity, which isindicated by lower basal and exercise catechola-mine levels in plasma.[56,68,99]
(3) Continuing stimulation of regional sympatheticnerves produces first a constrictor effect, followedby an ‘autoregulatory response’ (with partial or to-tal recovery of blood flow) and a hyperaemic phaseafter the cessation of the stimulation.[54]
In addition, reduction of the mesenteric bloodflow may be an important factor in the productionof GI disturbances associated with exercise, but onits own it fails to explain other clinical findings.
Postprandially, mesenteric blood flow is in-creased,[54] and the ingestion of food attenuates thereduction of blood flow induced by moderate tosevere exercise.[66] It would be expected that the
Running-Related GI Dysfunction 369
© Adis International Limited. All rights reserved. Sports Med 1998 Dec; 26 (6)

administration of food during exercise wouldimprove symptoms; however, runners as a rule vol-untarily abstain from exercise in the 3- to 5-hourpostprandial period.[5,7,10]
In addition, GI disturbances, should the reduc-tion of SBF be the main factor responsible, wouldoccur more commonly in higher intensity sportsand events, where the athletes reach higher heartrates and V
.O2max, such as middle distance races.
However, exercise-related diarrhoea, urgency andparticularly GI bleeding occur more frequently inmarathon and ultramarathon races where oxygenuptake and heart rate are far from reaching theirmaximum values.
Furthermore, some runners experience abdomi-nal distress at the beginning of a run[9] when bloodflow to the viscera should, theoretically, not becompromised.
2.3 Hormones
Gastrin, motilin, somatostatin, glucagon, pan-creatic polypeptide and VIP, which are increasedduring exercise,[100] may produce GI symptoms viadifferent mechanisms.
2.3.1 Vasoactive Intestinal Polypeptide (VIP)Mesenteric ischaemia[101] and mechanical stim-
ulus of the intestinal mucosa[19,102] evoke VIPrelease. VIP is a powerful stimulant of intestinalsecretion,[103,104] promotes colonic contraction, de-creases intestinal absorption in the dog[103] andprovokes a secretory type of diarrhoea.[105-107]
2.3.2 MotilinMotilin initiates migrating motor complexes[108]
and stimulates contraction of the intestinal musclefrom the rabbit[109] and human in vivo[110] and invitro.[111]
2.3.3 Peptide YYDuring exercise, splanchnic vasoconstriction is
associated with local release of peptide YY[112]
which increases small intestinal motility and con-traction.[113]
2.4 Prostaglandins (PG)
Eicosanoids are metabolites originating fromthe conversion of membrane phospholipids toarachidonic acid and the subsequent metabolisminto cyclooxygenase products (PG, thromboxanesand prostacyclin) and lipoxygenase products(leukotrienes). Mechanical stimuli[114] and smoothmuscle stretch[115,116] release PG. Thus, runningand the ‘up and down’ movement of the abdominalviscera stretching and distending the intestinal wallmay be responsible for the increase in systemic PGfound after marathon races.[117]
Evidence of increased PG synthesis can be dem-onstrated for virtually every recognised diarrhoeaillness.[118] PGE and PGF accelerate intestinal tran-sit time[119] and inhibit colonic contraction.[120,121]
In the dog, PGE2 induces giant migrating contrac-tions often associated with defecation.[122]
On the other hand, PGE2 decreases lower oe-sophageal sphincter pressure and oesophageal con-tractions.[123] PG stimulates intestinal fluid andelectrolyte accumulation in the gut lumen (en-teropooling effect) producing secretory diarrhoea,vomiting[124] and cramps.[118]
Runners taking NSAIDs and aspirin (both in-hibitors of PG production) have less positive FOBafter running than their nonmedicated counter-parts.[28,32,36]
In addition, loperamide, which is frequentlyused by runners to alleviate their symptoms, abol-ishes PG-induced diarrhoea.[125] Calmodulin, a cal-cium binding protein, mediates metabolism frommembrane phospholipids to arachidonic acid andsubsequently PG and leukotrienes. One of the anti-diarrhoeal effects of loperamide is obtained byblocking calmodulin.[126]
Therefore, running-associated vomiting, ab-dominal cramps, diarrhoea, urge to defecate andgastroesophageal reflux may be explained by anincreased production of PG by the GI tract. Fur-thermore, GI histological changes and GI bleedingmay be due to the release of leukotrienes (LCT4),which produce intense vasoconstriction of venulesand arterioles, leading to sluggish blood flow, cap-illary stasis, plasma leakage[127,128] and damage to
370 Gil et al.
© Adis International Limited. All rights reserved. Sports Med 1998 Dec; 26 (6)

measurements have not yet been made on athleteswith GI symptoms.
2.6.2 Colonic MotilityColonic contractions shifted from sporadic, iso-
lated, 1 to 4 contractions per minute (cpm) to reg-ular, propagated, 4 to 9 cpm in 6 of 10 volunteersrecorded with a solid-state transducer during a 1-hour run on a treadmill at 70 to 80% maximumheart rate. Five of the volunteers had previouslyexperienced runner’s diarrhoea.[149] The rise incolonic activity may have accounted for the symp-toms. In the fasted dog, exercise decreased the fre-quency of colonic migrating motor complexes(MMCs), but had no effect on the total or meanduration, or the cycle length of contractile states.In the fed dog, exercise disrupted MMCs andincreased the total duration of contractions thatwere organised as nonmigrating motor complexes.Exercise, in both fasted and fed states, inducedgiant migrating contractions, defecation and massmovements.[150]
2.7 Psychological Factors
Stress-related GI dysfunction has been postu-lated since the beginning of the century.[151] Stressdelays orocaecal transit[152] and inhibits fastingMMCs in the small bowel,[153,154] but increasesmyoelectrical[155] and colonic activity,[156] acceler-ating transit time in humans and experimental ani-mals.[157]
Many athletes experiencing GI symptoms believethat they are aggravated by ‘nerves’ and anxi-ety.[9,10] Up to 57% of athletes with runner’s diar-rhoea complain of GI symptoms before competi-tions; of these, 32% had similar symptoms whenemotionally distressed.[4]
The interaction between the brain and the guthas received much attention in the past few dec-ades. It has been observed that stress-induced GIsecretory and motor responses are mediated by en-dogenous release of corticorelin (corticotropin-releasing factor)[158,159] among others. During ex-ercise, plasma cortisol is increased, but this findingalso occurs in other sports such as cycling.[99]
Table III. Effect of physical exercise on whole-gut transit time
Population Diet Exercise Method Transit time Reference9M active71.5y
Controlsa Inactivity × 2wk 20 ROM × 3 daysAx-ray on fourth day
Delayed 142
14 (8M, 6F): 3groups (A, B and C)28y
Supervised Group A: Jogging 1h/day × 9wkGroup B: Light exercise (<50%V.O2max)
2.5-3h/day × 6wk free diet 0.5h/day × 3wkGroup C: 30-40 min/day light exercise(<50% V
.O2max) × 7wk
10 ROM3 times dailyStool x-ray
UnchangedUnchanged
Unchanged
143
10M sedentary35y
Constanta Walk: 4.5 km/h × 3 daysmax HR 109 beats/min
ROM × 3 daysAx-ray on fourth day
Unchanged 144
20M Specific diet 3 days’ pause3 days’ moderate activity
20 ROM Unchanged 145
10 (6M, 4F)30y
Measured onfourth daya
Rest/cycle/run × 1h/day × 1wk66% max HR50% V
.O2max
50 ROM, MTT-SStool x-ray
Accelerated 146
11M soccer players,9M sedentary
Constanta Soccer training/inactivity 10 ROM × 8 daysAx-ray on ninth day
Unchanged 147
a No specific dietary supervision.Ax-ray = abdominal x-ray; F = female; M = male; max HR = maximum heart rate; MTT-S = mean transit time given single doses of ROM;ROM = radiopaque markers; V
.O2max = maximal oxygen consumption; y = mean age in years.
372 Gil et al.
© Adis International Limited. All rights reserved. Sports Med 1998 Dec; 26 (6)

measurements have not yet been made on athleteswith GI symptoms.
2.6.2 Colonic MotilityColonic contractions shifted from sporadic, iso-
lated, 1 to 4 contractions per minute (cpm) to reg-ular, propagated, 4 to 9 cpm in 6 of 10 volunteersrecorded with a solid-state transducer during a 1-hour run on a treadmill at 70 to 80% maximumheart rate. Five of the volunteers had previouslyexperienced runner’s diarrhoea.[149] The rise incolonic activity may have accounted for the symp-toms. In the fasted dog, exercise decreased the fre-quency of colonic migrating motor complexes(MMCs), but had no effect on the total or meanduration, or the cycle length of contractile states.In the fed dog, exercise disrupted MMCs andincreased the total duration of contractions thatwere organised as nonmigrating motor complexes.Exercise, in both fasted and fed states, inducedgiant migrating contractions, defecation and massmovements.[150]
2.7 Psychological Factors
Stress-related GI dysfunction has been postu-lated since the beginning of the century.[151] Stressdelays orocaecal transit[152] and inhibits fastingMMCs in the small bowel,[153,154] but increasesmyoelectrical[155] and colonic activity,[156] acceler-ating transit time in humans and experimental ani-mals.[157]
Many athletes experiencing GI symptoms believethat they are aggravated by ‘nerves’ and anxi-ety.[9,10] Up to 57% of athletes with runner’s diar-rhoea complain of GI symptoms before competi-tions; of these, 32% had similar symptoms whenemotionally distressed.[4]
The interaction between the brain and the guthas received much attention in the past few dec-ades. It has been observed that stress-induced GIsecretory and motor responses are mediated by en-dogenous release of corticorelin (corticotropin-releasing factor)[158,159] among others. During ex-ercise, plasma cortisol is increased, but this findingalso occurs in other sports such as cycling.[99]
Table III. Effect of physical exercise on whole-gut transit time
Population Diet Exercise Method Transit time Reference9M active71.5y
Controlsa Inactivity × 2wk 20 ROM × 3 daysAx-ray on fourth day
Delayed 142
14 (8M, 6F): 3groups (A, B and C)28y
Supervised Group A: Jogging 1h/day × 9wkGroup B: Light exercise (<50%V.O2max)
2.5-3h/day × 6wk free diet 0.5h/day × 3wkGroup C: 30-40 min/day light exercise(<50% V
.O2max) × 7wk
10 ROM3 times dailyStool x-ray
Unchanged 143
10M sedentary35y
Constanta Walk: 4.5 km/h × 3 daysmax HR 109 beats/min
ROM × 3 daysAx-ray on fourth day
Unchanged 144
20M Specific diet 3 days’ pause3 days’ moderate activity
20 ROM Unchanged 145
10 (6M, 4F)30y
Measured onfourth daya
Rest/cycle/run × 1h/day × 1wk66% max HR50% V
.O2max
50 ROM, MTT-SStool x-ray
Accelerated 146
11M soccer players,9M sedentary
Constanta Soccer training/inactivity 10 ROM × 8 daysAx-ray on ninth day
Unchanged 147
a No specific dietary supervision.Ax-ray = abdominal x-ray; F = female; M = male; max HR = maximum heart rate; MTT-S = mean transit time given single doses of ROM;ROM = radiopaque markers; V
.O2max = maximal oxygen consumption; y = mean age in years.
372 Gil et al.
© Adis International Limited. All rights reserved. Sports Med 1998 Dec; 26 (6)

Pre-competition diarrhoea may be a result ofincreased colonic function due to stress. However,it is questionable whether stress causes GI symp-toms during habitual training sessions.
2.8 Diet
Athletes in general ingest higher amounts ofcarbohydrates and fibre than the sedentary popula-tion.[160] Dietary fibre increases faecal bulk, co-lonic filling, bacterial growth and metabolism inthe colon, thus decreasing transit time and increas-ing the frequency and volume of defecation.
This is supported by the findings of Binghamand Cummings,[143] who stated that when diet isconstant, exercise has no effect on intestinal func-tion.
On the other hand, physically more active peo-ple have higher caloric intakes. Resting orocaecaltransit is faster in high caloric consumers inde-pendently of the composition of the diet.[161]
However, there appears to be no relationshipbetween diarrhoea and dietary fibre or milk in ath-letes with symptoms.[4,10]
2.9 Miscellaneous
2.9.1 InfectionsSwain[162] described a case report of a runner
experiencing ‘typical’ symptoms of runners’ diar-rhoea with urgency, cramps, loose stools and stoolguaiac positive. After extensive tests, stool micro-biology showed Entamoeba histolytica. The pa-tient was treated with antibiotics and the symptomsresolved. Other infections such as Giardia mayalso give similar symptoms.[12] There is a paucityof data in the literature regarding infection, andconclusions must remain speculative.
2.9.2 Ascorbic AcidIt is well known that sportsmen and women
ingest high, and sometimes exceedingly high,amounts of vitamins and mineral supplements.Large amounts of ascorbic acid (vitamin C) maybe the source of GI complaints.[163] However, againno data are available.
2.9.3 Lactose Intolerance and Irritable Bowel SyndromeA survey showed that nervous diarrhoea before
competition was more common in runners who hadsymptoms of lactose intolerance, but there was norelationship with symptoms during or after run-ning.[9]
The same study reported that irritable bowel–like symptoms were related to the need to stop fora bowel motion while training. Irritable bowel syn-drome was found in 14% of runners, a number sim-ilar to that in other population surveys.[9]
2.9.4 DehydrationDehydration is not uncommon during long
training sessions, when runners avoid ingestingfluid due to the difficulties of drinking while run-ning and the unpleasant sensation of a full stomach.Dehydration reduces blood volume, thus aggravat-ing the reduced blood flow to the GI tract that oc-curs during exercise.
Rehrer et al.[71] found that 3.5 to 4% of body-weight loss was associated with an increased inci-dence of GI symptoms during exercise.
3. Conclusions
The effect of exercise on human physiology hasreceived much attention for the past few decades,but the GI tract has often been overlooked. Run-ning produces a variety of GI symptoms in a widenumber of individuals, affecting performance and,in the more severe cases, causing GI ischaemiawith blood loss and anaemia. Studies are neededin order to evaluate the incidence of such disordersin other modes of physical activity.
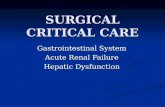
Figure 1 shows the different hypotheses on theaetiology of running-related GI symptoms. It ismost likely that an interaction of different mecha-nisms affects colonic motility, thus producing GIdysfunction. The mechanical action of runningmust be involved. Reduction of SBF has widelybeen hypothesised as the main factor; however,how severely this occurs is questionable. PG andother GI hormones are also probably involved.How other functions of the GI tract, such as absorp-
Running-Related GI Dysfunction 373
© Adis International Limited. All rights reserved. Sports Med 1998 Dec; 26 (6)

tion and permeability, respond to exercise remainsspeculative.
Clearly, the finishing line is still far away, andmore extensive research into the subject is war-ranted to improve our understanding of such a com-mon symptom.
References1. Scobie BA. Athletes’ diarrhoea [letter]. N Z J Sports Med 1970;
6: 312. Fogoros RN. ‘Runner’s trots’: gastrointestinal disturbances in
runners. JAMA 1980; 243 (17): 17433. Sullivan SN. The gastrointestinal symptoms of running. N Engl
J Med 1981; 304 (15): 9154. Sullivan SN, Wong C, Heindenheim P. Does running cause gas-
trointestinal symptoms? A survey of 93 randomly selectedrunners compared with controls. N Z Med J 1994; 107 (984):328-31
5. Keefe EB, Lowe DK, Goss R, et al. Gastrointestinal symptomsof marathon runners. West J Med 1984; 141 (4): 481-4
6. Sullivan SN. Exercise-associated symptoms in triathletes. PhysSports Med 1987; 15 (9): 106-10
7. Worobetz LJ, Gerrard DF. Gastrointestinal symptoms duringexercise in enduro athletes: prevalence and speculations onthe aetiology. N Z Med J 1985; 98 (784): 644-6
8. Riddoch C, Trinnick T. Gastrointestinal disturbances in mara-thon runners. Br J Sports Med 1988; 22: 71-4
9. Priebe W, Priebe J. Runner’s diarrhoea – prevalence and clinicalsymptomatology. Am J Gastroenterol 1984; 79: 827-8
10. Sullivan SN, Wong C. Runner’s diarrhoea: different patterns andassociated factors. J Clin Gastroenterol 1992; 14 (2): 101-4
11. Brouns F, Beckers E. Is the gut an athletic organ? Digestion,absorption and exercise. Sports Med 1993; 15 (4): 242-57
12. Green GA. Gastrointestinal disorders in the athlete. Clin SportsMed 1992; 11 (2): 453-68
13. Halvorsen FA, Lyng JL, Ritland S. Gastrointestinal bleeding inmarathon runners. Scand J Gastroenterol 1986; 21: 493-7
14. Moses FM. The effect of exercise on the gastrointestinal tract.Sports Med 1990; 9 (3): 159-72
15. Rehrer NJ, Meijer GA. Biomechanical vibration of the abdom-inal region during running and bicycling. J Sports Med PhysFitness 1991; 31 (2): 231-4
Running
Increased or decreased colonic motility
GI symptoms
↓GI absorption
GI permeability
Endotoxaemia
Miscellaneous ascorbic acid (vitamin C) infections diet psoas caecal volvulus IBS
Mechanicalfactors
Hormonesand
prostaglandins
Stress
Secretion of hormones and prostaglandins
↓Blood flow
↓
↓
Fig. 1. Potential aetiological factors of running-associated gastointestinal symptoms. GI = gastrointestinal; IBS = irritable bowelsyndrome; ↓ = decreased; ↑ = increased.
374 Gil et al.
© Adis International Limited. All rights reserved. Sports Med 1998 Dec; 26 (6)

16. Peters HP, Van Schelven FW, Verstappen PA, et al. Gastrointes-tinal problems as a function of carbohydrate supplements andmode of exercise. Med Sci Sports Exerc 1993; 25: 1211-24
17. Fahrenkrug J. Nervous release of VIP in the gastrointestinaltract of the cats: possible physiological implications. J Phys-iol (Lond) 1978; 284: 291-305
18. Hubel KA. Intestinal nerves and ion transport: stimuli, reflexes,and responses. Am J Physiol 1985; 248: G261-71
19. Hossdorf T, Burger M, Karoff C, et al. Radioimmunoassay forvasoactive intestinal polypeptide (VIP) in plasma before andduring endoscopic examinations. Hepatogastroenterology1982; 29 (4): 146-50
20. Porter AW. Case report: marathon running and the caecal slapsyndrome. Br J Sports Med 1982; 16 (3): 178
21. Porter AW. Non-steroidal anti-inflammatory drugs and ethanol.Br J Sports Med 1982; 16: 265
22. Dawson M. Psoas muscle hypertrophy: mechanical cause forjogger’s trots. BMJ 1985; 291: 787-8
23. Pevett TL, ME Wilkins, WC Gamble. Caecal volvulus, a differ-ent twist for the serious runner. N Engl J Med 1985; 312:1262-3
24. Rudzki SJ, Hazard H, Collinson D. GI blood loss in triathletes:its aetiology and relationship to sports anaemia. Aust J SciMed Sport 1995; 27 (1): 3-8
25. Halvorsen F, Ritland S. Gastrointestinal problems related toendurance event training. Sports Med 1992; 14 (3): 157-63
26. Baska RS, Moses FM, Deuster PA. Cimetidine reduces runningassociated GI bleeding: a prospective observation. Dig DisSci 1990; 35 (8): 56-60
27. Robertson JD, Maughan RJ, Davidson RJ. Faecal blood loss inresponse to exercise. BMJ 1987; 295: 303-5
28. Baska RS, Moses FM, Graeber G, et al. Gastrointestinal bleed-ing during an ultramarathon. Dig Dis Sci 1990; 35 (2): 276-9
29. Schwartz AE, Vanagunas A, Kamel PL. Endoscopy to evaluategastrointestinal bleeding in marathon runners. Ann InternMed 1990; 113: 632-3
30. McCabe ME, Peura DA, Kadakia SC, et al. GI blood loss asso-ciated with running a marathon. Dig Dis Sci 1986; 31 (11):1229-32
31. Porter AW. Do some marathon runners bleed into the gut? BMJ1983; 287: 1427
32. McMahon LF, Ryan MJ, Larson D, et al. Occult gastrointestinalblood loss in marathon runners. Ann Intern Med 1984; 100(6): 846-7
33. Worme JD, Doubt TJ, Singh A, et al. Dietary patterns, gastro-intestinal complaints, and nutrition knowledge of recreationaltriathletes. Am J Clin Nutr 1990; 51 (4): 690-7
34. Stewart JG, Ahlquist DA, Mc Gill DB, et al. Gastrointestinalblood loss and anaemia in runners. Ann Intern Med 1984;100: 843-5
35. Yges C, Chicharro JL, Lucia A, et al. Monoclonal antibodiesfor exercise-induced fecal occult blood detection – compari-son with Hemofec. Can J Appl Physiol 1995; 20 (1): 78-88
36. Wilhite J, Mellion MB. Occult gastrointestinal bleeding in en-durance cyclists. Phys Sports Med 1990; 18 (8): 75-8
37. Dobbs TW, Atkins M, Ratcliff, et al. Gastrointestinal bleedingin competitive cyclists. Med Sci Sport Exerc 1988; 20 (2)Suppl. 5: S78
38. Selby G, Frame D, Eichner ER. Effort-related blood loss inyoung distance runners during a competitive season. Med SciSport Exerc 1988; 20 (2) Suppl. 5: S78
39. Moses FM, Baska RS, Peura DA, et al. Effect of cimetidine onmarathon associated GI symptoms and bleeding. Dig Dis Sci1991; 36 (10): 1390-4
40. Alquist DA, McGill DB, Schwartz S, et al. HemoQuant, a newquantitative assay for faecal hemoglobin: comparison withhaemoccult. Ann Intern Med 1984; 101: 297-302
41. Schentag JJ. False positive ‘Hemoccult’ reaction with cimeti-dine [letter]. N Engl J Med 1981; 303: 110
42. Macrae F, St John DJ, Caligiore P, et al. Optimal conditions forhaemoccult testing. Gastroenterology 1982; 83: 860-3
43. Lampe JW, Slavin JL, Apple FS. Iron status of active womenand the effect of running a marathon on bowel function andgastrointestinal blood loss. Int J Sports Med 1990; 12 (2):173-9
44. Papaioannides D, Giotis Ch, Karagiannis N, et al. Acute uppergastrointestinal haemorrhage in long-distance runners. AnnIntern Med 1984; 101: 719
45. Cooper BT, Douglas SA, Firth LA, et al. Erosive gastritis andgastrointestinal bleeding in a female runner. Gastroenterol-ogy 1987; 92: 2019-23
46. Gaudin C, Zerath E, Guezennec CY. Gastric lesions secondaryto long distance running. Dig Dis Sci 1990; 35 (10): 1239-43
47. Heer M, Repond F, Hany A, et al. Acute colitis in a female longdistance runner. Gut 1987; 28: 896-9
48. Cantwell JD. Gastrointestinal disorders in runners. JAMA1981; 246 (13): 1404
49. Beaumont AC, Teare JP. Subtotal colectomy following mara-thon running in a female patient. J R Soc Med 1991; 84:439-40
50. Rubin RB, Saltzman JR, Zawacki JK. Bicycle racing,Raynaud’s phenomenon, and gastrointestinal bleeding. Am JGastroenterol 1994; 89 (2): 291-2
51. Moses FM, Breuer TG, Peura DA. Running-associated proxi-mal haemorrhagic colitis. Ann Intern Med 1988; 108: 385-6
52. Fisher RL, McMahon LF, Ryan MJ, et al. Gastrointestinalbleeding in competitive runners. Dig Dis Sci 1986; 31 (11):1226-30
53. Schoch DR, Sullivan AL, Grand RJ, et al. Gastrointestinalbleeding in an adolescent runner. J Pediatr 1987; 111 (2):302-3
54. Granger DN, Richardson, Kvietys PR. Intestinal blood flow.Gastroenterology 1980; 78: 837-63
55. Shepherd JT, Vanhoutte PM. Role of the venous system in cir-culatory control. Mayo Clin Proc 1978; 53 (4): 247-55
56. Clausen JP. Effect of physical training on cardiovascular adjust-ments to exercise in man. Physiol Rev 1978; 57: 779-815
57. Rowell LB, Blackmon JR, Bruce RA. Indocyanine green clear-ance and estimated hepatic blood flow during mild to maxi-mal exercise in upright man. J Clin Invest 1964; 43: 1677-760
58. Rowell LB, Blackmon JR, Martin RH, et al. Hepatic clearanceof indocyanine green in man under thermal and exercisestress. J Appl Physiol 1965; 20 (3): 384-94
59. Rowell LB, Brengelmann GL, Blackmon JR, et al. Splanchnicblood flow and metabolism in heat-stressed man. J ApplPhysiol 1968; 24 (4): 475-84
Running-Related GI Dysfunction 375
© Adis International Limited. All rights reserved. Sports Med 1998 Dec; 26 (6)

60. Kenney WL, Ho CW. Age alters regional distribution of bloodflow during moderate-intensity exercise. J Appl Physiol 1995;79 (4): 1112-9
61. Clausen JP, Klausen K, Rasmussen B, et al. Central and periph-eral circulatory changes after training of the arms or legs. AmJ Physiol 1973; 225 (3): 675-82
62. Ahlborg G, Weitzberg E, Sollevi A, et al. Splanchnic and renalvasoconstrictor and metabolic responses to neuropeptide Y inresting and exercising man. Acta Physiol Scand 1992; 145 (2):139-49
63. Ahlborg G. Lactate and glucose exchange across the forearms,legs, and splanchnic bed during and after prolonged leg exer-cise. J Clin Invest 1982; 69: 45-9
64. Ahlborg G, Felig P, Hagenfeldt L, et al. Substrate turnover dur-ing prolonged exercise in man: splanchnic and leg metabo-lism of glucose, free fatty acids and amino acids. J Clin Invest1974; 53: 1080-8
65. Rehrer NJ, Smets A, Reynaert H, et al. Direct measurement ofsplanchnic blood flow during exercise in man. J Am CollSports Med 1987; 24 (5): S165
66. Qamar MI, Read AE. Effects of exercise on mesenteric bloodflow in man. Gut 1987; 28: 583-7
67. Flamm SD, Taki J, Moore R, et al. Redistribution of regionaland organ blood volume and effect of cardiac function in re-lation to upright exercise intensity in healthy human subjects.Circulation 1990; 81: 1550-9
68. Jost J, Weiss M, Weicker H. Sympathoadrenergic regulation andthe adrenoceptor system. J Appl Physiol 1990; 68 (3): 897-904
69. Mailman D. Blood flow and intestinal absorption. Fed Proc1982; 41 (6): 2096-100
70. Orhi SK, Bjarnason I, Pathi V, et al. Cardiopulmonary bypassimpairs small intestine transport and increases gut permeabil-ity. Ann Thorac Surg 1993; 55 (5): 1080-6
71. Rehrer NJ, Janssen GM, Brouns F, et al. Fluid intake and gas-trointestinal problems in runners competing in a 25-km raceand a marathon. Int J Sports Med 1989; 10 Suppl. 1: S22-5
72. Sato N, Takenobu K, Motoaki S, et al. Measurement ofhemoperfusion and oxygen sufficiency in gastric mucosa invivo. Gastroenterology 1979; 76: 814-9
73. Gores GJ, Flarsheim LE, Dawson TL, et al. Swelling, reductivestress, and cell death during chemical hypoxia in hepatocytes.Am J Physiol 1989; 257: C347-54
74. Kingham JG, Whormell PJ, Lohery CA. Small intestinal per-meability: effects of ischaemia and exposure to acetyl salicy-late. Gut 1976; 17: 354-61
75. Chiu CJ, McArdle AH, Brown R, et al. Intestinal mucosal lesionin low flow states. Arch Surg 1970; 101: 478-83
76. Bulkley GB, Kvietys PR, Parks DA, et al. Relationship of bloodflow and oxygen consumption to ischaemic injury in the ca-nine small intestine. Gastroenterology 1985; 89: 852-7
77. Parks DA, Grogaard B, Granger DN. Comparison of partial andcomplete arterial occlusion models for studying intestinalischaemia. Surgery 1982; 92: 896-901
78. Parks DA, Bulkley GB, Granger DN, et al. Ischaemic injury inthe cat small intestine: role of superoxide radicals. Gastroen-terology 1982; 82: 9-15
79. Granger DN, Rutili G, McCord JM. Superoxide radicals in thefeline intestinal ischaemia. Gastroenterology 1981; 81: 22-9
80. Morishita T, Guth P. Effect of exogenous acid on the rat gastricmucosal microcirculation in haemorrhagic shock. Gastroen-terology 1987; 92: 1958-64
81. Wilcox MG, Howard TJ, Plaskon LA, et al. Current theories ofpathogenesis and treatment of nonocclusive mesenteric isch-aemia. Dig Dis Sci 1995; 40 (4): 709-16
82. Suvannapura A, Levens NR. Local control of mesenteric bloodflow by the renin-angiotensin system. Am J Physiol 1988; 255(3): G267-74
83. Bulkley GB, Oshima A, Bailey RW, et al. Control of gastricvascular resistance in cardiogenic shock. Surgery 1985; 98(2): 213-23
84. Bailey RW, Bulkley GB, Hamilton SR, et al. Pathogenesis ofnonocclusive ischaemic colitis. Ann Surg 1986; 203 (6): 590-9
85. Aldigier JC, Huang H, Dalmay F, et al. Angiotensin-convertingenzyme inhibition does not suppress plasma angiotensin IIincrease during exercise in humans. J Cardiovasc Pharmacol1993; 21 (2): 289-95
86. Ferrari R, Ceconi C, Rodella A, et al. Temporal relations ofendocrine response to exercise. Cardioscience 1991; 2 (2):131-9
87. Luger A, Deuster PA, Debolt JE, et al. Acute exercise stimulatesthe renin-angiotensin-aldosterone axis: adaptive changes inrunners. Horm Res 1988; 30 (1): 5-9
88. Szabo S. Mechanisms of gastric mucosal injury and protection.J Clin Gastroenterol 1991; 13 Suppl. 2: S21-34
89. Weitzberg E, Hemsen A, Lundberg JM, et al. ET-3 is extractedby and induces potent vasoconstriction in human splanchnicand renal vasculatures. J Appl Physiol 1995; 79 (4): 1255-9
90. Fukumura D, Kurose I, Miura S, et al. Role of endothelin-1 inrepeated electrical stimulation-induced microcirculatory dis-turbance and mucosal damage in the rat stomach. J Gas-troenterol Hepatol 1996; 11 (3): 279-85
91. Dobi I, Kekesi V, Toth M, et al. Endothelin-induced long-lastingmesenteric vasoconstriction: a hypothetical mechanism ofnon-occlusive intestinal infarction. Acta Chir Hung 1991; 32(3): 199-208
92. Maeda S, Miyauchi T, Waku T, et al. Plasma endothelin-1 levelin athletes after exercise in a hot environment: exercise-induced dehydration contributes to increases in plasmaendothelin-1. Life Sci 1996; 58 (15): 1259-68
93. Ahlborg G, Weitzberg E, Lundberg J. Metabolic and vasculareffects of circulating endothelin-1 during moderately heavyprolonged exercise. J Appl Physiol 1995; 78 (6): 2294-300
94. Appenzeller O, Wood SC. Peptides and exercise at high and lowaltitudes. Int J Sports Med 1992; 13 Suppl. 1: S135-40
95. Bounous G, McArdle AH. Marathon runners: the intestinalhandicap. Med Hypotheses 1990; 33: 261-4
96. McArdle W, Katch FI, Katch VL. Exercise physiology: energy,nutrition and human performance. Philadelphia: Lea & Febi-ger, 1991: 302
97. Sullivan SN. The effect of running on the gastrointestinal tract.J Clin Gastroenterol 1984; 6: 461-5
98. Jordan PH, Boulafendis D, Guinn GA. Factors other than majorvascular occlusion that contribute to intestinal infarction. AnnSurg 1970; 171: 189-94
99. Bloom SR, Johnson RH, Park DM, et al. Differences in themetabolic hormonal response to exercise between racing cy-clists and untrained individuals. J Physiol 1976; 258: 1-18
376 Gil et al.
© Adis International Limited. All rights reserved. Sports Med 1998 Dec; 26 (6)

100. Sullivan SN, Champion MC, Christophides ND, et al. Gastro-intestinal regulatory responses in long-distance runners. PhysSportsmed 1984; 12 (7): 78-82
101. Modlin IM, Bloom SR, Mitchell S. Plasma vasoactive intestinalpolypeptide (VIP) levels and intestinal ischaemia. Ex-perientia 1978; 34: 535-6
102. Barbezat GO, Grossmann MI. Intestinal secretion: stimulationby peptides. Science 1971; 174: 422-4
103. Eklund S, Jodal M, Lundgren O, et al. Effects of vasoactiveintestinal polypeptide on blood flow, motility and fluid trans-port of the gastrointestinal tract of the cat. Acta Physiol Scand1979; 105 (4): 461-8
104. Mailman D. Effects of vasoactive intestinal polypeptide on in-testinal absortion and blood flow. J Physiol 1978; 279: 121-32
105. Kane MG, O’Dorisio TM, Krejs GJ. Production of secretorydiarrhoea by intravenous infusion of vasoactive intestinalpolypeptide. N Engl J Med 1983; 309: 1482-5
106. Krejs GJ, Fordtran J. Effect of VIP on water and ion transportin the human jejunum. Gastroenterology 1980; 78: 722-7
107. Racusen LC, Binder HJ. Alteration of large intestinal electro-lyte transport by vasoactive intestinal polypeptide in the rat.Gastroenterology 1977; 73: 790-6
108. Telford GL, Condon RE, Szurszewski JH. Opioid receptors andthe initiation of migrating myoelectric complexes. Am JPhysiol 1989; 256 (1): 672-7
109. Adachi H, Toda N, Nayashi S, et al. Mechanism of the excit-atory action of motilin on isolated rabbit intestine. Gastroen-terology 1981; 80: 783-8
110. Rennie JA, Christophides ND, Bloom SR, et al. Stimulation ofhuman colonic activity by motilin [abstract]. Gut 1979; 20:A912
111. Suzuki T, Takahashi I, Itoh Z. Motilin and gallbladder: newdimensions in physiology. Peptides 1981; 2: 229-33
112. Ahlborg G, Lundberg JM. Splanchnic release of neuropeptide Yduring prolonged exercise with and without beta-adrenoceptorblockade in healthy man. Clin Physiol 1991; 11 (4): 343-51
113. Buell MG, Harding RK. Effects of peptide YY on intestinalblood flow distribution and motility in the dog. Regul Pept1989; 24 (2): 195-208
114. Beubler E, Juan H. PGE release, blood flow and transmucosalwater movement after mechanical stimulation of the rat jeju-nal mucosa. Naunyn Schmiedebergs Arch Pharmacol 1978;305: 91-5
115. Bennett A, Friedman CA, Vane JR. Release of prostaglandinsE1 from the rat stomach. Nature 1967; 216: 873-6
116. Gallavan RH, Jacobson ED. Prostaglandins and the splanchniccirculation. Proc Soc Exp Biol Med 1982; 170: 391-7
117. Demers LM, Harrison TS, Halbert DR, et al. Effect of pro-longed exercise on plasma prostaglandin levels. Prostaglan-dins Med 1981; 6 (4): 413-8
118. Hawkey CJ, Rampton DS. Prostaglandins and the gastrointes-tinal mucosa: are they important in its function, disease ortreatment? Gastroenterology 1985; 89: 1162-88
119. Rush BD, Ruwart MJ. The role of accelerated colonic transit inprostaglandin-induced diarrhoea and its inhibition by pro-stacyclin. Br J Pharmacol 1984; 83 (1): 157-9
120. Konturek SJ, Pawlik W. Physiology and pharmacology of pros-taglandins. Dig Dis Sci 1986; 31 (2) Suppl. 2: 6S-19S
121. Hunt RH, Dilawary JB, Misiewicz JJ. The effect of prostaglan-din F2α and E2 on the motility of the sigmoid colon. Gut 1975;16: 47-9
122. Staumont G, Fioramonti J, Frexinos J, et al. Changes in colonicmotility induced by sennosides in dogs: evidence of prosta-glandin mediation. Gut 1988; 29: 1180-7
123. Occhipinti M. Prostaglandins and gastrointestinal function.Adv Pediatr 1978; 25: 205-21
124. Milton-Thompson GJ, Cummings JH, Newman A, et al. Co-lonic and small intestinal response to intravenous prostaglan-din F2α and E2 in man. Gut 1975; 1: 42-6
125. Lange AP, Secher NJ, Amery W. Prostaglandin-induced diar-rhoea treated with loperamide or diphenoxylate: a double-blind study. Acta Med Scand 1977; 202 (6): 449-54
126. Goodman G, Gilman A. The pharmacological basis of therapeu-tics. New York: Pergamon Press, 1985: 302
127. Samuelson B. Leukotrienes: mediators of immediate hypersen-sitivity reactions and inflammation. Science 1983; 220: 568-75
128. Hua XY, Dahlen SE, Lundberg S, et al. Leukotrienes C4, D4and E4 cause widespread and extensive plasma extravasationin the guinea-pig. Naunyn Schmiedebergs Arch Pharmacol1985; 330: 136-41
129. Whittle BJ. Prostaglandins and leukotrienes in gastrointestinaldiseases. In: Domschke W, Dammann HG, editors. Prosta-glandins and related compounds. New York: Springer-Verlag,1988: 16
130. Barclay GR, Turnberg LA. Effect of moderate exercise on saltand water transport in the human jejunum. Gut 1988; 29:816-20
131. Williams JH, Milton Mager JR, Jacobson ED. Relationship ofmesenteric blood flow to intestinal absortion of carbohy-drates. J Lab Clin Med 1964; 63: 853-63
132. Peters HP, Akkermans LM, Bol E, et al. Gastrointestinal symp-toms during exercise: the effect of fluid supplementation.Sports Med 1995; 20 (2): 65-75
133. Fordtran JS, Saltin B. Gastric emptying and intestinal absorp-tion during prolonged severe exercise. J Appl Physiol 1967;23 (3): 331-5
134. Gisolfi CV, Spranger KJ, Summers RW, et al. Effects of cycleexercise on intestinal absorption in humans. J Appl Physiol1991; 71 (6): 2518-27
135. Bosenberg AT, Brock-Utne JG, Gaffin SL, et al. Strenuous ex-ercise causes systemic endotoxemia. J Appl Physiol 1988; 65(1): 106-8
136. Cammack JN, Read W, Cann A, et al. Effect of prolonged ex-ercise on the passage of a solid meal through the stomach andthe small intestine. Gut 1982; 23: 957-62
137. Keeling WF, Martin B. Gastrointestinal transit during mild ex-ercise. J Appl Physiol 1987; 63 (3): 978-81
138. Keeling WF, Harris A, Martin BJ. Orocecal transit during mildexercise in women. J Appl Physiol 1990; 68 (4): 1350-3
139. Meshkinpour H, Kemp C, Fairshter R. Effect of aerobic exer-cise on mouth-to-cecum transit time. Gastroenterology 1989;96: 938-41
140. Soffer EE, Summers RW, Gisolfi C. Effect of exercise on intes-tinal motility and transit time in trained athletes. Am J Physiol1991; 260: G698-702
141. Koffler KH, Menkes A, Redmon RA, et al. Strength trainingaccelerates gastrointestinal transit in middle-aged and oldermen. Med Sci Sports Exerc 1992; 24 (4): 415-9
Running-Related GI Dysfunction 377
© Adis International Limited. All rights reserved. Sports Med 1998 Dec; 26 (6)

142. Liu F, Toda Y. Brief physical inactivity prolongs colonic transittime in elderly men. Int J Sports Med 1993; 14: 465-7
143. Bingham SA, Cummings JH. Effect of exercise and physicalfitness on large intestinal function. Gastroenterology 1989;97: 1389-99
144. Robertson G, Meshkinpour H, Cohen A, et al. Effects of exer-cise on total and segmental colon transit [abstract]. Gastroen-terology 1990; 98 (5): A385
145. Coenen C, Wegener M, Wedman B, et al. Does physical exerciseinfluence bowel transit time in healthy young men? Am JGastroenterol 1992; 87 (3): 292-5
146. Oettle GJ. Effect of moderate exercise on bowel habit. Gut1991; 32: 941-4
147. Sesboue B, Arhan P, Devroede G, et al. Colonic transit in soccerplayers. J Clin Gastroenterol 1995; 20 (3): 211-4
148. Rao KA, Evans DF. Gastrointestinal problems in athletes.Sports Exerc Injury 1995; 1: 183-90
149. Cheskin LJ, Crowell MD, Kamal N, et al. The effects of acuteexercise on colonic motility. Gastrointest Motil 1992; 4: 173-7
150. Dapoigny M, Sarna SK. Effect of physical exercise on colonicmotor activity. Am J Physiol 1991; 260: G646-52
151. Cannon WB. The movements of the intestines studied by meansof the Roentgen rays. Am J Physiol 1902; 6: 251-77
152. O’Brien JD, Thompson GD, Holly J, et al. Stress disturbs hu-man gastrointestinal transit via a beta-1 adrenoceptor medi-ated pathway [abstract]. Gastroenterology 1985; 88: 1520
153. Valori RM, Kumar D, Wingate DL. Effects of different types ofstress and ‘prokinetic’ drugs on the control of the fasting mo-tor complexes in humans. Gastroenterology 1986; 90 (6):1890-900
154. McRae S, Younger K, Thompsom DG, et al. Sustained mentalstress alters human jejunal motor activity. Gut 1982; 23 (5):404-9
155. Narducci F, Snape WJ, Battle WM, et al. Increased colonic mo-tility during exposure to a stressful situation. Dig Dis Sci1985; 30: 40-4
156. Barone FC, Deegan JF, Fowler PJ, et al. A model of stress-in-duced increased faecal output and colonic transit. Gastroen-terology 1986; 90: 1337
157. Williams CL, Villar RG, Peterson JM, et al. Stress-inducedchanges in intestinal transit in the rat: a model for irritablebowel syndrome. Gastroenterology 1988; 94: 611-21
158. Lenz HJ, Raedler A, Greten H, et al. Stress-induced gastroin-testinal secretory and motor responses in rats are mediated byendogenous corticotropin-releasing factor. Gastroenterology1988; 95 (6): 1510-7
159. Bueno L, Gue M. Evidence for the involvement of corticotropin-releasing factor in the gastrointestinal disturbances inducedby acoustic and cold stress in mice. Brain Res 1988; 441 (1-2):1-4
160. Van Erp-Barrt AM, Saris WH, Binkhorst RA, et al. Nationwidesurvey on nutritional habits in elite athletes: energy, carbohy-drate and fat intake. Int J Sports Med 1989; 10 Suppl. 1: S3-7
161. Harris A, Lindeman AK, Martin BJ. Rapid orocaecal transit inchronically active persons with high energy intake. J ApplPhysiol 1991; 70 (4): 1550-3
162. Swain RA. Exercise induced diarrhoea: when to wonder. MedSci Sports Exerc 1994; 26 (5): 523-6
163. Sharman IM. Gastrointestinal disturbances in runners. Br JSports Med 1982; 16 (3): 179
Correspondence and reprints: Dr Etsuro Yazaki, GI ScienceResearch Unit, 26 Ashfield Street, London E1 2AJ, England.E-mail: [email protected]
378 Gil et al.
© Adis International Limited. All rights reserved. Sports Med 1998 Dec; 26 (6)