AESTHETICS Readers’ Choice 27th Annual 100...dental exam, smile analysis, and oral cancer...
4
R R DENTISTRYTODAY.COM VOLUME 32 NO. 7 THE NATION’S LEADING CLINICAL NEWS MAGAZINE FOR DENTISTS JULY 2O13 TWO PEER-REVIEWED CE CREDITS Management of Plaque-Related Soft-Tissue Trauma Ahmad Soolari, DMD, MS, et al pg. 96 RESTORATIVE Effective Cavity Liner Randy S. Weiner, DMD, pg. 136 BUYERS’ GUIDE Fiber Posts and Pins, pg. 138 27th Annual Special section begins on page 41 P R O D U C T S Readers’ Choice Jack S. Roth, DDS pg. 108 ENDODONTICS AESTHETICS Peter Harnois, DDS pg. 120 AESTHETICS Ross W. Nash, DDS pg. 114 Stephen Abrams, DDS pg. 104 TECHNOLOGY TOP 100 PR0DUCTS JULY 2013
Transcript of AESTHETICS Readers’ Choice 27th Annual 100...dental exam, smile analysis, and oral cancer...
![Page 1: AESTHETICS Readers’ Choice 27th Annual 100...dental exam, smile analysis, and oral cancer screening (which included the use of the VELscopeVx [DenMat]), we presented the patient](https://reader042.fdocuments.us/reader042/viewer/2022013021/5f0e7a3d7e708231d43f7021/html5/page/1.jpg)
000000000000000000000000R R
DENTISTRYTODAY.COM
VOLUME 32 NO. 7 THE NATION’S LEADING CLINICAL NEWS MAGAZINE FOR DENTISTS JULY 2O13
TWO PEER-REVIEWED CE CREDITSManagement of Plaque-Related Soft-Tissue Trauma Ahmad Soolari, DMD, MS, et al pg. 96
RESTORATIVEEffective Cavity LinerRandy S. Weiner, DMD, pg. 136
BUYERS’ GUIDEFiber Posts and Pins, pg. 138
TOPTOPTOPTOPTOPTOP27th Annual
Special section begins on page 41
PRODUCTS
Readers’ Choice
Jack S. Roth, DDSpg. 108
ENDODONTICS
AESTHETICS
Peter Harnois, DDSpg. 120
AESTHETICS
Ross W. Nash, DDSpg. 114
Stephen Abrams, DDSpg. 104
TECHNOLOGY
111111111TOP
10
0 P
R0
DU
CTS
JULY
20
13
![Page 2: AESTHETICS Readers’ Choice 27th Annual 100...dental exam, smile analysis, and oral cancer screening (which included the use of the VELscopeVx [DenMat]), we presented the patient](https://reader042.fdocuments.us/reader042/viewer/2022013021/5f0e7a3d7e708231d43f7021/html5/page/2.jpg)
120
Full-prep veneers remain the standardin our dental education, if not ourpractices. Not until the last decade
have thin veneer techniques been intro-duced to students as an appropriate treat-ment methodology, when indicated.
Today, our patients’ increasing dental IQis driving their demand for a less invasiveapproach to aesthetic treatment. This articlewill present a case report demonstrating thelatest generation of thin veneers (Lumineers[DenMat]). This clinical treatment approachrepresents the opportunity for responsibleaesthetics, while always assessing the re -quirement for the removal of healthy toothstructure. DenMat’s new approach and edu-cational platform for Lumineers, calledThinnovation, is not just about no-prepara-tion dentistry, though we must always con-sider the concept of choosing the best possi-ble approach for each patient, based on indi-vidual needs and circumstances.
CASE REPORTDiagnosis and Treatment Planning
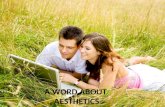
A 28-year-old female patient, Ashley, present-ed to our office. She had completed 3 years oforthognathic treatment with her oral max-illofacial surgeon and her orthodontist. Shespecifically sought a dentist who offered no-prep style veneers. Her chief complaint washer smile or, in her words, the lack of “show-ing teeth” when smiling. In addition, she didnot like the quality of the teeth/smile that didshow (Before Image and Figure 1).
The patient presented with a postortho-dontic removable upper Essix-style retainer,and with healthy periodontium and stableocclusion, showing no temporomandibular
joint disorder (TMD) symptoms or brux-ing/clenching. Full dental records were per-formed and a LUMISmile (DenMat) picturetaken to produce a digital smile make -over. Her principal aesthetic issues includedmultiple diastemas, peg lateral incisors, andhyperplastic gingival tissues that coveredthe gingival one third of the maxillary (peg)lateral incisors (teeth Nos. 7 and 10). Also evi-dent was stained, mottled, and hypocalcifiedenamel on all upper teeth.
At her initial appointment, it was appar-ent that she had already done her homework.She had requested information from her oralsurgeon about the current landscape of porce-lain veneer options and already knew aboutthin veneers, specifically Lumineers. She hadfollowed up by visiting DenMat’s patientWeb site (lumineers.com) to learn moreabout what was possible with minimal-prepveneer systems. She already knew what shewanted. This experience is increasingly com-mon. As a general dentist practicing aestheticdentistry for the past 31 years, I have foundthat the majority of new patients have someidea of what they seek clinically. Today’spatients are more empowered with theknowledge available to them and often havegone beyond what they’ve seen on televisionor heard from friends to visit Web sites and
educate themselves. Our role is to help themdetermine appropriate treatment options andto outline the probable outcome based on thecurrent state of their dentition. Giving pa -tients all possible options, and then lettingthem decide, has proven to be a consistentlysuccessful beginning to case acceptance.
Ashley’s first appointment was morefocused on how her new smile could look, interms of shapes and shades, than it was talk-ing about the difference between minimal- orno-prep veneers (such as Lumineers) and tra-ditionally prepped ve neers. She knew that shewanted an aesthetic solution that minimizedthe removal of her tooth structure. One of herfirst comments to me was, “I don’t have thatmuch tooth structure as it is, so I don’t wantmy teeth made any smaller!”
As part of the aesthetic consult, LUMI -Smile photos were taken to provide a digitalsmile makeover in less than 30 minutes. (TheSNAP Digital Imaging system is another use-ful diagnostic tool that could be used here.) Acomprehensive smile analysis was conduct-ed, including completion of a Smile AnalysisForm by the patient. From this information,the patient communicated that she did notlike to smile due to her small, misshapen,and discolored teeth. After completing a full
Peter Harnois,DDS
A New Perspective on MinimallyInvasive Veneer Techniques
continued on page 124Figure 1. Pre-op smile retracted, frontal view.
Before Image. Pre-op smile retracted, frontal view. After Image. The final smile.
AESTHETICS
BEFORE AFTER
DENTISTRYTODAY.COM • JULY 2013
![Page 3: AESTHETICS Readers’ Choice 27th Annual 100...dental exam, smile analysis, and oral cancer screening (which included the use of the VELscopeVx [DenMat]), we presented the patient](https://reader042.fdocuments.us/reader042/viewer/2022013021/5f0e7a3d7e708231d43f7021/html5/page/3.jpg)
AESTHETICS124
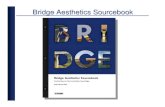
dental exam, smile analysis, and oralcancer screening (which included theuse of the VELscopeVx [DenMat]), wepresented the patient with her LUMI -Smile before and after digital images(Figures 2a and 2b).
Our patients’ responses at thisstage are often emotional, and thispatient was no different. The case pro-posal for 8 Lumineers for teeth Nos. 5to 12, with a post-treatment removablere tainer/nightguard, was accepted.
Clinical ProtocolTreatment started in early December2012, with a prophylaxis. A one-hourchairside whitening was done (Lumi -brite and Sapphire light [Both by Den -Mat]), followed by one week of homewhitening using a 35% carbamide per-oxide gel (Lumibrite) with customtrays (30 minutes per day for one weekwas prescribed, and followed). Ourpatient’s teeth were whitened from2M1 to OM3/OM2, and the porcelainshade the patient selected was OM2.(Note: Clinicians can use any effectivewhitening system and technique oftheir choosing. For example, with theEPIC laser technique [BIOLASE Tech -nology], treatments can be performedin as little as 30 minutes.) Possible lasergingivoplasty was also discussed withthe patient at this time, though sheexpressed hesitation with the proce-dure so a final decision was postponed.
One week after whitening andshade selection, enamel-contouringprocedures were begun. Enamel con-touring has long been considered asomewhat gray area in achieving thedesired outcome sought by a patient.The problem has been that traditionalprep is well defined, but enamel con-touring is not. There are no set princi-ples of smile design. Beauty is in theeye of the beholder, and there is noright or wrong. The new Thin no -vation approach is based on the prin-ciples of smile design and utilizesminimally invasive concepts of toothpreparation to achieve the desiredresult. For the first time, the Thinno -vation concepts of enamel contouringstrive to define the proper principlesof contouring to achieve the aesthetic,natural lifelike result that the patientseeks from the doctor.
Initially, it is our job to obtain thenecessary information from the pa tient.We need to listen and photo documenteach person’s individual pre-op situa-tion. LUMISmile allows the practitionerto show each patient an individual digi-
tal smile makeover and is a tremen-dously successful visual starting pointfor discussing with the pa tient what ispossible. In more ad vanced cases, livemodels, intraoral mock-ups, and ap -proved provisionals are tremendousdiagnostic tools that Thinnovation al -lows a doctor to em ploy. In this pa -tient’s case, enamel contouring was notonly what she sought from this den-tist’s office, but a viable option for treat-ment utilizing the following Thinno -vation concepts of enamel contouring:correct size discrepancies, adjust oc -clusal plane cants, adjust midline cants,adjust suprabulges and incisal bevel.
Understanding smile design con-cepts will dictate what to contour. Anyimperfection is magnified if not con-
toured. In Ashley’s case, there were cer-tain bulges and line angles that, if notproperly contoured, would have lookedthick, bulky, and unnatural in the endresult. Her natural teeth had a facialbulge to them that needed to be reducedto elongate her teeth and close thediastemas and achieve the natural lookshe wanted. A very important conceptfor the doctor to grasp is that Lumineersis an additive cosmetic procedure.Properly informing the patient thatsmoothing the “bumps” off of her teethto achieve a natural result made perfectsense to her. The fact that I could alsoinform her that enamel contouringwould not induce any biological harmto her teeth made her feel even betterabout the prescribed treatment.
After she signed the informed con-sent form, we focused on 3 clinicalobjectives. First, an incisal bevel wouldbe created to allow for design of the pa -tient’s veneers with proper form andfunction with her existing occlusion.The heights of contour on the facial as -pect would be reduced so all teethwould slope in toward the incisal as -pect from the facial height of contour.Finally, all the line angles would bereduced and rounded, and facial embra-sures would be deepened where therewas interproximal contact of teeth toallow for well-defined line angles and anatural depth of field to the facialembrasures. All of this was accom-plished without any patient discom-fort, local anesthetic, or temporization.
As mentioned, the patient was ini-tially reluctant to trim tissue with laser,so we contoured her enamel first andthen showed her what a difference itwould make if we could expose the nat-ural tooth structure still under herhyperplastic tissue. Also, I wanted toper form an aesthetic crown lengthen-ing (in general), since the patientshowed her attached gingiva when shesmiled. Once she saw and understoodthat, we performed the laser gingivo-plasty using a diode laser (SOL DiodeLaser [DenMat]) at one W continuouswave setting, un covering the remainingclinical crown of teeth Nos. 5 to 12.(Note: There are numerous other dentaldiode lasers suitable for this proceduresuch as Picasso Lite [AMD LASERS],EPIC 10 [BIOLASE Tech nology], SIRO -Laser Advance [Sirona Dental Systems]Odyssey Navigator [Ivoclar Vivadent],and so on.) This created a more naturalresult and a more symmetrical gingivaldisplay in general (Figures 3 and 4). Welet healing occur over one week (Fig ures5a and 5b). Final impressions were thentaken along with records and photos.
In preparation for Lumineersplacement, 2 full-arch impressionswere taken using a vinyl polysiloxane(VPS) impression material (Splash![DenMat]). In addition, a face-bow(Panadent), stick-bite, and a closed-tray bite registration were also taken.Then, all was sent to DenMat’s full-service dental lab in California. In ad -dition, 8 post-contouring photos weretaken and submitted through an on -line Web portal. An Essix .040 thick-ness removable retainer was fabricat-ed for the patient to wear full-timeuntil the placement of her veneers.
Once the laboratory team receivedthe materials from our office, the im -pressions were scanned to produce digi-tal models for fabrication of the first setof digital designs. Three days later, digi-
DENTISTRYTODAY.COM • JULY 2013
A New Persepective on Minimally...continued from page 120
Figure 2a. Before. Patient’s before image,which is sent to DenMat digitally.
a
Figure 2b. After. Patient’s LUMISmile(DenMat) digital after, received in the sameconsult appointment from DenMat to give thepatient an idea of her eventual result.
b
Figure 3. Frontal retracted contoured/prelaser. Figure 4. Immediate postlaser.
Figure 5a. Right lateral, postlaser after oneweek of healing.
Figure 5b. Left lateral, postlaser at oneweek.
a b
![Page 4: AESTHETICS Readers’ Choice 27th Annual 100...dental exam, smile analysis, and oral cancer screening (which included the use of the VELscopeVx [DenMat]), we presented the patient](https://reader042.fdocuments.us/reader042/viewer/2022013021/5f0e7a3d7e708231d43f7021/html5/page/4.jpg)
AESTHETICS 125
JULY 2013 • DENTISTRYTODAY.COM
tally designed previews were e-mailed tome for review. After the design previewswere altered, per my instructions, anapproved set of previews (Figures 6 to 10)were sent for final fabrication of theveneers. These approved digital previewswere made possible by implementingthe previously discussed smile designconcepts and proper enamel contouringto achieve the desired lifelike aestheticresult the patient was seeking. The com-pleted Lumineers were sent 13 days later.
Placement Appointment Lumineers were placed following thesteps in “The Doctor’s Guide to Lumi -neer Placement.” The lab-etched Lu mi -neers were treated with porcelain con-ditioner and prime. The teeth werethen polished with porcelain laminatepolishing paste found in the LumineersPlacement Kit (DenMat). Using Ultra -Bond (DenMat) try-in paste, I placedteeth Nos. 7 and 8 with the supremewhite shade and teeth Nos. 9 and 10with shade B-O. Our patient selectedthe supreme white shade for her OM2Cerinate veneers placement.
Her teeth were polished againwith porcelain laminate polishingpaste. The arch was isolated with Sap -phire whitening system cheek retrac-tors and isolated (Paint-On Dam[DenMat] placed on lingual aspect ofteeth Nos. 4 to 13).
Teeth Nos. 5 to 12 were etchedwith 30% phosphoric acid, rinsed,and dried. Five coats of Tenure A and B(DenMat) self-cure adhesive were ap -plied to the teeth and dried. Next, onecoat of Tenure S was applied to bothteeth and to the Lumineers, thenthinned with air.
The Lumineers were loaded andplaced in sequence of teeth Nos. 8 and 9using a Lumigrip and supreme whiteUltraBond. After wiping off excess ce -ment, teeth Nos. 7 and 10 were placed.Using a 2-mm tack-curing tip attachedto a Sapphire curing light, teeth Nos. 8and 9 were spot-cured for one second.Teeth Nos. 6 and 11 were then placed.Teeth Nos. 7 and 10 were then tack-curedfor one second. Teeth Nos. 5 and 12 wereplaced. Teeth Nos. 5, 6, 11, and 12 weretack-cured for one second and remain-ing material was wiped off with brushesdipped in Tenure S. Final curing of 5 sec-
onds facially and lingually was conduct-ed with a 9-mm light-curing tip.
Using a bur and finishing system(designed by DenMat for this restorativesystem), the remaining resin ce mentwas removed. This was accomplishedusing the mosquito diamond; 12 and 30fluted carbides on the facial aspect; andthe football-shaped diamond, alongwith the 12 and 30 fluted carbides, onthe L aspect. A finishing kit was used forfinal bite adjustment, and all contactswere opened (Cerisaw [Den Mat]) andsmoothed (Cerisander [DenMat]). Thefinal polish was completed with a pol-ishing cup (Dialite [Brasseler USA]) andporcelain laminate polishing paste. Fullalginate im pressions were also taken forthe fabrication of a new maxillary Essix.040 retainer/guard.
As the patient experience is defin-itive, her statement affords an appro-priate conclusion: “My smile looks na -tural, but more importantly, it feelsnatural. My teeth don’t look bulky andmy bite feels no different than prior tohaving Lumineers placed. I am get-ting compliments left and right onhow amazing my smile looks!” (Fig -ures 11 to 14, and After Image).
CLOSING COMMENTSMinimally invasive Lumineers with a
high level of natural aesthetics wereselected for this case, consistent withboth expressed patient objectives andclinical assessment. The goal was todeliver an aesthetic smile makeoverwhile preserving the most toothstructure possible.
Digital design was used, as well aspretreatment patient imaging, whichsupports predictable results. Patientveneers are fabricated as thin as 0.3 mm,therefore requiring minimal reductionof healthy tooth structure. The currentgeneration of leucite-reinforced porce-lain allows for very thin (0.3 mm)pressed veneers that are also strong (216MPa). The manufacturer also provides avariety of fabrication processes frompressed monochromatic to layeredpolychromatic restorations.
It’s important to note that lightenamel contouring was needed on thiscase in order to achieve naturally beau-tiful, lifelike results. The distinctionbetween no-preparation, minimal-prep aration, and traditional full-prepa-ration veneer techniques is often mis-understood and miscommunicated.What makes a veneer restoration min-imally invasive? The author suggeststhat “minimally invasive” applies toany veneer prep technique as long asthe least amount of tooth structure is
being removed on that particular caseor tooth while still delivering func-tional, aesthetic results.
It takes a multidisciplinary ap -proach to anterior aesthetics to ensurethat all tools at our disposal are beingused to preserve natural tooth structurewhile still achieving the desired aesthet-ic results. In this particular case, thatmultidisciplinary approach includedorthognathic surgery, detailed treatmentplanning and risk assessment, soft-tissuerecontouring, enamel contouring, and alaboratory partner that delivered anultra-thin set of aesthetic veneers.�
Dr. Harnois practices general and cosmetic den-tistry in Hinsdale and Chicago, Ill. He graduatedwith honors from the University of Illinois at Chi -cago College of Dentistry in 1982, where he thenalso served as an assistant clinical professor ofOral Diagnosis from 1983 to 1989. He is thepresident of the Illinois Chapter of the AmericanAcademy of Facial Esthetics (AAFE) and a mem-ber of the American Academy of Cosmetic Den -tistry, the World Clinical Laser Institute, the Amer -ican Dental Association, the Illinois State DentalSociety, and the Chicago Dental Society. He isalso a Fellow and faculty member of the AAFE.Dr. Harnois is a nationally recognized speak erwho lectures for NuCalm; the AAFE on Botox anddermal fillers; and for DenMat on Lumineers,Snap-On Smile, and oral cancer detection. Hecan be reached at [email protected].
Disclosure: Dr. Harnois is a nonpaid consultantfor DenMat Holdings. He received no compen-sation for writing this article.
Figure 6. Frontal view (solid). Figure 7. Right lateral view (solid). Figure 8. Left lateral view (solid).
Figure 10. Frontal trans view (transparent). Figure 11. Finished frontal view retracted.Figure 9. Occlusal view (solid).
Figure 13. Left lateral view retracted. Figure 14. Finished smile nonretracted.Figure 12. Right lateral view retracted.
Digital design was used, aswell as pretreatment patientimaging, which supports predictable results.