Aesthetic Surgery of the Orbits and Eyelids
31
Aesthetic Surgery of the Orbits and Eyelids Joseph A. Broujerdi, MD, DMD INTRODUCTION The term blepharoplasty derives from the Greek term blephron meaning eyelid and plastos meaning formed. 1 Ali ibn Isa (AD 940–1010) wrote 2 ; Gather a fold of lid skin between a couple of fingers, or raise it up with a hook, and lay the fold between two small wooden bars or rods as long as the lid and as broad as a lancet. Bind their ends very tight together. The skin between these small pieces of wood, deprived of nutrient, dies in about ten days, the en- closed skin falls off, leaving no scar. —(The Tadhkirat of Ali ibn Isa of Baghdad) Reading this passage enlightens one that ancient humans’ ideas were not far fetched compared with the modern-day search for the fountain of youth. Aesthetic surgery of the eyelids has advanced with new instrumentation, tech- nology, innovation, research, and good practice of evidence-based medicine. If the eyes are the window to the soul, then the periorbital tissue is the frame for this window. Aesthetic surgery of the eyelid and surrounding structures aims to keep a youthful frame for the soul. The practice of periocular rejuvenation has moved from skin, muscle, and fat resection of the eyelids only to incorporate a more complex lift, suspension, and volumization of the midface and brow structures. Our improved understanding of the anatomy and pathophysiology of the aging process has assisted in this paradigm shift. The demand from our patients to look natural and youthful has forced us to reevaluate our practice methods and incorporate new advances and tech- niques into our practice. PERIORBITAL AND EYELID EVALUATION A complete evaluation of the patient for oculoplas- tic procedure is the most important step. The initial conversation with the patient should access what their desires are, psychological readiness for cosmetic surgery (eg, acceptance of surgical downtime, risks, and finances), if the patient has realistic expectations, and any ophthalmologic conditions or past surgeries that might change management of the patient (eg, keratorefractive surgery, which may cause dry eyes syndrome after eyelid procedures). Have the patient present pictures of themselves at a more youthful stage in their life so you may evaluate the aging process that has taken place. The medical history should also identify any conditions that might place the patient at greater risks, such as coagulopathies, hypertension, thyroid disease, and neuromuscular conditions. Take into consideration that patients Aesthetic Plastic Surgery Institute, 9401 Wilshire Boulevard Suite 1105, Beverly Hills, CA 90212, USA E-mail address: [email protected] KEYWORDS Aesthetic surgery Orbits Eyelids KEY POINTS A complete evaluation of the patient for oculoplastic procedure is important. The paradigm in oculoplastic surgery has shifted to more conservative eyelid skin, muscle, and fat resection as well as more periorbital soft tissue lift, suspension, and volumization. The effects of facial aging are dependent not only on gravity but also on both intrinsic (gender, genetic) and extrinsic (environmental) factors. Oral Maxillofacial Surg Clin N Am 24 (2012) 665–695 http://dx.doi.org/10.1016/j.coms.2012.07.005 1042-3699/12/$ – see front matter Ó 2012 Published by Elsevier Inc. oralmaxsurgery.theclinics.com
Transcript of Aesthetic Surgery of the Orbits and Eyelids

Aesthetic Surgery of the Orbitsand Eyelids
Joseph A. Broujerdi, MD, DMDKEYWORDS
� Aesthetic surgery � Orbits � Eyelids
KEY POINTS
� A complete evaluation of the patient for oculoplastic procedure is important.
� The paradigm in oculoplastic surgery has shifted to more conservative eyelid skin, muscle, and fatresection as well as more periorbital soft tissue lift, suspension, and volumization.
� The effects of facial aging are dependent not only on gravity but also on both intrinsic (gender,genetic) and extrinsic (environmental) factors.
INTRODUCTION lift, suspension, and volumization of the midface
clinics.com
The term blepharoplasty derives from the Greekterm blephron meaning eyelid and plastosmeaning formed.1 Ali ibn Isa (AD 940–1010) wrote2;
Gather a fold of lid skin between a couple offingers, or raise it up with a hook, and lay thefold between two small wooden bars or rodsas long as the lid and as broad as a lancet.Bind their ends very tight together. The skinbetween these small pieces ofwood, deprivedof nutrient, dies in about ten days, the en-closed skin falls off, leaving no scar.
—(The Tadhkirat of Ali ibn Isa of Baghdad)
Reading this passage enlightens one thatancient humans’ ideas were not far fetchedcompared with the modern-day search for thefountain of youth. Aesthetic surgery of the eyelidshas advanced with new instrumentation, tech-nology, innovation, research, and good practiceof evidence-based medicine.
If the eyes are the window to the soul, then theperiorbital tissue is the frame for this window.Aesthetic surgery of the eyelid and surroundingstructures aims to keep a youthful frame for thesoul. The practice of periocular rejuvenation hasmoved from skin, muscle, and fat resection ofthe eyelids only to incorporate a more complex
Aesthetic Plastic Surgery Institute, 9401 Wilshire BoulevaE-mail address: [email protected]
Oral Maxillofacial Surg Clin N Am 24 (2012) 665–695http://dx.doi.org/10.1016/j.coms.2012.07.0051042-3699/12/$ – see front matter � 2012 Published by E
and brow structures. Our improved understandingof the anatomy and pathophysiology of the agingprocess has assisted in this paradigm shift. Thedemand from our patients to look natural andyouthful has forced us to reevaluate our practicemethods and incorporate new advances and tech-niques into our practice.
PERIORBITAL AND EYELID EVALUATION
A complete evaluation of the patient for oculoplas-tic procedure is the most important step. The initialconversation with the patient should access whattheir desires are, psychological readiness forcosmetic surgery (eg, acceptance of surgicaldowntime, risks, and finances), if the patient hasrealistic expectations, and any ophthalmologicconditions or past surgeries that might changemanagement of the patient (eg, keratorefractivesurgery, which may cause dry eyes syndrome aftereyelid procedures). Have the patient presentpictures of themselves at a more youthful stagein their life so you may evaluate the aging processthat has taken place. The medical history shouldalso identify any conditions that might place thepatient at greater risks, such as coagulopathies,hypertension, thyroid disease, and neuromuscularconditions. Take into consideration that patients
rd Suite 1105, Beverly Hills, CA 90212, USA
lsevier Inc. oralmaxsurgery.the

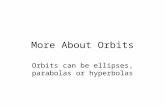
Fig. 2. Patient with long forehead.
Broujerdi666
are in your office for consultations because theywant to have elective cosmetic surgery notbecause they need to be at your office. You shouldalso consider having an ophthalmologist andoptometrist in your area to whom you can refer.Almost all patients in need of periorbital rejuvena-tion need a basic ophthalmologic evaluation andclearance before their surgery. Do not undertakeunnecessary risks and perform your due dili-gences thoroughly.An aesthetically pleasing object to the trained
eye has symmetry and balance and is propor-tionate. On your initial evaluation of the patient,start with architectural framework of the orbito-maxillofacial structures, the position and fullnessof the soft tissue, and the texture and quality ofthe periorbital skin.A full surgical ophthalmologic examination is
discussed elsewhere in this issue by Powell et al,but for the sake of completeness pertinent detailsare included in this article.
Examination of the Forehead and Eyebrow
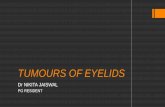
The forehead is described with 3 major aestheticsubunits: the forehead, brows, and temples. Inevaluating the forehead, start with hairline posi-tion. The forehead should on average measure 5to 6 cm from the glabella to the trichion and shouldbe one-third of the facial height. A patient witha low hairline is a good candidate for an opencoronal or anterior hairline brow-lift procedure ifthere is brow ptosis (Fig. 1). A patient with a highhairline is a good candidate for an endoscopic,limited incision, direct or transblepharoplasty(palpebral) brow-lift procedure if there is a browptosis (Fig. 2). The forehead should have a naturalcurvature; consider autologous fat transfer if thiscurvature has been lost because of the agingprocess. Look for temporal hollowing with agingand consider autologous fat transfer as well.
Fig. 1. Patient with short forehead.
Evaluate your patient for forehead rhytids andfurrows and whether they are dynamic or static;consider toxins or endoscopically assisted oropen partial muscle resection with your brow lift.Normal brow position was described by Gunter
and Antrobus3:
1. The medial brow is at or below the level of theorbital rim
2. The medial border of the eyebrow is above themedial canthus
3. The eyebrow should rise gently, with a gentlepeak at least two-thirds of the way to its lateralend, and with this peak usually above the laterallimbus
4. The lateral tail of the brow should be higher thanthe medial end
5. The male brow is at the level of the supraorbitalrim medially and below laterally.
The brow itself is divided into 3 subunits: lateral,medial, and central. The youthful lid-brow junctionshould have a natural convexity contour. Thisshape is in part because of the subgaleal fat aswell as the retro-obicularis oculi fat (ROOF) pads.With age, there is loss of volume and descent oftissue. Gunter and Antrobus3 also describe howthe eyebrow and the nasojugal fold should createan oval, with the pupil at the center. If the distanceof the brow to pupil is reduced, then there is browptosis, and if the distance between the pupil andnasojugal fold is increased, then there is midfaceptosis or hypoplasia. In a normal head positionwithprimary gaze, thedistancebetween thecentralupper lidmargins and thepalpebral fold is one-thirdthe distance from the lid margin to the eyebrow. Adecrease in the distance of the eyebrow to the lidmargin indicates brow ptosis, and an increase inthedistance from the fold to the lidmargin indicateseyelid ptosis.4 One can also measure the distance

Fig. 4. Patient with right upper eyelid ptosis.
Aesthetic Surgery of the Orbits and Eyelids 667
between the central upper lid margin and the infe-rior edge of the central eyebrow in a normal gazeposition called the brow upper lid; this distance isnormally 10 mm. One can also measure thedistance between the central inferior eyebrowsand the inferior limbus (called the brow inferiorlimbus distance) in a normal primary gaze; thismeasurement is normally 22mm.5 Another methodfor measuring brow ptosis or asymmetry is touse the ocular asymmetry measuring device(Bausch and Lomb Storz Instruments) designedby Putterman and Chalfin.6
Examination of the Upper Eyelid
When one evaluates the upper eyelid, one shouldlook for excessive skin (dermatochalasia), herni-ated orbital fat, prolapsed lacrimal gland,abnormal eyelid crease, blepharoptosis, andretraction (Fig. 3). Excessive skin of the uppereyelid is easily assessed, and herniated nasaland central fat pads are identified by lifting theskin and pushing the eye. This maneuver inten-sifies the herniation of fat pockets and distin-guishes edema of the eyelid from herniation oforbital fat. The position of the lacrimal gland isidentified by elevating the temporal eyebrowskin; if the gland is prolapsed, one notices theherniated position of the gland. The upper eyelidcrease is identified by elevating the eyebrow andmarking the central crease. One can intensify thecrease by asking the patient to look up anddown from a central gaze position. An upper eyelidcreaser can be used to identify the position of orthe new proposed position of the eyelid crease.The distance from the central upper eyelid marginto the upper eyelid crease is referred to as themargin crease distance.7 This distance ismeasured to be from 8 to 10 mm. A lid ptosisshould be suspected if the distance is decreased(Fig. 4). Also, identifying the upper lid crease
Fig. 3. Female patient with dermatochalasia andherniated orbital fat pads.
allows the surgeon to determine how much skinshould be removed and if a brow-lift procedureneeds to accompany a blepharoplasty.
Identifying ptosis preoperatively saves thesurgeon and patient grief and potential litigationsin the future. There are several methods to accessptosis. One method is by measuring the palpebralfissure width at a normal gaze, which is thedistance from the central lower lid margin to theupper lid margin.7 The normal distance is 10 mmand this measurement is not significantly specificbut can identify ptosis. Margin reflex distance ismeasured by shining a light at the pupils ata normal gaze position and measuring thedistance of the reflected corneal light reflex tothe central upper lid margin.7 This distance isusually between 4 and 4.5 mm. A distance lessthan that measurement determines the amount indistance required to elevate the upper lid duringptosis repair. Upper eyelid ptosis can also be iden-tified by blocking the brow on the examined side,having the patient lift the opposite side, and askingthe patient to look to the extreme down gaze froma normal gaze position.8 If the distance betweenthe lower and upper central lid margin is lessthan 2 mm, then a ptosis should be suspected.Patients with ptosis are not able to lift the upperlid because the forehead muscles are blocked.
Upper eyelid retraction could be a sign of thyroiddisease. A palpebral fissure width test can identifyan excessive distancebetween the eyelids. Promptophthalmologic and endocrine evaluation is rec-ommendedbefore proceeding to elective cosmeticsurgery.
Examination of the Lower Eyelid
The lower eyelid examination should include eval-uation for excessive skin (dermatochalasia), herni-ated orbital fat pads, lid retraction, and laxity(Fig. 5). Excess skin is evaluated by asking the

Fig. 5. (A) Frontal view, patient with bilateral lower lid dermatochalasia, herniated orbital fat pads, lateral lidretraction with laxity, and bilateral upper lid ptosis. (B) Left lateral view, patient with lower lid dermatochalasia,herniated orbital fat pads with inferior descent of lid-cheek junction, malar hypoplasia, and ptosis.
Broujerdi668
patient to look up, and the amount of excess skinis evaluated for either skin resection or laser resur-facing and tightening. The herniated orbital fatpads are evaluated in the nasal, central, andtemporal positions by placing pressure over theeyelid and noting herniation of the fat in each posi-tion. This maneuver distinguishes edema versusherniated fat. The examiner should also considerhypertrophied obicularis oculi muscle.Lower eyelid retraction is evaluatedbyhaving the
patient and examiner at the same eye level andshining a light into the patient’s pupil. The distantfrom the corneal light reflex to the central lower lidmargin is measured. This distance is usually 5.5mm and the lower lid is at the level of the lowerlimbus of the eye or just slightly below it. Anydistance greater or below the lower limbus is anindication for lid retraction and the surgeon shouldbe prepared for reconstruction. This examination isreferred to as the marginal reflex distance 2.9
Lower lid laxity is evaluated with a snap backtest. The lower lid is pinched between the 2 fingersand allowed to snap back into position. The laxity,the time it takes to snap back, and possible ever-sion of the lid are assessed. If there is any indicationof lid laxity, one should consider a concomitantlower lid suspension procedure. The examinershould also assess the laxity of the lateral andmedial canthal tendons by pulling on the canthaltendon; if the complex moves easily and lateral ormedial fissures are rounded off easily, then a can-thal tuck should also be considered as part of thetreatment plan.
Examination of the Midface
The examination of the midface should start witha skeletal evaluation. Hypoplastic maxillary andzygomatic bones should be noted with a negativevector at the lid-cheek junction. If indicated, I
obtain a cone beam computed tomography(CBCT) scanof thepatient to analyze the facial skel-etal pattern and distinguish whether skeletalaugmentation is necessary. The position of theglobe should also be determined with an exoph-thalmometry instrument to distinguish betweena true negative vector or an exophthalmos. Theamount and position of the midfacial fat compart-ments should be evaluated. The surface anatomyof the cheek forms a Y, where the center is the sub-obicularis oculi fat (SOOF). Above the SOOF is thelid-cheek junction formed by the orbital retainingligament. Medial to the SOOF is the nasojugalgroove (tear trough),which is formedby the junctionof the levator labii superioris muscle fibers and thepreseptal orbicularis oculi muscle fibers, with skinand subcutaneous fat overlying it. Recent anatomicstudies by Haddock and colleagues10 have shownthat the tear trough is formed between the presep-tal fibers of pars palpebrarum and pars orbitalis ofthe orbicularis oculi muscle and the levator labiisuperiorismuscle ismuch inferior to the tear trougharea. These investigators also explain that the teartrough deformity is the atrophy of the overlyingskin and subcutaneous fat and attenuation of theorbital retaining ligaments in the valley of the orbi-cularis oculi muscle with bulging of the postseptalorbital nasal fat pads to exacerbate the deformity.Lateral to the SOOF is the palpebral-malar groove,which separates the malar fat pad and SOOF.Continuation of the nasojugal groove into the mid-face forms themidcheek furrow, which is the sepa-ration of the malar fat pad from the nasolabial fatpad. The presence of tear trough deformity withmalar bags and festoons is an indication ofhypoplasia, inferior descent, and separation of themidfacial fat compartments. There is alwaysa combination of volume loss and separation withinferior descent of attached tissue. The tear troughdeformity is classified as class I to III, class I being

Aesthetic Surgery of the Orbits and Eyelids 669
volume loss medially (loss of subcutaneous fat andherniation of nasal fat pad), class II volume lossmedial and centrally (volume loss in SOOF andattenuation of the lid-cheek junction), and class IIIvolume loss medial, central, and laterally (volumeloss in the malar fat pads with inferior descent)with complete orbital hollowing.11 The skin shouldalso be evaluated for signs of aging, including atro-phic skin changes, dyschromia, rhytids, and loss ofskin elasticity (Fig. 6).
The Rest of the Examination
The visual fields, acuity, and ocular motility shouldbe evaluated, as described elsewhere in this issue.The eyes should also be evaluated for tear secre-tion with a Schirmer test. Patients with low secre-tions are prone to postoperative complications.This test is also described elsewhere in this issue.The cornea should be evaluated and a test forBell phenomenon performed. The eyelid is closedtightly by the patient, the examiner pries the lidopen slightly, and the position of the iris is noted.If the iris has not elevated, then the test is abnormaland the patient is prone to postoperative irritationof the eye. Because the patient is not able toelevate the eyeball superiorly and protect it, therisk of postoperative irritation increases.
Photography
The standard photography for periorbital surgery isto obtain a frontal periorbital view in a normal,upward, and downward gaze as well as periorbitallateral and oblique views preoperatively and post-operatively. In addition, I also obtain a full-frontal,basal, bilateral oblique, and lateral views of thepatient preoperatively, 1 week, 1 month, 3 months,and 6 months postoperatively. I also take a three-dimensional (3D) surface image of the patientbefore and after surgery via the 3dMDface system(3dMD, Atlanta, GA).The 3dMDface System
Fig. 6. (A) Frontal view, patient with periorbital hypoplasdeformity, and midface hypoplasia with ptosis. (B) Left la
consists of 6machine vision cameras synchronizedto fire at the same time, within a 1.5-millisecondwindow. 3dMDsystems are based on an advancedsoftware technique called active stereo photo-grammetry, which momentarily projects a uniquelight pattern on the subjectwhile the image is taken.3dMD software then identifies the same uniquepoint frommultiple images and uses simple geom-etry and complex algorithms to calculate the coor-dinates of the point and construct the 3D facialshape in a TSB file format. In certain cases, Icombine DICOM (Digital Imaging andCommunica-tions in Medicine) files from a CBCT study with theTSB files to form a 3D surface image froma 3dMFface system using 3dMDvultus softwareto obtain a true skeletal facial image of a patient.These complete data assist me in preoperativeplanning, and the 3dMDvultus software allows meto perform virtual surgery on both skeletal andsoft tissue components (Fig. 7).
RELEVANT SURGICAL ANATOMY OFPERIORBIT
Detailed orbital anatomy is described elsewhere inthis issue, and only relevant surgical anatomy isdiscussed in this section. The 7 facial skeletalstructures that form the orbital framework (maxilla,zygoma, ethmoid, frontal, lacrimal, palatine, sphe-noid) provide a platform for the attachment of thesoft tissue (Fig. 8). The main sensory nerves ofthe periorbital structures are branches of thetrigeminal nerve (V2, V3) and exit the facial bonesvia foramina, notches, or along the bone to providesensation. The supraorbital nerve exits the orbit viaa notch or foramina on the frontal bone. The supra-trochlear and infratrochlear nerves exit the orbitthrough a notch. The zygomaticofrontal nervesexit the frontal bone via its foramina, and zygoma-ticofacial nerves also exit the zygomatic bone viaits foramina. The infraorbital nerve exits the maxilla
ia, upper and lower lid dermatochalasia, tear troughteral view.

Fig. 7. (A) 3D surface image preoperative frontal view by 3dMDface system, patient with malar and paranasalhypoplasia and a negative vector. (B) 3D surface image fused with 3D computed tomography scan image, beforeleft oblique view. (C) Before left lateral view. (D) Frontal view, patient after malar and paranasal Medpore (PorexSurgical, Stryker) implant. (E) Postoperative left oblique view. (F) Postoperative left later view.
Broujerdi670
via its foramina. The motor nerve supply is mostlythrough the facial nerve and its branches (zygo-matic and frontal).On the frontal bone above the supraorbital ridge
is the orbital ligamentous adhesion, where thedeep galea aponeurotica adheres to the bone.This galea invests the frontalis with the procerus,depressor supraciliary, and corrugator muscles.Just above this ligamentous attachment and belowthe galea, the galeal fat pad exits, which allows forthe smooth gliding of the muscles of facial expres-sion. As we age, this fat pad atrophies and createsa flatness and droop to the appearance of the
forehead. At the temporal crest, the orbital liga-mentous adhesions become the temporal ligamen-tous adhesions and run superior-posterior tobecome the superior temporal septum, where thetemporalis muscle and its fascia insert. Over thesupraorbital ridge, the orbicularis retaining liga-ment exits where the orbital septum attaches toand it assists in the attachment of the obicularisoculi muscle. The preseptal fat in the lateral browarea between the orbital septum and the obicularisoculi is called the retro-obicularis oculi fat. This fatlayer provides a lateral fullness to the brow, andwith aging, the fat pad loses its volume and assists

Fig. 9. Orbital anatomy, midsagittal section, uppereyelid.
Fig. 8. Orbital anatomy, orbital bones.
Aesthetic Surgery of the Orbits and Eyelids 671
in the dropping appearance of the brow. The obicu-laris retaining ligament also runs along the lateralorbital ridge and down to the inferior orbital rim.The lateral attachments are thick and are knownas the lateral brow thickening and lateral orbitalthickening. On the internal aspect of the orbitalrim over the lateral orbital thickening is the site ofattachment for the lateral canthal ligament. At thelateral brow area, the temporalis muscle with itsdeep fascia travels through the infratemporalfossa, and just above this, the sentinel vein piercesthrough the galea aponeurotic layer into the looseareolar fat and crosses over to the supraorbitalridge. Above the loose areolar tissue, the partialtemporal fascia (superficial temporal fascia)houses the frontal branches of the facial nerve.The partial temporal fascia is also in continuationwith the superficial musculoaponeurotic system(SMAS) layer in the face.
At the midfacial level just below the orbital re-taining ligament, the zygomatic cutaneous liga-ment originates from the zygomatic bone andhas attachments on the obicularis oculi muscleand on to the subcutaneous structures. Betweenthese 2 ligaments, the SOOF resides, and aboveit are the pars orbitalis fibers of the obicularis oculimuscle. Between the SOOF and the preperiostealfat and periosteum is the potential prezygomaticspace. Just below the space laterally, the zygo-matic major and zygomatic minor muscles origi-nate and medially the levator labii superiorisoriginates. These groups of muscles are deeperto the obicularis oculi muscle. Just inferior to theSOOF and superficial to the muscles are the malarfat pad medially and lateral-inferiorly the nasola-bial fat pad.
The surgical zones of the eye and periorbit aredivided into zones 0 to 6: zone 0 is the globe andall structures behind the orbital septum; zones Iand II are the upper and lower eyelid and any struc-ture to the orbital septum; zones III and IV are the
medial and lateral canthus and all structures poste-rior to the ligaments; zone V is all the contagiousstructures. The aperture of the eyelids measures28 to 30mmhorizontally and 10 to 12mmvertically.Both the horizontal and vertical aperture candecrease with aging because of laxity of theaponeurotic, canthal, tarsal, and retinacularattachments. The upper lid margin rests 2 mmbelow the upper limbus of the iris, and the lowerlid margin rests at the lower limbus of the iris. Thelateral commissure of the eyelid is positioned 2mm higher than the medial side; with aging, thereis definitive laxity of the canthal attachment appa-ratus and there are changes in the lateral commis-sure of the lid. The periorbital skin is thin, withminimal subcutaneous fat; this predisposes theskin to wrinkling, stretching, with age. The obicula-ris oculi muscle is a sphincter muscle divides into2: the pars palpebrarum and pars orbitalis. Theobicularis oculi muscle is innervated on its deepsurface by the zygomatic branches of the facialnerve. The pars palpebrarum is further dividedinto the preseptal and pretarsal sections. Thepars orbitalis is attached circumferential to theorbital retaining ligament superiorly and inferiorlyand laterally to the lateral thickening ligaments.Inferiorly, this attachment is known as the lid-cheek junction. Medially the muscle fibers connectdirectly to the orbital wall and canthal tendon ina complex anatomic arrangement linked to thelacrimal sac.
The upper eyelid fold is created by the dermalattachment of the levator aponeurotic extensionsthrough the obicularis oculi muscle (Fig. 9). Theseattachments start at the lid margin and terminateabove the superior tarsal plate, which forms the

Broujerdi672
supratarsal fold. The supratarsal plate is about 10mm long and is suspended by the lateral andmedial canthal tendons. Posteriorly, the supratar-sal plate is suspended by the Whitnall ligament inthe orbit. The lateral and medial extensions ofthe Whitnall ligament are known as the medialand lateral horns, which connect to the canthaltendons. Posterior to the Whitnall ligament andattached to the levator apo neurosis is the levatorpalpebral superioris muscle, which is innervatedby the branches of the oculometer nerve. Justbeneath the levator aponeurosis is the Mullermuscle, which also attaches to the posteriorborder of the supratarsal plate. This muscle isinnervated by the sympathetic nervous systemtraveling with arterial system. The superior septumorbitale at its inferior leg attaches to the levatoraponeurosis at the superior tarsal plate junctionand at its superior leg attaches to the orbital peri-osteum and arcus marginalis. Posterior to theseptum are the fat pads. Medially, the nasal fatpad (pale yellow) is divided from the central fatpad (rich yellow) by the superior trochlear muscle,which rotates around the pulley attached to theorbital roof by the trochlea. There is no lateral fatpad. This space is occupied by the lacrimal gland.The lower lid has 3 main layers: the anterior
lamella is formed by the skin and obicularis oculimuscle (Fig. 10); the middle lamella is formed bythe inferior tarsal plate (which is 2–5 mm high), theinferior orbital septum, and the orbital fat pads;the posterior lamella is formed by the capsulopal-pebral fascia, which is an extension of the inferiorrectus muscle, the counterpart to the levatoraponeurosis and the palpebral conjunctiva. Thecapsulopalpebral fascia splints around the inferioroblique muscle and attaches to the Lockwood
Fig. 10. Orbital anatomy, midsagittal section, lowereyelid.
ligament, then fibers ascend forward to attach tothe inferior tarsal plate and septum orbitally. Thisfascia has the same function as the upper lidlevator. The orbital septum joins the orbital rim peri-osteum and forms the arcusmarginalis. There are 3distinctive fat pads in the lower lid. The medial fatpad isdivided from the central fat padby the inferiorobliquemuscle and the central fat pad is separatedfrom the lateral fat pad by the capsulopalpebralfascia.The vascular supply to the periorbital structures
is mostly derived from the internal carotid systemvia the ophthalmic artery and partly by the externalcarotid system via the infraorbital, angular, andsuperficial temporal artery. The ophthalmic arterygives off the lacrimal, supraorbital, and supratro-chlear and dorsal nasal arteries. The upper andlower eyelids are supplied via the lateral palpebralartery (a branch of the lacrimal artery) and medialpalpebral artery (a branch of the ophthalmicartery). The lateral and medial palpebral arteriesanastamose to form the marginal arcade artery.The venous system parallels the arterial bloodsupply. The lymphatic drainage of the periorbitalis in the inferior lateral direction to the preauricular,parotid, and submandibular lymph nodes.
THE AGING PERIORBIT
The effects of facial aging are dependent not onlyon gravity but also on both intrinsic (gender,genetic) and extrinsic (environmental) factors.The intrinsic component is a complex dynamicchange that occurs over time in the hard tissue(bone, teeth) and soft tissue (eg, skin, ligaments,muscle, fat) of the face. At the skeletal level, thereis a reduction of facial height and loss of bonyprominences (convexity to concavity), mostmarked in themaxilla andmandible; this is stronglycorrelated with loss of teeth.12–15 There is alsoa decrease in soft tissue thickness with age.16
There are significant changes to the facial muscleswith aging; morphologically, the muscle thins out,and histologically, there is an atrophy of musclefibers and increase in intracellular matrix.17 Arecent morphologic study of the upper pretarsalobicularis oculi muscle18 revealed that the musclelayer remained intact with aging; this be isolated tothe eyelids. The facial fat compartments also gothrough an inferior migration and volume losswith the aging process.19 The retaining fibers andligaments of the face become attenuated and laxerwith the aging process as well.20 Histomorpho-metric analysis has revealed statistically signifi-cant thinning of the cutis. Elastic and collagenfibers in the cutis undergo degeneration processesduring aging.21

Aesthetic Surgery of the Orbits and Eyelids 673
The process of aging is interdependent of allcomponents and affects the tissues at all levels.The process reveals the separate components ofthe periorbital structures with aging such as thebrow ptosis, blepharoptosis, lateral commissuredroop, lid-cheek junction, periorbital hallowing,tear trough deformity, malar bags, and nasolabialfold (Fig. 11).
The Forehead and Brow
The forehead forms redundant tissue with atrophicchanges in the skin. The anterior hairline recedes.Deep furrows and rhytids form in horizontal andvertical directions. The subgaleal and ROOF fatpads lose their volume; this shows up as concavityin the central midforehead area. The ROOF alsodescends inferiorly because of loss of attenuationof the retaining ligaments. This change createsa brow ptosis, with loss of convexity of the supra-brow ridge and lateral hooding.
In the temporal area, the temporal fat pads losesits volume and creates a hollowing shape to thelateral forehead area. The bony ridges of thefrontal bones undergo remodeling, with loss ofconvexity and formation of concavities withatrophy and thinning of the muscles.
The Upper Eyelid
The supratarsal fold loses its definition. If the fatpads are herniated, they stretch the skin andcreate dermatochalasia and push the lid fold infe-riorly. If there is excessive atrophy of the fat pads,it pushes back the lid fold superiorly and gives thepatient a hollow look. In the case of senile ptosis,the tarsal fold does move superiorly. The lacrimalgland can droop and create a ptotic look to thelateral lid-brow junction.
The Lower Eyelid
There is an atrophic change to the lower eyelidskin, with thinning of the dermis with rhytid forma-tions and dyschromia. Both the lateral and medial
Fig. 11. (A) The aging face, frontal view. (B) The aging fa
canthal attachments become lax and stretch outwith a decrease in the eyelid fissures, rounding,and inferior displacement of the lateral canthus.The tarsal plates become lax and create a liddroop, with entropion and occasionally ectropion.Herniated fat pads can create puffiness to thelower lids with dermatochalasia. Also fat padatrophy can create hollowness to the periorbital,with retraction of the globe into the socket andlid laxity. The orbital retaining ligaments becomeattenuated and pull the lid-cheek junction inferi-orly. This situation increases the distance betweenthe lid margin and the lid-cheek junction, giving theappearance of tear trough deformity.
The Midface
Theagingprocessworks at all different layers of themidfacial tissues, starting with bony changes in themaxilla and zygoma, with a decrease in verticalheight and loss of bony prominence in themidface.The retaining ligaments become attenuated andthe fat pads atrophy. As a consequence, there isa vertical droop in the midfacial tissue and loss ofvolume and separation of midface fat pads, withformation of nasojugal, palpebral-malar, and naso-labial grooves. The buccal fat pad also goesthrough the same transformation, which leads clin-ically to the formation of frowns and marionettelines. The muscles of facial expression alsobecome attenuated and stretched with the agingprocess, leading to downturning of the lip commis-sure and elongation of the upper lip with atrophicand hypoplastic changes.
THE BROW AND FOREHEAD IN PERIORBITALREJUVENATION
The evaluation of the forehead unit was describedearlier. There are multiple surgical options for browand forehead rejuvenation in combination witheyelid procedures for obtaining an aestheticallynatural and youthful appearance to the periorbitalstructure. According to the literature,20 there is
ce, right oblique view.

Broujerdi674
no 1 single procedure favored for brow and fore-head rejuvenation. In general, patients with browptosis with a low hairline are candidates forcoronal or endoscopic brow lift and patients witha high hairline or prominent forehead are candi-dates for either anterior hairline, limited incision,or direct or transblepharoplasty (palpebral). Eachtechnique has its indications, with its advantagesand disadvantages, with no one technique supe-rior to the others.20 In general, open proceduresallow for excision of redundant skin, whereas theendoscopic technique allows for repositioning ofthe redundant tissue. The selection of an appro-priate technique is dependent on an accuratediagnosis, the patient’s expectations, and thesurgeon’s skills.With aging, not only is there a descent of the fore-
head and brow structures but also a loss of volumein the forehead and brow is apparent. The foreheadloses its soft tissue convexity, with development ofdeep furrows, and at the forehead-brow-lid junc-tion the loss of volume and convexity leads tobrow ptosis and an aged look. One should alsoconsider volume replenishment with autologousfat transfer with brow-lift procedures. This proce-dure restores the youthful and natural appearanceto both forehead and brow.
Coronal Brow Lift
This technique has made a comeback after itlost popularity with the introduction of theendoscopic approach. The open approach al-lows for excision of redundant tissue and im-proved longevity.
Advantages:
1. Direct access to anatomic structures for resec-tion and anchorage
2. Camouflage of scar in the hairline3. Direct excision of redundant tissue4. Longevity of the lift.
Disadvantages:
1. Long scar2. Risk of alopecia3. Elevation of the anterior hairline4. Paresthesia of forehead and scalp.
The frontal incision is placed 5 cm posterior andparallel to the anterior hairline in a beveled direc-tion to allow for hair growth into the scar. Thetemporal incision is designed in a zigzag fashion,starting with the first zigzag at the top of the supe-rior sulcus of the ear, moving in an anterior direc-tion and the third moving in an anterior directionand meeting the frontal incisions. This designallows for better camouflage and parting of the
hair when wet. The temporal dissection is at thelevel of the glistening layer of the deep temporalfascia with release of the temporal and orbital liga-mentous attachments as well as the lateral browand orbital thickening ligaments. Preserving thesentinel vein reduces postoperative swelling andbleeding. This dissection preserves the fontalbranches of the facial nerve. Interiorly, the dissec-tion is in a subgaleal plane until 1 to 2 cm above thesupraorbital rim, then it sharply dissects to a sub-periosteal plane. With subperiosteal dissectionrelease, the arcus marginalis with preservationand release of the supraorbital neurovascularbundle forms its foramina or notch. The galea isscored in a horizontal direction. The galea is metic-ulously incised and the muscle is partially resectedwithout injuring the neurovascular bundle. Thescalp flap is elevated and secured temporallywith staples to verify the position of the brow,and the excess scalp is marked and excised. Irecommend securing the temporal-parietal fasciato the deep temporal fascia in the temporal regionwith permanent sutures before layered closure ofthe scalp flap. I also advocate the use of drainsand compression dressing to prevent hematomaformation.
Anterior Hairline Brow Lift
The major indication for this technique is a long(greater than 6–7 cm) forehead. The incision isplaced along the hairline in a beveled fashionto allow hair growth into the scar line. Laterally,the incision is curved in to the temporal scalp.The remainder of the dissection is similar tothe coronal brow lift. The excess skin is excisedin a beveled fashion parallel to the initialincision.
Advantages:
1. Direct access to anatomic structures for resec-tion and anchorage
2. Camouflage of scar in the hairline3. Direct excision of redundant tissue4. Longevity of the lift5. Prevents elevation of the forehead.
Disadvantages:
1. Long scar2. Risk of alopecia3. Scar along the anterior hairline4. Paresthesia of forehead and scalp.
Limited Incision Brow Lift
The limited incision brow lift is indicated for correc-tion of brow ptosis without lifting the central fore-head. The incisions are placed 2 to 3 cm behind

Aesthetic Surgery of the Orbits and Eyelids 675
the temporal hairline perpendicular to the vector ofpull. The incisions are 3 to 5 cm as indicated. Thedissection and release of attaching tissue in thetemporal, lateral forehead, and periorbital regionare similar to the coronal lift. The vector of lift isin a superior-posterior direction, and redundanttissue is excised in full thickness. Permanentsutures are placed between superficial fasciaand the deep fascia for fixation and anchorage.Scalp closure is performed in a layered fashion(Fig. 12).
Advantages:
1. Direct access to anatomic structures foranchorage
2. May be combined with upper blepharoplastyand transpalpebral resection of the corrugators
3. Avoids injury to the deep division supraorbitalnerve
4. Elevation of the lateral brow segment5. No elevation of the forehead.
Disadvantages:
1. Limited access to the forehead muscles2. Risk of alopecia along the scar3. Difficulty in addressing deep forehead rhytids.
Endoscopic Brow Lift
The endoscopic brow lift has the ability to lift thebrow, reposition the forehead, and address thedeep forehead rhytids and minimize the complica-tions of scalp paresthesia, alopecia, and a longscar. There is a need for additional endoscopicinstrumentation (4 mm, 30� endoscope camera)and ability to create an optical cavity with the peri-orbital, forehead, and lateral brow structures. Theincisions are 1 to 2 cm long in the hair-bearing scalpand 1 to 2 cm behind the hairline. A total of 5 inci-sions are recommended: 1 central, 2 lateral, and2 temporal. The dissection is similar to the coronal
Fig. 12. (A) Preoperative frontal view, patient with age-reldermatochalasia with brow ptosis. (B) Postoperative frontupper blepharoplasty, autologous fat transfer to the perresurfacing.
lift, with use of endoscopic instrumentation andcamera to create a surgical cavity and releaseadhering tissues. The vector of pull is in a supe-rior-posterior and medial direction. The brow andforehead lift anchorage is provided by screw orcortical tunneling at 45� and suture fixation of thesuperficial fascia to the screw device as well assuture fixation of the superficial fascia to the deepfascia laterally in the temporal region for optimalresults.22 Drilling of the frontal bone should notexceed a depth of more then 3 to 4 mm becauseof risk of penetration of the inferior cortical layerand dural tear.23 Mitek anchors (2 mm depth) withsuture fixation can also be used. The periosteumneeds 6 to 12 weeks for adhering back to thebone surface, and the fixation technique mustprovide anchorage until the periosteum fusesback to the bone.21 Screw fixation is either by re-sorbable material or removable titanium screwsthat have holes to secure the superficial fascia tothe screw for anchorage. The fixation screws canbe removed in the office postoperatively with localanesthesia. Other types of resorbable screw havefixation prongs to the scalp, for example Endotine(Coapt System, Palo Alta, CA), which allows forrapid anchorage without suture material. Thisdevice has been reported to be palpable for up to15months and is recommended for patientswhosescalp is thicker than 5 to 6 mm (Fig. 13).24–26
Advantages:
1. Direct visualization of forehead muscle2. Minimal incision3. Less chance for forehead and scalp pares-
thesia.
Disadvantages:
1. Technical learning curve2. Additional cost3. Need for fixation onto scalp.
ated skin changes, periorbital hypoplasia, upper eyelidal view, patient status after limited incision brow lift,iorbital soft tissue and erbium fractionated laser skin

Fig. 13. (A) Preoperative frontal view, patient with brow ptosis. (B) Postoperative frontal view, patient statusafter endoscopic brow lift and sliding genioplasty.
Broujerdi676
Direct Brow Lift
The ideal candidate for a direct brow lift is a patientwith deep forehead rhytids or male pattern hairloss or receding hairline. The incision is placed inthe deep furrows of the forehead or superiorbrow margin. The dissection enters the subgalealplane to release the attaching periorbital tissuesand allow access to the forehead musculature.The forehead flap is redraped in a desired vector,redundant tissue is excised from the inferior flap,and the forehead flap is anchored with permanentsutures to the superior periosteum. The incisionand dissection can be limited to the brow regiononly for brow elevation.
Advantages:
1. Ease of access to the brow structures and fore-head muscles
2. Correction of brow asymmetry.
Disadvantages:
1. Visible scaring2. Paresthesia of forehead and scalp.
Transpalpebral Brow Lift
Transpalpebral brow lift is performed through anupper eyelid blepharoplasty incision. A blepharo-plasty may also be performed at the same time.The ideal candidate is a patient with high orreceding hairline or who is balding.27,28 This tech-nique has been described in patients with recur-rent brow ptosis or asymmetry after a brow-liftprocedure. After the blepharoplasty incision ismade, the obicularis oculi muscle is incised trans-versally and the dissection is in a submuscularplane carried in a superior direction above thesupraorbital rim and lateral to the neurovascularbundle. Medially, the corrugators and procerusare excised. Browpexy is performed by fixatingthe undersurface of the obicularis oculi muscle to
the periosteum with resorbable sutures in a des-ired vector. Care should be taken to preventskin dimpling at the site of suture fixation. Meticu-lous hemostasis is required with this technique aswell.
Advantages:
1. Ease of access to the brow structures and fore-head muscles
2. Correction of brow asymmetry3. Short operating time.
Disadvantages:
1. Highly vascularized surgical field2. Paresthesia of forehead and scalp.
Postoperative Care and Complications
Scalp and hairline incisions are dressed with anti-biotic ointment. If drains are used, they can beremoved in 24 to 72 hours postoperatively. Papertape is used on the forehead and lateral browarea to minimize edema, with a head wrap, whichcan be removed in 72 hours. Patients should sleepwith their bedhead elevated for a minimum of 2weeks. Patients should be given artificial tearsand ophthalmic ointment in case dry eyes or la-gophthalmos develops. Ice packs over the fore-head and eyes should be used routinely toreduce postoperative edema. Patient should notparticipate in strenuous activity for the first 2weeks. Any suture removal is performed after 7days. The most common complications afterbrow lift are;
� Alopecia� Dissatisfaction� Scarring� Asymmetry� Sensory loss� Infection

Fig. 14. Markings for upper blepharoplasty.
Aesthetic Surgery of the Orbits and Eyelids 677
� Lagophthalmos� Motor deficiency� Abnormal contour� Hematoma
REJUVENATION OF THE UPPER EYELID
The key to a successful surgical outcome is inpreoperative diagnosis and planning your surgicaltechnique. The natural youthful appearance of theupper eyelid was described earlier. The keycomponents are:
1. Fullness, volume, and convexity of the lid-browjunction
2. The upper eyelid crease is more often in a lowposition
Routinely ask your patients to bring a photo-graph of themselves at a youthful stage that showsthe periorbital area for comparison. Evaluate yourpatients for brow ptosis caused by either volumeloss or a combination of volume loss and descentof soft tissue attachment. These patients developflatness to the lid-brow junction or lateral hooding.This flatness can be addressed with brow volumi-zation or lift at the same time as the upper bleph-aroplasty procedure. Look for abnormally highupper lid crease and ptosis. A patient with highupper lid crease has either had aggressive muscleand fat resection upper eyelid surgery or hascongenital or senile ptosis. A patient with high lidcrease position without ptosis needs volumizationand lowering of the lid crease. Patients with ptosisexcessively use their frontalis muscle and developasymmetry of the brow position, forehead rhytids,and deep furrows. Evaluate your patient forconcomitant blepharoplasty and levator aponeu-rosis repair or Muller muscle-conjunctival resec-tion. A phenylephrine test with 2.5% strengthidentifies patients who benefit form Muller muscleresection. A levator suspension is usually per-formed under local anesthesia or intravenous (IV)sedation so that the patient can open and closethe eyelid for repositioning of the lid during ptosisrepair. If ptosis is not diagnosed in the initial eval-uation, after eyelid surgery, ptosis becomesevident and can lead to an unhappy patient.Consult your ophthalmologist for a second opinionand work with an oculoplastic surgeon as needed.Description of ptosis repair is beyond the scope ofthis article, but its recognition is vital for propersurgical planning and achieving a natural youthfulappearance after surgery.
There is a paradigm shift in aestheticoculoplastic surgery in preservation of muscleand volumization. Fagien29 describes preservingthe preseptal obicularis oculi muscle during upper
blepharoplasty by creating an accordion effect orbulking of the muscle during skin closure to createan improved supratarsal and lid-brow junctionvolume. Demasceno and colleagues30 have foundthat muscle resection causes more postoperativesymptoms and presents worse initial aestheticoutcome. However, the aesthetic outcome is thesame when the preseptal orbicularis oculi muscleis excised or preserved. There is also a lack ofconsensus in the literature regarding preseptalobicularis oculi muscle resection during upperblepharoplasty, but most surgeons preservemuscle.28
Upper Blepharoplasty
Proper skin marking is essential for a goodoutcome. The inferior margin is marked at about8 to 10 mm centrally, 6 to 8 mm medially (nasal),and 7 to 9 mm laterally from the lid margin paralle-ling the skin crease. The inferior margin should liebetween the medial extent of the punctum andlateral extent of the lateral commissure of theeyelid. Excess skin is pinched with a forceps until2 mm lagophthalmos is seen and then markedsuperiorly. The superior margin is parallel to thearch of the inferior extent of the brow, medially itcurves inferiorly to meet the inferior margin, andlaterally it extends out about 1 cm from the lateralcommissure of the eyelid. The inferior and superiormargins are connected with a curvilinear linemark laterally (Fig. 14). Sclera shields areused to protect the globe, and 1% xylocaine with1/100,000 epinephrine is infiltrated with a 32-gauge needle for anesthesia and hemostasis. Afterwaiting 10 minutes for hemostasis, incisions are

Broujerdi678
made with a 15-c blade. Hemostasis is achievedwith electrocautery during each step throughoutthe procedure. The marked skin is excised viaa de-epithelialization technique with a sharp blade.The excised skin should be saved for comparison.If preseptal obicularis oculi muscle excision isplanned, Westcott scissors are used to removea 1-mm-thick strip of muscle to expose the orbitalseptum. Digital pressure is placed over the orbit toidentify the nasal and central fat pads. If muscleresection is not planned, Westcott scissors areused to make a buttonhole through the muscleand septum over the fat pads (Fig. 15). Each fatpad is teased out, clamped with a forceps,excised, and then cauterized. The fat should besaved for comparison with the contralateral side.Make sure that you have achieved meticuloushemostasis before moving to the next step. Next,the skin flaps are approximated with multiple inter-rupted 6-0 fast absorbing gut suture at high-tension areas. The skin is closed with a 6-0 nylonsuture running in subcuticular fashion, with theends sticking out for removal in 1 week (Fig. 16).
Revision Upper Blepharoplasty
Most patients who present for revision blepharo-plasty are unhappy with their results for one ofthe following reasons:
1. Loss of periorbital volume with hollowing of theupper eyelid sulcus
2. High orbital lid crease3. Dermatochalasia4. Hypopigmentation of scar with marked transi-
tion between the upper lid and darker thick sub-brow skin.
Review operative records and photographs aspart of your initial evaluation of the patient. Haveyour patient bring a photograph of them ata younger age as well. Evaluate your patient for
Fig. 15. Herniated nasal fat pad after gentle push onthe globe.
brow ptosis, volume loss, and blepharoptosis.Have your ophthalmologist perform a routine eyeexamination and rule out ptosis of the lids. Bewatchful of dry eye syndrome after surgery. Thegoals of revision blepharoplasty should includethe following (Fig. 17):
1. Autologous fat transfer to the brow to volumizethe lid-brow junction
2. Lowering of the lid crease by marking the infe-rior margin at about 8 mm from the lid margin
3. Minimal to no skin excision centrally and medi-ally; skin excision mostly laterally to elevate thelateral hooding
4. Preserving preseptal obicularis oculi muscleand creating a bulking effect with skin closure
5. Autologous fat transfer to the nasal and centralpreseptal area as needed
6. Laser skin resurfacing or chemical peel of thesubbrow skin after surgery can assist insmoothening the transition zone.
Asian Eyelid Surgery
The first description of Asian eyelid surgery datesback to the late nineteenth century in Japan byMikamo, who used conjunctival-dermal sutureligation to create a supratarsal double eyelidfold.31 By the early twentieth century, in Japanafter World War I, Marou32 described the first inci-sional Asian eyelid procedure. After World War II,in 1955, Millard’s article subtitled “Oriental to occi-dental” coined the term “Westernization of theAsian eyelid”.33 Sayoc and Fernandez in the1960s independently described suturing thedermis of the superior skin flap to the tarsal plate;Flowers later modified this technique and it hasbecome a widely accepted and published tech-nique for Asian eyelid surgery.34–36
The Asian eyelid blepharoplasty is not to west-ernize the Asian eye but to beautify oneself, havethe ability to wear eye makeup without smudgingand also to have aesthetically bigger eyes. TheAsian cranium is a brachiocephalic to mesoce-phalic type, with flat and broad midface featureswith shallow orbits. These features give the eyesa puffy appearance compared with Whites.37 Themajor anatomic difference between Asians’ andWhites’ upper eyelids are (Fig. 18A);
1. Point of fusion of the levator aponeurosis withorbital septum just above the tarsal palate inAsians as opposed to 5 to 10 mm above thetarsal plate in Whites38
2. Excessive orbital fat with distribution of the pre-aponeurotic fat compartment hanging over thefusion point of the aponeurosis and the septum

Fig. 16. (A) Preoperative frontal view, patient with dermatochalasia of the upper eyelid with herniated orbital fatpads. (B) Preoperative left lateral view. (C) Postoperative frontal view, patient status after upper blepharoplasty.(D) Postoperative left lateral view.
Fig. 17. (A) Preoperative frontal view, patient status after upper blepharoplasty with recurrent dermatochalasia.(B) Preoperative view, left lateral view. (C) Postoperative frontal view, patient status after revision upper bleph-aroplasty and cell-assisted fat transfer. (D) Postoperative left lateral view.
Aesthetic Surgery of the Orbits and Eyelids 679

Fig. 18. (A) Midsagittal section of Asian upper eyelid with no crease. The orbital septum is not fused to thelevator aponeurosis above the tarsal plate. (B) Medial epicanthoplasty as described by Flowers.36
Broujerdi680
3. Lack of fibrous attachments across the levatoraponeurosis to the orbicularis oculi and thedermis of the eyelid
4. Excessive and laxity of the upper eyelid skincaused by overhanging of the preaponeuroticfat over the fusion point
5. Medial epicanthal folds.
The Asian eyelid and periorbita have beendescribed as double eyelid folds, no eyelid fold,medial epicanthal folds, lateral hooding, or havinghigh medial brows. The Asian medial epicanthalfolds have been classified into 4 categories byFlowers 39: type I, in which the medial canthus isexposed; type II, in which the medial canthusand fold form the same line; type III, in which thecanthal fold covers the medial canthuscompletely; and type IV or pseudo I, in which theeyelid fold completely covers the lid margin, anda tight band of skin covers the medial corner.Flowers described a modified version of the V-Wmedial epicanthoplasty by Ochida40 for thecorrection of the Asian medial epicanthal folds(see Fig. 18B). There are other description of Z-plasty or Y-V-plasty in the literature as well.41,42
In the preoperative evaluation, pay close attentionto the position of the medial brow in patients withblepharoptosis. It is common for Asian patients
with eyelid ptosis to develop a persistent medialbrow elevation and lateral brow ptosis. This char-acteristic gives the appearance of a straightbrow as opposed to an arched brow. A standardAsian blepharoplasty without correction of theeyelid ptosis, lateral brow ptosis with brow lift,and release of the medial insertions of the frontalismuscle leads to an unaesthetic outcome and anunhappy patient.The goals in Asian eyelid surgery are outlined as
follows (Fig. 19):
1. Create an upper eyelid crease that is lower inposition relative to Whites’
2. Correction of the medial epicanthal canopy3. Create a high arched lateral brow relative to the
medial brow4. Removal of excessive skin and fat.
The steps in Asian blepharoplasty are describedas follows:
1. Skin markings in a lazy S-shape, the tip downmedially and tip up laterally, vertical height cen-trally at 2 mm, the inferior margin of the markingat the level of the superior edge of the tarsalplate centrally
2. Skin excision with 2 to 3 mm of the pretarsalobicularis oculi muscle

Fig. 19. (A) Preoperative 3D frontal view, Asian upper eyelid with medial epicanthal fold, malar, and mandibularangle hyperplasia. (B) Preoperative 3D fused left oblique view. (C) Preoperative 3D left lateral view. (D) Preoper-ative frontal view. (E) Postoperative frontal view, patient status after upper Asian blepharoplasty with medial ep-icanthoplasty, Malar and mandibular angle reduction. (F) Postoperative 3D frontal view. (G) Postoperative 3Dfused left oblique view. (H) Postoperative 3D left lateral view.
Aesthetic Surgery of the Orbits and Eyelids 681

Broujerdi682
3. Opening of the orbital septum in a horizontalfashion with excision of the preaponeurotic fat
4. Suturing of the dermis of superior margin to thelevator aponeurosis and then to the dermis ofthe inferior margin
5. Skin closure.
Postoperative Care and Complications
Cold compresses are applied with a saline-soakedgauze and ice over the gauze for the first 48 hourson and off. This practice reduces the postoperativeedema. Make sure the patient is able to count theirfingers and is not complaining of severe pain, whichare the signs for retrobulbar hemorrhage. If a patientis diagnosed with retrobulbar hematoma, a bedsideopeningof the incision shouldbeperformed immedi-ately, diuresis is initiatedwithmanitol, and IV steroidsstarted to reduce edema and retinal and optic nervedamage. An emergent ophthalmologic consultationis required, and the patient should be taken to theoperating room emergently for exploration andcontrol of bleeding. If patients complain of dryeyes, initiate artificial tears as needed throughoutthe day and ophthalmic ointment during sleep.Patientsmay initially have lagophthalmos,withexpo-sure keratitis. Patients should sleep with the head oftheirbedelevatedandshouldnotparticipate instren-uous activity for the first 2weeks. Any suture removalis performed after 7 days. Antibiotic ointment overthe eyelid incisions should be avoided because ofpossibility of granuloma formation. Reading shouldbe minimized to no more than 5 to 10 minutes everyhour to reduce eye strain and sclera edema forma-tion.Other complications includewounddehiscenceor infection, temporary eyelash eversion, and epithe-lial suture cyst formation.
REJUVENATION OF THE LOWER EYELID
In evaluating patients for lower lid blepharoplasty,you should also assess the position of the lowerlids, degree of laxity of the lower lids, the positionof the lid-cheek junction, and volume of midfacialtissue. There are multiple surgical approaches tothe rejuvenation of the lower eyelid, including thetransconjunctival or supraciliary approach anda combination as described by Fagien43 with orwithout addressing the lateral suspension of thelower eyelids and midfacial tissue. The bestapproach is dependent on the effects of aging onthe periorbital tissue and the surgeon’s technicalability. Lateral canthal dystopia can be correctedwith either canthopexy for mild to moderatedystopia and release of the canthal attachmentwith canthoplasty for moderate to severedystopia.44,45 Themaingoals in lower eyelid rejuve-nation are:
1. Restore the horizontal length of the eyelidfissure
2. The position of the lower lid is restored at thelower limbus or just below it
3. The lateral canthal attachment is higher thenthe medial canthal attachment
4. There is a smooth transition between lower lidand cheek
5. The lid-cheek junction is elevated and thecheek develops a natural convexity.
Transconjunctival Approach
With the transconjunctival technique, the surgeoncan address the herniated fat pads, resuspensionof the lateral canthal tendon, excision of the lateralobicularis oculi muscle, elevation of the midfacialtissue, and restoration of the lower lid height witha graft.After administration of 1% xylocaine with 1/
100,000 epinephrine and waiting for 10 minutesfor both hemostasis and anesthesia, a transcon-junctival incision is made in the palpebral conjunc-tiva halfway between the fornix and inferior tarsalplate with a Colorado needle. The dissectionshould carry through the capsulopalpebral fasciaand be retracted superiorly. Next, the fat pads areidentified with digital pressure. The orbital septumis opened directly over each fat pad with Westcottscissors, and the nasal, central, and temporal fatpads are teased out, clamped, excised, andcauterized. Care should be taken not to injure theinferior oblique muscle, which separates the nasaland central fat pads. The amount of excised fatdiffers in each patient and the surgeon shouldsave each fat pad for comparison with the contra-lateral side. Also, the excised fat pads can beused as autogenous fat transfer to the SOOF ortear trough area, with suture fixation or insertioninto an elevated pocket.46,47 Hemostasis ismeticu-lously checked and the palpebral conjunctiva maybe closed with a fat-absorbing gut suture, with theknots placed internally so as not to irritate thecornea (Fig. 20).
Canthoplasty
If a lateral canthal suspension is necessary as partof the lower blepharoplasty, a canthopexy or can-thoplasty can be performed in conjunction with thetransconjunctival approach. The canthopexy isdiscussed later with the subciliary and combina-tion approach. A canthoplasty is performed byreleasing the lateral canthal thickening attachmentwith a lateral canthotomy. A 0.8-cm to 1.0-cm inci-sion is made in the lateral canthus and the skinflaps are elevated. Westcott scissors are used to

Fig. 20. (A) Preoperative frontal view, patient with upper and lower dermatochalasia and brow ptosis. (B) Post-operative frontal view, patient status after upper and lower blepharoplasty, limited incision brow lift and endo-nasal rhinoplasty.
Aesthetic Surgery of the Orbits and Eyelids 683
sever the lateral canthus. The lateral retainingligament is exposed for 0.5 to 1 mm by excisingthe conjunctival and skin epithelium dependingon how lax and droopy the lower lid is. The lateralobicularis oculi muscle is incised elliptically,exposing the lateral orbital periosteum. A 4-0 polypropylene suture is used for a 3-point fixa-tion from the inferior to the superior lateral
Fig. 21. (A) Preoperative frontal view, patient with upperlower lid laxity, brow ptosis, midfacial hypoplasia, and ptosfrontal view, patient status after upper blepharoplasty, locanthoplasty, endoscopic brow and midface lift with autol
retaining ligament then to the edge of the lateralorbital periosteum in a more posterior superiorposition relative to its insertion. Make sure yourknot is buried and does not penetrate throughthe skin or conjunctiva. The edges of the obicula-ris oculi muscle are approximated with resorb-able sutures and the skin closed with fastabsorbing gut sutures (Fig. 21).
and lower dermatochalasia, herniated orbital fat pads,is. (B) Preoperative right lateral view. (C) Postoperativewer lid transconjunctival blepharoplasty with lateralogous fat transfer. (D) Postoperative right lateral view.

Broujerdi684
If a midfacial lift is deemed necessary you mayaccess the orbital rim and midface through yourtransconjunctival approach. After removal of theherniated fat pads, the capsulopalpebral fascia isretracted superiorly and the lid margin inferiorly.A malleable retractor is used to identify the inferiororbital rim. A Colorado tip is used to incise the peri-osteum 1 to 2mmbelow the orbital rim in a presep-tal fashion. A periosteal elevator is used to elevatethe midfacial periosteum, including the attach-ments for the orbital retaining ligament, zygomaticligaments, and soft tissue. Care should be taken topreserve the inferior orbital nerve and vasculatureemerging out of the foramina. Next, permanentsutures such as 4-0 polypropylene are used toelevate the periosteum below the orbital retainingligaments and suture fixated to the arcus margina-lis of the inferior orbital rim. Autologous fat transfercan be performed to volumize the SOOF and themalar and nasolabial fat pads. If the midfacialdescent is severe, consider performing an endo-scopic midface lift with volumization in conjunctionwith your blepharoplasty (Fig. 22).
Subciliary Approach
The subciliary technique should be consideredwhen the patient has formed excessive lower lidskin with hypertrophy of the obicularis oculi muscleor attenuation and elongation. This approachmay also be used in conjunction with the
Fig. 22. (A) Preoperative frontal view, patient with upper alower lid laxity, lateral lower lid retraction, midfacial hypo(C) Postoperative frontal view, patient status after upperplasty with lateral canthoplasty, CO2 fractionated laser rfat transfer. (D) Postoperative right lateral view.
transconjunctival approach. A lateral canthopexymay also be performed simultaneously.After administration of 1% xylocaine with
1/100,000 epinephrine and waiting for 10 minutesfor both hemostasis and anesthesia, an incisionis made just below the lashes frommedial to lateralthen extending out to the lateral canthal skin.Dissection is carried down to the preseptal obicu-laris oculi muscle, and the skin flap is elevated inan inferior and lateral direction. Westcott scissorsare used to penetrate the obicularis oculi muscle,and an incision is made along the incision line.The superior flap is elevated and the fat pads areidentified with digital pressure. Westcott scissorsare used to open the orbital septum and the fatpads teased out and clamped, cut, and cauter-ized. Next, a strip of the preseptal obicularis oculimuscle is excised from the inferior flap margin asdeemed necessary. The skin flap is elevated ina superior lateral direction and marked. Excessskin is excised and the incision line closed witha 6-0 nylon suture in a running fashion (Fig. 23).
Canthopexy
Canthopexy may be performed simultaneouslywith the subciliary approach. After the skin flap iselevated and the lateral obicularis oculi muscleexposed, an elliptical muscle is excised, exposingthe retinaculum at the commissure, which is justbelow the muscle. The inferior flap with obicularis
nd lower dermatochalasia, herniated orbital fat pads,plasia, and ptosis. (B) Preoperative right lateral view.blepharoplasty, lower lid transconjunctival blepharo-esurfacing, endoscopic midface lift with autologous

Fig. 23. (A) Preoperative frontal view, patient with lower lid dermatochalasia, herniated orbital fat pads, lowerlid laxity, midfacial hypoplasia, and ptosis. (B) Preoperative right oblique view. (C) Postoperative frontal view,patient status after lower lid subciliary blepharoplasty with lateral canthopexy, endoscopic midface lift withautologous fat transfer. (D) Postoperative right oblique view.
Aesthetic Surgery of the Orbits and Eyelids 685
oculi muscle is elevated from the retinaculum,which allows for the elevation of the muscle. A4-0 polypropylene suture is used to elevate thesuperior obicularis oculi muscle to the incisionand retinaculum at the commissure via a mattresssuture in a superior lateral vector to the lateralorbital rim area. Next, the obicularis muscle inferiorto the excision is elevated and sutured to its supe-rior edge and the retinaculum ligament below itwith a resorbable suture in a 3-point fixation tech-nique. Excess skin is excised and closed asdescribed earlier.
Combination of Transconjunctival andSubciliary Approach
A combination of the transconjunctival and subcili-ary approach has been described. This techniquecan be used when the patient requires a combina-tion of midfacial lift, excision of obicularis oculimuscle, excision of excessive skin, or cantho-plasty/canthopexy.
Postoperative Care and Complications
Cold compresses are applied with a saline-soakedgauze and ice over the gauze for the first 48 hourson and off. This procedure reduces the postoper-ative edema. Make sure the patient is able to counttheir fingers and is not complaining of severe pain,
which are the signs for retrobulbar hemorrhage. Alateral canthotomy is performed bedside ifa patient is diagnosed with retrobulbar hematoma,diuresis is initiated with manitol, and IV steroidsstarted to reduce edema and retinal and opticnerve damage. An emergent ophthalmologicconsultation is required and the patient shouldbe taken to the operating room emergently forexploration and control of bleeding. If patientscomplain of dry eyes, initiate artificial tears asneeded throughout the day and ophthalmic oint-ment during sleep. The patient should sleep withthe head of their bed elevated and should notparticipate in strenuous activity for the first 2weeks. Any suture removal is performed after 7days. Antibiotic ointment over the eyelid incisionsshould be avoided because of the possibility ofgranuloma formation. Reading should be mini-mized to no more than 5 to 10 minutes everyhour to reduce eye strain and sclera edema forma-tion. Homeopathic over-the-counter medicationssuch as arnica gel and pills are recommendedto reduce ecchymosis and its duration. Othercomplications that can occur are ectropion andlid retraction with an external approach. Carefulpreoperative evaluation for horizontal lid laxityand minimal skin excision are the best preventivemeasures. Immediate postoperative tarsorraphysuture and lid massage improve the outcome. If

Broujerdi686
the patients continue to have problems, then skingrafting, tarsal strip procedures, cheek lift, andvolumization may be necessary. Loss of eyelashesand suture cysts are also possible postoperatively.
THE MIDFACE IN PERIORBITALREJUVENATION
The aging process affects the midfacial tissueby slight resorption of midfacial bone convexity,attenuation of the retaining ligaments andinvesting fascial tissue, loss of volume andatrophy of midfacial fat compartments, attenua-tion and atrophy of muscle of facial expression,and atrophy of the dermatocutis complex withformation of rhytids and furrows. Not all of thesecomponents are affected in the aging facesimultaneously and to the same degree. Evaluateyour patients and determine which componentsneed to be addressed in your surgical plan. Anatural and youthful midface has the followingcharacteristics:
1. The transition point between the lower eyelidand cheek is at the lid-cheek junction, whichis concave and smooth, with no hollowness orflattening.
Fig. 24. (A) Preoperative right oblique view, patient with mPostoperative right oblique view, patient status after sublateral view.
2. The midface has a convex surface and itsheight of contour is located at the most superiorand lateral point, where the malar complex andthe arch transition.
3. The transition point between the cheek and theupper lip is at the nasolabial region, which isconcave and smooth without furrows anddeep grooves.
I have classified patients in need of midfacialprocedures into 5 categories:
I. Volumization with subdermal fillers or autoge-nous fat (Fig. 24)
II. Volumization and fascial lift (Fig. 25)III. Fascial liftIV. Osteoplasty with implant augmentation or
autogenous or cadaver bone (see Fig. 7)V. Combination of volumization, fascial lift, and
osteoplasty.
Patients in categories I and IV are generally youngpatients with congenital facial hypoplasia; patientsin category II are going through the normal agingprocess; patients in category III are slightly obeseor have hyperplastic tissues; and patients in cate-gory V are going through a normal or acceleratedaging process and have facial bone hypoplasia.
alar hypoplasia. (B) Preoperative right lateral view. (C)dermal fillers to the midface. (D) Postoperative right

Fig. 25. (A) Preoperative frontal view, patient with periorbital, perioral, face, and neck age-related changes. (B)Preoperative right oblique view. (C) Preoperative right lateral view. (D) Postoperative frontal view, patient statusafter upper and lower lid transconjunctival blepharoplasty, endoscopic brow and midface lift, face and neck liftwith SMAS and platysmal plication and autologous fat transfer. (E) Postoperative right oblique view. (F) Postop-erative right lateral view.
Aesthetic Surgery of the Orbits and Eyelids 687
For facial bone osteoplasty, I routinely use Medpor(Porex Surgical, Stryker) implants with fixation.48
The orbital rim, malar, paranasal, or a combinationof these anatomic implants can be used. Facial vol-umization is discussed in the following sections.
Endoscopic Midface Lift
The midface can be addressed simultaneouslywith lower blepharoplasty or brow-lift procedures.The endoscopic midface procedure addresses thefollowing areas: lid-cheek junction, tear troughdeformity, palpebral-malar groove, nasolabialfolds, downturning of the commissure of the lip,central upper lip area, and alar base with nasaltip (Fig. 26). I perform a modification of Ramirez’sendoscopic assisted midfacial lift.49 I perform
a wider transvestibular incision, with wider dissec-tion and incorporation of the alar base cinch suturewith V-Y closure.50 The technical steps aredescribed as follows:
� Temporal brow incision as described forendoscopic brow lift
� Deep temporal fascial dissection withsentinel vein identification and preservation
� Release of zygo-orbicular ligament� Forehead and brow dissection and muscleresection for a forehead and brow lift asneeded
� Subciliary or transconjunctival incisionswith removal of fat pads
� Release of arcus marginalis and orbitalretaining ligaments

Fig. 26. (A) Preoperative 3D frontal view, patient with upper and lower lid dermatochalasia, lower lid laxity, browptosis, midfacial hypoplasia, ptosis, and retrogenia. (B) Preoperative 3D fused left oblique view. (C) Preoperative3D left lateral view. (D) Postoperative 3D frontal view, patient status after upper and lower lid transconjunctivalblepharoplasty, endoscopic brow and midface lift, autologous fat transfer, and sliding genioplasty. (E) Postoper-ative 3D fused left oblique view. (F) Postoperative 3D left lateral view.
Broujerdi688
� Maxillary vestibular incision from firstmolar tofirst molar with subperiosteal dissection
� Release of zygomatic and mesenteric liga-ments with dissection of the buccal fatpads
� Connection of the temporal and zygomatic-maxillary pockets via subperiosteal dissec-tion over the zygomatic arch
� Facial bone osteoplasty as needed� Midfaceelevationandsuture fixationofSOOF,malar fat pad, and buccal fat pad to the deep
temporal fascia in a superior-posterior vectorwith a 4-0 polypropylene suture
� Autologous fat transfer as needed� Canthopexy or canthoplasty as needed� Closure of temporal incision� Closure of lower eyelid incisions with or
without skin resection� Alar base cinch suture and V-Y maxillary
vestibular closure� If combined with brow lift, drains are
routinely used.

Aesthetic Surgery of the Orbits and Eyelids 689
Postoperative Care and Complications
Scalp incisions are dressed with antibiotic oint-ment. If drains are used, they can be removed in24 to 72 hours postoperatively. Paper tape isused on the midface and lateral brow area to mini-mize edema, with a head wrap, which can beremoved in 72 hours. Drains are removed within48 to 72 hours. Have patients sleep with their bed-head elevated for a minimum of 2 weeks. Patientsshould be given artificial tears and ophthalmicointment in case dry eyes or lagophthalmosdevelops. Ice packs over the forehead, midface,and eyes should be used routinely to reduce post-operative edema. Oral rinse with cholorohexadinegluconate with strict oral hygiene and a soft dietare recommended. There should be no suctionon straws for the first week. Patients may showerfully after 72 hours. Patient should not participatein strenuous activity for the first 2 weeks. Anysuture removal is performed after 7 days. Postop-erative complications of endoscopic midface liftare similar to the brow-lift procedure.
PERIORBITAL REJUVENATION WITHAUTOLOGOUS FAT TRANSFER
The use of autologous fat for correction of contourirregularities in reconstructive facial surgery datesback to the late nineteenth century.51 The resultswere unpredictable, with fat resorption and localregional adverse effects such as cyst and fibroustissue formation. The procedure fell out of favoruntil after the 1980s with the advent of liposuc-tion.52 The procedure was still unpredictable, withnear-complete resorption of the fat, until Cole-man53 described the atraumatic technique of lip-oaspirate harvest and injection techniques topreserve the fragile adipocytes. This techniquehas reduced the fat resorption rate and has madethe facial volumization technique with autologousfat a more predictable procedure. The techniqueis described as:
� harvesting with low negative pressure� purifying the lipoaspirate by washing outwith normal saline and centrifugation
� placing minimal amounts of adipocytes inmultiple tunnels.
Recent studies on fat tissue indicate that itcontainsnotonlyadipocytesbut alsopreadipocytes,endothelial cells, fibroblasts, and adipose-derivedadult mesenchymal stem cells (ADSCs), which aremultipotent cells that are capable of differentiatinginto neural, cartilage, bone, fat, and connectivetissues.54 Fat tissue contains the largest amount ofmultipotent and adult stem cells per area compared
withbonemarrowandother tissues.This finding indi-cates that isolatedADSCs fromfat tissuecanprovidea basis for regenerative medicine. Scientificevidence suggest that ADSCs produce and secretecytokines such as platelet-derived growth factor,transforming growth factor b, vascular endothelialgrowth factor, epidermal growth factor, and insulin-likegrowth factor. Thesegrowth factors induceauto-crine and paracrine effects in their surroundings,promoting angiogenesis andwound healing. ADSCscan be isolated from lipoaspirate via an enzymaticdigestion technique and centrifuged to separatethe multipotent cells into stromal vascular fraction(SVF) cells.55 In the laboratory, the SVF cells shouldadhere to a Petri dish, grow and replicate, andproduce CD34 and CD 90 cell surface markers toidentify as ADSCs. This technique can be performedin an accredited office-based outpatient surgicalcenter under good manufacturing practice andmust adhere to the Code of Federal Regulations(CFR) (US Food and Drug Administration [FDA]CFR title 21 part 1271) for use in a physician’s prac-tice. The SVF contains millions of isolated ADSCsthat could be used for tissue regeneration. Studieshave shown that enriched fat graft with SVF hasincreased adipose cell survival and retention of thegraft via increased vascularization.56 Other applica-tions of ADSCs include direct injection of SVF intothe dermis with increases in extracellular collagen,elastin production, and fibroblast, which reducewrinkles and improve skin quality.57 ADSCs areunder investigation in the orthopedic, cardiovas-cular, urology, endocrinology, and neurology fields.
The latest technique in facial volumization withautologous fat transfer is cell-assisted lipotransfer(CAL). CAL is the enrichment of autologous fatgraft with ADSCs. The technique involves removalof 300 to 500 mL of lipoaspirate via a tumescentsuction-assisted liposuction technique. The har-vested lipoaspirate is washed with normal salinethrough a filter and centrifuged. This procedureyields approximately 100 mL harvest lipoaspirateready for use. Approximately 25 to 50 mL of thewashed, filtered, and centrifuged lipoaspirate istreated with collagenase for enzymatic separationof the SVF cells from the adipose cells. The iso-lated SVF cells are then mixed with the remaining50 mL prepared lipoaspirate for injections ordirectly injected into the dermis for aesthetic facialvolumization or regenerative skin changes. Theenriched lipoaspirate is injected via 1-mL Luerlock syringes and a blunt cannula into the fore-head, temporal fat pads, ROOF, supraorbital rim,glabella, SOOF, malar and nasolabial fat pads, orother desired areas. Also, the SVF is injecteddirectly into the dermis in an area approximately1 cm2 by creating a wheel under the skin (Fig. 27).

Fig. 27. (A) Preoperative frontal view. Patient status after upper blepharoplasty and neck lift presents with recur-rent upper lid dermatochalasia, jowls, platysmal diastasis, age-related skin and soft tissue atrophy. (B) Preopera-tive left oblique view. (C) Preoperative left lateral view. (D) Postoperative frontal view, patient status afterrevision upper blepharoplasty, revision neck lift with suture suspension, cell-assisted fat transfer to the face.(E) Postoperative left oblique view. (F) Postoperative left lateral view.
Broujerdi690
THE ROLE OF SUBDERMAL FILLERS INPERIORBITAL REJUVENATION
For any particular reason, patients might notchoose autogenous volumization or might not be
good or healthy candidates for aesthetic surgicalrejuvenation. Subdermal fillers are alternative toautogenous volumization, and both patients andphysicians may levitate toward them. The inject-able industry is a billion-dollar market in the United

Aesthetic Surgery of the Orbits and Eyelids 691
States and is growing daily. The number oneproce-dure performed by aesthetic surgeons across thecountry is injectables. On the market there aremultiple injectable products, and each subdermalfiller has its advantages and disadvantages foruse in a particular anatomic area. It is beyond thescope of this article to review all products that areFDA-approved in the market. Please review theinsert in each product for indications, directions,and use. The products are divided into synthetic,nonsynthetic, resorbable, and nonresorbable. Theresorbable nonpermanent nonsynthetic biode-gradable fillers on the market and FDA-approvedare bovine collagen (xenograft) (eg, Zyderm/Zyplast), porcine collagen (xenograft) (eg, Evo-lence), and human collagen (autologous graft) (eg,Dermalogen). The resorbable nonpermanentsynthetic biodegradable fillers on the market andFDA-approved are hyaluronic acid (eg, Restylaneor Juvederm), calcium hydroxylapatite beads (eg,Radiesse), and poly-L-lactic acid (eg, Sculptra).The permanent synthetic nonbiodegradable fillerson the market and FDA-approved are poly(methylmethacrylate)microspheres (eg, Artefill) andacrylichydrogel (eg, DermaLive and DermaDeep).
The most common areas for subdermal fillerinjections are the temporal area, the brow, thetear trough, malar pads and the nasolabial folds,the nose, lips, marionette lines, prejowls, jaw line,and the chin. Each area has an ideal product forinjection volumization depending on its properties;for example, hyaluronic acid is ideal for tear troughdeformity because the material flows well, hasa low viscosity, and the soft tissue is thin andunforgiving. Calcium hydroxylapatite is ideal formalar augmentation because the product is highlyviscous, the tissues are thick, and longevity isneeded (see Fig. 24).
The classification of complications of subdermalfillers include immediate, long-term, allergic reac-tion, and poor technique. After injection, patientsmay develop swelling, edema, erythema, andbruising immediately. This is a normal outcomeafter injection, and the recommended treatmentis palliative care and use of homeopathic medica-tions, gels, and creams. Long-term complicationsinclude dissatisfaction with results and granulomaformation, which could be caused by infection orforeign body reaction. The recommended treat-ment is steroid injection, antihistamines, anddigital pressure.58 Patients who develop anallergic reaction should be treated with steroids,antihistamines, and palliative care. Allergiesshould be reported and documented. For knownproducts such as Zyderm/Zyplast, preinjectionallergic testing should be performed. With poorinjection techniques or using dermal filler for an
anatomic area that is not recommended, a patientcan develop beading, ridging, and nodule forma-tion. Instruct patients to perform deep tissuemassage immediately to disperse the product oruse dissolving or digesting enzymes such as hyal-uronidase (Vitrase) for hyaluronic acid.59 Othercomplications such as intravascular and perivas-cular injections have been described. Patientsmay develop embolic events and skin necrosis. Ifembolic events with neurologic symptoms arepresent, immediate emergent evaluation andtreatment are recommended. If a patient developsvascular insufficiency, the initial signs are poorcapillary refill of the tissue followed by epidermol-ysis and hyperemia. Skin necrosis and scarringcan ensue. The recommended treatment is recog-nition and treatment with enzymatic degradationintravascularly or vascularly if indicated, followedby aspirin therapy, nitropaste application, warmcompresses, and local wound care as needed. Ifpatients develop paresthesia after injection, enzy-matic degradation if indicated followed by steroidtherapy is recommended. The best method ofprevention of neurovascular injury is to use a bluntsyringe for injections and inject while movingforward to push away the neurovascular structureor advance aspirate, then inject in incrementswhile pulling out.60
LASER SKIN RESURFACING IN PERIORBITALREJUVENATION
Laser skin resurfacing can be used as an adjunct toperiorbital rejuvenation. I routinely incorporate laserresurfacing with transconjunctival blepharoplasty toinduce skin contractures as well as rejuvenation.This adjunct has allowed me to decrease thenumber of occasions for performing skin resectionwith lower blepharoplasty unless the patient pres-ents with a significant amount of skin excess, laxity,and hypertrophic obicularis oculi muscle. I performthe laser skin resurfacing on the same surgical dayor wait until the patient’s edema and ecchymosishave subsided. The decision is based on theamount of swelling and bruising immediately afterthe treatment (see Fig. 22).
Whether a conservative treatment plan such asbotulin toxin and dermal fillers is planned orcomplete surgical rejuvenation, laser resurfacingcan be used to improve outcome and treat theatrophic changes in the skin. These age-relatedatrophic skin changes are (Fig. 28)16:
� Decrease in the thickness of the dermis withloss of type I collagen
� Decrease in elastin protein with loss of skinelasticity

Fig. 28. (A) Preoperative frontal view, patient with age-related skin atrophy. (B) Postoperative frontal view,patient status after CO2 fractionated laser resurfacing.
Broujerdi692
� Increase in the thickness of the epidermallayer with a decrease in the basal layer
� Discoloration of the skin (dyschromia) withincreased rate of hyperpigmentation
� Sun damage with formation of actinic kera-tosis spots.
The 2 wavelengths of laser in common use forskin resurfacing are pulsed carbon dioxide (CO2)at 10,600 nm and erbium:yttrium aluminum garnet(YAG) at 2940 nm. Laser physics are beyond thescope of this article, but both CO2 and erbiu-m:YAG laser are both absorbed by water mole-cules (chromophore) in the tissue and createselective photothermolysis.61 These ablativelasers remove all of the epidermis and varyingthicknesses of the dermis. Healing is from theskin appendages. Fractionated photothermolysiswith ablation or ablation-fractionated laser (AFL)is the new treatment of skin rejuvenation.62 AFLcreates alternating columns of ablative photother-molysis of the epidermis and dermis called micro-thermal zones and nontreated columns. Thisselective treatment allows for faster healing fromthe side tissues and decreased complications ofablative lasers. This situation means less down-time and fewer complications, but results arecomparable with the ablative lasers.Patient selection, prelaser preparation, and
postlaser follow-up of the patient are crucial in ob-taining optimal results and avoiding unhappypatients and the risk of potential litigation. Patientswith Fitzpatrick type I to III are the ideal candidatesfor laser resurfacing. I routinely pretreat mypatients with 4% to 8% hydroquinone and Retin-A 0.025% cream for a minimum of 2 weeks beforetheir ablative laser treatment. This strategyreduces postoperative hyperpigmentation andpossible increase in healing potential and allowsthe skin to peel its dead, sun-damaged stratumcorneum layer off for even penetration of the laserphotons.63,64 Orringer and colleagues65 found no
evidence of enhanced collagen formation, accel-erated re-epithelialization, or quicker resolution ofpostoperative erythemia with tretinoin pretreat-ment before laser resurfacing. In my practice, Istop the creams 3 days before laser treatment toallow the inflammation to subside. Make sureyour patients are not taking isotretinoin for 6 to12 months before laser resurfacing, because itincreases the risk of hypertrophic scarring byreducing the skin appendages for healing.66 Onecan argue that with AFL treatment the healing isnot completely dependent on the skin append-ages but from the surrounding untraumatizedepithelium. I routinely use antiviral antibioticsprophylactically against herpes simplex virus.Make sure your patients do not have active skininfection or multiple acne vulgaris lesions. Avoidsmokers, because their healing potential is poor.The procedure is performed under sedation or
topical and local facial anesthetic block. I use non-reflective metal corneal shields to protect the eyes.Prevent oxygen pooling around your drapes withwet towels around the patient if supplementaloxygen is given in an open circuit. This strategyprevents laser fires. Use smoke evacuators withfilters and a cooling device for patient comfort.Follow the American National Standard Instituteand Occupational Safety Health and Administra-tion laser safety standards.Postoperatively, pain is generally not an issue
with AFL treatments because the patient is notleft with totally raw skin; patients complain of anintense burning sensation only after the first2 hours. Immediately after treatment, apply Aqua-phor cream mixed with small amounts of topicalanesthetic on the treated areas. This strategyrelieves the patient of the intense burning thatensues after laser treatment. Patients are in-structed to keep a thin layer of Aquaphor continu-ously until the skin spontaneously peels off. Thisevent usually happens within 3 to 7 days after laserdepending on the intensity of the treatment.

Aesthetic Surgery of the Orbits and Eyelids 693
Patients are given strict instructions to avoid sunand strenuous activity. Use of sun-blocking agentswith zinc oxide and titanium oxide is crucialbecause theses agents block all ultraviolet rays.Patients are started on 4% to 8% hydroquinonewith or without 1% hydrocortisone cream afterthey have peeled to reduce hyperpigmentation,inflammation, edema, and potential scarring.Patients with intense itching are prescribed 1%hydrocortisone cream with oral hydroxyzine.Patients are instructed to use skin moisturizersthroughout the day to keep the skin hydrated afterthey have peels. Patients are also allowed to usemineral-based makeup several days after peeling.
REFERENCES
1. von Graefe CF. De rhinoplastic, P 13. Berlin: Reime;
1818.
2. Wood C. The Tadhkirat of Ali ibn Isa of Baghdad
(trans). Chicago: Northwestern University; 1936.
p. 98, 115, 118–9.
3. Gunter J, Antrobus S. Aesthetic analysis of the
eyebrow. Plast Reconstr Surg 1997;99:1808–16.
4. Warren R. Non-endoscopic limited incision brow lift.
In: Aston SJ, Steinbrech DS, Walden JL, editors.
Aesthetic plastic surgery. Philadelphia: Saunders
Elsevier; 2009. p. 263–73.
5. Putterman AM. Evaluation of the cosmetic oculo-
plastic surgery patient. In: Fagien S, editor. Putter-
man’s cosmetic oculoplastic surgery. 4th edition.
Philadelphia: Saunders Elsevier; 2008. p. 21–30.
6. Putterman AM, Chalfin J. Ocular asymmetry
measuring device. Ophthalmology 1979;86:1203–8.
7. Putterman AM, Urist MJ. Muller muscle-conjunctiva
resection. Arch Ophthalmol 1975;94:619–23.
8. Olson JJ, Putterman AM. Loss of vertical palpebral
fissure height on downgaze in acquired blepharop-
tosis. Arch Ophthalmol 1995;113:1293–7.
9. Putterman AM. Basic oculoplastic surgery. In:
Peyman GA, Sanders DR, Goldberg MF, editors.
Principles and practice of ophthalmology. Philadel-
phia: WB Sanders; 1980. p. 2248–50.
10. Haddock NT, Saadeh PB, Boutros S, et al. The tear
trough and lid/cheek junction: anatomy and implica-
tions for surgical correction. Plast Reconstr Surg
2009;123(4):1332–40 [discussion: 1341–2].
11. Flowers RS. Tear trough implants for correction of tear
trough deformity. Clin Plast Surg 1993;20:403–15.
12. Levine RA, Garza JR, Wang PT, et al. Adult facial
growth: applications to aesthetic surgery. Aesthetic
Plast Surg 2003;27(4):265–8.
13. Bartlett SP, Grossman R, Whitaker LA. Age-related
changes of the craniofacial skeleton: an anthropo-
metric and histologic analysis. Plast Reconstr Surg
1992;90(4):592–600.
14. Farkas LG, Eiben OG, Sivkov S, et al. Anthropo-
metric measurements of the facial framework in
adulthood: age-related changes in eight age cate-
gories in 600 healthy white North Americans of Euro-
pean ancestry from 16 to 90 years of age.
J Craniofac Surg 2004;15(2):288–98.
15. Vleggaar D, Fitzgerald R. Dermatological implica-
tions of skeletal aging: a focus on supraperiosteal
volumization for perioral rejuvenation. J Drugs Der-
matol 2008;7(3):209–20.
16. Kahn DM, Shaw RB. Overview of current thoughts
on facial volume and aging. Facial Plast Surg
2010;26(5):350–5.
17. Penna V, Stark GB, Eisenhardt SU, et al. The aging
lip: a comparative histological analysis of age-
related changes in the upper lip complex. Plast Re-
constr Surg 2009;124(2):624–8.
18. Lee H, Park M, Lee J, et al. Histopathologic findings
of the orbicularis oculi in upper eyelid aging: total or
minimal excision of orbicularis oculi in upper bleph-
aroplasty. Arch Facial Plast Surg 2011. [Epub ahead
of print].
19. Gierloff M, Stohring C, Buder T, et al. Aging changes
of the midfacial fat compartments: a computed
tomographic study. Plast Reconstr Surg 2012;
129(1):263–73.
20. Elkwood A, Matarasso A, Rankin M, et al. National
plastic surgery survey: brow lifting techniques and
complications. Plast Reconstr Surg 2001;108:
2143–50.
21. Romo T, Sclafani AP, Yung RT, et al. Endoscopic
foreheadplasty: a histologic comparison of perios-
teal refixation after endoscopic versus bicorporal
lift. Plast Reconstr Surg 2000;105:1111–7.
22. Honig JF, Frank MH, Knutti D, et al. Video
endoscopic-assisted brow lift: comparison of the
eyebrow position after Endotine tissue fixation
versus suture fixation. J Craniofac Surg 2008;19(4):
1140–7.
23. Walden JL, Orseck MJ, Aston SJ. Current methods
for brow fixation: are they safe? Aesthetic Plast
Surg 2006;30(5):541–8.
24. Evans GRD, Kelishadi SS, Ho KU, et al. “Heads
up” on brow lift with Coapt Systems’ Endotine
Forehead technology. Plast Reconstr Surg 2003;
113:1504–5.
25. Chowdhury S, Malhotra R, Smith R, et al. Patient and
surgeon experience with the Endotine forehead
device for brow and forehead lift. Ophthal Plast
Reconstr Surg 2007;23(5):358–62.
26. Langsdon PR, Metzinger SE, Glickstein JS, et al.
Transblepharoplasty brow suspension: an
expanded role. Ann Plast Surg 2008;60(1):2–5.
27. Tyers AG. Brow lift via the direct and trans-
blepharoplasty approaches. Orbit 2006;25(4):261–5.
28. Hoorntje LE, Lei B, Stollenwerck GA, et al. Resec-
ting orbicularis oculi muscle in upper eyelid

Broujerdi694
blepharoplasty–a review of the literature. J Plast Re-
constr Aesthet Surg 2010;63(5):787–92.
29. Fagien S. Upper blepharoplasty: volume enhance-
ment via skin approach: lowering the lid crease. In:
Fagien S, editor. Putterman’s cosmetic oculoplastic
surgery. 4th edition. Philadelphia: Saunders Elsev-
ier; 2008. p. 87–103.
30. Damasceno RW, Cariello AJ, Cardoso EB, et al.
Upper blepharoplasty with or without resection of
the orbicularis oculi muscle: a randomized double-
blind left-right study. Ophthal Plast Reconstr Surg
2011;27(3):195–7.
31. Mikamo K. A technique in the double eyelid opera-
tion. J Chugaishinpo 1896;17:1197.
32. Maruo M. Plastic reconstruction of a “double eyelid”
operation in 1523 cases. Jpn J Ophthalmol 1929;24:
393.
33. Millard R Jr. Oriental peregrination. Plast Reconstr
Surg 1955;16:331.
34. Soyoc BT. Plastic reconstruction of the superior
palpebral fold in slit eyes. Am J Ophthalmol 1954;
38:556.
35. Fernandez LR. Double eyelid operation in the
Oriental in Hawaii. Plast Reconstr Surg 1960;25:257.
36. Flowers RS. Anchor blepharoplasty. Clin Plast Surg
1993;20(2):193–207.
37. Onizuka T, Iwanami M. Blepharoplasty in Japan.
Aesthetic Plast Surg 1984;8:97–100.
38. Kakizaki H, Leibovitch I, Selva D, et al. Orbital
septum attachment on the levator aponeurosis in
Asians: in vivo and cadaver study. Ophthalmology
2009;116(10):2031–5.
39. Flowers RS. Surgical treatment of the epicanthal
fold. Plast Reconstr Surg 1983;73:751.
40. Uchida K. The Uchida method for the double eyelid
operation in 1523 cases. Jpn J Ophthalmol 1926;30:
593.
41. Park JI. Modified Z-epicanthoplasty in the Asian
eyelid. Arch Facial Plast Surg 2000;2:43–7.
42. Kao YS, Lin CH, Fang RH. Epicanthoplasty with
modified Y-V advancement procedure. Plast Re-
constr Surg 1998;102:1835–41.
43. Fagien S. Lower blepharoplasty: blending the lid/
cheek junction with orbicularis muscle and lateral
retinacular suspension. In: Fagien S, editor. Putter-
man’s cosmetic oculoplastic surgery. 4th edition.
Philadelphia: Saunders Elsevier; 2008. p. 161–79.
44. Dailey RA, Chavez MR. Lateral canthoplasty with
acellular cadaveric dermal matrix graft (AlloDerm)
reinforcement. Ophthal Plast Reconstr Surg 2012;
28(1):e29–31.
45. Lessa S, Nanci M. Simple canthopexy used in trans-
conjunctival blepharoplasty. Ophthal Plast Reconstr
Surg 2009;25(4):284–8.
46. Grant JR, Laferriere KA. Periocular rejuvenation:
lower eyelid blepharoplasty with fat repositioning
and the suborbicularis oculi fat. Facial Plast Surg
Clin North Am 2010;18(3):399–409.
47. Momosawa A, Kurita M, Ozaki M, et al. Transcon-
junctival orbital fat repositioning for tear trough
deformity in young Asians. Aesthet Surg J 2008;
28(3):265–71.
48. Schendel SA, Broujerdi JA. Facial bone sculpturing.
In: Ward Booth Peter, Hausamen Jarg-Erich,
Schendel Stephen A, editors. Maxillofacial surgery.
2nd edition. St Louis (MO): Churchill Livingstone/
Elsevier; 2007. p. 1404–22.
49. Ramirez OM. Three-dimensional endoscopic mid-
face enhancement: a personal quest for the ideal
cheek rejuvenation. Plast Reconstr Surg 2002;
109(1):329–40 [discussion: 341–9].
50. Schendel SA, Williamson LW. Muscle reorientation
following superior repositioning of the maxilla.
J Oral Maxillofac Surg 1983;41(4):235–40.
51. Neuber G. Uber die Wiederanheilung vollstandig
vom Korper getrennter, die ganze Fettschicht en-
thaltender Hautstucke. Zbl F Chirurgie 1893;30:16
[in German].
52. Illouz YG. The fat cell “graft”. A new technique to
fill depressions. Plast Reconstr Surg 1986;78:
122–3.
53. Coleman SR. Long-term survival of fat transplants:
controlled demonstrations. Aesthetic Plast Surg
1995;19:421–5.
54. Strem BM, Hicok KC, Zhu M, et al. Multipotential
differentiation of adipose tissue-derived stem cells.
Keio J Med 2005;54:132–41.
55. Yoshimura K, Shigeura T, Matsumoto D, et al.
Characterization of freshly isolated and cultured
cells derived from the fatty and fluid portions of
liposuction aspirates. J Cell Physiol 2006;208:
64–76.
56. Ma Z, Han D, Zhang P, et al. Utilizing muscle-
derived stem cells to enhance long-term retention
and aesthetic outcome of autologous fat grafting:
pilot study in mice. Aesthetic Plast Surg 2011;
36(1):186–92.
57. Kim JH, Jung M, Kim HS, et al. Adipose-derived
stem cells as a new therapeutic modality for ageing
skin. Exp Dermatol 2011;20(5):383–7.
58. Saylan Z. Facial fillers and their complications. Aes-
thet Surg J 2003;23:221–4.
59. Goodman GJ, Bekhor P, Rich M, et al.
A comparison of the efficacy, safety, and longevity
of two different hyaluronic acid dermal fillers in the
treatment of severe nasolabial folds: a multicenter,
prospective, randomized, controlled, single-blind,
within-subject study. Clin Cosmet Investig Derma-
tol 2011;4:197–205.
60. Sclafani AP, Fagien S. Treatment of injectable soft
tissue filler complications. Dermatol Surg 2009;
35(Suppl 2):1672–80.

Aesthetic Surgery of the Orbits and Eyelids 695
61. Papadavid E, Katsambas A. Lasers for facial
rejuvenation: a review. Int J Dermatol 2003;
42(6):480–7.
62. Saedi N, Petelin A, Zachary C. Fractionation: a new
era in laser resurfacing. Clin Plast Surg 2011;38(3):
449–61.
63. McDonald WS, Beasley D, Jones C. Retinoic acid
and CO2 laser resurfacing. Plast Reconstr Surg
1999;104(7):2229–35.
64. Goldman MP. The use of hydroquinone with facial
laser resurfacing. J Cutan Laser Ther 2000;2(2):73–7.
65. Orringer JS, Kang S, Johnson TM, et al. Tretinoin
treatment before carbon-dioxide laser resurfacing:
a clinical and biochemical analysis. J Am Acad Der-
matol 2004;51(6):940–6.
66. Ong MW, Bashir S. Fractional laser resurfacing for
acne scars: a review. Br J Dermatol 2012;166(6):
1160–9.