Open access to clinical trials through prospective clinical trials registries

Original article
Advancing non-invasive neuromodulation clinicaltrials in children: Lessons from perinatal stroke
Adam Kirton
Departments of Pediatrics and Clinical Neurosciences, Cumming School of Medicine, Hotchkiss Brain Institute andAlberta Children's Hospital Research Institute, 2888 Shaganappi Trail NW, Calgary, AB T3B6A8, Canada
Keywords:
Neuroplasticity
Developmental plasticity
Brain stimulation
Cerebral palsy
Perinatal stroke
Transcranial magnetic stimulation
Transcranial direct current stimula-
tion
Clinical trials
a b s t r a c t
Applications of non-invasive brain stimulation including therapeutic neuromodulation are
expanding at an alarming rate. Increasingly established scientific principles, including
directional modulation of well-informed cortical targets, are advancing clinical trial
development. However, high levels of disease burden coupled with zealous enthusiasm
may be getting ahead of rational research and evidence. Experience is limited in the
developing brain where additional issues must be considered. Properly designed and
meticulously executed clinical trials are essential and required to advance and optimize
the potential of non-invasive neuromodulation without risking the well-being of children
and families. Perinatal stroke causes most hemiplegic cerebral palsy and, as a focal injury
of defined timing in an otherwise healthy brain, is an ideal human model of developmental
plasticity. Advanced models of how the motor systems of young brains develop following
early stroke are affording novel windows of opportunity for neuromodulation clinical tri-
als, possibly directing neuroplasticity toward better outcomes. Reviewing the principles of
clinical trial design relevant to neuromodulation and using perinatal stroke as a model, this
article reviews the current and future issues of advancing such trials in children.
© 2016 European Paediatric Neurology Society. Published by Elsevier Ltd. All rights
reserved.
1. First principles of neuromodulationclinical trials
Non-invasive brain stimulation applications are exploding.There is great and justified concern that the rate of growth inthe number of brains being stimulated is already far exceedingthe level of science that supports the approach. There are
major issues of unregulated use across broad and oftenvulnerable populations with immoral marketing of unproven,
potentially dangerous devices. Examples range from shame-less promotion of enhanced gaming performance to teenagersto do it yourself tDCS machines being made in people's base-ments. Ethical issues specific to the application of brain
stimulation in children must also be considered. For thesereasons, and in order to advance the responsible scientificstudy of neuromodulation in the developing brain, severalprinciples merit discussion here.
It is highly unlikely that introducing a focal magnetic fieldor local current into a functional area of human cortex will
E-mail address: [email protected].
Official Journal of the European Paediatric Neurology Society
e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 2 1 ( 2 0 1 7 ) 7 5e1 0 3
http://dx.doi.org/10.1016/j.ejpn.2016.07.0021090-3798/© 2016 European Paediatric Neurology Society. Published by Elsevier Ltd. All rights reserved.

magically create new, clinically relevant function. Instead, an
endogenous substrate for neuroplasticity thatmight be alteredby such neuromodulation seems a much more likely mecha-nism by which brain stimulation might produce lasting, ther-apeutic alterations in brain function. This fundamentaltenet also helps correct for the known and large heterogeneitybetween subjects inevitably enrolled in such trials. That a TMSmeasurement as simple as the rest motor threshold can rangefrom 20 to over 60% of maximum stimulator output across asample of normal subjects of the same age and gender pointsto anevenmore enormous inter-subject variability in clinicallydiseased populations. However, if such subjects share funda-
mental neuroplasticity mechanisms within their cortex (e.g.long termpotentiation) and are induced to activate them in thecontext of desired, functional activity, the potential for neu-romodulation is likely greater.
In a similar context, an informed cortical target for mod-ulation is also essential. Identification of such functionallyrelevant cortical regions is often difficult. As outlined below,studies of enhancement of motor learning with brain stimu-lation and have often logically targeted the primary motorcortex. This has logically extended to clinical populationswithmotor disability, targeting the motor cortex and related
network components in common populations of motordisability such as adult stroke hemiparesis.1 Importantly, thisevolving process has not rested on such simplistic anatomicallocalization alone. Instead, neurophysiological models havebeen developed to first understand what happens to the sys-tem of interest in the disease state. These often include largebodies of evidence from preclinical animal models combinedwith human studies using advanced neuroimaging and otherneurophysiology tools. Such an example for perinatal strokewill be presented below.
Such models not only identify potential targets but also a
desired direction for change. For example, the lesioned motorcortexmay be underactivewhile the homologous region of thecontralateral, non-lesioned hemisphere may be relativelyoveractive. Such a model of “imbalanced interhemisphericmotor inhibition” is probably over simplified but is well sup-ported by large volumes of neurophysiological evidence andhas driven the majority of non-invasive brain stimulationtrials in adult stroke.1,2 Recent summative evidence of rTMStherapeutic trials highlights this point by comparing modal-ities and targets across a wide range of such conditions.3
Importantly, each these three principles of modulating aninformed target in a specific direction during activation of endoge-
nous plasticity are arguably still not well defined in relativelyconcrete examples like adult stroke. In fact, such principlesare often not entirely obvious (or even theoretically welldefined) in many other stimulation clinical trials. While suchfailure should raise immediate concerns of validity, theirpresence is relatively sparse in the most defined therapeuticnon-invasive brain stimulation population: adult majordepression. High frequency rTMS of the dominant dorsolat-eral prefrontal cortex (DPFC) is FDA and Health Canadaapproved and rapidly expanding as an insured service. Whilebased on some human evidence of regional dysfunction in
this broad, highly connected areawith functional implicationsfor some symptomology, it could be argued that the ability ofdepression to satisfy the above criteria is modest at best.
This raises a final principle consideration of disease spec-
ificity. As a very common, disabling, and highly studied dis-ease, major depression carries well-defined diagnostic andclassification criteria. Despite this, there are innumerablefactors, both measureable and unknown, that would likelyinfluence response to neuromodulation. In contrast, autism isa heterogeneous disorder of social and communicationdevelopment that is likely due to hundreds of different geneticdisorders in addition to other etiologies. This does not meanthat informed, symptom-specific targeting of cortical regionsto enhance other therapies or learning is impossible. Howev-er, the breadth of heterogeneity must be acknowledged and
adjusted for whenever possible if meaningful trials are to bedesigned. Trials of autism due to one specific mutation bringlimitations of recruitment and sample size and are still notideal; consider the phenotypic variability of tuberous sclerosisalone. However, striving for disease specificity wheneverpossible will likely advance progress in paediatric neuro-modulation trials much faster. Extricating the very specificforms of perinatal stroke from the more complex world ofcerebral palsy for motor learning neuromodulation trialsprovides a practical example.
2. Perinatal stroke
You will not likely incur a higher period of risk for ischaemicstroke than the week you are born.4 A term newborn carries arisk >1:3500,5 three-fold higher than a week in the life of adiabetic, hypertensive, smoking adult and eight-fold above alladults.6 An additional 50% of perinatal stroke presents later in
infancy.7 Perinatal stroke is the leading cause of hemiplegiccerebral palsy (HCP) and most survivors suffer additionalneurological sequelae including intellectual disabilities, lan-guage impairments, developmental and behavioural disor-ders, and epilepsy.8e10 Frequent occurrence combined withlifelong morbidity generates large global burdens. Identifica-tion of a causative factor remains elusive in most cases11 andwith no means of prevention, perinatal stroke and HCP willburden thousands of children for decades to come.
An essential first step in improving outcomes from peri-natal brain injury is to understand the underlying disease. We
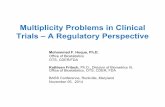
have defined distinct clinical-radiographic perinatal strokesyndromes,11,12 refining perinatal stroke research towardspecific disease states. Two main types predominate. Theseare summarized in Fig. 1. We have validated this imaging-based classification system and demonstrated it's researchapplications including the prediction of long-term neurolog-ical outcomes,12,13 recognition of novel risk factors,14e16 im-aging markers of disease processes, and new targets fortherapeutic interventions.14,17Arterial ischaemic strokes (AIS)are large brain injuries secondary to occlusion of major cere-bral arteries. Some present at birth with acute seizures (calledsymptomatic neonatal AIS) while others are not recognized
until infancy when hemiparesis becomes evident (calledarterial presumed perinatal ischaemic stroke).7,18e20 Incontrast, periventricular venous infarctions (PVI) are subcor-tical white matter lesions acquired well before birth. Sec-ondary to germinal matrix bleeds with subsequent medullaryvenous infarction, these lesions occur in utero before 34 weeks
e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 2 1 ( 2 0 1 7 ) 7 5e1 0 376

gestation.21e26 MRI work by our group and others can detectthese remote foetal bleeds, facilitating accurate diag-nosis.12,26,27 Our recent work has begun elucidating the path-
ophysiological and plasticity mechanisms in PVI.12,14,27 Ourimaging and population-based data12 suggest AIS and PVIprevalence are similar. Most relevant here, both AIS and PVIinjure primary components of the motor system early in life,resulting in HCP. This commonality of focal motor injury in ahealthy brain, combined with distinct differences in lesiontiming and location, makes perinatal stroke the ideal humanmodel for the study of developmental plasticity.
3. Perinatal stroke outcomes
Neurodevelopmental deficits occur in ~75% of perinatal strokesurvivors.8,10,19,28e34 Hemiparetic CP is the most commonterm-born cerebral palsy35 and stroke is the leading cause.36,37
Motor deficits are the most prominent and disabling
symptom, present in 30e60% of acute symptomaticNAIS31,38,39 and >80e90% of presumed perinatal ischaemicstrokes including PVI.12,18,19,31 Clinical, laboratory, and EEG
variables are limited in their abilities to predict motoroutcome,9,10,29,34,40 but neuroimaging has improved the earlyidentification of the most affected children.31,33,34,41e44 Weand others have described how corticospinal tract diffusionMRI in NAIS45,46 and structural MRI in PPIS12 can predictmotoroutcomes in infancy. This has opened the window for inter-vention earlier in development. Deficits in language, vision,cognition, behaviour and epilepsy also occur, present in20e60%8,10,18,19,47e49 of arterial strokes. The morbidity ofperinatal stroke lasts a lifetime, amplifying the burden onchild, family, and society.50 Physical disability contributes
across this realm of consequences and current interventionshave limited efficacy.51 There is therefore an urgent need fornew treatment strategies founded upon our best possibleunderstanding of the neurophysiology that underlies theclinical dysfunction.
Fig. 1 e Developmental plastic motor organization following perinatal stroke. (A) Arterial perinatal strokes (NAIS or APPIS)acquired near term result in damage to cortical and subcortical structures. (B) Periventricular venous infarction (PVI) areacquired in utero prior to 34 weeks gestation resulting in isolated injury to the subcortical white matter. Both lesionsdamage corticospinal tracts, leading to contralateral hemiparetic CP. (C) Animal and human evidence has constructedworking models of developmental motor organization following such early unilateral injury. Control of the weak right hand(W) often relies on both contralateral corticospinal pathways from the left (lesioned) motor cortex (LM1) and ipsilateralprojections from the unlesioned (right) motor cortex (RM1, dashed line). These two inputs compete to establish synapseswith anterior horn spinal motor neuron pools (circles) during development. Each M1 may also influence the other via IHI(coloured dashed arrows). The relative interhemispheric balance is associated with clinical function with contralateralcontrol associated with better function. Interventions that promote the success of contralateral (or inhibit the success ofipsilateral) upper motor neuron systems to compete for spinal motor neurons could result in better motor function.
e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 2 1 ( 2 0 1 7 ) 7 5e1 0 3 77

4. Plastic organization following unilateralperinatal brain injury: an integrated model
In 1936, Kennard described better outcomes in younger pri-mates following unilateral motor cortex lesions.52 This Ken-nard principle has fostered efforts to understand and harnessage-related plasticity. Common occurrence and focal injury inan otherwise healthy brain makes perinatal stroke an ideal
humanmodel. Terms like “repair” and “reorganization” implythe existence of inherent restorative mechanisms thatevolutionary models suggest would not exist.53 Instead, plas-tic adaptation may represent alterations of normal, ongoingdevelopmental processes occurring after injury. Elegant ani-mal work and human studies have solidified a model thatcreates novel avenues for therapeutic interventions in hemi-paretic CP.54e56 The model consists of 3 primary components(see Fig. 1): The lesioned (A) and non-lesioned (B) motor cortex(and their intra and inter-hemispheric connections) and theirinfluence on spinal motor neuron pools (C).
A. The lesioned hemisphere: contralateral projections tothe paretic hand. Adult stroke and animal studies sug-gest that, on average, motor control in the lesionedhemisphere is associated with better function.57e61 A
small childhood stroke study showed that recruitmentof perilesional motor area may be associated withhigher function.62 We have further correlated thepresence of contralateral projections from the lesionedhemisphere with better function.63,64 Rare hemipareticCP studies have shown decreased excitability in thelesioned hemisphere65 while maintained motor activa-tions approximate typical motor areas.66 PVI-like le-sions have associated this contralateral arrangementwith better function.67 Small studies have suggestedrehab-induced clinical gains may be associated withincreases in lesioned motor cortex activations in
HCP.68,69 Enhancing motor control in the lesionedhemisphere should favour improved function.
B. Role of the unlesioned hemisphere: ipsilateral pro-jections to the paretic hand. Abnormal projections fromthe unlesioned hemisphere to the paretic hand arecommon in hemiparetic CP70e75 but inconsistent intheir physiology.70e73,76e78 Ipsilateral projections arepresent in equal proportion at birth but are subse-quently withdrawn during normal development.79
Ipsilateral projections likely arise from homologous re-gions of primary motor cortex (M1).67,76,77,13 Our work
suggests the same in both childhood64,78 and perinatalstroke.81 In HCP,70e74,77,13 arterial,73e75,82,174 and PVI-likelesions67,73,74 ipsilateral projections are associated withpoorer motor function. Over-activity of the non-lesioned M1 may be associated with larger defi-cits.67,73,82 In the largest TMS study of perinatal stroke(n ¼ 52), we recently described the neurophysiology ofthe contralesional hemisphere, validating many ofthese observations (Zewdie et al., under review).
Recruitment of ipsilateral projections may thereforerepresent an example of maladaptive plastic organization
not compatible with normal hand function. A patho
logically overactive contralesional M1 controlling the ipsi-
lateral weak hand represents a potential therapeutic targetin hemiparetic CP.55,84 Decreasing pathological over-activity of non-lesioned M1 may enhance motor learningin adult stroke.85e88 In the original Kennard experiments,lesioning the contralesional M1 months after initial injuryin young primates improved function of the originallyparetic limb.52 Complex cortical motor circuits within andbetween the hemispheres also mediate neuroplasticityincluding interhemispheric inhibition (IHI)89,90 and intra-cortical inhibitory and facilatory circuits.65,91,92 Alterationsin these have provided insight to adult stroke recov-
ery.93e97 Each of these model components representneurophysiological outcomes measurable with moderntechnologies (below).98We havemeasured such systems inchildren with paediatric99 and perinatal81 stroke, confirm-ing their relevance to clinical function.C. Synaptic competition model. The target of these devel-
oping upper motor neuron systems are the spinal lowermotor neurons, control of which determines function.Continuous competition between contralateral andipsilateral corticospinal tract projections to establishsynapses with these cells occurs through development
with eventual contralateral domination andwithdrawalof ipsilateral projections.54,55 Primate studies confirm aprotracted developmental period for such organ-ization56,100e102 spanning childhood and into adult-hood.103 Injury likely reduces the normal contralateraladvantage, allowing ipsilateral projections to establishcontrol in more severe hemiparetic CP.
Cortical stimulation or inhibition can modulate this pro-cess. Pharmacological inhibition of M1 alters spinal motorneuron innervation and enhances ipsilateral pro-jections104,105 as seen in hemiparetic CP.55 Daily M1 elec-
trical stimulation can also preserve the corticospinalconnections normally withdrawn during early develop-ment in cats.106 These findings complement evidence ofactivity-dependent enhancement of corticospinal connec-tions in animal,105 histopathological,107 and neurophysio-logical studies.71,79 Interventional strategies to enhancecontralateral (or inhibit ipsilateral) corticospinal pro-jections might therefore enhance motor development andfunction.56 This might be achieved in two ways e stimu-lation of the lesioned M1 or inhibition of the unlesionedM1. The latter approach carries stronger animal evidence56
with authors concluding that: “activity-dependent pro-
cesses later in development can be harnessed to restore amore normal pattern of corticospinal connectivity andfunction.”
5. The window of opportunity indevelopmental neuroplasticity
Modern definitions of CP suggest deficits are static and non-progressive.108 However, neonates with stroke usuallydemonstrate no observable neurological deficits.109 Asym-metry is not appreciated until 4e6 months12,19 with the fullseverity typically appreciated years later.110 Consistent with
e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 2 1 ( 2 0 1 7 ) 7 5e1 0 378

the model above, progressive loss of contralateral control
through early developmentmay result in imbalance of corticalcontrol and motor networks, resulting in impaired function.Both animal100,111 and TMS studies of motor development byourselves99 and others73,112 agree that plastic motor organi-zation continues well beyond adolescence. New trials areproving that the plasticity of even the aged adult brain ismodifiable with multiple interventions.113 Whether or not theoptimal window for interventional modulation suggested inanimal models falls within the earliest years of humandevelopment remains to be determined. Before brain stimu-lation can be advanced toward this very young age of possible
maximal plasticity, the neurophysiology, efficacy, and safetyof modulatory interventions must first be established in olderchildren. Hence, school age children represent the ideal pop-ulation in which brain stimulation and modulation of brainplasticity should be explored. Before invasive, permanent in-terventions (e.g. stem cells)114 can be advanced, non-invasivemeans need to demonstrate efficacy of the approach whileelucidating the neurophysiological principles on which theyare based.
6. Therapeutic neuromodulation inhemiparetic CP
6.1. Intensive motor learning, manual therapy
Owing to an increasing number of clinical trials, evidence foremerging hemiparetic CP therapies is increasing. Constraintinduced movement therapy (CIMT) promotes functional use
of an impaired limb by constraint of the less-impaired limbcoupled with repetitive motor practice.113,115e118 In adultstroke, 2 weeks of CIMT can generate gains lastingyears.113,118,119 Multiple paediatric trials support CIMT effec-tiveness in hemiparetic CP.51,120e128 Consistent with themodel below, functional imaging suggests CIMT shifts motorfunction toward the lesioned hemisphere.68,129e132 CIMT-induced cortical reorganization has been demonstrated inadults with fMRI130,133e135 and TMS129,136e142 and small hem-iparetic CP studies.68,69,132 CIMT limitations include a some-what invasive nature and the exclusion of bimanual learning.
Bimanual approaches can also improve function in hemi-paretic CP trials.143,144 Hand-arm Intensive Bimanual Therapy(HABIT) is an evidence-based, safe, valid, and effective motorlearning therapy in children with hemiparetic CP.124,144e147
Efficacy appears equal to CIMT144 but the absence ofconstraint facilitates functional bimanual motor learning andremoves the complications of casting in our outpatient pop-ulation. Comparisons of CIMT and HABIT suggest possiblegreater achievement of self-directed goals with HABIT.144
Models for intensive motor learning may combine ap-proaches with early CIMT (e.g. week 1) to induce new func-tions in the paretic limb followed immediately (week 2) by
bimanual therapy to encourage incorporation of new functioninto more functional tasks.
How such therapies are delivered has also evolved. Inten-sive, camp-based models are increasingly popular, both forpsychosocial and programming benefits but also to deliverhigh doses of structured motor learning therapy that may
optimize use-dependent changes in brain plasticity and
function. Such programs should be based on best availableevidence and structured according to standardized elementssuch as the TiDIER criteria.105 Consistency of intensity, dosing,and methodology can be increased by strict adherence to amanual of operations by a limited number of trained thera-pists.144 Structured home programs based on the same prin-ciples with ongoing therapist support may be provided duringlonger-term follow-up periods. Therapy programs should bedesigned and delivered by experienced paediatric occupa-tional therapists. The cost of using such highly qualifiedpersonnel for so many hours of 1:1 therapymay be restrictive.
We recently used final year therapy students supervised by 2experienced paediatric OT's to deliver such therapy in campmodel with good success, broader knowledge translation tolearners, and much lower costs.
Providing such intensive, goal-directed, evidence-basedtherapy to all participants provides numerous potential ad-vantages. These go beyond the primary principle above thatan endogenous substrate for plastic change may well be anessential requirement for brain stimulation to be effective.That all subjects receive individualized, “best available”treatment facilitates randomization to such additional in-
terventions where there is equipoise regarding efficacy andminimal, but not zero, risk of adverse events. It creates op-portunity for active, motivated participation focused on aimsthat matter to the individual patient. Limitations include thedosage of therapy achieved over focused time frames wherethe optimal number of hours, both total and divided betweenfocused and more general training, remain to be determined.The balance of unimanual versus bimanual and the timing ofhow the two should be integrated is also imprecise and inneed of better evidence. Lastly, the potential psychologicaland social benefits of such group-based participation with
grouping of participants by developmental level should not beunderestimated. This may be optimized by inclusion of groupactivities within camp based day programs or, alternatively,incorporated into smaller time frames within after schoolprograms, possibly with the addition of group weekends ses-sions. When asked, most children with hemiparesis have notpreviously met a peer with the same disability. Workingtogether to achieve personal goals alongside similarlyaffected, motivated peers likely carries large psychosocialbenefits, themore accuratemeasurement of which is a goal offuture trials.
As outlined below, we have completed two clinical trials of
non-invasive brain stimulation in children with perinatalstroke and hemiparesis. This included a total of 68 partici-pants between the ages of 6 and 18 years: 45 in an rTMS trial105
and 24 in a tDCS intervention (unpublished). All participatedin child-centred, goal-directed, age-appropriate intensivemotor learning programs over 2 weeks.
6.2. Non-invasive brain stimulation: repetitivetranscranial magnetic stimulation (rTMS)
TMS given repeatedly can produce lasting changes in brainfunction. rTMS studies have established this principle inhealth and disease over the past 20 years148e150 with recentevidence-based summaries of therapeutic efficacy.3 High
e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 2 1 ( 2 0 1 7 ) 7 5e1 0 3 79

frequency rTMS (~10 Hz) stimulates cortex which both ani-
mal151e154 and adult148 stroke studies suggest can facilitatemotor function. Similarly, low frequency rTMS (~1 Hz) typi-cally inhibits cerebral cortex though there are exceptions toboth these rules.155e157 rTMS is amenable to randomized,sham-controlled clinical trials.158 Accumulating evidencesuggests rTMS can modulate neural networks159 to enhancemotor function in chronic adult stroke.160,161 Limitations ofrTMS include very focal administration and burdensome,immobile hardware that prevents simultaneous rehabilitationand co-activation of endogenous motor learning systems.
Despite both the high burden of motor disability and
greater brain plasticity in children, rTMS studies have beenlimited. Completed rTMS studies have reported favourabletolerability with no significant adverse events.162e164 DailyrTMS for weeks in animals,165 adults with stroke149,160,166e170
and our recent paediatric stroke trials63,81,160,171 further sup-port this safety. Evidence from our group and others hasshown no adverse effect of non-lesioned M1 inhibitory rTMSon normal (unaffected) hand function in hemiparetic sub-jects.57,63 We completed the first paediatric rTMS randomizedtrial where 8 days of non-lesional inhibitory rTMS improved
hand function in with chronic subcortical stroke acquired
during childhood.63
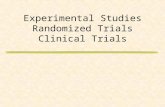
We recently completed the PLASTIC CHAMPS trial(Fig. 3).172 This was a factorial, controlled randomized trialdesigned to test the ability of contralesional, inhibitory rTMSand CIMT to enhance motor learning in children with peri-natal stroke and hemiparesis. Forty-five children aged 6e18years completed all outcome measures from baseline to 6months. There were no serious adverse events or drop outsand tolerability measures were favourable. An additive effectof rTMS and CIMT was observed on the primary objectiveoutcome of change in AHA at 6 months where the addition of
both therapies more than doubled the chances of a clinicallysignificant improvement (Fig. 2). Subjective, psychosocial andquality of life gains were also observed. This trial alsoconfirmed the feasibility of measuring both baseline ANDpost-intervention plastic neurophysiology using advancedimaging and TMS neurophysiology (see below). This trialprovides class II evidence for rTMS and CIMT enhancement ofmotor learning therapy while supporting the overall safetyand feasibility of conducting non-invasive stimulation trialsin children with perinatal stroke-induced hemiparesis.
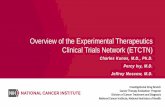
Fig. 2 e Timeline of evaluations, interventions, and outcomes. Baseline neurophysiology and motor function studies areperformed within a month of intervention. HABIT therapy (90 min) with TDCS or sham (first 30 min) intervention occursdaily for 10 consecutive weekdays. Both Jebsen Taylor hand function test (JT) and safety outcomes (S) are evaluated daily. Alloutcomes are repeated the week following intervention. Patients enter a home maintenance therapy program with clinicaloutcomes retested at 2 and 6 months. See text for details. Abbreviations: fMRI: Functional MRI; rsfMRI: Resting state fMRI;TMS: Transcranial magnetic stimulation; TDCS Transcranial direct current stimulation; HABIT: Hand-arm bimanualintensive therapy; AHA: Assisting Hand Assessment; COPM: Canadian occupational performance measure; TST: TDCSsafety test; JT: Jebsen Taylor Test of Hand Function; MA: Melbourne Assessment of Unilateral Upper Extremity Function; BB:Box and blocks test; PP: Perdue pegboard test; PMAL: Paediatric Motor Activity Log; QOL: Quality of life measures.
e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 2 1 ( 2 0 1 7 ) 7 5e1 0 380

6.3. Non-invasive brain stimulation: transcranial directcurrent stimulation (tDCS)
tDCS applies scalp electrodes (anode and cathode) to generateweak direct currents (1e2 mA) that induce polarity-dependent
changes in brain excitability.173 tDCS induces regional, tran-
sient modulation of resting membrane potential and corticalneuronal excitability.174 In general, anodal stimulation increases
cortical excitability while cathodal stimulation decreases it.
Modern commercial tDCS systems are painless, inexpensive,
and portable, allowing patients to remain mobile during activerehabilitation. tDCS safety and tolerability in adults is well
established with thousands of tested and published safety
guidelines.175e177 Seizure or other serious adverse events have
notbeenreported.Subjectsmayreportmild, transient tinglingoritchingduring thefirstminuteof tDCScurrent escalation.177This
sensation can be mimicked in sham experiments, making tDCS
amenable to blinded, randomized trials.178 A published
consensus statement endorses the ability of tDCS to enhancemotor learning (and other brain functions) in healthy and
diseased adults179 but does not even mention the developing
brain. tDCS can enhance motor learning in both animals and
healthy adults when administered briefly over the motor
cortex.180e183 Adult studies have not only demonstrated
enhancedmotor skill learning with contralateral anodal or ipsi-
lateral cathodal tDCSbut are also elucidating themechanismsof
neuroplasticity involved.180,181 The duration of effect clearly
outlasts tDCS interventionsbyhours todays inadosedependent
fashion, confirming a therapeutic potential.85,86,184e186
Recent trials provide Class I evidence that tDCS canenhance motor recovery in adults with chronic stroke (seeTable 1).2,85e87,187,188 Though fundamental mechanisms maydiffer, the same approach outlined above estimulating thelesioned, or inhibiting the unlesioned hemisphere, (or both)2eappears to enhance motor function. For example, Lindenberget al.2 studied 20 chronic, hemiparetic stroke patients. Fivedays of structured therapy (60min)was combinedwith 30minof bilateral anodal (lesioned M1) and cathodal (non-lesioned
M1) tDCS. Outcomes included validated strokemotor functionmeasures and pre and post-intervention fMRI neurophysi-ology. Collectively, such studies support the feasibility, safety,and potential of our proposed study and provide a solidfoundation for design, stimulation parameters, and outcomemeasures. They also highlight directions for advancement e
Fig. 3 e PLASTIC CHAMPS trial flow and primary results. (Top) Recruited participants have all motor measures and TMSneurophysiology measured at baseline. They then enter a day camp for 10 consecutive weekdays, all receiving intensivemotor learning therapy and randomized to rTMS and CIMT or not. Outcomes are repeated at 1 week and clinical measures at2 and 6 months. (Bottom) Main results demonstrated additive benefits of rTMS and CIMT on AHA scores at 6 months (left)with large and sustained gains in COPM across all treatment groups (right). (Modified from Kirton et al, Neurology 2016).174
e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 2 1 ( 2 0 1 7 ) 7 5e1 0 3 81

Table 1 e Summary of tDCS clinical trials in adult stroke.
Study Stroke population N Site tDCS Training Outcome measures Results summary
Hummel, 200587 Chronic 6 AAS
25 cm2; 1 mA; 20 min JTT practice JTT, TMS JTT improved with AA, outlaststim period. AA increasedcortical excitability
Hummel, 200588 Chronic 1 AAS
25 cm2; 1 mA; 20 min JTT, pinch force, reactiontime, TMS
Improved JTT, reaction time,and increase corticalexcitability
Fregni, 200589 Chronic 6 AACUS
35 cm2; 1 mA; 20 min JTT practice JTT Improved JTT with AA and CU
Hummel, 2006267 Chronic 11 AAS
25 cm2; 1 mA; 20 Pinch force, reaction time AA shortened reaction time andincreased pinch force relativeto S
Hesse, 2007268 Subacute 10 AA 1.5 mA; 7 min; 30 days Robot FM 3/10 improved in FMBoggio, 2007269 Chronic 9 AA
CUS
5 days JTT Both AA and CU improved JTTcompared to sham
Celnik, 2009270 Chronic 9 AASPNS
49 cm2; 1 mA; 20 min Key stroke tDCS þ PNS improved keystroke accuracy compared tosham conditions or tDCS alone.Maintained 1 and 6 days aftertraining.
Kim 2009271 Subacute 10 AAS
25 cm2; 1 mA; 20 min BBT, finger acceleration AA improved BBT and fingeracceleration to a greater extentthan S. BBT improvementslasted at least 60 min post-stim
Kim 2010272 Subacute 19 AACUS
25 cm2; 2 mA; 20 min; 10days
30 min of OT FM, BI CU led to greater FMimprovements compared to S
Lindenberg 20102 Chronic 20 AA þ CUS
16 cm2; 1.5 mA; 30 min;10 days
PT/OT; 5 days FM; WMFT Real tDCS improved FM andWMFT compared to S.Improvements lasted at least 1week
Mahmoudi 2011195 Subacute to Chronic 10 AA þ CUAACUAA
35 cm2, 1 mA; 20 min JTT Improvements with AA þ CU,AA and CU. No improvementswith AA (extra-ceph) or S
Nair 2011273 Chronic 14 CUS
1 mA; 30 min; 5 days OT for 60 min/day; 5days
ROM, FM, fMRI CU resulted in greaterimprovements in ROM and FMthan sham. Effects lasted atleast one week. Decreased fMRIactivation in contralesionalmotor region
Hesse 2011274 Subacute 96 AACUS
35 cm2; 2 mA; 20 min;daily
20 min robot; 30sessions
FM, muscle strength andtone, BI, BBT
All groups improved, no effectbetween interventions
european
journal
of
paedia
tric
neurology
21
(2017)75e103
82

Bolognini 2011275 Chronic 14 AA þ CUS
35 cm2; 2 mA; 40 min CIMT 14 days JTT, pinch and gripstrength, MALS, FM, TMS
JTT, strength, MALS, FMimproved with tDCS. Increasedlesioned M1 excitability
Stagg 2012276 Chronic 13 AACUS
35 cm2, 1 mA; 2 min Reaction time AA improved reaction time,and CU to a lesser extentcompared to S.
Lindenberg 2012277 Chronic 10 AA þ CU 1.5 mA; 30 min PT/OT 60 min/day; 10days (re-assess at 5days)
FM, WMFT Larger improvements in thefirst week compared to thesecond week
Takeuchi 2012278 Chronic 27 1 Hz rTMSAArTMS þ AA
25 cm2; 1 mA; 20 min Finger tapping, pinch force,TMS
rTMS-tDCS enhanced pinchforce, but had no effect onfinger tapping. Changes in TCI
Rossi 2013279 Acute 50 AAS
35 cm2; 2 mA; 20 min; 5days
FM, NIHSS Both groups improved, but nodifference between AA and S
Zimerman 2012280 Chronic 12 CUS
25 cm2; 1 mA; 20 min Finger tapping; TMS CU enhance motor skillcompared to S. Correlationbetween SICI andenhancement.
Wu 2013281 Subacute 90 CA (S1)S (S1)
25 cm2; 1.2 mA; 20 min;5x/wk # 4 wk
PT; 30 min twice a day,5x/wk # 4wk
MAS, FM, BI More clinical importantdifferences with active tDCScompared to sham post-treatment and at 4 week followup.
Ochi 2013282 Chronic 18 AACU
35 cm2; 1 mA; 10 min; 5days
Robot-assisted armtraining; 5 days
FM, MAS, MAL Both tDCS conditions improvedFM and MAS, but not MAL
Lefebvre 2013283 Chronic 18 AA þ CUS
35 cm2; 1 mA; 30 min Training circuit task Grip force, PPT, circuit task tDCS enhanced circuit taskonline learning, with retentionat 1 week. Improved PPT scoreswith tDCS
Fusco 2013284 Subacute 9 AA þ CUAACUS
35 cm2; 1.5 mA; 15 min 9-hole peg test; pinch force;grip strength
AA improved 9-hole peg test,CU improved strength. Noimprovements with bilateral.
Lefebvre 2014285 Chronic 19 AA þ CUS
35 cm2; 1 mA; 20 min Precision grip movements,PPT
Grip and PPT improved withtDCS compared to S
Khedr 2013286 Subacute 40 AACUS
35 cm2; 2 mA; 25 min; 6days
Therapy 1 h after tDCS;30 min
NIHSS, BI, muscle strength;TMS
All groups improved (smallerimprovements in musclestrength). No differencebetween AA and CU, but bothbetter than S. Increased corticalexcitability in lesioned M1
O'Shea 2014287 Chronic 13 AACUAA þ CUS
35 cm2; 1 mA; 20 min Reaction time AA þ CU had no effect onreaction time compared tosham, whereas AA and CU didquicken RT.
(continued on next page)
european
journalofpaedia
tric
neurology
21
(2017)75e103
83

Table 1 e (continued )
Study Stroke population N Site tDCS Training Outcome measures Results summary
Giacobbe 2013288 Chronic 12 AAS
2 mA; 20 min 20 min robotic practice Robot; TMS Movement speed improved.Smoothness improved withtDCS. tDCS after practicereduced speed. Increasedcortical excitability
Fusco 2014289 Subacute 16 AAS
? PT ? Both AA and S improveddexterity. No chance in handforce
Lee 2014290 Subacute 59 CUSCU þ training
25 cm2, 2 mA; 20 min; 15days
VR therapy, 30min/day MAS, manual muscle test,manual function test, FM,BBT, BI
Both groups improved manualmuscle and function and FMand BI scores. Change in FMwas higher in CU þ traininggroup
Cha 2014291 Chronic 20 AAS
35 cm2; 1 mA; 20 min; 20days
30 min/day BBT; grip strength; FM Both groups improved outcomescores. tDCS improved BBT andFM more than training alone
Fusco 2014290 Subacute 11 CUS
35 cm2; 1.5 mA; 10 min;10 days (1/day)
45min# 2/day# 10 days 9-hole peg test; pinchstrength, FM, grip strength;BI
No added benefit of CUcompared to S
Au-Yeung 2014292 Chronic 10 AACUS
35 cm2; 1 mA; 20 min; 1day
PPT, pinch strength CU improved PPT, but not pinchstrength. No improvement withAA or S
Gillick 2015293 Congenital hemiparesis 13 AA þ CUS
35 cm2; 0.7 mA; 10 min;
Goh 2015294 Chronic 10 AA5 Hz-rTMS-A
1 mA; 20 min TMS; Trail making test;reaction time; pinch force
Increased cortical excitabilitywith AA. No change in motoroutcomes
Di Lazzaro 2014295 Acute 14; 20 AA þ CUS
35 cm2; 2 mA; 40 min; 5days
CIMT þ therapy; 1.5 hper day
ARAT; 9-hole peg test; gripstrength; MAL; NIHS; TMS
No change in motor outcomes.tDCS reduced IHI imbalance at3 months post stroke.
Lefebvre 2015296 Chronic 19 AA þ CUS
35 cm2; 1 mA; 30 min Trained circuit task PPT, circuit task Greater improvement in circuittask and PPT with real tDCS.
Sattler 2015297 Acute 20 AA þ PNSS þ PNS
35 cm2, 1.2 mA; 13min; 5days
JTT, 9-hole peg test, gripstrength, FM, hand tapping;TMS
Greater improvements at 2 and4 week follow up with AAcompared to sham.Improvements on secondaryoutcome measures too with AAcompared to S
Cho 201556 Chronic 27 AA 35 cm2; 2 mA; 20 min; 18days (3 # 6weeks)
Mirror therapy or none(control); 18 days (3 # 6weeks)
BBT. FM, JTT, grip strength Control groups improved gripstrength and JTT. Greaterimprovements in BBT and gripstrength with tDCS
Rocha 2016298 Chronic 21 AACUS
35 cm2; 1mA; 13min (forAA) or 9 min (for CU); 3x/wk for 4 wks
CIMT; 6 h/day for 3 wk1 h of PT daily 3x/wk for4 wk
FM, MAL, grip strength Increase in FM for active tDCSgroups. All groups equallyimproved MAL and gripstrength.
european
journal
of
paedia
tric
neurology
21
(2017)75e103
84

Straudi 2016299 Acute - Chronic 23 AA þ CUS
35 cm2, 1 mA, 30 min; 10days
Robot-assisted therapy;10 days
FM, BBT, MAL Both groups improved FM, butno difference between AA andS. Patients with chronicsubcortical strokes benefitedmore than those with acute andcortical stroke however.
Allman 2016300 Chronic 24 AAS
35 cm2; 1 mA; 20 min; 9days
Motor training; 1hr perday
FM, ARAT, WMFT ARAT WMFT showedimprovements up to 3 monthspost-training with AA
Triccas 2015301 Subacute e Chronic 22 AAS
Cunningham 2015302 Chronic 12 AAS
35 cm2; 1 mA; 30 min perstimulation
CIMT þ therapy;30 min # 2/day x 3/weekfor 5 weeks
FM; 9-hole peg test; TMS tDCS improved motoroutcomes. Increasedexcitability in thecontralesional hemisphere.
Lee 2015303 Chronic 24 AA?S
?? Physical therapy FM Real stimulation plus therapyimproved FM scores to a greaterextent compared to therapyalone
Chen 2016304 Subacute e Chronic 5 AA þ CU 16 cm2; 1.5 mA; 30 min;10 days
1 h OT/day; 10 days FM, rsfMRI FM scores improved. Increasedconnectivity betweenipsilesional M1 andcontralesional PMC
Mortensen 2016305 Chronic 15 AAS
35 cm2; 1.5 mA; 20; 5days
OT; 30 min/day 5 days JTT, grip strength Both groups improved JTT. AAimproved grip strengthcompared to sham (no longerpresent 1wk post). Trend for JTTretention with AA
Legend: AA e anodal stimulation, affected hemisphere, CU e cathodal stimulation, unaffected hemisphere, FM e Fugl-Meyer motor score, AAT e Aachener aphasia test.
european
journalofpaedia
tric
neurology
21
(2017)75e103
85

larger, more homogeneous populations, evidence-based
therapy, more integrated neurophysiological outcomes and,of course, studying the more plastic paediatric population.
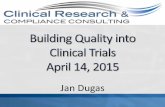
We recently demonstrated the ability of tDCS to enhancemotor learning in typically developing children. One previousstudy had demonstrated early evidence of safety, tolerability,and neurophysiological effects of brief tDCS applications tomotor cortex in children.189 We conducted a 4 arm, blinded,sham-controlled trial of motor cortex tDCS to enhance motorlearning in children aged 6e18 years.190 Subjects repeatedlyperformed a motor learning task (Purdue Pegboard) with theirleft hand over three days. They were randomly assigned to
receive 20 min of contralateral anodal (1 mA), ipsilateralcathodal (1 or 2 mA) or sham tDCS during the first 20 min.Learning curves were strongly enhanced with active treat-ment with effects retained 6 weeks later and additional gainsin untrained motor function of both hands (Fig. 4). We believethis provides important proof-of-principle evidence toadvance further studies in hemiparetic CP and other diseasepopulations.
Though there ismuchneed for additional investigation, themost informed primary target in hemiparetic children withperinatal stroke currently is the contralesional M1. A cathodal
approach is supportedby theaboveevidence for tDCSeffects innormal children190 and probable effect of the similar approachwith inhibitory rTMS in the same population.172 Stimulationover intact (non-lesioned) brain also maximizes safety withmore predictable distribution of tDCS currents compared tochildren with large arterial lesions.191,192 Methods should bebased in the best accumulated evidence from previous studiesof cathodal tDCS in addition to those cited above includingadultmotor learning,179e181 adult stroke rehabilitation2,86,87,188
and studies of electrode montages in stroke.193 Soft, replace-able 25 cm2 electrodes would typically be placed on clean, dry
areas of the scalp with the cathode placed over the non-lesioned M1. This location would ideally be individualized foreach subject using TMS and/or task fMRI and targeted withneuronavigation.Consistentwithprevious tDCSstrokestudiesexamining electrode placement,193 the reference electrodewould be placed over the contralateral orbit. Using available,programmable, and current-controlled stimulators allowsautomatic ramp up slowly over 30 s to the treatment current,typically 1.0 mA tDCS or shamwould usually be administeredduring the first 20e30 min of motor learning therapy and on adaily basis in a camp-based model. Experienced techniciansshould apply and monitor all systems, being on hand for im-
mediate trouble-shooting. Some tDCS systems can blind theadministrator though it is only essential that cliniciansadministering therapy and those performing the outcomemeasures are blinded to treatment allocation.
We recently completed a phase 1/2, randomized, sham-controlled, double-blind, clinical trial to test whether theaddition of tDCS to intensive motor therapy was associatedwith larger gains in clinical function. Participants completed agoal-directed, peer-supported after school camp model ofmotor learning therapy for 2 weeks, randomized to receivecontralesional, cathodal tDCS (1 mA) or sham during the first
20 min of each day. Primary outcomes were the COPM (sub-jective) and AHA (objective) in addition to multiple safety andtolerabilitymeasures (see discussion below)measured out to 2
months post-intervention. The final results were presented at
the 2016 International Stroke Conference in Los Angeles inFebruary 2016 and is currently submitted for publication. Insummary, interventions were well tolerated with no seriousadverse events and all safety outcomes were satisfied. Sig-nificant tDCS effects were observed on COPM, but not AHAoutcomes, suggesting possible benefit and providing impor-tant data for the execution of a larger, more definitive trial.
7. Systematic approach to clinical trialdesign: CONSORT
Any trial is only as good as the methods on which it rests.Thankfully, the importance of this fundamental concept hasevolved over recent decades to carefully define the essentialcriteria of valid clinical trials and their reporting. The CON-
SORT (ConsolidatedStandardsofReportingTrials) statement isan evidence-basedminimumset of standards for the reportingof randomized clinical trials.194 First initiated in 1996, the cur-rent version was last updated in 2010 and the most up to dateversion including recent modifications are available online.These include a 25 item checklist as well as a template flowdiagram to account for participant movement through a trial.An accompanying “explanation and elaboration” statementfurther defines each element and is available in multiple for-mats.Multiple extensions have also beendeveloped to addressdesigns beyond simple two group parallel designs such as
cluster, non-inferiority, and pragmatic trials.Use of the CONSORT guidelines has been associated with
improved reporting of clinical trials.195 The website receives>17,000 hits per month. More importantly, over 600 journalshave endorsed the CONSORT guidelines. While the primarymotive for applying the CONSORT guidelines should be thebest possible trial, it is fair to say that no future clinical trialwill likely be published in any reputable journal withoutcareful adherence. It is therefore reasonable to suggest thatapplication of the CONSORT guidelines is both an extremelyhelpful and scientifically essential process in the design,
execution, and reporting of any clinical trial. With this inmind, the outline of the guidelines will be applied below toreview several essential elements of trial design as they relateto non-invasive brain stimulation trials in children. Outcomemeasures, the largest single issue, are discussed separatelyfollowing this.
7.1. Populations
Where participant populations exist and how they areaccessed for recruitment will primarily depend on the inclu-sion and exclusion criteria (discussed next). However, beforethese criteria are applied, the sample to be screened should becarefully selected to represent, as best as possible, the popu-lation of interest as a whole. Reductions from the true popu-
lation toward the sample studied will inevitably introduceselection and other biases, the number and calibre of whichdecrease the translatability of any ultimate findings propor-tionately. Therefore, the optimal starting point is a large,complete, population-based sample of subjects with the con-dition of interest. Asmentioned elsewhere, disease-specificity
e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 2 1 ( 2 0 1 7 ) 7 5e1 0 386

will be a major determinant of this population. For example,from a population-based sample of cerebral palsy (somethingalready difficult to find), perhaps 30% of these will be hemi-paretic and perhaps 75% of these will have confirmed peri-natal stroke as the cause.
We began building the Alberta Perinatal Stroke Project (APSP)in 2007. This is a large population-based cohort of MRI-
confirmed perinatal stroke consented to research nownumbering nearly 800 subjects all living within the Canadianprovince of Alberta (population of ~4.2 million). This requiredanexhaustive reviewofover 80 ICDcodes, 6000medical charts,structured imaging review, patient contact and inperson clinicassessments. The effort took over 7 years and is still ongoing.
The yield for clinical trials however was immense, providing alarge unbiased sample from which candidates could berandomly recruited, optimizing translatability to the diseasepopulation as awhole. As outlined in the following sections onselection criteria and recruitment, this apparently very largenumber shrinks rapidly as these realities are introduced,further biasing the sample along the way.
7.2. Selection criteria
Further reduction of the eligible population for recruitmentwill occur with application of inclusion and exclusion criteria.Their selection must rest on the primary research question
Fig. 4 e tDCS motor learning trial methods and results. Motor training of the non-dominant hand over 3 days is shown inthe top bars with subjects randomized to 1 of 4 tDCS treatment montages (including sham). Active treatment groupsshowed markedly steeper learner curves (bottom) with sustained effects at 6 weeks. (Modified from Ciechanski and Kirton,Cerebral Cortex 2016).192
e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 2 1 ( 2 0 1 7 ) 7 5e1 0 3 87

being asked; if this has to be compromised by changing
criteria to suit other needs, the question should instead bechanged. Once true to the primary question, additional issuesof confounders, known response predictors, clinical realities(i.e. minimum function levels), clinical significance or need(i.e. maximal function levels), safety, and ability to complymust be considered. Criteria should be strictly quantified orqualified according to established metrics when possible.
The following provides an example of potentially relevantinclusion and exclusion criteria for a combined intensivemotor learning and neurostimulation trial in hemiparetic CP.
7.2.1. Inclusion criteria
1. Symptomatic hemiparetic CP (Paediatric Stroke OutcomeMeasure (PSOM) > 0.5) AND Manual Abilities ClassificationSystem (MACS)196 grade IeIV AND child/parent perceivedlimitations in function)
2. Clinical and MRI-confirmed perinatal stroke syndrome(NAIS, APPIS, PVI)
3. Active wrist extension >20$, finger extension >10$
4. Can lift the affected arm 15 cm above a table surface andgrasp light objects
5. Term birth (>36 weeks) and current age 5e18 years6. Informed consent/assent
7.2.2. Exclusion criteria
1. Other neurological disorder not related to perinatal stroke2. Multifocal stroke3. Severe hemiparesis (no voluntary contraction in paretic
hand, MACS level V)
4. Severe spasticity in the affected limb (Modified AshworthScale >3)
5. Severe developmental delay or other inability to complywith study protocol
6. Unstable epilepsy (>1 seizure/month or >2 medicationchanges last 6 months)
7. Any TMS171 or MRI contraindication including implantedelectronic devices
8. Botox, orthopaedic surgery, or other invasive mechanicaltherapy in past 6 months
9. Constraint, brain stimulation or other modulatory therapy
in past 6 months
7.3. Randomization
Methods for randomization within clinical trials are complexand beyond the scope of this discussion. However, severalfundamental issues to be considered relate predominantly totrial design and a priori knowledge of response predictors andother potential confounders. Options including block orminimized randomization may help ensure balance oftreatment allocation across subgroups of patients. Such
subgroups may be easily defined (e.g. site A versus site B) ormore complicated such as predefined factors known orhighly suspected to be associated with the outcomes of in-terest or potential response to treatment. Examples mightinclude factors such as age, level of baseline disability, orcorticospinal tract arrangement. However, it should be
emphasized that the relationship of these factors to the
ability to respond to an intervention are incompletely, if atall, understood. Therefore, despite these specific consider-ations, it should be remembered that simple randomizationshould usually correct for such differences across treatmentgroups.
Most forms of randomization can be performed simplyusing patient codes and computer-based or online softwareadministered by an unbiased study member such as thestatistician. Concealment of randomization must be assuredand multiple means are available. Development, storage, andbreaking of codes by an unbiased third party may be reason-
able. Treatment administrators can sometimes be automati-cally blinded, such as modern, programmable tDCS systems.Stimulation trials in children are likely moving toward multi-centre studies, introducing additional considerations.Randomization in permuted blocks, with the number ofblocks matching the number of participating sites, mayfacilitate even distribution within sites. Multi-site trials on theother hand, may require a central randomization and treat-ment allocation process. Expertise from experienced clinicaltrialists and statisticians may be particularly helpful.
7.4. Recruitment
Failure to recruit complete samples on time is one of themostcommon reasons for trials to be delayed or not completed atall. Estimates of attainable sample sizes must be realistic (i.e.pessimistic). Hard numbers from established populations arerequired rather than blind estimates of prevalence based onpublished epidemiological data. What may appear as large,easily adequate number of potential subjects often reduces
dramatically when realistic limitations are estimated. Exam-ples include presence of exclusion criteria, inability to confirmall inclusion criteria, geographical factors, failure to recruitrates, and attrition with drop-outs possible at all stages (whomust be included within intention to treat analyses if occursfollowing randomization).
7.5. Informed consent and assent
Consenting children and parents to novel, experimental trialsof brain stimulation requires special attention. Potentialbenefits may be easily over-estimated by families of disabledchildren due to lack of alternative therapies, being“impressed” by technology, or other reasons. Risk must alsobe fairly disclosed based on best available evidence. Our labhas completed nearly 3 million stimulations on over 250childrenwithmany conditions without serious adverse event.This provides direct evidence to families of minimal risk theycan trust however such examples are not always available.Theoretical risks must be presented in context with estimatesof relative risk and potential harm. An ability to understand
randomization may be difficult to communicate and may beforgotten months later when final results are shared withfamilies. Both parents and children, in our experience, maysometimes harbour feelings of disappointment or evenmistrust when discovering they were in the sham group, evenwhen they may have made substantial clinical gains. Honest,
e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 2 1 ( 2 0 1 7 ) 7 5e1 0 388

clear, and repeated explanations are all that can reasonably be
offered.
7.6. Structure and flow
Structuring a complex, multifaceted intervention withnumerous requirements for space, infrastructure, and highly
qualified personnel requires organized structure. An exampleof the sequence, timeline and flow of our recently completedcontrolled trial of tDCS in school-aged children is shown inFig. 2. Factors considered include family convenience wheretiming of drop offs and pick-ups, time of year (school yearversus summer), and extracurricular activities may affectcompliance and participation. Including unique activitiesmaydiversify therapy while optimizing fun for participants. Ex-amples in our experience include virtual reality, cooking,therapeutic arts, horticultural therapy, and video gaming (e.g.rockband). Balancing focused motor training with more gen-
eral and group activities as well as breaks and relaxation canbe challenging. It is essential to include input from experts inpaediatric therapy, child life, and subjects and their familiesfor optimal planning.
7.7. Sham-control and blinding
Effective sham techniques are well established for non-invasive stimulation methods. For rTMS, this includesaltering coil direction or use of commercially available shamcoils. For tDCS, devices can often be ramped on for all subjectsto produce the typically transient scalp sensations experi-enced, and then ramped off for the sham group. Such sham-ming has been proven effective,178 including in children.172,190
Cross-over design trials carry a risk of subjects detecting dif-ferences when they switch groups and interventions in naı̈vesubjects only avoid this potential problem. Ideally, all in-
vestigators, those administering treatments, outcome asses-sors, parents and children remain blinded. Thoseadministering tDCSmaynot be if they are otherwise separatedfrom the outcome measures and therapy. Modern tDCS sys-tems can also be programmed to randomize and administeraccordingly, allowing the administrator to remain blinded.
7.8. Analysis and sample size
Statistical analysis will of course depend on the researchquestions to be addressed. In most circumstances, analysiswill be intention to treat, accounting for all subjects ran-domized whether they complete the trial or not. Additionalper protocol analyses may be performed and reported but thisis not usually done in isolation. Collaborator expertise inclinical trials and biostatistical methods are an essentialrequirement. Variables for calculation of sample size shouldbe extrapolated from the most relevant literature. Estimates
are typically based on application of the first order analysismethod to the main hypothesis using the primary outcome.Estimated samples should be comparable or proportional toprevious trials in similar populations.
All studies need to be registered prior to consent of the firstpatient (www.clinicaltrails.gov).
8. Outcome measures
Selection of outcome measures is likely one of the mostessential components of clinical trial design. Standardized,unbiased administration and interpretation by qualified ex-perts blinded to treatment allocation and other clinical in-formation is required but often challenging. Additionalissues specific to considering neurostimulation in-
terventions in children include a relative paucity of vali-dated measures, heterogeneous populations (e.g. CP versushemiparetic CP versus perinatal stroke hemiparesis), andvariable effects of age and developmental level to name justa few. However, these limitations are being overcomethrough a variety of creative means to facilitate evaluationof such interventions. Measures used in similar previoustrials should be considered in anticipation of comparabilityand eventual pooling of data in meta-analyses. At the sametime, careful review of how well certain measures were ableto demonstrate change (or not) and other limitations in
those same trials may be good reasons to consider addi-tional or alternative outcomes. Outcome measures can beconsidered under headings of clinical/functional, safety, andneurophysiological.
8.1. Clinical outcomes: motor function
A rigorous, evidence-based approach to clinical motoroutcome selection should be adopted. Testing should beperformed by a team of experienced experts that may include
paediatric occupational and physical therapists, develop-mental paediatricians, paediatric neurologists and physiat-rists, and clinical trialists. More specific outcomes mayrequire additional expertise such as child psychology re-searchers when considering psychosocial and quality of lifeoutcomes. Multidimensional evaluations should consider thebody structure and function, activity and participation do-mains of the WHO International Classification of Func-tioning, Disability and Health (ICF), considering bothunimanual and bimanual performance.197 Tools with estab-lished clinimetric properties in the population of interest (i.e.
hemiparetic CP) are selected to evaluate diverse upper ex-tremity functions relevant to daily living in children.198,199
Measures need to be both child and family friendlyincluding sensitivity to time and fatigue. Measurement ofboth uni- and bi-lateral function of both limbs are requiredfor normative data, evaluation of different clinical functions,and safety (including screening for changes in unaffectedhand function). Testing should be video-taped for qualityassurance, inter-rater validation, and additional offlineanalysis. Motor outcomes are measured at baseline, and 1week, 2 months post-intervention.
With these principles in mind, the following three po-
tential primary outcome measures might be considered in aclinical trial of intensive motor learning therapy combinedwith non-invasive brain stimulation in hemiparetic chil-dren. An additional list of possible secondary outcomes andtheir supporting evidence and attributes are summarized inTable 2.
e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 2 1 ( 2 0 1 7 ) 7 5e1 0 3 89

Table 2 e Examples of potential functional outcome measures for clinical trials of neuromodulation in hemiparetic CP.
Measure Target Application and evidence-base
Canadian Occupational Performance Measure (COPM) Individual goals for therapy Individualized, family-centred tool identified child and family-perceived difficulties and personalimprovement goals for self-care, productivity (school), and activities. The same experienced OTscreened potential goals with child and parents with consensus defining those goals that were bothfunctionally relevant and reasonably achievable. Scaled scores for performance and satisfaction of eachgoal were obtained (1 lowest, 10 highest). Such subjective, patient-centred measures are increasinglyconsidered essential in paediatric hemiparetic CP trials. The COPM is validated for paediatrichemiparetic CP trials across our age range. Sensitivity to change has been established with an increasein COPM scores of %2 units considered clinically significant.
Assisting Hand Assessment (AHA) Bimanual function The AHA is an established evidence-based standard for the objective quantification of bilateral handfunction in children with hemiparetic CP. Certified occupational therapists administer a structured,play-based assessment of spontaneous bimanual hand use followed by itemized scoring of the video-taped session. This Rasch-built evaluation carries the strongest evidence of inter-rater, intra-rater, andtest-retest reliabilities, test-validity, and responsiveness to change for bimanual tasks in hemiparetic CPchildren within our age range. Sensitivity to change and excellent clinimetric properties have beenestablished in paediatric hemiparetic CP trials. Consistent with validated methods, AHA scores areexpressed as logit units with an increase of %5 units considered clinically significant.
Melbourne Assessment of UnilateralUpper Limb Function (MA)
Unimanual function The MA is a validated, criterion-referenced functional measure designed to detect change inhemiparetic children. Trained therapists evaluate upper extremity motor tasks with performanceranked for each creating a total maximal score of 122 points (reported as percentage). Validation studieshave correlated MA with clinically relevant functional outcomes in school-aged children.
Jebsen Taylor Test of Hand Function (JTTHF) Unimanual function 1. Standardized timed test of unimanual upper extremity functional activities evaluating efficiency ofmovement. Important for comparability as the most common outcome measure used in adult stroketDCS clinical trials and recent paediatric CP studies.
AbilHAND Manual function Designed to assess manual function in children with cerebral palsy, the AbilHAND scores 21 commonmanual activities in children at 3 levels of difficulty with summary logit unit scores. This measure is notspecific to hemiparetic children but has been used in other paediatric CIMT trials.
Grip and pinch strength (GS, PS) Motor function GS is a simple, quick measure of hand motor function quantifiable with a dynamometer employed inmany paediatric hemiparetic CP and adult rTMS stroke trials. Unaffected hand GS and PS are alsopotential safety outcomes.
Box and blocks (BB) Dexterity This test of unimanual dexterity will be applied on both sides as in previously reported paediatric CIMTtrials. Assessment of the unaffected limb provides a safety measure (described above).
Purdue pegboard test (PPT) Dexterity 2. Performed bilaterally to measure manual dexterity and is commonly used in paediatric CIMT studies,and was the primary outcome in our healthy tDCS motor learning trial in children.
Paediatric Motor Activity Log (PMAL) Daily activity 3. Commonly used in hemiparetic CP studies with test-retest stability and sensitivity to change.Completed by parents.
PedsQL Cerebral Palsy Module (3.0) Quality of Life Condition specific and validated, age-adjusted child and parental reports assessed domains of dailyactivities, school activities, movement/balance, pain/hurt, fatigue, eating activities, and speech/communication.
APSP Parental Outcome Measure (POM) Parental psychology Measures adverse parental psychological outcomes in parents of children with perinatal strokeincluding unique symptoms of maternal guilt and blame.
european
journal
of
paedia
tric
neurology
21
(2017)75e103
90

8.1.1. Primary objective motor outcome: Assisting HandAssessment (AHA)
This is currently the established standard for the objectivequantification of bilateral hand function in children withhemipareticCP.199ARasch-built evaluation, theAHAcarriesthe strongest evidence of inter-rater, intra-rater, and test-retest reliabilities, test-validity, and responsiveness tochange for bimanual tasks in hemiparetic school-agedchildren.199e204 Sensitivity to change and excellent clini-
metric properties have been established in multiple pedi-atricHCPclinical trials.120,144,205e207Onepotential limitationof theAHAisadrop inscorewhennewunimanual functionshave not yet been incorporated into the bimanual tasksbeingmeasured (i.e. scoresmay drop despite new function).Our trained therapistshave successfullyexecuted>200AHAmeasurements within multiple clinical trials172 with excel-lent compliance and robust data.
8.1.2. Primary subjective motor outcome: Canadianoccupational performance measure (COPM)
Subjective outcome measures are now considered a valid,potentially essential outcome measure in rehabilitationtrials including children with hemiparetic CP.51,208 It couldbe argued that any gains shown in objective tests of motorfunction (e.g. strength, dexterity) are meaningless if thepatients themselves have not perceived the achievementof a personal goal or some other personal satisfaction. Forthese reasons, individualized, patient-centered, goaldirected tools such as the COPM have been developed andvalidated. Applied by an experienced pediatric OT incombinationwith child and parents, the COPM can identify
child and family-perceived difficulties in categories of self-care, productivity (school), and activities.209e213 Validatedfor both school-aged children214,215 and pediatric hemi-paretic CP trials,208,214,216e218 the COPM has been a robustmeasure in our previous perinatal stroke trials.172 We havealso recently characterized how COPM goals are set in thispopulation and their relationship to success in suchinterventional trials (Haspels et al., 2016, unpublisheddata).
8.1.3. Novel “real-life, continuous” motor outcome:actigraphic symmetry index (ASI)
No existing motor outcome measure can quantify contin-uous use of the upper extremities during the normal ac-tivities of real life. We recently proposed to overcome thislimitation using actigraphy. Lightweight wrist accelerom-eters can constantly measure and store subtle movements(e.g. fitbit). Such systems can also track movements indisabled persons including those with CP.219 In upcoming
trials, we will use the Actiwatch2 system to record meanmovements every 15 seconds for 48 hour epochs of time(baseline, 2 months, 6 months) as well as continuously
during the 2 week intervention phase. Importantly, we will
do this bilaterally (2 watches), allowing the generation of asymmetry index between the affected and unaffectedlimbs. Our preliminary data has established the feasibilityand accuracy of these methods in school-aged children(Cole et al., unpublished data).
Many additional clinical outcome measures can beconsidered depending on the nature of the trial. Examples,including their supporting evidence and primary targets, aresummarized in Table 2.
8.2. Safety outcomes
With limited non-invasive neuromodulation data in thedeveloping brain, careful and complete application of safetyoutcomes is paramount within clinical trials. Adult guidelinesand safety reviews are available for both TMS171 and tDCS175
and are certainly applicable. However, issues unique to chil-
dren need to be screened for and rates of tolerability and po-tential adverse events documented. Safety issues should beidentified a priori by experienced investigators but also atarms-length by a data safety and monitoring board (DSMB).Interim safety analyses may be incorporated into trial designat set time points (e.g. after certain numbers of subjects havecompleted outcomes). These analyses, as well as any seriousadverse events, should be reviewed by the DSMB and insti-tutional ethics boards requirements according to established,pre-defined protocols.
Safety can be considered under the following headings.
8.2.1. Serious adverse events
Typical definitions of SAE are adverse events or reactionsthat results in death, is life-threatening, requires hospi-talisation or prolongation of existing hospitalisation, re-sults in persistent or significant disability or incapacity, oris a congenital anomaly or birth defect. Fortunately, SAEreports in non-invasive brain stimulation have beenexceedingly rare across decades of use.
8.2.2. Function-specific adverse effects
Unique undesired outcomes may occur in specific studies.In the case of modulation trials for hemiparetic CP, oneexample is provided by the known control of both upperextremities by the non-lesioned hemisphere. Subse-quently, inhibitory stimulation of the contralesional motorcortex might include theoretical consideration of reducinghand function in the unaffected hand or in the target
affected hand, particularly in those with prominent ipsi-lateral corticospinal arrangements. Therefore, primarysafety outcomes in our brain stimulation trials haveincluded regular measures of both affected and unaffectedhand function across time points for each subject andwithin interim safety analyses.
e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 2 1 ( 2 0 1 7 ) 7 5e1 0 3 91

8.2.3. Side effects
Any intervention capable of having biological effects mustalso have the risk of side effects. Extrapolating from themuch larger volume of evidence from the adult brainstimulation world and published guidelines,171 a reason-able list of side effects to be specifically screened for can begenerated. These include feelings of headache or neck painwith TMS with the addition of itching or burning sensa-tions for tDCS. However, symptoms specific to young age
groupsmay exist, such as TMS-induced vasovagal syncopein adolescents.220,221 Each anticipated subjective symptomcan be screened for and quantified including scale severity,duration, need for treatment, etc using a simple form.Screening and documentation should be repeated overtime to assess for persistence or tolerance.
8.2.4. Tolerability
A standardized safety and tolerability evaluation for TMS
in children has been developed63,222 and is easily adaptedfor different population and modalities including tDCS.190
Subjects are asked to rank order their stimulation experi-ence amongst 7 other common childhood experiences.
Optimizing safety requires attention to each of the aboveissues. Brain stimulation studies in children should be per-formed by experienced personnel in a secure environment.Immediate access to medical care should be available in theunlikely occurrence of a serious adverse event. Written stan-dardized operating procedures, for both experimentalmethods and handling adverse events, should be imple-
mented and staff tested for their familiarity with these.Our single centre experience has administered nearly 3
million stimulations to over 280 children in the past 8 years.Ages ranged from 8months to 19 years (median 11.2) with thevast majority being school-aged. The most common condi-tions were perinatal stroke/cerebral palsy (70), mild traumaticbrain injury (TBI, 68), or typically developing (53). Multi-disciplinary neurophysiological studies included single- andpaired-pulse TMS methods. Therapeutic clinical trials usedrepetitive TMS (rTMS) and anodal/cathodal motor cortextDCS. Prospectively collected safety and tolerability data on all
subjects included the paediatric TMS safety and tolerabilitymeasure, child and parental interviews, and data safety andmonitoring boards. There were no serious adverse events.Tolerability between TMS (402,680 stimulations) and rTMS(2.1million stimulations) was comparable and rated similar toa long car ride. Although >100 had brain injuries and/or epi-lepsy, no seizures occurred. Headache following a TMSneurophysiology protocol was more common in perinatalstroke (40%) than typically developing (13%) participants butwas mild and self-limiting. Mild neck pain with was relativelycommon but comparable between perinatal stroke (22%),
depression (19%), and TBI (19%). Tolerability improved overtime with rates of headache, neck pain, and unpleasanttingling decreasing by >50% at repeat testing. Of 51 children
receiving tDCS, scalp itching in 55% was mild, transient, and
comparable to shamwith no drop-outs. Neither low frequencyrTMS or cathodal tDCS of the non-lesioned hemispheredecreased function of either hand in children with hemi-paretic cerebral palsy.We believe this data supports that brainstimulation is safe and well tolerated in children.
9. Neurophysiological outcomes
Advanced neurotechnologies have greatly advanced the abil-ity to understand developmental plasticity in real patients.This includes baseline measures to evaluate natural processand how they relate to function but also the opportunity toexplore the potential mechanisms of intervention-inducedchange. Combining modern technologies allows the compre-hensive, integrated study of brain structure and function
personalized to each individual. Clinically relevant examples ofsuch integration are increasingly available in adults223 butawaiting full exploration in children. Summarized here areleading applications of single- and paired-pulse TMS, imagingincluding task and resting state fMRI and diffusion tensorimaging (DTI), and robotics.
9.1. Transcranial magnetic stimulation (TMS)
First described in 1985,224 most TMS studies are publishedsince 2008 but only <3% include children. Focused magneticfields applied across neuronal membranes result in focaldepolarisations of human cortex according to Faraday's Law.With narrow spatial resolution, TMS can affect discrete
functional areas,225 offering non-invasive, painless mappingof motor systems.67,76,77,226 Tools relevant to the current studyinclude “single-pulse” measurements such as motor evokedpotentials (MEP) which quantify motor pathway neurophysi-ology from cortex to muscle. Motor thresholds and stim-uluseresponse curves reflect corticospinalexcitability.72,222,227 Paired-pulse TMS employs multiplestimuli to elucidate interactions between different brainareas.90,92,225,228e232 TMS is safe and well tolerated in chil-dren,162,222,233 supported by animal studies106,151,234e238 andpublished guidelines.171 Application is safe in adult
stroke85e87,148,149,160,161,166,228 and supported by our safetywork in children with stroke.66,72,81,220 TMS-related seizureshave not been described in children162 including administra-tion over seizure foci.239,240
Modern technologies include single pulse systems forexcitability and pathways as well as paired-pulse methodscapable of probing cortical excitatory, inhibitory, and otherphysiological functions. Neuronavigation systems such asBrainsight (Rogue Research, Montreal) allow real time co-registration of coil location with individual subject MRI inthree dimensions, including overlay of functional imagingtargets. We have successfully demonstrated each of these
methods in children with stroke.99 Single pulse TMS candetermine bilateral M1 excitability.99,241 Motor evoked poten-tials are recorded from hand muscle, often the first dorsalinterosseous (FDI), bilaterally. The motor “hotspot” is definedover M1 as the area producing consistent, high amplitudeMEP. Resting motor threshold (RMT) is then defined as the
e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 2 1 ( 2 0 1 7 ) 7 5e1 0 392

stimulator intensity required to produce MEP % 50 mV in 5/10
trials. Our studies63,78 suggest stroke side MEP are obtainablein >80% of subjects. Activated motor thresholds are also ob-tained during ~20% of maximal FDI activation via visualfeedback. Motor maps can also be created in the lesioned andunlesioned hemisphere. We recently added a TMS Roboticsystem (Axilum, Strasbourg) that should greatly facilitateexecution of such outcomes.
Additional potential TMS neurophysiological outcomesinclude: (1) Stimulus response curves (rest and active). BilateralM1 excitability is quantified by measuring MEP amplitudesacross 5 escalating stimulus intensities such as 100/110/120/
130/140/150% of RMT. (2) Interhemispheric Inhibition (IHI). Bidi-rectional IHI (lesioned to unlesioned hemisphere and vice-versa) applies stimuli to both M1 in quick succession withmethods described elsewhere.63,90,96,242e244 Paired-pulse TMSapplies a suprathreshold conditioning stimulus (CS) con-tralaterally immediately prior to a test stimulus (TS) withinterstimulus intervals of 10 and 40 ms. The decrease in TSMEP quantifies IHI. (3) Short interval intracortical inhibition (SICI).M1 SICI can be determined according to established paired-pulse methods.91,245 For example, after suprathreshold CS,SICI effects are typically seenwith an interstimulus interval of
2 ms. These and other TMS measures of cortical neurophysi-ology can define baseline function as well as changes occur-ring secondary to interventions.
9.2. Functional MR (fMRI) and the resting state (rsfMRI)
Functional MRI extrapolates regional brain activity fromchanges in blood oxygen-dependent signal. Two fMRI mo-
dalities have provided valuable insight to motor physiology,development, and stroke recovery. Task-dependent fMRIcompares regional activity between on and off states duringperformed motor tasks. Task fMRI has established funda-mental principles of development and stroke recoveryincluding the roles of each hemisphere (above). Small hemi-paretic CP studies have demonstrated similar utility andsupport ourmodel. However, task fMRI only studies individualbrain areas rather than the integrated neural networks.
“A connectivity-based system perspective is much closer to theneurobiology underlying brain physiology compared to analyzing
anatomically segregated regions (i.e. traditional fMRI).”246 Restingstate fMRI (rsfMRI) is a recent advance that facilitates suchnetwork analysis.247 Simple acquisition of fMRI data duringpatient rest can be analyzed by both exploratory andhypothesis-driven methods to create models of functionaland effective network connectivity.246,248 Such rsfMRI ap-proaches now provide invaluable insight to brain plasticitymechanisms in adult stroke.246,249,250 Resting state motornetworks are measurable in young children251 but are rela-tively unstudied in perinatal stroke. The stark contrast pro-vided by arterial (cortical lesions at term) and PVI (preterm,subcortical) creates an ideal human model to explore motor
network development after perinatal brain injury. Further-more, changes in functional networks likely represent anessential measure of intervention-induced plasticity.Recently, such approaches have been validated in adultswhere change induced by brain stimulation interventionsmay be demonstrated using rsfMRI.223,252
9.3. Diffusion tensor imaging (DTI)
Diffusion MRI acquires microscopic information on structuralbrain connections. DTI measures preferential water moleculediffusion (Brownian motion) along axonal axes, providingunique structural and physiological information in thedeveloping and diseased brain.253 DTI non-invasively mea-sures neural fibre composition, integrity, and orientationwhile tractography creates three dimensional reconstructionsof large white matter tracts.254 DTI can evaluate the motor
system including corticospinal tract integrity.257 In adultstroke, corticospinal tract DTI measures correlate with motoroutcomes.258,259 DTI utility has been demonstrated acrossnumerous childhood neurological disorders257 and can besynergistically integrated with fMRI and TMS to createcomprehensive, in vivo models of brain structure and func-tion.86 Perinatal stroke DTI studies are few260 though CP ap-plications261,262 support feasibility. We recently demonstratedour ability to evaluate corticospinal tract integrity in perinatalstroke using DTI.263
9.4. Robotics
Robots have further advanced the ability to measure complexclinical function indisabledpatients.Robotic technologiessuchas the KINARM (Kinesiological Instrument for Normal andAltered Reaching Movement) can assess limb movements atthe shoulder and elbow. Unique advantages complimentary totheabovemodalitiesareconferred. Forexample,positionsenseis probably a major contributor to disability in hemipareticpatients. However, a lack of objective measures of such func-tion has limited study. Using KINARM, the characteristics of
positionsensesdysfunctionare increasinglywell characterizedin adult stroke18,19 We have shown that the samemethods arewell tolerated by children where a standardized, validatedassessment of sensorimotor function can include two tasksthat specifically target proprioception. Position sense can bemeasured using a positionmatching task; the robot moves theaffected arm to random spatial locations and the subject thenattempts to mirror match the positions with the unaffectedarm. To measure kinaesthesia; the robot moves the affectedarm. Subjects are required to move the good arm to matchspeed, amplitude and direction. Both tasks are completed first
with vision occluded and again without the blindfold to deter-mine their ability to compensate with vision. Using thesemethods, we recently demonstrated the common occurrenceof such deficits in children with perinatal stroke and their as-sociation with clinical function.264 Such robotic outcomes willbe available tool in identifying new modulation targets andassessing outcomes from the interventional trials tat result.
10. Future directions
The translational pipeline from proof of principle through thephases of early stage clinical trials to the accumulation ofmultiple, positive, multicentre fully powered trials must beconsidered. The prolonged nature, and associated high costs,are likely comparable to drug development in some regardsthough potentially more economical. For example, rTMS for
e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 2 1 ( 2 0 1 7 ) 7 5e1 0 3 93

adult major depression has driven the field of therapeutic
non-invasive neuromodulation. Despite many positive ran-domized controlled trials spanning more than a decade, theintervention is only just now becoming an insured service inmany developed countries. The extremely common occur-rence, poor response rates to current medications, anddisabling nature of major depression have likely driven thisprocess relatively quickly. In comparison, treating differentforms of cerebral palsy in children may not carry the sameweight, further slowing the process. This should notdiscourage effort but is a considered reason to optimize thedesign, exaction, and progress of early clinical trials.
The economics of such interventions in children have notbeen studied and remain difficult to estimate with such alimited number of trials to date. However, camp-basedintensive motor learning is both a likely prerequisite forneuromodulation in children with motor disability as well asbeing an expensive, resource-intensive endeavour. Full dayprograms may be required to reach adequate dosing. Highlyqualified personnel are many for such programs, includingskilled therapists to both deliver treatment and administeroutcomes. We have tried to mitigate some of these costs withafter-school therapy programs and incorporating student
therapists to administer therapy under the guidance of moreexperienced therapists. Home-based therapy programs areincreasing in popularity for these reasons and may becomefeasible as portable, simple stimulation devices are developed.Such tDCS systems are already being designed includingpatient-friendly operation and ability for remote program-ming and monitoring by study investigators. However, homeprograms may risk removing the substantial psychosocialbenefits young people may receive from participating in campbased programs. These issues will need to be carefullyweighed in the design of future trials.
Neuromodulation trials in children with cerebral palsybring the possibility of precision medicine to paediatricrehabilitation. While predictors of response to such in-terventions have not yet beenwell defined, there is little doubtthat individual factors such as age, baseline disability, lesiontype or location, and corticospinal tract arrangement likelyplay a role.265 A recent review suggested a possible systematicapproach to classify hemiparetic children based on clinical(e.g. mirrormovements), TMS (corticospinal tract orientation),and imaging (corticospinal tract integrity) variables.266 Theseare logical steps that are yet to be validated but carry the po-tential to bring personalized medicine to the rehabilitation of
children with hemiparetic CP.
Conflict of interest
None.
r e f e r e n c e s
1. Hsu WY, Cheng CH, Liao KK, Lee IH, Lin YY. Effects ofrepetitive transcranial magnetic stimulation on motor
functions in patients with stroke: a meta-analysis. Stroke2012;43(7):1849e57.
2. Lindenberg R, Renga V, Zhu LL, Nair D, Schlaug G.Bihemispheric brain stimulation facilitates motor recoveryin chronic stroke patients. Neurology 2010;75:2176e84(1526e632X (Electronic)).
3. Lefaucheur J-P, Andr!e-Obadia N, Antal A, Ayache SS,Baeken C, Benninger DH, et al. Evidence-based guidelines onthe therapeutic use of repetitive transcranial magneticstimulation (rTMS). Clin Neurophysiol 2014;125(11):2150e206.http://dx.doi.org/10.1016/j.clinph.2014.05.021.
4. Mineyko A, Kirton A. The black box of perinatal ischemicstroke pathogenesis. J Child Neurol 2011;26(9):1154e62.
5. Nelson KB. Perinatal ischemic stroke. Stroke 2007;38:742e5(1524e4628 (Electronic)).
6. Petty GW, Brown Jr RD, Whisnant JP, Sicks JD, O'Fallon WM,Wiebers DO. Ischemic stroke subtypes: a population-basedstudy of incidence and risk factors. Stroke 1999;30:2513e6(0039e2499 (Print)).
7. Raju TN, Nelson KB, Ferriero D, Lynch JK. Ischemic perinatalstroke: summary of a workshop sponsored by the NationalInstitute of child health and human development and theNational Institute of neurological disorders and stroke.Pediatrics 2007;120:609e16.
8. DeVeber G, MacGregor D, Friefeld S, Chan A, Meanery B,Domi T. Neurological outcome in survivors of neonatalarterial ischemic stroke. Pediatr Res 2003;53(4):537A.
9. Mercuri E, Cowan F, Gupte G, Manning R, Laffan M,Rutherford M, et al. Prothrombotic disorders and abnormalneurodevelopmental outcome in infants with neonatalcerebral infarction. Pediatrics 2001;107(1098e4275):1400e4.
10. Sreenan C, Bhargava R, Robertson CM. Cerebral infarction inthe term newborn: clinical presentation and long- termoutcome. J Pediatr 2000;137(0022e3476):351e5.
11. Kirton A, deVeber G. Advances in perinatal ischemic stroke.Pediatr Neurol 2009;40:205e14.
12. Kirton A, deVeber G, Pontigon AM, MacGregor D, Shroff M.Presumed perinatal ischemic stroke: vascular classificationpredicts outcomes. Ann Neurol 2008;63(4):436e43.
13. Domi T, deVeber G, Shroff M, Kouzmitcheva E,MacGregor DL, Kirton A. Corticospinal tract pre-walleriandegeneration: a novel outcome predictor for pediatric strokeon acute MRI. Stroke 2009;40:780e7.
14. Kirton A, Shroff M, Pontigon AM, deVeber G. Risk factors andpresentations of periventricular venous infarction vs arterialpresumed perinatal ischemic stroke. Arch Neurol2010;67:842e8 (1538e3687 (Electronic)).
15. Tan M, Shroff M, Pontigon A, deVeber G, Kirton A. Role ofoccipital bone compression of the superior sagittal sinus inthe pathophysiology of neonatal cerebral sinovenousthrombosis. Thromb Haemost 2007;5(2):577.
16. Kirton A, Armstrong-Wells J, Chang T, deVeber G, Rivkin MJ,Hernandez M, et al. Symptomatic neonatal arterial ischemicstroke: the international pediatric stroke study. Pediatrics2011;128:e1402e10 (1098e4275 (Electronic)).
17. Payne ET, Wei XC, Kirton A. Reversible wall enhancement inpediatric cerebral arteriopathy. Can J Neurol Sci2011;38:139e40 (0317e1671 (Print)).
18. DeVetten G, Coutts SB, Hill MD, Goyal M, Eesa M, O'Brien B,et al. Acute corticospinal tract Wallerian degeneration isassociated with stroke outcome. Stroke J Cereb Circ2010;41(4):751e6. http://dx.doi.org/10.1161/STROKEAHA.109.573287.
19. Tan MA, Miller E, Shroff MM, Deveber GA, Kirton A.Alleviation of neonatal sinovenous compression to enhancecerebral venous blood flow. J Child Neurol. 2013May;28(5):583e8. http://dx.doi.org/10.1177/0883073812449689. Epub 2012 Jul 17.
e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 2 1 ( 2 0 1 7 ) 7 5e1 0 394

20. Trauner DA, Chase C, Walker P, Wulfeck B. Neurologicprofiles of infants and children arter perinatal stroke. PediatrNeurol 1993;9:383e6.
21. Golomb MR, MacGregor DL, Domi T, Armstrong DC,McCrindle BW, Mayank S, et al. Presumed pre- or perinatalarterial ischemic stroke: risk factors and outcomes. AnnNeurol 2001;50(0364e5134):163e8.
22. Uvebrant P. Hemiplegic cerebral palsy. Aetiology andoutcome. Acta Paediatr Scand Suppl 1988;345:1e100(0300e8843 (Print)).
23. de Vries LS, Roelants-van Rijn AM, Rademaker KJ, van HI,Beek FJ, Groenendaal F. Unilateral parenchymalhaemorrhagic infarction in the preterm infant. Eur J PaediatrNeurol 2001;5:139e49 (1090e3798 (Print)).
24. de Vries LS, Rademaker KJ, Groenendaal F, Eken P, vanHaastert IC, Vandertop WP, et al. Correlation betweenneonatal cranial ultrasound, MRI in infancy andneurodevelopmental outcome in infants with a largeintraventricular haemorrhage with or without unilateralparenchymal involvement. Neuropediatrics 1998;29:180e8(0174e304X (Print)).
25. Ghi T, Simonazzi G, Perolo A, Savelli L, Sandri F, Bernardi B,et al. Outcome of antenatally diagnosed intracranialhemorrhage: case series and review of the literature.Ultrasound Obstet Gynecol 2003;22:121e30 (0960e7692 (Print)).
26. Elchalal U, Yagel S, Gomori JM, Porat S, Beni-Adani L,Yanai N, et al. Fetal intracranial hemorrhage (fetal stroke):does grade matter? Ultrasound Obstet Gynecol 2005;26:233e43(0960e7692 (Print)).
27. Takanashi J, Barkovich AJ, Ferriero DM, Suzuki H, Kohno Y.Widening spectrum of congenital hemiplegia:periventricular venous infarction in term neonates.Neurology 2003;61:531e3 (1526e632X (Electronic)).
28. Takanashi J, Tada H, Barkovich AJ, Kohno Y. Magneticresonance imaging confirms periventricular venousinfarction in a term-born child with congenital hemiplegia.Dev Med Child Neurol 2005;47:706e8 (0012e1622 (Print)).
29. Kirton A, Wei X. Teaching neuroimages: confirmation ofprenatal periventricular venous infarction withsusceptibility-weighted MRI. Neurology 2010;74(12):e48.
30. Abels L, Lequin M, Govaert P. Sonographic templates ofnewborn perforator stroke. Pediatr Radiol 2006;36:663e9(0301e0449 (Print)).
31. deVeber G, Andrew M. Canadian pediatric ischemic strokestudy group cerebral sinovenous thrombosis in children. NEngl J Med 2001;345(0028e4793):417e23.
32. Fitzgerald KC, Williams LS, Garg BP, Carvalho KS,Golomb MR. Cerebral sinovenous thrombosis in the neonate.Arch Neurol 2006;63:405e9 (0003e9942 (Print)).
33. Lee J, Croen LA, Lindan C, Nash KB, Yoshida CK, Ferriero DM,et al. Predictors of outcome in perinatal arterial stroke: apopulation-based study. Ann Neurol2005;58(0364e5134):303e8.
34. deVeber G, MacGregor D, Curtis R, Mayank S. Neurologicoutcome in survivors of childhood arterial ischemic strokeand sinovenous thrombosis. J Child Neurol2000;15(0883e0738):316e24.
35. Mercuri E, Barnett A, Rutherford M, Guzzetta A, Haataja L,Cioni G, et al. Neonatal cerebral infarction and neuromotoroutcome at school age. Pediatrics2004;113(1098e4275):95e100.
36. Mercuri E, Rutherford M, Cowan F, Pennock J, Counsell S,Papadimitriou M, et al. Early prognostic indicators ofoutcome in infants with neonatal cerebral infarction: aclinical, electroencephalogram, and magnetic resonanceimaging study. Pediatrics 1999;103(0031e4005):39e46.
37. Hagberg B, Hagberg G, Beckung E, Uvebrant P. Changingpanorama of cerebral palsy in Sweden. VIII. Prevalence and
origin in the birth year period 1991e94. Acta Paediatr2001;90:271e7 (0803e5253 (Print)).
38. Nelson KB, Lynch JK. Stroke in newborn infants. LancetNeurol 2004;3(1474e4422):150e8.
39. Nelson KB. Can we prevent cerebral palsy? N Engl J Med2003;349:1765e9 (1533e4406 (Electronic)).
40. Mercuri E, Jongmans M, Bouza H, Haataja L, Rutherford M,Henderson S, et al. Congenital hemiplegia in children atschool age: assessment of hand function in the non-hemiplegic hand and correlation with MRI. Neuropediatrics1999;30:8e13 (0174e304X (Print)).
41. deVeber G., Kirton A., CPISR Study Group. Arterial ischemicstroke in children. Ann Neurol n.d.;60(S10):115.
42. Goldenberg NA, Knapp-Clevenger R, Manco-Johnson MJ.Elevated plasma factor VIII and D-dimer levels as predictorsof poor outcomes of thrombosis in children. N Engl J Med2004;351(1533e4406):1081e8.
43. Mercuri E, Anker S, Guzzetta A, Barnett A, Haataja L,Rutherford M, et al. Neonatal cerebral infarction and visualfunction at school age. Arch Dis Child Fetal Neonatal Ed2003;88(1359e2998):F487e91.
44. Bava S, Archibald SL, Trauner DA. Brain structure inprenatal stroke: quantitative magnetic resonance imaging(MRI) analysis. J Child Neurol 2007;22:841e7 (0883e0738(Print)).
45. Boardman JP, Ganesan V, Rutherford MA, Saunders DE,Mercuri E, Cowan F. Magnetic resonance imagecorrelates of hemiparesis after neonatal and childhoodmiddle cerebral artery stroke. Pediatrics2005;115(1098e4275):321e6.
46. Ganesan V, Ng V, Chong WK, Kirkham FJ, Connelly A. Lesionvolume, lesion location, and outcome after middle cerebralartery territory stroke. Arch Dis Child1999;81(0003e9888):295e300.
47. De Vries LS, Van der Grond J, Van Haastert IC,Groenendaal F. Prediction of outcome in new-born infantswith arterial ischaemic stroke using diffusion-weightedmagnetic resonance imaging. Neuropediatrics2005;36(1):12e20. http://dx.doi.org/10.1055/s-2005-837544.
48. Kirton A, Shroff M, Visvanathan T, deVeber G. Quantifiedcorticospinal tract diffusion restriction predicts neonatalstroke outcome. Stroke J Cereb Circ 2007;38(3):974e80. http://dx.doi.org/10.1161/01.STR.0000258101.67119.72.
49. Lynch JK. Cerebrovascular disorders in children. Curr NeurolNeurosci Rep 2004;4(1528e4042):129e38.
50. McLinden A, Baird AD, Westmacott R, Anderson P,deVeber G. Early cognitive outcome after neonatal stroke. JChild Neurol 2007 Sep;22(9):1111e6.
51. Westmacott R, MacGregor D, Askalan R, deVeber G. Lateemergence of cognitive deficits after unilateral neonatalstroke. Stroke 2009;40:2012e9 (1524e4628 (Electronic)).
52. Taylor TN, Davis PH, Torner JC, Holmes J, Meyer JW,Jacobson MF. Lifetime cost of stroke in the United States.Stroke 1996;27(9):1459e66.
53. Hoare B, Imms C, Carey L, Wasiak J. Constraint-inducedmovement therapy in the treatment of the upper limb inchildren with hemiplegic cerebral palsy: a Cochranesystematic review. Clin Rehabil 2007;21(8):675e85.
54. Kennard MA. Age and other factors in motor recovery fromprecentral lesions in monkeys. Am J Physiol 1936;115:137e46.
55. Trevathan WR. Introduction to evolutionary medicine. In:Trevathan WR, Smith EO, McKenna JJ, editors. Evolutionarymedicine, vol. 1. New York: Oxford University Press Inc; 1999.p. 3e6.
56. Eyre JA, Smith M, Dabydeen L, Clowry GJ, Petacchi E,Battini R, et al. Is hemiplegic cerebral palsy equivalent toamblyopia of the corticospinal system? Ann Neurol2007;62(5):493e503.
e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 2 1 ( 2 0 1 7 ) 7 5e1 0 3 95

57. Eyre JA. Corticospinal tract development and its plasticityafter perinatal injury. Neurosci Biobehav Rev 2007;31:1136e49(0149e7634 (Print)).
58. Martin JH, Friel KM, Salimi I, Chakrabarty S. Activity- anduse-dependent plasticity of the developing corticospinalsystem. Neurosci Biobehav Rev 2007;31(8):1125e35. http://dx.doi.org/10.1016/j.neubiorev.2007.04.017.
59. Werhahn KJ, Conforto AB, Kadom N, Hallett M, Cohen LG.Contribution of the ipsilateral motor cortex to recovery afterchronic stroke. Ann Neurol 2003;54:464e72 (0364e5134(Print)).
60. Foltys H, Krings T, Meister IG, Sparing R, Boroojerdi B,Thron A, et al. Motor representation in patients rapidlyrecovering after stroke: a functional magnetic resonanceimaging and transcranial magnetic stimulation study. ClinNeurophysiol 2003;114:2404e15 (1388e2457 (Print)).
61. Ward NS, Cohen LG. Mechanisms underlying recovery ofmotor function after stroke. Arch Neurol2004;61(0003e9942):1844e8.
62. Calautti C, Leroy F, Guincestre JY, Marie RM, Baron JC.Sequential activation brain mapping after subcortical stroke:changes in hemispheric balance and recovery. Neuroreport2001;12:3883e6 (0959e4965 (Print)).
63. Rossini PM, Calautti C, Pauri F, Baron JC. Post-stroke plasticreorganisation in the adult brain. Lancet Neurol2003;2:493e502 (1474e4422 (Print)).
64. Cioni G, Montanaro D, Tosetti M, Canapicchi R,Ghelarducci B. Reorganisation of the sensorimotor cortexafter early focal brain lesion: a functional MRI study inmonozygotic twins. Neuroreport 2001;12:1335e40 (0959e4965(Print)).
65. Kirton A, Chen R, Friefeld S, Gunraj C, Pontigon AM,deVeber G. Contralesional repetitive transcranial magneticstimulation for chronic hemiparesis in subcortical paediatricstroke: a randomised trial. Lancet Neurol 2008;7(6):507e13.
66. Kirton A, deVeber G, Gunraj C, Chen R. Cortical excitabilityand interhemispheric inhibition after subcortical pediatricstroke: plastic organization and effects of rTMS. ClinNeurophysiol 2010;121:1922e9 (1872e8952 (Electronic)).
67. Berweck S, Walther M, Brodbeck V, Wagner N, Koerte I,Henschel V, et al. Abnormal motor cortex excitability incongenital stroke. Pediatr Res 2008;63:84e8.
68. Staudt M, Gerloff C, Grodd W, Holthausen H, Niemann G,Krageloh-Mann I. Reorganization in congenital hemiparesisacquired at different gestational ages. Ann Neurol2004;56:854e63 (0364e5134 (Print)).
69. Staudt M, GroddW, Gerloff C, Erb M, Stitz J, Krageloh-Mann I.Two types of ipsilateral reorganization in congenitalhemiparesis: a TMS and fMRI study. Brain2002;125(0006e8950):2222e37.
70. Juenger H, Linder-Lucht M, Walther M, Berweck S, Mall V,Staudt M. Cortical neuromodulation by constraint-induced movement therapy in congenital hemiparesis: anFMRI study. Neuropediatrics 2007;38:130e6 (0174e304X(Print)).
71. Walther M, Juenger H, Kuhnke N, Wilke M, Brodbeck V,Berweck S, et al. Motor cortex plasticity in ischemic perinatalstroke: a transcranial magnetic stimulation and functionalMRI study. Pediatr Neurol 2009;41(3):171e8.
72. Farmer SF, Harrison LM, Ingram DA, Stephens JA. Plasticityof central motor pathways in children with hemiplegiccerebral palsy. Neurology 1991;41:1505e10 (0028e3878(Print)).
73. Carr LJ, Harrison LM, Evans AL, Stephens JA. Patterns ofcentral motor reorganization in hemiplegic cerebral palsy.Brain 1993;116:1223e47 (Pt 5)(0006e8950 (Print)).
74. Maegaki Y, Maeoka Y, Ishii S, Shiota M, Takeuchi A,Yoshino K, et al. Mechanisms of central motor
reorganization in pediatric hemiplegic patients.Neuropediatrics 1997;28:168e74 (0174e304X (Print)).
75. Nezu A, Kimura S, Takeshita S, Tanaka M. Functionalrecovery in hemiplegic cerebral palsy: ipsilateralelectromyographic responses to focal transcranial magneticstimulation. Brain Dev 1999;21:162e5 (0387e7604 (Print)).
76. Vandermeeren Y, Sebire G, Grandin CB, Thonnard JL,Schlogel X, De Volder AG. Functional reorganization of brainin children affected with congenital hemiplegia: fMRI study.Neuro Image 2003;20(1):289e301.
77. Yue Cao, Vikingstad EM, Huttenlocher PR, Towle VL,Levin DN. Functional magnetic resonance studies ofreorganization of the human hand sensorimotor area afterunilateral brain injury in the perinatal period. Proc Natl AcadSci U. S. A 1994;91:9612e6.
78. Macdonell RA, Jackson GD, Curatolo JM, Abbott DF,Berkovic SF, Carey LM, et al. Motor cortex localization usingfunctional MRI and transcranial magnetic stimulation.Neurology 1999;53:1462e7 (0028e3878 (Print)).
79. Thickbroom GW, Byrnes ML, Archer SA, Nagarajan L,Mastaglia FL. Differences in sensory and motor corticalorganization following brain injury early in life. Ann Neurol2001;49(0364e5134):320e7.
81. Eyre JA, Taylor JP, Villagra F, Smith M, Miller S. Evidence ofactivity-dependent withdrawal of corticospinal projectionsduring human development. Neurology 2001;57:1543e54(0028e3878 (Print)).
82. Nirkko AC, Rosler KM, Ozdoba C, Heid O, Schroth G,Hess CW. Human cortical plasticity: functional recoverywith mirror movements. Neurology 1997;48:1090e3(0028e3878 (Print)).
84. Ragazzoni A, Cincotta M, Borgheresi A, Zaccara G,Ziemann U. Congenital hemiparesis: different functionalreorganization of somatosensory and motor pathways. ClinNeurophysiol 2002;113:1273e8 (1388e2457 (Print)).
85. Rutten GJ, Ramsey NF, van Rijen PC, Franssen H, vanVeelen CW. Interhemispheric reorganization of motor handfunction to the primary motor cortex predicted withfunctional magnetic resonance imaging and transcranialmagnetic stimulation. J Child Neurol 2002;17:292e7(0883e0738 (Print)).
86. Staudt M. (Re-)organization of the developing human brainfollowing periventricular white matter lesions. NeurosciBiobehav Rev 2007;31(8):1150e6.
87. Hummel F, Cohen LG. Improvement of motor function withnoninvasive cortical stimulation in a patient with chronicstroke. Neurorehabil Neural Repair 2005;19:14e9 (1545e9683(Print)).
88. Hummel F, Celnik P, Giraux P, Floel A, Wu WH, Gerloff C,et al. Effects of non-invasive cortical stimulation on skilledmotor function in chronic stroke. Brain 2005;128:490e9(1460e2156 (Electronic)).
89. Fregni F, Boggio PS, Mansur CG, Wagner T, Ferreira MJ,Lima MC, et al. Transcranial direct current stimulation of theunaffected hemisphere in stroke patients. Neuroreport2005;16(0959e4965):1551e5.
90. Takeuchi N, Tada T, Toshima M, Chuma T, Matsuo Y,Ikoma K. Inhibition of the unaffected motor cortex by 1 Hzrepetitive transcranical magnetic stimulation enhancesmotor performance and training effect of the paretic hand inpatients with chronic stroke. J Rehabil Med 2008;40:298e303(1650e1977 (Print)).
91. Schambra HM, Sawaki L, Cohen LG. Modulation ofexcitability of human motor cortex (M1) by 1 Hz transcranialmagnetic stimulation of the contralateral M1. ClinNeurophysiol 2003;114:130e3 (1388e2457 (Print)).
92. Pal PK, Hanajima R, Gunraj CA, Li JY, Wagle-Shukla A,Morgante F, et al. Effect of low-frequency repetitive
e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 2 1 ( 2 0 1 7 ) 7 5e1 0 396

transcranial magnetic stimulation on interhemisphericinhibition. J Neurophysiol 2005;94(3):1668e75.
93. Mall V, Berweck S, Fietzek UM, Glocker FX, Oberhuber U,Walther M, et al. Low level of intracortical inhibition inchildren shown by transcranial magnetic stimulation.Neuropediatrics 2004;35:120e5 (0174e304X (Print)).
94. Garvey MA, Ziemann U, Bartko JJ, Denckla MB, Barker CA,Wassermann EM. Cortical correlates of neuromotordevelopment in healthy children. Clin Neurophysiol2003;114:1662e70 (1388e2457 (Print)).
95. Liepert J, Hamzei F, Weiller C. Motor cortex disinhibition ofthe unaffected hemisphere after acute stroke. Muscle Nerve2000;23:1761e3 (0148e639X (Print)).
96. Murase N, Duque J, Mazzocchio R, Cohen LG. Influence ofinterhemispheric interactions on motor function in chronicstroke. Ann Neurol 2004;55:400e9 (0364e5134 (Print)).
97. Liepert J, Restemeyer C, Kucinski T, Zittel S, Weiller C. Motorstrokes: the lesion location determines motor excitabilitychanges. Stroke 2005;36(1524e4628):2648e53.
98. Cicinelli P, Pasqualetti P, Zaccagnini M, Traversa R, Oliveri M,Rossini PM. Interhemispheric asymmetries of motor cortexexcitability in the postacute stroke stage: a paired-pulsetranscranial magnetic stimulation study. Stroke2003;34:2653e8 (1524e4628 (Electronic)).
99. Liepert J, Storch P, Fritsch A, Weiller C. Motor cortexdisinhibition in acute stroke. Clin Neurophysiol2000;111:671e6 (1388e2457 (Print)).
100. Ziemann U, Corwell B, Cohen LG. Modulation of plasticityin human motor cortex after forearm ischemic nerve block.J Neurosci 1998;18:1115e23 (0270e6474 (Print)).
101. Kirton A, deVeber G, Gunraj C, Friefeld S, Chen R. Corticalexcitability and interhemispheric inhibition in subcorticalpediatric stroke: chronic reorganization and effects ofcontralesional inhibitory rTMS. Brain Stimul 2008;1(3):271.
102. Armand J, Olivier E, Edgley SA, Lemon RN. Postnataldevelopment of corticospinal projections from motor cortexto the cervical enlargement in the macaque monkey. JNeurosci 1997;17:251e66 (0270e6474 (Print)).
103. Koh TH, Eyre JA. Maturation of corticospinal tracts assessedby electromagnetic stimulation of the motor cortex. Arch DisChild 1988;63:1347e52 (1468e2044 (Electronic)).
104. Chakrabarty S, Martin JH. Postnatal development of themotor representation in primary motor cortex. J Neurophysiol2000;84:2582e94 (0022e3077 (Print)).
105. Guzzetta A, Staudt M, Petacchi E, Ehlers J, Erb M, Wilke M,et al. Brain representation of active and passive handmovements in children. Pediatr Res 2007;61:485e90(0031e3998 (Print)).
106. Martin JH, Lee SJ. Activity-dependent competition betweendeveloping corticospinal terminations. Neuroreport1999;10:2277e82.
107. Martin JH, Kably B, Hacking A. Activity-dependentdevelopment of cortical axon terminations in the spinal cordand brain stem. Exp Brain Res 1999;125:184e99.
108. Salimi I, Martin JH. Rescuing transient corticospinalterminations and promoting growth with corticospinalstimulation in kittens. J Neurosci 2004;24:4952e61 (1529e2401(Electronic)).
109. Scales DA, Collins GH. Cerebral degeneration withhypertrophy of the contralateral pyramid. Arch Neurol1972;26:186e90 (0003e9942 (Print)).
110. Bax M, Goldstein M, Rosenbaum P, Leviton A, Paneth N,Dan B, et al. Proposed definition and classification ofcerebral palsy, April 2005. Dev Med Child Neurol2005;47(8):571e6.
111. Kirton A, deVeber G. Cerebral palsy secondary to perinatalischemic stroke. Clin Perinatol 2006;33:367e86 (0095e5108(Print)).
112. Bouza H, Rutherford M, Acolet D, Pennock JM,Dubowitz LM. Evolution of early hemiplegic signs in full-term infants with unilateral brain lesions in the neonatalperiod: a prospective study. Neuropediatrics 1994;25:201e7(0174e304X (Print)).
113. Li Q, Martin JH. Postnatal development of corticospinal axonterminal morphology in the cat. J Comp Neurol2001;435:127e41 (0021e9967 (Print)).
114. Eyre JA, Miller S, Clowry GJ, Conway EA, Watts C. Functionalcorticospinal projections are established prenatally in thehuman foetus permitting involvement in the developmentof spinal motor centres. Brain 2000;123:51e64 (Pt1)(0006e8950 (Print)).
115. Wolf SL, Winstein CJ, Miller JP, Thompson PA, Taub E,Uswatte G, et al. Retention of upper limb function in strokesurvivors who have received constraint-induced movementtherapy: the EXCITE randomised trial. Lancet Neurol2008;7(1):33e40.
116. Daly JJ, Wolpaw JR. Brainecomputer interfaces inneurological rehabilitation. Lancet Neurol 2008;7(11):1032e43.http://dx.doi.org/10.1016/S1474-4422(08)70223-0.
117. Taub E, Crago JE, Uswatte G. Constraint-induced movementtherapy: a new approach to treatment in physicalrehabilitation. Rehabil Psychol 1998;43(2):152e70.
118. Taub E, Uswatte G, Pidikiti R. Constraint-induced movementtherapy: a new family of techniques with broad applicationto physical rehabilitation e a clinical review. J Rehabil Res Dev1999;36(3):237e51.
119. Taub E, Uswatte G, Elbert T. New treatments inneurorehabilitation founded on basic research. Nat RevNeurosci 2002;3(3):228e36.
120. Wolf SL, Winstein CJ, Miller JP, Taub E, Uswatte G, Morris D,et al. Effect of constraint-induced movement therapy onupper extremity function 3 to 9 months after stroke: theEXCITE randomized clinical trial. J Am Med Assoc2006;296:2095e104 (1538e3598 (Electronic)).
121. Hakkennes S, Keating JL. Constraint-induced movementtherapy following stroke: a systematic review of randomisedcontrolled trials. Aust J Physiother 2005;51(4):221e31.
122. Eliasson AC, Krumlinde-sundholm L, Shaw K, Wang C.Effects of constraint-induced movement therapy in youngchildren with hemiplegic cerebral palsy: an adapted model.Dev Med Child Neurol 2005;47(4):266e75.
123. Taub E, Ramey SL, DeLuca S, Echols K. Efficacy of constraint-induced movement therapy for children with cerebral palsywith asymmetric motor impairment. Pediatrics2004;113(1098e4275):305e12.
124. Taub E, Griffin A, Nick J, Gammons K, Uswatte G, Law CR.Pediatric CI therapy for stroke-induced hemiparesis inyoung children. Dev Neurorehabilitation 2007;10(1):3e18.
125. Willis JK, Morello A, Davie A, Rice JC, Bennett JT. Forced usetreatment of childhood hemiparesis. Pediatrics2002;110:94e6 (1098e4275 (Electronic)).
126. Charles J, Gordon AM. Development of hand-arm bimanualintensive training (HABIT) for improving bimanualcoordination in children with hemiplegic cerebral palsy. DevMed Child Neurol 2006;48:931e6 (0012e1622 (Print)).
127. Deluca SC, Echols K, Law CR, Ramey SL. Intensive pediatricconstraint-induced therapy for children with cerebral palsy:randomized, controlled, crossover trial. J Child Neurol2006;21(11):931e8.
128. Sung IY, Ryu JS, Pyun SB, Yoo SD, Song WH, Park MJ. Efficacyof forced-use therapy in hemiplegic cerebral palsy. Arch PhysMed Rehabil 2005;86(11):2195e8.
129. Sakzewski L, Ziviani J, Boyd R. Systematic review and meta-analysis of therapeutic management of upper-limbdysfunction in children with congenital hemiplegia.Pediatrics 2009;123(6):e1111e22.
e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 2 1 ( 2 0 1 7 ) 7 5e1 0 3 97

130. Brady K, Garcia T. Constraint-induced movement therapy(CIMT): pediatric applications. Dev Disabil Res Rev2009;15(2):102e11.
131. Liepert J, Bauder H, Wolfgang HR, Miltner WH, Taub E,Weiller C. Treatment-induced cortical reorganization afterstroke in humans. Stroke 2000;31(0039e2499):1210e6.
132. Schaechter JD, Kraft E, Hilliard TS, Dijkhuizen RM, Benner T,Finklestein SP, et al. Motor recovery and corticalreorganization after constraint-induced movement therapyin stroke patients: a preliminary study. Neurorehabil NeuralRepair 2002;16:326e38 (1545e9683 (Print)).
133. Wittenberg GF, Chen R, Ishii K, Bushara KO, Eckloff S,Croarkin E, et al. Constraint-induced therapy in stroke:magnetic-stimulation motor maps and cerebral activation.Neurorehabil Neural Repair 2003;17:48e57 (1545e9683 (Print)).
134. Sutcliffe TL, Gaetz WC, Logan WJ, Cheyne DO, Fehlings DL.Cortical reorganization after modified constraint-inducedmovement therapy in pediatric hemiplegic cerebral palsy. JChild Neurol 2007;22:1281e7 (0883e0738 (Print)).
135. Johansen-Berg H, Dawes H, Guy C, Smith SM, Wade DT,Matthews PM. Correlation between motor improvementsand altered fMRI activity after rehabilitative therapy. Brain2002;125:2731e42 (0006e8950 (Print)).
136. Hodics T, Cohen LG. Functional neuroimaging in motorrecovery after stroke. Top Stroke Rehabil2005;12(1074e9357):15e21.
137. Hodics T, Cohen LG, Cramer SC. Functional imaging ofintervention effects in stroke motor rehabilitation. Arch PhysMed Rehabil 2006;87:S36e42 (12 Suppl 2).
138. Liepert J, Miltner WH, Bauder H, Sommer M, Dettmers C,Taub E, et al. Motor cortex plasticity during constraint-induced movement therapy in stroke patients. Neurosci Lett1998;250:5e8 (0304e3940 (Print)).
139. Liepert J, Graef S, Uhde I, Leidner O, Weiller C. Training-induced changes of motor cortex representations in strokepatients.ActaNeurol Scand2000;101:321e6 (0001e6314 (Print)).
140. Liepert J. Motor cortex excitability in stroke before and afterconstraint-induced movement therapy. Cogn Behav Neurol2006;19(1):41e7.
141. Hamzei F, Liepert J, Dettmers C, Weiller C, Rijntjes M. Twodifferent reorganization patterns after rehabilitativetherapy: an exploratory study with fMRI and TMS.Neuroimage 2006;31:710e20 (1053e8119 (Print)).
142. Liepert J. Transcranial magnetic stimulation inneurorehabilitation. Acta Neurochir Suppl 2005;93:71e4(Journal Article).
143. Ro T, Noser E, Boake C, Johnson R, Gaber M, Speroni A, et al.Functional reorganization and recovery after constraint-induced movement therapy in subacute stroke: case reports.Neurocase 2006;12(1):50e60.
144. Tarkka IM, Kononen M, Pitkanen K, Sivenius J, Mervaalat E.Alterations in cortical excitability in chronic stroke afterconstraint-induced movement therapy. Neurol Res2008;30(5):504e10.
145. Gordon AM, Schneider JA, Chinnan A, Charles JR. Efficacy ofa hand-arm bimanual intensive therapy (HABIT) in childrenwith hemiplegic cerebral palsy: a randomized control trial.Dev Med Child Neurol 2007;49(11):830e8.
146. Gordon AM, Hung YC, Brandao M, Ferre CL, Kuo HC, Friel K,et al. Bimanual training and constraint-induced movementtherapy in children with hemiplegic cerebral palsy: arandomized trial. Neurorehabil Neural Repair2011;25(8):692e702.
147. Gordon AM, Chinnan A, Gill S, Petra E, Hung YC, Charles J.Both constraint-induced movement therapy and bimanualtraining lead to improved performance of upper extremityfunction in children with hemiplegia. Dev Med Child Neurol2008;50(12):957e8.
148. Skold A, Josephsson S, Eliasson AC. Performing bimanualactivities: the experiences of young persons with hemiplegiccerebral palsy. Am J Occup Ther 2004;58(4):416e25.
149. Kuhnke N, Juenger H, Walther M, Berweck S, Mall V,Staudt M. Do patients with congenital hemiparesis andipsilateral corticospinal projections respond differently toconstraint-induced movement therapy? Dev Med Child Neurol2008;50(12):898e903.
150. Khedr EM, Ahmed MA, Fathy N, Rothwell JC. Therapeutictrial of repetitive transcranial magnetic stimulation afteracute ischemic stroke. Neurology 2005;65(3):466e8.
151. Naeser MA, Martin PI, Nicholas M, Baker EH, Seekins H,Kobayashi M, et al. Improved picture naming in chronicaphasia after TMS to part of right Broca's area: an open-protocol study. Brain Lang 2005;93:95e105.
152. Pascual-Leone A, Tormos JM, Keenan J, Tarazona F,Canete C, Catala MD. Study and modulation of humancortical excitability with transcranial magnetic stimulation. JClin Neurophysiol 1998;15(0736e0258):333e43.
153. Plautz EJ, Barbay S, Frost SB, Friel KM, Dancause N,Zoubina EV, et al. Post-infarct cortical plasticity andbehavioral recovery using concurrent cortical stimulationand rehabilitative training: a feasibility study in primates.Neurol Res 2003;25:801e10 (0161e6412 (Print)).
154. Adkins-Muir DL, Jones TA. Cortical electrical stimulationcombined with rehabilitative training: enhanced functionalrecovery and dendritic plasticity following focal corticalischemia in rats. Neurol Res 2003;25:780e8 (0161e6412(Print)).
155. Kleim JA, Bruneau R, VandenBerg P, MacDonald E,Mulrooney R, Pocock D. Motor cortex stimulation enhancesmotor recovery and reduces peri-infarct dysfunctionfollowing ischemic insult. Neurol Res 2003;25:789e93(0161e6412 (Print)).
156. Teskey GC, Flynn C, Goertzen CD, Monfils MH, Young NA.Cortical stimulation improves skilled forelimb use followinga focal ischemic infarct in the rat. Neurol Res 2003;25:794e800(0161e6412 (Print)).
157. Pascual-Leone A, Amedi A, Fregni F, Merabet LB. The plastichuman brain cortex. Annu Rev Neurosci 2005;28:377e401.
158. Maeda F, Keenan JP, Tormos JM, Topka H, Pascual-Leone A.Modulation of corticospinal excitability by repetitivetranscranial magnetic stimulation. Clin Neurophysiol2000;111:800e5 (1388e2457 (Print)).
159. Chen R, Classen J, Gerloff C, Celnik P, Wassermann EM,Hallett M, et al. Depression of motor cortex excitability bylow-frequency transcranial magnetic stimulation. Neurology1997;48(0028e3878):1398e403.
160. Lisanby SH, Gutman D, Luber B, Schroeder C, Sackeim HA,Sham TMS. Intracerebral measurement of the inducedelectrical field and the induction of motor-evoked potentials.Biol Psychiatry 2001;49(5):460e3.
161. Speer AM, Benson BE, Kimbrell TK, Wassermann EM,Willis MW, Herscovitch P, et al. Opposite effects of high andlow frequency rTMS on mood in depressed patients:relationship to baseline cerebral activity on PET. J AffectDisord 2009;115:386e94 (1573e2517 (Electronic)).
162. Takeuchi N, Chuma T, Matsuo Y, Watanabe I, Ikoma K.Repetitive transcranial magnetic stimulation ofcontralesional primary motor cortex improves handfunction after stroke. Stroke 2005;36(12):2681e6.
163. Mansur CG, Fregni F, Boggio PS, Riberto M, Gallucci-Neto J,Santos CM, et al. A sham stimulation-controlled trial ofrTMS of the unaffected hemisphere in stroke patients.Neurology 2005;64(10):1802e4.
164. Quintana H. Transcranial magnetic stimulation in personsyounger than the age of 18. JECT 2005;21:88e95 (1095e0680(Print)).
e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 2 1 ( 2 0 1 7 ) 7 5e1 0 398

165. Rossini PM, Desiato MT, Caramia MD. Age-related changesof motor evoked potentials in healthy humans: non-invasiveevaluation of central and peripheral motor tracts excitabilityand conductivity. Brain Res 1992;593:14e9.
166. Lin KL, Pascual-Leone A. Transcranial magnetic stimulationand its applications in children. Chang Gung Med J2002;25(7):424e36.
167. Liebetanz D, Fauser S, Michaelis T, Czeh B, Watanabe T,Paulus W, et al. Safety aspects of chronic low-frequencytranscranial magnetic stimulation based on localized protonmagnetic resonance spectroscopy and histology of the ratbrain. J Psychiatr Res 2003;37:277e86 (0022e3956 (Print)).
168. Naeser MA, Martin PI, Nicholas M, Baker EH, Seekins H,Helm-Estabrooks N, et al. Improved naming after TMStreatments in a chronic, global aphasia patientecase report.Neurocase 2005;11:182e93.
169. Kauffmann CD, Cheema MA, Miller BE. Slow right prefrontaltranscranial magnetic stimulation as a treatment formedication-resistant depression: a double-blind, placebo-controlled study. Depress Anxiety 2004;19:59e62 (1091e4269(Print)).
170. Klein E, Kolsky Y, Puyerovsky M, Koren D, Chistyakov A,Feinsod M. Right prefrontal slow repetitive transcranialmagnetic stimulation in schizophrenia: a double-blindsham-controlled pilot study. Biol Psychiatry 1999;46:1451e4(0006e3223 (Print)).
171. Padberg F, Zwanzger P, Thoma H, Kathmann N, Haag C,Greenberg BD, et al. Repetitive transcranial magneticstimulation (rTMS) in pharmacotherapy-refractory majordepression: comparative study of fast, slow and sham rTMS.Psychiatry Res 1999;88:163e71 (0165e1781 (Print)).
172. Pascual-Leone A, Rubio B, Pallardo F, Catala MD. Rapid-ratetranscranial magnetic stimulation of left dorsolateralprefrontal cortex in drug-resistant depression. Lancet1996;348:233e7 (0140e6736 (Print)).
173. Wassermann EM. Risk and safety of repetitive transcranialmagnetic stimulation: report and suggested guidelines fromthe international workshop on the safety of repetitivetranscranial magnetic stimulation, June 5e7, 1996.Electroencephalogr Clin Neurophysiol 1998;108(1):1e16.
174. Kirton A, Andersen J, Herrero M, Nettel-Aguirre A, Carsolio L,Damji O, et al. Brain stimulation and constraint for perinatalstroke hemiparesis: the PLASTIC CHAMPS trial. Neurology2016 May 3;86(18):1659e67. http://dx.doi.org/10.1212/WNL.0000000000002646. Epub 2016 Mar 30.
175. Zaghi S, Acar M, Hultgren B, Boggio PS, Fregni F. Noninvasivebrain stimulation with low-intensity electrical currents:putative mechanisms of action for direct and alternatingcurrent stimulation. Neuroscientist 2010;16:285e307(1089e4098 (Electronic)).
176. Nitsche MA, Paulus W. Excitability changes induced in thehuman motor cortex by weak transcranial direct currentstimulation. J Physiol 2000;527:633e9. Pt 3(0022e3751 (Print)).
177. Brunoni AR, Amadera J, Berbel B, Volz MS, Rizzerio BG,Fregni F. A systematic review on reporting and assessmentof adverse effects associated with transcranial direct currentstimulation. Int J Neuropsychopharmacol 2011:1e13(1469e5111 (Electronic)).
178. Nitsche MA, Cohen LG, Wassermann EM, Priori A, Lang N,Antal A, et al. Transcranial direct current stimulation: stateof the art 2008. Brain Stimul 2008;1:206e23 (1935e861X(Print)).
179. Poreisz C, Boros K, Antal A, Paulus W. Safety aspects oftranscranial direct current stimulation concerning healthysubjects and patients. Brain Res Bull 2007;72:208e14(0361e9230 (Print)).
180. Gandiga PC, Hummel FC, Cohen LG. Transcranial DCstimulation (tDCS): a tool for double-blind sham-controlled
clinical studies in brain stimulation. Clin Neurophysiol2006;117:845e50 (1388e2457 (Print)).
181. Reis J, Robertson EM, Krakauer JW, Rothwell J, Marshall L,Gerloff C, et al. Consensus: can transcranial direct currentstimulation and transcranial magnetic stimulation enhancemotor learning and memory formation? Brain Stimul2008;1:363e9 (1935e861X (Print)).
182. Reis J, Schambra HM, Cohen LG, Buch ER, Fritsch B, Zarahn E,et al. Noninvasive cortical stimulation enhances motor skillacquisition over multiple days through an effect onconsolidation. Proc Natl Acad Sci USA 2009;106(5):1590e5.
183. Fritsch B, Reis J, Martinowich K, Schambra HM, Ji Y,Cohen LG, et al. Direct current stimulation promotes BDNF-dependent synaptic plasticity: potential implications formotor learning. Neuron 2010;66:198e204 (1097e4199(Electronic)).
184. Boggio PS, Alonso-Alonso M, Mansur CG, Rigonatti SP,Schlaug G, Pascual-Leone A, et al. Hand functionimprovement with low-frequency repetitive transcranialmagnetic stimulation of the unaffected hemisphere in asevere case of stroke. Am J Phys Med Rehabil 2006;85:927e30(0894e9115 (Print)).
185. Vines BW, Nair DG, Schlaug G. Contralateral and ipsilateralmotor effects after transcranial direct current stimulation.Neuroreport 2006;17:671e4 (0959e4965 (Print)).
186. Hummel FC, Heise K, Celnik P, Floel A, Gerloff C, Cohen LG.Facilitating skilled right hand motor function in oldersubjects by anodal polarization over the left primary motorcortex. Neurobiol Aging 2010 Dec;31(12):2160e8. http://dx.doi.org/10.1016/j.neurobiolaging.2008.12.008. Epub 2009Feb 6.
187. Nitsche MA, Schauenburg A, Lang N, Liebetanz D, Exner C,Paulus W, et al. Facilitation of implicit motor learning byweak transcranial direct current stimulation of the primarymotor cortex in the human. J Cogn Neurosci 2003;15:619e26(0898e929X (Print)).
188. Nitsche MA, Paulus W. Sustained excitability elevationsinduced by transcranial DC motor cortex stimulation inhumans. Neurology 2001;57:1899e901 (0028e3878 (Print)).
189. Hummel FC, Voller B, Celnik P, Floel A, Giraux P, Gerloff C,et al. Effects of brain polarization on reaction times andpinch force in chronic stroke. BMC Neurosci 2006;7:73(1471e2202 (Electronic)).
190. Boggio PS, Nunes A, Rigonatti SP, Nitsche MA, Pascual-Leone A, Fregni F. Repeated sessions of noninvasive brainDC stimulation is associated with motor functionimprovement in stroke patients. Restor Neurol Neurosci2007;25:123e9 (0922e6028 (Print)).
191. Moliadze V, Schmanke T, Andreas S, Lyzhko E, Freitag CM,Siniatchkin M. Stimulation intensities of transcranial directcurrent stimulation have to be adjusted in children andadolescents. Clin Neurophysiol Off J Int Fed Clin Neurophysiol2015;126(7):1392e9. http://dx.doi.org/10.1016/j.clinph.2014.10.142.
192. Ciechanski P, Kirton A. Transcranial direct-currentstimulation can enhance motor learning in children. CerebCortex N. Y N 2016;1991. http://dx.doi.org/10.1093/cercor/bhw114.
193. Kessler SK, Minhas P, Woods AJ, Rosen A, Gorman C,Bikson M. Dosage considerations for transcranial directcurrent stimulation in children: a computational modelingstudy. PloS One 2013;8(9):e76112. http://dx.doi.org/10.1371/journal.pone.0076112.
194. Gillick BT, Kirton A, Carmel JB, Minhas P, Bikson M. Pediatricstroke and transcranial direct current stimulation: methodsfor rational individualized dose optimization. Front HumNeurosci 2014;8:739. http://dx.doi.org/10.3389/fnhum.2014.00739.
e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 2 1 ( 2 0 1 7 ) 7 5e1 0 3 99

195. Mahmoudi H, Borhani HA, Petramfar P, Jahanshahi S,Salehi Z, Fregni F. Transcranial direct current stimulation:electrode montage in stroke. Disabil Rehabil 2011;33:1383e8(1464e5165 (Electronic)).
196. Schulz KF, Moher D, Altman DG. CONSORT 2010 comments.Lancet Lond Engl 2010;376(9748):1222e3. http://dx.doi.org/10.1016/S0140-6736(10)61879-X.
197. Plint AC, Moher D, Morrison A, Schulz K, Altman DG, Hill C,et al. Does the CONSORT checklist improve the quality ofreports of randomised controlled trials? A systematicreview. Med J Aust 2006;185(5):263e7.
198. Arner M., Beckung E., Eliasson A., Krumlinde-sundholm L.,Rosenbaum P., Rosblad B. Manual ability classificationsystem for children with cerebral palsy. Available at: http://www.macs.nu/.
199. World Health Organization International classification offunctioning, disability and health (ICF). Genevea (Switzerland):World Health Organization; 2001.
200. Gilmore R, Sakzewski L, Boyd R. Upper limb activitymeasures for 5- to 16-year-old children with congenitalhemiplegia: a systematic review. Dev Med Child Neurol2010;52(1):14e21.
201. Greaves S, Imms C, Dodd K, Krumlinde-sundholm L.Assessing bimanual performance in young children withhemiplegic cerebral palsy: a systematic review. Dev MedChild Neurol 2010;52(5):413e21.
202. Krumlinde-sundholm L, Holmefur M, Kottorp A,Eliasson AC. The Assisting Hand Assessment: currentevidence of validity, reliability, and responsiveness tochange. Dev Med Child Neurol 2007;49(4):259e64.
203. Krumlinde-sundholm L, Eliasson A-C. Development of theassisting hand assessment: a Rasch-built measure intendedfor children with unilateral upper limb impairments. Scand JOccup Ther 2003;10(1):16e26.
204. Holmefur M, Krumlinde-sundholm L, Eliasson AC. Interraterand intrarater reliability of the assisting hand assessment.Am J Occup Ther 2007;61(1):79e84.
205. Holmefur M. The Assisting Hand Assessment: continueddevelopment, psychometrics and longitudinal use. Stockholm:Karolinska Institutet; 2009.
206. Holmefur M, Aarts P, Hoare B, Krumlinde-sundholm L. Test-retest and alternate forms reliability of the assisting handassessment. J Rehabil Med 2009;41(11):886e91.
207. Eliasson AC, Shaw K, Ponten E, Boyd R, Krumlinde-sundholm L. Feasibility of a day-camp model of modifiedconstraint-induced movement therapy with and withoutBotulinum toxin a injection for children with hemiplegia.Phys Occup Ther Pediatr 2009;29(3):311e33.
208. Gilmore R, Boyd R, Sakzewski L. A systematic review of theclinimetric properties of upper limb activity measures for 5-to 16-year-old children with congenital hemiplegia. Dev MedChild Neurol 2008;50(Suppl. 4) (Journal Article):66.
209. Sakzewski L, Ziviani J, Boyd RN. Best responders afterintensive upper-limb training for children with unilateralcerebral palsy. Arch Phys Med Rehabil 2011;92:578e84(1532e821X (Electronic)).
210. Wallen M, Ziviani J, Herbert R, Evans R, Novak I. Modifiedconstraint-induced therapy for children with hemiplegiccerebral palsy: a feasibility study. Dev Neurorehabil2008;11(2):124e33.
211. Law M, Baptiste S, McColl M, Opzoomer A, Polatajko H,Pollock N. The Canadian occupational performancemeasure: an outcome measure for occupational therapy.Can J Occup Ther Rev Can Ergother 1990;57(2):82e7.
212. Law M, Polatajko H, Pollock N, McColl MA, Carswell A,Baptiste S. Pilot testing of the Canadian occupationalperformance measure: clinical and measurement issues.Can J Occup Ther Rev Can Ergother 1994;61(4):191e7.
213. McColl MA, Paterson M, Davies D, Doubt L, Law M. Validityand community utility of the Canadian occupationalperformance measure. Can J Occup Ther Rev Can Ergother2000;67(1):22e30.
214. Carswell A, McColl MA, Baptiste S, Law M, Polatajko H,Pollock N. The Canadian occupational performancemeasure: a research and clinical literature review. Can JOccup Ther Rev Can Ergother 2004;71(4):210e22.
215. Hanna K, Rodger S. Towards family-centred practice inpaediatric occupational therapy: a review of the literature onparent-therapist collaboration. Aust Occup Ther J2002;49(1):14e24.
216. Cusick A, Lannin NA, Lowe K. Adapting the Canadianoccupational performance measure for use in a paediatricclinical trial. Disabil Rehabil 2007;29(10):761e6.
217. Sakzewski L, Boyd R, Ziviani J. Clinimetric properties ofparticipation measures for 5- to 13-year-old children withcerebral palsy: a systematic review. Dev Med Child Neurol2007;49(3):232e40. http://dx.doi.org/10.1111/j.1469-8749.2007.00232.x.
218. Wallen M, O'Flaherty SJ, Waugh M-CA. Functional outcomesof intramuscular Botulinum toxin type a and occupationaltherapy in the upper limbs of children with cerebral palsy: arandomized controlled trial. Arch Phys Med Rehabil2007;88(1):1e10.
219. Ostensjo S, Oien I, Fallang B. Goal-oriented rehabilitation ofpreschoolers with cerebral palsyea multi-case study ofcombined use of the Canadian occupational performancemeasure (COPM) and the goal attainment scaling (GAS). DevNeurorehabil 2008;11(4):252e9.
220. Martin A, Burtner PA, Poole J, Phillips J. Case report: ICF-levelchanges in a preschooler after constraint-inducedmovement therapy. Am J Occup Ther 2008;62(3):282e8.
221. Grap MJ, Hamilton VA, McNallen A, Ketchum JM, Best AM,Arief NYI, et al. Actigraphy: analyzing patient movement.Heart Lung 2011;40(3):e52e9.
222. Kirton A, deVeber G, Gunraj C, Chen R. Neurocardiogenicsyncope complicating pediatric transcranial magneticstimulation. Pediatr Neurol 2008;39:196e7 (0887e8994(Print)).
223. Gillick BT, Rich T, ChenM, Meekins GD. Case report ofvasovagal syncope associated with single pulse transcranialmagneticstimulationinahealthyadultparticipant.BMCNeurol2015;15:248. http://dx.doi.org/10.1186/s12883-015-0510-2.
224. Garvey MA, Gilbert DL. Transcranial magnetic stimulation inchildren. Eur J Paediatr Neurol 2004;8(1090e3798):7e19.
225. Sarfeld AS, Diekhoff S, Wang LE, Liuzzi G, Uludag K,Eickhoff SB, et al. Convergence of human brain mappingtools: neuronavigated TMS parameters and fMRI activity inthe hand motor area. Hum Brain Mapp 2012May;33(5):1107e23. http://dx.doi.org/10.1002/hbm.21272.Epub 2011 Apr 21.
226. Barker AT, Jalinous R, Freeston IL. Non-invasive magneticstimulation of human motor cortex. Lancet 1985;1:1106e7(0140e6736 (Print)).
227. Theodore WH. Handbook of transcranial magneticstimulation. Edited by A. Pascual-Leone, N.J. Davey, J.Rothwell, E.M. Wasseran, B.K. Puri, Arnold, London, 2001.pound 110 sterling, ISBN 0340720093. Epilepsy Behav2002;3(1525e5050 (Print)):404.
228. Jang SH, Byun WM, Chang Y, Han BS, Ahn SH. Combinedfunctional magnetic resonance imaging and transcranialmagnetic stimulation evidence of ipsilateral motor pathwaywith congenital brain disorder: a case report. Arch Phys MedRehabil 2001;82:1733e6 (0003e9993 (Print)).
229. Carr LJ. Development and reorganization of descendingmotor pathways in children with hemiplegic cerebral palsy.Acta Paediatr Suppl 1996;416:53e7 (0803e5326 (Print)).
e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 2 1 ( 2 0 1 7 ) 7 5e1 0 3100

230. Duque J, Hummel F, Celnik P, Murase N, Mazzocchio R,Cohen LG. Transcallosal inhibition in chronic subcorticalstroke. Neuroimage 2005;28:940e6 (1053e8119 (Print)).
231. Brasil-Neto JP, Cammarota A, Valls-Sole J, Pascual-Leone A,Hallett M, Cohen LG. Role of intracortical mechanisms in thelate part of the silent period to transcranial stimulation ofthe human motor cortex. Acta Neurol Scand 1995;92:383e6(0001e6314 (Print)).
232. Hallett M. Transcranial magnetic stimulation. Negativeeffects. Adv Neurol 1995;67:107e13 (0091e3952 (Print)).
233. Terao Y, Ugawa Y. Basic mechanisms of TMS. J ClinNeurophysiol 2002;19:322e43 (0736e0258 (Print)).
234. Heinen F, Glocker FX, Fietzek U, Meyer BU, Lucking CH,Korinthenberg R. Absence of transcallosal inhibitionfollowing focal magnetic stimulation in preschool children.Ann Neurol 1998;43:608e12.
235. Gilbert DL, Garvey MA, Bansal AS, Lipps T, Zhang J,Wassermann EM. Should transcranial magnetic stimulationresearch in children be considered minimal risk? ClinNeurophysiol 2004;115(1388e2457):1730e9.
236. Valero-Cabre A, Rushmore RJ, Payne BR. Low frequencytranscranial magnetic stimulation on the posterior parietalcortex induces visuotopically specific neglect-like syndrome.Exp Brain Res 2006:1e8 (0014e4819 (Print)).
237. Valero-Cabre A, Payne BR, Rushmore J, Lomber SG, Pascual-Leone A. Impact of repetitive transcranial magneticstimulation of the parietal cortex on metabolic brainactivity: a 14C-2DG tracing study in the cat. Exp Brain Res2005;163:1e12 (0014e4819 (Print)).
238. Bolay H, Gursoy-Ozdemir Y, Unal I, Dalkara T. Alteredmechanisms of motor-evoked potential generation aftertransient focal cerebral ischemia in the rat: implicationsfor transcranial magnetic stimulation. Brain Res2000;873:26e33.
239. Eyre JA, Flecknell PA, Kenyon BR, Koh TH, Miller S. Acuteeffects of electromagnetic stimulation of the brain oncortical activity, cortical blood flow, blood pressure andheart rate in the cat: an evaluation of safety. J NeurolNeurosurg Psychiatry 1990;53:507e13.
240. Edgley SA, Eyre JA, Lemon RN, Miller S. Excitation of thecorticospinal tract by electromagnetic and electricalstimulation of the scalp in the macaque monkey. J Physiol1990;425:301e20 (0022e3751 (Print)).
241. Theodore WH, Hunter K, Chen R, Vega-Bermudez F,Boroojerdi B, Reeves-Tyer P, et al. Transcranial magneticstimulation for the treatment of seizures: a controlled study.Neurology 2002;59:560e2 (0028e3878 (Print)).
242. Tassinari CA, Cincotta M, Zaccara G, Michelucci R.Transcranial magnetic stimulation and epilepsy. ClinNeurophysiol 2003;114:777e98 (1388e2457 (Print)).
243. Magnetic stimulation in clinical neurophysiology. vol. 2.Philadelphia, PA: Elsevier; 2005
244. Daskalakis ZJ, Christensen BK, Fitzgerald PB, Roshan L,Chen R. The mechanisms of interhemispheric inhibition inthe human motor cortex. J Physiol 2002;543:317e26(0022e3751 (Print)).
245. Di LV, Oliviero A, Profice P, Insola A,Mazzone P, Tonali P, et al.Direct demonstration of interhemispheric inhibition of thehuman motor cortex produced by transcranial magneticstimulation. Exp Brain Res 1999;124:520e4 (0014e4819 (Print)).
246. Ferbert A, Priori A, Rothwell JC, Day BL, Colebatch JG,Marsden CD. Interhemispheric inhibition of the humanmotor cortex. J Physiol 1992;453:525e46.
247. Roshan L, Paradiso GO, Chen R. Two phases of short-intervalintracortical inhibition. Exp Brain Res 2003;151:330e7(0014e4819 (Print)).
248. Grefkes C, Fink GR. Reorganization of cerebral networksafter stroke: new insights from neuroimaging with
connectivity approaches. Brain 2011;134:1264e76 (1460e2156(Electronic)).
249. Friston KJ, Frith CD, Fletcher P, Liddle PF, Frackowiak RS.Functional topography: multidimensional scaling andfunctional connectivity in the brain. Cereb Cortex1996;6:156e64 (1047e3211 (Print)).
250. Stephan KE, Friston KJ. Analyzing effective connectivity withfMRI. Wiley Interdiscip Rev Cogn Sci 2010;1:446e59.
251. Rehme AK, Eickhoff SB, Wang LE, Fink GR, Grefkes C.Dynamic causal modeling of cortical activity from the acuteto the chronic stage after stroke. Neuroimage2011;55:1147e58 (1095e9572 (Electronic)).
252. Carter AR, Astafiev SV, Lang CE, Connor LT, Rengachary J,Strube MJ, et al. Resting interhemispheric functionalmagnetic resonance imaging connectivity predictsperformance after stroke. Ann Neurol 2010;67:365e75(1531e8249 (Electronic)).
253. de Bie HM, Boersma M, Adriaanse S, Veltman DJ, Wink AM,Roosendaal SD, et al. Resting-state networks in awake five-to eight-year old children. Hum Brain Mapp 2012;33:1189e201(1097e0193 (Electronic)).
254. Polania R, Nitsche MA, Paulus W. Modulating functionalconnectivity patterns and topological functionalorganization of the human brain with transcranial directcurrent stimulation. Hum Brain Mapp 2011;32:1236e49(1097e0193 (Electronic)).
257. Rollins NK. Clinical applications of diffusion tensor imagingand tractography in children. Pediatr Radiol 2007;37:769e80(0301e0449 (Print)).
258. Moller M, Frandsen J, Andersen G, Gjedde A, Vestergaard-Poulsen P, Ostergaard L. Dynamic changes in corticospinaltracts after stroke detected by fibretracking. J NeurolNeurosurg Psychiatry 2007;78:587e92 (1468e330X(Electronic)).
259. Radlinska B, Ghinani S, Leppert IR, Minuk J, Pike GB, Thiel A.Diffusion tensor imaging, permanent pyramidal tractdamage, and outcome in subcortical stroke. Neurology2010;75:1048e54 (1526e632X (Electronic)).
260. Heller SL, Heier LA, Watts R, Schwartz TH, Zelenko N,Doyle W, et al. Evidence of cerebral reorganization followingperinatal stroke demonstrated with fMRI and DTItractography. Clin Imaging 2005;29(4):283e7. http://dx.doi.org/10.1016/j.clinimag.2004.09.003.
261. Yoshida S, Hayakawa K, Yamamoto A, Okano S, Kanda T,Yamori Y, et al. Quantitative diffusion tensor tractographyof the motor and sensory tract in children with cerebralpalsy. Dev Med Child Neurol 2010;52:935e40 (1469e8749(Electronic)).
262. Glenn OA, Ludeman NA, Berman JI, Wu YW, Lu Y, Bartha AI,et al. Diffusion tensor MR imaging tractography of thepyramidal tracts correlates with clinical motor function inchildren with congenital hemiparesis. AJNR Am J Neuroradiol2007;28(9):1796e802. http://dx.doi.org/10.3174/ajnr.A0676.
263. Hodge J, Carlson H, Goodyear B, wei x. Kirton A DTIquantification of corticospinal tract integrity in perinatalstroke. Proc Neuro DevNet Brain Dev Conf 2011;30.
264. Kuczynski AM, Dukelow SP, Semrau JA, Kirton A. Roboticquantification of position sense in children with perinatalstroke. Neurorehabil Neural Repair 2016 Jan 7.pii: 1545968315624781. [Epub ahead of print].
265. Juenger H, Kuhnke N, Braun C, Ummenhofer F, Wilke M,Walther M, et al. Two types of exercise-inducedneuroplasticity in congenital hemiparesis: a transcranialmagnetic stimulation, functional MRI, andmagnetoencephalography study. Dev Med Child Neurol2013;55:941e51 (1469e8749 (Electronic)).
266. Jaspers E, Byblow WD, Feys H, Wenderoth N. Thecorticospinal tract: a Biomarker to categorize upper limb
e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 2 1 ( 2 0 1 7 ) 7 5e1 0 3 101

functional potential in unilateral cerebral palsy. Front Pediatr2015;3:112. http://dx.doi.org/10.3389/fped.2015.00112.
267. Hummel FC, Cohen LG. Non-invasive brain stimulation: anew strategy to improve neurorehabilitation after stroke?Lancet Neurol 2006;5:708e12 (1474e4422 (Print)).
268. Hesse S, Werner C, Schonhardt EM, Bardeleben A, Jenrich W,Kirker SG. Combined transcranial direct current stimulationand robot-assisted arm training in subacute stroke patients:a pilot study. Restor Neurol Neurosci 2007;25:9e15 (0922e6028(Print)).
269. Boggio PS, Rigonatti SP, Ribeiro RB, Myczkowski ML,Nitsche MA, Pascual-Leone A, et al. A randomized,double-blind clinical trial on the efficacy of cortical directcurrent stimulation for the treatment of majordepression. Int J Neuropsychopharmacol 2007:1e6(1461e1457 (Print)).
270. Celnik P, Paik N-J, Vandermeeren Y, Dimyan M, Cohen LG.Effects of combined peripheral nerve stimulation and brainpolarization on performance of a motor sequence task afterchronic stroke. Stroke 2009;40(5):1764e71. http://dx.doi.org/10.1161/STROKEAHA.108.540500.
271. Kim DY, Ohn SH, Yang EJ, Park C-I, Jung KJ. Enhancing motorperformance by anodal transcranial direct currentstimulation in subacute stroke patients. Am J Phys MedRehabil Assoc Acad Physiatr 2009;88(10):829e36. http://dx.doi.org/10.1097/PHM.0b013e3181b811e3.
272. Kim D-Y, Lim J-Y, Kang EK, You DS, Oh M-K, Oh B-M, et al.Effect of transcranial direct current stimulation on motorrecovery in patients with subacute stroke. Am J Phys MedRehabil Assoc Acad Physiatr 2010;89(11):879e86. http://dx.doi.org/10.1097/PHM.0b013e3181f70aa7.
273. Nair DG, Renga V, Lindenberg R, Zhu L, Schlaug G.Optimizing recovery potential through simultaneousoccupational therapy and non-invasive brain-stimulationusing tDCS. Restor Neurol Neurosci 2011;29(6):411e20. http://dx.doi.org/10.3233/RNN-2011-0612.
274. Hesse S, Waldner A, Mehrholz J, Tomelleri C, Pohl M,Werner C. Combined transcranial direct current stimulationand robot-assisted arm training in subacute stroke patients:an exploratory, randomized multicenter trial. NeurorehabilNeural Repair 2011;25(9):838e46. http://dx.doi.org/10.1177/1545968311413906.
275. Bolognini N, Vallar G, Casati C, Latif LA, El-Nazer R,Williams J, et al. Neurophysiological and behavioral effectsof tDCS combined with constraint-induced movementtherapy in poststroke patients. Neurorehabil Neural Repair2011;25(9):819e29. http://dx.doi.org/10.1177/1545968311411056.
276. Stagg CJ, Bachtiar V, O'Shea J, Allman C, Bosnell RA,Kischka U, et al. Cortical activation changes underlyingstimulation-induced behavioural gains in chronic stroke.Brain J Neurol 2012;135(Pt 1):276e84. http://dx.doi.org/10.1093/brain/awr313.
277. Lindenberg R, Zhu LL, Ruber T, Schlaug G. Predictingfunctional motor potential in chronic stroke patients usingdiffusion tensor imaging. Hum Brain Mapp 2012;33:1040e51(1097e0193 (Electronic)).
278. Takeuchi N, Tada T, Matsuo Y, Ikoma K. Low-frequencyrepetitive TMS plus anodal transcranial DCS preventstransient decline in bimanual movement induced bycontralesional inhibitory rTMS after stroke. NeurorehabilNeural Repair 2012;26(8):988e98. http://dx.doi.org/10.1177/1545968311433295.
279. Rossi C, Sallustio F, Di Legge S, Stanzione P, Koch G.Transcranial direct current stimulation of the affectedhemisphere does not accelerate recovery of acute strokepatients. Eur J Neurol 2013;20(1):202e4. http://dx.doi.org/10.1111/j.1468-1331.2012.03703.x.
280. Zimerman M, Heise KF, Hoppe J, Cohen LG, Gerloff C,Hummel FC. Modulation of training by single-sessiontranscranial direct current stimulation to the intact motorcortex enhances motor skill acquisition of the paretic hand.Stroke 2012;43(8):2185e91. http://dx.doi.org/10.1161/STROKEAHA.111.645382.
281. Wu D, Qian L, Zorowitz RD, Zhang L, Qu Y, Yuan Y. Effects ondecreasing upper-limb poststroke muscle tone usingtranscranial direct current stimulation: a randomized sham-controlled study. Arch Phys Med Rehabil 2013;94(1):1e8. http://dx.doi.org/10.1016/j.apmr.2012.07.022.
282. Ochi M, Saeki S, Oda T, Matsushima Y, Hachisuka K. Effectsof anodal and cathodal transcranial direct currentstimulation combined with robotic therapy on severelyaffected arms in chronic stroke patients. J Rehabil Med2013;45(2):137e40. http://dx.doi.org/10.2340/16501977-1099.
283. Lefebvre S, Laloux P, Peeters A, Desfontaines P, Jamart J,Vandermeeren Y. Dual-tDCS enhances online motor skilllearning and long-term retention in chronic stroke patients.Front Hum Neurosci 2013;6. http://dx.doi.org/10.3389/fnhum.2012.00343.
284. Fusco A, De Angelis D, Morone G, Maglione L, Paolucci T,Bragoni M, et al. The ABC of tDCS: effects of anodal, bilateraland cathodal montages of transcranial direct currentstimulation in patients with stroke-a pilot study. Stroke ResTreat 2013;2013:837595. http://dx.doi.org/10.1155/2013/837595.
285. Lefebvre S, Thonnard J-L, Laloux P, Peeters A, Jamart J,Vandermeeren Y. Single session of dual-tDCS transientlyimproves precision grip and dexterity of the paretic handafter stroke. Neurorehabil Neural Repair 2014;28(2):100e10.http://dx.doi.org/10.1177/1545968313478485.
286. Khedr EM, Shawky OA, El-Hammady DH, Rothwell JC,Darwish ES, Mostafa OM, et al. Effect of anodal versuscathodal transcranial direct current stimulation on strokerehabilitation: a pilot randomized controlled trial.Neurorehabil Neural Repair 2013;27(7):592e601. http://dx.doi.org/10.1177/1545968313484808.
287. O'Shea J, Boudrias M-H, Stagg CJ, Bachtiar V, Kischka U,Blicher JU, et al. Predicting behavioural response to TDCS inchronic motor stroke. Neuroimage 2014;85:924e33. http://dx.doi.org/10.1016/j.neuroimage.2013.05.096.
288. Giacobbe V, Krebs HI, Volpe BT, Pascual-Leone A, Rykman A,Zeiarati G, et al. Transcranial direct current stimulation(tDCS) and robotic practice in chronic stroke: the dimensionof timing. Neuro Rehabil 2013;33(1):49e56. http://dx.doi.org/10.3233/NRE-130927.
289. Fusco A, Iosa M, Venturiero V, De Angelis D, Morone G,Maglione L, et al. After vs. priming effects of anodaltranscranial direct current stimulation on upper extremitymotor recovery in patients with subacute stroke. RestorNeurol Neurosci 2014;32(2):301e12.
290. Fusco A, Assenza F, Iosa M, Izzo S, Altavilla R, Paolucci S,et al. The ineffective role of cathodal tDCS in enhancing thefunctional motor outcomes in early phase of strokerehabilitation: an experimental trial. Biomed Res Int2014;2014:1e9. http://dx.doi.org/10.1155/2014/547290.
291. Cha H-K, Ji S-G, Kim M-K, Chang J-S. Effect of transcranialdirect current stimulation of function in patients withstroke. J Phys Ther Sci 2014;26(3):363e5. http://dx.doi.org/10.1589/jpts.26.363.
292. Au-Yeung SSY, Wang J, Chen Y, Chua E. Transcranial directcurrent stimulation to primary motor area improves handdexterity and selective attention in chronic stroke. Am J PhysMed Rehabil 2014;93(12):1057e64. http://dx.doi.org/10.1097/PHM.0000000000000127.
293. Gillick BT, Feyma T, Menk J, Krach LE, Usset M, Vaith A, et al.Safety and feasibility of transcranial direct current
e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 2 1 ( 2 0 1 7 ) 7 5e1 0 3102

stimulation in pediatric hemiparesis: a randomizedcontrolled pilot study. Phys Ther 2015 Mar;95(3):337e49.http://dx.doi.org/10.2522/ptj.20130565. Epub 2014 Nov 20.
294. Goh H-T, Chan H-Y, Abdul-Latif L. Aftereffects of 2noninvasive brain stimulation techniques on corticospinalexcitability in persons with chronic stroke: a pilot study. JNeurol Phys Ther JNPT 2015;39(1):15e22. http://dx.doi.org/10.1097/NPT.0000000000000064.
295. Di Lazzaro V, Rothwell JC. Corticospinal activity evoked andmodulated by non-invasive stimulation of the intact humanmotor cortex: corticospinal activity and the human motorcortex. J Physiol 2014;592(19):4115e28. http://dx.doi.org/10.1113/jphysiol.2014.274316.
296. Lefebvre S, Dricot L, Laloux P, Gradkowski W,Desfontaines P, Evrard F, et al. Neural substrates underlyingstimulation-enhanced motor skill learning after stroke. BrainJ Neurol 2015;138(Pt 1):149e63. http://dx.doi.org/10.1093/brain/awu336.
297. Sattler V, Acket B, Raposo N, Albucher J-F, Thalamas C,Loubinoux I, et al. Anodal tDCS combined with radial nervestimulation promotes hand motor recovery in the acutephase after ischemic stroke. Neurorehabil Neural Repair2015;29(8):743e54. http://dx.doi.org/10.1177/1545968314565465.
298. Rocha S, Silva E, Foerster !A, Wiesiolek C, Chagas AP,Machado G, et al. The impact of transcranial direct currentstimulation (tDCS) combined with modified constraint-induced movement therapy (mCIMT) on upper limb functionin chronic stroke: a double-blind randomized controlledtrial. Disabil Rehabil 2016;38(7):653e60. http://dx.doi.org/10.3109/09638288.2015.1055382.
299. Straudi S, Fregni F, Martinuzzi C, Pavarelli C, Salvioli S,Basaglia N. tDCS and robotics on upper limb strokerehabilitation: effect modification by stroke duration and
type of stroke. Biomed Res Int 2016;2016:5068127. http://dx.doi.org/10.1155/2016/5068127.
300. Allman C, Amadi U, Winkler AM, Wilkins L, Filippini N,Kischka U, et al. Ipsilesional anodal tDCS enhances thefunctional benefits of rehabilitation in patients after stroke.Sci Transl Med 2016;8(330):330re1. http://dx.doi.org/10.1126/scitranslmed.aad5651.
301. Triccas LT, Burridge JH, Hughes A, Verheyden G, Desikan M,Rothwell J. A double-blinded randomised controlled trialexploring the effect of anodal transcranial direct currentstimulation and uni-lateral robot therapy for the impairedupper limb in sub-acute and chronic stroke. Neuro Rehabil2015;37(2):181e91. http://dx.doi.org/10.3233/NRE-151251.
302. CunninghamDA,VarnerinN,MachadoA, Bonnett C, Janini D,Roelle S, et al. Stimulation targeting higher motor areas instroke rehabilitation: a proof-of-concept, randomized,double-blinded placebo-controlled study of effectiveness andunderlying mechanisms. Restor Neurol Neurosci2015;33(6):911e26. http://dx.doi.org/10.3233/RNN-150574.
303. Lee D-G, Lee D-Y. Effects of adjustment of transcranial directcurrent stimulation on motor function of the upperextremity in stroke patients. J Phys Ther Sci2015;27(11):3511e3. http://dx.doi.org/10.1589/jpts.27.3511.
304. Chen JL, Schlaug G. Increased resting state connectivitybetween ipsilesional motor cortex and contralesionalpremotor cortex after transcranial direct current stimulationwith physical therapy. Sci Rep 2016;6:23271. http://dx.doi.org/10.1038/srep23271.
305. Mortensen J, Figlewski K, Andersen H. Combinedtranscranial direct current stimulation and home-basedoccupational therapy for upper limb motor impairmentfollowing intracerebral hemorrhage: a double-blindrandomized controlled trial. Disabil Rehabil2016;38(7):637e43. http://dx.doi.org/10.3109/09638288.2015.1055379.
e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 2 1 ( 2 0 1 7 ) 7 5e1 0 3 103