
Advances in Transfusion and Blood Conservation Arman Kilic, MD Division of Cardiac Surgery,...
41
Advances in Transfusion and Blood Conservation Arman Kilic, MD Division of Cardiac Surgery, Department of Surgery, Johns Hopkins Hospital, Baltimore, MD No relevant financial relationships to disclose.
-
Upload
anna-atkins -
Category
Documents
-
view
216 -
download
2
Transcript of Advances in Transfusion and Blood Conservation Arman Kilic, MD Division of Cardiac Surgery,...
Advances in Transfusion and Blood Conservation
Arman Kilic, MDDivision of Cardiac Surgery, Department of Surgery,
Johns Hopkins Hospital, Baltimore, MD
No relevant financial relationships to disclose.
Overview
1. Why should we care?
2. What is the evidence?
3. How should we (healthcare professional, institution) proceed with regards to blood transfusion practice?
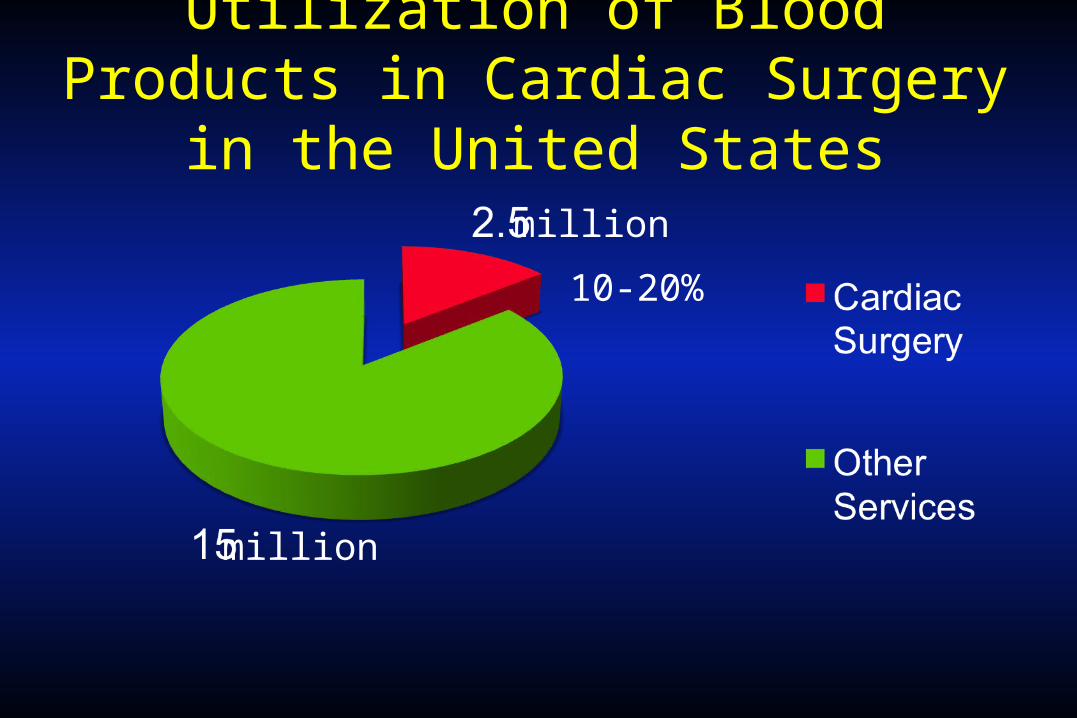
Utilization of Blood Products in Cardiac Surgery in the United States
million
million
10-20%
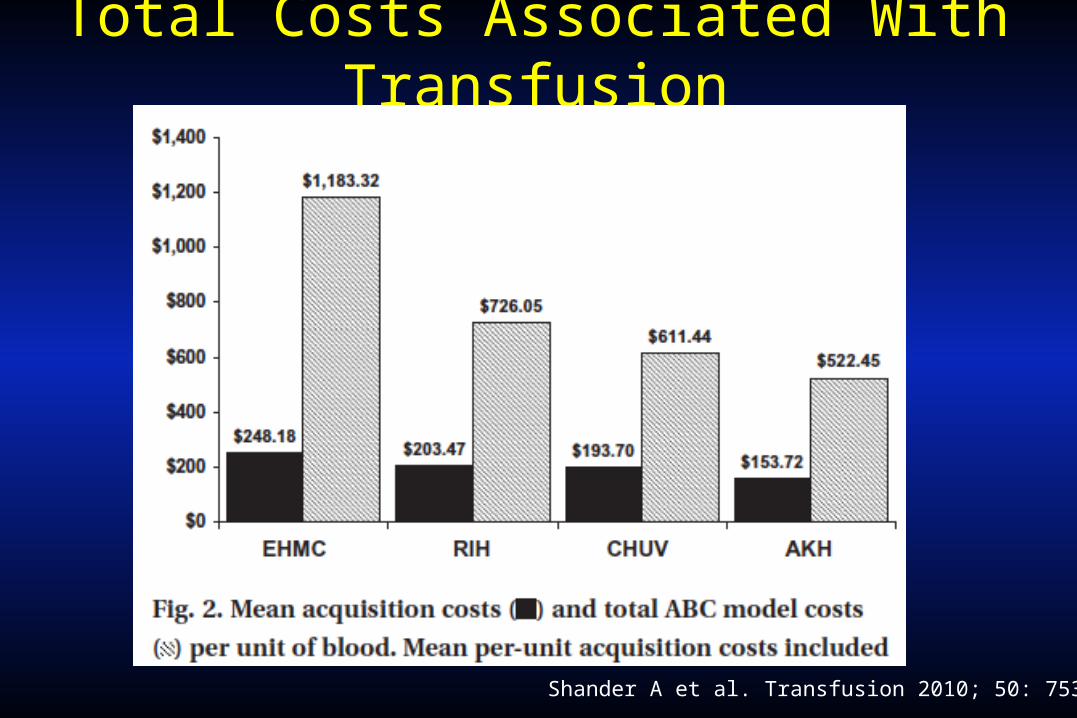
Total Costs Associated With Transfusion
Shander A et al. Transfusion 2010; 50: 753-65.
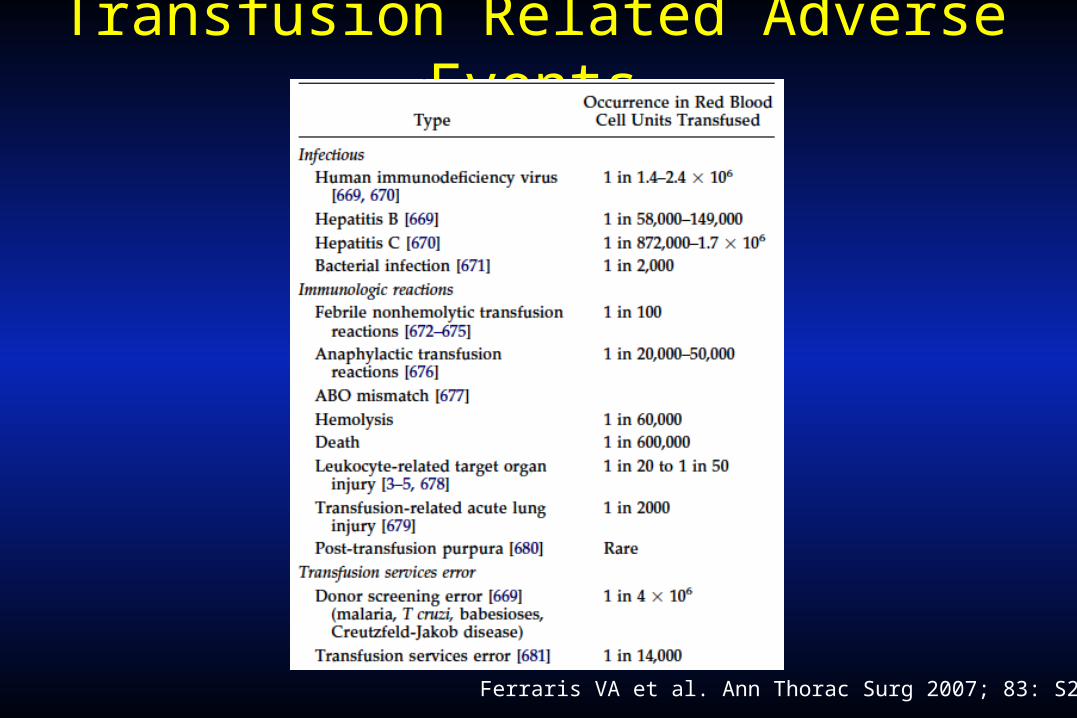
Transfusion Related Adverse Events
Ferraris VA et al. Ann Thorac Surg 2007; 83: S27-86.
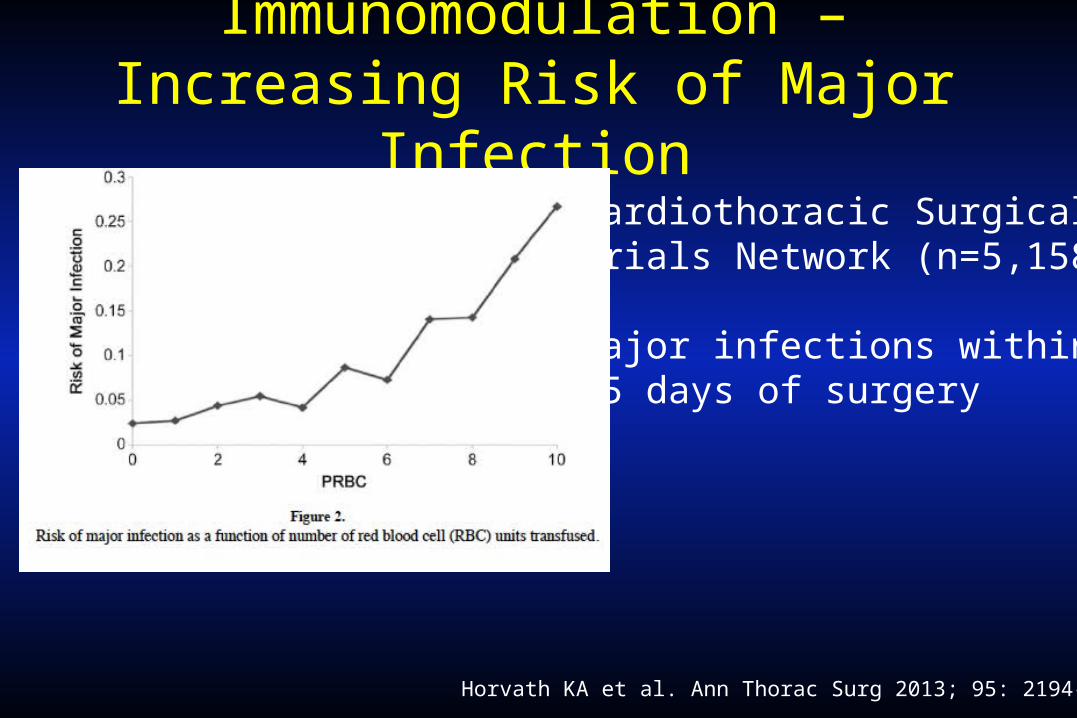
Immunomodulation – Increasing Risk of Major Infection
Horvath KA et al. Ann Thorac Surg 2013; 95: 2194-201.
Cardiothoracic SurgicalTrials Network (n=5,158)
Major infections within 65 days of surgery
Other Postoperative Morbidity Associated with Transfusions in Cardiac Surgery
• Atrial fibrillation• Respiratory failure• ARDS• Reintubation• Prolonged mechanical ventilation• Acute renal failure • Neurologic adverse events• Gastrointestinal complications
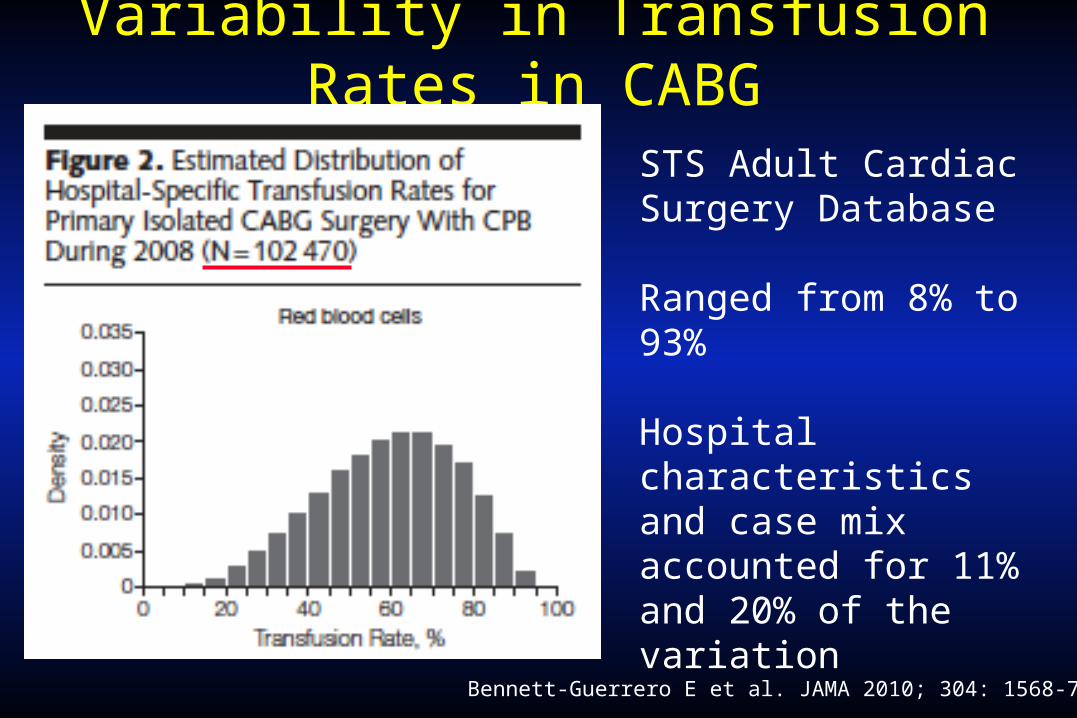
Variability in Transfusion Rates in CABG
Bennett-Guerrero E et al. JAMA 2010; 304: 1568-75.
STS Adult Cardiac Surgery Database
Ranged from 8% to 93%
Hospital characteristics and case mix accounted for 11% and 20% of the variation
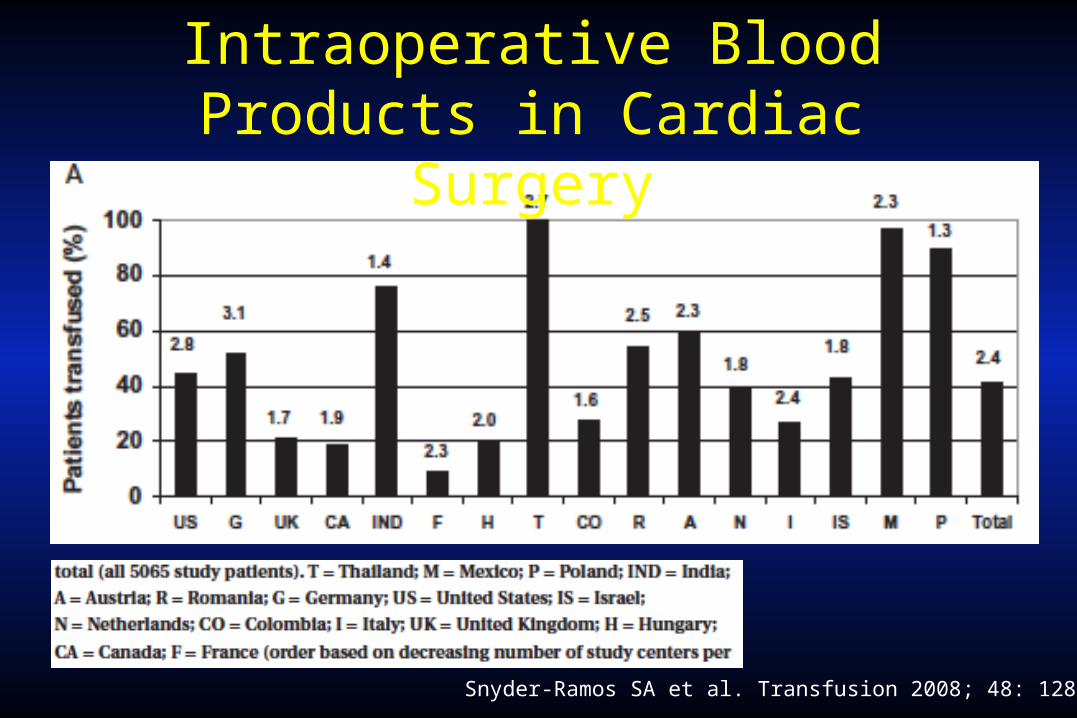
Utilization of Intraoperative Blood Products in Cardiac Surgery
Snyder-Ramos SA et al. Transfusion 2008; 48: 1284-99.
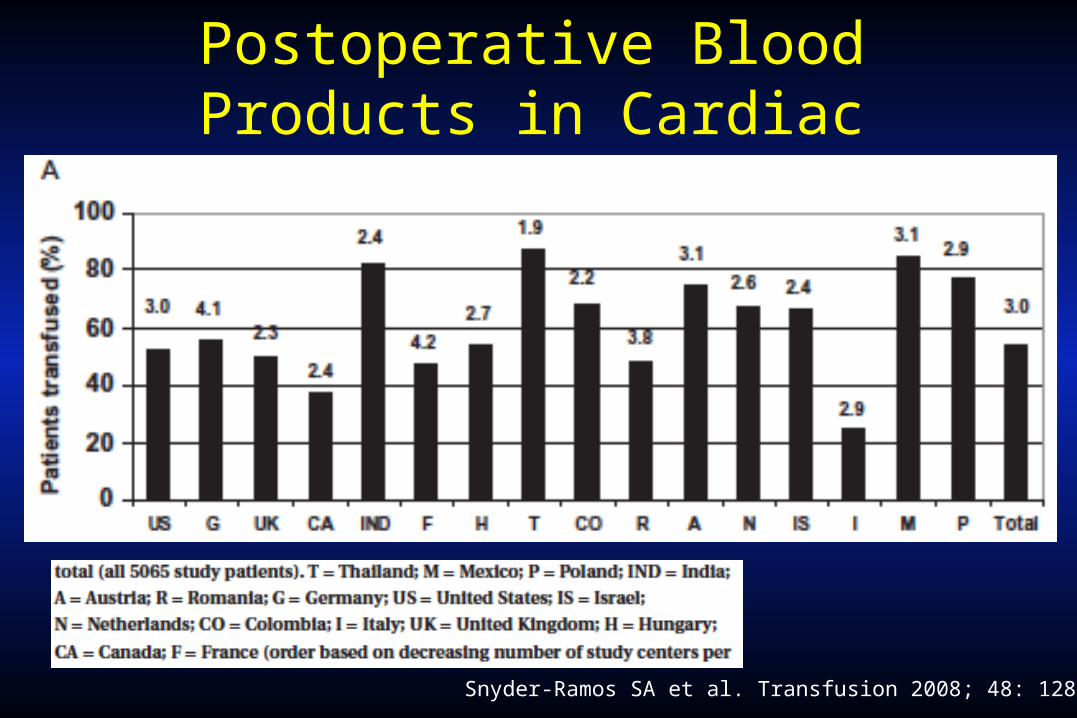
Utilization of Postoperative Blood Products in Cardiac Surgery
Snyder-Ramos SA et al. Transfusion 2008; 48: 1284-99.
Overview
1. Why should we care?
2. What is the evidence?
3. How should we (healthcare professional, institution) proceed with regards to blood transfusion practice?
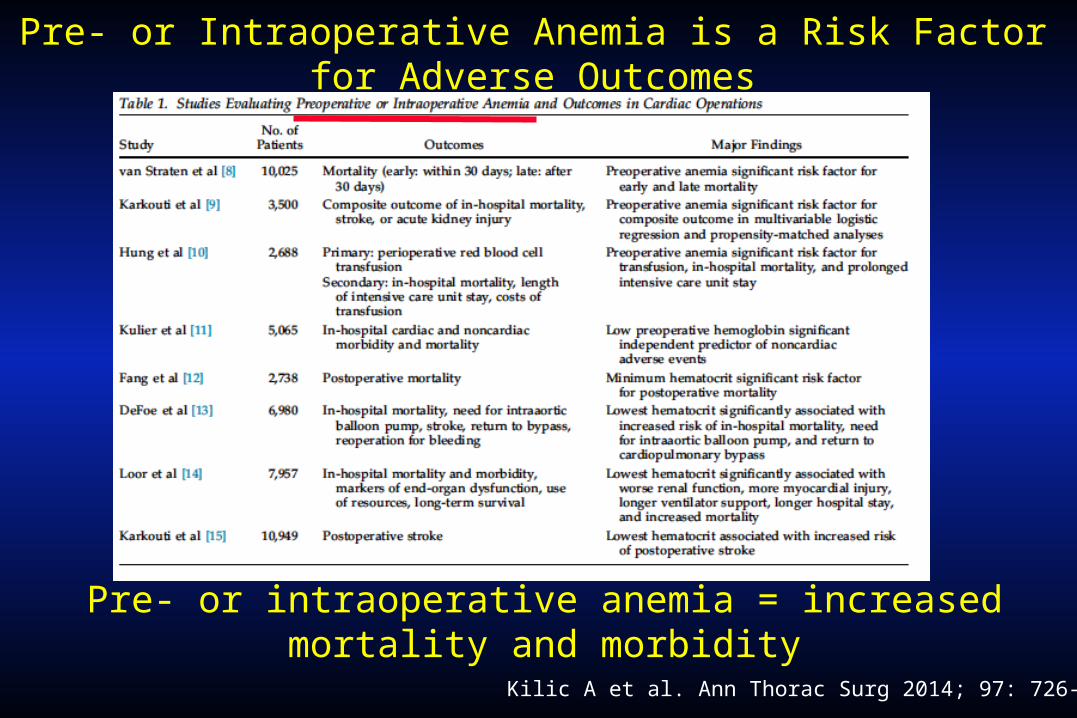
Pre- or Intraoperative Anemia is a Risk Factor for Adverse Outcomes
Kilic A et al. Ann Thorac Surg 2014; 97: 726-34.
Pre- or intraoperative anemia = increased mortality and morbidity
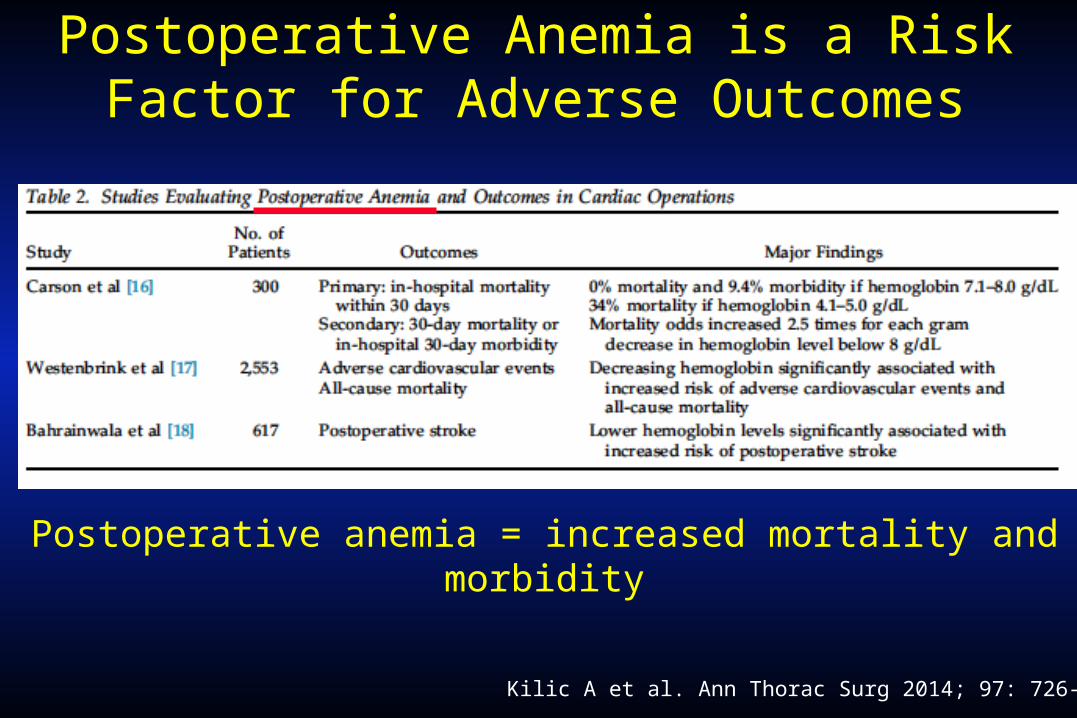
Postoperative Anemia is a Risk Factor for Adverse Outcomes
Kilic A et al. Ann Thorac Surg 2014; 97: 726-34.
Postoperative anemia = increased mortality and morbidity
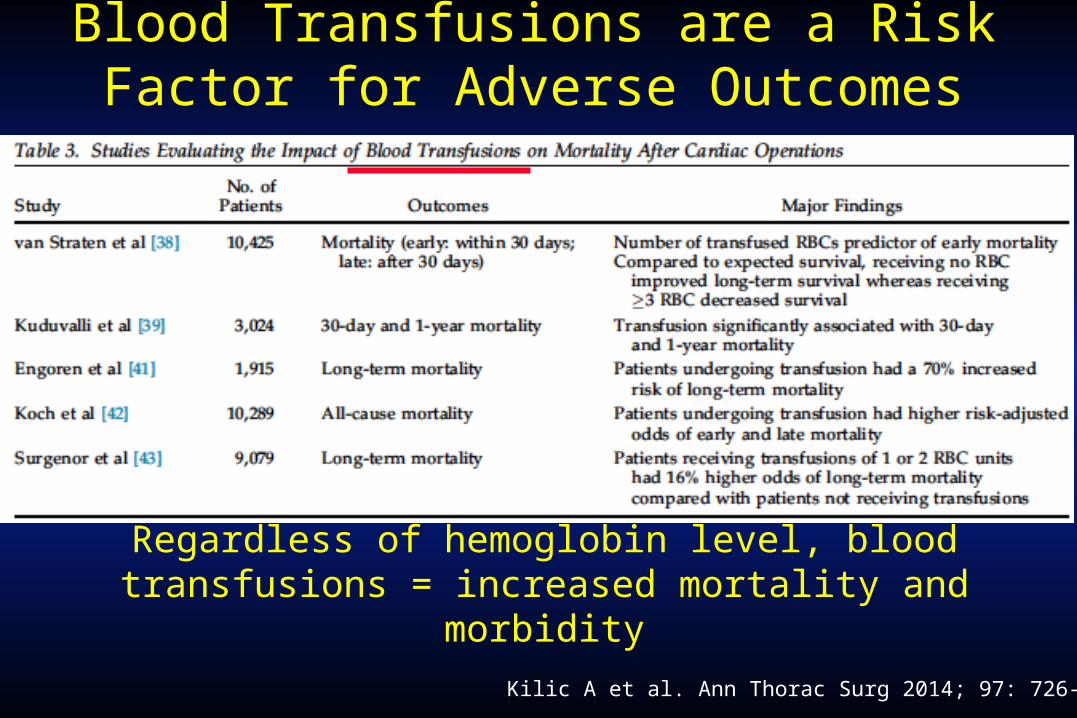
Blood Transfusions are a Risk Factor for Adverse Outcomes
Kilic A et al. Ann Thorac Surg 2014; 97: 726-34.
Regardless of hemoglobin level, blood transfusions = increased mortality and morbidity
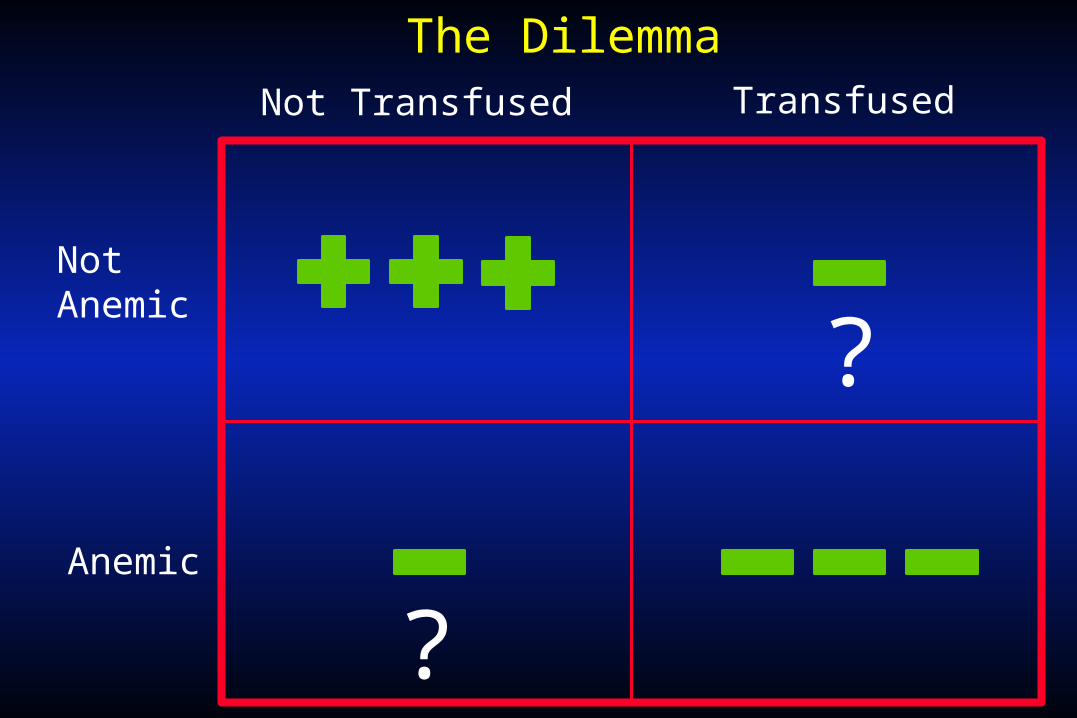
Not Transfused Transfused
NotAnemic
Anemic
?
?
The Dilemma
The Answer
There are 5 randomized controlled trials that specifically address blood transfusions in the face of anemia:
•TRICC•FOCUS•UGI bleed•TRACS•TITRe2
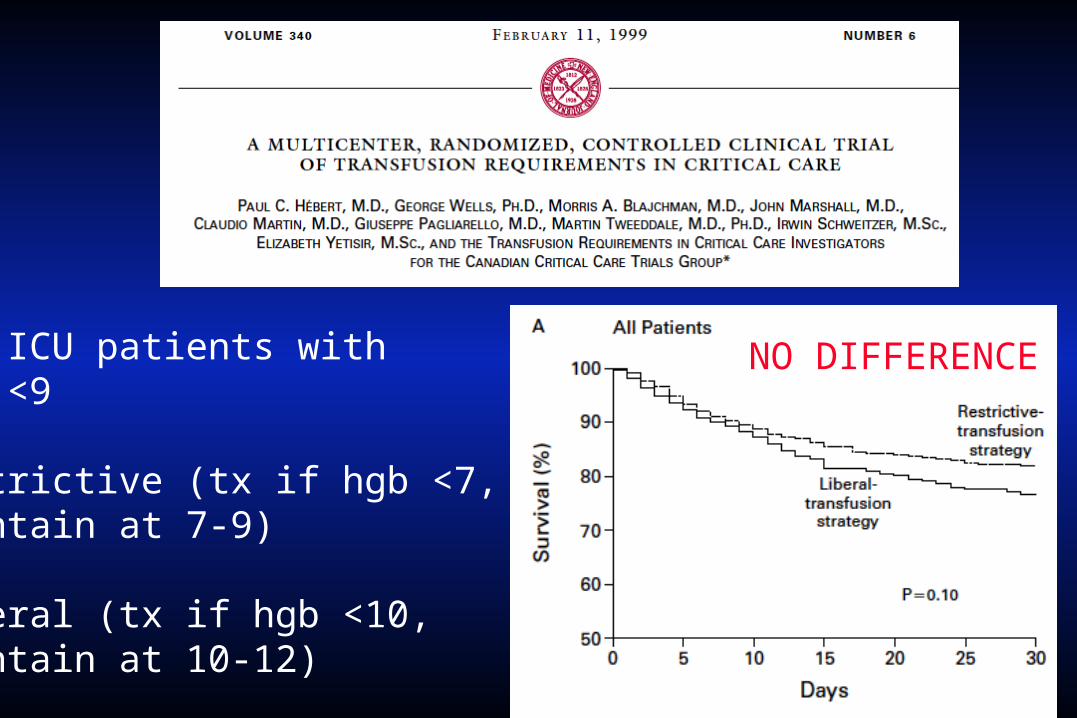
838 ICU patients with hgb <9
Restrictive (tx if hgb <7, maintain at 7-9)
Liberal (tx if hgb <10, maintain at 10-12)
NO DIFFERENCE
2,016 hip fracture patients, hgb <10 (mean age = 81 years!!)
Restrictive (tx if hgb <8)
Liberal (tx if hgb <10)
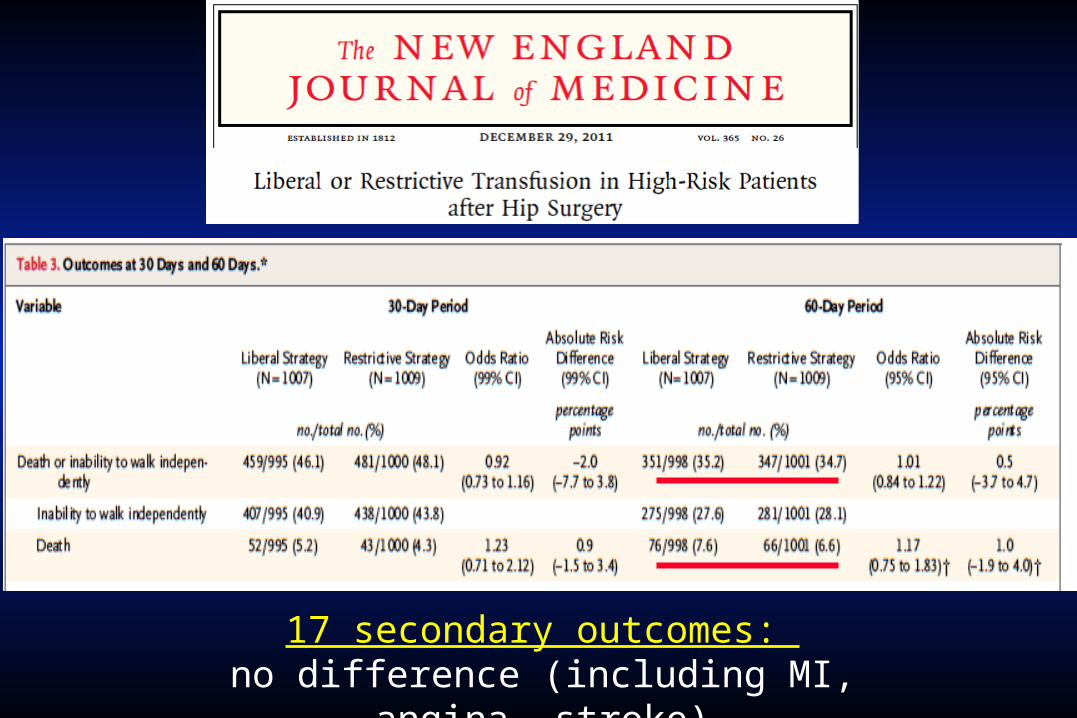
17 secondary outcomes: no difference (including MI, angina, stroke)
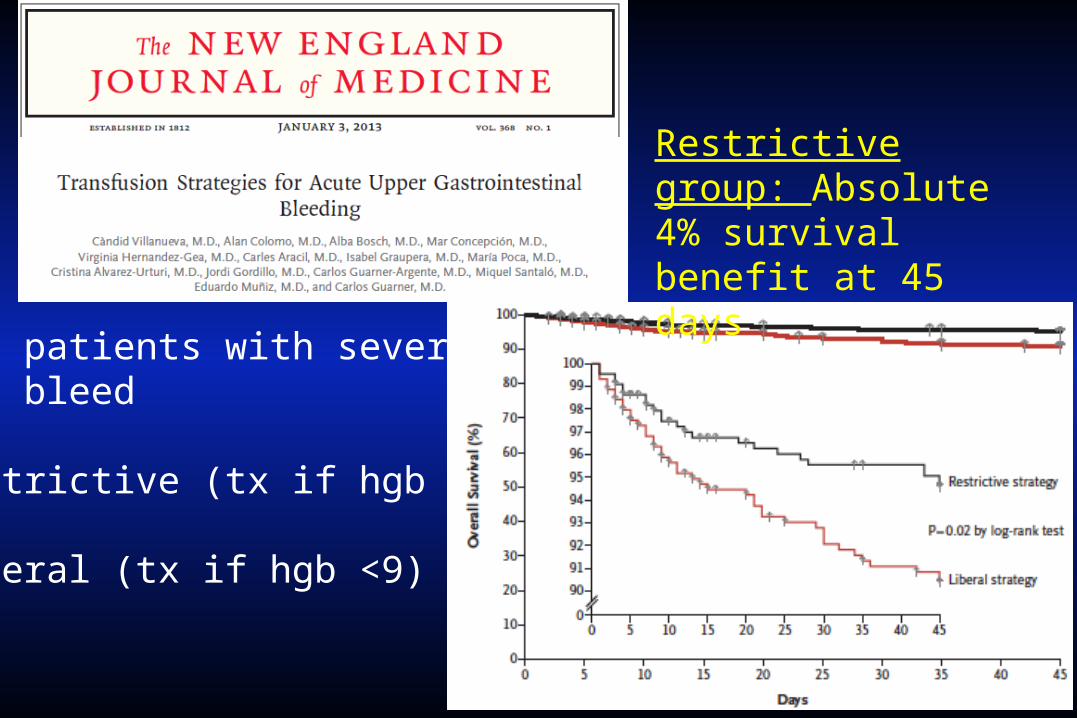
921 patients with severeUGI bleed
Restrictive (tx if hgb <7)
Liberal (tx if hgb <9)
Restrictive group: Absolute 4% survival benefit at 45 days
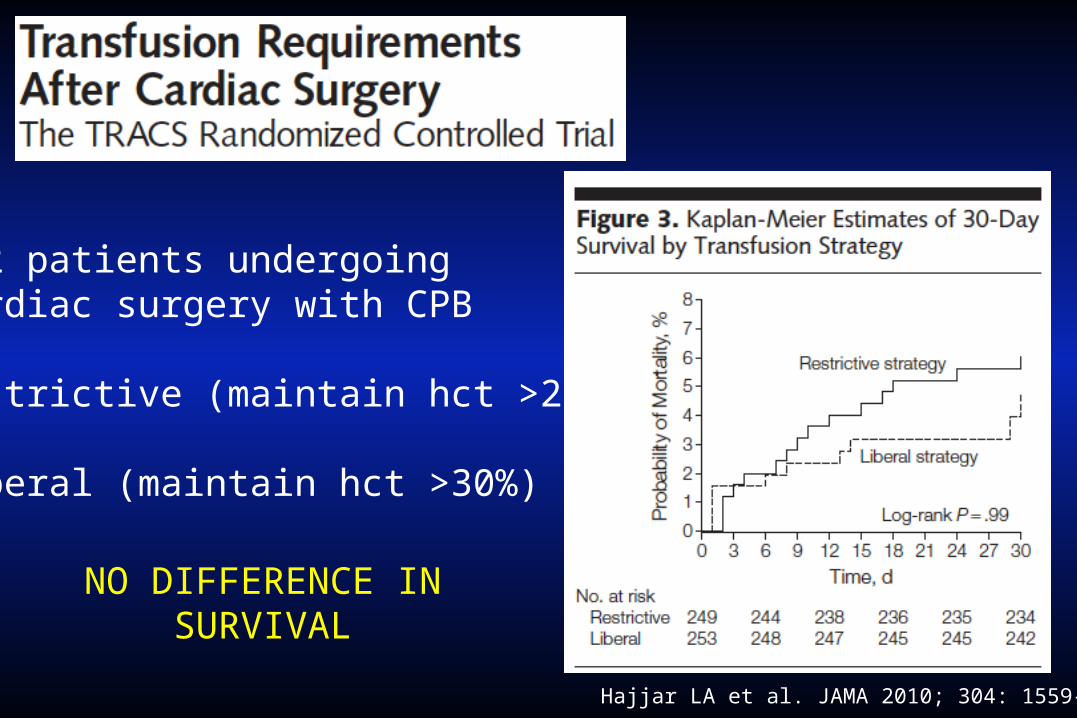
512 patients undergoing cardiac surgery with CPB
Restrictive (maintain hct >24%)
Liberal (maintain hct >30%)
Hajjar LA et al. JAMA 2010; 304: 1559-67.
NO DIFFERENCE IN SURVIVAL
2,003 patients undergoing nonemergent cardiac surgery with hgb <9
Restrictive (tx if hgb <7.5)
Liberal (tx if hgb <9)
TITRe2 Trial
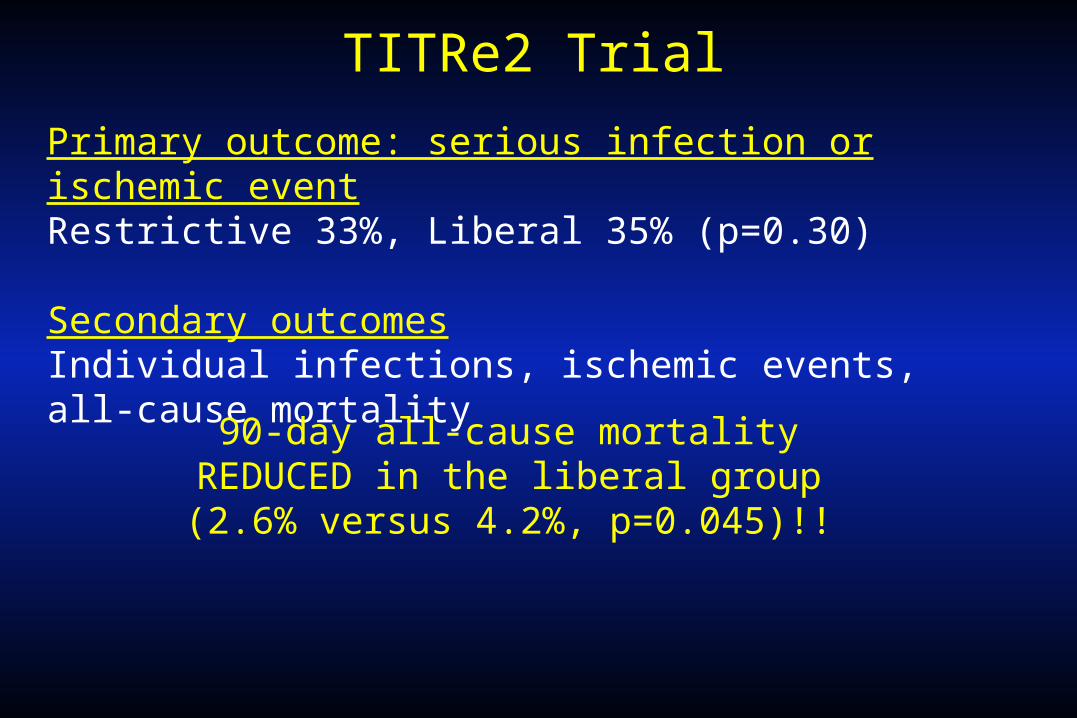
TITRe2 Trial
Primary outcome: serious infection or ischemic eventRestrictive 33%, Liberal 35% (p=0.30)
Secondary outcomesIndividual infections, ischemic events, all-cause mortality
90-day all-cause mortality REDUCED in the liberal group (2.6% versus 4.2%, p=0.045)!!
Overview
1. Why should we care?
2. What is the evidence?
3. How should we (healthcare professional, institution) proceed with regards to blood transfusion practice?
Ferraris VA et al. Ann Thorac Surg 2007; 83: S27-86.
Ferraris VA et al. Ann Thorac Surg 2011; 91: 944-82.
Ferraris VA et al. Ann Thorac Surg 2011; 91: 944-82.
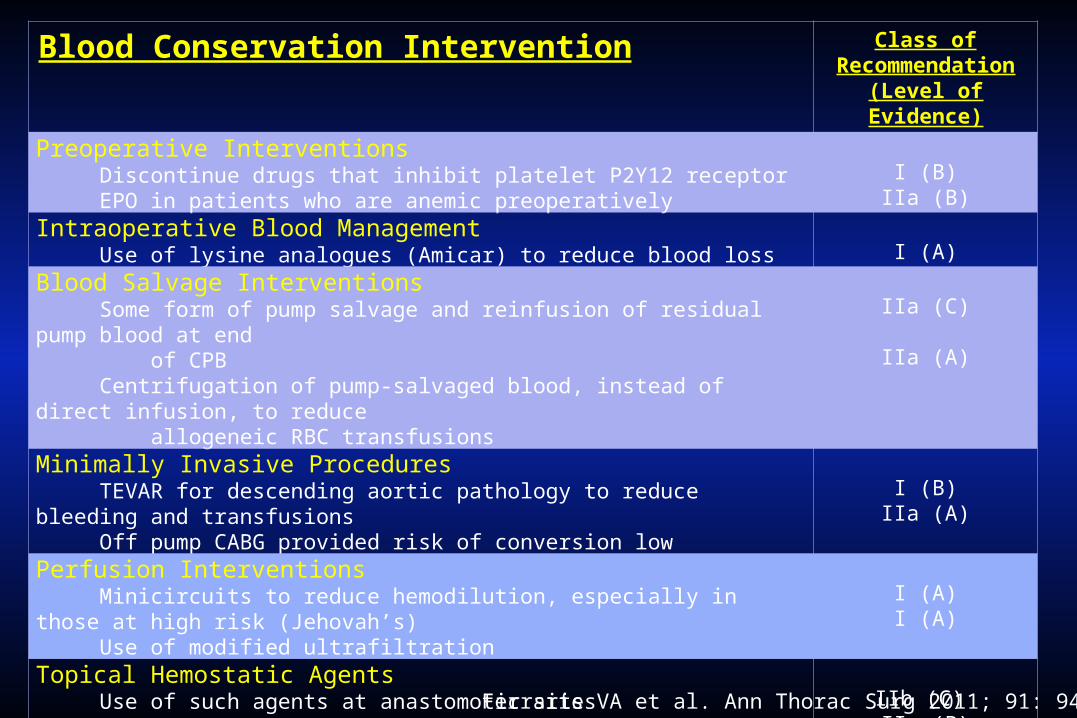
Blood Conservation Intervention Class of Recommendation
(Level of Evidence)
Preoperative Interventions Discontinue drugs that inhibit platelet P2Y12 receptor EPO in patients who are anemic preoperatively
I (B)IIa (B)
Intraoperative Blood Management Use of lysine analogues (Amicar) to reduce blood loss I (A)
Blood Salvage Interventions Some form of pump salvage and reinfusion of residual pump blood at end of CPB Centrifugation of pump-salvaged blood, instead of direct infusion, to reduce allogeneic RBC transfusions
IIa (C)
IIa (A)
Minimally Invasive Procedures TEVAR for descending aortic pathology to reduce bleeding and transfusions Off pump CABG provided risk of conversion low
I (B)IIa (A)
Perfusion Interventions Minicircuits to reduce hemodilution, especially in those at high risk (Jehovah’s) Use of modified ultrafiltration
I (A)I (A)
Topical Hemostatic Agents Use of such agents at anastomotic sites Antifibrinolytic agents poured into the surgical wound after CPB to limit CT drainage
IIb (C) IIa (B)
Creation of a Multidisciplinary Blood Management Team IIa (B)
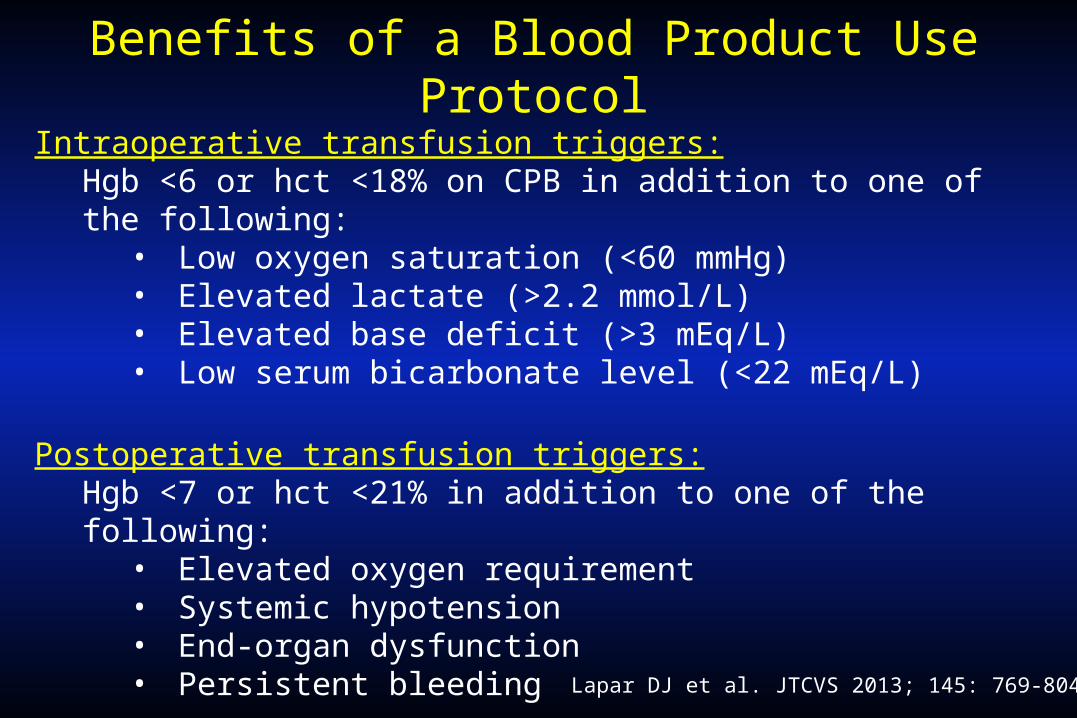
Benefits of a Blood Product Use Protocol
Lapar DJ et al. JTCVS 2013; 145: 769-804.
Intraoperative transfusion triggers:Hgb <6 or hct <18% on CPB in addition to one of the following:
• Low oxygen saturation (<60 mmHg)• Elevated lactate (>2.2 mmol/L)• Elevated base deficit (>3 mEq/L)• Low serum bicarbonate level (<22 mEq/L)
Postoperative transfusion triggers:Hgb <7 or hct <21% in addition to one of the following:
• Elevated oxygen requirement• Systemic hypotension• End-organ dysfunction• Persistent bleeding
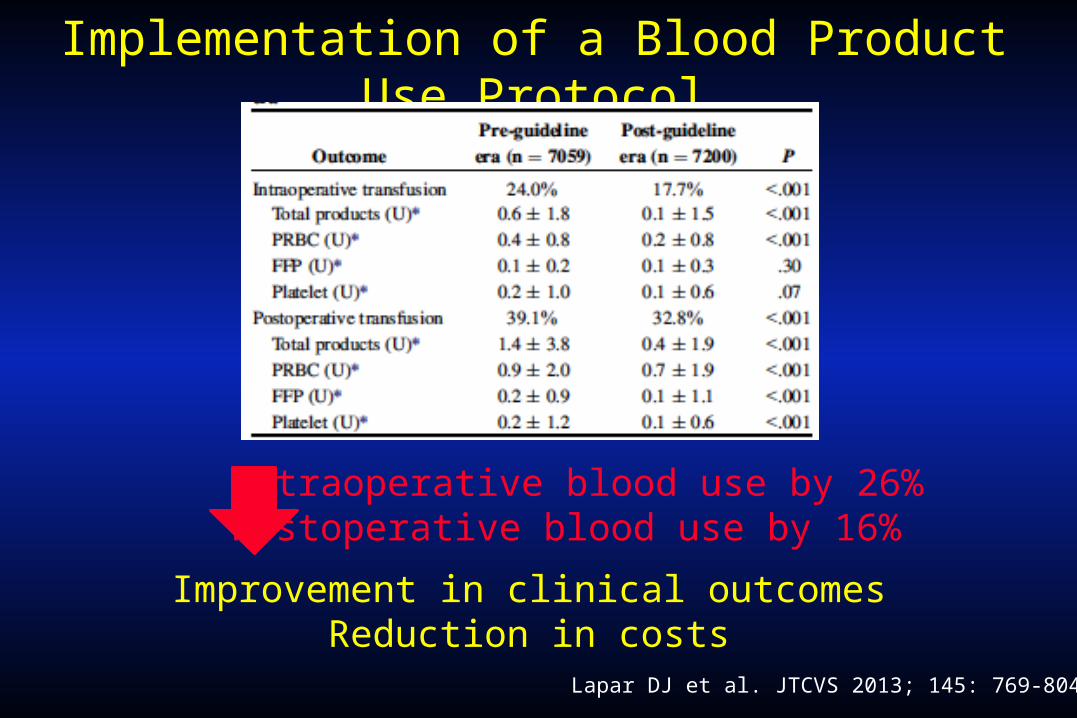
Implementation of a Blood Product Use Protocol
Lapar DJ et al. JTCVS 2013; 145: 769-804.
Intraoperative blood use by 26%Postoperative blood use by 16%
Improvement in clinical outcomesReduction in costs
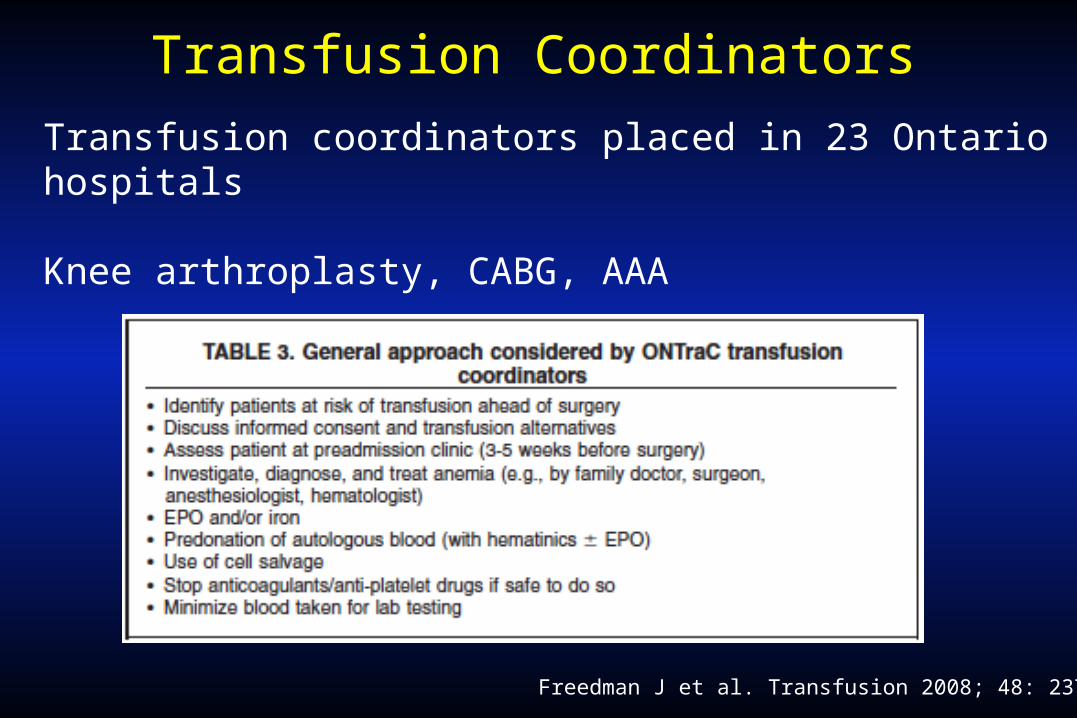
Transfusion Coordinators
Freedman J et al. Transfusion 2008; 48: 237-50.
Transfusion coordinators placed in 23 Ontario hospitals
Knee arthroplasty, CABG, AAA
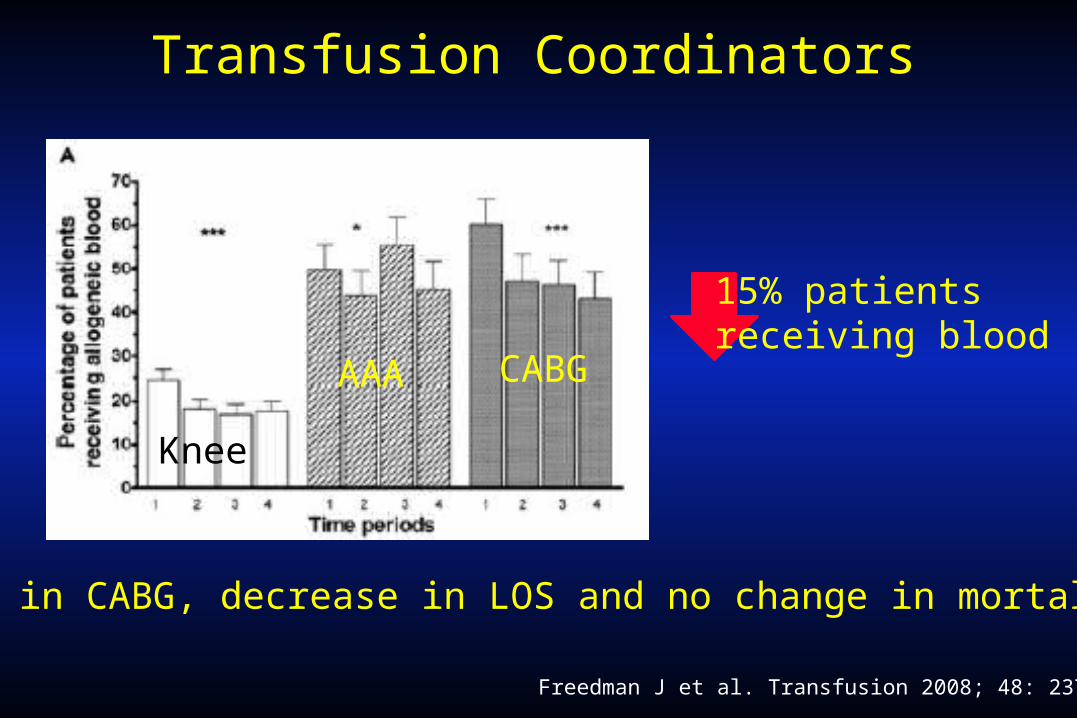
Transfusion Coordinators
Freedman J et al. Transfusion 2008; 48: 237-50.
CABG
Knee
AAA
And in CABG, decrease in LOS and no change in mortality
15% patients receiving blood
Disclosure of Transfusion Behavior
Beaty CA et al. Ann Thorac Surg 2013; 96: 2168-74.
Transfusion trigger of hgb <8 g/dl
3 time periods
• No feedback
• Weekly feedback of group transfusion behavior
• Weekly feedback with identification of individual
surgeon transfusion behavior
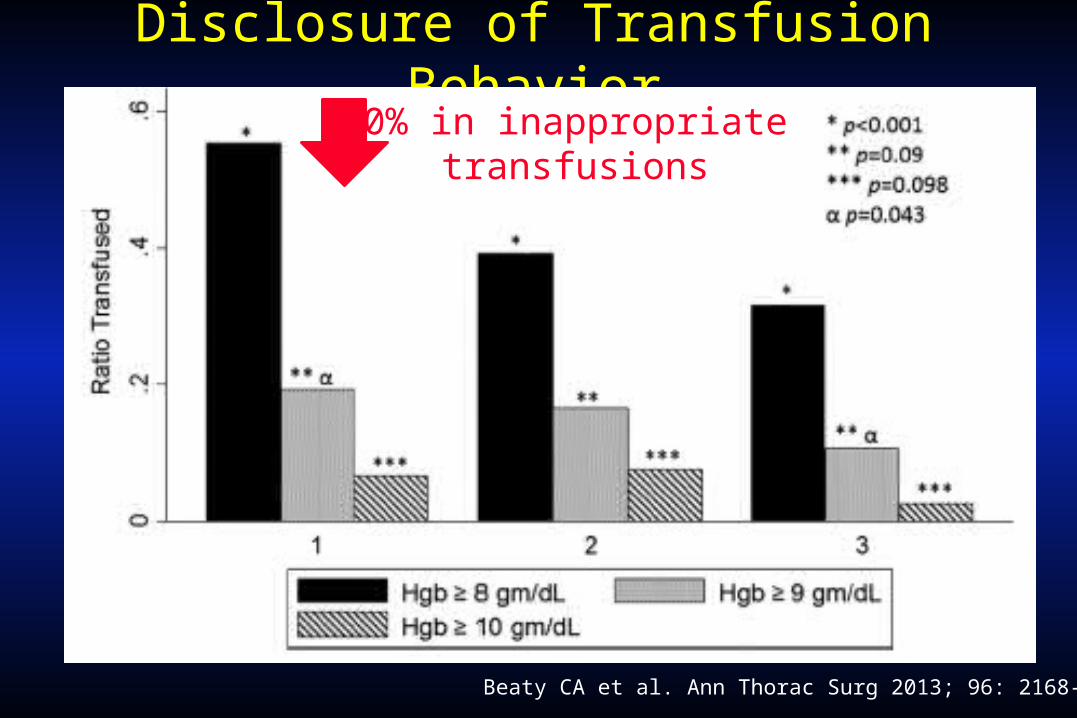
Disclosure of Transfusion Behavior
Beaty CA et al. Ann Thorac Surg 2013; 96: 2168-74.
50% in inappropriate transfusions

Take Home Point #1
Blood transfusions can be lifesaving.
Take Home Point #2
Pre-, intra-, and postoperative anemia are independently associated with worse outcomes in cardiac surgery.
Take Home Point #3
Blood transfusions are independently associated with worse outcomes in cardiac surgery.
Take Home Point #4
Blood transfusions cost money.
Take Home Point #5
Multiple evidence-based blood conservation techniques (preoperatively, intraoperatively, and postoperatively) should be employed.
Take Home Point #6
Most importantly, every institution needs a multidisciplinary, agreed upon transfusion protocol with continued monitoring of adherence.
Acknowledgements
Glenn Whitman, M.D.
Advances in Transfusion and Blood Conservation
Arman Kilic, MDDivision of Cardiac Surgery, Department of Surgery,
Johns Hopkins Hospital, Baltimore, MD


















