
ADVANCED PPE NERMINE CHOUMANE PRESENTED...
136
ADVANCED PPE NERMINE CHOUMANE PRESENTED TO: Dr. Diana Malaeb, Pharm D Chair LEBANESE INTERNATIONAL UNIVERSITY SCHOOL OF PHARMACY FALL 2012
Transcript of ADVANCED PPE NERMINE CHOUMANE PRESENTED...
ADVANCED PPE
NERMINE CHOUMANE
PRESENTED TO: Dr. Diana Malaeb, Pharm D Chair
LEBANESE INTERNATIONAL UNIVERSITY
SCHOOL OF PHARMACY
FALL 2012

4/24/2013

OUTLINE
I. Background
II. Journal club evaluation
a. Journal evaluation
b. Title evaluation
c. Authors evaluation
d. Abstract
e. Introduction
1. Trial funding
2. Rationale
3. Objective
4. Hypothesis
5. Reference

OUTLINE
f. Methods
1. Study design
2. Study population
3. Randomization & Treatment
4. Outcomes
a. Efficacy
b. Microbiology
c. Pharmacokinetic
5. Safety
6. Statistical analysis
OUTLINE
g. Result
1. Patient
2. Clinical outcomes
3. Safety
4. Microbiology
5. Pharmacokinetic
h. Discussion
1. Author’s comments
2. Strengths
3. Limitations
4. Author’s conclusion
III. Conclusion
IV. Other studies
A VIEW OVER

BACKGROUND
• Clostridium difficile (C. difficile) is a gram positive, spore‐forming anaerobic bacillus
• It is the leading cause of healthcare‐associated diarrhea
• It is the primary infective cause of antibiotic-associated diarrhea
• It has been responsible for a large number of outbreaks in hospitals
BACKGROUND
• CDI appears to be increasing in populations that are at low & high risk
• This can be attributed to emergence of hypervirulentstrain of C. difficile
(NAP1/BI/027)
North American pulse-field gel electrophoresis type 1 (NAP1),
Restriction endonuclease type BI,
Polymerase chain reaction ribotype 027

BACKGROUND – SIGNS & SYMPTOMS -
• CDI may be asymptomatic, but if symptoms are present, they may range in severity from mild-moderate diarrhea to life‐threatening pseudomembranous colitis
• Patients with healthcare‐associated CDI may experience ≥ 1of the following complications:
1. Clinical dehydration
2. Hypokalemia
3. Mild gastrointestinal bleeding
4. Ileus

BACKGROUND – COMPLICATIONS -
• Complications of severe CDI include:
1. Bowel perforation
2. Hypotension
3. Renal failure
4. Sepsis & Death
• CDI has been associated with:
1. Additional diagnostic and interventional procedures
2. Additional length of stay in hospital
3. Higher total hospital costs
BACKGROUND – TRANSMISSION -
• Transmission of C. difficile occurs primarily
through the fecal‐oral route following transient
contamination of the hands of healthcare
workers and patients/residents
• Contamination of the care environment also
plays a major role in the spread of C. difficile

BACKGROUND – RISK FACTORS -
• Risk Factors for CDI:
1. History of antibiotic use, particularly fluoroquinolones
2. Bowel disease/surgery
3. Chemotherapy
4. Prolonged hospitalization
5. Treatment with PPI
6. Immunosuppressive therapy
7. History of CDI
8. Recent surgery
9. Increased age
BACKGROUND – DIAGNOSIS -
• A patient is identified as a CDI case if:
1. S/He has diarrhea, fever, abdominal pain and/or ileus,
+a laboratory confirmation of a positive toxin assay for C. difficile
OR
2. S/He has a diagnosis of pseudomembranes on sigmoidoscopyor colonoscopy or histological/pathological diagnosis of CDI
OR
3. S/He has a diagnosis of toxic megacolon
• Toxin testing is most important clinically, but is hampered by its lack of sensitivity
• To overcome this problem =>
2-step method that uses EIA detection of glutamate
dehydrogenase (GDH) as initial screening and then uses the
cell cytotoxicity assay or toxigenic culture as the confirmatory
test for GDH-positive stool specimens only
• Results appear to differ based on the GDH kit used; therefore, until more data are available on the sensitivity of GDH testing, this approach remains an interim recommendation
BACKGROUND – DIAGNOSIS -
BACKGROUND – PREVENTION -
• Transmission of CDI can be prevented by strict
adherence to routine practices and additional
precautions
• Practices that are critical to prevent transmission of
CDI include:
1. Appropriate use of personal protective
equipment (PPE)
2. Hand hygiene
3. Appropriate cleaning and disinfection of
environmental surfaces and equipment
BACKGROUND – PREVENTION -
• Administration of currently available probioticsis not recommended to prevent primary CDI
=> limited data + potential risk of bloodstream
infection
• Minimize the frequency and duration of antimicrobial therapy and the number of antimicrobial agents prescribed, to reduce CDI risk

BACKGROUND– TREATMENT -
• Medical Management of Clostridium difficile Infection:
Do not treat symptom‐free carriers of C. difficile
Discontinue antibiotics if possible, or consider changing to a lower CDI risk group of antibiotics such as aminoglycosides,TMP/SMX, tetracyclines, and/or metronidazole
Do not use antidiarrheals (e.g. loperamide [Immodium], diphenoxylate [Lomotil])
Supportive therapy with intravenous fluids and electrolytes may be sufficient to relieve symptoms
BACKGROUND– TREATMENT -
When severe or complicated CDI is suspected, initiate empirical treatment as soon as the diagnosis is suspected
If the stool toxin assay result is negative, the decisionto initiate, stop, or continue treatment must be individualized
Gastric acid suppression &(PPIs) have also been recognized as a risk factor for CDI and should be used selectively
Antimicrobial has been shown to be the single most successful strategy for preventing CDI
Dosages must be given orally in order to be fully effective in the gut
BACKGROUND– TREATMENT -
DOC if initial M-M CDI =>
Metronidazole 500 mg po tid for 10–14 days
DOC if initial Severe CDI =>
Vancomycin 125 mg po qid for 10–14 days
DOC if Severe complicated CDI =>
Vancomycin 500mg po qid /500 mg in 100 ml NS per rectum q.6hrs (if ileus is present)
+/-
Metronidazole 500 mg IV q.8hrs
BACKGROUND– TREATMENT -
If Severely ill patients =>
Colectomy
If first recurrence of CDI =>
Treat with the same regimen as for the initial
episode
If second or later recurrence of CDI =>
vancomycin therapy using a tapered and/or pulse regimen
BACKGROUND– OLDER TREATMENT -
Rifampin
Nitazoxanide
Rifaximin
Tigecycline
BACKGROUND– OTHER TREATMENT -
IVIG =>
Currently the only available antibody that could potentially be used for
treatment of CDI; Retrospective analyses have examined the use of IVIG single or repeated doses of 125 to 400 mg/kg in severe or recurrent CDI and have not shown a benefit
Monoclonal Antibodies
Use of 2 monoclonal antibodies against toxins A and B administered together in a Phase 2, randomized clinical trial
=> Lower recurrence rate in the monoclonal antibody group Vs
placebo
Vaccines =>
C. difficile toxoid-based vaccine being developed by Sanofi Pasteur is currently being studied in a Phase 2, randomized trial
Fidaxomicin
recently approved for treatment of this infection in the USA in May, 2011,
and in Europe in December, 2011


4/24/2013
A VIEW OVER

Fidaxomicin Vancomycin
Brands Dificid® - Vancocin® HCL Pulvules
- Vancocin ®HCL
- Vancoled®
- Vancolon®
Dosage form/
Strength
- Oral tablet 200mg - IV Powder for Solution:
1, 5, 10, 500, 750mg
- Oral Powder for
suspension: 250mg/5ml,
500mg/6ml
- Oral Capsule: 125, 250mg
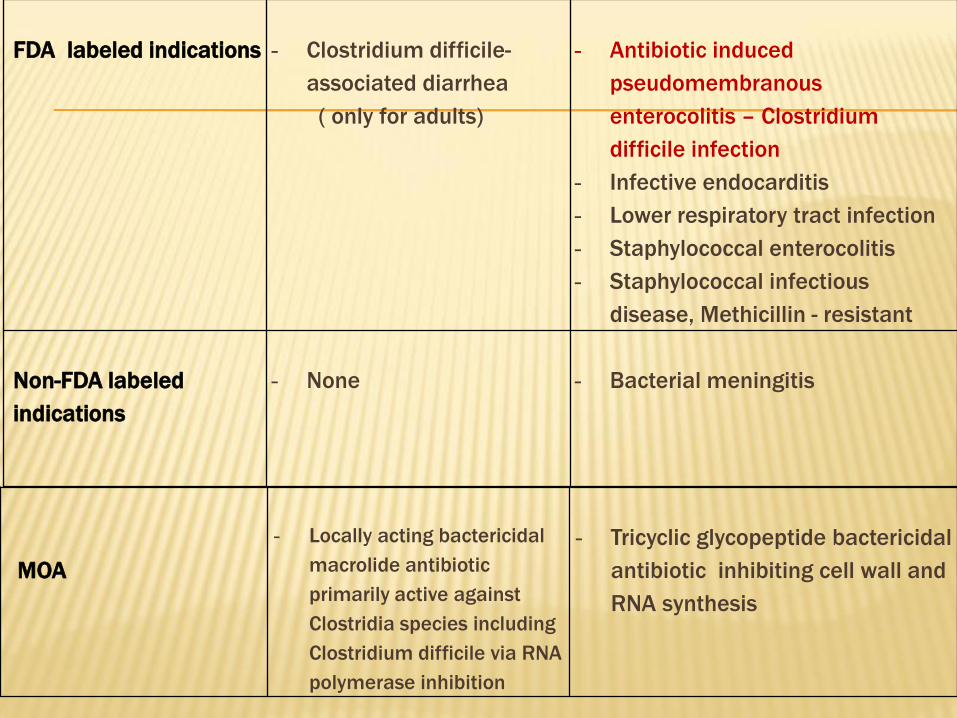
FDA labeled indications - Clostridium difficile-
associated diarrhea
( only for adults)
- Antibiotic induced
pseudomembranous
enterocolitis – Clostridium
difficile infection
- Infective endocarditis
- Lower respiratory tract infection
- Staphylococcal enterocolitis
- Staphylococcal infectious
disease, Methicillin - resistant
Non-FDA labeled
indications
- None - Bacterial meningitis
MOA
- Locally acting bactericidal
macrolide antibiotic
primarily active against
Clostridia species including
Clostridium difficile via RNA
polymerase inhibition
- Tricyclic glycopeptide bactericidal
antibiotic inhibiting cell wall and
RNA synthesis
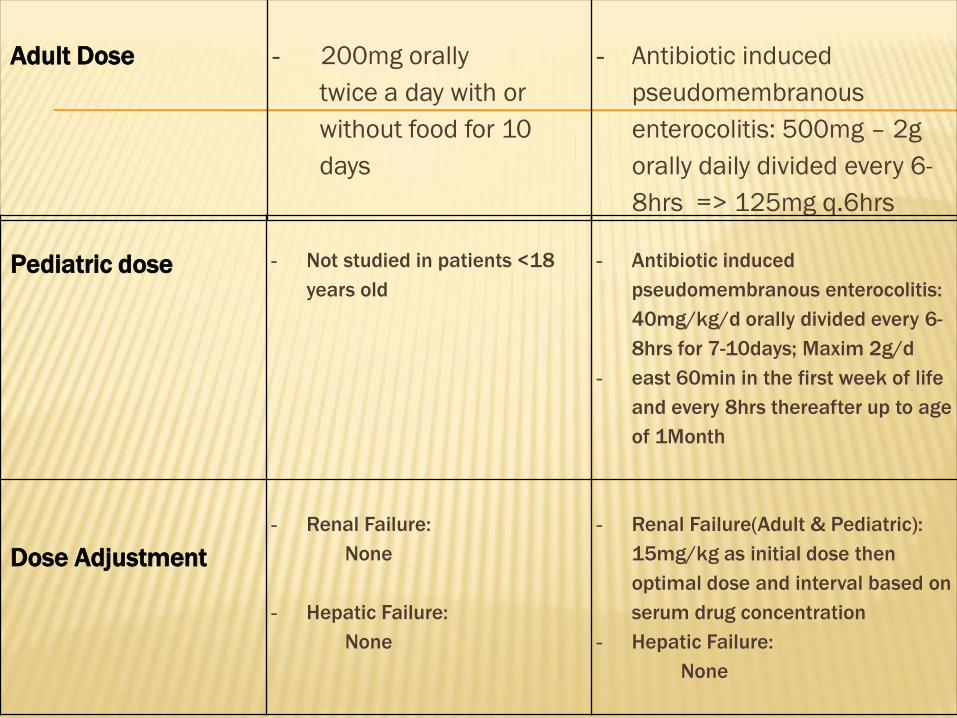
Adult Dose - 200mg orally
twice a day with or
without food for 10
days
- Antibiotic induced
pseudomembranous
enterocolitis: 500mg – 2g
orally daily divided every 6-
8hrs => 125mg q.6hrs
Pediatric dose - Not studied in patients <18
years old
- Antibiotic induced
pseudomembranous enterocolitis:
40mg/kg/d orally divided every 6-
8hrs for 7-10days; Maxim 2g/d
- east 60min in the first week of life
and every 8hrs thereafter up to age
of 1Month
Dose Adjustment
- Renal Failure:
None
- Hepatic Failure:
None
- Renal Failure(Adult & Pediatric):
15mg/kg as initial dose then
optimal dose and interval based on
serum drug concentration
- Hepatic Failure:
None

If missed a
dose/forget to use
your medicine
- Use it as soon as you can
- If it’s almost time for your
next dose, wait until then
to use the medicine and
skip the missed dose
- Do not use extra medicine
to make up for a missed
dose
- Use it as soon as you can
- If it’s almost time for your
next dose, wait until then to
use the medicine and skip
the missed dose
Do not use extra medicine to
make up for a missed dose
Storage & Stability - Store the medicine in a
closed container at room
temperature, away from
heat, moisture and direct
light
- Keep it away from children
and never share your
medicine with anyone
- Store the medicine in a closed
container at room
temperature, away from heat,
moisture and direct light
- Keep it away from children
and never share your
medicine with anyone
- After reconstitution, may
refrigerate for 14 days

Absorption - Minimal - Minimal
PPB - 31% - 55%
T1/2 - Drug: 11.7hrs
- Metabolite (OP-
1118): 11.2hrs
- 6hrs
Excretion - Feces >92%
- Urine= 0.59%
- Urine = 80-90%
Metabolism - Independent of
CYP450
- Independent of
CYP450

CI- Not determined - Allergy to corn/corn products
- Hypersensitivity to Vancomycin
Caution- Fidaxomicin is minimally
absorbed and should not
be used for treatment of
systemic infections
- Use of Fidaxomicin in the
absence of C.difficile
infection is not expected to
benefit patients and may
promote development of
drug resistant bacteria
- Drug eruption, pruritus, and
rash reported rarely
- Not effective by the oral route
for other types of infections
- Rapid bolus administration
may cause hypotension and
cardiac arrest (rare); administer
in diluted solution over a period
not <60 min
- Ototoxicity reported; caution
with underlying hearing loss
and amynoglycosides; Caution
with renal insufficiency and
adjust dose with renal
dysfunction
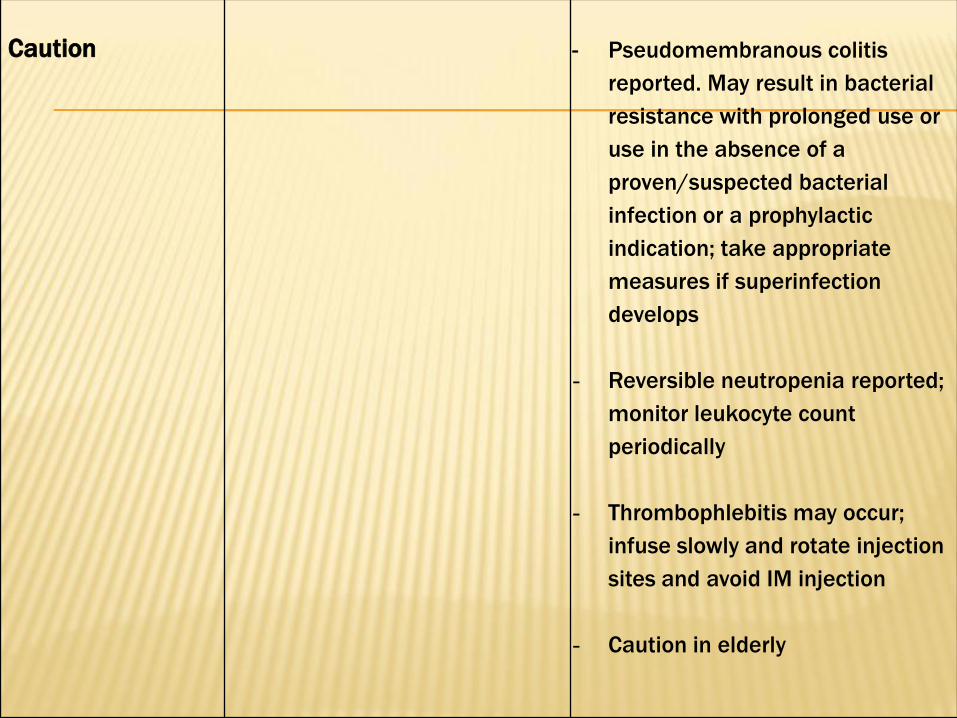
Caution - Pseudomembranous colitis
reported. May result in bacterial
resistance with prolonged use or
use in the absence of a
proven/suspected bacterial
infection or a prophylactic
indication; take appropriate
measures if superinfection
develops
- Reversible neutropenia reported;
monitor leukocyte count
periodically
- Thrombophlebitis may occur;
infuse slowly and rotate injection
sites and avoid IM injection
- Caution in elderly
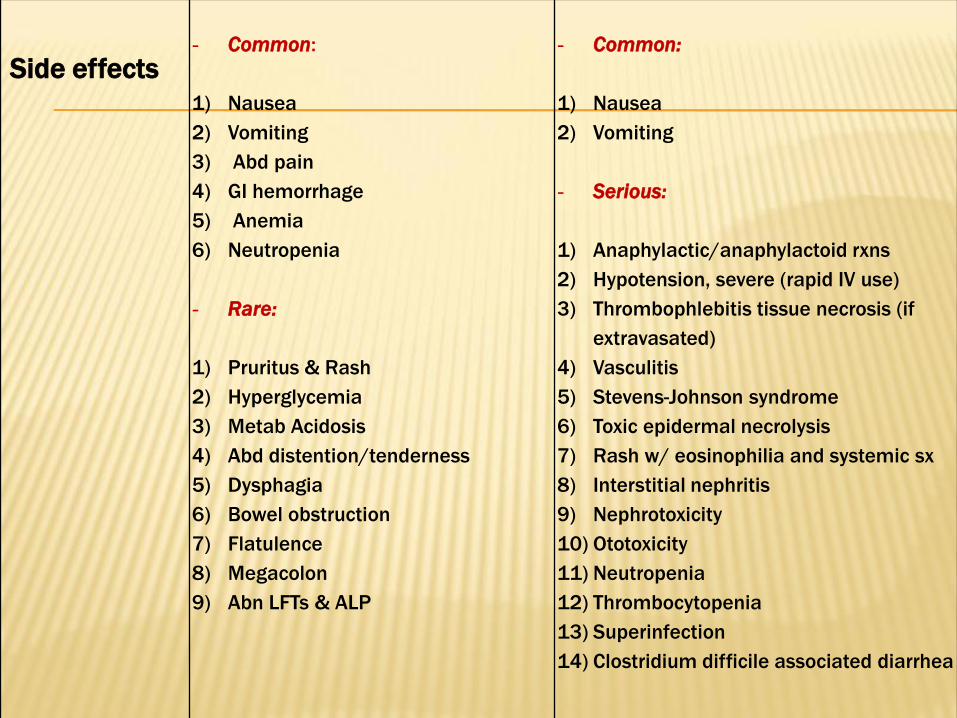
Side effects- Common:
1) Nausea
2) Vomiting
3) Abd pain
4) GI hemorrhage
5) Anemia
6) Neutropenia
- Rare:
1) Pruritus & Rash
2) Hyperglycemia
3) Metab Acidosis
4) Abd distention/tenderness
5) Dysphagia
6) Bowel obstruction
7) Flatulence
8) Megacolon
9) Abn LFTs & ALP
- Common:
1) Nausea
2) Vomiting
- Serious:
1) Anaphylactic/anaphylactoid rxns
2) Hypotension, severe (rapid IV use)
3) Thrombophlebitis tissue necrosis (if
extravasated)
4) Vasculitis
5) Stevens-Johnson syndrome
6) Toxic epidermal necrolysis
7) Rash w/ eosinophilia and systemic sx
8) Interstitial nephritis
9) Nephrotoxicity
10) Ototoxicity
11) Neutropenia
12) Thrombocytopenia
13) Superinfection
14) Clostridium difficile associated diarrhea
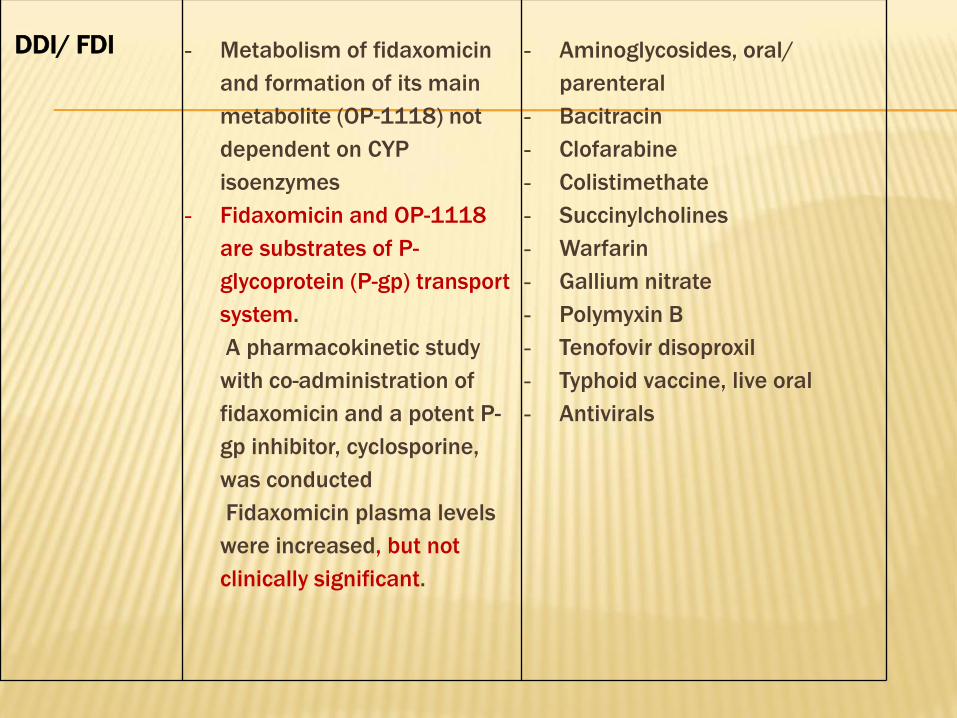
DDI/ FDI - Metabolism of fidaxomicin
and formation of its main
metabolite (OP-1118) not
dependent on CYP
isoenzymes
- Fidaxomicin and OP-1118
are substrates of P-
glycoprotein (P-gp) transport
system.
A pharmacokinetic study
with co-administration of
fidaxomicin and a potent P-
gp inhibitor, cyclosporine,
was conducted
Fidaxomicin plasma levels
were increased, but not
clinically significant.
- Aminoglycosides, oral/
parenteral
- Bacitracin
- Clofarabine
- Colistimethate
- Succinylcholines
- Warfarin
- Gallium nitrate
- Polymyxin B
- Tenofovir disoproxil
- Typhoid vaccine, live oral
- Antivirals

Pregnancy &
Lactation
- Category B
- Unknown if crosses
placenta and if it’s
excreted in human milk
- Category C
- In breastfeeding, infant risk
cannot be ruled out
Monitor - Resolution of S&S of
Clostridium difficile
infection is indicative of
efficacy
- Hypersensitivity reactions (eg,
Stevens-Johnson syndrome,
vasculitis)
- Infusion reactions (eg,
hypotension, arrhythmias, "red
neck")
- Thrombophlebitis
- Ototoxicity
- Renal function
- Diarrhea
- Pseudomembranous colitis
- Neutropenia
- Superinfection infusion
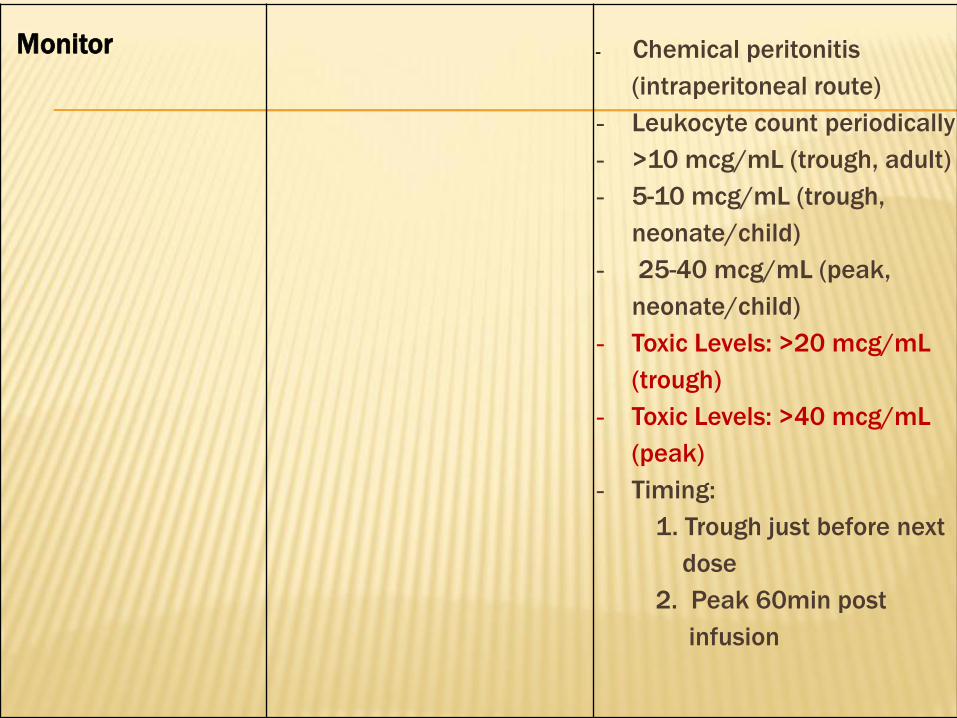
Monitor - Chemical peritonitis
(intraperitoneal route)
- Leukocyte count periodically
- >10 mcg/mL (trough, adult)
- 5-10 mcg/mL (trough,
neonate/child)
- 25-40 mcg/mL (peak,
neonate/child)
- Toxic Levels: >20 mcg/mL
(trough)
- Toxic Levels: >40 mcg/mL
(peak)
- Timing:
1. Trough just before next
dose
2. Peak 60min post
infusion

JOURNAL CLUB EVALUATION
• The New England Journal of Medicine (NEJM) is
an English-Language peer reviewed medical
journal published by the Massachusetts
Medical Society
• It describes itself as the oldest continuously
published medical journal in the world
• Established in 1812

JOURNAL CLUB EVALUATION
• The journal publishes weekly editorials, papers on original research, review articles, correspondence, and case reports
• It has the highest impact factor of the journals of clinical medicine => IF, 2010= 53.486
• Issues/Year: 52
• It requires that articles it publishes not have been published or released elsewhere
• The article was published in february 3, 2011 -----> up to date
• Journal homepage: www.nejm.org
JOURNAL CLUB EVALUATION
• Editors:
Walter Prentice Bowers, 1921–1937
Robert Nason Nye, 1937–1947
Joseph Garland, 1947–1967
Franz J. Ingelfinger, 1967–1977
Arnold S. Relman, 1977–1991
Jerome P. Kassirer, 1991–1999
Marcia Angell, 1999–2000
Jeffrey M. Drazen, 2000–present
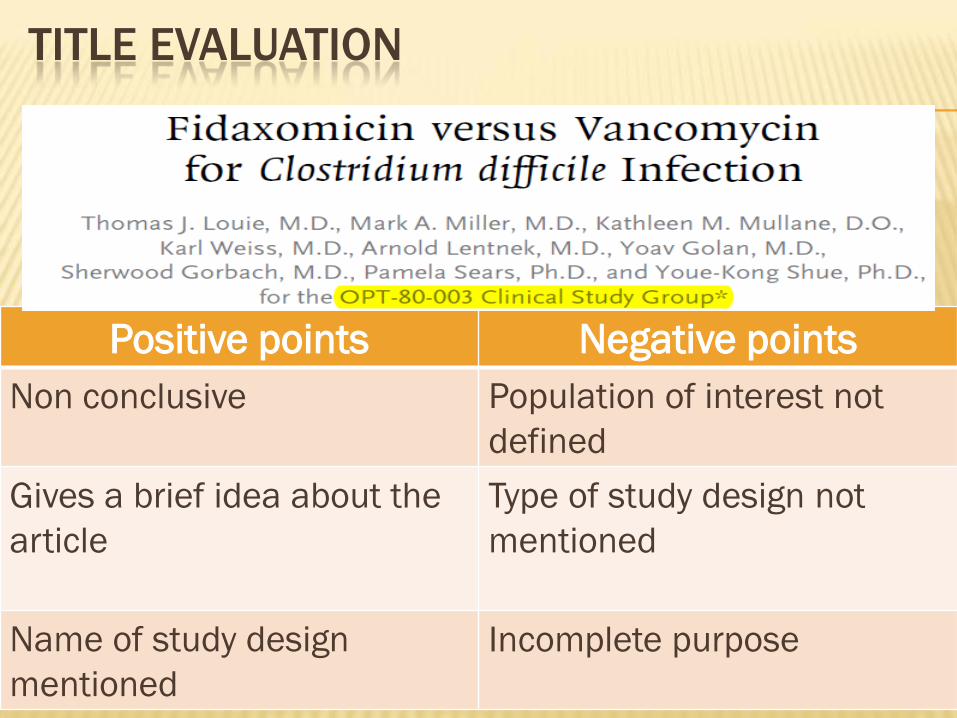
TITLE EVALUATION
Negative pointsPositive points
Population of interest not
defined
Non conclusive
Type of study design not
mentioned
Gives a brief idea about the
article
Incomplete purposeName of study design
mentioned

AUTHORS EVALUATION
Contributors
Thomas J. Louie, M.D
. Professor of : 1. Medicine
2. Microbiology, Immunology &
Infectious Diseases
. MD at University of Alberta
. Involved in clinical trials with the focus around the evolution
of new antimicrobial agents and biologic response modifiers
in seriously ill patients with infections
AUTHORS EVALUATION
Kathleen M. Mullane, D.O
. Internal Medicine – Certified
. Infectious Disease Medicine - Board Eligible
. Practice Affiliations: UNIVERSITY OF CHICAGO
. Hospital affiliations: 1. University of Chicago
Medical Center
2. Loyola University Medical
Center
3. University Hospital
AUTHORS EVALUATION
1- Pamela Sears, Ph.D., inventor of Fidaxomicin patent &
employee of & owning stock options in OPTIMER
pharmaceuticals
2- Youe-Kong Shue, Ph.D., employee of & owning stock options in
OPTIMER pharmaceuticals
3- Sherwood Gorbach, M.D., part-time employee of OPTIMER
pharmaceuticals & holding a patent on lactobacillus GG
probiotic & B-glucan
4- Karl Weiss, M.D., honoraria & consulting fees from
pharmaceutical companies
AUTHORS EVALUATION
5- Thomas J. Louie, M.D., specialised in infectious
disease
6- Mark A. Miller, M.D.,
7- Arnold Lentnek, M.D.,
8- Yoav Golan, M.D.,

AUTHORS EVALUATION
The authors are highly educated (PhD,D.O.&
M.D.) & are reputable source of trust in medical
field
× Most of the authors work at OPTIMER
pharmaceuticals which is the funder & producer
of Fidaxomicin
× No biostatician nor pharmacists
(the source of drug information & counseling)

ABSTRACT EVALUATION

ABSTRACT EVALUATION
Divided into 4 sections
Brief & provide a summarized idea about the article
Primary & secondary end points mentioned
Methodology matches the one of article
Target & number of population identified
Dose & duration of treatment mentioned
Statistical analyses listed
P value listed
Objective listed in the background

ABSTRACT EVALUATION
× Mean Age group unspecified
× Study design type not listed
× Not all reporting tools are identified
× Adverse events not listed
INTRODUCTION EVALUATION
49
INTRODUCTION EVALUATION
Trial Funding
• Trial was funded by “OPTIMER PHARMACEUTICALS”
• It’s the producer of Fidaxomicin that was previously named “OPT-80”
• Most of the members of the clinical study group are employees
• Dr. Pamela Sears (the inventor) works at OPT
Authors’ interference & Bias cannot be eliminated

INTRODUCTION EVALUATION
Rationale:
• Incidence & severity of CDI are increasing
• Recurrent relapses of patients after old therapy
• Nowadays, young-healthy & peripartum women are at a high risk
• Emergence of hypervirulent CD strain NAP1/BI/027
• Reduced rates of clinical response & increased rates of recurrence seen in more recent studies are causes of concern

INTRODUCTION EVALUATION
Objective :
To evaluate the results of a phase 3 noninferiority
study comparing Fidaxomicin with Vancomycin in
629 patients with Clostridium difficile infection
× Not clearly identified and retrieved
INTRODUCTION EVALUATION
General Overview about the MO and the
drugs:
Clostridium difficile background well presented
Fidaxomicin defined in details
INTRODUCTION EVALUATION
Fidaxomicin (previously called OPT-80)
is a new macrocyclic antibiotic that is more active
in vitro than vancomycin by a factor of 8 against
C.difficile, including NAP1/B1/027 strains
Has minimal systemic absorption and high fecal concentration and limited activity in vitro/vivo against normal gut flora
× Vancomycin was not described clearly
× Alternative treatments were absent

INTRODUCTION EVALUATION
• Hypothesis :
• H0: NO DIFFERENCE BETWEEN FIDAXOMICIN &
VANCOMYCIN
• H1: FIDAXOMICIN IS SUPERIOR TO VANCOMYCIN
REJECTED OR ACCEPTED?!!!

INTRODUCTION EVALUATION
References:
• 36 references are identified
• Majority are 1ry literatures : case studies, articles….
• Secondary literatures: NEJM, AAC, CGH, JCM
Trustful & highly informative sources
Provide powerful relevance with
topic: microbiology,gastroenterology,infectious
diseases…
Wide medical background extending to other
fields on medicine(gynecology)
Other cited clinical trials & articles were also
involved

METHODS EVALUATION

STUDY DESIGN EVALUATION
The OPT-80-003 Clinical Trial Study Group, is a
• Prospective
• Multicenter
• Double-blinded
• Randomized
• Parallel group trial
Conducted between May 9, 2006 & August 21, 2008
Sponsored by “Optimer Pharmaceuticals”
Data analysis performed by authors & others in OPT
who provided a written manuscript & submitted it
Included patients from different states of USA and Canada
STUDY DESIGN EVALUATION
Done according to ethical principles of the
Declaration of Helinski & Current Good Clinical
practices
Study protocol approved by the institutional review
boards
All patients provided an informed consent
Data monitored & retrieved by INC research

Exclusion CriteriaInclusion Criteria
Life-threatening/fulminant CDI. ≥16 years old with CDI
. CDI → 1) Diarrhea: >3 unformed bowel
movement daily before
randomization
2) CD toxin A/B/Both in stool
specimen, 48hrs before
randomization
Toxic Megacolon
Patient could have received 4 doses of
Metronidazole/Vancomycin/, 24 hrs before
randomization
Previous treatment with FidaxoNo other concurrent treatment
(oral bacitracin,fusidic acid or rifaximin)
History of Ulcerative colitis/Crohn’s disease
>1 CDI occurrence in 3 Months before start
of study

STUDY POPULATION EVALUATION
Inclusion & Exclusion criteria are adequate
All participants provided written informed consent
Number of Patient screened = 629
Wide age group (>16 YO) CDI can affect all age
groups
The study included patients from USA (52 states)
and from Canada ( 15 states)

STUDY POPULATION EVALUATION
Multicenter hence:
High patient variability
Results can be generalized
× Patient characteristics not listed
× More expensive
× More effort to ensure compliance to clinical
protocol across all centers
RANDOMIZATION & TREATMENT EVALUATION
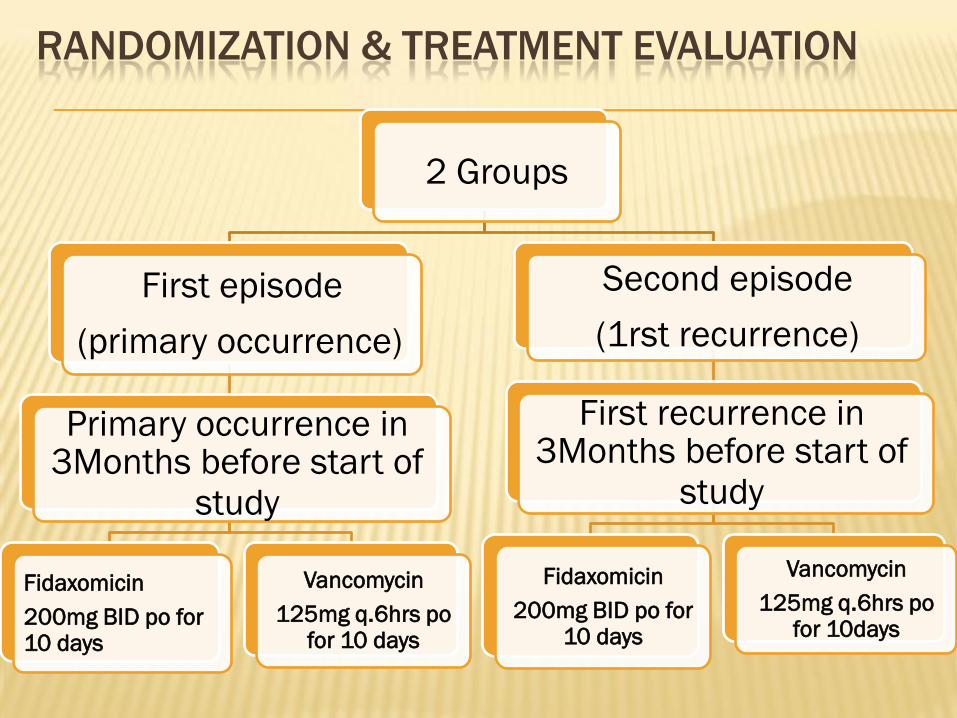
2 Groups
First episode
(primary occurrence)
Primary occurrence in 3Months before start of
study
Fidaxomicin
200mg BID po for 10 days
Vancomycin
125mg q.6hrs pofor 10 days
Second episode
(1rst recurrence)
First recurrence in 3Months before start of
study
Fidaxomicin
200mg BID po for 10 days
Vancomycin
125mg q.6hrs pofor 10days
RANDOMIZATION & TREATMENT EVALUATION
The Independent Ethics Committee or
Institutional Review Board at each study site
approved the protocol
The study was conducted in accordance with
the ethical principles in the Declaration of
Helsinki, consistent Good Clinical Practices &
applicable regulatory requirements
RANDOMIZATION & TREATMENT EVALUATION
An interactive voice-response system
& a Computer generated randomization
schedule provided randomization # and
medication kit # for each patient
Placebo & Fidaxomicin & Vancomycin were
overencapsulated to look the same

RANDOMIZATION & TREATMENT EVALUATION
Daily assessment during 10 days course of
therapy for clinical cure/failure
If Clinical cure, patient followed for recurrence
with:
1. Weekly assessment for 28 days after last dose
of study medication had been given
2. Immediate patient-initiated reassessment by
study team if diarrhea recurred

RANDOMIZATION & TREATMENT EVALUATION
Doses & frequency of administration are within the normal
range
Route of administration(PO) was compatible with the drug
recommendation
Following up patients due to high recurrence of CDI
Randomization was done accurately by highly technical
methods
Rational division of patients into 1st & 2nd episode
OUTCOME EVALUATION – EFFICACY -
Primary efficacy variable :
Rate of clinical cure in MITT & PP population at the
end of therapy or at the time of early withdrawal
from the study => Resolution of Sx + no need for further Tx
MITT = Modified intention-to-treat population with CDI
+ randomization + at least 1 dose of study
medicine
PP = Per-protocol population consist of MITT patients +
treatment for at least 3 days if treatment failure or at
least 8 days if clinical cure; in both cases, patients had
adherence to the protocol and underwent an end-of-therapy
evaluation

OUTCOME EVALUATION – EFFICACY -
Secondary efficacy variable :
1) Recurrence of CDI during the 4 week period after the end
of the course of therapy
2) Global cure in MITT & PP population
1ry & 2ry end points are clearly identified
They are also rational because our aim in
CDI treatment is to evaluate clinical
cure, recurrence & global cure for
better monitoring & follow up of patients
OUTCOME EVALUATION – MICROBIOLOGY -
Fecal samples for toxin assays to verify CDI were done:
• At early end of treatment
• At end of treatment
• At time of diagnosis of recurrence
Tests performed at individual study sites:
• R.M. Alden Research Laboratory
C.difficile isolation & susceptibility with the use of CLSI M11-A7 agar dilution method
• Edward Hines,Jr,Veterans Affairs Hospital
Restriction-endonuclease typing
OUTCOME EVALUATION – PHARMACOKINETIC -
Blood samples:
Before & 3-5h after the 1st dose on day 1 & at the
end of therapy/early end of visit
SAFETY EVALUATION
Involves patients who received ≥ 1 dose & ≥ 1 assessment after
this dose
Assessed from the day informed consent was provided to the last
dose or visit
It inludes:
1. Physical examination
2. Electrocardiography (ERT)
3. Clinical lab testing (Hematologic & Biochemical tests & Urinalysis)
Adverse events:
Classified according to “ Medical Dictionary for Regulatory Activities “but
adverse events reported > 1 for a patient was counted only once
SAFETY EVALUATION
An adverse event can be reported more than
once for a patient
But: each patient was counted only once in the
incidence count for a particular adverse event
Safety evaluations were scheduled on basic
time
Assessment methods are accurate

STATISTICAL ANALYSIS EVALUATION
The trial was designed as a noninferiority study
One sided lower 97.5% CI was used in the analysis of primary endpoints with a noninferiority margin of
-10% points
If the lower boundary of CI limit was within -10% point
margin Clinical noninferiority was demonstrated
Secondary endpoints of recurrence and overall cure, were analyzed by post hoc hypothesis with the use of two sided tests of populations at a significance level of 0.05

STATISTICAL ANALYSIS EVALUATION
The post hoc analyses assesses treatment
differences according to :
1. Age
2. Inpatient VS outpatient status
3. Prior occurrence of CDI VS no prior occurrence
4. Disease severity (mild, moderate & severe)
5. Strain type
The time to resolution of diarrhea analysed with
the use of Kaplan-Meier method & Gehan-Wilcoxon
test for comparison of resolution time curves

STATISTICAL ANALYSIS EVALUATION
All summary statistics are presented as:
1. Means ± SD for continuous variables
2. Numbers & percentages for categorical variables
Post hoc analyses detects patterns & relationships btw subgroups of sampled population using a proper statistical method
Two sided looks at where most of the population are likely to lie
One sided looks at the percentage of units that are greater or less than a certain point

RESULTS EVALUATION
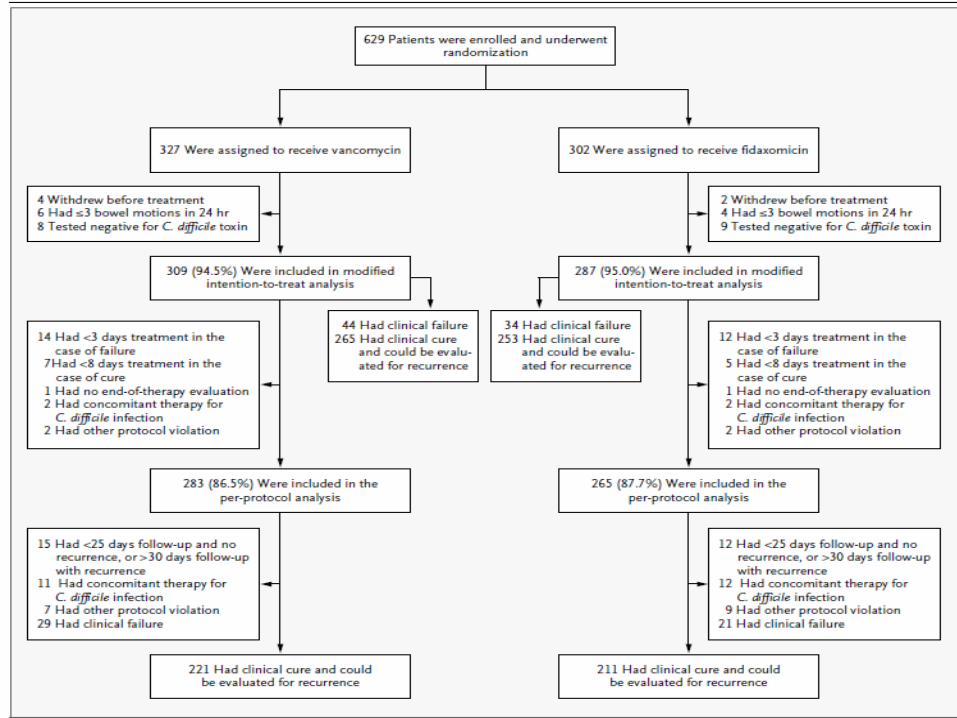
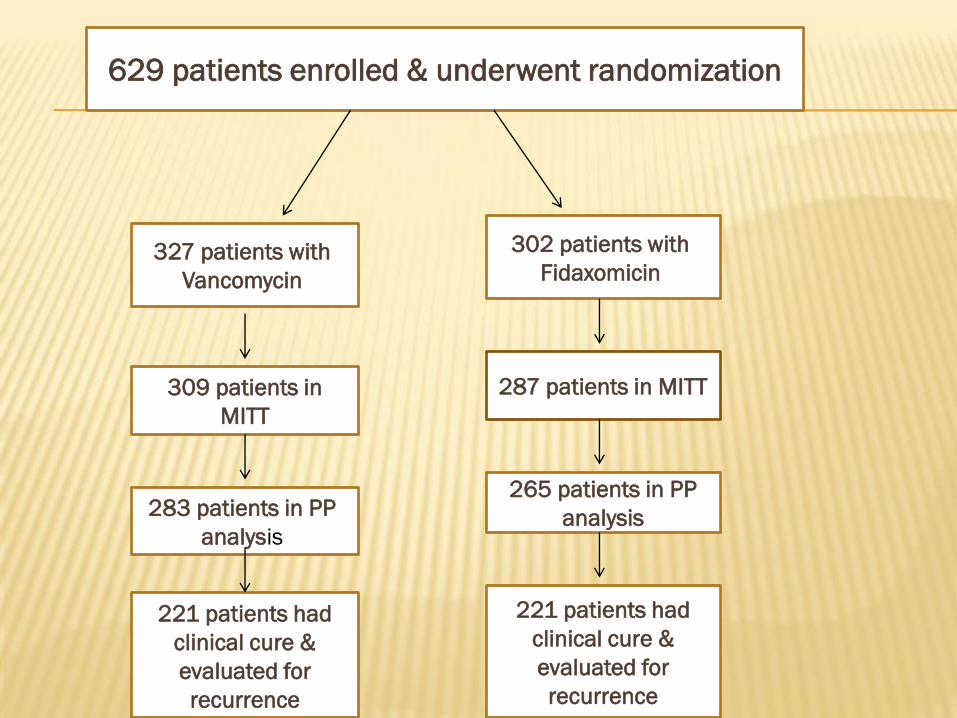
629 patients enrolled & underwent randomization
327 patients with
Vancomycin
302 patients with
Fidaxomicin
309 patients in
MITT
287 patients in MITT
283 patients in PP
analysis
265 patients in PP
analysis
221 patients had
clinical cure &
evaluated for
recurrence
221 patients had
clinical cure &
evaluated for
recurrence

MITT
596
PP
548
Vanco
309
Fidaxo
309
Vanco
283
Fidaxo
265
91.4% adhered to
Tx
91.7% adhered to
TX
96.1% adhered to
Tx
95.8% adhered to
Tx
221 cured =>
%78.1
221 cured =>
83.4%
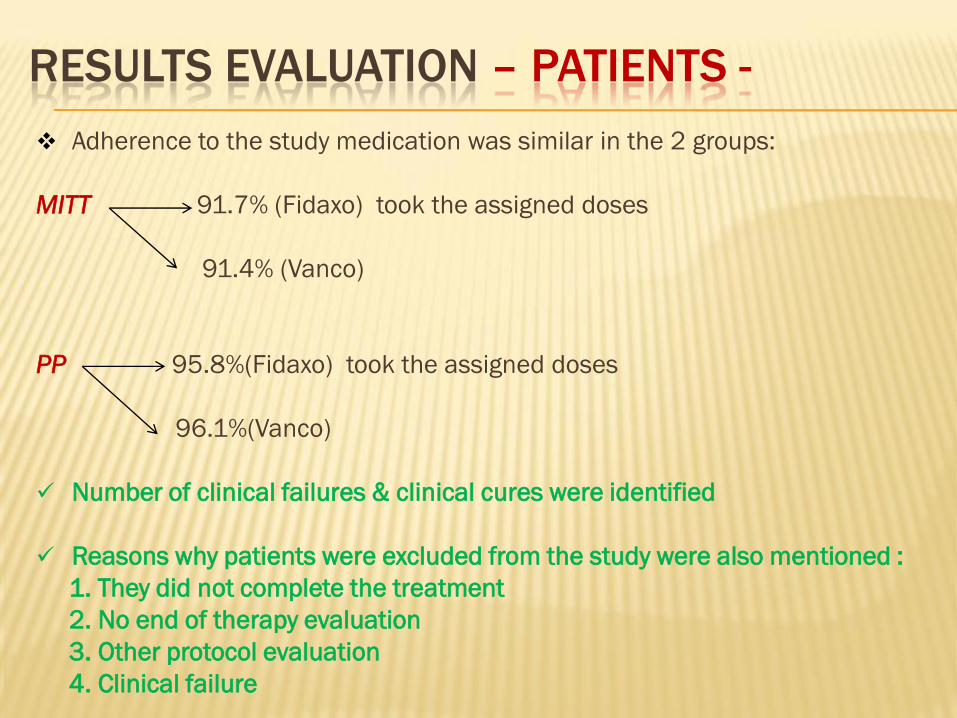
RESULTS EVALUATION – PATIENTS -
Adherence to the study medication was similar in the 2 groups:
MITT 91.7% (Fidaxo) took the assigned doses
91.4% (Vanco)
PP 95.8%(Fidaxo) took the assigned doses
96.1%(Vanco)
Number of clinical failures & clinical cures were identified
Reasons why patients were excluded from the study were also mentioned :
1. They did not complete the treatment
2. No end of therapy evaluation
3. Other protocol evaluation
4. Clinical failure
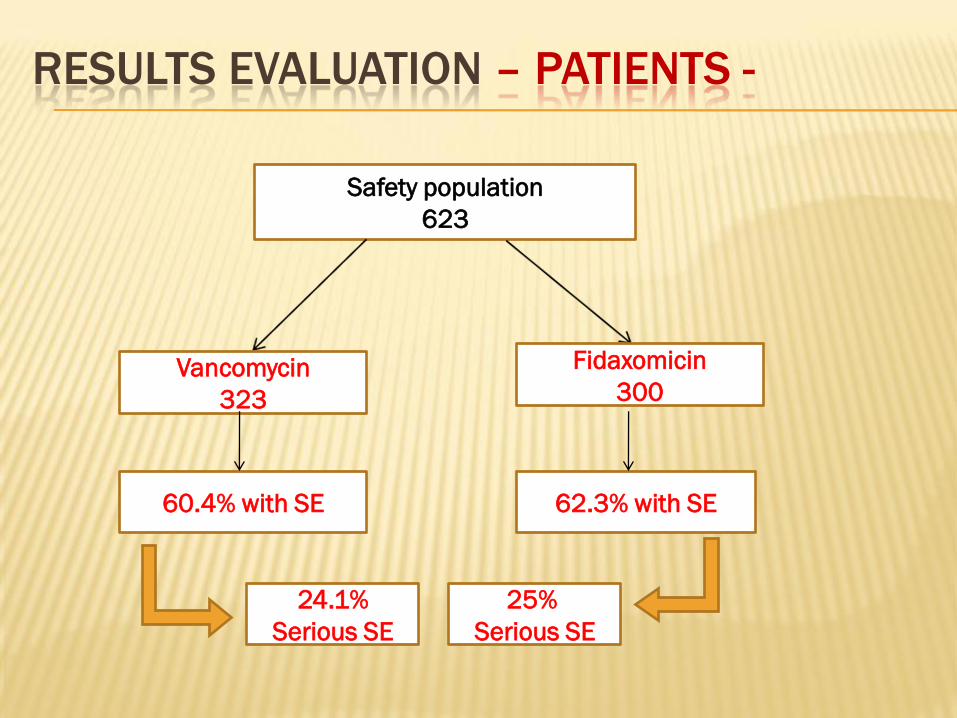
RESULTS EVALUATION – PATIENTS -
Safety population
623
Vancomycin
323
Fidaxomicin
300
60.4% with SE 62.3% with SE
24.1%
Serious SE
25%
Serious SE

Comparison was done at the level of:
1. Age
2. Gender
3. Number of unformed stools per day
4. Response to MTZ
5. Treatment of CDI
6. Previous episodes of CDI
7. BI/NAP1/027 strain (%)
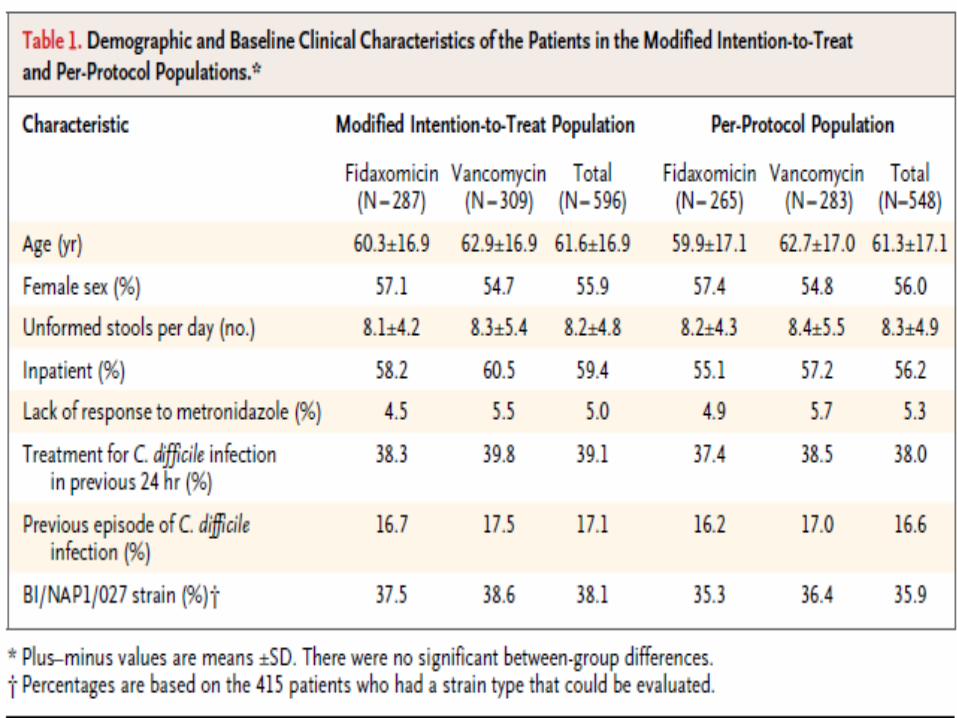
RESULTS EVALUATION – PATIENTS -
RESULTS EVALUATION – PATIENTS -
1. Results showed no significant
difference between groups with respect to
baseline characteristics
2. Patients characteristics clearly
tabulated, well elaborated & informative
3. Number of patients enrolled in this
study is correct (MITT n= 596)
RESULTS EVALUATION – PATIENTS -
4. Mean±SD for continuous variables mentioned
5. % & # for categorical variables mentioned

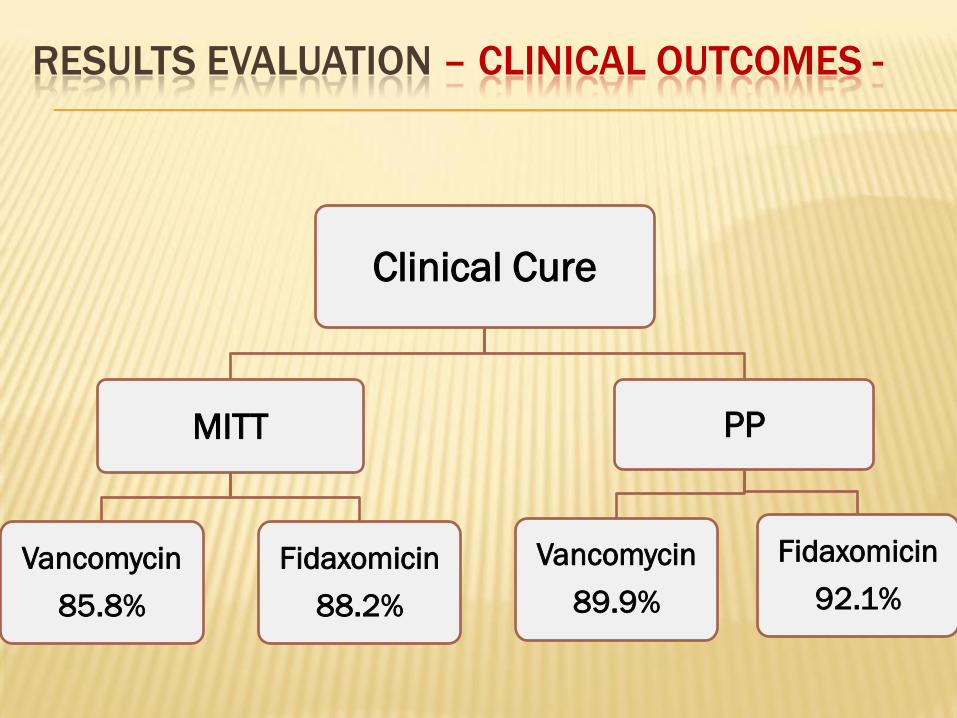
Clinical Cure
MITT
Vancomycin
85.8%
Fidaxomicin
88.2%
PP
Vancomycin
89.9%
Fidaxomicin
92.1%
RESULTS EVALUATION – CLINICAL OUTCOMES -

MITT= 85.8 - 88.2= -2.4% points
PP = 89.8 – 92.1= -2.3% points
CI = 97.5% with a noninferiority margin of -10%
In MITT & PP population, we have
respectively a reduction of 2.4% and 2.3%
points in Clinical cure with Vanco vs Fidaxo
We are 97.5% confident that MITT & PP population
have met the criteria for Clinical cure
RESULTS EVALUATION – CLINICAL OUTCOMES -
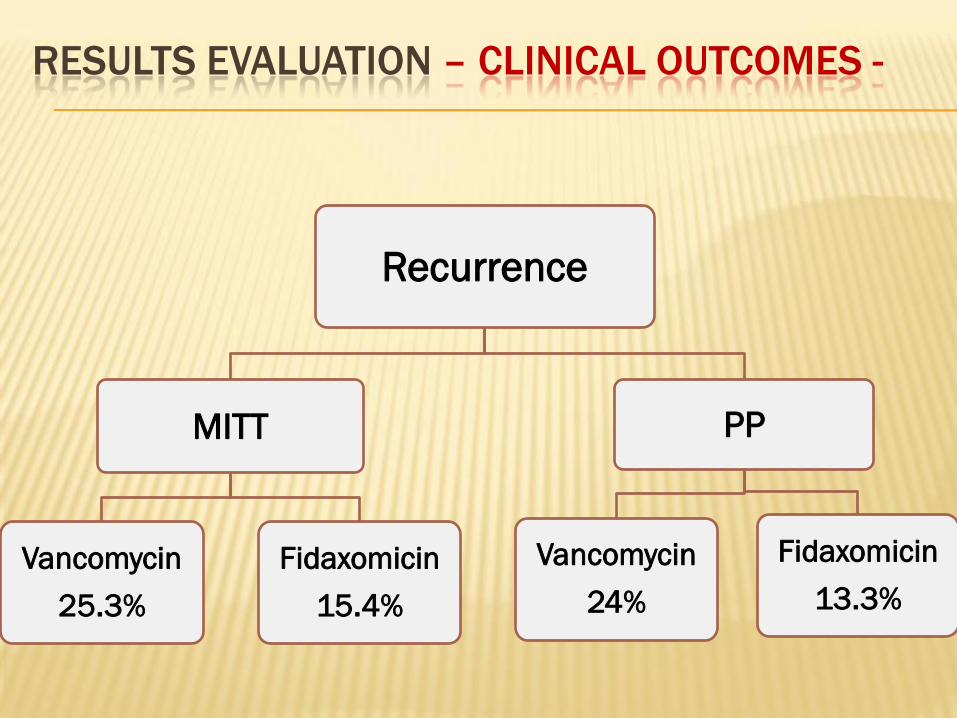
Recurrence
MITT
Vancomycin
25.3%
Fidaxomicin
15.4%
PP
Vancomycin
24%
Fidaxomicin
13.3%
RESULTS EVALUATION – CLINICAL OUTCOMES -

MITT= 15.4 - 25.3= -9.9% points
CI = 95% (-16.6 to -2.9), p= 0.005
PP = 13.3 – 24= -10.7% points
CI = 95% (-17.9 to -3.3), p= 0.004
In MITT & PP population, we have
respectively a reduction of 9.9% and 10.7%
points in Recurrence with Fidaxo vs Vanco
We are 95% confident that Tx with Fidaxo was associated with a
significant lower rate of recurrence than was with Vanco in both
MITT & PP populations
RESULTS EVALUATION – CLINICAL OUTCOMES -

Global Cure
MITT
Vancomycin
64.1%
Fidaxomicin
74.6%
PP
Vancomycin
67.1%
Fidaxomicin
77.7%
RESULTS EVALUATION – CLINICAL OUTCOMES -
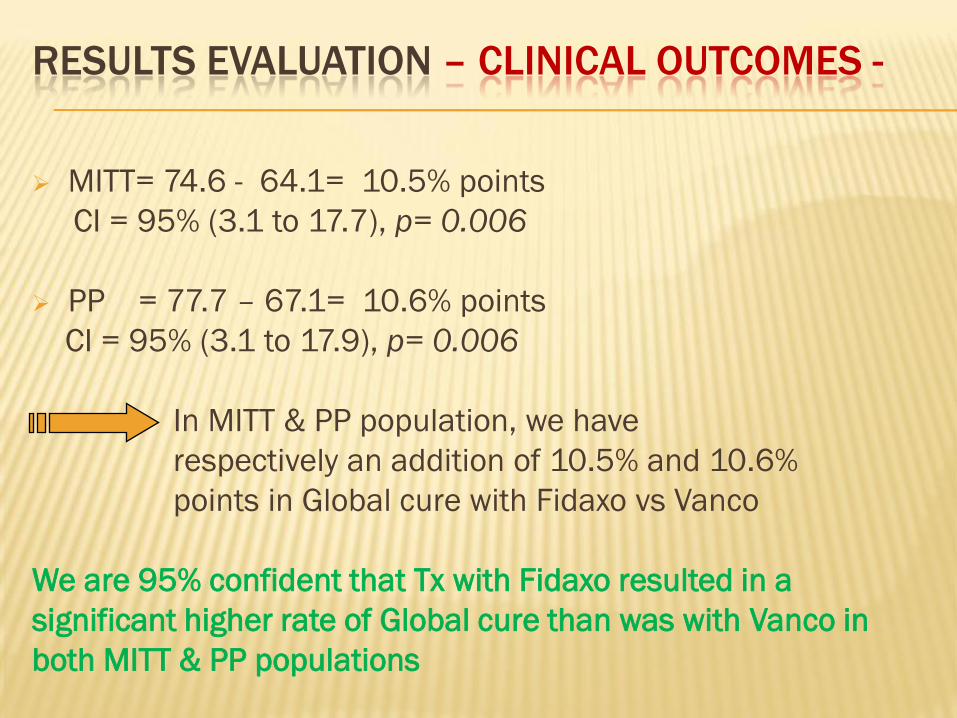
MITT= 74.6 - 64.1= 10.5% points
CI = 95% (3.1 to 17.7), p= 0.006
PP = 77.7 – 67.1= 10.6% points
CI = 95% (3.1 to 17.9), p= 0.006
In MITT & PP population, we have
respectively an addition of 10.5% and 10.6%
points in Global cure with Fidaxo vs Vanco
We are 95% confident that Tx with Fidaxo resulted in a
significant higher rate of Global cure than was with Vanco in
both MITT & PP populations
RESULTS EVALUATION – CLINICAL OUTCOMES -
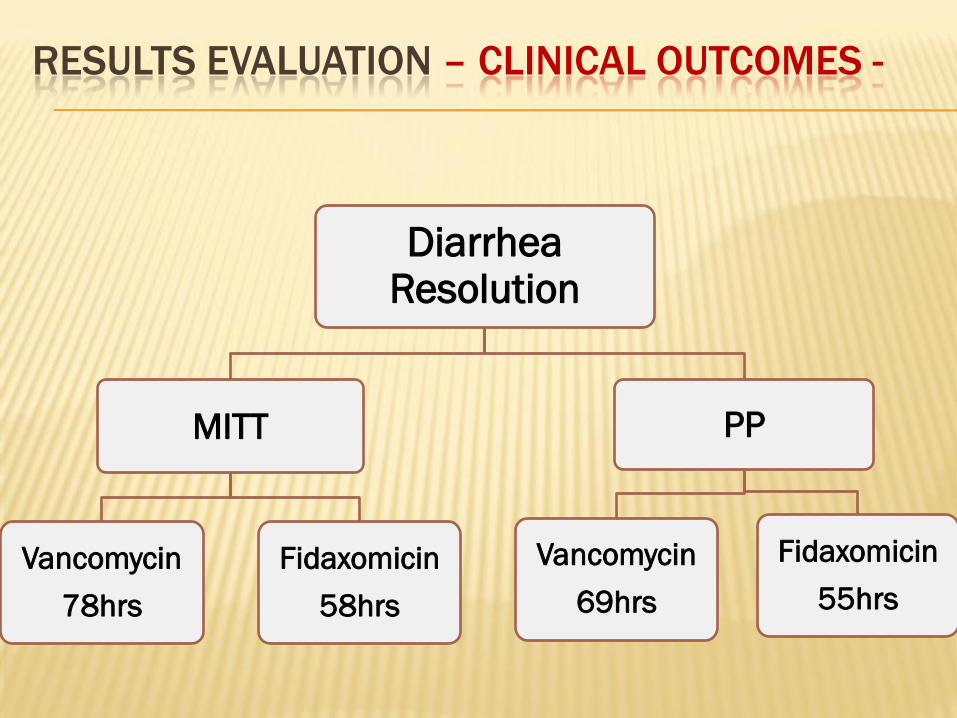
Diarrhea Resolution
MITT
Vancomycin
78hrs
Fidaxomicin
58hrs
PP
Vancomycin
69hrs
Fidaxomicin
55hrs
RESULTS EVALUATION – CLINICAL OUTCOMES -

Shorter duration of diarrhea resolution
with Fidaxo vs Vanco in MITT & PP
population
RESULTS EVALUATION – CLINICAL OUTCOMES -
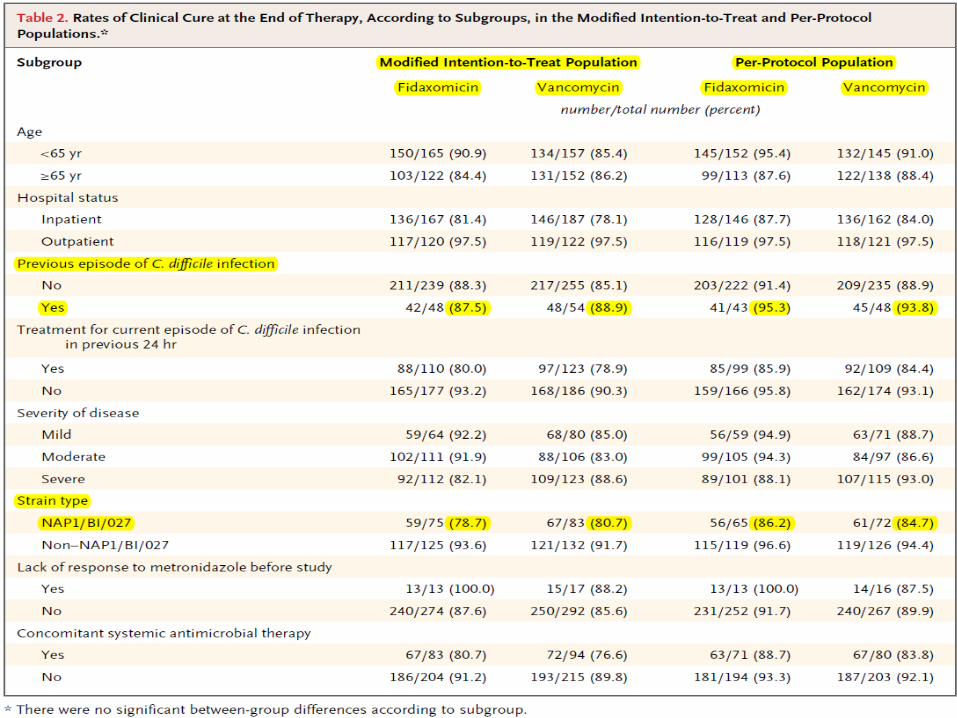

Subgroup analyses of Clinical cure rates according to different
characteristics showed No significant difference between
treatments in both MITT & PP populations according to subgroup
Ex.1:
RESULTS EVALUATION – CLINICAL OUTCOMES -
Patient with previous episode of CDI
MITT
Vancomycin
88.9% cured
Fidaxomicin
87.5% cured
PP
Vancomycin
93.8% cured
Fidaxomicin
95.8% cured
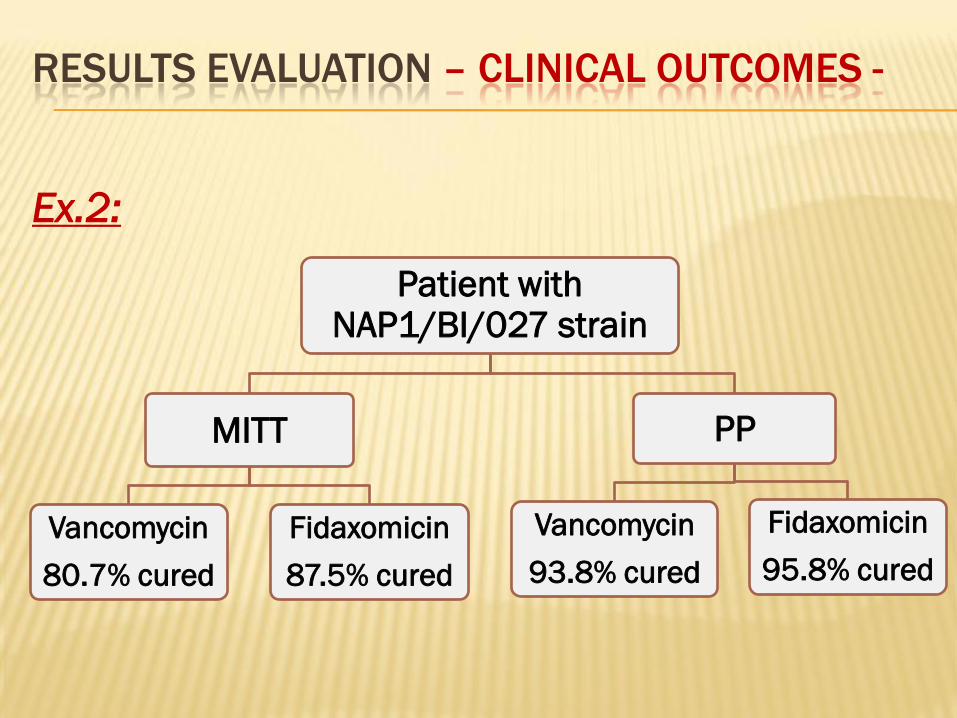
Ex.2:
RESULTS EVALUATION – CLINICAL OUTCOMES -
Patient with NAP1/BI/027 strain
MITT
Vancomycin
80.7% cured
Fidaxomicin
87.5% cured
PP
Vancomycin
93.8% cured
Fidaxomicin
95.8% cured
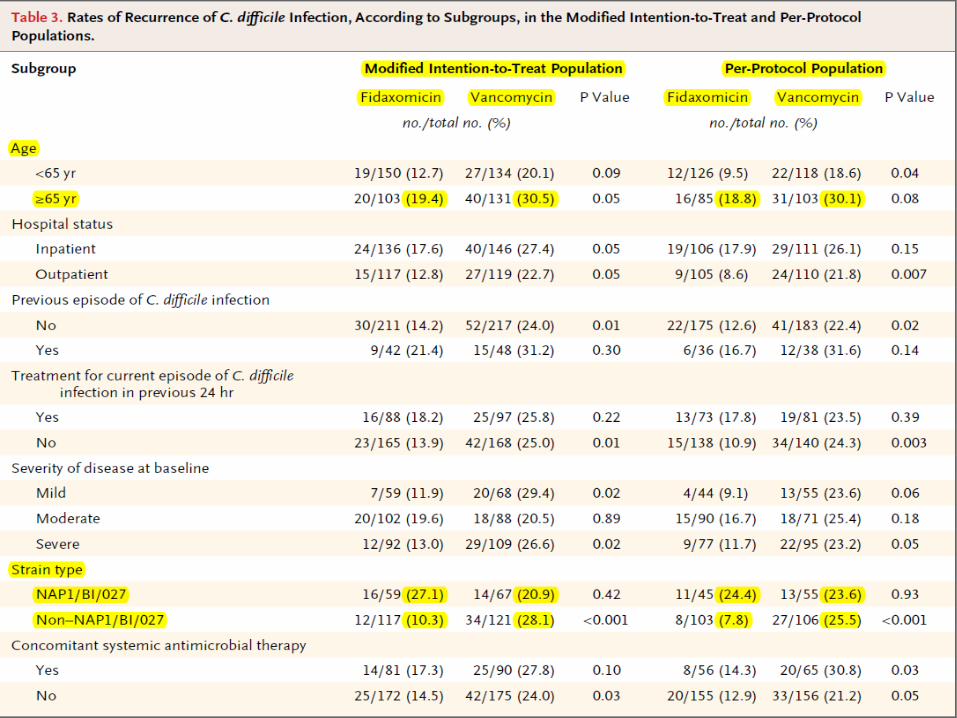

Subgroup analyses of Recurrence rates according to different
characteristics showed that Fidaxo was associated with lower
rates of recurrence vs Vanco in both MITT & PP populations
according to subgroup
Ex.1:
RESULTS EVALUATION – CLINICAL OUTCOMES -
Patient ≥65 years old
MITT
Vancomycin
30.5% RR
Fidaxomicin
19.4%RR
PP
Vancomycin
30.1% RR
Fidaxomicin
18.8% RR

Ex.2:
RESULTS EVALUATION – CLINICAL OUTCOMES -
Patient with Non-NAP1/BI/027 strain
MITT
Vancomycin
28.1% RR
Fidaxomicin
10.3% RR
PP
Vancomycin
25.5% RR
Fidaxomicin
7.8% RR

BUT: Similar rate of recurrence in pts with
NAP1/BI/027 strain ≠ Non-NAP1/BI/027
RESULTS EVALUATION – CLINICAL OUTCOMES -
Patient with NAP1/BI/027 strain
MITT
Vancomycin
20.9% RR
Fidaxomicin
27.1% RR
PP
Vancomycin
23.6% RR
Fidaxomicin
24.4% RR

RESULTS EVALUATION – SAFETY -
No significant difference in rate of ADR (mild GI & nonspecific sx) or serious adverse events 9.7% (Fidaxo) & 9% (Vanco)
Occurrence of adverse events were 62.3% (Fidaxo) & 60.4% (Vanco)
Occurrence of serious adverse events were 25% (Fidaxo) & 24.1% (Vanco)
More serious adverse events related to lab tests results in Fidaxo(4.7%) vs Vanco(1.2%)
No subjects discontinued the study as a result of intolerance or allergy

RESULTS EVALUATION – MICROBIOLOGY -
In vitro, antimicrobial activity against CDI showed minimum inhibitory concentrations:
1. ≤ 0.25mcg/ml for Fidaxomicin
2. 2 mcg/ml for Vancomycin
No relationship between MIC & clinical outcome (cure or recurrence)
This test only gives info about microbiologic characteristics of both Antibiotics

RESULTS EVALUATION –PHARMACOKINETIC-
Mean plasma concentration of Fidaxomicin at day1:
22.8 ± 26.5ng/ml (range 0.4 to 185)
No plasma accumulation was found between day 1 & the end of therapy
Mean end of therapy fecal concentration:
1225 ± 795 mcg/g (range 31.7 to 4640)
4900 times as high as minimum inhibitory
concentration
RESULTS EVALUATION
• 1. Fidaxomcin rapidly kills C.diff (bacteriocidal)
whereas Vancomycin inhibits growth
(bacteriostatic)
2. Fidaxomicin has prolonged Antibiotic effect
preserves bacteroides in the fecal flora which
are markers of normal anaerobic microflora
3. Microflora maintain “ COLONIZATION
RESISTANCE” & prevent further emergence of
CDI

DISCUSSION EVALUATION
DISCUSSION EVALUATION
Author’s Comments:
• The clinical profile of CDI has worsened in the past decade
Increased mortality & morbidity
• Emergence of new & more virulent strains (BI/NAP1/027)
• CDI became more serious illness in North America & Europe, even in countries with low incidence of B1/NAP1/027
• Initial approach of treatment is to discontinue the Antibiotic that precipitated the infection
• Standard treatment are Metronidazole (MZD) & Vancomycin
DISCUSSION EVALUATION
• MTZ is efficiently absorbed & small amount reaches the colon Disadvantage in mucosal & luminal
infections
• Systemic SE include:
Nausea– HA – Taste perversion – Peripheral neuropathy
• MTZ is associated with more failure & higher recurrence in severely ill patients as compared to Vancomycin
• Oral MTZ or Vancomycin induces the emergence of Vancomycin resistant enterococcus (VRE)
DISCUSSION EVALUATION
• 20-30% of patients have recurrent course of
illness of CDI
• Retreatment with MTZ or Vancomycin resolves
the condition in most patients, however, 1/3
have >1 recurrence
• Severe illness & deaths are associated with
relapses

DISCUSSION EVALUATION
Narrow antimicrobial
spectrum
Against CD, Staph &
Enterococci
Bactericidal
Low systemic SE
45% reduction in recurrences
Improved Global cure
Poorly absorbed
from intestine
Similar rate of recurrence &
cure for strains B1/NAP1/027
Post-antibiotic effect
Preserves intestinal flora
FDA approved in May 2011 for the treatment of C.
difficile-associated diarrhea in patients aged ≥18 years
Fidaxomicin
DISCUSSION EVALUATION
Strengths:
• Prospective, multicenter, double-blinded,
randomized, parallel group trial
• Well defined dose and dosage form
• Presence of comparable studies supporting
safety & efficacy
• Organized & informative tables & figures
DISCUSSION EVALUATION
• P values, SD & CI are mentioned
• Recurrence monitoring
• Informed Consent
• Inclusion & Exclusion criteria were highly
relevant to CDI
• Primary & secondary end points were clearly
identified
DISCUSSION EVALUATION
Limitations:
• Cannot generalize results to adolescents in case
of Fidaxomicin
• No biostatistic investigators
• Small sample size

CONCLUSION EVALUATION
Author’s conclusion:
Fidaxomicin & Vancomycin have similar
effectiveness with respect to the clinical
resolution of acute diarrheal disease due
to CDI but more sustained/durable
resolution of disease is achieved with
Fidaxomicin
CONCLUSION EVALUATION
Author’s conclusion well correlated
with the study objective
CONCLUSION
The incidence and hospitalizations due to C. difficile infection and disease have grown at an alarming rate
The mainstays of treatment for some time have been metronidazole and vancomycin
Last year, FDA approved a new antibiotic for the treatment of CDI, Fidaxomicin in adults (>18 yo )
It is currently indicated for mild to moderate CDI
It has been shown not to be inferior to vancomycin but it has not been shown to be superior
CONCLUSION
One potential advantage: it does not alter the normal flora of the bowel as much as vancomycindoes, which may explain why the risk of recurrent disease was lower with fidaxomicin
Fidaxomicin can be used instead of Vancomycindue to lower rate of recurrence hence lower costs & improved rate of global cure
But Further studies are required to generalize Fidaxomicin in adolescents & worlwide

OTHER STUDIES

Prospective
Multicenter
Double-blind
Randomised, non-inferiority trial
From 45 sites in Europe & 41 sites in the USA & Canada
Between April 19, 2007, & Dec 11, 2009
Identical in design and procedures to previous study
Aim => To compare the efficacy of fidaxomicin and
vancomycin in Europe, as well as in Canada &
USA

Primary efficacy variable :
Rate of clinical cure in MITT & PP population at the
end of therapy or at the time of early withdrawal
from the study => Resolution of Sx + no need for further Tx
Secondary efficacy variable :
1) Recurrence of CDI during the 4 week period after the end of the course of therapy
2) Global cure in MITT & PP population
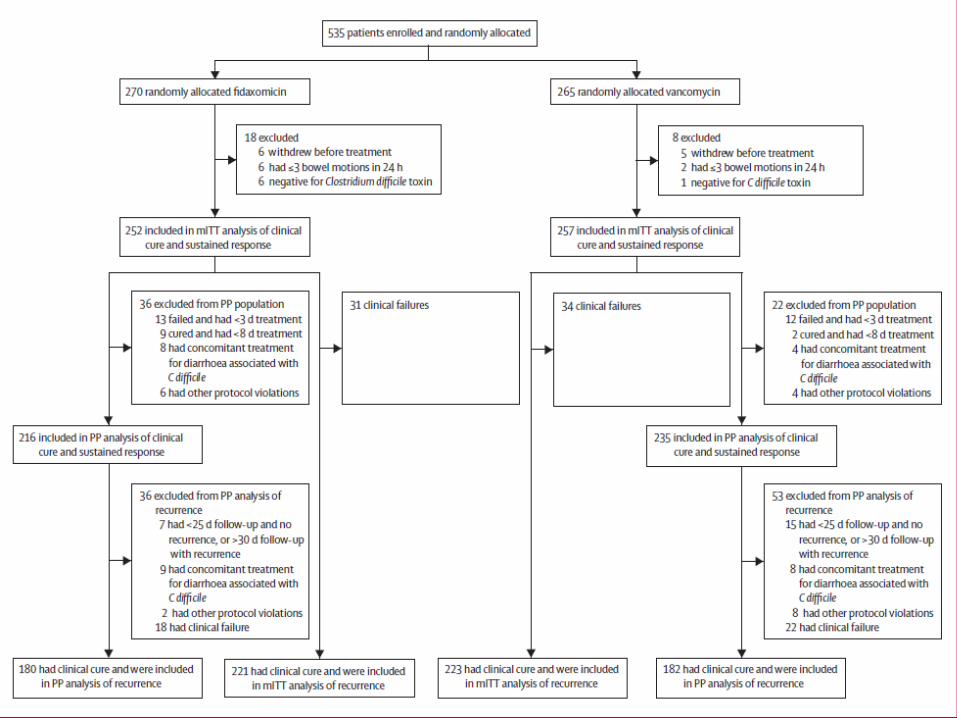
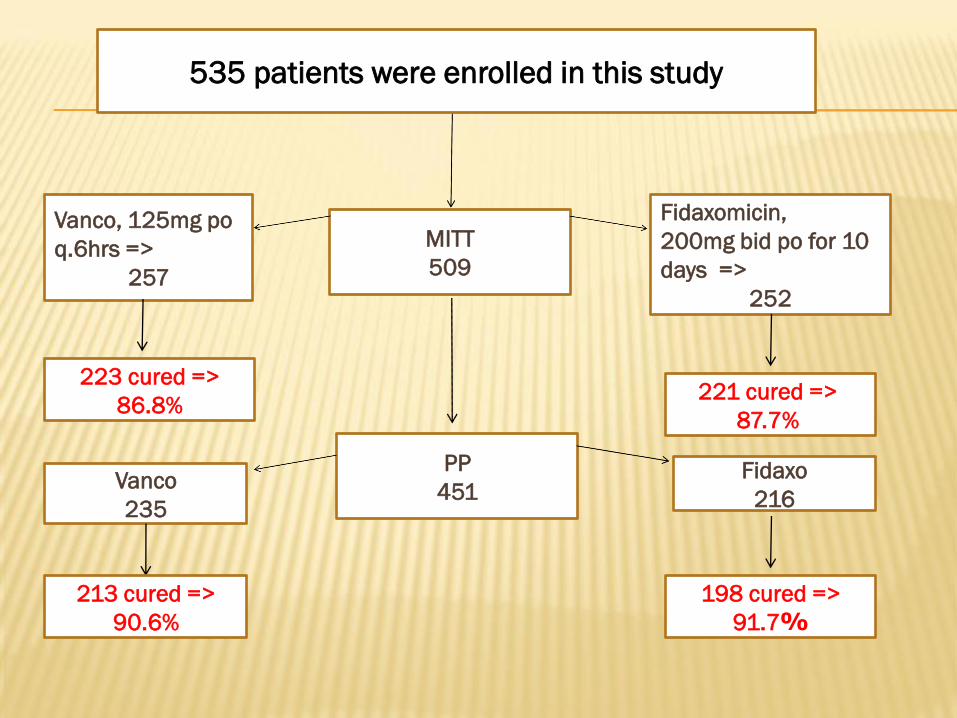
MITT
509
PP
451
Vanco, 125mg po
q.6hrs =>
257
Fidaxomicin,
200mg bid po for 10
days =>
252
Vanco
235
Fidaxo
216
223 cured =>
86.8%221 cured =>
87.7%
213 cured =>
90.6%
198 cured =>
%91.7
535 patients were enrolled in this study
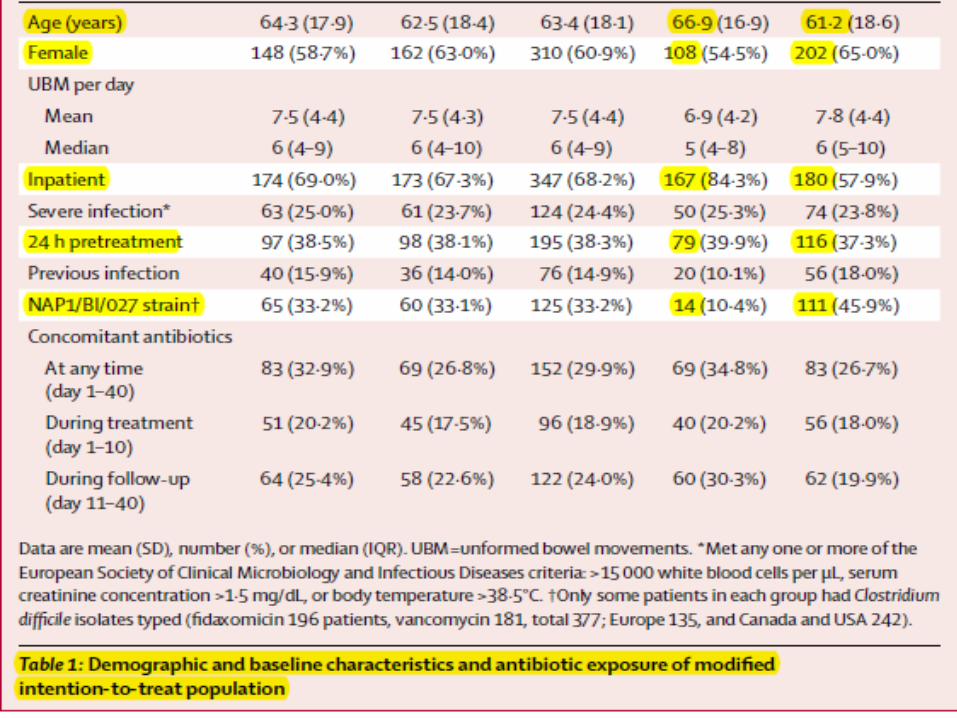
A greater proportion of patients were inpatients at the time of enrolment in Europe than in Canada and the USA
Fewer patients in Europe than in Canada & USA had a previous episode of C difficile infection in the preceding 3 months
Treatment of other infections with concomitant antibiotics was more common in Europe than it was in Canada & USA
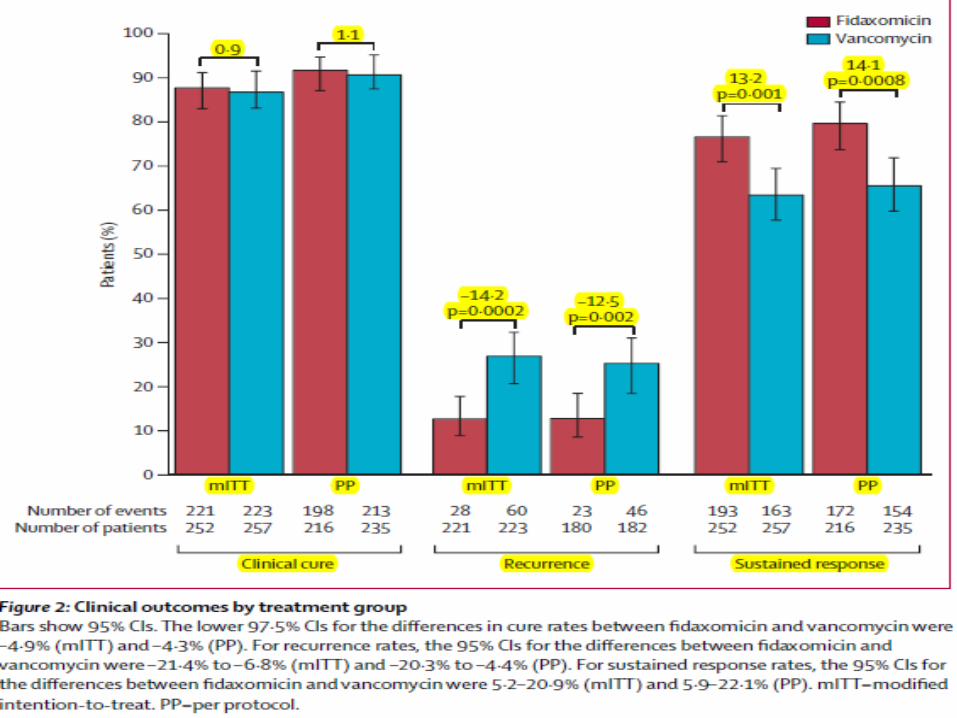
Fidaxomicin was non-inferior to vancomycin for clinical cure rate
=>These findings match those from a study done in just Canada and the USA
Treatment with fidaxomicin was associated with a lower rate of recurrence in the 4 weeks after completion of treatment than was vancomycin
=> This difference was larger than that in the previous study
Sustained response rates were also higher in subgroups treated with fidaxomicin than in those given vancomycin
Clinical cure with the two drugs was not significantly different for any subgroup with the exception of patients exposed to concomitant antibiotics during treatment
=> Exposure to concomitant antibiotics during
treatment reduced the clinical cure rate of
patients given vancomycin, but had no apparent
effect on those treated with fidaxomicin
=> This could indicate that intestinal microflora have
a role in initial response, and not just resistance
to recurrence
Trends in time to resolution of diarrhea were not
significantly different in treatment groups
However,with patients who received concomitant
antibiotics, longer times to resolution was noticed than
those who did not
Occurrence of treatment-emergent adverse events did
not differ between groups
All strains were susceptible to both fidaxomicin &
vancomycin
In Canada & USA, the most prevalent group was BI,
but in Europe, Y was most common
In summary, fidaxomicin was non-inferior to
vancomycin in initial clinical response
Patients successfully treated with fidaxomicin
were less likely to have recurrence of disease
within 4 weeks after treatment completion
=> superior sustained response for
fidaxomicin.

References

REFERENCES

REFERENCES
The Lancet Infectious Diseases,Volume 12, Issue 4, April 2012, Pages 281–289, Fidaxomicin versus vancomycin for infection with Clostridium difficile in Europe, Canada, and the USA: a double-blind, non-inferiority, randomised controlled trial
The American Journal of Geriatric Pharmacotherapy Volume 10, Issue 1, February 2012, Pages 14–24 Clostridium Difficile Infection in Older Adults: A Review and Update on its Management
The American Journal of Geriatric Pharmacotherapy Volume 10, Issue 4, August 2012, Pages 258–263. A Year in Review: New Drugs for Older Adults in 2011

REFERENCES
International Journal of Infectious Diseases Volume 15, Issue 7, July 2011, Pages e438e448,Use of alternative or adjuvant pharmacologic treatment strategies in the prevention and treatment of Clostridium Difficile infection
Journal of Infection Available online 24 October 2012, Clostridium difficile: A European perspective
The Journal for Nurse Practitioners Volume 7, Issue 7, July August 2011, Pages 602–603, Clostridium difficile Treatment
First Consult ,Clostridium difficile infection
Clinical Practice Guidelines for Clostridium difficile Infection in Adults:2010 Update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA), May 2010, vol.31, no.5



















