
Advanced Pharmacology Respiratory Pharmacology Handout Samples/Advanced... · 1 Unit 5 ©2014...
27
1 ©2014 Barkley & Associates Unit 5 Advanced Pharmacology Respiratory Pharmacology Thomas W. Barkley, Jr., PhD, ACNP‐BC, FAANP President, Barkley & Associates www.NPcourses.com and Professor of Nursing Director of Nurse Practitioner Programs California State University, Los Angeles Robert Fellin, PharmD, BCPS Faculty, Barkley & Associates Pharmacist, Cedars‐Sinai Medical Center Los Angeles, CA ©2014 Barkley & Associates Unit 5 Allergic Rhinitis Allergic rhinitis (hay fever) – resembles the common cold: Tearing Sneezing Nasal congestion Postnasal drip Itchy throat Due to antigen (allergen) exposure Pollen, mold spores, dust mites, certain foods, animal dander Genetic predisposition http://www.theage.com.au
Transcript of Advanced Pharmacology Respiratory Pharmacology Handout Samples/Advanced... · 1 Unit 5 ©2014...

1
©2014 Barkley & AssociatesUnit 5
Advanced PharmacologyRespiratory Pharmacology
Thomas W. Barkley, Jr., PhD, ACNP‐BC, FAANPPresident, Barkley & Associates
www.NPcourses.comand
Professor of NursingDirector of Nurse Practitioner ProgramsCalifornia State University, Los Angeles
Robert Fellin, PharmD, BCPSFaculty, Barkley & Associates
Pharmacist, Cedars‐Sinai Medical CenterLos Angeles, CA
©2014 Barkley & AssociatesUnit 5
Allergic Rhinitis Allergic rhinitis (hay fever) – resembles the
common cold:
Tearing
Sneezing
Nasal congestion
Postnasal drip
Itchy throat
Due to antigen (allergen) exposure
Pollen, mold spores, dust mites, certain foods, animal dander
Genetic predisposition
http://www.theage.com.au

2
©2014 Barkley & AssociatesUnit 5
Allergic Rhinitis Seasonal vs. perennial allergic rhinitis
Pathophysiology: Inflammation of the mucous membranes in the nose, throat and airways
Normal nasal mucosa has many mast cells and basophils (try to recognize environmental agents as the enter the body)
Allergic rhinitis patients have more mast cells
Histamine (chemical mediator of inflammation): responsible for many of the symptoms of allergic rhinitis
H1-receptors: Responsible for allergic symptoms
©2014 Barkley & AssociatesUnit 5
H1-receptor Antagonists/AntihistaminesFIRST Generation Agents:
brompheniramine (Dimetapp), chlorpheniramine (Chlor-Trimeton), clemastine (Tavist), cyproheptadine (Periactin), dexchlorpheniramine (Polaramine), dimenhydrinate (Dramamine), diphenhydramine (Benadryl), hydroxyzine (Atarax, Vistaril), promethazine (Phenergan)
Adverse Effects: sedation, dry mouth, headache, dizziness, urinary retention, thickening of bronchial secretions, nausea, vomiting, hypotension, tachycardia, QT prolongation
Comments: All equally effectiveOften combined with decongestant/antitussiveMost effective when taken prophylactically to prevent allergic symptomsAbility to reverse acute allergic symptoms is limitedCaution with alcohol and other CNS depressantsSome patients experience paradoxical excitation

3
©2014 Barkley & AssociatesUnit 5
H1-receptor Antagonists/AntihistaminesSECOND Generation Agents:
azelastine (Astelin), cetirizine (Zyrtec), desloratadine (Clarinex), fexofenadine (Allegra), levocetirizine (Xyzal), loratadine (Claritin), olopatadine (Patanase, Patanol)
Adverse Effects: dry mouth, headache, dizziness, drowsiness, bitter taste (olopatadine), nausea, hypotension, sedation (less than 1st
generation)
Comments: Azelastine: intranasal formulationMost effective when taken prophylactically to prevent allergic symptomsAbility to reverse acute allergic symptoms is limitedAll equally effectiveCaution with alcohol and other CNS depressantsSome patients experience CNS stimulation (nervousness, insomnia, tremor, etc.)Considered less effective than 1st generation agents
©2014 Barkley & AssociatesUnit 5
Nasal DecongestantsAgents: naphazoline (Privine), oxymetazoline (Afrin), phenylephrine (Neo-
Synephrine), pseudoephedrine (Sudafed)
MOA: sympathomimetic, alpha-adrenergic activity
Adverse Effects: Intranasal: transient nasal irritation, burning, sneezing, nasal dryness, rebound congestionAll: headache, nervousness, insomnia, headache, dry mouth, CNS excitation, tremors, dysrhythmias, tachycardia, difficulty in voiding
Comments: Provide immediate relief for acute allergy symptomsIntranasal: duration should not exceed 3 to 5 days as tolerance developsTolerance: gradually switch to intranasal corticosteroidsOral products do not produce rebound congestionProlonged use: hypersecretion of mucus, worsening nasal congestionOnset of action: intranasal much faster than oral agentsDo not relive sneezing, tearing

4
©2014 Barkley & AssociatesUnit 5
Intranasal GlucocorticoidsAgents: beclomethasone (Beconase AQ), budesonide (Rhinocort
Aqua), ciclesonide (Omnaris), flunisolide (Nasalide), fluticasone (Flonase), mometasone (Nasonex), triamcinolone acetonide (Nasacort AQ)
MOA: reduce inflammation, edema; cause vasoconstriction
Adverse Effects:
transient nasal irritation, burning, sneezing, nasal dryness, epistaxis
Comments: DOC for allergic rhinitisMinimal adverse effectsAll administered by metered-spray deviceAll equally effectiveMay take 3-4 weeks to achieve peak responseMost effective when taken in advance of expected allergen exposure
©2014 Barkley & AssociatesUnit 5
Miscellaneous AgentsAgents: cromolyn (NasalCrom), ipratropium (Atrovent), montelukast
(Singulair)
MOA: mast cell stabilizer, anti-inflammatory (cromolyn)anticholinergic agent (ipratropium)leukotriene receptor antagonist (montelukast)
Adverse Effects: nasal burning, irritation (cromolyn)nasal irritation, burning, sneezing, nasal dryness, cough, HA (ipratropium)HA, nausea, diarrhea (montelukast)
Comments: Reserved for patients unresponsive to other therapiesMay take 4 weeks to achieve peak responseMost effective when taken in advance of expected allergen exposureLimited effectiveness/less effective than other agentsRole of montelukast remains to be defined

5
©2014 Barkley & AssociatesUnit 5
Antitussives: OpioidsAgents: codeine, (Robitussin-AC), dextromethorphan (Benylin,
Delsym), hydrocodone (Hycodan)
MOA: suppress the cough reflex via CNS
Adverse Effects:
lightheadedness, sedation, nausea, headache and dizziness
Comments: Most effective agents available for cough suppressionSuppression of cough obtained at doses lower than those needed for analgesiaDextromethorphan max dose: 120 mg/dayDextromethorphan: most frequently used antitussive (OTC cough & cold products)Use of codeine/hydrocodone has diminishedCodeine/hydrocodone: controlled substances
©2014 Barkley & AssociatesUnit 5
Antitussives: Non-OpioidsAgents: benzonatate (Tessalon Perles)
MOA: anesthetizes the stretch receptors in the lungs, thus suppressing cough
Adverse Effects:
nausea, dizziness, headache, sedated, somnolence
Comments: Benzonatate requires prescriptionWell tolerated with minimal adverse effectsDo not crush/chew benzonatate = numbing of the mouth and pharynxChemically related to local anesthetics

6
©2014 Barkley & AssociatesUnit 5
ExpectorantsAgents: guaifenesin (Robitussin)
MOA: increases the volume and reduces the viscosity of secretions in the trachea and bronchi
Adverse Effects:
nausea, vomiting
Comments: Most effective OTC expectorant (?)
Common ingredient in many OTC cough and cold preparationsMaximum dose: 2400 mg/24 hours
©2014 Barkley & AssociatesUnit 5
FDA Statements: OTC Cold Products Not appropriate to take data from adults
and apply it to children under 12 years of age
Products containing decongestants, antihistamines and antitussives are NOT effective in children < 6 years of age – and may cause serious side effects
FDA: strongly recommend NOT using such OTC products in children < 2 years of age
More studies about how these medicines affect children are needed
www.sharp.com

7
©2014 Barkley & AssociatesUnit 5
Mucolytics
©2014 Barkley & AssociatesUnit 5
N-Acetylcysteine (Mucomyst)Indications: Adjuvant therapy in patients with abnormal or viscid
mucous secretions in acute and chronic broncho-pulmonary disease
MOA: exerts mucolytic action through its free sulfhydryl group which opens up the disulfide bonds in the mucoproteins thus lowering mucous viscosity
Dose: 1 mL of 20% solution or 2 mL of 10% solution via nebulizer 4 times/day
AdverseEffects:
Nausea, vomiting, bronchospasm
Comments: Patients should receive a bronchodilator prior to administration
8
©2014 Barkley & AssociatesUnit 5
Dornase Alfa (Pulmozyme)Indications: Adjunct management of CF to reduce the frequency
of respiratory infections, and to improve pulmonary function
MOA: recombinant Human Deoxyribonuclease (rHDNase); selectively cleaves DNA of neutrophils thereby decreasing mucous viscosity
Dose: 2.5mg nebulized inhalation daily
AdverseEffects:
chest pain, pharyngitis, cough dyspnea, hemoptysis, wheezing, rash, conjunctivitis
Comments: Should not be used routinely as a mucolytic outside cystic fibrosis patients
©2014 Barkley & AssociatesUnit 5
Drugs for Lower Pulmonary Disorders

9
©2014 Barkley & AssociatesUnit 5
Pulmonary Drugs via Inhalation Aerosol – suspension of minute liquid droplets or fine sold
particles suspended in gas Major Advantage: Delivers drugs to the immediate site of
action (reducing systemic effects) An oral drug would have to be given in a higher dose to
have an equivalent therapeutic dose All inhalation agents have the potential to produce
systemic effects (e.g., anesthetics, paint thinners, etc.)
©2014 Barkley & AssociatesUnit 5
Devices for Inhalation Metered Dose Inhalers (MDIs) – use a propellant to deliver
a measured dose of drug to the lungs during each breath of drug emitted from the MDI
Dry Powder Inhalers (DPIs) – small device that is activated by inhalation to deliver a fine powder directly to the bronchial tree
Nebulizers – small machines that vaporize a liquid medication into a fine mist that can be inhaled, using a face mask of handheld device

10
©2014 Barkley & AssociatesUnit 5
Methods of Aerosol DeliveryPopulation Optimal technique Therapeutic issues
MDI Age > 5 years
old
Actuation during slow deep inhalation followed by 10 second breath holding
Open mouth technique
Close mouth technique
Deposition of 50~80% of actuated dose in oral-pharynx
Spacer and
Valve holding chamber
Age > 4 years old Actuation during slow deep inhalation followed by 10 second breath holding
Bulky to carry
Decrease oral-pharyngeal deposition & decrease risk of thrush
Nebulizer For patient who cannot use MDI or a face mask
Slow tidal breathing with occasional deep breaths
Using a “blow-by”technique is not appropriate
Output is dependent on device and operating parameters
Use of face mask decreases delivery to lungs by 50%
Expert Panel Report: NHLBI Guidelines for the Diagnosis and Management of Asthma - Summary Report 2007http://www.nhlbi.nih.gov/guidelines/asthma/asthgdln.htm
©2014 Barkley & AssociatesUnit 5
Disadvantages of Aerosols Precise dose received by the patient is difficult to measure Optimally, only 10-50% actually reaches the lower
respiratory tract Swallowing medication may cause systemic SE Rinse mouth thoroughly after use
http://www.myrespiratorysupply.com http://www.aafa.org www.parknicollet.com

11
©2014 Barkley & AssociatesUnit 5
Which Method of Drug Delivery is Superior?
Metered-Dose Inhaler
Dry Powder Inhaler
Nebulizer
Pharmacology for Nurses: A Pathophysiologic Approach (4th Edition)
©2014 Barkley & AssociatesUnit 5
Asthma“Chronic inflammatory disorder of the airways… causing recurrent episodes of wheezing, breathlessness, chest tightness and coughing…that is reversible either spontaneously or with treatment.” 22.9 million people in the US have asthma One of the most common chronic diseases of childhood Variability in response to medications requires
individualization of therapy

12
©2014 Barkley & AssociatesUnit 5
Asthma Increased responsiveness of the trachea and bronchi to stimuliNarrowing of airways
http://www.lincoln.ne.gov/city/health/environ/pollu/dirtair.htm
©2014 Barkley & AssociatesUnit 5
Asthma: Pathophysiological Characteristics
Hypertrophy of smooth muscle Mucosal edema and hyperemia Thickening of epithelial
basement membrane Hypertrophy of mucus gland Acute inflammation Plugging of airways by thick,
viscous mucus
http://www.asthmainschools.com/index.php?option=com_content&view=article&id=59&Itemid=51

13
©2014 Barkley & AssociatesUnit 5
Asthma
Most important allergens are encountered indoors!
Dust, pets, roaches, molds, cigarette smoke, exercise, etc.
Labs/Diagnostics
Signs and symptoms (intermittent dyspnea, cough & wheezing)
Physical exam & Patient history
PFT values (spirometry)
Chest x-ray findings: hyperinflation
2007 Asthma Guidelines: National Heart, Lung and Blood Institute
©2014 Barkley & AssociatesUnit 5
Classification of Asthma Severity
Components of Severity
Asthma Severity
Intermittent
Persistent
Mild Moderate Severe
Symptoms < 2 days/week >2 days/week Daily Throughout the day
Nighttime awakening < 2 x/month 3-4 x/month > 1 x/week, not nightly Often 7 x/week
Short acting β agonist for symptom control < 2 day/week > 2 days/week Daily Several times a day
Interference with normal activities none Minor Some Extreme
Lung functionFEV1 > 80% > 80 % 60-80 % < 60%
FEV1/ FVC normal normal Reduced < 5% Reduced > 5%
Risk Exacerbation requiring oral systemic corticosteroids 0-1 / year > 2 / year
Recommended Step for Initiating therapy
Step 1 Step 2
Step 3 Step 4 or 5
Consider short course of oral systemic corticosteroids
Expert Panel Report: NHLBI Guidelines for the Diagnosis and Management of Asthma - Summary Report 2007http://www.nhlbi.nih.gov/guidelines/asthma/asthgdln.htm

14
©2014 Barkley & AssociatesUnit 5Expert Panel Report: NHLBI Guidelines for the Diagnosis and Management of Asthma - Summary Report 2007
http://www.nhlbi.nih.gov/guidelines/asthma/asthgdln.htm
Management of Asthma
©2014 Barkley & AssociatesUnit 5
Beta-Agonists/SympathomimeticsIndications: DOC for acute bronchoconstriction;
Intermittent symptoms;Exercise-Induced Bronchospasm (EIB)
Agents: Short acting agents (SABA’s):albuterol (Proventil), levalbuterol (Xopenex), metaproterenol(Alupent), pirbuterol (Maxair), terbutaline (oral; Brethine)
MOA: cause bronchial smooth muscle relaxationAdverseEffects:
dose-related tachycardia, tremor, palpitations, nausea, headache, hypokalemia
Comments: Scheduled daily use not recommendedQuick onset of actionDuration of action: 5-6 hoursLevalbuterol is NOT superior to other agentsDPI’s not indicated for acute severe exacerbations

15
©2014 Barkley & AssociatesUnit 5
Inhaled Corticosteroids (ICS)Indications: Preferred therapy for long-term control of persistent
asthma in all patientsAgents: beclomethasone (Beclovent), budesonide (Pulmicort),
ciclesonide (Alvesco), flunisolide (Aerospan), fluticasone (Flovent), mometasone (Asmanex)
MOA: anti-inflammatory; inhibits inflammatory cells and release of inflammatory mediators
Adverse Effects: headache, pharyngitis, dysphonia, oral candidiasis
Comments: Administer on scheduled basis, not “prn”NOT used to treat an acute asthma attackRinse mouth thoroughly after inhalationBudesonide is preferred in pregnancySystemic adverse effects can occur with any ICS
©2014 Barkley & AssociatesUnit 5
Beta-Agonists/SympathomimeticsIndications: Treatment and prevention of bronchospasm only as
concomitant therapy inhaled corticosteroid;Exercise-Induced Bronchospasm (EIB)
Agents: Long acting (LABA’s): arformoterol (Brovana)*, formoterol (Foradil), indacaterol (Arcapta)*, salmeterol(Serevent)
MOA: cause bronchial smooth muscle relaxationAdverse Effects: tachycardia, tremor, palpitations, nausea, headache,
hypokalemiaComments: DO NOT act quickly
NOT for acute symptom managementDuration of action: 12 hoursShould not be used as monotherapy *FDA labeled only for COPD

16
©2014 Barkley & AssociatesUnit 5
MethylxanthinesIndications: Alternative, not preferred, therapy for mild persistent
asthma or as adjunct therapy with ICSAgents: aminophylline (IV),
theophylline (oral; Theo-Dur)MOA: bronchodilation through smooth muscle relaxation
Adverse Effects:
nausea, vomiting, headache, insomnia, tremor,
irritability, restlessness, tachycardia, seizures
Comments: Clinical utility limited by low therapeutic indexMany drug-drug interactionsMetabolism/clearance is age dependentMonitor dug levels
©2014 Barkley & AssociatesUnit 5
Mast Cell StabilizersIndications: Alternative, but not preferred for mild persistent
asthma; Exercise induced bronchospasm (EIB)
Agents: cromolyn (Intal)
MOA: anti-inflammatory; prevents bronchoconstriction; blocks the release of histamine
AdverseEffects:
Relatively non-toxic; taste disturbances, cough
Comments: Not a substitute for ICSNot as effective as beta-agonist for EIBAs effective as theophylline or leukotriene antagonistsMay take up to 4 weeks to achieve benefit

17
©2014 Barkley & AssociatesUnit 5
Leukotriene ModifiersIndications: Alternative, but not preferred for mild persistent asthma;
Exercise induced bronchospasm (EIB)Agents: montelukast (Singulair), zafirlukast (Accolate), zileuton
(Zyflo)MOA: inhibit bronchoconstriction; may prevent airway edema
and smooth muscle contractionAdverse Effects: abdominal pain, dizziness, rash, dyspepsia,
hepatotoxicityComments: Not all patients report a benefit with treatment
Difficult to predict who will respondSeveral drug interactionsZileuton: hepatotoxicity; monitor LFT’sLess effective than low dose ICSNot as effective as LABA’s when added to ICS
©2014 Barkley & AssociatesUnit 5
AnticholinergicsIndications: Adjunct therapy in acute asthma exacerbation not
completely responsive to beta agonistAgents: ipratropium bromide (Atrovent)MOA: blocks acetylcholine at parasympathetic sites in
bronchial smooth muscle causing bronchodilationAdverse Effects: Rare: mydriasis, dry mouth, taste disturbances
Comments: ipratropium + beta agonists = greater and prolonged bronchodilation than using either agent separatelyAdditional long-term studies are needed to determine its role in asthma*Not FDA labeled for asthma

18
©2014 Barkley & AssociatesUnit 5
Systemic CorticosteroidsIndications: Acute severe exacerbations not responding completely to
initial inhaled beta-agonist therapyAgents: prednisone (Deltasone), methylprednisolone (Solu-
Medrol), prednisolone (Millipred)MOA: anti-inflammatory; inhibits inflammatory cells and release
of inflammatory mediatorsAdverse Effects: nausea, hyperglycemia, psychosis, weight gain,
osteoporosisComments: IV therapy offers no therapeutic advantage over oral
administrationDuration of therapy: 5-10 daysHigh-dose regimens do not enhance outcomes and are associated with higher rate of side effectsShould not be used as chronic maintenance therapy
©2014 Barkley & AssociatesUnit 5
Recombinant Anti-IgE AntibodyIndications: Treatment of allergic asthma not well controlled on oral
corticosteroids or ICSAgent: omalizumab (Xolair)
MOA: binds to the mast cells limiting the of release of mediators in response to allergen exposure
Dose: Based on baseline total serum IgE level & weightAdverseEffects:
injection site reaction, headache, pharyngitis, sinusitis, thrombocytopenia, anaphylaxis
Comments: Do not abruptly stop systemic or ICS upon initiation of therapySubcutaneous injectionCost of therapy is significantDue to the potential for anaphylaxis, patients should be observed for 2 hours after injection

19
©2014 Barkley & AssociatesUnit 5
Asthma Action Plan
http://www.pedipress.com/dap_using4zone_actionplan.html
Individualize for each patient
Allows for self-management
Teaches patients to recognize triggers/ early signs of deterioration
Allows early institution of therapy for acute exacerbations
Improves outcomes
©2014 Barkley & AssociatesUnit 5
COPDChronic Bronchitis:Excessive secretion of
bronchial mucus – Present 3 months or more in each of 2 consecutive years
Emphysema:Abnormal permanentenlargement of air spaces
distal to the terminal bronchiole
– Destruction of the alveoli
http://my.clevelandclinic.org/disorders/chronic_obstructive_pulmonary_disease/hic_understanding_copd.aspx

20
©2014 Barkley & AssociatesUnit 5
COPD Diagnostics Symptoms (dyspnea at rest or on exertion, cough with or
without sputum production, progressive limitation of activity)
Spirometry showing airflow limitation that is incompletely reversible with inhaled bronchodilator
FEV1 and all other measurements of expiratory airflow reduced
TLC, FRC and RV may be increased
Absence of an alternative explanation for the symptoms and airflow limitation
2014 GOLD Guidelines for COPD: Global Strategy for Diagnosis, Management and Prevention of COPD
©2014 Barkley & AssociatesUnit 5
Classification of COPDClassification of Severity of Airflow Limitation in COPD
(Based on Post-Bronchodilator FEV1)
In patients with FEV1/FVC < 0.70:
GOLD 1: Mild FEV1 ≥ 80% predicted
GOLD 2: Moderate 50% ≤ FEV1 < 80% predicted
GOLD 3: Severe 30% ≤ FEV1 < 50% predicted
GOLD 4: Very Severe FEV1 < 30% predicted
http://www.goldcopd.org/uploads/users/files/GOLD_Report_2014_Jan23.pdf

21
©2014 Barkley & AssociatesUnit 5
Global Strategy for Diagnosis, Management and Prevention of COPD
Combined Assessment of COPD
Risk
(GOLD
Classification of Airflow Lim
itation)
Risk
(Exacerbation history)
≥ 2or > 1 leadingto hospitaladmission
1 (not leadingto hospitaladmission)
0
Symptoms
(C) (D)
(A) (B)
CAT < 10
4
3
2
1
CAT > 10
BreathlessnessmMRC 0–1 mMRC > 2
http://www.goldcopd.org/uploads/users/files/GOLD_Report_2014_Jan23.pdf
©2014 Barkley & AssociatesUnit 5
Management of COPD Smoking cessation Avoid irritants and allergens Pulmonary rehabilitation Immunizations Influenza vaccine Pneumococcal vaccine
Pharmacotherapy Bronchodilators Theophylline Corticosteroids Antibiotics Oxygen

22
©2014 Barkley & AssociatesUnit 5
Beta-Agonists/SympathomimeticsIndications: DOC for intermittent symptoms of COPD
Beta-agonist = anticholinergicAgents: Short acting agents (SABA’s):
albuterol (Proventil), levalbuterol (Xopenex), pirbuterol (Maxair)
MOA: cause bronchial smooth muscle relaxationAdverseEffects:
dose-related tachycardia, tremor, palpitations, nausea, headache, hypokalemia
Comments: Improve symptoms; do not slow decline of COPDScheduled daily use may be requiredQuick onset of actionLevalbuterol is NOT superior to other agentsFrequently used in combination with anticholinergic (Combivent)
©2014 Barkley & AssociatesUnit 5
AnticholinergicsIndications: DOC for COPD; use tiotropium for frequent and persistent
symptomsNOT used as monotherapy for acute exacerbations
Agents: Short acting: ipratropium bromide (Atrovent)Long acting: tiotropium (Spiriva), aclidinium (Tudorza)
MOA: blocks acetylcholine at parasympathetic sites in bronchial smooth muscle causing bronchodilation
Adverse Effects: Rare: mydriasis, dry mouth, taste disturbances
Comments: Improve symptoms; do not slow decline of COPDSlower onset and more prolonged effect compared with beta-agonistConsider tiotropium when patients require short acting agents on a scheduled basisFrequently used in combination with beta-agonist
23
©2014 Barkley & AssociatesUnit 5
Beta-Agonists/SympathomimeticsIndications: Frequent and persistent symptoms of COPD; utilized when
patients require short acting agents on a scheduled basisAgents: Long acting (LABA’s): arformoterol (Brovana)*, formoterol
(Foradil), indacaterol (Arcapta)*, salmeterol (Serevent)MOA: Cause bronchial smooth muscle relaxationAdverse Effects:
Tachycardia, tremor, palpitations, nausea, headache, hypokalemia
Comments: NOT for acute symptom managementMore convenient: 12 hour durationUseful for nocturnal symptomsNo dose titration; standard dosage for all agentsImprove symptoms and reduce exacerbations*FDA labeled for COPD
©2014 Barkley & AssociatesUnit 5
MethylxanthinesIndications: Adjunct therapy for patients who have not achieved
optimal response to ipratropium/beta-agonist
Agents: theophylline (oral; Theo-Dur)MOA: bronchodilation through smooth muscle relaxation;
respiratory stimulant; reduces diaphragmatic fatigue
AdverseEffects:
nausea, vomiting, headache, insomnia, tremor, irritability, restlessness, tachycardia, seizures
Comments: Clinical utility limited by low therapeutic indexMany drug-drug interactionsMonitor dug levelsConsidered only for those who are intolerant or unable to use an inhaled bronchodilator

24
©2014 Barkley & AssociatesUnit 5
Inhaled Corticosteroids (ICS)Indications: Symptomatic patients with a FEV1 < 50% & repeated
exacerbations (Stage III and IV)Agents: beclomethasone (Beclovent), budesonide (Pulmicort),
ciclesonide (Alvesco), flunisolide (Aerospan), fluticasone (Flovent), mometasone (Asmanex)
MOA: anti-inflammatory; inhibits inflammatory cells and release of inflammatory mediators
Adverse Effects: headache, pharyngitis, dysphonia, oral candidiasis
Comments: Does not modify long-term decline of FEV1 in COPDReduces frequency of exacerbations Combination therapy with LABA > either agent aloneNot all patients will benefit from ICSRinse mouth thoroughly after inhalationSystemic adverse effects can occur with any ICS
©2014 Barkley & AssociatesUnit 5
Systemic CorticosteroidsIndications: Acute exacerbation;
Chronic therapy should be avoided if possible
Agents: prednisone (Deltasone), methylprednisolone (Solu-Medrol), prednisolone (Millipred)
MOA: anti-inflammatory; inhibits inflammatory cells and release of inflammatory mediators
AdverseEffects:
nausea, hyperglycemia, psychosis, weight gain, osteoporosis
Comments: Clinical benefit in chronic management not evident and risk of toxicity is extensiveNOT considered as routine maintenance therapyIf required, use lowest effective dose
25
©2014 Barkley & AssociatesUnit 5
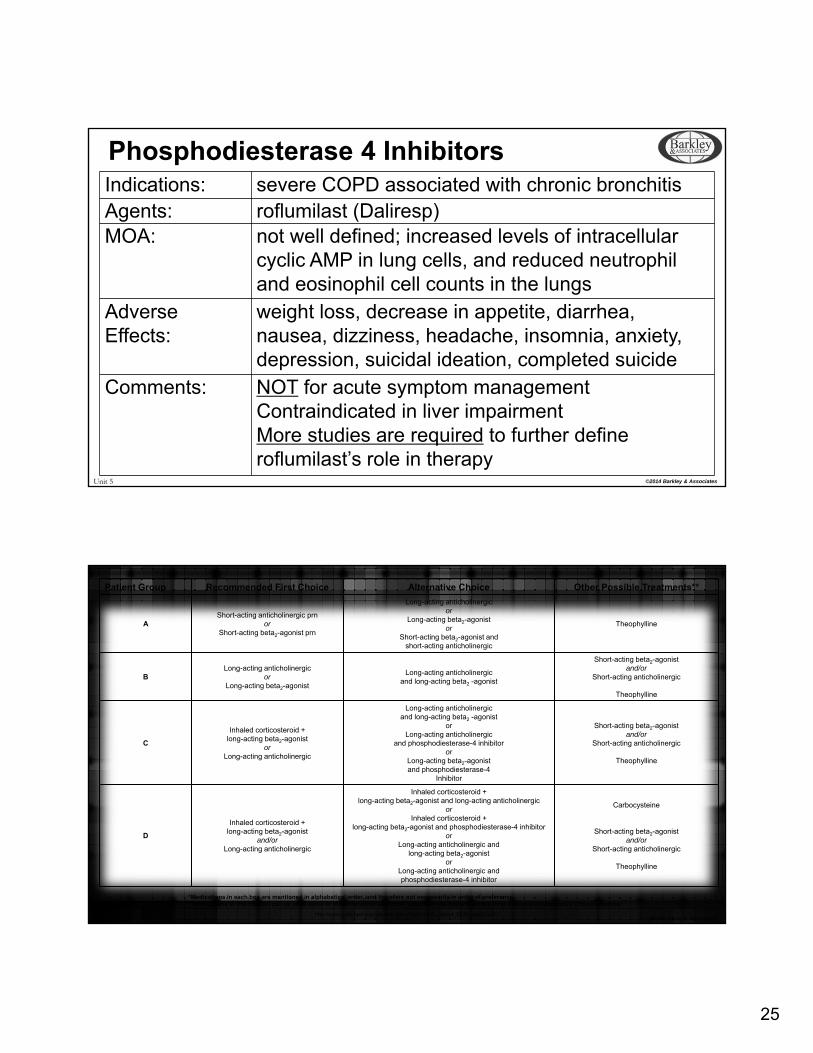
Phosphodiesterase 4 InhibitorsIndications: severe COPD associated with chronic bronchitisAgents: roflumilast (Daliresp)MOA: not well defined; increased levels of intracellular
cyclic AMP in lung cells, and reduced neutrophil and eosinophil cell counts in the lungs
Adverse Effects:
weight loss, decrease in appetite, diarrhea, nausea, dizziness, headache, insomnia, anxiety, depression, suicidal ideation, completed suicide
Comments: NOT for acute symptom managementContraindicated in liver impairmentMore studies are required to further define roflumilast’s role in therapy
©2014 Barkley & AssociatesUnit 5
Patient Group Recommended First Choice Alternative Choice Other Possible Treatments**
AShort-acting anticholinergic prn
or Short-acting beta2-agonist prn
Long-acting anticholinergic or
Long-acting beta2-agonist or
Short-acting beta2-agonist andshort-acting anticholinergic
Theophylline
BLong-acting anticholinergic
or Long-acting beta2-agonist
Long-acting anticholinergicand long-acting beta2 -agonist
Short-acting beta2-agonist and/or
Short-acting anticholinergic
Theophylline
C
Inhaled corticosteroid +long-acting beta2-agonist
or Long-acting anticholinergic
Long-acting anticholinergicand long-acting beta2 -agonist
orLong-acting anticholinergic
and phosphodiesterase-4 inhibitor or
Long-acting beta2-agonistand phosphodiesterase-4
Inhibitor
Short-acting beta2-agonist and/or
Short-acting anticholinergic
Theophylline
D
Inhaled corticosteroid +long-acting beta2-agonist
and/orLong-acting anticholinergic
Inhaled corticosteroid +long-acting beta2-agonist and long-acting anticholinergic
orInhaled corticosteroid +
long-acting beta2-agonist and phosphodiesterase-4 inhibitoror
Long-acting anticholinergic andlong-acting beta2-agonist
orLong-acting anticholinergic andphosphodiesterase-4 inhibitor
Carbocysteine
Short-acting beta2-agonist and/or
Short-acting anticholinergic
Theophylline
*Medications in each box are mentioned in alphabetical order, and therefore not necessarily in order of preference**Medications in this column can be used alone or in combination with other options in the Recommended First Choice and Alternative Choice columns
http://www.goldcopd.org/uploads/users/files/GOLD_Report_2014_Jan23.pdf

26
©2014 Barkley & AssociatesUnit 5
Pneumonia
©2014 Barkley & AssociatesUnit 5
Pneumonia: Signs/Symptoms Fever Shaking chills Purulent sputum Lung consolidation on physical exam Malaise Increased fremitus
www.med-ed.virginia.edu

27
©2014 Barkley & AssociatesUnit 5
Management of Pneumonia Strep. pneumoniae: most common etiological agent for community
acquired pneumonia (CAP)
Outpatient Management of CAP:
Healthy patients (< 60 years old with NO comorbidities)
Macrolide (azithromycin, clarithromycin, erythromycin)
Doxycycline
Patients with other health problems (e.g., COPD, diabetes, heart failure, cancer or > 65 years old)
Respiratory fluoroquinolone (moxifloxacin, gemifloxacin or levofloxacin
Beta-lactam (amoxicillin-clavulanate, cefuroxime) plus a macrolide or doxycycline
©2014 Barkley & AssociatesUnit 5
The End


















