Adult Medicine PRN Focus Session -An Update to the ...
22
Adult Medicine PRN Focus Session-An Update to the Management of Acute Bacterial Skin and Skin Structure Infections: What is the Utility of the New Agents? Activity Number: 0217-0000-16-120-L01-P, 1.50 hours of CPE credit; Activity Type: An Application-Based Activity Monday, October 24, 2016 1:30 p.m. to 3:00 p.m. Great Halls 1 & 2 Moderator: Kurt Wargo, Pharm. D., BCPS Regional Dean and Associate Professor of Pharmacy, Wingate University Hendersonville Health Sciences Center, Hendersonville, North Carolina Agenda 1:30 p.m. Acute Bacterial Skin and Skin Structure Infections: A Review of The Pathophysiology and Epidemiology and Relevance of Current Guidelines Douglas N. Fish, Pharm. D., FCCP, BCPS Professor and Chair, Department of Clinical Pharmacy, Department of Pharmacy, University of Colorado Anschutz Medical Campus, Skaggs School of Pharmacy and Pharmaceutical Sciences, Aurora, Colorado 2:00 p.m. The Treatment of ABSSSIs Caused by MRSA: Should New Agents Be First-line Therapy? Sandy J. Estrada, Pharm. D., BCPS Pharmacy Clinical Specialist, Infectious Diseases; PGY2 Infectious Diseases Program Director, Lee Memorial Health System, Fort Meyers, Florida 2:30 p.m. The Treatment of ABSSSIs Caused by MRSA: If It Ain’t Broke, Don’t Try and Fix It! Katherine T. Lusardi, Pharm. D., BCPS, AQ-ID Antimicrobial Stewardship Pharmacist, UAMS Medical Center, Little Rock, Arkansas Conflict of Interest Disclosures Sandy J. Estrada: Clinical Investigator: (The Medicines Company), Speaker’s Bureau: (The Medicines Company, Theravance, Merck) Douglas N. Fish: Consultancies: (Theravance), Grants: (Merck) Katherine T. Lusardi: Stocks: (Gilead Sciences, Inc) Kurt Wargo: no conflicts to disclose Learning Objectives 1. Discuss the pathophysiology and epidemiology of ABSSSIs. 2. Apply the most current guideline recommendations to the treatment of their patients. 3. Describe new agents approved since the release of 2014 guidelines. 4. Compare and contrast the new agents for the treatment of ABSSSIs caused by MRSA. 5. Determine the role of new agents in the treatment of ABSSSIs caused by MRSA. 6. Discuss advantages of new agents over older alternatives. 7. Compare and contrast advantages and disadvantages of new agents in relation to older alternatives. © American College of Clinical Pharmacy 1
Transcript of Adult Medicine PRN Focus Session -An Update to the ...
Adult Medicine PRN Focus Session-An Update to the Management of Acute Bacterial Skin and Skin Structure Infections: What is the Utility of the New Agents? Activity Number: 0217-0000-16-120-L01-P, 1.50 hours of CPE credit; Activity Type: An Application-Based Activity
Monday, October 24, 2016 1:30 p.m. to 3:00 p.m. Great Halls 1 & 2
Moderator: Kurt Wargo, Pharm. D., BCPS Regional Dean and Associate Professor of Pharmacy, Wingate University Hendersonville Health Sciences Center, Hendersonville, North Carolina
Agenda
1:30 p.m. Acute Bacterial Skin and Skin Structure Infections: A Review of The Pathophysiology and Epidemiology and Relevance of Current Guidelines Douglas N. Fish, Pharm. D., FCCP, BCPS Professor and Chair, Department of Clinical Pharmacy, Department of Pharmacy, University of Colorado Anschutz Medical Campus, Skaggs School of Pharmacy and Pharmaceutical Sciences, Aurora, Colorado
2:00 p.m. The Treatment of ABSSSIs Caused by MRSA: Should New Agents Be First-line Therapy? Sandy J. Estrada, Pharm. D., BCPS Pharmacy Clinical Specialist, Infectious Diseases; PGY2 Infectious Diseases Program Director, Lee Memorial Health System, Fort Meyers, Florida
2:30 p.m. The Treatment of ABSSSIs Caused by MRSA: If It Ain’t Broke, Don’t Try and Fix It! Katherine T. Lusardi, Pharm. D., BCPS, AQ-ID Antimicrobial Stewardship Pharmacist, UAMS Medical Center, Little Rock, Arkansas
Conflict of Interest Disclosures Sandy J. Estrada: Clinical Investigator: (The Medicines Company), Speaker’s Bureau: (The Medicines Company, Theravance, Merck) Douglas N. Fish: Consultancies: (Theravance), Grants: (Merck) Katherine T. Lusardi: Stocks: (Gilead Sciences, Inc) Kurt Wargo: no conflicts to disclose
Learning Objectives 1. Discuss the pathophysiology and epidemiology of ABSSSIs.2. Apply the most current guideline recommendations to the treatment of their patients.3. Describe new agents approved since the release of 2014 guidelines.4. Compare and contrast the new agents for the treatment of ABSSSIs caused by MRSA.5. Determine the role of new agents in the treatment of ABSSSIs caused by MRSA.6. Discuss advantages of new agents over older alternatives.7. Compare and contrast advantages and disadvantages of new agents in relation to older alternatives.
© American College of Clinical Pharmacy 1

8. Compare and contrast costs associated with new agents compared to older alternatives.9. Develop plans to optimize old alternatives in order to achieve similar outcomes to the new agents.
Self-Assessment Questions
Self-assessment questions are available online at www.accp.com/am
© American College of Clinical Pharmacy 2

2016 ACCP Annual Meeting
Acute Bacterial Skin and Skin Structure Infections:
A Review of the Pathophysiology and Epidemiology, and Relevance of
Current Guidelines
Douglas N. Fish, PharmD, FCCP, BCPS‐AQ ID
Skaggs School of Pharmacy and pharmaceutical Sciences, Anschutz Medical Campus
Aurora, Colorado
October 24, 2016
2016 ACCP Annual Meeting
Conflict of Interest
• Advisory Board: Theravance
• Grant Funding/Research Support: Merck
2016 ACCP Annual Meeting
Learning Objectives
• Discuss the pathophysiology and epidemiology ofAcute Bacterial Skin and Skin Structure Infections (ABSSSIs)
• Apply the most current guideline recommendations to the treatment of patients
• Describe agents approved since the release of the2014 IDSA guidelines
2016 ACCP Annual Meeting
Epidemiology of ABSSSIs
• Among most common infections seen in both community and hospital settings
• Incidence of ABSSSIs increased from 32.1 to 48.1/1,000 population between 1997 and 2005
• Most infections are mild and treated in outpatient settings
• ~6.5 million office visits/year
• Approximately 3‐5% of all office visits involve SSTIs
• Increasing incidence of Group A streptococcal infections,including necrotizing infections
• Increasing incidence of infections due to drug‐resistant bacteria, particularly methicillin‐resistant S. aureus (MRSA)
Dryden MS. J Antimicrob Chemother 2010;65(Suppl 3):iii35‐44. Cardona AF, Wilson SE. Clin Infect Dis 2015;61(Suppl 2):S69‐78.Tong SYC, et al. Clin Microbiol Rev 2015;28:603‐661.
2016 ACCP Annual Meeting
Epidemiology of ABSSSIs• ED visits for ABSSSIs increased from 1.2 million to 3.4 millionbetween 1992 and 2005
• May account for up to 7‐10% of all hospital admissions
• Hospital admissions due to ABSSSIs increased in U.S. from 675,000 to 870,000 between 2000 and 2004 (29% increase)
• In UK, three‐fold increase in hospitalizations for abscesses andcellulitis from 1991‐2006
• In Australia, 48% increase in hospitalizations due to cutaneous abscesses from 1999‐2008
• Many potential complications including thrombophlebitis, abscess, osteomyelitis, septic arthritis, sepsis
• 10‐34% of all S. aureus bacteremias originate from ABSSSI
Dryden MS. J Antimicrob Chemother 2010;65(Suppl 3):iii35‐44. Cardona AF, Wilson SE. Clin Infect Dis 2015;61(Suppl 2):S69‐78.Tong SYC, et al. Clin Microbiol Rev 2015;28:603‐661.
2016 ACCP Annual Meeting
Pathophysiology of ABSSSIs• Skin infections occur as a result of breaches in the skin barrier,either macroscopic or microscopic
• S. aureus infections best characterized
• Neutrophils and macrophages involved in primary response tobacterial invasion
• Host response evaded by multiple bacterial mechanisms including:
• Blocking of leukocyte chemotaxis
• Sequestration of host antibodies
• Formation of polysaccharide capsules or biofilms to escape leukocyte detection
• Resisting destruction after ingestion by phagocytes
David MZ, Daum RS. Clin Microbiol Rev 2010;23:616‐687.Tong SYC, et al. Clin Microbiol Rev 2015;28:603‐661.
© American College of Clinical Pharmacy 3

2016 ACCP Annual Meeting
Pathophysiology of ABSSSIs
• Multiple virulence factors in S. aureus including:
• Panton‐Valentine Leukocidin (PVL) in CA‐MRSA = lyses WBCs
• Alpha‐hemolysin = toxin forms pores in human cells, facilitatespenetration of skin layers, associated with more severe cutaneous lesions
• Phenol‐soluble modulins (PSMs) = proteins lyse cells including leukocytes and erythrocytes, facilitate colonization and invasion
• Arginine catabolic mobile element (ACME) = provides protection against microbicidal compounds produced by skin
• Regulatory locus referred to as agr controls the expression of PVL, alpha‐hemolysin, PSMs, and other toxins
David MZ, Daum RS. Clin Microbiol Rev 2010;23:616‐687.Tong SYC, et al. Clin Microbiol Rev 2015;28:603‐661.
2016 ACCP Annual Meeting
Pathophysiology/Etiology of ABSSSIs• Predisposing factors generally include:
• Trauma (e.g., abrasions, penetrating wounds, insect bites)
• Disruptions of the cutaneous barrier (e.g., leg ulcers, wounds,fissured webs, dermatosis, pressure ulcers)
• Chronic inflammation (e.g., eczema, radiation therapy)
• Lymphedema, venous insufficiency
• Preexisting skin infections (e.g., tinea, varicella)
• Injection drug use
• Prevalence = 28‐32%
• Obesity
• Immunosuppression (e.g., diabetes, alcohol abuse)
• Risk of ABSSSI increased 1.6‐fold in Type 1 and 1.3‐fold and Type 2 DM
• Risk of hospitalization or other complications increased 5‐fold in DM
Dryden MS. J Antimicrob Chemother 2010;65(Suppl 3):iii35‐44. Cardona AF, Wilson SE. Clin Infect Dis 2015;61(Suppl 2):S69‐78.Tong SYC, et al. Clin Microbiol Rev 2015;28:603‐661.
2016 ACCP Annual Meeting
Etiology of ABSSSIs
• Retrospective study performed in patients at Kaiser Permanente of Northern California between 2006 and 2009
• Over 3 million covered lives in the system
• 648,699 infections among 495,458 unique patients• 52% female, 78% adults, mean SD age = 41 23
• Hospitalization in 6% of patients• Only 23% of patients cultured, but 58% of cultures were positive
• 2% of patients with positive blood cultures
• 39% of blood isolates were S. aureus
• 41% of S. aureus isolates were MRSA
Ray GT et al. DiagnMicrobiol Infect Dis 2013;76:24‐30.
2016 ACCP Annual Meeting
Etiology of ABSSSI: Trends in S. aureus and MRSA
0
10
20
30
40
50
60
1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
All S. aureus
MSSA
MRSA
% of Cultured ABSSSI Episodes
Ray GT et al. DiagnMicrobiol Infect Dis 2013;76:24‐30.
2016 ACCP Annual Meeting
Overview of the Skin and Skin Structures• Epidermis
• Avascular proliferative layer, constantly regenerating protein and lipid
• About as thick as a sheet of paper
• Dermis
• Contains blood vessels, lymphatics, and fibroblasts
• Eccrine sweat glands, sebaceous glands, and hair follicles originate here
• Subcutaneous tissue
• Effective cushion and energy storage reserve of variable thickness
• Directly overlies fascia and muscle tissues
Skin and skin structure infections may include any and all layers of the skin as well as fascia and muscle
2016 ACCP Annual Meeting
Classifications of Skin Infections
• Primary: involve areas of previously healthy skin,usually involve only one pathogen
• Secondary: occur in areas of previously damaged skin, often polymicrobial
• Complicated: involve deeper skin structures (e.g. fascia, muscle), require significant surgical intervention, and/or occur in patients with compromised immune function (e.g. diabetes, HIVinfection)
Dryden MS. J Antimicrob Chemother 2010;65(Suppl 3):iii35‐44. Cardona AF, Wilson SE. Clin Infect Dis 2015;61(Suppl 2):S69‐78.Tong SYC, et al. Clin Microbiol Rev 2015;28:603‐661. Stevens DL, et al. Clin Infect Dis 2014;59:e10‐52.
© American College of Clinical Pharmacy 4

2016 ACCP Annual Meeting
ABSSSI Classification:Uncomplicated vs. Complicated
Uncomplicated (Primary) Complicated (Secondary)
Superficial: – Impetigo
Deeper: – Erysipelas
– Cellulitis
Hair follicle associated:– Folliculitis
– Furunculosis
Abscess: – Carbuncle
– Other cutaneous abscesses
Acute wound infections:– Traumatic
– Bite-related
– Post-operative
Chronic wound infections:– Diabetic foot infections
– Venous stasis ulcers
– Pressure sores
Perianal cellulitis ± abscess
DiNubile M et al. J Antimicrob Chemother. 2004;53(Suppl 2):ii37‐50.
2016 ACCP Annual Meeting
Etiology of ABSSSIs: Kaiser Permanente, 2006‐2009Type of Infection
% of episodes
Pathogens (% of positive cultures)
All S. aureus
MRSA β‐hemolytic streptococci
Other Gram (+) bacteria
E. coli Other Gram (‐) bacteria
Anaerobic bacteria
Cellulitis and abscess
63% 81 45 9 4 3 9 <1
Folliculitis 14% 88 32 5 3 1 10 <1
Impetigo 8% 88 13 18 2 1 6 0
Other Misc.
7% 80 27 12 3 3 15 <1
Carbuncle/ furuncle
4% 91 56 4 2 2 5 0
Surgical Site
3% 52 17 6 11 16 32 2
Wound Infection
1% 68 18 12 5 4 31 0
All ABSSSIs 80% 40 9 9 3 4 14 <1
Ray GT et al. Diagn Microbiol Infect Dis 2013;76:24‐30.
2016 ACCP Annual Meeting
Association Between Types of ABSSSI and Incidence of MRSA
0
10
20
30
40
50
60
70
80
Impetigo UncomplicatedSSSI
UncomplicatedSSSI withabscess
ComplicatedSSSI
MRSA
MSSA
65%
62%
40%
7%13%
36%
6%
16%
MRSA = 8% of all S. aureus
Tong SYC, et al. Clin Microbiol Rev 2015;28:603‐661.
% of Po
sitive Cultures MRSA = 31% MRSA = 85%
MRSA = 83%
2016 ACCP Annual Meeting
Patient Case #1J.J. is a 44 year‐old male who presents to the ED with a swollen and painful right lower leg after scratching it on a barbed wire fence. The right calf has a ~6 x 4 cm lesion without a well demarcated border which is diffusely red, erythematous, warm to the touch, and painful. No ulcers, blisters, drainage, or areas of necrosis are noted. His PMH is noncontributory and he has NKDA. He has a fever of 100.2oF, otherwise no other systemic findings. J.J. is diagnosed with cellulitis of the right lower leg.
Which of the following antibiotic regimens would be MOST appropriate for treatment of J.J.’s infection?
a. Oral cephalexin x 5 days
b. Oral trimethoprim/sulfamethoxazole x 10 days
c. Intravenous vancomycin x 7 days
d. Intravenous cefazolin x 10 days
2016 ACCP Annual Meeting
Practice Guidelines for the Diagnosis and Management of Skin and Soft
Tissue Infections: 2014 Update by the Infectious Diseases Society of America
Stevens DL, Bisno AL, Chambers HF, et al. Clin Infect Dis 2014;59:e10‐52.
Published June 18, 2014
2016 ACCP Annual Meeting
SSTI Management Definitions• Nonpurulent SSTIs:
• Mild infection: no focus of purulence or systemic signs of infection
• Moderate infection: systemic signs of infection [temperature >38°C, tachycardia (heart rate >90 beats per minute), tachypnea (respiratory rate >24 breaths per minute) or abnormal white blood cell count (<12 000 or<400 cells/µL)]
• Severe infection: failure of oral antibiotics or systemic signs of infection, orthose who are immunocompromised, or those with clinical signs of deeperinfection such as bullae, skin sloughing, hypotension, or evidence of organ dysfunction
• Purulent SSTIs:• Mild infection: incision and drainage
• Moderate infection: systemic signs of infection as above
• Severe infection: patients who have failed incision and drainage plus oralantibiotics, those with SIRS and hypotension, or immunocompromised patients
Stevens DL et al. Clin Infect Dis 2014;59:e10-52.
© American College of Clinical Pharmacy 5

2016 ACCP Annual Meeting
Management of ABSSSIs: IDSA 2014 Guidelines
Nonpurulent Infections(Examples: Cellulitis, erysipelas, necrotizing infections)
Mild Infection Moderate Infection Severe Infection
Oral Antibiotics:Penicillin VK
Cephalosporin (e.g. cephalexin)DicloxacillinClindamycin
IV Antibiotics:Penicillin GCefazolin
Ceftriaxone(Nafcillin)
Clindamycin
Emergent Surgical Inspection Debridement
Specimens for Culture & Susceptibility Testing
Empiric IV Antibiotics:Vancomycin +
Piperacillin/tazobactamStevens DL et al. Clin Infect Dis 2014;59:e10-52.
2016 ACCP Annual Meeting
2014 IDSA Guidelines: Outpatient Treatment of ABSSSI
• For non‐purulent cellulitis, empirical therapy for infectiondue to β‐hemolytic streptococci is recommended in mild infections
• β‐Lactam (e.g. PCN VK, cephalexin, dicloxacillin) 500 mg PO QID
• Clindamycin 300‐450 mg PO TID
• IV therapy with similar agents for moderate infections
• Empiric coverage for MRSA is recommended in patients who do not respond to β‐lactam therapy
• May also be considered in those with systemic toxicity, IVDUs,penetrating trauma
• Duration of therapy = 5 daysStevens DL et al. Clin Infect Dis 2014;59:e10-52.
2016 ACCP Annual Meeting
Patient Case #1 RevisitedJ.J. is a 44 year‐old male who presents to the ED with a swollen and painful right lower leg after scratching it on a barbed wire fence. The right calf has a ~6 x 4 cm lesion without a well demarcated border which is diffusely red, erythematous, warm to the touch, and painful. No ulcers, blisters, drainage, or areas of necrosis are noted. His PMH is noncontributory and he has NKDA. He has a fever of 100.2oF, otherwise no other systemic findings. J.J. is diagnosed with cellulitis of the right lower leg.
Which of the following antibiotic regimens would be MOST appropriate for treatment of J.J.’s infection?
a. Oral cephalexin x 5 days
b. Oral trimethoprim/sulfamethoxazole x 10 days
c. Intravenous vancomycin x 7 days
d. Intravenous cefazolin x 10 days
2016 ACCP Annual Meeting
Patient Case #2Y.K. is a 69 year‐old female presents with an erythematous area on her left upper arm which is warm to the touch and edematous. The affected area is approximately 4 in2 with poorly defined borders, and has an area in the center which is ulcerated and draining a brownish, purulent fluid. Her temperature is 102.3°F and WBCs are elevated at 12,000; her other vital signs are normal. Her medical history is significant for HTN, DL, and depression. She has NKDA.
Y.K. is diagnosed with cellulitis. Following incision & drainage, what is the most appropriate empiric antibiotic treatment for this patient?
a. Oral dicloxacillin x 10 days
b. Oral trimethoprim/sulfamethoxazole x 5 days
c. Intravenous vancomycin x 7 days
d. Intravenous cefazolin x 10 days
2016 ACCP Annual Meeting
Etiology of ABSSSIs: Kaiser Permanente, 2006‐2009Type of Infection
% of episodes
Pathogens (% of positive cultures)
All S. aureus
MRSA β‐hemolytic streptococci
Other Gram (+) bacteria
E. coli Other Gram (‐) bacteria
Anaerobic bacteria
Cellulitis and abscess
63% 81 45 9 4 3 9 <1
Folliculitis 14% 88 32 5 3 1 10 <1
Impetigo 8% 88 13 18 2 1 6 0
Other Misc.
6% 80 27 12 3 3 15 <1
Carbuncle/ furuncle
4% 91 56 4 2 2 5 0
Surgical Site
3% 52 17 6 11 16 32 2
Wound Infection
1% 68 18 12 5 4 31 0
All ABSSSIs 80 40 9 9 3 4 14 <1
Ray GT et al. Diagn Microbiol Infect Dis 2013;76:24‐30.
2016 ACCP Annual Meeting
Management of ABSSSIs: IDSA 2014 Guidelines
Purulent Infections(Examples: Abscess, cellulitis, furuncle, carbuncle)
Mild Infection Moderate Infection Severe Infection
Incision & Drainage
Oral Antibiotics:TMP/SMXDoxycycline
Empiric IV Antibiotics:VancomycinLinezolid
DaptomycinTelavancinCeftaroline
Stevens DL et al. Clin Infect Dis 2014;59:e10-52.
No Antibiotics
Incision & DrainageSpecimens for C/S
Incision & DrainageSpecimens for C/S
© American College of Clinical Pharmacy 6

2016 ACCP Annual Meeting
2014 IDSA Guidelines: Outpatient Treatment of ABSSSI• Empirical therapy for MRSA is recommended for purulent cellulitis (e.g. cellulitis associated with purulent drainage or exudate in the absence of adrainable abscess) in outpatients
• Antibiotics include:• TMP‐SMX 1‐2 DS tabs PO BID
• Doxycycline 100 mg PO BID
• Alternative agents include minocycline (200 mg x 1, then100 mg PO BID) and linezolid (600 mg PO BID)
• Duration of therapy = 5 days
Stevens DL et al. Clin Infect Dis 2014;59:e10-52.
2016 ACCP Annual Meeting
Patient Case #2 RevisitedY.K. is a 69 year‐old female presents with an erythematous area on her left upper arm which is warm to the touch and edematous. The affected area is approximately 4 in2 with poorly defined borders, and has an area in the center which is ulcerated and draining a brownish, purulent fluid. Her temperature is 102.3°F and WBCs are elevated at 12,000; her other vital signs are normal. Her medical history is significant for HTN, DL, and depression. She has NKDA.
Y.K. is diagnosed with cellulitis. Following incision % drainage, what is the most appropriate empiric antibiotic treatment for this patient?
a. Oral dicloxacillin x 10 days
b. Oral trimethoprim/sulfamethoxazole x 5 days
c. Intravenous vancomycin x 7 days
d. Intravenous cefazolin x 10 days
2016 ACCP Annual Meeting
Patient Case #3F.S., a 49 year‐old male, presents to the ED with cellulitis on his back. The lesion is a 3 cm‐diameter abscess with necrotic edges, a 4 cm halo of erythema, and warm to the touch with drainage of yellowish purulent material. Two similar, smaller lesions are also present. The PMH is significant for hypertension, T2DM, and obesity. F.S. has a temperature of 101.9oF andWBC of 14,500. F.S. was initially seen by his PCP 5 days ago for a self‐reported “spider bite” on his back; at that time an I & D of a 1 x 2 cm abscess was performed and he was started on PO clindamycin.
Which of the following antibiotic regimens would be most appropriate for F.S at this time?
a. Oral amoxicillin/clavulanate x 10 days
b. Intravenous vancomycin x 5 days
c. Oral trimethoprim/sulfamethoxazole x 7 days
d. Intravenous ceftaroline x 5 days
2016 ACCP Annual Meeting
Management of ABSSSIs: IDSA 2014 Guidelines
Purulent Infections(Examples: Abscess, cellulitis, furuncle, carbuncle)
Mild Infection Moderate Infection Severe Infection
Incision & Drainage
Oral Antibiotics:TMP/SMXDoxycycline
Empiric IV Antibiotics:VancomycinLinezolid
DaptomycinTelavancinCeftaroline
Stevens DL et al. Clin Infect Dis 2014;59:e10-52.
No Antibiotics
Incision & DrainageSpecimens for C/S
Incision & DrainageSpecimens for C/S
2016 ACCP Annual Meeting
Treatment of ABSSSI in Hospitalized Patients
• Empiric antibiotics for hospitalized patients with complicated infections (e.g., deeper infections,surgical/traumatic wound infection, major abscesses, cellulitis, infected ulcers/burns) should cover MRSA pending cultureresults:
• Vancomycin 30‐40 mg/kg/d• Dosed to troughs of 15‐20 mg/L
• Linezolid 600 mg IV/PO Q12H• Daptomycin 4 mg/kg IV Q24H• Telavancin 10 mg/kg IV Q24H• Ceftaroline 600 mg IV Q12H
• Duration of therapy = 7‐14 days
Stevens DL et al. Clin Infect Dis 2014;59:e10-52.
2016 ACCP Annual Meeting
Patient Case #3 RevisitedF.S., a 49 year‐old male, presents to the ED with cellulitis on his back. The lesion is a 3 cm‐diameter abscess with necrotic edges, a 4 cm halo of erythema, and warm to the touch with drainage of yellowish purulent material. Two similar, smaller lesions are also present. The PMH is significant for hypertension, T2DM, and obesity. F.S. has a temperature of 101.9oF andWBC of 14,500. F.S. was initially seen by his PCP 5 days ago for a self‐reported “spider bite” on his back; at that time an I & D of a 1 x 2 cm abscess was performed and he was started on PO clindamycin.
Which of the following antibiotic regimens would be most appropriate for F.S at this time?
a. Oral amoxicillin/clavulanate x 10 days
b. Intravenous vancomycin x 5 days
c. Oral trimethoprim/sulfamethoxazole x 7 days
d. Intravenous ceftaroline x 5 days
© American College of Clinical Pharmacy 7

2016 ACCP Annual Meeting
Antibiotic Options for Treatment of MRSA ABSSSIs in Hospitalized Patients
• Traditional “older” agents• Vancomycin – approved 1958• Clindamycin – approved 1968• Quinupristin/dalfopristin (Synercid) – approved 1999• Linezolid (Zyvox) – approved 2000• Daptomycin (Cubicin) – approved 2003• Tigecycline (Tygacil) – approved 2005
• Newer agents• Telavancin (Vibativ) – approved 2009• Ceftaroline (Teflaro) – approved 2010• Dalbavancin (Dalvance) – approved May 23, 2014• Tedizolid (Sivextro) – approved June 20, 2014• Oritavancin (Orbactiv) – approved August 6, 2014
2016 ACCP Annual Meeting
Antibiotic Options for Treatment of MRSA ABSSSIs in Hospitalized Patients
• Traditional “older” agents• Vancomycin – approved 1958• Clindamycin – approved 1968• Quinupristin/dalfopristin (Synercid) – approved 1999• Linezolid (Zyvox) – approved 2000• Daptomycin (Cubicin) – approved 2003• Tigecycline (Tygacil) – approved 2005
• Newer agents• Telavancin (Vibativ) – approved 2009• Ceftaroline (Teflaro) – approved 2010• Dalbavancin (Dalvance) – approved May 23, 2014• Tedizolid (Sivextro) – approved June 20, 2014• Oritavancin (Orbactiv) – approved August 6, 2014
2016 ACCP Annual Meeting
ABSSSI Pathophysiology, Epidemiology, and Current Guidelines:
Key Takeaways• ABSSSIs are among the most common infections &increasing in both frequency and severity
• MRSA remains a key pathogen, being more common inpurulent and complicated infections
• The 2014 IDSA guidelines base need for empiric antibioticsand specific drug selection on purulent vs. nonpurulentinfection, severity, and risk of MRSA
• Newer agents for the treatment of ABSSSI are either notwell defined or not addressed at all in the 2014 IDSA guidelines, creating controversy regarding appropriate roles
© American College of Clinical Pharmacy 8

2016 ACCP Annual Meeting
The Treatment of ABSSSIs caused by MRSA: Should New Agents be First Line Therapy
Sandy J. Estrada, Pharm.D., BCPS (AQID)
Lee Memorial Health System
Fort Myers, FL
10/24/2016
2016 ACCP Annual Meeting
Conflict of Interest
• Speaker’s Bureau: Merck, Theravance, The Medicines Company
• Research Funding: The Medicines Company
2016 ACCP Annual Meeting
Learning Objectives
• Compare and contrast the new agents for the treatment of ABSSSIscaused by MRSA
• Determine the role of new agents in the treatment of ABSSSIs caused by MRSA
• Discuss advantages of new agents over older alternatives
2016 ACCP Annual Meeting
Why Do We Need New Agents?
• MRSA Rates remain high nationally
• Increased Vancomycin MICs
• Higher vancomycin doses increase nephrotoxicity
• Vancomycin tolerance affects susceptiblity of other agents
2016 ACCP Annual Meeting
Newly Approved Antimicrobials • Telavancin
• Approved: September 11, 2009
• Label expansion for concurrent S. aureus bacteremia
• Dalbavancin• Approved: May 23, 2014
• Tedizolid phosphate• Approved: June 20, 2014
• Oritavancin• Approved: August 6, 2014
• All indicated to treat ABSSSI
2016 ACCP Annual Meeting
Case
• ZT is 38 year old male with a history of non‐healing surgical wound on his left foot
• Culture from 3 weeks ago grew MRSA• Vancomycin MIC 2 mcg/ml; Linezolid MIC 2 mcg/ml• Patient completed 10 days of oral linezolid
• PMH: Diabetes, obesity• PSH: Left second toe amputation• Social history: non‐contributory except that he is a business owner and is reluctant to be hospitalized or come for daily iv antimicrobial infusion
• At office visit today, there is purulent drainage from the wound and nosignificant improvement from the last vist
• Would you consider a “new” ABSSSI antimicrobial for ZT?
© American College of Clinical Pharmacy 9

2016 ACCP Annual Meeting
The Old or the New: Factors to Consider• Guidelines
• Primary Literature
• Resistance
• Pharmacoecomomics
• Patient Satisfaction
2016 ACCP Annual Meeting
Tedizolid Summary Features and Properties
Indication
Complicated skin and skin structure infections in adults
Mechanism of action
Oxazolidinone antibacterial; inhibits ribosomal translation
Resistant Spectrum of Activity
MRSA, VISA/hVISA, VRSA/VRE, DAP-NS SA/Ent, LR-Ent
Dosage and administration
Dose 200 mg
Frequency Daily for 6 days
Preparation and administration
Oral IV: NS 250 mL; 1 hour infusion
Renal Adjustment (CrCl <30 ml/min)Hemodialysis
None
Ent=enterococcusDAP=daptomycinLR=linezolid resistant
2016 ACCP Annual Meeting
Tedizolid Pharmacokinetics • Tedizolid phosphate is rapidly converted to tedizolid by serum phosphatasein vivo
ParameterTedizolid
200 mg daily
Cmax 1.8 mcg/ml
Tmax (oral) 3 hours
AUC0-inf 21.6 mcg x hr/ml
Protein binding 85-90%
Half-life 11 hours
Volume of distribution
108 L
Elimination18% urine82% feces
Bioavailability 91%
Tissue Penetration -1x serum concentration for adipose and muscle
-40x in epithelial lining fluid (ELF)
2016 ACCP Annual Meeting
Enhanced Activity in vitro with Tedizolid
Organism MIC 90 mcg/mlStaphylococcus aureus
MSSA 0.25-0.50
MRSA 0.25-1.0
Streptococcus pyogenes 0.25-0.50
Streptococcus agalactiae 0.25-0.50
Streptococcus pneumoniae 0.25-0.50
Enterococcus faecalis
Non-VRE & VRE 0.5
Enterococcus faecium
Non-VRE & VRE 0.5
Clostridium species 2
Peptostreptococcus sp. 0.5
Increases stability against some linezolid resistant isolates
Tedizolid is approximately 4-8x more potent than linezolid
Brown SD et al. Antimicrob Agents Chemother 2010;5:2063–9
2016 ACCP Annual Meeting
Comparable Outcomes with Shorter Duration of Therapy
Clinical ResponseTedizolid
N=332Linezolid
N=335
Early at 48-72 hours
Cessation of lesion spread 264 (79.5%) 266 (79.4%)
Reduction in lesion size >20% 259 (78%) 255 (76.1%)
Sustained clinical success at end of therapy
Cessation of lesion spread 230 (69.3%) 241 (71.9%)
Reduction in lesion size >20% 268 (80.7%) 271 (80.9%)
Clinical Success 7-14 days post therapy
Investigator’s assessment 284 (85.5%) 288 (86%)
Prokocimer P et al. JAMA. 2013;309(6):559-569
Tedizolid 200 mg PO daily x 6 days vs Linezolid 600 mg PO BID x 10 days
2016 ACCP Annual Meeting
Less GI Toxicity with Tedizolid in Phase III Trials
EventTedizolid
N=662Linezolid
N=662
>1 serious event 12 (1.8) 13 (2.0)
Discontinuation 3 (0.5) 6 (0.9)
GI Disorders 105 (16) 153 (23)
Nausea 54 (8.2) 81 (12.2)
Vomiting 19 (2.9) 37 (5.6)
Diarrhea 26 (3.9) 35 (5.3)
Nervous System 65 (9.8) 67 (10.1)
Headache 41 (6.2) 39 (5.9)
Dizziness 12 (1.8) 14 (2.1)
Number (%) of Patients
Prokocimer P et al. JAMA. 2013;309(6):559-569
© American College of Clinical Pharmacy 10

2016 ACCP Annual Meeting
Less Hematologic Changes with Tedizolid
1.9
3.4
2.6
3.4
1.6
6.86.4
7.3
0
1
2
3
4
5
6
7
8
Day 7-9 Day 11-13 Last ActiveDose
Through LastActive Dose
0.8
1.5
0.8
1.5
2.5 2.4 2.5
3.9
0
1
2
3
4
5
6
7
8
Day 7-9 Day 11-13 Last ActiveDose
Through LastActive Dose
Absolute Neutropenic Count < Lower Limit of Normal
Platelet Count < Lower Limit of Normal
Pat
ient
s, %
Tedizolid Linezolid
2016 ACCP Annual Meeting
Low Probability of MAO‐I Adverse Effects
• Tedizolid shows weak and reversible MAO inhibitor activity in vitro• MAO‐A: IC50 = 8.7 uM
• MAO‐B: IC50= 5.7 uM
• Tedizolid Cmax (fCmax) is seven‐fold lower than IC50 for MAO‐A/B
• No adverse effects observed with tyramine and pseudoephedrinechallenges
• No increased serotonin activity after tryptophan challenge in mice using 30x human equivalent doses of tedizolid
Flanagan S, et al. Antimicrob Agents Chemother. 2013;57(7):3060-3066
2016 ACCP Annual Meeting
Telavancin Summary Features and Properties
Indication
Complicated skin and skin structure infections in adults; including patients with concurrent S. aureus bacteremia
Mechanism of action
Lipoglycopeptide; inhibition of cell-wall synthesis and disruption of bacterial membrane function
Resistant Spectrum of Activity
MRSA, VISA/hVISA, DAP-NS LR-SA
Dosage and administration
Dose 10 mg/kg
Frequency Daily
Preparation and administration IV: D5W 250 mL; 1 hour infusion
Renal Adjustment CrCl 30-50 ml/min = 7.5 mg/kg Q24hCrCl 10-30 ml/min = 10 mg/kg Q48h
Ent=enterococcusDAP=daptomycinLR=linezolid resistant
2016 ACCP Annual Meeting
Telavancin In vitro Activity against Methicillin‐Resistant S. aureus (MRSA)
1. Pace JL, et al. Antimicrob Agents Chemother. 2003;47(11):3602‐3604. 2. Clinical and Laboratory Standards Institute (CLSI). Approved Standard – 9th ed., CLSI document M7 A9, CLSI, 940 West Valley Rd.,Suite 1400, Wayne, PA. 19087 2012.
Vancomycin
Linezolid
Telavancin
Growth control10
9
8
7
6
5
4
3
2
1
0
0 4 8 12 16 20 24
Log (CFU
/mL)
Time (hours)
11
12
2016 ACCP Annual Meeting
Telavancin in vitro ActivityTelavancin MIC (µg/mL)
Organism No. tested MIC90
S. aureus (all) 9,610 0.06
MSSA 4,959 0.06
MRSA 4,651 0.06
Vancomycin ≤1 µg/mL 4,561 0.06
Vancomycin = 2-4 µg/mL 90 0.06
Daptomycin ≤0.5 µg/mL 4,607 0.06
Daptomycin = 1-2 µg/mL 43 0.06
Multidrug resistant (MDR) 1,371 0.06
Mendes RE, et al. Antimicrob Agents Chemother. 2015;59:1811-1814.
2016 ACCP Annual Meeting
ATLAS 1&2: Telavancin Phase 3 Studies in cSSSI
1. VIBATIV (telavancin) Prescribing Information. Theravance Biopharma Antibiotics, Inc. December 2014. 2. Stryjewski ME, et al. Clin Infect Dis. 2008;46(11):1683-1693. 3. FDA Briefing Document/FDA Anti-Infective Drugs Advisory Committee Meeting November 19, 2008.
Primary objective
• To compare the efficacy and safety of VIBATIV to vancomycin in the treatment of adults with complicated Gram-positive cSSSI with emphasis on patients with infections due to MRSA at a test-of-cure (TOC) visit 7-14 days after completion of therapy
• 1794 patients (AT population; 129 centers in 21 countries)
Adult patients with cSSSI with MRSA suspected or confirmed as primary cause
Require IV antibiotic treatment for ≥7 days
• Comparators
Telavancin 10 mg/kg IV q24h
Vancomycin 1g q12h†
• Treatment duration
7 to 14 days
© American College of Clinical Pharmacy 11

2016 ACCP Annual Meeting
ATLAS 1&2: Cure RatesPooled clinical cure rates from Phase 3 clinical trialsPooled clinical cure rates from Phase 3 clinical trials
Cure Rate, %
1. VIBATIV (telavancin) Prescribing Information. Theravance Biopharma Antibiotics, Inc. December 2014. 2. Stryjewski ME, et al. Clin Infect Dis. 2008;46(11):1683-1693. 3. FDA Briefing Document/FDA Anti-Infective Drugs Advisory Committee Meeting November 19, 2008.
65
70
75
80
85
90
All Treated Clinically Evaluable
Telavancin
Vancomycin
2016 ACCP Annual Meeting
ATLAS 1&2 Adverse Events
VIBATIV 10 mg/kgN=929
%
VancomycinN=938
%
Taste disturbance 33 7
Nausea 27 15
Vomiting 14 7
Foamy urine 13 3
Pruritus 6 13
VIBATIV (telavancin) Prescribing Information. Theravance Biopharma Antibiotics, Inc. December 2014.
2016 ACCP Annual Meeting
Dalbavancin Summary Features and Properties
Indication
Complicated skin and skin structure infections in adults
Mechanism of action
Glycopepetide antibacterial inhibits peptidoglycan synthesis
Resistant Spectrum of Activity
MRSA, VISA/hVISA, DAP-NS SA/Ent, LR-Ent
Dosage and administration
Dose 1000mg day 1; 500mg day 8 or 1500 mg day 1
Frequency Once weekly
Preparation and administration D5W only (1-5 mg/ml) 30 minute IV infusion
Renal Adjustment (CrCl <30 ml/min) 750mg day 1; 375 mg day 8 OR 1175 mg IV x 1
Ent=enterococcusDAP=daptomycinLR li lid i t t
2016 ACCP Annual Meeting
Dalbavancin Activity Against Gram Positive Pathogens MIC 90 mcg/ml
Organism Dalbavancin VancomycinStaphylococcus aureus 0.06 1
MRSA 0.06 2
VRSA 1.0-2.0 >4
Streptococcus pyogenes 0.03 1
Streptococcus agalactiae 0.12 0.5
Viridans group streptococcus 0.016-0.03 0.5
Streptococcus pneumoniae 0.03 0.5
Enterococcus faecalis 0.06 2
Enterococcus faecium 0.12 1
VanA VRE 32-128 512
VanB/C VRE 0.12-1 512
Clostridium species 0.5 1
Listeria species 0.06
2016 ACCP Annual Meeting
Similar Early Response Rates with Dalbavancin
Assessment at 72 hours
Dalbavancin 2 doses
Vancomycin/ linezolid
Absolute Difference (95% CI)
No lesion spread
DISCOVER 1 83.3% 81.8% 1.5 (-4.6-7.9)
DISCOVER 2 76.8% 78.3% -1.5(-7.4-4.6)
Both Trials 79.7% 79.8% 0.1 (-4.5-4.2)
Early >20% reduction of infection area
DISCOVER 1 89% 90.9% -1.0 (-5.7-4.0)
DISCOVER 2 87.6% 85.9% 1.7 (-3.2-6.7)
Both Trials 88.6% 88.1% 0.6 (-2.9-4.1)
Boucher, HW et al. N Engl J Med 2014;370:2169-79
2016 ACCP Annual Meeting
Dalbavancin: One Dose vs Two Doses
Outcome Dalbavancin 1Dose
Dalbavancin 2 Doses
Absolute Difference (95% CI)
Response at 48-72h 81.4% 84.2% -2.9 (-8.5-2.8)
Day 14 clinical success 84% 84.8% -0.9(-6.3, 4.6)
Day 28 clinical success 84.5% 85.1% -0.6 (-6, 4.8)
Dunne MW, et al. Clin Infect Dis 2016;62:545-551.
© American College of Clinical Pharmacy 12

2016 ACCP Annual Meeting
Limited and Comparable Adverse Effects Profile
Adverse EffectDalbavancin N=1178 (%)
Comparators*N=1224 (%)
Serous adverse effect 109 (6.1%) 80 (6.5%)
Drug discontinuation 53 (3%) 35 (2.8%)
Nausea 98 (5.5%) 78 (6.4%)
Vomiting 50 (2.8%) 37 (3%)
Diarrhea 79 (4.4%) 72 (5.9%)
Headache 83 (4.7% 59 (4.8%)
Rash 48 (2.7%) 30 (2.4%)
Puritus 38 (2.1%) 41.3.3%)
ALT 3x ULN 12 (0.8%) 2 (0.2%)
*Comparators include: Vancomycin, Linezolid, Cefazolin, and Cephalexan
2016 ACCP Annual Meeting
Oritavancin Summary Features and Properties
Indication
Complicated skin and skin structure infections in adults
Mechanism of action
Glycopeptide antibacterial; inhibits peptidoglycan synthesis
Resistant Spectrum of Activity
MRSA, VISA/hVISA, VRSA/VRE, DAP-NS SA/Ent, LR-SA/Ent
Dosage and administration
Dose 1200mg once
Frequency One time dose
Preparation and administration D5W 1000 mL only3-hour IV infusion
Renal Adjustment (CrCl <30 ml/min
None
Ent=enterococcusDAP=daptomycinLR=linezolid resistant
Corey RG, et al. N Engl J Med 2014;370:2180-90.
2016 ACCP Annual Meeting
Oritavancin Mechanism of Action
•Oritavancin exhibits three distinct mechanisms of action•Binds to peptidoglycan precursors to inhibittransglycosolation step of cell wall biosynthesis
•Binds to peptide bridging segments to inhibitcross‐linking
•Disrupts bacterial membrane integrity, leadingto depolarization, permeabilization and cell death
2016 ACCP Annual Meeting
Oritavancin in vitro Activity MIC 90 mcg/ml
Organism Oritavancin VancomycinStaphylococcus aureus
MSSA 0.12 1
MRSA 0.12 2
VRSA 1.0 >4
Streptococcus pyogenes 0.25 1
Streptococcus agalactiae 0.25 0.5
Streptococcus pneumoniae 0.008 0.5
Enterococcus faecalis
Non-VRE 0.06 2
VRE 1.0 512
Enterococcus faecium
Non-VRE 0.03 1
VRE 0.25 512
Clostridium species 1.0 1
2016 ACCP Annual Meeting
Oritavancin Displays PotentConcentration Dependent Killing
• Antimicrobial effect on NRS384 CA‐MRSA (USA300)
2016 ACCP Annual Meeting
Potential Affects on Concomitant Medications
• Despite the absence of hepatic metabolism, oritavancin affects CYP 450 system
• Non‐specific weak inhibitor• CYP2C9 and CYP2C19
• Warfarin AUC increased 31%
• Ratio of omeprazole to 5‐OH‐omeprazole increased 15%
• Contraindication• Use of IV heparin within 48 hours of oritavancin administration
• aPTT remains falsely elevated
© American College of Clinical Pharmacy 13
2016 ACCP Annual Meeting
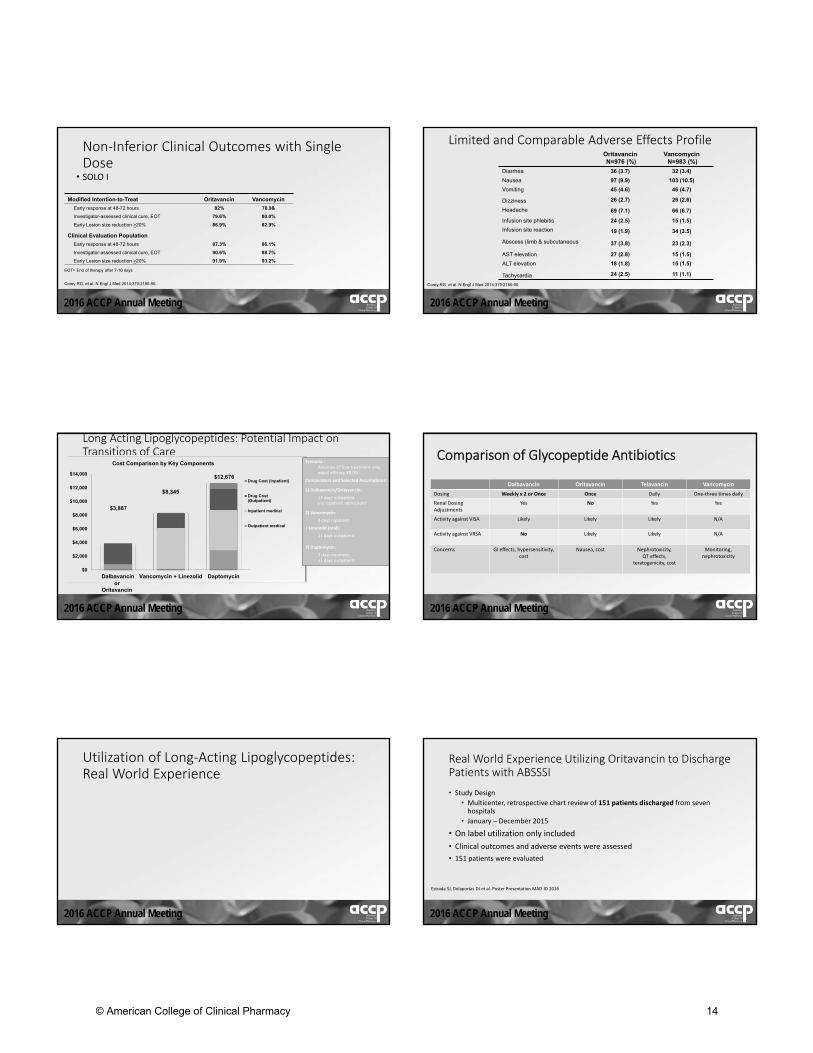
Non‐Inferior Clinical Outcomes with Single Dose
• SOLO I
Modified Intention-to-Treat Oritavancin Vancomycin
Early response at 48-72 hours 82% 78.9&
Investigator-assessed clinical cure, EOT 79.6% 80.0%
Early Lesion size reduction >20% 86.9% 82.9%
Clinical Evaluation Population
Early response at 48-72 hours 87.3% 86.1%
Investigator-assessed clinical cure, EOT 90.6% 88.7%
Early Lesion size reduction >20% 91.9% 93.2%
EOT= End of therapy after 7-10 days
Corey RG, et al. N Engl J Med 2014;370:2180-90.
2016 ACCP Annual Meeting
Limited and Comparable Adverse Effects Profile OritavancinN=976 (%)
Vancomycin N=983 (%)
Diarrhea 36 (3.7) 32 (3.4)
Nausea 97 (9.9) 103 (10.5)
Vomiting 45 (4.6) 46 (4.7)
Dizziness 26 (2.7) 26 (2.6)
Headache 69 (7.1) 66 (6.7)
Infusion site phlebitis 24 (2.5) 15 (1.5)
Infusion site reaction 19 (1.9) 34 (3.5)
Abscess (limb & subcutaneous 37 (3.8) 23 (2.3)
AST elevation 27 (2.8) 15 (1.5)
ALT elevation 18 (1.8) 15 (1.5)
Tachycardia 24 (2.5) 11 (1.1)
Corey RG, et al. N Engl J Med 2014;370:2180-90.
2016 ACCP Annual Meeting
Long Acting Lipoglycopeptides: Potential Impact on Transitions of Care
$3,887
$8,345
$12,676
$0
$2,000
$4,000
$6,000
$8,000
$10,000
$12,000
$14,000
Dalbavancin Vancomycin + Linezolid Daptomycin
Cost Comparison by Key Components
Drug Cost (Inpatient)
Drug Cost(Outpatient)
Inpatient medical
Outpatient medical
Scenario : Assumes 1st line treatment only, equal efficacy 88.9%1
Comparators and Selected Assumptions:
1) Dalbavancin/Oritavancin:
14 days outpatient(no inpatient admission)
2) Vancomycin:
3 days inpatient
+ Linezolid (oral):
11 days outpatient
3) Daptomycin:
3 days inpatient, 11 days outpatient
orOritavancin
2016 ACCP Annual Meeting
Comparison of Glycopeptide Antibiotics
Dalbavancin Oritavancin Telavancin Vancomycin
Dosing Weekly x 2 or Once Once Daily One‐three times daily
Renal Dosing Adjustments
Yes No Yes Yes
Activity against VISA Likely Likely Likely N/A
Activity against VRSA No Likely Likely N/A
Concerns GI effects, hypersensitivity, cost
Nausea, cost Nephrotoxicity, QT effects,
teratogenicity, cost
Monitoring, nephrotoxicity
2016 ACCP Annual Meeting
Utilization of Long‐Acting Lipoglycopeptides: Real World Experience
2016 ACCP Annual Meeting
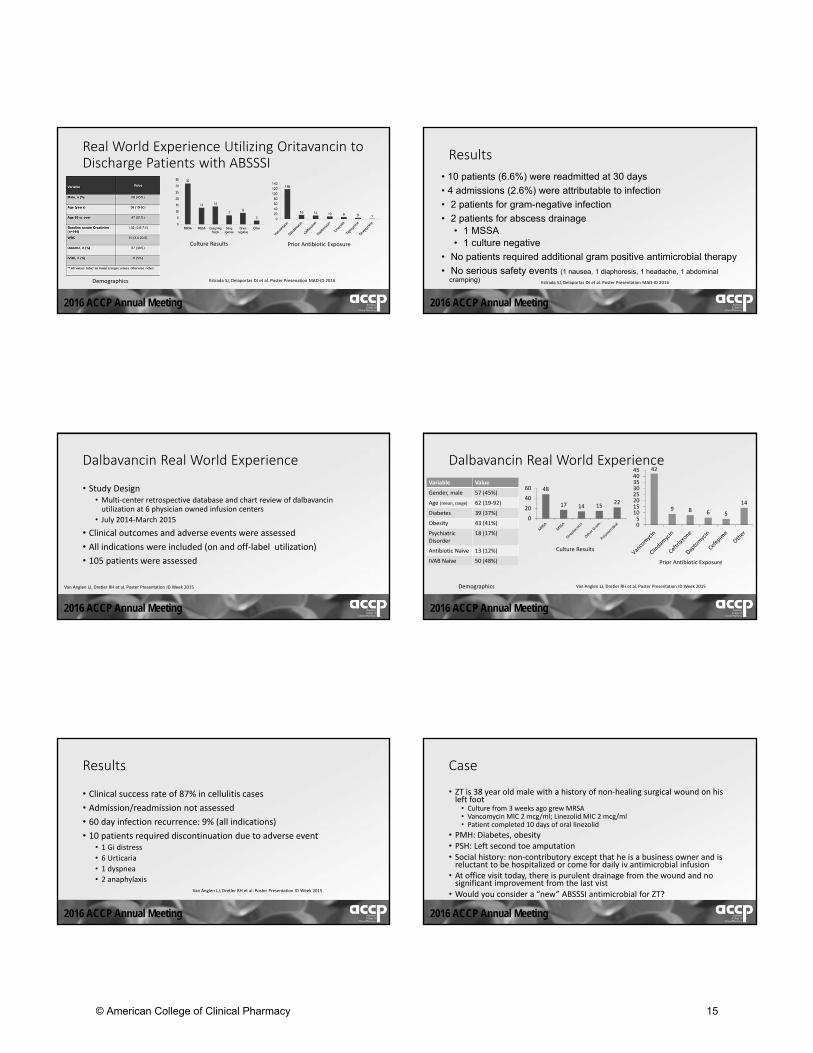
Real World Experience Utilizing Oritavancin to Discharge Patients with ABSSSI
• Study Design
• Multicenter, retrospective chart review of 151 patients discharged from seven hospitals
• January – December 2015
• On label utilization only included
• Clinical outcomes and adverse events were assessed
• 151 patients were evaluated
Estrada SJ, Delaportas DJ et al. Poster Presentation MAD‐ID 2016
© American College of Clinical Pharmacy 14
2016 ACCP Annual Meeting
Real World Experience Utilizing Oritavancin to Discharge Patients with ABSSSI
Demographics
Culture Results Prior Antibiotic Exposure
Estrada SJ, Delaportas DJ et al. Poster Presenation MAD‐ID 2016
2016 ACCP Annual Meeting
Results
• 10 patients (6.6%) were readmitted at 30 days
• 4 admissions (2.6%) were attributable to infection
• 2 patients for gram-negative infection
• 2 patients for abscess drainage• 1 MSSA• 1 culture negative
• No patients required additional gram positive antimicrobial therapy
• No serious safety events (1 nausea, 1 diaphoresis, 1 headache, 1 abdominal cramping) Estrada SJ, Delaportas DJ et al. Poster Presentation MAD‐ID 2016
2016 ACCP Annual Meeting
Dalbavancin Real World Experience
• Study Design• Multi‐center retrospective database and chart review of dalbavancinutilization at 6 physician owned infusion centers
• July 2014‐March 2015
• Clinical outcomes and adverse events were assessed
• All indications were included (on and off‐label utilization)
• 105 patients were assessed
Van Anglen LJ, Dretler RH et al. Poster Presentation ID Week 2015
2016 ACCP Annual Meeting
Dalbavancin Real World Experience
Variable Value
Gender, male 57 (45%)
Age (mean, range) 62 (19‐92)
Diabetes 39 (37%)
Obesity 43 (41%)
Psychiatric Disorder
18 (17%)
Antibiotic Naïve 13 (12%)
IVAB Naïve 50 (48%)
48
17 14 1522
0
20
40
60
42
9 8 6 5
14
051015202530354045
Demographics
Culture Results
Prior Antibiotic Exposure
Van Anglen LJ, Dretler RH et al. Poster Presentation ID Week 2015
2016 ACCP Annual Meeting
Results
• Clinical success rate of 87% in cellulitis cases
• Admission/readmission not assessed
• 60 day infection recurrence: 9% (all indications)
• 10 patients required discontinuation due to adverse event• 1 Gi distress
• 6 Urticaria
• 1 dyspnea
• 2 anaphylaxisVan Anglen LJ, Dretler RH et al. Poster Presentation ID Week 2015
2016 ACCP Annual Meeting
Case
• ZT is 38 year old male with a history of non‐healing surgical wound on his left foot
• Culture from 3 weeks ago grew MRSA• Vancomycin MIC 2 mcg/ml; Linezolid MIC 2 mcg/ml• Patient completed 10 days of oral linezolid
• PMH: Diabetes, obesity• PSH: Left second toe amputation• Social history: non‐contributory except that he is a business owner and is reluctant to be hospitalized or come for daily iv antimicrobial infusion
• At office visit today, there is purulent drainage from the wound and nosignificant improvement from the last vist
• Would you consider a “new” ABSSSI antimicrobial for ZT?
© American College of Clinical Pharmacy 15

2016 ACCP Annual Meeting
Role in Therapy‐ Discussion
• Tedizolid• Reduce duration of therapy
• Preserved activity against linezolid resistant organisms
• Less MAOI activity
• Telavancin• Patients with concurrent bacteremia
• Preserved activity against resistant organisms
• Once daily option for outpatient setting
2016 ACCP Annual Meeting
Role in Therapy ‐ Discussion
• Dalbavancin/Oritavancin• Shift IV therapy more into the outpatient setting
• Limit/reduce hospitalizations and healthcare costs
• Awaiting data on treatment of more serious infections
© American College of Clinical Pharmacy 16

2016 ACCP Annual Meeting
The Treatment of ABSSSIs Caused by MRSA: If It Ain’tBroke, Don’t Try to Fix It!
Katherine Lusardi, PharmD, BCPS‐AQ ID
UAMS Medical Center, Hospital Pharmacy
Little Rock, AR
24 October 2016
2016 ACCP Annual Meeting
Conflict of Interests
• Shareholder in Gilead Sciences, Inc.
2016 ACCP Annual Meeting
Learning Objectives
1. Compare and contrast advantages and disadvantages of new agentsin relation to older alternatives.
2. Compare and contrast costs associated with new agents compared to older alternatives.
3. Develop plans to optimize old alternatives in order to achieve similaroutcomes to the new agents.
2016 ACCP Annual Meeting
Audience Response
• Area of practice?• Hospital, OP, ED
• 340b Hospitals?
• Who has ED programs in place where this would work?
• Who wishes they could have effective ED avoidance programs?
2016 ACCP Annual Meeting
Old vs. NewOne is Silver and the Other Gold
2016 ACCP Annual Meeting
Old and NewOld
• Clindamycin
• Daptomycin
• Doxycycline
• Linezolid
• Tetracycline
• TMP/SMX
• Vancomycin
New
• Ceftaroline
• Dalbavancin
• Oritavancin
• Tedizolid
• Televancin
© American College of Clinical Pharmacy 17

2016 ACCP Annual Meeting
New Agents ‐ Advantages
• “One and done”
• Compliance
• Less line requirements
• Patient assistance options
Various monographs
2016 ACCP Annual Meeting
New Agents ‐ Disadvantages
• Broader coverage than necessary
• Adverse effects
• Drug/lab interactions
• Administration concerns
• Logistics
• Paperwork
• Cost
Various monographs
2016 ACCP Annual Meeting
Old Agents ‐ Advantages
• Practitioner comfort
• Mostly PO options
• Well studied
• Cost
• Mostly generic
Various monographs
2016 ACCP Annual Meeting
Old Agents ‐ Disadvantages
• Adverse effects
• Drug interactions
• Line requirements
• Increasing resistance
• Compliance
Various monographs
2016 ACCP Annual Meeting
Pricing
Drug MedispanAWP
ASP (Average Sales
Price)
Cost/14 days
Oritavancin 1200 mg 3480.00 2957.04 3480.00
Dalbavancin 1500 mg 5364.00 4564.80 5364.00
Ceftaroline 600 mg 183.10 148.80 5126.80
Televancin 750 mg 449.93 376.28 6299.02
Tedizolid 200 mg 371.70 (PO)
255.40 (IV)
5203.8
Drug MedispanAWP
ASP Cost/14days
Daptomycin 500 mg 543.59 452.00 7610.26
Linezolid 600 mg 96.00 (IV)183.00 (PO)
47.337 (IV)
5124.00
SMX/TMP DS 1.85 ‐‐ 103.60
Clindamycin 300 mg 1.29 ‐‐ 72.24
Doxycycline 100 mg 5.53 ‐‐ 154.84
Minocycline 100 mg 1.67 ‐‐ 46.76
Vancomycin 1000 mg 19.20 5.96 537.60
https://www.cms.gov/Medicare/Medicare‐Fee‐for‐Service‐Part‐B‐Drugs/McrPartBDrugAvgSalesPrice/2016ASPFiles.html
2016 ACCP Annual Meeting
New Agents on Trial
• Oritavancin vs vancomycin = non‐inferior2‐3
• SOLO‐I & SOLO‐II
• Dalbavancin vs vancomycin = non‐inferior4
• Discover I & Discover II
• Ceftaroline vs vancomycin + aztreonam = non‐inferior5‐6
• Canvas 1 & Canvas 2
• Televancin vs vancomycin = non‐inferior7
• Atlas 1 & Atlas 2
• Tedizolid vs Linezolid = non‐inferior8‐9
• Establish 1 & Establish 2
© American College of Clinical Pharmacy 18

2016 ACCP Annual Meeting
Study Comparators2‐9
• Outcomes assessed • New agents were all non‐inferior
• Early treatment response
• Follow up out to 28 days, readmission not assessed
• Change in ABSSSI trial design
• Study structure• Different, but limited comparators
• For long acting agents, >45% of patients in studies were treated inpatient• Mean hospitalization 8+ days
2016 ACCP Annual Meeting
Optimization of Older Agents
2016 ACCP Annual Meeting
Appropriate Assessment is Key
• Some infections are not serious enough• Role of antibiotics
• Role of IV antibiotics
• Some infections are too serious• Role of PO antibiotics
• Role of ED/CDU/OU
• Role of hospital admission
2016 ACCP Annual Meeting
Appropriate Assessment
• Prospective study of ABSSSI presentations to ED• 619 patients enrolled
• 94 (15.2%) admitted to hospital, Avg LOS = 4 Days• More likely to have systemic signs of infection (SIRS), infected wounds, non‐abscess based infections
• Larger infected areas were more likely to be admitted• 30 (31.9%) admitted patients had infected areas > 78.5cm2
• 6.9% of non‐admitted patients had infected areas > 78.5cm2
• Reasons for admission• 85% needed IV abx
• 24.5% needed surgical interventionTalan DA, et al. West J Emerg Med. 2015; 16: 89‐97
2016 ACCP Annual Meeting
Susceptibilities for MRSA11‐17
National Databases Local (Arkansas) Susceptibility
Clindamycin 60.3 – 79.8 =
Daptomycin 99.7 – 100 =
Linezolid 99.9 – 100 =
Tetracycline 94.1 – 94.9 <
TMP‐SMX 93.4 – 98.3 =
Vancomycin (MIC90 = 1) 99.9 – 100 =
Ceftaroline 95.4 >
Dalbavancin 99.6 ?
Oritavancin 98.4 ?
Tedizolid 100 ?
Telavancin 100 ?
2016 ACCP Annual Meeting
Appropriate Treatment
• Subset analysis of a rapid diagnostic prospective clinical trial
• Primary outcomes were failure at 7 days and reported ABSSSIrecurrence at 1 and 3 months
• 272 Patients consented and enrolled• 1 week failure: 10.2%
• 1 month recurrence: 22.4%
• 3 month recurrence: 19.9%
• Risk of recurrence: contact with pt with ABSSSI, use of packing, history of ABSSSI
May LS, et al. West J Emerg Med. 2015; 642‐652.
© American College of Clinical Pharmacy 19

2016 ACCP Annual Meeting
Appropriate Treatment
• Prospective study comparing TMP/SMX and doxycycline for MRSAABSSSI
• 34 Patients enrolled from ED visit, no hospital admissions included• Abscesses drained and packed
• Follow up visit at 2‐5 days, phone f/u at 10‐14 days and 28‐35 days
• 23 (68%) had MRSA, all was susceptible to TMP/SMX and doxycycline
• Infection/erythema diameter was 7.2+4.9 cm
• Primary outcome was failure• 3 (9%) had failure at 10‐14 days and were hospitalized
• All failures were in TMP/SMX group, but not significant differencesCenizal MJ, et al. AAC.2007; 2628‐2630
2016 ACCP Annual Meeting
Appropriate Treatment
• Retrospective comparison between tetracyclines and B‐lactams• 282 included community onset MRSA ABSSSI
• 90 received tetracyclines (minocycline, doxycycline)
• 192 received B‐lactams (amoxicillin/clavulanate, cephalexin)
• 91% required I&D (half by surgical service)
• Median lesion diameter 4 cm
• Overall success was 90.1%• Tetracycline: 96%
• B‐lactam: 87%
• B‐lactam therapy was only independent risk factor for failure
Ruhe JJ, et al. AAC. 2007; 3298‐3303.
2016 ACCP Annual Meeting
Appropriate Treatment
• Retrospective review of antibiotic therapy for CA‐MRSA
• 531 episodes of CA‐MRSA in 492 patients• 361 patients with abscesses (~80% had I&D)
• 312 (%) received active antibiotics
• 219 (%) received inactive antibiotics
• 45 (8.5%) had treatment failure through follow up days 14‐30• No association of failure with lesion size
• Only predictor of failure was inactive treatment• Note: 190 pts with inactive treatment still had success
Ruhe JJ, et al. CID. 2007; 777‐784.
2016 ACCP Annual Meeting
Appropriate Treatment
• Daptomycin – evaluated in Phase 3 trials, at 4mg/kg for cSSTI• 10% of patients had MRSA
• Success compared to
• Post‐marketing patient databases: CORE 2004 & CORE 2005• 52‐63% of patients had MRSA
• 667 (66.7%) patients with cSSTI
• Clinical success rates 93‐96%
Seaton RA. J Antimicrob Chemo. 2008; S3: iii15‐iii23.
2016 ACCP Annual Meeting
ED Avoidance: CDU/OU
• 213 pts referred to CDU• 39 (18.3%) patients hospitalized
• 181 patients not enrolled in study
• 32 (15%) patients discharged on IV abx (ceftriaxone, ampicillin/sulbactam,clindamycin, vancomycin)
• Followed up in 48‐72 hours with PCP, wound care, or ID doctor
• IV LOT 3.4 days
• 96.9% treatment success rate
• Conclusion: hospitalization avoided, 109 days moved from IP to OP
Rentala M. Am J Emerg Med. 2016; 1273‐1275.
2016 ACCP Annual Meeting
ED Avoidance: CDU/OU
• Pediatric ED Evaluation of 8234 cases• 2200 Admitted to hospital
• Mean age 27.3 months
• 304 Admitted to OU
• 192 patients evaluable per study• Mean age 47 months, less likely to have abscesses
• 43 (22.4%) Failed OU stay and were admitted from OU with average LOS 2.9 days• More likely to present with fever, and more resources used
Mistry RD, et al. J Emerg Med. 2015; 855‐863.
© American College of Clinical Pharmacy 20
2016 ACCP Annual Meeting
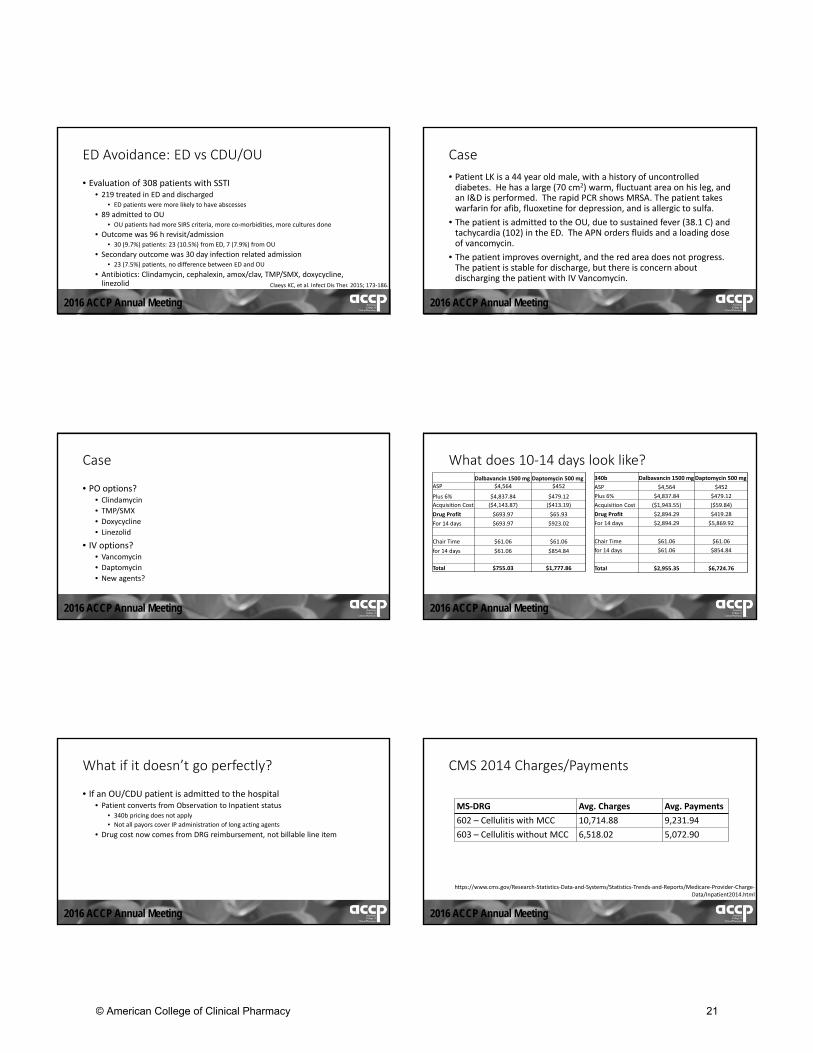
ED Avoidance: ED vs CDU/OU
• Evaluation of 308 patients with SSTI• 219 treated in ED and discharged
• ED patients were more likely to have abscesses
• 89 admitted to OU• OU patients had more SIRS criteria, more co‐morbidities, more cultures done
• Outcome was 96 h revisit/admission• 30 (9.7%) patients: 23 (10.5%) from ED, 7 (7.9%) from OU
• Secondary outcome was 30 day infection related admission• 23 (7.5%) patients, no difference between ED and OU
• Antibiotics: Clindamycin, cephalexin, amox/clav, TMP/SMX, doxycycline,linezolid Claeys KC, et al. Infect Dis Ther. 2015; 173‐186.
2016 ACCP Annual Meeting
Case
• Patient LK is a 44 year old male, with a history of uncontrolled diabetes. He has a large (70 cm2) warm, fluctuant area on his leg, andan I&D is performed. The rapid PCR shows MRSA. The patient takes warfarin for afib, fluoxetine for depression, and is allergic to sulfa.
• The patient is admitted to the OU, due to sustained fever (38.1 C) andtachycardia (102) in the ED. The APN orders fluids and a loading doseof vancomycin.
• The patient improves overnight, and the red area does not progress.The patient is stable for discharge, but there is concern about discharging the patient with IV Vancomycin.
2016 ACCP Annual Meeting
Case
• PO options?• Clindamycin
• TMP/SMX
• Doxycycline
• Linezolid
• IV options?• Vancomycin
• Daptomycin
• New agents?
2016 ACCP Annual Meeting
What does 10‐14 days look like?Dalbavancin 1500 mg Daptomycin 500 mg
ASP $4,564 $452
Plus 6% $4,837.84 $479.12
Acquisition Cost ($4,143.87) ($413.19)
Drug Profit $693.97 $65.93
For 14 days $693.97 $923.02
Chair Time $61.06 $61.06
for 14 days $61.06 $854.84
Total $755.03 $1,777.86
340b Dalbavancin 1500 mgDaptomycin 500 mg
ASP $4,564 $452
Plus 6% $4,837.84 $479.12
Acquisition Cost ($1,943.55) ($59.84)
Drug Profit $2,894.29 $419.28
For 14 days $2,894.29 $5,869.92
Chair Time $61.06 $61.06
for 14 days $61.06 $854.84
Total $2,955.35 $6,724.76
2016 ACCP Annual Meeting
What if it doesn’t go perfectly?
• If an OU/CDU patient is admitted to the hospital• Patient converts from Observation to Inpatient status
• 340b pricing does not apply
• Not all payors cover IP administration of long acting agents
• Drug cost now comes from DRG reimbursement, not billable line item
2016 ACCP Annual Meeting
CMS 2014 Charges/Payments
MS‐DRG Avg. Charges Avg. Payments
602 – Cellulitis with MCC 10,714.88 9,231.94
603 – Cellulitis without MCC 6,518.02 5,072.90
https://www.cms.gov/Research‐Statistics‐Data‐and‐Systems/Statistics‐Trends‐and‐Reports/Medicare‐Provider‐Charge‐Data/Inpatient2014.html
© American College of Clinical Pharmacy 21

2016 ACCP Annual Meeting
ED Avoidance: Limitations
• Heavy on quick turn around paperwork• Insurance verification
• Coding and billing
• Potential to delay treatment
• If patient is admitted, potential to lose money
• Role of drug restriction
2016 ACCP Annual Meeting
Summary
• New agents are expensive compared to old agents, but may have LOSbenefit when used appropriately.
• Effective use of new agents will take well designed protocols that notall hospitals have ready. Many times, old agents will work for plenty of patients.
• No new agent has been prove superior.
• Assess infections appropriately for severity, placing patients into theappropriate treatment environment.
• Utilize agents in situations that justify the high cost of new agents
2016 ACCP Annual Meeting
The Treatment of ABSSSIs Caused by MRSA: If It Ain’tBroke, Don’t Try to Fix It!
Katherine Lusardi, PharmD, BCPS‐AQ ID
UAMS Medical Center, Hospital Pharmacy
Little Rock, AR
24 October 2016
2016 ACCP Annual Meeting
References1. 2016 ASP Drug Pricing Files. Centers for Medicare and Medicaid. https://www.cms.gov/Medicare/Medicare‐Fee‐for‐Service‐Part‐B‐
Drugs/McrPartBDrugAvgSalesPrice/2016ASPFiles.html. Accessed 10 September 2016.
2. Corey GR, Kabler H, Mehra P, et al. Single‐dose oritavancin in the treatment of acute bacterial skin infections. N Engl J Med. 2014; 370: 2180‐2190.
3. Corey GR, Good S, Jiang H, et al. Single‐dose oritavancin versus 7‐10 days of vancomycin in the treatment of gram‐positive acute bacterial skin and skin structure infections: the SOLO II noninferiority study. Clin Infect Dis. 2015; 254‐262.
4. Boucher HW, Wilcox M, Talbot GH, Puttagunta S, Das AF, Dunne MW. Once‐weekly dalbavancin versus daily conventional therapy for skin infection. N Engl J Med. 2014;370(23):2169‐2179.
5. Wilcox MH, Corey GR, Talbot GH, et al. CANVAS 2: the second Phase III, randomized, double‐blind study evaluating ceftaroline fosamil for the treatment of patients with complicated skin and skin structure infections. J Antimicrob Chemother. 2010; S4: iv53‐iv65.
6. Corey GR, Wilcox MH, Talbot GH, et al. CANVAS 1: the first Phase III, randomized, double‐blind study evaluating ceftaroline fosamil for the treatment of patients with complicated skin and skin structure infections. J Antimicrob Chemother. 2010; S4: iv41‐iv51.
7. Stryjewski ME, Graham DR, Wilson SE, et al. Telavancin versus vancomycin for the treatment of complicated skin and skin‐structure infections caused by gram‐positive organisms. ClinInfect Dis. 2008; 43: 1683‐1693.
8. Prokocimer P, De Anda C, Fang E, et al: Tedizolid phosphate vs linezolid for treatment of acute bacterial skin and skin structure infections: the ESTABLISH‐1 randomized trial. JAMA. 2013;309: 559‐569.
9. Moran GJ, Fang E, Corey GR, et al: Tedizolid for 6 days versus linezolid for 10 days for acute bacterial skin and skin‐structure infections (ESTABLISH‐2): a randomised, doubleblind, phase3, non‐inferiority trial. Lancet Infect Dis . 2014; 14: 696‐705
10. Talan DA, Salhi BA, Moran GJ, et al. Factors associated with decision to hospitalize emergency department patients with skin and soft tissue infection. West J Emerg Med. 2015; 16: 89‐97.
11. McCurdy SP, Jones RN, Mendes RE, Puttagunta S, Dunne MW. In Vitro Activity of Dalbavancin against Drug‐Resistant Staphylococcus aureus Isolates from a Global Surveillance Program. Antimicrob Agent Chemother. 2015; 59(8): 5007‐5009.
12. Sader HS, Farrell DJ, Flamm RK, Jones RN. Activity of ceftaroline and comparator agents tested against Staphylococcus aureus from patients with bloodstream infections in US medicalcentres (2009–13). J Antimicrob Chemother. 2015; 70(7): 2053‐2056.
2016 ACCP Annual Meeting
References13. Mendes RE, Sader HS, Flamm RK, Farrell DJ, Jones RN. Telavancin In Vitro Activity against a Collection of Methicillin‐Resistant Staphylococcus aureus Isolates, Including Resistant Subsets, from the United
States. AntimicrobAgent Chemother. 2015; 59(3): 1811‐1814.
14. Mendes RE, Farrell DJ, Sader HS, Flamm RK, Jones RN. Activity of oritavancin against Gram‐positive clinical isolates responsible for documented skin and soft‐tissue infections in European and US hospitals(2010–13). J AntimicrobChemother. 2015; 70(2): 498‐504.
15. Mendes RE, Farrell DJ, Sader HS, Flamm RK, Jones RN. Baseline Activity of Telavancin against Gram‐Positive Clinical Isolates Responsible for Documented Infections in U.S. Hospitals (2011‐2012) as Determined by the Revised Susceptibility Testing Method. Antimicrob Agent Chemother. 2014; 59(1): 702‐706.
16. Mendes RE, Sader HS, Flamm RK, Farrell DJ, Jones RN. Oritavancin Activity against Staphylococcus aureus Causing Invasive Infections in U.S. and European Hospitals: a 5‐Year International SurveillanceProgram. AntimicrobAgent Chemother. 2014; 58(5): 2921‐2924.
17. Pfaller MA, Flamm RK, Jones RN, Farrell DJ, Mendes RE. Activities of Tedizolid and Linezolid Determined by the Reference Broth MicrodilutionMethod against 3,032 Gram‐Positive Bacterial Isolates Collected in Asia‐Pacific, Eastern Europe, and Latin American Countries in 2014. AntimicrobAgent Chemother. 2016; 60(9): 5393‐5399.
18. May LS, ZocchiM, Zatorski C, et al. Treatment failure outcomes for emergency department patients with skin and soft tissue infections. West J EmergMed. 2015; 16: 642‐652.
19. Cenizal MJ, Skiest D, Luber S, et al. Prospective randomized trial of empiric therapy with trimethoprim‐sulfamethoxazole or doxycycline for outpatient skin and soft tissue infections in an area of high prevalence of methicillin resistant Staphylococcus aureus. AntimicrobAgent Chemother. 2007; 2628‐2630.
20. Ruhe JJ, Menon A. tetracyclines as an oral treatment option for patients with community onset skin and soft tissue infections caused by methicillin‐resistant Staphylococcus aureus. Antimicrob AgentChemother. 2007; 3298‐3303.
21. Ruhe JJ, Smith N, Bradsher RW, Menon A. Community‐onset methicillin‐resistant Staphylococcus aureus skin and soft‐tissue infections: impact of antimicrobial therapy on outcome. Clin Infect Dis. 2007;44:777‐784.
22. Seaton RA. Daptomycin: rationale and role in the management of skin and soft tissue infections. J AntimicrobChemother . 2008; S3: iii15‐iii23.
23. RentalaM, Andrews S, Tiberio A, Alagappan K, Tavdy T, et al. Intravenous Home Infusion Therapy Instituted From a 24‐Hour Clinical Decision Unit For Patients With Cellulitis. Am J Emerg Med. 2016; 1273‐1275.
24. Mistry RD, Hirsch AW, Woodford AL, Lundy M. Failure of emergency department observation unit treatment for skin and soft tissue infections. J EmergMed. 2015; 49: 855‐863.
25. Claeys KC, Lagnf AM, Patel TB, et al. Acute bacterial skin and skin structure infections treated with intravenous antibiotics in the emergency department or observation unit: experience at the DetroitMedical Center. Infect Dis Ther. 2015; 4: 173‐186.
26. Inpatient Charge Data FY 2014. Centers for Medicare and Medicaid. https://www.cms.gov/Research‐Statistics‐Data‐and‐Systems/Statistics‐Trends‐and‐Reports/Medicare‐Provider‐Charge‐Data/Inpatient2014.html. Accessed 10 September 2016.
© American College of Clinical Pharmacy 22