Adult Antimicrobial Treatment Guide -...
26
1 Adult Antimicrobial Treatment Guide 2 nd Edition, October 2012 Doses are based on normal renal function This guide refers to non-pregnant adults unless stated otherwise. Useful contact numbers: Extension Bleep Microbiology results 5457 Medical Microbiologists: Dr Anan Ghazy 5401 Dr Adnan Aali 5456 Dr Priya Khanna 5452 Infectious Diseases Pharmacist: Kam Cheema 5541 321 Infectious Diseases Team: Registrars 250 Consultants (Dr Sandhu/Lynn/Ash) Via switchboard Medicines information 5303
Transcript of Adult Antimicrobial Treatment Guide -...
1
Adult Antimicrobial Treatment Guide
2nd Edition, October 2012
Doses are based on normal renal function This guide refers to non-pregnant adults unless stated otherwise.
Useful contact numbers:
Extension Bleep
Microbiology results 5457
Medical Microbiologists:
Dr Anan Ghazy 5401
Dr Adnan Aali 5456
Dr Priya Khanna 5452
Infectious Diseases Pharmacist:
Kam Cheema 5541 321
Infectious Diseases Team:
Registrars 250
Consultants (Dr Sandhu/Lynn/Ash) Via switchboard
Medicines information 5303
2
Drugs in RED are contra-indicated in penicillin allergy
Drugs in AMBER should be prescribed with caution and only if penicillin allergy is less severe
Drugs in GREEN are considered safe
IN PATIENTS WITH PENICILLIN ALLERGY THE SYMPTOMS OF THE
REACTION MUST BE DOCUMENTED ON THE DRUG CHART
Severe penicillin allergy = anaphylactic reactions. These patients
must not be given any beta-lactam agents (RED & AMBER).
Less severe penicillin allergy = e.g. rash only. These patients may be
given carbapenems and cephalosporins (AMBER) if there is no
satisfactory alternative and the benefits outweigh the risks of cross
sensitivity.
3
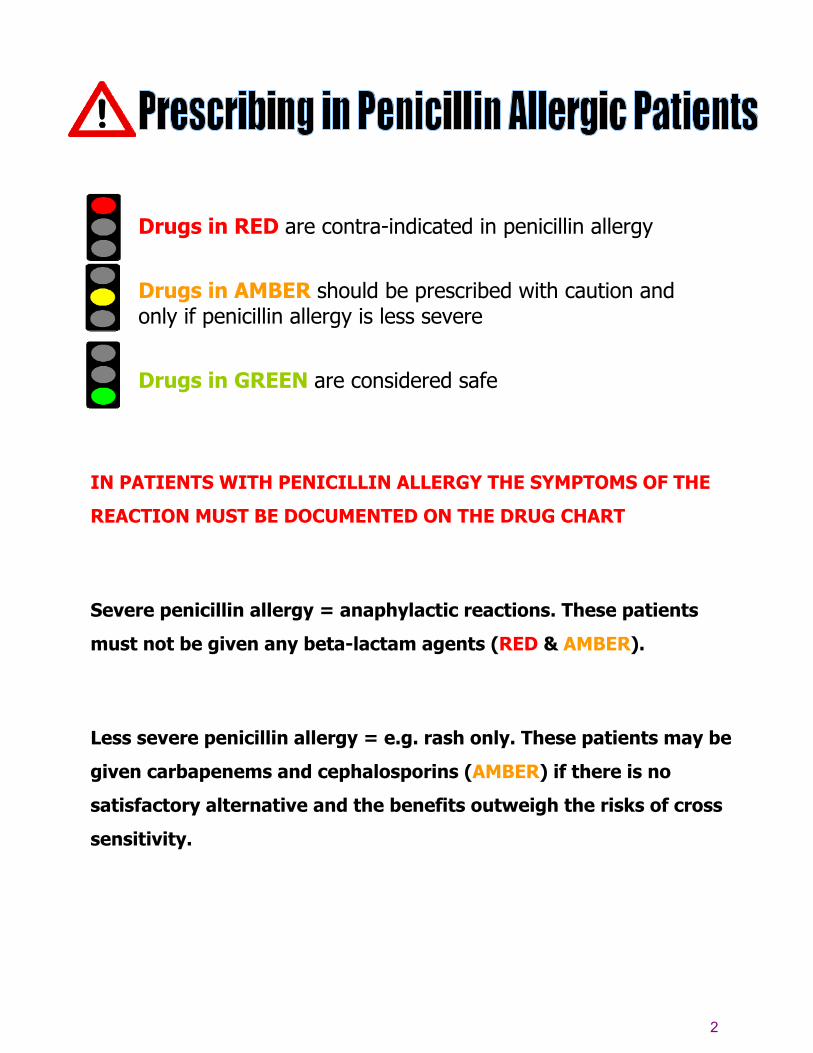
Guidance on prescribing antibiotics
STEP 1 (Start Smart) Send microbiology samples
Empiric choice of Antibiotic (See appropriate guidelines) Use oral therapy whenever possible
STEP 2 (then Focus) 48 hour REVIEW
Check l) response to empiric antibiotic ll) microbiology culture and sensitivity results
No or poor response to empiric antibiotic
Fair to good response to empiric antibiotic
STOP Discuss with micro-biologists
Consider alternative regimen
Known organism
YES NO
Switch to more specific, narrow spectrum antibiotic, as sensitivities
indicate Use oral whenever possible or consider OPAT
Switch to oral equivalent regimen
if possible
4
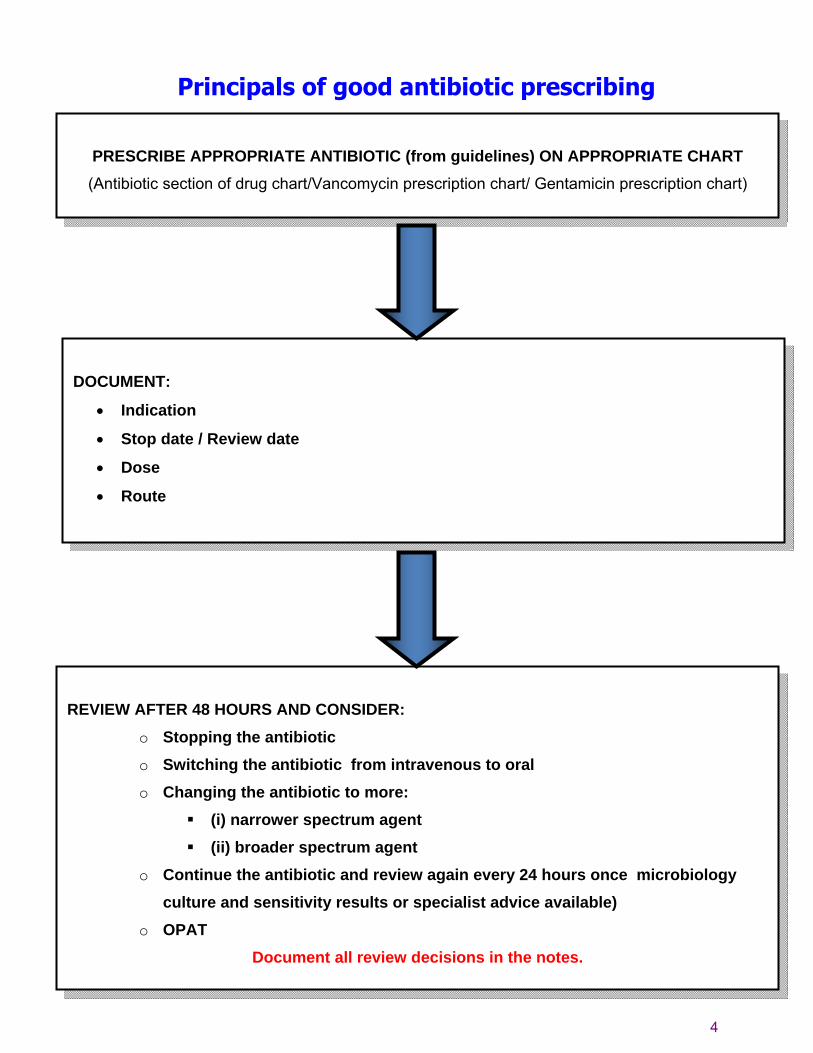
Principals of good antibiotic prescribing
PRESCRIBE APPROPRIATE ANTIBIOTIC (from guidelines) ON APPROPRIATE CHART (Antibiotic section of drug chart/Vancomycin prescription chart/ Gentamicin prescription chart)
DOCUMENT:
• Indication
• Stop date / Review date
• Dose
• Route
REVIEW AFTER 48 HOURS AND CONSIDER:
o Stopping the antibiotic o Switching the antibiotic from intravenous to oral o Changing the antibiotic to more:
(i) narrower spectrum agent (ii) broader spectrum agent
o Continue the antibiotic and review again every 24 hours once microbiology culture and sensitivity results or specialist advice available)
o OPAT Document all review decisions in the notes.
5
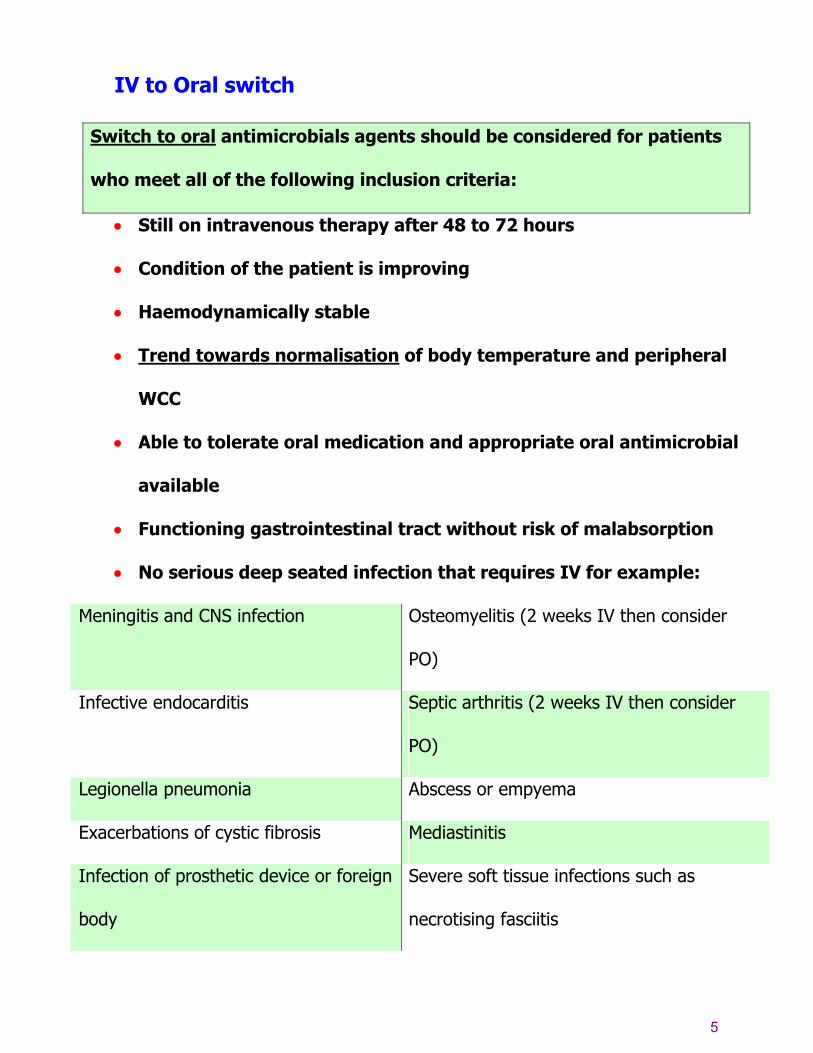
IV to Oral switch
Switch to oral antimicrobials agents should be considered for patients
who meet all of the following inclusion criteria:
• Still on intravenous therapy after 48 to 72 hours
• Condition of the patient is improving
• Haemodynamically stable
• Trend towards normalisation of body temperature and peripheral
WCC
• Able to tolerate oral medication and appropriate oral antimicrobial
available
• Functioning gastrointestinal tract without risk of malabsorption
• No serious deep seated infection that requires IV for example:
Meningitis and CNS infection Osteomyelitis (2 weeks IV then consider
PO)
Infective endocarditis Septic arthritis (2 weeks IV then consider
PO)
Legionella pneumonia Abscess or empyema
Exacerbations of cystic fibrosis Mediastinitis
Infection of prosthetic device or foreign
body
Severe soft tissue infections such as
necrotising fasciitis

6
Indications to continue IV therapy
• Continuing serious sepsis ( 2 or more of the following):
• Temperature >38oC or <36oC
• Tachycardia >90/min
• Tachypnoea >20 breaths/min
• WCC >12 or <4
• Febrile with neutropenia (WCC < 1.0)
Antimicrobials for which oral absorption is very good
Antimicrobial Percentage
oral
absorption
Notes
Ciprofloxacin
70 IV Ciprofloxacin only necessary when patient is NBM. Oral dosing
sustains high plasma concentrations for longer than IV.
400mg BD IV ≡ 750mg BD PO & 200mg BD IV ≡ 500mg BD PO
Clarithromycin 55 Use oral whenever possible despite erratic absorption - IV causes
phlebitis (rate not >5mg/min)
Clindamycin 90
Co-amoxiclav 60 - 85 1.2g TDS IV ≡ 625mg TDS PO & 600mg TDS IV ≡ 375mg TDS PO
Cotrimoxazole 90- 100
Flucloxacillin 50
Fluconazole 90
Linezolid 100
Metronidazole 100
Voriconazole 100
7
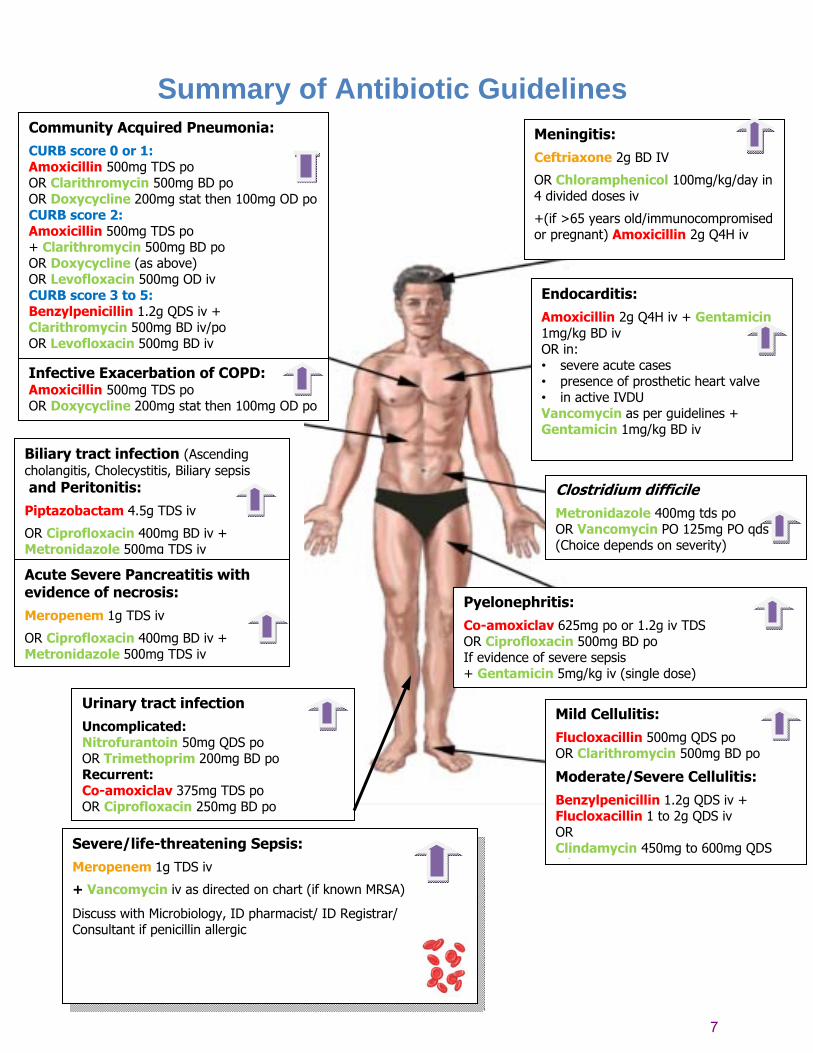
Summary of Antibiotic Guidelines
Meningitis:
Ceftriaxone 2g BD IV
OR Chloramphenicol 100mg/kg/day in 4 divided doses iv
+(if >65 years old/immunocompromised or pregnant) Amoxicillin 2g Q4H iv
Community Acquired Pneumonia:
CURB score 0 or 1: Amoxicillin 500mg TDS po OR Clarithromycin 500mg BD po OR Doxycycline 200mg stat then 100mg OD po CURB score 2: Amoxicillin 500mg TDS po + Clarithromycin 500mg BD po OR Doxycycline (as above) OR Levofloxacin 500mg OD iv CURB score 3 to 5: Benzylpenicillin 1.2g QDS iv + Clarithromycin 500mg BD iv/po OR Levofloxacin 500mg BD iv
Infective Exacerbation of COPD: Amoxicillin 500mg TDS po OR Doxycycline 200mg stat then 100mg OD po
Endocarditis:
Amoxicillin 2g Q4H iv + Gentamicin 1mg/kg BD iv OR in: • severe acute cases • presence of prosthetic heart valve • in active IVDU Vancomycin as per guidelines + Gentamicin 1mg/kg BD iv
Biliary tract infection (Ascending cholangitis, Cholecystitis, Biliary sepsis and Peritonitis:
Piptazobactam 4.5g TDS iv
OR Ciprofloxacin 400mg BD iv + Metronidazole 500mg TDS iv
Clostridium difficile
Metronidazole 400mg tds po OR Vancomycin PO 125mg PO qds (Choice depends on severity)
Pyelonephritis:
Co-amoxiclav 625mg po or 1.2g iv TDS OR Ciprofloxacin 500mg BD po If evidence of severe sepsis + Gentamicin 5mg/kg iv (single dose)
Mild Cellulitis:
Flucloxacillin 500mg QDS po OR Clarithromycin 500mg BD po
Moderate/Severe Cellulitis:
Benzylpenicillin 1.2g QDS iv + Flucloxacillin 1 to 2g QDS iv OR Clindamycin 450mg to 600mg QDS i /
Severe/life-threatening Sepsis:
Meropenem 1g TDS iv
+ Vancomycin iv as directed on chart (if known MRSA)
Discuss with Microbiology, ID pharmacist/ ID Registrar/ Consultant if penicillin allergic
Acute Severe Pancreatitis with evidence of necrosis:
Meropenem 1g TDS iv
OR Ciprofloxacin 400mg BD iv + Metronidazole 500mg TDS iv
Urinary tract infection
Uncomplicated: Nitrofurantoin 50mg QDS po OR Trimethoprim 200mg BD po Recurrent: Co-amoxiclav 375mg TDS po OR Ciprofloxacin 250mg BD po

8
Respiratory CONDITION DRUG DOSE DURATION Infective Exacerbation of COPD No radiological signs of consolidation. Only use antibiotics if real evidence of infection.
Amoxicillin OR Doxycycline
500mg TDS po 200mg stat then 100mg OD po
5 days 5 days
CURB score-0-1 Amoxicillin OR Clarithromycin OR Doxycycline
500mg TDS po 500mg BD po As above
5 days 5 days 5 days
CURB score-2 Amoxicillin + Clarithromycin OR Doxycycline OR Levofloxacin
500mg TDS po/iv 500mg BD po/iv 200mg stat then 100mg OD po 500mg OD iv
7 days 7 days 7 days
Community acquired pneumonia – Most patients can have oral therapy, IV only needed if severe (CURB-65 >3, or if unable to take orally. Send sputum and blood cultures in all cases. For severe pneumonia send urine cultures for legionella and pnemococcus. (Contact Microbiology if haemoptysis, multilobar infiltrates, cavitation, leucopenia +/- after a flu-like illness)
CURB score-3-5 Benzylpenicillin + Clarithromycin Or in cases of: • severe sepsis requiring ITU/HDU admission • influenza • substance misuse Co-amoxiclav + Clarithromycin OR Levofloxacin
1.2g QDS iv 500mg BD iv/po 1.2g TDS iv 500mg BD iv/po 500mg BD iv
7 days 7 days 7 days 7 days 7 days
Aspiration pneumonia Treatment should be with the relevant antibiotics as above but ensure there is adequate anaerobic cover + Metronidazole 400mg po / 500mg iv TDS. Co-amoxiclav and Piptazobactam have activity against anaerobes: there is no need to add Metronidazole. Early onset, mild to moderate: Doxycycline
As above
7 days
Pneumonia- hospital acquired Infection after hospital stay >3days. Evidence of new consolidation on CXR plus evidence of infection. Send sputum and blood cultures.
Severe: Piptazobactam OR Ciprofloxacin + Clarithromycin ADD Vancomycin (if MRSA+ve)
4.5g TDS iv 400mg BD iv 500mg BD iv iv (see page 13)
7 days 7 days
CURB-65 Score 1 point for each • Confusion
• Urea> 7 mmol/l
• Respiratory rate > 30/min
• Shock (systolic BP <
90mmHg, diastolic BP <
60mmHg)
• Age > 65 years
9
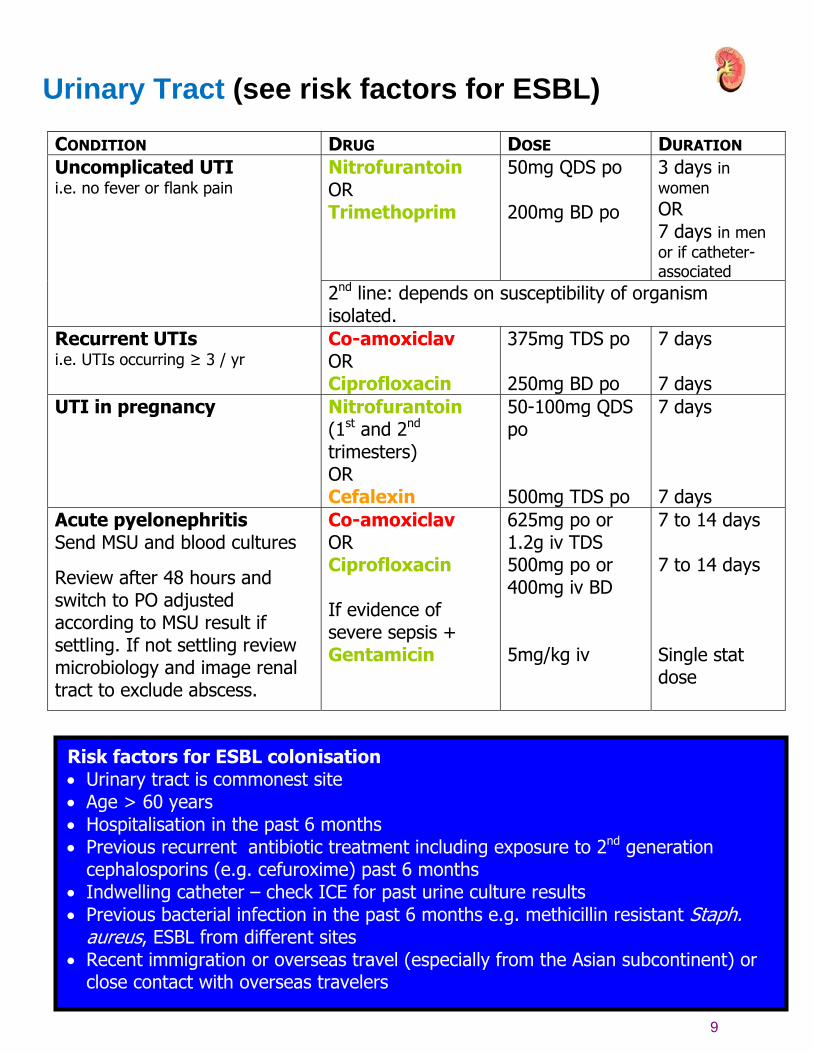
Urinary Tract (see risk factors for ESBL)
CONDITION DRUG DOSE DURATION Nitrofurantoin OR Trimethoprim
50mg QDS po 200mg BD po
3 days in women OR 7 days in men or if catheter-associated
Uncomplicated UTI i.e. no fever or flank pain
2nd line: depends on susceptibility of organism isolated.
Recurrent UTIs i.e. UTIs occurring ≥ 3 / yr
Co-amoxiclav OR Ciprofloxacin
375mg TDS po 250mg BD po
7 days 7 days
UTI in pregnancy Nitrofurantoin (1st and 2nd trimesters) OR Cefalexin
50-100mg QDS po 500mg TDS po
7 days 7 days
Acute pyelonephritis Send MSU and blood cultures
Review after 48 hours and switch to PO adjusted according to MSU result if settling. If not settling review microbiology and image renal tract to exclude abscess.
Co-amoxiclav OR Ciprofloxacin If evidence of severe sepsis + Gentamicin
625mg po or 1.2g iv TDS 500mg po or 400mg iv BD 5mg/kg iv
7 to 14 days 7 to 14 days Single stat dose
Risk factors for ESBL colonisation • Urinary tract is commonest site • Age > 60 years • Hospitalisation in the past 6 months • Previous recurrent antibiotic treatment including exposure to 2nd generation
cephalosporins (e.g. cefuroxime) past 6 months • Indwelling catheter – check ICE for past urine culture results • Previous bacterial infection in the past 6 months e.g. methicillin resistant Staph.
aureus, ESBL from different sites • Recent immigration or overseas travel (especially from the Asian subcontinent) or
close contact with overseas travelers

10
Gastrointestinal
CONDITION DRUG DOSE DURATION Biliary tract infection Ascending cholangitis Cholecystitis Biliary sepsis
Piptazobactam OR Ciprofloxacin + Metronidazole If less severe penicillin allergy contact microbiology for advice
4.5 g TDS iv 400mg BD iv 500mg TDS iv
7 days
Peritonitis Piptazobactam OR Ciprofloxacin + Metronidazole If less severe penicillin allergy contact microbiology for advice
4.5 g TDS iv 400mg BD iv 500mg TDS iv
7 days
Acute severe Pancreatitis No antibiotics unless evidence of necrosis:
Acute severe Pancreatitis with evidence of necrosis
Meropenem OR Ciprofloxacin + Metronidazole
1g TDS iv 400mg BD iv 500mg TDS iv
7 to 14 days and then review
Clostridium difficile diarrhoea
Stop precipitating antibiotic therapy if possible- See guidelines page 16
Helicobacter pylori eradication
See appropriate section of the latest edition of the British National Formulary
11
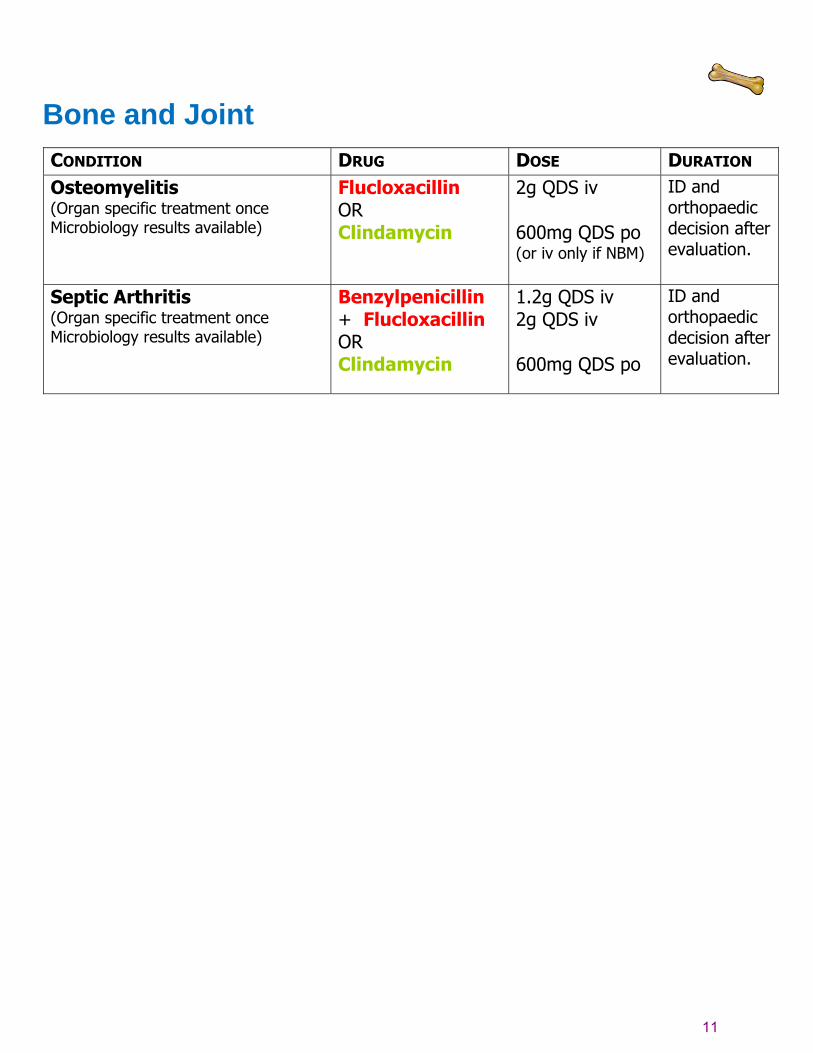
Bone and Joint
CONDITION DRUG DOSE DURATION Osteomyelitis (Organ specific treatment once Microbiology results available)
Flucloxacillin OR Clindamycin
2g QDS iv 600mg QDS po (or iv only if NBM)
ID and orthopaedic decision after evaluation.
Septic Arthritis (Organ specific treatment once Microbiology results available)
Benzylpenicillin + Flucloxacillin OR Clindamycin
1.2g QDS iv 2g QDS iv 600mg QDS po
ID and orthopaedic decision after evaluation.
12
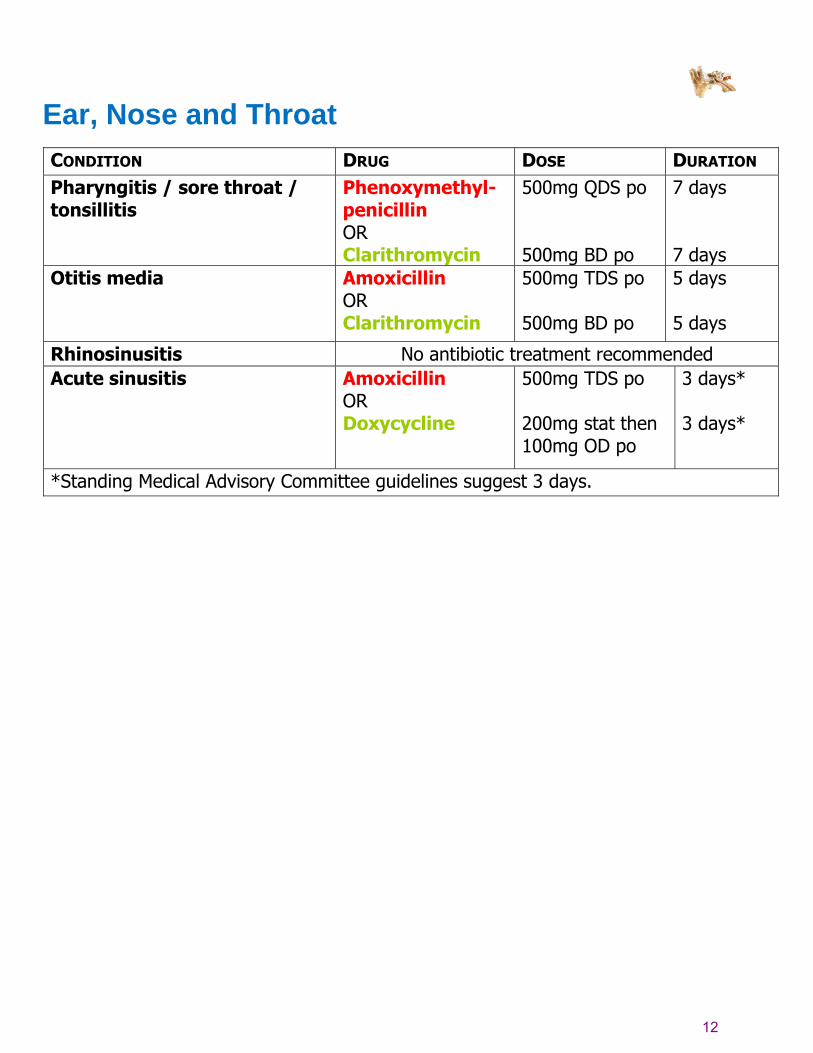
Ear, Nose and Throat
CONDITION DRUG DOSE DURATION Pharyngitis / sore throat / tonsillitis
Phenoxymethyl-penicillin OR Clarithromycin
500mg QDS po 500mg BD po
7 days 7 days
Otitis media Amoxicillin OR Clarithromycin
500mg TDS po 500mg BD po
5 days 5 days
Rhinosinusitis No antibiotic treatment recommended Acute sinusitis Amoxicillin
OR Doxycycline
500mg TDS po 200mg stat then 100mg OD po
3 days* 3 days*
*Standing Medical Advisory Committee guidelines suggest 3 days.
13
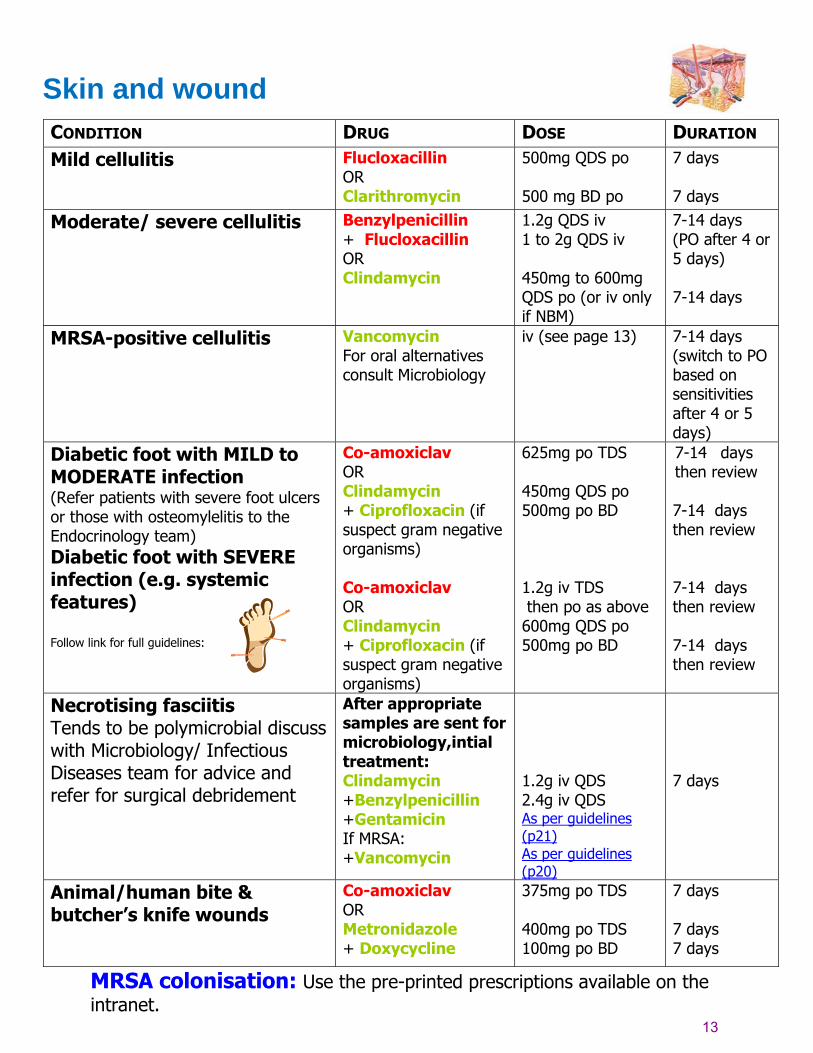
Skin and wound
CONDITION DRUG DOSE DURATION Mild cellulitis Flucloxacillin
OR Clarithromycin
500mg QDS po 500 mg BD po
7 days 7 days
Moderate/ severe cellulitis Benzylpenicillin + Flucloxacillin OR Clindamycin
1.2g QDS iv 1 to 2g QDS iv 450mg to 600mg QDS po (or iv only if NBM)
7-14 days (PO after 4 or 5 days) 7-14 days
MRSA-positive cellulitis Vancomycin For oral alternatives consult Microbiology
iv (see page 13)
7-14 days (switch to PO based on sensitivities after 4 or 5 days)
Diabetic foot with MILD to MODERATE infection (Refer patients with severe foot ulcers or those with osteomylelitis to the Endocrinology team) Diabetic foot with SEVERE infection (e.g. systemic features) Follow link for full guidelines:
Co-amoxiclav OR Clindamycin + Ciprofloxacin (if suspect gram negative organisms) Co-amoxiclav OR Clindamycin + Ciprofloxacin (if suspect gram negative organisms)
625mg po TDS 450mg QDS po 500mg po BD 1.2g iv TDS then po as above 600mg QDS po 500mg po BD
7-14 days then review 7-14 days then review 7-14 days then review 7-14 days then review
Necrotising fasciitis Tends to be polymicrobial discuss with Microbiology/ Infectious Diseases team for advice and refer for surgical debridement
After appropriate samples are sent for microbiology,intial treatment: Clindamycin +Benzylpenicillin +Gentamicin If MRSA: +Vancomycin
1.2g iv QDS 2.4g iv QDS As per guidelines (p21) As per guidelines (p20)
7 days
Animal/human bite & butcher’s knife wounds
Co-amoxiclav OR Metronidazole + Doxycycline
375mg po TDS 400mg po TDS 100mg po BD
7 days 7 days 7 days
MRSA colonisation: Use the pre-printed prescriptions available on the intranet.
14
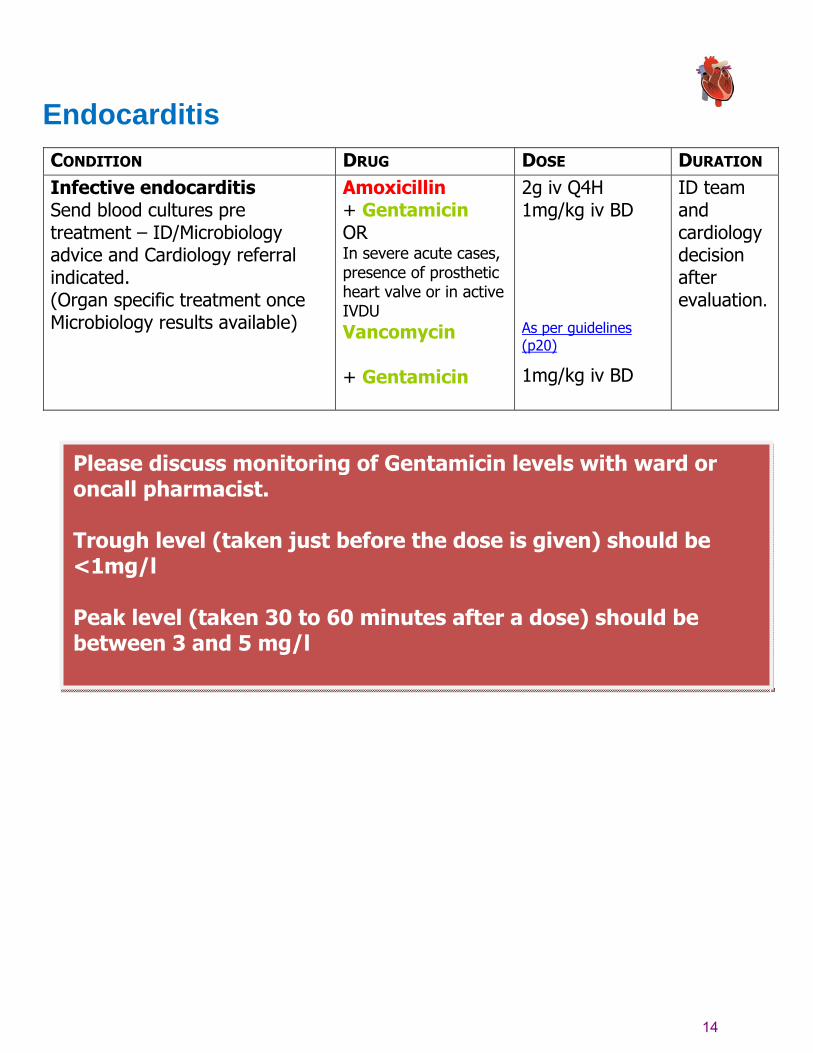
Endocarditis
CONDITION DRUG DOSE DURATION Infective endocarditis Send blood cultures pre treatment – ID/Microbiology advice and Cardiology referral indicated. (Organ specific treatment once Microbiology results available)
Amoxicillin + Gentamicin OR In severe acute cases, presence of prosthetic heart valve or in active IVDU Vancomycin + Gentamicin
2g iv Q4H 1mg/kg iv BD
As per guidelines (p20)
1mg/kg iv BD
ID team and cardiology decision after evaluation.
Please discuss monitoring of Gentamicin levels with ward or oncall pharmacist. Trough level (taken just before the dose is given) should be <1mg/l Peak level (taken 30 to 60 minutes after a dose) should be between 3 and 5 mg/l

15
Sexual Health (Refer patients with STDs to the GU clinic on 8 North) CONDITION DRUG DOSE DURATION Vaginal candidiasis Clotrimazole
OR Fluconazole
500mg pessary 150mg po
STAT STAT
Acute epididymo-orchitis Ciprofloxacin
500mg BD po 10 to 14 days
Pelvic Inflammatory disease Ceftriaxone + Metronidazole + Doxycycline OR Ofloxacin + Metronidazole
500mg im 400mg BD po 100mg BD po 400mg BD po 400mg BD po
STAT 14 days 14 days 14 days 14 days
HIV There is an oncall HIV consultant for advice about treatment of patients (contact via switchboard). Advice regarding post exposure prophylaxis should be accessed via 0ccupational Health or the A&E department if out of hours.
16
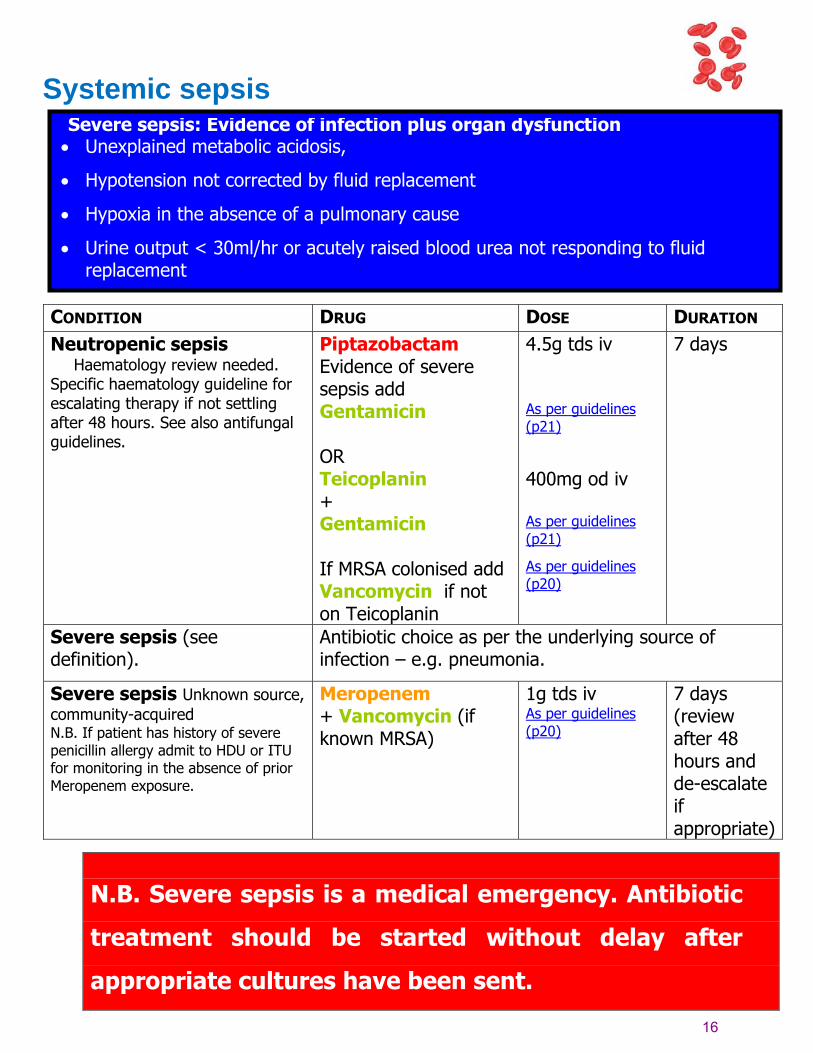
Systemic sepsis
CONDITION DRUG DOSE DURATION Neutropenic sepsis Haematology review needed. Specific haematology guideline for escalating therapy if not settling after 48 hours. See also antifungal guidelines.
Piptazobactam Evidence of severe sepsis add Gentamicin
OR Teicoplanin + Gentamicin If MRSA colonised add Vancomycin if not on Teicoplanin
4.5g tds iv As per guidelines (p21)
400mg od iv As per guidelines (p21)
As per guidelines (p20)
7 days
Severe sepsis (see definition).
Antibiotic choice as per the underlying source of infection – e.g. pneumonia.
Severe sepsis Unknown source, community-acquired N.B. If patient has history of severe penicillin allergy admit to HDU or ITU for monitoring in the absence of prior Meropenem exposure.
Meropenem + Vancomycin (if known MRSA)
1g tds iv As per guidelines (p20)
7 days (review after 48 hours and de-escalate if appropriate)
N.B. Severe sepsis is a medical emergency. Antibiotic
treatment should be started without delay after
appropriate cultures have been sent.
Severe sepsis: Evidence of infection plus organ dysfunction • Unexplained metabolic acidosis,
• Hypotension not corrected by fluid replacement
• Hypoxia in the absence of a pulmonary cause
• Urine output < 30ml/hr or acutely raised blood urea not responding to fluid replacement
17
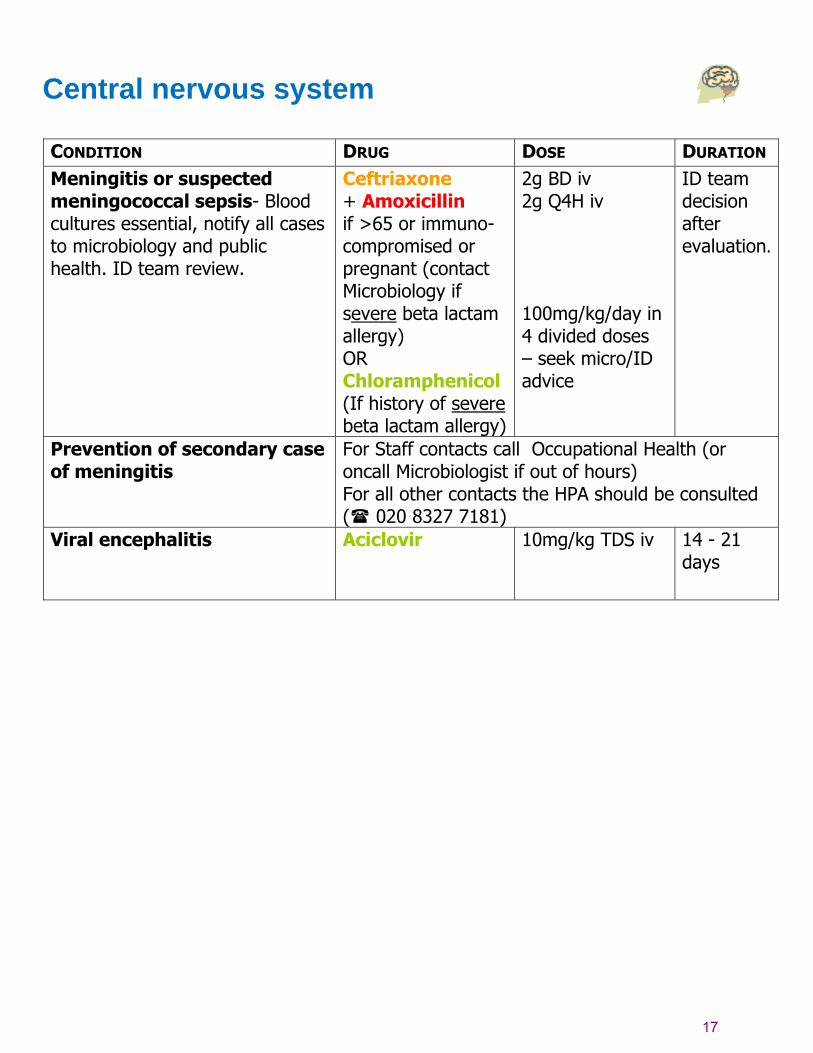
Central nervous system
CONDITION DRUG DOSE DURATION Meningitis or suspected meningococcal sepsis- Blood cultures essential, notify all cases to microbiology and public health. ID team review.
Ceftriaxone + Amoxicillin if >65 or immuno-compromised or pregnant (contact Microbiology if severe beta lactam allergy) OR Chloramphenicol (If history of severe beta lactam allergy)
2g BD iv 2g Q4H iv 100mg/kg/day in 4 divided doses – seek micro/ID advice
ID team decision after evaluation.
Prevention of secondary case of meningitis
For Staff contacts call Occupational Health (or oncall Microbiologist if out of hours) For all other contacts the HPA should be consulted ( 020 8327 7181)
Viral encephalitis Aciclovir 10mg/kg TDS iv
14 - 21 days

18
Travel related infections
Patients with infections relating to recent overseas travel should be referred to the
Infectious Diseases team
N.B. Severe malaria is a medical emergency. After
rapid clinical assessment and confirmation of the
diagnosis, full doses of parenteral anti-malarial
treatment should be started without delay with any
effective malarial first available
See malaria treatment algorithm:
MalariaAlgorithm07.pdf

19
Restricted antibiotics
Unless part of the approved Trust guideline the following antimicrobials are only to be prescribed with Microbiology/Infectious Diseases approval:
x Amikacin x Carbapenems (e.g. Meropenem, Imipenem & Ertapenem) x Cephalosporins (e.g. Ceftazidime & Ceftriaxone) x Ciprofloxacin Injection x Piptazobactam x Teicoplanin x Vancomycin
The following antimicrobials are only to be prescribed with Microbiology/Infectious Diseases approval:
x Fosfomycin x Liposomal Amphotericin x Caspofungin Injection x Flucytosine x Daptomycin x Linezolid x Tigecycline x Temocillin x Voriconazole
20
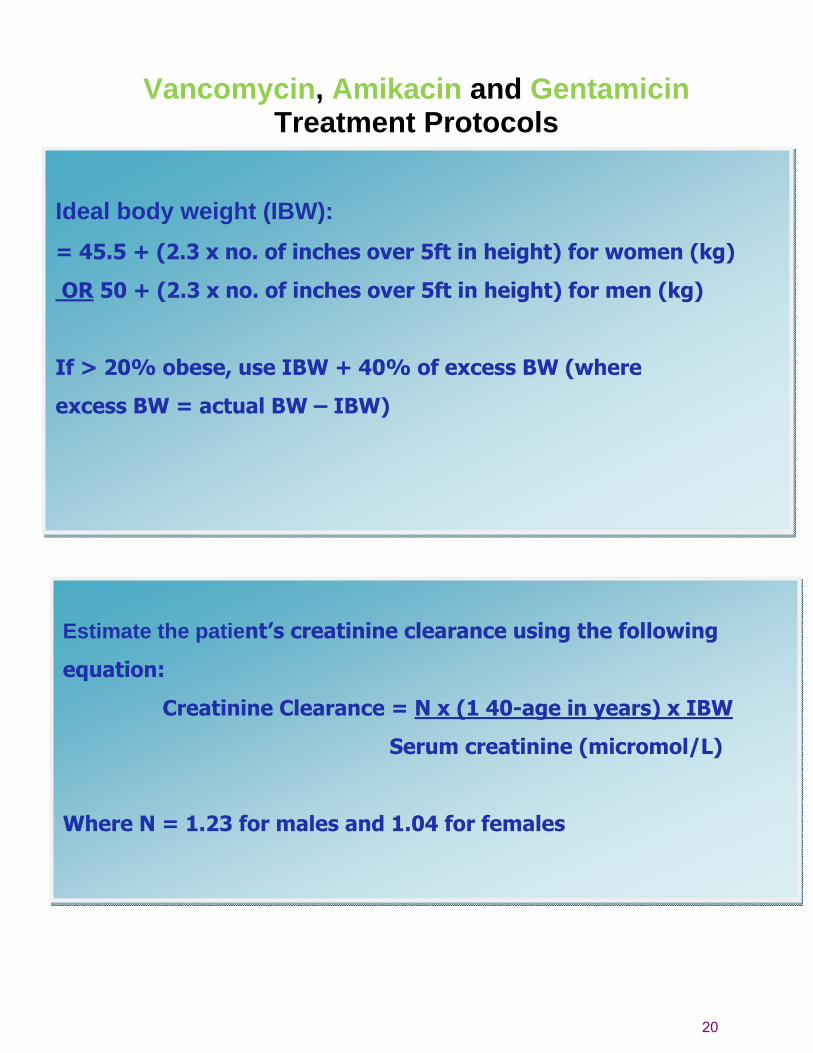
Vancomycin, Amikacin and Gentamicin Treatment Protocols
Ideal body weight (IBW): = 45.5 + (2.3 x no. of inches over 5ft in height) for women (kg) OR 50 + (2.3 x no. of inches over 5ft in height) for men (kg)
If > 20% obese, use IBW + 40% of excess BW (where
excess BW = actual BW – IBW)
Estimate the patient’s creatinine clearance using the following
equation:
Creatinine Clearance = N x (1 40-age in years) x IBW
Serum creatinine (micromol/L)
Where N = 1.23 for males and 1.04 for females

21
Vancomycin Treatment Protocol
(use separate Vancomycin prescription) DOSE
ADMINISTRATION
The infusion rate should not exceed 10mg/min (e.g. 1g over 100 to 120 minutes). Final concentration should not exceed 5mg/ml.
MONITORING N.B. Remember to write dosing and sampling times on the request form AIM for a trough Vancomycin level of 10-15mg/L (except endocarditis)
• Measure first trough level immediately before the 3rd or 4th dose. • Measure trough levels every 3 to 4 days. • Repeat the trough level before the 3rd or 4th dose
o Following a dose adjustment o If renal function changes
• There is no need to monitor peak Vancomycin levels, except in patients with bacterial endocarditis (aim for trough level of 15-20mg/L in endocarditis) INTERPRETING RESULTS
• Unless specifically advised, it is not necessary to wait for the results of the level before administering the dose
• In general, if the trough level is high, increase the dose interval; if the trough level is low, reduce the dose interval or increase the dose.
• If in doubt seek advice from Medicines Information, ext 5303, or the ward Pharmacist.
Creatinine clearance
(ml/min)
Weight
<60kg
Weight
>60kg
<20 Give a 1g dose- take a level every 24 hours-redose with 1g when the
level is less than 10mg/L
20-39 750mg daily 1g daily
40-59 500mg twice daily 750mg twice daily
60-100 750mg twice daily 1g twice daily
>100 1g twice daily 1.25g twice daily
22
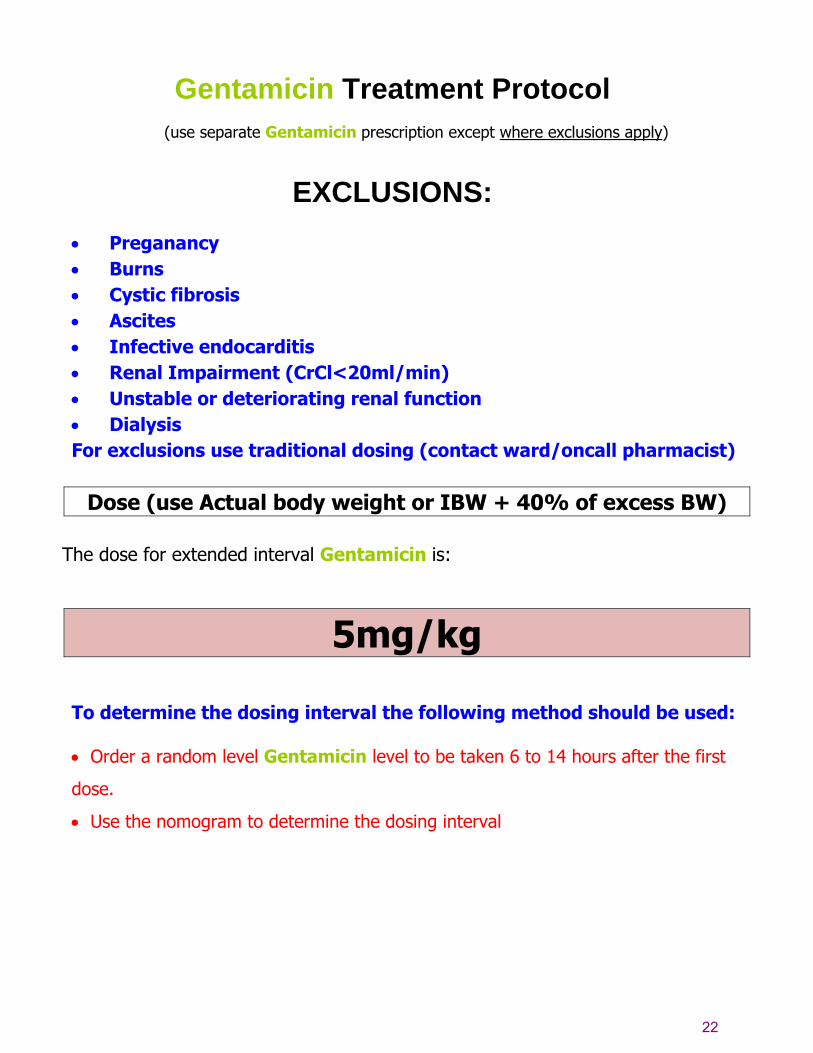
Gentamicin Treatment Protocol
(use separate Gentamicin prescription except where exclusions apply)
EXCLUSIONS:
• Preganancy • Burns • Cystic fibrosis • Ascites • Infective endocarditis • Renal Impairment (CrCl<20ml/min) • Unstable or deteriorating renal function • Dialysis For exclusions use traditional dosing (contact ward/oncall pharmacist)
Dose (use Actual body weight or IBW + 40% of excess BW)
The dose for extended interval Gentamicin is:
5mg/kg To determine the dosing interval the following method should be used: • Order a random level Gentamicin level to be taken 6 to 14 hours after the first
dose.
• Use the nomogram to determine the dosing interval

23
ADMINISTRATION
Each extended interval dose should be given as an infusion, over 1 hour, in 100ml
of either dextrose 5% or sodium chloride 0.9%.
MONITORING
You do not need to measure peak levels.
Measure the predose (trough) levels TWICE weekly if renal function stable
Predose Gentamicin level should be ≤ 1mg/L.
Check serum creatininine regularly as appropriate: in elderly patients and
those with fluctuating renal function this may be required daily.
DURATION
Should be given for maximum of 5 days – for any longer duration please contact Microbiology. Back
24
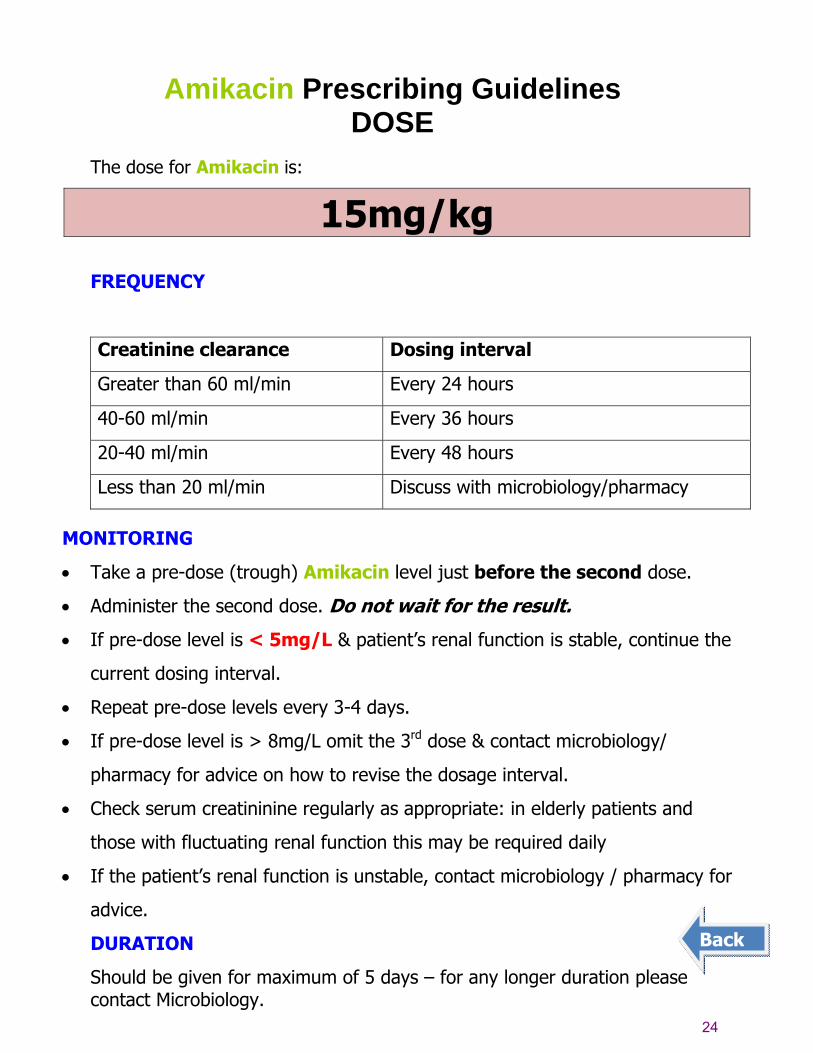
Amikacin Prescribing Guidelines
DOSE The dose for Amikacin is:
15mg/kg
FREQUENCY
Creatinine clearance Dosing interval
Greater than 60 ml/min Every 24 hours
40-60 ml/min Every 36 hours
20-40 ml/min Every 48 hours
Less than 20 ml/min Discuss with microbiology/pharmacy
MONITORING
• Take a pre-dose (trough) Amikacin level just before the second dose.
• Administer the second dose. Do not wait for the result.
• If pre-dose level is < 5mg/L & patient’s renal function is stable, continue the
current dosing interval.
• Repeat pre-dose levels every 3-4 days.
• If pre-dose level is > 8mg/L omit the 3rd dose & contact microbiology/
pharmacy for advice on how to revise the dosage interval.
• Check serum creatininine regularly as appropriate: in elderly patients and
those with fluctuating renal function this may be required daily
• If the patient’s renal function is unstable, contact microbiology / pharmacy for
advice.
DURATION
Should be given for maximum of 5 days – for any longer duration please contact Microbiology.
Back

25
Management of Clostridium difficile (C.diff) guidelines
Clostridium difficile infection (CDI) 1st/2nd episode
Diarrhoea and one of the following: Positive C.diff toxin test or results of C.diff test pending and clinical suspicion of CDI
Symptoms/signs: not severe CDI
Metronidazole PO 400mg tds 14 days
Symptoms/signs: severe CDI • WCC>15 • Acute rising creatinine • T>38.5oC • or signs/symptoms of severe colitisVancomycin PO 125mg PO qds 14 days
Daily assessment (include review of fluids/electrolytes)
Symptoms improving Diarrhoea should resolve in 1-2 weeks Recurrence occurs in ~ 20% after 1st
episode: 40% after 2nd episode
Symptoms not improving or worsening
Should not normally be deemed a treatment failure until received at least one week of treatment. However, if evidence of severe CDI continues or worsens:
Surgery & ID consultation
AND switch to: Vancomycin 250mg PO/NG qds +
Metronidazole 500mg IV tds 14 days
Symptoms not improving or worsening
Should not normally be deemed a treatment failure until received at least one week of treatment. However, if evidence of severe CDI: WCC>15 • Acute rising creatinine • T>38.5oC
or signs/symptoms of severe colitis
Switch to oral Vancomycin 125mg PO/NG qds 14 days
Ideally stop non-C.diff antibiotics to allow normal intestinal flora to be re-established.
Discontinue any other diarrhoea-causing medication if possible.
Suspected cases must be isolated.
Back
Further ID/GI/Surgery multi-disciplinary review (see next page)
N.B. As PO Vancomycin is not absorbed it is not necessary to measure blood levels.

26
Recurrent Clostridium difficile diarrhoea ≥ 3rd episode
Further ID/GI/Surgery multi-disciplinary review Consider the following: 1 Vancomycin 500mg PO/NG qds 2 IV Immunoglobulin 400mg/kg single dose (consider repeat) 3 Surgical Intervention 4 Intracolonic Vancomycin (500mg in 100ml saline every 4 to 12 hourly) Given as retention enema; 18 gauge Foley catheter with 30ml balloon inserted per rectum: vancomycin instilled; catheter clamped for 60 minutes; deflate and remove
Manage acute disease as per algorithm:
1 Vancomycin 125mg qds PO/NG qds 14 days
2 ID referal is MANDATORY
3 tapering Vancomycin regimen e.g.:
o Vancomycin 125mg every 6 hours for 7 days followed by o Vancomycin 125mg every 12 hours for 7 days followed by o Vancomycin 125mg every day 7 days followed by o Vancomycin 125mg every other day for 7 days followed by o Vancomycin 125mg every 3 days for 7 days then stop.
Warning:
After resolution of Clostridium difficile, any further antibiotic
use in the next 3 months, should be discussed with Micro/ID