Adherence & HIV Variability in intervention and standard care impacts treatment outcomes in HAART...
36
Adherence & HIV Variability in intervention and standard care impacts treatment outcomes in HAART adherence intervention trials: A meta-analysis or RCTs Marijn de Bruin Wageningen & Maastricht University, the Netherlands
-
Upload
brittney-hopkins -
Category
Documents
-
view
221 -
download
0
Transcript of Adherence & HIV Variability in intervention and standard care impacts treatment outcomes in HAART...

Adherence & HIV
Variability in intervention and standard care impacts treatment outcomes in HAART adherence intervention
trials: A meta-analysis or RCTs
Marijn de BruinWageningen & Maastricht University, the Netherlands
The treatment of HIV• HIV/AIDS & treatment
• High adherence levels important
• Many patients do not achieve or maintain that
• Treatment escalation: viral resistance, opp. infections
Supporting adherence important health care objective

Behavior change interventions
• (Non)Adherence is a behavior
• Causes behavior: ‘determinants’– Knowledge, attitude, planning, forget, lack of support
• Determinants can be influenced by methods / techniques
• When tailored or based on participation more effective

Behavior change interventions
• Active content of interventions:Effective techniques * Important determinants
• HIV: large number of adherence interventions
• Meta-analysis useful to compile research:– Overall effect?– What explains these effects?
• Previous meta’s: small-medium ES, not possible to explain why

Intervention care
50
60
70
80
90
100
1 2 3
50
60
70
80
90
100
1 2 3
Expected: Larger effects caused by more comprehensive interventions
% patients with VL undetectable or adherence >95%Study phase

Intervention care
50
60
70
80
90
100
1 2 3
50
60
70
80
90
100
1 2 3
But that’s funny (part 1)…
But that’s funny… (2)
• Standard care to controls own study more comprehensive than effective interventions
• Possible explanation: SoC different between clinics

Intervention care
Standard care
50
60
70
80
90
100
1 2 3
50
60
70
80
90
100
1 2 3
Variability in standard care…
• Wagner & Kanouse also argued that standard care may vary and impact treatment outcomes (2003, JAIDS)
• If so, intervention effects cannot be accurately interpreted, compared, nor generalized to other settings without controlling for this variability
• Rarely some form of control for SoC content (i.e. active versus passive controls)
Meta 1: Content & effectiveness SC
• Obtain descriptions standard care provided to controls
• Determine the active ingredients
• Examine relation standard care and outcomes

Methods
• Embase, Psycinfo, Medline, trials 1996-2007
• Excl: DOT; focus only on psychiatric, IDU’s, adolescents
• 29 studies included, 95% authors responded
• Standard care checklist, outcomes & other predictors
• Coding manual incl. taxonomy with 41 BCT’s targeting important adherence determinants (adapted from Abraham & Michie, 2008, HP; Bartholomew, Intervention Mapping, 2006).

Determinant # Technique
Knowledge 1 Provide general information
Tailoring
Individualization
2Increase memory & understand.
Awareness 3 Risk communication
Tailoring
4 Self-monitoring of behaviour
5 Self-report of behaviour
6Electronic monitoring of behaviour
7 Reflective listening
8 Delayed feedback of behaviour
Objectively measured
Subjectively measured
9 Direct feedback of behaviour
10 Feedback of clinical outcomes

Social influence
11 Provide info peer behaviour
12 Social comparison peers
13 Norm important other
Attitude 14 Reevaluation, self-evaluation
15 Persuasive communication
Tailoring
16 Reward behavioural progress
17 Reward motivational progress
Self-efficacy
18 Modeling
19 Verbal persuasion
Tailoring
20 Practice, guided practice
21 Plan coping response
Participation
22 Graded tasks, goal setting
Participation
23 Reattribution, ext. attribution
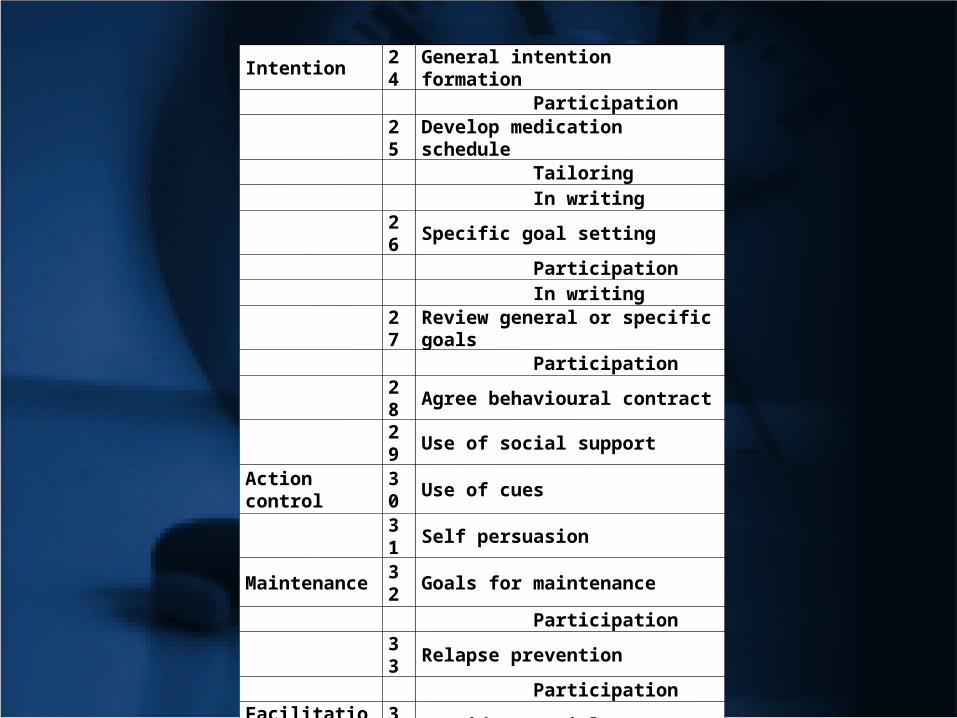
Intention 24 General intention formation Participation
25 Develop medication schedule Tailoring In writing
26 Specific goal setting Participation In writing
27 Review general or specific goals Participation
28 Agree behavioural contract29 Use of social support
Action control 30 Use of cues
31 Self persuasion
Maintenance 32 Goals for maintenance
Participation33 Relapse prevention
ParticipationFacilitation 34 Provide materials
35 Continuous professional support36 Individualize regimen37 Cope with side effects38 Reduce environmental barriers

Example of definition
Determinant: Attitude
16. Reinforcement of behavioural progress:Includes praise and encouragement as well as material rewards,
but the reward/incentive must be explicitly linked to the achievement of specified goals. Also includes use of self-reward strategies.
NB Different from technique #17 in the sense that this technique
reinforces behavioural progress while technique #17 concerns reinforcement of motivational progress.

So does anything happen in the control groups?» ?
DeterminantStandard care activities (coded as techniques)
Coded techniques
Knowledge
Information about HIV, medication and adherence Provide general information
Use of illustrative materials to transfer information Increase memory & understanding
Handing out brochure or written information Additional channel: Brochure
Awareness
Information about consequences of non-adherence Risk communication
Encourage use of 7-day pill box Direct feedback of behavior
Feedback of CD4 & viral load Feedback of clinical outcome
Feedback of MEMS-results* Delayed feedback of behavior
AttitudeInformation about the importance of adherence Persuasive communication
Encourage medication adherence Persuasive communication
Self-efficacy
Encourage storing spare doses in different places Verbal persuasion
Plan ahead for holidays and weekends Plan coping responses
Discuss general barriers and ways to overcome them Plan coping responses
Determine cause non-adherence & generate solutions Plan coping responses
Intention
Develop a medication intake schedule Develop medication schedule
Tailor schedule to patients’ lifestyle Tailor medication schedule
Write down dosing schedule (time, medication, number of pills) Medication schedule in writing
Encourage patients to organize social support Use of social support
Action controlIdentify daily habits and plan intake at these times Use of cues
Encourage use of alarm devices Use of cues
Facilitation
Provide information about side effects & how to deal with them Cope with side effects
Inquire about side-effects & if any, appropriate steps taken Cope with side effects
Delivery of medication at home Provide materials
Social worker helps with housing, unemployment, legal issues Reduce environmental barriers
Design new regimens when regimen is too complex Individualize regimen
Patients with adherence problems return more frequently Tailoring of number of visits
Told to contact health care professional in case of any problems Continuous professional support
Follow-up telephone calls to inquire about difficulties Continuous professional support

DeterminantStandard care activities coded as applications of behavior change techniques
Coded techniques
Knowledge
Information about HIV, medication and adherence
Provide general information
Use of illustrative materials to transfer information
Increase memory & understanding
Handing out brochure or written information Additional channel: Brochure
Awareness
Information about consequences of non-adherence Risk communication
Encourage use of 7-day pill box Direct feedback of behavior
Feedback of CD4 & viral load Feedback of clinical outcome
Feedback of MEMS-results* Delayed feedback of behavior

Attitude
Information about the importance of adherence
Persuasive communication
Encourage medication adherence Persuasive communication
Self-efficacy
Encourage storing spare doses in different places Verbal persuasion
Plan ahead for holidays and weekends Plan coping responses
Discuss general barriers and ways to overcome them Plan coping responses
Determine cause non-adherence & generate solutions Plan coping responses
Intention
Develop a medication intake schedule Develop medication schedule
Tailor schedule to patients’ lifestyle Tailor medication schedule
Write down dosing schedule (time, medication, number of pills)
Medication schedule in writing
Encourage patients to organize social support Use of social support

Action control
Identify daily habits and plan intake at these times Use of cues
Encourage use of alarm devices Use of cues
Facilitation
Provide information about side effects & how to deal with them Cope with side effects
Inquire about side-effects & if any, appropriate steps taken Cope with side effects
Delivery of medication at home Provide materials
Social worker helps with housing, unemployment, legal issues
Reduce environmental barriers
Design new regimens when regimen is too complex Individualize regimen
Patients with adherence problems return more frequently
Tailoring of number of visits
Told to contact health care professional in case of any problems
Continuous professional support
Follow-up telephone calls to inquire about difficulties
Continuous professional support
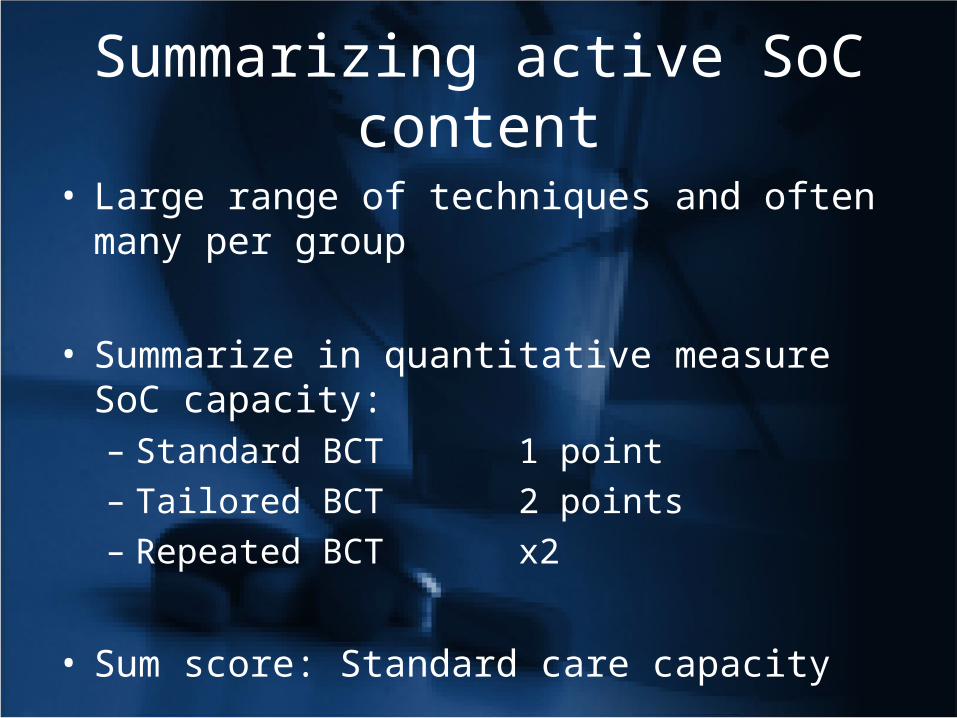
Summarizing active SoC content
• Large range of techniques and often many per group
• Summarize in quantitative measure SoC capacity:– Standard BCT 1 point– Tailored BCT 2 points– Repeated BCT x2
• Sum score: Standard care capacity
• Reliability standard care tool: Cronbachs alfa .90

Holzemer
Pradier
Levy
Tuldra
Servellen
Knobel
Wagner
Rathbun
Goujard
Weber
Remien
de Bruin
Andrade
Fairley
Wohl
McPherson-Baker
DiIorio
Murphy
0 5 10 15 20 25 30
Figure 1. Variability in standard care capacity
Variability in SoC capacity provided to controls (de Bruin et al., 2009, Health Psychology)

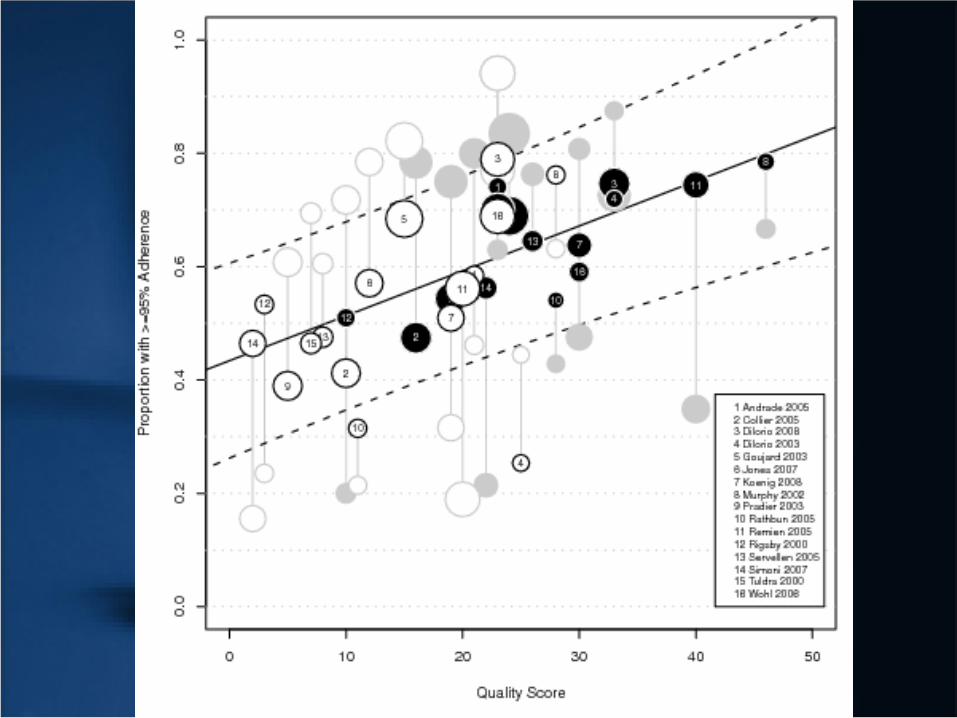
0 5 10 15 20 25 30
0.2
0.3
0.4
0.5
0.6
0.7
0.8
Standard Care Quality
Pro
port
ion
with
Und
etec
tabl
e V
iral L
oad
Relation SoC capacity & viral suppression
Capacity p = .002
Range explains 34% points VL
Ethnicity p=.006
23% lower chance undetectable

Conclusions
• Capacity of adherence support in HIV-clinics varies considerably between settings and is an important predictor of % patients with undetectable viral load
• Meta-analyses that control for SoC variability when examining the effects of interventions more accurate?

Meta-2: Objectives
1. Reliably assess SoC and intervention care capacity
2. Examine relationship with adherence >95% and viral load undetectable
3. Examine whether difference in outcomes intervention and controls is best explained by difference in content (rather than the full content of intervention manuals)

Intervention care
Standard care
50
60
70
80
90
100
1 2 3
50
60
70
80
90
100
1 2 3

Methods• Same search & exclusion procedure
• Randomized controlled trials EU & USA 1996-2009
• Contacted all authors for (30/31):– Intervention & standard care protocols and materials– Characteristics all patients– Viral load and adherence data
• Blinded coders: Kappa .75

Descriptives
• 25/31 RCTs in USA
• 18 treatment experienced patients
• 24 focus specifically on Afr-Am or Hispanic patients
• ½ studies used self-report, other MEMS-caps
• Not all studies measured viral load or adherence; some dropout due to missing SoC or intervention
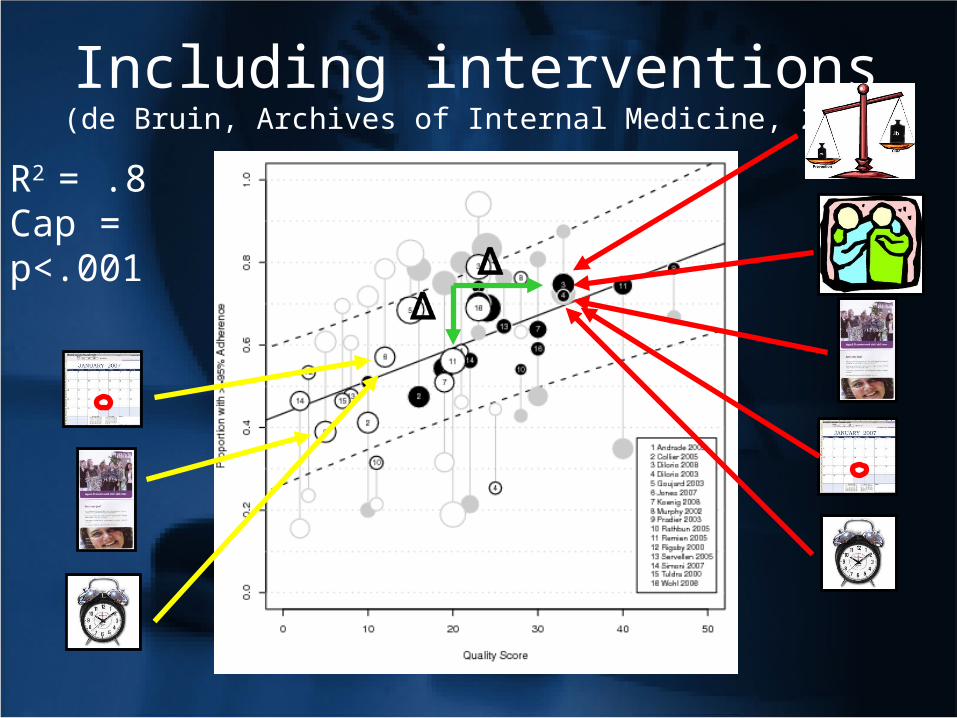
Including interventions(de Bruin, Archives of Internal Medicine, 2010)
R2 = .8Cap = p<.001

Intervention care
Standard care
50
60
70
80
90
100
1 2 3
50
60
70
80
90
100
1 2 3

“Unique intervention capacity”
R2 = .78Cap VL p = .02Cap ad p <.01

Checks
• Deleting lower quality studies did not affect results• No evidence of publication bias
Strongest additional predictors• Non-caucasian 27% lower chance undetectable• MEMS 50% point lower adherence than self-reports• Methodological checks (e.g. dropout, intensity)
Excluding n.s. predictors did not affect the outcomes

And
rade
Kno
bel
Col
lier
Rig
sby
Gou
jard
Jone
s200
7
Dilo
rio20
08
Pra
dier
Woh
l
Hol
zem
er
Java
nbak
ht
Rat
hbun
Tul
dra
Koe
nig
Ser
velle
n
Sm
ith
Mur
phy2
002
Rem
ien
Rat
e D
iffer
ence
And
rade
Kno
bel
Col
lier
Rig
sby
Gou
jard
Jone
s200
7
Dilo
rio20
08
Pra
dier
Woh
l
Hol
zem
er
Java
nbak
ht
Rat
hbun
Tul
dra
Koe
nig
Ser
velle
n
Sm
ith
Mur
phy2
002
Rem
ien
Rat
e D
iffer
ence
00.
050.
10.
150.
20.
250.
30.
350.
4
Expected Rate Differences under Difference Levels of Standard Care
Expected ratedifference forRemien under:
Low SCQ
Medium SCQ
High SCQ

Conclusions (1)• Capacity of qualitatively sound adherence care crucial for
treatment success (40-50% undetectable VL)
• SoC often suboptimal, but content high quality adherence care known
• Limited evidence of (cost)effectiveness interventions on top of “current best practice”: Implement?
• Additional predictors, e.g. ethnicity, adherence measurement

Conclusions (2)Without accurate SoC reports, intervention effects cannot beinterpreted What was the unique content?compared Different testing conditions?generalized How does SoC map onto other settings?
• Replicate findings• Future meta’s should control for SoC variability• Intervention & SoC reports should improve
• Future meta’s should control for SoC variability• Intervention and SoC reports should improve

Questions raised…
• What does this mean for previous meta’s?
• And for interventions already published?
• And for health care based on this work?
[email protected] University, the Netherlands







![Interventions for enhancing adherence to treatment in ... · [Intervention Review] Interventions for enhancing adherence to treatment in adults with bronchiectasis Amanda McCullough](https://static.fdocuments.us/doc/165x107/5f3f3db211fb1568232d56e7/interventions-for-enhancing-adherence-to-treatment-in-intervention-review.jpg)