ADDRESSING DISPARITIES IN BEHAVIORAL …...Nintendo Wii Sports in older adults with SSD (three 35...
85
Improving the lives of 10 million older adults by 2020 | © 2019 National Council on Aging National Coalition on Mental Health and Aging and National Council on Aging PRESENT ADDRESSING DISPARITIES IN BEHAVIORAL HEALTH CARE FOR OLDER ADULTS 2019-2020 August 21, 2019
Transcript of ADDRESSING DISPARITIES IN BEHAVIORAL …...Nintendo Wii Sports in older adults with SSD (three 35...

Improving the lives of 10 million older adults by 2020 | © 2019 National Council on Aging
National Coalition on Mental Health and Aging
and
National Council on Aging
PRESENT
ADDRESSING DISPARITIES IN BEHAVIORAL HEALTH CARE FOR OLDER ADULTS
2019-2020
August 21, 2019

Improving the lives of 40 million older adults by 2030 | © 2019 National Council on Aging | ncoa.org | @NCOAging
Mission:
To provide opportunities for professional, consumer and government organizations to work together towards improving the availability and quality of mental health preventive and treatment strategies to older Americans and their families through education, research and increased public awareness.
Visit: www.ncmha.org

Improving the lives of 40 million older adults by 2030 | © 2019 National Council on Aging | ncoa.org | @NCOAging
History, Membership and Activities:
•Formed in 1991 by a group of organizations from the aging and mental health fields
•Comprised of 100 national and state associations, state coalitions, and governmental agencies, e.g., SAMHSA and ACL.
•Co-sponsor events to highlight challenges of mental health and aging
• Identify new approaches to addressing problems.
Improving the lives of 40 million older adults by 2030 | © 2019 National Council on Aging | ncoa.org | @NCOAging
NCOA: Who We AreWe believe every person deserves to age well
OUR VISION A just and caring society in which each of us, as we age, lives with dignity, purpose, and security
OUR MISSION Improve the lives of millions of older adults, especially those who are struggling
Improving the lives of 10 million older adults by 2020 | © 2019 National Council on Aging
NCOA’s Center for Healthy Aging
• Goal: Increase the quality and years of healthy life for older adults and adults with disabilities
• Two national resource centers funded by the Administration for Community Living ❑ Chronic Disease Self-Management
Education (CDSME)❑ Falls Prevention
• Other key areas: Behavioral health, physical activity, immunizations, oral health
Improving the lives of 40 million older adults by 2030 | © 2019 National Council on Aging | ncoa.org | @NCOAging
Webinar Series on “Addressing Disparities in Behavioral Health Care
for Older Adults”• Following the May 20th National Older Adult Mental Health Awareness
Day (OAMHD) events, NCMHA developed a plan to collaborate with interested government agencies, private sector groups, and experts to maintain the momentum and recommendations generated from OAMHD.
• A series of webinars during 2019/2020 that target specific topics with a practical focus and accompanying tools/resources to address the needs of older adults with mental health conditions, as well as state/local efforts/best practices.
• A special feature of the webinars will be that the sessions will coincide with monthly, weekly and daily national mental health or aging observances.

Improving the lives of 40 million older adults by 2030 | © 2019 National Council on Aging | ncoa.org | @NCOAging
Key Objectives of the Webinar Series
• Identify specific approaches that address disparities in behavioral health care for older adults
• Ensure that older adults with mental health and addiction-related conditions are integrated within all MH awareness raising, policy, programmatic and research efforts going forward.
• Raise awareness among primary care, mental health, other health service providers and the aging network about the impact of suicide, opioid use, and interrelated problems, and impact provider practice patterns for older adults.
• Identify specific tools such as geriatric assessment, questions –suicide ideation, firearm presence, opioid use and other screening tools – and detailed guidance.
Improving the lives of 40 million older adults by 2030 | © 2019 National Council on Aging | ncoa.org | @NCOAging
Webinar Series Roll Out – 2019-2020
July 23, 2019 (2:00 PM EDT) – National Minority Mental Health Month
“Integrating Culturally Relevant Mental Health Services in Primary Care Medicine for Older Adults (Co-sponsored by the Amer. Psychological Assoc.)
August 21 (12:00 PM EDT) – Senior Citizen’s Day
“Prevention and Health Promotion for Late-Life Mental Health Disorders”
September 18 (12 PM EDT) – Suicide and Healthy Aging Month
“Strategies for Reducing Suicide in Older Adults”
October 10 (2:00 PM EDT) – World Mental Health Day
“Home & Community-Based Mental Health Services: Meeting the Needs of Older Adults”

Improving the lives of 40 million older adults by 2030 | © 2019 National Council on Aging | ncoa.org | @NCOAging
Webinar Series Roll Out – 2019-2020
November 13 – Family Caregivers and Alzheimer’s Awareness Month
“The Invisible Health Care Provider: Family Caregivers of Individuals with Dementia”
January 23, 2020 (12:00 PM EST) – Mental Health Wellness Month
“Solutions to Behavioral Health Workforce Shortages & Lack of Funding”
February 27 (2:00 PM EST) – Eating Disorders and Mental Health Month
“Bridging the Science-Practice Gap: Potential Opportunities for Geriatric Mental Health”
March 26 (3:00 PM EDT) – National Brain Injury Awareness Month
“Traumatic Brain Injury and Mental Illness Among Older Adults: The Problem and New Management Approaches”

Improving the lives of 40 million older adults by 2030 | © 2019 National Council on Aging | ncoa.org | @NCOAging
Today’s Webinaron “Senior Citizen’s Day”
“Prevention and Health Promotion for Late-Life Mental Health Disorders”
Presenter: Amanda Leggett, Ph.D.
Dr. Leggett is a Research Assistant Professor in the Program for Positive Aging and Geriatric Psychiatry Section of the Psychiatry
Department, at the University of Michigan

Prevention and Health Promotion for
Late-Life mental Health Disorders
Amanda Leggett, PhD
Research Assistant Professor
Department of Psychiatry, Geriatric Psychiatry Section

1. Why prevention?
2. Prevention terminology
3. Risk and protective factors
4. Pharmacological prevention
5. Psychological prevention
6. Other forms of prevention
and intervention
7. Conclusions and future
directions
An ounce of prevention is worth a pound of cure
Benjamin Franklin

Why prevention?


PKU (Phenylketonuria)
• An intellectual and seizure disorder
• Early diagnosis and special diet can lead to normal lifespan and mental development

But what about mental disorders?
Depression is prevalent in older adults
6-10% in primary care
settings
30% in medical and
long-term care settings
(Hindi et al., 2011)

may be more reversible
Subsyndromalstates
Leading cause of years lived with disability worldwide
Mental and substance use
disorders(Whiteford et al., 2013)

Excess mortality after myocardial infarction, stroke and cancer
Depression results in (Hindi et al., 2011)

Major risk factor for suicide
Especially in older white
men(Van Orden & Conwell, 2011)

Shrinking number of specialty geriatric mental health providers

Importance of prevention:Reducing other downstream
negative outcomes
•Cognitive decline
•Better pain control
•Caregiver burden
•Cardiovascular and cerebrovascular health
•Healthcare costs

Whiteford, H. A., Degenhardt, L., Rehm, J., Baxter, A. J., Ferrari, A. J., Erskine, H. E., ... & Vos, T. (2013). Global burden of disease attributable to mental
and substance use disorders: Findings from the Global Burden of Disease Study 2010. Lancet, 382(9904), 1575–1586. (PubMed ID: 23993280)

Prevention terminology
Caplan’s (1964) public health framework:
Primary
Secondary
Tertiary

Gordon’s (1987) framework (adopted by the Institute of Medicine):
aimed at an entire populationUniversal
Selected
Indicatedfocus on individuals who already
show early signs or symptoms of a
disorder
target those at high risk

SAMHSA.Gov

Preventionconundrum
If individuals in the control group donot develop the clinical disorder at acertain rate, difficult to see effect inthe group without avery large sample size.
Statistical
significance

Risk and Protective Factors

Risk factors- associated with increased likelihood of a negative outcome
-Early childhood adverse events
-Low SES
-Insomnia
Protective factors-associated with lower likelihood of negative outcome
-Social support
-Self-efficacy
-Higher income
-Mature coping style
-Mastery
Individual, family, community level
-Stress
-Disability
-Isolation
-Bereavement
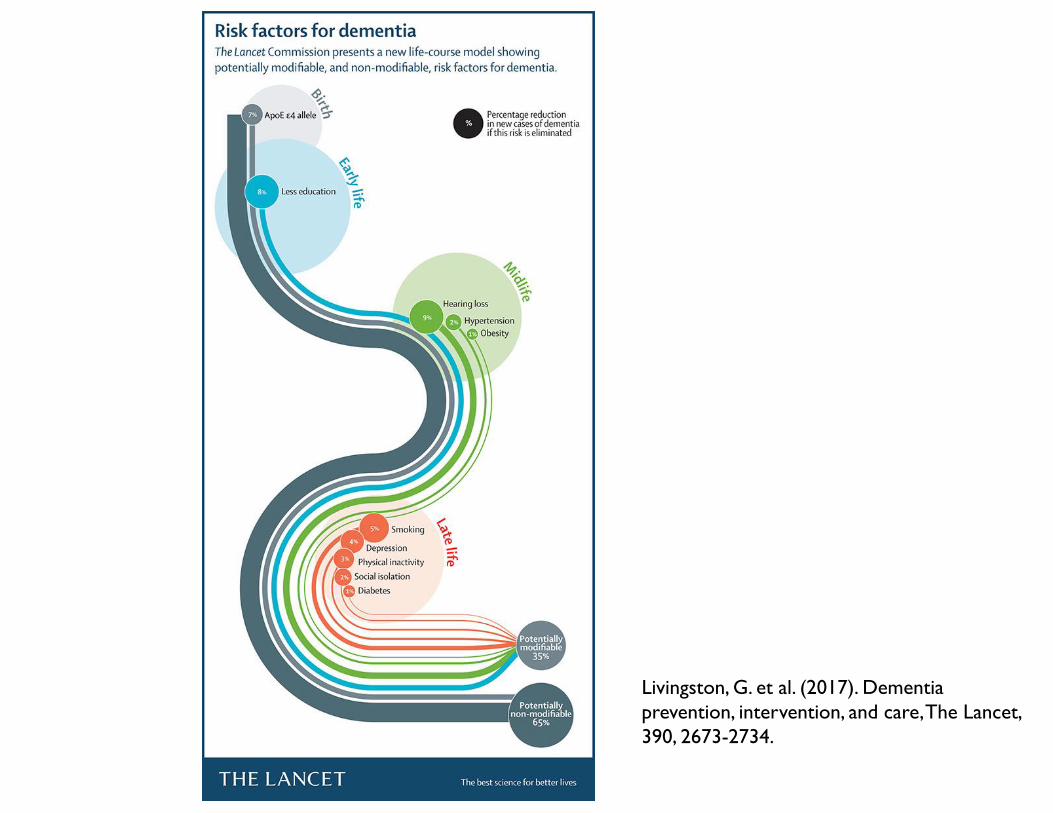
Livingston, G. et al. (2017). Dementia
prevention, intervention, and care, The Lancet,
390, 2673-2734.

Potential Brain Mechanisms for Preventative Strategies in Dementia
Livingston, G. et al. (2017). Dementia
prevention, intervention, and care, The Lancet,
390, 2673-2734.
Pharmacological prevention

For example…
Preventing relapse
•Reynolds et al. (2006): adults (age 70+) who recovered from MDD and then received two years of paroxetine (Paxil) were less likely to develop a new episode of MDD

Following medical crisis
•Robinson et al. (2008): Adults (age 50-90) who had suffered a stroke in the past 3 months; a 12-month trial
Escitalopram
(Lexapro)
8.5%
Problem-
solving
therapy (PST)
11.9%
Placebo
22.4%
NNT = 8

Limitations of Pharmacological Prevention
Results are mixed
Ethical concerns- prescribing without diagnosed disorder?
Less effective for mild symptoms
Side-effects (e.g. fall risk, cognitive impairment)
Older adults already take many medications
Non-pharmacological treatment preferred by older adults
Psychological intervention
Cognitive Behavioral Therapy Approach
targets dysfunctional thoughts
and levels of activity, aiming to
restructure one’s thoughts and
ultimately change behavior

“Coping with Stress” Course
in nursing home residents with SSD
(13 sessions over 7 weeks) (Konnert, Dobson and Stelmach, 2009)
Scores on the Geriatric Depression Scale
declined significantly and were significantly
better compared to the control group
No significant improvement on CES-D and DASMIE scales
Baseline to 6 months post-treatment
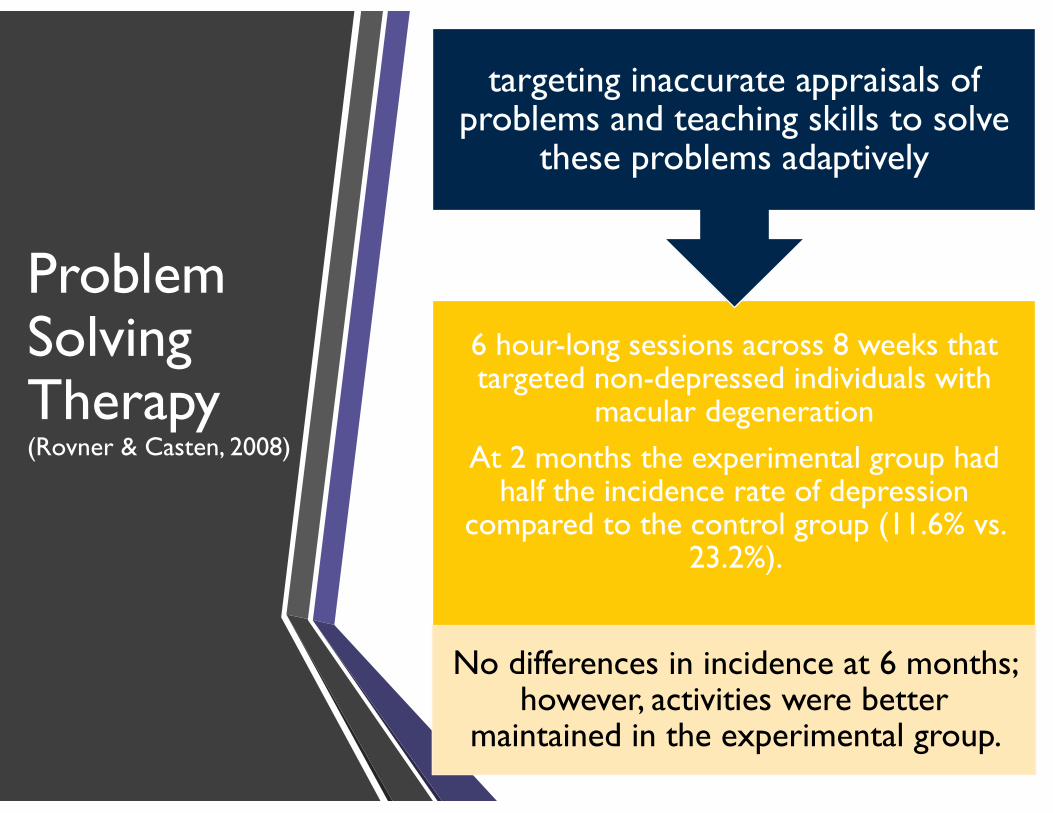
Problem Solving Therapy(Rovner & Casten, 2008)
6 hour-long sessions across 8 weeks that targeted non-depressed individuals with
macular degeneration
At 2 months the experimental group had half the incidence rate of depression
compared to the control group (11.6% vs. 23.2%).
No differences in incidence at 6 months; however, activities were better
maintained in the experimental group.
targeting inaccurate appraisals of problems and teaching skills to solve
these problems adaptively

Other forms of prevention and intervention

Stepped Care
•Van’tVeer-Tazelaar et al. (2009) older adults (75 yrsor older) in primary care over three 4-month periods
• Watchful waiting
• Bibliotherapy (Coping with Depression) with nurse visit and follow-up
• 7 session Problem Solving Therapy
• Primary care referral for antidepressant treatment
Reduced odds
of developing
an anxiety or
depressive
disorder by half
over a year
.12 vs .24

Care management & Suicide Prevention (Alexopoulos et al., 2009)
Primary care patients (age
60+) with minor or
major depression
Care Managers gave recommendations to physicians and helped patients
maintain treatment adherence
More likely to receive
antidepressant and/or
psychotherapy (85-89% vs 49-
62%)
2.2 times greater
decline in suicidal ideation
Internet based
• Spek et al. (2008) adults 50 and over with SSD;10 week Coping with Depression group Course vs. 8 session Internet-based CBT self-help vs. Wait list control
• 62% of internet based below threshold
• 45% of group CBT below threshold
• 38% of waitlist control below threshold

Light therapy
•Re-Timer (30 mins a day for 2 weeks older adults with SSD and poor sleep quality)
•Feasibility and acceptability
• 91% reported it very easy to use
• 93% adhered to the intervention
• 64% would continue to wear
•No adverse events
Depressive symptoms declined and self-reported
sleep improved significantly

Brief Behavioral Treatment of
Insomnia (BBTI): Education about
sleep regulation, what influences sleep,
behaviors that inhibit or promote sleep
•Germain et al. (2006) 60+ yrs with diagnosed insomnia✓Spend only the amount of time
in bed one expects to sleep
✓Wake up at the same time each day
✓Only go to bed when sleepy
✓Get out of bed if not sleeping
• Improved: nighttime awakenings, sleep latency, quality, and efficiency, anxiety and depressive symptoms
Reminiscence and Life Review
• Pot and colleagues (2010): 50 to 90yrs with SSD; 12 two-hour sessions vs. control group which watched a successful aging video
• Discuss life experiences, sensory recall, etc.
• Houses the individual lived in or smells from one’s past
• Significant improvement in depressive symptoms relative to control group
• Not anxiety- both groups improved
• Meta-analysis: reduced depressive symptoms in those with SSD (d-0.37) (Bohlmeijer et al., 2003)

“Exergame” Intervention
•Rosenberg et al. (2010): 12 week Nintendo Wii Sports in older adults with SSD (three 35 minute sessions a week; no control group).
•Depressive symptoms significantly declined
• Reduction maintained at 24-week follow-up
• 37% of participants’ symptom scores declined by 50% or more
•Anxiety scores declined across the intervention, but not significantly

The Silver Song ClubA health promotion example
• Coulton et al. (2015): 14-week 60+ yrs choral intervention (90-minute rehearsals) vs. a normal activity control group
• 6 months: had significantly improved mental-health related quality of life scores (Mean difference= 2.35)
• Cost effective

Social activities-easy to implement, high impact
(Forsman et al., 2011)

Mind-Body

Tai Chi
• Lavretsky et al. (2011): adults 60+ with MDD who only partially responded to escitalopram (Lexapro); 10 week tai chi intervention vs. 10 week health education group• Reduction and remission in depressive
symptoms• improved health-related quality of life• decreased inflammation (C-reactive
protein)
• Also associated with improved cognitive abilities like delayed recall (Lam et al., 2012)

Meditation
• Lavretsky et al. (2013) Dementia caregivers with mild depressive symptoms
• Kirtan Kriya vs. listening to relaxing music for 12 minutes a day for 8 weeks
• 65% showed 50% reduction in depressive sympomts (vs. 31%)
• 43% improvement in telomerase activity (vs. 3.7%)

Conclusions and Future Directions
Conclusions
Pharmacotherapy• efficacy in preventing
recurrence of
depression
• yet antidepressants
and benzodiazepines
are associated with a
number of negative
side-effects for older
adults
Psychotherapy• reduces the
incidence of
depressive and
anxiety disorders
• therapy sessions
are lengthy and
may require travel
to a therapist.
Psychosocial• promoting mental
health
• more indicated and
selective studies are
needed to show
whether psychosocial
prevention can
reduce incidence of
disorder

Limitations
Few studies consider prevention of new incidence over time
Studies need an adequate follow-up period
Very large samples required to detect differences when rate of conversion to disorder is low
Most studies have limited racial and socioeconomic diversity
Future Directions
•A better understanding of risk factors can enable us to target the most vulnerable
•Disabilities, mobility and cognitive capabilities & resiliencies, wisdom, and strength
•Patient centered outcomes research
•Making informed health care decisions, outcomes that matter to patients
•Values and preferences of older adults

Future Directions
•How to reach rural elderly?
• Innovations in technology
•Reach elders with mobility, transportation, or economic difficulties
•Allow individuals to work at own pace
•Shared globally
• Inexpensive
•Reusable
•Downside: crisis assistance and ethical concerns

Future Directions
•Can prevention use biomarkers to target etiology of mental disorder?
•Need for interventions that can be carried out by more than just mental health specialists!
•Work through primary care physicians or social services
•Lay counselor approach in low- and middle-income countries (Dias et al., 2019)

Negative Valence Systems
• Loss
• Fear
Positive Valence Systems
• Reward responsiveness
• Reward learning
Cognitive Systems
• Attention
• Working memory
Systems for Social Processes
• Attachment
• Social communication
Arousal/Regulatory Systems
• Arousal
• Circadian Rhythms
Sensorimotor Systems
• Motor actions
• Habit
Helpful Reviews & Reports
• Bohlmeijer, E., Smit, F., & Cuijpers, P. (2003). Effects of reminiscence and life review on late-life depression: a meta-analysis, 18, 1088-1094.
• Butler et al. (2018) Does Cognitive training prevent cognitive decline?: A systematic review. Annals of Internal Medicine, 168, 63-68.
• Fan & Wong (2019) Effect of cognitive training on daily function in older people without major neurocognitive disorder: a systematic review. Geriatrics, 4, 44.
• Forsman, A.K., Nordmyr, J., & Wahlbeck, K. (2011). Psychosocial interventions for the promotion of mental health and the prevention of depression among older adults. Health Promotion International, 26, 85-107.
• Fournier, J. C., et al. 2010. “Antidepressant Drug Effects and Depression Severity: A Patient-level Meta-analysis.” Journal of the American Medical Association (JAMA), 303(1): 47–53.
• Kim et al. (2017). Cognitive stimulation as a therapeutic modality for dementia: a meta-analysis. Psychiatry Investigation, 14, 626-639
• Lee, S.Y., Franchetti, M.K., Imanbayev, A., Gallo, J.J., Spira, A.P., & Lee, H.B. (2012). Non-pharmacological prevention of major depression among community-dwelling older adults: A systematic review of the efficacy of psychotherapy interventions. Archives of Gerontology and Geriatrics, 55, 522-529.
• McDaid, D., Park, A., & Wahlbeck, K. (2019). The economic case for the prevention of mental illness. Annual Review of Public Health, 40, 373-89.
• World Health Organization (2004). Prevention of Mental Disorders: Effective Interventions and Policy Options. Retrieved from: https://www.who.int/mental_health/evidence/en/prevention_of_mental_disorders_sr.pdf

References
• (2014, March 11). Metrics: Disability-Adjusted Life Year (DALY). Retrieved from https://www.who.int/healthinfo/global_burden_disease/metrics_daly/en/
• Alexopoulos GS, Reynolds CF, Bruce ML, et al. (2009). Reducing suicidal ideation and depression in older primary care patients: 24-month outcomes of the PROSPECT study. American Journal of Psychiatry, 166:882–90.
• Anderson, C. (2012, July 25). Geriatric mental health workforce faces a growing shortage. Retrieved from https://www.healthcarefinancenews.com/news/geriatric-mental-health-workforce-faces-growing-shortage
• Andrews G, Issakidis C, Sanderson K, et al. (2004) Utilising survey data to inform public policy: comparison of the cost-effectiveness of treatment of ten mental disorders. British Journal of Psychiatry, 184:526–33.
• Baglioni C, Battagliese G, Feige B, et al. (2011). Insomnia as a predictor of depression: a meta-analytic evaluation of longitudinal epidemiological studies. J Affect Disord, 135:10–19.
• Bahar-Fuchs A., Clare L., Woods B. (2013). Cognitive training and cognitive rehabilitation for mild to moderate Alzheimer’s disease and vascular dementia. Cochrane Database of Systematic Reviews. Issue 6. Art. No.: CD003260. DOI: 10.1002/14651858.CD003260.pub2.
• Baker, M. K., et al. (2007). “Efficacy and Feasibility of a Novel Tri-modal Robust Exercise Prescription in a Retirement Community: A Randomized, Controlled Trial.” Journal of the American Geriatrics Society 55(1): 1–10.
• Belleville S. (2008). Cognitive training for persons with mild cognitive impairment. Int Psychoger, 20:57–66.
• Bohlmeijer, E., Smit, F., & Cuijpers, P. (2003). Effects of reminiscence and life review on late-life depression: a meta-analysis, 18, 1088-1094.
• Butler M, McCreedy E, Nelson VA, Desai P, Ratner E, Fink HA, et al. (2018) Does Cognitive training prevent cognitive decline?: A systematic review. Annals of Internal Medicine, 168, 63-68.
• Clare L, Woods RT, Moniz Cook ED, Orrell M, Spector A. (2003). Cognitive rehabilitation and cognitive training for early-stage Alzheimer's disease and vascular dementia. Cochrane Database Syst Rev, CD003260.
• Cohen A, Houck PR, Szanto K, et al. (2006). Social inequalities in response to antidepressant treatment in older adults. Arch Gen Psychiatry, 63:50–6.
• Coulton et al. (2015). Effectiveness and cost-effectiveness of community singing on mental health-related quality of life of older people: randomized controlled trial. The British Journal of Psychiatry, 207, 250-255.
• Denihan, A., et al. (2000). “Three-year Prognosis of Depression in the Community-dwelling Elderly.” British Journal of Psychiatry176: 453–7.
• Dias A, Azariah F, Anderson SJ, et al (2018). Preventing major depression in older adults living in low- and middle-income countries: a randomized controlled trial of problem solving therapy. JAMA Psychiatry.
• Espiritu RC, Kripke DF, Ancoli-Israel S, et al. (1994). Low illumination experienced by San Diego adults: association with atypical depressive symptoms. Biol Psychiatry, 35:403–407
• Fan & Wong (2019) Effect of cognitive training on daily function in older people without major neurocognitive disorder: a systematic review. Geriatrics, 4, 44.
• Forsman, A. K., Schierenbeck, I., and Wahlbeck, K. (2011). “Psychosocial Interventions for the Prevention of Depression in Older Adults: Systematic Review and Meta-analysis.” Journal of Aging and Health, 23: 387–416.
• Fournier, J. C., et al. (2010). “Antidepressant Drug Effects and Depression Severity: A Patient-level Meta-analysis.” Journal of the American Medical Association, 303(1): 47–53.
• Germain A, Moul DE, Franzen PL, Miewald JM, Reynolds CF, Monk TH, et al. (2006). Effects of a brief behavioral treatment for late-life insomnia: preliminary findings. J Clin Sleep Med, 2(4):403-406.
• Hampstead BM , Brown GS (2013) Using neuroimaging to inform clinical practice for the diagnosis and treatment of mild cognitive impairment. Clin Geriatr Med 29, 829–845.
• Hindi F, Dew MA,Albert SM, Lotrich FE, Reynolds CF. (2011). Preventing depression in later life: state of the art and science circa 2011. In Prevention in Mental Health: Lifespan Perspective, ed. DV Jeste, C Bell, 34:67–78. Philadelphia: Saunders
• Huckans M, Hutson L, Twamley E, Jak A, Kaye J, Storzbach D. (2013). Efficacy of cognitive rehabilitation therapies for mild cognitive impairment (MCI) in older adults: working toward a theoretical model and evidence-based interventions. NeuropsycholRev, 23(1):63–80.
• Jeste, D. (2002). Preventing Mental Illness Is No Fantasy. Retrieved from https://psychnews.psychiatryonline.org/doi/full/10.1176/pn.47.17.psychnews_47_17_3-a
• Kim et al. (2017). Cognitive stimulation as a therapeutic modality for dementia: a meta-analysis. Psychiatry Investigation, 14, 626-639
• Kim et al. (2017). Cognitive stimulation as a therapeutic modality for dementia: a meta-analysis. Psychiatry Investigation, 14, 626-639
• Konnert, C., Dobson, K., and Stelmach, L. (2009). “The Prevention of Depression in Nursing Home Residents: A Randomized Clinical Trial of Cognitive–Behavioral Therapy.” Aging & Mental Health, 13(2): 288–99.
• Laborde-Lahoz P, El-Gabalawy R, Kinley J, Kirwin PD, Sareen J, Pietrzak RH (2015) Subsyndromal depression among older adults in the USA: prevalence, comorbidity, and risk for new-onset psychiatric disorders in late life. Int J Geriatr Psychiatry 30:677–685.
• Lam LC, Chau RC, Wong BM, et al. (2012). A 1-year randomized controlled trial comparing mind body exercise (tai chi) with stretching and toning exercise on cognitive function in older Chinese adults at risk of cognitive decline. J Am Med Dir Assoc,13:568, e15−e20

• Lamkin, P. (2018). Smart Wearables Market To Double By 2022: $27 Billion Industry Forecast. Retrieved from https://www.forbes.com/sites/paullamkin/2018/10/23/smart-wearables-market-to-double-by-2022-27-billion-industry-forecast/#5418c7a52656
• Lavretsky H, Alstein LL, Olmstead RE, et al. (2011). Complementary use of tai chi chih augments escitalopram treatment of geriatric depression: a randomized controlled trial. Am J Geriatr Psychiatry, 19:839–850
• Lavretsky H, Epel E. S., Siddarth P. et al. (2013). “A pilot study of yogic meditation for family dementia caregivers with depressive symptoms: effects on mental health, cognition, and telomerase activity,” International Journal of Geriatric Psychiatry, vol. 28, no. 1, pp. 57–65.
• Lee, S.Y., Franchetti, M.K., Imanbayev, A., Gallo, J.J., Spira, A.P., & Lee, H.B. (2012). Non-pharmacological prevention of major depression among community-dwelling older adults: A systematic review of the efficacy of psychotherapy interventions. Archives of Gerontology and Geriatrics, 55, 522-529.
• Leggett, A.N., Conroy, D.A., Blow, F.C., Kales, H.C. (2018). Bright light as a preventive intervention for depression in late-life: A pilot study on feasibility, acceptability, and symptom improvement. AJGP, 26, 598-602.
• Lieverse R, Van Someren EJ, Nielen MM, Uitdehaag BM, Smit JH, HoogendijkWJ. (2011). Bright light treatment in elderly patients with non-seasonal major depressive disorder: a randomized placebo-controlled trial. Arch general psychiatry. 68:61–70. doi: 10.1001/archgenpsychiatry.2010.183
• Livingston, G. et al. (2017). Dementia prevention, intervention, and care, The Lancet, 390, 2673-2734.
• McDaid, D., Park, A., & Wahlbeck, K. (2019). The economic case for the prevention of mental illness. Annual Review of Public Health, 40, 373-89.
• Mikami, K., et al. (2011). “Increased Frequency of First-episode Post-stroke Depression After Discontinuation of Escitalopram.” Stroke, 42(11): 3281–3.
• National Institute of Mental Health (2019). NIMH Strategic Plan for Research. Retrieved from: https://www.nimh.nih.gov/about/strategic-planning-reports/strategic-objective-3.shtml
• National Research Council and Institute of Medicine. (2009). Preventing Mental, Emotional, and Behavioral Disorders Among Young People: Progress and Possibilities. Washington DC: The National Academies Press.
• Papp, K.V., Walsh, S.J., & Snyder, P.J. (2009). Immediate and delayed effects of cognitive interventions in healthy elderly: A review of current literature and future directions, Alzheimer's & Dementia, 5(1), 50-60, doi: 10.1016/j.jalz.2008.10.008.
• Pot, A. M., et al. (2010). “The Impact of Life Review on Depression in Older Adults: A Randomized Controlled Trial.” International Psychogeriatrics, 22(4): 572–81.
• Rai, Yates, & Orrell (2018). Cognitive stimulation therapy for dementia. Clinical Geriatric Medicine, 34, 653-665
• Reynolds, C. F., et al. (2006). “Maintenance Treatment of Major Depression in Old Age.” The New England Journal of Medicine, 354(11): 1130–8.
• Riemersma-van der Lek RF, Swaab DF, Twisk J, Hol EM, Hoogendijk WJ, Van Someren EJ. (2008). Effect of bright light and melatonin on cognitive and noncognitive function in elderly residents of group care facilities: a randomized controlled trial. JAMA. 299:2642–55. doi: 10.1001/jama.299.22.2642
• Robinson, R. G., et al. (2008). “Escitalopram and Problem- solving Therapy for Prevention of Post-stroke Depression: A Randomized Controlled Trial.” JAMA 299(20): 2391–2400.
• Rosenberg, D., et al. (2010). “Exer-games for Sub-syndromal Depression in Older Adults: A Pilot Study of a Novel Intervention.” American Journal of Geriatric Psychiatry 18(3): 221–6.
• Rovner, B. W., and Casten, R. J. (2008). “Preventing Late-life Depression in Age-related Macular Degeneration.” American Journal of Geriatric Psychiatry 16: 454–9.
• Rush AJ. (2007) Limitations in efficacy of antidepressant monotherapy. J Clin Psychiatry, 68(Suppl 10):8–10.
• Schoevers RA, Smit F, Deeg DJ, et al. (2006). Prevention of late-life depression in primary care: do we know where to begin? Am J Psychiatry, 163:1611–21.
• Smit F, Ederveen A, Cuijpers P, et al. (2006) Opportunities for cost-effective prevention of late-life depression: an epidemiological approach. Arch Gen Psychiatry, 63: 290–6.
• Spector A, Orrell M, Woods B. (2010). Cognitive stimulation therapy (CST): effects on different areas of cognitive function for people with dementia. Int J Geriatr Psychiatry, 25: 1253–1258.
• Spek, V., et al. (2008). “One-year Follow-up Results of a Randomized Controlled Clinical Trial on Internet-based Cognitive Behavioural Therapy for Sub-threshold Depression in People Over 50 Years.” Psychological Medicine 38(5): 635–40.
• Substance Abuse and Mental Health Services Administration. Retrieved from https://www.samhsa.gov/
• Sumaya, IC, Rienzi, BM, Deegan, JF, Moss, DE. (2001). Bright light treatment decreases depression in institutionalized older adults a placebo-controlled crossover study. J Gerontol A Biol Sci Med Sci, 56: M356–60.
• Thivierge S, Simard M, Jean L, et al. (2008). Errorless learning and spaced retrieval techniques to relearn instrumental activities of daily living in mild Alzheimer’s disease: a case report study. Neuropsychiatr Dis Treat, 4: 987–999.
• Van Orden, K. & Conwell, Y. (2011). Suicides in late life. Current Psychiatry Reports, 13, 234-241.
• Van’tVeer-Tazelaar, P. J., et al. (2009). “Stepped-care Prevention of Anxiety and Depression in Late Life: A Randomized Controlled Trial.” Archives of General Psychiatry 66(3): 297–304.
• Whiteford, H. A., Degenhardt, L., Rehm, J., Baxter, A. J., Ferrari, A. J., Erskine, H. E., ... & Vos, T. (2013). Global burden of disease attributable to mental and substance use disorders: Findings from the Global Burden of Disease Study 2010. Lancet, 382(9904), 1575–1586.
• Woods B, Aguirre EP, Spector AE, Orrell M. (2012). Cognitive stimulation to improve cognitive functioning in people with dementia. Cochrane Database Syst Rev, 2:CD005562.

What about cognition?

Cognition Focused
Cognitive Stimulation
Cognitive Rehabilitation
Cognitive Training

•COGNITIVE
STIMULATION
•Engagement in a range of activities and discussions
•Typically conducted in groups
•Goal – Improve general cognitive and social functioning
(Kim et al., 2017; Rai et al., 2018)

Evidence for cognitive stimulation therapy
Improvements in self-reported quality of life
Small improvement in general cognitive performance
Cost-effectiveness compared to medications
No improvement in mood or behavioral symptoms
(Kim et al., 2017; Rai et al., 2018; Spector, Orrell, &
Woods, 2010; Woods, Aguirre, Spector, & Orrell &, 2012)

Goal –Improve performancein a specific domain of cognitive function
COGNITIVE
TRAINING
Guided practice on a set of standardized tasks that aim to address specific aspects of cognition such as memory, language, or attention
(Belleville, 2008; Butler et al., 2018; Clare & Woods,
2003; Huckans et al., 2013; Papp et al., 2009)

•COGNITIVE
REHABILITATION
•A collaboration between client, family member (where appropriate) and professionals aimed at devising and carrying out an individually-planned intervention
Goal – Improve personally-relevant areas of cognitive functioning that impact everyday life
(Bahar-Fuchs et al., 2013; Hampstead et al.,
2013; Huckans et al., 2013; Kurz, Pohl,
Ramsenthaler, & Sorg, 2009; Thivierge, Simard,
Jean, & Grandmaison, 2008)

Evidence for cognitive rehabilitation and training
Small improvement in general cognitive performance
Can help change targeted behaviors, may improve instrumental activity of daily living function
Inconsistent results on specific cognitive domains
Studies have not considered conversion to dementia over time
(Butler et al., 2018; Fan & Wong, 2019; Hampstead et al., 2013;
Huckans et al., 2013)

Childhood Aggression
• Community level efforts work!
• Behavioral strategies
• Reducing TV and video game exposure
• Group public feedback with group rewards
• Cooperative games
(Institute of Medicine, 2009)
Current treatments aren’t preventing all disability
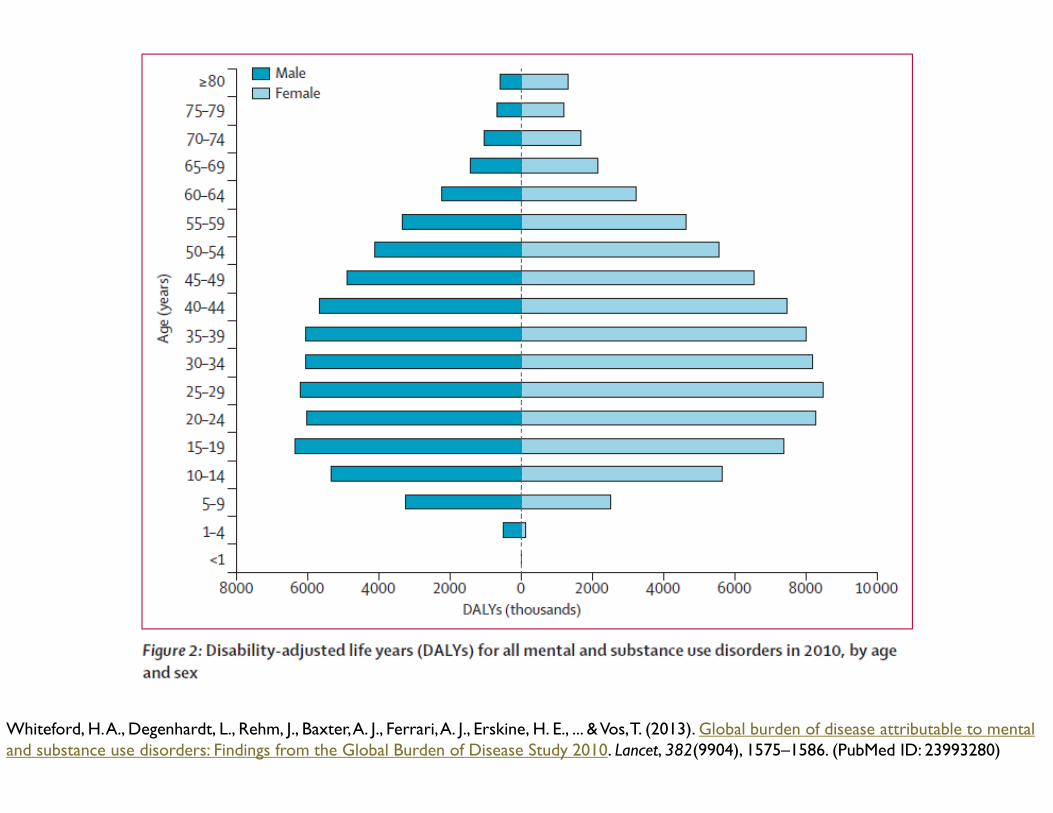
Whiteford, H. A., Degenhardt, L., Rehm, J., Baxter, A. J., Ferrari, A. J., Erskine, H. E., ... & Vos, T. (2013). Global burden of disease attributable to mental
and substance use disorders: Findings from the Global Burden of Disease Study 2010. Lancet, 382(9904), 1575–1586. (PubMed ID: 23993280)

Effort• Number Needed to Treat
• Number if individuals who would need to receive an intervention to avoid one new case of illness
Effect• Attributable fraction
• Cases that would be prevented if a risk factor was eliminated
0
25
50
75
100
No intervention Intervention
NNT
% of condition
that result in
death
25% survive regardless
of intervention
50% survive
because of
intervention
25% die regardless
of intervention
NNT= 100/50 = 2

Pharmacological Prevention
Antidepressants effective in the treatment of depression even among the oldest old (Trappler & Cohen, 1998)
Most older adults recover, but many relapse
Prophylactic antidepressant use as maintenance/relapse prevention

Exercise
• Baker et al. (2007): retirement community residents with no to mild depressive symptomatology
• 10-week exercise program vs. wait-list control
• Three 1-hour sessions a week of:
• high intensity resistance training
• moderate-intensity aerobic training
• balance training
• No differences were found
• Symptoms were low to begin with
• But participants with more symptoms at baseline improved most

Tai Chi
•Lam et al (2012): tai chi offered for 1 year for older adults at risk for cognitive decline vs. stretching/toning exercise group
•Greater preserved cognitive abilities, improvement in delayed recall, and depression scores
•But no change in global cognition test scores

Sleep as a Mechanism for Prevention

•Sleep disturbance and mood are strongly associated• Incidence of depression over time 13.1% in individuals with insomnia
symptoms vs. 4% among those without insomnia symptoms (Baglioni et al., 2011)
•Circadian rhythm disturbances- etiological role?
•Healthy older adults not exposed to enough daily light

Improving the lives of 10 million older adults by 2020 | © 2019 National Council on Aging
Any Questions?
Please type your questions into the chat box on the lower left hand side of your screen.