

Addressing bone loss in shoulder instability lennard funk
39
-
Upload
wrightington-upper-limb-unit -
Category
Health & Medicine
-
view
244 -
download
10
Transcript of Addressing bone loss in shoulder instability lennard funk

www.wrightington.com
Basil Vandegriend, 2006
2
www.wrightington.com
How best to measure Glenoid Bone Loss?
1. X-Rays
2. MRI
3. CT
4. Arthroscopy
3

www.wrightington.com
How much glenoid loss for Bony Reconstruction?
1. 5%
2. 10%
3. 20%
4. 25%

www.wrightington.com
What is a significant Hill-Sachs Lesion?
1. 4cm long
2. 20% humeral head surface
3. 40% humeral head surface
4. Engaging at Arthroscopy

GLENOID BONE LOSS
6

www.wrightington.com
Where does 20-25% come from?
Itoi Cadaveric Studies - JBJS, 2000: Stability of repaired cadaveric shoulders
With no glenoid removed With 21% anterior glenoid removed ER and ABER
Yamamoto & Itoi - AJSM, 2009 Stability ratio mechanical test 8 cadavers At 20% stability ration greatly decreased
Yamamoto - JBJS, 2010 Same study (with 5 more shoulders)!!
7

www.wrightington.com
Pear
8
Inverted Pear

www.wrightington.com 9
• Glenoid loss 20-30% • FU 34 months • 15% Recurrence rate
“requiring surgery”
• ‘Inverted Pear’ • FU 27 months • 67% Recurrence rate
(89% contact athletes)

HUMERAL HEAD BONE LOSS
10

www.wrightington.com
What is a significant Hill-sachs lesion?
Bigliani & Flatow (1996) [quoted in Cetik (2007)]:
Mild - <20% Moderate - 20-45% Severe - >45%
11
> 30% = Needs Treatment

www.wrightington.com
What is a significant Hill-sachs lesion?
Balg & Bouileau (2008) in ISIS: Visible on AP X-Ray in External Rotation
12

www.wrightington.com
Funky Pizza Method
13

www.wrightington.com
Remplissage“Fill-in / padding” Eugene Wolf (2008)
14

www.wrightington.com
Indications for Remplissage
Wolf (2008): Combined glenoid bone defect & large Hill-Sachs
Burkart (2009): Moderate to large Hill-Sachs (>3 mm depth) with bony glenoid loss of >25% Borderline cases where glenoid defect is close to 25% but Hill-Sachs is small to moderate in size
Boileau (2010):
Large, Calandra Grade 3 Hill-Sachs, without glenoid bone-loss
15

Assessing Bone Loss
16
www.wrightington.com
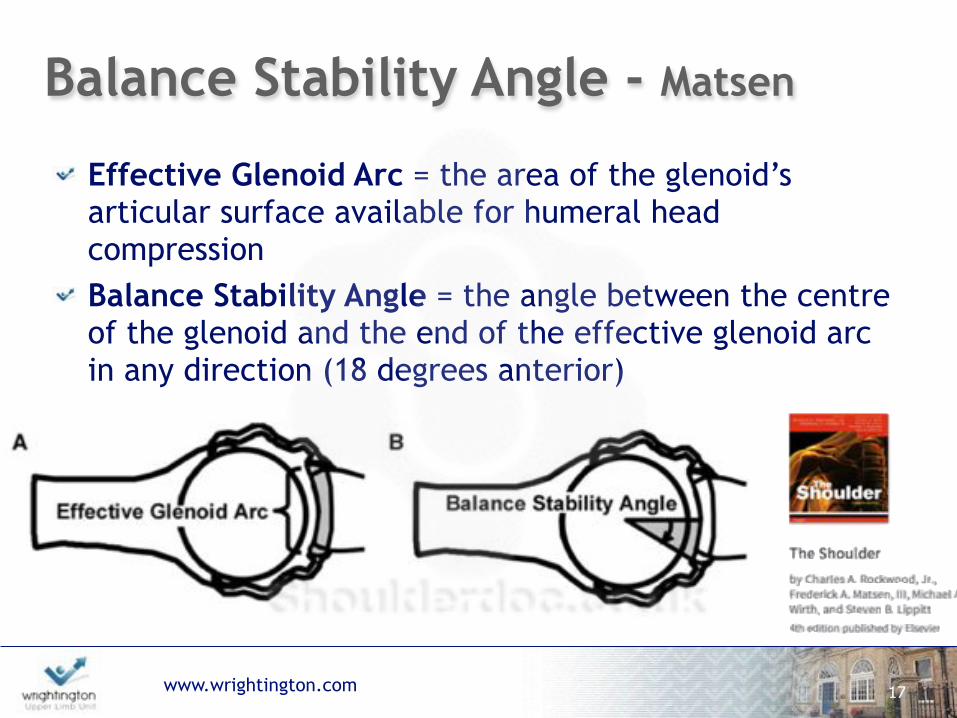
Balance Stability Angle - Matsen
Effective Glenoid Arc = the area of the glenoid’s articular surface available for humeral head compression Balance Stability Angle = the angle between the centre of the glenoid and the end of the effective glenoid arc in any direction (18 degrees anterior)
17

www.wrightington.com
‘Glenoid Track’ - Itoi & Yamamoto
Yamamoto - Cadaver
Metzger - MRI/MRA
Omori - In-vivo
18
Yamamoto N, Itoi E, Abe H, et al. JSES 2007 Metzger et al. AAOSM, 2010 Omori et al. AJSM. March 2014.
Defined as the contact area between the glenoid and the humeral head while keeping the arm in maximum external rotation, maximum horizontal extension, and 0° to 90° of abduction relative to the trunk. "If a Hill-Sachs lesion extends medially over the glenoid track, there is a risk of engagement.

www.wrightington.com
Largest Track (contact) found in full ABER = 84% of glenoid width
19
‘Glenoid Track’

www.wrightington.com 20
‘Glenoid Track’If the medial margin of a Hill-Sach’s lesion lies outside the glenoid track, this will cause an engaging Hill-Sach’s. "Bony defect of the glenoid will narrow the glenoid track, which can cause the medial margin of a relatively small Hill-Sach’s lesion to be outside the glenoid track

www.wrightington.com
1. Measure the diameter (D) of the inferior glenoid, either by arthroscopy or from 3D CT scan.
2. Determine the width of the anterior glenoid bone loss (d). 3. Calculate the width of the glenoid track (GT) by the following
formula: GT=0.83D-d 4. Calculate the width of the HSI, which is the width of the Hill-
Sachs lesion (HS) plus the width of the bone bridge (BB) between the rotator cuff attachments and the lateral aspect of the Hill-Sachs lesion: HSI = HS + BB.
5. If HSI > GT, the HS is off track, or engaging. If HSI < GT, the HS is on track, or non-engaging.
21

www.wrightington.com
Normal Glenoid Track
22
83%

www.wrightington.com
Anterior Glenoid Deficiency
23
D
83%

www.wrightington.com
The Formula:
24
1. Measure the diameter (D) of the inferior glenoid, either by arthroscopy or from 3D CT scan (of Opposite shoulder).
2. Determine the width of the anterior glenoid bone loss (d).
3. Calculate the width of the glenoid track (GT) by the following formula: GT=0.83D-d
4. Calculate the width of the HSI, which is the width of the Hill-Sachs lesion (HS) plus the width of the bone bridge (BB) between the rotator cuff attachments and the lateral aspect of the Hill-Sachs lesion: HSI = HS + BB.
5. If HSI > GT, the HS is off track, or engaging. If HSI < GT, the HS is on track, or non-engaging.
D
83%

www.wrightington.com
The Formula:
25
1. Measure the diameter (D) of the inferior glenoid, either by arthroscopy or from 3D CT scan.
2. Determine the width of the anterior glenoid bone loss (d).
3. Calculate the width of the glenoid track (GT) by the following formula: GT=0.83D-d
4. Calculate the width of the HSI, which is the width of the Hill-Sachs lesion (HS) plus the width of the bone bridge (BB) between the rotator cuff attachments and the lateral aspect of the Hill-Sachs lesion: HSI = HS + BB.
1. If HSI > GT, the HS is ‘off track’, or engaging.
2.If HSI < GT, the HS is ‘on track’, or non-engaging.

www.wrightington.com
Treatment Paradigm
26
Group Glenoid Defect Hill-Sachs Recommended
Treatment
1 <25% On Track Arthroscopic Bankart
2 <25% Off Track Arthroscopic Bankart + Remplissage
3 >25% On Track Latarjet
4 >25% Off TrackLatarjet +
Remplissage / Humeral Bone Graft

Decision Making
27

www.wrightington.com
Balg & Bouileau, JBJSB, 2007:
Instability Severity Score!
28

www.wrightington.com
Balg & Bouileau, JBJSB, 2007:
No difference between: Gender (p=0.32) Type of Sports (p=0.31)
Difference between: Age (p=0.001) Level of sport (p=0.03) Shoulder laxity (p=0.03) Hill-Sachs lesion (p=0.002)
29

www.wrightington.com
My approach to Latarjet:
30
Considerations:

www.wrightington.com
Pragmatic 1:
24yr male footballer First Traumatic Dislocation
31

www.wrightington.com
Final repair

www.wrightington.com
Sugaya Technique
Sugaya et al. 2005

www.wrightington.com
Pragmatic 2:
28yr male Multiple recurrent traumatic dislocations with reducing force. Dislocating dressing & sleep Now avoidance Unable to work as nurse
34

www.wrightington.com

www.wrightington.com 36
“Soap and water and common sense are the best disinfectants”
William Osler

www.wrightington.com
Thank You
37

www.wrightington.com
Clinical (Classification)
MR Arthrogram
Glenoid
Bankart
Repair(scope / open)
Deficiency
Latarjet / Eden-Hybinette
Humeral Head
Large Hill-Sachs
Remplissage / Allograft
Capsule
HAGL
Repair(open / Scope)
Hyperlax
Shift / Plication

www.wrightington.com


















