Eugm 2012 oneill - perspective on the current environment for adaptive clinical trials - 2012 eugm

Adaptive Clinical Trials: A Necessary Step toward
Personalized Medicine
Adaptive Clinical Trials: A Necessary Step toward
Personalized Medicine Donald A. Berry
[email protected] A. Berry

22
Financial DisclosureFinancial Disclosure
Part owner Berry Consultants, LLCDesigns adaptive trials for Pharmaceutical companiesMedical device companiesNIH-sponsored cooperative groups
Part owner Berry Consultants, LLCDesigns adaptive trials for Pharmaceutical companiesMedical device companiesNIH-sponsored cooperative groups

33
Janet Woodcock, Director CDER FDAJanet Woodcock,
Director CDER FDA
“Improved utilization of adaptive
and Bayesian methods” could help
resolve low success rate of and
expense of phase 3 clinical trials
“Improved utilization of adaptive
and Bayesian methods” could help
resolve low success rate of and
expense of phase 3 clinical trials

44
FDA’s Critical Path Opportunities Report (2006)
FDA’s Critical Path Opportunities Report (2006)
“uncovered a consensus that the two most important areas for improving medical product development are biomarker development and streamlining clinical trials.”
“uncovered a consensus that the two most important areas for improving medical product development are biomarker development and streamlining clinical trials.”
http://www.fda.gov/ScienceResearch/SpecialTopics/CriticalPathInitiative/default.htm

55
For example, in 2010, the Biomarkers Consortium–a public-private partnership that includes the NIH, the FDA, patient groups, and pharmaceutical and biotech–initiated a groundbreaking trial in breast cancer to predict drug responsiveness based on the presence or absence of genetic and biological markers, … I-SPY 2 (ClinicalTrials.gov NCT01042379).

66
"Our current approach [to trials] is horribly inefficient, and we need to do something better," says Roger Lewis, an emergency medicine physician at Harbor-University of California, Los Angeles, Medical Center. Lewis helps advise a company called Berry Consultants …

77
Lewis and Berry, along with emergency medicine physician William Barsan at the University of Michigan, will be studying whether "adaptive" trial designs that incorporate new information in midcourse can answer medical questions. They also want to learn what concerns researchers might have about this approach.

88
Current use of Bayesian adaptive designs
Current use of Bayesian adaptive designs
MDACC (> 300 trials) Device companies (> 25 PMAs)* Drug companies (Most of
top 40; many biotechs)**
MDACC (> 300 trials) Device companies (> 25 PMAs)* Drug companies (Most of
top 40; many biotechs)** *http://www.fda.gov/MedicalDevicesDeviceRegulationandGuidance/GuidanceDocuments/ucm071072.htm**http://www.fda.gov/downloads/DrugsGuidanceCompliance RegulatoryInformation/Guidances/UCM201790.pdf

99
Example: Troxacitabine in AML* (endpoint: CR by day 50)
Example: Troxacitabine in AML* (endpoint: CR by day 50)
RANDOMIZE
RANDOMIZE
IdarubicinAra-C
IdarubicinAra-C
Trox Idarubicin
Trox Idarubicin
TroxAra-C Trox
Ara-C
n = 25
n = 25
n = 25
Standard designStandard design
Adaptiverandomizationto learn, while
effectivelytreating
patients in trial
Adaptiverandomizationto learn, while
effectivelytreating
patients in trial
Our designOur design
* Giles JCO 2003

1010
Adaptive RandomizationAdaptive Randomization
Assign with higher probability to better performing therapies
TI dropped after 24th patient Trial stopped after 34 patients
Assign with higher probability to better performing therapies
TI dropped after 24th patient Trial stopped after 34 patients

1111
Summary of AML trial results
Summary of AML trial results
CR by 50 days:IA 10/18 = 56%TA 3/11 = 27%TI 0/5 = 0%
CR by 50 days:IA 10/18 = 56%TA 3/11 = 27%TI 0/5 = 0%

1212
Some areas of application of Bayesian adaptive drug trialsSome areas of application of Bayesian adaptive drug trials Migraine Oncology Rh Arthritis Lupus Diabetes Obesity Stroke Gastroparesis
Migraine Oncology Rh Arthritis Lupus Diabetes Obesity Stroke Gastroparesis
Spinal Cord Injury HIV Hepatitis C Pre-term labor Constipation Overactive bladder Libido Alzheimer’s
Spinal Cord Injury HIV Hepatitis C Pre-term labor Constipation Overactive bladder Libido Alzheimer’s

1313
Simulations Usually RequiredSimulations Usually Required To find operating characteristics: Type I error rate Power Sample size distribution
Prospective design essential Longitudinal modeling Many scenarios Accrual rate matters
To find operating characteristics: Type I error rate Power Sample size distribution
Prospective design essential Longitudinal modeling Many scenarios Accrual rate matters

1414
"Our current approach [to trials] is horribly inefficient, and we need to do something better," says Roger Lewis, an emergency medicine physician at Harbor-University of California, Los Angeles, Medical Center. Lewis helps advise a company called Berry Consultants …

1515
Lewis and Berry, along with emergency medicine physician William Barsan at the University of Michigan, will be studying whether "adaptive" trial designs that incorporate new information in midcourse can answer medical questions. They also want to learn what concerns researchers might have about this approach.

1616
Bayesian adaptive trialsBayesian adaptive trialsStopping early (or late)EfficacyFutility
Dose finding (& dose dropping)Seamless phasesPopulation findingAdaptive randomizationRamping up accrual
Stopping early (or late)EfficacyFutility
Dose finding (& dose dropping)Seamless phasesPopulation findingAdaptive randomizationRamping up accrual

1717
Why?Why?
Smaller trials (usually!)More accurate conclusionsCan focus on better
treatment of patients in trials
Smaller trials (usually!)More accurate conclusionsCan focus on better
treatment of patients in trials

1818
Three Recent Examples of Smaller Sample Size UsingThree Recent Examples of Smaller Sample Size Using
Bayesian predictive probabilities
Longitudinal modeling
Bayesian predictive probabilities
Longitudinal modeling

1919
A Bayesian statistical design was used with arange in sample size from 600 to 1800 patients.

2020
From “Methods”From “Methods”
“These interim analyses were not the standard type in which the trial results are announced when a boundary is crossed. Rather, the decision to discontinue enrollment was based on a prediction that future follow-up was likely to give a meaningful answer.”
“These interim analyses were not the standard type in which the trial results are announced when a boundary is crossed. Rather, the decision to discontinue enrollment was based on a prediction that future follow-up was likely to give a meaningful answer.”

2121

2222
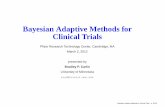
Time to Chronic Failure by Randomization Group (Updated)
Time to Chronic Failure by Randomization Group (Updated)
64%
16%
TCool 103
69 69 66 63 62 61 54 52 37 15 3 2
AAD 56 39 29 19 16 13 11 10 7 2 0 0 0• Circles in the graph represent censored patients
THERMOCOOL
Free
dom
from
Chr
onic
Fai
lure
Days into Effectiveness Follow-up
64%
16% AAD
0 30 60 90 120 150 180 210 240 270 300 330 3600.0
0.2
0.4
0.6
0.8
1.0

Adaptive Design-Key Features
Response-Adaptive RandomizationUses interim data and Bayesian techniques to modify the treatment allocation
probabilities in favor of more informative treatment arms.• Maximize information about dose-response relationship• increases the probability of success in Phase 3 by bringing the correct dose forward
into Phase 3
Predefined Decision RulesFrequent interim analyses allows determination of futility or success• Allows Ph2a and Ph2b to be combined in a single trial• Succeed efficiently and fail efficiently
Trial simulationsDefine operating characteristics (false + rate, statistical power, and sample size
distributions)
Uses accumulating data to decide on how to modify aspects of the study without undermining the validity and integrity of the trial.
Robert Lenz, San Diego, Oct 5, 2009

Response-Adaptive Randomization
New Patient
Randomizationto placebo or optimal
dose
Find optimal
dose1
2
Sufficientinformation
obtained
Futility
Decision
Continue until max. sample size reached
6
9
8
7
10
Ongoing Pts Data
3 Estimation of Dose-Response
5
Longitudinal model predicts final outcome
4
Robert Lenz, San Diego, Oct 5, 2009

Response-Adaptive RandomizationA
DA
S-C
og S
core
Doses (mg)0 5 10 15 20 30 35
Area of the D-R relationship we want greatest information about
Robert Lenz, San Diego, Oct 5, 2009

Goal is to Find the ED90 and MEDA
DA
S-C
og S
core
Doses (mg)0 5 10 15 20 30 35
MED ED90
ED90: smallest dose that produces 90% of the maximal efficacy over the doses studied
MED: minimally effective dose; operationally defined as the smallest dose that produces at least 1.75 point improvement over placebo in ADAS-Cog
Robert Lenz, San Diego, Oct 5, 2009

Adaptive Randomization
• The probability of allocating the subsequent subject to a particular dose is proportional to the reduction in the variance of ED90 achieved when a subject is allocated to that dose.
• The allocation ratio will be altered in such as way as to maximize the information (minimize the variance) about the MED and ED90.
• Randomization probabilities are updated every 2 weeks.
Robert Lenz, San Diego, Oct 5, 2009

Normal Dynamic Linear Model
• Normal Dynamic Linear Model is used to describe the dose-response relationship.
• This is a very versatile and flexible model that allows for non-monotonic response functions.
• Allows borrowing strength from neighboring doses (don’t treat each dose as entirely independent), thereby narrowing the probability distribution around the dose.
• Thus, increasing the number of doses increases information about the entire dose-response curve, not just a single dose.
Robert Lenz, San Diego, Oct 5, 2009

Simulations: Sensitivity Analyses
• The primary simulation is based on the best guesses of accrual rate and correlation between early (week 4 and 8) and final time point (week 12) for the ADAS-Cog scores.
• Maximum sample size is 400
• When considering all the simulated D-R curves, very favorable operating characteristics
• False positive rate less than 5%• False negative rate < 20%
• Average sample size across D-R relationships is 319
Robert Lenz, San Diego, Oct 5, 2009

Model estimates of ACAScog(every two weeks)
30

31

32

33

34

35

36

37

38

39

40

41

42

43

44

45

46

47

48

49

50

May 14, 2009: Stop for futility
51
N = 322Completers = 238

Same as previous, but dropping incomplete patients52

53
Final

Sample sizes
54

55

56

57

58

59

60

61

62

63

64

65

66

67

68

69

70

71

72

73

74

May 14, 2009: Stop for futility75

76
Final

7777
Adaptive Phase II/III TrialAdaptive Phase II/III Trial

7878
IoM Report on Cancer Cooperative Groups 2010

7979
Example from Critical Path Initiative
Example from Critical Path Initiative
Type II diabetesSeamless Phase II/III: Dose
finding plus confirmationSample size 200 - 1566Active comparator & placeboPrimary endpoint:
Clinical Utility Index (12 months)
Type II diabetesSeamless Phase II/III: Dose
finding plus confirmationSample size 200 - 1566Active comparator & placeboPrimary endpoint:
Clinical Utility Index (12 months)

8080
Some DetailsSome DetailsPhase II: 7 doses experimental drug
plus placebo plus active controlPhase III1 or 2 doses experimental drugSample size via predictive power
considering available Phase II dataAdaptive transition: Bayesian
predictive probsBoth phases driven by CUI
Phase II: 7 doses experimental drug plus placebo plus active control
Phase III1 or 2 doses experimental drugSample size via predictive power
considering available Phase II dataAdaptive transition: Bayesian
predictive probsBoth phases driven by CUI

8181
Clinical Utility IndexClinical Utility Index
Dose-response modeling Longitudinal modelingDose-response modeling Longitudinal modeling
Exp – AC12 mos
Exp – AC12 mos
Exp – P6 mos
Exp – P6 mos
0 0 0 0

8282
Adaptive Biomarker TrialAdaptive Biomarker Trial

8383
EXAMPLE
TRIAL

8484
Savings possible in sample size when
using biomarkers …
Savings possible in sample size when
using biomarkers …

8585
Berry et al. SABCS 2009

8686

I‐SPY2: The Cartoon(Press conference* slides)
*<http://ispy2.org>

Standard Phase 2 Cancer Drug Trials
Experimental armExperimental armPopulationof patients
Outcome:Tumor
shrinkage?
Populationof patients
Outcome:Longer timedisease free
RANDOMIZE

Standard Phase 2 Cancer Drug Trials
Experimental drugExperimental drug
Outcome:Longer timedisease free
RANDOMIZE
Outcome:Tumor
shrinkage?
Populationof patients
Populationof patients
Consequence:34% success rateof Phase 3 Trials

I‐SPY2 TRIAL
Outcome:Complete response at surgery
Populationof patients
ADAPTIVELY
RANDOMIZE

I‐SPY2 TRIAL
Outcome:Complete response at surgery
Arm 2 graduates to small focused Phase 3 trial
Populationof patients
ADAPTIVELY
RANDOMIZE

I‐SPY2 TRIAL
Outcome:Complete response at surgery
Populationof patients
Arm 3 dropsfor futility
ADAPTIVELY
RANDOMIZE

I‐SPY2 TRIAL
Outcome:Complete response at surgery
Arm 5 graduates to small focused Phase 3 trial
Populationof patients
RANDOMIZE
ADAPTIVELY

I‐SPY2 TRIAL
Outcome:Complete response at surgery
Arm 6 isadded tothe mix
Populationof patients
RANDOMIZE
ADAPTIVELY
Goal: Greater than 85% success rate in
Phase 3, with focus onpatients who benefit

9595

9696
I-SPY2 Adaptive Design ProcessI-SPY2 Adaptive Design Process PI: Laura Esserman, UCSF Sponsored by FNIH: NCI, FDA,
industry, academia, Coordinated with FDA (CDER,
CBER & CDRH) from inception Current status: 20 centers, ~50
patients, experimental drugs so far: neratinib, ABT888, AMG386
PI: Laura Esserman, UCSF Sponsored by FNIH: NCI, FDA,
industry, academia, Coordinated with FDA (CDER,
CBER & CDRH) from inception Current status: 20 centers, ~50
patients, experimental drugs so far: neratinib, ABT888, AMG386

9797
I-SPY 2 EffectsI-SPY 2 Effects Match drugs (& combos) with
biomarker signatures Graduate drug/biomarker pairs to
smaller (n < 300), more focused, more successful Phase 3
Descendents of I-SPY 2 in melanoma, colorectal cancer, Alzheimer’s, acute heart failure, …
Match drugs (& combos) with biomarker signatures
Graduate drug/biomarker pairs to smaller (n < 300), more focused, more successful Phase 3
Descendents of I-SPY 2 in melanoma, colorectal cancer, Alzheimer’s, acute heart failure, …

9898
Software?Software?
SAS ADAPT?SAS ADAPT?

Copyright © 2010 Berry Consultants, LLC, SAS Institute Inc., and Tessella Inc. All rights reserved.
BeST: Solution for Smarter Clinical Trials

Solution Design
Trial Simulation Engine
Design Specs
SAS Analysis
Simulation Simulation Results
JMP/SASReview &
Visualization
Design Selection/ Iteration
FinalDesign
Trial ExecutionEngine
Data Source
TrialData
Results
SAS Analysis
Simulation Actual trial Dashboard
DSMB

101101
Also, Selected Short Subject …Also, Selected
Short Subject …

102102
Designing a clinical trial is making a decision
Designing a clinical trial is making a decision
Motivated by dinner with Joel Tsevat and
John Perentisis …
Motivated by dinner with Joel Tsevat and
John Perentisis …

103103
Decision analysis as a medical research paradigm
Decision analysis as a medical research paradigm
Why do we carry out clinical trials of experimental products?(1) To see if they are safe and effective.(2) To see if the results are unusual
assuming product is ineffective.(3) To deliver good medicine to patients.
Does your answer matter?

104104
Standard Approach to Choosing Sample SizeStandard Approach to Choosing Sample Size
Consider time to event. Want 25% reduction in hazards Type I error 5%, two-sided Power 80% Accrual rate 2/month Median for control: 8 months Follow-up after accrual: 12 months
Answer: n = 650
Consider time to event. Want 25% reduction in hazards Type I error 5%, two-sided Power 80% Accrual rate 2/month Median for control: 8 months Follow-up after accrual: 12 months
Answer: n = 650
Where are the questions about the disease? the population? Is this
CABG or a rare pediatric cancer?
Where are the questions about the disease? the population? Is this
CABG or a rare pediatric cancer?

105105
We need a new paradigm!
We need a new paradigm!

106106
Choosing sample size using decision analysisChoosing sample size
using decision analysis Goal: Effective overall treatment of
patients, both those who come after the trial and those in the trial
Example formalizing this goal: Maximize expected number of successes over all patients
Goal: Effective overall treatment of patients, both those who come after the trial and those in the trial
Example formalizing this goal: Maximize expected number of successes over all patients

107107
Compare Joffe/Weeks JNCI Dec 18, 2002
Compare Joffe/Weeks JNCI Dec 18, 2002
“Many respondents viewed the main societal purpose of clinical trials as benefiting the participants rather than as creating generalizable knowledge to advance future therapy. This view, which was more prevalent among specialists such as pediatric oncologists that enrolled greater proportions of patients in trials, conflicts with established principles [from Belmont Report] of research ethics.”
“Many respondents viewed the main societal purpose of clinical trials as benefiting the participants rather than as creating generalizable knowledge to advance future therapy. This view, which was more prevalent among specialists such as pediatric oncologists that enrolled greater proportions of patients in trials, conflicts with established principles [from Belmont Report] of research ethics.”
We must rethink the “established principles
of research ethics”
We must rethink the “established principles
of research ethics”

108108
“More ethical” approach:Maximize overall benefit“More ethical” approach:Maximize overall benefit
What is “overall”?All patients who will be treated
with therapies assessed in trialCall it N, “patient horizon”Enough to know magnitude of N:
100? 1000? 1,000,000?
What is “overall”?All patients who will be treated
with therapies assessed in trialCall it N, “patient horizon”Enough to know magnitude of N:
100? 1000? 1,000,000?

109109
Goal: maximize expected number of successes in N Either one- or two-armed trial Suppose n = 1000 is right for one trial & N = 1,000,000 Then for other N’s use n =
Goal: maximize expected number of successes in N Either one- or two-armed trial Suppose n = 1000 is right for one trial & N = 1,000,000 Then for other N’s use n =
1000
1,000,000

110110
Prior distributions?Prior distributions?

111111
Optimal allocations in a two-armed trialOptimal allocations in a two-armed trial

112112
√N3√N
2 √N2

113113
ConclusionsConclusions Standard clinical research paradigm
doesn’t apply to rare populations Decision analysis addresses right
questions, hypothesis testing does not Bayesian adaptive approach balances
experimentation and treating trial participants effectively
Bayesian attitude uses all info “All info” includes longitudinal info and
borrowing adult info to children
Standard clinical research paradigm doesn’t apply to rare populations
Decision analysis addresses right questions, hypothesis testing does not
Bayesian adaptive approach balances experimentation and treating trial participants effectively
Bayesian attitude uses all info “All info” includes longitudinal info and
borrowing adult info to children