Adam Aluisio NIH/FIC Research Scholar University of Nairobi/University of Washington
17
Male partner HIV-1 testing and antenatal clinic attendance associated with reduced infant HIV-1 acquisition and mortality Adam Aluisio NIH/FIC Research Scholar University of Nairobi/University of Washington
-
Upload
wynter-haney -
Category
Documents
-
view
22 -
download
2
description
Male partner HIV-1 testing and antenatal clinic attendance associated with reduced infant HIV-1 acquisition and mortality. Adam Aluisio NIH/FIC Research Scholar University of Nairobi/University of Washington. Vertical transmission & infant mortality. - PowerPoint PPT Presentation
Transcript of Adam Aluisio NIH/FIC Research Scholar University of Nairobi/University of Washington

Male partner HIV-1 testing and antenatal clinic attendance
associated with reduced infant HIV-1 acquisition and mortality
Adam AluisioNIH/FIC Research Scholar
University of Nairobi/University of Washington
Vertical transmission & infant mortality
• Risk of mother-to-child transmission of HIV-1• With interventions <2%• Without interventions 15-45%
• Infant mortality in sub-Saharan Africa• Overall ~100/1000• HIV-1 infected infants ~1/3

Partner involvement in PMTCT
Farquhar, C., et al., JAIDS, 2004.

Objectives
• Determine the role of male partner involvement in:–Mother-to-child transmission of HIV-1 –Infant mortality
Methods• Women enrolled at ~32 weeks gestation with
1 year follow-up – Encouraged to invite partners for antenatal clinic
attendance and optional VCT services
– Male partner data gathered from all female participants
– Infants examined monthly and tested for HIV-1 at birth, 1, 3, 6, 9 and 12 months postpartum
Statistical analysis• Correlates of male partner attendance
– Pearson X2 , independent sample t tests & logistic regression
• MTCT of HIV-1 & HIV-1-free survival– Kaplan-Meier – Cox regression
• Adjusting for maternal viral load and infant feeding modality
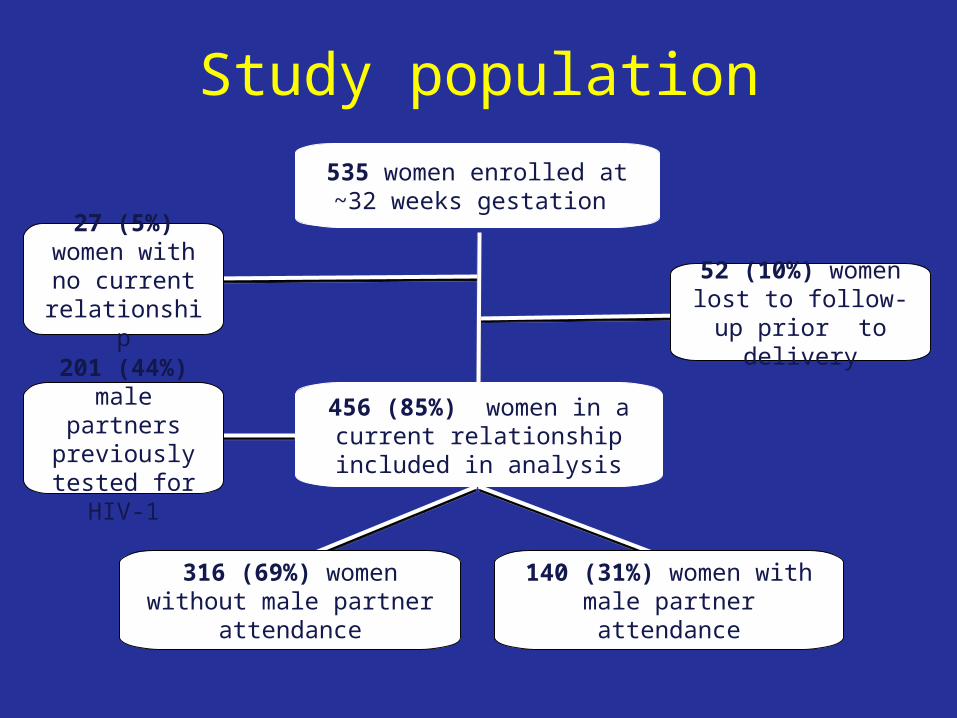
Study population535 women enrolled at ~32 weeks
gestation
316 (69%) women without male partner attendance
140 (31%) women with male partner attendance
456 (85%) women in a current relationship included in analysis
52 (10%) women lost to follow-up prior to
delivery
201 (44%) male partners previously
tested for HIV-1
27 (5%) women with no current
relationship

Attending male population
Characteristics (N=140) Median (IQR)/Freq (%)
Age (years) 31 (27-35)
Duration of relationship (years) 4 (2-7)
Female partner disclosed serostatus 138 (99%)
Discussed PMTCT of HIV-1 interventions with partner* 76 (72%)
Previously tested for HIV-1 as per female participant 128 (91%)
Participant tested in study 75 (54%)
Positive HIV-1 result among those tested 42 (56%)
* N=106
Correlates of male clinic attendance• Female disclosed serostatus to the male partner
– (99% of attending males v. 69% of non-attending males)
• Reported partner discussion of PMTCT interventions – (76% of attending males v. 40% of non-attending males)
• Male partner previously tested for HIV-1 as per female report – (91% of attending males v. 23% of non-attending males)– aOR=20.2; 95% CI 9.5-42.9; P=<0.001
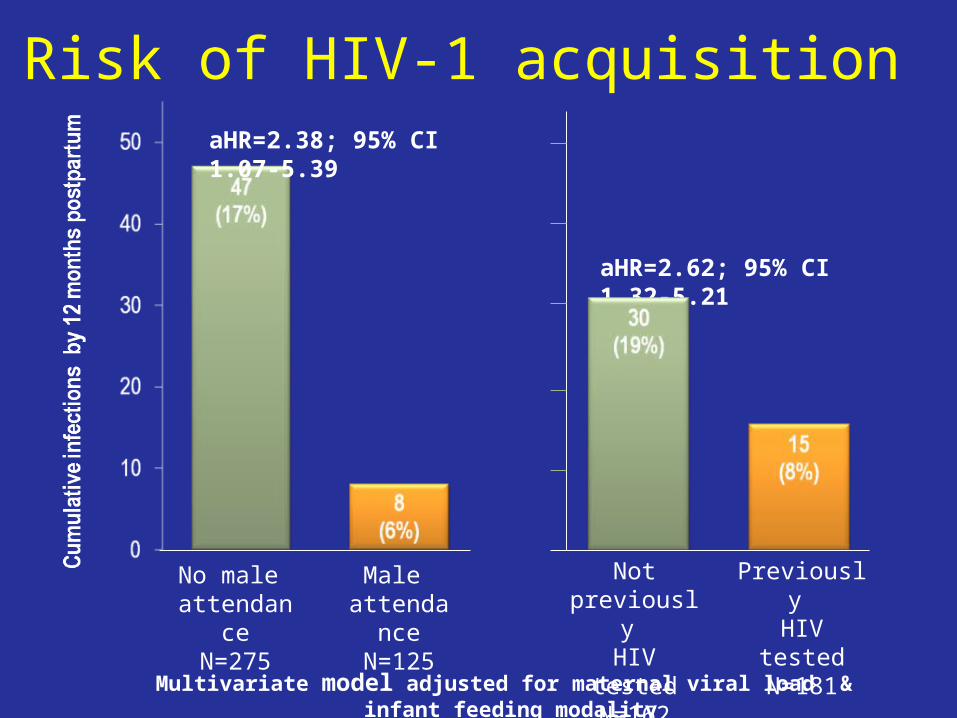
Risk of HIV-1 acquisition
Multivariate model adjusted for maternal viral load & infant feeding modality
aHR=2.62; 95% CI 1.32-5.21
No male attendance
N=275
Male attendance
N=125
Not previously HIV tested
N=162
Previously HIV tested
N=181
aHR=2.38; 95% CI 1.07-5.39

HIV-1-free survival P
rop
ort
ion
of
infa
nts
ali
ve &
HIV
-1 n
eg
ativ
e
Log rank P = <0.001 Yes (- - -)
No (____)
Log rank P = 0.015

HIV-1-free survival
1Multivariate model adjusted for maternal viral load & infant feeding modality
Correlate N aHR (95% CI)1 P value
Male attendance 296 0.41 (0.22-0.79) 0.007
Previous male HIV-1 testing 258 0.47 (0.27-0.81) 0.006

Summary & implications • Male partner involvement associated with:
– reduced risk of MTCT of HIV-1 – increased HIV-1-free survival
• Maternal-child health support– financial, physical or emotional
• Increasing male antenatal clinic attendance and VCT utilization – increase HIV-1 testing, prevention & treatment
www.pepfar.gov/press/81257.htm
AcknowledgmentsUniversity of NairobiDorothy Mbori-NgachaRose BosireRuth NduatiElizabeth ObimboPhelgona OtienoDalton WamalwaChristine Gichuhi
Fred Hutch Cancer Research CenterJulie OverbaughSandy Emery
University of WashingtonCarey FarquharGrace John-StewartBarbara Lohman-PayneBarbra Richardson
Support from NIH: NICHD and Fogarty International Center
Thank you to all study staff and participants

Male partner involvement factors• Male partner clinic attendance• Previous male partner HIV-1 testing as per female report
– Highly associated X2 (1)=139.1; P=<0.001– To avoid multi-co-linearity and to represent the affect of each individual
factor, the factors were analyzed independently in multivariate models.– Male partner ANC attendance for HIV-1 positive women is promoted in
PMTCT of HIV-1 guidelines to achieve greater HIV-1 testing, therefore identifying the specific factor is of less public health importance than identifying that both factors should be undertaken to increase diagnoses and treatment of HIV-1 infected individuals while concurrently improving infant health.

Infant feeding
• Mother choosing to breastfeed at time of enrollment and infant exposure to breast milk during the first year of life highly associated–X2 (1)=113.3; P=<0.001–OR=12.4; 95% CI 7.5-20.5; P =<0.001

Male partner perspective of PMTCT/ANC
• Attitude Towards PMTCT– Generally approved of PMTCT interventions (99%)– Approved of infant feeding alternatives (82%)
• Perception of obstacles to attending ANC/PMTCT services– Lack of information/knowledge on the existence of
services or necessity to go there (49%)– Being too busy/no time (37%)
Theuring, S., et al., AIDS Behav, 2009.