ACUTE RHEUMATIC FEVER (ARF) I.U. CERRAHPAŞA MEDICAL FACULTY DEPARTMENT OF PEDIATRICS DIVISION OF...
53
ACUTE RHEUMATIC FEVER (ARF) I.U. CERRAHPAŞA MEDICAL FACULTY DEPARTMENT OF PEDIATRICS DIVISION OF PEDIATRIC CARDIOLOGY PROF. DR. AYŞE GÜLER EROĞLU
-
Upload
cleopatra-lang -
Category
Documents
-
view
225 -
download
1
Transcript of ACUTE RHEUMATIC FEVER (ARF) I.U. CERRAHPAŞA MEDICAL FACULTY DEPARTMENT OF PEDIATRICS DIVISION OF...

ACUTE RHEUMATIC FEVER (ARF)
I.U. CERRAHPAŞA MEDICAL FACULTY
DEPARTMENT OF PEDIATRICS
DIVISION OF PEDIATRIC CARDIOLOGY
PROF. DR. AYŞE GÜLER EROĞLU

DEFINITION
* ARF, which consists of delayed nonsupurative sequelae of upper respiratory tract infection with group A ß-hemolytic streptococci, is a diffuse inflammatory disease of the connective tissue involving the heart, joints, brain, blood vessels, and subcutaneous tissue.

INCIDENCE
* Worldwide, it is the most common cause of acquired heart disease in children and young adults.
* Although the incidence of ARF has declined sharply over the past six decades in the developed countries, particularly developing countries continue to experience a high incidence of this disease.
* There is no difference in the incidence of ARF between males and females (chorea is more common in females).

EPIDEMIOLOGY
* Crowding in inadequate housing is probably the main risk factor for acquiring streptococcal infection and resulting ARF.
* The high incidence of streptococcal respiratory infections in the winter and spring probably accounts for the frequency of onset of ARF in these seasons.
* ARF is more common in people with genetic predisposition.
* Initial attacks of ARF are encountered most commonly in children between the ages of 5 and 15 years old.

EPIDEMIOLOGY
* An untreated group A streptococcal infections of the upper respiratory tract may result in ARF.
* A relatively small number of M types are the most common and dangerous rheumatogenic pharyngeal strains.
* The necessity for the preceding streptococcal infection to occur in the upper respiratory tract rather than skin is well documented.

CrowdingWinter5 – 15 years old
Socioeconomic standarts School
Group A ß-hemolyticstreptococci ARF
Upper respiratory tract infection
Penicilline (-)
1-5 (3) weeks
(%2)
EPIDEMIOLOGY

PATHOGENESIS
* ARF results from the interaction of three main factors– A causative agent (group A ß-hemolytic streptococci)
– An organ site dependence (upper respiratory tract)
– A vulnerable host
* How the organism causes rheumatic fever is still unclear.
*The most popular theory of pathogenesis is autoimmunity.

Grup A Streptococcus
Serotypes; M3, M18
Susceptile Host Positive forHLA-DR 4,2,1,3,7Allotype D8 /17
Tissue/OrganInflammation
Joints HeartBrain VascularConnective tissue
Immune Reaction
Cross-Reactive Antibody and / or Cell-Mediated Immunity
ACUTE RHEUMATİC FEVER
PATHOGENESIS

Latency period between the occurrence of the streptococcal pharyngitis and the onset of the clinical manifestations of ARF.

PATHOLOGY
* ARF is characterized pathologically by two main lesions in the connective tissues occuring particularly around small blood vessels in heart, brain, joints and skin.
* The first and the earliest lesion is exudative, degenerative, and inflammatory. This lesion contributes to transitory manifestations of ARF and responds to antiinflammatory agents. This early phase lasts 2 to 3 weeks and is followed by the second lesion.

PATHOLOGY
*The second characteristic lesion of ARF is a proliferative one that may persist for many months and years. Aschoff’s nodules are characteristic proliferative lesion of ARF. The proliferative lesion probably does not respond to the antiinflammatory agents.
* Pericardium-serofibrinous pericarditis*Myocardium-Aschoff’s nodules, interstitial
inflammation*Endocardium-mitral and aortic valvulitis and rarely
tricuspid or pulmonary valvulitis* Joints-artritis heals without residual manifestations* Subcutaneous nodules-heal rapidly without sequelae

J o n e s C r i t e r ia
Major Manifestations
• Polyarthritis• Carditis• Sydenham’s chorea• Erythema marginatum• Subcutaneous nodules
Minör Manifestations
Clinical • Fever • ArthralgiaLaboratory • Elevated acute phase reactans
Erythrocyte sedimentationC-reactive protein
• Prolonged P-R interval (> 0.16")
Supporting evidence of antecedentgroup A Streptococcal infection
• Elevated ASO • Positive throat culture or • Rapid streptococcal antigen test

If supported by evidence of preceding group A streptococcal
infection, the presence of two major manifestations or of one
major and two minor manifestations indicates a high
probability of ARF.
DIAGNOSIS

* History of streptococcal pharyngitis, 1 to 5 weeks (average, 3 weeks) before the onset of symptoms, is common. The latent period may be as long as 2 to 6 months (average, 4 months) in cases of isolated chorea.
* Pallor, malaise, easy fatigability, and other history, such as epistaxis (5% to 10%) and abdominal pain, may be present.
* Family history of ARF frequently is positive.
HISTORY

* Arthritis, the most common manifestation of ARF (70% of cases), usually involves large joints (e.g., knees, ankles, elbows, wrists). Often more than one joint, is involved, with a characteristic migratory nature of the arthritis. Swelling, heat, redness, severe pain, tenderness, and limitation of motion are common.
* The arthritis responds dramatically to salicylate therapy; if patients treated with salicylates (with documented therapeutic levels) do not improve in 48 hours, the diagnosis of ARF probably is incorrect.
ARTHRITIS

•Juvenile rheumatoid arthritis is often misdiagnosed as ARF. The following findings suggest juvenile rheumatoid arthritis rather than ARF: involvement of peripheral small joints, symmetrical involvement of large joints without migratory arthritis, pallor of the involved joints, a more indolent course, no evidence of preceding streptococcal infection, and the absence of prompt response to salicylate therapy within 24 to 48 hours.
DIFFERENTIAL DIAGNOSIS
* Other collagen vascular diseases (systemic lupus erythematosus, mixed connective tissue disease); reactive arthritis, including poststreptococcal arthritis; serum sickness; and infectious arthritis (such as gonococcal) occasionally require differentiation.
* Virus-associated acute arthritis (rubella, parvovirus, hepatitis B virus, herpes viruses, enteroviruses) is much more common in adults.
* Hematologic disorders, such as sicklemia and leukemia, should be considered in the differential diagnosis.
* Poststreptococcal reactive artritis
DIFFERENTIAL DIAGNOSIS

CARDITIS
* Frequency in ARF is 50 % (in our patients 75,4 %)* ARF may frequently involve all three layers.
Pancarditis Endocarditis: Mitral regurgitation, aortic regurgitation, mitral stenosis (late sequelae)Myocarditis: Tachycardia (out of proportion to the fever that persist during sleep), congestive heart failure (CHF)Pericarditis : Friction rub, pericardial effusion, chest pain, and ECG changes

•S1 is normal or diminished.•S2 may split widely.•S3 commonly present and loud.•Regurgitant systolic murmurs at the apex , grade 2 to 4/6, transmits to left axilla•A mid-diastolic apical murmur due to edematous cusps (Carey-Coombs)
MITRAL REGURGITATION (MR)
* MR occurs in about 50-70% of patients with rheumatic carditis. * In our patients with ARF is seen in about 78% and occurs in about 92% of patients with rheumatic carditis
MITRAL REGURGITATION
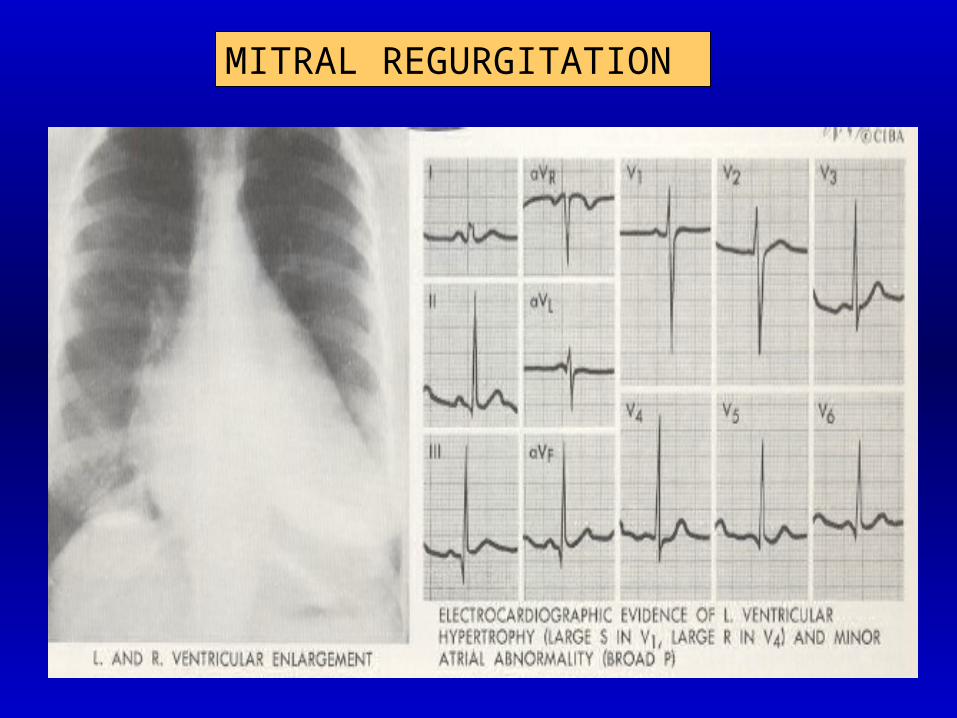
ECG: Normal in mild cases
Left ventricular hypertrophy (LVH) with or without
left atrial enlargement (LAH)
Atrial fibrillation is rare in children
X-ray: LV and the LA enlarge
Pulmonary vascularity usually is normal
Echo: The two dimentional echo shows dilated LV and LA
Color, Doppler studies can assess the severity of MR
MITRAL REGURGITATION
* AR occurs in about 20% of patients with rheumatic carditis. (In our patients isolated AR is seen in about 2% and associatedwith MR 85%)
* It can be an isolated finding but is usually associated with MR.
AORTIC REGURGITATION
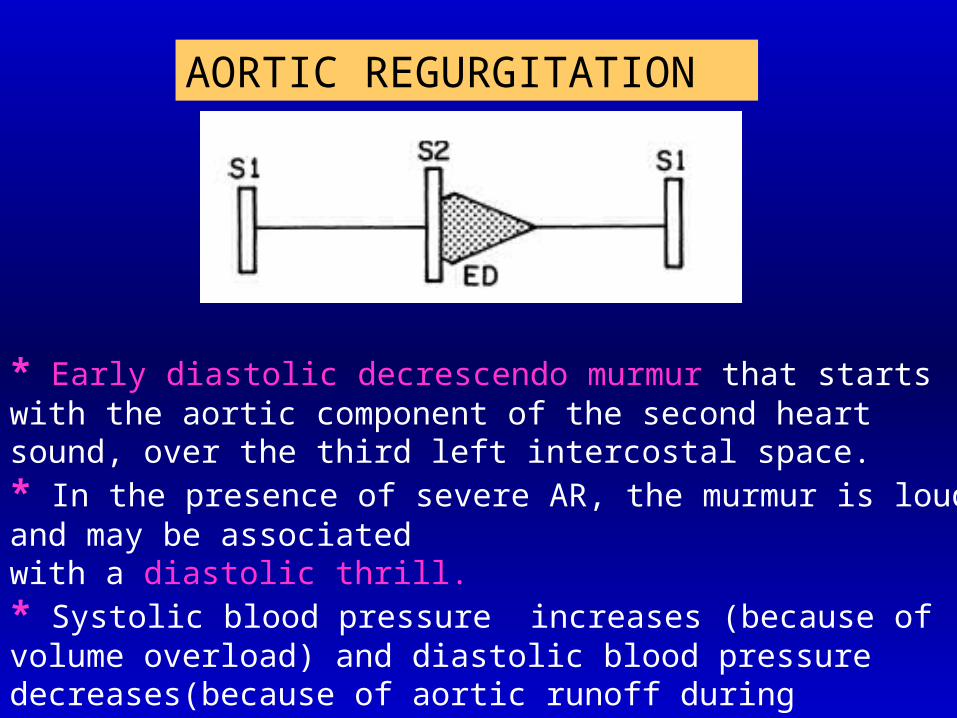
* Early diastolic decrescendo murmur that starts with the aortic component of the second heart sound, over the third left intercostal space.* In the presence of severe AR, the murmur is loud and may be associated with a diastolic thrill.* Systolic blood pressure increases (because of volume overload) and diastolic blood pressure decreases(because of aortic runoff during diastole)* In such cases, the increased pulse pressure due to the aortic runoff lesion is reflected by bounding peripheral pulses.
AORTIC REGURGITATION
AORTIC REGURGITATION
ECG: Normal in mild cases In severe cases, LVH usually is present. LAH may be present.X-ray: Cardiomegaly involving the LV is present A dilated ascending aorta and/or a prominent
aortic knob frequently are present. Pulmonary venous congestion develops if LV failure supervenes.Echo: The LV dimention is increased, but the LA remains normal in size.
Color, Doppler studies can assess the severity of AR

AORTIC REGURGITATION
MYOCARDITIS
Myocarditis is usually accompanied by valvulitis and leads to:1) Tachycardia (out of proportion to the fever) that persists during sleep.2) Rapid cardiac enlargement.3) Congestive heart failure

PERICARDITIS
* Pericarditis is encountered in only 5 to 10% of patients with carditis. In our patients is seen in about 10% and associated with valvulitis.
* Pericarditis (friction rub, pericardial effusion, chest pain, and ECG changes) may be present.
* Differential diagnosis; Isolated pericarditis is usually due to an etiology other than ARF (viral and other pericarditis, collagen vascular diseases).


SYDENHAM'S CHOREA
Frequency 10-15 % Girls > BoysLatency period 1-6 months (4 months)
It is a neuropsychiatric disorder consisting of both neurologic signs (choreic movement and hypotonia) and psychiatric signs (e.g., emotional lability, hyperactivity, seperation anxiety, obsessions and compulsions).

* The adventitious movements, weakness, and hypotonia continue for an average of 7 months (up to 17 months) before slowly waning in severity.
* Recently, elevated titers of “antineuronal antibodies” recognizing basal ganglion tissues have been found in over 90% of patients. The levels of the antineuronal antibody titer are positively related to the severity of choreic movements.
* These findings suggest that chorea may be related to dysfunction of basal ganglia and cortical neuronal components. * Differential diagnosis: congenital choreoathetosis, habitual spasms, brain tumors, behavior problems
SYDENHAM'S CHOREA

Cardiac involvement of 25 patients with chorea in the Division of Pediatric Cardiology in Cerrahpaşa Medical Faculty
17 girls, 8 boysCarditis clinically (+) 7 (% 28)Carditis clinically (Ø) 18--In 14 of these patients (78%),carditis was detected with echocardiography (silent carditis)
Isolated MR : 9Isolated AR : 3MR + AR : 2

ERYTHEMA MARGINATUM
* Frequency in ARF is 5-6 % (in our patients 2.6 %)
* Erythema marginatum is a macular, nonpruritic rash with a serpiginous erythematous border surronding normal- looking skin. They are most commonly located on the trunk and proximal limbs and do not involve the face.
* Erythema marginatum is not pathognomonic, having been reported in drug reactions and glomerulonephritis.
SUBCUTANEOUS NODULES
* Recent studies report a frequency of less than 5 % (in our patients 4,7 %)
* The nodules are located on the extensor surface of the joints, particularly the elbows, knuckles, knees and ankles. Occasionally they are found on the scalp and over the spine. They vary in size from 0.5 to 2 cm and are painless and freely movable.
* Subcutaneous are not pathognomic of ARF, since they occur in juvenile rheumatoid arthritis and systemic lupus erithematozus.

Major manifestations in 400 patients with ARF in the Division of Pediatric Cardiology in Cerrahpaşa Medical Faculty
1965-74 1988-98 ToplamMajor belirti N % N % N % %
Carditis (isolated) 105 56,1 68 32 173 43,3Arthritis (isolated) 29 15,5 44 21 73 18,5 69,1Corea (isolated) 13 7 17 8 30 7,5
Carditis+Arthritis 22 11,8 76 36 98 24,5Carditis+Chorea 4 2,1 2 0,9 6 1,5 29,6Carditis+Nodules 4 2,1 1 0,5 5 1,3Carditis+Eritema 2 1,1 2 0,5
Carditis+Arthritis+Nodules 2 1,1 3 1,4 5 1,3Carditis+Eritema+Nodules 1 0,5 1 0,3Carditis+Arthritis+Chorea 1 0,5 2 0,9 3 0,8 3,5Carditis+Arthritis+Eritema 1 0,5 2 0,9 3 0,8Carditis+Chorea+Nodules 1 0,5 1 0,3
Carditis+Arthritis+Nodules+Eritema 1 0,5 1 0,3 0,35 major manifestations 0 0
Clinical findings * Arthralgia refers to joint pain without the objective changes of arthritis. It must not be considered a minor manifestation when arthritis is present.
•Fever (usually with a temperature of at least 102°F [38.8°C]) is present early in the course of untreated rheumatic fever. The classical form is very rare nowadays.Laboratory findings*Elevated acute-phase reactants (elevated C-reactive protein levels and elevated erythrocyte sedimentation rate) are objective evidence of an inflammatory process.
* A prolonged PR interval on the ECG is neither specific for ARFnor an indication of active carditis.
MINOR MANIFESTATIONS

Supporting evidence of antecedentgroup A streptococcal infection
* Elevated ASO * Positive throat culture or * Rapid streptococcal antigen test

Antistreptolysin O (ASO) titer is well standardized and therefore is the most widely used test. It is elevated in 80% of patients with acute rheumatic fever and in 20% of normal individuals. Only 67% of patients with isolated chorea have an elevated ASO titer.
A single low ASO titer does not exclude acute rheumatic fever.

Department of Pediatrics in Cerrahpaşa Medical FacultyASO levels in ARF and other arthritisi
N X <200 >200 >400 >800 >1200 % % % % %
FMF(1976-78) 26 1007 15,4 84,6 61,5 41,0 34,6
Henoch-Schönlein(1977-86) 76 904 14,4 85,5 75,0 48,7 29,0
JRA (1967-79) 70 653 34,3 65,7 52,9 35,7 22,9
Non ARF arthritis 172 777 22,7 77,3 57,0 43,0 27,3
ARF (1965-74) 162 963 7,4 92,6 74,1 42,0 25,1
The antideoxyribonuclease B test is favored over other tests. Titers of 240 Todd units or greater in children and 120 Todd units or greater in adults are considered elevated.
The Streptozyme test (Wampole Laboratories) is a relatively simple slide agglutination test, but it is less standardized and less reproducible than the other antibody tests. It should not be used as a definitive test for evidence of antecedent group A streptococcal infection.

A diagnosis of acute rheumatic fever is highly probable
when either two major manifestations or one major and two
minor manifestations, plus evidence of antecedent
streptococcal infection, are present.
DIAGNOSIS

* Two major manifestations are always stronger than one major plus two minor manifestations.
* Arthralgia cannot be used as a minor manifestation in the presence of arthritis.
* The absence of evidence of an antecedent group A streptococcal infection is a warning that ARF is unlikely (except when chorea is present). The patients who show no evidence of cardiac involvement on initial examination should be monitored closely for evidence of carditis over the following 2 to 3 weeks.
DIAGNOSIS

* The heart murmurs of ARF must be differentiated from functional murmurs, mitral valve prolapse, myocarditis, pericarditis and congenital heart diseases.
* The possibility of the early suppression of full clinical manifestations should be sought during the history taking. Subtherapeutic doses of aspirin may suppress full manifestations.
DIFFERENTIAL DIAGNOSIS
* In 1884 Laseque noted, ‘ARF is a disease that licks the joints but bites the heart’* Only carditis can cause permanent cardiac damage (Rheumatic heart disease). Signs of mild carditis disappear rapidly in weeks, but those of severe carditis may last for 2 to 6 months.
* Arthritis subsides within a few days to several weeks, even without treatment, and does not cause permanent damage.
* Chorea gradually subsides in 6 to 7 months or longer and usually does not cause permanent neurologic sequelae.
CLINICAL COURSE

Onat T, Ahunbay G: Long-term prognosis of rheumatic mitral regurgitation:Presentation of yearly prognostic regressions in relation to affecting factors.The Turkish Journal of Pediatrics 31: 185-199, 1989
PROGNOSİS

Onat T, Ahunbay G: Long-term prognosis of rheumatic mitral regurgitation:Presentation of yearly prognostic regressions in relation to affecting factors.The Turkish Journal of Pediatrics 31: 185-199, 1989

Onat T, Ahunbay G: Long-term prognosis of acute rheumatic carditis with combined aortic and mitral regurgitation The Turkish Journal of Pediatrics 31: 185-199, 1989

TREATMENT
* Streptococcal eradication and prophylaxis
* Treatment of clinical manifestations
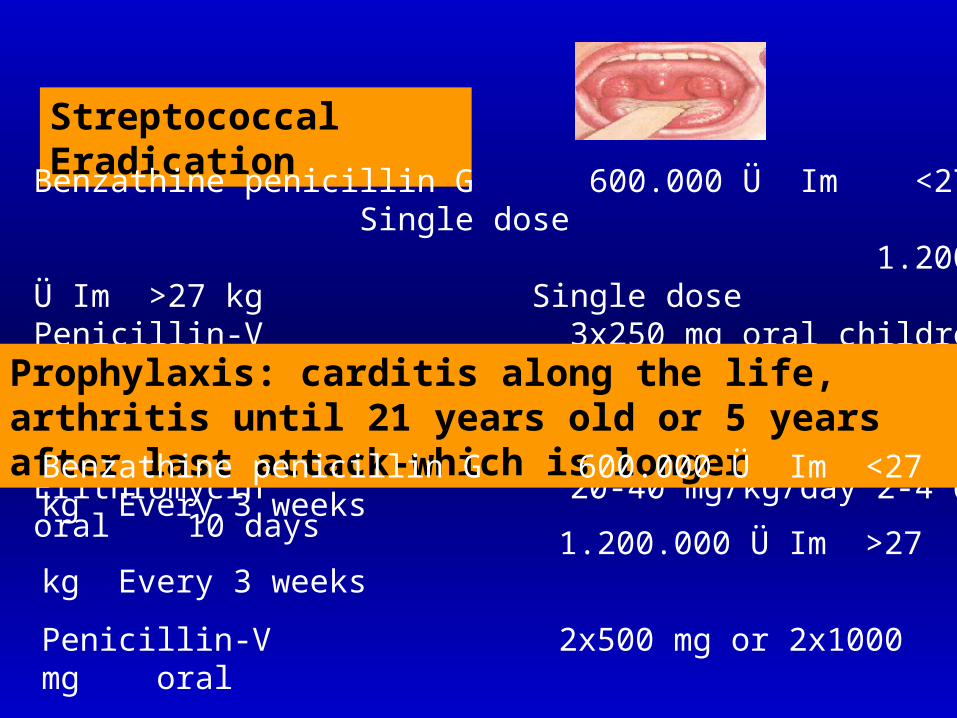
Streptococcal Eradication
Benzathine penicillin G 600.000 Ü Im <27 kg Single dose 1.200.000 Ü Im >27 kg Single dosePenicillin-V 3x250 mg oral children 10 days 3x500 mg oral adolescents, adults 10 days Erithromycin 20-40 mg/kg/day 2-4 doses oral 10 days
Prophylaxis: carditis along the life, arthritis until 21 years old or 5 years after last attack-which is longer
Benzathine penicillin G 600.000 Ü Im <27 kg Every 3 weeks 1.200.000 Ü Im >27 kg Every 3 weeks
Penicillin-V 2x500 mg or 2x1000 mg oral
Sulfadiazine 1.0 gr oral
Erithromycin 2x250 mg oral

Treatment of Clinical Manifestations
Carditis
Oral prednisolon 2 mg/kg/day (mak.60 mg) 2-3 wk. After improvement, the therapy is with drawn gradually over 4 to 6 weeks
Salicylate 90-100 mg/kg/day (4 dose) 2- 3 wk. After improvement, therapy is with drawn gradually over 3 weeks
The serum salicylate level should be about 25 mg/dL and should not exceed 30 mg/dL
Arthritis Alone
Antiinfinflammatory agents should be delayed until a proper clinical and laboratory diagnosis has been established.Neither salicylates nor corticosteroids guarantee termination of the disease and its cardiac damage.

General Guidelines for Bed Rest and Indoor Ambulation
Mild Carditis *
Arthritis Alone
Moderate Carditis **
Severe Carditis ***
Bed rest
Indoor ambulation
3-4 wk
3-4 wk
1-2 wk
1-2 wk
4-6 wk
4-6 wk
As long as CHF is present
2-3 mo
* Questionable cardiomegaly.** Definite but mild cardiomegaly.*** Marked cardiomegaly (>0,56) or heart failure.

Management of Sydenham's chorea
Haloperidol 3 x 0.5 mg (3 x 2.0 mg)
Phenobarbital 15-30 mg (every 6-8 h.)
Valproate 15-20 mg/kg/day
Anti-inflammatory agents are not needed in patients with isolated chorea.
Without the prophylaxis, about 25% of patients with isolated chorea (without carditis) develop rheumatic valvular heart disease in 20-year follow-up.