Acute respiratory failure
31
Acute Respiratory Failure Associate professor Ahmed Elmadana ver. 1.0.1 SI “Dnipropetrovs`k Medical Academy of MHU” Department of Anesthesiology and Intensive Care Medicine
-
Upload
elmadana1988 -
Category
Health & Medicine
-
view
56 -
download
2
Transcript of Acute respiratory failure

Acute Respiratory Failure
Associate professor Ahmed Elmadana
ver. 1.0.1
SI “Dnipropetrovs`k Medical Academy of MHU”Department of Anesthesiology and Intensive Care Medicine

Dept. Anesthesiology and Intensive Care Medicine DSMA, 2015
Definition
Acute respiratory failure is a rapidly progressive pathological state, when respiratory system can not support optimal blood gases tension, or do it thanks to the compensatory resources.

Dept. Anesthesiology and Intensive Care Medicine DSMA, 2015
Classification ARF by prof. A.I.Treshchinsky
Acute Respiratory FailureI.Ventilation ARF
centrogenic neuromuscular thoracic-abdominal
II.Parenchimal ARF obstructive constrictive obstructive and constrictive restrictive diffusion distributive and shunt

Dept. Anesthesiology and Intensive Care Medicine DSMA, 2015
Definition of the subgroups
Ventilation ARF – the kind of ARF, develops as a result of violation of the act of breathing.
Parenchimal ARF – the kind of ARF, develops as a result of pathological changes into the upper respiratory tract and lungs tissues.

Dept. Anesthesiology and Intensive Care Medicine DSMA, 2015
Ventilation ARF
centrogenic neuromuscular thoracic and abdominal

Dept. Anesthesiology and Intensive Care Medicine DSMA, 2015
Causes of the Centrogenic ARF Ischemia into the aria of the respiratory center
systemic hypoperfusion (any shock) local disturbance of the cerebral perfusion
Hypoxia of the respiratory center neurons ischemia Severe anemia hemiglobinemia, carboxyhemoglobinemia and other stations,
when hemoglobin can not conjunction with oxygen highly expressed disturbances of acid-base balance, in which
disrupted affinity of hemoglobin with oxygen Mechanical destruction of the respiratory center zone

Dept. Anesthesiology and Intensive Care Medicine DSMA, 2015
Causes of the Neuromuscular ARF
Violation of the passage of impulses from the respiratory center to the respiratory muscles by nerve trunks Injury of the spinal cord (rupture, compression, contusion) Injury of nerve trunks
Impairment of the synaptic transmission of impulses from neuron to respiratory muscles myasthenia gravis (deficit neurotransmitter, receptor deficiency) using of muscles relaxants the action of bacterial toxins (botulism, leptospirosis and others)

Dept. Anesthesiology and Intensive Care Medicine DSMA, 2015
Causes of the thoracic, abdominal and combined ARF
Thoracic: abnormal contents in the pleural cavity (pneumothorax, hydrothorax,
hemothorax or pyothorax) violation of the integrity of the skeleton of the chest (bilateral multiple rib
fractures with the formation of the symptom "floating" of the chest and paradoxical breathing)
violation of the integrity of the pleural cavity (open pneumothorax) Abdominal:
increase the volume of content the abdomen (ascites, intestinal bloating in acute intestinal obstruction, intestinal paresis or mesenteric thrombosis, pregnancy)
Combined thoracic and abdominal: diaphragmatic hernia rupture of the diaphragm

Dept. Anesthesiology and Intensive Care Medicine DSMA, 2015
Causes of the obstructive ARF Pathological contents of the upper respiratory tract
solid foreign bodies fluid (blood, phlegm, pus, water)
Narrowing of the upper respiratory tract due to edema edema of bronchial mucosa (irritating substances, an allergic
reaction) edema of the vocal cords (trauma, allergic reaction to insects bites) external compression of the trachea or bronchi
Violation of the position of structures relative to each other subsidence the tongue on the back of the throat

Heimlich maneuver

Heimlich maneuver in special situationsFor newborns and infants
Self-helping

Dept. Anesthesiology and Intensive Care Medicine DSMA, 2015
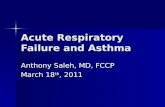
Subsidence the tongue, triple maneuver by P.Safar Triple maneuver includes:
1.Tilt the head2.Moving forward the jaw (chin lift )3.Open the mouth

Dept. Anesthesiology and Intensive Care Medicine DSMA, 2015
Causes of constrictive ARF laryngospasm bronchospasm spasm of bronchiolas

Obstructive and constrictive ARF

Obstructive and constrictive ARF
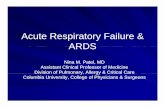
Changing in bronchi with bronchial asthma
Bronchi with asthma:1 – spasm2 – edema of mucosa3 - hypersecretion
Normal bronchus

Dept. Anesthesiology and Intensive Care Medicine DSMA, 2015
Causes of restrictive ARF Interstitial edema of lungs
acute left ventricular heart insufficiency Inhalation poisoning of irritation substances Aspiration pneumonitis (Mendelson’s syndrom)
Local edema of lung’s tissue pneumonia
Local lesion of extensibility of the lung tissue atelectasis pneumosclerosis, pneumofibrosis

Dept. Anesthesiology and Intensive Care Medicine DSMA, 2015
Mechanisms of physiological and pathological bypass
Mosaic statusof pulmonary elements
Actively functioning pulmonary element
Редуцированный легочной элемент
Внутрилегочной шунт
Альвеолярное «мертвое
пространство»
Reducedpulmonary element
Pulmonary bypass Alveolar “dead space”

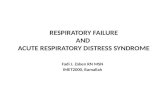
Kinds of bypass
1. normal alveoli2. alveoli with exudate
or transudate3. compression of the lung4. restriction5. obstruction6. violation of the pulmonary circulation7. violation of the diffusion of gases through the alveolar capillary membrane

Distributive and shunt ARF
ventilation
perfusion
In vertical position
вентиляция In horisontal position
perfusion

The main types of intensive care of ARF
1.Restoring and maintaining airway2.Oxygen therapy3.Assisted or mandatory artificial
lungs ventilation4.Extracorporeal gas exchange

Methods of intensive care of ARF1. Restoring and maintaining of airway:
• non-invasive (triple maneuver by P.Safar, oropharyngeal or nasopharyngeal cannula)
• half-invasive (laryngeal mask, esophageal obturator “Combitube”)
• invasive (endotracheal intubation, bronchoscopy)• surgical (cricoidotomy, tracheostomy)• medical (bronchodilators, dissolution of sputum)
2. Oxygen therapy:• with facemask• with nasal catheters• through endotracheal tube or laryngeal mask
3. Artificial lungs ventilation:• assisted (spontaneous breathing saved)• mandatory (spontaneous breathing not saved or depressed by medication)
4. Extracorporeal gas exchange

Principles of the oxygen therapy
1. Dosing100 % oxygen can be use during short time. For prolonged using concentration of oxygen must be decreasing to the minimal effective level
2. ConditionIn view of the damaging effect on the mucous membrane of the trachea and bronchi dry oxygen, it requires humidification
3. ContinuityMode with periodic cessation of oxygen therapy is less favorable than the continuous supply of oxygen due to the disruption of compensatory mechanisms


Indications for intubation and respiratory support• Protect the airway
for example, facial trauma or burns, unconscious patient• Treat profound hypoxaemia
for example, pneumonia, cardiogenic pulmonary edema, acute respiratory distress syndrome
• Postoperative carefor example, after cardiothoracic surgery and other major,complicated, or prolonged surgery
• Allow removal of secretionsfor example, myasthenia gravis, Guillain-Barré syndrome
• Rest exhausted patientsfor example, severe asthma
• Avoid or control hypercapniafor example, acute brain injury, hepatic coma,chronic obstructive airways disease

Ventilatory support should be considered if :
Respiratory rate > 40 /min or <8 /minVital capacity <10-15 ml/minPaO2 <11 kPa on FiO2 > 0.4PaCO2 high with respiratory acidosis (pH<7.2)VD/VT >60%QS/QT >15-20%ExhaustionConfusionSevere shockSevere LVFRaised ICP

Initial ventilator set-up
• Check for leaks• Check oxygen on • FIO2 0.6-1
• Volume Tidal - 7-12ml/kg• Rate - 10-15/min• I:E ratio - 1:2• Peak Pressure < 40 cm H2O
• PEEP - 0-5 cm H2O

Respiratory support
• Oxygen supplementation₋ Nasal cannula₋ Venturi mask₋ Partial rebreathing mask₋ Nonrebreathing mask (reservoir bag)₋ Face mask
• Continuous Positive Airway Pressure• Bag ventilation• Laryngeal mask• ET intubation• Mechanical ventilation

Peak airway pressure is measured at the airway opening (Pao) and is routinely displayed by mechanical ventilators. It represents the total pressure needed to push a volume of gas into the lung and is composed of pressures resulting from inspiratory flow resistance (resistive pressure), the elastic recoil of the lung and chest wall (elastic pressure), and the alveolar pressure present at the beginning of the breath (positive end-expiratory pressure [PEEP].
Resistive pressure is the product of circuit resistance and airflow. In the mechanically ventilated patient, resistance to airflow occurs in the ventilator circuit, the endotracheal tube, and, most importantly, the patient’s airways.
Elastic pressure is the product of the elastic recoil of the lungs and chest wall (elastance) and the volume of gas delivered. For a given volume, elastic pressure is increased by increased lung stiffness (as in pulmonary fibrosis) or restricted excursion of the chest wall or diaphragm (eg, in tense ascites or massive obesity).
End-expiratory pressure in the alveoli is normally the same as atmospheric pressure. However, when the alveoli fail to empty completely because of airway obstruction, airflow limitation, or shortened expiratory time, end-expiratory pressure may be positive relative to the atmosphere.
Modes of Mechanical Ventilation
Volume-cycled ventilation•V/C - volume-control•SIMV - synchronized intermittent mandatory ventilation
Pressure-cycled ventilation•PCV - pressure control ventilation•PSV - pressure support ventilation
Noninvasive positive pressure ventilation (NIPPV)•CPAP - continuous positive airway pressure•BiPAP - bilevel positive airway pressure

Extracorporeal membrane oxygenation
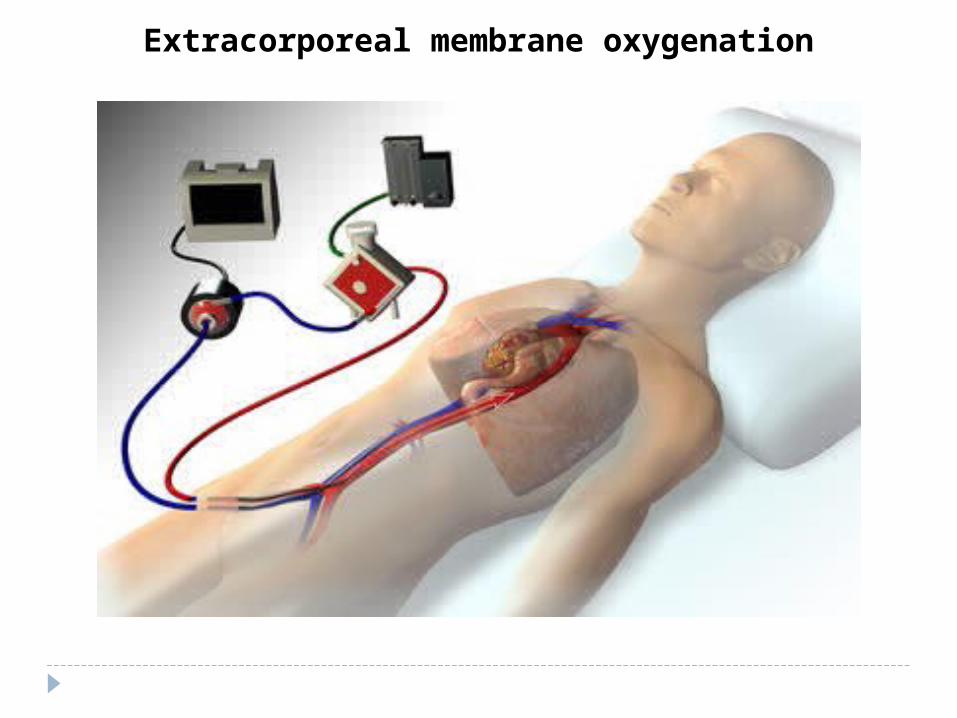
Extracorporeal membrane oxygenation