Acute respiratory conditions in childhood
50
Acute respiratory conditions in childhood part I. Peter Čižnár Seminar, 5 year General Medicine
Transcript of Acute respiratory conditions in childhood

Acute respiratory conditions in childhood
part I.
Peter Čižnár
Seminar, 5 year General Medicine

Contents
• Anatomy and function
• Breathing patterns
• Physical examination
• Acute respiratory symptom
• Respiratory distress
• Respiratory failure
• Most common acute infections
Aim: to understand the difference between child and adultto recognize dangerous and potentially life-threatening symptomsto diagnose and treat most common acute infections

Main function of the respiratory system
• to supply sufficient oxygen to meet metabolic demands and remove carbon dioxide
• Ventilation
• Perfusion
• Diffusion
V/Q = ventilation/perfusion ratio
amount of air reaching the alveoli per minute to the
amount of blood reaching the alveoli per minute
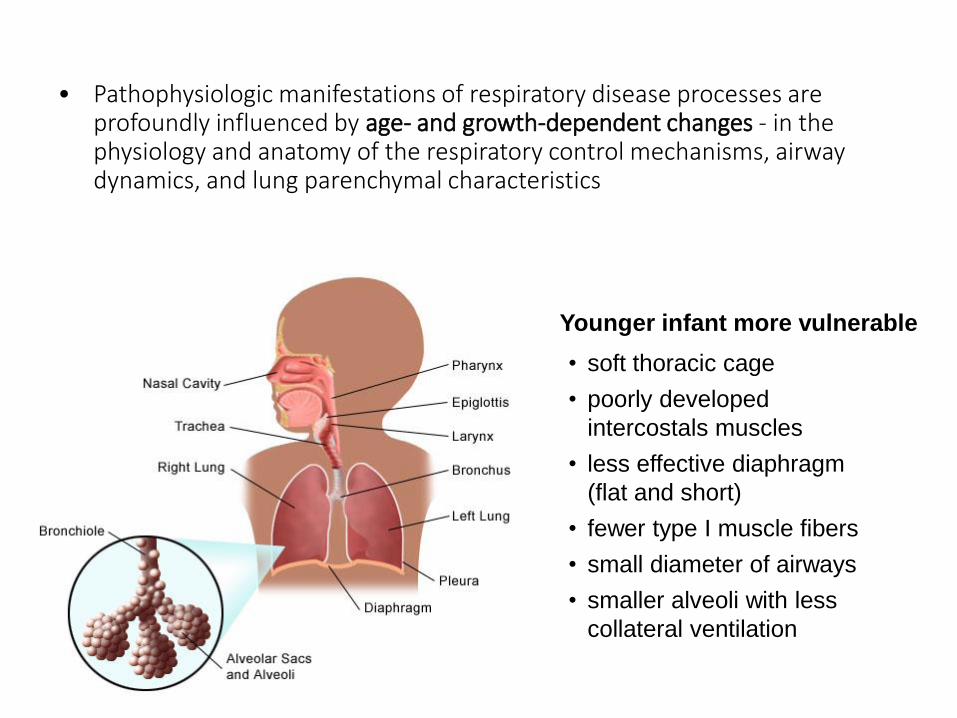
• Pathophysiologic manifestations of respiratory disease processes are profoundly influenced by age- and growth-dependent changes - in the physiology and anatomy of the respiratory control mechanisms, airway dynamics, and lung parenchymal characteristics
• soft thoracic cage
• poorly developed
intercostals muscles
• less effective diaphragm
(flat and short)
• fewer type I muscle fibers
• small diameter of airways
• smaller alveoli with less
collateral ventilation
Younger infant more vulnerable

Functional anatomy: Development of sinuses
Frontal: from 2-4y, but rarely site of
infection until 6th-10th year
Ethmoid (anterior, posterior): at birth
Maxillary: from birth, but clinical
significance only after 3rd year
Sfenoidal: present from birth, clinical
significance after 5th-8th year
Pneumatization of sinuses

Functional anatomy: Airway and lung development

Functional anatomy: Lungs
Right lung: 3 lobes (upper, middle, lower)
- occupies 55% of total lung volume
Left lung: 2 lobes (upper, lower)
- inferior division of upper lobe – lingula
(analogue to middle lobe on the right)
• Three basic faces: – convex costal, opposed to the rib cage– concave diaphragmatic– mediastinal
• Lungs are embedded in a separate pleural cavity and by the mediastinum
• Except the hilum, visceral pleura covers the lung´s outer surface - extends also into thefissures, demarking pulmonary lobes

• Conducting tubes bring inhaled gases to a large highly vascularized gas exchange surface (100 m2 in adult human)
• Efficient transport of gases at alveolo-capilar membrane
• Late evolutionary mechanism for efficient gas exchange
of terrestrial organisms
Functional anatomy: Lungs

Anatomy of the airways
• 2 functional compartments:• proximal conducting zone
(bronchial tree)
• distal respiratory zone (alveolar region)
• Basic structure already present at birth
• Dichotomous branching (avg 23 generations) is variable
• More peripheral lose cartilage and become bronchioles, distal to terminal bronchiole is „acinus“ (all airways participate in gas exchange)
Transitional
bronchioles
Co
nd
uctin
g a
irw
ays
Acin
ar
airw
ays

Microstructure of the airways
• Airways are lined with a continuous epithelium that gradually changes from ciliated pseudostratified columnar epithelium (bronchi) to ciliated simple cuboidal epithelium (bronchioles)
• At alveolar region abruptly become become sqamous
• Ciliated cells dominate, responsible for propelling mucus
epithelium is not made of single cell type, but a mosaic of several cell types
1) Ciliated epithelium
2) Goblet cell
3) Gland
4) Cartilage
5) Smooth muscle cell
6) Clara cell
7) Capillary
8) Basal membrane
9) Surfactant
10) Type I epithelial cell
(pneumocyte)
11) Alveolar septum
12) Type II epithelial cell
(pneumocyte)
Smooth muscles varies with
anatomic location.
Muscle contraction ↑ airway
rigidity – airway resistance
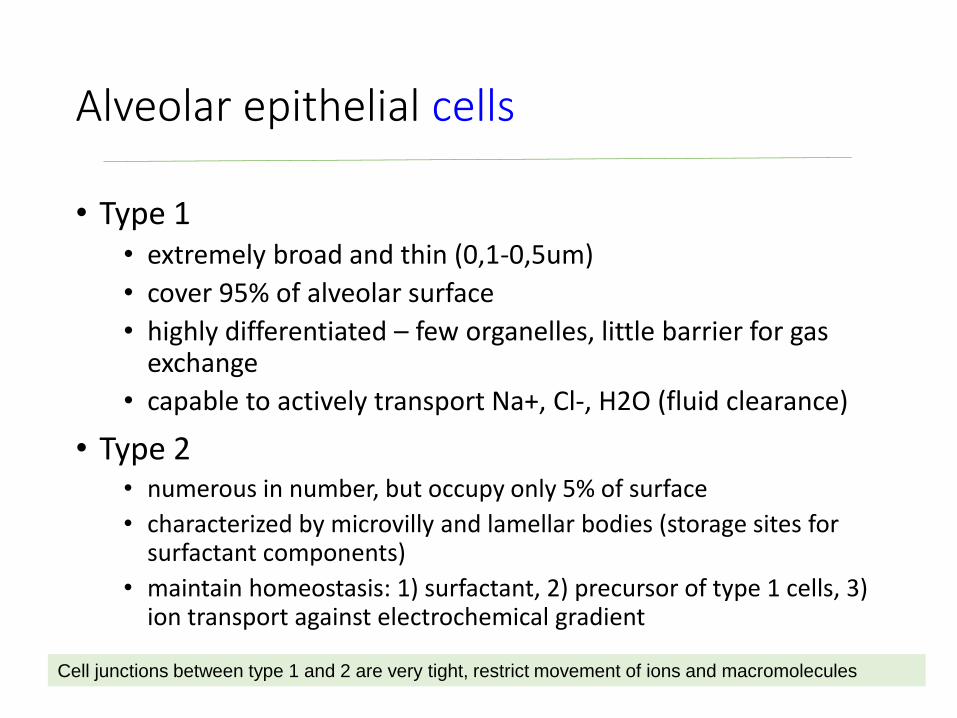
Alveolar epithelial cells
• Type 1• extremely broad and thin (0,1-0,5um)
• cover 95% of alveolar surface
• highly differentiated – few organelles, little barrier for gas exchange
• capable to actively transport Na+, Cl-, H2O (fluid clearance)
• Type 2• numerous in number, but occupy only 5% of surface
• characterized by microvilly and lamellar bodies (storage sites for surfactant components)
• maintain homeostasis: 1) surfactant, 2) precursor of type 1 cells, 3) ion transport against electrochemical gradient
Cell junctions between type 1 and 2 are very tight, restrict movement of ions and macromolecules

Surfactant
• Biophysical activities:• keep lung open (alveolar stability)
• decrease the work of breathing
• prevent alveolar edema
• Innate host defense and injury sesponse
Complex substance with multiple functions in alveoli and small airways
Composition
• sat. phosphatidylcholines 50%
• unsaturated phosphatid. 20%
• phosphatidyl glycerol 8%
• other phosphatidyl lipids 6%
• neutral lipids 8%
• proteins (SP-A, B, C, D) 8%
Alveolar surfactant life cycle1. synthesis → 2. secretion → 3. form
transition (tubular myelin) → 4. cathabolism
(degradation) → 5. recyclation

Lung defense mechanisms• Large particles (>10um) are filtrated by upper airways (nose)
• Smaller particles (5-10um) may reach trache and bronchi, deposited on mucosa
• Respirable fraction <1um reach alveoli (deposited or exhaled)
• Mucocilliary transport – continuously move a thin layer of mucus
1 cell 200 cillia beat 7-22x/s
• Immune mechanisms: alveolar macrophages, PMN, secretory IgA
• Reflexes: sneezing, cough, bronchoconstriction

Systematic approach
• The lung can be considered to be formed from six “trees”(abnormalities of bronchial venous drainage are notknown, so in practice only five trees):
• bronchial• arterial (systemic and pulmonary)• venous (systemic and pulmonary)• lymphatic
Three areas wherein malformations may affect the respiratory system:
(1) the heart and great vessels(2) the chest wall (including respiratory neuromuscular apparatus)(3) the abdomen


Hospital admissions in 1-14 year old
zdroj: CDC, 2007Kovács a spol., 2010

Respiratory diseases
Classification:
• I. Anatomic
Upper Respiratory Diseases (nose, throat - nasopharynx, paranasal sinuses)
Lower Respiratory Diseases (larynx, bronchi, lungs, pleura)
• II. Etiologic
Congenital (malformations, immaturity)
Acquired• Infectious• Non-infectious (allergic/immunologic, neoplastic, anatomic – aspiration,
herniation, metabolic etc.)
• III. Progression
Acute
Chronic

Pathologic breathing patterns
• Periodic breathing - A respiratory pattern consisting of regular oscillations in breathing amplitude, commonly seen in neonates
- Typically, a respiratory pattern in which ≥3 apneas lasting ≥3 seconds occur, separated by <20 seconds of respiration
- Usually absent in the 1st 48 hours of life; more frequent during REM (active) sleep versus non-REM (quiet) sleep; Less common in prone versus supine position
In full-term infants• amount of periodic breathing usually <4% of total sleep time
• amount gradually decreases through the 1st year of life
• by 1 year of age, the mean amount of periodic breathing is <1% of total sleep time
In premature infants• amount of periodic breathing is higher than in full-term infants
• amount correlates inversely with gestational age
Don’t confuse periodic breathing with obstructive and/or central apnea!

Pathologic breathing patterns
Periodic breathing cont’d
• can be seen in healthy infants, children, and adults
• abnormalities, in any component of the breathing control system, may result in an increased amount of periodic breathing
• Possible etiologies• delay in detecting changes in blood gas values by the chemoreceptors• increased chemoreceptor gain
• Associated conditions• Apnea of prematurity or infancy
• Familial history of sudden infant death syndrome (SIDS)
• Anemia of prematurity
• Hypoxemia
• Hypochloremic alkalosis

Pathologic breathing patterns
• Kussmaul (acidotic) breathing• rapid, deep and labored breathing (air hunger)
• respiratory compensation fo MA (diarrhoea, DKA)
• Biot’s breathing
– completely irregular breathing pattern
– continually variable rate and depth
– lesions in the respiratory center in brainstem
• Cheyn-Stokes breathing
– alternate periods of apnea (no breathing) changing smoothly into periods of hyperbreathing (HF, low Na)

Symptoms of respiratory diseases
• coughing
• wheezing
• chest tightness
• noisy breathing
• fever
• shortness of breath
• cyanosis
Signs of pulmonary disease• breath (normal, bronchial, none)
• adventitious breath sounds (wheeze, crepitation, pleural rub, none)
• percussion (hyperresonance, dullness, tympanic)
• fremitus (normal, increased, decreased, none)
Physical examination
• observation (inspection)
• palpation
• percussion
• auscultation

Inspection (observation)
Observe before touching the child !
• Chest movement• symetrical or spliting of one side
• Chest shape• overblown or barrel shaped
• pectus excavatum (hollow chest)
• pectus carinatum (pigeon chest)
• Harrison’s sulcus (diaphragmatic tug)
• Respiratory rate
• Type of respiratory movement• eupnoea, tachypnoea, dyspnea, ortopnea
• Finger clubbing, petechiae (traumatic in severe cough)
Avoid anxiety (keep the mother hold the infant or small child)
Clothing should be removed to inspect the thorax

Physiology of the respiratory system
AGE HR BP RR
Premature newborn 120 - 170 55-75 / 35- 45 40 - 70
0-3 m 100 – 150 65-85 / 45- 55 35 – 55
3-6 m 90 – 120 70-90 / 50-65 30 – 45
6-12 m 80 – 120 80-100 / 55-65 25 - 40
1-3 y 70 - 110 90-105 / 55-70 20 – 30
3-6 y 65 – 110 95-110 / 60-75 20 – 25
6-12 y 60 – 95 100-120 / 60-75 14 – 22
> 12 y 55 - 85 110-135 / 65-85 12 – 18
Respiratory rate has a greater range in children compared to adults (more responsive
to exercise, emotions, illness)
Determine by: observing chest movement or by chest auscultation!

Inspection (observation)
RESPIRATION• general appearance – inability to feed, smile, lack of consolability• respiratory rate - tachypnea• colour – pallor, cyanosis• nasal component – nasal flaring (enlargement of both nasal openings during
inspiration)
• audible breath sounds – grunting (repetitive, short expiratory sounds), wheezing (musical expiratory sound), stridor (high-piched, inspiratory noise), obstruction (lack of breath sounds)
• work of breathing • nasal flaring (excessive movement of nares)• grunting, retractions
• supraclavicular – soft tissue over clavicles
• intercostal - indrawing of the skin between ribs
• subcostal – just below the costal margin
Observe before touching the child !

Palpation and percussion
• Palpation less useful in infants and toddlers• search masses or areas of tenderness
• tactile fremitus – a vibratory sensation during crying or speaking (increased in consolidation, decreased in atelectasis)
• Percussion by tapping lightly with middle finger of the middle phalanx of the opposite hand (pleximeter)
• percuss entire chest comparing symmetric sites
• reduced resonance (dullness) – presence of consolidation (pneumonia, pleural effusion, position of heart and liver)
• Increased resonance (hyper-resonance) – retention of air
Hands should be warm !
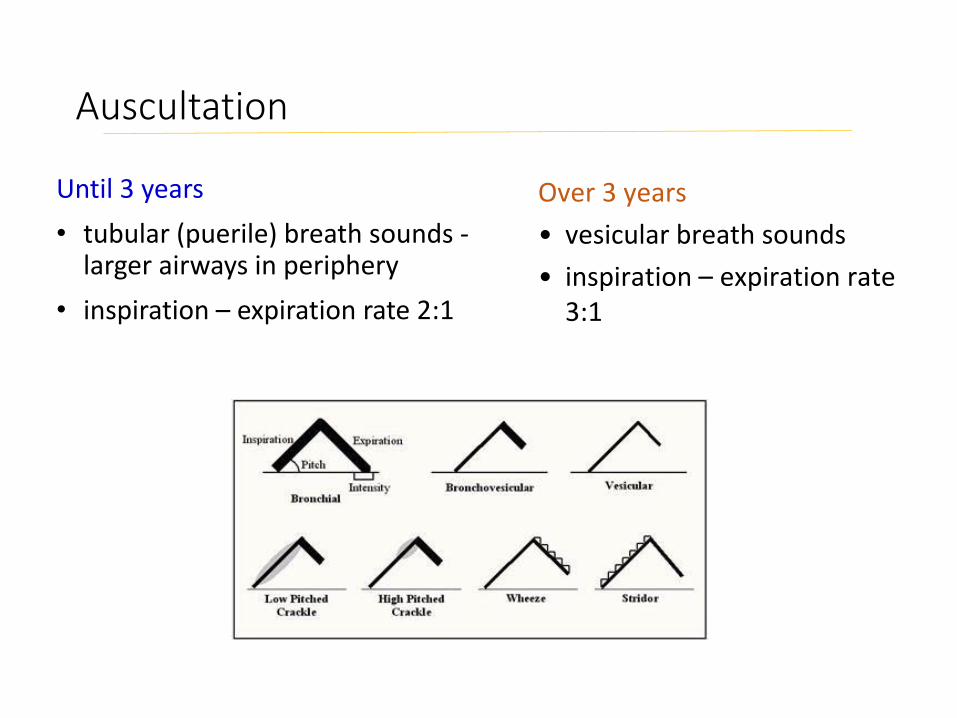
Auscultation
Until 3 years
• tubular (puerile) breath sounds -larger airways in periphery
• inspiration – expiration rate 2:1
Over 3 years
• vesicular breath sounds
• inspiration – expiration rate 3:1

Auscultation
Adventitious breath sounds
• Continuous • wheezy – continuous musical sound
• air movement through a narrowed airway caused by edema, excessive mucus production, bronchospasm
• rhonchi• low pitched wheeze, or gurgle, produced by airflow through liquids of various
viscosity in the airways
• Discontinuous• Crackles (rale), crepitation
• like rubbing of a lock of hair over head – snapping open of previously collapsed airways or alveoli (crepitation indux)
• pleural rub rare in childhood

Acute Respiratory Symptoms
• Tachypnea (rapid breathing)
• Dyspnea (shortness of breath): subjective sensation of difficult, laboured, uncomfortable breathing
• occur through 1) increased respiratory muscle work, 2) stimulation of neuroreceptors throughout the respiratory tract, or 3) stimulation of peripheral and central chemoreceptors
• physical finding: grunting, flaring of the nasal alae, retractions of the supraclavicular, intercostals and subcostal areas
• differential diagnosis: central (e.g.psychiatric), respiratory, cardiovascular
• Labs - selectively based upon history and physical examination: CBC with differential, electrolytes, BUN, Cr, cultures (blood, urine, sputum), swabs (throat, NPW), ABG, CXR, EKG

Acute Respiratory Symptoms
• Hypoxia: the most worrisome sign and clinical endpoint O2 sat. are helpful, but remember that they represent the ratio of oxygenated haemoglobin to total haemoglobin; O2 sat. can still be normal in the face of anemia or CO poisoning
• Cyanosis: means that carboxyhemoglobin is at least 5g/100mL of blood, or that O2 sat. have dropped below 85% (polycythemic patients can appear cyanotic when an anemic patient would be acyanotic, simply due to the content of carboxyhemoglobin)
• Central cyanosis (e.g. cyanotic congenital heart disease)
• Peripheral cyanosis (e.g. severe respiratory disease): sign of decreased peripheral perfusion or impaired gas diffusion

Acute Respiratory Symptoms
• Cough: most important reflex mechanism protecting the airways and lung, may be voluntary or generated by reflex irritation (nose, sinus, pharynx, larynx, trachea bronchi and bronchioles)
Loss of cough reflex leads to aspiration
• Productive cough (moist)
• Dry cough
• Chest pain: variety of sources, virtually any structure in the chest can cause pain (lungs, ribs, chest wall muscles, diaphragm, joints between the ribs and sternum)
• Etiology: injury, infection, irritation
Occasionally, pain can be referred from another area (such as the abdomen), or may also be a manifestation of stress or anxiety
Chest pain in children is rarely caused by the heart

Respiratory distress, RDS, ARDS
Respiratory distress syndrome (RDS):- a common breathing disorder affecting newborns, most often preterm babies,
nearly all newborns who are born before 28 weeks of pregnancy- less often can can affect full term newborns- due to low surfactant production lungs collapse - develops in the first 24 hours, over time become bronchopulmonary dysplasia
Acute respiratory distress syndrome (ARDS)*:- a disease characterized by severe diffuse inflammation and hypoxemia
that can affect both adults and children
Pediatric Acute respiratory distress syndrome (PARDS):- a heterogeneous syndrome with a variety of causes- not required bilateral infiltrates on chest imaging ....
* Ferguson ND, Fan E, Camporota L, et al. The Berlin definition of ARDS: An expanded rationale, justification, and supplementary material. Intensive Care Med. 2012;38:1573–1582

Respiratory distress
• in patient with abnormalities of CNS or neuromuscular disease the respiratory failure can be present without respiratory distress (not be able to mount sufficient effort)
• a child who appears in respiratory distress might not have a respiratory illness
CAVE ! ! !
Diagnosed from signs:• cyanosis, nasal flaring, grunting, tachypnea, wheezing,
chest wall retractions, stridor

Definition of acute respiratory distress
• when breathing does not match the body’s metabolic demand for oxygen due to failure of oxygenation and/or ventilation
• typically characterized by signs of increased work of breathing - tachypnea, use of accessory muscles, retractions, in very young children head bobbing, nasal flaring, grunting
• respiratory rate may be increased or inappropriately slow for the clinical condition (warning sign of respiratory distress and impending respiratory arrest)
• abnormal pattern of respiration is a sign of respiratory distress that may offer clues to etiology

Causes of acute respiratory distress
Respiratory tract• Infection• Asthma, anaphylaxis• Foreign body or liquid
aspiration• Airway anomalies• Inhalation of biological
or chemical substances• Chest wall trauma• Thoracic cavity
condition• Pulmonary condition
Cardiovascular• Congenital heart disease• Acute heart failure• Myocarditis, pericarditis• Arrythmia• Myocardial infartion,
cardiac tamponade, shock
Nervous system• Depressed ventilation• Hypotonia• Pulmonary aspiration in
airway reflexes loss

Causes of acute respiratory distress
Metabolic and endocrine diseases
• Metabolic acidosis• diabetic ketoacidosis• severe dehydratation• Sepsis• Toxic ingestions• Inborn errors of
metabolism
• Hyperthyroidism• Hypothyroidism• Hyperammonemia• Hypocalcemia
(laryngospasm)
Hematologic• Decreased oxigen capacity
• Acute severe anemia(blood loss, hemolysis, methemoglobinemia, carbone monoxide)
• Acute chest syndrome (in sickle cell disease)
Gastrointestinal• Gastrointestinal reflux with
pulmonary aspiration
• Hypoventilation in abdominal distension or pain (bowel obstruction, perforation, trauma)

Acute Respiratory Failure• Failure to deliver adequate O2 (hypoxia), or remove CO2 (hypercapnia)
• 50% of deaths in children under 1 year (soft thoracic cage, poorly developed intercostalsmuscles, less effective diaphragm - flat and short, fewer type I muscle fibers, small diameter of airways, smaller alveoli with less collateral ventilation)
• patients with chronic disease during an intercurrent acute illness (e.g. influenza) or surgery
• previously healthy children (pneumonia, epiglottitis, acute asthma, aspiration)
Finding Causes Examples
Type I Hypoxia
PaO2
normal PaCO2
Ventilation / perfusion defect Pneumonia, atelectasis, bronchopulmonary
dysplasia, pulmonary embolus, ARDS
Diffusion impairment Pulmonary edema, interstitial pneumonia, ARDS
Shunt Pulmonary a-v malformation
Type II Hypoxia
Hypercapnia
PaO2
PaCO2
Hypoventilation Neuromuscular disease (polio, G-B sy), severe
respiratory obstruction (epiglottitis,
bronchiolitis, asthma), head trauma, sedation
Therapy: at the ICU, oxygen supplementation, intubation, mechanical ventilation
Normocapnic vs hypercapnic hypoxia

Premenná 0 bodov 1 bod 2 body 3 body
Počet dychov
< 2 mesiace ≤ 60 61-69 ≥ 70
2-12 mes. ≤ 50 51-59 ≥ 60
2. rok ≤ 40 41-44 ≥ 45
3. rok ≤ 34 35-39 ≥ 40
4-5 rokov ≤ 30 31-35 ≥ 36
6-12 rokov ≤ 26 27-30 ≥ 31
> 12 rokov ≤ 23 24-27 ≥ 28
Retrakciehrudníka
žiadne subkostálne alebo interkostálne
≥2 : subkostálne, interkostálne, substernálne alebo súhyby nosných stien (dojča)
≥3 : sub-, interkostálne, substernálne,suprasternál-ne, supraklavikulárne alebo súhyby nosných stien / súhybyhlavy (dojča)
Dyspnoe
0-2 roky normálny orálny príjem, aj vokalizácia, aktívne
≥1 : ťažkosti s kŕmením, sťažená vokalizácia alebo agitovanosť
≥2 : ťažkosti s kŕmením, sťažená vokalizácia alebo agitovanosť
orálny príjem zastavený, bez vokalizácie, útlm alebo zmätenosť
2-4 roky normálny orálny príjem aj vokalizácia, hrá sa
≥1 : znížená chuť do jedla, kašeľ pri hre, hyperaktivita
≥2 : znížená chuť do jedla, intenzívny kašeľ pri hre, hyperaktivita
odmieta orálny príjem, odmieta hru alebo útlm a zmätenosť
>4 roky počíta do ≥10 na jedno nadýchnutie
počíta do 7-9 na jedno nadýchnutie
počíta do 4-6 na jedno nadýchnutie
počíta do <3 na jedno nadýchnutie
Auskultácia normálne dýchanie, bez piskotov
piskoty na konci expíria piskoty počas celého expíria
Insp.aj expir.piskoty alebo oslabené dýchanie
Re
spir
ačn
é s
kóre
(R
S)

Respiratory distress - infections
• Uvulitis
• Epiglottitis
• Retropharyngeal abscess
• Peritonsillar abscess
• Croup (laryngitis)
• Tracheitis
• Bronchiolitis
• Pneumonia
Symptoms: redness, swelling, spots, sore throat, difficult swallowing, chocking, horse voice
Cause? : infection (viral, bacterial), allergy, hereditary angioedema, acid reflux or vomiting
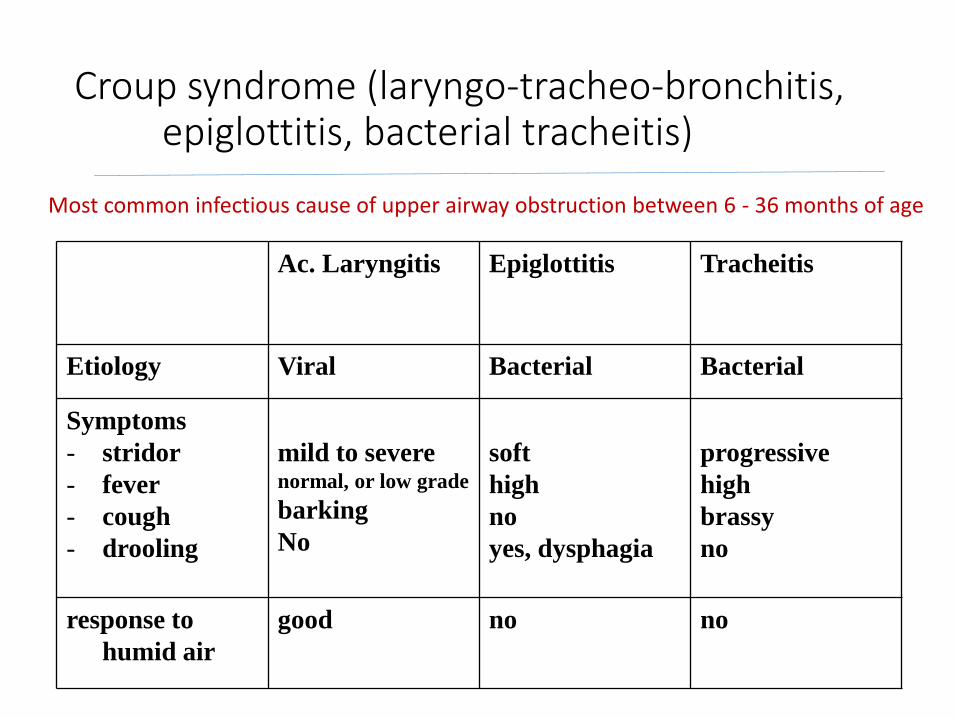
Croup syndrome (laryngo-tracheo-bronchitis, epiglottitis, bacterial tracheitis)
Ac. Laryngitis Epiglottitis Tracheitis
Etiology Viral Bacterial Bacterial
Symptoms
- stridor
- fever
- cough
- drooling
mild to severenormal, or low grade
barking
No
soft
high
no
yes, dysphagia
progressive
high
brassy
no
response to
humid air
good no no
Most common infectious cause of upper airway obstruction between 6 - 36 months of age

Acute laryngitis - treatment
• mist inhalation (humid air, saline)• nebulized racemic
epinephrine (adrenaline)• oral hydratation (only small sips
of liquid – water, ORS)
• oxygen• corticosteroids (i.m., rectal)• minimal handling• in epiglottitis – manipulate as
little as possible!!, remain child sitting
• needle cricothyroidotomy• antibiotics• ICU
Always admit to hospital if:
• actual or suspected epiglottitis
• progressive stridor, severe stridor at rest
• respiratory distress
• hypoxemia
• restlessness
• cyanosis
• pallor
• depressed sensorium or high fever in a toxic-appearing child

Acute bronchitis(obstructive or wheezing bronchitis)
• primary viral upper respiratory infection (parainfluenza, influenza, RS virus, adenovirus)
• - secondary bacterial infection (Streptococcus pneumoniae, Moraxella catarrhalis, or H. influenzae)
• Symptoms: Physical findings vary with the age of the patient and the stage of the disease.
• in infants: No or low grade fever, expiratory dyspnea, wheezing, shortness of breath. Within several days, the cough becomes productive.
• older children: whistling sounds during respiration (rhonchi), soreness of the chest, dry cough, occasionally by shortness of breath.
• Treatment: symptomatic (inhalation of bronchodilators, corticosteroids in severe bronchial obstruction, mucolytics)

Bronchiolitis
• Pathology: inflammatory obstruction of the small airways
• Age: during the first 2 yr of life, peak incidence at approximately 6 mo
• Etiology: respiratory syncytial virus (RSV) in more than 50% of cases, parainfluenza virus, mycoplasma, some adenoviruses.
• Clinical picture: starts as a mild upper respiratory tract infection with serous nasal discharge and fever of 38.5-39°, gradual development of respiratory distress with paroxysmal wheezy cough, dyspnea, and irritability, difficult feeding.
• Physical examination: Tachypnea (60-80 breaths/min), hyperexpandedchest, extreme distress, fine crackles at the end of inspiration and in early expiration.
• Complications: critical period first 48-72 hr after the onset of dyspnea, apneic spells, respiratory acidosis, dehydratation, case fatality rate is less than 1%;
• Treatment: hospitalization, supportive therapy (cool humidified oxygen), sitting position (30-40 dg), parental fluid replacement, Ribavirin (inhalation) – steroids – bronchodilatation ?

Pneumonia
Classification by etiology
Community acquired (CAP) • Nosocomial acquires (NAP)• Pneumonia of chronically sick• Ventilator associated pneumonia• Pneumonia in immunocompromised
bakterial viral fungal mixed
typical atypical
A.
B.
Streptococcus pneumoniaStaphylococcus aureusgroup A Streptococcus
Mycoplasma pneumoniaeChlamydia pneumoniae

Pathogen detection among children with CAP requiring hospitalization
BMC Infectious Diseases 17(1), Dec 2017
• Respiratory syncytial virus (RSV) (22.9%)
• Human rhinovirus (HRV) (22.1%)
• M. pneumoniae (15.8%)
• Coinfection in 34.6% • 71.3% mixed viral-bacterial
infections
• Mixed infections more• in age < 6 months• in admissions to PICU
N=846 patients with CAP

PneumoniaC. Radiology classification
Lobar pneumonia Bronchopneumonia Intertitial pneumonia
> 4 years: the frontal posteroanterior (PA) upright chest view
younger children: position does not affect the size of the cardiothoracic shadow, use the anteroposterior (AP) supine view

Deň č. 1.
Zatienenie ľavého pľúcneho poľa s
presunom stredových štruktúr doprava
Deň č. 2.
Stav po drenáži hrudníka s odsatím
cca 100ml výpotku
Exudative left side pleuropneumonia with lower lobe atelectasis

Exudative left side pleuropneumonia with lower lobe atelectasis
Deň č. 21.
Nález s nehomogénnym ložiskovým
zatienením v ľavom dolnom pľúcnom poli
Deň č. 22.
CT nález pneumatokély v ľavom dolnom pľúcnom poli
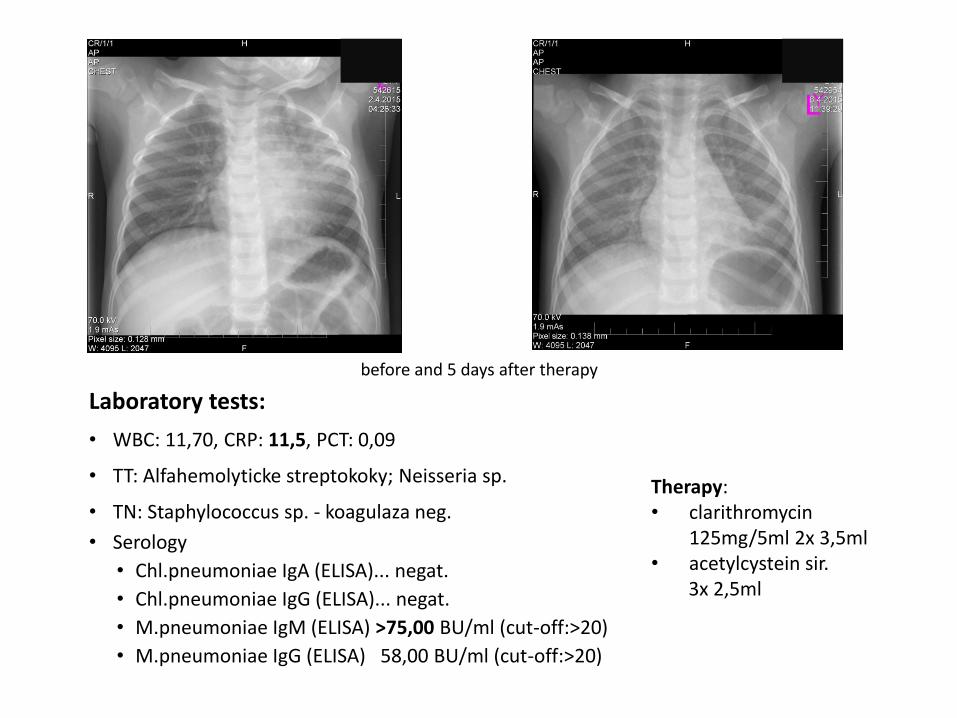
Laboratory tests:
• WBC: 11,70, CRP: 11,5, PCT: 0,09
• TT: Alfahemolyticke streptokoky; Neisseria sp.
• TN: Staphylococcus sp. - koagulaza neg.
• Serology
• Chl.pneumoniae IgA (ELISA)... negat.
• Chl.pneumoniae IgG (ELISA)... negat.
• M.pneumoniae IgM (ELISA) >75,00 BU/ml (cut-off:>20)
• M.pneumoniae IgG (ELISA) 58,00 BU/ml (cut-off:>20)
Therapy: • clarithromycin
125mg/5ml 2x 3,5ml• acetylcystein sir.
3x 2,5ml
before and 5 days after therapy

Conclusions
Respiratory distress may develop in children due to multiple etiologiesthat result in one of the following final common pathways
• Hypoxemia
• Hypercarbia
• Difficulty with mechanics of respiration, typically from airway obstruction, muscle weakness or discomfort
• Disordered control of ventilation in which respiration may be depressed or stimulated
Respiratory distress in response to hypoxemia or hypercarbia can rapidly progress to life-threatening respiratory failure
Neonates, infants, and young children are at particular risk given their high oxygen consumption and decreased respiratory reserve







![Chronic Pancreatitis Associated Acute Respiratory Failuremedcraveonline.com/MOJI/MOJI-05-00149.pdf · Chronic Pancreatitis Associated Acute Respiratory ... [1,2]. Acute respiratory](https://static.fdocuments.us/doc/165x107/5ca432de88c993ad338b9ab4/chronic-pancreatitis-associated-acute-respiratory-f-chronic-pancreatitis-associated.jpg)