Acute peri-operative left heart failureleft heart failure - Acute... · Acute peri-operative left...
46
Acute peri-operative left heart failure left heart failure Alexandre Mebazaa, Hôpital Lariboisière, Université Paris 7 U942 Inserm
Transcript of Acute peri-operative left heart failureleft heart failure - Acute... · Acute peri-operative left...

Acute peri-operative left heart failureleft heart failure
Alexandre Mebazaa, Hôpital Lariboisière, Université Paris 7p ,
U942 Inserm

Conflict of InterestConflict of Interest
Lecture fee: Orion
No other conflicts for this lectureNo other conflicts for this lecture

Acute peri-operative heart failureheart failure
Systolic heart failure, mostly after CPB
Diastolic heart failure: post-operativeDiastolic heart failure: post operative period of any surgery
Right ventricular failureg

Practical Recommendations On The Management of Perioperative Heart Failure g
In Cardiac Surgery
Chairpersons: F Follath, W Toller, A MebazaaMebazaa
Faculty: A Pitsis, A Rudiger, D Longrois, S-E Ricksten, I Bobek, SG De Hert, G Wieselthaler, U Schirmer, LK von Segesser, M Sander, D Poldermans, M Ranucci, P Wouters, M Seeberger, ER Schmid, W Weder
Mebazaa et al Crit Care 2010

Practical Recommendations On The Management of Perioperative Heart Failure g
In Cardiac Surgery
EpidemiologyRi k S ifi iRisk StratificationCardioprotective agentsCardioprotective agentsMonitoringPharmacological treatmentClinical scenariosClinical scenariosMechanical circulatory support
Mebazaa et al Crit Care 2010

« Medical » Cardiogenic Shock in ICU: EFICA t d S t Ad i iEFICA study, Symptoms on Admission
SBP H 93 139SBP mmHg 126 93 139 <0.0001DBP mmHg 71 54 77 <0.0001
Zannad F, Mebazaa A, et al. Eur J Heart Fail. 2006
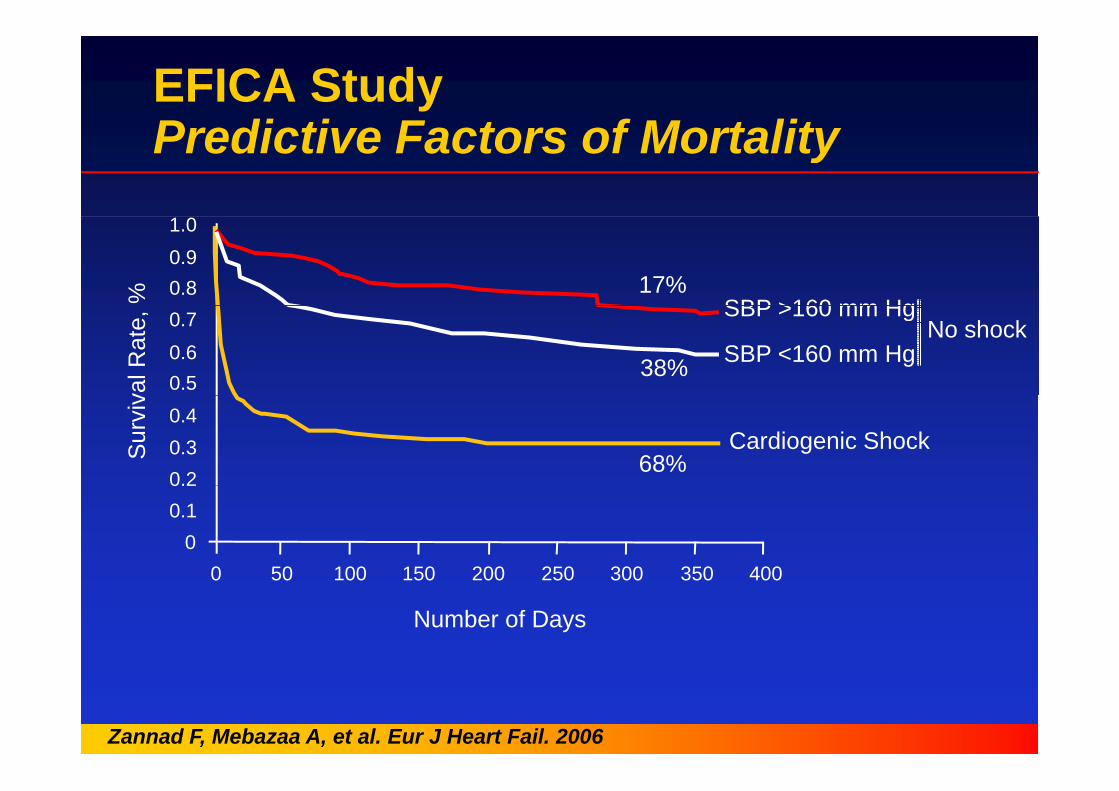
EFICA StudyP di ti F t f M t litPredictive Factors of Mortality
0.80.91.0
SBP >160 mm Hg% 17%
0.50.60.7
SBP <160 mm Hg
SBP >160 mm Hg
val R
ate,
38%No shock
0.20.30.4
Cardiogenic ShockSur
viv
68%
00.10.2
0 50 100 150 200 250 300 350 4000 50 100 150 200 250 300 350 400
Number of Days
Zannad F, Mebazaa A, et al. Eur J Heart Fail. 2006

Survival rates of ICU-patients with different acute heart failure syndromes over timeacute ea t a u e sy d o es o e t e

Risk stratification in cardiac surgerycardiac surgery
Group recommendations:
‐Indicators of major clinical risk in the perioperative period are: unstable coronary syndromes, decompensated HF, significant arrhythmias and severe valvular diseasearrhythmias and severe valvular disease‐Clinical risk factors include history of heart disease, compensated HF, cerebrovascular disease, presence of diabetes p , , pmellitus, renal insufficiency and high‐risk surgery‐the EuroScore® predicts perioperative cardiovascular alteration
llin cardiac surgery well‐BNP measure before surgery is an additional factor of risk stratificationstratification
Mebazaa et al Crit Care 2010
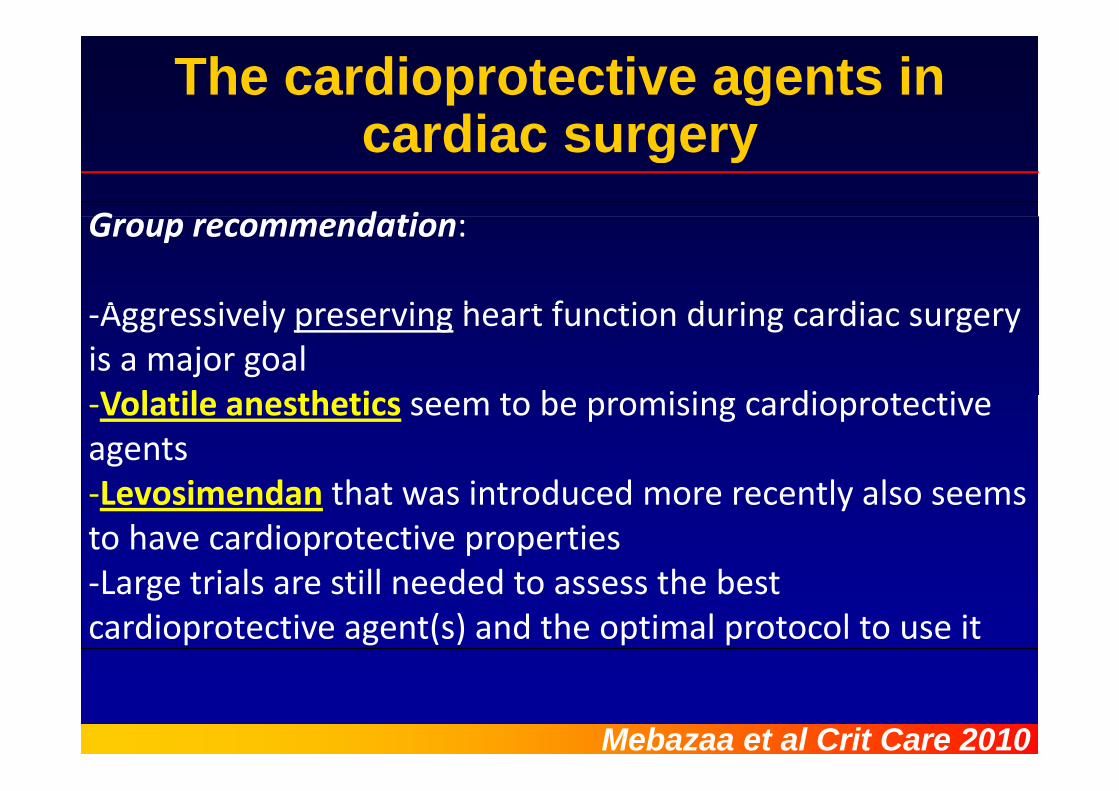
The cardioprotective agents in cardiac surgerycardiac surgery
G d tiGroup recommendation:
A i l i h t f ti d i di‐Aggressively preserving heart function during cardiac surgery is a major goalV l til th ti t b i i di t ti‐Volatile anesthetics seem to be promising cardioprotectiveagentsL i d th t i t d d tl l‐Levosimendan that was introduced more recently also seems to have cardioprotective propertiesL t i l till d d t th b t‐Large trials are still needed to assess the best cardioprotective agent(s) and the optimal protocol to use it
Mebazaa et al Crit Care 2010
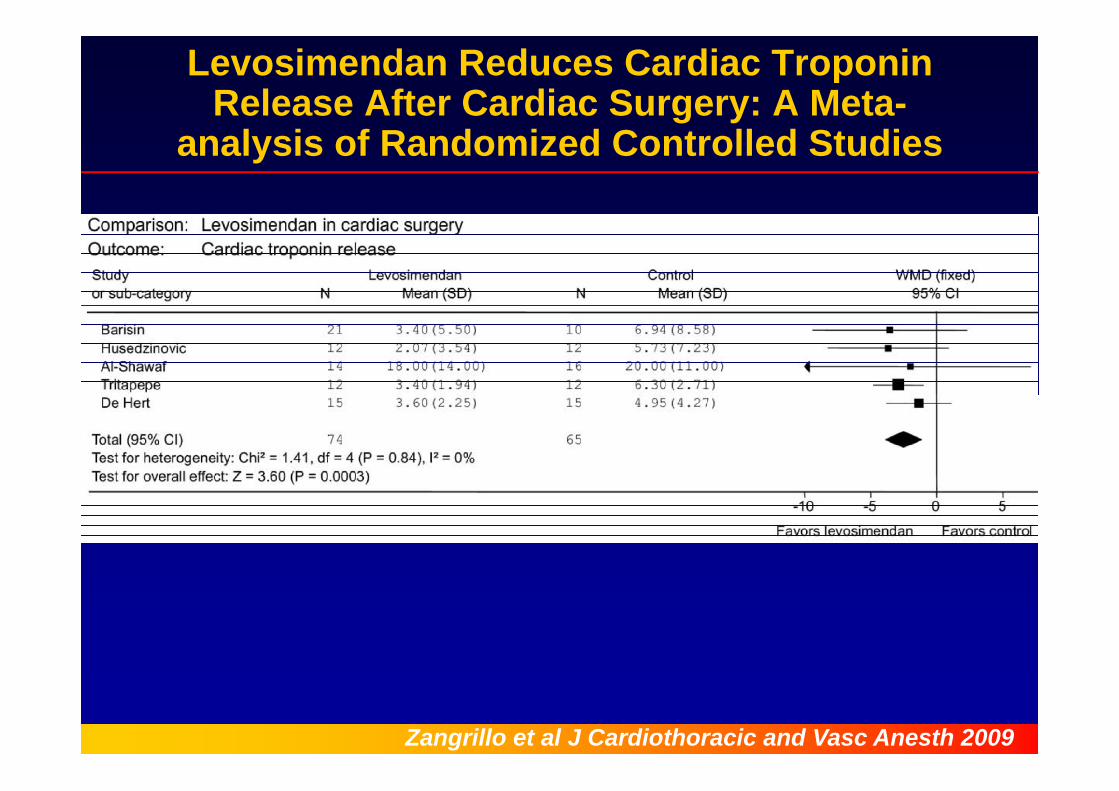
Levosimendan Reduces Cardiac Troponin Release After Cardiac Surgery: A Meta-
analysis of Randomized Controlled Studies
Zangrillo et al J Cardiothoracic and Vasc Anesth 2009
Monitoring in cardiac surgeryMonitoring in cardiac surgeryGroup recommendation:p‐Monitoring is aimed to early detect and assess the mechanism(s) of perioperative cardiovascularmechanism(s) of perioperative cardiovascular dysfunction V l t t i id ll d b “d i ”‐Volume status is ideally assessed by “dynamic” measures of haemodynamic parameters before and after volume challenge rather than single measures ‐Heart function is first assessed by echocardiographyy g p yfollowed by PAC, especially in case of right heart dysfunctiondysfunction
Mebazaa et al Crit Care 2010
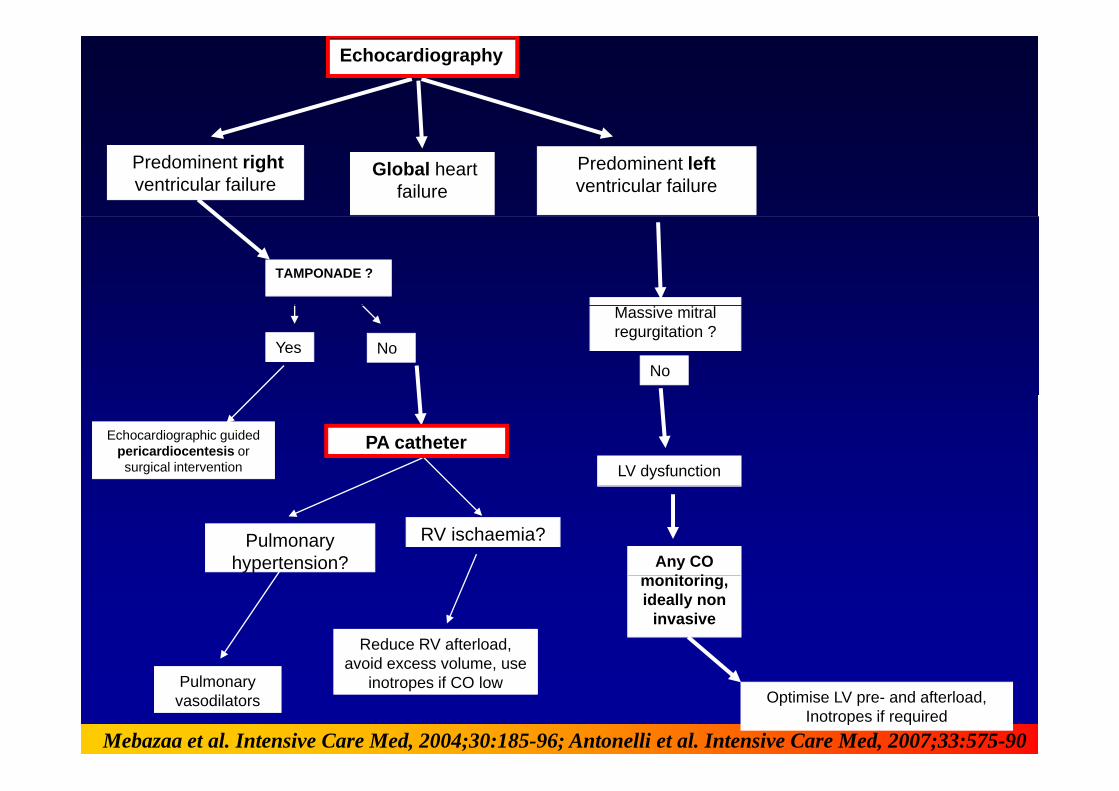
Echocardiography
Predominent rightventricular failure
Predominent leftventricular failure
Global heart failure
TAMPONADE ?
Yes
Massive mitral regurgitation ?
NoNo
Echocardiographic guided pericardiocentesis or surgical intervention
PA catheterLV dysfunction
Pulmonary hypertension?
RV ischaemia?Any CO
it i
Reduce RV afterload, avoid excess volume use
monitoring,ideally non
invasive
Pulmonary vasodilators
avoid excess volume, use inotropes if CO low
Mebazaa et al. Intensive Care Med, 2004;30:185-96; Antonelli et al. Intensive Care Med, 2007;33:575-90
Optimise LV pre- and afterload,Inotropes if required

Intensive Care Medicine, 2006; 32:9-10

The « pyramid » of echocardiography skills in ICU
Cholley,Vieillard-Baron, Mebazaa, ICM 2006

Management of post-operative hemodynamic failure
SBP < 85mmHg
hemodynamic failureSBP < 85mmHg
Oliguria (<0.5ml/Kg/hour)Clinical signs of tissue hypoperfusion
Heart rate
Volemia VesseltoneMyocardial
functionfunction
Pharmacologic treatment of cardiac dysfunction in the perioperative period of
cardiac surgery (1)Group recommendation‐In case of myocardial dysfunction consider the following 3 options either alone or combined:1)Milrinone decreases PCWP and SVR while stroke volume (SV) and heart rate (HR) increase less than with other inotropes2)Dobutamine improves SV and HR while PCWP moderately decreases3)Levosimendan increases SV and decreases SVR. It also reduces the time to extubation and ICU LOS compared to dobutamine
Mebazaa et al Crit Care 2010
Pharmacologic treatment of cardiac dysfunction in the perioperative period of
‐ Norepinephrine should be used in case of low bloodcardiac surgery (2)
Norepinephrine should be used in case of low blood pressure due to vasoplegia, to maintain an adequate perfusion pressure Volaemia should be repeatedlyperfusion pressure. Volaemia should be repeatedly assessed to ensure that the patient is not h l i hil dhypovolaemic while under vasopressors
‐ Optimal use of inotropes or vasopressors in the perioperative period of cardiac surgery is still controversial and needs further large multinational controversial and needs further large multinational studies
Mebazaa et al Crit Care 2010
Clinical scenarios of cardiac dysfunctiondysfunction
Group recommendation :pThe classification of cardiac impairment in the perioperative period of cardiac surgery should be based 1) on the time of p g y )occurrence:‐precardiotomy (A)p y‐failure to wean (B)‐postcardiotomy (C)and 2) on the haemodynamic severity of the condition of the patient‐crash and burn (1)‐sliding fast (2)‐stable but inotrope dependent (3)
Mebazaa et al Crit Care 2010

Mechanical Circulatory Supporty
Cli i l i C l d d iClinical scenarios Commonly used devicesIABP
I ll 2 5/5A. precardiotomy CS Impella 2.5/5Percutaneous (tranfemoral) ECMO
TandemHeartIABP
B. failure to wean
IABPImpella 5ECMO
Centrifugal pumps as LVAD RVAD BVADCentrifugal pumps as LVAD, RVAD,BVADAbiomed BVS 5000, AB 5000, Thoratec PVAD
Long term implantable devicesIABP
C. postcardiotomy CS
IABPImpella 5ECMO
Centrifugal pumps* as LVAD, RVAD, BVADg p p , ,Percutaneous pulsatile devices** as LVAD, RVAD,BVADLong term implantable devices 1st, 2nd and 3rd generation
Mebazaa et al Crit Care 2010

Acute peri-operative heart failureheart failure
Systolic heart failure, mostly after CPB
Diastolic heart failure: post-operativeDiastolic heart failure: post operative period of any surgery
Right ventricular failureg

Patient’s historyPatient s history
• Men, 72 y.o.• smoker, quit 15 y ago• no diabetes• no diabetes• Admitted for knee surgery• major risk factor: father of an
anesthesiologist!anesthesiologist!
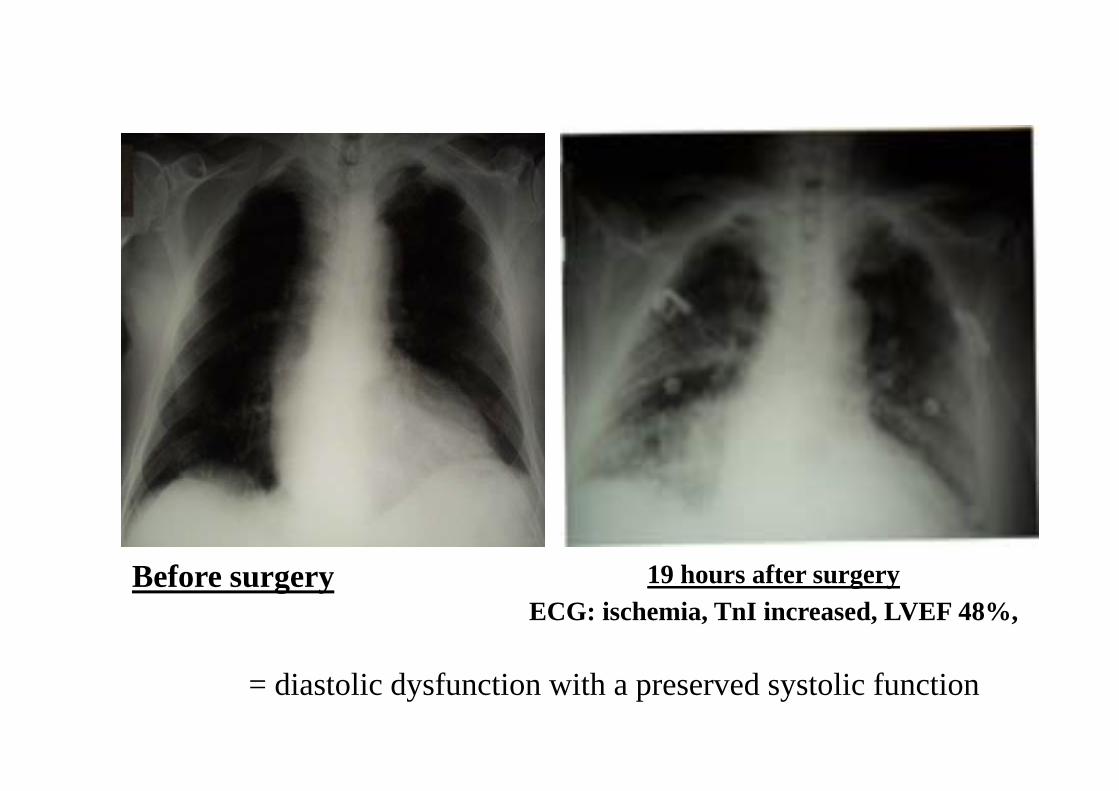
Before surgery 19 hours after surgeryBefore surgery 19 hours after surgeryECG: ischemia, TnI increased, LVEF 48%,
= diastolic dysfunction with a preserved systolic function

↑ Myocardial oxygen
consumption
↓ Coronary oxygen delivery
Increase in body temperature Anemia
MYOCARDIAL
+ +
MYOCARDIAL ISCHEMIA
↓diastolic coronary↓ filli i
TACHYCARDIA
↓ filling time
+
LEFT VENTRICULARDIASTOLIC DYSFUNCTION
Hypovolemia, Pain
Treatment by:diuretics morphine
blood transfusionβ-blockers
PULMONARY CONGESTION
β

Diastolic heart failure in anaesthesia and ICU
Pirracchio et al. Br. J. Anaesth.2007; 98: 707-721


Acute peri-operative heart failureheart failure
Systolic heart failure, mostly after CPB
Diastolic heart failure: post-operativeDiastolic heart failure: post operative period of any surgery
Right ventricular failureg

Right ventricular failure
following CPBfollowing CPB
Mechanims?
Mebazaa et al. Intensive Care Med, 2004;30:185-96

Pulmonary stenosis

Right coronary stenosis

Pulmonary stenosis and RC stenosis
1971

Dilated Right Ventricle !
TR

Auto-aggravation of CO decrease in ARVFRight Ventricular Failure
Reduction in CO + RV dilatation + reduction in LV preloadp
tricuspid regurgitation hypotensiontricuspid regurgitation hypotension
decrease in RCPPdecrease in RCPPorgan's hypoperfusion
+ congestion (acidosis )
greater reduction in CO
+ congestion (acidosis, ...)
greater reduction in CO
Mebazaa et al. Intensive Care Med, 2004;30:185-96

DANGER
Volume loading can be harmfulVolume loading can be harmful
It may worsen liver and kidneyti if RV f ti i tcongestion if RV function is not
previously restoredpreviously restored

volume loading CO is oftenPA
g CO is oftenunchanged
ARVFRAP
RVTR
Increase in AP
CONGESTION
Increase in AP,transaminases and
creatinine
CONGESTION

In AHF-induced liver congestion
• What is/are the mechanism(s) of:
– Increased transaminases?
– Increased alkaline phosphatase ?

AHF i d d li ti
The cardio-hepatic syndromeAHF-induced liver congestion
(increased BNP)
Bile ductcompression
Bile ductcompression
Normalcompression(increased AP)
compression(increased AP)
+++++
+ +++++
and cytolysis(increased transaminases)

In case of RVF, « tailored therapy » i d dis recommended
Low BP: NE is needed to improve right coronary perfusion pressure and organ perfusion pressureHigh PAP: Inhaled NOLow CO/cardioprotection: levosimendan is an optionp

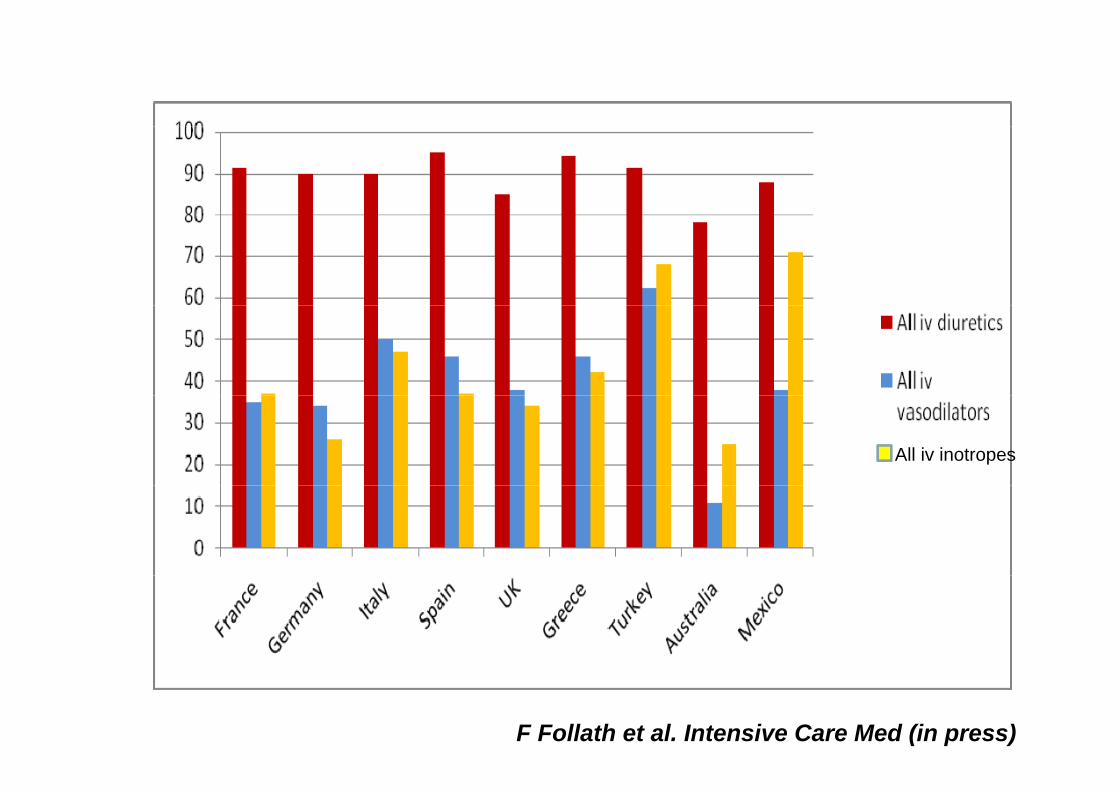
Acute Heart Failure: Global Survey of Standard Treatment
The ALARM-HF StudyThe ALARM-HF Study
F Follath et al. Intensive Care Med (in press) A Mebazaa Intensive Care Med (in press)
All iv inotropes
F Follath et al. Intensive Care Med (in press)

0.6
ty Epinephrine4
0.5
mor
tali Epinephrine
Norepinephrine
0.3
0.4
spita
l m0.
20
In-h
os
Whole cohort
Dopamine
Dobutamine
0.1
Whole cohort
Diuretics
0 5 10 15 20 25 30
0.0 Levosimendan
Diuretics
Vasodilatators0 5 10 15 20 25 30
DaysA Mebazaa Intensive Care Med (in press)

SBP < 100 mmHg SBP 100-119 mmHg
SBP 120-159 mmHg SBP > 160 mmHg
A Mebazaa Intensive Care Med (in press)

Does post-discharge treatment influence short-
d l t t ?and long-term outcome ?

All-Cause Mortality by Beta-Blocker Useat Baseline and Discharge
All-Cause Mortality by Beta-Blocker Useat Baseline and Discharge (n=1000+ patients)at Baseline and Discharge
1.0
at Baseline and Discharge
1.0
( p )va
l 0.9Baseline
Discharge
val 0.9
Baseline
Discharge
of s
urvi
v
0.8 No / Yes
Yes / Yes
of s
urvi
v
0.8 No / Yes
Yes / Yes
babi
lity
o
0.7No / No
Yes / No
babi
lity
o
0.7No / No
Yes / No
0.6Prob
0.6Prob
0.00 30 60 90 120 150 180
0.00 30 60 90 120 150 1800 30
Days since start of study drug infusion60 90 120 150 1800 30
Days since start of study drug infusion60 90 120 150 180

Effects of beta-blockers on patients admitted for acute respiratory failure (n=300+ patients)for acute respiratory failure (n 300+ patients)
No/YesYes/Yes
No/Yes
CARDIAC CAUSES NON-CARDIAC CAUSES
No/No
Yes/YesNo/Yes
No/No
Yes/No
Yes/No
Noveanu et al Crit Care 2010

In summaryIn summary
• In case of low CO in post-operative CPB period:p– Understand the mechanism (echo, PAC)
Give an appropriate treatment– Give an appropriate treatment
• Do not forget to give a post-discharge treatmenttreatment









![Acute heart failure [MBBS]](https://static.fdocuments.us/doc/165x107/58f9ac181a28abe55c8b45d9/acute-heart-failure-mbbs-58f9ddbd15ebc.jpg)