The Use of Procalcitonin as a Sepsis Marker in a Community ...
Upload
taemCategory
view
393download
0description

28-Nov-14
1
SEPSIS MARKERS IN
CLINICAL USE
Methee Chayakulkeeree, MD, PhD Division of Infectious Diseases and Tropical Medicine
Department of Medicine
Faculty of Medicine Siriraj Hospital
Mahidol University
Systemic Inflammatory Response Syndrome
(SIRS)
Criteria
• Two or more of the following are required
Body temperature > 38 °C or < 36 °C
Heart rate > 90 beats/min
Respiratory rate > 20 breaths/min (or arterial pCO2 < 32 mmHg, indicating hyperventilation)
White blood cell count > 12.0 x109/L or < 4.0 x109/L (or > 10% immature forms)
• Sepsis = Infection + SIRS
• Severe sepsis = Sepsis + evidence of organ dysfunction
Crit Care Med 1992;20:864-74., Crit Care Med 2003;31:1250-6.

28-Nov-14
2
Diagnostic Criteria for Sepsis
General variables
• Fever (> 38.3°C)
• Hypothermia (core temperature < 36°C)
• HR > 90/min or > 2 SD above normal value for age
• Tachypnea
• Altered mental status
• Significant edema or positive fluid balance (> 20 mL/kg over 24 hr)
• Hyperglycemia (plasma glucose > 140 mg/dL or 7.7
mmol/L) in the absence of diabetes
Inflammatory variables
• Leukocytosis (WBC count > 12,000 /μL)
• Leukopenia (WBC count < 4000 /μL)
• Normal WBC count with > 10% immature forms
• Plasma C-reactive protein > 2 SD above normal value
• Plasma procalcitonin > 2 SD above the normal value
Hemodynamic variables
• Arterial hypotension (SBP < 90 mm Hg, MAP < 70 mm
Hg, or an SBP decrease > 40 mm Hg in adults or < 2 SD below normal for age)
Organ dysfunction variables
• Arterial hypoxemia (Pao2/Fio2 < 300)
• Acute oliguria (urine output < 0.5 mL/kg/hr for at least 2 hrs despite adequate fluid resuscitation)
• Creatinine increase > 0.5 mg/dL or 44.2 μmol/L
• Coagulation abnormalities (INR > 1.5 or aPTT > 60 s)
• Ileus (absent bowel sounds)
• Thrombocytopenia (platelet count < 100,000 /μL)
• Hyperbilirubinemia (plasma total bilirubin > 4 mg/dL or 70 μmol/L)
Tissue perfusion variables
• Hyperlactatemia (> 1 mmol/L)
• Decreased capillary refill or mottling
Infection, documented or suspected, and some of the following:
Surviving Sepsis Campaign Guidelines. Crit Care Med. 2013;41:580-637.
Severe sepsis = sepsis-induced tissue
hypoperfusion or organ dysfunction
• Sepsis-induced hypotension
• Lactate above upper limits laboratory normal
• Urine output < 0.5 mL/kg/hr for > 2 hrs despite adequate fluid resuscitation
• Acute lung injury with Pao2/Fio2 < 250 in the absence of pneumonia as infection source
• Acute lung injury with Pao2/Fio2 < 200 in the presence of pneumonia as
infection source
• Creatinine > 2.0 mg/dL (176.8 μmol/L)
• Bilirubin > 2 mg/dL (34.2 μmol/L)
• Platelet count < 100,000 μL
• Coagulopathy (international normalized ratio > 1.5)
Surviving Sepsis Campaign Guidelines. Crit Care Med. 2013;41:580-637.

28-Nov-14
3
Two phases of sepsis: Sequential Model
Hyper-inflammatory phase: SIRS
Immunosuppressed phase: Compensatory anti-inflammatory response syndrome
(CARS)
Contrib Microbiol 2011;17:1–11., Chest 1997;112:235–43.
Pro-inflammatory cytokines: TNF, IL-1β, IL-6, CRP, PCT
Anti-inflammatory cytokines: IL-10
Two phases of sepsis: Concurrent Model
Infect Dis Clin North Am 1999;13:413–26.

28-Nov-14
4
Sepsis Biomarkers • Acute phase proteins
CRP
Procalcitonin (PCT)
Pentraxin3 (PTX3)
Lipopolysaccharide binding protein (LBP)
• Cytokines & chemokines IL-1RA, IL-1b, IL-2, IL-6, MCP-1
TNF-a, TNFR1/2
HMGBP1
• Cell surface markers Soluble CD14 (presepsin)
Neutrophil CD64 index (CD64in)
mHLA-DR (monocyte HLA-DR levels)
CD-163
• Receptor markers VEGF
Soluble VEGF-receptor 1 (sFLT)
Soluble urokinase plasminogen activator
(suPAR)
sTREM-1
RAGE (soluble receptor for advanced
glycationend products)
• Coagulation Activated partial thromboplastin time (aPTT)
waveform analysis
Protein C receptor
Thrombomodulin
• Endothelial damage Heparin binding protein
E-selectin
Neopterin
ICAM-1, VCAM-1
Angiopoietin-1 and -2
Syndecan-1 and -2
• Vasodilation Copeptin (AVP precursor)
• Cell damage MicroRNA
Microparticles
• Cell repair Procollagen III amino propeptide
inflammation
coagulation
Tissue damage
and repair
Pro-inflammatory cytokines during
hyper-inflammatory phase of sepsis
PAMPs = Pathogen Associated Molecular Patterns
DAMPs = Damage Associated Molecular Patterns
Crit Rev Clin Lab Sci, 2013; 50: 23–36

28-Nov-14
5
Interleukin-6 (IL-6)
• A pro-inflammatory cytokine
• More reliably measurable in plasma than TNF and IL-1β
• Not specific for sepsis (like TNF and IL-1β)
• Autoimmune rheumatic disorders
• Major role as a biomarker of sepsis appears to be
prognostic, not diagnostic
• Elevated levels of IL-6 in septic patients are associated
with an increase in mortality
Br J Surg 1994;81:1306–8., Intensive Care Med 2002;28:1220–5., Crit Care Med 2004;32:2173–82.
C- reactive protein (CRP)
• One of a group of acute phase reactants
• A well-established biomarker of infection and inflammation
• Inflammatory or infectious disease
• Atherosclerosis
• Cardiovascular disease
• High sensitivity, low specificity
• Also use for monitoring in pediatric and post-operative
patients
N Eng J Med 1999;340:448–54.

28-Nov-14
6
Procalcitonin (PCT)
• A peptide precursor of the hormone calcitonin
• Composed of 116 amino acids with a half-life of 25 to 30 hours
• Produced by parafollicular cells (C cells) of the thyroid and the
neuroendocrine cells of the lung and the intestine
• Level in healthy individuals is below the limit of detection (10 pg/mL)
• Rises in a response to a pro-inflammatory stimulus, especially of
bacterial origin (not in viral infection or non-infectious inflammations)
• Produced mainly by the cells of the lung and the intestine
• High procalcitonin levels produced during infections are not followed
by a parallel increase in calcitonin or a decrease in serum calcium
levels.
Lancet Infect Dis 2013;13: 426–35

28-Nov-14
7
Procalcitonin-guided interventions against
infections in ICU: an RCT
Procalcitonin-guided interventions against
infections in ICU: an RCT
Crit Care Med 2011; 39:2048 –2058

28-Nov-14
8
Conclusion from the study
• A strategy with escalation of broad spectrum
antimicrobials in the intensive care unit guided by daily
procalcitonin measurements as used in this trial did NOT
improve survival and did lead to an increased use of
broad-spectrum antimicrobials, which is concerning in
regard to toxicity, resistance, and economics.
• We observed deleterious effects on organ function and
length of stay in the intensive care unit and the strategy
cannot be recommended.
Crit Care Med 2011; 39:2048 –2058
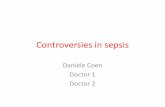
Biomarkers of activated neutrophils and
monocytes in sepsis
Neutrophil Macrophage

28-Nov-14
9
Four Promising Biomarkers for Acute
Infection
•sTREM-1
•suPAR
•ProADM
•sCD14 (Presepsin)
LBP and sCD14 (Presepsin)
• Elevated levels of LBP can identify patients with infection, but this protein effectively neutralizes LPS, and may even be anti-inflammatory
• Therefore, LBP may be less discriminating than other biomarkers with regard
to risk of developing severe sepsis
• Recently, there has been interest in measuring a soluble form of CD14
(Presepsin) as a biomarker of sepsis.
• Soluble CD14 levels were shown to be comparable to PCT for diagnosis of bacterial infection and correlated with the degree of severity in septic patients
J Infect Chemother 2012;18:891–7., J Infect Chemother 2011;17:764–9.

28-Nov-14
10
Soluble CD14-subtype (sCD14-ST)
• CD14 is a 13 kDa protein that is present in macrophage,
monocyte, and granulocyte cells and their cell
membranes
• Responsible for intracellular transduction of endotoxin
signals
• Its soluble fraction is present in blood and is thought to be
produced in association with infections
J Infect Chemother 2011;17:764–9.
sCD14 in Clinical Use
Annals of Intensive Care 2013, 3:22.

28-Nov-14
11
sCD14 Value in Different Conditions
J Infect Chemother 2011;17:764–9.
sCD14 and Other Biomarkers in Sepsis
Infection vs. non-infection SIRS: infection vs. sepsis
J Infect Chemother 2011;17:764–9.

28-Nov-14
12
sCD14 and APACHE II Score
J Infect Chemother 2011;17:764–9.
sCD14 in Emergency Department
Critical Care 2013, 17: R244

28-Nov-14
13
sCD14 in Emergency Department
Critical Care 2013, 17: R244
Diagnosis of sepsis Predicting severe sepsis
Multicenter, Randomized ALBIOS Trial - sCD14 and Organ Failure
Intensive Care Med. 2014 Oct 16
Total 997 patients 1 = <597 ng/L 2 = 597-1397 ng/L
3 = >1397 ng/L

28-Nov-14
14
ALBIOS Trial: Appropriateness of ATB Therapy and sCD14
Intensive Care Med. 2014 Oct 16
ALBIO Trial: Day 1 sCD14 Concentration and Mortality
Intensive Care Med. 2014 Oct 16

28-Nov-14
15
ALBIOS Trial: Changes in sCD14 and Mortality
Intensive Care Med. 2014 Oct 16
D1-2 1st : < -14.9
2nd : -14.9-13.7
3rd : > 13.7
D1-7 1st : < -38.4
2nd : -38.4- 15.8
3rd : > 15.8
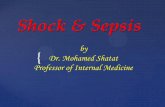
Burn Sepsis
Burns. 2014;40:664-9

28-Nov-14
16
Burns. 2014;40:664-9
Burn Sepsis
Abdominal Sepsis Intra-abdominal infections Sample size: Healthy 70, SIRS 30, Sepsis 20, Severe sepsis 10
Clin Chem Lab Med 2013;51:2053-62

28-Nov-14
17
sCD14 in Sepsis vs SIRS (non-infection)
Area under ROC sCD14: 0.996
PCT: 0.912 CRP: 0.857
WBC: 0.777
Clin Chem Lab Med 2013;51:2053-62
Biomarkers in Febrile Neutropenia in
Pediatric Oncology Patients
Cytokine 2013:62:34-37

28-Nov-14
18
sCD14-ST in Adult Febrile Neutropenia
• Preliminary data from Siriraj Hospital
• Total = 25
• Male 12 (48%), female 13 (52%)
• Mean age 43 ± 11 years
• Underlying diseases
• AML 14 (56%)
• ALL 4 (16%)
• CML 1 (4%)
• NHL 5 (20%)
• Other 1 (4%)
Bacteremia and Biomarkers
sCD14-ST Procalcitonin
*
*
*

28-Nov-14
19
Summary
• Biomarkers are promising for use for diagnosis and
prognosis in sepsis as well as initiation and determination
of antimicrobial therapy
• Biomarkers available for clinical use include PCT, CRP,
IL6 and sCD14
• Increasing data of sCD14-ST for clinical use in intensive
care and emergency department
THANK YOU FOR YOUR
ATTENTION