ACS NSQIP 30 Day Outcomes Supports Implementation of a Surgical Checklist
31
S NSQIP 30 Day Outcomes Supports plementation of a Surgical Checkli Scott Ellner, DO, MPH, FACS Cynthia Ross-Richardson, MS, BSN, RN, CNOR Saint Francis Hospital and Medical Center University of Connecticut Integrated Surgery Residency May 21, 2012 Changing Culture
description
ACS NSQIP 30 Day Outcomes Supports Implementation of a Surgical Checklist. Changing Culture. Scott Ellner, DO, MPH, FACS Cynthia Ross-Richardson, MS, BSN, RN, CNOR Saint Francis Hospital and Medical Center University of Connecticut Integrated Surgery Residency May 21, 2012. Objectives. - PowerPoint PPT Presentation
Transcript of ACS NSQIP 30 Day Outcomes Supports Implementation of a Surgical Checklist

ACS NSQIP 30 Day Outcomes Supports Implementation of a Surgical Checklist
Scott Ellner, DO, MPH, FACSCynthia Ross-Richardson, MS, BSN, RN, CNOR
Saint Francis Hospital and Medical CenterUniversity of Connecticut Integrated Surgery Residency
May 21, 2012
Changing Culture

Objectives
• Discuss the use of a validated safety attitudes questionnaire to understand behavior in the surgical environment
• Discuss OR team training to change culture
• Discuss the implementation and use of the AORN surgical checklist
• Discuss the use of the American College of Surgeons National Surgical Quality Improvement Program to assess 30-day postoperative complications

Demographics
• 600 Bed tertiary care facility• Level 2 Trauma Center• UConn Surgical Residency• 8,000 General surgery cases/yr.• 30 Operating rooms
ACS NSQIP since 2007ACS TQIP since 2011
SFHMC Hartford, Connecticut

Operating Room TeamOperating Room Team
Circa 1914

Operating Room Team
Circa 2012

Shame and Blame


American College of SurgeonsNational Surgical Quality Improvement
Program
• Evidence-based• Risk-adjusted• Data driven
= Improved Surgical Outcomes
Shukri F. Khuri, MD

30-Day Adverse Event Rate
20.14%
0.99%2.81%
7.61%6.74%
3.33%
0%
5%
10%
15%
20%
25%
All 30-dayMorbidity
DVT/PE HAP SSI Transfusion UTI
3,314 General Surgery Cases Collected by 2010

Post-Operative Urinary Tract Infections
Observed Rate: 2.41%Expected Rate: 1.47%O/E Ratio: 1.64Status: Needs Improvement
2009

Patient Safety Project
• Implementation and compliance with AORN (WHO) checklist
• Pilot project 75 general surgery cases compared to historical controls to reduce post-operative 30-day complications as measured by NSQIP
• Team Training Sessions to Change Culture

Metrics/Outcomes
• Reduce NSQIP 30 day post-operative outcomes– Urinary Tract
Infection– Surgical Site Infection– Hospital Acquired
Pneumonia– Thromboembolic
events– Transfusion rate
• No Retained Foreign Bodies
• Assess Safety Attitudes – Likert Scale
• Circulating Nurse Exits
• Compliance with AORN Checklist
• Qualitative Observations

Identifying Culture
Communication
Behavior
Rituals
Tolerance

Safety Attitudes Questionnaire
21. The culture in the ORs here makes it easy to learn from the errors of others.
1 2 3 4 5 N/A
46. All the personnel in the ORs here take responsibility for patient safety.
1 2 3 4 5 N/A
12. In the OR, it is difficult to discuss errors.
1 2 3 4 5 N/A

SAQ Participants
N=161

Overall SAQ Results

Pre-Training Observations of Team Communication
• Language Barriers• Shared commitment• Assumptions • Efficiency• Interruptions• Side conversation
• Multi-tasking• Complacency • Personal Issues • Workload/Staff
fluctuation• Fatigue and stress• Disruptive behavior


Why Team Training?
• Enhances communication
• Addresses improper behavior
• Helps to build trust
• Gives all employees a voice
• Improves the overall safety culture
• Encourages leadership

Team Training Tool
• Session 1 – Crucial Conversations
• Session 2 – Getting What You Want: Communication Strategies That Help You Get What You Need
• Session 3 – When the Going Gets Tough: Achieving a Positive Outcome

Launch of Team Training
SafetyPool of Shared
Meaning
Violence
Silence
Safety
Safety

Checklist Introduction

Barriers
1) Complacency2) Resistance 3) Exposing failures4) Challenging years of
embedded culture5) Compliance6) Training7) Uneasy Leadership

OR Change Agents
• OR Ambassadors
• OR Observers
• Executive Leadership

Observed Qualitative Results
Good Teamwork. Specimen sent to Pathology with follow-up during case
No equipment malfunctions. Staff in room joined together to announce Time-Out and Debrief
Anesthesia initiating the Time-Out
No site marked for hernia. Circulatorrecognized and asked surgeon to mark.
Joking by surgeon at expense of female personnel
CRNA brought open cup of Coffee, raised sheet to coverview of anesthesia area
Patient paged overhead by surgical floor while in surgery

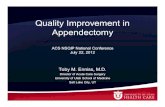
Quantitative Results
20.14%
0.99%2.81%
7.61% 6.74%
3.33%
6.85%
0.00% 0.00%
5.48%
0.00%2.74%
0%
5%
10%
15%
20%
25%
All 30-dayMorbidity
DVT/PE HAP SSI Transfusion UTI
Pre-Intervention Post-Intervention
N= 75 general surgery cases

Post-Operative Urinary Tract Infections
Observed Rate: 1.23%Expected Rate: 1.43%O/E Ratio: 0.86Status: As Expected 2011
2009

Post-Operative Pneumonia
Observed Rate: 0.65%Expected Rate: 1.24%O/E Ratio: 0.52Status: Exemplary
2011
2009

Circulating Nurse Exits
• Average 9 exits (4 hour case)*
• Observed range 0-25 exits (average 3 exits)
• Checklist Compliance 97%
• Increase in the number of OR exits led to higher rates of patient morbidity
*Christian et al. Surgery 2006

Take Home Points
•Acknowledge the need for change•Measure baseline attitudes – SAQ•Implement team training curriculum•Observe and audit checklist utilization•Recognize and address barriers•Provide resources for sustainability•Identify metrics to demonstrate change

Thank You