ACoRN Workbook “2012 Update” · ACoRN Workbook “2012 Update” _____ Name: ACoRN Neonatal...
19
ACoRN Workbook – version 1.4.01 February 2013 (2012 Update) © ACoRN Neonatal Society ACoRN Workbook “2012 Update” _____________________________________ Name: ACoRN Neonatal Society Société néonatale “ACoRN” A Canadian non-profit Society Vancouver, British Columbia www.acornprogram.net
Transcript of ACoRN Workbook “2012 Update” · ACoRN Workbook “2012 Update” _____ Name: ACoRN Neonatal...

ACoRN Workbook – version 1.4.01 February 2013 (2012 Update) © ACoRN Neonatal Society
ACoRN Workbook
“2012 Update”
_____________________________________ Name:
ACoRN Neonatal Society Société néonatale “ACoRN”
A Canadian non-profit Society Vancouver, British Columbia
www.acornprogram.net

ACoRN Workbook – version 1.4.01 February 2013 (2012 Update) © ACoRN Neonatal Society

ACoRN Workbook – version 1.4.01 February 2013 (2012 Update) © ACoRN Neonatal Society
The ACoRN Process

ACoRN Workbook – version 1.4.01 February 2013 (2012 Update) © ACoRN Neonatal Society

ACoRN Workbook – version 1.4.01 February 2013 (2012 Update) © ACoRN Neonatal Society
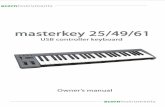
The Resuscitation Sequence
Ensure 100% O2, positive pressureventilation, chest compressions, and
epinephrine correctly administered (^) Repeat epinephrine Ensure vascular access Consider volume expansion Draw venous blood gas
Transillumination Consider needle aspiration
Call for help Access equipment Provide warmth Position Clear airway (^) Stimulate Administer O2 as needed
Establish monitors:- pulse oximetry (pre-ductal)- cardiorespiratory- blood pressure
Ineffective breathing HR < 100 bpm
No
Yes
No
HR > 60 bpm Initiate chest compressions
(^) with 100% O2
Administer epinephrine (^)
Consider intubation at any point indicated by a caret (^)
HR > 100 bpm
HR < 60 bpm
HR < 60 bpm
HR < 60 bpm
Initiate/continue positive pressure ventilation (^)
Consider pneumothorax
HR < 60 bpm
ACoRN PrimarySurvey
Ineffective breathing Heart rate < 100 bpm Central cyanosis
Yes

ACoRN Workbook – version 1.4.01 February 2013 (2012 Update) © ACoRN Neonatal Society
The Respiratory Sequence
Vascular access Chest radiograph Blood gas Consider consultation
Respiratory Laboured respiration * Respiratory rate > 60/min * Receiving respiratory support *
Recheck patent airway/breathing Administer O2 as needed to maintain SpO2 88-95% Establish/continue monitors:
- pulse oximetry (pre-ductal)- cardiorespiratory- blood pressure- oxygen analyzer
Calculate ACoRN Respiratory Score if spontaneously breathing
Yes
No
Respiratory Sequence
Focused history Physical examination Review diagnostic tests done Establish working diagnosis
Consider chest drain and followup chest radiograph
Consider surfactant
RDS Pneumothorax (1) TTN Mild respiratory distress
Reassess diagnosis and management if unresolved within 4 hours
Mild respiratory distress (ACoRN score < 5) lasting < 4 hours
Severe respiratory distress (score > 8) Apnea or gasping Receiving ventilation
Moderate respiratory distress (score 5 to 8) Persistent or new respiratory distress
Intubate if not already intubated Optimize ventilation
Consider/adjust respiratory support (CPAP or PPV)
Repeat ACoRN Respiratory Score if spontaneously breathing Optimize oxygenation Optimize respiratory support (adjust ventilator/CPAP settings, wean, or discontinue)
Problem List
Supportive care
Aspiration Pneumonia PPHN Other
(1) drainage of a symptomatic pneumothorax takes precedence over returning to the Problem List

ACoRN Workbook – version 1.4.01 February 2013 (2012 Update) © ACoRN Neonatal Society
The Respiratory Score (p. 3-7):
Score 0 1 2
Respiratory rate 40 to 60/min 60 to 80/min > 80/min
Oxygen requirement1 none ≤ 50% > 50%
Retractions none mild to moderate
severe
Grunting none with stimulation continuous at rest
Breath sounds on auscultation easily heard
throughout decreased barely heard
Prematurity > 34 weeks 30 to 34 weeks < 30 weeks
1 A baby receiving oxygen prior to the setup of an oxygen analyzer should be assigned a score of “1”
Adapted from Downes JJ, Vidyasagar D, Boggs TR Jr, Morrow GM 3rd. Respiratory distress syndrome of newborn infants. I. New clinical scoring system (RDS score) with acid-base and blood-gas correlations. Clin Pediatr 1970; 9(6):325-31. Total score: Mild: < 5; Moderate: 5 to 8; Severe: > 8 Interpretation of blood gas results (p. D-4):
1. Normal, acidosis or alkalosis? 2. Respiratory, metabolic, mixed or
compensated?
Blood gas values (p. D-4):
pH PCO2 BD Interpretation
↓ ↑ Normal Respiratory acidosis
↓ Normal ↑ Metabolic acidosis
↑ ↓ Normal Respiratory alkalosis
↑ Normal ↓ Metabolic alkalosis
Normal Acceptable values for acute respiratory distress
pH 7.35 to 7.45 7.25 to 7.40
PCO2 35 to 45 mmHg 45 to 55 mmHg
BD - 4 to + 4 mmol/L

ACoRN Workbook – version 1.4.01 February 2013 (2012 Update) © ACoRN Neonatal Society
The Cardiovascular Sequence

ACoRN Workbook – version 1.4.01 February 2013 (2012 Update) © ACoRN Neonatal Society
Signs of circulatory stability / instability (p. 4-8):
Tolerance to various degrees of desaturation in newborns with cyanotic heart disease, assuming normal hemoglobin levels and cardiac output (p. 4-35):
SpO2 Degree of desaturation Stable Circulatory instability or anemia
> 75% mild to moderate usually well tolerated usually tolerated
65 to 75% marked usually tolerated not well tolerated
< 65% severe poorly tolerated poorly tolerated
Sign Stable Unstable
Level of alertness, activity and tone alert, active and looking well,
normal tone listless, lethargic and/or
distressed, decreased tone
Skin colour, and temperature well perfused, peripherally warm pale, mottled, peripherally cool
Capillary refill time ≤ 3 seconds centrally and peripherally
> 3 seconds
Pulses easy to palpate weak, absent
Mean blood pressure ≥ gestational age in weeks < gestational age in weeks
Heart rate 100 to 160 bpm > 160 bpm
Urine output ≥ 1 mL/kg/hour < 1 mL/kg/hour

ACoRN Workbook – version 1.4.01 February 2013 (2012 Update) © ACoRN Neonatal Society
The Neurology Sequence

ACoRN Workbook – version 1.4.01 February 2013 (2012 Update) © ACoRN Neonatal Society
Therapeutic Hypothermia / Normothermia for HIE
The following Alerting Signs identify babies who require observation for the development of hypoxic ischemic encephalopathy.
When indicated, therapeutic hypothermia should only be initiated after: completion of Neonatal Resuscitation (NRP), and the ACoRN Primary Survey and Sequences consultation with the clinical transport coordinator and following a strict protocol.
Therapeutic normothermia involves active thermal management to avoid hyperthermia. The aim of therapeutic normothermia is to maintain the axillary temperature between 36.0oC and 36.5oC.
Criteria for Initiation of Therapeutic Hypothermia (Appendix F): The following must all be met prior to initiating therapeutic hypothermia
NRP and ACoRN Sequences completed
At risk of HIE Alerting Sign present
Moderate to severe HIE present as per the Clinical Assessment of Neurological Dysfunction table
Gestational age is ≥ 35 weeks
Postnatal age is ≤ 6 hours
No absolute contraindications (e.g. cardiorespiratory instability, severe coagulopathy, etc)
Tertiary level consultation obtained

ACoRN Workbook – version 1.4.01 February 2013 (2012 Update) © ACoRN Neonatal Society
Clinical assessment of neurological dysfunction (p. 5-9, F-5):
The presence of moderate or severe HIE is defined as seizures or signs present in at least three of the six categories below, or by the regionally recommended scoring system.
Category Mild Moderate Severe
Level of alertness “hyperalert” lethargy stupor or coma
Spontaneous activity normal decreased activity no activity
Posture mild distal flexion
arms flexed, legs extended
arms and legs extended
Tone normal hypotonic flaccid
Primitive reflexes weak suck, strong Moro
weak suck, incomplete Moro
absent suck, absent Moro
Autonomic (one of) Pupils Heart rate Respirations
dilated reactive
tachycardia
normal
constricted
bradycardia
periodic breathing
dilated or non-reactive
variable heart rate
apnea
Seizures none absent or present absent or decerebrate Adapted from Sarnat HB et al: Neonatal encephalopathy following fetal distresss: A clinical and encephalographic study. Arch Neurol 33:695,1976. Jitteriness versus Seizures (p. 5-4):
Adapted from Volpe JJ. Neurology of the Newborn. 5th Edition. Philadelphia: WB Saunders Company, 2008 Documentation of abnormal movements (p. 5-31):
Time/ duration
Suppress by holding
Origin/ spread
Eye/mouth movements
Level of alertness Autonomic changes
Other signs
09:00 h 20 sec
No Right arm, then all extremities
Eyes deviated to left Normal crying, auditory and visual responses when not seizing
No No
Observation Jitteriness Seizures
Abnormal gaze or eye movement no yes
Movements exquisitely sensitive to stimuli yes no
Predominant movement tremor clonic jerking
Movements cease with passive flexion yes no
Autonomic changes (e.g., tachycardia, increase in blood pressure, or apnea)
no yes

ACoRN Workbook – version 1.4.01 February 2013 (2012 Update) © ACoRN Neonatal Society
The Surgical Conditions Sequence

ACoRN Workbook – version 1.4.01 February 2013 (2012 Update) © ACoRN Neonatal Society
The Fluid & Glucose Management Sequence

ACoRN Workbook – version 1.4.01 February 2013 (2012 Update) © ACoRN Neonatal Society
Guide for enteral and intravenous fluid administration (p. 7-4):
Postnatal age Baseline milk intake (if not breastfed on cue)
Baseline intravenous intake (if not feeding)
Day 1 (72 mL/kg/day)
up to 6 mL/kg1 q 2h (9 mL/kg q 3h)
D10%W at 3 mL/kg/hour
Day 2 (96 mL/kg/day)
up to 8 mL/kg q 2h (12 mL/kg q 3h)
D10%W at 4 mL/kg/hour
Day 3 (120 mL/kg/day)
up to 10 mL/kg q 2h (15 mL/kg q 3h)
D10%W with 20 mmol/L of NaCl at 5 mL/kg/hour
≥ Day 4 (144 mL/kg/day)
up to 12 mL/kg q 2h (18 mL/kg q 3h)
D10%W with 20 mmol/L of NaCl at 6 mL/kg/hour (± other electrolytes)
1 If hypoglycemic, start with 8 mL/kg q 2h.
Suggested steps for increasing glucose intake if blood glucose checks remain < 2.6 mmol/L or < 47 mg/dL (p. 7-15):
Steps Enterally fed IV dextrose infusion
Baseline Breastfeed on cue, or
Feed every 2 to 3 hours
D10%W, 3 mL/kg/hour (5 mg/kg/minute of glucose)
Step 1 Feed measured volume 8 mL/kg every 2 hours, or
Start IV dextrose infusion at baseline
D10%W, 4 mL/kg/hour (6.7 mg/kg/minute of glucose)
Step 2 Go to IV dextrose infusion step 1, and proceed from there
D12.5%W, 4 to 5 mL/kg/hour (8.3 to 10.4 mg/kg/minute of glucose)
Obtain consultation and investigations
Consider central access if on > D12.5%W
Consider glucagon or other pharmacological intervention if > D12.5%W is needed

ACoRN Workbook – version 1.4.01 February 2013 (2012 Update) © ACoRN Neonatal Society
The Thermoregulation Sequence

ACoRN Workbook – version 1.4.01 February 2013 (2012 Update) © ACoRN Neonatal Society
The Infection Sequence

ACoRN Workbook – version 1.4.01 February 2013 (2012 Update) © ACoRN Neonatal Society
Notes re Infection Sequence
A well term baby born to an asymptomatic mother with a negative prenatal GBS screen or > 4 hours of intrapartum antibiotics, does not need specific intervention. Such a baby has no Alerting Signs for infection, and does not enter the Infection Sequence
A baby who has ACoRN alerting signs with * should have diagnostic testing for sepsis and antibiotic therapy; except term and late preterm babies with mild respiratory distress lasting < 4 hours who are otherwise well and have no risk factors for infection.
First-line antibiotics in sepsis occurring in the first 3 days of life are ampicillin and an aminoglycoside (usually gentamicin). If meningitis cannot be ruled out in an unwell baby, cefotaxime should be added.
Notes re Transport
The sending facility needs to prepare the following material to go with the baby:
a copy of o prenatal, labour and delivery records o the mother’s chart with all relevant neonatal history o the baby’s chart o laboratory data
radiographs o note on the last chest radiograph if the endotracheal tube has been repositioned and no new
radiographs have been taken
clearly labeled specimens if requested, for example o the baby’s blood cultures (aerobic ± anaerobic) o a maternal blood sample o a cord blood sample from the placenta, useful mainly for a direct antibody (Coombs’) test
the placenta, wrapped in a sealed plastic bag or placed in a bucket with a lid (no additives or preservatives)
signed consent forms for transport, admission and care at the receiving hospital, and for transfusion of blood products
contact information for the baby’s parents and family physician.

ACoRN Workbook – version 1.4.01 February 2013 (2012 Update) © ACoRN Neonatal Society
Transport Neonatal Pre-Transport Communication Sheet
Date & time: Physician calling: Phone
Institution calling: City Phone
Institution accepting: City Phone
Information about the newborn
Name: Reason for consultation:
Date of birth Time Sex Birth weight Gestation Apgar score Eye prophylaxis? 1 min: 5 min: Vitamin K? Resuscitation: Congenital anomalies:
Respiration Cardiac massage Medications / route
Spontaneous: Yes ( ) No ( ) Manual ventilation: Yes( ) No ( ) Oxygen: Yes ( ) % No ( )
Intubated: Time ETT size ______ Suctioned for meconium: Yes ( ) No ( )
Yes ( ) No ( )
Time: Started: ____
Ended: ________
ET/EV ET/EV ET/EV ET/EV
Cord gases:
Postnatal course: Curent condition:
HR: RR: BP: Capillary refill: sec FiO2: IPPV: SpO2: Physical exam:
IV access / solutions Medications / route: RX – results Blood glucose (time) Blood gases (time)
Information about the mother:
Name: Age: G: P: LMP / EDC /
Blood group: Rh: VDRL: Rubella: HBsAG: TB: HIV:
GBS: Pos ( ) Neg ( ) Unknown ( ) Other
Focused history:
Labor / birth:
Fetal monitoring: Yes ( ) No ( ) Internal ( ) External ( ) Auscultation ( ) Normal ( ) Abnormal ( )
Scalp blood gases Duration: 1st stage 2d stage SROM ( ) AROM ( ) Duration: Color: AFV: Medications: Analgesia /anesthesia:
Birth: Cesarean ( ) Vaginal ( ) Forceps ( ) Vacuum ( ) Presentation:
Complications:
Date: Name & position:
Adapted: PPPESO. Neonatal Transport. Perinatal Nursing Guidelines (3rd Ed). Ottawa, ON: Perinatal Partnership Program of Eastern and Southeastern Ontario, 2001.