
Acma presentation april 2013 4.8.13 sf
20
Central Texas Health Care in 2013: Organizing Our Delivery System ACMA Meeting April 2013
Transcript of Acma presentation april 2013 4.8.13 sf

Central Texas Health Care
in 2013: Organizing Our Delivery System
ACMA MeetingApril 2013

2
Why Reform the Delivery System?
• There are 50 million uninsured Americans• Health care costs are a factor in 55% of personal
bankruptcies.• Health care costs have been growing at 2-3 times
the rate of inflation for 3 decades.• Quality and safety rankings are below most
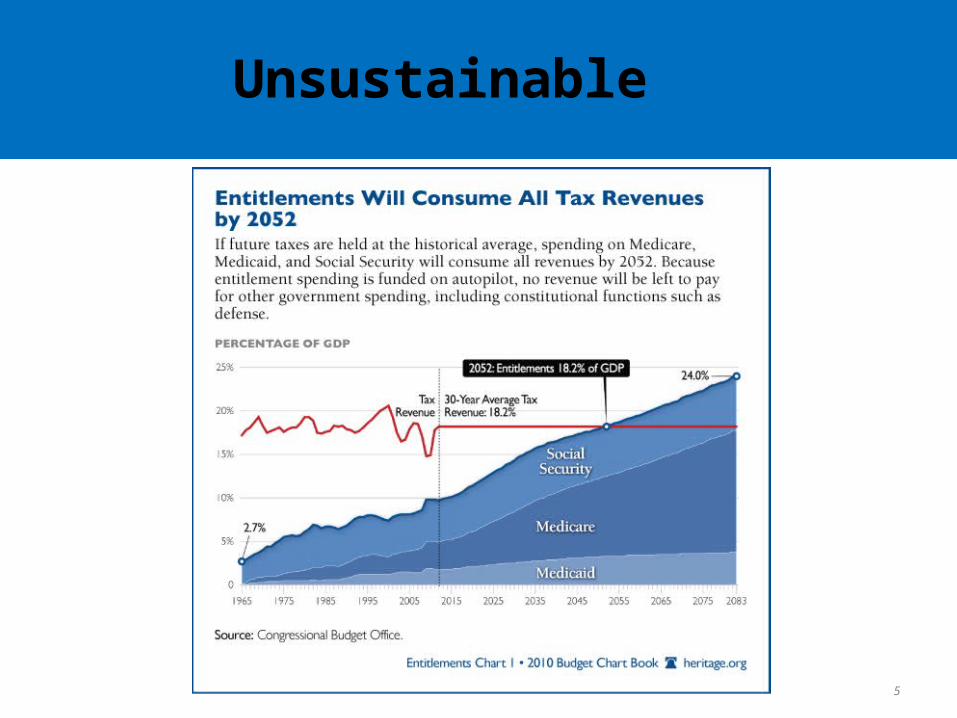
developed and industrialized nations.• Medicare and Medicaid costs “unsustainable.”• Health care continues to consume a larger
proportion of our nation’s GDP (currently 18%)

Unsustainable

Unsustainable
5
Unsustainable

Follow the Money
• 1% of the population accounts for 25% of health costs;
• 10% of the population accounts for 70% of health costs;
• 78% of national health care expenditures can be attributed to chronic illness.
On order of $2 trillion.

7
Enter Insurance Reform (ACA)
• Expansion of insurance coverage– Medicaid expansion (not in Texas)– Employer mandate; small business tax credit– Individual mandate ($95/1% $695/2.5%)– Insurance Exchanges (2014) and tax credit (400% FPL)
• Insurance Regulation and Reform– Do away with lifetime maximums– Do away with pre-existing conditions– Do away with rescissions (being dropped once you’re sick)– Guaranteed deductible-free preventive care– Minimum Medical Loss Ratio (MLR)
HMMMM….
8
• Quality & Safety– Pay for value programs to turn focus toward quality
improvement.– Encourage and reward use of information technology.– Research to support “evidence based care.”
• Cost Efficiency– Emphasis of preventative & chronic condition management
to reduce downstream costs.– Accountable Care Organizations (ACOs) - pay for value not
for volume.• ACO concept is now new. Examples of Clinically Integrated
Networks: Advocate Physician Partners; Kaiser Permanente; Cleveland Clinic.
Enter Insurance Reform (ACA)

Volume Based System• Proprietary Pricing• Broad Payer Networks• Episodic Patient Care• Disparate Providers• Hospital Focus• Practice Pattern
Variation• Provider Centered Care• Fragmented Hospital IT
Value Based System• Transparent Pricing• Performance Based
Networks• Cross-Continuum of Care• Clinically Integrated
Providers• Health System Focus• Evidence Based Care• Person Centered Care• Cross-Continuum Based
IT
Delivery System Transformation

10
Volume Based Reimbursement

11
• Real change will require us to fundamentally change the way care is delivered.– Aligned Incentives– Enhanced communication and managed transitions– Risk-stratified interventions – getting the most
resources to the sickest patients– Organized care
The Right Care at the Right Place at
the Right Time
Value Based Care

Key Attributes of a Clinically Integrated Network Physician Driven and Governed
Structured Quality Initiatives
IT Infrastructure for Quality Data Measurement and Reporting
Incentive payments
CLINICAL INTEGRATION
A network of physicians willing to demonstrate a high degree of interdependence and cooperation through a program of initiatives designed to control costs and ensure quality, which is supported by an infrastructure that allows the physicians to evaluate and modify practice patterns.
-- Hogan Marren, Ltd.
Defining Clinical Integration

Key Attributes of an ACO• Person Centered Care
• Physician Driven
• Coordinated Care Across the Continuum
• Practice Consistent Evidence Based Medicine (Clinical Integration)
• Responsible for Cost and Quality of a Population
• Rewarded, financially, for Performance
ACCOUNTABLE CARE
ORGANIZATION
A network of physicians,
hospitals and ancillary providers that share clinical
and financial responsibility for providing care to
patients across the continuum.
Defining ACO


Seton Healthcare
Family
Seton Health Alliance
Community Physicians
• Building clinically integrated network of health care
providers
• Selected as one of 32 Pioneer ACOs in 2012
• Commericial ACO contracts begining in 2013
Seton Health Alliance ACO

• 1-5% of Population• Advanced Care Coordination Clinic
(ACCC) High Risk Chronic
• 10-15% of Population• Embedded Nurse
Navigator-PCP Care Coordination
Moderate Risk Chronic
• Estimated 80% of Population
• Care Gap Management
Healthy and Low Risk
Tran
siti
on
s (1
0%)
Ho
me
& P
ost
Acu
te
Em
erg
ency
Dep
artm
ent
Pre
ven
t In
pat
ien
t A
dm
its
En
d o
f L
ife
(5%
) P
allia
tive
Car
e P
rog
ram
Risk Stratified Interventions
17
• 10,397 active patients• 200+ participating
providers• 30+ facility and agency
partners• 36 locations• 9 cities• 11 counties• 14,000 square miles
Seton Health Alliance ACO

18
Transitions & Post Acute Network
Goals:• Improve transitions and handoffs across the continuum;• Strengthen provider-provider communication across the
continuum;• Reduce preventable readmissions.
Process: Utilized Request for Information; Grow network of physician groups and facilities/agencies aligned with mission and objectives
Current Network:• 5 Physician Practices (hospitalist/post acute)• 18 Skilled Nursing Facilities• 3 Rehabilitation Hospitals• 12 Home Health Agencies• 1 Physician Home Service Provider

19
Charting the Journey
Plan well before you take the journey.
Remember the carpenter’s rule:
measure twice, cut once.

20
Meredith Duncan
Director of Operations, Seton Health Alliance
Contact Information


















