Acknowledgments Robert I. McLachlan, FRACP, PhD · Curatio PowerPoint TemplateControversies in Male...
12
Curatio PowerPoint TemplateControversies in Male Hypogonadism Bradley D. Anawalt, MD 1 The General Practice Education Day Healthed / Generation Next August 22 nd Sydney Update on Androgen Deficiency Robert I. McLachlan, FRACP, PhD Director, Andrology Australia Principal Research Fellow, Hudson Institute of Medical Research Consultant Andrologist, Monash IVF Group Disclosures None David Handelsman: ANZAC Institute, Sydney Gary Wittert: T4DM study Univ Adelaide Carolyn Allan: Hudson Institute, Melbourne Endocrine Society Australia Working Party Acknowledgments Recent concepts and interventions • Sex hormone actions • ‘At risk’ groups – challenges in detection • Controversies in management • Treatment options & monitoring Androgen Deficiency (AD) No unequivocal clinical features nor agreed serum biomarkers of androgen sufficiency • Diagnosis requires synthesis of clinical features and biochemistry • Androgen deficiency is a syndromic diagnosis not one defined by blood levels: – Statistical population-based distribution (e.g. serum calcium) – Therapeutic targets (e.g. cholesterol) Bhasin S et al. Steroids. 2008;73:1311. Androgen deficiency in adults General – sense of well being, poor concentration – tiredness, poor stamina – mood change - depression, irritability Sexual – libido – ejaculate volume – erectile failure Organ specific features – muscle mass and strength – osteoporosis and fracture – increased fat mass – cardiovascular & metabolic Androgen deficiency in adults General – sense of well being, poor concentration – tiredness, poor stamina – mood change - depression, irritability Sexual – libido – ejaculate volume – erectile failure Organ specific features – muscle mass and strength – osteoporosis and fracture – increased fat mass – cardiovascular & metabolic Symptoms screening tools like AMS not helpful
Transcript of Acknowledgments Robert I. McLachlan, FRACP, PhD · Curatio PowerPoint TemplateControversies in Male...

Curatio PowerPoint TemplateControversies in Male Hypogonadism
Bradley D. Anawalt, MD
1
The General Practice Education DayHealthed / Generation Next
August 22nd Sydney
Update on Androgen Deficiency
Robert I. McLachlan, FRACP, PhD
Director, Andrology Australia
Principal Research Fellow, Hudson Institute of Medical Research
Consultant Andrologist, Monash IVF Group
Disclosures
None
David Handelsman: ANZAC Institute, Sydney
Gary Wittert: T4DM study Univ Adelaide
Carolyn Allan: Hudson Institute, Melbourne
Endocrine Society Australia Working Party
Acknowledgments
Recent concepts and interventions
• Sex hormone actions
• ‘At risk’ groups – challenges in detection
• Controversies in management
• Treatment options & monitoring
Androgen Deficiency (AD)
No unequivocal clinical features nor agreed serum biomarkers of androgen sufficiency
• Diagnosis requires synthesis of clinical features and biochemistry
• Androgen deficiency is a syndromic diagnosis not one defined by blood levels:
– Statistical population-based distribution (e.g. serum calcium)
– Therapeutic targets (e.g. cholesterol)
Bhasin S et al. Steroids. 2008;73:1311.
Androgen deficiency in adults
General– sense of well being, poor concentration– tiredness, poor stamina – mood change - depression, irritability
Sexual– libido – ejaculate volume– erectile failure
Organ specific features– muscle mass and strength– osteoporosis and fracture– increased fat mass– cardiovascular & metabolic
Androgen deficiency in adults
General– sense of well being, poor concentration– tiredness, poor stamina – mood change - depression, irritability
Sexual– libido – ejaculate volume– erectile failure
Organ specific features– muscle mass and strength– osteoporosis and fracture– increased fat mass– cardiovascular & metabolic
Symptoms screening tools
like AMS not helpful

Curatio PowerPoint TemplateControversies in Male Hypogonadism
Bradley D. Anawalt, MD
2
Androgen deficiency in adults
General– sense of well being, poor concentration– tiredness, poor stamina – mood change - depression, irritability
Sexual– libido – ejaculate volume– erectile failure
Organ specific features– muscle mass and strength– osteoporosis and fracture– increased fat mass– cardiovascular & metabolic
What mediates these
diverse actions?
Direct pathway
(muscle)
Estradiol
Diversification pathway (brain, bone)
D Handelsman www.ENDOTEXT.org
aromatase
(0.2%)
Androgen receptor
Estrogen receptors
DHT
GnRH
LH Amplification pathway (prostate, skin)
Inactivation pathway
5a-reductase
(5-10%)
Hepatic oxidation &
conjugation
Renal excretion
Androgen receptorY
Testosterone6 mg/day
Testosterone: Three hormones in one
Testosterone is the molecule of choice for
physiological androgen replacement
Implications of ‘Three hormones in one’
Testosterone Therapy in Men with Androgen Deficiency Syndromes: Endocrine Society Clinical Practice Guideline
Published Online: July 02, 2013
J Clin Endo Metab 2010, 95, 2536
Use, misuse and abuse of androgens. The Endocrine Society of Australia consensus guidelines for androgen prescribing Med J Australia 2000 ;172:220
Conway A, Handelsman DJ, Lording DW, Stuckey B, Zajac JD
.
Update in preparation .......
Androgen replacement is warranted at ANY age when deficiency due to
Defined testicular or hypothalamo-pituitary disease
Benefit of physiological replacement is based on evidence of safety & efficacy
Challenge: to identify the patients
Hypothalamo-pituitary-testicular axis
GnRH
Inhibin B
Pituitary
LH, FSH
pulsatile
Testosterone
Estradiol
Hypothalamus
Testis
Behaviour
Prostate
Muscles
Skin & Hair
Lipids
Bone marrowPrimary testicular
failure
Secondary testicular
failure

Curatio PowerPoint TemplateControversies in Male Hypogonadism
Bradley D. Anawalt, MD
3
Basic approach to androgen deficiency
Think of it: history and examination
1st Blood: Serum total testosterone (fasting)
between 0800 and 1000hr : circadian variation
Adjust time frame for shift workers
Wittert G. Curr Opin Endocrinol Diabetes Obes. 2014 ;21 239.
Confirmatory blood testing
Repeat total T
30% normalize on repeat
Serum LH: primary vs secondary testicular failure
Serum SHBG and calculated free T
Elevation: age, hyperthyroidism, liver
disease, anti-epileptic therapies
Suppression: obesity, insulin resistance,
androgen exposure
When a pathological cause of AD suspected
Low T, low LH ? Pituitary failure
• Serum prolactin (prolactinoma)
• Iron studies (haemochromatosis)
• Pituitary function : cortisol, FT4, TSH, growth hormone
• Hypothalamo-pituitary MRI
Low T, high LH Primary testicular failure
• Karyotype suspected Klinefelters Syndrome
• Y chromosome microdeletion in infertility context
Classic Androgen deficiency
Primary (high LH) impaired testis function
Klinefelter’s syndrome
Infertile men
Testicular damage vascular, cancer Rx
Secondary (low LH) hypothalamo-pituitary
Prolactinoma
Congenital GnRH deficiency (rare)
Commonest chromosomal disorder 1:600 males
Commonest cause of undiagnosed androgen deficiency
Almost all androgen deficient as adults- Benefit from replacement
70% escape diagnosis lifelong Bojesen JCEM 2003
detection strategies a major challenge
Reject your stereotypical images of KS
Klinefelter’s Syndrome – 47XXY
From: Nieschlag and Behre, 2007
gynecomastia
abdominal obesity
small testicular
volume
reduced body hair
horizontal pubic
hairline
varicose veins
narrow shoulders
Classical KS
in textbooks
Profound learning
difficulties

Curatio PowerPoint TemplateControversies in Male Hypogonadism
Bradley D. Anawalt, MD
4
From: Nieschlag and
Behre, 2007
gynecomastia
abdominal obesity
small testicular
volume
reduced body hair
horizontal pubic
hairline
varicose veins
narrow shouldersNot always!!
may appear entirely normal and
adequately virilised when clothed
Classical KS
in textbooks
Profound learning
difficulties
From: Nieschlag and
Behre, 2007
gynecomastia
abdominal obesity
small testicular
volume
reduced body hair
horizontal pubic
hairline
varicose veins
narrow shouldersNot always!!
may appear entirely normal and
adequately virilised when clothed
Classical KS
in textbooks
~10,000 missed KS males in Australia
Failure to systemically examine male
genitalia : flaw in education & practice
From: Nieschlag and
Behre, 2007
gynecomastia
abdominal obesity
small testicular
volume
reduced body hair
horizontal pubic
hairline
varicose veins
narrow shouldersNot always!!
may appear entirely normal and
adequately virilised when clothed
Classical KS
in textbooks
~10,000 missed KS males in Australia
Failure to systemically examine male
genitalia : flaw in education & practice
Klinefelter’s syndrome: The most overlooked cause of
androgen deficiency. St John B & McLachlan RI
Endocrinology Today 2015; 4(1): 8-14
Small testes found on routine
genital examination
Small testes found on routine
genital examination
All types of practice
Male health evaluation
requires full history &
routine physical exam
Male infertility : IVF programs
Male factor infertility accounts for ~30%
Spermatogenic failure is most common cause
Azoospermia : ~14% are Klinefelters
Androgen deficiency ~ 1 in 8 infertile men

Curatio PowerPoint TemplateControversies in Male Hypogonadism
Bradley D. Anawalt, MD
5
Male infertility : IVF programs
Male factor infertility accounts for ~30%
Spermatogenic failure is most common cause
Azoospermia : ~14% are Klinefelters
Androgen deficiency ~ 1 in 8 infertile men
Now it gets tricky.....
Low testosterone associated with
• Chronic disease
• Obesity
• Diabetes
• ? Age per se
When if ever is testosterone treatment warranted?
Now it gets tricky.....
Low testosterone associated with
• Chronic disease
• Obesity
• Diabetes
• ? Age per se
When if ever is testosterone treatment warranted?
All share common
non specific
symptoms with
androgen deficiency
1936 University of Washington Olympic Gold Medal Crew
Courtesy J Amory
1936 University of Washington Olympic Gold Medal Crew50-Year Reunion
Courtesy J Amory

Curatio PowerPoint TemplateControversies in Male Hypogonadism
Bradley D. Anawalt, MD
6
Low “T” - How to Sell Disease Schwartz & Woloshin JAMA June 3rd 2013
‘A man on TV is selling me a miracle cure that will
keep me young forever. It’s called Androgel for
treating something called ‘Low T’, a
pharmaceutical company–recognized condition
affecting millions of men with low testosterone,
previously known as getting older.’
—The Colbert Report,1st December 2012
Healthy Man StudySartorius G et al Clin Endocrinol 2012 ;77:755
Testosterone
Age (years)
40 50 60 70 80 90
Se
rum
Te
sto
ste
ron
e (
nm
ol/
L)
0
5
10
15
20
25
30
35
40
n=325 men, 2900 serum specimens
35
Healthy Man StudySartorius G et al Clin Endocrinol 2012 ;77:755
Testosterone
Age (years)
40 50 60 70 80 90
Se
rum
Te
sto
ste
ron
e (
nm
ol/
L)
0
5
10
15
20
25
30
35
40
n=325 men, 2900 serum specimens
Serum T did not vary with age
T
Symptoms
Age
1
2
Barometer of
Health
hypothesis
2
1 2
1
Andropause
hypothesis
Disease
1 2
>60%
population
Wu FCW et al. J Clin Endocrin Metab 93(7): 2737-2745 (2008)
European Male Aging Study (EMAS) Relationship
between Age and Testosterone in 3220 Men
40-44 45-49 50-54 55-59 60-64 65-69 70-74 75-79

Curatio PowerPoint TemplateControversies in Male Hypogonadism
Bradley D. Anawalt, MD
7
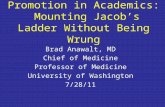
Wu FCW et al. J Clin Endocrin Metab 93(7): 2737-2745 (2008)
European Male Aging Study (EMAS) Relationship
between Age and Testosterone in 3220 Men
40-44 45-49 50-54 55-59 60-64 65-69 70-74 75-79
BMI <25
BMI 25-29
BMI ≥30
T
Symptoms
Age
2
Barometer of
Health hypothesis
2
1 2
1Andropause
hypothesis
Disease
2 A
22 B
T
Symptoms
Age
2
Barometer of
Health hypothesis
2
1 2
1Andropause
hypothesis
Disease
2 A
22 B? Testosterone
as adjunct in
management
Philosophy of Testosterone Treatment
Physiological replacement (‘natural therapy’)
Replicate normality in HYPOGONADAL men
Definition and identification of subjects
----------------------------------------------------------------------------
Pharmacological treatment (as a drug)
Dose for desired effect in EUGONADAL men
Risk : benefit ratio
Serum T 6.4 nM: maybe testosterone will help?
What is your goal?
Does testosterone
work?
Are there better
approaches?
When is enough
too much?

Curatio PowerPoint TemplateControversies in Male Hypogonadism
Bradley D. Anawalt, MD
8
20 40
Serum testosterone rises as body weight fallsGrossmann M JCEM 2011, 96, 2341
Ageing, overweight men with type 2 diabetes and low T levels
→ lifestyle measures such as weight loss and exercise
Serum T
levels
Weight loss
Testosterone as a drug – emerging
therapeutic roles requiring RCT data
1. Metabolic syndrome & diabetes
2. Frailty – age or disease related sarcopenia
3. Depression
4. Cardiovascular health
Testosterone for Prevention of
Type 2 Diabetes in High Risk Men:
placebo-controlled RCTWittert G http://www.t4dm.org.au/
Hypothesis:
Reduce onset/reverse Type 2 DM in men with low T,
over and above a lifestyle program
Secondary endpoints:
• body composition
• systemic & vascular inflammation
• mood, QOL, psychosocial function
• adherence to the lifestyle program
~420 randomised
Target 1000
T
Symptoms
Age
2
Barometer of
Health hypothesis
2
1 2
1Andropause
hypothesis
Disease
2 A
22 B? Testosterone
as adjunct in
management
T
Symptoms
Age
2
Barometer of
Health hypothesis
2
1 2
1Andropause
hypothesis
Disease
2 A
22 BCompelling case
for RCTs on
specific endpoints
• efficacy
• safety
Current climate in TRT in aging men
Testosterone Replacement Therapy Faces FDA Scrutiny
Garnick M. JAMA , 2015: 313, 563
Disease Mongering of Age-Associated Declines in Testosterone and Growth Hormone Levels
Perls T & Handelsman DJ
J American Geriatrics Society, 2015 in press
PBS support threshold in men > 40 yr without a defined testicular or pituitary cause lowered to 6nM

Curatio PowerPoint TemplateControversies in Male Hypogonadism
Bradley D. Anawalt, MD
9
Cardiovascular risk : evidence is contradictory and inconclusive
Observational studies
In older men: increased and decreased CV events
Mostly retrospective studies, non-randomised, multiple biases and confounders
RCTs
↑ CV events with high dose Te therapy in frail old men
Unconfirmed in another RCT in similar men
Meta-analysis: 3,000 mainly older men - ↑ in range of CV events ..many limitations to data
US FDA review : no increase of major CV events in testosterone-treated men.
But FDA mandates labelling of US testosterone products to warn about a possible increased risk of heart attack and stroke
-----------------------
• Use with caution, if at all, in older men, especially with known cardiovascular disease.
• Unstable cardiac disease or recent CV (within 6-12 months) constitute contraindications
Dr ‘No Testosterone’? Dr ‘Not first option and not
without deep reflection’
Managing Homer
• Lifestyle
– Diet
– Exercise
• Medical
– diabetes, hypertension, dyslipidemia
• Psychosexual issues
– Judicious use of PDE5 inhibitors
• Consideration of androgen therapy
– Realistic benefits – RCT data low quality
– Risks - ? cardiovascular
:
Testosterone does not enhance efficacy of sildenafil in erectile dysfunction: RCT data
• 40-70 years
• Total T <10 nM
• Optimal sildenafil dose
• Testosterone / placebo gel for 14 weeks
Testosterone no added benefit to sildenafil alone
Spitzer M Ann Intern Med 2012 57:681

Curatio PowerPoint TemplateControversies in Male Hypogonadism
Bradley D. Anawalt, MD
10
Testosterone preparations
1940
1954
1977
1992
1995
1998
2004
2004
2002
2004
Testosterone preparations
Courtesy of M Zitzmann, Munster
Reandron
Testosterone replacement: individualized approach
Tailored to clinical setting
induction virilisation vs replacement in adulthood
Compliance
Age
0 1 2
Serum
Te
(nM)
10
20
30
T gel, patch,
axilla,cream
Days Weeks
0 2 4 6 8 10
T esters im
T undecanoate im‘Reandron’
T implant
Normal range
Testosterone Preparations
No oral or synthetic formulations Handelsman MJA 2012:196, 642 ↑
2↑↑012
Adoption of Reandron Australia 2006-2010
Issues with T undecanoate
15 years experience Europe, 10 yr in Australia
Widey reported in long term use Zitzmann M J Sex Med 2013: 10:579 Wang C J Androl 2010;31:457
Inject 4ml slowly – 2 mins !
Post injection cough ~1:50 injection; mild/mod.
Midddleton Eur J Endocrinol 2015 Jan 30
Monitoring androgen therapy
‘Age-appropriate’ general medical care
lipids, blood pressure, weight
Special considerations:elderly: avoid long acting formulations - polycythemia
prostate health
cardiovascular health
sleep apnea – prior history or risk factors
Desire for fertility is a contraindication

Curatio PowerPoint TemplateControversies in Male Hypogonadism
Bradley D. Anawalt, MD
11
Systematic reviews of prostate cancer risk
Testosterone therapy in hypogonadal men and prostate cancer risk: a systematic review.
Shabsigh R Int J Impot Res 2009;21:9
44 studies: No increased prostate cancer risk
Effect of testosterone replacement therapy on prostate cancer: systematic review & meta-analysis.
Cui Y Prostate Cancer Prostatic Dis 2014;17:132
22 RCTs, n= 2351: no increase in short-term
Long-term data are warranted
Key messages
1. Native testosterone is preferred sex steroid
2. Focus on identifying established deficiency
3. Low T level are frequently associated with common comorbidities - these ought be the primary focus
4. RCT data on testosterone as a ‘drug’ awaited
5. Testosterone therapy is readily monitored:
convenience = compliance
www.andrologyaustralia.org
Clinical summary guides
Courses for GPsaccredited education provider through RACGP
Course description Type
RACGP QI
&CPD Point
s
Younger male healthmale infertility, testicular cancer,
Klinefelters, PE, prostatitis
Online ALM
(Free)
40 Category
130 PRPD
points
Older male health androgen deficiency, erectile
dysfunction & co-morbid
disease, prostate disease.
Online ALM
(Free)
40 Category
130 PRPD
points
Aboriginal and
Torres Strait
Islander males
Tailored knowledge and skills to
initiate dialogue and
engagement
Male Health
Education
DVD
(Free)
4 Category 2 2 Core
points
Men’s sexual and
reproductive health
Postgraduate Unit Dept. of
General Practice, Monash Univ.
Distance
education
(Fee-
payable)
Contact the
Coordinator

Curatio PowerPoint TemplateControversies in Male Hypogonadism
Bradley D. Anawalt, MD
12
Many thanks!