
Acknowledgements
28
Laurence Weinberg Staff Anaesthetist, Austin Hospital, Victoria Clinical Fellow, Department of Surgery, The University of Melbourne. Length of stay after open radical prostatectomy with intravenous lignocaine followed by 24-hour subcutaneous infusion: blinded, randomized, placebo controlled multicentre trial
-
Upload
quinlan-brooks -
Category
Documents
-
view
15 -
download
0
description
Length of stay after open radical prostatectomy with intravenous lignocaine followed by 24-hour subcutaneous infusion: blinded, randomized, placebo controlled multicentre trial. - PowerPoint PPT Presentation
Transcript of Acknowledgements

Laurence WeinbergStaff Anaesthetist, Austin Hospital, Victoria Clinical Fellow, Department of Surgery, The
University of Melbourne.
Length of stay after open radical prostatectomy with intravenous lignocaine followed by 24-hour
subcutaneous infusion: blinded, randomized, placebo controlled multicentre trial

Acknowledgements
o ANZCA: Project Grant
o University of Melbourne Story D, Gordon I, Christophi C
o Co-investigators Rachbuch C, Beilby D, Trinca J, Howard W, Yeomans M, Yanezas M, James K, McNicol L

Intravenous Lignocaine
• Clear advantages: abdominal surgery• Lower pain scores • Opioid sparing effects• Enhances functional recovery • Reduces immune alterations• Decreases length of hospital stay

Subcutaneous Lignocaine
• Neuropathic pain• Ischaemic pain
Limited data for ACUTE postoperative pain

Hypothesis
Intraoperative IV lignocaine + 24 hrs post-operative SC lignocaine Enhances recovery Shortens length of hospital stay after open radical retropubic prostatectomy

Study Design
• Prospective randomised multicentre• Blinded• Inclusion criterion Adults (age > 18 years < 75 years) Elective open radical prostatectomy ASA I-III patients
• Exclusion criterionx Creatinine > 200 umoll/L, Abn LFT’s x Chronic opioid usex Allergy: morphine, LAx Cardiac conduction defects/Class I anti-arrhythmic agents

Study Design
• Human Research Ethics approval• Consenting patients randomised 2 groups• GA: standardized, no regional anaesthesia
• All patients: 1. Induction: Propofol: 1-3 mg/kg; Fentanyl 3 ug/kg2. Maintenance: Volatile anaesthesia: 0.6-1 MAC, Fentanyl infusion 2.5 ug/kg/hr3. Surgical closure: Paracetamol IV 1 g, Ketorolac 30 mg 4. Postoperatively: Morphine PCA, 1 mg boluses, 5 min lockout QID paracetamol, NSAID, Acute Pain Service

Study Design
• Lignocaine group: Pre-induction• Loading dose IV: 1.5 mg/kg• Intraop infusion IV: 1.5 mg/kg/hr
Study Design
• Lignocaine group:• Post-op SUBCUT infusion: 1.5 mg/kg/hr
Study Design
• Control group:• Normal saline: equal volume delivered in the
same way

Study Design
• Primary outcome1. Length of hospital stay
• Secondary outcomes1. GI function2. Time to mobilise3. Rescue analgesia and anti-emetic therapy4. Visual Analogue Scores for pain (VAS) 0 to 100mm5. Morphine consumption: 24 hours 6. Patient satisfaction7. Opioid & lignocaine side effects8. Lignocaine plasma levels: PACU & 24 hours9. Adverse events

Statistics analyses
• Power analyses: based on a PILOT STUDY* for patients undergoing open radical prostatectomy (2007/8) who received PCA morphine alone: mean hospital stay 4.5 days (SD 26.4 hrs)
• Sample size: 18 hour difference in hospital stay, power 0.8, significance level of 0.05, 38 patients per group
• Analyses: intention-to-treat bases
* Weinberg L, et al. Anaesthesia & Intensive Care 2010; 38: A1116

Consort diagram
Total patients consentedN = 85
Total patients consentedN = 85
Patients excludedN = 10
Laparoscopic retropubic prostatectomy N = 9Procedure aborted (anaphylaxis) N = 1
Patients excludedN = 10
Laparoscopic retropubic prostatectomy N = 9Procedure aborted (anaphylaxis) N = 1
Inclusion critreria metN = 75
Randomised
Inclusion critreria metN = 75
Randomised
Placebo GroupN = 38
Placebo GroupN = 38
Lignocaine GroupN = 37
Lignocaine GroupN = 37
Intention to treatIntention to treat Intention to treatIntention to treat

Demographics
Lignocaine Group Placebo GroupPatients (n) 37 38
Age* (yrs) 61 (6.3, 44-70) 60.0 (7.6, 38-71)
Weight* (kg) 85 (14.1, 52-117) 83 (11.9, 60-123)
Body mass index* (kg/m2) 28 (5.05, 16.9-42.2) 26 (3.53, 21.2-35.9)
ASA Class - I / II / III 24 / 13 / 0 26 / 12 / 0
Gleason Scores 7 (0.86) 7 (0.62)
PSA 8.7 (5.02) 7.8 (4.85)
* Data presented as SD, range
Hospital Stay
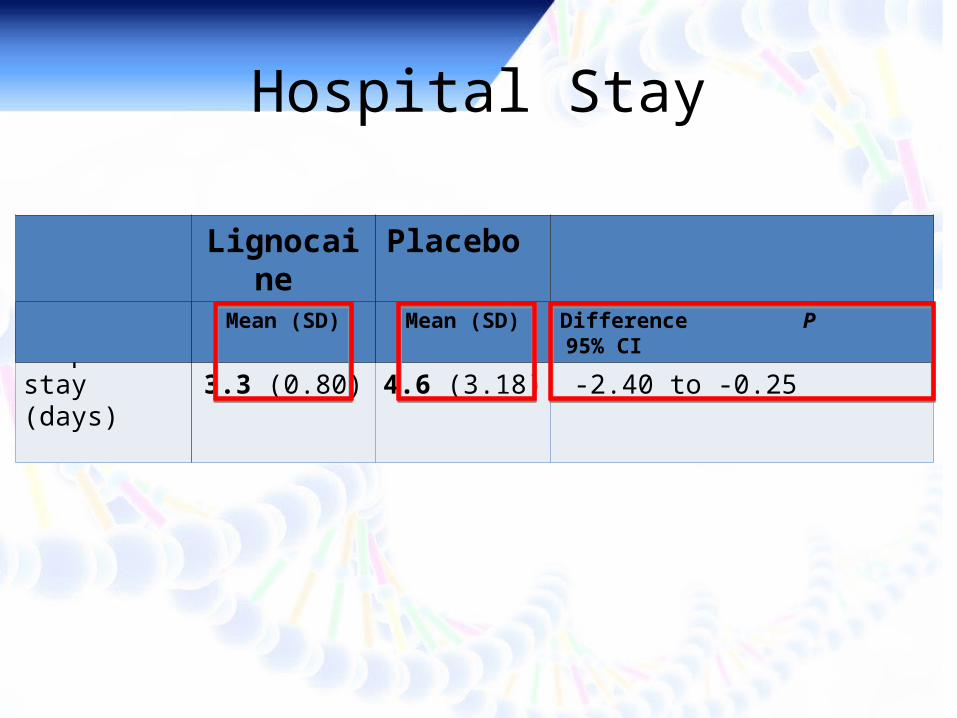
Hospital stay (days) 3.3 (0.80) 4.6 (3.18) -1.3 0.017 -2.40 to -0.25
Lignocaine Placebo Mean (SD) Mean (SD) Difference P 95% CI

Operative variables
Surgery duration (min) 155.7 (34.2) 141.6 (44.6) 0.13 (-4.27, 32.47)
Lowest intraop temp (0C) 35.5 (0.5) 35.6 (0.5) 0.41 (-0.34, 0.14)
Blood loss (ml) 1050.8 (750.9) 940.3 (651.1) 0.50 (-218, 439)
Blood Tx* (% patients) 5.4% 7.9% 1.00* (-16.0%, 10.9%)
Colloids (total) 843.9 (926.6) 742.6 (713.8) 0.60 (-281, 483)
Crystalloids (total) 3281.1 (1094.6) 2552.6 (1173.5) 0.007 (206, 1251)
Lignocaine Placebo Mean (SD) Mean (SD) P 95% CI
• For comparison of means, standard two-sample t-tests were used • Uses Fisher's Exact Test due to comparison of proportions with small sample size
Postoperative variables
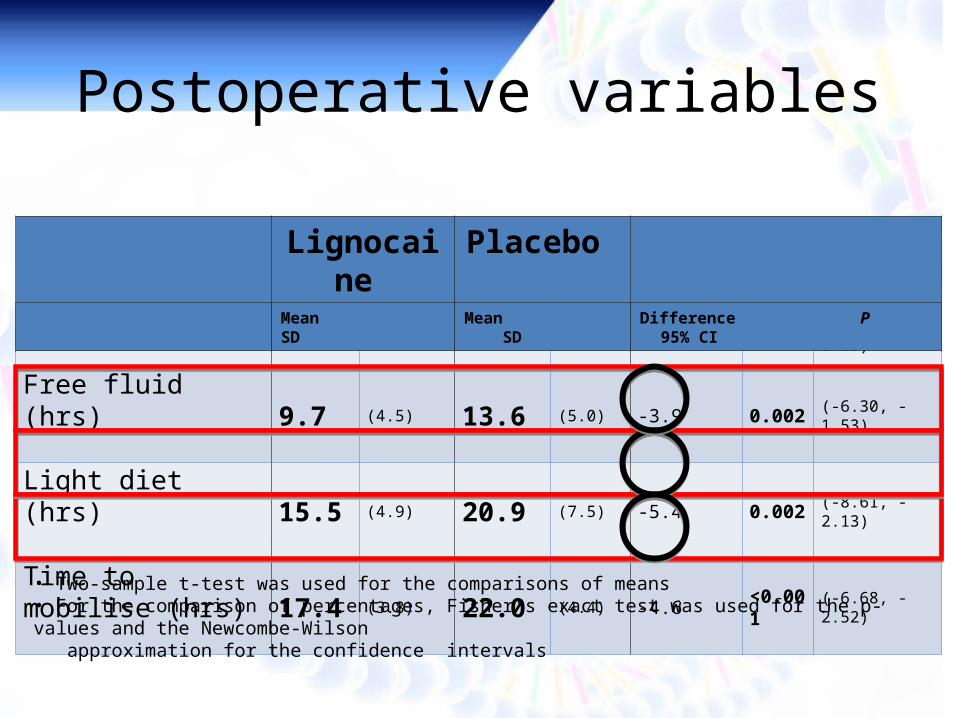
Oral sips (hrs) 7.2 (3.6) 8.6 (4.3) -1.4 0.17 (-3.39, 0.60)
Free fluid (hrs) 9.7 (4.5) 13.6 (5.0) -3.9 0.002 (-6.30, -1.53)
Light diet (hrs) 15.5 (4.9) 20.9 (7.5) -5.4 0.002 (-8.61, -2.13)
Time to mobilise (hrs) 17.4 (3.8) 22.0 (4.4) -4.6 <0.001 (-6.68, -2.52)
Lignocaine Placebo Mean SD Mean SD Difference P 95% CI
• Two-sample t-test was used for the comparisons of means • For the comparison of percentages, Fisher’s exact test was used for the p-values and the Newcombe-Wilson approximation for the confidence intervals

Adverse Effects (% patients)
Nausea/Vomiting 51.4% 44.7% 0.6
Pruritis 16.2% 23.7% 0.6
Dizziness 37.1% 54.1% 0.17
Visual disturbances 11.4% 16.2% 0.7
Peri-oral numbness 5.9% 5.4% 1.0
Muscle weakness 2.9% 8.1% 0.6
Paraesthesia 9.1% 8.1% 1.0
Constipation 10.8% 26.3% 0.14
Lignocaine Placebo P

Post-op Complications
Hypotension requiring medical intervention
5.4% 2.6% 0.6
Other cardiovascular 0.0% 0.0% 1.0
Respiratory depression 0.0% 0.0% 1.0
Pneumonia 0.0% 0.0% 1.0
Intra-abdominal sepsis 0.0% 2.6% 1.0
Wound healing 0.0% 0.0% 1.0
Renal 0.0% 0.0% 1.0
Lignocaine Placebo P

Pain Rest
MEAN
Lignocaine Placebo
19.3 mm 37.3 mm
Difference: 18 mm
95% CI: 7.3 – 28 mm
P = 0.001

Cumulative Morphine
Lignocaine Placebo
38.3 mg 52.3 mg
MEAN
Difference: 13.9 mg
95% CI: 2.2 - 25.7
P = 0.02

Cumulative Morphine
Lignocaine Placebo
1.4 mg/hr 2.0 mg/hr
MEAN SLOPE
Difference: -0.62
95% CI: -0.14 to -0.02
P = 0.02

Adverse events
• SC cannulae: nil complications• Inadvertent administration of lignocaine

Lignocaine Levels
Recovery*
1.36 (0.48) 0.5 – 2.19 < 0.5 0.00 <0.001* (0.63-0.94)
24-hours 3.20 (0.95) 1.1 – 4.96 < 0.5
Lignocaine (ug/mL) Placebo (ug/mL)
Mean (SD) Range Mean SD P 95% CI
• * Uses Mann-Whitney of medians (adjusted for ties) due to non-Normal data • Not appropriate for formal analyses of the 24-hour data as all values in placebo were recorded as < 0.5 .

Conclusions
IV lignocaine followed by 24-hr SC infusion
• Shorter length of stay (1.3 days)• Accelerated acute rehabilitation
Free fluid (3.9 hrs) Diet (5.4 hrs) Mobilisation (4.6 hrs)
• Less 24-hour morphine use• Lower pain scores• Safety factors: paramount

Future directions
• Plasma levels & pain scores• Cancer recurrence• Chronic pain• Utility in laparoscopic radical prostatectomy

Thank you 谢谢
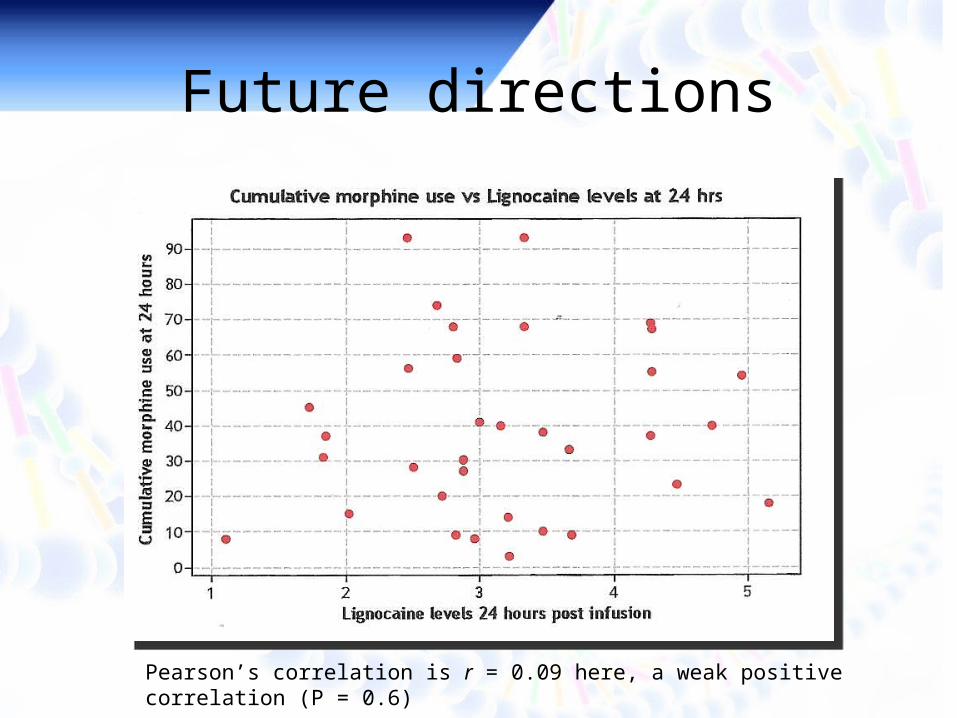
Future directions
Pearson’s correlation is r = 0.09 here, a weak positive correlation (P = 0.6)


















