Acid-Base Disorders · Acid-Base Disorders Mara Nitu, MD,* Greg Montgomery, MD,† Howard Eigen,...
12
Acid-Base Disorders Mara Nitu, MD,* Greg Montgomery, MD, † Howard Eigen, MD § Author Disclosure Drs Nitu, Montgomery, and Eigen have disclosed no financial relationships relevant to this article. This commentary does not contain a discussion of an unapproved/ investigative use of a commercial product/ device. Objectives After completing this article, readers should be able to: 1. Understand the mechanisms for regulating acid-base physiology. 2. Know the differential diagnosis of metabolic acidosis associated with high anion gap and plan for initial management. 3. Know the differential diagnosis of normal anion gap metabolic acidosis. 4. Describe pulmonary compensatory changes in metabolic acidosis and alkalosis. 5. Understand how various diuretics can lead to acid-base imbalance. 6. Describe renal compensatory changes in respiratory acidosis and alkalosis. Case Study A 16-year-old girl who has no significant previous medical history presents to the emer- gency department with a 4-day history of nausea, vomiting, fever, chills, diarrhea, leg cramps, abdominal pain, and headaches. She is finishing her menstrual period and ar- rives with a tampon in place, which she reports that she inserted yesterday. Her vital signs include a heart rate of 165 beats/min, respiratory rate of 28 breaths/min, blood pressure 65/30 mm Hg, and oxygen saturation of 100% on 4 L/min of oxygen. The most likely diag- nosis for this patient is toxic shock syndrome, which was later confirmed with a positive antibody test. The initial arterial blood gas (ABG) values are: ● pH, 7.24 ● Partial pressure of oxygen (PO 2 ), 138 mm Hg ● Partial pressure of carbon dioxide (PCO 2 ), 19 mm Hg ● Bicarbonate (HCO 3 ), 8 mEq/L (8 mmol/L) ● Base excess (BE), 18 mEq/L (18 mmol/L) Such findings are suggestive of metabolic acidosis with respi- ratory compensation. Further laboratory results are: ● Serum sodium (Na ), 133 mEq/L (133 mmol/L) ● Potassium (K ), 4.2 mEq/L (4.2 mmol/L) ● Chloride (Cl ), 109 mEq/L (109 mmol/L) ● HCO 3 , 12 mEq/L (12 mmol/L) ● Anion gap (AG), 12 mEq/L (12 mmol/L) ● Blood urea nitrogen (BUN), 49 mg/dL (17.5 mmol/L) ● Creatinine, 3.96 mg/dL (350 mol/L) ● Calcium, 5.2 mg/dL (1.3 mmol/L) ● Albumin, 2.0 g/dL (20 g/L) The apparently normal AG is misleading. After correcting the AG for hypoalbuminemia, the adjusted AG is 17 mEq/L (17 mmol/L). Lactic acidemia due to shock, one of the likely causes for *Associate Professor of Clinical Pediatrics, Section of Pediatric Pulmonology, Critical Care and Allergy; Medical Director, PICU/ Riley Hospital for Children; Medical Co-Director of Lifeline Transport Team, Indianapolis, IN. † Assistant Professor of Clinical Pediatrics, Section of Pulmonology, Critical Care and Allergy; Medical Director, Pediatric Bronchoscopy Laboratory, James Whitcomb Riley Hospital for Children, Indianapolis, IN. § Billie Lou Wood Professor of Pediatrics, Associate Chairman for Clinical Affairs; Director, Section of Pediatric Pulmonology, Critical Care and Allergy, James Whitcomb Riley Hospital for Children, Indianapolis, IN. Abbreviations ABG: arterial blood gas AG: anion gap BE: base excess BUN: blood urea nitrogen Ca 2 : calcium Cl : chloride CNS: central nervous system DKA: diabetic ketoacidosis GI: gastrointestinal H : hydrogen HCO 3 : bicarbonate K : potassium Mg 2 : magnesium Na : sodium NH 3 : ammonia NH 4 : ammonium PCO 2 : partial pressure of carbon dioxide PO 2 : partial pressure of oxygen RTA: renal tubular acidosis Article fluids and electrolytes 240 Pediatrics in Review Vol.32 No.6 June 2011
Transcript of Acid-Base Disorders · Acid-Base Disorders Mara Nitu, MD,* Greg Montgomery, MD,† Howard Eigen,...
Acid-Base DisordersMara Nitu, MD,* Greg
Montgomery, MD,†
Howard Eigen, MD§
Author Disclosure
Drs Nitu,
Montgomery, and
Eigen have disclosed
no financial
relationships relevant
to this article. This
commentary does not
contain a discussion
of an unapproved/
investigative use of a
commercial product/
device.
Objectives After completing this article, readers should be able to:
1. Understand the mechanisms for regulating acid-base physiology.2. Know the differential diagnosis of metabolic acidosis associated with high anion gap
and plan for initial management.3. Know the differential diagnosis of normal anion gap metabolic acidosis.4. Describe pulmonary compensatory changes in metabolic acidosis and alkalosis.5. Understand how various diuretics can lead to acid-base imbalance.6. Describe renal compensatory changes in respiratory acidosis and alkalosis.
Case StudyA 16-year-old girl who has no significant previous medical history presents to the emer-gency department with a 4-day history of nausea, vomiting, fever, chills, diarrhea, legcramps, abdominal pain, and headaches. She is finishing her menstrual period and ar-rives with a tampon in place, which she reports that she inserted yesterday. Her vital signsinclude a heart rate of 165 beats/min, respiratory rate of 28 breaths/min, blood pressure65/30 mm Hg, and oxygen saturation of 100% on 4 L/min of oxygen. The most likely diag-nosis for this patient is toxic shock syndrome, which was later confirmed with a positive antibodytest.
The initial arterial blood gas (ABG) values are:
● pH, 7.24● Partial pressure of oxygen (PO2), 138 mm Hg● Partial pressure of carbon dioxide (PCO2), 19 mm Hg● Bicarbonate (HCO3
�), 8 mEq/L (8 mmol/L)● Base excess (BE), �18 mEq/L (18 mmol/L)
Such findings are suggestive of metabolic acidosis with respi-ratory compensation.
Further laboratory results are:
● Serum sodium (Na�), 133 mEq/L (133 mmol/L)● Potassium (K�), 4.2 mEq/L (4.2 mmol/L)● Chloride (Cl�), 109 mEq/L (109 mmol/L)● HCO3
�, 12 mEq/L (12 mmol/L)● Anion gap (AG), 12 mEq/L (12 mmol/L)● Blood urea nitrogen (BUN), 49 mg/dL (17.5 mmol/L)● Creatinine, 3.96 mg/dL (350 �mol/L)● Calcium, 5.2 mg/dL (1.3 mmol/L)● Albumin, 2.0 g/dL (20 g/L)
The apparently normal AG is misleading. After correctingthe AG for hypoalbuminemia, the adjusted AG is 17 mEq/L(17 mmol/L).
Lactic acidemia due to shock, one of the likely causes for
*Associate Professor of Clinical Pediatrics, Section of Pediatric Pulmonology, Critical Care and Allergy; Medical Director, PICU/Riley Hospital for Children; Medical Co-Director of Lifeline Transport Team, Indianapolis, IN.†Assistant Professor of Clinical Pediatrics, Section of Pulmonology, Critical Care and Allergy; Medical Director, PediatricBronchoscopy Laboratory, James Whitcomb Riley Hospital for Children, Indianapolis, IN.§Billie Lou Wood Professor of Pediatrics, Associate Chairman for Clinical Affairs; Director, Section of Pediatric Pulmonology,Critical Care and Allergy, James Whitcomb Riley Hospital for Children, Indianapolis, IN.
Abbreviations
ABG: arterial blood gasAG: anion gapBE: base excessBUN: blood urea nitrogenCa2�: calciumCl�: chlorideCNS: central nervous systemDKA: diabetic ketoacidosisGI: gastrointestinalH�: hydrogenHCO3
�: bicarbonateK�: potassiumMg2�: magnesiumNa�: sodiumNH3: ammoniaNH4: ammoniumPCO2: partial pressure of carbon dioxidePO2: partial pressure of oxygenRTA: renal tubular acidosis
Article fluids and electrolytes
240 Pediatrics in Review Vol.32 No.6 June 2011
increased AG metabolic acidosis, is confirmed by a highserum lactate value of 6.9 mg/dL (0.8 mmol/L). One hourlater, the ABG values are:
● pH, 7.06● PO2, 63 mm Hg● PCO2, 47 mm Hg● HCO3
�, 13.2 mEq/L (13.2 mmol/L)● BE, �16 mEq/L (16 mmol/L)
This ABG panel reveals metabolic acidosis withoutrespiratory compensation due to developing respiratoryfailure.
IntroductionThe loss of acid-base balance is an expression of variousconditions encountered frequently in clinical practice.Changes in hydrogen ion concentration can lead tounraveling of the protein tertiary structure, thereby caus-ing enzyme dysfunction, enzyme loss, and cell death.Understanding the physiology behind various distur-bances in acid-base balance is necessary for determining acorrect diagnosis and management plan.
Maintaining acid-base homeostasis involves the lungs,kidneys, and a very complex system of buffers, all aimingto maintain the normal pH (7.35 to 7.45) of the arterialblood. Lowering the arterial pH below 7.35 is termedacidosis, and an increase of the arterial pH above 7.45constitutes alkalosis.
Metabolic acidosis is associated with a low pH and lowHCO3
� concentration. Metabolic alkalosis is associatedwith a high pH and high HCO3
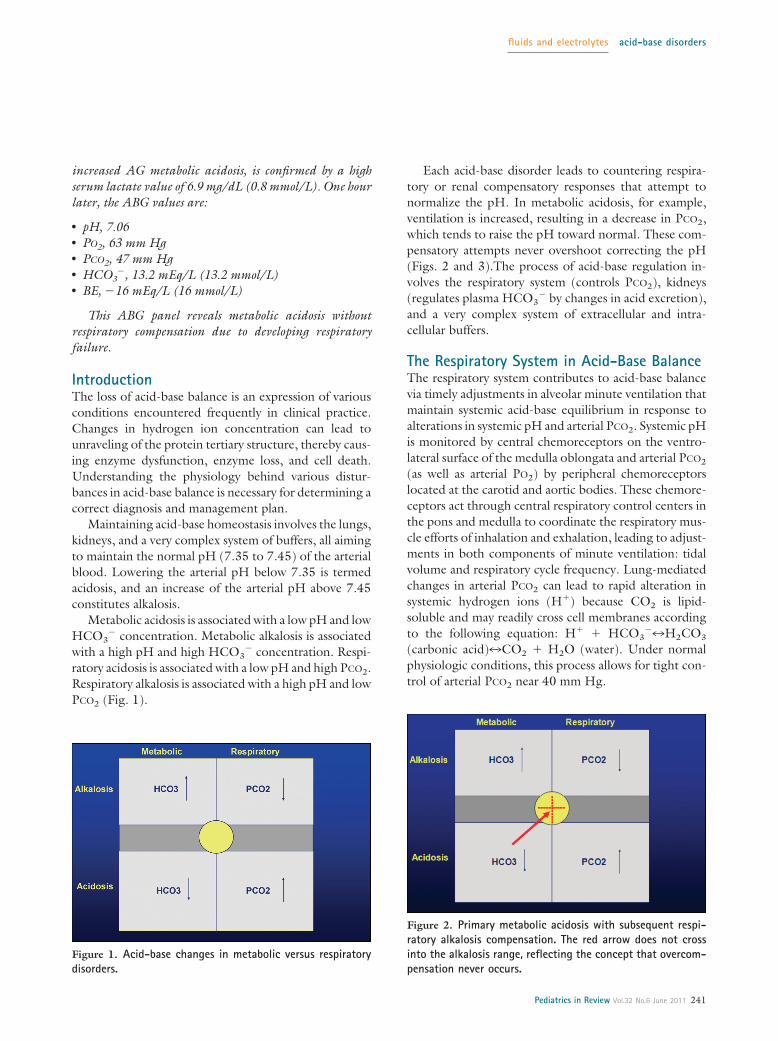
� concentration. Respi-ratory acidosis is associated with a low pH and high PCO2.Respiratory alkalosis is associated with a high pH and lowPCO2 (Fig. 1).
Each acid-base disorder leads to countering respira-tory or renal compensatory responses that attempt tonormalize the pH. In metabolic acidosis, for example,ventilation is increased, resulting in a decrease in PCO2,which tends to raise the pH toward normal. These com-pensatory attempts never overshoot correcting the pH(Figs. 2 and 3).The process of acid-base regulation in-volves the respiratory system (controls PCO2), kidneys(regulates plasma HCO3
� by changes in acid excretion),and a very complex system of extracellular and intra-cellular buffers.
The Respiratory System in Acid-Base BalanceThe respiratory system contributes to acid-base balancevia timely adjustments in alveolar minute ventilation thatmaintain systemic acid-base equilibrium in response toalterations in systemic pH and arterial PCO2. Systemic pHis monitored by central chemoreceptors on the ventro-lateral surface of the medulla oblongata and arterial PCO2
(as well as arterial PO2) by peripheral chemoreceptorslocated at the carotid and aortic bodies. These chemore-ceptors act through central respiratory control centers inthe pons and medulla to coordinate the respiratory mus-cle efforts of inhalation and exhalation, leading to adjust-ments in both components of minute ventilation: tidalvolume and respiratory cycle frequency. Lung-mediatedchanges in arterial PCO2 can lead to rapid alteration insystemic hydrogen ions (H�) because CO2 is lipid-soluble and may readily cross cell membranes accordingto the following equation: H� � HCO3
�7H2CO3
(carbonic acid)7CO2 � H2O (water). Under normalphysiologic conditions, this process allows for tight con-trol of arterial PCO2 near 40 mm Hg.
Figure 1. Acid-base changes in metabolic versus respiratorydisorders.
Figure 2. Primary metabolic acidosis with subsequent respi-ratory alkalosis compensation. The red arrow does not crossinto the alkalosis range, reflecting the concept that overcom-pensation never occurs.
fluids and electrolytes acid-base disorders
Pediatrics in Review Vol.32 No.6 June 2011 241
The Kidneys in Acid-Base BalanceThe kidney’s role in acid-base balance consists of reab-sorbing filtered HCO3
� and excreting the daily acid loadderived principally from the metabolism of sulfur-containing amino acids. Ninety percent of filteredHCO3
� is reabsorbed in the proximal tubules, primarilyby Na�-H� exchange, and the remaining 10% is reab-sorbed in the distal nephron, primarily via hydrogensecretion by a proton pump (H�-ATPase). Under nor-mal conditions, no HCO3
� is present in the final urine.The excretion of the daily H� load occurs in the distal
tubule. Once excreted in the urine, the H� must bebound to a buffer to avoid excessive urine acidificationand promote further excretion. The two primary buffersin the urine are ammonia (NH3), which is excreted andmeasured as ammonium (NH4
�) and phosphate (re-ferred to and measured as titratable acidity). The kidneyssynthesize and excrete NH3, which combines with H�
excreted by the collecting duct cells to form NH4�:
H��NH3�NH4�. NH3 diffuses freely across mem-
branes; NH4�does not. Failure to produce and excrete
sufficient NH4�, therefore, leads to the development of
metabolic acidosis.
Extracellular and Intracellular Buffers inAcid-Base BalanceThe most important buffer in the extracellular fluid isHCO3
�, due both to its relatively high concentrationand its ability to vary PCO2 via changes in alveolar venti-lation. Chemoreceptor analysis of arterial pH and PCO2
allows for centrally mediated adjustments in minute ven-
tilation to maintain arterial PCO2. The HCO3� interacts
with H�, as demonstrated in the following formula:H� � HCO3
�7H2CO37CO2 � H2O. This reactionserves as the basis for the Henderson-Hasselbalch equa-tion: pH�6.1 � log (HCO3
�/0.03 � PCO2). Althoughthis equation describes a patient’s acid-base status, itdoes not provide insight into the mechanism of theacid-base disorder.
The Henderson-Hasselbalch equation lists PCO2 andHCO3
� as independent predictors of acid-base balance,but in reality they are interdependent (as suggested bythe chemical reaction H� � HCO3
� described previ-ously). Furthermore, the Henderson-Hasselbalch equa-tion does not account for other important nonbicarbon-ate buffers present in the body, such as the primaryintracellular buffers of proteins, organic and inorganicphosphates, and hemoglobin. In addition, bone is animportant site for buffering of acid and base loads.
Laboratory Assessment of Acid-Base BalanceAcid-base balance is assessed by blood gas analysis andserum measurement of several important electrolytes,leading to the calculation of the AG. Blood gas analyzersmeasure the pH and the PCO2 directly. The HCO3
�
value is calculated from the Henderson-Hasselbalchequation. The BE value also is calculated as the amountof base/acid that should be added to a sample of wholeblood in vitro to restore the pH to 7.40 while the PCO2 isheld at 40 mm Hg. The PCO2 not only points to the typeof disorder (respiratory or metabolic) but also corre-sponds to the magnitude of the disorder.
The AG method was developed to include othernonbicarbonate buffers in the analysis. Based on theprinciple of electroneutrality, the sum of the positivecharges should equal the sum of the negative charges asfollows: Na��K��Mg2� (magnesium) �Ca2� (cal-cium) �H��Cl�� HCO3
�� protein �� PO43� (phos-
phate)� OH�� SO42� (sulfate)� CO3
2�� conjugatebase�. Sodium, chloride, and HCO3
� are measuredeasily in the serum. Therefore, the AG is calculated by theformula AG�{Na�} � {Cl�� HCO3
�}. A normal AG is12�2 mEq/L (12 mmol/L). Some clinicians and somepublished reports include potassium as a measured cationin the calculation of AG, which raises the normal value by4 mEq/L (4 mmol/L).
The AG is defined as the difference between theunmeasured plasma anions and the unmeasured plasmacations. Clinically, an elevated AG is believed to reflect anincrease of unmeasured anions and, therefore, a meta-bolic acidosis. This concept is explained by the fact thatunmeasured cations (Mg2� � Ca2� � H�) are more
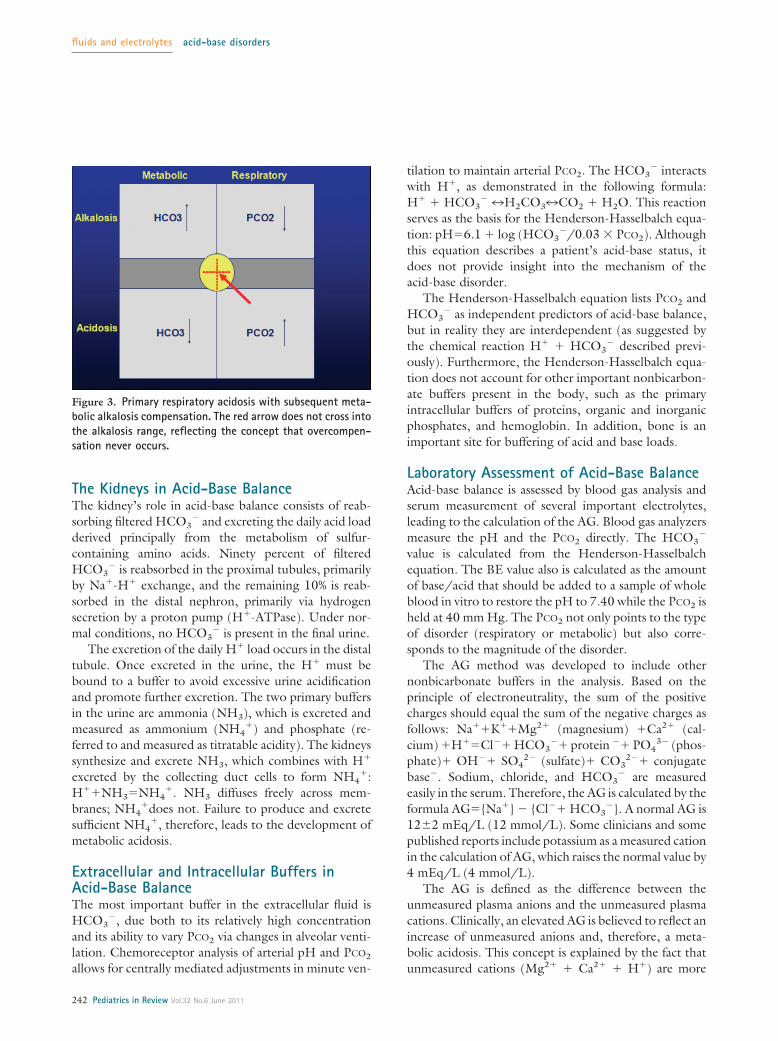
Figure 3. Primary respiratory acidosis with subsequent meta-bolic alkalosis compensation. The red arrow does not cross intothe alkalosis range, reflecting the concept that overcompen-sation never occurs.
fluids and electrolytes acid-base disorders
242 Pediatrics in Review Vol.32 No.6 June 2011
tightly controlled and the unmeasured anions have agreater tendency to fluctuate. Theoretically, the AG alsocan increase following a decrease in serum K�, Ca2�, orMg2�, but the normal concentration of these cations isso low that a reduction does not have a significant clinicalimpact on the AG.
In general, these principles hold true for the previ-ously healthy individual who develops an acute illness.However, for the critically ill host whose plasma proteinconcentrations are greatly reduced, the low protein val-ues hide an associated increase in unmeasured anions.Without the correction for hypoalbuminemia, it is possi-ble to overlook a true high AG acidosis, mistakenlyassuming it to be a normal AG acidosis.
According to the Figge formula, each 1-g/dL reduc-tion in the serum albumin concentration is expected toreduce the AG by 2.5 mEq/L:
Adjusted AG�observed AG � (2.5 �
[normal albumin � observed albumin]
Metabolic Acid-Base DisturbanceMetabolic Acidosis
Metabolic acidosis is defined as an acid-base imbalancethat leads to anion excess (low HCO3
� concentration)and subsequently to an arterial pH below 7.35. Severalmechanisms can lead to metabolic acidosis: excess acidproduction, increased acid intake, decreased renal acid ex-cretion, increased HCO3
� loss from the gastrointestinal(GI) tract, and excess HCO3
� excretion in the kidney.For a patient who has intact respiratory function,
developing metabolic acidosis leads to respiratory com-pensation by hyperventilation. Each 1-mEq/L reductionin plasma HCO3
� concentration prompts a 1.2-mm Hgcompensatory fall in the PCO2. Clinically, the patient’srespiratory rate increases within the first hour of the onsetof metabolic acidosis, and respiratory compensation isachieved within 24 hours. Failure of the respiratory sys-tem to compensate for metabolic acidosis is an ominoussign that should trigger careful evaluation of the patient’smental status and cardiorespiratory function.
Calculating the AG is a very useful initial step indiagnosing various causes of metabolic acidosis.
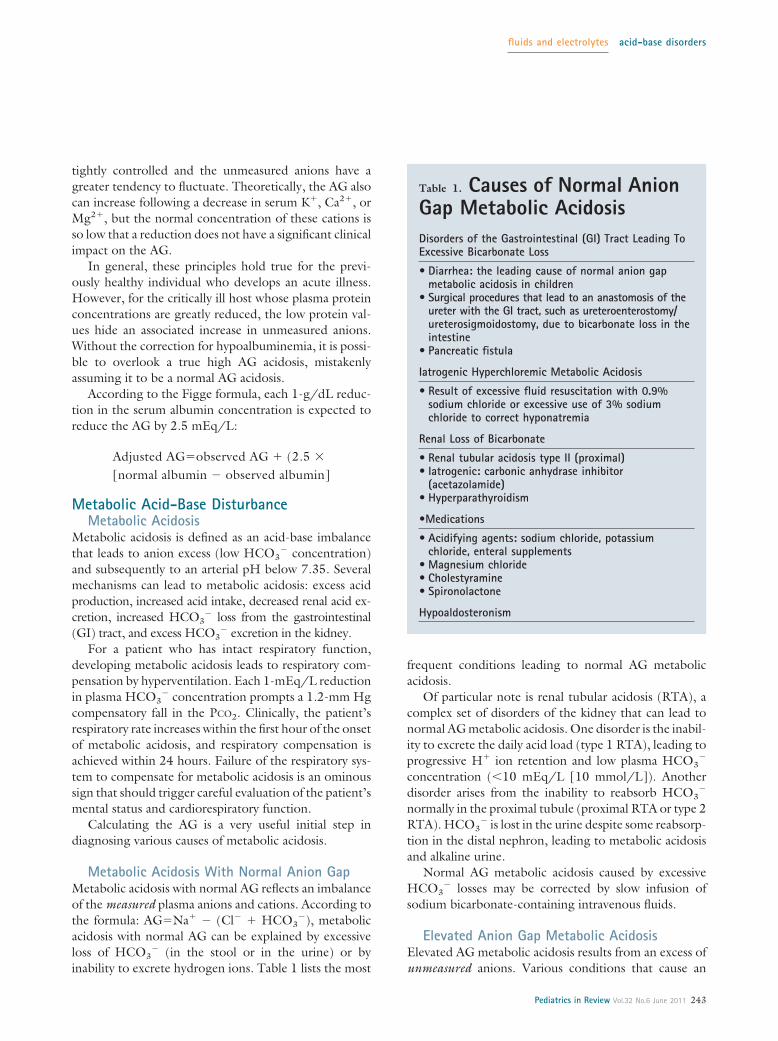
Metabolic Acidosis With Normal Anion GapMetabolic acidosis with normal AG reflects an imbalanceof the measured plasma anions and cations. According tothe formula: AG�Na� � (Cl� � HCO3
�), metabolicacidosis with normal AG can be explained by excessiveloss of HCO3
� (in the stool or in the urine) or byinability to excrete hydrogen ions. Table 1 lists the most
frequent conditions leading to normal AG metabolicacidosis.
Of particular note is renal tubular acidosis (RTA), acomplex set of disorders of the kidney that can lead tonormal AG metabolic acidosis. One disorder is the inabil-ity to excrete the daily acid load (type 1 RTA), leading toprogressive H� ion retention and low plasma HCO3
�
concentration (�10 mEq/L [10 mmol/L]). Anotherdisorder arises from the inability to reabsorb HCO3
�
normally in the proximal tubule (proximal RTA or type 2RTA). HCO3
� is lost in the urine despite some reabsorp-tion in the distal nephron, leading to metabolic acidosisand alkaline urine.
Normal AG metabolic acidosis caused by excessiveHCO3
� losses may be corrected by slow infusion ofsodium bicarbonate-containing intravenous fluids.
Elevated Anion Gap Metabolic AcidosisElevated AG metabolic acidosis results from an excess ofunmeasured anions. Various conditions that cause an
Table 1. Causes of Normal AnionGap Metabolic AcidosisDisorders of the Gastrointestinal (GI) Tract Leading ToExcessive Bicarbonate Loss
• Diarrhea: the leading cause of normal anion gapmetabolic acidosis in children
• Surgical procedures that lead to an anastomosis of theureter with the GI tract, such as ureteroenterostomy/ureterosigmoidostomy, due to bicarbonate loss in theintestine
• Pancreatic fistula
Iatrogenic Hyperchloremic Metabolic Acidosis
• Result of excessive fluid resuscitation with 0.9%sodium chloride or excessive use of 3% sodiumchloride to correct hyponatremia
Renal Loss of Bicarbonate
• Renal tubular acidosis type II (proximal)• Iatrogenic: carbonic anhydrase inhibitor
(acetazolamide)• Hyperparathyroidism
•Medications
• Acidifying agents: sodium chloride, potassiumchloride, enteral supplements
• Magnesium chloride• Cholestyramine• Spironolactone
Hypoaldosteronism
fluids and electrolytes acid-base disorders
Pediatrics in Review Vol.32 No.6 June 2011 243

accumulation of unmeasured anions, leading to high AGmetabolic acidosis, are listed in Table 2.
When faced with an elevated AG metabolic acidosis,calculating the osmotic gap may help determine theunderlying condition. Similar to the AG, the osmotic gapis the difference between the measured serum osmolalityand the calculated value. The calculated serum osmo-lality is: 2 � [Na�] � glucose/18 � BUN/2.8. Anormal osmotic gap should be 12�2 mOsm/L. A highosmotic gap is a sign of an excess of an unmeasuredosmotic active substance such as ethylene glycol (anti-freeze), methanol (wood alcohol), or paraldehyde.
KetoacidosisKetoacidosis describes accumulation of ketone bodies(beta-hydroxybutyrate and acetoacetic acid) followingexcessive intracellular use of lipids as a metabolic sub-strate. This metabolic shift occurs during starvation orfasting or as a reflection of a lack of appropriate metabolicsubstrate for energy production (during specific dietswhere carbohydrates are replaced with lipids). Hyper-ketotic diets sometimes are employed for intractableepilepsy in an effort to decrease the seizure threshold.
Diabetic ketoacidosis (DKA) results from a decreasein insulin production that leads to an inability to trans-port glucose into the cell. The cell shifts to lipid metab-olism, despite the surrounding hyperglycemia (also de-scribed as “starvation in the middle of the plenty”). Thediagnosis of DKA is confirmed by the findings of hyper-glycemia, a high AG acidosis, ketonuria, and ketonemia.
The earliest symptoms of DKA are related to hyper-glycemia. Older children and adolescents typically pres-ent with polyuria (due to the glucose-induced osmoticdiuresis), polydipsia (due to the increased urinary losses),fatigue, and weight loss. Hypovolemia may be severe ifurinary losses are not replaced, with the presentationof very dry mucous membranes and prolonged capillaryrefill time. As a result of worsening metabolic acidosis,the patient develops hyperventilation and deep (Kuss-maul) respirations, representing respiratory compensa-tion for metabolic acidosis. Hyperpnea develops from anincrease in minute volume (rate � tidal volume) or fromincreased tidal volume alone without an increase in respi-ratory rate. When DKA is being managed, the patient’schest excursion and respiratory rate should be observedcarefully to determine if hyperpnea is present. In infants,hyperpnea may be manifested only by tachypnea.
Without prompt medical attention, DKA can prog-ress to cerebral edema and cardiorespiratory arrest.Neurologic findings, ranging from drowsiness, lethargy,and obtundation to coma, are related to the severity ofhyperosmolality or to the degree of acidosis. Treatmentof DKA includes sensitive correction of the underlyinginsulin, volume, and electrolyte deficiencies.
Lactic AcidosisLactic acidosis, another cause of an elevated AG, occurswhen cells shift to anaerobic pathways for energy pro-duction as a result of tissue hypoxia due to inappro-priate tissue perfusion, inappropriate oxygen supply, ormitochondrial dysfunction (as seen in inborn errors ofmetabolism or ingestion of drugs or toxins). The clinicalpresentation may involve seizures or symptoms consis-tent with the initial disorder that led to lactic acidosis,such as cyanosis, signs and symptoms suggestive of tissuehypoperfusion, and hypotension. As lactic acidosis wors-ens, further hemodynamic compromise occurs. Manage-ment should be targeted to restoring adequate tissueperfusion and oxygen supply by treating the underlyingcause of the lactic acidosis.
Inborn Errors of MetabolismSeveral inborn errors of metabolism can present withhigh AG metabolic acidosis. Based on the affected met-abolic pathway, the increased AG is caused by a differentchemical substance: urea cycle defects present with hy-perammonemia; or inborn errors of amino acids, carbo-hydrate, or organic acid metabolism present either withketoacidosis, lactic acidosis (as in Krebs cycle defects), orincreased organic acids production. Symptoms often arenonspecific and include poor feeding, failure to thrive,seizures, and vomiting.
Table 2. Causes of Elevated AnionGap Metabolic AcidosisKetoacidosis
• Starvation or fasting• Diabetic ketoacidosis
Lactic Acidosis
• Tissue hypoxia• Excessive muscular activity• Inborn errors of metabolism
Ingestions
• Methanol• Ethylene glycol• Salicylates• Paraldehyde
Renal Failure
• Uremia
fluids and electrolytes acid-base disorders
244 Pediatrics in Review Vol.32 No.6 June 2011

Managing inborn errors of metabolism involves iden-tifying the defective or deficient enzyme and limiting theintake of the metabolic substrate that requires the use ofthat particular enzyme. In selected cases, dialysis may bethe appropriate tool for removing the excess anion.
IngestionsIngestions of various chemical substances are anothercause of metabolic acidosis with an elevated AG. Sali-cylate overdose is well known to cause increased AGmetabolic acidosis by interfering with cellular metabo-lism (uncoupling of oxidative phosphorylation). Earlysymptoms of salicylate overdose include tinnitus, fever,vertigo, nausea, vomiting, and diarrhea. More severeintoxication can cause altered mental status, coma, non-cardiac pulmonary edema, and death. Most patientsshow signs of intoxication when the plasma salicylateconcentration exceeds 40 mg/dL. Treatment of salicy-late ingestion involves promoting alkaline diuresis toenhance renal salicylate excretion. In severe cases, dialysismay be required (generally considered when plasma sa-licylate concentrations exceed 80 mg/dL in acute intox-ication and 60 mg/dL in chronic ingestions).
Toluene inhalation also can lead to metabolic acidosiswith an increased AG. In patients who experience tolu-ene ingestion (glue sniffing), the overproduced hippu-rate is both filtered and secreted by the kidneys, leadingto rapid elimination in the urine. As a result, the AG maybe near-normal or normal at the time of presentation andthe patient might be diagnosed mistakenly as having anormal AG acidosis.
Ethylene glycol (antifreeze), methanol, and paralde-hyde ingestion lead to an increased AG metabolic acido-sis and an increased osmotic gap. Both the AG and theacidosis due to methanol and ethylene glycol ingestionsresult from metabolism of the parent compound. Nei-ther may be seen in patients early in the course ofingestion or when there is concurrent ingestion of etha-nol. Ethanol combines competitively with alcohol dehy-drogenase, thereby slowing the metabolism of methanolor ethylene glycol to their toxic metabolites and slowingthe appearance of both the acidosis and the high AG.This effect explains why ethanol administration is used inthe medical management of methanol and ethylene gly-col ingestions, along with fomepizole (alcohol dehydro-genase inhibitor). Management of ethylene glycol andmethanol toxicity also involves hemodialysis, which re-moves both the ingested substance and the metabolicbyproducts from the serum.
Massive ingestions of creams containing propyleneglycol (eg, silver sulfadiazine) also can lead to increasedAG metabolic acidosis.
Renal FailureRenal failure causes an increased AG metabolic acidosisdue to the failure to excrete H�. Normally, eliminationof the serum acid load is achieved by urinary excretion ofH�, both as titratable acidity and as NH4
�. Titratableacid is a term used to describe acids such as phosphoricacid and sulfuric acid present in the urine. The termexplicitly excludes NH4
� as a source of acid and is part ofthe calculation for net acid excretion. The term titratableacid was chosen based on the chemical reaction of titra-tion (neutralization) of those acids in reaction with so-dium hydroxide.
As the number of functioning nephrons declines inchronic kidney disease and the glomerular filtration ratedecreases to below 25% of normal, the patient developsprogressive high AG metabolic acidosis (hyperchloremiamay occur transiently in the initial phases of renal failure).In addition to the decrease in NH4
� excretion, decreasedtitratable acidity (primarily as phosphate) may play a rolein the pathogenesis of metabolic acidosis in patients whoexperience advanced kidney disease. Of course, dialysisoften is employed to correct the severe fluid and electro-lyte imbalances generated by renal failure.
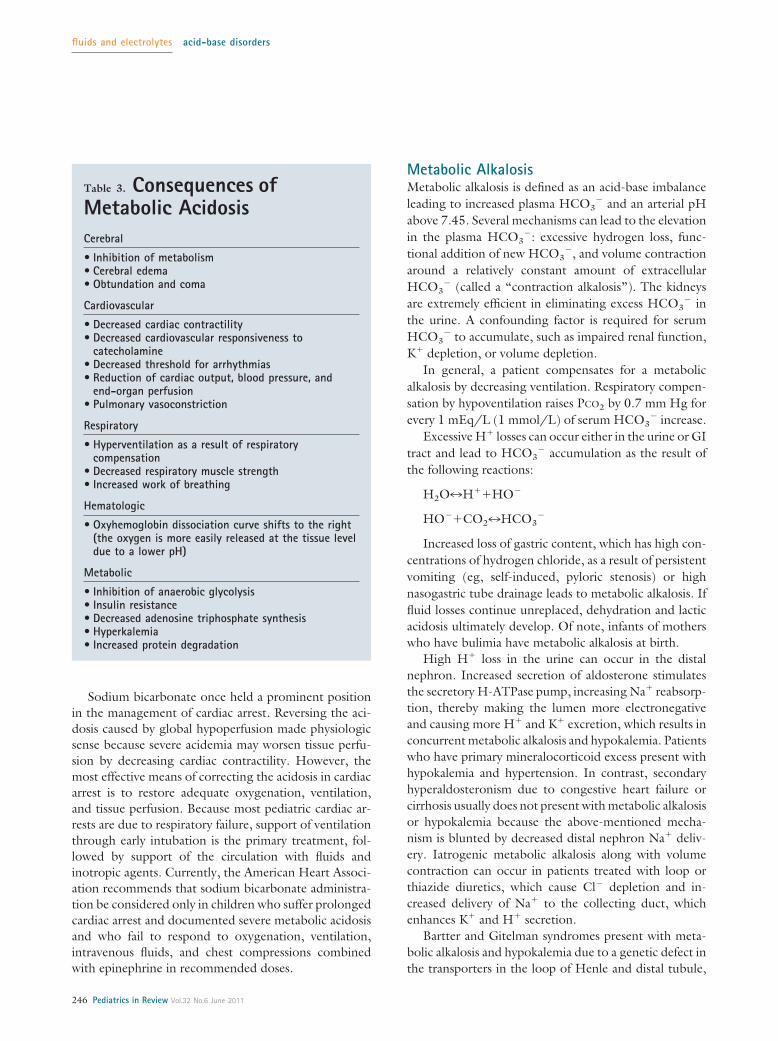
Management of Metabolic AcidosisRegardless of the cause, acidemia, if untreated, can leadto significant adverse consequences (Table 3).
Use of HCO3� therapy to adjust the pH for pa-
tients who have metabolic acidosis is controversial. Slowinfusion of sodium bicarbonate-containing intravenousfluids can be used in cases of normal AG metabolicacidosis to replenish excessive HCO3
� losses (eg, as aresult of excessive diarrhea). However, infusing sodiumbicarbonate-containing fluids for increased AG meta-bolic acidosis has questionable benefit and should not beused clinically.
As discussed, HCO3� combines with H�, leading to
H2CO3 that subsequently dissociates to CO2 and H2O.Infusing HCO3
� decreases serum pH and raises CO2 andH2O. Neither the cell membranes nor the blood-brainbarrier is very permeable to HCO3
�; CO2 diffuses freely tothe intracellular space, where it combines with H2O, lead-ing to H2CO3 and worsening of the intracellular pH.Administering intravenous sodium bicarbonate to a patientwho has an increased AG metabolic acidosis can lead to afalse sense of security because the underlying problem ishidden by an artificially improved serum pH.
fluids and electrolytes acid-base disorders
Pediatrics in Review Vol.32 No.6 June 2011 245
Sodium bicarbonate once held a prominent positionin the management of cardiac arrest. Reversing the aci-dosis caused by global hypoperfusion made physiologicsense because severe acidemia may worsen tissue perfu-sion by decreasing cardiac contractility. However, themost effective means of correcting the acidosis in cardiacarrest is to restore adequate oxygenation, ventilation,and tissue perfusion. Because most pediatric cardiac ar-rests are due to respiratory failure, support of ventilationthrough early intubation is the primary treatment, fol-lowed by support of the circulation with fluids andinotropic agents. Currently, the American Heart Associ-ation recommends that sodium bicarbonate administra-tion be considered only in children who suffer prolongedcardiac arrest and documented severe metabolic acidosisand who fail to respond to oxygenation, ventilation,intravenous fluids, and chest compressions combinedwith epinephrine in recommended doses.
Metabolic AlkalosisMetabolic alkalosis is defined as an acid-base imbalanceleading to increased plasma HCO3
� and an arterial pHabove 7.45. Several mechanisms can lead to the elevationin the plasma HCO3
�: excessive hydrogen loss, func-tional addition of new HCO3
�, and volume contractionaround a relatively constant amount of extracellularHCO3
� (called a “contraction alkalosis”). The kidneysare extremely efficient in eliminating excess HCO3
� inthe urine. A confounding factor is required for serumHCO3
� to accumulate, such as impaired renal function,K� depletion, or volume depletion.
In general, a patient compensates for a metabolicalkalosis by decreasing ventilation. Respiratory compen-sation by hypoventilation raises PCO2 by 0.7 mm Hg forevery 1 mEq/L (1 mmol/L) of serum HCO3
� increase.Excessive H� losses can occur either in the urine or GI
tract and lead to HCO3� accumulation as the result of
the following reactions:
H2O7H��HO�
HO��CO27HCO3�
Increased loss of gastric content, which has high con-centrations of hydrogen chloride, as a result of persistentvomiting (eg, self-induced, pyloric stenosis) or highnasogastric tube drainage leads to metabolic alkalosis. Iffluid losses continue unreplaced, dehydration and lacticacidosis ultimately develop. Of note, infants of motherswho have bulimia have metabolic alkalosis at birth.
High H� loss in the urine can occur in the distalnephron. Increased secretion of aldosterone stimulatesthe secretory H-ATPase pump, increasing Na� reabsorp-tion, thereby making the lumen more electronegativeand causing more H� and K� excretion, which results inconcurrent metabolic alkalosis and hypokalemia. Patientswho have primary mineralocorticoid excess present withhypokalemia and hypertension. In contrast, secondaryhyperaldosteronism due to congestive heart failure orcirrhosis usually does not present with metabolic alkalosisor hypokalemia because the above-mentioned mecha-nism is blunted by decreased distal nephron Na� deliv-ery. Iatrogenic metabolic alkalosis along with volumecontraction can occur in patients treated with loop orthiazide diuretics, which cause Cl� depletion and in-creased delivery of Na� to the collecting duct, whichenhances K� and H� secretion.
Bartter and Gitelman syndromes present with meta-bolic alkalosis and hypokalemia due to a genetic defect inthe transporters in the loop of Henle and distal tubule,
Table 3. Consequences ofMetabolic AcidosisCerebral
• Inhibition of metabolism• Cerebral edema• Obtundation and coma
Cardiovascular
• Decreased cardiac contractility• Decreased cardiovascular responsiveness to
catecholamine• Decreased threshold for arrhythmias• Reduction of cardiac output, blood pressure, and
end-organ perfusion• Pulmonary vasoconstriction
Respiratory
• Hyperventilation as a result of respiratorycompensation
• Decreased respiratory muscle strength• Increased work of breathing
Hematologic
• Oxyhemoglobin dissociation curve shifts to the right(the oxygen is more easily released at the tissue leveldue to a lower pH)
Metabolic
• Inhibition of anaerobic glycolysis• Insulin resistance• Decreased adenosine triphosphate synthesis• Hyperkalemia• Increased protein degradation
fluids and electrolytes acid-base disorders
246 Pediatrics in Review Vol.32 No.6 June 2011

respectively, the same locations as those inhibited byloop and thiazide diuretics.
In addition to H� loss, metabolic alkalosis also can beinduced by the shift of H� into the cells.
As discussed previously, hypokalemia is a frequent find-ing in patients who have metabolic alkalosis. Hypokalemiaby itself causes intracellular acidosis and increased serumalkalosis by the following mechanism: intracellular K�
shifts into the serum to replete the extracellular stores, andto maintain electroneutrality, H� enters the cells. Hydro-gen movement into the cells lowers the intracellular pHand leaves unbuffered excess HCO3
� in the serum. Theintracellular acidosis in renal tubular cells promotes H�
secretion and, therefore, HCO3� reabsorption.
Metabolic alkalosis due to functional addition of“new” HCO3
� can occur by several mechanisms: de-creased renal excretion of HCO3
�, posthypercapnicalkalosis, or excessive intake or administration of alkali.
Decreased Renal Bicarbonate ExcretionRenal failure can lead to metabolic alkalosis because thekidneys fail to excrete excess HCO3
�.
Posthypercapnic AlkalosisChronic respiratory acidosis (retention of CO2) leads to acompensatory increase in hydrogen secretion and anensuing increase in the plasma HCO3
� concentration tocorrect the pH. When the PCO2 is decreased rapidly bymechanical ventilation of a patient who has chronicrespiratory acidosis, the ensuing metabolic alkalosis isslow to disappear. Because Cl� loss often is present inposthypercapnic alkalosis, repleting the Cl� deficit maybe essential to correct the alkalosis.
Furthermore, the acute fall in PCO2 in a person whohas chronic respiratory acidosis raises the cerebral intra-cellular pH acutely, a change that can induce seriousneurologic abnormalities and death because CO2 candiffuse freely across the blood-brain barrier out of theintracellular space, leading to severe alkalosis. Accord-ingly, the PCO2 must be reduced gradually in mechani-cally ventilated patients who present initially with chronichypercapnia.
Excessive Intake or Administration of AlkaliAlkali administration does not induce metabolic alkalosisin healthy people because the healthy kidney can excreteHCO3
� rapidly in the urine. However, metabolic alka-losis can occur if very large quantities of HCO3
� areadministered acutely or if the ability to excrete HCO3
�
is impaired. The administration of large quantities ofcitrate is known to lead to metabolic alkalosis. Examples
of large administrations of citrate are infusion of morethan 8 units of banked blood or fresh frozen plasmaor administration of citrate as an anticoagulant duringdialysis.
Contraction AlkalosisContraction alkalosis occurs when relatively large vol-umes of HCO3
�-free fluid are lost, a situation frequentlyseen with administration of intravenous loop diuretics.Contraction alkalosis also may occur in other disorders inwhich a high-Cl�, low-HCO3
� solution is lost, such assweat losses in cystic fibrosis, loss of gastric secretions inpatients who have achlorhydria, and fluid loss from fre-quent stooling by patients who have congenital chlori-dorrhea, a rare congenital secretory diarrhea.
Regardless of the cause, alkalosis, if untreated, canlead to significant adverse consequences (Table 4).
Management of Metabolic AlkalosisThree general principles apply to the therapy of meta-bolic alkalosis: correct true volume depletion, correct K�
depletion, and correct Cl� depletion (in Cl�-responsivemetabolic alkalosis). For patients who have true volume
Table 4. Consequences ofUntreated AlkalosisCerebral
• Cerebral vasoconstriction with reduction of cerebralblood flow
• Tetany, seizures, lethargy, delirium, and stupor
Cardiovascular
• Vasoconstriction of the small arterioles, includingcoronary arteries
• Decreased threshold for arrhythmias
Respiratory
• Compensatory hypoventilation with possiblesubsequent hypoxemia and hypercarbia (respiratoryfailure)
Hematologic
• Oxyhemoglobin dissociation curve shifts to the left(the oxygen is bound more tightly to theoxyhemoglobin)
Metabolic and Electrolyte Imbalances
• Stimulation of anaerobic glycolysis• Hypokalemia• Decreased plasma ionized calcium• Hypomagnesemia and hypophosphatemia
fluids and electrolytes acid-base disorders
Pediatrics in Review Vol.32 No.6 June 2011 247

depletion, fluid administration of normal saline replacesthe Cl� and free water deficits. Potassium chloride ad-ministration for patients who have concurrent hypokale-mia is an important component of treatment. This agentbecomes particularly helpful in patients who are edema-tous due to heart failure or cirrhosis and cannot receivesodium chloride because an infusion can increase thedegree of edema. Another method for treating metabolicalkalosis in an edematous patient is to administer acet-azolamide, a carbonic anhydrase inhibitor, which causesa mild increase in production of urine that has highHCO3
� content, thus reacidifying the blood.Correcting metabolic alkalosis (usually diuretic-
induced) may be particularly important for intubatedpatients who have chronic respiratory acidosis. Thehigher pH caused by the metabolic alkalosis subse-quently impairs the respiratory drive and leads to hypo-ventilation that exacerbates hypoxemia, delaying wean-ing and extubation. In these patients, metabolic alkalosisusually is corrected by enteral supplements of potassiumchloride or sodium chloride. Very rarely, in the intensivecare unit setting, the metabolic alkalosis can be so severethat it impairs weaning from mechanical ventilation. Inthese circumstances, intravenous infusion of hydrogenchloride can correct the alkalosis.
Measuring the urinary Cl� is the preferred method forassessing the renal response to Cl� therapy. For patientsexperiencing Cl� depletion (urinary Cl� �10 mEq/L[10 mmol/L]) (eg, GI losses, diuretic therapy, and sweatlosses in cystic fibrosis), every attempt should be made tocorrect hypochloremia. Conditions that cause metabolicalkalosis due to high aldosterone concentrations are un-responsive to Cl� and are associated with high urine Cl�
concentrations.Minimizing continuing acid and chloride losses by
excessive nasogastric fluid drainage with a histamine2
blocker or proton pump inhibitor also may be helpful.
Respiratory Acid-Base DisturbancesAs noted, chemoreceptor analysis of arterial pH andPCO2 allows for centrally mediated adjustments in min-ute ventilation to maintain arterial PCO2 near 40 mm Hg.Primary respiratory disturbances in acid-base equilibriummay result from different pathologic scenarios. ArterialPCO2 rises abnormally (respiratory acidosis) if systemicCO2 production exceeds the ventilatory capacity or whenefficient ventilation is inhibited by intrinsic or acquiredconditions. Conversely, arterial PCO2 decreases abnor-mally (respiratory alkalosis) in response to physiologicdisorders that result in excessive ventilation. Both respi-ratory acidosis and alkalosis may appear in association
with other metabolic acid-base disturbances, often mak-ing accurate diagnosis and treatment of the underlyingdisease difficult to achieve.
Respiratory AcidosisRespiratory acidosis occurs when arterial PCO2 increasesand arterial pH decreases due to a reduction in alveolarminute ventilation or, less commonly, an excessive in-crease in CO2 production. Acute respiratory acidosisoccurs with an acute elevation in PCO2 as a result ofsudden limitation or failure of the respiratory system.Chronic respiratory acidosis is due to more indolentincreases in PCO2 as a consequence of systemic diseaseover the course of several days. Reduction in minuteventilation can result from depression of central nervoussystem (CNS) respiratory drive, anatomic obstruction ofthe respiratory tract, or intrinsic or acquired impairmentsof normal thoracic excursion (Table 5).
Table 5. Common Causes ofRespiratory Acidosis inChildrenCentral Nervous System Depression
• Medication effects– Sedative: benzodiazepines, barbiturates– Analgesic: narcotics– Anesthetic agents: propofol
• Central nervous system disorders– Head trauma– Infection– Tumor– Congenital central hypoventilation
Impairments of Thoracic Excursion or VentilatoryEfficiency
• Chest wall/lung disorders– Asphyxiating thoracic dystrophy– Progressive thoracic scoliosis– Thoracic trauma– Acute lung injury/pneumonia– Pneumothorax/parapneumonic effusion– Severe obesity
• Nerve/muscle disorders– Congenital myopathies– Spinal cord injury– Toxin exposure: organophosphates, botulism– Guillain-Barre syndrome
Respiratory Tract Obstruction
• Upper airway obstruction– Adenotonsillar hypertrophy
• Status asthmaticus
fluids and electrolytes acid-base disorders
248 Pediatrics in Review Vol.32 No.6 June 2011

The body’s compensatory changes in response toacute respiratory acidosis initially are limited to bufferingvia systemically available cellular HCO3
� stores. Becauseof this limitation, serum HCO3
� concentrations riseacutely by only 1 mEq/L (1 mmol/L) for every 10-mmHg elevation in arterial PCO2. In response to chronicrespiratory acidosis, the kidney retains HCO3
� andsecretes acid, an alteration in function that takes sev-eral (3 to 5) days to have a noticeable physiologic ef-fect. Eventually, in chronic respiratory acidosis, serumHCO3
� concentrations ultimately rise by approximately3.5 mEq/L (3.5 mmol/L) for every 10-mm Hg eleva-tion in arterial PCO2.
Respiratory acidosis can affect both the CNS andcardiovascular system adversely. CNS effects include in-creased cerebral blood flow and increased intracranialpressure, which can present clinically as disorientation,acute confusion, headache, and mental obtundation.Cardiovascular effects include peripheral vasodilationand tachycardia. Severe hypoventilation leads to higherarterial PCO2 and more severe hypoxemia. Hypoxemiamay be partially compensated by improved tissue extrac-tion of oxygen via an acute acidosis-mediated rightwardshift in the oxyhemoglobin dissociation curve and releaseof oxygen to the tissues. However, as respiratory acidosispersists, a reduction in red blood cell 2,3 diphospho-glycerate (an organophosphate created in erythrocytesduring glycolysis) results in a shift of the curve to the leftand an increase of hemoglobin affinity for oxygen.
Management of Respiratory AcidosisTreatment of respiratory acidosis usually focuses on cor-recting the primary disturbance. Immediate discontinu-ation of medications that suppress central respiratorydrive or administration of appropriate reversal agentsshould be considered. Noninvasive ventilation or intuba-tion with mechanical ventilation may be necessary toachieve adequate alveolar ventilation and appropriatereduction in arterial PCO2. As arterial PCO2 is corrected,individuals who experience excessive Cl� depletion maysubsequently suffer poor renal clearance of HCO3
�,leading to a concomitant state of metabolic alkalosis.
Respiratory AlkalosisRespiratory alkalosis occurs when there is reduction inarterial PCO2 and elevation in arterial pH due to excessivealveolar ventilation. Causes of excessive alveolar ventila-tion include medication toxicity, CNS disease, intrinsiclung diseases, and hypoxia (Table 6).
Compensatory changes in response to respiratory al-kalosis involve renal excretion of HCO3. As in respira-
tory acidosis, renal compensation improves as the disor-der persists. Serum HCO3
� concentrations decline by2 mEq/L (2 mmol/L) for every 10-mm Hg decrease inarterial PCO2 in acute respiratory alkalosis. In chronicrespiratory alkalosis, serum HCO3
� concentrations de-cline by 4 mEq/L (4 mmol/L) for every 10-mm Hgdecrease in arterial PCO2.
Adverse Effects of Respiratory AlkalosisAdverse systemic effects of respiratory alkalosis includeCNS and cardiovascular disturbances. Respiratory alka-losis often provokes increased neuromuscular irritability,manifested as paresthesias or carpopedal spasms. In ad-dition, cerebral blood vessels vasoconstrict acutely andimpede adequate cerebral blood flow. Myocardial con-tractility may be diminished and cardiac arrhythmias mayoccur. The oxyhemoglobin dissociation curve shifts tothe left in response to acute respiratory alkalosis, impair-ing peripheral oxygen delivery.
Management of Respiratory AlkalosisTreatment of respiratory alkalosis centers on correctingthe underlying systemic cause or disorder. Close assess-ment of oxygenation status and correction of hypoxemiavia oxygen administration is paramount. Acute hyper-ventilation syndrome often is treated simply by havingthe patient breathe into a paper bag. To prevent highaltitude-associated respiratory alkalosis, slow ascent toallow for acclimatization is recommended; administra-
Table 6. Common Causes ofRespiratory Alkalosis inChildrenMedication Toxicity
• Salicylate overdose• Central nervous system stimulants
– Xanthines (eg, caffeine)– Analeptics (eg, doxapram)
Central Nervous System Disorders
• Central nervous system tumor• Head injury/stroke• Hyperventilation syndrome: stress/anxiety
Respiratory Disorders
• Pneumonia• Status asthmaticus• Pulmonary edema• Excessive mechanical or noninvasive ventilation• Hypoxia/high altitude
fluids and electrolytes acid-base disorders
Pediatrics in Review Vol.32 No.6 June 2011 249
tion of acetazolamide before ascent should be consid-ered. The only cure for acute mountain sickness, once ithas developed, is either acclimatization or descent. How-ever, symptoms of acute mountain sickness can be re-duced with acetazolamide and pain medications forheadaches.
Suggested ReadingBrandis K. Acid-Base Physiology. Accessed March 2011 at: http://
www.anaesthesiamcq.com/AcidBaseBook/ABindex.phpCarrillo-Lopez H, Chavez A, Jarillo A, Olivar V. Acid-base disor-
ders. In: Fuhrman B, Zimmerman J, eds. Pediatric CriticalCare. 3rd ed. Philadelphia, PA: Mosby Elsevier; 2005:958–989
Grogono AW. Acid-Base Tutorial. 2010. Accessed March 2011 at:http://www.acid-base.com
Kraut JA, Madias NE. Approach to patients with acid-base disor-ders. Respiratory Care. 2001;46:392–403
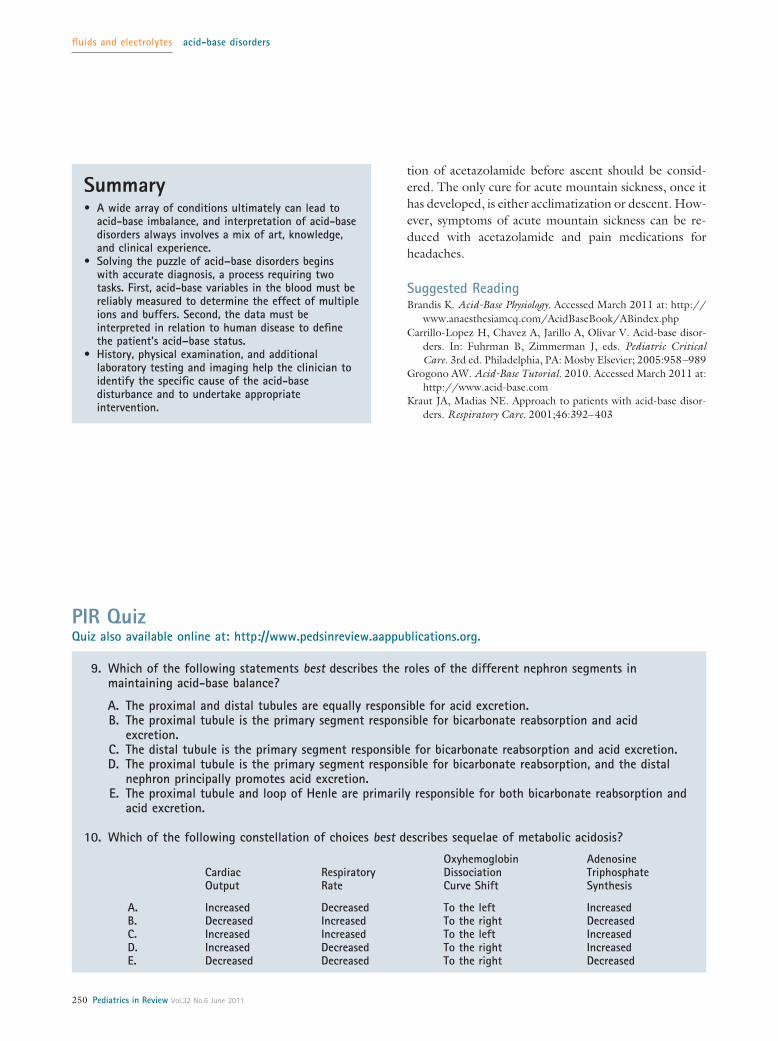
Summary• A wide array of conditions ultimately can lead to
acid-base imbalance, and interpretation of acid-basedisorders always involves a mix of art, knowledge,and clinical experience.
• Solving the puzzle of acid–base disorders beginswith accurate diagnosis, a process requiring twotasks. First, acid-base variables in the blood must bereliably measured to determine the effect of multipleions and buffers. Second, the data must beinterpreted in relation to human disease to definethe patient’s acid–base status.
• History, physical examination, and additionallaboratory testing and imaging help the clinician toidentify the specific cause of the acid-basedisturbance and to undertake appropriateintervention.
PIR QuizQuiz also available online at: http://www.pedsinreview.aappublications.org.
9. Which of the following statements best describes the roles of the different nephron segments inmaintaining acid-base balance?
A. The proximal and distal tubules are equally responsible for acid excretion.B. The proximal tubule is the primary segment responsible for bicarbonate reabsorption and acid
excretion.C. The distal tubule is the primary segment responsible for bicarbonate reabsorption and acid excretion.D. The proximal tubule is the primary segment responsible for bicarbonate reabsorption, and the distal
nephron principally promotes acid excretion.E. The proximal tubule and loop of Henle are primarily responsible for both bicarbonate reabsorption and
acid excretion.
10. Which of the following constellation of choices best describes sequelae of metabolic acidosis?
CardiacOutput
RespiratoryRate
OxyhemoglobinDissociationCurve Shift
AdenosineTriphosphateSynthesis
A. Increased Decreased To the left IncreasedB. Decreased Increased To the right DecreasedC. Increased Increased To the left IncreasedD. Increased Decreased To the right IncreasedE. Decreased Decreased To the right Decreased
fluids and electrolytes acid-base disorders
250 Pediatrics in Review Vol.32 No.6 June 2011
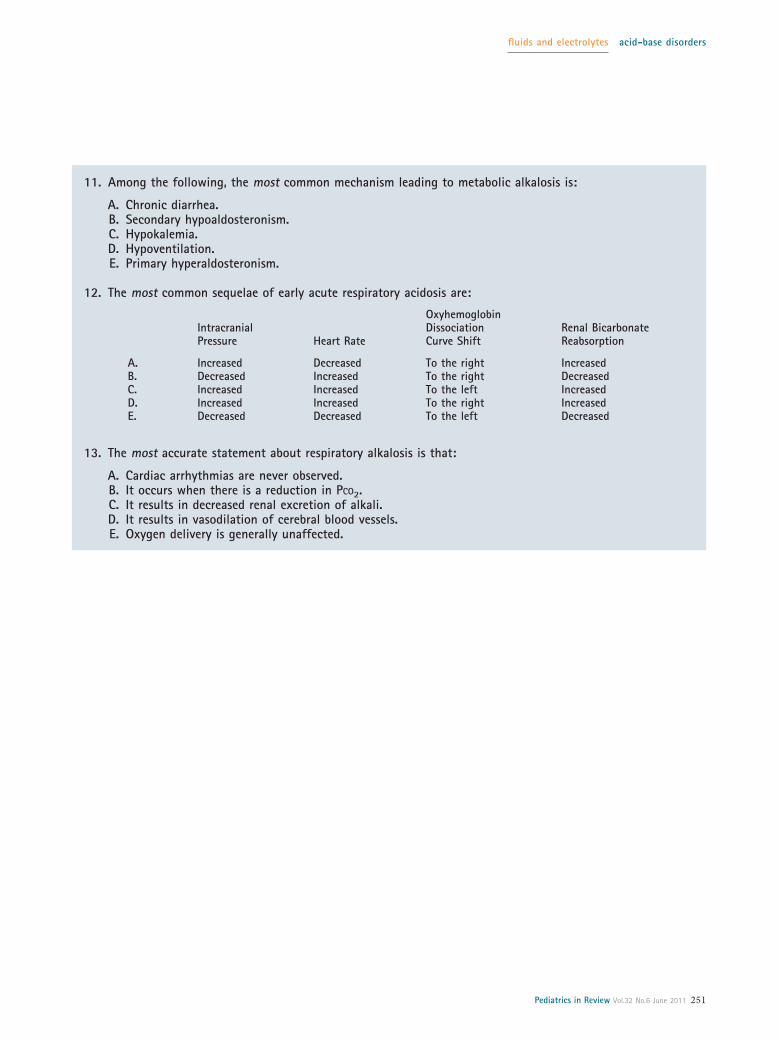
11. Among the following, the most common mechanism leading to metabolic alkalosis is:
A. Chronic diarrhea.B. Secondary hypoaldosteronism.C. Hypokalemia.D. Hypoventilation.E. Primary hyperaldosteronism.
12. The most common sequelae of early acute respiratory acidosis are:
IntracranialPressure Heart Rate
OxyhemoglobinDissociationCurve Shift
Renal BicarbonateReabsorption
A. Increased Decreased To the right IncreasedB. Decreased Increased To the right DecreasedC. Increased Increased To the left IncreasedD. Increased Increased To the right IncreasedE. Decreased Decreased To the left Decreased
13. The most accurate statement about respiratory alkalosis is that:
A. Cardiac arrhythmias are never observed.B. It occurs when there is a reduction in PCO2.C. It results in decreased renal excretion of alkali.D. It results in vasodilation of cerebral blood vessels.E. Oxygen delivery is generally unaffected.
fluids and electrolytes acid-base disorders
Pediatrics in Review Vol.32 No.6 June 2011 251


















