
ACCS Anaesthetic Trainees Wales Workbook · ACCS Anaesthetic Trainees Wales Workbook ... FRIDAY...
33
Final Version approved 31 st July 2017 ACCS Anaesthetic Trainees Wales Workbook August 2017 For Wales Deanery CT 1&2 ACCS Anaesthetic Trainees ACCS – Wales
Transcript of ACCS Anaesthetic Trainees Wales Workbook · ACCS Anaesthetic Trainees Wales Workbook ... FRIDAY...
Final Version approved 31st July 2017
ACCS Anaesthetic
Trainees
Wales
Workbook August 2017
For Wales Deanery CT 1&2 ACCS Anaesthetic Trainees
ACCS – Wales
2
Contents
Introduction 3
Specialist Training Committee (STC) 4
ACCS Website & Social Media 6
Induction 7
Teaching 7
National ACCS Trainees Day 11
Study Leave 11
Looking After Yourself (Your Health) 11
Professional Support Unit 12
Career Changes 12
ACCS Curriculum 13
Training requirements for EM post 16
Training requirements for AM post 17
Training requirements for ITU post 18
Training requirements for Anaesthetics post 19
ARCP 27
Career info:
Dual Accreditation in Intensive Care Medicine 28
Sub-specialty Pre-Hospital Emergency Medicine training 31
3
Introduction
Since the introduction of the new ACCS curriculum in May 2010 ACCS training is described
under the headings of:
1. Common Competences
2. Major Presentations
3. Acute Presentations
4. Anaesthesia in ACCS
5. Practical Procedures
Some of this training must be obtained in a particular module, but other competences can be
achieved in any of the modules, provided that all are achieved by the end of year 2. This system
can make it difficult for trainees and trainers to keep track of what competencies remain
outstanding, and the ACCS workbook is designed to make this process easier.
The workbook gives trainees and trainers a central document where all the required
competencies and clinical procedures can be recorded, and correct paperwork identified. It
aims to clarify the ACCS Curriculum: anything that is not clear should be discussed with your
Educational Supervisor.
Trainees should ensure they are registered with RCOA and that they have access to the relevant
e-portfolio.
http://www.rcoa.ac.uk/trainee-e-portfolio/e-portfolio-contacts
Trainees should use the RCOA e-portfolio for the anaesthesia-specific forms during the
anaesthetic block. For the ICM block they should discuss with their Educational Supervisor
which forms to use, those from their e-portfolio or paper copies downloaded from the FICM
website which could be scanned in.
Paper forms should be completed during the EM/AM posts. Copies of these forms are found on
the Wales Deanery and AWSEM websites. These can both be printed and filled in by hand or
can be emailed to the trainer for electronic completion. If completed electronically please print
and ensure the trainer has signed the form.
4
Each time the trainee completes a 6-month module within the ACCS programme a Structured
Training Report (StR) should be completed by the Module Clinical Supervisor. All “paperwork”
whether on e-portfolio or paper, should be summarised on the paper checklists in this
workbook. Supervisors’ signatures in the workbook are not necessary – “see e-portfolio” etc is
acceptable.
At the ARCP the trainee should submit this workbook summarising the acquired competences,
along with the paper or e-portfolio evidence.
ARCP Checklists are available on the AWSEM website:
http://www.awsem.org.uk/training/wpba-arcps/st1-ct1-st2-ct2/
The Specialist Training Committee
Specialty Training Manager, Wales Deanery: Zoe Dummett
Email: [email protected]
Head of School Emergency Medicine, ACCS STC Chair, acting ACCS TPD
Amanda Farrow, EM Consultant, Bridgend Email: [email protected]
Specialty Leads
ACCS Lead for Anaesthesia: Rachel Walpole, Consultant Anaesthetist, Newport
Email: [email protected]
ACCS Lead for Acute Medicine: Llifon Edwards, Consultant Physician, Newport
Email: [email protected]
ACCS Lead for Intensive Care Medicine: Alison Ingham, Consultant Anaesthetist & Intensivist,
Bangor
Email: [email protected]
ACCS Lead for Emergency Medicine: Ranga Mothukuri, EM Consultant Morriston
Email: [email protected]
5
Hospital Leads
University Hospital of Wales, Cardiff: Melvyn Jenkins-Welch, Ana Consultant
Email: [email protected]
Morriston Hospital, Swansea: Ranga Mothukuri, EM Consultant
Email: [email protected]
Royal Gwent Hospital, Newport: Rachel Walpole, Consultant Anaesthetist
Email: [email protected]
Ysbyty Gwynedd, Bangor: Alison Ingham, Consultant Anaesthetist & Intensivist, Bangor
Email: [email protected]
Wrexham Maelor Hospital: Ash Basu, EM Consultant Email: [email protected]
Nevill Hall, Abergavenny: Ed Curtis, Consultant Anaesthetist
Email: [email protected]
Princess of Wales, Bridgend: Amanda Farrow, EM Consultant Email: [email protected]
Core TPD for Anaesthesia: (responsible for ACCS Anaesthetic CT3 trainees) Graeme Lilley
Email: [email protected]
Trainee Representatives:There are 2 elected trainee representatives, one from CT/ST1 and one
from CT/ST2. They represent trainees’ views at Specialist Training Committee meetings. Please
contact one of them if there are issues you wish to bring to the attention of the STC.
2017 Representatives are:
CT/ST2: Pip Falkner ACCS EM Trainee NHH Email: [email protected]
CT/ST1: Will be elected in September 2017
6
Wales ACCS Website and Social Media
Wales Deanery website ACCS page
https://www.walesdeanery.org/specialties/acute-care-common-stem-accs
AWSEM Website ACCS page
http://www.awsem.org.uk/
ACCS Wales Whats app group
A whats app group of trainees and trainers set up to aid communication ( please contact the
trainee rep if you wish to be added)
ACCS Wales Facebook Group
A closed group, please search for ACCS Wales and join the group, it is open to everyone. You
are welcome to use it to share information or to put questions to other members of the group.
ACCS Wales Twitter account
Please follow @ACCSWales
Junior Anaesthetists of Wales (JAW) – www.junioranaesthetistsofwales.org.uk Welsh School of Anaesthesia www.welshschool.co.uk
National ACCS Website and Social Media
The National ACCS Website can be found here: www.rcoa.ac.uk/accs. It is a useful source of
information including a trainee’s guide, FAQs, links to the curriculum etc. There are National
ACCS Trainee Representatives who sit on the National Intercollegiate ACCS Training Committee,
and they can be contacted via the website.
Follow ACCS Training on twitter @icaccst
7
ACCS Induction
All CT1 trainees are invited to the ACCS Induction day which is usually held in early September.
The day will outline the curricular requirements for the CT1 and 2 years and is a great
opportunity to meet members of the STC and other trainees.
All CT2 trainees will be invited to attend the “Core Anaesthetic Trainees CT1” Induction day
which is also usually held in early September. The day is run by the School of Anaesthesia and
includes talks on the curriculum, the primary FRCA, the E-portfolio and the professional support
unit. It is compulsory to attend the day.
ACCS Teaching
Local ACCS Teaching opportunities for ACCS Anaesthetic Trainees:
Morriston Hospital
Anaesthetics:
Primary Teaching is held on a Wednesday Morning (Dr Beth Hale is the lead)
Finals Teaching is held on a Thursday Morning (Drs Anna Roberts/Katy Beard/Stuart Jenkins are the leads)
The department holds a list of audit days, which are full days and during these audits/M&M are discussed.
Audit Leads are Drs Ors Takats and Christine Range, and Dr Jo Quigley is the lead for M&M. EM:
Departmental induction at start of post (2 hours each day, Mon – Fri) - Protected time
Weekly afternoon teaching on Wednesday from 2pm-5pm - Protected time. Topics
include ATLS, ALS, APLS.
Board round teaching every handover shift in the morning – Important learning points
from cases
Clinical Governance Forum first Friday of every month where audits are presented, M&M
is discussed. Trainees advised to attend.
Sepsis teaching for all juniors when they start
AM:
8
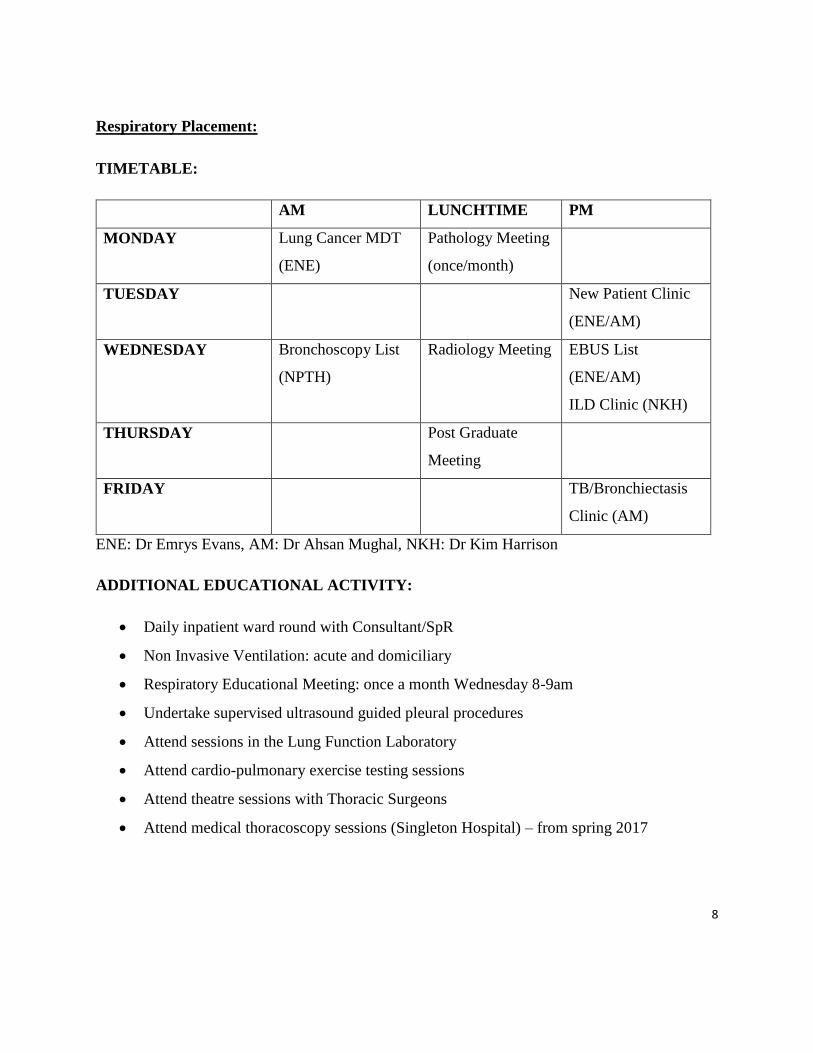
Respiratory Placement:
TIMETABLE:
AM LUNCHTIME PM
MONDAY Lung Cancer MDT
(ENE)
Pathology Meeting
(once/month)
TUESDAY New Patient Clinic
(ENE/AM)
WEDNESDAY Bronchoscopy List
(NPTH)
Radiology Meeting EBUS List
(ENE/AM)
ILD Clinic (NKH)
THURSDAY Post Graduate
Meeting
FRIDAY TB/Bronchiectasis
Clinic (AM)
ENE: Dr Emrys Evans, AM: Dr Ahsan Mughal, NKH: Dr Kim Harrison
ADDITIONAL EDUCATIONAL ACTIVITY:
Daily inpatient ward round with Consultant/SpR
Non Invasive Ventilation: acute and domiciliary
Respiratory Educational Meeting: once a month Wednesday 8-9am
Undertake supervised ultrasound guided pleural procedures
Attend sessions in the Lung Function Laboratory
Attend cardio-pulmonary exercise testing sessions
Attend theatre sessions with Thoracic Surgeons
Attend medical thoracoscopy sessions (Singleton Hospital) – from spring 2017
9
ALSO:
Ad hoc teaching sessions can be arranged with the Respiratory Consultants (or other members of
the Respiratory Team including Pharmacists, Clinical Nurse Specialists, Physiotherapists etc).
To arrange this please discuss with Dr E Evans.
Am: Gastroenterology placement:
Wed (8:30 am - 09:30 am) - Gastro departmental meeting
45 mins of educational activity - case presentation / journal club (Gastro / General
Medicine related)
15 mins - administrative issues (team rota discussion / any other business)
Mon (13:00 -14:00 hrs) - CMT teaching programme (also open to ACCS trainees on
medical rotation)
First 3 Mondays of the month - teaching on various medical conditions / specialities
Last Monday of the month - Clinical Skills Lab Procedural training training for 1
procedure every month - Ascitic Drain / Intercostal drain insertion / LP / Central venous
cannulation
Thursday (13:00 - 14:00) - Grand Round (with audit / mortality meeting once in 2
months)
Nevil Hall Hospital
Anaesthetics:
Wednesday: afternoon teaching on anaesthetic topics plus 1 hour dedicated ICU teaching.
Thursday MDT paediatric resuscitation scenarios with the emergency dept,
6 monthly emergency front of neck access course (CICO)
Monthly departmental audit/ CPD/ morbidity & mortality meeting
After 1 month in anaesthetics: critical incident training in theatres and the simulation lab which includes
20 scenarios to be covered.
Initial assessment of anaesthetic competencies
Medicine
Tuesday morning 1 hour - clinical teaching Thursday lunchtime 1 hour – hospital grand round Thursday afternoon 2 hour – clinical bedside teaching From September departmental (acute medicine) teaching session for 2 hours every fortnight
EM Thursday morning weekly 8-9
10
Royal Gwent Hospital
Grand Round – Wednesday Lunchtime
Anaesthetics: Novice Teaching – multiple sessions per week over about 6 weeks. Following this, move
onto Primary FRCA teaching – once weekly lasting 3-4 hours. Usually consultant led, sometimes
senior trainees. After passing the Primary, you go to Final teaching – same length of time but on
different day of the week. Weekly simulation sessions (usually critical incident sims). Weekly
departmental lunchtime meeting – opportunity for trainees to present on topics. Monthly QI and audit
day. CICO courses run every few months. Rota’d to attend the paediatric ED simulations (one
trainee). Joint Obs-Anaes meeting (monthly) – usually presenting on recent cases/projects. Usually
senior trainees presenting. Weekly Critical Incident reflection meeting – trainees encouraged to attend
and discuss incidents/difficulties.
ITU: Thursday afternoon teaching programme which contains governance meetings such as M&M (2 monthly) , quarterly research meetings, as well as a weekly journal club and an hour (or longer) consultant led teaching for the trainees on basic ICU topics. We also frequently have external speakers for an hour or so on topics related to intensive care medicine. Additionally we have recently started a weekly consultant led lunchtime teaching session for 30-45 minutes (generally on Tuesday or Wednesday) on basic ICU topics as well. Medicine: CT1/2 in cardiology have cardiology teaching ? Thursday mornings. Respiratory team teaching is Friday Lunchtime. EM: 2 full days induction off rota
1 day x-ray course – off rota
Monthly full day teaching day – taken off rota
Aim for 15min daily teaching at boardround, pre written cases for discussion Departmental in situ SIM programme
University Hospital of Wales - TBC
11
Wrexham Maelor Hospital
ANAES : Thurs (09:00 - 12:00) - weekly departmental teaching program (3hrs) - year long program structured around the core anaesthetic syllabus. Thurs (08:30 - 09:00) - Journal club - trainees are encouraged to pick, present and critique a topic that they find interesting or has changed their practice in some way. ITU : Wed (17:30 - 18:30) - weekly education slot (1hr), changes weekly between hot topics, journal club, case presentations, M&M... Daily (Mon-Fri) - Teaching ward rounds from 10:15 Biweekly (Mon/Thurs) - ITU MDT meetings 11:30
Ysbyty Gwynedd Hospital
Weekly Grand Round on Friday lunchtime Weekly radiology teaching Wed lunchtime Monthly ECG teaching 1st Tues of month Monthly VC of Medical teaching from Royal College Physicians of Edinburgh Annual Trauma Team Training day Twice yearly CICO course Extensive programme of other events provided by Postgraduate Dept including things like Breaking Bad News Anaesthetics: ( usually attend both Anaesthetics and ITU teaching in both posts) Wednesday 2-5 pm Thursday 5:30 – 6:30 pm joint anaesthesia / ICM departmental meeting including M&M ITU: Wednesday 1-2 pm Medicine: CMT teaching Thursday 1-2 pm EM: Junior EM teaching the 1st, 2nd and 4th Thursday every month from 1300-1700, and the Patient Safety/M&M meeting will be the penultimate Tuesday of every month at 0800.
12
Regional ACCS Teaching opportunities for all ACCS Trainees:
1. ACCS Regional Teaching Programme
Five themed days rotating around ACCS training sites (Unconscious Patient, Shock &
Sepsis, Major Trauma, Cardiology and Respiratory emergencies). The days are multi-
disciplinary and mapped to the curriculum. They involve some classroom teaching
sessions, as well as simulation and practical procedures. Reflective logs on learning
points from teaching days can be linked to the curriculum to evidence sign-off of the
various CMPs and CAPs. The training day timetable will be sent out separately. You will
need to apply for study leave. It is anticipated you will be most likely to attend these
days during the CT1 year during your EM/AM posts.
2. ACCS Practical Procedures Day
Usually held in Princess of Wales Hospital, Bridgend and North Wales. Useful for sign-
off of some practical procedures or just for practice.
Anaesthetic Teaching opportunities for all ACCS Anaesthetic Trainees:
SWABS – South Wales Anaesthetic Basic Sciences is run on a regular basis at hospitals
across South Wales and provided exam focused lecture-style teaching which may be
useful to attend in your CT2 year.
North Wales Regional Teaching – Fortnightly (all day) North Wales regional teaching which is shared amongst all 3 sites. It is a year long program based around the FRCA anaesthetic syllabus.
Primary FRCA teaching : Trainees should aim to sit the FRCA Primary MCQ Examination by the
end of CT2 and must achieve both parts of the Primary by the end of CT3.
Transfer Training:
The Critical Care Network runs regular Transfer Courses for trainees. WAG requires that a trainee supervising an interhospital transfer must have attended the course, so it is desirable to achieve this before ST3 if possible. It is NOT a curriculum or ARCP requirement for CT1-2, however the transfer module must be signed off for the BLTC at the end of CT3 (CT2b), and this can either be achieved by attending the Transfer Course OR during a supervised intra-hospital transfer.
To register for a place on the course please contact: South Wales: [email protected]
North Wales: sue.o'[email protected]
13
Relevant Local Courses
AWAG Emergency Medicine Airway Day - run by All Wales Airway Group(AWAG) and
EM Consultants once a year in Cardiff usually in Autumn.
https://allwalesairwaygroup.co.uk/page/home
TREATs course – excellent trauma day run in Morritson @treatscourse on Twitter
National ACCS Trainee Day
This is held annually at the Royal College of Anaesthetists in London. It is free (and includes a
very nice lunch!). Presentations usually focus around curriculum and ARCP issues, and career
options and advice (PHEM, combining ITU with other specialties etc).
Study Leave
Please see the link below to the Wales Deanery study leave policy.
https://www.walesdeanery.org/sites/default/files/archive_files/Documents/QA/All_Wales_
Study_Leave_Policy_-_January_2015.pdf
Looking after Yourself
Medicine is a stressful profession, and Core Training can be particularly difficult because of
frequent changes of post, a steep learning curve, and exam pressures.
The GMC makes clear that a good doctor looks after their own health and well-being as well as
that of their patients.
If you find yourself struggling then either your Educational Supervisor or any Consultant that
you feel able to talk to should be your first source of support. However if you feel unable to
confide in a senior colleague, you may wish to make use of the BMA helpline; it is not necessary
to be a BMA member to use it:
BMA Counselling & Doctor Adviser Service: 0845 9200169
Alternatively, Health for Health Professionals Wales offers free Psychotherapy referral to any
doctor in Wales. It is a confidential service funded by the Welsh Government.
http://www.hhpwales.co.uk
Tel 0800 0582738 between 9am and 5pm Mon-Fri, calls free from a landline.
14
Professional Support Unit
https://psu.walesdeanery.org/
The Professional Support Unit is a service provided by the Wales Deanery to support trainees
who are struggling for any reason; common referrals are to help with examination difficulties,
improve organisational or communication skills, or for health and personal issues. The service is
confidential. Most referrals are made by Educational Supervisors (with trainee consent) but
trainees may refer themselves.
Career Changes
Thoughts of specialty change are inevitable in ACCS training. It is NOT possible to change to an
alternative parent specialty without repeating the application / interview process. If you are
considering changing specialty, you can discuss your options with the appropriate ACCS
Specialty Lead or the ACCS TPD. Many ACCS trainees have changed routes in the past; many
others have had their doubts but then happily continued on the original path.
15
ACCS Curriculum
The ACCS Curriculum can be found on RCOA ACCS website https://www.rcoa.ac.uk/accs/2012-
curriculum
ACCS training is described under the headings of:
1. Common Competences: ( ACCS curriculum pages 26-73)
These are competencies that should be acquired by all doctors during their training
period starting within the undergraduate career and developed throughout
postgraduate training. For ACCS trainees, competence to at least level 2 descriptors will
be expected prior to progression into further specialty training. Many of these
competencies are an integral part of clinical practice and as such will be assessed
concurrently with the clinical presentations and procedures assessments. Trainees
should use these assessments to provide evidence that they have achieved the
appropriate level. Descriptors of the required performance at each level can be found in
the curriculum. At least 50% of the common competencies must be signed off at level 2
or above by the end of the CT2 ACCS year. For a few common competencies alternative
evidence should be used e.g. assessments of audit and teaching, completion of courses,
management portfolio, which can be used to record management and leadership
competencies.
2. Major Presentations (CMPs)
These are seen as the cornerstone of the clinical skills of ACCS trainees and they should all be signed off by the end of the second year.
Two must be completed in the Emergency Medicine placement and must be summatively assessed using the Mini-CEX descriptor tool or a summative CbD (see Curriculum pages 222-228). Summative tools are available for Major trauma, Shock, Altered level of consciousness and Sepsis.
The other four WPBAs can be achieved in any post but two are usually assessed in each of the Acute Medicine & ICM placement. It is usually recommended that Septic Patient is signed off in the ICM placement. The knowledge, skills and behaviours to be achieved for each presentation are listed in the curriculum.
16
3. Acute presentations (CAPs)
There are 38 Acute Presentations (APs) which need to be signed off by the end of the second year of ACCS. These are generally most applicable to AM and EM and whilst a minimum of 10 in AM and 10 in EM should be signed off, trainees should be strongly encouraged to complete them all during those placements. There are 5 APs that require the trainee to complete specific summative WBAs in the EM attachment. Up to 5 APs can be covered by a single ACAT in either EM or AM. The knowledge, skills and behaviours to be achieved for each presentation are listed in the curriculum.
4. Anaesthesia in ACCS
During the Anaesthesia component of ACCS, trainees first achieve the Initial Assessment of
Competency (IAC) and then go on to complete the 8 Core Units of Training that comprise the
Introduction to Anaesthesia. All trainees should use the RCOA guide for novices found here.
Paper certificate and further information can be found here.
Logbook : All trainees should maintain a logbook of all their Anaesthetic cases. This should be a
summary report by age, specialty, ASA grade and level of supervision. There is an electronic
logbook available from the Royal College of Anaesthetists that is free to download, and trainees
are strongly advised to use this for their records, as it will generate the required reports.
5. Intensive Care Medicine
During Basic training in ICM, the trainee works under direct supervision for the majority
of the time, being introduced to the knowledge and skills required for ICM. A broad-
based outline knowledge of the wide range of problems which are seen in ICM is
necessary at Basic level. Greater understanding and expertise can then be built upon
this during higher stages of training should trainees wish to pursue ICM as a career.
6. Practical Procedures
There is a list of 44 Practical Procedures in the ACCS Curriculum. 39 out of 44 (ideally all)
are expected to be completed by the end of the second year, and all by the end of the
third year. 17 are associated with the Anaesthetic Initial Assessment of Competence,
and 11 are associated with ICM training.
17
Workplace Based Assessments:
The CMPs and CAPs and most of the common competences are assessed using the ACCS
workplace-based assessments (WBAs):
Mini-Clinical Evaluation Exercise (M-CEX)
Direct Observation of Procedural Skills (DOPS)
Multi-Source Feedback (MSF) : please use the paperwork specific to the specialty being
assessed or alternatively use the RCOA e-portfolio and ask your Anaesthetic ES who will have
access to liaise with the placement supervisor. One should be completed during each six month
post. A minimum of 12 responses is required.
Case-Based Discussion (CBD)
Acute Care Assessment Tool (ACAT and ACAT-EM)
Audit Assessment
Teaching Observation
18
TRAINING REQUIREMENTS FOR EACH POST
Emergency Medicine
During your EM post you are required to complete the following WPBAs as a minimum:
1. 2 summative WPBAs ( CBD or Mini-Cex) by a Consultant for 2 Major Presentations
2. 5 summative WPBAs ( CBD or Mini-Cex) by a Consultant for the following 5 Acute
Presentations ( Abdominal pain, Breathlessness, Chest Pain, Head Injury and Mental
Health)
3. One ACAT by a Consultant to cover a max of 5 Acute Presentations
4. Your WPBA should include 1 ACAT, 3 CBD and 4 Mini-cex as a minimum
5. You should cover a minimum total of 10 Acute Presentations by WPBAs
6. 5 DOPs to include Airway maintenance, Wound management, Primary Survey and
Fracture / joint manipulation
7. MSF – 12 responses minimum and 3 Consultants ( this can be done in the RCOA e-
portfolio or on RCEM MSF forms)
8. You will be required to have an Educational Supervisors report completed at the end
of the post which will be submitted for your ARCP.
All the required forms can be found here:
http://www.awsem.org.uk/training/wpba-arcps/st1-ct1-st2-ct2/
19
Acute Medicine Training Requirements
During your AM post you are required to complete the following WPBAs as a minimum:
1. 2 formative WPBAs ( CBD or Mini-Cex) for 2 Major Presentations
2. 3 ACATs by a Consultant to cover a max of 5 Acute Presentations
3. Your WPBA should include 3 ACAT, 3 CBD and 3 Mini-cex as a minimum
4. You should cover a minimum total of 10 Acute Presentations by WPBAs
5. 5 DOPs
6. MSF – 12 responses minimum and 3 Consultants ( this can be done in the RCOA e-
portfolio or on RCEM MSF forms)
7. You will be required to have an Educational Supervisors report completed at the end
of the post which will be submitted for your ARCP.
All the required forms can be found here:
http://www.awsem.org.uk/training/wpba-arcps/st1-ct1-st2-ct2/
20
ITU Training Requirements
During your ITU post you are required to complete the following as a minimum:
1. 2 WPBAs ( CBD or Mini-Cex) for 2 Major Presentations ( unless they have all been
completed in previous posts)
2. Your WPBA should include 4 CBD, 3 Mini-cex and 6 DOPS as a minimum
3. You need to complete an ITU logbook
4. You will be required to achieve the 11 specific ITU competences listed below
a. Demonstrates aseptic peripheral venous cannulation
b. Demonstrates aseptic arterial cannulation (+ local anaesthetic)
c. Obtains an arterial blood gas sample safely, interprets results correctly
d. Demonstrates aseptic placement of central venous catheter
e. Connects mechanical ventilator and selects initial settings
f. Describes Safe Use of Drugs to Facilitate Mechanical Ventilation
g. Describes Principles of Monitoring Respiratory Function
h. Describes the Assessment of the patient with poor compliance during Ventilatory Support
(‘fighting the ventilator’)
i. Prescribes safe use of vasoactive drugs and electrolytes
j. Delivers a fluid challenge safely to an acutely unwell patient
k. Describes actions required for accidental displacement of ETT or tracheostomy
5. MSF – 12 responses minimum and 3 Consultants ( this can be done in the RCOA e-portfolio
or on RCEM MSF forms)
6. You will be required to have an Educational Supervisors report completed at the end of the
post which will be submitted for your ARCP.
7. All the required forms can be found here: http://www.awsem.org.uk/training/wpba-
arcps/st1-ct1-st2-ct2/ or here: https://www.ficm.ac.uk/curriculum-assessment-
training/assessment-forms
21
Anaesthesia curriculum and assessments for ACCS Anaesthetic Trainees
During the Anaesthetic Module, all ACCS trainees should complete the Introduction to Anaesthetic
Practice.
It comprises:
1. The Initial Assessment of Competence (IAC), followed by:
2. 8 Units of Anaesthetic Core Training as listed in Appendix 2 below.
The IAC is a set of 19 core competencies which must be achieved before working without immediate
supervision. Once the IAC is achieved, the trainee moves on to complete the 8 Core Units of Training
that make up the Introduction to Anaesthesia. This will require a minimum of a further 7 WPBAs – see
Appendix 2 for details. Each Unit of Training apart from ‘Management of cardiac arrest in adults and
children’ requires 1x DOPS, 1x ACEX, 1x CBD, and achievement of all the Clinical Learning Outcomes.
A CUT form must be completed for each of the 8 Units of Training, confirming that the trainee has
achieved all the minimum clinical learning outcomes.
The CUT form for ‘Management of cardiac arrest in adults and children’ may be signed if the trainee has
a valid ALS/APLS certificate. If they do not have a certificate the College recommends use of simulation
to assess the trainee.
The Initial Assessment of Competence
This is a summative assessment
▪ The aim should be to achieve the IAC within the first three months.
▪ Each assessment must be a single assessment event and therefore trainees must complete a minimum
of 19 separate assessment events to achieve their IAC.
▪ Assessments for the IAC can only be signed off by consultants.
▪ The IAC certificate must be signed by two consultants.
▪ The IAC must be completed satisfactorily and the IAC certificate signed before a trainee can work with
distant supervision.
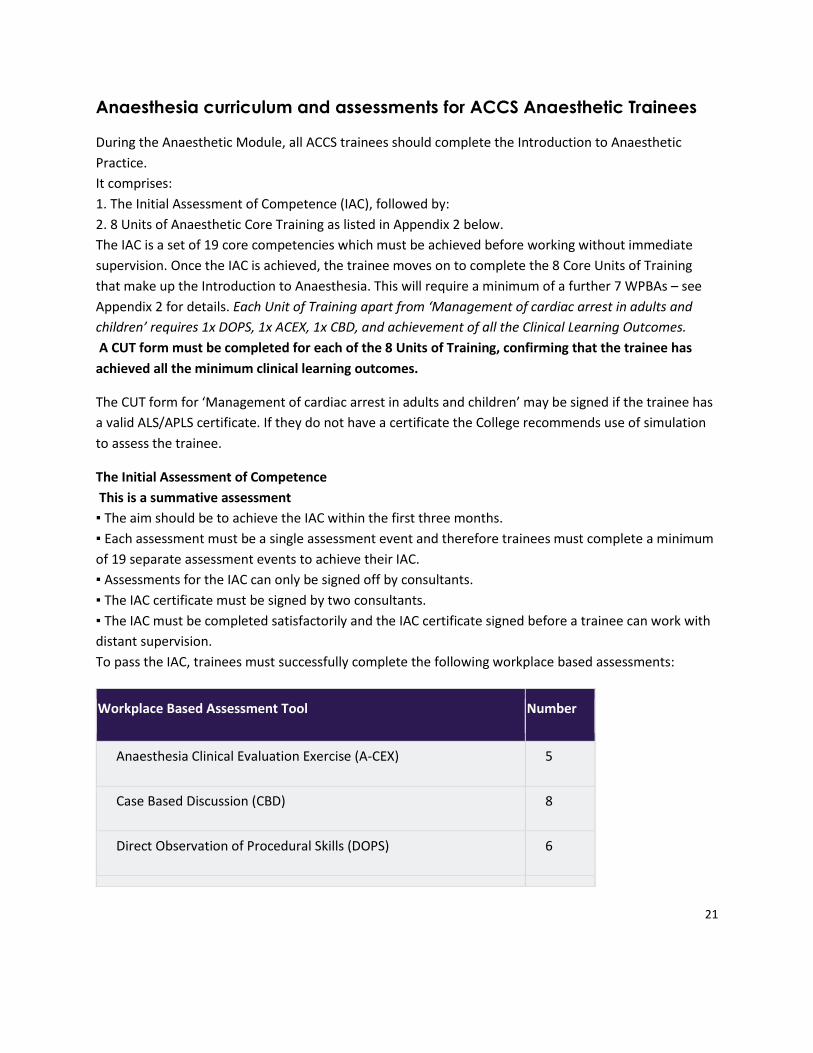
To pass the IAC, trainees must successfully complete the following workplace based assessments:
Workplace Based Assessment Tool Number
Anaesthesia Clinical Evaluation Exercise (A-CEX) 5
Case Based Discussion (CBD) 8
Direct Observation of Procedural Skills (DOPS) 6
22
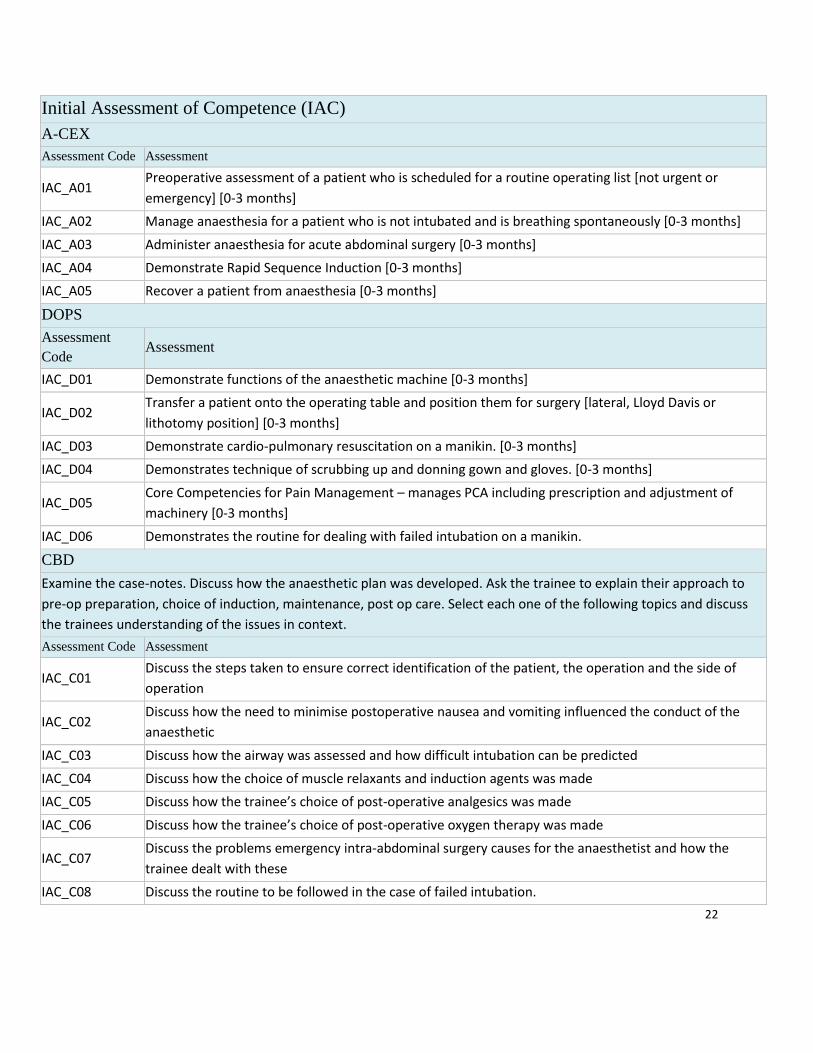
Initial Assessment of Competence (IAC)
A-CEX
Assessment Code Assessment
IAC_A01 Preoperative assessment of a patient who is scheduled for a routine operating list [not urgent or
emergency] [0-3 months]
IAC_A02 Manage anaesthesia for a patient who is not intubated and is breathing spontaneously [0-3 months]
IAC_A03 Administer anaesthesia for acute abdominal surgery [0-3 months]
IAC_A04 Demonstrate Rapid Sequence Induction [0-3 months]
IAC_A05 Recover a patient from anaesthesia [0-3 months]
DOPS
Assessment
Code Assessment
IAC_D01 Demonstrate functions of the anaesthetic machine [0-3 months]
IAC_D02 Transfer a patient onto the operating table and position them for surgery [lateral, Lloyd Davis or
lithotomy position] [0-3 months]
IAC_D03 Demonstrate cardio-pulmonary resuscitation on a manikin. [0-3 months]
IAC_D04 Demonstrates technique of scrubbing up and donning gown and gloves. [0-3 months]
IAC_D05 Core Competencies for Pain Management – manages PCA including prescription and adjustment of
machinery [0-3 months]
IAC_D06 Demonstrates the routine for dealing with failed intubation on a manikin.
CBD
Examine the case-notes. Discuss how the anaesthetic plan was developed. Ask the trainee to explain their approach to
pre-op preparation, choice of induction, maintenance, post op care. Select each one of the following topics and discuss
the trainees understanding of the issues in context.
Assessment Code Assessment
IAC_C01 Discuss the steps taken to ensure correct identification of the patient, the operation and the side of
operation
IAC_C02 Discuss how the need to minimise postoperative nausea and vomiting influenced the conduct of the
anaesthetic
IAC_C03 Discuss how the airway was assessed and how difficult intubation can be predicted
IAC_C04 Discuss how the choice of muscle relaxants and induction agents was made
IAC_C05 Discuss how the trainee’s choice of post-operative analgesics was made
IAC_C06 Discuss how the trainee’s choice of post-operative oxygen therapy was made
IAC_C07 Discuss the problems emergency intra-abdominal surgery causes for the anaesthetist and how the
trainee dealt with these
IAC_C08 Discuss the routine to be followed in the case of failed intubation.
23
The compulsory WPBAs listed for the IAC can be used as evidence towards signing off the units in ‘The
Introduction to Anaesthetic practice’ as mapped out below in Appendix 2. A further 7 assessments are
the minimal additional requirement to complete the Introduction to Anaesthesia. See Appendix 2 for
details.
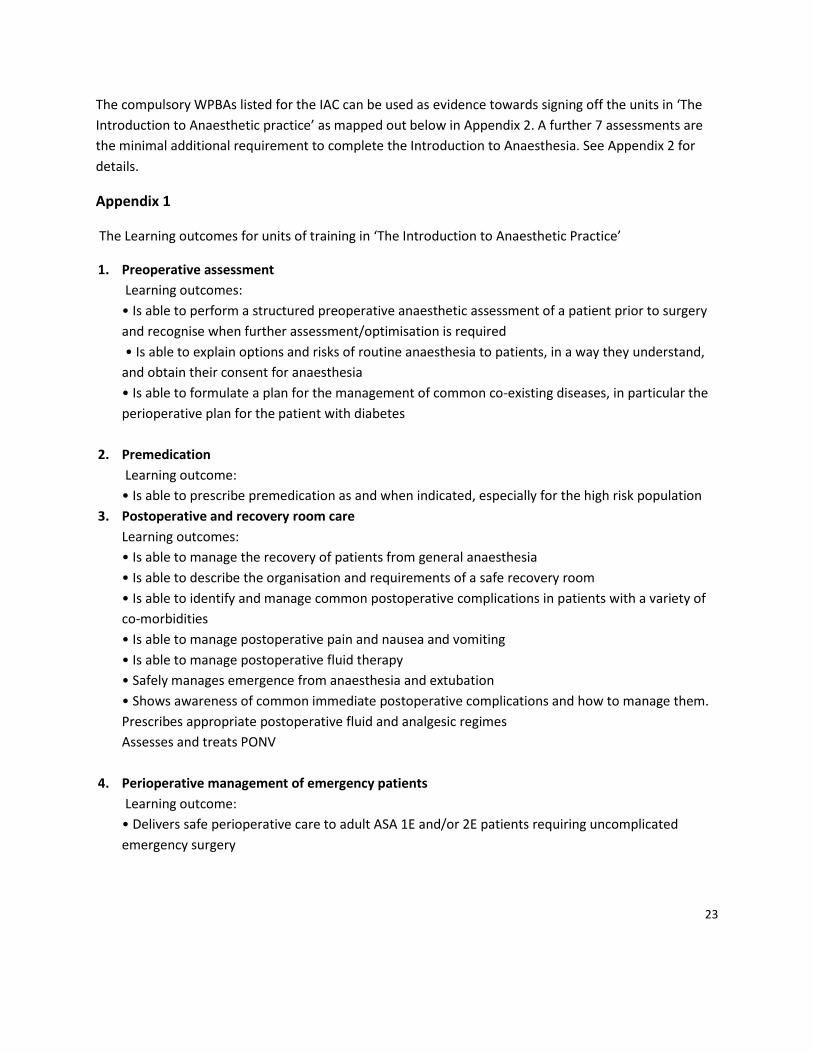
Appendix 1
The Learning outcomes for units of training in ‘The Introduction to Anaesthetic Practice’
1. Preoperative assessment
Learning outcomes:
• Is able to perform a structured preoperative anaesthetic assessment of a patient prior to surgery
and recognise when further assessment/optimisation is required
• Is able to explain options and risks of routine anaesthesia to patients, in a way they understand,
and obtain their consent for anaesthesia
• Is able to formulate a plan for the management of common co-existing diseases, in particular the
perioperative plan for the patient with diabetes
2. Premedication
Learning outcome:
• Is able to prescribe premedication as and when indicated, especially for the high risk population
3. Postoperative and recovery room care
Learning outcomes:
• Is able to manage the recovery of patients from general anaesthesia
• Is able to describe the organisation and requirements of a safe recovery room
• Is able to identify and manage common postoperative complications in patients with a variety of
co-morbidities
• Is able to manage postoperative pain and nausea and vomiting
• Is able to manage postoperative fluid therapy
• Safely manages emergence from anaesthesia and extubation
• Shows awareness of common immediate postoperative complications and how to manage them.
Prescribes appropriate postoperative fluid and analgesic regimes
Assesses and treats PONV
4. Perioperative management of emergency patients
Learning outcome:
• Delivers safe perioperative care to adult ASA 1E and/or 2E patients requiring uncomplicated
emergency surgery
24
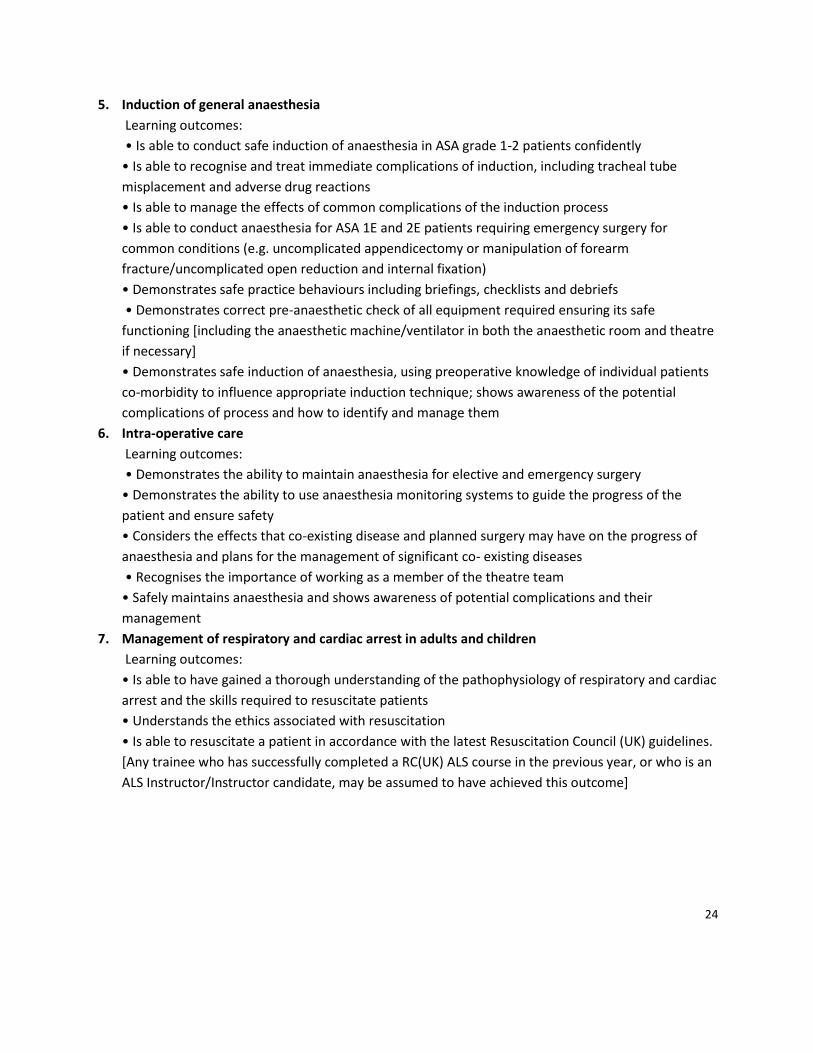
5. Induction of general anaesthesia
Learning outcomes:
• Is able to conduct safe induction of anaesthesia in ASA grade 1-2 patients confidently
• Is able to recognise and treat immediate complications of induction, including tracheal tube
misplacement and adverse drug reactions
• Is able to manage the effects of common complications of the induction process
• Is able to conduct anaesthesia for ASA 1E and 2E patients requiring emergency surgery for
common conditions (e.g. uncomplicated appendicectomy or manipulation of forearm
fracture/uncomplicated open reduction and internal fixation)
• Demonstrates safe practice behaviours including briefings, checklists and debriefs
• Demonstrates correct pre-anaesthetic check of all equipment required ensuring its safe
functioning [including the anaesthetic machine/ventilator in both the anaesthetic room and theatre
if necessary]
• Demonstrates safe induction of anaesthesia, using preoperative knowledge of individual patients
co-morbidity to influence appropriate induction technique; shows awareness of the potential
complications of process and how to identify and manage them
6. Intra-operative care
Learning outcomes:
• Demonstrates the ability to maintain anaesthesia for elective and emergency surgery
• Demonstrates the ability to use anaesthesia monitoring systems to guide the progress of the
patient and ensure safety
• Considers the effects that co-existing disease and planned surgery may have on the progress of
anaesthesia and plans for the management of significant co- existing diseases
• Recognises the importance of working as a member of the theatre team
• Safely maintains anaesthesia and shows awareness of potential complications and their
management
7. Management of respiratory and cardiac arrest in adults and children
Learning outcomes:
• Is able to have gained a thorough understanding of the pathophysiology of respiratory and cardiac
arrest and the skills required to resuscitate patients
• Understands the ethics associated with resuscitation
• Is able to resuscitate a patient in accordance with the latest Resuscitation Council (UK) guidelines.
[Any trainee who has successfully completed a RC(UK) ALS course in the previous year, or who is an
ALS Instructor/Instructor candidate, may be assumed to have achieved this outcome]
25
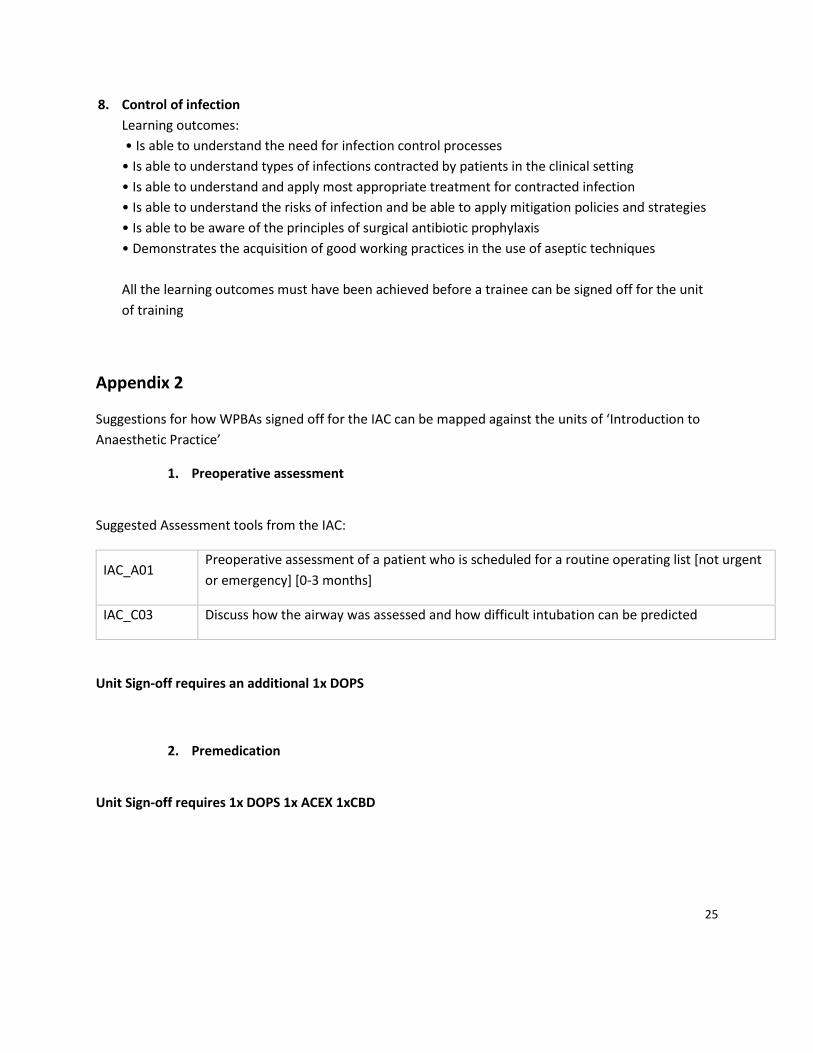
8. Control of infection
Learning outcomes:
• Is able to understand the need for infection control processes
• Is able to understand types of infections contracted by patients in the clinical setting
• Is able to understand and apply most appropriate treatment for contracted infection
• Is able to understand the risks of infection and be able to apply mitigation policies and strategies
• Is able to be aware of the principles of surgical antibiotic prophylaxis
• Demonstrates the acquisition of good working practices in the use of aseptic techniques
All the learning outcomes must have been achieved before a trainee can be signed off for the unit
of training
Appendix 2
Suggestions for how WPBAs signed off for the IAC can be mapped against the units of ‘Introduction to
Anaesthetic Practice’
1. Preoperative assessment
Suggested Assessment tools from the IAC:
IAC_A01 Preoperative assessment of a patient who is scheduled for a routine operating list [not urgent
or emergency] [0-3 months]
IAC_C03 Discuss how the airway was assessed and how difficult intubation can be predicted
Unit Sign-off requires an additional 1x DOPS
2. Premedication
Unit Sign-off requires 1x DOPS 1x ACEX 1xCBD
26
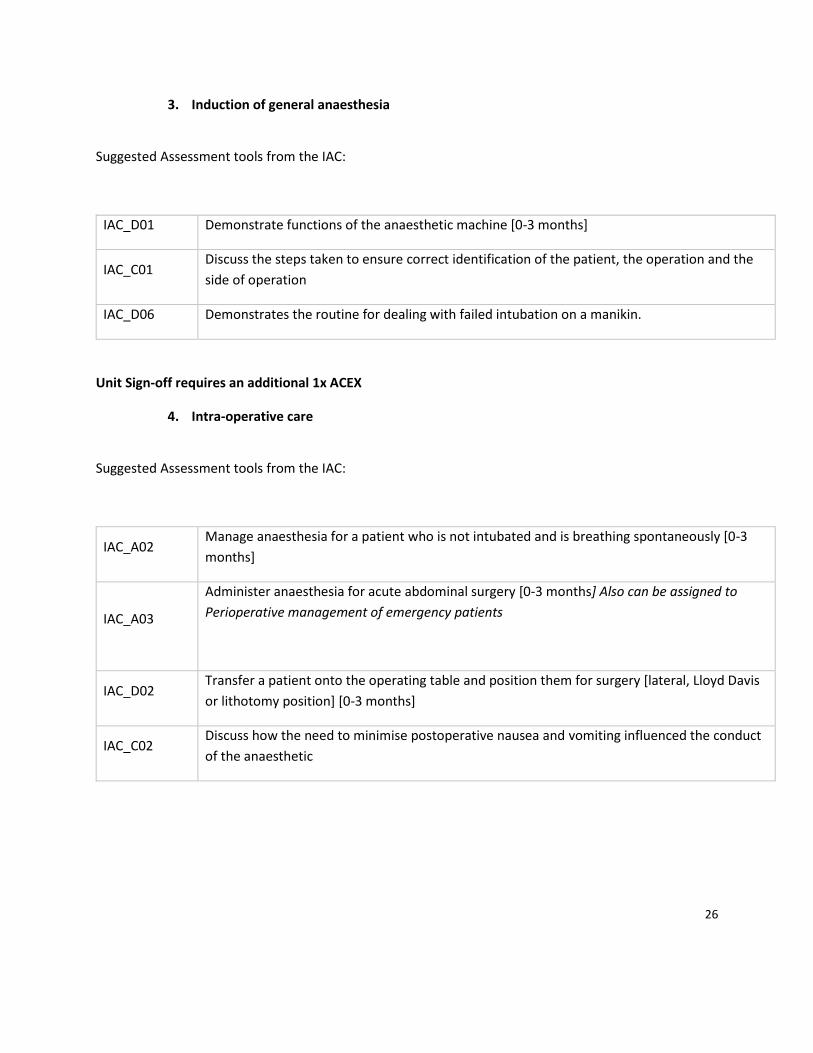
3. Induction of general anaesthesia
Suggested Assessment tools from the IAC:
IAC_D01 Demonstrate functions of the anaesthetic machine [0-3 months]
IAC_C01 Discuss the steps taken to ensure correct identification of the patient, the operation and the
side of operation
IAC_D06 Demonstrates the routine for dealing with failed intubation on a manikin.
Unit Sign-off requires an additional 1x ACEX
4. Intra-operative care
Suggested Assessment tools from the IAC:
IAC_A02 Manage anaesthesia for a patient who is not intubated and is breathing spontaneously [0-3
months]
IAC_A03
Administer anaesthesia for acute abdominal surgery [0-3 months] Also can be assigned to
Perioperative management of emergency patients
IAC_D02 Transfer a patient onto the operating table and position them for surgery [lateral, Lloyd Davis
or lithotomy position] [0-3 months]
IAC_C02 Discuss how the need to minimise postoperative nausea and vomiting influenced the conduct
of the anaesthetic
27
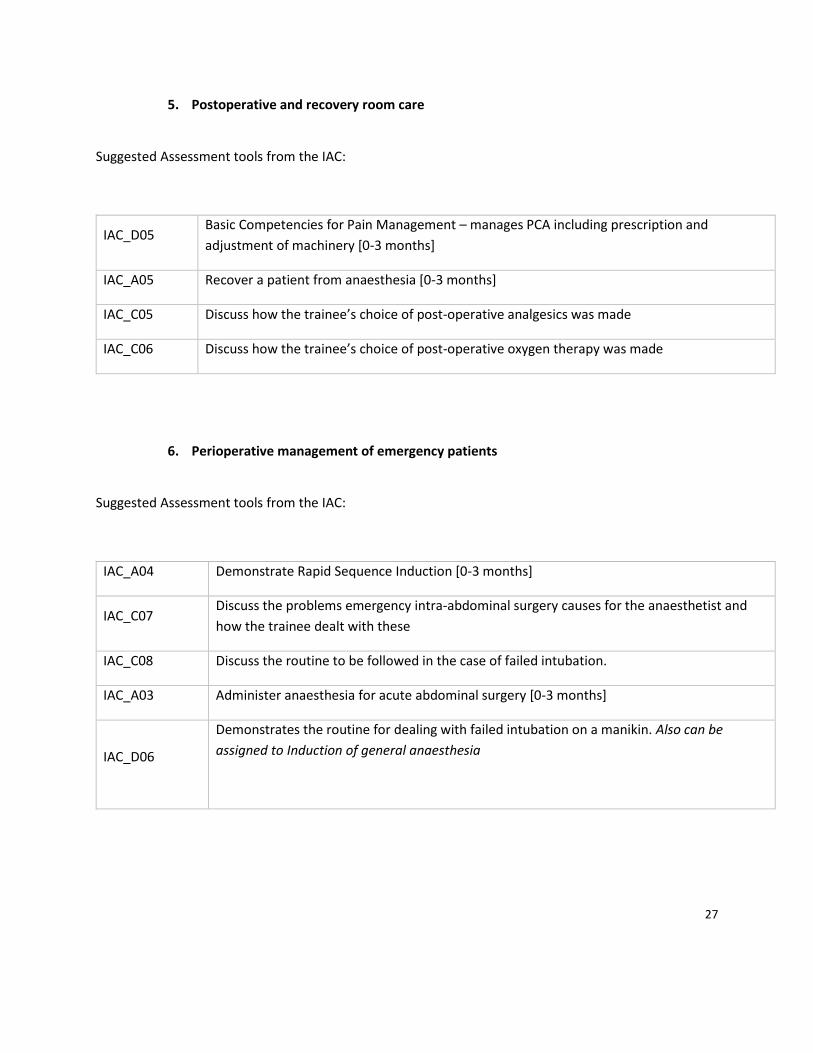
5. Postoperative and recovery room care
Suggested Assessment tools from the IAC:
IAC_D05 Basic Competencies for Pain Management – manages PCA including prescription and
adjustment of machinery [0-3 months]
IAC_A05 Recover a patient from anaesthesia [0-3 months]
IAC_C05 Discuss how the trainee’s choice of post-operative analgesics was made
IAC_C06 Discuss how the trainee’s choice of post-operative oxygen therapy was made
6. Perioperative management of emergency patients
Suggested Assessment tools from the IAC:
IAC_A04 Demonstrate Rapid Sequence Induction [0-3 months]
IAC_C07 Discuss the problems emergency intra-abdominal surgery causes for the anaesthetist and
how the trainee dealt with these
IAC_C08 Discuss the routine to be followed in the case of failed intubation.
IAC_A03 Administer anaesthesia for acute abdominal surgery [0-3 months]
IAC_D06
Demonstrates the routine for dealing with failed intubation on a manikin. Also can be
assigned to Induction of general anaesthesia
28
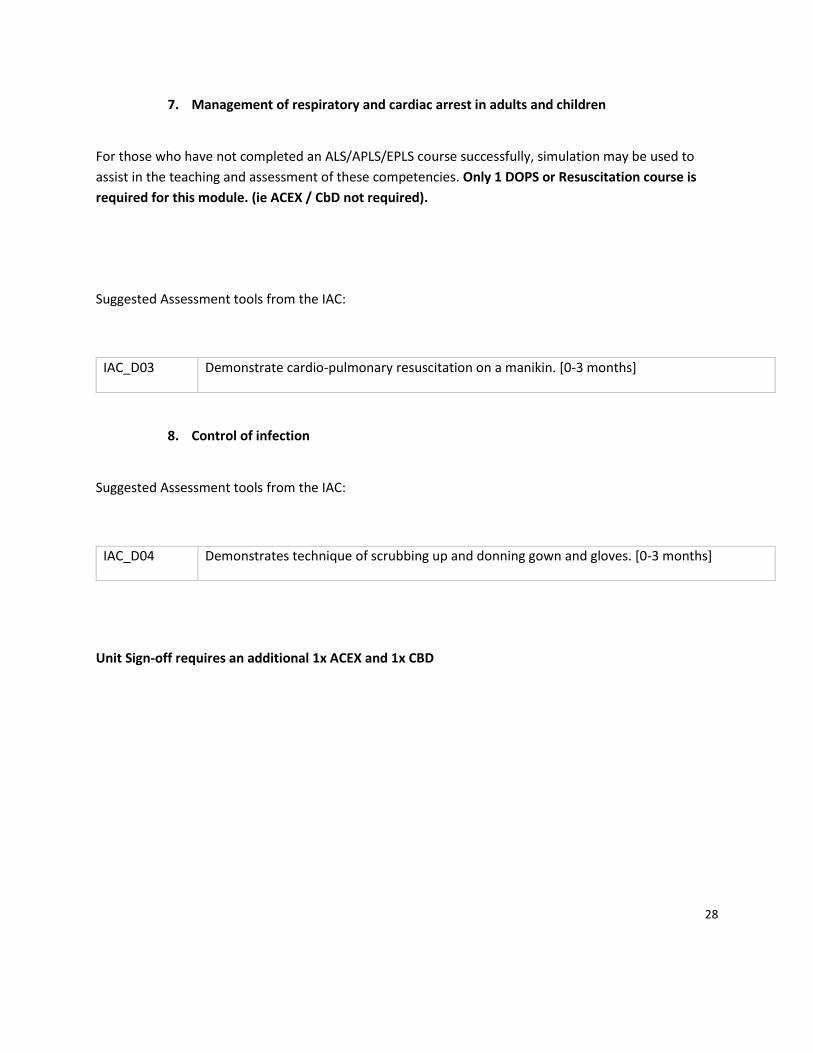
7. Management of respiratory and cardiac arrest in adults and children
For those who have not completed an ALS/APLS/EPLS course successfully, simulation may be used to
assist in the teaching and assessment of these competencies. Only 1 DOPS or Resuscitation course is
required for this module. (ie ACEX / CbD not required).
Suggested Assessment tools from the IAC:
IAC_D03 Demonstrate cardio-pulmonary resuscitation on a manikin. [0-3 months]
8. Control of infection
Suggested Assessment tools from the IAC:
IAC_D04 Demonstrates technique of scrubbing up and donning gown and gloves. [0-3 months]
Unit Sign-off requires an additional 1x ACEX and 1x CBD
29
ARCP (Annual Review of Competence Progression)
The ARCP is the annual review of trainees' progress. Detailed information relating to the Annual Review of Competency Progression, (ARCP) is documented in the Gold Guide. All trainees should make themselves familiar with this document as well as local Deanery/LETB processes.
Checklists can be found on the ACCS page on AWSEM website.
http://www.awsem.org.uk/training/wpba-arcps/st1-ct1-st2-ct2/
ARCPs are usually held towards the end of June of early July.
We usually hold ARCPs in South and North Wales to minimise travel for the trainees.
The ARCP has two broad functions:
1) Fitness to Progress
The ACCS ARCP is the mechanism for reviewing and recording evidence and a means whereby the evidence of the outcome of assessments is recorded to provide a record of a trainee’s progress within their training post including Out Of Programme Training (OOPT). It makes judgements about the competencies acquired by a trainee and their suitability to progress to the next stage of training and provides a final statement of the trainee's attainment of the curricular competencies and thereby the completion of the stages of the training programme.
2) Fitness to Practice
The ACCS ARCP also gives advice to the Deanery Revalidating Officer about revalidation of the
trainee to enable a recommendation to the GMC.
30
A Career in Intensive Care Medicine
Dr Alison Ingham - ICM lead for ACCS
Intensive Care Medicine (ICM) is an exciting and dynamic career choice (I’m biased of course!).
Hopefully you will enjoy your ACCS ICM placement so much, you will be thinking about further
training in ICM. If so, here is how you go about it.
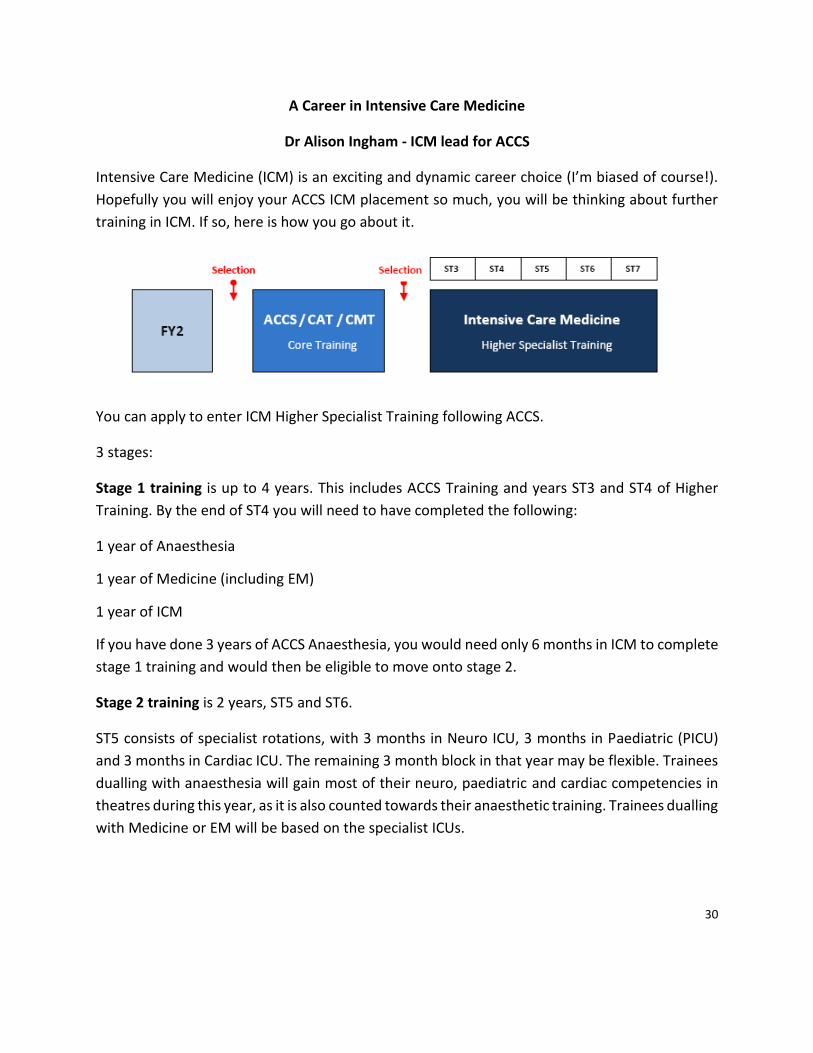
You can apply to enter ICM Higher Specialist Training following ACCS.
3 stages:
Stage 1 training is up to 4 years. This includes ACCS Training and years ST3 and ST4 of Higher
Training. By the end of ST4 you will need to have completed the following:
1 year of Anaesthesia
1 year of Medicine (including EM)
1 year of ICM
If you have done 3 years of ACCS Anaesthesia, you would need only 6 months in ICM to complete
stage 1 training and would then be eligible to move onto stage 2.
Stage 2 training is 2 years, ST5 and ST6.
ST5 consists of specialist rotations, with 3 months in Neuro ICU, 3 months in Paediatric (PICU)
and 3 months in Cardiac ICU. The remaining 3 month block in that year may be flexible. Trainees
dualling with anaesthesia will gain most of their neuro, paediatric and cardiac competencies in
theatres during this year, as it is also counted towards their anaesthetic training. Trainees dualling
with Medicine or EM will be based on the specialist ICUs.
31
ST6 is a “special skills” year and is only undertaken by ICM single CCT trainees. Dual trainees will
spend this year in their partner specialty. The special skills year could include research, teaching
and training or further time in a specialist ICU.
During stage 2 training, you will also have to pass the FFICM exam.
Stage 3 Training: This is one year during which you will start working in a more senior role and
learning the skills needed to become a consultant.
Dual Training:
You can dual train with the following specialties:
Acute Medicine, EM, Anaesthesia, Renal Medicine & Respiratory Medicine
Luckily, getting a dual CCT does not double your training time. Instead it increases it from 7 to 8.5
years. Parts of your training will count towards both specialities and your training programme
will be tailored by the appropriate Training Programme Directors. Application is stepped. This
means that although you can apply for both specialties at the same time, you can only hold one
offer, so application for the second specialty will be needed the following year. It does not matter
which specialty you accept first, but both must be in the same Deanery.
Unfortunately you will have to keep two portfolios, one for each specialty. You may also have to
get used to being at different stages of training in your two specialties – for example you might
have finished stage one training in ICM (ST4) but still be finishing your ST3 year in your partner
specialty.
So why choose Wales?
Wales is a diverse country that will give you a great lifestyle as you build your future career. Wales
offers something for everyone, from cosmopolitan towns and cities to stunning coastal locations.
With affordable housing and welcoming communities it is an ideal place to achieve a work-life
balance. It even has its own language, although it is not necessary to learn it to pursue training,
employment or to live here. Wales is covered by a single Deanery which puts high quality training
at the heart of medical careers.
32
The ICM specialist training scheme in Wales is funded directly by the Deanery which allows us to
choose posts which will best benefit the trainee. This enables us to provide excellent posts in
Anaesthesia and Medicine as well as ICM.
Currently hospitals training at ST3-4 level are in Swansea, Newport, Bangor, Wrexham, Cardiff
and Royal Glamorgan with the ST5 year based in Cardiff. Other hospitals also provide training and
placements may take in other units depending on the trainee’s needs. The ST6 year will be
tailored according to whether the trainee is dual or single accrediting and the ST7 year is likely to
be mainly in South Wales.
The Specialist Training Committee and Deanery make support of the trainee central to their
business and you can look forward to a carefully developed scheme that allows you to grow in
experience and confidence as the years go by. You will experience a variety of Intensive Care
Units and will emerge from the scheme a rounded and mature professional with the ability to
take on a consultant role in both large and small hospitals.
Further Information
If you would like to talk to someone in more detail about ICM training, please contact Dr Dallison,
Dr Evans or myself. There will also be an ICM Faculty Tutor at each hospital within Wales who
provide ACCS training, who will also be able to help you.
Dr Matt Dallison [email protected] Regional Advisor for ICM
Dr Alison Ingham [email protected] Deputy Regional Advisor
Dr Teresa Evans [email protected] Training Programme Director
33
Pre- Hospital Emergency Medicine (PHEM) Training
Pre-hospital Emergency Medicine is emerging from a time when volunteer doctors did their best in difficult circumstances to professional, well governed and funded pre-hospital services. In Wales the Emergency Medical Retrieval and Transfer Service (EMRTS) delivers consultant led critical care to the whole of Wales for primary taskings and time critical inter-hospital transfers. Sub-specialty training in PHEM is available to trainees of EM, Anaesthetics, ICM and AM. The application is usually within the ST4-5 year of training and is through a national recruitment system. The training programme is either a year full time or longer if the training is blended with your base specialty. The exit exam is the Fellowship of Immediate Medical Care (FIMC RCSEd). For more details please visit the Faculty website http://www.ibtphem.org.uk/IBTPHEM/Welcome.html In the meantime enjoy the ACCS programme and it will equip you well for a PHEM career. Consider attending clinical governance days and relevant courses around PHEM and make sure you don’t get travel sick. More information about PHEM training in Wales please contact the Wales Deanery PHEM TPD Ian Bowler https://www.walesdeanery.org/specialties/pre-hospital-emergency-medicine


















