Accounting for the cost of scaling-up health interventions
8
HEALTH ECONOMICS Health Econ. 13: 1117–1124 (2004) Published online 25 February 2004 in Wiley InterScience (www.interscience.wiley.com). DOI:10.1002/hec.880 COSTING METHODOLOGY Accounting for the cost of scaling-up health interventions Benjamin Johns a, * and Rob Baltussen a,b On behalf of WHO-CHOICE a Global Programme on Evidence for Health Policy (GPE/EQC), World Health Organization, Switzerland b Institute for Medical Technology Assessment (iMTA), Erasmus Medical Centre Rotterdam, The Netherlands Summary Recent studies such as the Commission on Macroeconomics and Health have highlighted the need for expanding the coverage of services for HIV/AIDS, malaria, tuberculosis, immunisations and other diseases. In order for policy makers to plan for these changes, they need to analyse the change in costs when interventions are ‘scaled-up’ to cover greater percentages of the population. Previous studies suggest that applying current unit costs to an entire population can misconstrue the true costs of an intervention. This study presents the methodology used in WHO- CHOICE’s generalised cost effectiveness analysis, which includes non-linear cost functions for health centres, transportation and supervision costs, as well as the presence of fixed costs of establishing a health infrastructure. Results show changing marginal costs as predicted by economic theory. Copyright # 2004 John Wiley & Sons, Ltd. Keywords health; cost-effectiveness; coverage; scaling-up; costs Introduction Recent studies such as the Commission on Macroeconomics and Health have highlighted the need for expanding the coverage of services for HIV/AIDS, malaria, tuberculosis, immunisa- tions and other diseases [1]. In order for policy makers to plan for these changes, they need to analyse the change in costs when interventions are ‘scaled-up’ to cover greater percentages of the population. They, for example, may be interested in the cost of extending health interventions to the poorest people in their country, who often live in rural or remote areas previously uncovered [2]. Without a means of determining the costs of expanding health interventions into such areas, policy makers cannot assess the desirability or feasibility of scaling-up interventions. Previous costing studies have shown that rural health centres have higher cost per patient treated than urban health centres [3,4], and comparisons of EPI programmes imply that very high levels of population coverage increase the cost per vaccine given [5–7]. Additionally, Kumaranayake and Watts show increasing aver- age costs for HIV/AIDS curative and preventive interventions moving from current to 25% coverage level in sub-Saharan Africa [8]. However, little empirical work has been done on the cost of scaling up interventions, because, in general, costing studies have been point-in-time Copyright # 2004 John Wiley & Sons, Ltd. Received 26 March 2003 Accepted 7 October 2003 *Correspondence to: Global Programme on Evidence for Health Policy (GPE/EQC), World Health Organization, CH-1211 Geneva 27, Switzerland. E-mail: [email protected]
-
Upload
benjamin-johns -
Category
Documents
-
view
214 -
download
0
Transcript of Accounting for the cost of scaling-up health interventions

HEALTH ECONOMICS
Health Econ. 13: 1117–1124 (2004)
Published online 25 February 2004 in Wiley InterScience (www.interscience.wiley.com). DOI:10.1002/hec.880
COSTING METHODOLOGY
Accounting for the cost of scaling-up health interventions
Benjamin Johnsa,* and Rob Baltussena,b
On behalf of WHO-CHOICE
aGlobal Programme on Evidence for Health Policy (GPE/EQC), World Health Organization, Switzerlandb Institute for Medical Technology Assessment (iMTA), Erasmus Medical Centre Rotterdam, The Netherlands
Summary
Recent studies such as the Commission on Macroeconomics and Health have highlighted the need for expanding thecoverage of services for HIV/AIDS, malaria, tuberculosis, immunisations and other diseases. In order for policymakers to plan for these changes, they need to analyse the change in costs when interventions are ‘scaled-up’ to covergreater percentages of the population. Previous studies suggest that applying current unit costs to an entirepopulation can misconstrue the true costs of an intervention. This study presents the methodology used in WHO-CHOICE’s generalised cost effectiveness analysis, which includes non-linear cost functions for health centres,transportation and supervision costs, as well as the presence of fixed costs of establishing a health infrastructure.Results show changing marginal costs as predicted by economic theory. Copyright# 2004 John Wiley & Sons, Ltd.
Keywords health; cost-effectiveness; coverage; scaling-up; costs
Introduction
Recent studies such as the Commission onMacroeconomics and Health have highlightedthe need for expanding the coverage of servicesfor HIV/AIDS, malaria, tuberculosis, immunisa-tions and other diseases [1]. In order for policymakers to plan for these changes, they need toanalyse the change in costs when interventions are‘scaled-up’ to cover greater percentages of thepopulation. They, for example, may be interestedin the cost of extending health interventions to thepoorest people in their country, who often live inrural or remote areas previously uncovered [2].Without a means of determining the costs of
expanding health interventions into such areas,policy makers cannot assess the desirability orfeasibility of scaling-up interventions.
Previous costing studies have shown thatrural health centres have higher cost per patienttreated than urban health centres [3,4],and comparisons of EPI programmes imply thatvery high levels of population coverage increasethe cost per vaccine given [5–7]. Additionally,Kumaranayake and Watts show increasing aver-age costs for HIV/AIDS curative and preventiveinterventions moving from current to 25%coverage level in sub-Saharan Africa [8].However, little empirical work has been done onthe cost of scaling up interventions, because, ingeneral, costing studies have been point-in-time
Copyright # 2004 John Wiley & Sons, Ltd.Received 26 March 2003Accepted 7 October 2003
*Correspondence to: Global Programme on Evidence for Health Policy (GPE/EQC), World Health Organization, CH-1211Geneva 27, Switzerland. E-mail: [email protected]

measurements that do not include increases incoverage over time [9].
The few theoretical studies on the subject showthat average costs, or cost per recipient, canseriously misconstrue the true costs of an inter-vention and lead to erroneous conclusions on thecost effectiveness of interventions. While the WorldDevelopment Report 1993 acknowledged that cost-effectiveness ratios would vary with populationcoverage, it left no methodology for evaluatingthese differences. For example, they evaluated EPIprogrammes at only two coverage levels, using apercentage mark-up to account for the differencein cost [2].
Over theorised that factors influencing the costof expanding coverage included the transportationcosts of supervisory trips and drug re-supply, andthe recruitment and training of health personnel inremote areas [10]. Further, capital costs mayincrease in remote areas because the items neededfor building have to be shipped greater distances.Thus, he predicted an eventually increasingmarginal cost curve, resulting in a U-shapedaverage cost curve.
The cost component of the Commission onMacroeconomics and Health (CMH) calculatedthe cost of scaling-up by multiplying an averagecost per patient by the predicted future number ofpatients, and adding a percentage of these costs toaccount for training and upgrading the overallhealth system [11–13].
As part of its WHO-CHOICE project,a WHOhas undertaken an effort to assess the overall costsand effects of a wide variety of health interven-tions, including the cost of scaling-up [14]. WHO-CHOICE is performing this assessment for a rangeof interventions for 14 sub-regions of the worldbased on the Global Burden of Disease epidemio-logical patterns [15]. The provision of sub-regionalestimates allows interventions to be classified intobroad categories that have broad validity acrossthe region – e.g. those that are very cost-effective,those that are cost-effective, and those that arecost-ineffective. Policy makers can then ask if thereare good reasons why very cost-effective interven-tions are not done in their setting, while at thesame time cost-ineffective interventions are beingdone.
As a first step in the process of assessing costs,WHO-CHOICE reviewed the literature on the costof scaling-up [Johns B, Tan Torres T. Predictingthe cost of scaling-up health interventions: asystematic review. Submitted manuscript, 2003].
This study identifies a number of broad areaswhere economies or diseconomies of scale exist inhealth interventions: geography and transporta-tion, fixed costs of establishing a health infra-structure, human resources, and managementtransition costs. This study also finds that therehas been no method developed for accounting forthese components of scaling-up in different settingsand/or for different types of health interventions.Without taking into account these factors, anyattempt to assess the cost of scaling-up healthinterventions could misconstrue the true costs ofthese interventions. Since each of the above factorsinteract differently with different interventions,failing to account for these factors could affectthe relative cost-effectiveness of interventions atdifferent levels of coverage.
The objective of this paper is to describe amethodology to estimate the cost of scaling-up foruse in cost-effectiveness in general and for WHO-CHOICE’s generalised cost effectiveness analysis(GCEA) in particular. It defines a methodologyfor accounting for the spatial aspects of scaling-upbased on the literature review.
Methods
The assumptions used in WHO-CHOICE’s GCEAaffect what and how costs are counted. Impor-tantly, GCEA analysis ask which interventionspotentially are the most cost effective, and there-fore assumes a standard capacity utilisation rate of80% [16].b This prevents an (unfair) comparison ofthe cost-effectiveness of programmes that arecurrently run very inefficiently to those that arerun efficiently. Thus, while the total costs ofprogramme management are included, costs toimprove management techniques are not included.
Four issues are distinguished in the accountingthe costs of scaling up. Firstly, as mentionedabove, several studies suggest that rural healthcentres have higher cost per patient due to lowercapacity utilisation (discussed in Health CentreUnit Costs). Second, scaling-up health care pro-grammes into more remote areas also involvesshipping supplies and equipment over longerdistances and through more difficult terrain.Fielder shows, for example, that the cost ofshipping a kilogram of vitamin A capsules todifferent provinces in Nepal can have an almostsix-fold difference in cost ([17] analysed in Johns
Copyright # 2004 John Wiley & Sons, Ltd. Health Econ. 13: 1117–1124 (2004)
B. Johns and R. Baltussen1118

and Tan Torres (2003)) (discussed in Transporta-tion Costs). Third, studies also show that admin-istrative regions tend to have fixed cost, in terms ofmedia outreach, training, or basic administration,regardless of the population covered [18–20](discussed in Fixed Costs). Finally, as programmesare scaled-up, the supervision and managementbecome more complicated, requiring more re-sources devoted to these activities [11,21] (dis-cussed in Supervision Costs). An example of theresults for each section are presented for the AfrDc
and AmrAd regions, both to demonstrate theresults of the analysis and to suggest how theresults differ in developing and developed coun-tries.
1. Health Centre Unit Costs: For equity reasons,it is assumed that there is a health centre accessiblewithin 1 h to all of the covered population [22].Thus, every person is assumed to be able to accessa health centre within 1 h of travel time [23–25].e Aunique Geographical Information System compo-nent was designed such that the square kilometrewith the highest population density in a countrywas assumed to have a health centre.f Thepopulation served by this health centre was takenout the grid, and the process re-started. In thissystem, 1 h travel time assumes access to motorvehicle transport where paved roads exist, other-wise all travel is assumed to occur by foot.
Thus, as coverage expands, the catchment areaof each additional health centre tends to havefewer people, indicating that capacity utilisationdecreases [26]. Since the overhead costs aredistributed among fewer patients, the cost perpatient will be higher for these health centres.Capacity utilisation equals the actual number ofpatients seen divided by the number of patientsthat would be seen at standard capacity. Theactual number of patients seen is calculated as thepopulation of the catchment area multiplied bythe number of visits per capita per year [[26,27],author consultation with WHO]. The number ofpatients that would be seen at standard capacityequals the number of health workers multiplied bythe number of patients seen per health worker perday [26] multiplied by the number of working daysin a year.
For example, the smallest health centre with twohealth workers in Denmark is assumed to be ableto handle 37 patients per day at standard capacity,with 230 working days in a year [27, Adam T,Ebener S, Johns B, Evans DB. Cost of Scaling upHealth Interventions at Primary Facilities: Multi-
Country Analysis. Forthcoming manuscript,2003]. The average person is assumed to attend aclinic 6 times per year [27]. Thus, a catchment areawith 1500 inhabitants would operate at thestandard capacity of 80% (((1500*6)/(37*230))>1), while a catchment area with 1000people would operate at a capacity of 71%(((1000*6)/(37*230))=0.71). This model assumesthat health centres are not over-utilised, sinceareas with high population can either increase thesize of health facilities or construct new facilities.
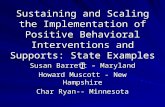
Figure 1 shows the results of this analysis for theWHO epidemiological sub region AfrD andAmrA. As can be seen in the figure, in the centralurban areas, health centres are used at the targetcapacity, but as the population coverage expandsinto rural areas, the capacity utilisation dropsdramatically. On the basis of these capacityutilisation data, the cost per patient at variouscoverage levels is then predicted using econometricmodels [28, Adam et al., 2003].g Also, the AfrDregion sees a decline in capacity utilisation at anearlier level of population coverage, at around65% coverage, than the AmrA region, which doesnot see declines in capacity utilisation until almost90% coverage. Two factors determine this differ-ence: the population of AmrA is more concen-trated in urban areas, and it has greater access toroads, thus the size of the catchment areas in ruralsections can be geographically larger (and thusinclude more people) than those in AfrD. Thesharp drop in marginal capacity utilisation afterthese points indicates that covering the entirepopulation would be very expensive; however,since WHO-CHOICE evaluates interventions onlyup to 95% coverage, this paper does not evaluateat what point trekking clinics or health posts with
0%
20%
40%
60%
80%
100%
0% 20% 40% 60% 80% 100%
Percentage of the Population Covered
Cap
acit
y U
tili
sati
on
Marginal AfrD
Average AfrD
Marginal AmrA
Average AmrA
Figure 1. Marginal and average capacity utilisation for health
centres
Accounting for the Cost of Scaling-up Health Interventions 1119
Copyright # 2004 John Wiley & Sons, Ltd. Health Econ. 13: 1117–1124 (2004)

occasional staffing would be more appropriatethan health centres.
2. Transportation costs: The calculation of thecost of transportation is based on a Lim*aao andVenables study showing the percentage change inprice of a good based on the distance it travels, thetransportation infrastructure, the average GDPper capita of a country, and other variablesrelating to the availability of seaports, neighbour-ing trade partners, etc. [29]. This method is appliedonly to traded goods, since they need to be shippedthroughout a country, while local goods arealready present in a place, or have relatively lowtransport costs [16,30].h
To calculate the average distance a good travels,the straight line distance between the centre of thecapital city of a country and each of the healthcentres (as discussed in Health Centre Unit Costs)is calculated. The Lim*aao and Venables priceelasticity for distance was then used with thisestimated distance to calculate the cost of trans-portation [31]. While this method does notnecessarily mean that higher coverage rates willhave higher shipping distances, especially if thereare major urban centres outside of the capital city,the results for AfrD and AmrA shown in Figure 2show that this is the trend, as it is for most regionsof analysis. While the differences in the y-interceptshown in Figure 2 for these two regions reflects thediffering sizes of countries in the two regions, thesimilarity in slope suggests that distance travelledwill increase similarly (although not identically) inmany different regions.
3. Fixed costs: It is assumed that each provincehas a set level, or fixed, overhead cost associatedwith the administration of a program. Forexample, a media outreach campaign using pro-vincial television will require a certain number ofbroadcasts no matter how many people are in theprovince. With fixed costs associated with eachprovince, there are diseconomies of scale becauseeach additional province is assumed to containfewer people. In this model, the most populousprovince is assumed to be covered first, then thesecond most populous, and so on. Figure 3presents the results of this analysis for the AfrDand AmrA regions. The dotted line indicatesconstant economies of scale (i.e. what wouldhappen if every province covered had the samepopulation), while the solid lines shows the resultspredicted in this model. The figure shows that theAmrA region will have greater diseconomies ofscale than the AfrD region. However, this is not ageneral trend between developed and developingcountries; the results are specific to the populationdistribution and administrative structure of in-dividual countries.
4. Supervision costs: The distance travelledin a supervision visit also increases with highercoverage. At the national and provincial level, thisis calculated as twice the distance that a tradedgood is transported since supervision visits con-stitute a round trip. Thus, the number ofprogramme staff involved in supervision activitiesneeds to increase both in proportion to theincreased distances covered and to account for
0
500
1000
1500
2000
0% 20% 40% 60% 80% 100%
Percentage of the Population Covered
Dis
tan
ce (
Km
s)
Average TravelDistance AfrD
Average TravelDistance AmrA
Figure 2. Average distance to the capital city
0%
25%
50%
75%
100%
0% 20% 40% 60% 80% 100%
% Population Covered
% P
rovi
nces
Co
vere
d
AfrD
AmrA
Constant
Figure 3. Number of provinces covered vs population served.
The dotted line shows constant economies of scale, the solid line
shows the population covered as predicted in this model
B. Johns and R. Baltussen1120
Copyright # 2004 John Wiley & Sons, Ltd. Health Econ. 13: 1117–1124 (2004)

the increased number of provinces, since eachprovince is assumed to need an equal number ofsupervision visits.
Results
This section presents findings on the cost ofinterventions to demonstrate the effects of employ-ing the model. Figure 4 shows the average andmarginal costs for an outreach intervention toeducate community health workers on nutritionand hygiene for the WHO epidemiological subregion AfrD and AmrA. The costs presented hereexclude health centre costs, to illustrate the effectsof the use of the fixed costs, transportation andsupervision aspects of the model on the total cost.Costs were calculated for each 10% level ofpopulation coverage. The figure shows that lowestaverage cost per capita occurs at around 45%coverage for AfrD, while the sharpest increase incosts occurs between 90% and 100% populationcoverage. For AmrA the pattern is similar, exceptthat the lowest average cost is at lower coveragelevels (at about 30%), and the slope of themarginal cost curve is steeper through the mid-range of coverage. The primary reason for this isthat the population of the provinces in AfrD aremore equally distributed than those of AmrA; thefixed costs of the program are spread more evenly.This figure is similar to the findings presented inthe Over study, which also shows diseconomies ofscale starting at about a 30% coverage level [10].
Table 1 shows the total costs per capita for aniron supplementation programme and an iron
fortification programme for the WHO epidemio-logical sub regions AfrD and AmrA. The resultsare presented for the three geographic coveragelevels commonly used for WHO-CHOICE’s ana-lysis. These interventions have two very differentcost structures; thus, scaling up is expected toaffect the costs in different ways. Iron fortification
AfrD Region
AmrA Region
$0.00
$0.10
$0.20
$0.30
$0.40
10% 30% 50% 70% 90%
Population Coverage LevelC
ost
per
Cap
ita
AverageCosts
MarginalCosts
$0.20
$0.30
$0.40
$0.50
$0.60
$0.70
$0.80
$0.90
10% 30% 50% 70% 90%
Population Coverage Level
Co
stp
er C
apita
AverageCosts
MarginalCosts
Figure 4. Marginal and average cost for hygiene outreach. In
Year 2000 International $ (Health centre costs excluded). Costs
represent the amount needed per average year of programme
implementation
Table 1. Cost per capitaa for two select interventions in year 2000 International $
Coverage level (%) Average cost per capita Increase in costs/capita per % increase in population covered
Ironsupplementation
Ironfortification
Ironsupplementation
Ironfortification
AfrD region50 $ 0.10 $ 0.1380 $ 0.24 $ 0.10 $ 0.0047 $ �0.01395 $ 0.31 $ 0.09 $ 0.0048 $ �0.001AmrA region50 $ 0.28 $ 0.1180 $ 0.44 $ 0.09 $ 0.0054 $ �0.000995 $ 0.55 $ 0.08 $ 0.0073 $ �0.0002
aCosts are average annual discounted programme costs of implementing an intervention during 10 years. Note that a straightcomparison of cost per capita across interventions is misleading in deciding whether an intervention is of low cost or moreexpensive at a population level, because there is variation in the target populations for each of these interventions.
Accounting for the Cost of Scaling-up Health Interventions 1121
Copyright # 2004 John Wiley & Sons, Ltd. Health Econ. 13: 1117–1124 (2004)

shows economies of scale up through 95%population coverage because the relatively highcentral costs are spread across more people, withonly some flattening of the average cost curve dueto increased costs at the district level. Ironsupplementation, on the other hand, requiressupervision and implementation at the healthcentre level, and thus shows rising costs ascoverage expands. This shows that the model isadaptable to different types of interventions.
Discussion
The methods described in this paper represent afirst effort to account for the cost associated withincreasing geographic coverage of health interven-tions. As such, several assumptions were made andare further discussed below. Analysts adapting thismethod should take into account these assump-tions and fit them to their own setting wherenecessary.
The method assumes goods are shipped fromthe capital city – as opposed to a port or entrypoint for traded goods – of the country, whichimpacts two issues. First, this assumption over-estimates costs for countries with multiple entrypoints for goods, while for countries with oneentry point, this assumption may underestimatecosts. The capital city is selected as the bestcompromise to estimate the average cost oftransport at the sub-regional level since it is oftenthe point of central warehousing.
Second, this method uses distance to estimatetransport cost. This may not capture the difficultyin accessing certain areas in a country with poortransportation infrastructure, difficult terrain, orboth. Also, the data used to calculate the priceelasticity of transportation are only available atthe country level. Developments in the GISdatabase indicate that in the future, a moredetailed level of analysis will be possible [23]. Forexample, time of travel studies may becomeavailable and replace the variables for distanceand the transportation index used in the Lim*aaoand Venables study. Alternatively, a differentmethod based more closely on GIS data could bedeveloped.
This method accounts only for spatial factors inthe scaling-up of interventions and, in the absenceof data, does not account for variation in the priceof local goods within a country. While mean salary
figures were used in the calculation of total costs,countries’ inability to recruit and retain health careworkers in remote areas indicate that current mid-level estimates of wages may in fact underestimatethe true costs of successfully scaling up a program.More research is needed in this area.
This model is intended for use in differentsettings. While the examples in this paper areaggregated up to a regional level, the samemethods could be used for country level analysis.As the examples presented show, by usingobserved data from a country, it accounts for thedifferences in the spatial distribution of thepopulation, transportation infrastructure, andadministrative organisation. Much of this data isavailable at the country level. GIS data onpopulation distribution and transportation infra-structure are needed to implement this model andare becoming increasingly available. In addition,data on patient utilisation of health centres [27]and the capacity of a minimally sized healthfacility are needed to model health centre distribu-tions. While this model utilises averages derivedfrom the literature for the latter data [Adamet al., 2003], countries could do their ownassessment. Finally, while existing econometricmodels can be employed to show the increase inaverage costs for health centres as capacityutilisation falls, countries could also make theirown estimates based on observed data in theircountry.
This method represents a significant improve-ment in the estimation of the costs of scaling-upinterventions. While previous studies scaled costup linearly, this method accounts for an increase inmarginal costs as coverage increases, which fits inwith economic theories on economies of scale [15].Allowing some costs to be fixed regardless of thesize of the population reached – for example,television broadcasts – has incorporated econo-mies of scale. On the other hand, using higher costfor transport, supervision, and health centre carehas included diseconomies of scale at highercoverage levels. This is an important step forshowing the impact of higher coverage on costsand outcomes.
Acknowledgements
The authors thank Chris Murray, David Evans, andTessa Tan Torres for guidance throughout this project.
B. Johns and R. Baltussen1122
Copyright # 2004 John Wiley & Sons, Ltd. Health Econ. 13: 1117–1124 (2004)

We are also grateful to Raymond Hutubessy, TaghreedAdam, Dan Chisholm, and Moses Aikins for their inputin the development of the methods used, and to NatalySabharwal and Steeve Ebener for their work inprocessing the data necessary for the development ofthis method. The comments by two anonymous refereeson an earlier draft of this paper are gratefully acknowl-edged. The views expressed are those of the authorsalone and not necessarily those of the organization theyrepresent.
Notes
a. WHO seeks to provide the evidence decision-makersneed to set priorities and improve the performance oftheir health systems. The Global Programme onEvidence for Health Policy (GPE) is assemblingregional databases on the costs, impact on popula-tion health and cost-effectiveness of key healthinterventions. This work known as WHO-CHOICEstarted in 1998 with the development of standardtools and methods. The objectives of WHO-CHOICEare:
* develop a standardised method for cost-effectivenessanalysis that can be applied to all interventions indifferent settings;
* develop and disseminate tools required to assessintervention costs and impacts at the populationlevel;
* determine the costs and effectiveness of a wide rangeof health interventions, presented with probabilisticuncertainty analysis;
* summarise the results in regional databases that willbe available on the Internet;
* assist policy-makers and other stakeholders tointerpret and use the evidence.
b. Capacity utilisation is defined as the ratio ofproductive use of an input over the total potentialproductive use of an input. For WHO-CHOICE’spurposes, capacity utilisation was assumed to be80%. However, analyst adapting this method shouldadjust the capacity utilisation level to that appro-priate for their setting.
c. The AfrD region includes Algeria, Angola, Benin,Burkina Faso, Cameroon, Cape Verde, Chad, Co-moros, Equatorial Guinea, Gabon, Gambia, Ghana,Guinea, Guinea-Bissau, Liberia, Madagascar, Mali,Mauritania, Mauritius, Niger, Nigeria, Sao TomeAnd Principe, Senegal, Seychelles, Sierra Leone, andTogo.
d. The AmrA region includes Canada, the United Statesof America, and Cuba.
e. Health centres are defined as a place for outpatientclinical visits with at least one full time doctor andnurse on the staff.
f. The documentation of this component is in prepara-tion. WHO plans to make this software freelyavailable to the public.
g. Results of this analysis are presented on the WHO-CHOICE website: http://www.who.int/evidence/cea.
h. Note that for certain traded items, such as drugs thatrequire cold chain storage, this model will notcapture the full cost of transport. Thus, the costsfor distributing these items should be calculatedindependently.
References1. Commission on Macroeconomics and Health.
Macroeconomics and health: investing in health foreconomic development. Report of the Commissionon Macroeconomics and Health. Center for Inter-national Development at Harvard University.http://www.cid.harvard.edu/cidcmh/CMHReportpdf, World Health Organization, 2001.
2. World Bank. World Development Report 1993:Investing in Health. Oxford University Press: NewYork, 1993.
3. Berman P, Brotowasisto, Nadjib M et al. The costsof public primary health care services in ruralIndonesia. Bull World Health Organ 1989; 67(6):685–694.
4. Berman P. Cost efficiency in primary health care:studies of health facilities in Indonesia. HealthPolicy Plan 1989; 4(4): 316–322.
5. Brenzel L, Claquin P. Immunization programs andtheir costs. Soc Sci Med 1994; 39(4): 527–536.
6. Phonboon K, Shepard DS, Ramaboot S et al.The Thai expanded programme on immunization:role of immunization sessions and their cost-effectiveness. Bull World Health Organ 1989; 67(2):181–188.
7. Robertson RL, Davis JH, Jobe K. Service volumeand other factors affecting the costs of immuniza-tions in the Gambia. Bull World Health Organ 1984;62(5): 729–736.
8. Kumaranayake L, Watts C. HIV/AIDS preventionand care interventions in Sub-Saharan Africa: aneconometric analysis of the costs of scaling-up.The S Afr J Econ (Special Edition) 2000; 68(5):1012–1032.
9. Foster SO, McFarland DA, John AM. Measles.In Disease Control Priorities in Developing Coun-tries, Jamison DT, Mosley WH, Measham AR et al.(eds). Oxford University Press: New York, 1993;161–187.
10. Over M. The effect of scale on cost projections for aprimary health care program in a developingcountry. Soc Sci Med 1986; 22(3): 351–360.
11. Hanson K, Ranson K, Oliveira-Cruz V, Mills A.Constraints to scaling up health interventions: a
Accounting for the Cost of Scaling-up Health Interventions 1123
Copyright # 2004 John Wiley & Sons, Ltd. Health Econ. 13: 1117–1124 (2004)

conceptual framework and empirical analysis. WHOCommission on Macroeconomics and Health.www.cmhealth.org/docs/wg5 paper13.pdf (Work-ing Group 5, Paper 13), 2001.
12. Kumaranayake L, Kurowski C, Conteh L. Costs ofscaling up priority health interventions in low-incomeand selected middle-income countries: methodologyand estimates. London School of Hygiene andTropical Medicine. www.cmhealth.org/docs/wg5 paper18.pdf (Working group 5 Paper 18),2001.
13. Oliveira-Cruz V, Hanson K, Mills A. Approaches toovercoming health systems constraints at the periph-eral level: a review of the evidence. London School ofHygiene and Tropical Medicine, WHO Commissionon Macroeconomics and Health. www.cmhealth.org/docs/wg5 paper14.pdf (Working Group 5 Pa-per 14), 2001.
14. Hutubessy RCW, Baltussen RMPM, Tan Torres-Edejer T et al. Generalised cost-effectiveness analy-sis: an aid to decision making in health. Appl HealthEcon Health Policy 2002; 1(2): 89–95.
15. Murray CJL, Lopez AD. The Global Burden ofDisease: A Comprehensive Assessment of Mortalityand Disability from Diseases, Injuries, and RiskFactors in 1990 and Projected to 2020. HarvardUniversity Press: Cambridge, MA, 1996.
16. Baltussen RM, Adam T, Tan Torres T, HutubessyRC, Acharya A, Evans DB, Murray CJ. GeneralizedCost-Effectiveness Analysis: A Guide. http://www.who.int/evidence/cea. World Health Organization,Global Programme on Evidence for Health Policy:Geneva, 2002.
17. Fiedler JL. The Nepal National Vitamin A Pro-gram:cost estimates for 2000 and alternative config-urations of a nationwide program. Partners forHealth Reformplus Project. Abt Associates Inc:Bethesda, MD, 2001. Special Initiatives Report, No.41. Partners for Health Reformplus.
18. Fiedler JL, Dado DR, Maglalang H et al. Costanalysis as a vitamin A program design andevaluation tool: a case study of the Philippines.Soc Sci Med 2000; 51(2): 223–242.
19. Mills A, Broomberg J, Lavis J et al. The costs ofHIV/AIDS prevention strategies in developing coun-tries. World Health Organization (document no.GPA/DIR/93.2): Geneva, 1993.
20. Saitowitz R, Hendricks M, Fiedler J et al. Aproposed vitamin A supplementation programmefor South Africa}design, coverage and cost. S AfrMed J 2001; 91(9): 755–760.
21. Seshadri SR. Constraints to scaling up healthinterventions: country case study: India. www.cmhealth.org/docs/wg5 paper16.pdf. WHO Com-mission on Macroeconomics and Health: 2001.
22. De Winter ER. Are we ignoring population densityin health planning? The issues of availability andaccessibility. Health Policy Plan 1992; 7(2): 191–193.
23. Perry B, Gesler W. Physical access to primary healthcare in Andean Bolivia. Soc Sci Med 2000; 50(9):1177–1188.
24. Khan MM, Ali D, Ferdousy Z et al. A cost-minimization approach to planning the geographi-cal distribution of health facilities. Health PolicyPlan 2001; 16(3): 264–272.
25. Stock R. Distance and the utilization of healthfacilities in rural Nigeria. Soc Sci Med 1983; 17(9):563–570.
26. Doherty J, Rispel L, Webb N. Developing a plan forprimary health care facilities in Soweto, SouthAfrica. Part II: Applying locational criteria. HealthPolicy Plan 1996; 11(4): 394–405.
27. World Bank. World Development Indicators 2000.World Bank: Washington, DC, 2000.
28. Adam T, Evans DB, Murray CJL. Econometricestimation of country-specific hospital costs. Cost-effectiveness Res Allocation 2003; 1(3).
29. Limao N, Venables AJ. Infrastructure, geographicaldisadvantage, transport costs, and trade. WorldBank Econ Rev 2001; 15: 451–479.
30. Dinwiddy C, Teal F. Principles of Cost-BenefitAnalysis for Developing Countries. Cambridge Uni-versity Press: Cambridge, 1996.
31. Roncek DW. Learning more from tobit coefficients:extending a comparative analysis of political pro-test. Am Soc Rev 1992; 57: 503–507.
B. Johns and R. Baltussen1124
Copyright # 2004 John Wiley & Sons, Ltd. Health Econ. 13: 1117–1124 (2004)