ACB ACB News The Editor is responsible for the final content; advertisers are responsible for the...
48
In this issue Welcome Professor Ian Young, ACB President Council Report Focus Reports ACB Workforce Survey A Day of Fertility and Screening at Exeter Hull, City of Culture 2017 AKI Flags ACB Golf Society The Association for Clinical Biochemistry & Laboratory Medicine | Issue 647 | June 2017 ACB News
Transcript of ACB ACB News The Editor is responsible for the final content; advertisers are responsible for the...

In this issue
WelcomeProfessorIan Young,ACB President
Council Report
Focus Reports
ACB WorkforceSurvey
A Day ofFertility andScreeningat Exeter
Hull, City of Culture2017
AKI Flags
ACB GolfSociety
The Association for Clinical Biochemistry & Laboratory Medicine | Issue 647 | June 2017
ACBNews


About ACB NewsThe Editor is responsible for the finalcontent; advertisers are responsible for thecontent of adverts. Views expressed are not necessarily those of the ACB.
Lead EditorMr Ian HanningDepartment of Clinical BiochemistryHull Royal InfirmaryAnlaby RoadHull HU3 2JZEmail: [email protected]
Associate Editors Mrs Sophie BarnesDepartment of Clinical Biochemistry12th Floor, Lab BlockCharing Cross HospitalFulham Palace RoadLondon W6 8RFEmail: [email protected]
Dr Gina Frederick Pathology Laboratory, Level 5Royal Derby HospitalUttoxeter RoadDerby DE22 3NEEmail: [email protected]
Dr Derren Ready Public Health England National Infection ServiceMicrobiology Reference Services61 Colindale AvenueLondon NW9 5EQ Email: [email protected]
Situations Vacant AdvertisingPlease contact the ACB Office:Tel: 0207-403-8001 Fax: 0207-403-8006Email: [email protected]
Display Advertising & InsertsPRC Associates Ltd1st Floor Offices115 Roebuck RoadChessingtonSurrey KT9 1JZTel: 0208-337-3749 Fax: 0208-337-7346Email: [email protected]
ACB Administrative OfficeAssociation for Clinical Biochemistry & Laboratory Medicine130-132 Tooley StreetLondon SE1 2TUTel: 0207-403-8001 Fax: 0207-403-8006Email: [email protected]
ACB PresidentProfessor Ian YoungTel: 028 90632743 Email: [email protected]: @ACBPresident
ACB Home Pagehttp://www.acb.org.uk
Printed by Swan Print Ltd, BedfordISSN 1461 0337© Association for Clinical Biochemistry &Laboratory Medicine 2017
ACBNewsIssue 647 • June 2017
The monthly magazine for clinical science
Issue 647 | June 2017 | ACB News
Front cover: Professor Ian Young,incoming President of the ACB,with Dr Gwyn McCreanor, Past President
General News page 4
Practice FRCPath Style Calculations page 20
Microbiology News page 22
Council News page 23
Focus News page 24
Trainees News page 28
Meeting Reports page 31
BIVDA News page 40
Obituaries page 42
ACB News Crossword page 45
Situations Vacant page 46
4 | General News
Issue 647 | June 2017 | ACB News
HealthcareScience WeekHealthcare Science week has come andgone already. There was a lot of activityacross the country to raise the profile ofHCSs to colleagues and patients. For aflavour of what took place have a look atthe HCS week calendar and get inspiredfor next year: http://www.nhsemployers.org/campaigns/healthcare-science-week-2017/hcs-week-2017-calendar �
SudokuThis month’s puzzle
Last month’s solution
The NHS Five YearForward ViewThe next steps for the NHS Five YearForward View document were publishedon 31st March 2017. See here for furtherinformation: https://www.england.nhs.uk/publication/next-steps-on-the-nhs-five-year-forward-view/It concentrates on the delivery of urgent
and emergency care, general practice,cancer and mental health over the nexttwo years. STPs are mentioned in terms oftheir role in integration of services andensuring funding efficiencies.The report refers to scientists twice, once
around strengthening workforce and thesecond reference relates to PHE scientistsand outbreaks. It mentions pathology onceand alludes to needing to deliver a fast,high quality service and ensuringefficiencies. �
NHS ImprovementThe ACB has been invited to join theNational Pathology Optimisation DeliveryGroup which is being chaired by AdrianNewland. This group has the remit ofdeveloping and coordinating a number ofworkstreams aiming to progress theimplementation of the recommendationsof the Carter Report. We have beenreassured that quality assurance will be acornerstone of any reconfiguration ofservices. �
CondolencesThe Association has been advised of thedeaths of Professor Roger Ekins (seeObituary on page 42), Professor StephenJeffcoate (see Obituary on page 44) and Dr Daniel Simpson. Dr Simpson a RetiredMember from Edinburgh, passed away on15th April 2017. He joined the Associationin 1965. �


6 | General News
Issue 647 | June 2017 | ACB News
This report criticises the short-sightednessof successive governments for failing toplan effectively for the long-term future ofthe health service and adult social care.The Committee makes it clear that a tax-funded, free-at-the-point-of-use NHS isthe most efficient way of delivering healthcare and should remain in place. For thatprinciple to remain, however, many aspectsof the way the NHS delivers healthcare willhave to change.The Committee concludes that a culture
of short-termism seems to prevail in theNHS and adult social care and that theDepartment of Health has been unwillingor unable to look beyond the next fewyears. It recommends that a new,independent Office for Health and CareSustainability should be established tolook at health and care needs for the next15-20 years and report to Parliament onthe impact of changing demographicneeds, the workforce and skills mix in the
NHS and the stability of health and socialcare funding relative to demand.The report highlights that the failure to
implement a comprehensive long-termstrategy to secure the appropriatelyskilled, well-trained and committedworkforce that the health and care system will need is the biggest internalthreat to the sustainability of the NHS. The report highlights the problems ofover-burdensome regulation, unnecessarybureaucracy, a prolonged period of payrestraint, low levels of morale andretention problems.Click on the link to read the report
and see the written evidence submitted by the ACB: https://www.publications.parliament.uk/pa/ld201617/ldselect/ldnhssus/151/151.pdfOr watch Lord Patel, Committee Chair, on YouTube here:https://www.youtube.com/watch?v=kBDGqGY19is �
Consultant Clinical ScientistAppointments
This is a reminder that if you are appointing to a Consultant post,Job Description Review and College representation on the Appointments Committee
(AAC) can be requested by emailing [email protected], including date, time and venue for the AAC.
Following advertisement and date setting, the College will identify an assessor (this applies to England, Wales and Northern Ireland). These assessors are full members
of the AAC and will advise on the suitability of the training and experience ofcandidates for appointment, and feedback information from the AppointmentsCommittee to the College. This enables the name of the successful applicant
to be reported in the College Bulletin as well as helping to collect important data for future workforce planning.
See here for further details: https://www.rcpath.org/profession/workforce.html �
House of Lords Select Committee on theLong-term Sustainability of the NHS andAdult Social Care


8 | General News
Issue 647 | June 2017 | ACB News
ACB Golf Society Future MeetingsSummer MeetingVenue: Dunston Hall, Norwich
https://www.qhotels.co.uk/our-locations/dunston-hall/ Date: Friday, date to be confirmed
Autumn Meeting2nd Dutch-British Biochemists Open
Venue: The Netherlands, course to be confirmedDate: Friday 22nd September 2017
If you wish to play in either of these events and are not on the ACB Golf Society mailing list please contact:
Ian Watson by email: [email protected] or tel: 07889324549
Latest VenturePublications Book Launched at Focus 2017
Karen Mitchell (left), Paul Newland(middle) and Patricia Wilkie (right) at theFocus launch of the latest VenturePublications book, Neonatology andLaboratory Medicine, by Sarah Heap, Jim Gray and Andrew Ewer. �
New ACB President
Professor Ian Young has stepped into therole of ACB President. Past President GwynMcCreanor comments: ‘I have been ACBPresident for two years until the AGM on5th May 2017 and I have enjoyed everyminute of it. It is such an honour to takeon the role and it’s wonderful to workwith so many excellent ACB Members.Now that I have demitted office, I continue as Past President for a furtheryear. Professor Young is Professor ofMedicine at Queens University Belfast andChief Scientific Advisor to the Departmentof Health in Northern Ireland. He is goingto have a busy and challenging two yearsahead and I hope he enjoys the role asmuch as I did.’ �


10 | General News
Issue 647 | June 2017 | ACB News
. . . But where do you gofrom here? The aim of the flag is to alert clinical staffto patients with the condition. One of theproblems is that the AKI flag may begenerated on the same patient onnumerous samples over a period of time.We have overcome this problem by use ofa search on Winpath and an Excelspreadsheet with a macro.A search is run on Winpath every day at
4am for all AKI flags on samples from theprevious day. The output from this searchis a .csv file with fields for HospitalNumber, Consultant, Ward, Patient Name,Age, Date of Sample, Time of Sample,Gender, Serum Creatinine, AKI Grade andLaboratory Number.The AKI nurses were finding that, while
the results of the search were useful,
it took considerable amounts of time toselect out the newly flagged patients. In order to overcome this a macro was
written for an Excel spreadsheet. Themacro is linked to a button on thespreadsheet so all the nurses have to dowhen they arrive in the morning is loadthe spreadsheet and press the button.The actions performed by the macro are
as follows:
� The search results (as a .csv file) areloaded into the spreadsheet at row4001, to avoid any conflicts with data inthe top lines.
� The newly loaded data is then copiedand pasted at row 200.
� The entire top block of data is sorted indescending date order.
� A “remove duplicates” action isperformed using Hospital number and
So you’ve generated anAKI Flag . . .Michael Colley, Great Western Hospital, Swindon

General News | 11
Issue 647 | June 2017 | ACB News
AKI grade. This results in only the mostrecent sample with a given AKI gradeon each patient being retained.
� These are again sorted by date and AKIgrade, both in descending order and byPatient Name in ascending order.
� Where AKI3 is present this ishighlighted in RED, AKI2 in Pink andAKI1 remains white.
� Any data lower on the spreadsheetthan row 3000 is deleted in order toprevent the sheet from becoming toolarge. The relevant data is in the toprows.
� The button disappears from thespreadsheet so that it is evident that ithas been activated, though reloadingthe spreadsheet and repressing thebutton does not change the datadisplayed.
� The spreadsheet is automatically saved,replacing the previous version.
This process has saved the nursesconsiderable time and proved a positiveasset to them. The Winpath search and Macro Code are
available on request. �
ACB South West & Wessex Regional Scientific Meeting
Jointly organised with the Supra-Regional Assay Service
for Trace Elements
Trace ElementsFriday 6th October 2017Oake Manor Golf Club, Taunton
Further information to follow.
We are looking for some speakers from the South-West & Wessex Region and also Wales to take part in the programme. If you are interested please contact Paul Cook on
[email protected] via the ACB Regional meetings website:
http://www.acb.org.uk

The first of two ACB National WorkforceSurveys issued by the ACB in 2016 had theaim of providing an updated and morecomprehensive set of ACB workforce data.1,365 invitations to participate in thesurvey were distributed to Ordinary,Honorary, Federation, and TemporaryRetired members, with 622 (45.6%)members completing the survey.
Workforce DemographicsThere was observed a marked gender biasamong the workforce; 63.3% ofrespondents were female. A bimodaldistribution of age ranges was alsoevident, with peaks at 31-40 years and 51-60 years. A large majority ofrespondents (91.2%) described theirethnicity as white (British, Irish or Other),and 5.4% considered themselves to have adisability. A majority of participants(84.0%) stated that their positon was fulltime, and a permanent post (86.3%). Ofthe 16% who are working part time, 84%are female. (See chart below).
Banding, Job Role, and Area ofWorkOf those surveyed, 92% stated that theywere employed by the NHS, as opposed tothe private sector (2.5%) or an NHS/privatesector collaboration (5.5%). The majorityof survey participants stated that theirprincipal area of work was ClinicalBiochemistry (75.8%), with Microbiology(7.8%), ‘Other’ (4.4%), and Immunology(3.5%) the next most common areas ofwork. Pay banding as categorised by jobtitles are given in the table opposite.
Planned Retirement DateOver one-fifth (21.4%) of participantsindicated that they intended to retire inthe next 5 years. This included 50% of theparticipants who stated they were head oftheir department, 38.6% of those workingat ‘Consultant’ Afc pay grades and 41.2%of Medical Staff. This is likely to representa substantial proportion of the moreexperienced members of the profession.
12 | General News
Issue 647 | June 2017 | ACB News
Report on the 2016 ACB Workforce SurveysJonathan Scargill, Salford Royal NHS Foundation Trust

Registration and FRCPath StatusNearly all participants stated that theywere HCPC registered (77.3%), GMCregistered (11.4%), or working towardregistration (8.7%). FRCPath statusappeared largely appropriate for paybandings, with the majority of consultantgrade staff having completed FRCPath,and more junior grades havingcommenced or yet to start on FRCPathqualification.
Lost, New and Vacant Posts Survey 2016The second survey issued by the ACB in2016 was a repeat (and further extended)survey of previous surveys on lost, new andvacant posts issued in 2010 and 2013. One hundred and fifty-nine invitations toparticipate in the survey were distributedto individuals who had identifiedthemselves as the head of their
department by the first workforce survey.The response rate (38.3%) was lower
than previous years; the 2013 survey wasresponded to by 50.2% of those contacted.The 317 members of staff described byheads of department in this surveyrepresent less than a quarter of the 1359Ordinary, Federation, Honorary, andTemporary Retired members of the ACB.Questions were based around changes tostaffing structures in the departments ofthe participants over the last 3 years.Around a quarter of participants (24.6%)said that their department had mergedwith another in the last 3 years, andaround two-thirds (65.6%) that they hadseen some change to the staffing structureof their department, a marked increase onthe 2013 survey (49.5%). Over one-third(35.7%) of participants said that they hadbeen unable to recruit to posts. All ofthese stated that this was due to lack of
General News | 13
Issue 647 | June 2017 | ACB News

applicants, or a lack or suitablyqualified/experienced candidates. The survey demonstrated a small netincrease in posts, mostly due to areduction in the number of lost postscompared to previous surveys. It should benoted that the 2013 survey did not includemedical posts, and asked about postslost/created/vacant over 2 years ratherthan 3 (see chart above).The data suggest that there is a
tendency for new posts to be advertised atlower grades compared to those lost. This may represent the loss of higher-banded posts in restructuring ofdepartments, with lower graded postsadvertised as the end-point of this exercise(see chart below).
Future PlansThe surveys conducted provide vitalinformation about the future challengesthe profession faces and it is important toformalise the generation of this data andencourage a higher response rate toproduce more accurate information. A strategy for this will be debated at theACB Education, Training and WorkforceCommittee meeting in May. The Association also needs to ensure thatthe information is disseminated to thosewho are involved in recruitment at a locallevel. Heads of Departments need to know
the problems highlighted in this report toencourage them to secure the fundingnow for posts to ensure there is not aworkforce shortfall in the future. Manyoccupants of senior positions intend toretire within the next few years and it islikely that there will not be sufficientnumbers of candidates to fill these roles.The information also needs to reach localLETBs to ensure that the professionrecruits the correct number of candidatesto ensure posts can be filled. There arereports of posts being lost as there are notenough suitable candidates applying forroles which may be in response toinsufficient trainees being recruited. It is noted that the ACB is not a verydiverse group and this has been thesubject of work undertaken by RachelWilmot. Rachel has presented her data tothe ACB Executive and in collaborationwith the Science Council and support fromthe Executive will plan how the associationcan increase the diversity of ourprofession. The data generated from this survey
have identified several areas for theAssociation to consider. By publishingthese data it is hoped that there isincreased visibility of the currentworkforce issues and that departmentsconsider this information when reviewingservice needs. �
14 | General News
Issue 647 | June 2017 | ACB News

General News | 15
Issue 647 | June 2017 | ACB News
Trade Union Statement to Members
The Statement to Members issued in connection with the Union’s annual return for period ended 31st December 2016
as required by Section 32A of the Trade Union and Labour Relations (Consolidation) Act 1992 can be found on the website:
http://www.acb.org.uk/trade-union-statement
Information from the Chief ScientificOfficer (England)Committee Member Application:NHS England’s Chief Scientific Officer’s Leadership, Improvement and Advice Group
NHS England’s Office of the Chief ScientificOfficer is recruiting Senior HealthcareScientists to join the CSO Leadership,Improvement and Advice (LIA) group. This group brings together key leadersfrom across the system to ensurehealthcare science can be at the forefrontof transformational change. There are four vacancies available.
For further details and full invitation letterplease email [email protected] marking‘LIA Group’ in the subject heading. The closing date for final expressions of
interest is 2nd June and interviews will beheld in person on the 21st June at SkiptonHouse, London. Successful applicants are advised that
they should be available to attend astrategy group meeting on 4th July. �
Women in Science andEngineering Awards2017 – NominationsNow Open!The Women in Science and Engineering(WISE) Awards is a unique annual event, a special opportunity to recognise inspiringorganisations and individuals activelyaddressing the core concerns of WISE:promoting science, technology,engineering and mathematics to girls andwomen. This year the Office of the Chief Scientific
Officer are sponsoring a WISE Technology &Engineering in Health Award whichchampions a woman who uses science,technology and engineering to improvehealth. Visit their website for more details on the
award categories and criteria and find outhow to apply: https://www.wisecampaign.org.uk/wise-awards/wise-awards-2017The closing date for nominations is
23rd June 2017. The award ceremony willtake place on the evening of 9th Novemberin London. �
Book ReviewsPlease note that following discussion at the last Annals Editors’ meeting, ACB News will take over book reviews – the first such review will appear in the August Edition.

16 | General News
Issue 647 | June 2017 | ACB News
Dr Chris Chase is celebratingthe Pathology Laboratory atHull Royal Infirmary’s part in welcoming everyone tothe City of Culture
Hull is the 2017 City of Culture and we arecelebrating our small part in promotingthe city. Our laboratory sits next to themain railway line, a few hundred yardsfrom Hull’s main train station. If you haveever travelled to Hull by train then youmay have seen us running around in ourwhite lab coats; occasionally we may evenwave to the London bound trains.We are all very excited that Hull is the2017 City of Culture, as in our lunch breakswe can race to the City Centre and admirethe ever-changing art installations, such asa giant wind turbine blade, cascadingweeping poppies or Lego daffodils. Hull
has so much to offer: lots of museums,galleries, stunning architecture and awonderful waterfront area with bars andrestaurants. Hull is certainly not dull (‘Ull is never dull’).We have entered the spirit with our own
contribution, a seventy foot sign attachedto the front of the building looking outover the railway line simply boasting OUR CULTURE: YOUR CARE.Our laboratory is a large silver metallic
structure built originally as a laundry andis Hull’s answer to the Pompidou Centre. It houses Blood Sciences andHistopathology (Microbiology is still in theadjoining tower block) and we have asmaller Blood Science and Virologylaboratory at our sister hospital at CastleHill which sits in beautiful countrysidenestling at the foot of the YorkshireWolds. Nearly two hundred staff work in the
Hull building, working day and night to
Our Lab in the City of CultureDr Chris Chase, Pathology Training Manager, Hull & East YorkshireHospitals NHS Trust

General News | 17
Issue 647 | June 2017 | ACB News
service the Hull and East YorkshireHospitals NHS Trust and GPs in the city andin the East Riding of Yorkshire, processingmillions of samples per year.We have been working hard to develop
a pathology wide culture of Equality,Respect, and Integrity, which we proudly wear on our purple lanyardsaround our necks. This emphasises oursense of teamwork and reinforces ourpatient-focussed approach.We are passionate about training and
education and believe that everyone,regardless of banding, can be empoweredthrough learning. We have developed
strong links with local Universities such asHull, Sheffield Hallam and York College.We have a large number of Trainees andwill soon be embarking on theapprenticeship pathways. Hull is the Cityof Culture and we are proud to have ourown culture of education and training, a culture of inclusivity and opportunity forall and to be a centre of excellence.So when your train is slowing down to
enter the station in Hull, give us a wave.Welcome to the City of Culture where youcan gaze at a life size statue of the poetPhilip Larkin and see a copy of AmyJohnson’s plane that flew to Australia. �
ACB Golf Society ReportIan Watson, Secretary, ACB Golf Society
A select group, including new membersRobert Hill and Ahmed Waise, joinedGraham White, who had organised theevent, Pete Wood, Bill Fraser and myself on7th April – a glorious Spring day – at theexcellent Donnington Grove ChampionshipCourse in Berkshire.While the fairways were quite generous
and there was not much in the way ofwater hazards, the course was liberallysupplied with large bunkers and trees topenalise wayward shots.As the weather in the North had been
pretty wet it was a pleasant surprise for meto find the course in great condition andthat there was plenty of run-on for shotsrather than being plugged in the mud! The front 9 was moderately hilly once we
had crossed the A34 bridge after the firsthole; the back 9 was less physicallystrenuous, but judging from the scoresperhaps not topographically – or shouldthat be psychologically?The Nearest the Pin on the par 3 15th
was won by Bill Fraser with a beautifullyflighted shot over the water and largebunker; the winner of the Stablefordcompetition was also Bill Fraser winning asleeve of balls, with Graham White and IanWatson second equal.The Summer meeting will be at Dunston
Hall, Norwich: https://www.qhotels.co.uk/our-locations/dunston-hall/ Dates are currently being finalised so if
you are not on the emailing list and wish toplay contact me on: [email protected] �
Update on FITJust a reminder that the NICE report on Faecal Immunochemical Testing (FIT) in England isdue out in June: Quantitative faecal immunochemical tests to guide referral for colorectalcancer in primary care, In development [GID-DG10005}.We await with baited breath! �

18 | General News
Issue 647 | June 2017 | ACB News
Inaugural Meetingof the Oxford NHSGenomics MedicineCentre: 27th June2017The 100,000 Genomes Project willtransform the way patients with raredisease or cancer are diagnosed andtreated.The Oxford NHS GenomicMedicine Centre (Oxford NHS GMC) iscelebrating its launch with an eventjointly hosted by Oxford Academic HealthScience Network (Oxford AHSN) on the27th June at the Oxford Belfry nearThame. The event will include importantupdates on the progress of this excitingarea of development within the regionand speakers will discuss a variety oftopics to facilitate understanding anddevelopment of key areas of the OxfordNHS GMC and provide an overview ofcurrent national and regional activities.Find out more and register here:https://www.eventbrite.co.uk/e/oxford-nhs-genomic-medicine-centre-launch-event-tickets-34065528914 �
Healthcare ScienceEducation Event:Where are we nowand where are wegoing?The Healthcare Science EducationWorking Group at Great Ormond StreetHospital along with Healthcare Scientistsfrom Trusts across London are hosting anEducation in Healthcare Science event on21st July 2017. This event will discuss education within
Healthcare Science, where we are now,where we're going and how to maximisethe impact of the opportunities ahead of us. This meeting will showcase current
work and facilitate discussions aboutreaching across boundaries in education.Find out more and register for the event here:https://www.eventbrite.com/e/healthcare-science-education-where-are-we-now-and-where-are-we-going-tickets-33931393712?aff=es2 �

General News | 19
Issue 647 | June 2017 | ACB News
EditorialIan Hanning
Just as I was checking the first proof for the June edition I received a letter from Dr JohnLines, former Editor of ACB News. He welcomed me ‘to the Guild of ACB News Editors,from the oldest living member to {me} as the newest member’.The recent cyber attacks on the NHS brought back memories of a ‘communication issue’
in the late 1960s. The story is reproduced below. �

20 | Practice FRCPath Style Calculations
Issue 647 | June 2017 | ACB News
Recent European guidelines advise treatment with urea as a second-line treatment for thesyndrome of inappropriate antidiuresis (SIADH), with the aim of inducing an osmoticdiuresis. A 65-kg man with a stable serum sodium concentration (after fluid restriction) of125 mmol/L is commenced on urea 15 g/day. Calculate the anticipated increase in serumosmolality, stating the assumptions made. NB: the formula of urea is CO(NH2)2.
FRCPath, Autumn 2015
Urea is evenly distributed throughout body water.
Urea empirical formula = CH4N2O, calculate MW:
C = 12H4 = 4 x 1 = 4N2 = 2 x 14 = 28O = 16MW = 60
Number of mmol urea administered = wt urea (g) x 1000 = 15 x 1,000 = 250 mmolMW urea 60
Assume total body water is 60% of body weight:
Total body water = Body wt (kg) x 60 = 65 x 60 = 39 L100 100
Urea concentration in body water = Urea load (mmol) = 250 = 6.4 mmol/LBody water (L) 39
Since urea is undissociated and serum urea is in equilibrium with urea in other fluidcompartments, the increase in serum osmolality due to 15 g urea administration isapproximately 6 mmol/L.
Assumptions:• That all the administered urea is absorbed (if given orally) and evenly distributed
throughout total body water without any excretion. In practice a steady state wouldeventually be achieved (half-life is probably about 2 h) but there would befluctuations depending on dosing interval used. If given as a single bolus then thetheoretical peak is 6 mmol/L but levels would fall rapidly before the next dose due tourinary excretion.
• That the patient has a normal total body water content for his weight. The lowsodium suggests that this may not be the case.
Deacon’s Challenge No 190 - Answer

Practice FRCPath Style Calculations | 21
Issue 647 | June 2017 | ACB News
Question 191You need to make up a phosphate buffer with a pH of 7.4 and a total phosphateconcentration of 40 mmol/L. Calculate the amounts of sodium dihydrogen phosphateand disodium monohydrogen phosphate that need to be weighed into 1 litre ofwater, given that the pKa is 6.82 (atomic weights: Na 23, P 31).
FRCPath, Autumn 2015

22 | Microbiology News
Issue 647 | June 2017 | ACB News
The Diggle Microbiology ChallengeThese multiple-choice questions, set by Dr Mathew Diggle, are designed withTrainees in mind and will help with preparation for the Microbiology Part 1FRCPath exam.
Question 1 from FebruaryA 26 year old pregnant woman (17/40 gestation) consulted her General Practitioner(GP) because her 2 year old son has a vesicular rash on his hands and in his mouth. The mother is concerned about her unborn child. The GP is experienced and confidentof his diagnosis of hand foot and mouth disease, but telephones you regarding furthermanagement.
Choose the most appropriate advice:
A) Phone the local CCDC to find out if there is a current epidemic B) Reassure the mother that there is no risk to the pregnancy C) Refer the lady for foetal ultrasound scan D) Send a vesicle fluid from the child for EM studies E) Send blood for serological examination
AnswerB) There is no need to phone the local CCDC as enteroviruses are continually circulatingin the population and no prophylaxis/vaccination is available.
Infection with enteroviruses is not associated with any particular foetal consequence,and the GP is experienced and confident in his diagnosis. An ultrasound scan would bewarranted in the case of a more serious antenatal infection such as parvovirus, to checkfor signs of foetal hydrops. Vesicle fluid from HFMD is not routinely sent for EM studies,although EM could be used to diagnose infections with Molluscum contagiosum andthose caused by Orf virus. Blood could be requested for serological investigation if theGP was not confident of the diagnosis. VZV can cause a vesicular rash, but this typicallyappears on the trunk and spreads. The serological investigation of blood forenterovirus exposure is not warranted in pregnancy.
Question 2A 22-year old female medical student recently returned from Tanzania presents with ahistory of haematuria. On investigation schistosomal serology is shown to be positive.
Select the treatment of choice:
A) Albendazole B) Ivermectin C) Mebendazole D) Praziquantel E) Suramin
The answer to Question 2 will appear in the next issue of ACB News – enjoy! �

Council News | 23
Issue 647 | June 2017 | ACB News
As always at Council we have our topics ofthe day. At the last council meeting inMarch we spent time discussing three maintopics, namely:
1. Spotlight on the Scientific Committee2. Our communications Strategy3. Membership
Scientific Committee
I am sure most of you may have read therecent article in February, giving you aninsight into the Director of the ScientificAffairs, Chris Chaloner. Our focus atCouncil was on what the ScientificCommittee stands for and how it benefitsand relates to the membership. Chrishighlighted some of the key areas of theirwork, focussing on standardisation ofpractice, producing guidance material thathelps us all do our day job, and the role ofAMALCs, the monographs for individualanalytes. He acknowledged the intent toreally expand these into areas across allspecialities emphasising the need forsupport from Trainees and experts in allspecialities across laboratory Medicine, to create an “Amalcopaedia”, and also notforgetting to keep the current documentsup to date.
Communication Strategy
The role and potential use of the ACB appwas discussed. For those who have notdownloaded it yet, it is available for bothAndroid and IOS. This will incorporatemeetings held by the ACB, and has alreadybeen developed to support Focus 2017.Discussion centred on the expectation ofreaching the membership more frequentlyto share information to and from the ACB,giving a voice to all our members.
The website was a key topic, and this wasfelt to be evolving well in line with ouraims. The meetings calendar has been welltested and will ensure meeting clashes donot occur, also giving members theopportunity to plan CPD activities well inadvance, either attending local regionalmeetings or looking further afield.Training and Education was also at theforefront of our strategy and we are tryingto explore ways of disseminatingknowledge at all levels with the use of IT,without necessarily expecting themembership to travel too far, definitelyone for the future.
Membership
The final topic of discussion was themembership which has taxed (forgive thepun!) our outgoing Director of Finance. It was acknowledged that we havedecreasing numbers, due to decreasedintake and retirement from the profession.It was agreed that whilst it was notcurrently critical, a strategic view isrequired to ensure we continue to growand develop to meet the future needs ofthe membership. Finally, do you fancy writing an
AMALC or reviewing one? It is worth 5 CPD points if you write one, and it is agreat way to learn and be part of our very own “Amalcopaedia”. If so pleasecontact Chris Chaloner on email:[email protected]. As always, if there is anything you would
like to discuss with me or indeed have anyideas you would like to put forward onany issue, please contact me [email protected] �
Council Meeting: March 2017Paul Newland, Director for Publications and Communications

For the first time, Focus was held over 2days rather than 3, the theme being ‘thepatient journey’. It started with theconference reception in the War Galleriesat the Royal Armouries on the Wednesdayevening. This was an informal drinksreception for Trainees and conferencedelegates, followed by the Focus Fringe atthe Wardrobe Bar. The evening providedan excellent opportunity to meet, catch-upand socialise with colleagues, make newcontacts and network with other membersof our profession.The sun was shining over Leeds for the
first day of the ACB Focus 2017Conference. The scientific programme forthe conference looked excellent and thespeakers certainly did not disappoint. Wewere welcomed at the opening ceremony
by our immediate Past President, GwynMcCreanor, followed by the Transatlanticplenary lecture given by Professor MikeBennett from the Children’s Hospital ofPhiladelphia who spoke about geneticcauses of hyperinsulinism. After a veryuseful revision of the pathology anddiagnosis of hyperinsulinism, ProfessorBennett went on to explain some of hisgroup’s recent research into theinvolvement of short-chain 3-hydroxyacyl-coA dehydrogenase (SCHAD). Two parallel sessions followed the
tea-break with talks relating to the impactof service organisation on access or ‘gamechangers’. Highlights included Dr StephenGibbons’ excellent talk on laboratorymedicine for transgender patients, which
24 | Focus News
Issue 647 | June 2017 | ACB News
Focus in Leeds UpdateJames Pethick, Sandwell and West Birmingham Hospitals; ThomasMorris, St George’s Hospital, London; and Ellie McLaughlan, LeedsGeneral Infirmary
Dr Gwyn McCreanor presents the ACB FoundationAward to Dr Bill Bartlett
Dr Gwyn McCreanor presents the TransatlanticAward to Professor Mike Bennett

focused on how clinical biochemistry canmove forward to ensure a high quality,inclusive service for these patients. Dr Maurice O’Kane gave an interestingtalk about the challenges faced in the areaof point of care testing, and theimportance of clinically-drivencommissioning. Delegates then attended parallel
symposia regarding delivery of patient-oriented services or researchpresentations for the ACB Medal Award.All the candidates presented work of anexceptional standard, with the awardgoing to Rebecca Stead for her researchinto MNKs as novel markers of type 2diabetes mellitus risk. Congratulations alsoto Edmund Wilkes as the runner up. The day finished with the Foundation
Lecture given by Dr Bill Bartlett who spokeabout the importance of understandingvariation for critical evaluation of ourmethods and for interpretation of testresults. On Thursday evening, the delegates
gathered at the impressive New Dock Hallfor the conference dinner. As well as adelicious meal, this was an opportunity tosocialise with friends and colleagues, withmany of us chatting or dancing into theearly hours!The final day of the conference
commenced with the Flynn Lecturedelivered by President of the Royal Collegeof Pathologists, Dr Suzy Lishman. Her talktook the theme of the meeting to everypatient journey’s ultimate destination,giving a brief and detailed history ofautopsy, the challenges facing the practicein today’s climate and the benefits thatconsented autopsies can provide togrieving families, physician education,patient care and diagnostics for futurepatients.Two industry sponsored workshops took
place between the Flynn lecture and thefirst parallel session of the day. The
Nephrocheck early AKI workshop ledseamlessly into the first talk at themanaging patient and professionalknowledge parallel session. The firstlecture delivered by Dr Andrew Lewingtondelved into renal function biomarkers andthe benefits of detecting AKI at an earlystage to reduce patient harm andmortality. This was followed by an eye-opening presentation from ProfessorSteve Ball detailing 3 cases ofhyponatraemia with different outcomes as a result of differences in treatment.International guidelines forhyponatraemia treatment were discussedand highlighted the importance ofappropriate management ofhyponatraemia. The third presentationfocused on dehydration in the elderly. The audience were presented with thefindings of a systematic review ofpublished data and primary research forthe best, non-invasive screening methodfor dehydration in the elderly without the
Focus News | 25
Issue 647 | June 2017 | ACB News
Dr Lance Sandle presents the Flynn Lecture Awardto Dr Suzy Lishman

need for performing labour intensiveserum osmolality. The final presentation inthis parallel session was on dynamiccortisol test interpretation, and based onthe results of a UK NEQAS survey.The attended poster rounds returned on
Thursday and Friday, with groups ofdelegates able to listen to explanationsfrom the authors and ask questions in the
presence of senior colleagues whoprovided further insight into each topic via a microphone linked to individualheadphones.The final afternoon of the conference
was another parallel session. Themetabolic medicine session touched onmanagement of inherited metabolicdiseases as well as the management of
26 | Focus News
Issue 647 | June 2017 | ACB News
Delegates at the Attended Poster Sessions
Delegates at the Exhibition

nutritional deficiencies following bariatricsurgery and phenotypes of diabetes. In theclinical cases session, six excellent caseswere presented ranging from vitamin Adeficiency to bizarre serial amylasemeasurements, unusual metabolism andsteroid biosynthesis. The clinical cases
session was promptly followed by a well-attended closing ceremony of what isarguably one of the most successful Focusconferences in recent years, and a tributeto the Organising Committee. We arealready looking forward to the next Focusmeeting in Manchester in 2018. �
Focus News | 27
Issue 647 | June 2017 | ACB News
The Conference Dinner in the New Dock Hall
Industry sponsored workshops were well attended

The annual ACB Training Day at Focus2017 took place on Wednesday the 3rd ofMay at the Royal Armouries in Leeds. It isaimed at members of the profession whoare working towards their FRCPathexaminations, regardless of their stage oftraining. As a relatively junior Trainee inthe field (second year STP student), I wasinitially reluctant to attend the TrainingDay because sitting the FRCPath examsseems a long way off in the future. First Ineed to complete all of my OLATcompetencies and MSc requirements!However, my training supervisor and otherTrainees who had attended the day inprevious years assured me that it would beof great benefit to my overall training and
professional development. I would benefitwhen I do eventually sit my FRCPath examsand, more immediately, when I have myOSFE at the end of my STP training nextyear. The morning session, organised by the
ACB Education Committee and overseenby Hazel Borthwick (ACB Deputy Directorfor Education, Training and Workforce),was on FRCPath OSPE preparation with amock examination designed to simulateand give a flavour of the real exam. It wasemphasised by the organising team thatthe mock was not an examination ofcurrent knowledge but a means forcandidates to become more familiar withthe process so they feel comfortable when
28 | Trainees News
Issue 647 | June 2017 | ACB News
Trainees Report on AnnualTraining Day at FocusThomas Morris, St George’s Hospital, London; James Pethick, Sandwelland West Birmingham Hospitals; and Ellie McLaughlan, Leeds GeneralInfirmary
Trainees taking part in the mock OSPE

the real examination comes around.Roughly a month before the Training Dayan email was sent out listing the topicsthat the questions in the OSPE would bebased on. The reason for this was toensure that all delegates, regardless oftheir stage of training or currentknowledge, could prepare for thequestions, get as much out of the mockexamination as possible and learn fromthe experience in a positive manner. I personally found this very useful as itgave me an incentive to go away, lookthrough my notes and reinforce what Ihad previously learnt.Hazel and Frances Boa began the
morning session by giving an introductionto the FRCPath examination. This coveredthe different parts and what is examinedat each stage, based on Miller’s pyramid ofcompetence (knows, knows how, showshow, does). Participants were then giventhe opportunity to ask questions about theexamination process. Following this, themock OSPE examination started.Candidates were divided into small groups
across seven different tables, with eachtable associated with a poster thatcontained laboratory based data and aseries of short questions related to thatdata. Each candidate had 10 minutes toanswer the questions. At the end of thistime, the different groups switched tablesand moved on to the next poster until allof the candidates had rotated round allthe posters. The topics that were coveredon the posters were: enzyme activitycalculations, blood gases, serumelectrophoresis and myeloma, EQAinterpretation, vitamin D LC-MS/MS dataanalysis, xanthochromia investigation andthe diagnosis of haemochromatosis. Aftercompleting the OSPE, candidates weregiven a well-deserved break, beforereturning to run through the answers indetail and have any queries answered. This concluded the morning session of theTraining Day. I found this part of theTraining Day extremely valuable as it gaveme an insight into what to expect in thereal life OSPE and the level of knowledgeand understanding that is required to pass
Trainees News | 29
Issue 647 | June 2017 | ACB News
Trainees workshop

30 | Trainees News
Issue 647 | June 2017 | ACB News
this part of the process. What I particularlyenjoyed about the mock was thatcandidates were able to go round thedifferent posters in small groups, thismeant that if you were unsure on a certainquestion or did not understand part of theposter you could ask someone in yourgroup for help and advice.The afternoon session was organised by
the Supra-regional Assay Service (SAS) andinvolved clinical teaching from the teamsthat perform specialist work. The teachingsessions had three themes: porphyria,specialist endocrine and proteins. The porphyria element was delivered by Dr Mike Badminton (SAS Porphyria Service,University of Wales), the specialistendocrine by Mrs Sophie Barnes (ImperialCollege Healthcare NHS Trust) and Dr Julian Barth (Leeds Teaching HospitalNHS Trust), and proteins by Dr JoannaSheldon (Protein Reference Unit, St George's Hospital). This was an informalsession where Trainees were givenbackground information by each of theorganisers in the form of posters orhandouts. The background informationcontained all of the important points“distilled” by the experts. This informationwas used during the session and was alsointended to be used in the future as
revision notes or even teaching material.After reading through the distilled points,a selection of case studies and clinicalquestion booklets were handed out by theSAS teams. Trainees then had theopportunity to work through these casesand questions in a self-directed learningmanner, either individually orcollaboratively in small groups. The expertsfrom the SAS labs were constantlycirculating and on hand to answer anyquestions and enable all Trainees,regardless of the level of knowledge orexpertise, to benefit from the session. The final part of the session was given bythe SAS experts and was a summary of themain learning points, the key conceptsfrom each topic and the "take home"messages. This was also an additionalopportunity for any final questions to beanswered. I found this session immenselyuseful as it went over a number of topicsthat are not well covered in standardtextbooks and allowed me to gain furtherknowledge into these specialistpathologies. The session also provided me with an opportunity to get to knowthe experts in the SAS labs and made me appreciate the excellent and rewarding work that goes on in thesedepartments. �

Meeting Reports | 31
Issue 647 | June 2017 | ACB News
The ACB South West and Wessex RegionalScientific Meeting was held in conjunctionwith the Regional Annual GeneralMeeting on the 6th March 2017 at thePrincess Elizabeth Orthopaedic Centre,Royal Devon and Exeter Hospital (RD&E).The meeting was attended by delegatesfrom across the region including two STP Trainees in Clinical Biochemistry.The meeting began with a short AGM
presided over by Dr Anthea Patterson –Royal Cornwall Hospital (RCH). Dr Patterson provided feedback from thelast council meeting including theappointment of officers into the SouthWest and Wessex ACB RegionalCommittee. The Committees now includeDr Anthea Patterson as Chair, Joe Bailey(Torbay) as Secretary, Miss Anna Barton(RCH) and Dr Angie Cooper (Derriford) asJoint Meetings Secretary and Treasurer, Dr Mandy Perry (RD&E) and Oliver Robert(Derriford) as Ordinary Members. RecentlyMary Stapleton (North Devon) wasappointed as audit lead, and Kristen Lilly(Derriford) as our new Immunologistrepresentative.
Infertility
Following the short AGM, Joanne Carey,Senior Embryologist at the PeninsulaReproductive Centre Exeter, gave anengaging talk on infertility. Joanne beganby giving an overview of the commoncauses of infertility in both males andfemales, with erectile dysfunction,retrograde ejaculation and azoospermiathe common aetiology in males; and
tubular factor, primary ovarian failure,endometriosis, PCOS, and ovulatory factorrelated to age, the common causes infemales. Further detailed discussion wasprovided on the various treatment optionsincluding the use of clomiphene citrate toenhance stimulation of ovulation, and thedifferent fertility techniques such asintrauterine insemination andintracytoplasmic sperm injection. The risksassociated with different treatmentmethods including ovarianhyperstimulation syndrome, multiplebirths and the chromosomal abnormalitiesarising from forced fertilization werepresented.
Non-Invasive Prenatal Testing
This section of the talk was provided byProfessor Neil Avent of PlymouthUniversity. Professor Avent began byproviding a historical perspective of non-invasive prenatal testing including thediscovery by Dennis Lo in the 1990s thatcell free foetal DNA was present in thematernal circulation. Foetal cell free DNAaccounts for 10-15% of cell free DNApresent in the maternal circulation andoriginates from the placenta as the endproduct of apoptosis of placental tissuecells. The highlight of this presentationwas the application of foetal cell free DNAin RhD typing of foetus thereby allowingthe provision of anti-D prophylaxis to RhDnegative mothers pregnant with a RhDpositive foetus. The potential futureapplication of cell free DNA in the area ofprenatal diagnosis of trisomies using next
Conception to Birth: A Day of Fertility andScreening at ExeterDaniel Isemede, Torbay Hospital, Torquay

32 | Meeting Reports
Issue 647 | June 2017 | ACB News
generation sequencing was addressed dueto the 99% diagnostic rate for Trisomy 21using this method.
Gestational Diabetes
Following on from the exciting discussionon the clinical application of NextGeneration Sequencing as a tool in non-invasive prenatal testing was a jointpresentation on an equally exciting topicof gestational diabetes mellitus (GDM)presented by Joy Norgate and Dr BeaKnight: both specialist midwifes at theRD&E. The importance of early diagnosisof GDM was highlighted and the fact thatGDM is present in 18% of pregnancies. Ms Norgate and Dr Knight provided anoverview of current diagnostic criteria inthe UK and risk factors for GDM. Currentscreening is based on the oral glucosetolerance test (OGTT) which involves theconsumption of 75 g of glucose loadfollowing an overnight fast. However, in some hospitals Lucozade is used instead.With the sugar tax set to be introduced inthe coming future, the use of Lucozademay thus present a diagnostic dilemmastressing the need for standardisation ofOGTT.
Pre-eclampsia and BiochemicalMarkers
Following the lunch break was anengaging talk on the screening anddiagnosis of pre-eclampsia presented byProfessor Kevin Spencer, King GeorgeHospital. This session was particularlyexciting as pre-eclampsia, according toProfessor Spencer, is the most commoncomplication of pregnancy with 5-7% ofcases associated with significant foetal andmaternal morbidity. Even more exciting tonote is that pre-eclampsia tends to presentin the 2nd and 3rd trimester with evidenceof organ pathophysiology. There is a lackof validated prophylactic treatment andsuitable biomarkers for screeningpurposes. An ideal biomarker needs to
occur at an early stage when trophoblasticinvasion of the placental arteries can beengineered with treatment. Placentalgrowth factor (PLGF) is a recent biomarkerassociated with pre-eclampsia and thismarker is reduced in early, mid and latepre-eclampsia making it an ideal candidatebiomarker for screening.
Rhesus D
Dr Wayne Thomas, ConsultantHaematologist at Derriford Hospital, gavea detailed overview of the significance ofanti-D development in pregnancy. Anti-Dis highly immunogenic and in 90% ofpatients, transfusion of 1 unit of RhDpositive red cells into a RhD negativepersons will result in the formation of anti-D antibodies. Dr Thomas stressed theimportance of timely prophylactictreatment with anti-D in RhD negativemums carrying a RhD positive pregnancyas 1:6 women will form anti-D. Dr Thomasagain hinted at the significance ofprenatal testing of the foetus using cellfree DNA to determine its RhD phenotypeas this could be informative in deciding onthose needing anti-D prophylaxis.
Advances in Neonatal Diabetes
The penultimate lecture of the day wasdelivered by Dr Tim McDonald (RD&E).Neonatal diabetes occurs in three forms.50% of cases have transient neonataldiabetes mellitus (TNDM), 40% havepermanent neonatal diabetes (PNDM), and10% are syndromic. TNDM typicallypresents within the first few months of lifewith complete remission between 6-18months and reoccurs at some stage later inlife. Dr McDonald explained the specificgenetic abnormalities responsible forTNDM including the 6q24-relatedmethylation defect which occurs in 50% ofcases and a gain of function in the β-cellresponsible for the majority of the otherhalf of cases. KATP channel related TNDMresponds well to treatment with

Meeting Reports | 33
Issue 647 | June 2017 | ACB News
sulphonylurea. The take home messagefrom Dr McDonald was that neonataldiabetes presenting within the first sixmonths of life is likely to be due to amonogenetic cause as research into HLAanalysis suggested that T1DM wasuncommon before 6 months of life.
Neonatal Blood Spot Screening
Final presentation of the day wasdelivered by Dr Helena Kemp, SouthmeadHospital, Bristol. Dr Kemp gave aninteresting update on the newborn blood spot screening service and theimprovements in service delivery since the
introduction of screening for PKU in the1960s. We were reminded of theimportance of adequate sample collectionand sample quality and the financialimpact of having a repeat test due to poorsample quality or as a result ofcontamination. She also presented thefindings from a recent study whichconcluded that <20 µL of blood spot couldpotentially result in false negative with upto 30% negative bias. The day concluded well and thanks go
out to the Organising Committee: Dr Angie Cooper (Derriford) and Miss Anna Barton (RCH). �

The ACB ROI Scientific Meeting was heldon January 27th 2017 at St Vincent’sUniversity Hospital and was officiallyopened by Dr Graham Lee, ACB ROIRegion Chair, ACB Council Representativeand ACB Regional Tutor.
National Clinical Programme forPathology
Dr Mary Keogan, Clinical Lead for theNational Clinical Programme forPathology, provided the opening address.She outlined the origins of the NationalClinical Programme for Pathology and thekey achievements to date includingdefinition of the 10 Principles forLaboratory Modernisation, developmentof the National Laboratory Handbook (Vol. 1), formation of a Point of CareConsultative Group and initiation of theReference Interval Harmonisation Project.
The National Medical LaboratoryInformation System (MedLIS) project offersa unique opportunity to improve thedelivery of laboratory medicine, healthcarequality, efficiency and outcomes forpatients in the Irish healthcare system. Sheconcluded by highlighting the critical rolethat Pathology plays in the patient carepathway and the need for increasedclinical input to drive the delivery ofPathology Services.
Pathology Networks
The morning session provided attendeeswith different perspectives on PathologyNetworks; appropriately titled ‘Networks – a blessing or a curse’.Dr Cathy Street, Consultant Clinical
Biochemist, offered a unique personalinsight into Pathology Services in England.She outlined the key themes of the Carter
ACB ROI Scientific Meeting Micheál Ryan, St John’s Hospital, Limerick
34 | Meeting Reports
Issue 647 | June 2017 | ACB News
Speakers at the meeting included (from left to right) Dr Pat Twomey, Dr Chris Fourie, Dr Graham Lee, Dr Cathy Street, Dr Mike Ryan and Dr Mary Keogan

Independent Reviews (both 2005/2008)based on consolidation of Pathologyservices in England. The aim of thisconsolidation of Pathology services was toprovide improved service quality,responsiveness and cost effectiveness.She indicated how the transformation of
pathology services has moved quite slowlywith issues surrounding; differentiation of‘hot’ and ‘cold’ work, logistics between the‘hub and spoke’ laboratories,underestimation of costs associated withdevelopment/reconfiguration of PathologyNetworks, and the unrealistic models fordelivery of Pathology services which havebeen devised. These issues have impactedon staff morale within laboratories leadingto the loss of many experienced staffmembers. Dr Street also highlighted the pathology-
related concerns raised by Royal College ofPathologists in their response to LordCarter’s independent report, ‘Operationalproductivity and performance in EnglishNHS acute hospitals: UnwarrantedVariations’. The RCPath had indicated thatthe instruction to consolidate is ‘unlikelyto save money and is likely to cost more inthe long-term, put the lives and well-beingof patients at risk and increase litigation’.She questioned if the transformation ofPathology services has truly been clinicallyled and asserted that the establishment ofmanaged Pathology Networks has resultedin greater losses than gains with adiminished quality of service providing notangible benefit to patients and staff.Dr Chris Fourie, of LTS Consulting,
provided a very different perspective, as a consultant supporting consolidationand transformation of Pathology Servicesin England. LTS works with NHSImprovement for a number of Trusts andprivate Pathology service providers. LTS are supporting the NHSI to define theroadmap for Pathology through asummary of the current state of Pathologyservices and by setting a clear set of
benchmarks. He suggested that financeand clinical input can be the key enablersor constraints to service delivery withmajor opportunities in the operationalaspects of Pathology service delivery. He outlined the recipe for success in
terms of Pathology Service Consolidationwhich includes; Clinical Leadership, whichplays a key role, Executive Participation,Logistics, Integration of Technology andChange Management Support. He alsointroduced PinpointBPS which is aperformance management system thatprovides Laboratory Management withdetailed analytics and structured processdocumentation.Dr Pat Twomey, Consultant Chemical
Pathologist (in the absence of Dr DavidJames, Clinical Director, SouthwestPathology Services, SPS), provided asuccinct overview of how Pathologyservices can be delivered through a publicprivate partnership. SPS, formed in 2012, is a joint venture between Taunton andSomerset NHS Foundation Trust, YeovilDistrict Hospital NHS Foundation Trust andIntegrated Pathology Partnerships (iPP).SPS delivers full laboratory services to apopulation of 500,000 patients and over100 GP practices in Somerset. Dr Twomeyoutlined the key ingredients for asuccessful Pathology Network and the co-operation that can be achieved in apublic-private partnership.Dr Mike Ryan, Consultant Chemical
Pathologist, Northern HSC Trust,completed the session with a highlyengaging overview of PathologyNetworking in Northern Ireland and itsprogress to date. He outlined thechallenges that laboratories face such asrapid advances in technology, the changesin the QA and regulatory environment,unnecessary risks associated with variationin practice, the clinical demand for moreeffective ICT and constrained resources. He was firm in his belief that informationtechnology is the key to transforming
Meeting Reports | 35
Issue 647 | June 2017 | ACB News

Pathology services and that many of thechallenges are now drivers for themodernisation of the Pathology Service. He presented the three proposals for
modernising Pathology services inNorthern Ireland currently in the publicconsultation domain. They include;consolidation of ‘cold’ testing activity,infrastructure development in terms of IT and logistics and an integratedmanagement structure. He asserted that a‘root and branch’ change is required to theway the Pathology Service is delivered andstressed that ‘there is no right answer butthere is a wrong answer: that we do notchange!’
Screening Programme Updates
Moving away from ‘Pathology Networks’,the afternoon session was dedicated toROI Screening Programme Updates, bothin Colorectal Cancer and CongenitalHypothyroidism (CHT). Dr Diarmuid O’Donoghue, Clinical
Director of the National Colorectal CancerScreening Programme(www.bowelscreen.ie), provided an updateon the implementation of this programme,which commenced in 2013. In the ROI,bowel (colon, rectal or colorectal) cancer isthe second most common newly diagnosed
cancer among men and women. Thenumber of new cases of colorectal cancerwill increase by 79% in men and 56% inwomen by 2020. The BowelScreencolorectal screening programme will offerfree screening to men and women aged55-74 on a two-yearly cycle. To developcapacity for the entire population, theprogramme has been introduced on aphased basis, starting with men andwomen aged 60-69.Dr O’Donoghue outlined the screening
options available, in particularhighlighting the advantages of the FIT(faecal immunochemical test) over theguaiac test, including its superiordiagnostic performance for the detectionof pre-cancerous lesions. Round 1 resultsof the screening programme wereprovided, including the number of lettersof invitations sent (0.5 millionapproximately), uptake rate (40%),positive result percentage (5%),percentage of those with a positive FITthat attended for colonoscopy (93%) andif the colonoscopy was offered within 4weeks (82%). Dr O’Donoghue concludedby indicating some of the challenges thisscreening programme faces in terms ofimproving the participation rate, the need
36 | Meeting Reports
Issue 647 | June 2017 | ACB News

to expand the program to the 55-74 year-old age group and the associatedfunding required. Dr Nuala Murphy, Consultant Paediatric
Endocrinologist, provided an update onthe Newborn Screening Programme forCongenital Hypothyroidism (CHT) whichcommenced in 1979. She provided anoverview of the screening programmestructure which utilises the ‘heel-prick test’(Guthrie) method to screen for CHT andreferred to the 2014 ESPE ConsensusGuidelines which define the biochemicalcriteria used in the decision to initiatetreatment for CHT.If CHT is suspected, an appropriate
action plan for the infant is initiated,
which includes repeat TFTs, a technetiumthyroid scan and subsequent consultationwith a Consultant PaediatricEndocrinologist with the aim to commencethyroxine treatment by day 10 of life. Dr Murphy concluded her presentation byreferring to the debate surroundingoptimal TSH ‘cut-offs’ employed using the‘heel-prick test’ which differ betweennational screening programmes. Sheoutlined the potential reasons for anincrease in incidence of ‘true’ CHTincluding the use of lower TSH ‘cut-offs’,changes in ethnic populations,misclassification of transient CHT, andexposure to environmental toxins. �
Meeting Reports | 37
Issue 647 | June 2017 | ACB News

38 | Meeting Reports
Issue 647 | June 2017 | ACB News
The latest ACB Southern Region Scientificmeeting, ‘A meeting from the SASEndocrinology Group, Dedicated to thememory of Professor Roger Ekins’ wasjointly organised by the University ofWestminster with a fantastic programmearranged by Sophie Barnes and the SASEndocrinology group. The meetingincluded an interesting and movingpersonal tribute from Dr Richard Chapmanwho worked closely with Professor Ekinsthroughout his career. Richard took theaudience through this career from hispioneering work in the development ofcompetitive binding immunoassaytechniques to the development of the first‘direct’ free hormone assay, undoubtedlyshaping the use of this methodology as weknow it today.The day started with a fascinating talk
from Dr Gary Woodward who walked usthrough random forests and machinelearning with the use of a free statisticalpackage to aid in the interpretation ofurine steroid profiles, aptly entitled‘Modelling a Biochemist’s brain’. He reassured us we’re not all out of a jobjust yet but clearly demonstrated howbiochemistry, computer science andstatistics can all work together to help thelaboratory achieve new efficiencies. The focus on steroids continued with
Dr Norman Taylor showcasing the work ofhis team to produce a serum based steroidprofile by LC-MS/MS with his talk‘Multicomponent serum and urine steroid
analysis: learning afresh’. The excellentteam work in his department was evidentthroughout his talk and it was fascinatingto learn about new findings in patientswith adrenal cell carcinomas and the vitalinformation the serum steroid profile canunlock.Sophie Barnes, Chair of the SAS
Endocrinology Group, was next to speakand shared her expertise in ‘Renin activityby LC-MS/MS’. The audience welcomedreminders about the many drugs thataffect the interpretation of renin andaldosterone measurement and wereinterested to hear about the benefitsprovided by the use of LC-MS/MS tomeasure renin activity.Dr Julian Barth finished the morning
session with his talk ‘Challenges in theinterpretation of serum testosterone’ andconfirmed there are certainly many! It was a stark reminder that this ‘routine’test is confounded by many factors whichthe Clinical Biochemists in the audienceneed to consider when providinginterpretative advice. Lunch was served and offered a chance
for networking amongst colleagues andwith the representatives from thegenerous sponsors of the meeting: Abbott, Randox, Shimadzu and Waters.The Southern Region AGM was quorateand proceeded with updates from each ofthe committee members.After lunch Dr Sue Oddy gave a talk on
the ‘SAS Thyroid service – new
A Southern RegionScientific Meetingincluding a Tribute toProfessor Roger EkinsRebecca Powney, Southern Region Meetings Secretary

Meeting Reports | 39
Issue 647 | June 2017 | ACB News
developments’ as she shared someinteresting cases that demonstrated thevariety of thyroid function testinterferences including: assay interference;familial dysalbuminaemichyperthyroxinaemia; and macro-TSH. It was great to hear about the advances inthe measurement of free hormones andsee the latest equilibrium dialysis chamberfirst hand as it was passed round the room.Dr Chris Boot continued the interestingstart to the afternoon with his talk‘Copeptin (CT-proAVP) in the investigationof polyuria/polydipsia syndrome’. Chrisshared his experience of running the SASCopeptin service and the advantages ofusing this analyte to aid in the diagnosis ofdiabetes insipidus. He shared somepromising work on the use of hypertonicsaline infusion tests, which his Trust use inpreference to water deprivation testsfollowing a risk assessment of bothdynamic function tests. After a quickrefuel and networking over the afternooncoffee break Dr Gwen Wark gave her talk‘Proinsulin and C-peptide’ and shared herexpertise in the measurement of proinsulinand C-peptide and the factors to consider,
both in relation to sample stability andbetween method variability. The morerecent use of urinary C-peptide/creatinineratios was discussed and the improvementsin diagnostic performance offered. Themeeting finished with a talk from Dr DavidChurch on ‘Insulin: Assays, Analogues andAntibodies’ and some excellent work oninsulin autoimmune syndrome. He clearlydemonstrated the importance ofunderstanding the methods we use in thelaboratory and how this can have a drasticimpact on patient care. The day ended with a drinks reception,
the latest addition to the Southern Regionsocial programme, offering a greatopportunity for delegates to network andcatch up on these increasingly rareoccasions outside of the laboratory.I’d like to take this opportunity to thank
all of the local organisers and sponsors ofSouthern Region scientific meetings whohave put together some fantasticprogrammes for our members. If you areinterested in organising a meeting orwould like to know more about the role ofthe Meetings Secretary, please get in touchon [email protected] �
This month I am going to have more of anewsy style article for ACB readers ratherthan a specific theme as it has been amixed time for industry since the Aprilissue of ACB News. The most significant thing (other than
the calling of a General Election of course)was the publication of the EU IVDRegulation after a gestation period thatan elephant would be impressed by! Atone stage it even looked like it was goingto be scrapped and the process re-startedbut it was finally published on 5th May inthe Official Journal. The clock has startedticking for the 5 year transition to EU law.Eek! There is an enormous amount for usto do as an industry with uplifting ofproducts into higher risk categories(estimated as a one-off cost of £25-50,000
per test with ongoing costs for vigilance)as just one aspect of the increased burden.For you, the users of our products, therewill also be uncertainty: Will you loseaccess to some older products? (Probablymore likely to be true for virology andmicrobiology). What will be the impact onin-house manufacture? Much is unknownstill and will also rely on the outcomes onnegotiations for the dreaded Brexit (sorry,but I still keep thinking this was a baddream nearly a year later).During May there was the very upbeat
Focus meeting in Leeds followed by ourown 25th Anniversary celebrations andofficial opening of our new office byMaggie Throup, parliamentary candidatefor re-election to Erewash in Derbyshire.Maggie’s success in the 2015 election
40 | BIVDA News
Issue 647 | June 2017 | ACB News
Industry Insights: June 2017Doris-Ann Williams, Chief Executive, BIVDA
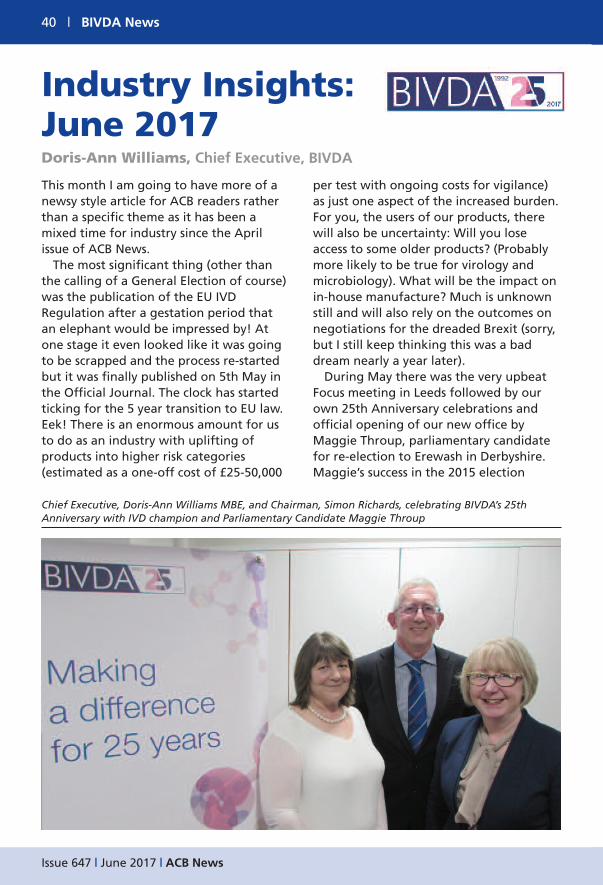
Chief Executive, Doris-Ann Williams MBE, and Chairman, Simon Richards, celebrating BIVDA’s 25thAnniversary with IVD champion and Parliamentary Candidate Maggie Throup

BIVDA News | 41
Issue 647 | June 2017 | ACB News
meant we had a real voice for IVDs inParliament and significantly on the HealthSelect Committee. Maggie also helpedensure IVDs were protected from theramifications of the Health Service MedicalSupplies (Costs) Act 2017 which gainedRoyal Assent on 27th April just prior todissolution of Parliament.Purdah has seen chaos wreaked across
events planned during May includinglosing speakers from our Spring GeneralMeeting and several other events such asthe Access track at the NICE Conferenceand the 6th UK Diagnostic Forum inOxford. BIVDA also had a parliamentaryroundtable on the implementation of CRPin primary care postponed and a LifeScience Industry APPG event on Brexit wasa casualty. (Purdah is the six week periodprior to an election which is governed byrules to prevent voting to be biased by theoutgoing Government for example, bymaking substantive announcements ofinvestments nationally or in anyconstituency).Our Spring Meeting included
presentations on the IVD Regulation; the new European Medical TechnologyIndustry code for sponsorship ofhealthcare professionals (which we areadopting from 1st January 2018); the LifeScience Industry Register (to be hosted bythe Academy of Healthcare Science) whichwill meet the needs of the NHS intraceability and professional standards forindustry interfacing with the NHS; newservices available to the IVD industry fromNICE (for a fee – jury is out on whetherthese will be affordable as the pricing isthe same as for the pharma sector); andthe final talk was from Cancer Research UKon their focus for the future and whatthey hope to see from the industrialstrategy.
The Life Sciences Industrial Strategy andAccelerated Access Review Implementationwere due to be announced at the end ofMay and have both been additionalcasualties of the election. It is likely bothwill come out as soon as possible afterJune 8th assuming the ConservativeGovernment is, or I should say as you readthis, has been re-elected! Furthercasualties, much closer to the heart ofBIVDA is the delay to the announcementof the successfully funded new NIHR MICs(MedTech & IVD Co-operatives) which arereplacing the Diagnostics Evidence Co-Operatives and Healthcare TechnologyCo-Operatives. However I have beenassured by Dr Tony Soteriou at DH thatletters have been written and a newMinister for any Government is likely to bevery keen to announce the good news asearly as he/she can in June.I was also delighted to be asked to be an
External Trustee for UK NEQAS and verymuch look forward to attending themeetings and supporting the organisation.I also became a non-Executive Director forthe Australian start-up company AtomoDiagnostics who have an innovativeplatform for lateral flow which WHO andGates Foundation both see as having animpact on care in remote developingworld locations. So the summer at BIVDA is going to be
dedicated to analysing the newGovernment and ensuring our outreach ismaximised to Ministers, re-organisingcancelled events and working with thenewly appointed MICs focussed on IVDs.We are also recruiting for a new GeneralManager and External Affairs Assistant,planning educational seminars formembers and continuing business as usual! �
42 | Obituaries
Issue 647 | June 2017 | ACB News
Professor Roger Ekins, FRS, who diedpeacefully on 26th July 2016, aged 89, willbe remembered for his pioneering work inhormone measurement by saturationanalysis and his scintillating personality. A Cambridge graduate who trained as aPhysicist, Roger spent his professional lifeas a Clinical Biochemist manqué. A meeting in his honour organised jointlyby the Association for Clinical Biochemistryand Laboratory Medicine, SupraRegionalAssay Service (SAS) Endocrinology Group,and the University of Westminster washeld in London on the 31st March thisyear. Working at the Middlesex Hospital in
London in the late 1950s Roger developeda method for measuring thyroxine inblood utilising the binding properties ofnaturally occurring thyroxine bindingglobulin. This was similar to work in theUSA by Berson and Yalow who used insulinantibodies to measure insulin. Roger calledhis technique saturation analysis; Yalowand Berson called their methodimmunoassay. Immunoassay won out andbecame a clinical biochemistry work-horseapplicable in hospital laboratories andelsewhere to almost any substance,hormone, drug, protein to which anantibody with the appropriate bindingcharacteristics can be developed. Rogernarrowly missed out on the 1977 NobelPrize for Physiology and Medicineawarded to Rosalyn Yalow, also a Physicistby training. Spurred on by a professional rivalry that
he cherished throughout his working life,Roger continued, among other things, todevelop methods for measuring hormonesand other trace substances in blood. He was one of the first to recognise the
potential provided by monoclonalantibodies for developing new methodsthat did not involve the use of radio-isotopes, for measuring hormonesand other trace substances. His work inthis field with some of the world’s leadingreagent manufacturers led to himreceiving the Edwin Ullman Award fromthe American Association of ClinicalChemists in 1998. In 1974 Roger’s laboratory was one of
only six to be recognised by theDepartment of Health as able to provide aNational rather than just local endocrineservice. It was designated a SAS Laboratoryand funded centrally. Much of Roger’s clinical work was
carried out in collaboration with clinicalendocrinologists at the Middlesex Hospital,London where he spent most of his career.As a result Roger achieved internationalstatus as an Endocrinologist and authority
Roger Ekins FRS – Pioneerfor Hormone Measurements

Obituaries | 43
Issue 647 | June 2017 | ACB News
on the physiological applications ofhormone assays. In particular, he definedthe mechanisms that underlie crucialeffects exerted by maternal hormones onthe early development of the fetal brain. In the 1980s Roger pioneered a
technology of microarrays that permitssimultaneous measurement of theconcentrations of thousands of substances,such as hormones, viruses and genes, froma drop or two of blood, leading to hisreceipt of a Prince of Wales Award forInnovation. He was elected FRS in 2001and in 2006 the Department of Healthgave him a Lifetime Achievement Award
making him the first scientist to receiveone.To those who knew him, Roger was a
kind, gentle man with an enthusiasm thatwas infectious. He was a memorableteacher not only in his own institution butothers such as the University of Surrey inGuildford where his lectures were alwayswell attended. This was not far from his country cottage in Friday Street, a delightful hamlet in the Surrey Hillswhere he and his lovely wife entertainedtheir friends and students fortunateenough to be invited. �
JH and HJ

44 | Obituaries
Issue 647 | June 2017 | ACB News
Stephen Jeffcoate, or Steve as he wasknown to colleagues, was the eldest son ofObstetrician Professor Sir NormanJeffcoate. His mother was Manx andfollowing bomb damage to the familyhome in Liverpool he spent part of the waron the Isle of Man. He went to schools inLiverpool before obtaining a First ClassHonours degree in Medical Sciences atCambridge UniversityHe completed medical studies at
St Thomas’s Hospital in London beforefocusing on a career in ClinicalBiochemistry, with a particular interest inEndocrinology. He was an acknowledgedexpert in the then emerging technique ofimmunoassay. He also developed aninterest in quality assessment andestablished an early proficiencymonitoring scheme for LH, FSH andprolactin. In 1975 he moved to ChelseaHospital for Women as Professor ofBiochemical Endocrinology.With funding from the Department of
Health and the World Health Organisationhe organised an international effort tostandardise methods of immunoassay forreproductive hormones. The work becamethe basis for a WHO Special Programmefor Research in Human Reproduction. The WHO Collaborating Centre at Chelseawas responsible for provision ofradioimmunoassay reagents to 150laboratories around the world along withan EQA scheme and courses in radio-immunoassay both in London and abroad.Steve also set up a linked programme
(Chelsea Kits) which provided reagents forLH, FSH and Prolactin to the majority of
Clinical Biochemistry laboratories in the UK during the 1980s.Whilst the WHO Centre continued its
activities for over 20 years, in 1986 Stevemoved on to become head of thehormone section of the National Institutefor Biological Standards and Control.He was a member of a WHO ExpertCommittee on Biological Standardisationand helped establish UK, EU and WHOguidelines for the standardisation ofrecombinant hormones.Steve had many and varied interests and
in 1993 he took early retirement to pursuehis interests in ecology, particularlybutterfly conservation, and long distancewalking. He was a co-author of theMillennium Atlas of Butterflies in Britainand Ireland and became Chair of thecharity Butterfly Conservation. Hecompleted several long distance walksincluding Nice to Geneva. During this timehe also helped to devise CPA standards forEQA Schemes. He had retained a fondnessfor the Isle of Man where he spent a lot oftime in his later years and served as Chairof the Manx Wildlife Trust for three years.To his colleagues, whether junior or his
peers, he provided support andencouragement along with an insightfulmind and great sense of fun. His activitiesin standardisation and quality assurancestill influence current practice in medicallaboratories. �
MD
Also see: https://www.theguardian.com/society/2017/may/02/stephen-jeffcoate-obituary
Professor Stephen Jeffcoate:A Man of Quality 6th June 1939 – 31st March 2017

Crossword | 45
Issue 647 | June 2017 | ACB News
Last month’s solution
ACB News CrosswordSet by RugosaAcross 8 Odd smidgen could provide diagnostic
information on examination (4)9 Attribute of 11/17/27/23 that is
surprising (or terrific) since withouterror (10)
10 See 1 Down11/17/27/23 Our validation predicated work is, in a
way, embodied with ado in veterinarylab science (8-5,10,8)
12 Violent fall causes impaired vision (8)14 Set out treatises about 6 signs of
distension (6)16 Condition: left back in the lurch (4)17 See 1118 Entertain a large number (4)19 Tone down bad humour (6)21 Smears – lousy laundresses no use! (8)23 See 1126 Carriage made ascent (6)27 See 1128 Uniform flush (4)
Down1 & 10 across Irate lecturer has original method of
seeking support for 11/17/27/23(10,6)
2 Never eat correctly, so weaken (8)3 No fret about aftermaths of chest condition (6)4 Locate quote verbally (4)5 Just served up some French first class
bun treats (8)6 Straight in with typical masculine
arrogance (6)7 Element of last waltz in first composition (4)13 Tries out 22 (5)15 Summarised way crab tasted (10)17 A Brit lab ordered US hypnotic (8)18 If so, dry death unlikely (8)20 Without extra time, extemporisation could
cause fatality (6)22 Attempts 13 (6)24 Distressing xeroderma but no order for
test (4)25 Ancient being interrogates roughly
without treating (4)
46 | Situations Vacant
Issue 647 | June 2017 | ACB News
To advertise your vacancy contact:ACB Administrative Office,
130-132 Tooley Street, London SE1 2TUTel: 0207 403 8001 Fax: 0207 403 8006 Email: [email protected]
Deadline: 26th of the month prior to the month of publicationTraining Posts: When applying for such posts you should ensure that appropriate supervision and training support will be
available to enable you to proceed towards HCPC registration and the FRCPath examinations. For advice, contact your Regional Tutor. The Editor reserves the right to amend or reject advertisements deemed unacceptable to the Association.
Advertising rates are available on request.