Acasereportfrom HenriMondorhospital - AFIIM · Acasereportfrom HenriMondor"hospital...
14
A case report from Henri Mondor hospital Ismahen Ben Yaacoub, Julie Mayer, Alain Luciani, Hicham Kobeiter, Alain Rahmouni, JeanFrançois Deux
Transcript of Acasereportfrom HenriMondorhospital - AFIIM · Acasereportfrom HenriMondor"hospital...

A case report fromHenri Mondor hospital
Ismahen Ben Yaacoub, Julie Mayer, AlainLuciani, Hicham Kobeiter, AlainRahmouni, Jean-‐François Deux

Mr B., 48 year-‐old
• Medical history :
– Appendicectomy
– Family history (sister) of primiJve dilatedcardiomyopathy with EF=30%
– Current smoker (15 cigarets/day)
• Experienced 2 lipothymies with transient chest pain
• AdmiYed in the emergency unit 15 days ago during thesecond event:
– Biology -‐, Electrocardiogram -‐, chest x-‐ray -‐
– No hospitalizaJon, no treatment
• Stress echocardiography scheduled

Rest TTE4 chamber view
3D SA views

Rest TTE• What do you see ?
• An intraLV tumorregarding lateral segmentHyperechogenicity Fine limitaJonsMobile Located betweentrabeculaJons
• An inferobasalhypokinesis
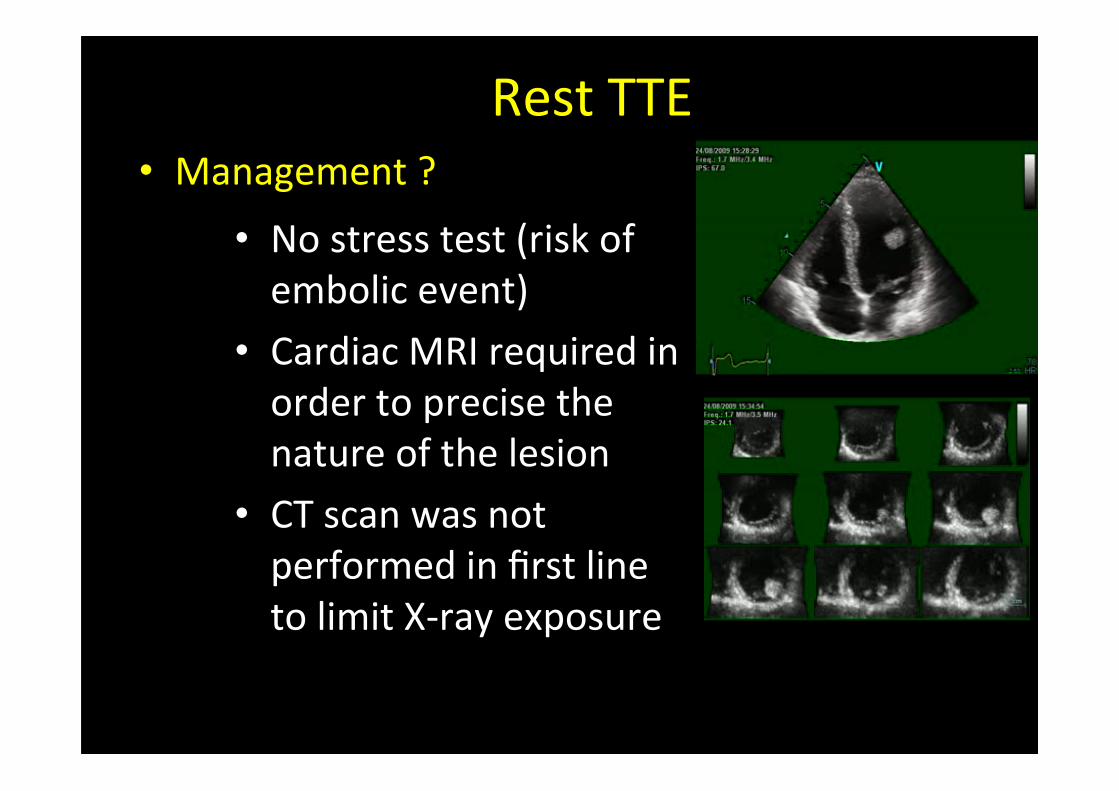
Rest TTE• Management ?
• No stress test (risk ofembolic event)
• Cardiac MRI required inorder to precise thenature of the lesion
• CT scan was notperformed in first lineto limit X-‐ray exposure

Cardiac MRI
• Cine MR (SSFP sequence)

Cardiac MRI
• What do you see ?
• An intraLV tumor:
• mobile lesion
• broad-‐based lesion
• An hykokinesis of theinferior wall

Black blood imaging
• FSE T1w • STIR T2w

Gadolinium injecJon
• Perfusion
• 3D LE
• BB T1
• PSIR

Finally…
• Intra LV tumor + inferior myocardial infarcJon
• Your diagnosis ?
• First hypothesis: it is a MI with a thrombus !• Possible but:
• Thrombus is located near necrosis andnot strictly in contact with the MI
• MRI detected an enhancement of the« thrombus » : it is possible butunfrequent, usually enhancemet isevidenced in old marginated thrombus

Second hypothesis• MR evidenced 2 disJnct lesions: a MI and acardiac tumor !
• The tumor as a bening appearance on MRexaminaJon
• Can we link these 2 diagnosis ?
• Yes, if we suppose that MI has an embolic origin
• Benin tumor + coronary embols the mostevident diagnosis is ….
CARDIAC MYXOMA

Other examinaJons
• Brain MRI:– Small high signalareas detected inthe white matersuggesJng emboliclesions
• Coronarography examinaJon:

The paJent was transferred in cardiacsurgery
• A 4 cm gelaJnous ovoid lesion was excised
• The lesion was located in the lem ventriculebetween trabeculaJons
• A pedunculated stalk was evidenced duringsurgery
• Histological analysis: cardiac myxoma

Cardiac myxoma
• Most commun primary cardiac tumor of the heart
• ≈ 5% of myxomas are located in ventricules
• Embolic phenomena: second most commun clincalmanifestaJon (30-‐40% of paJents)
• But coronary embolizaJon are rare (0.06%), morefrequent in the inferior territory (63% of cases)
• MRI:– hypo/iso intense on T1W, hyperintense on T2W– Heterogenous enhancement amer gadolinim injecJon
• Therapy: surgical excision
Grebenc et al; Radiographics 2000;20:1073-103