
ABSTRACT - IRCOBI...Stalnaker et al. (1979) and Terriere et al. (1979) analyzed force deflection...
16
ASSESSMENT OF THORACIC INJURY CRITERIA FOR SE IMPACT Shashi Kuppa, Rolf Eppinger, Matt Maltese -National Highway Traffic Saty Administration, USA Ram Naik - Conrad Technologies Inc. ABSTRACT Frank Pintar, Narayan Yoganandan - Medical Col le ofWisconsin Roger Saul, Joseph McFadden, - Vehicle Research and Test Center A series of34 side impact tests conduc ted at the Medil College ofWisconsin and at Ohio State University using post - mortem human subjects in a Heidelberg type sied, were exaned for the purpose of developing and assessing thoracic injury criteria for side impact. The ef fects of three test conditions we invest igated: test speed (24 or 32 kph), impact rce (padded or rigid), a pelvic offset (present or absent). The post-mortem human subjects were instrunted with accelerometers on the ribs and spine and ehest bands around the thorax and abdomen to characterize their mechanical response during the impact. Ld cells at the walls measured the iact force at the level of the thorax, abdomen, pelvis, and lower extremity. The resulting injuries were determined through radiography and detailed autopsy and ei r severity was coded acrding to the AIS 90 Sle. Rib actures were the most comn injury type with injury severity ranging om AIS=O to AIS=5. Chest deflections were derived by using the ehest band data to comte the ehest ntours at every millisecond during the event. The test data were analyd using stastical technies such as ANOVA, l inear reession, Jostic regression, d categorical analysis. veral existing candidates for side imct injury critia were evaluated such as Thoracic Trauma Index (TTI), Average Spinal Aeleration (ASA), ehest deflection, ehest velocity, ehest VC, peak and average contact force, st ored energy criteria (SEC) and energy storing rate criteria (ESRC) r their injury prediction abil ity. The age of the subject was found t o influence injury severity while gender and mass were und to have I ittle or no influence on injury respon. Acceleratis filtered with SAE Class 1 80 filters were tter predictors of injury than accelerations filtered with SAE class 600, < or FIRl 00 fi lters. Maxim normalized ehest deflection (dxn) was a beer predictor of rib fractures (R2=0.54, p-lue=0.0001 ) and injury severity bed on AIS (score p-value=0.000 1 , Gamma=O. 7 1 ) than any other existing injury eriteria with TTI being the next best predictor ofinjury severity based on AIS (score p-value=0.0012, Gamma=0.64). Maximum normalized resultant upper spine acceleration (rspul 80n) was the best individual predictors of injury severity based on rib actures and maxim AIS levels with a p- value=0.0001 . A model using a line combination of age, dxn, and rspul 80n was a siif icantly better predictor of rib fractures and injury based on AIS (p - value=0.000 l , Gamma=0.86). Silarly, a model using a linear combition of age and the product of dxn and rspu 1 80n was also a good predictor of injury severity (p-value=0.000 l , Gamma=0.85). KEYWORDS: side impact, injury criteria, thorax DESPITE THE IMPLEMENTATION of a federal standard r side iact in 1 990, the biomechanics community has not accepted a universal injury criterion r the thorax. The EU injury criteria utilizes the ehest deflection and VC as the side impact injury criteria while the US standards use TTI r side impact regulation. The Thoracic Trauma dex (TTI) is a ehest acceleration based asurement which was developed using data from 84 cadaver sied tests (Eppinr, 1984 , Morgan et al. , 1986). IRCOBI Co+fere+ce - Montpeer (France), September 2000 13 1
Transcript of ABSTRACT - IRCOBI...Stalnaker et al. (1979) and Terriere et al. (1979) analyzed force deflection...

ASSESSMENT OF THORACIC INJURY CRITERIA FOR SIDE IMPACT
Shashi Kuppa, Rolf Eppinger, Matt Maltese -National Highway Traffic Safety Administration, USA Ram Naik - Conrad Technologies Inc.
ABSTRACT
Frank Pintar, Narayan Yoganandan - Medical College ofWisconsin Roger Saul, Joseph McFadden, - Vehicle Research and Test Center
A series of34 side impact tests conducted at the Medical College ofWisconsin and at Ohio State University using post-mortem human subjects in a Heidelberg type sied, were exarnined for the purpose of developing and assessing thoracic injury criteria for side impact. The effects of three test conditions were investigated: test speed (24 or 32 kph), impact surface (padded or rigid), and pelvic offset (present or absent). The post-mortem human subjects were instrumented with accelerometers on the ribs and spine and ehest bands around the thorax and abdomen to characterize their mechanical response during the impact. Load cells at the walls measured the impact force at the level of the thorax, abdomen, pelvis, and lower extremity. The resulting injuries were determined through radiography and detailed autopsy and their severity was coded according to the AIS 90 Scale. Rib fractures were the most common injury type with injury severity ranging from AIS=O to AIS=5. Chest deflections were derived by using the ehest band data to compute the ehest contours at every millisecond during the event.
The test data were analyzed using statistical techniques such as ANOV A, linear regression, Jogistic regression, and categorical analysis. Several existing candidates for side impact injury criteria were evaluated such as Thoracic Trauma Index (TTI), Average Spinal Acceleration (ASA), ehest deflection, ehest velocity, ehest VC, peak and average contact force, stored energy criteria (SEC) and energy storing rate criteria (ESRC) for their injury prediction ability. The age of the subject was found to influence injury severity while gender and mass were found to have Iittle or no influence on injury response. Accelerations filtered with SAE Class 1 80 filters were better predictors of injury than accelerations filtered with SAE class 600, 60 or FIRl 00 filters. Maximum normalized ehest deflection ( dmaxn) was a better predictor of rib fractures (R2=0.54, p-value=0.000 1 ) and injury severity based on AIS (score p-value=0.000 1 , Gamma=O. 7 1 ) than any other existing injury eriteria with TTI being the next best predictor ofinjury severity based on AIS (score p-value=0.0012, Gamma=0.64). Maximum normalized resultant upper spine acceleration (rspul 80n) was the best individual predictors of injury severity based on rib fractures and maximum AIS levels with a pvalue=0.0001 . A model using a linear combination of age, dmaxn, and rspul 80n was a significantly better predictor of rib fractures and injury based on AIS (p-value=0.000 l , Gamma=0.86). Sirnilarly, a model using a linear combination of age and the product of dmaxn and rspu 1 80n was also a good predictor of injury severity (p-value=0.000 l , Gamma=0.85).
KEYWORDS: side impact, injury criteria, thorax
DESPITE THE IMPLEMENTATION of a federal standard for side impact in 1990, the biomechanics community has not accepted a universal injury criterion for the thorax. The EU injury criteria utilizes the ehest deflection and VC as the side impact injury criteria while the US standards use TTI for side impact regulation. The Thoracic Trauma Index (TTI) is a ehest acceleration based measurement which was developed using data from 84 cadaver sied tests (Eppinger, 1984, Morgan et al., 1986).
IRCOBI Co11fere11ce - Montpellier (France), September 2000 131

Stalnaker et al. ( 1 979) and Terriere et al. ( 1 979) analyzed force deflection data of the struck side half thorax in a series of cadaver lateral drop tests onto an unpadded or padded force plate. They found ehest compression to correlate better with thoracic injury than thoracic accelerations. Using the results from these studies, EU applies a threshold on maximum ehest deflection (42 mm) and maximum VC ( 1 .0) in their regulation.
Lau and Viano ( 1 986) analyzed data from 123 frontal impacts to anesthetized rabbits from which they proposed the Viscous Criterion, an injury criterion based on the product of peak ehest deformation velocity and peak normalized ehest deflection to predict thoracic soft tissue injury. Viano ( 1 989) analyzed the data from a number of cadaver impactor tests in side impact and found that the peak viscous response VCmax and peak ehest compression were better predictors of thoracic injury than acceleration based criteria.
Wang ( 1 989) performed an analytical study of the mathematical and physical properties of the viscous criterion and proposed energy concepts such as Stored Energy Cri terion (SEC) and Energy storing Rate Criterion (ESRC), Dissipated Energy Criterion (DEC), and Energy Dissipating Rate Criterion (EDRC) as candidates for thoracic injury assessment. Through mathematical manipulation, the SEC was found to be proportional to the square of ehest compression while the ESRC is proportional to the square of ehest viscous criterion
Cavanaugh et al. ( 1 993) reported the results of seventeen sied tests using the Heidelberg type sled setup with unembalmed cadavers and found that ehest compression, Viscous Criterion (VC), and Average Spine Acceleration (ASA) were more predictive of thoracic injury than acceleration and force based criteria. According to Cavanaugh, ASA is a measure of rate of change of momentum transfer and is effective in predicting the injury reducing abilities of soft padding.
Pintar et al. ( 1 997) analyzed the data from a series of twenty-six human cadaver sled tests using the Heidelberg type sied system with thorax, abdomen, and pelvic wall to better understand side impact injury tolerance. The cadavers were instrumented with accelerometers and ehest bands from which thoracic deflections were computed. The resulting injuries were mainly rib fractures with injury severity ranging from AIS=O to AIS=5. Assessment of existing injury criteria using logistic regression suggested TTI to be a better predictor of injury than ASA or maximum normalized ehest deflection (C). A new injury criteria TTI*C, a product of maximum normalized ehest deflection and TTI yielded the best statistical outcome compared to any of the existing criteria examined. This study had a !arge enough sample size, however there was not a detailed analysis of all existing injury criteria.
Chung et al. analyzed the data from limited stroke high energy impacts to six cadaveric subjects at the level of the sixth rib. This study suggested that ehest deflection and the energy generated in a lateral velocity pulse impact correlated with the number of rib fractures better than acceleration or the viscous response of the struck side rib cage. Injury criteria based on acceleration (TTI, R2=0.033) or the viscous response (VCmax, R2=0.007) did not correlate with the number ofrib fractures. Chest deflection or stored energy criteria correlated well to the number ofrib fractures. However, this was a very small sample size (6 tests) and all the oadaveric subjects had serious or severe injuries.
The current study is an extension of the Pintar ( 1 997) study. Thirty four side impact sied test data using post-mortem human subjects conducted at the Medical College of Wisconsin and Ohio State University were analyzed using various statistical analysis procedures. Existing thoracic and abdominal injury criteria such as TTI, ASA, ehest deflection, VC, Stored Energy Criteria (SEC), and Energy Storing Rate Criteria (ESRC) were cornputed for each test and the injury predictive ability of these existing criteria were evaluated for the available data. Further, using regression methods, new injury functions were developed and their injury predictive ability was assessed.
TEST METHODOLOGY
A series of 34 human cadaver tests with ehest band instrumentation was conducted to assess impact injury tolerance under side impact loading conditions (Appendix). Testing was conducted at the Medical College of Wisconsin (MCW) and at Ohio State University (OSU). A Heidelberg type side impact sied test apparatus configured for left sided impacts was utilized at both test centers. The human subjects at MCW were unembalmed fresh and frozen human cadavers while those at OSU 132 IRCOBI Conference - Montpellier (France}, September 2000

were all fresh cadavers. The cardiovascular system of the cadavers was pressurized to approximately in-vivo conditions. The pulmonary system was pressurized prior to impact and then left open to atmospheric pressure (Pintar, 1996).
Instrumentation of the eadaver included the following: triaxial aeeelerometers fixed to T 1 or T2 vertebra, T l 2 vertebra, and saerum, uniaxial aecelerometer fixed to the left lateral portion of rib 4 and rib 8 to measure medial-lateral aeeeleration and aecelerometer fixed to sternum to measure anteriorposterior acceleration. The load wall was instrumented to measure impact forees at the levels of mid thorax, abdomen, and pelvis. Both the test centers instrumented the surrogflte with two 40 ehannel ehest bands at the level of rib 4 and the 7'h rib. Side impact tests were conducted under a variety of different configurations: two different veloeities, 24 kph and 32 kph; flat rigid wall; flat wall with 1 0 cm of Ethafoam LC200 padding; and rigid or padded wall with pelvie load plate offset by 1 2 cm to represent an armrest.
Following the tests, the human subj ects were radiographed and necrop sied to delineate any trauma to the hard and soft tissues that oeeurred during the impact event. The injury severity was coded according to the AIS 90 manual (Abbreviated Injury Scale, 1990). AIS was assigned to rib fractures as follows: 1 rib fraeture: AIS 1 ; 2-3 rib fraetures: AIS 2; > 3 rib fractures on only one side of ehest: AIS 3 , > 3 rib fractures on both sides AIS 4. In each case, the presence of haemo/pneumo thorax or flail ehest increased the AIS level by 1 . A haemo'pneumo thorax was assumed when there were pleural tears caused by the fractured ribs. A flail ehest was eonsidered to be an unstable ehest wall which was determined by the individual pathologist at each test center.
Details of the test apparatus, eadaver preparation, and instrumentation are provided in Pintar et al. ( 1 996, 1997).
DATA ANALYSIS
Transducer data were processed using various filter classes and the appropriate filter classes were applied for computing existing injury criteria. The rib and spinal acceleration signals were filtered with SAE Channel Class 600, 1 80, and 60 filters, and FIRl 00 filters. Resultant upper and lower spinal aeeelerations were eomputed. The thoracie, abdominal, and pelvie force signals were filtered with SAE Class 600 and 1 80 filters. The accelerations and forces were normalized using the equal velocity-equal stress scaling procedure outlined by Eppinger et al. ( 1 984) as shown in Equation 1 .
033
acceleratiol\um = acceleration * ( mass l
75 kg) (75 k ) 0.66
forc� = force * __ g
mass (1)
where mass = mass o f subj e et in k g. stanclard mas s = 75 kg
The FIRI OO filtered peak rib 4, rib 8, and T l2 lateral aecelerations (rlu l OO, rll I OO, splIOO) and the age and mass of the subject were used to compute the Thoraeic Trauma Index (Eppinger, 1984) given by Equation 2.
1 . rrass TTI = 1.4 * age+ -(nb100+ spll00)*--2 75 kg
(2)
where ribl 00 is the rraxirrrum of (1.3 * rlul 00- 2.02) and r11100
The SAE Class 1 80 filtered Tl2 lateral aeceleration (sp l l 80) was used to compute Average Spinal Aeceleration ASA l O, ASA1 5, andASA20 as defined by Cavanaugh ( 1993). The average spinal aceelerations were normalized for age and mass using Equation 3 .
A SA = A SA * age
* mass
45 75 kg
IRCOBI Conference - Montpellier (France), September 2000
(3)
133

25% 75%
20% 80%
Figure 1: Location of ehest deflection computation along the ehest band .
Using the curvature data from each ehest band, ehest band contours were computed at every millisecond during the impact phase of the event. The origin of each contour was chosen at the point at which the band crossed the spine. Proceeding clockwise from the origin around the band, and considering the entire circumferential distance as 1 00%, distances were computed between 20% and 80% points, 25% and 75% points, and 30% and 70% points along the band (Figure 1 ) for every millisecond during the irnpact event. Chest deformation time histories between the pairs of points were calculated as the difference in the distance between the two points before impact and at every millisecond during the impact event. Therefore, 6 deflections, 3 from the top band and 3 from the bottom band, were computed The ehest deflections were filtered with SAE Oass 600 filters and differentiated to obtain rate of deformations and VC using the method recommended by SAE (Jl 733). The deflections were normalized using the original ehest width before the irnpact event at the location of deflection computation (Equation 4).
TEST RESULTS
D fl . deflection e ectlon= = -------
ehest width at time 0 (4)
Among the 34 sied tests, 1 3 were conducted at the Ohio State University (OSU) and 2 1 were conducted at the Medical College of Wisconsin (MCW). Figure 2 presents the number of tests in each test condition. Only 5 tests were conducted with the presence of pelvic offset (pelvic load wall offset by 1 2 cm to represent an armrest).
8 �---------------�
_ _ _ _ _ _ _ _ _ _ _ _ _ _ o 9.�v- •�<;w _ _ _
0 · r·_._. __ ,_,_ RHF PHF RLF PLF RHO RLO PLO
Test Condition
Figure 2: Number oftests conducted at different test centers and different test conditions. R=rigid wall, P= padded wall, H=high impact velocity (32 kph), L=low irnpact velocity (24 kph), F=flat wall, O=pelvic offset.
134 IRCOBI Co11ference - Mo11tpellier (France), September 2000

The maximum AIS injury (MAIS) for all subjects was due to the number of rib fractures and associated soft tissue injury (hemo/pneumo thorax). The mean age of the subjects in this data set was 68.5± 12 .5 years. The mean age ofsubj ects who sustained MAIS � 3 severity injury is 72±9 years while those sustaining less than MAIS=3 severity injury had an average age of 56.5±1 6 years (Figure 3). The average mass of the subject was 73±21 kg. There were 6 female subjects in the high speed tests and 2 in the low speed tests.
Among the six computed ehest deflections for each subject, the location of the maximum normalized deflection for the 34 tests was evenly distributed at the level of top and bottom band. However, the maximum normalized deflection was better correlated to the maximum normalized deflection computed at the top band (R2=0.9) than to the maximum normalized deflection computed at the bottom oond (R2=0. 7).
The majority of the subjec ts ( 19) s ustain ed maximum AIS l evel inj ury of MAIS � 4 (Figure 4 ). Eight of the 34 subjects sustained MAIS<3 injury severity and seven subjects sustained MAIS=3 injury severity. Figure 5 presents the mean number ofrib fractures along with the corresponding standard deviation for each test condition. Some subjects experienced greater than 35 rib fractures. However, a number of these fractures were deemed minor and the subject was coded to sustain AIS=4 severity thoracic injury due to rib fractures. The average number of rib fractures sustained by the subjects tested at 32 kph is 1 9± 1 1 while that for subjects tested at 24 kph is 6.5±6. There were 1 1 abdominal injuries of AIS=2 severity which all occurred in the high speed tests into a rigid or padded flat wall. In six of the high speed flat wall tests, the subject sustained AIS=2 shoulder injuries. There were 2 pelvic fractures (AIS=2) in the high speed-rigid flat wall tests and 2 pelvic fractures (AIS=2) in pelvic offset condition with rigid wall. The presence of padding bad minimal influence on injury severity while the test speed significantly influenced injury severity (Figures 3 and 5). Details of the test results are presented in the Appendix.
.-.
100 90 80
„ 70 i 60 � so
< = 48 sJ 30 � 20
10 0
� tlil��J , ;x
1 , • 1 -<
1'; 1;
RHF PHF RLF PLF RHO RLO PLO
Test Conlitim
Figure 3: Mean age and standard deviation of subjects at time of death versus test condition and injury severity. R=rigid wall, P= padded wall, H=high impactvelocity (32 kph), L=low impact velocity (25 kph), F=flat wall, O=pelvic offset.
IRCOBI Conference - Montpellier (France), September 2000 135

0 1 2 3 MAIS
4 5
Figure 4: Number of tests versus rnaximum AIS injury (MAIS) sustained by the cadaveric subject.
RHF PHF RLF PLF RHO RLO PLO Test Condition
Figure 5: Average Number ofrib fractures versus test condition.
ANALYSIS PROCEDURE
Statistical analyses were conducted using Statistical Analysis Software, SAS (SAS Institute, 1 990) and JMP (SAS Institute, 1 998). The response or dependent variable considered was the injury severity in the form of either ( 1 ) total number of rib fractures (rbfx) as a continuous variable, (2) Injury severity as a dichotomous nominal variable (cat l ) of the form MAIS<3 and MAIS>=3 , (3) Injury severity as a dichotomous nominal variable (cat2) of form MAIS<4 and MAIS>=4, (4) Injury severity as an ordinal variable (cat3) in the form MAIS<3 , MAIS=3, and MAIS>=3. The explanatory variables examined were derivatives of measured mechanical parameters such as accelerations, deflections, and forces, as weil as subject characteristics such as age, mass, and gender.
Analysis of variance and correlation analyses were conducted to identify any biases in the data and to determine the relationship between the explanatory variables such as peak and average forces, accelerations, and deflections under different test conditions and anthropometric characteristics. The normality of the distribution of the explanatory and response variables was examined using ShapiroWilk W test and from quantile normal plots (SAS Institute, 1 998). Outliers in the data were estimated using Mahalanobis distance measures. When an outlier was identified, test data was examined carefully to justify removing data from data set.
Analysis of variance was conducted to identify the characteristics of the subject (age, mass, and gender) which had significant influence on injury outcome and acted as confounders to models using mechanical parameters as explanatory variables. Then, all s ubsequent models using inj ury outcome as the response variable included the effect of the identified confounders. Initial models consisted of
136 IRCOBI Conference - Montpellier (France), September 2000

the confounding variables and individual mechanical parameters. These models helped identify mechanical parameters having no influence on injury outcome thereby reducing the number of variables for further analysis. Multivariate and discriminant analyses were then conducted using stepwise regression to identify combination of mechanical parameters along with confounders which demonstrated improved predictive ability and goodness of fit measures.
When total number of rib fractures was considered as the response variable, linear regression was conducted. The effect of high er order terrns and interaction effects were assessed for each model. The predictive ability of each model was assessed using the p-value of the F-statistics of the total model. The R2 and adjusted R2 value, which is a measure of the variance around the mean of the response variable which is explained by the model, was used in assessing the goodness of fit of the model. The higher the R2 associated with the model, the better is its predictive ability. The effect of individual parameters in the model was assessed using chi-square statistics.
When dichotomous and ordinal categories of max im um AIS level injury - MAIS ( cat 1 , cat2 or cat3) were used as the response variables, logistic regression was used. Details of the methods of using logistic regression with impact biomechanics data is detailed by Kuppa et al. ( 1 998) and Hosmer ( 1989). The goodness of fit ofthe füll model was assessed using the p-value ofthe -2*loglikelihood ratio as well as the score statistics. The lower the p-value of the model, the better is its goodness offit. The predictive ability of the model was assessed using Goodman-Kruskal which is like R2 in regression analysis, where, a Gamma value of 1 indicates perfect predictive ability while a zero indicates no predictive ability of the model. Higher val ues of Gamma indic ate better p redictive ability of the model. Details on the computation of Goodman-Kruskal Gamma are provided in Kuppa et al. ( 1998). Model building strategies outlined by Hosmer and Lemoshow (1 989) were used. The effect of higher order terms and interaction was also assessed for each model.
In some of the 34 tests, due to the unavailabil ity of certain measured mechanical data, some explanatory variables were missing. The missing data was not imputed. Instead, injury predicting models did not consider those tests which did not contain values of the explanatory variable under consideration. Therefore, the number of observations (n) is less than 34 in some models presented in Tables 1 -4.
RESULTS OF ANALYSIS
IDENTIFICATION OF OUTLIERS AND CONFOUNDERS: The Mahalanobis distance measure suggested test 3577 was an outlier because of excessive number of rib fractures ( 45). However, the maximum AIS level, MAIS, which provides a better measure of the overall consequence of the injuries was only 4 . Careful examination of the autopsy report for this test indicated that many of the rib fractures in this test were minor or hairline. Eliminating these minor fractures, the total number of observed rib fractures for this test were adjusted to 32. No other test data was considered as an outlier and no data was removed from the analysis.
The analysis of variance using age, gender, mass, test condition, and test center indicated age of the subject at the time of death had a significant influence on injury severity in the form of number of rib fractures or the categorical MAIS (p=0.005), while gender of the subjects (p=022) and mass of the subject (p=0.9) had minimal influence on injury outcome. There was no significant difference in injury outcome between the two test centers for the same test condition in terrns of mean rib fractures and mean AIS level (p-value=0.2).
ANALYSIS WITH NUMBER OF RIB FRACTURES AS RESPONSE VARIABLE: Table 1 lists some of the best models identified using linear regression with number of rib fractures as the response variable. Since age was found to have significant influence on injury outcome, it was introduced into subsequent analyses as a confounder. Regression analysis suggested that acceleration data filtered with SAE Class 1 80 filter were better predictors of rib fractures than the corresponding accelerations filtered with SAE Class 60, SAE Class 600 or FIR 100 filters. Normalized deflections and accelerations were better predictors of injury than non normalized deflections. In all cases, the interaction terms and nonlinear effects in a model did not improve the R2 and p-value significantly and so were deemed unnecessary.
The mechanical parameters which best correlated to the number of rib fractures were maximum IRCOBI Conference - Montpellier (France}, September 2000 137

normalized deflection ( drnaxn) (R2=0.54) , maximum normalized resultant upper spine acceleration (rspu 1 80n) (R2=0.56), and rnaximum normalized lower spine acceleration (spl l 80n) (R2=0.46). The injury criteria, TTI (R2=0.34), ASAlO (R2=0.32), Vmax (R2=0.3 1 ) and VCrnax (R2=0.29) were not significant predictors of the number of rib fractures for this data set. Maximum thoracic, abdominal, and pelvic force (thx_f, abd_f, and pel_f) and the corresponding rate of loading (thx_fr, abd_fr, pel_fr), energy terms (SEC, ESRC) and rate of deflection (vmax) were also poor predictors ofinjury (R2<0.25).
-c§ 200 00 =i �150 � !,.)
:e 1 0 0 .s i' � 50 §' s 0 � 20
1 1 1 1 1 1
-- - � , - s:mrx +- 1s rJ,rx-- ·:2s rbf� : ........ ... ... ......... ... , 1 1 1 1 •"" -.... 1 1 1 1 1 ... ... 1 • 1 1 1 „ - - „ - „ „ „ - - - - - • - - - - -�-- - - - - - „ - „ „ „ „ - „ „ - - - - - ... „ - - - - - ..... „ - - „ - „
1 1 - ........ 1 1
: ... ... '{. _ : 1 1 ' ' -. �-- ' ' 1 1 "' '- M 1 1 1 : : 2. � : : „ „ � � „ „ - - „ „ ; „ „ „ „ "" „ T - „ „ „ 1 - „ - - „ - i „ - - - - -y ..::..- - „ „ .,. .. „ „ - - „ -
: "'- : 3 : 1 6 13 : 12 : ... ... ...... � . � . . . '""'· ' - -. • ' ......,_,_ • • 17 l 9 """· 3315 •
0 : : � 21: : J : - - - - - - r - - - „ - - + - „ „ - - -� - -11>--- - .! - - - „o. .. � 1�11 - - -:- -
30
• 1 "'� 1 1 1 " ' � . 0 •
40
1 2 1 � 1
: 1 � 50
. . --..,_,
60 70 80 age at time of death (years)
90 1 0 0 Figure 6 : Age o f the subject versus normalized maximum upper spine resultant acceleration (rspu 1 80n) for 5 , 1 5 , and 25 rib fractures. Test data are shown on the plot as the number of rib fractures sustained by the subject in each test. R2=0.54 Model 1 2.
� 250 - .
1 1 1 1 1 1
: - s:mrx +- 1s rl>rx-- : 2s mrX Q .._ _ 1 1 1 1 1 1 1 � 200 „ - - „ „ „;„�..>-'-=..-�-... - „ - - - -:- - - - - - -:- - - - - - -:- - - - - - -:- - - - - - � - „ - - - -oft 1 -- ... - � „ ... : : : :
� 1 - ... „ � 1 1 1
: 1 : : - ... -- ... ! : : 150 - - - - - - ; - - - - - - ; - - -.- - - - - - -:- - - - - - i3lr� ·m.::.-_- - � - - - - - -� ...._____, , , 1 • o' ... _...,
:----- � � 5 : 11 : • 1 2 1 : - - ... = 100 0 1 1 1 1 0 1 9 1
-:3 - - - - - - � - - - - - -� - - - - -� -� -� - 11� - -11- i5l� - - - , - - - - - -
• � 2 . ---.· - 116 • ' � 1 1 1 1 1 � 1 t 1 1 1 1 1 --...... 1
50 - - - - - -� - - - - - -�- - - - _ _ :_ - - - - _ _ :_ - - - - - d- _1 _ _ -�- -� -� - - - -'C : : : t : : : ... � 1 1 1
e O -+---+--<----+-+------t-�: --+-� 20 30 40 50 60 70 80 90 1 0 0 age at time of death (years)
Figure 7: Age of the subject versus normalized maximum ehest deflection (dmaxn*300mm) for 5, 1 5, and 25 rib fractures. Test data are shown on the plot as the number of rib fractures sustained by the subject in each test. R2=0. 5 1 .Model 1 1 .
Stepwise regression identified the linear combination of normalized resultant upper spine acceleration filtered to SAE Class 1 80 (rspu 180n), maximum normalized deflection (drnaxn), and the confounding variable, age, tobe a very good predictor ofthe number of rib fractures (Model 1 5 : R2::::0.64, p-value =0.0001 ) . A linear combination of age and a product o f peak normalized deflection and peak norrnalized resultant upper spine acceleration (rspu 1 80n *chnaxn) also correlated well with number of rib fractures (Model 1 4 : R2=0.63, p-value=0.000 1 ) . Figures 6 and 7 display linear regression lines of maximum normalized resultant upper spine acceleration (rspul 80n, Model 12-Table 1 ) and maximum deflection ( dmaxn*chest width of a 5<Yh percentile male =300 mm, Model 1 1 -Table 1 ), respectively, versus age for 5 , 1 5 , and 25 number ofrib fractures.
138 IRCOBI Conference - Montpellier (France), September 2000

Table 1 : Linear regression results using number of rib fraetures (rbfx) as the response. S d b . . R2 f h d 1 orte >y mereasmg o t e mo e .
No. model
1 5 .3 5+0. 1 4asa l 5n
2 - 1 4. 82+0.35age+5 .98vcmax
3 - 1 7 „49+0.36age+0.56vmax
4 - 1 0.2+0 . l 3ttin
5 2 .38+0.23*asa l On
6 -20.96+0.33 age+O. l 5spl l 80n
7 -30.94+0.43age+0.28rspu 1 OOn
8 2 .5+0.59asa 1 On*dmaxn
9 -5.22+0.264ttin*dmaxn
1 0 - l 2.26+0. l 8age+O. l rblu l 80n
1 1 -37.56+0.32age+7 6.46dmaxn
1 2 -2 7.43+0.37age+0.23rspu 1 80n
1 3 -22.5+0.27age+O. l 7rspu l 80n+0.04rlu l 80n
1 4 -23.91 +0.35*age+0.50*rsp u 1 80n* dmaxn
15 -37.45++0.35age+45.3dmaxn+0.15rspu180n
where: dmaxn: maximum normalized ehest defleetion
n p-value of Ri Adj. R 2 F-stat
3 3 0.0024 0.26 1 2 0 . 2374
34 0 . 0045 0 . 2939 0.2484
34 0.002 1 0.3274 0.284
33 0.0004 0.34 1 3 0 .3201
33 0.0002 0.3565 0 .3358
33 0.0001 0.4583 0.4222
34 0.0001 0.46 5 1 0.4306
33 0.0001 0.4765 0.4596
3 3 0.000 1 0.4883 0.47 1 8
3 2 0.000 1 0.4896 0.4544
34 0.0001 0.5395 0.5098
3 4 0.0001 0.5624 0.5342
32 0.000 1 0.6032 0.5606
34 0.0001 0.6329 0.6092
34 0.0001 0.6389 0.6028
spu180n: maximum normalized lateral upper spine aeeeleration (SAE Class 1 80 filter) rspul80n: maximum normalized resultant upper spine aeeeleration (SAE Class 1 80 filter) rspulOOn: maximum normalized resultant upper spine aeeeleration (FIR 1 00 filter) spl180n: maximum normalized lateral lower spine acceleration (SAE Class 1 80 filter) rblu180n: maximum normalized lateral upper rib aeeeleration (SAE Class 180 filter) asalO: asa l O (Cavanaugh, 1 993) normalized as in Equation 3 . asa15: asa 1 5 (Cavanaugh, 1 993) normalized as i n Equation 3 . tti: defined in Equation 2 vmax: maximum rate of ehest deflection vcmax: maximum VC
ANALYSIS USING CATEGORIES OF MAXIMUM AIS LEVELS: Since the response variables catl and cat2 are eategorical, and eat3 is ordinal, logistic regression was used. The analyses using maximum AIS level ( MAIS) categorized as (1) cat l : MAIS<3 and MAIS � 3 are presented in Table 2 . The results using cat2: ( MAIS<4 and MAIS�4) and eat3 : (MAIS<3, MAIS=3 and MAIS>3) as response variables are very similar to those using catl and are presented in Table 3 and 4. Tables 2-4 provide the basic results of each model. The probability of injury (P) is obtained using Equation 5 . The definitions of the independent variables used in the model are provided in Table 1 .
P = 1 �-logit) , where logit is ofform a + l:: bixi + e (5)
The trends observed in the logistic regression models were similar to those in the linear regression analysis with number of rib fractures as the response. Again, because the age of the subjeet at the time of death was determined to be a significant confomder, it was included as an explanatory variable in all the subsequent models. Normalized deflections and aecelerations were better predictors of injury than the non normalized deflections. Maximum values of deflection, forces, and accelerations were better predictors of injury than average values. ASA 1 0 was a better predictor of injury than ASA 15 or ASA20. TTI (score p=0.0016) was a signifieantly better predictor of injury than ASA l O (score p=0.01 5). The best individual predictors of injury were maximum normalized deflection ( dmaxn) ( score p=0.0005) and normalized resultant upper spine acceleration filtered at SAE Class 1 80 (rspu 1 80n) (seore p=0.0003). For injuries greater than AIS=3, dmaxn (p=0.000 1 ) was IRCOBI Co11ference - Montpellier (France), September 2000 139

a better predictor of injury than rspu l 80n (p=0.0005). The best predictors of injury were a linear combination of age, dmaxn, and rspu 1 80n (score p-value=0.000 1 , Gamma=0.858) and a linear combinationof age and rspu 1 80n*dmaxn (score p-value=0.0001, Gamma=0.847).
Interaction effects and higher order nonlinear terms were found not to influence injury response significantly. The results with nominal and ordinal response variables suggest that response can be well characterized by a linear combination of explanatory variables obtained from logistic regression.
The probability o f AIS�4 thoracic injury versus the linear combination of maximum normalized ehest deflection (dmaxn), and maximum normalized resultant upper spine acceleration (rspu 1 80n) of Model 1 2 in Table 4 for a 30, 45, and 60 year old subject is presented in Figure 8 .
Table 2: Logistic Regression Results Using c atl : (MAIS<3 and M AIS�3) as the response Sorted by increasing Goodman-Kruskall Gamma value of the model.
No. Logit of Model n -2logLR score P- Gamma Value
1 - 1 . 0 1 7+0.048asa 1 5 3 3 6 . 1 42 0.05 0.508
2 -2. 1 96+0.09 l asa 1 0 3 3 9 .594 0.0 1 56 0 .6 1 3 -8 .58+0. 1 1 age+0.037spl l 80n 3 3 1 2.873 0.0025 0 .75
4 -9 .66+0 .066TTI 3 3 14 .86 0.00 1 6 0 .8
5 - 1 0 . 1 +O. l 2age+0.03 rblu l 80n 3 2 1 7 .043 0.0009 0 .833 6 -4. 1 2+0.089*TTl*dm axn 3 3 1 4.447 0.00 1 1 0.84
7 - 1 5.36+0. 1 8age+0.083spu l 80n 34 1 8 .4 1 0.0007 0.865
8 - 1 4.91+0.14age+l 9.75dmaxn 34 1 7.59 0.0005 0.865
9 - l 6.57+0. l 8age+0. 1 1 rspu 1 OOn 34 1 9.45 0.0003 0.875
1 0 - 1 7 . 54+0. 1 9age+0.069rspu 1 80n+0.02 l rb l u 1 80n 34 2 1 .093 0.00 1 2 0.896
1 1 - 1 5.67+0 . 1 8age+0.084rspu1 80n 34 20.2 0.0003 0.904
1 2 -l 7.1 3+0.18age+8.S l d m a x n+0.06 1 rspu 1 80n 34 20.98 0.0006 0.913
13 -15. l 9+0. I 88age+O.l 86 * dmax n * rspu I 80n 34 2 1 . 1 2 0.0003 0.923
The definitions of the variables used in the models are provided in Table 1 .
Table 3: Logistic regression results using cat2: ( MAIS<4 and MAIS �4) as the response Sorted by increasing Goodman-Kruskall Gamma value of the model.
No. Logit of Model n -2logLR score P- Gamma Value
1 - l .02+0.02asa 1 5 3 3 3 .2 3 0.0886 0.544
2 -5. 705+0.053age+0.028spl 1 80n 3 3 8 .505 0.0225 0 .55
3 -5 .2 1 2+0.04 1 9age+O.O 1 89rblu 1 80n 3 2 9 .0 1 0.0 1 94 0.578
4 - 1 . 9 l 7+0.044asa 1 0 3 3 6.724 0.0 1 69 0 .58 1
5 - 5 .03 1 3 +0 . 028TTI 3 3 8.867 0.0056 0.647
6 - 1 1 .66+0 . 1 age+0.08 8rspu 1 OOn 34 1 4.08 0.0037 0.655
7 - 1 0.073+0 .09age+0.067spu 1 80n 34 1 4.85 0.0026 0.66
8 - 1 2.34+0. l Oage+0.082rspu l 80n 34 1 9.84 0.0005 0.778
9 -7 .23+0. 1 1 *TTl*dmaxn 3 3 20 .61 0.000 1 0.805
10 -1 9.96+0.08age+3 8.88dmaxn 34 24.42 0.0001 0.854
1 1 - 1 9.492+0.1 65age+0.323 * d maxn * rspu 1 8 0n 34 27.59 0.0001 0.875
1 2 -41 .29+0.20age+49.9 1 d m a x n+0. 1 24rspu1 80n 34 32.309 0.0001 0.931
140 IRCOBI Conference - Montpellier (France), September 2000

Table 4: Logistie regression results using eat3: (MAIS<3, MAIS=3, and MAIS>3) as the response. S d b . . G od Krusk 11 G 1 f h d 1 orte >Y mereasmg 0 man- a amma va ue o t e mo e .
No.
1 2 3 4 5 6
7 8 9
1 0 1 1
1 2
Logit ofModel fo r MAIS 4+
- 1 . 1 1 7+0.02 1 asa 1 5 -2. l 488+0.049asa 1 0 -7 . 64+0.08age+0.028sp l 1 80n -5 .969+0. 0 3 3TTI -7. 7+0.0729age+0 .0208rblu l 80n - 1 3 .86+0. 1 3age+0.094rspu 1 OOn
- 1 1 .98+0. l I age+0.068spu 1 80n -16.51 3+0. l l age+ 24.66dmaxn -6. 1 +0.089*TTI*dmaxn - 1 3 . 77+0.12a2e+0.079rspul 80n
- 1 5.66+0.148age+0.22 * dmaxn * rspu 180n - 1 9.97+0.137a2e+ l 7 .96dmaxn+0.057rspu 1 80n
�0.8 ·� -
' - - - - - - - - - - - - - - - ·:;sö ·;e-� - - - -
:old
n -21ogLR score P-
Value 3 3 4. 1 1 7 0.0461 33 8.567 0.0077 33 1 2.953 0.0049 3 3 1 2.681 0.00 1 2 32 1 5 .42 1 0.0023 34 2 1 .4 1 7 0.0005
34 2 1 .0 1 4 0 . 0005 34 26.587 0.0001 3 3 22.923 0.0001 34 26.429 0.0001 34 3 2 . 6 1 9 0.0001 34 32.698 0.0001
� 0.6 „ - - „ - - - - - - - - „ - - -:- - - - „ „ ... - „ - - „ - - � - - „ - „ "'o1a. „ „ „ „ „ „ „ � < � 0.4 =
,/:J. e 0.2 �
' '
0 --1--�---=:;;..-..-:�-====��--i�����--1 s 10 IS 20
l i .96dmaxnf-0.0Si rspul80n
Gamma
0.305 0.53 0.57
0 .637 0.642 0.675
0 . 7 1 0.761 0.762 0.778 0.847 0.858
Figure 8: Probabi lity of AIS �4 thoraeie injury for a 30 year, 45 year and 60 year old subject as a funetion of maximum normalized defleetion ( dmaxn) and maximum normalized resultant upper spine aeeeleration (rspu l 80n) from Model 1 2 of Table 4.
= 1 8 0 .....--�����������������----. S --'-,
: AIS 3 t: -..... AI� 4+
s 160 � - - - - - -· - - - - - - - - � - - - - - - - - � - - - - - - - � - - - - - - - - · - - - - - - - - � - - - - - - -
0 (f'l „ 140 � � 120 -
20
• 1 1 1 1 1
30
1 1 1 1 1 : „ „ „ „ „ „ „ -� „ „ „ „ „ „ -�J- „ ... „ „ „ ... „ l .. ""4„ „ „ � „ -� a„ ... „ „ „ ... 1 1 � 1 1 't 1
40 50
1 1 4 1
' 4 ' 4 ' - - - �- - - - - �- - � -�4- - - - -�- - - - - - -' 0 : 4 � 3 ! - - - - - - - - � - -4 - - - -
8 :
60 70 80 90 age at time of death (years)
Figure 9: Lines of 30% prob ability of AIS� 3 and AIS� 4 thoraeie injury as a funetion of age of the subject and maximum ehest defleetion (normalized ehest defleetion * ehest width of a 501h pereentile male=300 mm) (Model 8, Table 4). The maximum AIS injury of the test data points are also presented in the figure. IRCOBI Conference - Montpellier (France), September 2000 141

lli 60 Cl) Cl::: s 40 EI 20 :z::
� 0 -+--+�-+---�-+---�-+---�-+---�-t---�-t-_,_---1 � 20 30 40 50 60 70 80 90
age at time of death (years)
Figure 10: Lines of 30% prob ability of AIS� 3 and 4 thoracie injury as a function of age of the subjects and maximum normalized resultant upper spine aeeeleration (Model 1 0, Table 4). The maximum AIS of the test data points are also presented in the figure.
The 30% probability of AIS � 3 and AIS�4 thoracie injury lines as a funetion of maximum ehest defleetion (dmaxn*300) and age ofthe subjeet (Model 8 of Table 4) are presented in Figure 9. The 30% prob ability of AIS � 3 and AIS �4 thoracie injury as a function of maximum normalized resultant upper spine acceleration (rspu I 80n) and age of the subjeet (Model 1 0 of Table 4) are presented in Figure 1 0 . The 30% probabi lity of AIS � 4 thoraeic injury lines for a 30, 45, and 60 year old as a linear eombination of dmaxn*300 and rspu l 80n (Model 1 2 of Table 4) are presented in Figure 1 1 . The sample data has an average subjeet age of 68.5 years, with rspul 80n ranging between 20-120 g's (Figure 1 0) and dmaxn*300 ranging between 50- 1 5 0 mm (Figure 9). Within this range of data it was found that the hyperbolie funetion of Model 1 1 in Table 4 is almost linear and is similar to the 30% probability of injury lines presented in Figure 1 1 .
i 250 ,,...... = = � 200 � � 150 r:: � ... � 100 - - - -öl'd' - - � - - - - - - - - - � - - - - - - - - - -:- -� : 45 year !;i : old
� 50 +----+---�+----+-�---;�---� � � � � 100 1�
nonn. upper spine accel (rspul80n) Figure 1 1 : 30% prob ability of AIS�4 thoraeie injury for a 30, 45, and 60 year old as a funetion of maximum ehest deflection and maximum normalized resultant upper spine aceeleration (Model 1 2, Table 4). DISCUSSION
A detailed statistieal analysis was eonducted using data from 34 side impact sied tests to evaluate and develop injury eriteria. Thoracic and abdominal soft tissue injury was minimal and was also assoeiated with low AIS levels. The maximum AIS was determined by the number of rib fractures and associated soft tissue injury (pneumothorax) due to rib fraetures. Analyses were conducted using the number of rib fraetures as well as the categorical maximum AIS levels. The variable "number of rib
142 IRCOBI Conference - Montpellier (France), September 2000

fractures" (rbfx) used in this data set included all observed rib fractures but does not distinguish between severe fraetures ( eompound or displaeed rib fractures) from the minor fractures (hairline, simple, or ineomplete fractures ). In some tests a number of the rib fractures noted were hairline fractures which would have minor if no injury consequence. On the other hand, the reported MAIS levels in the data set provided a good estimate of the overall severity of the injuries sustained by the subject, which even included associated soft tissue injury. Therefore, the results using logistie regression models using MAIS categories may pertain roore to the severity of injury (i.e. threat-to-life) than the linear regression rib fracture models which are a more mechanistie outcome deseriptor.
In this data set, the age of the subjeet at the time of death had signifieant influence on the injury severity while gender of the subjeet did not influenee injury severity. The non-signifieanee of gender may be assoeiated with the small sample size of the female subjects (8 females) in this data set. Since this data set has very few soft tissue injuries, it is reasonable that injury eriteria such as VC, whieh are particularly developed as soft tissue injury criteria, were not significant predictors of injury. The proeedure for VC computation is plagued with amplifieation of measurement errors due to the differentiation of deflections. This may also contribute to the non-signifieanee of VC as an injury predictor.
The ehest defleetions were computed from ehest bands wrapped extemally around the body. Therefore the eomputed deflections include the deformation of the skin and flesh as weil as the ribs. The analysis in this paper only considers total deflection whieh includes the deformation of the flesh and skin. In order to obtain the rib deflections, which may be a roore appropriate injury predietors than total deflection, a portion of the skin and flesh thiekness may have to be subtraeted from the total defleetions. The eomputed ehest defleetions are the ehest deflections along the total width of the thorax as shown in Figure 1 . However, the side impaet dummies measure only half thorax ehest defleetions. Therefore, in order to apply the developed injury eriteria on the dumrnies, either the ehest defleetions would need to be adjusted to represent half thorax deflections or the dummies be modified to measure füll thorax defleetions.
Maximum normalized ehest deflection ( dmaxn) was found tobe a better predictor of injury than any other existing injury eriteria with TTI being the next best predictor of injury severity based on AIS. A 30% probability of AIS � 4 injury is associated with TTI= 1 5 5 and an ASA1 0=27 which are similar results as that reported by Morgan ( 1 986) and Cavanaugh ( 1 993). The model using the product of TTI and maximum normalized deflection (dmaxn) was a reasonably good predictor of injury (Gamma=0.76, p-value=0.0001) as was noted by Pintar et al. ( 1 996).
The model using a linear combination of age, and the product of maximum normalized defleetion and resultant normalized upper spine acceleration, dmaxn*rspu1 80n, (Model 1 1 , Table 4) was as good a predictor of injury as the model using a linear combination of age, dmaxn, and rspu 1 80n (Model 12, Table 4) . This is because within the range of data, the hyperbolie function of the produet of rspu 1 80n and dmaxn in Model 1 1 is approximately linear and sirni.lar to the linear function of Model 1 2 . This data set exhibited mainly linear behavior between the response and explanatory variables. There was no signifieance of nonlinear effects or interaction terms and so were not included in any of the injury predictor models.
The model using a linear eombination of age, maximum normalized resultant upper spine acceleration (rspu 1 80n), and normalized deflection ( dmaxn) was the best predictor of thoraeic injury (p=0.000 1 , Gamma=0.858) among all those exarnined. This result is similar to that observed in analysis of frontal impact sied tests (Kuppa et al., 1 998). For a 45 year old, 50'h pereentile male oeeupant, a ehest deflection of 1 30 mm and a resultant upper spine acceleration of 90 g' s is associated with a 30% probability of AIS�3 injury.
FUTURE RESEARCH
Though this data set is signifieantly !arger than previous research efforts where ehest defleetions were measured, a !arger data set could obviously offer better insights and predictive relationships. Therefore, future research will concentrate on increasing the number of observations in the data set. Changes to eadaveric subject preparation are also being investigated in order to make the frequency and severity of soft tissue injuries more in line with field observations. Efforts will also be made to
IRCOBI Co11ference - Montpellier (France), September 2000 I 43
combine the sled test data from Wayne State University (Cavanaugh, 1 993) and the previous Heidelberg tests (Morgan, 1 986). Application of the developed injury criteria to side impact test dummies will also be examined.
REFERENCES
Cavanaugh, J. M „ et al„ "Injury and Response ofthe Thorax in Side Impact Cadaveric Tests ," ThirtySeventh Stapp Car Crash Conference, SAE Paper No. 933 1 27, 1 993, pp 1 99-222.
Chung, J„ et al„ "Thoracic Injury Mechanisms and Biomechanical Responses in Lateral Velocity Pulse Impacts," Forty-Third Stapp Car Crash Conference, SAE Paper No. 99SC04, 1 999, pp. 39-54.
Eppinger, R. H„ Marcus, J. H„ Morgan, R. M„ " Developrnent of Dummy and Injury Index for NHTSA's Thoracic Side Impact Protection Research Program," SAE Paper No. 840885, Government/Industry Meeting and Exposition, Washington D.C„ 1 984.
Hosmer, D. W„ and Lemeshow, S„ (1 989) Applied Logistic Regression, John Wiley and Sons. Kuppa, S„ Eppinger, R„ "Development of an Improved Thoracic Injury Criterion," Proceedings of the Forty-Second Stapp Car Crash Conference, SAE Paper No. 983153, 1 998, pp. 1 39-1 54.
Lau I. V„ Viano, D.C„ "The Viscous Criterion -Bases and Applications of an Injury Severity Index for Soft Tissues," Proceedings of the Thirtieth Stapp Car Crash Conference, SAE Paper No. 861882, 1986, pp. 1 23- 142.
Morgan, R. M„ Marcus, J. H , and Eppinger, R. H „ ''Side Impact - the Biofidelity of NHTSA's Proposed ATD ad Efficacy of TTI," SAE Paper No. 86 1 877, Thirtieth Stapp Car Crash Conference, 1986.
Pintar, F. A„ et al„ "Instnnnentation of Human Surrogates for Side Impact," Fortieth Stapp Car Crash Conference, SAE Paper No. 96241 2, 1996.
Pintar, F .A„ et al„ "Chest Band Analysis of Human Tolerance of Side Impact," Forty-First Stapp Car Crash Conference, SAE Paper No. 973320, 1 997.
SAS/ST AT Users Guide, Volume 2, Version 6, 41h Edition, The SAS Institute Inc„ Cary, NC, 1990.
JMP Statistics and Graphics Guide, Version 3, First Edition, The SAS Institute lnc„ Cary, NC, 1995.
Stalnaker, R L„et al„ "Modification of Part 572 Dummy for Lateral Impact According to Biomechanical Data," Proceedings of the Twenty-Third Stapp Car Crash Conference, SAE Paper No. 79 1 03 1 , 1 979, pp. 843-872.
Terriere, C„ et al„ "Synthesis of Human Tolerances Obtained from Lateral Impact Simulations," Seventh International Conference on Experimental Safety Vehicles, 1 979,pp. 359-373.
Wang, J. T„ "Analytical Studies of lnjury Criteria for the Thorax," Journal of Biomechanical Engineering, Vol. 1 1 1 , 1 989.
144 IRCOBI Conference - Montpellier (France), September 2000

;;; � g � � � II> 1 � ::: 'S � �· ... � ;:i ::: � � C-:i � � �
� 1-...>
�
�
�
....
"'"
CJI
AP
PE
ND
IX:
Su
mm
ary
of
Tes
t D
ata
Te
st n
o.
sex
a
ge
ma
ss
MA
IS
rbfx
ts
tcfn
th
x
f ab
d
f p
el
f th
x
fr a
bd
fr
p
el
fr d
ma
xn
v
ma
x
vc
ma
x
yrs
k
g
N
N
N
N/m
s N
/ms
N/m
s m
im
m/s
312
0
M
73
8
9
4
15
RL
F
55
34
19
19
34
51
24
4
55
3
26
0
.47
7
35
.1
312
2
M
27
7
2
0
0
RL
F
68
53
19
63
8
613
5
27
13
02
4
91
0.3
64
12
.2
31
55
M
55
7
6
3 1
1
RL
F
48
66
5
22
7
32
57
5
94
4
35
2
90
0
.39
4
7.3
32
76
M
7
0
71
0
0
PL
F
34
85
19
14
56
12
147
17
5 3
90
0
.17
6
5.2
32
77
M
5
6
64
2
2
P
LF
14
94
0
162
5
49
45
5
09
7
0
56
6
0.3
00
4
.4
32
78
M
5
0
93
2
3
PH
F
129
81
31
12
6
84
1 5
28
16
5 3
66
0
.29
9
16.8
33
20
F
8
2
74
4
3
3
PH
F
57
74
3
414
8
49
0
20
1 15
6
70
1 0
.47
7
11.
0
33
21
F
75
4
2
4
25
P
HF
6
100
3
70
7
84
24
14
7
93
3
94
0
.43
7
9.2
33
22
M
7
3 7
2
4
12
RH
F
42
55
9
62
9
99
50
4
31
113
4
45
39
0
.48
4
26
.1
33
23
F
5
9
81
4
21
PH
F
85
89
4
33
2
86
58
3
03
2
30
9
49
0
.45
8
9.2
33
24
M
7
7
75
4
3
4
RH
F
95
58
5
80
9
172
30
5
16
132
0
190
0
0.4
90
2
2.2
33
25
M
6
3
61
4
16
RH
F
84
32
3
89
3
158
87
9
19
87
7
23
07
0
.32
5
19.9
34
22
M
4
4
83
2
3
RH
F
160
97
3
32
8 9
74
5
1318
2
62
7
31
0.3
95
10.9
34
23
M
4
9
62
4
5
RH
F
69
58
3
25
3
172
29
2
89
3
03
3
44
9
0.4
10
9.7
M
78
8
8
4
13
RL
O
36
50
4
86
10
66
4
155
5
79
9
17
0.3
59
8
.3
M
84
7
6
4
15
RL
O
38
79
5
51
143
08
4
98
3
47
16
40
0
.33
5
6.9
M
79
9
3
3 12
R
HO
4
36
0
1914
2
06
32
3
66
13
81
210
1 0
.312
7
.2
M
74
7
7
5 2
2
RH
F
72
97
2
03
6
179
28
9
77
3
24
3
25
8
0.4
12
11.
8
F
74
5
2
4
45
R
HF
7
615
4
63
9
129
69
2
91
38
9
110
4
0.4
03
1
5.6
F
73
5
1 4
2
9
RH
F
92
16
56
75
2
66
89
3
54
2
35
1 1
105
6
0.3
97
14
.9
M
98
4
13
R
HF
1
110
9
45
46
17
09
2
59
3
177
2
66
61
0.3
26
13
.2
M
56
3
16
PH
F
68
60
4
07
5
103
78
18
7
11
8
59
3
0.2
58
6
.2
F
45
4
9
P
HF
6
913
4
70
0
102
91
176
13
6
63
1 0
.37
5
12.2
M
4
30
R
HF
10
38
6
49
69
16
417
4
94
3
45
4
03
1 0
.45
8
16.4
M
4
20
P
HF
4
77
6
22
94
6
09
7
218
15
6
67
3
0.4
23
7
.8
M
4
17
PH
F
78
94
3
73
2
84
88
3
72
1
54
6
22
0
.417
9
.3
M
10
PL
F
412
1 2
25
3
513
7
99
6
5
38
0
0.4
09
6
.7
M
11
P
HF
7
48
0
34
95
8
65
7
31
1
181
50
0
0.4
12
8
.8
M
4
PL
O
34
43
7
17
90
48
14
9
46
2
48
6
0.1
91
4.1
M
PL
O
30
35
6
15
74
09
16
8 18
9
37
1 0
.27
0
4.6
F
PL
F
36
89
2
181
78
35
8
7
57
6
34
0
.318
6
.6
F
RL
F
49
57
2
98
1 5
73
3
22
7
44
3 8
70
0
.37
4
9.2
M
RL
F
57
27
2
45
4
88
38
3
84
18
96
7
41
0.3
64
6
.7
M
PL
F
412
5
196
9
79
08
14
4
134
9
41
0.3
05
6
.2
test
con
figu
ratio
n:--
R=r
igid
, P=p
addi
ng, H
=32
kph
im�
ct, L
=24
kph
impa
ct, O=
offs
et w
all,
F=fla
t wal
l rb
fx:
num
ber o
f rib
frac
ture
s; th
x_f:
max
. tho
racic
forc
e; a
bd
_f:
max
. abd
omin
al fo
rce;
pel
_f:
max
. pel
vic
forc
e;
thx_
fr:
max
. rat
e of
thor
acic
load
ing;
abd
_fr
: m
ax. r
ate
ofab
dom
inal
load
ing;
pel
_fr
: m
ax. r
ate
ofpe
lvic
load
ing;
m/s
8.9
2.1
1.9
0.5
0.9
1. 1
3.2
3.1
5.1
2.8
3.2
3.1
2.2
2.1
1.4
1.4
1.2
2.6
2.3
3.1
2.2
0.8
1.6
2.8
2.0
2.6
1.5
2.1
0.4
0.9
1.3
2.2
1. 7
1.2
TT
I
188
85
160
154
125
153
170
191
27
5
156
25
5
213
158
172
188
20
2
23
2
215
212
30
0
156
183
24
7
25
4
210
142
170
129
116
153
164
195
155
dm
ax
n: m
axim
um n
onnaliz
ed d
efle
ctio
n; v
max
: m
axim
um e
hest
vel
ocity
; vcm
ax:
max
imum
ches
t VC
; TT
I: th
orac
ic tr
aum
a in
dex;
- """
0\ ;;; � g <§, � � 1 � ::: �
"" ::::: �- -;;; § (')
� c..:i � � c:::- � N
� �
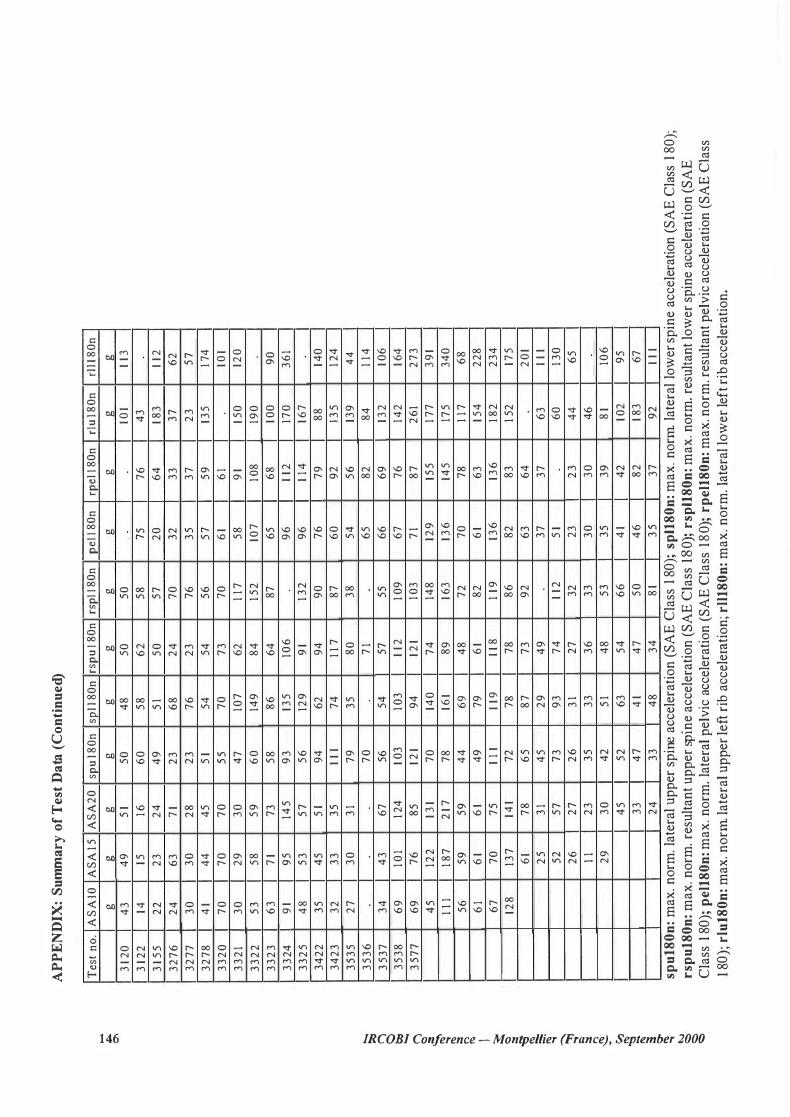
AP
PE
ND
IX:
Summ
ary
of
Tes
t D
ata (
Co
nti
nu
ed)
Tes
t n
o.
AS
AIO
A
SA
15
AS
A2
0
spu
l80
n
spl l
80
n
rsp
u l
80
n
rsp
l l 8
0n
p
ell
80
n
rpe
l l 8
0n
rl
u 1
80
n
rll1
80
n
g
g
g
g
g
g
g
g
g
g
g
312
0
43
4
9
51
5
0
48
5
0
50
10
1 1
13
312
2
14
15
16
60
5
8
62
5
8
75
7
6
43
315
5 2
2
23
2
4
49
5
1 5
0
57
2
0
64
18
3 1
12
32
76
2
4
63
7
1 2
3
68
2
4
70
3
2
33
3
7
62
32
77
3
0
30
2
8
23
7
6
23
7
6
35
3
7
23
5
7
32
78
4
1 4
4
45
5
1
54
5
4
56
5
7
59
13
5
174
33
20
7
0
70
7
0
55
7
0
73
7
0
61
61
101
33
21
30
2
9
30
4
7
107
6
2
117
5
8
91
150
12
0
33
22
5
3
58
5
9
60
14
9
84
15
2
107
10
8 19
0
33
23
6
3
71
73
5
8
86
6
4
87
6
5 6
8
100
9
0
33
24
91
95
14
5
93
13
5
106
9
6
112
17
0
36
1
33
25
4
8
53
5
7
56
12
9
91
132
9
6
114
16
7
34
22
3
5
45
5
1
94
6
2
94
9
0
76
7
9
88
14
0
34
23
3
2
33
3
5
11
1
74
1
17
8
7
60
9
2
1 35
12
4
35
35
2
7
30
3
1 7
9
35
8
0
38
5
4
56
13
9
44
35
36
7
0
71
65
8
2
84
1
14
35
37
3
4
43
6
7
56
54
5
7
55
6
6
69
13
2
106
35
38
6
9
101
124
10
3 10
3 1
12
109
6
7
76
14
2
164
35
77
6
9
76
8
5
121
94
12
1 10
3 7
1 8
7
26
1 2
73
45
12
2
131
70
14
0
74
14
8
129
15
5
177
3
91
11
1
187
2
17
78
16
1 8
9
163
136
14
5
175
3
40
56
5
9
59
4
4
69
4
8
72
7
0
78
1
17
68
61
61
61
49
7
9
61
82
6
1 6
3
154
2
28
67
7
0
75
1
11
1
19
11
8
119
13
6
136
18
2
23
4
128
13
7
141
72
7
8
78
8
6
82
8
3
15
2
175
61
78
6
5
87
7
3
92
6
3
64
2
01
25
3
1 4
5
29
4
9
37
3
7
63
1
11
52
5
7
73
9
3
74
1
12
51
6
0
130
26
2
7
26
3
1 2
7
32
2
3
23
4
4
65
11
2
3
35
3
3
36
3
3
30
3
0
46
29
3
0
42
5
1 4
8
53
3
5
39
8
1 10
6
45
5
2
63
54
6
6
41
42
10
2
95
33
4
7
41
47
5
0
46
8
2
183
67
24
3
3
48
3
4
81
35
3
7
92
1
11
spu
180
n: m
ax. n
orm
. late
ral u
pper
spine
acce
lerat
ion
(SA
E Cl
ass 1
80);
spl1
80
n: m
ax. n
orm
late
ral l
ower
spin
e acc
elera
tion
(SA
E Cl
ass 1
80);
rsp
u18
0n
: max
. nor
m. r
esul
tant
uppe
r spin
e acc
elera
tion
(SA
E Cl
ass 1
80);
rsp
l18
0n
: max
. nor
m. r
esul
tant
low
er sp
ine a
ccele
ratio
n (SA
E Cl
ass 1
80);
pel
180
n: m
ax. n
orm
. late
ral p
elvic
acce
lerat
ion
(SA
E Cl
ass 1
80);
rpel
180
n: m
ax. n
orm
. res
ulta
nt pe
lvic
acce
lerat
ion
(SA
E Cl
ass
180)
; rlu
l80
n: m
ax. n
orm
late
ral u
pper
left
rib ac
celer
atio
n; rl
l18
0n
: max
. nor
m. la
tera
l low
er le
ft rib
acce
lerat
ion.


















