Abnormalities in cord blood mononuclear cytokine production as a predictor of later atopic disease...
4
EDITORIAL Abnormalities in cord blood mononuclear cytokine production as a predictor of later atopic disease in childhood The escalating prevalence of atopic disease over recent decades [1–6], with associated spiralling social and eco- nomic costs [7–10], has emphasized the urgent need for action which will avert or reverse this trend. Of particular interest is the growing need for the development of primary prevention strategies. Essential to this approach is a clear understanding of the immunological processes in early life which promote TH2-polarized atopic sensitization. Envir- onmental factors implicated in this process, including changes in patterns of childhood infection [11–14], allergen exposure, and dietary intake [15], are currently being addressed. A means of identifying children at risk is important for targeted prevention. Currently the most reli- able way of predicting allergy is atopic heredity, but with the rising disease prevalence, the risk is still substantial for previously unaffected families. For many years there has been a search for a reliable marker for allergy prediction. Although elevated cord blood IgE (CB-IgE) is associated with the development of atopy, asthma [16–18], and ele- vated IgE at 5 years [18], after more than 20 years of research [19–21], it is now widely accepted that CB-IgE is of less value than a positive family history in predicting allergy, and is not of value as a screening test [22]. The paper by Kondo et al. in this issue reports the first long-term prospective study of clinical symptoms in child- ren in relation to capacity to generate IFNg responses at birth [23], and provides tantalizing hints of another possible prognostic marker, i.e. peri-natal T-cell function. Current developments in this area of research started in 1992, when this same group were the first to document allergen-specific proliferative responses in cord blood [24], an observation which promoted a surge of interest in cellular immune responses during the neonatal period. The findings from this and other research in this area have altered current concepts of initial allergen sensitization, which is now generally accepted to begin in utero. In this context, recent work by our own group confirms definitively (by microsatellite genotyping), that these allergen-specific responses by cord blood mononuclear cells (CBMC), noted previously as positive lymphoproliferation by many groups [24–28] are due to allergen-specific fetal T cells, as opposed to maternally-derived contaminants [29]. This work by our group shows that virtually all neonates display TH2-skewed allergen-specific responses at birth [29,30]. In the early post-natal period these TH2 responses are quickly restricted [30,31] by maturing TH1 immunity (a process know as immune deviation) and by 5 years of age normal patterns of TH1 immunity appear established in non-atopic individuals [32]. The central question is: why does this process fail in atopic individuals? There has been accumulating evidence of immaturity in aspects of immune function in atopic children, starting with an earlier report by our group that IFNg responses are defective in T-cell clones isolated from ‘high risk’ infants (with atopic heredity), compared with low risk infants [33]. It is now clear that while many immune functions are normally less mature at birth, these maturational deficien- cies may be more marked in individuals who go on to develop atopy. A large number of studies [25,30,34–37] have documented defective polyclonal IFNg responses by CBMCs from neonates either at risk of atopy, or those who later develop disease. Based on current data from many of the groups cited above, Fig. 1 shows a hypothetical model for the post-natal maturation of polyclonal IFNg responses. Although all neonates have reduced capacity for mitogen stimulated IFNg responses [38–41], this appears more marked in atopic individuals at birth, as discussed above [25,30,34– 37]. In normal non-atopic infants, IFNg responses to mitogenic polyclonal stimulation gradually increase over the first year of life, but at 2 years are still well below adult levels [38]. By 4–5 years of age most normal children have polyclonal IFNg responses approaching adult levels [38]. In contrast, infants with atopic heredity show a more delayed increase in IFNg responses in the early post- natal period, with the capacity for IFNg remaining sig- nificantly reduced compared with low risk children [33]. During this period, responses to vaccine antigen are also weaker in infants with higher serum IgE levels [42]. It is likely that the IFNg responses during this period are important for normal post-natal immune deviation of fetal TH2 responses. Clearly, these observed defects in TH1 immune responses provide a very attractive explana- tion for the persistence of the fetal TH2 responses [30] seen during childhood in association with atopic disease. Other work by our group has shown that the first 2 years of life is a critical period for the development of T helper memory patterns [31,43]. Targeting these TH1 defects in atopic individuals during this early period may provide potential for disease prevention. The developmental patterns of allergen-specific memory are less clear. Very few studies have examined 1313 q 1998 Blackwell Science Ltd Clinical and Experimental Allergy, 1998, Volume 28, pages 1313–1316
Transcript of Abnormalities in cord blood mononuclear cytokine production as a predictor of later atopic disease...

EDITORIAL
Abnormalities in cord blood mononuclear cytokine productionas a predictor of later atopic disease in childhood
The escalating prevalence of atopic disease over recentdecades [1–6], with associated spiralling social and eco-nomic costs [7–10], has emphasized the urgent need foraction which will avert or reverse this trend. Of particularinterest is the growing need for the development of primaryprevention strategies. Essential to this approach is a clearunderstanding of the immunological processes in early lifewhich promote TH2-polarized atopic sensitization. Envir-onmental factors implicated in this process, includingchanges in patterns of childhood infection [11–14], allergenexposure, and dietary intake [15], are currently beingaddressed. A means of identifying children at risk isimportant for targeted prevention. Currently the most reli-able way of predicting allergy is atopic heredity, but withthe rising disease prevalence, the risk is still substantial forpreviously unaffected families. For many years there hasbeen a search for a reliable marker for allergy prediction.Although elevated cord blood IgE (CB-IgE) is associatedwith the development of atopy, asthma [16–18], and ele-vated IgE at 5 years [18], after more than 20 years ofresearch [19–21], it is now widely accepted that CB-IgE isof less value than a positive family history in predictingallergy, and is not of value as a screening test [22].
The paper by Kondoet al. in this issue reports the firstlong-term prospective study of clinical symptoms in child-ren in relation to capacity to generate IFNg responses atbirth [23], and provides tantalizing hints of another possibleprognostic marker, i.e. peri-natal T-cell function. Currentdevelopments in this area of research started in 1992, whenthis same group were the first to document allergen-specificproliferative responses in cord blood [24], an observationwhich promoted a surge of interest in cellular immuneresponses during the neonatal period. The findings fromthis and other research in this area have altered currentconcepts of initial allergen sensitization, which is nowgenerally accepted to beginin utero. In this context,recent work by our own group confirms definitively (bymicrosatellite genotyping), that these allergen-specificresponses by cord blood mononuclear cells (CBMC),noted previously as positive lymphoproliferation by manygroups [24–28] are due to allergen-specific fetal T cells, asopposed to maternally-derived contaminants [29]. Thiswork by our group shows that virtually all neonates displayTH2-skewed allergen-specific responses at birth [29,30]. Inthe early post-natal period these TH2 responses are quicklyrestricted [30,31] by maturing TH1 immunity (a process
know as immune deviation) and by 5 years of age normalpatterns of TH1 immunity appear established in non-atopicindividuals [32]. The central question is: why does thisprocess fail in atopic individuals?
There has been accumulating evidence of immaturity inaspects of immune function in atopic children, starting withan earlier report by our group that IFNg responses aredefective in T-cell clones isolated from ‘high risk’ infants(with atopic heredity), compared with low risk infants [33].It is now clear that while many immune functions arenormally less mature at birth, these maturational deficien-cies may be more marked in individuals who go on todevelop atopy. A large number of studies [25,30,34–37]have documented defective polyclonal IFNg responses byCBMCs from neonates either at risk of atopy, or those wholater develop disease.
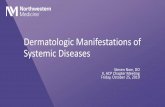
Based on current data from many of the groups citedabove, Fig. 1 shows a hypothetical model for the post-natalmaturation of polyclonal IFNg responses. Although allneonates have reduced capacity for mitogen stimulatedIFNg responses [38–41], this appears more marked inatopic individuals at birth, as discussed above [25,30,34–37]. In normal non-atopic infants, IFNg responses tomitogenic polyclonal stimulation gradually increase overthe first year of life, but at 2 years are still well below adultlevels [38]. By 4–5 years of age most normal children havepolyclonal IFNg responses approaching adult levels [38].In contrast, infants with atopic heredity show a moredelayed increase in IFNg responses in the early post-natal period, with the capacity for IFNg remaining sig-nificantly reduced compared with low risk children [33].During this period, responses to vaccine antigen are alsoweaker in infants with higher serum IgE levels [42]. It islikely that the IFNg responses during this period areimportant for normal post-natal immune deviation offetal TH2 responses. Clearly, these observed defects inTH1 immune responses provide a very attractive explana-tion for the persistence of the fetal TH2 responses [30] seenduring childhood in association with atopic disease. Otherwork by our group has shown that the first 2 years of life isa critical period for the development of T helper memorypatterns [31,43]. Targeting these TH1 defects in atopicindividuals during this early period may provide potentialfor disease prevention.
The developmental patterns of allergen-specificmemory are less clear. Very few studies have examined
1313q 1998 Blackwell Science Ltd
Clinical and Experimental Allergy,1998, Volume 28, pages 1313–1316

allergen-specific responses at birth. One small study [25]suggested that low IFNg responses to allergen (bLG) byCBMCs was associated with atopic eczema at 1 year of age.In their present study Kondoet al. [23] document the firstlong-term follow-up (to 6 years of age) on children who hadpreviously had their cord blood cytokine responses ana-lysed. In contrast with the many previous studies of cordblood IFNg, this study measured allergen-stimulatedresponses rather than mitogen-induced responses. Theydemonstrate that low level CBMC IFNg responses to foodallergens are associated with atopic disease at 6 years, andalso with higher cord blood IgE levels. These findings areconsistent with the discussion above.
Clearly, all of these observations are fuelling speculationthat cord blood cytokine responses may represent a markerfor identification of children who are likely to developatopy. Currently this is unfortunately not the case. Whilethere is little doubt from the cited literature that impairedcapacity for neonatal cytokine production (particularlyIFNg) correlates consistently with the development ofatopy in small population studies, this is, as yet, of novalue in predicting atopy at an individual level. It isimportant to stress that, in this context, these cytokinemeasurements are largely experimental, with no currentdiagnostic application. As such, there are no standardizedmethods for detection. Different laboratories use widelyvarying culture conditions; with differences in stimulationmethods, allergens, cell numbers, culture media, culture
durations and methods of detection. There are no ‘normal’values forin vitro cytokine responses, which do not conformto a gaussian distribution, usually show a wide variationbetween individuals, and may be affected by other peri-natalfactors such as trauma and sepsis. The problems with usingsuch measures for prediction in individuals are obvious.Given this, the consistency of the observed deficiencies inIFNg responses by ‘at risk’ neonates is quite remarkable andobviously indicates a very significant underlying geneticdefect. While these observations do not bring us muchcloser to predicting accurately individual atopy, researchin this area remains very important, and has considerablyenhanced current understanding of the kinetics of immuneresponses during the early life period, in both atopic andnon-atopic children.
Thus, the combined efforts of the many groups studyingearly life cytokine responses, have been central to develop-ing a clearer picture of the disease mechanisms which areinitiated during this period. This area of research now needsto extend to examine immunological effects of potentialenvironmental influences, and how these interact withunderlying genetic factors, with a view to interventionbefore persistent TH2 immunity is established. There is anurgent need for more precise data on the nature of the IFNg
defect, which appears an increasingly likely target for earlyintervention and disease prevention. Increasingly, it isbecoming clear that this will only be possible throughcollaborative efforts.
1314 S. L. Prescott and P. G. Holt
q 1998 Blackwell Science Ltd,Clinical and Experimental Allergy, 28, 1313–1316
Fig. 1. Post-natal maturation of polyclonalIFNg responses in atopic and non-atopicinfants.

References
1 Peat J, van den Berg R, Green Wet al.Changing prevalence ofasthma in Australian school children. Br Med J 1994;308:1591–6.
2 Ninan T, Russell G. Respiratory symptoms and atopy inAberdeen school children: evidence from two surveys 25years apart. Br Med J 1992; 304:873–5.
3 Nakagomi T, Itaya H, Tominaga T, Yamaki M, Hisamatsu S,Nagagomi O. Is atopy increasing? Lancet 1994 343.
4 Shaw R, Crane J, O’Donnell T, Porteous L, Coleman E.Increasing asthma prevalence in a rural New Zealand adoles-cent population 1975–89. Arch Dis Child 1990; 65:1319–23.
5 Manfreda J, Becker A, Wang P, –Z, Roos L, Anthonisen N.Trends in physician diagnosed asthma prevalence in Manitobabetween 1980 and 1990. Chest 1992; 103:151–7.
6 von Mutius E, Weiland S, Fritzsch C, Duhme H, Keil U.Increasing prevalence of hayfever and atopy in Leipzig, EastGermany. Lancet 1998; in press.
7 Weiss K, Gergen P, Hodgson T. An economic evaluation ofasthma in the United States. N Engl J Med 1992; 326:862–6.
8 Lenny W. The burden of pediatric asthma. Pediatric Pulmonol1997; 15:13–6.
9 Krahn M, Berka C, Langlois P, Detsky A. Direct and indirectcosts of asthma in Canada. CMAJ 1996; 154:821–31.
10 Smith D, Malone D, Lawson K, Okamoto L, Battista C,Saunders W. A national estimate of the economic costs ofasthma. Am J Resp Crit Care Med 1997; 156:787–93.
11 Martinez FD, Stern DA, Wright AL, Taussig LM, Halonen M.Association of non-wheezing lower respiratory tract illnessesin early life with persistently diminished serum IgE levels.Group Health Med Associates Thorax 1995; 50:1067–72.
12 Magnussen H, Jorres R, Nowak D. Effect of air pollution on theprevalence of asthma and allergy: lessons from the Germanunification. Thorax 1993; 48:879–81.
13 Mutius E, Martinez F, Fritzsch C, Nicolai T, Roell G, ThiemannH. Prevalence of asthma and atopy in two areas of West andEast Germany. Am J Respir Crit Care Med 1994; 149:358–64.
14 Bjorksten B. Risk factors in early childhood for the develop-ment of atopic diseases. Allergy 1994; 49:400–7.
15 Weiss S. Diet as a risk factor for asthma. New York: Wiley1997.
16 Croner S, Kjellman NIM. Development of atopic disease inrelation to family history and cord blood IgE levels. Elevenyear follow–up in 1654 children. Pediatr Allergy Immunol1990; 1:14–20.
17 Kjellman N, –I, Croner S. Cord blood IgE determination forallergic prediction – a follow–up to seven years of age in 1651children. Ann Allergy 1984; 53:167–71.
18 Hansen LG, Halken S, Host A, Møller K, Østerballe O.Prediction of allergy from family history and cord blood IgElevels. Pediatr Allergy Immunol 1993; 4:34–40.
19 Kjellman N–I, Johansson S. IgE and atopic allergy in new-borns and infants with a family history of atopic disease. ActaPaedt Scand 1976; 65:601–7.
20 Michel FB, Bousquet J, Greillier P, Robinet–Levy M,Coulomb Y. Comparison of cord blood immunoglobulin E
concentrations and maternal allergy for the prediction ofatopic diseases in infancy. J Allergy Clin Immunol 1980;65:422–30.
21 Magnusson C. Maternal smoking influences cord serum IgEand IgD levels and increases the risk for subsequent infantallergy. J Allergy Clin Immunol 1986; 78:898–904.
22 Kjellman NIM. IgE in neonates is not suitable for generalallergy risk screening. Pediatr Allergy Immunol 1994; 5:1–4.
23 Kondo N, Kobayashi Y, Shinoda S, Takenaka R, Teramoto T,Fukao T, Matsui E, Kasahara K, Yokoyama Y. Reducedinterferon gamma production by antigen stimulated cordblood mononuclear cells as a risk factor of allergic disorders.Clin Exp Allergy 1998; 28:1340–4.
24 Kondo N, Kobayashi Y, Shinoda S, Kasahara K, Kameyama T,Iwasa S, Orii T. Cord blood lymphocyte responses to foodantigens for the prediction of allergic disorders. Arch Dis Child1992; 67:1003–7.
25 Warner JA, Miles EA, Jones AC, Quint DJ, Colwell BM,Warner JO. Is deficiency of interferon gamma production byallergen triggered cord blood cells a predictor of atopiceczema? Clin Exp Allergy 1994; 24:423–30.
26 Piccinni MP, Mecacci F, Sampognaro S, Manetti R, ParronchiP, Maggi E, Romagnani S. Aeroallergen sensitization canoccur during fetal life. Int Arch Allergy Immunol 1993;102:301–3.
27 Piastra M, Stabile A, Fioravanti G, Castagnola M, Pani G, RiaF. Cord blood mononuclear cell responsiveness to beta–lacto-globulin: T–cell activity in ‘atopy prone’ and ‘non–atopy–prone’ newborns. Int Arch Allergy Immunol 1994; 104:358–65.
28 Miles EA, Warner JA, Jones AC, Colwell BM, Bryant TN,Warner JO. Peripheral blood mononuclear cell proliferativeresponses in the first year of life in babies born to atopicparents. Clin Exp Allergy 1996; 26:780–8.
29 Prescott S, Macaubas C, Holt B, Smallacombe T, Loh R, Sly P,Holt P. Transplacental priming of the human immune system toenvironmental allergens: universal skewing of initial T–cellresponses towards Th–2 cytokine profile. J Immunol 1998;160:4730–7.
30 Prescott S, Macaubas C, Smallacombe T, Holt B, Sly P, Loh R,Holt P. Reciprocal age-related patterns of allergen specific T–cell immunity in normal versus atopic infants. EuropeanRespiratory Rev 1998; in press.
31 Yabuhara A, Macaubas C, Prescott SLJ, Venaille TJ, Holt B,Habre W, Sly PD, Holt PG. Th–2–polarised immunologicalmemory to inhalant allergens in atopics is established duringinfancy andearly childhood. Clin Exp Allergy1997; 27:1261–9.
32 Macaubas C, Prescott S, Smallacombe T, Yabuhara A,Venaille T, Holt B, Sly P, Holt P. Peri-natal and early child-hood cytokine responses to environmental allergens. NewYork: Marcel Dekker Inc. In press.
33 Holt PG, Clough JB, Holt BJ, Baron–Hay MJ, Rose AH,Robinson BWS, Thomas WR. Genetic ‘risk’ for atopy isassociated with delayed post-natal maturation of T cell com-petence. Clin Exp Allergy 1992; 22:1093–9.
34 Rinas U, Horneff G, Wahn V. Interferong production by cordblood mononuclear cells is reduced in newborns with a family
CBMCs as predictors of atopic disease1315
q 1998 Blackwell Science Ltd,Clinical and Experimental Allergy, 28, 1313–1316

history of atopic disease and is independent from cord bloodIgE levels. Pediatr allergy Immunol 1993; 4:60–4.
35 Tang MLK, Kemp AS, Thorburn J, Hill D. Reduced interferongamma secretion in neonates and subsequent atopy. Lancet1994; 344:983–5.
36 Liao S, Liao T, Chiang B, Huang M, Chen C, Chou C, Hsieh K.Decreased production of IFNg and decreased production ofIL–6 by cord blood mononuclear cells of newborns with a highrisk of allergy. Clin Exp Allergy 1996; 26:397–405.
37 Martinez F, Stern D, Wright A, Holberg C, Taussig L, HalonenM. Association of interleukin–2 and interferon–g productionby blood mononuclear cells in infancy with parental allergyskin tests and with subsequent development of atopy. J AllergyClin Immunol 1995; 96:652–60.
38 Miyawaki T, Seki H, Taga K, Sato H, Taniguchi N. Dissociatedproduction of interleukin–2 and immune (gamma) interferonby phytohaemaglutinin stimulated lymphocytes in healthyinfants. Clin Exp Immunol 1985; 59:505–11.
39 Wilson CB, Westall J, Johnston L, Lewis DB, Dower SK,Alpert AR. Decreased production of interferon gamma byhuman neonatal cells – intrinsic and regulatory deficiencies.J Clin Invest 1986; 77:860–7.
40 Wakasugi N, Virelizer J. Defective interferon gamma produc-tion in the human neonate I Dysregulation rather than intrinsicabnormality. J Immunol 1985; 134:167–76.
41 Lewis DB, Larsen A, Wilson CB. Reduced interferon gammamRNA levels in human neonates – evidence for an intrinsic T–cell deficiency independent of other genes involved in T–cellactivation. J Exp Med 1986.
42 Prescott S, Holt P. Serum IgE levels are higher in infants withreduced lymphoproliferative responses to tetanus vaccination.Lancet 1998; 351:1489.
43 Prescott S, Macaubas C, Yabuhara A, Venaille T, Holt B,Habre W, Loh R, Sly P, Holt P. Developing patterns of T cellmemory to environmental allergens in the first two years of life.Int Arch Allergy Immunol 1997; 113:75–9.
S. L. PRESCOTT
P. G. HOLT
TVW Telethon Institute for Child Health ResearchPO Box 855
West Perth 6872Australia
1316 S. L. Prescott and P. G. Holt
q 1998 Blackwell Science Ltd,Clinical and Experimental Allergy, 28, 1313–1316