
ABMP Scar Tissue Management Part 1
8
ABMP Scar Tissue Management: Part 1-Introduction ©2020, Associated Bodywork & Massage Professionals 1 SCAR TISSUE MANAGEMENT Part 1: Introduction with Nancy Keeney Smith and Cathy Ryan SCAR TISSUE MANAGEMENT SERIES Part 1 Part 2 Part 3 Clinical Considerations • Edema • Techniques: Lymphatic system • Fibrosis • Techniques: Fascia and connective tissue Assessment and Treatment Guidelines • Assessment and evaluation • Stages of wound healing • Treatment protocols: Lymphatic system • Treatment protocols: Fascia and connective tissue Introduction • MT role in scar tissue management • Fascia and connective tissue • Lymphatic system • Wound healing: Normal and abnormal Course Outline ❶ Introduction ❷ MT role in scar tissue management ❸ Fascia and connective tissue ❹ Lymphatic system ❺ Wound healing and scar formation: Normal and abnormal SCAR TISSUE MANAGEMENT Part 1: Introduction What is the issue? What needs to change? How can our hands facilitate the needed changes? Richard Lebert, RMT The RMT Education Project www.rmtedu.com Course Outline ❶ Introduction ❷ MT role in scar tissue management ❸ Fascia and connective tissue ❹ Lymphatic system ❺ Wound healing and scar formation: Normal and abnormal SCAR TISSUE MANAGEMENT Part 1: Introduction 1 2 3 4 5 6
Transcript of ABMP Scar Tissue Management Part 1

ABMP Scar Tissue Management: Part 1-Introduction
©2020, Associated Bodywork & Massage Professionals 1
SCAR TISSUE
MANAGEMENT
Part 1: Introduction
with Nancy Keeney Smithand Cathy Ryan
SCAR TISSUEMANAGEMENT SERIES
Part 1 Part 2 Part 3
Clinical Considerations
• Edema
• Techniques: Lymphatic system
• Fibrosis
• Techniques:Fascia and connective tissue
Assessment and Treatment Guidelines
• Assessment and evaluation
• Stages of wound healing
• Treatment protocols:Lymphatic system
• Treatment protocols:Fascia and connective tissue
Introduction
• MT role in scar tissue management
• Fascia and connective tissue
• Lymphatic system
• Wound healing: Normal and abnormal
Course Outline
❶ Introduction
❷ MT role in scar tissue management
❸ Fascia and connective tissue
❹ Lymphatic system
❺ Wound healing and scar formation:
Normal and abnormal
SCAR TISSUE
MANAGEMENT
Part 1: Introduction
What is the issue?
What needs to change?
How can our hands facilitate the needed changes?
Richard Lebert, RMT
The RMT Education Project
www.rmtedu.com
Course Outline
❶ Introduction
❷ MT role in scar tissue management
❸ Fascia and connective tissue
❹ Lymphatic system
❺ Wound healing and scar formation:
Normal and abnormal
SCAR TISSUE
MANAGEMENT
Part 1: Introduction
1 2
3 4
5 6

ABMP Scar Tissue Management: Part 1-Introduction
©2020, Associated Bodywork & Massage Professionals 2
Fascia and Connective Tissue (CT)
Dense and Loose
Fiber and Fluid
Fluid-filled space observable
only in living/hydrated tissue
GC Guimberteau – Interior Architecture, Handspring 2015
SLIDING NETWORKLOOSE CT
Fluid-filled space observable
only in living/hydrated tissue
• Capable of viscosity changes
• Volume and viscosity have a role in:
• Reducing friction
• Creating space (fluid gap) between articulating tissues and structures
• Sliding
GC Guimberteau – Interior Architecture, Handspring 2015
SLIDING NETWORKLOOSE CT
Organization and distribution of intramuscular connective tissue in normal and immobilized sketch muscles. Jarvinen, T et. Al, V(2002). Journal of Muscle Research and Cell Motility 23: 245-254
A B
Superficial Fascia • Provides a passageway for
larger nerves, blood, and lymphatic vessels
Deep Fascia • Creates muscle containers
(epi, peri, endomysium)
• Comprises dense and loose connective tissue
From “Scar Tissue Management,” Smith & Ryan 2016, Handspring Publishing
www.handspringpublishing.com
7 8
9 10
11 12

ABMP Scar Tissue Management: Part 1-Introduction
©2020, Associated Bodywork & Massage Professionals 3
Course Outline
❶ Introduction
❷ MT role in scar tissue management
❸ Fascia and connective tissue
❹ Lymphatic system
❺ Wound healing and scar formation:
Normal and abnormal
SCAR TISSUE
MANAGEMENT
Part 1: Introduction • The lymph system plays a vital role in inflammation
management. Lymphatic dysfunction may contribute to
the development of pathophysiological scars.
• Excess swelling/edema creates a tensional pull on tissue.
Increased mechanical tension drives collagen deposition.
Inflammation
• 1,000 plus nodes
• One-way system
• Cleanses fluid
• Collects information
Lymph Nodes
University of Virginia discovery of lymph vessels
in the brain
Glymphatic system
60% active while we sleep
Lymph System Discoveries
Conference2015 Joint Conference on Acupuncture, Oncology, and Fascia
PresentationLymphatics and Cancer Biology
PresenterMelody A. Swartz, PhDWilliam B. Ogden Professor, Institute of Molecular Engineering, University of Chicago, Illinois
Video Links
https://oshercenter.org/joint-conference-2015-video-presentations/
https://www.youtube.com/watch?v=01bGsu3H4Y8&t=499s
• Lymph fluid is rich with information
• The lymph system is hardy
• Inflammation issues are showing signs
of autoimmune issues (research coming)
Lymphatics and Cancer Biology
Dr. Melody Swartz
13 14
15 16
17 18
ABMP Scar Tissue Management: Part 1-Introduction
©2020, Associated Bodywork & Massage Professionals 4
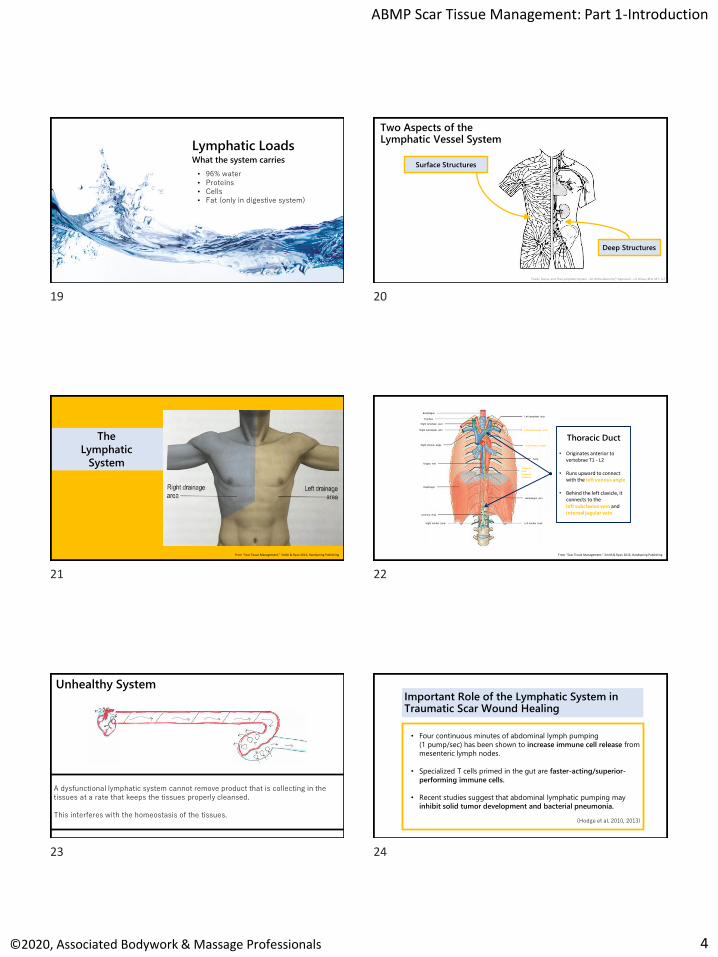
What the system carries
Lymphatic Loads
• 96% water• Proteins• Cells• Fat (only in digestive system)
Two Aspects of the Lymphatic Vessel System
Surface Structures
Deep Structures
Fluids, Fascia, and The Lymphatic System - An Ortho-Bionomy® Approach - Liz Olivas, BFA, MT, CLT
The
Lymphatic
System
From “Scar Tissue Management,” Smith & Ryan 2016, Handspring Publishing
2
Thoracic Duct
• Originates anterior to vertebrae T1 - L2
• Runs upward to connect with the left venous angle
• Behind the left clavicle, it connects to the left subclavian vein and internal jugular vein
Esophagus
Trachea
Right lymphatic duct
Right subclavian vein
Right venous angle
Azygos vein
Diaphragm
Cisterna chyli
Right lumbar trunk
Left lymphatic duct
Left subclavian vein
Left venous angle
Aorta
Thoracic
duct
(thoracic
portion)
Hemiazgos vein
Left lumbar trunk
From “Scar Tissue Management,” Smith & Ryan 2016, Handspring Publishing
Unhealthy System
A dysfunctional lymphatic system cannot remove product that is collecting in the tissues at a rate that keeps the tissues properly cleansed.
This interferes with the homeostasis of the tissues.
• Four continuous minutes of abdominal lymph pumping
(1 pump/sec) has been shown to increase immune cell release from
mesenteric lymph nodes.
• Specialized T cells primed in the gut are faster-acting/superior-
performing immune cells.
• Recent studies suggest that abdominal lymphatic pumping may
inhibit solid tumor development and bacterial pneumonia.
(Hodge et al. 2010, 2013)
Important Role of the Lymphatic System in Traumatic Scar Wound Healing
19 20
21 22
23 24

ABMP Scar Tissue Management: Part 1-Introduction
©2020, Associated Bodywork & Massage Professionals 5
Conference
2015 Joint Conference on Acupuncture, Oncology, and
Fascia
Presentation
Manual Therapy and Lymphatics
Presenter
Lisa Hodge, PhD
Associate Professor, Department of Cell Biology and
Immunology, University of North Texas Health Science
Center, Texas
Video Links
https://oshercenter.org/joint-conference-2015-video-presentations/https://www.youtube.com/watch?v=MFMk76jdjxM&t=127s
Manual Therapy and Lymphatics
Dr. Lisa Hodge
• 5–7 minutes of abdominal pumping gets the system moving
• This action initiates the lymph-immune system
Course Outline
❶ Introduction
❷ MT role in scar tissue management
❸ Fascia and connective tissue
❹ Lymphatic system
❺ Wound healing and scar formation:
Normal and abnormal
SCAR TISSUE
MANAGEMENT
Part 1: Introduction
Wound Healing and Scar Formation
Physiological (Normal)
and
Pathological (Abnormal)
Days 5 201510 25
InflammationLasts 1–4 days(may last weeks)
ProliferationTypically lasts 4–21 days (may last up to 6 weeks)
Starts within 48-72 hours of initial injury
RemodelingLasts from months to years
Normal Stages of Wound Healing
HomeostasisImmediate
Normal Stages of Wound Healing
Homeostasis
• Clot formation to control bleeding
Inflammation
• Immune cells clean the area
• Various cells begin the process of healing
Proliferation
• Scar forms to heal the wound gap and restore tissue integrity
Remodeling
• Stronger scar material (collagen) is produced to increase the strength of the healed tissue and restore function
Several factors can influence and impact the process.
25 26
27 28
29 30

ABMP Scar Tissue Management: Part 1-Introduction
©2020, Associated Bodywork & Massage Professionals 6
Primary Players in Skin and Connective Tissue/Fascia Remodeling and Collagen Production
• Fibroblasts
• Myofibroblasts
• Transforming Growth Factor: TGF-ß1
Can be influenced by
• Stress/anxiety
• Sympathetic nervous system/parasympathetic nervous system imbalance
• Neural hyperactivity or sensitization
• Excess or prolonged inflammation/edema
• Immobilization
• Tissue tension
• When collagen proliferation does not shut down,
abnormal scars will form.
• The physical hallmark of pathological scars is
excessive/anomalous (fibrotic) collagen.
• If (hyper) vascular/neural regression does not occur, the
scar and surrounding tissue function may be abnormal.
Abnormal Wound Healing
When collagen proliferation does not shut down, abnormal scars will form.
Abnormal Wound Healing
Keloid scar: abnormal collagen extends beyond the margin of the wound
Hypertrophic scar: abnormal scar within the wound margins (raised, pigmented)
From “Traumatic Scar Tissue Management,” Smith & Ryan 2016, Handspring Publishing
Abnormal Wound Healing
FibrosisFibrotic collagen: Fuzzy/rough, lacking normal crimp, dense, brittle, rigid,
pathological cross-links, and disorganized/chaotic arrangement
Healthy tissuespacious and well organized
Wound areadense and chaotic
Adapted from: Coelho, N. M., & McCulloch, C. A. (2016). Contribution of collagen adhesion receptors to tissue fibrosis. Cell and tissue research, 365(3), 521-538.
Wound healing doesn’t always
result in fibrosis.
So what happens?
How do we get there?
31 32
33 34
35 36
ABMP Scar Tissue Management: Part 1-Introduction
©2020, Associated Bodywork & Massage Professionals 7
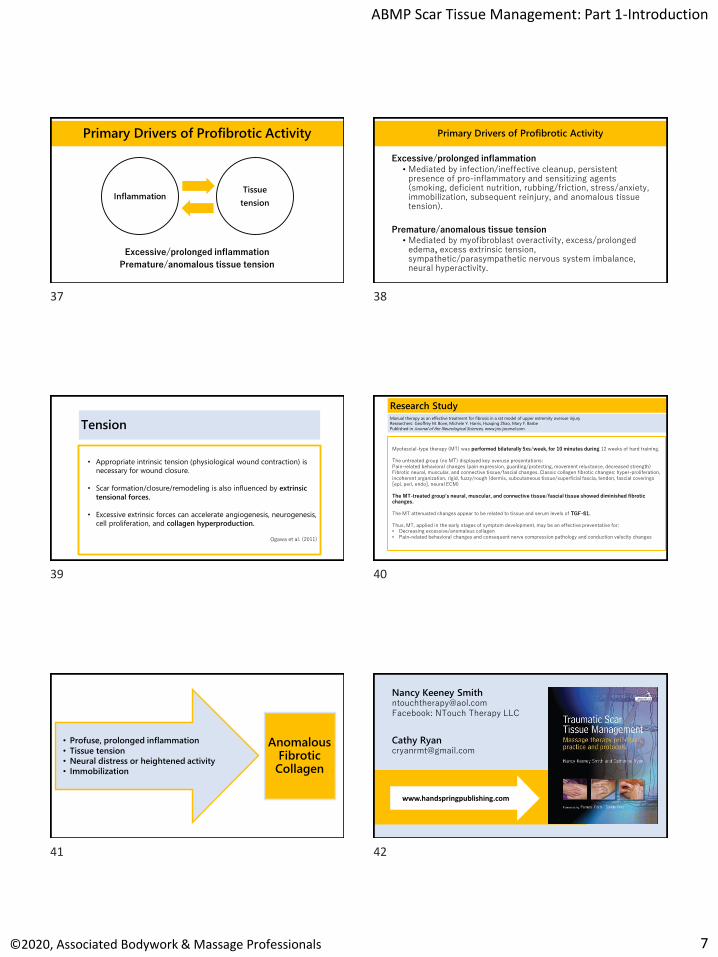
Primary Drivers of Profibrotic Activity
Excessive/prolonged inflammation
Premature/anomalous tissue tension
InflammationTissue
tension
Excessive/prolonged inflammation
• Mediated by infection/ineffective cleanup, persistent presence of pro-inflammatory and sensitizing agents (smoking, deficient nutrition, rubbing/friction, stress/anxiety, immobilization, subsequent reinjury, and anomalous tissue tension).
Premature/anomalous tissue tension • Mediated by myofibroblast overactivity, excess/prolonged
edema, excess extrinsic tension, sympathetic/parasympathetic nervous system imbalance, neural hyperactivity.
Primary Drivers of Profibrotic Activity
• Appropriate intrinsic tension (physiological wound contraction) is
necessary for wound closure.
• Scar formation/closure/remodeling is also influenced by extrinsic
tensional forces.
• Excessive extrinsic forces can accelerate angiogenesis, neurogenesis,
cell proliferation, and collagen hyperproduction.
Ogawa et al. (2011)
TensionManual therapy as an effective treatment for fibrosis in a rat model of upper extremity overuse injury
Researchers: Geoffrey M. Bove, Michele Y. Harris, Huaqing Zhao, Mary F. Barbe
Published in Journal of the Neurological Sciences, www.jns-journal.com
Research Study
Myofascial-type therapy (MT) was performed bilaterally 5xs/week, for 10 minutes during 12 weeks of hard training.
The untreated group (no MT) displayed key overuse presentations:Pain-related behavioral changes (pain expression, guarding/protecting, movement reluctance, decreased strength) Fibrotic neural, muscular, and connective tissue/fascial changes. Classic collagen fibrotic changes: hyper-proliferation, incoherent organization, rigid, fuzzy/rough (dermis, subcutaneous tissue/superficial fascia, tendon, fascial coverings [epi, peri, endo], neural ECM)
The MT-treated group’s neural, muscular, and connective tissue/fascial tissue showed diminished fibrotic changes.
The MT attenuated changes appear to be related to tissue and serum levels of TGF-ß1.
Thus, MT, applied in the early stages of symptom development, may be an effective preventative for:• Decreasing excessive/anomalous collagen • Pain-related behavioral changes and consequent nerve compression pathology and conduction velocity changes
Anomalous Fibrotic Collagen
• Profuse, prolonged inflammation
• Tissue tension
• Neural distress or heightened activity
• Immobilization
Cathy [email protected]
www.handspringpublishing.com
Nancy Keeney [email protected]: NTouch Therapy LLC
37 38
39 40
41 42
ABMP Scar Tissue Management: Part 1-Introduction
©2020, Associated Bodywork & Massage Professionals 8
Scar Tissue Management Series
Reference List
Benjamin, M., Kaiser, E., & Milz, S. (2008). Structure‐function relationships in tendons: a review. Journal of Anatomy, 212(3), 211-228.
Berrueta, L., Muskaj, I., Olenich, S., Butler, T., Badger, G. J., Colas, R. A., ... & Langevin, H. M. (2016). Stretching impacts inflammation resolution in connective tissue. Journal of Cellular Physiology, 231(7), 1621-1627.
Bialosky, J. E., Beneciuk, J. M., Bishop, M. D., Coronado, R. A., Penza, C. W., Simon, C. B., & George, S. Z. (2018). Unraveling the mechanisms of manual therapy: modeling an approach. Journal of Orthopaedic & Sports Physical Therapy, 48(1), 8-18.
Bishop, M. D., Torres-Cueco, R., Gay, C. W., Lluch-Girbés, E., Beneciuk, J. M., & Bialosky, J. E. (2015). What effect can manual therapy have on a patient's pain experience?. Pain Management, 5(6), 455-464.
Bouffard, N. A., Cutroneo, K. R., Badger, G. J., White, S. L., Buttolph, T. R., Ehrlich, H. P., ... & Langevin, H. M. (2008). Tissue stretch decreases soluble TGF‐β1 and type‐1 procollagen in mouse subcutaneous connective tissue: Evidence from ex vivo and in vivo models. Journal of Cellular Physiology, 214(2), 389-395.
Bouffard N et al 2009 Tissue stretch decreases procollagen-1 and TGF-β1 in mouse subcutaneous fascia. Abstract. 2nd Fascia Research Congress. Free University of Amsterdam, Amsterdam.
Bove, G., & Chapelle, S. (2012). Visceral mobilization can lyse and prevent peritoneal adhesions in a rat model. Journal of Bodywork and Movement Therapies.
Chaitow (2014) Fascial dysfunction – manual therapy approaches. Pencaitland, UK: Handspring Publishing.
Chaitow, L. (Ed.) (2018). Fascial dysfunction – manual therapy approaches. 2nd Ed. Handspring Publishing.
Corey, S. M., Vizzard, M. A., Bouffard, N. A., Badger, G. J., & Langevin, H. M. (2012). Stretching of the back improves gait, mechanical sensitivity and connective tissue inflammation in a rodent model. PloS one, 7(1), e29831.
Scar Tissue Management Series
Reference ListCowman, M. K., Schmidt, T. A., Raghavan, P., & Stecco, A. (2015). Viscoelastic properties of hyaluronan in physiological conditions. F1000Research, 4.
Crane, J. D., Ogborn, D. I., Cupido, C., Melov, S., Hubbard, A., Bourgeois, J. M., & Tarnopolsky, M. A. (2012). Massage therapy attenuates inflammatory signaling after exercise-induced muscle damage. Science Translational Medicine, 4(119), 119ra13-119ra13.
Franchi, M., Ottani, V., Stagni, R., & Ruggeri, A. (2010). Tendon and ligament fibrillar crimps give rise to left‐handed helices of collagen fibrils in both planar and helical crimps. Journal of Anatomy, 216(3), 301-309.
Fritz, S. (2016). Mosby's Fundamentals of Therapeutic Massage. Elsevier Health Sciences.
Fryer G, Fossum C (2009) Therapeutic mechanisms underlying muscle energy approaches. Physical therapy for tension type and cervicogenic headache: physical examination, muscle and joint management, Boston: Jones and Bartlett
Gracovetsky, S. (2016). Can fascia’s characteristics be influenced by manual therapy? Journal of Bodywork and Movement Therapies, 20:893–897
Guimberteau, J. C., & Delage, J. P. (2012, October). The multifibrillar network of the tendon sliding system. In Annales de chirurgie plastique et esthetique (Vol. 57, No. 5, pp. 467-481).
Guimberteau (2012) Scars and Adhesions Panel – Lecture notes from The 3rd International Fascia Research Congress, Vancouver, 28-30 March
Hodge LM, Bearden MK, Schander A et al (2010) Abdominal lymphatic pump treatment mobilizes leukocytes from the gastrointestinal associated lymphoid tissue into lymph. Lymphatic Research and Biology 8: 103-10.
Hodge LM, Bearden MK, Schander A et al (2013) Lymphatic pump treatment mobilizes leukocytes from the gut associated lymphoid tissue into lymph. Lymphatic Research and Biology 8(2): 103-110.
Scar Tissue Management Series
Reference List
Hicks, M. R., Cao, T. V., Campbell, D. H., & Standley, P. R. (2012). Mechanical strain applied to human fibroblasts differentially regulates skeletal myoblast differentiation. Journal of Applied Physiology, 113(3), 465-472.
Huang, C., Holfeld, J., Schaden, W., Orgill, D., & Ogawa, R. (2013). Mechanotherapy: revisiting physical therapy and recruiting mechanobiology for a new era in medicine. Trends in Molecular Medicine, 19(9), 555-564.
Kanazawa, Y., Nomura, J., Yoshimoto, S., Suzuki, T., Kita, K., Suzuki, N., & Ichinose, M. (2009). Cyclical cell stretching of skin-derived fibroblasts downregulates connective tissue growth factor (CTGF) production. Connective Tissue Research, 50(5), 323-329.
Khan, K.M. and Scott, A. (2009) Mechanotherapy: how physical therapists’ prescription of exercise promotes tissue repair. British Journal of Sports Medicine 43, 247–252
Kisseleva, T., Cong, M., Paik, Y., Scholten, D., Jiang, C., Benner, C., ... & Evans, S. M. (2012). Myofibroblasts revert to an inactive phenotype during regression of liver fibrosis. Proceedings of the National Academy of Sciences, 109(24), 9448-9453.
Langevin, H. M. (2013). The science of stretch. The Scientist, 27(5), 32.
Langevin HM, Nedergaard M, Howe AK (2013) Cellular control of connective tissue matrix tension. Journal of Cellular Biochemistry, 114(8): 1714-9.
Matteini, P., Dei, L., Carretti, E., Volpi, N., Goti, A., & Pini, R. (2009). Structural behavior of highly concentrated hyaluronan. Biomacromolecules, 10(6), 1516-1522.
Ng, J. L., Kersh, M. E., Kilbreath, S., & Knothe Tate, M. (2017). Establishing the basis for mechanobiology-based physical therapy protocols to potentiate cellular healing and tissue regeneration. Frontiers in Physiology, 8, 303.
Ogawa, R. (2011). Mechanobiology of scarring. Wound Repair and Regeneration, 19, s2-s9.
Scar Tissue Management Series
Reference ListPohl, H. (2010). Changes in the structure of collagen distribution in the skin caused by a manual technique. Journal of bodywork and movement therapies, 14(1), 27-34.
Roman, M., Chaudhry, H., Bukiet, B., Stecco, A., & Findley, T. W. (2013). Mathematical analysis of the flow of hyaluronic acid around fascia during manual therapy motions. The Journal of the American Osteopathic Association, 113(8), 600-610.
Schleip R, Muller DG (2013) Training principles for fascial connective tissues: Scientific foundation and suggested practical applications. Journal of Bodywork and Movement Therapies, 17(1): 103-115
Simmonds, N., Miller, P., & Gemmell, H. (2012). A theoretical framework for the role of fascia in manual therapy. Journal of Bodywork and Movement Therapies, 16(1), 83-93.
Smith, N. & Ryan, C. (2016). Traumatic Scar Tissue Management – Massage Therapy Principles, Practice and Protocols. Pencaitland, UK: Handspring Publishing.
Stecco, C., Fede, C., Macchi, V., Porzionato, A., Petrelli, L., Biz, C., ... & De Caro, R. (2018). The fasciacytes: a new cell devoted to fascial gliding regulation. Clinical Anatomy, 31(5), 667-676.
Thompson, W. R., Scott, A., Loghmani, M. T., Ward, S. R., & Warden, S. J. (2016). Understanding mechanobiology: physical therapists as a force in mechanotherapy and musculoskeletal regenerative rehabilitation. Physical Therapy, 96(4), 560-569.
Threlkeld, A. J. (1992). The effects of manual therapy on connective tissue. Physical Therapy, 72(12), 893-902.
Tortora, G.J., Funke, B.R., Case, C.L. (2007). Introduction to Microbiology. San Francisco: Pearson Benjamin Cummings.
Tozzi, P., 2012. Selected fascial aspects of osteopathic practice. Journal of Bodywork and Movement Therapies, 16(4), 503e519.
Scar Tissue Management Series
Reference List
Troeger, J. S., Mederacke, I., Gwak, G. Y., Dapito, D. H., Mu, X., Hsu, C. C., ... & Schwabe, R. F. (2012). Deactivation of hepatic stellate cells during liver fibrosis resolution in mice. Gastroenterology, 143(4), 1073-1083.
Waters-Banker, C., Dupont-Versteegden, E. E., Kitzman, P. H., & Butterfield, T. A. (2014). Investigating the mechanisms of massage efficacy: the role of mechanical immunomodulation. Journal of Athletic Training, 49(2), 266-273.
Wynn, T. A. (2007). Common and unique mechanisms regulate fibrosis in various fibroproliferative diseases. The Journal of Clinical Investigation, 117(3), 524-529.
Zuther JE (2011) Lymphedema management: the comprehensive guide for practitioners, 2e. Stuttgart: Thieme
43 44
45 46
47


















