ABC’s of surgery Anesthetic/Allergy History Has the pt or anyone in the family ever had a reaction...
143
-
Upload
willa-logan -
Category
Documents
-
view
214 -
download
0
Transcript of ABC’s of surgery Anesthetic/Allergy History Has the pt or anyone in the family ever had a reaction...


ABC’s of surgery• Anesthetic/Allergy History
• Has the pt or anyone in the family ever had a reaction to anesthesia or allergy to anesthesia?
• Bleeding History• Has he or anyone in his family ever had any
problems with bleeding spontaneously, after being cut, or having surgery or a tooth extraction?

• Corticosteroid History • Have they taken IV or PO steroids in the last
year and if so, how much and for how long?
• Drugs Use including Herbals• Any medications they take including illicit,
OTC, or herbals
• Exercise Tolerance• Can they walk up 2 flights of stairs (= 4
METS)

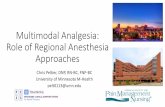
1. Cardiovascular – AHA/ACC 2009 guidelines, revised cardiac risk index, beta blocker recommendations
2. Pulmonary – risk reduction/DVT prophylaxis3. Endocrinology – adrenal insufficiency and diabetes4. Hematology- anemia and anticoagulation management5. Hepatology – Child-Pugh class and MELD score6. Neurology – seizures and other neurolgic disorders7. Nephrology – renal dysfunction and electrolyte goals8. Preoperative Testing9. Infectious Diseases- wound and endocarditis
prophylaxis10. Medications and Surgery

Need for emergencynoncardiac surgery? Yes
(Class I, LOE C)Operating room Perioperative surveillance
and postoperative risk stratification and risk factor
management
Active cardiac conditions* Evaluate and treat per
ACC/AHA guidelines
Consider operating room
No
Low risk surgery
Yes (Class I, LOE B)
Yes (Class I, LOE B)
Proceed with planned surgery
Functional capacity greater than or equal to 4 METs without symptoms.‡ Proceed with
planned surgeryYes (Class IIa, LOE B)
No
No
Step 2
Step 3
Step 1
Step 4

3 or more clinical risk factors?
1-2 clinical risk factors?
No clinical risk factors?
Vascular Surgery
Intermediate risk surgery
Class IIa,
LOE B
Consider testing if it will change management ¶
Proceed with
planned surgeryProceed with planned surgery with HR control ¶ (Class IIa, LOE B)
or consider noninvasive testing (Class IIb LOE B) if it will change with management
No or unknown Step 5
Vascular Surgery
Intermediate risk surgery
Class ILOE B

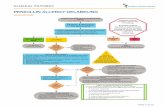
Class I Benefit >>> Risk
Procedure/ Treatment SHOULD be performed/ administered
Class IIa Benefit >> RiskAdditional studies with focused objectives needed
IT IS REASONABLE to perform procedure/administer treatment
Class IIb Benefit ≥ RiskAdditional studies with broad objectives needed; Additional registry data would be helpful
Procedure/Treatment MAY BE CONSIDERED
Class III Risk ≥ BenefitNo additional studies needed
Procedure/Treatment should NOT be performed/administered SINCE IT IS NOT HELPFUL AND MAY BE HARMFUL
shouldis recommendedis indicatedis useful/effective/
beneficial
is reasonablecan be useful/effective/
beneficialis probably
recommended or indicated
may/might be consideredmay/might be reasonableusefulness/effectiveness
is unknown /unclear/uncertain or not well established
is not recommendedis not indicatedshould notis not
useful/effective/beneficial
may be harmful
Applying Classification of Recommendations and Level of
Evidence
Alternative Phrasing:





4 C IT(Fore See IT)
1. HX of CHF2. HX of CVA3. HX of CAD4. HX of CKD
• CR >2.0
5. Insulin Dependent Diabetes6. Type of Surgery• intraperitoneal, intrathorcic, suprainguinal vascular
0 Risk Factors – 0.4% 2 Risk Factors – 7% 1 Risk Factor – 0.9% 3 Risk Factors –11%
Risk of Major Cardiac Event

Copyright ©2007 American College of Cardiology Foundation. Restrictions may apply.
Brilakis, E. S. et al. J Am Coll Cardiol 2007;49:2145-2150
Perioperative Stent Thrombosis Prevention Strategies

Can You… Can You…
1 Met Take care of yourself? 4 Mets
Climb a flight of stairs or walk up a hill?
Eat, dress, or use the toilet?
Walk on level ground at 4 mph (6.4 kph)?
Walk indoors around the house?
Do heavy work around the house like scrubbing floors or lifting or moving heavy furniture?
Walk a block or 2 on level ground at 2 to 3 mph (3.2 to 4.8 kph)?
Participate in moderate recreational activities like golf, bowling, dancing, doubles tennis, or throwing a baseball or football?
4 Mets Do light work around the house like dusting or washing dishes?
> 10 Mets
Participate in strenuous sports like swimming, singles tennis, football, basketball, or skiing?
MET indicates metabolic equivalent; mph, miles per hour; kph, kilometers per hour. *Modified from Hlatky et al, copyright 1989, with permission from Elsevier, and adapted from Fletcher et al.

Risk Stratification Procedure Examples
Vascular (reported cardiac Aortic and other major vascular surgery
risk often > 5%) Peripheral vascular surgery
Intermediate (reported Intraperitoneal and intrathoracic surgery
cardiac risk generally 1%-5%) Carotid endarterectomy
Head and neck surgery Orthopedic
surgery Prostate surgery
Low† (reported cardiac Endoscopic procedures
risk generally <1% Superficial procedure /Breast surgery
Cataract surgeryAmbulatory surgery
JACC 2009;54;e13-e118

Condition ExamplesUnstable coronary syndromes
Unstable or severe angina* (CCS class III or IV)†Recent MI‡
Decompensated HF (NYHA functional class IV; worsening or new-onset HF)Significant arrhythmias High-grade atrioventricular block
Mobitz II atrioventricular blockThird-degree atrioventricular heart blockSymptomatic ventricular arrhythmiasSupraventricular arrhythmias (including atrial
fibrillation) with uncontrolled ventricular rate (HR > 100 bpm at rest)
Symptomatic bradycardiaNewly recognized ventricular tachycardia
Severe valvular disease Severe aortic stenosis (mean pressure gradient > 40 mm Hg, aortic valve area < 1.0 cm2, or symptomatic)
Symptomatic mitral stenosis (progressive dyspnea on exertion, exertional presyncope, or HF) or MVA<1.5
cm2 CCS indicates Canadian Cardiovascular Society; HF, heart failure; HR, heart rate; MI, myocardial infarction; NYHA, New York Heart Association. *According to Campeau.10 †May include stable angina in patients who are unusually sedentary. ‡The ACC National Database Library defines recent MI as more than 7 days but within 30 days)
JACC 2009;54;e13-e118

2009 Perioperative Focused Update RecommendationsCirculation. Nov 2009;120:2123-2151
CLASS I1. Beta blockers should be continued in patients undergoing surgery
who are receiving beta blockers for treatment of conditions with ACCF/AHA Class I guideline indications for the drugs. (Level of Evidence: C)
CLASS II1. Beta blockers titrated to heart rate and blood pressure are probably
recommended for patients undergoing vascular surgery who are at high cardiac risk owing to coronary artery disease or the finding of cardiac ischemia on preoperative testing.4,5 (Level of Evidence: B)
2. Beta blockers titrated to heart rate and blood pressure are reasonable for patients in whom preoperative assessment for vascular surgery identifies high cardiac risk, as defined by the presence of more than 1 clinical risk factor.* (Level of Evidence: C)

3.Beta blockers titrated to heart rate and blood pressure are reasonable for patients in whom preoperative assessment identifies coronary artery disease or high cardiac risk, as defined by the presence of more than 1 clinical risk factor,* who are undergoing intermediate-risk surgery.6 (Level of Evidence: B)
CLASS IIb1.The usefulness of beta blockers is uncertain for patients who are undergoing either intermediate-risk procedures or vascular surgery in whom preoperative assessment identifies a single clinical risk factor in the absence of coronary artery disease.* (Level of Evidence: C)
2. The usefulness of beta blockers is uncertain in patients undergoing vascular surgery with no clinical risk factors* who are not currently taking beta blockers.7 (Level of Evidence: B)

CLASS III1.Beta blockers should not be given to patients undergoing surgery who have absolute contraindications to beta blockade. Level of Evidence: C
2. Routine administration of high-dose beta blockers in the absence of dose titration is not useful and may be harmful to patients not currently taking beta blockers who are undergoing noncardiac surgery.8 (Level of Evidence: B)
*Clinical risk factors include history of ischemic heart disease, history of compensated or prior heart failure, history of cerebrovascular disease, diabetes mellitus, and renal insufficiency (defined in the Revised Cardiac Risk Index as a preoperative serum creatinine of >2 mg/dL).9 ACC indicates American College of Cardiology; and AHA, American Heart Association.

Start beta blockers well in advance of surgery, not immediately preoperatively.
Titrate to heart rate of 50-70. Avoid systolic BP < 100 or HR < 50. Example – Bisoprolol 2.5 mg/day as
starting dose with titration of 1.25 mg/d. Continue for perhaps 30 days
postoperatively. Lancet 2008; 371:1839-1847 (POISE) and Ann Surg. 2009; 249:921-926 (DECREASE
IV).



• Obtain PFTs for patients with COPD or asthma if clinical evaluation cannot determine if the patient is at their
best baseline and that airflow obstruction is optimally reduced. In this case, PFTs may identify patients who will benefit from more aggressive preoperative management.
• Obtain PFTs for patients with dyspnea or exercise intolerance that remains unexplained after clinical evaluation. In this case, the differential diagnosis may include cardiac disease or deconditioning. The results of PFTs may change preoperative management.
• PFTs should not be used as the primary factor to deny surgery • PFTs should not be ordered routinely prior to abdominal
surgery or other high risk surgeriesAnn Intern Med. 2006 Apr 18;144(8):575-80

When to do ABGs
• Current data does not support the use of preoperative arterial blood gas analyses to stratify risk for postoperative pulmonary

Table 5—Proven Risk-Reduction Strategies
PreoperativeSmoking cessation 6–8 wk before undergoing surgeryInspiratory muscle training
IntraoperativeUse of neuromuscular agents other than pancuroniumPostoperativeIncentive SpirometryCPAP

Lung Resection

Abbreviations: CPET cardiopulmonary exercise test; Dlco diffusing capacity of the lung for carbon monoxide; LVRSlung volume reduction surgery; PPOpredicted postoperative; %PPOpercent predicted postoperative;V˙o2maxmaximal oxygen consumptionChest 2007;132;161S-177S

Inherited Thrombophilia› Factor V Leiden › Prothrombin Gene Mutation› Protein S deficiency› Protein C deficiency› Antithrombin Deficiency› Rare Disorders
Dysfibrinogenemia Acquired Disorders
› Malignancy› Presence of Central Venous
Catheter› Surgery, especially orthopedic› Trauma› Pregnancy› Hormone Replacement› Obesity (BMI >30)
› Drugs Tamoxifen,
Bevacizumab,Thalidomide, Lenalidomide
› Immobilization› CHF› Antiphopholipid Antibody› Myeloproliferative disorders
Polycythemia vera Essential
Thrombocythemia› Paroxysmal Nocturnal
Hemoglobuinuria› Inflammatory Bowel Disease› Nephrotic Syndrome› Multiple Myeloma› Marked Leukocytosis in acute
leukemia› HIV/AIDSUptodate 2010 : Overview of the Causes of
Venous Thrombosis

T – Thrombosis (previous)
H - Hereditary Thrombophilia
R- Renal Disease/Nephrotic Syndrome
O – Oral Contraceptive or Estrogen
M – Malignancy B – Bechet’s/IBD O – Obesity S – Stroke I – Immobilization S- Surgery

Table 5—Levels of Thromboembolism Risk and Recommended Thromboprophylaxis in Hospital Patients (Section 1.3)* Levels of Risk Approximate DVT Risk %† Suggested Thromboprophylaxis Options‡ Withou tThromboprophylaxis,
Low risk Minor surgery in mobile patients <10 No specific thromboprophylaxis Medical patients who are fully Early and “aggressive” ambulation mobile
Moderate risk Most general, open gynecologic 10–40 LMWH (at recommended doses), LDUH or urologic surgery patients bid or tid, fondaparinux Medical patients, bed rest or sick
Moderate VTE risk plus high Mechanical thromboprophylaxis§ bleeding risk
High riskHip or knee arthroplasty, HFS 40–80 LMWH (at recommended doses)Major trauma, SCI fondaparinux, oral vitamin K antagonist (INR 2–3)High VTE risk plus high bleeding Mechanical thromboprophylaxis§ risk *The descriptive terms are purposely left undefined to allow individual clinician interpretation.†Rates based on objective diagnostic screening for asymptomatic DVT in patients not receiving thromboprophylaxis.‡See relevant section in this chapter for specific recommendations.§Mechanical thromboprophylaxis includes IPC or VFP and/or GCS; consider switch to anticoagulant thromboprophylaxis when high bleeding risk decreases.CHEST June 2008 vol. 133 no. 6 suppl 381S-453S

CHEST June 2008 vol. 133 no. 6 suppl 381S-453S

1.0 General Recommendations
Hospital Thromboprophylaxis Policy1.2.1. For every general hospital, we recommend that a formal, active strategy that addresses the prevention of VTE be developed (Grade 1A).
1.2.2. We recommend that the local thromboprophylaxis strategy be in the form of a written, institution-wide thromboprophylaxis policy (Grade 1C).
1.2.3. We recommend the use of strategies shown to increase thromboprophylaxis adherence, including the use of computer decision support systems (Grade 1A), preprinted orders (Grade 1B), and periodic audit and feedback (Grade 1C). Passive methods such as distribution of educational materials or educational meetings are not recommended as sole strategies to increase adherence to thromboprophylaxis (Grade 1B).

Mechanical Methods of Thromboprophylaxis1.4.3.1. We recommend that mechanical methods of thromboprophylaxis be used primarily in patients at high risk for bleeding (Grade 1A), or possibly as an adjunct to anticoagulant-based thromboprophylaxis (Grade 2A).
1.4.3.2. For patients receiving mechanical methods of thromboprophylaxis, we recommend that careful attention be directed toward ensuring the proper use of, and optimal adherence with, these methods (Grade 1A).
Aspirin as Thromboprophylaxis1.4.4. We recommend against the use of aspirin alone as thromboprophylaxis against VTE for any patient group (Grade 1A).
Anticoagulant Dosing1.4.5. For each of the antithrombotic agents, we recommend that clinicians follow the manufacturer-suggested dosing guidelines (Grade 1C).Renal Impairment and Anticoagulant Dosing

1.4.6. We recommend that renal function be considered when making decisions about the use and/or the dose of LMWH, fondaparinux, and other antithrombotic drugs that are cleared by the kidneys, particularly in elderly patients, patients with diabetes mellitus, and those at high risk for bleeding (Grade 1A). Depending on the circumstances, we recommend one of the following options in this situation: avoiding the use of an anticoagulant that bioaccumulates in the presence of renal impairment, using a lower dose of the agent, or monitoring the drug level or its anticoagulant effect (Grade 1B).
Antithrombotic Drugs and Neuraxial Anesthesia/Analgesia or Peripheral Nerve Blocks1.5.1. For all patients undergoing neuraxial anesthesia or analgesia, we recommend appropriate patient selection and caution when using anticoagulant thromboprophylaxis (Grade 1A).
1.5.2. For patients receiving deep peripheral nerve blocks, we recommend that the same cautions considered for neuraxial techniques be applied when using anticoagulant thromboprophylaxis (Grade 1C).

2.0 General, Vascular, Gynecologic, Urologic, Laparoscopic, Bariatric, Thoracic, and Coronary Artery Bypass Surgery
2.1 General Surgery2.1.1. For low-risk general surgery patients who are undergoing minor procedures and have no additional thromboembolic risk factors, we recommend against the use of specific thromboprophylaxis other than early and frequent ambulation (Grade 1A).
2.1.2. For moderate-risk general surgery patients who are undergoing a major procedure for benign disease, we recommend thromboprophylaxis with LMWH, LDUH, or fondaparinux (each Grade 1A).
2.1.3. For higher-risk general surgery patients who are undergoing a major procedure for cancer, we recommend thromboprophylaxis with LMWH, LDUH three times daily, or fondaparinux (each Grade 1A).

2.1.4. For general surgery patients with multiple risk factors for VTE who are thought to be at particularly high risk, we recommend that a pharmacologic method (ie, LMWH, LDUH three times daily, or fondaparinux) be combined with the optimal use of a mechanical method (ie, graduated compression stockings [GCS] and/or IPC) [Grade 1C].
2.1.5. For general surgery patients with a high risk of bleeding, we recommend the optimal use of mechanical thromboprophylaxis with properly fitted GCS or IPC (Grade 1A). When the high bleeding risk decreases, we recommend that pharmacologic thromboprophylaxis be substituted for or added to the mechanical thromboprophylaxis (Grade 1C).

2.1.6. For patients undergoing major general surgical procedures, we recommend that thromboprophylaxis continue until discharge from hospital (Grade 1A). For selected high-risk general surgery patients, including some of those who have undergone major cancer surgery or have previously had VTE, we suggest that continuing thromboprophylaxis after hospital discharge with LMWH for up to 28 days be considered (Grade 2A).
2.2 Vascular Surgery2.2.1. For patients undergoing vascular surgery who do not have additional thromboembolic risk factors, we suggest that clinicians not routinely use specific thromboprophylaxis other than early and frequent ambulation (Grade 2B).2.2.2. For patients undergoing major vascular surgery procedures who have additional thromboembolic risk factors, we recommend thromboprophylaxis with LMWH, LDUH, or fondaparinux (Grade 1C).

2.3 Gynecologic Surgery2.3.1. For low-risk gynecologic surgery patients who are undergoing minor procedures and have no additional risk factors, we recommend against the use of specific thromboprophylaxis other than early and frequent ambulation (Grade 1A).
2.3.2. For gynecology patients undergoing entirely laparoscopic procedures, we recommend against routine thromboprophylaxis, other than early and frequent ambulation (Grade 1B).
2.3.3. For gynecology patients undergoing entirely laparoscopic procedures in whom additional VTE risk factors are present, we rec-ommend the use of thromboprophylaxis with one or more of LMWH, LDUH, IPC, or GCS (Grade 1C).2.3.4. For all patients undergoing major gynecologic surgery, we recommend that thromboprophylaxis be used routinely (Grade 1A).

2.3.5. For patients undergoing major gynecologic surgery for benign disease without additional risk factors, we recommend LMWH (Grade 1A), LDUH(Grade 1A), or IPC started just before surgery and used continuously while the patient is not ambulating (Grade 1B).
2.3.6. For patients undergoing extensive surgery for malignancy and for patients with additional VTE risk factors, we recommend routine thromboprophylaxis with LMWH (Grade 1A), or LDUH three times daily (Grade 1A), or IPC, started just before surgery and used continuously while the patient is not ambulating (Grade 1A). Alternative considerations include a combination of LMWH or LDUH plus mechanical thromboprophylaxis with GCS or IPC, or fondaparinux (all Grade 1C).

2.3.7. For patients undergoing major gynecologic procedures, we recommend that thromboprophylaxis continue until discharge from hospital (Grade 1A). For selected high-risk gynecology patients, including some of those who have undergone major cancer surgery or have previously had VTE, we suggest that continuing thromboprophylaxis after hospital discharge with LMWH for up to 28 days be considered (Grade 2C).
2.4 Urologic Surgery2.4.1. For patients undergoing transurethral or other low-risk urologic procedures, we recommend against the use of specific thromboprophylaxis other than early and frequent ambulation (Grade 1A).
2.4.2. For all patients undergoing major, open urologic procedures, we recommend that thromboprophylaxis be used routinely (Grade 1A).

2.4.3. For patients undergoing major, open urologic procedures, we recommend routine thromboprophylaxis with LDUH twice daily or three times daily (Grade 1B), GCS and/or IPC started just before surgery and used continuously while the patient is not ambulating (Grade 1B), LMWH (Grade 1C), fondaparinux (Grade 1C), or the combination of a pharmacologic method (ie, LMWH, LDUH, or fondaparinux) with the optimal use of a mechanical method (ie, GCS and/or IPC) [Grade 1C].
2.4.4. For urologic surgery patients who are actively bleeding, or who are at very high risk for bleeding, we recommend the optimal use of mechanical thromboprophylaxis with GCS and/or IPC at least until the bleeding risk decreases (Grade 1A). When the high bleeding risk decreases, we recommend that pharmacologic thromboprophylaxis be substituted for or added to the mechanical thromboprophylaxis (Grade 1C).

2.5 Laparoscopic Surgery2.5.1. For patients undergoing entirely laparoscopic procedures who do not have additional thromboembolic risk factors, we recommend against the routine use of thromboprophylaxis, other than early and frequent ambulation (Grade 1B).
2.5.2. For patients undergoing laparoscopic procedures in whom additional VTE risk factors are present, we recommend the use of thromboprophylaxis with one or more of LMWH, LDUH, fondaparinux, IPC, or GCS (all Grade 1C).
2.6 Bariatric Surgery2.6.1. For patients undergoing inpatient bariatric surgery, we recommend routine thromboprophylaxis with LMWH, LDUH three times daily, fondaparinux, or the combination of one of these pharmacologic methods with optimally used IPC (each Grade 1C).

2.6.2. For patients undergoing inpatient bariatric surgery, we suggest that higher doses of LMWH or LDUH than usual for nonobese patients be used (Grade 2C).
2.7 Thoracic Surgery2.7.1. For patients undergoing major thoracic surgery, we recommend routine thromboprophylaxis with LMWH, LDUH, or fondaparinux (each Grade 1C).2.7.2. For thoracic surgery patients with a high risk of bleeding, we recommend the optimal use of mechanical thromboprophylaxis with properly fitted GCS and/or IPC (Grade 1C).2.8 Coronary Artery Bypass Surgery2.8.1. For patients undergoing coronary artery bypass graft (CABG) surgery, we recommend the use of thromboprophylaxis with LMWH, LDUH, or optimally used bilateral GCS or IPC (Grade 1C).

2.8.2. For patients undergoing CABG, we suggest the use of LMWH over LDUH (Grade 2B).
2.8.3. For patients undergoing CABG with a high risk of bleeding, we recommend the optimal use of mechanical thromboprophylaxis with properly fitted bilateral GCS or IPC (Grade

3.0 Orthopedic Surgery
3.1 Elective Hip Replacement3.1.1. For patients undergoing elective total hip replacement (THR), we recommend the routine use of one of the following anticoagulant options: (1) LMWH (at a usual high-risk dose, started 12 h before surgery or 12 to 24 h after surgery, or 4 to 6 h after surgery at half the usual high-risk dose and then increasing to the usual high-risk dose the following day); (2) fondaparinux (2.5 mg started 6 to 24 h after surgery); or (3) adjusted-dose VKA started preoperatively or the evening of the surgical day (international normalized ratio [INR] target, 2.5; INR range, 2.0 to 3.0) (all Grade 1A).
3.1.2. For patients undergoing THR, we recommend against the use of any of the following: aspirin, dextran, LDUH, GCS, or venous foot pump (VFP) as the sole method of thromboprophylaxis (all Grade 1A).

3.1.3. For patients undergoing THR who have a high risk of bleeding, we recommend the optimal use of mechanical thromboprophylaxis with the VFP or IPC (Grade 1A). When the high bleeding risk decreases, we recommend that pharmacologic thromboprophylaxis be substituted for or added to the mechanical thromboprophylaxis (Grade 1C).
3.2 Elective Knee Replacement3.2.1. For patients undergoing TKR, we recommend routine thromboprophylaxis using LMWH (at the usual high-risk dose), fondaparinux, or adjusted-dose VKA (INR target, 2.5; INR range, 2.0 to 3.0) (all Grade 1A).
3.2.2. For patients undergoing TKR, the optimal use of IPC is an alternative option to anticoagulant thromboprophylaxis (Grade 1B).
3.2.3. For patients undergoing TKR, we recommend against the use of any of the following as the only method of thromboprophylaxis: aspirin(Grade 1A), LDUH (Grade 1A), or VFP (Grade 1B).

3.2.4. For patients undergoing TKR who have a high risk of bleeding, we recommend the optimal use of mechanical thromboprophylaxis with IPC (Grade 1A) or VFP (Grade 1B). When the high bleeding risk decreases, we recommend that pharmacologic thromboprophylaxis be substituted for or added to the mechanical thromboprophylaxis (Grade 1C).
3.3 Knee Arthroscopy3.3.1. For patients undergoing knee arthroscopy who do not have additional thromboembolic risk factors, we suggest that clinicians not routinely use thromboprophylaxis other than early mobilization (Grade 2B).
3.3.2. For patients undergoing arthroscopic knee surgery who have additional thromboembolic risk factors or following a complicated procedure, we recommend thromboprophylaxis with LMWH (Grade 1B).

3.2.4. For patients undergoing TKR who have a high risk of bleeding, we recommend the optimal use of mechanical thromboprophylaxis with IPC (Grade 1A) or VFP (Grade 1B). When the high bleeding risk decreases, we recommend that pharmacologic thromboprophylaxis be substituted for or added to the mechanical thromboprophylaxis (Grade 1C).
3.3 Knee Arthroscopy3.3.1. For patients undergoing knee arthroscopy who do not have additional thromboembolic risk factors, we suggest that clinicians not routinely use thromboprophylaxis other than early mobilization (Grade 2B).
3.3.2. For patients undergoing arthroscopic knee surgery who have additional thromboembolic risk factors or following a complicated procedure, we recommend thromboprophylaxis with LMWH (Grade 1B).

3.4 Hip Fracture Surgery3.4.1. For patients undergoing HFS, we recommend routine thromboprophylaxis using fondaparinux (Grade 1A), LMWH (Grade 1B), adjusted-dose VKA (INR target, 2.5; INR range, 2.0 to 3.0) [Grade 1B], or LDUH (Grade 1B).
3.4.2. For patients undergoing HFS, we recommend against the use of aspirin alone (Grade 1A).
3.4.3. For patients undergoing HFS in whom surgery is likely to be delayed, we recommend that thromboprophylaxis with LMWH or LDUH be initiated during the time between hospital admission and surgery (Grade 1C).
3.4.4. For patients undergoing HFS who have a high risk of bleeding, we recommend the optimal use of mechanical thromboprophylaxis (Grade 1A). When the high bleeding risk decreases, we recommend that pharmacologic thromboprophylaxis be substituted for or added to the mechanical thromboprophylaxis (Grade 1C).

3.5 Other Thromboprophylaxis Issues in Major Orthopedic Surgery3.5.1 Commencement of Thromboprophylaxis3.5.1.1. For patients receiving LMWH as thromboprophylaxis in major orthopedic surgery, we recommend starting either preoperatively or postoperatively (Grade 1A).
3.5.1.2. For patients receiving fondaparinux as thromboprophylaxis in major orthopedic surgery, we recommend starting either 6 to 8 h after surgery or the next day (Grade 1A).
Screening for Deep Vein Thrombosis Before Hospital Discharge3.5.2. For asymptomatic patients following major orthopedic surgery, we recommend against the routine use of DUS screening before hospital discharge (Grade 1A).

Duration of Thromboprophylaxis3.5.3.1. For patients undergoing THR, TKR, or HFS, we recommend thromboprophylaxis with one of the recommended options for at least 10 days (Grade 1A).
3.5.3.2. For patients undergoing THR, we recommend that thromboprophylaxis be extended beyond 10 days and up to 35 days after surgery (Grade 1A). The recommended options for extended thromboprophylaxis in THR include LMWH (Grade 1A), a VKA (Grade 1B), or fondaparinux (Grade 1C).
3.5.3.3. For patients undergoing TKR, we suggest that thromboprophylaxis be extended beyond 10 days and up to 35 days after surgery (Grade 2B). The recommended options for extended thromboprophylaxis in TKR include LMWH (Grade 1C), a VKA(Grade 1C), or fondaparinux (Grade 1C).

3.5.3.4. For patients undergoing HFS, we recommend that thromboprophylaxis be extended beyond 10 days and up to 35 days after surgery (Grade 1A). The recommended options for extended thromboprophylaxis in HFS include fondaparinux (Grade 1A), LMWH (Grade 1C), or a VKA (Grade 1C).
3.6 Elective Spine Surgery3.6.1. For patients undergoing spine surgery who do not have additional thromboembolic risk factors, we suggest that clinicians not routinely use specific thromboprophylaxis other than early and frequent ambulation (Grade 2C).
3.6.2. For patients undergoing spine surgery who have additional thromboembolic risk factors such as advanced age, malignancy, presence of a neurologic deficit, previous VTE, or an anterior surgical approach, we recommend that one of the following thromboprophylaxis options be used: postoperative LDUH (Grade 1B), postoperative LMWH (Grade 1B), or optimal use of perioperative IPC (Grade 1B). An alternative consideration is GCS (Grade 2B).

3.6.3. For patients undergoing spine surgery who have multiple risk factors for VTE, we suggest that a pharmacologic method (ie, LDUH or LMWH) be combined with the optimal use of a mechanical method (ie, GCS and/or IPC) (Grade 2C).
3.7 Isolated Lower-Extremity Injuries Distal to the Knee3.7.1. For patients with isolated lower-extremity injuries distal to the knee, we suggest that clinicians not routinely use thromboprophylaxis

4.0 Neurosurgery
4.0.1. For patients undergoing major neurosurgery, we recommend that thromboprophylaxis be used routinely (Grade 1A), with optimal use of IPC (Grade 1A). Acceptable alternatives to IPC are post operative LMWH (Grade 2A) or LDUH (Grade 2B).
4.0.2. For patients undergoing major neurosurgery who have a particularly high thrombosis risk, we suggest that a mechanical method (ie, GCS and/or IPC) be combined with a pharmacologic method (ie, postoperative LMWH or LDUH) (Grade 2B).

5.0 Trauma, Spinal Cord Injury, Burns
5.1 Trauma5.1.1. For all major trauma patients, we recommend routine thromboprophylaxis if possible (Grade 1A).
5.1.2. For major trauma patients, in the absence of a major contraindication, we recommend that clinicians use LMWH thromboprophylaxis starting as soon as it is considered safe to do so (Grade 1A). An acceptable alternative is the combination of LMWH and the optimal use of a mechanical method of thromboprophylaxis (Grade 1B).
5.1.3. For major trauma patients, if LMWH thromboprophylaxis is contraindicated due to active bleeding or high risk for clinically important bleeding, we recommend that mechanical thromboprophylaxis with IPC or possibly with GCS alone be used (Grade 1B). When the high bleeding risk decreases, we recommend that pharmacologic thromboprophylaxis be substituted for or added to the mechanical thromboprophylaxis (Grade 1C).

5.1.4. In trauma patients, we recommend against routine DUS screening for asymptomatic deep vein thrombosis (DVT) (Grade 1B). We do recommend DUS screening in patients who are at high risk for VTE (eg, in the presence of a spinal cord injury [SCI], lower-extremity or pelvic fracture, or major head injury), and who have received suboptimal thromboprophylaxis or no thromboprophylaxis (Grade 1C).
5.1.5. For trauma patients, we recommend against the use of an inferior vena cava (IVC) filter as thromboprophylaxis (Grade 1C).
5.1.6. For major trauma patients, we recommend the continuation of thromboprophylaxis until hospital discharge (Grade 1C). For trauma patients with impaired mobility who undergo inpatient rehabilitation, we suggest continuing thromboprophylaxis with LMWH or a VKA (target INR, 2.5; range, 2.0 to 3.0) (Grade 2C).

5.2 Acute Spinal Cord Injury5.2.1. For all patients with acute SCI, we recommend that routine thromboprophylaxis be provided (Grade 1A).
5.2.2. For patients with acute SCI, we recommend thromboprophylaxis with LMWH, commenced once primary hemostasis is evident (Grade 1B). Alternatives include the combined use of IPC and either LDUH (Grade 1B) or LWMH (Grade 1C).
5.2.3. For patients with acute SCI, we recommend the optimal use of IPC and/or GCS if anticoagulant thromboprophylaxis is contraindicated because of high bleeding risk early after injury (Grade 1A). When the high bleeding risk decreases, we recommend that pharmacologic thromboprophylaxis be substituted for or added to the mechanical thromboprophylaxis (Grade 1C).

5.2.4. For patients with an incomplete SCI associated with evidence of a spinal hematoma on CT or MRI, we recommend the use of mechanical thromboprophylaxis instead of anticoagulant thromboprophylaxis at least for the first few days after injury (Grade 1C).5.2.5. Following acute SCI, we recommend against the use of LDUH alone (Grade 1A).
5.2.6. For patients with SCI, we recommend against the use of an IVC filter as thromboprophylaxis (Grade 1C).
5.2.7. For patients undergoing rehabilitation following acute SCI, we recommend the continuation of LMWH thromboprophylaxis or conversion to an oral VKA (INR target, 2.5; range, 2.0 to 3.0) (Grade 1C).

5.3 Burns5.3.1. For burn patients who have additional risk factors for VTE, including one or more of the following: advanced age, morbid obesity, extensive or lower-extremity burns, concomitant lower-extremity trauma, use of a femoral venous catheter, and/or prolonged immobility, we recommend routine thromboprophylaxis if possible (Grade 1A).
5.3.2. For burn patients who have additional risk factors for VTE, if there are no contraindications, we recommend the use of either LMWH or LDUH starting as soon as it is considered safe to do so (Grade 1C).
5.3.3. For burn patients who have a high bleeding risk, we recommend mechanical thromboprophylaxis with GCS and/or IPC until the bleeding risk decreases (Grade 1A).

6.0 Medical Conditions
6.0.1. For acutely ill medical patients admitted to hospital with congestive heart failure or severe respiratory disease, or who are confined to bed and have one or more additional risk factors, including active cancer, previous VTE, sepsis, acute neurologic disease, or inflammatory bowel disease, we recommend thromboprophylaxis with LMWH (Grade 1A), LDUH (Grade 1A), or fondaparinux (Grade 1A).
6.0.2. For medical patients with risk factors for VTE, and for whom there is a contraindication to anticoagulant thromboprophylaxis, we recommend the optimal use of mechanical thromboprophylaxis with GCS or IPC (Grade 1A).

7.0 Cancer Patients
7.0.1. For cancer patients undergoing surgical procedures, we recommend routine thromboprophylaxis that is appropriate for the type of surgery (Grade 1A). Refer to the recommendations in the relevant surgical subsections.
7.0.2. For cancer patients who are bedridden with an acute medical illness, we recommend routine thromboprophylaxis as for other high-risk medical patients (Grade 1A).Refer to the recommendations in Section 6.0.
7.0.3. For cancer patients with indwelling central venous catheters, we recommend that clinicians not use either prophylactic doses of LMWH(Grade 1B). or minidose warfarin (Grade 1B) to try to prevent catheter-related thrombosis.

7.0.4. For cancer patients receiving chemotherapy or hormonal therapy, we recommend against the routine use of thromboprophylaxis for the primary prevention of VTE (Grade 1C).
7.0.5. For cancer patients, we recommend against the routine use of primary thromboprophylaxis to try to improve survival (Grade 1B).

Epidural catheters should not be placed until at least 12 hours after the last dose of prophylactic LMWH and 24 hours after high dose LMWH
If postoperative LMWH is to be used, the first dose should not be administered prior to 24 hours postoperatively if a twice-daily dosing regimen is planned, and not prior to six to eight hours postoperatively if a single-daily dosing regimen is planned
For both twice-daily and single-daily dosing regimens, if the patient has an indwelling epidural catheter postoperatively, the LMWH should not be initiated until at least two hours after catheter removal
single-daily dosing regimen, epidural catheters may be maintained, but the catheter should not be removed for at least 10 to 12 hours after the last LMWH dose
If a traumatic tap, for single-daily dosing regimen, epidural catheters may be maintained, but the catheter should not be removed for at least 10 to 12 hours after the last LMWH dose
If LMWH prophylaxis must be instituted in the presence of an indwelling catheter, low-dose epidural techniques should be used to permit careful monitoring of neurologic function.
Uptodate : Adverse effects of neuraxial analgesia and anesthesia for obstetrics


Salem et al. Perioperative glucocorticoid coverage. Ann Surg. 1994; 219:416-25.

Surgical Stress
Examples Steroid supplement
Comment
Minor Hernia repair 25 mg HCT IV or Prednisone 5 mg PO
Use cortrosyn stimulation if time (250 IV with cortisol at 30, 60 minutes; >/= 18 is normal). Always give baseline oral steroid dose if on steroids
Moderate GB removal,colon resection, THA
25 mg HCT q8h for 24 h
Major Whipple, total proctocolectomy,CABS
50 mg HCT q8h for 48 h

The initial insulin infusion rate can be estimated as between one-half and three-fourths of the patient’s total daily insulin dose expressed as units/h.
Regular insulin, 0.5–1 unit/h, is an appropriate starting dose for most type 1 diabetic patients.
Patients treated with oral antidiabetic agents who require perioperative insulin infusion, as well as insulin-treated type 2 diabetic patients, can be given an initial infusion rate of 1–2 units/h.
Diabetes Spectrum January 2002 Vol 15 no1 44-48

Diabetes Spectrum January 2002 vol 15 no1 44-48

Diabetes Spectrum January 2002 vol 15 no1 44-48

Box 1. Perioperative management of patients with insulin-dependent diabetes Need basal insulin at all times to avoid diabetic ketoacidosis Night before procedure Continue usual dose of p.m. glargine/NPH or a mixture (can recommend two thirds of usual dose if tightly controlled) the night before surgery (as long as taking usual oral intake the night before surgery) For insulin pump users, continue usual overnight basal rate Morning of procedure No boluses of short-acting hypoglycemics unless blood sugar is greater than 200 mg/dL and greater than 3 hours preoperatively May place on insulin drip OR give usual dose of glargine if routinely taken in morning For insulin pump users, continue usual basal rate and infuse D5 throughout operation If on NPH or other insulin mixture: No short-acting insulin within 3 to 4 hours of procedure (ie, no mixture preoperatively) Give half the usual intermediate-acting insulin, with D5, at controlled rate throughout procedure If doing operation without continuous D5, give no insulin preoperatively
Special situations Emergency surgery No bolus of short-acting hypoglycemics preoperatively. Frequent (every 30–60 minutes) monitoring of blood sugar throughout operation. Start insulin infusion if blood sugar is greater than 200 mg/dL Cardiac surgery Continue insulin infusion as needed to maintain blood glucose at 100 to 150 mg/dL in first 3 postoperative daysAbbreviations: D5–5%, dextrose containing solution; NPH, neutral protamine Hagedorn.
Medical Clinics of North America May 3, 2009 93:1031–1047


• The old adage of transfusing red cells such that the hemoglobin is greater than 10 g/dL and the hematocrit is more than 30% before surgery no longer applies.
• Updated guidelines from the American Society of Anesthesiology recommend transfusion if hemoglobin level is less than 6 g/dL, and that transfusion is rarely necessary when the level is more than 10 g/dL. • When hemoglobin concentrations fall between 6 and 10 g/dL, the guidelines state that transfusion decisions should be based on indication of organ ischemia, risk for or ongoing bleeding, intravascular volume status, and susceptibility to complications of inadequate oxygenation.
• The FOCUS trial in patients with hip fractures and underlying cardiovascular disease suggests that a hemoglobin level of 8 is safe for surgery.
• The authors recommend carefully evaluating each patient’s symptoms and signs and not basing the transfusion decision solely on a hemoglobin concentration. Those patients who are symptomatic from their anemia should be transfused as needed.
Medical Clinics of North America 2009 Sep;93(5):1095-104

Condition† Intervention
INR more than therapeutic range but < 5.0; no significant bleeding
Lower dose or omit dose; monitor more frequently and resume at lower dose when INR therapeutic; if only minimally above therapeutic range, no dose reduction may be required (Grade 1C).
INR ≥ 5.0, but < 9.0; no significant bleeding
Omit next one or two doses, monitor more frequently, and resume at an appropriately adjusted dose when INR in therapeutic range. Alternatively, omit dose and give vitamin K (1–2.5 mg po), particularly if at increased risk of bleeding (Grade 1C). If more rapid reversal is required because the patient requires urgent surgery, vitamin K (≤ 5 mg po) can be given with the expectation that a reduction of the INR will occur in 24 h. If the INR is still high, additional vitamin K (1–2 mg po) can be given (Grade 2C).
INR ≥ 9.0; no significant bleeding
Hold warfarin therapy and give higher dose of vitamin K (2.5–5 mg po) with the expectation that the INR will be reduced substantially in 24–48 h (Grade 1B). Monitor more frequently and use additional vitamin K if necessary. Resume therapy at an appropriately adjusted dose when INR is therapeutic.
Serious bleeding at any elevation of INR
Hold warfarin therapy and give vitamin K (10 mg by slow IV infusion), supplemented with FFP, PCC, or rVIIa, depending on the urgency of the situation; vitamin K can be repeated q12h (Grade 1C).
Life-threatening bleeding
Hold warfarin therapy and give FFP, PCC, or rVIIa supplemented with vitamin K (10 mg by slow IV infusion). Repeat, if necessary, depending on INR (Grade 1C).
Administration of vitamin KIn patients with mild to moderately elevated INRs without major bleeding, give vitamin K orally rather than subcutaneously (Grade 1A).
† If continuing warfarin therapy is indicated after high doses of vitamin K1, then heparin or low-molecular-weight heparin can be given until the effects of vitamin K1 have been reversed, and the patient becomes responsive to warfarin therapy. It should be noted that INR values > 4.5 are less reliable than values in or near the therapeutic range. Thus, these guidelines represent an approximate guide for high INRs.

Cleveland Clinic Journal of Medicine November 2009 vol. 76 Suppl 4 S37-S44

• High risk—bridging anticoagulation with therapeutic-dose subcutaneous LMWH or IV UFH
• Moderate risk—bridging anticoagulation with therapeutic-dose subcutaneous LMWH, therapeutic-dose IV UFH, or low-dose subcutaneous LMWH
• Low risk—bridging anticoagulation with low-dose subcutaneous LMWH or no bridging.
Cleveland Clinic Journal of Medicine November 2009 vol. 76 Suppl 4 S37-S44

Abnormal Results Differential Diagnosis
Prolonged prothrombin time Liver disease, vitamin K deficiency, severe factor VII deficiency
Prolonged partial thromboplastin time Deficiency of factor VIII, IX, XI, or XII; lupus anticoagulant; von Willebrand’s disease
Prolonged prothrombin time and partial thromboplastin time
Disseminated intravascular coagulation, deficiencies of factors II, V, or X; coagulation factor inhibitor
Prolonged bleeding time Von Willebrand’s disease, thrombocytopenia, functional platelet disorders
Thrombocytopenia Pseudothrombocytopenia, splenic sequestration, decrease production, increase destruction
Medical Clinics of North America 2003: 87:229-242

Work Up for Abnormal APTT1) Repeat Test2) Mixing study3) If correction, Factors VIII, IX, and XI4) If no correction, CLA and inhibitor
screen5) Optional: Factor XII, HMWK,
Prekallikrein
Western Journal Of Medicine 1989;150:51-58


Medical Clinics North America 2009 Jul;93(4):917-29

Initially developed by Child and Turcotte in 1964 to risk stratify patients undergoing shunt surgery for portal decompression
Current CTP scoring system is based upon five parameters: serum bilirubin, serum albumin, prothrombin time, ascites and encephalopathy
The sum of the points for each of these five parameters gives the total score and patients with chronic liver disease are placed into one of three CTP classes (A, B or C)

UpToDate: Model for End-stage Liver Disease (MELD)

MELD is a prospectively developed and validated chronic liver disease severity scoring system that uses a patient's laboratory values for serum bilirubin, serum creatinine, and the international normalized ratio for prothrombin time (INR) to predict survival.
MELD = 3.8[Ln serum bilirubin (mg/dL)] + 11.2[Ln INR] + 9.6[Ln serum creatinine (mg/dL)] + 6.4› Where Ln equals the natural logarithm› Most often calculated with a MELD score calculator.
http://www.mayoclinic.org/meld/mayomodel7.html

UpToDate: Model for End-stage Liver Disease (MELD)

The MELD score also has prognostic value in several clinical settings outside of liver transplantation including predicting mortality associated with: alcoholic hepatitis, hepatorenal syndrome, fulminant hepatic failure, sepsis in cirrhosis, acute variceal hemorrhage, surgical procedures in chronic liver disease patients, and the TIPS procedure


• The greatest risk factor for perioperative stroke is a history of prior stroke.
• There is evidence in the cardiac anesthesia literature that dropping the mean arterial pressure by at least 10 mm Hg from the preoperative baseline increases the risk for stroke by approximately four fold.
• The concept of keeping the blood pressure as close as possible to baseline in this patient population is important and should be considered the safest practice.
• Stroke prophylactic agents such as aspirin and warfarin should be maintained in the perioperative period, if at all possible.
Medical Clinics of North America September (2009) 93 1123–1130

• It is helpful to characterize spine disease as either chronic or acute.
• Preoperative assessment should focus on neurologic deficits and possible ventilatory compromise from phrenic nerve involvement or control of the airway as a result of cervical disease and restricted neck flexion/extension.
• Severe spine deformities necessitate pulmonary function testing to evaluate the extent of restrictive lung disease present. This information is also helpful to properly manage such ventilator settings and to evaluate for fitness of extubation following surgery.
Medical Clinics of North America September (2009) 93 1123–1130

• To manage pain preoperatively, and to avoid any symptoms of withdrawal, patients should be told to continue their current dose of narcotic medications and be specifically instructed to take them the morning of surgery.
• Some anticonvulsant medications now are commonly used for neuropathic pain syndromes—gabapentin, carbamazepine, and so on. The latter frequently induces a syndrome of inappropriate antidiurectic hormone secretion, thus a preoperative electrolyte panel would be important.
Medical Clinics of North America September (2009) 93 1123–1130

• Primary headache disorders include migraines, cluster, pseudotumor cerebri, hemicrania continuum, and exertional headaches.
• Secondary headaches are because of more ominous processes such as intracranial masses, giant cell arteritis, and hydrocephalus.
• An assessment of baseline intracranial pressure (ICP) should be provided for patients with pseudotumor cerebri, as cerebral perfusion pressure needs to be maintained at acceptable levels during general anesthesia. • Similarly, a general assessment of ICP must be made for patients with intracranial mass lesions.
• Antiepileptic drugs should be continued when applicable, and a history of recent steroid use for secondary headache disorders should be communicated.
Medical Clinics of North America September (2009) 93 1123–1130

• Patients with epilepsy are known to have an increased risk for perioperative seizure secondary to the choice of anesthetic or physiologic derangement.
• In evaluating the patient with epilepsy, it is important to obtain a complete history, including the type of seizure disorder and its characteristics so that the perioperative team can recognize if and when the patient has a seizure.
• The antiepileptic drugs (AED) regimen should be reviewed, drug levels should be drawn before surgery, and a therapeutic level obtained. The medications should be continued during the perioperative period.
• Most AEDs at toxic or even therapeutic levels may cause liver dysfunction and possibly bone marrow suppression. Liver function tests, a complete blood count, and a metabolic panel should be performed before surgery.Medical Clinics of North America September (2009) 93 1123–1130

• Patients with Duchenne and Becker muscular dystrophy suffer from a progressive loss of muscle mass. They are susceptible to multiple perioperative complications affecting the respiratory, cardiac, and musculoskeletal systems.
• Acute rhabdomyolysis can result from the use of certain inhalational anesthetic agents. Duchenne’s muscular dystrophy is a risk for malignant hyperthermia.
• Because of the risk association between muscular dystrophy and malignant hyperkalemia after paralysis with succinylcholine, the use of this depolarizing neuromuscular relaxant has fallen out of favor.
Medical Clinics of North America September (2009) 93 1123–1130

• Multiple Sclerosis (MS) may be divided into 4 subtypes: relapsing/remitting (80% of cases), primary progressive, secondary progressive, and progressive relapsing.
• The time course of the disease is important to elucidate any medications used for spasticity such as dantrolene or baclofen.
• If a patient is having an exacerbation of MS, surgery should be delayed if possible until the resolution of the acute symptoms. The stress of surgery and anesthesia alone may lead to an exacerbation, so patients should be counseled in this regard so as to make an informed decision to pursue elective surgery and for prophylaxis to prevent an exacerbation.
Medical Clinics of North America September (2009) 93 1123–1130

• In preparing the myasthenic patient for surgery, it is important to assess the severity and recent history of disease, current treatments, and any other concomitant illnesses. Review every planned medication since many medications exacerbate myasthenia.
• Preoperative pulmonary function testing can be very helpful to the perioperative team to determine the ability for a patient to be extubated after surgery.
• It is important to discriminate recent worsening neurologic symptoms between an MG exacerbation (myasthenic crisis) from pyridostigmine (cholinesterase) toxicity.
• An edrophonium test or careful assessment of the patient’s symptoms following an additional dose of cholinesterase inhibitor may be used to differentiate between the two entities.
• If a patient is having worsening symptoms, elective surgery should be postponed until more aggressive treatment such as immunotherapy or plasmapherisis can be performed. Medical Clinics of North America September (2009) 93 1123–1130

• GBS may lead to significant dysautonomia. • The presence of a dysautonomia should be made clear to the anesthesiologist so that preparations for hemodynamic fluctuation can be made.
• Blood pressure augmenting agents such as fludrocortisone and midodrine should be continued in the perioperative period, since hypotension tends to be more problematic and injurious intraoperatively.
Medical Clinics of North America September (2009) 93 1123–1130

• A pharmacogenetic disorder of skeletal muscle that presents as a hypermetabolic response to potent volatile anesthetic gases such as halothane, sevoflurane, desflurane and the depolarizing muscle relaxant succinylcholine
• The incidence of MH reactions ranges from 1:5,000 to 1:50,000–100,000 anesthesias.
Orphanet Journal of Rare Diseases 2007, 2:21

Preventive measures• Thorough anesthetic history to determine the possibility of the patient or a family member having experienced an MH episode.
• When suspicion of MH exists, family members should not be given trigger anesthetic agents, i.e. potent volatile anesthetic agents such as halothane, sevoflurane, desflurane, enflurane, isoflurane and succinylcholine, and testing is recommended.
• Patients with any form of myotonia should not receive succinylcholine.
• Patients with hypokalemic periodic paralysis, central core disease, Duchenne or Becker muscular dystrophy, paramyotonia, or myotonia fluctuans should not receive trigger agents.
• All patients receiving more than a brief general anesthetic should have their core temperature monitored.
• Young patients (below age 12 approximately) should not receive succinylcholine for elective procedures, in order to avoid the possibility of hyperkalemic response in a patient with undiagnosed muscular dystrophy.Orphanet Journal of Rare Diseases 2007, 2:21


Sodium >/= 130 meq/l Potassium < 5 Bicarbonate >/= 14-18 meq/l pH>/+ 7.25-7.30


• To minimize the risks of volume overload, electrolyte imbalances,and uremic bleeding, arrangements should be made for patients requiring dialysis to receive it within 24 hours of surgery.
• JNC VII recommends patients with CKD or diabetes have a blood pressure less than130/80 mmHg.
• Discontinuation of ACEI or ARA therapy for at least 10 hoursbefore general anesthesia is recommended to reduce the risk of postinduction hypotension
•An eGFR should be calculated to not only ensure that correct dosage adjustments are made for renally excreted medications but also to help quantify perioperative risk
Surgery in the Renal Patient
GFR (mL/min/1.73 m2) = 186 x (Pcr)-1.154 x (age)-0.203 x (0.742 if female) x (1.210 if African American)

• It is typically recommended that potassium levels be no more than 5 to 5.5 mmol/L. However, the preoperative potassium level needs to be evaluated in the context of its rate of change from previous levels, the potential blood transfusion requirements during surgery, and the potential for alterations in acid/base status perioperatively.
• Intraoperative hypotension and decreased renal perfusion is often considered a risk factor for the development of perioperative AKI
Surgery in the Renal Patient




Figure 1. Suggestions for adult preoperative testing. Y, usually indicated; M, usually indicated for males; S, may be requested (and reviewed) by surgeon as a part of the surgical workup; +/-, if situation is acute/severe. Unshaded area, timing of test typically is not critical; results from 90 days (and possibly 180 days) may be acceptable. Shaded Area, typically best to obtain within 30 days of surgery. Comments : 1) Times and test listings are suggestions: they are not absolute and should not preclude other testing in given settings; nor should they prevent a case from proceeding if the anesthesiologist and surgeon deem that to be appropriate. 2) Testing for a given disorder depends on the severity of the disorder in the context of planned surgery; i.e., are the tests likely to generate potentially clinically significant information and provide information that would be an important

Uptodate: Preoperative medical evaluation of the healthy patient
• Preoperative screening questionnaire - devised to detect pre-existing conditions shown to be associated with perioperative adverse events.

• Routine preoperative laboratory tests have not been shown to improve patient outcomes among healthy patients undergoing surgery.
• H&H(baseline) – recommended for ALL patients greater than 65 undergoing major surgery or younger patients undergoing a surgery that is expected to result in significant blood loss.• Renal Function – not recommended except in the following
• Age >50 undergoing intermediate or high risk surgery• Younger patients suspected of having renal disease• when hypotension is likely during surgery• when nephrotoxic medications will be used.
• Serum electrolytes, blood glucose, liver function, hemostasis, and urinalysis – NOT recommended in the healthy preoperative patient

• EKG - NOT recommend in the asymptomatic patient undergoing low risk surgical procedures
•Is Recommended for :• patients without perioperative clinical risk factor who require vascular surgical procedures• patients with preexisting cardiovascular disease who are undergoing surgery
• CXR - NOT recommended in the healthy patient•Is Recommended for:
• patients with cardiopulmonary disease • patients older than 50 years of age who are undergoing abdominal aortic aneurysm surgery or upper abdominal/thoracic surgery



Nature of Operation
Common Pathogens Recommended Antimicrobials
Adult Dosage Before Surgery
Cardiac Staphylococcus Aureus, S. Epidermidis
Cefazolin or Vancomycin 1-2 g IV21 g IV
Gastrointestinal Esophageal, gastroduodenal
Biliary tract
Colorectal 14
Appendectomy, Non-perforated
Enteric gram-neg bacilli, gram positive cocci
Enteric Gram-neg bacilli, enterococci, clostridia
Enteric Gram-neg bacilli, anaerobes, enterococci
Same as for colorectal
High Risk4 Only: cefazolin 5
High Risk4 Only: cefazolin 5
Oral: neomycin + erythromycin base7 OR + metronidaxole7Parenteral : cefoxitin5 or cefotetan5
OR cefazolin + metronidaxonle OR ampicillin/sulbactam5
cefoxitin5 or cefotetan5 OR cefazolin + metronidaxonle OR ampicillin/sulbactam5
1-2g IV
1-2g IV
1-2g IV
1-2g IV0.5g IV3g IV
1-2g IV1-2g IV0.5g IV3g IV
The Medical Letter Volume 7 (Issue 82) June 2009

Nature of Operation
Common Pathogens
Recommended Antimicrobials
Adult Dosage Before Surgery
Genitourinary Cystoscopy alone
Cystosocopy with manipulation or Upper Tract intrumentation10
Open or laparoscopic Surgery 11
Enteric Gram-neg Bacilli, enterococci
Enteric Gram- neg bacilli, enterococci
Enteric Gram-neg bacilli, enterococci
High Risk8 only: CiprofloxacinOR timethoprim-Sulfamethoxazole
Ciprofloxacin
OR trimethroprim-Sulfamethoxazole
Cefazolin5
500mg PO or 400mg IV1 DS tab
500mg PO or 400mg IV
1 DS tab
1-2g IV
Gynecologic and ObstetricVaginal, abdominal or laparoscopic hysterectomy
Cesarean section Abortion
Enteric gram-neg bacilli, anaerobes, Gp B strep, enterococci
Same as hysterectomySame as hysterectomy
Cefoxitin5, cefotetan5 or cefzaolin5 OR ampicillin/ sulbactam5
Cefazolin5Doxycycline
1-2gIV
3g IV
1-2g IV300mg PO
The Medical Letter Volume 7 (Issue 82) June 2009

Nature of Operation
Common Pathogens
Recommended Antimicrobials
Adult Dosage Before Surgery
Head and Neck SurgeryIncisions through oral or pharyngeal mucosa
Anaerobes, enteric gram—neg bacilli, S. aureus
ClindamycinOR cefazolin + metronidazole
600-900mg IV1-2g IV0.5 IV
Neurosurgery S.aureus, S.epidermidis
Cefaxolin or Vancomycin
1-2gIV1gIV
Ophthalmic S.epidermidis, S.aureus, streptococci, enteric gram –neg bacilli, Pseudomonas spp.
Gentamicin, tobramycinCiprofloxacin, gatifloacin,Levofloxacin, moxifloxacin, ofloxacin or neomycin-gramicidin-polymyxin B Cefazolin
Mulitple drops Topically over 2 to 24 hours
100mg subcon-juctivally
Orthopedic S.aureus, S.epidermitis
Cefazolin13 or Cefuoxime13 OR Vancomycin
1-2g IV1.5g IV1 g IV
Thoracic (Non-Cardiac)
S. asureus, S.epidermitis, stertococci, enteric gam-neg bacilli
Cefazolin or cefuroximeOR Vancomycin3
1-2g IV1.5g IV1g IV
The Medical Letter Volume 7 (Issue 82) June 2009

Nature of Operation
Common Pathogens
Recommended Antimicrobials
Adult Dosage Before Surgery
VascularArterial Surgery involving a prostesis, the abdomnial aorta, or a groin incision
Lower extremity amputaino for ischemia
S. aureus, S.epidermidis, enteric gram-negative bacilli
S. aureus, S. epidermidis, enteric gram-neg bacilli
Cefazolin or cefuroximeOR vancomycin3
CefazolinOR vancomycin3
1-2g IV1.5 g IV1g IV
1-2g IV1g IV
1. Parenteral prophylactic antimicrobials can be given as a single IV dose begun 60 minutes or less before the operation. For prolonged operations (>4hours), or those with major blood loss, additional intraoperative doses should be given at intervals 1-2 times the half-life of the drug (ampicillin/sulbactam q2-4 hours, cefazolin q2-5 hours, cefuroxime q3-4 hours, cefoxitin q2-3 hours, clindamycin q3-6 hours, vancomycin q6-12 hours, and metronidazole q6-8 hours [DW Bratzler et al. Clin Infect Dis 2004; 38:1706]) for the duration of the procedure in patients with normal renal function. If vancomycin or a fluoroquinolone is used, the infusion should be started 60-120 minutes before the initial incision in order to minimize the possibility of an infusion reaction close to the time of induction of anesthesia and to have adequate tissue levels at the time of incision. 2. Some consultants recommend an additional dose when patients are removed from bypass during open-heart surgery.3. Vancomycin can be used in hospitals in which methicillin-resistant S. aureus and S. epidermidis are a frequent cause of postoperative wound infection,patients previously colonized with MRSA, or for those who are allergic to penicillins or cephalosporins. Rapid IV administration may causehypotension, which could be especially dangerous during induction of anesthesia. Even when the drug is given over 60 minutes, hypotension mayoccur; treatment with diphenhydramine (Benadryl, and others) and further slowing of the infusion rate may be helpful. Some experts would give 15mg/kg of vancomycin to patients weighing more than 75 kg, up to a maximum of 1.5 g, with a slower infusion rate (90 minutes for 1.5 g). For operationsin which enteric gram-negative bacilli are common pathogens, many Medical Letter consultants would add another drug such as an aminoglycoside(gentamicin, tobramycin or amikacin).4. Morbid obesity, esophageal obstruction, decreased gastric acidity or gastrointestinal motility.5. For patients allergic to penicillins and cephalosporins, clindamycin with either gentamicin, ciprofloxacin, levofloxacin or aztreonam is a reasonablealternative.6. Age >70 years, acute cholecystitis, non-functioning gall bladder, obstructive jaundice or common duct stones.7. 1 g of neomycin plus 1 g of erythromycin at 1 PM, 2 PM and 11 PM or 2 g of neomycin plus 2 g of metronidazole at 7 PM and 11 PM the day beforean 8 AM operation.8. For a ruptured viscus, therapy is often continued for about five days.9. Urine culture positive or unavailable, preoperative catheter, transrectal prostatic biopsy, placement of prosthetic material.10. Shockwave lithotripsy, ureteroscopy.11. Including percutaneous renal surgery, procedures with entry into the urinary tract, and those involving implantation of a prosthesis. If manipulationof bowel is involved prophylaxis is given according to colorectal guidelines.12. Divided into 100 mg one hour before the abortion and 200 mg one half hour after.13. If a tourniquet is to be used in the procedure, the entire dose of antibiotic must be infused prior to its inflation..
The Medical Letter Volume 7 (Issue 82) June 2009


2008 VHD Focused Update Recommendations
Class IIa 1. Prophylaxis against infective endocarditis is reasonable for the following patients at highest risk for adverse outcomes from infective endocarditis who undergo dental procedures that involve manipulation of either gingival tissue or the periapical region of teeth or perforation of the oral mucosa4:
• Patients with prosthetic cardiac valves or prosthetic material used for cardiac valve repair. (Level of Evidence: B)
•Patients with previous infective endocarditis. (Level of Evidence: B)
• Patients with CHD. (Level of Evidence: B)
• Unrepaired cyanotic CHD, including palliative shunts and conduits. (Level of Evidence: B)
• Completely repaired congenital heart defect repaired with prosthetic material or device, whether placed by surgery or by catheter intervention, during the first 6 months after the procedure. (Level of Evidence: B)
• Repaired CHD with residual defects at the site or adjacent to the site of a prosthetic patch or prosthetic device (both of which inhibit endothelialization). (Level of Evidence: B)
• Cardiac transplant recipients with valve regurgitation due to a structurally abnormal valve. (Level of Evidence: C)

Class III 1. Prophylaxis against infective endocarditis is not recommended for nondental procedures (such as transesophageal echocardiogram, esophagogastroduodenoscopy, or colonoscopy) in the absence of active infection. (Level of Evidence: B)4

• High-risk patients were defined as those patients with underlying cardiac conditions associated with the highest risk of adverse outcome from infective endocarditis, not necessarily those with an increased lifetime risk of acquisition of infective endocarditis.
• Prophylaxis is no longer recommended for prevention of endocarditis for procedures that involve the respiratory tract unless the procedure is performed in a high-risk patient and involves incision of the respiratory tract mucosa, such as tonsillectomy and adenoidectomy.
• Prophylaxis is no longer recommended for prevention of infective endocarditis for GI or GU procedures, including diagnostic esophagogastroduodenoscopy or colonoscopy (Table 2).
Endocarditis Prophylaxis (continued)

Situation Agent Regimen: Single Dose 30 to 60 min Before Procedure
Adults Children Oral Amoxicillin 2 g 50 mg/kgUnable to take oral medication
Ampicillin 2 g IM or IV 50 mg/kg IM or IV
ORCefazolin or ceftriaxone 1 g IM or IV 50 mg/kg IM or IV
Allergic to penicillins or ampicillin—oral
Cephalexin 2 g 50 mg/kg
ORClindamycin 600 mg 20 mg/kg
ORAzithromycin or clarithromycin
500 mg 15 mg/kg
Allergic to penicillins or ampicillin and unable to take oral medication
Cefazolin or ceftriaxone 1 g IM or IV 50 mg/kg IM or IV
ORClindamycin 600 mg IM or IV 20 mg/kg IM or IV
IM indicates intramuscular; and IV, intravenous.*This table corresponds to Table 7 in the 2008 Focused Update Incorporated Into the ACC/AHA 2006 Guidelines for the Management of Valvular Heart Disease.2
Or use other first- or second-generation oral cephalosporin in equivalent adult or pediatric dosage.
Cephalosporins should not be used in an individual with a history of anaphylaxis, angioedema, or urticaria with penicillins or ampicillin.
Table 4. Regimens for a Dental Procedure*





Name or class of drug
Clinical considerations
Recommended strategy for surgery with prolonged NPO state
Beta blockers
Abrupt withdrawal can result in hypertension, tachycardia and myocardial ischemia.Perioperative initiation can prevent postoperative myocardial ischemic events in patients with signficantly increased cardiac risk, but may increase risk for stroke; perioperative initiation of beta blockers is not recommended for other patient populations.
Continue therapy up to and including day of surgery. Substitute IV propranolol, metoprolol or labetalol during NPO state
Alpha 2 agonistsWithdrawal can cause extreme hypertension and myocardial ischemia
Continue therapy up to and including day of surgery. Substitute transdermal clonidine or rarely IV methyl dopa.

Name or class of drug
Clinical considerations
Recommended strategy for surgery with prolonged NPO state
Calcium channel blockers
Conflicting evidence on whether there is an increased risk of bleeding
Continue therapy up to and including day of surgery. No IV substitution necessary unless poor hemodynamics (hypertension or arrythmia)
Ace inhibitors and angiotensin receptor blockers
Continuation can result in hypotension.
Continue therapy up to and including day of surgery if using for hypertension. Discontinue on day of surgery if using for CHF and baseline blood pressure is low. Use parenteral enalaprilat as needed in postoperative period.
DiureticsContinuation can result in hypovolemia and hypotension.
Continue therapy up to day of surgery but discontinue morning dose. Use parenteral forms as needed in postoperative period.

Name or class of drug
Clinical considerations
Recommended strategy for surgery with prolonged NPO state
Statins
Continuation may elevate risk of myopathy, but provides cardiovascular protection.
Continue statins up to and including day of surgery.
Non-statin lipid-lowering agents
Niacin and fibric acid derivatives may cause rhabdomyolysis. Bile acid sequestrants interfere with absorption of other medications.
Discontinue day before surgery. Resume with oral intake.


Name or class of drug
Clinical considerations
Recommended strategy for surgery with prolonged NPO state
Inhaled bronchodilators (beta agonists and anticholinergics)
No known adverse effects.
Continue therapy up to and including day of surgery. Use nebulized forms if patient unable to comply with inhalation maneuver.
Theophylline
No known adverse effects but very narrow range between therapeutic and toxic level.
Continue up to day before surgery. Discontinue the evening before surgery. Resume with PO intake. Use nebulized or inhaled beta agonist or anticholinergics
Leukotriene inhibitorsNo known adverse effects.
Continue therapy up to and including day of surgery and resume when patient able to take oral medications.


Name or class of drug
Clinical considerations
Recommended strategy for surgery with prolonged NPO state
H2 blockersNo known adverse effects.
Continue therapy up to and including day of surgery. Substitute IV forms available for prolonged postoperative NPO state.
Proton pump inhibitors
No known adverse effects.
Continue therapy up to and including day of surgery. Substitute IV H2 blockers for prolonged postoperative NPO state.


Name or class of drug
Clinical considerations
Recommended strategy for surgery with prolonged NPO state
Oral contraceptives
Continuation may increase risk of venous thromboembolism. Stopping can result in unwanted pregnancies.
Continue up to and including the day of surgery for procedures with low to moderate risk of venous thromboembolism. Stop 4-6 weeks before surgery for procedures with high risk for thromboembolism. Instruct on alternate forms of contraception and obtain serum pregnancy test immediately before surgery.
Hormone replacement therapy
Continuation may increase risk of venous thromboembolism.
Continue up to and including the day of surgery for procedures with low to moderate risk of venous thromboembolism. Stop 4-6 weeks before surgery for procedures with high risk for thromboembolism. Resume when tolerating oral medications.
Selective estrogen receptor modulators
Continuation may increase risk of venous thromboembolism.
Continue up to and including the day of surgery for procedures with low risk of venous thromboembolism. Stop 4-6 weeks before surgery for procedures with moderate to high risk for thromboembolism. Resume when tolerating oral medications When SERMs areused for breast cancer treatment consult oncologist.


Name or class of drug
Clinical considerations
Recommended strategy for surgery with prolonged NPO state
AntiepilepticNo known adverse effects.
Continue therapy up to and including day of surgery. Parenteral phenytoin or phenobarbital should be administered. These could be substituted for other antiepileptic with no parenteral substitute.
Levodopa/Carbidopa
Metabolite of Levodopa, dopamine can cause arrhythmias, hypotension or hypertension
Continue therapy up to the night before surgery and hold it the day of surgery. Resume with oral intake as soon as possible.
Dopamine agonists (Bromocriptine, pramipexole, and ropirinole)
Directly stimulate dopamine receptors and can cause arrhythmias or hypotension.
Continue therapy up to the night of surgery and hold it for at least 12 hrs before surgery. Resume with oral intake as soon as possible.

Name or class of drug
Clinical considerations
Recommended strategy for surgery with prolonged NPO state
Selegiline (selective MAO inhibitor)
At usual doses for Parkinson disease does not induce hypertension when tyramine containing foods are ingested.
Hold the medication the evening before surgery. Resume with oral intake.
PyridostigmineCan cause muscarinic side effects.
Continue therapy up to the night of surgery. For patients taking long acting preparations substitute short-acting preparations the night before surgery. Restart when hemodynamically stable. Parenteral substitutions are available. For IM substitution give 1/10th the usual oral dose and for IV substitution give 1/30th the usual dose.


Name or class of drug
Clinical considerations
Recommended strategy for surgery with prolonged NPO state
Opioids
Abrupt withdrawal can cause yawning, abdominal cramps, nausea, vomiting, diarrhea, insomnia, anxiety and salivation.
Continue therapy up to and including day of surgery. Rectal, transmucosal, transdermal and parenteral preparations available.
TramadolSeizures, drug interactions.
Substitute another analgesic until oral intake.
Nonsteroidal antiinflammatory drugs
Continuation may cause perioperative hemorrhage.
Hold for three days prior to surgery then resume with oral intake.


Name or class of drug
Clinical considerations
Recommended strategy for surgery with prolonged NPO state
Tricyclic antidepressants
Continuation may increase the potential for arrythmias. Abrupt withdrawal can lead to insomnia, nausea, headache, increased salivation and increased sweating.
If patients on high doses, continue up to and through surgery. For patients on low doses or if periooperative arrythmia is likely, shoud discontinue for 7 days prior to surgery. Resume with oral intake. No parenteral substitution available.
Serotonin reuptake inhibitors
Increased risk of bleeding.
Discontinue 3 weeks prior to high risk surgery (CNS Procedures)Resume with oral intake. No parenteral substitution available.

Name or class of drug
Clinical considerations
Recommended strategy for surgery with prolonged NPO state
Monoamine oxidase inhibitors
If continued, and direct acting sympathomimetic agents like ephedrine are used during anesthesia, can result in severe HTN. If agents like meperidine or dextromethorphan are used can result in "serotonin syndrome".
For emergency procedures a MAO-safe anesthetic technique should be used.Should be discontinued for 2 weeks prior to elective surgery.Resume with oral intake. No parenteral substitution available.
Lithium
Continuation may prolong the effect of muscle relaxants and due to impaired renal concentrating ability can cause hypovolemia and hypernatremia.
Continue therapy up to and including the day of surgery with close monitoring of electrolytes and volume status. Resume with oral intake. No parenteral substitution available.

Name or class of drug
Clinical considerations
Recommended strategy for surgery with prolonged NPO state
Valproic acidNo known adverse effects
Continue therapy up to and including day of surgery. Resume with oral intake. A parenteral formulation (valproate sodium) is available.
Antipsychotics
Some agents are associated with QT prolongation, and occasionally cause hypotension or arrythmias. No recent data available.
Continue therapy up to and including day of surgery. Parenteral formulations are available for haloperidol, chlorpromazine, aripriprazole, olanzapine, and ziprasidone. If prolonged NPO state is anticipated, depot formulations(eg haloperidol decanoate) could be considered, to begin well before surgery in consultation with psychopharmacologist.
Benzodiazepines
Abrupt withdrawal can result in agitation, HTN, delirium and seizures.
Continue therapy up to and including day of surgery. Parenteral diazepam, lorazepam and chlordiazepoxide are available for prolonged NPO state.
BuspironeNo known adverse effects.
Continue therapy up to and including day of surgery. No parenteral substitution available but parenteral diazepam, lorazepam or chlordiazepoxide can be used for prolonged NPO state.


Name or class of drug
Clinical considerations
Recommended strategy for surgery with prolonged NPO state
Aspirin and dipyridamole
Continuation may cause perioperative hemorrhage.Discontinuation may increase the risk of vascular complications.
Continue for surgeries where patients are at high risk for perioperative vascular complications and morbidity related to perioperative hemorrhage is not significant.Discontinue if perioperative bleeding could be catastrophic as in CNS surgery. If stopped, discontinue aspirin 7-10 days before surgery and discontinue dipyridamole at least 2 days before surgeryResume with oral intake.
Thienopyridines (clopidogrel, prasugrel, or ticlopidine)
When used after cardiac stenting procedure, if discontinued can cause cardiac ischemia perioperatively. If continued can result in bleeding complications.
Ideally elective procedures should be delayed until the mandatory period of platelet inhibition with these agents is completed. When used for long term stroke prophylaxis, should be discontinued 7-10 days.Resume with oral intake